Breastfeeding Patterns in Relation to Thumb Sucking and Pacifier Use
http://jhl.sagepub.com/Journal of Human Lactation
http://jhl.sagepub.com/content/early/2012/09/08/0890334412452933The online version of this article can be found at:
DOI: 10.1177/0890334412452933
published online 10 September 2012J Hum Lactand Donna T. Geddes
Vanessa S. Sakalidis, Tracey M. Williams, Catherine P. Garbin, Anna R. Hepworth, Peter E. Hartmann, Michael J. PaechUltrasound Imaging of Infant Sucking Dynamics during the Establishment of Lactation
Published by:
http://www.sagepublications.com
On behalf of:
International Lactation Consultant Association
can be found at:Journal of Human LactationAdditional services and information for
http://jhl.sagepub.com/cgi/alertsEmail Alerts:
http://jhl.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Sep 10, 2012OnlineFirst Version of Record >>
at University of Western Australia on October 15, 2012jhl.sagepub.comDownloaded from

Journal of Human LactationXX(X) 1 –9© The Author(s) 2012Reprints and permission: http://www. sagepub.com/journalsPermissions.navDOI: 10.1177/0890334412452933http://jhl.sagepub.com
Original Research
Well EstablishedInfants are believed to become more efficient at breastfeeding with age; how sucking patterns may influence this process is unclear. Similarly, breastfeeding consists of nutritive sucking (NS) and non-nutritive sucking (NNS); yet tongue movement during NNS on the breast is undocumented.
Newly ExpressedWe measured infant sucking dynamics during breastfeeding at early and established lactation and showed different tongue
452933 JHLXXX10.1177/0890334412452933Sakalidis et al.Journal of Human Lactation2012
Date submitted: February 21, 2012; Date accepted: June 4, 2012.
1School of Chemistry and Biochemistry, The University of Western Australia, Crawley, Western Australia2School of Medicine and Pharmacology, The University of Western Australia, Crawley, Western Australia
Corresponding Author:Vanessa S. Sakalidis, BHlth Sc(Hons), M310, School of Chemistry and Biochemistry, The University of Western Australia, 35 Stirling Hwy, Crawley, Perth, 6009, Western Australia Email: [email protected]
Ultrasound Imaging of Infant Sucking Dynamics during the Establishment of Lactation
Vanessa S. Sakalidis, BHlth Sc (Hons)1, Tracey M. Williams, BSc1, Catherine P. Garbin, CNM, IBCLC1, Anna R. Hepworth, BSc (Hons), DipEd1, Peter E. Hartmann, BSc, PhD1, Michael J. Paech, MBBS, DRCOG, FRCA, FANZCA, FFPMANZCA, FRANZCOG (Hon), DM2, and Donna T. Geddes, DMU, Post Grad Dip (Sci), PhD1
AbstractBackground: Infant sucking problems are frequently implicated in early weaning during breastfeeding, yet our understanding of early sucking dynamics is limited.Objective: This study aimed to describe infant sucking patterns during breastfeeding at secretory activation and determine whether they changed by the time of established lactation.Methods: Sucking patterns and milk intake of 15 breastfeeding infants were assessed on day 3.2 ± 0.8 and later at follow-up, 16.0 (11.3-22.8) days postpartum. Nipple diameters, tongue movement, nipple position, and suck rate during nutritive sucking (NS) and non-nutritive sucking (NNS) were measured from ultrasound scans of the intra-oral cavity during breastfeeding. Milk intake and LATCH scores were also recorded.Results: As the tongue lowered during a suck cycle, the nipple increased in size (P < .001), milk flowed into the intra-oral space and the nipple moved closer to the hard-soft palate junction (P < .001). During NS, nipple diameters and the mid-tongue movement were greater than during NNS (P < .001). As the infant aged, the mid-tongue lowered further (P = .002), suck rates became faster (P < .001) and milk intake increased (P = .004), however, no differences were seen for LATCH scores (P = .34).Conclusion: Differences in tongue movement between NS and NNS suggest that there is an altered sucking action when milk flow is absent. Similar sucking patterns at day 3 and during established lactation imply that infants have a mature sucking pattern in the early postpartum period.
Keywordsbreastfeeding initiation, infant physiology, infant feeding, sucking, ultrasound
at University of Western Australia on October 15, 2012jhl.sagepub.comDownloaded from

2 Journal of Human Lactation XX(X)
movement between NS and NNS, and similar tongue movement between early and established lactation, suggesting infants have a mature sucking pattern from the early postpartum period.
BackgroundInfant sucking and latching difficulties are commonly cited as reasons for ceasing breastfeeding during the initiation of lac-tation,1 yet there is little knowledge regarding sucking dynam-ics, specifically tongue movement, during this period. Secretory activation is the initiation of copious milk secretion occurring 30-40 hours after birth, triggered by the withdrawal of progesterone after delivery of the placenta.2 Rapid increases in milk secretion occur over this period, such that infant milk transfer increases from less than 100 mL/d on day 1 postpar-tum to between 500 mL and 750 mL by day 5, stabilizing to between 750 and 800 mL/d on average by 1 month postpar-tum.3 Although it is believed infants change their sucking dynamics and efficiency over time as a result of maturation, it is unknown how infant tongue movement changes in response to increased milk production during established lactation.
