Breast Cancer Therapy in Different Ethnic Groups
169
Differences Are Important: Breast Cancer Therapy in Different Ethnic Groups R.L.B. Costa et al PALOMA-3: Phase 3 Trial of Fulvestrant With or Without Palbociclib in Premenopausal and Postmenopausal Women With Hormone Receptor–Positive, Human Epidermal Factor Receptor 2–Negative Metastatic Breast Cancer That Progressed on Prior Endocrine Therapy H. Iwata et al. Editorial: R.L.B. Costa et al Special Article: ASCO Multidisciplinary Cancer Management Course: Connecting Lives, Cancer Care, Education, and Compassion in Zimbabwe S. Ndarukwa et al AN AMERICAN SOCIETY OF CLINICAL ONCOLOGY JOURNAL AUGUST 2017 | Volume 3, Issue 4
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Breast Cancer Therapy in Different Ethnic Groups

Differences Are Important: Breast Cancer Therapy in Different Ethnic Groups
R.L.B. Costa et al
PALOMA-3: Phase 3 Trial of Fulvestrant With or Without Palbociclib in
Premenopausal and Postmenopausal Women With Hormone Receptor–Positive,
Human Epidermal Factor Receptor 2–Negative Metastatic Breast Cancer
That Progressed on Prior Endocrine Therapy
H. Iwata et al. Editorial: R.L.B. Costa et al
Special Article: ASCO Multidisciplinary Cancer Management Course:
Connecting Lives, Cancer Care, Education, and Compassion in Zimbabwe
S. Ndarukwa et al
AN AMERICAN SOCIETY OF
CLINICAL ONCOLOGY JOURNAL
AUGUST 2017 | Volume 3, Issue 4

ContentsEDITORIAL
Differences Are Important: Breast Cancer Therapy in Different Ethnic GroupsRicardo L.B. Costa and William J. Gradishar (see article on page 289)................................................................. 281
COMMENTARY
Developing CSCO Lung Cancer Practice Guidelines Stratified by Resource Availability and Treatment ValueQing Zhou and Yi-Long Wu.................................................................................................................................... 285
ORIGINAL REPORTS
Breast Cancer
PALOMA-3: Phase III Trial of Fulvestrant With or Without Palbociclib in Premenopausal and PostmenopausalWomenWith Hormone Receptor–Positive, Human Epidermal Growth Factor Receptor 2–NegativeMetastatic BreastCancer That Progressed on Prior Endocrine Therapy—Safety and Efficacy in Asian PatientsHiroji Iwata, Seock-Ah Im, Norikazu Masuda, et al (see editorial on page 281)..................................................... 289
Decreased Survival With Mastectomy Vis-a-Vis Breast-Conserving Surgery in Stage II and III Breast Cancers:A Comparative Treatment Effectiveness StudyAmbakumar Nandakumar, Goura Kishor Rath, Amal Chandra Kataki, et al ........................................................... 304
Clinical Overestimation of HER2 Positivity in Early Estrogen and Progesterone Receptor–Positive Breast Cancerand the Value of Molecular Subtyping Using BluePrintEttienne J. Myburgh, Lizanne Langenhoven, Kathleen A. Grant, et al .................................................................... 314
Pediatric Oncology
Prediagnostic Intervals in Retinoblastoma: Experience at an Oncology Center in BrazilClarissa Campolina de Sa Mattosinho, Nathalia Grigorovski, Evandro Lucena, et al ............................................... 323
Pain Management and Use of Opioids in Pediatric Oncology in India: A Qualitative ApproachPaola Angelini, Katherine M. Boydell, Vicky Breakey, et al..................................................................................... 331
Journal of Global Oncology (ISSN 2378-9506) is published online only six times a year, bimonthly,by the American Society of Clinical Oncology, 2318 Mill Road, Suite 800, Alexandria, VA 22314.
Editorial correspondence should be addressed to Gilberto Lopes, MD, MBA, Journal of Global Oncology.Phone: 703-797-1900; Fax: 703-684-8720. E-mail: [email protected]. Internet: ascopubs.org/journal/jgo.
Journal of Global Oncology® is a registered trademark of American Society of Clinical Oncology, Inc.
continued on next page
August 2017Volume 3, Issue 4

Epidemiology
Cancer Care at Times of Crisis and War: The Syrian ExampleEman Sahloul, Riad Salem, Wessam Alrez, et al .................................................................................................... 338
Clinical Practice
Survey of Implementation of Antiemetic Prescription Standards in Indian Oncology Practices and Its Adherence tothe American Society of Clinical Oncology Antiemetic Clinical GuidelineVijay Patil, Vanita Noronha, Amit Joshi, et al .......................................................................................................... 346
Immunotherapy
Positive PD-L1 Expression Predicts Worse Outcome in Cutaneous AngiosarcomaAkira Shimizu, Kyoichi Kaira, Yuko Okubo, et al .................................................................................................... 360
Thoracic Oncology
Comparison of Symptom Score and Bronchoscopy-Based Assessment With Conventional ComputedTomography–Based Assessment of Response to Chemotherapy in Lung CancerLakshimikant Baburao Yenge, Digambar Behera, Mandeep Garg, et al ................................................................. 370
Health Services and Outcomes
Identifying and Prioritizing Gaps in Neuroendocrine Tumor Research: A Modified Delphi Process With Patientsand Health Care Providers to Set the Research Action Plan for the Newly Formed Commonwealth NeuroendocrineTumor CollaborationEva Segelov, David Chan, Ben Lawrence, et al ...................................................................................................... 380
Presentation, Treatment, and Outcomes of Haitian Women With Breast Cancer in Miami and Haiti: Disparities inBreast Cancer—A Retrospective Cohort StudyAlexandra Gomez, Vincent DeGennaro, Sophia H.L. George, et al ......................................................................... 389
REVIEW ARTICLE
Cervical Precancer Treatment in Low- and Middle-Income Countries: A Technology OverviewMauricio Maza, Celina M. Schocken, Katherine L. Bergman, et al ......................................................................... 400
SPECIAL ARTICLE
American Society of Clinical Oncology Multidisciplinary Cancer Management Course: Connecting Lives, CancerCare, Education, and Compassion in Zimbabwe—A Pilot for Efforts of Sustainable Benefit?Sandra Ndarukwa, Anna Mary Nyakabau, Anees B. Chagpar, et al ....................................................................... 409
CASE REPORTS
Colonic Mucosa-Associated Lymphoid Tissue Lymphoma Presented as Multiple Polyposis at Colonoscopy ina Nigerian Man: Case Report of a Rare Occurrence and Brief Review of LiteratureAderemi Oluyemi and Nicholas Awolola................................................................................................................. 418
DNA Repair Defect and RAS Mutation in Two Patients With Schistosoma mansoni–Associated Colorectal Cancer:Carcinogenesis Steps or Mere Coincidence?Gustavo Fernandes Godoy Almeida, Filipe Wanick Sarinho, Paula Carvalho de Abreu e Lima, et al....................... 423
August 2017 Volume 3, Issue 4

CORRESPONDENCE
Call for Breast Cancer Risk Factor Education in Countries With Limited Health Care ResourcesTara J. Rick and Judith J. Merinyo ........................................................................................................................ 427
High Epidermal Growth Factor Receptor Mutation Rates in Peruvian Patients With Non–Small-Cell Lung Cancer:Is It a Matter of Asian Ancestry?Joseph A. Pinto, Luis A. Mas, and Henry L. Gomez ............................................................................................... 429
Also in This Issue
Editorial RosterCurrent Abstracts
@JGO_ASCO
August 2017 Volume 3, Issue 4

jgo Editorial RosterEDITOR-IN-CHIEF
Gilberto Lopes, MD, MBA, Miami, FL
ASSOCIATE EDITORS
Otis Brawley, MD, Atlanta, GA
Mary Gospodarowicz, MD, Toronto, Canada
David Kerr, MD, DSc, Oxford, United Kingdom
Tezer Kutluk, MD, PhD, Ankara, Turkey
Rengaswamy Sankaranarayanan, MD, Lyon,France
D. Cristina Stefan, MD, PhD, Cape Town, SouthAfrica
SOCIAL MEDIA EDITOR
Gilberto Lopes, MD, MBA, Miami, FL
EDITORIAL BOARD
Isaac F. Adewole, MB, BS, Ibadan, Oyo, Nigeria
Nada A. S. Al Alwan, MD, PhD, Baghdad, Iraq
Benjamin O. Anderson, MD, Seattle, WA
Ami S. Bhatt, MD, PhD, Stanford, CA
Gouri Shankar Bhattacharyya, MD, PhD, DNB,MRCP, Kolkata, India
Jeannine M. Brant, PhD, APRN, AOCN, FAAN,Billings, MT
Philip E. Castle, PhD, MPH, Arlington, VA
Franco Cavalli, MD, Ticino, Switzerland
Eduardo L. Cazap, MD, PhD, Buenos Aires,Argentina
Linus Tsuhuang Chuang, MD, MPH,New York, NY
James Cleary, MB, BS, FAChPM, Madison, WI
C. Norman Coleman, MD, Chevy Chase, MD
Anil D’Cruz, Mumbai, India
Paul de Souza BSc(Med), MBBS, MPH, PhD,FRACP, Sydney NSW, Australia
Nagi S. El Saghir, MD, Beirut, Lebanon
Ahmed Elzawawy, MD, Port Said, Egypt
Kenneth Fleming, MB ChB, MA(Oxon), DPhil,FRCPath, FRCP, Oxford, United Kingdom, andBethesda, MD
Tamer M. Fouad, MD, PhD, Cairo, Egypt
Ophira Ginsburg, MSc, MD, Toronto, Canada
William J. Gradishar, MD, Chicago, IL
Serigne Gueye, MD, FWACS, Dakar, Senegal
Francisco Gutierrez-Delgado, MD, PhD, FACP,Oaxaca, Mexico
Abdul Rahman Jazieh, MD, MPH, Riyadh, SaudiArabia
Felicia Knaul, PhD, Coral Gables, FL
Patrick J. Loehrer, MD, Indianapolis, IN
Gary H. Lyman, MD, MPH, Seattle, WA
Danny Milner, MD, Boston, MA
Twalib Ngoma, MD, Dar es Salaam, Tanzania
Nir Peled, MD, PhD, FCCP, Petah Tikva, Israel
Surendra S. Shastri, MD, Mumbai, India
Yuankai Shi, MD, PhD, Beijing, China
Lawrence N. Shulman, MD, Philadelphia, PA
George W. Sledge Jr., MD, Stanford, CA
RichardSullivan,MD,PhD,London,UnitedKingdom
Edward L. Trimble, MD, MPH, Bethesda, MD
Daniel A. Vorobiof, MD, Johannesburg, SouthAfrica
Christopher P. Wild, PhD, Lyon, France
William C. Wood, MD, Atlanta, GA
Annie Young, Coventry, UK
Publisher:David SampsonManaging Editors:Ken G. KornfieldEmilie Gunn
Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

jgo Journal of Global Oncology
JOURNAL OF GLOBAL ONCOLOGY
(ISSN 2378-9506) is published online only sixtimesa year, bimonthly, by theAmericanSociety ofClinical Oncology, 2318 Mill Road, Suite 800,Alexandria, VA 22314.
EDITORIAL CORRESPONDENCE(manuscript-related inquiries):
Gilberto Lopes, MD, MBA, Editor-in-ChiefJournal of Global OncologyPhone: 703-797-1900; Fax: 703-684-8720E-mail: [email protected]; Internet: ascopubs.org/journal/jgo
AMERICAN SOCIETY OF CLINICAL ONCOLOGY(membership-related inquiries):
ASCO Member ServicesPhone: 703-299-0158Toll-free: 888-282-2552Fax: 703-299-0255E-mail: [email protected]: www.asco.orgHours: Monday-Friday, 8:30 a.m.-5:00 p.m.Eastern Time
CUSTOMER SERVICE
JGO Customer ServicePhone: 703-519-1430; Toll-free: 888-273-3508; Fax: 703-518-8155E-mail: [email protected]
ADVERTISING SALES
The Walchli Tauber Group, Inc.225 Old Emmorton Road, Suite 201Bel Air, MD 21015Phone: 443-512-8899; Fax: 443-512-8909www.wt-group.com
BUSINESS-TO-BUSINESS SALES
Rick WerdannSpringer Healthcare, LLC233 Spring StreetNew York, NY 10013Phone: 212-460-1523Mobile: 646-209-1840E-mail: [email protected]: www.SpringerHealthcare.com
FREE PUBLIC ACCESS
Journal of Global Oncology (JGO) provides freeonline access at ascopubs.org/journal/jgo.
PERMISSIONS REQUESTS
Licensing, Rights, and Permissions DivisionAmerican Society of Clinical OncologyPhone: 571-483-1722Fax: 703-518-5094E-mail: [email protected]
Licensing: All articles are published under a CC BY or CC BY-NC-ND Creative Commons license, found here:https://creativecommons.org/licenses/.
Copyright: Copyright © 2017 by American Society of Clinical Oncology unless otherwise indicated. All rights reserved. Nopart of this publication may be reproduced or transmitted in any form or by any means now or hereafter known, electronicor mechanical, including photocopy, recording, or any information storage and retrieval system, without permission inwriting from the Publisher. Printed in the United States of America. Journal of Global Oncology® is a registered trademarkof American Society of Clinical Oncology, Inc.
Support: Journal of Global Oncology has received support from the following funders and thanks them for their generouscontributions: CRDF Global; National Cancer Institute; and US Department of Agriculture. For information about supportingJournal of Global Oncology or other programs of the American Society of Clinical Oncology (ASCO), please contact the ConquerCancer Foundation of ASCO at (571) 483-1700 or visit www.conquercancerfoundation.org/corporate-foundation-giving.
Disclaimer:The ideas and opinionsexpressed in JGO donot necessarily reflectthose of the AmericanSociety of ClinicalOncology (ASCO). Themention of any product,service, or therapy inthis publication or inany advertisement inthis publication shouldnot be construed asan endorsement of theproducts mentioned. Itis the responsibility ofthe treating physicianor other health careprovider, relying onindependent experienceand knowledge of thepatient, to determinedrug dosages and thebest treatment for thepatient. Readers areadvised to check theappropriate medicalliterature and theproduct informationcurrently provided by themanufacturer of eachdrug to be administeredto verify approveduses, the dosage,method, and durationof administration, orcontraindications.Readers are alsoencouraged to contactthe manufacturer withquestions about thefeatures or limitationsof any products. ASCOassumes no responsibilityfor any injury or damageto persons or propertyarising out of or relatedto any use of thematerial contained inthis publication or to anyerrors or omissions.
Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

jgo Current Abstracts Volume 3, Issue 4 August 2017
PALOMA-3: Phase III Trial of Fulvestrant With or Without Palbociclib inPremenopausal and Postmenopausal Women With HormoneReceptor–Positive, Human Epidermal Growth Factor Receptor2–Negative Metastatic Breast Cancer That Progressed on PriorEndocrine Therapy—Safety and Efficacy in Asian Patients
abstract
Purpose To assess efficacy and safety of palbociclib plus fulvestrant in Asians with endocrinetherapy–resistant metastatic breast cancer.
Patients and Methods The Palbociclib Ongoing Trials in the Management of Breast Cancer 3 (PALOMA-3)trial, a double-blind phase III study, included 521 patients with hormone receptor–positive/humanepidermal growth factor receptor 2–negative metastatic breast cancer with disease progression onendocrine therapy. Patient-reported outcomes (PROs) were assessed on study treatment and at the end oftreatment.
Results This preplanned subgroup analysis of the PALOMA-3 study included premenopausal andpostmenopausal Asians taking palbociclib plus fulvestrant (n = 71) or placebo plus fulvestrant (n = 31).Palbociclib plus fulvestrant improved progression-free survival (PFS) compared with fulvestrant alone.Median PFS was not reached with palbociclib plus fulvestrant (95% CI, 9.2 months to not reached) butwas 5.8 months with placebo plus fulvestrant (95% CI, 3.5 to 9.2 months; hazard ratio, 0.485; 95% CI,0.270 to 0.869; P = .0065). The most common all-cause grade 3 or 4 adverse events in the palbociclibarm were neutropenia (92%) and leukopenia (29%); febrile neutropenia occurred in 4.1% of patients.Within-patient mean trough concentration comparisons across subgroups indicated similar palbociclibexposure between Asians and non-Asians. Global quality of life was maintained; no statistically sig-nificant changes from baseline were observed for patient-reported outcome scores with palbociclib plusfulvestrant.
Conclusion This is the first report, to our knowledge, showing that palbociclib plus fulvestrant improvesPFS in asian patients. Palbociclib plus fulvestrant was well tolerated in this study.
J Glob Oncol 3. © 2017 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
continued
Hiroji Iwata
Seock-Ah Im
Norikazu Masuda
et al
pp 289-303
Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

jgo Current Abstracts Volume 3, Issue 4 August 2017
Decreased Survival With Mastectomy Vis-a-Vis Breast-ConservingSurgery in Stage II and III Breast Cancers: A Comparative TreatmentEffectiveness Study
abstract
Purpose The primary purpose of hospital-based cancer registries is assessing patient care. Clinicalstage–based survival and treatment-based survival are some of the key parameters for such assessment.Because of the challenges in obtaining follow-up parameters, a separate study on patterns of care andsurvival was undertaken by the Indian National Cancer Registry Program. The results for cancer of thefemale breast are presented here.
Patients and Methods Data abstracted in a standardized patient information form were transmitted onlineto a central repository. Treatment patterns were assessed for 9,903 patients diagnosed between January1, 2006, and December 31, 2008, from 13 institutions. Survival analysis was restricted to 7,609 patientsfrom nine institutions wherein follow-up details (as of December 31, 2012) were available for at least60% of patients.
Results The overall 5-year survival rates with breast-conserving surgery (BCS) and mastectomy (MS)were 94.0% and 85.8%, respectively, for stage II disease (adjusted hazard ratio, 2.40; 95% CI, 1.8 to3.2) and 87.1% and 69.0%, respectively, for stage III disease (hazard ratio, 2.82; 95% CI, 2.2 to 3.7).Patients who had MS did better with systemic therapy (chemotherapy and/or hormone therapy), whereaspatients with BCS required just local radiation therapy to achieve best survival.
Conclusion This observational study in the natural setting of care of patients with cancer in India showedsignificantly decreased survival with MS when compared with BCS. The reasons for lower survival withMS and the biologic or scientific rationale of the necessity of systemic therapy to achieve optimal survivalin patients undergoing MS but not in those with BCS need further investigation.
J Glob Oncol 3. © 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
continued
AmbakumarNandakumar
Goura Kishor Rath
Amal Chandra Kataki
et al
pp 304-313
Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

jgo Current Abstracts Volume 3, Issue 4 August 2017
Clinical Overestimation of HER2 Positivity in Early Estrogen andProgesterone Receptor–Positive Breast Cancer and the Value ofMolecular Subtyping Using BluePrint
abstract
Purpose Human epidermal growth factor receptor 2 (HER2) positivity is an important prognostic andpredictive indicator in breast cancer. HER2 status is determined by immunohistochemistry and fluo-rescent in situ hybridization (FISH), which are potentially inaccurate techniques as a result of severaltechnical factors, polysomy of chromosome 17, and amplification or overexpression of CEP17 (cen-tromeric probe for chromosome 17) and/or HER2. In South Africa, HER2-positive tumors are excludedfrom a MammaPrint (MP; Agendia BV, Amsterdam, Netherlands) pretest algorithm. Clinical HER2 statushas been reported to correlate poorly with molecular subtype. The aim of this study was to investigate thecorrelation of clinical HER2 status with BluePrint (BP) molecular subtyping.
Methods Clinico-pathologic and genomic information was extracted from a prospectively collectedcentral MP database containing records of 256 estrogen receptor–positive and/or progesteronereceptor–positive tumors. Twenty-one tumors considered HER2 positive on immunohistochemistry or FISHwere identified for this study.
Results The median age of patients was 56 years (range, 34 to 77 years), with a median tumor size of16 mm (3 to 27 mm). Four (19%) tumors were confirmed HER2-enriched subtype, six (29%) were luminalA, and 11 (52%) were luminal B. The positive predictive values of HER2/CEP17 ratio ‡ 2 and HER2 copynumber ‡ 6 were only 29% and 40%, respectively. The differences in means for HER2/CEP17 ratio weresignificant between BP HER2-enriched versus luminal (P = .0249; 95% CI, 0.12 to 1.21) and MP high-risk versus low-risk tumors (P = .0002; 95% CI, 0.40 to 1.06).
Conclusion Of the 21 tumors considered clinically HER2 positive, only four were HER2-enriched subtypewith BP, indicating an overestimation of HER2 positivity. FISH testing has a poor positive predictive value.
J Glob Oncol 3. © 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
continued
Ettienne J. Myburgh
Lizanne Langenhoven
Kathleen A. Grant
et al
pp 314-322
Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

jgo Current Abstracts Volume 3, Issue 4 August 2017
Prediagnostic Intervals in Retinoblastoma: Experience atan Oncology Center in Brazil
abstract
Purpose Retinoblastoma is the most common intraocular malignancy of childhood. In most cases, parentsare the first to notice leukocoria and other symptoms before undergoing a prolonged period of stressbefore diagnosis. The purpose of this study was to determine prediagnostic intervals of patients withretinoblastoma at an oncology tertiary center (Instituto Nacional de Cancer) in Rio de Janeiro, Brazil, andrelate them to stage at diagnosis, eye salvage, and survival.
Methods Parents or caregivers of children with retinoblastoma registered between January 2006 andSeptember 2013 were interviewed using a semistructured individually applied questionnaire, concerningtheir trajectory before registration.
Results Out of 76 patients, 39 (51%) were girls, 52 (68%) had unilateral retinoblastoma, and 24 (32%)had bilateral retinoblastoma, totaling 100 affected eyes. The most common stage of diagnosis was theintraocular group, with 63 (83%) patients; nine (12%) were extraocular, and four (5%) had metastaticdisease. During the follow-up time of 376 24.5 months, 10 (13%) patients died and 70 (70%) eyes wereenucleated. Mean family interval was 1.6 6 2.6 months, mean medical interval was 5.0 6 6.2 months,mean referral interval was 0.2 6 1.4 months, and mean overall interval was 7.1 6 6.9 months. Inunivariate analysis, age at diagnosis, maternal education, medical interval, and overall interval weresignificantly related to advanced stage at diagnosis and survival. In multivariate analysis, maternaleducation and medical interval were significantly related to advanced stage at diagnosis and survival. Novariables affected eye salvage.
Conclusion Medical interval was responsible for 70% of the overall interval; therefore, programs orcampaigns targeting retinoblastoma early diagnosis should focus emphasize in medical awareness.
J Glob Oncol 3. © 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
continued
Clarissa Campolina de SaMattosinho
Nathalia Grigorovski
Evandro Lucena
et al
pp 323-330
Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

jgo Current Abstracts Volume 3, Issue 4 August 2017
Pain Management and Use of Opioids in Pediatric Oncology in India:A Qualitative Approach
abstract
Purpose Consumption of medical opium for pain relief in India is low, despite the country being one of themain world producers of the substance. We investigated obstacles to opioid use and physician per-ceptions about optimal pain management in pediatric oncology patients in India.
Methods Semistructured interviews were conducted with oncologists who work in pediatric oncologysettings. A mixed sampling strategy was used, including maximum variation and confirmation anddisconfirmation of cases, as well as snowball sampling. Key informants were identified. Interviews wereaudio recorded, transcribed verbatim, and analyzed by thematic analysis methodology.
Results Twenty-three interviews were performed across 20 Indian institutions. The main obstaclesidentified were lack of financial resources, inadequate education of health care providers on painmanagement, insufficient human resources (particularly lack of dedicated trained oncology nurses), pooraccess to opioids, and cultural perceptions about pain. Children from rural areas, treated in publichospitals, and from lower socioeconomic classes appear disadvantaged. A significant equality gap existsbetween public institutions and private institutions, which provide state-of-the-art treatment.
Conclusion The study illuminates the complexity of pain management in pediatric oncology in India,where financial constraints, lack of education, and poor access to opioids play a dominant role, but lackof awareness and cultural perceptions about pain management among health care providers and parentsemerged as important contributing factors. Urgent interventions are needed to optimize care in thisvulnerable population.
J Glob Oncol 3. © 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
continued
Paola Angelini
Katherine M. Boydell
Vicky Breakey
et al
pp 331-337
Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

jgo Current Abstracts Volume 3, Issue 4 August 2017
Cancer Care at Times of Crisis and War: The Syrian Example
abstract
Purpose As Syria enters its fifth year of conflict, the number of civilians killed and injured continues torise sharply. Along with this conflict comes the rapid decline of medical care, specifically cancer care. Todetermine physician and equipment availability, cancer screening and management, and possiblesolutions relative to various major cities, a survey was distributed to physicians inside Syria through thehelp of the humanitarian organization Syrian American Medical Society.
Methods Online surveys were distributed to both certified oncologists who work in cancer clinics andgeneral physicians who work in rural and mobile clinics inside Syria. Variables assessed were physicianspecialty, location, population, cost, regional situation (besieged versus government controlled), andresource availability and access. Results were stratified by location and physician specialty.
Results Survey results revealed a large shortage of specialized physicians and inhibited accessibility toscreening and management options in besieged areas compared with government-controlled regions.Physicians within both government-controlled and besieged cities reported limited or no targeted agents,radiation therapy, clinical trials, bone marrow transplantation, positron emission tomography scans,magnetic resonance imaging, and genetic testing.
Conclusion The Syrian civil war has resulted in suboptimal oncology care in the majority of the region. Inconsideration of specific deficiencies in cancer care, we recommend several solutions that may betterthe level of care in Syria: patient education on medical documentation and self-examination; onlineconsultation; and cheap, effective screening methods. The implementation of these recommendationsmay change the course of cancer care in a country that has deteriorated into the worst humanitarian crisisof the century.
J Glob Oncol 3. © 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
continued
Eman Sahloul
Riad Salem
Wessam Alrez
et al
pp 338-345
Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

jgo Current Abstracts Volume 3, Issue 4 August 2017
Survey of Implementation of Antiemetic Prescription Standards inIndian Oncology Practices and Its Adherence to the AmericanSociety of Clinical Oncology Antiemetic Clinical Guideline
abstract
Purpose Adherence to international antiemetic prophylaxis guidelines like those of ASCO can result inbetter control of chemotherapy-induced nausea and vomiting; however, the extent of implementation ofsuch guidelines in India is unknown. Therefore, this survey was planned.
Methods This study was an anonymized cross-sectional survey approved by the ethics committee. Surveyitems were generated from the clinical questions given in the ASCO guidelines. The survey was dis-seminated through personal contacts at an oncology conference and via e-mail to various communityoncology centers across India. The B1, B2, and B3 domains included questions regarding the optimalantiemetic prophylaxis for high, moderate, and low-minimal emetogenic regimens.
Results Sixty-six (62.9%) of 105 responded and 65 centers (98.5%) were aware of the publishedguidelines. The partial, full, and no implementation scores were 92.5%, 4.5%, and 3.0%, respectively.Full implementation was better for the low-minimal emetogenic regimens (34.8%) than the highlyemetogenic regimens (6.1%). The three most frequent reasons for hampered implementation of ASCOguidelines in routine chemotherapy practice cited by centers were a lack of sensitization (26 centers;39.4%), lack of national guidelines (12 centers; 18.2%), and lack of administrative support (10 centers;15.2%).
Conclusion Awareness regarding ASCO antiemetic guidelines is satisfactory in Indian oncology prac-tices; however, there is a need for sensitization of oncologists toward complete implementation of theseguidelines in their clinical practice.
J Glob Oncol 3. © 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
continued
Vijay Patil
Vanita Noronha
Amit Joshi
et al
pp 346-359
Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

jgo Current Abstracts Volume 3, Issue 4 August 2017
Positive PD-L1 Expression Predicts Worse Outcome in CutaneousAngiosarcoma
abstract
Purpose Programmed death-1 (PD-1) or programmed death ligand-1 (PD-L1) targeted therapies haveshown promising survival outcomes in several human neoplasms. However, it is unclear whether theexpression of PD-L1 can be correlated to any clinical and pathologic variables in patients with cutaneousangiosarcoma (CA). The aim of this study was to evaluate the clinicopathological significance of PD-L1expression in CA patients.
Materials and Methods Data from 52 patients with CA were retrospectively reviewed. PD-L1 expression,tumor proliferation determined by Ki-67 index, and immunohistochemical evaluation of tumor-infiltratinglymphocytes, CD4+ and CD8+, were used to determine correlation with clinicopathological variables.
Results PD-L1 was positively expressed in 40% of all patients. PD-L1 expression was significantlyassociated with tumor cell proliferation. Multivariate analysis confirmed that high levels of CD8+ tumor-infiltrating lymphocytes were a significant predictor in patients with clinical stage I CA and the positiveexpression of PD-L1 was an independent prognostic factor in predicting worse outcome.
Conclusion PD-L1 expression is a novel pathologic marker for predicting worse outcome in patients with CA.
J Glob Oncol 3. © 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
continued
Akira Shimizu
Kyoichi Kaira
Yuko Okubo
et al
pp 360-369
Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

jgo Current Abstracts Volume 3, Issue 4 August 2017
Comparison of Symptom Score and Bronchoscopy-BasedAssessment With Conventional Computed Tomography–BasedAssessment of Response to Chemotherapy in Lung Cancer
abstract
Purpose There is a paucity of literature on symptom score (SS) plus fiberoptic bronchoscopy (FOB) –basedresponse evaluation (RE) to chemotherapy for lung cancer. This study aimed to compare the reliability ofRE by SS, chest radiograph (CXR), and FOB with computed tomography (CT) –based assessment (Re-sponse Evaluation Criteria in Solid Tumors (RECIST) and WHO criteria) for lung cancer chemotherapy.Methods This was a prospective observational study involving treatment-naïve patients with lung cancerplanned for chemotherapy, with one or more lesions on FOB and CT. Patients underwent assessment twiceby SS, CXR, FOB, and CT (at baseline and after chemotherapy). Six symptoms (dyspnea, cough, chest pain,hemoptysis, anorexia, and weight loss) were noted on visual analog scale. Respiratory symptom burden(RSB) and total symptom burden (TSB) were calculated from the first four and all six symptoms, re-spectively, as the mean of individual SS. Bronchoscopic findings were recorded as per European Re-spiratory Society classification for tracheobronchial stenosis. Responses were classified as completeresponse (CR), partial response (PR), stable disease (SD), or progressive disease (PD) by each method.For FOB and SS, improvement or worsening by ‡ 20% was taken as PR or PD, respectively, whereas< 20% change was considered SD. Agreements were tested using Cohen’s k statistic.Results All individual SS, RSB, and TSB scores, and the number and distribution of FOB lesions improvedsignificantly after chemotherapy. Individually, CXR and SS had no or minimal agreement with FOB-basedand CT-based responses. RECISTand WHO criteria had strong agreement overall (Cohen’s k = 0.872) andperfect agreement for PD (Cohen’s k = 1.000). Cohen’s kvalues for FOB-based assessment with RECISTand WHO were 0.324 and 0.349, respectively for overall RE, and 0.462 and 0.501 for differentiatingresponders (CR and PR) from nonresponders (SD and PD), respectively. Cohen’s kvalues for PD were0.629 (FOB alone), 0.672 (FOB and RSB), 0.739 (FOB and TSB), and 0.764 (FOB and CXR).Conclusion CT-based assessment should remain the reference for objective RE of chemotherapy in lungcancer. A combination of FOB and CXR may be used as a surrogate to diagnose PD if CT is not feasible.
J Glob Oncol 3. © 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
continued
Lakshimikant BaburaoYenge
Digambar Behera
Mandeep Garg
et al
pp 370-379
Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
jgo Current Abstracts Volume 3, Issue 4 August 2017
Identifying and Prioritizing Gaps in Neuroendocrine TumorResearch: A Modified Delphi Process With Patients and Health CareProviders to Set the Research Action Plan for the Newly FormedCommonwealth Neuroendocrine Tumor Collaboration
abstract
Purpose Neuroendocrine tumors (NETs) are a diverse group of malignancies that pose challengescommon to all rare tumors. The Commonwealth Neuroendocrine Tumor Collaboration (CommNETS) wasestablished in 2015 to enhance outcomes for patients with NETs in Canada, Australia, and New Zealand.A modified Delphi process was undertaken involving patients, clinicians, and researchers to identify gapsin NETs research to produce a comprehensive and defensible research action plan.
Methods A three-round modified Delphi process was undertaken with larger representation than usual formedical consensus processes. Patient/advocate and health care provider/researcher expert panelsundertook Round 1, which canvassed 17 research priorities and 42 potential topics; in Round 2, thesepriorities were ranked. Round 3 comprised a face-to-face meeting to generate final consensus rankingsand formulate the research action plan.
Results The Delphi groups consisted of 203 participants in Round 1 (64% health care providers/researchers, 36% patient/advocates; 52% Canadian, 32% Australian, and 17% New Zealander), ofwhom 132 participated in Round 2. The top eight priorities were biomarker development; peptide re-ceptor radionuclide therapy optimization; trials of new agents in advanced NETs; functional imaging;sequencing therapies for metastatic NETs, including development of validated surrogate end points forstudies; pathologic classification; early diagnosis; interventional therapeutics; and curative surgery. Twomajor areas were ranked significantly higher by patients/advocates: early diagnosis and curative surgery.Six CommNETS working parties were established.
Conclusion This modified Delphi process resulted in a well-founded set of research priorities for thenewly formed CommNETS collaboration by involving a large, diverse group of stakeholders. This ap-proach to setting a research agenda for a new collaborative group should be adopted to ensure thatresearch plans reflect unmet needs and priorities in the field.
J Glob Oncol 3. © 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
continued
Eva Segelov
David Chan
Ben Lawrence
et al
pp 380-388
Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

jgo Current Abstracts Volume 3, Issue 4 August 2017
Presentation, Treatment, and Outcomes of Haitian Women WithBreast Cancer in Miami and Haiti: Disparities in Breast Cancer—ARetrospective Cohort Study
abstract
Purpose We compared a cohort of Haitian immigrants with residents in Haiti with breast cancer (BC) toevaluate the effects of location on presentation, treatment, and outcomes.
Patients and Methods Participants were Haitian women with BC living in Miami who presented to theUniversity of Miami/Jackson Memorial Hospital and women with BC living in Haiti who presented to theInnovating Health International Women’s Cancer Center. The primary outcome was the relationshipbetween location, cancer characteristics, and survival. The secondary objective was to compare ourresults with data extracted from the SEER database. Cox regression was used to compare survival.
Results One hundred two patients from University of Miami/Jackson Memorial Hospital and 94 patientsfrom Innovating Health International were included. The patients in Haiti, compared with the patients inMiami, were younger (mean age, 50.2 v 53.7 years, respectively; P = .042), presented after a longerduration of symptoms (median, 20 v 3 months, respectively; P < .001), had more advanced stage (44.7% v25.5% with stage III and 27.6% v 18.6% with stage IV BC, respectively), and had more estrogenreceptor (ER) –negative tumors (44.9% v 26.5%, respectively; P = .024). The percentage of women whodied was 31.9% in Haiti died compared with 17.6% in Miami. Median survival time was 53.7 months forwomen in Haiti and was not reached in Miami. The risk of death was higher for women in Haiti versuswomen in Miami (adjusted hazard ratio, 3.09; P = .0024).
ConclusionWomen with BC in Haiti experience a significantly worse outcome than immigrants in Miami,which seems to be related to a more advanced stage and younger age at diagnosis, more ER-negativetumors, and lack of timely effective treatments. The differences in age and ER status are not a result ofaccess to care and are unexplained.
J Glob Oncol 3. © 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
continued
Alexandra Gomez
Vincent DeGennaro
Sophia H.L. George
et al
pp 389-399
Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
jgo Current Abstracts Volume 3, Issue 4 August 2017
Cervical Precancer Treatment in Low- and Middle-Income Countries:A Technology Overview
abstract
Cervical cancer is the fourth leading cause of cancer-related death in women worldwide, with 90% ofcases occurring in low- and middle-income countries (LMICs). There has been a global effort to increaseaccess to affordable screening in these settings; however, a corresponding increase in availability ofeffective and inexpensive treatment modalities for ablating or excising precancerous lesions is alsoneeded to decrease mortality. This article reviews the current landscape of available and developingtechnologies for treatment of cervical precancer in LMICs. At present, the standard treatment of mostprecancerous lesions in LMICs is gas-based cryotherapy. This low-cost, effective technology is anexpedient treatment in many areas; however, obtaining and transporting gas is often difficult, andunwieldy gas tanks are not conducive to mobile health campaigns. There are several promising ablativetechnologies in development that are gasless or require less gas than conventional cryotherapy. Althoughfurther evaluation of the efficacy and cost-effectiveness is needed, several of these technologies are safeand can now be implemented in LMICs. Nonsurgical therapies, such as therapeutic vaccines, antivirals,and topical applications, are also promising, but most remain in early-stage trials. The establishment ofevidence-based standardized protocols for available treatments and the development and introduction ofnovel technologies are necessary steps in overcoming barriers to treatment in LMICs and decreasing theglobal burden of cervical cancer. Guidance from WHO on emerging treatment technologies is alsoneeded.
J Glob Oncol 3. © 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
continued
Mauricio Maza
Celina M. Schocken
Katherine L. Bergman
et al
pp 400-408
Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

jgo Current Abstracts Volume 3, Issue 4 August 2017
American Society of Clinical Oncology Multidisciplinary CancerManagement Course: Connecting Lives, Cancer Care, Education,and Compassion in Zimbabwe—A Pilot for Efforts of SustainableBenefit?
executivesum
mary
The burden of cancer in low- to middle-income countries is growing and is expected to rise dramaticallywhile resources to manage this disease remain inadequate. All authorities for the management of cancerrecommend multidisciplinary care. Educational efforts by international organizations to assist localprofessionals in caring for their patients tend to have a lasting impact because they empower localprofessionals and enhance their skills. A multidisciplinary cancer management course was designed byAmerican Society of Clinical Oncology staff and local experts to provide a roadmap for cross-specialtyinteraction and coordination of care in Zimbabwe. The outcome of the course was measured throughfeedback obtained from participants and impact on local workforce. The cancer management course wasrelevant to daily practice and fostered long-lasting partnerships and collaborations. Furthermore, itresulted in a more motivated local workforce and strengthened existing multidisciplinary practices.Cancer care is in a critical state in low- to middle-income countries. Educational efforts and collaborativepartnerships may provide a cost-effective strategy with sustainable benefits. A multidisciplinary ap-proach to optimize therapy is desirable. Evaluation of the course impact after a period of 6 months to1 year is needed to determine the sustainability and impact of such efforts.
J Glob Oncol 3. © 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
Sandra Ndarukwa
Anna Mary Nyakabau
Anees B. Chagpar
et al
pp 409-417
Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

editorial
Differences Are Important: Breast CancerTherapy in Different Ethnic GroupsSee accompanying article on page 289
Breast cancer is the most frequently diagnosedcancer and the second leading cause of cancerdeath amongAsianwomen.1-3Hormonal receptor(HR) –positive tumors are the most common typeof breast cancer, and treatment of metastaticdisease remains palliative. Endocrine therapy isthe cornerstone of treatment of patients with HR-positive metastatic breast cancer (MBC). In post-menopausal patients, aromatase inhibitors havebecome the treatment of choice in first-line ther-apy with a median progression-free survival (PFS)of approximately 10months.4-7Upon disease pro-gression, second-line treatment options includeother classes of aromatase inhibitors (steroidal ornonsteroidal), the estrogen receptor antagonistfulvestrant, and tamoxifen, which have modestefficacy (median PFS, 3 to 6 months).4,8-13 Morerecently, further understanding of mechanisms ofanti-estrogen therapy resistance (eg, cell cyclekinase aberrations) fostered improvement inMBC therapy. Antiestrogen therapies functionpartly through suppression of cyclin-dependentkinase 4 (CDK4) and cyclin-dependent kinase 6(CDK6) activity, and reactivation of these kinaseshas been implicated in endocrine resistance.14
Indeed, in the first-line setting, palbociclib (a small-molecule CDK4/6 inhibitor) has shown efficacyin patients with HR-positive, human epidermalgrowth factor receptor 2 (HER2) –negative, re-current or de novo MBC in combination withletrozole. The Palbociclib Ongoing Trials in theManagement of Breast Cancer (PALOMA) -2 trialis adouble-blindphase III trial inwhich themedianPFS was 24.8 months in the palbociclib plusletrozole group compared with 14.5 months inthe placebo plus letrozole group (hazard ratio[HR], 0.58; 95% CI, 0.46 to 0.72; P , .001).15
In addition, in the Mammary Oncology Assess-ment of LEE011’s (Ribociclib) Efficacy and Safety(MONALEESA-2) trial, ribociclib (another CDK4/6inhibitor) also improved the median PFS of pa-tients with HR-positive, HER2-negative, recurrentor de novo MBC who had not received treatment
of metastatic disease (HR, 0.56; 95% CI, 0.43 to0.72; P , .001).16 In the PALOMA-3 trial, thecombination of palbociclib with fulvestrant signif-icantly improved the median PFS in patients withHR-positive, HER2-negative MBC to 9.5 months,compared with 4.6 months among patients treat-ed with fulvestrant and placebo (HR, 0.46; 95%CI, 0.36 to 0.59; P , .001).17,18
In the article that accompanies this editorial, Iwataet al19 report the results of 105 Asian patientsenrolled onto the PALOMA-3 trial. This is indeed arelevant preplanned subgroup analysis, becauseethnic pharmacogenomic differences pertainingto pharmacokinetics, pharmacodynamics, effi-cacy, and tolerance are not well understood forCDK inhibitors among Asian patients. Remark-ably Asians have been under-represented inother large randomized studies assessing effi-cacy of CDK inhibitors (ie, MONALEESA-2 trial:68 of 668 patients were Asian; PALOMA-2 trial:95 of 666 patients were Asian).15,16 The premiseof interethnic variability is further corroborated byreports of differential drug metabolism of agentsother thanpalbociclib, such as tamoxifen, throughtheCYPcomplex. For instance, asmanyas30%ofwhites are poor metabolizers of tamoxifen giventhe predominance of the CYP2D6*4 allele (rareamongAsians); conversely, 38% to 70%of Asiansare intermediate metabolizers of tamoxifen givenCYP2D6*10 allele presence (rare among non-Asians).20,21 Similarly, polymorphisms in the pro-moter enhancer region of the TYMS gene, whichencodes thymidylate synthase, may account forlower capecitabine-induced toxicity rates amongAsians compared with whites.22,23
Furthermore, outside the realm the pharmaco-genomics studies, subgroup analyses of largerbreast cancer trials support distinct risk-benefitratios of selected targeted therapies amongAsians with breast cancer. In the Breast CancerTrials of Oral Everolimus-2 (BOLERO-2), certaintoxicities were more common among Asians
Ricardo L.B. Costa
William J. Gradishar
All authors: FeinbergSchool of Medicine andRobert H. LurieComprehensive CancerCenter of NorthwesternUniversity, Chicago, IL
Corresponding author:William J. Gradishar, MD,Division of Hematology/Oncology, Department ofMedicine, FeinbergSchool of Medicine, 676North St Clair, Ste 850,Chicago, IL 60611;e-mail: [email protected].
281 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
© 2017 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License

compared with non-Asians with HR-positive,HER2-negative MBC treated with the mamma-lian target of rapamycin inhibitor everolimus com-binedwith exemestane, including stomatitis (80%v 54%, respectively), rash (50% v 37%, respec-tively), dysgeusia (31% v 20%, respectively), andpneumonitis (23% v 15%, respectively).24 Inaddition, Asian patients with HER2-positiveMBC treatedwithHER2-targetedantibodies (tras-tuzumab and pertuzumab) combined with doce-taxel needed frequent chemotherapy dosereductions (47% for Asian v 13% for non-Asianpatients).25 A remarkable differential toxicitypro-file was also observed between Asians and non-Asians (edema, 26% v 5%; myalgia, 42% v 15%;febrile neutropenia, 19% v 7%; upper respiratorytract infection, 26% v 10%; decreased appetite,47% v 19%; and rash, 44% v 22%, respectively).These examples indicate that there is need toevaluate not only the efficacy, but also the safetyofnewagents indifferentethnicgroups,particularlyAsianpatients,who formasmall proportionofearly-phase and drug registry clinical trials.
The PALOMA-3 trial showed significant baselinedifferences betweenAsians andnon-Asians.19Forinstance, Asians weighed significantly less (meanweight, 57 v 75 kg in non-Asians; P , .0013)and were shorter (mean height, 156 v 163 cmin non-Asians; P , .0013). This is remarkablebecause lower weight (ie, body mass index)has shown positive correlation with an im-proved clinical benefit rate from fulvestrantfor the treatment of HR-positive MBC.26
The median PFS in Asians was not reached in thepalbociclib arm (95% CI, 9.2 to not reached) butwas 5.8months (95%CI, 3.5 to 9.5months) in theplacebo arm (HR, 0.485; 95% CI, 0.27 to 0.87;P 5 .0065).19 Asian patients treated with fulves-trant and placebo had similar PFS to patients inhistorical Asian and non-Asian controls.8,27 Inaddition, the magnitude of benefit among Asiansand non-Asians was similar for the primary endpoint of PFS in both groups (HR, 0.451; 95% CI,0.34 to 0.59; P , .001 for non-Asians). Theseefficacy results are in harmony with preliminaryanalysis of the MONALEESA-2 trial, which en-rolled 68 Asians; a preliminary subgroup analysisshowed that PFS was significantly prolongedwith ribociclib combined with letrozole for pa-tients treated in Asia (HR, 0.298; 95% CI, 0.134to 0.662) and outside Asia (HR, 0.602; 95% CI,0.457 to 0.792).28
Neutropenia is the most common treatment-related toxicity associated with palbociclib.29 In
both the PALOMA-2 and PALOMA-3 trials, themost common treatment-related grade 3 or 4toxicity was neutropenia (66.5% and 65%, re-spectively). Of note, infection is a rare complica-tion of CDK inhibitor–induced neutropenia, andno deaths were reported as a result of infection ineither trial, indicating the favorable safety pro-file of palbociclib. All patients in the PALOMA-3trial had trough pharmacokinetic samples fordetermination of palbociclib plasma concentra-tions on the first two cycles of treatment, andexposure to treatment was similar between Asiansand non-Asians. Palbociclib was well-toleratedamong Asians; none of the Asian patients dis-continued treatment as a result of toxicity, andmeasures of patient-reported outcomes showedno significant deterioration in global quality oflife. However, Asian patients had higher rates ofgrade 3 and 4 neutropenia compared with non-Asians (92% v 58%, respectively). In a phase Istudy of palbociclib plus letrozole in Japanesepatients, 83% had grade 3 or 4 neutropenia.30
Similar results were also seen with ribociclib inthe MONALEESA-2 trial, in which grade 3 or 4neutropenia was documented in 71% of the 35Asians patients treated with ribociclib and letro-zole.28 Interestingly, Asians in the PALOMA-3trial had an absolute neutrophil count 19% lowerthan non-Asians at baseline, but additional studiesare needed understand whether the increasedneutropenia rates inAsians are a function of lowerpretreatment WBC counts. Among non-Asians,neutropenia has not shown correlation withprior chemotherapy, tumor grade, body weight,or age.29,31
Taking into account all caveats inherent to ana-lyses of subpopulations of large clinical trials (eg,invariably small sample size, multiplicity of test-ing), the data presented by Iwata et al19 supportthe clinically meaningful efficacy of palbociclibfor the end point of PFS in Asians. However, thisreport and others indicate that Asians have ahigher risk of adverse events (eg, grade 3 and 4neutropenia) despite preserved patient-reportedoutcomes and quality of life; the reasons for thishave yet to be elucidated. In light of growingevidence of interethnic pharmacogenomic andsafety discrepancies between Asians and non-Asians observed in recently published clinical tri-als and observational studies, there is a clear needfor enhanced enrollment of Asians and otherethnic groups into clinical trials of new agents forthe treatment of MBC.
DOI: https://doi.org/10.1200/JGO.2017.009936Published online on jgo.org on April 11, 2017.
282 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

