Breast Cancer and Lactation History in Mexican Women
10
American Journal of Epidemiology Copyright © 1996 by The Johns Hopkins University School of Hygiene and Public Health All rights reserved Vol. 143, No. 6 Printed in U.S.A. Breast Cancer and Lactation History in Mexican Women Isabelle Romieu, 1 Mauricio Hernandez-Avila, 2 Eduardo Lazcano, 2 Lizbeth Lopez, 2 and Ricardo Romero-Jaime 3 The authors conducted a case-control study in Mexico City between September 1990 and December 1992 to determine whether a dose-response relation could be observed between duration of lactation and the risk of breast cancer. Cases, women aged 20-75 years, were identified through six hospitals in Mexico City (n = 349) and were interviewed to obtain data on risk factors for breast cancer, including a detailed history of lactation. Controls (n = 1,005) were selected from the general population using the Mexican national sampling frame. Parous women who had ever lactated had a reduction in breast cancer risk (age-adjusted odds ratio (OR) = 0.39, 95% confidence interval (Cl) 0.25-0.62). A small decreasing trend of breast cancer risk in relation to duration of lactation (p < 0.001) was observed. Compared with parous women who had never breast-fed, women who had breast-fed for 12-24 months had an age-adjusted odds ratio of 0.47 (95% Cl 0.27-0.83). A stronger protective effect was observed with lactation duration for the first live birth among pre- and postmenopausal women (for 4-12 months of lactation, OR = 0.56 (95 percent Cl 0.32-0.96) and OR = 0.48 (95 percent Cl 0.29-0.81) in pre- and postmenopausal women, respectively). Adjusting for potentially con- founding factors modified these results only slightly. The declining trend in fertility and lactation among Mexican women could lead to a major epidemic of breast cancer such as that observed in Western countries. Am J Epidemiol 1996;143:543-52. breast feeding; breast neoplasms; lactation Results from recent case-control studies suggest a significant protective effect of prolonged lactation on breast cancer that is independent of parity, essentially among premenopausal women (1-12). Two cohort studies (13, 14) and various case-control studies (15- 20) have failed to find such an inverse association. However, these studies were largely confined to post- menopausal women, and most failed to examine the effect of total duration of lactation (3, 11) or included few women with prolonged lactation. Until recently, prolonged lactation has been the norm among Mexican women. However, to date there are no data on the potential impacts of such a practice on breast cancer incidence. Therefore, as part of an ongoing multicenter case-control study, we examined Received for publication June 29,1994, and in final form June 30, 1995. Abbreviations: Cl, confidence interval; OR, odds ratio; SES, socioeconomic status. 1 Centra Pan-Americano de Ecologia Humana y Salud, Organiza- cion Pan-Americana de la Salud, Metepec, Mexico State, Mexico. 2 Centra de Investigaciones en Salud Publica, Instituto Nacional de Salud Publica, Cuernavaca, Morelos, Mexico. 3 Instituto Mexicano del Seguro Social, Mexico City, Distrito Fed- eral, Mexico. Reprint requests to Dr. Mauricio Hernandez-Avila, Instituto Na- cional de Salud Publica, Av. Universidad 655, Col. Santa Maria Ahuacatitlan, C.P. 62508 Cuernavaca, Morelos, Mexico. the relation between breast cancer and lactation his- tory, as well as whether a dose-response relation be- tween lactation duration and breast cancer could be observed in a population of women among whom prolonged lactation is highly prevalent. MATERIALS AND METHODS Cases We conducted a case-control study of breast cancer, diet, and different reproductive factors in Mexico City between September 1990 and December 1992. Newly incident cases of breast cancer were identified among women younger than 75 years of age who had been residents of the metropolitan area of Mexico City for at least 2 years. Cases were identified from six hospi- tals belonging to the two major health providers in Mexico City: the Social Security system, which pro- vides health care to the formally employed and their families, and the Ministry of Health hospitals, which provide health care to the population that is not in the formal sector or that is unemployed. Cases from the private sector were not included, because the hospital participation rate was low. The hospitals that partici- pated in our study provided medical care to 80 percent of cases reported to the Mexico City Tumor Registry. 543 by guest on September 5, 2016 http://aje.oxfordjournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Breast Cancer and Lactation History in Mexican Women

American Journal of EpidemiologyCopyright © 1996 by The Johns Hopkins University School of Hygiene and Public HealthAll rights reserved
Vol. 143, No. 6Printed in U.S.A.
Breast Cancer and Lactation History in Mexican Women
Isabelle Romieu,1 Mauricio Hernandez-Avila,2 Eduardo Lazcano,2 Lizbeth Lopez,2 andRicardo Romero-Jaime3
The authors conducted a case-control study in Mexico City between September 1990 and December 1992to determine whether a dose-response relation could be observed between duration of lactation and the riskof breast cancer. Cases, women aged 20-75 years, were identified through six hospitals in Mexico City (n =349) and were interviewed to obtain data on risk factors for breast cancer, including a detailed history oflactation. Controls (n = 1,005) were selected from the general population using the Mexican national samplingframe. Parous women who had ever lactated had a reduction in breast cancer risk (age-adjusted odds ratio(OR) = 0.39, 95% confidence interval (Cl) 0.25-0.62). A small decreasing trend of breast cancer risk in relationto duration of lactation (p < 0.001) was observed. Compared with parous women who had never breast-fed,women who had breast-fed for 12-24 months had an age-adjusted odds ratio of 0.47 (95% Cl 0.27-0.83). Astronger protective effect was observed with lactation duration for the first live birth among pre- andpostmenopausal women (for 4-12 months of lactation, OR = 0.56 (95 percent Cl 0.32-0.96) and OR = 0.48(95 percent Cl 0.29-0.81) in pre- and postmenopausal women, respectively). Adjusting for potentially con-founding factors modified these results only slightly. The declining trend in fertility and lactation amongMexican women could lead to a major epidemic of breast cancer such as that observed in Western countries.Am J Epidemiol 1996;143:543-52.
breast feeding; breast neoplasms; lactation
Results from recent case-control studies suggest asignificant protective effect of prolonged lactation onbreast cancer that is independent of parity, essentiallyamong premenopausal women (1-12). Two cohortstudies (13, 14) and various case-control studies (15-20) have failed to find such an inverse association.However, these studies were largely confined to post-menopausal women, and most failed to examine theeffect of total duration of lactation (3, 11) or includedfew women with prolonged lactation.
Until recently, prolonged lactation has been thenorm among Mexican women. However, to date thereare no data on the potential impacts of such a practiceon breast cancer incidence. Therefore, as part of anongoing multicenter case-control study, we examined
Received for publication June 29,1994, and in final form June 30,1995.
Abbreviations: Cl, confidence interval; OR, odds ratio; SES,socioeconomic status.
1 Centra Pan-Americano de Ecologia Humana y Salud, Organiza-cion Pan-Americana de la Salud, Metepec, Mexico State, Mexico.
2 Centra de Investigaciones en Salud Publica, Instituto Nacionalde Salud Publica, Cuernavaca, Morelos, Mexico.
3 Instituto Mexicano del Seguro Social, Mexico City, Distrito Fed-eral, Mexico.
Reprint requests to Dr. Mauricio Hernandez-Avila, Instituto Na-cional de Salud Publica, Av. Universidad 655, Col. Santa MariaAhuacatitlan, C.P. 62508 Cuernavaca, Morelos, Mexico.
the relation between breast cancer and lactation his-tory, as well as whether a dose-response relation be-tween lactation duration and breast cancer could beobserved in a population of women among whomprolonged lactation is highly prevalent.