Infants exhibit 2 types of sucking within a breastfeed: nutri-tive sucking (NS), during which milk is consumed; and non-nutritive sucking (NNS), during which only saliva is swallowed.4 During NS, intra-oral vacuum is believed to play an important role in milk removal,5-8 however, tongue move-ment during NNS on the breast has not been investigated. Conventional descriptions state that during NS, milk is stripped from the nipple by a peristaltic movement of the tongue, which compresses milk from the nipple (nipple base to tip).9-14 Recent ultrasound studies of term infants during established breast-feeding have suggested otherwise, showing that as the tongue is drawn downward, the nipple expands evenly and milk flows into the infant’s oral cavity. This movement corresponds with increasing vacuum and therefore supports the notion that vac-uum is important for effective milk removal.6,15
Unfortunately, the current knowledge of sucking dynam-ics and tongue movement during early lactation is based on bottle-feeding studies. Since the delivery of milk is markedly different for bottle-feeding and breastfeeding,16-18 the results of these studies cannot be generalized to breastfeeding. The aim of this study was to use ultrasound imaging to describe tongue movement during breastfeeding at secretory activa-tion (day 3) in infants born via uncomplicated vaginal birth and to determine whether the movement changed over time once lactation was established (follow-up, days 10-45). In addition, we aimed to compare tongue movement between NS and NNS during breastfeeding.
MethodsParticipants
Mothers intending to breastfeed were recruited from August 2008-April 2010 through either the prenatal birthing clinic or obstetric ward at King Edward Memorial Hospital
for Women, Perth, Western Australia. Only full-term, healthy infants (gestational age ! 38 wk) of mothers with an uncomplicated vaginal birth and who were successfully breastfeeding were included. Infants were excluded if they were < 38 weeks gestational age or had any condition that may affect feeding ability. Ethics approval was obtained from the Human Research Ethics Committee of the Women and Newborn Health Service of Western Australia. Mothers supplied written informed consent to participate in the study.
ProtocolTwo assessments of breastfeeding at different time points were made, the first on day 3 postpartum (range 2-4) and the second between days 10 and 45 postpartum (follow-up). The day 3 assessment was carried out at either the hospital or the mother’s home, and the follow-up assessment was performed at the mother’s home. Assessments consisted of ultrasound imaging of the infant’s intra-oral cavity during breastfeeding; evaluation of the breastfeed using the LATCH tool; and measurement of milk intake.
Ultrasound ImagingSubmental ultrasound scans of the midline of the infant’s intra-oral cavity were performed during breastfeeding using a portable ultrasound (Titan hand-carried Sonosite, Australia) with a broadband intracavity transducer (ICT/8-5MHz), as described previously.6,15 A small quantity of Parker Ultrasonic Gel (Fairfield, NJ, USA) was placed on the transducer before commencing the scan to provide good transmission of the ultrasound beam. The transducer was positioned along the midsagittal line of the infant’s body, and light pressure was used to maintain contact with the infant’s chin. The transducer was rotated until a midsagittal view of the nipple was displayed, along with the hard-soft palate junction (HSPJ) and the anterior and middle tongue; the tip of the tongue could not be visualized using this method. All scans were recorded to a PC notebook (Acer Travelmate 6293) using Compro VideoMate S350. Ultrasound scans began when the infant attached to the breast and ended when the infant finished feeding (2 scans ended earlier because of scanning difficulties).
Breastfeeding Evaluation via the LATCH ToolBreastfeeding characteristics were assessed by 1 researcher using the LATCH tool, which scores latch, audible swal-lowing, type of nipple, comfort, and hold (positioning) during breastfeeding on a 10-point scale.19,20
Milk IntakeAt each assessment, milk intake was determined by weighing the infant before and after breastfeeding using
at University of Western Australia on October 15, 2012jhl.sagepub.comDownloaded from

Sakalidis et al. 3
an Electronic Baby Weigh Scale (Medela AG, Baar, Switzerland). Milk intake (g) was calculated by subtracting the initial weight from the final weight. No correction for infant insensible water loss was made; therefore, milk intake may be underestimated by 3%-10%.21 The duration of the monitored feed was estimated by calculating the time between test weighs, which occurred immediately before and after the breastfeed.
Ultrasound Definitions and MeasurementA suck cycle was defined as starting when the mid-tongue (Figure 1a) was in apposition with the palate (tongue up, TU), followed by downward excursion of the tongue until the mid-tongue reached its lowest point (tongue down, TD; Figure 1b) and ending with the tongue in apposition with the palate again. Nutritive sucking was defined as suck cycles resulting in the delivery of milk into the oral cavity as imaged by ultrasound where the milk bolus appeared as a hypoechoic (black) area filled with echogenic (white)
flecks. Non-nutritive sucking was defined as suck cycles in which no milk was present on ultrasound (Figure 1c and d). For each infant, 3 consecutive suck cycles of the first and clearest imaging during both NS and NNS were selected for both day 3 and follow-up scans (3 suck cycles were not con-secutive). During each suck cycle, 2 frames were analyzed, 1 at TU and 1 at TD. Six anatomical measurements were made: nipple diameters at 2, 5, 10, and 15 mm from the tip of the nipple (Figure 2); depth of the intra-oral space (dis-tance from the hard-soft palate junction (HSPJ) to the sur-face of the posterior tongue); and distance from the nipple tip to the HSPJ. Measurements were made using Screen Calipers (version 3.2, Iconico, Inc., New York, 2006) using a PC notebook. All measurements were performed by 1 researcher, and this method has been validated and is described in detail elsewhere.15 Suck rates were determined by counting the number of sucks per burst on the ultrasound recording for the first 3 and last 3 minutes of the feed. A burst was defined as the periods of sucking (tongue mov-ing), between pauses (tongue resting).
