Breast Cancer Australian Study
208
PEEK PATIENT EXPERIENCE EXPECTATIONS KNOWLEDGE www.cc-dr.org 2018 Breast Cancer Australian Study PEEK Volume 1 Issue 5 February 2018
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Breast Cancer Australian Study

PEEK PA
TIEN
T
EXPE
RIE
NC
E
EXPE
CTA
TIO
NS
KNO
WLE
DG
E
www.cc-dr.org
2018
Breast CancerAustralian StudyPEEK Volume 1 Issue 5February 2018

This study was generously sponsored by AstraZeneca Australia.
AstraZeneca Australia provided arm’s length sponsorship for International Centre for Community-Driven Research to implement the PEEK protocol in breast cancer. The sponsor had no input into the methodology, data collection, data analysis of reporting.
The Centre for Community-Driven Research team for this study included:
Catherine Holliday Anne Holliday Farah Zaidi Josephine Byrne Hunter Baggen Kirilee Matters Sarah Due Katriona Smith Anne Sullivan Darron Webber

Contents
Summary of Results 4
Section 1: Introduction and methodology 23
Section 2: Demographics 37
Section 3: Symptoms and diagnosis 57
Section 4: Decision-making 71
Section 5: Treatment 84
Section 6: Communication and information 108
Section 7: Care and support 142
Section 8: Quality of life and experience in the health system 156
Section 9: Expectations and Messages 170
Section 10: Advice 191
Section 11: Discussion 197
Section 12: What’s next? 207

Summary of results
Breast Cancer 2018 Australian PEEK Study
Summary of results

Summary of results
Breast Cancer 2018 Australian PEEK Study
Executive summary The most common symptom leading to diagnosis in this patient population was breast lumps, however a number of women were asymptomatic when diagnosed. The most common diagnostic pathway described was self-detecting a lump or other breast abnormality, seeking attention from a general practitioner and being referred to mammogram, ultrasound and biopsy and it is important to note that the number of women with no symptoms whose diagnosis may have been delayed without mammography screening. Support at diagnosis was inadequate for many of the participants in this patient population with two thirds not receiving the support that they needed, and notably only about a third of those with stage IV disease had received enough support at diagnosis. In addition, 35% of all participants had not had any discussion about biomarkers and 33% were unsure about their biomarker status. The types of treatments experienced by this patient population were most commonly surgery and radiation therapy, followed by Tamoxifen, Cyclophosphamide (Endoxan), Paclitaxel, Docetaxel and Letrozole (Femara). Challenges described by participants in relation to side effects of treatment included fatigue and lower
energy levels, while changes to their relationships and family dynamics and anxiety had a significant impact on QoL. It is important to note that participants in this study with metastatic breast cancer had an increased level of anxiety in relation to disease progression. Participants in this patient population most commonly considered long term survival and outcomes followed by considerations about demonstrated effectiveness and outcomes when making decisions, and the decision-making proves was often shared between family, close friends and their treating clinician. Their information preference was to talk to someone and this was particularly relevant for patients with metastatic breast cancer. The majority of care and support for participants in this patient population study came from family and friends and this was followed by care and support from specialist breast nurses and general practitioners, and overall, patients received very good care, navigation and care coordination. However, participants with metastatic breast cancer and those in rural areas received poorer care coordination and communication.

Summary of results
Breast Cancer 2018 Australian PEEK Study
Section 1: Introduction and methodology
• Breast cancer is the third most commonly diagnosed cancer in Australia accounting for approximately 12% of newly diagnosed cancers. It is the most commonly diagnosed cancer in women with approximately 1 in 8 at risk of diagnosis before the age of 85.
• Breast cancer is classified into five main stages - stage 0 to stage IV - based on invasiveness, size and spread of disease.
• Patient Experience, Expectations and Knowledge (PEEK) is a research program developed by the Centre for Community-Driven Research (CCDR). The aim of PEEK is to conduct patient experience studies across several disease areas using a protocol that will allow for comparisons over time (both quantitative and qualitative components). PEEK studies give us a clear picture and historical record of what it is like to be a patient at a given point in time, and by asking patients about their expectations, PEEK studies give us a way forward to support patients and their families with treatments, information and care.
• In this PEEK study, 100 women with breast cancer throughout Australia participated in the study that included a structured interview and quantitative questionnaire. This study in breast cancer is therefore the largest study reported in Australia in the past five years that used structured interviews as part of the methodology. In addition PEEK is a comprehensive study covering all aspects of disease experience from symptoms, diagnosis, treatment, healthcare communication, information provision, care and support, quality of life, and future treatment and care expectations.
Section 2: Demographics and study population characteristics Demographics
• One hundred participants living in Australia with stage 0 to stage IV breast cancer were recruited into the study.
• The majority of participants were from New South Wales (n=24, 24.00%), Victoria (n24, n=24.00%), and Queensland (n=19, 19.00%). There were 56 participants (56.00%) from a major city and 44 participants (44.00%) from regional or rural areas.
• Subgroup analysis are included throughout the study. These include: disease stage, stage 0-I (n=20, 20.00%), stage II-III (n=30, 30.00%) and stage IV (n=50, 50.00%); metastatic disease (n=50, 50.00%) compared to those no metastases (n=50, 50.00%); by location, metropolitan (n=56, 56%) or regional/rural areas (n= 44, 44.00%); and by education status including those with university degree (n= 54, 54.00%) and those with high school or trade certificate (n=46, 46.00%).
Baseline Heath – SF36 score • The overall scores for the cohort were in the highest quintile for role limitations due to emotional problems. • The scores for physical functioning, and social functioning were in the second highest quintile indicating. • The scores for emotional well-being, pain, general health, and health change were in the middle quintile. • The scores for role limitations due to physical health, and energy/fatigue were in the second lowest quintile.
SF36 scores by disease stage • Those with stage IV disease scored significantly worse than stages 0 and I for role limitations due to physical
health, and social functioning. • Those with stage IV disease scored significantly worse than those with stages 0 and I and stages II and III for
emotional well-being, and general health. • There were no significant differences between groups for physical function, role limitations due to emotional
problems, energy/fatigue, pain or health change. SF36 scores by metastatic status
• Those with metastatic disease scored worse on the role limitations due to physical health, energy/fatigue, emotional well-being, social functioning and general health compared to those without metastases.
SF36 scores by location • There were no differences observed for any of the SF36 scales between those that live in metropolitan areas
compared to those that live in regional or rural areas. SF36 scores by education
• Those with a university degree scored statistically better on the physical functioning scale compared those with high school or trade certificate.

Summary of results
Breast Cancer 2018 Australian PEEK Study
Section 3: Experience of symptoms and diagnosis Symptoms at diagnosis
• In the online questionnaire participants were asked to recall all of the symptoms that they experienced and their quality of life while experiencing those symptoms. The most common symptom experienced was a breast lump, noted by 60 participants (60.00%), followed by a change in size, shape or feel of the breast (n=46, 46.00%), breast pain (n=36, 36.00%) and feeling tired/lower energy than usual (n=36, 36.00%). Skin changes including puckering, dimpling, rash or redness of skin, and ache or pain in bones were each noted by 23 participants (23.00%).
• In relation to sub-group variations, participants with stage 0-I breast cancer noted a change in size, shape or feel of their breast less frequently than the general cohort (25.00% compared to 46.00% in the general cohort). They also noted breast pain and feeling tired/less energy than usual less frequently (25.00% compared to 36.00% in the general cohort for both symptoms) and aches or pain in bones less frequently (10.00% compared to 23.00% in the general cohort).
• In the structured interview participants were asked to describe the symptoms that actually led to their diagnosis, as opposed to all the symptoms that they could recall. There were 39 women (39.00%) that described feeling a lump and seeking medical attention. This was the most common symptom experienced that led to diagnosis. The same number of participants (n=39, 39.00%) described not noticing any symptoms prior to diagnosis. Other symptoms included breast pain (n=9, 9.00%) and breast swelling, asymmetry or bruising (n=7, 7.00%).
• In relation to sub-group variations, participants with stage 0-I breast cancer described having no symptoms more frequently than the general cohort (55.00% compared to 39.00% in the general cohort).
• The most common diagnostic pathway described was self-detecting a lump or other breast abnormality, seeking attention from a general practitioner and being referred to mammogram, ultrasound and biopsy (n=48, 48.00%). There were an additional five participants (5.00%) that described self-detecting a lump or other breast abnormality, however being referred to ultrasound and biopsy directly. The next most common diagnostic pathway was through routine mammography which led to ultrasound and biopsy (n=32, 32.00%). There were also eight participants (8.00%) that described being diagnosed through their GP (through a routine check-up or other investigation) which led to mammography, ultrasound and biopsy.
• In relation to sub-group variations, participants with stage II-III breast cancer described self-detection leading to diagnosis more frequently than the general cohort (70.00% compared to 48.00% in the general cohort). Participants with stage 0-I breast cancer described diagnosis following a routine check-up or other investigation with their general practitioner more frequently (25.00% compared to 8.00% in the general cohort).
Support at diagnosis
• In the online questionnaire, participants were asked whether they felt supported at the time of diagnosis. There were 42 participants (42.00%) that indicated that they had no support at diagnosis, while 34 participants (34.00%) noted that they had enough support. An additional 24 participants (24.00%) indicated that they had some support but that it was not enough.
• In relation to sub-group variations, participants with stage 0-I breast cancer reported having no support at diagnosis less frequently than the general cohort (30.00% compared to 42.00% in the general cohort), however, this group also reported having enough support at diagnosis, more frequently than the general cohort (45.00% compared to 34.00% in the general cohort). Participants that were high school educated reported that they had enough support at diagnosis, less frequently than the general cohort (21.74% compared to 34.00% in the general cohort).

Summary of results
Breast Cancer 2018 Australian PEEK Study
Genetic/biomarker tests • Participants were asked whether they had ever had a discussion about genetic tests or tests to see if there
were biomarkers that might be relevant to their condition or treatment. There were 42 participants (42.00%) that indicated that they had brought up the topic for discussion with their doctor and 23 participants (23.00%) that reported that their doctor had brought up the topic for discussion. There were also 35 participants (35.00%) that indicated that no one had ever spoken to them about this.
• In relation to sub-group variations participants with stage 0-I and stage II-III breast cancer indicated that they had brought up the topic of biomarker or genetic testing less frequently than the general cohort, while participants with stage IV breast cancer brought up the topic more frequently (stage 0-I = 30.00%, stage II – III = 16.67%, stage IV = 62.00% compared to 42.00% in the general cohort). Participants with stage II-III breast cancer indicated that their doctor brought up the topic of biomarker/genetic testing, more frequently than the general cohort (46.67% compared to 23.00% in the general cohort). Participants with stage 0-I breast cancer reported that no one had brought up this topic with them, more frequently than the general cohort (55.00% compared to 35.00% in the general cohort).
• Participants were also asked about their interest in this type of test if it was available. The majority of participants noted that they had not had this test, but would like to (n=64, 64.00%). There were 20 participants (20.00%) that reported having this test and not paying out of pocket for it, while 13 participants (13.00%) indicated that they had not had this test and were not interested in it.
• In relation to sub-group variations, participants that were university educated indicated that they had not had this test but would like to, more frequently than the general cohort (75.93% compared to 64.00% in the general cohort), while participants that were high school educated indicated that they were not interested in this test, more frequently than the general cohort (23.92% compared to 13.00% in the general cohort).
Understanding of prognosis • Participants were asked whether anyone talked to them about prognosis. The most common theme noted
by 23 participants (23.00%) was that they had not been given a clear prognosis. This was followed by two themes noted by 14 participants (14.00%) each including the understanding that they would make a full recovery and are not likely to have a recurrence, and that they have a good prognosis with maintenance therapy. There were also 14 participants (14.00%) that were not able to describe prognosis, but rather focused on describing their treatment regime.
• In relation to sub-group variations, participants with stage 0-I breast cancer reported not being given a clear prognosis less frequently than the general cohort (5.00% compared to 23.00% in the general cohort). This group also reported having a good prognosis with a full recovery and little chance of recurrence, more frequently than the general cohort (60.00% compared with 14.00% in the general cohort). There were also no participants with stage IV breast cancer that reported this theme. Participants with stage I-III breast cancer reported having a good prognosis with maintenance therapy more frequently than the general cohort (40.00% compared to 14.00% in the general cohort), while participants with stage IV breast cancer reported this less frequently (2.00% compared to 14.00% in the general cohort).
Section 4: Experience of health professional communication
Conversations about treatments • Participants were asked to describe the conversations they have had about their breast cancer in relation to
treatment options. The most common theme was that participants felt as though they were informed and had time to make treatment decisions (n=40, 40.00%). In contrast, the next most common theme noted by 31 participants (31.00%) was that they felt as though they were not being given treatment options but rather being told what to do. In a similar theme that was noted by 11 participants, participants described being supported but feeling as though there were limited treatment options for them.
• There were a number of sub-group variations. Participants with stage II-III breast cancer reported being informed and having time to make treatment decisions, more frequently than the general cohort (50.00% compared to 40.00% in the general cohort). Participants with stage 0-I breast cancer indicated that they had not been given treatment options, less frequently than the general cohort (20.00% compared to 31.00% in the general cohort).

Summary of results
Breast Cancer 2018 Australian PEEK Study
Decision-making • The most common theme described by participants was that decisions about treatment were ultimately
made by talking with their partner/spouse and their family, including very close friends (n=32, 32.00%). This was followed by participants describing that they would consult with others, but ultimately the decision was their own (n=19, 19.00%). The final themes included decision-making between themselves and their clinician (n=17, 17.00%), decision-making between themselves and their partner/spouse (n=16, 16.00%) and decisions-making between their clinician as well as their clinician also (n=16, 16.00%).
• There were sub-group variations in relation to decisions about treatment that were ultimately made by talking with their partner/spouse and their family, including very close friends. Participants with stage 0-I breast cancer reported this less frequently than the general cohort (20.00% compared to 32.00% in the general cohort), while participants with stage II-III breast cancer reported this more frequently (43.33% compared to 32.00% in the general cohort). Participants in rural areas described decision-making as ultimately their own decision, more frequently than the general cohort (29.55% compared to 19.00% in the general cohort).
• Participants were asked about the things that they take into consideration when making decisions about treatment. There were two key themes in this section. The most common theme was that participants considered long term survival and outcomes (n=27, 27.00%) and this was followed by considerations about demonstrated effectiveness and outcomes (n=25, 25.00%). The remaining themes in this section included impact on quality of life (n=16, 16.00%), financial considerations (n=14, 14.00%), severity of side effects (n=13, 13.00%) and impact on their family (n=13, 13.00%).
• Participants with stage 0-I breast cancer reported considering demonstrated effectiveness and outcomes less frequently than the general cohort (10.00% compared to 25.00% in the general cohort). This group did not report considering the severity of side effects or the impact of treatment on their family. Participants with stage II-III breast cancer reported the impact on treatment in general and on their family more frequently than the general cohort (26.67% compared to 13.00% in the general cohort).
• In the final question about decision-making, participants were asked whether they felt the way they made decisions had changed over time since they were diagnosed. Close to half of all participants reported that the way that they make decisions had stayed the same (n=49, 49.00%). A quarter of all participants (n=25, 25.00%) reported that the way that they make decisions has changed and this related to them being more empowered and informed over time. There were also 19 participants (19.00%) that noted they had changed the way they make decisions as they are more cautious and considered.
• In relation to sub-group variations, participants with stage 0-I breast cancer reported being more empowered and informed, more frequently than the general cohort (45.00% compared to 25.00% in the general cohort). They also reported being more cautious and considered, less frequently than the general cohort (5.00% compared to 19.00% in the general cohort). Participants in rural areas reported making decisions in the same way less frequently than the general cohort (36.36% compared to 49.00% in the general cohort). They also reported changing the way they make decisions as they have a different outlook on life, more frequently than the general cohort (18.18% compared to 8.00% in the general cohort) and this theme was unique to participants in rural areas.
Section 5: Experience of treatment and health services
Treatments experienced
• The most common treatments were surgery (n=94, 94.00%) and radiation therapy (n=79, 79.00%). This was followed by Tamoxifen (n=43, 43.00%), Cyclophosphamide (Endoxan) (n=39, 39.00%), Paclitaxel (n=34, 34.00%), Docetaxel (Taxotere) (n=33, 33.00%) and Letrozole (Femara) (n=33, 33.00%).
• Participants were asked to rate their quality of life on a scale of 1 to 7 while using each specific treatment (with 1 being ‘Life was very distressing and 7 being ‘Life was great’). Mean quality of life scores ranges from 1.70 to 4.13, that is, all quality of life scores were with the ‘Life was very distressing’ to ‘Life was average’ range. The treatment that scored the least impact on quality of life was Exemestane (Aromasin) (mean score 4.13). Herceptin (mean score 3.60), Tamoxifen (mean score 3.51), Anastrozole (Arimidex) (mean score 3.47) and Letrozole (Femara) (mean score 3.24) all had a mean score of at least 3, that is in the ‘Life was a little distressing’ range. The remaining treatments had a mean quality of life score of 2.13 to 2.94, that is in the ‘Life was distressing’ range. There was one treatment scoring less than 2 (Docetaxel/Taxotere,) with a mean

Summary of results
Breast Cancer 2018 Australian PEEK Study
score of 1.70). • The treatments that had a mean effectiveness score of at least 4 (Effective) were Exemestane (Aromasin)
(average score 4.00), Doxorubicin (Adriamycin) (average score 4.04), radiation therapy (average score 4.04), Paclitaxel (average score 4.21), Herceptin (average score 4.33) and Anastrozole (Arimidex) (average score 4.36). The remaining treatments scored had a mean effectiveness score of at least 3, that is in the moderately effective range.
• When asked what side effects or symptoms participants could cope with, the most common theme was that participants felt as though they could cope with all side effects (n=21, 21.00%), however it was also often noted that this was because they had to (that, is they had no choice but to cope). There were also 16 participants (16.00%) that noted that there were no side effects that they could cope with, that is, they only noted that there were difficult side effects. In relation to specific side effects that participants felt they could cope with, the main themes were fatigue (n=10, 10.00%), nausea and vomiting (n=10, 10.00%). hair loss (n=9, 9.00%), radiation burns/blisters (n=9, 9.00%) and cramps (n=9, 9.00%).
• When asked what side effects or symptoms participants found difficult to cope with, the most common side effect that participants felt they could not cope with was pain (n=20, 20.00%). Within this theme, there were 10 participants that specifically spoke about bone pain, while the remaining 10 participants spoke about other pain. The next most difficult side effect was fatigue and lethargy (n=18, 18.00%). The remaining themes that were each noted by 9 participants (9.00%) included the psychological impact, restriction in mobility and change in physical appearance. Nausea and symptoms of menopause were noted as difficult side effects by 8 participants (8.00%).
Adherence to medication
• The most common theme in this section was that participants would continue with a therapy for as long as prescribed (n=36, 36.00%). This was followed by participants describing that they would not give up on any medication (n=16, 16.00%). There were 14 participants (14.00%) that spoke about continuing with a treatment for a month or more, and 10 participants (10.00%) that described sticking to a treatment for 2 to 3 months.
• There were two sub-group variations where participants with stage 0-I breast cancer described not giving up on a treatment less frequently than the general cohort (5.00% compared to 16.00% in the general cohort). This sub-group also described sticking with something for about a month or more less frequently than the general cohort (5.00% compared to 14.00% in the general cohort).
• Participants were asked what needed to change for them to feel like a treatment is working. The two most common themes were that participants needed to see test results or have some clinical indication that the treatment is working; and needing to feel better or do everyday tasks. These themes were both noted by 21 participants (21.00%). The next most common theme noted by 13 participants (13.00%) was that they were unable to describe the change needed to feel as though a treatment was working. Having no disease progression or no recurrence, needing to directly fix the symptoms that treatment is intended to fix, and needing pain to dissipate were each noted by 11 participants (11.00%).
Treatment at home or hospital
• Participants were asked, if there was an option to have treatment in a pill form at home or chemotherapy in hospital, which they would prefer. The majority of participants spoke about a preference for taking medication at home (n=71, 71.00%). Of the remaining participants, 26 (26.00%) described a preference for hospital and two (2.00%) were uncertain.
• The rationale for their choice was also analysed. The most common theme was that participants preferred having medication at home because it is more convenient and comfortable (n=36, 36.00%). The next most common theme was that the participant preferred treatment at hospital in case something went wrong, however it was also noted that this would depend on the type of treatment offered (n=10, 10.00%).
• As a follow-up question, participants were asked what support they would need to feel comfortable having treatment at home. The majority of participants (n=59, 59.00%) spoke about needing to have someone to call if they have a question or issue, especially out or hours. The next most frequent theme was the need to be checked regularly by a general practitioner or nurse at home (n=21, 21.00%) while an additional eight participants (8.00%) described needing check-ups but not necessarily at home.
Complementary therapies

Summary of results
Breast Cancer 2018 Australian PEEK Study
• There were 38 participants (38.00%) that described not using any complementary therapies and this was the most common theme. Massage was the most common complementary therapy, used by 22 participants (22.00%). In a consolidated theme, there were various complementary therapies that participants spoke about including acupuncture, reiki and reflexology (n=18, 18.00%). Taking vitamins and minerals (n=14, 14.00%), healthy diets (n-12, 12.00%), mindfulness (n=10, 10.00%) and yoga or light exercise (n=7, 7.00%) were also described as complementary therapies.
Service provision and affordability
• The vast majority of participants had access to a general practitioner (n=97, 97.00%), medical oncologist (m=96, 96.00%), surgeon (n=92.00%) and radiation oncologist (n=83, 83.00%) for the treatment of their breast cancer.
• The majority of patients had private healthcare insurance (n=82, 82.00%), 44 participants were treated as private patients, 27 (27.00%) as public patients and 28 (28.00%) equally as public and private patients. A little over half of the participants were treated in the private hospital system (n=56, 56.00%).
• The majority of participants have never missed medical appointments due to cost (n=76, 76.00%), and have never been unable to afford prescription medications (n=83, 83.00%). Half of participants have never had trouble paying for basic needs due to their diagnosis with breast cancer (n=50, 50.00%).
Changes to work status • The work status for a number of participants changed due to their diagnosis with breast cancer with about a
quarter of participants reducing the number of hours worked (n=26, 26,00%), and 21 (21.00%) quitting their jobs.
• Very few carers had to quit their job (n=3, 3.00%) or reduce the number of hours worked (n=5, 5.00%), however, carers have had to take leave either with pay (n=34, 34.00%), or without pay (n=10, 10.00%).
Section 6: Information and communication Access to information
• Participants were asked what information they had accessed in relation to their condition. Almost half of all participants described receiving information from local charities in Australia including (n=46, 46.00%) and an additional 29 participants (29.00%) spoke about receiving information from a McGrath Foundation or a specialist nurse. There were 39 participants (39.00%) that described seeking information from the internet, 17 (17.00%) that described receiving information from hospitals and 13 (13.00%) that spoke about receiving information from other patients. There were 11 participants, all of whom had stage IV breast cancer, that described a lack of information about metastatic breast cancer.
• In relation to sub-group variations, as noted there were 11 participants, all of whom had stage IV breast cancer, that described a lack of information about metastatic breast cancer. Participants with stage II-III breast cancer reported receiving information from local charities more frequently than the general cohort (60.00% compared to 46.00% in the general cohort) and participants with stage 0-I breast cancer reported receiving information from their oncologist more frequently than the general cohort (45.00% compared to 19.00%) in the general cohort). Rural participants described receiving information from their breast care nurse or McGrath nurse more frequently than the general population (40.91% compared to 29.00% in the general cohort).
Information that was helpful • There was a range of information that participants found helpful including Breast Cancer Network Australia’s
information and their My Journey Kit (n=13, 13.00%), information from other patients about their experience (n=13, 13.00%) and information provided by McGrath or specialist nurses (n=11, 11.00%). There were also 13 participants (13.00%) that noted that all information was helpful. In relation to specific topics, the most useful topic of information noted by 10 people (10.00%) was information about the participant’s specific type of cancer (that is, triple negative, ER positive, metastatic cancer etc.) and the side effects of treatment including what to expect (n=10, 10.00%).

Summary of results
Breast Cancer 2018 Australian PEEK Study
Information that was not helpful • The most common theme described by 28 participants (28.00%) was that all information is helpful and there
is nothing that is not helpful. The next most common theme was that unsolicited information, that is, people telling you what to do, sharing their opinions or platitudes was not helpful and this was described by 20 participants (20.00%). In a similar theme, nine participants (9.00%) described stories about the worst-case scenario or horrific stories as not helpful. There were also 13 participants (13.00%) that described information from non-reputable sources such as Facebook and the media as not helpful.
Information preferences • Participants were asked whether they had a preference for information online, talking to someone, in
written (booklet) form or through a phone App. The most common theme was that participants preferred to talk to someone in relation to information provision (n=36, 36.00%). This was followed by a preference for written or online information combined with talking to someone (n=32, 32.00%). When combined, these two main themes represent 68 participants (68.00%) that have some preference for talking to someone in relation to information provision. The next most common theme was online information (n=21, 21.00%).
• In relation to sub-group variations, participants a preference for talking to someone (with or without online information) increased with stage of disease, that is participants with stage IV breast cancer described his preference most frequently (78.00%) compared to stage II-III (63.34%) and stage 0-I (50.00%).
Timing of information
• The most common time that participants described being receptive to receiving information was at the time of diagnosis (n=17, 17.00%). This was followed by after surgery (n=16, 16.00%) and being most receptive when information is given gradually over time (n=14, 14.00%). An additional 11 participants (11.00%) described being most receptive to receiving information when they are away from the hospital or following appointments.
• In relation to sub-group variations, participants with stage 0-I breast cancer described being receptive to information at diagnosis more frequently than the general cohort, whereas participants with stage IV disease described this less frequently than the general cohort (50.00% for stage 0-I, 4.00% for stage IV and 17.00% for the general cohort). Participants with stage 0-I breast cancer also described being receptive to information after surgery less frequently than the general cohort (5.00% compared to 16.00% in the general cohort).
Health professional communication • Participants were asked to describe the communication that they had had with health professionals
throughout their experience. The most common theme was that participants were satisfied with communication (very good to excellent) (n=37, 37.00%). There were 32 participants (32.00%) that described poor communication. This was particularly in relation to the feeling that clinicians did not take the time to explain things and allow questions. In contrast, there were 21 participants (21.00%) that felt as though communication was overall good, however there were possibly some improvements to be made.
• There were a number of sub-group variations. Participants with stage 0-I breast cancer described being satisfied with communication (Good, possibly some improvements), more frequently than the general cohort (35.00% compared to 21.00% in the general cohort). Participants in metropolitan areas described having poor communication, less frequently than the general cohort, while participants in rural areas described this more frequently (19.64 for metropolitan participants, 47.73 for rural participants, compared to 32.00% in the general cohort)
• The most common theme was that participants spoke and trusted a number of health professionals (n=32, 32.00%). This was followed by their general practitioner as a single health professional that they spoke to about their condition (n=15, 15.00%). There were then various combinations of health professionals including oncologist plus general practitioner (n=13, 13.00%) and oncologist plus surgeon.
• Half of all participants spoke about being able to access a breast care, specialist of McGrath nurse (n=50, 50.00%) while an additional 27 participants (27.00%) spoke about care received from chemotherapy or general oncology nurses. There were 16 participants (16.00%) that indicated that they had not accessed a breast care nurse and the remaining participants were unsure whether they had accessed a specialist nurse or not.

Summary of results
Breast Cancer 2018 Australian PEEK Study
• There were two sub-group variations. Participants with stage IV breast cancer reported accessing specialist breast or McGrath nurses less frequently than the general cohort (26.00% compared to 50% in the general cohort) and participants in regional/rural areas also reported accessing specialist or McGrath nurses less frequently (27.27%).
Respect shown to patients • The majority of participant felt as though they had been treated respectfully throughout their experience in
the health system (n=69, 69.00%). There were five participants (5.00%) that did not feel as though they had been treated respectfully and an additional 26 participants (26.00%) that felt they were treated respectfully for the most part, except for one or two occasions.
Knowledge and confidence The Partners in Health questionnaire (PIH) measures an individual’s knowledge and confidence for managing their own health. The Partners in Health comprises a global score, 4 sub scales; knowledge, treatment, symptoms and coping. A higher score denotes a better understanding and knowledge of disease. Partners in health – overall score
• Overall, the participants scored in the top quintile for knowledge, adherence to treatment, and management of symptoms. The scores for coping and total score were in the second highest quintile.
Partners in health - by disease stage • Participants with very stage IV disease had a statistically significant worse score for the coping subscale
compared those with stage II-III disease.
Partners in health – by metastatic status • Participants with very metastatic disease had a statistically significant, worse scores for the adherence to
treatment, and coping subscales compared those without metastases.
Partners in health – by location • Participants living in regional or rural areas had had a statistically significant, worse scores for the adherence
to treatment, management of symptoms, coping and total score subscales compared those living in metropolitan areas.
Partners in health – by education • No differences were observed between those with university education and those with high school or trade
qualifications for any PIH subscale. Information given by health care professionals
• Information about treatment options (88.00%), and disease management (66.00%) were most frequently given to participants by healthcare professionals, and information about clinical trials (7.00%) and complementary therapies (18.00%) were give least often.
• Information patterns given to participants by was similar for all subgroups, however, those that had metastatic disease tended to get more information than those without, and those that live in metropolitan areas received more information than those in regional or remote areas

Summary of results
Breast Cancer 2018 Australian PEEK Study
Information searched for independently • Information about treatment options (58.00%), and interpreting test results (58.00%), were most often
searched for independently by participants, and clinical trials (23.00%) and hereditary and genetic concerns (29.00%) were least searched for.
• Stage IV participants tended to search for more information compared to other disease stages with over 60% of stage IV participants searching for information about disease cause, treatment options, complementary therapies, interpreting test results and psychological support. Those with stage 0-I disease tended to search for less information independently compared to other disease stages.
• Those with metastatic disease searched for more information than those without. • Those living in metropolitan areas searched for more information than those in regional and remote areas. • Those with university education searched for more information compared to those high school or trade
qualification. Gaps in Information
• The largest gaps in information, where information was neither given to patients nor searched for independently were for clinical trials (70.00%), and hereditary, genes and biomarkers (65.00%). Participants were given most information either from healthcare professionals or independently for treatment options (96.00%) and disease management (80.00%). Complementary therapies (43.00%) was the topic that was most searched for independently following no information from health professionals (49.00%).
Most trusted information sources • Across all participants, information from the participants’ hospital or clinic was most trusted, and
information from pharmaceutical companies was least trusted. Information from not for profit or charitable organisations and government sources were near equal in trust by participants. This order of preference was the same for all sub-groups.
Section 7: Experience of care and support
Coordination of care • Overall the cohort had a ‘care received’ score in the highest quintile, indicating very good care received. The
scores for navigation and care coordination fell in the second highest quintile indicating good scores. The total score and communication score were in the middle of the scale.
Coordination of care – by disease stage • Participants with stage IV disease had significantly worse scores for communication and total score
compared to those with stage 0-I disease and those with stage II-III disease.
Coordination of care – by metastatic status • Participants with metastases had significantly worse scores for the care coordination total score and
communication score compared to those without metastases.
Coordination of care – by location • Participants that live in regional or rural areas had significantly worse scores for the care coordination total
score, communication score and care received score compared to those that live in metropolitan areas.
Coordination of care – by education • No statistically significant differences were observed between those with university education and those
with high school or trade certificate any Care Coordination scores.

Summary of results
Breast Cancer 2018 Australian PEEK Study
Care and support • The majority of care and support received came from family and friends (n=65, 65.00%). This was followed
by care and support from specialist breast nurses and McGrath nurses (n=31, 31.00%) and the same number of participants (n=31, 31.00%) noted care and support from their general practitioner. There were 23 participants (23.00%) that described care and support from other patients and support services that connected patients with each other.
• There were a number of sub-group variations. Participants with stage II-III breast cancer spoke about receiving care and support from family and friends more frequently while participants with stage IV breast cancer spoke about this less frequently (83.33% stage II-III, 52.00% stage IV compared to 65.00% in the general cohort). Participants with stage IV breast cancer spoke about receiving care and support from specialist breast or McGrath nurses less frequently than the general cohort (22.00% compared to 40.00% in stage 0-III breast cancer). Participants in rural areas reported receiving care and support from their general practitioner, less frequently than the general cohort (20.45% compared to 31.00% in the general cohort).
Section 8: Experience of quality of life
Quality of life • The main theme was that breast cancer had a significant impact on multiple areas of an individuals’ quality
of life (n=38, 38.00%). This was followed by a description of a ‘new normal’ or not being the same person that they used to be (n=26, 26.00%). This theme included changes to their relationships and family dynamics. The next most common theme was the impact of fatigue and lower energy levels which impacted quality of life, and this was noted by 22 participants (22.00%). There were 18 participants (18.00%) that described the impact of being anxious or frightened, 16 participants (16.00%) that spoke about not letting breast cancer impact their quality of life, 15 participants (15.00%) that described needing to take advantage of the time they had and the relationships they had in order to maintain quality of life and finally, 10 participants (10.00%) that described the financial impact of breast cancer in relation to quality of life.
• Participants with stage II-III breast cancer noted the impact of fatigue more frequently than the general cohort (33.33% compared to 22.00% in the general cohort). This group also described not letting breast cancer impact their quality of life, more frequently than the general cohort (26.67% compared to 16.00% in the general cohort). Participants in rural areas noted that there was a ‘new normal’, more frequently than participants in the general cohort (36.36% compared to 26.00% in the general cohort).
Regular activities to maintain health • The main thing that participants needed to do to everyday to maintain their health was to rest or take things
slowly (n=44, 44.00%). This was followed by needing to put themselves first (n=25, 25.00%) and needing to focus on maintaining their mental health (n=23, 23.00%). There were also 20 participants (20.00%) that spoke about needing to be diligent in taking medication.
Impact on relationships • The main impact on relationships was in relation to people becoming distant or people not
understanding/knowing what to say. This was noted by 39 participants (39.00%). The next most common theme was in relation to participants being more assertive in their relationships and realising who their true friends are (n=36, 36.00%). There were also 19 participants (19.00%) that described relationships becoming stronger and an additional 11 participants (11.00%) that described no impact to personal relationships.
• There was one sub-group variation where participants in rural areas reported people becoming distant or not knowing what to say, more frequently than the general cohort (54.55% compared to 39.00% in the general population).
Anxiety and fear of progression • The Fear of Progression questionnaire measures the level of anxiety people experience in relation to their
conditions. The Fear of Progression questionnaire comprises a total score, with a higher score denoting increased anxiety. Overall the entire cohort had a median total score of 34.99, which is a score in the middle of the scale.

Summary of results
Breast Cancer 2018 Australian PEEK Study
Fear of progression – by disease stage • Participants with disease stage IV scored worse on the fear of progression total score compared to those
with stage 0-I disease.
Fear of progression – by metastatic status • Participants with metastases scored worse on the fear of progression total score compared to those without
metastases.
Fear of progression – by geographic location • There was no difference observed in the fear of progression total score between participants that live in
metropolitan areas and those that live in regional or rural areas.
Fear of progression – by level of education There was no difference observed in the fear of progression total score between participants with university qualifications and those with high school or trade certificates.
Section 9: Expectations of future treatment, care and support, information and communication Expectations of future treatments
• The most common expectation was that new treatments would have less side effects in general. This was noted by 37 participants (37.00%) and in this theme, there were no particular side effects mentioned. The next most common theme was the expectation that new treatments would be less invasive (n=27, 27.00%) and this included treatments being more personalised. There were 20 participants who noted the expectation that new treatments would be affordable (20.00%) and 14 participants that described the expectation or a cure or that their breast cancer would not be recurrent. There were a number of specific side effects that participants expected would be addressed through new treatments including fatigue, burns, hair loss, nausea, symptoms of menopause and weight gain. However, these were all noted by five participants or less.
• Participants were asked to rank which symptoms/aspects of quality of life would they want controlled in a treatment for them to consider taking it. The most important aspects reported were nausea and vomiting, and pain; the least important were hair loss and loss of appetite.
• Participants were asked to rank what is important for them overall when they make decisions about treatment and care. The most important aspects were safety of treatment/weighing up risks and benefits, and severity of side effects. The least important were cost, and including family in decision-making.
• Participants were asked to rank what is important for decision-makers to consider when they make decisions that impact treatment and care. The two most important values were access for all patients to all treatments and services, and quality of life; the least important was economic value to government.
Expectation of future information provision • The most common theme was that participants were satisfied with the current level of information and did
not have any recommendations (n=35, 35.00%). In relation to specific expectations there were 15 participants (15.00%) that described wanting more information that is specific to their type of cancer and respective treatment options. There were also 12 participants (12.00%) that described the expectation that information will be more readily available (including new research and clinical trials), and the same number of participants that described the expectation that there will be more information in relation to side effects.
• In relation to sub-group variations, participants with stage 0-I breast cancer were satisfied with the current level of information and did not have any recommendations, more frequently than the general cohort (45.00% compared to the general cohort 35.00%). There were also no participants in this group that described the expectation that there will be more information in relation to side effects.
Expectation of future healthcare professional communication • The most common theme was that participants were generally satisfied with health professional
communication and did not have any recommendations (n=33, 33.00%). There were 22 participants (22.00%) that expected future communication should be clearer and to understand this is all new information for patients, and 16 participants (16.00%) whose expectation was that communication should

Summary of results
Breast Cancer 2018 Australian PEEK Study
be more compassionate and empathetic. • Participants with stage II-III breast cancer reported being satisfied with communication, less frequently than
the general cohort (20.00% compared to 33.00% in the general cohort). This group also reported the expectation that communication would be compassionate and empathetic, more frequently (26.67% compared to 16.00% in the general cohort).
Section 9: Expectations of future treatment, care and support, information and communication Expectations of future treatments
• The most common expectation was that new treatments would have less side effects in general. This was noted by 37 participants (37.00%) and in this theme, there were no particular side effects mentioned. The next most common theme was the expectation that new treatments would be less invasive (n=27, 27.00%) and this included treatments being more personalised. There were 20 participants who noted the expectation that new treatments would be affordable (20.00%) and 14 participants that described the expectation or a cure or that their breast cancer would not be recurrent. There were a number of specific side effects that participants expected would be addressed through new treatments including fatigue, burns, hair loss, nausea, symptoms of menopause and weight gain. However, these were all noted by five participants or less.
• Participants were asked to rank which symptoms/aspects of quality of life would they want controlled in a treatment for them to consider taking it. The most important aspects reported were nausea and vomiting, and pain; the least important were hair loss and loss of appetite.
• Participants were asked to rank what is important for them overall when they make decisions about treatment and care. The most important aspects were safety of treatment/weighing up risks and benefits, and severity of side effects. The least important were cost, and including family in decision-making.
• Participants were asked to rank what is important for decision-makers to consider when they make decisions that impact treatment and care. The two most important values were access for all patients to all treatments and services, and quality of life; the least important was economic value to government.
Expectation of future information provision • The most common theme was that participants were satisfied with the current level of information and did
not have any recommendations (n=35, 35.00%). In relation to specific expectations there were 15 participants (15.00%) that described wanting more information that is specific to their type of cancer and respective treatment options. There were also 12 participants (12.00%) that described the expectation that information will be more readily available (including new research and clinical trials), and the same number of participants that described the expectation that there will be more information in relation to side effects.
• In relation to sub-group variations, participants with stage 0-I breast cancer were satisfied with the current level of information and did not have any recommendations, more frequently than the general cohort (45.00% compared to the general cohort 35.00%). There were also no participants in this group that described the expectation that there will be more information in relation to side effects.
Expectation of future healthcare professional communication • The most common theme was that participants were generally satisfied with health professional
communication and did not have any recommendations (n=33, 33.00%). There were 22 participants (22.00%) that expected future communication should be clearer and to understand this is all new information for patients, and 16 participants (16.00%) whose expectation was that communication should be more compassionate and empathetic.
• Participants with stage II-III breast cancer reported being satisfied with communication, less frequently than the general cohort (20.00% compared to 33.00% in the general cohort). This group also reported the expectation that communication would be compassionate and empathetic, more frequently (26.67% compared to 16.00% in the general cohort).

Summary of results
Breast Cancer 2018 Australian PEEK Study
Expectation of future care and support • Participants were asked whether there was anything they would like to see in relation to the care and
support they receive. The main theme was the recommendation was in relation to more support that connects patients with health professionals and other patients, whether this is online, phone, in-person or through support groups (n=32, 32.00%). This was followed by support for specialist nurses for breast cancer patients (n=17, 17.00%). There were also 16 participants (16.00%) that were satisfied with the level of care and support received and did not have any additional recommendations.
• Participants with stage 0-I breast cancer called for support that connects patients with health professionals and other patients, less frequently than the general cohort (5.00% compared to 32.00%). Participants with stage II-III breast cancer reported being satisfied with care and support received less frequently than the general cohort (3.33% compared to 16.00% in the general cohort).
Messages to decision-makers • The most common message described by over half of all participants was that treatments should be
available and affordable to those who need them (n=54, 54.00%). This was followed by the message to provide holistic care and empower the patient and this included personalising treatment (n=25, 25.00%). An additional 10 participants (10.00%) had the message that it is important to continue funding research and support services.
• There was one sub-group variation where participants with stage IV disease had the message that
treatments should be available and affordable to those who need them, more frequently than the general cohort (64.00% compared to 54.00% in the general cohort and 44.00% in stage 0-III participants).
Section 10: Advice to other patients and families
• Participants were asked what advice they would give to other people who are newly diagnosed with breast cancer and their families. The most common advice to newly diagnosed patients was to be informed (n=29, 29.00%). This was followed by asking for help and accepting help (n=200, 20.00%), and talking to other patients (n=17, 17.00%). There were also 15 participants (15.00%) whose advice was to take things step-by-step, 14 participants (14.00%) whose advice was to have a support person to both talk to and take to appointments, 12 participants (12.00%) whose advice was to remain positive and 10 participants (10.00%) whose advice was to do what is right for you and make your own decisions.

Summary
Breast Cancer 2018 Australian PEEK Study
Stage 0-I Stage II-III Stage IV Regional/ Rural Metropolitan University educated High school/ Trade educated
Baseline health Poorer role limitations due to physical health, and social functioning, emotional well-being, and general health.
Better physical functioning
Symptoms that led to diagnosis
No symptoms
Diagnostic pathway Routine check-up or other investigation
Self detection
Support at diagnosis No support at diagnosis Enough support at diagnosis
Enough support at diagnosis
Biomarker/genetic testing
Brought up the topic of biomarker or genetic testing
No one had brought up this topic
Brought up the topic of biomarker or genetic testing
Doctor brought up the topic of biomarker or genetic testing
Brought up the topic of biomarker or genetic testing
Table i: Sub-group variations

Summary
Breast Cancer 2018 Australian PEEK Study
Stage 0-I Stage II-III Stage IV Regional/ Rural Metropolitan University educated High school/ Trade educated
Description of prognosis
No clear prognosis
Good prognosis with a full recovery and little chance of recurrence
Good prognosis with a full recovery and little chance of recurrence Good prognosis with maintenance therapy
Discussions about treatments
Not given treatment options
Informed and having time to make treatment decisions
Decisions about treatment
Partner/spouse and their family
Partner/spouse and their family
Ultimately their own decision
Considerations when making decisions about treatment
Effectiveness and outcomes, severity of side effects or the impact of treatment on their family
Impact on treatment in general and on their family
Changes in approach to decision making
More empowered and informed More cautious and considered
Make decisions in the same way Different outlook on life
Adherence to medication
Not giving up on a treatment

Summary
Breast Cancer 2018 Australian PEEK Study
Stage 0-I Stage II-III Stage IV Regional/ Rural Metropolitan University educated High school/ Trade educated
Access to information Received information from their oncologist
Received information from local charities
A lack of information about metastatic breast cancer
Search for more information
Received information from breast care nurse
Preference for talking to someone
Search for more information
Search for more information
Timing of information Receptive to information at diagnosis Receptive to information after surgery
Receptive to information at diagnosis
Partners in Health Poorer outcome for the coping subscale and adherence to treatment
Poorer adherence to treatment, management of symptoms, coping and total score subscales
Health professional communication
Satisfied with communication (Good, possibly some improvements)
Poor communication
Poor communication
Care coordination Poorer communication, care coordination and total score
Poorer care coordination total score, communication score and care received

Summary
Breast Cancer 2018 Australian PEEK Study
Stage 0-I Stage II-III Stage IV Regional/ Rural Metropolitan University educated High school/ Trade educated
Care and support Family and friends Family and friends Specialist breast or McGrath nurses
Care and support from their general practitioner
Quality of life Impact of fatigue Not letting breast cancer impact their quality of life
New normal
Fear of Progression Worse fear of progression total score
Key Less frequently More frequently

Section 1
Breast Cancer 2018 Australian PEEK Study
Section 1 Introduction and methods

Section 1
Breast Cancer 2018 Australian PEEK Study
Section 1: Introduction and methodology
• Breast cancer is the third most commonly diagnosed cancer in Australia accounting for approximately 12% of newly diagnosed cancers. It is the most commonly diagnosed cancer in women with approximately 1 in 8 at risk of diagnosis before the age of 85.
• Breast cancer is classified into five main stages - stage 0 to stage IV - based on invasiveness, size and spread of disease.
• Patient Experience, Expectations and Knowledge (PEEK) is a research program developed by the Centre for Community-Driven Research (CCDR). The aim of PEEK is to conduct patient experience studies across several disease areas using a protocol that will allow for comparisons over time (both quantitative and qualitative components). PEEK studies give us a clear picture and historical record of what it is like to be a patient at a given point in time, and by asking patients about their expectations, PEEK studies give us a way forward to support patients and their families with treatments, information and care.
• In this PEEK study, 100 women with breast cancer throughout Australia participated in the study that included a structured interview and quantitative questionnaire. This study in breast cancer is therefore the largest study reported in Australia in the past five years that used structured interviews as part of the methodology. In addition PEEK is a comprehensive study covering all aspects of disease experience from symptoms, diagnosis, treatment, healthcare communication, information provision, care and support, quality of life, and future treatment and care expectations.

Section 1
Breast Cancer 2018 Australian PEEK Study
Introduction Breast cancer is the third most commonly diagnosed cancer in Australia accounting for approximately 12% of newly diagnosed cancers1 and it is the most commonly diagnosed cancer in women, with approximately 1 in 8 at risk of diagnosis before the age of 851. Early detection of breast cancer has led to excellent five-year survival rates of 90%1, however when the cancer spreads to other parts of the body (metastatic breast cancer), the five-year survival rates are significantly lower at 20%2. In 2014, there were over 16,500 new cases of breast cancer diagnosed, these were primarily in women, with less than 150 cases of breast cancer diagnosed in men3. There were almost 3,000 deaths from breast cancer in 2015, primarily in women, with less than 30 men dying from breast cancer3. In Australia in 2012, just under 66,000 people were living with breast cancer4. The fatal burden and non-fatal burden of breast cancer in females was found to be highest compared to other diseases5. Survival from breast cancer is influenced by many factors such as age, demographics, stage of tumour at time of diagnosis and the treatment received5. The 5-year survival rate in females with breast cancer was reported to be 90% with highest rate being among age group of 35-694. The survival rate is reportedly better for females with small tumours as compared to large tumours6. Females with the tumour size of 10 mm or less have been found to have 98% survival rate which decreases to 73% for females with a tumour size of 30 mm or more6. Survival was found to be higher among females whose lymph nodes were cancer free compared to females whose lymph nodes were not cancer free6. Breast cancer results when abnormal growth occurs in the cells lining breast ducts or lobules6. Symptoms of breast cancer include presence of a new lump in the breast or underarm area, swelling, pain, redness, irritation or dimpling on any part of breast, nipple discharge or any change in the size or shape of the breast7. However, some patients may not exhibit any of these symptoms8. There are several risk factors associated with breast cancer such as age, sex, affluence, family history, breast condition and endogenous oestrogens 9. Breast cancer can develop in both males and females but as noted the incidence in females is significantly higher than males6. Increasing age is one of the most predominant risk factors with 75% of cases occurring after the age of 509. Family history is a strong risk factor
and women with an affected first degree relative (mother, daughter or sister) are at twice the risk of developing breast cancer than those with no affected first degree relative9. Women with high breast density are reportedly at four to six times higher risk of developing breast cancer9. Risk of developing breast cancer is increased by presence of pre-invasive beast conditions such as lobular carcinoma in situ, ductal carcinoma in situ and atypical ductal hyperplasia9. Breast cancer is also known to be prevalent in societies with high socio-economic status9. In addition, high oestrogen levels among postmenopausal woman doubles their risk of developing breast cancer compared to women with low levels of circulating oestrogens9. Alcohol consumption of more than 2 standard drinks per day can increase risk of breast cancer significantly9. A systemic review revealed other risk factors such as diabetes mellitus, hormone replacement therapy and oral contraceptives which can significantly increase risk of developing breast cancer by almost 10-23%10. Breast cancer is classified into five main stages which further have sub stages11.
• The stage 0 refers to individual with pre-invasive cancer conditions like ductal carcinoma in situ or lobular carcinoma in situ.
• Stage I refers to early stage where lump is <2 cm with absence of cancer cells.
• Stage IIA and IIB (early) are early stages with presence of cancer cells. In Stage IIA and IIB, cancer cells have been found in one to three lymph nodes in the armpit.
• In stage IIIA, the size may range from >2 to <5 cm. Cancer cells are found in 4-9 lymph nodes in the armpit with enlarged lymph nodes are also enlarged which may be attached to each other or to the underlying tissue. This stage could also involve 1 or more lymph nodes present under the breastbone but none of lymph nodes in the armpit are involved.
• In stage IIIB, cancer cells start to spread to nearby muscles and skin with the cancer being of any size.
• In stage IIIC, cancer cells are found in 10 or more lymph nodes in the arm pit; or 1or more lymph nodes above or below the collarbone; or 1 or more lymph nodes under the breastbone and 1 or more lymph nodes in the armpit.
• Stage IV refers to cancer of any size where cancer cells are resent in other parts of the body.

Section 1
Breast Cancer 2018 Australian PEEK Study
Patient Experience, Expectations and Knowledge (PEEK) Patient Experience, Expectations and Knowledge (PEEK) is a research program developed by the Centre for Community-Driven Research (CCDR). The aim of PEEK is to conduct patient experience studies across several disease areas using a protocol that will allow for comparisons over time (both quantitative and qualitative components). PEEK studies give us a clear picture and historical record of what it is like to be a patient at a given point in time, and by asking patients about their expectations, PEEK studies give us a way forward to support patients and their families with treatments, information and care. The research protocol used in PEEK studies is independently driven by CCDR. PEEK studies include a quantitative and qualitative component. The quantitative component is based on a series of validated tools. The qualitative component is the result of two years of protocol testing by CCDR to develop a structured interview that solicits patient experience data and provides patients with the opportunity to provide advice on what they would like to see in relation to future treatment, information and care. The structured interview has also been designed so that the outcomes of PEEK studies can inform policy, research, health technology assessment, care, information, supportive care services and advocacy efforts. Methodology Participants To be eligible for the study, participants needed to have been diagnosed with stage 0 to stage IV breast cancer, have experienced the healthcare system in Australia, be 18 years of age or older, be able to speak English, and be able to give consent to participate in the study. Recruitment commenced on 3 October 2017 and the study closed for recruitment on 12 November 2017. Participants were recruited via email and social media through ICCDR. Ethics Ethics approval for this study was granted (as a low or negligible risk research study) by the Centre for Community-Driven Research Ethics Committee (Reference CS_Q4_03).
Data collection Data for the online questionnaire was collected using Zoho Survey (Zoho Corporation Pvt. Ltd. Pleasanton, California, USA, www.zoho.com/survey). Participants completed the survey from September 2017 to January 2018. There were six researchers who conducted telephone interviews and used standardised prompts throughout the interview. The interviews were recorded and transcribed verbatim. Identifying names and locations were not included in the transcript. All transcripts were checked against the original recording for quality assurance. Interview data was collected from September 2017 to January 2018. Online questionnaire (quantitative) The online questionnaire consisted of the 36-Item Short Form Health Survey (SF36)12, a modified Cancer Care Coordination Questionnaire for Patients (CCCQ)13, the Short Fear of Progression Questionnaire (FOP12)14, and the Partners in Health version 2 (PIH)15. In addition investigator derived questions about demographics, diagnosis, treatment received and future treatment decisions making were included. Structured Interview (qualitative) Interviews were conducted via telephone by a registered nurse or researcher with a background in psychology trained in qualitative research. The first set of interview questions guided the patient through their whole experience from when symptoms were noticed up to the present day. The next set of questions allowed patients to reflect on what they would like to see in the future in relation to treatment and care and asked them what their messages to decision-makers would be about the care and treatment patients with their condition receive. The interview also asks patients about the advice they would give to others recently diagnosed with their condition or disease. All interviews were recorded and transcribed verbatim.

Section 1
Breast Cancer 2018 Australian PEEK Study
Questionnaire analysis Statistical analysis was conducted using R included in the packages “car”, “dplyr” and “ggplot2” (R 3.3.3 GUI 1.69 Mavericks build (7328). The aim of the statistical analysis of the SF36, CCCQ, FOP12, and PIH responses was to identify variations by respondent type (by CHF class, and by location), and by co-morbidity or symptom type (hyperkalemia status, hypertension status, sleep problem status and anxiety status). Global scales and sub scales were calculated according to reported instructions12-14. For comparisons by CHF class, a one-way analysis of variance (ANOVA) analysis was conducted. A Tukey HSD test was used post-hoc to identify the source of any differences identified in the one-way ANOVA test. Where the assumptions for the one-way ANOVA were not met, a Kuskal-Wallis rank sum test on care was conducted with post hoc pairwise comparisons using Wilcoxon rank sum test. When the assumption of equal variances were not met, a Welch one-way test was used with post-hoc pairwise t-tests with no assumption of equal variances. For all other comparisons, a two-sample t-test was used when assumptions for normality and variance were met, or when assumptions were not met, a Wilcoxon rank sum test with continuity correction was used. Questions where participants were asked to rank preferences were analysed using weighted averages. Weights were applied in reverse, the most preferred option was given the largest weight equal to the number of options, the least preferred option was given the lowest weight of 1. Structured interviews analysis A content analysis was conducted using conventional analysis to identify major themes from structured interviews. Text from the interviews were read line-by-line by the lead researcher and then imported into NVivo 8 (QSR International). Each question within the interview was individually analysed. Initial categories and definitions were identified and registered in NVivo. The minimum coded unit was a sentence however
there were also paragraphs and phrases that were coded as a unit. A second researcher verified the codes and definitions, and the text was coded until full agreement was reached using the process of consensual validation. As a general rule, where a theme occurred less than 5 times it was not included in the study results. Data analysis and final reporting was completed on 26 February 2018. Position of this study A search was conducted in Pubmed (22 January 2018) to identify breast quality of life or patient experience studies that had been conducted in the past five years in Australia (Table 1.1 – 1.3). The search terms “Breast cancer”, “Quality of Life”, “Patient experience”, “Patient reported outcomes” and “interview” were used, excluding non-English articles, and review articles. Studies of less than five participants were excluded, and where the same cohort was reported more than one, one representative study was included. Sixty-eight studies were identified that explored patient reported experiences breast cancer, three studies used mixed methods (both qualitative and quantitative tools), 15 studies employed qualitative research methods and 50 quantitative research methods. Mixed methods The three mixed method studies are listed in table 1.1. The largest study of 1965 participants focused on information needs associated with sexual well-being, this study was mostly quantitative, the qualitative component comprised open ended questions in an online survey16. One study of 501 participants explored factors influencing decision making for breast reconstruction following mastectomy17 and one study of 49 participants explored patient preference for methods of imaging for breast cancer staging18. None of these studies included interviews in data collection.
Section 1
Breast Cancer 2018 Australian PEEK Study
Table 1.1: Mixed methods patient reported experience studies
Author Number of participants and tools Study focus Ussher et a, 201316
n=1965, online survey, mostly quantitative with qualitative component collected as open-ended questions.
Information needs associated with sexual well-being
Somogyi et al, 201517
n=501, factors influencing decision making online questionnaire
Breast reconstruction decision making
Hobbs et al, 201518
n=49, investigator patient preference questions, and open ended questions on survey
Patient preference for staging imaging
Qualitative studies
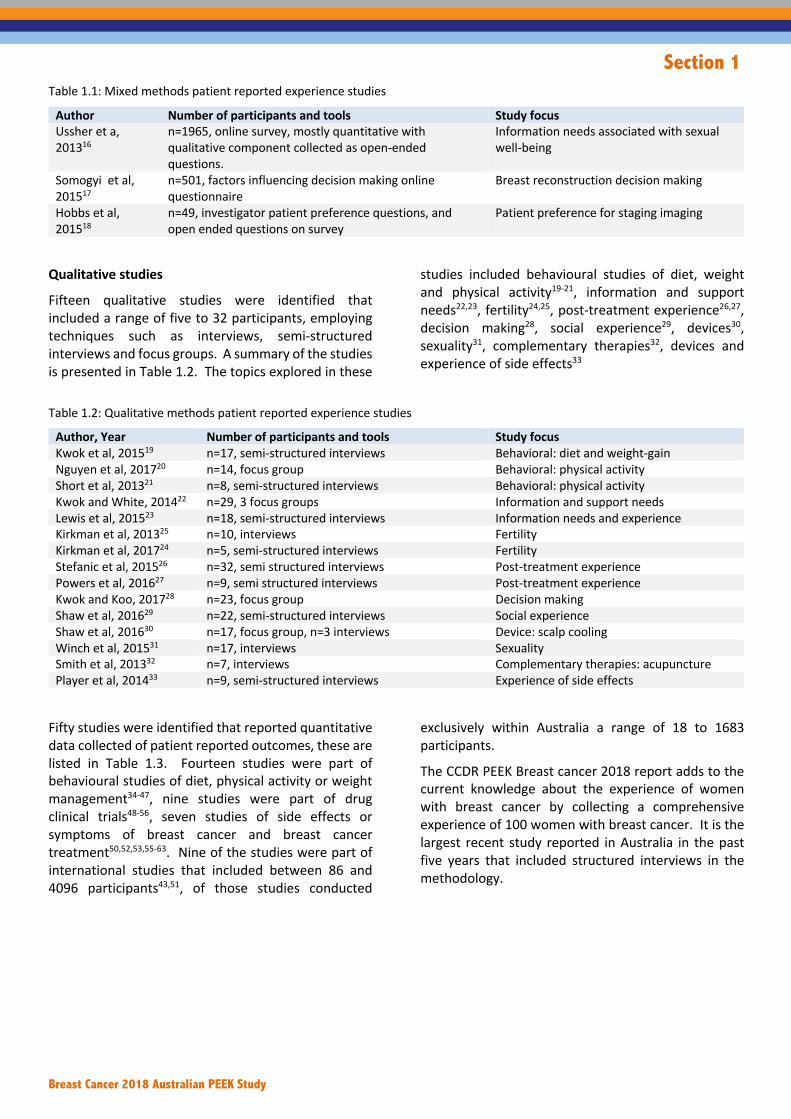
Fifteen qualitative studies were identified that included a range of five to 32 participants, employing techniques such as interviews, semi-structured interviews and focus groups. A summary of the studies is presented in Table 1.2. The topics explored in these
studies included behavioural studies of diet, weight and physical activity19-21, information and support needs22,23, fertility24,25, post-treatment experience26,27, decision making28, social experience29, devices30, sexuality31, complementary therapies32, devices and experience of side effects33
Table 1.2: Qualitative methods patient reported experience studies
Author, Year Number of participants and tools Study focus Kwok et al, 201519 n=17, semi-structured interviews Behavioral: diet and weight-gain Nguyen et al, 201720 n=14, focus group Behavioral: physical activity Short et al, 201321 n=8, semi-structured interviews Behavioral: physical activity Kwok and White, 201422 n=29, 3 focus groups Information and support needs Lewis et al, 201523 n=18, semi-structured interviews Information needs and experience Kirkman et al, 201325 n=10, interviews Fertility Kirkman et al, 201724 n=5, semi-structured interviews Fertility Stefanic et al, 201526 n=32, semi structured interviews Post-treatment experience Powers et al, 201627 n=9, semi structured interviews Post-treatment experience Kwok and Koo, 201728 n=23, focus group Decision making Shaw et al, 201629 n=22, semi-structured interviews Social experience Shaw et al, 201630 n=17, focus group, n=3 interviews Device: scalp cooling Winch et al, 201531 n=17, interviews Sexuality Smith et al, 201332 n=7, interviews Complementary therapies: acupuncture Player et al, 201433 n=9, semi-structured interviews Experience of side effects
Fifty studies were identified that reported quantitative data collected of patient reported outcomes, these are listed in Table 1.3. Fourteen studies were part of behavioural studies of diet, physical activity or weight management34-47, nine studies were part of drug clinical trials48-56, seven studies of side effects or symptoms of breast cancer and breast cancer treatment50,52,53,55-63. Nine of the studies were part of international studies that included between 86 and 4096 participants43,51, of those studies conducted
exclusively within Australia a range of 18 to 1683 participants.
The CCDR PEEK Breast cancer 2018 report adds to the current knowledge about the experience of women with breast cancer by collecting a comprehensive experience of 100 women with breast cancer. It is the largest recent study reported in Australia in the past five years that included structured interviews in the methodology.