MATERIALS AND METHODS
Cases
We conducted a case-control study of breast cancer,diet, and different reproductive factors in Mexico Citybetween September 1990 and December 1992. Newlyincident cases of breast cancer were identified amongwomen younger than 75 years of age who had beenresidents of the metropolitan area of Mexico City forat least 2 years. Cases were identified from six hospi-tals belonging to the two major health providers inMexico City: the Social Security system, which pro-vides health care to the formally employed and theirfamilies, and the Ministry of Health hospitals, whichprovide health care to the population that is not in theformal sector or that is unemployed. Cases from theprivate sector were not included, because the hospitalparticipation rate was low. The hospitals that partici-pated in our study provided medical care to 80 percentof cases reported to the Mexico City Tumor Registry.
543
by guest on September 5, 2016
http://aje.oxfordjournals.org/D
ownloaded from
544 Romieu et al.
Cases were selected among women attending thegynecologic clinic of the hospital for biopsy of a breastlump. A total of 506 women agreed to participate andcompleted an interview. All women for whom thebiopsy confirmed the diagnosis of breast cancer wereincluded as cases in the study (« = 349). The partic-ipation rate among the cases was 95 percent.
Controls
Controls were an age-stratified random sample ofresidents of the Mexico City metropolitan area, iden-tified from 3,694 households randomly selected fromthe National Household Sampling Frame (21). Theselected households were visited by interviewers, whoobtained a listing of women living there. Women aged25-80 years who had been residents of the MexicoCity area for at least 2 years were considered eligiblecontrols. Limited numbers for each age group wereestablished a priori to match the age distribution ofcancer cases. Of the households visited, there was noeligible control in 28.4 percent, and the eligible controlrefused to be interviewed in 14.6 percent. Only oneeligible control per household was included in thestudy.
Interviewers administered a questionnaire that askedabout sociodemographic variables, potential risk fac-tors for breast cancer (including lifestyle habits), andreproductive and gynecologic history; also includedwas a food frequency questionnaire. Information onlactation history included duration of lactation for eachlive birth, identification of breastfeeding as bilateral orunilateral, and reason for having breast-fed unilater-ally. Cases referred for a breast problem were inter-viewed at the hospital before the breast cancer diag-nosis to avoid influencing their responses to thequestionnaire due to knowledge of their disease. Infact, 40 percent (n = 151) of the women interviewedas potential cases were diagnosed as having a benignbreast disease. Controls were interviewed in theirhomes.
Analysis
The SAS (22) and Stata (23) systems were used fordatabase management and statistical analysis. Univa-riate statistics were calculated for all variables. Vari-ables measured on a continuous scale were explored interms of their original distribution as well as in cate-gories.
Analyses were performed for all women and for pre-and postmenopausal women separately. Informationon type of menopause (natural or surgical) was ob-tained by questionnaire. Natural menopause was de-
fined as 12 consecutive months of amenorrhea withoutan obvious cause.
The effect of lactation on the risk of breast cancerwas studied, examining the effect of ever having lac-tated, total duration of lactation, and duration of lac-tation for the first and second liveborn children. Anindex of socioeconomic status (SES) was developed assuggested by Bronfman et al. (24) by combining fivevariables (number of persons living in the house, num-ber of rooms in the house (excluding the kitchen andbathroom), availability of drinking water, sanitaryconditions, and education of the head of the family).
Odds ratios and 95 percent confidence intervalswere obtained from logistic regression models to eval-uate the association between breast cancer and lacta-tion and other potential risk factors, including age (in5-year groups), SES (low, medium, or high), age atmenarche (^11, 12, 13, 14, 15, or >16 years), age atfirst full-term pregnancy (<19, 20-29, or >30 years),parity (0, 1-2, 3-4, or S5), menopausal status (yes/no), and family history of breast cancer (yes/no). Mul-tivariate logistic regression was used to control forpotentially confounding factors (25). Testing for lineartrend in logit risks with increasing exposure was car-ried out using the likelihood ratio test under the as-sumption of a linear relation (25). To test for theexistence of a trend associated with duration of lacta-tion, we included a dichotomous variable for everhaving lactated and a continuous variable for durationof lactation (0, 1-3, 4-12, 13-24, 25-36, 37-60, or^61 months) simultaneously in logistic regressionmodels.