AUTHOR CONTRIBUTIONS
Manuscript writing: All authorsFinal approval of manuscript: All authors
AUTHORS’ DISCLOSURES OFPOTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided byauthors of this manuscript. All relationships are consideredcompensated. Relationships are self-held unless noted. I 5
Immediate Family Member, Inst 5 My Institution. Relation-ships may not relate to the subject matter of this manuscript.For more information about ASCO’s conflict of interest policy,please refer to www.asco.org/rwc or ascopubs.org/jco/site/ifc.
Ricardo L.B. CostaNo relationship to disclose
William J. GradisharNo relationship to disclose
REFERENCES
references
1. Siegel RL, Miller KD, Jemal A: Cancer statistics, 2016. CA Cancer J Clin 66:7-30, 2016
2. Bray F, McCarron P, Parkin DM: The changing global patterns of female breast cancer incidenceand mortality. Breast Cancer Res 6:229-239, 2004
3. Shin HR, Joubert C, Boniol M, et al: Recent trends and patterns in breast cancer incidence amongEastern and Southeastern Asian women. Cancer Causes Control 21:1777-1785, 2010
4. Howell A, Robertson JF, Abram P, et al: Comparison of fulvestrant versus tamoxifen for thetreatment of advanced breast cancer in postmenopausal women previously untreated with en-docrine therapy: Amultinational, double-blind, randomized trial. J Clin Oncol 22:1605-1613, 2004
5. Bonneterre J, Buzdar A, Nabholtz JM, et al: Anastrozole is superior to tamoxifen as first-line therapyin hormone receptor positive advanced breast carcinoma. Cancer 92:2247-2258, 2001
6. Paridaens RJ, Dirix LY, Beex LV, et al: Phase III study comparing exemestane with tamoxifen asfirst-line hormonal treatment of metastatic breast cancer in postmenopausal women: The Euro-pean Organisation for Research and Treatment of Cancer Breast Cancer Cooperative Group. J ClinOncol 26:4883-4890, 2008
7. Mouridsen H, Gershanovich M, Sun Y, et al: Superior efficacy of letrozole versus tamoxifen as first-line therapy for postmenopausal women with advanced breast cancer: Results of a phase III studyof the International Letrozole Breast Cancer Group. J Clin Oncol 19:2596-2606, 2001
8. Di Leo A, Jerusalem G, Petruzelka L, et al: Results of the CONFIRM phase III trial comparingfulvestrant 250 mg with fulvestrant 500 mg in postmenopausal women with estrogen receptor-positive advanced breast cancer. J Clin Oncol 28:4594-4600, 2010
9. Johnston SR, Kilburn LS, Ellis P, et al: Fulvestrant plus anastrozole or placebo versus exemestanealone after progression on non-steroidal aromatase inhibitors in postmenopausal patients withhormone-receptor-positive locally advanced or metastatic breast cancer (SoFEA): A composite,multicentre, phase 3 randomised trial. Lancet Oncol 14:989-998, 2013
10. Chia S, Gradishar W, Mauriac L, et al: Double-blind, randomized placebo controlled trial of ful-vestrant compared with exemestane after prior nonsteroidal aromatase inhibitor therapy in post-menopausal women with hormone receptor-positive, advanced breast cancer: Results from EFECT.J Clin Oncol 26:1664-1670, 2008
11. Lønning PE, Taylor PD, Anker G, et al: High-dose estrogen treatment in postmenopausal breastcancer patients heavily exposed to endocrine therapy. Breast Cancer Res Treat 67:111-116, 2001
12. Ingle JN, Suman VJ, Rowland KM, et al: Fulvestrant in women with advanced breast cancer afterprogression on prior aromatase inhibitor therapy: North Central Cancer Treatment Group TrialN0032. J Clin Oncol 24:1052-1056, 2006
13. Bines J, Dienstmann R, Obadia RM, et al: Activity of megestrol acetate in postmenopausal womenwith advanced breast cancer after nonsteroidal aromatase inhibitor failure: A phase II trial. AnnOncol 25:831-836, 2014
14. Miller TW, Balko JM, Fox EM, et al: ERa-dependent E2F transcription can mediate resistance toestrogen deprivation in human breast cancer. Cancer Discov 1:338-351, 2011
15. Finn RS, Martin M, Rugo HS, et al: Palbociclib and letrozole in advanced breast cancer. N Engl JMed 375:1925-1936, 2016
283 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

16. Hortobagyi GN, Stemmer SM, Burris HA, et al: Ribociclib as first-line therapy for HR-positive,advanced breast cancer. N Engl J Med 375:1738-1748, 2016
17. Turner NC, Ro J, Andre F, et al: Palbociclib in hormone-receptor-positive advanced breast cancer.N Engl J Med 373:209-219, 2015
18. Cristofanilli M, Turner NC, Bondarenko I, et al: Fulvestrant plus palbociclib versus fulvestrant plusplacebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer thatprogressed on previous endocrine therapy (PALOMA-3): Final analysis of the multicentre, double-blind, phase 3 randomised controlled trial. Lancet Oncol 17:425-439, 2016
19. IwataH, Im S-A,MasudaN, et al: PALOMA-3: Phase III trial of fulvestrant with or without palbociclibin premenopausal and postmenopausal women with hormone receptor–positive, human epi-dermal growth factor receptor 2–negative metastatic breast cancer that progressed on priorendocrine therapy—Safety and efficacy in Asian patients. J Glob Oncol 3:289-303, 2017
20. Lim HS, Ju Lee H, Seok Lee K, et al: Clinical implications of CYP2D6 genotypes predictive oftamoxifen pharmacokinetics in metastatic breast cancer. J Clin Oncol 25:3837-3845, 2007
21. Bradford LD: CYP2D6 allele frequency in European Caucasians, Asians, Africans and their de-scendants. Pharmacogenomics 3:229-243, 2002
22. Marsh S, Collie-Duguid ES, Li T, et al: Ethnic variation in the thymidylate synthase enhancer regionpolymorphism among Caucasian and Asian populations. Genomics 58:310-312, 1999
23. Haller DG, Cassidy J, Clarke SJ, et al: Potential regional differences for the tolerability profiles offluoropyrimidines. J Clin Oncol 26:2118-2123, 2008
24. Noguchi S, Masuda N, Iwata H, et al: Efficacy of everolimus with exemestane versus exemestanealone in Asian patients with HER2-negative, hormone-receptor-positive breast cancer in BOLERO-2. Breast Cancer 21:703-714, 2014
25. Swain SM, Im YH, Im SA, et al: Safety profile of pertuzumab with trastuzumab and docetaxel inpatients from Asia with human epidermal growth factor receptor 2-positive metastatic breastcancer: Results from the phase III trial CLEOPATRA. Oncologist 19:693-701, 2014
26. Gevorgyan A, Bregni G, Galli G, et al: Body mass index and clinical benefit of fulvestrant inpostmenopausal women with advanced breast cancer. Tumori 102:e11-e14, 2016
27. Yoo C, Kim SB, Ahn JH, et al: Efficacy of fulvestrant in heavily pretreated postmenopausal womenwith advanced breast cancer: A preliminary report. J Breast Cancer 14:135-139, 2011
28. Yap YS, Tseng LM, Blackwell KL, et al: First-line ribociclib 1 letrozole in postmenopausal Asianwomen with hormone receptor-positive (HR1), human epidermal growth factor receptor2-negative (HER2–) advanced breast cancer (ABC): A subgroup analysis from MONALEESA-2.Ann Oncol 27, 2016 (suppl 9; abstr LBA1)
29. Finn RS, Crown JP, Ettl J, et al: Efficacy and safety of palbociclib in combination with letrozole asfirst-line treatment of ER-positive, HER2-negative, advanced breast cancer: Expanded analyses ofsubgroups from the randomized pivotal trial PALOMA-1/TRIO-18. Breast Cancer Res 18:67, 2016
30. Tamura K, Mukai H, Naito Y, et al: Phase I study of palbociclib, a cyclin-dependent kinase 4/6inhibitor, in Japanese patients. Cancer Sci 107:755-763, 2016
31. FinnR, Crown J, Ettl J, et al: Clinical patterns of palbociclib associated neutropenia in the PALOMA-1/TRIO-18 trial. Ann Oncol 25:iv116-iv136, 2014 (suppl 4)
284 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

commentaries
Developing CSCO Lung Cancer PracticeGuidelines Stratified by ResourceAvailability and Treatment Value
China is the third-largest country by area and thelargest low- tomiddle-incomecountry in theworld.Economic growth and urbanization have resultedin sedentary lifestyles, increasingly Western die-tary habits, and increases in smoking rates, alco-hol consumption, and environmental pollution.These changes have led to increased rates ofnoncommunicable diseases such as cancer.1,2
According to data from GLOBOCAN 2012 (Esti-mated Cancer Incidence, Mortality and Preva-lence Worldwide in 2012), lung cancer accountsfor 21.3% of all cancers and 27.1% of all cancer-related deaths in China, making it the most com-mon cancer in terms of both incidence andmortality for women and men.3 Many lung cancertreatment guidelines have been developed, includ-ing the ASCO guidelines andNational Comprehen-sive Cancer Network Guidelines in the UnitedStates and the European Society for Medical On-cology guidelines. Asian countries such as Japanand South Korea have their own lung cancer treat-ment guidelines. In contrast, diagnosis and treat-ment of Chinese patients with lung cancer is stillmostly dependent on foreign guidelines. GivenChina’s vast population,widegeographicspan,anddiverse cultures and socioeconomic groups, can-cer treatments vary greatly, and one standard set ofguidelines will not suffice. Although medical care inwestern China has improved rapidly, the more de-veloped eastern areas continue to benefit most fromrecent progress in cancer treatment.4 Urban resi-dents generally have higher socioeconomic statusand better access to cancer care compared withrural residents. Patients with cancer in more de-veloped regions are more likely to have accessto essential drugs, therapies, and screenings. Butsome patients are overtreated through the off-labeluse of anticancer drugs,5 which can occur as aresult of poor socioeconomic status, shortage ofanticancer drugs, profitable prescriptions, unfamil-iarity with the latest medical developments, and alack of guidelines that suit all Chinese patients withcancer. At the same time, China is one of the mostactive regions for lung cancer research, which is
beneficial to patients with lung cancer worldwide.Expanding the benefits of lung cancer research tothe entire Chinese population is one of the mostprominent issues facing Chinese care providers.
Applying Western cancer research to Chinesepatients is problematic. Chinese patients withnon–small-cell lung cancer (NSCLC) differ fromWestern patients in multiple ways, including dif-ferent driver mutations, different etiologies,6-10
and different tolerances to treatment. Therefore,several top cancer experts from the Chinese So-ciety of Clinical Oncology (CSCO) have developed aset of lung cancer guidelines to promote standard-ization of lung cancer diagnosis and treatment inChina.TheCSCOguide referencesother guidelinesand the latest updates in lung cancer research; italso has modified treatment guidelines for Chinese-specific populations; the goal is to benefit Chinesepatients and offer practical instructions for doctorsin China who treat patients with lung cancer.
This guide includes both tables and text butmostly tables with supplementary text descriptions.The information in the tables has been made asclear and concise as possible for convenient citationand reference, and evidence and consensus areincluded along with diagnosis and treatmentsuggestions. Addendums are attached to tableswhen needed. The CSCO categories of evidenceand consensus are as follows: category 1 includesmulticenter randomized controlled clinical trialsandmay vary between global and Chinese clinicalpractice; category 2 includes single-center ran-domized controlled clinical trials or highly influ-ential translational medical research; category 3includes studies that raised new questions. Thetext portions of this guide include detailed de-scriptions and reviews of the latest evidence,which are based on proof and academic findingsto clarify current developments and to meet ahigher level of clinical and academic needs. Noveldrugs that are available in other countries but notyet approved in China are introduced in the text orsummarized in separate tables.
Qing Zhou
Yi-Long Wu
All authors: GuangdongLung Cancer Institute,Guangdong GeneralHospital, and GuangdongAcademy of MedicalSciences, Guangzhou,People’s Republic ofChinaCorresponding author:Yi-LongWu,MD,GuangdongLung Cancer Institute,Guangdong GeneralHospital and GuangdongAcademy of MedicalSciences, 106 ZhongshanEr Rd, Guangzhou510080, People’sRepublic of China; e-mail:[email protected].
285 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
© 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License

The most significant characteristic of this set ofguidelines is that it has two strategy levels focusedon both resource availability and treatment value:a basic strategy and an optional strategy. Basicstrategies are targeted to county-level hospitalsand above. These recommendations are funda-mental for diagnosis and treatment and are basedon a high level of evidence and consensus; mostimportantly, they are accessible. Optional strate-gies are higher-level choices that include moreeffective treatments available in better medicalcenters in more developed regions. Our previousretrospective study of a large number of patientsfrom an outpatient oncology database revealedmajor disparities in the treatment of patients withlung cancer in China. Therefore, it was importantto develop new guidelines for treatment that arestratified according to available resources andtreatment value.11 This stratification providesreasonable and actionable instructions for differ-ent levels of medical care providers, with the goalof tailoring the treatment of patients with lungcancer in China and reducing the burden of lungcancer.
Two examples can help explain the recommen-dation levels. First, for patients with stage IIIBNSCLC, the widely accepted standard treatmentis definitive concurrent chemoradiation therapy.12-17
However, given the technical conditions neces-sary for radiotherapy and the capacity for treat-ing radiation-related complications in China,the basic strategy in the CSCO guidelines onlyrecommends a combination of radiotherapy
and chemotherapy, either sequential or concur-rent. For institutions fully qualified to provideradiotherapy, concurrent chemoradiotherapyis recommended as an optional strategy. Asecond example is bevacizumab combinedwith platinum-based chemotherapy as first-linetherapy for metastatic NSCLC,18-20 which is aworldwide standard treatment strategy. How-ever, the cost of the drug (¥20,000 to ¥35,000per cycle for bevacizumab alone) is unafford-able for most families, so the CSCO guidelineslist this as an optional strategy. Examples offirst-line treatment of stage IV non–squamous-cell lung cancer without a driver gene are listedin Table 1.
The latestdiscoveriesand traits specific toChinesepeople still need to be included in this guide, alongwith other topics such as palliative care. To keepupwith the fast paceof researchanddiscoveries inthe field of lung cancer diagnosis and treatment,lung cancer experts from CSCO are scheduled toupdate the guidelines once a year, with a newguide planned for release each April. This is thefirst detailed set of lung cancer guidelines inChina. With appropriate publicity and promotion,the guidelines are expected to improve the diag-nosis and treatment of patients with lung cancer inChina.
Increasing numbers of domestically producednovel drugs to treat lung cancer are being investi-gated andwill eventually benefit Chinese patientswith lung cancer. In addition, more and better
Table 1. First-Line Treatment of Stage IV Non–Squamous-Cell Lung Cancer Without a Driver Gene.
Stage Stratification Basic Strategy Optional Strategy
Stage IV non–squamous-cell lung cancerwithout a driver gene
PS 5 0~1 Cisplatin or carboplatin-based doubletregimen:
1. Pemetrexedmaintenance therapyfor non-DP patientsafter approximately fourto six cycles cisplatin orcarboplatin 1pemetrexed inductionchemotherapy(category 1)
Cisplatin or carboplatin 1gemcitabine (category 1)
2. Carboplatin 1paclitaxel 1bevacizumab, thenbevacizumabmaintenance therapy(category 1)
Cisplatin or carboplatin 1 docetaxel(category 1)
Cisplatin or carboplatin 1 paclitaxel(category 1)
Cisplatin or carboplatin1 vinorelbine(category 1)
Cisplatin or carboplatin 1pemetrexed (category 1)
PS 5 2 Single regimen chemotherapyGemcitabine (category 2A)Paclitaxel (category 2A)Vinorelbine (category 2A)Docetaxel (category 2A)
Abbreviation: DP, disease progression; PS, performance status.
286 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

individual-initiated trials are in progress, andacademic organizations such as the Chinese Tho-racic Oncology Group have achieved better out-comes among Chinese patients with lung cancer.Together, these activities will eventually improve
diagnosis, treatment, and outcomes among pa-tients with lung cancer in China.
DOI: https://doi.org/10.1200/JGO.2016.006734Published online on jgo.org on October 12, 2016.
AUTHOR CONTRIBUTIONS
Manuscript writing: All authorsFinal approval of manuscript: All authors
AUTHORS’ DISCLOSURES OFPOTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided byauthors of this manuscript. All relationships are consideredcompensated. Relationships are self-held unless noted. I 5Immediate Family Member, Inst 5 My Institution. Relation-ships may not relate to the subject matter of this manuscript.For more information about ASCO’s conflict of interest
policy, please refer to www.asco.org/rwc or ascopubs.org/jco/site/ifc.
Qing ZhouNo relationship to disclose
Yi-Long WuHonoraria: AstraZeneca, Eli Lilly, Roche, Pierre Fabre,Pfizer, SanofiConsulting or Advisory Role: AstraZeneca, Roche, Merck,Boehringer IngelheimResearch Funding: Boehringer Ingelheim (Inst), Roche (Inst)
REFERENCES1. World Health Organization: Western Pacific Region: China. 2012. http://www.wpro.who.int/
countries/chn/en/
2. Ferlay J, Soerjomataram I, ErvikM, et al: GLOBOCAN2012 v1.0, Cancer Incidence andMortalityWorldwide:IARCCancerBaseNo. 11. Lyon, France, International Agency forResearch onCancer. http://globocan.iarc.fr
3. Zhang Y, Tao S, Shen H, et al: Inhalation exposure to ambient polycyclic aromatic hydrocarbonsand lung cancer risk of Chinese population. Proc Natl Acad Sci USA 106:21063-21067, 2009
4. Liu J, Chen G, Chi I, et al: Regional variations in and correlates of disability-free life expectancyamong older adults in China. BMC Public Health 10:446, 2010
5. Wang W, Zhu M, Guo D, et al: Off-label and off-NCCN guidelines uses of antineoplastic drugs inChina. Iran J Public Health 42:472-479, 2013
6. Wu YL, Zhong WZ, Li LY, et al: Epidermal growth factor receptor mutations and their correlation withgefitinib therapy in patients with non-small cell lung cancer: A meta-analysis based on updatedindividual patient data from six medical centers in mainland China. J Thorac Oncol 2:430-439, 2007
7. Mok TS: Personalized medicine in lung cancer: What we need to know. Nat Rev Clin Oncol 8:661-668, 2011
8. Jemal A, Bray F, Center MM, et al: Global cancer statistics. CA Cancer J Clin 61:69-90, 2011
9. World Health Organization: Report on the Global Tobacco Epidemic: The MPOWER package,2008. http://www.who.int/tobacco/mpower/mpower_report_full_2008.pdf
10. Loomis D, Grosse Y, Lauby-Secretan B, et al: The carcinogenicity of outdoor air pollution. LancetOncol 14:1262-1263, 2013
11. Yang LL, Zhang XC, Yang XN, et al: Lung cancer treatment disparities in China: A question in needof an answer. Oncologist 19:1084-1090, 2014
12. Albain KS, Swann RS, Rusch VW, et al: Radiotherapy plus chemotherapy with or without surgicalresection for stage III non-small-cell lung cancer: A phase III randomised controlled trial. Lancet374:379-386, 2009
13. Curran WJ Jr, Paulus R, Langer CJ, et al: Sequential vs. concurrent chemoradiation for stage IIInon-small cell lung cancer: Randomized phase III trial RTOG 9410. J Natl Cancer Inst 103:1452-1460, 2011
14. Belani CP, Choy H, Bonomi P, et al: Combined chemoradiotherapy regimens of paclitaxel andcarboplatin for locally advanced non-small-cell lung cancer: A randomized phase II locally ad-vanced multi-modality protocol. J Clin Oncol 23:5883-5891, 2005
287 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

15. Gandara DR, Chansky K, Albain KS, et al: Long-term survival with concurrent chemoradiationtherapy followed by consolidation docetaxel in stage IIIB non-small-cell lung cancer: A phase IISouthwest Oncology Group study (S9504). Clin Lung Cancer 8:116-121, 2006
16. Hanna NH, Neubauer M, Ansari R, et al: Phase III trial of cisplatin (P) plus etoposide (E) plusconcurrent chest radiation (XRT) with or without consolidation docetaxel (D) in patients (pts) withinoperable stage III non-small cell lung cancer (NSCLC): HOG LUN 01–24/USO-023. J Clin Oncol25:18s, 2007 (suppl; abstr 7512)
17. Mina LA, Neubauer MA, Ansari RH, et al: Phase III trial of cisplatin (P) plus etoposide (E) plusconcurrent chest radiation (XRT) with or without consolidation docetaxel (D) in patients (pts) withinoperable stage III non-small cell lung cancer (NSCLC): HOG LUN 01–24/USO-023—Updatedresults. J Clin Oncol 26:15s,2008 (suppl; abstr 7519)
18. Patel JD, Socinski MA, Garon EB, et al: PointBreak: A randomized phase III study of pemetrexedplus carboplatin and bevacizumab followed bymaintenance pemetrexed and bevacizumab versuspaclitaxel plus carboplatin and bevacizumab followed by maintenance bevacizumab in patientswith stage IIIB or IV nonsquamous non-small-cell lung cancer. J Clin Oncol 31:4349-4357, 2013
19. Barlesi F, Scherpereel A, Rittmeyer A, et al: Randomized phase III trial of maintenance bev-acizumab with or without pemetrexed after first-line induction with bevacizumab, cisplatin, andpemetrexed in advanced nonsquamous non-small-cell lung cancer: AVAPERL (MO22089). J ClinOncol 31:3004-3011, 2013
20. Barlesi F, Scherpereel A, Gorbunova V, et al: Maintenance bevacizumab-pemetrexed after first-line cisplatin-pemetrexed-bevacizumab for advanced nonsquamous nonsmall-cell lung cancer:Updated survival analysis of the AVAPERL (MO22089) randomized phase III trial. Ann Oncol 25:1044-1052, 2014
288 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

originalreport
PALOMA-3:Phase III Trialof FulvestrantWithor Without Palbociclib in Premenopausaland Postmenopausal WomenWith HormoneReceptor–Positive, Human EpidermalGrowth Factor Receptor 2–NegativeMetastatic Breast Cancer That Progressedon Prior Endocrine Therapy—Safety andEfficacy in Asian PatientsSee accompanying editorial on page 281
abstract
Purpose To assess efficacy and safety of palbociclib plus fulvestrant in Asians with endocrinetherapy–resistant metastatic breast cancer.
Patients and Methods The Palbociclib Ongoing Trials in the Management of Breast Cancer 3 (PALOMA-3)trial, a double-blind phase III study, included 521 patients with hormone receptor–positive/human epi-dermal growth factor receptor 2–negativemetastatic breast cancerwith disease progression on endocrinetherapy. Patient-reported outcomes (PROs) were assessed on study treatment and at the end of treatment.
Results This preplanned subgroup analysis of the PALOMA-3 study included premenopausal and post-menopausal Asians taking palbociclib plus fulvestrant (n = 71) or placebo plus fulvestrant (n = 31).Palbociclib plus fulvestrant improved progression-free survival (PFS) compared with fulvestrant alone.Median PFSwas not reachedwith palbociclib plus fulvestrant (95%CI, 9.2months to not reached) but was5.8monthswith placebo plus fulvestrant (95%CI, 3.5 to 9.2months; hazard ratio, 0.485; 95%CI, 0.270 to0.869; P = .0065). The most common all-cause grade 3 or 4 adverse events in the palbociclib arm wereneutropenia (92%) and leukopenia (29%); febrile neutropenia occurred in 4.1% of patients. Within-patient mean trough concentration comparisons across subgroups indicated similar palbociclib exposurebetween Asians and non-Asians. Global quality of life was maintained; no statistically significant changesfrom baseline were observed for patient-reported outcome scores with palbociclib plus fulvestrant.
ConclusionThis is the first report, to our knowledge, showing that palbociclib plus fulvestrant improvesPFSin asian patients. Palbociclib plus fulvestrant was well tolerated in this study.
J Glob Oncol 3. © 2017 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
INTRODUCTION
Breast cancer mortality rates in North Americanand Asian countries are comparable, with onestudy noting that approximately 50% to 75% ofAsian women have hormone receptor (HR) –
positive/human epidermal growth factor receptor2 (HER2) –negative breast cancer.1,2 ThemedianageofAsiansat the timeofbreast cancerdiagnosis
(45 to 50 years) is lower than that of Westernpatients (55 to 60 years), including those in theUnited States.3,4 Thus, the rate of premeno-pausal women with breast cancer is higher inAsian populations compared with non-Asianpopulations.5,6 Cancer therapy effectivenesscan also vary between Asians and non-Asians,and Asians may have a different adverse event
Hiroji Iwata
Seock-Ah Im
Norikazu Masuda
Young-Hyuck Im
Kenichi Inoue
Yoshiaki Rai
Rikiya Nakamura
Jee Hyun Kim
Justin T. Hoffman
Ke Zhang
Carla Giorgetti
Shrividya Iyer
Patrick T. Schnell
Cynthia Huang Bartlett
Jungsil Ro
Author affiliations andsupport information (ifapplicable) appear at theend of this article.Clinical trial information:NCT01942135.
Correspondingauthor:HirojiIwata, MD, PhD, AichiCancer Center Hospital,1-1, Kanokoden, Chikusa-ku, Nagoya, 464-8681,Japan; e-mail address:[email protected].
289 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
© 2017 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License

(AE) experience versus women from other regionsas a result of various reasons such as pharmaco-genomics and differences in the metabolism of aspecific drug.7
In patients with HR-positive/HER2-negative met-astatic breast cancer (MBC), endocrine therapy isthe mainstay of treatment8; however, major chal-lenges exist when treating patients who have de-veloped resistance to endocrine therapy withtamoxifen or aromatase inhibitors.9,10 Thus, treat-ments that can overcome endocrine therapy re-sistance and improve outcomes are essential.
Palbociclib, an oral small-molecule inhibitor ofcyclin-dependent kinases 4 and 6 (CDK4/6), pre-vents DNA synthesis by blocking the progressionof the cell cycle from the G1 to the S phase.11,12
The Palbociclib Ongoing Trials in the Manage-ment of Breast Cancer 3 (PALOMA-3) study in-cluded women with HR-positive/HER2-negativeadvanced breast cancer whose cancer had re-lapsedor progressedduringor afterprior endocrinetherapy.13,14 In the endocrine-resistant setting,palbociclib plus fulvestrant demonstrated im-proved efficacy versus fulvestrant plus placebo(median progression-free survival [PFS], 9.5 v4.6months, respectively; hazard ratio [HR], 0.46;95% CI, 0.36 to 0.59; P, .001).13 This subgroupanalysis evaluates the efficacy and safety of pal-bociclib plus fulvestrant versus placebo plus ful-vestrant in Asians and non-Asians enrolled ontoPALOMA-3, a placebo-controlled clinical study.
PATIENTS AND METHODS
Patients and Study Design
PALOMA-3, an international, multicenter, ran-domized, double-blind, placebo-controlled,parallel-group, phase III clinical trial, includedwomenwithHR-positive/HER2-negative advancedbreast cancer whose cancer had relapsed or pro-gressed (on the basis of histologic or cytologicconfirmation of recurrent local or distant diseaseprogression) during or within 12 months of com-pleting adjuvant endocrine therapy or while on orwithin 1 month from prior endocrine therapy foradvancedbreast cancerorMBC.13,14Onepreviousline of chemotherapy for advanced or metastaticdisease was allowed. Asian patients in this analysiswere defined as all patients who self-identifiedtheir race as Asian to investigators from the fol-lowing options provided on the case report form:white, black, Asian, or other. Asian patients wereincluded from eight study sites in Japan (n = 35),five sites in Korea (n = 43), and two sites in Taiwan(n = 4); 23 other Asian patients also were includedin this analysis.
Patients were randomly assigned 2:1 to receivepalbociclib plus fulvestrant or placebo plus fulves-trant. Patients receivedplacebo or palbociclib 125mg/d orally for 3 weeks followed by 1 week off;fulvestrant 500mgwas administered intramuscu-larly on days 1 and 15 of cycle 1 and then every28days (67days) thereafter starting fromday1ofcycle 1.13,14 In premenopausal patients, anyluteinizing hormone–releasing hormone (LHRH)agonist was administered starting at least 4 weeksbefore study therapy initiation. Patients who didnot receive goserelin as their LHRH agonist beforestudy entry were switched to goserelin from thetime of random assignment through the entirestudy treatment period. The primary objectivewas investigator-assessed PFS; secondary objec-tives included clinical benefit response (CBR),objective response rate (ORR), survival probabil-ities, safety and tolerability, and patient-reportedoutcomes (PROs). In April 2015, the independentdatamonitoring committee reviewed the results ofthe study and concluded that its primary objectivehad been met as the study crossed the prespeci-fied Haybittle-Peto efficacy stopping boundary(a = .00135).13 The updated results of the overallpopulation have been previously published, andthesedata (cutoff date:March16, 2015)were alsoused in this present analysis.13
An institutional review board/independent ethicscommittee approved the protocol; the studywas conducted in accordance with the Declara-tion of Helsinki. All patients provided written in-formed consent before any study procedureswere started. Additional patient eligibility criteriaand study design details have been describedpreviously.13,14
Assessments
PFS was defined as the time from the date ofrandom assignment to the date of first documen-tation of objective progression of disease or deathas a result of any cause in the absence of docu-mented progression of disease, whichever oc-curred first. CBR was defined as the overall rateof complete response, partial response, or stabledisease > 24 weeks according to the ResponseEvaluation Criteria in Solid Tumors (RECIST) ver-sion 1.1. Objective response was defined as theoverall complete response or partial responseaccording to RECIST version 1.1. Using x-ray,computed tomography, or magnetic resonanceimaging, tumor assessments were performed atbaseline and every 8 weeks for the first year andthen every 12weeks. The type, incidence, severity,and seriousness of AEs and the relationship of AEs
290 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

to studymedicationswere recorded.Severity of AEswas graded on the basis of the National CancerInstitute Common Terminology Criteria for AdverseEvents version 4.0. A serious AE was defined as anAE that results in death, is life threatening, requiresinpatient hospitalization or prolongation of existinghospitalization, results in persistent or significantdisabilityor incapacity,or results incongenitalanom-aly or birth defect. An AE could additionally beconsidered serious by the investigator if it jeop-ardized the patient or required intervention toprevent one of the other AE outcomes.
In addition, pharmacokinetic (PK) data and PROswere assessed by race. Trough PK samples fordetermination of palbociclib plasma concentra-tions were collected from all randomly assignedpatients on day 15 of cycles 1 and 2. PROs wereassessed using the European Organisation forResearch and Treatment of Cancer Quality of LifeQuestionnaire C30, a 30-item questionnairethat includes functional scales, symptom scales,and a global health status/quality-of-life (QOL)scale.15,16 For functional and global QOL scales,higher scores represent a better level of function-ing. For symptom-oriented scales, a higher scorerepresentsmore severe symptoms.PROquestion-naires were completed before dose on day 1 ofcycles 1 to 4, then on day 1 of every other sub-sequent cycle starting with cycle 6, and finally, atthe end of treatment. For PK assessments, a posthoc analysis was used for the comparison of racialsubgroups.
Statistical Analyses
Study assessments of efficacy, safety, and PROswere prespecified; efficacy subgroup analyses byvarious baseline variables, including race, werepreplanned in the protocol and statistical analysisplan. Statistical analyses by race were conductedfor exploratory purposes. Demographic and base-line disease characteristics were summarized bytreatment arm in a frequency table for Asians andnon-Asians. Quantitative baseline variables, in-cludingage,weight, andheight,were summarizedusing descriptive statistics (ie,median and range).Quantitative baseline variables were comparedbetween the two treatment arms using a Wilcoxontwo-sample test without adjusting for multiplicity.Efficacy analyseswereperformedusing the intent-to-treat principle. Kaplan-Meier estimates of me-dian PFS and the respective 95% CIs were pro-vided for both treatment groups. PFS databetween the treatment groups were comparedusing a log-rank test. HR was estimated fromthe Cox proportional hazards regression model.
The odds ratio estimator and the exact test wereused to compare the rates of binary efficacy endpoints. AEs were summarized using descriptivestatistics in Asians who took one or more doses ofstudy treatment. The within-patient averages ofthe palbociclib steady-state trough PK sampleswere summarized and compared across sub-groups. PRO analyses were based on the PRO-evaluable population (ie, patients in the intent-to-treat population with a baseline assessment andone or more postbaseline assessments before theend of study treatment). Completion rates weresummarized by cycle. Repeated-measures mixed-effects analyses were performed to compare on-treatment overall scores and changes from base-line between treatment groups while controllingfor baseline.
RESULTS
Patients
From October 7, 2013, to August 6, 2014, 105Asians were enrolled onto the study (74 and 31patients in the palbociclib and placebo arms, re-spectively; Fig 1). Demographic and baseline dis-ease characteristics were generally similarbetween Asians and non-Asians except for age,weight, and percentage of premenopausal or peri-menopausal patients. Asians, comparedwithnon-Asians, were generally younger (mean age, 53.7 v57.7 years, respectively; P = .0013) and weighedless (mean, 56.7 v74.6 kg, respectively;P, .001;Table 1). The percentage of premenopausal orperimenopausal women at baseline was higher inAsians (42%) compared with non-Asians (15%).Among Asians, demographic and baseline dis-ease characteristics were generally similar be-tween the palbociclib and placebo arms.
Efficacy
The degree of PFS improvement in the palbociclibarm versus the placebo arm was similar in Asiansand non-Asians (Fig 2). ThemedianPFS in Asianswas not reached in the palbociclib arm (95% CI,9.2 months to not reached) but was 5.8 months(95% CI, 3.5 to 9.2 months) in the placebo arm(HR, 0.485; 95% CI, 0.27 to 0.87; P = .0065). Innon-Asians, the median PFS was 9.5 months(95% CI, 7.6 to 11 months) in the palbociclibarm compared with 3.8 months (95% CI, 3.3 to5.5 months) in the placebo arm (HR, 0.451; 95%CI, 0.34 to0.59;P, .001). InAsians, theCBRwas70% (95% CI, 59% to 80%) with palbociclib plusfulvestrant and 52% (95% CI, 33% to 70%) withplacebo plus fulvestrant (odds ratio, 2.216; 95%CI, 0.85 to 5.7; Table 2). In non-Asians, the CBR
291 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

was 66% (95% CI, 60% to 71%) and 37% (95%CI, 29% to 46%) in the palbociclib and placeboarms, respectively (odds ratio, 3.234; 95%CI, 2.1to 5.0; P, .001). The ORR in Asians was 19% inthe palbociclib arm and 13% in the placebo arm.The sample size was underpowered to performany statistical analysis. However, the degrees ofimprovement for CBR and ORR in Asians weresimilar to those seen in non-Asians.
Safety
Theexposure to study treatmentswascomparablebetweenAsians and non-Asians (Table 3). AmongAsians, 100% of patients in the palbociclib armand 94% in the placebo arm experiencedtreatment-emergent AEs of any grade (Table 4).The most common AEs among Asians were neu-tropenia and leukopenia. Febrile neutropenia oc-curred in three Asians (4%) in the palbociclib arm,with two of these cases reported as a serious AE.On the basis of results that were unadjusted forsample size differences between Asians and non-Asians, non-Asians in the palbociclib arm gener-ally experienced similar treatment-emergent AEsat comparable incidences (, 10%); however, inAsians, compared with non-Asians, the incidenceof fatigue (19% v 44%, respectively) was lower,and the rates of neutropenia (92% v 78%, re-spectively), stomatitis (41% v 24%, respectively),rash (32% v 11%, respectively), and nasophar-yngitis (21% v 10%, respectively) were higher(Table 4).
The median number of treatment interruptionsper patient was not different between Asians andnon-Asians, regardless of treatment group. Thenumber of cycle delays per patient was higher inAsians than non-Asians, regardless of treatmentgroup. The median relative dose was lower inAsians than non-Asians in the palbociclib groupandsimilar betweenAsiansandnon-Asians in the
placebo group (Table 3). Fourteen non-Asianpatients (5.1%) in the palbociclib arm and fivenon-Asian patients (3.5%) in the placebo armdiscontinued palbociclib or placebo treatmentbecause of an AE.
In Asians, the overall incidence of serious AEs was14% (10 of 73 patients) in the palbociclib arm and23% (seven of 31 patients) in the placebo arm(Appendix Table A1). In non-Asians, the inci-denceof seriousAEswas13%(34of 272patients)and 16% (23 of 141 patients) in the palbocicliband placebo arms, respectively. In the placeboplus fulvestrant group, the incidence of seriousAEs inAsians (23%)was similar to the incidence innon-Asians (16%).
PK Results
Comparison of the within-patient mean steady-state palbociclib trough concentrations in Asiansand non-Asians demonstrated relative consis-tency in the central tendency and range of theobserved values across subpopulations, indicat-ing similar palbociclib exposure in these sub-populations (Fig 3). Geometric mean values ofthe within-patient mean steady-state palbociclibtrough concentration values were similar forAsians and non-Asians (85.7 and 74.8 ng/mL,respectively). A population PK-pharmacodynamic(PD) analysis performed to assess the exposure-response relationship for neutropenia withinPALOMA-3 showed that Asian race, baseline ALTlevel, and age were significant covariates on thebaseline absolute neutrophil count (ANC) values.Asian race, lower baselineALT level, and youngerage were associated with lower baseline ANCvalues. Importantly, race was not found to be acovariate on any of the model PD response pa-rameters. Generally, Asians in PALOMA-3 had abaselineANCvalue thatwas19% lower thannon-Asians (Appendix Table A2).
Asians Randomly Assigned(n = 105)
Ongoing(n = 68)
Discontinued• Patient died in follow-up• Other
(n = 6)*
(n = 5)
(n = 1)
Palbociclib + Fulvestrant(n = 74)
Placebo + Fulvestrant(n = 31)
Ongoing(n = 27)
(n = 4)*
(n = 1)(n = 1)
(n = 2)
Discontinued• Lost to follow-up• Withdrew consent to participate• Patient died in follow-up
Non-Asians Randomly Assigned (n = 416)
Ongoing(n = 234)
(n = 39)†
(n = 5)
(n = 31)
(n = 3)
Discontinued• Withdrew consent to participate• Patient died in follow-up• Other
Ongoing(n = 114)
Palbociclib + Fulvestrant(n = 273)
Placebo + Fulvestrant(n = 143)
(n = 29)‡
(n = 5)
(n = 19)
(n = 5)
Discontinued• Withdrew consent to participate• Patient died in follow-up• Other
Fig 1. Patientdisposition. (*) None of thepatients discontinuedtreatment because ofadverse events (AEs).(†) One patient (0.4%)discontinued treatmentbecause of AEs. (‡) Twopatients (1.4%)discontinued treatmentbecause of AEs.
292 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