Section 1
Breast Cancer 2018 Australian PEEK Study
Table 1.3: Qualitative studies Author N
umber
HRQoL
Symptom
s and diagnosis
Decision making
Treatment
Co mm
unication/Information
Care and support
Anxiety, depression, mood
Expectations
Behavioural/Lifestyle
Body image
Sexual function
Study focus
Anderson et al, 201547 55 X Behavioural: Wellness program #Beatty et al, 201764 121 X X X X X 43,4
8,49
,51
Stress
Bell et al, 201457 1205 X Side effects/symptoms *Bernhard et al, 201551 4096 X Drug clinical trial *Boyle et al, 201548 3074 X Drug clinical trial Brennan et al, 201665 47 X X X X Treatment satisfaction:
Surgery/device Brennan et al, 201666 68 X X Unmet needs/care coordination Buchan et al, 201641 41 X X Behavioural: physical activity Cinieri et al, 201754 50 X Drug clinical trial Corica et al, 201667 126 X X Treatment: Surgery/RT Cormie et al, 201335 62 X X Behavioural: physical activity Davis et al, 201458 1683 X X Side effects/symptoms Flitcroft et al, 201668 51 X Decision making #Garvey et al, 201669 41 X X Indigenous HRQoL *Gelmon et al, 201549 652 X Drug clinical trial Gho st al, 201362 432 X X Side effects/symptoms Hagstrom et al, 201642 39 X X Behavioural: physical activity Hau et al, 201359 688 X X X Side effects/symptoms Hayes et al, 201336 194 X X Behavioural: physical activity Hickey et al, 201670 38 X X Complementary therapies: clinical
trial Howes et al, 201671 400 X Treatment: Surgery Inglis et al, 201561 93 X Side effects/symptoms Juraskova et al, 201372 25 X X X X Complementary therapies: lubricant
clinical trial #*Kampshoff et al, 201643 574 X X Behavioural: physical activity Kokavec, 201673 37 X Community psycho-social education Lawler et al, 201744 53 X X X Behavioural: physical activity, diet,
weight Lawn et al, 201545 20 X X Behavioural: physical activity, diet,
weight Leung et al, 201474 412 X X Social support Leung et al, 201675 505 X X Social support Lewis et al, 201476 333 X Complementary therapies:
deodorant Loudon et al, 201437 18 X X Behavioural: physical activity #Marino et al, 201460 934 X X X Side effects/symptoms #Martin et al, 201540 72 X X Behavioural: physical activity Ng et al, 201677 143 X Treatment satisfaction: Surgery Oh et al, 201378 29 X X X Complementary therapies:
Acupuncture Panjari et al, 201479 274 X Psychological well-being for elderly *Phillips et al, 201652 86 X X Drug clinical trial Plummer and Chalmers, 201734
36 X X Behavioural: Health literacy, physical activity
Przezdziecki et al, 201380 279 X X X Body image Reeves et al, 201746 90 X X X X Behavioural: physical activity, diet,
weight *Ribi et al, 201653 1722 X Drug clinical trial *Saha et al, 201755 240 X Drug clinical trial

Section 1
Breast Cancer 2018 Australian PEEK Study
Author Num
ber
HRQoL
Symptom
s and diagnosis
Decision making
Treatment
Comm
unication/Information
Care and support
Anxiety, depression, mood
Expectations
Behavioural/Lifestyle
Body image
Sexual function
Study focus
Short et al, 201539 330 X X Behavioural: physical activity *Sledge et al, 201756 669 X Drug clinical trial Stefanic et al, 201463 43 X X Side effects/symptoms Sundaresan et al, 201581 161 X Treatment: Radiotherapy Tian et al, 201382 400 X X X QoL as a prognostic tool Tucker et al, 201683 119 X X X X X Sexuality *Turner et al, 201550 521 X Drug clinical trial Yee et al, 201438 71 X X X Behavioural: physical activity
*International studies, # Not exclusively breast cancer participants

Section 1
Breast Cancer 2018 Australian PEEK Study
References
1. Cancer_Australia. Treatment options for secondary (metastatic) breast cancer. n.d. https://canceraustralia.gov.au/affected- cancer/cancer-types/breast- cancer/treatment/treatment-options-breast-cancer- type/treatment-options-secondary-metastatic-breast- cancer (accessed 25 February 2018 2018). 2. Kaufman PA, Awada A, Twelves C, et al. Phase III open-label randomized study of eribulin mesylate versus capecitabine in patients with locally advanced or metastatic breast cancer taxane. J Clin Oncol 2015; 33(6): 594-601. 3. AIHW. Australian Cancer Incidence and Mortality (ACIM) books: breast cancer. 2017. <http://www.aihw.gov.au/acim-books>. (accessed 25 February 2018. 4. AIHW. Cancer in Australia 2017 5. AIHW. Burden of cancer in Australia. 2011; AUSTRALIAN BURDEN OF DISEASE STUDY SERIES Number 12. 6. AIHW. Breast cancer in Australia an overview. 2012. 7. CDC. Breast Cancer. 2017. https://www.cdc.gov/cancer/breast/basic_info/symptoms.htm (accessed 26 February 2018. 8. Cancer_Australia. Early detection of breast cancer. 2015. https://canceraustralia.gov.au/publications-and-resources/position-statements/early-detection-breast-cancer (accessed 26 February 2018. 9. National Breast and Ovarian Cancer Centre. Breast cancer risk factors: a review of the evidence [Internet]. Surry Hills: National Breast and Ovarian Cancer Centre. 2009. p. viii-x. 10. Anothaisintawee T, Wiratkapun C, Lerdsitthichai P, et al. Risk factors of breast cancer: a systematic review and meta-analysis. Asia Pac J Public Health 2013; 25(5): 368-87. 11. Cancer_Australia. Stages of Breast Cancer. 2017. https://breast-cancer.canceraustralia.gov.au/diagnosis/stages-breast-cancer (accessed 26 February 2018. 12. 36-Item Short Form Survey (SF-36) Scoring Instructions. n.d. https://www.rand.org/health/surveys_tools/mos
/36-item-short-form/scoring.html (accessed 10 February 2017. 13. Young JM, Walsh J, Butow PN, Solomon MJ, Shaw J. Measuring cancer care coordination: development and validation of a questionnaire for patients. BMC Cancer 2011; 11: 298. 14. Hinz A, Mehnert A, Ernst J, Herschbach P, Schulte T. Fear of progression in patients 6 months after cancer rehabilitation-a- validation study of the fear of progression questionnaire FoP-Q-12. Support Care Cancer 2015; 23(6): 1579-87. 15. Petkov J, Harvey P, Battersby M. The internal consistency and construct validity of the partners in health scale: validation of a patient rated chronic condition self-management measure. Qual Life Res 2010; 19(7): 1079-85. 16. Ussher JM, Perz J, Gilbert E. Information needs associated with changes to sexual well-being after breast cancer. J Adv Nurs 2013; 69(2): 327-37. 17. Somogyi RB, Webb A, Baghdikian N, Stephenson J, Edward KL, Morrison W. Understanding the factors that influence breast reconstruction decision making in Australian women. Breast 2015; 24(2): 124-30. 18. Hobbs MM, Taylor DB, Buzynski S, Peake RE. Contrast-enhanced spectral mammography (CESM) and contrast enhanced MRI (CEMRI): Patient preferences and tolerance. J Med Imaging Radiat Oncol 2015; 59(3): 300-5. 19. Kwok A, Palermo C, Boltong A. Dietary experiences and support needs of women who gain weight following chemotherapy for breast cancer. Support Care Cancer 2015; 23(6): 1561-8. 20. Nguyen NH, Hadgraft NT, Moore MM, et al. A qualitative evaluation of breast cancer survivors' acceptance of and preferences for consumer wearable technology activity trackers. Support Care Cancer 2017; 25(11): 3375-84. 21. Short CE, James EL, Plotnikoff RC. How social cognitive theory can help oncology-based health professionals promote physical activity among breast cancer survivors. Eur J Oncol Nurs 2013; 17(4): 482-9. 22. Kwok C, White K. Perceived information needs and social support of Chinese-Australian breast cancer survivors. Support Care Cancer 2014; 22(10): 2651-9.

Section 1
Breast Cancer 2018 Australian PEEK Study
23. Lewis S, Yee J, Kilbreath S, Willis K. A qualitative study of women's experiences of healthcare, treatment and support for metastatic breast cancer. Breast 2015; 24(3): 242-7. 24. Kirkman M, Apicella C, Graham J, et al. Meanings of abortion in context: accounts of abortion in the lives of women diagnosed with breast cancer. BMC Womens Health 2017; 17(1): 26. 25. Kirkman M, Stern C, Neil S, et al. Fertility management after breast cancer diagnosis: a qualitative investigation of women's experiences of and recommendations for professional care. Health Care Women Int 2013; 34(1): 50-67. 26. Stefanic N, Caputi P, Lane L, Iverson DC. Exploring the nature of situational goal-based coping in early-stage breast cancer patients: A contextual approach. Eur J Oncol Nurs 2015; 19(6): 604-11. 27. Powers N, Gullifer J, Shaw R. When the treatment stops: A qualitative study of life post breast cancer treatment. J Health Psychol 2016; 21(7): 1371-82. 28. Kwok C, Koo FK. Participation in treatment decision-making among Chinese-Australian women with breast cancer. Support Care Cancer 2017; 25(3): 957-63. 29. Shaw LK, Sherman KA, Fitness J, Breast Cancer Network A. Women's experiences of dating after breast cancer. J Psychosoc Oncol 2016; 34(4): 318-35. 30. Shaw J, Baylock B, O'Reilly A, et al. Scalp cooling: a qualitative study to assess the perceptions and experiences of Australian patients with breast cancer. Support Care Cancer 2016; 24(9): 3813-20. 31. Winch CJ, Sherman KA, Koelmeyer LA, Smith KM, Mackie H, Boyages J. Sexual concerns of women diagnosed with breast cancer-related lymphedema. Support Care Cancer 2015; 23(12): 3481-91. 32. Smith C, Carmady B, Thornton C, Perz J, Ussher JM. The effect of acupuncture on post-cancer fatigue and well-being for women recovering from breast cancer: a pilot randomised controlled trial. Acupunct Med 2013; 31(1): 9-15. 33. Player L, Mackenzie L, Willis K, Loh SY. Women's experiences of cognitive changes or
'chemobrain' following treatment for breast cancer: a role for occupational therapy? Aust Occup Ther J 2014; 61(4): 230-40. 34. Plummer LC, Chalmers KA. Health literacy and physical activity in women diagnosed with breast cancer. Psychooncology 2017; 26(10): 1478-83. 35. Cormie P, Pumpa K, Galvao DA, et al. Is it safe and efficacious for women with lymphedema secondary to breast cancer to lift heavy weights during exercise: a randomised controlled trial. J Cancer Surviv 2013; 7(3): 413-24. 36. Hayes SC, Rye S, Disipio T, et al. Exercise for health: a randomized, controlled trial evaluating the impact of a pragmatic, translational exercise intervention on the quality of life, function and treatment-related side effects following breast cancer. Breast Cancer Res Treat 2013; 137(1): 175-86. 37. Loudon A, Barnett T, Piller N, Immink MA, Williams AD. Yoga management of breast cancer-related lymphoedema: a randomised controlled pilot-trial. BMC Complement Altern Med 2014; 14: 214. 38. Yee J, Davis GM, Beith JM, et al. Physical activity and fitness in women with metastatic breast cancer. J Cancer Surviv 2014; 8(4): 647-56. 39. Short CE, James EL, Girgis A, D'Souza MI, Plotnikoff RC. Main outcomes of the Move More for Life Trial: a randomised controlled trial examining the effects of tailored-print and targeted-print materials for promoting physical activity among post-treatment breast cancer survivors. Psychooncology 2015; 24(7): 771-8. 40. Martin EA, Battaglini CL, Hands B, Naumann F. Higher-Intensity Exercise Results in More Sustainable Improvements for VO2peak for Breast and Prostate Cancer Survivors. Oncol Nurs Forum 2015; 42(3): 241-9. 41. Buchan J, Janda M, Box R, Schmitz K, Hayes S. A Randomized Trial on the Effect of Exercise Mode on Breast Cancer-Related Lymphedema. Med Sci Sports Exerc 2016; 48(10): 1866-74. 42. Hagstrom AD, Marshall PW, Lonsdale C, Cheema BS, Fiatarone Singh MA, Green S. Resistance training improves fatigue and quality of life in previously sedentary breast cancer
Section 1
Breast Cancer 2018 Australian PEEK Study
survivors: a randomised controlled trial. Eur J Cancer Care (Engl) 2016; 25(5): 784-94. 43. Kampshoff CS, Stacey F, Short CE, et al. Demographic, clinical, psychosocial, and environmental correlates of objectively assessed physical activity among breast cancer survivors. Support Care Cancer 2016; 24(8): 3333-42. 44. Lawler S, Maher G, Brennan M, Goode A, Reeves MM, Eakin E. Get Healthy after Breast Cancer - examining the feasibility, acceptability and outcomes of referring breast cancer survivors to a general population telephone-delivered program targeting physical activity, healthy diet and weight loss. Support Care Cancer 2017; 25(6): 1953-62. 45. Lawn S, Zrim S, Leggett S, et al. Is self-management feasible and acceptable for addressing nutrition and physical activity needs of cancer survivors? Health Expect 2015; 18(6): 3358-73. 46. Reeves M, Winkler E, McCarthy N, et al. The Living Well after Breast Cancer Pilot Trial: a weight loss intervention for women following treatment for breast cancer. Asia Pac J Clin Oncol 2017; 13(3): 125-36. 47. Anderson DJ, Seib C, McCarthy AL, et al. Facilitating lifestyle changes to manage menopausal symptoms in women with breast cancer: a randomized controlled pilot trial of The Pink Women's Wellness Program. Menopause 2015; 22(9): 937-45. 48. Boyle FM, Smith IE, O'Shaughnessy J, et al. Health related quality of life of women in TEACH, a randomised placebo controlled adjuvant trial of lapatinib in early stage Human Epidermal Growth Factor Receptor (HER2) overexpressing breast cancer. Eur J Cancer 2015; 51(6): 685-96. 49. Gelmon KA, Boyle FM, Kaufman B, et al. Lapatinib or Trastuzumab Plus Taxane Therapy for Human Epidermal Growth Factor Receptor 2-Positive Advanced Breast Cancer: Final Results of NCIC CTG MA.31. J Clin Oncol 2015; 33(14): 1574-83. 50. Turner NC, Ro J, Andre F, et al. Palbociclib in Hormone-Receptor-Positive Advanced Breast Cancer. N Engl J Med 2015; 373(3): 209-19. 51. Bernhard J, Luo W, Ribi K, et al. Patient-reported outcomes with adjuvant exemestane
versus tamoxifen in premenopausal women with early breast cancer undergoing ovarian suppression (TEXT and SOFT): a combined analysis of two phase 3 randomised trials. Lancet Oncol 2015; 16(7): 848-58. 52. Phillips KA, Regan MM, Ribi K, et al. Adjuvant ovarian function suppression and cognitive function in women with breast cancer. Br J Cancer 2016; 114(9): 956-64. 53. Ribi K, Luo W, Bernhard J, et al. Adjuvant Tamoxifen Plus Ovarian Function Suppression Versus Tamoxifen Alone in Premenopausal Women With Early Breast Cancer: Patient-Reported Outcomes in the Suppression of Ovarian Function Trial. J Clin Oncol 2016; 34(14): 1601-10. 54. Cinieri S, Chan A, Altundag K, et al. Final Results of the Randomized Phase II NorCap-CA223 Trial Comparing First-Line All-Oral Versus Taxane-Based Chemotherapy for HER2-Negative Metastatic Breast Cancer. Clin Breast Cancer 2017; 17(2): 91-9 e1. 55. Saha P, Regan MM, Pagani O, et al. Treatment Efficacy, Adherence, and Quality of Life Among Women Younger Than 35 Years in the International Breast Cancer Study Group TEXT and SOFT Adjuvant Endocrine Therapy Trials. J Clin Oncol 2017; 35(27): 3113-22. 56. Sledge GW, Jr., Toi M, Neven P, et al. MONARCH 2: Abemaciclib in Combination With Fulvestrant in Women With HR+/HER2- Advanced Breast Cancer Who Had Progressed While Receiving Endocrine Therapy. J Clin Oncol 2017; 35(25): 2875-84. 57. Bell RJ, Robinson PJ, Nazeem F, et al. Persistent breast pain 5 years after treatment of invasive breast cancer is largely unexplained by factors associated with treatment. J Cancer Surviv 2014; 8(1): 1-8. 58. Davis SR, Panjari M, Robinson PJ, Fradkin P, Bell RJ. Menopausal symptoms in breast cancer survivors nearly 6 years after diagnosis. Menopause 2014; 21(10): 1075-81. 59. Hau E, Browne L, Capp A, et al. The impact of breast cosmetic and functional outcomes on quality of life: long-term results from the St. George and Wollongong randomized breast boost trial. Breast Cancer Res Treat 2013; 139(1): 115-23.

Section 1
Breast Cancer 2018 Australian PEEK Study
60. Marino JL, Saunders CM, Emery LI, Green H, Doherty DA, Hickey M. Nature and severity of menopausal symptoms and their impact on quality of life and sexual function in cancer survivors compared with women without a cancer history. Menopause 2014; 21(3): 267-74. 61. Inglis H, Boyle FM, Friedlander ML, Watson SL. Dry eyes and AIs: If you don't ask you won't find out. Breast 2015; 24(6): 694-8. 62. Gho SA, Steele JR, Jones SC, Munro BJ. Self-reported side effects of breast cancer treatment: a cross-sectional study of incidence, associations, and the influence of exercise. Cancer Causes Control 2013; 24(3): 517-28. 63. Stefanic N, Caputi P, Iverson DC. Investigating physical symptom burden and personal goal interference in early-stage breast cancer patients. Support Care Cancer 2014; 22(3): 713-20. 64. Beatty L, Kemp E, Binnion C, et al. Uptake and adherence to an online intervention for cancer-related distress: older age is not a barrier to adherence but may be a barrier to uptake. Support Care Cancer 2017; 25(6): 1905-14. 65. Brennan ME, Flitcroft K, Warrier S, Snook K, Spillane AJ. Immediate expander/implant breast reconstruction followed by post-mastectomy radiotherapy for breast cancer: Aesthetic, surgical, satisfaction and quality of life outcomes in women with high-risk breast cancer. Breast 2016; 30: 59-65. 66. Brennan ME, Butow P, Spillane AJ, Boyle F. Patient-reported quality of life, unmet needs and care coordination outcomes: Moving toward targeted breast cancer survivorship care planning. Asia Pac J Clin Oncol 2016; 12(2): e323-31. 67. Corica T, Nowak AK, Saunders CM, et al. Cosmesis and Breast-Related Quality of Life Outcomes After Intraoperative Radiation Therapy for Early Breast Cancer: A Substudy of the TARGIT-A Trial. Int J Radiat Oncol Biol Phys 2016; 96(1): 55-64. 68. Flitcroft K, Brennan M, Costa D, Wong A, Snook K, Spillane A. An evaluation of factors affecting preference for immediate, delayed or no breast reconstruction in women with high-risk breast cancer. Psychooncology 2016; 25(12): 1463-9.
69. Garvey G, Cunningham J, He VY, et al. Health-related quality of life among Indigenous Australians diagnosed with cancer. Qual Life Res 2016; 25(8): 1999-2008. 70. Hickey M, Marino JL, Braat S, Wong S. A randomized, double-blind, crossover trial comparing a silicone- versus water-based lubricant for sexual discomfort after breast cancer. Breast Cancer Res Treat 2016; 158(1): 79-90. 71. Howes BH, Watson DI, Xu C, Fosh B, Canepa M, Dean NR. Quality of life following total mastectomy with and without reconstruction versus breast-conserving surgery for breast cancer: A case-controlled cohort study. J Plast Reconstr Aesthet Surg 2016; 69(9): 1184-91. 72. Juraskova I, Jarvis S, Mok K, et al. The acceptability, feasibility, and efficacy (phase I/II study) of the OVERcome (Olive Oil, Vaginal Exercise, and MoisturizeR) intervention to improve dyspareunia and alleviate sexual problems in women with breast cancer. J Sex Med 2013; 10(10): 2549-58. 73. Kokavec A. Community Based Psychosocial Education Can Improve Mood Disturbance in Breast Cancer Survivors at Various Stages of Their Recovery. Behav Cogn Psychother 2016; 44(6): 730-6. 74. Leung J, Pachana NA, McLaughlin D. Social support and health-related quality of life in women with breast cancer: a longitudinal study. Psychooncology 2014; 23(9): 1014-20. 75. Leung J, Smith MD, McLaughlin D. Inequalities in long term health-related quality of life between partnered and not partnered breast cancer survivors through the mediation effect of social support. Psychooncology 2016; 25(10): 1222-8. 76. Lewis L, Carson S, Bydder S, Athifa M, Williams AM, Bremner A. Evaluating the effects of aluminum-containing and non-aluminum containing deodorants on axillary skin toxicity during radiation therapy for breast cancer: a 3-armed randomized controlled trial. Int J Radiat Oncol Biol Phys 2014; 90(4): 765-71. 77. Ng SK, Hare RM, Kuang RJ, Smith KM, Brown BJ, Hunter-Smith DJ. Breast Reconstruction Post Mastectomy: Patient Satisfaction and Decision Making. Ann Plast Surg 2016; 76(6): 640-4.

Section 1
Breast Cancer 2018 Australian PEEK Study
78. Oh B, Kimble B, Costa DS, et al. Acupuncture for treatment of arthralgia secondary to aromatase inhibitor therapy in women with early breast cancer: pilot study. Acupunct Med 2013; 31(3): 264-71. 79. Panjari M, Robinson PJ, Davis SR, Schwarz M, Bell RJ. A comparison of the characteristics, treatment and outcome after 5 years, of Australian women aged 70+ with those aged <70 years at the time of diagnosis of breast cancer. J Geriatr Oncol 2014; 5(2): 141-7. 80. Przezdziecki A, Sherman KA, Baillie A, Taylor A, Foley E, Stalgis-Bilinski K. My changed body: breast cancer, body image, distress and self-compassion. Psychooncology 2013; 22(8): 1872-9. 81. Sundaresan P, Sullivan L, Pendlebury S, et al. Patients' perceptions of health-related quality of life during and after adjuvant radiotherapy for T1N0M0 breast cancer. Clin Oncol (R Coll Radiol) 2015; 27(1): 9-15. 82. Tian Y, Schofield PE, Gough K, Mann GB. Profile and predictors of long-term morbidity in breast cancer survivors. Ann Surg Oncol 2013; 20(11): 3453-60. 83. Tucker PE, Saunders C, Bulsara MK, et al. Sexuality and quality of life in women with a prior diagnosis of breast cancer after risk-reducing salpingo-oophorectomy. Breast 2016; 30: 26-31.
Section 1
Breast Cancer 2018 Australian PEEK Study
Abbreviations
DF DF Degrees of Freedom. The number of values in the final calculation of a statistic that are free to vary.
IQR Interquartile range. A measure of statistical dispersion, being equal to the difference between 75th and 25th percentiles, or between upper and lower quartiles.
F F-statistic. An F statistic is a value you get when you run an ANOVA test or a regression analysis to find out if the means between two populations are significantly different.
FOP Fear of Progression. Tool to measure anxiety related to progression. ICCDR Centre for Community-Driven Research MS Mean of Squares. Estimates of variance across groups
SD . . SD Standard Deviation. A quantity expressing by how much the members of a group differ from the mean value for the group.
SF 36 Short Form Health Survey 36 SS or c2 Sum of the Squares. The sum of squares is used as a mathematical way to find the
function which best fits (varies least) from the data. t t-Statistic. Size of the difference relative to the variation in your sample data. PEEK Patient Experience, Expectations and Knowledge PIH Partners in Health P Probability value. A small p-value (typically ≤ 0.05) indicates strong. A large p-value
(> 0.05) indicates weak evidence. QoL Quality of LIfe W Kendall's W statistic (sometimes called the Coefficient of Concordance) is a non
parametric statistic. It's used to assess agreement between different raters, and ranges from 0 to 1.

Section 2
Breast Cancer 2018 Australian PEEK Study
Section 2 Demographics

Section 2
Breast Cancer 2018 Australian PEEK Study
Section 2: Demographics and study population characteristics Demographics
• One hundred participants living in Australia with stage 0 to stage IV breast cancer were recruited into the study.
• The majority of participants were from New South Wales (n=24, 24.00%), Victoria (n24, n=24.00%), and Queensland (n=19, 19.00%). There were 56 participants (56.00%) from a major city and 44 participants (44.00%) from regional or rural areas.
• Subgroup analysis are included throughout the study. These include: disease stage, stage 0-I (n=20, 20.00%), stage II-III (n=30, 30.00%) and stage IV (n=50, 50.00%); metastatic disease (n=50, 50.00%) compared to those no metastases (n=50, 50.00%); by location, metropolitan (n=56, 56%) or regional/rural areas (n= 44, 44.00%); and by education status including those with university degree (n= 54, 54.00%) and those with high school or trade certificate (n=46, 46.00%).
Baseline Heath – SF36 score • The overall scores for the cohort were in the highest quintile for role limitations due to emotional
problems. • The scores for physical functioning, and social functioning were in the second highest quintile indicating. • The scores for emotional well-being, pain, general health, and health change were in the middle quintile. • The scores for role limitations due to physical health, and energy/fatigue were in the second lowest
quintile. SF36 scores by disease stage
• Those with stage IV disease scored significantly worse than stages 0 and I for role limitations due to physical health, and social functioning.
• Those with stage IV disease scored significantly worse than those with stages 0 and I and stages II and III for emotional well-being, and general health.
• There were no significant differences between groups for physical function, role limitations due to emotional problems, energy/fatigue, pain or health change.
SF36 scores by metastatic status • Those with metastatic disease scored worse on the role limitations due to physical health, energy/fatigue,
emotional well-being, social functioning and general health compared to those without metastases. SF36 scores by location
• There were no differences observed for any of the SF36 scales between those that live in metropolitan areas compared to those that live in regional or rural areas.
SF36 scores by education • Those with a university degree scored statistically better on the physical functioning scale compared
those with high school or trade certificate.

Section 2
Breast Cancer 2018 Australian PEEK Study
Demographics
One hundred participants living in Australia with stage 0 to stage IV breast cancer were recruited into the study. The majority of participants were from New South Wales (n=24, 24.00%), Victoria (n24, n=24.00%), and Queensland (n=19, 19.00%). There were 56 participants (56.00%) from a major city and 44 participants (44.00%) from regional or rural areas.
Subgroup analysis are included throughout the study, these include: disease stage, stage 0-I (n=20, 20.00%), stage II-III (n=30, 30.00%) and stage IV (n=50, 50.00%); metastatic disease (n=50, 50.00%) compared to those no metastases (n=50, 50.00%); by location, metropolitan (n=56, 56%) or regional/rural areas (n= 44, 44.00%); and by education status including those with university degree (n= 54, 54.00%) and those with high school or trade (n=46, 46.00%). Demographics of participants are listed in Table 2.1
Table 2.1: Demographics
Characteristic n= Percentage of Participants Stage n=100 0 10 10.00 I 10 10.00 II 16 16.00 III 14 14.00 IV 50 50.00 Type of breast cancer n=100 *Additional information Unsure 33 33.00 ER +ve 15 15.00 ER +ve, PR +ve 26 26.00 ER +ve, HER 2 +ve 7 7.00 ER +ve,HER2 +ve,PR +ve 2 2.00 HER 2 +ve 7 7.00 Triple Negative 10 10.00 BRCA +ve 3 3.00 Has breast cancer spread? N=100 Yes 50 50.00 No 50 50.00 Site of breast metastases n=50 (Can spread to more than one location) Bone 38 76.00 Lymph 21 42.00 Liver 14 18.00 Lung 11 22.00 Brain 5 10.00 Contralateral breast 3 6.00 Distal lymph nodes 3 6.00

Section 2
Breast Cancer 2018 Australian PEEK Study
Characteristic n= Percentage of Participants Location: State n=100 New South Wales 24 24.00 Victoria 24 24.00 Queensland 19 19.00 Western Australia 18 18.00 South Australia 6 6.00 Australian Capital Territory 5 5.00 Tasmania 3 3.00 Northern Territory 1 1.00 Geographical location n=100 Major City 56 56.00 Inner Regional 29 29.00 Outer Regional 15 15.00 Social Economic Indexes for Areas n=100 (1= most disadvantaged) 1 4 4.00 2 8 8.00 3 1 1.00 4 7 7.00 5 12 12.00 6 16 16.00 7 4 4.00 8 14 14.00 9 10 10.00 10 24 24.00 Gender n=100 Female 100 100.00 Age of participant n=100 35-44 10 10.00 45-54 43 43.00
55-64 28 28.00 65-74 17 17.00 75-84 2 2.00 Birth country n=100 Australia 86 86.00 United Kingdom 11 11.00 New Zealand 1 1.00 Peru 1 1.00 South Africa 1 1.00 Race n=99 Caucasian/White 94 94.95 Asian 1 1.01 Australian 1 1.01 European 1 1.01 Hispanic/Latino 1 1.01 Indian 1 1.01

Section 2
Breast Cancer 2018 Australian PEEK Study
Characteristic n= Percentage of Participants Highest level of education obtained n=100 Less than High School degree 7 7.00 Some College but no degree 13 13.00 Trade 6 6.00 Associate degree 9 9.00 Bachelor Degree 30 30.00 Graduate degree 15 15.00 High school degree or equivalent 20 20.00 My health Record Access n=100 No 67 67.00 Yes 8 8.00 I Don't know what "My health record" is 18 18.00 Not Sure 7 7.00 My health Record Use n=8 Good 1 12.50 Acceptable 4 50.00 Poor 2 25.00 Very Poor 1 12.50 Carer status n=68 (Can be carer to more than one category) Children 22 33.85 Parents 4 5.88 Friend 2 2.94 Siblings 1 1.47 I am not a carer 40 5.88
*Additional information: Biomarker status All participants Stage 0-1 Stage II-III Stage IV
Unsure 33 10 9 14
ER +ve 15 2 4 9
ER +ve,PR +ve 26 5 11 10
ER +ve,HER2 +ve 7 0 2 5
ER +ve,HER2 +ve,PR +ve 2 0 0 2
HER2 +ve 7 0 3 4
Triple negative breast cancer 10 3 1 6
BRCA +ve 3 0 1 2

Section 2
Breast Cancer 2018 Australian PEEK Study
Baseline health
The Short Form Health Survey 36 (SF36) measures baseline health, or the general health of an individual. The SF36 comprises nine sub scales: physical functioning, role limitations due to physical health, role limitations due to emotional problems, energy and fatigue, emotional well-being, social function, pain, general health, and health change from one year ago. A higher score denotes a better health/function.
Summary statistics for the entire cohort are displayed alongside the possible range of each scale in Table 2.2, where the scale has a normal distribution mean and sd are used as a central measure, otherwise the median and IQR are used. The overall scores for the cohort were in the highest quintile for role limitations due to emotional problems (Median = 100.00, IQR = 100.00). The scores for physical functioning (median = 70.00, IQR=35.00) and Social Functioning (median = 68.75,
IQR = 25.00) were in the second highest quintile for the cohort. The scores for emotional well-being (median = 60.00, IQR=24.00), pain (median = 57.50, IQR= 35.00), general health (median = 45.00, IQR = 26.25) and health change (median = 50.00, IQR = 31.25) were in the middle quintile indicating moderate scores. The scores for role limitations due to physical health (median = 25.00, IQR =75.00) and energy/fatigue (mean = 39.85, sd=18.73) were in the second lowest quintile.
Comparisons of SF36 have been made based on breast cancer stage (Figures 2.1 to 2.9, Tables 2.3 to 2.9), metastatic status (Figures 2.10 to 2.18, Tables 2.10 to 2.11), location (Figures 2.19 to 2.27, Tables 2.12 to 2.13), and education (Figures 2.28 to 2.36, Tables 2.14 to 2.15).
Table 2.2: SF36 summary statistics all participants
Scale Mean SD Median IQR Possible range
Physical functioning 65.00 23.80 70.00 35.00 0-100
Role limitations due to physical health
37.50 41.67 25.00 75.00 0-100
Role limitations due to emotional problems
59.67 44.27 100.00 100.00 0-100
Energy/fatigue* 39.85 18.73 40.00 30.00 0-100
Emotional well-being 64.20 14.63 60.00 24.00 0-100
Social functioning 63.88 24.09 68.75 25.00 0-100
Pain 56.48 24.92 57.50 35.00 0-100
General health 45.50 19.93 45.00 26.25 0-100
Health change 57.00 29.10 50.00 31.25 0-100
*Normal distribution use mean and SD
Comparisons of SF36 sub scales by disease stage
Comparisons of SF36 sub scales were made between participants by disease stage; Stages 0 and I, Stages II and III, and Stage IV. Boxplots of each SF36 scale by disease severity are displayed in Figures 2.1-2.9, and summary statistics are listed in Tables 2.3. A one-way ANOVA test was used with the assumptions for response variable residuals were normally distributed and variances of populations were equal. When the ANOVA test indicated a significant result, post hoc comparisons were made using the Tukey HSD test
(Tables 2.4 – 2.5). When the assumptions for normality of residuals was not met, a Kruskal-Wallis test was used, and when a significant result was indicated, it was followed by post hoc Wilcoxon rank sum tests between groups (Tables 2.6 – 2.7).
When assumptions for assumption of equal variances were not met, a Welch one-way test was used, and when a significant result was indicated, it was followed by pairwise t-tests with no assumption of equal variances (Tables 2.8 – 2.9).

Section 2
Breast Cancer 2018 Australian PEEK Study
A one way ANOVA test indicated a significant difference in the SF36 energy/fatigue scale between groups [F(2, 97) = 4.03 ,p = 0.0209] (Table 2.4). Post hoc comparisons using the Tukey HSD test did not indicate any significant differences between groups (Table 2.5).
A Kruskal-Wallis test indicated a significant difference between severity for the role limitations due to physical health [X2(2) = 7.60, p=0.0224] (Table 2.6). Post hoc pairwise comparisons using Wilcoxon rank sum test indicated a that the median score for Stage 0-I (median = 75.00, IQR = 100.00) were higher compared to the median score for Stage IV (median = 0.00, IQR = 50.00) p=0.0224 (Table 2.3 and 2.7).
A Welch one-way test indicated a significant difference between groups for emotional well-being [F(2, 39.44) = 8.48, p=0.0009] (2.8). Post hoc comparisons indicated that the median score for stage IV (mean = 58.60, sd = 10.00) was significantly lower than the median score for stage 0-I (mean = 71.00, sd = 16.50), p= 0.0064; and significantly lower than that for stage II-III (mean = 69.10, sd = 16.50) p= 0.0064 (Tables 2.3 and 2.9).
A Welch one-way test indicated a significant difference between groups for social functioning [F(2, 40.00) = 5.02, p=0.0113] (Table 2.8). Post hoc comparisons indicated that the median score for stage IV (mean = 57.00, sd = 17.00) was significantly lower than the median score for stage 0-I (mean = 74.40, sd = 25.20), p= 0.0260 (Table 2.3 and 2.9).
A Welch one-way test indicated a significant difference between groups for general health [F(2, 44.32) = 19.11, p<0.0001] (Table 2.8). Post hoc comparisons indicated that the median score for stage IV (mean = 35.90, sd = 14.20) was significantly lower than the median score for stage 0-I (mean = 58.80, sd = 15.40), p<0.0001; and significantly lower than that for stage II-III (mean = 52.70, sd = 23.00) p= 0.0012 (Tables 2.3 and 2.8).
No significant differences were observed for physical function, role limitations due to emotional problems, pain or health change.

Section 2
Breast Cancer 2018 Australian PEEK Study
Figure 2.1: Boxplot of SF36 physical functioning by disease stage
Figure 2.2: Boxplot of SF36 role limitations due to physical health by disease stage
Figure 2.3: Boxplot of SF36 role limitations due to emotional problems by disease stage
Figure 2.4: Boxplot of SF36 energy/fatigue by disease stage
Figure 2.5: Boxplot of SF36 emotional well-being by disease stage
2.6: Boxplot of SF36 social functioning by disease stage
Stage 0-I Stage II -III Stage IV
2040
6080
100
SF36 Physical Functioning
Stage 0-I Stage II -III Stage IV
020
4060
80100
SF36 Role Limitations Due to Physical Health
Stage 0-I Stage II -III Stage IV
020
4060
80100
SF36 Role Limitations Due to Emotional Problems
Stage 0-I Stage II -III Stage IV
020
4060
80
SF36 Energy/Fatigue
Stage 0-I Stage II -III Stage IV
3040
5060
7080
90
SF36 Emotional Well-being
Stage 0-I Stage II -III Stage IV
020
4060
80100
SF36 Social Functioning

Section 2
Breast Cancer 2018 Australian PEEK Study
Figure 2.7: Boxplot of SF36 pain by disease stage 2.8: Boxplot of SF36 general health by disease stage
Figure 2.9: Boxplot of SF36 health change by disease stage
Stage 0-I Stage II -III Stage IV
020
4060
80100
SF36 Pain
Stage 0-I Stage II -III Stage IV
2040
6080
SF36 General Health
Stage 0-I Stage II -III Stage IV
020
4060
80100
SF36 Health Change

Section 2
Breast Cancer 2018 Australian PEEK Study
Table 2.3 summary statistics SF36 by stage SF36 subscale Group Count Mean Sd Median IQR Physical function Stage 0-I 20 71.00 21.90 75.00 26.20
Stage II-III 30 65.70 28.50 70.00 43.80 Stage IV 50 62.20 21.30 67.50 25.00
Role limitations due to physical health
Stage 0-I 20 57.50 43.00 75.00 100.00 Stage II-III 30 43.30 44.50 25.00 100.00 Stage IV 50 26.00 36.10 0.00 50.00
Role limitations due to emotional problems
Stage 0-I 20 71.70 39.40 100.00 66.70 Stage II-III 30 61.10 45.60 100.00 100.00
Stage IV 50 54.00 45.10 33.30 100.00 Energy/Fatigue Stage 0-I 20 45.50 16.00 45.00 22.50
Stage II-III 30 44.70 22.40 45.00 32.50 Stage IV 50 34.70 16.00 37.50 23.80
Emotional well-being Stage 0-I 20 71.00 16.50 70.00 26.00 Stage II-III 30 69.10 16.50 70.00 23.00 Stage IV 50 58.60 10.00 56.00 12.00
Social Functioning Stage 0-I 20 74.40 25.20 75.00 50.00 Stage II-III 30 68.30 30.00 75.00 37.50 Stage IV 50 57.00 17.00 50.00 25.00
Pain Stage 0-I 20 63.40 24.90 57.50 37.5 Stage II-III 30 58.10 26.20 56.20 34.40 Stage IV 50 52.80 23.90 57.50 45.00
General health Stage 0-I 20 58.80 15.40 60.00 18.80
Stage II-III 30 52.70 23.00 57.50 30.00 Stage IV 50 35.90 14.20 35.00 20.00
Health change Stage 0-I 20 63.80 25.00 50.00 25.00 Stage II-III 30 55.80 33.90 50.00 68.80
Stage IV 50 55.00 27.70 50.00 50.00 Table 2.4: ANOVA table by disease stage
SF36 subscale Sum of squares
Df Mean square
F P
Energy/Fatigue Between Groups 2661 2 1330.30 4.03 0.0209* Within Groups 32062 97 330.50 Total 34323 99
* Statistically significant at p<0.05

Section 2
Breast Cancer 2018 Australian PEEK Study
Table 2.5: Post-hoc Tukey HSD test SF36 subscale Comparison Mean
difference Lower Upper P adjusted
Energy/Fatigue Stage II-III - Stage 0-I -0.83 -13.33 11.66 0.9862 Stage IV – Stage 0-I -10.80 -22.25 0.65 0.0688 Stage IV – Stage II-III -9.97 -19.96 0.03 0.0507
Table 2.6: Summary statistics and Kruskal-Wallis rank sum test for SF36 scales by disease stage
SF36 subscale X2 Df P Physical functioning 2.07 2 0.3558 Role limitations due to physical health 7.60 2 0.0224* Role limitations due to emotional problems 2.03 2 0.3624 Pain 2.37 2 0.3064 Health change 2.07 2 0.3554
* Statistically significant at p<0.05 Table 2.7: PosthocpairwisecomparisonsusingWilcoxonranksumtest,p-values
SF36 subscale Group Stages 0 and I Stages II and III Role limitations due to physical health
Stages II and III 0.4010
Stage IV 0.0230* 0.1310 * Statistically significant at p<0.05 Table 2.8: Welch One-way test by disease stage
SF36 subscale F Df1 Df2 P Emotional well-being 8.48 2.00 39.44 0.0009* Social functioning 5.02 2.00 40.00 0.0113* General health 19.11 2.00 44.32 <0.0001*
* Statistically significant at p<0.05 Table 2.9: Post-hocpairwiset-testwithnoassumptionofequalvariance,p-values
SF36 subscale Group Stages 0 and I Stages II and III Emotional well-being Stages II and III 0.6869
Stage IV 0.0064* 0.0064* Social functioning Stages II and III 0.4460
Stage IV 0.0260* 0.0980 General health Stages II and III 0.2679
Stage IV <0.0001* 0.0012* * Statistically significant at p<0.05

Section 2
Breast Cancer 2018 Australian PEEK Study
Comparisons of SF36 sub scales by metastatic status
Comparisons of SF36 subscales were made between those that had metastases compared with those that did not. Boxplots of each SF36 scale by metastatic status are displayed in Figures 2.10-2.18. A two-sample t-test was used when assumptions for normality and variance were met (Table 2.10), or when assumptions for normality and variance were not met, a Wilcoxon rank sum test with continuity correction was used (Table 2.11). A two sample t-test indicated that the mean score for the SF36 energy/fatigue scale was significantly higher for those without metastases (mean =45.00, sd = 19.90) compared to those with metastases (mean = 34.70, sd = 16.00) [t(98) = 2.85, p=0.0054] (Table 2.10).
A Wilcoxon rank sum test with continuity correction indicated a significant difference between those with
metastatic disease (median = 0.00, IQR =50.00) and those without (median = 50.00, IQR = 100.00) for role limitations due to physical health [W=1602.00, p=0.0100]; a significant difference between those with metastatic disease (median = 56.00, IQR =12.00) and those without (median = 70.00, IQR = 26.00) for emotional well-being [W=1813.50, p<0.0001]; a significant difference between those with metastatic disease (median = 50.00, IQR = 25.00) and those without (median = 75.00, IQR = 46.00) for social functioning [W=1730.50, p=0.0007]; and a significant difference between those with metastatic disease (median = 35.00, IQR = 20.00) and those without (median = 60.00, IQR = 30.00) for general health [W=1934.00, p<0.0001] (Table 2.11). In each case, those with metastatic disease scored worse than those without.
Figure 2.10: Boxplot of SF36 physical functioning by metastatic status
Figure 2.11: Boxplot of SF36 role limitations due to physical health by metastatic status
No metastases Metastases
2040
6080
100
SF36 Physical Functioning
No metastases Metastases
020
4060
80100
SF36 Role Limitations due to Physical Health

Section 2
Breast Cancer 2018 Australian PEEK Study
Figure 2.12: Boxplot of SF36 role limitations due to emotional problems by metastatic status
Figure 2.13: Boxplot of SF36 energy/fatigue by metastatic status
Figure 2.14: Boxplot of SF36 emotional well-being by metastatic status
Figure 2.15: Boxplot of SF36 social functioning by metastatic status
Figure 2.16: Boxplot of SF36 pain by metastatic status Figure 2.17: Boxplot of SF36 general health by metastatic status
No metastases Metastases
020
4060
80100
SF36 Role Limitations due to Emotional Problems
No metastases Metastases
020
4060
80
SF36 Energy/Fatigue
No metastases Metastases
3040
5060
7080
90
SF36 Emotional Well-being
No metastases Metastases
020
4060
80100
SF36 Social Functioning
No metastases Metastases
020
4060
80100
SF36 Pain
No metastases Metastases
2040
6080
SF36 General Health

Section 2
Breast Cancer 2018 Australian PEEK Study
Figure 2.18: Boxplot of SF36 health change by metastatic status
Table 2.10: Summary statistics and two sample t-test SF36 subscales by metastatic status SF36 subscale Group Count Mean SD t df P Energy/Fatigue Metastases 50 34.70 16.00 2.85 98 0.0054*
No metastases 50 45.00 19.90 * Statistically significant at p<0.05
Table 2.11: Summary statistics Wilcoxon rank sum test with continuity correction SF36 subscales by location SF36 subscale Group Count Median IQR W P Physical functioning Metastases 50 67.50 25.00 1442.50 0.1838
No metastases 50 72.50 45.00 Role limitations due to physical health
Metastases 50 0.00 50.00 1602.00 0.0100* No metastases 50 50.00 100.00
Role limitations due to emotional problems
Metastases 50 33.30 100.00 1406.00 0.2425 No metastases 50 100.00 66.70
Emotional well-being Metastases 50 56.00 12.00 1813.50 <0.0001* No metastases 50 70.00 26.00
Social functioning Metastases 50 50.00 25.00 1730.50 0.0007* No metastases 50 75.00 46.90
Pain Metastases 50 57.50 45.00 1452.50 0.1594 No metastases 50 57.50 35.00
General health Metastases 50 35.00 20.00 1934.00 <0.0001* No metastases 50 60.00 30.00
Health change Metastases 50 50.00 25.00 1373.00 0.3784 No metastases 50 50.00 50.00
* Statistically significant at p<0.05
No metastases Metastases
020
4060
80100
SF36 Health Change

Section 2
Breast Cancer 2018 Australian PEEK Study
Comparisons of SF36 sub scales by location
Comparisons of SF36 subscales were made between those that live in a metropolitan area compared with those that live in regional or rural areas. Boxplots of each SF36 scale by location are displayed in Figures 2.19-2.27. A two-sample t-test was used when
assumptions for normality and variance were met (Table 2.12), or when assumptions for normality and variance were not met, a Wilcoxon rank sum test with continuity correction was used (Table 2.13). No statistically significant differences were observed between these two groups for any SF36 sub scale (Tables 2.12 and 2.13).
Figure 2.19: Boxplot of SF36 physical functioning by location
Figure 2.20: Boxplot of SF36 role limitations due to physical health by location
Figure 2.21: Boxplot of SF36 role limitations due to emotional problems by location
Figure 2.22: Boxplot of SF36 energy/fatigue by location
Metropolitan Regional/Rural
2040
6080
100
SF36 Physical Functioning
Metropolitan Regional/Rural
020
4060
80100
SF36 Role Limitations due to Physical Health
Metropolitan Regional/Rural
020
4060
80100
SF36 Role Limitations due to Emotional Problems
Metropolitan Regional/Rural
020
4060
80
SF36 Energy/Fatigue

Section 2
Breast Cancer 2018 Australian PEEK Study
Figure 2.23: Boxplot of SF36 emotional well-being by location
Figure 2.24: Boxplot of SF36 social functioning by location
Figure 2.25: Boxplot of SF36 pain by location Figure 2.26: Boxplot of SF36 general health by location
Figure 2.27: Boxplot of SF36 health change by location
Metropolitan Regional/Rural
3040
5060
7080
90
SF36 Emotional Well-being
Metropolitan Regional/Rural
020
4060
80100
SF36 Social Functioning
Metropolitan Regional/Rural
020
4060
80100
SF36 Pain
Metropolitan Regional/Rural
2040
6080
SF36 General Health
Metropolitan Regional/Rural
020
4060
80100
SF36 Health Change

Section 2
Breast Cancer 2018 Australian PEEK Study
Table 2.12: Summary statistics and two sample t-test SF36 subscales by location SF36 subscale Group Count Mean SD T df p Energy/Fatigue Metropolitan 56 38.50 19.30 -0.77 98 0.4440
Regional/Rural 44 41.50 18.10 Table 2.13: Summary statistics Wilcoxon rank sum test with continuity correction SF36 subscales by location
SF36 subscale Group Count Median IQR W p Physical functioning Metropolitan 56 67.50 36.20 1219.00 0.9305
Regional/Rural 44 70.00 30.00 Role limitations due to physical health
Metropolitan 56 25.00 100.00 1360.00 0.3467 Regional/Rural 44 12.50 75.00
Role limitations due to emotional problems
Metropolitan 56 83.30 75.00 1249.50 0.8976 Regional/Rural 44 100.00 100.00
Emotional Well-Being Metropolitan 56 64.00 17.00 1360.50 0.3719 Regional/Rural 44 60.00 25.00
Social functioning Metropolitan 56 75.00 25.00 1374.50 0.315 Regional/Rural 44 50.00 28.10
Pain Metropolitan 56 57.50 33.10 1371.00 0.3312 Regional/Rural 44 56.20 37.50
General Health Metropolitan 56 45.00 40.00 1162.00 0.6280 Regional/Rural 44 42.50 27.50
Health change Metropolitan 56 50.00 50.00 1219.00 0.9279 Regional/Rural 44 50.00 25.00
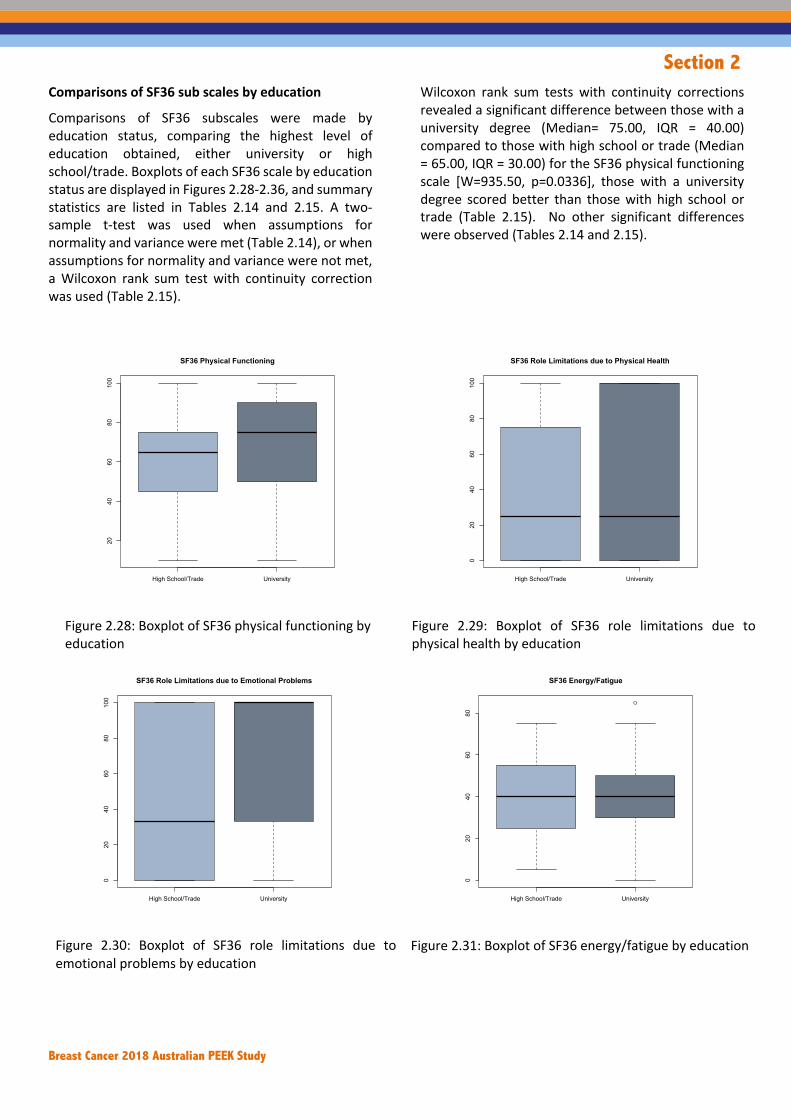
Section 2
Breast Cancer 2018 Australian PEEK Study
Comparisons of SF36 sub scales by education
Comparisons of SF36 subscales were made by education status, comparing the highest level of education obtained, either university or high school/trade. Boxplots of each SF36 scale by education status are displayed in Figures 2.28-2.36, and summary statistics are listed in Tables 2.14 and 2.15. A two-sample t-test was used when assumptions for normality and variance were met (Table 2.14), or when assumptions for normality and variance were not met, a Wilcoxon rank sum test with continuity correction was used (Table 2.15).
Wilcoxon rank sum tests with continuity corrections revealed a significant difference between those with a university degree (Median= 75.00, IQR = 40.00) compared to those with high school or trade (Median = 65.00, IQR = 30.00) for the SF36 physical functioning scale [W=935.50, p=0.0336], those with a university degree scored better than those with high school or trade (Table 2.15). No other significant differences were observed (Tables 2.14 and 2.15).
Figure 2.28: Boxplot of SF36 physical functioning by education
Figure 2.29: Boxplot of SF36 role limitations due to physical health by education
Figure 2.30: Boxplot of SF36 role limitations due to emotional problems by education
Figure 2.31: Boxplot of SF36 energy/fatigue by education
High School/Trade University
2040
6080
100
SF36 Physical Functioning
High School/Trade University
020
4060
80100
SF36 Role Limitations due to Physical Health
High School/Trade University
020
4060
80100
SF36 Role Limitations due to Emotional Problems
High School/Trade University
020
4060
80
SF36 Energy/Fatigue

Section 2
Breast Cancer 2018 Australian PEEK Study
Figure 2.32: Boxplot of SF36 emotional well-being by education
2.33: Boxplot of SF36 social functioning by education
Figure 2.34: Boxplot of SF36 pain by education 2.35: Boxplot of SF36 general health by education
Figure 2.36: Boxplot of SF36 health change by education
High School/Trade University
3040
5060
7080
90SF36 Emotional Well-being
High School/Trade University
020
4060
80100
SF36 Social Functioning
High School/Trade University
020
4060
80100
SF36 Pain
High School/Trade University
2040
6080
SF36 General Health
High School/Trade University
020
4060
80100
SF36 Health Change

Section 2
Breast Cancer 2018 Australian PEEK Study
Table 2.14: Summary statistics and two sample t-test SF36 subscales by education SF36 subscale Education Count Mean SD T df P Energy/Fatigue High school/Trade 46 39.60 18.30 -0.14 98 0.8892
University degree 54 40.10 19.30
Table 2.15: Summary statistics Wilcoxon rank sum test with continuity correction SF36 subscales by education SF36 subscale Education Count Median IQR W P Physical functioning High school/Trade 46 65.00 30.00 935.50 0.0336*
University degree 54 75.00 40.00
Role limitations due to physical health
High school/Trade 46 25.00 75.00 1238.50 0.9824
University degree 54 25.00 93.80
Role limitations due to emotional problems
High school/Trade 46 33.30 100.00 1049.00 0.1466
University degree 54 100.00 66.70
Emotional well-being High school/Trade 46 60.00 19.00 1076.00 0.2502
University degree 54 64.00 20.00
Social functioning High school/Trade 46 50.00 37.50 1029.50 0.1352
University degree 54 75.00 25.00
Pain High school/Trade 46 50.00 22.50 998.50 0.0895
University degree 54 67.50 44.40
General Health High school/Trade 46 40.00 30.00 1108.00 0.3540
University degree 54 45.00 37.50
Health change High school/Trade 46 50.00 62.50 1289.00 0.7373
University degree 54 50.00 25.00 * Statistically significant at p<0.05

Section 3
Breast Cancer 2018 Australian PEEK Study
Section 3 Symptoms and diagnosis

Section 3
Breast Cancer 2018 Australian PEEK Study
Section 3: Experience of symptoms and diagnosis Symptoms at diagnosis
• In the online questionnaire participants were asked to recall all of the symptoms that they experienced and their quality of life while experiencing those symptoms. The most common symptom experienced was a breast lump, noted by 60 participants (60.00%), followed by a change in size, shape or feel of the breast (n=46, 46.00%), breast pain (n=36, 36.00%) and feeling tired/lower energy than usual (n=36, 36.00%). Skin changes including puckering, dimpling, rash or redness of skin, and ache or pain in bones were each noted by 23 participants (23.00%).
• In relation to sub-group variations, participants with stage 0-I breast cancer noted a change in size, shape or feel of their breast less frequently than the general cohort (25.00% compared to 46.00% in the general cohort). They also noted breast pain and feeling tired/less energy than usual less frequently (25.00% compared to 36.00% in the general cohort for both symptoms) and aches or pain in bones less frequently (10.00% compared to 23.00% in the general cohort).
• In the structured interview participants were asked to describe the symptoms that actually led to their diagnosis, as opposed to all the symptoms that they could recall. There were 39 women (39.00%) that described feeling a lump and seeking medical attention. This was the most common symptom experienced that led to diagnosis. The same number of participants (n=39, 39.00%) described not noticing any symptoms prior to diagnosis. Other symptoms included breast pain (n=9, 9.00%) and breast swelling, asymmetry or bruising (n=7, 7.00%).
• In relation to sub-group variations, participants with stage 0-I breast cancer described having no symptoms more frequently than the general cohort (55.00% compared to 39.00% in the general cohort).
• The most common diagnostic pathway described was self-detecting a lump or other breast abnormality, seeking attention from a general practitioner and being referred to mammogram, ultrasound and biopsy (n=48, 48.00%). There were an additional five participants (5.00%) that described self-detecting a lump or other breast abnormality, however being referred to ultrasound and biopsy directly. The next most common diagnostic pathway was through routine mammography which led to ultrasound and biopsy (n=32, 32.00%). There were also eight participants (8.00%) that described being diagnosed through their GP (through a routine check-up or other investigation) which led to mammography, ultrasound and biopsy.
• In relation to sub-group variations, participants with stage II-III breast cancer described self-detection leading to diagnosis more frequently than the general cohort (70.00% compared to 48.00% in the general cohort). Participants with stage 0-I breast cancer described diagnosis following a routine check-up or other investigation with their general practitioner more frequently (25.00% compared to 8.00% in the general cohort).
Support at diagnosis
• In the online questionnaire, participants were asked whether they felt supported at the time of diagnosis. There were 42 participants (42.00%) that indicated that they had no support at diagnosis, while 34 participants (34.00%) noted that they had enough support. An additional 24 participants (24.00%) indicated that they had some support but that it was not enough.
• In relation to sub-group variations, participants with stage 0-I breast cancer reported having no support at diagnosis less frequently than the general cohort (30.00% compared to 42.00% in the general cohort), however, this group also reported having enough support at diagnosis, more frequently than the general cohort (45.00% compared to 34.00% in the general cohort). Participants that were high school educated reported that they had enough support at diagnosis, less frequently than the general cohort (21.74% compared to 34.00% in the general cohort).