RESULTS
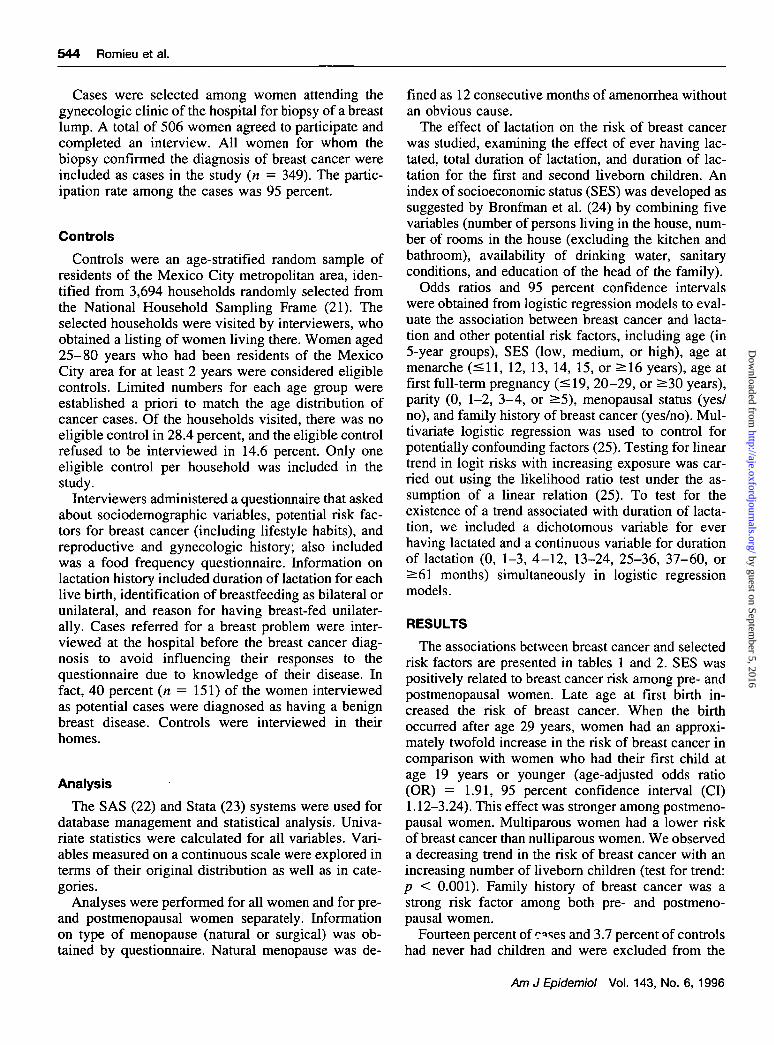
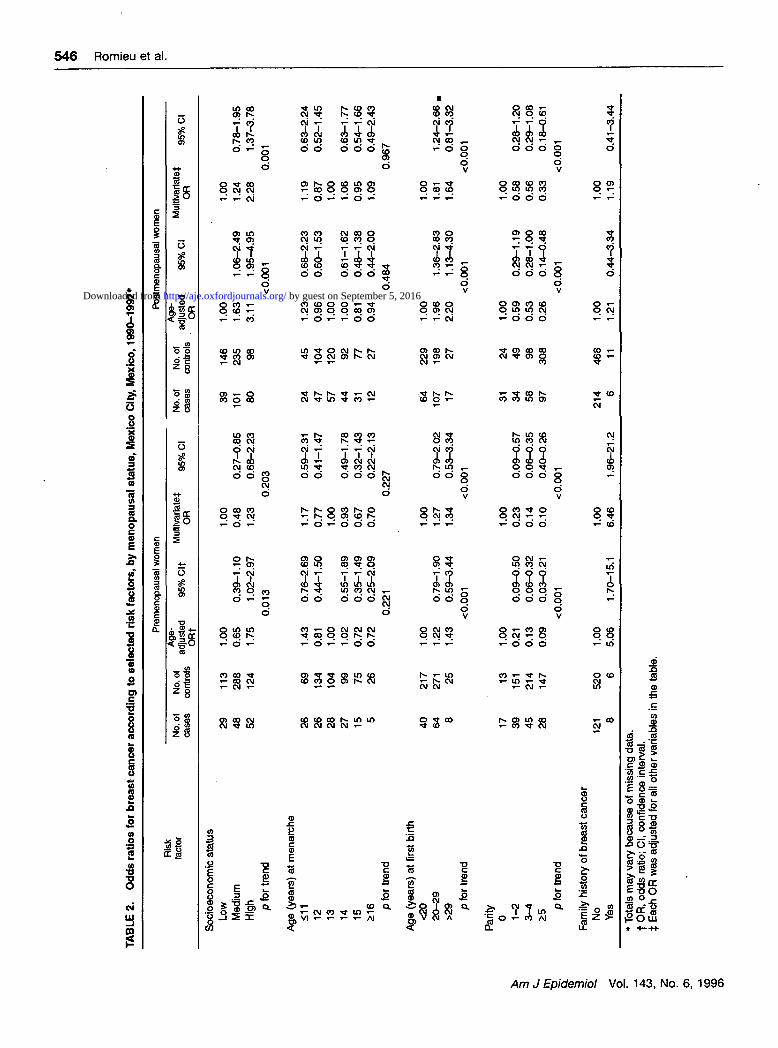
The associations between breast cancer and selectedrisk factors are presented in tables 1 and 2. SES waspositively related to breast cancer risk among pre- andpostmenopausal women. Late age at first birth in-creased the risk of breast cancer. When the birthoccurred after age 29 years, women had an approxi-mately twofold increase in the risk of breast cancer incomparison with women who had their first child atage 19 years or younger (age-adjusted odds ratio(OR) = 1.91, 95 percent confidence interval (CI)1.12-3.24). This effect was stronger among postmeno-pausal women. Multiparous women had a lower riskof breast cancer than nulliparous women. We observeda decreasing trend in the risk of breast cancer with anincreasing number of liveborn children (test for trend:p < 0.001). Family history of breast cancer was astrong risk factor among both pre- and postmeno-pausal women.
Fourteen percent of c<>ses and 3.7 percent of controlshad never had children and were excluded from the
Am J Epidemiol Vol. 143, No. 6, 1996
by guest on September 5, 2016
http://aje.oxfordjournals.org/D
ownloaded from
Breast Cancer and Lactation History 545
TABLE 1. Odds ratios for breast cancer according to selected1990-1992*
Riskfactor
Socioeconomic statusLowMedium.High
p for trend
Age (years) at menarche<1112131415>16
p for trend
Age (years) at first birth<2020-29>29
p for trend
Parity01-23- 1£5
p for trend
Menopausal statusNoYes
Family history of breast cancerNoYes
No. ofcases
68149132
507383714517
10417125
4873
103125
129220
33514
No. ofcontrols
259523223
11423822419215153
44646952
37200312455
526479
98817
risk factors, Mexico City
Age-adjusted 95% Clf
ORt
1.001.152.48
1.380.891.001.020.780.87
1.001.641.91
1.000.410.330.20
1.000.86
1.002.38
0.82-1.601.74-3.52
<0.001
0.90-2.120.61-1.30
0.70-1.490.51-1.190.47-1.60
0.193
1.24-2.171.12-3.24
< 0.001
0.24-0.700.20-0.550.12-0.32
<0.001
0.57-1.31
1.14-4.93
, Mexico,
Multivariate* g 5 % c |
1.000.891.84
1.250.821.001.020.820.93
1.001.571.58
1.000.410.360.25
1.000.99
1.002.42
0.63-1.271.26-2.70
0.001
0.80-1.980.55-1.22
0.68-1.530.53-1.280.48-1.77
0.387
1.17-2.110.90-2.75
< 0.005
0.24-0.720.21-0.600.15-0.41
<0.001
0.63-1.55
1.13-5.17
* Totals may vary because of missing data.t OR, odds ratio; Cl, confidence interval.$ Each OR was adjusted for all other variables in the table.
analysis of the relation between breast cancer andlactation. Among parous women who had been diag-nosed with breast cancer, 37 percent were premeno-pausal (n = 112) and 63 percent were postmenopausal(n = 189).
Parous women who had ever lactated had a breastcancer risk of 0.47 (95 percent CI 0.30-0.73) com-pared with parous women who had never lactated.Adjusting by age, the protective effect of lactationincreased slightly (OR = 0.39, 95 percent CI 0.25-0.62).,This effect was present among both premeno-pausal women (age-adjusted OR = 0.48,95 percent CI0.26-0.89) and postmenopausal women (age-adjustedOR = 0.29, 95 percent CI 0.14-0.59) (tables 3 and 4).
Duration of lactation, even short-term, was alsoassociated with a reduction in breast cancer risk.
Women who had breast-fed for up to 3 months had anage-adjusted odds ratio of 0.48 (95 percent CI 0.23-0.96) compared with parous women who had neverbreast-fed. Women who had breast-fed for 37-60months had an age-adjusted odds ratio of 0.27 (95percent CI 0.15-0.49), and women who breast-fed formore than 60 months had an odds ratio of 0.23 (95percent CI 0.13-0.39). After adjustment for SES, par-ity, age at first full-term pregnancy, family history ofbreast cancer, and menopausal status, results remainedsimilar; we also observed a significant decreasingtrend in the risk of breast cancer associated with totalduration of lactation (test for trend: p < 0.0005) (table3). This protective effect was more evident for post-menopausal women. Among premenopausal women, along duration of lactation did not substantially modify
Am J Epidemiol Vol. 143, No. 6, 1996
by guest on September 5, 2016
http://aje.oxfordjournals.org/D
ownloaded from
TA
BL
E 2
. O
dd
s r
ati
os
fo
r b
rea
st
can
cer
acco
rdin
g t
o s
ele
cte
d r
isk
fa
cto
rs, b
y m
en
op
au
sai
sta
tus
, M
exic
o C
ity,
Mexic
o,
19
90
-19
92
*
Ris
k(a
ctor
Pre
men
opau
sal
wom
enP
ostm
enop
ausa
l w
omen
No.