Figure 1. Example of a submental midsaggital ultrasound of the infant oral cavity during a breastfeed on day 3 showing the anterior and mid-tongue. During nutritive sucking (NS) at (a) tongue up, the nipple is evenly compressed from the tip to base, and the tongue is in contact with the hard and soft palate. As the tongue lowers at (b), the nipple has evenly expanded in size, moved closer to the HSPJ, and the mid-tongue has lowered, allowing milk to flow into the intra-oral space. During non-nutritive sucking (c), the nipple is less compressed at tongue up compared to NS, and (d) as the tongue is lowered, at tongue down the nipple has expanded to a lesser degree, and the mid-tongue lowered to a lesser extent compared to NS. Abbreviations: AT, anterior tongue; HP, hard palate; IOS, intra-oral space; J, hard-soft palate junction; M, milk; MT, mid-tongue; N, nipple; SP, soft palate.
at University of Western Australia on October 15, 2012jhl.sagepub.comDownloaded from
4 Journal of Human Lactation XX(X)
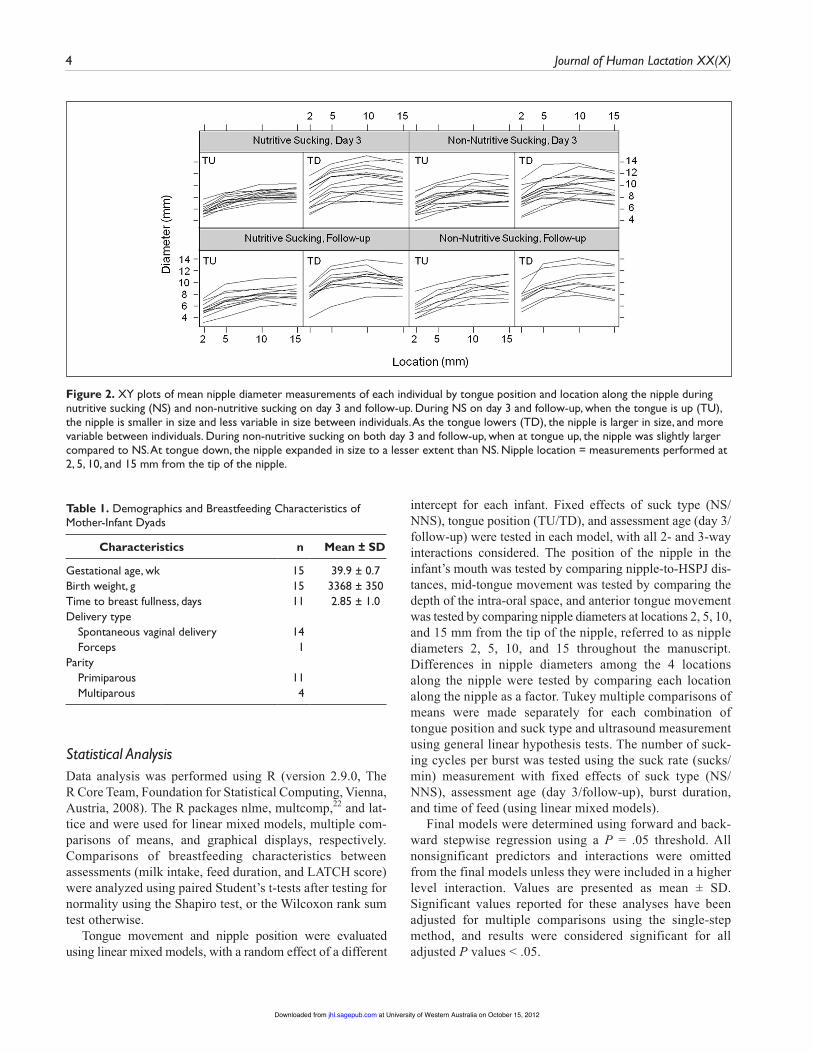
Statistical AnalysisData analysis was performed using R (version 2.9.0, The R Core Team, Foundation for Statistical Computing, Vienna, Austria, 2008). The R packages nlme, multcomp,22 and lat-tice and were used for linear mixed models, multiple com-parisons of means, and graphical displays, respectively. Comparisons of breastfeeding characteristics between assessments (milk intake, feed duration, and LATCH score) were analyzed using paired Student’s t-tests after testing for normality using the Shapiro test, or the Wilcoxon rank sum test otherwise.
Tongue movement and nipple position were evaluated using linear mixed models, with a random effect of a different
intercept for each infant. Fixed effects of suck type (NS/NNS), tongue position (TU/TD), and assessment age (day 3/follow-up) were tested in each model, with all 2- and 3-way interactions considered. The position of the nipple in the infant’s mouth was tested by comparing nipple-to-HSPJ dis-tances, mid-tongue movement was tested by comparing the depth of the intra-oral space, and anterior tongue movement was tested by comparing nipple diameters at locations 2, 5, 10, and 15 mm from the tip of the nipple, referred to as nipple diameters 2, 5, 10, and 15 throughout the manuscript. Differences in nipple diameters among the 4 locations along the nipple were tested by comparing each location along the nipple as a factor. Tukey multiple comparisons of means were made separately for each combination of tongue position and suck type and ultrasound measurement using general linear hypothesis tests. The number of suck-ing cycles per burst was tested using the suck rate (sucks/min) measurement with fixed effects of suck type (NS/NNS), assessment age (day 3/follow-up), burst duration, and time of feed (using linear mixed models).
Final models were determined using forward and back-ward stepwise regression using a P = .05 threshold. All nonsignificant predictors and interactions were omitted from the final models unless they were included in a higher level interaction. Values are presented as mean ± SD. Significant values reported for these analyses have been adjusted for multiple comparisons using the single-step method, and results were considered significant for all adjusted P values < .05.
