
Lactation MYTHBUSTERS!
109
Lactation MYTHBUSTERS! Katrina B. Mitchell, MD, IBCLC, PMH-C Breast Surgical Oncologist Lactation Consultant Perinatal Mental Health Provider Ridley Tree Cancer Center at Sansum Clinic Santa Barbara, CA
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Lactation MYTHBUSTERS!

Lactation MYTHBUSTERS!
Katrina B. Mitchell, MD, IBCLC, PMH-CBreast Surgical Oncologist
Lactation ConsultantPerinatal Mental Health Provider
Ridley Tree Cancer Center at Sansum Clinic
Santa Barbara, CA

No Disclosures

The great enemy of truth is very often not the lie -- deliberate, contrived, and dishonest – but the myth – persistent, persuasive, and unrealistic.
Too often we hold fast to the cliches of our forebears.-JFK, 1962
(Intro to James McKenna ‘Safe Infant Sleep’)

Massage

Why Do People Massage?
• People perceive localized prominent breast tissue and believe they can squeeze out milk like a tube of toothpaste
• Misunderstanding of breast anatomy and physiology
• In reality, ducts are innumerable and microscopic and interlacing, like fine lace or cobwebs
• When you massage, you just increase inflammatory fluid surrounding the ducts, cause capillary injury, and cause narrowing of ducts

fat (white)
fibrous tissue(pink)
Lobule with Central Duct
PLEASE DO NOT MASSAGE ME!

Larger ductsSmaller ducts feed into larger ducts
PLEASE DO NOT MASSAGE ME!

#ILCA2021
Another Look at What You’re Massaging

What Happens When You Massage?
• Increased tissue swelling
• Injured blood vessels • Inflammation• Pain• True obstruction of
milk flow
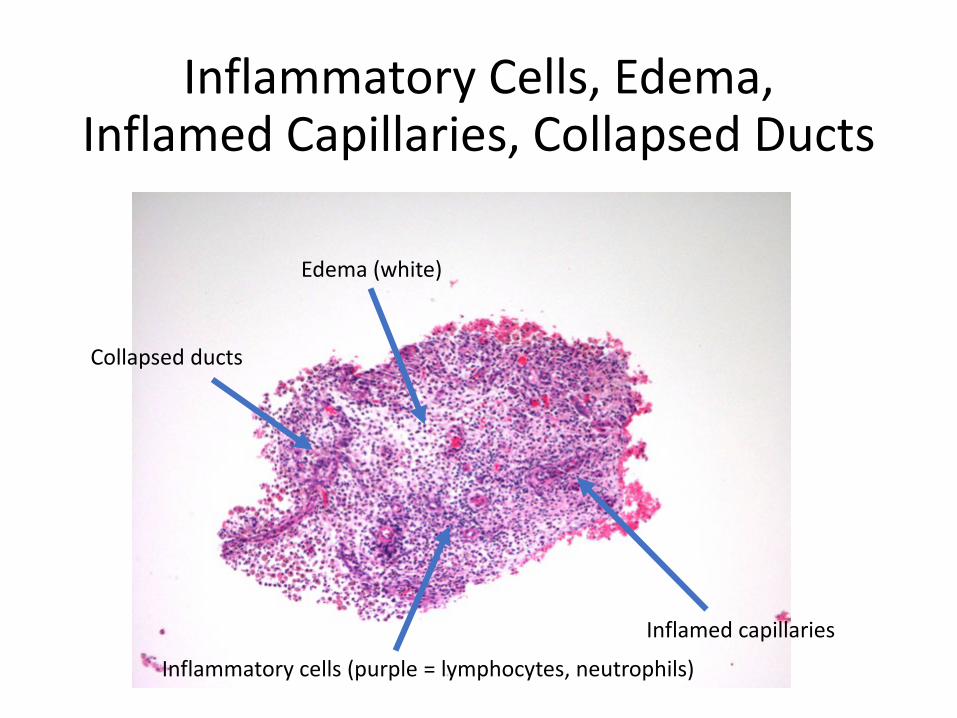
Inflammatory Cells, Edema, Inflamed Capillaries, Collapsed Ducts
Edema (white)
Collapsed ducts
Inflamed capillaries
Inflammatory cells (purple = lymphocytes, neutrophils)

ILCA 2021 Conference #ILCA2021
Bruising From Massage

ILCA 2021 Conference30 August – 30 November
#ILCA2021
MRI Appearance of Massage Damage

What Does Pumping and Massage Do?