Section 3
Breast Cancer 2018 Australian PEEK Study
Genetic/biomarker tests • Participants were asked whether they had ever had a discussion about genetic tests or tests to see if there
were biomarkers that might be relevant to their condition or treatment. There were 42 participants (42.00%) that indicated that they had brought up the topic for discussion with their doctor and 23 participants (23.00%) that reported that their doctor had brought up the topic for discussion. There were also 35 participants (35.00%) that indicated that no one had ever spoken to them about this.
• In relation to sub-group variations participants with stage 0-I and stage II-III breast cancer indicated that they had brought up the topic of biomarker or genetic testing less frequently than the general cohort, while participants with stage IV breast cancer brought up the topic more frequently (stage 0-I = 30.00%, stage II – III = 16.67%, stage IV = 62.00% compared to 42.00% in the general cohort). Participants with stage II-III breast cancer indicated that their doctor brought up the topic of biomarker/genetic testing, more frequently than the general cohort (46.67% compared to 23.00% in the general cohort). Participants with stage 0-I breast cancer reported that no one had brought up this topic with them, more frequently than the general cohort (55.00% compared to 35.00% in the general cohort).
• Participants were also asked about their interest in this type of test if it was available. The majority of participants noted that they had not had this test, but would like to (n=64, 64.00%). There were 20 participants (20.00%) that reported having this test and not paying out of pocket for it, while 13 participants (13.00%) indicated that they had not had this test and were not interested in it.
• In relation to sub-group variations, participants that were university educated indicated that they had not had this test but would like to, more frequently than the general cohort (75.93% compared to 64.00% in the general cohort), while participants that were high school educated indicated that they were not interested in this test, more frequently than the general cohort (23.92% compared to 13.00% in the general cohort).
Understanding of prognosis • Participants were asked whether anyone talked to them about prognosis. The most common theme noted
by 23 participants (23.00%) was that they had not been given a clear prognosis. This was followed by two themes noted by 14 participants (14.00%) each including the understanding that they would make a full recovery and are not likely to have a recurrence, and that they have a good prognosis with maintenance therapy. There were also 14 participants (14.00%) that were not able to describe prognosis, but rather focused on describing their treatment regime.
• In relation to sub-group variations, participants with stage 0-I breast cancer reported not being given a clear prognosis less frequently than the general cohort (5.00% compared to 23.00% in the general cohort). This group also reported having a good prognosis with a full recovery and little chance of recurrence, more frequently than the general cohort (60.00% compared with 14.00% in the general cohort). There were also no participants with stage IV breast cancer that reported this theme. Participants with stage I-III breast cancer reported having a good prognosis with maintenance therapy more frequently than the general cohort (40.00% compared to 14.00% in the general cohort), while participants with stage IV breast cancer reported this less frequently (2.00% compared to 14.00% in the general cohort).

Section 3
Breast Cancer 2018 Australian PEEK Study
Experience of symptoms before diagnosis
Participants were asked to recall all of the symptoms that they experienced before diagnosis and this was asked in the online questionnaire. Participants were also asked to recall their quality of life while experiencing those symptoms. The most common symptom experienced was a breast lump, noted by 60 participants (60.00%), followed by a change in size, shape or feel of the breast (n=46, 46.00%), breast pain (n=36, 36.00%) and feeling tired/lower energy than usual (n=36, 36.00%). Skin changes including puckering, dimpling, rash or redness of skin, and ache or pain in bones were each noted by 23 participants (23.00%).
In relation to sub-group variations, participants with stage 0-I breast cancer noted a change in size, shape or feel of their breast less frequently than the general cohort (25.00% compared to 46.00% in the general cohort). They also noted breast pain and feeling tired/less energy than usual less frequently (25.00% compared to 36.00% in the general cohort for both symptoms) and aches or pain in bones less frequently (10.00% compared to 23.00% in the general cohort).
Table 3.1: Symptoms experienced
Symptoms experienced All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n=30 % n=50 % n=50 %Breast lump 60 60.00 11 55.00 17 56.67 28 56.00 32 64.00
Change in size, shape or feel 46 46.00 5 25.00 13 43.33 18 36.00 28 56.00
Breast pain 36 36.00 5 25.00 11 36.67 16 32.00 20 40.00
Feeling tired/lower energy levels than usual 36 36.00 5 25.00 16 53.33 21 42.00 15 30.00
Skin changes including puckering, dimpling, rash or redness of skin
23 23.00 4 20.00 8 26.67 12 24.00 11 22.00
Ache or pain in bones 23 23.00 2 10.00 4 13.33 6 12.00 17 34.00
Fluid leaking from your nipple 10 10.00 0 0.00 0 0.00 0 0.00 10 20.00
Less of an appetite 10 10.00 1 5.00 5 16.67 6 12.00 4 8.00

Section 3
Breast Cancer 2018 Australian PEEK Study
Figure 3.1: Symptoms experienced Participants were asked to rate their quality of life while experiencing symptoms on a scale of 1 to 7, with 1 being life was very distressing, 4 being life was average and 7 being life was great. Mean quality of life while experiencing symptoms ranged from 2.20 to 5.04. The majority of scores were in the ‘3 = Life was a
little distressing’ range. In relation to quality of life while experiencing symptoms, the symptoms with the most impact on quality of life were fluid leaking from nipple (mean score 2.20), feeling tired/lower energy levels (3.33), breast lump (3.43) and breast pain (3.47).
Figure 3.2: Symptoms experienced and mean QoL
0
10
20
30
40
50
60
70
Breast lump Change in size,shape or feel of
breast
Breast pain Feelingtired/lower
energy levels thanusual
Skin changesincluding
puckering,dimpling, rash orredness of skin
Ache or pain inbones
Fluid leaking fromnipple
Less of anappetite
0.00
1.00
2.00
3.00
4.00
5.00
6.00
Fluid leakingfrom nipple
Feelingtired/lower
energy levelsthan usual
Breast lump Breast pain Change in size,shape or feel of
breast
Ache or pain inbones
Less of anappetite
Skin changesincluding
puckering,dimpling, a rash
or redness ofskin

Section 3
Breast Cancer 2018 Australian PEEK Study
Table 3.2: Symptoms experienced and mean QoL
In the structured interview, participants were asked to describe the symptoms that actually led to their diagnosis, as opposed to all the symptoms that they could recall. There were 39 women (39.00%) that described feeling a lump and seeking medical attention. This was the most common symptom experienced that led to diagnosis. Participant describes feeling a lump and seeking medical attention
Yes. I was actually scratching an itch and I felt it was my first diagnosis that was a palpable lump, it was very, very small. I think I was just very fortunate that it wasn't deep in the breast. I don't have huge breasts, but I've got enough there that, if it had been deeper into the breast, I wouldn't have noticed it. I think it was actually itchy. I think that's what gave me the itch without end. When I went to scratch it, it sort of had a pointy edge to it….That was just a little bit I noted. I actually hadn't had any mammograms done for eight years. That sort of prompted me to go off and get a referral for a mammogram and ultrasound which took me about six months to get around to, but I did eventually. Participant 18 Yes, I'm a regular breast checker. I check regularly in the shower. I was in the shower one day in mid May and I was just washing myself and I found a hardened area down on my left breast on the side. I was just pre-period and I thought, 'maybe it's just a bit of that I'll just leave it for a couple of days." Then I had my period and waited for a couple of days after that and it was still there and I just thought, "I don't like this.'' I went to the GP. The GP didn't think it would be anything, but she was more than happy to refer me for an ultra sound and a mammogram which I did. Participant 31
I noticed a lump but it didn't seem like--as the way they advertise it as a typical lump, as a frozen pea or a pimple or something like that. I thought I'd actually bumped myself because it was like it was a bruise, when the blood fills up underneath it, and it forms a bit of a lump, that's what it felt like but it didn’t go away and I was already due because I had turned 50, due to have a breast screening, so I booked that and I went in to have that and the lady when she was doing the breast screen, she said she could see something on there as well. Participant 79 The same number of participants (n=39, 39.00%) described not noticing any symptoms prior to diagnosis. Participant describes not noticing any symptoms prior to diagnosis
Well, I didn’t. Mine was picked up with a routine screening. I turned 65 and my GP suggested that we do a whole lot of baseline things and that included a mammogram and an ultrasound of my breasts. The results came back unclear and the radiologist suggested that I wait three months and then, go for another one. My GP, because she had a lot of breast cancer in her family, she was really unhappy with that. When the results came to her, I went down with my film and she said, “No, we’re not waiting that long. If there’s nothing, it shouldn’t be hanging over your head and if it is something, you need to it dealt with more quickly.” She got me in within a week to see a breast surgeon. The breast surgeon thought it was a bit unsure but she did a manual examination. She wasn’t very happy with that, noticed some dimpling. I had more ultrasounds and then, a biopsy. The biopsy came back positive. It was a lobular cancer, nobody could feel it. Even the surgeon couldn’t feel it. It was
Symptom experienced Mean QoL
Fluid leaking from nipple 2.20
Feeling tired/lower energy levels than usual 3.33
Breast lump 3.43
Breast pain 3.47
Change in size, shape or feel of breast 3.57
Ache or pain in bones 3.65
Less of an appetite 4.10
Skin changes including puckering, dimpling, a rash or redness of skin 5.04

Section 3
Breast Cancer 2018 Australian PEEK Study
almost a luck thing that I was diagnosed when I was. That’s right. everybody, I think, was a bit surprised when that came through, it’s malignant. It was four and a half centimetres so it was quite large. The ultrasound, really high-quality ultrasound, they thought it was around about three centimetres. When it actually came out and went to pathology, it was four and a half. I was extremely lucky. It didn’t get any further. Participant 2 Sure. Actually no, I can’t because I never noticed anything at all. In fact, even the tracing surgeons couldn’t feel anything. It was only picked up on a mammogram. Participant 68
I didn't actually notice anything though. My cancer was picked up with a baseline ultrasound. I didn't find a lump. My doctor didn't find a lump. I was told it is a normal check-up of your breast, you're too young for a mammogram but send you for an ultrasound. That's it. Participant 81 Other symptoms included breast pain (n=9, 9.00%) and breast swelling, asymmetry or bruising (n=7, 7.00%). In relation to sub-group variations, participants with stage 0-I breast cancer described having no symptoms more frequently than the general cohort (55.00% compared to 39.00% in the general cohort).
Table 3.3: Symptoms that led to diagnosis
Symptoms leading to diagnosis All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n=30 % n=50 % n=50 %Participant describes feeling a lump on their breast and seeking medical attention from their GP
39 39.00 8 40.00 14 46.67 22 44.00 17 34.00
Participant describes not having any symptoms
39 39.00 11 55.00 5 16.67 16 32.00 23 46.00
Participant describes having a family history of breast cancer
11 11.00 3 15.00 2 6.67 5 10.00 6 12.00
Participant describes having breast pain 9 9.00 1 5.00 5 16.67 6 12.00 3 6.00
Participant describes abnormal puckering or skin abnormality on breast
7 7.00 0 0.00 4 13.33 4 8.00 3 6.00
Participant describes having breast swelling/asymmetry or bruising
7 7.00 1 5.00 2 6.67 3 6.00 4 8.00
Participant describes having an inverted nipple
1 1.00 0 0.00 0 0.00 0 0.00 1 2.00
Participant describes having bone pain 1 1.00 0 0.00 0 0.00 0 0.00 1 2.00
Participant describes abnormal discharge 1 1.00 0 0.00 1 3.33 1 2.00 0 0.00
Symptoms leading to diagnosis All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant describes feeling a lump on their breast and seeking medical attention from their GP
39 39.00 25 44.64 14 31.82 19 35.19 20 43.48
Participant describes not having any symptoms
39 39.00 22 39.29 17 38.64 20 37.04 19 41.30
Participant describes having a family history of breast cancer
11 11.00 8 14.29 3 6.82 8 14.81 3 6.52
Participant describes having breast pain 9 9.00 4 7.14 5 11.36 6 11.11 3 6.52
Participant describes abnormal puckering or skin abnormality on breast
7 7.00 3 5.36 4 9.09 5 9.26 2 4.35
Participant describes having breast swelling/asymmetry or bruising
7 7.00 2 3.57 5 11.36 3 5.56 4 8.70
Participant describes having an inverted nipple
1 1.00 0 0.00 1 2.27 0 0.00 1 2.17
Participant describes having bone pain 1 1.00 1 1.79 0 0.00 1 1.85 0 0.00
Participant describes abnormal discharge 1 1.00 1 1.79 0 0.00 1 1.85 0 0.00

Section 3
Breast Cancer 2018 Australian PEEK Study
Figure 3.3: Symptoms that led to diagnosis Diagnostic pathway The most common diagnostic pathway described was self-detecting a lump or other breast abnormality, seeking attention from a general practitioner and being referred to mammogram, ultrasound and biopsy (n=48, 48.00%). There were an additional five participants (5.00%) that described self-detecting a lump or other breast abnormality, however being referred to ultrasound and biopsy directly. The next most common diagnostic pathway was through routine mammography which led to ultrasound and biopsy (n=32, 32.00%). There were also eight
participants (8.00%) that described being diagnosed through their GP (through a routine check-up or other investigation) which led to mammography, ultrasound and biopsy. In relation to sub-group variations, participants with stage II-III breast cancer described self-detection leading to diagnosis more frequently than the general cohort (70.00% compared to 48.00% in the general cohort). Participants with stage 0-I breast cancer described diagnosis following a routine check-up or other investigation with their general practitioner (25.00% compared to 8.00% in the general cohort).
Table 3.4: Diagnostic pathways
0
5
10
15
20
25
30
35
40
45
Participantdescribes feeling a
lump on their breastand seeking medicalattention from their
GP
Participantdescribes not having
any symptoms
Participantdescribes having afamily history of
breast cancer
Participantdescribes having
breast pain
Participantdescribes abnormal
puckering or sk inabnormality on
breast
Participantdescribes having
breastswel ling/asymetry
or bruising
Diagnostic pathway All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n=30 % n=50 % n=50 %Self detected lump or abnormality to GP to mammogram, ultrasound and biopsy
48 48.00 8 40.00 21 70.00 29 58.00 19 38.00
Mammogram, ultrasound and biopsy 32 32.00 5 25.00 7 23.33 12 24.00 20 40.00
GP to mammogram, ultrasound and biopsy 8 8.00 5 25.00 1 3.33 6 12.00 2 4.00
Other (including MRI and bone scan) 7 7.00 2 10.00 0 0.00 2 4.00 5 10.00
Self detected lump or abnormality to GP to ultrasound and biopsy
5 5.00 0 0.00 1 3.33 1 2.00 4 8.00

Section 3
Breast Cancer 2018 Australian PEEK Study
Support at diagnosis
In the questionnaire, participants were asked whether they felt supported at the time of diagnosis. There were 42 participants (42.00%) that indicated that they had no support at diagnosis, while 34 participants (34.00%) noted that they had enough support. An additional 24 participants (24.00%) indicated that they had some support but that it was not enough.
In relation to sub-group variations, participants with stage 0-I breast cancer reported having no support at diagnosis more frequently than the general cohort (30.00% compared to 42.00% in the general cohort), however, this group also reported having enough support at diagnosis, more frequently than the general cohort (45.00% compared to 34.00% in the general cohort). Participants that were high school educated reported that they had enough support at diagnosis, less frequently than the general cohort (21.74% compared to 34.00% in the general cohort).
Table 3.5: Support at diagnosis
Diagnostic pathway All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Self detected lump or abnormality to GP to mammogram, ultrasound and biopsy
48 48.00 29 51.79 19 43.18 25 46.30 23 50.00
Mammogram, ultrasound and biopsy 32 32.00 18 32.14 14 31.82 18 33.33 14 30.43
GP to mammogram, ultrasound and biopsy 8 8.00 5 8.93 3 6.82 5 9.26 3 6.52
Other (including MRI and bone scan) 7 7.00 3 5.36 4 9.09 4 7.41 3 6.52
Self detected lump or abnormality to GP to ultrasound and biopsy
5 5.00 1 1.79 4 9.09 2 3.70 3 6.52
Support at diagnosis All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n=30 % n=50 % n=50 %I/we had no support 42 42.00 6 30.00 13 43.33 19 38.00 23 46.00
I/we had enough support 34 34.00 9 45.00 11 36.67 20 40.00 14 28.00
I/we had some support but it wasn't enough 24 24.00 5 25.00 6 20.00 11 22.00 13 26.00
Support at diagnosis All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %I/we had no support 42 42.00 23 41.07 19 43.18 21 38.89 21 45.65
I/we had enough support 34 34.00 22 39.29 12 27.27 24 44.44 10 21.74
I/we had some support but it wasn't enough 24 24.00 11 19.64 13 29.55 9 16.67 15 32.61

Section 3
Breast Cancer 2018 Australian PEEK Study
Figure3.4: Support at diagnosis
Genetic and biomarker tests
Participants were asked whether they had ever had a discussion about genetic tests or tests to see if there were biomarkers that might be relevant to their condition or treatment. There were 42 participants (42.00%) that indicated that they had brought up the topic for discussion with their doctor and 23 participants (23.00%) that reported that their doctor had brought up the topic for discussion. There was
also 35 participants (35.00%) that indicated that no one had ever spoken to them about this. In relation to sub-group variations, participants with stage 0-I and stage II-III breast cancer indicated that they had brought up the topic of biomarker or genetic testing less frequently than the general cohort, while participants with stage IV breast cancer brought up the topic more frequently (stage 0-I 30.00%, stage II – III 16.67%, stage IV 62.00% compared to 42.00% in the general cohort). Participants with stage II-III breast cancer indicated that their doctor brought up the topic of biomarker/genetic testing, more frequently than the general cohort (46.67% compared to 23.00% in the general cohort). Participants with stage 0-I breast cancer reported that no one had brought up this topic with them, more frequently than the general cohort (55.00% compared to 35.00% in the general cohort).
Table 3.6: Genetic and biomarker tests
0
5
10
15
20
25
30
35
40
45
I/we had no support I/we had enough support I/we had some support but it wasn'tenough
Discussions about biomarker/genetic testing All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n= % n=50 % n=50 %I brought up the topic with my doctor for discussion
42 42.00 6 30.00 5 16.67 11 22.00 31 62.00
My doctor brought up the topic with me for discussion
23 23.00 3 15.00 14 46.67 17 34.00 6 12.00
No one has ever spoken to me about this type of test
35 35.00 11 55.00 11 36.67 22 44.00 13 26.00
Discussions about biomarker/genetic testing All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %I brought up the topic with my doctor for discussion
42 42.00 24 42.86 18 40.91 25 46.30 17 36.96
My doctor brought up the topic with me for discussion
23 23.00 16 28.57 7 15.91 10 18.52 13 28.26
No one has ever spoken to me about this type of test
35 35.00 16 28.57 19 43.18 19 35.19 16 34.78

Section 3
Breast Cancer 2018 Australian PEEK Study
Figure 3.5: Genetic and biomarker tests
Participants were also asked about their interest in this type of test if it was available. The majority of participants noted that they had not had this test, but would like to (n=64, 64.00%). There were 20
participants (20.00%) that reported having this test and not paying out of pocket for it, while 13 participants (13.00%) indicated that they had not had this test and were not interested in it. In relation to sub-group variations, participants that were university educated indicated that they had not had this test but would like to, more frequently than the general cohort (75.93% compared to 64.00% in the general cohort), while participants that were high school educated indicated that they were not interested in this test, more frequently than the general cohort (23.91% compared to 13.00% in the general cohort).
Table 3.7: Interest in genetic and biomarker tests
0
5
10
15
20
25
30
35
40
45
I brought up the topic with my doctor fordiscussion
No one has ever spoken to me aGout this type oftest
My doctor Grought up the topic with me fordiscussion
Biomarker/genetic testing experience All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n= % n=50 % n=50 %I have not had this test but would like to 64 64.00 14 70.00 17 56.67 31 62.00 33 66.00
I have had this test and did not have to pay out of pocket for it
20 20.00 2 10.00 5 16.67 7 14.00 13 26.00
I have not had this test and am not interested in it
13 13.00 3 15.00 6 20.00 9 18.00 4 8.00
I have had this test through a clinical trial 1 1.00 0 0.00 1 3.33 1 2.00 0 0.00
I have had this type of test and paid for it myself
2 2.00 1 5.00 1 3.33 2 4.00 0 0.00
Biomarker/genetic testing experience All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %I have not had this test but would like to 64 64.00 39 69.64 25 56.82 41 75.93 23 50.00
I have had this test and did not have to pay out of pocket for it
20 20.00 10 17.86 10 22.73 9 16.67 11 23.91
I have not had this test and am not interested in it
13 13.00 5 8.93 8 18.18 2 3.70 11 23.91
I have had this test through a clinical trial 1 1.00 1 1.79 0 0.00 0 0.00 1 2.17
I have had this type of test and paid for it myself
2 2.00 1 1.79 1 2.27 2 3.70 0 0.00

Section 3
Breast Cancer 2018 Australian PEEK Study
Figure 3.6: Interest in genetic and biomarker test
Communication and understanding of prognosis
Participants were asked whether anyone talked to them about prognosis. The most common theme noted by 23 participants (23.00%) was that they did not have a clear prognosis. Participant describes not having a clear prognosis
Well I don't even think my doctors' have told me my current prognosis. They always just say we hope that you live a long life. Haven't really been discussed I'm must say. Participant 33
No, the oncologist said, or well I can give you numbers if you want, but she said it's not going to be accurate. So I guess that's good as it gets? I always feel I'm never satisfied with what they tell me when I go for check-ups, because last time I went was not long after Olivia Newton John's recurrence, and I said something about that and I said, "Isn't it strange how it took them so long for her diagnosis to get discovered, her re-diagnosis." And I said, "Surely she's having the best medical check-ups and whatever." And she said, Oh no well the blood test doesn't necessarily show anything" so I thought, oh well why do we do it? I then lost faith in why am I going every six months and paying these hundreds of dollars for these tests that isn't necessarily going to show anything. Participant 63
I have stage IV invasive. I went in, knowing from the biopsy, that I had probably cancer. Prognosis is hard to say, no-one wants to put a number on it, but I would like to say that I'll live with this for a long, long time. Participant 88
This was followed by two themes noted by 14 participants (14.00%) each including the understanding that they would make a full recovery and are not likely to have a recurrence and that they have a good prognosis with ongoing or maintenance therapy. There were also 14 participants (14.00%) that were not able to describe prognosis, but rather focused on describing their treatment regime. Participant describes understanding that they have a good prognosis with ongoing or maintenance therapy
It's good. I've just had another 12-month check-up, and they've said it's all clear. And I'm on exemestane pills, I think it's called Exemestane, it's Aromasin is the one I take. I've been taking it for, no not two years three years, but I've got to take it for five years. And the oncologist said that as long as I take it for the five years, possibly an extra year he was talking about, then it should be good. because I don't have any breast tissue left at all. They've taken it all. Participant 25 Pretty good. In relation to breast cancer, I'm pretty confident. I have just passed my five year since diagnosis with the second one, and I honestly think I'm done with it. I think I'm good. I'm still on Letrozole. They're still tossing up whether to keep me on for five years or ten years. I think I'm going to decide on the five year and leave it at because I'm sick of it. Participant 39
0 10 20 30 40 50 60 70
I have not had this test but would like to
I have had this test and did not have to pay out of pocket for it
I have not had this test and am not interested in it
I have had this type of test and paid for it myself
I have had this test through a clinical trial

Section 3
Breast Cancer 2018 Australian PEEK Study
I've been told that I could go on for years and years and years both by the oncologist and by my GP because when I went back to the oncologist the week before last, they told me that the hormone blockers are having the effect that they hoped they would in the fact that the bone disease is starting to settle. It hasn't settled completely yet but they are expecting it to keep improving. It will never go away which I understand but I was never given a dire prognosis and I live with that hope that I'll go on for a lot of years yet to come. My GP says he's got patients that he treats that have been on these hormone blockers for 10 to 15 years, so he said to me he can't see why I'd be any different. Participant 58 Participant describes understanding that they will have a full recovery and are not likely to have a recurrence I'm expected to make a full recovery because that's early breast cancer, hopefully. This is my prognosis, I'm very lucky compared to others. Participant 3 It should be really good. Well, I was very lucky. There was no spread. They did an excision and they got the margins are really good. I've had the radiation. obviously, they're not going to say cured but I've obviously got a very good prognosis compared to so many women. Participant 12
My current prognosis is that I'm very unlikely to get breast cancer or any other cancer. It's been nearly five years; they always talk about that five-year period. But, I've just been tested every and each way; I've had markers done just recently and I'm actually sitting here with drain tubes in situ because I've just had more breast tissues removed for aesthetic reasons but also for comfort. My last surgery in STATE was a bit of a botchy job so I went to a surgeon up here and she's just made it all very streamlined and flash. Participant 49 In relation to sub-group variations, participants with stage 0-I breast cancer reported not being given a clear prognosis, less frequently than the general cohort (5.00% compared to 23.00%). This groups also reported having a good prognosis with a full recovery and little chance of recurrence, more frequently than the general cohort (60.00% compared with 14.00% in the general cohort). There were also no participants with stage IV breast cancer that reported this theme. Participants with stage II-III breast cancer reported having a good prognosis with maintenance therapy more frequently than the general cohort (40.00% compared to 14.00% in the general cohort), while participants with stage IV breast cancer reported this less frequently (2.00% compared to 14.00% in the general cohort).
Table 3.8: Understanding of prognosis
Understanding of prognosis All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n= % n=50 % n=50 %Participant describes not being given a clear prognosis.
23 23.00 1 5.00 7 23.33 8 16.00 15 30.00
Participant describes having a good prognosis: make a full recovery and not likely to have a recurrence
14 14.00 12 60.00 2 6.67 14 28.00 0 0.00
Participant describes having a good prognosis with maintenance therapy (i.e. continuing to take pills and following up with oncologist)
14 14.00 1 5.00 12 40.00 13 26.00 1 2.00
Participant description of prognosis is in relation to diagnosis and/or treatment regime rather than prognosis.
14 14.00 1 5.00 2 6.67 3 6.00 11 22.00
Participant is not able to describe their prognosis
8 8.00 0 0.00 3 10.00 3 6.00 5 10.00
Participant describes prognosis in relation to their cancer being incurable
7 7.00 0 0.00 0 0.00 0 0.00 7 14.00
Participant describes anxiety or uncertaintly in relation to recurrence
6 6.00 2 10.00 1 3.33 3 6.00 3 6.00
Participant describes conducting their own research to understand prognosis
6 6.00 0 0.00 4 13.33 4 8.00 2 4.00
Participant describes having a good prognosis: in remission
4 4.00 2 10.00 2 6.67 4 8.00 0 0.00
Participant describes receiving conflicting prognosis from various health professionals
4 4.00 3 15.00 1 3.33 4 8.00 0 0.00

Section 3
Breast Cancer 2018 Australian PEEK Study
Figure 3.7: Understanding of prognosis
Understanding of prognosis All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant describes not being given a clear prognosis.
23 23.00 14 25.00 9 20.45 14 25.93 9 19.57
Participant describes having a good prognosis: make a full recovery and not likely to have a recurrence
14 14.00 9 16.07 5 11.36 7 12.96 7 15.22
Participant describes having a good prognosis with maintenance therapy (i.e. continuing to take pills and following up with oncologist)
14 14.00 10 17.86 4 9.09 6 11.11 8 17.39
Participant description of prognosis is in relation to diagnosis and/or treatment regime rather than prognosis.
14 14.00 7 12.50 7 15.91 9 16.67 5 10.87
Participant is not able to describe their prognosis
8 8.00 3 5.36 5 11.36 3 5.56 5 10.87
Participant describes prognosis in relation to their cancer being incurable
7 7.00 2 3.57 5 11.36 2 3.70 5 10.87
Participant describes anxiety or uncertaintly in relation to recurrence
6 6.00 6 10.71 0 0.00 2 3.70 4 8.70
Participant describes conducting their own research to understand prognosis
6 6.00 4 7.14 2 4.55 2 3.70 4 8.70
Participant describes having a good prognosis: in remission
4 4.00 2 3.57 2 4.55 3 5.56 1 2.17
Participant describes receiving conflicting prognosis from various health professionals
4 4.00 2 3.57 2 4.55 3 5.56 1 2.17
0
5
10
15
20
25
Participantdescribes notbeing given a
clear prognosis.
Participantdescribes having a
good prognosis:make a full
recovery and notlikely to have a
recurrence
Participantdescribes having a
good prognosiswith maintenance
therapy (i.e.continuing to takepills and following
up withoncologist)
Participantdescription ofprognosis i s in
relation todiagnosis and/ortreatment regime
rather thanprognosis.
Participant is notable to describetheir prognosis
Participantdescribes
prognosis inrelation to their
cancer beingincurable
Participantdescribes anxietyor uncertaintly in
relation torecurrence
Participantdescribes
conducting theirown research to
understandprognosis
Participantdescribes having agood prognosis: in
remission
Participantdescribesreceiving
conflictingprognosis fromvarious healthprofessionals

Section 4
Breast Cancer 2018 Australian PEEK Study
Section 4 Decision-making

Section 4
Breast Cancer 2018 Australian PEEK Study
Section 4: Experience of health professional communication Conversations about treatments
• Participants were asked to describe the conversations they have had about their breast cancer in relation to treatment options. The most common theme was that participants felt as though they were informed and had time to make treatment decisions (n=40, 40.00%). In contrast, the next most common theme noted by 31 participants (31.00%) was that they felt as though they were not being given treatment options but rather being told what to do. In a similar theme that was noted by 11 participants, participants described being supported but feeling as though there were limited treatment options for them.
• There were a number of sub-group variations. Participants with stage II-III breast cancer reported being informed and having time to make treatment decisions, more frequently than the general cohort (50.00% compared to 40.00% in the general cohort). Participants with stage 0-I breast cancer indicated that they had not been given treatment options, less frequently than the general cohort (20.00% compared to 31.00% in the general cohort).
Decision-making • The most common theme described by participants was that decisions about treatment were ultimately
made by talking with their partner/spouse and their family, including very close friends (n=32, 32.00%). This was followed by participants describing that they would consult with others, but ultimately the decision was their own (n=19, 19.00%). The final themes included decision-making between themselves and their clinician (n=17, 17.00%), decision-making between themselves and their partner/spouse (n=16, 16.00%) and decisions-making between their clinician as well as their clinician also (n=16, 16.00%).
• There were sub-group variations in relation to decisions about treatment that were ultimately made by talking with their partner/spouse and their family, including very close friends. Participants with stage 0-I breast cancer reported this less frequently than the general cohort (20.00% compared to 32.00% in the general cohort), while participants with stage II-III breast cancer reported this more frequently (43.33% compared to 32.00% in the general cohort). Participants in rural areas described decision-making as ultimately their own decision, more frequently than the general cohort (29.55% compared to 19.00% in the general cohort).
• Participants were asked about the things that they take into consideration when making decisions about treatment. There were two key themes in this section. The most common theme was that participants considered long term survival and outcomes (n=27, 27.00%) and this was followed by considerations about demonstrated effectiveness and outcomes (n=25, 25.00%). The remaining themes in this section included impact on quality of life (n=16, 16.00%), financial considerations (n=14, 14.00%), severity of side effects (n=13, 13.00%) and impact on their family (n=13, 13.00%).
• Participants with stage 0-I breast cancer reported considering demonstrated effectiveness and outcomes less frequently than the general cohort (10.00% compared to 25.00% in the general cohort). This group did not report considering the severity of side effects or the impact of treatment on their family. Participants with stage II-III breast cancer reported the impact on treatment in general and on their family more frequently than the general cohort (26.67% compared to 13.00% in the general cohort).
• In the final question about decision-making, participants were asked whether they felt the way they made decisions had changed over time since they were diagnosed. Close to half of all participants reported that the way that they make decisions had stayed the same (n=49, 49.00%). A quarter of all participants (n=25, 25.00%) reported that the way that they make decisions has changed and this related to them being more empowered and informed over time. There were also 19 participants (19.00%) that noted they had changed the way they make decisions as they are more cautious and considered.
• In relation to sub-group variations, participants with stage 0-I breast cancer reported being more empowered and informed, more frequently than the general cohort (45.00% compared to 25.00% in the general cohort). They also reported being more cautious and considered, less frequently than the general cohort (5.00% compared to 19.00% in the general cohort). Participants in rural areas reported making decisions in the same way less frequently than the general cohort (36.36% compared to 49.00% in the general cohort). They also reported changing the way they make decisions as they have a different outlook on life, more frequently than the general cohort (18.18% compared to 8.00% in the general cohort) and this theme was unique to participants in rural areas.

Section 4
Breast Cancer 2018 Australian PEEK Study
Discussions about treatment
Participants were asked to describe the conversations they have had about their breast cancer in relation to treatment options. The most common theme was that participants felt as though they were informed and had time to make treatment decisions (n=40, 40.00%). Participants felt as though they were informed and had time to make treatment decisions
I met with the surgeon and he gave me, initially it was options in regards to surgery, of what I could do, then I took my option of what to do. After that, he then met with me to talk about treatment and the way forward. It wasn't about this is an option for you, this is what's going to happen, the chemotherapy. He said when I get back to CITY then I'll be assigned an oncologist and they will talk to me about where to from here. I met with my oncologist. He gave me three options of chemo. They all had different timeframes to them and different drugs. He basically left it to me to choose which option. I chose the option that I thought was going to be best for me. He broke it down into manageable chunks, so to speak. He said, "We'll get through the chemo and then towards the end then we'll talk about radiation and where to from here." Participant 5 When I went to see the surgeon first, she told me about the surgical options in terms of having either a lumpectomy or a mastectomy. Then when I went and saw the oncologist, she also then went through my results and saying the choice of whether I should also have chemotherapy or radiation. I did get a lot of information to all the different avenues. The ball was left in my court to say which I would like to pursue, really. Participant 41
Right. The diagnosis was devastating ...Tended to be in a total blur. I remember the first person I spoke to was actually at the breast screen place where a surgeon spoke to me and I barely remember anything of what he said, Basically. Fortunately I had a almost instant appointment with my GP. The GP was helpful and has been since. I'm very fortunate in that. Basically, and at time when I've needed ... particularly when I was going through that chemo and sick all the time. I saw perhaps too much of her. In terms of the treatment then, I was offered a chance to be on a trial because I'd never had any chemo before…it's a targeted form of chemotherapy like you've heard of Herceptin. It's a little bit like that. So I went for a second opinion, because I didn't have the trust. I felt
maybe they're just putting me on this trial because... but anyway, I went for a second opinion to another doctor. He said it was a perfectly fine option to take and so I started on the clinical trial. Participant 71 In contrast, the next most common theme noted by 31 participants (31.00%) was that they felt as though they were not being given treatment options but rather being told what to do. Participant describes not being given treatment options My GP first sent me to the surgeon and she took control, she did a lumpectomy. She didn't really give me any other options, she just said, "This is what we need to do, lumpectomy." That's what I did. After that, she referred me to the oncologist at the local cancer center. The radiotherapy oncologist, he just discussed again like, "This is what we should do." I did it. The medical oncologist they're like, "Once radiotherapy is finished, then I'm going to put you on Tamoxifen to help hopefully not get a recurrence." I wasn't given any real options, I was just told this is what needed to happen. maybe my breast cancer, I didn't need to make choices, it was straightforward, clean cut, "This is what you need to do." Participant 3 There weren't any. Basically, he said, "This is what is happening, this is what will happen and I've referred you to a surgeon." He put pictures, he put them up on the wall and said "Look at this, we can see that it's spreading. The only option is for us to remove the breast." You're in such a daze at that time. You’ll do anything they say. Later on, when I was talking to my husband, I'm 62 now, but never once discussed reconstruction, anything along those lines at all. I think I answered questions in your...in the survey that I answered the questions originally and they said, “Were you shown how to massage your scar?” I must have missed all that. I thought when you've had major surgery, you're in a daze. I again spoke to my husband and said, "Do you recall anybody offering me anything"? He said, “No.” I was reading the questions out to him. Participant 59
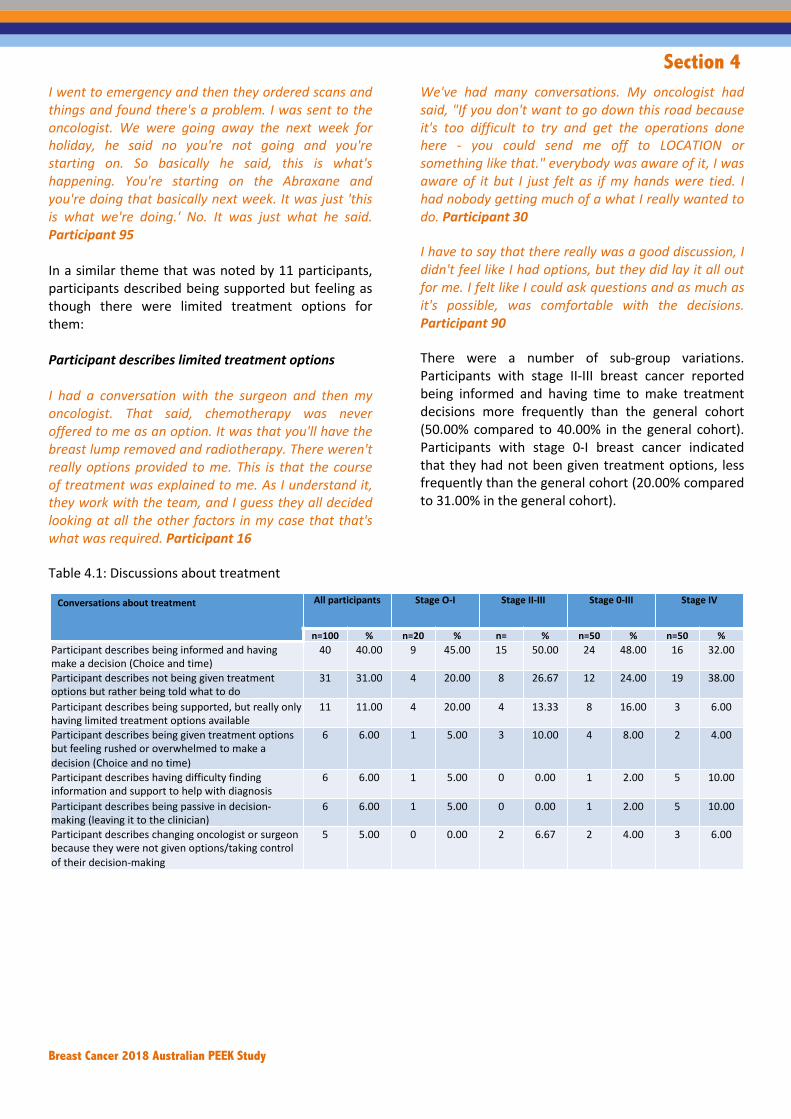
Section 4
Breast Cancer 2018 Australian PEEK Study
I went to emergency and then they ordered scans and things and found there's a problem. I was sent to the oncologist. We were going away the next week for holiday, he said no you're not going and you're starting on. So basically he said, this is what's happening. You're starting on the Abraxane and you're doing that basically next week. It was just 'this is what we're doing.' No. It was just what he said. Participant 95 In a similar theme that was noted by 11 participants, participants described being supported but feeling as though there were limited treatment options for them: Participant describes limited treatment options I had a conversation with the surgeon and then my oncologist. That said, chemotherapy was never offered to me as an option. It was that you'll have the breast lump removed and radiotherapy. There weren't really options provided to me. This is that the course of treatment was explained to me. As I understand it, they work with the team, and I guess they all decided looking at all the other factors in my case that that's what was required. Participant 16
We've had many conversations. My oncologist had said, "If you don't want to go down this road because it's too difficult to try and get the operations done here - you could send me off to LOCATION or something like that." everybody was aware of it, I was aware of it but I just felt as if my hands were tied. I had nobody getting much of a what I really wanted to do. Participant 30 I have to say that there really was a good discussion, I didn't feel like I had options, but they did lay it all out for me. I felt like I could ask questions and as much as it's possible, was comfortable with the decisions. Participant 90 There were a number of sub-group variations. Participants with stage II-III breast cancer reported being informed and having time to make treatment decisions more frequently than the general cohort (50.00% compared to 40.00% in the general cohort). Participants with stage 0-I breast cancer indicated that they had not been given treatment options, less frequently than the general cohort (20.00% compared to 31.00% in the general cohort).
Table 4.1: Discussions about treatment
Conversations about treatment All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n= % n=50 % n=50 %Participant describes being informed and having
make a decision (Choice and time)
40 40.00 9 45.00 15 50.00 24 48.00 16 32.00
Participant describes not being given treatment
options but rather being told what to do
31 31.00 4 20.00 8 26.67 12 24.00 19 38.00
Participant describes being supported, but really only
having limited treatment options available
11 11.00 4 20.00 4 13.33 8 16.00 3 6.00
Participant describes being given treatment options
but feeling rushed or overwhelmed to make a
decision (Choice and no time)
6 6.00 1 5.00 3 10.00 4 8.00 2 4.00
Participant describes having difficulty finding
information and support to help with diagnosis
6 6.00 1 5.00 0 0.00 1 2.00 5 10.00
Participant describes being passive in decision-
making (leaving it to the clinician)
6 6.00 1 5.00 0 0.00 1 2.00 5 10.00
Participant describes changing oncologist or surgeon
because they were not given options/taking control
of their decision-making
5 5.00 0 0.00 2 6.67 2 4.00 3 6.00

Section 4
Breast Cancer 2018 Australian PEEK Study
Figure 4.1: Discussions about treatment
Conversations about treatment All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant describes being informed and having
make a decision (Choice and time)
40 40.00 26 46.43 14 31.82 24 44.44 16 34.78
Participant describes not being given treatment
options but rather being told what to do
31 31.00 14 25.00 17 38.64 13 24.07 18 39.13
Participant describes being supported, but really only
having limited treatment options available
11 11.00 6 10.71 5 11.36 7 12.96 4 8.70
Participant describes being given treatment options
but feeling rushed or overwhelmed to make a
decision (Choice and no time)
6 6.00 5 8.93 1 2.27 3 5.56 3 6.52
Participant describes having difficulty finding
information and support to help with diagnosis
6 6.00 3 5.36 3 6.82 4 7.41 2 4.35
Participant describes being passive in decision-
making (leaving it to the clinician)
6 6.00 4 7.14 2 4.55 3 5.56 3 6.52
Participant describes changing oncologist or surgeon
because they were not given options/taking control
of their decision-making
5 5.00 3 5.36 2 4.55 4 7.41 1 2.17
0
5
10
15
20
25
30
35
40
45
Participant descr ibesbeing informed and
having make adecision (Choice and
time)
Participant descr ibesnot being given
treatment options butrather being told what
to do
Participant descr ibesbeing supported, but
really only havinglimited treatmentoptions available
Participant descr ibesbeing given treatment
options but feelingrushed or
overwhelmed to makea decision (Choice and
no time)
Participant descr ibeshaving diffi culty
finding informationand support to help
with diagnosis
Participant descr ibesbeing passive indecision-making(leaving it to the
clinician)
Participant descr ibeschanging oncologist orsurgeon because they
were not givenoptions/taking control
of their decision-making

Section 4
Breast Cancer 2018 Australian PEEK Study
Decision-making Who is involved in decision-making
Participants were asked who was involved in decisions made about treatment and care. The most common theme described by participants was that decisions about treatment were ultimately made by talking with their partner/spouse and their family, including very close friends (n=32, 32.00%). Decision-making including partner/spouse and family, including very close friends My husband came in to every appointment…my mum ended up being right on board and she likes to research and found out everything. She came and met all the doctors so that she could [laughs]. They would give her the good hands. Everyone almost gave her a hug and said they would look after her. She felt good. Okay. It was all the doctors and myself and what I actually liked is that when I was when they got all the biopsy when they took out the lumpectomy and that got all the information they needed. My surgeon, my oncologist, and my radiation oncologist, all met and discussed. So they made sure that the pathway was - everyone was on board. I like that the best. No one missed out on any information. Participant 32 My husband and mainly one of my daughters who lives at home now, they come to every single appointment. Pretty much, it's a decision that we all make together between the clinicians, myself, my husband, and my daughter. Participant 48 No, I talk with my family. I have one son and daughter-in-law that I am very close to and I talk to them. I talk to my partner of 25 years. He’s attended most of my appointments with me and I also talk to my palliative care physician. He has been extremely helpful in helping me. That what I should do or take as far as reducing pain and continuing on hopefully my reasonable last term. Participant 61 The next most common theme was participants describing that they would consult with others, but ultimately the decision was their own (n=19, 19.00%).
Participant describes consulting with others but ultimately the decision was their own Well, at that time I was just my decision. I didn't want to stress my family. Although my son, my youngest one, said, "Mum, I'll shave my head," and things like. I say, "No, no. I'm not going to have the chemo." I just didn't want to screw his year 12. He was, I didn't. I said, "No, no. I'm not going to have the chemo. I don't need it at this time." I just made the decision myself. Participant 21 I'm the one that makes the decision about my healthcare, that's the final decision. If I was to talk to my family about that, it would only be the logistics of a trial, or in keeping them up to date on what I'm looking at and why I'm doing that sort of thing. I don't sit down and say do you think this is a good idea. I have a best friend. I talk to her a lot about treatments. If I'm having trouble thinking, "What do you reckon? What would be better to do this or this?" She's the one that I go to to talk sort that out. I've got two sisters and her, so they are probably the ones that I'll go to to try and make sense what would be the better option. Participant 43 It's always my decision, but I do think about and talk to my family and take advice from the doctor. I always do my research though. Participant 96 The final themes included combinations of decision-making between themselves, clinicians and their partner/spouse. This included decision-making between themselves and their clinician (n=17, 17.00%), decision-making between themselves and their partner/spouse (n=16, 16.00%) and decisions-making between their clinician as well as their partner/spouse also (n=16, 16.00%). There were a number of sub-group variations in relation to decisions about treatment that were ultimately made by talking with their partner/spouse and their family, including very close friends. Participants with stage 0-I breast cancer reported this less frequently than the general cohort (20.00% compared to 32.00% in the general cohort), while participants with stage II-III breast cancer reported this more frequently (43.33% compared to 32.00% in the general cohort). Participants in rural areas described decision-making as ultimately their own decision, more frequently than the general cohort (29.55% compared to 19.00% in the general cohort).

Section 4
Breast Cancer 2018 Australian PEEK Study
Table 4.2: Decision-making process – who patients consult
Figure 4.2: Decision-making process – who patients consult
Who is involved in decision-making All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n=30 % n=50 % n=50 %Participant describes talking with their partner/spouse and/or family (or close friend) to make the final decisions
32 32.00 4 20.00 13 43.33 17 34.00 15 30.00
Participant describes consulting others but the decision is ultimately their own
19 19.00 4 20.00 6 20.00 10 20.00 9 18.00
Decision-making is between themselves and the clinician only
17 17.00 5 25.00 1 3.33 6 12.00 11 22.00
Participant describes talking with their partner/spouse to make the final decisions
16 16.00 3 15.00 6 20.00 9 18.00 7 14.00
Participant describes talking with their clinician and partner/spouse to make the final decisions
16 16.00 4 20.00 4 13.33 8 16.00 8 16.00
Who is involved in decision-making All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant describes talking with their partner/spouse and/or family (or close friend) to make the final decisions
32 32.00 20 35.71 12 27.27 17 31.48 15 32.61
Participant describes consulting others but the decision is ultimately their own
19 19.00 6 10.71 13 29.55 7 12.96 12 26.09
Decision-making is between themselves and the clinician only
17 17.00 10 17.86 7 15.91 11 20.37 6 13.04
Participant describes talking with their partner/spouse to make the final decisions
16 16.00 10 17.86 6 13.64 6 11.11 10 21.74
Participant describes talking with their clinician and partner/spouse to make the final decisions
16 16.00 10 17.86 6 13.64 13 24.07 3 6.52
0
5
10
15
20
25
30
35
Participant descr ibes talking withtheir partner/spouse and/or
family (or close friend) to makethe final decisions
Participant descr ibes consultingothers but the decision is
ultimately their own
Decision-making is betweenthemeselves and the clinician
only
Participant descr ibes talking withtheir partner/spouse to make the
final decisions
Participant descr ibes talking withtheir clinician and partner/spouse
to make the final decisions

Section 4
Breast Cancer 2018 Australian PEEK Study
What is considered when making decisions Participants were asked about the things that they take into consideration when making decisions about treatment. There were two key themes in this section. The most common theme was that participants considered long term survival and outcomes (n=27, 27.00%) and this was followed by considerations about demonstrated effectiveness and outcomes (n=25, 25.00%). Participant describes considering long term survival and outcomes Survival would be number one. I just want to do what's best for me to be healthy and to have a good quality of life because without that you can't have anything pretty much; because I want to be here for my kids as well. Participant 3 The percentage of not getting cancer again if I have a particular chemotherapy, that was a consideration. I also needed evidence which is why I didn't go on with radiotherapy because I didn't have any evidence. I was prepared to do anything so I wouldn't get breast cancer again. Participant 49 The only thing I really considered was what's going to give me the best chance of beating this disease and longevity. That was probably the most important thing to me. I was prepared to do anything, really, just to get rid of this cancer. Participant 56 Staying alive for my family. Long term results of the therapy. Participant 76 Participant describes considering demonstrated effectiveness and outcomes I look at the evidence. I look at the peer-review articles and whatever the evidence is out there. That's probably what I do. I tend to, before each appointment, do my own research so I know what we're talking about by the time we get there. I do ask their opinion. I do say, "If you were me, what would you do?" I always find that's a really good question because you can't escape answering that honestly. I also go with my intuition: what feels right for me. Participant 48
I mean obviously the side effects and impingement on the quality of life. And I mean I would always say what is the evidence base that it's going to actually be affective for me? Participant 52 I guess when you’re taking the drugs after you’ve taken the drug, I take into consideration whether it’s effective or not. Participant 61 The remaining themes in this section included impact on quality of life (n=16, 16.00%), financial considerations (n=14, 14.00%), severity of side effects (n=13, 13.00%) and impact on their family (n=13, 13.00%). Participant describes considering the impact on quality of life That I can continue the lifestyle that I want to…it's through my lifestyle that I have chosen the way that I've gone. I live quite an active lifestyle when I'm well. It's all about continued health after the treatment, not so much the immediate treatment like before they produce more options. It's quite truthful if hindsight is a wonderful thing. If I had a crystal ball back when I was 40 and if there was any chance of it coming back, I would have gone double mastectomy here and now. Participant 11 Well, staying here for one [laughs]. You kind of got to think about - and your quality of life, which when you're going through chemo is not much. Participant 51 Life, living. Trying to get the best out of what quality of life and how long you'll have. That's all the things to take in. Participant 78 Participant describes considering financial considerations Cost, definitely cost now, because this has just set us back so much it's not funny. It really makes you reassess the whole public-private situation. Depending on what, there's lots of things that come into play. I was advised a couple of months ago to have a procedure done in LOCATION on my back, and I just went "Yeah, what's the out of pocket, $1100, plus you've got to get to LOCATION, yeah no. Thank you, I won't do it, I'll find something else." So I look at how big an impact it is on my life, and how big an impact it's gonna be on the rest of the family as well. Participant 13

Section 4
Breast Cancer 2018 Australian PEEK Study
One of them we did make at the time was cost which I look back now. but I ended up stopping work and things like that. It was the cost. After we thought, "We just do it and we will try to make it all out. We just went with what was, but the doctor thought was the best way to go. We put a bit of trust in -- actually we put a lot of trust in them. Participant 32 Initially, I guess, is working, whether you can work, side-effects. I'm lucky, I've been through the public system. If I was in the private system, I'd be considering cost and implications on time and work. Participant 57 Participant describes considering severity of side effects The concern for me around chemotherapy, was around side effects and possible long-term effects. To be honest, I don't feel like potential long-term effects were appropriately explained to me when I made the decision. There is stuff I found out, subsequent to having the chemotherapy treatment. That you go, "Well, I think that should have been a factor in considering whether I did it or not." Participant 22 The effect on my body, the length of time that the treatment will take and any potential side effects, long term, as well. Then eventually, I suppose, we consider the cost of things as well, but the cost didn’t really factor into it that much. Participant 68 How long, in practice, going to have a disease, it's the first one. Then, I suppose, how it's going to affect me, what side effects will have and long-term side effects and that's pretty much all I thought about. Participant 72
Participant describes considering impact on family Well, what I thought about is how is it going to impact the people that I love. That was back then. Right now, I'm not sure whether I made the right decision or not. I'm still thinking about it. Back then I based the decision in how would impact my son which was still in a critical stage. Participant 21 How it's going to affect family? How it would affect my daily life? I want to be back to normal…I also, at the time when I was diagnosed had a son doing year 12. My biggest thing was I want to make this work for him. It's that difficult. I know he was aiming very high to go to where he needed to go. He did incredibly well. That was my biggest strain. Then I had another son who was in uni, but he was the number one. Participant 24 The impact it will have on my family and children, trying to make it as easy as possible for them. I suppose I was more looking at trying to alleviate the burden on everyone else to try and just get on with it and not have it hanging around and that sort of thing. In retrospect, looking back, saying you should put yourself first, but I suppose it doesn't always happen that way because you're concerned of making everyone else feel all right about it, I think. Which I know it's a little bit twisted. Participant 41 Mainly thing is my family, how they are going to react with things and how it’s going to affect the family. Participant 84. Participants with stage 0-I breast cancer reported considering demonstrated effectiveness and outcomes less frequently than the general cohort (10.00% compared to 25.00% in the general cohort). This group did not report considering the severity of side effects or the impact of treatment on their family. Participants with stage II-III breast cancer reported the impact on treatment in general and on their family more frequently than the general cohort (26.67% compared to 13.00% in the general cohort).