of
case
sN
o. o
fco
ntro
ls
Age
-ad
just
edO
Rt
95%
Clt
Mul
ttvar
iate
fO
R95
% C
lN
o. o
fca
ses
No.
of
cont
rols
Age
-ad
just
edO
R95
% C
lM
ultlv
aria
tef
OR
95%
Cl
6' w o co CO
Soci
oeco
nom
ic s
tatu
s
Low
Mediu
m
Hig
h p f
or
trend
Age
(ye
ars
) a
t m
enarc
he
511
12 13 14 15 £1
6 p f
or
trend
Age
(ye
ars
) at
first
birth
<20
20
-29
>29 p f
or
tre
nd
Parit
y0 1
-2 p f
or
trend
Fam
ily h
isto
ry o
f bre
ast
ca
nce
rN
oY
es
29 48 52 26 26 28 27 15 5 40 64 8 17 39 45 28 121 8
113
288
124
69 134
10499 75 26 217
271 25 13 151
214
147
520 6
1.00
0.65
1.75
1.43
0.81
1.00
1.02
0.72
0.72
1.00
1.22
1.43
1.00
0.21
0.13
0.09
1.00
5.06
0.39-1.10
1.02-2.97
0.013
0.76-2.69
0.44-1.50
0.55-1.89
0.35-1.49
0.25-2.09
0.221
0.79-1.90
0.59-3.44
<0.001
0.09-0.50
0.06-0.32
0.03-0.21
<0.001
1.70-15.1
1.00
0.48
1.23
1.17
0.77
1.00
0.93
0.67
0.70
1.00
1.27
1.34
1.00
0.23
0.14
0.10
1.00
6.46
0.27-0.85
0.68-2.23
0.203 0.59-2.31
0.41-1.47
0.49-1.78
0.32-1.43
0.22-2.13
0.227 0.79-2.02
0.53-3.34
<0.001
0.09-0.57
0.06-0.35
0.40-0.26
<0.001
1.96-21.2
39 101 80 24 47 57 44 31 12 64
107 17 31 34 58 97
214 6
146
23598 45 104
12092 77 27 229
198
27 24 49 98 308
468 11
1.00
1.63
3.11
1.23
0.96
1.00
1.00
0.81
0.94
1.00
1.96
2.20
1.00
0.59
0.53
0.26
1.00
1.21
1.06-2.49
1.95-4.95
< 0.001 0.68-2.23
0.60-1.53
0.61-1.62
0.48-1.38
0.44-2.00
0.484
1.36-2.83
1.13^.30
<0.001
0.29-1.19
0.28-1.00
0.14-0.48
<0.001
0.44-3.34
1.00
1.24
2.28
1.19
0.87
1.00
1.06
0.95
1.09
1.00
1.81
1.64
1.00
0.58
0.56
0.33
1.00
1.19
0.78-1.95
1.37-3.78
0.001 0.63-2.24
0.52-1.45
0.63-1.77
0.54-1.66
0.49-2.43
0.967 1.24-2.66
0.81-3.32
<0.001
0.28-1.20
0.29-1.08
0.18-0.61
<0.001
0.41-3.44
* T
ota
ls m
ay
vary
beca
use
of
mis
sing
da
ta.
t O
R,
od
ds
ratio
; C
l, c
onfid
ence
in
terv
al.
i E
ach
OR
was
ad
just
ed
for
all
oth
er
variable
s in
the
table
.
by guest on September 5, 2016http://aje.oxfordjournals.org/Downloaded from

Breast Cancer and Lactation History 547
TABLE 3. Odds ratios for breast cancer according to lactation experience, Mexico City,1990-1992*
Riskfactor
Ever lactatedNoYes
Total duration of lactation (months)01-34-1213-2425-3637-60>60
p for trend
No. of children breastfed01-23-4>4
p for trend
Duration of lactation with first livebirth (months)
01-34-12>12
p for trend
Duration of lactation with secondlive birth (months)
01-34-12>12
p for trend
No. ofcases
36265
36165942393475
367680
108
6656
14039
9043
10043
No. ofcontrols
58905
5867
17013288
141307
58231256399
133189430215
257123351167
Age-adjusted
ORf
1.000.39
1.000.480.590.470.600.270.23
1.000.550.450.28
1.000.700.530.24
1.001.090.670.53
95% Clf
0.25-0.62
0.23-0.960.34-1.000.27-0.830.33-1.080.15-0.490.13-0.39
<0.001
0.33-0.920.27-0.750.17-0.46
<0.001
0.45-1.080.37-0.770.15-0.39
< 0.001
0.71-1.680.48-0.940.34-0.82
< 0.001
Mexico,
Muttivariate* „ „ r |OR 9 5 / ° C I
1.000.54
1.000.470.610.520.720.330.31
1.000.570.520.39
1.000.680.620.28
1.001.000.750.65
0.33-0.89
0.23-0.950.35-1.050.29-0.920.39-1.320.18-0.620.16-0.57
<0.001
0.34-0.960.31-0.870.21-0.70
< 0.001
0.43-1.060.42-0.910.17-0.47
< 0.001
0.64-1.560.53-1.080.41-1.04
0.069
* Totals may vary because of missing data. No parous cases or controls were excluded from the analyses ofthe relation between breast cancer and lactation.
t OR, odds ratio; Cl, confidence interval.t Adjusted for age, socioeconomic status, family history of breast cancer, menopausal status, age at first
birth, and parity.