ILCA 2021 Conference30 August – 30 November
#ILCA2021

ILCA 2021 Conference30 August – 30 November
#ILCA2021
• Unlike galactocele or abscess (discrete fluid collection), this is mass without drainable fluid collection
• Results from massage of early inflammatory or infectious mastitis
• Capillary injury, edema, tissue inflammation, bleeding
• With or without overlying erythema
Johnson and Mitchell Breast J 2019
Lactational Phlegmon


Right Breast Phlegmon


ILCA 2021 Conference30 August – 30 November
#ILCA2021

ILCA 2021 Conference30 August – 30 November
#ILCA2021

What Should Be Done Instead?

Solutions to plugging

ILCA 2021 Conference #ILCA2021
Narrowed Duct Treatment• Breastfeed physiologically
• Avoid pump• Treat hyperlactation• Educate about normal
cellular distension
• ICE ICE ICE• Advil/Tylenol PRN
• Do NOT OVERFEED ON AFFECTED BREAST
• Backs up more cars in the traffic jam


30 August – 30 November
Cameron 2013, Cooper and Kowalsky 2015
Narrowed Duct Treatment• Therapeutic ultrasound
• Thermal and nonthermal effects, including acceleration of metabolic rate, reduction of pain, increased circulation
• Method• Frequency 1mHz,
intensity 2.0 W/cm2• 5-6.5 mins for area 2-3x
the head of the probe

NO MASSAGE

Massage = 9.0 Magnitude Earthquake

• Reduces swelling by assisting movement of lymph fluid, decreasing edema• Technique
• “Very gentle touch/traction of skin - “like petting a cat” • The purpose is to lift skin to allow flow of lymphatic drainage and vascular
decongestion• Ten small circles at junction of internal jugular and subclavian veins• Ten small circles in axilla • Continue with light touch massage from nipple towards clavicle, axilla
• Start during pregnancy if experiencing painful rapid breast growth, and use as needed postpartum for engorgement
PhysicianGuideToBreastfeeding.org
Lymphatic Drainage

Lymphatic massage


ILCA 2021 Conference30 August – 30 November
#ILCA2021
Narrowed Duct Treatment• Sunflower lecithin
prevention 5 g/daily• Poke root
(phytolocca) acutely• Image with breast
ultrasound if it doesn’t resolve
• Rule out fluid collection or mass
Johnson and Mitchell Breast J 2019

When in Doubt, Use Common Sense
There’s NO way massage, continuously pumping or feeding, wrapping in hot packs ETC will make this feel better

“Yeast”




Vasospasm of Nipple – NOT Yeast
• Cutaneous vasoconstriction of nipple that causes pain
• White->blue->red• Can last more than an hour
• Triggered by cold (hot shower to cold room), suck, pressure (pump)
• Pain usually worse after baby de-latches; may radiate throughout breast
• If persistent, can cause nipple ischemia -> trauma -> worsening pain
• Differentiate from other trauma
• E.g pumping or baby latching with mom engorged
Berens et al ABM Protocol # 26

Vasospasm
• Rx: HEAT at all times• Wool pads, hand
warmers, old wood sweater, old technical fleece etc etc
• Wound care for secondary trauma as needed
• SSRI vs. CalicumChannel Blocker for refractory pain

Contact Dermatitis: Not Yeast• May have history of eczema,
allergic tendency• Symptoms
• Itchy and/or painful nipple, areola
• Cracks, scabs• Erythematous• May have oozing of open
areas• Assess allergies
• Baby medication or food• Laundry detergent • Breast pad material• New nursing bra• Pump parts• Nipple crème, topical abx
• Tx• Remove allergen• 0.1% triamcinolone
Photo: Pam Berens, MD

Not Yeast
Berens et al ABM Protocol # 26
Presentation
After two weeks 0.1% triamcinolone cremeAfter one week 0.1% mometasone creme
Presentation

Not Yeast
Presentation
Three months later with some recurrence after cessation of steroid

Dermatitis, Not Yeast


ALWAYS Ask What Baby Ingested
• Well-defined, scaly plaque x 2-3 weeks with 14-month baby nursing
• Mom allergic to bananas
• Also common with antibiotics

Petroleum Allergy

Not Yeast
Demarcation between normal nipple and affected areola (nipple not involved = not Paget’s)

And Ask Where Baby is Touching
• 35F followed for nipple blebs, areola flaking/itching
• Persistent left nipple flaking 3 months after cessation breastfeeding; asymmetric c/w right nipple
• Punch biopsy: “changes associated with chronic rubbing”