Section 4
Breast Cancer 2018 Australian PEEK Study
Table 4.3: Considerations when making decisions
Considerations when making decisions-about treatment
All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n=30 % n=50 % n=50 %
Participant considers long term outcomes/survival27 27.00 7 35.00 7 23.33 14 28.00 13 26.00
Participant considers effectiveness/demonstrated outcomes
25 25.00 2 10.00 9 30.00 11 22.00 14 28.00
Participant considers the impact of the treatment on my quality of life
16 16.00 4 20.00 4 13.33 8 16.00 8 16.00
Participant considers the financial costs to them and their family
14 14.00 2 10.00 5 16.67 7 14.00 7 14.00
Participant considers the severity of side effects13 13.00 0 0.00 2 6.67 2 4.00 11 22.00
Participant considers the impact of treatment on themselves and their family in general
13 13.00 0 0.00 8 26.67 8 16.00 5 10.00
Considerations when making decisions-about treatment
All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %
Participant considers long term outcomes/survival 27 27.00 16 28.57 11 25.00 16 29.63 11 23.91
Participant considers effectiveness/demonstrated outcomes
25 25.00 15 26.79 10 22.73 16 29.63 9 19.57
Participant considers the impact of the treatment on my quality of life
16 16.00 7 12.50 9 20.45 5 9.26 11 23.91
Participant considers the financial costs to them and their family
14 14.00 8 14.29 6 13.64 8 14.81 6 13.04
Participant considers the severity of side effects 13 13.00 8 14.29 5 11.36 10 18.52 3 6.52
Participant considers the impact of treatment on themselves and their family in general
13 13.00 7 12.50 6 13.64 6 11.11 7 15.22

Section 4
Breast Cancer 2018 Australian PEEK Study
Figure 4.3: Considerations when making decisions
Changes in decision-making In the final question about decision-making, participants were asked whether they felt the way they made decisions had changed over time since they were diagnosed. Close to half of all participants reported that the way that they make decisions had stayed the same (n=49, 49.00%). Participant describes the way that they make decisions had stayed the same I think I approach them pretty much in the same way but I try to see more of the positive in those decisions whatever, will this have a good effect on me or not… I've had to choose things and I never ever thought I would have to do which it's amazing what you have to do when what you can do and you have to do it that's the thing. I think I've probably pretty much I'm using reasonably positive but yes. Participant 4
That's a really interesting question. No I don't think so to be honest. I think my primary factor will always be what clinical benefit is this going to give me. Participant 35 That's a good question, isn't it? I've always talked to my husband about things and I've always had the same GP for years and I've always felt very happy with him in the fact that he doesn't muck around, if he thinks there is a problem he acts on it straight away in the fact that he wasn't happy that I had to wait for a fine needle biopsy…would have had to wait three weeks and he said no, not good enough and rang around until he got me in to someone quickly…I don't think I've changed in my thoughts really except this is something new I've never had to deal with before. Participant 58
0
5
10
15
20
25
30
Participant considers long termoutcomes/survival
Participant considerseffectiveness/demonstrated
outcomes
Participant considers theimpact of the treatment on my
quality of life
Participant considers thefinancial costs to them and
their family
Participant considers theseverity of side effects
Participant considers theimpact of treatment on
themselves and their family ingeneral

Section 4
Breast Cancer 2018 Australian PEEK Study
A quarter of all participants (n=25, 25.00%) reported that the way that they make decisions has changed and this related to them being more empowered and informed. Participant describes the way that they make decisions has changed and this related to them being more empowered and informed Yes. I know a lot more now and I would ask more questions. I just…I don't know that it's possible to…it wasn't like I didn't read things. You start to assimilate all those pieces of information after a period of time. I'm just not sure it's possible to process the fact that you've got the diagnosis and then, all the technical information about what's going on, in the time that you have available. I don't think I regret any of the decisions that I’ve made. I would definitely think it through more thoroughly now than I did at that time. When you’re first getting diagnosed, you’ll almost do whatever the doctors tell you. Participant 22 Definitely it's changed. I think I'm a little bit more…no, just a bit more switched on, I think, and just a bit more aggressive in the way I make decisions, most definitely. Participant 45 Yes. I think it probably has. That depends on the type of people. I didn't question anything I was told that I needed to do either. I mean, looking in hindsight, I would've ensured I had more ongoing tests. To check the size and that sort of thing. I 'd be always happy for them to make those decisions. My oncologist used to tell me what I had to do. Just tell me where I need to show up and I'll do it. The problem was that I am one of those people that needed to know all of the information, so that's how I operate. Participant 93
There were also 19 participants (19.00%) that noted they had changed the way they make decisions as they are more cautious and considered. Participant describes the way that they make decisions has changed as they are more cautious and considered Probably now I think a bit more about decisions than I did before. before I didn't sort of maybe go into things as much. We sort of did quite a bit of research when we knew that I had breast cancer and sort of looked at the options, and the costs, and everything like that, and what was going to happen. So I think it has changed. I think a lot more about things before I do them I think now. Participant 25 I think I will take more time to consider everything rather than…I don't necessarily think my decisions would have changed in 2013. I think now the way I make decisions, I would have considered a few more things. I think having gone to some of the breast support networks at HOSPITAL, just the number of people who even saw second surgeons or sought second opinions. Participant 34 Yes, I think so, yes. I certainly have become more informed and reflective over time. You start to I guess negotiate with yourself what you are willing to put up with and where the line is between living just for the sake of living, and quality of life. Participant 70 In relation to sub-group variations, participants with stage 0-I breast cancer reported being more empowered and informed, more frequently than the general cohort (45.00% compared to 25.00% in the general cohort). They also reported being more cautious and considered, less frequently than the general cohort (5.00% compared to 19.00% in the general cohort). Participants in rural areas reported making decisions in the same way less frequently than the general cohort (36.36% compared to 49.00% in the general cohort). They also reported changing the way they make decisions as they have a different outlook on life, more frequently than the general cohort (18.18% compared to 8.00% in the general cohort) and this theme was unique to participants in rural areas.

Section 4
Breast Cancer 2018 Australian PEEK Study
Table 4.4: Decision-making over time
Figure 4.4: Decision-making over time
All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n=30 % n=50 % n=50 %No, it has stayed the same 49 49.00 8 40.00 16 53.33 24 48.00 25 50.00
Yes, more empowered and informed (more research)
25 25.00 9 45.00 8 26.67 17 34.00 8 16.00
Yes, more cautious and considered - there is a greater impact of their decisions
19 19.00 1 5.00 4 13.33 5 10.00 14 28.00
Yes, generally has a different outlook on life 8 8.00 1 5.00 3 10.00 4 8.00 4 8.00
All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %No, it has stayed the same 49 49.00 33 58.93 16 36.36 28 51.85 21 45.65
Yes, more empowered and informed (more research)
25 25.00 14 25.00 11 25.00 12 22.22 13 28.26
Yes, more cautious and considered - there is a greater impact of their decisions
19 19.00 11 19.64 8 18.18 11 20.37 8 17.39
Yes, generally has a different outlook on life 8 8.00 0 0.00 8 18.18 5 9.26 3 6.52
0
10
20
30
40
50
60
No, it has stayed the same Yes, more empowered and informed(more research)
Yes, more cautious and considered -there is a greater impact of their
decisions
Yes, generally has a different outlookon life

Section 5
Breast Cancer 2018 Australian PEEK Study
Section 5 Treatment and health service provision

Section 5
Breast Cancer 2018 Australian PEEK Study
Section 5: Experience of treatment
Treatments experienced
• The most common treatments were surgery (n=94, 94.00%) and radiation therapy (n=79, 79.00%). This was followed by Tamoxifen (n=43, 43.00%), Cyclophosphamide (Endoxan) (n=39, 39.00%), Paclitaxel (n=34, 34.00%), Docetaxel (Taxotere) (n=33, 33.00%) and Letrozole (Femara) (n=33, 33.00%).
• Participants were asked to rate their quality of life on a scale of 1 to 7 while using each specific treatment (with 1 being ‘Life was very distressing and 7 being ‘Life was great’). Mean quality of life scores ranges from 1.70 to 4.13, that is, all quality of life scores were with the ‘Life was very distressing’ to ‘Life was average’ range. The treatment that scored the least impact on quality of life was Exemestane (Aromasin) (mean score 4.13). Herceptin (mean score 3.60), Tamoxifen (mean score 3.51), Anastrozole (Arimidex) (mean score 3.47) and Letrozole (Femara) (mean score 3.24) all had a mean score of at least 3, that is in the ‘Life was a little distressing’ range. The remaining treatments had a mean quality of life score of 2.13 to 2.94, that is in the ‘Life was distressing’ range. There was one treatment scoring less than 2 (Docetaxel/Taxotere,) with a mean score of 1.70).
• The treatments that had a mean effectiveness score of at least 4 (Effective) were Exemestane (Aromasin) (average score 4.00), Doxorubicin (Adriamycin) (average score 4.04), radiation therapy (average score 4.04), Paclitaxel (average score 4.21), Herceptin (average score 4.33) and Anastrozole (Arimidex) (average score 4.36). The remaining treatments scored had a mean effectiveness score of at least 3, that is in the moderately effective range.
• When asked what side effects or symptoms participants could cope with, the most common theme was that participants felt as though they could cope with all side effects (n=21, 21.00%), however it was also often noted that this was because they had to (that, is they had no choice but to cope). There were also 16 participants (16.00%) that noted that there were no side effects that they could cope with, that is, they only noted that there were difficult side effects. In relation to specific side effects that participants felt they could cope with, the main themes were fatigue (n=10, 10.00%), nausea and vomiting (n=10, 10.00%). hair loss (n=9, 9.00%), radiation burns/blisters (n=9, 9.00%) and cramps (n=9, 9.00%).
• When asked what side effects or symptoms participants found difficult to cope with, the most common side effect that participants felt they could not cope with was pain (n=20, 20.00%). Within this theme, there were 10 participants that specifically spoke about bone pain, while the remaining 10 participants spoke about other pain. The next most difficult side effect was fatigue and lethargy (n=18, 18.00%). The remaining themes that were each noted by 9 participants (9.00%) included the psychological impact, restriction in mobility and change in physical appearance. Nausea and symptoms of menopause were noted as difficult side effects by 8 participants (8.00%).
Adherence to medication
• The most common theme in this section was that participants would continue with a therapy for as long as prescribed (n=36, 36.00%). This was followed by participants describing that they would not give up on any medication (n=16, 16.00%). There were 14 participants (14.00%) that spoke about continuing with a treatment for a month or more, and 10 participants (10.00%) that described sticking to a treatment for 2 to 3 months.
• There were two sub-group variations where participants with stage 0-I breast cancer described not giving up on a treatment less frequently than the general cohort (5.00% compared to 16.00% in the general cohort). This sub-group also described sticking with something for about a month or more less frequently than the general cohort (5.00% compared to 14.00% in the general cohort).
• Participants were asked what needed to change for them to feel like a treatment is working. The two most common themes were that participants needed to see test results or have some clinical indication that the treatment is working; and needing to feel better or do everyday tasks. These themes were both noted by 21 participants (21.00%). The next most common theme noted by 13 participants (13.00%) was that they were unable to describe the change needed to feel as though a treatment was working. Having no disease progression or no recurrence, needing to directly fix the symptoms that treatment is intended to fix, and needing pain to dissipate were each noted by 11 participants (11.00%).

Section 5
Breast Cancer 2018 Australian PEEK Study
Treatment at home or hospital
• Participants were asked, if there was an option to have treatment in a pill form at home or chemotherapy in hospital, which they would prefer. The majority of participants spoke about a preference for taking medication at home (n=71, 71.00%). Of the remaining participants, 26 (26.00%) described a preference for hospital and two (2.00%) were uncertain.
• The rationale for their choice was also analysed. The most common theme was that participants preferred having medication at home because it is more convenient and comfortable (n=36, 36.00%). The next most common theme was that the participant preferred treatment at hospital in case something went wrong, however it was also noted that this would depend on the type of treatment offered (n=10, 10.00%).
• As a follow-up question, participants were asked what support they would need to feel comfortable having treatment at home. The majority of participants (n=59, 59.00%) spoke about needing to have someone to call if they have a question or issue, especially out or hours. The next most frequent theme was the need to be checked regularly by a general practitioner or nurse at home (n=21, 21.00%) while an additional eight participants (8.00%) described needing check-ups but not necessarily at home.
Complementary therapies
• There were 38 participants (38.00%) that described not using any complementary therapies and this was the most common theme. Massage was the most common complementary therapy, used by 22 participants (22.00%). In a consolidated theme, there were various complementary therapies that participants spoke about including acupuncture, reiki and reflexology (n=18, 18.00%). Taking vitamins and minerals (n=14, 14.00%), healthy diets (n-12, 12.00%), mindfulness (n=10, 10.00%) and yoga or light exercise (n=7, 7.00%) were also described as complementary therapies.
Service provision and affordability
• The vast majority of participants had access to a general practitioner (n=97, 97.00%), medical oncologist (m=96, 96.00%), surgeon (n=92.00%) and radiation oncologist (n=83, 83.00%) for the treatment of their breast cancer.
• The majority of patients had private healthcare insurance (n=82, 82.00%), 44 participants were treated as private patients, 27 (27.00%) as public patients and 28 (28.00%) equally as public and private patients. A little over half of the participants were treated in the private hospital system (n=56, 56.00%).
• The majority of participants have never missed medical appointments due to cost (n=76, 76.00%), and have never been unable to afford prescription medications (n=83, 83.00%). Half of participants have never had trouble paying for basic needs due to their diagnosis with breast cancer (n=50, 50.00%).
Changes to work status • The work status for a number of participants changed due to their diagnosis with breast cancer with about
a quarter of participants reducing the number of hours worked (n=26, 26,00%), and 21 (21.00%) quitting their jobs.
• Very few carers had to quit their job (n=3, 3.00%) or reduce the number of hours worked (n=5, 5.00%), however, carers have had to take leave either with pay (n=34, 34.00%), or without pay (n=10, 10.00%).

Section 5
Breast Cancer 2018 Australian PEEK Study
Treatments experienced
Participants were asked in the questionnaire to identify the treatments that they had experienced. The most common treatments were surgery (n=94, 94.00%) and radiation therapy (n=79, 79.00%). This was followed by Tamoxifen (n=43, 43.00%), Cyclophosphamide (Endoxan) (n=39, 39.00%), Paclitaxel (n=34, 34.00%), Docetaxel (Taxotere) (n=33, 33.00%) and Letrozole
(Femara) (n=33, 33.00%). Treatments that were used and reported by less than 10 participants were not included in the tables and calculations. These included Carboplatin, Everolimus (Afinitor), Goserelin (Zoladex), Pertuzumab (Perjeta), Vinorelibine (Navelbine), Methotrexate (Ledertrexate, Methoblastin), Ribociclib, Mitomycin, Gemcitabine (Gemzar), Palbociclib (Ibrance), and Capecitabine (Xeloda).
Table 5.1: Treatments experienced
Treatment n= % Mean QoL score Range Mean effectiveness score
Range
Surgery 94 94.00 2.74 Low = 1, High = 5 3.89 Low = 1, High = 5
Radiotherapy 79 79.00 2.94 Low = 1, High = 6 4.04 Low = 1, High = 5
Tamoxifen 43 43.00 3.51 Low = 1, High = 6 3.30 Low = 1, High = 5
Cyclophosphamide (Endoxan) 39 39.00 2.21 Low = 1, High =4 3.79 Low = 1, High = 7
Paclitaxel 34 34.00 2.38 Low = 1, High = 4 4.21 Low = 2, High = 5
Docetaxel (Taxotere) 33 33.00 1.70 Low = 1, High = 4 3.94 Low = 1, High = 5
Letrozole (Femara) 33 33.00 3.24 Low = 1, High = 5 3.04 Low = 1, High = 4
Doxorubicin (Adriamycin) 29 29.00 2.38 Low = 1, High = 4 4.00 Low = 1, High = 5
Exemestane (Aromasin) 23 23.00 4.13 Low = 1, High = 6 4.00 Low = 1, High = 5
Flurouracil (5FU) 17 17.00 2.24 Low = 1, High = 4 3.88 Low = 3, High = 4
Anastrozole (Arimidex) 17 17.00 3.47 Low = 1, High = 5 4.36 Low = 4, High = 5
Epirubicin (Ellence) 15 15.00 2.13 Low = 1, High = 4 3.87 Low = 2, High = 5
Herceptin 15 15.00 3.60 Low = 2, High = 7 4.33 Low = 1, High = 5

Section 5
Breast Cancer 2018 Australian PEEK Study
Figure 5.1: Treatments experienced (% of all participants) As a follow-up question (within the online questionnaire), participants were asked to rate their quality of life on a scale of 1 to 7, while using each specific treatment (with 1 being ‘Life was very distressing and 7 being ‘Life was great’). Mean quality of life scores ranges from 1.70 to 4.13, that is, all quality of life scores were with the ‘Life was very distressing’ to ‘Life was average’ range. The treatment that scored the least impact on quality of life was Exemestane (Aromasin) (mean score 4.13). Herceptin
(mean score 3.60), Tamoxifen (mean score 3.51), Anastrozole (Arimidex) (mean score 3.47) and Letrozole (Femara) (mean score 3.24) all had a mean score of at least 3, that is in the ‘Life was a little distressing’ range. The remaining treatments had a mean quality of life score of 2.13 to 2.94, that is in the ‘Life was distressing’ range. There was one treatment scoring less than 2 (Docetaxel/Taxotere, with a mean score of 1.70).
0
10
20
30
40
50
60
70
80
90
100
Surgery Radiotherapy Tamoxifen Cyclophosphamide(Endoxan)
Paclitaxel Docetaxel (Taxotere) Letrozole (Femara) Doxorubicin(Adriamycin)
Exemestane(Aromasin)
Flurouracil (5FU) Anastrozole (Ar imidex) Epirubicin (Ellence) Herceptin

Section 5
Breast Cancer 2018 Australian PEEK Study
Figure 5.2: Treatments experienced and mean quality of life A second follow-up question was asked in relation to how effective the participant felt the treatment was on a scale of 1 to 5 (with 1 being ineffective and 5 being very effective). The treatments that had a mean effectiveness score of at least 4 (Effective) were Exemestane (Aromasin) (average score 4.00), Doxorubicin (Adriamycin) (average score 4.04),
Radiotherapy (average score 4.04), Paclitaxel (average score 4.21), Herceptin (average score 4.33) and Anastrozole (Arimidex) (average score 4.36). The remaining treatments scored had a mean effectiveness score of at least 3, that is in the moderately effective range.
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
4.50
Exemest
ane (A
romasi
n)
Hercepti
n
Tamoxife
n
Anastrozole (A
r imidex)
Letrozol
e (Fem
ara)
Radiothe
rapy
Surge
ry
Paclita
xel
Doxorubicin
(Adria
mycin)
Flurourac
il (5FU
)
Cyclop
hosphamide (
Endoxan
)
Epiru
bicin (E
llence)
Docetax
el (Ta
xotere)
Life was very distressing (Score = 1)
Life was distressing(Score = 2)
Life was a little distressing(Score = 3)
Life was average(Score = 4)
Life was good(Score = 5)
Life was very good(Score = 6)
Life was great(Score = 7)

Section 5
Breast Cancer 2018 Australian PEEK Study
Figure 5.3: Treatments experienced and effectiveness Side effects of treatment Participants were guided to reflect on the side effects that they had experienced from their various treatments. They were then asked two, separate questions in relation to the side effects that they felt they could cope with, and the side effects that were very difficult to cope with. The most common theme was that participants felt as though they could cope with all side effects (n=21, 21.00%), however it was also often noted that this was because they had to (that, is they had no choice but to cope). There were also 16 participants (16.00%) that noted no side effects that they could cope with, rather they only noted that there were difficult side effects. In relation to specific side effects that participants felt they could cope with, the main themes were fatigue (n=10, 10.00%), nausea and vomiting (n=10, 10.00%). hair loss (n=9, 9.00%), radiation burns/blisters (n=9, 9.00%) and cramps (n=9, 9.00%). There were a number of sub-group variations. Participants with stage IV disease reported having no side effects that they could cope with, only difficult
side effects more frequently than the general cohort (26.00% compared to 16.00% in the general cohort). Participants with stage 0-I breast cancer reported being able to cope with fatigue more frequently than the general cohort (20.00% compared to 10.00%). Participants from rural areas reported being able to cope with all side effects more frequently than the general cohort (31.82% compared to 21.00% in the general cohort).
Figure 5.4: Side effects that participants could cope with (% of all participants)
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
4.50
5.00
Letrozol
e (Fem
ara)
Tamoxife
n
Cyclop
hosphamide (
Endoxan
)
Epiru
bicin (E
llence)
Flurourac
il (5FU
)
Surge
ry
Docetax
el (Ta
xotere)
Exemest
ane (A
romasi
n)
Doxorubicin
(Adria
mycin)
Radiothe
rapy
Paclita
xel
Hercepti
n
Anastrozole (A
r imidex)
Ineffective(Score = 1)
Somewhat effective(Score = 2)
Moderately effective(Score = 3)
Effective(Score = 4)
Very effective(Score = 5)
0
2
4
6
8
10
12
Coping with allside effects
(because you haveto).
Nno side effectsthat were easy tocope with. Only
difficult sideeffects.
Fatigue (tiredness) Nausea andvomiting
Hair loss Radiation therapyburns or blisters
Cramps andassociated pain

Section 5
Breast Cancer 2018 Australian PEEK Study
Figure 5.5: Side effects that participants could cope with (Word cloud)

Section 5
Breast Cancer 2018 Australian PEEK Study
Table 5.2: Side effects that participants could cope with
Participant describes being able to cope with all side effects
Well, you cope with all of them, because you don't have a choice. I get up in the morning and it takes a minute or two to get my body organized to be able to walk, because my feet are sore, my hands are sore. but you cope with it because you just got to. You don't have a choice. Participant 5
Yes. Broadly speaking I've coped pretty well with all of them. I've got two kids... That's one thing that makes you just get on with it and cope with it because they need too as well. That's one aspect of it. The surgery was just really rest and time. The radiotherapy, I was uncomfortable and the logistics of getting there and all that were a pain. I was very very glad when it was over, that whole process. But really from when I finished, it's still a bit of fatigue and stuff now but the recovery of my skin was quite quick. It's amazing how the skin regenerates itself and some of the skin's been good. The tamoxifen, that's a bit challenging given the longevity of taking that drug and mentally that's challenging because you know what it means so you know that its with you for the long term. It's finding ways to deal with the side effects in a positive way which is what I'm exploring at the moment. Participant 31
I've had to cope with all of them but that doesn't mean I enjoyed coping with it because you just got to get on and live. Participant 50 Participant describes being able to cope with fatigue Probably the tiredness and feeling a bit unwell was probably the easiest to cope with. Participant 26 Which of the side effects I'm best able to cope with? I guess the feeling of exhaustion. That was fair to be able to deal with. I guess, it's the only one I could deal with. Participant 29 I think most of the side-effects you can get something to help with. Like tiredness, you can't…you just got to rest. Participant 60
Side effects that patients can cope with All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n= % n=50 % n=50 %Participant describes coping with all side effects (because you have to).
21 21.00 3 15.00 6 20.00 9 18.00 12 24.00
Participant describes no side effects that were easy to cope with. Only difficult side effects.
16 16.00 2 10.00 1 3.33 3 6.00 13 26.00
Participant describes fatigue (tiredness) 10 10.00 4 20.00 3 10.00 7 14.00 3 6.00
Participant describes nausea and vomiting 10 10.00 0 0.00 1 3.33 1 2.00 9 18.00
Participant describes hair loss 9 9.00 2 10.00 4 13.33 6 12.00 3 6.00
Participant describes radiation therapy burns or blisters
9 9.00 3 15.00 2 6.67 5 10.00 4 8.00
Participant describes cramps and associated pain 9 9.00 2 10.00 5 16.67 7 14.00 2 4.00
Side effects that patients can cope with All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant describes coping with all side effects (because you have to).
21 21.00 10 17.86 14 31.82 9 16.67 10 21.74
Participant describes no side effects that were easy to cope with. Only difficult side effects.
16 16.00 8 14.29 6 13.64 10 18.52 5 10.87
Participant describes fatigue (tiredness) 10 10.00 6 10.71 4 9.09 5 9.26 4 8.70
Participant describes nausea and vomiting 10 10.00 6 10.71 3 6.82 8 14.81 5 10.87
Participant describes hair loss 9 9.00 6 10.71 3 6.82 8 14.81 2 4.35
Participant describes radiation therapy burns or blisters
9 9.00 6 10.71 2 4.55 4 7.41 4 8.70
Participant describes cramps and associated pain 9 9.00 6 10.71 3 6.82 5 9.26 4 8.70

Section 5
Breast Cancer 2018 Australian PEEK Study
Participant describes being able to cope with nausea and vomiting My nausea and vomiting et cetera were really well-managed, and I had tethering dose of steroids. I had lots of antiemetic, so that part wasn't a big problem. Participant 34 Yes. Well, I'm still now. I still have constant nausea and headaches, and I can cope with that. Yes, all the doctors are good with the nausea tablets and things like that. Still, having to take medication to deal with it. There's nothing else unless you try other things. Participant 51 I think the nausea probably, I meant it wasn't pleasant, but you get through that, I guess because you expect to have you know to anticipate it and are ready for it. Participant 87 The most common side effect that participants felt they could not cope with was pain (n=20, 20.00%). Within this theme, there were 10 participants (that specifically spoke about bone pain, while the remaining 10 participants spoke about other pain. The next most difficult side effect was fatigue and lethargy (n=18, 18.00%). The remaining themes that were each noted by 9 participants (9.00%) included the psychological impact, restriction in mobility and change in physical appearance. Nausea and symptoms on menopause
were noted as difficult side effects by 8 participants (8.00%).
Figure 5.6: Side effects that participants found difficult to cope with (% of all participants)
0
5
10
15
20
25
Pain Bone pain Other pain (not bonepain)
Fatigue and lethargy(tiredness)
Psychological-impact(depression, stress)
Restriction in physicalmobility
Change in physicalappearance (includinghair loss and eyebrow
loss)
Other side effects thatparticipants couldn't
cope with
Nausea Symptoms ofmenopause

Section 5
Breast Cancer 2018 Australian PEEK Study
Figure 5.7: Side effects that participants found difficult to cope with (Word cloud) Table 5.3: Side effects that participants found difficult to cope with
Side effects that are difficult to cope with All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n= % n=50 % n=50 %Participant describes pain as being difficult to cope with
20 20.00 4 20.00 6 20.00 10 20.00 10 20.00
Bone pain 10 10.00 1 5.00 2 6.67 3 6.00 7 14.00
Other pain (not bone pain) 10 10.00 3 15.00 4 13.33 7 14.00 3 6.00
Participant describes fatigue and lethargy (tiredness) as being difficult to cope with
18 18.00 4 20.00 4 13.33 8 16.00 10 20.00
Participant describes the psychological-impact (depression, stress) as being difficult to cope with
9 9.00 2 10.00 4 13.33 6 12.00 3 6.00
Participant describes restriction in physical mobility as being difficult to cope with
9 9.00 0 0.00 2 6.67 2 4.00 7 14.00
Participant describes change in physical appearance (including hair loss and eyebrow loss) as being difficult to cope with
9 9.00 1 5.00 5 16.67 6 12.00 3 6.00
Participant describes other side effects that participants couldn't cope with
9 9.00 1 5.00 2 6.67 3 6.00 6 12.00
Participant describes nausea as being difficult to cope with
8 8.00 1 5.00 3 10.00 4 8.00 4 8.00
Participant describes symptoms of menopause as being difficult to cope with
8 8.00 0 0.00 4 13.33 4 8.00 4 8.00

Section 5
Breast Cancer 2018 Australian PEEK Study
Participant describes pain as being difficult to cope with
The pain of infections, that was hard. Pain does your head in after a while. Participant 9
Yes. Nerve pain. No, no. Nothing compared to that. Participant 10
I've had pain in my shoulder, pain in my arm, and to be told I didn't have any lymphoedema. I went to a lymphoedema conference, hopped on a plane and have everyone say, "Oh my gosh you've got lymphoedema why don't you get it treated?", that was hard to deal with but again you can ask and ask and ask and no one seems to do anything. Participant 50
Participant describes bone pain as being difficult to cope with
The bone pain because there were just days I couldn't control it. Participant 39
Chemo I think is the worst. Yes, just everything. Then having to give yourself the steroid injection a few days later, and then being awake night after night. Then I had sleeping tablets, so I could get some sleep and the bone pain. It was just all awful. Participant 65
Bone pain, I forgot to mention that too, deep, deep bone pain that nothing touches. There is no way, I stood in showers, I did everything I could think of. Participant 78
Participant describes fatigue and lethargy as being difficult to cope with
At times, I guess the tiredness at times. The frustration because you can't get on and do stuff you want to get on and do. Having said that, I kept very active all through my whole treatment even with radiation. The Tamoxifen definitely knocks you around a bit more in terms of how you're feeling? Participant 12
I found the fatigue and the bone pain, really difficult. I knew I should have been exercising, but I just found that by the time the third chemo came around, I just felt completely incapable of doing that, but I was still working and I continued to work throughout. That probably used up a fair amount of energy, and I do think I would have benefited from doing more exercise, or even doing something like yoga at that time. (continued after last question answered - all part of one response) I found writing very difficult, I found trying to sustain concentration for any period of time was really difficult. Participant 34
I think the fatigue that came from it is really hard because you really just you want to do things but you just can't. Your body doesn't respond the same way. Yes and the fatigue stays forever. It doesn't just stop when treatment stops. Participant 53
Side effects that are difficult to cope with All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant describes pain as being difficult to cope with
20 20.00 10 17.86 10 22.73 13 24.07 7 15.22
Bone pain 10 10.00 6 10.71 4 9.09 6 11.11 5 10.87
Other pain (not bone pain) 10 10.00 4 7.14 6 13.64 7 12.96 2 4.35
Participant describes fatigue and lethargy (tiredness) as being difficult to cope with
18 18.00 12 21.43 6 13.64 13 24.07 5 10.87
Participant describes the psychological-impact (depression, stress) as being difficult to cope with
9 9.00 3 5.36 3 6.82 5 9.26 2 4.35
Participant describes restriction in physical mobility as being difficult to cope with
9 9.00 6 10.71 3 6.82 3 5.56 7 15.22
Participant describes change in physical appearance (including hair loss and eyebrow loss) as being difficult to cope with
9 9.00 5 8.93 4 9.09 7 12.96 2 4.35
Participant describes other side effects that participants couldn't cope with
9 9.00 6 10.71 4 9.09 5 9.26 5 10.87
Participant describes nausea as being difficult to cope with
8 8.00 4 7.14 4 9.09 6 11.11 2 4.35
Participant describes symptoms of menopause as being difficult to cope with
8 8.00 4 7.14 4 9.09 2 3.70 5 10.87

Section 5
Breast Cancer 2018 Australian PEEK Study
Adherence to medications
Participants were asked how long they adhere with a therapy before they think it might not be working or give up on it. The most common theme in this section was that participants would continue with a therapy for as long as prescribed (n=36, 36.00%). Participants primarily spoke about adhering to treatment in consultation with their treating clinician.
Adherence to treatment in consultation with clinician
I always go by the doctor's advice and If I think it's not working I ask if I should give it up. I don't make my own decisions on that. Participant 3
I haven't given up on any treatment. I suppose that decision would be made in consultation with my doctors. I haven't given up on any treatment because you assume they are working and you can't see that it's working, although with the chemotherapy with me because I had chemotherapy before surgery, we could see on the scans that my tumour was shrinking and certainly that made us to continuing with that. I haven't given up on any treatments. Participant 23
I usually do it whole. I usually just see the whole course out. If it's medication and they're giving you a month or two months to do it, I would usually give it the whole time. You don't know. Sometimes medication would take up to a month to just start kicking in and then it works from there on. You've got to be open-minded and positive about everything. Participant 78
This was followed by participants describing that they would not give up on any medication (n=16, 16.00%).
Participant describes not giving up on any treatment
I pretty much haven’t given up on anything that had been suggested to me, to be honest. I'm facing back supplements now because that's what I was advised to do. In terms of everything that I was advised to do and take, I did. The only thing I did negotiate with my oncologist towards the end of the chemo, was a reduced thyroid dose because it was making me a bit crazy. In fact, I would say, taking the steroids was probably the worst bit about chemo. Notwithstanding the fact that are not probably managed a bunch of side effects. It made me quite wired and made it very difficult for me to sleep. Participant 22
I had been diagnosed with so many things since then that I have stuck to all my medications I've been given. If I give up…a lot of people give up on Tamoxifen. I've had enough of that, but I've heard the longer you're on that, the more your body copes with it. The symptoms become less. You have to give your body time to adjust to them too. You can't just say, "Oh well this isn't working." Like I said, I still had no cancer. To me, that drug was working. You know what I mean? Participant 24
No. It never been a factor. I've always given myself 100%. I made the decision at the beginning to do what they told me to do. I'd always kick myself if I did stop and I'd never know if I didn't keep going. Does that make sense what I'm trying to say? Participant 62
There were 14 participants (14.00%) that spoke about adhering to a treatment for a month or more, and 10 participants (10.00%) that described sticking to a treatment for 2 to 3 months.
There were two sub-group variations where participants with stage 0-I breast cancer described not giving up on a treatment less frequently than the general cohort (5.00% compared to 16.00% in the general cohort). This sub-group also described sticking with something for about a month or more less frequently than the general cohort (5.00% compared to 14.00% in the general cohort).

Section 5
Breast Cancer 2018 Australian PEEK Study
Figure 5.8: How long patients adhere to a therapy (% of all participants
Table 5.4: How long patients adhere to a therapy
0
5
10
15
20
25
30
35
40
As prescr ibed(adherence
depends on adviceof doctor)
Not giving up onany treatment
Continuing withtreatment for
about a month ormore
Continuing withtreatment forabout 2 to 3
months
Depending on sideeffects
As long as i t isworking
Continuing withtreatment for
about a week ortwo
Adherence to treatment All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n= % n=50 % n=50 %Participant describes continuing with treatment for as long as prescribed (adherence depends on advice of doctor)
36 36.00 9 45.00 9 30.00 18 36.00 18 36.00
Participant describes not giving up on any treatment 16 16.00 1 5.00 8 26.67 9 18.00 7 14.00
Participant describes continuing with treatment for about a month or more
14 14.00 1 5.00 4 13.33 5 10.00 9 18.00
Participant describes continuing with treatment for about 2 to 3 months
10 10.00 2 10.00 4 13.33 6 12.00 4 8.00
Participant describes adherence depending on side effects
9 9.00 0 0.00 3 10.00 3 6.00 6 12.00
Participant describes continuing with treatment for as long as it is working
7 7.00 4 20.00 2 6.67 6 12.00 1 2.00
Participant describes continuing with treatment for about a week or two
8 8.00 2 10.00 1 3.33 3 6.00 5 10.00
Adherence to treatment All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant describes continuing with treatment for as long as prescribed (adherence depends on advice of doctor)
36 36.00 22 39.29 14 31.82 20 37.04 16 34.78
Participant describes not giving up on any treatment 16 16.00 9 16.07 7 15.91 12 22.22 4 8.70
Participant describes continuing with treatment for about a month or more
14 14.00 10 17.86 4 9.09 6 11.11 8 17.39
Participant describes continuing with treatment for about 2 to 3 months
10 10.00 5 8.93 5 11.36 2 3.70 8 17.39
Participant describes adherence depending on side effects
9 9.00 5 8.93 4 9.09 6 11.11 3 6.52
Participant describes continuing with treatment for as long as it is working
7 7.00 4 7.14 3 6.82 4 7.41 3 6.52
Participant describes continuing with treatment for about a week or two
8 8.00 4 7.14 4 9.09 5 9.26 3 6.52

Section 5
Breast Cancer 2018 Australian PEEK Study
Impact of treatment
Participants were asked what needed to change for them to feel as though a treatment was working. The two most common themes were that participants needed to see test results or have some clinical indication that the treatment is working and needing to feel better and more energised. These themes were both noted by 21 participants (21.00%). The next most common theme noted by 13 participants was that they were unable to describe the change needed to feel as though a treatment was working. Having no disease progression or no recurrence, needing to directly fix the symptoms that the treatment is intended to fix, and needing pain to dissipate were each noted by 11 participants (11.00%).
Figure 5.9: What needs to change to know a treatment has worked
Table 5.5: What needs to change to know a treatment has worked
0
5
10
15
20
25
Test results or havesome clinical
indication
Feel better/energised Unable to descr ibewhat needs to change
No progression ofdisease
Directly fix thesymptoms that
treatment is intendedto fix.
Pain to dissipate
What needs to change for patients to feel like treatment has worked
All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n= % n=50 % n=50 %Participant describes needing to see test results or
have some clinical indication that the treatment is
working
21 21.00 5 25.00 4 13.33 9 18.00 12 24.00
Participant describes needing to feel
better/energised
21 21.00 5 25.00 8 26.67 13 26.00 8 16.00
Participant is unable to describe what needs to
change for them to feel like treatment is working
13 13.00 2 10.00 4 13.33 6 12.00 7 14.00
Participant describes having no progression of
disease or maintaining stable disease (no recurrence)
11 11.00 2 10.00 4 13.33 6 12.00 5 10.00
Participant describes treatment needing to directly
fix the symptoms that it is intended to fix. e.g if it is
to stop neuropathy, it should stop neuropathy
11 11.00 1 5.00 5 16.67 6 12.00 5 10.00
Participant describes needing pain to dissipate 11 11.00 2 10.00 2 6.67 4 8.00 7 14.00
What needs to change for patients to feel like treatment has worked
All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant describes needing to see test results or
have some clinical indication that the treatment is
working
21 21.00 12 21.43 9 20.45 15 27.78 6 13.04
Participant describes needing to feel
better/energised
21 21.00 13 23.21 8 18.18 9 16.67 12 26.09
Participant is unable to describe what needs to
change for them to feel like treatment is working
13 13.00 7 12.50 6 13.64 6 11.11 7 15.22
Participant describes having no progression of
disease or maintaining stable disease (no
recurrence)
11 11.00 4 7.14 7 15.91 3 5.56 8 17.39
Participant describes treatment needing to directly
fix the symptoms that it is intended to fix. e.g if it is
to stop neuropathy, it should stop neuropathy
11 11.00 8 14.29 3 6.82 8 14.81 3 6.52
Participant describes needing pain to dissipate 11 11.00 6 10.71 5 11.36 6 11.11 5 10.87

Section 5
Breast Cancer 2018 Australian PEEK Study
Participant describes needing to see test results or have some clinical indication that the treatment is working
There's no warranty or anything on it but I'd love to know if you could have a blood test to see what your hormones are like. Do you really need to be on it? Or is it over-precautionary, or whatever. You think the choice is to take the tablet or die. And that's' not always on the back of my mind. It pops into my head every now and then and I think, "Well, what can I do about it?" There's no complete treatment and answer. They can't say you're going to never get it back. Participant 36
I think just my cancer markers and my scan. The main reason you use your treatment is to reduce the cancer. If that's not happening, then there's no point in taking it. Participant 61
The main thing is the clinical markers, but that is obviously balanced with how I am feeling and whether the side effects are tolerable. I do need to see that it is not making me feel worse I guess is the short answer. Participant 70
Participant describes needing to feel better and energised
This is a hard one because I truly felt that most of my treatment has worked. I don't know how to answer that question because I hadn't given up on the treatment. You need treatment is going to give you energy, makes you feel good, that makes you feel like…you really need to feel you're well enough to go and do things. You want something that's going to energise you. To tell you, it's a great part of those things. Participant 24
Yes, that's right. Probably a general feeling of well-being, definitely. If I'm feeling more energized and not so…because that's one of the other things is that I'm still suffering quite a bit with fatigue. So if I felt that something was supposed to be helping me from a fatigue perspective and it wasn't getting any better, then I wouldn't continue it. Participant 56
I just want to feel like I can do the things that I want to do and not have the cancer dictate what I can do. I just want to get back to as much normalcy as possible, that's all. Participant 81
Participant describes having no disease progression or no recurrence
Yeah. Well for me it's very specific. It is for me to know that it's working is that I know that I'm continuing to have my tumours shrinking and not progressing. Yep, that's the only, I guess that's it. If you're talking about in terms of what's making it work. Participant 52
I think the main thing would be to keep it stable, you know not make it worse. That would be the main thing. It's probably the thing I worry about the most is not so much whether it will fix me but whether it will aggravate it and make it worse. Participant 74
I don't know how to answer that. I guess the only way of knowing it's worth is if your cancer doesn't come back. I guess you'll know everything has worked if there's no spread, no recurrence of the cancer. Participant 80
Participant describes needing to directly fix the symptoms/problem that treatment is intended to fix
Anything? I've got to feel the difference. obviously, the aspirin, I just take that because I know I've got prevent this clotting, so I'll just take that. The Lyrica they put me on, I've started on it. There's definitely a difference with my feet, so I stay on it. The fish oil when I went off it, literary I was struggling to walk so definitely back on it. I was on Rosehip, and I went off it, and I noticed absolutely no difference. Participant 39
That all depends on what you're taking the treatment for, isn't it? You couldn't apply that to all the treatments that you take because it all depends on what outcome that you're looking for really. That's not a straight forward question to ask. Yes, if I was looking for something to help with my mouth ulcers then I'd be looking for relief immediately of course and something like that. With chemotherapy, I'm looking for something to help kill cancer cells and try to do live a lifestyle to help just promote that chemotherapy to work. I don't drink alcohol or anything like that that's going to combat my body. I give it the best opportunity to work. I might look for immediate responses unless it's like a treatment that's successful, like mouth ulcers and stuff like that. Yes, it's all dependent on what it is that I'm doing and what outcome I'm looking for from it. Whether I persevere with it. Participant 43
I suppose I need to- If it’s an antibiotic I would want to know that the infection that it’s treating is clearing up. As if like those vitamins I just mentioned, I supposed I’d like to see that the experience the benefits of the product that they are advertising-- to know that it’s worth keeping continuingly. Participant 68

Section 5
Breast Cancer 2018 Australian PEEK Study
Participant describes needing pain to dissipate
Pain needs to be less. Some clear outcome. I got quite depressed and anxious at one point and took medication for that. obviously, you know whether you feel better or not on that, and that took a bit of mucking around to get the right one. Participant 9
Well. I'm hoping that the chemo I'm about to start will get rid of the symptoms that I'm sure are caused by the cancer, like pains at the top of my tummy and the pain in my shoulders and the pain in my lower back. I think what needs to improve is my quality of life or the symptoms. Participant 60
Just my temperature going down and just the pain level going down. The comfort. Yes. Participant 89
Treatment at home or hospital
Participants were asked, if there was an option to have treatment in a pill form at home or chemotherapy in hospital, which they would prefer. The majority of participants spoke about a preference for taking medication at home (n=71, 71.00%). Of the remaining participants, 26 (26.00%) described a preference for hospital and two (2.00%) were uncertain. The rationale for their choice was also analysed. The most common theme was that participants preferred having medication at home because it is more convenient and comfortable (n=36, 36.00%). Participant describes a preference for treatment at home as being more convenient and comfortable At home in tablet form, you're just more comfortable in your own home and you don't need to leave, put that energy that you put into walking out the front door, making sure you look presentable, for example, into the actual place. If it was safe to do at home without any medical professionals around you then you could just a tablet, that would be great; rather than having to go out and expend energy, especially if you're unwell. Participant 3 At home in a tablet form. That's purely about being in your own space and being around my family, being with my kids. Participant 31
The tablet. because it’s more convenient, easier to administer and would require no time, unless it had significant side effects. No time off work or away from family. Participant 68 The next most common theme was that the participant preferred treatment at hospital in case something went wrong, however it was also noted that this would depend on the type of treatment offered (n=10, 10.00%). Participant describes a preference for treatment at hospital in case something goes wrong It depends on the type of treatment. With my chemo, I definitely would not have that at home I'd be in the hospital. If something were to go wrong, I've got the necessary people there. With my other breast cancer treatment, I do have that in a tablet form at home, just depends on the treatment. Participant 5 I'd still want to go to hospital to have it done only for the fact that if something goes wrong when you're doing it, they're there. I had a couple of reactions. Just the itching and that stuff. They knew what to do right away. If that happened at home, I think I would have panicked. I didn't mind going and getting it done because I knew they were looking after me. I knew they wouldn't let me home unless I was okay. Participant 62 In hospital I think because I have access to…something may go wrong with the treatment they have access to things you don't have at home. Plus, I don't want family watching me going through this stuff at home and have the memory of all that. I have to say to have it done in hospital if I could. Participant 82 There was one sub-group variation with participant with stage 0-I breast cancer describing having medication at home because it is more convenient and comfortable more frequently than the general cohort (50.00% compared to 36.00% in the general cohort).

Section 5
Breast Cancer 2018 Australian PEEK Study
Table 5.6: Preference for treatment at home or hospital
Table 5.7: Preference for treatment at home or in hospital (rationale)
Preference for treatment at home or hospital All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n= % n=50 % n=50 %Home 71 71.00 15 75.00 24 80.00 39 78.00 32 64.00
Hospital 26 26.00 4 20.00 6 20.00 10 20.00 16 32.00
Unsure 2 2.00 1 5.00 0 0.00 1 2.00 1 2.00
Preference for treatment at home or hospital All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Home 71 71.00 45 80.36 26 59.09 40 74.07 31 67.39
Hospital 26 26.00 10 17.86 16 36.36 11 20.37 15 32.61
Unsure 2 2.00 1 1.79 1 2.27 2 3.70 0 0.00
Preference for treatment at home or hospital All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n= % n=50 % n=50 %Participant describes a preference for medication at home because it is more convenient/ comfortable
36 36.00 10 50.00 9 30.00 19 38.00 17 34.00
Participant describes a preference for hospital in case something goes wrong
10 10.00 4 20.00 3 10.00 7 14.00 3 6.00
Participant describes a preference depending on effectiveness of treatment
8 8.00 1 5.00 2 6.67 3 6.00 5 10.00
Participant describes a preference for hospital because they will be monitored more closely
7 7.00 2 10.00 0 0.00 2 4.00 5 10.00
Participant describes a preference for medication at home because it will give them more control
7 6.00 2 5.00 1 3.33 3 4.00 4 8.00
Participant describes a preference for medication at home because it is better for their family life/situation
6 6.00 0 0.00 4 13.33 4 8.00 2 4.00
Participant describes a preference for hospital because they don't want to feel isolated
6 6.00 0 0.00 0 0.00 0 0.00 6 12.00
Participant describes a preference for medication at home (no other explanation)
5 5.00 0 0.00 0 0.00 0 0.00 5 10.00
Participant describes a preference for medication at home because they are afraid of needles or have bad veins
5 5.00 1 5.00 4 13.33 5 10.00 0 0.00
Participant describes a preference for medication at home because they don't like hospitals
5 5.00 1 5.00 3 10.00 4 8.00 1 2.00
Participant describes a preference depending on duration and frequency of treatment
5 5.00 0 0.00 3 10.00 3 6.00 2 4.00
Participant describes a preference for medication at home but indicates concerns about needing someone to call if there is an issue
2 2.00 0 0.00 2 6.67 2 4.00 0 0.00

Section 5
Breast Cancer 2018 Australian PEEK Study
Figure 5.10: Preference for treatment at home or in hospital (rationale)
Preference for treatment at home or hospital All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant describes a preference for medication at home because it is more convenient/ comfortable
36 36.00 24 42.86 12 27.27 16 29.63 20 43.48
Participant describes a preference for hospital in case something goes wrong
10 10.00 3 5.36 7 15.91 4 7.41 6 13.04
Participant describes a preference depending on effectiveness of treatment
8 8.00 5 8.93 3 6.82 5 9.26 3 6.52
Participant describes a preference for hospital because they will be monitored more closely
7 7.00 3 5.36 4 9.09 3 5.56 4 8.70
Participant describes a preference for medication at home because it will give them more control
7 6.00 4 5.36 3 6.82 5 7.41 2 4.35
Participant describes a preference for medication at home because it is better for their family life/situation
6 6.00 3 5.36 3 6.82 2 3.70 4 8.70
Participant describes a preference for hospital because they don't want to feel isolated
6 6.00 2 3.57 4 9.09 4 7.41 2 4.35
Participant describes a preference for medication at home (no other explanation)
5 5.00 3 5.36 2 4.55 5 9.26 0 0.00
Participant describes a preference for medication at home because they are afraid of needles or have bad veins
5 5.00 4 7.14 1 2.27 3 5.56 2 4.35
Participant describes a preference for medication at home because they don't like hospitals
5 5.00 1 1.79 4 9.09 3 5.56 2 4.35
Participant describes a preference depending on duration and frequency of treatment
5 5.00 4 7.14 1 2.27 2 3.70 3 6.52
Participant describes a preference for medication at home but indicates concerns about needing someone to call if there is an issue
2 2.00 1 1.79 1 2.27 2 3.70 0 0.00
0
5
10
15
20
25
30
35
40
Preference for medicationat home: more
convenient/comfortable
Preference for hospital: incase something goes
wrong
Preference depending oneffectiveness of treatment
Preference for hospital:monitored more closely
Preference for medicationat home: more control

Section 5
Breast Cancer 2018 Australian PEEK Study
Support needed if treatment is at home
As a follow-up question, participants were asked what support they would need to feel comfortable having treatment at home. The majority of participants (n=59, 59.00%) spoke about needing to have someone to call if they have a question or issue, especially out or hours. The next most frequent theme was the need to be checked regularly by a general practitioner or nurse at home (n=21, 21.00%) while an additional eight participants (8.00%) described needing check-ups but not necessarily at home.
There was one sub-group variation. Participants with stage II-III breast cancer described needing to have someone to call if they have a question or issue, especially out or hours more frequently than the general cohort (73.33% compared to 59.00% in the general cohort).
Figure 5.11: Support needed to be treated at home
Participant describes needing to have someone to call if they have a question or issue, especially out or hours.
A doctor that I could access 24/7, if I needed to get any relief of sickness, vomiting or sickness resulting from taking medication. Just reassurance and someone that you could ring, 24 hour helpline, maybe, "I'm feeling this and this, is it normal? How long do I have to wait
before this'll subside? Do I need to go into hospital to get relief?" Just make sure you had 24 hour back-up.
You aren't left at home alone by yourself to deal with this, with the unknown. Participant 20
I suppose a phone number to someone that you could ring that would be there to talk to you. Since I was having chemo in the day I was able to phone the chemo ward, but in the evening, you were able to phone another ward and they would put you through to someone who could talk to you. I only did it once, but it was nice to know that that number was there if you needed it. And not necessarily being visited by anybody, but someone to just text you to check up on you. Participant 35
Probably someone that you could contact if you have any issues and that would have to be out of hours as well. Because that's another thing, to not have anyone to ask a question out of normal 8 to 4 hours and having to present at the emergency department along with heaps of other people for when you're dealing with something. Participant 72
Participant describes needing to be checked regularly by a general practitioner or nurse at home
The regular checking from the…my breast cancer nurse, or mammography nurse, or a regular checking with the…so a regular check it with one of those ladies. Participant 5
I think if you're going to be doing at home from that point of view then you'd probably do need someone who's visiting regularly to ensure that you're actually taking the medication and to keep an eye on things in terms of side effects as well because you still need that support at home in your own environment. Participant 40.
Probably regular visits from a nurse, breast care nurse or the cancer care nurse, to make sure that was going okay and maybe more regular visits with the oncologist as well if I wasn't seeing a practitioner every time maybe more regularly with the oncologist. Participant 7
0
10
20
30
40
50
60
70
Participant descr ibes
that they would need to
have someone to cal l if
they have a question or
issue (out of hours, 24/7
support)
Participant descr ibes
need to be checked
regularly by GP/ Nurse
Participant descr ibes
that they would need to
have regular check-ups
(not at home but at the
clinic/hospital)
Participant descr ibes
that they would need to
have support for their
family/friends
Participant descr ibes
needing an overall
support
Participant descr ibes
not needing support
Participant descr ibes
that they would need to
have a plan in case of
emergency, such as
knowing where the local
hospital (A&E or ED
department etc).