PROs
Questionnaire completion rateswere high at base-line and during treatment (from baseline to cycle12,> 90%of patients in each group completed allquestions on the European Organisation for Re-search and Treatment of Cancer Quality of LifeQuestionnaire C30). In Asians, no significant de-terioration from baseline in global QOL was ob-served within the palbociclib arm. Among theAsian subgroup in the study, no significant differ-ences between treatment arms were observed for
global QOL, functioning, pain, fatigue, or nauseaand vomiting (Appendix Fig A1A). Significantlygreater deterioration was observed in the pla-cebo arm versus the palbociclib arm for dyspnea(score, 1.2 v 9.2, respectively; P, .05; AppendixFig A1B).
DISCUSSION
CDK4/6 inhibitors are now an integral part ofthe management of HR-positive/HER2-negativeMBC.17 Palbociclib, the first-in-class CDK4/6
Table 1. Demographic and Baseline Disease Characteristics in the Asian and Non-Asian Populations Enrolled Onto the PALOMA-3 Trial
Characteristic
Asian Non-Asian
Palbociclib +Fulvestrant (n = 74)
Placebo +Fulvestrant(n = 31)
Total(n = 105)
Palbociclib +Fulvestrant (n = 273)
Placebo +Fulvestrant(n = 143+)
Total(n = 416)
Age, years, mean (range) 54 (34-82) 53 (39-79) 54* (34-82) 58 (30-88) 58 (29-80) 58 (29-88)
, 55 years 39 (53) 20 (65) 59 (56) 112 (41) 57 (40) 169 (41)
> 55 years 35 (47) 11 (35) 46 (44) 161 (59) 86 (60) 247 (59)
Menopausal status
Premenopausal orperimenopausal
31 (42) 13 (42) 44 (42) 41 (15) 23 (16) 64 (15)
Postmenopausal 43 (58) 18 (58) 61 (58) 232 (85) 120 (84) 352 (85)
Race
Asian 74 (100) 31 (100) 105 (100) 0 0 0
White 0 0 0 252 (92) 133 (93) 385 (93)
Black or other 0 0 0 21 (8) 10 (7) 31 (7)
Weight, kg, mean (range) 57 (36-83) 56 (35-71) 57* (35-83) 74 (45-142) 76 (43-127) 75 (43-142)
Height, cm, mean (range) 156 (140-167) 157 (145-174) 156* (140-174) 163 (142-183) 162 (122-180) 163 (122-183)
ECOG performance status
0 52 (70) 21 (68) 73 (70) 154 (56) 95 (66) 249 (60)
1 22 (30) 10 (32) 32 (31) 119 (44) 48 (34) 167 (40)
Measurable disease present 58 (78) 29 (94) 87 (83) 210 (77) 109 (76) 319 (77)
Documented sensitivity toprior hormonal therapy
58 (78) 26 (84) 84 (80) 216 (79) 110 (77) 326 (78)
Prior chemotherapy asmetastatic treatment, withor without priorneoadjuvant or adjuvanttherapy
21 (28) 14 (45) 35 (33) 92 (34) 50 (35) 142 (34)
No. of previous hormonalregimens for primarydiagnosis
1 22 (30) 11 (36) 33 (31) 112 (41) 66 (46) 178 (43)
. 1 52 (70) 20 (65) 72 (69) 161 (59) 77 (54) 238 (57)
Prior tamoxifen 54 (73) 23 (74) 77 (73) 156 (57) 81 (57) 237 (57)
Prior aromatase inhibitors 54 (73) 24 (77) 78 (74) 242 (89) 127 (89) 369 (89)
NOTE. Data presented as No. (%) unless otherwise noted.Abbreviations: ECOG, Eastern Cooperative Oncology Group; PALOMA-3, Palbociclib Ongoing Trials in the Management of Breast Cancer 3.*P < .0013 versus non-Asian.
293 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

inhibitor approved for the treatment ofHR-positiveMBC, has shown impressive PFS improvementwhen combined with either an aromatase inhibi-tor18 or selective estrogen receptor downregula-tor14 in both patients who are endocrine sensitiveand endocrine resistant. In the PALOMA-1 phaseII study and PALOMA-2 phase III study of patientswho had not previously received endocrine ther-apy, longer PFSwas reportedwith palbociclib plusletrozole versus letrozole alone.18,19 Similarly, inthe PALOMA-3 study, in patients who had pre-viously received endocrine therapy, palbociclibplus fulvestrant resulted in longer PFS than ful-vestrant alone.14Palbociclibhasbeenapproved inthe United States and has been used inmore than48,000 patients since February 2015.20 Palbociclib
is also approved by regulatory authorities for ad-vanced breast cancer in the following countries inAsia: Singapore, Malaysia, Macau, Hong Kong, andKorea. Inmanyof these countries, palbociclibwill bereviewed by health technology agencies, payers, orboth. The positive clinical value of palbociclib inAsian patients should be considered alongside theeconomic implications.
Substantial clinical experience has been accumu-lated in white patients. Although few Asians wereenrolled onto the PALOMA-1 study,21 21% ofpatients in thepalbociclib armand18%ofpatientsin the fulvestrant arm in PALOMA-3 were Asian.14
This study adds to the limited body of literatureassessing a CDK4/6 inhibitor in Asians and rep-resents the largest patient experience with
Table 2. Summary of Investigator-Assessed Best Overall Tumor Response by Treatment in Asian and Non-Asian Patients
Response
Asian Non-Asian
Palbociclib + Fulvestrant(n = 74)
Placebo + Fulvestrant(n = 31)
Palbociclib + Fulvestrant(n = 273)
Placebo + Fulvestrant(n = 143)
CBR (CR + PR + SD > 24 weeks),No. (%; 95% CI)
52 (70; 58.5 to 80.3) 16 (52; 33.1 to 69.8) 179 (66; 59.6 to 71.2) 53 (37; 29.1 to 45.5)
CR 0 1 (3) 0 3 (2)
PR 14 (19) 3 (10) 52 (19) 8 (6)
SD > 24 weeks 38 (51) 12 (39) 127 (47) 42 (29)
Odds ratio (95% CI) for CBR 2.216 (0.851 to 5.718) 3.234 (2.077 to 5.043)
P .0557 , .001
Objective progression 12 (16) 6 (19) 46 (17) 51 (36)
NOTE. Data presented as No. (%) unless otherwise noted.Abbreviations: CBR, clinical benefit response rate; CR, complete response; PR, partial response; SD, stable disease.
PFS
Prob
abili
ty (%
)
0
20
40
60
80
100
AsianHR, 0.48595% CI, 0.270 to 0.869P = .0065
Non-AsianHR, 0.45195% CI, 0.343 to 0.593P < .001
1 2 3 4 5 6 7 8 9 10 11 12
Time (months)No. at risk:
74 72 62 61 55 55 44 43 20 20 5 4 0
31 30 25 25 19 19 15 15 6 6 3 2 0Asian
Non-Asian143 135 87 80 64 61 44 43 16 16 10 5 2 1 0
273 261 219 212 192 189 158 154 71 65 27 19 7 7 1 0
13 14 15
Asian
PAL + FULMedian PFS, NR (95% CI, 9.2 months to NR)PCB + FULMedian PFS, 5.8 months (95% CI, 3.5 to 9.2 months)
Non-Asian
PAL + FULMedian PFS, 9.5 months(95% CI, 7.6 to 11.0 months)PCB + FULMedian PFS, 3.8 months(95% CI, 3.3 to 5.5 months)
Fig 2. Investigator-assessed progression-freesurvival (PFS) in Asian andnon-Asian patients. FUL,fulvestrant; HR, hazardratio;NR,not reached;PAL,palbociclib; PCB, placebo.
294 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

palbociclib in Asians. The present findings showthat palbociclib plus fulvestrant improved PFS inAsianswithHR-positive/HER2-negativeMBCwhoexperienced progression on prior endocrine ther-apy and that the safety profile of palbociclib plusfulvestrant in Asians was generally consistent withthat observed in non-Asians. Together, these find-ings suggest that palbociclib is beneficial in pa-tients who have not previously received endocrinetherapy and in Asians and non-Asians who expe-rienced relapse or progression during prior endo-crine therapy.
Differences in racial background can be associ-ated with variable efficacy outcomes and safetyprofiles.22 As a result of genetic variations in anenzyme responsible for doxorubicin meta-bolism,23 Asians have been shown to be moresusceptible to myelosuppression induced bydoxorubicin compared with whites.22 In addition,a higher incidence of febrile neutropenia withdocetaxel has been reported in Asians comparedwith whites.22 Genetic differences associated withrace also can lead to differences in treatmentresponse and efficacy. In Koreans with MBC,CYP2D6*10/*10 genetic polymorphisms havebeen associated with reduced plasma concentra-tions of the tamoxifen activemetabolites endoxifenand 4-hydroxytamoxifen, as well as reduced clin-ical benefit (complete response, partial response,or stable disease > 24 weeks) and significantlyshorter median time to progression (P = .0032).24
These racial variations highlight the importance ofevaluating the efficacy and safety of cancer med-ications within the Asian population.
Similar to findings from the present analysis, themost common AEs reported in the PALOMA-1study with palbociclib were neutropenia andleukopenia.14,18 In the PALOMA-3 study, non-hematologic AEs were predominantly mild ormoderate in severity. Moreover, an important dif-ference of treatment exposure was observed be-tween Asians and non-Asians in the palbociclibarm, with higher percentages of Asians experienc-ing dose interruptions, dose reductions, and cycledelays than non-Asians. Interestingly, the rates ofgrade 3 and grade 4 neutropenia were modestlyhigher in Asians than non-Asians. Because pal-bociclib exposure was similar in Asians and non-Asians, the increased rates of neutropenia cannotbe explained by differential drug exposure acrossracial subgroups. Asian race, lower baseline ALT,and younger age were all predictors of a lowerbaseline ANC value. The Asians in PALOMA-3, onaverage, were younger and had a lower baselineALT than the non-Asians, thus compounding ef-fects of the covariates. Overall, in the PALOMA-3patient population, a typical Asian patient (52years old at enrollment with a baseline ALT of17 U/L) had a baseline ANC value 19% lowerthan a typical non-Asian patient (58 years old atenrollment with a baseline ALT of 21 U/L), whichmaypartially explain thehigher rate of neutropenia
Table 3. Study Treatment Exposure and Duration
Treatment Factor
Asian Non-Asian
Palbociclib + Fulvestrant(n = 74)
Placebo + Fulvestrant(n = 31)
Palbociclib + Fulvestrant(n = 273)
Placebo + Fulvestrant(n = 143)
No. of cycles, median (range) 8 (1-15) 6 (1-15) 9 (1-18) 5 (1-18)
Duration of treatment, days, median (range) 237 (21-413) 168 (21-406) 231 (1-481) 119 (14-498)
Average daily dose administered, mg,median (range)
118 (80-129) 125 (125-125) 125 (80-131) 125 (106-129)
Patients with > 1 dose reduction 38 (52) 0 79 (29) 3 (2)
Relative dose,* %, median (range) 87 (51-102) 100 (88-100) 98 (25-107) 100 (70-107)
Patients with interruptions as a result of AEs 60 (82) 3 (10) 127 (47) 7 (5)
Patients with dose reduction as a result ofAEs
37 (51) 0 77 (28) 3 (2)
No. of interruptions per patient, median(range)
2 (1-28) 1 (1-5) 2 (1-15) 1 (1-8)
Patients with cycle delay as a result of AEs 37 (51) 0 86 (32) 3 (2)
No. of cycle delays per patient, median(range)
2 (1-4) 1 (1-1) 1 (1-6) 1 (1-2)
NOTE. Data presented as No. (%) unless otherwise noted.Abbreviation: AE, adverse event.*Relative dose = [(actual dose)/(intended dose)] 3 100%.
295 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Table 4. Treatment-Emergent AEs Among Asian and Non-Asian Patients (> 10% incidence in Asian palbociclib plus fulvestrant group)
AE
No. of Patients (%)
Asian Non-Asian
Palbociclib + Fulvestrant(n = 73)
Placebo + Fulvestrant(n = 31)
Palbociclib + Fulvestrant(n = 272)
Placebo + Fulvestrant(n = 141)
AllGrades
Grade3
Grade4
AllGrades
Grade3
Grade4
AllGrades Grade 3 Grade 4
AllGrades Grade 3
Grade4
Any AE 73 (100) 52 (71) 14 (19) 29 (94) 5 (16) 0 267 (98) 158 (58) 27 (10) 125 (89) 29 (21) 4 (3)
Hematologic
Neutropenia* 67 (92) 54 (74) 13 (18) 2 (7) 0 0 212 (78) 135 (50) 21 (8) 4 (3) 0 1 (0.7)
Leukopenia† 33 (45) 20 (27) 1 (1) 1 (3) 0 0 138 (51) 73 (27) 1 (0.4) 6 (4) 1 (0.7) 1 (0.7)
Thrombocytopenia‡ 19 (26) 2 (3) 0 — — — 54 (20) 4 (2) 2 (0.7) — — —
Anemia§ 18 (25) 2 (3) 0 3 (10) 2 (7) 0 78 (29) 8 (3) 0 16 (11) 1 (0.7) 0
Nonhematologic
Stomatitisk 30 (41) 1 (1) 0 3 (10) 0 0 64 (24) 1 (0.4) 0 20 (14) 0 0
Rash¶ 23 (32) 1 (1) 0 — — — 29 (11) 1 (0.4) 0 9 (6) 0 0
Nausea 22 (30) 0 0 7 (23) 0 0 90 (33) 0 0 40 (28) 1 (0.7) 0
Nasopharyngitis 15 (21) 0 0 3 (10) 0 0 26 (10) 0 0 9 (6) 0 0
Fatigue 14 (19) 0 0 6 (19) 0 0 121 (44) 8 (3) 0 43 (31) 2 (1) 0
Alopecia 13 (18) 0 0 2 (7) 0 0 45 (17) 0 0 9 (6) 0 0
Constipation 13 (18) 0 0 3 (10) 0 0 53 (20) 0 0 24 (17) 0 0
Decreased appetite 13 (18) 0 0 2 (7) 1 (3) 0 39 (14) 3 (1) 0 12 (9) 0 0
Headache 13 (18) 0 0 7 (23) 0 0 67 (25) 2 (0.7) 0 26 (18) 0 0
Vomiting 13 (18) 1 (1) 0 2 (7) 0 0 45 (17) 0 0 23 (16) 1 (0.7) 0
Diarrhea 12 (16) 0 0 3 (10) 0 0 62 (23) 0 0 29 (21) 1 (0.7) 0
Pyrexia 12 (16) 0 0 1 (3) 0 0 26 (10) 1 (0.4) 0 8 (6) 0 0
Cough 11 (15) 0 0 2 (7) 0 0 40 (15) 0 0 20 (14) 0 0
Hot flush 10 (14) 0 0 1 (3) 0 0 43 (16) 0 0 28 (20) 1 (0.7) 0
Pain in extremity 10 (14) 0 0 1 (3) 0 0 33 (12) 0 0 20 (14) 3 (2) 0
Dizziness 9 (12) 1 (1) 0 3 (10) 0 0 32 (12) 0 0 13 (9) 0 0
Musculoskeletalpain
9 (12) 0 0 — — — 17 (6) 1 (0.4) 0 12 (9) 1 (0.7) 0
Arthralgia 8 (11) 0 0 3 (10) 0 0 41 (15) 1 (0.4) 0 24 (17) 0 0
Back pain 8 (11) 0 0 3 (10) 0 0 43 (16) 4 (2) 0 26 (18) 3 (2) 0
Dyspepsia 7 (10) 0 0 2 (7) 0 0 24 (9) 0 0 7 (5) 0 0
Mucosalinflammation
7 (10) 0 0 — — — 7 (3) 0 0 5 (4) 0 0
Oropharyngeal pain 7 (10) 0 0 1 (3) 0 0 30 (11) 0 0 11 (8) 0 0
Pruritus 7 (10) 0 0 4 (13) 0 0 15 (6) 0 0 7 (5) 0 0
Abbreviation: AE, adverse event.*Event cluster consisting of the preferred terms (PTs) neutropenia and neutrophil count decreased.†Event cluster consisting of the PTs leukopenia and WBC count decreased.‡Event cluster consisting of the PTs platelet count decreased and thrombocytopenia.§Event cluster consisting of the PTs anemia, hematocrit decreased, and hemoglobin decreased.kEvent cluster consisting of the PTs aphthous stomatitis, cheilitis, glossitis, glossodynia, mouth ulceration, mucosal inflammation, oral pain, oropharyngeal discomfort,oropharyngeal pain, and stomatitis.
¶Event cluster consisting of the PTs dermatitis, dermatitis acneiform, rash, rash erythematous, rash maculopapular, rash papular, and rash pruritic.
296 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

observed in Asians. Importantly, race was notdemonstrated to be a covariate on any of the PDresponse parameters, suggesting that there wasno increased sensitivity to palbociclib-inducedneutropenia in Asians.
MBC in premenopausal women is not well studiedbecause clinical trials often exclude this patientpopulation. One phase II study of 73 patientswith HR-positive MBC showed that the efficacy offirst-line therapy with letrozole plus goserelin inpremenopausal patients was comparable with theefficacy of letrozole alone in postmenopausalpatients25; these findings support additional re-search into assessing the efficacy of othertreatments in combination with goserelin in pre-menopausal patients with breast cancer. MBC inpremenopausal women is rare in the Westernworld; however, higher incidences are seen inAsian countries and in developing countries suchasMexico, LatinAmerica, andEgypt, wherebreastcancer is more common in younger women and isfrequently diagnosed at later stages as a result ofsuboptimal access to health care.3,4,26-29 Palbo-ciclib plus fulvestrant improved PFS in both pre-menopausal and postmenopausal Asians inPALOMA-3. Because of the small number of pa-tients in this cohort, no formal statistical analysiscould be performed. Nevertheless, palbociclibplus fulvestrant in addition to an LHRH agonistcould be a reasonable treatment option for
younger patients with breast cancer who are pre-menopausal, including Asian patients.
Assessing PROs is important to comprehensivelydefine the risk-benefit profile of treatments. In thecurrent study, Asians in the palbociclib groupmaintainedgoodQOL throughout the study,whichis important in establishing the benefit-risk profileof combination therapy.
In conclusion, as observed in the full study pop-ulation, PFSwas longer inAsianswithHR-positive/HER2-negative MBC who received palbociclibplus fulvestrant versus those who received pla-cebo plus fulvestrant. Furthermore, QOL wasmaintained in Asians who received palbociclib.The safety profile of palbociclib was consistentwith that previously reported and was similar inAsians andnon-Asians. Theprotocol-defineddos-ing modification instructions for palbociclib, in-cluding adjusting dose on the basis of individualtolerability, enabled Asians to avoid discontinua-tion from the study as a result of an AE, allowingthem to stay on treatment as long as non-Asiansand thus maintain the same efficacy benefit fromcombination therapy. Overall, palbociclib plusfulvestrant seems to be a reasonable treatmentoption in Asians with HR-positive/HER2-negativeMBC that has progressed on prior endocrinetherapy.
DOI: https://doi.org/10.1200/JGO.2016.008318Published online on jgo.org on April 11, 2017.
AUTHOR CONTRIBUTIONS
Conception and design:Hiroji Iwata, Ke Zhang, Cynthia HuangBartlett, Jungsil RoCollection and assembly of data: Hiroji Iwata, Seock-Ah Im,Norikazu Masuda, Young-Hyuck Im, Kenichi Inoue,Yoshiaki Rai, Rikiya Nakamura, Jee Hyun Kim,
Ke Zhang, Carla Giorgetti, Cynthia Huang Bartlett,Jungsil Ro
Data analysis and interpretation: Hiroji Iwata, Seock-Ah Im,NorikazuMasuda, JustinT.Hoffman,KeZhang,CarlaGiorgetti,Shrividya Iyer, Patrick T. Schnell, Cynthia Huang Bartlett,Jungsil Ro
AsianNon-Asian
Plas
ma
Palb
ocic
lib C
once
ntra
tion
(ng/
mL)
0
50
100
150
200
250Fig 3. Plasma
palbociclib within-patientmean steady-state troughconcentration in Asian andnon-Asian patients.Diamonds represent thesubpopulation geometricmean values, and opencircles represent individualpatient values. The dashedline represents thearithmetic mean value of alldata from all patients. Thebox plot provides medianand25%and75%quartileswith whiskers to the lastpoint within 1.5 times theinterquartile range.
297 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Manuscript writing: All authorsFinal approval of manuscript: All authorsAccountable for all aspects of the work: All authors
AUTHORS’ DISCLOSURES OFPOTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided byauthors of this manuscript. All relationships are consideredcompensated. Relationships are self-held unless noted. I =Immediate Family Member, Inst = My Institution. Relation-ships may not relate to the subject matter of this manuscript.For more information about ASCO’s conflict of interest policy,please refer to www.asco.org/rwc or ascopubs.org/jco/site/ifc.
Hiroji IwataConsulting or Advisory Role: Chugai Pharma, Eisai,AstraZeneca
Seock-Ah ImConsulting or Advisory Role: AstraZeneca, Novartis, Roche,Spectrum Pharmaceuticals, PfizerResearch Funding: AstraZeneca
Norikazu MasudaHonoraria: Chugai Pharma, AstraZenecaResearch Funding:ChugaiPharma (Inst), Pfizer (Inst),Novartis(Inst), Eli Lilly (Inst), AstraZeneca (Inst), Kyowa-Kirin (Inst)
Young-Hyuck ImNo relationship to disclose
Kenichi InoueResearch Funding:Pfizer (Inst), Eli Lilly (Inst), Chugai Pharma,Daiichi-Sankyo (Inst), Taiho Pharmaceutical (Inst), MSD(Inst), Parexel (Puma) (Inst)
Yoshiaki RaiNo relationship to disclose
Rikiya NakamuraNo relationship to disclose
Jee Hyun KimNo relationship to disclose
Justin T. HoffmanEmployment: PfizerStock or Other Ownership: PfizerTravel, Accommodations, Expenses: Pfizer
Ke ZhangEmployment: Pfizer (former employer), Janssen Research andDevelopment (current employer)
Stock or Other Ownership: Pfizer
Carla GiorgettiEmployment: PfizerStock or Other Ownership: Pfizer
Shrividya IyerEmployment: PfizerStock or Other Ownership: Pfizer
Patrick T. SchnellEmployment: PfizerStock or Other Ownership: Pfizer
Cynthia Huang BartlettEmployment: PfizerStock or Other Ownership: Pfizer
Jungsil RoNo relationship to disclose
ACKNOWLEDGMENTWe thank Yanke Yu (Pfizer, La Jolla, CA) for analysis providedfor this article. We also thank the patients who participated inthe PALOMA-3 study, and the investigators, study nurses, andsite staff for their support of the trial. Medical writing supportwas provided by Anny Wu, PharmD, of Complete HealthcareCommunications, and was funded by Pfizer. Fulvestrant wasprovided by AstraZeneca, London, United Kingdom.
Affiliations
Hiroji Iwata, Aichi Cancer Center Hospital, Nagoya; Norikazu Masuda, National Hospital Organization, Osaka National Hospital,Osaka; Kenichi Inoue, Saitama Cancer Center, Saitama; Yoshiaki Rai, Sagara Hospital, Kagoshima City; Rikiya Nakamura, ChibaCancer Center, Chiba, Japan; Seock-Ah Im, Seoul National University Hospital, Cancer Research Institute, Seoul NationalUniversity College ofMedicine;Young-Hyuck Im, SamsungMedical Center, SungkyunkwanUniversity School ofMedicine, Seoul;Jee Hyun Kim, Seoul National University Bundang Hospital, Seongnam; Jungsil Ro, National Cancer Center, Goyang, Republic ofKorea; Justin T. Hoffman and Ke Zhang, Pfizer, La Jolla, CA; Carla Giorgetti, Shrividya Iyer, and Patrick T. Schnell, Pfizer, New York,NY; and Cynthia Huang Bartlett, Pfizer, Collegeville, PA.
Support
Supported by Pfizer, New York, NY.
Prior Presentation
Presented at the European Society for Medical Oncology Asia 2015 Congress, Singapore, December 18-21, 2015.
REFERENCES1. Jemal A, Bray F, Center MM, et al: Global cancer statistics. CA Cancer J Clin 61:69-90, 2011
2. Li J, Zhang BN, Fan JH, et al: A nation-wide multicenter 10-year (1999-2008) retrospective clinical epidemiologicalstudy of female breast cancer in China. BMC Cancer 11:364, 2011
3. American Cancer Society: Breast Cancer Facts & Figures 2015-2016. http://www.cancer.org/acs/groups/content/@research/documents/document/acspc-046381.pdf
298 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

4. Youlden DR, Cramb SM, Yip CH, et al: Incidence and mortality of female breast cancer in the Asia-Pacific region.Cancer Biol Med 11:101-115, 2014
5. Ghiasvand R, Adami HO, Harirchi I, et al: Higher incidence of premenopausal breast cancer in less developedcountries: Myth or truth? BMC Cancer 14:343, 2014
6. SiW, Li Y, Han Y, et al: Epidemiological and clinicopathological trends of breast cancer in Chinese patients during 1993to 2013: A retrospective study. Medicine (Baltimore) 94:e820, 2015
7. Swain SM, Im YH, Im SA, et al: Safety profile of pertuzumab with trastuzumab and docetaxel in patients from Asia withhuman epidermal growth factor receptor 2-positive metastatic breast cancer: Results from the phase III trialCLEOPATRA. Oncologist 19:693-701, 2014
8. Cardoso F, Costa A, Norton L, et al: ESO-ESMO 2nd international consensus guidelines for advanced breast cancer(ABC2). Ann Oncol 25:1871-1888, 2014
9. Early Breast Cancer Trialists’ Collaborative Group: Tamoxifen for early breast cancer: An overview of the randomisedtrials. Lancet 351:1451-1467, 1998
10. Ellis M: Overcoming endocrine therapy resistance by signal transduction inhibition. Oncologist 9:20-26, 2004 (suppl 3)
11. Marzec M, Kasprzycka M, Lai R, et al: Mantle cell lymphoma cells express predominantly cyclin D1a isoform and arehighly sensitive to selective inhibition of CDK4 kinase activity. Blood 108:1744-1750, 2006
12. Saab R, Bills JL, Miceli AP, et al: Pharmacologic inhibition of cyclin-dependent kinase 4/6 activity arrests proliferationin myoblasts and rhabdomyosarcoma-derived cells. Mol Cancer Ther 5:1299-1308, 2006
13. Cristofanilli M, Turner NC, Bondarenko I, et al: Fulvestrant plus palbociclib versus fulvestrant plus placebo fortreatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous en-docrine therapy (PALOMA-3): Final analysis of the multicentre, double-blind, phase 3 randomised controlled trial.Lancet Oncol 17:425-439, 2016
14. Turner NC, Ro J, Andre F, et al: Palbociclib in hormone-receptor-positive advanced breast cancer. N Engl J Med 373:209-219, 2015
15. European Organisation for Research and Treatment of Cancer Quality of Life Group: EORTC QLQ-C30 (version 3).http://www.eortc.be/qol/files/C30/QLQ-C30%20English.pdf
16. AaronsonNK, Ahmedzai S, BergmanB, et al: The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 85:365-376, 1993
17. Murphy CG, Dickler MN: The role of CDK4/6 inhibition in breast cancer. Oncologist 20:483-490, 2015
18. Finn RS, Crown JP, Lang I, et al: The cyclin-dependent kinase 4/6 inhibitor palbociclib in combinationwith letrozole versus letrozole alone as first-line treatment of oestrogen receptor-positive, HER2-negative, advanced breast cancer (PALOMA-1/TRIO-18): A randomised phase 2 study. Lancet Oncol 16:25-35, 2015
19. Finn RS, Martin M, Rugo HS, et al: PALOMA-2: Primary results from a phase III trial of palbociclib (P) with letrozole (L)compared with letrozole alone in postmenopausal women with ER+/HER2- advanced breast cancer (ABC). J ClinOncol 34, 2016 (suppl; abstr 507)
20. Pfizer: Pfizer 2015 Annual Review: Advances in Oncology. https://www.pfizer.com/files/investors/financial_reports/annual_reports/2015/assets/pdfs/pfi2015ar-advances-in-oncology.pdf
21. Pfizer: IBRANCE (palbociclib). http://labeling.pfizer.com/ShowLabeling.aspx?id=2191
22. Ling WH, Lee SC: Inter-ethnic differences: How important is it in cancer treatment? Ann Acad Med Singapore 40:356-361, 2011
23. Voon PJ, Yap HL, Ma CY, et al: Correlation of aldo-ketoreductase (AKR) 1C3 genetic variant with doxorubicinpharmacodynamics in Asian breast cancer patients. Br J Clin Pharmacol 75:1497-1505, 2013
24. Lim HS, Ju Lee H, Seok Lee K, et al: Clinical implications of CYP2D6 genotypes predictive of tamoxifen pharma-cokinetics in metastatic breast cancer. J Clin Oncol 25:3837-3845, 2007
25. Park IH, Ro J, Lee KS, et al: Phase II parallel group study showing comparable efficacy between premenopausalmetastatic breast cancer patients treated with letrozole plus goserelin and postmenopausal patients treated withletrozole alone as first-line hormone therapy. J Clin Oncol 28:2705-2711, 2010
26. Jung KW, Won YJ, Kong HJ, et al: Cancer statistics in Korea: Incidence, mortality, survival, and prevalence in 2011.Cancer Res Treat 46:109-123, 2014
27. Schlichting JA, Soliman AS, Schairer C, et al: Breast cancer by age at diagnosis in the Gharbiah, Egypt, population-based registry compared to the United States Surveillance, Epidemiology, and End Results Program, 2004-2008.BioMed Res Int 2015:381574, 2015
28. Villarreal-Garza C, Aguila C, Magallanes-Hoyos MC, et al: Breast cancer in young women in Latin America: An unmet,growing burden. Oncologist 18:26-34, 2013(suppl)
29. Villarreal-Garza C,Mohar A, Bargallo-Rocha JE, et al: Molecular subtypes and prognosis in youngMexicanwomenwithbreast cancer. Clin Breast Cancer 10.1016/j.clbc.2016.11.007 [epub ahead of print on November 23, 2016]
299 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

APPENDIX
A
-2.1
0.8
-1.7
1.3
-2.4 -2.4
-5.0
-0.1
-2.6
-0.2
-2.3
3.2
-10
-5
0
5
10
GlobalQOL
PhysicalFunctioning
RoleFunctioning
EmotionalFunctioning
CognitiveFunctioning
SocialFunctioning
Estim
ated
Ove
rall
Mea
nCh
ange
Fro
m B
asel
ine
Imp
rovem
ent
Palbociclib + Fulvestrant
Fulvestrant
B
-0.4
2.8
-0.1
1.2
-4.9
2.3
-0.9
3.4
1.52.5
-0.7
9.2
0.30.9
1.62.4
-10
-5
0
5
10
Fatigue Nausea/Vomiting
Pain Dyspnea* Insomnia AppetiteLoss
Diarrhea Constipation
Estim
ated
Ove
rall
Mea
nCh
ange
Fro
m B
asel
ine
Imp
rovem
ent
Palbociclib + Fulvestrant
Fulvestrant
Fig A1. Overall mean(SE) change from baselinein patient-reported scoreson the EuropeanOrganisation for Researchand Treatment of CancerQuality of LifeQuestionnaire C30 of (A)global quality of life (QOL)and function and (B)symptoms in Asianpatients. (*) P , .05 forpalbociclib plus fulvestrantversus placebo plusfulvestrant.
300 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Table A1. Serious AEs Among Asian and Non-Asian Patients
AE
No. of Patients (%)
Asian Non-Asian
Palbociclib +Fulvestrant (n = 73)
Placebo +Fulvestrant (n = 31)
Palbociclib +Fulvestrant (n = 272)
Placebo +Fulvestrant(n = 141)
Pneumonia 0 1 (3) 1 (0.4) 1 (1)
Febrile neutropenia 2 (3) 0 0 1 (1)
Neutropenia* 2 (3) 0 2 (1) 0
Suicide attempt 2 (3) 0 0 0
Breast cancer 0 1 (3) 0 0
Fracture 0 1 (3) 0 0
Nasopharyngitis 0 1 (3) 0 0
Osteonecrosis of jaw 0 1 (3) 0 0
Pyelonephritis 0 1 (3) 0 0
Road traffic accident 0 1 (3) 0 0
Viral upper respiratorytract infection
0 1 (3) 0 0
Pleural effusion 0 0 3 (1) 3 (2)
Ascites 0 0 0 3 (2)
Disease progression 1 (1) 0 1 (0.4) 0
Back pain 0 0 1 (0.4) 1 (1)
Cholelithiasis 0 0 1 (0.4) 0
Chronic obstructivepulmonary disease
0 0 1 (0.4) 1 (1)
Dyspnea 0 0 1 (0.4) 1 (1)
Peripheral edema 0 0 1 (0.4) 1 (1)
Pain 0 0 1 (0.4) 1 (1)
Vomiting 0 0 1 (0.4) 1 (1)
Pulmonary embolism† 0 0 3 (1) 0
Pyrexia 0 0 3 (1) 0
Deep vein thrombosis 0 0 2 (1) 0
Pathologic fracture 0 0 0 2 (1)
Acute otitis media 1 (1) 0 0 0
Cataract 1 (1) 0 0 0
Pharyngitis 1 (1) 0 0 0
Pyrexia 1 (1) 0 0 1 (1)
Urinary tract infection 1 (1) 0 0 0
Acute respiratory distresssyndrome
0 0 0 1 (1)
Adenocarcinoma gastric 0 0 0 1 (1)
Atypical pneumonia 0 0 0 1 (1)
Cerebral hemorrhage 0 0 0 1 (1)
Cerebrovascularaccident
0 0 0 1 (1)
Chest pain 0 0 0 1 (1)
Cholecystitis 0 0 0 1 (1)
(Continued on following page)
301 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
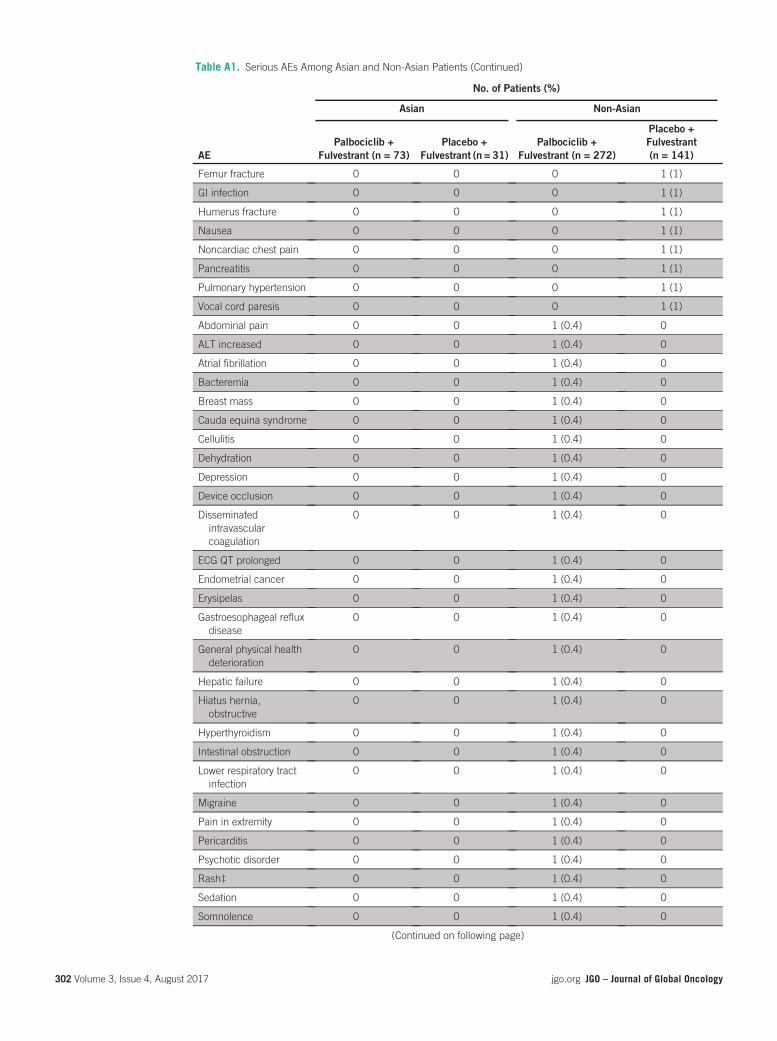
Table A1. Serious AEs Among Asian and Non-Asian Patients (Continued)
AE
No. of Patients (%)
Asian Non-Asian
Palbociclib +Fulvestrant (n = 73)
Placebo +Fulvestrant (n = 31)
Palbociclib +Fulvestrant (n = 272)
Placebo +Fulvestrant(n = 141)
Femur fracture 0 0 0 1 (1)
GI infection 0 0 0 1 (1)
Humerus fracture 0 0 0 1 (1)
Nausea 0 0 0 1 (1)
Noncardiac chest pain 0 0 0 1 (1)
Pancreatitis 0 0 0 1 (1)
Pulmonary hypertension 0 0 0 1 (1)
Vocal cord paresis 0 0 0 1 (1)
Abdominal pain 0 0 1 (0.4) 0
ALT increased 0 0 1 (0.4) 0
Atrial fibrillation 0 0 1 (0.4) 0
Bacteremia 0 0 1 (0.4) 0
Breast mass 0 0 1 (0.4) 0
Cauda equina syndrome 0 0 1 (0.4) 0
Cellulitis 0 0 1 (0.4) 0
Dehydration 0 0 1 (0.4) 0
Depression 0 0 1 (0.4) 0
Device occlusion 0 0 1 (0.4) 0
Disseminatedintravascularcoagulation
0 0 1 (0.4) 0
ECG QT prolonged 0 0 1 (0.4) 0
Endometrial cancer 0 0 1 (0.4) 0
Erysipelas 0 0 1 (0.4) 0
Gastroesophageal refluxdisease
0 0 1 (0.4) 0
General physical healthdeterioration
0 0 1 (0.4) 0
Hepatic failure 0 0 1 (0.4) 0
Hiatus hernia,obstructive
0 0 1 (0.4) 0
Hyperthyroidism 0 0 1 (0.4) 0
Intestinal obstruction 0 0 1 (0.4) 0
Lower respiratory tractinfection
0 0 1 (0.4) 0
Migraine 0 0 1 (0.4) 0
Pain in extremity 0 0 1 (0.4) 0
Pericarditis 0 0 1 (0.4) 0
Psychotic disorder 0 0 1 (0.4) 0
Rash‡ 0 0 1 (0.4) 0
Sedation 0 0 1 (0.4) 0
Somnolence 0 0 1 (0.4) 0
(Continued on following page)
302 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
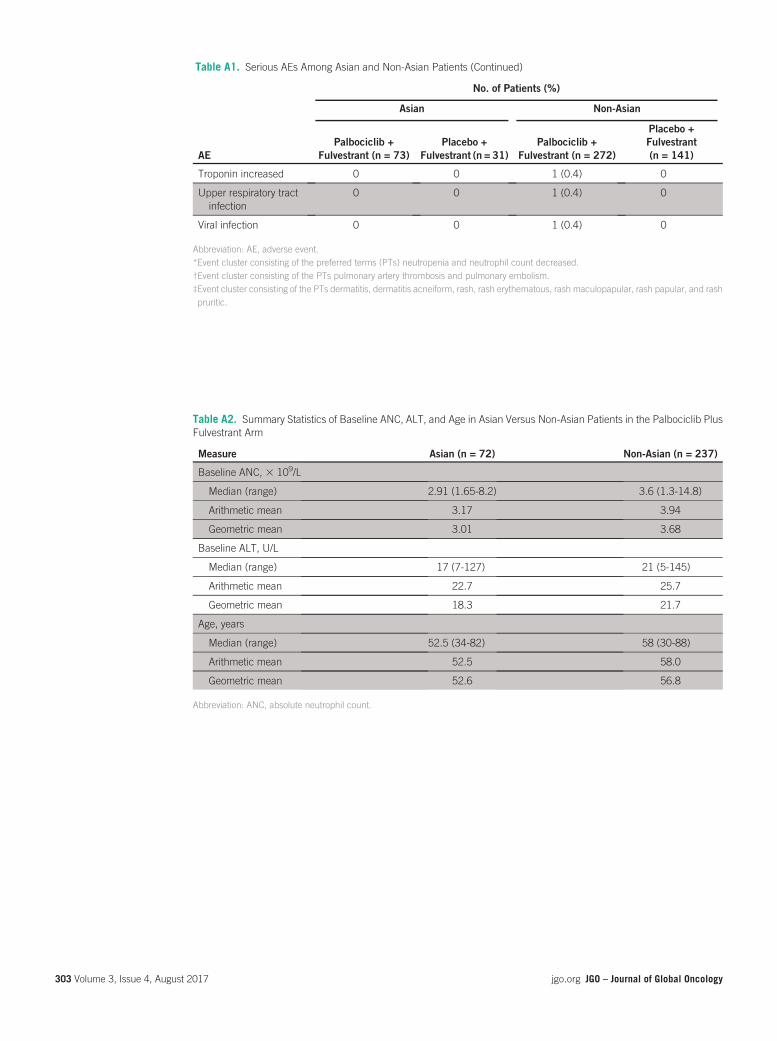
Table A1. Serious AEs Among Asian and Non-Asian Patients (Continued)
AE
No. of Patients (%)
Asian Non-Asian
Palbociclib +Fulvestrant (n = 73)
Placebo +Fulvestrant (n = 31)
Palbociclib +Fulvestrant (n = 272)
Placebo +Fulvestrant(n = 141)
Troponin increased 0 0 1 (0.4) 0
Upper respiratory tractinfection
0 0 1 (0.4) 0
Viral infection 0 0 1 (0.4) 0
Abbreviation: AE, adverse event.*Event cluster consisting of the preferred terms (PTs) neutropenia and neutrophil count decreased.†Event cluster consisting of the PTs pulmonary artery thrombosis and pulmonary embolism.‡Event cluster consisting of the PTs dermatitis, dermatitis acneiform, rash, rash erythematous, rash maculopapular, rash papular, and rashpruritic.
Table A2. Summary Statistics of Baseline ANC, ALT, and Age in Asian Versus Non-Asian Patients in the Palbociclib PlusFulvestrant Arm
Measure Asian (n = 72) Non-Asian (n = 237)
Baseline ANC, 3 109/L
Median (range) 2.91 (1.65-8.2) 3.6 (1.3-14.8)
Arithmetic mean 3.17 3.94
Geometric mean 3.01 3.68
Baseline ALT, U/L
Median (range) 17 (7-127) 21 (5-145)
Arithmetic mean 22.7 25.7
Geometric mean 18.3 21.7
Age, years
Median (range) 52.5 (34-82) 58 (30-88)
Arithmetic mean 52.5 58.0
Geometric mean 52.6 56.8
Abbreviation: ANC, absolute neutrophil count.
303 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

originalreport
Decreased Survival With MastectomyVis-a-Vis Breast-Conserving Surgery inStage II and III Breast Cancers: AComparative Treatment EffectivenessStudy
abstract
Purpose The primary purpose of hospital-based cancer registries is assessing patient care. Clinicalstage–based survival and treatment-based survival are some of the key parameters for such assessment.Because of the challenges in obtaining follow-up parameters, a separate study on patterns of care andsurvival was undertaken by the Indian National Cancer Registry Program. The results for cancer of thefemale breast are presented here.
Patients and Methods Data abstracted in a standardized patient information form were transmitted onlineto a central repository. Treatment patternswere assessed for 9,903patients diagnosed between January 1,2006,andDecember31,2008, from13 institutions. Survival analysiswas restricted to7,609patients fromnine institutions wherein follow-up details (as of December 31, 2012) were available for at least 60% ofpatients.
Results The overall 5-year survival rates with breast-conserving surgery (BCS) andmastectomy (MS) were94.0% and 85.8%, respectively, for stage II disease (adjusted hazard ratio, 2.40; 95%CI, 1.8 to 3.2) and87.1%and69.0%, respectively, for stage III disease (hazard ratio, 2.82; 95%CI, 2.2 to 3.7). Patientswhohad MS did better with systemic therapy (chemotherapy and/or hormone therapy), whereas patients withBCS required just local radiation therapy to achieve best survival.
Conclusion This observational study in the natural setting of care of patients with cancer in India showedsignificantly decreased survival withMSwhen comparedwith BCS. The reasons for lower survival withMSand the biologic or scientific rationale of the necessity of systemic therapy to achieve optimal survival inpatients undergoing MS but not in those with BCS need further investigation.
J Glob Oncol 3. © 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
INTRODUCTION
Worldwide, breast cancer is the most commoncancer among women, composing 25% of allfemale cancers.1 The annual estimated incidenceof new breast cancers in women in India is ap-proximately 100,000. Breast cancer has shown astatistically significant increase in incidence ratesover time in the Indian Population-Based CancerRegistries.2 Information on patterns of breast can-cer care and survival is essential in assessingcancer treatment services, and a hospital-basedcancer registry is central to this effort.3 There areseveral challenges in obtaining proper and accu-rate data on clinical stage–based survival in the
setting of a developing country. These includetreatment compliance and post-treatment follow-up, including relevant information on recurrenceand/or complications of disease.4 The main aimof this study was to obtain clinical stage–specifictreatment and survival information for breast can-cer in India.
Numerous studies from developed countries havecompared survival results of breast-conservingsurgery (BCS) and mastectomy (MS).5-8 Previouspublications from India on BCS and survival arefrom individual hospitals.9-11 The findings pooledand reported in this study were facilitated bya process of electronic transfer of data from
AmbakumarNandakumar
Goura Kishor Rath
Amal Chandra Kataki
P. Poonamalle Bapsy
Prakash C. Gupta
Paleth Gangadharan
Ramesh C. Mahajan
Manas NathBandyopadhyay
Kumara Swamy
Elizabeth Vallikad
Rudrapatna N.Visweswara
Francis Selvaraj Roselind
Krishnan Sathishkumar
Dampilla Daniel VijayKumar
Ankush Jain
Kondalli LakshminarayanaSudarshan
Author affiliations andsupport information (ifapplicable) appear at theend of this article.Corresponding author:Ambakumar Nandakumar,MD, MPH, National Centrefor Disease Informatics andResearch, Indian Council ofMedicalResearch, IIFloorofNirmal Bhawan, ICMRComplex, Poojanahalli Rd,Off NH-7, Adjacent toTrumpet Flyover of BIAL,Kannamangala Post,Bangalore 562110, India;e-mail: [email protected].
304 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
© 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License

collaborating institutions with the Internet asthe medium of transmission to a central repos-itory. An earlier version of this method, whichconstituted the basic design and frameworkfor obtaining information, has been describedpreviously.12
PATIENTS AND METHODS
Thirteen institutionsparticipated in thestudy (DataSupplement). A standardized patient informationform (PIF; Data Supplement) developed by oncol-ogists with specific expertise in breast cancerwas hosted on a Web site (www.hbccrindia.org).Printed forms with an instruction manual weresupplied to participants. Trained staff completedthe form throughacombination of patient-attendantinterviews; scrutiny of medical records, other rel-evant documents, and registers; and discussionswith concerned clinicians. Collaborating centerswere given individual login identifications andpasswords with instructions for online data entryto electronically transmit the data to a centralrepository, the National Centre for Disease Infor-matics and Research (NCDIR). Themandate andmission statements of this unique center (an out-come of the National Cancer Registry Program ofthe Indian Council of Medical Research) are pro-vided at the NCDIR Web site (www.ncdirindia.org). All participating institutions had the studyprotocol cleared by their respective institutionalethics committees, and patient consent was in-corporated into the individual patient medicalrecord.
Stage-based treatment patterns were examinedfor 9,903 newly diagnosed (between January 1,2006, and December 31, 2008) patients withinfiltrating duct carcinoma of the breast treatedat the participating institutions.However, survivalanalysis was restricted to 7,609 patients fromnine centers having at least 60% follow-up in-formation on their respective patients as of De-cember 31, 2012. The ultimate end point ofoverall survival (OS) was defined as the periodbetween the date of diagnosis and the date ofdeath (when death occurred before January 1,2013) from any cause. Patients who died on orafter January 1, 2013, were deemed alive forsurvival analysis. The number and proportion ofpatients with toxicity (on the basis of early andlate complications) and recurrence are basedon any one such reported event. The PIF pro-vided details of clinical TNM and stage group-ing at initial presentation of the patient. On thebasis of the lymph node status, pathologic TNM(pTNM) was also recorded. TNM on the basis
of histopathology findings (pTNM) supersededthe clinical TNM for the final stage grouping.13
Analysis was carried out separately for stages I,II, and III. Patients with stage IV disease (whichis exclusively a metastatic disease) and patientswhose stage was unknown were excluded fromthis study.
Surgical Treatment
Patients who had undergone lumpectomy with orwithout axillary lymph node clearance were de-fined as having received BCS, whereas patientswho had simple MS (with or without axillary lymphnode clearance) or radical MS were classified ashaving had MS.
Radiotherapy
Patients who had received radiotherapy (RT) tothe chest wall (> 45 Gy) with or without anadditional boost with radical intent were consid-ered as having received optimal RT, and thosewho received less than this dose were consid-ered as have received suboptimal RT. Patientstreated with palliative intent RT or RT givenonly to the axilla and/or supraclavicular nodeswere excluded. Few patients (1.6%) received RTthrough such techniques as intensity-modulatedRT or image-guided RT, so these factors weredisregarded.
Chemotherapy
Chemotherapy was considered as given if thepatient received it as neoadjuvant, concurrent,or adjuvant chemotherapy. Standard prescribedprotocols in use of specific chemotherapy drugswere followed. Anthracyclines with and withouttaxanes and/or other drug combinations were an-alyzed separately. Because few patients (n = 23)were given trastuzumab, no separate analysis wasdone on this.
Hormone Therapy
Patients who received neoadjuvant or adjuvantintervention with surgical oophorectomy, RT-ovarianablation, medical tamoxifen, or aromatase inhibitorswere considered as having received hormonetherapy (HT).
Receptor Status
Estrogen receptor (ER), progesterone receptor(PR), and human epidermal growth factor recep-tor 2 (HER2) status was determined in all patientsandwasclassified as triple negative, triple positive,ER and PR positive andHER2 negative, and othercombinations.
305 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Software Programs and Quality Checks
In-house Internet-based software programs (www.hbccrindia.org; www.ncdirindia.org) were mod-eled for data capture, checked for complete-ness and consistency, tracked patient follow-up,updated treatment information, and recordedfollow-updetails. Checksdoneondata varied fromdate checks to verifying discrepancies in clinicalinformation (Data Supplement). Lists of patientswith improbable data were sent back to concernedcenters for rectification. Further, a center-wiserandom sample of 10% of patients was listed, andcenters were asked to reabstract the medical re-cords for certain essential parameters; thematch-ing results were found to be 95% accurate.
Statistical Analysis
The Kaplan-Meier method14 and Cox proportionalhazards regression15 in the SPSS package (ver-sion 21; SPSS, Chicago, IL) were used to calculate5-year cumulative survival (FCS) rate and fatalityrisk (with statistical significance), respectively.
Multivariate analysis was performed using Coxproportional hazard regression analysis.
RESULTS
The Data Supplement provides patient, diagnos-tic, and treatment characteristics for the 9,903patients with breast cancer in whom patterns ofcare were examined and for the 7,609 patients inwhom survival analysis was also done. Overall, theFCS rate in 7,609 patients was 73.8%, varyingfrom 93.3% in patients with stage I disease to24.5% in patients with stage IV disease.
Stage I
BCS was performed in 198 (55.9%) of 354 pa-tients, and MS was performed in 146 (41.2%) of354patients. Themedian ages of womenwhohadBCS and MS were 52 and 57 years, respectively.The FCS rates were 95.5% for patients who hadBCS (alone or with other treatments) and 91.3%forpatientswhounderwentMS(aloneorwithothertreatments). The difference was not statisticallysignificant (hazard ratio [HR], 1.7; 95% CI, 0.7 to
Table 1. FCS and Cox Proportional HRs According to Type of Treatment in Stage II
Factor No. of Patients FCS (%) Unadjusted HR (95% CI) Adjusted* HR (95% CI)
Type of surgery
BCS 965 94.0 1.0 1.0
MS 1,785 85.8 2.40 (1.80 to 3.21) 2.37 (1.73 to 3.25)
RT dose, Gy
> 45 1,151 90.8 1.0 1.0
, 45 363 82.6 1.88 (1.38 to 2.56) 1.33 (0.94 to 1.89)
No RT 1,366 86.8 1.46 (1.14 to 1.86) 0.98 (0.75 to 1.28)
CT
Anthracyclines with or without taxanes 1,940 89.8 1.0 1.0
CMF 175 85.3 1.37 (0.91 to 2.06) 1.00 (0.65 to 1.56)
Other combinations 114 85.4 1.35 (0.77 to 2.37) 1.74 (0.98 to 3.08)
No CT 651 82.9 1.73 (1.36 to 2.21) 1.93 (1.49 to 2.50)
HT
HT given 1,358 91.6 1.0 1.0
No HT 1,522 84.3 1.93 (1.54 to 2.41) 1.65 (1.27 to 2.15)
Receptor status
Triple negative 661 86.8 1.0 1.0
Triple positive 195 89.1 0.78 (0.48 to 1.28) 0.91 (0.54 to 1.54)
ER and PR positive and HER2 negative 786 93.5 0.46 (0.32 to 0.65) 0.55 (0.37 to 0.83)
Other combinations† 1,238 84.7 1.16 (0.90 to 1.51) 1.05 (0.79 to 1.39)
Total 2,880 87.9
Abbreviations: BCS, breast-conserving surgery; CMF, cyclophosphamide, methotrexate, and fluorouracil; CT, chemotherapy; ER, estrogen receptor; FCS, 5-year cumulativesurvival; HER2, human epidermal growth factor receptor; HR, hazard ratio; HT, hormone therapy; MS, mastectomy; PR, progesterone receptor; RT, radiotherapy.*Adjusted for RT, CT, HT, and receptor status.†Information on receptor status available for only one or two of the three receptors.
306 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