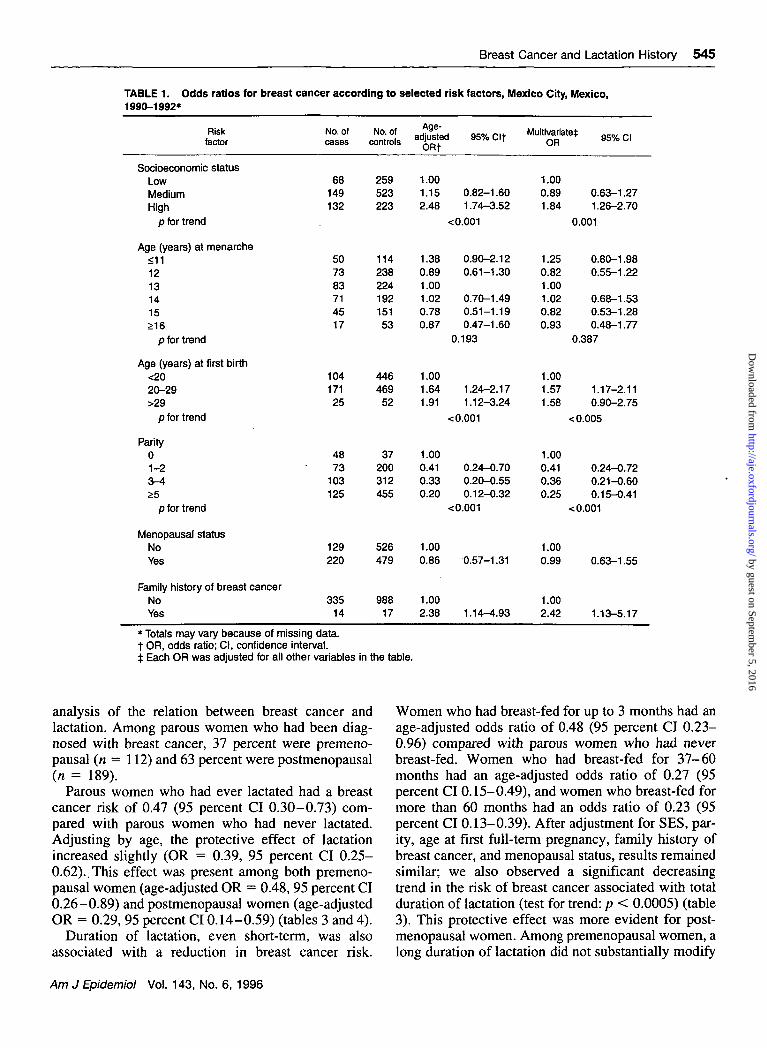
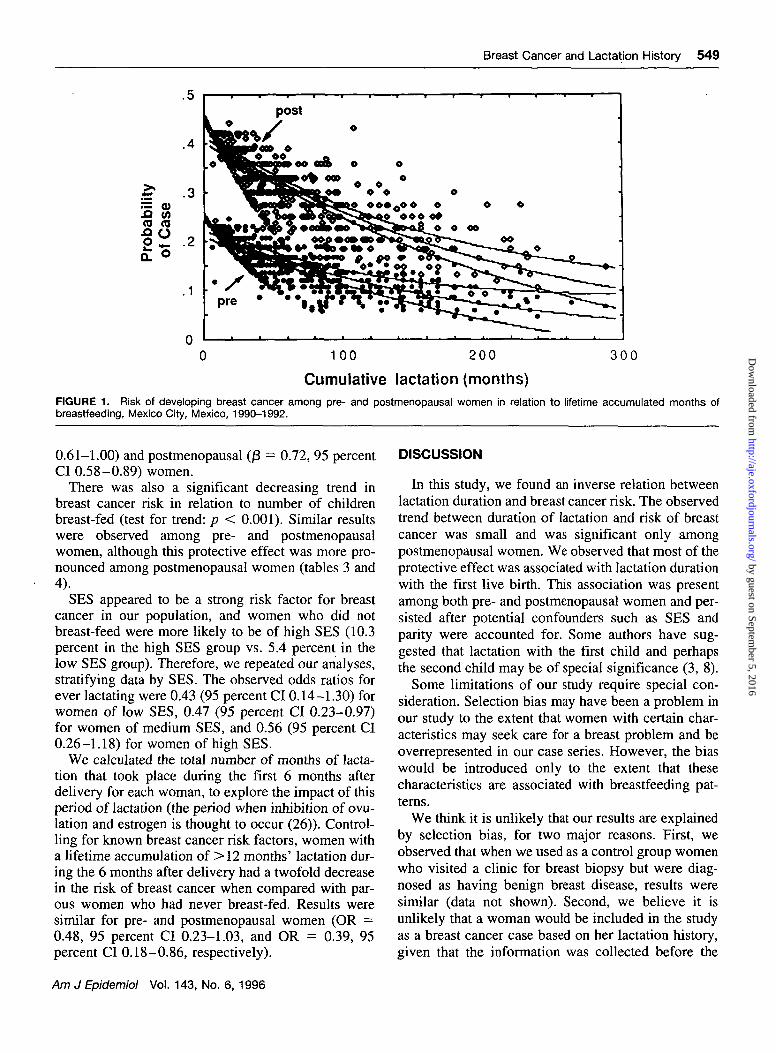
the results obtained for lactation up to 3 months induration (table 4, figure 1).
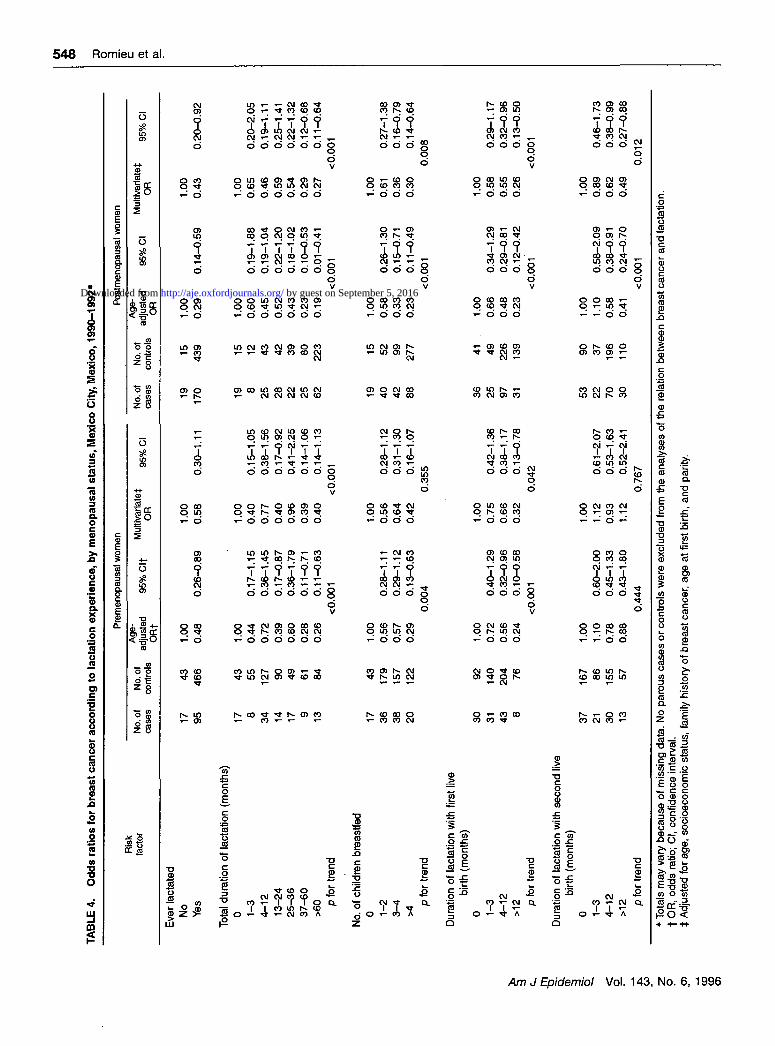
Long-term lactation was protective against breastcancer when lactation with the first live birth wasexamined. Women who had breast-fed their first childfor 4-12 months had an age-adjusted breast cancerrisk of 0.53 (95 percent CI 0.37-0.77). We observed asignificant decreasing trend in the risk of breast cancerwith increasing duration of lactation among pre- andpostmenopausal women (tests for trend: p < 0.001 andp < 0.001, respectively). Results remained similarafter adjustment for potentially confounding factors.Duration of lactation with the second liveborn childappeared to have a smaller impact on risk and was
significant only among postmenopausal women (ta-bles 3 and 4).
We conducted additional analysis to determine theimpact of lactation duration in months after accountingfor whether a woman had ever breast-fed. We ob-served a decreasing trend in breast cancer risk withadditional lactation time (/3 = 0.89, 95 percent CI0.79-0.99) that was significant among postmeno-pausal women (|3 = 0.85, 95 percent CI 0.74-0.98).When lactation duration with the first child was con-sidered, we observed a strong protective effect ofadditional lactation time (j3 = 0.74, 95 percent CI0.62-0.87) for all women. This effect was observedseparately for premenopausal (/3 = 0.79, 95 percent CI
Am J Epidemiol Vol. 143, No. 6, 1996
by guest on September 5, 2016
http://aje.oxfordjournals.org/D
ownloaded from
•s!