Section 5
Breast Cancer 2018 Australian PEEK Study
Use of complementary therapies
Participants were asked whether they had used any complementary therapies. There were 38 participants (38.00%) that described not using any complementary therapies and this was the most common theme: No, lots of people had lots of suggestions about different things that I could try but I felt so shitty and horrible I just didn’t have the headspace to really explore them. Participant 27 I personally am not one for complementary therapies, but nobody suggested I go out and get massages or anything like that. I never really do. I don't do alternative stuff either. I've never been one for taking St. John's Wort or Valerian or anything like that. Participant 44 No. They told me not to. They said straight out, "Do not try anything." Not with the drugs. They said, "If we could do this an easier way, we would, but we can't. So don't try anything." Participant 62
Massage was the most common complementary therapy, used by 22 participants (22.00%). In a consolidated theme, there were various complementary therapies that participants spoke about including acupuncture, reiki and reflexology (n=18, 18.00%). Taking vitamins and minerals (n=14, 14.00%), healthy diets (n-12, 12.00%), mindfulness (n=10, 10.00%) and yoga or light exercise (n=7, 7.00%) were also described as complementary therapies.
Figure 5.12: Use of complementary therapies (% of all participants)
Table 5.8: Use of complementary therapies
0
5
10
15
20
25
30
35
40
Participant descr ibes notusing any complementary
therapies
Participant descr ibesmassage and/or
physiotherapy as acomplementary therapy
Other includingacupuncture, i and
reflexology
Participant descr ibes takingvitamins or mineralsupplements as a
complementary therapy
Participant descr ibes diet asa complementary therapy
Participant descr ibesmindfulness as a
complementary therapy(meditation)
Participant descr ibes takingwalks or jogging or doing
yoga as complimentrytherapy
Use of complementary therapy All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n= % n=50 % n=50 %Participant describes not using any complementary therapies
38 38.00 6 30.00 13 43.33 19 38.00 19 38.00
Participant describes massage and/or physiotherapy as a complementary therapy
22 22.00 6 30.00 9 30.00 15 30.00 7 14.00
Other including acupuncture, reiki and reflexology18 18.00 1 5.00 8 26.67 9 18.00 9 18.00
Participant describes taking vitamins or mineral supplements as a complementary therapy
14 14.00 2 10.00 6 20.00 8 16.00 6 12.00
Participant describes diet as a complementary therapy
12 12.00 1 5.00 5 16.67 6 12.00 6 12.00
Participant describes mindfulness as a complementary therapy (meditation)
10 10.00 2 10.00 3 10.00 5 10.00 5 10.00
Participant describes taking walks or jogging or doing yoga as complementary therapy
7 7.00 3 15.00 3 10.00 6 12.00 1 2.00

Section 5
Breast Cancer 2018 Australian PEEK Study
Use of complementary therapy All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant describes not using any complementary therapies
38 38.00 24 42.86 14 31.82 16 29.63 22 47.83
Participant describes massage and/or physiotherapy as a complementary therapy
22 22.00 14 25.00 8 18.18 15 27.78 7 15.22
Other including acupuncture, reiki and reflexology 18 18.00 9 16.07 9 20.45 12 22.22 6 13.04
Participant describes taking vitamins or mineral supplements as a complementary therapy
14 14.00 6 10.71 8 18.18 9 16.67 5 10.87
Participant describes diet as a complementary therapy
12 12.00 8 14.29 4 9.09 9 16.67 3 6.52
Participant describes mindfulness as a complementary therapy (meditation)
10 10.00 7 12.50 3 6.82 9 16.67 1 2.17
Participant describes taking walks or jogging or doing yoga as complementary therapy
7 7.00 4 7.14 3 6.82 5 9.26 2 4.35

Section 5
Breast Cancer 2018 Australian PEEK Study
Service provision and affordability Details about the healthcare system where participants were treated for breast cancer and financial complications from treatment are listed in Tables 5.8 and 5.9. Participants had access to a general practitioner (n=97, 97.00%), medical oncologist (m=96, 96.00%), surgeon (n=92.00%) and radiation oncologist (n=83, 83.00%) for the treatment of their breast cancer (Table 5.9). The majority of patients had private healthcare insurance (n=82, 82.00%), 44 participants were treated as private patients, 27 as public patients and 28 as equally public and private patients (Table 5.10). The majority of participants were treated in the private hospital system (n=56, 56.00%) (Table 5.10).
The majority of participants have never missed medical appointments due to cost (n=76, 76.00%), and have never been unable to afford prescription medications (n=83, 83.00%) (Table 5.8). Half of participants have never had trouble paying for basic needs due to their diagnosis with breast cancer (n=50, 50.00%) (Table 5.10). The work status for a number of participants changed due to their diagnosis with breast cancer with about a quarter of participants reducing the number of hours worked (n=26, 26,00%), and 21 quitting their jobs (Table 5.9). Very few carers had to quit their job (n=3, 3.00%) or reduce the number of hours worked (n=5, 5.00%), however, carers have had to take leave either with pay (n=34, 34.00%), or without pay (n=10, 10.00%) (Table 5.10).
Table 5.9: Provider of treatment
What health professionals have you had access to in relation to your breast cancer? N=100 % General Practitioner (GP) 97 97.00 Medical Oncologist 96 96.00 Surgeon 92 92.00 Radiation oncologist 83 83.00 Counselling or psychological support 62 62.00 Physiotherapy 49 49.00 Plastic surgeon 46 46.00 Dietician 25 25.00 Geneticist 25 25.00 General cancer care coordinator (not breast specific) 10 10.00 Occupational therapy 10 10.00 Exercise physiologist 8 8.00 Lymphoedema clinic 4 4.00 Palliative care 4 4.00 Survivorship clinic 4 4.00 Wellness services (massage, tai chi, meditation, yoga) 4 4.00 Integrated cancer centre BRICC 1 1.00

Section 5
Breast Cancer 2018 Australian PEEK Study
Table 5.10: Service provision and affordability Private health insurance
Yes 82 82.00
No 18 18.00
Treated as public or private patient
Equally public and private 28 28.00
Private 44 44.00
Public 27 27.00
Don’t know 1 1.00
Primary hospital system treated in
Both public and private 18 18.00
Private 56 56.00
Public 26 26.00 Had to delay or cancel healthcare appointments due to affordability N=100 Never 76 76.00
Rarely 3 3.00
Sometimes 8 8.00
Often 0 0.00
Very often 13 13.00
Unable to fill prescription due to cost N=100
Never 83 83.00
Rarely 5 5.00
Sometimes 12 12.00
Often 0 0.00
Very often 0 0.00
Difficult to pay for basic needs as a result of breast cancer diagnosis
Not at all difficult 50 50.00
Slightly difficult 21 21.00
Somewhat difficult 8 8.00
Moderately difficult 6 6.00
Extremely difficult 15 15.00
Change in employment due to breast cancer (can choose more than one option)
I have taken leave without pay 30 30.00
I have taken leave with pay 28 28.00
I was retired or did not have a job when diagnosed 27 27.00
I have reduced the number of hours I work 26 26.00
I have had to quit my job 21 21.00
My work status has not changed 21 21.00
I have accessed my superannuation 4 4.00
Change in carer job status (can choose more than one option)
My carer had to quit their job 3 3.00
My carer has reduced the number of hours they work 5 5.00
My carer has taken leave with pay 34 34.00
My carer has taken leave without pay 10 10.00
My carer was retired or did not have a job when diagnosed 15 15.00
My carers work status has not changed 43 43.00

Section 6
Breast Cancer 2018 Australian PEEK Study
Section 6 Information and communication

Section 6
Breast Cancer 2018 Australian PEEK Study
Section 6: Information and communication Access to information
• Participants were asked what information they had accessed in relation to their condition. Almost half of all participants described receiving information from local charities in Australia including (n=46, 46.00%) and an additional 29 participants (29.00%) spoke about receiving information from a McGrath Foundation or a specialist nurse. There were 39 participants (39.00%) that described seeking information from the internet, 17 (17.00%) that described receiving information from hospitals and 13 (13.00%) that spoke about receiving information from other patients. There were 11 participants, all of whom had stage IV breast cancer, that described a lack of information about metastatic breast cancer.
• In relation to sub-group variations, as noted there were 11 participants, all of whom had stage IV breast cancer, that described a lack of information about metastatic breast cancer. Participants with stage II-III breast cancer reported receiving information from local charities more frequently than the general cohort (60.00% compared to 46.00% in the general cohort) and participants with stage 0-I breast cancer reported receiving information from their oncologist more frequently than the general cohort (45.00% compared to 19.00%) in the general cohort). Rural participants described receiving information from their breast care nurse or McGrath nurse more frequently than the general population (40.91% compared to 29.00% in the general cohort).
Information that was helpful • There was a range of information that participants found helpful including Breast Cancer Network
Australia’s information and their My Journey Kit (n=13, 13.00%), information from other patients about their experience (n=13, 13.00%) and information provided by McGrath or specialist nurses (n=11, 11.00%). There were also 13 participants (13.00%) that noted that all information was helpful. In relation to specific topics, the most useful topic of information noted by 10 people (10.00%) was information about the participant’s specific type of cancer (that is, triple negative, ER positive, metastatic cancer etc.) and the side effects of treatment including what to expect (n=10, 10.00%).
Information that was not helpful • The most common theme described by 28 participants (28.00%) was that all information is helpful and there
is nothing that is not helpful. The next most common theme was that unsolicited information, that is, people telling you what to do, sharing their opinions or platitudes was not helpful and this was described by 20 participants (20.00%). In a similar theme, nine participants (9.00%) described stories about the worst-case scenario or horrific stories as not helpful. There were also 13 participants (13.00%) that described information from non-reputable sources such as Facebook and the media as not helpful.
Information preferences • Participants were asked whether they had a preference for information online, talking to someone, in
written (booklet) form or through a phone App. The most common theme was that participants preferred to talk to someone in relation to information provision (n=36, 36.00%). This was followed by a preference for written or online information combined with talking to someone (n=32, 32.00%). When combined, these two main themes represent 68 participants (68.00%) that have some preference for talking to someone in relation to information provision. The next most common theme was online information (n=21, 21.00%).
• In relation to sub-group variations, participants a preference for talking to someone (with or without online information) increased with stage of disease, that is participants with stage IV breast cancer described his preference most frequently (78.00%) compared to stage II-III (63.34%) and stage 0-I (50.00%).
Section 6
Breast Cancer 2018 Australian PEEK Study
Timing of information • The most common time that participants described being receptive to receiving information was at the time
of diagnosis (n=17, 17.00%). This was followed by after surgery (n=16, 16.00%) and being most receptive when information is given gradually over time (n=14, 14.00%). An additional 11 participants (11.00%) described being most receptive to receiving information when they are away from the hospital or following appointments.
• In relation to sub-group variations, participants with stage 0-I breast cancer described being receptive to information at diagnosis more frequently than the general cohort, whereas participants with stage IV disease described this less frequently than the general cohort (50.00% for stage 0-I, 4.00% for stage IV and 17.00% for the general cohort). Participants with stage 0-I breast cancer also described being receptive to information after surgery less frequently than the general cohort (5.00% compared to 16.00% in the general cohort).
Health professional communication • Participants were asked to describe the communication that they had had with health professionals
throughout their experience. The most common theme was that participants were satisfied with communication (very good to excellent) (n=37, 37.00%). There were 32 participants (32.00%) that described poor communication. This was particularly in relation to the feeling that clinicians did not take the time to explain things and allow questions. In contrast, there were 21 participants (21.00%) that felt as though communication was overall good, however there were possibly some improvements to be made.
• There were a number of sub-group variations. Participants with stage 0-I breast cancer described being satisfied with communication (Good, possibly some improvements), more frequently than the general cohort (35.00% compared to 21.00% in the general cohort). Participants in metropolitan areas described having poor communication, less frequently than the general cohort, while participants in rural areas described this more frequently (19.64 for metropolitan participants, 47.73 for rural participants, compared to 32.00% in the general cohort)
• The most common theme was that participants spoke and trusted a number of health professionals (n=32, 32.00%). This was followed by their general practitioner as a single health professional that they spoke to about their condition (n=15, 15.00%). There were then various combinations of health professionals including oncologist plus general practitioner (n=13, 13.00%) and oncologist plus surgeon.
• Half of all participants spoke about being able to access a breast care, specialist of McGrath nurse (n=50, 50.00%) while an additional 27 participants (27.00%) spoke about care received from chemotherapy or general oncology nurses. There were 16 participants (16.00%) that indicated that they had not accessed a breast care nurse and the remaining participants were unsure whether they had accessed a specialist nurse or not.
• There were two sub-group variations. Participants with stage IV breast cancer reported accessing specialist breast or McGrath nurses less frequently than the general cohort (26.00% compared to 50% in the general cohort) and participants in regional/rural areas also reported accessing specialist or McGrath nurses less frequently (27.27%).
Respect shown to patients • The majority of participant felt as though they had been treated respectfully throughout their experience
in the health system (n=69, 69.00%). There were five participants (5.00%) that did not feel as though they had been treated respectfully and an additional 26 participants (26.00%) that felt they were treated respectfully for the most part, except for one or two occasions.

Section 6
Breast Cancer 2018 Australian PEEK Study
Knowledge and confidence The Partners in Health questionnaire (PIH) measures an individual’s knowledge and confidence for managing their own health. The Partners in Health comprises a global score, 4 sub scales; knowledge, treatment, symptoms and coping. A higher score denotes a better understanding and knowledge of disease. Partners in health – overall score
• Overall, the participants scored in the top quintile for knowledge, adherence to treatment, and management of symptoms. The scores for coping and total score were in the second highest quintile.
Partners in health - by disease stage • Participants with very stage IV disease had a statistically significant worse score for the coping subscale
compared those with stage II-III disease.
Partners in health – by metastatic status • Participants with very metastatic disease had a statistically significant, worse scores for the adherence to
treatment, and coping subscales compared those without metastases.
Partners in health – by location • Participants living in regional or rural areas had had a statistically significant, worse scores for the adherence
to treatment, management of symptoms, coping and total score subscales compared those living in metropolitan areas.
Partners in health – by education • No differences were observed between those with university education and those with high school or trade
qualifications for any PIH subscale. Information given by health care professionals
• Information about treatment options (88.00%), and disease management (66.00%) were most frequently given to participants by healthcare professionals, and information about clinical trials (7.00%) and complementary therapies (18.00%) were give least often.
• Information patterns given to participants by was similar for all subgroups, however, those that had metastatic disease tended to get more information than those without, and those that live in metropolitan areas received more information than those in regional or remote areas
Information searched for independently
• Information about treatment options (58.00%), and interpreting test results (58.00%), were most often searched for independently by participants, and clinical trials (23.00%) and hereditary and genetic concerns (29.00%) were least searched for.
• Stage IV participants tended to search for more information compared to other disease stages with over 60% of stage IV participants searching for information about disease cause, treatment options, complementary therapies, interpreting test results and psychological support. Those with stage 0-I disease tended to search for less information independently compared to other disease stages.
• Those with metastatic disease searched for more information than those without. • Those living in metropolitan areas searched for more information than those in regional and remote areas. • Those with university education searched for more information compared to those high school or trade
qualification.

Section 6
Breast Cancer 2018 Australian PEEK Study
Gaps in Information • The largest gaps in information, where information was neither given to patients nor searched for
independently were for clinical trials (70.00%), and hereditary, genes and biomarkers (65.00%). Participants were given most information either from healthcare professionals or independently for treatment options (96.00%) and disease management (80.00%). Complementary therapies (43.00%) was the topic that was most searched for independently following no information from health professionals (49.00%).
Most trusted information sources • Across all participants, information from the participants’ hospital or clinic was most trusted, and
information from pharmaceutical companies was least trusted. Information from not for profit or charitable organisations and government sources were near equal in trust by participants. This order of preference was the same for all sub-groups.

Section 6
Breast Cancer 2018 Australian PEEK Study
Access to information Participants were asked what information they had accessed in relation to their condition. Almost half of all participants described receiving information from local charities in Australia including (n=46, 46.00%) and an additional 29 participants (29.00%) spoke about receiving information from a McGrath Foundation or a specialist nurse. There were 39 participants (39.00%) that described seeking information from the internet, 17 (17.00%) that described receiving information from hospitals and 13 (13.00%) that spoke about receiving information from other patients. There were 11 participants, all of whom had stage IV breast cancer, that described a lack of information about metastatic breast cancer.
In relation to sub-group variations, as noted 11 participants, all of whom had stage IV breast cancer, that described a lack of information about metastatic breast cancer. Participants with stage II-III breast cancer reported receiving information from local charities more frequently than the general cohort (60.00% compared to 46.00% in the general cohort) and participants with stage 0-I breast cancer reported receiving information from their oncologist more frequently than the general cohort (45.00% compared to 19.00%) in the general cohort). Rural participants described receiving information from their breast care nurse or McGrath nurse more frequently than the general population (40.91% compared to 29.00% in the general cohort).
Table 6.1: Access to information
Information received All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n=30 % n=50 % n=50 %Participant describes receiving information from the charity sector (Cancer Council, BCNA, My Journey, Hopes and Hurdles package)
46 46.00 10 50.00 18 60.00 28 56.00 18 36.00
Participant describes searching the internet/online information
39 39.00 8 40.00 9 30.00 17 34.00 22 44.00
Participant describes receiving information from their breast care nurse or McGrath Foundation
29 29.00 7 35.00 8 26.67 15 30.00 14 28.00
Participant describes receiving written information from their oncologist (specialist)
19 19.00 9 45.00 5 16.67 14 28.00 5 10.00
Partiipant describes receiving information from hospitals
17 17.00 3 15.00 5 16.67 8 16.00 9 18.00
Participant describes support groups or other talking/connecting with patients as a source of information
13 13.00 4 20.00 3 10.00 7 14.00 6 12.00
Participant describes information from surgeon 13 13.00 4 20.00 4 13.33 8 16.00 5 10.00
Participant describes limited information available about metastatic/advanced or stage IV cancer
11 11.00 0 0.00 0 0.00 0 0.00 11 22.00
Participant describes receiving written information from their GP
10 10.00 3 15.00 0 0.00 3 6.00 7 14.00
Participant describes receiving too much information (information overload, feeling overwhelemed)
10 10.00 1 5.00 6 20.00 7 14.00 3 6.00
Participant describes receiving information from books given to them
9 9.00 5 25.00 1 3.33 6 12.00 3 6.00
Participant describes searching for research articles (more scientific)
4 4.00 3 15.00 1 3.33 4 8.00 0 0.00

Section 6
Breast Cancer 2018 Australian PEEK Study
Table 6.1: Access to information (cont.)
Figure 6.1: Access to information (% of all participants)
Information received All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n=30 % n=50 % n=50 %Participant describes receiving information from the charity sector (Cancer Council, BCNA, My Journey, Hopes and Hurdles package)
46 46.00 10 50.00 18 60.00 28 56.00 18 36.00
Participant describes searching the internet/online information
39 39.00 8 40.00 9 30.00 17 34.00 22 44.00
Participant describes receiving information from their breast care nurse or McGrath Foundation
29 29.00 7 35.00 8 26.67 15 30.00 14 28.00
Participant describes receiving written information from their oncologist (specialist)
19 19.00 9 45.00 5 16.67 14 28.00 5 10.00
Partiipant describes receiving information from hospitals
17 17.00 3 15.00 5 16.67 8 16.00 9 18.00
Participant describes support groups or other talking/connecting with patients as a source of information
13 13.00 4 20.00 3 10.00 7 14.00 6 12.00
Participant describes information from surgeon 13 13.00 4 20.00 4 13.33 8 16.00 5 10.00
Participant describes limited information available about metastatic/advanced or stage IV cancer
11 11.00 0 0.00 0 0.00 0 0.00 11 22.00
Participant describes receiving written information from their GP
10 10.00 3 15.00 0 0.00 3 6.00 7 14.00
Participant describes receiving too much information (information overload, feeling overwhelemed)
10 10.00 1 5.00 6 20.00 7 14.00 3 6.00
Participant describes receiving information from books given to them
9 9.00 5 25.00 1 3.33 6 12.00 3 6.00
Participant describes searching for research articles (more scientific)
4 4.00 3 15.00 1 3.33 4 8.00 0 0.00
0
5
10
15
20
25
30
35
40
45
50
Participant descr ibes receivinginformation from the charity sector(Cancer Council, BCNA, My Journey,
Hopes and Hurdles package)
Participant descr ibes searching theinternet/online information
Participant descr ibes receivinginformation from their breast care
nurse or McGrath Foundation
Participant descr ibes receivingwritten information from their
oncologist (specialist)
Partiipant describes receivinginformation from hospitals
Participant descr ibes support groupsor other talk ing/connecting with
patients as a source of information
Participant descr ibes informationfrom surgeon

Section 6
Breast Cancer 2018 Australian PEEK Study
Information that was helpful
After talking about all of the information that participants had received, they were then asked what information had been helpful. There was a range of information that participants found helpful including Breast Cancer Network Australia’s information and their My Journey Kit (n=13, 13.00%), information from other patients about their experience (n=13, 13.00%) and information provided by McGrath or specialist nurses (n=11, 11.00%).
Participant describes information from local charities as being helpful
Yes, I was given the My Journey Kit at breast screening on the day I was diagnosed in January. That had the books of so much information which, to this day, I still refer to. It has been absolutely brilliant. I've also asked the breast care nurse I was assigned through the hospital and the GP and surgeon. I've been given more than enough information. Since I had this My Journey Kit, etcetera, I haven't used Google nowhere near the time because I find if I can get it straight to the people that are caring for me and looking after me, they know my case history more than Google does [laughs]. It's much easier to speak to the people that are treating me than getting information off the Internet or even from other people. Sometimes it's nice to talk to people in the same situation, but with us all being different, I think I need to speak to the people that are in charge of my diagnosis and treatment. That's where I tend to go first [laughs]. Participant 4
Well, initially, I got online and did a lot of doctor googling. Then, of course, I've got the My Journey kit in the mail, which was absolutely wonderful. I went onto the breast Cancer BCNA Network and the McGrath Foundation and was able to access an awful lot of information from there. After my lumpectomy, I've got a visit from a McGrath breast care nurse in hospital. I also got a visit from a lady from the cancer council who gave me a little pillow to drive home with in the car to give me a bit of relief between the seatbelt on that side. I got an awful lot of support from that kind of area both written and personal. Participant 37
Well initially I was-- there was a breast clinic nurse here in breast care LOCATION and the nurse, before surgery I think, she gave me a fair bit of information and went through what would happen at surgery and different phases. Also, I have given the Hopes and Hurdles package, the Journey Kit the…what’s the first one? My Journey Kit and all that. After that, it's pretty much what I’ve been able to access on the internet and stuff like that. Also through BCNA, I read that, I've been on there. On the online service now, so I read other people’s experiences. Participant 64
There were also 13 participants (13.00%) that noted that all information was helpful. These participants valued the ability to access information on broad topic areas to support their decision-making.
Participant describes all information being helpful
Pretty much all of it. Everything like finding out about different types and different treatments. I just think knowledge and learning about it because you can make informed choices. Also, you know you are not alone, there's so many other people which shouldn't be comforting but it is because it's horrible that other people are also going through with this that they need to feel less alone. Participant 3
All of it. I think in the beginning it was I just wanted to know what sort of breast cancer I had and I guess I was looking for a reason of how it happened and what it meant. I was really caught up in this half hour spread like, what's going to happen now? How long have I got before it's going to come back? What trials are on now? That sort of information that was helpful to me. It's the unknown I think that scares everyone. I know I'm going to die, it will kill me unless there's some miraculous cure in the next five years. but I just wanted to know, do I have some time left? Participant 43
I just think everyone's been helpful. Everyone's tried to give you as much information. Even my family's try to find out as much as they can and try to help you that way. I think everyone. It's amazing how kind people are when you get cancer. People just are different. They treat you so differently to everyday life. Participant 78

Section 6
Breast Cancer 2018 Australian PEEK Study
Table 6.2: Information that was helpful
Information that has been helpful All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n=30 % n=50 % n=50 %Participant describes all information as being helpful 13 13.00 4 20.00 5 16.67 9 18.00 4 8.00
Participant describes BCNA or My Journey as helpful 13 13.00 4 20.00 6 20.00 10 20.00 3 6.00
Participant describes information from other patients about their experience as helpful
13 13.00 3 15.00 4 13.33 7 14.00 6 12.00
Participant describes their nurse or McGrath foundation as helpful
11 11.00 1 5.00 2 6.67 3 6.00 8 16.00
Participant describes information about their specific type of cancer as useful (for example triple negative, ER positive, metastatic cancer etc)
10 10.00 1 5.00 3 10.00 4 8.00 6 12.00
Participant describes information about side effects of treatment and what to expect as helpful
10 10.00 1 5.00 3 10.00 4 8.00 6 12.00
Participant describes their oncologist or specialist as helpful for information
10 10.00 2 10.00 2 6.67 4 8.00 6 12.00
Participant describes online information from Pamphlets, booklets, packages helpful
10 10.00 1 5.00 0 0.00 1 2.00 9 18.00
Participant describes not finding any particularly information as being helpful
9 9.00 1 5.00 4 13.33 5 10.00 4 8.00
Participant describes online information as helpful(website, google)
8 8.00 0 0.00 4 13.33 4 8.00 4 8.00
Information that has been helpful All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant describes all information as being helpful 13 13.00 6 10.71 7 15.91 6 11.11 7 15.22
Participant describes BCNA or My Journey as helpful 13 13.00 7 12.50 6 13.64 4 7.41 9 19.57
Participant describes information from other patients about their experience as helpful
13 13.00 8 14.29 5 11.36 5 9.26 8 17.39
Participant describes their nurse or McGrath foundation as helpful
11 11.00 4 7.14 7 15.91 3 5.56 8 17.39
Participant describes information about their specific type of cancer as useful (for example triple negative, ER positive, metastatic cancer etc)
10 10.00 7 12.50 3 6.82 5 9.26 5 10.87
Participant describes information about side effects of treatment and what to expect as helpful
10 10.00 6 10.71 4 9.09 8 14.81 2 4.35
Participant describes their oncologist or specialist as helpful for information
10 10.00 6 10.71 4 9.09 5 9.26 5 10.87
Participant describes online information from Pamphlets, booklets, packages helpful
10 10.00 7 12.50 3 6.82 7 12.96 3 6.52
Participant describes not finding any particularly information as being helpful
9 9.00 5 8.93 4 9.09 5 9.26 4 8.70
Participant describes online information as helpful(website, google)
8 8.00 6 10.71 2 4.55 5 9.26 3 6.52
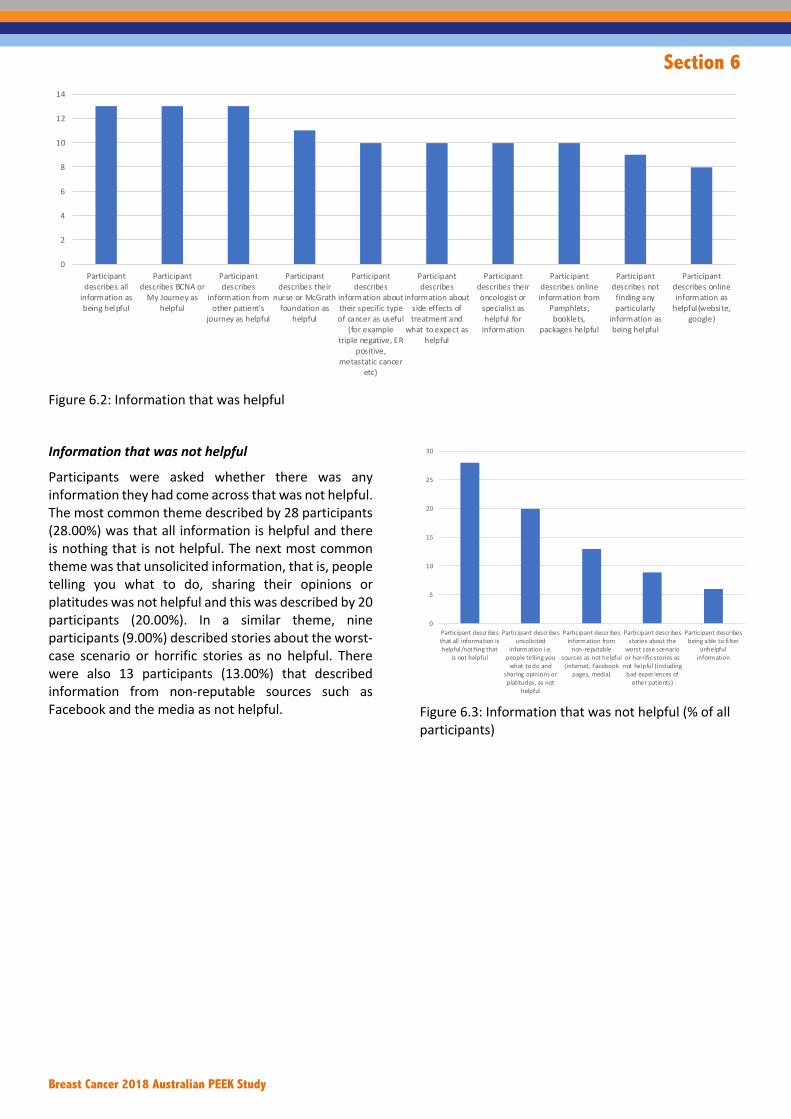
Section 6
Breast Cancer 2018 Australian PEEK Study
Figure 6.2: Information that was helpful
Information that was not helpful
Participants were asked whether there was any information they had come across that was not helpful. The most common theme described by 28 participants (28.00%) was that all information is helpful and there is nothing that is not helpful. The next most common theme was that unsolicited information, that is, people telling you what to do, sharing their opinions or platitudes was not helpful and this was described by 20 participants (20.00%). In a similar theme, nine participants (9.00%) described stories about the worst-case scenario or horrific stories as no helpful. There were also 13 participants (13.00%) that described information from non-reputable sources such as Facebook and the media as not helpful.
Figure 6.3: Information that was not helpful (% of all participants)
0
2
4
6
8
10
12
14
Participant
describes all
information as
being helpful
Participant
describes BCNA or
My Journey as
helpful
Participant
describes
information from
other patient's
journey as helpful
Participant
describes their
nurse or McGrath
foundation as
helpful
Participant
describes
information about
their specific type
of cancer as useful
(for example
triple negative, ER
positive,
metastatic cancer
etc)
Participant
describes
information about
side effects of
treatment and
what to expect as
helpful
Participant
describes their
oncologist or
specialist as
helpful for
information
Participant
describes online
information from
Pamphlets,
booklets,
packages helpful
Participant
describes not
finding any
particularly
information as
being helpful
Participant
describes online
information as
helpful (websi te,
google)
0
5
10
15
20
25
30
Participant descr ibesthat all information ishelpful/nothing that
is not helpful
Participant descr ibesunsolicited
information i.e.people telling you
what to do andsharing opinions orplatitudes, as not
helpful
Participant descr ibesinformation from
non-reputablesources as not helpful
(internet, Facebookpages, media)
Participant descr ibesstories about the
worst case scenarioor horrifi c stories as
not helpful (includingbad experiences of
other patients)
Participant descr ibesbeing able to fi lter
unhelpfulinformation
Participant descr ibesinformation that isnot specific to their
type of cancer asbeing not helpful
Participant descr ibesconflicting
information as nothelpful
Participant descr ibesinformation from
international sourcesnot helpful

Section 6
Breast Cancer 2018 Australian PEEK Study
Table 6.3: Information that was not helpful
Participant describes all information as being helpful Nothing really, no. I haven't come across that at all because every little bit that you can get, it's great in any way. Participant 5 Any of the information not helpful? None that I can tell you in my experience at all. My girlfriend, the one who's got cancer as well, she won't read anything. She doesn't want to know. I guess we are all different. Participant 29 I wouldn’t think no information…the more information the better even though at first I was overwhelmed with all the info. Over time, go back and read it again when my head's a bit clearer. It's all helpful. Yes. Participant 64
Participant describes unsolicited information, that is, people telling you what to do, sharing their opinions or platitudes, as not being helpful No, not really. I really don't like people preaching at you and saying, you should do this and you should do that, I guess. You should be doing this or you should be doing that. Participant 51 Other people who are not fully conversant with your condition, your diagnosis, giving advises to what they believe you should be doing. Participant 54
Information that is not helpful All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n=30 % n=50 % n=50 %Participant describes that all information is helpful/nothing that is not helpful
28 28.00 4 20.00 7 23.33 11 22.00 17 34.00
Participant describes unsolicited information i.e. people telling you what to do and sharing opinions or platitudes, as not helpful
20 20.00 4 20.00 6 20.00 10 20.00 10 20.00
Participant describes information from non-reputable sources as not helpful (internet, Facebook pages, media)
13 13.00 5 25.00 4 13.33 9 18.00 4 8.00
Participant describes stories about the worst case scenario or horrific stories as not helpful (including bad experiences of other patients)
9 9.00 2 10.00 3 10.00 5 10.00 4 8.00
Participant describes being able to filter unhelpful information
6 6.00 0 0.00 3 10.00 3 6.00 3 6.00
Participant describes information that is not specific to their type of cancer as being not helpful
4 4.00 2 10.00 1 3.33 3 6.00 1 2.00
Participant describes conflicting information as not helpful
4 4.00 3 15.00 0 0.00 3 6.00 1 2.00
Participant describes information from international sources not helpful
4 4.00 1 5.00 1 3.33 2 4.00 2 4.00
Information that is not helpful All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant describes that all information is helpful/nothing that is not helpful
28 28.00 14 25.00 14 31.82 16 29.63 12 26.09
Participant describes unsolicited information i.e. people telling you what to do and sharing opinions or platitudes, as not helpful
20 20.00 12 21.43 8 18.18 11 20.37 7 15.22
Participant describes information from non-reputable sources as not helpful (internet, Facebook pages, media)
13 13.00 6 10.71 7 15.91 6 11.11 7 15.22
Participant describes stories about the worst case scenario or horrific stories as not helpful (including bad experiences of other patients)
9 9.00 8 14.29 1 2.27 5 9.26 4 8.70
Participant describes being able to filter unhelpful information
6 6.00 4 7.14 2 4.55 3 5.56 3 6.52
Participant describes information that is not specific to their type of cancer as being not helpful
4 4.00 1 1.79 3 6.82 3 5.56 1 2.17
Participant describes conflicting information as not helpful
4 4.00 1 1.79 3 6.82 2 3.70 2 4.35
Participant describes information from international sources not helpful
4 4.00 2 3.57 2 4.55 2 3.70 2 4.35

Section 6
Breast Cancer 2018 Australian PEEK Study
I couldn't say anything. I've accepted and thought about whatever people have said to me along the way. I wouldn't say, there's, probably, more people, not health professionals, but there's people in everyday life that have been more unhelpful. [laughs] One woman in particular. She tried to tell me, I should go down the natural path, blah blah blah. I said to her, "Look, I'm sorry, but I just need to get this done." I've never been…I respect people who go down for help the natural products road, if they need to, but something like cancer. I don't believe it can. I believe you have to deal with it. That wasn't helpful. but it wasn't anything to do with any healthcare person. Participant 69 Participant describes stories about the worst-case scenarios as not being helpful Probably the blogs? When people just write about their own experiences sometimes they write about their horrible experiences but you don’t know what kind of cancer they have and they might have different side effects towards chemo. Participant 33 All these wonderful people that tell you all those terrible things that you don’t really want to hear. but not from any doctors or nurses or anyone like that. They have been from people. I'm sure they don't mean to be…what's the word I'm looking for? Nasty. You feel like saying, "Just shut up, I don't need to hear that." Whereas everybody else has been so good and as a friend of mine said to me, "These people that tell you to stay positive," she said, "they don't know what they are talking about." She said, "They haven't been through it," she said, "all you've got to do is turn up and do what they tell you to do." I thought that was pretty good advice and she's been through it. She had breast cancer eight years ago and had a mastectomy, so she knows what she's talking about. She's never told me sad stories about people she knows that have died or anything like that but other people when they find out, and they don't find out from me, but find out through the grapevine, the first thing they say is, "Oh yes, my friend died of that." You think I really needed to hear that? Participant 58 Yes. This is the third time I've said it. The online blog I said I don't like them. Some people love them but I don't like them. There's a lot of misinformation and they are a bit depressing if you read everybody's story. Participant 61
Participant describes information from non-reputable sources as not being helpful Just the hocus-pocus information that you come across sometimes; like on the less reputable sources or something. I've read something that sounded unbelievable like some sort of snake juice can cure your cancer, that nonsense. That's not helpful. I don't know if statistics are helpful or not. It's hard when you read or hear about other people not having such a good outcome prognosis. I guess that's reality but it brings you down, it scares you. So, I don't know if that's helpful but that's just reality, you can't really pick and choose your information, can you? I only want to hear the good stuff, I don't want to hear the bad stuff. Participant 3 Not really any of the information that is from reputable sources, designed to be consumed by people who’ve been diagnosed with cancer. Yes. As long as you stick to the credible path, that’s okay. I did, again, I had the point where I had to deliberately stop Googling things. I think walking that fine line between informing yourself enough to feel like you are genuinely in charge of your own treatment, and just becoming a full-time cancer patient Googler. Which was not something I wanted to do either. Participant 22

Section 6
Breast Cancer 2018 Australian PEEK Study
Information preferences (Format of information)
Participants were asked whether they had a preference for information online, talking to someone, in written (booklet) form or through a phone App. The most common theme was that participants preferred to talk to someone in relation to information provision (n=36, 36.00%). This was followed by a preference for written or online information combined with talking to someone (n=32, 32.00%). When combined, these two main themes represent 68 participants (68.00%) that have some preference for talking to someone in relation to information provision. The next most common theme was online information (n=21, 21.00%).
In relation to sub-group variations, participants a preference for talking to someone (with or without online information) increased with stage of disease, that is participants with stage IV breast cancer described his preference most frequently (78.00%) compared to stage II-III (63.34%) and stage 0-I (50.00%).
Figure 6.4: Information preferences – Format (% of all participants)
Table 6.4: Information preferences (Format)
0
5
10
15
20
25
30
35
40
Participant descr ibes apreference for talking
to someone
Participant descr ibes apreference forcombination ofonl ine/written
information andtalking to someone
Participant descr ibes apreference for online
information
Participant descr ibes apreference for wri tten
information
Participant descr ibeshaving no preference
Participant descr ibes apreference for a
phone app
Participant specificallydescribes not wanting
a phone app
Information preference All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n=30 % n=50 % n=50 %Participant describes a preference for talking to someone
36 36.00 6 30.00 5 16.67 11 22.00 25 50.00
Participant describes a preference for combination of online/written information and talking to someone
32 32.00 4 20.00 14 46.67 18 36.00 14 28.00
Combined themes of preference for talking to someone with or without written/online information
68 68.00 10 50.00 19 63.34 29 58.00 39 78.00
Participant describes a preference for online information
21 21.00 7 35.00 8 26.67 15 30.00 6 12.00
Participant describes a preference for written information
6 6.00 1 5.00 1 3.33 2 4.00 4 8.00
Participant describes having no preference4 4.00 2 10.00 1 3.33 3 6.00 1 2.00
Participant describes a preference for a phone app3 3.00 0 0.00 3 10.00 3 6.00 0 0.00
Participant specifically describes not wanting a phone app
2 2.00 0 0.00 1 3.33 1 2.00 1 2.00
Information preference All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant describes a preference for talking to someone
36 36.00 23 41.07 13 29.55 18 33.33 18 39.13
Participant describes a preference for combination of online/written information and talking to someone
32 32.00 16 28.57 16 36.36 17 31.48 15 32.61
Combined themes of preference for talking to someone with or without written/online information
68 68.00 39 69.64 29 65.91 35 64.81 33 71.74
Participant describes a preference for online information
21 21.00 11 19.64 10 22.73 10 18.52 11 23.91
Participant describes a preference for written information
6 6.00 4 7.14 2 4.55 3 5.56 3 6.52
Participant describes having no preference4 4.00 2 3.57 2 4.55 3 5.56 1 2.17
Participant describes a preference for a phone app3 3.00 3 5.36 0 0.00 2 3.70 1 2.17
Participant specifically describes not wanting a phone app
2 2.00 1 1.79 1 2.27 2 3.70 0 0.00

Section 6
Breast Cancer 2018 Australian PEEK Study
Participant describes a preference to talk to someone
I think I've got a preference to talking with someone, 'cause you can ask questions….some of the things that I've read to were really good that were talks because I thought I already had an idea or that I knew that there was lots of different things brought up, sometimes if you think you know about something, it's still okay to go over it again. 'Cause your brain's ... When you're going through all that confusion and emotion, plus you've got all the brain fog and it's a real whirlwind. It's really hard to pick up the information. Participant 7
I like talking to somebody. I suppose because of my work, I'm on computers all day, and I do buy online. I don't find reading information online enough because there's no one to answer my question. I don't find frequently ask questions ever really answer my frequently asked question. That thing doesn't appeal to me. I'm a very visual person and I don't need to see the flesh until then. You know what I'm saying? It's not the road life photos that I'm seeing. It's just the drawing I'm seeing. because some of it are tutorial drawings and not-- I need to see real life myself. Someone actually thoroughly goes through for the layman because I'm no medical person. I've got people that remember the ins and outs of that name. I'll go, "Really. I don't want to retain that. I don't need to retain it. It's not my job to retain it". All I know is that this is what happened? This is what we did to fix it? Now let's move on. Participant 11
Talking to someone. I hate the move to everything being online. And I know it's fantastic for people who are not in major cities, but you can not replace speaking to people and having someone who actually can take the time to listen to you, rather than just provide generic information. There's obviously a need for both. I'd be totally lost without the internet, I would ... it is invaluable. but you need someone else to help you interpret half of it, so yeah. Participant 52
Participant describes a preference for written or online information combined with talking to someone
Probably, a mixture of all but I do like -- I'm an oldie. I like the hard copy. Those books because they're there. You don't have to go online and search and find and then whatever. I can just pick up or I can mark some way where I was and when I go back. I like those books have been extremely helpful. Talking to someone of course because you do have questions along the way. Participant 12
It depends what I'm trying to research. Talking to somebody is really helpful if you're at the stage where you're trying to decide, "Will I do it or won't I do it." Really, I would read a lot of information before I talk to somebody. That's a very difficult question and there's no preference. I do all of those things. I would read about it. I'd probably talk to somebody. I definitely consider my family in what I'm going to do as well. Participant 61
I think you need to be given good information from the surgeons and oncologists that you talk to but I think you need to be also pointed towards good websites to read out and learn more stuff because when I was first diagnosed, we didn't know what the hormone make-up was and all that sort of stuff. I had no idea. I just thought I had a breast cancer. I didn't know that there's a multitude of different sorts. I found that very helpful to read to all those different things. Read up that if you got this type, then this sort of treatment regimen is generally was prescribed and if you got that type, usually it responds well with chemotherapy or this one doesn't respond to chemo so we won't be doing it, that sort of things. When I was going to my first appointment with the surgeon with a whole list of questions and she was like, "Good. You've been doing some homework." Participant 81
Participant describes a preference for online information
Online information I think because it’s easier and that you can get more of it not like if you’ve read the book and that’s it. but online information needs to keep on and on. Participant 1
I would probably say online information because I did a lot of it at night when I couldn't sleep earlier on. Participant 31
I think online. Provided it's accurate. Careful who you trust. Participant 37
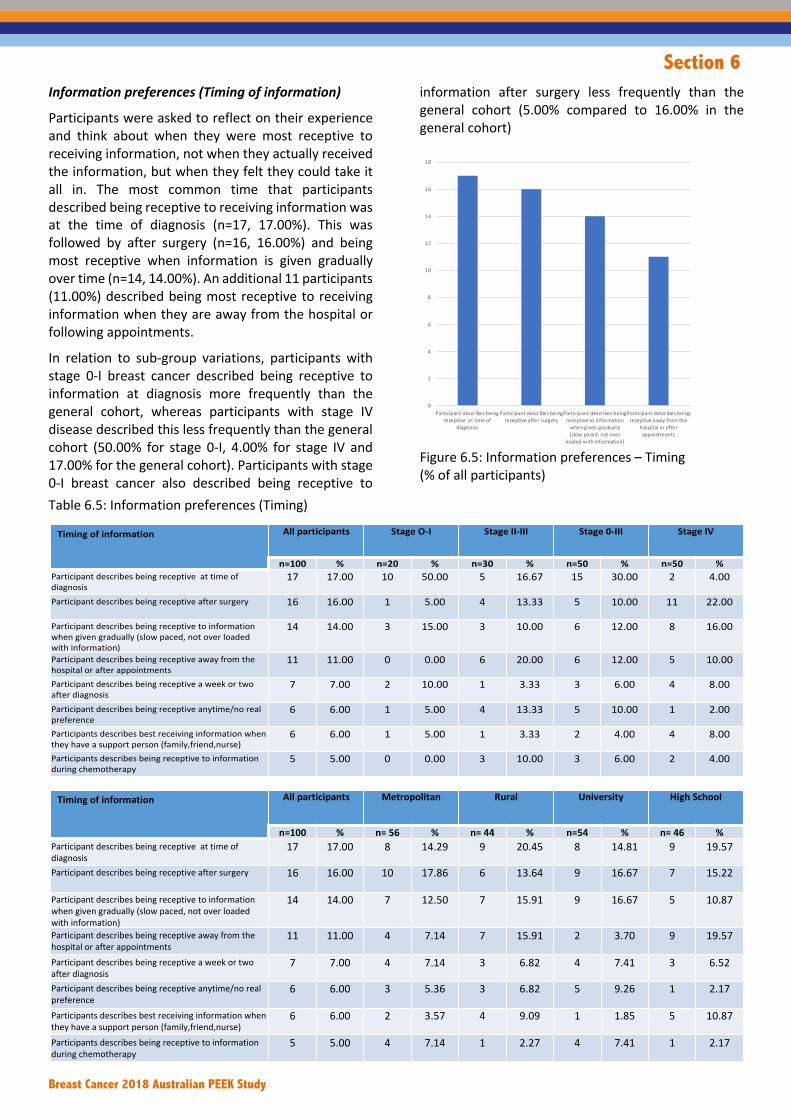
Section 6
Breast Cancer 2018 Australian PEEK Study
Information preferences (Timing of information)
Participants were asked to reflect on their experience and think about when they were most receptive to receiving information, not when they actually received the information, but when they felt they could take it all in. The most common time that participants described being receptive to receiving information was at the time of diagnosis (n=17, 17.00%). This was followed by after surgery (n=16, 16.00%) and being most receptive when information is given gradually over time (n=14, 14.00%). An additional 11 participants (11.00%) described being most receptive to receiving information when they are away from the hospital or following appointments.
In relation to sub-group variations, participants with stage 0-I breast cancer described being receptive to information at diagnosis more frequently than the general cohort, whereas participants with stage IV disease described this less frequently than the general cohort (50.00% for stage 0-I, 4.00% for stage IV and 17.00% for the general cohort). Participants with stage 0-I breast cancer also described being receptive to
information after surgery less frequently than the general cohort (5.00% compared to 16.00% in the general cohort)
Figure 6.5: Information preferences – Timing (% of all participants)
Table 6.5: Information preferences (Timing)
0
2
4
6
8
10
12
14
16
18
Participant descr ibes beingreceptive at time of
diagnosis
Participant descr ibes beingreceptive after surgery
Participant descr ibes beingreceptive to information
when given gradual ly(slow paced, not over
loaded with information)
Participant descr ibes beingreceptive away from the
hospital or afterappointments
Participant descr ibes beingreceptive a week or two
after diagnosis
Participant descr ibes beingreceptive anytime/no real
preference
Participants describes bestreceiving information
when they have a supportperson
(family,friend,nurse)
Participants describesbeing receptive toinformation during
chemotherapy
Timing of information All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n=30 % n=50 % n=50 %Participant describes being receptive at time of diagnosis
17 17.00 10 50.00 5 16.67 15 30.00 2 4.00
Participant describes being receptive after surgery 16 16.00 1 5.00 4 13.33 5 10.00 11 22.00
Participant describes being receptive to information when given gradually (slow paced, not over loaded with information)
14 14.00 3 15.00 3 10.00 6 12.00 8 16.00
Participant describes being receptive away from the hospital or after appointments
11 11.00 0 0.00 6 20.00 6 12.00 5 10.00
Participant describes being receptive a week or two after diagnosis
7 7.00 2 10.00 1 3.33 3 6.00 4 8.00
Participant describes being receptive anytime/no real preference
6 6.00 1 5.00 4 13.33 5 10.00 1 2.00
Participants describes best receiving information when they have a support person (family,friend,nurse)
6 6.00 1 5.00 1 3.33 2 4.00 4 8.00
Participants describes being receptive to information during chemotherapy
5 5.00 0 0.00 3 10.00 3 6.00 2 4.00
Timing of information All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant describes being receptive at time of diagnosis
17 17.00 8 14.29 9 20.45 8 14.81 9 19.57
Participant describes being receptive after surgery 16 16.00 10 17.86 6 13.64 9 16.67 7 15.22
Participant describes being receptive to information when given gradually (slow paced, not over loaded with information)
14 14.00 7 12.50 7 15.91 9 16.67 5 10.87
Participant describes being receptive away from the hospital or after appointments
11 11.00 4 7.14 7 15.91 2 3.70 9 19.57
Participant describes being receptive a week or two after diagnosis
7 7.00 4 7.14 3 6.82 4 7.41 3 6.52
Participant describes being receptive anytime/no real preference
6 6.00 3 5.36 3 6.82 5 9.26 1 2.17
Participants describes best receiving information when they have a support person (family,friend,nurse)
6 6.00 2 3.57 4 9.09 1 1.85 5 10.87
Participants describes being receptive to information during chemotherapy
5 5.00 4 7.14 1 2.27 4 7.41 1 2.17

Section 6
Breast Cancer 2018 Australian PEEK Study
Participant describes being most receptive to information at diagnosis
I think really right at the beginning because you're so hungry to know more to know absolutely everything to try and figure out your situation and try and figure out your own prognosis like I'm going to survive. I just remember that's all I did, spent the whole time reading, reading, reading, searching information. I think I was ready to then because you just want to know it consumes you but we can think about. I couldn't switch off I just wanted to know everything there was to know. Participant 3
When I got the first concrete diagnosis, then I just wanted to know everything that there ever was because I just wanted to know what my options were, what was going to happen, how long I was going to live or I'm so like, "Oh, my God." Once I got officially diagnosed, and they said yes, this is the type of cancer that you have, then that was when I wanted to know everything about it. Participant 25
I think at the beginning. I just wanted to learn as much about my type of cancer and actually even though I was pretty scared. I made it to get the facts and figures, read through and discuss it, as confronting as that was with advanced cancer. Participant 76
Participant describes being most receptive to information after surgery
Probably during my recovery time at home, when I was recovering from surgery…It was literally three weeks from diagnosis to surgery for me. During that time, I had to decide what to do, make arrangements to do it, extricate myself from work, tell a bunch of people, tell my kids, it was all just getting myself to that point where I could get to the hospital. I stayed in the hospital for five days. Partly by choice because I had small children and I wanted to have a rest. That was actually…that first part met the nurse, who was a fantastic support. She’d spent quite a bit of time with me in the hospital. Then came to visit a couple of times when I was home, post-surgery. Participant 22
After I found out or after surgery, when they told me how my chemo had worked for me. I sort of went, "Oh, thank God, okay, I can go forward now." Yes, it was just sort of the run up until then. Once you're going through treatment, you don't know if it's going to work or not. You're just sort of holding your breath, if you know what I mean. It's not until you walk into that office and-- you've had your operation. He's taken everything out to see what's left, and then you get that news, for me, that's when I was able to be more open and going, "Okay, I don't have to be so fearful now." Participant 45
Yes, I think it’s probably best a couple months after surgery. Once you’re recovering from surgery you don’t really need-- there’s enough there to cope with. You don’t need any more stuff in your head. There’s so much stuff going, your head's going 100 miles an hour and you're just trying to recover. I think probably, first three months after that is when I actually started going back and reading and understanding it more. Participant 64
Participant describes being most receptive to information gradually/over time
It was definitely ... I think it was a gradual thing. At the first part of the diagnosis, that was really difficult to take things in. I did get a pack, the breast cancer pack, which was like a big box that's got all the information in it and a diary. That was really helpful, too. I can't remember. Participant 7
I don't know, I think that's a difficult one. because it is so overwhelming in the beginning that you're not going to retain everything. I think having that information repeated, or a follow-up meeting after the initial diagnosis, to feel that there's no time limits. Where you've had your diagnosis, you've not yet started treatment. To have that follow-up appointment, maybe with the breast care nurse and a surgeon would be useful, going forward. Participant 34
When I'm most receptive about it? Definitely not in the beginning of it all. I think you need to have time just to sit and take it all. It's a bit of a surprise. Sometimes, I do have it. I don't still get it in my head that it's back. Participant 82
Participant describes being most receptive to information away from the hospital or following appointments
I think when you have gotten over the initial shock. The initial shock, it's pretty earth-shattering. When you're trying to get your head around it and then to receive information, that just becomes too much I think. When I got back into the surgery and it was then easy for me to go home and have a look at the material. Once I got the pathology report back from the surgery and was able to look at the pathology report and make sense of it, with the information that I had. That was very helpful for me to understand where I stood Basically and what my choices were here. Participant 22
That's why I always have my partner with me because while they're telling me stuff, you don't process it properly. Whereas I would take it more in when I went home and then spoke about it more with my partner. We would work out what we both heard and put it all together. It's more later on once you went home from the appointment. Participant 77

Section 6
Breast Cancer 2018 Australian PEEK Study
I needed to be able to take it home and digest it because of many things I did. I even just taped with the permission of the specialist that I've seen. I had recording in the background so I can really listen to everything they said at home. Yes because you are very overwhelmed at the time. That's why I've always made sure I have a support person with me or two to listen as well. Participant 81
Communication with health professionals
Participants were asked to describe the communication that they had had with health professionals throughout their experience. The most common theme was that participants were satisfied with communication (very good to excellent) (n=37, 37.00%). Where communication was excellent, participants described feeling as though they were considered as an individual and had access to health professionals to ask questions.
Participant describes excellent communication
It has been fantastic with all the help, and assistance, and information like if I've just got any query, I've rung up the surgeon or I rang out a breast care nurse, spoke to them. I could not fault anything like that, I've had the best assistance and being treated as an individual person, everybody's the same they have been treated as an individual but they'll not just say, "You're in this box, you've got this breast cancer and this is how we deal with it." Everybody is looking to my story, as I call it my journey my new normal but everybody has, of course, guided me along the way but listen to me and if I want to know something they've gone out of their way to be helped, so helpful and very understanding and understand that it is a life changing and it can even be worse for some people. I felt like that I was important, that they cared about me. They cared about what happened to me and what my next 10, 20, 30. However many years I'm lucky enough to be here but they made me feel like I was important. Participant 4 Brilliant. Fantastic. I've felt like everyone has been on the same page, everyone has -- I've been part of the team of making the decisions, but my particular case has been discussed Basically from the initial diagnosis, everyone needed to be involved in. My team has been pulled in and been part of the decision making. Right from the start, I was set up with the genetics counsellors. Once the surgeon knew that reconstruction might be a consideration, I went to the plastic surgeon. before chemo, I had already seen the plastic surgeon, the radio-oncologist, the genetics counsellors, everyone was referred right from the beginning, and all the supports were put in place right from the start. Participant 23
Fantastic, amazing. Amazing. My oncologist got a nurse and any problems, she'll just ring her. That's the oncologist nurse and the breast care nurse has been amazing as well, but I haven't bothered them because I haven't need to. When I've needed something like I needed a couple of questions and that stuff but I haven't -- They know a lot of people there by name and they wouldn't know me by name because I'm not in their face. Every time I've gone into hospital for different things, they've certainly come and seen me and been absolutely amazing. I know they are there but there's people that rely on them 24/7 where I haven't needed that. Participant 62 There were 32 participants (32.00%) that described poor communication. This was particularly in relation to the feeling that clinicians did not take the time to explain things and allow questions. Where there was poor communication, participants described not being seen as a person, not being able to ask questions or being dismissed. Participant describes poor communication There's been times I've never wanted to see my medical oncologist again because I felt like a small child who was asking too many questions [laughs]. That I should just take what she said and make a decision of it. It's not a very humorous situation, but to be absolutely dead pan face and go into a very sterile environment is possibly not the way most people who are dealing with breast cancer want to be because you just want to feel a bit loved. You don't want someone to fall over you and say, "Oh poor you," but you want to feel a bit like a person not just like a statistic or something that they're doing things to. Then medical oncologist was really poor at that communication. Although getting correct information and giving you statistics and outcomes, she couldn't be better at that information. but also not very good at…you couldn't interrupt with a question. You had to keep your questions until the end, which isn't very good. You go in with your questions on a list, but if you think of something as you're talking, you're not going to remember it at the end. That communication was really poor. Participant 17 Paternalistic, is that a word I could use? I felt a lot that I'd just been told this is your treatment, this is what's happening. And that's not necessarily a criticism I don't mean it like that at all. but I don't think, like for my oncologist, I don't think she has sat down with me and talked about my type or the stage or the this or the that. She just sort of said, "This is going to be your treatment" because she sees it every day and that's the treatment for that type. And I don't know how much

Section 6
Breast Cancer 2018 Australian PEEK Study
you need to know, really, to an extent. Knowledge is power to an extent, but it's that prime balance between having enough information but not having too much so that it scares you witless. Participant 35 Pretty awful. I'm so sorry. The radiation doctor is really good. The oncologist, he actually took five minutes to actually…you haven't got the time, she's seeing many people, and I don't know whatever. I'm a bit angry in my mind because I've had to ask and ask and ask about seeing a psychologist or seeing someone for counselling and getting no response from the oncologist. Never once has she asked me in two years then she asked me how I am. She just looks at me and to make an assessment on how I am by if I'm smiling or not smiling. I don't think there's been a lot of response there. The radiation doctor was more responsive and the breast care nurse is just so busy, one person can only do so much. I think there's a lot to be done in that area. I don't have anything else to say. Participant 50 In contrast, there were 21 participants (21.00%) that felt as though communication was overall good, however there were possibly some improvements to be made with one or two negative incidents reported. Participant describes overall good communication, with one or two negative experiences Mostly good, it's really only those two registrars that I've had no problem, every everyone else has been very knowledgeable and helpful and given me lots of their time, yes so overall good but just I spoiled it otherwise I would have said fantastic. Participant 3 It's been patchy, it would be fair to say. My surgeon doesn’t have a good bedside manner, but I pretty quickly decided that that didn't bother me. I just needed him to be a good surgeon, but it has been patchy. Though there have been times my oncologist has been fantastic and other times not. There have been times when information's been easy to get and then other times not. Yes, patchy would be all I could say. I will say though that, in terms of the care I received from the
nursing staff both in the hospital and then when I was an outpatient doing chemo, was exceptional. I felt really beautifully cared for. Participant 21 I had a terrible GP experience. I've had a wonderful experience with my now oncologist but a very bad experience with my previous oncologist. I have a fabulous relationship and experience with my palliative care physician. It depends, you're talking about. Participant 61 There were a number of sub-group variations. Participants with stage 0-I breast cancer described being satisfied with communication (Good, possibly some improvements), more frequently than the general cohort (35.00% compared to 21.00% in the general cohort). Participants in metropolitan areas described having poor communication, less frequently than the general cohort, while participants in rural areas described this more frequently (19.64 for metropolitan participants, 47.73 for rural participants, compared to 32.00% in the general cohort).
Figure 6.6: Communication with health professionals (% of all participants)
0
5
10
15
20
25
30
35
40
Participant descr ibesbeing satisfied with
communication (Verygood to excellent)
Participant descr ibes poorcommunication (Not
taking the time to explainthings/allowing questions)
Participant descr ibesbeing satisfied with
communication (Good,possibly some
improvements)
Participant descr ibessupportive
communication (Beingable to ask questions)
Participant descr ibesfeeling as though therewasn't communicationbetween specialist and
health professionals

Section 6
Breast Cancer 2018 Australian PEEK Study
Table 6.6: Communication with health professionals
Communication with health professionals All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n=30 % n=50 % n=50 %Participant describes being satisfied with communication (Very good to excellent)
37 37.00 8 40.00 9 30.00 17 34.00 20 40.00
Participant describes poor communication (Not taking the time to explain things/allowing questions)
32 32.00 6 30.00 9 30.00 15 30.00 17 34.00
Participant describes being satisfied with communication (Good, possibly some improvements)
21 21.00 7 35.00 8 26.67 15 30.00 6 12.00
Participant describes supportive communication (Being able to ask questions)
8 8.00 1 5.00 3 10.00 4 8.00 4 8.00
Participant describes feeling as though there wasn't communication between specialist and health professionals
7 7.00 2 10.00 4 13.33 6 12.00 1 2.00
Communication with health professionals All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant describes being satisfied with communication (Very good to excellent)
37 37.00 25 44.64 12 27.27 17 31.48 20 43.48
Participant describes poor communication (Not taking the time to explain things/allowing questions)
32 32.00 11 19.64 21 47.73 18 33.33 14 30.43
Participant describes being satisfied with communication (Good, possibly some improvements)
21 21.00 14 25.00 7 15.91 15 27.78 6 13.04
Participant describes supportive communication (Being able to ask questions)
8 8.00 4 7.14 4 9.09 4 7.41 4 8.70
Participant describes feeling as though there wasn't communication between specialist and health professionals
7 7.00 3 5.36 4 9.09 4 7.41 3 6.52

Section 6
Breast Cancer 2018 Australian PEEK Study
Who patients talk to about their condition
Participants were asked who they talked to most about their condition. The most common theme was that participants spoke to a number of health professionals (n=32, 32.00%). This was generally a combination of oncologist, nurse, general practitioner and/or surgeon. This was followed by their general practitioner as a single health professional that they spoke to about their condition (n=15, 15.00%). There were then various combinations of health professionals including oncologist plus general practitioner (n=13, 13.00%) and oncologist plus surgeon.
Figure 6.7: Who patients talk to (% of all participants)
Table 6.7: Who patients talk to
Access to specialist nurse care Half of all participants spoke about being able to access a breast care, specialist of McGrath nurse (n=50, 50.00%) while an additional 27 participants (27.00%) spoke about care received from chemotherapy or general oncology nurses. There were 16 participants (16.00%) that indicated that they had not accessed a breast care nurse and the remaining participants were unsure whether they had accessed a specialist nurse or not.
Figure 6.8: Access to specialist nurse care (% of all participants)
0
5
10
15
20
25
30
35
All healthprofessionals
(Combination ofmore than two health
professionals )
General Practitioner Oncologist plusGeneral Practitioner
Oncologist plussurgeon
Nurse
Who patients talk to All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n=30 % n=50 % n=50 %All health professionals (Combination of more than two health professionals )
32 32.00 6 30.00 9 30.00 15 30.00 17 34.00
General Practitioner 15 15.00 2 10.00 5 16.67 7 14.00 8 16.00
Oncologist plus general practitioner 13 13.00 3 15.00 3 10.00 6 12.00 7 14.00
Oncologist plus surgeon 8 8.00 2 10.00 3 10.00 5 10.00 3 6.00
Nurse 8 8.00 0 0.00 3 10.00 3 6.00 5 10.00
Who patients talk to All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %All health professionals (Combination of more than two health professionals )
32 32.00 20 35.71 12 27.27 16 29.63 16 34.78
General Practitioner 15 15.00 6 10.71 9 20.45 10 18.52 5 10.87
Oncologist plus general practitioner 13 13.00 8 14.29 5 11.36 9 16.67 4 8.70
Oncologist plus surgeon 8 8.00 4 7.14 4 9.09 4 7.41 4 8.70
Nurse 8 8.00 6 10.71 2 4.55 2 3.70 6 13.04
0
10
20
30
40
50
60
Participant descr ibes accessing a breast carenurse or McGrath nurse
Participant descr ibes accessing a generalnurse or chemo nurse
Participant descr ibes not accessing a breastcare nurse

Section 6
Breast Cancer 2018 Australian PEEK Study
Half of all participants spoke about being able to access a breast care, specialist of McGrath nurse (n=50, 50.00%) while an additional 27 participants (27.00%) spoke about care received from chemotherapy or general oncology nurses. There were 16 participants (16.00%) that indicated that they had not accessed a breast care nurse and the remaining participants were unsure whether they had accessed a specialist nurse or not. There were two sub-group variations. Participants with stage IV breast cancer reported accessing specialist breast or McGrath nurses less frequently than the general cohort (26.00% compared to 50% in the general cohort) and participants in regional/rural areas also reported accessing specialist or McGrath nurses less frequently (27.27%). It is important to note that in a previous question, there were more participants from regional/rural areas that received information from a specialist nurse, however after this interaction, there was little or no contact. Table 6.8: Access to specialist nurse care
Access to specialist nurse care All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n=30 % n=50 % n=50 %Participant describes accessing a breast care nurse or McGrath nurse
50 50.00 12 60.00 13 43.33 25 50.00 13 26.00
Participant describes accessing a general nurse or chemo nurse
27 27.00 5 25.00 8 26.67 12 24.00 8 16.00
Participant specifically describes not accessing a breast care nurse
16 16.00 2 10.00 7 23.33 9 18.00 3 6.00
Access to specialist nurse care All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant describes accessing a breast care nurse or McGrath nurse
50 50.00 26 46.43 12 27.27 20 37.04 18 39.13
Participant describes accessing a general nurse or chemo nurse
27 27.00 12 21.43 9 20.45 12 22.22 9 19.57
Participant describes not accessing a breast care nurse
16 16.00 3 5.36 9 20.45 5 9.26 7 15.22

Section 6
Breast Cancer 2018 Australian PEEK Study
Respect shown to patients in the health system
Participants were asked whether they had been treated with respect throughout their experience in the health system. The majority of participant felt as though they had been treated respectfully throughout their experience in the health system (n=69, 69.00%). There were five participants (5.00%) that did not feel as though they had been treated respectfully and an additional 26 participants (26.00%) that felt they were treated respectfully for the most part, except for one or two occasions.
Figure 6.9: Respect shown to patients (% of all participants)
Table 6.9: Respect shown to patients
0
10
20
30
40
50
60
70
80
Participant descr ibes being treatedwith respect
Participant descr ibes being treatedwith respect for most of the time,except for one or two occasions.
Participant descr ibes not beingtreated with respect
Respect shown to patients All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n=30 % n=50 % n=50 %Participant describes being treated with respect
69 69.00 13 65.00 18 60.00 31 62.00 38 76.00
Participant describes being treated with respect for most of the time, except for one or two occasions.
26 26.00 4 20.00 12 40.00 16 32.00 10 20.00
Participant describes not being treated with respect
5 5.00 2 10.00 0 0.00 2 4.00 3 6.00
Respect shown to patients All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant describes being treated with respect
69 69.00 37 66.07 32 72.73 38 70.37 31 67.39
Participant describes being treated with respect for most of the time, except for one or two occasions.
26 26.00 16 28.57 10 22.73 12 22.22 14 30.43
Participant describes not being treated with respect
5 5.00 3 5.36 2 4.55 3 5.56 2 4.35

Section 6
Breast Cancer 2018 Australian PEEK Study
Knowledge and confidence
The Partners in Health questionnaire (PIH) measures an individual’s knowledge and confidence for managing their own health. The Partners in Health comprises a global score, 4 sub scales; knowledge, treatment, symptoms and coping. A higher score denotes a better understanding of disease. Summary statistics for the entire cohort are displayed alongside the possible range of each scale in Table 6.10. Overall, the participants scored in the top quintile for knowledge (Median=27.00, IQR = 6.00), adherence to treatment (Median=15.00, IQR = 2.00), and management of symptoms (Median=21.00, IQR = 5.00). The scores for coping (Median=15.00, IQR = 6.25) and total score
(Median=80.00, IQR = 12.00) were in the second highest quintile.
Box plots display each of the Partners in Health sub-scales by disease stage, metastatic status, location of participants and education status (Figures 6.10 – 6.29).
Comparisons of PIH global and sub scales have been made based on disease stage (Figures 6.10 to 6.14, Tables 6.11 to 6.14), metastatic status (Figures 6.15 to 6.19, Table 6.15), location (Figures 6.20 to 6.24, Tables 6.16 and 6.17), and education status (Figures 6.25 to 6.29, Table 6.18).
Table 6.10: Summary statistics all participants Partners in Health
Scale Median IQR Possible range
Knowledge 27.00 6.00 0-32
Adherence to treatment 15.00 2.00 0-16
Management of symptoms 21.00 5.00 0-24
Coping 15.00 6.25 0-24
Total score 80.00 12.00 0-96
Comparisons of PIH sub scales by disease stage
Comparisons of PIH subscales were made disease severity. Summary statistics are listed in Tables 6.11 and 6.14. A one-way ANOVA test was used when assumptions for normality and variance were met (Table 6.12), or when assumptions for normality and variance were not met, a Kruskal-Wallis test sum correction test was used (Table 6.14).
A one way ANOVA test indicated a significant difference in the PIH coping scale between groups
[F(2,97) = 5.28, p = 0.0067] (Table 6.12). Post hoc comparisons using the Tukey HSD test indicated that the mean score for those with stage IV disease (mean = 13.50, sd = 4.44) was significantly lower than stage II-III disease (mean = 16.70, sd = 5.31), p=0.0125 (Table 6.13).
No other significant differences were observed (Table 6.14).