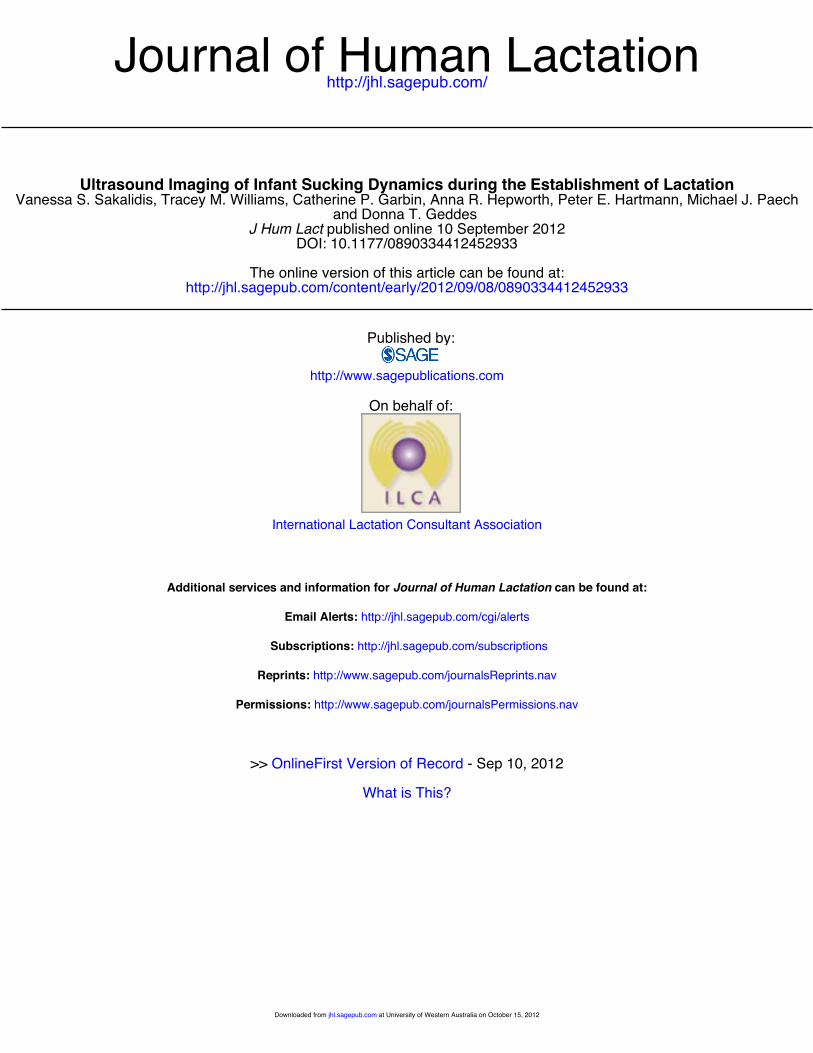
Figure 2. XY plots of mean nipple diameter measurements of each individual by tongue position and location along the nipple during nutritive sucking (NS) and non-nutritive sucking on day 3 and follow-up. During NS on day 3 and follow-up, when the tongue is up (TU), the nipple is smaller in size and less variable in size between individuals. As the tongue lowers (TD), the nipple is larger in size, and more variable between individuals. During non-nutritive sucking on both day 3 and follow-up, when at tongue up, the nipple was slightly larger compared to NS. At tongue down, the nipple expanded in size to a lesser extent than NS. Nipple location = measurements performed at 2, 5, 10, and 15 mm from the tip of the nipple.
Table 1. Demographics and Breastfeeding Characteristics of Mother-Infant Dyads
Characteristics n Mean ± SD
Gestational age, wk 15 39.9 ± 0.7Birth weight, g 15 3368 ± 350Time to breast fullness, days 11 2.85 ± 1.0Delivery type Spontaneous vaginal delivery 14 Forceps 1Parity Primiparous 11 Multiparous 4
at University of Western Australia on October 15, 2012jhl.sagepub.comDownloaded from
Sakalidis et al. 5
ResultsDemographics and Breastfeeding Characteristics
Fifteen women aged 33.4 years (SD 5.0), were included in the study. Infants (8 female, 7 male) were on average 3.2 days (SD 0.8) old at the first assessment (n = 15) and median 16.0 (interquartile range 11.25-22.75) days old at follow-up (n = 13) and had an Apgar score > 8 at both 5 and 10 minutes (Table 1). For the monitored feeds, milk intake was greater at follow-up (P = .004), however the feed duration (P = .63) and LATCH scores (P = .34) were similar between assess-ments (Table 2).
Sucking CharacteristicsNutritive Sucking
During NS, the start of the suck cycle was defined as the tongue compressing the nipple and resting against the hard and soft palate (Figure 1a). As the tongue lowered, the anterior portion lowered to a lesser degree than the
mid-tongue, nipple ducts opened as the nipple increased in diameter, and the nipple moved closer to the HSPJ (closest point occurred at TD). Milk was subsequently observed flowing into the intra-oral space (Figure 1b). The anterior portion of the tongue began to rise 1 or 2 frames before the mid-tongue reached its most inferior point and slightly com-pressed the base of the nipple. The rest of tongue then rose until it was back in contact with the palate, and the nipple moved further away from the HSPJ (furthest point occurred at TU). Milk was observed in the intra-oral space until the mid-tongue returned to the palate. Nutritive sucking was observed throughout feeds and was more commonly seen at the beginning and middle of the feed.
Non-nutritive SuckingDuring NNS, the tongue started the suck cycle by slightly compressing the nipple and resting up against the hard and soft palate (Figure 1c). As the tongue began to lower, the anterior portion descended less than the mid-tongue. The mid-tongue lowered to a lesser degree compared to during NS, the nipple moved closer to the HSPJ, and neither nipple
Table 2. Breastfeeding Characteristics on Day 3 and at Follow-up
Day 3 Follow-up
Mean SD Mean SD P
Milk intake on visit, mLa 15.0 10.5-25.0 52.0 42.0-68.0 .004Duration of feed, min 19.1 6.5 16.1 6.7 .63LATCH score, /10 9.2 0.75 9.4 0.70 .34Suck rate, sucks/min, nutritive sucking 68.0 14.8 74.0 17.1 .001Suck rate, sucks/min, non-nutritive sucking 77.8b 18.2 88.9b 23.9 .001
aData presented as median (interquartile range) for milk intake.bSignificance between nutritive sucking and non-nutritive sucking (P < .001).Note: Milk intake was analyzed using the Wilcoxon rank-sum test, Duration and LATCH were analyzed using Paired Student’s t-tests, and suck rate was analyzed using linear mixed models.