Dyad: dermatitis

Exclusive Pumping Milk Crust
After cessation of EP


Pump Trauma

THIS is Yeast• Not contagious
• Host microbiome/health issue• Risk factors for true candida
• Obese, diabetic, immunocompromised• Warm, less vascular (i.e. NOT the nipple)
• IMF, axilla, abdominal pannus

Pumping for Engorgement

30 August – 30 November

ILCA 2021 Conference30 August – 30 November
#ILCA2021
Engorgement and Hyperlactation
• No precise definition• Production of milk in excess
of what baby needs– Term infant needs 450-
1200ml• Doesn’t change over time
• Can be localized issue to one breast or one ductal system/quadrant
Lawrence and Lawrence Breastfeeding: A guide for the medical profession 2016; ABM protocol #33

ILCA 2021 Conference30 August – 30 November
#ILCA2021
Consequence of “Pumping to Prevent Milk Stasis”
• Unilateral iatrogenic hyperlactation
• Patient instructed to feed or pump to “keep breast empty” after first episode mastitis
• Developed recurrent mastitis until instructed to leave that breast full and feed left breast to right breast in a 3:1 or 4:1 ratio

Resolution

Told to “Pump to Empty”
24 hours after needle biopsy 1 week later
9 dayslater
Healed after cessation of
pumping

Soaking Nipples in Salt Water

DO NOT USE TOO SMALL FLANGESDO NOT SOAK IN EPSOM SALT!
Unroofed blistersto start proper wound care

Patient told this:• Soak breast in Epsom salt• Pump• Apply castor oil wraps with
heating pad on top• Patient said, “our kitchen
looked like a ‘Breaking Bad’ episode” …
• Massage• Pump• Do “Breast Gymnastics”
• Patient said, “I can only go so low ….”
And in General, If You Feel Silly Doing It, IT IS SILLY

Other Things to Avoid
• APNO• Hair dryers• Strange/dangerous
positions• Commercial
massagers/vibrating devices
• Nipple shells• Wet Tea Bags

Trauma Treatment• Lubricated, moist/closed healing
environment• Think surgical wound care, burns
• Do not “air dry” or soak in Epsom salt
• Hydrogel pads, balm without lanolin (lanolin allergenic), medihoney (baby may reject taste), polymem, mepilex
• Be mindful of coconut allergy in other products
• Your hospital may be able to stock mepilex
• PRN 0.1% triamcinolone for severe injury/pain
• APNO-NO-NO!• Expensive, has antifungal and
antibacterial that is not needed and potentiates allergy; relief in this compound is generally from the steroid

Pump Trauma Treatment
• Avoid nipple shells: cause nipple areolar complex edema, worsen trauma due to inability to deep latch

Some Wounds Need DebridementPresentation One week s/p
polymem
Two weeks s/p polymem
Four weeks s/p polymem

NEEDS DEBRIDEMENT
”Kitchen sink” wound care x 6 weeks
One week after polymem
Resolved at two weeks

Mastitis and Antibiotics

30 August – 30 November
48 hours later
• Ice/heat• Ibuprofen• NO MASSAGE• Don’t overfeed• TUS

30 August – 30 November
All Things Red Are Not Infectious!
• Hives• Dermatitis• DVT• Sprained Ankle• Other things that cause
fever• SIRS, ARDS, paraneoplastic
syndromes• Pancreatitis outcomes are
WORSENED with antibiotics

Bras

Acute dependent edema
Images: Casey Rosen-Carole, MD

Chronic dependent edema

Blebs

Nipple Bleb (“Milk Blister”)
• Painful inflammatory lesion on surface of nipple orifice; can be large or small, multiple or single
Mitchell and Johnson J Mam Gland Neoplasia 2020

Normal milk flow
Bacteria
Bacteria
Mammary epitheliumAreola
Nipple
(A) HEALTHY MAMMARY GLAND
Reduced milk flow
Bacteria
Bacteria
Mammary epithelium
obstruction
Blebs, cracking
Inflammation
(B) MASTITIS
• Bacteria: ≤3 log10 CFU/ml
• Heterogeneouspopulation
• Bacteria:> 4 log10 CFU/ml
• Homogeneous population
Decreased milk secretion
Duct section
Obstruction
Increasedpressure,
Increased edema
Difficultmilk secretion
Milk culture

Underlying Ductal Inflammation

Can Be Obvious

Or Subtle (“Cracked Nipple”)