Section 6
Breast Cancer 2018 Australian PEEK Study
Figure 6.10: Boxplot of PIH knowledge by disease stage Figure 6.11: Boxplot of PIH adherence to treatment by disease stage
Figure 6.12: Boxplot of PIH management of symptoms by disease stage
Figure 6.13: Boxplot of PIH coping by disease stage
Figure 6.14: Boxplot of PIH total score by disease stage
Stage 0 and I Stage II and III Stage IV
1520
2530
Partners in Health - Knowledge
Stage 0 and I Stage II and III Stage IV
810
1214
16
Partners in Health - Adherence to Treatment
Stage 0 and I Stage II and III Stage IV
1012
1416
1820
2224
Partners in Health - Management of Symptoms
Stage 0 and I Stage II and III Stage IV
510
1520
Partners in Health - Coping
Stage 0 and I Stage II and III Stage IV
5060
7080
90
Partners in Health - Total Score

Section 6
Breast Cancer 2018 Australian PEEK Study
Table 6.11: Summary statistics PIH coping scale by disease severity
PIH Scale Group Count Mean Sd Coping Stage 0-I 20 16.40 4.11
Stage II-III 30 16.70 5.31 Stage IV 50 13.50 4.44
Table 6.12: ANOVA table for PIH coping scale by disease stage
PIH Scale Sum of squares
Df Mean square
F P
Coping Between Groups 228.9 2 114.43 5.28 0.0067* Within Groups 2103.9 97 21.69 Total 2332.80 99
* Statistically significant at p<0.05
Table 6.13: Post hoc Tuckey HSD test for PIH coping scale by disease severity
PIH Scale Comparison Mean difference
Lower Upper P adjusted
Coping Stage II and III – Stage 0-I 0.27 -2.93 3.47 0.9785 Stage IV – Stage 0-I -2.86 -5.79 0.07 0.0576 Stage IV – Stage II-III -3.13 -5.69 -0.57 0.0125*
* Statistically significant at p<0.05
Table 6.14: Summary statistics and Kruskal-Wallis rank sum test by disease severity PIH Scale Group Count Median IQR X2 Df P Knowledge Stage 0-I 20 27.50 5.25 0.96 2 0.6186
Stage II-III 30 28.50 6.50 Stage IV 50 27.00 3.75
Adherence to Treatment
Stage 0-I 20 15.50 3.25 5.51 2 0.0636 Stage II-III 30 16.00 1.00
Stage IV 50 15.00 1.75 Management of Symptoms
Stage 0-I 20 20.50 4.25 0.08 2 0.9619 Stage II-III 30 21.50 5.00 Stage IV 50 21.00 5.00
Total Score Stage 0-I 20 79.50 8.50 1.75 2 0.4164 Stage II-III 30 82.00 14.50 Stage IV 50 79.50 12.00
Comparisons of PIH sub scales by metastatic status
Comparisons of PIH sub scales were made between participants comparing those that have metastatic disease with those that do. Boxplots are displayed in Figures 6.15 to 6.19. Two sample t-test assumptions for normality and variance were not met, a Wilcoxon rank sum test with continuity correction was used (Table 6.15). A Wilcoxon rank sum test with continuity correction indicated a significant difference in the Partners in Health – Adherence to Treatment scale [W
= 1541.00, p=0.0361] with those that had metastatic disease (Median = 15.00, IQR = 1.75) scoring lower than those without (Median = 16.00, IQR = 1.75); and a significant difference in the Coping scale [W= 1669.50, p=0.0037], those with metastatic disease (Median = 14.00, IQR = 4.00) scoring lower than those without metastatic disease (Median = 16.50, IQR = 8.00). No other statistically significant differences were observed between these two groups (Table 6.15).

Section 6
Breast Cancer 2018 Australian PEEK Study
Figure 6.15: Boxplot of PIH knowledge by metastatic status
Figure 6.16: Boxplot of PIH adherence to treatment by metastatic status
Figure 6.17: Boxplot of PIH management of symptoms by metastatic status
Figure 6.18: Boxplot of PIH coping by metastatic status
Figure 6.19: Boxplot of PIH total score by metastatic status
No Metastases Metastases
1520
2530
Partners in Health - Knowledge
No Metastases Metastases
810
1214
16
Partners in Health - Adherence to Treatment
No Metastases Metastases
1012
1416
1820
2224
Partners in Health - Management of Symptoms
No Metastases Metastases
510
1520
Partners in Health - Coping
No Metastases Metastases
5060
7080
90
Partners in Health - Total Score

Section 6
Breast Cancer 2018 Australian PEEK Study
Table 6.15: Summary statistics Wilcoxon rank sum test with continuity correction PIH subscales by metastatic status
PIH subscale Metastatic status Count Median IQR W P Knowledge No metastases 50 28.00 6.00 1378.50 0.3750
Metastases 50 27.00 3.75 Adherence to treatment
No metastases 50 16.00 1.75 1541.00 0.0361* Metastases 50 15.00 1.75
Management of symptoms
No metastases 50 21.00 5.00 1211.00 0.7884 Metastases 50 21.00 5.00
Coping No metastases 50 16.50 8.00 1669.50 0.0037* Metastases 50 14.00 4.00
Total score No metastases 50 81.50 12.20 1428.00 0.2189 Metastases 50 79.50 12.00
* Statistically significant at p<0.05
Comparisons of PIH sub scales by location
Comparisons of PIH sub scales were made between participants between those that live in metropolitan areas and those that live in regional or remote areas. Boxplots are displayed in Figures 6.20 to 6.24. Two sample t-test was used when assumptions for normality and variance were met (Table 6.16). When assumptions normality and variance were not met, a Wilcoxon rank sum test with continuity correction was used (Table 6.17). A two sample t-test indicated a significant difference in the coping scale [t(98)= 3.17, p-=0.0020] with those living in metropolitan areas (mean = 16.36, sd = 4.38) scoring higher than those in regional or rural areas (mean = 13.39, sd = 4.97).
A Wilcoxon rank sum test with continuity correction indicated a significant difference in the adherence to treatment score [W=1540.00, p=0.0255], with those living in metropolitan areas (median = 15.50, IQR = 2.00) scoring higher than those in regional or rural areas (median = 15.00, IQR = 4.00); and for the management of symptoms scale [W= 1644.50, p = 0.0038], with those living in metropolitan areas (median = 22.00, IQR = 4.00) scoring higher than those regional or rural (median = 19.00, IQR =7.50); and the total score [W= 1715.50, p= 0.008] with those living in metropolitan areas (median = 83.00, IQR = 8.25) scoring higher than those living in regional or rural areas (median = 76.00, IQR = 22.20).
Figure 6.20: Boxplot of PIH knowledge by location Figure 6.21: Boxplot of PIH adherence to treatment by location
Metropolitan Regional/Rural
1520
2530
Partners in Health - Knowledge
Metropolitan Regional/Rural
810
1214
16
Partners in Health - Adherence to Treatment

Section 6
Breast Cancer 2018 Australian PEEK Study
Figure 6.22: Boxplot of PIH symptoms by location Figure 6.23: Boxplot of PIH coping by location
Figure 6.24: Boxplot of PIH total score by location
Table 6.16: Summary statistics and two sample t-test PIH subscale by location
PIH subscale Location Count Mean sd t df p Coping Metropolitan 56 16.36 4.38 3.17 98 0.0020*
Regional/Remote 44 13.39 4.97 * Statistically significant at p<0.05
Table 6.17: Summary statistics Wilcoxon rank sum test with continuity correction PIH subscales by location PIH subscale Location Count Median IQR W p Knowledge Metropolitan 56 28.00 4.00 1460.00 0.1122
Regional/Remote 44 27.00 7.75 Adherence to treatment Metropolitan 56 15.50 2.00 1540.00 0.0255*
Regional/Remote 44 15.00 4.00 Management of symptoms
Metropolitan 56 22.00 4.00 1644.50 0.0038* Regional/Remote 44 19.00 7.50
Total score Metropolitan 56 83.00 8.25 1715.50 0.0008* Regional/Remote 44 76.00 22.20
* Statistically significant at p<0.05
Metropolitan Regional/Rural
1012
1416
1820
2224
Partners in Health - Managemnt of Symptoms
Metropolitan Regional/Rural
510
1520
Partners in Health - Coping
Metropolitan Regional/Rural
5060
7080
90
Partners in Health - Total Score

Section 6
Breast Cancer 2018 Australian PEEK Study
Comparisons of PIH sub scales by Education
Comparisons of PIH sub scales were made between participants based on highest education levels obtained; highschool/trade or university. Boxplots are displayed in Figures 6.25 to 6.29. Two sample t-test
assumptions for normality and variance were not met, a Wilcoxon rank sum test with continuity correction was used (Table 6.18). No statistically significant differences were observed between these two groups for any PIH sub scale (Tables 6.18).
Figure 6.25: Boxplot of PIH knowledge by education status
Figure 6.26: Boxplot of PIH adherence to treatment by education status
Figure 6.27: Boxplot of PIH symptoms by education status
Figure 6.28: Boxplot of PIH coping by education status
High school/Trade University
1520
2530
Partners in Health - Knowledge
High school/Trade University
810
1214
16
Partners in Health - Aherence to Treatment
High school/Trade University
1012
1416
1820
2224
Partners in Health - Management of Symptoms
High school/Trade University
510
1520
Partners in Health - Coping

Section 6
Breast Cancer 2018 Australian PEEK Study
Figure 6.29: Boxplot of PIH total score by education status
Table 6.18: Summary statistics Wilcoxon rank sum test with continuity correction PIH subscales by education level PIH subscale Group Count Median IQR W p Knowledge Trade or high school 46 27.00 5.75 1178.50 0.6613
University 54 27.50 5.00 Adherence to treatment
Trade or high school 46 15.00 2.75 1194.00 0.7310 University 54 15.00 2.00
Management of symptoms
Trade or high school 46 20.00 5.00 1053.50 0.1887 University 54 22.00 3.75
Coping Trade or high school 46 14.00 5.00 1032.00 0.1459 University 54 16.00 6.75
Total score Trade or high school 46 78.50 14.50 989.50 0.0799 University 54 82.00 12.80
High school/Trade University
5060
7080
90
Partners in Health - Total Score
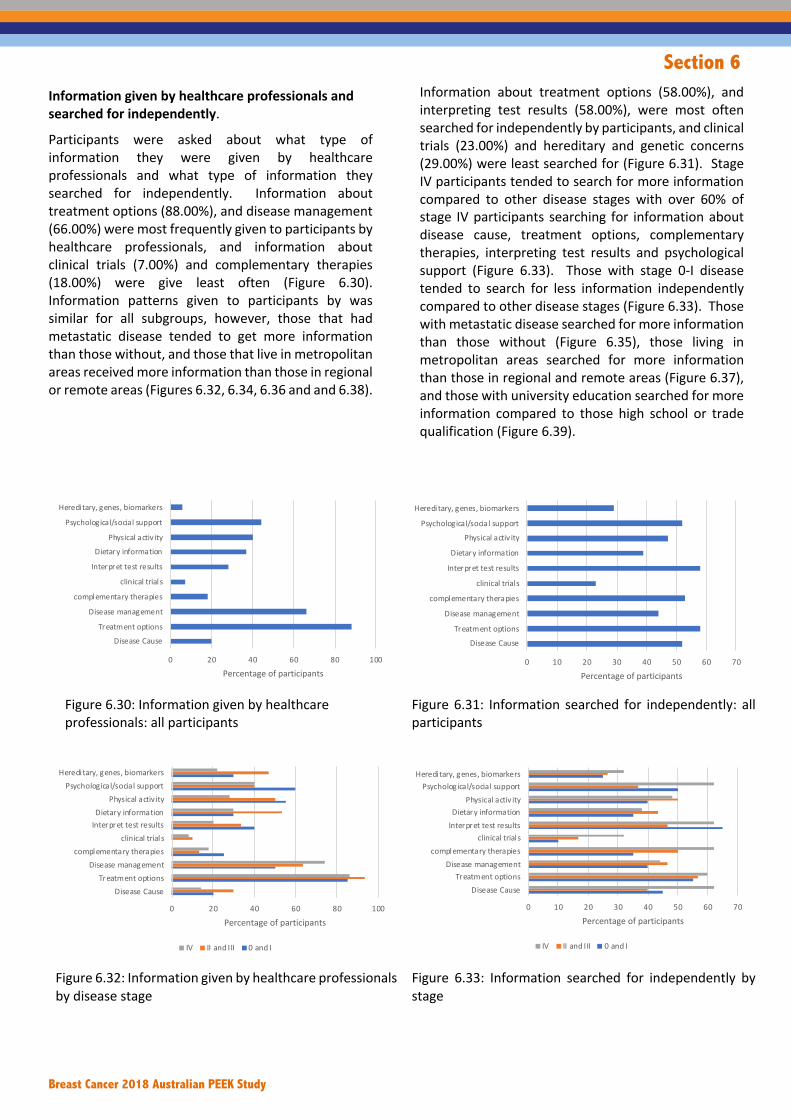
Section 6
Breast Cancer 2018 Australian PEEK Study
Information given by healthcare professionals and searched for independently.
Participants were asked about what type of information they were given by healthcare professionals and what type of information they searched for independently. Information about treatment options (88.00%), and disease management (66.00%) were most frequently given to participants by healthcare professionals, and information about clinical trials (7.00%) and complementary therapies (18.00%) were give least often (Figure 6.30). Information patterns given to participants by was similar for all subgroups, however, those that had metastatic disease tended to get more information than those without, and those that live in metropolitan areas received more information than those in regional or remote areas (Figures 6.32, 6.34, 6.36 and and 6.38).
Information about treatment options (58.00%), and interpreting test results (58.00%), were most often searched for independently by participants, and clinical trials (23.00%) and hereditary and genetic concerns (29.00%) were least searched for (Figure 6.31). Stage IV participants tended to search for more information compared to other disease stages with over 60% of stage IV participants searching for information about disease cause, treatment options, complementary therapies, interpreting test results and psychological support (Figure 6.33). Those with stage 0-I disease tended to search for less information independently compared to other disease stages (Figure 6.33). Those with metastatic disease searched for more information than those without (Figure 6.35), those living in metropolitan areas searched for more information than those in regional and remote areas (Figure 6.37), and those with university education searched for more information compared to those high school or trade qualification (Figure 6.39).
Figure 6.30: Information given by healthcare professionals: all participants
Figure 6.31: Information searched for independently: all participants
Figure 6.32: Information given by healthcare professionals by disease stage
Figure 6.33: Information searched for independently by stage
0 20 40 60 80 100
Disease CauseTreatment options
Disease management
complementary therapies
clinical trial s
Interpret test results
Dietary informationPhysical activ ity
Psychological/social support
Heredi tary, genes, biomarkers
Percentage of participants0 10 20 30 40 50 60 70
Disease CauseTreatment options
Disease management
complementary therapies
clinical trial s
Interpret test results
Dietary information
Physical activ ityPsychological/social support
Heredi tary, genes, biomarkers
Percentage of participants
0 20 40 60 80 100
Disease CauseTreatment options
Disease managementcomplementary therapies
clinical trial sInterpret test resultsDietary information
Physical activ ityPsychological/social support
Heredi tary, genes, biomarkers
Percentage of participants
IV II and III 0 and I
0 10 20 30 40 50 60 70
Disease CauseTreatment options
Disease managementcomplementary therapies
clinical trial sInterpret test resultsDietary information
Physical activ ityPsychological/social support
Heredi tary, genes, biomarkers
Percentage of participants
IV II and III 0 and I

Section 6
Breast Cancer 2018 Australian PEEK Study
Figure 6.34: Information given by healthcare professionals by metastatic status
Figure 6.35: Information searched for independently by metastatic status
Figure 6.36: Information given by healthcare professionals by location
Figure 6.37: Information searched for independently by location
Figure 6.38: Information given by healthcare professionals by education
Figure 6.39: Information searched for independently by metastatic status
Information gaps
The largest gaps in information, where information was neither given to patients nor searched for independently were for clinical trials (70.00%), and hereditary, genes and biomarkers (65.00%) (Figure 6.40). Participants were given most information either from healthcare professionals or independently for treatment options (96.00%) and disease management (80.00%) (Figure 6.40). Complementary therapies (43.00%) was the topic that was most searched for independently following no information from health professionals (49.00%) (Figure 6.40).
0 20 40 60 80 100
Disease CauseTreatment options
Disease managementcomplementary therapies
clinical trial sInterpret test resultsDietary information
Physical activ ityPsychological/social support
Heredi tary, genes, biomarkers
Percentage of participants
Metastases No metastases
0 10 20 30 40 50 60 70
Disease CauseTreatment options
Disease managementcomplementary therapies
clinical trial sInterpret test resultsDietary information
Physical activ ityPsychological/social support
Heredi tary, genes, biomarkers
Percentage of participants
Metastases No metastases
0 20 40 60 80 100 120
Disease CauseTreatment options
Disease managementcomplementary therapies
clinical trial sInterpret test resultsDietary information
Physical activ ityPsychological/social support
Heredi tary, genes, biomarkers
Percentage of participants
Regional/Remote Metropolitan
0 10 20 30 40 50 60 70 80 90
Disease CauseTreatment options
Disease managementcomplementary therapies
clinical trial sInterpret test resultsDietary information
Physical activ ityPsychological/social support
Heredi tary, genes, biomarkers
Percentage of participants
Regional/Rural Metropolitan
0 20 40 60 80 100
Disease CauseTreatment options
Disease managementcomplementary therapies
clinical trial sInterpret test resultsDietary information
Physical activ ityPsychological/social support
Heredi tary, genes, biomarkers
Percentage of participants
University High school/Trade
0 10 20 30 40 50 60 70 80
Disease CauseTreatment options
Disease managementcomplementary therapies
clinical trial sInterpret test resultsDietary information
Physical activ ityPsychological/social support
Heredi tary, genes, biomarkers
Percentage of participants
University High school/Trade

Section 6
Breast Cancer 2018 Australian PEEK Study
Figure 6.40: Proportion of information given by health care professionals and searched for independently.
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Disease CauseTreatment options
Disease managementcomplementary therapies
clinical trial s
Interpret test resultsDietary information
Physical activ ity
Psychological/social supportHeredi tary, genes, biomarkers
Info given NOT searched Info given AND searched
Info NOT given AND searched Info NOT given NOT searched

Section 6
Breast Cancer 2018 Australian PEEK Study
Most trusted information sources
Participants were asked to rank which information source that they most trusted, where 1 is the most trusted and 4 is the least trusted. A weighted average is presented in Figure 6.41. With a weighted ranking, the higher the score, the more trusted the source of information to the participant. Across all participants, information from the participants’ hospital or clinic
was most trusted, and information from pharmaceutical companies was least trusted, Information from not for profit or charitable organisations and government sources were near equal in trust by participants (Figure 6.41). This order of preference was the same for all sub-groups (Figures 6.42 – 6.45).
Figure 6.41: Most trusted information sources Figure 6.42: Most trusted information sources by disease stage
Figure 6.43: Most trusted information sources by metastatic status
Figure 6.44: Most trusted information sources by location
Figure 6.45: Most trusted information sources by education
0
0.5
1
1.5
2
2.5
3
3.5
4
Non-profit/charity Government Pharmaceutical Clinic/hospital
0
0.5
1
1.5
2
2.5
3
3.5
4
Non-profit/charity Government Pharmaceutical Clinic/hospital
0 and I II and III IV
0
0.5
1
1.5
2
2.5
3
3.5
4
Non-profit/charity Government Pharmaceutical Clinic/hospital
No metastases Metastases
0
0.5
1
1.5
2
2.5
3
3.5
4
Non-profit/charity Government Pharmaceutical Clinic/hospital
Metropolitan Regional/Remote
0
0.5
1
1.5
2
2.5
3
3.5
4
Non-profit/charity Government Pharmaceutical Clinic/hospital
High school/Trade University

Section 7
Breast Cancer 2018 Australian PEEK Study
Section 7 Care and support

Section 7
Breast Cancer 2018 Australian PEEK Study
Section 7: Experience of care and support Coordination of care
• Overall the cohort had a ‘care received’ score in the highest quintile, indicating very good care received. The scores for navigation and care coordination fell in the second highest quintile indicating good scores. The total score and communication score were in the middle of the scale.
Coordination of care – by disease stage • Participants with stage IV disease had significantly worse scores for communication and total score
compared to those with stage 0-I disease and those with stage II-III disease.
Coordination of care – by metastatic status • Participants with metastases had significantly worse scores for the care coordination total score and
communication score compared to those without metastases.
Coordination of care – by location • Participants that live in regional or rural areas had significantly worse scores for the care coordination total
score, communication score and care received score compared to those that live in metropolitan areas.
Coordination of care – by education • No statistically significant differences were observed between those with university education and those
with high school or trade certificate any Care Coordination scores.
Care and support • The majority of care and support received came from family and friends (n=65, 65.00%). This was followed
by care and support from specialist breast nurses and McGrath nurses (n=31, 31.00%) and the same number of participants (n=31, 31.00%) noted care and support from their general practitioner. There were 23 participants (23.00%) that described care and support from other patients and support services that connected patients with each other.
• There were a number of sub-group variations. Participants with stage II-III breast cancer spoke about receiving care and support from family and friends more frequently while participants with stage IV breast cancer spoke about this less frequently (83.33% stage II-III, 52.00% stage IV compared to 65.00% in the general cohort). Participants with stage IV breast cancer spoke about receiving care and support from specialist breast or McGrath nurses less frequently than the general cohort (22.00% compared to 40.00% in stage 0-III breast cancer). Participants in rural areas reported receiving care and support from their general practitioner, less frequently than the general cohort (20.45% compared to 31.00% in the general cohort).

Section 7
Breast Cancer 2018 Australian PEEK Study
Experience of coordination of care
A Care Coordination questionnaire was completed. The Care Coordination questionnaire comprises a total score, 2 sub scales (communication and navigation), and a single question for each relating to care-coordination and care received. A higher score denotes better care outcome. Summary statistics for the entire cohort are displayed alongside the possible range of each scale in Table 7.1. Overall the entire cohort had a median care received score of 9.0, which is in the highest quintile, indicating very good care received. The scores for navigation (mean = 26.10, sd = 4.48) and care coordination (median = 8.00, IQR = 3) fell in the second highest quintile indicating good
scores. The Total score (median = 68.00, IQR = 19.00) and communication (median = 41.00, IQR = 15.50) were in the middle of the scale.
Box plots display each of the Care Coordination scores by disease stage, metastatic disease status, location of participants, and education status (Figures 7.1 to 7.20).
Comparisons of Care Coordination scores have been made based on disease stage (Figures 7.1 to 7.5, Tables 7.2 to 7.7), metastatic disease status (Figures 7.6 to 7.10, Table 7.8), location (Figures 7.11 to 7.15, Tables 7.9 and 7.10), and education status (Figures 7.16 to 7.20, Tables 7.11 and 7.12).
Table 7.1: Summary statistics Total score - Communication and Navigation
Scale Mean SD Median IQR Possible range
Total score 67.19 12.59 68.00 19.00 20-100
Communication 41.09 9.84 41.00 15.50 13- 65
Navigation* 26.10 4.48 27.00 6.00 7-35
Care co-ordination 6.82 2.60 8.00 3.00 1-10
Care received 7.80 2.43 9.00 2.00 1-10
*Normal distribution, use mean and sd as central measure
Comparisons of Care Coordination scores by disease stage
Comparisons of Care Coordination subscales were made by disease stage. Summary statistics are listed in Table 7.2. A one-way ANOVA test was used with the assumptions for response variable residuals were normally distributed and variances of populations were equal. When the ANOVA test indicated a significant result, post hoc comparisons were made using the Tukey HSD test (Tables 7.3 to 7.4). When the assumptions for normality of residuals was not met, a Kruskal-Wallis test was used, and when a significant result was indicated, it was followed by post hoc Wilcoxon rank sum tests between groups (Table 7.5). When assumptions for assumption of equal variances were not met, a Welch one-way test was used, and when a significant result was indicated, it was followed by pairwise t-tests with no assumption of equal variances (Tables 7.6 – 7.7).
A one way ANOVA test indicated a significant difference in the care coordination communication score between groups [F(2,97) = 9.42, p = 0.0002], (Table 7.3). Post hoc comparisons using the Tukey HSD test indicated that the mean score for those with Stage IV disease (mean = 37.10, sd = 7.87) had a significantly lower score (p= 0.043) than those with Stage 0-I disease (mean = 45.00, sd = 11.20), and was lower than stage II-III disease (mean = 45.10, sd =9.46), p=0.0008 (Tables 7.2 and 7.4).
A Welch one-way test indicated a significant difference in the care coordination total score between groups [F(2, 40.60) = 5.62, p=0.0070]. Post hoc comparisons indicated that the median score for stage IV (mean = 63.10, sd = 9.52) was significantly lower than the median score for stage 0-I (mean = 72.10, sd =15.50 ), p= 0.0360; and significantly lower than that for stage II-III (median = 70.70, sd = 13.10) p= 0.0250 (Tables 7.2 and 7.7).
There were no differences observed between stages for navigation, care coordination or care received (Tables 7.2 and 7.5)

Section 7
Breast Cancer 2018 Australian PEEK Study
Figure 7.1: Boxplot of Care coordination total score by disease stage
Figure 7.2: Boxplot of Communication sub scale disease stage
Figure 7.3: Boxplot of Navigation sub scale disease stage
Figure 7.4: Boxplot of Care coordination question disease stage
Figure 7.5: Boxplot of Care received disease stage
STAGE 0 and I STAGE II and III STAGE IV
5060
7080
90
Care Coordination - Total Score
STAGE 0 and I STAGE II and III STAGE IV
2030
4050
60
Care Coordination - Communication
STAGE 0 and I STAGE II and III STAGE IV
1520
2530
35
Care Coordination - Navigation
STAGE 0 and I STAGE II and III STAGE IV
24
68
10
Care Coordination - Care Coordination
STAGE 0 and I STAGE II and III STAGE IV
24
68
10
Care Coordination - Received
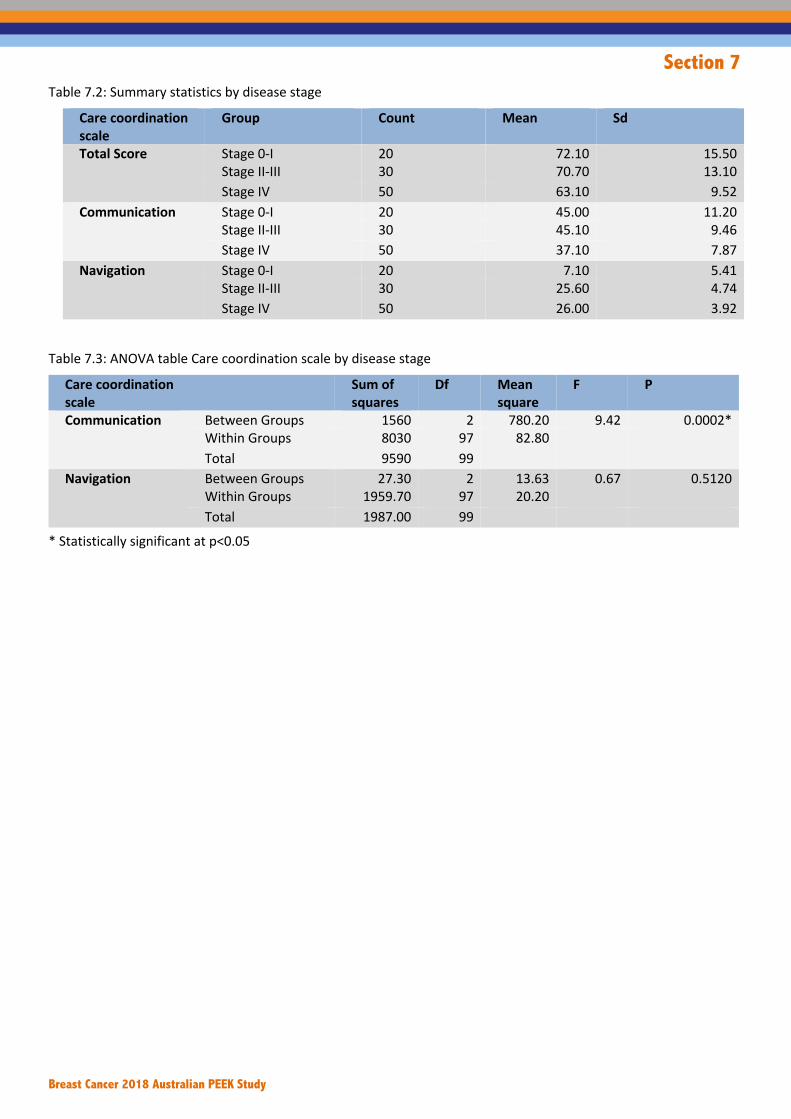
Section 7
Breast Cancer 2018 Australian PEEK Study
Table 7.2: Summary statistics by disease stage
Care coordination scale
Group Count Mean Sd
Total Score Stage 0-I 20 72.10 15.50 Stage II-III 30 70.70 13.10 Stage IV 50 63.10 9.52
Communication Stage 0-I 20 45.00 11.20 Stage II-III 30 45.10 9.46 Stage IV 50 37.10 7.87
Navigation Stage 0-I 20 7.10 5.41 Stage II-III 30 25.60 4.74 Stage IV 50 26.00 3.92
Table 7.3: ANOVA table Care coordination scale by disease stage
Care coordination scale
Sum of squares
Df Mean square
F P
Communication Between Groups 1560 2 780.20 9.42 0.0002* Within Groups 8030 97 82.80 Total 9590 99
Navigation Between Groups 27.30 2 13.63 0.67 0.5120 Within Groups 1959.70 97 20.20 Total 1987.00 99
* Statistically significant at p<0.05

Section 7
Breast Cancer 2018 Australian PEEK Study
Table 7.4: Post hoc Tuckey HSD test Care coordination by disease severity
Care coordination scale
Comparison Mean difference
Lower Upper P adjusted
Communication Stage II-III – Stage 0-I -0.07 -6.18 6.31 0.9996 Stage IV - Stage 0-I -7.86 -13.59 -2.13 0.0043* Stage IV - Stage II-III -7.93 -12.93 -2.93 0.0008*
* Statistically significant at p<0.05 Table 7.5: Summary statistics Kruskal-Wallis test sum correction test by disease stage
Care coordination scale
Group Count Median IQR X2 Df P
Care coordination
Stage 0-I 20 8.00 5.25 1.37 2 0.5029 Stage II-III 30 8.00 3.00 Stage IV 50 8.00 2.00
Care received Stage 0-I 20 8.00 3.25 0.62 2 0.7327 Stage II-III 30 9.00 2.75 Stage IV 50 9.00 2.00
Table 7. 6: Welch one-way test by disease stage. Care coordination scale F Df1 Df2 P Total Score 5.62 2 40.60 0.0070*
* Statistically significant at p<0.05 Table 7.7: Pairwise t-tests with no assumption of equal variances by disease stage
Care coordination scale Group Stages 0 and I Stages II and III Total Score Stages II and III 0.7420
Stage IV 0.0360* 0.0250* * Statistically significant at p<0.05
Comparisons of Care Coordination scores by metastatic status
Comparisons of Care Coordination scores were made between those that have metastatic disease and those that do not. Boxplots for each of the care coordination scales are displayed in Figures 7.6 to 7.10. Assumptions for normality and variance were not met, a Wilcoxon rank sum test with continuity correction was used (Table 7.8). Those that had metastases (median =
62.00, IQR = 13.50) had a significantly lower score [W = 1685.50, p=0.0026] than those without (median = 73.50, IQR = 22.50); those with metastatic disease (median = 37.00, IQR = 15.00) had a significantly lower communication score [W= 1869.50, p<0.0001] compared to those without metastases (median = 46.00, IQR = 15.50) .There were no statistically significant differences for navigation, care coordination and care received, between these groups.

Section 7
Breast Cancer 2018 Australian PEEK Study
Figure 7.6: Boxplot of Care coordination total score metastatic status
7.7: Boxplot of Care coordination Communication metastatic status
Figure 7.8: Boxplot of Care coordination Navigation metastatic status
Figure 7.9: Boxplot of Care coordination question metastatic status
Figure 7.10: Boxplot of Care Received metastatic status
No Metastases Metastases
5060
7080
90Care Coordination - Total Score
No Metastases Metastases
2030
4050
60
Care Coordination - Communication
No Metastases Metastases
1520
2530
35
Care Coordination - Navigation
No Metastases Metastases
24
68
10
Care Coordination - Care Coordination
No Metastases Metastases
24
68
10
Care Coordination - Care Received

Section 7
Breast Cancer 2018 Australian PEEK Study
Table 7.8: Summary statistics Wilcoxon rank sum test with continuity correction by metastatic status Care coordination scale Metastatic
disease Count Median IQR W p
Total score No metastatic disease
50 73.50 22.50 1686.50 0.0026*
Metastatic disease
50 62.00 13.50
Communication No metastatic disease
50 46.00 15.50 1869.50 <0.0001*
Metastatic disease
50 37.00 15.00
Navigation No metastatic disease
50 27.00 6.00 1266.50 0.9118
Metastatic disease
50 27.00 5.00
Care coordination No metastatic disease
50 8.00 3.00 1412.00 0.2585
Metastatic disease
50 8.00 2.00
Care received No metastatic disease
50 9.00 3.00 1347.50 0.4860
Metastatic disease
50 9.00 2.00
* Statistically significant at p<0.05 Comparisons of Care Coordination scores by Location
Comparisons of Care Coordination scores were made between participants that live in metropolitan areas compared to those that live in regional/rural. A two-sample t-test was used when assumptions for normality and variance were met (Table 7.9), or when assumptions for normality and variance were not met, a Wilcoxon rank sum test with continuity correction was used (Table 7.10). There was a significant difference between those that live in metropolitan
areas (median = 70.00, IQR =16.50) compared with those that live in regional /rural areas (median = 61.00, IQR = 16.20) for Total score [W=1591.50, p=0.0125]; and for communication [W=1617.00, P=0.0073) between metropolitan (median = 44.00, IQR = 13.00) and regional/rural (median = 37.00, IQR = 17.00); and for care received [W=1516.00, p=0.0403] for metropolitan (median = 9.00, IQR =2.00) and regional/rural (median =8.00, IQR =3.00). In each case, those that live in regional/rural areas had a lower score.
Figure 7.11: Boxplot of Care coordination total score by location
7.12: Boxplot of Care coordination Communication by location
Metropolitan Regional/Rural
5060
7080
90
Care Coordination - Total Score
Metropolitan Regional/Rural
2030
4050
60
Care Coordination - Communication

Section 7
Breast Cancer 2018 Australian PEEK Study
Figure 7.13: Boxplot of Care coordination Navigation by location
Figure 7.14: Boxplot of Care coordination question by location
Figure 7.15: Boxplot of Care Received by location Table 7.9: Summary statistics and Two sample t test by location
Care Coordination
Location Number Mean SD T df P
Navigation Metropolitan 56 26.71 4.36 1.56 98 0.1225 Regional/Rural 44 25.32 4.56
Table 7.10: Summary statistics Wilcoxon rank sum test with continuity correction by location
Care Coordination
Group Number Median IQR W P
Total Score Metropolitan 56 70.00 16.50 1591.50 0.0125* Regional/Rural 44 61.00 16.20
Communication Metropolitan 56 44.00 13.00 1617.00 0.0073*
Regional/Rural 44 37.00 17.00 Care coordination
Metropolitan 56 8.00 2.25 1488.50 0.0712 Regional/Rural 44 6.00 3.25
Care received Metropolitan 56 9.00 2.00 1516.00 0.0403*
Regional/Rural 44 8.00 3.00 * Statistically significant at p<0.05
Metropolitan Regional/Rural
1520
2530
35Care Coordination - Navigation
Metropolitan Regional/Rural
24
68
10
Care Coordination - Care Coordination
Metropolitan Regional/Rural
24
68
10
Care Coordination - Care Received

Section 7
Breast Cancer 2018 Australian PEEK Study
Comparisons of Care Coordination scores by education
Comparisons of Care Coordination scores were made between participants education levels, comparing those with high school or trade with those with university education. A two-sample t-test was used
when assumptions for normality and variance were met (Table 7.11), or when assumptions for normality and variance were not met, a Wilcoxon rank sum test with continuity correction was used (Table 7.12). No statistically significant differences were observed between these two groups for any Care Coordination scores (Tables 7.11 and 7.12).
Figure 7.16: Boxplot of Care coordination Total Score by education
7.17: Boxplot of Care coordination Communication by education
Figure 7.18: Boxplot of Care coordination Navigation by education
Figure 7.19: Boxplot of Care coordination question by education
High school/Trade University
5060
7080
90
Care Coordination - Total Score
High school/Trade University
2030
4050
60
Care Coordination - Communication
High school/Trade University
1520
2530
35
Care Coordination - Navigation
High school/Trade University
24
68
10
Care Coordination - Care Coordination

Section 7
Breast Cancer 2018 Australian PEEK Study
Figure 7.20: Boxplot of Care Received by education
Table 7.11: Summary statistics and Two sample t test by education status Care Coordination
Group Number Mean SD T Df P
Navigation High school/Trade 46 26.00 4.60 -0.29 98 0.7692 University 54 26.20 4.41
Table 7.12: Summary statistics Wilcoxon rank sum test with continuity correction by education status
Care Coordination
Group Number Median IQR W P
Total score High school/Trade 46 64.00 19.00 1180.50 0.6725
University 54 68.00 18.80
Communication High school/Trade 46 41.00 15.00 1198.00 0.7626
University 54 41.00 15.00 Care coordination
High school/Trade 46 7.50 5.00 1130.00 0.4338
University 54 8.00 2.00 Care received High school/Trade 46 9.00 3.00 991.50 0.0717
University 54 9.00 1.75
High school/Trade University
24
68
10Care Coordination - Care Received

Section 7
Breast Cancer 2018 Australian PEEK Study
Experience of care and support
Participants were asked what care and support they had received throughout their experience. The majority of care and support received came from family and friends (n=65, 65.00%).
Participant describes receiving support from family and friends
Friends like I said about there's been…I said to my husband, "We've had a friend who's covered everything." Like friends who haven't really come to see me but we've always been able to leave our dog with them or say, "Can you check the pets while we're away?" They’ve been very good in that practical support but not really good in the emotional support. Then other friends who have been really good in but there are, "Let's just meet for a coffee", or "I'll come round and bring my baby and you can just give him a hug." What I did find at first, and it really upset me, is everyone was asking my husband how I was and not many people were asking me how I was. He never thought to say, "So and so was asking after you." I just thought, "No one cares how I am." I'm just sitting here feeling awful and everyone is just going on about their day to day. Then when I said to him no one cares, he said, "So and so sent me this text." I go, "Thanks for telling me." The longer it's gone on probably the less some people have keeping in contact. But, there’s some people who have been there the whole way throughout. You know where your real friendships are. Participant 18
As far as friends go, they've been amazing. Couldn't be more supportive. As I said, we belong to a singing group and they've just been lovely, very supportive. They're not in my face all the time either. Family have been wonderful. When I was first diagnosed, it was just after Easter and all our daughters had been away and my husband was dreading ringing them and letting them know. My oldest daughter worked in the city and my husband rang her and she was here within two hours with coffee and cake. She said to me "Mum, coffee and cake fixes anything." Then my youngest daughter, who actually lives in LOCATION, but is a teacher, and she was up in LOCATION METEROPOLITAN on a school camp. She just said to her boss, "My mum needs me," and left and came here. Spent the day and night with us and went back to the camp the next day. And our other daughter worked late that night so she could spend the whole of the next day with me. Their support has been wonderful, but they don't mollycoddle me either, which is good. Participant 60
I've had support from my family, my sisters which has been great. Also, my friends and work colleagues, very supportive at work. When I was after the surgery and even continue on through chemo organizing meals and things like that. Friends that would take me to appointments and things when I wasn't allowed to drive myself before and after surgery and things like that. Just having people around me to talk to. I found that the cancer care nurses were a friend as well to have a chat to about how I was feeling, what was going on and they were very supportive. Participant 81
The next most common theme was care and support from specialist breast nurses and McGrath nurses (n=31, 31.00%) and the same number of participants (n=31, 31.00%) noted care and support from their general practitioner.
Participant describes receiving support from specialist breast nurses and McGrath nurses
The breast care nurse, she was really good. Can’t speak highly enough of the breast care nurses that I dealt with. Participant 21
The nurses are all so lovely and chatty. You're always looked after. In the room there would be four or six chairs with us getting chemo and the nurses would just have this chatter that's going around constantly while they were giving the treatment. It was almost worth sitting there feeling like throwing up if there are having a bit of a laugh at the bags, sort of thing. The next person is saying something else. That was all kind of nice, they made nice as possible. Considering what you're doing. Participant 40
Also the calls from my breast cancer nurse just to see how I was doing every now and again was good, was helpful. Participant 58
Well, I'll start with the breast care nurse, first of all. She has been brilliant. Her role in supporting me has been amazing. Participant 63
Participant describes receiving support from their general practitioner
I really don't feel like I've received a lot of support from my family. I think they just don't know what to do. I don't know how I feel. I suppose I haven't told them. I think probably more from the GP. My GP has been really good. Participant 75
GP's been wonderful and he's supportive and helpful. Participant 79
Yeah, lots of support from family and friends and a lovely family GP that is very supportive, definitely. Participant 90

Section 7
Breast Cancer 2018 Australian PEEK Study
There were 23 participants (23.00%) that described care and support from other patients and support services that connected patients with each other, and this included face-to-face support as well as charities that connected patients, and online support groups.
Participant describes receiving support from other patients (peer support)
I've Joined a support group and they meet twice a month, once a month for a Sunday lunch and once a month for a week night dinner. I've only been able to get to one of those so far but that was to meet other women in the same situation was really useful and helpful. A bit daunting to go into that scenario but it was good. There's a couple of breast care nurses who are attached to that support group who attend as well. Participant 32
Well, the other day I went to a workshop that was held here at our local hospital and it was a group called Look Good Feel better. I signed up for it and I went along with it. It was probably more for people that actually are going through chemotherapy and radiation treatment, losing their hair and all that sort of stuff. They gave us a bag full of cleansers and moisturizers and a bit of make-up so we could actually put our makeup on and look good. Then it was great to go and talk to other people. There's a whole group of us going through
exactly the same thing. Some were having treatment, some weren’t and having treatment. Those sort of groups are very important and the people that were running them were absolutely amazing. Most of them were all cosmeticians, but it was just fabulous too that there's not more things that we can get involved in, yes. I really would like to see some sort of support group where people go and talk to other people. Participant 73
Online. When you make a comment online about breast cancer, the replies and the compassion that even strangers show you is wonderful. Participant 87
There were a number of sub-group variations. Participants with stage II-III breast cancer spoke about receiving care and support from family and friends more frequently while participants with stage IV breast cancer spoke about this less frequently (83.33% stage II-III, 52.00% stage IV compared to 65.00% in the general cohort). Participants with stage IV breast cancer spoke about receiving care and support from specialist breast or McGrath nurses less frequently than the general cohort (22.00% compared to 40.00% in stage 0-III breast cancer). Participants in rural areas reported receiving care and support from their general practitioner, less frequently than the general cohort (20.45% compared to 31.00% in the general cohort).

Section 7
Breast Cancer 2018 Australian PEEK Study
Table 7.13: Care and support received
Figure 7.21: Care and support received (% of all participants)
Care and support received All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n=30 % n=50 % n=50 %Participant describes care and support from family and friends
65 65.00 14 70.00 25 83.33 39 78.00 26 52.00
Participant describes care and support from breast care or McGrath nurses
31 31.00 9 45.00 11 36.67 20 40.00 11 22.00
Participant describes care and support from their general practitioner
31 31.00 6 30.00 11 36.67 17 34.00 14 28.00
Participant describes care and support from a support group or other patients (including Look Good Feel Good, churches)
23 23.00 3 15.00 10 33.33 13 26.00 10 20.00
Participant describes not receiving significant support
23 23.00 0 0.00 8 26.67 8 16.00 15 30.00
Participant describes care and support from medical specialist (oncologists, surgeons, radiation therapists)
13 13.00 2 10.00 5 16.67 7 14.00 6 12.00
Participant describes home care help (cleaning, meals provided)
11 11.00 1 5.00 3 10.00 4 8.00 7 14.00
Care and support received All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant describes care and support from family and friends
65 65.00 36 64.29 29 65.91 36 66.67 29 63.04
Participant describes care and support from breast care or McGrath nurses
31 31.00 15 26.79 16 36.36 16 29.63 15 32.61
Participant describes care and support from their general practitioner
31 31.00 22 39.29 9 20.45 19 35.19 12 26.09
Participant describes care and support from a support group or other patients (including Look Good Feel Good, churches)
23 23.00 16 28.57 7 15.91 11 20.37 12 26.09
Participant describes care and support from medical specialist (oncologists, surgeons, radiation therapists)
13 13.00 9 16.07 4 9.09 9 16.67 4 8.70
Participant describes home care help (cleaning, meals provided)
11 11.00 5 8.93 6 13.64 4 7.41 7 15.22
0
10
20
30
40
50
60
70
Participant descr ibescare and support from
family and friends
Participant descr ibescare and support frombreast care or McGrath
nurses
Participant descr ibescare and support from
their GP (Generalpractitioner)
Participant descr ibescare and support from
a support group orother patients
(including Look GoodFeel Good, churches)
Participant descr ibesnot receiv ing
significant support
Participant descr ibescare and support from
medical specialist(oncologists, surgeons,
radiation therapists)
Participant descr ibeshome care help(cleaning, meals
provided)

Section 8
Breast Cancer 2018 Australian PEEK Study
Section 8 Quality of life

Section 8
Breast Cancer 2018 Australian PEEK Study
Section 8: Experience of quality of life
Quality of life • The main theme was that breast cancer had a significant impact on multiple areas of an individuals’ quality
of life (n=38, 38.00%). This was followed by a description of a ‘new normal’ or not being the same person that they used to be (n=26, 26.00%). This theme included changes to their relationships and family dynamics. The next most common theme was the impact of fatigue and lower energy levels which impacted quality of life, and this was noted by 22 participants (22.00%). There were 18 participants (18.00%) that described the impact of being anxious or frightened, 16 participants (16.00%) that spoke about not letting breast cancer impact their quality of life, 15 participants (15.00%) that described needing to take advantage of the time they had and the relationships they had in order to maintain quality of life and finally, 10 participants (10.00%) that described the financial impact of breast cancer in relation to quality of life.
• Participants with stage II-III breast cancer noted the impact of fatigue more frequently than the general cohort (33.33% compared to 22.00% in the general cohort). This group also described not letting breast cancer impact their quality of life, more frequently than the general cohort (26.67% compared to 16.00% in the general cohort). Participants in rural areas noted that there was a ‘new normal’, more frequently than participants in the general cohort (36.36% compared to 26.00% in the general cohort).
Regular activities to maintain health • The main thing that participants needed to do to everyday to maintain their health was to rest or take
things slowly (n=44, 44.00%). This was followed by needing to put themselves first (n=25, 25.00%) and needing to focus on maintaining their mental health (n=23, 23.00%). There were also 20 participants (20.00%) that spoke about needing to be diligent in taking medication.
Impact on relationships • The main impact on relationships was in relation to people becoming distant or people not
understanding/knowing what to say. This was noted by 39 participants (39.00%). The next most common theme was in relation to participants being more assertive in their relationships and realising who their true friends are (n=36, 36.00%). There were also 19 participants (19.00%) that described relationships becoming stronger and an additional 11 participants (11.00%) that described no impact to personal relationships.
• There was one sub-group variation where participants in rural areas reported people becoming distant or not knowing what to say, more frequently than the general cohort (54.55% compared to 39.00% in the general population).
Anxiety and fear of progression • The Fear of Progression questionnaire measures the level of anxiety people experience in relation to their
conditions. The Fear of Progression questionnaire comprises a total score, with a higher score denoting increased anxiety. Overall the entire cohort had a median total score of 34.99, which is a score in the middle of the scale.
Fear of progression – by disease stage • Participants with disease stage IV scored worse on the fear of progression total score compared to those
with stage 0-I disease.
Fear of progression – by metastatic status • Participants with metastases scored worse on the fear of progression total score compared to those
without metastases.
Fear of progression – by geographic location • There was no difference observed in the fear of progression total score between participants that live in
metropolitan areas and those that live in regional or rural areas.
Fear of progression – by level of education • There was no difference observed in the fear of progression total score between participants with university
qualifications and those with high school or trade certificates.