Table 3. Nipple Diameter Measurements (in mm) on Day 3 and at Follow-up
Day 3 Follow-up
BurstNipple
Location, mm Tongue Up Tongue Downa Tongue Up Tongue Downa
Nutritive sucking 2 5.5 ± 1.0 7.8 ± 2.2 5.4 ± 1.3 8.1 ± 1.5 5 7.1 ± 1.1 9.9 ± 2.4 7.1 ± 1.6 10.0 ± 1.8 10 8.2 ± 1.1 10.1 ± 2.6 8.2 ± 1.3 10.1 ± 1.8 15 8.3 ± 1.2 10.0 ± 2.5 8.4 ± 1.5 10.0 ± 1.6Non-nutritive sucking 2 6.1 ± 1.6 7.4 ± 1.9 5.6 ± 1.6 7.5 ± 1.8 5 7.7 ± 1.7 9.1 ± 2.0 7.3 ± 1.6 9.7 ± 2.2 10 8.6 ± 1.8 9.9 ± 2.0 9.0 ± 1.6 10.1 ± 2.2 15 8.4 ± 1.7 9.2 ± 2.0 9.3 ± 1.8 10.2 ± 2.4
aAll TU to TD differences are significant at P < .001. Data presented as mean ± SD. Nipple location = measurements performed at 2, 5, 10, and 15 mm from the tip of the nipple. Statistical analysis performed using Tukey pairwise comparisons.
at University of Western Australia on October 15, 2012jhl.sagepub.comDownloaded from

6 Journal of Human Lactation XX(X)
ducts nor milk flow was observed (Figure 1d). When the posterior tongue lowered to its most inferior point, the ante-rior portion began to rise. The rest of the tongue followed until it was in contact with the palate again, and the nipple ended further away from the HSPJ. Non-nutritive sucking was observed throughout feeds and was more commonly seen at the end of the feed.
Tongue, Nipple Movement, and Suck RatesAnterior tongue movement was related to suck type and position with a 2-way interaction. As the tongue lowered during a suck cycle, all nipple diameters significantly increased in size compared to during TU (Table 3, Figure 2, all P < .001). A larger range of tongue movement was seen during NS; at TU during NS, all nipple diameters were smaller than during NNS, and at TD, all nipple diameters were larger than during NNS (interaction: P < .001; Figure 3).
During NS and NNS, when the tongue was up, all nipple diameters were significantly larger along the nipple from the tip to base; they were smallest at the tip and largest at the base (all comparisons P < .001) except nipple diameters 10 and 15 (NS P = .88, NNS P = .91). Similarly, in the tongue down (TD) position, all nipple diameters were significantly larger in size along the nipple from the tip to base; they were smallest at the tip and largest at the base (all compari-sons P < .05) except for nipple diameter 5 and 15 (NS P = .91, NNS P = .58; Table 3).
Anterior tongue movement differed along the nipple, where significantly more movement occurred at nipple diameter 5 compared to the rest of the nipple (nipple
diameter 10, P = .03; nipple diameter 2, P = .03; nipple diameter 15, P < .001). The least movement occurred at nip-ple diameter 15.
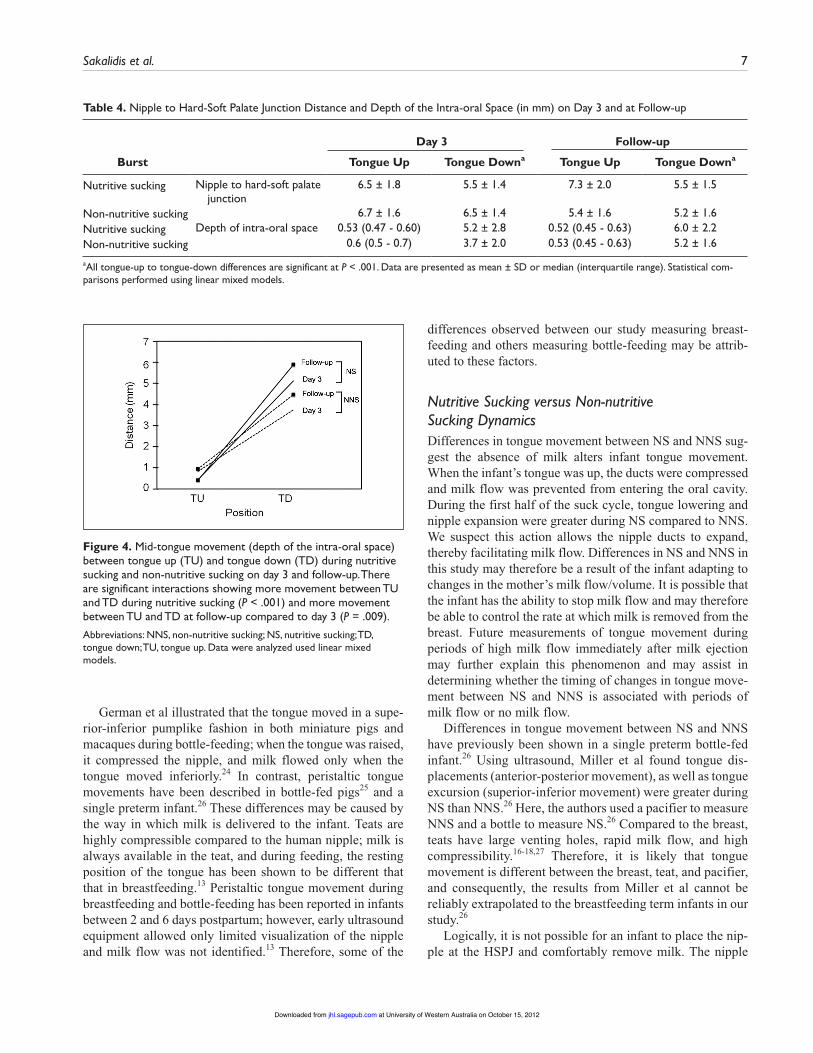
Mid-tongue movement was related to suck type, age, and position, with significant 2-way interactions. As the mid-tongue lowered, the depth of the intra-oral space signifi-cantly increased for both NS and NNS (Table 4; P < .001). There was more movement between TU and TD during NS than NNS (interaction; P < .001). Similarly, there was more movement between TU and TD at follow-up compared to day 3 (interaction P = .009; Figure 4).
