Conservative surgery and radiotherapy for early breast cancer
Upload
khangminh22Category
view
0download
0
VO
LU
ME
7, 2
02
0



Dear Colleagues,
ARCHIVES OF BREAST CANCER
Happy new year, 2021!
The year 2020 began when every single activity was affected by the Coronavirus pandemic. As a medical journal, we tried our best to publish more articles exploring the idea of confronting cancer patients and cancer research with an undesirable disaster, COVID-19.
Although everything was affected by the pandemic, we passed a successful year in 2020. We could accomplish all the three premeditated plans. Now, ABC benefited from a more powerful editorial board, more extensive indexings and, as a result, more articles in terms of both quality and quantity from different parts of the world. The result of these activities is reflected in doubling the number of citations of ABC articles in 2020 compared to 2019. The only unfortunate happening for the journal in 2020 was the loss of one of the most brilliant members of our editorial board, Professor Robidoux.
In 2021 we are planning to:1. Apply for indexing in Clarivate, Thompson-Reuters, and Scopus.2. Accept more articles and observe the preplanned average of 2 weeks as the submission-to-decision time. 3. Increase the number of published articles to 14 manuscripts per issue.ABC will invite all researchers to join this multidisciplinary scientific forum and select this journal as a
platform to publish their scientific papers. You will have an excellent experience with ABC's fast and easy publication process for your qualified researches!
Good luck in 2021!
Ahmad Kaviani, MDEditor-in-Chief,Archives of Breast Cancer

Executive Directors
S. Zand, M.D.Clinical ResearcherN. Mashoori, M.D. Breast Surgeon, Clinical ResearcherM. NeishabouryAnesthesiologist, Clinical Researcher
Editor-in-Chief
Department of Surgery, Tehran University of Medical Sciences
Office
K. DavoodzadehM. Tak
Technical Editors
V. Karimi
Associate EditorMojgan Karbakhsh, M.D.
Department of Community and Preventive Medicine, Tehran University of Medical Sciences
In the memory of the Distinguished Professors in the Editorial Board
Professor André Robidoux (1945-2020)Department of Surgical Oncology,University of Montreal, Canada
Professor Mohammad SafaeiKeshtgar (1962-2017)Department of Surgery,Royal Free Hospital,University College London, UK.
Dr. Ahmad Kaviani

Dr. David KragDepartment of Surgical Oncology, University of Vermont, Burlington, USA
Dr. Remy J SalmonDepartment of Surgical Oncology, Curie Institute, Paris, France
Dr. Yazid BelkacemiDepartment of |Radiation Oncology, Henri Mondor Breast Center, Paris, France
Dr. Farin KamangarDepartment of Epidemiology, Morgan State University, Baltimore, USA
Dr. Vincent Vinh-HungDepartment of Radiation Oncology, University Hospital of Martinique, France
Dr. Alfred FitoussiDepartment of Surgery, Curie Institute, Paris, France
Dr. Fiana NakhlisDepartment of Surgical Oncology, Dana-Farber Cancer Institute, Boston, USA
Dr. Abdul KasemDepartment of Surgery, King's College Hospital, University of London, UK
Dr. Kouki InaiDepartment of Pathology, Hiroshima University, Hiroshima, Japan
Dr. Giorgio TregliaDepartment of Nuclear Medicine, Oncology Institute of Southern Switzerland, Bellinzona, Switzerland
Dr. Siavash AtrchianDepartment of Radiation Oncology, University of British Columbia, Vancouver, Canada
Dr. Erica PatosckiDepartment of Surgical Oncology, University of Montréal, Canada
Dr. Mahsa MohebtashDepartment of Medical Oncology, Morgan State University, Baltimore, USA
Dr. Alain DaninoDepartment of Plastic & Reconstructive Surgery, University of Montreal, Canada
Dr. Peiman HaddadDepartment of Radiation Oncology, Tehran University of Medical Sciences, Tehran, Iran
Dr. Mehran HabibiDepartment of Surgery, Johns Hopkins Bayview campus, Baltimore, USA
Editorial Board
Dr. Rami YounanDepartment of Surgical Oncology, University of Montréal, Montréal, Canada
Dr. Fernando Collado-MesaDepartment of Radiology, University of Miami, USA
Dr. Farid MeybodiDepartment of Surgery,Westmead Breast Cancer Institute, New South Wales, Australia
Dr. Senarath EdirimanneDepartment of Surgery, University of Sydney, Australia
Dr. Masud YunesianDepartment of Epidemiology, Tehran University of Medical Sciences, Tehran, Iran
Dr. Sanjay WarrierDepartment of Surgery, University of Sydney, Sydney, Australia
Dr. Ghaith HeilatDepartment of Surgery, Yarmouk University, Jordan
Dr. Joseph Bou-MerhiDepartment of Plastic & reconstructive Surgery, University of Montreal, Canada
Dr. Keivan MajidzadehDepartment of Medical Genetics, Moatamed Cancer Institute, Tehran, Iran
Dr. Benoît CouturaudDepartment of Plastic & reconstructive Surgery, Curie Institute, Paris, France
Dr. Patricia ClarkDepartment of Surgery, Ironwood Cancer and Research Centers, Arizona, USA
Dr. Ashraf ShomaDepartment of Surgery, Mansoura University, Egypt
Dr. Alphonse TranDepartment of Nuclear Medicine, University of Montreal, Canada
Dr. Mahmoud Al-BalasDepartment of Surgery, Hashemite University, Jordon
Dr. Nazanin KhakpourDepartment of Surgical Oncology, Moffitt Cancer Center, New York, USA
Dr. Vignesh RavichandranComputational Biology, Memorial Sloan Kettering Cancer Center, New York, USA
Dr. Petros CharalampoudisDepartment of Surgery University College London, London, UK

Archives of Breast Cancer Volume 7, Issue 1, Feb. 2020
REMEMBRANCEOncology Loses a Pioneer 97iEditorial TeamDOI https://doi.org/10.32768/abc.20207397i-97ii
INVITED COMMENTARYCovid-19 and Cancer Patients: Delving into Burning Questions 1Sadaf AlipourDOI https://doi.org/10.32768/abc.2020711-3
REVIEW ARTICLEPhytoestrogens and Breast Diseases: A Matter of Concern for the Gynecologist 4Sadaf Alipour, Amirhossein EskandariDOI https://doi.org/10.32768/abc.2020714-9
CLINICAL EXPERIENCEGenetic Counseling in the Follow-up of Breast Cancer patients; Conversion of a 10Luminal Tumor to TNBC Hamid Ahmadi, Reza Hosseinpour, Behnaz Jahanbin, Keivan Majidzadeh-A, Farid Azmoudeh-ArdalanDOI https://doi.org/10.32768/abc.20207110-13
VIEWPOINT AND ALGORITHMModifications in Breast Cancer Guidelines in COVID-19 Pandemic; An Iranian Consensus 14Farhad Shahi, Mehrzad Mirzania, Mahdi Aghili, Mohammadreza Dabiri, Sharareh Seifi, Alireza Bary, Nafiseh Ansarinejad, Alireza Rezvani, Soroush Rad, Amirali Shahi, Ahmad Elahi, Ahmad KavianiDOI https://doi.org/10.32768/abc.20207114-21
ORIGINAL ARTICLEAccurate Detection of Breast Cancer Metastasis Using a Hybrid Model of Artificial 22Intelligence Algorithm Jafar Abdollahi, Atlas Keshandehghan, Mahsa Gardaneh, Yasin Panahi, Mossa Gardaneh DOI https://doi.org/10.32768/abc.20207122-28
Knowledge, Attitudes, and Practices toward Breast Cancer 29Hesam Adin Atashi, Mohammad Eslami Vaghar, Maedeh Olya, Parisa Mirzamohammadi, Hamid Zaferani Arani, Mohammad Hadizadeh, Seyed Mahmoud Reza Hashemi Rafsanjani, Ghoncheh AlizadehDOI https://doi.org/10.32768/abc.20207129-36
Associated Factors with Adopting Preventive Behaviors for Breast Cancer in Iran 37Marzieh Hajikarimbaba, Rahman Panahi, Leila Dehghankar DOI https://doi.org/10.32768/abc.20207137-43
CASE REPORTProgressive Metastatic Breast Phyllodes Tumor Turns into Spindle Cell Sarcoma: 44Report of Two Cases and Review of the Literature Nahid Nafissi, Seyed-Mohamad-Sadegh Mirahmadi, Majid Samsami, Nafiseh AnsarinejadDOI https://doi.org/10.32768/abc.20207144-48
Contents
Archives of Breast Cancer Volume 7, Issue 2, May. 2020
Contents
LETTER TO EDITORFrom Days of "Nonverbal Communication" to Days of “Masks” and "Evisit": 49 Effective Palliative and Cancer Care Communication in the Times of Covid-19 Mamak TahmasebiDOI https://doi.org/10.32768/abc.20207249-50
INVITED COMMENTARYImpact of Prioritization of Breast Cancer Patients Treatment in the Case of Long- 51term Existence of COVID-19 Sanambar SadighiDOI https://doi.org/10.32768/abc.20207251-53
REVIEW ARTICLEFDG PET Application for Management of Breast Cancer Patient: A Narrative Review 54Saeed Farzanehfar, Farahnaz Aghahoseini, Marzieh Peyman, Mehrshad AbbasiDOI https://doi.org/10.32768/abc.20207254-58
CLINICAL EXPERIENCEInflammatory Breast Cancer in a Very Young Genetically Susceptible Woman: 59Case Presentation in a Tumour Board Session, Discussion and Decision-Making Sadaf Alipour, Leila Bayani, Akram SeifollahiDOI https://doi.org/10.32768/abc.20207259-64
ORIGINAL ARTICLE Features of Breast Cancer in Iranian-born Migrant Women Treated in Australia 65Farid Meybodi, Meagan E BrennanDOI https://doi.org/10.32768/abc.20207265-71
Molecular Simulations Identify Target Receptor Kinases Bound by Astaxanthin to 72 Induce Breast Cancer Cell Apoptosis Mossa Gardaneh, Zahra Nayeri, Parvin Akbari, Mahsa Gardaneh, Hasan TahermansouriDOI https://doi.org/10.32768/abc.20207272-82
SHORT COMMUNICATIONThe role and application of metaphor in creatioThe Role and Application of 83Metaphor in Preventing Breast Cancer Phobian the phobia of breast cancer Malahat Shabani MinnabadDOI https://doi.org/10.32768/abc.20207283-87
CASE REPORTOvarian Cancer Metastatic to Breast and Axilla: A Case Report 88Mehdi Ghelichkhani, Nahid Naffisi, Zahra Rahimi, Farshid Ghasemi Meydansar,Masoud Haghighikian, Leila Sadeghi| DOI https://doi.org/10.32768/abc.20207288-92 Page 88-92
A Malignant phyllodes Tumor of the Breast; Presentation of an Uncommon Case 93and Review of the LiteratureSumaiya Iqbal, Juwairiya, Nowfala Nowshad, Khadeeja Mohammad DOI https://doi.org/10.32768/abc.20207293-96

Archives of Breast Cancer Volume 7, Issue 3, Aug. 2020
Contents
EDITORIALOncoplastic Breast Surgery – Pros and Cons for the Breast Surgical Oncologist 97Faina NakhlisDOI https://doi.org/10.32768/abc.20207397-99
CLINICAL EXPERIENCEPapillary Lesion of the Breast in a Young Girl Suspicious to Juvenile Papillomatosis, 100Clinical Decision Making in a Multi-disciplinary Team and Review of the Literature Marzieh Mohammadi Zavieh, Farid Azmude Ardalan, Farnaz Karimi, Nahid Sedighi, Ramesh Omranipour, Ahmad ElahiDOI https://doi.org/10.32768/abc.202073100-103
ORIGINAL ARTICLECharacteristics of Breast Cancer at First Presentation in Sudanese Patients Attending 104 the National Cancer Institute–University of Gezira (NCI–UG) Muna Ahmed Eltayeb, Areeg Faggad, Osama Sharafeldin Abbadi, Moawia Mohammed Ali ElhassanDOI https://doi.org/10.32768/abc.202073104-110
Clinicopathologic Features and Survival Analysis of Non-metastatic Breast Cancer 111Patients in Guatemala Hugo Castro-Salguero, Luis García Aceituno, Alba Kihn, Raúl Jiménez, Allan Ramos-EsquivelDOI https://doi.org/10.32768/abc.202073111-118
The Unique Mental Impacts of Breast-Conserving Surgery and Mastectomy According 119to a Multi-Centered Cross Sectional Survey Conducted in Japan Yuri Hazawa, Goro Kutomi, Hiroaki Shima, Toshio Honma, Tosei Ohmura, Asaka Wada, Toshihiko Mikami, Miki Hotta, Momoka Narumi, Tomohiro Ishinuki, Yoshika Kuno, Makoto Meguro, Ichiro Takemasa, Minoru Okazaki, Hideji Masuoka, Kazuaki Asaishi, Toshio Ohyanagi, Thomas T. Hui, Toru MizuguchiDOI https://doi.org/10.32768/abc.202073119-126
Concordance and Diagnostic Accuracy of Ultrasonography and Mammography 127Findings with Pathology Results in Breast Cancer Leila Ghafoor, Abbas Hajian, Yaser Hamidian, Seyed Hamed RohaniDOI https://doi.org/10.32768/abc.202073127-131CASE REPORTA Case Report of Spontaneous Thrombosis of an Iatrogenic Breast Pseudoaneurysm 132Masoumeh Gity, Batoul Seifi Nadergoli, Behnaz Moradi, mohammadreza chavoshiDOI https://doi.org/10.32768/abc.202073132-135
Large Malignant Phyllodes Tumor of the Breast: Case Report of a Young Female 137 and Review of Literature Melissa Kyriakos Saad, Imad El Hajj, Elias SaikalyDOI https://doi.org/10.32768/abc.202073136-142

Archives of Breast Cancer Volume 6, Issue 1, Feb. 2019
Contents
Archives of Breast Cancer Volume 7, Issue 4, Nov. 2020
LETTER TO EDITORA Plea for Defining a Uniform Standard Order in Reporting Details of a Whole 143 Breast Ultrasound: The Point of View of Two Breast Surgeons? Sadaf Alipour, Farzaneh GolfamDOI https://doi.org/10.32768/abc.202074143-144
INVITED COMMENTARYThe Challenge of Breast Density– Options for Management and Breast Cancer Screening 145 Meagan Brennan, Brooke Nickel, Nehmat HoussamiDOI https://doi.org/10.32768/abc.202074145-148
Fertility Preservation in Breast Cancer Patients Under Special Consideration of Ovarian 149Stimulation for Fertility Purposes Sebastian Findeklee; Sebastian Grewe, Klaus DiedrichDOI https://doi.org/10.32768/abc.202074149-154
ORIGINAL ARTICLEAssessment of Prognostic and Therapeutic Factors in Male Breast Cancer: An 155Observational Study of a Southwest Spanish Single Center Daniel Herrero, María Rocío Morales Herrero, José Luis López Guerra, Alberto Sánchez Camacho-Mejías, Irene Carrasco García, Paloma Santos Fernández, Carmen Victoria Almeida González, Marta Benavent Viñuales, Alejandro Falcón González, Álvaro Montaño Periáñez, Rosario González Mancha, Francisco Javier Salvador Bofill, Manuel Ruiz BorregoDOI https://doi.org/10.32768/abc.202074155-163
Prognostic Value of Androgen Receptor in Triple Negative Breast Cancer of Iranian Patients 164in Yazd Region Fatemeh Alsadat Nobakht, Mansour MoghimiDOI https://doi.org/10.32768/abc.202074164-167
Health System Barriers to the Discussion of Breast Reconstruction Options in 168Australia: Improving Access Through Appropriate Referral Kathy Flitcroft, Meagan Brennan, Andrew SpillaneDOI https://doi.org/10.32768/abc.202073168-177
Encysted Papillary Carcinoma of the Breast (EPC): A Follow-up Study to Investigate the Role 178of Sentinel Lymph Node Biopsy Ioannis Spyrou, Foivos Irakleidis, Stergios Douvetzemis, Hisham Hamed, Ashutosh KothariDOI https://doi.org/10.32768/abc.202074178-182
Quality of Life Assessment After Conserving Breast Surgery and Intraoperative 183Radiotherapy (IORT) in Breast Cancer Patients Using the BREAST-Q Questionnaire Marina Caldana, Davide Lombardi, Silvia Urbani, Francesca Pellini, Sara Mirandola, Eleonora Granuzzo, Giovanni Paolo PolliniDOI https://doi.org/10.32768/abc.202074183-188
Novel Approach Exploiting the Hyperspectral Imaging System for Breast Cancer Therapy 189and Diagnosis Mohamed Hisham Fouad Aref, Ibrahim H. Aboughaleb, Abou-Bakr M. Youssef, Yasser H. El-aSharkawyDOI https://doi.org/10.32768/abc.202074189-201
CASE REPORTPrimary Leiomyosarcoma of the Breast Papilla: A Case Report 202Matthäeus Bürger, Edson Marchiori, Maria Celia R. Djahjah, Ana Helena CorreiaDOI https://doi.org/10.32768/abc.202074202-206

We are so sad to know of the rapid loss of Professor André Robidux.
He was an exceptional educator, teaching the next generation of surgeons with enthusiasm and patience. He leaves behind a legacy of excellent patient care and a career in research, visionary and unparalleled. He was a cherished colleague who will never be forgotten by those who had the good luck to have know him.
bRemy J Salmon
After surgical training in the USA, he returned back to Canada, where he rose through the hierarchy, becoming the Medical Director of the Breast Cancer Research Group at the University of Montreal Hospital Center. He was a very well known scientist through his activities in the NSABP, where, as a Francophone, he played an essential role in the transition between Canada and France. If a transatlantic medical cooperation had been possible,
Doctor Robidoux had an exemplary surgical career and was recognized worldwide for his vision, innovation and dedication in the field of clinical research in breast cancer. The NSABP presented him with the “Distinguished Lifetime Achievement Award” to underline his impeccable commitment to oncology research.
Doctor Robidoux was a full professor in the department of surgery at the University of Montreal and holder of the Scotiabank Chair in Breast Cancer Diagnosis and Treatment from 2000 until recently. He died of cancer at the age of 72 on Saturday, July 25, surrounded by loved ones.
aErica Patocskai
He played a central role in the advances in breast cancer treatments over the past 40 years and treated thousands of women in Quebec with his remarkable expertise and integrity. Besides his outstanding achievements, he was greatly appreciated by his patients, colleagues and research team because of his dedication, great humanity and humility.
We will miss his friendly and warm presence, his insightful questions and his long-standing friendship. Scientific meetings will not be the same without him.
cMichel Alain Danino
But the memory that will mark his fellow surgeons is his sparkling, intelligent and mischievous gaze. For us, his colleagues, and his friends, he embodied for all of us a scientific and moral compass. But this probity was with him always associated with kindness.
The population of Dr. Robidoux's laboratory reflected his commitment to the need for international cooperation in scientific discovery and in the dissemination of learning in the breast cancer field. Many languages could be heard in the various labs and offices of Dr. Robidoux's Laboratory. He was appreciated not only for his remarkable knowledge but also for his incredible kindness. But above all, Dr.
On Saturday 25 July 2020, the breast oncology community lost Professor Andre Robidoux, whose pioneering contributions have shaped several aspects of the battle against breast cancer. It would have been possible to expand on his major academic contribution with 114 publications in peer-reviewed journals between 1982 and 2020, 2 books on the history of breast cancer research and his countless invitations as a visiting professor throughout the world.
it certainly would have taken place through it. On a human level, he regularly came to share his
experience at conferences in Paris and in the provinces, and it was always a renewed pleasure to discuss with him the progress of medicine and surgery, but also "things" of the world.
He had a benevolent behaviour to all his colleagues, especially towards young people and those training in his team, and his humour, which was clearly visible on his face, taught how to defuse the inevitable tensions in surgical units.
i
Oncology Loses a Pioneer
Open AccessRemembrance
DOI: 10.32768/abc.20207397i-97ii
Editorial Team. Arch Breast Cancer 2020; Vol. 7, No. 3: 97i-97ii
Professor André Robidoux(1948-2020)

Professor Andre Robidoux
Dr. Robidoux's scientific contributions have triggered the ever-expanding horizon of breast cancer research and led to paradigm shifts in our understanding of the genetic origin of this disease. His legacy will endure for generations to come. The plastic surgery community extends its condolences to his wife and family.
Named by many of his female patients "Pape"-which is the French word for Pope, Dr Andre Robidoux incarnated a figure of Hope for many of them. A native of the small French Canadian village of Sorel, he made his way to the Major Leagues of research on Breast Cancer, the NSABP "National Surgical Breast and Bowel project" organization.
eSaima Hassan
He called the Breast "The Noble Gland" in his discussions with peers, friends or patients as he devoted his professional career and lots of his time to studying and shaping research pertaining to breast cancer.
He will be remembered as a Milestone personality in the research on Breast Cancer having gone through breast cancer treatments from the original mutilating Halsted radical mastectomy to the more modern oncoplastic breast techniques, and from completely random systemic treatments to the most precise targeted therapies!
Robidoux lived for his patients. He was listening to their demands for morphologic rehabilitation. We, reconstructive surgeons, always found a rare openness in his person. He was thus one of the first to offer his patients immediate breast reconstructions and skin preservation, he accompanied and gave credit to all breast reconstruction development from cutaneous breast expansion to microsurgical reconstruction by deep inferior epigastric vessels flaps.
Always a great story-teller, he always had social talent and tricks in his pocket.
He will be missed by so many…
dRami Younan
Dr. Robidoux was a Full Professor in the Department of Surgery at University of Montreal, surgical oncologist at the Centre Hospitalier de l'Université de Montreal (CHUM), and clinical researcher at the Centre de Recherche (CR-CHUM).
Dr. Robidoux dedicated his career to the fight against breast cancer, and his objective was to improve the care for breast cancer patients in
In his mourning, this poem by Rudaki (859-941), the father of Persian poetry, is very befitting by loosing him:
I always considered him as a kind and compassionate father. In one sentence, he was a high-ranking and praiseworthy human in all personal and professional fields.
I am one of the last lucky surgeons to be able to work with Professor Robidoux for a while. For the first time, I met him in the summer of 2017 in his small office in the old building of Hotel Dieu in Hospital Montreal. I saw a courteous, kind, and very respectful senior whose great spirit thoroughly impressed me, the professor who was really much greater than his internationally renowned name, Professor Robidoux.
His mastery in the latest clinical studies in breast cancer and his creative and innovative thinking made him always very fascinating and enticing. The extent of his information was not limited to breast cancer or even medicine, and his accurate information on different subjects like the cultural and social backgrounds of different ethnicities all around the world was astonishing.
His ideas to draw a plan for the Archives of Breast Cancer were very instructive and inspiring for me, and I try my best to consider his recommendation in the journal.
and many thousands are lost from the wisdom of humankind.”
Quebec. Dr. Robidoux helped to bring clinical trials to thousands of breast cancer patients in Montreal. Amongst his many achievements, Dr. Robidoux was a recipient of the Distinguished Investigator Lifetime Achievement Award in 2010, in recognition of his extraordinary commitment to the NSABP and oncology research.
“From the number of two eyes (human beings), one is less,
Dr. Robidoux was a visionary and a prolific researcher. He contributed to two paradigm shifts in breast cancer surgery; 1) the change from aggressive, mutilating radical mastectomies to partial mastectomies; and 2) the use of neoadjuvant chemotherapy prior to surgery. He was a thoughtful clinician, a skillful surgeon, a kind mentor, and a warm human being. His passing leaves a huge loss for oncology, his colleagues, friends, and family.
fAhmad Kaviani
ii Editorial Team. Arch Breast Cancer 2020; Vol. 7, No. 3: 97i-97ii
a Chief of Surgical Oncology Service, CHUM, University of Montreal, Montreal, Canadab Retired Professor of Surgical Oncology, Curie Institute, Paris, Francec Chief of Plastic and Reconstructive Surgery Service, CHUM, University of Montreal, Montreal, Canadad Associate Professor, Surgical Oncology Service, CHUM, University of Montreal, Montreal, Canadae S cotiabank Chair in the Diagnosis and Treatment of Breast Cancer, Division of Surgical Oncology, Centre de
Recherche-CHUM, University of Montreal, Montreal, Canadad Editor-in-Chief, Archives of Breast Cancer, Professor of Surgery, Tehran University of Medical Sciences, Tehran, Iran

Apart from physicians who are directly involved in the management of the viral infection in Covid-19 patients, medical specialists also have to make medical decisions for diagnosis or treatment of other disorders in patients infected with, or at risk of the novel virus. At the same time, there are still no confirmed guidelines and even no proven scientific evidence. Cancer is one of the most significant challenges that patients and health care professionals have to face under these circumstances. Meanwhile, oncologic surgeons face several dilemmas:
Covid-19, caused by the 2019 novel coronavirus, is being transmitted across an increasing number of
1countries. It is a critical global public health threat because of its high transmission rate and potential
2fatality. On the last day of January 2020, the world health organization (WHO) announced a Public Health Emergency of International Concern
3(PHEIC). According to the WHO situation report, world statistics on 6 March 2020 were 98192 confirmed cases and 3380 deaths from the disease (https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/).
- Are cancer patients at risk of more severe disease or higher mortality? Cancer is an underlying disease
4, 5that puts patients at high risk of infections. Should they be admitted for surgery during the outbreak of this virus?
- What are the special considerations for the surgery of these patients during Covid-19 outbreak? What measures should be taken in the pre- and post-operative period, and throughout the operation?
- Are patients with cancer at higher risk of contracting Covid-19?
Are patients with cancer at higher risk of contracting Covid-19? Are cancer patients at higher risk of more severe disease and higher mortality?
Overall, this study showed a higher risk of Covid-19 infection and unfulfilling outcomes for patients. The authors recommended more strict personal protection for these patients and more aggressive management of the viral disease, if they showed symptoms of the novel coronavirus.
Another finding of this research was a higher rate of severe disease, ICU admission, and death in Covid-19 cases with underlying cancer. Cancer survivors had higher chances of unfavorable outcomes compared with patients with no history of cancer.
Despite insufficient evidence regarding the potential implication of Covid-19 in the context of malignancy, cancer is known to negatively affect the
4immune system. This can lead to critical unfavorable outcomes in patients undergoing chemotherapy. The National Clinical Research Center for Respiratory Disease and the National Health Commission of the People’s Republic of China have mutually launched a prospective cohort of Covid-19 cases confirmed by laboratory tests in order to follow the course of the disease. Reviewing features of 1590 patients with complete data to detect patients with underlying
6 cancer, Liang et al. found 18 cases. This means that 1% of the Covid-19 cases were afflicted by cancer. This rate is higher than that of cancer in the general Chinese population, which is around 0.3%. This may suggest that cancer patients are at higher risk of symptomatic Covid-19. Interestingly enough, 12 out of these 18 patients had no active cancer and were long-term cancer survivors. Moreover, cancer patients were older than others in that cohort.
This paper aims to address the above questions based on the best available evidence.
- What preventive measures should be taken by the medical team during surgery in cancer patients during Covid-19 epidemic?
Covid-19 and Cancer Patients: Delving into Burning Questions
a Breast Disease Research Center, Tehran University of Medical Sciences, Tehran, Iran
b Department of Surgery, Arash Women's Hospital, Tehran University of Medical Sciences, Tehran, Iran
a,bSadaf Alipour*
Open AccessInvited commentary
* Address for correspondence:Sadaf Alipour, MDAssociate Professor,Address: Arash Women's Hospital, Shahid Baghdarnia St.,Ressalat St., Tehran, Iran.Tel: +98 21 61192761Email: [email protected]
DOI: 10.19187/abc.2020711-3
1Alipour, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 1-3

Yu et al. also point to complete examinations for Covid-19, which should take place before operation on the cancer patient, stressing that the operating room should have a negative pressure system. They recommend having all the surgical equipment checked according to sterilization and disinfection protocols and using general anesthesia with tracheal intubation. The authors also state that surgical specimens should be considered infectious and
Li et al. also recommended performing an accurate assessment of the patients for Covid-19 before surgery of esophageal cancer. They opt for a 2-week isolation of the patient and checking body temperature twice daily, as well as testing for the virus. Most importantly, they emphasize that any modifiable condition which can increase the risk of post-operative infection or other complications should be corrected before surgery; this would prevent lengthening of the patient's stay at the hospital, thus minimizing the risk of further
7infections, including Covid-19.
What measures should be taken in the pre- and post-operative period, and during the cancer operation?
Approaching the subject in terms of anesthesiology, and insisting on performing only emergency surgeries, Wen and Li recommended a full assessment of the patient for infection with the novel coronavirus in order to detect asymptomatic/ undiagnosed cases. History of recent travels and close contact with people affected with Covid-19, as well as body temperature measurement and even chest CT scan, have been
9recommended before surgery by these authors.
Should patients with cancer be admitted for treatment and surgery during Covid-19 outbreak?
Currently, precise estimates are not available on when Covid-19 epidemic in different countries is going to “hopefully” terminate. The decision about cancer treatment should follow the general principles of cancer management.
To date, risks of the untreated malignancy while waiting for the Covid-19 epidemic to subside versus risks of exposure to this virus during admission for cancer treatment have not been studied. Therefore, the physician must decide based on each patient’s status and cancer conditions, as well as hospital settings. Liang et al. have proposed delaying the surgery or chemotherapy in stable cancer where
6Covid-19 is endemic. Li et al. have reviewed possible options for patients with esophageal cancer during Covid-19 outbreak, suggesting postponing
7the treatment, when possible. Also, Yu et al. suggested that if surgery is indicated for colorectal malignancy based on the characteristics of cancer, it should be done as soon as the hospital can accept admissions for elective surgeries. They opt for laparoscopic surgery (versus open surgery) under
8these conditions.
Previous coronavirus epidemics, including MERS and SARS, affected health care workers at a
10very high rate of around 20%. This seems possible for Covid-19, and thus all protective precautions are warranted for the medical staff while they provide care during the whole length of patient's stay at the
8hospital.
2. Rothan HA, Byrareddy SN. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. Journal of Autoimmunity. 2020:102433.
1. Lipsitch M, Swerdlow DL, Finelli L. Defining the Epidemiology of Covid-19- Studies Needed. New England Journal of Medicine. 2020.
In conclusion, in the light of the limited available evidence, cancer patients should be considered high risk for Covid-19. They must be protected against the virus by protective personal behaviors, including using physical, respiratory barriers and hygienic habits, and aggressive treatment if affected by the novel coronavirus. In stable conditions, patients should undergo operation according to their cancer characteristics in non-epidemic areas. If the conditions are endemic, stable cancer surgery can be postponed. Further studies would lead to more conclusive results and assist in making decisions on more evidence-based grounds.
8handled accordingly.
5. Rotstein C, Cummings KM, Nicolaou AL, Lucey J, Fitzpatrick J. Nosocomial infection rates at an oncology center. Infection Control & Hospital Epidemiology. 1988; 9:13-9.
3. Zhou D, Zhang P, Bao C, Zhang Y, Zhu N. Emerging Understanding of Etiology and Epidemiology of the Novel Coronavirus (COVID-19) infection in Wuhan, China. 2020.
References
None.Conflict of Interest
4. Kamboj M, Sepkowitz KA. Nosocomial infections in patients with cancer. The lancet oncology. 2009; 10:589-97.
What precautions are needed for the medical team during surgery in cancer patients during Covid-19 epidemic?
These few articles have been published investigating the conditions in China, which is witnessing the most severe epidemic for Covid-19. In other parts of the world, with a lower burden of the disease, waiting for two weeks –as the incubation period- cannot be recommended, except for the patients with a positive history of travel or close contact. Thus, taking a thorough history, and physical examination and a pre-operative x-ray of the chest would probably suffice. This is what we are doing under present conditions. If endemic diseases occur, the same approach as above would be necessary.
Covid-19 and cancer patients
2 Alipour, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 1-3
10. Peeri NC, Shrestha N, Rahman MS, Zaki R, Tan Z, Bibi S, et al. The SARS, MERS and novel coronavirus (COVID-19) epidemics, the newest and biggest global health threats: what lessons have we learned? International Journal of Epidemiology. 2020.
7. Li Y, Qin J, Wang Z, Yu Y, Wen Y, Chen X, et al. Surgical treatment for esophageal cancer during the outbreak of COVID-19. Zhonghua zhong liu za zhi [Chinese journal of oncology]. 2020; 42:E003.
8. Yu G, Lou Z, Zhang W. Several suggestion of operation for colorectal cancer under the outbreak of Corona Virus Disease 19 in China. Zhonghua wei chang wai ke za zhi= Chinese journal of gastrointestinal surgery. 2020; 23:9.
6. Liang W, Guan W, Chen R, Wang W, Li J, Xu K, et al. Cancer patients in SARS-CoV-2 infection: a nationwide analysis in China. The Lancet Oncology. 2020.
9. Wen X, Li Y. Anesthesia Procedure of Emergency Operation for Patients with Suspected or Confirmed COVID-19. Surgical Infections. 2020.
3Alipour, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 1-3
Covid-19 and cancer patients

disorders. In four consecutive studies concerning exogenous sex hormones and the breast as a matter of concern for gynecologists and other physicians who prescribe these medications, we have focused on
4OCP3, HRT , and the use of other synthetic sex
5hormones in women without any breast lesion as well as those affected by various breast disorders. As the last part of that quadruple research, we review the literature on the effect of phytoestrogens (PEs) on BC in the present work.
The structure of PEs is similar to 17-β-estradiol (E2), and are therefore recognized as plant-derived (phyto) estrogens. Due to this similarity, PEs may bind to estrogen receptors (ER) and suppress or,
6conversely, prompt estrogen-dependent conditions.
IntroductionBreast disease and specifically breast cancer
(BC) are affected by female sex hormones. While endogenous hormones affect the breast physiology and are involved in the pathophysiology of benign and malignant breast diseases, exogenous sex
1, 2 hormones may adversely affect the breast.Some considerations must be taken into account
while prescribing hormones for various gynecologic
ARTICLE INFO
Conclusion: Existing data generally supports the safety of phytoestrogen consumption regarding the risk of breast cancer in the general population, in women with benign breast disorders, in those at risk of breast cancer, and even in survivors of the cancer. However, due to insufficient evidence, prescription of high doses of phytoestrogens is still not recommended.
Methods: We carried out a thorough search of the existing literature using appropriate keywords with the aim of finding systematic reviews, reviews, cohort studies and clinical trials regarding the effects of phytoestrogens on the breast in the general population, breast cancer survivors, women at high risk of breast cancer and those with benign breast diseases.
Background: This study is the last part of a quadruple series investigating the relationship between breast disorders and the consumption of exogenous sex hormones. Due to the structural similarity of phytoestrogens to estrogen and the confusion associated with their possible estrogenic activity in the breast, this part aims at reviewing of the literature on the relationship between phytoestrogens and breast disorders.
Results: Many studies have approached the relationship between phytoestrogens and the risk of breast cancer or recurrence of the disease. Also, a few studies have considered the effects of phytoestrogens on benign breast disorders, BRCA genes, and the risk of breast cancer in high risk women. However, the variety of studies and the retrospective nature of many of them make it impossible to draw definite conclusions.
Accepted:
phytoestrogen
Revised:
Breast cancer
23 February 2020
Key words:
isoflavone
Received:
menopause,
16 February 2020
hot flush,
26 January 2020
estrogen,
* Address for correspondence: Amirhossein Eskandari, MDAddress: Central building of Ministry of health and Medical Education, Eyvanak Boulevard, Ghods Shahrak, Tehran, Iran.Tel: 0098-21-22507213E-mail: [email protected]
ABSTRACT
Phytoestrogens and Breast Diseases: A Matter of Concern for the Gynecologist
a Breast Disease Research Center, Tehran University of Medical Sciences, Tehran, Iran
b Department of Surgery, Arash Women's hospital, Tehran University of Medical Sciences, Tehran, Iran
c Deputy of Education, Ministry of Health, Tehran, Iran
a,b cSadaf Alipour , Amirhossein Eskandari*
Open AccessReview Article
DOI: 10.19187/abc.2020714-9
4 Alipour, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 4-9

We aimed to find valid data concerning the effects of PE on the breast in the general population, women with benign breast disorders (BBD), high-risk women, and breast cancer survivors. We carried out a comprehensive search in Google Scholar and PubMed using combinations of these keywords: “benign breast”, BRCA, “breast cancer”, “breast cancer survivor”, “family history”, fibroadenoma, fibrocystic, flax, high-risk, isoflavonoid, isoflavone, lignan, phytoestrogen, soy, and “systematic review”.
There are five main classes of PE, including isoflavonoids, coumestans, stilbenes, flavonoids and lignans, which are found in various plant foods such as soybeans, chickpeas, flax, mung beans, beans and
7-9lentils.The issue considered in this article warrants
attention from two different perspectives. First, hot flashes and other hormone-deprivation symptoms are common in BC survivors who undergo endocrine therapy or chemotherapy. Hormone replacement therapy is the most effective treatment for alleviation of these symptoms, but possible negative consequences for the cancer course prevents their use. Secondly, as PEs are often freely used by women or prescribed by physicians, the potential effects of such PE-containing foods on breast diseases and the potential risks they pose for BC need to be
10-12investigated.A variety of phytoestrogen-containing foods and
factory-based combinations and supplements of these compounds are available. Studies of PE in various forms and supplies are innumerable, but we did not aim to systematically review all of them. Our aim was to review the effects of dietary intake or supplemental prescription of these compounds on the breast.
Methods
Due to the bulk of the existing literature on the subject, we focused first on systematic reviews, then on solitary cohort studies and clinical trials as well as reviews. Thus, we extracted data from all relevant studies.
Results and Discussion1. Phytoestrogens in the general population1.1. Phytoestrogens and their effects on the breast
composition in the general populationMany estrogen compounds cause breast pain and
breast edema. Whether the same changes occur secondary to the use of phytoestrogens was investigated
13 14in two studies by Dastjerdi et al. , and Alipour et al. In these studies, placebo and isoflavone supplements were compared regarding their effects on breast exam and breast ultrasound but no significant differences were detected between the two groups in either study.
1.2. Phytoestrogens and the risk of breast cancer in the general population
Due to the high rate of PE consumption by Asians
and the low incidence of BC among them, the possibility of a protective effect for these compounds
11against BC has been put forward. Many studies have considered the effect of PE on BC risk. However, the designs of these studies and their findings are so diverse that conclusive results and definitive conclusions cannot be easily obtained.
Some researchers have considered the risk of BC as a function of the rate of consuming PE-containing foods and supplements. Some studies have studied one specific type of PEs while some others have considered all or multiple forms of PEs. Several works have investigated the association between PE consumption and specific subtypes of BC, while others have considered pre- versus post-menopausal BC.
Flaxseed which contains a large amount of lignans has been the subject of multiple studies. Calado et al. have reviewed the relevant literature and found several studies on mice, all of which showed a decrease in tumor load or growth in animals fed with
15flaxseed. Also, human studies have showed a reduced risk of breast cancer in women consuming higher amounts of flaxseed. This effect was more prominent in postmenopausal BC under certain conditions, and limited to postmenopausal ER+ tumors in one study. The researchers concluded that further research and especially clinical trials considering flaxseed and BC risk need to be conducted to confirm the association.
Peeters et al. carried out a review of 18 articles containing analytical epidemiological data about the effect of dietary PE on BC risk, showing that PE intake had no protective effect against BC, except for the use of PE in very high doses or in adolescence.7 Dong et al. systematically reviewed prospective studies on the potential relationship between soy
16isoflavone intake and BC incidence. Their meta-analysis suggested an indirect association only in Asians but failed to show any dependence on the
17dose of PE intake. Fritz et al. carried out a thorough review of the effect of PE on BC, reporting no increase in BC risk with the use of dietary PE. They also found that amounts of PE intake comparable to traditional Japanese food may have a protective role against the cancer. Nagata et al. reviewed all epidemiological studies investigating the effects of dietary soy on incidence of BC among Japanese women and mortality associated with it. They considered five cohorts and six case–control studies, the results of which varied from no effect to a strong inverse association between dietary soy and BC risk. They concluded that soy intake may cause BC risk
18 reduction in the Japanese population. Zhao et al. carried out a systematic review of all prospective cohort studies on the association between dietary isoflavones and BC risk. They conducted a meta-analysis of 16 eligible studies, showing no significant
19 association.Apart from these studies, two population‐based
5Alipour, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 4-9
Phytoestrogens and breast disorders

2. Phytoestrogens in BC survivorsPhytoestrogens have been investigated in
managing menopausal symptoms and particularly hot flashes in breast cancer survivors, although their beneficial effect in the general population is still
11uncertain. Two earlier clinical trials in 2000 and
122002 compared the effects of dietary PE in soy to placebo on managing hot flashes in BC survivors, detecting no significant differences. A systematic
24review by Flower et al. assessed the positive effects of flaxseed on menopausal symptoms, finding a non-significant reduction in hot flashes. In addition, a review of clinical trials in 2016 comparing PE with placebo for the treatment of hot flashes in BC
9 survivors did not find any significant effect for PE.Moreover, a recent review of different types of management of the symptoms in these patients did
25not find PE as an effective therapy.
An important issue which is still controversial is the safety of PE in BC prognosis. While some studies suggest the possibility of worsening BC by consuming PE due to its similarity to estrogens,
15, 26, 27many others support its protective role.
case‐control studies in 2004 reported a reduced risk of premenopausal BC due to high levels of dietary
20lignan and high intakes of isoflavonoids (for ER+
21tumors). Two other population‐based case‐control 22studies carried out in Canada in 2006 and 2013 x
compared the effects of consuming PE during adolescence, reporting a reduced risk of BC in adults with a higher intake. This effect was limited to postmenopausal BC, mainly ER+ BC in the latter.
In 2011, Dong et al. reviewed prospective studies examining the effect of soy isoflavones on the recurrence of BC among the survivors. They failed to observe a clear relationship, although a reduction in recurrence was more likely to be associated with the
16use of PE. In 2013 Fritz et al. performed a thorough review of all observational studies as well as randomized and uncontrolled trials concerning the association between dietary isoflavones and recurrence of BC in survivors. They showed that dietary use of soy was safe for BC survivors independent of tamoxifen use, possibly decreasing the rate of recurrence and mortality. However, they recommended against the consumption of high doses
17 of soy in this population due to insufficient evidence.In another concurrent systematic review by Chi et al., a systematic review and meta-analysis of five cohort studies showed a diminished rate of recurrence in BC survivors and lower mortality in postmenopausal women. These results were applicable to both hormone receptor-positive and negative tumors. However, a recent systematic review and meta-analysis of observational studies by Qiu et al. showed different results. They detected a slightly decreased survival in post-menopausal women with BC who were PE consumers before the disease, whereas PE
consumption following the disease had no effect on survival. They also demonstrated a lower recurrence rate in BC survivors who used dietary PE before or
28after the diagnosis.
3. Phytoestrogens in high-risk womenProspective studies on the use of PE in high risk
women for breast cancer have not been performed, and thus we cannot be certain whether the use of PE would have a protective or stimulating effect in this group. However, this can be indirectly inferred by considering some existing studies.
In order to investigate the risk of BC in regard to PE consumption in women with a positive family history, Powles et al. designed a prospective study including either three-year consumption of red clover or placebo in healthy women with a family history of BC. They measured mammographic density as a risk marker for BC, finding no significant difference in the
29two groups.
The Korean Hereditary Breast Cancer Study (KOHBRA) was designed to evaluate nutritional issues in BRCA mutation carriers. Among various dietary elements, Ko et al. found out that the use of soy-containing food lowered the risk of BC in gene-
32positive participants.
3.1. Positive family history of breast cancer
Other studies focused on the association between PE and BC by evaluating the mediating role of family history. For example, in a population-based case–control study by Thanos et al., a possible reverse association was found between PE intake during adolescence and future risk of BC. A family
22history of BC did not significantly affect this result. Also, the lack of association between PE intake and BC detected in the prospective population-based
30cohort study of Hedelin et al. was not affected by a family history of BC. In addition, in a nested case-control study (out of a large multiethnic cohort study) by Goodman et al., where PE levels were measured in pre-diagnosis urine specimens in postmenopausal BC cases and controls, the indirect association found between high PE use and BC was not mediated by any potential confounder, including
31family history of BC.
The effect of PE on BC risk in genetically positive women has been rarely investigated. In our review, we found only one study which had considered the subject among gene-positive women.
3.2. BRCA mutation careers
We also found a few animal studies or in vitro works on the effect of PE on the gene itself at the cellular-molecular level. Bernard et al. investigated the effect of daidzein and genistein, two isoflavones, on BRCA2 in BC cell lines, observing a down-regulation in some gene expressions, suggesting a
33possible preventive effect for these compounds.
6 Alipour, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 4-9
Phytoestrogens and breast disorders
Bosviel et al. studied whether genistein and daidzein could affect DNA methylation in mutated BRCA1 and BRCA2 genes in BC cell lines, reporting that these can de-methylate DNA and bring back the
34oncosuppressor expression of the genes. In a recent study on mice bred with BRCA1 gene, Donovan et al. fed animals with genistein-rich food from birth to 50 days. They found a decrease in methylation of BRCA1, suggesting that dietary genistein might
35have a therapeutic role.
4. Phytoestrogens in benign breast disorders
References
None.
BBD is frequent as many women refer to gynecology or breast clinics for breast pain, where fibrocystic changes (FCC) are the most common finding among them.36 In addition, fibroadenomas (FA) are among the most common benign breast
37lumps. In our review, we found a few clinical trials regarding the effects of PE on BBD. Wu et al. examined whether the rate of FCC was affected by soy products, finding a non-significant reduced risk
38of FCC with proliferation and FCC with atypia. Mirghafourvand et al. compared the effect of flaxseed on cyclical mastalgia, finding a significantly reduced mastalgia in the case group compared to
39controls after two months. Atkinson et al. measured the levels of equol, a bacterial metabolite of daidzein, in plasma of women with FCC and controls. However, they did not find any evidence in favour of
40a positive association between these conditions. Kişakeviç et al. investigated the effects of a 6-month use of phytoestrogens on breast pain and ultrasound-detected breast structure in perimenopausal and early-menopausal women with and without FCC. They detected a lowered ultrasound-detected tissue density and a reduced number of cysts and a decreased size after 3 months, as well as a decrease in severity and frequency of mastalgia in the case group
41after 6 months.
1. Yager JD, Davidson NE. Estrogen carcinogenesis in breast cancer. The New England journal of medicine. 2006; 354:270-82.
Conflict of Interest
In conclusion, PE has been broadly explored regarding its relation with BC, and to a lesser extent with other breast conditions. Studies are largely different in their designs and definitions, and the type, amount, and timing of PE consumption, in addition to ethnic dissimilarities in study cases preclude conclusive results. Nevertheless, the existing data are mostly in favor of the safety of these compounds in the general population as well as in women with BC or at risk of the disease. Due to insufficient evidence, prescription of high doses of PE for the latter two groups is still not recommended.
3. Alipour S, Eskandari A. Prescribing Oral Contraceptives in Women With Breast Diseases: A Matter of Concern for the Gynecologist. Archives of Breast Cancer. 2019:55-68.
6. Rietjens IM, Louisse J, Beekmann K. The potential health effects of dietary phytoestrogens. British journal of pharmacology. 2017; 174:1263-80.
8. Iqbal J, Abbasi BA, Khalil AT, Ali B, Mahmood T, Kanwal S, et al. Dietary isoflavones, the modulator of breast carcinogenesis: Current landscape and future perspectives. Asian Pacific Journal of Tropical Medicine. 2018; 11:186.
10. This P, De La Rochefordi A, Clough K, Fourquet A, Magdelenat H. Phytoestrogens after breast cancer. Endocrine-related cancer. 2001; 8:129-34.
4. Eskandari A, Alipour S. Hormone Replacement Therapy and Breast Diseases: A Matter of Concern for the Gynecologist. Archives of Breast Cancer. 2019:113-9.
7. Peeters P, Keinan-Boker L, Van der Schouw Y, Grobbee D. Phytoestrogens and breast cancer risk. Breast cancer research and treatment. 2003; 77:171-83.
13. Dastjerdi MV, Eslami B, Sharifi MA, Moini A, Bayani L, Mohammad-Khani H, et al. Effect of soy isoflavone on hot flushes, endometrial thickness, and breast clinical as well as sonographic features. Iranian journal of public health. 2018; 47:382.
14. Alipour S, Afshar S, Moini A, Dastjerdi MV, Saberi A, Bayani L, et al. Clinical and Ultrasonographic Changes of the Breast after Use of Soy Isoflavones. Asian Pacific Journal of Cancer Prevention. 2012; 13:6093-5.
15. Calado A, Neves PM, Santos T, Ravasco P. The
5. Alipour S, Eskandari A. Miscellaneous Exogenous Hormones and Breast Diseases: A Matter of Concern for the Gynecologist. Archives of Breast Cancer. 2019:150-5.
2. Clemons M, Goss P. Estrogen and the risk of breast cancer. New England Journal of Medicine. 2001; 344:276-85.
11. Quella SK, Loprinzi CL, Barton DL, Knost JA, Sloan JA, LaVasseur BI, et al. Evaluation of soy phytoestrogens for the treatment of hot flashes in breast cancer survivors: A North Central Cancer Treatment Group Trial. Journal of Clinical Oncology. 2000; 18:1068-.
9. Wiśniewska I, Jochymek B, Lenart-Lipińska M, Chabowski M. The pharmacological and hormonal therapy of hot flushes in breast cancer survivors. Breast Cancer. 2016; 23:178-82.
12. Van Patten CL, Olivotto IA, Chambers GK, Gelmon KA, Hislop TG, Templeton E, et al. Effect of soy phytoestrogens on hot flashes in postmenopausal women with breast cancer: a randomized, controlled clinical trial. Journal of Clinical oncology. 2002; 20:1449-55.
7Alipour, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 4-9
Phytoestrogens and breast disorders

19. Zhao T-T, Jin F, Li J-G, Xu Y-Y, Dong H-T, Liu Q, et al. Dietary isoflavones or isoflavone-rich food intake and breast cancer risk: A meta-analysis of prospective cohort studies. Clinical nutrition. 2019; 38:136-45.
20. McCann SE, Muti P, Vito D, Edge SB, Trevisan M, Freudenheim JL. Dietary lignan intakes and risk of pre‐and postmenopausal breast cancer. International journal of cancer. 2004; 111:440-3.
22. Thanos J, Cotterchio M, Boucher BA, Kreiger N, Thompson LU. Adolescent dietary phytoestrogen intake and breast cancer risk (Canada). Cancer Causes & Control. 2006; 17:1253-61.
effect of flaxseed in breast cancer: a literature review. Frontiers in nutrition. 2018; 5:4.
17. Fritz H, Seely D, Flower G, Skidmore B, Fernandes R, Vadeboncoeur S, et al. Soy, red clover, and isoflavones and breast cancer: a systematic review. PloS one. 2013; 8:e81968.
23. Anderson LN, Cotterchio M, Boucher BA, Kreiger N. Phytoestrogen intake from foods, during adolescence and adulthood, and risk of breast cancer by estrogen and progesterone receptor tumor subgroup among Ontario women. International journal of cancer. 2013; 132:1683-92.
18. Nagata C, Mizoue T, Tanaka K, Tsuji I, Tamakoshi A, Matsuo K, et al. Soy intake and breast cancer risk: an evaluation based on a systematic review of epidemiologic evidence among the Japanese population. Japanese journal of clinical oncology. 2014; 44:282-95.
16. Dong J-Y, Qin L-Q. Soy isoflavones consumption and risk of breast cancer incidence or recurrence: a meta-analysis of prospective studies. Breast cancer research and treatment. 2011; 125:315-23.
21. Linseisen J, Piller R, Hermann S, Chang‐Claude J. Dietary phytoestrogen intake and premenopausal breast cancer risk in a German case‐control study. International journal of cancer. 2004; 110:284-90.
27.Messina M. Impact of soy foods on the development of breast cancer and the prognosis of breast cancer patients. Complementary Medicine Research. 2016; 23:75-80.
26. Prasad P, Shayne M. Effect of Dietary Soy on Breast Cancer Recurrence and Mortality: A Review. J Nutr Food Sci. 2016; 6:2.
28. Qiu S, Jiang C. Soy and isoflavones consumption and breast cancer survival and recurrence: a
25. Li T, Yang J, Lv Y, Yin F, Xu L, Liu H, et al. Quantitative comparison of drug efficacy in treating hot flashes in patients with breast cancer. Breast cancer research and treatment. 2019; 173:511-20.
24. Flower G, Fritz H, Balneaves LG, Verma S, Skidmore B, Fernandes R, et al. Flax and breast cancer: A systematic review. Integrative cancer therapies. 2014; 13:181-92.
32. Ko K-P, Kim S-W, Ma SH, Park B, Ahn Y, Lee JW, et al. Dietary intake and breast cancer among carriers and noncarriers of BRCA mutations in the Korean Hereditary Breast Cancer Study. The American journal of clinical nutrition. 2013; 98:1493-501.
37. Ajmal M, Van Fossen K. Breast fibroadenoma. 2019.
30. Hedelin M, Löf M, Olsson M, Adlercreutz H, Sandin S, Weiderpass E. Dietary phytoestrogens are not associated with risk of overall breast cancer but diets rich in coumestrol are inversely associated with risk of estrogen receptor and progesterone receptor negative breast tumors in Swedish women. The Journal of nutrition. 2008; 138:938-45.
34. Bosviel R, Dumollard E, Déchelotte P, Bignon Y-J, Bernard-Gallon D. Can soy phytoestrogens decrease DNA methylation in BRCA1 and BRCA2 oncosuppressor genes in breast cancer? Omics: a journal of integrative biology. 2012; 16: 235-44.
36. Malherbe K, Fatima S. Fibrocystic Breast Disease. StatPearls [Internet]: StatPearls Publishing; 2019.
29. Powles TJ, Howell A, Evans DG, McCloskey EV, Ashley S, Greenhalgh R, et al. Red clover isoflavones are safe and well tolerated in women with a family history of breast cancer. Menopause international. 2008; 14:6-12.
31. Goodman MT, Shvetsov YB, Wilkens LR, Franke AA, Le Marchand L, Kakazu KK, et al. Urinary phytoestrogen excretion and postmenopausal breast cancer risk: the multiethnic cohort study. Cancer Prevention Research. 2009; 2:887-94.
systematic review and meta-analysis. European journal of nutrition. 2019; 58:3079-90.
35. Donovan MG, Selmin OI, Doetschman TC, Romagnolo DF. Epigenetic Activation of BRCA1 by Genistein In Vivo and Triple Negative Breast Cancer Cells Linked to Antagonism toward Aryl Hydrocarbon Receptor. Nutrients. 2019; 11:2559.
39. Mirghafourvand M, Mohammad-Alizadeh-Charandabi S, Ahmadpour P, Javadzadeh Y. Effects of Vitex agnus and Flaxseed on cyclic mastalgia: A randomized controlled trial. Complementary therapies in medicine. 2016;
33. Bernard-Gallon DJ, Satih S, Chalabi N, Rabiau N, Bosviel R, Fontana L, et al. Phytoestrogens regulate the expression of genes involved in different biological processes in BRCA2 knocked down MCF-7, MDA-MB-231 and MCF-10a cell lines. Oncology reports. 2010; 23:647-53.
38. Wu C, Ray RM, Lin MG, Gao DL, Horner NK, Nelson ZC, et al. A case-control study of risk factors for fibrocystic breast conditions: Shanghai Nutrition and Breast Disease Study, China, 1995–2000. American journal of epidemiology. 2004; 160:945-60.
8 Alipour, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 4-9
Phytoestrogens and breast disorders

41. Кишакевич І, Конар Р. Correction of dismetabolic manifestations in perimenopausal and early postmenopausal women with fibrocystic disease. Reproductive Endocrinology. 2016:82-6.
40. Atkinson C, Ray RM, Li W, Lin M-G, Gao DL, Shannon J, et al. Plasma equol concentration is not associated with breast cancer and fibrocystic breast conditions among women in Shanghai, China. Nutrition Research. 2016; 36:863-71.
24:90-5.
9Alipour, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 4-9
Phytoestrogens and breast disorders

A 33-year-old female was referred to our hospital with a complaint of left nipple retraction and mass
(HER2), protein overexpression and HER2 gene 2amplification. Patients suffering from TNBC face a
high risk of early metastasis and death within five years after diagnosis but high rates of complete pathological response occur following neoadjuvant
3, 4chemotherapy. One of the current criteria in the guidelines of the National Comprehensive Cancer Network (NCCN) for the test of BRCA1 and BRCA2 includes patients with TNBC diagnosed before the
5age of 60 years and no family history. Patients with BRCA mutations face an increased risk of getting cancers such as breast, ovary, pancreas, and
6melanoma. Some studies recommend bilateral risk-reducing mastectomy and bilateral salpingo-
5, 7, 8oophorectomy for these patients.
Case presentation
Breast cancer is the most common malignant disease among women across the world. A recent study found that conversion in breast cancer hormone receptors takes place during the metastatic
1progression. Triple-negative breast cancer (TNBC) is an aggressive subgroup of breast cancer. Accounting for 12% to 17% of breast cancers, TNBC is characterized by the lack of expression of estrogen receptor (ER) and progesterone receptor (PR), absence of human epidermal growth factor receptor 2
Introduction
ARTICLE INFO
Background: Triple-negative subtype does not have any of the receptors that are commonly found in breast cancer. Patients suffering from Triple-negative breast cancer are at risk of early metastasis and BRCA mutation. The conversion of the receptors during the metastatic progression or local recurrence of breast cancer is a well-known topic that affects the therapeutic measures and outcome. Confirmation of immunohistochemistry is essential in these conditions, but genetic evaluation is controversial.
Question: Does the patient need genetics counseling in a conversion setting? And does the new specimen need CISH/FISH techniques to confirm TNBC tumors?
Conclusion: There are no strong guidelines to recommend genetic counseling and BRCA testing for patients with breast cancer biomarkers conversion. Re-assessing the specimen for ER, PR, and HER-2 is necessary for this setting.
Case presentation: A woman suffering from primary luminal breast cancer presented with femoral bone metastasis in the follow-up after two years. Bone metastasis was compatible with the triple-negative subtype. This case was discussed at the weekly breast multidisciplinary team session of the Department of Breast Surgery, Tehran University of Medical Sciences.
conversion
04 February 2020
Received:
27 January 2020
Key words:
Revised:
16 February 2020Accepted:
genetic counseling,triple negative, IHC,
Breast cancer,
* Address for correspondence: Farid Azmoodeh Ardalan, MDProfessor of Pathology,Address: Pathology Department, Cancer Institute,Imam Khomeini Hospital Complex, Tehran 14197-33141, IranTel: +98 21 61192502Fax: +98 21 66923557e-mail: [email protected]
ABSTRACT
Genetic Counseling in the Follow-up of Breast Cancer patients; Conversion of a Luminal Tumor to TNBC
a Department of Surgery, Tehran University of Medical Sciences, Tehran, Iran
b Department of Pathology, Tehran University of Medical Sciences, Tehran, Iran
c Department of Genetics, Breast Cancer Research Center, Motamed Cancer Institute, ACECR, Tehran, Iran
a a b cHamid Ahmadi , Reza hosseinpour , Behnaz Jahanbin , Keivan Majidzadeh-A ,
bFarid Azmoudeh-ardalan*
Open AccessClinical Experience
DOI: 10.19187/abc.20207110-13
10 Ahmadi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 10-13

Radiation therapy continued with 10Gy/5fr electron to tumoral bed. By the completion of radiation therapy, the patient received hormone therapy (tamoxifen 20 mg/day). She followed up on a regular basis with clinical examination (every six months) and mammography (every 12 months). Two years after treating the primary tumor, she presented with progressive pain in the hip area. Investigations for the source of the pain with a bone scan, plain X-ray, and MRI showed a highly suspicious metastatic lesion in the right femoral head. CT scan of the thoracic and abdominopelvic cavity did not show any other metastatic lesion (PET was not affordable for the patient at that time).
The case was presented at the weekly breast multidisciplinary team session at the Department of Breast Surgery, Tehran University of Medical Sciences. The questions were as follows: Does the patient need genetic assessment because of TNBC in the metastatic lesions? And does the new specimen need CISH/FISH techniques to confirm TNBC tumors?
sensation for the past three months. The patient had no family history of breast or ovarian cancer. She was married and had a child. In her physical examination, a 30 mm fixed mass was palpated in the retro areolar region. The lymph nodes (LNs) in the axillary region were palpable. Mammography showed a spiculated mass with suspicious microcalcification (BIRADS 5). Malignancy was suggested in ultrasonographic evaluation (BIRADS 5) with cortical thickening in at least two LNs in the axilla. After a core needle biopsy from the breast lesion and fine needle aspiration (FNA) from the LNs, invasive ductal carcinoma with positive LNs was confirmed (Clinical T2, N1). Immunohistochemical (IHC) analysis of the specimen showed that the tumor was ER, PR, and HER2 positive with Ki67 %30. We recommended the patient to undergone adjuvant chemotherapy, but she preferred to do the surgery first. Central resection and axillary dissection were done. In permanent pathology reports, all surgical margins were free, and the tumor involved four out of ten lymph nodes. Metastatic workups were negative in thoracic and abdominal CT scan as well as whole-body bone isotope scan. After surgery, the patient received chemotherapy (Adriamycin and Taxol followed by Herceptin) and radiotherapy for the whole breast and supraclavicular region (50Gy/25fr).
Question
According to the recommend-ation of the multidisciplinary team, the patient underwent orthopedic surgery and femoral head replacement by an implant. The metastatic infiltrative carcinoma with breast origin pattern was approved in pathology evaluation although the IHC profile of the tumor was converted to ER, PR, and HER2 negative with a Ki67 45%.
DiscussionThe conversion of the receptors during the
metastatic progression or local recurrence of breast cancer is a common topic affecting the therapeutic
1measures and outcome. Up to 50% of treatment 9 plans have been changed due to this conversion.
Cejalvo et al. identified 47 genes that were expressed 10 differently in metastatic versus primary disease.
There are several possible mechanisms for the conversion of breast cancer hormone receptors expression. Technical errors and the variability in the accuracy of IHC reports may contribute to the difference of hormone receptors status between
11primary and metastatic tumors. Some studies have showed associations between changes in receptors and the duration from primary tumor diagnosis to metastasis, sites of metastasis, or breast cancer
12, 13subtypes, but some others contradict such reports. Tumor markers conversion could be a result of
14genetic drift during tumor progression. The negative conversion of tumor markers is a predictor of poor prognosis. Therefore, biomarker change evaluation in the metastatic site is a crucial concern that may not only affect the treatment options but also
1predict the prognosis of patients. For reassessment of PR and ER, pathology review and IHC may be sufficient. However, a repeat biopsy is also recommended, particularly when the specimen is small, and there is the possibility of some technical
9problems such as prolonged cold ischemic time. Some authors also recommend rebiopsy when there is any discrepancy between histomorphologic findings on H&E and the results of biomarkers (e.g., the potential technical error in tubular or mucinous
9, 15carcinoma with positive HER2 results). In-situ hybridization assays, such as Chromogenic in situ hybridization (CISH), Silver in situ hybridization (SISH), and fluorescent in situ hybridization (FISH) are also recommended for HER2 overexpression
16reassessment. Real-time qPCR is an alternative 15
option to evaluate breast cancer hormone receptors. Bone metastases may be biased by false-negative IHC results for both hormone receptors and HER-2
17-22due to decalcification. Therefore, we cannot be sure whether a genuine conversion in tumor markers has occurred or not, although bone and bone marrow samples can be used for the evaluation of HER2 status and compared with the status of the primary
23tumor. Although in situ hybridization may be helpful in this case, the possibility of DNA degradation during calcification cannot be excluded. This may result in false-negative ISH results as well. Therefore, a sufficient sample of tumoral tissue without decalcification should be available at the time of tissue processing and evaluation. There are often some softer parts in the metastatic bone samples which can be processed without decalcification. Also, other methods of calcification, e.g., using EDTA can be applied instead of acid.
11Ahmadi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 10-13
Genetics assessment in BC metastasis

References
Conflict of Interest
Multidisciplinary team (MDT) recommendation
Ethical Consideration
For this patient with breast cancer biomarkers conversion (luminal type in the primary tumor and triple-negative in bone metastasis), members of breast MDT in the Breast Surgery Department, Imam Hospital, Tehran University of Medical Sciences, did not recommend genetic counseling and BRCA testing. They thought that the evidence was not sufficient enough to support BRCA tests. In fact, this topic was so controversial among the members that they could not make a unanimous decision. They recommended talking to the patients and providing her with the latest findings of the studies. We suggested designing a survey to compare BRCA results between primary TNBC and breast cancer patients with triple-negative in metastatic lesions. Regarding re-assessing the specimen for ER, PR, and HER-2, the members recommended re-evaluating the profile using FISH or CISH methods.
1. Woo JW, Chung YR, Ahn S, Kang E, Kim E-K, Kim SH, et al. Changes in Biomarker Status in Metastatic Breast Cancer and Their Prognostic Value. J Breast Cancer. 2019;22(3):439-52.
The patients agreed to present her medical information anonymously by singing an informed consent.
3. von Minckwitz G, Schneeweiss A, Loibl S, Salat C, Denkert C, Rezai M, et al. Neoadjuvant
The authors have nothing to disclose.
2. Foulkes WD, Smith IE, Reis-Filho JS. Triple-negative breast cancer. New England journal of medicine. 2010;363(20):1938-48.
There is a consensus in the international guidelines over the necessity of genetic counseling for patients whose primary breast tumors are TNBC. Overall, about 15–20% of breast cancers are triple-negative. Among them, the majority of TNBC patients are young women or women with a mutation in the
2, 24, 25BRCA genes. This subtype differs from the others in the natural history of the disease and patients’ outcome. In fact, TNBC tumors grow and spread faster, have more limited treatment options, and have
24, 25a worse prognosis. National Comprehensive Cancer Network (NCCN) guideline recommended hereditary cancer testing for the patients diagnosed at
5 age <60 years with TNBC. The guidelines also recommend genetic testing in TNBC patients at any age, although this is applicable when the primary tumor is triple-negative. To the best of our knowledge, there is no definite recommendation for TNBC when it is found in metastasis, especially when the primary tumor is not TNBC.
4. Harbeck N. Neoadjuvant therapy in patients with triple negative and HER2 positive early breast cancer. The Breast. 2017;32:S18.
7. Dowdy SC, Stefanek M, Hartmann LC. Surgical r isk reduction: prophylact ic salpingo-oophorectomy and prophylactic mastectomy. American journal of obstetrics and gynecology. 2004;191(4):1113-23.
9. Nguyen TH, Nguyen VH, Nguyen TL, Qiuyin C, Phung TH. Evaluations of Biomarker Status Changes between Primary and Recurrent Tumor Tissue Samples in Breast Cancer Patients. BioMed research international. 2019;2019.
14. Kuukasjärvi T, Karhu R, Tanner M, Kähkönen M, Schäffer A, Nupponen N, et al. Genetic heterogeneity and clonal evolution underlying development of asynchronous metastasis in human breast cancer. Cancer research. 1997;57(8):1597-604.
13. Amir E, Clemons M, Purdie CA, Miller N, Quinlan P, Geddie W, et al. Tissue confirmation of disease recurrence in breast cancer patients: pooled analysis of multi-centre, multidisci-plinary prospective studies. Cancer treatment reviews. 2012;38(6):708-14.
6. Mersch J, Jackson MA, Park M, Nebgen D, Peterson SK, Singletary C, et al. Cancers associated with BRCA 1 and BRCA 2 mutations other than breast and ovarian. Cancer. 2015;121(2):269-75.
12. de Dueñas EM, Hernández AL, Zotano ÁG, Carrión RMP, López-Muñiz JIC, Novoa SA, et al. Prospective evaluation of the conversion rate in the receptor status between primary breast cancer and metastasis: results from the GEICAM 2009-03 ConvertHER study. Breast cancer research and treatment. 2014;143(3):507-15.
10. Cejalvo JM, de Dueñas EM, Galván P, García-Recio S, Gasión OB, Paré L, et al. Intrinsic subtypes and gene expression profiles in primary and metastatic breast cancer. Cancer research. 2017;77(9):2213-21.
11. Allred DC. Commentary: hormone receptor testing in breast cancer: a distress signal from Canada. Oncologist. 2008;13(11):1134-6.
8. Calderon‐Margalit R, Paltiel O. Prevention of breast cancer in women who carry BRCA1 or BRCA2 mutations: a critical review of the literature. International journal of cancer. 2004;112(3):357-64.
carboplatin in patients with triple-negative and HER2-positive early breast cancer (GeparSixto; GBG 66): a randomised phase 2 trial. The lancet oncology. 2014;15(7):747-56.
5. Network NCC. Genetic/familial High-Risk assessment: Breast, Ovary and pancratic (version 1.2020) [Available from: https://www. nccn.org/professionals/physician_gls/pdf/genetics_bop.pdf.
12 Ahmadi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 10-13
Genetics assessment in BC metastasis

17. Holdaway I, Bowditch J. Variation in receptor status between primary and metastatic breast cancer. Cancer. 1983;52(3):479-85.
18. Rasmussen BB, Kamby C. Immunohistochemical detection of estrogen receptors in paraffin sections from primary and metastatic breast cancer. Pathology-Research and Practice. 1989;185(6): 856-9.
15. Stefanovic S, Wirtz R, Deutsch TM, Hartkopf A, Sinn P, Varga Z, et al. Tumor biomarker conversion between primary and metastatic breast cancer: mRNA assessment and its concordance with immunohistochemistry. Oncotarget. 2017; 8(31):51416-28.
19. Kuukasjärvi T, Kononen J, Helin H, Holli K, Isola J. Loss of estrogen receptor in recurrent breast cancer is associated with poor response to endocrine therapy. Journal of Clinical Oncology. 1996;14(9):2584-9.
20. Lower EE, Glass EL, Bradley DA, Blau R, Heffelfinger S. Impact of metastatic estrogen receptor and progesterone receptor status on survival. Breast cancer research and treatment. 2005;90(1):65-70.
21. Broom RJ, Tang PA, Simmons C, Bordeleau L, Mulligan AM, O'MALLEY FP, et al. Changes in estrogen receptor, progesterone receptor and Her-2/neu status with time: discordance rates between primary and metastatic breast cancer. Anticancer research. 2009;29(5):1557-62.
22. Simmons C, Miller N, Geddie W, Gianfelice D, Oldfield M, Dranitsaris G, et al. Does confirmatory tumor biopsy alter the management of breast cancer patients with distant metastases? Annals of oncology. 2009;20(9):1499-504.
23. Amir E, Ooi W, Simmons C, Kahn H, Christakis M, Popovic S, et al. Discordance between receptor status in primary and metastatic breast cancer: an exploratory study of bone and bone marrow biopsies. Clinical oncology. 2008;20(10): 763-8.
24. Dent R, Trudeau M, Pritchard KI, Hanna WM, Kahn HK, Sawka CA, et al. Triple-negative breast cancer: clinical features and patterns of recurrence. Clinical cancer research. 2007;13(15): 4429-34.
25. Cleator S, Heller W, Coombes RC. Triple-negative breast cancer: therapeutic options. The lancet oncology. 2007;8(3):235-44.
16. Fabi A, Di Benedetto A, Metro G, Perracchio L, Nisticò C, Di Filippo F, et al. HER2 protein and gene variation between primary and metastatic breast cancer: significance and impact on patient care. Clinical Cancer Research. 2011;17(7): 2055-64.
13Ahmadi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 10-13
Genetics assessment in BC metastasis

IntroductionCoronavirus disease (COVID-19)In March 2020, the World Health Organization
1declared the novel Coronavirus infection a pandemic. Although all people are susceptible to infection, mortality rate is significantly higher in patients with
ARTICLE INFO
Background: In March 2020, the World Health Organization declared the novel COVID-19 infection a pandemic. Among high-risk patients infected by the virus, breast cancer patients are vulnerable to present more severe infections. Iran is among the countries with a high incidence of COVID-19 , and most of the routine activities of medical centers are affected by the epidemic disease. Thus, there is a need to make some modifications to international protocols for dealing with breast cancer in the affected countries.
Methods: The headings of breast cancer management protocols have been discussed among the university-affiliated professors in different disciplines involved in breast cancer management. The discussions were done through a “WhatsApp” group considering the tiles and the latest news about COVID-19. Under each title, we provide the consensus of all members in the related disciplines.
Recommendations and Conclusion: In each specialty, all members agreed to choose minimal intervention. The modifications aim to reduce the workload of the medical centers as well as to provide the least interface of the patients with the medical centers. The members know that some recommendations may interfere with the routine best-practice recommendations and decrease the quality measures in the patient's outcome. Therefore, these recommendations are valid just in epidemic COVID-19 situation in the country.
Received:
28 February 2020Revised:
15 March 2020 Accepted:
21 March 2020
CoronavirusKey words:
COVID-19breast cancer guidelines
* Address for correspondence: Ahmad Kaviani, MD Professor of Breast Surgery, Address: Imam Khomeini Hospital Complex, Tehran, 1419733141, IranTel: +98 21 88871785Fax: +98 21 88871698Email: [email protected]
ABSTRACT
Modifications in Breast Cancer Guidelines in COVID-19 Pandemic;An Iranian Consensus
a Breast Disease Research Center, Tehran University of Medical Sciences, Tehran, Iran
b Department of Hematology & Medical Oncology, Tehran University of Medical Sciences, Tehran, Iran
c Radiation Oncology Research Center ,Cancer Institute, Tehran University of Medical Sciences, Tehran, Iran
d Department of Hematology & Medical Oncology, Shahid Beheshti University of Medical Sciences, Tehran, Iran
e Chronic Respiratory Diseases Research Center, National Research Institute of Tuberculosis and Lung Diseases
(NRITLD), Shahid Beheshti University of Medical Sciences, Tehran, Iranf Department of Hematology & Medical Oncology, Mashhad University of Medical Sciences, Mashhad, Iran
g Department of Hematology & Medical Oncology, Iran University of Medical Sciences, Tehran, Iran
h Department of Hematology & Medical Oncology, Shiraz University of Medical Sience, Shiraz, Fars, Iran
i Hematology Research Center, Shiraz University of Medical Sience, Shiraz, Fars, Iranj Hematology, Oncology, and Hematopoietic Stem Cell Transportation Research Center, Tehran University of Medical Sciences, Tehran, Irank Faculty of Medicine, University of Montreal, Montreal, Canada
l Department of Surgery, Alborz University of Medical Sciences, Karaj, Alborz, Iranm Department of Surgery, Tehran University of Medical Sciences, Tehran, Iran
a,b b c b d,eFarhad Shahi , Mehrzad Mirzania , Mahdi Aghili , Mohammadreza Dabiri , Sharareh Seifi ,
f g h,i b,j kAlireza Bary , Nafiseh Ansarinejad , Alireza Rezvani , Soroush Rad , Amirali Shahi ,
l a,k,mAhmad Elahi , Ahmad Kaviani*
Open AccessShort Communication
DOI: 10.19187/abc.20207114-21
14 Shahi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 14-21

Discussion and Recommendations
Methods
1. Infection prevention and controlIn order to diminish the spread of the novel
The headings of breast cancer management protocols were discussed among university-affiliated professors in different disciplines (multidisciplinary approach) involved in breast cancer management. The discussions were done through a “WhatsApp” group considering the tiles and the latest news about COVID-19. Regarding each title, we considered the consensus of all members in the related disciplines. The admin of the group (first author) asked the members to comment on each title by direct questions and case presentations. Also, some items were added according to Frequently Asked Questions (FAQ) banks and databases asked by patients and health care professionals.
As the pandemic continues, the national health system of the country will be increasingly engaged in the management of this critical and potentially life-threatening infection. On the other hand, medical centers admit patients who show more severe presentation of COVID-19. Therefore, the risk of involvement of patients referred for other diseases is higher.
According to official statistics, Iran is in a dire situation as a result of the outbreak. As of 21 March 2020, about 20000 people have been infected by COVID-19 and about 2000 people have died due to the infection, based on the reports by the Iranian
9Ministry of Health.In this paper, we present modifications in the
approved breast cancer guidelines in an effort to reduce the frequency of hospital visits for breast cancer patients as the outbreak continues. The new guidelines will allow us to save the limited health care resources only for urgencies and emergencies and more importantly to protect our vulnerable breast cancer patients against COVID-19. A large group of Iranian medical physicians involved in the care of breast cancer patients in large academic centers have contributed to this project through a virtual discussion platform.
older age, immunocomprised status, or severe 2,3
comorbid diseases, most notably cancer. On the other hand, there is not enough evidence to make a conclusive association between cancer and COVID-
4,519. Breast cancer is the most common cancer in women with treatment ranging from surgery, systemic chemotherapy, hormonal therapy and radiation therapy to more novel targeted immunotherapies. These patients face higher likelihood of exposure to the virus due to their frequent visits to medical centers and imaging centers. Furthermore, the immune suppression associated with most cancer directed therapies confers greater risk of serious complications
6-8and mortality from infection with COVID-19.
For minimizing unessential visits to medical facilities it is advisable that screening procedures, such as mammography and clinical breast examinations, be postponed. This measure will help to reserve human resources available in hospitals and
10clinics for COVID-19 patients in need of urgent help.
Standard diagnostic procedures should still be pursued for diagnosis and staging of the disease prior to surgery. However, we recommend forgoing the placement of markers at the site of axillary lymph nodes and breast biopsies in advanced-stage disease given that this decision may lead to a higher mastectomy rate. We can minimize staging procedures before adjuvant therapy, especially for T0-
12T3, N0-N1, M0. These measures will decrease the burden on radiologic centers, minimize contacts and transports and save human resources.
Coronavirus (COVID-19), health care professionals should engage in rigorous handwashing and advise their patients to do the same. Social distancing should be reinforced for patients and their families until the pandemic subsides. Information regarding these preventative measures must be distributed among patients through social media or other online outlets and during every medical encounter. Maximum protective care for health care professionals and hospital employees who are in contact with cancer patients is crucial. Clinic staff may need additional training on the use of personal protective equipment (PPE). Breast cancer patients who refer to the hospitals are advised to protect themselves by personal protective equipment like masks and
10,11gloves.
3. Breast cancer staging
2. Breast cancer screening
Breast cancer patients requiring surgery after neoadjuvant chemotherapy are relatively immuno-deficient, which increases their risk of infection with COVID-19 and developing serious complications. Considering the fact that surgery is still a crucial part of breast cancer therapy, it should continue to be performed following standard protocols as long as it is within the hospital policies for pandemic crisis. It is
4. Breast cancer surgery
COVID-19 continues to spread faster than expected. Therefore, we need to reserve our limited hospital wards for COVID-19 patients. Most of our surgery wards are currently closed in order to provide care to COVID-19 patients. Our surgeons teams have reduced their elective surgeries to minimize the risk of their patients and health care workers contracting the infection. This is also due to considerable shortage of available non-Covid-19 ward beds and personel in the hospitals across the country including the major referral centers in Tehran.
4.1. Avoid hospital admissions
15Shahi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 14-21
BC guidelines modification in COVID-19 pandemic

4.4. Mastectomy in DCIS and T1-2 N0 patients
Immediate breast reconstruction should be avoided in the epidemic situation of COVID-19 regardless of the type of breast reconstruction. Flap reconstructions require 1-5 days of hospital admission, and the implant and expander reconstructions will slightly increase the risk of complications, which is not acceptable in a viral epidemic s i tuat ion. Al l secondary breast
We can consider Breast Conserving Surgery (BCS) followed by Accelerated Partial Breast Irradiation (APBI) or Intraoperative Radiation Therapy (IORT) for appropriated low risk patients. If the patient need whole breast irradiation it is recommended to do mastectomy in place of BCS or postpone radiotherapy up to 20 weeks after surgery. The latter is indicated in patients who are not high risk for local recurrence (microscopic positive margin, age
15less than 40 years).
We strongly recommend to stop all risk reducing surgeries for the patients even if there is a known genetic mutation (e.g. BRCA, CHECK, etc.) These operations can be done some months after subsiding the pandemic situation.
In the case of non-palpable early breast tumors, it is advisable to use markers to localize the tumors, as usual. However, routine preoperative wire or radioactive seed placement in patients who are scheduled for the operation after neoadjuvant therapies would raise the risk of COVID-19 infection by increasing the number of referrals to the hospital as well as the workload of hospitals. The latter also could exhaust hospital resources required to tend to COVID-19 patients.
4.5. Breast Reconstruction:
essential that we refrain from admitting patients in hospitals overnight. Therefore, it is strongly advisable that all breast surgeries be performed in a Day-Care
10,13,14unit except for patients with severe comorbidities.
4.3. Risk reducing surgeries
4.2. Tumor localization at the time of surgery in advance stages
Although in most references, breast-conserving surgery (BCS) followed by radiation has the same efficacy as mastectomy in the treatment of Ductal Carcinoma Insitu, during COVID-19 outbreak, the surgeon can consider mastectomy more frequently. The surgeon should fully inform the patients of the potential risk of contracting COVID-19 through frequent visits to medical centers to receive radiation following BCS. Overall, to decrease the frequency of hospital visits in early-stage node-negative invasive cancers as well as DCIS, we recommend substituting “mastectomy” for “breast-conserving surgery plus radiotherapy”
reconstructions should be canceled or postponed when the COVID-19 outbreak has subsided.
5. Neoadjuvant /Adjuvant systemic therapy
According to previous studies and ASCO recommendation, we don't postpone adjuvant chemotherapy and begin therapy as soon as possible. In advanced stages, triple negative patients and HER2 positive cases, there is survival benefit to start adjuvant chemotherapy sooner (especially under 30
16-21days). Hormone therapy, with or without anti HER2 treatment, is less toxic and can therefore be started earlier.
In Luminal A breast cancer patients, we recommend to follow “predict online” instead of “NCCN guideline” which minimizes the use of
22chemotherapy. We believe that intensive regimens are not suitable during epidemic days; therefore, we can use shorter chemotherapy regimens such as Docetaxel plus Cyclophosphamide instead of routine 8 courses anthracycline based regimens for low risk patients such as those with node-negative, hormone receptor-positive breast cancer or for the triple-negative breast cancer patients (T<10mm) with
10,23,24negative nodes.
It is clear that we must strictly follow safety precautions including personal protection, checking fever and other symptoms like cough and dyspnea for both patients and their families before each cycle of chemotherapy. We need better time management to shorten waiting times before chemotherapy and minimize the number of allowed visitors for each
10 patient.
We recommend to substitute every 3 weeks regimens instead of dose dense or weekly protocols. During chemotherapy, as per ASCO recommendation, using primary GCSF prophylaxis and even prophylactic antibiotics may make our patients less vulnerable to COVID-19 related complications. It is reasonable to use less glucocorticoid base premedication for chemotherapy induced nausea and
10vomiting prophylaxis.
Coming soon, all of our wards must provide services to COVID-19 patients. We must choose less toxic systemic therapy for breast cancer patients given that toxicity predisposes them to COVID-19 infection and that controlling the complications will become increasingly difficult due to limited human and medical resources. However according to ASCO recommendation “withholding critical anti-cancer
10therapy is not currently recommended”.
There is no evidence that bisphosphonate use can affect COVID-19 infection. However, we decided to stop adjuvant bisphosphonate injections (every 6 months) or even substitute by oral or subcutaneous forms. We made this decision as a means of minimizing contact between patients and health care professionals and not because of the side effects of bisphosphonate. Besides, we currently do not have
16 Shahi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 14-21
BC guidelines modification in COVID-19 pandemic

There is no need to stop hormone therapy during the COVID-19 epidemic, even if COVID-19 infection is proven or suspected, especially in an outpatient setting. For hormone-positive patients with comorbidities, we can offer neoadjuvant/adjuvant hormone therapy instead of chemotherapy in cases
10with proven or suspected COVID-19 infection.
6. Radiation therapy
adequate staff and resources to provide this service to our patients. We continue bisphosphonate use for metastatic patients as per the guidelines.
We should consider the general situation of the patient if the home infusion is socially feasible for the patients, and the medical center has enough equipment and human resources to securely cover the substitution of IV in-hospital chemotherapy by oral or at-home chemotherapy.
7. Treatment of metastasisIn metastatic patients, it is highly recommended to
use less aggressive and toxic treatment if possible. For negative hormone patients, oral chemotherapy drug administration is recommended instead of IV administration and single agent therapy is preferred over combination therapy. Holiday policy is more acceptable than maintenance chemotherapy. We should also try to minimize hospitalizing our patients especially for palliative treatments. For hormone-positive patients, hormone therapy is the preferred
10treatment except for catastrophic metastatic crisis. We recommend delayed use of CD4/6 inhibitors,
Radiotherapy will significantly increase the number of referrals to hospitals and, therefore, the risk of contracting COVID-19. Although it is not the standard of care, many T1-T2, N0 patients can be treated by mastectomy instead of BCT to avoid the 25-30 days visits required for radiation treatment. For patients receiving chemotherapy before RT, time interval does not influence survival rates. However, the possible interplay between the timing of chemotherapy and timing of RT needs further elucidation. In addition, the results should be evaluated further in different subgroups. Overall, we conclude that starting RT as soon as possible after BCS may not be necessary and delaying it up to 20
29weeks is reasonable. We must refer to local guidelines before making this decision to make sure
28that the patient is a suitable candidate for this option.
Radiation therapy can be pursued following routine local guidelines and protocols. However, we endorse considering more conservative radiation techniques such as hypofractionation or IORT for proper patients. After neoadjuvant chemotherapy, all favorable “clinically complete responder” patients can be potential candidates for more conservative radiation therapy. We can also omit tumor bed boost in older patients with sufficient clear margin and good
15,25-28prognostic factors.
given their risk of neutropenia. If a metastatic patient receives radiotherapy as a palliative treatment, it is highly recommended to use hypofractionated or single fraction radiation therapy. (20 Gy in 5 or 8 Gy in single fraction)
9. Sharing data among patients and health care providers
It is recommended to restrict follow-up visits and para clinic activities such as blood testing (especially tumor markers) and imaging except in the presence of symptoms. To reduce the number of hospital/clinic visits and relieve patients' anxiety, healthcare professionals are encouraged to be in touch with them via telephone or web-mediated consulting to support patients remotely and meet their needs. It is possible to learn about symptoms and solve many of our patients' problems without necessarily meeting them in
10person.
Unfortunately, before the COVID-19 epidemic, Cyberspace and the Internet were underutilized in our healthcare system and both patients and healthcare providers were unaware of the benefits of communication through these platforms. This epidemic has taught us the importance of developing sufficient infrastructure to improve the status of cyber networking in our healthcare system. Currently, many clinicians use social media platforms such as “WhatsApp”, “Telegram” and “Instagram” to communicate with their patients.
Nonetheless, we need to move forward and promote more specialized platforms or the so called “Telemedicine Apps” such as “Virtual Breast Clinic-http://rubanapp.com/”, which is currently being used in our center. In order to support our patients and control their anxiety, we can share with them the latest news on COVID-19 and published government guidelines on cyberspace. We can also share educational media and information concerning stress management, nutrition, early detection methods, self-protection and prevention measures such as proper
31-35hand washing techniques. We have summarized the recommendations in Table 1.
8. Follow-up and supportive care According to our local guideline published by
Iranian Society of Endocrine and Metabolism and Iranian Rheumatology Society, it is advisable to prescribe 50000 units of oral vitamin D per week for only 4 weeks in persons who did not check their plasma
30vitamin D level recently. According to ASCO recommendation “there is no evidence to use prophylactic antiviral therapy for COVID-19 in cancer
10patients”. We must inform our patients that they should seek medical attention in the event of fever (T>37.3), tachypnea (RR>20), dyspnea, hypoxia (O2 sat<93%) or dry cough although ASCO does not recommend COVID-19 testing in all cancer
10,31,32patients.
17Shahi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 14-21
BC guidelines modification in COVID-19 pandemic

Table 1. Recommendations to deal with breast cancer during COVID-19 pandemic outbreak
ReferencesRecommendation
Educate patients, health care providers to:
- Correct handwashing, avoid touching the eyes,
nose, and mouth
- Social distancing
- Use of personal protective equipment (PPE)
according to local guidelines
- Home quarentine according to local guidelines
- Cover mouth and nose with a tissue during cough
and wear a facemask if you are sick
- Clean and disinfect frequently touched surfaces
- Inform patients as well as healthcare professionals
about the symptoms of COVID-19
Drug therapy:
- Prescribe 50000 units of vitamin D per week for 4 weeks
for all breast cancer patients
(Suggested by our local guideline)
- No need to prophylactic antiviral therapy
- Postpone screening procedures, such as mammography
and clinical breast examinations
- Minimize staging procedures before adjuvant therapy
General Rules:
- Reschedule elective surgeries as necessary
- Limit visits to hospitals and day care clinics
- It is recommended not to postpone surgery
- Breast surgeries should be performed in a Day-Care
unit except for patients with severe comorbidities
Risk reducing surgery:
- postpone risk reducing surgery some month after
subsiding pandemic outbreak
Surgery for DCIS and early stage T1-2, N0:
- Consider mastectomy more frequently to avoid
radiotherapy (after full discussion with patients)
- Substitute IORT or APBI instead of whole breast RT
in appropriated patients or omission of RT in older
patients (>70 years) with good prognostic factor and good
peripheral margins
Tumor localization:
- Avoid routine preoperative wire or radioactive seed
placement except for non-palpable tumors
Breast Reconstruction:
- Avoid immediate breast reconstruction
- Do not use implant and expander reconstructions
- Delay secondary breast reconstructions
Timing:
- Do not delay anti-cancer therapy
- Initiate or continue systemic cancer treatment as your
curatives plans.
- Begin chemotherapy as soon as possible (<30 days) in advanced
stages, triple-negative patients and HER2 positive cases
- Screen patients for possible COVID-19 infection sign and
symptoms before each course of chemotherapy
.
10ASCO31-33CDC guidelines34Local guidelines
35NHS24ESMO
10ASCO
Suggested
12NCCN
Suggested
10ASCO11
CDC13-14ACS
Suggested
10ASCO
35NHS
Uptodate22Predict online
Suggested
Infection prevention and control
Screening
Breast cancer staging
Surgery
Neoadjuvant/Adjuvant
Chemotherapy
Title
18 Shahi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 14-21
BC guidelines modification in COVID-19 pandemic

- Delay or modify treatment in a patient with active infection
- Collect routine lab samples needed before each chemotherapy
at home
Choosing protocol:
- Minimize chemotherapy in Luminal A patients by following
“predict online” instead of “NCCN guideline”
- Substitute every-3-weeks regimens instead of dose dense or
weekly protocols
- Four courses Docetaxel plus Cyclophosphamide instead of
routine 8 courses Anthracycline-based regimens in low risk
patients such as: those with node-negative, hormone
receptor-positive breast cancer or smaller than 10 mm in
triple-negative breast cancer with negative nodes
- Consider home-care chemotherapy if it is feasible for the
patient and the health system
- Continue hormone therapy during the COVID-19 epidemic
even if COVID-19 infection is proven or suspected
Supportive treatments:
- Minimize glucocorticoids use for prevention of nausea
and vomiting
- Use GCSF as primary prophylaxis.
- Minimize infectious complications by using prophylactic
antibiotics
- Defer supportive zoledronic acid treatments
- Consider oral or subcoutaneous form if home infusion is
medically and logistically feasible specially for anti Her-2
- Change intravenous treatments to subcutaneous or oral if
there are alternatives
- Consider deferring supportive therapies such as densoumab
and zoledronic acid treatments (except for hypercalcaemia)
preferably by home care if feasible
- Consider treatment breaks for long-term treatments
(Holiday policy)
- Delay using CD4/6 inhibitors given their risk of neutropenia
- Use more conservative radiation technique such as
IORT or APBI techniques if available
- Delaying radiation therapy up to 20 weeks after surgery if
the patients have no high risk of local recurrence (positive margin)
age less than 40 years or if no systemic treatment is given
- Radiation can postpone in low risk patients as long as the
COVID-19 outbreak is kept to a minimum or the risk for
patients involvement is reasonably reduced
- For adjuvant breast RT use hypofractionated RT (42.6 Gy in
16 fractions) instead of conventional RT (50 GY in 25 fractions)
specially in node negative breast cancer
- Omit boost in patients with more than 50 years old and
clean surgical margins
- Offer omission of adjuvant breast radiotherapy to those
patients with low risk breast cancer who fulfil the NICE
Early Breast Cancer Guideline (2018) criteria
- Identify alternative arrangements to minimize patient
exposure/remote monitoring/follow-up
- Minimize face-to-face appointments
- Postpone routine follow-up visits
- Better schedule appointments to reduce waiting times (not to
arrive early –consider measures such as texting them when ready
10ASCO35NHS
Suggested
35NHS
Suggested
10ASCO35NHS
12NCCN
35NHS
Suggested
Palliative/ Metastatic
Radiotherapy
Followup
19Shahi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 14-21
BC guidelines modification in COVID-19 pandemic