4.2). Patients who receivedRT orHT in addition tosurgery (BCS or MS) had significantly better sur-vival compared with those who did not receive RTor HT (RT: FCS, 97.6% v 88.8%, respectively;HR, 4.0; 95% CI, 1.5 to 10.9; HT: FCS, 96.7%v 88.3%, respectively; HR, 3.0; 95% CI, 1.3 to 7.1).A combination of surgery (BCS or MS), RT, andHT with or without chemotherapy gave signifi-cantly better OS compared with all other single ormultimodality treatments (FCS, 99.0% v 90.7%,respectively; HR, 5.1; 95% CI, 1.2 to 21.7).Survival in stage I breast cancers was not influ-enced by age or receptor status.
Stage II
Of 2,880 patients with stage II disease, BCS wasperformed in 965 patients (33.5%), MS was per-formed in 1,785 patients (62.0%), and 130 pa-tients (4.5%) did not receive any type of surgery.The patient, diagnostic, and treatment character-istics of patients who received BCS and MS aregiven in the Data Supplement. Patients who had
BCS, compared with those who had MS, showedsignificantly better survival (FCS, 94.0% v 85.8%,respectively; Table 1). Patients withMS also had ahigher risk of death after adjusting for all othertypes of treatments and receptor status (HR, 2.4;95% CI, 1.7 to 3.3). Survival was significantlybetter in patients who had ER- and PR-positiveand HER2-negative disease than in patients withtriple-negative receptor status.
Analysis was done separately for the BCS andMS groups to examine the possible reasons forthe relatively poorer survival in patients with MS(Tables 2 and 3). For patients with BCS, inclusionof RT, which constitutes breast-conservation ther-apy (BCT), significantly increased the survivalcompared with patients who had not receivedRT. For patients who had MS, addition of bothchemotherapy andHT significantly increased sur-vival, whereas there was no improvement in sur-vival with addition of RT (Table 3).
The overall findings were similar when analysiswas done separately for stage IIA and IIB disease.
Table 2. FCS and Cox Proportional HRs According to Type of Treatment in Stage II Patients Who Received BCS
Factor No. of Patients FCS (%) Unadjusted HR (95% CI) Adjusted* HR (95% CI)
Type of surgery
BCS 965 94.0 1.0 1.0
RT dose, Gy
> 45 675 95.7 1.0 1.0
, 45 39 92.2 1.81 (0.55 to 5.94) 1.59 (0.42 to 6.02)
No RT 251 89.1 2.91 (1.70 to 5.00) 2.25 (1.19 to 4.24)
CT
Anthracyclines with orwithout taxanes
656 95.5 1.0 1.0
CMF 24 91.7 1.71 (0.41 to 7.16) 1.75 (0.35 to 8.64)
Other combinations 72 88.8 2.21 (0.92 to 5.33) 1.54 (0.60 to 3.94)
No CT 213 90.8 2.38 (1.33 to 4.24) 1.82 (0.92 to 3.62)
HT
HT given 432 95.8 1.0 1.0
No HT 533 92.4 1.93 (1.10 to 3.39) 0.97 (0.45 to 2.10)
Receptor status
Triple negative 306 91.2 1.0 1.0
Triple positive 75 95.1 0.47 (0.14 to 1.55) 0.45 (0.12 to 1.63)
ER and PR positive andHER2 negative
308 96.2 0.46 (0.23 to 0.92) 0.40 (0.16 to 0.99)
Other combinations† 276 94.2 0.74 (0.40 to 1.38) 0.67 (0.33 to 1.34)
Total 965 94.0
Abbreviations: BCS, breast-conserving surgery; CMF, cyclophosphamide, methotrexate, and fluorouracil; CT, chemotherapy; ER, estrogen receptor; FCS, 5-year cumulativesurvival; HER2, human epidermal growth factor receptor; HR, hazard ratio; HT, hormone therapy; PR, progesterone receptor; RT, radiotherapy.*Adjusted for RT, CT, HT, and receptor status.†Information on receptor status available for only one or two of the three receptors.
307 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

However, when examined by node status (N0[node negative] and N1 [node positive]), the dif-ference in the FCS rate between BCS and MSwas more pronounced in node-positive patients(11.6% [92.8% v 81.2%, respectively]) com-pared with node-negative patients (5.0% [95.0%v 90.0%, respectively]). Furthermore, node-positive MS patients showed significantly poorersurvival in the absence of administering optimalRT (HR, 2.7; 95% CI, 1.5 to 4.9), chemotherapy(HR, 1.97; 95% CI, 1.2 to 3.2), or HT (HR, 2.1;95% CI, 1.3 to 3.4) compared with MS patientswho had received optimal RT, chemotherapy,or HT.
Stage III
Of the 3,620 patients with stage III disease, 544(15.0%) underwent BCS, and 2,740 (75.7%) un-derwent MS. Three hundred thirty-six patients(9.3%) did not receive any surgical treatment.The patient, diagnostic, and treatment character-istics of patients who received BCS and MS aregiven in the Data Supplement. Table 4 lists theFCS rates and Cox proportional hazards HRs
according to type of treatment. The FCS ratewas 87.1% for BCS compared with 69.0% forMS. The risk of death for MS compared with BCSas expressed by the HR was significantly higher(HR, 2.6; 95% CI, 2.0 to 3.4) after adjusting forRT, chemotherapy, andHT.Onehundredninety-four patients received cyclophosphamide, meth-otrexate, and fluorouracil as chemotherapy andhad significantly poorer survival compared withpatients who received anthracyclines with or with-out taxanes as chemotherapy.
As in patients with stage II disease, the overallfindings were similar when analysis was doneseparately for stage IIIA and stage IIIB. Also asin patient with stage II disease, node-positive MSpatients (N1-3) had a significantly lower survivalwhenoptimalRTand/orHTwerenot administeredcompared with MS patients who had receivedthese therapies.
Table 5 compares the survival rates in this studywith those in other key reports. The survival benefitof BCS, especially in stage II and III breast cancer,seems to be greater in this study when compared
Table 3. FCS and Cox Proportional HRs According to Type of Treatment in Stage II Patients Who Received MS
Factor No. of Patients FCS (%) Unadjusted HR (95% CI) Adjusted* HR (95% CI)
Type of surgery
MS 1,785 85.8 1.0 1.0
CT
Anthracyclines with or without taxanes 1,210 87.4 1.0 1.0
CMF 125 87.5 0.90 (0.53 to 1.53) 0.97 (0.57 to 1.65)
Other combinations 39 84.4 1.24 (0.51 to 3.03) 1.21 (0.50 to 2.96)
No CT 411 80.3 1.61 (1.22 to 2.13) 1.75 (1.32 to 2.33)
HT
HT given 867 90.9 1.0 1.0
No HT 918 80.7 2.16 (1.66 to 2.83) 1.87 (1.37 to 2.53)
Receptor status
Triple negative 341 83.5 1.0 1.0
Triple positive 113 87.4 0.75 (0.42 to 1.35) 1.09 (0.59 to 2.03)
ER and PR positive and HER2 negative 457 92.0 0.42 (0.27 to 0.65) 0.60 (0.37 to 0.98)
Other combinations† 874 83.2 0.96 (0.71 to 1.31) 1.16 (0.84 to 1.61)
RT dose, Gy
> 45 430 85.1 1.0
, 45 270 82.5 1.20 (0.83 to 1.74)
No RT 1,085 87.0 0.88 (0.65 to 1.18)
Total 1,785 85.8
Abbreviations: CMF, cyclophosphamide, methotrexate, and fluorouracil; CT, chemotherapy; ER, estrogen receptor; FCS, 5-year cumulative survival; HER2, human epidermalgrowth factor receptor; HR, hazard ratio; HT, hormone therapy; MS, mastectomy; PR, progesterone receptor; RT, radiotherapy.*Adjusted for CT, HT, and receptor status.†Information on receptor status available for only one or two of the three receptors.
308 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

with others. The Data Supplement depicts theKaplan-Meier comparative survival curves for pa-tients who received BCS and MS separately forstage II and stage III disease. Therewasno survivaldifference between age groups in patients withstage II or stage III disease.
DISCUSSION
Several clinical trials have shown that BCS is asgood as MS in early-stage (stage II) breast cancer,althoughsomereportshave indicatedahigher rateof local recurrence in patients who have under-gone BCS.5,16,18,19 Other aspects that have beencompared are initial tumor size, patterns of re-currence, and time to locoregional recurrence ordistant metastases.6,20 These studies have shownthat there is no difference in survival between thetwo types of surgery. A national registry-basedstage-by-stage comparison has also shown equalsurvival for BCS and MS.21 A meta-analysis byYang et al22 showed that OS was not statistically
significant between patients who underwent MSand BCT.
However, recent publications from Canada23 andresults from the SEER database8 show bettersurvival of patients with BCT compared with MS.A report presented at the San Antonio BreastCancer Symposium in December 2015 on anobservational study of 37,000 women showeda better survival with BCT than with MS (76.8%v 59.7%, respectively).24
There have been single-institution reports fromIndia comparing survival in patients receivingBCS and those receiving MS.10,11 To our knowl-edge, this is the first multi-institutional study inIndia to provide insight into the extent of practiceof BCS vis-a-vis MS and the survival differencesbetween these two treatments. It is not a ran-domized clinical trial, but it nonetheless givesan accurate picture of the patterns of care andsurvival in the natural arena of selection of pa-tients with cancer for a specific type cancer
Table 4. FCS and Cox Proportional HRs According to Type of Treatment in Patients With Stage III Disease
Factor No. of Patients FCS (%) Unadjusted HR (95% CI) Adjusted* HR (95% CI)
Type of surgery
BCS 544 87.1 1.0 1.0
MS 2,740 69.0 2.82 (2.18 to 3.66) 2.56 (1.96 to 3.35)
RT dose, Gy
> 45 1,854 76.9 1.0 1.0
, 45 812 64.9 1.73 (1.49 to 2.01) 1.16 (0.98 to 1.37)
No RT 954 56.2 2.45 (2.12 to 2.83) 2.03 (1.73 to 2.38)
CT
Anthracyclines with orwithout taxanes
2,771 70.6 1.0 1.0
CMF 194 56.6 1.66 (1.33 to 2.08) 1.36 (1.08 to 1.72)
Other combinations 204 70.5 1.00 (0.75 to 1.34) 0.76 (0.56 to 1.03)
No CT 451 64.0 1.41 (1.18 to 1.69) 0.98 (0.81 to 1.19)
HT
HT given 1,541 78.0 1.0 1.0
No HT 2,079 61.9 2.03 (1.78 to 2.31) 1.72 (1.48 to 2.00)
Receptor status
Triple negative 823 69.2 1.0 1.0
Triple positive 223 75.6 0.70 (0.51 to 0.95) 0.88 (0.64 to 1.22)
ER and PR positive and HER2negative
778 80.3 0.58 (0.47 to 0.72) 0.76 (0.60 to 0.96)
Other combinations† 1,796 63.4 1.21 (1.04 to 1.42) 1.12 (0.95 to 1.32)
Total 3,620 69.1
Abbreviations: BCS, breast-conserving surgery; CMF, cyclophosphamide, methotrexate, and fluorouracil; CT, chemotherapy; ER, estrogen receptor; FCS, 5-year cumulativesurvival; HER2, human epidermal growth factor receptor; HR, hazard ratio; HT, hormone therapy; MS, mastectomy; PR, progesterone receptor; RT, radiotherapy.*Adjusted for CT, HT, and receptor status.†Information on receptor status available for only one or two of the three receptors.
309 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

treatment in the country. Observational studiessuch as the patterns of care studies or compar-ative treatment effectiveness studies have thefollowing several advantages: they are compre-hensive, have been externally validated, havebroader criteria for patient inclusion, are un-biased, and provide results in routine clinicalsettings.25 The strengths, opportunities, andlimitations of this study, which is identical to theone on cervical cancer, have been outlined pre-viously.26 The differences observed in survivalare a result of a combination of treatment mo-dality and selection criteria of patients. The latterare unknown and have not been taken into ac-count. However, there is no selection bias be-cause all patients who received cancer-directedtreatment in their respective institutions havebeen accounted for, and exclusion criteria arebased on scientific logic.26 Other limitations spe-cific to this study are that in a high proportion ofpatients (pattern of care, 33.4%; pattern of sur-vival, 28.6%) information on receptor status wasnot available andasubstantial number of patients
with stage I (10 patients), stage II (130 patients),and stage III disease (336 patients) did not re-ceive any surgical treatment. Because there wasno information as to why surgery was not done inthese patients, we were unable to provide theclinical or other rationale for this result.
This study is a foremost example of cancer regis-tration (through a national program of cancerregistries covering several cancer centers andmedical institutions) evaluating clinical parame-ters andprovidingcritical findings that couldhavean impact on patient care. A network of cancerhospitals linked to a central coordinating center(NCDIR)with a system to accruegoodclinical datathrough modern electronic information technol-ogy is in place.
The differences in survival that were observedbetween MS and BCS are significant and sub-stantial. The difference was 8.2% for patients withstage II disease and as high as 18.1% for patientswith stage III disease, with the results being thesameevenwhen separately analyzed according to
Table 5. International Comparison of Survival Rates
Study Study Type FIGO Stage Treatment No. of Patients 5-Year OS (%)
van Dongen et al,16 2000 Randomized trial I-II BCS 448 82
MS 420 85
Agarwal et al,8 2014 Retrospective(cancer-specific survival)
I-II BCS 92,671 97
MS 34,999 94
MS+RT 4,479 90
Onitilo et al,17 2015 Retrospective I-IIIA BCS 3,340 91
MS 1,995 84
Present study, 2015 Observational I BCS 198 96
MS 146 91
II BCS 965 94
MS 1,785 86
IIA BCS 577 96
MS 779 88
IIB BCS 388 92
MS 1,006 84
III BCS 544 87
MS 2,740 69
IIIA BCS 278 89
MS 1,200 73
IIIB BCS 202 87
MS 1,285 67
IIIC BCS 64 77
MS 255 58
Abbreviations: BCS, breast-conserving surgery; FIGO, International Federation of Gynecology and Obstetrics; MS, mastectomy; OS, overall survival; RT, radiotherapy.
310 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

stages IIIA and IIIB. The results presentedhere arethose of pooled data from several institutions. Thedata of individual centers were separately exam-ined to ascertain whether there were any varia-tions among institutions in the survival or theextent of survival difference between BCS andMS. A comparable survival pattern and differ-ence were observed in all institutions. Age andrate of recurrence or complications were alsosimilar between the two groups. The variation inother treatments impacting survival betweenpatients who had received BCS and MS showsthat for stage II disease, RT plays a major role forBCS but not for MS, although relatively more MSpatients received less RT and suboptimal RT. Theroles of chemotherapy and HT seem less impor-tant than RT for BCS, whereas these treatments(chemotherapy and HT) are more important forimproved survival in the MS group. The need forgreater systemic therapy in patients with MS incontrast to those who had BCS is difficult to explain.One could hypothesize that removal of the breast asa result of MS entails loss of patient immunity thatrequires additional systemic therapy.
A similar picture was observed in stage III dis-ease where patients who had MS did betterwhen they received a combination of RT, che-motherapy, and HT, whereas in patients whohad BCS, RT alone was sufficient to have equiv-alent survival. The proportions of patients withstage II and III disease in the pattern-of-care
group (all 13 institutions) who underwent BCSwere 29.5% and 12.8%, respectively (DataSupplement).
In conclucion, the findings justify further inves-tigation of the possible reasons for decreasedsurvival in patients with MS. The underlyingcause of death, including the events that leadto it, whether a result of early or late complica-tions of treatment, needs to be studied. A well-substantiated analysis of this parameter wouldrequire availability of accurate and complete in-formation on these characteristics in a majority ofpatients, which was not available in the currentstudy. Because obtaining such data is hugelychallenging in the routine Indian setting, a ran-domized study on the cause of death in patientswith breast cancer could provide insights. Suchstudies could take into account additional andfurther details of points that were not gatheredin this study, including information on individualcaregivers, socioeconomic status of patients, andadditional details on investigations done for stag-ing. There seems to be a need to promote aware-ness about the distinct advantages of BCS in thecontext of developing countries, and further stud-ies are required to examine the biologic or sci-entific rationale of the requirement of systemictherapy in patients with MS but not in those withBCS.
DOI: https://doi.org/10.1200/JGO.2016.004614Published online on jgo.org on October 12, 2016.
AUTHOR CONTRIBUTIONS
Conception and design: Ambakumar Nandakumar,Goura Kishor RathAdministrative support: Goura Kishor RathCollection and assembly of data: Ambakumar Nandakumar,Francis Selvaraj Roselind, Krishnan Sathishkumar, DampillaDaniel Vijay Kumar, Ankush Jain, Kondalli LakshminarayanaSudarshan
Data analysis and interpretation: Ambakumar Nandakumar,Goura Kishor Rath, Amal Chandra Kataki, P. PoonamalleBapsy, Prakash C. Gupta, Paleth Gangadharan, Ramesh C.Mahajan, Manas Nath Bandyopadhyay, Kumara Swamy,Elizabeth Vallikad, Rudrapatna N. VisweswaraManuscript writing: All authorsFinal approval of manuscript: All authorsAccountable for all aspects of the work: All authors
AUTHORS’ DISCLOSURES OFPOTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided byauthors of this manuscript. All relationships are consideredcompensated. Relationships are self-held unless noted.I = Immediate Family Member, Inst = My Institution.Relationships may not relate to the subject matter of thismanuscript. For more information about ASCO’s conflict of
interest policy, please refer to www.asco.org/rwc orascopubs.org/jco/site/ifc.
Ambakumar NandakumarNo relationship to disclose
Goura Kishor RathNo relationship to disclose
Amal Chandra KatakiNo relationship to disclose
P. Poonamalle BapsyNo relationship to disclose
Prakash C. GuptaNo relationship to disclose
Paleth GangadharanNo relationship to disclose
Ramesh C. MahajanNo relationship to disclose
Manas Nath BandyopadhyayNo relationship to disclose
Kumara SwamyNo relationship to disclose
311 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Elizabeth VallikadNo relationship to disclose
Rudrapatna N. VisweswaraNo relationship to disclose
Francis Selvaraj RoselindNo relationship to disclose
Krishnan SathishkumarNo relationship to disclose
Dampilla Daniel Vijay KumarNo relationship to disclose
Ankush JainNo relationship to disclose
Kondalli Lakshminarayana SudarshanNo relationship to disclose
ACKNOWLEDGMENTA list of collaborators from the respective participatingcenters is given in theAppendix. The study proposal/protocolwas approved and recommended for release of grants at thefollowing three different levels: first by the members of theerstwhile Steering Committee of the National Cancer Reg-istry Program and now the Research Area Panel on Cancer(RAP-Cancer) and Scientific Advisory Committee of theNational Centre for Disease Informatics and Research(NCDIR); second by the Scientific Advisory Group of theNon-Communicable Disease Division of the Indian Councilof Medical Research (ICMR); and third by the BiomedicalResearchBoard of the ICMR.Thechief principal investigatorof the study (A.N.) has been assisted by his team at NCDIR,by the members of RAP-Cancer, the directors and theirclinical and cancer registry colleagues at the cancer centersand medical colleges, and the concerned staff at ICMRheadquarters, New Delhi, India.
Affiliations
Ambakumar Nandakumar, Francis Selvaraj Roselind, Krishnan Sathishkumar, Dampilla Daniel Vijay Kumar, Ankush Jain,Kondalli Lakshminarayana Sudarshan, National Centre for Disease Informatics and Research; P. Poonamalle Bapsy, ApolloHospitals; Kumara Swamy, HealthCare Global–Bangalore Institute of Oncology; Elizabeth Vallikad, St John’s Medical College;Rudrapatna N. Visweswara, International Medical School–MS Ramaiah Medical College, Bangalore; Goura Kishor Rath, InstituteRotary Cancer Hospital, All India Institute of Medical Sciences, New Delhi; Amal Chandra Kataki, Dr B.B. Borooah CancerInstitute, Guwahati; Prakash C. Gupta, Healis-Sekhsaria Institute of Public Health, Navi Mumbai; Paleth Gangadharan, AmritaInstitute ofMedical Sciences andResearch Centre, Kochi; Ramesh C. Mahajan, Postgraduate Institute ofMedical Education andResearch, Chandigarh; and Manas Nath Bandyopadhyay, Cancer Centre Welfare Home and Research Institute, Kolkata, India.
Support
SupportedbytheNationalCentreforDiseaseInformaticsandResearch,apermanentinstituteoftheIndianCouncilofMedicalResearch,the premier medical research body of India and part of Department of Health Research, Ministry of Health and Family Welfare,Government of India. Three initial workshops to finalize the patient information form were supported by the WHO.
Written on behalf of the Patterns of Cancer Care and Survival Studies Group.
REFERENCES1. Torre LA, Bray F, Siegel RL, et al: Global cancer statistics, 2012. CA Cancer J Clin 65:87-108, 2015
2. National Centre for Disease Informatics and Research: Time trends in cancer incidence rates 1982-2010. Bangalore,India, National Centre for Disease Informatics and Research, National Cancer Registry Programme, Indian Council ofMedical Research, 2013
3. Young JL: The hospital-based cancer registry, in Jensen OM, Parkin DM, MacLennan R, et al (eds): Cancer Reg-istration: Principles and Methods. Lyon, France, International Agency for Research on Cancer, Scientific PublicationNo. 95, 1991, pp 177-184
4. Nandakumar A: Strategy for active follow-up in conduct of survival studies. Presented at the Annual ReviewMeeting ofNational Cancer Registry Programme of India, Dibrugarh, India, November 24-26, 1993
5. Veronesi U, Cascinelli N, Mariani L, et al: Twenty-year follow-up of a randomized study comparing breast-conservingsurgery with radical mastectomy for early breast cancer. N Engl J Med 347:1227-1232, 2002
6. Blichert-Toft M, Nielsen M, During M, et al: Long-term results of breast conserving surgery vs. mastectomy for early stageinvasive breast cancer: 20-year follow-up of theDanish randomizedDBCG-82TMprotocol. Acta Oncol 47:672-681, 2008
7. Cao JQ, Olson RA, Tyldesley SK: Comparison of recurrence and survival rates after breast-conserving therapy andmastectomy in young women with breast cancer. Curr Oncol 20:e593-e601, 2013
8. Agarwal S, Pappas L, Neumayer L, et al: Effect of breast conservation therapy vs mastectomy on disease-specificsurvival for early-stage breast cancer. JAMA Surg 149:267-274, 2014
9. Deo SVS, Samaiya A, Shukla NK, et al: Breast conservation therapy for breast cancer: Patient profile and treatmentoutcome at a tertiary care cancer centre. Natl Med J India 18:178-181, 2005
10. Narendra H, Ray S: Breast conserving surgery for breast cancer: Single institutional experience from Southern India.Indian J Cancer 48:415-422, 2011
312 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

11. Gadgil A, Roy N, Sankaranarayanan R, et al: Effect of comprehensive breast care on breast cancer outcomes: Acommunity hospital based study from Mumbai, India. Asian Pac J Cancer Prev 13:1105-1109, 2012
12. Nandakumar A, Gupta PC, Gangadharan P, et al: Geographic pathology revisited: Development of an atlas of cancer inIndia. Int J Cancer 116:740-754, 2005
13. Sobin L, Gospodarowicz M, Wittekind C: TNM Classification of Malignant Tumours (ed 7). Geneva, Switzerland,International Union Against Cancer, 2009
14. Kaplan EL, Meier P: Nonparametric estimation from incomplete observations. J Am Stat Assoc 53:457-481, 1958
15. Cox DR: Regression models and life tables. J R Stat Soc B 34:187-220, 1972
16. van Dongen JA, Voogd AC, Fentiman IS, et al: Long-term results of a randomized trial comparing breast-conservingtherapy with mastectomy: European Organization for Research and Treatment of Cancer 10801 trial. J Natl CancerInst 92:1143-1150, 2000
17. Onitilo AA, Engel JM, Stankowski RV, et al: Survival comparisons for breast conserving surgery and mastectomyrevisited: Community experience and the role of radiation therapy. Clin Med Res 13:65-73, 2015
18. Jacobson JA, Danforth DN, Cowan KH, et al: Ten-year results of a comparison of conservation with mastectomy in thetreatment of stage I and II breast cancer. N Engl J Med 332:907-911, 1995
19. FisherB, AndersonS,Bryant J, et al: Twenty-year follow-upof a randomized trial comparing totalmastectomy, lumpectomy,and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med 347:1233-1241, 2002
20. Lee S, Kim SW, Kim S-K, et al: Locoregional recurrence of breast conserving surgery after preoperative chemotherapyin Korean women with locally advanced breast cancer. J Breast Cancer 14:289-295, 2011
21. Ye JC, Yan W, Christos P, et al: Equivalent survival with mastectomy or breast-conserving surgery plus radiation inyoung women aged, 40 years with early-stage breast cancer: A national registry-based stage-by-stage comparison.Clin Breast Cancer 15:390-397, 2015
22. Yang SH, Yang KH, Li YP, et al: Breast conservation therapy for stage I or stage II breast cancer: A meta-analysis ofrandomized controlled trials. Ann Oncol 19:1039-1044, 2008
23. Fisher S, Gao H, Yasui Y, et al: Survival in stage I-III breast cancer patients by surgical treatment in a publicly fundedhealth care system. Ann Oncol 26:1161-1169, 2015
24. SieslingS: Ten-yeardata: Lumpectomyand radiotherapy trumpmastectomy. http://www.medscape.com/viewarticle/855810
25. Holzer S, Stewart A, Dudeck J: Assessing patterns of care, in Sankila R, Black R, Coebergh JW, et al (eds): Evaluationof Clinical Care by Registries. Lyon, France, International Agency for Research on Cancer, Technical PublicationNo. 37, 2003, pp 55-58
26. Nandakumar A, Rath GK, Kataki AC, et al: Concurrent chemoradiation for cancer of the cervix: Results of a multi-institutional study from the setting of a developing country (India). J Glob Oncol 1:11-22, 2015
APPENDIX Patterns of Cancer Care and Survival Studies GroupProject Management Group: Ambakumar Nandakumar (National Centre for Disease Informatics and Research [NCDIR],Bangalore), Francis Selvaraj Roselind (NCDIR), Krishnan Sathishkumar (NCDIR), Dampilla Daniel Vijay Kumar (NCDIR),Ankush Jain (NCDIR), and Kondalli Lakshminarayana Sudarshan (NCDIR).
Cancer Research Area Panel: Goura Kishor Rath (Institute Rotary Cancer Hospital, All India Institute ofMedical Sciences, NewDelhi), AmalChandraKataki (DrB.B.BorooahCancer Institute,Guwahati), P.PoonamalleBapsy (ApolloHospitals,Bangalore),PrakashC. Gupta (Healis-Sekhsaria Institute of Public Health,NaviMumbai), Paleth Gangadharan (Amrita Institute ofMedicalSciences and Research Centre, Kochi), Ramesh C. Mahajan (Postgraduate Institute of Medical Education and Research,Chandigarh), Manas Nath Bandyopadhyay (Cancer Centre Welfare Home and Research Institute, Kolkata), Kumara Swamy(HealthCare Global–Bangalore Institute of Oncology, Bangalore), Elizabeth Vallikad (St John’s Medical College, Bangalore),Rudrapatna N. Visweswara (International Medical School–MS Ramaiah Medical College, Bangalore).
Collaborators (institutes) supplying individual patient data (in descending order of the number of patients with cancer onwhom information was provided, first for survival studies and then for pattern of care only): Tata Memorial Hospital (TMH),Mumbai—R.A.Badwe;A.K.D’Cruz;B.Ganesh;VaniParmar; SudeepGupta;AshwiniBudrukkar;RakeshJalali; Arshi Khan;Sushama Saoba; Sharwari Joshi; Mitali Sapkal. Cancer Institute (WIA), Chennai—V. Shanta; R. Swaminathan; V. Sridevi;R. Rama; P. Shanthi; M.S. Kalyani. Regional Cancer Centre, Thiruvananthapuram—Paul Sebastian; Aleyamma Mathew;Preethi Sara George; Ratheesan K; Beela Sarah Mathew. Amrita Institute of Medical Sciences, Kochi—D.K. Vijaykumar;P. Gangadharan. Mahavir Cancer Sansthan, Patna—J.K. Singh;M. Singh; P. Jain; A. Kumari. HealthCare Global BangaloreInstitute of Oncology, Bangalore—B.S. Ajaikumar, Kumaraswamy, Raghavendra Rao M, M.Bandemegal, K.Murugan,N.Rao, R.S. Bilimagga, Gopinath K. S, R. Nayak. Dr B. Borooah Cancer Institute, Regional Cancer Centre, Guwahati—A.C. Kataki;MouchumeeBhattacharyya. AssamMedical College, Dibrugarh—K. AdhikariM;M.S. Ali; R. Akhtar; S.K. Bhuyan;I. Baruah; Sheila Neog. Cachar Cancer Hospital and Research Centre, Silchar—R. Kannan; R. Tapkire; G. Dutta; A. Das;G. Roy. Rajiv Gandhi Cancer Institute and Research Centre, New Delhi—S. Rawat; A. Mishra; A.K. Pahuja. PostgraduateInstitute ofMedical EducationandResearch, Chandigarh—S.Ghoshal; S.C. Sharma.KidwaiMemorial Institute of Oncology,Bangalore—M.Vijayakumar;K.RamachandraReddy;C.Ramesh;D.J. Jayaram.GovernmentMedicalCollegeandHospital,Nagpur—K.M. Kamble; V.N. Sagdeo; N. Jambhulkar. ICMRHeadquarters, NewDelhi—V.M. Katoch; D.K. Shukla; T. Kaur.
313 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

originalreport
Clinical Overestimation of HER2Positivity in Early Estrogen andProgesterone Receptor–Positive BreastCancer and the Value of MolecularSubtyping Using BluePrint
abstract
Purpose Human epidermal growth factor receptor 2 (HER2) positivity is an important prognostic andpredictive indicator in breast cancer. HER2 status is determined by immunohistochemistry and fluorescentin situ hybridization (FISH), which are potentially inaccurate techniques as a result of several technicalfactors, polysomyof chromosome17, andamplification or overexpression of CEP17 (centromeric probe forchromosome 17) and/or HER2. In South Africa, HER2-positive tumors are excluded from a MammaPrint(MP; Agendia BV, Amsterdam, Netherlands) pretest algorithm. Clinical HER2 status has been reported tocorrelate poorly with molecular subtype. The aim of this study was to investigate the correlation of clinicalHER2 status with BluePrint (BP) molecular subtyping.
Methods Clinico-pathologic and genomic informationwas extracted fromaprospectively collected centralMPdatabase containing records of 256 estrogen receptor–positive and/or progesterone receptor–positivetumors. Twenty-one tumors considered HER2 positive on immunohistochemistry or FISHwere identified forthis study.
Results Themedianageof patientswas56 years (range, 34 to77 years),with amedian tumor size of 16mm(3 to27mm). Four (19%) tumorswereconfirmedHER2-enriched subtype, six (29%)were luminal A, and11(52%) were luminal B. The positive predictive values of HER2/CEP17 ratio ‡ 2 and HER2 copy number ‡ 6were only 29% and 40%, respectively. The differences in means for HER2/CEP17 ratio were significantbetweenBPHER2-enriched versus luminal (P= .0249; 95%CI, 0.12 to 1.21) andMPhigh-risk versus low-risk tumors (P = .0002; 95% CI, 0.40 to 1.06).
Conclusion Of the 21 tumors considered clinically HER2 positive, only four were HER2-enriched subtypewith BP, indicating an overestimation of HER2 positivity. FISH testing has a poor positive predictive value.
J Glob Oncol 3. © 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
INTRODUCTION
Humanepidermal growth factor receptor 2 (HER2),orHER2/neu,hasbeenawell-recognizedoncogeneinvolved in the oncogenesis of several cancers. Inbreast cancer, it is an established prognostic andpredictivebiomarker.1Where theadjuvantmanage-ment of early HER2-positive breast cancer is con-cerned, significant improvements in disease-freeandoverallsurvivalhavebeenshownwiththeadditionof trastuzumab to chemotherapy for tumors. 1 cmand for node-positive disease.2-6 This benefitwas also seen for tumors , 1 cm when certainadverse prognostic features were present.7
Screening mammography has given rise to anincreased incidence of breast cancer diag-nosed at an earlier stage,8 of which an estimated15% to 20% are considered to be HER2 posi-tive.1 In southern Africa, the incidence of HER2-positive breast cancer is estimated at 25.2%.9
Although data before 2011 were limited byunder-reporting from private laboratories, theeffect of this was found to be , 4%.10 Becauseof the cost implications of trastuzumab on adeveloping economy, only a minority of thesepatients have access to trastuzumab at anystage of their disease. Significant disparity existsbetween patients who rely on state care and
Ettienne J. Myburgh
Lizanne Langenhoven
Kathleen A. Grant
Lize van der Merwe
Maritha J. Kotze
Author affiliations andsupport information (ifapplicable) appear at theend of this article.
Corresponding author:Ettienne J. Myburgh, MB,ChB, MMed (Surg), FCS(SA), MediclinicPanorama, RothschildBlvd, Suite 101,Panorama, Cape Town,SouthAfrica; e-mail: [email protected].
314 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
© 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License

those who have access to private medicalinsurance.
For patients who rely on state care, trastuzumabis only available in one of the nine South Africanprovinces. Insofar as private funders are con-cerned, reimbursement protocols are diverseand often require a significant copayment fromthe patient. It is not uncommon to administertrastuzumab only to a certain arbitrary financialpoint rather than according to standard of careguidelines, which currently suggest 1 year ofadjuvant therapy. In such a cost-conscious en-vironment, all attempts should be made to moreclearly define a subset of patients who may ben-efit from costly therapies, thereby improving ac-cess by all women regardless of financial or socialmeans.
Identifying patients with HER2-positive tumorshas relied largely on immunohistochemistry(IHC) and the use of fluorescent in situ hybridiza-tion (FISH). Unfortunately, several pitfalls exist inthe process. Notably, these include the variabilityin reporting of HER2 status by IHC assessmentonly, and theeffect ofpolysomyof chromosome17in breast tumor cells leading to inaccurate estima-tion of HER2 gene expression.11 Guidelines havebeen developed to improve the accuracy of report-ing, with the intent of selecting any patient whomightpossiblybenefit from targeted therapy.12Thishas led tomore equivocal cases being identified.13
In a cost-conscious environment, however, weshould focusour attentiononmodalities thatmightmaintain the positive predictive value (PPV) butalso improve the negative predictive value to avoidineffective and costly therapy.
In South Africa and Namibia, most health carefunders require reflex FISH testing on all HER2-positive tumors with 2+ or 3+ IHC staining, al-though some funders will accept tumors with3+ IHC staining for the funding of trastuzumab.
Since 2007, it has been possible to order Mam-maPrint (MP; Agendia BV, Amsterdam, Nether-lands) through local agents in South Africa, whichshipped the preparedmaterial to theNetherlands.MP is a 70-gene microarray-based genomic risk–assessment assay. In 2010, an 80-gene micro-array calledBluePrint (BP)wasadded to report theintrinsic molecular subtype of the tumor. TheHER2-enriched subtype is defined by the ERBB2,GRB7, PERLD1, and SYCP3 genes.14 Until early2016, the Agendia Breast Cancer Suite alsoincluded a separate single-gene microarray forthe estrogen receptor (ER), progesterone receptor(PR), andHER2 receptor, namely TargetPrint (TP).
After an initial health economic assessmentand the development of an MP pretest algorithm(MPA),15 this technology was introduced for early-stage ER/PR-positive, HER2-negative tumors inSouth Africa; to date, 256 tests have been done. In arecent publication, Pohl et al16 showed that MPaltered the treatment decision in 52%of patientsin this subgroup. With the recent publication of theresults from the EORTC-10041/BIG-3-04 MINDACT(Microarray In Node-Negative and 1 to 3 PositiveLymph Node Disease May Avoid Chemotherapy)trial, the safety of omitting adjuvant chemotherapy inlow-risk tumors, as determined by MP, has been wellestablished.17 As in the MINDACT trial, which in-cluded 9.5% HER2-positive tumors, a few such tu-morswere included in theSouthAfricanMPdatabase.
Internationally, several other genomic profilingassays have become available, notably OncotypeDX, which is the only other assay available to theSouth African private health sector through localagents. Although it has approximately 90% of themarket share in theUnited States,18 it is estimatedto hold roughly 40% of the market share in SouthAfrica. It does not report molecular subtyping.
Although recently published guidelines from ASCOrecommendedagainst theuse of any commerciallyavailable biomarkers in early HER2-positive breastcancer,19 there has been substantial evidence ofthe importanceofmolecular subtyping in treatmentdecision making rather than pure recurrence riskprediction,20,21 which would be more appropriatein the era where targeted biologic agents are beingdeveloped at a rapid pace.
Thenegative predictive value of single-geneHER2reporting has been shown in a cohort of patientswith HER2-negative tumors.22 In HER2-positivetumors, mRNA levels seem to be a good predictorof response to trastuzumab and chemotherapy inpatients with ER-positive disease.23
It iswell recognized that current strategies inHER2testing do not accurately determine all of themolecular pathways driving oncogenesis. Thismight be the reason why a complete pathologicresponsewas only seen in 31.7%of patients in theHER2-positive subset of the GeparQuattro dataset.24 Several publications have recently alludedto the fact that a significant proportion of tumorsreported to be HER2 positive using IHC/FISH(clinically HER2 positive [cHER2]) are not oftheHER2-enriched (HER2E) subtype.19,25,26 Thisindicates that other pathways might drive prolifera-tion, eg, downstream phosphatidylinositol 3-kinaseactivation through mechanisms such as loss ofPTEN, which induces resistance to trastuzumab.27
315 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