Nipple position was significantly related to suck type and position, but not age. As the tongue lowered, the nipple moved closer to the HSPJ (P < .001), but it never reached the junction itself. This pattern was the same for NS and NNS (P = .77; Table 4) and there was no difference in move-ment between assessments (P = .64).
Suck rate was related to suck type and age. Faster suck rates were recorded during NNS (P < .001) compared to NS, and both NS and NNS suck rates were faster at the follow-up assessment compared to the day 3 assessment (P < .001; Table 2). During NS, suck rates became faster by 0.3 sucks/minute with every burst across the feed (P = .01), but there was no difference for NNS (P = .19).
DiscussionThis study confirmed that infant sucking dynamics during secretory activation were similar to those observed during established lactation. Milk removal coincided with a lower-ing of the tongue, which has been previously associated with increasing vacuum, supporting the notion that vacuum is important for milk removal.6,23 During NNS, the tongue did not lower to the same degree as it did during NS, suggesting that the absence of milk alters tongue movement. Similar sucking patterns between day 3 and 45 postpartum suggest the infant has a mature sucking pattern in the early postpar-tum period.
Sucking MechanismOur results show milk flow occurs when the tongue is low-ered, rather than when the tongue is compressing the nipple.10 Furthermore, McClellen et al showed a pattern of tongue movement identical to that of infants in our study, in that when the tongue was lowered to its most inferior point, there was an even expansion of the nipple from the tip to the base (Figure 2, Table 3), along with nipple duct expansion and subsequent milk flow into the intra-oral space.15 Using simul-taneous measurement of vacuum and ultrasound, Geddes et al have shown inferior movement of the tongue corresponds with increasing vacuum and milk flow in established breast-feeding infants.6 Smith et al also used ultrasound to image infant sucking during breastfeeding and suggested that vac-uum created by enlargement of the oral cavity, rather than compression, would most likely result in milk flow.5
Figure 3. Anterior tongue movement (nipple diameter measurements) at each location along the nipple between tongue up and tongue down during nutritive sucking and non-nutritive sucking. There is a significant interaction showing more movement between tongue up and tongue down during nutritive sucking than non-nutritive sucking (P < .001). Abbreviations: NNS, non-nutritive sucking; NS, nutritive sucking; TD, tongue down; TU, tongue up. Nipple location = measurements performed at 2, 5, 10, and 15 mm from the tip of the nipple. Data were analyzed used linear mixed models.
at University of Western Australia on October 15, 2012jhl.sagepub.comDownloaded from
Sakalidis et al. 7
German et al illustrated that the tongue moved in a supe-rior-inferior pumplike fashion in both miniature pigs and macaques during bottle-feeding; when the tongue was raised, it compressed the nipple, and milk flowed only when the tongue moved inferiorly.24 In contrast, peristaltic tongue movements have been described in bottle-fed pigs25 and a single preterm infant.26 These differences may be caused by the way in which milk is delivered to the infant. Teats are highly compressible compared to the human nipple; milk is always available in the teat, and during feeding, the resting position of the tongue has been shown to be different that that in breastfeeding.13 Peristaltic tongue movement during breastfeeding and bottle-feeding has been reported in infants between 2 and 6 days postpartum; however, early ultrasound equipment allowed only limited visualization of the nipple and milk flow was not identified.13 Therefore, some of the
differences observed between our study measuring breast-feeding and others measuring bottle-feeding may be attrib-uted to these factors.
Nutritive Sucking versus Non-nutritive Sucking DynamicsDifferences in tongue movement between NS and NNS sug-gest the absence of milk alters infant tongue movement. When the infant’s tongue was up, the ducts were compressed and milk flow was prevented from entering the oral cavity. During the first half of the suck cycle, tongue lowering and nipple expansion were greater during NS compared to NNS. We suspect this action allows the nipple ducts to expand, thereby facilitating milk flow. Differences in NS and NNS in this study may therefore be a result of the infant adapting to changes in the mother’s milk flow/volume. It is possible that the infant has the ability to stop milk flow and may therefore be able to control the rate at which milk is removed from the breast. Future measurements of tongue movement during periods of high milk flow immediately after milk ejection may further explain this phenomenon and may assist in determining whether the timing of changes in tongue move-ment between NS and NNS is associated with periods of milk flow or no milk flow.
Differences in tongue movement between NS and NNS have previously been shown in a single preterm bottle-fed infant.26 Using ultrasound, Miller et al found tongue dis-placements (anterior-posterior movement), as well as tongue excursion (superior-inferior movement) were greater during NS than NNS.26 Here, the authors used a pacifier to measure NNS and a bottle to measure NS.26 Compared to the breast, teats have large venting holes, rapid milk flow, and high compressibility.16-18,27 Therefore, it is likely that tongue movement is different between the breast, teat, and pacifier, and consequently, the results from Miller et al cannot be reliably extrapolated to the breastfeeding term infants in our study.26
Logically, it is not possible for an infant to place the nip-ple at the HSPJ and comfortably remove milk. The nipple
Table 4. Nipple to Hard-Soft Palate Junction Distance and Depth of the Intra-oral Space (in mm) on Day 3 and at Follow-up
Day 3 Follow-up
Burst Tongue Up Tongue Downa Tongue Up Tongue Downa
Nutritive sucking Nipple to hard-soft palate junction
6.5 ± 1.8 5.5 ± 1.4 7.3 ± 2.0 5.5 ± 1.5
Non-nutritive sucking 6.7 ± 1.6 6.5 ± 1.4 5.4 ± 1.6 5.2 ± 1.6Nutritive sucking Depth of intra-oral space 0.53 (0.47 - 0.60) 5.2 ± 2.8 0.52 (0.45 - 0.63) 6.0 ± 2.2Non-nutritive sucking 0.6 (0.5 - 0.7) 3.7 ± 2.0 0.53 (0.45 - 0.63) 5.2 ± 1.6
aAll tongue-up to tongue-down differences are significant at P < .001. Data are presented as mean ± SD or median (interquartile range). Statistical com-parisons performed using linear mixed models.