CD g- < O 143 z p 6,1996
TAB
LE 4
. O
dd
s ra
tio
s fo
r b
reas
t ca
nce
r ac
cord
ing
to
lact
atio
n e
xper
ien
ce, b
y r
Ris
kfa
cto
r
Eve
r la
ctat
edN
oY
es
Tota
l dur
atio
n of
lact
atio
n (m
onth
s)0 1
-34
-12
13-2
425-3
637-6
0>
60 p
for
tren
d
No.
of c
hild
ren
brea
stfe
d0 1
-23
-4>4
p fo
r tr
end
Dur
atio
n of
lact
atio
n w
ith f
irst
live
birt
h (m
onth
s)0 1
-34-1
2>
12 p
for t
rend
Dur
atio
n of
lact
atio
n w
ith s
econ
d liv
ebi
rth
(mon
ths)
0 1-3
4-12
>1
2 p fo
r tre
nd
No
. of
ca
se
s
17 95 17 8 34 14 17 9 13 17 36
38
20 30
31 43 8 37 21 30 13
No
. of
con
tro
ls
43
466 43 55 1
27
90 49
61 84 43
179
157
122
92
140
20
47
6
167
86
155
57
nen
op
ausa
l sta
tus,
Mex
ico
City
, Mex
ico
, 199
0-19
92*
Pre
men
opau
sal
wom
en
Age
-ad
just
ecO
Rt
1.00
0.4
8
1.00
0.44
0.72
0.39
0.80
0.28
0.26
1.00
0.56
0.57
0.29
1.00
0.72
0.56
0.24
1.00
1.10
0.78
0.88
i 95
% C
lt
0.26
-0.8
9
0.17
-1.1
50.
36-1
.45
0.17
-0.8
70.
36-1
.79
0.11
-0.7
10.
11-0
.63
<0.0
01 0.28
-1.1
10.
29-1
.12
0.13
-0.6
30.
004 0.40
-1.2
90.
32-0
.96
0.10
-0.5
8<0
.001 0.
60-2
.00
0.45
-1.3
30.
43-1
.80
0.44
4
Mul
tivar
iate
t 95
% C
l
1.00
0.5
8
1.00
0.40
0.77
0.40
0.96
0.39
0.40
1.00
0.56
0.64
0.42
1.00
0.75
0.66
0.32
1.00
1.12
0.93
1.12
* T
otal
s m
ay v
ary
beca
use
of
mis
sing
dat
a. N
o p
arou
s ca
ses
or c
ontr
ols
wer
e ex
clud
ed fr
omt
OR
, od
ds r
atio
; Cl,
conf
iden
ce in
terv
aI.
| A
djus
ted
for a
ge, s
ocio
econ
omic
sta
tus,
fam
ily
0.30
-1.1
1
0.15
-1.0
50.
38-1
.56
0.17
-0.9
20.
41-2
.25
0.14
-1.0
60.
14-1
.13
<0.0
01 0.28
-1.1
20.
31-1
.30
0.16
-1.0
70.
355 0.
42-1
.36
0.38
-1.1
70.
13-0
.78
0.04
2 0.61
-2.0
70.
53-1
.63
0.52
-2.4
10.
767
No.
of
case
s
19 170 19 8 25 28 22 25
62 19 40
42
88 36
25
97
31 53 22
70
30
No.
of
cont
rols
154
39 15 12 43 42
39
80
22
3 15 52
99
277 41 49
22
613
9
90
37
196
11
0
Pos
tmen
opau
sal w
omen
Age
-ad
just
edO
R
1.00
0.2
9
1.00
0.6
00
.45
0.5
20
.43
0.2
30
.19
1.00
0.5
80
.33
0.2
3
1.00
0.6
60
.48
0.2
3
1.00
1.10
0.5
80
.41
95%
Cl
'
0.14
-0.5
9
0.19
-1.8
80.
19-1
.04
0.22
-1.2
00.
18-1
.02
0.10
-0.5
30.
01-0
.41
< 0
.001 0.26
-1.3
00.
15-0
.71
0.11
-0.4
9<
0.00
1
0.3
4-1
.29
0.2
9-0
.81
0.1
2-0
.42
< 0
.00
1
0.5
8-2
.09
0.3
8-0
.91
0.2
4-0
.70
< 0.
001
Mul
tivar
iat
OR
1.00
0.43
1.00
0.65
0.46
0.59
0.54
0.29
0.27
1.00
0.61
0.36
0.30
1.00
0.58
0.55
0.26
1.00
0.89
0.62
0.49
i the
ana
lyse
s of
the
rela
tion
betw
een
brea
st c
ance
r an
d la
ctat
ion.
hist
ory
of b
reas
t can
cer,
age
at f
irst
birt
h, a
nd
par
ity.
0.20
-0.9
2
0.20
-2.0
50
.19
-1.1
10.
25-1
.41
0.22
-1.3
20.
12-0
.68
0.11
-0.6
4<0
.001 0.
27-1
.38
0.16
-0.7
90.
14-0
.64
0.00
8 0.29
-1.1
70.
32-0
.96
0.13
-0.5
0<0
.001 0.
46-1
.73
0.38
-0.9
90.
27-0
.88
0.01
2
by guest on September 5, 2016http://aje.oxfordjournals.org/Downloaded from
Breast Cancer and Lactation History 549
.5
.4
J? .3(0 (0
5O n
.1
L ©
tot
* /pre
post
© •© _»
!§&•»»»«
K^MAIMMI
B3FSKS
• ••••?
•©
• ©
1©^S*•»
©
o ©© •©©•o«©• ,AA A©
»*"»|£;- * ? •
©©
$ © ©aSj©^^ .^£^»,©©V»^_
•» ©
0©
% X * ^ A . ©
* ^ —© © • ! r11 u>. '
100 200
Cumulative lactation (months)
3 0 0
FIGURE 1. Risk of developing breast cancer among pre- and postmenopausal women in relation to lifetime accumulated months ofbreastfeeding, Mexico City, Mexico, 1990-1992.
0.61-1.00) and postmenopausal (jECI 0.58-0.89) women.
There was also a significant decreasing trend inbreast cancer risk in relation to number of childrenbreast-fed (test for trend: p < 0.001). Similar resultswere observed among pre- and postmenopausalwomen, although this protective effect was more pro-nounced among postmenopausal women (tables 3 and4).
SES appeared to be a strong risk factor for breastcancer in our population, and women who did notbreast-feed were more likely to be of high SES (10.3percent in the high SES group vs. 5.4 percent in thelow SES group). Therefore, we repeated our analyses,stratifying data by SES. The observed odds ratios forever lactating were 0.43 (95 percent CI 0.14-1.30) forwomen of low SES, 0.47 (95 percent CI 0.23-0.97)for women of medium SES, and 0.56 (95 percent CI0.26-1.18) for women of high SES.