Conflict of InterestsThere is no conflict of interest to declare.
References1. Branswell H, Joseph A. WHO declares the
coronavirus outbreak a pandemic 2020 [Available from:https://www.statnews.com/2020/03/11/who-declares-the-coronavirus-outbreak-a-pandemic.]
2. Liang W, Guan W, Chen R, Wang W, Li J, et al. Cancer patients in SARS-CoV-2 infection: a nationwide analysis in China. Lancet Oncol. 2020;21(3):335-7.
3. Wang H, Zhang L. Risk of COVID-19 for patients with cancer. Lancet Oncol. 2020.
4. Xia Y, Jin R, Zhao J, Li W, Shen H. Risk of COVID-19 for cancer patients. Lancet Oncol. 2020.
5. Zhou F, Yu T, Du R, Fan G, Liu Y, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020.
9. Iranian Ministry of Health and Medical Education medical guidelines, Infographic / Existing Statistics of COVID-19 Patients - 20 March 2020 to 21 March 2020 [Available from: https://www. isna.ir/news/99010602727/]
10. Care of Individuals with Cancer During COVID-19. 2020 [Available from: https://www.asco.org /asco-coronavirus-information/care-individuals-cancer-during-covid-19.]
7. Kamboj M, Sepkowitz KA. Nosocomial infections in patients with cancer. Lancet Oncol. 2009;10(6):589-97.
11. National Center for Immunization and Respiratory Diseases (NCIRD) DoVD. Coronavirus Disease 2019 (COVID-19), Interim Clinical Guidance for Management of Patients with Confirmed
8. Li JY, Duan XF, Wang LP, Xu YJ, Huang L, et al. Selective depletion of regulatory T cell subsets by docetaxel treatment in patients with nonsmall cell lung cancer. J Immunol Res. 2014;2014:286170.
6 . L i n d e s y H . P r e v e n t i n g i n f e c t i o n i n immunocompromised cancer patients: Latest recommendations. Oncology Times. 2008;30(18): 25-6.
12. NCCN. Guideline v3.2020 BINV-1 2020 [Available from: https://www.nccn.org/ professionals/physician_gls/pdf/breast.pdf.]
20. Lohrisch C, Paltiel C, Gelmon K, Speers C, Taylor S, et al. Impact on survival of time from definitive surgery to initiation of adjuvant chemotherapy for early-stage breast cancer. J Clin Oncol. 2006;24(30):4888-94.
19. Shannon C, Ashley S, Smith I. Does timing of adjuvant chemotherapy for early breast cancer influence survival? Journal of clinical oncology. 2003;21(20):3792-7.
13. American College of Surgens, COVID-19: Guidance for Triage of Non-Emergent Surgical Procedures 2020 [Available from: https://www.facs.org/about-acs/covid-19/information-for-surgeons/triage]
18. Chavez-MacGregor M, Clarke CA, Lichtensztajn DY, Giordano SH. Delayed initiation of adjuvant chemotherapy among patients with breast cancer. JAMA oncology. 2016;2(3):322-9.
Coronavirus Disease (COVID-19). 2020. [Available from: https:/ /www.cdc.gov/ coronavirus/2019-ncov/hcp/clinical-guidance-management-patients.html.]
15. Caponio R, Ciliberti MP, Graziano G, Necchia R, Scognamillo G, et al. Waiting time for radiation therapy after breast-conserving surgery in early breast cancer: a retrospective analysis of local relapse and distant metastases in 615 patients. Eur J Med Res. 2016;21(1):32.
16. Salner AL, Smith S, Yu PP. Timing of adjuvant chemotherapy administration for early breast cancer. American Society of Clinical Oncology; 2018.
17. Gagliato Dde M, Gonzalez-Angulo AM, Lei X, Theriault RL, Giordano SH, et al. Clinical impact of delaying initiation of adjuvant chemotherapy in patients with breast cancer. J Clin Oncol. 2014;32(8):735-44.
14. American College of Surgens, COVID-19: Recommendations for Management of Elective Surgical Procedures 2020 [Available from: https:// www.facs.org/about-acs/covid-19/information-for-surgeons/elective-surgery.]
21. Kupstas AR, Hoskin TL, Day CN, Habermann EB,
to see them so they can wait in their car)
- Virtual attendance at MDT meetings
- Have discussions about patients and make decisions
in specific situation via cyberspace
- Encourage our teams to be in touch with patients via
internet such as “WhatsApp”, “Telegram” or “Instagram”
- Share educational media and information concerning
stress management, nutrition etc.
- Gather Frequently Asked Questions (FAQ) data banks
and educate nurses to answer our patients properly.
- Use “Telemedicine Apps” such as “Virtual Breast
Clinic-http://rubanapp.com/”
Sharing data between patients
and health care providers
20 Shahi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 14-21
BC guidelines modification in COVID-19 pandemic

27. Livi L, Borghesi S, Saieva C, Meattini I, Rampini A, et al. Radiotherapy timing in 4,820 patients with breast cancer: university of florence experience. International Journal of Radiation Oncology* Biology* Physics. 2009;73(2):365-9.
28. Associazione Italiana di Radioterapia Oncologica-La Radioterapia dei tumori della mammella: indicazioni e criteri guidada. Ed. 2013. 2016 [Available from:http://www.radioterapiaitalia.it/ allegato__1222_796.phtml.]
23. Nitz U, Gluz O, Clemens M, Malter W, Reimer T, et al. West German Study PlanB Trial: adjuvant four cycles of epirubicin and cyclophosphamide plus docetaxel versus six cycles of docetaxel and cyclophosphamide in HER2-negative early breast cancer. Journal of Clinical Oncology. 2019;37(10):799-808.
31. National Center for Immunization and Respiratory Diseases (NCIRD) DoVD. About Coronavirus Disease 2019 (COVID-19), 2020 [Available from: https:/ /www.cdc.gov/coronavirus/2019-ncov/about/index.html.]
26. Kim K, Chie EK, Han W, Noh D-Y, Ha SW. Impact of delayed radiotherapy on local control in node-negative breast cancer patients treated with breast-conserving surgery and adjuvant radiotherapy without chemotherapy. Tumori Journal. 2011;97(3):341-4.
22. Online PREDICT Tool, Version 1.2. [Available from:https://breast.predict.nhs.uk/]
Boughey JC. Effect of Surgery Type on Time to Adjuvant Chemotherapy and Impact of Delay on Breast Cancer Survival: A National Cancer Database Analysis. Ann Surg Oncol. 2019;26(10): 3240-9.
24. What should medical oncologists know about COVID-19? 2020 [Available from: https://www. esmo.org/newsroom/covid-19-and-cancer/q-a-on-covid-19.]
25. Kindts I, Laenen A, Depuydt T, Weltens C. Tumour bed boost radiotherapy for women after breast-conserving surgery. Cochrane Database Syst Rev. 2017;11:CD011987.
29. van Maaren MC, Bretveld RW, Jobsen JJ, Veenstra RK, Groothuis-Oudshoorn CG, et al. The influence of timing of radiation therapy following breast-conserving surgery on 10-year disease-free survival. Br J Cancer. 2017;117(2):179-88.
30. Instructions for taking vitamin D to combat corona 2020 [Available from:https://www.isna.ir/news/ 98121813751/.]
32. National Center for Immunization and Respiratory Diseases (NCIRD) DoVD. Coronavirus Disease 2019 (COVID-19), Interim Clinical Guidance for Management of Patients with Confirmed Coronavirus Disease (COVID-19). 2020. [Available from: https://www.cdc.gov/coronavirus /2019ncov/prepare/prevention.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoron
33. National Center for Immunization and Respiratory Diseases (NCIRD) DoVD. Interim Guidance for Healthcare Facilities: Preparing for Community Transmission of COVID-19 in the United States 2020. [Available from: https://www.cdc.gov/ coronavirus/2019-ncov/healthcare-facilities/ guidance- hcf.html.]
35. NHS Clinical guide for the management of cancer patients during the coronavirus pandemic 2020 [Available from:https://www.england.nhs.uk/ coronavirus/publication/specialty-guides/.]
34. Iranian Ministry of Health and Medical Education medical guidelines for COVID-19 2020 [Available from:http://dme.behdasht.gov.ir.]
avirus%2F2019-ncov%2Fabout%2Fprevention. Html]
21Shahi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 14-21
BC guidelines modification in COVID-19 pandemic

Although most cancers originate from a mutated single cell, tumors grow and gain heterogeneous cell populations, so they have no common genotypic/ phenotypic profile. This heterogeneity is translated
expected to be diagnosed with invasive BC with 1
62,930 women within situ BC in the United States. The mortality rate due to BC is estimated to be 42,260 deaths (41,760 women and 500 men). Sixty-two percent of BC patients are diagnosed with a tumor localized in the breast whose 5-year survival
2rate is 99%. However, the rate is reduced to 85% for those who have the cancer metastasized to the regional lymph nodes and it will be dramatically dropped to 27% if the cancer spreads to distant
3,4organs.
IntroductionBreast cancer (BC) is one of the most prevalent
cancer types among human populations with one out of eight women being reportedly affected during her lifetime. The increase of BC outbreak has been significant in the last fifty years causing the highest number of deaths among all cancer types. In 2019 alone, approximately 268,600 women were
ARTICLE INFO
Background: Breast cancer (BC) is a prevalent disease and a major cause of mortality among women worldwide. A substantial number of BC patients experience metastasis which in turn leads to treatment failure and death. The survival rate has been significantly increased due to more rapid detection and substantial improvements in adjuvant therapies including newer chemotherapeutic and targeted agents, and better radiotherapy techniques.
Conclusion: Our findings indicate that our MLP-GA hybrid algorithm can speed up diagnosis with higher accuracy rate than the individual patterns of algorithm.
Methods: In this study, we cross-compared the application of advanced artificial intelligence algorithms such as Logistic Regression, K-Nearest Neighbors, Discrete Cosine Transform, Random Forest Classifier, Support Vector Machines, Multilayer Perceptron, and Ensemble to diagnose BC metastasis. We further combined MLP with genetic algorithm (GA) as a hybrid method of intelligent analysis. The core data we used for comparison belonged to the images of both benign and malignant tumors collected from Wisconsin Breast Cancer dataset from the UCI repository.
Results: The application of several different algorithms to the collection of BC data indicated that these algorithms have comparable accuracy rate in detecting and predicting cancer. However, our hybrid algorithm showed superior accuracy, sensitivity and specificity compared to the individual algorithms. Two methods of comparison (Cross-Validation and Holdout) were applied to this study which produced consistent results.
metastasis,
specificity selection,
hybrid algorithm.
Key words:
classification algorithms,
machine learning,
Breast cancer,
Received:
Revised:
08 January 2020
15 December 2019
Accepted:
18 January 2020
*Address for correspondence: Yasin Panahi, PhDAddress: Pajoohesh Blv, Tehran-Karaj HWY, Tehran, 14965/161, IranTel: +98 21 44580344Fax: +98 21 44580395Email: [email protected],
ABSTRACT
Accurate Detection of Breast Cancer Metastasis Using a HybridModel of Artificial Intelligence Algorithm
a Deputy of Research and Technology, Ardabil University of Medical Sciences, Ardabil, Iran
b Department of Stem Cells and Regenerative Medicine, National Institute of Genetic Engineering and Biotechnology,
Tehran, Iranc Department of Biology, York University, Toronto, Canada
a b c a bJafar Abdollahi , Atlas Keshandehghan , Mahsa Gardaneh , Yasin Panahi* , Mossa Gardaneh
Open AccessOriginal Article
DOI: 10.19187/abc.20207122-28
22 Abdollahi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 22-28

to some cancer cell populations with invasive and 5
metastasizing capacity causing tumor malignancy. Metastasis is a biological hallmark of malignant
6tumors and the main cause of cancer mortality. Therefore, early detection can have extremely profound impact on overall patient outcome and survival.
BC is a systemic disease that may be treated via 7
surgery and chemo- and radiotherapy. Pathologically, a single factor alone cannot be attributed to BC, scince there are several factors that are proposed as BC risk factors including age, personal history, breast
8pathology, family history, and genetic predisposition. Also, interactions between environmental and genetic factors can induce susceptible genes such as BRCA1
9and BRCA2 to undergo mutation, which in turn leads to tumorigenesis.
Current diagnostic methods of tumor metastasis are developed as preclinical and clinical assays. Preclinical assays are used in ex-vivo samples and in in-vivo mice and comprise lab tests/histopathology, non-invasive blood tests, small animal imaging, molecular genetic imaging, and circulating tumor cells. Approaches used to detect metastatic lesions at clinical levels include biomarker tracking, imaging
10procedures, and circulating tumor cells. In fact, a diagnostic test is considered complete when it can
11achieve 100% sensitivity and specificity. None of these diagnostic methods meet this criterion and have not yet been successfully translatable from bench to bedside.
Some of these methods have been adopted for cancer diagnosis for more than 40 years. However, the biopsy-based histopathology is one of the most widely used methods to detect metastatic cells and classify cancer. Pathologists use histopathological images to accurately identify tumor cells. With this technique, they examine the microscopic structure of
12the patient's tissue. Of note, this is the gold standard for the detection and diagnosis of micrometastases in
13tissues suspected to have tumor cells. However, analysis of slides made from biopsies is a laborious task for a pathologist and requires sufficient time, remarkable skill and prudence. It is not an error-free
14task and might leave small metastases un-detected. In comparison, computer-aided histopathological analysis can play an important role in the detection
15and prediction of BC tumor cells. In this case, the use of Artificial Intelligence (AI) algorithms is an attempt to improve speed and accuracy of diagnosis.
Several AI algorithms have been developed and applied to cancer detection. Logistic Regression (LR) is a statistical and mathematical procedure that explores data sets with one or more free variants that hold a result, whereas K-Nearest Neighbors (KNN) is a supervised machine learning method used to solve classification and regression problems. Decision Tree Classifier (DTC) works by separating images into parts of differing importance and
MethodsIn this study, we used data of digitalized
pathologic images from Wisconsin Breast Cancer dataset [(https://archive.ics.uci.edu/ml/datasets/ Breast+Cancer+Wisconsin+(Diagnostic)] that included 357 benign and 212 malignant BC samples. We primarily reviewed the reports of the period 2006-2019 on diagnosis and classification of images collected from cancer tissues based on various algorithms. Our review indicated that application of an ML algorithm alone has not been precise and successful in detection and prediction of diseases. Next, we used 7 standardized and widely used algorithms to classify BC on our samples for comparison. K-Nearest Neighbors (KNNs) that uses the probability of density estimation based on nuclear methods, and Decision Tree (DT) employed for pattern extraction were the first two algorithms we applied. Our third algorithm was Forest Tree (FT) and we used a collection of FTs to classify cancer patients. We entered a set of data to each FT so the algorithm could start learning. For prediction, we used a new set of data so the FTs could predict the outcome.
Logistic Regression (LR) was the fourth algorithm employed in order to segregate benign tumors from malignant ones. For this, we applied 30 parameters as potential risk factors and compared the results using Receiver Operating Characteristics (ROP) in terms of the level of sensitivity and specificity. In MLP that simulates human brain
16performance , we used Gradient-based Multilayer Perceptron neural network as an MLP type widely applied to BC diagnosis. The next algorithm we used was SVC(Support Vector Classifier) the kernel of which was used for the classification of polished data
converts them into equivalent frequency coefficients. Random Forest Classifier (RFC) is another algorithm based on an ensemble learning method that creates a set of decision trees from randomly-selected subset of training set to aggregate votes and decide the final class of the test object. Support Vector Machines (SVM) is a supervised learning method that examines the data and sorts it into one of the two categories. Multilayer Perceptron (MLP), on the other hand, is a feed-forward artificial neural network that generates a set of outputs from a set of inputs. Finally, Ensemble techniques are machine learning techniques where more than one learner are constructed for a given task, and Multilayer Perceptron/Genetic Algorithm (MLP-GA) can more accurately detect tumor cells. Given that the individual use of AI algorithms may not lead to rapid and accurate detection of tumor cells, we attempted to cross-compare a number of these index algorithms in our study. We also combined MLP with genetic algorithm (GA) to create a hybrid pattern for boosted efficiency of detection.
23Abdollahi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 22-28
Artificial intelligence for detection of BC Metastasis

and enhanced precision of benign/malignant tumor diagnosis. After the basic algorithms, group learning algorithm was applied to develop a model of data classification with enhanced precision and performance compared to the basic algorithms.
Finally, in order to boost neural network algorithms such as MLP, we applied genetic algorithms (GAs) to add a new hybrid pattern of MLG-GA to individual algorithms. Indeed, we used GA to optimize initial weights in a neural network and determine optimal quantities of the parameters in both learning and detection processes of the system. We adopted two different strategies called Cross-Validation and Holdout to our comparison studies. We applied 569 samples in each experiment and devoted 60% for learning, 20% for evaluation, and 20% for the main tests. For this, we applied various criteria that included sensitivity, accuracy and specificity, True/False Positive Rates, Positive/ Negative Predictive Values, methods of data segregation, etc.
ResultsAlgorithms: an overviewFigure 1 shows a flow chart of the algorithms we
Data collected from DT and FT showed, respectively, 93% and 97% accuracy. Logistic Regression predicted cancer with 96% accuracy, 94% sensitivity and 95% specificity whereas MLP produced 95% accuracy. The accuracy figures for SVM and group learning were found, respectively, 96% and 93%. Figure 2 compares the accuracy rates based on the Holdout approach.
Comparison of algorithms for their accuracy of diagnosis
Table 1 compares the performance of different algorithms using the Holdout strategy. Data achieved through KNN indicated that Gaussian Nuclear Density Estimation based on Euclidean distance detects cancer with 93% accuracy.
applied in this study. It shows how our hybrid system is designed. We entered the data into our machine learning algorithms in 3 steps. In step one, basic algorithm was applied individually but in step 2 they were then used in groups. In step 3, we applied our hybrid system comprising of MLP and genetic algorithm (MLP-GA). The algorithms were ultimately evaluated for their performance in predicting the samples.
Table 1. Comparison of accuracy rates.
Recall F1-scorePrecision
0.96
0.96
0.97
0.93
0.95
0.93
0.93
0.98
0.00987
0.00987
0.00970
0.01101
0.00943
0.00966
0.00966
0.00543
0.97
0.97
0.97
0.94
0.95
0.94
0.94
0.98
0.96
0.96
0.97
0.94
0.95
0.94
0.94
0.98
0.96
0.96
0.97
0.94
0.95
0.94
0.94
0.98
LR
SVM
RFC
DTC
MLP
KNN
Ensemble
MLP-GA
AccuracyAlgorithm Standard deviation
Figure 1. A schematic flow chart of the algorithms.
.Diagnosis of BC was compared in rates among various algorithms with Holdout approach.
24 Abdollahi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 22-28
Artificial intelligence for detection of BC Metastasis

Comparison between these algorithms by the Cross-Validation strategy generated data that was nearly identical to those of the Holdout approach. This showed that the MLP-GA hybrid has the highest accuracy rate among all those algorithms used in our study (Table 2 and Figure 3).
We employed boxplot in order to demonstrate the accuracy rate of our algorithms in classifying cancer data using cross-Validation. Figure 4 shows the outcome of the boxplot analysis in the distribution of accuracy rates for the validation of the algorithms. A boxplot was drawn for each figure of diagnosis algorithms. The results indicate that all algorithms have a range of the least distance between 86 and 100 with an average of 94.
LRSVM R
FDTC
MLP
KNN
Encem
ble
MLP
-GA
0
20
40
60
80
100
Holdout
Acc
ura
cy (
%)
ACC
Precision
Recall
F1-score
Figure 2. Comparison of accuracy rates. Graph shows the percentage of accuracy for each algorithm using Holdout comparison approach. Each column represents at least two different comparison experiments carried out independently.
LRKNN
DTC RFC
SVMM
LP
Ensem
ble
MLP
-GA
0
20
40
60
80
100
Cross-validation
Acc
ura
cy (
%)
Figure 3. Comparison of accuracy rates. The graph shows the accuracy percentage for each algorithm using cross-validation comparison approach. Each column represents at least two different comparison experiments carried out independently.
Table 2. Comparison of accuracy rates.
0.93
0.93
0.92
0.95
0.93
0.96
0.94
0.997
0.01839
0.01282
0.01121
0.01204
0.01966
0.00966
0.01615
0.00015
LR
KNN
DTC
RFC
SVM
MLP
Ensemble
MLP-GA
AccuracyAlgorithm SD
25Abdollahi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 22-28
Artificial intelligence for detection of BC Metastasis
Diagnosis of BC was compared in rates among various algorithmswith Cross-Validation approach. LR, Logistic Regression;KNN, K-Nearest Neighbors; DTC, Decision Tree Classifier; RFC, Random Forest Classifier; SVM, Support Vector Machines;MLP, Multilayer Perceptron; MLP-GA, Multilayer Perceptron/Genetic Algorithm; SD, Standard Deviation.

We next applied randomized search (RS) and grid search (GS) methods in order to optimize estimating parameters and improve our results as well as find those parameters that affect the learning process in parallel. Figure 5 shows the result of comparison and evaluation for each algorithm using RS and GS. These findings indicate that our hybrid algorithm MLP_GA has a superior performance in optimization and search for parameters effective in rapid diagnosis of cancer with an accuracy rate of 98%.
In this study, we used various algorithms for classifying BC datasets. In order to select the best algorithm, we applied the timing criterion and its complexity as an element for comparing multiple algorithms for problem solving. Table 3 shows the results of comparing execution time complexity within various algorithms. As shown in Table 3, the MLP-GA algorithm has higher performance in terms of time complexity and in classifying datasets. Its execution time reached 0.04 with an accuracy rate of 98.3%.
We, therefore, used Confusion Matrix (CM) to show the overall performance of algorithms so we could evaluate their function or malfunction in the classification and diagnosis of datasets. Table 4
compares the performance of various algorithms using CM.
Hybrid algorithm MLP-GA with the highest level of accuracy and lowest deviation
The data indicate the high performance of our recommended algorithm MLP-GA so that its accuracy, sensitivity and specificity have reached, respectively, 98%, 98% and 94%. They also indicate that the algorithm MLP_GA has a superior performance and is capable of classifying all datasets.
We showed that our hybrid system has an accuracy rate of 99.7% which was the highest among all algorithms we studied (Table 2 and Figure 3). This system also showed a deviation rate of 0.00015 disease prediction, the lowest rate compared to those of other algorithms we studied.
DiscussionBreast cancer is a malignant tumor with different
phenotypes. We applied AI-based effective algorithms to breast tissue images and addressed the question of whether AI can help detect cancerous tissues and BC metastasis as a result. We particularly found that a
Figure 4. Comparison of accuracy rates among algorithms in the distribution of accuracy rates in validating classification data.
Figure 5. Comparison of accuracy rate of algorithms for optimization and search for parameters effective in cancer detection
26 Abdollahi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 22-28
Artificial intelligence for detection of BC Metastasis

combined algorithmic procedure of MLP-GA can more efficiently minimize errors of diagnosis.
All the algorithms we used to detect BC worked with reasonable accuracy and speed. However, they differ from one another in their composition and functionality. In order to benefit from their strength and enhance the efficiency of diagnosis, we created the MLP-GA hybrid algorithm that demonstrated maximum precision with minimum errors. Similar attempts have been already made to detect heart
23-25disease and Coronary Artery Disease. In an elegant study, Mobadersany et al. applied their convolutional neural networks to combine histology images and genomic biomarkers into a single unified framework and showed that this hybridized system is superior to current procedures in predicting the
26overall survival of glioma patients. Belciug and Gorunescu applied a hybrid neural network/genetic
Of the AI algorithms that we examined, ANN identifies patterns and processes that originate from the biological neural system and operates similar to the brain. ANN is comprised of a vast number of extraordinary interconnected processing elements called neurons that act in concert to solve a problem.
16It has been applied to BC detection and risk
18, 19assessment. K-Nearest neighbors algorithm is a non-parametric method used for classification and regression. This approach has also been applied to
20, 21BC detection. Random Forest or Random Decision Forest is considered a supervised learning algorithm that builds a forest by accident. Accidental Forest makes several Decision Trees and then links them to produce more accurate and reliable
22predictions. It has been applied to BC detection.
Our hybrid system, in line with the systems reported above, recommends precise therapeutic procedures for complex diseases, reduces errors in clinics and improves enrolment in clinical trials. Since AI technology is rapidly growing in medicine, it will practically address data sharing and privacy, the transparency of algorithms, standardization of data and cooperation in various operating systems. Our main objective in the near future is designing intelligent models for BC metastasis and image classification assisted by early diagnosis of cancer using AI particularly MLP.
In conclusion, our hybrid algorithm MLP-GA was found superior to our other algorithms in detecting BC incidence more reliably and accurately.
Conflict of Interests
References1. American Cancer Society: https://www. cancer.org/
content/dam/cancer-org/research/cancer-facts-and-statistics/breast-cancer-facts-and-figures/breast-cancer-facts-and-figures-2019-2020.pdf.
2. Cancer Facts & Figures 2018. Atlanta: American Cancer Society; 2018.
3. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA: A Cancer J Clin. 2018; 68(1):7-30.
None.
algorithm to detect BC occurrence and recurrence. They designed a multi-layer perceptron using a GA routine and found that this combination is superior to individual approaches in providing accurate
27classification of BC samples.
4. Breast Cancer Facts & Figures 2017-2018.
Table 3. Comparison of timing complexity in the classification of datasets.
Table 4. Comparison of performance among various algorithms using Confusion Matrix.
Recall
DTC
F1-score
MLP KNN Ensemble MLP-GA
Precision
RFC
0.120921
0.099941
0.442738
0.101936
0.117928
0.124924
0.112928
0.046721
l0.96
0.94
0.95
0.90
0.90
0.92
0
96
96
97
93
95
93
93
98
0.97
0.96
0.97
0.88
0.90
0.96
0
0.96
0.95
0.95
0.90
0.89
0.90
0
0.95
0.92
0.92
0.89
0.92
0.88
0.89
0.98
0.93
0.91
0.89
0.86
0.86
0.88
0
0.93
0.93
0.89
0.90
0.89
0.90
0
0.95
0.95
0.95
0.91
0.90
0.89
0
0.96
0.96
0.97
0.93
0.95
0.93
0.93
0.983
0.95
0.92
0.93
0.89
0.92
0.88
0.89
0.983
0.98
0.98
0.94
0.98
0.98
0.98
0
0.93
0.93
0.92
0.95
0.93
0.96
0.94
0.997
0.93
0.93
0.93
0.89
0.90
0.90
0
KNN
DT
RF
RG
SVM
MLP
Ensemble
MLP-GA
Accuracy
Sensitivity
Specificity
PPV
NPV
TPR
FPR
Accuracy
LR
Algorithm
Algorithm
SD
SVM
27Abdollahi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 22-28
Artificial intelligence for detection of BC Metastasis

5. Meacham C, Morrison S. Tumour heterogeneity and cancer cell plasticity. Nature. 2013. 501:328–337.
Atlanta: American Cancer Society, Inc.; 2017.
6. National Cancer Institute, 2019, https://www. cancer.gov/types/metastatic-cancer.
7. Sarıtaş AG, Yalav O, Kekeç Y, Sakman G, et al. Effect of neoadjuvant chemotherapy on estrogen receptor, progesterone receptor, Cerb-B2, vascular endothelial growth factor and Ki-67 in patients with locally advanced breast cancer. Cukurova Med J. 2019; 44(1):226-231.
8. Shah R, Rosso K, Nathanson SD. Pathogenesis, prevention, diagnosis and treatment of breast cancer. World J Clin Oncol. 2014;5(3):283–298.
9. Nathanson, KN, Wooster R, & Weber BL. Breast cancer genetics: what we know and what we need. Nature medicine, 2001; 7(5):552.
19. Ayer T, Alagoz O, Chhatwal J, Shavlik JW, Kahn CE Jr, Burnside ES. Breast cancer risk estimation with artificial neural networks revisited: discrimination and calibration. Cancer.
10. Menezes ME, Das SK, Minn I, Emdad L, Wang XY, Sarkar D, Pomper MG, Fisher PB. Detecting Tumor Metastases: The Road to Therapy Starts Here. Adv Cancer Res. 2016; 132: 1-44.
11. Mordente, A., Meucci, E., Martorana, G. E., & Silvestrini, A. Cancer Biomarkers Discovery and Validation: State of the Art, Problems and Future Perspectives. Adv Exp Med Biol. 2015; 867:9-26.
17. Saritas I. Prediction of Breast Cancer Using Artificial Neural Networks. J Med Syst (2012) 36: 2901.
13. Bird B, Romeo M, Laver N, & Diem M. Spectral detection of micro-metastases in lymph node histo-pathology. J Biophotonics. 2009; 2(1-2):37-46.
14. Spanhol FA, Oliveira LS, Petitjean C, Heutte L. A Dataset for Breast Cancer Histopathological Image Classification. IEEE Trans Biomed Eng. 2016; 63:1455-1462 .
12.Kumar R, Srivastava R, & Srivastava S. Detection and Classification of Cancer from Microscopic Biopsy Images Using Clinically Significant and Biologically Interpretable Features. J Med Eng. 2015:14.
16. Abdollahi J, Moghaddam BN, & Parvar ME. Improving diabetes diagnosis in smart health using genetic-based Ensemble learning algorithm. Approach to IoT Infrastructure. Future Gen Distrib Systems J. 2019; 1:23-30.
15. Aswathy M, & Jagannath M. Detection of breast cancer on digital histopathology images: Present status and future possibilities. Informatics in Medicine Unlocked. 2017; 8:74-79.
18.Sepandi M, Taghdir M, Rezaianzadeh A, Rahimikazerooni S. Assessing Breast Cancer Risk with an Artificial Neural Network. Asian Pac J Cancer Prev. 2018; 19(4):1017-1019.
2010;116(14):3310–3321.
22. Zhang H, Wang M. Search for the smallest random forest. Stat Interface. 2009; 2(3):381.
24. Verma L, Srivastava S, & Negi PC. A Hybrid Data Mining Model to Predict Coronary Artery Disease Cases Using Non-Invasive Clinical Data. J Med Syst. 2016, 40, 178 (2016).
25. Kolukisa B, Hacilar H, Goy G, Kus M, Bakir-Gungor B, Aral A, Gungor VC. Evaluation of classification algorithms, linear discriminant analysis and a new hybrid feature selection methodology for the diagnosis of coronary artery disease. 2018 IEEE International Conference on Big Data: 2232-2238.
23.Liu X, Wang X, Su Q, et al. A Hybrid Classification System for Heart Disease Diagnosis Based on the RFRS Method. Comput Math Methods Med. 2017; 2017:8272091.
26. Mobadersany P, Yousefi S, Amgad M, et al. Predicting cancer outcomes from histology and genomics using convolutional networks. Proc Natl Acad Sci U S A. 2018;115(13):E2970–E2979.
20. Altman N S. An introduction to kernel and nearest-neighbor nonparametric regression. The Am Stat. 1992; 46 (3): 175–185.
21. Sarkar M, Leong TY. Application of K-nearest neighbor's algorithm on breast cancer diagnosis problem. Proc AMIA Symp. 2000;759–763.
27.Belciug S, Gorunescu F. A hybrid neural network/genetic algorithm applied to breast cancer detection and recurrence. Expert Systems. 2013; 30(3):243-254.
28 Abdollahi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 22-28
Artificial intelligence for detection of BC Metastasis

the most common cancer in women in many 1, 2
countries such as Iran, Turkey, etc. The incidence 3of breast cancer was near 46.8 in 100,000 in 2012.
Based on a global report, 13,835,000 patients suffer from cancer and 458,400 deaths were caused by
3 breast cancer in 2010. In Iran, the incidence of breast cancer is 24% of the total of malignancies among women, that is approximately 36 per
4100,000. Although the incidence of breast cancer is
Breast cancer is the second cause of cancer-related mortality among women in the US. Also, it is
Introduction
ARTICLE INFO
Methods: The study was conducted on 210 of midwives aged 20-62 who participated in a seminar for clarifying the role of knowledge, attitudes and practices in breast cancer early detection and prevention. The data were collected using a standard questionnaire which has 4 sections with 55 items including age, educational level, number of family members, marital status, family history of breast cancer and their knowledge, attitude and practices about breast cancer screening. Data were analyzed using SPSS version 13.0.
Conclusion: An appropriate level of knowledge and practice of breast cancer screening was observed to help prevention among midwives. The findings can have remarkable practical implications as midwives can play an important role to broaden the breast-cancer-related knowledge of women.
Background: The incidence of breast cancer is rising rapidly worldwide. Midwives have an important role in early detection of the disease by providing the patients with awareness and an accurate Clinical Breast Examination (CBE) of the patients that are effective in early detections. This study investigated the knowledge, attitudes and practices of midwives toward breast cancer.
Results: About two-third of the participants (65.9%) had excellent knowledge about the signs and symptoms of breast cancer. The results revealed that 30.8% of respondents performed self-examination once a month. There was a significant correlation between the knowledge of breast cancer and adopting preventive practices (P = 0.02). The level of their attitude was significantly associated with a positive family history of breast cancer (P= 0.03). There was no significant relationship between marital status or family history of breast cancer with CBE.
Key words:
clinical breast examination,
preventionmidwives,
04 February 2020
09 January 2020Revised:
Accepted:
Received:
04 February 2020
Breast cancer,knowledge,
Address for correspondence: Hamid Zaferani Arani,Address: Young Researchers and Elite Club, Islamic Azad University, Tehran Medical Sciences, Tehran, Iran. Tel: +98 937 483 0246, Fax: +98 21 22748001, E-mail: [email protected]
ABSTRACT
Knowledge, Attitudes, and Practices toward Breast Cancer among Midwives in a Breast Cancer Educational Seminar in Tehran
a School of Medicine, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran
b Assistant Professor, School of Nursing and Midwifery, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran
c Cellular & Molecular Department, School of Advanced Sciences, Tehran Medical Sciences, Islamic Azad University, Tehran, Irand Cancer Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran
e Department of Cellular molecular biology, Faculty of new sciences, Tehran Medical Sciences, Islamic Azad University,
Tehran, Iran
a b a cHesam Adin Atashi , Mohammad Eslami Vaghar , Maedeh Olya , Parisa Mirzamohammadi , a b,d aHamid Zaferani Arani* , Mohammad Hadizadeh , Seyed Mahmoud Reza Hashemi Rafsanjani ,
eGhoncheh Alizadeh
Open AccessOriginal Article
DOI: 10.19187/abc.20207129-36
29Atashi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 29-36

rising, the mortality rate has decreased, due to early diagnosis and good treatment options. Insufficient screening examinations is a main reason for diagnosis of breast cancer in advanced stages which contributes to heavy burden of this cancer in Iranian
5women.The appropriate screening procedure has an
important role in early detection and diagnosis that can promote the treatment response. Early diagnosis can improve the effectiveness of the treatment and decrease the disease burden in all types of cancer,
6including breast cancer. It also plays a pivotal role in the prevention of breast cancer. The 5-year survival rate has reached approximately 85% with early detection, whereas the late detection can decrease the
7survival rate to 56%. Therefore, screening has an undeniable role in prolonging life expectancy and decreasing the complications and mortality rate of
8breast cancer. Screening methods include mammography, clinical breast examination (CBE),
.and breast self-examination (BSE). Despite the existence of advanced screening methods, some of techniques such as mammography (approximately 10% of cases) fail to diagnose of tumors or may show
1 0false-positive results. Today, BSE is not recommended as a screening method in early breast cancer detection. Most of the renowned algorithms have omitted BSE from the list of early detection measures, although it seems that it cannot be a global recommendation. In some limited-resource countries that have not incorporated the screening program in their health care system, BSE can spot large tumors and is considered a good method for breast cancer awareness. Obviously, it is an easy, cost-effective, and safe method of screening in these countries. Also, about 90% of patients with breast cancer detect their
10disease by self-examination. The clinical sign of tumor in BSE is any mass, swelling, discharge,
11, 12redness or any change in the breast. Despite its benefits, most women would rather not do BSE. Hence, educating people to do BSE seems to be necessary for countries that may not have access to the screening programs such as mammography and CBE.
Midwives can play an important role in BSE education. Indeed, understanding the beliefs and attitudes of midwifery students about breast cancer and BSE, and subsequently broadening their knowledge, can improve the early diagnosis of breast
1cancer and reduce breast-cancer-related deaths. On the other hand, in some countries, breast surgeons are inaccessible and in some cultures, women prefer not to refer to a male health center for CBE, which may
8reduce the referral rate to health care provider. Although many women in nearly all medical fields might have insufficient knowledge about breast cancer, midwives usually have enough information
9, 13about thismalignancy. Thus, they can play an important role in educating other women about breast cancer who refer to them for gynecologic
In the questionnaire, there are various items to assess the level of knowledge, attitude, and practices of the midwives toward breast cancer prevention and BSE. It consisted of 55 questions split into four parts. The first part consisted of 6 socio-demographic questions including age, educational level, number of family members, marital status, and family history of breast cancer. The second part comprised of 22 questions on the respondents’ knowledge of breast cancer including signs and symptoms (10 items) and risk factors (12 items). The third part consisted of 12 statements about attitudes toward breast cancer (breast cancer prevention, BSE, early detection and the odds of developing breast cancer). The final part consisted of 15 questions about the practice of midwives regarding breast cancer prevention.
Methods
In the section dedicated to breast cancer attitudes, the participants scored each statement using a 5-
The aim of this study is to investigate the knowledge, attitudes, and practices of midwives toward breast cancer screening and the association with socio-demographics among the Iranian female midwives who participated in a breast cancer prevention seminar in Tehran.
exams. Besides, if midwives educate other women well, they can also convey these experience to their
14other counterparts.
This analytic cross-sectional study was conducted among midwives who participated in a one-day seminar entitled "clarifying the duty of midwives in early detection and prevention of breast cancer”. The questionnaires were distributed among participants at the beginning of the seminar before presentations and collected 30 minutes after the end of the presentations. The study population consisted of 210 midwives who attended the event. Data collection was performed through a researcher-made questionnaire. The validity and reliability of the questionnaire were attested
15(Cronbach's alpha = 0.86).
With reference to the scoring of part two, every correct response received 1 point, while every incorrect response was scored 0. The total score ranged within 0-22. Respondents with scores 0-6 were assumed to have poor knowledge, those with scores 7-14 were considered to have moderate knowledge, and those with scores 15-22 were regarded to have excellent knowledge about breast cancer. In analyzing each section of part two, in the ‘Sign and Symptoms’ section, respondents with scores 0-3 were regarded as having poor knowledge, those with scores 4-6 as moderate, and those with scores 7-10 as excellent knowledge of breast cancer signs and symptoms. For the questions concerning Risk Factors, respondents with scores 0-4 were categorized as having poor knowledge, those with scores 5-8 as moderate, and those with scores 9-12 as excellent .
30 Atashi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 29-36
Midwives KAP toward breast cancer

ResultsSocio-demographic characteristics
point Likert scale (one to five for absolutely disagree, disagree, without no ideas, agree, and absolutely agree, respectively). The overall score of attitudes was calculated according to the total points acquired by the respondents regarding the 12 items. Respondents with scores 12-36 were considered to have negative beliefs, and those with scores 37-60 were assumed to have positive beliefs.
Evaluation of the final part involved calculating the percentage of correct and incorrect responses to questions about breast cancer prevention. Data were analyzed with descriptive statistics, chi-square test, one-way Analysis of Variance (ANOVA), independent-samples t-test, and logistic regression analysis by SPSS version 13. The significance level for the two-tailed test was set at P < 0.05.
From a total of 210 participants, 185 midwives returned their questionnaires. Among the respondents, there was one individual with a personal history of breast cancer. There was no divorced woman and the mean number of family members was 3.93 (± 1.33). In terms of the education level, nine (4.9%) of women had a diploma (a certificate in the field of midwifery) and the rest had an academic degree, two of whom had a PhD. The
The results for the ‘Signs and Symptoms’ section had a mean score of 6.60 (± 1.73), meaning that overall, the participants had relatively favorable knowledge of the signs and symptoms of breast cancer (weak (n=7,13%), moderate (n=27-50%), and excellent (n=122-65.9%). The three correct answers with the highest frequency in this part were suspicious mass (n=175, 94.6%), dimpling (n=171, 92.4%), and changes in the skin texture (n=167, 90.3%). Painful breasts near menstruation (n=176, 96.2%) and breast pain (n=93, 50.7%) were the factors that most of the respondents wrongly answered. No significant relationship was found between education level and knowledge about breast cancer signs and symptoms (P = 0.057); however, a significant relationship was found between the knowledge and family history (P = 0.020).
A considerable proportion of participants aged 40 years and above (80 members, 43.2%), had a bachelor's degree (148 members, 80%), were married (101 members, 54.6%), and did not have family history of breast cancer (141 members, 76.2%).Table 1 presents the demographic characteristics of the respondents.
knowledge about breast cancer sign and symptoms
age range of participants was between 20 and 62 years, with a mean age of 35.61 ± 11.81.
Table 1. Frequency distribution and percentage of socio-demographic characteristics of participants
PercentFrequency
20-2930-3940 ≤TotalMissingTotal
High school certificateAssociate degreeBachelor of scienceMaster of scienceDoctor of philosophyTotalMissingTotal
≤ 45 ˂other
SingleMarriedTotalMissing
YesNoTotalMissing
MotherSisterRelativesTotalMissing
37.316.843.297.32.7100
4.94.3807.61.197.82.2100
32.422.744.9
41.654.696.2
3
17.376.293.56.5
3.80.514.118.481.6
6931801805
185
98
148142
1814
185
604283
771011787
3214117312
712634151
Age, (years)
Educational level
Number of family members
Marital status
Family history
Family relationshipin patient with positive family history
Characteristics
31Atashi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 29-36
Midwives KAP toward breast cancer

Table 2 reports the participants’ knowledge of breast cancer signs and symptoms.
Knowledge of breast cancer risk factorsOur assessment of the participants’ knowledge
about risk factors showed a mean score of 7.67 (±2.13). The majority of respondents believed that unhealthy habits (n=174, 94.1%), lack of childbirth (n=161, 87%), and consumption of fatty food (n=156, 84.3%) were the main risk factors for breast cancer. Most of the respondents did not know that oral contraceptives (n=72, 38.9%) and delayed menarche (n=70, 37.8%) are risk factors for breast cancer development. Additionally, they believed that breastfeeding (n=168, 90.8%) and physical exercise (n=170, 91.9%) have protective effects on breast cancer prevention. Some respondents believed that breast imaging (n=78, 42.2%), BSE (n=50, 27.0%), and CBE (n=51, 27.6%) are not effective in breast cancer early detection (Table 3).
Overall, 13 (7%) midwives had weak, 108 (58.4%) had moderate, and 64 (34.6%) had excellent knowledge about breast cancer risk factors. It was observed that knowledge of breast cancer risk factors has no significant relationship with age (P = 0.09) and family history (P = 0.06). However, there was a
significant relationship between education level and knowledge of risk factors (P = 0.007). Table 3 summarizes the participants’ knowledge of breast cancer risk factors.
AttitudesThe mean score of midwives’ negative beliefs was
38.75 ± 3.30, and the mean score of midwives’ positive beliefs about risk factors was 38.65 ± 3.11. In contrast, the factors “early detection of breast mass is not valuable and just leads to stress” (n=174, 94.1%) and “BSE is a healthy habit” (n=183, 98.9%) had the maximum average value in the negative and positive attitudes, respectively. The highest scores in attitude belonged to the participants who were above 40 (47.35), had a high school certificate (40.75), were married (39.32), and had a positive family history of breast cancer (40). Figure 1 displays the comparison of demographic variables and attitudes. It was found that family history had a significant correlation with attitudes (P = 0.03). Similarly, marital status had a significant relationship with attitudes toward breast cancer screening, BSE, CBE, early detection of breast cancer, and its prevention (P = 0.009). There was no association between the total score of knowledge about breast cancer and attitudes (P = 0.466).
Table 2. Participants' knowledge about breast cancer signs and symptoms. (N= 185)
PercentFrequency
Correct answers
54.1
46.9
90.3
51.9
58.9
3.8
96.2
88.6
79.5
94.6
92.4
100
86
167
96
109
7
176
164
147
175
171
Breast Paresthesia
Feeling breast pain
Changing the skin form
Purulent discharge
Breast enlargement
Painful breast
Painful breast near menstruation
Bloody discharge
Wound on the nipple
Suspicious mass
Depression the part of breast skin
Characteristics
Table 3. Participants' knowledge toward breast cancer risk factors. (N= 185)
PercentFrequency
Correct answers
38.9
42.2
37.8
80
84.3
87.0
90.8
27.0
94.1
65.9
27.6
91.9
72
78
70
148
156
161
168
50
174
122
51
170
Taking OCP
Breast imaging
Delayed menarche
First childbirth between 40 to 45 years
Consumption of fatty foods
Lack of childbirth
Breastfeeding
BSE
Unhealthy habits (smoking, drinking, etc)
Late menopause
CBE
Regular daily exercise
Characteristics
32 Atashi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 29-36
Midwives KAP toward breast cancer

Practices of midwives regarding their breastsA total of 28 participants (15.1%) practiced
appropriately regarding breast cancer prevention, and 101 participants (54.6%) had harmful and risky practices in their lives (Table 4). Large number of participants said that they perform CBE (136 members, 73.5%). A total of 121 of respondents (67.5%) replied that they had not done mammography. Approximately 179 participants answered question on about doing mammography and a large proportion indicated that they practice it only as a check-up
(n=37, 20%). It was found that knowledge of breast cancer signs and symptoms had a significant correlation with family history (P=0.012) and educational level (P=0.045), and there was no correlation between marital status (P=0.388), age (P=0.466), risk factors (P=0.084) and positive attitudes toward practices regarding breast cancer (P=0.293). Table 5 outlines the correlation values of practice factors with some selected demographic variables. According to the results, marital status and family history had no impact on CBE.
Table 4. Participants' practice regarding their breasts
Table 5. Participants' practice regarding their breasts
Percent
Mammography
Frequency
CBEBSE
Taking vegetables and fruitsBSECBEMammographyRegular exercises
SmokingTaking fatty foods
Once in a monthMore than 2 times in a monthOnce in several monthsRarely
Immediately afterBetween 2 mensesA week before mensesAnytime they can
Exercise, nutrition, etc.Healthy food
-0.022 (0.381)
0.054 (0.229)
-0.066 (0.191)
0.067 (0.191)
-0.113 (0.046)
0.089 (0.083)
0.037 (0.292)
0.689 (0.125)
0.064 (0.002)
0.137 (0.011)
2.347 (0.001)
0.772 (0.835)
0.749 (0.356)
0.103 (0.459)
(0.429-1.108)
(0.064-0.527)
(0.137-0.772)
(2.347-24.211)
(0.772-1.233)
(0.749-1.109)
(0.103-2.795)
95.773.573.532.46.5
3.850.8
42.89.735.412.03
42.26.50.523.2
53.511.4
0.812 (0.389)
0.453 (0.065)
0.414 (0.048)
4.299 (0.004)
0.936 (0.610)
0.857 (0.159)
0.515 (0.420)
(0.505-1.305)
(0.195-1.051)
(0.173-0.992)
(1.593-11.598)
(0.725-1.207)
(0.692-1.062)
(0.103-2.579)
0.042 (0.278)
-0.050 (0.248)
-0.226 (0.002)
<0.001 (0.269)
-0.024 (0.359)
-0.118 (0.035)
-0.105 (0.062)
1771361365812
794
57134716
7812143
9921
-0.035 (0.312)
-0.054 (0.229)
-0.294 (0.001)
0.282 (<0.001)
-0.030 (0.328)
-0.162 (0.006)
0.080(0.120)
Appropriate practices
Harmful and risky habites
Performing BSE
BSE in relation to menses
Healthy daily habits
Age
Education level
Marital status
Family history
Knowledge of signs and symptoms
Knowledge of risk factor
Mean of attitude
0.978 (0.923)
0.530 (0.082)
0.786 (0.564)
2.349 (0.167)
0.951 (0.639)
0.912 (0.325)
2.682 (0.208)
(0.622-1.538)
(0.259-1.085)
(0.347-1.7800)
(0.700-7.878)
(0.769-1.175)
(0.759-1.096)
(0.578-12.442)
Characteristics
Variables OR (Sig.)
Correlation (Sig.)
CI OR (Sig.)
CI Correlation (Sig.)
OR (Sig.)
CI Correlation (Sig.)
Our results demonstrated that more than half of the participants (approximately 66%) had excellent knowledge about breast cancer signs and symptoms, while 13% had poor knowledge. Our findings revealed that “suspicious mass” and “painful breast”
Discussion had the highest and lowest frequency rate of the correct answers, respectively. It was observed that only women with an associate degree had negative beliefs regarding breast cancer screening tests, which may be related to this group’s overall lower-level knowledge. Ghazanfari et al. reported that the
33Atashi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 29-36
Midwives KAP toward breast cancer
In a research in Turkey about educational level on attitudes toward BSE, evaluating the attitude of the first- and fourth-year nursing and midwifery students, it was revealed that the first-year students did not have adequate information about BSE had more negative beliefs regarding the performance of BSE and the fourth-year students had positive
9attitudes to do BSE. Therefore, a college education can change negative attitudes toward more BSE to positive attitudes. In this study, based on our participants’ attitudes, only in its early-stage diagnosis, BSE can be helpful but it is not effective in reducing breast cancer mortality. This demonstrates the importance of educational attainment and how it can lead to increased knowledge of breast cancer risk
In our study, 13% of the participants had poor, 50% had moderate, and about 66% had good knowledge of breast cancer. Other studies on Iranian women indicated that about 12-28% of women had a good knowledge of breast cancer and 37% of them
4had no information about BSE. This difference in the knowledge of participants can imply the fact that many of our participants have academic education. In a study conducted in the United States-Mexico borderland, Mexican participants were reported to have a higher level of knowledge about breast cancer (86%) compared to U.S Latinas (71%), due to the fact that Mexican women have higher level of knowledge about breast cancer and they believed that BSE and CBE are the ways to early breast cancer diagnose and good treatment. This difference can be
16related to the age, education and insurance status , so about 90% of the breast cancer had been diagnosed by Mexican women themselves 10% of whom being
17in stage 1 of the breast cancer. In a study in the UK, half of the participants correctly answer 4 out of 5
18statements about breast cancer , because British women had broader knowledge about breast cancer, who can subsequently receive an early diagnosis and
19, 20good prognosis. Based on our findings and another study, there are significant correlations between educational level and breast cancer
4 knowledge and increase adoption of BSE.Despite the low level of knowledge about breast
cancer risk factors, awareness about breast cancer signs and symptoms was appropriate perhaps due to a few barriers for screening services and their
21important role to enhancing knowledge. In Iran, the lack of awareness is associated with geographic
22areas, occupations and education , and in Iran and other Asian countries educational level can affect the
4, 23performance of BSE and BCE.
factor of “early detection of breast mass has nothing but stress” had the highest average in negative attitudes. The most important inhibiting factors for breast cancer screening were women’s beliefs, attitudes towards preventive methods and their explanations about screening tests, shame, and the
15time-consuming nature of the practice.
factors. As reported by some studies, in most cases in developing countries like Iran the diagnose of
24cancers is delayed until later stages (> 2).
In our study, women aged over 40 years had the most positive beliefs regarding BSE and CBE. Previous studies in Iran demonstrated that 17-94% of women had positive attitudes toward BSE and screening tests, and 83.3% believed that BSE has a positive effect on the early diagnosis of breast cancer. In addition, 72% of participants believed that physical examination of breast and mammography
20, 27can be effective medical diagnostic procedures. Overall, 30.8% of participants in our study performed BSE once a month and 42.2% did it immediately after menopause. In a study from the
28US, 58% of women performed BSE -close to 51.5%- in our study, 33.3% of women over 40 years performed it and 31.8% knew how to do it correctly. Only 37% of participants were trained in BSE for which the healthcare staff was the most important
15, 20, 29source (38.2%). In North Ethiopia, about 6.5% of participants had ever practiced BSE, and only
306.25% of the respondents practiced BSE regularly. A study on 5000 women indicated that only 31% perform CBE because 60.9% of the participant ignore it and they are careless about it, 17.4% of participants have acceptable knowledge and 5.9%
29did not consider it necessary to diagnose the cancer.
A study on Nigerian nurses showed that just 40% of participants knew the appropriate time to perform
18BSE , while in nursing students in the USA about 77% recognized the correct time of BSE, and 80% of
20participants performed BSE satisfactorily. In some studies, the percentage of American and British people who had received one or all cancer screening methods (i.e., BSE, CBE, mammography) was
20, 25, 26higher than that in developing countries , because of good public education in advanced countries.
In Asian countries, the number of individuals performing BCE has grown with increasing
4, 23, 31knowledge of risk factors and age (30-50 years). In our study, we demonstrated that the level of knowledge is enhanced with higher ages , too. Generally, 39.6% of women had poor knowledge about mammography. Furthermore, 28.5% of women
4over 40 have done at least one mammography. Similarly, in our study, 32.5% of the participants aged over 40 have done at least one BSE in their life. In America, 31% of African-American citizens perform
14 4, 32, 33BSE once a month , while in Asia it is 10-20%. These differences can be attributed to various cultural barriers, and knowledge and beliefs regarding breast cancer in different societies. A high incidence of breast cancer in younger women has been reported in different studies and it is recommended that
30, 34mammography be performed from the age of 40.
The obstacles to BSE practice were found to be as follows: fear of being diagnosed with breast cancer,
34 Atashi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 29-36
Midwives KAP toward breast cancer

There were some limitations to this study such as the mere focus on midwifery students and graduated, so our results may not be generalizable to all health workers, and the sample size was small (n=210) considering the population of women in society and the incidence of breast cancer .
References
lack of self-confidence, lack of sufficient knowledge, lack of a family history of cancer, forgetfulness and
9laziness.
In conclusion, this study revealed a significant association between some socio-demographic characteristics and knowledge of breast cancer among midwives. According to the results, most of the participants had appropriate knowledge toward breast cancer prevention. The present study focused on the level of knowledge, attitudes and practices of midwives and their important role on educating other women to prevent breast cancer and reduce consequent burdens. Therefore, improving the midwives’ education about breast cancer can have a positive influence on other women’s health.
AcknowledgmentsWe appreciate the Cancer Research Center of
Shahid Beheshti University of Medical Sciences in Tehran for providing financial support.
Given the significance of knowledge about breast cancer and its important role in improving women’s health, we suggest that further studies be conducted on the knowledge about breast cancer among other health workers.
Conflict of InterestsThe authors declare no conflict of interests in this
study.
1. Gençtürk N, Demirezen E, Ay F. Health beliefs of midwifery students at Istanbul University about breast cancer and breast self-examination acknowledgements. Journal of Cancer Education. 2017;32(4):784-9.
2. Jazayeri SB, Saadat S, Ramezani R, Kaviani A. Incidence of primary breast cancer in Iran: Ten-year national cancer registry data report. Cancer epidemiology. 2015;39(4):519-27.
3. Jemal A, Center MM, DeSantis C, Ward EM. Global patterns of cancer incidence and mortality rates and trends. Cancer Epidemiology and Prevention Biomarkers. 2010;19(8):1893-907.
4. Tilaki KH, Auladi S. Awareness, attitude, and practice of breast cancer screening women, and the associated socio-demographic characteristics, in northern Iran. Iranian journal of cancer prevention. 2015;8(4).
5. Barati M, Shoar LM, Mohammadi Y, Dogonchi M. Factors Affecting Breast Self-examination Behavior Among Female Healthcare Workers in Iran: The Role of Social Support Theory. Journal
of Preventive Medicine and Public Health. 2019;52(4):224.
6. Lin L, Yan L, Liu Y, Yuan F, Li H, et al. Incidence and death in 29 cancer groups in 2017 and trend analysis from 1990 to 2017 from the Global Burden of Disease Study. Journal of hematology & oncology. 2019;12(1):96.
7. Kalliguddi S, Sharma S, Gore CA. Knowledge, attitude, and practice of breast self-examination amongst female IT professionals in Silicon Valley of India. Journal of family medicine and primary care. 2019;8(2):568.
8. Noroozi A, Jomand T, Tahmasebi R. Determinants of breast self-examination performance among Iranian women: an application of the health belief model. Journal of Cancer Education. 2011;26(2): 365-74.
9. Memis S, Balkaya NA, Demirkiran F, editors. Knowledge, attitudes, and behaviors of nursing and midwifery students regarding breast self-examination in Turkey. Oncology nursing forum; 2009.
10. Bebis H, Altunkurek SZ, Acikel C, Akar I, Altunkurek SZ. Evaluation of breast self-examination (BSE) application in first and second degree relatives of patients with breast cancer. Asian Pacific Journal of Cancer Prevention. 2013;14(8):4925-30.
11. Dagne AH, Ayele AD, Assefa EM. Assessment of breast self-examination practice and associated factors among female workers in Debre Tabor Town public health facilities, North West Ethiopia, 2018: Cross-sectional study. PloS one. 2019;14(8).
12. Balkaya NA, Memis S, Demirkiran F. The effects of breast self-exam education on the performance of nursing and midwifery students: A 6-month follow-up study. Journal of Cancer Education. 2007;22(2):77-9.
13. Hajian-Tilaki K, Auladi S. Health belief model and practice of breast self-examination and breast cancer screening in Iranian women. Breast cancer. 2014;21(4):429-34.
14. Chouliara Z, Papadioti-Athanasiou V, Power K, Swanson V. Practice of and attitudes toward breast self-examination (BSE): a cross-cultural comparison between younger women in Scotland and Greece. Health Care for Women International. 2004;25(4):311-33.
16. Banegas MP, Bird Y, Moraros J, King S, Prapsiri S, et al. Breast cancer knowledge, attitudes, and early detection practices in United States-Mexico border Latinas. Journal of Women's Health. 2012;21(1):101-7.
17. Zapka JG, Stoddard A, Maul L, Costanza ME.
15. Ghazanfari Z, Azattalab F. Knowledge, Attitude and Practice (Kap) Study Regarding Prevention of Breast Cancer in Working Women of Chaloos City. SSU_Journals. 2006;14(2):51-5.
35Atashi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 29-36
Midwives KAP toward breast cancer
24. Knaul F, Bustreo F, Ha E, Langer A. Breast cancer: why link early detection to reproductive health interventions in developing countries? salud pública de méxico. 2009;51:s220-s7.
22. Taleghani F, Kianpour M, Tabatabaiyan M. Barriers to breast self-examination among Iranian women. Iranian journal of nursing and midwifery research. 2019;24(2):108.
28. Budden L. Young women's breast self-examination knowledge and practice. Journal of Community Health Nursing. 1995;12(1):23-32.
20. O. Odusanya OOT, Olumuyiwa. Breast cancer knowledge, attitudes and practice among nurses in Lagos, Nigeria. Acta oncologica. 2001;40(7): 844-8.
25. Banning M. Black women and breast health: A review of the literature. European Journal of Oncology Nursing. 2011;15(1):16-22.
Interval adherence to mammography screening guidelines. Medical Care. 1991:697-707.
26. Pérez-Stable EJ, Otero-Sabogal R, Sabogal F, McPhee SJ, Hiatt RA. Self-reported use of cancer screening tests among Latinos and Anglos in a prepaid health plan. Archives of Internal Medicine. 1994;154(10):1073-81.
21. Hurst CP, Promthet S, Rakkapao N. Factors Associated with Breast Cancer Awareness in Thai Women. Asian Pacific Journal of Cancer Prevention. 2019;20(6):1825-31.
18. Lavelle K, Charlton A. Women's perception of risk of cancer. Bmj. 1998;317(7157):542.
29. Temiz M, Aslan A, İnandı T, Beshirov E, Beyaz F. Knowledge, attitudes, and behaviors of female teachers related to breast cancer and breast examination in southern Turkey. Breast Care. 2008;3(1):55-60.
19. Richards M, Westcombe A, Love S, Littlejohns P, Ramirez A. Influence of delay on survival in patients with breast cancer: a systematic review. The Lancet. 1999;353(9159):1119-26.
30. Abay M, Tuke G, Zewdie E, Abraha TH, Grum T, et al. Breast self-examination practice and associated factors among women aged 20–70 years attending public health institutions of Adwa town, North Ethiopia. BMC research notes. 2018;11(1):622.
23. Haji‐Mahmoodi M, Montazeri A, Jarvandi S, Ebrahimi M, Haghighat S, et al. Breast Self‐Examination: Knowledge, Attitudes, and Practices Among Female Health Care Workers in Tehran, Iran. The breast journal. 2002;8(4):222-5.
27. Marzouni HZ, Lavasani Z, Shalilian M, Najibpour R, Fakhr MS, et al. Women's awareness and attitude toward breast self-examination in dezful city, Iran, 2013. Iranian Red Crescent Medical Journal. 2015;17(1).
31. Yavari P, Pourhoseingholi MA. Socioeconomic factors association with knowledge and practice of breast self-examination among Iranian women.
34.Akhigbe AO, Omuemu VO. Knowledge, attitudes and practice of breast cancer screening among female health workers in a Nigerian urban city. BMC cancer. 2009;9(1):203.
33. Secginli S, Nahcivan NO. Factors associated with breast cancer screening behaviours in a sample of Turkish women: a questionnaire survey. International journal of nursing studies. 2006;43(2):161-71.
32. Avci IA. Factors associated with breast self-examination practices and beliefs in female workers at a Muslim community. European journal of oncology nursing. 2008;12(2):127-33.
Asian Pac J Cancer Prev. 2007;8(4):618-22.
36 Atashi, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 29-36
Midwives KAP toward breast cancer

37
Iranian women have been suffering from breast cancer a decade earlier, and 70% of the patients are
3diagnosed at an advanced stage. Later on, the studies that assessed the incidence rate of this cancer in Iran reported that the average age of the patients diagnosed with this cancer has decreased as
4compared to the other countries of the world.
According to 2019 statistics, breast cancer has an incidence of 11.6% among all types of cancer, accounting for 6.5% of mortalities worldwide. Also, as demonstrated by GLOBOCAN 2018, breast cancer
1Breast cancer is a major concern of global health
and is the leading cause of cancer deaths in women 2
worldwide. In comparison with other countries,
Introduction
ARTICLE INFO
Background: Considering the remarkable role of students in society and the relatively high prevalence of breast cancer in women, this study aimed to determine the factors related to adopting preventive behaviors for breast cancer in students.
Methods: This was a descriptive cross-sectional study. The study population consisted of 375 female students of Qazvin city, who were selected by stratified random sampling during the year 2019. Data collection tools included a demographic and contextual questionnaire and a valid and reliable questionnaire for measuring breast cancer preventive behaviors. Data were analyzed using SPSS 23 software program, descriptive statistics and logistic regression.
Results: Using there was a statistically significant relationship between adopting preventive behaviors against breast cancer and physical activity (P <0.001), so that the chances of adopting good preventive behaviors in students with "occasionally", "rarely" and "never" physical activity were respectively 0.410, 0.113, and 0.098 times chance for the students with daily physical activity. There was a significant relationship between breast cancer prevention and academic years (p= 0.027), so that the chances of adopting good-level preventive behaviors in the senior students was 1.498 times higher than the first year students. There was also a significant relationship between adopting preventive behaviors and employment (P = 0.017), so that the chances of adopting good-level preventive behaviors in unemployed students was 1.725 times higher than that of the employed students.
Conclusion: Students with lower education and less physical activity and the employed individuals less commonly adopted preventive behaviors. Therefore, it is necessary to pay more attention to these students in designing educational programs.
16 February 2020
Received:
19 January 2020Revised:
Accepted:06 February 2020
Key words:Preventive Behaviors, breast cancer,student
* Address for correspondence: Leila Dehghankar,Address: Qazvin University of Medical Sciences, School of Nursing & Midwifery. Social Determinants of Health Research CanterEmail: [email protected], [email protected]
ABSTRACT
Associated Factors with Adopting Preventive Behaviors for Breast Cancer in Iran
a Student Research Committee, School of Nursing & Midwifery, Qazvin University of Medical Sciences, Qazvin, Iran
b Department of Health Education & Promotion, School of Medical Sciences, Tarbiat modares University, Tehran, Iran
c Department of Nursing, Social Determinants of Health Research Center, School of Nursing & Midwifery, Qazvin University of Medical Sciences, Qazvin, Iran
a b cMarzieh Hajikarimbaba , Rahman Panahi , Leila Dehghankar*
Open AccessOriginal Article
Hajikarimbaba, et al. Arch Breast Cancer 2019; Vol. 7, No. 1: 37-43
DOI: 10.19187/abc.20207137-43

There are several risk factors reported as determinants of breast cancer including family history, reproductive behaviors, obesity, smoking, low physical activity and exposure to radiation,
11, 12stress, and anxiety. Unhealthy lifestyles (such as smoking, alcohol consumption, excessive exposure, inadequate personal hygiene, and inadequate diet) unfavorable environmental factors and genetics
13increase the risk of developing cancers.
incidence will rise from two million people in the year 2018 to more than three million people in 2046, which
5, 6demonstrates an increase of 46 percent. The World Health Organization (WHO) has predicted that cancer-related deaths will affect 24 million people by
7, 82035.
The lifestyle of students can be a good example of a healthy lifestyle in a community. On the other hand, the student population has significantly grown throughout the country in recent years. Therefore, it is important to identify the factors that influence students' compliance with healthier behaviors and
22, 23reduce risky behaviors. Given the importance of 24
breast cancer, the role of screening in its prevention
An international survey on breast cancer risk factors in the university students from 23 countries reported poorer knowledge of these students in comparison with older women. The findings emphasize the vital need for young women to have breast cancer prevention information to enhance
19, 20their behavior in order to prevent breast cancer. On the other hand, women play a key role in the development of any society. Therefore, more attention should be paid to their health care in a
21community.
By preventing and using screening, the incidence of cancer and the resulting mortality will be
14reduced. Studies show that with the early detection of cancer, the 5-year survival rate will be reduced by
1597%. It has been suggested that the appropriate method for breast cancer prevention and early detection is performing preventive behaviors which might include lifestyle modification and screening behaviors (mammography, cl inical breast
16examination and breast self-examination). Breast self-examination is inexpensive and easily accessible and does not require sophisticated and technical training. Clinical examination by a
17 physician is also helpful in early stages. Mammo-graphy is the most accurate test for early detection of
18breast cancer.
It is important to mention that there are numerous cases of breast cancer at the ages of 20 to 25 years in Iran; which might have some implications for screening programs for breast cancer by lowering the screening age at which average-risk and high-risk adults should start screening (e.g. from over 50 years
9to under 30 years of age). According to the latest surveys, about 8,500 new cases of breast cancer are
10registered each year in Iran out of whom 1,400 die.
This study was a cross-sectional study with a descriptive-analytical approach. The statistical population consisted of female students of Imam Khomeini International University in Qazvin in the academic year 2018-2019. We adopted stratified random sampling so that the number of subjects selected from each school was determined in proportion to the total number of undergraduate students in each school (as a class), and in each school the proportion of disciplines with the number of samples was specified according to the number of disciplines, i.e., quota sampling technique was used in the school. Students were selected by simple random sampling in each discipline and completed questionnaires.
Data collection
and the lower age of this cancer in Iran, research in 25
this area would be a priority. This study aimed to determine factors related to
the adoption of breast cancer prevention behaviors in students.
Methods
Inclusion criteria included being a female student, holding an undergraduate degree, studying at Imam Khomeini International University and having willingness to participate in the study. Exclusion criteria included physical and mental illnesses as claimed by the individual herself, having a history of mammary conditions and/or diseases (abnormal breast or cyst discharge, and cysts), a history of breast cancer in them or in a close relative (mother, sister, and aunt) and delivering incomplete questionnaires.
The second part was a valid and reliable questionnaire for measuring breast cancer prevention behaviors. It consisted of 4 questions about breast cancer preventive behavior. The scores considered for “always”, “often”, “sometimes” and “never” were 4, 3, 2, and 1, respectively. The minimum score was 4 and the maximum was 16. According to the mean scores, the average below 50% indicates poor preventive behavior, the average between 50 to 75% shows moderate preventive behavior and the average between 75 to 100
26represents good preventive behavior. Afterwards, this variable was regrouped into two levels of poor (earning less than 50% of the total score) and good (earning 50-100% of the total score) to be used in logistic regression. Content validity and reliability of this tool were assured in the study of Kalanfarma et al. Content validity was above 0.79 and Cronbach's
Questionnaires consisting of two parts were used for data collection. The first part was a demographic questionnaire which requested information about age, education, field of study, marital status, income, place of residence, employment status, and physical activity per week.
Adaptive behaviors for BC
38 Hajikarimbaba, et al. Arch Breast Cancer 2019; Vol. 7, No. 1: 37-43

After submitting a letter of introduction to Imam Khomeini International University, the questionnaires were distributed and completed. Data were entered into SPSS software and analyzed using descriptive statistics and logistic regression.
A total of 375 students were enrolled in this study. Of these, the highest number of students was in the age group 20-30 years including 182 students (48.5%). Also, 118 participants (31.5%) were freshmen and 319 participants (85.1%) were single. Table 1 shows other demographic information about
26alpha coefficient was estimated 0.76. Moreover, we sought the consultation of ten experts for the modification of items and validation of the questionnaire. It was then distributed to 30 students and Cronbach's alpha coefficient was calculated 0.81.
Results
Table 2 lists the factors associated with adopting breast cancer prevention behaviors in the students revealed through the logistic regression test. As the results show, physical activity was one of the factors related to adopting preventive behaviors against breast cancer (P <0.001), so that the chances of adopting good-level preventive behaviors in students with physical activity including "Occasionally", "rarely" and "never" were respectively 0.410, 0.113, and 0.098 times chance for the students with daily physical activity. Academic age was another factor associated with adopting preventive behaviors
the students.Results showed that the mean and standard
deviation of the overall score for adopting preventive behaviors against breast cancer was 1.82±8.92 out of 16. The prevalence of breast cancer prevention behaviors was poor in 150 (40%) and good in 225 (60%) of the students.
Table 1. Frequency distribution of the students according to demographic characteristics
%N
Under 20 years
years 20-30
Higher than 30 years
Single
Married
Divorced
Everyday
Most days
Sometimes
Rarely
Never
Freshmen
Sophomores
Juniors
Seniors
unemployed
employed
Under 1 million
1-2 million
2-3 million
Higher than 3 million
Qazvin
County
Village
Dormitory
Technical Engineering
Agriculture
Architecture
Science Research
Literature
Social sciences
48.3
48.5
3.2
85.1
14.4
0.5
8.5
23.5
33.6
28.3
6.1
31.5
31.2
22.9
14.4
86.4
13.6
9.3
36.8
28.3
25.3
33.1
27.7
1.6
37.6
16.3
5.9
10.9
14.9
22.4
29.6
181
182
12
319
54
2
32
88
126
106
23
118
117
86
54
324
51
35
138
106
95
124
104
6
141
61
22
41
56
84
111
Age
marital status
Physical activity
Academic years
Employment status
Income level
Residence
Field of study
Characteristics
39Hajikarimbaba, et al. Arch Breast Cancer 2019; Vol. 7, No. 1: 37-43
Adaptive behaviors for BC

Discussion
against breast cancer (P = 0.027), so that the chances of adopting good preventive behaviors in the fourth year students was 1.498 times higher than those in the first year. Employment was also another factor influencing the adoption of preventive behaviors for breast cancer (P = 0.017), so that the chances of adopting good preventive behaviors in the unemployed students was 1.725 times higher than the employed ones (Table 2). There was no significant relationship between breast cancer prevention behaviors and other variables.
The findings showed that the majority of the students had good breast cancer prevention
The purpose of this study was to determine factors associated with the adoption of breast cancer prevention behaviors among students.
The results of this study showed that physical activity was one of the factors related to adopting preventive behaviors of breast cancer, so that the chances of adopting good-level preventive behaviors
behaviors, which was in line with the results of Dafei 27 28
et al. and Montazeri et al. But Aghaeian et al. reported that the scores gained by the majority of women studied in Karaj were moderate concerning the adoption of preventive behaviors against breast
10cancer. Contrary to the results of the present study, Andsoy stated that nurses scored low on preventive
19behavior against breast cancer. It should be also noted that the results of the present study contradicts those of Nourizadeh et al. in which adopting preventive behaviors for breast cancer was reported
29at a low level. To explain, we can refer to differences in the sampling and the tools of measuring the behavior.
Table 2. Frequency distribution of the students according to demographic characteristics
Lower UpperExp(B)
95% C.I
Wald Sig.
Under 20 years
20-30 years
Higher than 30 years
Single
Married
Divorced
Freshmen
Sophomores
Juniors
Seniors
Daily
Most of the time
occasionally
Rarely
Never
Qazvin
County
Village
Dormitory
Under 1 million
1-2 million
2-3 million
Higher than 3 million
Technical Engineering
Agriculture
Architecture
Science Research
Literature
Social sciences
.351
.463
.524
.000
.546
.366
.637
.510
.148
.040
.026
.592
.249
.694
.389
.377
.398
.324
.748
.550
.305
.543
.767
1.099
11.369
2.389
.
1.935
1.538
3.523
4.838
1.137
.322
.370
2.172
11.577
2.355
2.468
2.564
2.753
3.480
5.072
3.247
1.506
2.359
3.876
4.329
2.677
1.033
.085
.085
.000
2.781
.007
.617
.856
54.990
.620
2.936
16.688
11.700
.796
.143
.293
.622
.049
.002
.001
.008
5.632
.010
1.861
.410
.910
.109
1.740
3.262
.115
.102
.309
.959
.771
.999
.027
.933
.432
.035
.000
.431
.087
.000
.001
.850
.705
.589
.430
1.000
.964
.972
.927
.344
.921
.172
.522
.340
.742
.017
.071
.621
2.294
1.119
.000
1.028
.750
1.498
1.571
.410
.113
.098
1.134
1.698
1.279
.979
.983
1.046
1.062
1.947
1.336
.678
1.131
1.725
4.097
-.476
.830
.113
-22.994
.027
-.288
.404
.452
-.891
-2.177
-2.328
.125
.530
.246
-.021
-.017
.045
.060
.666
.290
-.389
.123
.545
1.410
.291
.817
.387
28420.722
.323
.366
.436
.574
.520
.533
.681
.332
.979
.312
.472
.489
.494
.605
.488
.453
.407
.375
.413
.781
Age
Marital Status
Academic Yyear
Physical activity
Residence
Income level
Field of study
Job constant
Variable Levels B S.E.
Adaptive behaviors for BC
40 Hajikarimbaba, et al. Arch Breast Cancer 2019; Vol. 7, No. 1: 37-43
were higher in students with regular physical activity. Saremi et al. noted in their results that movement activities, physical activity, sports/leisure activities, and total physical activity play a preventive role in the prevalence of breast cancer in
30young women. Colditz et al. found that the incidence of breast cancer was lower in women with
31regular physical activity. Friedenreich et al. reported that the incidence rate of breast cancer
32decreases in women with physical activity. Given the possible reasons for this relationship, these two variables can be referred to as ‘homogeneity’. Moreover, doing physical activity is a form of preventive behavior.
The results showed that the factor of academic years was related to the adoption of preventive behaviors against breast cancer, so that the chances of adopting good-level preventive behaviors in the fourth year students were higher than the first year students. In the study conducted by Matos et al. in Brazil, it was found that educated people with higher economic status had higher rates of breast cancer
28screening. There was a significant relationship between breast self-examination and the level of
38education in the studies conducted by Karimi , 39 37 40
Ziaeefard , and Godazandeh. Baba pour et al. , 41 42Anvari et al. and Rastad et al. also showed that
people with higher level of education were more aware of breast cancer screening behaviors. But the
43results of the study by Raisi et al. were inconsistent with the findings of the present study due probably to the fact that all participants in the study had university education and thus developed greater awareness.
Since this study was conducted only among a sample of students at Imam Khomeini International University in Qazvin, its results cannot be generalized to students in other parts of the country. Therefore, it is recommended that this study be conducted on a wider scale in Iran, especially among medical students, and compare its results with non-
The results showed that employment was another factor associated with adopting preventive behaviors against breast cancer, so that the chances of adopting good-level preventive behaviors were higher in the unemployed students than the employed ones. In their study conducted in Turkey, Demirkiran et al. stated that the occupation of individuals has a significant impact on the prevention of breast
33 34cancer. In the study of soltanahmadi , Salimi 35 36 37
Pormehr , Farshabaf , and Godazandeh , breast self-examination was found to have a statistically significant relation with employment, so that having a job increased the rate of preventive behaviors against breast cancer. This discrepancy can be explained by differences in the tools of measurement and the age of the subjects. Beyond this, the occupation of individuals has a great impact on adopting preventive behavior.
medical students. Other limitations of this study were the relatively small sample size, lack of access to students on academic leave, lack of similar studies, and self-reported data collection.
As conclusion, the results indicate that lower prevalence of breast cancer prevention behaviors was higher in students with lower education and less physical activity, and those who were employed. Therefore, it is necessary to pay more attention to these students in the design of educational programs. Further studies are suggested to elucidate how the relevant factors influence the adoption of preventive behaviors in breast cancer.
AcknowledgmentsThis study was conducted with the support of the
Vice-Chancellor for Research and Technology of Qazvin University of Medical Sciences (Code of Ethics (IR.QUMS.REC.1397.193)), with the assistance of Imam Khomeini International University of Qazvin and the cooperation of its female students. Their efforts are appreciated.
Conflict of InterestsThere is no conflict of interest to declare.
References
3. Khadijah Kalan Farman Farma, Zahra Jalili, Iraj Zareban, and Mahnaz Shahraki Pour . Effect of education on preventive behaviors of breast cancer in female teachers of guidance schools of Zahedan city based on health belief model. J Educ Health Promot. 2014; 3: 77.
4. Akbari ME, Sayad S, Sayad S, et al. Breast Cancer Status in Iran: Statistical Analysis of 3010 Cases between 1998 and 2014. Int J Breast Cancer. 2017;2017:2481021.
6. Motahare Pilevarzadeh ,Mehrbanoo Amirshahi, R o g h a i y e h A f s a rg h a r e h b a g h , H o s e i n Rafemanesh, Seyed Mehdi Hashemi, Abbas Balouchi. REVIEW Global prevalence of depression among breast cancer patients: a
5. Observatory TGC (2018) GLOBOCAN. Breast Cancer 2019. http://gco.iarc.fr/today/data/ factsheets/cancers/20-Breast-factsheet.pdf 2. Siegel RL, Miller KD, Jemal A Cancer statistics 2019; 69(1):7–34
2. Khiyali Z1, Aliyan F, Kashfi SH, Mansourian M, Khani Jeihooni A. Educational Intervention on Breast Self-Examination Behavior in Women Referred to Health Centers: Application of Health Belief Model. Asian Pac J Cancer Prev. 2017 26;18(10):2833-2838.
1. Muhammad Abdul Hadi , Mohamed Azmi Hassali ,Asrul Akmal Shafie, Ahmed Awaisu. Knowledge and Perception of Breast Cancer among Women of Various Ethnic Groups in the State of Penang: A Cross-Sectional Survey. Med Princ Pract 2010;19:61–67 .
41Hajikarimbaba, et al. Arch Breast Cancer 2019; Vol. 7, No. 1: 37-43
Adaptive behaviors for BC

7. DeSantis C, Siegel R, Bandi P, Jemal A. Breast cancer statistics, 2011. CA Cancer J Clin 2011;61:409-418
systematic review and meta analysis . Breast Cancer Research and Treatment 2019 ; 176:519–533.
8. Behjat Marzbani , Javad Nazari , Farid Najafi , Behnaz Marzbani , Sara Shahabadi , Mahin Amini , Mehdi Moradinazar , Yahya Pasdar , Ebrahim et al. Dietary patterns, nutrition, and risk of breast cancer: a case-control study in the west of Iran . Epidemiol Health. 2019;41: e2019003.
9. Behzad Baradaran , Khalil Hajiasgharzadeh. Breast Cancer Among Young Women in Iran .International Journal of Women’s Health and Reproduction Sciences 2019; 7(2).
11 .Haj ian–Ti laki KO, Kaveh-Ahangar T. Reproductive factors associated with breast cancer risk in northern Iran. Med Oncol 2011; 28: 441-6. 10. Hajian-Tilaki KO, Gholizadehpasha AR, Bozorgzadeh S, Hajian-Tilaki E. Body mass index and waist circumference are predictor biomarkers of breast cancer risk in Iranian women. Med Oncol 2011; 28: 1296-301
12. Yazdani-Charati R, Hajian-Tilaki K, Sharbatdaran M. Comparison of pathologic characteristics of breast cancer in younger and older women. Caspian J Intern Med 2019; 10(1): 42-47.
10. Aghaeian N, Farahaninia M, Janmohamadi S, Haghani H. Association between health literacy and preventive behaviors of breast cancer in women. Journal of Health Literacy. Summer 2019; 4(2):9-17.
14. Torkizade S, Soltanian Z, DavariDolatabadi N. Awareness of female nursing, midwifery and para medicine students of Hormozgan University of Medical Sciences in relation to the risk factors, prognosis and prevention of breast cancer. Journal of Modern Medical Information Sciences. 2017; 3 (1) :22-28. [Persian]
13. Onsory K, Ranapoor S. Breast Cancer and the Effect of Environmental Factors Involved. NCMBJ. 2011; 1 (4) :59-70.
16. Khazaee-Pool et al.: Breast cancer-preventive behaviors: exploring Iranian women’s experiences. BMC Women's Health 2014 14:41.
17. Bozorgi N, Khani S, Elyasi F, Moosazadeh M, Janbabaei G, Shojaee L. A Review of Strategies to Promote Breast Cancer Screening Behaviors in Women . J Mazandaran Univ Med Sci. 2018; 28 (165) :243-255 .[Persian]
15. Miri M, Moodi M, Moasheri B, Sourgi Z, Hami J. A Applied Health Belief Model (H.B.M) in Adopting Preventive Behaviors in Breast Cancer by Female Teachers of Birjand. jha. 2004; 7 (17) :51-57 URL: http://jha.iums.ac.ir/ article-1-86-en.html
18. Monfared A, Ghanbari A, Jansar Hosseini L,
22. Smith DR. A systematic review of tobacco smoking among nursing students. Nurse Education in Practice. 2007; 7(5): 293-302.
19. Andsoy II, Gul A. Breast, cervix and colorectal cancer knowledge among nurses in Turkey. Asian Pacific Journal of Cancer Prevention 2014;15:2267-72.
24. Vakili M, Pirdehghan A, Adimi M, Sadeghian M, Akhondi M. Epidemiology and trend of cancer in Yazd, a central province of Iran, 2005-2009. Journal of research in health sciences. 2014; 14(3): 210-3.
25. Didarloo a, Shorkhabi z, Pourali R. survey of knowledge, worry and screening behavior towards breast cancea among female students of urmia university of medical sciences, in 2014. Journal of Urmia Nursing And Midwifery Faculty. 2016;14(3):201-12. [Persian]
23. Dehghankar L, Hajikarimbaba M, Panahi R. Health Literacy and Factors Related to It Among Female Students of Imam Khomeini International University in Qazvin, Iran. sjsph. 2019; 17 (3) :295-306 .[Persian]
28. Matos JC, Pelloso SM, Carvalho MD. Factors associated with secondary breast cancer prevention in Maringá. Paraná State, Brazil. Cadernos de saúde pública 2011; 27: 888-98
26. Kalan FarmanFarma K, Zareban I, Jalili Z, Shahraki pour M, Lotfi B. The Effect of Education on Condition of Knowledge, Attitude and Preventive Behaviors of Breast Cancer in Female Teachers at Guidance Schools in Zahedan. Journal of Torbat Heydariyeh University of Medical Sciences 2013;1:65-73
Norozi N. Status of Screening by Mammography and its Related Factors in the General Population of Women in Rasht . IJN. 2017; 30 (107) :32-41.
21. Tehrani H, Rahmani M, Jafari A. Health literacy and Its relationship with general health of women referring to health care centers. Journal of Health Literacy. Fall 2018; 3(3): 42-48.
20. Early J, Armstrong SN, Burke S, Thompson DL. US female college students’ breast health knowledge, attitudes, and determinants of screening practices: new implications for health education. Journal of American College Health 2011; 59:640-7
29. Nourizadeh R, Bakhtari aghdam F, Sahebi L. A survey on the knowledge and beliefs and behaviors of women referring to health centers in Tabriz regarding breast cancer and its screening methods, 2010. Iranian Journal of Breast
2 7 . D a f e i M , D e h g h a n i A , M o m e n i Z , Kalanfarmanfarma K, Koohgardi M, Jalali M et al . Study of breast cancer knowledge, attitude, and preventive behaviors among women referring to health-treatment centers in Yazd, Iran, 2015. Pajouhan Scientific Journal 2017; 15: 46-53. [Persian]
Adaptive behaviors for BC
42 Hajikarimbaba, et al. Arch Breast Cancer 2019; Vol. 7, No. 1: 37-43

32. Friedenreich C, Cust A. Physical activity and breast cancer risk: impact of timing, type and dose of activity and population subgroup effects. Br J Sports Med. 2008; 42(8):636-47.
30. Saremi A, Moradzadeh R, Mohammadi Bonchenari S. Physical Activity and Breast Cancer Prevalence: A Case Control Study in Arak, Iran (2017-2018) .Iranian Quarterly Journal of Breast Disease. 2019; 12(1):29-38.
34. soltanahmadi Z, Abbaszadeh A, Tirgari B. [A survey on the rate and causes of wo men’s participation or nonparticipation in breast and cervical cancers screening programs]. Iran J Obstetr Gynecol Infertil 2010; 13: 37-46. [Persian]
35. Salimi PS, Kariman N, Sheykhan Z, Alavi MH. [Investigation of breast cancer screening tests performance and affecting factors in women referred to Ardebil’s health and medical centers]. J Ardebil Univ Med Sci 2010; 10: 310-8. [Persian]
36. Farshbaf KA, Shahnazi M, Ghahvechi A, Thorabi H. [Performance conditions of breast cancer screening methods and its efficient factors among women referring to health centers of Tabriz]. Iran J Nurs Res 2009; 4: 27-38. [Persian]
31. Colditz G, Hankinson S. The nurse's health study: lifestyle and health among women. Nat Rev Cancer. 2005; 5(5):388-96.
Diseases 2010; 3: 43-51. [Persian]
37.GodazandehGh.A, Khani H, Khalilian AR, Atarod Z, FirozJaei MA, Partovi A, TayebiFard H. Knowledge and practice of above 15 years old females towards breast cancer prevention in Sari township, 2004. Journal of Mazandaran University of Medical Sciences 2006;16: 74-64
38.Karimi H, Sam Sh. Effect of breast self-examination (BSE) education on increasing women’s knowledge and practice, Ramsar. Journal of Babol University of Medical Sciences 2005; 7: 68-1.
39. Ziaeefard Z, AbdollahiKh, ZahediR,RahmanianS, Rahmnian K. knowledge of breast self-examination and mammography women marred over 20 years old referred to health center in south Iran. Journal of Jahrom university medical science 2011; 10:49-55.
40. Baba pour N, Nasiri R, Mir rajaee AS. Evaluation of the knowledge, attitude and performance of female personnels of Mashhad Azad university hospitas about breast cancer. Journal of Medical Sciences of Islamic azad university of Mashhad 2014;4(1):1-22. [Persian]
33. Demirkiran F, Ozgun H, Eskin M, Turk G, Cam R, Ozgun O, Demirkiran AE Cognition of breast cancer among gestational age Turkish women: a cross-ectional study. Asian Pacific Journal of Cancer Prevention 2011; 12:277-82.
43. Raisi M, Javadzadeh S , Sharifi Rad Gh , Yarmohammadi P. Knowledge, Attitude and Practice of Female Employees of Isfahan University of Medical Sciences about Breast Self-Examination. Journal of Health System Research 2011 ; 1 (2:) 747-744. [Persian]
41. Anvari K, Mosavi H, Kavosi F, Silian Tosi M. Assessment of knowledge, attitude and practice of female students of Mashhad University of Medical Sciences regarding risk factors, early diagnosis and methods of breast cancer prevention. Iranian Journal of Breast Disease 2012;6(2,3):32-43. [Persian]
42. Rasta H, SHokohi L, Dehghani L, Motamed jahromi M. Knowledge and practice of Fasa women about breast cancer in 7342. Journal of Fasa University of Medical Sciences 2013;3 (7) 16-82. [Persian]
43Hajikarimbaba, et al. Arch Breast Cancer 2019; Vol. 7, No. 1: 37-43
Adaptive behaviors for BC

44
1to malignant phyllodes tumors (PTs). As some tumors show similar characteristics of PTs and fibroadenoma, there is not a distinct boundary between FA and PT and it is still a considerable challenge to differentiate PTs from FAs due to
2morphology integration. In 1883, Johannes Müller introduced cystosarcoma
3phyllodes in mammary tissue with leaf shape growth. As the phyllodes tumors (PTs) can have different
IntroductionBreast fibro-epithelial lesions encompass a wide
variety of tumors from benign fibroadenomas (FAs)
ARTICLE INFO
Background: Breast fibroepithelial lesions encompass a wide variety of tumors from benign fibroadenomas to malignant phyllodes tumors (PTs). Local recurrence was reported in 20% of all subgroups and 20-25% risk of distant metastasis though superaggressive tumors are rare. Two young patients with nonresponsive, frequent recurrences of phyllodes tumors turned into the aggressive metastatic sarcoma are presented.
Case Presentation: Case 1: A 34-year-old married woman referred with the chief complaint of a mass and pain in her right breast. There was a 3cm well defined mass in right breast. An intermediate grade benign phyllodes tumor was confirmed in biopsy. Patient underwent surgical wide excision, radiotherapy. Three weeks later the mass recurred in her right breast with severe pain and nonproductive cough without hemoptysis. A single lung metastasis is conformed in the CT scan. Total mastectomy and thoracoscopic metastasectomy was performed and spindle cell sarcomas in both specimens is confirmed. Chemotherapy was done. Two weeks after chemotherapy she presented with multiple bilateral lung metastasises and thoracic wall involvement. No regression in metastasis was seen receiving the second line chemotherapeutic agents. Case 2: A 17-year-old young girl was referred to the breast clinic with a 2 cm firm mobile mass in left breast. The histopathology of the mass was benign phyllodes tumor. (1.5 cm margins) The tumor recurred 3 months later treated. During radiotherapy, the patient referred to the emergency department with the complaint of dyspnea and sever pleural effusion. The cytology reported malignant cells. CT-guided biopsy showed a high grade sarcoma. During chemotherapy, large ulcer in the site of the breast was appeared and mastectomy with Latissmus dorsi flap was performed and angiosarcoma was confirmed. Despite the second and third line chemotherapy the disease was progressed and multiple lung metastasis were confirmed in chest CT scan.
Conclusion: It seems that some subtypes of breast sarcomas could have an extremely an aggressive behavior which threatens the life of the patients in a short period of time. Further studies is suggested to discriminate the aggressive subtypes at the first step.
08 November 2019
10 January 2020
18 December 2019
Received:
Revised:
Accepted:
breast sarcoma,Phyllodes tumor,
early recurrence
Key words:
* Address for correspondence: Nafiseh Ansarinejad, MDAddress: department of hematology-oncology, Rassoul Akram Hospital. Sattarkhan-Niayesh Avenue, Teharn, IranTel: +98 21 64352390Fax: +98 21 64352486Email: [email protected]
ABSTRACT
Progressive Metastatic Breast Phyllodes Tumor Turns into Spindle Cell Sarcoma: Report of Two Cases and Reviewof the Literature
a Breast department, Rasoul-Akram Hospital, Iran university of medical sciences, Tehran, Iran
b School of Medicine, Iran University of Medical Sciences, Tehran, Iran
c Department of Surgery, Shahid Beheshti university of medical sciences, Tehran, Iran
d Department of Hematology and Oncology, Iran University of Medical Sciences, Tehran, Iran
a b c dNahid Nafissi , Seyed-Mohamad-Sadegh Mirahmadi , Majid Samsami , Nafiseh Ansarinejad*
Open AccessCase Report
Nafissii, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 44-48
DOI: 10.19187/abc.20207144-48