In a publication by Prat et al,26 only 47% of patientswith cHER2 tumors had the HER2E subtype. In theNeoadjuvant Breast Registry Symphony Trial, only33 (44%) of the 75 patients with ER/PR-positivecHER2-positive disease had the HER2E subtype.20
To further investigate the role of genomic profilingbeyond standard HER2 reporting, this study wasundertaken to evaluate the value of molecular sub-typing in HER2 assessment of ER/PR-positivebreast cancers.
METHODS
This study was performed in accordance with theethical standards laid out in the 1964 Declarationof Helsinki. Ethical approval was granted by theHealth and Research Ethics Committee of the Uni-versity of Stellenbosch (reference number N09/06/166). All patients consented to their clinico-pathologic data being stored in a central data-base and used for later analysis.
Study Population
Detailed records of 256 tumors from southernAfrican patients, referred for MP analysis since2007, have been prospectively collected in a cen-tral database. Referrals were from oncologists andsurgeons in both private and public practicesin South Africa and Namibia. Histology and FISHtesting was done by several nationally accreditedprivatepathology laboratories, andnocentral reviewwas done. MP risk scoring and ER, PR, and HER2receptor status were determined as previously de-scribed.22Recordsof the tumors thathadBPassaysperformed were considered and provided informa-tion on patient age and sex; tumor type, grade, andsize; ER, PR, and HER2 status; nodal status; MPrisk; and the molecular subtype as determined byBP.Most also hadTP results for ER, PR, andHER2.
Inclusion Criteria
Patients with equivocal or positiveHER2 testing asdefined by the 2013 American Society of ClinicalOncology/College of American Pathologists con-sensus guidelines,12 including HER2 staining in-tensity of 3+ (IHC), HER2/centromeric probe forchromosome 17 (CEP17) ratio > 2 (FISH), orHER2 copy number > 4 (FISH).
Statistical Analysis
Characteristics are described as the median(range) for quantitative/numerical data and ascount (percentage) for qualitative/categorical data.Because the variancesof thegroups inboth theMPand the BP result groups were clearly different,Welch two-sample t testswereused to compare the
mean values of both HER2/CEP17 ratio and HER2copy number between each of the BP and MPresults. To ensure valid results, both HER2/CEP17ratio andHER2copynumberwere log-transformedto approximate normality before analysis, becauseof data skewness. Diagnostic measures were esti-mated from scratch. Functions fromR, freely avail-able from www.r-project.org, were used for thestatistical analysis.
RESULTS
From the database, 21 tumors were identified byour selection criteria (Table 1). The demographicdata of the study population are summarized inTable 2. Patients were all women, with a medianage of 56 years (range, 34 to 77 years), and withhistologically confirmed infiltrating ductal carcino-mas, which were moderately to strongly ER pos-itive. Seven of the tumors were PR negative. Thehistologic grades of differentiation were predom-inantly grade 2 (10 tumors, 47%) and grade 3(eight tumors, 38%); two tumorsweregrade1,andone was of unknown differentiation. The mediantumor size was 16 mm (range, 3 to 27 mm). Six(29%) patients with nodal involvement were in-cluded, five of whomhadmacrometastases to onenode, and one patient with isolated tumor cellsonly.
FISH tests were done in 20 patients, amongwhomseven (35%) tests reported only the HER2/CEP17ratio because they were done before 2013.
Eleven (52%) tumors had IHC HER2 staining in-tensity of 3+, of which seven (64%) were positiveon FISH testing, three (27%) were negative, andone was not sent for FISH analysis. Nine (42%)patients with HER2 staining intensity of 2+ in-cluded eight (89%) who were considered HER2positive and one equivocal on FISH applying theASCO 2013 criteria.12 Of the eight positives, six(75%) showed a HER2/CEP17 ratio > 2 and two(25%) had ratios, 2 but copy number. 6. One(5%) tumor remained equivocal after FISH. One(5%) patient, with HER2 staining intensity of 1+and luminal subtype, had overexpression ofHER2mRNAonTPand subsequently showed anHER2/CEP17 ratio of 2.98 on reflex FISH testing.
Of note, referringphysicians requested reflexFISHanalyses for another five of the patients. In onepatient, the initial HER2/CEP17 ratio was equivo-cal based on ASCO 2007 guidelines,27a and thesame result was found after reflex FISH. In fourpatients, FISH was repeated after BP reported lumi-nal subtype and in three of them, the HER2/CEP17
316 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
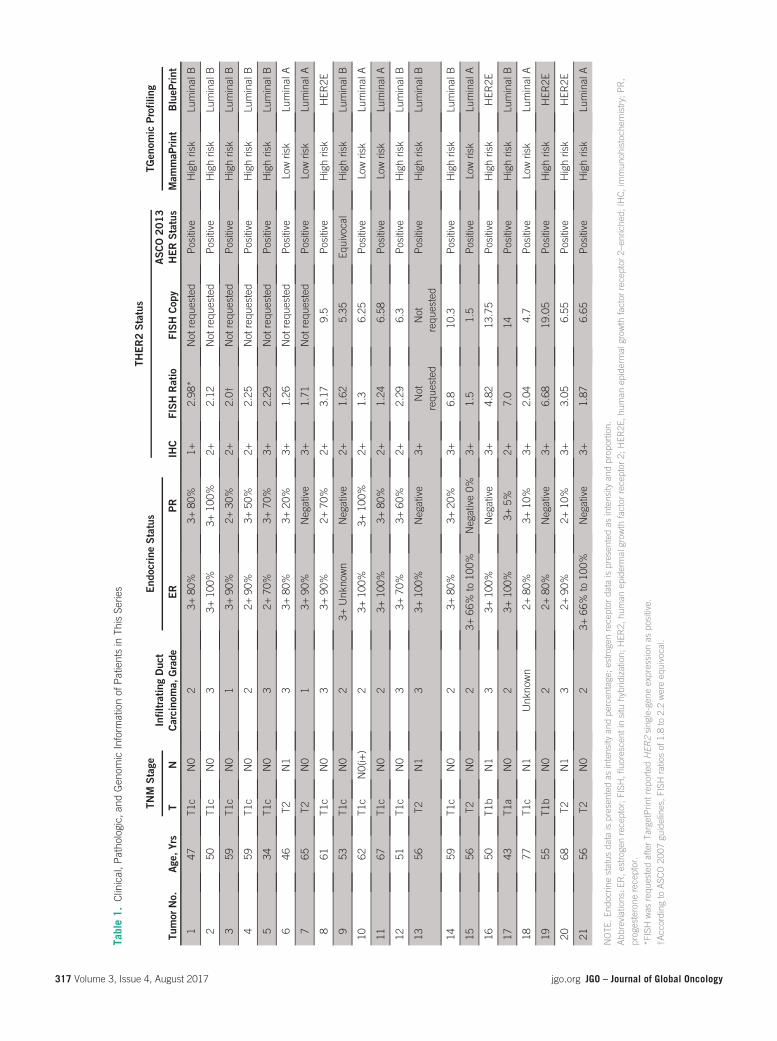
Table1.
Clinical,P
atho
logic,
andGen
omicInform
ationof
Patientsin
ThisSe
ries
TNM
Stage
End
ocrin
eStatus
THER2Status
TGen
omic
Profiling
Tumor
No.
Age
,Yrs
TN
InfiltratingDuc
tCarcino
ma,
Grade
ER
PR
IHC
FISHRatio
FISHCop
yASCO2013
HERStatus
Mam
maP
rint
BlueP
rint
147
T1c
N0
23+
80%
3+80
%1+
2.98
*Not
requ
ested
Positive
Highrisk
LuminalB
250
T1c
N0
33+
100%
3+10
0%2+
2.12
Not
requ
ested
Positive
Highrisk
LuminalB
359
T1c
N0
13+
90%
2+30
%2+
2.0†
Not
requ
ested
Positive
Highrisk
LuminalB
459
T1c
N0
22+
90%
3+50
%2+
2.25
Not
requ
ested
Positive
Highrisk
LuminalB
534
T1c
N0
32+
70%
3+70
%3+
2.29
Not
requ
ested
Positive
Highrisk
LuminalB
646
T2N1
33+
80%
3+20
%3+
1.26
Not
requ
ested
Positive
Lowrisk
LuminalA
765
T2N0
13+
90%
Neg
ative
3+1.71
Not
requ
ested
Positive
Lowrisk
LuminalA
861
T1c
N0
33+
90%
2+70
%2+
3.17
9.5
Positive
Highrisk
HER
2E
953
T1c
N0
23+
Unk
nown
Neg
ative
2+1.62
5.35
Equivoca
lHighrisk
LuminalB
1062
T1c
N0(i+)
23+
100%
3+10
0%2+
1.3
6.25
Positive
Lowrisk
LuminalA
1167
T1c
N0
23+
100%
3+80
%2+
1.24
6.58
Positive
Lowrisk
LuminalA
1251
T1c
N0
33+
70%
3+60
%2+
2.29
6.3
Positive
Highrisk
LuminalB
1356
T2N1
33+
100%
Neg
ative
3+Not
requ
ested
Not
requ
ested
Positive
Highrisk
LuminalB
1459
T1c
N0
23+
80%
3+20
%3+
6.8
10.3
Positive
Highrisk
LuminalB
1556
T2N0
23+
66%
to10
0%Neg
ative0%
3+1.5
1.5
Positive
Lowrisk
LuminalA
1650
T1b
N1
33+
100%
Neg
ative
3+4.82
13.75
Positive
Highrisk
HER
2E
1743
T1a
N0
23+
100%
3+5%
2+7.0
14Positive
Highrisk
LuminalB
1877
T1c
N1
Unk
nown
2+80
%3+
10%
3+2.04
4.7
Positive
Lowrisk
LuminalA
1955
T1b
N0
22+
80%
Neg
ative
3+6.68
19.05
Positive
Highrisk
HER
2E
2068
T2N1
32+
90%
2+10
%3+
3.05
6.55
Positive
Highrisk
HER
2E
2156
T2N0
23+
66%
to10
0%Neg
ative
3+1.87
6.65
Positive
Highrisk
LuminalA
NOTE
.End
ocrin
estatus
data
ispresen
tedas
intensity
andpe
rcen
tage;e
strogenreceptor
data
ispresen
tedas
intensity
andprop
ortion.
Abb
reviations:E
R,e
strogenreceptor;F
ISH,fluorescent
insitu
hybridization;
HER
2,hu
man
epidermal
grow
thfactor
receptor
2;HER
2E,h
uman
epidermal
grow
thfactor
receptor
2–en
riche
d;IHC,immun
ohistoch
emistry;
PR,
progesterone
receptor.
*FISH
was
requ
estedafterTa
rgetPrin
trep
ortedHER
2sing
le-gen
eexpression
aspo
sitive.
†According
toASC
O20
07gu
idelines,F
ISH
ratiosof
1.8to
2.2wereeq
uivocal.
317 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

ratios were discordant and in the fourth, the copynumber was discordant (Table 3).
On the basis of the ASCO 2013 guidelines,12 20(95%) patients would have been consideredHER2positive and one inconclusive, requiring furthertesting.
On BP analysis with MP risk, only four (19%)tumors were HER2E subtype, six (29%) were low-risk luminal, and 11 (52%) were high-risk luminal(Fig 1).
Assuming that BP accurately identifies HER2Esubtype and taking into account the initial FISHanalysis in 20 patients, as well as the results of fivereflex tests (n = 25), an HER2/CEP17 ratio > 2hadasensitivity of 100%(fourof four), but aPPVofonly 29% (four of 14) and a Matthews correlationcoefficient of 0.387. Similarly, in 14 FISH testswhere the HER2 copy number was reported, a
value> 6 had a sensitivity of 100% (four of four),but a PPV of only 40% (four of 10) and aMatthewscorrelation coefficient of 0.40. The difference inmeans of theHER2/CEP17 ratiowas significant forHER2E versus luminal tumors (P = .0249; 95%CIfor true difference in log-transformedmeans, 0.12to 1.21 logs; Fig 2).
Using the 2013 ASCO guidelines to predict HER2positivity and excluding one equivocal result, thePPV was only 20% (four of 20). Interestingly, thedifference in means of the HER2/CEP17 ratio washighly significant for MP high-risk versus low-risktumors (P = .0002; 95% CI for true difference inlog-transformed means, 0.40 to 1.06). In thisinstance, a ratio . 2 has a specificity of 92%, aPPV of 0.85, and a negative predictive value of0.83 for a high-risk MP result.
DISCUSSION
The current series is limited by small numbers as aresult of the exclusion of cHER2-positive patientsfromMPfunding in southernAfrica, inaccordancewith the MPA initially described by Grant et al.15
Valuable informationcouldneverthelessbegleanedfrom the 21 HER2-positive tumors extracted fromthe MP database, which indicated a possible over-estimation of HER2 status. Only four of the patientshad HER2E tumors, suggesting a good response totrastuzumab treatment. Themajority, however, hadluminal A or B disease, with a significantly lowerreported response to chemotherapy and doubtfulbenefit from trastuzumab.19,24,25 The six low-riskluminalA tumorswouldbeexpected to respondwellto endocrine therapy only.
Published data from South Africa on 109 ER/PR-positive, HER2-negative tumors showed a highrisk-to-low risk ratio of 39% versus 61%,16
whereas 68%of patients in the current serieswerehigh risk on MP, indicating that FISH positivitymight predict a higher likelihood of a high-riskresult but has poor PPV for HER2E.
Table 2. Characteristics of Study Participants and Tumors
Characteristic No. (%)
Median age at diagnosis in years (range) 56 (34-77)
Median tumor size in millimeters (range) 16 (3-27)
Histologic grade of differentiation, n = 21
1 2 (10)
2 10 (47)
3 8 (38)
Unknown 1 (5)
Nodal status, n = 21
N0 15 (71)
N0(i+) (isolated tumor cells) 1 (4)
N1 5 (25)
MammaPrint plusBluePrint genomicprofile,n=21
Low-risk luminal 6 (29)
High-risk luminal 11 (52)
HER2 type 4 (19)
NOTE. All values are expressed as no. (%) unless indicated otherwise.
Table 3. Summary of Fluorescent In Situ Hybridization Results in Five Patients for Whom Reflex Testing Was Undertaken
Initial HER2 Status Reflex FISH Genomic Profiling
Tumor No. IHC FISH Ratio FISH Copy FISH Ratio FISH Copy MammaPrint BluePrint
2 2+ 2.12 Not requested 1.01 Not requested High risk Luminal B
3 2+ 2.0* Not requested 2 Not requested High risk Luminal B
4 2+ 2.25 Not requested 1.04 Not requested High risk Luminal B
10 2+ 2.29 Not requested 1.72 Not reported Low risk Luminal A
21 3+ 1.87 6.65 1.47 3.07 Low risk Luminal A
Abbreviations: FISH, fluorescent in situ hybridization; HER2, human epidermal growth factor receptor 2; IHC, immunohistochemistry.*According to ASCO 2007 guidelines, FISH ratios of 1.8 to 2.2 were equivocal.
318 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

If results from the Neoadjuvant Breast RegistrySymphony Trial20 are considered, a pathologiccomplete response (pCR) was seen in 53% ofHER2E subtypes versus 38% in cHER2-positivepatients. In IHC/FISH ER/PR-positive, HER2-positive patients, reclassified as luminal A or Busing BP, the pCR was only 3%. The difference inpCR in cHER2 versus HER2E tumors can beexplained by the dilutional effect of the large pro-portion of patients with luminal disease in thecHER2group. If these results were applied to thecurrent cohort, the expected benefit of trastuzu-mab would be even less, considering the largepercentage of patients with luminal breast cancer.Furthermore, it seems that omitting anti-HER2therapy in patients with non-HER2E tumors doesnot have an impact on survival.26
Fromourdata analysis, it was clear that thecurrentASCO guidelines for HER2/CEP17 ratio and copynumber has a poor PPV. It is possible that usinghigher cut-off values might reduce the numberof luminal tumors selected; some authors have
reported a better response to trastuzumab withcopy number . 1228 and higher HER2/CEP17ratio,29 although the HER2E tumors in this serieshave copy numbers ranging from 6.55 to 19.05and HER2/CEP17 ratios from 3.17 to 6.68.
A significant difference in the log-transformedmean HER2/CEP17 ratio and copy number wasobserved for HER2E tumors compared with theluminal tumors. The small numbers andskewnessresulted in wide confidence intervals with signif-icant overlap, which precluded further analysis ofthe series. Because of this, reporting the actualmean values will not be a reflection of the truecenter of the data set. It is, however, a phenom-enon that could be explored in a future largerseries.
The fact that the four patients had contradictoryHER2/CEP17 ratios or copy number on repeattesting is a further indication of the discrepanciesin the current testing practice. Despite the smalldata set andwide confidence intervals, thePPV forboth HER2/CEP17 ratio and copy number re-mains poor.
Two node-negative tumors in this series were, 10 mm; one was found to be high-risk luminaland one HER2E. In these small tumors, the impor-tance of accurate HER2 determination is of evengreater consequence. It is generally accepted thatsmall node-negative tumorshaveagoodprognosis,but there remains a small number of patients withpoor outcomes. Little prospective information isavailable in T1a/b tumors, and only the BreastCancer International Research Group 006 trial(BCIRG-006) allowed inclusion of node-negative
25
20
15
10
5
0HER2E cHER2+
Tumor Subtype
No.
of T
umor
s
Luminal
IHC FISH Equiv
4 4 Low Risk (4)
Low Risk (2)
High Risk(11)
15
2
High Risk Low Risk
2
3
4
5
6
7
MammaPrint
HER2
/CEP
17 R
atio
HER2E Luminal
2
3
4
5
6
7
BluePrint
HER2
/CEP
17 R
atio
Fig 1. Reclassificationoftumors reported to beclinically positive for humanepidermal growth factorreceptor 2 (cHER2+) usingimmunohistochemistry(IHC)/fluorescent in situhybridization (FISH) intoHER2-enriched (HER2E)and luminal subtypes.Equiv, equivocal.
Fig 2. Strip plots ofhuman epidermal growthfactor receptor 2 (HER2)/centromeric probe forchromosome 17 (CEP17)ratios on log-scale for bothMammaPrint risk andBluePrint subtyping.Distributions are closer tonormality, but variancesremain different. Thedifference in means of theHER2/CEP17 ratio wassignificant for molecularsubtype (P = .0249; 95%CI, 0.12 to 1.21 logs)and MammaPrint risk(P = .0002; 95% CI, 0.40to 1.06 logs).
319 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

tumors, 10mm.6 However, with reported 5-yeardistant recurrence–free survival of 98% in un-treatedHER2-positive T1a/b tumors,30 the benefitfrom adjuvant chemotherapy and trastuzumab ispossibly outweighed by the toxicity of treatment31
in this subgroup of patients. Even with alternativechemotherapy regimens, toxicity remains high,with limited benefit in patients with tumors, 10 mm.32 It might therefore be helpful tosubmit all node-negative cHER2 tumors , 10 mmfor MP/BP testing to select those patients mostlikely to gain benefit.
The numbers and demographic characteristics ofthe study population are limitedby the referral biasimposed by the pre-existing MPA15 and conser-vative selection of patients by referring physicians.This is reflected in the small percentage of HER2-positive tumors contained in the database. Fur-thermore, the study focused on a subgroup ofER/PR-positive tumors only. In most of the pub-lished series evaluating HER2-positive tumors,both hormone receptor–positive and hormonereceptor–negative tumors were included, and adifference in response to trastuzumab betweenthese two groups was reported.19 Additionally,
the predictive value of MP/BP needs furthervalidation in selecting patients for trastuzumabtreatment.
Despite the limitations of this study, it is in line withsimilar reports of larger series. As a preliminaryinvestigation, it warrants the development of ex-panded referral guidelines and further evaluationof molecular subtyping in patients with cHER2-positive tumors.
On the basis of our findings in this study and therecent evidence from literature of the overestima-tion of HER2 positivity as determined by clinicalguidelines, further evaluation of molecular sub-typing in theworkupofHER2-positive tumors shouldbeconsidered,33 includingER/PR-negative, cHER2-positive tumors , 10 mm. Institutional protocols,such as the MPA applied as a cost-saving strategyin thesouthernAfricancontext,15,16 shouldbeadapt-ed to include patients with ER/PR-positive, cHER2-positive disease with limited nodal involvement tomatch the demographic characteristics of those re-ported in the MINDACT trial.
DOI: https://doi.org/10.1200/JGO.2016.006072Published online on jgo.org on November 16, 2016.
AUTHOR CONTRIBUTIONS
Conception and design: Ettienne J. Myburgh, LizanneLangenhoven, Maritha J. Kotze
Collection and assembly of data: Ettienne J. Myburgh,Kathleen A. Grant, Maritha J. Kotze
Data analysis and interpretation: Ettienne J. Myburgh, Lize Vander Merwe
Manuscript writing: All authorsFinal approval of manuscript: All authorsAccountable for all aspects of the work: All authors
AUTHORS’ DISCLOSURES OFPOTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided byauthors of this manuscript. All relationships are consideredcompensated. Relationships are self-held unless noted. I =Immediate Family Member, Inst = My Institution. Relation-ships may not relate to the subject matter of this manuscript.For more information about ASCO’s conflict of interest policy,please refer to www.asco.org/rwc or ascopubs.org/jco/site/ifc.
Ettienne J. MyburghConsulting or Advisory Role: Stellenbosch University
Lizanne LangenhovenNo relationship to disclose
Kathleen A. GrantNo relationship to disclose
Lize Van der MerweNo relationship to disclose
Maritha J. KotzeLeadership: GknowmixStock or Other Ownership: Genecare Molecular Genetics(dormant) (I), Gknowmix
Patents, Royalties, Other Intellectual Property: Inventor(unrelated to current publication): M.J. Kotze. South AfricanMedical Research Council. A method of diagnosing patientswith cardiovascular disease or a genetic predisposition forcardiovascular disease. South African patent 2001/5419,July 2, 2001; and M.J. Kotze, S.J. van Rensburg, R. Rooney,P.D. Haug. University of Stellenbosch. In vitro method ofdiagnosing a demyelinating disease subtype. South Africanpatent ZA2008/08511, September 29, 2008. (Inst)
ACKNOWLEDGMENTWe thank ElizabethMurray, Rika Pienaar, and Yadhir Baitchufor highlighting HER2 discrepancies resolved by microarraysand for assistance with data review, as well as all the clini-cians who referred patients and ensured the integrity of thedata.
Affiliations
Ettienne J. Myburgh University of Stellenbosch, Tygerberg; Lizanne Langenhoven, Mediclinic Panorama Hospital, Cape Town;Kathleen A. Grant, Cape Peninsula University of Technology; Lize van der Merwe, University of Western Cape, Bellville; andMaritha J. Kotze,University ofStellenboschandNationalHealthLaboratoryService,TygerbergHospital,CapeTown,SouthAfrica.
320 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

SupportSupported by the Strategic Health Innovation Partnerships (SHIP) Unit of the South AfricanMedical Research Council (MRC) withfunds from the South African Department of Science and Technology (Research Grant No. S003665), the National ResearchFoundationofSouthAfrica(GrantNo.86417),andtheCapePeninsulaUniversityofTechnology (CPUT)researchfund.TheSupportProgram for Industry Innovation provided financial support toward development of a laboratory interface for Agendia in theNetherlands to provide South African patients access to the MP test.
REFERENCES1. Hudis CA: Trastuzumab—Mechanism of action and use in clinical practice. N Engl J Med 357:39-51, 2007
2. Joensuu H, Bono P, Kataja V, et al: Fluorouracil, epirubicin, and cyclophosphamide with either docetaxel orvinorelbine, with or without trastuzumab, as adjuvant treatments of breast cancer: Final results of the FinHer Trial.J Clin Oncol 27:5685-5692, 2009
3. SpielmannM, Roche H, Delozier T, et al: Trastuzumab for patients with axillary-node-positive breast cancer: Results ofthe FNCLCC-PACS 04 trial. J Clin Oncol 27:6129-6134, 2009
4. Gianni L, Dafni U, Gelber RD, et al: Treatment with trastuzumab for 1 year after adjuvant chemotherapy in patients withHER2-positive early breast cancer: A 4-year follow-up of a randomised controlled trial. Lancet Oncol 12:236-244, 2011
5. Perez EA, Romond EH, Suman VJ, et al: Four-year follow-up of trastuzumab plus adjuvant chemotherapy for operablehuman epidermal growth factor receptor 2-positive breast cancer: Joint analysis of data from NCCTG N9831 andNSABP B-31. J Clin Oncol 29:3366-3373, 2011
6. Slamon D, Eiermann W, Robert N, et al: Adjuvant trastuzumab in HER2-positive breast cancer. N Engl J Med 365:1273-1283, 2011
7. Rodrigues MJ, Peron J, Frenel JS, et al: Benefit of adjuvant trastuzumab-based chemotherapy in T1ab node-negativeHER2-overexpressing breast carcinomas: A multicenter retrospective series. Ann Oncol 24:916-924, 2013
8. Schmidt F, Hartwagner KA, Spork EB, et al: Medical audit after 26,711 breast imaging studies: Improved rate ofdetection of small breast carcinomas (classified as Tis or T1a,b). Cancer 83:2516-2520, 1998
9. Dickens C, Duarte R, Zietsman A, et al: Racial comparison of receptor-defined breast cancer in southern Africanwomen: Subtype prevalence and age-incidence analysis of nationwide cancer registry data. Cancer EpidemiolBiomarkers Prev 23:2311-2321, 2014
10. Singh E, Underwood JM, Nattey C, et al: South African National Cancer Registry: Effect of withheld data from privatemedical health systems on cancer incidence estimates. S Afr Med J 105:107-109, 2015
11. Hanna WM, Ruschoff J, Bilous M, et al: HER2 in situ hybridization in breast cancer: Clinical implications of polysomy17 and genetic heterogeneity. Mod Pathol 27:4-18, 2014
12. Wolff AC, HammondMEH,Hicks DG, et al: Recommendations for human epidermal growth factor receptor 2 testing inbreast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guidelineupdate. J Clin Oncol 31:3997-4013, 2013
13. Lim TH, Lim AS, Thike AA, et al: Implications of the updated 2013 American Society of Clinical Oncology/College ofAmerican Pathologists guideline recommendations on human epidermal growth factor receptor 2 gene testing usingimmunohistochemistry and fluorescence in situ hybridization for breast cancer. Arch Pathol Lab Med 140:140-147,2016
14. KrijgsmanO, RoepmanP, Zwart W, et al: A diagnostic gene profile for molecular subtyping of breast cancer associatedwith treatment response. Breast Cancer Res Treat 133:37-47, 2012
15. Grant KA, Apffelstaedt JP, Wright CA, et al: MammaPrint Pre-screen Algorithm (MPA) reduces chemotherapy inpatients with early-stage breast cancer. S Afr Med J 103:522-526, 2013
16. Pohl H, Kotze MJ, Grant KA, et al: Impact of MammaPrint on clinical decision-making in South African patients withearly-stage breast cancer. Breast J 22:442-446, 2016
17. Cardoso F, van’t Veer LJ, Bogaerts J, et al: 70-Gene signature as an aid to treatment decisions in early-stage breastcancer. N Engl J Med 375:717-729, 2016
18. Cook K: Genomic Health has sickly stock chart. Forbes, 2013. www.forbes.com/sites/zacks/2013/10/07/genomic-health-has-sickly-stock-chart/
19. Harris LN, Ismaila N, McShane LM, et al: Use of biomarkers to guide decisions on adjuvant systemic therapy forwomenwith early-stage invasive breast cancer: American Society of Clinical Oncology clinical practice guideline. J ClinOncol 34:1134-1150, 2016
20. Whitworth P, Stork-Sloots L, de Snoo FA, et al: Chemosensitivity predicted by BluePrint 80-gene functional subtypeandMammaPrint in the prospectiveNeoadjuvant Breast Registry Symphony Trial (NBRST). Ann Surg Oncol 21:3261-3267, 2014
21. Yao K, Goldschmidt R, Turk M, et al: Molecular subtyping improves diagnostic stratification of patients with primarybreast cancer into prognostically defined risk groups. Breast Cancer Res Treat 154:81-88, 2015
321 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
22. Grant KA, Pienaar FM, Brundyn K, et al: Incorporating microarray assessment of HER2 status in clinical practicesupports individualized therapy in early-stage breast cancer. Breast 24:137-142, 2015
23. Denkert C, Huober J, Loibl S, et al: HER2 and ESR1 mRNA expression levels and response to neoadjuvant tras-tuzumab plus chemotherapy in patients with primary breast cancer. Breast Cancer Res 15:R11, 2013
24. Untch M, Rezai M, Loibl S, et al: Neoadjuvant treatment with trastuzumab in HER2-positive breast cancer: Resultsfrom the GeparQuattro study. J Clin Oncol 28:2024-2031, 2010
25. Gluck S, de Snoo F, Peeters J, et al: Molecular subtyping of early-stage breast cancer identifies a group of patients whodo not benefit from neoadjuvant chemotherapy. Breast Cancer Res Treat 139:759-767, 2013
26. Prat A, Carey LA, Adamo B, et al: Molecular features and survival outcomes of the intrinsic subtypes within HER2-positive breast cancer. J Natl Cancer Inst 106:dju152, 2014
27. Gajria D, Chandarlapaty S: HER2-amplified breast cancer: Mechanisms of trastuzumab resistance and novel targetedtherapies. Expert Rev Anticancer Ther 11:263-275, 2011
27a. Wolff AC, HammondME, Schwartz JN, et al: American Society of Clinical Oncology/College of American Pathologistsguideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. J Clin Oncol 25:118-145, 2007
28. Borley A, Mercer T, Morgan M, et al: Impact of HER2 copy number in IHC2+/FISH-amplified breast cancer onoutcome of adjuvant trastuzumab treatment in a large UK cancer network. Br J Cancer 110:2139-2143, 2014
29. Kogawa T, Fouad TM, Liu DD, et al: High HER2/centromeric probe for chromosome 17 fluorescence in situ hy-bridization ratio predicts pathologic complete response and survival outcome in patients receiving neoadjuvantsystemic therapy with trastuzumab for HER2-overexpressing locally advanced breast cancer. Oncologist 21:21-27,2016
30. Yap KH, Tripathy D: A review of the management of T1a/bN0 HER2-overexpressed breast cancer. Am J HematolOncol 11:11-15, 2015
31. Fehrenbacher L, Capra AM, Quesenberry CP Jr, et al: Distant invasive breast cancer recurrence risk in humanepidermal growth factor receptor 2-positive T1a and T1b node-negative localized breast cancer diagnosed from 2000to 2006: A cohort from an integrated health care delivery system. J Clin Oncol 32:2151-2158, 2014
32. Tolaney SM, Barry WT, Dang CT, et al: Adjuvant paclitaxel and trastuzumab for node-negative, HER2-positive breastcancer. N Engl J Med 372:134-141, 2015
33. Kotze MJ, Murray EM, Luckhoff HK, et al: Clinical dilemma of contradictory HER2 status in breast cancer resolved bymicroarrays. Breast 24:S45, 2015 (suppl 1; abstr 55)
322 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

originalreport
Prediagnostic Intervals inRetinoblastoma: Experience atan Oncology Center in Brazil
abstract
Purpose Retinoblastoma is the most common intraocular malignancy of childhood. In most cases, parentsare the first to notice leukocoria and other symptoms before undergoing a prolonged period of stress beforediagnosis. The purpose of this study was to determine prediagnostic intervals of patients with retino-blastoma at an oncology tertiary center (Instituto Nacional de Cancer) in Rio de Janeiro, Brazil, and relatethem to stage at diagnosis, eye salvage, and survival.
Methods Parents or caregivers of children with retinoblastoma registered between January 2006 andSeptember 2013 were interviewed using a semistructured individually applied questionnaire, concerningtheir trajectory before registration.
Results Out of 76patients, 39 (51%)weregirls, 52 (68%)hadunilateral retinoblastoma, and24 (32%)hadbilateral retinoblastoma, totaling 100 affected eyes. The most common stage of diagnosis was the in-traocular group, with 63 (83%) patients; nine (12%) were extraocular, and four (5%) had metastaticdisease. During the follow-up time of 376 24.5 months, 10 (13%) patients died and 70 (70%) eyes wereenucleated. Mean family interval was 1.6 6 2.6 months, mean medical interval was 5.0 6 6.2 months,mean referral intervalwas0.261.4months, andmeanoverall intervalwas7.166.9months. In univariateanalysis, age at diagnosis, maternal education, medical interval, and overall interval were significantlyrelated to advanced stage at diagnosis and survival. In multivariate analysis, maternal education andmedical interval were significantly related to advanced stage at diagnosis and survival. No variablesaffected eye salvage.
Conclusion Medical interval was responsible for 70% of the overall interval; therefore, programs orcampaigns targeting retinoblastoma early diagnosis should focus emphasize in medical awareness.
J Glob Oncol 3. © 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
INTRODUCTION
Retinoblastoma is the most common intraocu-lar malignancy of childhood, usually first detectedby parents.1 Population-based studies show ahigher incidence of retinoblastoma in some coun-tries, such as Brazil,2 where approximately 400children are diagnosed each year.3
In developed countries, retinoblastoma is usuallydiagnosed in early intraocular stages, and thesurvival rate is. 90%.4,5 However, in developingcountries, approximately 40% of the childrenaffected still die at young age of metastaticdisease.6,7
In developing countries, the diagnosis of retino-blastoma is usually made at advanced stages,lowering ocular and patient survival.8 The sur-vival of patientswith retinoblastoma in these coun-tries is influenced by socioeconomic and cultural
factors, resulting in late diagnosis. There is also ashortageofmodern treatments in thesecountries.9,10
Early detection permits the use of treatments thatpreserve theeyes,minimizingmorbidity.8,11Whenthere is lack of knowledge about the disease, thetime to make the diagnosis is longer, delayingreferral to a specialized treatment center. Thisallows the disease to become more advancedand reduces the chances for healing.12
Prognosis of most pediatric tumors is related totumorbiology13; in retinoblastoma, latediagnosis is amajor determinant for disease dissemination.9,14
At least 50% of the 5,000 to 8,000 new casesworldwide will present symptoms of extraoculardisease.7
The outcome of patients with retinoblastoma in de-veloping countries is highly influenced by the lackof early diagnosis.15 Therefore, understanding the
Clarissa Campolina de SaMattosinho
Nathalia Grigorovski
Evandro Lucena
Sima Ferman
Anna Tereza MirandaSoares de Moura
Arlindo Freire Portes
All authors: InstitutoNacional de Cancer;Universidade Estacio deSa; and UniversidadeEstadualdoRiodeJaneiro,Rio de Janeiro, Brazil.Presented at theInternational Society ofOcular Oncology Meeting,Paris, France, June16-19,2015; and the CongressoInternational daSociedade Brasileira deOftalmologia, Rio deJaneiro, Brazil, July24-26, 2014.The views and opinionsexpressed in this article arethose of the authors and donot necessarily reflect theofficial views of theInstituto Nacional deCancer, UniversidadeEstacio de Sa, orUniversidade Estadual doRio de Janeiro.Corresponding author:Clarissa Campolina de SaMattosinho,MD,RuaPraiado Flamengo 374/1501,Rio de Janeiro, RJ CEP22210-065, Brazil;e-mail: [email protected].
323 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
© 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License

particularities of prediagnostic intervals is crucial tolaunch campaigns focused on the real sources ofdelays. The purpose of this study was to determinethe duration of segments composing prediagnosticintervals of patients with retinoblastoma and relatethose intervalswith advancedstageat diagnosis, eyesalvage, and patient survival.
METHODS
Parents or caregivers of children with retinoblas-toma treated at an oncology tertiary center (Insti-tuto Nacional de Cancer) in Rio de Janeiro, Brazil,between January 2006andSeptember 2013wereinterviewed about their trajectory before registra-tion. Most interviews were conducted taking ad-vantage of previously scheduled consultations inthe ocular oncology outpatient unit. Patients whodid not have booked consultations throughout thedatacollectionperiodwere invited toparticipatebytelephone. Three attempts at contact were madeat different times and dates using all phone num-bers available from the patient chart. Althoughsome invitations were conducted by telephone,all interviews were performed face to face. Re-spondents were always parents or the child’s legalcaregiver who previously signed the consent form.Therewasnodifference in procedure according tothe parent’s educational level. The interview didnot require reading or writing abilities, because allquestions were orally spoken and answers weretranscribed by the investigator himself. In cases ofdeceased patients, all interviews were conductedafter the child’s death. Those parents were alsoinvited to participate in the study by telephone orduring scheduled appointments for siblings whowere still being screened for retinoblastoma.
The report of prediagnostic history was recorded in auniformformatusingasemistructuredquestionnaire.The only open question was relative to first perceivedsign, the answer to which was literally copied andthencategorizedaccordingtothemost frequentsignscited in the literature on this subject as leukocoria,strabismus, red eye, low vision, and others.16
Respondents were asked about the sequence ofevents from the initial moment when someonenoticed something different in the child’s eyesuntil registration. Socioeconomic data were ob-tained from all patients during the interview,assessing place of residency, maternal education(years spent in school), number of people perhousehold, and private health insurance.
According to the Aarhus statement regarding pre-diagnosticpatientpathways, emphasiswasgiven tothe initialocularsymptomsnotedandprediagnostic
intervals. Diagnosis date was defined as the regis-tration date, using criteria suggested by the Euro-pean Network of Cancer Registries.17 Prediagnosticintervals were defined by such decisive dates as themoment of perception of first symptom, first consul-tation after perception, and date of referral to theoncology care institution.
Prediagnostic intervals definitions used in thisstudy are as follows: Family interval is the timebetween first symptom noticed and first consulta-tion with a doctor. Medical interval is the timebetween the first consultation and referral to theoncology tertiary center. Referral interval is thetime between referral and registration in the on-cology tertiary center. Overall interval is the timebetweenperceptionof the first symptomsanddateof registration (family plus medical plus referral).The following clinical parameters were taken frompatient charts: laterality, date of birth, date ofregistration, stage at registration, treatment infor-mation, and eye and patient survival.
The International Retinoblastoma Staging Sys-tem18 (0, I, II, III, IV) was used and categorizedfor statistical analyses as follows: intraocular dis-ease (stage 0, I, II), extraocular disease (stage III),metastatic disease (stage IV). For some compar-isons we used the term advanced stage at diag-nosis (stage III plus stage IV). For eachaffectedeyewe used the International Classification of Retino-blastoma grouping system (A, B, C, D, E).
Statistical analysis was performed using Epi Info 7.Bivariate andmultivariate analysis consisted of logis-tic regression,usinga5%significance level and95%CIs.The informedconsentwasprovided toparentsorcaregivers of the children surveyed. The study wasaccepted by the local ethics committee.
RESULTS
Out of 94 registered patients with retinoblastomaduring the study period, eight patients receivedinitial treatment outside of our institution and wereexcluded, one parent refused to participate, andnine parents could not be reached through tele-phone numbers provided in patient charts. Par-ents or caregivers of76patientswereavailableandaccepted the invitation to the interview.
Table 1 shows descriptive statistics of all 76patients, and Table 2 shows the extent of prediag-nostic intervals. Leukocoria was cited in associa-tion with other signs in six cases, and strabismuswas associated with red eye in one case.
In bivariate analysis (Table 3), mean maternaleducation was significantly related to advancedstage at diagnosis (P = .016) and survival (P = .003).
324 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Other than maternal education, none of the socio-economic characteristics (people per household,place of residency, coverage by private health in-surance) carried a significant difference with out-comes (advanced stage at diagnosis, enucleation,and survival). Medical interval, overall interval, andage at diagnosis were significantly related to ad-vanced stage at diagnosis and survival. Enucle-ation was not significantly affected by any of thosevariables.
Multivariate analysis is shown in Table 4 by logisticregression. Maternal education was selected byvirtue of significant association in bivariate analy-sis. All prediagnostic intervals were also included,because they were part of the study purpose. Ageat diagnosis and overall interval were excludedfrom this analysis because those variables werehighly correlated with other interval variables(family, medical, and referral intervals), and usingthem all together could produce collinearity, with aconsequent loss of statistical significance. Medi-cal interval and maternal education were signifi-cantly related to advanced stage at diagnosis andsurvival.
Out of 100 affected eyes, 70% were enucleated.Among bilateral cases (n = 24), three patients hadbilateral enucleations, four patients had both eyespreserved, and 17 patients had one eye enucle-ated. Among unilateral cases (n = 52), 47 patientswere enucleated and only five patients had the eyepreserved. All 10 deaths (13%) were caused bydiseaseprogression or relapses; therewasno toxicdeath. Mean interval from diagnosis to interviewwas 3.26 2.2 years (range, 0 to 7 years; median,3 years). The mean follow-up time was 37 624.5 months.
DISCUSSION
Prediagnostic intervals of pediatric cancers havebeen regularly reported for more than 50 years;they are a source of sorrow for physicians andparents,14 differing widely between tumor types.Determinants of prediagnostic intervals, such asparental attention, health care structure, and phy-sician awareness, are difficult to assess.14
A systematic review of 98 papers about prediag-nostic intervals in pediatric malignancies pointedout the often false general belief that a long delaybefore diagnosis always leads to worse progno-sis.14 Brasme et al14 established that delayeddiagnosis was associated with poor outcome forretinoblastoma and possibly for leukemia, neph-roblastoma, and rhabdomyosarcoma. Besidesthose, pediatric cancer prediagnosis interval
Table 1. Socioeconomic and Clinical Characteristics of Patients With Retinoblastoma(n = 76) in a Tertiary Oncology Center in Rio de Janeiro, Brazil (2006 to 2013)
Characteristic No. (%)
Socioeconomic characteristics
Sex
Male 37 (49)
Female 39 (51)
Age, months
Mean 6 SD 21.7 6 14.6
Median 18
Range 1.0-58
Maternal education, No. of years spent inschool, mean 6 SD
10.9 6 3.9
Place of residency
Urban area 55 (72)
Rural area 19 (25)
Other states 2 (3)
No. of people per household, mean6 SD 4.5 6 1.5
Private health insurance 28 (37)
Clinical characteristics
Laterality
Unilateral 52 (68)
Bilateral 24 (32)
Presenting signs*
Leukocoria 54 (71)
Strabismus 23 (30)
Red eye 3 (4)
Low vision 3 (4)
Others 3 (4)
Stage at diagnosis (IRSS)
Intraocular (0, I, II) 63 (83)
Extraocular (III) 9 (12)
Metastatic (IV) 4 (5)
Advanced (III + IV) 13 (17)
Eye staging by ICR (n = 100 eyes)
A 7 (7)
B 19 (19)
C 14 (14)
D 11 (11)
E 49 (49)
Positive family history 3 (4)
Vital status
Alive 66 (87)
Deceased 10 (13)
Abbreviations: IRC, International Classification of Retinoblastoma; IRSS, International RetinoblastomaStaging System; SD, standard deviation.*Total above 100% considering presenting signs associations.
325 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

lengths depend more on the tumor’s biology thanon parental or medical factors. Median overallinterval revealed a wide variation among tumortypes, from approximately 3 weeks in leukemiaand neuroblastoma to approximately 5 to 6 weeksin lymphoma and rhabdomyosarcoma, and themedian overall interval was 13 weeks for soft-tissue sarcomas.14
Even thoughrecognizing that longdiagnosticdelay isnot necessarily associated with poor outcomes, itmight be a relief for family and doctors.14 Delayeddiagnosis is a source of regret for physicians andparents and a prominent cause of malpractice law-suits.14 Therefore, the authors suggested suitableways to achieve early diagnosis, including takinginto account parent complaints, never ignoringpersisting symptoms, and thoroughly investigatingsigns or symptoms that are not comprehended.14
The term delay in diagnosis is commonly used todescribe an undefined period between symptomonset and definitive diagnosis. This term has neg-ative connotations, implies criticism, and is oftenused to assign blame.19,20 Authors frequentlyused an arbitrary time point defined by their
observations to qualify the moment when a delaybecomes unacceptable or excessive.19 Usingmore neutral terms, such as prediagnostic inter-val, is now advised.20 This period is typically sub-divided into twocomponents, the first onebetweenonset of symptoms and first consultation and thesecond one between first consultation and diag-nosis. This study also divided the second periodinto two parts: before and after referral to theoncology tertiary center.
Our study relied on parent recall of events that tookplace many months or even years before, possiblyintroducing amemory bias. However, most studiesabout prediagnostic intervals are based on chartinformation that may have missing information.Because parents were all personally interviewed,and events related to childhoodcancer often causedeep family scars, the results may be more accu-rate than those extracted essentially from chartinformation. The systematic review previouslymentioned about delayed diagnosis of pediatriccancer published in 201214 found only two studiesthat included semistructured interviews with par-entswhose childrenhadadiagnosis of cancer.21,22
In both studies, time to diagnosis was important forparents, independently of time between diagnosisand the interview. Parental experiences during thisperiod may affect their reaction to diagnosis, treat-ment, and trust in the health care system.14
Although Brazil is a country with large continentaldistances and enormous geographical barriers,most patients (72.3%) were living within the met-ropolitan area of the city of Rio de Janeiro, thesecond most populous city in Brazil, with approx-imately 6.3 million inhabitants. Even those livingin rural areas were not extremely isolated. The
Table 2. Prediagnostic Interval Lengths, Measured inMonths, of Patients With Retinoblastoma(n = 76) in Rio de Janeiro, Brazil (2006 to 2013)
Interval Mean 6 SD Median Range
Family interval 1.6 6 2.6 1.0 0-13
Medical interval 5.0 6 6.2 2.5 0-34
Referral interval 0.2 6 1.4 0 0-12
Overall interval 7.1 6 6.9 5.0 0-35
NOTE: Overall interval = family + medical + referral.Abbreviations: SD, standard deviation.
Table 3. Bivariate Analysis Between Socioeconomic Features, First Signs, and Prediagnostic Intervals With Outcomes(Advanced Stage at Diagnosis, Enucleation, and Survival)
Measure
Advanced Stage at Diagnosis Enucleation Survival
OR 95% CI P OR 95% CI P OR 95% CI P
Age at diagnosis 1.07 1.03 to 1.12 .002* 0.98 0.95 to 1.01 .192 1.05 1.01 to 1.10 .028*
Maternal education 0.83 0.71 to 0.97 .016* 1.09 0.96 to 1.24 .184 0.77 0.65 to 0.91 .003*
Private health insurance 0.28 0.06 to 1.37 .116 1.6 0.56 to 4.57 .38 0.43 0.08 to 2.23 .314
Leukocoria 0.9 0.25 to 3.3 .874 1.8 0.64 to 5.08 .267 0.56 0.14 to 2.23 .41
Strabismus 0.65 0.16 to 2.6 .538 0.61 0.22 to 1.72 .353 2.67 0.69 to 10.32 .153
Family interval 1.00 0.99 to 1.01 .31 1.06 0.9 to 1.3 .44 1.00 0.995 to 1.01 .43
Medical interval 1.00 1,00 to 1,01 .02* 0.99 0.99 to 1.03 .21 1.00 1.001 to 1.008 .014*
Referral interval 1.02 0.99 to 1.04 .23 1.019 0.97 to 1.07 .97 1.04 0.999 to 1.08 .06
Overall interval 1.14 1.04 to 1.25 .005* 0.98 0.91 to 1.05 .52 1.15 1.05 to 1.27 .0046*
Abbreviations: OR, odds ratio.*P , .05.
326 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
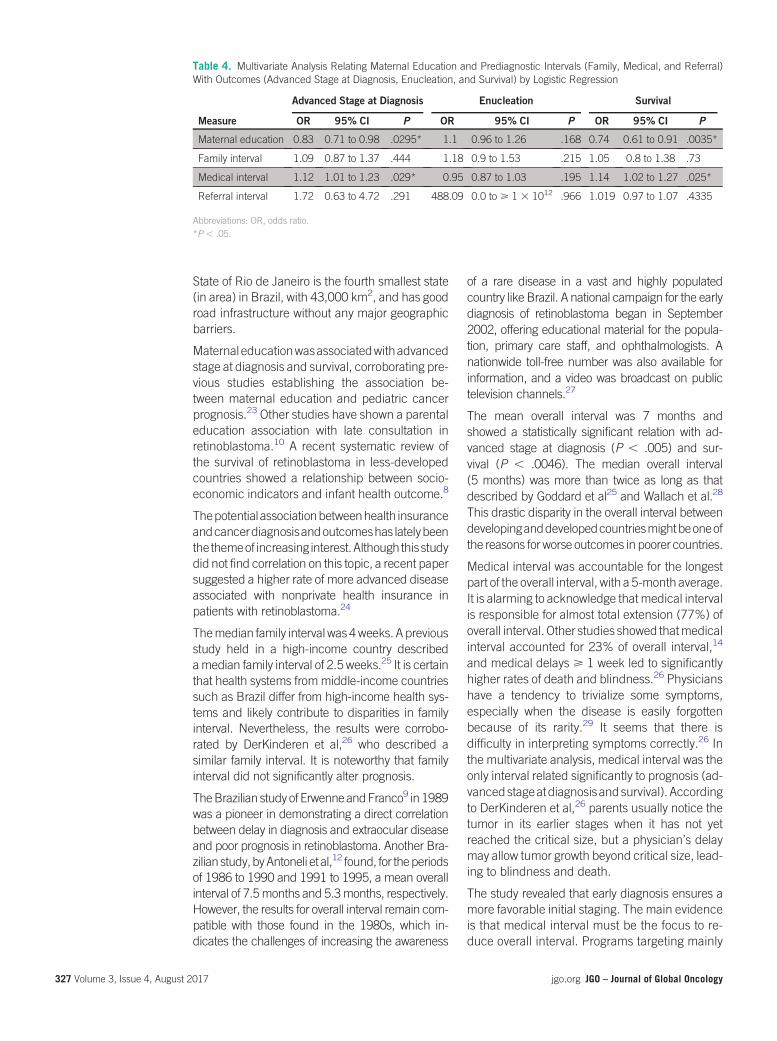
State of Rio de Janeiro is the fourth smallest state(in area) in Brazil, with 43,000 km2, and has goodroad infrastructure without any major geographicbarriers.
Maternal educationwasassociatedwithadvancedstage at diagnosis and survival, corroborating pre-vious studies establishing the association be-tween maternal education and pediatric cancerprognosis.23 Other studies have shown a parentaleducation association with late consultation inretinoblastoma.10 A recent systematic review ofthe survival of retinoblastoma in less-developedcountries showed a relationship between socio-economic indicators and infant health outcome.8
Thepotential associationbetweenhealth insuranceandcancerdiagnosisandoutcomeshas latelybeenthe themeof increasing interest.Although thisstudydid not find correlation on this topic, a recent papersuggested a higher rate of more advanced diseaseassociated with nonprivate health insurance inpatients with retinoblastoma.24
Themedian family interval was4weeks. A previousstudy held in a high-income country describedamedian family interval of 2.5 weeks.25 It is certainthat health systems from middle-income countriessuch as Brazil differ from high-income health sys-tems and likely contribute to disparities in familyinterval. Nevertheless, the results were corrobo-rated by DerKinderen et al,26 who described asimilar family interval. It is noteworthy that familyinterval did not significantly alter prognosis.
TheBrazilian study of ErwenneandFranco9 in1989was a pioneer in demonstrating a direct correlationbetween delay in diagnosis and extraocular diseaseand poor prognosis in retinoblastoma. Another Bra-zilian study,byAntoneli et al,12 found, for theperiodsof 1986 to 1990 and 1991 to 1995, a mean overallinterval of 7.5months and 5.3months, respectively.However, the results for overall interval remain com-patible with those found in the 1980s, which in-dicates the challenges of increasing the awareness
of a rare disease in a vast and highly populatedcountry like Brazil. A national campaign for the earlydiagnosis of retinoblastoma began in September2002, offering educational material for the popula-tion, primary care staff, and ophthalmologists. Anationwide toll-free number was also available forinformation, and a video was broadcast on publictelevision channels.27
The mean overall interval was 7 months andshowed a statistically significant relation with ad-vanced stage at diagnosis (P , .005) and sur-vival (P , .0046). The median overall interval(5 months) was more than twice as long as thatdescribed by Goddard et al25 and Wallach et al.28
This drastic disparity in the overall interval betweendevelopinganddevelopedcountriesmightbeoneofthe reasons for worse outcomes in poorer countries.
Medical interval was accountable for the longestpart of the overall interval, with a 5-month average.It is alarming to acknowledge that medical intervalis responsible for almost total extension (77%) ofoverall interval. Other studies showed thatmedicalinterval accounted for 23% of overall interval,14
and medical delays > 1 week led to significantlyhigher rates of death and blindness.26 Physicianshave a tendency to trivialize some symptoms,especially when the disease is easily forgottenbecause of its rarity.29 It seems that there isdifficulty in interpreting symptoms correctly.26 Inthe multivariate analysis, medical interval was theonly interval related significantly to prognosis (ad-vancedstageatdiagnosis andsurvival). Accordingto DerKinderen et al,26 parents usually notice thetumor in its earlier stages when it has not yetreached the critical size, but a physician’s delaymay allow tumor growth beyond critical size, lead-ing to blindness and death.
The study revealed that early diagnosis ensures amore favorable initial staging. The main evidenceis that medical interval must be the focus to re-duce overall interval. Programs targeting mainly
Table 4. Multivariate Analysis Relating Maternal Education and Prediagnostic Intervals (Family, Medical, and Referral)With Outcomes (Advanced Stage at Diagnosis, Enucleation, and Survival) by Logistic Regression
Measure
Advanced Stage at Diagnosis Enucleation Survival
OR 95% CI P OR 95% CI P OR 95% CI P
Maternal education 0.83 0.71 to 0.98 .0295* 1.1 0.96 to 1.26 .168 0.74 0.61 to 0.91 .0035*
Family interval 1.09 0.87 to 1.37 .444 1.18 0.9 to 1.53 .215 1.05 0.8 to 1.38 .73
Medical interval 1.12 1.01 to 1.23 .029* 0.95 0.87 to 1.03 .195 1.14 1.02 to 1.27 .025*
Referral interval 1.72 0.63 to 4.72 .291 488.09 0.0 to > 1 3 1012 .966 1.019 0.97 to 1.07 .4335
Abbreviations: OR, odds ratio.*P , .05.
327 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