We calculated the total number of months of lacta-tion that took place during the first 6 months afterdelivery for each woman, to explore the impact of thisperiod of lactation (the period when inhibition of ovu-lation and estrogen is thought to occur (26)). Control-ling for known breast cancer risk factors, women witha lifetime accumulation of >12 months' lactation dur-ing the 6 months after delivery had a twofold decreasein the risk of breast cancer when compared with par-ous women who had never breast-fed. Results weresimilar for pre- and postmenopausal women (OR =0.48, 95 percent CI 0.23-1.03, and OR - 0.39, 95percent CI 0.18-0.86, respectively).
0.72, 95 percent DISCUSSION
In this study, we found an inverse relation betweenlactation duration and breast cancer risk. The observedtrend between duration of lactation and risk of breastcancer was small and was significant only amongpostmenopausal women. We observed that most of theprotective effect was associated with lactation durationwith the first live birth. This association was presentamong both pre- and postmenopausal women and per-sisted after potential confounders such as SES andparity were accounted for. Some authors have sug-gested that lactation with the first child and perhapsthe second child may be of special significance (3, 8).
Some limitations of our study require special con-sideration. Selection bias may have been a problem inour study to the extent that women with certain char-acteristics may seek care for a breast problem and beoverrepresented in our case series. However, the biaswould be introduced only to the extent that thesecharacteristics are associated with breastfeeding pat-terns.
We think it is unlikely that our results are explainedby selection bias, for two major reasons. First, weobserved that when we used as a control group womenwho visited a clinic for breast biopsy but were diag-nosed as having benign breast disease, results weresimilar (data not shown). Second, we believe it isunlikely that a woman would be included in the studyas a breast cancer case based on her lactation history,given that the information was collected before the
Am J Epidemiol Vol. 143, No. 6, 1996
by guest on September 5, 2016
http://aje.oxfordjournals.org/D
ownloaded from
550 Romieu et al.
diagnosis of breast cancer and the interviewers werenot aware of the hypothesis being tested.
SES could act as a confounder or an effect modifierin that it was associated with risk of breast cancer,frequency of breastfeeding, and parity. However, ourresults were affected little when we stratified womenaccording to their socioeconomic level.
Because cases were interviewed at the clinics andcontrols in their homes, differences may have beenintroduced in responses by participants. However, theobservation that results were similar when hospitalcontrols were analyzed suggests that this source ofbias is unlikely as an explanation for our findings. Ifthis bias did occur, lactation histories would probablybe more complete among breast cancer cases, leadingto underestimation of the real protective effect oflactation.
Our results are concordant with those of recentstudies that have reported a protective effect of lacta-tion on breast cancer risk (1-12). Some previous stud-ies found a protective effect among parous womenregardless of menopausal status (1, 7-9), whereas oth-ers found this effect in premenopausal women only (2,10-12). In these studies, a significant dose-responseeffect was observed, although the minimal durationnecessary to achieve a significant reduction in riskvaried considerably (11). Earlier case-control studies(15-18) and two recent cohort studies (13, 14) did notfind a protective effect of lactation. It has been sug-gested that failure to examine the relation betweenlactation and breast cancer risk according to meno-pausal status, as well as potential misclassification ofdata on lactation history, may explain discordant find-ings between studies (11).
In our study, a large number of women had breast-fed for an extended period (mean = 46 months, stan-dard deviation 54 months), which resulted in highpower for studying a dose-response effect of lactationon breast cancer risk. We observed a significant pro-tective effect for as few as 3 months of lactation and amajor protective effect after 36 or more months oflactation.
However, among premenopausal women, we didnot observe a significant decreasing trend in breastcancer risk in relation to total duration of lactation,although we did observe a strong protective effectwhen lactation duration with the first child was con-sidered. Several factors may explain this. First, in ourpopulation, parity and duration of lactation werestrongly correlated (r = 0.71), and therefore the spe-cific effects of these factors on breast cancer risk weredifficult to disentangle. Duration of lactation with thefirst child was less correlated with parity (r = 0.37),and its effect could be more accurately determined.
Second, the timing of lactation with the first child maybe more important, because during the first pregnancyand lactation, the mammary cells undergo maturation,which may be protective against the carcinogenic pro-cess. In our population, women were more likely tolactate at an early age (mean = 21 years, standarddeviation 5 years). It has been suggested that this is aprotective factor which could act due to both thetiming of exposure and the latency effect (12).
Newcomb et al. (11) reported that no association ofrisk and lactation duration was observed for womenwho had lactated less than 10 years before diagnosis.This could partly explain the strong protective trendobserved among premenopausal women in relation tolactation duration with the first child, given the rela-tively young age of the premenopausal breast cancercases in our population (median age, 39 years). How-ever, because data were sparse, we could not fullyexplore the modifying effect of age at first lactation.
Different hypotheses may explain the protective ef-fect of lactation. Direct action on the pituitary gland oron ovarian activity would change the woman's post-partum hormonal status, which would reduce estrogenlevels through suppression of ovulation. As a result,total cumulative exposure to estrogen would be re-duced, which could inhibit initiation or growth ofbreast cancer (3, 27). The strong protective effect onbreast cancer risk that we observed using cumulativemonths of lactation in the early postpartum period (^6months) tends to support this hypothesis.
Another hypothesis to explain the protective effectof lactation is that it may "flush out" carcinogens (3).Experimental studies that have evaluated the inductionof breast tumors in mice have documented more tu-mors in nipple-excised breasts than in normal breasts.The obstruction of the nipple resulted in prolongedexposure to carcinogens (28-30), whereas on thesuckled side, the carcinogen was excreted in the milk.Some authors have also observed that exogenouschemicals are secreted into the breast ducts of non-lactating women, suggesting that normal physiologicsecretory activity may result in exposure of breastepithelium to ingested or inhaled environmental car-cinogens (31). Furthermore, comparisons of patientswho had breast-fed unilaterally with patients who hadbreast-fed from both breasts indicate a significant in-creased risk of cancer in the unsuckled breast (32).
Because breastfeeding is highly prevalent in Mex-ico, the reason for not breastfeeding could be associ-ated with an underlying risk factor for breast cancer.Byers et al. (2) have suggested that successful lacta-tion could be seen as an indicator of a normally bal-anced endocrine system, and unsuccessful lactation,conversely, as a correlate of an underlying hormonal
Am J Epidemiol Vol. 143, No. 6, 1996
by guest on September 5, 2016
http://aje.oxfordjournals.org/D
ownloaded from

Breast Cancer and Lactation History 551
imbalance that might cause increased subsequent riskof breast cancer. However, even if parous women whohad not breast-fed had an underlying risk of breastcancer, this would not explain the dose-response rela-tion that was observed between duration of lactationand breast cancer.
During the interview, we did not collect informationon the use of hormones to suppress lactation andreasons for not breastfeeding. However, in Mexico,hormonal treatments to suppress lactation are seldomused, and lactation is promoted throughout the publichealth sector. Published articles on studies conductedin Mexico mention that the most frequent reasons fornot breastfeeding reported by mothers are: a percep-tion of insufficient milk, a lack of confidence, a lack ofknowledge regarding the nutritional value of maternalmilk, rejection by the infant, a lack of postpartumbreastfeeding guidance, the practice of providing arti-ficial milk to new mothers in some health institutions,and health problems of the mother or the child (33).