On the recent physical examination, there was a mass in the lower outer quadrant of her right breast 5 cm far from the border of the nipple-areola complex, measured about 3 cm. The well-defined mass was firm in palpation and had a lobulated margin. Ultrasonography showed a 30- mm benign mass with a regular border in the lower outer quadrant of the right breast, mostly suggesting fibroadenoma. A core needle biopsy was performed, and the pathologist reported it as an intermediate grade benign phyllodes tumor. Preoperative investigations, including Chest X-ray, were performed. All the lab tests and radiology findings were normal except for
natural histories, World Health Organization (WHO) suggested the classification of PTs into three forms, including benign, premalignant (borderline), and
4malignant lesions. Furthermore, there is no correlation between tumor categories with its clinical manifestation. It is also hard to distinguish between subgroups with radiological and histopathological
5findings.PTs are rare biphasic fibro-epithelial tumors that
account for 0.3 to 1% of all primary breast 6neoplasms. The PTs invasion is unpredictable. Local
recurrence was reported in 20% of all subgroups of breast PTs. Although distant metastasis commonly occurs in the malignant and borderline subgroups (20-25%), it can be rarely found in benign breast PTs. The common sites of distant metastasis are lung and bone as a consequence of hematogenous spreading of
7, 8the tumor cells. The breast PTs challenge women 9
mostly in the age range of 35 to 55.
Case No1: Case Presentation
A 34-year-old married woman was referred to the surgical oncology outpatient clinic of Rasoul-e-Akram hospital with the chief complaint of a mass in her right breast. The patient had two children, and had her first childbirth at the age of 20. She had a family history of gastric cancer in her father and her paternal aunt. The patient had a personal history of multiple sclerosis (MS) and minor depression and used Gabapentine, Assentra, Doxepin, and Azaram to control the neurologic and psychologic symptoms. Also, she had a history of breast pain and breast cysts in both breasts approved by ultrasonography and an examination by her family physician.
Regarding the low efficacy of adjuvant treatment, the primary line of treatment is the aggressive removal of the tumor and its adjacent healthy tissue during surgical intervention. Although chemoth-erapy and radiotherapy are not approved as main adjuvant treatments, radiotherapy is shown to have
8limited benefits in selected patients.In this article, we present two uncommon cases of
young females with frequent early recurrences of phyllodes tumor along with the phyllodes tumors turned into the aggressive metastatic sarcoma.
the breast mass.
Case No 2:
According to the histopathology report, she underwent surgical excision of the mass with a one- cm margin from each side of the tumor. The histopathological evaluation of the surgical specimen revealed a high-grade malignant phyllodes tumor with a focally positive margin. The records of the patient were presented in the Multidisciplinary Tumor Board (MDT). Since the patients strongly preferred not to do a mastectomy, the recommendation of the panel of experts was radiation therapy and close follow-ups. The patient received 50 Gy to the whole breast, followed by a boost dose of 16 Gy to lumpectomy bed totally in 33 fractions. There was no significant complication for the irradiation rather than redness and skin burning.
Three weeks after the last session of radiotherapy, the patient referred back to the clinic because of palpation of mass in her right breast near the location of the primary excised tumor. The mass was palpable on the physical examination. Also, she suffered from severe pain with radiation to the axilla and nonproductive cough without hemoptysis. Magnetic Resonance Imaging (MRI) of the breasts was performed and the recurrence of the tumor was suggested. Also, in the Computed Tomography (CT) scan of the chest, a single metastasis of the lung was confirmed. According to the second discussion in MDT, the brain MRI was performed though it did not show any abnormality compared to the previous multiple brain MRIs for the follow-up of multiple sclerosis. The patient underwent a total mastectomy and thoracoscopic metastasectomy by means of lung-wedge resection. Histopathological evaluation of the surgical specimen revealed spindle cell sarcomas in both specimens. The patient referred to the medical oncology department for chemotherapy. She received Ifosfamide and Adriamycin for four courses as the first line of chemotherapy agents. Two weeks after the concluding session of chemotherapy, the patient returned to the emergency department of the hospital with complaints of chest pain and dyspnea. Computed tomography (CT) scan showed multiple bilateral lung metastases and thoracic wall involvement. By the progression of the disease, the chemotherapy regimen was changed to Gemcitabine and Docetaxel based on the opinion of MDT. Unfortunately, there was no regression in metastasis by receiving three sessions of the second line chemotherapeutic agents. Finally, the patient referred to the supportive care department and received supportive care. The patient died 12 months after the diagnosis of her disease.
A 17-year-old young girl was referred to the breast clinic of Rasoul-e-Akram hospital with the chief complaint of a mass palpation in her left breast. In the past medical history of the patient, there was neither any risk factor for the breast cancer nor any
Phyllodes tumor progression to agressive sarcoma
45Nafissii, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 44-48
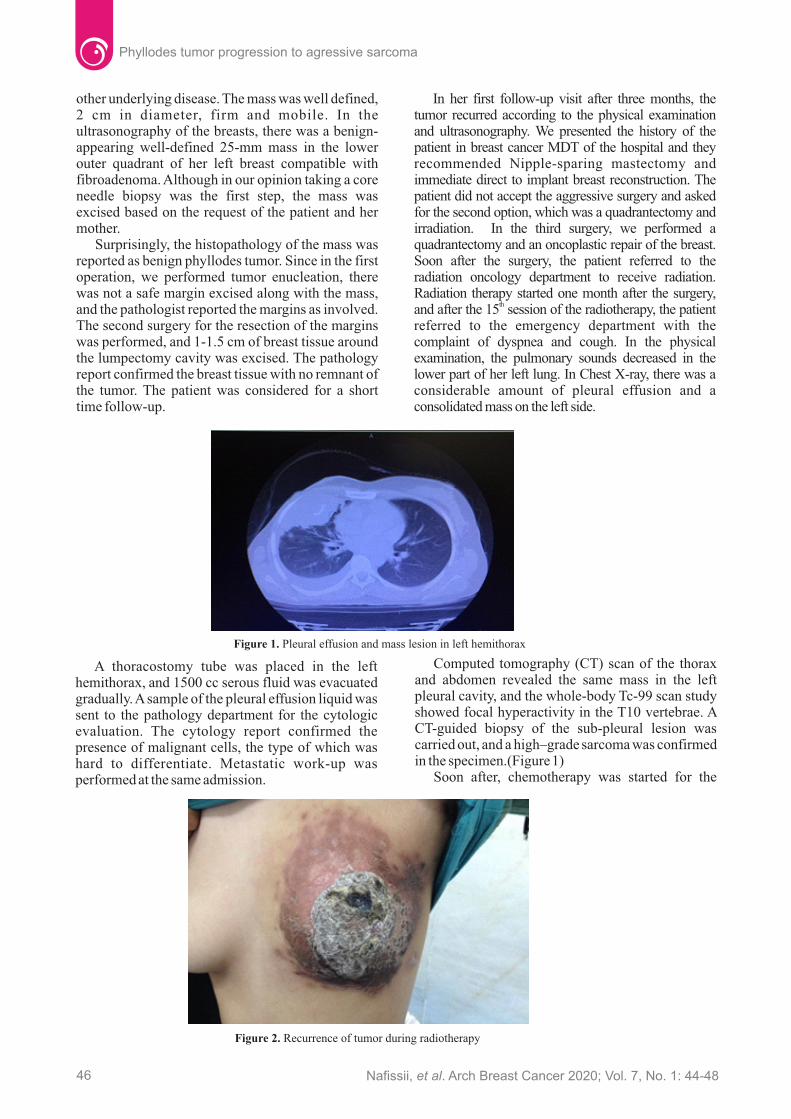
Surprisingly, the histopathology of the mass was reported as benign phyllodes tumor. Since in the first operation, we performed tumor enucleation, there was not a safe margin excised along with the mass, and the pathologist reported the margins as involved. The second surgery for the resection of the margins was performed, and 1-1.5 cm of breast tissue around the lumpectomy cavity was excised. The pathology report confirmed the breast tissue with no remnant of the tumor. The patient was considered for a short time follow-up.
other underlying disease. The mass was well defined, 2 cm in diameter, firm and mobile. In the ultrasonography of the breasts, there was a benign-appearing well-defined 25-mm mass in the lower outer quadrant of her left breast compatible with fibroadenoma. Although in our opinion taking a core needle biopsy was the first step, the mass was excised based on the request of the patient and her mother.
In her first follow-up visit after three months, the tumor recurred according to the physical examination and ultrasonography. We presented the history of the patient in breast cancer MDT of the hospital and they recommended Nipple-sparing mastectomy and immediate direct to implant breast reconstruction. The patient did not accept the aggressive surgery and asked for the second option, which was a quadrantectomy and irradiation. In the third surgery, we performed a quadrantectomy and an oncoplastic repair of the breast. Soon after the surgery, the patient referred to the radiation oncology department to receive radiation. Radiation therapy started one month after the surgery,
thand after the 15 session of the radiotherapy, the patient referred to the emergency department with the complaint of dyspnea and cough. In the physical examination, the pulmonary sounds decreased in the lower part of her left lung. In Chest X-ray, there was a considerable amount of pleural effusion and a consolidated mass on the left side.
Figure 2. Recurrence of tumor during radiotherapy
Figure 1. Pleural effusion and mass lesion in left hemithorax
A thoracostomy tube was placed in the left hemithorax, and 1500 cc serous fluid was evacuated gradually. A sample of the pleural effusion liquid was sent to the pathology department for the cytologic evaluation. The cytology report confirmed the presence of malignant cells, the type of which was hard to differentiate. Metastatic work-up was performed at the same admission. Soon after, chemotherapy was started for the
Computed tomography (CT) scan of the thorax and abdomen revealed the same mass in the left pleural cavity, and the whole-body Tc-99 scan study showed focal hyperactivity in the T10 vertebrae. A CT-guided biopsy of the sub-pleural lesion was carried out, and a high–grade sarcoma was confirmed in the specimen.(Figure 1)
Phyllodes tumor progression to agressive sarcoma
46 Nafissii, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 44-48

patient with the regimen of ifosfamide and Adryamicime. Following two sessions of chemotherapy, the patient returned with the complaint of a large mass in her left breast. In clinical examination, there was a 7*4*6 cm large mass, which was impending to become a large ulcer in her breast.(Figure 2) There was significant lymphadenopathy in her left axillary region. The patient underwent radical mastectomy with the resection of all skin and pectoralis muscles. The lymph nodes in the first level of the axilla were excised as well. Latissimus dorsi muscle flap was used for the coverage of the surgery defect. (Figure 3)The pathology reported the tumor as a high-grade angiosarcoma with large reactive lymph nodes. The patient referred to the medical oncology department to continue chemotherapy.
phyllodes tumors with a mean age of 39.6±7.6 years. Of them, 22, 9, 6 patients had benign, borderline and malignant PTs, respectively. The median duration of local recurrence was 20 months. In this series, only one patient with malignant PT was reported with
13 lung metastasis.
Distant metastasis in breast sarcoma is an outstanding finding which predicts the overall
7survival. The time lapse between the surgery to distant metastasis in breast PTs is reported from 2 to 57 months (average 21 months). Although an early metastasis is not common in breast PTs, our patient showed the signs and symptoms of lung metastasis in a month after the first surgery. The common sites of metastasis are lung (75.7%), bone (18.9%), brain (10.8%), and liver (5.4%). The mean survival of breast PTs patients with distant metastasis was reported as long as 7 months in a study by Mitus and colleagues. The longest survival is seen in patients with bone metastasis, and the shortest survival can be
7seen after brain metastasis. Despite the short survival, our patient did not have any metastatic lesion in her brain.
Regardless of the tumor subgroup, the first-line treatment of PTs is a surgery including lumpectomy, wide local excision, and total mastectomy. Recent reports confirmed the safety of a more conservative
Figure 3. Mastectomy and coverage of the defect by Latissmus dorsi flap
Discussion
A systematic review by Lu et al. in 2019 illustrates that the age and the size of the phyllodes tumor are not related to the rate of local recurrence though the breast-conserving surgery and margin involvement are significantly associated with a higher rate of local recurrence. The local recurrence rates from 8 percent in benign phyllodes tumor, 13 percent in borderline tumors, and 18 percent in the malignant sarcomas. Most tumors relapses occur within two years after the surgery, and it is not common for a tumor to recur in a limited period of time (less than one month) as observed in our
12patients. Tan et al. evaluated 37 patients with breast
Breast sarcoma is typically a rare phenomenon that may present similar symptoms to other primary breast malignancies. Primary breast sarcoma is divided into three subgroups of primary breast sarcoma, aroused sarcoma from the post-irradiated breast (secondary to the irradiation), and malignant phyllodes tumors (cystosarcoma phyllodes). Malignant phyllodes tumor is a biphasic malignant stromal neoplasm consisting of epithelial and spindle cell elements, which demonstrates a wide
10, 11variety of morphologies. Phyllodes tumor of the breast is reported in the younger age compared to the
9 typical breast carcinoma in the case of our patients.
The oncologist started Gemcitabine and Docetaxel as the second line of chemotherapy. The response to these agents was satisfactory and all the pleural and pulmonary lesions disappeared after the third session.
Two months after the completion of the chemotherapy, the patient referred with the complaint of a mass in the left axilla. A biopsy was obtained from the new mass, which was reported as spindle sarcoma with prominent vascular differentiation. A few weeks later, multiple round masses on the thoracic wall and latissimus dorsi flap appeared. (Figure 4) Also, there were multiple lung metastases in the CT scan of the thorax. The patient was referred to the palliative care department of the hospital and died four months afterwards.
Figure 4. Local recurrence of the tumore in less than 4 weeks
47Nafissii, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 44-48
Phyllodes tumor progression to agressive sarcoma

References
The written consent was signed by the patients when they were alive to report their medical history and to anonymously publish the images in medical literature for educational and research purposes.
In the reported patients, the early local recurrence can be justified by insufficient surgical treatments in the first operation but the distant metastasis was not related to the surgical treatment. It seems that some subtypes of breast sarcomas could have an extremely aggressive behavior which threatens the life of the patients in a short period of time. Further studies is suggested to discriminate the aggressive subtypes at the first step. The outcome of the patients may differ by selecting more aggressive local treatments and a different systemic therapies.
Ethical Consideration
NoneConflict of Interests
2. Lee AH, Hodi Z, Ellis IO, Elston CW. Histological features useful in the distinction of phyllodes tumour and fibroadenoma on needle core biopsy of the breast. Histopathology. 2007;51(3):336-44.
4. Zhang Y, Kleer CG. Phyllodes Tumor of the Breast: Histopathologic Features, Differential Diagnosis, and Molecular/Genetic Updates.
1. Pareja F, Geyer FC, Kumar R, Selenica P, Piscuoglio S, et al. Phyllodes tumors with and without fibroadenoma-like areas display distinct genomic features and may evolve through distinct pathways. NPJ Breast Cancer. 2017; 3:40.
3. Telli ML, Horst KC, Guardino AE, Dirbas FM, Carlson RW. Phyllodes tumors of the breast: natural history, diagnosis, and treatment. J Natl Compr Canc Netw. 2007;5(3):324-30.
surgical approach in the treatment of phyllodes tumors. Nowadays, in most protocols, breast conservation with a sufficient margin is an acceptable treatment. MacDonald et al. reported that the size of the tumor could be influenced by surgeon’s decisions regarding the limitation of
14recurrence and cosmetic outcome. They stated that thirty-six percent of the patients with a tumor of larger than 5 cm could undergo breast-conserving surgery. Nevertheless, 75% of patients with tumors of smaller than 5 cm can be treated safely to avoid
14total mastectomy. , All in all, it is more of consensus that mastectomy versus breast-conserving surgery is significantly associated with a lower rate of local recurrence and distant metastasis, particularly in
7, 12, 13malignant PTs. Also, adequate surgical margin reduced the rate of local recurrence, particularly in malignant PTs though it did not have any impact on
9, 12, 13 distant metastasis.
8. Guerrero MA, Ballard BR, Grau AM. Malignant phyllodes tumor of the breast: review of the literature and case report of stromal overgrowth. Surg Oncol. 2003;12(1):27-37.
13. Tan EY, Tan PH, Yong WS, Wong HB, Ho GH, et al. Recurrent phyllodes tumours of the breast: pathological features and clinical implications. ANZ J Surg. 2006;76(6):476-80.
14. Macdonald OK, Lee CM, Tward JD, Chappel CD, Gaffney DK. Malignant phyllodes tumor of the female breast: association of primary therapy with cause-specif ic survival f rom the Surveillance, Epidemiology, and End Results (SEER) program. Cancer. 2006;107(9):2127-33.
6. Abdelkrim SB, Trabelsi A, Bouzrara M, Boudagga MZ, Memmi A, et al. Phyllodes Tumors of the Breast: A Review of 26 Cases. World J Oncol. 2010;1(3):129-34.
Arch Pathol Lab Med. 2016;140(7):665-71.
7. Mitus JW, Blecharz P, Walasek T, Reinfuss M, Jakubowicz J, et al. Treatment of Patients with Distant Metastases from Phyllodes Tumor of the Breast. World J Surg. 2016;40(2):323-8.
9. Amir RA, Rabah RS, Sheikh SS. Malignant Phyllodes Tumor of the Breast with Metastasis to the Pancreas: A Case Report and Review of Literature. Case Rep Oncol Med. 2018;2018: 6491675.
10. Confavreux C, Lurkin A, Mitton N, Blondet R, Saba C, et al. Sarcomas and malignant phyllodes tumours of the breast--a retrospective study. Eur J Cancer. 2006;42(16):2715-21.
5. McKenna AM, Pintilie M, Youngson B, Done SJ. Quantification of the morphologic features of fibroepithelial tumors of the breast. Arch Pathol Lab Med. 2007;131(10):1568-73.
11. Wang F, Jia Y, Tong Z. Comparison of the clinical and prognostic features of primary breast sarcomas and malignant phyllodes tumor. Jpn J Clin Oncol. 2015;45(2):146-52.
12. Lu Y, Chen Y, Zhu L, Cartwright P, Song E, et al. Local Recurrence of Benign, Borderline, and Malignant Phyllodes Tumors of the Breast: A Systematic Review and Meta-analysis. Ann Surg Oncol. 2019;26(5):1263-75.
Phyllodes tumor progression to agressive sarcoma
48 Nafissii, et al. Arch Breast Cancer 2020; Vol. 7, No. 1: 44-48

Especially in cancer care, decoding nonverbal cues is essential for the physicians, as psychological and spiritual distresses put a huge strain on the patient and his/her family. Nonverbal expressions are not only a window into the emotional state but contain clues for physical symptoms such as pain. They inform the physician about the patient's personality, family dynamics, and unique characteristics which are essential to provide the best care personalized to
2the patient's needs.
Language is considered as the main tool of communication, but in fact, the majority of communications is nonverbal. During a patient-physician visit, health related information is being transferred not only by spoken words, but also by the tone of voice, facial expression, pauses, sighs as well
1as other behaviors and body gesture.If we consider words as the verbal part of
communication, whatever remains would be nonverbal. We, physicians, are trained to look for nonverbal and behavioral clues to achieve an effective communication (e.g. blushed face, lowered eyebrows or tightened fists).
Health communication is a two-way street. As care providers we should not only be able to effectively recognize our patients' emotions and attitudes, but to be mindful of our own facial expressions and body language especially during critical conversations especially when it comes to bad news. For the sake of the patients and their families, physicians must be aware of their own
3nonverbal behavior and what it may unfold. Obviously, negative body posture, the lack of eye-to- The situation would be even more complicated by
the newly suggested method of patient visit, known as telemedicine or eVisit. What would happen to nonverbal parts of communication when you receive a voice or text message from your patient? Have you ever thought about receiving emotions through Emojis?
It has been famously said that “eyes are the window to the soul” and a physician can uncover many symptoms and emotions simply by looking at the patient’s eyes. Even this window is distorted these days by goggles or shields. I find myself often looking at a reflection of my own mask-covered face rather than my patient’s eyes.
These days, a simple smoothing of the throat causes distraction and a clearing reminds us of “Covid-19”. This constant fear, by nature, changes our feelings and behaviors.
My first high-tech visit was with a 68-year-old lady with advanced metastatic breast cancer. I met
Digital Communication
Wearing personal protective equipment not only covers facial expression, but also affects non-verbal behavior. To avoid any accidental exposure from surroundings and surfaces, many patients consciously control their slightest body movements.
I had not noticed the vital role of nonverbal c o m m u n i c a t i o n a n d b e h a v i o r a l c u e s i n communication with patients until the Covid-19 era, when covering the face with a mask became essential and part of a new normal. “Listening” to all those nonverbal signs had been always an important part of my interaction with patients in the palliative care clinic. Now, in this Covid-19 era, I have to understand my patients behind those paper masks. I am unable to detect the tremor of my patient’s chin before bursting into tears or to see the grinding of the teeth to fully evaluate the severity of the pain.
eye contact, and screen gaze have a negative impact 4
on the patient-physician communication.
49
From Days of "Nonverbal Communication" to Days of “Masks” and "EVisit": Effective Palliative and Cancer Care Communication in the Times of Covid-19
a Gynecologist/Palliative Medicine Fellow, Cancer Institute, Tehran University of Medical Sciences, Tehran, Iran
aMamak Tahmasebi*
Open AccessLetter to Editor
Address for correspondence: Mamak Tahmasebi, MDAssociate Professor,Address: Imam Khomeini Hospital, Cancer Institute, Gharib St., 1419733141, Tehran, Iran Tel: +98 21 6658 1542Email: [email protected]
Tahmasebi, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 49-50
DOI: 10.19187/abc.20207249-50

Palliative care in COVID-19 outbreak
References1. Knapp M L, Hall JA, Horgan TG. Nonverbal
Communication in Human Interaction, 8th edition. Cengage Learning, Boston, MA.2013.
3. Blanch-Hartigana D, Eedenb M, Verdam MGE, et al. Effects of communication about uncertainty and oncologist gender on the
What are the advantages and disadvantages of e-Visit which is an online discussion between a clinician and a patient via the Internet?
2. Kissane D W, Bultz BD, Butow PN, et al. Oxford Textbook of Communication in Oncology and Palliative Care, 2nd edition. Oxford University Press. 2017.
her son at my clinic in the hospital. He asked me to prescribe some medicine for his mother's sleep. As I enquired about her other symptoms, he instantly made a video call with her mother. She was lying on a mattress on the floor while her bare chest was visible. Before I could say a word, her daughter who was holding the phone, pleaded for a pill for her mother's mood and also some medication to improve her appetite. Even through the phone, a nasty malignant wound on the site of the mastectomy incision was obvious. My insistence for talking to her was rewarded and the first word she uttered was PAIN.
Lots of questions before setting up an e-Clinic should be answered. Feasibility and accessibility of appropriate infrastructure and broadband connectivity just put us on the doorstep. Security, privacy, and healthcare quality all need a professional support team. Health care providers and even patients and their caregivers should receive suitable training to be able to replace a face-to-face visit with an online communication. Finally, the financial mechanism between patients and the health care system should be
4,5redefined accordingly.
Patient-physician communication is one of the most important and complex processes in palliative and cancer care and now has become further complicated by technology during tele-health visits. Presence of infrastructural, cultural barriers, and lack of propensity to adapt to technology both by patients and physicians are all crucial factors that will influence an effective communication. Assessing patients’ feedback on digital and nondigital communication should be seen as a practical approach to improving patient-physician interaction. Adding digital communication training to the medical education curriculum would also be one of the universities' responsibilities. It is inevitable to note that the medicine in future will be different from what we have been trained for.
Are we ready for stepping into the new era of digital communication?
Conflict of InterestNone.
physician-patient relationship. Patient Education and Counseling 2019;102(9):1613-1620.
4. Kee JWY, Khoo HS, Lim I, Koh MYH. Communication Skills in Patient-Doctor Interactions. Learning from Patient Complaints. Health Professions Education 2018;4(2):97-106.
5. Finn NB, Bria WF. Digital Communication in Medical Practice. Springer. 2009.
Tahmasebi, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 49-5050

Considering the high infection rate of COVID-19 and the shortages encountered by health care systems around the globe, as the pandemic was established, national and international guidelines have quickly emerged to deal with the problem. The American Society of Breast Surgeons developed and ASCO followed protocols that categorized breast cancer patients into three priority levels of the urgency of
5care. Three levels of treatment triage have been specified based on how much especial therapy would be imminen t fo r cancer pa t i en t s . These recommendations range from priority A for patients whose condition meets the need for immediate surgery to priority C for patients who can wait for the standard treatment until the end of the pandemic. Besides, priority B is considered to be between those two extremes and permits prescription of alternative less aggressive therapies for some months. For example, a 55-year-old woman with a newly diagnosed hormone receptor-positive early breast
After the official announcement of the first patient with a new SARS-COVID-2 disease to the
1world in December 2019 , every society around the globe has experienced the spread of the fatal
2disease. As the coronavirus pandemic has been continuing relentlessly, starting from China cancer centers, health systems have been facing complex situations and unprecedented challenges in protecting their caregivers as well as their vulnerable
3patients. At the same time, Iranian oncologists have faced serious problems in making decisions for the treatment of breast cancer patients as the most prevalent cancer among women and the first killer
4among cancer patients.
However, like any decision made in a challenging situation, prioritization of the patients will still give rise to some controversies and consequences. On one hand, in the first round of the pervasive epidemic of coronavirus disease, health care professionals have suffered from a lack of specific equipments to deal with this highly contagious virus, and the health systems have been overwhelmed by shortages of health care facilities and staff.
Even though health system resources have limitations, there is an essential need to consider the logistic demands in order to provide the best practice and care for our cancer patients in the Corona era. Three months is a short period on the scale of accomplishing tremendous improvements. However, there are numerous practical and
On the other hand, cancer patients suffered from suspension, early cessation, or even uncommenced standard treatment. As time is passing by and the authorities are adopting the three different distancing strategies including contact tracing measures, isolation of infected individuals, and the physical distancing of population, would it be really justified to postpone anti-cancer therapies from the cancer patients anymore?
The question that comes to the mind is the feeling of a patient for whom standard treatment is postponed to an indefinite time in the future. Although no one knows how long the outbreak will continue, and there is no sign of the disappearance of the virus in the short-run, at the moment, there are reports that the rate of new COVID infection is slowing down in many parts of the world. Is it the right time to revisit the prioritization of breast cancer and put patients back on the board? They seem to have the right to receive the verified excellence of treatment now.
cancer will receive pills as neoadjuvant hormonal therapy instead of chemotherapy or surgery until the pandemic would be over. Our colleagues in Iran followed international guidelines and developed
6similar national guidelines.
51
Impact of Prioritization of Breast Cancer Patients Treatment inthe Case of Long-term Existence of COVID-19
a Medical Oncology Department, Cancer Institute, Tehran University of Medical Sciences, Tehran, Iran
aSanambar Sadighi*
Open AccessInvited commentary
Address for correspondence: Sanmbar Sadighi, MDAddress: Cancer Institute, Imam Khomeni Hospital, KeshavarzBlvd, Tehran, IranTel: +98 21 61195804Email: [email protected]
Sadighi, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 51-53
DOI: 10.19187/abc.20207249-50

COVID-19 and BC patients treatments
affordable steps that can be taken to protect staff and patients in implementing procedures, such as using COVID-clear rooms for COVID-free patients or minimizing COVID-exposed staff entry to operating rooms.
A retrospective study of patients with cancer in China suggested that recurrent hospital visits and admissions are potential risk factors for COVID-19
3infection. There are also reports of high infectivity rates among health care workers who might have few
8or even no symptoms. Although unnecessary visits should be discouraged in the COVID outbreak, cancer patients' problems who lose their communication with the health-care-system might be more serious. For instance, there are reports of an alarming decline
9in the diagnosis of cancer in the viral pandemic. Patients avoid meeting their family doctors due to the fear of exposure to the virus. Even switching to telehealth creates more trouble as patients are deprived of physical examination that may be
9associated with the early diagnosis of cancer .
However, Telemedicine creates a great opportunity in the transition of in-patients follow up visits of known cases without compromising the care for these patients. It also provides resources for following preventive and therapeutic measures as well as the psychosocial well-being of the patients. Telemedicine free appointments via WhatsApp are currently available in Iran, providing opportunities for patients to discuss their questions with professionals in the field, although it is yet not possible to take drug prescriptions or laboratory orders in this way.
Considering social distancing as an individual's daily life responsibility in the COVID era, and also stringent adherence of the cancer patients to wearing masks and high-standard hygiene, health authorities could look at this lock-down period as a window of opportunity to improve their services. As a result, cancer patients will gain even better outcomes than before. Services are easy to perform, such as tracking cases through nasopharynx RT-PCR testing and checking the blood for protective antibody levels, especially among health care workers.
Another problem oncologists are facing in the COVID outbreak is triage for palliative treatments. For instance, based on the Radiation Advances triage system, palliative radiation therapy is applicable to an advanced case of a tumor with cord-compression as Tier 1, but it would differ for another patient who is in the same situation with an imminent but
7incomplete compression considered as Tier 2 . What would be the short and long term physical and psychosocial outcomes of such a prioritization schedule?
Practical recommendations, as previously announced by National Comprehensive Cancer Network (NCCN), should be strictly executed in
10academic and private clinics and hospitals. Some of
4. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians. 2018;68(6):394-424.
1. Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). 16-24 F e b r u a r y 2 0 2 0 . 2 0 2 0 [ Av a i l a b l e a t : https://www.hoint/docs/defaultsource/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf.]
2. Coronavirus disease (COVID-19) Pandemic. 2020.
5. The American Society of Breast Surgeons (ASBrS) Recommendations for Prioritization,
None
Furthermore, there is a need to establish a centralized website to hold regular virtual meetings with hospital staff to share and check their attitudes toward the latest guidelines of protective behavior and make sure about the management of their daily and long-term stresses. Lastly, considering over-crowded cancer day clinics in Iran, it would be helpful to improve the appointment system to prevent the crowdedness of patients and their companions in closed spaces in clinics or hospitals.
References
those measures include contacting patients one day before the next visit and asking them about COVID symptoms or exposure; developing an especially dedicated clinic for evaluation and testing of suspicious cancer patients; increasing the awareness of patients and their families about safety measures by spreading pamphlets about COVID-19. Moreover, safety should be the very most important priority in all health organizations, and health care workers should be equipped with appropriate personal protection equipments(PPE).
Conflict of Interest
3. Liang W, Guan W, Chen R, Wang W, Li J, et al. Cancer patients in SARS-CoV-2 infection: a nationwide analysis in China. The Lancet Oncology. 2020;21(3):335-7.
In sum, it seems that academic institutions and private hospitals are in a crucial position to meet the new challenges brought by the COVID-19 outbreak as an opportunity to reach a new balance between offering effective, compassionate care for cancer patients and maintaining the safety of their health professional teams. Also, at every single center, "a task force group" can be formed to list and classify all diagnostic, therapeutic, and rehabilitation measures taking into account the possibility of the second outbreak of the COVID-19. If it is delayed, patients will be deprived of receiving adequate medical care during Corona's second epidemic.
Sadighi, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 51-5352

6. Shahi F, Mirzania M, Dabiri M, Seifi S, Bary A, et al. Modifications in Breast Cancer Guidelines in COVID19 Pandemic; An Iranian Consensus. Archives of Breast Cancer. 2020:14-7.
8. Omranipour R, Mahmoodzadeh H, Hadjilooei F, Alipour S. Recommendations For Breast Surgical Care During Covid-19 Outbreak In Iran: Setting Priorities Of Management
9. Dinmohamed AG, Visser O, Verhoeven RH, Louwman MW, van Nederveen FH, et al. Fewer cancer diagnoses during the COVID-19 epidemic in the Netherlands. The Lancet Oncology. 2020.
10. Cinar P, Kubal T, Freifeld A, Mishra A, Shulman L, et al. Safety at the time of the COVID-19 pandemic: how to keep our oncology patients and healthcare workers safe. Journal of the National Comprehensive Cancer Network. 2020;1(aop):1-6.
Treatment and Triage of Breast Cancer Patients during the COVID-19 Pandemic 2020 [Available at: https://www.breastsurgeons. org/management/practice/covid19]
7. Yerramilli D, Xu AJ, Gillespie EF, Shepherd AF, Beal K, et al. Palliative Radiotherapy for Oncologic Emergencies in the setting of COVID-19: Approaches to Balancing Risks and Benefits. Advances in Radiation Oncology. 2020.
COVID-19 and BC patients treatments
Sadighi, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 51-53 53
the diseases based on the visible shape of the pathology and the changes it causes in organs. Mammography, ultrasonography, and MRI provided
2 3high sensitivity and flexibility to guide biopsies , and high specificity for breast tumor imaging,
4respectively. The drawback of functional imaging with lower spatial resolution hindered the scintigraphy images for years. Four decades later professor Abbas Alavi and the team he led used FDG
5as a new functional brain imaging tracer ; FDG was developed to a potent tumor agent and brought a remarkable advance in the field of oncologic imaging. PET scanners provide superior spatial resolution due to their crystal structure and
6coincidence acquisition method. Attenuation is lower due to higher photon energy positrons emit. Furthermore, the method benefitted from attenuation corrections using real patient attenuation map provided by gamma emission and transmission data by CT. PET imaging has achieved such a position that many clinicians consider it as a final or even
IntroductionFunctional imaging has comprised a considerable
1part of medical imaging procedures for 50 years. Many essential physiological facts have been established through functional imaging, and its use has extended into clinical practice. Perfusion imaging, renal function studies, bone scintigraphy and many other functional images have become very common. Breast specific imaging was developed with a focus on MIBI as a surrogate of thallium 201, an important tumor agent. In the advent of state-of-the-art CT scanners, the fine details of anatomy illustrated by cross sectional images, reversed the trend among clinicians to use CT images to focus on
ARTICLE INFO
Background: The application of FDG PET/CT scan for assessment of patients with breast cancer is increasing. The cost effectiveness of the application could be different in a developing country with limited PET scanners and treatment priorities
Method: Open discussions of the PET reviewers from 2 out of 4 PET centers of Tehran, the capital city of Iran, were organized to provide insight into their opinions on the indications of FDG PET in breast cancer patients.
Conclusion: We suggest reserving the use of FDG PET for selected cases of suspected but not proven recurrent disease and in patients with high risk of metastasis before high risk surgery.
Results: The sensitivity of FDG PET scan is high for detection of distant metastases; however, assessment of lymph node pathology and the local extension of the breast cancer are questionable. Considering the cost of the procedure itself and the downstream diagnostic procedures, its application and diagnostic accuracy are hindered for breast cancer screening, staging, and assessment of response to treatment and prognosis. The advantages and disadvantages of FDG PET CT and dedicated breast FDG PET scan have been briefed in different clinical scenarios with a focus on limitations faced by a developing country.
Revised:
Accepted:
10 May 2020Received:
23 May 2020
PET,
29 May 2020
narrative review
FDG,
Key words:Breast cancer,
Address for correspondence: Mehrshad Abbasi, MDAssociate ProfessorAddress: Department of Nuclear Medicine, Vali-Asr HospitalTehran University of Medical Sciences, Tehran 1419731351,IranTel: +98 21 61192405 Fax: +98 21 66575103Email: [email protected]
54 Farzanehfar, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 54-58
ABSTRACT
FDG PET Application for management of breast cancer patient: a narrative review
a Department of Nuclear Medicine, Vali-asr Hospital, Tehran University of Medical Sciences, Tehran, Iran
a a a aSaeed Farzanehfar , Farahnaz Aghahoseini , Marzieh Peyman , Mehrshad Abbasi*
Open AccessReview Article
DOI: 10.19187/abc.20207254-58

perfect imaging modality, a view we are to oppose for different reasons in the current paper with particular attention to the field of breast cancer.
The use of whole body FDG PET for breast cancer screening is discouraging. Many biological cancer-related characteristics may influence the degree of uptake in a sizable breast malignant lesion. Well-differentiated cancers as well as certain histopathological subtypes, including those with indolent behavior, infiltrative pattern of growth and low cellular density such as infiltrative lobular carcinoma and tubular carcinoma do not take up FDG to the same extent as many FDG avid tumors
7do. Other factors such as receptor status and specific mutation have a controversial correlation with degree of FDG uptake for a given histopathology
8subtype. It is worth noting that a screening tool should have the capability of detection of very small size and non-palpable malignant lesions in the early stage of development. This may be the most important drawback for current PET scanners with sensitivity of less than 60% for malignant lesions <1 cm to be considered as the imaging modality of choice for breast cancer screening. The overall sensitivity for primary lesion ranges from 48 to 96; with lower performances reported from studies
9including smaller lesions. However, metabolic criteria derived from FDG PET scan may have a complementary role in improving risk stratification of incidentally-detected breast lesions in PET/CT scan in non-breast cancer patients.10 To sum up, the use of whole body PET for screening is questioned.
Screening
Methods
Even so, particular cases may benefit from screening by breast dedicated PET scans, with higher spatial resolution for limited breasts’ field in contrast
The narrative data for this study was accumulated through open discussions among the authors. There are 4 PET scanners installed in Tehran, the capital city of Iran, and the authors of the paper are nuclear physicians in the most advanced (i.e. FA) and the most up to date ( i.e. SF and MA) centers there. The essential topics were selected first and then the authors provided their scholarly opinions on the topics. Through directed literature search, the discussed material was approved with scientific citations or changed accordingly.
The application of PET can be categorized into different strata summarized as screening, initial staging, follow up for recurrence, re-staging, and response to treatment and prognosis. With a focus on a developing country, the following overall views could be considered for aforementioned applications in the field of breast cancer:
Results and discussion Initial Staging
14, 15FDG accumulates in invasive ductal cancers , breast dedicated PET scanners developed to do breast
16, 17screening. However, there is no global consensus to support the benefit of dedicated breast FDG PET. The accuracy of the dedicated breast PET images are
18high, i.e., 0.95, ranging from 0.82 to 1.0 , and considerably superior to the accuracy of mammography . The reason why dedicated PET scans did not take place as a screening tool is that the cost to a breast dedicated PET scan is 10 times of a mammography alongside the fact that instrumentation
19is expensive and not widely available.
to whole body PET imaging, including young high risk genetically predisposed patients or contralateral breasts predisposed to higher-grade tumors with
11-13more aggressive clinical courses.
Due to whole body nature, FDG PET scan is 20, 21useful for detection of metastasis , and in certain
22scenarios for detection of LN invasions. The role for whole body FDG PET/CT in T staging is limited. In breast cancer, FDG illustrates axillary LN invasions in about two thirds of the cases involved,
23which is not an accountable figure considering the detection rate of more than 95% achieved by sentinel LN biopsy. Although PET/CT is not a suitable substitute for routine axillary N staging, in patients who are at high risk for axillary metastasis, PET-detected positive nodes may be proceeded for US-guided biopsy, and hence, obviate the need for sentinel node biopsy in patients with biopsy-proven
24nodal involvement. Furthermore, currently, distant metastasis at the time of primary tumor diagnosis is very rare as a result of powerful screening and
25diagnostic methods. Lastly, the need for systemic therapy in low T tumors does not obviate definitive surgery. Consequently, the evaluation of distant metastasis could be postponed until after definitive surgery. Potential use of PET for certain locally advanced breast cancers is advocated for the assessment of prognosis and to monitor future
26, 27therapy. It should also be considered that breast 28
cancer is the most frequent cancer in females; initial staging of many common cancers by PET scan is hindered due to financial considerations. Some patients may benefit from initial staging by FDG PET scan, but the overall health system and community may not afford the cost, considering the fact that the procedure is not definitely cost
19effective. In the era of individualized practice however, physicians may consider a particular patient eligible for FDG PET scan e.g. an old patient with comorbidities with a small tumor in which detection of an axillary or internal mammary LN or a distant metastasis may change the approach, or a young patient with large breast tumors, where the detection of a distant metastasis may change the plan for neoadjuvanttherapy.
Application of PET in breast cancer
Farzanehfar, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 54-5855

FDG accumulates in recurrence sites and metastasis very sensitively; but the inflammation at surgery site is highly metabolic for weeks and granulation tissues for months. Specificity of the findings could be optimized with clinical reasoning concerning the possibility of malignancy as the
29reason for the findings. There are two definite scenarios where FDG PET provides future insight for the clinician: First, the recurrence is biochemically suspected but conventional images do not document its site. The oncologist/surgeons actively search for recurrence sites and then closely follow up the patient if the images are not indicative of the site of
30recurrence. Particularly, when metastasis is difficult to follow up with conventional anatomical imaging
31like intramedullary bone metastasis it could be
32optimally assessed by FDG PET scan. Furthermore, in certain situations, the conventional images including lung and abdominopelvic CT scans and bone scans point to a suspicious recurrence site. The extent of the finding is not so that the biopsy could be indicated or metastasis/recurrence confirmed. FDG uptake may support the clinician's decision to follow up or act on the findings. One of the major privileges of the FDG PET in this setting could be discrimination of post-radiation and post-surgery
33changes including fibrosis from recurrent tumors. Although granulation tissue, as mentioned above, and inflammation and fibrosis in early stages may
34, 35occur with high FDG uptake , the absence of high metabolic activity remarkably reduces the possibility
33of malignancy. The PET is reimbursed for breast cancer recurrence follow up in many health systems.
In a scenario where the patient may benefit from a second surgery which could be e i ther a metastasectomy at liver or lung, or local recurrence completion surgery, precise assessment of distant metastases would be a must. Obviation of surgery of a site in presence of another metastasis elsewhere is de facto. Obviously, repeated surgeries are more costly both for the patient and the health system, and detection of another recurrence site, which is considered as the strength of whole body sensitive
33, 36FDG PET scan , dramatically changes the decision to opt for surgery. In the era when there is a growing desire to eradicate disease more powerfully by surgeries in patients with metastasis and with the advent of effective chemotherapy agents, FDG PET may provide a rather complete map of the
37recurrence/metastasis sites to plan for the most reasonable action. It is noteworthy to mention when a malignant disease becomes systemic, certain malignant cells may disseminate and develop to very small nests bellow the spatial resolution of PET or visible but ignorable. Consequently, although the sensitivity of FDG PET is considered high, the extent
Follow up for Recurrence
Re-stagingIn a developing country like Iran where there are
only 8 PET scanners installed and less than 10 are planned for forthcoming years, considering the import limitations, the request for PET scans plausibly should be limited. In this country, about 100 PET scans could be performed a day and there
44are more than 18000 new cancer cases a year. Regarding the fact that screening, initial staging, and follow up of breast cancers patients could be done delicately with other imaging methods, FDG PET/CT scan could be preserved for patients with suspected but not confirmed recurrent disease and particular cases before proceeding to surgery with high risk of metastases which precludes a difficult or life threatening surgery in a high risk patient with various comorbidities.
Reference 1. Papanicolaou AC. Fundamentals of functional
brain imaging: A guide to the methods and their
NoneConflict of Interest
of the systemic diseases is higher than what is visualized.
Response to treatment and prognosisIn certain malignancies including lymphoma,
FDG uptake provides particular insight into the effectiveness of therapy. This finding could change
38the chemotherapy line or intensify the treatment. At the end of treatment, a PET scan without abnormal FDG uptake site confirms the completeness of the treatment and obviates further investigations for
39months. Nevertheless, the absence of FDG uptake does not exclude the possibility of recurrence and the necessity to follow up. This application is not highlighted for breast cancer. The local surgical tumor eradication is directly observed by the surgeon and pathologist, and the effect of systemic therapies
26, 40could be assessed by anatomical images. For example, the number and size of lesions in lung and liver metastases could be optimally followed by lung and 3 phase liver CT scans. There are particular scenarios in which FDG PET plays a remarkable
41role. After curative surgeries or ablations of bone and liver metastases by surgery, external beam radiat ion, radiofrequency, or microwave, discrimination of post therapy changes from remnant, or recurrent tumor is difficult using conventional
42images. The effectiveness of surgery with or without RF on a set of liver metastases could be optimally
43documented by FDG PET scan. The assessment of prognosis is another less useful application of FDG PET according to which high grade or more invasive tumors present with higher FDG uptake requiring
37more intensive treatments , an application which is neither robust nor cost effective in breast cancer setting.
56 Farzanehfar, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 54-58
Application of PET in breast cancer

3. Yeow K-M, Tan C-F, Chen J-S, Hsueh C. Diagnostic sensitivity of ultrasound‐guided needle biopsy in soft tissue masses about superficial bone lesions. Journal of ultrasound in medicine. 2000;19(12):849-55.
applications to psychology and behavioral neuroscience: CRC Press; 1998.
13. Hosono M, Saga T, Ito K, Kumita S, Sasaki M, et al. Clinical practice guideline for dedicated breast PET. Annals of nuclear medicine. 2014;28(6):597-602.
8. Buck A, Schirrmeister H, Kühn T, Shen C, Kalker T, et al. FDG uptake in breast cancer: correlation with biological and clinical prognostic parameters. European journal of nuclear medicine and molecular imaging. 2002;29(10):1317-23.
10. Bakhshayeshkaram M, Salehi Y, Abbasi M, Beni RH, Seifi S, et al. A preliminary study to propose a diagnostic algorithm for PET/CT-detected incidental breast lesions: application of BI-RADS lexicon for US in combination with SUVmax. European radiology. 2019;29(10):5507-16.
2. Rudin S, Kuhls A, Yadava G, Josan G, Wu Y, et al. New light-amplifier-based detector designs for high spatial resolution and high sensitivity CBCT mammography and fluoroscopy: SPIE; 2006.
6. España S, Herraiz J, Vicente E, Vaquero JJ, Desco M, et al. PeneloPET, a Monte Carlo PET simulation tool based on PENELOPE: features and validation. Physics in Medicine & Biology. 2009;54(6):1723.
9. Paydary K, Seraj SM, Zadeh MZ, Emamzadehfard S, Shamchi SP, et al. The evolving role of FDG-PET/CT in the diagnosis, staging, and treatment of breast cancer. Molecular Imaging and Biology. 2019;21(1):1-10.
11. Lee MV, Katabathina VS, Bowerson ML, Mityul MI, Shetty AS, et al. BRCA-associated cancers: role of imaging in screening, diagnosis, and management. Radiographics. 2017;37(4):1005-23.
4. Avril N, Schelling M, Dose J, Weber WA, Schwaiger M. Utility of PET in breast cancer. Clinical Positron Imaging. 1999;2(5):261-71.
5. Alavi A, Reivich M, Jones S, Greenberg J, Wolf A. Functional imaging of the brain with positron emission tomography. Nuclear medicine annual 19821982.
7. Groheux D, Espié M, Giacchetti S, Hindié E. Performance of FDG PET/CT in the clinical management of breast cancer. Radiology. 2013;266(2):388-405.
12. Even-Sapir E, Inbar M. PET in women with high risk for breast or ovarian cancer. The Lancet Oncology. 2010;11(9):899-905.
14. Song B-I, Lee S-W, Jeong SY, Chae YS, Lee WK, et al. 18F-FDG uptake by metastatic axillary lymph nodes on pretreatment PET/CT as a prognostic factor for recurrence in patients with
17. Miyake KK, Nakamoto Y, Togashi K. Current status of dedicated breast PET imaging. Current Radiology Reports. 2016;4(4):16.
20. Hoh CK, Hawkins RA, Glaspy JA, Dahlbom M, Tse NY, et al. Cancer detection with whole-body PET using 2-[18F] fluoro-2-deoxy-D-glucose. Journal of computer assisted tomography. 1993;17(4):582-9.
19. Naseri M, Farzanehfar S, Ranjbar S, Parvizi M, Abbasi M. An Overview on Positron Emission Mammography in Breast Cancer Detection and Follow up: Particular Concerns in Iran as a Developing Country. Archives of Breast Cancer. 2017:39-41.
22. Jung NY, Kim SH, Kang BJ, Park SY, Chung MH. The value of primary tumor 18 F-FDG uptake on preoperative PET/CT for predicting intratumoral lymphatic invasion and axillary nodal metastasis. Breast Cancer. 2016;23(5):712-7.
24. Gil‐Rendo A, Zornoza G, García‐Velloso M, Regueira F, Beorlegui C, et al. Fluorodeoxyglucose positron emission tomography with sentinel lymph node biopsy for evaluation of axillary involvement in breast cancer. British Journal of Surgery: Incorporating European Journal of Surgery and Swiss Surgery. 2006;93(6):707-12.
26. Groheux D, Mankoff D, Espié M, Hindié E. 18 F-FDG PET/CT in the early prediction of pathological response in aggressive subtypes of
25. Lebon V, Alberini J-L, Pierga J-Y, Diéras V, Jehanno N, et al. Rate of distant metastases on 18F-FDG PET/CT at initial staging of breast cancer: comparison of women younger and older than 40 years. Journal of Nuclear Medicine. 2017;58(2):252-7.
invasive ductal breast cancer. Journal of Nuclear Medicine. 2012;53(9):1337-44.
15. Song B-I, Hong CM, Lee HJ, Kang S, Jeong SY, et al. Prognostic value of primary tumor uptake on F-18 FDG PET/CT in patients with invasive ductal breast cancer. Nuclear medicine and molecular imaging. 2011;45(2):117-24.
16. Avril N, Sassen S, Roylance R. Response to therapy in breast cancer. J Nucl Med. 2009;50(Suppl 1):55S-63S.
18. Narayanan D, Berg WA. Dedicated breast gamma camera imaging and breast PET: current status and future directions. PET clinics. 2018;13(3): 363-81.
21. Lin A, Ma S, Dehdashti F, Markovina S, Schwarz J, et al. Detection of distant metastatic disease by positron emission tomography with 18F-fluorodeoxyglucose (FDG-PET) at initial staging of cervical carcinoma. International Journal of Gynecologic Cancer. 2019;29(3):487-91.
23. Marino MA, Avendano D, Zapata P, Riedl CC, Pinker K. Lymph Node Imaging in Patients with Primary Breast Cancer: Concurrent Diagnostic Tools. The oncologist. 2020;25(2):e231.
Farzanehfar, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 54-5857
Application of PET in breast cancer

30. Zangheri B, Messa C, Picchio M, Gianolli L, Landoni C, et al. PET/CT and breast cancer. European journal of nuclear medicine and molecular imaging. 2004;31(1):S135-S42.
breast cancer: review of the literature and recommendations for use in clinical trials. European journal of nuclear medicine and molecular imaging. 2016;43(5):983-93.
27. Groheux D, Giacchetti S, Delord M, Hindié E, Vercellino L, et al. 18F-FDG PET/CT in staging patients with locally advanced or inflammatory breast cancer: comparison to conventional staging. Journal of Nuclear Medicine. 2013; 54(1):5-11.
28. Key TJ, Verkasalo PK, Banks E. Epidemiology of breast cancer. The lancet oncology. 2001;2(3):133-40.
29. Evangelista L, Mansi L, Burei M, Saladini G. Pitfalls and artifacts of FDG PET/CT in recurrent breast cancer patients. Clinical and Translational Imaging. 2017;5(2):169-82.
31. Kosmas C, Koumpou M, Nikolaou M, Katselis J, Soukouli G, et al. Intramedullary spinal cord metastases in breast cancer: report of four cases and review of the literature. Journal of neuro-oncology. 2005;71(1):67-72.
32.Phi l l ips M, Horgan K, Scarsbrook A, Rengabashyam B, editors. Clinical Impact of PET-CT on patient management in metastatic breast cancer2017: European Congress of Radiology 2017.
33. Lim HS, Yoon W, Chung TW, Kim JK, Park JG, et al. FDG PET/CT for the detection and evaluation of breast diseases: usefulness and limitations. Radiographics. 2007;27(suppl_1):S197-S213.
38. Gil‐Rendo A, Martínez‐Regueira F, Zornoza G, García‐Velloso MJ, Beorlegui C, et al. Association between [18F] fluorodeoxyglucose uptake and prognostic parameters in breast
37. Eubank WB, Mankoff DA, editors. Evolving role of positron emission tomography in breast cancer imaging. Seminars in nuclear medicine; 2005: Elsevier.
34. Avril N, Menzel M, Dose J, Schelling M, Weber W, et al. Glucose metabolism of breast cancer assessed by 18F-FDG PET: histologic and immunohistochemical tissue analysis. Journal of Nuclear Medicine. 2001;42(1):9-16.
36. Dose J, Bleckmann C, Bachmann S, Bohuslavizki K, Berger J, et al. Comparison of fluorodeoxyglucose positron emission tomography and ‘conventional diagnostic procedures’ for the detection of distant metastases in breast cancer patients. Nuclear medicine communications. 2002;23(9):857-64.
35. Adejolu M, Huo L, Rohren E, Santiago L, Yang WT. False-positive lesions mimicking breast cancer on FDG PET and PET/CT. American Journal of Roentgenology. 2012;198(3):W304-W14.
cancer. British Journal of Surgery: Incorporating European Journal of Surgery and Swiss Surgery. 2009;96(2):166-70.
40.Alexander MT, Schmitz SCT, Kenneth EP, Claudette EL, Wouter VV, et al. Monitoring tumor response to neoadjuvant chemotherapy using MRI and 18F-FDG PET/CT in breast cancer subtypes. PloS one. 2017;12(5).
42. Eubank W, Mankoff D, Takasugi J, Vesselle H, Eary J, et al. 18fluorodeoxyglucose positron emission tomography to detect mediastinal or internal mammary metastases in breast cancer. Journal of clinical oncology. 2001;19(15):3516-23.
43.Nielsen K, van Tilborg AA, Scheffer HJ, Meijerink MR, de Lange-de Klerk ES, et al. PET-CT after radiofrequency ablation of colorectal liver metastases: suggestions for timing and image interpretation. European journal of radiology. 2013;82(12):2169-75.
44. Jazayeri SB, Saadat S, Ramezani R, Kaviani A. Incidence of primary breast cancer in Iran: Ten-year national cancer registry data report. Cancer epidemiology. 2015;39(4):519-27.
41. Almuhaideb A, Papathanasiou N, Bomanji J. 18F-FDG PET/CT imaging in oncology. Annals of Saudi medicine. 2011;31(1):3-13.
39. Avril S, Muzic Jr RF, Plecha D, Traughber BJ, Vinayak S, et al. 18F-FDG PET/CT for monitoring of treatment response in breast cancer. Journal of nuclear medicine: official publication, Society of Nuclear Medicine. 2016;57(Suppl 1):34S.
58 Farzanehfar, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 54-58
Application of PET in breast cancer

an inflammation over the breast; the diagnosis is thus frequently problematic or delayed because even the ultrasound (US) and mammogram may not show typical signs of malignancy, including a mass. Indeed, an important reason for delay in IBC diagnosis is that it can easily be misdiagnosed as a breast infection. The course of IBC is usually aggressive, and it may progress very rapidly over several weeks or months, leading to the diagnosis of a stage 3 or 4 cancer in the interval between two
1 screening mammographies. A clear association has not been proved between BRCA mutations and IBC, but it has been seen that patients with this type of cancer are younger than their non-IBC counterparts
3among BRCA positive patients.
The standard treatment of IBC includes neoadjuvant chemotherapy, modified radical mastectomy (MRM), and post-surgical radiation. Other treatments include endocrine therapy and
IntroductionInflammatory breast cancer (IBC) is a very poor-
prognosis type of breast cancer and the 5-year survival is around 40-50%. The incidence is low, comprising between 1 to 5% of all breast cancers in
1women. By definition, it is an invasive ductal carcinoma that invades and grows in skin lymphatic channels. IBC is considered T4d in TNM ACR classification of breast cancer regardless of tumor size. Therefore, the lowest stage of an IBC would be stage 3, even without lymph node metastases at the
2time of diagnosis. Its presentation does not follow the classical breast mass, and it commonly appears as
ARTICLE INFO
Case presentation: In this article, we present a case of inflammatory breast cancer in a very young woman who was positive for BRCA2 genes.
Question: The possibility to perform nipple sparing or skin sparing mastectomy and immediate breast reconstruction, and the indication for prophylactic contralateral mastectomy as discussed in the tumor board are presented in this article.
Conclusion: Neither of the more conservative techniques of mastectomy was appropriate for this case. Also, the prognosis of the patient mostly depends on the course of the ipsilateral tumor and prophylactic mastectomy would be wise only if the subsequent course of the disease is favourable.
Background: Inflammatory breast cancer is a very aggressive type of breast cancer which invades skin lymphatics. The standard treatment includes neoadjuvant chemotherapy followed by modified radical mastectomy and post-surgical radiation. Preserving the skin or nipple are not considered reasonable due to the involvement of the dermal lymphatics and therefore skin sparing or nipple- sparing mastectomy are not usually carried out for this type of breast cancer.
Accepted:
inflammatory breast cancer;
Received:
29 April 2020
27 May 2020
Key words:
Revised:
Breast reconstruction;
tumour board decision
17 May 2020
Address for correspondence: Sadaf Alipour, MDAddress: Arash Women's Hospital, Shahid Baghdarnia Street, Ressalat Street, Tehran, Iran- Postal code: 16539115911Tel: +98 21 611192761Fax: +98 21 66581526Email: [email protected]
59
ABSTRACT
Inflammatory Breast Cancer in a Very Young Genetically SusceptibleWoman: Case Presentation in a Tumour Board Session, Discussion and Decision-Making
a Breast Disease Research Center, Tehran University of Medical Sciences, Tehran, Iran b Department of Surgery, Arash Women's Hospital, Tehran University of Medical Sciences, Tehran, Iranc Department of Radiology, Arash Women's Hospital, Tehran University of Medical Sciences, Tehran, Irand Department of Pathology, Arash Women's Hospital, Tehran University of Medical Sciences, Tehran, Iran
a,b c dSadaf Alipour* , Leila Bayani , Akram Seifollahi
Open AccessCase Experience
Alipour, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 59-64
DOI: 10.19187/abc.20207259-64

targeted therapy, which are individualized based on 1
tumor characteristics. Mastectomy is done as standard MRM, because preserving the skin or nipple is not considered reasonable due to the involvement of
4the dermal lymphatics. Therefore, an important difference in the treatment of localized IBC or not-IBC tumors is that neoadjuvant chemotherapy and post-mastectomy radiotherapy are performed regardless of tumor size and axillary involvement, and that sentinel lymph node dissection and breast conserving surgeries should not be performed for IBC.
Case presentationA 29-year-old woman attended the breast clinic
with a red swollen left breast. She explained that the changes had occurred in the breast since 3 days before, with no pain. She had undergone biannual
We present a case of IBC in a very young woman. She was tested for BRCA genes, and the result was positive. Due to the young age of the patient and her request, other types of surgery including nipple-sparing mastectomy (NSM) or skin-sparing mastectomy (SSM) and the possibility of IBR, as well as the indication for prophylactic contralateral mastectomy were discussed on the tumor board. These debates and a concise literature review are presented in this article. The patient has offered her consent for the publication of her case as a manuscript or any scientific presentation provided that her name is not mentioned.
The accepted approach to reconstruction after mastectomy for locally advanced breast cancers and
5 IBC is a delayed one, because of the poor prognosis and concerns about possibility of delays in the main treatments, inadequate margin resection while preserving the skin, and probability of higher recurrence with immediate breast reconstruction
5, 6(IBR). However, surgeries other than MRM and even IBR have been studied for cases of IBC.
breast exam and US in the past two years, and the results showed fibrocystic changes with multiple small simple cysts in large, slightly asymmetric breasts. Her family history was positive; as her mother had been diagnosed with a premenopausal, unilateral invasive breast cancer at the age of 48.
In the present breast exam, the left side was markedly enlarged. The nipple was flat, and the skin over the nipple areola complex (NAC) was very thick and dry. The entire breast was erythematous and edematous without significant tenderness. No distinct mass was detected. Round mobile enlarged lymph nodes were palpated in the left axillary fossa.
Considering a faint possibility of mastitis, broad spectrum antibiotics were begun, but a breast US was performed instantly. The US revealed multiple sites of tissue distortions with severe posterior shadowing in the left breast, multiple foci of microcalcifications, skin thickening and multiple suspicious left axillary lymph nodes. The right breast was unremarkable. (Figure 1) The mammogram showed extremely dense breasts (ACR category d) with cutaneous and subcutaneous edema on the left side, but no distinct mass. (Figure 2) US-guided core needle biopsy of breast lesions and axillary adenopathies were performed.
A breast MRI with and without intravenous contrast showed severely diffuse enhancement and abnormal enhancement of the nipple, which were interpreted as involvement of the entire breast with malignancy.(Figure 3)A low suspicious (B4) mass
The histologic exam of the biopsy specimens showed invasive ductal carcinoma, and the axillary node was positive for malignancy. Immunohistochemistry was showed positive for estrogen receptors (ER) and progesterone receptors (PR), HER2 was 2+ with a negative FISH assay, and the Ki67 was 35-40%. Therefore, based on breast exam and microscopic assessment, the diagnosis was an ER +, PR +, HER2 –, IBC of the left breast.
Figure 1. Ultrasound shows multiple sites of tissue distortion in the left breast.
60 Alipour, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 59-64
Figure 2. Mammography shows extremely dense breasts with cutaneous and subcutaneous edema in the left side.
CPM in inflammatory BC with BRCA

Nowadays, immediate reconstruction after mastectomy is gaining more attention, because it has been shown to be oncologically safe, and novel techniques are leading to better cosmetic results .12 However, the higher rate of wound infection in IBR has been shown to cause a higher rate of systemic
13recurrence in a study by Beecher et al., a result 14
which has been contradicted by Mousa et al. IBR can be performed using autologous tissue or a prosthesis. In the latter case, the implant is ideally covered by acellular dermal matrices to improve the
15results and lessen the complications. A main weakness of this technique is that if radiation is
Despite the complete clinical response of the tumor, the board decided against SSM or NSM, and MRM with delayed reconstruction was recommended. The decision about contralateral prophylactic mastectomy was left to the patient: she could have it done during the left MRM, or at time of reconstruction; the second option was prioritized by the members. The reason for this recommendation is described in the discussion.
Skin sparing mastectomy and nipple sparing mastectomy
SSM is normally carried out for cases of early breast cancer only, because it is postulated to be accompanied by a high rate of recurrence in locally
7advanced disease. However, reviewing 67 cases of SSM and IBR with autologous tissue, of whom 25 were locally advanced cancers, Foster et al. did not find a significant difference regarding cosmetic
8results and the rate of recurrence.
NSM is appropriate for tumors that are at least 2 cm far from the NAC, but Ryu et al. have shown it to
9be safe for tumors closer to the NAC. Factors that increase the rate of post-operative complications in NSM and SSM in addition to large ptotic breasts include smoking, obesity, and breast irradiation. In both SSM and NSM, there is a possibility of leaving breast tissue behind nipple areola complex because of the small incisions used, which makes the
10procedure more challenging technically. This raises concerns about local recurrence. However, Peled et al. showed that SSM did not affect local recurrence in locally advanced breast cancer, and that the major threat in these patients is the distant recurrence of the
11disease.
Discussion
The oncologic safety of SSM and NSM in cases that have undergone neoadjuvant chemotherapy is under debate. Studies have recently been carried out to evaluate this issue and found out that locoregional recurrence and recurrence over the nipple were not significantly higher, and that disease-free and overall
9survival rates were acceptable.
board while reviewing the history of the patient and going through all paraclinical results.
Immediate breast reconstruction
was reported in the right breast, but microscopic assessment of the US-directed biopsy showed a benign lesion.
Metastasis work up was carried by CT scans of the chest, abdomen and pelvis, and whole body bone scan; no distant metastases were seen. Brain MRI was requested by the oncologist due to the headaches of the patient, and it was normal.
Neoadjuvant chemotherapy was initiated; she received 8 cycles of docetaxel, epirubicin, and cyclophosphamide. She had a good clinical response, and the breast physical and US exam were normal after the 8 cycles.
1. The patient desired IBR. Considering the tumor type, were NSM or SSM possible for the patient? Could we recommend immediate reconstruction?2. Given that the patient was very young and genetically high risk, should we advise contralateral prophylactic mastectomy? In other words, would the patient get benefits from contralateral mastectomy considering her risk of metastasis and cancer-related events?
The patient was referred for consultations about fertility preservation and genetic assessment. She decided against at first but genetic testing was performed. She asked for markers to be put in the breast lesions before any other treatment in order to undergo breast conserving surgery later, but it was refused because the inflammatory picture hindered breast preservation.
The two questions were discussed on the tumor
Left-sided mastectomy was planned for the patient. However, two major questions arose, which were put to debate on the tumor board of the Cancer Institute, Tehran University of Medical Sciences.
The result of the genetic test was received while the patient was under chemotherapy, showing that the patient was positive for BRCA2; this was checked in her mother also, with a positive result.
Questions
Figure 3. MRI shows severely diffuse enhancement of the left breast and abnormal enhancement of the nipple.
61Alipour, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 59-64
CPM in inflammatory BC with BRCA

Newman et al. assessed IBR in locally advanced breast cancer and showed that completion of IBR did not affect recurrence, although the adjuvant treatments were delayed because of the additional
22procedure. They recommended against the use of implants and emphasized that autologous reconstruction should be performed in these patients.
One of the major drawbacks of IBR is the delay it may cause in the completion of adjuvant therapies. Henry et al. conducted a study on 76 cases of mastectomy to assess this probability, and showed that adjuvant treatments had been deferred for around 90 days in the 44 breast cancer patients who
21had undergone IBR compared to the 32 who did not.
Wang et al. assessed the rate of IBR in patients with non-metastatic T4 breast cancer, and detected a low (10%) albeit increasing rate (from around 4% to
2318% between 1998 and 2015) of IBR. They did not find any association between IBR or prophylactic contralateral mastectomy and survival. They concluded that IBR could be an oncologically safe
23 procedure in IBC. Patel et al. investigated the effect of IBR on mortality rate among 1472 cases of IBC
5who had undergone mastectomy. IBR had been performed for 44 patients; these were mostly younger, showed less comorbidities, and had a higher income. Their results did not show any association between IBR and mortality. Nakhlis et al. assessed 240 cases of non-metastatic IBC, of whom 13 and 27 had undergone IBR and delayed breast
4reconstruction (DBR), respectively. The rate of recurrence, whether locoregional or distant, was more than 92% in the IBR group and 37% in the DBR cases, but the sample size of the IBR patients was too small to be judged for significance. Simpson et al. studied 60 patients with IBC for consequences of
6breast reconstruction. Here, the reconstructive procedure had not been performed in most of the patients (39 cases), bur 16 had undergone IBR, and DBR had been performed for 5 others. The rate of local complications was much higher in the IBR group (37.5% vs 2.6% and 0% in DBR and no reconstruction cases, respectively), and radiation had begun later. However, the rate of recurrence and mortality did not differ among the groups. Chen et al.
Interestingly, dissection of the axillary lymph nodes and the number of dissected nodes have been shown to be directly associated with the rate of post-operative complications when IBR is performed
20using tissue expanders.
needed after surgery, the prosthesis may undergo 1 6
contrac t ion and deformity. The ra te of postoperative complications including infection and the need to removal of the implant also increase with
1 7 , 1 8irradiation. Under these circumstances, reconstruction is recommended to be performed in the delayed setting. Also, a tissue expander can be placed and inflated, and get deflated at the time of
19irradiation.
As conclusion, because of the inflammatory nature of the breast cancer, neither NSM nor SSM was appropriate for this patient; and MRM was the best approach as in other cases of IBC. IBC is a poor-prognosis type of breast cancer, and its association with BRCA mutations has not been documented. However, our case was positive for the mutation, and despite this genetic susceptibility, immediate contralateral prophylactic mastectomy was not recommended. The rationale was that the prognosis of the IBC is expected mostly to depend on the course of the present disease. The recommendation was to perform the contralateral procedure only after a 2-years interval for observing the patient for local or distant recurrence.
reviewed 3374 non-metastatic IBC cases between 1998 and 2013, and found out that the rate of autologous or implant-based breast reconstruction and contralateral prophylactic mastectomy was
24increasing over the years for these patients. They de tec ted no s ign i f i can t e ffec t o f b reas t reconstruction on the patients' survival. Their data did not show the rate of IBR and DBR, but the authors argued that IBR should be safe in IBC from the point of view of oncologic concerns.
Our patient was genetically positive, a case where prophylactic mastectomy is normally recommended. However, the greatest advantage of this procedure is before cancer diagnosis. This patient was not aware of her genetic susceptibility previously. Her tumor was IBC and she had to undergo chemotherapy before surgery, and radiation afterwards; the chemotherapy and a longer, more complex operation could increase the post-operative complications and cause deferral of the irradiation. Considering the poor prognosis of the present tumor, a waiting time of 2 years before proceeding to a contralateral surgery seemed reasonable in order to observe the patient for local or distant recurrence. In other words, the prognosis of the patient was mostly expected to depend upon the course of the present cancer, and not on a contralateral cancer. These were explained to the patient, and she decided to delay the contralateral procedure.
On the other hand, there were several reasons for prioritizing delayed reconstruction over the immediate technique. The patient was thin with large breasts, so reconstruction would only be possible by an implant. As radiation was part of the treatment plan, prosthesis reconstruction was not a good choice. The tumor was IBC and very diffuse throughout the breast and over the skin before chemotherapy, with the proliferation index being high. These considerations, along with the fact that NSM and SSM are not yet totally approved techniques for IBC, lead to a decision against these procedures.
Patient-oriented discussion
62 Alipour, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 59-64
CPM in inflammatory BC with BRCA
The patient has signed informed consent for the presentation of her documents in this article.
References
Acknowledgments
Ethical Consideration
5. Patel SA, Ng M, Nardello SM, Ruth K, Bleicher RJ. Immediate breast reconstruction for women having inflammatory breast cancer in the United States. Cancer medicine. 2018; 7:2887-902.
8. Foster RD, Esserman LJ, Anthony JP, Eun-sil SH, Do H. Skin-sparing mastectomy and immediate breast reconstruction: a prospective cohort study for the treatment of advanced stages of breast carcinoma. Annals of Surgical Oncology. 2002; 9:462-6.
Conflicts of interestThere is no conflict of interest to declare.
2. Fouad TM, Barrera AMG, Reuben JM, Lucci A, Woodward WA, Stauder MC, et al. Inflammatory breast cancer: a proposed conceptual shift in the UICC–AJCC TNM staging system. The Lancet Oncology. 2017; 18:e228-e32.
3. Gutierrez Barrera AM, Fouad TM, Song J, Webster R, Elsayegh N, Wood AL, et al. BRCA mutations in women with inflammatory breast cancer. Cancer. 2018; 124:466-74.
4. Nakhlis F, Regan MM, Chun YS, Dominici LS, Caterson S, Bellon JR, et al. Patterns of breast reconstruction in patients diagnosed with inflammatory breast cancer: The Dana‐Farber Cancer Institute's Inflammatory Breast Cancer Program experience. The Breast Journal. 2020; 26:384-90.
1. Irakleidis F, Tan PH. Inflammatory Breast Cancer; Diagnostic and Therapeutic Challenges. Therapy. 2019; 2:126.
6. Simpson AB, McCray D, Wengler C, Crowe JP, Djohan R, Tendulkar R, et al. Immediate reconstruction in inflammatory breast cancer: challenging current care. Annals of surgical oncology. 2016; 23:642-8.
7. Medina-Franco H, Vasconez LO, Fix RJ, Heslin MJ, Beenken SW, Bland KI, et al. Factors associated with local recurrence after skin-sparing mastectomy and immediate breast reconstruction for invasive breast cancer. Annals of surgery. 2002; 235:814.
9. Ryu JM, Nam SJ, Kim SW, Lee SK, Bae SY, Yi HW, et al. Feasibility of nipple-sparing mastectomy with immediate breast reconstruction in breast cancer patients with tumor-nipple
I would like to acknowledge the professors, fellows, and residents of the tumor board of the Cancer Institute of Iran, as well as the patients who confidently attend the tumor board, and generously let us share the data on their disease.
distance less than 2.0 cm. World journal of surgery. 2016; 40:2028-35.
11. Peled AW, Wang F, Foster RD, Alvarado M, Ewing CA, Sbitany H, et al. Expanding the indications for total skin-sparing mastectomy: is it safe for patients with locally advanced disease? Annals of surgical oncology. 2016; 23:87-91.
10. Galimberti V, Vicini E, Corso G, Morigi C, Fontana S, Sacchini V, et al. Nipple-sparing and skin-sparing mastectomy: review of aims, oncological safety and contraindications. The Breast. 2017; 34:S82-S4.
16.Vandeweyer E, Deraemaecker R. Radiation therapy after immediate breast reconstruction with implants. Plastic and reconstructive surgery. 2000; 106:56-8; discussion 9-60.
12.Malata C, McIntosh S, Purushotham A. Immediate breast reconstruct ion af ter mastectomy for cancer. British journal of surgery. 2000; 87:1455-72.
14. Mousa M, Barnea Y, Arad U, Inbal A, Klausner J, Menes T. Association between postoperative complications after immediate alloplastic breast reconstruction and oncologic outcome. Clinical breast cancer. 2018; 18:e699-e702.
13. Beecher S, O'Leary D, McLaughlin R, Sweeney K, Kerin M. Influence of complications following immediate breast reconstruction on breast cancer recurrence rates. British Journal of Surgery. 2016; 103:391-8.
17. Jagsi R, Jiang J, Momoh AO, Alderman A, Giordano SH, Buchholz TA, et al. Complications after mastectomy and immediate breast reconstruction for breast cancer: a claims-based analysis. Annals of surgery. 2016; 263:219.
21. Henry L, Morris L, Downs R, Schwarz R. The impact of immediate breast reconstruction after mastectomy on time to first adjuvant treatment in women with breast cancer in a community setting. The American Journal of Surgery. 2017; 213:534-8.
15. Bertozzi N, Pesce M, Santi P, Raposio E. One-stage immediate breast reconstruction: a concise review. BioMed research international. 2017; 2017.
18. Pu Y, Mao T-C, Zhang Y-M, Wang S-l, Fan D-L. The role of postmastectomy radiation therapy in patients with immediate prosthetic breast reconstruction: A meta-analysis. Medicine. 2018; 97.
20. Verma R, Klein G, Dagum A, Khan S, Bui DT. The Effect of Axillary Lymph Node Sampling during Mastectomy on Immediate Alloplastic Breast Reconstruction Complications. Plastic and Reconstructive Surgery Global Open. 2019; 7.
19. Kronowitz SJ, Hunt KK, Kuerer HM, Babiera G, McNeese MD, Buchholz TA, et al. Delayed-immediate breast reconstruction. Plastic and reconstructive surgery. 2004; 113:1617-28.
CPM in inflammatory BC with BRCA
63Alipour, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 59-64

23. Wang M, Chen H, Wu K, Ding A, Zhang P, Zhang M. Post-mastectomy immediate breast reconstruction is oncologically safe in well-selected T4 locally advanced breast cancer: a large population-based study and matched case–control analysis. Breast cancer research and treatment. 2019; 176:337-47.
22. Newman LA, Kuerer HM, Hunt KK, Ames FC, Ross MI, Theriault R, et al. Feasibility of immediate breast reconstruction for locally advanced breast cancer. Annals of surgical oncology. 1999; 6:671-5.
24. Chen H, Wu K, Wang M, Wang F, Zhang M, Zhang P. A standard mastectomy should not be the only recommended breast surgical treatment for non-metastatic inflammatory breast cancer: A large population-based study in the Surveillance, Epidemiology, and End Results database 18. The Breast. 2017; 35:48-54.
64 Alipour, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 59-64
CPM in inflammatory BC with BRCA

65
in immigrant women. Australia has a population mammography screening program that is targeted to women aged 50–74. Women can attend on request
4from the age of 40. Participation in the screening program is lower among the immigrant population compared to Australian-born women, possibly due
5 to cultural and language barriers. In addition to fewer screen-detected cancer than Australian-born women, there is some evidence to suggest that other aspects of breast cancer patterns vary among different cultural groups in Australia. For example, women born in Arabic-speaking countries are younger than Australian-born women and they are
IntroductionBreast cancer is the most common cancer
affecting females in most countries around the 1-3
world, including Australia and Iran. While there is much information available about breast cancer in Australia overall, less is known about breast cancer
ARTICLE INFO
Methods: Women were eligible for this retrospective audit if treated for breast malignancy with country of birth recorded. Demographic, tumour and surgical data were extracted and analysed. Data for Iranian-born women were compared to data for Australian-born (comparison group 1) and women born in countries other than Australia or Iran (comparison group 2, referred to as ‘other’).
Background: While there is much information available about breast cancer in Australia overall, less is known about breast cancer in immigrant women and specifically Iranian-born women. Understanding this group is important to provide appropriate screening, treatment and support interventions. The aim of this study was to describe breast cancer presentation, tumour and treatment characteristics in Iranian-born women in Australia.
Conclusions: Iranian-born women treated for breast cancer in Australia were younger, had higher-grade tumours and were less likely to have a screen-detected cancer than Australian-born women or women born in other countries. Strategies to encourage screening participation in Iranian-born women are required. Support for these women is required as they are more likely to receive toxic treatments (chemotherapy and extended adjuvant endocrine therapy) due to younger age and higher grade tumours.
Results: 2086 women were eligible: Iranian-born n=27, Australian-born n=894 and Other n=1165. Iranian-born women were younger, mean age of 53.9 (five years younger in overall mean, SD 11.98, F=3.171, p=0.042). Iranian-born women were significantly less likely to present with a screen-detected cancer (X2= 11.481, p=0.003) and more likely to have a high-grade cancer (X2=14.383, p=0.006). There was no difference in mastectomy rate (X2=1.698, p=0.428).
surgical oncology
Breast neoplasms,
immigrants,
Iran,
Key words:
Australia,
23 April 2020
01 May 2020Accepted:
Revised: 09 April 2020Received:
Address for correspondence: Farid Meybodi, MD, FRACS Address: Westmead Breast Cancer Institute I Level 1, Block F I Westmead Hospital Westmead NSW 2145 Phone: +61432499525Fax: +61285691039Email: [email protected]
ABSTRACT
Features of Breast Cancer in Iranian-born Migrant Women Treated in Australia
a Westmead Breast Cancer Institute, Westmead Hospital, NSW, Sydney, Australia
b Western Clinical School, School of Medicine, Faculty of Medicine and Health, University of Sydney, Sydney, Australia
c School of Medicine Sydney, University of Notre Dame Australia, Darlinghurst, Sydney, Australia
a,b a,b,cFarid Meybodi* , Meagan E. Brennan
Open AccessOriginal Article
Meybodi, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 65-71
DOI: 10.19187/abc.20207265-71

Corresponding data were gathered for Australian-born women (comparison group 1) and for women born in countries other than Australia or Iran (comparison group 2, referred to as ‘other’) who were treated during the same time period. Area of disadvantage decile was included in demographic data and this was determined using Australian
Demographic data were extracted (patient age, country of birth, religion, marital status, postcode of residence). Tumour and surgical data were extracted (method of detection, histological type, size, grade, and receptor status of cancer as well as breast conservation vs mastectomy, re-excision, breast reconstruction and contralateral prophylactic surgery).
This study was a retrospective audit of a prospectively maintained database at the major referral hospital in Western Sydney. The database was searched to identify cases that met eligibility criteria: female, aged over 18, treated for DCIS or invasive breast cancer and born in Iran. Cases could not be included where country of birth was not recorded and cases were excluded when key pathological factors such as tumour type, size and grade were missing.
Western Sydney, the setting for this study, has a very diverse population. Over 40% of the population has a country of birth other than Australia and 45% speak a language other than English at home (twice
7the New South Wales state average). There is no single country or region of birth making up the population. Immigrants to Sydney come from many different Asian and Middle Eastern countries as well as European countries and New Zealand. The number of immigrants settling in Western Sydney increased by 21% over the five-year period from 2011 to 2016. Iranian-born women make up a significant proportion of this population, with an estimated total of 12,500 Iranian-born people living
7,8in Western Sydney. In Australia overall, there are more than 58,000 Iranian-born people and the population increased by 69% during the five year
9period between 2011 and 2016. Understanding breast cancer in the Iranian-born population is important in order to plan screening interventions and to provide culturally appropriate support to women and their families when breast cancer is diagnosed.
more likely to have high-grade and HER2 positive 6
cancer.
The aim of this study was to describe breast cancer presentation, tumour and treatment characteristics in Iranian-born women treated in Western Sydney. A further aim was to compare the features in Iranian-born women to those for women born in Australia or other (non-Australian, non-Iranian) countries.
Methods
Institutional ethics approval was obtained (Western Sydney HREC, 2019/ETH10761).
There were 2086 eligible cases identified: women treated for DCIS or invasive breast cancer (2011–2017) with country of birth information available. They were born in Iran (n=27, 1.3%), Australia (n=894, 42.9%), and other countries (n=1165, 55.8%). Eighty-one different countries of birth were noted, and Iran was the 12th most common (Table 1).
10government postcode tables based on census data.Analysis was conducted using SPSS Statistics
Version 24. Descriptive statistics were used to summarise each factor in each of the three groups. Chi-square analysis was performed to evaluate differences between groups. A p-value ≤0.05 was considered significant.
Results
DemographicsPatient demographics are shown in Table 2. The
mean age for the cohort overall was 58.6 years and Iranian-born women were significantly younger, mean 53.9 years (SD 11.98, F=3.171, p=0.042). In the Iranian-born group, 14.8% were over the age of 65 and none over the age of 80, compared to 70.7%
2and 29.3% for the cohort overall (X =17.299, p=0.027). There was no difference in menopausal
2status between the three groups (X =2.735, p=0.603). 59.3% of Iranian-born women nominated English as their preferred language and 33.3% nominated Farsi. Iranian-born women, categorised by postcode of
BC in Iranian-born in Australia
Table 1. Country of birth of women treated for DCIS
or invasive breast cancer (N=2086)
%N
894
139
134
109
85
63
46
34
32
30
28
27
25
25
24
22
22
21
21
20
285
2086
42.9
6.7
6.4
5.2
4.1
3
2.2
1.6
1.5
1.4
1.3
1.3
1.2
1.2
1.2
1.1
1.1
1
1
1
12.2
100
Australia
Philippines
China
United Kingdom
Lebanon
India
New Zealand
Fiji
Sri Lanka
Malta
Hong Kong
Iran
South Korea
Turkey
Italy
Iraq
Vietnam
Croatia
Malaysia
Afghanistan
Other
TOTAL
Country
66 Meybodi, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 65-71

Table 2. Demographic data for women born in Iran, Australia and other countries (N=2086 women)
(SD 11.63)
P
58.6 yrs
20 to 94 yrs
20-3536-5051-6566-80>80Total
EnglishFarsiArabicOtherUnknownTotal
AnglicanCatholicOther ChristianMuslimHinduBuddhistSikhAtheist/ AgnosticNoneJewishOtherUnknownTotal
MarriedDefactoDivorcedNever MarriedSeparatedSingleWidowedUnknownTotal
Group 1-2Group 3-4Group 5-6Group 7-8Group 9-10UnknownTotal
Underweight (<18.5)Healthy weight (18.5-24.9)Overweight (25-29.9)Obese (≥30)UnknownTotal
NeverCurrentPreviousUnknownTotal
Pre-menopausalPeri-menopausalPost-menopausalUnknownTotal
YesNoUnknownTotal
19134027
16901127
01560000305727
15160203027
33498027
0
5
1
31827
8210727
5118327
1016127
17.299
777.666
612.256
53.386
19.208
23.487
259.253
2.735
40.198
0.027
<0.001
<0.001
<0.001
0.014
0.001
<0.001
0.603
<0.001
3.4%21.8%42.5%27.6%4.7%
100.0%
99.1%0.0%0.6%0.3%0.0%
100.0%
27.7%33.3%17.8%0.4%0.0%0.4%0.0%3.1%9.6%0.0%0.3%7.2%
100.0%
57.6%4.4%13.4%7.9%4.1%1.5%10.3%0.8%
100.0%
20.0%13.9%19.8%23.9%22.4%0.0%
100.0%
0.4%
12.4%
15.8%
26.6%44.7%100.0%
20.4%3.6%65.0%11.1%
100.0%
20.0%9.5%66.1%4.4%
100.0%
46.5%51.0%2.5%
100.0%
2328054428533
1165
75865732915
1165
4836227198636311241341387
1165
80127924752101279
1165
2961551712622810
1165
9
179
165
2006121165
619173901391165
2559576253
1165
38475427
1165
2.0%24.0%46.7%24.5%2.8%
100.0%
65.1%0.5%4.9%28.2%1.3%
100.0%
4.1%31.1%23.3%8.4%5.4%5.4%0.9%2.1%11.5%0.1%0.3%7.5%
100.0%
68.8%2.3%7.9%4.0%4.5%0.9%10.9%0.8%
100.0%
25.4%13.3%14.7%22.5%24.1%0.0%
100.0%
0.8%
15.4%
14.2%
17.2%52.5%100.0%
53.1%1.5%33.5%11.9%
100.0%
21.9%8.2%65.4%4.5%
100.0%
33.0%64.7%2.3%
100.0%
2.6%23.2%44.9%25.7%3.6%
100.0%
79.6%0.7%3.0%16.0%0.8%
100.0%
14.2%31.7%20.9%5.2%3.0%3.2%0.5%2.5%10.7%0.0%0.5%7.6%
100.0%
63.8%3.2%10.5%5.7%4.4%1.1%10.6%0.8%
100.0%
22.9%13.5%16.9%23.2%23.5%0.0%
100.0%
0.6%
14.1%
14.7%
21.1%49.4%100.0%
38.8%2.4%47.0%11.7%
100.0%
21.0%8.7%65.7%4.6%
100.0%
38.8%58.8%2.4%
100.0%
5448493753675
2086
1660156233316
2086
29666143510863671152223111
1582086
133167218118912322216
2086
4772823524844890
2084
13
295
307
44110302086
809519812452086
439181137195
2086
810122650
2086
3.7%33.3%48.1%14.8%0.0%
100.0%
59.3%33.3%0.0%3.7%3.7%
100.0%
0.0%3.7%18.5%22.2%0.0%0.0%0.0%0.0%11.1%0.0%18.5%25.9%100.0%
55.6%3.7%22.2%0.0%7.4%0.0%11.1%0.0%
100.0%
11.1%11.1%14.8%33.3%29.6%0.0%
100.0%
0.0%
18.5%
3.7%
11.1%66.7%100.0%
29.6%7.4%37.0%25.9%100.0%
18.5%3.7%66.7%11.1%
100.0%
37.0%59.3%3.7%
100.0%
3019538024742894
8860530
894
248298159404028860364894
51539120713713927
894
1781241772132000
892
4
111
141
238400894
1823258199894
1798559139894
41645622894
Age Group
Preferred language
Religion
Marital status
Area of disadvantagedecile*
Body Mass Index
Use of oral contraceptivepill
Menopausal status
Familyhistory of breast cancer
Characteristic
Age
Iran (N=27)
Mean
Australia (N=894)
(SD 12.44) (SD 12.44)53.9 yrs
35 to 71 yrs
Other country (N=1165)
59.1 yrs
21 to 94 yrs
Total (N=2086)
58.3 yrs
20 to 94 yrs
N
Age range
N N% % % N %
(SD 11.98) 0.042F=3.171
*Unknown cases excluded from analysis
67Meybodi, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 65-71
BC in Iranian-born in Australia
2X value*

Table 3. Tumour characteristics for malignancy in women born in Iran, Australia and other countries (N=2088 tumours) 2X value* PTotalAustralia Other country
Unilateral cancerBilateral synchronous cancerUnknownTotal
Screen-detectedSymptomaticUnknownTotal
PalpableNot palpableUnknownTotal
DCISInvasive cancerUnknownTotal
LowIntermediateHighUnknownTotal
<20mm20-50mm >50mmUnknownTotal
Ductal NSTInvasive lobularTubularMedullaryMetaplasticMixedTypePapillaryMucinousOtherUnknownTotal
Grade 1Grade 2Grade 3UnknownTotal
pT1pT2pT3UnknownTotal
PositiveNegativeUnknownTotal
PositiveNegativeUnknownTotal
PositiveNegativeUnknownTotal
YesNoUnknownTotal
YesNoUnknownTotal
208440
2088
104796081
2088
17472331082088
293176332
2088
267017225293
130126136293
129217233267142546823
1763
35570166344
1763
844773121341763
144126656
1763
135834560
1763
19513741941763
40112551071763
45315061292088
99.8%0.2%0.0%
100.0%
50.1%46.0%3.9%
100.0%
83.7%11.2%5.2%
100.0%
14.0%84.4%1.5%
100.0%
8.9%23.9%58.7%8.5%
100.0%
44.4%43.0%0.3%12.3%100.0%
73.3%9.8%1.9%0.1%0.3%4.0%2.4%3.1%3.9%1.3%
100.0%
20.1%39.8%37.6%2.5%
100.0%
47.9%43.8%0.7%7.6%
100.0%
81.7%15.1%3.2%
100.0%
77.0%19.6%3.4%
100.0%
11.1%77.9%11.0%
100.0%
22.7%71.2%6.1%
100.0%
21.7%72.1%6.2%
100.0%
0.124
11.481
4.268
5.659
4.789
2.509
10.376
14.383
7.501
1.442
0.156
3.290
0.634
1.008
0.940
0.003
0.118
0.059
0.310
0.643
0.846
0.006
0.112
0.486
0.925
0.193
0.728
0.604
99.8%0.2%0.0%
100.0%
54.6%42.3%3.0%
100.0%
82.6%12.8%4.6%
100.0%
12.1%86.6%1.3%
100.0%
5.6%20.4%64.8%9.3%
100.0%
41.7%44.4%0.9%13.0%100.0%
73.0%9.8%2.1%0.3%0.3%4.3%2.2%3.0%3.9%1.3%
100.0%
23.6%38.1%36.1%2.2%
100.0%
49.7%43.5%0.1%6.7%
100.0%
80.6%15.9%3.5%
100.0%
76.5%19.7%3.7%
100.0%
9.5%78.5%12.0%100.0%
23.1%71.0%5.9%
100.0%
22.2%72.0%5.8%
100.0%
89320
895
48937927895
73911541895
10877512895
6227010108
4548114108
5667616223317233010775
18329528017775
385337152775
62512327775
59315329775
7460893775
17955046775
19964452895
116420
1166
54856652
1166
98711564
1166
18296420
1166
204710114182
8476022182
7079317043823313813964
16740137026964
4484251180964
79514128964
74618830964
119745100964
21868660964
25084076
1166
99.8%0.2%0.0%
100.0%
47.0%48.5%4.5%
100.0%
84.6%9.9%5.5%
100.0%
15.6%82.7%1.7%
100.0%
11.0%25.8%55.5%7.7%
100.0%
46.2%41.8%0.0%12.1%100.0%
73.3%9.6%1.8%0.0%0.4%3.9%2.4%3.2%3.9%1.3%
100.0%
17.3%41.6%38.4%2.7%
100.0%
46.5%44.1%1.1%8.3%
100.0%
82.5%14.6%2.9%
100.0%
77.4%19.5%3.1%
100.0%
12.3%77.3%10.4%100.0%
22.6%71.2%6.2%
100.0%
21.4%72.0%6.5%
100.0%
270027
1015227
213327
324027
01113
12003
1930000200024
5513124
11110224
212124
194124
221124
419124
422127
100.0%0.0%0.0%
100.0%
37.0%55.6%7.4%
100.0%
77.8%11.1%11.1%
100.0%
11.1%88.9%0.0%
100.0%
0.0%33.3%33.3%33.3%100.0%
33.3%66.7%0.0%0.0%
100.0%
79.2%12.5%0.0%0.0%0.0%0.0%8.3%0.0%0.0%0.0%
100.0%
20.8%20.8%54.2%4.2%
100.0%
45.8%45.8%0.0%8.3%
100.0%
87.5%8.3%4.2%
100.0%
79.2%16.7%4.2%
100.0%
8.3%87.5%4.2%
100.0%
16.7%79.2%4.2%
100.0%
14.8%81.5%3.7%
100.0%
Uni/bilateral breast cancer
Method ofDetection
Palpability
Type of malignancy
Grade DCIS (n=293)
Size DCIS (n=293)
Histology invasive cancer (n=1763)
Grade Invasive cancer (n=1763)
Size Invasive cancer (n=1763)
ER Status (n=1763) invasive cancer
PR Status (n=1763) invasive cancer
HER2 Status (n=1763) invasive cancer
Multifocal (n=1763) invasive cancer
Multifocality, all tumours (n=2088)
Tumour characteristic Iran
N N N N% % % %
*Unknown cases excluded from analysis
68 Meybodi, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 65-71
BC in Iranian-born in Australia

There was no difference in the type of tumour between country of birth groups (DCIS versus
2invasive cancer, X =4.268, p=0.118) or in grade or 2 2
size of DCIS (X =4.789, p=0.310 and X =2.509, p=0.643). For invasive cancer, there was no difference in histological type or size of tumour
2 2(X =10.376, p=0.846 and X =7.501, p=0.112). However, Iranian-born women had higher grade
Iranian women were less likely to be overweight 2
or obese (X =23.487, p=0.001) and less likely to have 2ever used the oral contraceptive pills (X 259.253,
p<0.001) than the other two groups.
Tumour characteristics
residence, had significantly less disadvantage than 2
the other two groups (X =19.208, p=0.014). This indicates that Iranian-born women were living in higher socio-economic suburbs than the other groups.
Tumour characteristics are shown in Table 3. Iranian-born women were less likely to present with a screen-detected breast cancer (37%) compared to Australian-born (54.6%) or other women (50.1%,
2X = 11.481, p=0.003). However, palpability of the 2
tumour was no different between groups (X = 4.268, p=0.118).
invasive cancers. Grade 3 cancers were present in 54.2% of Iranian-born women, compared to 36.1% of Australian-born women and 38.4% of others
2(X =14.383, p=0.006). There was no difference in ER, PR or HER2 receptor status or in multifocality of tumours.
Discussion
Surgical treatmentFactors related to surgical treatment are shown in
Table 4. There was no difference in final operation between groups (breast conservation vs mastectomy
2(X =1.698, p=0.428) or re-excision rate after initial
2breast conservation (X =1.579, p=0.454). The rate of immediate reconstruction after mastectomy was significantly lower in the ‘other’ group compared to
2Iranian or Australian-born women (X =20.304, p<0.001). This group was also less likely to undergo
2contralateral prophylactic mastectomy (X =27.5384, p<0.001.)
This study compares breast cancer variables in Iranian-born women treated in Australia (n=27) with Australian-born women (n=894) and those born in other countries (n=1165). The present study showed that Iranian-born women were younger than the other
Table 4. Surgical treatment factors for malignancy in women born in Iran, Australia and other countries (n=2086 women) 2X value* PTotalAustralia Other country
Breast conservationMastectomyUnknownTotal
Standard wide local excisionTherapeutic mammaplasty Wide excision and local flapUnknownTotal
YesNoUnknownTotal
Breast conservationMastectomyUnknownTotal
No immediate reconstructionImmediate reconstructionUnknownTotal
No CPMCPMUnknownTotal
No immediate reconstructionImmediate reconstructionUnknownTotal
14306506
2086
129113270
1430
258115517
1430
13227586
2086
4672910
758
6461120
758
38740
112
68.60%31.20%0.30%
100.00%
90.30%9.20%0.50%0.00%
100.00%
18.00%80.80%1.20%
100.00%
63.40%36.30%0.30%
100.00%
61.60%38.40%0.00%
100.00%
85.20%14.80%0.00%
100.00%
33.90%66.10%0.00%
100.00%
2.464
2.133
1.579
1.698
20.304
27.5384
4.000
0.292
0.711
0.454
0.428
<0.001
<0.001
0.135
70.10%29.80%0.10%
100.00%
89.20%10.40%0.50%0.00%
100.00%
18.00%80.70%1.30%
100.00%
64.80%35.10%0.10%
100.00%
52.50%47.50%0.00%
100.00%
78.00%22.00%0.00%
100.00%
27.50%72.50%0.00%
100.00%
6272661
894
5596530
627
1135068
627
5793141
894
1651490
314
245690
314
1950069
7873735
1165
7186540
787
1446349
787
7284325
1165
2961360
432
393390
432
1821039
67.60%32.00%0.40%
100.00%
91.20%8.30%0.50%0.00%
100.00%
18.30%80.60%1.10%
100.00%
62.50%37.10%0.40%
100.00%
68.50%31.50%0.00%
100.00%
91.00%9.00%0.00%
100.00%
46.20%53.80%0.00%
100.00%
1611027
1420016
115016
1512027
66012
84012
1304
59.30%40.70%0.00%
100.00%
87.50%12.50%0.00%0.00%
100.00%
6.30%93.80%0.00%
100.00%
55.60%44.40%0.00%
100.00%
50.00%50.00%0.00%
100.00%
66.70%33.30%0.00%
100.00%
25.00%75.00%0.00%
100.00%
Initial operation (n=2086)
Initial breast conservation type (n=1430)
Re-excision after breast conservation (n=1430)
Final Operation(n=2086)
Reconstruction after mastectomy (n=758)
Contralateral prophylactic mastectomy (n=758)(unilateral cancer undergoing ipsilateral mastectomy)
Reconstruction after CPM (n=112)
Tumour characteristic Iran
N N N N% % % %
*Unknown cases excluded from analysis
69Meybodi, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 65-71
BC in Iranian-born in Australia

The Iranian-born population in Australia (median age 35 years) is younger than other migrants (median age 44 years) and the Australian population overall
9(median age 38 years). This may partly explain the younger age of the Iranian-born women in the present study.
Australia has a free national screening program that targets women aged 50–74 and allows women aged 40–49 to attend on request. The overall participation rate in the screening program for women who speak a language other than English at home is <49%, compared to around 55% in English-
5speaking women. This is thought to be related to cultural and language issues which prevent the screening message from reaching women in minority groups or make breast screening challenging for cultural reasons. No specific information is available about rates of screening attendance specifically in women born in Iran. Lower screening attendance may explain why symptomatic rather than screen-detected cancers are more common in Iranian-born women. Lower attendance may be due to language and cultural barriers, however it could also be due to the younger cohort. The present study found that 37% of cancers in Iranian-born women occurred before the age of 50, so these women were younger than the age when they are formally invited to commence screening. Another hypothesis is that screening attendance in Iranian-born women is good (and some may be attending for screening between ages 40 and 50 on request) but there could be more interval cancers because high-grade cancers are more common. Further research is needed to examine this.
Programs to ensure that the screening message is reaching its target age group in cultural minority groups as well as the overall Australian population is essential. Some such programs are in place such as the Pink Sari program that targets women in Indian
11and Sri Lankan communities. It may also be appropriate to invite Iranian-born women to start screening at a younger age than Australian-born women. The trade-offs of this in terms of recall rate and cost would need to be examined.
The proportion of high-grade tumours in Iranian women has implications for treatment and support. Information about treatment with chemotherapy was not available in this study. It is hypothesised that Iranian-born women were more likely to be recommended for chemotherapy than the other groups as they were younger as well as having higher grade tumours. This means that culturally appropriate education and support is particularly important for
groups, with a mean age of 53.9 (around five years younger than the overall cohort) and 85% of Iranian-born women under the age of 66. Iranian-born women were less likely to be overweight or obese, and less likely to live in a disadvantaged area. They were less likely to present with a screen-detected cancer and more likely to have a high-grade cancer.
these women as they may be more likely to have more toxic treatment with more significant side effects than non-Iranian-born women.
Previous research in Australia has shown that unmet needs are higher in cancer survivorship for women from culturally and linguistically diverse
12,13backgrounds compared to Australian-born women. Iranian-born women may therefore be at higher risk of unmet long-term needs, especially if they have received more toxic treatments such as chemotherapy. Iranian-born women, with higher-grade cancers, are also more likely to be recommended for extended adjuvant endocrine therapy with its consequent side effects, which are frequently more significant in
14younger cancer survivors. Therefore, support is required in the long-term, not just at the time of initial cancer treatment. Patient-reported outcome measures were not part of this study; however, this is a recommended area for future research gain further insight into the cancer experience of Iranian-born women.
This study has several limitations. The number of Iranian-born women was very small in comparison to women in the other groups. The retrospective study design brings bias, and there was missing information for some variables. The non-Australian-born comparison group was extremely heterogeneous (women born in 79 different countries), which may limit conclusions about that group. Many women in the Iranian-born and the ‘other’ group had limited English and were interviewed with health care interpreters so the accuracy the background information provided may have been sub-optimal. Patient-reported outcomes were not included in this study. This information would provide additional insight into the cancer experience of Iranian-born women.
In conclusion, this study showed that Iranian-born women treated for breast cancer in Australia were younger, had higher-grade tumours and were less likely to have a screen-detected cancer than Australian-born women or women born in other countries. Strategies to encourage screening participation in Iranian-born women are required. Support for these women during cancer treatment and in survivorship is required as they are more likely to have received toxic treatments such as chemotherapy and extended adjuvant endocrine therapy due to their younger age and higher-grade tumours. Further research into patient-reported outcomes is required to understand the lived experience of cancer in these women.
Iranian-born women in this study were less likely to live in a geographic area of economic disadvantage than women in the comparator groups. They may, therefore, have a higher level of education and be receptive to educational and support material about breast cancer.
70 Meybodi, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 65-71
BC in Iranian-born in Australia