Multiple Blebs in Setting of Hyperlactation, Subacute Mastitis



Another Chronically Traumatized Bleb

Chemical Trauma: Gentian Violet

Fat Globules

This is Biofilm/Inflammatory Debris
• Often overpumping
• Hyperlactation

Mam
mar
y du
ct –
NO
mas
titis
Mam
mar
y du
ct -
MA
STITI
SS.
epi
derm
idis
biof
ilm

Normal milk flow
Bacteria
Bacteria
Mammary epitheliumMammary
areola
Nipple
(A) HEALTHY MAMMARY GLAND
Inflammation
• Bacteria: ≤3 log10 CFU/ml
• Heterogeneouspopulation
Reduced milk flow
Bacteria
Bacteria
Mammary epithelium
obstruction
Nippleblebs
(B) MASTITIS
• Bacteria:> 4 log10 CFU/ml
• Homogeneouspopulation
Decreased milk secretion
Obstruction
Local symptoms: erythema, induration, and pain
Systemic symptoms: Fever, tachycardia, flu-like symptoms
(A) Acute mastitis by S. aureus
toxins
Predisposing factors
(B) Subacute mastitis by CNS or streptococci
Tendency to chronic/recurrent mastitis
No breast rednessNo systemic symptoms
Widely underdiagnosed
No toxin productionThick biofilmsAntibiotic resistance
Local symptoms:engorgement,
pain (needle-like, burning), cramps, decreased secretion

Treat
• Pump only what baby needs, or don’t pump at all if possible
• Treat hyperlactation
• Probiotics vs. antibiotics (may resolve on its own with treatment of hyperlactation)
• Mental health

“Flat Nipples”

Nipples are Erectile Tissue
• Be mindful of language around new moms
• Use positive language and don’t pathologize mom or baby body parts
• Every nipple that isn’t completely fixed by cancer, scarring, or severe congenital bands is able to be made erect

Patient Told Nipples “Flat”


Placental Encapsulation

Placental Encapsulation Reduces Milk Production
• Placenta is full of progesterone
• ”PRO” “Gestation” (growing a baby)
• Placenta delivery and drop in progesterone stimulates increase in prolactin
• ”PRO” ”Lactation” (making milk)

Freezer Stashes

Freezing
• Freezing reduces calories, fat content, nutrients, antibodies
• Anxiety producing• Hyperlactation risks

”High Lipase”

No Evidence to Support “High Lipase”
• All fatty acids will break down in stored milk, and this doesn’t mean “lipase” is high
• Breast is a modified sweat gland and all mammals produce smells
• Most often, “high lipase” is “diagnosed” when a baby won’t take a bottle …

”10-10-10”

10-10-10 and others …• 10 mins each breast, ten mins
pumping, 10 ml formula• Feeding at breast should never
be timed (burns calories, fatigues mom and baby, doesn’t stimulate breast well)
• Baby either needs a lot more formula or none at all
• Nipple shields• Pacifier at the breast• Help mom evert nipple, feed
side lying, reduce breast edema• Syringes
• Exhausting for long term use! • “Marathon, not a sprint”

Pain

Pain
• Pumping incorrectly• Baby clamping from
hyper or hypolactation or large breasts
• DMERs/nursing aversion
• Vasospasm• Engorgement

Increasing Production

More Time on Breast Does Not Always =
More Milk• Babies respond to
volume/flow/calories, not undressing, tickling, trying to keep awake
• Bili lights = dehydrating, can put baby and mom’s breasts further behind
• De-couple/”divide and conquer” in early days to stimulate breasts and keep baby nourished to nurse well

Trash the Pump and
Dump!


ILCA 2021 Conference30 August – 30 November
#ILCA2021
Take Home Points
• NO MASSAGE• Do not feed to “keep breast empty” as
this worsens hyperlactation• Physiologic feeding
• Wear a good bra• Don’t soak nipples in salt water• HATI resolves vast majority of mastitis
without antibiotics • Heat, Advil, Tylenol, ICE ICE ICE• Not all things red are infectious
• Blebs are microbiome disruption, inflammation - NOT LATCH TRAUMA
• “Fat globules” are the same• P.S. NONE OF IT IS YEAST!!!!!!

Please reach out with questions at any time!Katrina Mitchell, MD, IBCLC, PMH-C, FACS
Santa Barbara, CA646-709-6048, [email protected]
PhysicianGuideToBreastfeeding.Org
Thank You




