Lactation appears to play an important role in pro-tecting women from breast cancer. Because of changesin women's lifestyles, lactation is decreasing in Mex-ico, and young women tend not to breast-feed or toshorten the duration of lactation (34). In associationwith the strong decline in the fertility rate, this de-creasing trend in lactation may be responsible for theincreasing incidence of breast cancer observed in theMexican population. Although a better understandingof the physiologic changes that occur during lactationis necessary to determine the main mechanism bywhich lactation may protect women from breast can-cer, breastfeeding is certainly a cost-effective inter-vention that should be promoted to protect the healthof both mother and infant.
ACKNOWLEDGMENTS
This work was supported by funding from the AmericanInstitute for Cancer Research (United States), the HealthMinistry of Mexico, the Pan-American Health Organiza-tion, and the Division of Environmental Health and InjuryControl, Centers for Disease Control and Prevention, At-lanta, Georgia.
REFERENCES
1. Lubin JH, Burns PE, Blot WJ, et al. Risk factors for breastcancer in women from North Alberta, Canada, as related toage at diagnosis. J Natl Cancer Inst 1982;68:211-17.
2. Byers T, Graham S, Rzepka T, et al. Lactation and breastcancer: evidence for a negative association in premenopausalwomen. Am J Epidemiol 1985;121:664-74.
3. McTiernan A, Thomas DB. Evidence for a protective effect oflactation on risk of breast cancer in younger women: results
from a case-control study. Am J Epidemiol 1986; 124:353-8.4. Katsouyanni K, Trichopoulos D, Boyle P, et al. Diet and
breast cancer: a case-control study in Greece. Int J Cancer1986;38:815-20.
5. Rosero-Bixby L, Oberle MW, Lee NC. Reproductive historyand breast cancer in a population of high fertility, Costa Rica,1984-85. Int J Cancer 1987;40:747-54.
6. Tao SC, Yu MC, Ross RK, et al. Risk factors for breast cancerin Chinese women of Beijing. Int J Cancer 1988;42:495-8.
7. Yuan JM, Yu MC, Ross RK, et al. Risk factors for breastcancer in Chinese women of Shanghai. Cancer Res 1988;48:1949-53.
8. Siskind V, Schofield F, Rice D, et al. Breast cancer andbreastfeeding: results from an Australian case-control study.Am J Epidemiol 1989;130:229-36.
9. Layde PM, Webster LA, Baughman AL, et al. The indepen-dent association of parity, age at first full term pregnancy, andduration of breast feeding with the risk of breast cancer. J ClinEpidemiol 1989;42:963-73.
10. Yoo K-Y, Tajima K, Kuroishi T, et al. Independent protectiveeffect of lactation against breast cancer: a case-control study inJapan. Am J Epidemiol 1992;135:726-33.
11. Newcomb PA, Storer BE, Longnecker MP, et al. Cancer of thebreast in relation to lactation history. N Engl J Med 1994;330:81-7.
12. Yang CP, Weiss NS, Band PR, et al. History of lactation andbreast cancer risk. Am J Epidemiol 1993;138:1050-6.
13. Kvale G, Heuch I. Lactation and cancer risk: Is there a relationspecific to breast cancer? J Epidemiol Community Health1987;42:30-7.
14. London SJ, Colditz GA, Stampfer MJ, et al. Lactation and riskof breast cancer in a cohort of US women. Am J Epidemiol1990;132:17-26.
15. MacMahon B, Lin TM, Lowe CR, et al. Lactation and cancerof the breast: a summary of an international study. Bull WorldHealth Organ 1970;42:185-94.
16. Kalache A, Vessey MP, McPherson K. Lactation and breastcancer. Br Med J 1980,280:223-4.
17. MacMahon B, Purde M, Cramer D, et al. Association of breastcancer risk with age at first and subsequent births: a study inthe population of the Estonian Republic. J Natl Cancer Inst1982;69:1035-8.
18. Brinton LA, Hoover R, Fraumeni JF. Reproductive factors inthe aetiology of breast cancer. Br J Cancer 1983;69:1035-8.
19. Duffy SW, Roberts MM, Elton RA. Risk factors for breastcancer: relevance to screening. J Epidemiol CommunityHealth 1983;37:127-31.
20. Brignone G, Cusimano R, Dardanoni G, et al. A case-controlstudy on breast cancer risk factors in a Southern Europeanpopulation. Int J Epidemiol 1987;16:356-61.
21. Gutierrez G, Sepulveda J, Tapia R, et al. Encuesta NacionalSeroepidemioldgica. I. Diseno conceptual y metodologia. (InSpanish). Salud Publica de Mexico 1988;30:836-52.
22. SAS Institute, Inc. SAS procedures guide. Release 6.03 ed.Cary, NC: SAS Institute, Inc, 1988.
23. Stata Corporation. 1993 Stata reference manual. Release 3.1,6th ed. College Station, TX: Stata Corporation, 1993.
24. Bronfman M, Guiscafre H, Castro V, et al. Estrategias paramejorar los patrones terapeuticos utilizados en diarrea agudaen unidades de atencion medica primaria. II. Medicion de ladesigualdad: una estrategia metodologica, analisis de las car-acteristicas socioeconomicas de la muestra. (In Spanish). ArchInvest Med (Mex) 1988; 19:351-60.
25. Breslow NE, Day NE. Statistical methods in cancer research.Vol 1. The analysis of case-control studies. Lyon, France:International Agency for Research on Cancer, 1980. (IARCscientific publication no. 32).
26. Gray HG, Campbell OM, Apelo R, et al. Risk of ovulationduring lactation. Lancet 1990;l:25-9.
27. Henderson BE, Ross RK, Pike MC, et al. Endogenous hor-mones as a major factor of human cancer. Cancer Res 1982;42:3232-9.
Am J Epidemiol Vol. 143, No. 6, 1996
by guest on September 5, 2016
http://aje.oxfordjournals.org/D
ownloaded from

552 Romieu et al.
28. Kelsey JL, Berkowitz GS. Breast cancer epidemiology. Can-cer Res 1988;48:5615-23.
29. Marchant J. Chemical induction of breast tumors in mice ofthe C57BI strain: the influence of pseudo-pregnancy, preg- 32.nancy and lactation on induction by methylcholanthrene. Br JCancer 1961;15:568-73. 33.
30. Brancifion C, Bonser GM, Cashera F. Chemically inducedmammary tumours following unilateral excision of the nipplesin pseudo-pregnant and lactating breeding BALB/c mice. Br J 34.Cancer 1962,16:232-7.
31. Petrakis NL, Mason L, Lee R, et al. Association of race, age,
menopausal status and cerumen type with breast fluid secre-tion in nonlactating women, as determined by nipple aspira-tion. J Natl Cancer Inst 1975;54:829-34.Ing R, Ho JHC, Petrakis NL. Unilateral breast-feeding andbreast cancer. Lancet 1977;2:124-7.Ysunza A. El abandono de la lactancia materna en Mexico. HSu causalidad. (In Spanish). La Rev Invest Clin (Mex) Suppl1986;38:97-102.Ysunza A. El abandono de la lactancia matema en Mexico. I.Tendencias recientes. (In Spanish). La Rev Invest Clin (Mex)Suppl 1986;38:41-6.
Am J Epidemiol Vol. 143, No. 6, 1996
by guest on September 5, 2016
http://aje.oxfordjournals.org/D
ownloaded from