The authors have no conflicts of interest to declare.
Conflicts of interest
References
3. World Health Organization. Cancer country profiles 2014. https://www.who.int/cancer/ country-profiles/en/#J.
5. Australian Institute of Health and Welfare. BreastScreen Australia monitoring report 2018. Vol Cancer series no. 112. Cat. no. CAN 116. Canberra: AIHW; 2018.
6. Heilat GB, Brennan ME, Kanesalingam K, Sriram N, Meybodi F, French J. Presentation, tumour and treatment features in immigrant women from Arabic-speaking countries treated for breast cancer in Australia. ANZ J Surg. 2020;90(3):325-331.
7. Western Sydney Regional Organisation of Counc i l s . Commun i ty p ro f i l e . 2016 ; https://profile.id.com.au/wsroc.
9. Australian Government (Department of Home Affairs). Iran-born community information summary. 2016; https://www.homeaffairs. gov.au/mca/files/2016-cis-iran.PDF. Accessed April 2020.
11. Service MHC. About Pink Sari. https://www. mhcs.health.nsw.gov.au/about-us/campaigns-and-projects/completedprojects/about-pink-sari-project. Accessed March 2020.
2. Australian Institute of Health and Welfare. Cancer in Australia 2017. Vol Cancer series no.101. Cat. no. CAN 100. Canberra: AIHW; 2017.
4. Australian Government (Department of Health). BreastScreen Australia. http://www.cancerscreening. gov.au/internet/screening/publishing.nsf/Content/breast-screening-1. Accessed January 2020.
12. Butow PN, Bell ML, Aldridge LJ, et al. Unmet needs in immigrant cancer survivors: a cross-sectional population-based study. Support Care Cancer. 2013;21(9):2509-2520.
13. Butow PN, Aldridge L, Bell ML, et al. Inferior health-related quality of life and psychological well-being in immigrant cancer survivors: a population-based study. Eur J Cancer. 2013;49(8):1948-1956.
10. Australian Bureau of Statistics. Socio-economic indexes for areas (SEIFA). Australian Bureau of Statistics; 2013.
1. Farhood B, Geraily G, Alizadeh A. Incidence and Mortality of Various Cancers in Iran and Compare to Other Countries: A Review Article. Iran J Public Health. 2018;47(3):309-316.
8. .ID. Greater Western Sydney Region Iranian population. 2011; https://profile.id.com.au/ s_greater-western-sydney-2019/iranian-population#n-473.
14. Brennan ME, Boyle FM, Butow PN, Spillane AJ. Evaluation of a survivorship care plan:
Long-term use, care coordination and quality of life in breast cancer survivors. Breast Cancer Management. 2015;4(4):145-157.
71Meybodi, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 65-71
BC in Iranian-born in Australia
Astaxanthin (AST) is a red carotenoid pigment and a natural product of microalgae Haematococcus pluvialis with unique structural and chemical
5characteristics. AST is a powerful scavenger capable
particularly chemoresistance contributes to breast cancer (BC) recurrence post-surgery followed by
2 secondary tumor formation and distant metastasis.Natural compounds that can help chemo-sensitization of tumors without raising unwanted side effects have
3,4drawn attention for some time.
IntroductionInduction of cell death pathways constitutes the
1basis of cancer chemotherapy. Drug resistance
ARTICLE INFO
Background: We investigated molecular mechanisms behind astaxanthin-mediated induction of apoptosis in breast cancer cell lines toward combination therapy against cancer drug resistance.
Results: Astaxanthin induced cell death in all three breast cancer cell lines was examined so that its IC50 in two HER2-amplifying lines SKBR3 and BT-474 stood, respectively, at 36 and 37 µM; however, this figure for MCF-7 was significantly lowered to 23 µM (P<0.05). Astaxanthin-treated SKBR3 cells showed apoptotic death upon co-staining. Our in silico examinations showed that some growth-promoting molecules are strongly bound by astaxanthin via their specific amino acid residues with their binding energy standing below -6 KCa/Mol. Next, astaxanthin was combined with either graphene oxide or carboxylated multi-walled carbon nanotube, with the latter affecting SKBR cell survival more extensively than the former (P<0.05). Finally, astaxanthin co-induced tumor suppressors p53 and PTEN but downregulated the expression of growth-inducing genes in treated cells.
Conclusions: These findings indicate astaxanthin carries' multitarget anti-tumorigenic capacities and introduce the compound as a suitable candidate for combination therapy regimens against cancer growth and drug resistance. Development of animal models to elucidate interactions between the compound and tumor microenvironment could be a major step forward towards the inclusion of astaxanthin in cancer therapy trials.
Methods: Breast cancer cell lines were treated with serial concentrations of astaxanthin to determine its IC50. We used drug-design software to predict interactions between astaxanthin and receptor tyrosine kinases or other key gene products involved in intracellular signaling pathways. Changes in gene expression were examined using RT-PCR. The effect of astaxanthin-nanocarbons combinations on cancer cells was also evaluated.
Key words:Breast cancer, astaxanthin,
receptor tyrosine kinase,apoptosis,
31 May 2020Accepted:
Received:
17 May 2020
23 May 2020Revised:
Address for correspondence: Mossa GardanehNational Institute of Genetic Engineering and Biotechnology, Pazhoohesh Blvd, Tehran-Karaj HWY Kilometer 15,PO BOX 14965/161, Tehran-IranTel: +98 21 4458 0344 Fax: +98 21 4458-0395 Email: , [email protected] [email protected]
72 Gardaneh, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 72-82
ABSTRACT
Molecular Simulations Identify Target Receptor Kinases Bound by Astaxanthin to Induce Breast Cancer Cell Apoptosis
a Department of Stem Cells and Regenerative Medicine, Division of Medical Biotechnology, National Institute of
Genetic Engineering and Biotechnology, Tehran, Iranb Department of Biology, York University, Toronto, Canada
c Department of Chemistry, Ayatollah Amoli Branch, Islamic Azad University, Amol, Iran
a a a b cMossa Gardaneh* , Zahra Nayeri , Parvin Akbari , Mahsa Gardaneh , Hasan Tahermansouri
Open AccessOriginal Article
DOI: 10.19187/abc.20207272-82

In mouse models of cancer, the potential of AST in inducing apoptosis among tumor cells has been demonstrated. As an example, the compound inhibits tumorigenesis in rat colon via inducing apoptosis. AST can do this by controlling ERK-2, AKT, MMPs-
242/9, COX-2 and NFkB genes. In another study, AST inhibited colon carcinogenesis by regulating
25inflammatory cytokines. In hamster model of mouth cancer, dietary AST inhibited NFkB and Wnt/β-catenin by inhibiting Erk/MAPK and PI3K/AKT,
23eventually leading to apoptosis. Based on its anti-inflammatory and anti-oxidant properties, AST was able to reduce proliferation and migration of BC cells
26compared to control normal breast epithelial cells. The anti-invasive and anti-metastatic potential of AST has been shown in increasing metastasis-
6of degrading free radicals in aqueous solvents. It is a free oxygen inhibitor and an effective inhibitor of
7lipid peroxidation. Cancer incidence is rare among North American
tribes who traditionally consume salmon fish (a rich 8source of AST). AST induces reduction of mouse
9tumor cells and synthesis of DNA. The compound
10also reduces mouse mammary tumor cells by 40%. Among eight carotenoids tested, AST most
11effectively inhibited the invasion of hepatoma cells. AST inhibits growth among human cancer cell lines too. For example, two human colon cancer cell lines incubated with AST for 4 days lost their growth
12significantly compared to their controls. The inhibiting effect of AST on human prostate cancer
13cells has also been reported. Finally, AST can prevent UV damage on DNA of skin fibroblasts,
14melanocytes and intestine cells.
The anti-proliferative effects of AST on cancer 17cells of breast, liver and lung have been shown in
parallel with a stronger growth inhibitory effect of 16
AST compared to other carotenoids. Also, AST differentially affects cancer cells without harming
17normal ones. AST indeed protects wild-type cells
18,19 20 21against oxidative stress, ultraviolet, neurotoxins, 22
and cell-tissue inflammation via inhibiting apoptosis. In contrast, it forces cancer cells to commit apoptosis. AST-treated cancer cells show a significant peak of hypodiploid, indicative of apoptosis with typical characteristics including modified mitochondrial morphology, transmembrane potential and respiratory chain and regulated levels of Bcl-2, Bax, Bad, Bcl-
17,23xL.
The anti-oxidant properties of AST restore superoxide dismutase (SOD) and catalase (CAT), thereby reducing intracellular O2− production and reversing lipopolysaccharide-induced toxicity and
15reactive oxygen species production in cancer cells. Such properties can also arrest cell cycle progression, inhibit cell proliferation and induce apoptosis by activating Nrf2-mediated anti-oxidant defense
16system. Unlike other carotenoids, there exists no report on the pro-oxidative properties of AST.
In this study, we examined the effect of AST on the fate of BC cell lines and the changes it causes in expression levels of some key genes involved in BC cell tumorigenicity. We tested AST potential in binding to key growth signaling molecules including receptor tyrosine kinases, examined its impact on gene expression, and used nano particles to potentiate anti-tumorigenic effects of the carotenoid.
specific miRNAs and suppressing the expression of 27
MYC transcription factor.
To make a stock solution of AST, 53.1 mg of its powder (Santa Cruz Biotechnology Inc., USA) was dissolved in 9 mL DMEM and 1 mL DMSO to obtain a 10 mM solution. This solution was filtered and stored at -20 ℃ until use. The cells were seeded in 96-well plates with 5000-7000 cells per well in 100-150 µL medium and incubated for 24 hrs before treatment began. Serial dilutions of AST were added to the cells followed by cell incubation for 5 hrs. We used AST doses of 8, 16, 24, 36, 40, 50, 65, 80 µM and then tested cell viability in each cell line using the MTT Viability assay. Each dose was tested in triplicate wells for each cell line and the whole experiment was repeated three times. Due to the lethal properties of DMSO as a solvent, and to determine AST independent effect, the cells were also treated with DMSO for the equivalent volumes in parallel.
Three BC cell lines namely MCF-7, BT-474 and SKBR3 plus MCF-10, a breast epithelial line as a control, were obtained from the cell bank in NIGEB and fed with Dulbecco’s Modified Eagle Medium (DMEM) supplemented with 10% FBS and incubated in 37 ℃ and 5% Co .2
Cell culture
We used MTT assay to measure cell viability as a percentage of untreated WT control cells. Briefly, a 5-mg/mL stock of MTT solution in PBS was formed from which 20 µL was added to 80 µL cell medium in each well of 96-well plates and incubated for 4 hrs. The medium was then replaced with 100 µL DMSO for another 30-min shaking-incubation at dark before reading absorbance in 580 nM (excitation) and 620 nM (emission) using an ELISA reader. An average of the produced figures in various doses of AST was used to determine AST effective dose.
Cell treatment
Since acridine orange (AO) co-applied with ethidium bromide (EB) stains nuclear DNA green in live cells and orange in dead cells, we followed the standard co-staining method to measure the percentage of viable SKBR3 cells. Cell groups were
Methods
Cell co-staining and live cell count
Cell death analyses
AST and BC cell apoptosis
Gardaneh, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 72-82 73

suspended at a normal counting concentration from which 50 µL was mixed with 50 µL of the stain in 96-well plates and subjected to counting under fluorescent light. Images were captured using a fluorescence microscope coupled with a Nikon digital camera. Six random microscopic fields per well were selected to count an average of 120 cells counted for each cell group in triplicates (three wells per group). Green cells and orange cells were considered, respectively, as living and dead cells. The data collected from three independent experiments were then expressed as the percentage of living cells by dividing the number of living cells by the number of total cells counted (living + dead).
Bioinformatic analysis of astaxanthin interactions with target molecules
+Three classes of luminal B, HER2 and basal
like/triple negative are considered as the main subtypes in BC. First, we used KEGG (Kyoto Encyclopedia of Genes and Genomes) database to identify molecular pathways involved in BC tumorigenesis. In this database, diseases are considered as induced molecular network systems. The aim of using this database was to reach a common signaling pathway among BC subtypes and, therefore, to reach therapeutic aims and target proteins. The next step was to determine the structure of selected proteins from Protein Data Bank (www.rcsb.org).
In order to prepare protein structures, we used the AutoDockTools software (http://autodock.scripps. edu/resources/adt). We omitted ligands and water molecules from the structure of each protein without deleting cofactors. The AST structure was captured
from Chemspider (http://www.chemspider.com/) and ATB site developed by the University of Queensland, Australia (https://atb.uq.edu.au) was utilized to design and optimize the AST molecular structure. We ultimately examined molecular docking using AutoDockTools. In this procedure, we first converted pdb files of ligands and proteins to pdbqt. Then, we applied the AutoGrid program in order to obtain a map for docking simulation. To do this, after defining proteins and ligands, Grid box in the active site of each protein was adjusted. In the next step, AutoDock was used for simulation using genetic algorithm as the searching parameter. In order to obtain dock scores, the docking protocol used in the study consisted of 200 independent runs along with population size=150 and the Lamarckian genetic algorithm was applied for all docking runs reported in Kcal/mol. Finally, the figures of interactions between AST and the selected proteins were portrayed through Discovery Studio Visualization software.
Reverse transcription (RT) PCR 28
RT-PCR was carried out as reported. Briefly, total RNA was extracted, DNase treated, and used (2µg) for cDNA synthesis. To amplify target DNA fragments, the cDNA samples were first denatured at 95 °C for 2 min before amplification. Table 1 shows the primer pairs we used for each gene candidate. PCR reactions were carried out for 30 cycles consisting of denaturation at 95 °C for 45”, annealing at various temperatures. Gel electrophoresis and band intensity measurements were duplicated as
28reported.
Table 1. Primer sequences for RT-PCR
Accession #Anneal. Temp
FR
FR
FR
FR
FR
FR
FR
FR
FR
TCCTTTGGAAAACCTGCAGA TGCTCTCCACGTTGCACA
CAATTCAGGACCCACACGAC CCTCTGGTCCTGGTATGAAGA
CTTGTGAAGGTCCTTGCCC GAGCCCCATGAAGTTCTCCA
AGGATGTGGACCAACGTGAG GTGCGTTCGATGACAGTGG
CATCAAAGAAGGCTGGCTCC ACGGAGAAGTTGTTTAAGGGG
ATCAGCCCCTTCGAACATCA ACAGGTCAGTCTCCATCAGG
ACATTCAACCCACACAAGAGG TCGAACTTGAATGGTGCTTCG
CCCCTCCTGGCCCCTGTCATCTTCGCAGCGCCTCACAACCTCCGTCAT
GTCTCCTCTGACTTCAACAGCGGTCTCCTCTGACTTCAACAGCG
NM_005228.5
NM_000314.7
NM_000875.5
NM_005163.2
NM_001626.6
NM_002746.3
NM_002745.4
NM_001126118.1
NM_002046
52.2ºC × 20”
53.2ºC × 20”
53ºC × 20”
54.2ºC × 20”
53.8ºC × 60”
52ºC × 20”
53.4ºC × 60”
54.8 ºC × 60”
56ºC × 60”
188
173
225
133
153
172
254
265
130
EGFR
PTEN
IGF1R
AKT1
AKT2
ERK1
ERK2
P53
GAPDH
Primer SequenceName Size (bp)
74 Gardaneh, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 72-82
AST and BC cell apoptosis

where C0 and Ce are, respectively, the initial and
Two carbon nanomaterials were used to combine with AST: graphene oxide (GO) and carboxylated multi-walled carbon nanotube (MWCNT-COOH). Their characteristics were as follows:
The concentration of AST was performed by Unico UV-2100 Model variable-wavelength UV-Vis spectrophotometry. Field emission scanning electron microscope (FESEM) was taken using an MIRA3\\TESCAN-XMU model. Fourier transform infrared spectroscopy (FT-IR) was recorded using KBr tablets on a Thermo Nicolet Nexus 870 FTIR spectrometer.
In order to load AST on nanotubes, 30 mg of GO or MWCNT-COOH was dispersed into 15 mL ethanol containing 100 mg/L of AST for 4 h. The amounts of absorbed AST were calculated as the difference between the initial and final concentrations when the equilibrium was reached. After 4h, the AST concentration in the aqueous solutions was determined by UV-Vis spectroscopy. The adsorption (%) was obtained as follows:
1. MWCNT-COOH: %95 purity, OD: 10-30 nm, Length: 0.5-2 μm, Neutrino Co., Ltd.2. GO nanoplatelets (99%, Thickness 3.4-7 nm with 6-10 Layers).
Combination of astaxanthin and carbon nanomaterials
final concentrations (mg/L) of AST in the aqueous solution.
We measured viability of AST-treated BC cell lines and found that the compound kills the cells at its lethal dose within 5 hours of treatment. Our results showed that IC50s for BT-474, SKBR3 and MCF-7 are, respectively, 36, 37 and 23 µM with no significant effect on normal controls MCF-10 (Figure 1). We also found that the cell death is dose dependent and accelerated beyond a range of the drug dose (Fig. 1B-D).
Data in the figures are represented as the mean ± standard error of the mean (SEM) of three or more separate experiments. Student’s T-test was used to analyze differences between two groups. Differences among three or more groups were analyzed by one-way analysis of variance (ANOVA), followed by a post hoc Duncan Multiple-comparisons Test (P<0.05, statistically significant; P<0.01, highly significant).
Statistical analyses
Morphological changes towards apoptosis post-treatment with astaxanthin
Cell co-staining using acridine orange and ethidium bromide reveals altered morphologies typical of apoptosis among cell samples (Figure 2). Over 29% of SKBR3 cells treated with 36 µM AST
ResultsDeath induction in breast cancer cell lines by
astaxanthin
Figure 1. The effect of astaxanthin on survival of breast cancer cell lines. Each column represents an average of three independent experiment carries out in triplicates. Symbols * and ** indicate statistical differences between each column with its counterpart in
control, whereas symbols # and ## show differences between each column of AST-treated cells and its control treated with DMSO.
Gardaneh, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 72-82 75
AST and BC cell apoptosis

The KEGG database encompasses data of genomics, biological pathways, human diseases, drugs and chemicals (Figure 3.1). The KEGG pathway analysis introduced PI3K/AKT and MAPK/ERK as the common signaling pathways that are actively present in all BC subtypes, hence their targeting can be translated to control all BC subgroups. To perform the docking studies, the following protein structures were captured from Protein Data Bank (PDB): AKT1 (1UNQ) and AKT2 (1O6L) as key proteins involved in the PI3K/AKT pathway, IGFR (5FXS) and EGFR (2RGP) as common receptors involved in cancer development, and ERK1 (4QTB) and ERK2 (3SA0) as principal proteins included in the MAPK/ERK pathway (Figure 3.2).
underwent apoptosis compared to their untreated controls (P<0.05), whereas this rate increased to 46% in the presence of 40 µM AST (P<0.01).
Strong binding between astaxanthin and key intracellular molecules
Following the preparation of ligands and proteins, docking was carried out in order to simulate drug-
Figure 2. Apoptotic death amongst SKBR3 cells treated with two astaxanthin doses. Each column represents an average of
three independent experiments carries out in triplicates by random counting of microscopic fields as detailed in Methods.
Symbols * and ** indicate statistical differences between each column with its control counterpart.
Figure 3.1. The KEGG database representing molecular pathways involved in breast cancer tumorigenesis.
76 Gardaneh, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 72-82
AST and BC cell apoptosis

Altered expression of growth signaling genes in astaxanthin-treated SKBR3 cell line
Simulation by docking showed that the lowest binding energies of AST with AKT1 and AKT2 were -8.49 and -10.69 between, respectively, two amino acids THR160, PHE161 in AKT1and three amino acids GLY235, TYR231 and ASN233 within AKT2. IGF1R with -11.37 and EGFR with -9.48 binding energies form an H bound with AST in, respectively, amino acids VAL1132 and MET766. Finally, AST interaction with ERK1/2 shows binding energies of -10.38 and -11 involving, respectively, amino acids TRY81, ARG84 in ERK1 and THR160, ARG67 in ERK2 (Figure 3). We also tested AST binding to various sites in random within the CD44 receptor protein but did not find favorable binding sites in the receptor structure.
receptors bindings. Table 2 shows the information related to five conformers with the least binding energy for each protein. These results indicate that AST can strongly bind to each of these proteins via their specific amino acid residues, leading to their inhibition.
Changes in mRNA expression of genes involved in growth pathways and tumor suppressor gene PTEN were monitored in SKBR3 cells. As shown in Figure 4, expression of RTKs, EGRF and IGFR, and other cell growth-promoting genes AKT1, AKT2, ERK1 and ERK2 was reduced upon AST treatment of the cells and most of these changes were statistically significant compared to untreated controls (Fig. 4; P<0.01). In contrast, the expression of tumor suppressors p53 and PTEN that promote apoptosis against cell growth, significantly increased upon AST treatment (P<0.01).
Figure 3.2. Astaxanthin reaction with a number of cell growth pathway proteins. See text for details.
Table 2. Binding energy for 5 initial conformers of target proteins.
-8.49
-10.69
-10.38
-11.00
-11.37
-9.48
AKT1
AKT2
ERK1
ERK2
IGF1R
EGFR
Protein Lowest Binding Energy (KCal/mol)Figure 4. Altered expression of key genes under
astaxanthin treatment. The gel image shows RT-PCR products. The intensity of the gel bands was
measured as outlined in Methods to produce the graph. Each column in the graph represents two I
ndependent RT-PCR experiments. Symbols * and ** show statistical differences between each column
and its control counterpart.
Gardaneh, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 72-82 77
AST and BC cell apoptosis

After producing our nano-drugs, cancer cell lines
On this basis, the adsorption percentage by GO and MWCNT-COOH was calculated to be 68% and 93%, respectively. This shows that MWCNT-COOH has significantly adsorbed AST in comparison to GO. Since AST is an almost non-polar molecule, π-π interactions play important roles in its adsorption process. On the other hand, the abundant polar groups in GO cause less adsorption of GO than MWCNT-COOH.
Acceleration of SKBR3 cell death using nano-astaxanthin
Figure 5 shows Field Emission Scanning Electron Microscope (FESEM) images and Fourier Transform InfraRed (FT-IR) spectroscopy of GO and MWCNT-COOH. FESEM images of GO and MWCNT-COOH were presented in Figure 5A. It is evident from these images that GO sheets illustrate the sheet-like structure with large thickness, smooth surface, and wrinkled edge. In addition, FESEM image of MWCNT-COOH shows that MWCNTs are curved, rope-like and highly tangled and agglomerated with each other. These results clearly confirm the morphology of MWCNT-COOH and GO.
The chemical structures of GO and MWCNT-COOH were determined by FT-IR analysis as presented in Figure 5B. In this figure, the peaks at 1700-1735 (C=O) and 1000-1200 (C-O) cm-1 are assigned to the C=O stretching vibration and C-O stretching mode which clearly shows carboxylic groups on the MWCNT-COOH and GO. In addition, the absorption peaks at 3300-3500 and 1500-1640 cm-1 obviously indicating stretching vibration of hydroxyl groups and the C=C vibration, respectively. These results show that plenty of hydroxyl and carboxyl groups were located on both carbon materials, particularly on GO.
SKBR3 and MCF-7 were treated, respectively, with 20 and 24 µM AST alone or nano-AST compounds. As shown in Fig. (5C), the percentage of the cells killed by GO-AST was comparable to the percentage of those killed by AST alone. However, the combination of AST+MWCNT-COOH accelerated cell death in both lines so that the difference with those under AST alone became significant (Figure 5C; P<0.05). Also, MCF-7 cells suffered more death than SKBR3 lines after treatment with AST+ MWCNT-COOH (P<0.05).
The strong binding of AST to key RTKs and downstream molecules also indicates the unexplored anti-neoplastic capacity of the photochemical compound. Overexpression or dysfunction of EGFR
DiscussionIn this study, we showed that AST significantly
reduces viability and induces apoptosis in three different BC cell lines. Based on the levels of HER2
29we have previously detected in these cell lines , it is conceivable from our current data that AST impact on cell survival might conversely correlate with HER2 content.
According to the KEGG database, several key molecules are involved in the cells’ survival and growth; therefore, among them, we selected EGFR, IGF1R, AKT, ERK1/2, and PTEN for analysis. Our data in silico indicated strong binding of AST to these molecules. These observations primarily suggest that although HER2 is a determinant receptor in cancer cell growth, AST binding to alternative molecules on the row may eventually overcome HER2 pro-growth function by providing a bypassing route toward disruption of growth signals. This might explain the reduced levels of viability among HER2-amplifying BC cell lines upon receiving higher doses of AST.
Figure 5. Acceleration of BC cell death treated with nano-astaxanthin compounds. The two images on the left show electron microscopy and adsorption spectroscopy, respectively. The right graph shows survival of treated BC cells. Each column
represents an average of three independent experiments carried out in triplicates by random counting of microscopic fields as detailed in Methods. Symbols * and ** indicate statistical differences between each column with its control counterpart, whereas symbol ‡ shows difference between nano-AST and AST alone and symbol # shows differences between nano-AST
and nano particle control.
78 Gardaneh, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 72-82
AST and BC cell apoptosis

(HER1 in humans) due to mutations plays a role in 30
tumorigenesis. Ligand binding can activate EGFR 31molecules to homo- or hetero-dimerize with HER2
or another EGFR member and these changes induce EGFR auto-phosphorylation in several of its tyrosine residues. These changes initiate downstream signaling pathways including MAPK, AKT and JNK,
32leading to DNA synthesis and cell proliferation plus cell migration. Conversely, inhibition of EGFR signaling may inhibit tumor formation or growth. Inhibitors of the EGFR oncogene have been developed against various cancer types that include several small molecules and antibodies e.g. gefitinib. However, the use of these therapeutics is likely to cause resistance in cancer cells through increasing
33the activity of key molecules such as STAT3.
In addition to inhibitory binding to key molecules of the common cell growth pathways, AST treatment also induced mRNA expression of p53 in our SKBR3
37,38 cells. Similar to hepatoma and colon cancer. AST-mediated dose-dependent induction of phospho-p53 leading to induced cell cycle arrest and enhanced apoptosis has been shown in BC lines MCF-7 with wild-type p53 and MDA-MB-231 that carries mutant
39p53. P53 can act as both an oncogene and a tumor suppressor so that its mutations are largely translated to tumor aggression, whereas its restoration leads to tumor regression. AST-mediated induction of p53 expression adds to the multitarget potential of the carotenoid against tumorigenesis, with its therapeutic benefits exceeding those of the anti-cancer
40dexamethasone. An extension of our study would examine how changes in p53 mRNA levels correlate with alterations in protein levels and activity.
We showed that beside EGFR, AST also strongly binds the insulin-like growth factor 1 (IGF-1) receptor (IGF1R). This receptor promotes cell growth by interacting IGF-1 and IGF-2, and IGF1R amplification and/or overexpression has implications in chemo- and radio-resistance and metastasis in
34,35several cancer types including BC. Indeed, triple-negative BC (TNBC) cells overexpress IGF1R at considerable levels, leading to elevated proliferation,
36 aggressive subtypes, and survival of all TNBCs.Cross-talks between EGFR and IGF1R prevent EGFR inhibitors from activity and so allow EGFR signaling to resume in the presence of these inhibitors. Our analysis in silico indicated that AST can strongly bind to a number of amino acid residues in these molecules. Simultaneous inhibition of EGFR and IGF1R by AST indicates the potential of the compound in blocking EGFR-IGF1R cross-talks and bypassing drug resistance caused upon utilizing inhibitors. Therefore, the anti-tumorigenic potency of the compound can be explored along with chemical inhibitors or chemotherapy drugs against BC.
Astaxanthin further downregulated the expression of Phosphatase and Tensin Homolog (PTEN). The
In conclusion, our in silico experiments showed that AST promotes induction of apoptotic cell death by interactions with key genes of tumorigenesis. When combined with nanotubes, the cell death rate amongst cancer cells increases significantly, an important development in breaking drug resistance in BC tumors. These anti-tumorigenic effects of AST provide a glimpse of a global picture of the effect of phytochemicals on BC therapy and/or prevention. Animal studies focusing on AST and nano-AST-mediated changes in expression of tumor suppressors, RTKs and growth pathway molecules as well as AST interactions with anti-metastatic miRNAs will consolidate our findings in the actual tumor cells and tumor microenvironment and assess AST utilities against tumor chemoresistance and metastasis in combined modes of clinical BC therapy.
AcknowledgementThis study was funded by a grant (541) from
National Institute of Genetic Engineering and
PTEN interacts with p53 to regulate EMT and cell 46 migration. Our study on SKBR3 cells showed that
AST induces p53 expression and, in parallel, restores lost levels of PTEN. In vivo studies using patient-derived xenograft HER2 models of BC similar to
29what we have developed before could provide deeper insights into the ultimate impact of PTEN-
+p53 co-induction by AST on HER2 BC tumor growth and outcome.
PTEN tumor suppressor gene, via its phosphatase activity, plays a role in cell cycle regulation and
41prevents cells from overgrowth and rapid division. The phosphatase activity of PTEN preferentially dephosphorylates PIP3 and so results in the inhibition of the AKT/PKB signaling pathway that regulates
42,43 cell growth, survival, and migration. Conversely, PTEN mutations contribute to the development of many cancers, with loss of PTEN tumor suppressor commonly occurring in human cancer particularly in
44prostate cancer and reduction of its expression in 45
BC. These add to the importance of PTEN induction by AST as an anti-tumor measure.
In fact, combined versus individual disruption of p53 and PTEN induces TNBC growth with clear activating impact on PI3K/AKT signaling, changes that lead to distinct mesenchymal features and poor
47clinical outcome. Compared to the wild-type p53
48expressed in MCF-7 , MDA-MB-231 carries mutant p53, which confers survival advantage to the
49TNBC cell line by suppressing apoptosis. Due to these differences, higher doses of AST are needed to
39kill MDA-MB-231 cells. If applied in TNBC line MDA-MB-231 and therapy-resistant TNBC tumor models carrying either wild-type or mutant p53, our in silico strategy might shed more light on the impact of PTEN-p53 interactions, upon AST treatment, on cancer cell growth and ultimately on tumor fate.
Gardaneh, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 72-82 79
AST and BC cell apoptosis

Biotechnology (NIGEB) in Tehran, Iran. The authors thank all colleagues and students who assisted us in completing this study.
The authors declare no conflict of interest.
6. Bagchi D, Garg A, Krohn RL, Bagchi M, Tran MX, Stohs SJ. Oxygen free radical scavenging abilities of vitamins C, E, β-carotene, pycnogenol, grape seed proanthocyanidin extract and astaxanthins in vitro. Res Commun Mol Pathol Pharmacol. 2001; 95:179-189
12. Onogi N, Okuno M, Matsushima‐Nishiwaki R, Fukutomi Y, Moriwaki H, Muto Y, Kojima S. Antiproliferative effect of carotenoids on human colon cancer cells without conversion to retinoic acid. Nutr Cancer. 1998; 32:20-24
8. Bates C, Van Dam C, Horrobin DF, Morse N, Huang YS, Manku MS. Plasma essential fatty acids in pure and mixed-race American Indians on and off a diet exceptionally rich in salmon. Prostaglandins Leukot Med. 1985; 17:77-84
2. Chuthapisith S, Eremin J, El-Sheemey M, Eremin O. Breast cancer chemoresistance: emerging importance of cancer stem cells. Surg Oncol. 2009; 19:27-32
5 . Guer in M, Hunt ley ME, Ola izo la M. Haematococcus astaxanthin: applications for human health and nutrition. Trends Biotechnol. 2003; 21:210-216
13. Ni X, Yu H, Wang S, Zhang C, & Shen S.
10. Kim HW, Park JS, Chew BP. B-carotene and astaxanthin inhibit mammary tumor cell growth and induce apoptosis in mice in vitro FASEB J. 2001; 15:298-298
4. Wang P, Li H, Yang YJ, Wang L, Lee SC. Overcome Cancer Cell Drug Resistance Using Natural Products. Evidence-Based Complement Alternat Med. 2015; 767136.
References1. Zheng HC. The molecular mechanisms of
chemoresistance in cancers. Oncotarget. 2017; 8:59950-59964, doi:10.18632/oncotarget.19048
3. Turrini E, Ferruzzi L, Fimognari C. Natural compounds to overcome cancer chemoresistance: toxicological and clinical issues. Expert Opin Drug Metab Toxicol. 2014; 10:1677-90.
7. Naguib YM. Antioxidant activities of astaxanthin and related carotenoids. Agri Food Chem. 2000; 48:1150-1154
9. Sun S, Gross MD, Iijima K, Jyonouchi H. Anti-tumor activity of astaxanthin on Meth-A tumor cells and its mode of action. FASEB J. 1998; 12:966-966
11. Kozuki Y, Miura Y, Yagasaki K. Inhibitory effects of carotenoids on the invasion of rat ascites hepatoma cells in culture. Cancer Lett. 2000; 151:111-115
Conflict of Interest
22. Kim YJ, Kim YA, Yokozawa T. Protection against oxidative stress, inflammation, and apoptosis of high-glucose-exposed proximal tubular epithelial cells by astaxanthin. J Agric Food Chem. 2009; 57:8793-8797
23. Kavitha K, Kowshik J, Kishore TK, Baba AB, Nagini S. Astaxanthin inhibits NF-κB and Wnt/β-catenin signaling pathways via inactivation of Erk/MAPK and PI3K/Akt to induce intrinsic apoptosis in a hamster model of oral cancer. Biochimica et Biophysica Acta (BBA) - General Subjects. 2013; 1830:4433-4444
16. Zhang X, Zhao WE, Hu L, Zhao L, Huang J. Carotenoids inhibit proliferation and regulate expression of peroxisome proliferators-activated receptor gamma (PPARgamma) in K562 cancer cells. Arch Biochem Biophys. 2011; 512:96–106
14. Lyons NM, O'Brien NM. Modulatory effects of an algal extract containing astaxanthin on UVA-irradiated cells in culture. J Dermatol Sci. 2002; 30:73-84
Astaxanthin Inhibits PC-3 Xenograft Prostate Tumor Growth in Nude Mice. Mar Drugs. 2017; 15:66
18. Dong LY, Jin J, Lu G, Kang XL. Astaxanthin attenuates the apoptosis of retinal ganglion cells in db/db mice by inhibition of oxidative stress. Marine Drugs. 2013; 11:960-974
17. Song XD, Zhang JJ, Wang MR, Liu WB, Gu XB, Lv CJ. Astaxanthin induces mitochondria-mediated apoptosis in rat hepatocellular carcinoma CBRH-7919 cells. Bullet Pharmaceut Bullet. 2011; 34:839-844
19. Song X, Wang B, Lin S, Jing L, Mao C, Xu P, Lv C, Liu W, Zuo J. Astaxanthin inhibits apoptosis in alveolar epithelial cells type II in vivo and in vitro through the ROS‐dependent mitochondrial signaling pathway. J Cell Mol Med. 2014; 18:2198-2212
15. Franceschelli S, Pesce M, Ferrone A, de Lutiis MA, Patruno A, Grilli A, et al. Astaxanthin treatment confers protection against oxidative s t r ess in U937 ce l l s s t imula ted wi th lipopolysaccharide reducing O2- production. PLoS ONE, 2014; 9:e88359.
20. Hama S, Takahashi K, Inai Y, Sakamoto R, Yamada A, Tsuchiya H, Kanamura K, Yamashita E, Kogure K. Protective effects of topical application of a poorly soluble antioxidant as taxanthin l iposomal formulat ion on ultraviolet-induced skin damage. J Pharmacol Sci. 2012; 101(8):2909-16
21. Ye Q, Huang B, Zhang X, Zhu Y, Chen X. Astaxanthin protects against MPP+-induced oxidative stress in PC12 cells via the HO-1/NOX2 axis. BMC Neurosci. 2012; 13:156
24. Nagendraprabhu P, Sudhandiran G. Astaxanthin inhibits tumor invasion by decreasing extracellular
80 Gardaneh, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 72-82
AST and BC cell apoptosis

25. Yasui Y, Hosokawa M, Mikami N, Miyashita K, Tanaka T. Dietary astaxanthin inhibits colitis and colitis-associated colon carcinogenesis in mice via modulation of the inflammatory cytokines. Chem Biol Interact. 2011; 193:79-87
31. Wieduwilt MJ, Moasser MM. The epidermal growth factor receptor family: biology driving targeted therapeutics. Cell Mol Life Sci. 2008; 65(10):1566-84
35. Brahmkhatri VP, Prasanna C, Atreya HS. Insulin-like growth factor system in cancer: novel targeted therapies. Biomed Res Int. 2015; 538019
29. Gardaneh M, Shojaei S, Kaviani A, Behnam B. GDNF induces RET-SRC-HER2-dependent growth in trastuzumab-sensitive but SRC- independent growth in resistant breast tumor cel ls . Breast Cancer Res Treat . 2017; 162(2):231-241
33. Wen W, Wu J, Liu L, Tian Y, Buettner R, Hsieh MY, Home D, Dellinger TH, Han ES,Jove R, Yim JH. Synergistic anti-tumor effect of combined inhibition of EGFR and JAK/STAT3 pathways in human ovarian cancer Mol Cancer. 2015; 14(1):100
26. McCall B, McPartland CK, Moore R, Frank-Kamenetskii A, Booth BW. Effects of Astaxanthin on the Proliferation and Migration of Breast Cancer Cells In Vitro. Antioxidants (Basel). 2018; 7(10):135
27. Kim HY, Kim YM, Hong S. Astaxanthin suppresses the metastasis of colon cancer by inhibiting the MYC-mediated downregulation of microRNA-29a-3p and microRNA-200a. Sci Rep. 2019; 9(1):9457
matrix production and induces apoptosis in experimental rat colon carcinogenesis by modulating the expressions of ERK-2, NFkB and COX-2. Invest New Drugs. 2011; 29:207-224
28. Gardaneh M, Gholami M, Maghsoudi N. Synergy between glutathione peroxidase-1 and astrocytic growth factors suppresses free radical generation and protects dopaminergic neurons against 6-Hydroxydopamine. Rejuven Res. 2011; 14:195-204
30. Zhang H, Berezov A, Wang Q, Zhang G, Drebin J, Murali R, Greene MI. ErbB receptors: from oncogenes to targeted cancer treatment. J Clin Invest. 2007; 117:2051–8
32. Oda K, Matsuoka Y, Funahashi A, Kitano H. A comprehensive pathway map of epidermal growth factor receptor signaling. Mol Systems Biol. 2005; 1:2005.0010
34. Denduluri SK, Idowu O, Wang Z, Liao Z, Yan Z, Mohammed MK, Ye J, Wei Q, Wang J, Zhao L, Luu HH. Isulin-like growth factor (IGF) signaling in tumorigenesis and the development of cancer drug resistance. Genes Dis. 2015; 2(1):13-25, 2015
42. Leslie NR, Downes CP. PTEN function: how normal cells control it and tumour cells lose it. Biochem J. 2004; 382(Pt 1):1-11
36. Soljic M, Mrklic I, Tomic S, Omrcen T, Sutalo N, Bevanda M, Vrdoljak E. Prognostic value of vitamin D receptor and insulin-like growth factor receptor 1 expression in triple-negative breast cancer. J Clin Pathol. 2018; 71(1):34-9
37. Liu X, Song M, Gao Z, Cai X, Dixon W, Chen X, Cao Y, Xiao H. Stereoisomers of astaxanthin inhibit human colon cancer cell growth by inducing G2/M cell cycle arrest and apoptosis. J Agr Food Chem. 2016; 64(41):7750-7759
38. Messina CM, Manuguerra S, Renda G, Santulli A. Biotechnological Applications for the Sustainable Use of Marine By-products: In Vitro Antioxidant and Pro-apoptotic Effects of Astaxanthin Extracted with Supercritical CO 2 from Parapeneus longirostris. Marine Biotech. 2019; 1-12.
39. Sowmya PR, Arathi BP, Vijay K, Baskaran V, Lakshminarayana R. Astaxanthin from shrimp efficiently modulates oxidative stress and allied cell death progression in MCF-7 cells treated synergistically with beta-carotene and lutein from greens. Food Chem Toxicol. 2017; 106(Pt A):58-69
40. Wang M, Zhang J, Song X, Liu W, Zhang L, Wang X, Lv C. Astaxanthin ameliorates lung fibrosis in vivo and in vitro by preventing transdifferentiation, inhibiting proliferation, and promoting apoptosis of activated cells. Food Chem Toxicol. 2013; 56:450–458
47. Liu JC, Voisin V, Wang S, Wang DY, Jones RA, Datti A, Uehling D, Al-awar R, Egan SE, Bader GD, Tsao M, Mak TW, Zacksenhaus E. Combined deletion of Pten and p53 in mammary epithelium accelerates triple-negative breast
41. Jerde TJ. Phosphatase and tensin homologue: novel regulation by developmental signaling J Sign Transduct. 2015; 282567.
43. Hopkins BD, Hodakoski C, Barrows D, Mense SM & Parsons, RE. PTEN function: the long and the short of it. Trends Biochem Sci. 2014; 39(4):183-90
44. Jamaspishvili T, Berman DM, Ross AE, Scher HI, De Marzo AM, Squire JA, Lotan TL. Clinical implications of PTEN loss in prostate cancer. Nat Rev Urol. 2018; 15(4):222-234
45. Zhang HY, Liang F, Jia ZL, Song ST & Jiang ZF. PTEN mutation, methylation and expression in breast cancer patients. Oncol Lett. 2013; 6(1):161-168
46. Martin P, Liu YN, Pierce R, Abou-Kheir W, Casey O, Seng V, Camacho D, Simpson RM, Kelly K. Prostate epithelial Pten/TP53 loss leads to transformation of multipotential progenitors and epithelial to mesenchymal transition. Am J Pathol. 2011; 179(1):422–435
Gardaneh, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 72-82 81
AST and BC cell apoptosis

epithelium accelerates triple-negative breast cancer with dependency on eEF2K. EMBO Mol Med. 2014; 6(12):1542–1560
48. Lu X, Errington J, Curtin NJ, Lunec J, Newell DR. The impact of p53 status on cellular sensitivity to antifolate drugs. Clin Cancer Res. 2001; 7:2114–2123
49. Hui L, Zheng Y, Yan Y, Bargonetti J, Foster DA. Mutant p53 in MDA-MB-231 breast cancer cells is stabilized by elevated phospholipase D activity and contributes to survival signals generated by phospholipase D. Oncogene. 2006; 25:7305–10
82 Gardaneh, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 72-82
AST and BC cell apoptosis

ations about cancer. Physicians, the media, and patients and their families use descriptive language and metaphors to express and convey the impact and experience of the disease. Conceptual metaphors play an important role in understanding the different aspects of emotional concepts when it is difficult to
4express them. Sontag in his book diseases and metaphors suggested that cancer metaphors emerged under the influence of military metaphors. Expressions like alien cells attack the body, defensive defects, surgery, radiography, chemotherapy, attack and counter-attack are examples of the effects of
5 military metaphors on cancer metaphors. This may be why the metaphors used in most cases have a harsh and scary nature which create a sense of fear of cancer. Thus, understanding military metaphors are effective in our awareness of breast cancer metaphors. Examples of these metaphors have been seen in published articles on breast cancer including the following: "Women who are survivors of breast
IntroductionBreast cancer has a long history as a disease in
civilized society and medical science. However, women avoid talking about it with their families, but this issue has attracted much attention in the past 25
1,2year. Cancer can change almost every aspect of a person's life. Analysis of how patients talk about themselves and how they feel is especially important
3in raising awareness among these patients. Research shows dissatisfaction of many breast cancer patients with the way in which words are used to describe it in the process of treatment. Images and metaphors are generally used in health community in communic-
ARTICLE INFO
Methods: This study investigated metaphors associated with breast cancer using data from SID, magiran, and noormags databases.
Results: The results showed that a number of medical concepts of cancer are expressed using conceptual metaphors, and that Persian speakers use different metaphors to express medical concepts related to breast cancer, such as "breast cancer is bad", "breast cancer results in an inactive life", and so on. These metaphors can have both positive and negative effects on common perceptions of breast cancer. The use of metaphors to address diseases, especially breast cancer, can cause feelings of fear and phobia among patients directly or indirectly, leading to a lack of timely referral for early treatment, fear of stigma or loneliness and death.
Conclusion: The findings of this research can inform experts, researchers and doctors that the use of words can be both curative and destructive. Thus, they should consider this issue in their careers and statements.
Background: Specialists, researchers, patients, and even their families use metaphors to describe diseases. Metaphors are known to be central tools in both communication and thinking. Crucially, even though many metaphors become conventionalized, metaphor choices are seldom neutral.
18 May 2020Accepted:
conceptual metaphors, breast cancer phobia
Key words:Breast cancer,
28 April 2020Received:
Revised:
10 May 2020
Address for correspondence: Malahat Shabani MinaabadAssistant Professor of Linguistics,Address: Department of Linguistics, Payame Noor University, PO BOX 19395-3697 Tehran, Iran.Email: [email protected]
83Shabani Minaabad, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 83-87
ABSTRACT
The Role and Application of Metaphor in Preventing Breast Cancer Phobia
a Department of Linguistics, Payame Noor University, Tehran, Iran
aMalahat Shabani Minaabad*
Open AccessShort communication
DOI: 10.19187/abc.20207283-87

cancer sometimes feel they have lost their femininity", written in an article about women with breast cancer. This reveals several metaphors for the readers instilling fear and panic in them about breast cancer. According to research, the word cancer is the
6most terrifying word for people among the diseases. Research have shown that metaphors can affect people's emotions, creating anxiety and fear which in turn interfere with proper treatment. Thus, care must be taken by doctors and experts in the use of words and metaphors if treatment is going to work for cancer patients, especially those suffering from breast
7cancer. Ever since the book Illness as Metaphor was published by Sontag, there has been a good deal of empirical and theoretical research on the role of metaphors in disease especially cancer all around the world. However, the effect of metaphors on fear of cancer has not received enough attention in Iran.
Lakoff and Johnson in 1980 initiated a new strand of research on metaphors by publishing their seminal work Illness and Metaphor. They developed a conceptual metaphor theory (CMT) in which conceptual metaphors include cognitive maps or a set of domains of dominant goals, most of which are subjective, abstract and complex, and less well-thought-out. Taking advantage of these metaphors, doctors can easily express their own complex emotional feelings and experiences. Medical language experts believe that the language of medicine has little clarity as medicine is not just a science, but rather science mixed with art influenced
4 by emotions and many abstract variables. Emotional experiences can hardly be expressed precisely in scientific language, so it is these metaphors that connect new emotional experiences to old ones and help us understand the complex pattern of emotions. Therefore, medical professionals widely use conceptual metaphors to make communication easier. These metaphors are often used with euphemisms for a dangerous situation. For example, the aim of a study published in 2008 was described as follows: the paper aims to investigate the relationship between HER2 / neu, p53, ER and PR genes with survival rate in patients with breast cancer
2in Mashhad. As can be seen, the metaphor survival used in the study is a military conceptual metaphor. Here survival depicts cancer as a battlefield or war for the individual. In the literature on breast cancer, malignant and benign have been widely used, which apparently divides cancer patients into bad and good. This necessitates attention to metaphors used in medical articles and discourses especially in the case of breast cancer. Thus, the present research aimed to examine the metaphors used for cancer, especially breast cancer. Specifically, the role and application of metaphors in creating fear and panic regarding breast cancer will be investigated. The aim of this study is to draw researchers and specialists' attention as well as that of the public to potential emotional
1. The full texts of the articles were available. 2. The journals were approved by Iran Ministry of Health.3.Journals publishing articles only on breast diseases and cancer.
Exclusion criteria1. Lack of access to the full text of the articles 2. Specialized scientific journals or journals that did not have scientific approval from the Ministry of Health or the Ministry of Science.
ResultsIn this study, 10 articles were randomly selected
from the articles published in breast cancer journals
In this research, Pragglejaz Metaphor Identifica-tion Procedure (MIP) (2007) was used to identify
8words or phrases used metaphorically in the text. The entire article was first scanned to gain an overview of the entire text of the reviewed article. The target units or words within the whole text were determined. In this study, words such as breast cancer, breast metastasis, etc. were used to identify potential metaphors. Every word or metaphor found in the text was then examined to determine its meaning along with its metaphorical meaning in other texts. In this research, words such as invasive treatments, survival etc. were found to have other meanings such as conflict, aggression, and war. Finally, the metaphors were found and listed.
(b) perceptions of breast cancer (c) factors contributing to the wide application of a metaphor
MethodsTo collect data, metaphors used in breast cancer
articles were studied. Research articles were examined to find conceptual metaphors associated with cancer. The researcher looked for key words like breast cancer, cancer, invasive treatments for breast disease, metastasis, chemotherapy for breast cancer, mastectomy and radiation therapy for breast cancer. Investigation of all texts required an enormous amount of time, so the number of key words was reduced to make data collection manageable. The metaphors found in the research articles are listed in Table 1. Inclusion and exclusion criteria for the articles under investigation were as follows:
Inclusion criteria
effects of words on people and creating fears in individuals and society. The question raised in this research is as follows:
1. What does the use of cancer metaphors in contemporary Persian reveal about?
(a) dominant views on the phenomena that are most frequently described as breast cancers
Metaphors in BC phobia
84 Shabani Minaabad, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 83-87

Breast cancer is invasiveIn sentences containing these metaphors, cancer is
seen as an enemy, or a wild beast that intends to invade and attack individuals. This metaphor depicts the feeling of fear and stress caused by the attack of an attacker in people. This invader is sometimes the breast cancer itself, sometimes a tissue specialist or a doctor, sometimes chemotherapy or radiation therapy. For example, the following sentence is an example of
9, 10,11this metaphor : "Postoperative pathology may be similar to the initial pathology report or may be more severe and even invasive cancer".
Breast cancer threatens the lives of all human
from magiran, Sid, and noormags databases and searched for metaphors and words associated with breast cancer. Table 1 presents the specifications of the articles and the number of metaphors and then summarizes the metaphors and words found.
The following metaphors were found in the articles reviewed:
Breast cancer destroys the sense of femininityIn the sentences containing this metaphor, it is
stated that women who suffer from breast cancer lose part of their femininity or all of their senses and sometimes have marital problems. The following is an example of this:
Breast cancer causes a person to feel amputated by losing one or both breasts. This lack of an organ in
In sentences containing this metaphor, cancer is considered as an entity or an object that seeks to kill all members of human society. According to this metaphor, no one is safe from the risk of being killed by breast cancer anywhere and under any circumstances. The following is an example of this:
beings
Despite many advances in medical science and the development of human knowledge in the prevention and treatment of various diseases, cancer is still the most serious disease that unfortunately threatens the lives of many people and the risk of catching it exists for a large number of people from
12human society.
Table 1. Reseach articles reviewed in the present study
F1-score
8
6
4
8
6
4
10
5
11
6
Article information
Seyed Nouri T, Zahmatkash T, Molayi T, Akbari P, Haghi Z, Mohseni Azad P. Assessment the Risk of breast
cancer using Gail model. Iranian Journal of Breast Disease Research.2009;1(2):53-57.
Yazdani F. The effects of yoga on function scales quality of life in women with breast cancer undergoing
radiation therapy: A randomized clinical trial. Avicenna Journal of Nursing and Midwifery Care. 2015;23(1):
49-62.
Najafi R, Amiri F, Roshnayi G, Abbasi M, Razi M. Factors Affecting Survival in Patients with Breast
Cancer in Hamedan Province from 2001 to 2018. Iranian Journal Breast Disease Research. 2019; 12 (4) :31-
38.
Abbasi, Zahra, and Mojgan Karbakhsh. Re: Delivering Bad News: When My Patient Was My Own Mother.
Archives of Breast Cancer (2019): 47-48.
Mohammadpour M, Yaseri M, Mahmoudi M, Entezar Mahdi R. Estimation of Survival in Women
Diagnosed with Breast Cancer with Cure Survival in West-Azerbaijan and East-Azerbaijan Provinces.
Scientific Journal of School of Public Health and Institute of Public Health Research . 2018; 16 (1) :63-74
Ghasemi M, Raeisi S, Aslani M. Study of BATF2 gene expression in breast cancer samples and association
with clinical factors and patient survival. Iranian Journal of Obstetrics, Gynecology and Infertility, 2020.
Hosseini Seyedeh M, Khaledifar B. Quality of life, pain and acceptance of treatment in women with breast
cancer in stages 1 and 2 in Chaharmahal and Bakhtiari province. Iranian Journal of Breast Disease Research.
2013; 6 (4) : 52-59
Ahmadzadeh, Laya, Maryam Vaezi, Sheida Sodagar, and Gholam Reza Golmohammad Nazhad. The Effect
of Acceptance and Commitment Therapy Adopted for Couples Compared with Integrative Couple Therapy
on Marital Conflicts of Couples with Breast Cancer. Iranian Quarterly Journal of Breast Disease.2019; 12
(3):47-54
Dehghani S, Salimi M, Nikonahad Lotfabadi N.Evaluation of anti-tumor effect of chemical compound [N-
'((5-nitrothiophen-2-YL) methylene)-2(phenylthio)benzohydrazide] in mouse model of breast cancer.
Journal of Cellular and Molecular Research (Iranian Journal of Biology), 2019; 32 (2): 205-215.
Hosseini M, Mellati A, Mousavi S, Moghimi M, Ramezani A. Relation between Proteome of Women with
Invasive Ductal Breast Cancer and Body Mass Index.Journal of Zanjan University of Medical Sciences &
Health Services. 2017; 25 (109) :74-84
85Shabani Minaabad, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 83-87
Metaphors in BC phobia

In such metaphors, it is suggested that people with breast cancer become stagnant or inactive in their lives, jobs and so on. In these metaphors and words, people are told that they will suffer from some kind of physical disability following breast cancer and surgeries such as breast resection (mastectomy), which in turn causes fear and panic about breast cancer. The following is an example of this metaphor: Breast cancer has caused a passive life in people.
Specialists, doctors and researchers working in the field of health and treatment of patients with breast cancer use metaphors to make unfamiliar and abstract concepts available to the general public. These metaphors actually act as frames where words take on meaning. According to many studies, the use of words has an emotional and cognitive load affecting people's mental health and well-being. Some studies have shown that metaphors used in texts about cancer can express different aspects of the
4disease and the experience of patients. In this study, it was found that the use of words associated with breast cancer can cause negative feelings and interference with the treatment, creating fear and phobia. In a study conducted to investigate the effectiveness of metaphorical therapy on people's irrational beliefs, the findings showed that metaphorical therapy could neutralize a patient's reactions without raising his or her anxiety and inform the patient through awareness or help to reconstruct the conditions and in some way use
13cognitive reconstruction. In fact, metaphors somehow create a false and irrational beliefs that form the basis of people's ideas about cancer in general and breast cancer in particular. Due to the use
Breast cancer is synonymous to a passive lifestyle
Discussion
women causes a change in their mental image, a decreased sense of femininity, a decreased sense of attraction specially sexual attraction as well as anxiety, depression, arousal, embarrassment, accompanied by fear of relapse, the thought of rejection and thoughts of death. With these words or metaphors, the person feels that with surgeries such as breast removal, she can no longer be like the person in the past to her spouse. In this case, the fear will overcome the person with the diagnosis of breast cancer, leading to actions such as rejecting treatment and surgery, denial of the disease and so on.
The study revealed that cancer is used as a metaphor in Persian. It also revealed that the use of metaphors associated with breast cancer is of particular importance in terms of their semantic load and their ability to create certain feelings and emotions in people. It was also found that metaphors associated with breast cancer have a wide use. The results of this research are in accordance with the
4-6, 10-15results reported by previous results.
of these metaphors and words, doctors and researchers have reconstructed people's cognitive and emotional beliefs about breast cancer. Another study found that metaphors gave rise to culturally appropriate treatment methods in individuals, which in turn alter emotional beliefs by reducing depression
14and increasing resilience in individuals. Therefore, it can be said that by reconstructing and paying attention to people's metaphors, it is possible to increase people's adaptability and, self-esteem in
15dealing with diseases. The findings of this study are informative in that they provide insight to experts and researchers when reporting their research findings on breast cancer in articles and conversations with patients and their families. Conducting experimental research in the future can focus on the effect of metaphorical therapy on reducing anxiety and fear among people with breast cancer.
References
3. Kennifer SL, Alexander SC, Pollak KI, Jeffreys AS, Olsen MK, Rodriguez KL, Arnold RM, Tulsky JA. Negative emotions in cancer care: Do oncologists' responses depend on severity and type of emotion? Patient Education Counseling. 2009;76(1):51–56.
7. Potts A, Semino E. Cancer as a Metaphor. Metaphor and Symbol. 2019 Apr 3;34(2):81-95.
9. Mohammadpour M, Yaseri M, Mahmoudi M, Entezar Mahdi R. Estimation of Survival in Women Diagnosed with Breast Cancer with Cure Survival in West-Azerbaijan and East-Azerbaijan Provinces. sjsph. 2018; 16 (1) :63-74.
10. Ghasemi, Mohammad, Raeisi, Somayeh, Aslani, Mojgan. Study of BATF2 gene expression in breast cancer samples and its association with clinical factors and patient survival rate. Iranian
2. Moradi M, Homayi Shandiz F, Shamsian A A, Eftekharzadeh M I, Hedayati M M, Bidkhoori H. The relationship between HER2 / neu and p53 genes and estrogen and progesterone receptors with survival rates in Iranian women with breast cancer. Iranian Journal of Breast Disease Research. 2008; 1 (2): 7-17.
4. Wahhabis M, Izadifar R. The use of metaphor in the expression of cancer. Comparative Linguistics Research, 2019; 9 (18): 207-224.
5. Sontag, S. Illness and its metaphors and AIDS and its metaphors. 1979, London: Penguin Books.
6. Altmann C. To use a metaphor at a time like this would be obscene": a study of cancer, poetry and metaphor. Colloquy: text theory critique. 2008 ;15:7-35.
8. Pragglejaz Group . MIP: A method for identifying metaphorically used words in discourse. Metaphor and symbol,2007, 22(1), 1-40.
1. Adams, J. 2010. Motivational narratives of assessments of the body after cosmetic surgery. Qualitative Health Research, 20(6): 755–67.
86 Shabani Minaabad, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 83-87
Metaphors in BC phobia

11. Hosseini M, Mellati A, Mousavi S, Moghimi M, Ramezani A. Relation between Proteome of Women with Invasive Ductal Breast Cancer and Body Mass Index. J Adv Med Biomed Res. 2017; 25 (109) :74-84.
12. Dehghani S, Salimi M, Nikonadel Tatefabadi, N. Evaluation of the anti-tumor effect of chemical compound N ((Five-Nitrothiophene-2- (YL Methylene) -2 (Phenylthio) benzohydride in breast cancer mouse model. Journal of Cellular and Molecular Research (Iranian Journal of Biology), 2020; 32 (2): 205-215 .
Journal of Obstetrics, Gynecology and Infertility, 2020; (24): 1-18.
14. Ghamari Kivi H, Rezaii Sharif A, Esmaeli Ghazi Valoii F. The Effectiveness of Metaphorical Cognit ive and Behavioral Therapy on Depression and Resilience in Divorced Women. Socialworkmag. 2016; 5 (1) :5-12
13. Kamasi S, Zaki A, Saeedi M, Borhani Moghani, M. The effect of metaphor and individual therapy on the irrational beliefs of drug addicts. Journal of Principles of Mental Health, 2016; 18 (4): 189-195.
15. Dehghan Manshadi M, Zarei I, Asgari M, Naziri Q. Investigating the effectiveness of metaphorical therapy and therapeutic forgiveness on the dimensions of adjustment after women's divorce. Journal of Psychological Methods and Models, 2017; 8 (27): 29-48.
87Shabani Minaabad, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 83-87
Metaphors in BC phobia

Most breast metastasis cases present as a solitary nodule and share some significant histological features including a metastatic lesion with a fibrous pseudocapsule showing a relatively well circumsc-ribed growth pattern, and the absence of an in situ
1carcinoma. The most common histologic feature of ovarian cancer metastatic to breast is papillary serous
4, 5adenocarcinoma. In mammography, the two main patterns observed in breast metastases are well circumscribed and spheroidal intramammary masses without spiculation or calcification, and architectural
2, 4, 6distortion and other skin changes. Breast metastases on ultrasound are either hypoechoic or isoechoic and
about 60% of women have a dissemination of disease which is usually limited to peritoneal cavity
3in 85% of patients. In advanced stages of the disease, ovarian cancer can be metastatic to liver,
3lungs and pleura.
Metastases to breast and axilla from extramammary sites are uncommon and have been reported in only 2%
1of breast malignancies. They most commonly originate from melanomas, lung cancer, sarcomas and
2renal carcinomas. Ovarian cancers metastatic to breast and axillary lymph nodes are extremely rare and only
3account for 0.03%-0.6% of all breast neoplasms.
Introduction
Ovarian cancer has the highest mortality rate among gynecological cancers and happens mostly in postmenopausal women. At the time of diagnosis,
ARTICLE INFO
Case presentation: A 67-year-old woman with a history of ovarian cancer, undergoing chemotherapy presented with redness and swelling in her left breast and pathologic axillary lymph nodes. Work ups revealed ovarian cancer metastases to breast and axillary lymph nodes. She underwent chemotherapy with second line chemotherapeutics. The results were satisfying and the patient is well.
Background: Metastases to breast and axilla from extramammary sites are uncommon and have been reported in only 2% of breast malignancies. Ovarian cancer metastatic to breast and axillary lymph nodes is extremely rare and only accounts for 0.03%-0.6% of all breast neoplasms. The most common histologic feature of ovarian cancer metastatic to breast is papillary serous adenocarcinoma. Differentiating the secondary breast malignancies from primary ones is crucial as the treatment and prognosis are different, which could avoid many unnecessary procedures. Prognosis is generally poor because most patients have simultaneous spread of the disease.
Conclusion: The history of cancer in patients with a breast mass, even if clinically benign, may give rise to potential metastases. Screening with physical examination and serial mammography for patients with ovarian cancer could be beneficial. Early and accurate diagnosis of breast metastatic tumors is critical for proper management and preventing unnecessary and possibly harmful procedures.
30 March 2020Revised:
Received:
Accepted:23 April 2020
28 April 2020
Key words:Ovarian cancer, breast metastasis,axillary metastasis
Address for correspondence: Mehdi Ghelichkhani, MDAddress: Department of Surgery, Rassoul AkramHospital. Sattarkhan-Niayesh Avenue, Teharn, IranTel: +98 21 64352390Fax: +98 21 64352486E-mail: [email protected]
89 Ghelichkhani, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 88-92
ABSTRACT
Ovarian Cancer Metastatic to Breast and Axilla: A Case Report
a Department of Surgery, Iran University of Medical sciences, Tehran, Iran
b Student Research Committee, School Of Medicine, Iran University of Medical sciences, Tehran, Iran
c Department of Medical Oncology and Hematology, Shahid Beheshti University of Medical Sciences, Tehran, Iran
a a b aMehdi Ghelichkhani* , Nahid Nafissi , Zahra Rahimi , Farshid Ghasemi Meydansar ,
a cMasoud Haghighikian , Leila Sadeghi
Open AccessCase Report
DOI: 10.19187/abc.20207288-92

In the physical examination, pathologic axillary lymph nodes were present. The primary diagnosis was
Case presentation
In 2017, she presented with abdominal pain. Abdominal wall mass guided core needle biopsy found papillary-like fragments composed of atypical cells with mildly pleomorphic hyperchromatic irregular nuclei and eosinophilic cytoplasm with focal calcifications. The tumor cells were immunopositive for CK7, ER, WT-1 and PAX-8, and immunonegative for CK20, TTf-1, CDX2, GATA3, Mammaglobin A and Calretinin markers. Analyses besides histomorphology and immunohistochemistry findings suggested left ovarian serous carcinoma. She received three sessions of Avastin (Bevacizumab) based chemotherapy and then underwent surgery in February, 2018. The patient continued to receive chemotherapy with Avastin for four more sessions after the surgery. Positron emission tomography (PET) scan was done and to complete the therapy, eight more Avastin based chemotherapy sessions were planned; however, after seven sessions, swelling and erythema appeared in the left breast (Figure 1).
2have well circumscribed margins.
A 67-year-old woman who was previously diagnosed with mullerian serous ovarian carcinoma in 2017, presented to our care unit in July 2019 with swelling and redness in her left breast.
Differentiating the secondary breast malignancies from primary ones is crucial as the treatment and prognosis are different, which could avoid many unnecessary procedures. Prognosis is generally poor because most patients have simultaneous spread of
2the disease.
In her previous screening mammography in 2017, scattered areas of fibroglandular density and benign calcifications were found in both breasts. There was no evidence of skin or nipple retraction or pathologic adenopathy.
In this study, we are presenting a 67-year-old woman with breast and axillary lymph node metastases from ovarian cancer.
breast cancer metastasis to axillary lymph nodes. Left axillary lymph node needle biopsy was done. The results showed nests of large epithelioid cells with subsequent immunohistochemistry (IHC): PAX-8: Positive, WT-1: Negative, TTf-1: Negative, Chromogranin: Positive, synoptophysin: Negative, ER: positive 50%, PR: Negative, HER-2: Equivocal (2+), CK: Positive, GATA-3: Negative and KI67: 80%. The findings suggested that the lesion was a metastatic carcinoma of ovarian origin. Direct digital bilateral mammography (DDR), mediolateral-oblique (MLO) and cranial-caudal (CC) views, bilateral breast sonography and left breast skin lesion biopsy were done to confirm the diagnosis.
The mammogram (Figure 2) revealed mild skin thickening in the left breast, compared to her previous mammography. Pathologic high density enlarged lymph nodes were seen in the left axillary region. No pathology was detected in the breast parenchyma.
In the sonography with 15 MHZ probe, echogenicity of both fibroglandular tissue appeared normal, but mildly ductal ectasia in both breasts, a lipoma of 9mm at 6 o'clock of left breast and skin thickening in central portion of left breast were found. Also, some lymph nodes with cortical thickness of up to 31 mm in the left axillary region and 13 mm in the right axillary region were seen.
Left breast skin lesion biopsy revealed dermal tumor emboli and intravascular involvement by high grade papillary carcinoma. IHC findings including positive PAX-8 and negative GATA-3 in both biopsies of axillary lymph node and breast skin were more in favor of metastatic ovarian carcinoma.
Figure 1. Swelling and erythema on patient's left breast
Figure 2. Axillary lymph node in mediolateral oblique (MLO) view of mammography
89Ghelichkhani, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 88-92
Ovarian cancer metastasis to breast and axilla

After biopsies and during preparation for chemotherapy, she developed symptoms (such as coughs and chest pain) similar to a cold. Radiology scan revealed pleural effusion. The fluid was discharged by thoracoscopy, pleurodesis was done and cytology confirmed malignant pleural effusion. Then the patient underwent chemotherapy with keytruda and topotecan. The outcomes were satisfying and there was no pathology in her breasts and axillary region or any side effects except ascites (Figure 3). The follow up continued for 3 months after interventions and the patient showed a very good clinical response.
The present report describes a case of ovarian cancer metastasis to the breast and axilla. Metastases to breast from extramammary primary sites are rare. It regularly happens among age groups at risk for primary breast carcinomas. Malignant melanoma, lung cancer, lymphoma, ovarian cancer, soft tissue sarcoma, gastrointestinal and genitourinary tumors, and some sporadic tumors such as thyroid neoplasm, osteosarcoma, and cervical, vaginal and endometrial carcinoma, are the most common tumors to metastasize to the breast from extramammary
2, 7locations. The most common symptom among patients is a palpable breast mass, although the lesion can also be found in regular mammography
8incidentally.
A solitary tumor is the most common type of clinical presentation of metastatic breast cancer (85% of patients) and only 4% of patients have
10diffuse involvement. The upper outer quadrant is the most common location for metastatic lesions
11(62% of patients).
Metastatic breast tumors are typically firm, superficial, well-circumscribed by a fibrous pseudocapsuleand movable masses with the overlying
1, 9skin generally of normal consistency. Previous studies indicated that calcifications are extremely rare and can
3, 8 only be seen in metastatic papillary carcinomas.
Discussion
For differential diagnosis of ovarian cancer metastasis to breast, a considerable number of immunohistochemical markers have been reported to be useful including ER, PAX8, CK7, CK20, GATA3, CA125, WT-1, GCDFP-15, and mesothelin. WT-1 exists in 70% of ovarian carcinomas and 95% of serous papillary carcinomas; however, it is found
15in less than 10% of breast cancers. In addition, Mesothelin is found in more than 90% of serous papillary ovarian carcinomas, but it is poorly
16 expressed in 3–14% of breast cancer cases.
Previous studies suggested fine needle aspiration (FNA) of the lesion is a proper and cost-effective
7, 12diagnostic approach. On the contrary, Smymiotis et al. discouraged FNA as it was not helpful in differentiating primary breast carcinoma from
13metastatic tumors. When examined microscopically, metastases usually do not have an invasive ductal or
9in situ component.
It is critical to differentiate breast metastases precisely from primary breast cancer because the prognosis and treatment are significantly different. Breast surgeries and radiation therapy can be unnecessary for metastases. In addition, chemother-apeutic treatments used in secondary tumors are different from primary breast lesions. Some studies suggest that ovarian metastasis to the breast should be treated as a systemic disease with proper
17chemotherapeutics. Conservative breast surgery is generally best reserved for patients who do not respond to systemic therapy and need palliation. In addition, a study of 169 patients with extramammary metastases to the breast found a considerably higher survival rate in patients undergoing breast metastasis
8 surgical resection.
The result of the previous reviews are not sufficient to provide a meaningful survival rate in this patient
While no marker should be considered to be 100% precise, these markers, alongside a comparison of the pathology of the primary tumor and the suspicious breast tumor, can help to distinguish breast metastases from primary cancer. Routine pathologic examination and considering clinical history may also be helpful to differentiate primary breast cancer from metastatic cancer.
The most common type of breast metastases from 1 ovarian tumors is papillary serous adenocarcinoma
which is not a common pattern of the majority of invasive breast carcinomas.
Immunohistochemical studies may also be helpful for diagnosis in some cases. Use of tumor markers such as expression of C7 and CK20 for adenocarcinoma, TTF-1 for lung cancer, aFP for hepatocellular carcinoma (HCC), Ki-67 cell proliferation marker, ER/PR, BRST-2 and HER-2/neuoncoprotein for primary breast cancer, can be beneficial for locating the origins of metastatic breast tumors without specific morphological
8, 14feature.
Figure 3. Abdominal CT scan demonstrating ascites
90 Ghelichkhani, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 88-92
Ovarian cancer metastasis to breast and axilla

Metastases to breast can mimic primary breast cancer. While breast metastases of ovarian cancer are uncommon, screening with physical examination and serial mammography for patients with ovarian cancer could be beneficial. The history of cancer in patients with a breast mass, even if clinically benign, may give rise to the possibility of potential metastases and may need further evaluation. A combination of patient’s clinical history, and radiologic, microscopic, pathologic and immunohistochemical features, could distinguish a primary breast mass from metastases. Early and accurate diagnosis of breast metastatic tumors is critical for proper management and preventing unnecessary and possibly harmful procedures in patients. Considering the poor prognosis of metastatic lesions, treatments should be individualized. Further work is necessary to confirm whether surgical resection of metastasis to the breast will bring a survival benefit in selected patients.
Ethical Consideration
group, due to the rarity of these metastases and the small number of patients. However, studies suggest that breast metastases and specifically from ovarian
18origins have an exceedingly worse prognosis. Patients have a median survival time of 10 months
8from the time their breast metastasis is diagnosed.Further clinical studies on ovarian cancer
metastasis to the breast should be conducted to establish new specific markers for a more precise histopathological diagnosis based on biopsy specimens and to assess the real need for surgical intervention in terms of short and long-term prognosis compared to a palliative chemotherapy.
Conflict of Interest
References
2. Antuono L, Angela F, Luca N, Giovanni M, Enrico C. Breast metastasis from ovarian cancer: A case report. Radiol Case Rep. 2018; 13(6):1166-9.
The patient gave a written consent to the authors to publish this case report about her condition and treatment.
None.
1. Delair D, Corben A, Catalano J, Vallejo C, Brogi E, et al. Non-mammary metastases to the breast and axilla: A study of 85 cases. Modern pathology : an official journal of the United States and Canadian Academy of Pathology, Inc. 2012;26.
4. Klein R, Brown A, Gomez-Castro C, Chambers S, Cragun J, et al. Ovarian Cancer Metastatic to
3. Della Corte L, Giampaolino P, Fabozzi A, Cieri M, Zizolfi B, et al. Breast metastasis two years after pelvic surgery and adjuvant chemotherapy for serous ovarian cancer. Gynecological Endocrinology. 2019;35(3):211-3.
7. Akçay MN. Metastatic disease in the breast. Breast (Edinburgh, Scotland). 2003;11:526-8.
9. Vergier B, Trojani M, De Mascarel I, Coindre J-M, Le Treut A. Metastases to the breast: Differential diagnosis from primary breast carcinoma. Journal of Surgical Oncology. 1991;48(2):112-6.
11. Moore DH, Wilson DK, Hurteau JA, Look KY, Stehman FB, et al. Gynecologic cancers metastatic to the breast. Journal of the American College of Surgeons. 1998;187(2):178-81.
15. Lee B, Hecht J, Pinkus J, Pinkus G. WT1, Estrogen Receptor, and Progesterone Receptor as Markers for Breast or Ovarian Primary Sites in Metastatic Adenocarcinoma to Body Fluids. American journal of clinical pathology. 2002;117:745-50.
16. Lee A. The histological diagnosis of metastases to the breast from extramammary malignancies. Journal of clinical pathology. 2008;60:1333-41.
6. Balaji R, Ramachandran K, Anila KR. Ovarian Carcinoma Metastasis to the Breast and Imaging Features With Histopathologic Correlation: A Case Report and Review of the Literature. Clinical Breast Cancer. 2009;9(3):196-8.
8. Williams S, Ehlers R, Hunt K, Yi M, Kuerer H, et al. Metastases to the breast from nonbreast solid neoplasms: Presentation and determinants of survival. Cancer. 2007;110:731-7.
17. Özsaran AA, Dikmen Y, Terek MC, Ulukus M, Özdemir N, et al. Bilateral metastatic carcinoma of the breast from primary ovarian cancer. Archives of Gynecology and Obstetrics. 2000;264(3):166-7.
14. Lee SK, Kim W, Kim SH, Hur S, Kim S, et al. Characteristics of Metastasis in the Breast From Extramammary Malignancies. Journal of surgical oncology. 2010;101:137-40.
the Breast Presenting as Inflammatory Breast Cancer: A Case Report and Literature Review. Journal of Cancer. 2010;1:27-31.
13. Smymiotis V, Theodosopoulos T, Marinis A, Goula K, Psychogios J, et al. Metastatic disease in the breast from nonmammary neoplasms. European journal of gynaecological oncology. 2005;26:547-50.
10. Kayikçioğlu F, Boran N, Ayhan A, Güler N. Inflammatory Breast Metastases of Ovarian Cancer: A Case Report. Gynecologic Oncology. 2001;83(3):613-6.
12. Gupta D, Merino M, Farhood A, Middleton L. Metastases to breast simulating ductal carcinoma in situ: Report of two cases and review of the literature. Annals of diagnostic pathology. 2001;5:15-20.
5. Tempfer C, Fizazi N, Ergonenc H, Solass W. Metastasis of ovarian cancer to the breast: A report of two cases and a review of the literature. Oncology Letters. 2016;11.
91Ghelichkhani, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 88-92
Ovarian cancer metastasis to breast and axilla

18.Micha JP, Goldstein BH, Epstein HD, Rettenmaier MA, Brown JV, III. Ovarian cancer metastatic to the breast. Gynecologic Oncology. 2006;102(2):386-90.
92 Ghelichkhani, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 88-92
Ovarian cancer metastasis to breast and axilla

Case Presentation A previously healthy 38-year-old Philipino lady,
unmarried and nulliparous with a family history of fibroadenoma, presented with a mass in the right breast for the last year. Over the preceding 6 months, the mass had been progressively increasing in size and was painful. The pain markedly increased during menstruation. There was no nipple discharge, bone
rapid increase in the size of the tumor or if the radiographic finding shows heterogeneous hypoechoic internal echoes without calcification. Moreover, once a phyllodes has been diagnosed, it is recommended to have a high degree of suspicion for malignancy despite a benign core biopsy.
IntroductionPhyllodes tumors are very rare and closely
resemble fibroadenomas, making their detection even more difficult. Diagnosis and proper management are crucial because of the malignant potential and tendency to recur. Phyllodes tumor bears specific clinical characteristics and should be considered by the clinician as a differential diagnosis for the breast lumps if clinical suspicion arises by the
ARTICLE INFO
Conclusion: Phyllodes tumor bears specific clinical characteristics and should be considered as a differential diagnosis in any mass lesion of the breast.. Diagnosis and management are crucial in phyllodes tumor because of their malignant potential recurrence. Clinicians should be competent in distinguishing between fibroadenoma and a phyllodes tumor. Lastly, given the rarity of phyllodes tumors, there is a need to establish guidelines to incorporate regular follow up for early detection of distant metastasis.
Background: Phyllodes tumours are rare fibroepithelial neoplasm of connective tissue of the breast accounting for 0.3-1% of all breast tumours with 10% of them being malignant. They resemble fibroadenomas clinically and can be mistakenly ignored.
Case presentation: A 38-year-old unmarried Philipino lady presented to the primary health center with a mass in the right breast for the past year. Over the preceding 6 months, it had progressively increased in size and pain. On examination, a 5 x 3 cm firm and lobulated mass was palpated in the right upper outer quadrant. Ultrasound scan showed a solid 4.25 x 3.3 x 2.4 cm mass with heterogeneous mixed echopattern. She was referred to Surgery department where an ultrasound-guided core biopsy showed a lesion suspicious for benign phyllodes tumor. An excision biopsy revealed three foci of malignant Phyllodes on the background of fibroadenoma. A staging CT was performed which showed no evidence of lymph node involvement or distant metastasis. A simple mastectomy was performed and histopathology confirmed the diagnosis of malignant phyllodes tumor. Postoperatively, the patient is on regular follow up in the breast clinic and physiotherapy department.
malignanciesphyllodes tumor,Breast cancer, Key words:
02 April 2020Revised:
Accepted:
Received:
21 April 2020
27 April 2020
Address for correspondence: Sumaiya Iqbal, InternshipAddress: Latifa Women and Children's Hospital, Dubai HealthAuthority Jaddaf Dubai, United Arab Emirates.Tel: +971569400124E-mail: [email protected]
ABSTRACT
Malignant phyllodes Tumor of the Breast; Presentation of an Uncommon Case and Review of the Literature
a Department of Obstetrics and Gynecology, Latifa Women and Children's Hospital, Dubai, UAE b Medical Education, Dubai Medical University, Dubai, UAE
a b a aSumaiya Iqbal* , Juwairiya Iqbal , Nowfala Nowshad , Khadeeja Mohammad
Open AccessCase Report
DOI: 10.19187/abc.20207293-96
93Iqbal, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 93-96

Due to rapid progression of clinical symptoms
pain, weight loss or night sweats. The medical, surgical and social history was insignificant. Her quality of life and occupation as a nurse was severely affected as she was unable to lift her right hand due to pain.
On physical examination, the right breast had a mass of dimensions 5x3 cm at 10 o’clock position. It was firm, lobulated, fixed to the underlying tissue and tender to touch. The overlying skin was erythematous. There was no peau’d orange, nipple discharge or nipple retraction in either breast. No lymph nodes were palpable. The left breast was unremarkable. Liver and spleen were not palpable. General examination was unremarkable.
Ultrasound of the right breast is shown in Figure 1 revealed a solid, well circumscribed, lobulated mass with mixed echo pattern suggestive of fibroadenoma with atypical radiologic features. Bilateral axillary lymph nodes were nonspecific. Therefore, the patient was classified as BIRADS Iva.
Core biopsy in Figure 2 demonstrates the cores of the breast tissue with papillary protrusions of stromal connective tissue with a leaf‐like appearance. There was no evidence of mitosis or cytological atypia.
and atypical findings obtained from Ultrasound, there was a high suspicion for malignancy. Therefore, excision biopsy was recommended by the Multidisciplinary team (MDT). Excision biopsy showed a foci of malignant phyllodes tumor accounting for 15-17% of the neoplasm. The epithelium, as seen in Figure 3, was arranged in broad leaf like clefts with scattered multinucleated bizarre stromal cells showing moderate pleomorphism and hyperchromasia.
Increased mitotic activity with mitoses up to 14-16 per 10 HPF were identified with some abnormal mitosis as seen in Figure 4.
A staging CT scan of chest, abdomen and pelvis was performed which showed no evidence of lymph node involvement and no distant metastasis.
Following some discussion with Multidisciplinary team including a breast surgeon, an oncologist and a pathologist regarding the small size of the patient’s breast, a total mastectomy of right breast was performed and the specimen weighing 19.7gm and measuring 4.5x3.5x3cm was sent to histopathology.
Immunohistochemical analysis done by a panel of cytokeratins (CKs) showed that CKAE1/AE3 was negative in stroma and CD34 was positive in stromal cells.
Figure 1. Ultrasound demonstrates a solid 4.25 x 3.3 x 2.4 cm well-circumscribed lobulated mass with a heterogeneous
mixed echopattern and, casting a posterior shadow.
Figure 2. Core biopsy showing the cores of the breast tissue with papillary protrusions of stromal connective tissue
producing a leaf‐like appearance.
Figure 3. Excision biopsy revealing scattered multinucleated bizarre stromal cells that show moderate pleomorphism and hyperchromasia.
Figure 4. Excision biopsy showing increased mitotic activity with some abnormal mitosis.
94 Iqbal, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 93-96
Malignant phyllodes tumour of breast

No evidence of residual malignant phyllodes tumor was found. There was benign fibroepithelial changes with stromal fibrosis, with few ectatic ducts and microcalcification seen.
Discussion
The patient had a good postoperative recovery and was able to return to work as a nurse. Two weeks post discharge, she was followed up in breast clinic where she complained of pain and hypersensitivity of the right chest wall. Clinically, the scar had healed with no signs of infection. The patient was reassured and scheduled for an appointment with physiotherapy department. She was put on a follow up plan with breast surgery clinic after 3 months.
Phyllodes tumours are rare fibroepithelial neoplasm of the connective tissue of breast accounting for <1% of all breast malignancies and has an
1incidence of about 2.1 per million. In 1838, Johannes Muller coined the term cystosarcoma-phyllodes based on leaf-like projections extending into cystic spaces and sarcoma-like stroma of the tumor. However, since up to 70% of phyllodes tumor are benign, the term “cystosarcoma” was removed and the tumor is now
2referred to simply as phyllodes tumors. Malignant phyllodes tumor (PT) is characterized
Phyllodes tumors are benign breast tumors found predominantly in females aged between 35 and 55
3(median 45). The size of the tumor is variable, from 1 cm to 41 cm (on average from 4 cm to 7 cm) and the
4skin is bright, stretched, and diminished. It has an initial phase of slow growth followed by the second phase of rapidly accelerating growth over a period of
2weeks to months. It may be associated with changes of overlying skin including atrophy, skin thinning, bloody nipple discharge, or nipple retraction, if the areolar region is involved.
According to the World Health Organization (WHO) classification of 2012, phyllodes tumor is classified as benign, borderline, or malignant as
6shown in Table 1.
On mammography and ultrasound, phyllodes tumors lack distinguishing characteristics and, thus, findings are not specific. Breast ultrasound usually shows a mass with size>=3,irregular shape, microlobulated borders, complex internal echo pattern, and hypervascularity, while internal cystic
5areas on MRI are suggestive of phyllodes tumor. Mammography demonstrates a very dense mass compared to the surrounding parenchyma.
Table 1. Three-Tiered Grading System for Phyllodes Tumors Based On 2012 World Health Organization Classification.
MalignantBorderline
Mild
Mild
<5
Absent
Well-defined
Marked
Marked
>10
Present
Infiltrative
Moderate
Moderate
5-9
Absent or focal
Well-defined or focal infiltrative
Stromal cellularity
Stromal atypia
Mitosis (per 10 HPF)
Stromal overgrowth
Tumor margin
BenignHistologic features
found that adjuvant radiotherapy for borderline and malignant tumors yielded superior 10-year local
9control rates; but no survival benefits. Chemotherapy is reserved for highly selected patients with large, high-risk, or recurrent malignant phyllodes tumors. However, hormonal therapy is not used to treat phyllodes tumors.
The survival rate for malignant phyllodes tumors is reported as approximately 60–80% at 5
10years. After the tumor has metastasized, the average 11net survival is 30 months.
In conclusion, PTs are a rare cause of rapidly enlarging painless breast masses in middle age women. Further workup should be considered when a patient suspects that the lesion is growing in size within 6 months to a year. Ultrasound usually shows heterogeneous hypoechoic internal echoes without calcifications. Our case highlighted the fact that it is difficult to diagnose phyllodes based on a core biopsy due to the subjective nature of interpretation of the degree of stromal cellularity as well as the degree of atypia. Even if a phyllodes is diagnosed on
by marked stromal cellularity and nuclear pleomorphism, stromal overgrowth, and more than 10 mitoses per 10 HPF. The presence of heterologous s a r c o m a t o u s e l e m e n t s ( l i p o s a r c o m a , chondrosarcoma, and osteosarcoma) alone qualifies
7a PT as malignant.In our case, the histopathologic features of the
tumor include the arrangement of epithelium in broad leaf like clefts with scattered multinucleated bizarre stromal cells showing moderate pleomorphism. Increased mitotic activity with mitoses up to 14-16 per 10 HPF are identified with some abnormal mitoses. These findings are compatible with those from malignant phyllodes tumors.
The mainstay of phyllodes tumour management has traditionally consisted of surgical excision with wide tumour-free margins, generally defined by some
8authors as at least 10 mm. Axillary lymph node dissection is not necessary. Adjuvant radiation therapy may benefit borderline or malignant tumors, but not benign ones. Belkacemi et al. in an analysis of the cases collected from the Rare Cancer Network
95Iqbal, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 93-96
Malignant phyllodes tumour of breast

6. Lakhani SR. WHO Classification of Tumours of the Breast: International Agency for Research on Cancer; 2012.
7. Zhang Y, Kleer C. Phyllodes Tumor of the Breast: Histopathologic Features, Differential Diagnosis, and Molecular/Genetic Updates. Archives of Pathology & Laboratory Medicine. 2016;140(7):665-671.
5. Duman L, Gezer N, Balcı P, Altay C, Başara I, Durak M et al. Differentiation between Phyllodes Tumors and Fibroadenomas Based on Mammographic Sonographic and MRI Features. Breast Care. 2016;11(2):123-127
9. Belkacemi Y, Bousquet G, Marsiglia H, Ray-Coquard I, Magne N, et al. Phyllodes tumor of
8. Tan BY, Acs G, Apple SK, Badve S, Bleiweiss IJ, et al. Phyllodes tumours of the breast: a consensus review. Histopathology. 2016;68(1):5-21.
The patient has given written informed consent to publish this case (including publication of images).
core biopsy, an excision biopsy is always required to determine if it is a benign or malignant phyllodes
12tumour. Surgical management is the mainstay of 1 3
treatment while adjuvant treatment with chemotherapy; radiotherapy or hormonal therapy currently have no clear evidence of benefit and
14remain controversial. Therefore, we recommend physicians to be vigilant of phyllodes tumors and consider them in the differential diagnosis should the clinical suspicion be raised.
AcknowledgementsWe acknowledge Dr. Hajer for proofreading the
manuscript.
Ethical Consideration
Conflict of InterestThe authors have no conflicts of interest to
declare.
References1. Altedlawi Albalawi I. A huge phyllodes tumor in
the breast: a case report. Electronic Physician. 2018;10(6):6951-6955
2. Amir RA, Rabah RS, Sheikh SS. Malignant Phyllodes Tumor of the Breast with Metastasis to the Pancreas: A Case Report and Review of Literature. Case Rep Oncol Med. 2018: 6491675.
3. Barrio AV, Clark BD, Goldberg JI, Hoque LW, Bernik SF, et al. Clinicopathologic features and long-term outcomes of 293 phyllodes tumors of the breast. Ann Surg Oncol. 2007;14(10):2961-70
4. Vargas-Hernandez VM, Aguilar VMV. Phyllodes Tumors (Cys tosarcoma Phyl lodes) : A Diagnostic and Therapeutic Challenge. World J Breast Cancer Res. 2019; 2(2): 1016
14. Câmara S, Gonzàlez-Farré X, Vargas-Moniz J. Giant phyllodes tumour – Case report, oncoplastic treatment and literature controversies. Revista de Senología y Patología Mamaria. 2017;30(2):79-84
13. Altedlawi Albalawi I. A huge phyllodes tumor in the breast: a case report. Electronic Physician. 2018;10(6):6951-6955
11. Yoshidaya F, Hayashi N, Takahashi K, Suzuki K, Akiyama F, et al. Malignant phyllodes tumor metastasized to the right ventricle: a case report. Surg Case Rep. 2015;1(1):121.
the breast. Int J Radiat Oncol Biol Phys. 2008;70(2):492-500.
12. Yan Z, Gudi M, Lim S. A large benign phyllodes tumour of the breast: A case report and literature review. International Journal of Surgery Case Reports. 2017;39:192-19
10. Demian G, Fayaz S, El-Sayed Eissa H, Nazmy N, Samir S, George T et al. Phyllodes tumors of the breast: Analysis of 35 cases from a single institution. Journal of the Egyptian National Cancer Institute. 2016;28(4):243-248
96 Iqbal, et al. Arch Breast Cancer 2020; Vol. 7, No. 2: 93-96
Malignant phyllodes tumour of breast

As the role of local therapy in multidisciplinary management breast cancer has been evolving over the past few of decades, so has the concept of oncoplastic surgery. While the safety of breast conserving therapy, or BCT, which consists of lumpectomy and adjuvant breast radiotherapy, for invasive and in situ breast carcinomas is well-
1,2established , the idea of a lumpectomy for larger lesions has been a challenge, even when neoadjuvant systemic therapy could be expected to downsize the lesion of interest.
As for the issue of local control, achieving clear surgical margins is a priority in ensuring the safety of BCT. A large number of studies have addressed this in both invasive breast cancer and ductal carcinoma in situ (DCIS), consistently demonstrating low re-excision rates in patients undergoing oncoplastic breast conserving surgery (4-12%), with breast conservation successfully achieved in greater than
5-890% of cases. These findings can reassure us as surgeons of the reliability of preoperative clinical and imaging assessment of the malignancy planned for resection, and it is, undoubtedly, at least in part,
Oncoplastic surgery encompasses a number of procedures combining oncologic and reconstructive techniques utilized in the surgical management of larger breast lesions, and this strategy has been
3,4 perfected and evaluated over the last 2 decades. In this process, there have been a number of outstanding challenges related oncoplastic surgery, especially relevant for the surgical oncologist: 1) the oncologic safety and the degree of local control associated with a lumpectomy for a larger lesion; 2) the optimal timing for a reconstructive procedure to overcome the potential cosmetic deformities resulting from excising a larger volume of tissue.
attributable to more “generous” excisions taking place in anticipation of a reconstructive operation.
Factors that have been found to be associated with 2
higher re-excision rates are BMI of least 25 kg/m and above, presence of mammographic calcifications, presence of DCIS in the lumpectomy specimen and
5,9invasive lobular histology. This is an important observation for patient counselling since the management of positive margins could be a challenge in cases when an immediate oncoplastic reconstructive procedure is performed during the same operation, as the latter extensively rearranges the breast tissue. In situations like these, when positive margins are reported after the operation, there is not clear guidance in the existing literature as to how a re-excision can be reliably performed, as the margins of interest would be difficult to be identified within extensively rearranged breast tissue. There is only anecdotal evidence related to intraoperative margin assessment (to enable margin clearance) and to intraoperative margin orientation (to facilitate initial lumpectomy wall identification for a possible subsequent re-excision). If there is no certainty about identifying the margin to be re-excised, the patient would likely require a mastectomy. Therefore, it may be more practical to complete the lumpectomy, with or without re-excisions, if necessary, and confirm the negative margin status and to plan the reconstructive procedure on a different date.
Additionally, there has been mounting evidence of excellent long-term local control achieved by oncoplastic surgery. In a single-institution retrospective analysis by Crown et al. which included 71 patients who underwent oncoplastic breast surgery, at a mean follow-up of 32.1 months, the local recurrence rate was 1.4%, and over 90% of patients reported excellent or good cosmetic
8outcomes. A larger retrospective study by Mansell et al. included 980 patients from an institutional prospective database, of whom 104 underwent an oncoplastic procedure, 558 had standard breast
10conservation and 318 had mastectomies. It is
97
Oncoplastic Breast Surgery – Pros and Cons for the Breast Surgical Oncologist
a Department of surgical oncology, Women and Brigham Hospital, Harvard Medical School, Boston, USA
aFaina Nakhlis*
Open AccessEditorial
Address for correspondence: Faina Nakhlis, MDAddress: 1153 Centre St, Jamaica Plain, MA 02130, USATel: +1 617-983-7777Fax: +1 617-983-7779Email: [email protected]
Nakhlis. Arch Breast Cancer 2020; Vol. 7, No. 3: 97-99
DOI: 10.32768/abc.20207397-99
Pro and cons for OBS
Admittedly, there is controversy regarding the optimal timing oncoplastic reconstructive procedure and adjuvant radiation. If the reconstruction is performed prior to radiation, a lower rate of radiation-related wound healing complications might be expected; however, subsequent radiation may affect the treated breast in a way that would compromise its symmetry with the contralateral breast, whether or not the latter had undergone an oncoplastic procedure. On the other hand, postponing of the oncoplastic reconstructive procedure until after radiation may be more optimal in achieving symmetry, but possibly at the price of a greater risk of healing issues associated with radiation. As these procedures become more prevalent, there will be a better consensus on the most appropriate timing of the reconstructive operation with respect to adjuvant radiotherapy.
Another consideration is the safety of the oncoplastic approach following neoadjuvant chemotherapy. In a study by Adamson et al., among 429 patients who underwent an oncoplastic procedure,
14122 underwent neoadjuvant chemotherapy. In this study, the neoadjuvant chemotherapy group consisted of younger patients (median age 52 years vs. 57 years), but they had more advanced tumors, and there was no difference in the postoperative complication rates observed.
An important aspect of the oncoplastic approach is the possibility of the already mentioned significant tissue rearrangement potentially resulting in difficulty in interpreting future mammographic studies; however, a study by Piper et al. demonstrated that at up to 5 years following oncoplastic procedures and standard lumpectomies there were no differences in mammographic recalls and in the number of
15 imaging-prompted biopsies. As the comfort level with oncoplastic surgery has increased overtime, it is not surprising that the utilization of this approach has
16significantly grown.
noteworthy that the patients who underwent an oncoplastic procedure had larger and higher grade tumors, and fewer of them were estrogen and progesterone receptor positive, yet the 5-year local recurrence rates were very low in all 3 study groups (3% in the oncoplastic group, 3.4% in the standard lumpectomy group and 2% in the mastectomy
1 0group). Subsequently, other studies have corroborated the oncologic safety of the oncoplastic
11-13 approach.
In summary, there is a convincing body of evidence to-date as to the oncologic safety of the oncoplastic approach to breast cancer, as it appears that more generous excisions and meticulous negative margin achievement result in outcomes similar to those seen with standard BCT. It may be more rational to complete the oncoplastic lumpectomy to ensure the negative margin status, and to proceed with the reconstructive procedure at a later date, in order to
3. Anderson BO, Masetti R, Silverstein MJ. Oncoplastic approaches to partial mastectomy: an overview of volume-displacement techniques. Lancet Oncol. 2005; 6:145-157.
Conflict of Interest
1. Morrow M, Strom EA, Bassett LW, et al. Standard for breast conservation therapy in the management of invasive breast carcinoma. CA Cancer J Clin. 2002; 52:277-300.
None.
2. Morrow M, Strom EA, Bassett LW, et al. Standard for the management of ductal carcinoma in situ of the breast DCIS. CA Cancer J Clin. 2002; 52:256-276.
References
10. Mansell J, Weiler-Mithoff EW, Stallard D, et al. Oncoplastic breast conservation surgery is oncologically safe when compared to wide local excision and mastectomy. The Breast . 2017;32: 179-185.
5. Benjamin MA, Siannott C, Bawa S, et al. Re-excision rate after partial mastectomy in oncoplastic breast conserving surgery. Annals of Plastic Surgery. 2019;82(suppl. 3):S170-S172.
7. Clough KB, Gouveia PF, Benyahi D, et al. Positive margins after oncoplastic surgery for breast cancer. Ann Surg Oncol. 2015; 22:4247-4253.
9. Amabile M, Mazouni C, Guimond C, et al. Factors predictive of re-excision after oncoplastic breast conserving surgery. Anticancer Research. 2015;35:4229-3234.
facilitate reliable margin identification, if a re-excision is necessary. Finally, it remains unclear whether the timing of oncoplastic reconstruction is more optimal when performed before or after adjuvant radiation therapy. Therefore, it is best for the patient to have this discussion with a plastic surgeon prior to any surgical interventions to facilitate shared decision-making.
4. Strach MC, Prasanna T, Kirova YM, et al. The importance of a multidisciplinary breast cancer patient pathway in the era of oncoplastic and reconstructive surgery. Critical Reviews in Oncology/Hematology. 2019; 134:10-21.
8. Crown A, Handy N, Rocha FG, Grumley JW. Oncoplastic reduction mammaplasty, an effective and safe method of breast conservation. The American Journal of Surgery. 2018;215: 910-915.
6. Carter SA, Lyons GR, Kuerer HM, et al. Operative and oncologic outcomes in 9861 patients with operable breast cancer: single-institution analysis of breast conservation and oncoplastic reconstruction. Ann Surg Oncol. 2016; 23:3190-3198.
11. Chakravorty A, Shrestha AK, Sanmugalingam N, et al. How safe is oncoplastic breast conservation? Comparative analysis with standard breast
Nakhlis. Arch Breast Cancer 2020; Vol. 7, No. 3: 97-9998