parent education about retinoblastoma may not besuccessful in all settings, because families did nottake long to notice the first signs and seek medicalhelp. Physicians were responsible for the longer partof prediagnostic intervals. Apparently, there is a lackof knowledge and awareness about retinoblastomaamong first-contact physicians in theBrazilianhealthsystem, especially in Rio de Janeiro. This problemwas also described in a Mexican study by Leal-Lealet al30 showing that medical students, just weeksfrom starting a primary care program, were not ableto make a timely retinoblastoma diagnosis.30
No association was found between prediagnosticintervals and globe salvage. This is consistent withother studies, such as those of Abramson et al1
and Butros et al,31 who did not related prediag-nostic intervals with ocularmorbidity in retinoblas-toma. Recently, new therapeutic modalities suchas intra-arterial chemotherapy are being imple-mented, enhancing globe salvage rates.
Even though early diagnosis in retinoblastoma de-pends also on socioeconomic factors intrinsic toeach country, actions to promote early diagnosisand referral may have impact especially in low-income countries.6 The partnership, known astwinning, between institutions from developedcountries providing support to build and trainlocal teams, associated with monetary funding,is essential to achieve better outcomes in less-developed countries.32 Twinning experiences haveproven successful worldwide, with several exam-ples of improvement in outcomeswith cancer world-wide.32-35 Nevertheless, the partnership betweenhigh-income countries and upper-middle–income
countries, such as Brazil, has more limited in-formation, and even less in the retinoblastomafield.36 A successful collaboration program wascreated in 1995 between a tertiary care, publicpediatric hospital in Argentina (upper-middle–income country) and a major specialized pro-gram in a world leading referral center for reti-noblastoma in theUnitedStates.36Thispartnershipshowed impressive results in Argentina and also inother countries, because it became a training cen-ter for Latin America specialists, with partial sup-port from the Fund for Ophthalmic Knowledge.36
This partnership allowed the implementation ofintra-arterial chemotherapy in our center, con-siderably improving the eye salvage rate. If pro-grams like this, between Argentina and the UnitedStates, were implemented in Brazil, other aspectsof retinoblastoma care, such as diagnostic pro-cess and medical awareness, would undoubtedlybe improved.
In conclusion, even though the study was basedon a limited number of patients from a singleinstitution, medical education about retinoblas-toma seems to be an important key to facilitatingthe recognition of first symptoms and shorteningthe overall interval. It is important to note thatmedical interval is highly influenced by healthsystem organization and structure. The resultsshould not be seen as a report to cast blamebut as a guide to implement campaigns andresources in medical education concerningretinoblastoma.
DOI: https://doi.org/10.1200/JGO.2016.005595Published online on jgo.org on October 12, 2016.
AUTHOR CONTRIBUTIONS
Conception and design: Clarissa Campolina de Sa Mattosinho,Nathalia Grigorovski, Sima Ferman, Arlindo Freire Portes
Administrative support: Anna Tereza Miranda Soares de MouraCollection and assembly of data: Clarissa Campolina de SaMattosinho, Nathalia Grigorovski, Evandro Lucena, SimaFerman, Arlindo Freire Portes
Data analysis and interpretation: Clarissa Campolina de SaMattosinho, Nathalia Grigorovski, Sima Ferman, Anna TerezaMiranda Soares de Moura, Arlindo Freire PortesManuscript writing: All authorsFinal approval of manuscript: All authorsAccountable for all aspects of the work: All authors
AUTHORS’ DISCLOSURES OFPOTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided byauthors of this manuscript. All relationships are consideredcompensated. Relationships are self-held unless noted. I =Immediate Family Member, Inst = My Institution. Relation-ships may not relate to the subject matter of this manuscript.
For more information about ASCO’s conflict of interest policy,please refer to www.asco.org/rwc or ascopubs.org/jco/site/ifc.
Clarissa Campolina de Sa MattosinhoNo relationship to disclose
Nathalia GrigorovskiNo relationship to disclose
Evandro LucenaNo relationship to disclose
Sima FermanNo relationship to disclose
Anna Tereza Miranda Soares de MouraNo relationship to disclose
Arlindo Freire PortesNo relationship to disclose
ACKNOWLEDGMENTWe thank the multidisciplinary team treating retinoblastomain our center for their support and hard work.
328 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

REFERENCES1. Abramson DH, Beaverson K, Sangani P, et al: Screening for retinoblastoma: Presenting signs as prognosticators of
patient and ocular survival. Pediatrics 112:1248-1255, 2003
2. de Camargo B, de Oliveira Santos M, Rebelo MS, et al: Cancer incidence among children and adolescents in Brazil:First report of 14 population-based cancer registries. Int J Cancer 126:715-720, 2010
3. Stiller CA, ParkinDM:Geographic and ethnic variations in the incidence of childhood cancer. BrMedBull 52:682-703,1996
4. Moll AC, Kuik DJ, Bouter LM, et al: Incidence and survival of retinoblastoma in TheNetherlands: A register based study1862-1995. Br J Ophthalmol 81:559-562, 1997
5. MacCarthy A, Birch JM, Draper GJ, et al: Retinoblastoma: Treatment and survival in Great Britain 1963 to 2002. Br JOphthalmol 93:38-39, 2009
6. Chantada GL: Retinoblastoma: Lessons and challenges from developing countries. Ellsworth Lecture 2011. Oph-thalmic Genet 32:196-203, 2011
7. Kivela T: The epidemiological challenge of the most frequent eye cancer: Retinoblastoma, an issue of birth and death.Br J Ophthalmol 93:1129-1131, 2009
8. Canturk S, Qaddoumi I, Khetan V, et al: Survival of retinoblastoma in less-developed countries impact of socio-economic and health-related indicators. Br J Ophthalmol 94:1432-1436, 2010
9. Erwenne CM, Franco EL: Age and lateness of referral as determinants of extra-ocular retinoblastoma. OphthalmicPaediatr Genet 10:179-184, 1989
10. Chantada G, Fandi~no A, Manzitti J, et al: Late diagnosis of retinoblastoma in a developing country. Arch Dis Child 80:171-174, 1999
11. Rodrigues KE, de CamargoB: Diagnostico precoce do cancer infantil: Responsabilidade de todos [in Portuguese]. RevAssoc Med Bras (1992) 49:29-34, 2003
12. Antoneli CBG, Steinhorst F, Ribeiro K de CB, et al: O papel do pediatra no diagnostico precoce do retinoblastoma [inPortuguese]. Rev Assoc Med Bras (1992) 50:400-402, 2004
13. Saha V, Love S, Eden T, et al: Determinants of symptom interval in childhood cancer. ArchDis Child 68:771-774, 1993
14. Brasme J-F, MorfouaceM, Grill J, et al: Delays in diagnosis of paediatric cancers: A systematic review and comparisonwith expert testimony in lawsuits. Lancet Oncol 13:e445-e459, 2012
15. Chantada GL, Qaddoumi I, Canturk S, et al: Strategies to manage retinoblastoma in developing countries. PediatrBlood Cancer 56:341-348, 2011
16. Abramson DH, Frank CM, Susman M, et al: Presenting signs of retinoblastoma. J Pediatr 132:505-508, 1998
17. Weller D, Vedsted P, Rubin G, et al: The Aarhus statement: Improving design and reporting of studies on early cancerdiagnosis. Br J Cancer 106:1262-1267, 2012
18. Linn Murphree A: Intraocular retinoblastoma: The case for a new group classification. Ophthalmol Clin North Am 18:41-53, viii, 2005
19. Lethaby CD, Picton S, Kinsey SE, et al: A systematic review of time to diagnosis in children and young adults withcancer. Arch Dis Child 98:349-355, 2013
20. Barr RD: “Delays” in diagnosis: Amisleading concept, yet providing opportunities for advancing clinical care. J PediatrHematol Oncol 36:169-172, 2014
21. Clarke JN, Fletcher PC: Parents as advocates: Stories of surplus suffering when a child is diagnosed and treated forcancer. Soc Work Health Care 39:107-127, 2004
22. Dixon-Woods M, Findlay M, Young B, et al: Parents’ accounts of obtaining a diagnosis of childhood cancer. Lancet357:670-674, 2001
23. Dang-Tan T, Franco EL: Diagnosis delays in childhood cancer: A review. Cancer 110:703-713, 2007
24. Green AL, Chintagumpala M, Krailo M, et al: Correlation of insurance, race, and ethnicity with pathologic risk in acontrolled retinoblastoma cohort: A Children’s Oncology Group study. Ophthalmology 123:1817-1823, 2016
25. Goddard AG, Kingston JE, Hungerford JL: Delay in diagnosis of retinoblastoma: Risk factors and treatment outcome.Br J Ophthalmol 83:1320-1323, 1999
26. DerKinderen DJ, Koten JW, Van Romunde LK, et al: Early diagnosis of bilateral retinoblastoma reduces death andblindness. Int J Cancer 44:35-39, 1989
27. Epelman S, EpelmanC, ErwenneC, et al: National campaign for early diagnosis of retinoblastoma inBrazil. J Clin Oncol22, 2004 (suppl 14; abstr 8561)
28. Wallach M, Balmer A, Munier F, et al: Shorter time to diagnosis and improved stage at presentation in Swiss patientswith retinoblastoma treated from 1963 to 2004. Pediatrics 118:e1493-e1498, 2006
29. Balmer A, Gailloud C: Retinoblastoma: Diagnosis and treatment. Dev Ophthalmol 7:36-100, 1983
329 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

30. Leal-Leal CA, Dilliz-Nava H, Flores-Rojo M, et al: First contact physicians and retinoblastoma in Mexico. Pediatr BloodCancer 57:1109-1112, 2011
31. Butros LJ, Abramson DH, Dunkel IJ: Delayed diagnosis of retinoblastoma: Analysis of degree, cause, and potentialconsequences. Pediatrics 109:E45, 2002
32. Rodriguez-Galindo C, Wilson MW, Chantada G, et al: Retinoblastoma: One world, one vision. Pediatrics 122:e763-e770, 2008
33. Leander C, Fu LC, Pe~na A, et al: Impact of an education program on late diagnosis of retinoblastoma in Honduras.Pediatr Blood Cancer 49:817-819, 2007
34. Howard SC, PedrosaM, LinsM, et al: Establishment of a pediatric oncology program and outcomes of childhood acutelymphoblastic leukemia in a resource-poor area. JAMA 291:2471-2475, 2004
35. Howard SC, Marinoni M, Castillo L, et al: Improving outcomes for children with cancer in low-income countries in LatinAmerica: A report on the recent meetings of the Monza International School of Pediatric Hematology/Oncology(MISPHO)-part I. Pediatr Blood Cancer 48:364-369, 2007
36. Chantada GL, Dunkel IJ, Schaiquevich PS, et al: Twenty-year collaboration between North American and SouthAmerican retinoblastoma programs. J Glob Oncol 2:347-352, 2016
330 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

originalreport
Pain Management and Use of Opioids inPediatric Oncology in India: A QualitativeApproach
abstract
Purpose Consumption of medical opium for pain relief in India is low, despite the country being one of themainworld producers of the substance.We investigated obstacles to opioid use and physician perceptionsabout optimal pain management in pediatric oncology patients in India.
Methods Semistructured interviews were conducted with oncologists who work in pediatric oncologysettings. A mixed sampling strategy was used, including maximum variation and confirmation and dis-confirmation of cases, aswell as snowball sampling. Key informantswere identified. Interviewswereaudiorecorded, transcribed verbatim, and analyzed by thematic analysis methodology.
Results Twenty-three interviews were performed across 20 Indian institutions. The main obstaclesidentified were lack of financial resources, inadequate education of health care providers on painmanagement, insufficient human resources (particularly lack of dedicated trained oncology nurses), pooraccess to opioids, and cultural perceptions about pain. Children from rural areas, treated in publichospitals, and from lower socioeconomic classes appear disadvantaged. A significant equality gap existsbetween public institutions and private institutions, which provide state-of-the-art treatment.
Conclusion The study illuminates the complexity of painmanagement in pediatric oncology in India, wherefinancial constraints, lack of education, and poor access to opioids play a dominant role, but lack ofawareness and cultural perceptions about pain management among health care providers and parentsemerged as important contributing factors. Urgent interventions are needed to optimize care in thisvulnerable population.
J Glob Oncol 3. © 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
INTRODUCTION
Pain affects patients with cancer at all stages ofdisease and treatment. Pain control is recognizedby theWorld Health Organization as paramount tochanging the quality of life of patients and theirfamilies.1
Cancer prevalence has increased in low-incomecountries, where 80% of pediatric patients withcancer live.2 With increasing improvement in othercauses of mortality (eg, infection, malnutrition),the relative burden of pediatric cancer continuesto grow.2 According to the Central IntelligenceAgency,3 in 2011, the population of India was1.2 billion, with almost one third younger than15 years of age. The overall incidence of canceris 38 to 124 per million children per year4,5 andhas increased at a faster rate than that in Westerncountries in past decades. This rise can be ex-plained by the increased number of cancer reg-istries, improved availability of diagnostic tools,and improved awareness of cancer among
physicians, all of which have tackled the problemsof underdiagnosis and underascertainment.4,6
The estimated actual incidence of pediatric can-cermay be evenhigher than these current figures.
India is one of the main producers of medicalopium.7 In 1985, the government issued restric-tions through the Narcotic Drugs and PsychotropicSubstances Act (NDPSA) on opioid prescriptionand distribution8 to prevent their diversion andmisuse, which led to a drop in opioid consumptionbymore than97%.7Otherdocumentedchallengesto pain control in India include difficult access topoints of distribution and poor education of healthcare providers in pain management and pallia-tive care.9-13 Despite these known issues, fewpublished studies explored the views of medicalprofessionals in pain management, medicationprescription, and education14-16 and none in pe-diatric oncology. This article explores the barriersto use of opioids and delivery of optimal pain
Paola Angelini
Katherine M. Boydell
Vicky Breakey
Purna A. Kurkure
Marian A. Muckaden
Eric Bouffet
Brijesh Arora
Paola Angelini and EricBouffet, The Hospital forSick Children, Toronto;Vicky Breakey, McMasterUniversity, Hamilton,Ontario, Canada; KatherineM. Boydell, University ofNew SouthWales, Sydney,New South Wales,Australia; and Purna A.Kurkure, Marian A.Muckaden, and BrijeshArora, Tata MemorialHospital, Mumbai, India.Presented at theInternational Society ofPediatric Oncology,Boston, MA, October22-24, 2010.
Corresponding author:Paola Angelini, MD,Division of PaediatricHaematology andOncology, The Hospital forSick Children, 555University Ave, Toronto,Ontario M5G 1X8,Canada; e-mail: [email protected].
331 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
© 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License

control to improve the lives of children with cancerin India.
METHODS
A qualitative approach was adopted that usedsemistructured interviews (Data Supplement) thatallowed us to explore and identify unanticipatedproblems and select a small subset of physiciansas the target for the study to reduce the risk of biasfrom a low response rate. The research partici-pants were pediatric oncologists who practice inpediatric units in India and were representative ofsex, type and place of training (general pediatricsversus pediatric hematology/oncology, Westerncountries versus India), and location of practice(rural areas versus cities, public versus privatehospitalswithin four states) and includedpediatrichematology/oncology, palliative care, surgery, andradiation oncology specialists. A mixed-samplingstrategy that included maximum variation andconfirmation and disconfirmation cases as wellas snowball sampling were used. When available,palliative care specialists were interviewed. Keyinformants were identified in the host institution.Author P.A. attended the palliative care clinic atTata Memorial Hospital, Mumbai, India, as well asconducted 1 day of home visits.
The semistructured interview was offered in per-son after preliminary contact on the phone toexplain the purpose and methodology of the in-terview and to obtain consent. All interviews wereconducted by the same interviewer over 1 month,recorded, transcribed verbatim, and analyzedwith a thematic analysis methodology. A classicset of coding strategies for qualitative thematicanalysis as outlined by Braun and Clarke17 wasused as follows: Investigators read and reread alltranscripts to familiarize themselves with the dataand tracked initial and emergent ideas (by usingextensive memo writing); relevant features of thedata were labeled systematically across the entiredata set to generate initial codes; data were col-lated by relevant code; codes were collated intolarger potential groupings, again to gather all therelevant data within a particular theme; groupingswere reviewed by checking to see if they wereconsistent with coded extracts (level 1) and theentire data set (level 2), and thematic maps weregenerated for analysis; and a written account wasproduced by selecting compelling extracts andexemplars and by relating the analysis to the re-search objectives and relevant research literature.The study was approved by the Research EthicsBoard of The Hospital for Sick Children, Toronto,Ontario, Canada.
RESULTS
All 23 physicians contacted agreed to participatein the study (Table 1). Numerous interrelatedissues emerged, which were financial issues, lackof education and awareness among health careproviders and the general population, lack ofhuman resources, and poor availability of opioids.Their relative importance varied based on geo-graphic area and type of hospital (public versusprivate).
Financial Issues
Financial issues dominated the discussions at alllevels (family, hospitals, andgovernment).Despitethe existence of a public health care system, themajority (71%) of health care expenditure is out ofpocket at the time of service.18,19 Morphine is in-expensive because opium is produced and man-ufactured locally, but indirect costs represent a
Table 1. Interviewee Demographics and SocialCharacteristics
CharacteristicNo. of Interviewees
(N = 23)
Sex
Male 13
Female 10
City
Mumbai 8
Chennai 3
Delhi 5
Jaipur 4
Pune 2
Barshi 1
State
Maharastra 11
Tamil Nadu 3
Rajasthan 4
Delhi 5
Hospital*
Government 6
Charitable 4
Private 10
Specialty
Medical/pediatric oncology 16
Palliative care 4
Radiation oncology 2
Surgery 1
*The total is not 23because in somecases,more thanonephysicianwas interviewed in one hospital.
332 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

heavy burden on families: “If they come from aremote village, for them to come back and followup [to modify morphine doses or receive a newprescription] is next to impossible. They’ll mort-gage land” (interviewee number 19 [Int#19]). Atthe hospital level, financial issues affect patientcare, particularly in public hospitals:
The payment to the doctors...is not very attractive.The nurses come here, get some training, andthey want to push off to a better hospital. So this isalso one reason that it becomes difficult for us totrain them. (Int#19)
Many physicians maintain private practice ormove to private hospitals with attractive salaries.
Lack of Education
Pain management and palliative care have onlyrecently been introduced into medical collegecurricula. “If you could introduce this [support-ive care training] as a basic training for...doctorswho are already in service, I think it will make a bigdifference” (Int#23). Frequent rotations throughvarious departments and limited use of opioidslimit opportunities for nurses and junior physiciansto gain experience in pain management. Many in-terviewees believed that they could not trust theirnurses to properly monitor patients as a result oflack of time and training. As one physician ex-plained, “[Intravenous] morphine actually requiresa lot of monitoring. Sisters [nurses] are not trainedhere for IVmorphinemonitoring. That’s why I avoidit” (Int#4). The fear of addiction or severe adverseeffects, particularly respiratorydepression, seemedto increase with limited experience. The use ofvisual or numeric scales tomonitor pain is sporadicand limited to the most affluent institutions (ie,private hospitals).
Lack of Awareness
Lack of awareness is widespread among physi-cians and parents: “I really don’t have toomuch ofthe trouble of pain” (Int#14).
Most of our pain episodes are related to the initialeither tumor mass or ALL [acute lymphoblasticleukemia] fresh diagnosis having body ache. Weundertreat pain very significantly. I realize it issomehow not part of the process of assessing apatient. (Int#1)
In most public hospitals, invasive procedures areperformed without conscious sedation, and post-operative pain ismanaged onpatient request or byusing standardized protocols without the monitor-ing and tailoring of treatment. Parents are noteducated to recognize signs of pain:
It is not a question of lack of time, rather lack ofawareness....They very rarely complain aboutthings. A child will be irritable and cranky, andthey think it is normal because of the overalldisease rather thanpain as such. Theydon’t knowthat painkillers are available and often associatemorphine with terminal disease and death andrefuse it. (Int#1)
Lack of Human Resources
“There is always a huge mismatch between thenumbers and the caregivers, and that is the chiefreason why our quality is not as it should be”(Int#21). According to The World Bank, the num-ber of physicians per 1,000 patients was 0.7 in2012 (compared with 2.1 in Canada).20 Man-power is particularly scarce in public hospitals,and this (togetherwith financial issues) creates thegap in the quality of care between private andpublic facilities. Such a shortage of health careproviders and consequent shortage of time ded-icated to each patient imposes prioritization: Phy-sicians rarely ask about pain, and patients prefertalking about more important subjects, such astreatment or prognosis. “They think that if I will talkmore about pain, they will just treat pain and theywill not be able to give treatment for my child’sdisease” (Int#23). Manpower shortage dictatesthe organization of work. “The staff population isso moving around that someone who is starting tolearn the process usually leaves the departmentbecause his time here is over” (Int#1). “[Nurses]usually last a longer period than the residents in aparticular ward. Over that period of time, they endup getting a significant expertise. My focus is to tryto empower thenurses” (Int#1). “The trendhere isnot to let the nurses take their own decision...thenurses should have more authority to change thedose” (Int#1). “Nurses are more meant to takeorders...they are too busy” (Int#3). In public hos-pital inpatient units, one nurse may take careof.50patients. Thehugeworkload leads tounduedelays inmanagement and therapeutic adjustmentand makes the use of some drugs (eg, intravenousmorphine) unsuitable. In the smaller centers, thesituation is even gloomier: “We don’t have compe-tent doctors in the district areas and rural areas”(Int#18).
Poor Availability of Opioids
A broad choice of opioids in various formulationsare available in the country, including morphine,pentazocine, meperidine, and fentanyl. However,“the licensing is sodifficult that peopledon’t apply.Unless you have all five licenses, no institute canbuy and dispensemorphine” (Int#19). As a result,
333 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

opioids are available only in a few pharmacies andhospitals, and the dispensation procedure is tor-tuous. Pharmacists and physicians are afraid ofbeing considered accountable for misuse or di-version and the heavy legal implications: “Sistershave to take specific precautions with respect tothis, and I am not very comfortable” (Int#5).“When the drug controller comes, you have toaccount for even half a tablet. In a public hospital,nobody wants to take such responsibilities”(Int#17). Most institutions have access to only oralmorphine and sometimes to fentanyl patches,which are expensive. The limited distribution net-work forces families to undergo long travels, whichincreases the financial burden. This also limits thepossibility for physicians and nurses to gain expe-rience in the use of opioids and thus generates avicious cycle. Physicians sometimes have to pre-scribe inappropriate drugs, such as pethidine orcrude opium tablets: “At times I askmy patients tohave the crude opium” (Int#22).
Successful Experiences
Despite the overwhelming difficulties, successfulexperiences were also identified. In a hospice inChennai, a physician reported high-quality painmanagement: “[Nurses] are round the clock. Wedepend on them to tell us what is what….We havegiven them the freedom to escalate or give the [asneeded] dosage” (Int#17). Adequate pain controlis achieved in most situations with oral morphineand plays an important educational role: “Therewas a stigma attached with the hospice that who-ever enters it dies....We are consciously encour-aging admitting patients who are not so sick andsending them home several times” (Int#17).
DISCUSSION
The main findings of this study are summarizedin the words of one interviewee: “The first majorproblem which I would rank is poverty. Secondthing would be illiteracy. The third thing would bethe sheer numbers, and this automatically trans-lates into lack of trainedmanpower. The last wouldbe availability of drugs” (Int#21).
Poverty
India adopted a public sector–led model of healthcare, but given inadequate investment from thegovernment (, 1% of the gross domestic productis devoted to health care), the private system hasexpanded and now providesmore than one half ofmedical care at unaffordable costs for uninsuredpeople (themajority).19 ThePlanningCommissionof India in 2010 recommended an increase in
health expenditures to 2.5%of the gross domesticproduct to achieve universal health care by 2022.21
In addition, nontransmittable diseases must be-come a priority, although the agenda has so farbeen dominated by maternal health and infectiousdiseases.
Illiteracy
Lackof education is reported inmany studies.22-24
Indian physicians reported lack of education inpain control and palliative care as well as in med-ical and oncology education, particularly amongnurses and general practitioners. “A nurse who istrained in this can do wonders” (Int#5). Someinterviewees suggested the creation of ad hocguidelines for junior physicians. Many programshave used the World Health Organization lad-der25-27 and have included a training programfor physicians and other operators (nurses andvolunteers), often in more than one session (eg,yearly).25 In Uganda, a highly effective model wascreatedbynursepractitioners aspart of apalliativecare plan, and because these nurses were onlyallowed toprescribepalliative caredrugs, theyalsofulfilled the need for dedicated staff.25 Theseexamples show how a change of approach tonursing and a long-established culture of subor-dinate relationship of nurses to physicians is pos-sible. In India, recent initiatives (eg, the introductionof oncology and pain management in the under-graduate medical curriculum, creation of fellow-ships in palliative care, the formation of the IndianAssociation of Palliative Care, workshops on pedi-atric cancer targeted to family physicians) are likelyto bring improvement.
Sheer Numbers
The size of the country, the high percentage ofpopulation living in rural areas, and the scarcity ofhealth care providers call for the development of amodel of decentralized care. In rural settings inUganda and Malaysia, programs that involvenurses trained and enabled to prescribe drugsfor palliation25,27 are successful in reaching almostall patients with cancer in need of palliation. Tra-ditional healers and even trained volunteers haveproven to be useful health care providers.6,25,28 Anexample of this comes from the cancer registry ofBarshi, the only rural cancer registry of India, in aremote village in Maharastra. Its nine employeesvisit . 500 villages regularly, educate the popula-tion about cancer, and identify individuals withsymptoms and refer them to the hospital clinic orto camps held periodically where they can under-go diagnostic procedures. In this area, no general
334 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

practitioner exists; the employees of the registry arethe only health care providers.
Availability of Drugs
Poor availability of opioids in India dates back tothe late 1980s when the government issued theNDPSA to fightmisuse and diversion ofmorphine.India is still amajor world producer,manufacturer,and exporter of opium and opioids. Through judi-cial cases, physicians and nongovernmental or-ganizations have tried to liberalize the use ofmedical opium.29-32 A recent amendment of theNDPSA to reduce the number of licenses neededhas effectively improved the availability of opioidsin 13 states, but more is needed. The state ofKerala is unique in the Indian landscape becausepalliative care services were started in the late1990s by volunteers who created the Neighbor-hood Network in Palliative Care, and this initiativewas followed by a state policy (Pain and PalliativeCare policy) in 2008 that was implemented by theState National Rural Health Mission. This projectfocuses on primary level care, including homecare and free delivery ofmedications and devices.Key to the success has been an awareness cam-paign from themedia,whichhas resulted in strongcommunity support, integrationwithin the govern-ment health care system, and capacity building atthe medical level.33 Relatively minor changes,such as the possibility to prescribe drugs for 1 to3 months, an increase in the number of phar-macies that distribute opioids, and improvedaccess to sustained-release formulations ofmorphine (now barely available), can translateinto major improvements.25,34,35 Tables 2 and3 summarize the contradictions of the Indianlandscape and suggested solutions from theinterviewees.
The issues described are not unique to pain con-trol but represent major priorities for the develop-ment of health care in India. Is it still worth it to askthe question and look for obstacles to pain controlin India? The interviewees challenged the studyquestion itself. Two of the most senior physiciansinterviewed said that pain control is not a priority inIndia and identified lack of access tomedical care,which leads to a missed diagnosis of approxi-mately 80% of childhood cancer (“If you giveme a million dollars, I would spend it on gettingthose 80% patients in rather than spending anydollar on pain management” [Int#9]) and infec-tions (“Most important [problem in India] I wouldsay [is] infection” [Int#25]) as the most commoncauses of childhood death.
Despite our efforts to choose a sample represen-tative of the diversity of Indian reality, our choicesled to multiple biases. We chose not to use trans-lators but to interview only physicians, who areusually fluent in English. Because physicians ap-pear to play a major role in pain management, weare confident that we got a comprehensive over-view of the issues. In settingswhere nurses play anindependent role, physicians and nurses havesimilar perspectives.36,37 Our choice may haveled to an underestimation of patient-related cul-tural issues, which were only reported by physi-cians. We mostly explored the urban reality.Whereas 70% of the Indian population lives inrural areas,3 only one interviewwasconducted in arural hospital, and threemorewere done in Jaipur,the only oncology referral center in Rajasthan,which highlights the issues experienced by therural population. We interviewed only allopathicphysicians. Because alternative medicine practi-tioners outnumber trained practitioners, the ques-tion of whether to involve them in pain control
Table 2. Contradictions in the Indian System
Societal Feature Contrast
Family-centered, rural society Health care centralized in the big cities
Strict regulations to avoid misuse Some physicians are forced to prescribeinappropriate opioids or opium tabletsbecauseof severe limitations in availabilityof medical opium
Belief that few children need palliative care Survival rate is below Western standards,and the child population is huge
Low education of parents Complex mixture of health care providers(including alternative medicine andunlicensed physicians), difficult tonavigate
Governmenthospitalswith ahugenumberofpatients and limited resources (affects themajority of patients)
Private hospitals with state-of-the-artfacilities and availability of humanresources (few patients can afford)
335 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

and palliative care is legitimate; however, thiswould have complicated the study beyond ourintention and can be the object of a futureinvestigation.
This study provides an overview of the barriersto opioid use in India and suggests areas for
improvement. Physicians must advocate for painmanagement at all levels—government, healthcare provider, and even family—to improve thelives of children with cancer.
DOI: https://doi.org/10.1200/JGO.2016.003483Published online on jgo.org on November 2, 2016.
AUTHOR CONTRIBUTIONS
Conception and design: Paola Angelini, Katherine M. Boydell,Marian A. Muckaden, Brijesh AroraProvision of study materials or patients: Purna A. Kurkure,Brijesh Arora
Collection and assembly of data: Paola AngeliniData analysis and interpretation: Paola Angelini, Katherine M.Boydell, Vicky Breakey, Purna A. Kurkure, Eric Bouffet,Brijesh Arora
Manuscript writing: All authorsFinal approval of manuscript: All authors
AUTHORS’ DISCLOSURES OFPOTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided byauthors of this manuscript. All relationships are consideredcompensated. Relationships are self-held unless noted. I =Immediate Family Member, Inst = My Institution. Relation-ships may not relate to the subject matter of this manuscript.For more information about ASCO’s conflict of interest policy,please refer to www.asco.org/rwc or ascopubs.org/jco/site/ifc.
Paola AngeliniNo relationship to disclose
Katherine M. BoydellNo relationship to disclose
Vicky BreakeyNo relationship to disclose
Purna A, KurkureNo relationship to disclose
Marian A. MuckadenNo relationship to disclose
Eric BouffetResearch Funding: Roche
Brijesh AroraNo relationship to disclose
ACKNOWLEDGMENTWe thank the physicians who participated in the study and thepatients and their families.
REFERENCES1. World Health Organization: Cancer Pain Relief. With a Guide to Opioid Availability (ed 2). Geneva, Switzerland, World
Health Organization, 2006
2. Howard SC,MetzgerML,Wilimas JA, et al: Childhood cancer epidemiology in low-income countries. Cancer 112:461-472, 2008
3. Central Intelligence Agency: The world factbook, 2011. http://cia.gov/library/publications/the-world-factbook/geos/in.html
4. Arora RS, Eden TO, Kapoor G: Epidemiology of childhood cancer in India. Indian J Cancer 46:264-273, 2009
5. Indian Cancer Society: India Cancer Incidence and Patterns in Urban Maharashtra: Incidence and Distribution ofCancer 2001. http://ghdx.healthdata.org/record/india-cancer-incidence-and-patterns-urban-maharashtra-incidence-and-distribution-cancer-2001
Table 3. Possible Solutions According to the Interviewees
Suggested Solutions Interview Quotes
Increase availability “The problem with morphine is availability.” (Int#7)
Increase awareness of physicians and nurses “The big obstacle is awareness.” (Int#1)
Increase number of health care providers “We need manpower.” (Int#21)“The issue is numbers.” (Int#18)
Have dedicated oncology nurses “A nurse who is trained in this can do wonders!” (Int#5)“My focus is to try to empower the nurses.” (Int#1)
Provide simple guidelines for physicians “Easily available guidelines, which any person canunderstand. It is something we canwork out.” (Int#1)
Focus on people in the community and in therural areas (decentralize care)
“Weneed to havemore trained personnel going out intothe smaller places....We don’t have that much skilleddoctors in the...rural areas.” (Int#18)
Educate the parents “Literacy is themajor barrier. If the family is literate, theywill understand...they will listen to us.” (Int#19)
Abbreviation: Int#, interviewee number.
336 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

6. SwaminathanR, SankaranarayananR: Under-diagnosis and under-ascertainment of casesmay be the reasons for lowchildhood cancer incidence in rural India. Cancer Epidemiol 34:107-108, 2010
7. Joranson DE, Rajagopal MR, Gilson AM: Improving access to opioid analgesics for palliative care in India. J PainSymptom Manage 24:152-159, 2002
8. Banerjee AK: Commentaries on the National Drugs and Psychotropic Substances Act, 1985 (ed 2). New Delhi, India,Ashoka Law House, 1993
9. Koshy RC, Rhodes D, Devi S, et al: Cancer pain management in developing countries: A mosaic of complex issuesresulting in inadequate analgesia. Support Care Cancer 6:430-437, 1998
10. JoransonDE, RyanKM: Ensuring opioid availability:Methods and resources. J PainSymptomManage33:527-532, 2007
11. Chaturvedi SK: Ethical dilemmas in palliative care in traditional developing societies, with special reference to theIndian setting. J Med Ethics 34:611-615, 2008
12. Soyannwo O: Cancer pain—progress and ongoing issues in Africa. Pain Res Manag 14:349, 2009
13. Omoti CE, Halim NK: Adult malignant lymphomas in University of Benin Teaching Hospital, Benin City, Nigeria—incidence and survival. Niger J Clin Pract 10:10-14, 2007
14. LeBaron V, Beck SL, Maurer M, et al: An ethnographic study of barriers to cancer pain management and opioidavailability in India. Oncologist 19:515-522, 2014
15. Human Rights Watch: Unbearable pain: India’s obligation to ensure palliative care, 2009. https://www.hrw.org/report/2009/10/28/unbearable-pain/indias-obligation-ensure-palliative-care
16. Cleary J, De Lima L, Eisenchlas J, et al: Formulary availability and regulatory barriers to accessibility of opioids for cancer pain inLatinAmericaand theCaribbean:A report fromtheGlobalOpioidPolicy Initiative (GOPI).AnnOncol24: xi41-xi50,2013(suppl11)
17. Braun V, Clarke V: Using thematic analysis in psychology. Qual Res Psychol 3:77, 2006
18. Prinja S, Kaur M, Kumar R: Universal health insurance in India: Ensuring equity, efficiency, and quality. Indian JCommunity Med 37:142-149, 2012
19. Reddy KS: India’s aspirations for universal health coverage. N Engl J Med 373:1-5, 2015
20. World Bank: Physicians (per 1,000 people), 2014. http://data.worldbank.org/indicator/SH.MED.PHYS.ZS
21. Singh Z: Universal health coverage for India by 2022: A utopia or reality? Indian J Community Med 38:70-73, 2013
22. Hwang WS, Tsai YF, Chang HC, et al: A prospective study of pain treatment for patients with advanced cancer whoreceive hospice home care. Zhonghua Yi Xue Za Zhi 65:331-335, 2002
23. LjungmanG, Kreuger A, Gordh T, et al: Treatment of pain in pediatric oncology: A Swedish nationwide survey. Pain 68:385-394, 1996
24. Jeon YS, Kim HK, Cleeland CS, et al: Clinicians’ practice and attitudes toward cancer pain management in Korea.Support Care Cancer 15:463-469, 2007
25. Logie DE, Harding R: An evaluation of a morphine public health programme for cancer and AIDS pain relief in sub-Saharan Africa. BMC Public Health 5:82, 2005
26. Devi BC, Tang TS: Documenting pain as the fifth vital sign: A feasibility study in an oncology ward in Sarawak,Malaysia.Oncology 74:35-39, 2008 (suppl 1)
27. Devi BC, Tang TS, Corbex M: Setting up home-based palliative care in countries with limited resources: A model fromSarawak, Malaysia. Ann Oncol 19:2061-2066, 2008
28. Joranson DE, Gilson AM, Dahl JL, et al: Pain management, controlled substances, and state medical board policy: Adecade of change. J Pain Symptom Manage 23:138-147, 2002
29. Ghooi RB, Ghooi SR: A mother in pain. Lancet 352:1625, 1998
30. Ghooi RB, Ghooi SR: Freedom from pain—A mirage or a possibility? Experience in attempts to change laws andpractices in India. J Pain Palliat Care Pharmacother 17:1-9, 2003; discussion 11-12
31. Rajagopal MR, Joranson DE: India: Opioid availability. An update. J Pain Symptom Manage 33:615-622, 2007
32. Rajagopal MR, Joranson DE, Gilson AM:Medical use, misuse, and diversion of opioids in India. Lancet 358:139-143, 2001
33. Rajagopal MR: The current status of palliative care in India. Cancer Contr 57-62, 2015
34. Leong L, Ninnis J, Slatkin N, et al: Evaluating the impact of pain management (PM) education on physician practicepatterns—A continuing medical education (CME) outcomes study. J Cancer Educ 25:224-228, 2010
35. Leon MX, De Lima L, Florez S, et al: Improving availability of and access to opioids in Colombia: Description andpreliminary results of an action plan for the country. J Pain Symptom Manage 38:758-766, 2009
36. Ljungman G, McGrath PJ, Cooper E, et al: Psychosocial needs of families with a child with cancer. J Pediatr HematolOncol 25:223-231, 2003
37. Ljungman G, Kreuger A, Gordh T, et al: Pain in pediatric oncology: do the experiences of children and parents differfrom those of nurses and physicians. Ups J Med Sci 111:87-95, 2006
337 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

originalreport
Cancer Care at Times of Crisis and War:The Syrian Example
abstract
Purpose As Syria enters its fifth year of conflict, the number of civilians killed and injured continues to risesharply. Along with this conflict comes the rapid decline of medical care, specifically cancer care. Todetermine physician and equipment availability, cancer screening and management, and possible so-lutions relative to various major cities, a survey was distributed to physicians inside Syria through the helpof the humanitarian organization Syrian American Medical Society.
Methods Online surveys were distributed to both certified oncologists who work in cancer clinics andgeneral physicians who work in rural and mobile clinics inside Syria. Variables assessed were physicianspecialty, location, population, cost, regional situation (besieged versus government controlled), andresource availability and access. Results were stratified by location and physician specialty.
Results Survey results revealed a large shortage of specialized physicians and inhibited accessibility toscreening and management options in besieged areas compared with government-controlled regions.Physicians within both government-controlled and besieged cities reported limited or no targeted agents,radiation therapy, clinical trials, bone marrow transplantation, positron emission tomography scans,magnetic resonance imaging, and genetic testing.
Conclusion The Syrian civil war has resulted in suboptimal oncology care in the majority of the region. Inconsideration of specific deficiencies in cancer care, we recommend several solutions that may better thelevel of care in Syria: patient education on medical documentation and self-examination; online con-sultation; and cheap, effective screening methods. The implementation of these recommendations maychange the course of cancer care in a country that has deteriorated into theworst humanitarian crisis of thecentury.
J Glob Oncol 3. © 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
INTRODUCTION
Patients with cancer who live in developing na-tions receive suboptimal care. In Syria, cancer careis considered expensive, lacks multidisciplinaryteams, and is offered only in limited areas. Newerchemotherapies, targeted therapies, subspecialtyoncology services, interventional procedures,microinvasive surgeries, bone marrow transplan-tation programs, modern imaging, and clinicaltrials are limited, and health insurance coverageis not available. In 2008, the National CancerInstitute documented 9,468 new cases of cancerin Syria.1 In a more focused study, 1,802 newcases of cancer were diagnosed in Aleppo, thesecond largest governate in Syria (970 men, 832women). In 1998, an overall crude incidence rateof 72.8per 100,000person-yearswas reported forthis population, thereby calling for the importanceof established and reliable cancer programs inSyria.2 The study found breast and bladder can-cers as the leading types, which accounted for
one third of all cancer cases. Lung and bladdercancers and leukemias were the most commonmalignancies among males, whereas breast andcervical cancers and leukemias were the mostcommon among females.2
Syria has quickly devolved into the worst human-itarian andmedical crisis of the century. By 2016,over 250,000 people have been killed, and over5 million have fled the violence, torture, and rapeand to take refuge in the neighboring countries ofTurkey, Jordan, and Lebanon.3 In 2015, theUnited Nations High Commissioner for Refugeesregistered over 4 million Syrian refugees and es-timated 7.6 million internally displaced inside thecountry.4 International medical and humanitarianorganizationshavenot beenallowed to enter Syria,which leavesmillions to face severe deficiencies inmedical care. The United Nations High Commis-sioner for Refugees reported that over 10.8millionpeople who live under siege suffer from a shortageof food, shelter, and medical aid. Among these
Eman Sahloul
Riad Salem
Wessam Alrez
Tayseer Alkarim
Ammar Sukari
Wasim Maziak
M. Bassel Atassi
Eman Sahloul, OaklandUniversity WilliamBeaumont School ofMedicine, Rochester;Ammar Sukari, WayneState University, Detroit,MI; Riad Salem,Northwestern University,Chicago; M. Bassel Atassi,Little Company of MaryHospital/Chicago MedicalSchool, Evergreen Park,IL;Wessam Alrez, AlrahmaCancer Center, EastGhuta; Tayseer Alkarim,Medical Oncology,Damascus, Syria; andWasim Maziak, FloridaInternational University,Miami, FL.Corresponding author:M. Bassel Atassi, MD,Little Company of MaryHospital/Chicago MedicalSchool, 2800 95th St,Evergreen Park, IL 60527;e-mail: [email protected].
338 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
© 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License