Section 8
Breast Cancer 2018 Australian PEEK Study
Experience of quality of life Participants were asked whether their condition has had an impact on their quality of life. The main theme was that breast cancer had a significant impact on multiple areas of an individuals’ quality of life (n=38, 38.00%). Within this theme, participants spoke about the impact of specific side effects, as well as the financial, emotional and physical implications of breast cancer. Participant describes a significant impact on quality of life It's had a huge effect because of the long term ongoing side effects. Chemo triggered fibromyalgia and inflammatory arthritis so that's a long-term issue that I now have to deal with. I'm on pain meds and all sorts of meds, not only meds relating to the breast cancer. I can’t work anymore because my fatigue is so much that I can’t do more than a few hours work. It's affected my ability to take care of all the things I used to within the family home like my parenting role has altered. Participant 28 It had an enormous impact on my quality of life. I was a very active person. Sports wise, I would play golf three times a week probably. I worked a great deal. I'm not able to play golf at all because of the risk of fractures. I do have quite a few fractures without playing golf. I've had times where I used to swim a lot. I can't swim anymore. It had an enormous effect on my quality of life. There are a few things that I can do and I try to be effective as I can but it has an enormous effect. Participant 63 Look, it's huge. It changes your life completely. When I was diagnosed, I think November 2013, so 2014 was treatment all year…Now, still, it's just the hardest part is the memory loss and the cognitive function which has impacted my life enormously. I guess from trying to get my words out and if I have to write something or send an email or even a text message, it doesn't make sense. I don't know what I've written, but if I read it back sometimes it's not even a couple of words being spelled. Then, just reading a book, you don't remember what you read yesterday, so you read the back of the book to trigger what the story is about. Then it's like, "Oh yes, that's right. That's what it was about." I could never go back and do the job that I was doing. I could never go back to work. I was extremely organized and on top of everything. Now, I'm not organised. I'm late for everything. It does. I'm at a point now where I need to go back to work because financially, I don't think there's enough support there in that aspect. In saying
that, all my medical expenses were pretty much covered for through the public system, but it's not working for those years that you just got to be on Centrelink benefits. Now I'm on a disability support pension because of my hands and because of stress disorder. Those things affect your life now every day. I think maybe putting more after your treatment that you can still access the counselling. All of that things can still help you to move forward. It's not like you've finished your treatment and it's gone. You might not have the cancer, but you've got all these other things that you're trying to cope with every day. Participant 67 This theme was followed by a description of a ‘new normal’ or not being the same person that they used to be (n=26, 26.00%). This theme included changes to their relationships and family dynamics. Participant describes needing to adjust to a ‘new normal’ Some of us for and against. [laughs] In the initial 12 months I didn't work so if you talk about my family they were glad to have me home. To drop them off at school and pick them up. They actually verbalised that quite a bit they said, "You're home" because I work. but for me, it's completely impacted my life. It still does. My quality of life. My body will never be the same. I think I'm still struggling to adjust to the new normal. I want to go back. it's just my head. The psychological impact everything and the fear of recurrence that's what...Yes I would say it impacts. Participant 33 I suppose there's different stages. During the treatment, it affects the family significantly because I couldn't be doing a lot. They would see me flaked out on the couch in the afternoon when I came home from primary school and things like that, which wasn't the best to see me like that. Now see you down the track, you wouldn't know any different. Now, it doesn't have any impact on the family. It's what I call my new normal is I've got numbness down from my shoulder to my elbow, but no one else knows about because why would you. And numbness across my chest and like things that too. They’re just things that I've got used to. It's not hampering how I live or how I operate. It's just different. How I live now with being a bit tired, I just take things a bit slower than I used to. I lose words sometimes when I'm talking. I don't know that's the chemo or older age [laughs] It's more adapting to it. because I'm getting every six months, there's is a little bit of anxiousness that comes in the preceding weeks before that, which I'll put to the back of my mind when I'm further away from that appointment. Yes, that's a

Section 8
Breast Cancer 2018 Australian PEEK Study
good phrase. It is scanxiety. I had mine last week. It was due in another ten days, and I just brought it forward because I'm like, "Come on. I'm not my hanging out. Just let's just get it done". Participant 42 It affects my quality of life because I'm not all the time in the right space to be the best mum because I'm either always in pain, I'm always frustrated so I'd say had this not happened we would be a lot better off. Have to always going to appointments and stuff because that makes it hard on my job and then it's definitely affected me so that a follow-on to affect the kids. Participant 92 The next most common theme was the impact of fatigue and lower energy levels which impacted quality of life, and this was noted by 22 participants (22.00%). Participant describes the impact of fatigue and lower energy levels I try very hard for it not to affect my family. My quality of life, the fatigue is the worst thing. I've had to adjust. So I'm a teacher….so I've gone to part time so that I can get two afternoons off. And I don't do anything fun, I just come home and nap. I have to sleep those two afternoons just to recharge so that when the kids come home from school it's homework and dinner. So yeah, quality of life the joint pain isn't great. Silly things, like I love baking and sewing and it's much harder to do those sort of things. But that's just getting older anyways. But I don't want to moan about it really. Participant 36 Yes, absolutely. I used to be a hugely athletic person who could do so many things. I was completely…I still am social but I was very social and I'm absolutely exhausted half the time. I can hardly do…I managed to live a very fulfilled life, but I had so much energy and saw people all the time. I just had to socialize anywhere near as much. I always had people over. I just haven't got enough energy. It puts a lot of pressure on your family. It's horrible for your family. Just for you, they get involved. Not well. They go through all those ups and downs. They go through all those new diagnosis. Participant 59 I've never felt the same again. My own energy levels, yes. Probably I'm more fatigued at the end of the day. I can still look after myself and the family. I probably experience more fatigue at the end of the day or week and it's definitely a new version of myself. Participant 78
There were 18 participants (18.00%) that described the impact of being anxious or frightened, and this was in relation to many aspects including fear of recurrence, the uncertainty of their prognosis or concerns about family members. Participant describes the impact of being anxious or frightened I guess, the biggest impact is concern of is it going to come back? If so, where? They told me if I get it back again, I haven't had a hope in hell. I guess that's my biggest concern. It's always in the back of your mind. If you know what I mean. This ex-doctor I had of mine, he came up and told me he got annoyed with me over something. He said, "You do realize that your cancer has gone to your brain?" That really crushed me. I shouldn't put any attention on him because he's a nasty piece of work. That was pretty terrible. Participant 30 Now, it's just a burden, I think for me. Then I worry about my daughters and their future, because they're young and I just worry whether one of them now doesn't want to get married and have children. My youngest one wants to have children and wants to hurry up and get married and things like that and have them before the whole breast cancer strikes her down. I know that's on their mind over time, so that really upsets me. That's mainly my main concern. I don't know whether I'd be able to return to work. I have been out of work since March. Yes. I really don't know where I'm going to end up. Very unknown while still waiting at the moment. Participant 31 It affects my quality of life when I'm not well. Hugely. but when you're feeling well, it doesn't really impact. Now I've had the liver Mets diagnosis, I guess it's like, I feel like it's like a hangman's noose hanging over not just me but my kids as well. Participant 62

Section 8
Breast Cancer 2018 Australian PEEK Study
There were 16 participants (16.00%) that spoke about not letting breast cancer impact their quality of life, 15 participants (15.00%) that described needing to take advantage of the time they had and the relationships they had in order to maintain quality of life and finally, 10 participants (10.00%) that described the financial impact of breast cancer in relation to quality of life. Participant describes needing to take advantage of the time and relationships So it has an impact and obviously also like I said to you before, I felt a bit slower and I'm having to stop and not cut down on doing things and committing to things and all that stuff. But in a way that there's been impact on my quality of life but its also an improvement in my quality of life because I've actually being much more mindful about saying, "No, don't have the capacity to do that," or "No we'll be too tired to do that," and just doing the things that I really want to do with the kids and my partner and not doing the things that really will get ourselves tied up in being busy all the time and really what for. So I'm really quite mindful about that part of the impact of it too. Participant 32 It's changed their view on life. We don't take things for granted. We don't sweat the small stuff anymore. We enjoy each day as it comes. Instead of saying that we must do that one day, we're actually doing it. It makes you reflect and appreciate life more. Participant 79 How does it affect my life? I think I said before, I make sure I really live my life now, and tell the people in my life I love them rather than being complacent about everyone and assuming that, yes, we are all going to be here tomorrow. I try to make each day mean something and be grateful for what I've got. Yes, it's changed in that way. Participant 87 Participant describes the financial impact Financially, I think we ... I think that time we get back to that was thing that I think I found difficult. I think in a hindsight, I probably-- I don't know what I maybe putting a bit more insurance or something, whether that would have helped, or something, or rather. I don't know. Participant 9
That's the other thing. If I have treatment when I see my specialist it's on Medicare, if I don't, if I just go to see him when I'm not having treatment like when I see the oncologist for breast cancer, I think that's $450 now. I might be banging on about money but money is a big, a big thing. 2013 I was diagnosed….Our out of pocket expenses without our private medical cover was for our tax was over $10,000. In just one and that was probably a bad year, but it puts a strain on what you claim to do. I think my husband puts away a $100 a week into a medical fund just to try and pay medical bills and for that year that didn’t cover it. Now it does, because as I said, I see him three months in but I get a bone strength treatment which means then its bulk billed. You can’t bill bulk bill PET scans and they’re over $1000. LOCATION actually, now has a PET scanner which before you had to go to METROPOLITAIN AREA. They do have. I think when we first went away they didn’t have and in STATE, they just send you up to the big city hospitals which is all bulk billed. I know I’m banging on about - but money might have been the one thing that has affected us. Participant 61 I suppose just taking the oomph out of me. It's really had a huge impact. I'm working but I don't have that get up and go anymore. Just lost my, not that I've ever-- Just lost my zest for life, I suppose. That then impacts on my kids and my husband. My capacity to earn money is less now. The job I was doing was a lot better pay than what I'm doing now. Now, I just wouldn't have the confidence to go for that kind of role again because of the chemo. Participant 65 In relation to sub-group variations, participants with stage II-III breast cancer noted the impact of fatigue more frequently than the general cohort (33.33% compared to 22.00% in the general cohort). This group also described not letting breast cancer impact their quality of life, more frequently than the general cohort (26.67% compared to 16.00% in the general cohort). Participants in rural areas noted that there was a ‘new normal’, more frequently than participants in the general cohort (36.36% compared to 26.00% in the general cohort).

Section 8
Breast Cancer 2018 Australian PEEK Study
Table 8.1: Quality of life
Quality of life All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n=30 % n=50 % n=50 %Participant describes breast cancer as a significant impact to multiple areas of their life
38 38.00 6 30.00 11 36.67 17 34.00 21 42.00
Participant describes a 'new normal' or not being the same person they used to be (including impact on relationships/change to family dynamics)
26 26.00 6 30.00 7 23.33 13 26.00 13 26.00
Participant describes fatigue or lower energy levels (being tired)
22 22.00 3 15.00 10 33.33 13 26.00 9 18.00
Participant describes being anxious or frightened about their cancer (including family members being concerned or anxious)
18 18.00 5 25.00 6 20.00 11 22.00 7 14.00
Participant describes not letting breast cancer impact their quality of life
16 16.00 3 15.00 8 26.67 11 22.00 5 10.00
Participant describes needing to take advantage of time and relationships while they have them
15 15.00 1 5.00 6 20.00 7 14.00 8 16.00
Participant describes financial challenges in relation to quality of life
10 10.00 1 5.00 4 13.33 5 10.00 5 10.00
Quality of life All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant describes breast cancer as a significant impact to multiple areas of their life
38 38.00 24 42.86 14 31.82 19 35.19 19 41.30
Participant describes a 'new normal' or not being the same person they used to be (including impact on relationships/change to family dynamics)
26 26.00 10 17.86 16 36.36 11 20.37 15 32.61
Participant describes fatigue or lower energy levels (being tired)
22 22.00 11 19.64 11 25.00 8 14.81 14 30.43
Participant describes being anxious or frightened about their cancer (including family members being concerned or anxious)
18 18.00 12 21.43 6 13.64 10 18.52 8 17.39
Participant describes not letting breast cancer impact their quality of life
16 16.00 12 21.43 4 9.09 11 20.37 5 10.87
Participant describes needing to take advantage of time and relationships while they have them
15 15.00 9 16.07 6 13.64 12 22.22 3 6.52
Participant describes financial challenges in relation to quality of life
10 10.00 4 7.14 6 13.64 5 9.26 5 10.87

Section 8
Breast Cancer 2018 Australian PEEK Study
Figure 8.1: Quality of life (% of all participants)
Everyday activities to manage health Participants were asked what some of the things are that they needed to do regularly to maintain their health. The main thing that participants needed to do to everyday to maintain their health was to rest or take things slowly (n=44, 44.00%). Participant describes needing to rest or take things slowly Yes. There’s nothing much that I can’t do. As I said the tiredness affects me. We have a lady come in and just vacuum and mop the floors and do the bath and I can do it, it’s just that it’s totally exhausting. Participant 61 Well, I still need to rest. If I get up and go in the morning and maybe going and do the food shopping or do some washing and things like that, I'm exhausted come lunch time. I still need to have a rest to recharge myself to then still get ready for when I pick the kids up and all of that sort of things. Participant 67 It's mostly keeping the fatigue at bay. That's the main thing, your life revolves around naps and energy levels. You've really got to time every part of your day around when you have the energy to do things. Participant 96
The next most frequent theme was needing to put themselves first (n=25, 25.00%) and needing to focus on maintaining their mental health (n=23, 23.00%): Participant describes needing to focus on maintaining their mental health I need to look after myself. I need to prioritize my health, which I didn't do. It wasn't done and I now don't dismiss things. If something comes up like a new lump or an ache or whatever, I go and get it checked. If I have that feeling like, no, I don't want this dismissed, I'm a bit more insistent with my doctor about what I want done. I just think if I had have been a bit more persistent initially and prioritized my health initially, I would have much better outcome or much better prognosis, but I didn't. I prioritize my health now and my needs. Participant 44 I have to commit myself in my head and keep pushing myself to feel and do everything I said I wanted to do and sometimes I just have to understand that that's actually not going to happen and forgive myself for not doing that. Participant 48
0
5
10
15
20
25
30
35
40
Participant descr ibesbreast cancer as a
significant impact tomultiple areas of their life
Participant descr ibes a'new normal' or not being
the same person theyused to be (including
impact onrelationships/change to
family dynamics)
Participant descr ibesfatigue or lower energy
levels (being tired)
Participant descr ibesbeing anxious or
frightened about theircancer (including fami ly
members beingconcerned or anxious)
Participant descr ibes notletting breast cancer
impact their quali ty of life
Participant descr ibesneeding to take
advantage of time andrelationships while they
have them
Participant descr ibesfinancial challenges in
relation to quality of life

Section 8
Breast Cancer 2018 Australian PEEK Study
What you need to do is you need to keep things as normal as what they were pre-cancer diagnosis. You need to be able to go to the gym, socialise with your friends, and not always discuss breast cancer. You don’t always want to have every topic discussed on your health or how you’re feeling or whatever, you really need to put yourself first a bit. Participant 94 There were also 20 participants (20.00%) that spoke about needing to be diligent in taking medication. Participant describes needing to be diligent in taking medication All I need to do is take one tablet a day, and just got to my two appointments a year at HOSPITAL NAME, once
with my breast surgeon and once with my oncologist. Participant 46 I need to take the drugs morning and night. And I try to stay in control of my emotions which at the moment is a daily struggle. Participant 62 I don't think I have any control over my breast cancer. The only thing I have control over is the pain. I'm taking a large dose of pain and nerve blockers. I have to do that otherwise I would be in so much pain that I wouldn't be able to function at all. The question is control your breast cancer. I don't have any control over the breast cancer. Participant 63
Table 8.2: Everyday activities to manage health
Everyday activities All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n=30 % n=50 % n=50 %Participant describes needing to rest or take things slowly as not to get too tired
44 44.00 8 40.00 17 56.67 25 50.00 19 38.00
Participant describes putting themselves first and/or taking care of themselves more diligently (prioritising)
25 25.00 4 20.00 5 16.67 9 18.00 16 32.00
Participant describes maintaining good mental health (including meditation)
23 23.00 7 35.00 8 26.67 15 30.00 8 16.00
Participant describes needing to be diligent about taking medication/treatment
20 20.00 2 10.00 7 23.33 9 18.00 11 22.00
Participant describes limited arm strength/arm pain or impact or lymphedema
15 15.00 4 20.00 4 13.33 8 16.00 7 14.00
Participant describes not needing to do anything in particular
15 15.00 4 20.00 4 13.33 8 16.00 7 14.00
Everyday activities All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %
Participant describes needing to rest or take things slowly as not to get too tired
44 44.00 24 42.86 20 45.45 23 42.59 21 45.65
Participant describes putting themselves first and/or taking care of themselves more diligently (prioritising)
25 25.00 16 28.57 9 20.45 14 25.93 11 23.91
Participant describes maintaining good mental health (including meditation)
23 23.00 14 25.00 9 20.45 9 16.67 14 30.43
Participant describes needing to be diligent about taking medication/treatment
20 20.00 12 21.43 8 18.18 11 20.37 9 19.57
Participant describes limited arm strength/arm pain or impact or lymphedema
15 15.00 5 8.93 10 22.73 7 12.96 8 17.39
Participant describes not needing to do anything in particular
15 15.00 7 12.50 8 18.18 9 16.67 6 13.04

Section 8
Breast Cancer 2018 Australian PEEK Study
Figure 8.2: Everyday activities to manage health (% of all participants)
Impact on relationships with family and friends Participants were asked whether having breast cancer has had an impact on their relationships with family and friends. The main impact on relationships was in relation to people becoming distant or people not understanding/knowing what to say. This was noted by 39 participants (39.00%).
Participant describes people becoming distant or people not understanding/knowing what to say
Yes, I do. Some people have no idea and some people just peeled away. Family's not been too bad, although my immediate family and that my husband and children, they've been really good and very supportive. They were fine. Broader family…they didn't know what to do, so they did nothing. Often, my sister, I was nine weeks into chemo or nine sessions into the chemo and on Christmas day my sister, we had Christmas here at our place, which is what we normally did. She walked in and said to me, "You don't look real good." And I said, "No, I'm on chemo." She seemed a bit surprised at that. Sometimes there nothing you can say. People don't, not everybody copes with illness as well. Some people are very good and some people are quite bothered by it. They don't cope well with it at all. I was equally surprised by some of the people who were just missing in action. Yes, and the people who ran up and said, "Oh,
you have to remain positive and you have to eat this and that. I wanted to scream at them. [laughs] There is nothing that would get me going more than this, if you stay positive, you'll get well. Well, I'm sorry but there is no evidence for this. There is no evidence for the, if you eat three lots of quinoa a day, it will kill your cancer. Participant 3 Yes, because a lot of them are scared. I've got three sisters, they're scared because they think they're going to get it, but they’re not….I had surgery in May this year and people were just so cruel because it didn't affect them but when we were trying to ask for help, I was getting the same thing, "Oh well you look so well." and the best one I got was that I should be more caring of my husband because he's had a major heart attack in June last year and he needs you to be strong for him. I've had to have major surgery on my breast two weeks before hand and people think it's just for the cancer, they don't know what happens afterwards if you have a breast reconstruction or follow up from the breast reconstruction, they just look at you and say, "You look well." I do have one lady coming to the house and said she can't understand why I wasn't capable of cleaning the house myself and I just smiled at her and asked her to leave because people are scared and they don't know what to say half the time. That's it, I have nothing else to say. Participant 51
0
5
10
15
20
25
30
35
40
45
50
Participant descr ibesneeding to rest or take
things slowly as not to gettoo tired
Participant descr ibesputting themselves first
and/or tak ing care ofthemselves more
diligently (prioritising)
Participant descr ibesmaintaining good mental
health (includingmeditation)
Participant descr ibesneeding to be diligent
about takingmedication/treatment
Participant descr ibeslimited arm strength/arm
pain or impact orlymphoedema
Participant descr ibes notneeding to do anything in
particular

Section 8
Breast Cancer 2018 Australian PEEK Study
That's put a bit of a strain on intimate relationship. With friends and other family members, it's funny that cancer can, I feel, be a bit alienating. People often stay away because they're afraid. They don't know what to say, so they don't say anything. I think that some people probably distance themselves from me, being afraid that perhaps I'd die. It's hard to repair some of those relationships unfortunately after an experience like cancer. Participant 82 The next most common theme was in relation to participants being more assertive in their relationships and realising who their true friends are (n=36, 36.00%). Participant describes being more assertive in their relationships and realising who their true friends are I think yes, but not always negatively because I think it just makes you more aware of the value of things and the value of your relationships and how ... Your life turns on a six pin so, they all sound like clichés these things, but if you have an argument with someone don't go to bed on it because you don't know what's going to happen. And I think it has improved it in some ways and in some cases I've actually stopped seeing people because…not because there's been any drama, but just because actually I don't need that old they didn't even text me in the whole time to say are you okay. And I know that people find it hard to deal with, but I'm much more selective now. Much more selective about who I give my time to and who I spend my time with. Participant 36 Probably yes. I suppose somehow you do find out who your friends are, don't you? I mean I'm amazingly lucky to discover that I have some really great friends but there are some people who just haven’t been able to deal with it. At the same time people who you don't think have come out of the woodwork and been more supportive, it really has been a learning curve. Participant 41
Most definitely, I think going through something like that you see who your real friends are. It's affecting my family. but because the outcome was good, yes, it's not an ongoing thing. It's like shocked when I was diagnosed. but you know you get through it, and you just do what you got to do, I guess. Participant 46 There were also 19 participants (19.00%) that described relationships becoming stronger and an additional 11 participants (11.00%) that described no impact to personal relationships. Participant describes relationships becoming stronger Yes, sometimes. I think I've got to try [laughs] because my daughter will say to me, "Mum, you're not going to use that breast cancer as an excuse." She just reminds me to try and stop bringing it up all the time, that's all. No, no. I think, if anything, it's fine, it's been a lot positive. I think I've got some perspective. Possibly maybe not been that terribly good a couple years ago, but now I'm feeling a bit more positive about things. Participant 9 My mum did a lot of it I relied my mom and my sister. So in the immediate family I think probably brought my husband and myself closer. We feel that we’re on each other’s time and supporting each other for the one goal. Participant 33 I think it's made them stronger. It hasn't been a negative. It's been a positive and that you realize that your family and friends are there for you. Participant 58 There was one sub-group variation where participants in rural areas reported people becoming distant or not knowing what to say, more frequently than the general cohort (54.55% compared to 39.00% in the general population).

Section 8
Breast Cancer 2018 Australian PEEK Study
Table 8.3: Impact on relationships
Figure 8.3: Impact on relationships (% of all participants)
Impact on relationships All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n=30 % n=50 % n=50 %Participant describes an impact on relationships: People becoming distant or people not understanding/knowing what to do or say/changes in relationship dynamics
39 39.00 7 35.00 10 33.33 17 34.00 22 44.00
Participant describes being more assertive or realising who your real friends/family are
36 36.00 8 40.00 14 46.67 22 44.00 14 28.00
Participant describes some relationships becoming stronger/appreciating relationships more
19 19.00 3 15.00 4 13.33 7 14.00 12 24.00
Participant describes no impact on personal relationships
11 11.00 3 15.00 5 16.67 8 16.00 3 6.00
Participant describes impact on intimacy with partner/spouse
9 9.00 1 5.00 4 13.33 5 10.00 4 8.00
Impact on relationships All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant describes an impact on relationships: People becoming distant or people not understanding/knowing what to do or say/changes in relationship dynamics
39 39.00 15 26.79 24 54.55 18 33.33 21 45.65
Participant describes being more assertive or realising who your real friends/family are
36 36.00 23 41.07 13 29.55 22 40.74 14 30.43
Participant describes some relationships becoming stronger/appreciating relationships more
19 19.00 13 23.21 6 13.64 10 18.52 9 19.57
Participant describes no impact on personal relationships
11 11.00 5 8.93 6 13.64 7 12.96 4 8.70
Participant describes impact on intimacy with partner/spouse
9 9.00 2 3.57 7 15.91 4 7.41 5 10.87
0
5
10
15
20
25
30
35
40
45
Participant descr ibes animpact on relationships:
People becomingdistant or people not
understanding/knowingwhat to do or
say/changes inrelationship dynamics
Participant descr ibesbeing more assertive orrealising who your real
friends/family are
Participant descr ibessome relationships
becomingstronger/appreciating
relationships more
Participant descr ibes noimpact on personal
relationships
Participant descr ibesimpact on intimacy with
partner/spouse

Section 8
Breast Cancer 2018 Australian PEEK Study
Experience of anxiety related to disease progression
The Fear of Progression questionnaire measures the level of anxiety people experience in relation to their conditions. The Fear of Progression questionnaire comprises a total score, with a higher score denoting increased anxiety. Summary statistics for the entire cohort are displayed alongside the possible range of the scale in Table 8.4. Overall the entire cohort had a mean total score of 34.99, which is a score in the middle of the scale.
Boxplots of Fear of Progression Total Score (FOPTS) by disease stage, metastatic status, location, and education status are displayed in Figures 8.5 to 8.8.
Comparisons of FOPTS were made by disease stage, metastatic status, location, and education status. A one-way ANOVA test with post hoc Tukey HSD tests were used to compare disease stage (Table 8.6). For all other comparisons, a two-sample t-test was used when assumptions for normality and variance were met (Table 8.8), or when assumptions for normality and variance were not met, a Wilcoxon rank sum test with continuity correction was used (Table 8.9).
A one way ANOVA test indicated a significant difference in the fear of progression total score between groups [F(2, 97) = 3.25, p = 0.0429] (Table 8.5). Post hoc comparisons using the Tukey HSD test indicated that the mean score for those with stage IV disease (mean = 37.00, sd = 6.75) was significantly higher than any stage 0-I disease (mean = 31.60, sd = 8.98), p = 0.0480 (Tables 8.5 and 8.7).
A Wilcoxon rank sum test with continuity correction indicated that those with metastases (median = 37.00, IQR = 11.00) had a higher fear of progression compared to those without metastases (median = 30.00, IQR = 13.20) [W= 879.50, p=0.0105] (Table 8.9) . There were no significant differences by location or education status (Table 8.8). In addition to the fear of progression questionnaire, participants were asked if they become anxious if they di not experience side effects of treatment as it makes them feel that the treatment is not working. The majority of participants never (n=54, 54.00%), seldom (n=28, 28.00%), sometimes (n=15, 15.00%), often (n=3, 3.00%) and no one felt this very often.
Table 8.4: Fear of Progression Total Score
Scale Mean Sd Possible range
Total score 34.99 8.63 12-60
Figure 8.5: Boxplot of FOPTS by Disease stage Figure 8.6: Boxplot of of FOPTS by metastatic status
Stage 0 and I Stage II and III Stage IV
2030
4050
60
Fear of Progression - Total Score
No Metastases Metastases
2030
4050
60
Fear of Progression - Total Score

Section 8
Breast Cancer 2018 Australian PEEK Study
Figure 8.7: Boxplot of FOPTS by location Figure 8.8: Boxplot of FOPTS by education
Table 8.5: Summary statistics for FOPTS by disease severity
FOPTS: Disease severity
Group Count Mean Sd
Disease stage Stage 0-I 20 31.60 8.98 Stage II-III 30 33.90 10.40 Stage IV 50 37.00 6.75
Table 8.6: ANOVA table for FOPTS by disease stage
FOPTS: Disease severity
Sum of squares
Df Mean square
F P
Disease Severity Between Groups 463 2 231.49 3.252 0.0429* Within Groups 6904 97 71.19 Total 7367 99
Table 8.7: Post hoc Tuckey HSD test FOPTS by disease stage
FOPTS: Disease severity
Comparison Mean difference
Lower Upper P adjusted
Disease Severity
Stage II-III – Stage 0-I 2.22 -3.58 8.01 0.6352 Stage IV – Stage 0-I 5.35 0.04 10.66 0.0480* Stage IV – Stage II-III 3.13 -1.50 7.77 0.2470
* Statistically significant at p<0.05 Table 8.8: Summary statistics and two sample t-test FOPTS
FOPTS Group Count Mean SD t df P Location Metropolitan 56 34.80 8.20 -0.31 98 0.7554
Regional/Rural 44 35.3 9.22 Education High school/Trade 46 33.80 8.14 -1.32 98 0.1899
University 54 36.00 8.96 * Statistically significant at p<0.005
Metropolitan Regional/Rural
2030
4050
60Fear of Progression - Total Score
High school/Trade University
2030
4050
60
Fear of Progression - Total Score
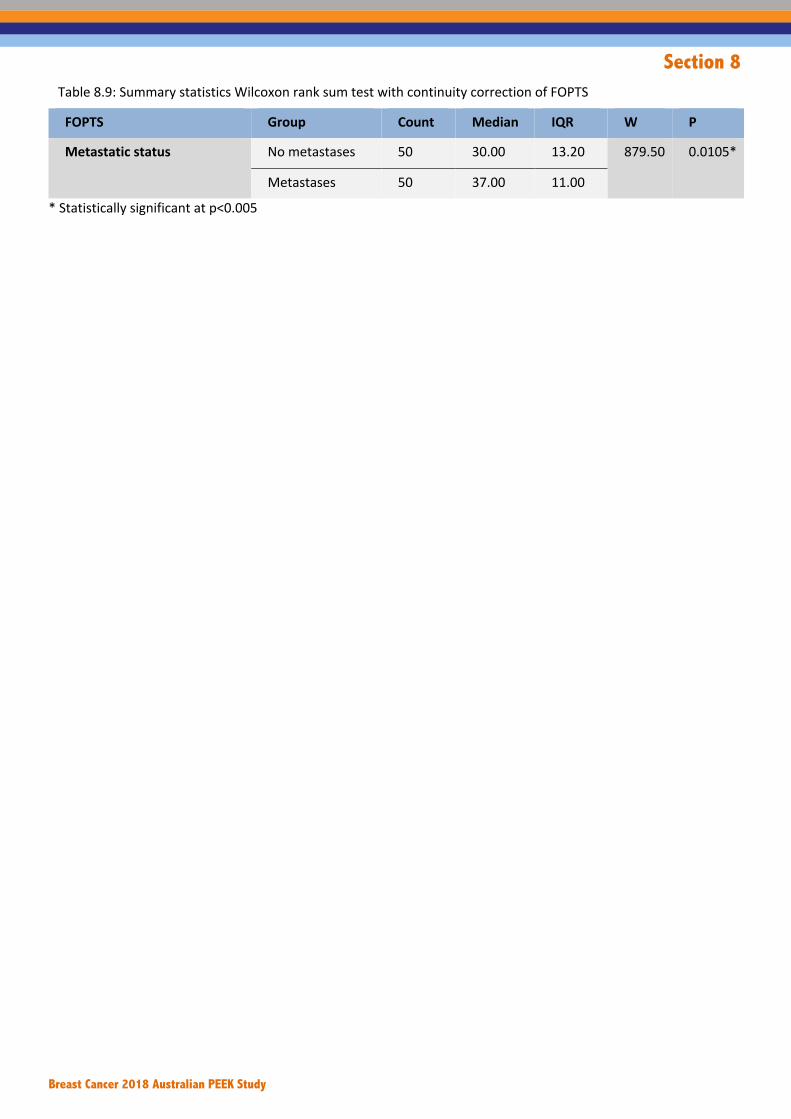
Section 8
Breast Cancer 2018 Australian PEEK Study
Table 8.9: Summary statistics Wilcoxon rank sum test with continuity correction of FOPTS
FOPTS Group Count Median IQR W P
Metastatic status No metastases 50 30.00 13.20 879.50 0.0105*
Metastases 50 37.00 11.00
* Statistically significant at p<0.005

Section 9
Breast Cancer 2018 Australian PEEK Study
Section 9 Expectations and messages

Section 9
Breast Cancer 2018 Australian PEEK Study
Section 9: Expectations of future treatment, care and support, information and communication Expectations of future treatments
• The most common expectation was that new treatments would have less side effects in general. This was noted by 37 participants (37.00%) and in this theme, there were no particular side effects mentioned. The next most common theme was the expectation that new treatments would be less invasive (n=27, 27.00%) and this included treatments being more personalised. There were 20 participants who noted the expectation that new treatments would be affordable (20.00%) and 14 participants that described the expectation or a cure or that their breast cancer would not be recurrent. There were a number of specific side effects that participants expected would be addressed through new treatments including fatigue, burns, hair loss, nausea, symptoms of menopause and weight gain. However, these were all noted by five participants or less.
• Participants were asked to rank which symptoms/aspects of quality of life would they want controlled in a treatment for them to consider taking it. The most important aspects reported were nausea and vomiting, and pain; the least important were hair loss and loss of appetite.
• Participants were asked to rank what is important for them overall when they make decisions about treatment and care. The most important aspects were safety of treatment/weighing up risks and benefits, and severity of side effects. The least important were cost, and including family in decision-making.
• Participants were asked to rank what is important for decision-makers to consider when they make decisions that impact treatment and care. The two most important values were access for all patients to all treatments and services, and quality of life; the least important was economic value to government.
Expectation of future information provision • The most common theme was that participants were satisfied with the current level of information and did
not have any recommendations (n=35, 35.00%). In relation to specific expectations there were 15 participants (15.00%) that described wanting more information that is specific to their type of cancer and respective treatment options. There were also 12 participants (12.00%) that described the expectation that information will be more readily available (including new research and clinical trials), and the same number of participants that described the expectation that there will be more information in relation to side effects.
• In relation to sub-group variations, participants with stage 0-I breast cancer were satisfied with the current level of information and did not have any recommendations, more frequently than the general cohort (45.00% compared to the general cohort 35.00%). There were also no participants in this group that described the expectation that there will be more information in relation to side effects.
Expectation of future healthcare professional communication • The most common theme was that participants were generally satisfied with health professional
communication and did not have any recommendations (n=33, 33.00%). There were 22 participants (22.00%) that expected future communication should be clearer and to understand this is all new information for patients, and 16 participants (16.00%) whose expectation was that communication should be more compassionate and empathetic.
• Participants with stage II-III breast cancer reported being satisfied with communication, less frequently than the general cohort (20.00% compared to 33.00% in the general cohort). This group also reported the expectation that communication would be compassionate and empathetic, more frequently (26.67% compared to 16.00% in the general cohort).

Section 9
Breast Cancer 2018 Australian PEEK Study
Expectation of future care and support • Participants were asked whether there was anything they would like to see in relation to the care and
support they receive. The main theme was the recommendation was in relation to more support that connects patients with health professionals and other patients, whether this is online, phone, in-person or through support groups (n=32, 32.00%). This was followed by support for specialist nurses for breast cancer patients (n=17, 17.00%). There were also 16 participants (16.00%) that were satisfied with the level of care and support received and did not have any additional recommendations.
• Participants with stage 0-I breast cancer called for support that connects patients with health professionals and other patients, less frequently than the general cohort (5.00% compared to 32.00%). Participants with stage II-III breast cancer reported being satisfied with care and support received less frequently than the general cohort (3.33% compared to 16.00% in the general cohort).
Messages to decision-makers • The most common message described by over half of all participants was that treatments should be
available and affordable to those who need them (n=54, 54.00%). This was followed by the message to provide holistic care and empower the patient and this included personalising treatment (n=25, 25.00%). An additional 10 participants (10.00%) had the message that it is important to continue funding research and support services.
• There was one sub-group variation where participants with stage IV disease had the message that
treatments should be available and affordable to those who need them, more frequently than the general cohort (64.00% compared to 54.00% in the general cohort and 44.00% in stage 0-III participants).

Section 9
Breast Cancer 2018 Australian PEEK Study
Expectations of future treatment Participants were asked a series of questions about their expectations for future treatments, information, health professional communication, and care and support.
When asked about their expectations of future treatment, there were a number of themes that emerged. The most common expectation was that new treatments would have less side effects in general. This was noted by 37 participants (37.00%) and in this theme, there were no particular side effects mentioned. Participant’s expectation is that new treatments would have less side effects in general A cure. Unfortunately, I think that's a bit like world peace, I'm not sure it's going to be achieved. The new treatments, what I'd like to see is things with less side effects. I've met younger women who the only hormone blocker they can take is tamoxifen and they just won't take it because of the side effects. I can actually understand that it can really ruin your quality of life. It's very daunting when you think about wasting another five years of your life on by taking some dreadful tablet that makes you miserable every hour of the day. I'd like to see better treatments with less horrible side effects and more follow-ups to your side effects. You shouldn't have to work to get followed up to your side effects. I found the attitude from the breast clinics was that if they ignored you saying, "This is happening. Oh, that's happening" That it would go away. I found it really frustrating. I didn't feel that I was listened to or I felt that they were treating me like a hysterical idiot, which I'm not. At times, not all the time. Participant 18 I think we just need better drugs, for what they do for your ongoing treatment. More research into the drugs that they're giving us, so that we don't have so many side effects, because the side effects are sometimes worse. I was talking to my GP, and he said the guys that have prostate cancer, they also take tamoxifen, but he said mostly, they don't last more than a few months, because they can't stand the side effects. We need obviously, more research into side effects. Participant 52 That was the main thing for me. Some of the treatments, sometimes, you wonder whether they're actually helping. They make you so sick, the chemo. At the same time look I understand that's the best that they have for now. If that works that works. (nice not to have the side effects) absolutely, yes. It would be nice
just to have that. All the good bits and take away the bad. Participant 94 The next most common theme was the expectation that new treatments would be less invasive (n=27, 27.00%) and this included treatments being more personalised. Participant’s expectation is that new treatments would be less invasive A cure, that's not likely. I don't know, I just think they need to, all the reading I've done on immunotherapy sounds really, really promising, and they need to try and find a way to not make radiotherapy and chemo the gold standard. So look for other gold standards, because the number of people I know that have lifelong side effects from those two treatments, yes it gives us more life, but in my case, the life it's given me is compromised by the treatment I had anyway, so it gives with one hand, takes with the other. So yeah, to have treatments that are a little less invasive, and maybe part of it is to get to the point where you can have the first few rounds of your chemo under hospital supervision, and then have something that can be administered at home, because in those early stages the running back and forth to appointments is horrendous. You're just constantly on the go. Participant 13 One day it'd be nice to know that women don’t need to have their breast removed. obviously, we have immune therapies and targeted therapies. Hopefully, one day there won’t be surgical interventions. Yes, I think less side effects. I would like to see patients being treated really holistically. I think integrated therapy has got to be a key and fundamental parts of that journey. Participant 48 I'd maybe like to see ... if you had the same type of breast cancer as me, maybe you didn't need to go through the chemo side of things. I was told or advised to go through chemo just as a preventative and I think maybe the surgery, radium and septum treatments because it targeted my gene that I had. I think that might have been sufficient but any clinical trials that can help speed up the diagnosis and not so much trauma to your body, I guess. Particpant 76

Section 9
Breast Cancer 2018 Australian PEEK Study
There were 20 participants who noted the expectation that new treatments would be affordable (20.00%) and 14 participants that described the expectation or a cure or that their breast cancer would not be recurrent. While some participants noted that they wanted a cure, most also realised that this might not be realistic. Participant talks about a cure however most also realised that this might not be realistic Cure. [laughs] I really don't know. I think that any new improvement is great. I'd hope that if there was anything new, if ever they found that this drug wasn't working, that they'd tell me about it straight away which I'm sure they would, because the doctor said to me on the first visit that sometimes the cancer can work its way around these hormone blockers. And he said if that happens, we just change the drug. Participant 59
From the treatments, one that works there is no treatment out there at the moment that cures metastatic breast cancer. I would like to see a treatment for metastatic breast cancer that actually cure this. Anybody living with metastatic breast cancer are just waiting for it to jump to the next place. Participant 62 For it to be gone. I'd like that but I'm not a fool. I'd like just for my treatment, I would hope they would give me few more years. Participant 83 There were a number of specific side effects that participants expected would be addressed through new treatments including fatigue, burns, hair loss, nausea, symptoms of menopause and weight gain. However, these were all noted by five participants or less.
Table 9.1: Expectations of future treatment
Expectations of future treatments All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n= % n=50 % n=50 %Participant's expectation is that new treatments have lesser side effects in general (when side effect is not mentioned)
37 37.00 10 50.00 10 33.33 19 38.00 17 34.00
Participant's expectation is that new treatments won't be so intrusive (more targeted approach)
27 27.00 6 30.00 12 40.00 18 36.00 9 18.00
Participant's expectation is that new treatments will be accessible and affordable
20 20.00 2 10.00 7 23.33 9 18.00 11 22.00
Participant describes treatment to be a cure (not be recurrent)
14 14.00 5 25.00 3 10.00 8 16.00 6 12.00
Participant's expectation is that new treatments won't involve chemotherapy and/or its its side effects
10 10.00 0 0.00 4 13.33 4 8.00 6 12.00
Participant describes that new treatment approach should be holistic and empower patients (give choices)
10 10.00 0 0.00 6 20.00 6 12.00 4 8.00
Other 9 9.00 0 0.00 3 10.00 3 6.00 6 12.00
Expectations of future treatments All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant's expectation is that new treatments have lesser side effects in general (when side effect is not mentioned)
37 37.00 22 39.29 15 34.09 21 38.89 16 34.78
Participant's expectation is that new treatments won't be so intrusive (more targeted approach)
27 27.00 12 21.43 15 34.09 17 31.48 10 21.74
Participant's expectation is that new treatments will be accessible and affordable
20 20.00 12 21.43 8 18.18 11 20.37 9 19.57
Participant describes treatment to be a cure (not be recurrent)
14 14.00 7 12.50 7 15.91 6 11.11 8 17.39
Participant's expectation is that new treatments won't involve chemotherapy and/or its its side effects
10 10.00 7 12.50 3 6.82 7 12.96 3 6.52
Participant describes that new treatment approach should be holistic and empower patients (give choices)
10 10.00 4 7.14 6 13.64 5 9.26 5 10.87
Other 9 9.00 7 12.50 2 4.55 6 11.11 3 6.52

Section 9
Breast Cancer 2018 Australian PEEK Study
Figure 9.1: Expectations of future treatment (% of all participants)
Values when making decisions about treatment Symptoms/aspects of quality of life important for treatments Participants were asked to rank which symptoms/aspects of quality of life would they want controlled in a treatment for them to consider taking it, were 1 is the most important and 10 is the least
important. A weighted average is presented in Figure 9.2. With a weighted ranking, the higher the score, the greater value it is to participants. The most important aspects reported were nausea and vomiting, and pain; the least important were hair loss and loss of appetite. Figures 9.3 and 9.4 show the weighted rank by disease stage and metastatic status, the symptoms and aspects of quality of life are similar within sub groups and follow much the same pattern as the entire cohort.
0
5
10
15
20
25
30
35
40
Participant'sexpectation is that
new treatmentshave lesser side
effects in general(when side effect is
not mentioned)
Participant'sexpectation is that
new treatmentswon't be so
intrusive (moretargeted approach)
Participant'sexpectation is that
new treatments willbe accessible and
affordable
Participantdescribes treatmentto be a cure (disease
wi ll not berecurrent)
Participant'sexpectation is that
new treatmentswon't involve
chemotherapyand/or its its side
effects
Participantdescribes that new
treatment approachshould Ge holistic
and empowerpatients (give
choices)
Other
0 1 2 3 4 5 6 7 8
Nausea/vomiting
Hair loss
Pain
Loss of appetite
Diarrhoea
Constipation
Mouth ulcers
Tiredness and Fatigue

Section 9
Breast Cancer 2018 Australian PEEK Study
Figure 9.2: Symptoms/aspects of quality of life important for treatments all participants (weighted rank)
Figure 9.3: Symptoms/aspects of quality of life important for treatments by disease stage
Figure 9.4: Symptoms/aspects of quality of life important for treatments by metastatic status
Values that are important to patients when making decisions Participants were asked to rank what is important for them overall when they make decisions about treatment and care, where 1 is the most important and 8 is the least important. A weighted average is presented in Figure 9.5. With a weighted ranking, the
higher the score, the greater value it is to participants. The most important aspects were safety of treatment/weighing up risks and benefits, and severity of side effects. The least important were cost, and including family in decision-making. Figures 9.6 and 9.7 show the weighted rank by disease stage and metastatic status, the values for making treatment decisions are similar within sub groups and are similar to the overall cohort.
Figure 9.5: Values important when making decisions (weighted rank)
0 1 2 3 4 5 6 7 8
Nausea/vomiting
Hair loss
Pain
Loss of appetite
Diarrhoea
Constipation
Mouth ulcers
Tiredness and Fatigue
IV II and III 0 and I
0 1 2 3 4 5 6 7 8
Nausea/vomiting
Hair loss
Pain
Loss of appetite
Diarrhoea
Constipation
Mouth ulcers
Tiredness and Fatigue
Metastases No metastases
0 1 2 3 4 5 6 7 8
Weighing up the ri sks and benefits
Severity of side effects
Time impact of treatment on quality of life
How treatment administered
How personal ised the treatment is
Including family in treatment decisions
My ability to fol low and stick to a treatment
Financial costs to me and my family

Section 9
Breast Cancer 2018 Australian PEEK Study
Figure 9.6: Values important when making decisions (by stage of disease)
Figure 9.7: Values important when making decisions (by location)
Values that are important to patients when others are making decisions on their behalf
Participants were asked to rank what is important for decision-makers to consider when they make decisions that impact treatment and care, where 1 is the most important and 5 is the least important. A weighted average is presented in Figure 9.8. With a weighted ranking, the higher the score, the greater value it is to
participants. The two most important values were access for all patients to all treatments and services, and quality of life; the least important was economic value to government. Figures 9.9 and 9.10 show the weighted rank by disease stage and metastatic status, the values for making decisions on their behalf are similar within sub groups and are similar to the overall cohort.
Figure 9.8: Values to consider on behalf of patients/families (weighted rank)
0 1 2 3 4 5 6 7 8
Weighing up the ri sks and benefits
Severity of side effects
Time impact of treatment on quality of life
How treatment administered
How personal ised the treatment is
Including family in treatment decisions
My ability to fol low and stick to a treatment
Financial costs to me and my family
IV II and III 0 and I
0 1 2 3 4 5 6 7 8
Weighing up the ri sks and benefits
Severity of side effects
Time impact of treatment on quality of life
How treatment administered
How personal ised the treatment is
Including family in treatment decisions
My ability to fol low and stick to a treatment
Financial costs to me and my family
Metastases No metastases
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5
Economic value government/tax payers
Economic value patients/their families
Quality of life for patients
Compassion
Access to all for all treatments/services

Section 9
Breast Cancer 2018 Australian PEEK Study
Figure 9.9: Values to consider on behalf of patients/families (weighted rank by disease stage)
Figure 9.10: Values to consider on behalf of patients/families (weighted rank by metastatic status)
Expectation of information provision Participants were asked what they would like to see in the future in relation to information provision. The most common theme was that participants were satisfied with the current level of information and did not have any recommendations (n=35, 35.00%).
Participant describes being satisfied with the current level of information: no recommendations
No. I think I had all the information. I had booklets and booklets, and pamphlets and everything. All that sort of thing that I'd been given, I'd been given information. (It's all relevant) Yes. I think a lot of it has been by mouth too, which I find best for me. Participant 10
I think everything that I wanted to know was covered, yes I can't say that I needed more information on anything. If I needed information my doctors would always point me in the right direction or give me handouts so I can’t fault that really I think there’s a lot of information about breast cancer and also other cancers. Participant 32
I can't think of anything, really. Nothing that I can really think of. There's was just so much information. I can honestly say I didn't think for one minute that I was short of any info that I needed at all, the information that I needed wasn't available, I didn't feel that at any point in time. In fact, sometimes there was too much information. I suppose in the beginning, you want as much information as you can get but sometimes there's so much information that you have information overload. No. I wouldn't say there's anything that I can think of that I would have needed more. Participant 57
In relation to specific expectations there were 15 participants (15.00%) that described wanting more information that is specific to their type of cancer and respective treatment options.
Participant describes expecting information that is specific to their type of cancer and respective treatment options
It's interesting because I'm currently thinking about how the Cancer Council displays all their information that my oncologist offers. It's just an array of booklets and you just have to look at every single booklet, not that applies to you. The internet was probably better because you can just see which one applies for you. That was a bit confusing when I saw all those booklet all over the wall. They had every type of cancer there was and mine was breast cancer. That was a bit confusing and I thought everything at once. Just a simple way of getting information. That is a physical way of displaying it but I think the internet was probably easier to look at and if I just had one booklet, one booklet would have just been good. Participant 33
I think you could do a fair bit of hunting online to get -- Well, that you asked me what do you know what your prognosis is. The answer to that question is particularly difficult to get a clear view on and it's not unusual where if you've got something that might tell you then they don't want you to do it without your doctor present like any or counsellor. Some of the things that I would quite happily go hard and fast and look at, they're saying, “Well you shouldn't do that on your own you should do that with someone with you. I guess that prognosis thing would be a really an easy way to deal with answering that question or getting that question for yourself to the level of satisfaction that you need because everybody might some people might not want to know what I want to know. Because I keep going to my breast surgeon. I don't want to do another test. I’m
0 1 2 3 4 5
Economic value government/tax payers
Economic value patients/their families
Quality of life for patients
Compassion
Access to all for all treatments/services
IV II and III 0 and I
0 1 2 3 4 5
Economic value government/tax payers
Economic value patients/their families
Quality of life for patients
Compassion
Access to all for all treatments/services
Metastases No metastases

Section 9
Breast Cancer 2018 Australian PEEK Study
happy to do a clinical trials though. I just want to make the best life decisions for me and the information I need to make the best life decisions for me are a better understanding of the things that could go wrong or that you're less well on. We have this five years I guess survival rate and then we have five years survival without disease rate and all those sorts of things but along that journey, I'm making decisions based on what I have now. As I said, I'd hate to find out in six months I had cancer again and I should have been able to make it different. How do you make the right decisions for you? Why did I go to work? Why didn't I just go and travel the world? Should I do that? Making those decisions is really hard because you can't put your hand on exactly. And maybe the information’s not there and I thought well maybe there's more information than I know that would help me. Anyway, so that would be nice. Participant 47
The only thing is, I always wondered why some people have chemotherapy and some people don't. I know people with breast cancer have had the surgery, radiation and chemo. What's the difference why I didn't know I didn't need it, or apparently I did. Why didn't I need it compared to the lady in the chair next to me? Do you know what I mean? Not to be explained to and maybe they don't tell you do that because I didn't need it but still it would be something that… is it something that should be offered to everybody, because I don't know much about chemotherapy. But is it something that should be offered to everyone, or is it just offered to certain people or what is the reasoning of having it or not having it? If you know what I mean. Participant 71
There were also 12 participants (12.00%) that described the expectation that information will be more readily available (including new research and clinical trials), and the same number of participants that described the expectation that there will be more information in relation to side effects.
Participant describes the expectation of having readily available information
A lot of the information is not readily available to everybody. I think that's probably a bit of an issue. I think that there is a lot of work being done out there and there's a lot of stuff being published in the professional journals that could be made more accessible to the general public. It's not all so technical that nobody could understand it. It would just need to be written slightly differently. It doesn't need to be at that super-duper scientific level. Also, just some more widespread education about the huge amount of policy peer reviewed medical stuff, which is freely available on the internet. Like the Cochrane reviews used by medicos
all the time, and just free in Australia. There's a lot of that sort of stuff which I think in general, not just for breast cancer, but for all human problems, that I just think there needs to be more education in that way. Certainly the crackpots get their information out there pretty readily. When you go onto the internet looking for information, you often have to dig down a fair way before you get something that's really relevant and reputable. Participant 2
Something else when you mentioned at the start about clinical trials and all that sort of thing, that is something I would be very interested in. I've since registered to be part of a study, but nothing been followed up. I think that could be…with clinical trials, that should be advertised or shared more. Participant 41
I guess I would like to know if there is any research ... anymore stuff being discovered like I saw on Facebook, it was saying for inflammatory cancer that there researching that rheumatoid arthritis treatment could help in addition to existing treatment. So I was gonna, when I see my surgeon, ask him what he knows about that, or the oncologist. You know, have you heard about this, that the treatments of rheumatoid arthritis is being tested now on inflammatory breast cancer and how could you access that treatment. Participant 68
Participant describes the expectation of having specific information about side effects
I'd love to see more information of side effects of the drugs that you take afterwards. I found that the chemist would give you a bit but there wasn't a lot of information on that. I really think that needs to be more. Maybe for some people, they need to read that before they decide that they’ll have treatment because they need to know that these things are going to happen. Chemist always gives you this and that but that's not a lot of information. You do need it more clearly. That would be the biggest thing. Participant 24
Yes, I think just a little bit more information, but then yes, a little bit of more information of what could go wrong, like the chemo side effects. I know that they give you a piece of paper these are your side effects, but I didn't have what was printed. What happened to me was just not unusual, but it wasn't common. I have actually thought, if they told you everything that could go wrong, you would never do it. You would, I'm going to take my chances. I'm such a black and white person that's my problem. I'm very down the line. Participant 36

Section 9
Breast Cancer 2018 Australian PEEK Study
I obviously do come across a little gaps like because I still do have in two of my fingers on the finger nails, just sort of numbing sensations and that's from the chemo. The fact that you get told you lose your hair and that you don't get notified that your eyelashes and eyebrows could go too. When you going to put mascara on and you're thinking there's nothing there, that's a little bit frightening. It's the little things like that, they sort of didn't touch on quite, like all the side effects. Participant 46
In relation to sub-group variations, participants with stage 0-I breast cancer were satisfied with the current level of information and did not have any recommendations, more frequently than the general cohort (45.00% compared to the general cohort 35.00%). There were also no participants in this group that described the expectation that there will be more information in relation to side effects
Table 9.2: Expectations of information provision
Expectations of future information All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n= % n=50 % n=50 %Participant does not have a specific recommendation as they were generally happy with the information provided
35 35.00 9 45.00 8 26.67 17 34.00 18 36.00
Participant describes the expectation that there will be more information specific to them and their treatment
15 15.00 4 20.00 6 20.00 10 20.00 5 10.00
Participant describes the expectation that information will be more readily available (including new research, trials)
12 12.00 3 15.00 4 13.33 7 14.00 5 10.00
Participant describes the expectation that there will be more information in relation to side effects
12 12.00 0 0.00 6 20.00 6 12.00 6 12.00
Participant describes expectation of information being given in more structured manner (in simpler terms)
6 6.00 0 0.00 2 6.67 2 4.00 4 8.00
Participant describes the expectation that there will be more information in relation to diet and nutrition
5 5.00 1 5.00 0 0.00 1 2.00 4 8.00
Participant describes the expectation that information in relation to psychological support will be offered
4 4.00 1 5.00 2 6.67 3 6.00 1 2.00
Participant describes being given too much information (overwhelming)
4 4.00 1 5.00 1 3.33 2 4.00 2 4.00
Participant describes expectation of information specifically related to metastatic breast cancer
4 4.00 0 0.00 0 0.00 0 0.00 4 8.00
Expectations of future information All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant does not have a specific recommendation as they were generally happy with the information provided
35 35.00 17 30.36 18 40.91 19 35.19 16 34.78
Participant describes the expectation that there will be more information specific to them and their treatment
15 15.00 10 17.86 5 11.36 8 14.81 7 15.22
Participant describes the expectation that information will be more readily available (including new research, trials)
12 12.00 8 14.29 4 9.09 6 11.11 6 13.04
Participant describes the expectation that there will be more information in relation to side effects
12 12.00 5 8.93 7 15.91 7 12.96 5 10.87
Participant describes expectation of information being given in more structured manner (in simpler terms)
6 6.00 3 5.36 3 6.82 2 3.70 4 8.70
Participant describes the expectation that there will be more information in relation to diet and nutrition
5 5.00 3 5.36 2 4.55 4 7.41 1 2.17
Participant describes the expectation that information in relation to psychological support will be offered
4 4.00 3 5.36 1 2.27 2 3.70 2 4.35
Participant describes being given too much information (overwhelming)
4 4.00 2 3.57 2 4.55 1 1.85 3 6.52
Participant describes expectation of information specifically related to metastatic breast cancer
4 4.00 4 7.14 0 0.00 2 3.70 2 4.35

Section 9
Breast Cancer 2018 Australian PEEK Study
Figure 9.11: Expectations of information provision (% of all participants)
Expectation of health professional communication Participants were asked whether there was anything they would like to see improved in the future in relation to the way that health professionals communicate with patients. The most common theme was that participants were generally satisfied with health professional communication and did not have any recommendations (n=33, 33.00%). Participant describes being satisfied with communication: no recommendations No, I think the communication, in my experience, is excellent. I think it might be harder for people living out of town. I'm in LOCATION, and all the specialists were right on hand. It would be harder in different situations, but I can't think of any way in which the communication could be improved. Participant 1 Not really. I think everybody I had was pretty good. The oncologist, the first time I met him, I didn't like him because he hadn't told me anything. Then when I went back to see him the next time, he said, "Well, I didn't
tell you at the first time because you're so so." Now, I'm going to give you more information and each time, he only gave me a bit more. He just said that's the way he does it. I think I was lucky. I've had different stories of other people who weren't so lucky but I was lucky with the people I had. Participant 25 Not really, I really can't think of anything that they're not doing, that I think they should be doing. They've just been terrific...honestly, I could not fault anyone. I think that everybody has just been, from day one, everybody's been so supportive and reassuring and very informative. I don't feel like anything has been held back from us. They're not telling me there's going to be a miracle. Sure, I'm praying for one, but they don't tell you there's going to be a miracle cure. I'd rather they didn't because, if there is not, there is not. You've got to be realistic about things. You can't live on a cloud and hope that you're going to float away. Participant 59
0
5
10
15
20
25
30
35
40
Participant doesnot have a specificrecommendation
as they weregenerally happy
with theinformation
provided
Participantdescribes the
expectation thatthere will be more
informationspecific to them
and theirtreatment
Participantdescribes the
expectation thatinformation willbe more readi ly
available(including newresearch, trials)
Participantdescribes the
expectation thatthere will be more
information inrelation to side
effects
Participantdescribes
expectation ofinformation being
given in morestructuredmanner (in
simpler terms)
Participantdescribes the
expectation thatthere will be more
information inrelation to dietand nutrit ion
Participantdescribes the
expectation thatinformation in
relation topsychological
support will beoffered
Participantdescribes beinggiven too much
information(overwhelming)
Participantdescribes
expectation ofinformation
specifically relatedto metastaticbreast cancer

Section 9
Breast Cancer 2018 Australian PEEK Study
There were 22 participants (22.00%) that expected future communication should be clearer and to understand this is all new information for patients, and 16 participants (16.00%) whose expectation was that communication should be more compassionate and empathetic. Participant describes expecting clear information that acknowledges this is all new for patients Yes. I definitely think that oncologists you get like half an hour of their time and they're just…you get quite a massive charge for half an hour of their time and you come out knowing what they think is important. But you don't even know what is important because you don't know that that might happen. I think with the medical oncology stuff it needs to be a more open frank discussion but in a friendly format, rather than a very condition-driven format. Participant 17 Yes, it's the things that they...there should be more communication about your scans and what is showing up on the scans of…you left a little bit on the dark and you don't hit this until you're going to see your own oncologist. There's quite of movement out there, do not let the patient have a look until the doctors has a look. Then you don't have the questions in your head that you should be asking about the tests. Participant 62 Just more information, probably, and why the treatment that you're getting, why you're getting that treatment, and as to why you're not offered something else, if you know what I mean. We’re going to do this, but the reason is because of this, this, and this. Participant 71
Participant describes expecting compassionate and empathetic communication Apart from the one …and her after surgery care which has been dealt with and that was just a one-off. Everyone else was being brilliant. But, yes, just professional communication between the health professionals. And also, just more of a professional and compassionate approach to communicating with the patient. Not having those conversations then arguing in front of me because that really does affect my confidence in the people that are looking after me. Participant 23 More empathy. The fact that you are a person, not a breast cancer. You're not a number. Just more empathy. Participant 55 It must be hard from a male's perspective. I do have a male surgeon to start with and then I ended up with a female doing the lymph node. There is such a huge difference in like he's very professional at his job. He did a very nice job and everything. But I felt he'd come around with his little entourage, and he wouldn't direct the questions at me. He'd get them to direct the questions at me. Whereas the other doctor, the female one, she's brilliant because she'd just talk to you like a woman down the street would be talking to you. She had more empathy towards me, whereas, it's like men being gynaecologists, they really don't get it when it comes to women. Even though they study it and that. Whereas a woman understands what's going on and can have more empathy towards them. That's the only thing. I think there needs to be more female doctors in the breast care. There's probably a lot. Participant 79 Participants with stage II-III breast cancer reported being satisfied with communication, less frequently than the general cohort (20.00% compared to 33.00% in the general cohort). This group also reported the expectation that communication would be compassionate and empathetic, more frequently (26.67% compared to 16.00% in the general cohort).