14. Adamson K, Chavez-MacGregor M, Caudle A, et al. Neoadjuvant chemotherapy does not increase complications in oncoplastic breast-conserving surgery. Ann Surg Oncol. 2019; 26:2730-2737.
16. Jonczyk MM, Jean J, Graham R, Chatterjee A. Surgical trends in breast cancer: a rise in novel operative treatment options over a 12 year analysis. Breast Cancer Research and Treatment. 2019;173:267-274.
12. De Lorenzi F, Bella JD, Maisonneuve P, et al. Oncoplastic breast surgery for the management of ductal carcinoma in situ (DCIS): is it oncologically safe? A retrospective cohort study. EJSO.2018;44:957-962.
13. Semprini G, Cattin F, Vaienti L, et al. Oncoplastic surgery and cancer relapses: cosmetic and oncologic outcomes in 489 patients. The Breast. 2013; 22:946-951.
conserving surgery. EJSO.2012;38:395-398.
15. Piper M, Peled AW, Sbitany H, et al. Comparison of mammographic findings following oncoplastic mammoplasty and lumpectomy without reconstruction. Ann Surg Oncol (2016) 23:65-71
Pro and cons for OBS
Nakhlis. Arch Breast Cancer 2020; Vol. 7, No. 3: 97-99 99

IDP is a benign, circumscribed, intra-ductal proliferation consisting of fibro-vascular cores covered by benign myoepithelial and outer epithelial layer. IDPs can be generally categorized into two types: central IDPs which involve large, central lactiferous ducts, and peripheral IDPs which involve the terminal duct lobular units. Central IDPs are mostly solitary, and peripheral IDPs tend to be multiple. Although multiple peripheral IDPs have been sometimes referred to as papillomatosis, this appellation is discouraged because of its inconsistent usage for different types of lesions. Clinically, central IDPs have variable sizes and present with
carcinoma). These lesions demonstrate papillary 1morphology.
ARTICLE INFO
Background: Papillary lesions of the breast are a heterogeneous group of neoplasms, the diagnosis and treatment of which is challenging. Typically surgical excision is recommended for papillary lesions after core needle biopsy (CNB) to rule out concurrent malignancy when a diagnosis of papilloma with atypia is yielded on CNB. For papilloma without atypia, however, making a decision about excision versus observation is challenging.
Conclusion: Histoathology review of CNB specimen in rare and high risk lesions may have some advantages. On the other hand, in high risk circumstances, the excision of the lesion is recommended. Thus, in this case, the multi-disciplinary team recommended excision of the lesion.
Case Presentation: A 14-year-old female with nipple discharge, and a 2 cm mass in the right breast, with the pathology of intra-ductal papilloma without atypia on CNB presented. The question to be answered by multi-disciplinary team was the best management of this papillary lesion and whether the follow up was adequate or excision was mandatory.
Question: What is the best plan for management of the young patient according to the primary pathology report of Juvenile Papillomatosis?
breast,
Revised:
atypia
Papillary lesion,
Received:
19 July 2020
4 August 2020
28 July 2020Accepted:
Key words:
Address for correspondence: Ahmad Elahi, MDAddress: Imam Ali Hospital Comlex, Alborz University of Medical Sciences, Karaj, Iran.Tel:+98 2188663937Email: [email protected]
ABSTRACT
Papillary Lesion of the Breast in a Young Girl Suspicious to Juvenile Papillomatosis, Clinical Decision Making in a Multi-disciplinary Team and Review of the Literature
a Department of Surgery, Tehran University of Medical Sciences, Tehran, Iranb Department of Pathology, Tehran University of Medical Sciences, Tehran, Iranc Department of Pathology, Alborz University of Medical Sciences, Alborz, Karaj, Irand Department of Radiology, Tehran University of Medical Sciences, Tehran, Irane Breast Cancer Research Center, Tehran University of Medical Sciences, Tehran, Iranf Department of Surgery, Alborz University of Medical Sciences, Alborz, Karaj, Iran
a b dc Marzieh Mohammadi Zavieh , Farid Azmude Ardalan , Farnaz Karimi , Nahid Sedighi , a,e f
Ramesh Omranipour , Ahmad Elahi*
Open AccessClinical Experience
Papillary lesions (PL) of the breast are a heterogeneous group of neoplasms, which include intra-ductal papilloma (IDP), IDP with usual ductal hyperplasia, IDP with atypical ductal hyperplasia, as well as IDP with ductal carcinoma in situ (DCIS), papi l lary DCIS and papi l lary carc inoma (encapsulated papillary carcinoma and solid-papillary
Introduction
DOI: 10.32768/abc.202073100-103
100 Mohammadi Zavieh, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 100-103

Surgical excision is often conducted for papillary lesions after CNB to rule out concurrent malignancy when a diagnosis of papilloma with atypia is yielded
8at CNB. However, for PLs without atypia, making a decision about excision versus observation is a dilemma for the surgeon.
nipple discharge that is often bloody. Peripheral IDPs are most frequently identified as small masses or densities on mammography. Both lesions may have micro-calcifications because of infarction and/or sclerosis followed by dystrophic calcium
2-4 deposition.
Ultrasonography revealed a 27 x 15 x 24 mm iso-echoic mass with lobulated margin in the right breast
Case presentation
Papillary lesions are challenging to diagnose and treat. PLs are usually identified by mammography and ultrasonography and subsequently diagnosed by
5core needle biopsy and/or vacuum-assisted biopsy. Imaging-guided core needle biopsy (CNB) provides reliable diagnosis of breast lesions, but papillary lesions detected at percutaneous biopsy may be
6difficult to interpret histologically. In addition, limited material and sampling error at CNB may lead to neglecting the presence of atypia or malignancy
7within or adjacent to the lesion.
The patient was a 14-year-old female presented with right breast spontaneous nipple discharge and mass. She had nipple discharge in the last 18 months, which was bloody in the beginning and then turned to serous discharge. She did not take any medication and had no family history of breast cancer. On physical examination, there was no distinct mass but a 2 x 2 cm thickening area was noted under the nipple-areolar complex. There was no spontaneous nipple discharge though a single duct serous discharge was detected on compression.
QuestionThe best management of the disease in a 14-year-
old female patient with a symptomatic papillary breast lesion (surgical excision vs. follow up) was the main concern faced by the Multi-disciplinary Team(MDT).
Discussion Juvenile papillomatosis of breast or Swiss cheese
disease is a rare lesion, which is more common in adolescence and young people (with mean age under 23). The disease typically presents with painless mass that, on physical examination, is circumscribed, easily movable, and most often considered to be a fibroadenoma. These lesions appear to be well-
9circumscribed but they are not encapsulated. Patients usually present with mass; however,
10hemorrhagic discharge and pain are rarely seen. Our patient had nipple discharge which was not bloody. The size of juvenile papillomatosis reportedly ranges between 1 and 8 cm, but the lesion was 3 cm in our patient.
retro-areolar region (BIRADS 4b). Because of the young age of the patient, MRI was requested, which showed a 30 x 12 x 18 mm sub-areolar mass with irregular margins, there was an iso to hyper-intensity and heterogeneous enhancement pattern with rapid washout kinetics in right retro-areolar area in T2 (BIRADS 4b). She underwent core needle biopsy, and the pathology diagnosis of florid papillary hyperplasia (compatible with juvenile papillomatosis) was reported. There was no sign of atypia or malignancy.
Juvenile papillomatosis is a clinicopathological entity, first described by Rosen et al. Pathologic examination demonstrates a constellation of benign lesions and proliferations including dilation of ducts, multiple intraductal papillomas, usual ductal
Figure1. Intra-ductal papilloma. A. Papillary fronds lined by a continuous layer of cuboidal myopepithelial cells (long black arrows) underlying a layer of columnar epithelial cells (short red arrows). H&E, 200x. B. Cytokeratin 5/6 highlights myoepithelial cells. Some
epithelial cells are also stained (arrows). CK5/6 immunostain, 200x. C. P63 shows positive nuclear reaction in myoepithelial cells. P63 immunostain, 200x.
101Mohammadi Zavieh, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 100-103
Papillary lesions of the breast

well-developed stroma, two cell types without cytological atypia but florid epithelial hyperplasia in some foci in favor of intra-ductal papilloma with florid usual ductal hyperplasia” as can be seen in Figure 1. Then the patient went under routine follow up.
The written consent was signed by the patient and her parents.
examination illustrated “dilated ducts, intra-ductal papilloma with complex intricate branching fronds with
In conclusion, it seems that it is better to review the CNB specimen when the primary report is among rare diseases of the breast and the patient is in high-risk group for papillomas. Surgical excision is recommended for the latter group
Conflict of InterestNone.
Ethical Consideration
2. Muttarak M, Lerttumnongtum P, Chaiwun B, Peh WC. Spectrum of papillary lesion of breast: clinical, imaging, and pathologic correlation. AJR AM J Roentgenol. 2008; 191(3) 700-707.
3. Daniel BL, Gardner RW, Birdwell RL, Newels KW, Jonson D. magnetic resonance of IDP of the breast, magn Reson imaging. 2003; 21(8): 887-892
4. Yang WT, Suen M, Metreweli C. sonographic features of benign papillary neoplasms of the breast: review of 22 patients. J ultrasound med. 1997;16(3):161-168.
5. Wyss P, Varga Z, Rossle M, Rageth CJ. Papillary lesions of the breast: outcomes of 156 patients managed without excisional biopsy. Breast J. 2014;20(4):394-401.
7. Youk JH, Kim E-K, Kwak JY, Son EJ, Park B-W, et al. Benign papilloma without atypia diagnosed at US-guided 14-gauge core-needle biopsy: clinical and US features predictive of upgrade to malignancy. Radiology. 2011;258(1):81-8.
8. Wen X, Cheng W. Nonmalignant breast papillary
References1. Schmitt SJ, Collins LC. Biopsy interpretation of
the breast. Vol4. Philadelphia, PA: Wolters Kluwer/ Lippincott Williams & Wilkins; 2019. Biopsy interpretation series. Epstein JI, series ed.
6. Carder PJ, Khan T, Burrows P, Sharma N. Large volume "mammotome" biopsy may reduce the need for diagnostic surgery in papillary lesions of the breast. J Clin Pathol. 2008;61(8):928-33.
Ultrasonography is an optimal tool for diagnosis. MRI also aids in diagnosis by showing small internal
12cyst on T2. In our patient ultrasonography and MRI revealed an irregular mass in retro-areolar region, which was not compatible with the pathology of juvenile papillomatosis. Therefore, the MDT recommended the review of the patient’s slides. Subsequently, a diagnosis of intraductal papilloma with usual ductal hyperplasia was rendered.
In some situation, surgical excision is recommended for papillary lesions following CNB to rule out concurrent malignancy when a diagnosis of papilloma
8with atypia is yielded at CNB. However, for the papillary lesions without atypia, decision-making regarding excision versus observation are conflicting. In fact, as 17-24% of the lesions can be underestimated
13by CNB, some authoroties prefer to remove the lesions surgically. Others, however, support follow-up with repeated imaging owing to the low rate of
14malignancy of benign papillomas. Different studies reported a malignancy risk of 2-7% associated with benign papillary lesions. The rate of upstaging of the lesions in surgical excision is quite variable among published studies. There is a risk of 7.5% for the upstaging of papillary lesions without atypia. This risk
15rises to more than 30% in papillary lesions with atypia. Recently, there has been a tendency toward risk stratification instead of a uniform surgical approach for papillary lesions without atypia. According to previous studies, low-risk situations that could be followed are
15,16listed in Table 1. If there was a high-risk circumstance, excision of the lesion is prudent.
hyperplasia, cystic changes, apocrine metaplasia, fibroadenomatoid hyperplasia and sclerosing
11adenosis.
Our patient had two high-risk factors, the first being the size of mass which was about 3 cm and secondly the observation that she experienced nipple discharge.
MDT recommendationsAfter imaging review, the lesion in MRI was found
to be a BIRADS 4a lesion, and the MDT decided to review the CNB specimen histopathology result for precise interpretation due to the discrepancy between imaging and pathology. Pathology review demonstrated “intra-ductal papilloma with usual ductal hyperplasia.” The MDT recommended the excision of the lesion because it was symptomatic and the lesion was about 3 cm in size which made her follow up with a higher risk of missing an underlying malignancy. As the patient and her family were concerned about follow-up too, she underwent excisional biopsy. Postoperative pathology
The patient’s concern about malignancy is an important point that should be considered in decision-making. Patients should be informed about the low risk of malignancy in cases with benign papillary lesions without atypia, and should be part
16of the decision-making process. Our patient and her family were concerned about malignancy.
Table 1. Low-risk situations which could be considered for follow-up with imagingSize less than 1 cmAge under 50-55 yearsLesions discovered incidentallyImaging concordanceLow BIRADSCentral papilloma (located less than 5 cm from the nipple)Asymptomatic lesions
102 Mohammadi Zavieh, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 100-103
Papillary lesions of the breast

lesions at core-needle biopsy: a meta-analysis of underestimation and influencing factors. Ann Surg Oncol. 2013;20(1):94-101.
10. Rosen PP, Lyngholm B and et al. juvenile papillomatosis of the breast and family history of breast carcinoma. Cancer. 1982
11. Rosen PP, Kimmel M. Juvenile papillomatosis of the breast. A follow up of 41 patients having biopsied before 1979. Am J Clin Pathol.1990
12. Ohlinger R et al, juvenile papillomatosis (JP) of the female breast (Swiss cheese disease) ---role of breast sonography. 2005
13. Cyr AE, Novack D, Trinkaus K, Margenthaler JA, Gillanders WE, et al. Are we overtreating papillomas diagnosed on core needle biopsy? Annals of surgical oncology. 2011;18(4):946-51.
14. Sohn V, Keylock J, Arthurs Z, Wilson A, Herbert G, et al. Breast papillomas in the era of percutaneous needle biopsy. Annals of Surgical Oncology. 2007;14(10):2979-84.
9. Marc E. Lippmann; Disease of the breast/ fifth edition/chapter 9/ page 81/ juvenile papillomatosis
15. Khan S, Bear HD. Can we now reach a consensus on the management of benign papillary breast lesions? 2019.
16. MacColl C, Salehi A, Parpia S, Hodgson N, Ramonas M, et al. Benign breast papillary lesions diagnosed on core biopsy: upgrade rate and risk factors associated with malignancy on surgical excision. Virchows Archiv. 2019;475(6):701-7.
103Mohammadi Zavieh, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 100-103
Papillary lesions of the breast

In Sub-Saharan Africa, BC occurs at young age at 4
presentation and is diagnosed at advanced stage.
are marked geographical variations in incidence rates, with BC being highest in the high-income countries (HICs) and lowest in the low- and middle-income countries (LMICs). The actual incidence of BC in Sudan is unknown because of the lack of a national cancer registry. Data from hospital-based registry revealed that BC is the most common cancer
2in Sudan. A report by the Khartoum Cancer Registry showed that the incidence of BC in Khartoum state
3was 25.1 per 100,000.
IntroductionBreast cancer (BC) is the most commonly
1reported cancer among women worldwide. According to Globocan (2018), the age at which BC
1occurs worldwide was 43.1/100,000. However, there
ARTICLE INFO
Methods: In this cross-sectional study, we included all BC patients treated at the NCI-UG from January to December 2013. Patients' demographic, clinical and pathological data were retrieved from the hospital records and analyzed using SPSS version 20, and associations between these factors were tested as well.
Results: A total of 232 cases were included in this research. The majority (97.8%) of subjects were females and 2.2% were males. The median age at diagnosis was 50 years (range, 22-90). The mean time between identification of symptoms and diagnosis was 13 months (SD=16.1). Clinical stages I, II, III, and IV represented 6.9%, 37.0%, 40.9% and 15.2%, respectively. Advanced stage at diagnosis was associated with longer duration between identifying the symptoms to diagnosis (P=0.006). Also the level of education of BC patients was significantly associated with clinical stage at presentation (P = 0.01).
Conclusions: Sudanese patients with BC present at a younger age and with more advanced stage at diagnosis than those in developed countries. Patients' education level and duration from identification of BC symptoms to diagnosis significantly impact the stage at the time of presentation. In limited resource setting, early diagnosis of symptomatic BC is crucial in reducing the disease burden.
Background: Little information is available about breast cancer (BC) in Sudan. Therefore, the present study aimed to provide baseline information about the demographic features and tumor characteristics, and also to investigate the associations between demographic variables and presentation stage in BC patients attending the National Cancer Institute-University of Gezira (NCI-UG), Sudan.
Sudanese women,
18 July 2020
advanceed stage, sub-Saharan Africa
25 July 2020
Key words:
Revised:
Received:
Breast neoplasm,
delayed presentation,
Accepted:
04 April 2020
Address for correspondence: Moawia Mohammed Ali Elhassan, MDAssociate Professor of OncologyAddress: Clinical and Radiation Oncologist, National Cancer Institute-University of Gezira, Wad Madani, Sudan PO Box 20Tel: +24 9121262156 E-mail: [email protected]
104
ABSTRACT
Characteristics of Breast Cancer at First Presentation in Sudanese Patients Attending the National Cancer Institute–University ofGezira (NCI–UG)
a Department of biochemistry, Faculty of Medicine, Gezira University, Sudan
b Department of molecular biology, National Cancer Institute, University of Gezira, Sudan
c Department of biochemistry, Faculty of Medicine, Omdurman Islamic University, Sudanc Department of Radiation Oncology, National Cancer Institute, University of Gezira, Sudan
a b cMuna Ahmed Eltayeb , Areeg Faggad , Osama Sharafeldin Abbadi ,dMoawia Mohammed Ali Elhassan*
Open AccessOriginal Article
DOI: 10.32768/abc.202073104-110
Eltayeb, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 104-110

Methods
Women in this region may be aware of a breast lump for many months and not to seek medical advice until they observe complications like pain, ulcer, foul-smelling purulent discharge or symptoms of metastatic disease. Delayed presentation has been attributed to lack of early detection programs, low levels of community awareness and poor health care systems infrastructure. Undue delay is sometimes ascribed to physicians who misdiagnose the
5symptoms. The majority of Sudanese women with BC present with locally advanced disease (stage III) or worse metastatic disease (stage IV) that is difficult
6-8to treat resulting in death. It has been reported that approximately two-thirds of Sudanese women noticed symptoms of their cancer for at least 12 months prior to diagnosis which is typical in many
5, 7countries in Sub-Saharan Africa.
SettingSudan is a low-income country with approximately
40 million inhabitants. Health care in Sudan is delivered at three levels: Primary care is provided through primary health care unit, dressing stations and family health centers; the rural hospitals provide the secondary health care; and the tertiary care level is provided through teaching, general and specialized hospitals. The NCI-UG, located in Gezirastate, central Sudan, serves approximately 5 million people in Gezira and other patients from nearby states. Treatmens available at the NCI include radiotherapy, chemotherapy, and palliative care. Cancer diagnosis and treatments are available to patients for free at public cancer centers.
Study design
Data collectionA pre-designed data form was used for data
collection. The data regarding demographics, clinical characteristics, pathology, background medical history (diabetes mellitus, hypertension, and ischemic heart diseases), family history (FH) of BC,
We performed a one-year cross-sectional study to investigate the demographic features, tumor characteristics and associations between various demographic variable and stage at presentations in all BC patients treated at the NCI-UG from January to December 2013. The patients with incomplete records (missing information on stage, or histopathology) were excluded.
In Sudan, data on the epidemiology of BC is 2,6-8
limited. Therefore, we conducted this study to provide baseline information about the demographic features, tumor characteristics, and the associations between various demographic variable and stage at presentations in BC patients treated at the National Cancer Institute-University of Gezira (NCI-UG), Sudan.
and disease clinical stage were obtained from patient medical files. The patients with first or second degree relatives with BC were considered positive for FH of BC. Tumor characteristics including histological types, grade, lymphovascular invasion (LVI), estrogen receptor (ER) and progesterone receptor (PR) status in addition to human epidermal growth factor receptor 2 (HER2) were obtained from histopathology reports attached to patients’ folders. All records were retrieved from the NCI-UG Records, Statistical and information Unit.
Results
Tumor characteristics
Patient Characteristics
Ethical considerations
The data was coded and analyzed by SPSS, version 20. Patient characteristics were described as frequencies and percentages for categorical variables or as median (range) and mean (SD) for numerical variables. Chi-square test and ANOVA test were used for comparisons and statistical analysis of association. A P value of 0.05 or less was assumed to be statistically significant.
A total of 232 patients were included in the study. The median age at diagnosis was 50 years (range, 22-90). The vast majority (97.4%) of the patients were females. The majority of the patients were unemployed (85%). More than half (59%) of women with BC were postmenopausal while 41% were premenopausal. The median age of menarche was 14 years (range, 10-18). Approximately 20% (45 cases) of patients had background medical history of diabetes mellitus (21 cases), hypertension (21 cases), and ischemic heart diseases (3 cases). 55% of our patients were from rural areas and only 15% had family history of BC. Table 1 illustrates the main demographic characteristics of the study population according to patients’ residence.
Statistical analysis
Ethical approval was obtained from the Ethics Committee at the NCI-UG. Subsequently, the proposal was reviewed by the Oncology Research Committee at the Sudan Medical Specialization Board.
Histopathology examination of tumors revealed invasive ductal carcinoma as the most common type (70.3%) followed by infiltrating lobular carcinoma (12.9%) and malignant phyllode tumors (5.2%). Other subtypes represented a small percentage of the cases. Tumor characteristics are presented in Table 2. Tumor tissues were found to be hormone receptors (HR) positive i.e. ER positive and/or PR positive in 102 (44%) cases while 89 (38.8%) cases presented as HR negative i.e. both ER-negative and PR-negative. Information on ER and PR status was not available in 40 (17%) cases. Only few (67/232; 28.9%) patients
BC presentation in Sudan
105Eltayeb, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 104-110

documented in 18 patients. At time of diagnosis, 58% of cases had palpable regional lymph node and 37(16%) patients had metastat ic disease. Mammography as part of triple assessment was conducted for about 36.2% of the patients. Data on the time interval between identification of symptoms by the patients and diagnosis was available for 220 patients (Figure 1). The mean time between identifying the symptoms by BC patients and diagnosis was 13 months (SD=16.1). Only 15 (6.8%) out of 220 patients had less than one-month duration
Breast mass was the most frequently reported clinical presentation (86%). Less frequent symptoms included breast pain (6%), nipple discharge (5%) and axillary mass (3%). Only 30 patients were diagnosed with tumors less than 2 cm (T1), 84 patients had tumor size 2-5cm (T2) and 67 patients with tumor bigger than 5 cm. Approximately, 30% (n= 68) of our patients presented with ulcerated tumor and/or fixed to skin or chest wall. The tumor size was not
were tested for HER2 status as shown in Table 2.Presenting symptoms
Table 1. Demographic characteristics of breast cancer patients according to residence
Characteristics RuralN (%)
UrbanN (%)
TotalN (%)
P Value
Sex
Age
Duration of symptoms
Menopausal Status
F/H of Breast cancer
Education level
FemaleMaleTotal
MeanSD
MeanSD
Pre-menopausalPost-menopausalTotal
YesNoTotal
IlliteratePrimarySecondaryHighTotal
122 (54.0%)4 (80.0%)
126(54.5%)
50.114.4
13.514.3
52 (56.9%)70 (52.6%)122 (54.0%)
18 (43.9%)104(58.1%)122 (55.5%)
55 (73.3%)50 (56.0%)16 (35.6%)5 (22.7%)
126 (54.8%)
104 (46.0%)1 (20.0%)
105 (45.5%)
51.612.3
12.518.2
41 (44.1%)63(46.4%)
104 (46.0%)
23 (56.1%)75 (41.9%)98 (44.5%)
20 (26.7%)30 (43.2%)29 (64.4%)17 (77.3%)104 (45.2%)
226 (100%)5 (100%)
231 (100%)
93 (100%)133 (100%)226 (100%)
41 (100%)179 (100%)220 (100%)
75 (100%)88 (100%)45 (100%)22 (100%)230 (100%)
0.24
0.37
0.71
0.64
0.07
0.001
- N; number, F/H, Family history; SD, Standard deviation - Missing data not included in the analysis
Table 2. Pathological characteristics of breast cancer patients (232 cases)
Characteristics Frequency Percentage
Histopathology
Grade
Presence of LVI
Presence of DCIS
HR status
HER2 status
Invasive Ductal CarcinomaInvasive Lobular carcinoma Malignant phyllodes tumorOthers
IIIIIIUnknown
YesNoUnknown
YesNoUnknown
Positive (ER +ve and/or PR +ve)Negative (ER –ve and PR –ve)Unknown
PositiveNegativeUnknown
163301227
19978729
469195
1328191
1029040
3235165
70.3%12.9%5.2%11.6%
8.2%41.8%37.5%12.5%
19.8%39.3%40.9%
5.6%12.1%82.3%
44.0%38.8%17.2%
13.8%15.1%71.1%
LVI: lymphovascular invasion; DCIS: ductal carcinoma in situ; HR: hormone receptor; ER: estrogen receptor; PR: progesterone receptor; HER2: Human epidermal growth factor receptor 2
BC presentation in Sudan
106 Eltayeb, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 104-110

Figure 1. Distribution of BC Patients (220 cases) According to Time between Recognition of Symptoms and Diagnosis
Table3. Comparison of different characteristics amongst disease stage at presentation
Stage IV Total P value
Age
Sex
Level of Education
Residence
Marital Status
Symptoms duration
Parity
F/H of breast cancer
Menopausal Status
Mean SD
FemaleMaleTotal
illiteratePrimarySecondaryHigherTotal
RuralUrbanTotal
MarriedSingleWidowed/DivorcedTotal
MeanSD
NulliparousParousTotal
YesNoTotal
PremenopausalPostmenopausalTotal
48.812.2
15 (6.6%)0
15 (6.5%)
2 (2.7%)6 (6.8%)6 (12.8%)1 (4.8%)15 (6.5%)
6 (4.7%)9 (8.6%)15 (6.5%)
12 (7.5%)2 (8%)
1 (2.2%)15(6.5%)
6.76.5
3 (6.2%)9 (5.6%)12 (5.7%)
3 (7.3)10 (5.6)
13 (5.9%)
7 (7.5%)8 (6.0%)15 (6.6%)
49.012.8
82 (36.1%)3 (60.0%)85 (36.6%)
16 (21.3%)35 (39.8%)23 (48.9%)11 (52.4%)85 (36.6%)
45 (35.7%)40 (38.1%)85 (36.6%)
60 (37.5%)12 (48.0%)13 (28.3%)
85(36.8)
9.9 13.2
20 (41.7%)56 (34.8%)76 (36.4%)
17 (41.5%)64 (35.6%)81 (36.7%)
35 (37.6%)48 (35.8%)83 (36.7%)
52.113.7
93 (41.0%)2 (40.0%)95 (41.0%)
42 (56.0%)31 (35.2%)13 (27.7%)8 (38.1%)94(40.7)
55 (43.7%)39 (37.1%)94 (40.7%)
65 (40.6%)6 (24.0%)23 (50.0%)94(40.7%)
13.8 17.5
19 (39.6%)71 (44.1%)90 (43.1%)
14 (34.1%)77 (42.8%)91 (41.2%)
36 (38.7%)56 (41.8%)92 (40.5%)
52.414.8
37 (16.3%)0
37 (15.9%)
15 (20.0 %)16 (18.2%)5 (10.6%)1 (4.8%)
37 (16.0%)
20 (15.9%)17 (16.2%)37 (16.0%)
23 (14.4)5 (20.0%)9 (20.0%)37(16%)
20.5 18.2
6 (12.5%)25 (15.5%)31 (14.8%)
7 (17.1%)29 (16.1%)36 (16.3%)
15 (16.0%)22 (16.4%)37 (16.2%)
227 (100%)5 (100%)
232(100%)
75 (100%)88 (100%)47 (100%)21 (100%)231(100%)
126 (100%)105 (100%)231 (100%)
160 (100%)25 (100%)46 (100%)231(100%)
48 (100%)161(100%)209 (100%)
41 (100%)180 (100%)221 (100%)
93(100%)134 (100%)227 (100%)
0.37
059
0.01
0.61
0.32
0.006
0.82
0.77
0.11
of symptoms before diagnosis.
Slightly more than half of cases had locally advanced BC i.e. Stage III (40.9%) or metastatic disease i.e. Stage IV (15.9%). Stage I and II were seen in 6.5% and 36.6% of our cases, respectively. Higher stage at diagnosis was associated with longer duration between identifying the symptoms by patients and diagnosis (P=0.006) as shown in Table 3 and Figure 2. Level of education was significantly associated with clinical stage at presentation (P= 0.01) as seen in Table 3.
Clinical stage
Discussion Male breast cancer accounted for 2.2% of our
Worldwide, BC accounts for 24.2% of female 1cancer burden. In Central Sudan, BC is the most
common cancer representing 34% of all female 9
cancers. Epidemiological characteristics of BC appear to be different in LMICs compared to HICs, with notably large proportions of young patients and
8,10-12aggressive forms of the disease. In the present study, the average age at diagnosis (50 years) is consistent with previous reports from Sub-Saharan Africa including Sudan, but approximately 10 years
13earlier than women in HICs. The low frequency of grade 1 tumors observed in the current study is
13consistent with a previous report from Sudan.
Characteristics Stage I Stage II Stage III
Figure 2. Distribution of mean duration between identification of symptoms by patients and diagnosis according to stage at diagnosis
BC presentation in Sudan
107Eltayeb, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 104-110

It has been reported that African women living in the rural areas are particularly vulnerable to late-stage diagnosis, partially due to the high cost of transportation and time taken to reach a secondary or
6a tertiary health care facility. In the current study, women from rural areas presented more often with stage III or IV disease than women from urban areas. In our limited resources setting, the reason for the high rate of late-stage diagnosis among BC patients from rural areas is not well understood and needs further studies.
study population. This finding is within the range that was reported previously for patients from Sudan
11, 14and other African countries, but higher than 15,1
populations in HICs. Considering that blacks living in the United States had higher male-to-female ratio than their white counterparts, it is plausible to suggest that genetic background plays an important role in this phenomenon. The significant role of BRCA1/2 as an etiological factor of male BC in
16central Sudan was highlighted in a previous study.In this study, more than half of the patients
presented with locally advanced (Stage III) or metastatic tumors (Stage IV). This has also been
4,12observed in other African countries. This is largely attributed to modifiable factors such as poor BC knowledge, illiteracy, and limited health care
4 infrastructure with no screening program for BC.The level of education in the current study was able to demonstrate significant association with clinical stage at presentation. Several other studies have previously reported that education has a significant impact on stage at diagnosis and the prognosis of this
4, 17devastating disease. A possible explanation for the result in the current study is that well educated women are more likely to live in more developed cities and subsequently have a better access to health care services.
Mammography screening increases the detection of early-stage BC. In this study, only 40% of our patients had access to mammography. This is because, during the study period, there was no functioning mammography machine outside the capital, Khartoum. The impact of screening mammography in BC stage at diagnosis has been
18, 19examined in several studies. Taplin and colleagues used data that included 1.5 million women aged 50 years or older to examine differences in screening implementation among women with late-stage and early-stage breast cancer. They found that late-stage cancers were higher among women with an absence
18of screening. A study conducted in Sudan showed that implementation of BC awareness and breast examination program that uses local volunteer women could increase the early detection of BC in
20rural areas. In our limited resource setting, lack of national program for BC screening as well as shortage of health educational programs on BC could be contributing factors to the advanced stages
The authors have no conflicts of interest to declare.
Our study suffers from several limitations including its retrospective nature and reliance on medical records. Moreover, it is a single institution’s data; we therefore cannot make conclusions for all parts of Sudan. However, the NCI-UG is one of the only two referral oncology hospitals in central Sudan; therefore, the current data provide a background for the epidemiology of BC within this region.
at presentation.
In Africa, there are considerable uncertainties 24
regarding the frequency of ER/PR subtypes. In previous BC series from Sudan considering the rate of ER/PR status, researchers reported inconsistent findings, although recent studies have suggested
6, 8, 13, 25,26increased ER/PR positivity. This difference probably reflects enhanced quality control procedures in our setting. In this study, 44% were ER and/or PR positive while 38.8% were ER-negative and PR-negative. Information on ER and PR status was not available in 40 (17%) cases.
In conclusion, we found that BC patients tend to be younger and present with more advanced stages at diagnosis than those in HICs. This study shows that the level of patient education and the duration from recognition of BC symptoms by the patients to diagnosis have a significant impact on stage at which the patients present. Our study showed that achieving earlier diagnosis of symptomatic BC is an important step in reducing the morbidity and mortality from this devastating disease.
The earlier BC is identified, the better chance in reducing the mortality from this disease. Studies have shown that a shorter time between the recognition of BC symptoms and the first medical consultation is associated with early-stage
21,22disease. Yet, delayed presentation of BC patients is typical of many African countries, including
5, 7, 23Sudan. We found the average duration between recognition of symptoms to diagnosis was 13 months, which is almost similar to previous studies
7, 23from Sudan. In our study, higher stage at diagnosis was significantly associated with longer duration between identification of symptoms by the patients and diagnosis. It has been reported that late stage diagnoses could be avoided if all patients with BC symptoms would present to a doctor within 1
22month. In the current study, a small number of patients (6.8%) identified the symptoms less than one month before diagnosis.
Conflict of interest
References 1. Bray F, Ferlay J, Soerjomataram I, Siegel RL,
Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and
BC presentation in Sudan
108 Eltayeb, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 104-110

7 . Alawad AA, Alsh iekh AA, Alha j AM. Demographic Characteristics and Review of Patients with Locally Advanced Breast Cancer in Sudan. AFRIMEDIC Journal. 2013;4(2):5-8.
5. Scheel JR, Anderson S, Foerster M, Galukande M, McCormack V. Factors Contributing to Late-Stage Breast Cancer Presentation in sub-Saharan Africa. Current Breast Cancer Reports. 2018.
6. Elgaili EM, Abuidris DO, Rahman M, Michalek AM, Mohammed SI. Breast cancer burden in central Sudan. International journal of women's health. 2010;2:77-82.
mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians. 2018;68(6):394-424.
2. Elamin A, Ibrahim ME, Abuidris D, Mohamed KE, Mohammed SI. Part I: cancer in Sudan-burden, distribution, and trends breast, gynecological, and prostate cancers. Cancer medicine. 2015;4(3): 447-56.
3. Saeed IE, Weng HY, Mohamed KH, Mohammed SI. Cancer incidence in Khartoum, Sudan: first results from the Cancer Registry, 2009-2010. Cancer medicine. 2014;3(4):1075-84.
4. McKenzie F, Zietsman A, Galukande M, Anele A, Adisa C, Parham G, et al. Drivers of advanced stage at breast cancer diagnosis in the multicountry African breast cancer - disparities in outcomes (ABC-DO) study. International journal of cancer. 2018;142(8):1568-79.
8. Mariani-Costantini R, M.M.A. E, Aceto GM, M o h a m e d a n i M A , Aw a d e l k a r i m K D . Epidemiology, Pathology, Management and Open Challenges of Breast Cancer in Central Sudan: A Prototypical Limited Resource African Setting. In: Pham PV, editor. Breast Cancer - From Biology to Medicine: IntechOpen; 2017.
9 . Elhassan M. Access to Treatment for Gynaecological Malignancies in Sudan. South Afr J Gynaecol Oncol. 2018;10(2):21-3.
11. Ndom P, Um G, Bell EM, Eloundou A, Hossain NM, Huo D. A meta-analysis of male breast cancer in Africa. Breast. 2012;21(3):237-41.
10. Corbex M, Bouzbid S, Boffetta P. Features of breast cancer in developing countries, examples from North-Africa. European journal of cancer. 2014;50(10):1808-18.
12.Kantelhardt EJ, Muluken G, Sefonias G, Wondimu A, Gebert HC, Unverzagt S, et al. A Review on Breast Cancer Care in Africa. Breast care. 2015;10(6):364-70.
14. Elhaj A, Awadelkarim KD. Male breast cancer patients: a retrospective study of patients
13. Awadelkarim KD, Arizzi C, Elamin EO, Hamad HM, De Blasio P, Mekki SO, et al. Pathological, clinical and prognostic characteristics of breast cancer in Central Sudan versus Northern Italy: implications for breast cancer in Africa. Histopathology. 2008;52(4):445-56.
16. Awadelkarim KD, Aceto G, Veschi S, Elhaj A, Morgano A, Mohamedani AA, et al. BRCA1 and BRCA2 status in a Central Sudanese series of breast cancer patients: interactions with genetic, ethnic and reproductive factors. Breast cancer research and treatment. 2007;102(2):189-99.
18. Taplin SH, Ichikawa L, Yood MU, Manos MM, Geiger AM, Weinmann S, et al. Reason for late-stage breast cancer: absence of screening or detection, or breakdown in follow-up? Journal of the National Cancer Institute. 2004;96(20): 1518-27.
20. Abuidris DO, Elsheikh A, Ali M, Musa H, Elgaili E, Ahmed AO, et al. Breast-cancer screening with trained volunteers in a rural area of Sudan: a pilot study. The Lancet Oncology. 2013;14(4): 363-70.
21. Neal RD, Tharmanathan P, France B, Din NU, Cotton S, Fallon-Ferguson J, et al. Is increased time to diagnosis and treatment in symptomatic cancer associated with poorer outcomes? Systematic review. British journal of cancer. 2015;112 Suppl 1:S92-107.
22. Arndt V, Sturmer T, Stegmaier C, Ziegler H, Dhom G, Brenner H. Patient delay and stage of diagnosis among breast cancer patients in Germany -- a population based study. British journal of cancer. 2002;86(7):1034-40.
characteristics and treatment outcome at the National Cancer Institute (NCIUG) - Central Sudan. Pan Arab Journal of Oncology. 2012;5(1).
15. Anderson WF, Althuis MD, Brinton LA, Devesa SS. Is male breast cancer similar or different than female breast cancer? Breast cancer research and treatment. 2004;83(1):77-86.
23. Salih AM, Alfaki MM, Alam-Elhuda DM, Nouradyem MM. Factors Delaying Presentation of Sudanese Breast Cancer Patients: an Analysis Using Andersen’s Model. Asian Pac J Cancer Prev. 2016;17(4):2105-10.
17. Wang K, Li X, Zhou C, Ren Y, Wang XB, He JJ. Socio-economic factors influencing tumor presentation and treatment options in Chinese breast cancer patients. Asian Pac J Cancer Prev. 2013;14(1):267-74.
24. Eng A, McCormack V, dos-Santos-Silva I. Receptor-defined subtypes of breast cancer in indigenous populations in Africa: a systematic review and meta-analysis. PLoS medicine. 2014;11(9):e1001720.
25. Gismalla MD, Elhassan MM, Abass MO. Clinical and pathological factors predicting axillary nodal metastasis in breast cancer patients of central Sudan: A single institution
19. Jacobellis J, Cutter G. Mammography screening and differences in stage of disease by race/ethnicity. American journal of public health. 2002;92(7): 1144-50.
BC presentation in Sudan
109Eltayeb, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 104-110

experience. . Saudi J Health Sci 2019;8:146-50.26. Salim OE, Mukhtar SI, Mohammed BI, Salih N,
Hamad K. Breast cancer in Africa, are we dealing with a different disease Sudan Med J 2014;50(1):1-24.
BC presentation in Sudan
110 Eltayeb, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 104-110

low incidence-to-mortality ratio, which it is often related to delays in diagnosis and to the
2unavailability of surgical or medical treatment.
Clinical characteristics and outcomes of BC patients vary depending on the study population. Previous studies have acknowledged that Hispanic patients feature different tumor subtypes and share poor long-term outcomes in comparison to non-
3,4 Hispanic populations.Guatemala is a low-middle income country
(LMIC) with 17 million habitants, mainly composed 5by mestizos (60.1%) and indigenous (39.3%) people.
Like some other countries in Central America,
IntroductionBreast cancer (BC) is the most common
malignancy and the major cause of cancer-related 1death among women worldwide. In developing
countries, the burden of this disease is reflected in the
ARTICLE INFO
Conclusion: The majority of patients with non-metastatic BC are diagnosed with advanced disease and many of them are younger than 50 years old. OS in this cohort of Guatemalan patients is lower than that reported in developed countries.
Background: Breast cancer (BC) is a leading cause of cancer related death worldwide. Unfortunately, data concerning clinicopathologic features of this malignancy in non-developed countries is scarce. This study aims to characterize a cohort of Guatemalan female patients with non-metastatic BC and to determine risk factors for overall survival (OS).
Methods: We retrieved data on consecutive patients from the Instituto Guatemalteco de Seguridad Social that were treated from 2008 to 2014. Clinical features and long-term outcomes were retrieved from medical records. Univariate and multivariate Cox regression analyses were conducted to identify variables associated with OS.
Results: 954 BC patients were identified during the time frame. A total of 436 women (46%) were younger than 50 years old. BC molecular subtypes categorized 537 patients (56.3%) with luminal A disease, 186 (19.5%) patients with triple negative tumors, 153 cases (16.1%) with HER-2 enriched tumors, and 78 patients (8.2%) with luminal B tumors. Clinical stage at presentation was stage I: 4.7% (n=45); stage II: 48.1% (n=459), and stage III: 47.2% (n=450). The overall 5-year survival rate was 75.2% (95% Confidence Interval: 72.0–78.3). In the multivariate analysis clinical stage, triple negative tumors and HER2 enriched tumors were independently associated with poor survival.
Received:
Accepted:
survival
03 June 2020
12 August 2020
Key words:
Guatemala;
Revised:
18 August 2020
Brest cancer;
Address for correspondence: Hugo Castro, MD. Address: Grupo Médico Angeles, 2da calle 25-19 zona 15, Vista Hermosa I; Edificio Multimedica, of 10-15, Guatemala City, Guatemala.Tel: (+502) 2385-7572E-mail: [email protected]
111
ABSTRACT
Clinicopathologic Features and Survival Analysis of Non-metastaticBreast Cancer Patients in Guatemala
a Grupo Médico Ángeles, Guatemala City, Guatemala
b Social Security Institute of Guatemala, Guatemala City, Guatemala
c Nacional Institute of Cancer of Guatemala, Guatemala City, Guatemalad School of Medicine, University of Costa Rica, San José, Costa Rica
a b c b dHugo Castro-Salguero* , Luis García Aceituno , Alba Kihn , Raúl Jiménez , Allan Ramos-Esquivel
Open AccessOriginal Article
Castro, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 111-118
DOI: 10.32768/abc.202073111-118

Given the expected increase of BC incidence and mortality in the coming years, and the relevance of these unknown data to Health care providers, we decided to conduct this study in order to describe clinical characteristics of non-metastatic BC patients from Guatemala and to identify clinical determinants of OS.
MethodsWe retrospectively reviewed the clinical records
of all patients diagnosed with non-metastatic BC at the Instituto Guatemalteco de Seguridad Social (IGSS) between January 2008 and December 2014. The IGSS is a referral center that provides health services to about 17% of the Guatemalan employed
7population. All cases were histologically confirmed by excisional or core needle biopsy before treatment. All patients were classified according to the American Joint Committee on Cancer Staging
8Manuel (TNM), Seventh Edition. For eligible patients we collected clinical data from medical records.
The adjuvant/neoadjuvant treatment regimens were decided by the medical oncologist in charge, and consisted of one of the following regimens: a) four cycles of adriamycin 60 mg/m2 and cyclophosphamide 600 mg/m2 (AC) every 21-days followed by paclitaxel 80 mg/m2 weekly for 12 weeks or for 4 cycles of docetaxel 75 mg/m2 every 21-days; b) 4 cycles of neoadjuvant AC followed by surgery and 4 cycles of adjuvant docetaxel
Patients were evaluated to receive neoadjuvant therapy in a multidisciplinary session. Patients with clinical response to neoadjuvant treatment were evaluated before each chemotherapy cycle, those with stable disease considered to be inoperable underwent radiotherapy followed by surgery. Pathological complete response (pCR) was considered to be the absence of any tumor cells both in the tumor and
13lymph nodes (ypTis or ypT0 and ypN0).
Guatemala has undergone an epidemiological and demographic transition, and the incidence and mortality of BC is increasing, with few data reported on the clinical characteristics and determinants of
6overall survival (OS) and disease-free survival.
The BC pathologist in charge assessed histological subtype, nuclear grade, and interpreted the immunohistochemical (IHC) analysis of all cases in formalin-fixed paraffin-embedded tissues from incisional biopsies taken for diagnosis. Estrogen receptor (ER), progesterone receptor (PR), Ki-67 index, and expression and/or HER2 gene amplification were conducted following current
9, 10recommendations. HER2 was deemed positive based on American Society of Clinical Oncology
11(ASCO) guideline. Breast cancer intrinsic subtypes 12
were specified based on St Gallen 2015 Consensus. Tumor size and lymph node involvement were reported in the pathological specimen after surgery.
(recommended for high risk patients based on the presence of at least one of the following characteristics: four or more positive axillary nodes, grossly evident extracapsular nodal extension, large primary tumors, and very close (< 1mm) or positive deep margins of resection of the primary tumor); c) dose-dense chemotherapy (recommended for women suffering from advanced or inflammatory breast cancer); d) platinum-based regimen (recommended for patients with TNT); e) six cycles of cyclophosphamide 600 mg/m2, methotrexate 40 mg/m2 and 5-fluorouracil 600 mg/m2 (CMF regimen); f) 4 cycles of AC adjuvant (recommended in low risk patients); g) endocrine therapy (tamoxifen, anastrozol or letrozol). Patients with HER2 positive tumors received trastuzumab for 52 weeks in the adjuvant setting.
Routine follow-up of these patients comprised clinical examination every three months during the first three years and yearly thereafter. An annual mammography was performed on all included patients.
Statistical analysisContinuous variables are presented as means and
standard deviations (SD). Categorical variables are presented as frequencies. The comparisons between continuous variables were made by the ANOVA test. The Chi-square test was run to evaluate the statistical association between categorical variables. The Kaplan-Meier method was used to determine the probability of OS and DFS. Follow-up was determined from the date of diagnosis to the date of last follow-up or death from any cause. Recurrence was defined by the clinical or histopathological evidence of metastatic disease as measured by the RECIST 1.1 criteria. The survival curves were compared by the log-rank test. Univariate and multivariate Cox’s regression analyses were performed to determine the hazard ratio (HR) with 95% confidence interval (95%CI) for OS. The multivariate model included only those variables with p values less than 0.10 in the univariate analysis. A p value less than 0.05 was assumed to be statistically significant. The statistical analysis was performed using SPSS version 22 for Mac (SPSS, Inc., Chicago, IL, USA).
ResultsGeneral characteristicsA total of 954 patients were identified during the
time frame. Table 1 summarizes the clinical characteristics of the population and categorized based on breast cancer intrinsic subtype, as assessed by IHC. In total, 436 women (46%) were younger than 50 years old, and only 72 patients (7.5%) were older than 70 years. The majority of patients (n=725, 76%) were diagnosed with advanced disease (stages IIB to IIIC).
Breast cancer in Guatemala
112 Castro, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 111-118

Median OS and DFS according to clinical stage, breast cancer subtype, and tumor grade are provided in Table 2. The results of the univariate and multivariate analyses for OS are depicted in Table 3. Figure 2 depicts the rate of OS according to breast cancer intrinsic subtype. 5-year OS according to clinical stage was 88.1% (95%CI: 78 – 97%) for stage I, 87.4% (95%CI: 84 – 90%) for stage II, and 60% (55 – 64%) for stage III. (Figure 3)
Overall median survival time after breast cancer diagnosis was 112 months (95%CI: 95.3 – 128.8), and the overall 5-year survival rate was 75.2% (95% CI: 72.0 – 78.3).
Most common distant sites at recurrence included lung (n=114; 44.7%), bone (75; 29.4%), central nervous system (n=47; 18.4%), and liver (n=38; 14.9%). Local recurrent disease was presented in 35 (13.7%) cases.
events were confirmed by biopsy. The majority of patients with recurrent events (n=167; 65.5%) were treated with chemotherapy, followed by best supportive care in 34 patients (13.3%), and hormonal therapy in 27 patients (10.6%). Only 15.6% of patients with hormone-receptor positive disease at recurrence were treated with hormonal therapy.
Pathological complete response was achieved by 27% and 33% of patients with HER2 positive tumors and TNT, respectively. The OS analysis showed that patients achieving pCR had better OS than their counterparts (Hazard ratio: 0.56; 95%CI: 0.36-0.88; p=0.001).
Long-term outcomes
A total of 678 (71.0%) patients were treated with adjuvant chemotherapy, and 277 patients (29%) underwent neoadjuvant therapy. Among patients receiving preoperative chemotherapy, we identified 72 patients (26%) with pCR, and 183 patients (66%) with partial response. A total of 8 cases (3%) had p rogres s ive d i sease du r ing neoad juvan t chemotherapy.
Median OS among patients with pCR was 100 months (95% CI: 46.9-153.0), while patients without pCR had a median OS time of 73 months (95%CI: 59.7 – 86.3 months). (Figure 1)
Medical therapy and response to neoadjuvant chemotherapy
After a median follow up of 52 months, a total of 242 patients died (25.4%) and 255 (26.8%) had a recurrent event. Only 28.4% of these recurrent
Table 1. Demographic characteristics of patients included in the study with breast cancer
Characteristic Luminal A(n=537; 56.3%)
Luminal B(n=78; 8.2%)
All (n=954) HER2(n=153; 16.1%)
Triple Negative(n=186; 19.5%)
P Value
Age(Years, SD)
Clinical stage (%)
Histological Type (%)
Nuclear grade (%)
Body Mass Index (%)
Treatment (%)
Age
IAIBIIAIIBIIIAIIIBIIIC
DuctalLobularUnknown
LowIntermediateHighUnknown
ObeseOverweightNormalUnderweightUnknown
Adjuvant chemotherapyNeoadjuvant chemotherapyChemotherapy + RadiotherapySurgery aloneSurgery +endocrine therapyNeoadjuvant and adjuvant chemotherapy Unknown
52.4 ± 12.5
5 (0.5)40 (4.2)
184 (19.3)275 (28.8)318 (33.3)119 (12.5)13 (1.4)
893 (93.6)59 (6.2)2 (0.2)
122 (12.8)403 (42.2)310 (32.5)119 (12.5)
232 (24.3)362 (37.9)336 (35.2)12 (1.3)12 (1.3)
549 (57.5)
184 (19.3)
36 (3.8)
8 (0.8)82 (8.6)
93 (9.7)
2 (0.3)
54.0 ± 12.2
5 (0.9)25 (4.7)
117 (21.8)158 (29.4)174 (32.4)54 (10.1)4 (0.7)
490 (91.2)47 (8.8)
0 (0)
91 (16.9)258 (48.2)109 (20.2)79 (14.7)
132 (24.6)208 (38.7)183 (34.1)
7 (1.3)7 (1.3)
329 (61.3)
85 (15.8)
20 (3.7)
2 (0.4)72 (13.4)
28 (5.2)
1 (0.2)
52.08 ± 12.9
0 (0)2 (2.6)
13 (16.6)26 (33.3)27 (34.8)9 (11.4)1 (1.3)
74 (94.9)4 (5.1)0 (0)
6 (7.7)38 (48.7)23 (29.5)11 (14.1)
21 (26.9)26 (33.3)26 (33.3)1 (1.3)4 (5.2)
43 (55.1)
12 (15.4)
1 (1.3)
0 (0.0)8 (10.3)
13 (16.7)
1 (1.3)
51.05 ± 12.9
0 (0)9 (5.9)
24 (15.7)35 (22.9)49 (32.0)30 (19.6)6 (3.9)
150(98.0)1 (0.7)2 (1.3)
10 (6.5)48 (31.4)85 (55.5)10 (6.5)
30 (19.6)58 (37.9)64 (41.8)1 (0.7)0 (0)
85 (55.6)
30 (19.6)
5 (3.3)
3 (2.0)1 (0.7)
29 (19.0)
0 (0.0)
49.37 ± 11.9
0 (0)4 (2.2)
30 (16.0)56 (30.1)68 (36.6)26 (14.0)2 (1.1)
179 (96.2)7 (3.8)0 (0)
15 (8.1)59 (31.7)93 (50.0)19 (10.2)
49 (26.3)70 (37.7)63 (33.9)3 (1.6)1 (0.5)
92 (49.5)
57 (30.6)
10 (5.4)
3 (1.6)1 (0.5)
23 (12.4)
0 (0.0)
< 0.001
0.016
< 0.001
< 0.001
0.158
< 0.001
Breast cancer in Guatemala
113Castro, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 111-118

Figure 1.
Figure 2.
Breast cancer in Guatemala
114 Castro, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 111-118

Figure 3.
Table 2. Overall survival and disease-free survival according to clinical stages, intrinsic breast cancer subtypes, and tumor grade.
Variable P ValueMedian Disease-Free Survival (months)
(95% CI)
Median Overall Survival (months)
(95% CI)
5 years OverallSurvival rate
(95% CI)
P Value
Clinical stage
Intrinsicbreast cancer subtype
IA IB IIA IIB IIIA IIIB IIIC Luminal ALuminal BHER2 positiveTriple negative
Histological grade I or IIIII
33 (27.9 – 38.1)35 (17.3 – 52.7)30 (26.6 – 33.4)24 (19.9 – 28.1)21 (16.7 – 25.3)16 (10.0 – 22.0)
31 (25.9 -36.0)35 (24.8 – 45.2)19 (13.3 – 24.6)16 (21.2 – 26.9)
30 (26.4 – 33.6)19 (15.4 – 22.6)
< 0.001
< 0.001
< 0.001
97 (72.9 – 121.1)Not reached*Not reached*
85 (72.7 – 127.6)51 (34.0 – 67.9)35 (28.3 – 41.6)
112 (non calculable**)78 (non calculable**)
Not reached*72 (57.5 – 86.5)
112 (95.2 – 128.8)85 (73.6 – 96.4)
80 (47 – 100)89 (79 – 98)88 (82 – 93)86 (81 – 90)71 (65 – 76)39 (29 – 48)44 (16 – 71)
83 (79 – 86)68 (56 – 79)69 (61 – 77)59 (51 – 66)
83 (79 - 87)60 (53 - 66
< 0.001
< 0.001
< 0.001
*Not reached: Longer follow-up is needed in order to achieve the median overall survival in this subgroup.**Non-calculable: The formula for the estimation of the 95% confidence interval was not applicable due to large sample variation.
Table 3. Univariate and multivariate analysis of overall survival for the entire population
Variable Univariate analysis Multivariate analysis
1.00 (0.99-1.01)
Reference3.56 (1.66-7.57)3.79 (2.81-5.10)0.45 (0.35-0.58)1.28 (0.97-1.70)2.55 (1.94-3.34)
Age (years)Clinical stage I II IIIER positiveHER2 positiveTriple negative
0.98< 0.001
< 0.0010.081
< 0.001
Reference2.72 (1.83 – 4.05)5.44 (3.66 – 8.10)1.11 (0.68 – 1.81)1.87 (1.21 – 2.89)3.32 (1.88 – 5.89)
<0.001
0.670.005
<0.001
P ValueHazard ratio (95% CI) P ValueHazard ratio (95% CI)
115Castro, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 111-118
Breast cancer in Guatemala

Although BC mortality in Guatemala ranks among the lowest worldwide1, the 5-year OS is considerably lower than that reported in developed
23countries. Similarly, the 5-year OS by subtype was lower than previously reported, particularly in TN
23and HER2 positive tumors. These differences can be attributed to the unavailability of medical therapies or delays in referral and treatment initiation in our cohort, as previous authors have already
24noticed, but also can be a reflection of the over-representativeness of young patients with high grade and TN tumors, since some authors have argued that young age at diagnosis is independently related to
25worse long-term prognosis.
Our study also revealed a high proportion of patients younger than 50 years old. This percentage is higher than that reported for American populations
16according to the SEER Registry (46% vs. 19%) , but similar to the percentage previously reported in
21Mexican patients. Similarly, Hispanic patients living in USA usually are younger than their White
17counterparts. This finding is of paramount importance for screening purposes in our country.
Our findings also showed that the percentage of patients with TN tumors (19.5%) is higher than that
16,17reported for Caucasian (10-12.5%) and Asian 18populations (8%) , and similar to that reported in
19 20Mexico (23.1%) and Costa Rica (17.1%) Indeed, clinical characteristics of patients with TN tumors are very similar to Mestizo populations reported
21elsewhere , such as young age at diagnosis, and high grade histological differentiation. These differences in BC subtypes among ethnic groups can reflect variations in the prevalence of risk factors, as well as
22a consequence of intrinsic genetic variations.
Our study also described the results of neoadjuvant chemotherapy in operable BC patients. Although the percentage of patients undergoing preoperative treatment was similar to that reported in
26, 27other cohorts (19.3%) , our data suggest that neoadjuvant therapy was underused, since the majority of patients in our cohort had locally
Our study reports, for the first time, a clinical depiction of a cohort of Guatemalan patients with non-metastatic BC. These findings show that the majority of cases presented with large tumors and lymph nodal metastases. It has been postulated that lack of access to health services and lack of screening policies are responsible for the high incidence of locally advanced tumors in this particular
14population. Indeed, only one-third of patients were diagnosed at an early stage, suggesting a lack of BC awareness and little access to screening and health care services. Previous authors have reported that adherence to mammography guidelines is considerably low among Guatemalan females as a consequence of a lack of insurance coverage and low
15 education.
Discussion
Other authors declare no conflicts of interest.
advanced disease. In concordance with previous 28
reports , our data showed an OS improvement in favor of those patients who achieved pCR, a finding that must be interpreted cautiously because of the small sample size undergoing neoadjuvant chemotherapy in our cohort.
The Guatemalan government´s expenditure on health care is among the lowest of Central American
29countries. This, and other challenges such as the
30low health insurance coverage , and the low prevalence of screening, are among the main barriers this country faces in order to reduce the burden of BC. Other needs that must be fulfilled include the lack of national cancer centers and protocols, the lack of trained personnel, and poor access to primary
14,30care in rural areas.
In summary, our studied population is diagnosed at locally advanced stages, indicating the need to increase awareness about BC among Guatemalan women and to improve the screening program for earlier detection of the disease. Given the high percentage of BC patients under the age of 50, we recommend starting screening mammography prior this age.
This work was partly funded by Roche Servicios S.A.
Hugo Castro has received honoraria from Roche, Novartis, Bayer, Pfizer, consulting for Roche and Bayer. Allan Ramos-Esquivel has received honoraria from Roche and Pfizer, consulting for Roche, Bayer, and Novartis; and travel and accommodations expenses from Bayer, Roche, Novartis, and Johnson & Jonhson.
Our findings cannot accurately reflect the prognosis and clinical characteristics of all Guatemalan patients affected with BC due to its unicenter design. Besides, its retrospective design could bias the results due to some missing data from clinical records. For instance, we did not have access to other potential confounder variables associated
3 1with prognosis, such as smoking , alcohol
32 33consumption , or previous hormone use. Despite these caveats, our study provides a first clinical picture that can contribute to improve health policies in Guatemala. Further national efforts must be carried out to better describe the epidemiology of cancer patients in our country.
Conflict of Interest
Financial Support
References1. World Health Organization. International Agency
for Research on Cancer. [Available at: https:// gco.iarc.fr/ today/data/factsheets/cancers/10_8_9-Colorectum-fact-sheet.pdf.]
Breast cancer in Guatemala
116 Castro, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 111-118
2. Hu K, Ding P, Wu Y, Tian W, Pan T, Zhang S. Global patterns and trends in the breast cancer inc idence and mor ta l i ty according to sociodemographic indices: an observational study based on the global burden of diseases. BMJ Open 2019;9:e028461.
5. Instituto Nacional de Estadística ,Guatemala. [Available from: https://www.ine.gob.gt]
6. Sierra MS, Soerjomataram I, Antoni S, Laversanne M, Piñeros N, de Vries E, et al. Cancer patterns and trends in Central and South America. Cancer Epidemiol 2016; 44 Suppl 1; S23-S42.
8. Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol 2010; 17(6): 1471-1474.
4. Lara-Medina F, P´rez-Sánchez V, Saavedra-Pérez D, Blake-Cerda M, Arce C, Motola-Kuba D, et al. Triple‐negative breast cancer in Hispanic patients. Cancer 2011; 117: 3658-3669.
3. Hines LM, Risendal B, Byers T, Mengshol S, Lowery J, Singh M. Ethnic disparities in breast tumor phenotypic subtypes in Hispanic and non-Hispanic white women. J Womens Health (Larchmt). 2011 Oct; 20(10):1543-50.
10. Dowsett M, Nielsen TO, A'Hern R, Bartlett J, Coombes RC, Cuzick J, Ellis M, Henry NL, Hugh JC, Lively T, McShane L, Paik S, Penault-Llorca F, et al. Assessment of Ki67 in breast cancer: recommendations from the International Ki67 in Breast Cancer working group. J Natl Cancer Inst. 2011;103:1656–64.
9. Hammond ME, Hayes DF, Dowsett M, Allred DC, Hagerty KL, Badve S, Fitzgibbons PL, Francis G, Goldstein NS, Hayes M, Hicks DG, Lester S, Love R, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer (unabridged version) Arch Pathol Lab Med. 2010;134:e48–72.
7. Becerril-Montekio, López-Dávila. Sistema de Salud de Guatemala. Salud Pub Mex 2011; 53:S197-S-208.
11. Wolff AC, Hammond ME, Hicks DG, Dowsett M, McShane LM, Allison KH, Allred DC, Bartlett JM, Bilous M, Fitzgibbons P, Hanna W, Jenkins RB, Mangu PB, et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J Clin Oncol. 2013;31:3997–4013.
12. Coates AS, Winer EP, Goldhirsch A, Gelber RD, Gnant M, Piccart-Gebhart M, Thürlimann B, Senn HJ, Panel Members Tailoring therapies--improving the management of early breast
20. Srur-Rivero N, Cartin-Brenes M. Breast cancer characteristics and survival in a Hispanic population of Costa Rica. Breast Cancer (Auckl) 2014; 8:103-108.
16. Lund MJ, Butler EN, Hair BY, et al. Age/race differences in HER2 testing and in incidence rates for breast cancer triple subtypes: a population-based study and first report. Cancer. 2010; 116: 2549‐2559.
18. Kurebayashi J, Moriya T, Ishida T, et al. The prevalence of intrinsic subtypes and prognosis in breast cancer patients of different races. Breast. 2007;16:S72–S77.
19. Lara-Medina F, Pérez-Sánchez V, Saavedra-Pérez D, Blake-Cerda M, Arce C, Motola-Kuba D, et al. Triple-negative breast cancer in Hispanic patients. Cancer 2011; 117: 3658-3669
21. Parise CA, Bauer KR, Caggiano V. Variations in b reas t cancer sub types wi th age and race/ethnicity. Crit Rev Oncol Hematol 2010; 44-52.
24. Piñeros M, French S, Frazier L, Laversanne M, Barnoya J, Garrido C, et al. Advancing Reliable Data for Cancer Control in the Central America Four Region. J Global Oncol 2018; 4.1-11.
25. Maggard MA, O´Connel JB, Lane KE, Liu JH, Etzioni DA, Ko CY. Do young breast cancer
13. von Minckwitz G, Untch M, Blohmer JU, Costa SD, Eidtmann H, Fasching PA, et al. Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J Clin Oncol. 2012; 30:1796-804.
14. Justo N, Wilking N, Jonsson B, Luciani S, Cazap E. A Review of Breast Cancer care and Outcomes in Latin America. 2013; 18: 248-256.
23. DeSantis CE, Ma J, Gaudet MM, Newman LA, Miller KD, Sauer AG, et al. Breast cancer statistics 2019; CA A Cancer ] Clin 2019; 69:438-451.
17.Swede H, Gregorio DI, Tannenbaum SH, Brockmeyer JA, Ambrosone C, Wilson LL, et al. Prevalence and Prognostic Role of Triple-Negative Breast Cancer by Race: A surveillance study. Clin Breast Cancer 2011; 11:332-341.
22. Gaudet MM, Gierach GL, Carter BD, et al. Pooled analysis of nine cohorts reveals breast cancer risk factors by tumor molecular subtype. Cancer Res. 2018;78:6011-6021.
cancer: St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2015. Ann Oncol. 2015;26: 1533–46.
15. Graves KD, Huerta E, Cullen J, Kaufman E, Sheppard V, Luta G, et al. Perceived Risk of Breast Cancer among Latinas Attending Community Clinics: Risk Comprehension and Relationship with Mammography Adherence. Cancer Causes Control 2008; 19:1373-82.
117Castro, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 111-118
Breast cancer in Guatemala

31. Duan W, Li S, Meng X, Sun Y, Jia C. Smoking and survival of breast cancer patients: a meta-analysis of cohort studies. Breast 2017; 33:117-124.
26. Zhang L, King J, Wu XC, Hsieh MC, Chen VW, Yu Q, et al. Racial/ethnic differences in the utilization of chemotherapy among stage IIII breast cancer patients, stratified by subtype: Findings from ten National Program of Cancer Registries states. Cancer Epidemiol 2019; 58:1-7.
27. Puig CA, Hoskin TL, Day CN, Habermann EB, Boughey JC. National Trends in the Use of Neoadjuvant Chemotherapy for Hormone Receptor-Negative Breast Cancer: A National Cancer Data Base Study.Ann Surg Oncol 2017; 24: 1242-1250.
patients have worse outcomes? J Surg Res 2003; 113:109-113.]
28.Cortazar P, Zhang L, Untch M, Mehta K, Constantino JP, Wolmark N. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet 2014; 384:164-172.
29.World Health Organization: Global health expenditure database.
30. Goss PE, Lee BL, Badovinac-Crnjevic T, et al. Planning cancer control in Latin America and the Caribbean. Lancet Oncol 2013; 14:391-436.
33. Newcomb PA, Egan KM, Trentham-Dietz A, et al. Prognostic use of hormone therapy and mortality after breast cancer. Cancer Epidemiol Biomarkers Prev 2008; 17:864-8.
32. Vrieling A, Buck K, Heinz J, Obi N, Benner A, Flesch-Janys D, et al. Pre-diagnostic alcohol consumption and postmenopausal breast cancer survival: a prospective patient cohort study. Breast Cancer Res Treat 2012; 136: 195–207.
Breast cancer in Guatemala
118 Castro, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 111-118

119
Health-related quality of life (HRQOL) has become a fundamental goal of breast cancer
1management. The mortality rate of breast cancer is decreasing, whereas the incidence rate of breast cancer is on the rise. At present, one in eight women
Introduction
ARTICLE INFO
Background: Improving health-related quality of life (HRQOL) has become a fundamental goal of breast cancer management. This study aimed to examine the differences between the QOL outcomes of breast-conserving surgery (BCS) and mastectomy. We also established structural equation models for BCS and mastectomy to elucidate their unique effects on QOL.
Methods: Between July 2019 and November 2019, 254 patients, who were scheduled to visit one of four clinics, were recruited for this study. We evaluated HRQOL using various questionnaires, such as the BREAST-Q, EQ-5D-5L, and Hospital Anxiety and Depression Scale (HADS). The relationships among the examined clinical indicators were evaluated using structural equation modeling (SEM).
Results: The QOL scores of the BCS group were better than those of the mastectomy group (0.85±0.129 vs. 0.81±0.12, P=0.020). Also, anxiety (2.94±2.95 vs. 3.81±3.08, P=0.025) and depression (2.55±2.77 vs. 3.74±3.19, P=0.002) were less severe in the BCS group than in the mastectomy group. Furthermore, the relationships among QOL status and mental health status were more complex in the BCS group than in the mastectomy group (Chi-square minimization p-value: 0.231 vs. 0.469, respectively). Also, depression directly affected QOL in the mastectomy group (R=-0.47), but not in the BCS group.
Conclusions: There were differences in QOL and mental health between the BCS and mastectomy groups. SEM is useful for identifying such differences, which can be used to develop strategies for improving QOL.
Revised: 25 June 2020
01 August 2020
Received:
Accepted:
Key words:
mastectomy,
27 July 2020
Quality of life,
structural equation modeling .
breast-conserving surgery,
Address for correspondence: Toru Mizuguchi, M.D., Ph.D.Address: Department of Nursing and Surgical Science, Sapporo Medical University Postgraduate School of Health Science, Sapporo 060-8556, JapanTel: +81-11-611-2111 Fax: +81-11-612-5525E-mail: [email protected]
ABSTRACT
The Unique Mental Impacts of Breast-Conserving Surgery and Mastectomy According to a Multi-Centered Cross Sectional Survey Conducted in Japan
a Department of Nursing and Surgical Science, Sapporo Medical University Postgraduate School of Health Science, Sapporo, Japanb Department of Surgery, Surgical Science and Oncology, Sapporo Medical University Postgraduate School of Medicine, Sapporo, Japanc Department of Breast Surgery, Sapporo Breast Surgical Clinic, Sapporo, Japand Department of Surgery, Higashi-Sapporo Hospital, Sapporo, Japane Department of Breast Surgery, Sapporo Kotoni Breast Clinic, Sapporo, Japanf Department of Liberal Arts and Sciences, Center for Medical Education, Sapporo Medical Universityg Department of Surgery, Division of Pediatric Surgery, Stanford University School of Medicine, Stanford, CA, USA
a b b c d bYuri Hazawa , Goro Kutomi , Hiroaki Shima , Toshio Honma , Tosei Ohmura , Asaka Wada ,e e a a aToshihiko Mikami , Miki Hotta , Momoka Narumi , Yoshika Kuno , Tomohiro Ishinuki ,
d b c e eMakoto Meguro , Ichiro Takemasa , Minoru Okazaki , Hideji Masuoka , Kazuaki Asaishi , f g a, bToshio Ohyanagi , Thomas T. Hui , Toru Mizuguchi*
Open AccessOriginal Article
Hazawa, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 119-126
DOI: 10.32768/abc.202073119-126

are diagnosed with breast cancer, and the 5-year 2
survival rate of the disease was reported to be >90%. Thus, the number of breast cancer survivors is increasing. Therefore, determining the patients’ QOL status and the factors that affect it are essential for improved decision-making regarding the treatment of breast cancer.
The type of surgical procedure used to treat breast cancer has no impact on survival among patients
3, 4with early stage cancer. Therefore, breast-conserving surgery (BCS) is preferable to radical mastectomy for early stage breast cancer. On the other hand, it is unclear whether BCS and
5–8mastectomy produce different HRQOL outcomes. In general, BCS is less invasive than mastectomy, and hence, the postoperative QOL of patients that undergo BCS might be better than that of patients who undergo mastectomy. However, previous studies have reported conflicting results regarding the QOL outcomes of patients that underwent BCS or mastectomy, and the reasons for these discrepancies are unclear.
The BREAST-Q is one of the best measures for assessing the HRQOL of breast cancer patients. It has been validated and translated into thirty different
9, 10languages. The 5-level EuroQol 5-dimension version (EQ-5D-5L) is also a useful assessment tool for estimating QOL and provides a QOL score, which can be used to calculate quality-adjusted life-year and incremental cost-effectiveness ratio
11–14 values. The Hospital Anxiety and Depression Scale (HADS) is an assessment tool that is commonly used to evaluate mental health status after
15, 16surgery, including general outpatients. We evaluated QOL from multiple viewpoints because mental status is closely related to QOL in breast cancer patients, and the relationships among QOL
1, 17indicators are complex. To evaluate QOL in breast cancer pa t i en t s , we combined the th ree questionnaires mentioned above and attempted to elucidate the complex relationships between the factors that affect QOL.
Structural equation modeling (SEM) is used to elucidate complex relationships among multiple
18variables and involves simultaneously solving systems of linear equations. The QOL of breast cancer patients is affected by a complex range of factors, and hence, is difficult to understand. SEM might offer a general structure for assessing the QOL of breast cancer patients and help to visualize the relationships among clinical and social factors.
Study subjectsMethods
This study aimed to examine the differences between the QOL outcomes of BCS and mastectomy. Second, we established structural equation models for BCS and mastectomy to elucidate the unique characteristics of these procedures.
14The EQ-5D-5L questionnaire, whose Japanese 11, 12
version has been validated in previous studies,was applied in interviews to estimate QOL utility values. The five aspects evaluated by the EQ-5D-5L are mobility (MO), self-care (SC), usual activities (UA), pain/discomfort (PD), and anxiety/depression (AD), each of which has five levels of severity. Level 1 shows that the patient can do the relevant activity without any difficulty or feels comfortable. Level 5 shows the patient performs the relevant activity with difficulty or feels uncomfortable. Using a scoring function developed for Japan, these health status
EQ-5D-5L questionnaire
Between July 2019 and November 2019, 254 patients, who were scheduled to make outpatient visits to one of four clinics, were recruited for this cross-sectional study after providing informed consent. The four clinics were Sapporo Medical University Hospital, Sapporo Breast Surgical Clinic, Higashi-Sapporo Hospital, and Sapporo Kotoni Breast Clinic, which belong to the Sapporo breast medical team union. Patients who had undergone BCS or mastectomy for breast cancer more than three months ago and agreed to respond to the relevant questionnaires were eligible for this study. We recruited as many eligible patients as possible during the study period. The study protocol complied with the Declaration of Helsinki and was approved by the internal review board of Sapporo Medical University (approval ID: 312-68; approval date: July 11, 2019). Informed consent was obtained from all study subjects.
The procedures in this study complied with the ethical standards of the institutional review board of Sapporo Medical University, Sapporo, Japan (312-68) and the 1964 Declaration of Helsinki and its amendments or comparable ethical standards.
Informed consentInformed consent was sought from all study
participants.
Ethical approval
BREAST-Q questionnaireThe BREAST-Q mastectomy module and breast-
conserving therapy module (postoperative) each consist of the following 6 domains: BQ1: psychological well-being, BQ2: sexual well-being, BQ3: satisfaction with breasts, BQ4: physical well-being: chest, BQ5: satisfaction with the medical
19 team, and BQ6: adverse effects of radiotherapy.Each domain consists of 4 to 12 items and 3 to 5 scales. The score for each scale is converted to a 100-point scale using a conversion table. Thus, the score for each scale ranges from 0 (very dissatisfied) to 100 (very satisfied). The Japanese BREAST-Q, version 2.0, was used in this study.
Mastectomy vs. BCS mental impact
120 Hazawa, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 119-126

SEM of the BCS (Figure 1) and mastectomy (Figure 2) groups were performed. In the BCS group, the following standardized direct effects on QOL were detected: physical well-being (chest): 0.510, HADS-anxiety: -0.350, and time since surgery: 0.11 (Figure 1). The squared multiple correlations coefficient for the relationships among QOL and the factors in the model were 0.541. Some BREAST-Q domains were correlated with each other, and the model was complex (Figure 1), but exhibited very good fit values (CMIN: 0.231, RMSEA: 0.044, CFI:
Results
HADS-depression, the QOL utility value, and the time since surgery were used to identify the roles of the variables. Model fit was evaluated using the following standards proposed by McDonald and
21Ho : a good model fit is indicated by a chi-square minimization p-value of >0.05, a comparative fit index (CFI) of >0.95, and a root mean square error of approximation (RMSEA) of <0.05. Over a hundred models were compared, and the one with the smallest Akaike's Information Criterion (AIC) witha normed fit index (NFI) and a Tucker-Lewis Index (TLI) close to 1.000 was selected. The subscale internal consistency and variance values for single indicator latent variables were specified to reduce the measurement error in the model.
The QOL questionnaire scores are shown in Table 2. The scores for psychological well-being (56.9±23.4 vs. 46.5±19.1, P<0.001), sexual well-being (43.4±19.5 vs. 25.6±20.3, P<0.001), satisfaction with breasts (59.7±18.2 vs. 41.3±16.6, P<0.001), QOL (0.8549±0.1279 vs. 0.8168±0.1287, P=0.020), HADS-anxiety (2.94±2.95 vs. 3.81±3.08, P=0.025), and HADS-depression (2.55±2.77 vs. 3.74±3.19, P=0.002) differed significantly between the groups. On the other hand, the scores for physical well-being (chest), satisfaction with the medical team, and the adverse effects of radiotherapy did not differ significantly between the groups.
The clinical backgrounds of the patients are shown in Table 1. A total of 254 patients were recruited for this study after providing written informed consent. There were no differences in the treating institution, body mass index (BMI), age, time since surgery, the incidence of lymphedema, the current management strategy, progesterone receptor (PgR) status, human epidermal growth factor receptor 2 (HER2) status, the Ki-67 index, marital status, child status, housing status, or employment status between the BCS and mastectomy groups. There were significant differences between the groups in the TNM stage (P<0.001); the frequencies of reconstruction (1.7% vs. 13.0%, P=0.001), axial lymph node dissection (26.7% vs. 38.4%, P=0.049), radiotherapy (68.1% vs. 18.1%), and ER positivity (88.6% vs. 78.5%, P=0.034); and economic status (P=0.040).
Hospital Anxiety and Depression Scale questionnaire in Japanese
The HADS is a 14-item self-reported questionnaire which evaluates depression (7 items) and anxiety (7
16items) over the preceding week. Each item is evaluated on a 4-point Likert Scale (0–3), e.g., “I can laugh and see the funny side of things” (0: most of the time; 3: not at all). Each subscale score is obtained by summing the scores for each item on the subscale (subscale ranges: 0–21), with higher scores indicating greater severity. Following previous research, the mean subscale values were interpreted as follows: 0–7: “normal”, 8–10: “mild”, 11–15: “moderate”, and
2016–21: “severe”. The reliability statistic for anxiety and depression was 0.852.
parameters were changed into utility values from 0 to 1, where 0 indicated death and 1 showed full health. A utility value calculator is available on the EQ-5D homepage (https://euroqol.org/), and the coefficients for each of the five dimensions (MO, SC, UA, PD,
11and AD) are described in the literature. We registered our decision to use the EQ-5D-5L before the patients were recruited (ID: 26966).
Statistical analysis
Clinical outcomes of interestPhysical and pathological data were collected
from the questionnaires or the participants’ medical records after providing informed consent. The distributions of each clinical variable are analyzed by Kolmogorov–Smirnov test.
QOL-related variables and clinical variables were used to create structural equation models using the Amos software (IBM SPSS Amos, Version 20.0, IBM-SPSS, Inc., Armonk, New York, United States). SEM is used to estimate theoretical models of the correlations between individual variables within a given population. It can be used to visualize the relationships among variables in order to better understand the overall global situation in specific
18conditions. Standardized effects with corresponding 95% confidence intervals were measured using the bootstrapping method. In this study, the six subdomains of the BREAST-Q, HADS-anxiety,
SPSS (version 22, IBM-SPSS, Inc., Armonk, New York, United States) was used to analyze the data. The independent sample t-test was run for comparisons between the groups. We used to Levene’s test assess the equality of variances for each variable in comparisons between the two groups. We performed descriptive statistical analyses and the chi-square test to compare the groups’ demographic data. The results are presented as mean±SD values. P-values of <0.05 are considered to be significant.
Structural equation modeling
121Hazawa, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 119-126
Mastectomy vs. BCS mental impact
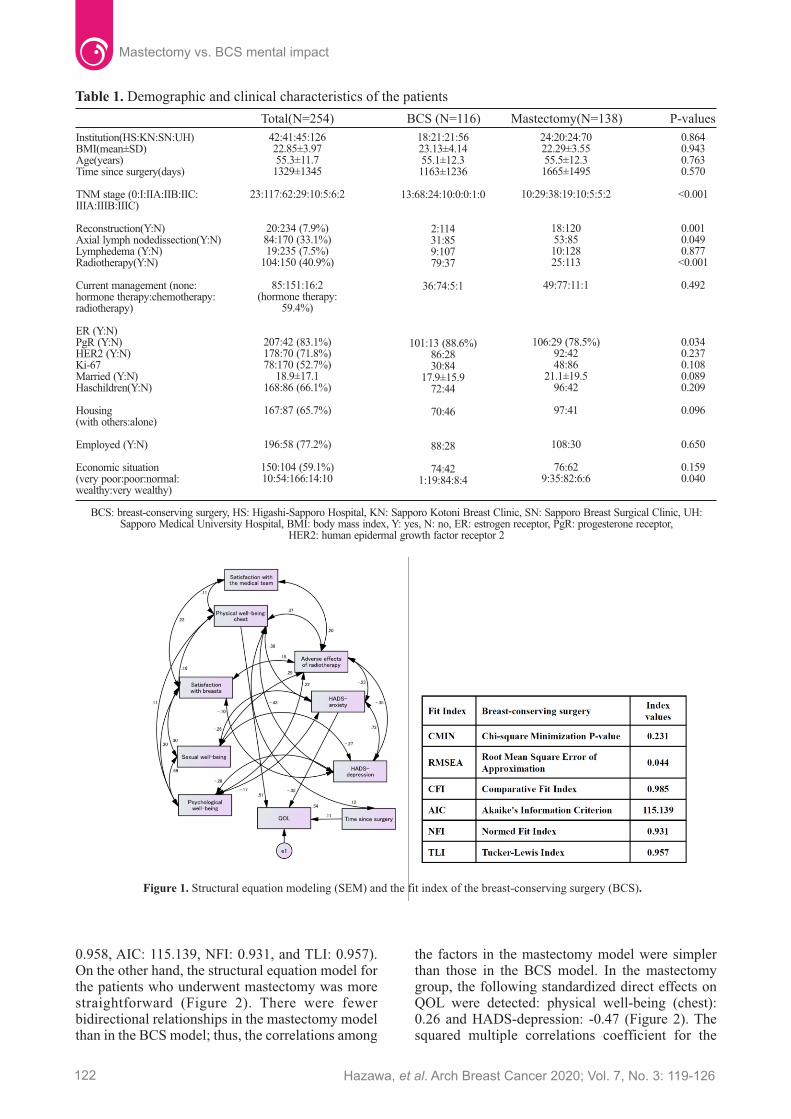
Table 1. Demographic and clinical characteristics of the patients
Total(N=254) BCS (N=116) Mastectomy(N=138) P-values
Institution(HS:KN:SN:UH)BMI(mean±SD)Age(years)Time since surgery(days)
TNM stage (0:I:IIA:IIB:IIC:IIIA:IIIB:IIIC)
Reconstruction(Y:N)Axial lymph nodedissection(Y:N)Lymphedema (Y:N)Radiotherapy(Y:N)
Current management (none:hormone therapy:chemotherapy:radiotherapy)
ER (Y:N)PgR (Y:N)HER2 (Y:N)Ki-67Married (Y:N)Haschildren(Y:N)
Housing(with others:alone)
Employed (Y:N)
Economic situation(very poor:poor:normal:wealthy:very wealthy)
42:41:45:12622.85±3.9755.3±11.7
1329±1345
23:117:62:29:10:5:6:2
20:234 (7.9%)84:170 (33.1%)19:235 (7.5%)
104:150 (40.9%)
85:151:16:2(hormone therapy:
59.4%)
207:42 (83.1%)178:70 (71.8%)78:170 (52.7%)
18.9±17.1168:86 (66.1%)
167:87 (65.7%)
196:58 (77.2%)
150:104 (59.1%)10:54:166:14:10
18:21:21:5623.13±4.1455.1±12.31163±1236
13:68:24:10:0:0:1:0
2:11431:859:10779:37
36:74:5:1
101:13 (88.6%)86:2830:84
17.9±15.972:44
70:46
88:28
74:421:19:84:8:4
24:20:24:7022.29±3.5555.5±12.3
1665±1495
10:29:38:19:10:5:5:2
18:12053:8510:12825:113
49:77:11:1
106:29 (78.5%)92:4248:86
21.1±19.596:42
97:41
108:30
76:629:35:82:6:6
0.8640.9430.7630.570
<0.001
0.0010.0490.877
<0.001
0.492
0.0340.2370.1080.0890.209
0.096
0.650
0.1590.040
0.958, AIC: 115.139, NFI: 0.931, and TLI: 0.957). On the other hand, the structural equation model for the patients who underwent mastectomy was more straightforward (Figure 2). There were fewer bidirectional relationships in the mastectomy model than in the BCS model; thus, the correlations among
the factors in the mastectomy model were simpler than those in the BCS model. In the mastectomy group, the following standardized direct effects on QOL were detected: physical well-being (chest): 0.26 and HADS-depression: -0.47 (Figure 2). The squared multiple correlations coefficient for the
BCS: breast-conserving surgery, HS: Higashi-Sapporo Hospital, KN: Sapporo Kotoni Breast Clinic, SN: Sapporo Breast Surgical Clinic, UH: Sapporo Medical University Hospital, BMI: body mass index, Y: yes, N: no, ER: estrogen receptor, PgR: progesterone receptor,
HER2: human epidermal growth factor receptor 2
Figure 1. Structural equation modeling (SEM) and the fit index of the breast-conserving surgery (BCS).
Mastectomy vs. BCS mental impact
122 Hazawa, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 119-126

relationships among QOL and the factors in the model were 0.290. The model also displayed very good fit values (CMIN: 0.469, RMSEA: <0.001, CFI: 1.000, AIC: 86.834, NFI: 0.928, and TLI: 1.001).
DiscussionWe investigated HRQOL using the BREAST-Q,
EQ-5D-5L, and HADS in 254 breast cancer patients and revealed the relationships that affect the QOL of breast cancer patients treated with mastectomy or BCS. We found that the QOL outcomes of the BCS group were better than those of the mastectomy group. Also, the BCS group exhibited less severe anxiety and depression than the mastectomy group. On the other hand, the relationships between QOL status and mental status were more complex in the BCS group than in the mastectomy group. Our study indicates the importance of intervening to ameliorate anxiety in patients who undergo BCS and depression in patients who undergo mastectomy. The absolute values obtained from the questionnaires could aid the development of future study protocols.
Eltahir et al. compared BREAST-Q scores between patients who underwent mastectomy alone
In the current study, the breast reconstruction rate was only 7.9%, whereas it was 67.2% in the study
22conducted by Eltahir et al. The low reconstruction rate seen in the present study might have been due to the fact that our study population was composed of Japanese women. Sim et al. reported various breast
and those who underwent reconstruction after mastectomy, and their results were quite similar to
22those obtained in the present study. In the current study, the scores for psychosocial well-being, sexual well-being, and satisfaction with breasts differed significantly between the groups, although breast reconstruction did not affect the BREAST-Q or QOL utility score (data not shown). However, the absolute values for each BREAST-Q subdomain were markedly lower in the present study than in the previous study, which included patients that underwent prophylactic mastectomy, some of whom might not have had cancer. As the present study demonstrated that anxiety and depression affected the QOL of breast cancer patients both directly and indirectly, it is reasonable that our QOL values were lower than those seen in the previous study, as our subjects might have been worried about future life-threatening cancer progression or recurrence.
Figure 2. Structural equation modeling (SEM) and the fit index of the mastectomy.
Table 2. Scores for each questionnairein the total,breast-conserving surgery, and mastectomy groups
Total(N=254)All Patients BCS (N=116) Mastectomy(N=138) P-values
Bq1 (N=245, 96.5%)BQ2 (N=122, 48.0%)BQ3 (N=160, 63.0%)BQ4 (N=219, 86.2%)BQ5 (N=241, 94.9%)BQ6 (N=126, 49.6%)QOL (N=250, 98.4%)HADS-anxiety (N=247,97.2%)HADS-depression (N=247, 97.2%)
51.3±21.733.3±21.853.6±19.776.6±18.987.1±17.477.6±22.60.83±0.123.41±3.053.19±3.06
56.9±23.443.4±19.559.7±18.278.4±17.488.8±14.177.2±21.9
0.8549±0.12792.94±2.952.55±2.77
46.5±19.125.6±20.341.3±16.674.8±20.285.7±19.879.0±25.5
0.8168±0.12873.81±3.083.74±3.19
<0.001<0.001<0.0010.1580.1590.7120.0200.0250.002
123Hazawa, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 119-126
Mastectomy vs. BCS mental impact

We found that ER-positive breast cancer was significantly more common in the BCS group than in the mastectomy group (88.6% vs. 78.5%, P=0.034). One possible reason for this is that the ER-positive patients in the BCS group achieved better survival outcomes than the ER-negative patients. Furthermore, the ER-negative patients in the mastectomy group had more advanced cancer than those in the BCS group (Table 1; P<0.001). Another possible reason is that hormone status affected decisions regarding treatment. We could not reach a definitive conclusion about this due to the study’s cross-sectional nature, although hormone status might be associated with QOL and other indicators.
reconstruction rates, ranging from 7.6% to 60.0%, 23
for different ethnicities. Lagendijk et al. reported that breast reconstruction improved the QOL of
24breast cancer patients after surgery. However, we did not observe any improvement in QOL after breast reconstruction (data not shown), except in the satisfaction with breasts subdomain (P=0.046). Similarly, a Polish study failed to demonstrate that
25reconstruction had a QOL advantage over BCS. The impact of breast reconstruction on QOL might depend on ethnic factors, such as race and religion. We need to investigate whether breast reconstruction improves QOL under our specific circumstances.
On the other hand, we also found that the ER-positive rate was higher than the PgR-positive rate in this study. Basic research has demonstrated that ER-
26 dependent pathways induce PgR expression.Therefore, theoretically, the ER-positive rate should always be higher than the PgR-positive rate, and the pathological information obtained in this study fit this theory.
Versions of the EQ-5D-5L tariff in various 11, 27
languages have been developed and validated. However, the problem with this tariff is that it involves discontinuous scores with a gap between 1.000 and 0.900, especially in the Japanese and
27,28Korean versions. Therefore, the QOL scores produced by the EQ-5D-5L could be underestimated in patients with slight health problems. However, different studies, including our study, have produced
24, 27quite similar values, which demonstrates that the EQ-5D-5L exhibits excellent reproducibility. The greatest advantage of the EQ-5D-5L is that it involves a simple questionnaire containing only five questions, which does not take a long time to complete.
The HRQOL of breast cancer patients might alter after surgery, depending on the type of surgery performed, the QOL domains examined, or the time
7, 29to the QOL evaluation. Our structural equation model for all patients was complicated, which indicated that QOL after breast surgery is influenced by various factors. On the other hand, the structural equation model for the mastectomy group was simpler, but did not exhibit reduced “goodness of
Funding
SEM is a multivariate statistical framework, which can be used to reveal the complex relationships
18among factors. We created various models and selected the one that exhibited the best fit. Huang et al. stated that preoperative communication with patients who undergo BCS regarding the advantages
31and disadvantages of using SEM is important. Our findings supported their conclusion that patients who undergo BCS need support to ameliorate their anxiety to improve their QOL. However, in these patients, the effects of chest-related physical well-being were more marked than those of anxiety. Our structural equation model indicated that physical support could have a positive impact on the QOL of patients that undergo BCS. On the other hand, depression had a strong direct effect on QOL in the mastectomy group. As depression was correlated with anxiety in the mastectomy group, medication or consultations with mental health specialists could help to improve the QOL of patients that undergo
32mastectomy.The main limitation of this study was that due to
its cross-sectional nature, we were unable to determine the exact relationships between clinical outcomes and their causes. Although most of the data had a normal distribution, it could not be proven whether the study population accurately represented the parent set. Furthermore, the results obtained for the Japanese population might not be generalizable to breast cancer patients from other geographic areas.
In conclusion, QOL and mental health differed between breast cancer patient that underwent BCS and those who underwent mastectomy. SEM is useful for identifying differences between patients who undergo BCS and those who undergo mastectomy. The management of anxiety is important for supporting patients who undergo BCS. On the other hand, managing depression is important for supporting patients who undergo mastectomy. This study provides some fundamental information that will aid the planning of future studies.
fit”. Our findings clearly indicate that QOL models for breast cancer patients need to be specific to BCS or mastectomy. Fehlauer et al. also reported that the HRQOL of breast cancer patients is affected by a complex range of factors, including age, physical
30functions, and psychological well-being. Our study suggested that the QOL of breast cancer patients should be divided according to the type of surgical procedure performed.
Acknowledgments The authors thank the registration team of
Sapporo Medical University Hospital, Sapporo Beast Surgical Clinic, Higashi-Sapporo Hospital, and Sapporo Kotoni Breast Clinic.
This study was supported by a Grant-in-Aid for
Mastectomy vs. BCS mental impact
124 Hazawa, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 119-126