scarcities is cancer care. An estimated 200,000Syrians have died as a result of chronic diseasessuch as cancer because of a lack of access totreatment and qualified physicians.5
Functioning medical clinics have become rareand expensive. Patients with poor prognoses areturned away due to limited funding; those withbetter prognoses are turned away due to costlytreatments. Since2013, themajority of healthcarefacilities have been destroyed, which leaves only47% of Syria’s hospitals and health centers par-tially functional.6 The Global Health Observatoryreported that in 2008, 31,000 physicians prac-ticed in Syria, with approximately 15 physiciansper 10,000 capita.7 Since then, . 15,000 physi-cians have fled Syria. For example, only one on-cologist remains in the large countryside of EastGhouta, with a reported 500,000 inhabitants.8
Furthermore, since May 2014, of the 5,000 phy-sicians who practiced in East Aleppo before theconflict, only 40 remain to serve 2.5 millionpeople.8
Although cancer incidence in low- and middle-incomecountries is low, survival rates of thosewithcancer are worse, with 72% of cancer deathsoccurring in low- and middle-income countries.9
This occurs not only because patients receiveaffordable/available treatment rather than optimaltreatment but alsobecauseof latediagnosis.9Withconflict comes a progressive increase in povertyand a decrease in health care; these are nowevident in Syrian patients with cancer. Challengesto the problem are evident and include delayeddiagnosis, lack of screening programs or continu-ity of care, treatment interruptions due to displace-ment and costs, threats tomedical personnel, anddestruction of infrastructure. The current inci-dence is difficult to establish inside Syria becausea representative sample of the population beforeand after the conflict are currently unavailable.Incidence may actually seem to decrease duringthe conflict due to increased undiagnosed casesas a result of thebreakdownof diagnostic services;even if carcinogenic materials are used in theconflict, their effect will likely take years beforebecomingapparent for epidemiologic surveillanceto document. This reality guided the context of thisstudy, which is focused on resource availabilityand general cancer management.
We investigatedhowconflict influencesavailabilityof, access to, and quality of cancer care in Syria.We have identified the most common cancers,explored existing diagnostic tools and treatmentoptions, identified preventive screeningmeasures
and follow-up efforts, compared government-controlled areas to besieged areas, comparedgeneral clinics to specialized cancer clinics, andproposed plausible solutions from an oncologicperspective.
METHODS
This is a cross-sectional study among several phy-sicianswhopractice invarious locationswithinSyria.Data were collected through self-administered,online, anonymous, translated Google question-naires from certified oncologists and surgeonswho work in cancer clinics inside besieged andgovernment-controlled major countrysides of Syriaand general physicians who work in various loca-tions in Syria, including rural and mobile clinics.Clinics were selected from the Syrian AmericanMedical Society database.
A 30-question survey was generated and distrib-uted to general practicing physicians who work inrural and mobile clinics inside Syria (Data Supple-ment). A 70-question Web-based survey was dis-tributed to Syrian oncology practitioners in sevenmajor Syrian countrysides: four government-controlled major cities (Damascus, Latakia, Homs,and West Aleppo) and three besieged large cities(East Ghouta, East Aleppo, and Idlib; Data Supple-ment). Analyses of Aleppowere separated into eastand west because the armed conflict has dividedthe city into east, which is currently under opposi-tion control, and west, which remains under gov-ernment control.10
Because of the small participant pool, the infor-mation gathered is considered pilot data for futurecancer research in Syria. Variables assessedwerephysician specialty, location, population, cost,regional situation (ie, besieged versus govern-ment controlled), resource access, and resourceavailability.
RESULTS
Cancer Clinics Inside Syria
Physician availability. The survey results indicatethat 20 oncologists work in the capital city ofDamascus. In the neighboring besieged EastGhouta countryside, one oncology-certified phy-sician is reported. In East Aleppo, where 500,000people reside, no treating oncologists are available,and thus, all patients with cancer often are trans-ferred to Turkey for treatment. In contrast, fourcertified oncologists are available in government-controlled West Aleppo, but access to them frombesieged East Aleppo is limited and dangerous. Anoncology pharmacist is available only in the cancerclinic in Homs, although all participants denied
339 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

having one available. In Idlib, the cancer clinicreportedly has only two general physicians andmore than 10 midwives at any given time. In theentire city, there are no certified oncologists andonly one student who at the time had 1 year oftraining in oncology. Furthermore, all participantsnoted that the cancer centers take care of bothadults and children. Results based on city/countryside and population are summarized inTable 1; populations are as reported by surveyparticipants in the area.
Resource and treatment availability. Basic diag-nostic tools are available in all clinics, includinglaboratory blood tests, biopsies, andbasic imagingstudies. Although magnetic resonance imaging isavailable in major cities, it is limited in besiegedareas. Radiation therapy is only available in Dam-ascus and Latakia, which restricts access to manypatients who live under siege or are required tocross military checkpoints. Positron emission to-mography scanners are only available in Damas-cus and require self-pay. Advanced services suchas interventional radiology and genetic testing arenot available. More-advanced options such asbone marrow transplantations and clinical trialsare also not available. Patients who can afford thecosts are referred to neighboring countries. How-ever, most patients do not have the capability oftraveling or paying for such expensive treatments,which leaves this population of patients with can-cer without treatment opportunity.
Chemotherapy was reported to be available in allcities, although the medications are extremelydifficult to import into besieged areas. Surveyparticipants from government-controlled citieslisted trastuzumab, rituximab, sorafenib, and ima-tinib as available treatment options; besiegedareas did not have access to targeted therapies,except EastGhoutawhere theparticipant reportedthe availability of imatinib.With regard tomortality,only Homs and East Ghouta responded. The par-ticipant fromHoms stated that 30 people died as aresult of cancer in 2013, and 22 died in 2014. In
East Ghouta, 20 people who died as a result ofcancer in 2013, and 41 died in 2014. Breastcancer was the most common malignancy re-ported in this study, with all survey participantsranking it first among other cancers. Hematologic,colon, and lung cancers were the next most com-mon, respectively.
Patient screening and follow-up. Only Damascusoffered preventive screening measures such asmammograms, colonoscopies, and Papanicolaousmears. Only two clinics reported an establishedfollow-up system after treatment completion. OnlyHoms and East Ghouta used computerized doc-umentation systems; all others reported having touse written documentation.
Online consultation. Survey participants had differ-ent opinions on the value of Internet and onlineconsultation, which they found was of limited valueto physicians working in hematology/oncology atcancer clinics inside Syria, except East Aleppo.Their reasons indicated include limited Internetaccess and sufficient knowledge on cancer cases,whereas general physicians found online consul-tation beneficial formanaging patientswith cancer.Table 2 summarizes the resource availability inSyria and compares it to that in US cancer clinics.
General Medical Clinics Inside Syria
The survey targeted three areas of northern Syria:East Aleppo, Idlib, and Hama. These areas werechosen because they are the largest cities outsidegovernment control but still under conflict. Threesurvey participants were general surgeons, onewas an orthopedic surgeon, and three were gen-eral practitioners.
Physician availability. Participants from Hamaand East Aleppo admitted that mistakes in di-agnosis were made as a result of poor resourceavailability and no specialized physicians. AnAmerican oncologist who volunteered in one ofthe clinics in Idlib explained that the clinic hadonly two general physicians and 10 nurses. The
Table 1. Comparison of Physician Availability in Seven Syrian Countrysides/Cities Relative to Population
City/Countryside Population Hematologist Oncologist Surgical Oncologist Specialized Pathologist
Damascus (the capital) . 1,000,000 20 2 Yes
Idlib 500,000-1,000,000 1 0 Yes
Homs City 500,000-1,000,000 Unknown 0 No
East Aleppo 500,000 0 0 No
East Ghouta 500,000 1 0 Yes
West Aleppo 500,000-1,000,000 4 2 Yes
Latakia 500,000-1,000,000 5 0 No
340 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

physician also reported that in the entire city,there were no certified oncologists and onlyone student who had 1 year of training in oncol-ogy. Physician availability in other areas waslimited to general practitioners.
Resource and treatment availability. Survey par-ticipants from East Aleppo and Idlib stated thatcomputed tomography scans are limited to certainlocations, whereas in Hama, they are available. Ofthe three countrysides, only Idlib confirmed theavailability of chemotherapydrugs.All participantsstated that no government-run hospitals existed inthe areas that were safe to travel to and no non-government organization (NGO)–based clinics toassist with patients with cancer; consequently,these patients are referred to Turkish cancercenters. All participants noted that patients oftenleave Syria for cancer treatment in neighboringcountries but return because of the high treat-ment costs.
Patient screening and follow-up. All participantsstated that no screening protocols, colonoscopies,andmammograms are available. If physicians aresuspicious of possible cancer because of indica-tors such as unintentional weight loss or a visiblemass, they either perform a biopsy on the massesor refer patients to Turkey for further investigation.Follow-ups are rare due to limited resources and
no system for keeping medical records in theclinics. Only participants in East Aleppo confirmedthat approximately 10 to 30 patients with cancercame to their general clinics in 2014 and 12 to 35in 2015, whereas participants from Hama andIdlib had no records of how many patients withcancer had come in.
Cost of Treatment in Syria
Besides limited resources, cost of cancer care isprohibitive to attaining treatment. The survey re-sults suggest thatmonthly cancer costs range from$100 to $1,000; thus, centers can only buy limitedamounts and cheaper alternatives of drugs. Al-though these numbers seem reasonable for can-cer treatment, a 2013article inAl-Akhbar reportedthat the median salary of working Syrians hasplummeted to $150 per month, whereas the costof basic goods have increased 300%.11,12 Onechemotherapy course costs roughly the same asthe annual per capita, translating to Americanpatients paying $47,000 for that same course.Although besieged participants are supportedby NGOs, funding is insufficient. In Damascusand Homs, there are no large NGOs, and patientspay out of pocket. There are two treatment centersin Damascus that patients are referred to for free;however, this government option is not available forpeople in political opposition areas or under siege.
Table 2. Summary of the Available Resources Compared With the United States
Resource
Syrian Cancer Center
Major Cities* Besieged Areas†Average US
Cancer Center Advanced US Cancer Center
Blood transfusions 3 3 3 3
G-CSF 3 Limited 3 3
Chemotherapy 3 Limited 3 3
Targeted agents Limited X 3 3
Onsite blood tests 3 3 3 3
Radiation therapy Limited X 3 3
Specialized surgeon Limited X Limited 3
Clinical trials X X Limited 3
Bone marrow transplantation X X X 3
Interventional radiology laboratory X X 3 3
Supportive services 3 3 3 3
PET scan Limited X 3 3
MRI 3 Limited 3 3
Genetic testing X X 3 3
Screening Limited X 3 3
Abbreviations: G-CSF, granulocyte colony-stimulating factor; MRI, magnetic resonance imaging; PET, positron emission tomography.*Damascus, Homs, Latakia, West Aleppo.†Idlib, East Aleppo, East Ghouta.
341 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

DISCUSSION
Cancer Care in a War Zone and Besieged Cities
The most common malignancy. Breast cancer isnow the most commonly diagnosed cancer inwomen and the second leading cause of cancerdeathamongwomen13; it is also themost commonmalignancy among Syrians as reported by surveyparticipants. In accordance with the study results,multiple essential diagnostic and treatment op-tions were found inadequate or unavailable. Earlydetection is the single most important factor insurviving breast cancer because the less ad-vanced the disease, the easier and less costly itis to treat.13 According to the American CancerSociety, 98% of women who receive their diagno-sis and are treated early are still alive 5 years latercompared with 84%of womenwhose disease hasspread to the lymph nodes before treatment startsand 28% whose cancer has spread to distantorgans.13 As indicated by the study results, mag-netic resonance imaging was either unavailable orlimited to certain regions and, thus, could not beused to supplement traditional diagnostic proce-dures in identifying locoregional extensions inyounger patients.14 Although radiotherapy andlumpectomy have equal benefits to total mastec-tomy in early stages of the disease, the lack ofradiation therapy and specialized breast surgeonsmay translate to an overly aggressive surgery.15,16
Targeted agents, such as trastuzumab, are of nobenefit to Syrian patients with human epidermalgrowth factor receptor 2 amplifications because oflimited availability and expense17; only surveyparticipants from East Ghouta, Homs, and Dam-ascus reported having access to trastuzumab.Furthermore, oncotype diagnostic testing is notavailable to guide treatment in patients with early-stage breast cancer who could benefit from oravoid chemotherapy.18
Challenges
Deficiencies in the standard of care and first-linetreatment.Aside frombreast cancermanagement,deficiency of first-line treatment options for manyother malignancies exist in Syria. As mentioned
previously, targeted and newer chemotherapeu-tic agents are scarce and thus of insufficientbenefit for patients with any kind of cancer. Thebenefits of radiation therapy for the managementof head and neck19 and stage III lung cancers20;adjuvant therapy forbreast,16 anal,21 andprostatecancers22; and neoadjuvant therapy for gastro-esophageal and rectal cancers23 and other ma-lignancies are not available in any of the Syriancountrysides besides Damascus and Latakia.Once again, this shortage causes a significantloss of therapeutic and survival benefits. In addi-tion, autologous stem cell transplantation for mul-tiple myelomas24 as well as allogeneic stem celltransplantation for acute leukemias,25 eligiblemyelodysplastic syndromes,26 and aplastic ane-mias27 are not available as treatment options inSyria.
Lack of specialized physicians. The Radiation Re-search Program at the National Cancer Instituterecommends that each city must have at least twosurgical oncologists, two radiation oncologists,and two hematologist oncologists.1 As shown inTable 3, Damascus was the only city that met theNational Cancer Institute recommendations,whereas all other cities had either zero or one ofthe specialized physicians listed.
Limited screening.More than one third of cancersare preventable, and another one third are poten-tially curableprovided theyaredetectedearly.28,29
In Syria, however, the technology and experiencefor screening are lacking, which calls for a re-construction in the country’s approach to earlydetection.
Limited follow-up. As observed in the survey re-sults, patient follow-up is inadequate in Syria fortwo chief reasons: Volunteer physicians treat pa-tients for limited amounts of time, and computer/chart systems have not been established. Unlesspatients personally maintain a meticulous andaccurate medical history, no records are keptfor blood test and biopsy results and drug treat-ments anddosages.WHO recommendscollectionof the following information whenever possible30:
Table 3. Summary of Survey Results From Seven General Physicians in East Aleppo, Hama, and Idlib
City/Countryside Blood Transfusions
ChemotherapyDrugs
ScreeningMammograms
ScreeningColonoscopies CT Scan
PatientFollow-up
East Aleppo Whole blood and PRBCs No No No Limited No
Hama No No No No Yes No
Idlib Whole blood and PRBCs No No No Limited No
Abbreviations: CT, computed tomography; PRBCs, packed red blood cells.
342 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

demographicandsocioeconomicdata (eg,patientname [identification], sex, date of birth, place ofbirth), financial data related to the payment of feesformedical servicesandhospital accommodation,and clinical patient data.
Plausible Solutions
As demonstrated in the study results, a wide dis-crepancy exists among Syrian cities and country-sides with regard to basic diagnostics, specializedphysicians, radiation therapy, chemotherapeuticagents, and even a safe commute. AlthoughDamascus and Latakia have suboptimal cancermanagement options, they remain acceptablecompared with other areas, which essentially in-cludes the rest of Syria. Thus, solutions to currentcancer care in Syria depends on geographic loca-tion and political affiliation. Opposition areas, forinstance, not only face the worst fortune in can-cer care but also must survive the least livableconditions. If an internationally protected zone isestablished, a specialized cancer center that re-ceives referrals from other areas of the countrycould provide basic diagnostics and treatmentoptions, radiation therapy, a diagnostic pathologylaboratory, and chemotherapeutic agents to solvethe cancer epidemic in Syria.
Online consultation. Physicians who work in gen-eral medical clinics inside Syria found online con-sultation and Internet access beneficial to thetreatment of patients with cancer. Such opportu-nities for telehealth and electronic medical con-sultation will give Syrian and volunteer physiciansbroader treatment options and allow for accu-rate diagnoses.31 The Syrian American Medical
Society has developed telemedicine strategies tosupport physicians through video cameras,Skype, and satellite Internet to ensure high-quality care to patients with trauma injuries andchronic disease.32 The current survey has helpedto solidify the significance of maintaining a con-nection with physicians inside areas where med-ical access and consultation are limited.
Patient education. In an environment where tan-gible resources and therapies are not available,patients must participate in maintaining their ownhealth and remain aware of their exposure topossible risk factors. In breast cancer, for in-stance, the development of culturally sensitivelocal education programs that teach women thesignificance of self-examination can result in atide-changing decrease in mortality rates.33 Suchan initiative can function as a mode of early de-tection and thus reduce the typical presentationof an advanced disease stage in disadvantagedareas.
Conclusion
A structured initiative that focuses on patient/physician education, equipment, and availabilityof specialized physicians and that creates referralfacilities in safe zones can positively change thecourse of cancer care inside Syria. Long-termadjustments are needed to ensure the sustainabil-ity of medical care. Such actions may alter thedisastrous outcomes in a country that faces theworst medical and humanitarian crisis of thecentury.
DOI: https://doi.org/10.1200/JGO.2016.006189Published online on jgo.org on August 31, 2016.
AUTHOR CONTRIBUTIONS
Conception and design: Eman Sahloul, Riad Salem, WasimMaziak, Bassel AtassiCollection and assembly of data: Eman Sahloul, Wessam Alrez,Tayseer Alkarim, Ammar Sukari, Bassel AtassiData analysis and interpretation: Eman Sahloul, Bassel AtassiManuscript writing: All authorsFinal approval of manuscript: All authorsAccountable for all aspects of the work: All authors
AUTHORS’ DISCLOSURES OFPOTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided byauthors of this manuscript. All relationships are consideredcompensated. Relationships are self-held unless noted.I = Immediate Family Member, Inst = My Institution. Rela-tionshipsmaynot relate to the subjectmatter of thismanuscript.For more information about ASCO’s conflict of interest policy,please refer to www.asco.org/rwc or ascopubs.org/jco/site/ifc.
Eman SahloulNo relationship to disclose
Riad SalemNo relationship to disclose
Wessam AlrezNo relationship to disclose
Tayseer AlkarimNo relationship to disclose
Ammar SukariNo relationship to disclose
Wasim MaziakNo relationship to disclose
Bassel AtassiNo relationship to disclose
343 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
REFERENCES1. National Cancer Institute Radiation Research Program: Human Resources for Treating New Cancer Cases in Syria.
http://rrp.cancer.gov/programsResources/lowIncome/syria.pdf
2. Mzayek F, Asfar T, Rastam S, et al: Neoplastic diseases in Aleppo, Syria. Eur J Cancer Prev 11:503-507, 2002
3. Alghothani N, Alghothani Y, Atassi B: Evaluation of a short-term medical mission to Syrian refugee camps in Turkey.Avicenna J Med 2:84-88, 2012
4. United Nations High Commissioner for Refugees: Syria regional refugee response: Regional overview. http://data.unhcr.org/syrianrefugees/regional.php
5. Murugen J: Syria’s other crisis, 2013. http://globalpublicsquare.blogs.cnn.com/2013/09/30/syrias-other-crisis
6. United Nations Office for the Coordination of Humanitarian Affairs, Consolidated Appeal Process: Syria Crisis Hu-manitarian Response (SHARP and RRP) 2014. http://www.unocha.org/cap/appeals/syria-crisis-humanitarian-response-sharp-and-rrp-2014
7. World Health Organization: Global Health Observatory data repository. http://apps.who.int/gho/data/?theme=home&vid=19200andtheme=country
8. Save the Children: A devastating toll: The impact of three years of war on the health of Syria’s children. http://www.savethechildren.org/atf/cf/%7b9def2ebe-10ae-432c-9bd0-df91d2eba74a%7d/save_the_children_a_devastating_toll.pdf
9. International Network for Cancer Treatment and Research: Cancer in developing countries. http://www.inctr.org/about-inctr/cancer-in-developing-countries
10. BBC News: Syria: Mapping the conflict. http://www.bbc.com/news/world-middle-east-22798391
11. Al-Akhbar English: The poor get poorer in Syria. http://english.al-akhbar.com/content/poor-get-poorer-syria
12. Axios International: Cancer treatment and care in developing countries. http://www.cancer.org/acs/groups/content/@nho/documents/document/globalfactsandfigures2007rev2p.pdf
13. American Cancer Society: Global cancer: Facts & figures 2007. https://www.cancer.org/acs/groups/content/@nho/documents/document/globalfactsandfigures2007rev2p.pdf
14. Oseledchyk A, Kaiser C, Nemes L, et al: Preoperative MRI in patients with locoregional recurrent breast cancer:Influence on treatment modalities. Acad Radiol 21:1276-1285, 2014
15. Zhou J, Enewold L, Zahm SH, et al: Breast conserving surgery versus mastectomy: The influence of comorbidities onchoice of surgical operation in the Department of Defense health care system. Am J Surg 206:393-399, 2013
16. Darby S, McGale P, Correa C, et al: Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and15-year breast cancer death: Meta-analysis of individual patient data for 10,801 women in 17 randomised trials.Lancet 378:1707-1716, 2011
17. Romond EH, Perez EA, Bryant J, et al: Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breastcancer. N Engl J Med 353:1673-1684, 2005
18. Albain KS, Barlow WE, Shak S, et al: Prognostic and predictive value of the 21-gene recurrence score assay inpostmenopausal women with node-positive, oestrogen-receptor-positive breast cancer on chemotherapy: A retro-spective analysis of a randomised trial. Lancet Oncol 11:55-65, 2010
19. Salama JK, Haddad RI, Kies MS, et al: Clinical practice guidance for radiotherapy planning after induction che-motherapy in locoregionally advanced head-and-neck cancer. Int J Radiat Oncol Biol Phys 75:725-733, 2009
20. O’Rourke N, Roque I Figuls M, Farre Bernado N, et al: Concurrent chemoradiotherapy in non-small cell lung cancer.Cochrane Database Syst Rev (6):CD002140, 2010
21. Graf R, Wust P, Hildebrandt B, et al. Impact of overall treatment time on local control of anal cancer treated withradiochemotherapy. Oncology 65:14-22, 2003
22. Pollack JM: Radiation therapy options in the treatment of prostate cancer. Cancer Invest 18:66-77, 2000
23. Roh MS, Colangelo LH, O’Connell MJ, et al: Preoperative multimodality therapy improves disease-free survival inpatients with carcinoma of the rectum: NSABP R-03. J Clin Oncol 27:5124-5130, 2009
24. Kyle RA, Rajkumar SV: Multiple myeloma. N Engl J Med 351:1860-1873, 2004
25. Cornelissen JJ, van Putten WLJ, Verdonck LF, et al: Results of a HOVON/SAKK donor versus no-donor analysis ofmyeloablative HLA-identical sibling stem cell transplantation in first remission acute myeloid leukemia in young andmiddle-aged adults: Benefits for whom? Blood 109:3658-3666, 2007
26. Appelbaum FR, Anderson J: Allogeneic bone marrow transplantation for myelodysplastic syndrome: Outcomesanalysis according to IPSS score. Leukemia 12:S25-S29, 1998 (suppl 1)
27. Peinemann F, Grouven U, Kroger N, et al: First-line matched related donor hematopoietic stem cell transplantationcompared to immunosuppressive therapy in acquired severe aplastic anemia. PLoS One 6:e18572, 2011
28. Kanavos P. The rising burden of cancer in the developing world. Ann Oncol 17:viii15-viii23, 2006 (suppl 8)
344 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
https://www.cancer.org/acs/groups/content/@nho/documents/document/globalfactsandfigures2007rev2p.pdf
29. Shibuya K, Mathers CD, Boschi-Pinto C, et al: Global and regional estimates of cancer mortality and incidence by site:II. Results for the global burden of disease 2000. BMC Cancer 2:37, 2002
30. International Atomic Energy Agency: Millions of cancer victims in developing countries lack access to life-savingradiotherapy. https://www.iaea.org/PrinterFriendly/NewsCenter/PressReleases/2003/prn200311.html
31. Van Gurp J, van Selm M, van Leeuwen E, et al: Teleconsultation for integrated palliative care at home: A qualitativestudy. Palliat Med 30:257-269, 2015
32. Syrian American Medical Society: Annual Report 2014-2015. https://www.sams-usa.net/foundation/images/SyrianAmerican Medical Society Annual Report 2015.pdf
33. Anderson BO, Yip C-H, Smith RA, et al: Guideline implementation for breast healthcare in low-income and middle-income countries: Overview of the Breast Health Global Initiative Global Summit 2007. Cancer 113:2221-2243, 2008(suppl 8)
345 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

originalreport
Survey of Implementation of AntiemeticPrescription Standards in IndianOncology Practices and Its Adherenceto the American Society of ClinicalOncology Antiemetic Clinical Guideline
abstract
Purpose Adherence to international antiemetic prophylaxis guidelines like those of ASCO can result inbetter control of chemotherapy-induced nausea and vomiting; however, the extent of implementation ofsuch guidelines in India is unknown. Therefore, this survey was planned.
Methods This study was an anonymized cross-sectional survey approved by the ethics committee. Surveyitems were generated from the clinical questions given in the ASCO guidelines. The survey was dis-seminated through personal contacts at an oncology conference and via e-mail to various communityoncology centers across India. The B1, B2, and B3 domains included questions regarding the optimalantiemetic prophylaxis for high, moderate, and low-minimal emetogenic regimens.
Results Sixty-six (62.9%) of 105 responded and 65 centers (98.5%) were aware of the publishedguidelines. The partial, full, and no implementation scores were 92.5%, 4.5%, and 3.0%, respectively.Full implementation was better for the low-minimal emetogenic regimens (34.8%) than the highlyemetogenic regimens (6.1%). The three most frequent reasons for hampered implementation of ASCOguidelines in routine chemotherapy practice cited by centers were a lack of sensitization (26 centers;39.4%), lack of national guidelines (12 centers; 18.2%), and lack of administrative support (10 centers;15.2%).
Conclusion Awareness regarding ASCO antiemetic guidelines is satisfactory in Indian oncology practices;however, there is a need for sensitization of oncologists toward complete implementation of these guidelinesin their clinical practice.
J Glob Oncol 3. © 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
INTRODUCTION
Chemotherapy-induced nausea and vomiting(CINV) is one of the most common and mostdistressing complications of chemotherapy.1 Ithas a detrimental effect on the quality of life ofpatients and their functional well-being.2-4 Un-controlled nausea or vomiting is also associatedwith frequent hospital andemergencydepartmentvisits, is resource consuming,5-8 and can lead toimpaired compliance with chemotherapy.1,9,10
There has been significant progress in the devel-opment of newer antiemetics and the use of com-binations of antiemetics. The optimal combinationthat is required depends on the emetogenic po-tential of the specific chemotherapy regimen
used. Clinical guidelines have been publishedby professional bodies, such as ASCO and theEuropean Society for Medical Oncology, for thesame.11,12 These guidelines have been shownto control the rate and severity of CINV13-16; how-ever, adherence rates internationally are variable(29% to 57.3%).13,14 In India, there are no na-tional guidelines, and oncologists rely most com-monly on ASCO clinical updates and the NationalComprehensive Cancer Network recommenda-tions, with the extent of implementation largelyunknown. To address this gap, the present surveywas planned with the primary objective of evaluat-ing the proportion of cancer centers that have fullyimplemented the ASCO antiemetics clinical prac-tice guideline11 standards in routine chemotherapy
Vijay Patil
Vanita Noronha
Amit Joshi
Purvish Parikh
Atanu Bhattacharjee
Santam Chakraborty
Sunny Jandyal
Vamshi Muddu
Anant Ramaswamy
K. Govinda Babu
Nilesh Lokeshwar
Sachin Hingmire
Nikhil Ghadyalpatil
Shripad Banavali
Kumar Prabhash
Author affiliations appear atthe end of this article.
Corresponding author:Kumar Prabhash, MD,Department of MedicalOncology, Tata MemorialHospital, Parel, Mumbai400012, India; e-mail:[email protected].
346 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
© 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License

practice. Secondary objectives were to determinethe proportion of centers that implement theseguidelines partially, to determine the standards thatare most commonly and least commonly imple-mented in each category of chemotherapy drugsaccording to emetogenicity, and to determine thedifficulties that are faced in implementing thesestandards.
METHODS
Survey Instrument
A written survey on the basis of the standardsaccording to the ASCO antiemetics clinical prac-tice guideline was designed.11We had conducteda similar survey previously and based the presentstudy on the earlier experience.17 Survey itemswere generated from the clinical questions in theguidelines and in the same order. The first andsecond clinical questions, which dealt with anti-emetic prophylaxis in high and moderate emeto-genic chemotherapy regimens, respectively, werefurther broken down into six subquestions each.These questions enquired about the use of an NKreceptor antagonist, 5HT3 antagonist, dexameth-asone, and their schedules. The remaining surveyquestions were based on statements in the guide-line. Because our intent was to focus on imple-mentation of the ASCO guidelines in a relativelyhomogenous population of adults with solid tu-mors, the survey did not include questions relatedto pediatric patients, hematologic malignancies,bone marrow transplant centers, patients beingtreated with radiation, and breakthrough emesis.
The survey included questions regarding institu-tional antiemetic policy (domain A); optimal anti-emetic prophylactic regimen for highly emetogenicantineoplastic drugs (domain B1); optimal anti-emeticprophylactic regimen formoderately emeto-genic antineoplastic drugs (domain B2); optimalantiemetic prophylactic regimen for low-minimalemetogenic antineoplastic drugs (domain B3);and antiemetic use in special situations (domainC). Response options in the survey included afour-itemLikert scale (always, usually, rarely, andnever), a binary scale (yes or no), or a multiple-choice format, depending on the type of question.In addition, we inquired about the important factorsthat prevented the center from fully implement-ing the standards. This response was in the formof a multiple-choice item along with a free-textoption. The survey instrument is shown in theAppendix.
In addition, some questions regarding the natureof oncology practice were also added. These ques-tions addressed the following items: state in which
the center was located, setting of practice (urbanor rural), teaching status (yes or no), funding source(public or private), and approximate number of pa-tients seen daily.
Survey Distribution
This was an anonymized cross-sectional survey.The survey was designed on Google forms (Goo-gle, Mountain View, CA). Oncologists that admin-ister chemotherapy were identified from the ICON(Indian Cooperative Oncology Network) databaseand invited to participate in this survey. Individualemails with a link to the survey form were sent torecognized cancer center chemotherapy units,and oncologists in these units were requested tocomplete the survey between October 22, 2015,and January 10, 2016. The invitation for the surveywas restricted to a single oncologist from each unit.If a center had a single team, only one of theoncologists was contacted. The center’s team wasconsidered a single unit. If a center had multiplechemotherapy units that functioned independentlyof each other and had policies independent of eachother, then one oncologist from the unit was invitedand was considered an independent entity in thesurvey
In addition, the survey instrument in PDF formatwas distributed through personal contacts in anational biennial joint conference of the ISMPO(IndianSociety ofMedical andPediatricOncology)and the Indian Society of Oncology that was heldfromNovember 6 to 8, 2015, atHotel GrandHyatt,Mumbai, India. Only members from units thatwere not invited (for lack of a valid e-mail address),or who were invited but had not completed thesurvey online, were given the option of completingthe survey at the conference.
Electronic responses were automatically capturedin a Google spreadsheet that was linked to theonline form, and responses collected on the PDFversion were manually entered into the samesheet.
Survey Population
The survey population consisted of adult oncologypractices that administer chemotherapy on a reg-ular basis. This included regional cancer centers,dedicated corporate cancer centers, cancerwingsof medical colleges, hospitals, and private oncol-ogy day care centers. As much as possible, only asingle oncologist was contacted from each center.If multiple oncologists from one center participated,they were asked to collaborate and submit a singleresponse.
347 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Ethics
The protocol was approved by the ICON ethicscommittee. ICON is an autonomous body of ISMPO,with a primary mandate for research.
Sample Size
The exact number of oncology centers in whichchemotherapy is administered in the country isunknown. As convenience sampling was used forthis survey, and formal sample size calculationswere not performed.
Statistical Analysis
To calculate the completeness of the implemen-tation of guidelines, we counted the number ofcorrect responses for each major question do-main. The correct responses to these questionswere decided before the start of the survey by theinvestigators (V.P. and K.P.) in accordance withthe target guidelines. The correct response foreach of the survey instrument questions is docu-mented in the Appendix. A domain standard wasconsidered to be fully implemented if . 90% ofthe items had correct responses for the givenstandard. It was considered partially implementedif between 50% and 90% of the items had correctresponses for the given standard. When , 50%had correct responses for the given standard, itwas considered not implemented. Thus, the for-mula for calculating the percentage implementa-tion rate for each domain was:
% Implementation rate in given domain ¼ðnumber of itemswith correct reponse=number
of items for a given domainÞ3 100
The detailed scoring system and calculation of thepercentage implementation rate is shown in theAppendix. A facility was considered to have fullyimplemented ASCO guidelines if it scored a per-cent implementation rate that exceeded 90% inthe B (B1, B2, and B3 combine) domains. Thepercentage of 90% was decided by consensusamong the investigators.
Descriptive data regarding frequencies of imple-mentation for a given standard as well as thedomain are presented. We have calculated thenumber and proportion of oncology centers thathave fully implemented each standard as well asthe full domain. Frequency of major reasons fornonimplementation of a given standard are pre-sented. Linear regression analysis was performedto identify factors that predicted low implementa-tion scores in B1, B2, and B3 domains.
RESULTS
Baseline Details of Participating Centers
Sixty-six (62.9%)of105centersparticipated in thesurvey. Details about these centers are listed inTable 1. Themajority of these centers (60; 90.9%)were located in urban areas, were dedicated can-cer centers (55; 83.3%), and were teaching in-stitutes (45; 68.2%). The median number ofpatients seen per physician was 40 (interquartilerange, 30 to 50 patients). The average number ofpatients seen per physician was 54.5 in the gov-ernment sector, whereas it was 33.8 in the privatesector (P = .009). Sixty-five (98.5%) of 66 centerswere aware of the presence of international anti-emetic guidelines.
Implementation of Standards
The target of partial, full, andno implementation ofstandards was seen in 92.5% (95% CI, 83.0% to97.0%), 4.5% (95% CI, 1.1% to 13.2%), and3.0% (95% CI, 0.3% to 11.2%) of centers, re-spectively, as shown in Figure 1. Only two centershad all standards implemented fully, whereasone center had . 90% standards implemented.Full implementation was better for the low-minimalemetogenic regimens (34.8% of centers; 95% CI,24.5% to 46.9%) than the highly emetogenic reg-imens (6.1% of centers; 95% CI, 2% to 15.1%).
Details about the implementation of each individ-ual standard in each domain are listed in theAppendix (Appendix Tables A1 to A6). In the B1domain (high antiemetic prophylaxis), the rec-ommendations with lowest compliance werethe use of olanzapine when aprepitant is notused (nine centers; 13.6%), appropriate useof 5HT3 antagonist on days 2 and 3 (13 centers;19.7%), and use of dexamethasone on days 2 and3 (44centers; 66.7%).Similarly, inB2domain, theappropriate use of 5HT3 and dexamethasone ondays 2 and 3 was significantly lacking (AppendixTables A2 and A3).
Factors Adversely Impacting Implementation
The three most frequently cited reasons for ham-pered implementation of ASCOguidelines in routinechemotherapy practice were a lack of sensitization(26 centers; 39.4%), lack of national guidelines (12centers; 18.2%), and lack of administrative support(10 centers; 15.2%). (Appendix Table A7). None ofthe following factors—place of practice, fundingsource, presence of dedicated cancer center,and patient load—were independently associ-ated with low implementation scores in B1, B2,or B3 domains (Appendix Tables A8 to A10).
348 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
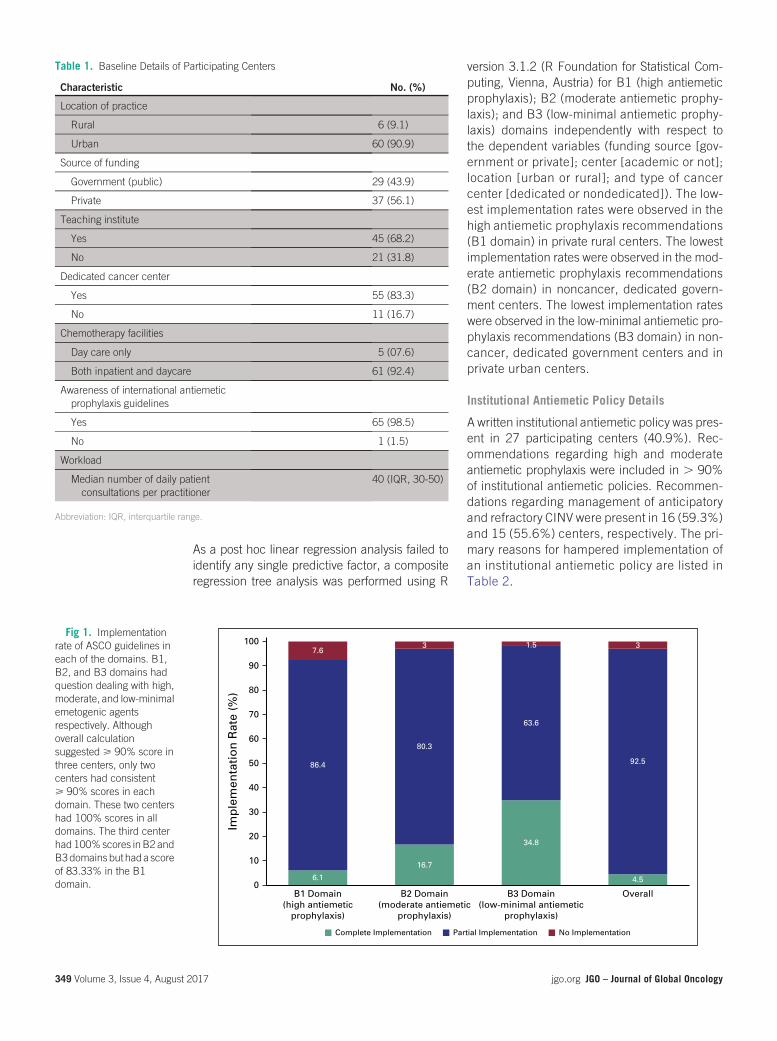
As a post hoc linear regression analysis failed toidentify any single predictive factor, a compositeregression tree analysis was performed using R
version 3.1.2 (R Foundation for Statistical Com-puting, Vienna, Austria) for B1 (high antiemeticprophylaxis); B2 (moderate antiemetic prophy-laxis); and B3 (low-minimal antiemetic prophy-laxis) domains independently with respect tothe dependent variables (funding source [gov-ernment or private]; center [academic or not];location [urban or rural]; and type of cancercenter [dedicated or nondedicated]). The low-est implementation rates were observed in thehigh antiemetic prophylaxis recommendations(B1 domain) in private rural centers. The lowestimplementation rates were observed in the mod-erate antiemetic prophylaxis recommendations(B2 domain) in noncancer, dedicated govern-ment centers. The lowest implementation rateswere observed in the low-minimal antiemetic pro-phylaxis recommendations (B3 domain) in non-cancer, dedicated government centers and inprivate urban centers.
Institutional Antiemetic Policy Details
A written institutional antiemetic policy was pres-ent in 27 participating centers (40.9%). Rec-ommendations regarding high and moderateantiemetic prophylaxis were included in . 90%of institutional antiemetic policies. Recommen-dations regarding management of anticipatoryand refractory CINV were present in 16 (59.3%)and 15 (55.6%) centers, respectively. The pri-mary reasons for hampered implementation ofan institutional antiemetic policy are listed inTable 2.
Table 1. Baseline Details of Participating Centers
Characteristic No. (%)
Location of practice
Rural 6 (9.1)
Urban 60 (90.9)
Source of funding
Government (public) 29 (43.9)
Private 37 (56.1)
Teaching institute
Yes 45 (68.2)
No 21 (31.8)
Dedicated cancer center
Yes 55 (83.3)
No 11 (16.7)
Chemotherapy facilities
Day care only 5 (07.6)
Both inpatient and daycare 61 (92.4)
Awareness of international antiemeticprophylaxis guidelines
Yes 65 (98.5)
No 1 (1.5)
Workload
Median number of daily patientconsultations per practitioner
40 (IQR, 30-50)
Abbreviation: IQR, interquartile range.
6.1
16.7
34.8
4.5
86.4
80.3
63.6
92.5
7.63 1.5 3
0
10
20
30
40
50
60
70
80
90
100
B1 Domain(high antiemetic
prophylaxis)
Imp
lem
enta
tio
n R
ate
(%)
B2 Domain(moderate antiemetic
prophylaxis)
B3 Domain(low-minimal antiemetic
prophylaxis)
Overall
Complete Implementation Partial Implementation No Implementation
Fig 1. Implementationrate of ASCO guidelines ineach of the domains. B1,B2, and B3 domains hadquestion dealing with high,moderate, and low-minimalemetogenic agentsrespectively. Althoughoverall calculationsuggested > 90% score inthree centers, only twocenters had consistent> 90% scores in eachdomain. These two centershad 100% scores in alldomains. The third centerhad 100%scores inB2 andB3domainsbuthada scoreof 83.33% in the B1domain.
349 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Knowledge and Practice in Special Situations
Details of the responses to special situations arelisted in Appendix Tables A11 and A12). In situ-ations that pertained tomultiday regimens, 31.8%(21)of centers startedantiemetics1daybefore thestart of chemotherapy, 74.2% (49) of centersselected antiemetic protocol for each day on thebasis of the emetogenic risk class of chemother-apy administered, and 63.6% (42) of centerscontinued antiemetic therapy for 2 days after thechemotherapy was completed. In protocols thatpertained to chemoradiation, 82.8% (53) of cen-ters selected antiemetics, taking into account theriskof emesis of both radiationandchemotherapy.Participating centers were divided in their pro-tocols regarding the emetogenic risk of weeklycisplatin (30 to 40 mg/m2) administered concur-rently with radiation. Of centers, 53.1% (34) con-sidered it as highly emetogenic and the remainingconsidered this protocol moderately emetogenic.
DISCUSSION
The profile and distribution of cancer centers inIndia presents several unique challenges in man-aging the complications of chemotherapy, including
CINV.Although75%to80%of thepopulation staysin rural areas, cancer centers are predominantlylocated inmajor cities.18Thus, amajorityofpatientsdo not have ready access to medical care, and thisadds to the challenge in deciding the appropriateantiemetic regimen. Compounding the issue is theaverage number of patients seen by individualoncologists, which has been reported to be muchhigher than in the West.19-22 In fact, this factor wasmentioned as one of the factors that hinderedappropriate antiemetic prophylaxis (12.3% ofcenters).
Selection of the optimal antiemetic regimen con-sists of gauging the emetogenic potential of che-motherapy regimens and then deciding theappropriate antiemetic prophylaxis consider-ing the factors that are unique to each country.Whereas international evidence-based guidelineshave been formulated for the selection of appro-priate antiemetic prophylaxis, there are minorvariations depending on local oncologic practice.In general, treatment guidelines formulated indeveloped countries are difficult to implement indeveloping countries.17 Unfortunately, many de-veloping countries, suchas India, donot have theirown guidelines for antiemetic prophylaxis. Hence,most oncologists in India use international guide-lines, such as the ASCO antiemetic guidelines.This is also reflected in the current study, where98.5% of the responding centers were aware andhad knowledge of these guidelines.
Overall, an encouraging finding in our study wasthe fact that 97.0%of centers had.50%of ASCOantiemetic clinical guideline standards imple-mented in routine practice; however, only threecenters implemented . 90% of standards andonly two centers implemented all standards fully.Guidelines regardinghighemetogenicprophylaxiswere the least implemented (only four centers;6.1%). Our survey identified three major areas ofconcern relating to the ASCO antiemetic guide-lines: the absence of olanzapine when aprepitantis not used (86.4%), overuse of 5HT3 antagonistfor delayed emesis (80.3%), andabsence of dexa-methasone for delayed emesis (33.3%). Whereasit may be argued that the ASCO antiemetic guide-lines did not offer olanazapine as an option, areference was made about its role in a scenarioprecluding aprepitant.11 On this basis, the inves-tigators decided that olanzapine is an essentialcomponent of an antiemetic regimen when apre-pitant cannot be used. Overuse of 5HT3 antag-onist for delayed emesis (71.1% in aprepitant usersand 57.1% in nonusers) and inappropriate use ofdexamethasone on days 2 and 3 postchemotherapy
Table 2. Details of Domain A: Institutional Antiemetic Policy
Characteristic No. (%)
Number of centers having institutional antiemetic policy
Yes 27 (40.9)
No 39 (59.1)
Details included in institutional policy 27
Recommendations for highly emetogenic agents 26 (96.3)
Recommendations for moderately emetogenic agents 25 (92.6)
Recommendations for low emetogenic agents 22 (81.5)
Recommendations for minimal emetogenic agents 14 (51.9)
Recommendations for anticipatory CINV 16 (59.3)
Recommendations for breakthrough CINV 18 (66.7)
Recommendations for refractory CINV 15 (55.6)
Factors hampering the development of institutionalantiemetic policy
39*
Lack of administrative support 9 (23.1)
Lack of sensitization 21 (53.8)
Lack of national guidelines 3 (7.7)
Lack of consensus among practitioners 4 (10.3)
Practicing international guidelines 6 (15.4)
Funding constraints 5 (12.8)
High number of patients 7 (17.9)
Abbreviation: CINV, chemotherapy-induced nausea and vomiting.*Participants would choose more than a single option in response to this question and hence the total ofresponses is more than 39.
350 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