Figure 4. Mid-tongue movement (depth of the intra-oral space) between tongue up (TU) and tongue down (TD) during nutritive sucking and non-nutritive sucking on day 3 and follow-up. There are significant interactions showing more movement between TU and TD during nutritive sucking (P < .001) and more movement between TU and TD at follow-up compared to day 3 (P = .009). Abbreviations: NNS, non-nutritive sucking; NS, nutritive sucking; TD, tongue down; TU, tongue up. Data were analyzed used linear mixed models.
at University of Western Australia on October 15, 2012jhl.sagepub.comDownloaded from

8 Journal of Human Lactation XX(X)
should be positioned so that milk is able to flow into the oral cavity, without the nipple triggering the large number of sen-sory cells harbored on the soft palate that stimulate the gag reflex.28 Our measurements show that the nipple never reached the HSPJ for both NS and NNS, suggesting that although correct positioning and attachment appear to be important for the mother’s comfort, using the HSPJ as a landmark for assessment of positioning may not be clinically useful (Table 4).
During NS, the infants’ mid-tongue lowered further and they sucked significantly slower compared to during NNS, indicating that lowering of the tongue is necessary first to allow the infant to create an adequate vacuum to enable milk removal, and second, to accommodate the milk bolus in the oral cavity. During NNS, only a small amount of saliva is swallowed, and therefore the tongue is not required to lower to the same extent as NS, which supports our findings that the tongue is moving less and does not compress the nipple to the same extent during NNS. These results also agree with external observations of the feeding infant showing that the excursion of the infant’s jaw movement is shorter and more rapid during NNS compared to during NS.29 We have shown that tongue movement changes during periods of no milk flow, and it is possible that low milk flow, infant fatigue, and or satiety could play a role in changes in tongue movement.
Maturation of Sucking DynamicsThe similarity in tongue movement patterns over the 2 assess-ments (day 3 and follow-up) supports the idea that the new-born sucking pattern is mature in the early postpartum period. Our findings with respect to diameters along the nipple and their changes as the tongue lowers agree with those of McClellan et al, who used the same measurement technique in breastfeeding infants aged between 1-5 months.15 The small-est tongue movements occur at the base of the nipple (nipple diameter 15), and the anterior portion of the tongue lowered and rose slightly before the remainder of the tongue. It is speculated that this action assists in both maintaining a base-line vacuum (seal to the breast) and clearing the bolus from the oral cavity.15 Despite the large range of ages of the follow-up visit, there was a uniformity in infant tongue movement of breastfeeding infants, suggesting that healthy term infants at day 3 postpartum have a mature and intact sucking dynamic.
This study has shown that infants positioned the nipple in a similar location within the mouth (nipple to HSPJ mea-surement) at day 3 and follow-up. It is interesting that there does not appear to be a change from the initiation of lacta-tion to established lactation (up to 6 months), indicating that there is a particular position conducive to effective milk removal.6,15,30
We have shown the degree of movement of the mid-tongue increased after the establishment of lactation, which could be a result of the infant accommodating for a larger milk bolus at follow-up, since milk intake increased and
milk volume available to the infant would have theoretically increased after secretory activation. However, since it is cur-rently not possible to measure milk flow on the breast, this hypothesis remains unconfirmed. More efficient feeding has been the major marker of infant maturation, and increased tongue movement, more rapid NS rates, and increased milk intake at the follow-up assessment support this finding (Table 2). It has been suggested that faster sucking may allow the infant to effectively coordinate sucking, swallow-ing, and breathing as milk flow increases over the first month postpartum.31 It is possible that the increased effi-ciency is a result of maturation of the brainstem in the abil-ity to coordinate rhythmic sucking, in comparison to the reflexive sucking responses in a newborn.31,32 Although it is not possible to state definitively, our results suggest 2 pos-sible mechanisms for more efficient feeding. The first is that the infant may be able to adapt to the mother’s milk volume/flow, and the second is that the infant is able to obtain more milk per suck.32 Measurement of milk flow rates from the breast and 3D analysis of the intra-oral cavity would be required to confirm this hypothesis.
Limitations to our study include the large age range of the follow-up visit and that we were unable to measure milk flow from the breast. Given the similarity of tongue movement between day 3 and follow-up and in older infants, we expect this age range did not influence our results, however we do not know about the sucking dynamics in the first 2 days of life. Measurement of milk flow from the breast is not cur-rently possible; however, our evaluation of total milk intake and feed duration provided a proxy measure for milk flow.
ConclusionDuring the establishment of lactation, infant sucking dynam-ics during breastfeeding were similar to those observed in later lactation. Milk removal coincided with downward movement of the tongue and supports the notion that vac-uum is implicated in milk removal. The pattern of tongue movement differs for NS and NNS; however, it is not differ-ent during secretory activation compared to during estab-lished lactation, suggesting infants have a mature sucking pattern from the early postpartum period.
AcknowledgmentsWe thank the breastfeeding mothers and infants for their time and participation in the study. We also thank Mrs. Desiree Cavill and Mrs. Tracy Bingham for their work in recruitment and data collection.
Declaration of Conflicting InterestsThe authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FundingThe authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This
at University of Western Australia on October 15, 2012jhl.sagepub.comDownloaded from

Sakalidis et al. 9
study was funded by an unrestricted grant from Medela AG, Baar, Switzerland; and a grant from the Women and Infants Research Foundation, Western Australia.