Conflicts of interest
Scientific Research from the Ministry of Education, Culture, Sports, Science, and Technology, Japan (No. 20K10404 to Mizuguchi T); Astellas Pharma, Inc., Tokyo, Japan; Daiichi Sankyo Company, Tokyo, Japan; Noguchi Hospital, Otaru, Japan; Doki-kai Tomakomai Hospital, Tomakomai, Japan; Yamaoka Clinic, Sapporo, Japan; Tsuchida Hospital, Sapporo, Japan; and Hokkaido Hepatitis B Litigation Orange Fund.
1. Ghislain I, Zikos E, Coens C, Quinten C, Balta V, Tryfonidis K, et al. Health-related quality of life in locally advanced and metastatic breast cancer: methodological and cl inical issues in randomised controlled trials. Lancet Oncol. 2016; 17(7): e294-e304.
The authors declare that they have no conflicts of interest.
4. Veronesi U, Cascinelli N, Mariani L, Greco M, Saccozzi R, Luini A, et al. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N Engl J Med. 2002; 347(16): 1227-32.
7. Shimozuma K, Sonoo H, Ichihara K, Miyake K, Kurebayashi J, Ota K, et al. The Impacts of Breast Conserving Treatment and Mastectomy on the Quality of Life in Early-stage Breast Cancer Patients. Breast Cancer. 1995; 2(1): 35-43.
References
3. Fisher B, Anderson S, Bryant J, Margolese RG, Deutsch M, Fisher ER, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med. 2002; 347(16): 1233-41.
5. Kiebert GM, de Haes JC, van de Velde CJ. The impact of breast-conserving treatment and mastectomy on the quality of life of early-stage breast cancer patients: a review. J Clin Oncol. 1991; 9(6): 1059-70.
6. Ohsumi S, Shimozuma K, Morita S, Hara F, Takabatake D, Takashima S, et al. Factors associated with health-related quality-of-life in breast cancer survivors: influence of the type of surgery. Jpn J Clin Oncol. 2009; 39(8): 491-6.
8. van der Steeg AF, De Vries J, Roukema JA. The value of quality of life and health status measurements in the evaluation of the well-being of breast cancer survivors. Eur J Surg Oncol. 2008; 34(11): 1225-30.
9. Cohen WA, Mundy LR, Ballard TN, Klassen A, Cano SJ, Browne J, et al. The BREAST-Q in
2. Morley R, Leech T. Optimal assessment tools in assessing breast surgery: patient reported outcome measures (PROMs) vs. objective measures. Gland Surg. 2019; 8(4): 416-424.
12. Koide R, Kikuchi A, Miyajima M, Mishina T, Takahashi Y, Okawa M, et al. Quality assessment using EQ-5D-5L after lung surgery for non-small cell lung cancer (NSCLC) patients. Gen Thorac Cardiovasc Surg. 2019; 67(12): 1056-1061.
16. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983; 67(6): 361-70.
20. Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosom Res. 2002; 52(2): 69-77.
22.Eltahir Y, Werners LL, Dreise MM, van Emmichoven IA, Jansen L, Werker PM, et al. Quality-of-life outcomes between mastectomy alone and breast reconstruction: comparison of patient-reported BREAST-Q and other health-
18. Stein CM, Morris NJ, Hall NB, Nock NL. Structural Equation Modeling. Methods Mol Biol. 2017; 1666: 557-580.
surgical research: A review of the literature 2009-2015. J Plast Reconstr Aesthet Surg. 2016; 69(2): 149-62.
10. Saiga M, Taira N, Kimata Y, Watanabe S, Mukai Y, Shimozuma K, et al. Development of a Japanese version of the BREAST-Q and the traditional psychometric test of the mastectomy module for the assessment of HRQOL and patient satisfaction following breast surgery. Breast Cancer. 2017; 24(2): 288-298.
11. Shiroiwa T, Fukuda T, Ikeda S, Igarashi A, Noto S, Saito S, et al. Japanese population norms for preference-based measures: EQ-5D-3L, EQ-5D-5L, and SF-6D. Qual Life Res. 2016; 25(3): 707-19.
13. Kikuchi A, Koide R, Iwasaki M, Teramoto M, Satohisa S, Tamate M, et al. Assessing quality of life using the brief cancer-related worry inventory for gynecological surgery. World J Obstet Gynecol 2019; 8(1): 1-7.
14. Brooks R. EuroQol: the current state of play. Health Policy. 1996; 37(1): 53-72.
15. Lim CC, Devi MK, Ang E. Anxiety in women with breast cancer undergoing treatment: a systematic review. Int J Evid Based Healthc. 2011; 9(3): 215-35.
17. Hutter N, Vogel B, Alexander T, Baumeister H, Helmes A, Bengel J. Are depression and anxiety determinants or indicators of quality of life in breast cancer patients? Psychol Health Med. 2013; 18(4): 412-9.
19. Pusic AL, Klassen AF, Scott AM, Klok JA, Cordeiro PG, Cano SJ. Development of a new patient-reported outcome measure for breast surgery: the BREAST-Q. Plast Reconstr Surg. 2009; 124(2): 345-53.
21. McDonald RP, Ho MH. Principles and practice in reporting structural equation analyses. Psychol Methods. 2002; 7(1): 64-82.
125Hazawa, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 119-126
Mastectomy vs. BCS mental impact

related quality-of-life measures. Plast Reconstr Surg. 2013; 132(2): 201e-209e.
23. Sim N, Soh S, Ang CH, Hing CH, Lee HJ, Nallathamby V, et al. Breast reconstruction rate and profile in a Singapore patient population: a National University Hospital experience. Singapore Med J. 2018; 59(6): 300-304.
24. Lagendijk M, van Egdom LSE, van Veen FEE, Vos EL, Mureau MAM, van Leeuwen N, et al. Patient-Reported Outcome Measures May Add Value in Breast Cancer Surgery. Ann Surg Oncol. 2018; 25(12): 3563-3571.
25. Szutowicz-Wydra B, Wydra J, Kruszewski WJ, Ciesielski M, Szajewski M, Walczak J, et al. Same Quality of Life for Polish Breast Cancer Patients Treated with Mastectomy and Breast Reconstruction or Breast-Conserving Therapy. Pol Przegl Chir. 2016; 88(5): 264-269.
26. Kunc M, Biernat W, Senkus-Konefka E. Estrogen receptor-negative progesterone receptor-positive breast cancer - "Nobody's land" or just an artifact? Cancer Treat Rev. 2018; 67: 78-87.
27. Liu L, Li S, Wang M, Chen G. Comparison of EQ-5D-5L health state utilities using four country-specific tariffs on a breast cancer patient sample in mainland China. Patient Prefer Adherence. 2017; 11: 1049-1056.
32. Yi JC, Syrjala KL. Anxiety and Depression in Cancer Survivors. Med Clin North Am. 2017; 101(6): 1099-1113.
29. Arndt V, Stegmaier C, Ziegler H, Brenner H. Quality of life over 5 years in women with breast cancer after breast-conserving therapy versus mastectomy: a population-based study. J Cancer Res Clin Oncol. 2008; 134(12): 1311-8.
31. Huang CC, Lien HH, Tu SH, Huang CS, Jeng JY, Chao HL, et al. Quality of life in Taiwanese breast cancer survivors with breast-conserving therapy. J Formos Med Assoc. 2010; 109(7): 493-502.
28. Teckle P, McTaggart-Cowan H, Van der Hoek K, Chia S, Melosky B, Gelmon K, et al. Mapping the FACT-G cancer-specific quality of life instrument to the EQ-5D and SF-6D. Health Qual Life Outcomes. 2013; 11: 203.
30. Fehlauer F, Tribius S, Mehnert A, Rades D. Health-related quality of life in long term breast cancer survivors treated with breast conserving therapy: impact of age at therapy. Breast Cancer Res Treat. 2005; 92(3): 217-22.
Mastectomy vs. BCS mental impact
126 Hazawa, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 119-126

127
Despite the advancement of the diagnostic and treatment tools, the median 5-years survival for the disease varies (58-85%), with regard to the fact that most survivors are treated when diagnosed in the
1lower stage of the disease. The suspected risk factors for breast cancer include the positive family history of the disease, long term estrogen exposure, first child birth after 35 years of age, white race, Asian or Hispanic race, obesity, genetic predisposition, and the age above 50 years. The latter is the most important risk factor orchestrating the cellular breast changes
3,4towards the dysplasia and malignancy. Currently, suspicious patients for breast cancer are screened by radiologic studies, including ultrasonography(US),
ARTICLE INFO
Background: Ultrasonography and mammography are two radiologic approaches for screening breast cancer; however, the pathology report is required for the ultimate diagnosis of malignancy. This study aimed to assess the concordance of ultrasonography (US) and mammography with the pathology in breast cancer.
Methods: A cross-sectional study was conducted to assess the breast US and the mammography findings based on the BI-RADS model in comparison with the definitive pathology reports in a single medical center. The sensitivity, the specificity, positive (PPV) and negative predictive value (NPV) and also the concordance between the US and the mammography data were analyzed.
Results: In this study, 126 patients were included. The sensitivity, specificity, PPV, and NPV for the US were 69.8, 71.9, 75.6 and 81.3 and for mammography were 91.9, 76.6, 80.8 and, 94.6 percent, respectively. The ROC-curve for either the US or the mammography showed that the BI-RADS 4 was accompanied with the highest sensitivity and specificity for the screening of the malignant breast lesions regarding the final diagnosis. Although an overall higher correlation between mammography report and presence of a malignant lesion was observed, the total relative concordance between the results of US and mammography as screening tools proved to be statistically significant (P<0.01).
Conclusion: Both the US and the mammography were sensitive and specific screening tools, particularly for the malignant breast lesions. Furthermore, when evidence of the BI-RADS≥4 in either the mammography or the US was present, utilization of the other test could be ignored before biopsy.
mammography;
pathology; BI-RADS;breast cancer;
Ultrasonography;
screening
Key words:
Received:
Accepted:01 August 2020
06 August 2020
Revised: 23 June 2020
Address for correspondence: Abbas Hajian. MDAddress: Department of General Surgery, Kashan University of Medical Sciences, Kashan, Iran Tel: +989121302268Email: [email protected]
ABSTRACT
Concordance and Diagnostic Accuracy of Ultrasonography and Mammography Findings with Pathology Results in Breast Cancer
a Department of General Surgery, Kashan University of Medical Sciences, Kashan, Iran b Department of Radiology, Kashan University of Medical Sciences, Kashan, Iran
a *a b aLeila Ghafoor , Abbas Hajian , Yaser Hamidian , Seyed Hamed Rohani
Open AccessOriginal Article
Ghafoor, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 127-131
The breast cancer is the first cause of cancer-related death among females between 20 and 44
1,2years. The incidence of new cases reached 7778 patients per year, and the specific age-related incidence reported 22.6 (95%CI 22.1-23.1) patients per every 100,000 females, with an age-standardized
2rate (ASR) of 27.4 (95%CI 22.5-35.9) in Iran.
Introduction
DOI: 10.32768/abc.202073127-131

mammography, and magne t i c r e sonance imaging(MRI). However, the diagnosis should be confirmed by the pathology reports . The ultrasonography is a non-invasive screening procedure specifically for finding the lesions in the dense breasts. The sensitivity of the US as an operator-dependent tool is about 70-90% and specificity has
5,6been reported to be widely different. On the other hand, the sensitivity and specificity of mammography
7,8vary between 55-90% and 70-97%, respectively. Concurrent use of US and mammography can
9decrease the false-negative reports to about 0.06% although in larger or more advanced tumors, the accuracy of either the US or mammography for estimating the size of the tumor has been decreased. Because of very low false-negative results of the screening studies, today, the concurrent use of the US and the mammography has been accepted as a common approach for breast tumor evaluation,
10preoperatively. Some studies have revealed that mammography had more advantageous results than did the US for demonstrating the tumor characte-ristics; however, some others have contradicted this
2,11result. Considering the review articles, the breast characteristics of every patient could be a guide to select which single available radiologic approach would be better for the patient. For example, in breasts with lower fat mass, the US and the MRI are more accurate than the mammography. This study was conducted to evaluate US and mammography findings for the breast lesions with regard to the pathologic reports.
MethodsThe data was obtained from the registered
medical files of the females pursuing breast examination either for the screening or diagnostic purposes (following symptoms), from May 2017 to October 2018. Ethical approval was obtained from the research ethics committee of the university (P/39/6/1/3264). The participants were randomly selected from the total of 630 registered medical files. Overall, from 252 files met inclusion criteria, and 126 samples were included through systematic random sampling. All the participants signed a written consent form for anonymous use of their data for research purposes. Exclusion criteria included the presence of inflammatory disease either locally in the breast (granulomatous mastitis) or systemic (like rheumatoid arthritis), positive history of breast, axillary or chest wall biopsy, previous thoracic surgery or irradiation, previous chemotherapy through the past 12 months of examination, presence of active skin and joint disease, ongoing pregnancy or consumption of oral contraceptives, tamoxifen or corticosteroids and need for axillary lymph node dissection. All patients were examined by a single general surgeon in a single public referral health care center. Females underwent breast examination, US
2. Positive family history of the breast cancer in a male relative.
5. Patients who insisted to have a breast biopsy.
4. Patients who were considered to be unable to return for timely follow-up.
3. Discordance between physical examination and radiologic report.
1. Positive family history of breast cancer in either first or second degree relatives.
Demographic data in addition to US, mammogr-aphy and the pathologic reports were used for analysis and interpretation. Frequency of categorical variables, central tendency statistics for continuous variables, sensitivity, specificity, Positive Predictive Value (PPV) and Negative Predicative Value (NPV) of US and the mammography were calculated using SPSS version 21. Independent sample T test, Fisher exact test, Chi-square were used to examine the association of the variables. The Youden’s index (sensitivity+specificity-1) was applied for dichotomous diagnostic tests. Statistical analysis for agreement indexes including Kendall’s, Gamma and
and mammography study, and the breast mass biopsy was taken with core needle biopsy or open incisional or excisional approaches. The Breast Imaging-Reporting and Data System (BI-RADS) was considered for radiologic findings introduction. It is an accepted international scaling system to assess the breast mass characteristics and applied as a guide for the next step in clinical approach.7The current study considered data of the US and the mammography reports with BI-RADS 0-V. The breast US had been performed by a single radiologist. The reports of both US and mammography were interpreted for all participants by the two attending physicians of the radiology department with over 12 years of experience. Finally, all reports are reviewed and corrected according to the revisions of an experienced radiologist who was an expert in breast imaging. After every patient underwent US and mammography, she was considered a candidate for the breast mass biopsy. Based on the guidelines for the management of breast cancer, BI-RADS≥4 needs further pathology assessment while, in this study, biopsy was also taken from patients with BI-RADS 2 and 3. The reason for the latter was one of the following considerations:
Breast biopsy was performed using one of the two following approaches by the surgeon: core needle biopsy (CNB) with the sterile 14 gauge biopsy needle (TSK ACECUT-Japan) under radiologic guide, or the surgical approach through incisional or excisional mass resection in the operating room. Specimens were sent to the reference hospital laboratory both in formalin and normal saline. The pathologic study as the definitive gold standard for making the diagnosis was performed by a single attending pathologist. The pathologic reports were classified as benign or malignant.
US & mammography concordance
128 Ghafoor, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 127-131

benign lesions (BI-RADS 2 and 3).The divergence between radiologic and pathologic reports was for the suspicious and/or the malignant lesions. Although mammography reports for the malignant masses (BI-RADS 5) were also fully compatible with those of the pathology, US revealed a lower diagnostic accuracy (94.3%) for distinguishing the malignant lesions(p<0.01). The source of most disagreements between radiologic findings and those of the pathology was for the suspicious lesions (BI-RADS 4). As Table 1 shows, the concordance between pathology reports and US/mammography for malignant lesions were 94.2/71.4% respectively (P<0.001). Overall, the results showed that mammography reports had the highest accuracy to diagnose malignancy in BI-RADS 5 subgroup (100%) and US, with BI-RADS 4 (94.3%). Table-2 shows sensitivity, specificity, PPV, NPV and, the Youden’s index for study findings.
The mean age (±SD) of 126 the participants was 55.2±13.9. Of all, 42(33.3%) of the study sample had positive family history of breast cancer. Considering the pathology report as the gold standard for cancer diagnosis, eventually, 76(60.3%) specimens were categorized as benign and the rest 50(39.7%) showed evidence of malignancy. Breast ultrasonography and mammography findings based on the BI-RADS are shown in Table 1.
As demonstrated in Table1, both US and mammography results demonstrated complete concordance with those of pathologic signs for th
Results
Kappa were also run. To demonstrate the precise convergence of data, the ROC curve was customized. The significance level of p was considered 0.05 or the lower. Also the findings were
12reported in line with the STROCSS criteria.
Table 1. The concordance of US and mammography results with pathology reports
Ultrasonography
BI-RADSBenign Malignant Total Benign Malignant Total
MammographyP valuePermanent pathologic report
n (%; in row/ in column)
0-12345Total
000
33(94.3/66.0)17(94.4/34.0)50(100/39.7)
048(100/38.1)25(100/19.8)35(100/27.8)18(100/14.3)126(100/100)
048(100/63.2)25(100/32.9)
2(5.7/2.6)1(5.6/1.3)
76(100/60.3)
050(100/65.8)22(100/28.9)4(28.6/5.3)
0(0)76(100/60.3)
000
10(71.4/20.0)40(100/80.0)50(100/39.7)
050(100/39.7)22(100/17.5)14(100/11.1)40(100/31.7)126(100/100)
N/A0.70.8
<0.001<0.01
Table 2 shows lower sensitivity and NPV for higher BI-RADS. This is while specificity and PPV showed an opposite pattern of association. The overall sensitivity, specificity, PPV, and NPV for US (mammography) were 69.8 (91.9), 71.9 (76.6), 75.6 (80.8), and 81.3 (94.6) percent, respectively. The Youden’s index to detect breast lesions was 0.46 for US and 0.68 for mammography. Customizing ROC curve for mammography and pathology reports demonstrated that for BI-RADS 4, we had the highest overall sensitivity (94.3%) and specificity (94.5%) for screening malignancy. ROC curve for
US and pathology showed the highest overall sensitivity (68-92%) and specificity (73-96%) for the BI-RADS 3 and 4. Considering the permanent pathology study for each patient, the convergence of the US and the mammography resul ts is demonstrated in Table 3.
The colored cells in Table 3 show concordance between US and mammography results considering pathology reports as the gold standard, within each BI-RADS stratum. The overall concordance between radiology and pathology (shown as grey in Table 3) was observed in 42 subjects (33.3%).
Table 2. Diagnostic statistics for US and mammography for breast malignancy considering pathology as the gold standard findings
BI-RADSRadiologic modality Sensitivity
% (95% confident interval)
Specificity 1PPV 2NPV Youde's index
P forYoude’s index
Ultrasonography
Mammography
2345
2-5
2345
2-5
20.5(14.3-27.7)72.6(65.7-80.5)95.8(93.2-98.6)98.6(96.9-99.4)71.9(65.2-77.7)
32.0(20.9-45.2)80.0(73.5-88.4)94.5(92.3-96.8)
10076.6(70.2-83.8)
46.7(38.3-55.4)71.0(66.6-76.4)92.3(88.2-96.4)92.3(87.4-97.3)75.6(70.2-80.8)
51.9(42.5-61.1)78.8(73.4-81.9)92.5(88.6-96.4)
10080.8(73.8-87.5)
96.2(94.1-97.3)92.4(89.1-95.7)67.9(59.3-73.8)22.6(11.8-34.6)69.8(61.6-76.3)
10098.0(96.8-99.2)94.3(92.4-96.3)75.4(68.8-80.1)91.9(87.3-95.6)
88.2(83.8-93.4)92.9(89.1-95.3)80.4(74.6-87.8)63.7(55.3-72.6)81.3(72.2-90.4)
10098.3(96.5-99.1)95.8(94.6-97.2)84.8(81.3-87.6)94.6(92.3-96.8)
<0.01
0.160.650.630.400.46
0.320.780.880.750.68
1: Positive Predictive Value 2: Negative Predictive Value
129Ghafoor, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 127-131
US & mammography concordance

Table 3. The convergence of breast US with mammography in BI-RADS model based on pathology as the gold standard findings
This study examined diagnostic accuracy and concordance of US and mammography stratified by BI-RADS and considering pathology reports as the gold standard on 126 study participants, of which 60% proved to be benign and 40% malignant. Since 1960 when mammography was first implemented, early discovery of asymptomatic breast cancer has increased and conclusively mortality rate has dropped to 25% accompanied with a 90% increase in true-
1positive findings. Mammography is more accurate than physical examination to find masses and detect micro-calcification. Fortunately, recent results have shown that three-dimensional mammography could be even more powerful to diagnose breast malignancies and is also associated with a lower false-positive reports in comparison with the traditional
1type. Although there are numerous studies in the medical literature on sensitivity and specificity of breast US and mammography based on definite pathology as the gold standard, the concordance between these two radiologic modalities has been less frequently investigated. This paper revealed a higher sensitivity for mammography (75.4-100%) in comparison with US (22.6-96.2%), the fact that has been confirmed by previous studies (33-56% for the
13,14US versus 36-88% for mammography). Moreover, in each BI-RADS category, mammography was more sensitive than US. Additionally, sensitivity of both the US and mammography was lower for higher BI-
Furthermore, overall complete or relative compatibility (pink and grey cells in Table3: 66+42) was observed for 108(85.7%) of cases. Furthermore, mammography over-diagnosed 12.7% of the benign lesions as malignant while the US study underestimated 1.6% of malignant lesions as the benign one.
Discussion
This study was conducted on available patients records in a single medical center with a limited number of participants. Lack of simultaneous application of US and mammography was another limitation. Moreover, symptomatic and asymptomatic patients seeking breast screening were pooled and thus not analyzed as separate groups.
In conclusion, both ultrasonography and
13,14RADS while an opposite result was found for specificity which was in line with some other
13,15studies. However, some studies have disputed this finding claiming that US was more sensitive than
16-18 mammography The differences in conclusions might be attributable to patients' characteristics in different studies (such as sample size, menopausal status of patients, genetics, and some breast characteristics, for example large breasts or breasts with higher fat composition) and/or other factors (such as instruments and equipment, and also operators’ technical skills). MRI has also been introduced as a screening instrument and its concordance with US and mammography has been
17-19studied. The current study showed a relative concordance
between US and mammography based on pathologic reports. It also revealed that findings from mammography had both a higher overall correlation with pathology and a lower underestimation of the disease in comparison to US. The US results were accompanied with over 12% overestimation of the benign lesions as malignant. However, more data needs to be carried out but this study argues that implementation of both US and mammography in breast lesions with the BI-RADS≥4 would not be necessary, when one of them is performed. Moreover, in BI-RADS 2 and 3, complete concordance with pathology was observed and no further invasive assessments were required.
130 Ghafoor, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 127-131
US & mammography concordance
relative concordancete concordance

All authors admitted to having no financial or professional benefits to in this study.
5. Devolli-Disha E, Manxhuka-Kerliu S, Ymeri H, Kut l lovc i A. Compra t ive accuracy of mammography and ultrasound in women with breast symptoms according to age and breast density. Bosn J basic Med Sci.2009; 9:131-6.
mammography were shown to be sensitive and specific imaging modalities for screening breast lesions, particularly for malignancy. The relative concordance rate between these two screening modalities was acceptable. However, the overall performance of mammography was better than that of US in all breast lesions, especially for the malignant ones. US exhibited some over-diagnosis of benign lesions as malignant ones. Invasive biopsy taken in suspected cases with the BI-RADS 2 and 3 is not recommended, based on the results of the current study.
9. Kim MJ, Kim EK, Kwak JY, Park BW and et al. Sonography surveillance for detection of contralateral metachronous breast cancer in an Asian population. AJR AM J Roentgenol.2009; 192(1):221-8.
6. Flobbe K, Bosch AM, Kesseles AG, Beets GL and et al. The additional diagnosis value of ultrasonography in the diagnosis of breast cancer; Arch Intern Med.2003;163(10):1194-9.
2. Jazayeri SB, Saadat S, Ramezani R, Kaviani A. Incidence of primary breast cancer in Iran: Ten-year national cancer registry data report. Cancer Epidemiol. 2015;39(4):519-527.
Conflicts of Interests
References1. Brunicardi CH, Anderesen DK, Billiar TR, Dunn
DL and et al. Schwartz’s principles of surgery 10th edition. Mc Graw Hill: Newyork. 2019;11(17):541-612.
3. Reeder JG and Vogel VG. Breast cancer prevention. Cancer treatment and research.2008; 141:149-64.
4. Lee IM, Shiroma EJ, Lobelo F, Puska P and et al. Effect of physical inactivity on major non-communicable disease worldwide: an analysis of burden of disease and life expectancy. The Lancet. 2012; 380(9838):219-29.
7. Geller BM, Vacek PM, Skelly J and Harvey SC. The use of additional imaging increased specificity and decreased sensitivity in screening mammography. J Clin Epidemiol.2005; 58(9):942-50.
8. Kriege M, Brekelmans CT, Obdeijn IM, Boetes C and et al. Factors affecting sensitivity and specificity of screening mammography and MRI on women with inherited risk for breast cancer. Breast cancer Res Treat.2006;100:109-19.
10. Siqueira FM, Rezende CA and Barra A.
11.Shoma A, Moutamed A, Ameen M and Abdelwahab A. Ultrasound for accurate measurement for invasive breast cancer tumor size. Breast J.2006;12:252-6.
15.Haghighatkhah HR. Evaluation of concordance of mammography and ultrasono-graphy reports with histopathology reports in benign and malignant breast disease. IJBD.2009; 2(2):27-32.
17. Yeh E, Slantez P, Kopans DB, Rafferty E and et al. Prospective comparison of mammography, sonography and MRI in patients undergoing neoadjuvant chemotherapy for palpable breast cancer. American J of Roentgenology.2005; 184(3): 868-77.
Correlation between clinical examination, mammography and ultrasonography with histopathological exam in determination of tumor size in breast cancer. Rev Bras Ginecol Obstet.2008;30:107-12.
12. Agha R, Abdall-Razak A, Crossley E, Dowlut N, Iosifidis C and Mathew G, for the STROCSS Group. The STROCSS 2019 Guideline: Strengthening the Reporting of Cohort Studies in Surgery. International Journal of Surgery.2019; 72:156-65.
13. Ko ES, Lee HA, Kim WC, Noh MS and et al. Triple negative breast cancer: correlation between imaging and pathological findings. European Radiology.2010; 20(5):1111-7.
14. Boyd NF, Guo H, Martin LJ, Sun L and et al. Mammography density and the risk and detection of breast cancer. NEJM.2007; 356(3):227-36.
16. Berg WA, Zhang Z, Lehrer D, Jong RA and et al. detection of breast cancer with addition annual screening ultrasound or a single screening MRI to mammography in women with elevated breast cancer risk. JAMA.2012;307(13) :1394-404.
18.Group MS. Screening with magnetic resonance imaging and mammography of a UK population at high familial risk of breast cancer: a prospect ive mult i center cohort s tudy (MARIBS). The Lancet.2005;365(9473):1769-78.
19. Lord S, Lie W, Craft P, Cawson J and et al. A systematic review of the effectiveness of magnetic resonance imaging as an addition to mammography and ultrasound in screening of women at high risk of breast cancer. European J of cancer.2007; 43(13):1905-17.
131Ghafoor, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 127-131
US & mammography concordance

132
Here we discussed an iatrogenic pseudoaneurysm following breast mass CNB which was treated conservatively.
Case presentationA 29-year-old woman with chief complaint of
nontender palpable breast mass was referred for further evaluations. Sonography showed a vascular, hypoechoic, well-circumscribed mass measuring 9×5 mm in the right breast upper outer quadrant. The lesion had a low suspicious feature (BIRADS 4a) and was candidate for tissue sampling.
Due to a suspicious history of bleeding disorders, platelets level and coagulation tests were checked and the result was normal. No drug history was recorded. Local anesthesia of skin and parenchyma around the lesion was done by 1% lidocaine without epinephrine. The surrounding tissue was checked to evaluate any probable vessel in the biopsy route. A biopsy was performed with a 14-gauge cutting needle and a throw of 22 millimeters under the guide of sonography.
Profuse bleeding occurred while doing the biopsy
IntroductionCore needle biopsy (CNB) is increasingly used as
a diagnostic method for histologic examination of breast pathologies before the main surgery. Cost-effectiveness, accessibility, minimal rate of complications and short Procedure duration are major factors to make CNB a popular method. Although hematoma is the most common c o m p l i c a t i o n i n C N B , l i m i t e d c a s e s o f
1pseudoaneurysm have been published. A pseudoaneurysm is a blood-containing false lumen that is connected to the main arterial lumen with a na r row neck . They cou ld ra re ly happen spontaneously in patients with severe atherosclerotic changes, although most cases are posttraumatic.
ARTICLE INFO
Conclusion: Although hematoma is a more common complication of breast biopsy, other complications including pseudoaneurysm should be kept in mind. Ultrasound is a useful technique for both the diagnosis and non-surgical treatment of the disease. Ultrasound-guided compression and follow up exams could be helpful to prevent invasive procedures.
Background: Pseudoaneurysm of the breast is a very uncommon disease mostly occurring following traumatic injuries including biopsy. Increasing the use of core needle biopsy in breast pathologies could lead to more cases of the iatrogenic pseudoaneurysm.
Case presentation: Here we described a breast pseudoaneurysm case that occurred after core needle biopsy. The diagnosis was made by color doppler ultrasonography and MRI with contrast. Ultrasound-guided compression was used to treat the lesion. The lesion was followed up with ultrasonography and finally it was resolved.
Received:
Pseudoaneurysm,
Revised:
Accepted:01 July 2020
17 May 2020
06 July 2020
Key words:
iatrogenic, breast,thrombosis
Address for correspondence: Mohammadreza Chavoshi, MDShariati Hospital, Ale Ahmad Highway, Tehran, Iran Tel: +98-9143133658Fax: +98-2166581577E-mail: [email protected]
ABSTRACT
A Case Report of Spontaneous Thrombosis of an Iatrogenic Breast Pseudoaneurysm
a Department of Radiology, Tehran University of Medical Sciences, Tehran, Iran
b Department of Radiology, Tabriz University of Medical Sciences, Tabriz, Iran
a b a a Masoumeh Gity , Batoul Seifi Nadergoli , Behnaz Moradi , Mohammadreza Chavoshi*
Open AccessCase Report
Gity, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 132-135
DOI: 10.32768/abc.202073132-135

The next day control sonography showed a 21×16 mm echo-free to hypoechoic mass with a 2 mm narrow neck at 11 o’clock of the right breast adjacent to previous mass.
Color Doppler investigations showed that the blood flow was turbulent inside the mass and there was to-and-fro spectral waveform in the neck of the lesion. (Figure 1)
and after the first sampling. Sonography showed a hematoma evident as a 20×15 mm hypoechoic lesion at the biopsy site. Immediate compression was done using the ultrasound transducer followed by manual compression for 30 minutes. No more bleeding was observed.
monitoring and conservative proceedings were advised.
Control Doppler ultrasonography 30 days after the biopsy showed a 12×7 mm heterogeneous mass with an anechoic center (Figure 3a). The color
Due to the formation of hematoma and inflammatory changes in the surrounding tissue, evaluation of the initial mass was not possible with ultrasound. On the other hand, definite pathology of the tumor was unknown since the biopsy failed. Therefore, MRI was done to further evaluate the mass. The MRI was performed after 20 days and revealed an oval-shaped mass in the upper outer quadrant of the right breast with intermediate T1 and heterogeneous high and low signal intensity on T2 images measuring 21×16×15 mm (Figure 2a). The mass shows intense rapid enhancement on dynamic series and is related to early drainage (Figure 2b). The diagnosis was an iatrogenic pseudoaneurysm so
Doppler image showed a whirling flow but power Doppler images showed vascularity which connected the mass to an adjacent vessel (Figure 3b).
Control MRI was done after 6 months. The results showed that the PA size had decreased (Figure 4) and
Figure 1. a) A heterogeneous hypoechoic mass with a turbulent flow. b) Spectral color Doppler revealed a to-and-fro waveform in the neck
Figure 2. a) T1W MRI without contrast shows an intermediate intensity mass in the upper outer quadrant of the right breast. b) T1W MRI with contrast shows intense rapid enhancement after contrast injection. Since the
pseudoaneurysm happened in about 2 cm of the mass, the mass is not obvious in this cut.
Breast pseudoaneurysm
133Gity, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 132-135

DiscussionA pseudoaneurysm or false aneurysm most
frequently occurs following a traumatic injury due to a puncture or tear in the arterial wall, after which blood is collected in adjacent tissue connected to the
1, 2vessel. Pseudoaneurysms do not have an arterial 1
wall and are contained by perivascular tissue. Pseudoaneurysm occurs mostly in females, old people, those suffering from atherosclerosis, and those treated by anticoagulation therapy such as
1-5warfarin, heparin, or aspirin. Pseudoaneurysm is uncommon but could be non-traumatic and spontaneous pr imari ly among those with atherosclerotic disease or receiving anticoagulation
3, 6therapy or both.Pseudoaneurysm in radiology is an obvious
complication of vascular catheterization and 1-5percutaneous core needle biopsy of a solid organ.
Breast pseudoaneurysm is diagnosed by mammo-graphy as a circumscribed mass which is adjacent to a
7blood vessel or extending from it, but an ultrasound can confirm the mass to be a pseudoaneurysm. An anechoic mass with echogenic rim, adjacent to an
6, 7artery requires ultrasound examination. Color and
its dimensions were 12×6 mm. The surgeon suggested the conservative Management. The lesion was completely resolved in the next ultrasound follow-up after 2 months.
Since sonography displays real-time images, immediately focused compression of a hematoma can be observed. Iatrogenic pseudoaneurysms caused by large-diameter sheaths and needles could not be thrombosed by compression possibly due to a wide neck. Although compression has been applied as a first-line treatment, it may often bring about no desirable outcome.
Spontaneous resolution of breast pseudoaneurysms 3, 6, 13 has also been reported. It is theorized that small
pseudoaneurysms may be more common than initially
Other treatments observed in the literature 2include percutaneous alcohol injection, thrombin
8, 10, 11 12injection, micro coil embolization and surgical 1, 4, 5
correction. However, surgical treatment is mostly recommended in cases of underlying breast malignancy. Since pseudoaneurysms in the breast are uncommon, they are in general treated in the same way as are pseudoaneurysms in other organs.
power Doppler imaging shows the adjacent artery, connecting neck, and communicating blood flow within the pseudoaneurysm with a turbulent flow and classic “ying-yang” sign on color Doppler imaging. The spectral Doppler imaging will show the “to-and-
3, 6, 8, 9 fro” waveform. In follow-up sonography as a result of clot formation there will be a hypoechoic lesion without any blood flow. Since some cases are secondary to traumatic injury the CT with contrast can be the first modality that shows pseudoaneurysm.
Figure 3. a) A hypoechoic heterogeneous mass in control US. b) Feeding artery of the mass.
Figure 4.T1W MRI with and without contrast after 6 months shows a decrease in the size of the mass
Breast pseudoaneurysm
134 Gity, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 132-135

7. Beres R, Harrington D, Wenzel M. Percutaneous repair of breast pseudoaneurysm: sonographically guided embolization. AJR American journal of roentgenology. 1997;169(2):425-7.
10. Buck RM, Ladner JR, Wuerdeman MF, Kitley
2. Bazzocchi M, Francescutti GE, Zuiani C, Del Frate C, Londero V. Breast pseudoaneurysm in a woman after core biopsy: percutaneous treatment with alcohol. American Journal of Roentgenology. 2002;179(3):696-8.
The written consent was signed by the patient.
References
5. Wilkes AN, Needleman L, Rosenberg AL. Pseudoaneurysm of the breast. AJR American journal of roentgenology. 1996;167(3):625-6.
thought, but the small size, small neck, and absence of underlying anticoagulation lead to a spontaneous resolution before clinical identification.
Pseudoaneurysm, as a potential complication of the breast biopsy, needs to be considered. Mapping the vessels near the lesion by color flow evaluation before the biopsy can help prevent complications like pseudoaneurysm or hematoma in interventions. If pseudoaneurysm occurs, ultrasound-guided compression and follow up exams could be helpful to prevent invasive procedures. However, if the lesion is still present, performing an additional procedure such as embolization or surgery should be considered.
Conflict of Interest
4. Dixon A, Enion D. Pseudoaneurysm of the breast: case study and review of literature. The British journal of radiology. 2004;77(920):694-7.
8. Eli E, Ansari H, Williams J, Carter M, Friedman P. Successful treatment of a two centimeter breast pseudoaneurysm with thrombin injection. The breast journal. 2012;3(18):292-3.
Ethical Consideration
1. Azorín Samper MdC, Hernandorena González M, Ibáñez Arias A, Díaz Sierra S, Bertolo Domínguez M, et al. A case report of pseudoaneurysm after a core needle biopsy of breast cancer. The Breast Journal. 2020;26(2):252-4.
3. Bitencourt A, Cohen MP, Graziano L, Souza JA, Marques EF, et al. Pseudoaneurysm after ultrasound-guided vacuum-assisted core breast biopsy. The breast journal. 2012;18(2):177.
None
6. El Khoury M, Mesurolle B, Kao E, Mujoomdar A, Tremblay F. Spontaneous thrombosis of pseudoaneurysm of the breast related to core biopsy. American Journal of Roentgenology. 2007;189(6):W309-W11.
9. Sohn Y-M, Kim MJ, Kim E-K, Chung SH, Kwak JY, et al. Pseudoaneurysm of the breast during vacuum-assisted removal. 2009.
12. Sasada S, Namoto-Matsubayashi R, Yokoyama G, Takahashi H, Sakai M, et al. Case report of pseudoaneurysm caused by core needle biopsy of the breast. Breast Cancer. 2010;17(1):75.
CA. A novel treatment for breast pseudoaneurysm in the anticoagulated patient. The Breast Journal. 2020.
13. Al Hadidy AM, Al Najar MS, Farah GR, Tarawneh ES. Pseudoaneurysm of the breast after blunt trauma: Successful treatment with ultrasound‐guided compression. Journal of Clinical Ultrasound. 2008;36(7):440-2.
11. McNamara Jr M, Boden T. Pseudoaneurysm of the breast related to 18-gauge core biopsy: successful repair using sonographically guided thrombin injection. American Journal of Roentgenology. 2002;179(4):924-6.
135Gity, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 132-135
Breast pseudoaneurysm

136
categorized it into benign, borderline, and malignant tumors on the basis of his topathological characteristics. Malignant phyllodes tumor is an uncommon but aggressive breast malignancy and constitutes nearly 25% of all phyllodes tumors. Although malignant phyllodes tumor typically occurs in the fourth to sixth decades of life, it can also occur in younger women. In a study by Abusalem et al., it was estimated that one out of 26 phyllodes tumor patients was malignant in patients 20-29 years
4, 5of age. Patients usually present with a spectrum of complaints starting with a palpable mass or abnormal mammogram and reaching architecture
IntroductionPhyllodes tumors are uncommon fibroepithelial
neoplasm of the breast, accounting for 0.3 to 0.5% of 1all female breast neoplasms , with an incidence rate
of about 2.1 per million mostly occuring in women 2, 3aged 45 to 49 years. The term ‘‘phyllodes tumor”
by the World Health Organization (WHO) has
ARTICLE INFO
Conclusion: Management of malignant phyllodes tumor remains debatable, especially when it comes to the effect of adjuvant radiotherapy and chemotherapy. From a surgical perspective, whether phyllodes tumors should be considered as epithelial breast cancers or as soft tissue sarcoma is another debate. On the other hand, although challenging, accurate identification of phyllodes tumor initially may aid in decreased recurrence.
Case Presentation: A 23-year-old female patient Gravida 0 Para 0, previously healthy, with no family history of breast or ovarian cancer was referred to our institution for managing a right breast mass increasing in size over a period of 1 month associated with reddish-brown discoloration of the skin. Breast ultrasound showed an isodense oval mass measuring approximately 16x14x12cm in the right lower outer quadrant of her breast. Core biopsy and FNA done revealed a low grade phyllodes tumor. MRI of breasts showed a huge mass of the right breast occupying all quadrants, measuring 15x14.5 cm in its greatest axis with involvement of the pectoralis major muscle, with no evidence of suspicious axillary lymphadenopathy. Distant metastatic work-up with CT scan of chest abdomen and pelvis and a PET scan did not show distant metastasis. Hence, the patient underwent right total mastectomy with a final pathology compatible with malignant phyllodes tumor. She is on regular follow up and 18 months post-surgery is still disease free.
Background: Phyllodes tumors are rare fibroepithelial neoplasm of the breast, representing 0.3 to 0.5% of all female breast neoplasms. The term ‘‘phyllodes tumor” by the World Health Organization (WHO) categorizes it into benign, borderline, and malignant tumors based on histopathological characteristics. Malignant phyllodes tumor is an uncommon but aggressive breast malignancy and accounts for approximately 25% of all phyllodes tumors.
Revised:
Received:
Accepted:21 July 2020
15 June 2020
29 July 2020
Key words:
breast cancer,Phyllodes tumor,
management
Address for correspondence: Melissa Kyriakos Saad, MDAddress: General surgeru department, Saint Georges Hospital University Medical Center, Ashrafieh, Beirut, P.O.Box 166 378,LebanonEmail: [email protected]
ABSTRACT
Large Malignant Phyllodes Tumor of the Breast: Case Report of a Young Female and Review of Literature
a Saint George Hospital University Medical Center, Beirut, Lebanon
a a aMelissa Kyriakos Saad* , Imad El Hajj , Elias Saikaly
Open AccessCase Report
Kyriakos Saad, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 136-142
DOI: 10.32768/abc.202073137-142
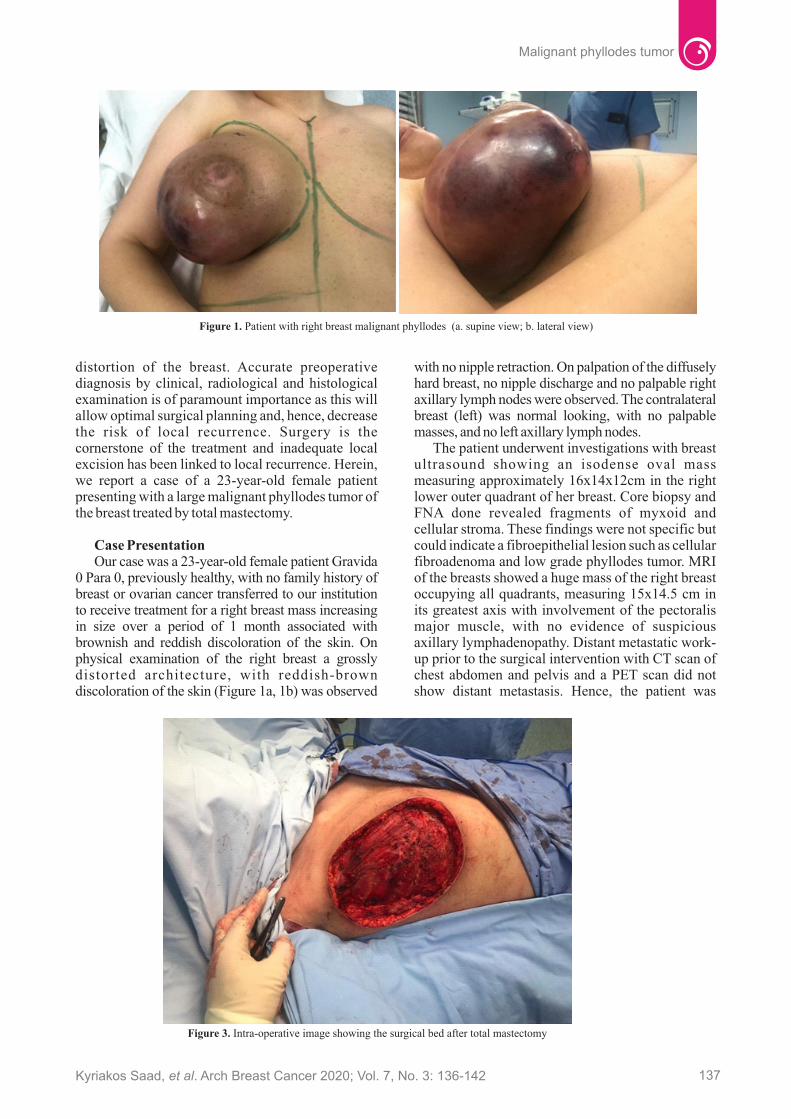
Case PresentationOur case was a 23-year-old female patient Gravida
0 Para 0, previously healthy, with no family history of breast or ovarian cancer transferred to our institution to receive treatment for a right breast mass increasing in size over a period of 1 month associated with brownish and reddish discoloration of the skin. On physical examination of the right breast a grossly distorted architecture, with reddish-brown discoloration of the skin (Figure 1a, 1b) was observed
distortion of the breast. Accurate preoperative diagnosis by clinical, radiological and histological examination is of paramount importance as this will allow optimal surgical planning and, hence, decrease the risk of local recurrence. Surgery is the cornerstone of the treatment and inadequate local excision has been linked to local recurrence. Herein, we report a case of a 23-year-old female patient presenting with a large malignant phyllodes tumor of the breast treated by total mastectomy.
with no nipple retraction. On palpation of the diffusely hard breast, no nipple discharge and no palpable right axillary lymph nodes were observed. The contralateral breast (left) was normal looking, with no palpable masses, and no left axillary lymph nodes.
The patient underwent investigations with breast ultrasound showing an isodense oval mass measuring approximately 16x14x12cm in the right lower outer quadrant of her breast. Core biopsy and FNA done revealed fragments of myxoid and cellular stroma. These findings were not specific but could indicate a fibroepithelial lesion such as cellular fibroadenoma and low grade phyllodes tumor. MRI of the breasts showed a huge mass of the right breast occupying all quadrants, measuring 15x14.5 cm in its greatest axis with involvement of the pectoralis major muscle, with no evidence of suspicious axillary lymphadenopathy. Distant metastatic work-up prior to the surgical intervention with CT scan of chest abdomen and pelvis and a PET scan did not show distant metastasis. Hence, the patient was
Figure 1. Patient with right breast malignant phyllodes (a. supine view; b. lateral view)
Figure 3. Intra-operative image showing the surgical bed after total mastectomy
137Kyriakos Saad, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 136-142
Malignant phyllodes tumor

bloodstream and lymphatic metastasis occurs rarely. The most frequently reported sites for metastases are
9the lung, soft tissue, bone, and pleura. The rate of metastases is 25%–31% for malignant and borderline tumors, whereas it is 4% for all types of
10phyllodes masses. Guidelines for cases of ma l ignan t phy l lodes tumor by Na t iona l Comprehensive Cancer Network include complete surgical resection with negative margins of at least 1 cm and preferably 1 to 2 cm due to the morphologic characteristic of the tumor. The presence of a pseudo capsule containing finger-like or pseudopodia-like projections around the phyllodes tumor tissue is likely, which, if not surgically excised, leads to a local recurrence. Therefore, the tumor with 1–2-cm width of normal tissue should be removed including
11, 12these pseudopodia of tumors. Total mastectomy is in general not suggested due to poor cosmetic outcomes, unless negative margins cannot be conducted or if the tumor is too large to be completely excised. Adjuvant radiation therapy is debatable in preventing tumor recurrence. Radiation has been found to prevent recurrence of borderline and malignant phyllodes tumor after surgical interventions (breast-conserving surgery and mastectomy) with no impact on disease-free
13survival. Furthermore, adjuvant radiation therapy is suggested for recurrent and malignant phyllodes tumor. Patients with high risk for recurrence, including those with histological margin less than 5
14, 15mm may be candidates for radiotherapy. On the other hand, routine adjuvant systemic therapy after initial excision is not recommended. Chemotherapy for locally recurrent tumor is contentious. Burton et al. reported effective palliation for patients suffering from metastatic disease with chemotherapy based on cisplatin and etoposide. As far as we know, this is the youngest reported case of malignant phyllodes tumor of the breast with this size. In our case, despite the large size of the tumor negative surgical margins of 1.6 cm were achieved by total mastectomy, with no recurrence at 18 months of follow-up. In our
scheduled for right total mastectomy.The patient went through a right total mastectomy
with partial excision of the pectoralis major where the tumor was involved (Figure 3, 4). Primary closure was possible without the need for autologous flap for closure. The final histopathogic result was consistent with features of malignant phyllodes tumor measuring 16.5x15x14cm, with clear negative surgical margins 1.6cm away from the tumor and the deepest surgical margin being 2mm away from the tumor. Post-surgical follow-up showed good wound healing, revealing no flap necrosis (Figure 5). She is on regular follow up and 18 months post-surgery is disease free with no evidence of local recurrence or distant recurrence by PET scan.
Extensive studies have been done regarding the treatment of common breast malignancies. However, the optimal management for rare breast tumors including phyllodes tumor has not been well established. Due to its rarity, the current medical literature lacks a sound treatment plan, especially when it comes to the effect of chemotherapy or radiotherapy on managing malignant phyllodes tumor of the breast. Most management protocols depend on retrospective case series. Irrespective of their histologic classification, phyllodes tumors have an unpredictable clinical outcome. Age, tumor size, surgical approach, mitotic activity, stromal overgrowth and surgical margin have been found to be important factors in diagnosis and prediction of
6recurrence. Kaprisi et al. found that tumor size and surgical margins were predictive of local
7recurrence, which is very important for treatment of phyllodes tumors to be successful. A review of the literature reveals a local recurrence rate >40% for all
8pathological types. On the contrary, different studies showed a local recurrence rate of less than 20% depending on the tumor subtype. Furthermore, a delay in treatment increases the possibility of distant metastases. Metastasis usually occurs via the
Discussion
Figure 4. Surgical Specimen excised Figure 5. Surgical Scar
138 Kyriakos Saad, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 136-142
Malignant phyllodes tumor

review of the English medical literature we identified 16 cases of large malignant phyllodes tumors of the breast, above 10cm in largest dimension (Table 1), with a size range of 10 to 40cm, with a mean age of 44 years old. Table 1 shows that the most common site of metastasis is lungs 6/16
(37.5%), followed by brain 3/16 (18.7%). Hence, appropriate surgery is the cornerstone and the first step towards successful treatment of phyllodes tumor.
In conclusion, management of malignant
Table 1. Comparison the studies evaluated malignant phyllodes tumor
40x38x16
40x30x10
33x32x22
32x32x17
31.5x15.6
30x20x13
20x20x25
Right
Right
Right
Left
Right
Left
Left
Radical mastectomy (tumor dissected off with right 6th rib and
pectoralis major)(primary closure
not possible)
Modified radical mastectomy (1/9 LNs)
Simple mastectomy
Radical mastectomy with split thickness
graft
Simple mastectomy
Simple mastectomy
Simple mastectomy with left chest wall defect was coveredtemporarily with
INTEGRA replacedwith split thickness
skin graft 5 weeks later
1. All margins involved 2. Post-op PET scan : tumor infiltrating the
5th and 6th ribs3. 6 weeks post-operative :
re-admitted for pleural effusion deceased due to pulmonary
complications
Free of recurrence at 18 months follow up
Free of recurrence at 1 year follow up
2 months after surgery: 1. CT chest : pulmonary nodules
• Biopsy : Lung metastasis• 4 months after chemotherapy: progression of lung metastasis
2. Headache and grand mal seizure: brain metastasis
(6x5x5 cm cerebral mass) underwent resection
3. Post-operatively dyspnea: intrathoracic progression
of disease 4. Succumbed to disease 20 months after first diagnosis
1. 3 weeks post-op: complaint of headache Right parietal tumor –
right craniotomy: metastatic malignant phyllodes tumor
2. 7 weeks post-op • LR: 6 new masses were
found, the largest measuring6 cm and a mass was palpated
in the right axilla: • FNA: enlarged pleomorphic
cells, epithelioid cells – identical to original tumor.
3. Patient deceased before initiating treatment
Free of recurrence 1 year after surgery
NA
None
Chemotherapy (adriamicyn and
ifosfamide)/radiotherapy
Chemotherapy (doxorubicin
and ifosfamide)Radiotherapy
6 cycles (AdriamycinVR,
ifosfamide, and mesna)4 cycles
(gemcitabine and docetaxel)
Patient deceased before any therapy could be initiated
Radiotherapy
None
O.ECW*, K. 16CK, 2017
A. Testori 17et al., 2015
R.Krishnamoorthy 18et al., 2014
AP.Gregston 19 et al., 2019
N. Roberts, 20D.M. Runk, 2015
I. Albalawi,212018
MA. Sbeih22 et al., 2015
53
33
35
32
50
41
41
Core biopsy inconclusive CT chest and
abdomen:large tumor with extension
to rib and pleura
PET: positive ALNSkeletal & lung
xray normal
FNA: borderline phyllodes Core biopsy: biphasic neoplasm with
malignant stromal component.CT brain
and chest & US abdomen no metastasis
Chest CT scan: large solid mass occupying the entire
left breast
Core needle biopsy:malignant neoplasm
with carcinomatous and sarcomatous elements, the cells showed focal marked pleomorphism (>10 mitoses/10HPF)
with focal necrosis (ER/PR positive; HER2 negative) CT of chest
positive for bilateral chest massesPET Scan: result
not mentioned
True cut biopsy malignant phyllodes tumor CT scanchest, abdomen and pelvis
normal Isotopes scan normal
Core biopsy: fascicular pseudoangiomatous stromal
hyperplasia or phyllodes tumorLeft ALN biopsy: chronic
lymphadenitis without neoplastic cells CT chest
and abdomen : no metastasis
Author/year Age Size(cm) Tumor Site
Pre-operativework-up
Type of Surgery
Adjuvanttreatment
Recurrence
˿
139Kyriakos Saad, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 136-142
Malignant phyllodes tumor

20x14x9.7
16.5x15x14
15.5x13.5x13
15x15
15x15
15
14x14x10
13x11x7
12
10x10
Right
Right
Right
Right
Left
Left
Right
Right
Right
Right
Radical mastectomy with pectoralis major
excision+ axillary lymph nodes dissection
(no positive ALNs)
Total mastectomy with partial
excision of pectoralis major (with primary
closure of defect)
Modified Radical Mastectomy + TRAM
flap (1/32 ALNs)
Simple mastectomy
Modified Radical Mastectomy
Simple mastectomy
Simple mastectomy without ALND
Partial mastectomy
Modified radical mastectomy
Simple mastectomy+ ALN excision
No LR 17 months after surgery
No LR after 18 months follow-up
PET scan: no distant metastasis
Free of LR at 3 years follow-up and free of distant metastasis (lung metastasis
resolved)
1. After 9 months Lung metastasis
2. Died of disease after 18 months of primary
diagnosis
3 months' post-op: · No LR
· Huge cystic nodule in the brain
· Contrast enhanced computed tomography (CECT) of chest, abdomen and pelvis showed lesions in lower lobe of left lung of 3.9 × 3.6 cm of +40
(HU) in posterobasal segment and right adrenal gland of 5.8 × 5.1 cm of +30HU
· 20 days' later patient succumbed to disease
· 19 months post-op: left pleural effusion/left
pleural mass · Patient deceased of disease 21 months after diagnosis
NA
1. Free margins but <1mm: re-excision margins
2. CT scan and bone scan negative for metastasis
Post-op CT chest and abdomen scan: no liver
or lung mets Follow-up NA
1. Lung metastasis increased in size
(progressive disease)2. Patient died 4 months
post-surgery due to respiratory failure
None
None
Chemotherapy (doxorubicin
and ifosfamide)
Radiotherapy (50Gy), Chemotherapy
(Cyclophosphamide)
None
Radiotherapy
None
Radio
None
4 cycles (FEC therapy :
cyclophosphamide, epirubicin, fluorouracil)
M.Takenaka 23et al., 2011
Our Case, 2020
SH.Moon 24et al., 2019
T.Saito 25et al., 1998
S. Khanal 26et al., 2018
J. Kaya,A. Betensley,
272013
J.Alves 28et al., 2011
A.Abdulkareem, 292019
M.Sani 30et al., 2008
S.Suzuki-Uematsu,312010
57
23
48
54
37
48
38
37
44
52
Core bx low grade myofibroblastic sarcoma)
CT suspicion of chest wall invasion MRI no ALN
CEA/Ca 15-3 normal Excisional marked stromal hypercellularity without an
epithelial component
Core biopsy &FNA: fragments of myxoid
and cellular stroma, may indicate a fibroepithelial lesion such as cellular fibroadenoma and low grade phyllodes tumor
CT chest abdomen& pelvis negative for metastasis
PET scan negative for metastasis
Core needle biopsy: malignant phyllodes
tumorCT chest metastatic LNs to Right axilla &
multiple solitary pulmonary nodules on right lungFNA of LNs positive
for metastasis PET scan
NA
Chest X-ray: negative US abdomen & pelvis
negative True-cut: necrotic areas with
fibrocollagenous tissue with proliferation of oval to elongated spindle cells
showing mild degree of atypia
NA
Core biopsy: biphasic neoplasm with malignant
stromal componentChest X-ray & Abdomen ultrasound negative for
distant metastasis
Core biopsy: Epithelial and stromal components Epithelial is benign, the
mesenchymal part showed spindle cell with increased
cellularity (mitotic rate 5/10 HPF) no atypia or necrosis
FNA: benignbreast lesion
CT chest (bilateral lung nodules)Core needle biopsy
(proliferation of atypical spindle-shaped cells with
marked coagulation necrosis ,no
epithelial components : sarcoma vs phyllodes)
140 Kyriakos Saad, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 136-142
Malignant phyllodes tumor

1. Rowell MD, Perry RR, Hsiu JG, Barranco SC. Phyllodes tumors. Am J Surg. 1993;165(3):376-9.
3. Salvadori B, Cusumano F, Del Bo R, Delledonne V, Grassi M, et al. Surgical treatment of phyllodes tumors of the breast. Cancer. 1989;63(12):2532-6.
10. Khosravi-Shahi P. Management of non metastatic
4. Reinfuss M, Mitus J, Duda K, Stelmach A, Rys J, et al. The treatment and prognosis of patients with phyllodes tumor of the breast: an analysis of 170 cases. Cancer. 1996;77(5):910-6.
A written informed consent was obtained from the patient to publish the case as well as any associated images
None.
8. Parker SJ, Harries SA. Phyllodes tumours. Postgrad Med J. 2001;77(909):428-35.
References
7. Mishra SP, Tiwary SK, Mishra M, Khanna AK. Phyllodes tumor of breast: a review article. ISRN Surg. 2013;2013:361469.
6. Briggs RM, Walters M, Rosenthal D. Cystosarcoma phylloides in adolescent female patients. Am J Surg. 1983;146(6):712-4.
Conflict of Interest
2. Bernstein L, Deapen D, Ross RK. The descriptive epidemiology of malignant cystosarcoma phyllodes tumors of the breast. Cancer. 1993;71(10):3020-4.
9. Yagishita M, Nambu Y, Ishigaki M, Okada T, Yamanouchi K, et al. [Pulmonary metastatic malignant phyllodes tumor showing multiple thin walled cavities]. Nihon Kokyuki Gakkai Zasshi. 1999;37(1):61-6.
5. Abusalem OT, Al-Masri A. Phyllodes Tumors of the Breast. Mater Sociomed. 2011;23(4):200-5.
phyllodes tumor remains debatable, especially when it comes to the role of adjuvant radiotherapy and chemotherapy. From a surgical perspective, whether phyllodes tumors should be considered as epithelial breast cancers or as soft tissue sarcoma is another debate. On the other hand, although challenging, accurate identification of phyllodes tumor initially may aid in decreasing the rate of local recurrence. Finally, due to rarity of such a disease, combining the observations of clinicians treating malignant phyllodes tumor in an international database will be beneficial to patients.
Acknowledgements
Special thanks to the General Surgery Department at Saint George Hospital University Medical Center and the National Breast Care Center at Sister Rosary Hospital
Ethical Consideration
19. Gregston AP, Metter DM, Osborne CRC, Pippen J, Jr. Giant malignant phyllodes tumor with metastasis to the brain. Proc (Bayl Univ Med Cent). 2019;32(1):116-8.
phyllodes tumors of the breast: review of the literature. Surg Oncol. 2011;20(4):e143-8.
20. Roberts N, Runk DM. Aggressive malignant phyllodes tumor. Int J Surg Case Rep. 2015;8C:161-5.
23. Takenaka M, Toh U, Otsuka H, Takahashi H, Iwakuma N, et al. Giant malignant phyllodes tumor: a case report . Kurume Med J . 2011;58(2):67-72.
14. Barth RJ, Wells WA, Mitchell SE, Cole BF. A prospective, multi-institutional study of adjuvant radiotherapy after resection of malignant phyllodes tumors. Annals of surgical oncology. 2009;16(8):2288-94.
13. Zeng S, Zhang X, Yang D, Wang X, Ren G. Effects of adjuvant radiotherapy on borderline and malignant phyllodes tumors: A systematic review and meta-analysis. Mol Clin Oncol. 2015;3(3):663-71.
16. Ong E, Kong C. CASE REPORT: MASSIVE RUPTURED MALIGNANT PHYLLODES TUMOUR. Journal of Health and Translational Medicine. 2017;20(1):18-20.
24. Moon SH, Jung JH, Lee J, Kim WW, Park HY, et al. Complete remission of giant malignant phyllodes tumor with lung metastasis: A case r e p o r t . M e d i c i n e ( B a l t i m o r e ) .
12. Kataria K, Dhar A, Ranjan P, Kumar A, Islam S, et al. Radical mastectomy SANS axillary lymph node dissection for large phyllodes tumor: a guarantee against recurrence. Indian Journal of Surgery. 2019;81(6):520-4.
15. Chaney AW, Pollack A, McNeese MD, Zagars GK. Adjuvant radiotherapy for phyllodes tumor of breast. Radiat Oncol Investig. 1998;6(6):264-7.
17. Testori A, Meroni S, Errico V, Travaglini R, Voulaz E, et al. Huge malignant phyllodes breast tumor: a real entity in a new era of early breast cancer. World J Surg Oncol. 2015;13:81.
21. Albalawi IA. A huge phyllodes tumor in the breast: a case report. Electron Physician. 2018;10(6):6951-5.
18. Krishnamoorthy R, Savasere T, Prabhuswamy VK, Babu R, Shivaswamy S. Giant malignant phyllodes tumour of breast. Case Rep Oncol Med. 2014;2014:956856.
11. Badwe RA, Kataria K, Srivastava A. Surgical Resection of Phyllodes Tumour: a Radical Approach as a Safeguard Against Local Recurrence. Indian J Surg. 2015;77(2):161-3.
22. Sbeih MA, Engdahl R, Landa M, Ojutiku O, Morrison N, et al. A giant phyllodes tumor caus ing u lce ra t ion and severe b reas t disfigurement: case report and review of giant phyllodes. J Surg Case Rep. 2015;2015(12).
141Kyriakos Saad, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 136-142
Malignant phyllodes tumor

26. Khanal S, Singh YP, Bhandari A, Sharma R. Malignant phyllodes tumor with metastases to lung, adrenal and brain: A rare case report. Ann Med Surg (Lond). 2018;36:113-7.
25. Saito T, Kato K, Kawamori J, Yoshinobu T, Sato T, et al. Radiotherapy to pulmonary metastases of a malignant phyllodes tumor of the breast. International Journal of Clinical Oncology. 1998;3(5):337-41.
2019;98(22):e15762.
30. Sani M, Leow V, Zaidi Z. Malignant phyllodes tumour: a case report. The Internet Journal of Surgery. 2008;21(2).
27. Kaya J, Betensley A. Is It Mass or Effusion: A Case of a Large Pleural Metastasis of Malignant Phyllodes Tumor of the Breast. Chest. 2013;144(4):484A.
28. Souza JAd, Marques EF, Guatelli C, Girao DS, Queroz T, et al. Malignant phyllodes tumor of the breast: case report. Revista da Associação Médica Brasileira. 2011;57(5):495-7.
31. Suzuki-Uematsu S, Shiraishi K, Ito T, Adachi N, Inage Y, et al. Malignant phyllodes tumor composed almost exclusively of a fibrosarcomatous component: a case report and review of malignant phyllodes tumors with metastases. Breast cancer. 2010;17(3):218-24.
29. Abdulkareem AA. Malignant breast phyllodes: Literature review of management and case report. Saudi Journal of Laparoscopy. 2019; 4(1):1.
142 Kyriakos Saad, et al. Arch Breast Cancer 2020; Vol. 7, No. 3: 136-142
Malignant phyllodes tumor

Breast Imaging Reporting and Data System (BIRADS) was introduced by the American College of Radiology (ACR) in 1993 and has since undergone several modifications. It offers a common language between radiologists for describing breast lesions, and between radiologists and clinicians to communicate their findings. The first version of BIRADS considered only mammography interpretation and report, but the subsequent versions have included
1ultrasound and MRI of the breast as well. BIRADS for ultrasound is evolving continuously in order to
2provide a constant and helpful guide for radiologists. Using BIRADS and the ultrasound lexicon have improved interobserver agreement between breast radiologists in interpreting breast ultrasound
3findings. While BIRADS for ultrasound was 2
introduced in the fourth version of BIRADS in 2003 , some items have been added or modified in the fifth version in 2013. Briefly, these consist of the addition of a subsection entitled “general considerations” which provides general data like image quality or anatomic considerations; deletion of the “lesion boundary” descriptor; defining “posterior features” instead of “posterior acoustic features” and “intraductal calcifications, calcifications in a mass and calcifications outside of a mass” in lieu of "macrocalcifications”; inclusion of new descriptors under “special cases”; rearrangement of several terms under “associated features” instead of “surrounding tissue”; re-definition of terms describing vascularity;
4and adding descriptors related to elastography.
Checklists or templates for a structured report are also developing quickly with the aim to offer
2consistent and reusable data formats , and provide accuracy and comprehensiveness concurrently with
5simplicity for the clinician. Particularly they aim to ease comparisons between successive imaging reports coming from different radiologists, as one of
6the main objectives of BIRADS. A structured breast ultrasound report would provide a consistent form for clinicians that can also lessen the risk of
5malpractice. Whole breast ultrasound is used as a helpful
adjunct to screening mammography, and the practice 7parameters have been defined by ACR. The
description of each finding in this modality includes a large number of details, and consequently it may show itself as a complex report.
As oncologic and breast surgeons who regularly benefit from breast ultrasound reports for management purposes of our patients, we believe that the outline and the order in which the descriptors come in the written report are extremely important in making it more easily understandable, and allowing a more practical and straightforward comparison with subsequent reports. In fact, the organization of the radiologist notes in the report might make it clear and user-friendly, or ambiguous and complex. We can imagine a whole breast ultrasound which delineates several masses, and, according to BIRADS, describes dimensions, localization, shape, orientation, margin, boundary, echo pattern, posterior features, and the effects on the surrounding tissues for each mass. Along with other findings, the whole report is categorized as BIRADS 3. The clinician who sees this report and the follow-up ultrasound performed some time later in another center would have to compare each individual finding between the two reports. If findings and
143
A Plea for Defining a Uniform Standard Order in Reporting Details of a Whole Breast Ultrasound: The Point of View of Two Breast Surgeons?
a Breast Disease Research Center, Tehran University of Medical Sciences, Tehran, Iran
b Department of Surgery, Arash Women's Hospital, Tehran University of Medical Sciences, Tehran, Iran
c Mostafa Khomeini Hospital, Shahed University, Tehran, Iran
a,b cSadaf Alipour* , Farzaneh Golfam
Open AccessLetter to Editor
Address for correspondence: Sadaf Alipour, M.D.Address: Breast Disease Research Center- Sadaf Building (Building of Cancer Institute Clinics)- Cancer Institute- Imam Khomeini Hospital Complex, Keshavarz BLV, Tehran, Iran. Tell: +98 21 61192761Email: [email protected]
Alipour, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 143-14
DOI: 10.19187/abc.202073143-144

User-friendly breast ultrasound reports
details are written and explained in different orders and manners, the comparison would be both time-consuming and ambiguous.
Unity among different reports of the whole breast ultrasound to make them easily understandable and comparable can only be provided by standardization of the written report format. This means that in order to make the breast ultrasound report more helpful for the clinicians, a uniform framework with a simple and reasonably arranged order of mentioning the findings and details ought to be defined as a complement to the present standards and descriptors of BIRADS. We believe that this format could also positively affect the practice of radiologists when comparing their findings with previous breast ultrasound reports of the same patient. Also, adding a summary about the findings to the final impression at the end of the reports could make it easier for the clinicians to follow the report.
Meanwhile, a study is being conducted at Tehran University of Medical Sciences to design and suggest a suitable outline; the results will be hopefully published in near future.
Conflicts of InterestThere is no conflict of interest to declare.
References 1. Mendelson E, Böhm-Vélez M., Berg W.,
Whitman G., Feldman M., Madjar H. ACR BI-RADS ultrasound. In ACR BI-RADS Atlas, Breast Imaging Reporting and Data System. Fifth ed. Reston, VA, USA: American College of Radiology, 2013; 1-173
2. Burnside ES, Sickles EA, Bassett LW, Rubin DL, Lee CH, Ikeda DM, Mendelson EB, Wilcox PA, Butler PF, D'Orsi CJ. The ACR BI-RADS® experience: learning from history. Journal of the American College of Radiology. 2009;6(12): 851-60.
3. Lazarus E, Mainiero MB, Schepps B, Koelliker SL, Livingston LS. BI-RADS lexicon for US and mammography: interobserver variability and positive predictive value. Radiology. 2006;239(2):385-91.
4. Spak DA, Plaxco JS, Santiago L, Dryden MJ, Dogan BE. BI-RADS® fifth edition: A summary of changes. Diagnostic and interventional imaging. 2017;98(3):179-90.
5. Kahn Jr CE, Langlotz CP, Burnside ES, Carrino JA, Channin DS, Hovsepian DM, Rubin DL. Toward best practices in radiology reporting. Radiology. 2009;252(3):852-6.
6. Levy L, Suissa M, Chiche JF, Teman G, Martin B. BIRADS ultrasonography. European journal of radiology. 2007;61(2):202-11.
7. The American College of Radiology: ACR practice parameter for the performance of whole-breast ultrasound for screening and
staging, available at: [https://www.acr.org/-/media/ACR/Files/Practice-Parameters/ USWholeBreast.pdf ]
Alipour, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 143-144144

Breast density is now well established as an 1
independent risk factor for breast cancer. Dense breast tissue, as measured on mammography, also has a masking effect, making breast cancer more difficult to detect. It reduces the sensitivity of mammography and increases the likelihood of an interval cancer (malignancy presenting with
1symptoms between screening rounds).While the risk and the diagnostic challenges
associated with dense breast tissue are understood, the way it should be managed remains less clear. There is increasing pressure from consumer groups for women to be notified of their breast density. These community groups, representing women at risk of breast cancer, or with a history of breast cancer, have lobbied strongly, and across most of the United States notification is now mandated by legislation. This means that every woman with dense breasts must be sent a letter by her radiologist informing her of her breast density.
However, evidence-based risk management guidelines are lacking, leading to confusion and anxiety. This Commentary will discuss the breast cancer risk associated with breast density and the options for cancer screening. On the basis of this, it will propose recommendations for the assessment and management of women with dense breasts. Options include the use of supplemental screening with tomosynthesis, ultrasound and/or MRI or varying the screening interval.
What is breast density?Breast density is a measurement of the proportion
of stroma and epithelium (which appears opaque/
white on a mammogram) relative to fatty tissue (which appears lucent/black on a mammogram). Density is a mammographic measurement. High mammographic density may be associated with clinical density (i.e. breasts that feel lumpy to palpation); however, there is a poor correlation between density measured by clinical examination
2 and imaging. The American College of Radiology (ACR) BiRADS system is a widely accepted method for classifying density into four categories, A (almost entirely fatty) to D (extremely dense,) as can
3be seen in Table 1. Categorisation can be made by visual estimation or using programs to calculate density from digital mammography images (automated measurement). Measurements can be difficult to reproduce and may vary between
4observers and time intervals. There is no universally accepted method for density estimation.
Breast density is determined by several factors. Young women (20’s and 30’s) tend to have very dense breast tissue and there is a trend for density to decrease with increasing age, breast feeding and post-menopausal status. Obesity is associated with
5lower breast density.
What is the risk of breast cancer in dense breasts?Although the estimates vary, women with high
breast density (>75%) have a risk of developing cancer 4.7 times higher than women of the same age
1with density <10% , or a risk 2.3 higher for women 5
with a density of <25% compared to density 75%. As a comparison, the risk ratio associated with two first-degree relatives with breast cancer is estimated at 3.8, a single first-degree relative with breast
145
The Challenge of Breast Density– Options for Management andBreast Cancer Screening
a Sydney Medical School, Faculty of Medicine and Health, University of Sydney, NSW
b School of Medicine, Sydney, University of Notre Dame, Sydney, NSW
a,b a aMeagan Brennan* , Brooke Nickel , Nehmat Houssami
Open AccessInvited Commentary
Address for correspondence: Prof Meagan Brennan, PhDAddress: University of Notre Dame,160 Oxford St, Darlinghurst NSW AustraliaTel +61 2 8204 4400Email: [email protected]
Brennan, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 145-148
3Table 1. Categories of Breast Densitya. The breasts are almost entirely fattyb. There are scattered areas of fibroglandular density c. The breasts are heterogeneously dense, which may obscure small massesd. The breasts are extremely dense, which lowers the sensitivity of mammography
DOI: 10.19187/abc.202073145-148

cancer younger than 50 years at 2.7, previous benign breast biopsy 1.9, a second-degree relative with
6breast cancer 1.7 and nulliparity 1.3.The prevalence of mammographic density in the
screening population has been reported at 43% in a cohort aged 40-74, (with dense tissue defined as being in the highest two (of four) categories of density, i.e. Category C or D); 57% for women aged
540-44 decreasing to 28% for women aged >85.
How can breast density be managed?There are no treatments currently recommended
to reduce density. Incidental reduction in density has been observed in women with breast cancer after withdrawal of hormone replacement therapy and during treatment with tamoxifen. A reduction is also seen in pre-menopausal women with BRCA mutations undergoing risk reducing salpingo-oophorectomy.
There is uncertainty about whether density-guided supplemental screening improves health outcomes. Population screening programs in the UK and Australia have not recommended any change to screening on the basis of breast density and do not
7, 8routinely notify women of their density.The most important initial management strategy
for women with dense breasts is education and support. Women should be given explanation of what mammographic density is, what their individual risk may be and reassurance that dense breasts are common, and that density will usually naturally reduce with age. Density can be explained as a risk factor for breast cancer that can be managed but not changed, similar to having a family history in
close relatives. The decreased accuracy of mammography in dense breasts can be explained and there are several options to manage this:
(1) following age-related population mammo-graphic screening recommendations without any additional interventions; (2) screening with mammography more frequently (annually rather than biennially);(3) considering breast tomosynthesis (3-D mammography) in place of standard (2-D) mam-mography if 2-D is the usual as in many screening programs;(4) screening with mammography (tomosynthesis or standard 2-D) combined with supplemental screening modalities, such as screening ultrasound and/or MRI.
What supplemental screening is available? Supplemental imaging for women with dense
breasts and normal mammography can increase the cancer detection rate, but there is limited evidence on whether this improves health outcomes beyond that from mammography alone. There are also potential harms to this approach as with all breast cancer screening, including false-positive examinations, potential overdiagnosis and additional cost. Therefore, careful discussion is required in order to formulate a strategy that is acceptable to the woman (Table 2).
1. Breast tomosynthesisDigital 2-D mammography is the standard form
of mammography and that used for screening in the Australian and UK screening programs and
Table 2. Managing breast density – individualised breast cancer screening1. Assess traditional breast cancer risk factors
• Risk factors should be assessed at the age of 40. • Consider potentially significant risk factors such as family history or personal history of breast cancer, previous atypical breast biopsy (lesions such as atypical ductal hyperplasia or lobular neoplasia).• Include lesser risk factors such as nulliparity, elevated age at first birth and lifestyle factors (alcohol intake, physical activity and BMI)
2. Assess breast density• The first screening mammogram at age 40 should include an assessment of mammographic density at baseline and this information can be used for planning. • If density is BI-RADS category C or D, this carries an increased risk of cancer and masking.
3. Patient education and support• Discuss the risk factors, how breast density fits in with the other risk factors
4. Discuss screening interval• Consider mammographic screening more frequently than every two years, or • Consider 2-yearly mammography with supplemental screening
5. Discuss supplemental breast cancer screening • If increased breast density exists with other risk factors, consider supplemental screening, which may include breast tomosynthesis, ultrasound and/or MRI. • Consider issues of local availability and patient acceptability. • Include information about supplemental screening: cancer detection is increased; however, the trade-offs are higher recall rate, biopsy rate and risk of overdiagnosis.
6. Continually re-assess the plan• Breast density changes over time and tends to decrease with age. • After menopause, breast density will usually decrease as a gradual process and supplemental imaging may not be needed in the long-term, should the density category reduce. • It is expected that evidence-based guidelines for managing breast density will become available in the next few years and advice to patients can be updated accordingly.
Breast density challenge
Brennan, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 145-148146

tomosynthesis is used for work-up of abnormalities only. Breast tomosynthesis (3-D mammography) is a newer imaging technology. The patient experience is similar; however, tomosynthesis will acquire a series (a ‘stack’) of images rather than a single image. In the screening setting, 3-D mammography is able to detect more cancers than 2-D mammography, but with higher expense, longer reporting time, higher radiation dose and a possible increase in recall rate in settings with a low background recall rate. There is also concern that the additional cancers identified with tomosynthesis may represent overdiagnosis of indolent cancers rather than detection of additional
9clinically significant cancers. For women with dense breast tissue, the incremental cancer detection rate is higher than for women with non-dense tissue so 3-D mammography appears to have advantages in
10, 11 this sub-group.
2. UltrasoundSupplemental ultrasound following negative
mammography has been shown to increase the number of cancers detected (4.2 per 1000) in women with dense breasts. However, significant numbers of false positives are found. The biopsy rate was five
12times higher when ultrasound was added , and the positive predictive value from combined mammogram and ultrasound was only half of that for ultrasound
13alone (22% vs 11%) in a key study.
Supplemental whole-breast ultrasound is usually by hand-held ultrasound. Automated technology is also being evaluated, which appears to have a benefit of being less operator-dependent and requiring less
14physician time.
3. Magnetic resonance imagingThere is little available evidence on which to form
recommendations about the use of MRI in women with dense breast tissue as their only risk factor. However, a recent large-scale randomised controlled trial demonstrated that the use of supplemental MRI in women with extremely dense breast tissue (Category D) and normal results on mammography resulted in the diagnosis of significantly fewer interval cancers than mammography alone. In that study, there was an increased risk of false positives and it is unknown whether the additional cancers
15detected were clinically significant. The cost of MRI is also a challenge in many settings. Abbreviated MRI protocols are being evaluated and these have the potential to be more acceptable to
16women and to be available at a lower cost.
4. Screening intervalThere is no evidence to inform the ideal screening
interval for women with dense breasts. Currently, some screening programs that recommend biennial or triennial mammography may recommend annual mammography for women above population risk of
breast cancer based on their family history. As the risk of cancer related to dense breasts is similar to this, it may be reasonable to recommend annual screening; however, this has not been specifically studied and it not routinely available in the UK or Australia.
Should women be notified of their breast density?As it is a risk factor for breast cancer, the case for
density notification is strong. There is a powerful ethical argument for density to be disclosed to patients and this is being demanded by women around the world. However, in the US, notification legislation has not been accompanied by clinical guidelines or by support and educational materials for general practitioners and patients. This has led to anxiety among women and confusion about what to do with the information. There is also an increase in supplemental screening without compelling evidence to support it and with the potential for increasing anxiety further with false positive
17examinations and overdiagnosis. With density notification likely to become routine in many countries, it is important that support and education is in place for women and their doctors.
Proposed individualised screening recommendationsBreast cancer screening is likely to become more
tailored, with assessment of all risk factors, including density, and development of an appropriate personalised screening regimen for the patient. The current ‘one-size-fits-all’ approach to population screening requires review.
On the current evidence, it is difficult to justify definitive recommendations for additional screening based on breast density alone. However, when breast density exists in combination with other risk factors such as multiple affected relatives and/or previous atypical breast biopsy, supplemental screening can be discussed (Table 2).
In conclusion, an appropriate screening regimen can be developed in consultation with the well-informed patient after detailed assessment of risk factors. There may be no change to general population screening recommendations for women with dense breasts and no other risk factors. For others, supplemental imaging with tomosynthesis, ultrasound and/or MRI can be considered. All of these options can increase the cancer detection rate but have trade-offs such as higher false positive and biopsy rate, risk of overdiagnosis and higher cost.
FundingNH received funding via the National Breast
Cancer Foundation (NBCF) Australia, Breast Cancer Research Leadership Fellowship.
Conflicts of InterestNone.
Brennan, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 145-148 147
Breast density challenge

References1. Boyd NF, Guo H, Martin LJ, Sun L, Stone J, et al.
Mammographic density and the risk and detection of breast cancer. N Engl J Med. 2007;356(3):227-36.
2. Alipour S, Bayani L, Saberi A, Alikhassi A, Hosseini L, et al. Imperfect correlation of mammographic and clinical breast tissue density. Asia Pac J Cancer Prev. 2013;14:3685-8.
3. American College of Radiology (ACR). ACR BI-RADS Atlas 5th Edition. ACR; 2013.
4. Melnikow J, Fenton JJ, Whitlock EP, Miglioretti DL, Weyrich MS, et al. Supplemental Screening for Breast Cancer in Women With Dense Breasts: A Systematic Review for the U.S. Preventive Services Task Force. Ann Intern Med. 2016;164(4):268-78.
5. Wang AT, Vachon CM, Brandt KR, Ghosh K, editors. Breast density and breast cancer risk: a practical review. Mayo Clinic Proceedings; 2014: Elsevier.
6. Lee CI, Chen LE, Elmore JG. Risk-based Breast Cancer Screening: Implications of Breast Density. Med Clin North Am. 2017;101(4):725-41.
7. Cancer Australia. Position statement on breast density and screening within the BreastScreen Australia Program. 2016; Guidelines for preventive activities in general practice. The Red Book, 9th Edition. 2020.
8. UK National Screening Committee. Additional screening with ultrasound after negative mam-mography screening in women with dense breasts. United Kingdom: UK National Screening Committee; 2019.
9. Brennan ME. Breast tomosynthesis: a fine balance between benefits and harms in breast cancer screening. The Medical journal of Australia. 2019;211(8):349.
10. Conant EF, Barlow WE, Herschorn SD, Weaver DL, Beaber EF, et al. Association of Digital Breast Tomosynthesis vs Digital Mammography With Cancer Detection and Recall Rates by Age and Breast Density. JAMA Oncol. 2019;5(5): 635-42.
11. Marinovich ML, Hunter KE, Macaskill P, Houssami N. Breast cancer screening using tomosynthesis or mammography: a meta-analysis of cancer detection and recall. JNCI: Journal of the National Cancer Institute. 2018; 110(9):942-9.
12. Scheel JR, Lee JM, Sprague BL, Lee CI, Lehman CD. Screening ultrasound as an adjunct to mammography in women with mammographically dense breasts. American journal of obstetrics and gynecology. 2015;212(1):9-17.
13. Berg WA. Tailored supplemental screening for breast cancer: what now and what next? American Journal of Roentgenology. 2009;192(2):390-9.
14. Zanotel M, Bednarova I, Londero V, Linda A,
Lorenzon M, et al. Automated breast ultrasound: basic principles and emerging clinical applications. La radiologia medica. 2018;123(1): 1-12.
15. Bakker MF, de Lange SV, Pijnappel RM, Mann RM, Peeters PH, et al. Supplemental MRI screening for women with extremely dense breast tissue. New England Journal of Medicine. 2019;381(22):2091-102.
16. Kuhl CK. Abbreviated magnetic resonance imaging (MRI) for breast cancer screening: rationale, concept, and transfer to clinical practice. Annual Review of Medicine. 2019;70: 501-19.
17. Houssami N, Lee CI. The impact of legislation mandating breast density notification–Review of the evidence. The Breast. 2018;42:102-12.
Brennan, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 145-148148
Breast density challenge

Importance of fertility preserving methodsA. Socio-demographic changes in societyIn the industrialized countries, two developments
have been observed over the last few decades that have shifted the focus of research and reproductive medicine to maintaining fertility. With regard to social life, there is a trend of postponing the realization of the desire to have children to an ever later phase of life or a childbirth does not take place at all due to existing biological limits. In Germany, for example, between 1993 and 2013, the age of women at the birth of their first child rose from
1around 25 to 29.3 years. It is well-known for a long period of time that women’s fertility decreases
2 steadily at the age of approximately 30 years.However, the optimum fertility is around 25 years. At the same time, there is an almost constant increase in life expectancy in cancer patients, especially in women with breast cancer. One reason for this observation is the progress made in oncologic therapy, which is reflected in improved long-term survival in cancer. However, these successes are accompanied by a loss of fertility due to premature ovarian insufficiency, triggered by gonadotoxic side
3, 4effects of chemotherapy and radiation. At the same time, many women report that they still want to have children despite being diagnosed with cancer. Up to every 7 patient would even be willing to accept a loss in oncologic safety if she could still give birth to a
5child.
B. Epidemiologic aspects of breast cancerBreast cancer is the most common malignancy in
women around the world with 1.6 million new breast cancer patients being identified each year
6worldwide. Overall, 4-6 % of the women diagnosed are under the age of 40, and about one out of five
7women possesses a premenopausal hormonal status . Advancement in the adjuvant systemic and locoregional therapy has resulted in a significantly improved forecast.
The function of the ovaries can be damaged by the therapy resulting in a loss of germ cells and later on in infertility. The question of maintaining fertility is of great importance regarding the self-determination of the patients. The potential use of treatments for fertility preservation has to be a compromise between risks and costs of the therapy. The overall forecast, family planning, gonadotoxic effects of the planned therapy and psychological compounds should be considered before doctors make an indication for fertility preservation.
An interdisciplinary collaboration of an oncologist, gynecologist, psychologist, radiologist, radiation therapist and reproductive specialist is indispensable.
Fertility preserving methods for breast cancer patients
A. General considerationsOvaries contain a limited number of gametes
compared to testes with a maximum of 6.000.000 follicles at 20 weeks of gestation. At birth, there are only 1,000,000 follicles left, and at entry of puberty there are only 300.000 follicles. Finally, the stock of follicles is exhausted by entry in the menopause. During the stage of fertility only 300–500 oocytes ovulate.
149
Fertility Preservation in Breast Cancer Patients Under SpecialConsideration of Ovarian Stimulation for Fertility Purposes
a Kinderwunschzentrum Niederrhein, Madrider Straße 6; D-41069 Mönchengladbach, Germany
b Department of Gynecology, Obstetrics and Reproductive Medicine, Saarland University Hospital, Kirrberger
Straße 100, Building 9, D-66421 Homburg, Germanyb Fertility Center Dr. Sebastian Grewe and Dr. Olaf Drost - Bremer Zentrum für Fortpflanzungsmedizin (BZF),
Bremen, Germanyd Schleswig-Holstein University Medical Center, Lübeck, Germany
a,b c dSebastian Findeklee* , Sebastian Grewe , Klaus Diedrich
Open AccessInvited Commentary
Address for correspondence: Sebastian Findeklee, MDAddress: Kinderwunschzentrum Niederrhein, Madrider Straße 6, D-41069 Mönchengladbach, GermanyTel: +49 6841-1628000Fax: +49 6841-1628110Email: [email protected]
Findeklee, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 149-154
DOI: 10.19187/abc.202073149-154