Section 9
Breast Cancer 2018 Australian PEEK Study
Table 9.3: Expectations of health professional communication
Expectations of future professional communication
All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n= % n=50 % n=50 %Participant does not have a specific recommendation as they were generally happy with the communication that they had
33 33.00 7 35.00 6 20.00 13 26.00 20 40.00
Participant's recommendation is that communication should be clearer and to understand this is all new information for patients
22 22.00 4 20.00 5 16.67 9 18.00 13 26.00
Participant's recommendation is that communication should be empathetic and compassionate
16 16.00 2 10.00 8 26.67 10 20.00 6 12.00
Participant's recommends better communication between different health professionals
8 8.00 0 0.00 7 23.33 7 14.00 1 2.00
Participant recommends communication to be personalised and holistic approach
7 7.00 2 10.00 2 6.67 4 8.00 3 6.00
Participant's recommendation is that communication should be consistent (includes being able to see the same doctor each time, someone that knows your medical history)
6 6.00 4 20.00 1 3.33 5 10.00 1 2.00
Participant's recommendation more options for treatment should be communicated to themmore options
4 4.00 2 10.00 1 3.33 3 6.00 1 2.00
Participant recommends more communication post treatment
3 3.00 0 0.00 3 10.00 3 6.00 0 0.00
Participant recommends more better communication of test results/patient records to patients themselves
3 3.00 1 5.00 1 3.33 2 4.00 1 2.00
Expectations of future professional communication
All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant does not have a specific recommendation as they were generally happy with the communication that they had
33 33.00 17 30.36 16 36.36 18 33.33 15 32.61
Participant's recommendation is that communication should be clearer and to understand this is all new information for patients
22 22.00 9 16.07 13 29.55 13 24.07 9 19.57
Participant's recommendation is that communication should be empathetic and compassionate
16 16.00 13 23.21 3 6.82 12 22.22 4 8.70
Participant's recommends better communication between different health professionals
8 8.00 6 10.71 2 4.55 3 5.56 5 10.87
Participant recommends communication to be personalised and holistic approach
7 7.00 3 5.36 4 9.09 4 7.41 3 6.52
Participant's recommendation is that communication should be consistent (includes being able to see the same doctor each time, someone that knows your medical history)
6 6.00 2 3.57 4 9.09 3 5.56 3 6.52
Participant's recommendation more options for treatment should be communicated to themmore options
4 4.00 2 3.57 2 4.55 2 3.70 2 4.35
Participant recommends more communication post treatment
3 3.00 1 1.79 2 4.55 2 3.70 1 2.17
Participant recommends more better communication of test results/patient records to patients themselves
3 3.00 1 1.79 2 4.55 1 1.85 2 4.35

Section 9
Breast Cancer 2018 Australian PEEK Study
Figure 9.12: Expectations of health professional communication (% of all participants) Expectation of care and support Participants were asked whether there was anything they would like to see in relation to the care and support they receive. The main theme was the recommendation was in relation to more support that connects patients with health professionals and other patients, whether this is online, phone, in-person or through support groups (n=32, 32.00%). Participant describes the expectation of having more support that connects patients with health professionals and other patients I was fortunate that I had time. At the time I was diagnosed I thought, "Oh my God it's going to grow while I'm sitting here waiting to see the surgeon in three weeks". And I was really nervous but I think having the reassurance and the time to go through all those steps is important. And having somebody that you can reach out to at any time is important because I think that some of the charities they say you can go online anytime and post a question or make a phone call and somebody can be there at the other end of the line reassuring you. I know the medical team, then you have the breast care nurses they are good as well. Participant 15 I've heard from different people that they've had people visit them in hospital from different organizations. I actually had someone from the local breast cancer group come and visit me and she was really nice. She had similar cancer to me, 10 years previously, and she was great. She totally found me in the hospital the first time, then spoke to me and that
was really good. I had a lot of people who said no, they didn't have that. Have it clear on how much it's going to cost you and things like that, things like how much time you're going to have off work. Participant 25 Patient organizations, charities, I think they need to make the first approach, that's my opinion. I just sit here feeling sorry for myself. You know what I mean? If I desperately need answers, I'll go and find them, but if I'm feeling lonely or, well, "I'll just sit here." I think that they need to make the approach to the people and make themselves available, personally. Even if just as a phone number. It would make it easier because maybe that's another side effect of organizing anything is just that impossible. You can't concentrate for any length of time. I've always been a big reader. I don't read that much anymore. Participant 60 This theme was followed by support for specialist nurses for breast cancer patients (n=17, 17.00%). Participant describes support for specialist nurses I think there's nothing really I can put my finger on because from my perspective, I had everything given to me and I was wrapped around with the greatest of care and support available. I don't know what else additional can be put in place really. I just have to say McGrath breast care nurse is absolute key to all of this they are just fantastic. If I didn't have my two nurses, I wouldn't have to go to meetings or treatments or stuff like that. They were just there every step of the way. Participant 5
0
5
10
15
20
25
30
35
Participant does not have a specificrecommendation as they were generallyhappy with the communication that they
had
Participant's recommendation is thatcommunication should be clearer and to
understand this is al l new informationfor patients
Participant's recommendation is thatcommunication should Ge empathetic
and compassionate
Participant's recommends Gettercommunication Getween different
health professionals
Participant recommends communicat ionto Ge personalised and holistic approach
Participant's recommendation is thatcommunication should Ge consistent(includes being aGle to see the same
doctor each time, someone that knowsyour medical history)

Section 9
Breast Cancer 2018 Australian PEEK Study
I think as far as a breast care nurses go, it would be wonderful if they had more run. They were more available. I found that that was never the place for me. It was really hard to try and get anyone to call me back. I know because when I compared it to when I was going privately, obviously it's private, but the breast care nurses was so lovely and so warming and loving. Whereas after that, I didn't get any of that. I didn't get anything. That would be nice. Participant 45 Metastatic breast care nurses. We have one at the LOCATION now, but there certainly wasn't one when I started. So I didn't ... I wasn't even ... I mean, the breast care nurse eventually called me I think about two months into my treatment. But I had a friend who was diagnosed and treated six months before me, and she kept asking me why I hadn't seen the breast care nurse. So that was obviously because they don't actually deal with women who've got metastatic breast cancer. And so, I mean the LOCATION have a metastatic breast care nurse, but I believe she only works one day a week, and ...I see her at the support groups, but again, I don't feel like I have ... she's, the impression I get is so over worked dealing with some of the other women in the group who've got far more pressing problems than I have. So I think ... I think any major oncology centre should have a metastatic breast care nurse who can help patients negotiate through the system. And I think especially for women who's first diagnosis is advanced breast cancer. You feel, when you have that double whammy of a diagnosis, to be told basically there isn't actually, you're not actually eligible for the breast care nurse, is very confusing and it takes a while for you to figure out yourself how to get around the system and what you need and ... and it makes you feel like you don't fit in. We often just don't fit the system. And I know it's all to do with the pathway, that early breast cancer goes through the surgeons, and then you get fed in through the wards and the breast care nurses pick
you up there. but they need to really look at that, because it's ... yeah. It's a big hole at the moment. Participant 53 There were also 16 participants (16.00%) that were satisfied with the level of care and support received and did not have any additional recommendations. Participant describes being satisfied with care and support: no recommendations I can't think of anything. My experience has been that I've had all the care for what I needed. I think that people living out of town, in country areas, need the facilities that we've got, but it's hard, isn't it? Participant 1 As I said I had a lot of support especially with friends. A lot of people maybe aren't in that position. Then they would obviously need support. I don't know how people do it if they're on their own or if they're trying to hold down a job or young children. I just don't know how they do it. Whereas that hasn't really been a factor luckily for me. Participant 19 I think, everybody is treated like I am, I couldn't ask for any more. I feel that if I wanted any more support, I'm sure I could go to the organization my friend goes to. She just said they've been wonderful with her, just so supportive. Participant 59 Participants with stage 0-I breast cancer called for support that connects patients with health professionals and other patients, less frequently than the general cohort (5.00% compared to 32.00%). Participants with stage II-III breast cancer reported being satisfied with care and support received less frequently than the general cohort (3.33% compared to 16.00% in the general cohort).

Section 9
Breast Cancer 2018 Australian PEEK Study
Table 9.4: Expectations of care and support
Expectations of future care and support All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n= % n=50 % n=50 %Participant's recommendation is for more support services that connect patients with health professionals and other patients (online, phone, in-person, support groups)
32 32.00 1 5.00 12 40.00 13 26.00 19 38.00
Participant's recommendation is that specialist nurses are important in breast cancer/care coordination
17 17.00 5 25.00 4 13.33 9 18.00 8 16.00
Participant does not have a specific recommendation as they were generally happy with the care and support that they had
16 16.00 4 20.00 1 3.33 5 10.00 11 22.00
Participant's recommendation is that specialist centres/specialist care is important in breast cancer
8 8.00 2 10.00 3 10.00 5 10.00 3 6.00
Participant's recommendation is for holistic care including making information about all treatment options available
8 8.00 4 20.00 4 13.33 8 16.00 0 0.00
Participant's recommendation opportunities for patients to talk to or connect with other patients
6 6.00 3 15.00 3 10.00 6 12.00 0 0.00
Participant's recommendation for Wellness centers
5 5.00 1 5.00 3 10.00 4 8.00 1 2.00
Participant's recommendation for care and support services to target young women (under 50)
3 3.00 1 5.00 2 6.67 3 6.00 0 0.00
Participant's recommendation for more funding (affordable healthcare)
3 3.00 1 5.00 1 3.33 2 4.00 1 2.00
Participant's recommendation for having services for follow up and after treatment
3 3.00 0 0.00 0 0.00 0 0.00 3 6.00
Expectations of future care and support All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant's recommendation is for more support services that connect patients with health professionals and other patients (online, phone, in-person, support groups)
32 32.00 16 28.57 16 36.36 13 24.07 19 41.30
Participant's recommendation is that specialist nurses are important in breast cancer/care coordination
17 17.00 8 14.29 9 20.45 10 18.52 7 15.22
Participant does not have a specific recommendation as they were generally happy with the care and support that they had
16 16.00 9 16.07 7 15.91 11 20.37 5 10.87
Participant's recommendation is that specialist centres/specialist care is important in breast cancer
8 8.00 4 7.14 4 9.09 4 7.41 4 8.70
Participant's recommendation is for holistic care including making information about all treatment options available
8 8.00 5 8.93 3 6.82 4 7.41 4 8.70
Participant's recommendation opportunities for patients to talk to or connect with other patients
6 6.00 5 8.93 1 2.27 1 1.85 5 10.87
Participant's recommendation for Wellness centers
5 5.00 3 5.36 2 4.55 1 1.85 4 8.70
Participant's recommendation for care and support services to target young women (under 50)
3 3.00 1 1.79 2 4.55 3 5.56 0 0.00
Participant's recommendation for more funding (affordable healthcare)
3 3.00 0 0.00 3 6.82 1 1.85 2 4.35
Participant's recommendation for having services for follow up and after treatment
3 3.00 2 3.57 1 2.27 1 1.85 2 4.35

Section 9
Breast Cancer 2018 Australian PEEK Study
Figure 9.13: Expectations of care and support (% of all participants)
0
5
10
15
20
25
30
35
Participant'srecommendation for
more supportservices (online,
phone, in-person,support
groups)
Participant'srecommendation is
that specialist nursesare important in
breast cancer/carecoordination
Participant does nothave a specific
recommendation asthey were generallyhappy with the care
and support thatthey had
Participant'srecommendation is
that specialistcentres/specialist
care is important inbreast cancer
Participant'srecommendation is
for holistic careincluding making
information about alltreatment options
available
Participant'srecommendationopportunities for
patients to talk to orconnect with other
patients
Participant'srecommendation for
Wel lness centers
Participant'srecommendation for
care and supportservices to target
young women (under50)
Participant'srecommendation for
more funding(affordablehealthcare)
Participant'srecommendation forhaving services forfol low up and after
treatment

Section 9
Breast Cancer 2018 Australian PEEK Study
Messages to decision-makers about the treatment and care that people affected by breast cancer
Participants were asked what their message to people who make decisions about their condition would be. The most common message described by over half of all participants was that treatments should be available and affordable to those who need them (n=54, 54.00%). This was followed by the message to provide holistic care and empower the patient and this included personalising treatment (n=25, 25.00%). An additional 10 participants (10.00%) had the message that it is important to continue funding research and support services. There was one sub-group variation where participants with stage IV disease had the message that treatments should be available and affordable to those who need them, more frequently than the general cohort (64.00% compared to 54.00% in the general cohort and 44.00% in stage 0-III participants). Treatments should be available and affordable to those who need them To put patients first. The money thing, that's difficult but probably it didn't affect me, but you know how you read that there's some wonderful drug, but it's not on the PBS so it's not accessible to everyone. It costs thousands of dollars, but it could save their life. but they can't afford it. I don't know what the answer is because…the government, for example, have to make it as easy as possible on the poor people going through it because we all pay taxes. I don't know. I was lucky because it didn't really affect me. Participant 3 I would like to say that every patient gets to see a breast care nurse or have access to a breast care nurse, and that all drugs are available to everybody. Participant 49 More consideration for the overall treatments. I was lucky with my surgeon and my doctors where they would admit me into hospital so that some of the treatments weren’t costing anything. While I’m in the hospital it was free. If I was an outpatient it was an arm and a leg. I was lucky to have good people like that. The radiation isn’t covered in your health insurance. I would hate to be in that position where you have to say, "Well, I can’t have treatment because I can’t afford it." I’m sure there’s a lot of people who are. I know that my health insurance and what we paid out was over $110,000. That was an eight-month period. One of the injections was over $6000. That's hard to imagine. It's not just the treatment. The treatment is expensive.
Then for someone like me to go to LOCATION to live there for six weeks. You’re running through households. It is expensive. It's not anybody's fault. It’s just something you don’t consider when you’re making those decisions. Participant 94 Provide holistic care and empower the patient Think about the whole person, their whole situation. everybody's situation is different. People cope with the physical changes, trying to think of how to put it? The physical changes differently. I know some people have actually found it really quite difficult to cope with the physical changes. With other people, it's not such a big difference. I think one of the things is how people around you react to it? That's a big factor. Also your age, that makes a difference too. The difference in your age when diagnosed should be taken into account because it's very different to be diagnosed with breast cancer in your 30's than it is to be diagnosed in the 70's. It's just a very different experience. Your support services will be different and your needs will be very different. If you're trying to juggle small children and breast cancer treatment, I saw many people coming into chemo with pre-schoolers with them because they had no one to leave them with. That's really difficult with baby in a pram. Your heart just goes out to them because it's maybe one of the things that places like HOSPITAL could think about is occasional care because they do have a lot of young women coming in there. Participant 2 That it's a journey. People need different kinds of information and different kinds of support at each part of the journey but the person needs to be looked at holistically. For example, all the breast cancer, pink lady all the runs and the activities. I've never heard the message to do with all that gym stuff and everybody walking around and doing all that running, the message that that can actually help you out kind of. Helps your quality of life and help you feel better. If you hear that message it helps your quality of life and helps you feel better and maybe they don't feel confident enough to say that it can mitigate it. Seems like that would be really helpful. That holistic approach to treatment. The mixed messages making sure that different conditions are not giving you mixed messages. Participant 16 I think to do like you are doing now and talk to the people that it affects most directly rather than make these decisions, if this is actually what's happening 'cause I couldn't tell you if it was or not but rather than making decisions on their behalf. Actually get the information at the coal face. Participant 69

Section 9
Breast Cancer 2018 Australian PEEK Study
Continue funding research and support services Put money into research. You never know you when you're going to find it. Fabulous thing. They can't just stop the research. They have to continue putting money in research. Participant 24 Please more funding, for the clinics, breast care nurses, all the support services. A lot of funding does get thrown at it but it's not enough. Yes, that was what I was just thinking that the squeaky wheel gets the most attention, doesn't it? You just got to keep squeaking. Participant 27 Well, they're doing pretty good really with lots of funding, aren't they. The fact that of lot of that treatment is through the PBS, because I look at some of the price of some of those drugs. If I was going to pay full price, that would be horrendous. I suppose keep doing what you're doing because there's a lot of people out there that get affected by it. Participant 42

Section 9
Breast Cancer 2018 Australian PEEK Study
Table 9.5: Messages to decision-makers
Figure 9.14: Messages to decision-makers (% of all participants)
Messages to decision-makers All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n=30 % n=50 % n=50 %Participant's message is that treatments should be available and affordable to those who need them
54 54.00 9 45.00 13 43.33 22 44.00 32 64.00
Participant's message is to provide holistic care and empower the patient (Personalised treatment)
25 25.00 7 35.00 6 20.00 13 26.00 12 24.00
Participant's message is to continue funding for research and support services.
10 10.00 0 0.00 7 23.33 7 14.00 3 6.00
Participant's message is to provide more information about options
9 9.00 4 20.00 1 3.33 5 10.00 4 8.00
Participant's message is to support better communication between clinicians and patients
7 7.00 1 5.00 2 6.67 3 6.00 4 8.00
Messages to decision-makers All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant's message is that treatments should be available and affordable to those who need them
54 54.00 30 53.57 24 54.55 27 50.00 27 58.70
Participant's message is to provide holistic care and empower the patient (Personalised treatment)
25 25.00 13 23.21 12 27.27 16 29.63 9 19.57
Participant's message is to continue funding for research and support services.
10 10.00 5 8.93 5 11.36 5 9.26 5 10.87
Participant's message is to provide more information about options
9 9.00 6 10.71 3 6.82 4 7.41 5 10.87
Participant's message is to support better communication between clinicians and patients
7 7.00 3 5.36 4 9.09 4 7.41 3 6.52
0
10
20
30
40
50
60
Participant's message is thattreatments should be
available and affordable tothose who need them
Participant's message is toprovide hol istic care and
empower the patient(Personalized treatment)
Participant's message is tocontinue funding for research
and support services.
Participant's message is toprovide more information
about options
Participant's message is tosupport better
communication betweenclinicians and patients

Section 10
Breast Cancer 2018 Australian PEEK Study
Section 10 Advice to other patients and families
Section 10
Breast Cancer 2018 Australian PEEK Study
Section 10: Advice to other patients and families
• Participants were asked what advice they would give to other people who are newly diagnosed with breast cancer and their families. The most common advice to newly diagnosed patients was to be informed (n=29, 29.00%). This was followed by asking for help and accepting help (n=20, 20.00%), and talking to other patients (n=17, 17.00%). There were also 15 participants (15.00%) whose advice was to take things step-by-step, 14 participants (14.00%) whose advice was to have a support person to both talk to and take to appointments, 12 participants (12.00%) whose advice was to remain positive and 10 participants (10.00%) whose advice was to do what is right for you and make your own decisions.

Section 10
Breast Cancer 2018 Australian PEEK Study
Advice to others diagnosed with breast cancer
Participants were asked what advice they would give to other people who are newly diagnosed with breast cancer and their families. The most common advice to newly diagnosed patients was to be informed (n=29, 29.00%). This was followed by asking for help and accepting help (n=200, 20.00%), and talking to other patients (n=17, 17.00%). There were also 15 participants (15.00%) whose advice was to take things step-by-step, 14 participants (14.00%) whose advice was to have a support person to both talk to and take to appointments, 12 participants (12.00%) whose advice was to remain positive and 10 participants (10.00%) whose advice was to do what is right for you and make your own decisions. Be informed Run for the hills. [laughter] It's a hard one, isn't it. Gather as much information as you can from any source you can. Don't feel pressured to make decisions and don't think that because one oncologist said something that that's it. You have the right to explore other options. Participant 28 My advice would be just to get all the information you can about the journey you're about to undertake. Just in terms of I did make a very quick decision about having a double mastectomy, and I don't regret having that. I got my diagnosis and walked out 40 minutes later saying, "Yes, let's book it in two weeks time". I'm glad I did that because I did find extra tumors that didn't show up on any ultrasounds or on a mammogram. I'm just saying sit there and take time to take all the information in. I was more of the mental state that I just wanted it out. Let's get it done. Participant 41 Just try to relax. As you're going through it, maybe take a little bit more time with-- It's hard, because if you're Stage 1, you can take a bit more time with what your treatment options are, whereas when they're saying to you, "You're Stage 3 and you need to do this," you kind of don't. So, maybe it depends on-- Yes, where they're at and you would need to take a bit more time with that sort of thing. Certainly, try some of the alternative things. I found, listening to the chemotherapy nurses, they had lots of advice which was good, about you had to take your steroids, and when you would take them, and all this sort of thing. Basically, and take on a lot of that advice I suppose, because they know. Participant 52
Ask for help and accept help The best advice that was given to me that I will pass on to anyone was, if people text you, saying- or phone you or speak to you saying, "I'm here to help." Generally, they mean it. It's a very rare person that comes and says, "I'm coming around to do this." So if you need help, pick up the phone to those people and say, "Could you help me in this way?" That was said to me by a lady who has faced four breast cancer. That stuck out in my mind and every time we had a hurdle, we needed to get our dog from one place to another and someone had asked, "Can I pick you up from the airport?" I will be like, "Actually, we are sorted for that but would you mind helping me out in this way?" No one minded helping, they just gave the help I needed without me asking them. Yes, so I will pass that piece of advice on because that was the best advice they had given me. Participant 17 Absolutely, accept help. Accept all the help that, if you're offered it. A lot of people would say to me, if there's anything I can do, give me a call. At first I just thought, they are just saying that. In the end it was ... you would talk to these people and then you'd say, if you could just come to my home on Wednesday morning and vacuum the floors for me, or take the dogs for a walk or just something simple like that, that would be fantastic. And people love it because they feel like they are doing something to support you and it's organised and it does help so much. It does it makes your friends feel like they're doing something to help you. Whereas, you don't want to bother people but if I could redo my cancer, the chemo part again. I possibly will now. But the things that I would be doing differently would definitely be things like that. Can someone come and just do a lot of washing twice a week. You just can't do anything and the kids shouldn't be expected…there's only so much they can step up. They shouldn't be expected to do everything as well. Things will behind and then everyone feels shitty because the house is a mess and kids aren't getting to practice or getting to after school things. They can't have their friends over. It's just stuff like is just -- If someone said to you, if there's anything I can do to help, have a list of things in your head, whether it's drive the kids to school, pick them up twice a week. Anything like that just -- I would say to people, think of those things that's practical, take people up on their offers. Participant 43

Section 10
Breast Cancer 2018 Australian PEEK Study
I guess the biggest tips I’d give for families and friends of people affected would be to keep communicating with the person that’s ill and their family; ask what maybe would be helpful for them. I guess for someone who's going through treatment not being afraid to ask for help if you need it. I didn't ask for help, and it was horrible. People would want to help, but they don't know what to do. That would be my advice. Participant 81 Talk to other patients I think what's worked for me was finding a group to belong to. I felt very isolated at the beginning and because of that one person I knew who had breast cancer, you know I don't have anybody in my family who had just died, I was very isolated at the beginning. I was very alone and people who knew what was going on with me were super positive. "You'll be fine." "They've told you early." My friends at work and my family. You do put on that happy face and say "Yes. Yes. I'm fine. I'm fine. I'm coping well." but you're actually underneath. So finding those support people whether it's the breast care nurses or the support networks like BCNA to belong to and talk to other ladies who are going through it. I found more reassurance than some of the doctor's appointments. Participant 15 I think it's about ensuring you have the best healthcare team you can around you. So ask other people who've been treated for breast cancer who they would recommend. Get in contact with a support group, speak to other women who've had breast cancer and their families. Yeah. I think this is it, I know there are a lot of support and services out there, but even having been as connected to the support group and the metastatic breast care nurse, I know I haven't taken advantage of many of them because at times it's all just too difficult even to access the support services. It's too much of a burden mentally, thinking these things through. And so yeah. Participant 53 Join online forums, there are an endless source of information, many of which do come from well-informed sources because some of the women affected by breast cancer on those forums are themselves, medical practitioners. Ensure that you have a line of communication through a nurse to your oncologist, through a breast nurse so that you don't have to suffer from symptoms for weeks and weeks until or months even until your next appointment with your oncologist. You don't have to do that, you can call somebody and say, this isn't working for me, I'm really sick. Somebody can make decisions about that
for you and advice you and stay positive, I guess. Participant 61 Take things step-by-step I think just to break it down into manageable sizes. Even though you know you've been diagnosed and you've got your surgery and your potential two lots of treatment, you break it down. I put it into surgery and then when I did chemo, I had first three months and then in that first three months, each three weeks and then second three months each week. You just break it down into manageable bite size chunks, and you know you've got a journey and it's a journey at different stages. You don't try and compact everything into one and think about what you going to do in 12 months-time and where you going to be at. Participant 5 I do advise them to accept the help that's going to be offered. Not to be afraid to ask for help. Don't rush back to work if you don't have to. Allow your body time to heal, and it's okay to cry. Participant 55 Just keep plodding along probably would be the advice I'd give because doctors aren't infallible, they don't know everything. I'm just trying to keep things as normal as possible and do what we always do. Just a bit slower. Participant 60 Have a support person My advice would be-- Yes, trying to make a decision right there, what you are going to do, so you're not really listening to the details. You're analysing your whole circumstances and you're not paying attention to what's out there, what's going to happen. My advice would be to get someone, go with someone, be with someone else that can really be a support, has a clear head that can take all these for you and then access all that help. Whether be financial or emotional or anything, just take it all, don't think. If it's there and it's available, you actually reach out because if you don't, then it comes back to haunt you later on. Yes, that's what I've learned. Participant 21 I would just say offer to go with people to appointments, offer to go with them to their radiotherapy, and do normal things as well. While I was having my radiotherapy, I stayed...because I live 100 miles away from where the hospital is. I stayed with a friend who lives in that town where the hospital is. In a way, that was good because we could just chat, and we would just do different things. She was making a quilt. She went to work. Say doing normal things as well but just being there just having someone

Section 10
Breast Cancer 2018 Australian PEEK Study
there.It's also being on your own. I'm not on my own, but you end up spending a lot of time on your own waiting for your radiotherapy and waiting for your doctor. It's just nice to have someone there. Participant 74 I can’t really -- maybe just I kind of wish I had taken notes, or had an advocate take notes for me. Probably just wish maybe I’d... I think what the breast care nurse was thinking about doing was starting.. where
should we go to appointments with people. And having something like that, someone to take notes or that could listen when you’re not really able to. I mean my mum went but she was really overwhelmed too. But having someone that has an understanding go, that can then kind of recap to you. I took in the notebooks to write things down, but I wasn’t in any good state to be taking notes. Maybe that would be something, If I had my time again I would do. Participant 90
Table 10.1: Advice from patients
Advice to other patients All participants Stage O-I Stage II-III Stage 0-III Stage IV
n=100 % n=20 % n=30 % n=50 % n=50 %Participant's advice is to be informed (Ask questions)
29 29.00 6 30.00 7 23.33 13 26.00 16 32.00
Participant's advice is to ask for help (accept help) and be open about what they feel
20 20.00 3 15.00 6 20.00 9 18.00 11 22.00
Participant describes talking to other patients (either individually or by support group or online)
17 17.00 4 20.00 5 16.67 9 18.00 8 16.00
Participant's advice is to take things step-by-step (one thing at a time, take things slow)
15 15.00 2 10.00 0 0.00 2 4.00 13 26.00
Participant's advice is to have a support person to talk to such as family, friends (including someone who would go to appointments with them)
14 14.00 0 0.00 8 26.67 8 16.00 6 12.00
Participant's advice is to remain positive 12 12.00 5 25.00 2 6.67 7 14.00 5 10.00
Participant's advice is to do what is right for them and make their own decisions (focus on themselves)
10 10.00 1 5.00 8 26.67 9 18.00 1 2.00
Advice to other patients All participants Metropolitan Rural University High School
n=100 % n= 56 % n= 44 % n=54 % n= 46 %Participant's advice is to be informed (Ask questions)
29 29.00 19 33.93 10 22.73 16 29.63 13 28.26
Participant's advice is to ask for help (accept help) and be open about what they feel
20 20.00 7 12.50 13 29.55 10 18.52 10 21.74
Participant describes talking to other patients (either individually or by support group or online)
17 17.00 9 16.07 8 18.18 10 18.52 7 15.22
Participant's advice is to take things step-by-step (one thing at a time, take things slow)
15 15.00 9 16.07 6 13.64 10 18.52 5 10.87
Participant's advice is to have a support person to talk to such as family, friends (including someone who would go to appointments with them)
14 14.00 7 12.50 7 15.91 8 14.81 6 13.04
Participant's advice is to remain positive 12 12.00 9 16.07 3 6.82 5 9.26 7 15.22
Participant's advice is to do what is right for them and make their own decisions (focus on themselves)
10 10.00 5 8.93 5 11.36 5 9.26 5 10.87

Section 10
Breast Cancer 2018 Australian PEEK Study
Figure 10.1: Advice from patients (% of all participants)
0
5
10
15
20
25
30
35
Participant's adviceis to be informed(Ask questions)
Participant's adviceis to ask for help(accept help) and
be open aboutwhat they feel
Participantdescribes talking to
other patients(either individually
or by supportgroup or online)
Participant's adviceis to take things
step-by-step (onething at a time,
take things slow)
Participant's adviceis to have a
support person totalk to like family,friends (including
someone whowould go to
appointments withthem)
Participant's adviceis to remain
positive
Participant's adviceis to do what i s
right for them andmake their own
decisions (focus onthemselves)

Section 11
Breast Cancer 2018 Australian PEEK Study
Section 11 Discussion

Section 11
Breast Cancer 2018 Australian PEEK Study
Symptoms, risk and diagnosis The most common symptom of breast cancer among women is breast lump with other symptoms commonly reported including nipple abnormalities, breast pain and breast skin abnormalities.1 Other less common symptoms are a change in the appearance of nipples, nipple discharge, breast contour abnormalities, breast ulceration and infection or inflammation of breast.1 Breast cancer can also lead to psychological distress, lymphoedema, fatigue, estrogen deprivation, insomnia and cognitive impairments.2,3 Non-breast symptoms indicating disease include axillary pain or axillary lump, oedema of upper limbs, neck lump or other lymph node involvement .1 In this PEEK study the most common symptom leading to diagnosis was breast lumps, however a number of women were asymptomatic when diagnosed. Other symptoms that led to diagnosis included pain, breast swelling, asymmetric breasts and bruising. These symptoms are consistent with the literature, although it is important to note that there were a number of women with no symptoms whose diagnosis may have been delayed without mammography screening. Support at diagnosis was inadequate for many of the participants in this PEEK study, with two thirds not receiving the support that they needed, and notably only about a third of those with stage IV disease had received enough support at diagnosis. This lack of support coupled with an unclear diagnosis results in a significant gap in service provision for this sub-group and an area for future interventions. The risk factors associated with breast cancer include high fat diet, lack of physical exercise and alcohol consumption.4 Consumption of food with trans fatty acids can increase lipid levels in the blood, stimulate inflammation, cause vascular endothelium dysfunction, increase abdominal obesity and insulin and body weight resistance.4 The risk of breast cancer is influenced by increased intake of high glycaemic index products.4,5 As noted, the risk of breast
cancer increases with increasing alcohol consumption,4,6 however overall risk can be decreased through physical activity and this is especially relevant for women who have undergone or are undergoing menopause. 4,7 In this PEEK study the most common diagnostic pathway described was self-detecting a lump or other breast abnormality, seeking attention from a general practitioner and being referred to mammogram, ultrasound and biopsy. The next most common diagnostic pathway was through routine mammography which led to ultrasound and biopsy. Early screening can help in reducing breast cancer related mortality and deaths.4 Mammography is one such procedure which is commonly used and helps in evaluating local stage of disease and response to treatment.4,8 Ultrasonography can be used as an additional tool for diagnosis of breast cancer 4,9. Magnetic resonance imaging (MRI) is another non-invasive procedure used for diagnosis of breast cancer to provide highly accurate imaging of the lesion; the disadvantage of MRI is that is an expensive and invasive procedure 4,9. Breast self-examination is a cheap and easy procedure which woman can conduct at home 4,10,11 and helps woman to learn about basic structure of breast and detect atypical structures in mammary gland 4,12. Some modern and non-standard diagnostic procedures are high-definition digital mammography, contrast-enhanced spectral mammography, optical mammography, radio thermometry mammography and positron emission tomography.4 These methods however require more research before being integrated into diagnostic practice. 4 Treatment The aim of surgery is excision of tumour with adequate margins or greater than 1mm. If local excision of not achievable or the tumour is large, multifocal or at the choice of the patient, a mastectomy is performed13. Neo-adjuvant therapies are used to reduce tumour size and

Section 11
Breast Cancer 2018 Australian PEEK Study
breast conservation14. Pathological staging of the axilla is dependent on clinical presentation, clinically negative sentinel lymph node biopsy is usually conducted at the time of surgery14. Axillary lymph node dissection is used for clinically positive or if the sentinel lymph node is positive in clinically negative patients14. For early breast cancer, following local excision with clear margins, it is standard for five weeks treatment with whole breast radiotherapy, this may also be offered to women with DCIS15. Following mastectomy, radiotherapy may be given to the chest wall for those with high risk of recurrence (four or more involved lymph nodes, involved margins), or at intermediate risk of recurrence (one to three involved lymph nodes, grade 3 disease, oestrogen receptor negative and aged under 40)15. For locally advanced breast cancer, treatment is mastectomy followed by radiation. Adjuvant treatment is determined by pathological outcomes, the biology of the tumour including histological grade, hormone receptor status and the amplification status of the HER2 gene in addition to lymph node status14. Five year Tamoxifen treatment is standard for pre-menopausal treatment of oestrogen receptor positive causes13, and aromatase inhibitors for post-menopausal women16, women who become post-menopausal benefit from changing to aromatase inhibitors17. There is benefit in continuing hormonal therapies to ten years, those who remain pre-menopausal continue with tamoxifen17 and post-menopausal the aromatase inhibitor letrozole18. The use of bisphosphonates reduces the risk of distance recurrence in post-menopausal women19. For HER2 positive, the monoclonal antibody tzastuzumab19 is used. Combination chemotherapy for early breast cancer only gives a small improvement on survival because the curative rate of surgery and hormone therapy in this group is high20. Chemotherapy is used in hormone receptor negative disease, hormone resistant disease, HER2 positive, and rapidly progressive
disease14. For early and locally advance breast cancer with positive lymph nodes, docetaxel chemotherapy is recommended15. On progression of advanced breast cancer, a sequence of single agent and combinations are used including single agent docetaxel, single agent vinorelbine, single agent capecitabine and combination gemcitaboine and paclitaxel21. Her 2 positive have a poor prognosis, these are treated with a combination of taxane chemotherapy with the monoclonal antibody tratuzumab22, following progression with trastuzumab, the kinase inhibitor lapatinib is used in combination with capecitabine23. Trastuzumab is used in early or locally advanced disease for one year unless disease progression occurs15, and in advanced breast cancer until disease progression unless progression is restricted to the central nervous system21 The aim of treatment in advanced breast cancer is disease control, symptom palliation and improvement in survival14. Hormonal treatment is used in oestrogen receptor positive women, the type is dependent on menopausal status14. Following resistance to hormone treatment, the hormone therapy exemestane is used with an enzyme inhibitor everolimus24. Radiation is used in advanced breast cancer in patients with bone metastases and pain, and in patients with brain metastases whole brain radiotherapy with or without resection21. The types of treatments experienced by participants was recorded in PEEK study, with the most common treatments being surgery and radiation therapy, followed by Tamoxifen, Cyclophosphamide (Endoxan), Paclitaxel, Docetaxel and Letrozole (Femara). Biomarkers In Australia, immunohistochemical assays to determine oestrogen receptor (ER) and progesterone receptor (PR) status are routinely performed on invasive breast carcinomas and are often performed on ductal carcinoma in situ1. The receptor status provides prognosis information and prediction of response to

Section 11
Breast Cancer 2018 Australian PEEK Study
endocrine therapy2,3 4. HER2 (human epidermal growth factor receptor 2) status is recommended for early invasive cancers and for metastatic or recurrent disease, it is a prognostic factor and also predicts response to biological therapies5. There is a subgroup of patients for whom the benefit of chemotherapy is not known, these included tumours that are ER positive, HER2 negative and node negative6. A number of commercially available products offer multi-gene profiling assays to predict which of these patients are at high risk of recurrence and should therefore be offered chemotherapy6. A systematic review of these products indicated that of the three major profiling assays, two lacked enough clinical evidence and were not actionable in the treatment of patients6. Two other markers of interest are Ki67 and CK, these, along with ER and PR are widely available, rapid, and inexpensive and they provide prognostic information7. Ki67 is a proliferation protein, high expression correlates with a poor outcome and conversely low expression correlates with a good outcome8. The assays have poor reproducibility and there is controversy defining the threshold for high and low expression, however it may be used when the values are high or low8. CK is important in Triple negative breast cancers (those that are ER, PR and HER2 negative) have very poor outcomes, CK expression may correlate with recurrence in triple negative breast cancers9. For the participants who took part in this PEEK study, 35% had not had any discussion about biomarkers and 33% were unsure about their biomarker status, however a large proportion of these would have had the minimum receptor testing. This may indicate that there is a lack of communication of disease results between surgeon and patient, and it is a topic that the majority of the participants were interested in.
Complementary therapies The advancements in the treatment of breast cancer and improvements in survival come with ongoing side effects which need to be managed, and one area of practice that has the potential to alleviate symptoms and side effects is complementary therapies.25 The evidence to support the complete resolution of symptoms is inconclusive, however studies point to a reduction of symptoms experienced that result in few to no side effects of complementary therapies.26 Some of the main symptoms and side effects of breast cancer that have been the focus on complementary therapies include psychosocial distress, lymphoedema, insomnia, fatigue, and cognitive impairments.27 Participants commonly described fatigue as having an impact on quality of life and something that they needed to manage in their everyday life. A study by Pinto and Azumbuja (2011) suggested that the prevalence of fatigue in breast cancer survivors ranged from 25 to 99 percent and that it is commonly associated with depression, insomnia and psychological distress.28 Some of the complementary therapies that have been investigated in small studies and shown to alleviate fatigue include massage therapy,29,30, traditional chinese medicine,31,32 foot reflexology33 biofield therapies such as polarity therapy, Reiki, and therapeutic touch34,35, mind–body interventions36 and yoga.37 Despite the challenges described by participants in relation to fatigue, over a third of participants in this PEEK study described not using any complementary therapies and this was the most common theme, with massage being the most common complementary therapy used by around one fifth of participants. The evidence supporting the use of complementary therapies is limited and often inconclusive, however there is a general consensus that they have the potential to be used for symptom management in the late effects of treatment for breast cancer

Section 11
Breast Cancer 2018 Australian PEEK Study
and may be of benefit to this patient population.25 Quality of life There were a number of aspects of (Quality of Life) QoL that participants in this PEEK study identified including changes to their relationships and family dynamics, fatigue and lower energy levels, and anxiety. It is important to note that participants in this study with metastatic breast cancer had an increased level of anxiety in relation to disease progression. QoL is particularly important in relation to metastatic breast cancer patients whose QoL has been observed to be severely reduced with a negative impact on psychosocial and physical functioning, ability to work, family life and relationships.38-43 Metastatic breast cancer patients often experience anxiety and depression and psycho-social support is essential for improvement of QOL. 44 Self-management and self-care can support patients with breast cancer to manage their own care and improve quality of life45. Physical activity is considered as a universally accepted self-management technique and it has been demonstrated to have a positive effect on QoL45. Physical activity has been observed to improve symptoms related to breast cancer such as fatigue46,47, psychological problems and physical functioning47,48 and overall improvements on QoL.45 In this PEEK study, when asked what were some of the things participants needed to do to maintain their health, the main theme was to rest or take things slowly and there were very few participants that described gentle physical exercise. Physical exercise therefore presents a cost effective and simple intervention to support QoL in this population of patients. This however is just one, simple intervention to support patients in managing their QoL and as treatment for metastatic cancer in particular, moves towards prolonging survival, it must also include alleviation of symptoms and improvements in QoL.38 This will need to include comprehensive care support systems,
acknowledging both physical and psycho-social support needs such as patient navigation which is a tool that has been observed to eliminate barriers to treatment and help breast cancer patients in obtaining better quality care and QoL.49 Health professional communication/decision-making Treatment decision making in oncology requires a balance between efficacy and toxicity in order to maintain QoL. Women with breast cancer have an identifiable role to play in taking part in decision making, however there is often an imbalance between health providers and patients in shared decision-making process and it has been reported not all women wish to be actively involved in shared decision making. 50 When making decisions about treatment, participants in this PEEK study most commonly considered long term survival and outcomes followed by considerations about demonstrated effectiveness and outcomes when making decisions, and the decision-making proves was often shared between family, close friends and their treating clinician. Shared decision making can be supported by patient decision aids which help provide personalised treatment options to women with breast cancer, enhance their knowledge of disease and boost their confidence regarding the decision they make.51 There is a particular need to support patients with metastatic breast cancer as their prognosis is known to be poorer and differences in treatment expectations between patients and clinicians have been reported.52 Some of the contributing factors in treatment expectations include previous experience with side effects, having young children, younger age and their level of education. 52

Section 11
Breast Cancer 2018 Australian PEEK Study
Information and Education There are various factors that influence access to health information, information preferences, and uptake of information for patients with breast cancer including level of education, age, prior knowledge, clinical complications, and comorbidities.53 In a study by Tucker et al. (2017) it was observed that, compared to woman with early stage breast cancer, women with metastatic breast cancer preferred information through telephone education sessions or scientific conferences. Additionally, the most accessed materials were government websites, scientific publications and printed patient materials.54 In this PEEK study, participants had a preference for talking to someone in relation to information provision, and this was followed by a preference for written or online information combined with talking to someone. Consistent with the literature, participants with metastatic breast cancer described a preference for telephone information more frequently than other sub-groups which may be due to their increased information needs and lack of certainty in relation to prognosis. An exploratory qualitative study observed that the cancer patients have a desire to receive more information in relation to their specific condition, in a more detailed manner. 60 This was also identified in this PEEK study as an area for improvement in relation to information provision. Support and psychosocial care The majority of care and support for participants in this PEEK study came from family and friends and this was followed by care and support from specialist breast nurses and general practitioners, and overall, the participants in this PEEK study, received very good care, navigation and care coordination. However, participants with metastatic breast cancer received poorer care coordination and communication. There are number of interventions present to help patients suffering from psychological
distress including include Cognitive and Behavioural Cancer Stress Management interventions (improves depressive symptoms, anxiety, self-efficacy, fatigue, social functioning, perceived social support, and benefit finding)55,56, Supportive-Expressive Therapy (improves in depressive symptoms, hopelessness and helplessness, trauma symptoms)57,58 and Meaning-Centered Psychotherapy (Improves quality of life, depressive symptoms, and hopelessness).59 A systematic review conducted in 2016 by Youl et al. assessed the psychosocial impact on breast cancer patients based on residential status and indigenous status. The information needs among women from rural areas was found to be different, specifically the existence of perceived stigma regarding accessing mental health information which presented a barrier to accessing information.61 Other barriers faced by women in rural areas were lack of access to supportive care, lack of information available regarding psychosocial impact and lesser access to treatment options.61 The medical team was reported to be the primary source of professional support for women from both metropolitan and rural areas and a lack of community-based programs in rural areas was also identified as an area of concern 61. In this PEEK study, participants in rural areas received poorer care coordination and communication and this may be an area for future investigation and intervention. Summary: Characterisation of the study population The most common symptom leading to diagnosis in this patient population was breast lumps, however a number of women were asymptomatic when diagnosed. The most common diagnostic pathway described was self-detecting a lump or other breast abnormality, seeking attention from a general practitioner and being referred to mammogram, ultrasound and biopsy and it is important to note that the number of women with no symptoms whose diagnosis may have been delayed without

Section 11
Breast Cancer 2018 Australian PEEK Study
mammography screening. Support at diagnosis was inadequate for many of the participants in this patient population with two thirds not receiving the support that they needed, and notably only about a third of those with stage IV disease had received enough support at diagnosis. In addition, 35% of all participants had not had any discussion about biomarkers and 33% were unsure about their biomarker status. The types of treatments experienced by this patient population were most commonly surgery and radiation therapy, followed by Tamoxifen, Cyclophosphamide (Endoxan), Paclitaxel, Docetaxel and Letrozole (Femara). Challenges described by participants in relation to side effects of treatment included fatigue and lower energy levels, while changes to their relationships and family dynamics and anxiety had a significant impact on QoL. It is important to note that participants in this study with metastatic breast cancer had an increased level of anxiety in relation to disease progression. Participants in this patient population most commonly considered long term survival and outcomes followed by considerations about demonstrated effectiveness and outcomes when making decisions, and the decision-making proves was often shared between family, close friends and their treating clinician. Their information preference was to talk to someone and this was particularly relevant for patients with metastatic breast cancer. The majority of care and support for participants in this patient population study came from family and friends and this was followed by care and support from specialist breast nurses and general practitioners, and overall, patients received very good care, navigation and care coordination. However, participants with metastatic breast cancer and those in rural areas received poorer care coordination and communication.
References
1. Koo MM, Von Wagner C, Abel GA, McPhail S, Rubin GP, Lyratzopoulos G. Typical and atypical presenting symptoms of breast cancer and their associations with diagnostic intervals: Evidence from a national audit of cancer diagnosis. Cancer epidemiology 2017; 48: 140. 2. Henneghan AM, Harrison T. Complementary and Alternative Medicine Therapies as Symptom Management Strategies for the Late Effects of Breast Cancer Treatment. Journal of Holistic Nursing 2015; 33(1): 84-97. 3. Pinto AC, de Azambuja E. Improving quality of life after breast cancer: Dealing with symptoms. Maturitas 2011; 70(4): 343-8. 4. Kolak A, Kamińska M, Sygit K, et al. Primary and secondary prevention of breast cancer. Annals of agricultural and environmental medicine : AAEM 2017; 24(4): 549. 5. Research. WCRFAIfC. Food, nutrition, physical activity and the prevention of cancer: a global perspective. Washington, DC, 2007. 6. Cao Y, Willett WC, Rimm EB, Stampfer MJ, Giovannucci EL. Light to moderate intake of alcohol, drinking patterns, and risk of cancer: Results from two prospective US cohort studies. BMJ (Online) 2015; 351: <xocs:firstpage xmlns:xocs=""/>. 7. Neilson HK, Conroy SM, Friedenreich CM. The Influence of Energetic Factors on Biomarkers of Postmenopausal Breast Cancer Risk. Current nutrition reports 2014; 3: 22. 8. Luczynska E, Heinze-Paluchowska S, Hendrick E, et al. Comparison between Breast MRI and Contrast-Enhanced Spectral Mammography. Med Sci Monitor 2015; 21: 1358-67. 9. Mehnati P, Tirtash MJ. Comparative Efficacy of Four Imaging Instruments for Breast Cancer Screening. Asian Pacific journal of cancer prevention : APJCP 2015; 16(15): 6177. 10. Akhtari-Zavare M, Latiff LA, Juni MH, Said SM, Ismail IZ. Knowledge of female undergraduate students on breast cancer and breast self-examination in Klang Valley, Malaysia. Asian Pacific Journal of Cancer Prevention 2015; 16(15): 6231-5.

Section 11
Breast Cancer 2018 Australian PEEK Study
11. Godavarty A, Rodriguez S, Jung YJ, Gonzalez S. Optical imaging for breast cancer prescreening. Breast Cancer: Targets and Therapy 2015; 7: 193-209. 12. Akhtari-Zavare M, Juni MH, Md Said S, Ismail IZ. Beliefs and behavior of Malaysia undergraduate female students in a public university toward breast self-examination practice. Asian Pacific Journal of Cancer Prevention 2013; 14(1): 57-61. 13. Moran MS, Schnitt SJ, Giuliano AE, et al. Society of Surgical Oncology-American Society for Radiation Oncology consensus guideline on margins for breast-conserving surgery with whole-breast irradiation in stages I and II invasive breast cancer. J Clin Oncol 2014; 32(14): 1507-15. 14. Yeo B, Turner NC, Jones A. An update on the medical management of breast cancer. BMJ 2014; 348: g3608. 15. NICE. Early and locally advanced breast cancer: diagnosis and treatment. Clinical Guidance CG80 2009. 16. Dowsett M, Cuzick J, Ingle J, et al. Meta-analysis of breast cancer outcomes in adjuvant trials of aromatase inhibitors versus tamoxifen. J Clin Oncol 2010; 28(3): 509-18. 17. Davies C, Pan H, Godwin J, et al. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial. Lancet 2013; 381(9869): 805-16. 18. Goss PE, Ingle JN, Martino S, et al. Randomized trial of letrozole following tamoxifen as extended adjuvant therapy in receptor-positive breast cancer: updated findings from NCIC CTG MA.17. J Natl Cancer Inst 2005; 97(17): 1262-71. 19. Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med 2005; 353(16): 1659-72. 20. Early Breast Cancer Trialists' Collaborative G, Clarke M, Coates AS, et al. Adjuvant chemotherapy in oestrogen-receptor-poor breast cancer: patient-level meta-analysis
of randomised trials. Lancet 2008; 371(9606): 29-40. 21. NICE. Advanced breast cancer: diagnosis and treatment 2009. 22. Slamon DJ, Leyland-Jones B, Shak S, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med 2001; 344(11): 783-92. 23. Geyer CE, Forster J, Lindquist D, et al. Lapatinib plus capecitabine for HER2-positive advanced breast cancer. N Engl J Med 2006; 355(26): 2733-43. 24. Baselga J, Campone M, Piccart M, et al. Everolimus in postmenopausal hormone-receptor-positive advanced breast cancer. N Engl J Med 2012; 366(6): 520-9. 25. Henneghan A, Harrison T. Complementary and Alternative Medicine Therapies as Symptom Management Strategies for the Late Effects of Breast Cancer Treatment. Journal of Holistic Nursing 2015; Volume 33 Number 1(March): 84–97. 26. Greenlee H, Balneaves L, Carlson L, et al. Clinical Practice Guidelines on the Use of Integrative Therapies as Supportive Care in Patients Treated for Breast Cancer. J Natl Cancer Inst Monogr 2014; Nov; 2014(50): 346–58. 27. Wanchai A, Armer J, Stewart B. Complementary and alternative medicine use among women with breast cancer: a systematic review. Clin J Oncol Nurs 2010 Aug;14(4):E45-55. doi: 10.1188/10.CJON.E45-E55. 28. Pinto A, de Azambuja E. Improving quality of life after breast cancer: Dealing with symptoms. . Maturitas 2011 I; (70, 343-348. doi:10.1016/j.maturitas.2011.09.008). 29. Russell NC, Sumler S-S, Beinhorn CM, Frenkel MA. Role of massage therapy in cancer care. Journal of Alternative and Complementary Medicine 2008; 14, 209-214. doi:10.1089/acm.2007.7176. 30. Fernandez-Lao C, Cantarero-Villanueva I, Diaz-Rodriguez L, Cuesta-Vargas AI, Fernandez-Delas-Penas C, Arroyo-Morales M. Attitudes towards massage modify effects of manual therapy in breast cancer survivors: A randomised clinical trial with crossover design.

Section 11
Breast Cancer 2018 Australian PEEK Study
European Journal of Cancer Care (2012). ; 21: 233-41. 31. Lee EJ, Frazier SK. The efficacy of acupressure for symptom management: A systematic review. Journal of Pain and Symptom Management 2011; 42, 589-603. 32. Qi F, Li A, Inagaki Y, et al. Chinese herbal medicines as adjuvant treatment during chemo- or radio-therapy for cancer. BioScience Trends 2010; 4: 297-307. 33. Lee J, Han M, Chung Y, Kim J, Choi J. Effects of foot reflexology on fatigue, sleep and pain: A systematic review and meta-analysis. . Journal of Korean Academy of Nursing 2011; 41, 821-833. 34. Mustian KM, Roscoe JA, Palesh OG, et al. Polarity therapy for cancer-related fatigue in patients with breast cancer receiving radiation therapy: A randomized controlled pilot study. . Integrative Cancer Therapies 2011; 10(1): 27-37. 35. Tsang KL, Carlson LE, Olson K. Pilot crossover trial of Reiki versus rest for treating cancerrelated fatigue. . Integrative Cancer Therapies, 2007; 6, 25-35. 36. Kwekkeboom KL, Cherwin CH, Lee JW, Wanta B. Mind-body treatments for the pain-fatigue-sleep disturbance symptom cluster in persons with cancer. Journal of Pain and Symptom Management 2010; 39: 126-38. 37. Cramer H, Lange S, Klose P, Paul A, Dobos G. Can yoga improve fatigue in breast cancer patients? A systematic review. Acta Oncologica 2012; 51: 559-60. 38. Kriegel S, Myers J, Befort C. Cancer changes everything!’.Exploring the lived experiences of women with metastatic breast cancer. Int J Palliat Nurs 2014(20): 334–42. 39. Reed E, Simmonds P, Haviland J. Quality of life and experience of care in women with metastatic breast cancer: a cross-sectional survey. . J Pain Symptom Manage 2012; 43: 747–58. 40. Irvin W, Muss H, Mayer D. Symptom management in metastatic breast cancer. . Oncologist 2011; 16: 1203–14. 41. Sarenmalm E, Thoren-Jonsson A, Gaston-Johansson F. Making sense of living under the shadow of death:
adjusting to a recurrent breast cancer illness. Qual Health Res 2009; 19: 1116–30. 42. Willis K, Lewis S, Ng F. The experience of living with metastatic breast cancer-a review of the literature. . Health Care Women Int 2014; 36: 514–42. 43. Vilhauer R. A qualitative study of the experiences of women with metastatic breast cancer. . Palliat Support Care 2008; 6: 249–58. 44. Lee Mortensen G, Madsen IB, Krogsgaard R, Ejlertsen B. Quality of life and care needs in women with estrogen positive metastatic breast cancer: a qualitative study. Acta oncologica (Stockholm, Sweden) 2017: 1. 45. Van Dijck S, Nelissen P, Verbelen H, Tjalma W, Gebruers N. The effects of physical self-management on quality of life in breast cancer patients: A systematic review. The Breast 2016; 28: 20-8. 46. Heim M, v d Malsburg M, Niklas A. Randomized controlled trial of a structured training program in breast cancer patients with tumor related chronic fatigue. . Onkologie 2007; 30:429e34. 47. Mock V, Pickett M, Ropka M, Muscari LE, Stewart K, Rhodes V. Fatigue and quality of life outcomes of exercise during cancer treatment. Cancer Pract 2001; 9:119e27. 48. Wang Y, Boehmke M, Wu Y, Dickerson S, Fisher N. Effects of a 6-week walking program on Taiwanese women newly diagnosed with early-stage breast cancer. . Cancer Nurs 2011; 34:E1e13. 49. Baik SH, Gallo LC, Wells KJ. Patient navigation in breast cancer treatment and survivorship: A systematic review. Journal of Clinical Oncology 2016; 34(30): 3686-96. 50. Mahmoodi N, Sargeant S. Shared decision-making - Rhetoric and reality: Women's experiences and perceptions of adjuvant treatment decision-making for breast cancer. Journal of health psychology 2017: 1359105316689141. 51. Savelberg W, van Der Weijden T, Boersma L, Smidt M, Willekens C, Moser A. Developing a patient decision aid for the treatment of women with early stage breast cancer: the struggle between simplicity and

Section 11
Breast Cancer 2018 Australian PEEK Study
complexity. BMC medical informatics and decision making 2017; 17(1): 112. 52. Lux MP, Bayer CM, Loehberg CR, et al. Shared decision-making in metastatic breast cancer: Discrepancy between the expected prolongation of life and treatment efficacy between patients and physicians, and influencing factors. Breast Cancer Research and Treatment 2013; 139(2): 429-40. 53. Martinez K, Kurian A, Hawley S, Jagsi R. How can we best respect patient autonomy in breast cancer treatment decisions? Breast Cancer Manag 2015; 4(1): 53–64. 54. Tucker C, Martin P, Jones R. Health information needs, source preferences and engagement behaviours of women with metastatic breast cancer across the care continuum: protocol for a scoping review. BMJ Open 2017; 7(2): e013619. 55. Matthews H, Grunfeld E, Turner A. The efficacy of interventions to improve psychosocial outcomes following surgical treatment for breast cancer: a systematic review and meta-analysis. . Psycho-Oncology 2017; 26(5): 593e607. 56. Jassim G. Psychological interventions for women with non-metastatic breast cancer. . Cochrane Database Syst Rev 2015; (5):CD008729. 57. Kissane D. Supportive-expressive group therapy for women with metastatic breast cancer: survival and psychosocial outcome from a randomized controlled trial. . Psycho-Oncology 20007; 16(4): 277e86. 58. Spiegel D. Effects of supportive-expressive group therapy on survival of patients with metastatic breast cancer. . Cancer 30e8 2007; 110((5):11). 59. Breitbart W. Meaning-centered group psychotherapy: an effective intervention for improving psychological well-being in patients with advanced cancer. . J Clin Oncol 2015; 33(7): 749e54. 60. Muntlin Athlin Å, Browall M, Wengström Y, Conroy T, Kitson AL. Descriptions of Fundamental Care needs in cancer care - an exploratory study. Journal of clinical nursing 2018.
61. Youl PH, Dasgupta P, Youlden D, et al. A systematic review of inequalities in psychosocial outcomes for women with breast cancer according to residential location and Indigenous status in Australia. Psycho-Oncology 2016: 1157-67.

Section 12
Breast Cancer 2018 Australian PEEK Study
Section 12 Next steps

Section 12
Breast Cancer 2018 Australian PEEK Study
Next steps At the end of each PEEK study, CCDR identifies three key areas that, if improved, would significantly increase the quality of life and/or the ability for individuals to better manage their own health. In relation to the breast cancer community, these three areas are:
• Information that is more specific to the various sub-types of breast cancer and supports education in relation to biomarkers and their relevance to treatment
• Interventions to address the gaps in care coordination and communication for metastatic breast cancer patients and patients in rural areas
• Interventions that reduce the impact of pain and fatigue of patients with breast cancer
2018 breast cancer metrics
Data collected in this PEEK study also provides a basis on which future interventions and public health initiatives can be based. Some of the 2018 breast cancer metrics that the sector can work together to improve upon are provided in Table 12.1 Table 12.1: Breast cancer 2018 Metrics Area of evaluation 2018 data Baseline health Physical functioning Role limitations die to physical health Role limitations due to emotional problems Energy/fatigue Emotional well-being Social functioning Pain General health Health change
Mean 65.00 37.50 59.67 39.85* 64.20 63.88 56.48 45.50 57.00
Median 70.00 25.00 100.00 40.00 60.00 68.75 57.50 45.00 50.00
Percentage of participants that have accessed My Health Record 8.00% Percentage of participants that have a discussion about biomarkers/genetic tests
65.00%
Knowledge of condition and treatments (Partners in Health) Knowledge Adherence to treatment Management of symptoms Coping Total score
Mean 26.26 19.49 19.90 15.05 75.70
Median 27.00 15.00 21.00 15.00 80.00
Care Coordination and care received Communication Navigation Care coordination Care received Care coordination - Total score
Mean 41.09 26.10* 6.82 7.80 67.10
Median 27.00 26.00 8.00 9.00 68.00
Fear of progression Total Score
Mean 34.99
Median 36.00
*Normal distribution, use mean as measure of central tendency