References 1. Li R, Fein SB, Chen J, Grummer-Strawn LM. Why mothers
stop breastfeeding: mothers’ self-reported reasons for stopping during the first year. Pediatrics. 2008;122:S69-76.
2. Pang WW, Hartmann PE. Initiation of human lactation: secre-tory differentiation and secretory activation. J Mammary Gland Biol Neoplasia. 2007;12:211.
3. Saint L, Smith M, Hartmann PE. The yield and nutrient content of colostrum and milk of women from giving birth to 1 month post-partum. Br J Nutr. 1984;52:87-95.
4. Lucas A, Lucas PT, Baum JD. Pattern of milk flow in breast-fed infants. Lancet. 1979;314:57-58.
5. Smith WL. Imaging evaluation of the human nipple during breast-feeding. Arch Pediatr Adolesc Med. 1988;142:76.
6. Geddes DT, Kent JC, Mitoulas LR, Hartmann PE. Tongue movement and intra-oral vacuum in breastfeeding infants. Early Hum Dev. 2008;84:471-477.
7. Colley JRT, Creamer B. Sucking and swallowing in infants. BMJ. 1958;2:422-423.
8. Hytten FE. Observations on the vitality of the newborn. Arch Dis Child. 1951;26:477.
9. Ardan G, Kemp F, Lind J. A cineradiographic study of breast-feeding. Br J Radiography. 1958;XXX1:156-162.
10. Woolridge M. The anatomy of infant sucking. Midwifery. 1986;2:164-171.
11. Hayashi Y, Hoashi E, Nara T. Ultrasonographic analysis of sucking behavior of newborn infants: the driving force of suck-ing pressure. Early Hum Dev. 1997;49:33-38.
12. Bosma J, Hepburn L, Josell S, Baker K. Ultrasound demonstra-tion of tongue motions during suckle feeding. Dev Med Child Neurol. 1990;32:223-229.
13. Weber J, Woolridge M, Baum J. An ultrasonographic study of the organisation of sucking and swallowing by newborn infants. Dev Med Child Neurol. 1986;28:19-24.
14. Ardran G, Kemp F, Lind J. A cineradiographic study of breast-feeding. Br J Radiol. 1958;XXX1:156-162.
15. McClellan H, Sakalidis V, Hepworth A, Hartmann P, Geddes D. Validation of nipple diameter and tongue movement measure-ments with B-mode ultrasound during breastfeeding. Ultra-sound Med Biol. 2010;36:1797-1807.
16. Meier P. Suck-breath patterning during bottle and breast-feeding for preterm infants. In: David TJ (ed). Major con-troversies in infant Nutrition. International congress and symposium series 215. London: Royal Society of Medicine: 1996; pp.9-20.
17. Mizuno K, Ueda A. Changes in sucking performance from non-nutritive sucking to nutritive sucking during breast- and bottle-feeding. Pediatr Res. 2006;59:728-731.
18. Mathew OP, Bhatia J. Sucking and breathing patterns during breast and bottle-feeding in term neonates. Effects of nutrient delivery and composition. Am J Dis Child. 1989;143:588-592.
19. Jensen D, Wallace S, Kelsay P. LATCH: a breastfeeding chart-ing system and documentation tool. J Obstet Gynecol Neonat Nurs. 1994;23:27-32.
20. Chang Z, Heaman M. Epidural analgesia during labor and delivery: effects on the initiation and continuation of effective breastfeeding. J Hum Lact. 2005;21:305-314.
21. Arthur PG, Hartmann PE, Smith M. Measurement of the milk intake of breast-fed infants. J Pediatr Gastroenterol Nutr. 1987;6:758-763.
22. Hothorn T, Bretz F, Westfall P. Simultaneous inference in gen-eral parametric models. Biom J. 2008;50:346-363.
23. Geddes DT, Sakalidis VS, Hepworth AR, et al. Tongue move-ment and intra-oral vacuum of term infants during breastfeed-ing and feeding from an experimental teat that released milk under vacuum only. Early Hum Dev. 2012;88:443-449.
24. German R, Crompton A, Levitch L, Thexton A. The mecha-nism of suckling in two species of infant mammal: miniature pigs and long-tailed macaques. J Exp Zool. 1992;261:322-330.
25. Thexton A, Crompton A, Owerkowicz T, German R. Correla-tion between intraoral pressures and tongue movements in the suckling pig. Arch Oral Biol. 2004;49:567-575.
26. Miller JL, Kang SM. Preliminary ultrasound observation of lin-gual movement patterns during nutritive versus non-nutritive sucking in a premature infant. Dysphagia. 2007;22:150-160.
27. Goldfield EC, Richardson MJ, Lee KG, Margetts S. Coordina-tion of sucking, swallowing, and breathing and oxygen satu-ration during early infant breast-feeding and bottle-feeding. Pediatr Res. 2006;60:450-455.
28. Miller AJ. Oral and pharyngeal reflexes in the mammalian ner-vous system: their diverse range in complexity and the pivotal role of the tongue. Crit Rev Oral Biol Med. 2002;13:409.
29. Walker M. Functional assessment of infant breastfeeding pat-terns. Birth. 1989;16:140-147.
30. Jacobs LA, Dickinson JE, Hart PD, Doherty DA, Faulkner SJ. Normal nipple position in term infants measured on breastfeed-ing ultrasound. J Hum Lact 2007;23:52-59.
31. Qureshi MA, Vice FL, Taciak VL, Bosma JF, Gewolb IH. Changes in rhythmic suckle feeding patterns in term infants in the first month of life. Dev Med Child Neurol. 2002;44: 34-39.
32. Kelly B, Huckabee M-L, Jones R, Frampton C. The first year of human life: coordinating respiration and nutritive swallowing. Dysphagia. 2007;22:37-43.
at University of Western Australia on October 15, 2012jhl.sagepub.comDownloaded from
Copyright © 2022 FDOKUMEN