The determining factors in the admission of a cytotoxic caused amenorrhea include the age of the woman at the time of the therapy, the ovarian reserve and the applied chemotherapy regimen. The gonadotoxic effect of the commonly used chemotherapies is shown in Table 1. As can be seen, there is a correlation between the cumulative dose of the radiation of the pelvis in the case of metastatic disease and damage of the ovarian function.
Damage to ovaries caused by oncologic therapy clinically appears as an ovarian dysfunction followed by abnormal estrous cycle. If the stock of follicles is irreversibly damaged due to adjuvant therapy, a secondary amenorrhea results including the proof of a lack of estrogen, a thin endometrial lining in sonography and loss of antral follicles (ovarian atrophy). Gonadotrophins can be measured in a hypergonadotropic range and Anti-Mullerian-Hormone (AMH) is beneath detection limit.
The current study situation concerning the duration of amenorrhea with partial damage to the stock of follicles appears inhomogeneous and varies
8highly between different authors.Sukuvanich et al. published the first prospective
study examining the effects of different chemotherapy regimens evaluating the probability of amenorrhea post therapy depending on the women’s age at the start
9of the therapy. In the period from 1998 to 2002, 466 women aged between 20 and 45 years were examined. The rate of amenorrhea was determined at 6, 12 and 24 months after termination of therapy.
Overall, 111 women out of the examined collective received the AC–regimen (Dexorubicin, Cycloph-osphamid, Paclitaxel),76 women were treated according the CMF–regimen (Cyclophosphamid, Methotrexat, 5-Fluorouracil) and 143 received the ACT–regimen (Doxorubicin, Cyclophosphamid, Paclitaxel). Also, 136 women gained other cytostatics (ACR-, FAC-, FACT-, as well as not further defined regimens).
The patients were divided into categories with respect to their age: 20-34 years (n=112), 35-39 years (n=142) and >40 years (n=212). The probability of amenorrhea was examined as well as the presumption of recurrent menses following amenorrhea. In only 11% of women aged 20-34 amenorrhea was reported six months after completed chemotherapy. Results slightly varied between different chemotherapy regimens. In relation to recurrence of menstruation following secondary amenorrhea the CMF-regimen showed worse outcomes than in the other chemotherapy schemes. All in all, the risk of premature ovarian insufficiency caused by chemotherapy in patients suffering from breast cancer appears to be low. However, regarding fertility preservation-especially in patients suffering from estrogen-sensitive breast cancer-it should be considered that a longer adjuvant endocrine therapy might be necessary. Meanwhile, the stock of ovarian follicles could be reduced, particularly if the therapy is initiated in the second half of the fourth life decade.
As the transposition of the ovaries out of the pelvis prior to radiotherapy as an additional fertility preserving technique is not a relevant issue for breast cancer patients we do not report on it in this review article.
B. Medical protection of ovarian functionIn breast cancer patients, GnRH analogues
(GnRHa), such as Leuprorelin, Buserelin or Goserelin, are used as medicamentous fertility-protective therapy. A depot injection is carried out every 28 or 84 days with a GnRHa during the entire period of chemotherapy (starting shortly before the initiation of chemotherapy, ending approximately 2 weeks after completion of chemotherapy). In this case, there might be a downregulation of the ovary with consecutively reduced intake of cytostatics. The main side effects are climacteric complaints. If the therapy lasts more than 6 months, the so-called add-back therapy with an estrogen and a progestin is recommended to counteract the serious consequences of a sexual hormone deficiency such as
10osteoporosis. During the last years there has been a lively debate about the pros and cons of applying GnRH analogues in women with hormone receptor-positive breast cancer. GnRHa treatment was considered to desensitize the tumor for the following endocrine therapy that is obligatory in hormone receptor-positive diseases, worsening the patient`s prognosis. However, in recent years there has been increasing evidence that GnRHa can in fact reduce the risk of premature ovarian insufficiency (POI) without being associated with a deterioration of prognosis - regardless of the hormone receptor status. In 2012, a meta-analysis of seven randomized studies with predominantly breast cancer patients showed that the administration of a GnRHa during chemotherapy can
Findeklee, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 149-154
Table 1. Gonadotoxicity of several agents applied in breast cancer patients
high risk (POI risk >= 80%)
intermediate risk (POI risk 20-80%)
low risk (POI risk < 20%)
unclear risk
CyclophosphamidBusulfanMelphalan
platin derivatesAdriamycin
Vincristin5-FluorouracilMethotrexatActinomycin D
TrastuzumabPertuzumabtyrosine kinase inhibitorsPembrolizumabCDK4/6 inhibitorsPARP inhibitorsPDL1 antagonists
Fertility preservation breast cancer
150

significantly reduce the risk of premature ovarian 11
insufficiency. Therefore, GnRHa as fertility preserving agents are recommended in the guideline of the German AGO (Arbeitsgemeinschaft
12Gynäkologische Onkologie) group. Nevertheless, the application of GnRHa solely for preserving fertility cannot be regarded as an effective strategy for preserving female fertility. For this reason, this approach is not recommended by the guidelines of the American Society for Reproductive Medicine (ASRM).
C. Ovarian stimulation and cryopreservation of oocytes
Carrying out ovarian stimulation is aimed at gathering mature oocytes (MII-stage) to preserve them in fertilized or unfertilized conditions to create a fertility reserve. The required treatment should be implemented promptly to avoid any delay of oncologic treatment. The aim is to retrieve as many oocytes as possible. At the same time, the risk of ovarian hyperstimulation should be avoided.
Often there are several years between fertility protection and the wish to attempt pregnancy; therefore, even women in a steady relationship should think about cryopreservation of unfertilized oocytes to ensure independence of the women in the case of separation from the partner. In this situation, the opportunity of 'splitting' should be discussed with the patient in which fertilized and unfertilized oocytes are cryopreserved. The later use of fertilized oocytes is only permitted after approval of both partners.
Procedures for ovarian stimulation can be initiated regardless of the time of menstrual cycle
13-16(“random-start-stimulation”). A total of two weeks should be scheduled for the treatment. Starting ovarian stimulation in the luteal phase takes on average 1-2 days more than starting it in the follicular phase. To increase the number of obtained oocytes in individual cases double stimulation could be proceeded. Double ovarian stimulation protocols are developed to allow ovarian stimulation and retrieving
17-19oocytes twice in the same menstrual cycle.
The success of this method and the number of retrieved oocytes during a menstrual cycle depends on ovarian reserve (antral follicle count, AMH concentration) and the patient's age. Vitrification represents an effective method for cryopreservation of oocytes achieving satisfying survival and
20fertilization rates. The birth rate of cryopreserved oocytes depends on the age of the women. The application rate of cryopreserved oocytes is low based on current studies and according to Diaz-
21Garcia, stands at 4.8%.In Germany, embryo cryopreservation for fertility
preservation is forbidden by law following the embryo protecting law “Embryonenschutzgesetz” enacted in 1990. In other countries, embryo cryopreservation is permitted by law and it is an
established method for fertility preservation. The pregnancy rates after fertility preservation using cryopreserved 2PN-cells (pronucleus stage) or cryopreserved embryos are comparable.
The German-IVF-Register has reported the viability rate of 90,2% using thawed oocytes and a
22pregnancy rate of 20,1% per embryo transfer. The antagonist protocol represents the preferred method for ovarian stimulation during fertility preservation including ovulation trigger by GnRH agonists. Depending on the stage of menstrual cycle, different protocols are used at the beginning of the treatment.
Starting in the early or middle follicular phase, the stimulation of oocytes can be performed with the aid of FSH, FSH/LH or HMG by default. From a follicle size of >13mm a prematurely ovulation is prevented through the application of an GnRH antagonist like Ganirelix or Cetrorelix. Finally, ovulation is triggered via a GnRH agonist (e.g. Triptorelin) after sonographic detection of 3 follicles >17mm or a leading follicle > 20mm (Figure 1).
In contrast, commencing the treatment in the late follicle phase, an ovulation induction with HCG is performed if the sonographic examination reveals a follicle size >13mm. Subsequently, the stimulation is carried out following the “luteal phase scheme”. Initiating the stimulation after ovulation has occurred, the stimulation is performed with FSH, FSH/LH or HMG introducing the antagonist after a new follicle reaches a size >13mm, following triggering ovulation by a GnRH agonist.
It is assumed that ovarian stimulation methods in patients suffering from hormone receptor-positive breast cancer could lead to hyperproliferation of tumor cells going along with supraphysiological serum concentrations of estrogen. In this situation stimulation protocols are complemented by aromatase inhibitors
23(off-label-use) like Letrozol. Thereby, serum concentrations of estrogen during the treatment for fertility preservation could be reduced by half (also at agonist flair-up). As far as known, fetal outcome and pregnancy rates are unaffected by addition of
23-26 aromatase inhibitors, it seems to be unlikely that stimulation with gonadotrophins could have a negative effect on patients' prognosis, especially considering
Figure 1. Scheme for ovarian cancer stimulation with the aim of oocyte cryopreservation in hormone receptor positive
in breast cancer patients.
Fertility preservation breast cancer
151Findeklee, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 149-154

the fact that the increase in the estrogen serum concentration during fertility preservation occurs over a period of approximately one week.
Further protocols are used for stimulation to retrieve oocytes such as double stimulation or progesterone primed ovarian stimulation.
D. Cryopreservation of ovarian tissueA further method for fertility preservation is the
ovarian tissue cryopreservation. The ovarian cortex is removed surgically and is cryopreserved afterwards. Upon completion of oncologic treatment and a recurrence and metastasis free interval of at least three years, the ovarian tissue can be thawed and transplanted back to the patient on the ovary or close to the ovary in the pelvic wall (see Figure 2). Using this technique the patients still have the opportunity to achieve spontaneous pregnancy. Up to now about 180 live births have been reported
27following ovarian tissue transplantation .
During the operation, as much ovarian tissue as needed should be removed. A wedge excision including the ovarian stroma with a high number of dormant follicles and its subsequent cryopreservation
28is the most established method. The advantage of this method is that it can be performed at any time during the menstrual cycle, so it does not require any delay in the initiation of oncologic treatmen
Greatest concern about this method is the fear of potential reimplantation of malignant cells. To reduce the risk, the removed ovarian tissue should be appropriately examined histologically to exclude
malignant involvement. Due to the subtype of breast cancer, the risk for malignant cells in ovarian tissue has been reported to be low (ductal carcinoma) to
29, 30medium (lobular carcinoma).
Previous data has showed that the use of cryopreserved ovarian tissue in everyday clinical practice is low, although this may increase in the next
21few years. There are often several years between removal of ovarian tissue and transplantation.
The removal and subsequent transplantation of ovarian tissue can be regarded as the fertility preserving method of choice if the oncologic treatment has to be commenced immediately within few days.
In conclusion, fertility preservation is an emerging field in the treatment of breast cancer in young women to maintain reproductive health which carries a vital psychological significance for the self determination of the patient. For this reason, the possibilities of fertility preservation should be discussed with each woman of reproductive age diagnosed with breast cancer. The network FertiProtekt, for example, carried out 1.323 consultations in 2018 and 908 interventions for fertility preservation were done. Most women (About 40 percent of women) with the diagnosis of cancer who were sent to one of the cooperating oncofertility centers for fertility counseling suffered from breast cancer. Table 2 gives an overview of the value of existing fertility preserving methods available for breast cancer patients.
FundingThe study received no funding.
Conflict of InterestsThe authors declare no conflict of interest.
References1. Weiss T. Ökonomische Bestimmungsgrößen der
Fertilität in westlichen Industrieländern. Bundesinstitut für Bevölkerungsforschung; 1996.
2. Menken J, Trussell J, Larsen U. Age and infertility. Science. 1986;233(4771):1389-94.
3. Anderson R, Wallace W, Baird D. Focus on Fertility Preservation Ovarian cryopreservation for fertility preservation: indications and outcomes. Reproduction. 2008;136:681-9.
4. Mattle V, Behringer K, Engert A, Wildt L. Female fertility after cytotoxic therapy–protection of
Figure 2. Laparoscopic transplantation of thawed ovarian tissue into a peritoneal pocket after completion of
oncological therapy.
Table 2. Value of the different fertility preserving methods being available for breast cancer patients
Ovarian tissue transplantationCryopreservation of immature oocytesCryopreservation of mature oocytes (MII)Cryopreservation of pronucleus stageCryopreservation of embryos
Method Time frame Pregnancy rate Status
immediatelyimmediately10-14 days10-14 days10-14 days
20-25% (tissue activity rate 70-80%)10-15%10-15%25-35%25-35%
establishedexperimental
has to be optimizedestablished, standardestablished, standard
Fertility preservation breast cancer
Findeklee, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 149-154152
ovarian function during chemotherapy of malignant and non‐malignant diseases. European Journal of Haematology. 2005;75:77-82.
5. Lee MC, Gray J, Han HS, Plosker S. Fertility and reproductive considerations in premenopausal patients with breast cancer. Cancer Control. 2010;17(3):162-72.
6. Ghoncheh M, Pournamdar Z, Salehiniya H. Incidence and mortality and epidemiology of breast cancer in the world. Asian Pacific Journal of Cancer Prevention. 2016;17(S3):43-6.
7. Radecka B, Litwiniuk M. Breast cancer in young women. Ginekologia polska. 2016;87(9):659-63.
8. Goldhirsch A, Gelber R, Castiglione M. The magnitude of endocrine effects of adjuvant chemotherapy for premenopausal breast cancer patients. Annals of Oncology. 1990;1(3):183-8.
9. Sukumvanich P, Case LD, Van Zee K, Singletary SE, Paskett ED, et al. Incidence and time course of bleeding after long‐term amenorrhea after breast cancer treatment: A prospective study. Cancer. 2010;116(13):3102-11.
10. Kleinstein J. GnRH-Analoga und Add-back-Verfahren. J Gyn Endokrinol 2008;2(2):40-3.
11. von Wolff M, Dian D. Fertility preservation in women with malignant tumors and gonadotoxic treatments. Deutsches Ärzteblatt International. 2012;109(12):220.
12. Arbeitsgemeinschaft Gynäkologische Onkologie. Kommission Mamma. Diagnostik und Therapie früher und fortgeschrittener Mammakarzinome; 2020.
13. Cakmak H, Katz A, Cedars MI, Rosen MP. Effective method for emergency fertility preservation: random-start controlled ovarian stimulation. Fertility and sterility. 2013;100(6): 1673-80.
14. von Wolff M, Capp E, Jauckus J, Strowitzki T, Germeyer A, et al. Timing of ovarian stimulation in patients prior to gonadotoxic therapy: an analysis of 684 stimulations. European journal of obstetrics & gynecology and reproductive biology. 2016;199:146-9.
15. von Wolff M, Dittrich R, Liebenthron J, Nawroth F, Schüring AN, et al. Fertility-preservation counselling and treatment for medical reasons: data from a multinational network of over 5000 women. Reproductive biomedicine online. 2015;31(5):605-12.
16. von Wolff M, Thaler CJ, Frambach T, Zeeb C, Lawrenz B, et al. Ovarian stimulation to cryopreserve fertilized oocytes in cancer patients can be started in the luteal phase. Fertility and sterility. 2009;92(4):1360-5.
17. Moffat R, Pirtea P, Gayet V, Wolf JP, Chapron C, et al. Dual ovarian stimulation is a new viable option for enhancing the oocyte yield when the time for assisted reproductive technnology is
limited. Reproductive biomedicine online. 2014;29(6):659-61.
18. Turan V, Bedoschi G, Moy F, Oktay K. Safety and feasibility of performing two consecutive ovarian stimulation cycles with the use of letrozole-gonadotropin protocol for fertility preservation in breast cancer patients. Fertility and sterility. 2013;100(6):1681-5.
19. Zhang J. Luteal phase ovarian stimulation following oocyte retrieval: is it helpful for poor responders? Reproductive Biology and Endocrinology. 2015;13(1):76.
20. Lawrenz B, Jauckus J, Kupka M, Strowitzki T, von Wolff M. Efficacy and safety of ovarian stimulation before chemotherapy in 205 cases. Fertility and sterility. 2010;94(7):2871-3.
21. Diaz-Garcia C, Domingo J, Garcia-Velasco JA, Herraiz S, Mirabet V, et al. Oocyte vitrification versus ovarian cortex transplantation in fertility preservation for adult women undergoing gonadotoxic treatments: a prospective cohort study. Fertility and sterility. 2018;109(3):478-85.
22. Blumenauer U, Czeromin D, Fehr K, Fiedler C, Gnoth J-S, et al. German IVF-Registry (D·I·R). Journal of Reproductive Medicine and Endocrinology 2018;6:279-315.
23. Oktay K, Turan V, Bedoschi G, Pacheco FS, Moy F. Fertility Preservation Success Subsequent to Concurrent Aromatase Inhibitor Treatment and Ovarian Stimulation in Women With Breast Cancer. J Clin Oncol. 2015;33(22):2424-9.
24. Haas J, Bassil R, Meriano J, Samara N, Barzilay E, et al. Does daily co-administration of letrozole and gonadotropins during ovarian stimulation improve IVF outcome? Reproductive Biology and Endocrinology. 2017;15(1):70.
25. Kim J, Turan V, Oktay K. Long-Term Safety of Letrozole and Gonadotropin Stimulation for Fertility Preservation in Women With Breast Cancer. J Clin Endocrinol Metab. 2016;101(4): 1364-71.
26. Sharma S, Ghosh S, Singh S, Chakravarty A, Ganesh A, et al. Congenital malformations among babies born following letrozole or clomiphene for infertility treatment. PloS one. 2014;9(10):e108219.
27. Findeklee S, Radosa JC, Takacs Z, Hamza A, Sima R, et al. Fertility preservation in female cancer patients: current knowledge and future perspectives. Minerva Ginecol. 2019;71(4):298-305.
28. Regan MM, Walley BA, Francis PA, Fleming GF, Lang I, et al. Concurrent and sequential initiation of ovarian function suppression with chemotherapy in premenopausal women with endocrine-responsive early breast cancer: an exploratory analysis of TEXT and SOFT. Ann Oncol. 2017;28(9):2225-32.
153Findeklee, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 149-154
Fertility preservation breast cancer

Fertility preservation breast cancer
29.Dolmans MM, Masciangelo R. Risk of transplanting malignant cells in cryopreserved ovarian tissue. Minerva Ginecol. 2018;70(4): 436-43.
30.Deutsche Gesellschaft für Gynäkologie und Geburtshilfe (DGGG) DGfRD, Deutsche Gesellschaft für Urologie (DGU). Leitlinie: Fertilitätserhaltung bei onkologischen Therapien. Level S2k, AWMF Register Nr. 015/082;2017.
Findeklee, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 149-154154

IntroductionMale breast cancer (MBC) accounts for less than
1% of all breast cancer (BC) diagnosed annually in 1, 2western countries. The incidence in the United
States (US) has been increasing in recent decades from 0.85 cases per 100,000 men in the mid-70s to
ARTICLE INFO
Background: Male breast cancer (MBC) accounts for less than 1% of breast cancer, requiring extrapolation of results from studies in women. The aim of the study is to evaluate prognostic and therapeutic factors with special focus in endocrine treatment (ET) on the disease outcome.
Methods: Observational, retrospective, single-center study of 53 MBC treated between January 1997 and December 2018 participated in the study. Among the participants, 48 patients had a performance status (PS) 0-1 (91%), 48 were hormone-receptor-positive (91%) and 4 were human epidermal growth factor 2 receptor (HER2) positive (8%). A total of 45 patients (85%) were treated with ET, with 36 patients (68%) receiving treatment in an adjuvant setting. The association analysis was performed using Chi-square test and survival was estimated using Kaplan-Meier with SPSS v25.
Results: The cohort had a median age of 68 years old (range: 40-88). We found that 84% had a non-metastatic breast cancer. A breast cancer gene (BRCA) analysis was carried out in 43% of the patients, showing BRCA2 mutated in 26.1% of those analyzed, without obtaining a benefit in overall survival (P=0.698). The analysis showed higher 5-year overall survival (OS) for PS 0 (P=0.010), absence of vascular invasion (P=0.033), Ki67 ≤14% (P=0.041) and absence of metastasis at diagnosis (p<0.0001). Patients receiving adjuvant ET above 5 years had a longer median OS (89 vs 69.6 months, P=0.024), disease-free survival (DFS), and distant relapse (84 vs 48 months; P=0.005, and P=0.002, respectively).
Conclusions: Several prognostic factors for male breast cancer have been described. Noteworthy, patients receiving adjuvant ET above 5 years had a higher OS and DFS. BRCA did not show prognostic value in OS in this cohort. Further studies with larger sample size are necessary.
Received:
26 August 2020Revised:
15 September 2020Accepted:
24 September 2020
Key words:Breast cancer,BRCA,endocrine therapy,men,prognosis.
Address for correspondence: Daniel Herrero Rivera, M.D. Address: Department of Medical Oncology, Virgen del Rocío University Hospital. Manuel Siurot Avenue, s/n. 41013, Seville,Spain. Tel & Fax: +34 95 501 2272 Email: [email protected]
155
ABSTRACT
Assessment of Prognostic and Therapeutic Factors in Male Breast Cancer: An Observational Study of a Southwest Spanish Single Center
a Department of Medical Oncology, University Hospital Virgen del Rocío, Seville, Spain
b Department of Radiation Oncology, University Hospital Virgen del Rocío, Seville, Spain
c Instituto de Biomedicina de Sevilla (IBIS/HUVR/CSIC/Universidad de Sevilla), Seville, Spaind Statistics and Research Methodology Unit University Hospital Virgen del Rocío, Seville, Spain
a a b,cDaniel Herrero Rivera* , María Rocío Morales Herrero , José Luis López Guerra ,a a aAlberto Sánchez-Camacho Mejías , Irene Carrasco García , Paloma Santos Fernández ,
d a,c aCarmen Victoria Almeida González , Marta Benavent Viñuales , Alejandro Falcón González , a a a,cÁlvaro Montaño Periáñez , Rosario González Mancha , Francisco Javier Salvador Bofill ,
a,cManuel Ruiz Borrego
Open AccessOriginal Article
Herrero Rivera, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 155-163
DOI: 10.19187/abc.202073155-163

1.44 cases per 100,000 men in 2011 according to 3
Surveillance, Epidemiology and End Result (SEER) while in Northern European countries it has remained stable in a similar period around 0.4 cases per
4100,000 men. In Southern Europe, Portugal showed 5an incidence of 1.77 cases per 100,000 men in 2011.
Mortality in the western world has decreased in the last decades. For instance, Spain reports a decrease from 0.74 deaths per 100,000 men in 2012 to 0.64
6deaths per 100,000 men in 2017.One of the main risk factors is the age, with the
average age at diagnosis being slightly older in men 4than in women. Other risk factors reported are
7family history, breast cancer gene (BRCA) germline mutations, especially BRCA2, having a cumulative
8risk for developing BC above 6% , and the existence of hyperestrogenism favored by alterations such as Klinefelter syndrome, testicular disorders, obesity, liver dysfunction, etc.
Compared with female BC, the MBC immunoh-istochemical expression is similar although it seems that there is a higher proportion of hormone-sensitive tumors and a higher expression of the androgen receptor suggesting higher endocrine treatment (ET)
9options.The treatment applied to MBC has been limited
by the small sample size represented in clinical trials, with no men appearing in the vast majority. Therefore, treatment decisions are based on studies
10conducted in women. The aim of this study is to analyze the prognostic
value of clinical and therapeutic characteristics, focusing on ET due to lack of evidence in some indications, and their differences from female BC. This study is one of the largest in Spain with the largest sample size recorded in the Andalusian region. Additionally, the impact of BRCA mutations on survival has been assessed. This research is presented in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting checklist.
MethodsPatients and designAn observational retrospective cohort study of 53
MBC patients between January 1997 and December 2018 in an Andalusian single center participated in the study. The sample size is the largest possible since it is a low incidence disease.
Inclusion criteria consisted of male patients of any age histologically diagnosed with BC with an intent to receive treatment. Exclusion criteria included cases with only partial clinical data available. Finally, 13 out of 66 patients were excluded for this reason. In addition, 6 patients receiving adjuvant ET were excluded because ET was not completed. Stage was assessed according to the 8th American Joint
11Committee on Cancer (AJCC) Staging Classification.The functional status of the patients was
evaluated using the Eastern Cooperative Oncology 12
Group (ECOG) performance status (PS) scale. Patients with localized disease who underwent
surgery initially, were followed every 3-6 months during the first 2-3 years and then every 6 months until the first 5 years. A physical and analytical examination was performed with the study of tumor biomarkers, as well as annual mammography, and bone densitometry every 2 years for those patients undergoing ET. Additionally, patients with advanced disease also underwent chest and abdomen computerized tomography every 2-4 months.
The patients were considered to be estrogen receptor (ER) positive and the progesterone receptor (PR) positive when there was ≥1% of immunohistochemical expression. The status of the human epidermal growth factor 2 receptor (HER-2) was initially determined by immunohistochemistry (IHC), considering the values of 3+ as positive, 2+ equivocal, and 1+ as negative. In equivocal cases, fluorescent in situ hybridization (FISH) was performed. Values of ≥2.3 for FISH were classified as positive, <1.8 as negative and values between 1.8-2.3 were classified as equivocal. If the values were not reported, especially before 2010, it was defined as an unknown value. The BRCA 1/2 mutational study was performed using direct sequencing and detection methods with amplification of the DNA by Polymerase chain reaction (PCR).
The information collected in this research has been obtained exclusively from human participants with the approval of a Spanish ethics board (ID EMS/dgc) in accordance with the 1964 Declaration of Helsinki and its later amendments.
Ethical StatementAll persons listed as authors have given their
approval for the submission of the paper.The information collected in this research has been
obtained exclusively from human participants with the approval of a Spanish ethics board (ID EMS/dgc) in accordance with the 1964 Declaration of Helsinki and its later amendments. The results of this study will not affect the standard management of men with breast cancer. Due to the retrospective nature of the study, formal consent was not required but all authors declared that patients’ personal data have been secured. No animals were involved in this study.
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Statistical analysisOverall survival (OS) was defined as time from
diagnosis to death due to any cause. Cancer specific survival (CSS) was defined as time from diagnosis to death due to BC. Disease-free survival (DFS) was defined as those patients rendered disease free and alive until a new event. Events in the analysis of DFS
Prognosis in male breast cancer
Herrero Rivera, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 155-163156

only 1 patient being non luminal HER2 positive. Stage II was the most common stage (41%) followed by stage 0-I (19%) and stage III (19%). Additionally, 57% had nodal infiltration and up to 23% of all patients had ≥4 affected nodes. Only 14% (n = 8) presented with distant metastases at diagnosis, with 50% of the patients showing this at bone level and the rest at visceral level.
Oncological treatmentA total of 47 patients (89%) underwent surgery,
which was mastectomy in 87% of the patients. Also, 25 patients (47%) received adjuvant RT with a dose ≥50 Gy in 76% of the irradiated cases while 85% received ET at some point during the follow up. Of the participants, 36 patients received adjuvant ET containing tamoxifen in 89% of cases, while only 11% received aromatase inhibitors (AIs) exclusively. After distant relapse, 13 patients received ET with tamoxifen as one of the treatments in 54% of the patients. LHRH agonists were administered in 10 patients (19%), which was guided in many patients (n=9) by presenting prostate cancer simultaneously. In addition, 3 men received cyclin inhibitors (2 with Ribociclib and 1 with Palbociclib) and 13 bisphosphonates (68% of stage IV patients).
On the other hand, 26 patients (49% of all cases) received CT, administered with neoadjuvant intention in 3 patients based on anthracyclines (epirubicin / doxorubicin every 3 weeks) and taxanes (docetaxel every three weeks/ paclitaxel weekly), with one of the patients receiving trastuzumab due to his amplified HER2 status. In relation to adjuvant CT, 16 patients received treatment, 12 of them based on anthracyclines and taxanes, with one patient receiving CMF (cyclophosphamide, methotrexate and fluorouracil) probably related to a history of arrhythmia, one patient receiving FEC (fluorouracil, epirubicin and cyclophosphamide) x6 cycles, one patient receiving 4 cycles of capecitabine, and lastly one patient receiving Carboplatin AUC2 + paclitaxel 80 mg / m2 x 6 cycles. After distant relapse, 14 patients received some CT-based treatment.
Statistical analysisIrrespective of the treatment modality, the OS and
CSS rates for all patients at 5 years were 58.5% and 63.3% respectively. Table 2 and 3 shows all parameters that were evaluated in the univariate analysis. PS 0 (OR: 0.20; P= 0.010; CI95%, 0.06–0.67), absence of vascular invasion (OR: 0.26; P= 0.033; CI95%, 0.07–0.92), Ki67≤14% (OR: 0.16; P= 0.041; CI95%, 0.03-0.83), and absence of distant metastasis at diagnosis (OR: 0.31; P <0.001; CI95%, 0.20–0.48) were associated with better OS at 5 years. In contrast, patients who did not undergo surgery (OR: 2.94; P= 0.003; CI95%, 1.97-4.37) were associated with worse prognosis. Absence of vascular invasion, Ki67≤14%, absence of distant metastasis, and no treatment with CT also showed
included any locoregional or distant failure, or death from any cause. Locoregional relapse was defined as local failure at the primary site or any nodal failure after treatment. Finally, distant relapse was defined as the recurrence of neoplastic disease at a location other than the primary tumor, and distant disease-free survival (DDFS) as the time from diagnosis until distant event or death. Categorical variables were expressed as frequencies and percentages and continuous variables as the median and range. The associations between the patient factors (age, familiar history of breast or ovarian cancer, ECOG, smoking status, cardiovascular disease, history of alcoholism, BRCA status), disease factors (histological and immunohistochemical characteristics, stage), and treatment factors (surgery, radiotherapy [RT], chemotherapy [CT], ET) and the survival outcome at 5 years were assessed using the Chi-squared statistical test. Multivariate analysis was not used due to the limited sample size. Survival was estimated by the Kaplan-Meier (KM) method using log-rank test to compare different variables. A p value of 0.05 or less was considered statistically significant. Data was analyzed using SPSS v.25 software (SPSS Inc, Chicago, IL, USA).
ResultsCharacteristics of the 53 patients are shown in
Table 1. The cohort consisted of 53 men with a median age of 68 years (range, 40-88 years). They had some comorbidities such as history of cardiac disease (47%) or thromboembolic events (9%). Among the participants, 77% were current or former smokers and 17% had history of alcoholism. Most patients (90%) had a PS 0-1 and 12 patients (23%) had a family history of breast or ovarian cancer and BRCA 1/2 mutations were examined in 43% (n=23) patients of the sample. BRCA positive mutations were observed in 26% (n=6) of BRCA patients assessed, increasing this percentage to 42% (n=5) in those patients who had a family history of breast or ovarian cancer. The mutations observed were of BRCA2 type in these patients. The median follow-up time for all patients was 73 months, being less than 1 year in only 3 patients due to premature death caused by the BC disease.
Tumor characteristics Histological characteristics were as follows: 89%
had infiltrating carcinoma (n = 47) while the rest had non-infiltrating histology (ductal carcinoma in situ, micropapillary and apocrine carcinoma), 60% grade 1-2 of modified Bloom Richardson classification (n = 32), 42% vascular invasion (n = 22), 26% in situ component associated (n = 14), 47% primary tumor size less than 2 cm (n = 25), and 64% had Ki67 proliferation index > 14 (n = 34). Also, 91% had a luminal tumor phenotype with 91% positive ER expression and 87% positive PR expression. In addition, 3 patients (6%) had HER2 positive status with
Prognosis in male breast cancer
Herrero Rivera, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 155-163 157

Table 1. Patient characteristicsVariables N (%)
Age, years
aHistory of cardiac disease
Smoking status
Performance status
Infiltrating carcinoma
ER status
PR status
HER2 status
Ki 67 proliferation index (%)
Primary tumor size (cm)
Number positives nodes
Metastasis at diagnosis
Stage at diagnosis
BRCA mutation
Surgery
ePathological margins
Type of endocrine therapy Adjuvant (N=36)
Metastatic (N=13)
LHRH agonist
<70≥70
NoYes
CurrentFormerNever
012
NoYes
NegativebPositive
Unknown
NegativecPositive
Unknown
NegativedPositive
Unknown
≤14>14
Unknown
≤2>2
Unknown
01-3 ≥4
Unknown
NoneBone
Visceral
0 and I II III IV
Unknown
NegativePositive
Unknown
No Yes
Margins free of tumorTumor at margins
Unknown
TamoxifenAIs
TamoxifenAis
NoYes
Unknown
32 (60)21 (40)
28 (53)25 (47)
6 (12)32 (65)11 (22)
33 (62)15 (28)5 (9)
6 (11)47 (89)
4 (7)48 (91)1 (2)
6 (11)46 (87)1 (2)
46 (87)3 (6)4 (7)
12 (23)34 (64)7 (13)
25 (47)24 (45)4 (8)
20 (38)18 (34)12 (23)3 (6)
45 (85)4 (7)4 (7)
10 (19)22 (41)10 (19)8 (15)3 (5)
17 (32)6 (11)
30 (57)
6 (11)47 (89)
41 (77)5 (9)7 (13)
32 (89)4 (11)
7 (54)6 (46)
42 (79)10 (19)1 (2)
Abbreviations: ER, estrogen receptor; PR, progesterone receptor; HER2, human epidermal growth factor receptor 2; AIs, aromatase inhibitors. a. History of cardiac disease includes pathologies such as ischemic heart disease, arrhythmias, valvulopathies, heart failure or hypertensive heart diseaseb. It is considered ER positive if ≥1% of tumor cells demonstrate positive nuclear staining by immunohistochemistry.c. It is considered PR positive if ≥1% of tumor cells demonstrate positive nuclear staining by immunohistochemistry.d. HER2 is positive when there is overexpression by immunochemistry or FISH in equivocal cases.e. All patients with tumor at margins were treated by mastectomy.
Prognosis in male breast cancer
Herrero Rivera, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 155-163158

Figure 1. Kaplan-Meier curve for overall survival (A) and disease-free survival (B) in male breast cancer depending on the lymph node involvement, showing better survival in patients with less lymph node metastasis.
Figure 2. Kaplan-Meier curves showing the effect of the duration of ET intake and its prognostic impact on overall survival (A), disease free-survival (B) and distant disease free-survival (C) in male breast cancer.
There is a statistically significant increase in survival with ET for at least 5 years.
Herrero Rivera, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 155-163
Prognosis in male breast cancer
159

better CSS at 5 years (P <0.05), while negative PR expression and not receiving surgery were associated with worse CSS (OR: 11.1; P= 0.022; CI95% 1.18-105.24; and OR: 3.38; P= 0.004; CI 95% 2.14-5.34, respectively). KM estimated better OS in patients with better PS at diagnosis (median OS for PS 0 = 88 months; PS 1 = 45 months; PS 2 = 39 months; P<0.001), early stages (median OS for stages 0-IA = 92 months; stages IB-III = 75 months; stage IV= 20 months; P<0.001), low lymph node involvement, (median OS for no lymph node involvement = 70 months; 1-3 lymph nodes = 66 months; ≥4 lymph nodes = 57 months; P=0.035; Figure 1), absence of metastasis at diagnosis (median OS 79 months vs 20 months, P< 0.001) compared with those with metastasis. Those who received adjuvant ET for at least 5 years (median OS 89 months vs 69.6 months, P=0.024; Figure 2) showed better results. The size of primary tumor at diagnosis did not show better OS by KM test (median OS for <2cm = 70 months vs ≥2cm = 64 months, P= 0.219).
Figure 3 shows the absence of impact in OS for those patients analyzed according to BRCA mutational status with the KM estimation.
Having PS 0 (OR: 0.18; p = 0.014; CI95%, 0.05-0.66) or Ki67≤14% (OR: 0.05; P= 0.001; CI95%, 0.01-0.45) were associated with better DFS at 5 years while those treated with adjuvant ET < 5 years (OR: 34.00; P= 0.001; CI95%, 3.25-355.41) had lower DFS. KM analysis estimated a better median DFS when having Ki67≤14% vs >14% (84 months vs 48 months, P= 0.004), early stages (median DFS for stages 0-IA = 91 months; stages IB-III = 57 months; stage IV= 10 months; P<0.001), lower lymph node involvement, (median DFS for no lymph node involvement = 75 months; 1-3 lymph nodes = 54 months; ≥4 lymph nodes = 48 months; P<0.001;
Figure 1) or receiving adjuvant ET for at least 5 years (84 months vs 48 months, P= 0.005; figure 2).
Sixteen patients (33%) experienced relapse after treatment for curative intention (3 [19%] were local, and 13 [81%] were distant). Patients with histological grade 1-2 (OR: 0.04; P = 0.001; CI95% 0.01-0.27), absence of vascular invasion (OR: 0.14; P= 0.026; CI95% 0.03-0.82), Ki67≤14% (OR: <0.1; P= 0.017), absence of lymph node involvement (OR: <0.1; P= 0.001) and early disease stages 0-II (OR: 0.07; P= 0.001; CI95% 0.01-0.36), absence of in situ component associated (OR: 0.19; P = 0.047; CI95% 0.04-0.94) showed better DDFS. In contrast, patients having adjuvant ET < 5 years (OR: 8.00; P = 0.034; CI95% 1.25-51.13) had an increased risk of distant relapse and shorter DDFS (84 months vs 48 months, P = 0.002; Figure 2).
DiscussionThere are many publications about the clinical
characteristics of MBC. However, the scientific information related to the treatment outcome is scarce, probably due to the small samples assessed.
In agreement with the literature, our study has found similarities in relation to conventional prognostic factors such as the early pathological stage, the low histological grade, having positive hormonal receptors, the absence of lymph node involvement or having low levels of proliferation
13index Ki67 associated with better outcome. However, one of the main prognostic factors that has been described in MBC, the size of primary tumor, was not found to be significantly associated with survival in our cohort. In addition and unlike
14-16previous published studies , cardiovascular risk factors such as smoking habit or having a history of cardiovascular or thromboembolic disease did not
Figure 3. Description of the BRCA status in the cohort studied (A) and Kaplan-Meier curve for overall survival (B) without being able to demonstrate positive or negative impact for the mutated state
Prognosis in male breast cancer
Herrero Rivera, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 155-163160

associate with poorer prognosis. These results are probably due to the limited sample size.
Our study included patients that were diagnosed and treated between 1997 and 2018 and many of them did not have a genomic platform test, nor met the criteria for this assessment. Currently, these platforms are a very useful tool in the prognostic assessment of the risk of recurrence in early
17hormone-sensitive BC and perhaps its application could have modified the type of adjuvant treatment administered and therefore the reported survival results.
As in other studies on men, there was a higher percentage of hormone-sensitive tumors (91%) and negative HER2 (87%) in our sample compared to what has been described in several studies in women 18, 19
with worse results in 5-year OS in our cohort compared to MBC and BC in women reported in the American National Cancer Database (58% vs. 74%
20and 83% respectively). Similar to the study of 21Anderson et al. based on data collected from the
SEER database, there was a BC peak incidence between 62 and 73 years with a median age of 68 years, differing from women who usually had 2 incidence peaks at 52 and 71 years.
The analysis of mutations in the BRCA genes was carried out in 43% of the patients, finding mutations in 11% of this subset, which was BRCA2 in all of them. These results are similar to those described in previous studies where 10-14% of men with BC had
18, 22BRCA2 mutations. Nevertheless, the hypothesis that mutations in BRCA 2 could associate with worse prognosis in MBC, could not be validated in our cohort although there is controversy on this subject
23currently. The vast majority of the patients with BRCA2 mutations (83.3%) had a family history of breast or ovarian cancer, which is a higher rate than in
24previous published cohorts. Most of the patients underwent mastectomy
versus breast conservative surgery (BCS) (87% vs. 13%) in agreement with Cloyd et al. who reported a series of 5425 MBC patients where 87% underwent
25mastectomy between 1983 and 2009. These data clearly differ from the management performed in women, where in the early stages, the percentage of
26conservative surgeries is around 53%. BCS does not appear to decrease MBC CSS at 5 years
27compared to mastectomy. In the absence of randomized studies, the addition
of adjuvant ET in MBC is supported by several retrospective studies, where improvement in OS is
28shown. The administration of adjuvant tamoxifen (89% of the patients) did not show a significant association with OS, CSS or DFS at 5 years compared with AIs exclusively. These results differ from other studies such as Eggemann et al., where tamoxifen seemed to decrease mortality and increase
29survival compared to AIs. Additionally, the subgroup treated with AIs exclusively did not
receive GnRH agonists, which could improve the efficacy of AIs by blocking the estrogenic effect of
30testicular origin. Interestingly, the duration of ET for at least 5 years
showed an improvement in the 5-year DFS,a decrease in the risk of distance relapse and a better 5-year OS. One of the potential explanations for these findings is the fact that 58% of MBC patients who received adjuvant ET for less than 5 years died before completing the adjuvant treatment, while the remaining 42% did not complete the 5-year prescription due to low adherence. This finding is in
31agreement with some previous studies.The main limitation of the present study is the
small sample that can influence the statistical analysis. Our future intention is to contact nearby hospital centers to obtain a larger sample and to have results that are as close as possible to reality. Secondly, it was not possible to perform a multivariate analysis that could allow us to eliminate possible confounding factors that may have an impact on the outcome. Finally, the effect of cyclin inhibitors was not evaluated because all patients receiving this treatment had started it recently.
In conclusion, we found a greater hormonal sensitivity in MBC. Additionally, there was a lower percentage of BCS in MBC compared to women despite having a similar survival in early stages. BRCA mutational state did not show a prognostic impact on the outcome. ET played a significant role, and the duration, at least 5 years, was important for the prognosis. No differences were found with the intake of tamoxifen or AIs exclusively in the adjuvant setting although the sample size was limited for this analysis.
The absence of consensus regarding the best therapeutic option, together with the advent of new treatments in clinical practice, means the lack of knowledge about the best therapeutic option to apply both in adjuvant setting and in advanced stages of the disease, and therefore conducting studies on this population is needed.
Conflicts of InterestAll authors have completed the ICMJE uniform
disclosure form. The authors have no conflicts of interest to declare.
References1. White J, Kearins O, Dodwell D, Horgan K,
Hanby AM, et al. Male breast carcinoma: increased awareness needed. Breast Cancer Research. 2011;13(5):219.
2. Society AC. Cancer Facts & Figs (2018) Atlanta: American Cancer Society. 2018.
3. Institute NC. Surveillance, Epidemiology, and End Results Program SEER Cancer Statistics Review, 1975–2011. 2011.
4. Miao H, Verkooijen HM, Chia K-S, Bouchardy
Herrero Rivera, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 155-163
Prognosis in male breast cancer
161

C, Pukkala E, et al. Incidence and Outcome of Male Breast Cancer: An Internat ional Population-Based Study. Journal of Clinical Oncology. 2011;29(33):4381-6.
5. André S, Pereira T, Silva F, Machado P, Vaz F, et al. Male breast cancer: Specific biological characteristics and survival in a Portuguese cohort. Mol Clin Oncol. 2019;10(6):644-54.
6. Estadística INd. Tasas estandarizadas de mortalidad por causa de muerte (causas más frecuentes), sexo y nivel de estudio.
7. Brinton LA, Richesson DA, Gierach GL, Lacey JV, Jr., Park Y, et al. Prospective evaluation of risk factors for male breast cancer. J Natl Cancer Inst. 2008;100(20):1477-81.
8. Tai YC, Domchek S, Parmigiani G, Chen S. Breast Cancer Risk Among Male BRCA1 and BRCA2 Mutation Carriers. JNCI: Journal of the National Cancer Institute. 2007;99(23):1811-4.
9. Rudlowski C. Male Breast Cancer. Breast Care. 2008;3(3):183-9.
10. Leon-Ferre RA, Giridhar KV, Hieken TJ, Mutter RW, Couch FJ, et al. A contemporary review of male breast cancer: current evidence and unanswered questions. Cancer and Metastasis Reviews. 2018;37(4):599-614.
11. Giuliano AE, Edge SB, Hortobagyi GN. Eighth Edition of the AJCC Cancer Staging Manual: Breast Cancer. Annals of Surgical Oncology. 2018;25(7):1783-5.
12. Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982;5(6):649-55.
13. Nicolini A, Ferrari P, Duffy MJ. Prognostic and predictive biomarkers in breast cancer: Past, present and future. Seminars in Cancer Biology. 2018;52:56-73.
14. Padron-Monedero A, Koru-Sengul T, Tannenbaum SL, Miao F, Hansra D, et al. Smoking and survival in male breast cancer patients. Breast Cancer Research and Treatment. 2015;153(3):679-87.
15. Reiner AS, Navi BB, DeAngelis LM, Panageas KS. Increased risk of arterial thromboembolism in older men with breast cancer. Breast cancer research and treatment. 2017;166(3):903-10.
16. Bradshaw PT, Stevens J, Khankari N, Teitelbaum SL, Neugut AI, et al. Cardiovascular Disease Mortality Among Breast Cancer Survivors. Epidemiology. 2016;27(1):6-13.
17. Nitz U, Gluz O, Christgen M, Kates R, Clemens M, et al. Reducing chemotherapy use in clinically high-risk, genomically low-risk pN0 and pN1 early breast cancer patients: five-year data from the prospective, randomised phase 3 West German Study Group (WSG) PlanB trial. Breast cancer research and treatment. 2017;165.
18. Fentiman IS. Male breast cancer is not congruent with the female disease. Critical Reviews in
Oncology/Hematology. 2016;101:119-24.19. Cardoso F, Bartlett JMS, Slaets L, van Deurzen
C H M , v a n L e e u w e n - S t o k E , e t a l . Characterization of male breast cancer: results of the EORTC 10085/TBCRC/BIG/NABCG International Male Breast Cancer Program. Annals of Oncology. 2017;29(2):405-17.
20. Greif JM, Pezzi CM, Klimberg VS, Bailey L, Zuraek M. Gender Differences in Breast Cancer: Analysis of 13,000 Breast Cancers in Men from the National Cancer Data Base. Annals of Surgical Oncology. 2012;19(10):3199-204.
21. Anderson WF, Althuis MD, Brinton LA, Devesa SS. Is Male Breast Cancer Similar or Different than Female Breast Cancer? Breast Cancer Research and Treatment. 2004;83(1):77-86.
22. Couch FJ, Farid LM, DeShano ML, Tavtigian SV, Calzone K, et al. BRCA2 germline mutations in male breast cancer cases and breast cancer families. Nature Genetics. 1996;13(1):123-5.
23. Deb S, Jene N, Kconfab I, Fox SB. Genotypic and phenotypic analysis of familial male breast cancer shows under representation of the HER2 and basal subtypes in BRCA-associated carcinomas. BMC Cancer. 2012;12:510-.
24. Diez O, Cortés J, Domènech M, Pericay C, Brunet J, et al. BRCA2 germ-line mutations in Spanish male breast cancer patients. Annals of Oncology. 2000;11(1):81-4.
25. Cloyd JM, Hernandez-Boussard T, Wapnir IL. Outcomes of Partial Mastectomy in Male Breast Cancer Patients: Analysis of SEER, 1983–2009. Annals of Surgical Oncology. 2013;20(5):1545-50.
26. Hershman DL, Buono D, Jacobson JS, McBride RB, Tsai WY, et al. Surgeon characteristics and use of breast conservation surgery in women with early stage breast cancer. Ann Surg. 2009;249(5):828-33.
27. Zaenger D, Rabatic BM, Dasher B, Mourad WF. Is Breast Conserving Therapy a Safe Modality for Early-Stage Male Breast Cancer? Clinical Breast Cancer. 2016;16(2):101-4.
28. Fogh S, Hirsch AE, Goldberg SI, Rosenberg CL, Taghian AG, et al. Use of Tamoxifen With Postsurgical Irradiation May Improve Survival in Estrogen and Progesterone Receptor– Positive Male Breast Cancer. Clinical Breast Cancer. 2011;11(1):39-45.
29. Eggemann H, Ignatov A, Smith BJ, Altmann U, von Minckwitz G, et al. Adjuvant therapy with tamoxifen compared to aromatase inhibitors for 257 male breast cancer patients. Breast Cancer Research and Treatment. 2013;137(2):465-70.
30. Reinisch M, Seiler S, Hauzenberger T, Schmatloch S, Strittmatter H-J, et al. 273PD_PRFinal analysis of the Male-GBG54 study: A prospective, randomised multi-centre phase II study evaluating endocrine treatment with either tamoxifen +/- gonadotropin releasing hormone analogue
Prognosis in male breast cancer
Herrero Rivera, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 155-163162

(GnRHa) or an aromatase inhibitor + GnRHa in male breast cancer patients. Annals of Oncology. 2018;29(suppl_8).
31. Xu S, Yang Y, Tao W, Song Y, Chen Y, et al. Tamoxifen adherence and its relationship to mortality in 116 men with breast cancer. Breast Cancer Research and Treatment. 2012;136(2): 495-502.
Herrero Rivera, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 155-163
Prognosis in male breast cancer
163

studies have reported that disease-free survival decrease significantly for patients with TNBC
3-5compared with non-TNBC. The treatment strategies do not target other tissues in the body and thus, in contrast to other anti-cancer treatments, other organs are not adversely affected. In this regard, immunotherapy has been used as one of the known targeted therapies for breast cancer, in which monoclonal antibodies are used against the hormonal receptors expressed by the breast cancer
6cells. A study found that tumor grade and stage were relatively higher among AR negative cases compared to AR positive ones, but the difference was not statistically significant in Iranian TBNC
7patients. There was no significant correlation be tween AR s ta tus and age , tumor s ize , histopathologic type of tumor, or lymph node involvement. However, AR had a statistically
ARTICLE INFO
Background: Triple negative breast cancer (TNBC) is a heterogeneous disease group with a higher recurrence risk and poorer prognosis. In this study, we aimed to investigate the frequency and prognostic value of androgen receptor (AR) expression in tissues of TNBC patients.
Methods: In this study a total of 60 TNBC patients treated between 2011 - 2016 in Shahid Sadoughi and Mortaz Hospital were included and their medical records were analyze. The available paraffin blocks were assessed immunohistochemically to determine AR expression. Tumors with ≥10% nuclear staining were considered AR-positive, while the ones with <10% staining were considered AR-negative. The association between AR expression, and clinical-pathologic characteristics and prognosis in TNBC was analyzed.
Results: The result showed that AR expression in TBNC correlated with high risk of recurrence but no significant correlation with the age, grade, tumor size, lymph node status, type of diagnosis, tumor location, and Ki-67 level was observed. Positive immunoreactivity for AR was observed in 19 out of 60 (11%) specimens. No correlation was observed between the AR expression and the age, grade, tumor size, lymph node status, type of diagnosis, tumor location, and Ki-67 level. The AR-positive patients exhibited high risk of recurrence (P=0.016) and death (P=0.015) in comparison with the AR-negative patients.
Concusions: AR may not be a suitable biomarker and treatment target for the Iranian Yazd patients with TNBC.
Received:
29 August 2020Revised:
17 October 2020Accepted:
20 October 2020
Key words:Androgen receptor (AR),TNBC, Immunohistochemistry
Address for correspondence: Fatemeh Alsadat Nobakht, MDAddress: Department of Pathology, Shahid Sadoughi hospital, Yazd, IranTel: +98 9122129551Fax: +98 3538235014Email: [email protected]
164
ABSTRACT
Prognostic Value of Androgen Receptor in Triple Negative Breast Cancer of Iranian Patients in Yazd Region
a Department of Pathology, Shahid Sadoughi University of Medical Sciences, Yazd, Iran
a aFatemeh Alsadat Nobakht* , Mansour Moghimi
Open AccessOriginal Article
IntroductionTriple-negative breast cancer (TNBC) comprises
110-17% of breast cancer. Since TNBC was insensitive to endocrine or target therapy, it was said to have poor prognosis among different molecular
2subtypes. Many studies have been done on sub-classifying TNBC to find the relation between prognostic and therapeutic factors. In Iran, breast cancer is the most common type of cancer among
3women comprising 24.4% of all malignancies. Most
Nobakht, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 164-167
DOI: 10.19187/abc.202073164-167

significant positive association with a lower tumor grade and lymphovascular invasion in Iranian
8TBNC. Naimi et al. in 2020 claimed that there was not any correlation between the AR expression and grade, stage, lymph node status, and Ki-67 level. The AR-positive patients exhibited higher age and larger tumor size at the time of diagnosis in comparison with the AR-negative patients. Low percentage of Iranian TNBC patients expressed AR and no significant correlation was observed between its expression and most of the clinicopathological
9parameters. Several studies have explored the potential significance of AR for therapeutic management of both primary and advanced disease, especially in TNBC due to the lack of any other targets. The main aim of the present study was to evaluate the prognostic value of AR expression and its correlation with the clinicopathologic properties of Iranian TNBC patients in Yazd region.
MethodsBreast cancer patients diagnosed with stage I–III
TNBC, at Shahid Sadoghi Yazd and Mortaz Hospital between 2011 and 2016, were eligible for this analysis. This retrospective study was conducted at the Pathology Department of Shahid Sadoghi Yazd
University of Medical Sciences. Patients were analyzed based on several variables such as: age, pathological parameters (tumor size, grading, necrosis, lymph nodes status, tumor histology, Ki-67, lympho-vascular invasion, androgen receptor expression). Survival analysis was estimated by the Kaplan Meier method. The association between categorical variables was estimated by the Chi square test. The Cox multivariate proportional hazard regression model was used to evaluate the effects of the prognostic factors on survival. Significant differences in probability of surviving between the strata were evaluated by log-rank test. Hazard ratios and 95% confidence intervals (CIs) were estimated from regression coefficients. A significance level of 0.05 was chosen to assess the statistical significance. Statistical analyses were performed using Statistical Package for Social Sciences (SPSS) software (version19, SPSS, Inc, Chicago, IL).
ImmunohistochemistryThe 3–5 mm sections were incubated at 60 ºC (40
min) for de-paraffinization. Then, the samples were immersed in xylene and rehydrated in the decreasing ethanol solutions. To inhibit activation of the
Table 1. Clinicopathological characteristics of TNBC patientsclinicopathological parameters Information
Age(years)
Tumor location
Tumor size(cm)
Margin involvement
Lymph node involvement (LNI)
Ki67%
Recurrence
Histology
Survival
Grade
Ki67
LeftRightUnknown
YesNoUnknown
N0 (LNI Numbers=0)N1 (LNI Numbers <3)N2 (LNI Numbers <9)N3 (LNI Numbers >9)
<20%<60% &>20%>60%unknown
YesNo
DuctalMedullaryMucinous
>(5years)<(5years)
G1G2G3
knownunknown
Mean47.18
132126
Mean3.58
142719
41775
11161419
753
5091
555
02436
4119
STD11.35
STD2.6
Range25-71
Range0.2-15
165Nobakht, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 164-167
Prognosis of AR in TNBC

CA) were employed for the detection. Mouse anti-rabbit horseradish peroxidase-conjugated secondary antibody was incubated for 40 min at room temperature. The color was developed using diaminobenzidine (DAB) as a chromogen. The slides were extensively washed with PBS after each
6step.
ResultsSixty TNBC patients were investigated in this
study. Table 1 illustrates the pathological
endogenous peroxidases, the samples were incubated in 0.3% hydrogen peroxide. The antigen retrieval of the samples was done by heating in an 830-W microwave oven (60°C, 15 min) in 10 mmol /L sodium c i t ra te buffer (pH=6.0) . Subsequently, the slides were incubated with rabbit anti-human androgen receptor monoclonal antibody (Clone SP107, Master Diagnostica, Granada, Spain) at 4ºC overnight. The primary antibody was replaced with PBS for the negative control. HRP Polymer and DAP Plus Chromogen (Thermo Fisher Scientific,
Table 2. Correlations between AR expression and tumor location, margin, recurrence, histology, survivalparametersPathological parameters AR Immunoreactivity (No. of patients (%))
AR-Positive AR-Negative Total
P-Value
Tumor location
Margin involvement
Recurrence
Histology
Survival
RightLeft
YesNo
YesNo
DuctalMedullaryMucinous
> (5 years)< (5 years)
7(33.3%)5(38.5%
7(36.8%)7(25.9%)
5(71.4%)14(26.4%)
17(34.0%)2(22.2%)0(0.0%)
15(27.3%)4(80.0%)
14(66.7%)8(61.5%)
12(63.2%)20(74.1%)
2(28.6%)39(73.6%)
33(66.0%)7(77.8%)1(100%)
40(72.7%)1(20.0%)
21(100%)13(100%)
19(100%)27(100%)
7(100%)53(100%)
50(100%)9(100%)1(100%)
55(100%)5(100%)
0.750
0.686
0.016
0.619
0.015
Table 3. Association between AR expression and tumor size, lymph node involvement, grade and Ki67parameters
Clinic pathological parameters AR Immunoreactivity (No. of patients (%))
AR-Positive AR-Negative Total
P-Value
Lymph node involvement (LNI)
Tumor size (TS)
Grade
Ki67%
Age
N0 (LNI Numbers=0)N1 (LNI Numbers<3)N02(LNI Numbers<9)N03(LNI Numbers>9)
TS<3cm3≤TS≤6TS>6
G2G3
<20%<60% & >20%>60%
<47>47
14 (34.1%)1(14.3%)3(42.9%)1(20.0%)
9(33.3%)9(36.0%)1(12.5%)
9(37.0%)10(28.0%)
2(18.0%)6(37.0%)3(21.4%)
8(25.0%)11(39.0%)
27(65.9%)6(85.7%)4(57.1%)4(80.0%)
18(66.7%)16(64.0%)7(87.5%)
15(63.0%)26(72.0%)
9(82.0%)10(63.0%)11(78.6%)
24(75.0%)17(61.0%)
41(100%)7(100%7(100%)5(100%)
27(100%)25(100%)8(100%)
24(100%)36(100%)
11(100%)16(100%)14(100%)
32(100%)28(100%)
0.612
0.477
0.428
0.460
0.235
characteristics of the patients.Association of AR Expression with pathological
Parameters in TNBC Patients The patients were divided into two groups
according to the AR expression (Table 2). Overall, 19 patients (32%) exhibited positive immunostaining for the AR according to the utilized scoring method. Also, 41 patients were negative for AR immunostaining. The correlation between AR expression and pathological parameters was investigated. As illustrated in Table 2, 3, patient’s survival with positive expression of AR was less than those with
negative expression (P=0.015). Also, AR positivity was associated with a higher risk of disease recurrence (P=0.016). Totally AR expression in TBNC correlated with a high risk of recurrence and death. No significant differences (P>0.05) were detected in age, grade, tumor size, lymph node, type of diagnosis tumor location, and Ki-67 level between these two groups.
DiscussionAndrogen receptor is a novel emerging prognostic
biomarker in breast cancer. However, there is limited
166 Nobakht, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 164-167
Prognosis of AR in TNBC

information about the correlation between the AR expression and pathological features of TNBC patients, especially in the Iranian population. Previous studies found AR to play an effective role in
10-12the mammary tumors' development and growth. Therefore, AR has gained much attention as a potential target for TNBC treatment.
In this study, androgen receptor expression and its correlation with pathological features of TNBC were investigated. Although, other studies reported a higher percentage of AR-positive TNBC patients, the AR expression was a less common feature in our patients. Among 60 TNBC specimens involved in this study, only 19 (32%) were positive for AR expression. Therefore, it can be concluded that the expression of this receptor in TNBC patients in Iranian population in Yazd regions is lower than that in other regions. AR-positive patients had lower survival rates. Also, the AR expression was correlated with the higher recurrence in comparison with the AR-negative group. However, no significant correlation was observed between other pathological features with AR expression.
In conclusion, optimizing breast cancer therapies to increase cure rates in early stages is necessary in medical oncology. Currently, the studies on treatment strategies for different kinds of cancers are focusing on targeted therapies as specific behavior for destroying the tumor cells. Iranian TNBC patients in Yazd religion exhibited a significantly lower percentage (32%) of AR-positive cases in comparison with other studies in other nationalities. Therefore, AR may not be an appropriate biomarker and potential therapeutic target for the Iranian Yazd patients with TNBC. To validate this finding, we recommend more comprehensive studies with a larger sample size and evaluation of the AR expression with TNBC patients’ survival. However, this study confirmed that AR positivity was associated with a higher risk of recurrence and death in agreement with most studies conducted in this regard.
Conflict of InterestNone.
References1. Reis‐Filho J, Tutt A. Triple negative tumours: a
critical review. Histopathology. 2008;52(1):108-18.
2. Dent R, Trudeau M, Pritchard KI, Hanna WM, Kahn HK, et al. Triple-negative breast cancer: clinical features and patterns of recurrence. Clin Cancer Res. 2007;13(15 Pt 1):4429-34.
3 . S a d j a d i A , N o u r a i e M , G h o r b a n i A , A l imohammad ian M, Ma lekzadeh R . Epidemiology of breast cancer in the Islamic Republic of Iran: first results from a population-based cancer reg is t ry. EMHJ-Eas te rn
Mediterranean Health Journal, 15 (6), 1426-1431, 2009. 2009.
4. Aghili M, Lashkari M, Farrokhpey AH, Izadi S. Triple-negative breast cancer survival in Iranian patients. Acta Medica Iranica. 2013:560-6.
5. Perez EA. Breast cancer management: opportunities and barriers to an individualized approach. Oncologist. 2011;16 Suppl 1:20-2.
6. Bernard-Marty C, Lebrun F, Awada A, Piccart MJ. Monoclonal antibody-based targeted therapy in breast cancer: current status and future directions. Drugs. 2006;66(12):1577-91.
7. Mohammadizadeh F, Sajadieh S, Sajjadieh H, Kasaei Z. Androgen receptor expression and its relationship with clinicopathological parameters in an Iranian population with invasive breast carcinoma. Adv Biomed Res. 2014;3:132.
8. Jam S, Abdollahi A, Zand S, Khazaeipour Z, Omranipour R, et al. Androgen Receptor Expression in Triple-Negative Breast Cancer. Archives of Breast Cancer. 2019:92-5.
9. Naimi A, Sultan M, Amjadi E, Goli P, Kefayat A. Androgen Receptor Expression and Its Cor re la t ion wi th Cl in icopa tho log ica l Parameters in Iranian Patients with Triple Negative Breast Cancer. Iranian Journal of Pathology. 2020:239-44.
10. Kono M, Fujii T, Lim B, Karuturi MS, Tripathy D, et al. Androgen Receptor Function and Androgen Receptor-Targeted Therapies in Breast Cancer: A Review. JAMA Oncol. 2017;3(9):1266-73.
11. Ricciardelli C, Bianco-Miotto T, Jindal S, Butler LM, Leung S, et al. The magnitude of androgen receptor positivity in breast cancer is critical for reliable prediction of disease outcome. Clinical Cancer Research. 2018;24(10):2328-41.
12. Aleskandarany MA, Abduljabbar R, Ashankyty I, Elmouna A, Jerjees D, et al. Prognostic significance of androgen receptor expression in invasive breast cancer: transcriptomic and protein expression analysis. Breast cancer research and treatment. 2016;159(2):215-27.
167Nobakht, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 164-167
Prognosis of AR in TNBC

overcome them. These recommendations have wider relevance for different health conditions and a range of practice settings.
There is growing evidence of the significant quality of life (QoL) benefits of breast reconstruction
1-5(BR) following mastectomy. Reflecting this solid evidence base, offering BR to all clinically eligible women undergoing mastectomy for breast cancer has been acknowledged as best practice in guidelines and recommendations in many developed
6-9countries. BR may be performed at the same time as mastectomy – immediate BR (IBR), or deferred to a separate surgical procedure at a later date – delayed BR (DBR). Cancer Australia, the peak Australian government cancer advisory body, has stated that it is “not appropriate to perform a mastectomy without first discussing with the patient the options of
10 immediate or delayed breast reconstruction.” Yet in Australia, the latest estimate of the national IBR rate
ARTICLE INFO
Background: This study aimed to document referral-based barriers impeding Australian women's informed decision-making about breast reconstruction (BR) and to propose a designated BR referral pathway to help overcome these barriers.
Methods: Semi-structured, in-depth interviews were conducted with ten women previously treated for breast cancer, 9 breast and reconstructive surgeons and 6 health professionals [n=25] who had identified problems with referrals for BR.
Results: Referral-based barriers to BR discussion were identified at three different levels: from a public or private screening centre to a General Practitioner (GP) or breast surgeon; from a GP to a breast surgeon; and from one breast surgeon (without BR skills) to another breast or plastic reconstructive surgeon (with BR skills). A lack of designated referral pathways has meant that clinically eligible women who are interested in considering immediate BR have been denied this opportunity.
Conclusions: Streamlining referral processes, along with patient and clinician education, would help to ensure that women are at least seen by the most appropriate clinicians to discuss BR options and to maximise their opportunity for BR should they choose that option. Designated referral pathways could also be useful in ensuring that preference-sensitive treatment decisions are facilitated in settings with varying degrees of resources and in a range of clinical conditions.
Received:
01 September 2020Revised:
17 October 2020Accepted:
24 October 2020
Key words:Breast reconstruction, informed choice,breast cancer, referral pathways,health care reform, patient preferences
Address for correspondence: Dr Kathy Flitcroft MA(Govt), PhD Address: The University of Sydney, Northern Clinical SchoolReserve Rd, Royal North Shore HospitalSt Leonards NSW, 2065 AustraliaPhone: +612 433455121; Fax: +612 99549938.Email: [email protected];
ABSTRACT
Health System Barriers to the Discussion of Breast ReconstructionOptions in Australia: Improving Access Through Appropriate Referral
a The University of Sydney, Northern Clinical School, Sydney, Australia
b Breast & Surgical Oncology, The Poche Centre, Sydney, Australiac The University of Notre Dame, Sydney,128-140 Broadway Chippendale NSW 2007, Australiad Westmead Hospital, Hawkesbury Rd Westmead NSW 2145, Australia
a,b a,c,d a,bKathy Flitcroft* , Meagan Brennan , Andrew Spillane
Open AccessOriginal Article
IntroductionThe importance of clear patient referral pathways
is often overlooked and is an under-researched health policy issue. Referral practices should aim to provide the patient with prompt referral to a full range of high quality services that are best suited to address the patient's needs. This case study of breast reconstruction (BR) practices in Australia documents the impact of inappropriate referral systems and suggests policy mechanisms to
DOI: 10.19187/abc.202073168-177
Flitcroft, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 168-177168

11 12is 18.3%. This compares with 27.4% in France, 13
26% in the United States of America (USA) and 1421% in the United Kingdom (UK).
Over 18,000 Australian women were newly 15diagnosed with invasive breast cancer in 2018 and
around 40% were expected to require or choose 10
mastectomy as their surgical treatment. Not all are medically suitable for BR. It may be contraindicated in women with extensive disease and relatively contraindicated in those with significant co-morbidities or risk factors for complications (such as diabetes, smoking and morbid obesity). BR is a preference-sensitive treatment option, with women
16citing a wide range of reasons for their choice. Not all women who are clinically eligible will choose this option. It is estimated that overall around 50% of
17,18women would choose BR if given the opportunity. Among women who do choose BR, there are pros and cons for IBR versus DBR and decisions will be influenced by personal assessments of what each individual values. From a health services position, the most important consideration is that all women are aware of all options and can make an informed decision about BR, including the option of no BR (NBR). This discussion does not always happen.
A National Mastectomy and Breast Reconstruction Audit (NMBRA) of over 19,000 women was conducted in England using prospectively collected
14data over a 15 month period in 2008-2009. It found that of women undergoing mastectomy only, 35% felt they had not received the right amount of information
14about BR. A 2015 survey of Breast Cancer Network Australia (BCNA) members, reported 61% of participants having an initial discussion about BR prior to mastectomy (meaning IBR was still not an option for
1939% of these women). A more recent study of BR in Australia provided clear examples of the impact of
20unmet informational needs. Furthermore, the link between inadequate information and low BR rates has been confirmed in two studies: a study from the Netherlands revealed that being informed about IBR
21 increased the odds of receiving IBR fourteen-fold,while a Malaysian study concluded that their low BR rate of 20.6% “can be attributed to the low referral
22rate.”In Australia, general and breast surgeons are
trained to perform resectional breast cancer surgery, such as wide local excision, simple mastectomy and axillary surgery, but not BR. Oncoplastic surgeons are qualified to both remove the cancer and reconstruct the breast with local pedicled flaps or breast implants, and to perform symmetrisation surgery for the other breast. Free-flap BR, which requires vascular anastomosis, is mostly performed by plastic reconstructive surgeons who are generally not trained to surgically remove breast cancer and associated lymph nodes. Hence, the type of surgeon a woman is initially referred to may make a difference to their reconstructive options.
There are four potential pathways for a woman diagnosed with breast cancer to be referred to a surgeon. BreastScreen Australia, the national public breast cancer screening body in Australia, determines breast cancer screening policy and invites women aged 50-74 to attend free biennial mammographic screening (women aged 40-49 or 75 years and older are also eligible to participate on request, but are not invited to participate). In 2015-16, the participation rate was 55% of women aged
2350-69. There is no mandated national policy for referral for treatment when cancer is diagnosed, so while BreastScreen Australia sets the national policy, each state or regional jurisdiction implements the policy in different ways.
A second potential pathway is for a woman to be diagnosed through a private breast cancer screening centre. While there is a Medicare rebate for screening mammograms, many private imaging clinics charge more than the Medicare Schedule Fee, so that women must pay out-of-pocket costs. Data are not available to quantify the amount of private
23screening. Reasons for women choosing to have a mammogram outside BreastScreen Australia include faster results, convenience, the availability of ultrasounds or a lack of awareness that they would be eligible for free screening through BreastScreen
24Australia. General Practitioners (GPs) may also choose to refer their patients to private centres because they are unclear of the eligibility criteria for public screening, they have links with private radiology clinics or because they believe the service quality is superior in the private setting where
23ultrasound is also available.
The third pathway is for women presenting with symptoms of breast cancer, who are investigated by their GP outside the screening program. Once a diagnosis has been made, the GP will make a surgical referral in consultation with the patient. GPs have a major role to play in directing women who require mastectomy to surgeons who will offer, at a minimum, information about breast reconstruction options. Referral may be to a breast surgeon who has undergone varying levels of specialist training in breast surgery, to an oncoplastic breast surgeon who has undergone oncoplastic training in addition to their specialist breast training, or to a general surgeon who performs breast surgery but has not undergone any additional specialist breast training. In metropolitan or large regional centres, there are likely to be several surgeons to choose from. In more remote or rural areas, there will be fewer choices.
The final pathway is referral between surgeons. Some general and breast surgeons who do not perform BR will discuss the options with women prior to mastectomy and refer women interested in BR to other surgeons who can offer that expertise.
This article aims to document the referral-based barriers impeding Australian women’s informed
Flitcroft, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 168-177 169
Referral pathways breast reconstruction

agreement. Each participant was assigned a sequential reference number, with a prefix of W for women, HP for health professional and S for surgeon to ensure confidentiality. Responses from interviewees were classified into broad topic-based categories, agreed on by all authors, to reflect the range of views on particular issues. Where data was considered to be relevant to more than one topic, it was included in all relevant categories. This sub-set of interviews were specifically analysed to investigate referral barriers, which are fundamental to the issue of informed patient choice. Data for this sub-study are based on participant responses to the “BR discussion”, “Patient choice”, and “Decision-making” categories (see Appendix 2).
Ethics statementEthics approval was obtained from the Human
Research Ethics Committee (HREC) of St Vincent’s & Mater Health, Sydney, Australia, in April 2015 (14/181).
ResultsDiscussion of BR options may be compromised in
all four referral pathways. Table 1 provides examples, supported by participant quotations, of the first and second pathways outlined above: initial referral following screen-detected breast malignancy
decision-making about BR. It also proposes a designated BR referral pathway to help overcome these barriers.
MethodsThis research is part of a larger qualitative study
of 90 participants interviewed for the Improving Breast Reconstruction Equity of Access through Stakeholder consultation and Translation into policy and practice (I-BREAST) study (see Appendix 1 for further information on the I-BREAST participants and interview processes).
This article is based on responses from a sub-set of 25 I-BREAST participants (28%) who described instances where lack of appropriate referral has acted as a barrier to informed choice. The interview schedules did not specifically ask about referral processes, but this issue emerged as one of interest from the interviews with 10 women treated for breast cancer, 9 surgeons and 6 health professionals. Written consent was obtained from all interview participants.
Data management and analysisInterviews were digitally recorded and de-
identified. They were uploaded and transcribed verbatim for data analysis by an independent transcription company that had signed a confidentiality
Table 1. Initial referral following screen-detected breast malignancy (public or private)†
Examples Quotes
Referral from public screening centres (Pathway 1)Patients referred to a surgeon from the public BreastScreen service are able to choose which surgeon they see. There is a risk that surgeons who attend BreastScreen clinics (who may not perform BR) might channel newly diagnosed women to their own private practices or those of their colleagues (who may not discuss or offer BR). One oncoplastic surgeon commented:
Another oncoplastic surgeon working in a different state noted:
A BCN working in an Inner regional area commented:
Referral from private screening centres (Pathway 2)Women at private centres may be seen by a breast physician who will refer them to a surgeon. One BCN noted that the breast physicians:
A 40 year old woman attending a private screening clinic for investigation of a breast lump was diagnosed with two small, low grade invasive cancers in one breast. She was sent a list of ten surgeons by the clinic and told to contact one of them for an appointment. With no further information provided, she chose a surgeon who worked in a public hospital nearby as she could not afford the additional costs associated with surgery in a private hospital, despite having private health insurance. This surgeon told the women she required a bilateral mastectomy and did not offer BR. The woman asked:
I mean, there was a lot of fuss – and I’m sure it’s the same in other states – about surgeons using BreastScreen as an opportunity to obtain private work. [S10, Major city]
BreastScreen – my experience with it is you go and they say, “It’s up to you to go and find a doctor,” or “Your GP will refer you,” but that’s not how ours is run ... I spoke to three [GPs] that said if their patients go to BreastScreen, if they get a positive result or recall or need something else done, they never see the patients again [until after treatment]. [S15, Major city]
…there's one breast surgeon that actually works for BreastScreen, and [s/he] of late has been getting a lot of referrals. I'm not quite sure how that works. One or two of the surgeons have been quite frustrated with that fact. [HP24, Inner regional]
…know the surgeons. And I’m sure they share it around, but if the patient says she wants to go privately, then nine out of 10 will be coming here. [HP30, Major city]
“Can I, should I be seeing a plastic surgeon about a reconstruction?” And he said, “No, let’s deal with this first and then I can recommend you to someone afterwards.” [W21, Major city]
Referral pathways breast reconstruction
Flitcroft, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 168-177170
†Regions classified according to the Australian Statistical Geography Standard (ASGS) 2016. Australian Bureau of Statistics.1270.0.55.005 - Australian Statistical Geography Standard (ASGS): Volume 5 - Remoteness Structure, July 2016. Latest issue 16/03/2018http://www.abs.gov.au/ausstats/[email protected]/mf/1270.0.55.005 [accessed 12 April 2019]. BCN = breast care nurse; BR = breast reconstruction; GP = general practitioner.

either through the publicly-funded BreastScreen Australia (pathway 1), or through private screening or radiology practices (pathway 2).
Table 2 outlines the referral processes when a diagnosis of symptomatic breast malignancy has been made by a GP (pathway 3). Table 3 provides examples of secondary referrals from one breast surgeon who does not perform BR to another breast or plastic reconstructive surgeon who does perform BR, as well as incidences of ‘non-referral’ where the initial surgeon does not refer their patient on (pathway 4).
In metropolitan areas, it is common for high volume oncoplastic-trained breast surgeons to work with a few highly skilled plastic surgeons who do free flaps to provide a full reconstruction armamentarium [S1, S19]. In other settings, breast surgeons may work routinely with plastic surgeons [S23, S30], and
even have regularly-scheduled combined operating lists [S27]. Such settings allow for a full range of BR options to be discussed and implemented.
For women living outside major cities, difficulty in obtaining referral to appropriate services is exacerbated. Our interviews have demonstrated that some breast surgeons appear reluctant to refer the patients to other surgeons or collaborate with them to increase the range of options for their patients. In these cases, either no BR may be offered or the type of reconstruction offered may be limited to what a particular surgeon can do (see Table 3).
In response to the referral issues raised by women, surgeons and health professionals, we have proposed an optimal BR referral pathway (see Figure 1). This suggested pathway will not disadvantage women who are satisfied with the current referral arrangements, but will benefit the women who have
Table 2. Initial referral following diagnosis of symptomatic breast malignancy by a GP (Pathway 3)†Examples Quotes
Three metropolitan oncoplastic surgeons from different states suggested that not all GPs are aware of where to refer women:
A BCN commented on the need for more GP education:
This may be a particular problem in rural and remote areas, where there is a high GP turnover:
Conversely, more stable GP practices may rely on long-established referral patterns:
One regional GP even refused to refer a woman to a non-local surgeon:
A potential problem for GPs is the lack of reconstructive surgeons who work in the public system in some regional areas, meaning there is nowhere locally to refer public patients for BR. This issue was described by a public patient who was told by the general surgeon:
But the same way that breast surgeons and plastic surgeons need to learn about the changes in breast surgery, well GPs need to learn that as well. [S7, Queensland]
I think the general practitioners need to be better educated as to who is reputable and who is not … All the GP knows is I've got a woman with breast cancer; I’ll refer her off to Joe Blow. [S24, South Australia]
The general practitioners, the referrers have to understand who they’re inviting to manage their patients. And many a time, the referrer is happy to just get the patient off their hands. They don’t always think through the entire ramification of that referral. [S5, NSW]
… we do need to do some more education around the breast nurse service, and that has been on our books for a little while to actually go around and speak to GPs and educate [them] about what we can provide, so that’s also an opportunity to talk about what kinds of surgery are available, because most of them wouldn’t know. [HP4, Inner regional]
… this is classed as remote and they do their six months stint … it's very hard to get a GP for longer than a year up here. [W13, Outer regional]
We would have a large number of male Anglo-Saxon 55 to 65 GPs in X, so I think they get a bit stuck in their referrals. [HP7, Metropolitan]
He refused to give me the referral and told me that I shouldn’t think I should be treated any differently and told me I should remain locally. I then went back to the breast surgeon and … I demanded a referral. [W14, Inner regional]
"You are an ideal candidate for immediate reconstruction, because you don't have to have chemo. You don't have to have radium [sic] and you don't have to have cancer drugs." I was getting very excited. And, then he said, "Unfortunately, we're not offering that service anymore here … because the surgeon left in February …You have to go private if you want it … He said, "There's a seven-year waiting list now [in the public system]" and that was with a surgeon, and now, we haven't got a surgeon. [W22, Outer regional]
†Regions classified according to the Australian Statistical Geography Standard (ASGS) 2016. Australian Bureau of Statistics.1270.0.55.005 - Australian Statistical Geography Standard (ASGS): Volume 5 - Remoteness Structure, July 2016. Latest issue 16/03/2018http://www.abs.gov.au/ausstats/[email protected]/mf/1270.0.55.005 [accessed 12 April 2019]. BCN = breast care nurse; BR = breast reconstruction; GP = general practitioner.
Flitcroft, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 168-177 171
Referral pathways breast reconstruction

Table 3. Secondary referrals from a breast surgeon who does not perform BR to one who does (Pathway 4)†Examples Quotes
Some health professionals working in areas where public BR is not available, may be tempted not to refer their patients for this service. A BCN reported that BR is rarely raised by the breast surgeons s/he works with. If the patient brings it up, the BCNs will say:
A breast physician commented:
Yet, one woman from a rural town stressed the importance of patients considering options outside their local area:
“Non-referral” patterns are not confined to rural or remote areas where there are fewer plastic breast reconstructive surgeons, but also occur in major hospitals in largely populated areas. For example, a BCN working in one capital city confirmed the reluctance of some surgeons to refer their patients on: [Once a surgeon has a referral, do they tend to pass them on?]
A private patient attending a general surgical practice in a major city, on hearing she needed a mastectomy, asked:
Two metropolitan surgeons – one oncoplastic and one plastic – mentioned the adage that “if all you have is a hammer, every problem looks like a nail.” [S8, S13]. This view is supported by a private patient who reported:
One plastic surgeon who worked in both public and private sectors commented:
The reverse is also true for some plastic surgeons whose preference may be to do autologous BR only. This may lead to pressure on patients to have surgical options they do not want:
Even when plastic reconstructive and breast surgeons are co-located in the same hospital, there is the possibility of non-referral, as noted in this oncoplastic surgeon’s comment:
One woman reported that she had to forcefully request a transfer to a different hospital in the same city where she could have IBR:
Another woman in the same initial hospital reported that she:
One oncoplastic surgeon with access to autologous BR in their local area still chose to refer patients to a more dedicated and consistent out-of-area service:
“We need to mention that at this first meeting. We need to start working it out from here.” But it wouldn’t be something that’s routinely mentioned. … I think because it’s not available in the public system in X … it’s just not on the horizon … because it’s not there, it’s not mentioned. [HP5, Major city]
… in the end, because there was nobody doing them [Brs], I didn’t even refer people. So, then there was the vast volume of people that weren’t registered as on the waiting list, but were. So, now what I do is I refer everybody that wants to go so that they can’t - the bureaucrats can’t say that there’s no waiting list problem. [HP36, Outer regional]
I think they need to have the ability to know that there is a second opinion … you feel like you really should stay with your small country town because that's the right thing to do … [were the surgeons reluctant to refer you?] That was not even an option … There was no option at all. [W16, Inner regional]
“No, they don’t, no, very, very rarely, and particularly if they’re referred privately.” [HP7, Major city]
“Well, what about reconstructive surgery?” and he just said, “Well, we don't offer that here” and went on to try and book me in to go ahead with the mastectomy … And that's all I had offered. [W1, Major city]
I feel like the surgeon gave me the option that he thought would be best for me, and when I said, “I really don’t want that, what’s the second option.” He gave me that but it’s still his speciality. I would have liked him to say, “This is the full range of options – this is what, out of those, I think would be best for you and these are the reasons why.” [W5, Major city]
… the reality is, in this capital or corporate world that we live in, if you’re a breast surgeon and the patient is undecided and they’re private, then you’re probably going to push them towards an implant breast reconstruction because you make more money, than sending it to someone else and then they make the money. So, in the private world, it’s very fraught with danger because of the conflict of interest with payment. [S30, Major city]
So I've had a discussion with him. I still really would just like to have simple implants. But I know that the gold standard for me is an autologous breast reconstruction with probably a DIEP, which I'm not keen on. It's such big surgery. [W15, Inner regional]
Or I’ll say to the patient “Look, time is the issue, it’s unlikely we’re going to get a plastic surgeon to coordinate all of this within the next few weeks. Therefore, we’re going to go with the cancer first.” So that’s where offering them an implant buys me time. [S5, Major city]
I wasn’t being encouraged in any way, shape or form to even consider reconstruction. [W18, Major city]
… was not allowed immediate reconstruction because I had to have chemo and radiotherapy and I had to have nodes removed from the left side. [W19, Major city]
… it has to be coordinated with everything else. So, I’ve found that it hasn’t been the case here and that is why I think a lot of the time I actually do refer my patients to places I know in X. It’s a shame but they have to go interstate to get that service. [So, more plastic surgeons working in the public system] will be a welcome thing in the context that they actually work in collaboration with the breast surgeons. [S28, Major city]
†Regions classified according to the Australian Statistical Geography Standard (ASGS) 2016. Australian Bureau of Statistics. 1270.0.55.005 - Australian Statistical Geography Standard (ASGS): Volume 5 - Remoteness Structure, July 2016. Latest issue 16/03/2018 http://www.abs.gov.au/ausstats/[email protected]/mf/1270.0.55.005 [accessed 12 April 2019]. BCN = breast care nurse; BR = breast reconstruction; DIEP = deep inferior epigastric perforator flap; IBR = immediate breast reconstruction.
Referral pathways breast reconstruction
Flitcroft, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 168-177172

not been able to access fully informed discussion of BR options, a pre-requisite for informed decision-making.
DiscussionAlthough current referral pathways are effective
for many women, these interviews have provided examples of the different ways that non-designated referral patterns may block informed discussion of BR options, with severe outcomes for some
20individuals. While BreastScreen Australia’s policy respects a woman’s autonomy of choice, it does not provide advice about how a woman should choose her treating team. A brief discussion of the possibility of BR for those women likely to require mastectomy would help to make a more informed choice. There are opportunities, before the referral is made, for the consultant surgeon, breast physician or breast care nurse/counsellor to raise the idea of BR with general treatment information at this time. If women are aware that BR exists as an option, it may empower them to raise it in discussions with their GP or chosen surgeon.
Similarly, women who undergo screening at private screening centres and/or women who do not have a regular GP should be equally entitled to discuss their surgery options with a surgeon who is either part of a team that can provide all options, including implant-based and autologous BR, or is prepared to refer women elsewhere for this discussion. Simply handing a woman pathology reports stating they have breast cancer, and then sending them off to choose their own surgeon without some form of guidance, as happened with W21 (Table 1), seems grossly inadequate. Arguably, it is little better than directing women to surgical colleagues who do not offer a full range of options for women who may require mastectomy as part of their breast cancer treatment and are unwilling to refer that patient on to those who do, as illustrated by the
experience of W14 (Table 1), who had to demand a referral from one surgeon offering only mastectomy to another capable of performing BR.
The term ‘postcode lottery’ has been used to describe the haphazard way in which where you live
11determines access to health services. Important medical decisions and treatment opportunities may be influenced by the ‘luck of the draw’ unless more dedicated, systematic and equitable procedures are introduced. For example, some hospitals where BR is performed will not accept ‘out of area’ referrals, so that women living outside those hospital catchment areas may have extremely long waiting times, as noted by W22 (Table 2).
These Australian experiences appear to align with those of the UK, where Potter and colleagues concluded that “women’s experiences of BR seem to be largely determined by the centre to which they are initially referred for breast cancer diagnosis and treatment, and the resources and skills of the
24surgeons practicing at that centre.” The designated referral pathway we have developed (Figure 1) aims to overcome referral barriers and embodies principles of equitable access. The adoption of this, or a similar pathway, would improve a woman’s chances of making a fully informed choice about breast cancer surgery as an evaluation of the English
14NMBRA noted.One of the challenges is how to make the initial
referrer aware of the range of services offered by local surgeons and what ‘appropriate referral’ means for their patients. It is difficult for GPs to predict which patients will require or choose mastectomy, and hence when access to BR is a relevant consideration. This is particularly problematic as women who present with symptoms (and go through the GP rather than the BreastScreen pathway) are most likely to have more extensive disease requiring mastectomy. There can be sensitivities and subtleties in determining appropriate referral, so further education of health professionals
Flitcroft, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 168-177 173
Referral pathways breast reconstruction
Figure 1. Ideal breast cancer referral pathway for potential mastectomy patients.

about these nuances is essential. One surgeon interviewed [S30] raised the issue of
‘conflict of interest’ as a barrier to women’s choice. Potential conflicts of interest may arise when clinicians place their own desire for performing surgery (and obtaining the fee) ahead of the patient’s need for optimal reconstruction in cases when this would require onward referral to another surgeon. As noted earlier, it is usually the initial surgeon who controls what BR options a woman is offered. While some are happy to refer their patients to other surgeons for full discussion of all options, our study has shown this is not always the case. Screening services may also facilitate potential conflicts of interest by encouraging referrals to surgeons who work at the screening service.
In 2015, Cancer Care Ontario produced a breast cancer treatment pathway map, which covered all aspects of breast cancer including prevention, screening, diagnosis, treatment and post-treatment issues. It mandated that all women with operable breast cancer requiring mastectomy be referred to a plastic surgeon, who performs all BR procedures in Canada, to discuss BR options prior to the
25mastectomy. In response to this mandate for BR discussion as part of the treatment pathway, an updated overview of BR procedures has been published to specifically inform primary care physicians and their patients about BR options,
26outcomes and complication rates. There is the potential for Australia to follow a similar referral pathway and produce its own educational information relevant to the Australian setting.
For example, a publication by the National Cancer Expert Reference Group, titled Optimal Care
27Pathway for Women with Breast Cancer has been endorsed by Cancer Australia and the Cancer Council Australia. Each state and territory has been invited to adopt and co-badge its recommendations for local use. In relation to BR, this document states: “Women should be fully informed of their options and offered the option of immediate or delayed reconstructive
27surgery if appropriate.” These recommendations specify the training and experience required of the breast and plastic surgeons performing BR and state that breast surgeon referrals should be directed to members of Breast Surgeons of Australia and New
27Zealand Inc. (BreastSurgANZ). However, this document stops short of suggesting changes to current referral processes to support the practical implementation of this recommendation.
This recommendation to refer women to members of the representative surgical group may provide the simplest way of increasing the likelihood that the topic of BR is at least discussed prior to mastectomy, as the Cancer Australia statement
10recommends. BreastSurgANZ, as the national professional body representing breast surgeons and training oncoplastic surgeons, strongly supports
Cancer Australia’s statements, and encourages the discussion of all BR options with clinically eligible and interested patients prior to mastectomy. BreastSurgANZ members, many of whom are trained in implant-based BR, must also be prepared to promptly refer women who are interested in autologous/free flap BR methods to other breast reconstructive surgeons. Monitoring compliance with this endorsement is difficult, but setting expectations for members is likely to be useful. Figure 1 provides a possible optimal referral pathway in terms of BR.
In addition, there are several parallel policy and practice changes that should be considered including: credentialing and appointment of surgeons attending BreastScreen to ensure they provide BR or work in a multidisciplinary team that does; encouragement of general discussion at BreastScreen about BR as a possible component of future treatment; the development of a GP awareness program about ‘what to look for in a breast cancer surgeon’; a greater focus on BR as part of breast cancer patient support and education for women facing mastectomy; further engagement with breast cancer advocacy groups such as Breast Cancer
28Network Australia and BR-specific groups such as 29
Reclaim Your Curves, which promote and empower women to ask their surgeons about BR opportunities; and multidisciplinary team discussion of local access issues (surgeon availability, refusal to accept ‘out of area’ referrals and hospital resources that impact on waiting times) so that local solutions may be developed. The increasing use of neoadjuvant chemotherapy (chemotherapy before surgery) provides an opportunity for patients to take more time exploring their BR options. Distance does not need to be a barrier to discussion of BR options, as a l is t of discussion prompts could be emailed/posted to the patient in advance of a telephone/internet-based discussion, from the GP’s office if it is not available in the patient’s home.
This research has some limitations that should be acknowledged. This study has used a convenience, purposive sampling method that may not be representative and is subject to selection bias. Participants were from metropolitan, regional and rural areas across mainland Australia, so the responses represent different geographical settings. The location of surgeons interviewed was informed by an earlier survey of BCNs, so we had some information on where possible problems with referral procedures existed and were able to focus on those geographical areas. While not comprehensive in its coverage, we believe this study provides a useful snapshot of current practice.
Our focus in this article on negative examples of BR referral practices may be considered a potential limitation, as we have not presented any commentary from respondents who thought the current system
Referral pathways breast reconstruction
Flitcroft, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 168-177174

worked well. While we acknowledge that many GPs and surgeons are already performing best practice in terms of BR referral, the purpose of this article is to highlight the difficulties women face in accessing BR when this is not the case. Secondly, as we have argued in the Discussion, the current referral processes work well for some women, but by documenting instances where they have not worked well for other women, we hope to have demonstrated the somewhat random outcomes which we believe are inequitable and need to be addressed.
It is possible that some practices may have changed since 2015 when the first interviews were conducted. Recall bias may also be an issue for patients sharing their stories about events that happened several years before.
In conclusion, worldwide evidence-based guidelines strongly recommend women undergoing mastectomy have a pre-operative discussion about breast reconstruction (BR) while immediate BR is still an option. Inequity in accessing fully-informed BR discussion in Australia has been previously
19documented. This article is the first to report on the role referral processes play in perpetuating that inequity.
Designated referral pathways are required to overcome barriers to BR in Australia. GPs and surgeons should be aware of the advantages of BR for eligible women, as well as the relatively few contraindications to BR. Streamlining of the referral processes, along with patient and clinician
education, would go a long way towards ensuring that women are at least seen by the most appropriate clinicians to discuss BR options and to maximise their opportunity for BR should they choose that option.
This study found instances, even in metropolitan areas that are well staffed and resourced, where women were referred to surgical practices who did not even discuss options for immediate BR with their patients. A lack of designated referral pathways has meant that clinically eligible women who are interested in considering immediate BR are denied this opportunity, because of lack of adequate information about their BR options, paternalistic attitudes by their surgeons who believe they know what is best for their patient, or a refusal to refer women on to other surgeons because of a fear of losing their patients.
We have argued that these surgeons have an ethical responsibility to refer women to other services or practices that do offer a discussion of BR options, even if these women do not live near available services. The introduction of designated referral pathways for BR would provide practical support for informed decision-making to help redress this issue in Australia. A similar optimal pathway approach could be adapted by different countries with varying degrees of health system resources and for a range of clinical conditions. Figure 2 illustrates a generic version of an optimal referral pathway for preference-sensitive treatment options.
Figure 2. The importance of designated referral pathways for preference-sensitive treatments
Conflict of InterestsAS is former President of Breast Surgeons of
Australia and New Zealand.
Funding StatementThis work was supported by The Friends of the
Mater Foundation (FOTM), North Sydney, Australia.
AcknowledgementsWe are grateful for the assistance of the
Consumer Advisory Panel (CAP) who advised on the interview component of this study. CAP members provided input into draft questionnaires and participant information to be sent to women with breast cancer, breast care nurses (BCNs) and breast surgeons. Once data collection was complete, CAP
Flitcroft, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 168-177 175
Referral pathways breast reconstruction

members were also invited to review and comment on the draft of this article. We also thank the interview participants.
References1. Chen W, Lv X, Xu X, Gao X, Wang B. Meta-
analysis for psychological impact of breast reconstruction in patients with breast cancer. Breast Cancer. 2018;25(4):464-9.
2. Fanakidou I, Zyga S, Alikari V, Tsironi M, Stathoulis J, et al. Mental health, loneliness, and illness perception outcomes in quality of life among young breast cancer patients after mastectomy: the role of breast reconstruction. Quality of Life Research. 2018;27(2):539-43.
3. Howes BH, Watson DI, Xu C, Fosh B, Canepa M, et al. Quality of life following total mastectomy with and without reconstruction versus breast-conserving surgery for breast cancer: A case-controlled cohort study. J Plast, Reconstr, Aesthetic Surg. 2016;69(9):1184-91.
4. National Clinical Audit Support Programme. A national audit of provision and outcomes of mastectomy and breast reconstruction surgery for women in England. London: The Information Centre NHS; 2011.
5. Platt J, Zhong T. Patient-Centered Breast Reconstruction Based on Health-Related Quality-of-Life Evidence. Clinics in Plastic Surgery. 2018;45(1):137-43.
6. Biganzoli L, Marotti L, Hart C, Cataliotti L, Cutuli B, et al. Quality indicators in breast cancer care: An update from the EUSOMA working group. Eur J Cancer. 2017;86:59-81.
7. National Breast and Ovarian Cancer Centre (NBOCC) and the Royal Australasian College of Surgeons (RACS). National Breast Cancer Audit – Public Health Monitoring Report on 2007 Data. Sydney; 2009.
8. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines) Breast Cancer. 2017.
9. National Institute for Health and Care Excellence (NICE). NICE Guidelines. Breast Cancer (Early & Locally Advanced) London: NICE; 2009.
10. Cancer Australia. Influencing best practice in breast cancer. Practice 11. 2016.
11. Flitcroft K, Brennan M, Costa D, Spillane A. Regional variation in immediate breast reconstruction rates in Australia. Br J Surg Open 2017;1:114-21.
12. Régis C, Le J, Chauvet MP, Le Deley MC, Le Teuff G. Variations in the breast reconstruction rate in France: A nationwide study of 19,466 patients based on the French medico-administrative database. Breast. 2018;42:74-80.
13.Sisco M, Du H, Warner JP, Howard MA, Winchester DP, et al. Have we expanded the equitable delivery of postmastectomy breast
members were also invited to review and comment on the draft of this article. We also thank the interview participants.
???
Spyrou, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 9-14
reconstruction in the new millennium? Evidence from the national cancer data base. J Am Coll Surg. 2012;215(5):658-66.
14. Jeevan R, Cromwell DA, Browne JP, Caddy CM, Pereira J, et al. Findings of a national comparative audit of mastectomy and breast reconstruction surgery in England. J Plast, Reconstr, Aesthetic Surg. 2014;67(10):1333-44.
15.Cancer Australia. Breast Cancer in Australia [Available from: https://breast-cancer.canceraustralia. gov.au/statistics.
16. Flitcroft K, Brennan M, Spillane A. Making decisions about breast reconstruction: A systematic review of patient-reported factors influencing choice. Quality of Life Research. 2017:1-33.
17. Brennan ME, Spillane AJ. Uptake and predictors of post-mastectomy reconstruction in women with breast malignancy - Systematic review. Eur J Surg Oncol. 2013;39:527-41.
18. Matrai Z, Kenessey I, Savolt A, Ujhelyi M, Bartal A, et al. Evaluation of patient knowledge, desire, and psychosocial background regarding postmastectomy breast reconstruction in Hungary: a questionnaire study of 500 cases. Med Sci Monit. 2014;20:2633-42.
19. Somogyi R, Webb A, Baghdikian N, Stephenson J, Edward K, et al. Understanding the factors that influence breast reconstruction decision making in Australian women. Breast. 2015;24(2):124-30.
20. Flitcroft K, Brennan M, Spillane A. The impact on Australian women of lack of choice of breast reconstruction options: A qualitative study. Psycho-oncology. 2019;28(3):547-2.
21. de Ligt KM, van Bommel ACM, Schreuder K, Maduro JH, Vrancken Peeters MTFD, et al. The effect of being informed on receiving immediate breast reconstruction in breast cancer patients. Eu J Surg Oncol. 2018;44(5):717-24.
22.Ishak A, Yahya MM, Halim AS. Breast Reconstruction After Mastectomy: A Survey of Surgeons’ and Patients’ Perceptions. Clinical Breast Cancer. 2018;18(5):e1011-e21.
23. Australian Institute of Health and Welfare (AIHW). BreastScreen Australia monitoring report 2014-2015 Canberra: AIHW; 2017.
24. Potter S, Mills N, Cawthorn S, Wilson S, Blazeby J. Exploring inequalities in access to care and the provision of choice to women seeking breast reconstruction surgery: a qualitative study. Br J Cancer. 2013;109(5):1181-91.
25. Cancer Care Ontario (CCO). Breast cancer treatment pathway map. Version 2015.11 ed. Toronto, Ontario: CCO; 2015.
26. Somogyi RB, Ziolkowski N, Osman F, Ginty A, Brown M. Breast reconstruction: Updated overview for primary care physicians. Can Fam Physician. 2018;64(6):424-32+e255-e64.
27.National Cancer Expert Reference Group.
Referral pathways breast reconstruction
Flitcroft, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 168-177176

Optimal Care Pathway for Women with Breast Cancer. Melbourne: Victorian Department of Health and Human Services; 2016.
28.Breast Cancer Network Australia (BCNA). [Available from: https://www.bcna.org.au/
29. Reclaim Your Curves (RYC). [Available from: https://www.reclaimyourcurves.org.au/.
Referral pathways breast reconstruction
Flitcroft, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 168-177 177

accounts for less than 3% of all cases of breast cancer 1, 2 and typically occurs in postmenopausal women.
EPC is also described as encapsulated or intra cystic papillary carcinoma. In the literature, it has been considered as a variant of Ductal Carcinoma in-Situ (DCIS), given its discrete nodular growth, its lack of stromal reaction, as well as its indolent clinical
3, 4behaviour. However, unlike classic DCIS, EPCs lack myoepithelial cells which, in many cases, can lead to the conclusion that some EPCs are, in fact, invasive carcinomas with an expansile growth pattern
5(Figures 1a & 1b). The latter hypothesis is further
ARTICLE INFO
Background: Encysted papillary carcinoma (EPC) is a rare breast neoplasm that mainly affects postmenopausal women. The purpose of this study was to examine whether a sentinel node biopsy would be deemed necessary in patients with a diagnosis of EPC and to determine if evidence of invasiveness can be diagnosed on a core needle biopsy with sufficient confidence to guide decision making for upfront axillary SLNB.
Methods: The available data of patients with EPC of the breast were reviewed at a tertiary breast cancer unit over a period of 10 years (2009-2019) and the concordance between core needle biopsy and final histology was assessed. We also carried out a detailed review of the available literature to inform best practice guidance for management of the axilla.
Results: During the study, a total of 37 EPC patients were identified, of whom 10 were excluded as they declined further treatment, providing us a study sample of 27 patients. The median age at diagnosis was 72 years (range 47-97) and the vast majority of patients (96%) were Estrogen Receptor (ER) positive. Of the 27 patients treated, 17 (63%) underwent a diagnostic axillary Sentinel Lymph Node Biopsy (SLNB). On the final histology, 13/27 (48%) proved to have invasive disease. A total of 5 (18%) patients had evidence of metastasis in the axillary nodes, of whom only 7% had macro-metastatic disease that warranted further axillary treatment. None of the treated patients had evidence of recurrence or distant metastatic disease, to date (median of 5 years of follow up).
Conclusion: Encysted papillary carcinoma is associated with a low incidence of axillary node involvement. SLNB should only be carried out when there is evidence of invasive cancer. An algorithm was developed to help guide management of the axilla in cases diagnosed with EPC on diagnostic core needle biopsy.
Received:
05 September 2020Revised:
21 September 2020Accepted:
28 September 2020
Key words:Encysted papillary carcinoma (EPC), sentinel lymph node biopsy (SLNB)
Address for correspondence: Ioannis Spyrou, MDAddress:Tel:Fax:Email: [email protected]
178
ABSTRACT
Encysted Papillary Carcinoma of the Breast (EPC): A Follow-up Studyto Investigate the Role of Sentinel Lymph Node Biopsy
a The Breast Unit, Guy's and St Thomas' NHS Foundation Trust, London, UK
a a a a aIoannis Spyrou* , Foivos Irakleidis , Stergios Douvetzemis , Hisham Hamed , Ashutosh Kothari
Open AccessOriginal Article
Spyrou, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 178-182
IntroductionEncysted papillary carcinoma (EPC) of the breast
is a rare breast cancer subtype. It is characterised by a papillary carcinoma which is located within a well-circumscribed cystic or distended mammary duct. It
DOI: 10.19187/abc.202073178-182

substantiated by their ability to metastasise to axillary lymph nodes in a small number of cases and the even
1rarer occurrence of distant metastatic disease.In 2012, the WHO working group acknowledged
the potential of minimal invasion in these non-aggressive lesions. However, despite the lack of myoepithelial cells around these lesions, EPC is referred to as an in-situ disease for the purposes of staging. However, there is no consensus on how to stage EPC in available literature and therefore unsurprisingly there is a lack of agreement on how to
6manage it.
Encysted papillary carcinoma presents most commonly as a palpable lump in 70-80% of cases, nipple discharge, or then as an incidental finding on breast imaging. It appears as a lobulated or well circumscribed lesion on mammogram or as a complex cyst with vascular flow on ultrasound
7(Figure 2). Almost 50% of EPCs have been
8identified in the retro-areolar region. Traditionally, patients diagnosed with EPCs have good prognosis in both in situ and invasive subgroups. They are slow
growing tumours with a 10-year survival rate of 9, 10
100% and a disease-free survival rate of 91%. Recent data have demonstrated significant
discrepancies in the management of the axilla following diagnosis of EPC. The largest study to date, based on the SEER database (total of 2649 patients, from 2000 to 2009), and published in 2016, showed a 5.5% incidence of axillary lymph node involvement in all EPCs. Therefore, a sentinel lymph node biopsy (SLNB) was recommended for all patients with EPC, as the node positive patient cohort
11possessed the worse overall prognosis. Another study from Nottingham (302 Papillary Carcinomas, including 208 EPCs, from 1990 to 2010), published in 2011 demonstrated that 3% of patients with EPC had evidence of micro-metastatic disease in the axillary nodes. This study suggested that management of axillary lymph nodes in EPCs should be similar to that of conventional DCIS, where synchronous SLNB should only be performed along with a mastectomy or in cases with evidence of invasive disease on final histology, following breast
12conserving surgery. Another review of 917 patients between 1988 and 2005 from the California Cancer Registry (CCR), published in 2008 showed a less than 8% incidence of axillary lymph node involvement and therefore, recommended SLNB for
13all patients with EPC. The purpose of this study was to examine whether
a sentinel node biopsy would be deemed necessary in patients with a diagnosis of an encysted papillary carcinoma and to determine if evidence of invasiveness can be diagnosed on a core needle biopsy with sufficient confidence to guide decision making for upfront axillary SLNB.
MethodsThe available data of patients diagnosed with
EPC of breast were reviewed at a tertiary breast cancer unit over a period of 10 years (2009-2019) and the concordance between core needle biopsy and final histology was assessed. Patients' level data were retrieved from the hospital electronic medical
a b
Figures 1a & 1b. Breast core biopsy (a) and wide local excision (b) of EPC (Hematoxylin and Eosin stain original magnification x 40). Core biopsy revealed an intermediate grade EPC. Final histology of the same patient revealed
a Grade 2 invasive carcinoma of No Special Type (NST) adjacent to the EPC.
Figure 2. Breast ultrasound image showing a mixed echogenic lesion [solid component (arrow) within
a well circumscribed cystic lesion]. Cytology of fluid aspirate revealed atypical cells suspicious of malignancy. A core biopsy
of the residual solid component revealed a papillary lesion with atypia, highly suggestive of an EPC.
???
179Spyrou, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 178-182

biopsy revealed a papillary lesion (B3) that was confirmed as an EPC following an excision biopsy. Overall, 27 patients (73%) underwent treatment and the remaining 10 (17%) were either deemed as very high risk for general anaesthesia due to co-morbidities or declined any form of treatment.
Of the 27 patients who received treatment, only 2 (7%) had evidence of invasive disease on their core biopsy. Also 2 (7%) patients had features suspicious for invasion. Consequently, these 4 patients (14%) underwent a synchronous SLNB. Twenty-six (96%) patients were strongly Estrogen Receptor (ER) positive. Twenty-two (81%) of the 27 underwent a Wide Local Excision (WLE) and 5/27 (19%) chose to undergo a mastectomy with synchronous SLNB. A total of 13/27 (48%) treated patients had invasive disease on their final histological specimen and 8/27 (30%) of them had associated DCIS (Table 1).
records. Furthermore, a comprehensive review of the PubMed database (with “encysted papillary carcinoma” as the search tem) was performed. Particular consideration was given to the California Cancer Registry review (2008), the SEER database analysis (2016) and the study from the University Nottingham (2011) to determine the appropriate clinical assessment and management of patients with breast EPC.
ResultsBetween 2009 and 2019, there were a total of 37
patients diagnosed with EPC of the breast. The median age at diagnosis was 72 years (range 47-97) and the vast majority of patients (96%) were Estrogen Receptor (ER) positive.
In 36 out of 37 patients (96%), EPC was diagnosed in core biopsy. In 1 (4%) patient, the core
Table1. Characteristics of treated EPC patients(n=27)Variabeles (%)nInvasion based on core biopsy
Estrogen Receptor (ER)
Type of Breast Surgical Treatment
Invasion based on final histology
Associate DCIS*
Sentinel Lymph Node Biopsy (SLNB)
Axillary metastasis
Distant metastasis
2232
261
225
1314
819
17102
322
027
YesNoSuspicious
PositiveNegative
Breast Conserving Surgery (BCS)Mastectomy (MX)
YesNo
YesNo
YesNo
Yes (Macro-metastasis)Yes (Micro-metastasis)No
YesNo
7.485.27.4
96.33.7
81.518.5
48.151.9
29.670.4
63377.4
11.181.5
0100
*DCIS: Ductal Carcinoma in Situ
Seventeen (63%) out of the 27 patients underwent a diagnostic SLNB to stage the axilla. This included patients who underwent a diagnostic SLNB at the time of their primary surgery either due to evidence or suspicion of invasive disease on their core biopsy or then due to the fact that they opted for a mastectomy. The remaining patients underwent a diagnostic SLNB following the diagnosis of invasive disease on their final histology. There was a 90 year old lady, who had invasive disease diagnosed on her final histology, but following a multi-disciplinary team discussion a SLNB was not deemed necessary, considering her advanced age, her low risk of recurrence and strong ER positivity. Two (7%) patients had evidence of macro-metastatic disease on SLNB and underwent a subsequent completion axillary clearance (cANC). Three (11%) patients had evidence of micro-metastatic disease in the nodes, which did not warrant
any further surgical intervention based on current breast cancer management guidelines. After a median follow up of 5 years, none of the treated patients developed locoregional recurrence or distant metastases (Table 1).
DiscussionThere are a limited number of published clinical
studies on EPC. Most of the studies are case reports or small case series from single institutions.
The perception that EPC is a malignancy of 1
elderly post-menopausal women , was supported by data from the current study, where the median age at diagnosis was 72 years. However, a recent clinical study involving 900 patients showed that 3.5% of
13them were male patients. The vast majority of published case series on EPC have not included male patients.
???
180 Spyrou, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 178-182

There is significant controversy regarding potential invasiveness of EPC and its ability to spread to the axilla. As a consequence, the management of this disease does not conform to agreed guidelines. In general, regardless of the therapeutic surgical strategy, the prognosis of EPC is
12generally excellent.
The California Cancer Registry (CCR) in a review of 917 cases showed that 7.8% of cases had regional disease, with either direct spread into adjacent tissues or axillary lymph nodes. They failed to specify the exact proportion of patients with micro-metastatic and macro-metastatic axillary nodal disease. The incidence of axillary lymph node involvement, despite being quite low, led to the recommendation to proceed with a diagnostic axillary sentinel lymph node biopsy (SLNB) in all patients with EPC, regardless of the presence of
13invasive disease within the diagnosed EPC.
In another important study from the Surveillance, Epidemiology, and End Results (SEER) registry including 2,649 female patients with EPC, axillary involvement was a key component. They reported that 5.5% of patients had axillary lymph node involvement. This study also showed that despite the low probability, EPC can spread to the axillary nodes. However, this study failed to clarify whether patients with axillary nodal involvement had largely micro-metastatic or then macro-metastatic disease. Analysis on whether axillary spread occurred in cases of pure EPC or in cases associated with DCIS or lymphovascular space invasion, was also missing. They did underline the significance of the lymph node status in EPC, since all patients with a pathologic negative axilla had a better overall survival rate. Consequently, they recommended that a SLNB should be performed for all patients with a
11 diagnosed EPC.Furthermore, a study of 208 patients, published
by the university of Nottingham showed that 3% of cases with EPC had axillary lymph node micro-
metastasis. According to this study, EPC, which is entirely surrounded by a layer of myoepithelial cells is considered an in-situ lesion. They recommended that this histological subtype should be regarded as papillary carcinoma in situ and should be treated similarly to DCIS. Moreover, this important study demonstrated that the outcome of patients with pure EPC or EPC associated with microinvasion or suspicion of invasion are not different, and both have
12excellent prognosis with local therapy alone. In a case report published in 2017, a 70 year old
female presented with a 120mm mass on ultrasound which on biopsy proved to be an EPC and was treated with a WLE and SLNB showing macrometastasis in one of the two lymph nodes excised. She subsequently underwent ALNC. The final histology of the breast specimen showed encysted papillary carcinoma of pre-dominantly intermediate nuclear pleomorphic
14grade with no evidence of conventional invasion. A magnetic resonance imaging following the operation showed that there was no other lesion in the breast, proving that the macrometastasis was caused exclusively by the EPC. This article was published as a case report emphasizing the rarity of lymph node metastasis is EPC.
In agreement with our study is a recent review by 15
Wang et al. 99 cases of Papillary carcinoma were evaluated, 43 of whom had EPC. It was proved that in these cases there was minimal lymph node involvement even in tumours with invasive component. The patients’ long term survival was outstanding as shown in our current study. This review concluded that there is no indication for routine SLNB in patients with papillary carcinoma treated with Wide local excision surgery.
In summary, there is a distinct lack of consensus for performing SLNB in patients with the diagnosis of EPC. The decision of upfront surgery to the axilla should be based on clinical indications guided by the histopathological characteristics of the EPC on core biopsy. These should be balanced against the
Figure 3. Treatment algorithm for patients diagnosed with EPC of breast on core biopsy. (Mx: Mastectomy, WLE: Wide Local Excision, SLNB: Sentinel Lymph Node Biopsy)
181Spyrou, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 178-182
???

potential risks and associated morbidity following an axillary intervention, such as upper l imb lymphoedema, longstanding shoulder stiffness and significant neurovascular injury. In light of this, we have developed a comprehensive treatment algorithm to help guide axil lary surgical interventions and potentially reduced morbidity [Figure 3]. We believe that a synchronous SLNB should not be the intervention of choice in all patients with the diagnosis of EPC. Synchronous SLNB should only be considered in patients with EPC that is associated with unequivocal evidence of invasion or in cases with a high suspicion of invasion. SLNB should also be the appropriate surgical approach in patients undergoing a mastectomy, as their primary breast treatment. Consequently, in the vast majority of patients with EPC and no evidence of invasion on core biopsy, SLNB should not be performed, unless they undergo a mastectomy as opposed to breast conserving surgery (BCS). Finally, in patients undergoing BCS with no proven invasion or suspicion of invasion on core biopsy, SLNB should only be performed as a second standalone diagnostic procedure, when invasion is reported following a wide excision on the breast final histology.
In conclusion, encysted papillary carcinoma is a rare malignant neoplasm of the breast with excellent prognosis that affects older, postmenopausal women. Patients with EPC require Sentinel Lymph Node Biopsy (SLNB) for staging of axilla, only if there is evidence or suspicion of invasion in their core biopsy or final histology specimen or if they are undergoing a mastectomy as their primary treatment. Routine axillary surgery in all cases undergoing BCS should be avoided. Based on our own experience, and a comprehensive review of available evidence, we have proposed an algorithm for the role of SLNB following a diagnosis of EPC.
Conflict of InterestNone.
References1. Mulligan AM, O'Malley FP. Papillary lesions of
the breast: a review. Adv Anat Pathol. 2007;14(2):108-19.
2. Solorzano CC, Middleton LP, Hunt KK, Mirza N, Meric F, et al. Treatment and outcome of patients with intracystic papillary carcinoma of the breast. Am J Surg. 2002;184(4):364-8.
3. Collins LC, Schnitt SJ. Papillary lesions of the breast: selected diagnostic and management issues. Histopathology. 2008;52(1):20-9.
4. Esposito NN, Dabbs DJ, Bhargava R. Are encapsulated papillary carcinomas of the breast in situ or invasive? A basement membrane study of 27 cases. Am J Clin Pathol. 2009;131(2):228-42.
5. Hill CB, Yeh IT. Myoepithelial cell staining patterns of papillary breast lesions: from
intraductal papillomas to invasive papillary carcinomas. Am J Clin Pathol. 2005;123(1):36-44.
6. Wei S. Papillary Lesions of the Breast: An Update. Arch Pathol Lab Med. 2016;140(7):628-43.
7. Liberman L, Feng TL, Susnik B. Case 35: intracystic papillary carcinoma with invasion. Radiology. 2001;219(3):781-4.
8. Eiada R, Chong J, Kulkarni S, Goldberg F, Muradali D. Papillary lesions of the breast: MRI, ultrasound, and mammographic appearances. AJR Am J Roentgenol. 2012;198(2):264-71.
9. Lefkowitz M, Lefkowitz W, Wargotz ES. Intraductal (intracystic) papillary carcinoma of the breast and its variants: a clinicopathological study of 77 cases. Hum Pathol. 1994;25(8):802-9.
10. Stamatakos M, Stefanaki C, Stasinou T, Papantoni E, Alexiou I, et al. Intracystic Papillary Carcinoma of the Breast in Males. In Search of the Optimal Treatment for this Rare Disease. Breast Care (Basel). 2011;6(5):399-403.
11. Mogal H, Brown DR, Isom S, Griffith K, Howard-McNatt M. Intracystic papillary carcinoma of the breast: A SEER database analysis of implications for therapy. Breast. 2016;27:87-92.
12. Rakha EA, Gandhi N, Climent F, van Deurzen CH, Haider SA, et al. Encapsulated papillary carcinoma of the breast: an invasive tumor with excellent prognosis. Am J Surg Pathol. 2011;35(8):1093-103.
13. Grabowski J, Salzstein SL, Sadler GR, Blair S. Intracystic papillary carcinoma: a review of 917 cases. Cancer. 2008;113(5):916-20.
14. J. Kratz SP, N. Barnes Manchester Royal Infirmary, Central Manchester University Hospitals,Adult Histopathology Dept., United Kingdom, 2017.
15. Wang Y, Lu S, Graves T, Ouseph MM, Resnick MB, et al. Can Sentinel Lymph Node Biopsy Be Spared in Papillary Carcinoma of the Breast? Clin Breast Cancer. 2017;17(2):127-33.
???
182 Spyrou, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 178-182

183
(lumpectomy/quadrantectomy) with adjuvant radiotherapy is the standard treatment for women with early-stage breast cancer, and it has proved to be equivalent to mastectomy in terms of overall
2-4survival and local recurrence of disease. The purpose of adjuvant radiotherapy is to reduce the risk of local disease recurrence. Adjuvant radiotherapy treatment can be delivered intra or post-operative; patients considered at low risk of local recurrence are
5candidates for IORT , which is a technique of partial irradiation of the breast by applying a single dose of
ARTICLE INFO
Background: In women undergoing breast surgery, Measurement of Patient Related Outcome Measures (PROMs) is important for improving the process of care, focusing on the patient's perspective. BREASTQ is a validated patient-reported outcome measure used increasingly in aesthetic and recostructive surgery. Only recently a breast conserving therapy module (BREASTQ-BCT) has been available. The aim of this study was to assess patient satisfaction and quality of life using BREAST-Q questionnaire in patients undergoing breast conserving surgery (BCS) plus IORT.
Methods: Women undergoing BCS plus IORT for an early-stage breast cancer for at least a year were invited by telephone to partecipate. We scheduled dedicated outpatient visits to our center. The medical interviewer collected medical history information and administered the BREASTQ-BCT in paper format. Data were inserted in a de-identified database. Univariate regression analysis was used to identify clinicopathological variables associated with "satisfaction with breast" domain score.
Results: Overall, 38 women completed the questionnaire. The domains of the questionnaire that obtained the lowest scores were ‘satisfaction with IORT information’ and ‘satisfaction with breasts’ (median score 59, IQR 55-73 and 51-69.5). Weight of specimen and vascular invasion were risk factors for lower ‘Satisfaction with breasts’ at univariate analysis. There was a moderate-strong correlation between 'satisfaction with the breasts' and 'psychosocial wellbeing' and 'Sexual wellbeing'.
Conclusions: In this retrospective study, without a pre-operative questionnaire, changes in individuals’ satisfaction and quality of life could not be identified. A prospective study comparing BCS plus external RT group and BCS plus IORT group could be informative.
Received:
18 September 2020Revised:
17 October 2020Accepted:
23 October 2020
Key words:Breast cancer, patient-reported outcome measures, BREAST-Q, breast conserving surgery, intraoperative radiotherapy,IORT.
Address for correspondence: Caldana Marina, MDAddress: Verona Integrated University HospitalP.le A. Stefani, 1 - 37126 Verona, ItalyTel: +39 045 812 7322Fax: +39 045 812 7752Email: [email protected]
ABSTRACT
Quality of Life Assessment After Conserving Breast Surgery and Intraoperative Radiotherapy (IORT) in Breast Cancer Patients Using the BREAST-Q Questionnaire
a Operative Unit of Breast Surgery Complex, Breast Unit, Oncologic Surgery Department, AOUI, Verona, Italy
a a a a aMarina Caldana* , Davide Lombardi , Silvia Urbani , Francesca Pellini , Sara Mirandola , a aEleonora Granuzzo , Giovanni Paolo Pollini
Open AccessOriginal Article
IntroductionBreast cancer is the most common cancer in
women in all age groups worldwide and its incidence 1is slightly increasing. Breast conserving surgery
Caldana, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 183-188
DOI: 10.19187/abc.202073183-188

radiation (20 Gy, 50 Kv), administered at the time of surgery. Two randomised controlled trials, TARGIT-
6 7A and ELIOT , have shown that IORT is non-inferior to External Beam Radiation Therapy (EBRT) in terms of local recurrence rate when delivered to patients with early breast cancers and specific tumour characteristics. IORT also has
8additional advantages in terms of organization.Although breast cancer is the leading cause of
cancer-related mortality in women, this trend is slightly decreasing, and advances in diagnostic and therapeutic management of breast cancer have produced significant improvements in disease-
9related survival. Currently, more than 60% of women with breast cancer live 20 years after initial
10diagnosis. Therefore, the assessment of patient satisfaction with the surgical result, quality of life after surgery and well-being in a psychosocial context are of vital importance in women undergoing breast surgery. Measurement of Patient Related Outcome Measures (PROMs) after breast surgery is now
11, 12included in clinical trials as an endpoint , and it is believed to be important for improving the process of
13care, focusing on the patient's perspective.
In 2009 the Memorial Sloan Kettering Cancer Center developed a questionnaire to elicit and quantify the patient's perception of the result after
14breast surgery, the BREASTQ. Several modules have been developed for the evaluation of patients undergoing radical mastectomy, reconstructive and reductive/additive breast surgery, and more recently
15, 16for BCT as well. The BREASTQ-BCT Module includes five domains that explore satisfaction with the breast, effects of radiotherapy, physical, sexual and psychological well-being. Furthermore, the four domains analyze the satisfaction in relation to the information provided and the relationship with the surgeon and medical team/nurses/administrative staff. Each domain is divided into multiple questions, to which patients answer according to a numerical rating scale. Several clinical trials used the BREASTQ Modules for the assessment of patient satisfaction
17, 18after radical mastectomy or reconstructive surgery , while only a few apply this PROM to the evaluation of
16patients undergoing BCT. In particular, patients undergoing IORT have never been evaluated through
19the BREASTQ-BCT Module.
We designed a transversal observational study which, through individual administration of the BREASTQ-BCT Questionnaire and through retrospective collection of clinical and anamnestic data, aimed to evaluate the quality of life of breast cancer patients after BCS associated with IORT, at least one year after surgery. This cross-sectional study is, to the best of our knowledge, the first study which implements the use of BREASTQ-BCT Module for quality of life assessment in patients undergoing IORT.
MethodsStudy populationWomen aged 18-74 who underwent breast
conserving surgery plus IORT for an early-stage (T1-T2) breast cancer between 2011 and november 2017 were included in the study. Patients who developed distant metastases were excluded, as were women who underwent modified radical mastectomy for local recurrence of disease since BCT.
The patients subjected to IORT were identified through the computerized operating register (Ormaweb). Subsequently, through the company filing software (Opera), the telephone numbers, personal data and an amnestic data of the patients were recovered.
Enrollment of eligible patients took place by telephone contact. We scheduled dedicated outpatient visits to our center. After signing the informed consent and data protection module, the medical interviewer collected medical history information and administered the BREASTQ-BCT in paper format, which the patient completed independently. The questionnaire was anonymous.
Clinical pathological data were collected through consultation of electronic medical records and documents. Data were inserted in a de-identified Excel worksheet (Microsoft Excel version 97-2003). Permission to use the Italian version of the BREAST-Q BCT Module was obtained from the Mapi
20Research Trust Institute.BREASTQ-BCT module was developed for BCS
with external adjuvant radiotheraphy. Effects of radiotherapy domain included questions not applicable to intraoperative radiation therapy, so we modified the domain eliminating these questions.
Ethical approvalAll procedures performed in studies involving
human partecipants were in accordance with ethical standard of the institutional and/or national reserarch commettee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The Ethics Committee of Verona and Rovigo approved the study (Prot. n. 20876/2017). Informed consent was obtained from all individual participants included in the study.
Data AnalysisThe result from the BREASTQ-BCT postoperative
questionnaire was analysed according to the user instructions provided by the MAPI Research Trust. The resulting score for each domain was converted to a Q-score (range 0-100) by the use of a manual scoring table, as recommended by the MAPI Research Trust. The analyses were carried out using the Microsoft Excel/SPSS spreadsheet. We used descriptive statistic including mean and standard deviation and median/IQR for parametric and non parametric data, respectively. Univariate regression analysis was used
QOL after BC treatment
184 Caldana, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 183-188

available for other intercurrent medical conditions. In additon, 9 women had accepted to participate but did not come to the appointment. In total, 38 women completed the questionnaire and were included in the analyses.
The mean age at the time of study was 64.95 (SD= 5.04). The mean age at the time of surgery was 60.62 (SD=5.79). The mean body mass index (BMI) was 26.07 (SD=4.20). The mean time from breast cancer surgery to participation in the study was 56.66 months (SD=26.84). The mean tumor diameter, evaluated by definitive histological examination, was 11.32 mm (SD=5.15). The mean surgical pathology specimen weight was 103.87 gr (SD=69.46).
The scores for each BREASTQ-BCT Module domain are summarized in Table 1. The highest scoring domain were ‘satisfaction with members of
to identify clinicopathological variables associated with "satisfaction with breast" domain score. Statistical significance was assumed to be p<0.05.
After testing for normality, Spearman’s rho correlation coefficients were calculated between ‘Satisfaction with Breasts’ and all other domains. They were tested at a two-sided 5% significance level. The study was conducted after obtaining the approval of the Ethics Committee.
ResultsThere were 77 eligible women and they were
contacted by phone. Overall, 15 women were not contactable because the phone number was not registered in the databases or because they did not answer the call. Also, 13 women were not interested in participating in the study and 2 women were not
Table 1. Results of BREAST-Q BCT moduleQuestion Number of participants who
replied the question (n)Median (IQR)Mean (95% CI)
Satisfaction with breastsEffetcs of radiotherapyPsychosocial wellbeingSexual wellbeingPhysical wellbeingSatisfaction with informationInformation about IORTSatisfaction with surgeonSatisfaction with medical teamSatisfaction with other members of office staff
38383823383635383838
61.7 (57.2-66.1)86.3 (81.5-91.1)79.6 (73.8-85.3)63.3 (54.7-62.0)58.3 (59-73.7)
66.3 (51.6 -68.4)60 (51.6-68.4)
92.4 (88.4-96.4)94 (89.8-96.4)
93.8 (88.4-99.1)
59 (51-69.5)87 (78-100)80 (64-100)62 (48-76.5)61 (53-66)62 (58-80)59 (55-73)
100 (86-100)100 (100-100)100 (100-100)
Table 2. Univariate linear regression analyses of 'satisfaction with breasts' from the BREAST-Q BCT moduleVariable N p valueCoefficient (Standard Error)Constant (Standard Error)
Age, yearsAge at surgery, yearsBMI, Kg/M2Family history of BCTumor location on pre-op imagingUpper Outer QuadrantSuperior Sagittal planeUpper Inner QuadrantLower Outer QuadrantInferior Sagittal PlaneLower Inner QuadrantTumor diameter on pre-op imagingSurgeryAxillary surgeryRe-excision of marginsPatholog y size, mmWeight of specimen, gHistologyIDCILCOtherMixedDCIS componentLymph-vascular invasionAdjuvant CTTime from surgery, monthsPost-operative complications
72.4 (30.2)62.9 (24.6)43.0 (17.8)60.45 (3.3)63.0 (10.6)
57.7 (6.4)62.2 (2.4)
61.0 (5.8)53.0 (4.2)55.0 (10.3)
66.1 (3.5)63.1 (2.3)62.2 (2.61)64.2 (5.7)61.2 (2.5)
3838383839
3939
393939
3939383939
- 0.16 (0.46)- 0.02 (0.4)0.72 (0.67)3.2 (4.84)
- 0.9 (11.05)6.33 (13.63)- 0.17 (12.19)- 5.5 (12.93)- 13.5 (14.93)- 2.0 (18.29)0.37 (0.58)
- 14.22 (14.6)- 3.72 (10.47)0.07 (0.46)0.08 (0.03)
6.14 (10.62)/
7.86 (11.65)27 (17.79)
- 7.31 (4.62)- 22.06 (9.9)- 1.8 (6.08)
- 0.04 (0.08)3.82 (6.88)
0.7250.9600.2880.513
0.9350.6450.9890.6730.3730.9140.523
0.3370.7240.7510.029
0.567/
0.5040.1380.1230.0320.7690.6300.582
BC: Breast cancer, IDC: Infiltranting ductal carcinoma, I LC: Infiltranting lobular carcinoma, DCIS: Ductal carcinoma In Situ , CT: chemotherapy.
185Caldana, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 183-188
QOL after BC treatment

medical team’, ‘satisfaction with members of office staff’ and ‘satisfaction with breast surgeon’, all showing a median of 100 (IQR=100-100, 100-100 and 100-86). The lowest scoring domain were ‘satisfaction with IORT information’ and ‘satisfaction with breasts’, both with a median score of 59 (IQR=55-73 and 51-69.5). The median score for ‘Effects of radiotheraphy ‘ domain was 87 (IQT= 78-100).
In our study the weight of specimen and vascular invasion were risk factors for lower ‘satisfaction with breasts’ in univariate analysis (Table 2).
There was a statistically significant positive correlation between ‘satisfaction with Breasts’ and ’psychological wellbeing’, ‘sexual wellbeing’, ‘satisfaction with Information’, ‘satisfaction about IORT’ and ‘satisfaction with medical team’. Only ‘sexual wellbeing’ demonstrated a strong correlation. ‘psychological wellbeing’ and ‘Satisfaction with information’ demonstrated a moderate correlation. Other domains demonstrated a weak correlation (Table 3).
DiscussionBreast conserving therapy is the most commonly
performed treatment for early-stage breast cancer today. The long-term oncologic safety and efficacy of this approach have been well described. Measurement of Patient Related Outcome Measures (PROMs) is of vital importance in women undergoing breast surgery, and it is believed to be important for improving the process of care, focusing on the patient's perspective.
BREASTQ, a validated patient-reported outcome measure, has been used increasingly in aesthetic and
21recostructive surgery , and only recently has a breast
17conserving surgery-specific module been available.Therefore, only a few studies have addressed
Patient Related Outcome Measures (PROMs) 16, 22following BCT.
This was the first study to implement the use of BREASTQ-BCT Module for quality of life assessment in patients undergoing IORT. In our study ‘Satisfaction with Breasts’ showed one of the lowest scores, which is lower than that reported in the literature (Table 4).
Table 3. Correlation between different domains of the BREAST-Q questionnaireDomain 1 Domain 2 Statistical significance
(p value)Correlation coefficient
Satisfaction with breasts Effects of radiotherapyPsychosocial wellbeingSexual wellbeingPhysical wellbeingSatisfaction with informationInformation about IORTSatisfaction with surgeonSatisfaction with medical teamSatisfaction with other members of office staff
r = 0,20s
r = 0,54s
r = 0,73s
r = 0,11s
r = 0,58s
r = 0,36s
r = 0,21s
r = 0,32s
r = 0,14s
p = 0,22p= 0,00p= 0,05p= 0,50p= 0,00p = 0,02p= 0,19p= 0,05p= 0,38
Table 4. Comparison with data from the literature.Our studyMean (SD)
16O'ConnellMean (SD)
22VrouweMean (SD)
24LagendijkMean (SD)
25RoseMedian
23DahlbäckMedian
Satisfaction with breastsPsychosocial wellbeingSexual wellbeingPhysical wellbeing
61.7 (±14.2)79.6 (±18.3)63.3 (±24.9)58.3 (±11.6)
69 (±20)78 (±22)56 (±21)76 (±18)
59.3 (±21.1)73.5 (±21.2)53.3 (±19.5)74 (±19.1)
66826081
65.7 (±22.4)70.1 (±21.4)57.5 (±20.3)71.2 (±18.9)
74825878
BREAST-Q usually is used in conjunction with the pre-operative baseline questionnaire. Our study is retrospective, and without the pre-operative baseline questionnaire, changes in an individuals’ satisfaction and quality of life could not be identified. It is possible that a lower satisfaction score reflects a lower score already preoperatively. We must also note that several patients were operated on when there was not much attention paid on oncoplastic surgery, which may have impacted the results.
We saw low scores also in the field 'information about IORT'. The reason could be that, especially in the first years of experience, counseling with the radiotherapist was aimed more at evaluating the possible indication to intraoperative radiotherapy
rather than informing the patient about the side effects of intraoperative radiotherapy.
In our study, the lowest response rate was obtained for ‘sexual wellbeing’. Only 60.5% (23/38) of participants completed that domain of questionnaire. This lack of response has also been reported in other
16, 23studies. The low response rates may be due to feelings of unease, cultural taboo or perceived irrelevance of the domain.
The mean score of that domain, in our study, was 63.3 (SD=24.9). ‘sexual wellbeing’ scores are also quite low in other studies (Table 4). Further research into the scores for this domain in women who are not undergoing breast surgery is required to determine whether these results simply reflect the sexual
186 Caldana, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 183-188
QOL after BC treatment

wellbeing of women in the general population.Numerous studies have attempted to identify
variables that lead to a poor aesthetic outcome following breast conservation therapy. Variables such as age, race, body mass index, breast size, tumor location, tumor size, tumor palpability, resection volume, surgical technique, reexicision, scar visibility, delayed wound healing, seroma, hematoma, infection, axillary dissection, radiation technique and dose, chemotheraphy and hormone therapy have documented as predictors of aesthetic outcome
16, 22following breast conservation therapy.
In a recent study, which analyzed the initial experience of the BREASTQ-BCT Module in a group of 200 patients, the risk factors for low score at the univariate analysis were observed to be BMI at time of surgery, change in BMI since surgery, type of axillary surgery, nodal status, size of tumour on ultrasound (mm), weight of specimen (g) and delayed wound healing (> 30 days). BMI at the time of surgery, type of axillary surgery and delayed wound healing remained independent risk factors in
16multivariate analysis.We evaluated several clinicopathological chara-
cteristics; the only two that have been shown to be risk factors for lower ‘Satisfaction with breasts’ (p <0.05) in univariate analysis included weight of specimen and lymph-vascular invasion.
The significance of lymphovascular invasion may be justified because this item is more commonly found in larger tumours requiring wider excision. We observed that there was a weak positive correlation between tumor size and weight of specimen r= 0.34, p=0.06). However, our data did not show a correlation between tumor size and lymph-vascular invasion (r=0.02, p= 0.88).
There was a positive correlation between 'Satisfaction with the breasts' and some domains of BREAST-Q. The strongest correlations was with "psychosocial wellbeing" and "sexual wellbeing", which supports the importance of improving the care process, focusing on the patient's perspective and quality of life. The absence of a correlation with 'Effects of radiotherapy' in this IORT-group suggests the need to compare these results with a group undergoing external radiation therapy.
In conclusion, this is the first study to use the complete BREASTQ-BCT module in IORT setting. The domains of the questionnaire that obtained the lowest scores were ‘Satisfaction with IORT information’ and ‘Satisfaction with breasts’.
Weight of specimen and vascular invasion were risk factors for lower ‘satisfaction with breasts’ in univariate analysis. There was a moderate-strong correlation between 'satisfaction with the breasts' and ‘psychosocial wellbeing’ and ‘sexual wellbeing’.
An important limitation of this study is the small sample size; however, it may be interesting to continue with the collection of data and compare it
with an ‘external radiotherapy’ group to evaluate whether intraoperative irradiation involves a different aesthetic outcome and above all if it has an impact on the quality of life. It would be interesting to perform this comparison through a prospective study, so that the preoperative BREASTQ-BCT Module can also be used to compare it with the postoperative one.
Conflict of InterestThe authors declare that they have no conflict of
interest.
References1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre
LA, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394-424.
2. Fisher B, Redmond C, Poisson R, Margolese R, Wolmark N, et al. Eight-year results of a randomized clinical trial comparing total mastectomy and lumpectomy with or without irradiation in the treatment of breast cancer. New England Journal of Medicine. 1989;320(13): 822-8.
3. Veronesi U, Cascinelli N, Mariani L, Greco M, Saccozzi R, et al. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N Engl J Med. 2002;347(16):1227-32.
4. Treatment of Early-Stage Breast Cancer: NIH Consensus Statement Online. 1990;8:1-19. Available at: http://odp.od.nih.gov/ consensus/ cons/081/081_statement.htm. .
5. Correa C, Harris EE, Leonardi MC, Smith BD, Taghian AG, et al. Accelerated Partial Breast Irradiation: Executive summary for the update of an ASTRO Evidence-Based Consensus Statement. Pract Radiat Oncol. 2017;7(2):73-9.
6. Vaidya JS, Wenz F, Bulsara M, Tobias JS, Joseph DJ, et al. Risk-adapted targeted intraoperative radiotherapy versus whole-breast radiotherapy for breast cancer: 5-year results for local control and overall survival from the TARGIT-A randomised trial. Lancet. 2014;383(9917):603-13.
7. Veronesi U, Orecchia R, Maisonneuve P, Viale G, Rotmensz N, et al. Intraoperative radiotherapy versus external radiotherapy for early breast cancer (ELIOT): a randomised controlled equivalence trial. The lancet oncology. 2013;14(13):1269-77.
8. Harris EE, Small Jr W. Intraoperative radiotherapy for breast cancer. Frontiers in oncology. 2017;7:317.
9. Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015; 136(5):E359-86.
QOL after BC treatment
187Caldana, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 183-188

to Referral for Partial Breast Reconstruction. Plast Reconstr Surg. 2018;141(1):1-9.
23. Dahlbäck C, Ullmark JH, Rehn M, Ringberg A, Manjer J. Aesthetic result after breast-conserving therapy is associated with quality of life several years after treatment. Swedish women evaluated with BCCT. core and BREAST-Q™. Breast cancer research and treatment. 2017;164(3):679-87.
24. Lagendijk M, van Egdom L, van Veen F, Vos E, Mureau M, et al. Patient-reported outcome measures may add value in breast cancer surgery. Annals of surgical oncology. 2018;25(12):3563-71.
25. Rose M, Svensson H, Handler J, Hoyer U, Ringberg A, et al. Patient-reported outcome after oncoplastic breast surgery compared with conventional breast-conserving surgery in breast cancer. Breast Cancer Res Treat. 2020;180(1): 247-56.
10. Breast Cancer. Available at http://about-cancer.cancerresearchuk.org/about-cancer/ breast-cancer/survival.
11. Hopwood P, Haviland JS, Sumo G, Mills J, Bliss JM, et al. Comparison of patient-reported breast, arm, and shoulder symptoms and body image after radiotherapy for early breast cancer: 5-year follow-up in the randomised Standardisation of Breast Radiotherapy (START) trials. Lancet Oncol. 2010;11(3):231-40.
12. Corica T, Nowak AK, Saunders CM, Bulsara M, Taylor M, et al. Cosmesis and Breast-Related Quality of Life Outcomes After Intraoperative Radiation Therapy for Early Breast Cancer: A Substudy of the TARGIT-A Trial. Int J Radiat Oncol Biol Phys. 2016;96(1):55-64.
13.Javid SH, Lawrence SO, Lavallee DC. Prioritizing Patient-Reported Outcomes in Breast Cancer Surgery Quality Improvement. Breast J. 2017;23(2):127-37.
14. Pusic AL, Klassen AF, Scott AM, Klok JA, Cordeiro PG, et al. Development of a new patient-reported outcome measure for breast surgery: the BREAST-Q. Plast Reconstr Surg. 2009;124(2):345-53.
15. Vrouwe SQ, Somogyi RB, Snell L, McMillan C, Vesprini D, et al. Patient-reported outcomes following breast conservation therapy and barriers to referral for partial breast reconstruction. Plastic and Reconstructive Surgery. 2018;141(1):1-9.
16. O'Connell RL, DiMicco R, Khabra K, O'Flynn EA, deSouza N, et al. Initial experience of the BREAST-Q breast-conserving therapy module. Breast Cancer Res Treat. 2016;160(1):79-89.
17. Lagendijk M, van Egdom LSE, Richel C, van Leeuwen N, Verhoef C, et al. Patient reported outcome measures in breast cancer patients. Eur J Surg Oncol. 2018;44(7):963-8.
18. Retrouvey H, Kerrebijn I, Metcalfe KA, O’Neill AC, McCready DR, et al. Psychosocial Functioning in Women with Early Breast Cancer Treated with Breast Surgery With or Without Immediate Breast Reconstruction. Annals of surgical oncology. 2019;26(8):2444-51.
19. Acquadro C, Conway K, Giroudet C, Mear I. Linguistic validation manual for health outcome assessments: Mapi Institute; 2012.
20. Klassen AF, Pusic AL, Scott A, Klok J, Cano SJ. Satisfaction and quality of life in women who undergo breast surgery: a qualitative study. BMC women's health. 2009;9(1):11.
21. Cohen WA, Mundy LR, Ballard TN, Klassen A, Cano SJ, et al. The BREAST-Q in surgical research: a review of the literature 2009–2015. Journal of Plastic, Reconstructive & Aesthetic Surgery. 2016;69(2):149-62.
22. Vrouwe SQ, Somogyi RB, Snell L, McMillan C, Vesprini D, et al. Patient-Reported Outcomes following Breast Conservation Therapy and Barriers
188 Caldana, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 183-188
QOL after BC treatment

189
IntroductionCancer is the second leading cause of death after
heart disease as it continues to threaten the lives of 1, 2millions worldwide. In males, the most leading
cause of cancer death is lung cancer. However, in females, breast cancer is mostly the leading cause of
ARTICLE INFO
Background: Breast malignant growth is the most widely recognized disease in women in both highly and less developed nations where early detection is vital for life-saving and fast recovery. Recently, Photonic technologies has played a vital role in medical applications. Their satisfactory and viable implementation in therapy and diagnosis requires reliable information on the optical properties of human tissues. This study presents an outline of recent outcomes on the magnitude of breast tissue optical properties.
Methods: We established two different system setups utilizing hyperspectral (HS) camera and multiple excitation source lights with wavelength (380~1050 nm) for this investigation. The first setup (Transmission Mode) was applied for light transmission measurement of ex-vivo breast sample. Thereby, we made calculations of sample absorption. The second setup (Reflection Mode) was used for the measurement of breast sample light diffuse reflectance. The outcomes of both setups were used to select the optimum spectral image to differentiate between the normal and tumoral regions in the ex-vivo breast sample by exploring the optical properties spectroscopy in the Near and visible (NIR-VIS) spectrum. Finally, we applied the custom system on the case study technique for breast tumor detection.
Results: Experimental investigations results showed that due to the various excitation wavelength light source (380~1050 nm) generates variable depths of penetration depth in the ex-vivo breast sample. Consequently, experimental results of the diffuse reflectance (Ŗd) provide the optimum spectral image at 600 nm for the diagnostic applications. However, the statistical calculation of the normalized signal validated the outcome at wavelength 680 nm. Additionally, we noticed the optimum spectral image for therapy applications at 700 nm by measurement of breast tissue transmission (Ţ) and attenuation absorption (Ą) calculation. Moreover, the statistical calculation of the normalized signal validated the outcome at wavelength 760 nm.
Conclusions: The proposed novel approach successfully provided promising results of the investigated breast sample optical properties in both diagnostic and therapy applications to assist the pathologist and the surgeon. The trail outcomes of the investigated case study were impressive for selecting optimum wavelength for diagnostic and treatment (680, 760 nm), respectively.
Received:
07 October 2020Revised:
26 October 2020Accepted:
29 October 2020
Key words:Breast cancer,hyperspectral imaging system, tissue optical properties, breast diagnosis & therapy,optical spectroscopy
Address for correspondence: Mohamed Hisham Aref, MSc.Address: Building 3, Block No 7078, El-Mokattam,Cairo, EgyptPostal Code: 11571Tel:+2 01221997009 Email: [email protected]
ABSTRACT
Novel Approach Exploiting the Hyperspectral Imaging System for Breast Cancer Therapy and Diagnosis
a Biomedical Engineering Department, Military Technical College, Cairo, Egyptb System & Biomedical Engineering Department, Cairo University, Giza, Egypt
a a bMohamed Hisham Aref* , Ibrahim H. Aboughaleb , Abou-Bakr M. Youssef ,aYasser H. El-Sharkawy
Open AccessOriginal Article
Aref, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 189-201
DOI: 10.19187/abc.202073189-201

3mortality. Breast cancer is the most widely recognized malignant disease in women in both
3, 4highly and less developed nations. More than 8% of women will endure this disease during their
5lifetime. Breast cancer is a malignant tumor that is established from cells in the breast some times with
6no symptoms in early stages.
Breast cancer rate increases with age from the 3rd 7
to the 5th decade. Of all breast malignant growth, 90 to 95% cases are found through breast self-
8assessment. As indicated by the World Health Organization (WHO) in 2018, it is evaluated that 627,000 women died from breast malignant growth, which is roughly 15% of all malignant deaths among
9women.Numerous common imaging techniques can be
utilized for breast malignant growth analysis such as 10, 11 7, 12X-ray Mammograms, Breast Ultrasound , and
13, 14Breast MRI. However, it is strengthened by several components such as the Contrast to Noise
15Ratio , spatial resolution, and Signal to Noise Ratio 16
of each device.The regular imaging technique for breast
screening and examinations in various countries is 17x-ray mammography. However, its sensitivity is
~74% and is reduced down to ~50% in dense breast, 18
beside manipulating x-ray radiation dosages while Breast MRI provides high sensitivity but its specificity is relatively poor. Additionally, it is characterized by being costly and long examination
19, 20time.
Currently, biopsy is the best technique for tumor identification, which incorporates the resection of tissue from the breast lesions which is then analyzed
21by a pathologist. However, it is expensive, tedious (staining, slicing, and microscopic examination) and requires exceptionally prepared specialists and
22pathologists.Whole tumor resection is challenging as a result
of the absence of perfect intraoperative tumor margin 23
imaging systems. Thus, in up to 37% of female patients encountering breast conserving surgery procedure, the tumor exists in the resection margins
24, 25of the resected specimen. This increases the risks
26of tumor recurrence and long recovery endurance. Now, a pathologist, who examins the tissue under an advanced microscope, assesses the resection margins a few days after a surgery. In this manner, there are few prompt analysis can give direct
27information to the specialist in real-time surgery.Lately, numerous scientists have set up various
methods for resection margins evaluation during breast-conserving surgery (frozen section analysis, ultrasound, imprint cytology, and sample radiography) to decrease the amount of tumor-
28-30positive resection margins. On the other hand, none of these techniques have been available and effective for clinical use. The “frozen setion analysis” could be done within ~30 mins, with a
sensitivity and specificity of 83% and 95%, 28
respectively.The main drawbacks of the technique involves
the necessity for a particular pathologist, risk of false negatives (FN), and the impracticability of
29, 30examining the entire surface of resection margins In the imprint cytology technique diagnose could be established within ~15 mins, with a sensitivity and specificity of 72% and 97%, respectively. The information elucidation errors, sample surface irregularity, and dryness are the drawbacks of this
28technique.
Hyperspectral imaging (HSI) is also called imaging spectroscopy, which reveals the novelty that integrates typical imaging and spectroscopy modalities to secure both spatial and spectral data of
31, 32an item. Imaging spectroscopy has been accessible as a far off detecting innovation since the
3 31960s. Several studies discussed the HSI
34capabilities in distinguishing red meats quality , and its relevance in excellence and safety inspections of
35the grains and nuts. Moreover, utilizing HSI in the near-infra red (NIR) wavelengths in agriculture and
36food crops has produced superior results.
Furthermore, for the medical applications exploiting HSI, subsequent studies revealed the eff iciency of HSI in non-invasive t issue
37examinations , in the tumor detection in ex-vivo 38
samples of head and neck for human being tissues , the usage of HSI with non-contact endoscopic system
39 40to detect colorectal cancer , detection of skin cancer ,
27, 40and breast tissue.
A study was conducted to highlight the unique properties of HSI in radiofrequency ablation
41(RFA). Aref et al. showed that HSI could be a powerful tool in distinguishing thermal ablation of 10 samples of the ex-vivo bovine liver due to the variations of the optical properties, with the trials
41showing an ideal spectral image (720±18.92 nm).
Moreover, the HSI system was exploited to determine malignant growth in the ex-vivo breast samples. The outcomes of the segmented spectral regions (420~620 nm) were efficient to distinguish the cancerous region from the normal tissue with 95%,and 96% sensitivity, and specificity,
42 respectively. Additionally, the HSI system was exploited for breast cancer detection over broadband spectral range (400~1650 nm) with two different classifier algorithms providing high sensitivity and
27specificity.The breast tissue interacts with light according to
its optical properties (type/size/density/color) to provide several mechanisms such as transmission,
43, 44absorption, and diffuse reflectance. The main concern in this experiment was measuring the sample transmission to calculate the absorption to identify and characterize the breast samples regarding its spectral signature, as illustrated in Figure 1.
Hyperspectral imaging system in BC
190 Aref, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 189-201

MethodsThe main protocol used in this study is as follows:• Sample investigation and tissue characterization.• HS image for the ex-vivo breast sample.• Measuring sample transmission transmission.• Calculation of the sample absorption from the measured transmission.• Measuring for sample diffuse reflection.• Selection of the optimum wavelength for therapy.• Selection of the spectral image to differentiate between the tumor and normal regions in the diagnostic applications. (Table 1)
In the proposed approach, we established a system that could provide promising outcomes regarding breast sample optical properties in both diagnostic and therapy applications. After exploring breast tissue optical properties (Transmission, absorption, and diffuse reflection), we could select the optimum wavelength for breast tissue therapy and diagnostic applications to assist the pathologist during the tissue investigation and reduce the time of examination and the surgeon during the breast biopsy and mastectomy process.
Figure 1. The light interaction (absorption / diffuse reflection / reflectance) of ex-vivo breast tissue sample highlighting the substitution of the breast tissue cells
Table 1. Patient’s charachterictics
Patient ID Age(years)
aBreast structure bTumor size cGrade
1
2
3
4
5
6
7
8
9
10
52
49
55
44
46
50
53
56
58
60
Extremely dense
Scattered dense
Heterogeneouslydense
Mostly fatty
Scattered dense
Heterogeneouslydense
Heterogeneously dense
Heterogeneously dense
Heterogeneously dense
Extremely dense
Stage 1 (<2cm)
Stage 2 (<4cm)
Stage 2 (<4cm)
Stage 2 (<4cm)
Stage 3 (>4cm but confined to the breast)
Stage 3 (>4cm but confined to the breast)
Stage 1 (<2cm)
Stage 3 (>4cm but confined to the breast)
Stage 2 (<4cm)
Stage 2 (<4cm)
Grade I
Grade I
Grade II
Grade II
Grade I
Grade II
Grade I
Grade II
Grade II
Grade I
a Breast Structure Type: Mostly fatty; Scattered density; Heterogeneously density; Extreme densityb Tumor Stage: Stage 1 – A breast tumor is smaller than 2 centimeters in diameter and the cancer has not spread beyond the breast; Stage 2 – A breast tumor measures 2 to 4 centimeters in diameter or cancerous cells have spread to the lymph nodes in the underarm area; Stage 3 – More widespread cancer is found; however, it is confined to the breast, surrounding tissues.c Tumor Grade: Grade I - Well differentiated; Grade II - Moderately differentiated
Hyperspectral imaging system in BC
191Aref, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 189-201

The main framework of the proposed system is subdivided into two individual setups utilizing hyperspectral HS camera. Both setups exploited polychromatic source light with wavelength (380~1050 nm). The first setup (Transmission Mode) was applied for light transmission measurement of the ex-vivo breast sample. Thereby, calculations of sample absorption, as displayed in Figure 2-a. Second setup (Reflection
Mode) were exploited for the measurement of breast sample light diffuse reflectance, as illustrated in figure 2-b.The results for the two setups were used to determine the opt imum wavelength to differentiate between the normal and tumor regions in the ex-vivo breast samples using the optical properties spectroscopy in the Near and visible (NIR-VIS) spectrum.
Figure 2. (a) System setup#1 (Transmission Mode - Ţ) Measuring the optical properties (Transmission and absorption) of the ex-vivo breast sample,(1) The HS camera used (Surface Optics,SOC710, USA) , (2) Polychromatic source light
(Derungs, 150 W, 400~1000 nm,Germany), (3) The investigated ex-vivo breast sample , (4) Computer and image processing software (b) system setup#2 (Reflection Mode - Ŗd) Measuring the optical properties (Diffuse Reflection)
of the ex-vivo Breast Sample, (c) Acquired RGB images for some of the ex-vivo breast samples in the experiments
Pathology examination and sample slicing for malignancyBefore the experimental investigation, the
procedure validation was achieved from Ain Shams University - Ethics Committee. Overall, 10 patients who with breast cancer who had been underwent mastectomy were selected. Subsequently, after
careful examination and evaluation, the breast tumor samples were selected from arbitrary patients.
The investigated ex-vivo breast samples were crudely cut into slices with approximate sizes (2.5×3 cm), sample thickness 4~6 mm, then transported in icebox full of deionized saline. The samples were approximately (2.5×3 cm) slices at lab temperature
Hyperspectral imaging system in BC
192 Aref, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 189-201
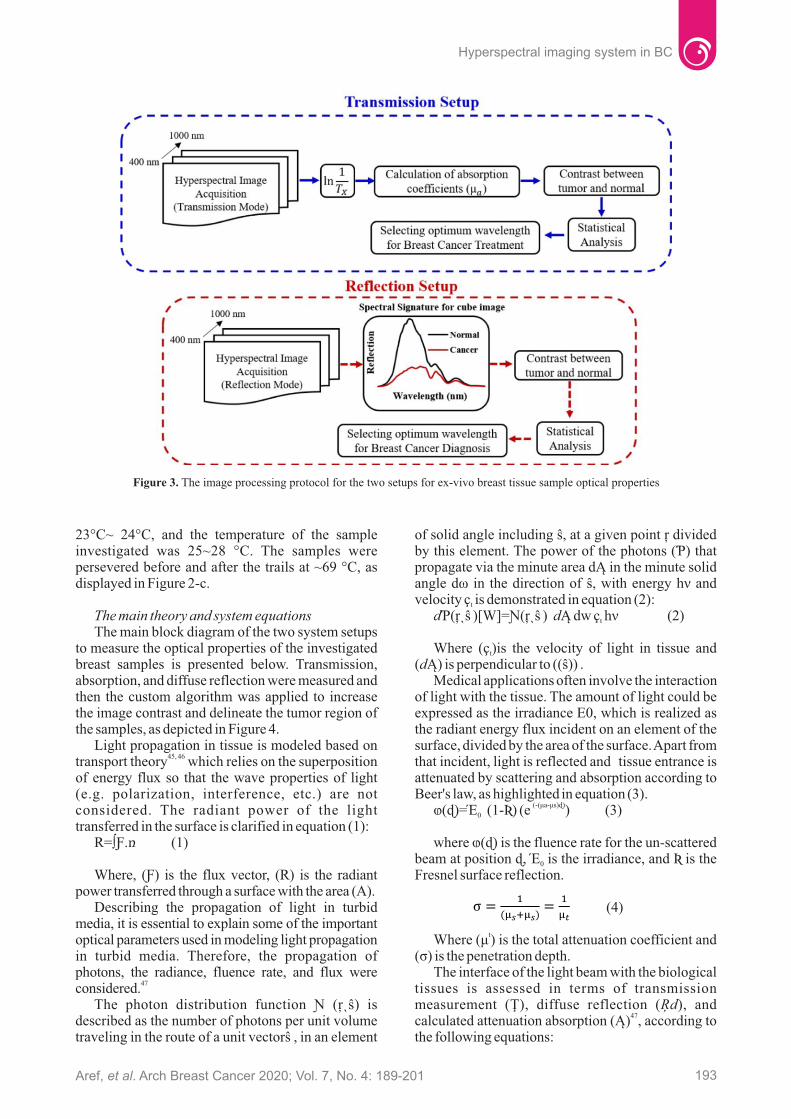
23°C~ 24°C, and the temperature of the sample investigated was 25~28 °C. The samples were persevered before and after the trails at ~69 °C, as displayed in Figure 2-c.
The main theory and system equationsThe main block diagram of the two system setups
to measure the optical properties of the investigated breast samples is presented below. Transmission, absorption, and diffuse reflection were measured and then the custom algorithm was applied to increase the image contrast and delineate the tumor region of the samples, as depicted in Figure 4.
Light propagation in tissue is modeled based on 45, 46
transport theory which relies on the superposition of energy flux so that the wave properties of light (e.g. polarization, interference, etc.) are not considered. The radiant power of the light transferred in the surface is clarified in equation (1):
R=∫Ƒ.ռ (1)
Where, (Ƒ) is the flux vector, (R) is the radiant power transferred through a surface with the area (A).
Describing the propagation of light in turbid media, it is essential to explain some of the important optical parameters used in modeling light propagation in turbid media. Therefore, the propagation of photons, the radiance, fluence rate, and flux were
47considered.The photon distribution function Ɲ (ŗˎŝ) is
described as the number of photons per unit volume traveling in the route of a unit vectorŝ , in an element
of solid angle including ŝ, at a given point ŗ divided by this element. The power of the photons (Ƥ) that propagate via the minute area dĄ in the minute solid angle dω in the direction of ŝ, with energy հν and velocity ç is demonstrated in equation (2):t
dƤ(ŗˎŝ )[W]=Ɲ(ŗˎŝ ) dĄ dᴡ ç հν (2)t
Where (ç )is the velocity of light in tissue and t
(dĄ) is perpendicular to ((ŝ)) .Medical applications often involve the interaction
of light with the tissue. The amount of light could be expressed as the irradiance E0, which is realized as the radiant energy flux incident on an element of the surface, divided by the area of the surface. Apart from that incident, light is reflected and tissue entrance is attenuated by scattering and absorption according to Beer's law, as highlighted in equation (3).
(-(μa-μs)ɖ)ⱷ(ɖ)=Έ (1-Ʀ) (e ) (3)0
where ⱷ(ɖ) is the fluence rate for the un-scattered beam at position ɖ, Έ is the irradiance, and Ʀ is the 0
Fresnel surface reflection.
(4)
tWhere (μ ) is the total attenuation coefficient and (σ) is the penetration depth.
The interface of the light beam with the biological tissues is assessed in terms of transmission measurement (Ţ), diffuse reflection (Ŗd), and
47calculated attenuation absorption (Ą) , according to the following equations:
Figure 3. The image processing protocol for the two setups for ex-vivo breast tissue sample optical properties
193Aref, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 189-201
Hyperspectral imaging system in BC

(5)
(6)
Where and are the light intensities measured by diffuse reflectance/transmittance with the breast sample and the standard reflecting optical white plate, respectively. The exemplifies the background light intensity distinguished by reflectance/transmittance without a sample on the reflecting plate.
Spectral planning and ProcurementTo capture the necessary HSI data, we used HS
camera (Surface Optics, SOC710, USA) with spectral resolution 3.1 nm equivalent to 600 × 502 pixels for the spectral group (HS Cube captured in 3.65 sec). The HSI was comprised of overall 128 spectral groups in range 379~1050 nm, incorporated with a lens with range (400~1000 nm). The camera was used with a lens (Schneider,400~1000 nm, Germany). The light assembly for the HS image scan was used with polychromatic source light (150 W, 400~1000 nm).
Several scanned images for investigating the sample were acquired, and then statistical analysis
was done for the spectral signature to select the ideal spectral image, followed by the custom algorithm.
A basic advancement in HSI imaging, before image procurement, is a level field correction for data standardization. A white equalization and dim current measurements were utilized to gain relative
48reflectance from the sample. The dark cube was captured by closing the HS camera lens with its cap to avoid any light getting into the sensor. Information from a dark image and white balance estimations were utilized to correct the deliberate material image. The fundamental reason for this amendment was to wipe out artifacts and noise impacts on the sample tissue, as clarified in equation (7):
(7)
Where RF(ϑ)is the relative reflectance of the object image, Im(ϑ) is the captured image, Id(ϑ) is the dark acquired image with the lens shut with the cap, and Iw(ϑ) is the acquired image of the whiteboard.
We applied normalization on the captured image to remove the unwanted spectral impact from the polychromatic light. The original captured images vary depending on the light, the irregular shape of the sample, and temperature variations, so spectral images ought to be normalized including pixel normalization, as demonstrated in equation (8).
(8
(10)
Where the Area of Histogram is ( ), the class width is ( ), and the frequency density is ( ).
ResultsIn this section, we illustrate the fundamental
investigation outcomes. The primary objective of these examinations is to highlight the system capability to discriminate between the normal and malignant tumor regions of the investigated ex-vivo breast samples utilizing the biological tissues optical properties.
We established two different system setups utilizing hyperspectral (HS) camera and various excitation source light with wavelength (380~1050 nm) for this investigation. The first setup involved light transmission (Ţ) measurement of ex-vivo breast sample to provide the necessary data for breast tumor therapy. The second setup involved the measurement of breast sample light diffuse reflectance (Ŗ ), which provided d
the crucial information for breast tumor detection.The outcomes of the two setups were used to
select the optimum wavelength which could differentiate between the normal and cancer specific regions in the investigated breast sample by exploring the optical properties spectroscopy in the
Although, normalization alters an m-dimensional grayscale previous image
I :{A} with intensity assessments in the previous
range minimum (min ) to maximum (max ) previous previous
into a new image I :{A} with intensity values in the range new
minimum (min ) to maximum (max ).new new
Next, applying the moving average filter, the arithmetic means filter at kernel value 10 for noise
49reduction and image enhancement, we have:
(9)
Where ‘S’ is the noisy image, f(X×Y) is the restored image, and “ ŕ ” and “ c “ for the row and column coordinates respectively, within a window ‘W’ of size ‘ ’ where the process takes place.
A histogram is comparable in appearance to a bar graph and it is a graphical display of information that arranges a lot of information to visualize/count the quantity of events of information (frequency) over units of discrete intervals, named buckets or bins. Basically, the equation for histogram circumvents the territory of the bars and it is assessed using the summation of the result of the class interval's width and comparing frequency thickness of each class, as explained in equation (10):
Hyperspectral imaging system in BC
194 Aref, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 189-201

Near and visible (NIR-VIS) spectrum.The raw data displayed in figure 4-a, b, and c show
the typical spectral values over the selected taken points on the malignant and normal regions. However, the raw data was normalized to neglect the variation of the intensity and focusing on the spectral change to display the spectroscopic point measurements, as
demonstrated in figure 4-c, d, and e.Regarding the first setup (Transmission Mode)
for light transmission (Ţ) measurement of ex-vivo breast sample, we acquired 7-spectral images (400~1000 nm) with resolution 100 nm regarding the 128-frames to reduce the time consumption of image processing, as displayed in figure 5.
Figure 4. (a) The Diffuse reflectance (Ŗ) measurements of both the normal (black line) and cancer (red line) ex-vivo breast sample over the whole spectrum range; (b) The Transmission (Ţ) measurements of both the normal (black line) and cancer (red line) ex-vivo breast samples over the whole spectrum range, (c) The Absorption (Ã) Calculations of both the
normal (black line) and cancer (red line) ex-vivo breast samples over the whole spectrum range, (d) The Diffuse reflectance (Ŗ) measurements after applying normalization to the raw data to neglect the intensity effect and focus on the wavelength
differentiation; (e) The Transmission (Ţ) measurements after applying normalization to the raw data to neglect the intensity effect and focus on the wavelength differentiation; (f) The Absorption (Ã) Calculations after applying normalization to the
raw data to neglect the intensity effect and focus on the wavelength differentiation.
Figure 5. The Multiple Excitation Wavelength Light Source (380~1050 nm) generates Variable Transmitted Light through the ex-vivo Breast Sample,(a) Breast Sample at 400 nm,(b) Breast Sample at 500 nm,(c) Breast Sample at 600 nm, (d) Breast Sample at 700 nm, (e) Breast Sample at 800 nm, (f) Breast Sample at 900, (g) Breast Sample at 1000 nm, (h) Conceded Image for the 7
wavelengths,(i) Conceded Image for the Image enhancement applying normalization and moving average filter (K=10) at scanned spectral images from (400 nm) to (1000 nm) with resolution 100 nm.
195Aref, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 189-201
Hyperspectral imaging system in BC

The Conceded Image of the scanned spectral images (400~1000 nm) with resolution 100 nm were used af ter applying image enhancement , normalization and moving average filter (K=10) to differentiate between the malignant and normal tissue at variable Transmitted (Ţ) Light through the ex-vivo Breast Sample as compared with the data from figure 45-b and figure 4-e as the spectral signature guidance to select the distinct spectral image, as presented in figure 6-a.
The Conceded Image of the attenuation absorption (Ą) to the spectral images (400~1000 nm) with resolution 100 nm was used after applying image enhancement, normalization, and moving average filter (K=10) to differentiate between the malignant and normal of ex-vivo Breast Sample as compared with the data from figure 4-c and figure 4-f as the spectral signature guidance to select the distinct spectral image, as exhibited in figure 6-b.
The second setup (Reflection Mode) was used for the measurement of breast sample light diffuse reflectance (Ŗd), as illustrated previously in figure 2-b. The experiment spectral signature demonstrated that the lowest measured diffuse reflection (Ŗd) at wavelength 400 nm and the highest at wavelength 560 nm could highly discriminate between the normal tissue and the malignant region, as can be seen in figure 7.
The Conceded Image of the sample light diffuse reflectance (Ŗd) at spectral images (400~1000 nm) with resolution 100 nm was used after applying image enhancement, normalization, and moving average filter (K=10) to remove the background noise to differentiate between the malignant and normal of ex-vivo Breast Sample as compared with the spectral signature in figure 4-a and figure 4-d, as displayed in figure 8.
Figure 6. (a) The Conceded Image after Image enhancement for Variable Transmitted Light through the ex-vivo Breast Sample applying normalization and moving average filter (K=10) at scanned spectral images from (400 nm)
to (1000 nm) with resolution 100 nm to differentiate between the malignant and normal tissue; (b) The Calculated Absorption Coefficient (Ą) from Variable Transmitted Light through the ex-vivo Breast Tissue
under investigation at scanned spectral images from (400 nm) to (1000 nm) with resolution 100 nm to differentiate between the malignant and normal
Hyperspectral imaging system in BC
196 Aref, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 189-201

Figure 7. The measured diffuse reflectance (Ŗd) of the breast sample, (a) Breast Sample at 400 nm,(b) Breast Sample at 500 nm,(c) Breast Sample at 600 nm, (d) Breast Sample at 700 nm, (e) Breast Sample at 800 nm, (f) Breast Sample at 900,
(g) Breast Sample at 1000 nm, (h) Conceded Image for the 7 spectral images,(i) Conceded Image after the Image Enhancement applying normalization and moving average filter (K=10) at scanned spectral images from (400 nm) to
(1000 nm) with resolution 100 nm.
Figure 8. Conceded Image for the measured diffuse reflectance of the breast sample after Image Enhancement applying normalization and moving average filter (K=10) at scanned spectral images from
(400 nm) to (1000 nm) with resolution 100 nm.
From figure 7 and 8, we could select the optimum spectral image by measured light diffuse reflectance (Ŗd), which had enough contrast to discriminate between the normal tissue and the malignant region which was at wavelength 600 nm. However, the results from the spectral signature in figure 4-a and
figure 4-d at wavelength 560 nm validated the outcome.
The HS image at wavelength (400 nm) represented the DC image which could not discriminate between the normal and the tumor regions, as shown in figure 9-a. The ideal HS image
197Aref, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 189-201
Hyperspectral imaging system in BC

was at wavelength (600 nm) applied for ideal distinction between the normal and the tumor regions, as verified and calculated previously and displayed in figure 9-b. The subtracted image at figure 9-c is considered to be the ideal information for the specialized which could be used to identify the normal region (highly illuminated in the left) and the tumor regions (the more darker regions).
Finally, figure 9-d illustrates the contour mapping of the variable regions of the malignant breast which could be delineated according to the variable threshold value.
DiscussionCancer is the second leading cause of death after
heart disease as it continues to threaten the lives of 1, 2millions worldwide. Breast malignant growth is
one of the most broadly perceived dangerous tumors in the world and the primary source of death among
3women. There is an expanding interest in improving breast cancer identification techniques using clinical imaging instruments because effective treatment of breast cancer relies upon its correct and early
24diagnosis. Fundamentally, we can recognize early
50tumors before the tumor metastasizes.We investigated the optical properties of the breast
tissue utilizing the capability of the hyperspectral camera in the (NIR-VIS) spectrum. A set of spectrum images among (400~1000 nm) from recently excised breast tissues were investigated using two
approaches: (1) (Transmission Mode) was applied for light transmission (Ţ) measurement and (2) (Reflection Mode) used for measurement of breast sample light diffuse reflectance (Ŗd). The outcomes of both methods were used to select the optimum wavelength to differentiate between the normal and tumor regions in the ex-vivo breast sample by exploring the optical properties spectroscopy in the (NIR-VIS) spectrum, as demonstrated in figure 4.
The raw data displayed in the graph of figure 4-a,b, and c showed the typical spectral values over the selected taken points on the malignant and normal regions. However, the raw data was normalized to neglect the variation of the intensity and focusing on the spectral change to display the spectroscopic point measurements, as demonstrated in figure 4-c, d, and e
Figure 5 shows the first setup (Transmission Mode) for light transmission (Ţ) measurement of ex-vivo breast sample. We acquired 7-spectral images (400~1000 nm) with resolution 100 nm regarding the 128-frames to reduce the time of image processing. We noticed that the optimum spectral image was highly contrasted at wavelength 700 nm for light transmission (Ţ) measurement and verified in the attenuation absorption (Ą) as shown in figure 6-b. However, the results of the statistical analysis regarding the raw data signal in figure 4- c indicate the optimum wavelength at 600 nm, although the normalized data from Figure 4-f was more clearly identified in wavelength 760 nm, as illustrated in table 2.
Figure 9. The ex-vivo breast Investigated Sample, (a) The HS Image of the breast sample at 400 nm , (b) The HS Image of the breast sample at 600 nm, (c) The subtracted Image between the (400 nm and 600 nm) to remove the DC background noise,
(d) The Contour Mapping of the variable threshold regions of the tumors in the breast sample.
Hyperspectral imaging system in BC
198 Aref, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 189-201

Figure 7 and Figure 8 displaying the acquired images regarding the second setup (Reflection Mode) to measure the Diffuse reflectance (Ŗd) measurements which emphasize the differentiation between the normal tissue and cancer region at wavelength 600 nm. Additionally, the statistical analysis of the raw data from figure 4-a show high contrast at wavelength 560 nm and after normalization it was more identified at 680 nm, as can be seen in table 3.
After selecting the optimum wavelength to differentiate between the normal and malignant tissue of the breast samples in the diagnostic applications by measuring the light diffuse reflection (Ŗd) at wavelength 600 nm, we removed the ground noise by spectral subtraction of spectral image at 400 nm to increase the contrast image, as shown in figure 9-c. Finally, figure 9-d illustrates the contour mapping of the variable regions of the breast malignant which could be used to delineate the cancerous regions in with variable threshold.
In conclusion, the results of this prospective approach revealed the HSI capability to be a feasible method to differentiate between the normal tissue and breast tumor, by providing vital information on the measurements of breast tissue optical properties in both the diagnostic and therapy applications. The experimental results by measurement of the diffuse reflectance (Ŗd) showed the optimum spectral image at 600 nm for the diagnostic applications. However, the statistical calculation of the normalized signal validated the outcome at wavelength 680 nm. Additionally, the optimum spectral image was obtained at 700 nm for the therapy applications by the measurement of breast tissue transmission (Ţ) and absorption (Ą) calculation. Moreover, the statistical calculation of the normalized signal validated the outcome at wavelength 760 nm. In future work, we will update the system hardware such as the HS camera and increase the source light wavelength range. Additionally, we will use a Q-
switched pulsed laser at a custom optical system (760 nm) for breast tumor ablation without normal tissue damage.
Conflicts of interestThe authors declare no conflict or competing
interests.
Ethics approvalAll experimental and investigation trails were
approved and validated by “Ain Shams University” Medical College Ethics Committee.
References1. Murphy SL, Xu J, Kochanek KD. National vital
statistics reports. National vital statistics reports. 2013;61(4).
2. Heron MP. Statistics, National Vital Statistics Reports Deaths: leading causes for 2017. 2019.
3. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394-424.
4. DeSantis CE, Miller KD, Dale W, Mohile SG, Cohen HJ, et al. Cancer statistics for adults aged 85 years and older, 2019. CA Cancer J Clin. 2019;69(6):452-67.
5. Cheng H-D, Shan J, Ju W, Guo Y, Zhang L. Automated breast cancer detection and classification using ultrasound images: A survey. Pattern recognition. 2010;43(1):299-317.
6. Saravanan D, Joseph D, Vaithyasubramanian S. Effective Utilization of Image Information Using Data Mining Technique. Recent Trends and Advances in Artificial Intelligence and Internet of Things: Springer; 2020. p. 207-15.
7. Brem RF, Lenihan MJ, Lieberman J, Torrente J. Screening breast ultrasound: past, present, and future. American Journal of Roentgenology. 2015;204(2):234-40.
Table 2. The Measurement of Breast tissue transmission (Ţ) to highlight the highest contrast between the normal and cancer regions over the spectrum range.
Table 3. The measured diffuse reflectance (Ŗd) of the ex-vivo breast sample of the breast tissue to highlight the highest contrast between the normal and cancer tissue at the various spectrum range
4009.38.00.954.495
40040.223.311.95
0
44012.68.42.9812.73
440174.280.166.504.243
48025.09.4
11.0422.63
480695.3270.8300.1312.02
52051.610.529.033.54
5201777.9466.9927.0319.09
56082.612.249.782.83
5602334.9607.2
1221.6325.46
60089.612.654.423.54
6002420.5727.1
1197.362.12
64083.512.350.310.71
6401933.9745.8840.0837.48
68066.712.538.3542.43
6801236.6711.9
370.9579.903
72059.012.033.2342.43
720783.6372.5290.7030.406
76049.911.8
26.9769.31
760729.8499.8162.6365.56
80036.411.0
17.9655.15
800570.4383.2132.3426.16
84028.010.112.6741.01
840241.0175.146.6322.63
88026.69.6
12.0525.46
880311.6221.663.6728.99
92018.78.96.9518.38
920144.3100.231.1828.99
Wavelength (nm)Breast tissue transmission (Ţ)Cancer tissue transmission (Ţ)Standard Deviation (Şd)(Şd) after Normalization
Wavelength (nm)Breast tissue reflection (Ŗd)Cancer tissue reflection (Ŗd)Standard Deviation (Şd)(Şd) after Normalization
199Aref, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 189-201
Hyperspectral imaging system in BC

8. Team TACSmaec. Breast Cancer Early Detection and Diagnosis 2019 [Available from: https:// www.cancer.org /cancer /breas t -cancer / screening- tests-and-early-detection/american-cancer-society-recommendations-for-the-early-detection-of-breast-cancer.html.
9. International Agency for Research on Cancer (IARC). Latest global cancer data: Cancer burden rises to 18.1 million new cases and 9.6 million cancer deaths in 2018. [Available from: www.who.int › cancer › PRGlobocanFinal.pdf.
10. Boyd NF, Martin LJ, Yaffe MJ, Minkin S. Mammographic density and breast cancer risk: current understanding and future prospects. Breast Cancer Res. 2011;13(6):223.
11. Gøtzsche PC, Jørgensen KJ. Screening for breast cancer with mammography. Cochrane database of systematic reviews. 2013(6).
12. Kelly KM, Dean J, Comulada WS, Lee S-J. Breast cancer detection using automated whole breast ultrasound and mammography in radiographically dense breasts. European radiology. 2010;20(3):734-42.
13. Hambly NM, Liberman L, Dershaw DD, Brennan S, Morris EA. Background parenchymal enhancement on baseline screening breast MRI: impact on biopsy rate and short-interval follow-up. AJR Am J Roentgenol. 2011;196(1):218-24.
14. Brennan S, Liberman L, Dershaw DD, Morris E. Breast MRI screening of women with a personal history of breast cancer. AJR Am J Roentgenol. 2010;195(2):510-6.
15. Mehnati P, Tirtash MJ. Comparative Efficacy of Four Imaging Instruments for Breast Cancer Screen ing . As ian Pac J Cancer Prev. 2015;16(15):6177-86.
16. Gutierrez RM, Cerquera E, Mañana G. MPGD for breast cancer prevention: a high resolution and low dose radiation medical imaging. Journal of Instrumentation. 2012;7(07):C07007.
17. Grosenick D, Rinneberg H, Cubeddu R, Taroni P. Review of optical breast imaging and spectroscopy. J Biomed Opt. 2016;21(9):091311.
18. Pisano ED, Gatsonis C, Hendrick E, Yaffe M, Baum JK, et al. Diagnostic performance of digital versus film mammography for breast-cancer screening. N Engl J Med. 2005;353(17): 1773-83.
19. Hylton N. Magnetic resonance imaging of the breast: opportunities to improve breast cancer management. J Clin Oncol. 2005;23(8):1678-84.
20. Lord S, Lei W, Craft P, Cawson J, Morris I, et al. A systematic review of the effectiveness of magnetic resonance imaging (MRI) as an addition to mammography and ultrasound in screening young women at high risk of breast cancer. European journal of cancer. 2007;43(13): 1905-17.
21. Your Guide to the Breast Cancer Pathology
Report 2014 [Available from: ht tps: / / www.breastcancer.org/cms_files/47/Breastcancerorg_Pathology_Report_Guide_2014.pdf.
22. Sahu A. Hyperspectral Imaging to Discern Malignant and Benign Canine Mammary Tumors: Temple University; 2012.
23. Ouyang Y, Tsui P-H, Wu S, Wu W, Zhou Z. Classification of Benign and Malignant Breast Tumors Using H-Scan Ultrasound Imaging. Diagnostics. 2019;9(4):182.
24. Alrahbi S, Chan PM, Ho BC, Seah MD, Chen JJ, e t a l . Extent of margin involvement , lymphovascular invasion, and extensive intraductal component predict for residual disease after wide local excision for breast cancer. Clinical Breast Cancer. 2015;15(3):219-26.
25. Merrill AL, Coopey SB, Tang R, McEvoy MP, Specht MC, et al. Implications of New Lumpectomy Margin Guidelines for Breast-Conserving Surgery: Changes in Reexcision Rates and Predicted Rates of Residual Tumor. Ann Surg Oncol. 2016;23(3):729-34.
26. Vos EL, Jager A, Verhoef C, Voogd AC, Koppert LB. Overall survival in patients with a re-excision following breast conserving surgery compared to those without in a large population-based cohort. European journal of cancer. 2015;51(3):282-91.
27. Kho E, Dashtbozorg B, De Boer LL, Van de Vijver KK, Sterenborg HJ, et al. Broadband hyperspectral imaging for breast tumor detection using spectral and spatial information. Biomedical optics express. 2019;10(9):4496-515.
28. Esbona K, Li Z, Wilke LG. Intraoperative imprint cytology and frozen section pathology for margin assessment in breast conservation surgery: a systematic review. Annals of surgical oncology. 2012;19(10):3236-45.
29. Keating JJ, Fisher C, Batiste R, Singhal S. Advances in intraoperative margin assessment for breast cancer. Current Surgery Reports. 2016;4(4):15.
30. St John ER, Al-Khudairi R, Ashrafian H, Athanasiou T, Takats Z, et al. Diagnostic Accuracy of Intraoperative Techniques for Margin Assessment in Breast Cancer Surgery: A Meta-analysis. Ann Surg. 2017;265(2):300-10.
31. Adão T, Hruška J, Pádua L, Bessa J, Peres E, et al. Hyperspectral imaging: A review on UAV-based sensors, data processing and applications for agriculture and forestry. Remote Sensing. 2017;9(11):1110.
32. Bioucas-Dias JM, Plaza A, Camps-Valls G, Scheunders P, Nasrabadi N, et al. Hyperspectral remote sensing data analysis and future challenges. IEEE Geoscience and remote sensing magazine. 2013;1(2):6-36.
33 . Robles -Kel ly A, Huynh CP. Imaging spectroscopy for scene analysis: Springer Science
Hyperspectral imaging system in BC
200 Aref, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 189-201

& Business Media; 2012.34. Xiong Z, Sun D-W, Zeng X-A, Xie A. Recent
developments of hyperspectral imaging systems and their applications in detecting quality attributes of red meats: A review. Journal of food engineering. 2014;132:1-13.
35. Moghaddam TM, Razavi SM, Taghizadeh M. Applications of hyperspectral imaging in grains and nuts quality and safety assessment: a review. Journal of Food Measurement and Characterization. 2013;7(3):129-40.
36. Dale LM, Thewis A, Boudry C, Rotar I, Dardenne P, et al. Hyperspectral imaging applications in agriculture and agro-food product quality and safety control: A review. Applied Spectroscopy Reviews. 2013;48(2):142-59.
37. Denstedt M, Bjorgan A, Milanič M, Randeberg LL. Wavelet based feature extraction and visualization in hyperspectral tissue characterization. Biomedical optics express. 2014;5(12): 4260-80.
38. Lu G, Little JV, Wang X, Zhang H, Patel MR, et al. Detection of head and neck cancer in surgical specimens using quantitative hyperspectral imaging. Clinical Cancer Research. 2017;23(18): 5426-36.
39. Han Z, Zhang A, Wang X, Sun Z, Wang MD, et al. In vivo use of hyperspectral imaging to develop a noncontact endoscopic diagnosis support system for malignant colorectal tumors. Journal of biomedical optics. 2016;21(1):016001.
40. Neittaanmäki‐Perttu N, Grönroos M, Tani T, Pölönen I, Ranki A, et al. Detecting field cancerization using a hyperspectral imaging system. Lasers in surgery and medicine. 2013;45(7):410-7.
41. Aref MH, Aboughaleb IH, El-Sharkawy YH. Tissue characterization utilizing hyperspectral imaging for liver thermal ablation. Photodiagnosis and Photodynamic Therapy. 2020;31:101899.
42. Aboughaleb IH, Aref MH, El-Sharkawy YH. Hyperspectral imaging for diagnosis and detection of ex-vivo breast cancer. Photodiagnosis and Photodynamic Therapy. 2020;31:101922.
43. Tuchin V. Tissue optics and photonics: Light-tissue interaction II. Journal of Biomedical Photonics and Engineering. 2016;2(3):030201.
44. Tuchin VV. Tissue optics and photonics: biological tissue structures. Journal of Biomedical Photonics & Engineering. 2015;1(1).
45. DiPerna RJ, Lions P-L. Ordinary differential equations, transport theory and Sobolev spaces. Inventiones mathematicae. 1989;98(3):511-47.
46.Rinzema K, Murrer L, Star W. Direct experimental verification of light transport theory in an optical phantom. JOSA A. 1998;15(8): 2078-88.
47. Yavari N. Optical spectroscopy for tissue diagnostics and treatment control. 2006.
48. Md Noor SS, Ren J, Marshall S, Michael K.
Hyperspectral image enhancement and mixture deep-learning classification of corneal epithelium injuries. Sensors. 2017;17(11):2644.
49. Kumar V, Gupta P. Importance of statistical measures in digital image processing. International Journal of Emerging Technology and Advanced Engineering. 2012;2(8):56-62.
50. Saika K, Sobue T. Cancer statistics in the world. Gan to kagaku ryoho Cancer & chemotherapy. 2013;40(13):2475-80.
201Aref, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 189-201
Hyperspectral imaging system in BC

202
1-3documented in the literature, and less than one-third of these cases are located in the nipple papillary region. Most patients with primary leiomyosarcoma of the breast are female, although at least four cases
4in males have been reported. The disease usually appears in postmenopausal women aged 50–80
5years; in rare cases, it appears in young girls. Most primary breast sarcomas expand rapidly, with advancing borders that confer a well-circumscribed gross appearance, with or without histological invasion. This appearance differs from that of most invasive breast carcinomas, which typically exhibit stellate or ill-defined borders macroscopically and
6widely infiltrative borders at the microscopic level.
ARTICLE INFO
Background: Breast leiomyosarcoma is a rare subtype of breast sarcoma, constituting 5–10% of the cases. Less than one-third of reported cases are located in the nipple papillary region, making it an extraordinarily rare malignancy, responsible for less than 0.1% of all malignant breast tumors. As no radiological criteria allow definitive diagnosis of papillary leiomyosarcoma, histopathological and immunohistochemical examination of suspicious lesions is required. The prognosis is generally optimistic compared with those for other breast sarcomas.
Case presentation: A 54-year-old previously healthy woman reported the appearance of a nodule in her right nipple in the preceding 9 months, associated with pruritus. Physical examination revealed that the lesion had a cystic consistency and measured approximately 3.0 cm. Imaging examinations showed no involvement of the adjacent breast parenchyma or axillary region and the lesion was classified as Breast Imaging-Reporting and Data System (BI-RADS) category IV. The lesion was excised, and the histopathological diagnosis was well-differentiated leiomyosarcoma of the mammary papilla, with immunohistochemical examination showing positivity for smooth-muscle tissue antigens. A staging CT examination was performed, showing no evidence of distant metastasis. After 2 years of follow-up, the patient shows no sign of tumor recurrence.
Conclusion: Although rare, leiomyosarcoma must be included in differential diagnosis of breast masses, especially those involving the periareolar region. Due to its good prognosis, reporting on this type of tumor is important to guide therapeutic planning, and to identify and track possible complications of its underdiagnosis.
Received:
21 September 2020Revised:
04 October 2020Accepted:
14 October 2020
Key words:Leiomyosarcoma,breast papilla, magnetic resonance imaging
Address for correspondence: Matthäeus Cunha Bürger, MD Address: Rua Firmino Gameleira, 360, Apto 301. Olaria. CEP 21021.450. Rio de Janeiro, BrazilTel: +55 22 981465921. Email: [email protected]
ABSTRACT
Primary Leiomyosarcoma of the Breast Papilla: A Case Report
a Department of Radiology, Clementino Fraga Filho University Hospital, Federal University of Rio de Janeiro, Rio de Janeiro, RJ, Brazilb Department of Pathological Anatomy, Clementino Fraga Filho University Hospital, Federal University
of Rio de Janeiro, Rio de Janeiro, RJ, Brazil
a a aMatthäeus Cunha Bürger* , Edson Marchiori , Maria Celia R. Djahjah , a bNathalie Cruz da Silva Bürger , Ana Helena Correia
Open AccessCase Report
IntroductionBreast sarcoma is an uncommon neoplasm, with
an incidence rate of 0.5–1%. Breast leiomyosarcoma is a rare subtype of breast sarcoma, constituting 5–10% of breast sarcoma cases. Fewer than 70 cases of this extraordinarily rare malignancy are
Cunha Bürger, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 202-206
DOI: 10.19187/abc.202073202-206

Morphologically, the typical histological features of circumscription, pronounced cellularity, and a composition of fusiform spindle cells with blunt-end nuclei lead to the suspicion of primary breast sarcoma. Confirmation by an immunohistochemical profile of smooth-muscle actin, vimentin, and desmin positivity is helpful. We report a case of primary leiomyosarcoma of the mammary papilla in a 54-year-old woman. After excision and central resection of the breast, the patient is well, with no sign of tumor recurrence.
Case presentationA 54-year-old woman presented at the mastology
ambulatory service due to the emergence of a nodule in her right nipple in the preceding 9 months, associated with pruritus. No bleeding, papillary discharge or family history of breast cancer was noted. Physical examination revealed that the right
nipple was enlarged and piriform, and had a cystic consistency and a diameter of about 3 cm. The axilla was free on palpation. Mammography showed a single high-density oval mass with well-defined margins, a diameter of 3.4 cm, and no associated calcification in the papillary region of the right breast. Magnetic resonance imaging showed an oval mass in the right nipple with a circumscribed margin, heterogeneous signal intensity (predominantly high on T2 and short tau inversion recovery sequences, intermediate on T1 sequences), and intense heterogeneous contrast enhancement (Figure 1). No involvement of the adjacent breast parenchyma or axillary region was observed. The lesion was classified as BI-RADS category IV. Its clinical and radiological characteristics, in particular its superficial and non-infiltrative nature, associated with the absence of lymph node dissemination, favored surgical excision.
Figure 1. Magnetic resonance imaging of the breast demonstrated an oval mass in the right nipple with a circumscribed margin, with (A) high signal intensity on a STIR sequence; (B) intermediate intensity on a T1 sequence; and (C) intense and heterogeneous
enhancement by contrast with no effect on the adjacent breast parenchyma, as demonstrated by maximum intensity projection reconstruction. (D) Colored parametric map showing the increased permeability of the lesion.
The mammary papilla was excised, and macroscopic examination revealed a whitish, firm-elastic, lobulated, well-defined tumor measuring 4.0 × 3.0 × 3.0 cm, juxtaposed to the overlying skin. Histopathological analysis revealed a well-differentiated leiomyosarcoma of the papilla, with spindle cells containing possible atypical nuclei and up to three mitotic figures/10 high-magnification fields, without tumor necrosis (Figure 2 and 3). Immunohistochemical examination showed positivity for smooth-muscle tissue antigens (e.g., actin and desmin) and negativity for carcinoma markers (p63 and cytokeratin pool), melanoma markers (S-100 and Melan A), and the vascular/myofibroblastic marker CD34, confirming the diagnosis (Figure 3).
A metastatic work-up, which included computed tomographic (CT) examination of the chest and abdomen, revealed no metastatic disease. A periareolar incision was made to expand the resection margins in the right breast, and the anterior scar and papillary region of the nipple were removed, with the creation of a 5-cm margin associated with central breast resection. Left breast reduction surgery was performed for aesthetic purposes (Figure 4). As lymphatic spread and nodal metastasis are not typical features of leiomyosarcomas, no sentinel lymph-node biopsy or axillary lymph-node dissection was performed. After 2 years of follow-up with annual mammography, the patient shows no sign or symptom of tumor recurrence.
203Cunha Bürger, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 202-206
Leiomyosarcoma of breast

Figure 2. Section showing a well-defined fusocellular neoplasia in the nipple region (hematoxylin and eosin stain, ×40).
Figure 3. (A) Section showing that the neoplasia is composed of fusocellular bundles, and detailed view showing a mitotic figure (arrow). Marked cytological atypia (B) and immunohistochemical positivity for actin (A and B) are evident
(hematoxylin and eosin stain, ×100). (C) Section showing immunohistochemical positivity for smooth muscle markers, including anti–smooth muscle anti-actin (×400).
Figure 4. Photograph of the postoperative result, following removal of the right periareolar region. Left breast reduction surgery was performed for aesthetic purposes.
204 Cunha Bürger, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 202-206
Leiomyosarcoma of breast

DiscussionThe exact origin of breast leiomyosarcomas is
debated. These entities belong to the subgroup of spindle-cell breast tumors, which generally arise from the smooth-muscle cells lining blood vessels or from stromal mesenchymal cells, reflecting the controversy surrounding their etiology. Most cases, including ours, are located near the areola and likely originate from the blood vessels and musculature in
6this anatomical region.Differentiation between breast sarcoma and
breast carcinoma is important, especially when the lesion presents as a mass. Breast sarcomas are unilateral (rarely bilateral), well-defined, large (5–6 cm) painless firm masses, typically diagnosed in
7patients aged about 50 years. They grow rapidly, with preferential hematogenous dissemination. Chest CT examination should be performed for all newly diagnosed patients, as the lungs are the predominant metastatic sites. Like sarcomas that appear elsewhere, breast sarcomas are usually treated with surgery and sometimes chemotherapy. With proper treatment, the prognosis is usually
7good. Breast carcinomas are diagnosed in patients
8aged about 60 years ; most of these lesions are minor and show preferential dissemination through the lymphatic and hematogenous pathways. Thus, the presence of lymphadenopathy in association with a mass in the breast should increase the likelihood of carcinoma over sarcoma. A wide range of treatments, including surgery, radiation therapy, chemotherapy and hormone therapy, are available for breast carcinoma. The prognosis is variable according to the staging and is good for lesions that are detected
8early.As no radiological criteria allow the definitive
diagnosis of papillary leiomyosarcoma, histopathological and immunohistochemical examination of lesions in
4suspected cases is required. The presence of a rapidly growing mass with indistinct or circumscribed margins and a heterogeneous or complex echotexture, and the absence of axillary lymphadenopathy, favor the
9diagnosis of sarcoma. The histopathological differential diagnosis is made with fusocellular metaplastic carcinoma, phyllodes tumor, myofibroblastoma and leiomyoma of the breast.
Leiomyosarcoma presents prominent cell atypia, 10atypical mitosis, vascular invasion, and necrosis.
Patients are usually asymptomatic, but they may experience itching, increased breast volume, pain,
11and hardening of the nipple or nodule.
Tumor size is an important prognostic factor, given that the overall survival rate is better for patients with tumors less than 5 cm in diameter. Dissemination is mainly hematogenous: cells spread to the lungs, bones, liver and central nervous system,
12with only discreet lymphatic spread. Albeit rare, the association of metastasis with a large, rapidly growing breast leiomyosarcoma signifies aggressive
13behavior.The initial treatment in the early stage of this
disease is operative, consisting of local resection or mastectomy. As leiomyosarcoma tends to recur locally, local resection is inadequate unless wide negative margins are achieved. For maximum effectiveness, a negative margin of at least 3 cm is recommended; however, a 2-cm margin can be
1utilized for breast conservation therapy. In our case, we achieved a 5-cm resection margin. Furthermore, given the mainly hematogenous dissemination route of metastasis, no case of a x i l l a r y l y m p h - n o d e i n v a s i o n h a s b e e n documented; thus, lymph node dissection may be
1unnecessary. We performed conservative breast surgery, as supported by reports on a few cases showing no difference in outcome between patients who underwent such surgery with the achievement of microscopically negative margins and those who
14 underwent mastectomy. Chemotherapy does not effectively treat breast sarcomas, although combined r eg imens may r e su l t i n some
15improvement. The use of adjuvant radiotherapy for leiomyosarcoma is based on the therapeutic principles established for soft-tissue sarcomas of the extremities. Several authors have suggested the use of radiotherapy for patients with positive
14surgical margins. Other prognostic factors that should be evaluated for radiotherapy are tumor size, infiltrative features, and histopathological grading. Given the rarity of leiomyosarcoma, available data are too limited to guide the use of radiotherapy and
15, 16chemotherapy. In our case, considering the limited extent of the disease, no radiotherapy or chemotherapy was administered.
The prognosis of breast leiomyosarcoma is generally optimistic relative to that of other breast sarcomas. However, because of the prolonged risk of
1recurrence, long-term follow-up may be indicated. Most available data on breast leiomyosarcoma derive from case reports and small case series, and the natural history of this disease and its response to different therapeutic modalities have not been well established.
Reporting on this type of tumor is important to determine the most appropriate management plan for the patient, to identify and track possible complications of its underdiagnosis and avoid overtreatment, aiming for the best disease-free result.
Ethical considerationsThe patient has provided written informed
consent to the publication of this case (including the publication of images).
Conflict of interestThe authors declare that they have no conflict of
interest.
205Cunha Bürger, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 202-206
Leiomyosarcoma of breast
References1. Amberger M, Park T, Petersen B, Baltazar GA.
Primary breast leiomyosarcoma with metastases to the lung in a young adult: Case report and literature review. Int J Surg Case Rep. 2018;47:34-7.
2. Felix C, Bispo M, Chagas C. Pancreatic Metastasis from Primary Leiomyosarcoma of the Breast. GE Port J Gastroenterol. 2019;26(3):223-5.
3. Wong LC, Huang PC, Luh SP, Huang CS. Primary leiomyosarcoma of the nipple-areola complex: report of a case and review of literature. J Zhejiang Univ Sci B. 2008;9(2):109-13.
4. Assis JOd, Pimentel ACdA, Chambo Filho A, Cintra LC, Scardini R. Leiomiossarcoma de mama: relato de caso. Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(4):255-8.
5. Rane SU, Batra C, Saikia UN. Primary leiomyosarcoma of breast in an adolescent girl: a case report and review of the literature. Case Rep Pathol. 2012;2012:491984.
6. Testori A, Meroni S, Voulaz E, Alloisio M, De Sanctis R, et al. Primary breast leiomyosarcoma and synchronous homolateral lung cancer: a case report. J Thorac Dis. 2017;9(12):E1054-E9.
7. Oktay Y, Fikret A. Leiomyosarcoma of the breast. J Surg Case Rep. 2011;2011(7):1.
8. Alkabban FM, Ferguson T. Cancer, breast. StatPearls [Internet]: StatPearls Publishing; 2019.
9. Smith TB, Gilcrease MZ, Santiago L, Hunt KK, Yang WT. Imaging features of primary breast sarcoma. AJR Am J Roentgenol. 2012;198(4): W386-93.
10. Munitiz V, Rios A, Canovas J, Ferri B, Sola J, et al. Primitive leiomyosarcoma of the breast: case report and review of the literature. Breast. 2004;13(1):72-6.
11. Minami S, Matsuo S, Azuma T, Uga T, Hayashi T, et al. Parenchymal leiomyoma of the breast: a case report with special reference to magnetic resonance imaging findings and an update review of literature. Breast Cancer. 2011;18(3): 231-6.
12. Al-Benna S, Poggemann K, Steinau HU, Steinstraesser L. Diagnosis and management of primary breast sarcoma. Breast Cancer Res Treat. 2010;122(3):619-26.
13. Singh G, Sharma D, Goyal S. Primary Leiomyosarcoma of Breast Presenting with Metastasis: An Atypical Presentation with Dismal Prognosis. Indian J Med Paediatr Oncol. 2017;38(4):535-7.
14. Lim SZ, Ong KW, Tan BK, Selvarajan S, Tan PH. Sarcoma of the breast: an update on a rare entity. J Clin Pathol. 2016;69(5):373-81.
15. Pollard SG, Marks PV, Temple LN, Thompson HH. Breast sarcoma. A clinicopathologic review
of 25 cases. Cancer. 1990;66(5):941-4.16. Parisi G, Signor MA, Finato N, Ceschia T, Magli
A. Breast leiomyosarcoma with myxoid aspects. Breast J. 2018;24(6):1086-7.
206 Cunha Bürger, et al. Arch Breast Cancer 2020; Vol. 7, No. 4: 202-206
Leiomyosarcoma of breast
Copyright © 2022 FDOKUMEN