(42.1% overuse in aprepitant users and 67.0%underuse in aprepitant nonusers) were the majordeficiencies in implementation of moderate an-tiemetic prophylaxis. Guidelines were fully imple-mented in the low and minimal risk setting in90.9% and 42.4% centers, respectively. Of cen-ters, 57.6% used antiemetics with agents that hadminimal risk of emetogenesis. Overuse of 5HT3antagonist for delayed emesis prophylaxis andunderuse of dexamethasone for the same arethe main issues in published work from otherdeveloped countries.23-26
Our survey also highlights the variable practices inoncology centers regarding antiemetics for multi-drug chemotherapy and antiemetic prophylaxisfor concurrent chemoradiation. One of the factorsthis survey did not touch upon was patient riskfactor adjusted antiemetic regimens. It is a knownfact that female patients and patients who hadprevious episodes of intractable vomiting areat a high risk of emesis and that modificationin selection of antiemetic regimens might bewarranted.13,27,28
As previously noted, the major factors that hin-dered wider implementation of ASCO antiemeticguidelines is the lack of sensitization, despite amajority of centers being aware of the existence ofsuch guidelines. In this context, lack of sensitiza-tion means lack of concern, or apathy, regardingchemotherapy-induced nausea and vomiting.Awareness and knowledge unfortunately do notalways translate into action, and emetic prophy-laxis seems to be one example. The authors
therefore decided to organize a biannual contin-uous medical education program for practicingoncologists and oncology trainees on antiemeticprophylaxis under the aegis of ICON. The programwould stress the recommendations which wereminimally implemented as per our survey. Wehope to improve the antiemetic prophylaxis forpatientswho receivechemotherapy in thecountry.
Another factor that impaired implementation ofASCO antiemetic guidelines was lack of nationalantiemetic prophylaxis guidelines. Presence ofnational guidelines or better institutional policymandates physicians adhere to such guide-lines or policies. These guidelines and policiesare medico-legally and ethically binding. There-fore, it was decided by the authors to providea simple, single-page algorithm for appropriateselection of antiemetic prophylaxis. Cost of anti-emetic regimens was also factored in the algo-rithm. The algorithm was drafted by the authors(V.P. and K.P.) and was debated by the othermembers before a final algorithm was drafted(Fig 2). The algorithm is primarily for centers thatdo not have institutional antiemetic guidelines. Asper our survey, 50% (33 centers) of respondingcenters belong to this category. In addition, thealgorithm can be an effective supplement even forthose centers where the antiemetic guidelines donot have recommendations for all situations asoutlined in the algorithm. We plan to design com-prehensive antiemetic guidelines for the Indiansubcontinent in partnership with such Indian on-cology associations as ICON and ISMPO.
Minimal
None
LowHigh
Yes No
Yes No
Can afford NK-1 antagonist?
Day 1: Dexa 12 mg IV/oral orgranisetron 1 mg IV/oral orondansetron 8 mg IV/oralor metoclopramide 10 mg IV/oral
Emetogenic Potential
Moderate
Day 1: Inj dexa 12 mg IV plus NK-1antagonist* plus inj 5HT3antagonist†Days 2-4: NK-1 antagonist* days 2and 3 plus dexa 8 mg IV/oral day
Day 1: Inj dexa 20 mg IV plusolanzapine 10 mg oral plus injpalonosetron 0.25 mg
Days 2-4: Olanzapine 10 mg oral
Can afford NK-1 antagonist?
Day 1: Inj dexa 12 mg IV plus NK-1antagonist* plus inj 5HT3antagonist†
Days 2-3: NK-1 antagonist*
Day 1: Inj dexa 12 mg IV plus inj5HT3 antagonist†
Days 2-3: dexa 8 mg oral or 5HT3antagonist†
Fig 2. Evidence-basedalgorithm for quickselection of appropriateantiemetic regimen. (*)NK-1 antagonist schedule:aprepitant 125 mg day 1and 80 mg days 2 and 3orally or fosaprepitant 150mg IV day 1 only. (†) 5HT3antagonist: granisetron 1mg IV/oral or ondansetron 8mg IV/oral or palonosetron0.25 mg IV day 1 only.Emetogenic potential:High: AC/EC, carmustine(. 250 mg/m2),cisplatin (any dose),cyclophosphamide(. 1.5 g/m2), dacarbazine,doxorubicin (> 60 mg/m2),epirubicin (. 90 mg/m2),ifosfamide (> 2 g /m2),mechlorethamine.Moderate (NK-1 antagonistpreferred): carboplatin,carmustine (< 250mg/m2),dactinomycin,daunorubicin, doxorubicin(, 60 mg/m2), epirubicin(< 90 mg/m2), ifosfamide(, 2 g /m2), irinotecan,methotrexate(> 250 mg/m2). Moderate:cyclophosphamide(< 1.5 g/m2), IFN-alpha(> 10 million U/m2),oxaliplatin, temozolomide.Low: carfilzomib, liposomaldoxorubicin, etoposide,eribulin, FU, floxuridine,gemcitabine, INF-alpfa (. 5to . 10 million units/m2),
351 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

In conclusion, awareness regarding the ASCOantiemetic clinical guidelines is satisfactory inIndian oncology practices; however, there is a needfor further sensitization of oncologists towardcomplete implementation of the guidelines in their
clinical practice. Developing national guidelinesthat are specific for India may help in the stan-dardization of antiemetic regimens.
DOI: https://doi.org/10.1200/JGO.2016.006023Published online on jgo.org on November 9, 2016.
AUTHOR CONTRIBUTIONS
Conception and design: Vijay Patil, Kumar PrabhashProvision of study materials or patients: Vijay Patil, K. GovindaBabuCollection and assembly of data: Vijay Patil, Vanita Noronha,Sunny Jandyal, Vamshi Muddu, Nilesh Lokeshwar, SachinHingmire, Nikhil Ghadyalpatil, Shripad BanavaliData analysis and interpretation:Vijay Patil, Amit Joshi, PurvishParikh, Atanu Bhattacharjee, Santam Chakraborty, AnantRamaswamy, K. Govinda Babu, Kumar PrabhashManuscript writing: All authorsFinal approval of manuscript: All authorsAccountable for all aspects of the work: All authors
AUTHORS’ DISCLOSURES OFPOTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided byauthors of this manuscript. All relationships are consideredcompensated. Relationships are self-held unless noted. I =Immediate Family Member, Inst = My Institution. Relation-ships may not relate to the subject matter of this manuscript.For more information about ASCO’s conflict of interest policy,please refer to www.asco.org/rwc or ascopubs.org/jco/site/ifc.
Vijay PatilNo relationship to disclose
Vanita NoronhaNo relationship to disclose
Amit JoshiNo relationship to disclose
Purvish ParikhNo relationship to disclose
Atanu BhattacharjeeNo relationship to disclose
Santam ChakrabortyNo relationship to disclose
Sunny JandyalNo relationship to disclose
Vamshi MudduNo relationship to disclose
Anant RamaswamyNo relationship to disclose
K. Govinda BabuNo relationship to disclose
Nilesh LokeshwarConsulting or Advisory Role: Bristol-Myers Squibb, Eisai,Dr. Reddy’s LaboratoriesTravel, Accommodations, Expenses: Dr. Reddy’s Laboratories
Sachin HingmireNo relationship to disclose
Nikhil GhadyalpatilNo relationship to disclose
Shripad BanavaliNo relationship to disclose
Kumar PrabhashNo relationship to disclose
Affiliations
Vijay Patil, Vanita Noronha, Amit Joshi, Santam Chakraborty, Sunny Jandyal, Anant Ramaswamy, Shripad Banavali, and KumarPrabhash, Tata Memorial Hospital; Purvish Parikh, Asian Institute of Oncology at Somaiya Ayurvihar: Cancer Care; NileshLokeshwar, Global Hospital, Mumbai; Atanu Bhattacharjee, Chiltern International; K. Govinda Babu, Kidwai Memorial Institute ofOncology, Bangalore; Vamshi Muddu, Apollo Hospital; Nikhil Ghadyalpatil, Yashoda Hospital, Hyderabad; and Sachin Hingmire,Deenanath Mangeshkar Hospital and Research Center, Pune, India.
REFERENCES1. Hesketh PJ: Chemotherapy-induced nausea and vomiting. N Engl J Med 358:2482-2494, 2008
2. Pirri C, Bayliss E, Trotter J, et al: Nausea still the poor relation in antiemetic therapy? The impact on cancer patients’quality of life and psychological adjustment of nausea, vomiting and appetite loss, individually and concurrently as partof a symptom cluster. Support Care Cancer 21:735-748, 2013
3. Bloechl-DaumB, Deuson RR, Mavros P, et al: Delayed nausea and vomiting continue to reduce patients’ quality of lifeafter highly and moderately emetogenic chemotherapy despite antiemetic treatment. J Clin Oncol 24:4472-4478,2006
4. Perwitasari DA, Atthobari J, MustofaM, et al: Impact of chemotherapy-induced nausea and vomiting on quality of life inIndonesian patients with gynecologic cancer. Int J Gynecol Cancer 22:139-145, 2012
ixabepilone, methotrexate(. 50 to , 250 mg/m2),mitomycin, mitoxantrone,pemetrexed, topotecan,taxanes. Minimal:bevacizumab, bleomycin,cetuximab, methotrexate(< 50 mg/m2), nivolumab,panitumumab,pertuzumab, ramucirumab,temsirolimus, trastuzumab,vinca alkaloids. dexa,dexamethasone; FU,fluorouracil; IFN, interferon;inj, injection; IV,intravenous; NK-1,neurokinin-1; PO, orally.
352 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

5. Moore S, Tumeh J, Wojtanowski S, et al: Cost-effectiveness of aprepitant for the prevention of chemotherapy-inducednausea and vomiting associated with highly emetogenic chemotherapy. Value Health 10:23-31, 2007
6. Humphreys S, Pellissier J, Jones A: Cost-effectiveness of an aprepitant regimen for prevention of chemotherapy-induced nausea and vomiting in patients with breast cancer in the UK. Cancer Manag Res 5:215-224, 2013
7. Ihbe-Heffinger A, Ehlken B, Bernard R, et al: The impact of delayed chemotherapy-induced nausea and vomiting onpatients, health resource utilization and costs in German cancer centers. Ann Oncol 15:526-536, 2004
8. Aseeri M, Mukhtar A, Al Khansa S, et al: A retrospective review of antiemetic use for chemotherapy-inducednausea and vomiting in pediatric oncology patients at a tertiary care center. J Oncol Pharm Pract 19:138-144,2013
9. Parikh PM, Charak BS, Banavali SD, et al: A prospective, randomized double-blind trial comparing metoclopramidealone with metoclopramide plus dexamethasone in preventing emesis induced by high-dose cisplatin. Cancer 62:2263-2266, 1988
10. Parikh PM, Shah SR, Shah SC, et al: Preliminary experience with use of a selective 5HT3 receptor antagonist(ondansetron) to prevent high dose chemotherapy induced emesis. Indian J Cancer 33:17-20, 1996
11. Basch E, Prestrud AA, Hesketh PJ, et al: Antiemetics: American Society of Clinical Oncology clinical practice guidelineupdate. J Clin Oncol 29:4189-4198, 2011 [Erattum: J Clin Oncol 32:2117, 2014]
12. Roila F, Herrstedt J, Aapro M, et al: Guideline update for MASCC and ESMO in the prevention of chemotherapy- andradiotherapy-induced nausea and vomiting: Results of the Perugia consensus conference. Ann Oncol 21:v232-v243,2010 (suppl 5)
13. Aapro M, Molassiotis A, Dicato M, et al: The effect of guideline-consistent antiemetic therapy on chemotherapy-induced nausea and vomiting (CINV): The Pan European Emesis Registry (PEER). Ann Oncol 23:1986-1992,2012
14. Gilmore JW, Peacock NW, Gu A, et al: Antiemetic guideline consistency and incidence of chemotherapy-inducednausea and vomiting in US community oncology practice: INSPIRE Study. J Oncol Pract 10:68-74, 2014
15. Caracuel F, Mu~noz N, Ba~nos U, et al: Adherence to antiemetic guidelines and control of chemotherapy-inducednausea and vomiting (CINV) in a large hospital. J Oncol Pharm Pract 21:163-169, 2015
16. Fujii H, IiharaH, IshiharaM, et al: Improvement of adherence to guidelines for antiemeticmedication enhances emeticcontrol in patients with colorectal cancer receiving chemotherapy of moderate emetic risk. Anticancer Res 33:5549-5556, 2013
17. Patil VM, Chakraborty S, Bhattacharjee A, et al: Survey of the state of implementation of the American Society ofClinical Oncology/Oncology Nursing Society Safety Standards for chemotherapy administration in India. J Oncol Pract11:365-369, 2015
18. Sirohi B: Cancer care delivery in India at the grassroot level: Improve outcomes. Indian J Med Paediatr Oncol 35:187-191, 2014
19. Akscin J, Barr TR, Towle EL: Benchmarking practice operations: Results from a survey of office-based oncologypractices. J Oncol Pract 3:9, 2007
20. Towle EL, Barr TR, Senese JL: The National Practice Benchmark for Oncology, 2013 report on 2012 data. J OncolPract 9:20s-38s, 2013
21. Barr TR, Towle EL: National oncology practice benchmark: An annual assessment of financial and operationalparameters-2010 report on 2009 data. J Oncol Pract 7:2s-15s, 2011 (suppl 2)
22. Noronha V, Tsomo U, Jamshed A, et al: A fresh look at oncology facts on south central Asia and SAARC countries.South Asian J Cancer 1:1-4, 2012
23. Van Laar ES, Desai JM, Jatoi A: Professional educational needs for chemotherapy-induced nausea and vomiting(CINV): Multinational survey results from 2388 health care providers. Support Care Cancer 23:151-157, 2015
24. Molassiotis A, Brearley SG, Stamataki Z: Use of antiemetics in the management of chemotherapy-related nausea andvomiting in current UK practice. Support Care Cancer 19:949-956, 2011
25. Yu S, Burke TA, Chan A, et al: Antiemetic therapy in Asia Pacific countries for patients receivingmoderately and highlyemetogenic chemotherapy–A descriptive analysis of practice patterns, antiemetic quality of care, and use of anti-emetic guidelines. Support Care Cancer 23:273-282, 2015
26. Almazrou S, Alnaim L: Evaluation of adherence to chemotherapy-induced nausea and vomiting guidelines. Anobservational study. J Cancer Ther 3:613-620, 2012
27. Hesketh PJ, Aapro M, Street JC, et al: Evaluation of risk factors predictive of nausea and vomiting with currentstandard-of-care antiemetic treatment: Analysis of two phase III trials of aprepitant in patients. Support Care Cancer18:1171-1177, 2010
28. Warr DG, Street JC, Carides AD: Evaluation of risk factors predictive of nausea and vomiting with current standard-of-care antiemetic treatment: Analysis of phase 3 trial of aprepitant in patients receiving adriamycin-cyclophosphamide-based chemotherapy. Support Care Cancer 19:807-813, 2011
353 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

29. Reference deleted.
30. Reference deleted.
31. Reference deleted.
APPENDIX
Table A1. Response to B1 Domain of Survey
Domain B1 Question (n = 66)
Response
Always Usually Rarely Never
Do you routinely use aprepitant or fosaprepitant,unless contraindicated, for highly emetogenicantineoplastic agents?
33 (50.0) 25 (37.9) 7 (10.6) 1 (1.5)
Correct response: 58 (87.9) Incorrect response: 8 (12.1)
Do you routinely use olanzapine, unlesscontraindicated, for highly emetogenicantineoplastic agents if aprepitant orfosaprepitant is not used?
3 (4.5) 6 (9.1) 31 (47.0) 26 (39.4)
Correct response: 9 (13.6) Incorrect response: 57 (86.4)
Do you routinely administer 5HT3 antagonist(for example, ondansetron or granisetron),unless contraindicated, for highly emetogenicantineoplastic agents?
59 (89.4) 6 (9.1) 0 1 (1.5)
Correct response: 65 (98.5) Incorrect response: 1 (1.5)
Do you routinely administer dexamethasone,unless contraindicated, for highly emetogenicantineoplastic agents?
57 (86.4) 8 (12.1) 0 1 (1.5)
Correct response: 65 (98.5) Incorrect response: 1 (1.5)
Do you prescribe 5HT3 antagonist on days 2 and3 of single day chemotherapy regimen of highemetogenic potential?
37 (56.1) 16 (24.2) 5 (7.6) 8 (12.1)
Incorrect response: 53 (80.3) Correct response: 13 (19.7)
Do you prescribe dexamethasone on days 2 and3 of single day chemotherapy regimen of highemetogenic potential?
22 (33.3) 22 (33.3) 18 (27.3) 4 (6.1)
Correct response: 44 (66.7) Incorrect response:22 (33.3)
NOTE. Data are given as No. (%). The actual responses are shown and, in addition, the scoring of responses as correct and incorrect inaccordance with guidelines is also shown.
354 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Table A2. Response to B2 Domain of Survey
Domain B2 Question (n = 38)
Response
Always Usually Rarely Never
Do you routinely use aprepitant orfosaprepitant, unless contraindicated, formoderately emetogenic antineoplasticagents?
32 (84.2) 6 (16.8) NA NA
Correct response: 38 (100) Incorrect response: NA
Do you routinely administer 5HT3antagonist(for example, ondansetron or granisetron),unless contraindicated, for moderatelyemetogenic antineoplastic agents?
30 (78.9) 8 (21.1) 0 (0) 0 (0)
Correct response: 38 (100) Incorrect response: 0 (0)
Doyou routinelyadministerdexamethasone,unless contraindicated, for moderatelyemetogenic antineoplastic agents?
25 (65.8) 11 (28.9) 2 (5.3) 0 (0)
Correct response: 36 (94.7) Incorrect response: 2 (5.3)
Do you prescribe 5HT3 antagonist on days 2and 3 of single day chemotherapyregimen of moderately emetogenicpotential?
12 (31.6) 15 (39.5) 7 (18.4) 4 (10.5)
Incorrect response: 27 (71.1) Correct response: 11 (28.9)
Do you prescribe dexamethasone on days 2and 3 of single day chemotherapyregimen of moderately emetogenicpotential?
3 (7.9) 13 (34.2) 17 (44.7) 5 (13.2)
Incorrect response: 16 (42.1) Correct response: 22 (57.9)
NOTE. Data are given as No. (%). Table shows data regarding those centers who routinely administer NK-1 receptor antagonist in routinepractice. The actual responses are shown, as is the scoring of responses as correct and incorrect in accordance with guidelines.Abbreviation: NA, not applicable, as only centers that routinely administer NK-1 receptor antagonist are selected.
355 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Table A3. Response to B2 Domain of Survey
Domain B2 Question (n = 28)
Response
Always Usually Rarely Never
Do you routinely use aprepitant orfosaprepitant, unless contraindicated, formoderately emetogenic antineoplasticagents?
NA NA 5 (17.9) 23 (82.1)
Incorrect response: NA Correct response: 28 (100)
Do you routinely administer 5HT3antagonist(for example, ondansetron or granisetron),unless contraindicated, for moderatelyemetogenic antineoplastic agents?
22 (78.6) 6 (21.4) 0 (0) 0 (0)
Correct response: 28 (100) Incorrect response: 0 (0)
Doyou routinelyadministerdexamethasone,unless contraindicated, for moderatelyemetogenic antineoplastic agents?
15 (53.6) 09 (32.1) 3 (10.7) 1 (3.6)
Correct response: 24 (85.7) Incorrect response: 4 (14.3)
Do you prescribe 5HT3 antagonist on days 2and 3 of single day chemotherapyregimen of moderately emetogenicpotential?
5 (17.9) 11 (39.3) 6 (21.4) 6 (21.4)
Incorrect response: 16 (57.1) Correct response: 12 (42.9)
Do you prescribe dexamethasone on days 2and 3 of single day chemotherapyregimen of moderately emetogenicpotential?
3 (10.7) 6 (21.4) 13 (46.5) 6 (21.4)
Correct response: 9 (32.1) Incorrect response: 19 (67.9)
NOTE. Data are given as No. (%). The table shows data regarding those centers that do not routinely administer NK-1 receptor antagonist inroutine practice. The actual responses are shown as is the scoring of responses as correct and incorrect in accordance with guidelines.Abbreviation: NA, not applicable as only centers that routinely do not administer NK-1 receptor antagonist are selected.
Table A4. Guideline Implementation Rate in B2 Domain
Domain
Implementation
Complete(score > 90%)
Partial(score 50%-90%)
No Implementation(score 0%-49.9%)
B2 domain (with NK-1 receptor antagonist;n = 38)
10 (26.3) 28 (73.7) 0 (0)
B2 domain (without NK-1 receptorantagonist; n = 28)
1 (3.6) 25 (89.3) 2 (7.1)
B2 domain (total; n = 66) 11 (16.7) 53 (80.3) 2 (3.0)
NOTE. Data are given as No. (%).
Table A5. Choice of 5HT-3 Antagonist in B2 Domain
Choice of 5HT-3 Antagonist No. (%)
Ondansetron 19 (28.8)
Granisetron 18 (27.3)
Palonosetron 29 (43.9)
356 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Table A6. Response to B3 Domain of Survey
Domain B3 Question (n = 66)
Response
Dexamethasone 5HT3 Antagonist Domperidone Aprepitant or Fosaprepitant None
Optimal antiemetic regimen to preventnauseaandvomiting from lowemetogenicantineoplastic agents
12 (18.2) 41 (62.1) 7 (10.6) 0 6 (9.1)
Correct response: 60 (90.9) Incorrect response: 6 (9.1)
Optimal antiemetic regimen to preventnausea and vomiting from minimalemetogenic antineoplastic agents
6 (9.1) 17 (25.8) 15 (22.7) 0 28 (42.4)
Incorrect response: 38 (57.6) Correct response: 28 (42.4)
NOTE. Data are given as No. (%).
Table A7. Factors That Hamper Implementation of ASCO Guidelines in Routine Chemotherapy Practice
Factors That Hamper Implementation of ASCO Antiemetic Policy (n = 66)*
Lack of administrative support 10 (15.2)
Lack of sensitization 26 (39.4)
Lack of national guidelines 12 (18.2)
Lack of consensus among practitioners 1 (01.5)
Practicing other international or institutional guidelines 5 (07.6)
Funding constraints 11 (16.7)
High number of patients 8 (12.1)
NOTE. Data are given as No. (%).*Participants would choose more than a single option in response to this question and, hence, the total of responses is more than 66.
Table A8. Impact of Various Factors on Center Ability to Implement Standards for High Emetogenic Prophylaxis
Variable Mean P
Location
Urban 58.33 .327
Rural 64.72
Source of funding
Government (public) 66.09 .343
Private 62.61
Teaching institute
Yes 63.49 .660
No 64.44
Dedicated cancer center
Yes 63.94 .679
No 65.15
Patient load (daily patients seen per physician)
< 40 62.60 .563
. 40 66.67
357 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Table A9. Impact of Various Factors on Center Ability to Implement Standards for Moderate Emetogenic Prophylaxis
Variable Mean P
Location
Urban 70.67 .246
Rural 80.83
Source of funding
Government (public) 71.55 .835
Private 71.62
Teaching institute
Yes 69.56 .221
No 75.95
Dedicated cancer center
Yes 71.73 .867
No 70.91
Patient load (daily patients seen per physician)
< 40 72.80 .958
. 40 69.60
Table A10. Impact of Various Factors on Center Ability to Implement Standards for Low and Minimal EmetogenicProphylaxis
Variable Mean P
Location
Urban 65.00 .305
Rural 83.33
Source of funding
Government (public) 74.13 .157
Private 60.81
Teaching institute
Yes 70.00 .161
No 59.52
Dedicated cancer center
Yes 68.18 .334
No 59.09
Patient load (daily patients seen per physician)
< 40 68.29 .112
. 40 64.00
358 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Table A11. Factors That Prompt a Modification in the Prophylactic Antiemetic Regimen or Its Doses in Chemotherapy Practice
Situation
Factor
AgeUncontrolledComorbidities
Moderate RenalDysfunction
Child PughB Liver Dysfunction QTc Prolongation No Knowledge
Modification of antiemetic regimen 25 (37.9) 36 (54.5) 21 (31.8) 18 (27.3) 34 (51.5) 8 (12.1)
Modification in doses of antiemeticagents regimen
22 (33.3) 36 (54.5) 27 (40.9) 23 (34.8) 29 (43.9) 9 (13.6)
NOTE. Data are given as No. (%). The participants would choose more than a single option in response to this question and hence the total of responses are more than 66.Abbreviation: QTc, corrected QT interval.
Table A12. Responses of Participants in Special Situations
Special Situation No. (%)
Multiday chemotherapy, the optimal treatment of nausea and vomiting includes (n = 66)*
Start antiemetics 1 day before 21 (31.8)
Each day antiemetics are selected on the basis of the emetogenic risk class ofchemotherapy administered
49 (74.2)
Continue antiemetic for 2 days after chemotherapy is over 42 (63.6)
For chemoradiation, the selection of antiemetics takes into account which factors (n = 64)†
Risk of emesis with radiation 1 (01.6)
Risk of emesis with chemotherapy 10 (15.6)
Both 53 (82.8)
Emetogenic potential regimen used while using concurrent weekly cisplatin (30-40 mg/m2)with radiation (n = 64)†
High 34 (53.1)
Moderate 30 (46.9)
*Participants would choose more than a single option in response to this question and hence the total of responses are more than 66.†Two participants did not respond to chemoradiation-related survey items, hence the number is 64.
359 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
originalreport
Positive PD-L1 Expression PredictsWorse Outcome in CutaneousAngiosarcoma
abstract
Purpose Programmed death-1 (PD-1) or programmed death ligand-1 (PD-L1) targeted therapies haveshown promising survival outcomes in several human neoplasms. However, it is unclear whether theexpression of PD-L1 can be correlated to any clinical and pathologic variables in patients with cutaneousangiosarcoma (CA). The aim of this study was to evaluate the clinicopathological significance of PD-L1expression in CA patients.
Materials and Methods Data from 52 patients with CA were retrospectively reviewed. PD-L1 expression,tumor proliferation determined by Ki-67 index, and immunohistochemical evaluation of tumor-infiltrating lymphocytes, CD4+ and CD8+, were used to determine correlation with clinicopathologicalvariables.
Results PD-L1 was positively expressed in 40% of all patients. PD-L1 expression was significantly as-sociated with tumor cell proliferation. Multivariate analysis confirmed that high levels of CD8+ tumor-infiltrating lymphocytes were a significant predictor in patients with clinical stage I CA and the positiveexpression of PD-L1 was an independent prognostic factor in predicting worse outcome.
Conclusion PD-L1 expression is a novel pathologic marker for predicting worse outcome in patients with CA.
J Glob Oncol 3. © 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
INTRODUCTION
Angiosarcoma is an extremely rare neoplasm thataccounts for less than 2% of all soft tissue sarco-mas.1Cutaneous angiosarcoma (CA) is an aggres-sive neoplasm arising from vascular or lymphaticendothelial cells and has a dismal outcome. The5-yearoverall survival rateofCAhasbeen reported torange from10%to30%.2,3AlthoughCAcanoccuranywhere in the body, it is frequently localized tothe head and neck regions. It has been challeng-ing todetermine the etiological factors for CAof theface and scalp because it affects a small per-centage of the population. In Japan, a combinedapproach with chemotherapy and radiotherapyhas been preferred as the first-line treatment ofCA, insteadof surgical resection.However, there isno established biomarker to predict the prognosisof CA in affected patients. Therefore, the need fora biomarker to define patients selected for surgeryshould be warranted.
Studies have reported the importance of tumor-infiltrating lymphocytes (TILs) in determining pa-tient outcomes in angiosarcoma.4-6Recently, Fujiiet al4 demonstrated that high levels of CD8+ TILs
are closely correlated with an improved prognosisand a longer disease-free period of distant metas-tases in patients with CA, suggesting that immu-notherapy using TILs could be a novel treatmentapproach for angiosarcoma.4 Recent clinical trialstargeting programmed death-1 (PD-1) or pro-grammed death ligand-1 (PD-L1) have exhibited apromising survival outcome in patients with cancerssuch as lung cancer and malignant melanoma.PD-L1 belongs to the B7 superfamily that down-regulates T-cell activation through the PD-1 recep-tor and has a negative effect on the immuneresponse.7-9 Although there are several studies onthe expression of PD-L1 and its prognostic signifi-cance in different human neoplasms, the clinico-pathological significance of PD-L1 expression in softtissue sarcomas is not well understood. Kim et al10
reported that PD-1-positive TILs and PD-L1 expres-sion were significantly correlated with the progres-sion and poor survival outcomes in soft tissuesarcomas. In their study, the positive expression ofPD-L1 after surgical resection was closely relatedto poor prognosis in various soft tissue sarcomas.However, less than 5% of patients in the study hadangiosarcoma and 80% of samples from those
Akira Shimizu
Kyoichi Kaira
Yuko Okubo
Daisuke Utsumi
Masahito Yasuda
Takayuki Asao
Masahiko Nishiyama
Kenzo Takahashi
Osamu Ishikawa
Akira Shimizu, KyoichiKaira, Masahito Yasuda,Takayuki Asao, MasahikoNishiyama, and OsamuIshikawa, GunmaUniversity GraduateSchool of Medicine,Maebashi, Gunma; andYuko Okubo, DaisukeUtsumi, and KenzoTakahashi, GraduateSchool of Medicine,University of the Ryukyus,Nishihara, Okinawa,Japan.A.S., K.K., and Y.O.contributed equally to thiswork. A.S. is alsoa corresponding author forthis work.
Corresponding author:Kyoichi Kaira, MD, PhD,Department of OncologyClinical Development,Gunma UniversityGraduate School ofMedicine, Showa-machi,Maebashi, Gunma,371-8511, Japan; e-mail:[email protected].
360 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
© 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License

patients exhibited positive PD-L1 staining. There-fore, prognostic significance of PD-L1 expressionin patients with angiosarcoma could not be clearlydetermined. Shen et al11 found that PD-L1 expres-sion positively correlated with TILs in osteosarcomaand thus could be a promising immunotherapeuticapproach to treat thedisease.Whenconsidering thepossible clinical importance of immune checkpointinhibitors targeting PD-L1/PD-1 in a disease associ-ated with poor outcomes, further studies on PD-L1expression can help understand its potential immu-notherapeutic and prognostic roles in treating CA.On thebasis of the clinical and therapeutic evidencethat correlates PD-L1 expression to predicting out-comes in other human neoplasms, we conductedthe current study to evaluate the clinicopathologicalsignificance of PD-L1 expression and TILs in CA.
MATERIALS AND METHODS
Patients
We identified and retrospectively examined 52consecutive patients who were positively diag-nosed with CA at the Gunma University and Uni-versity of the Ryukyus hospitals between October1987 and September 2014. We obtained 52paraffin-embedded tissue samples (from biopsyor surgical resection) and patient medical recordsfrom the two hospitals. This study was approvedby the institutional review board of Gunma Uni-versity and the ethical committee for clinical stud-ies at University of the Ryukyus. The approachused for the evaluation and resection of thesetumors has been described previously.4
There is no established method to clinically clas-sify tumor stages in CA. Therefore, as describedpreviously, we tentatively classified patients withCA into three stages: stage I for those with cuta-neous tumors, stage II for those with lymph nodemetastases, and stage III for those with distantmetastases, on the basis of the clinical evaluationbefore treatment.4
Immunohistochemical Staining
For PD-L1 and Ki-67, immunohistochemical stain-ing was performed according to the proceduresdescribed in previous studies.12,13 Rabbit mono-clonal antibodies against PD-L1 (1:100 dilution;Abcam, Cambridge, MA) and Ki-67 (1:40 dilution;Dako, Glostrup, Denmark) were used. The expres-sion of PD-L1 was considered positive whenmem-brane staining was observed. A semiquantitativescoring method was used for PD-L1: 1, 0% to 5%;2, 5% to 10%; 3, 10% to 25%; and 4, . 25% ofcells were positive. Tumors with score . 2 weregraded as positive.
Ahighly cell-rich area of the immunostained tissuesections was evaluated for Ki-67. Approximately1,000 nuclei were counted on each slide. Pro-liferative activity was assessed as the percentage ofKi-67-stained nuclei (Ki-67 labeling index) in thesample. The median value of the Ki-67 labelingindex was evaluated, and tumor cells with valuesgreater than the median value were defined ascells with high expression. Immunohistochemicalstaining was done for CD4+ (1:40 dilution; Dako)and CD8+ (1:200 dilution; Abcam) TILs in thetumor specimens. After evaluating the specimensentirely, the number of CD4+ and CD8+ TILs werecounted in the selected hot spot in a 3400 mag-nified field (0.26 mm2 field area). We determinedthe median number of CD4+ and CD8+ TILs asthe cutoff point for CD4+ and CD8+ TIL density.The tissue sections were examined in a blindedfashion by at least two of the authors, using lightmicroscopy.
Statistical Analyses
Probability values of,.05 indicated a statisticallysignificant difference as determined by Fisher’sexact test. The correlation between different vari-ables was analyzed using the nonparametricSpearman’s rank test. The Kaplan-Meier methodwas used to estimate survival as a function of time,and survival differences were analyzed by the log-rank test. Overall survival (OS) was determined asthe time elapsed from definite diagnosis to deathfrom any cause. Progression-free survival (PFS)was defined as the time elapsed between definitediagnosis and the disease progression or deathas a result of disease. Multivariate analyses wereperformed using a stepwise Cox proportional haz-ards model to identify independent prognosticfactors. Statistical analyses were performed usingGraphPad Prism 4 (Graph Pad Software, SanDiego, CA) and JMP 8 (SAS Institute, Cary, NC)for Windows.
RESULTS
Patient Demographics
Table 1 summarizes patient demographics ac-cording to the expression of PD-L1 in patients withCA. Themedian agewas 76 years (range, 57 to 91years). The primary site of the lesion was the scalpin 34 patients, face in 13, neck in four, and leg inone. Thirty-nine patients were classified as havingstage I disease, two as stage II, and 11 as stage III.Surgical resection had been done in 17 patients,radiotherapy in 45, and systemic chemotherapy in30. As a chemotherapeutic regimen, 26 patientswere treated with taxane agents including docetaxel
361 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

(n = 25). The median follow-up period was12.3 months (range: 1.6 to 92.1 months).
Immunohistochemical Analyses
Fifty-two primary lesions of CA were analyzed usingimmunohistochemical techniques. Figure 1 showsthe representative immunohistostained images ofPD-L1 expression (on the basis of a scoring scaleof 1 to 4) and CD4+ and CD8+ TILs. PD-L1
immunostaining was observed to be localizedpredominantly on the plasma membrane in theangiosarcoma cells. The rate of positive PD-L1 ex-pression was 40% (in 21 of 52 patients) and themean 6 SD score for PD-L1 was 1.8 6 0.8. Thepercentages of PD-L1 immunohistostains scoring1, 2, 3, and 4 were 60% (31 of 52), 15% (eight of52), 13% (seven of 52), and 12% (six of 52),respectively. On the basis of the analyses of CA
Table 1. Patients’ Demographics According to PD-L1 Expression
Variable
PD-L1 Expression
Patients, No.(N = 52) Positive (n = 21) Negative (n = 31) P
Age (years) .259
< 75 24 12 12
. 75 28 9 19
Sex . .999
Male 33 13 20
Female 19 8 11
Primary site . .999
Parietal 26 11 15
Nonparietal 26 10 16
Tumor size (mm) . .999
< 45 27 11 16
. 45 25 10 16
Clinical stage .747
1/2 39 15 24
3 13 6 7
Lymph node metastasis .549
Yes 32* 2 1
No 18* 17 30
Distant metastasis . .999
Yes 29* 4 6
No 22* 16 25
Ki-67 expression .025
High 26 15 11
Low 26 6 18
CD4 expression .781
High 24 9 15
Low 28 12 16
CD8 expression .403
High 24 8 16
Low 28 13 15
CD4+CD8 expression .582
High 25 9 16
Low 27 12 15
Abbreviation: PD-L1, programmed death ligand-1.*These variables lack data from some patients.
362 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
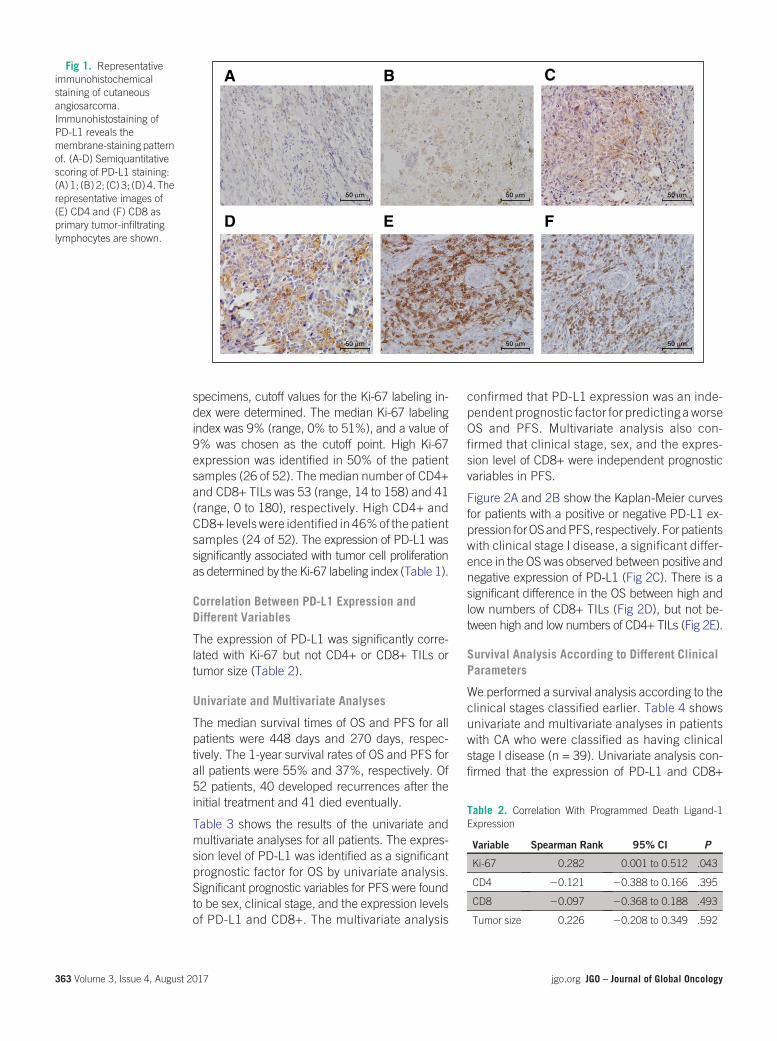
specimens, cutoff values for the Ki-67 labeling in-dex were determined. The median Ki-67 labelingindex was 9% (range, 0% to 51%), and a value of9% was chosen as the cutoff point. High Ki-67expression was identified in 50% of the patientsamples (26 of 52). The median number of CD4+and CD8+ TILs was 53 (range, 14 to 158) and 41(range, 0 to 180), respectively. High CD4+ andCD8+ levels were identified in 46%of the patientsamples (24 of 52). The expression of PD-L1 wassignificantly associated with tumor cell proliferationas determined by the Ki-67 labeling index (Table 1).
Correlation Between PD-L1 Expression andDifferent Variables
The expression of PD-L1 was significantly corre-lated with Ki-67 but not CD4+ or CD8+ TILs ortumor size (Table 2).
Univariate and Multivariate Analyses
The median survival times of OS and PFS for allpatients were 448 days and 270 days, respec-tively. The 1-year survival rates of OS and PFS forall patients were 55% and 37%, respectively. Of52 patients, 40 developed recurrences after theinitial treatment and 41 died eventually.
Table 3 shows the results of the univariate andmultivariate analyses for all patients. The expres-sion level of PD-L1 was identified as a significantprognostic factor for OS by univariate analysis.Significant prognostic variables for PFS were foundto be sex, clinical stage, and the expression levelsof PD-L1 and CD8+. The multivariate analysis
confirmed that PD-L1 expression was an inde-pendent prognostic factor for predicting aworseOS and PFS. Multivariate analysis also con-firmed that clinical stage, sex, and the expres-sion level of CD8+ were independent prognosticvariables in PFS.
Figure 2A and 2B show the Kaplan-Meier curvesfor patients with a positive or negative PD-L1 ex-pression forOSandPFS, respectively. For patientswith clinical stage I disease, a significant differ-ence in the OS was observed between positive andnegative expression of PD-L1 (Fig 2C). There is asignificant difference in the OS between high andlow numbers of CD8+ TILs (Fig 2D), but not be-tween high and low numbers of CD4+ TILs (Fig 2E).
Survival Analysis According to Different ClinicalParameters
We performed a survival analysis according to theclinical stages classified earlier. Table 4 showsunivariate and multivariate analyses in patientswith CA who were classified as having clinicalstage I disease (n = 39). Univariate analysis con-firmed that the expression of PD-L1 and CD8+
A B C
D E F
50 µm
50 µm
50 µm
50 µm
50 µm
50 µm
Table 2. Correlation With Programmed Death Ligand-1Expression
Variable Spearman Rank 95% CI P
Ki-67 0.282 0.001 to 0.512 .043
CD4 20.121 20.388 to 0.166 .395
CD8 20.097 20.368 to 0.188 .493
Tumor size 0.226 20.208 to 0.349 .592
Fig 1. Representativeimmunohistochemicalstaining of cutaneousangiosarcoma.Immunohistostaining ofPD-L1 reveals themembrane-staining patternof. (A-D) Semiquantitativescoring of PD-L1 staining:(A) 1; (B) 2; (C) 3; (D) 4. Therepresentative images of(E) CD4 and (F) CD8 asprimary tumor-infiltratinglymphocytes are shown.
363 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

levels was a significant prognostic factor for OSand PFS. The expression of PD-L1 and CD8+levels was also found to be an independent pre-dictor for worse prognosis, by multivariate analy-sis. In patients with CA who were classified ashaving clinical stages II or III disease, no statisti-cally significant differences in the OS (P = .422)and PFS (P = .751) were observed between pa-tients with positive and negative PD-L1 expression.
Of the 29 patients who initially underwent chemo-therapy, 24 were administered docetaxel; five re-ceived other regimens. We performed the survivalanalysis of these 29 patients. No statistically sig-nificant difference was found in the OS (P = .095)and PFS (P = .102) between patients with positive
(median OS, 263 days; median PFS, 133 days)and negative (median OS, 676 days; median PFS,423 days) PD-L1 expression.
DISCUSSION
Immune checkpoint inhibitors targeting PD-1 orPD-L1 have been available to treat human neo-plasms, including malignant melanoma and lungcancer, in Japan and other countries. Severalstudies have focused on the prognostic signifi-cance of PD-L1 expression in certain cancers.13-18
The positive rate of PD-L1 expression was 50% inbreast cancer, 39.2% in pancreatic cancer,42.2% in gastric cancer, 25% in hepatocellularcarcinoma, 43.9% in esophageal cancer, and
Table 3. Univariate and Multivariate Survival Analysis in All Patients
Variable
Overall Survival Progression-Free Survival
Univariate Multivariate Univariate Multivariate
MST (days) P HR 95% CI P MST P HR 95% CI P
Age (years) 0.931 .567
< 75 347 123
. 75 495 328
Sex 0.356 1.136 0.782 to 1.706 .511 .011 1.602 1.060 to 2.581 .024
Male 356 165
Female 583 477
Primary site .123 .939
Parietal 347 200
Nonparietal 583 235
Tumor size (mm) .794 .577
< 45 495 321
. 45 387 165
Clinical stage .083 1.142 0.768 to 1.658 0.497 .001 1.745 1.191 to 2.510 .005
1/2 583 335
3 326 50
PD-L1 .002 1.638 1.138 to 2.362 .008 .014 1.593 1.117 to 2.281 .011
Positive 276 123
Negative 638 369
Ki-67 .112 .188
High 356 200
Low 583 264
CD4 .725 .231
High 448 235
Low 495 135
CD8 .135 1.231 0.892 to 1.725 0.208 .049 1.448 1.039 to 2.055 .028
High 482 321
Low 323 221
Abbreviations: HR, hazard ratio; MST, median survival time; PD-L1, programmed death ligand-1.
364 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Positive PD-L1 (n = 21)
Negative PD-L1 (n = 31)
0 1,000 2,000 3,000
10
20
30
40
50
60
70
80
90
100
OS (%
)P = .002
A
0 500 1,000 1,500 2,000
10
20
30
40
50
60
70
80
90
100Positive PD-L1 (n = 21)
Negative PD-L1 (n = 31)
P = .014
Time (days)Time (days)
PFS
(%)
B
0 1,000 2,000 3,000
10
20
30
40
50
60
70
80
90
100
P < .001
Time (days)
OS (%
)
Negative PD-L1 (n = 24)
Positive PD-L1 (n = 15)C
0 1,000 2,000 3,000
10
20
30
40
50
60
70
80
90
100
P = .043
P = .112
Time (days)
OS (%
)
Low CD8 (n = 21)
High CD8 (n = 18)D
0 1,000 2,000 3,000
10
20
30
40
50
60
70
80
90
100
P = .717
Time (days)
OS (%
)
Low CD4 (n = 19)
High CD4 (n = 20)
Low Ki-67 (n = 26)
High Ki-67 (n = 26)E F
0 1,000 2,000 3,000
10
20
30
40
50
60
70
80
90
100 Score, 1
Score, 2
Score, 3
Score, 4
Legend
Time (days)
OS (%
)
G
0 1,000 2,000 3,000
10
20
30
40
50
60
70
80
90
100
Time (days)
OS (%
)
365 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

66.3% in renal cell carcinoma.13-18PD-L1 expres-sion may predict worse outcomes in these carci-nomas. Another study also identified PD-L1expression as an independent indicator of poorprognosis in soft tissue sarcoma.10 In 105 patientswith soft tissue sarcoma, a positive PD-L1 expres-sion was seen in 65%, and PD-L1 expression wassignificantly associated with advanced clinicalstage, distant metastases, and advanced clinico-pathological variables.10 However, that study in-cluded only five patients with angiosarcoma, andit was unclear whether the increased expressionof PD-L1 could be a significant predictor for poorprognosis in patients with angiosarcoma as well.Recently, D’Angelo et al19 documented the clin-icopathological significance of TILs and PD-L1expression in 50 soft tissue sarcoma specimens:14 gastrointestinal stromal tumors, five synovialsarcomas, four leiomyosarcomas, three spindlecell sarcomas, three angiosarcomas, and 21 othercancers. They reported that the expression ofPD-L1 was not observed in three angiosarcomaspecimens without the description of primary site.They concluded that the expression of PD-L1 waslow in sarcoma, and there was no associationbetween PD-L1 expression and survival. In con-trast, our study revealed that the positive rate ofPD-L1 expression in CA was almost similar to thatin human epithelial tumors and was an indepen-dent prognostic factor for worse outcome. Be-cause PD-1/PD-L1 therapy has been recognizedto be effective in patients with advanced can-cers,20 it is clinically important to examine thePD-L1 expression in tumor tissues before PD-1/PD-L1 immunotherapy. In fact, 36% of patientswith positive PD-L1 tumors responded to anti-PD1immunotherapy, whereas patients with negativePD-L1 tumors did not.21
In the current study, we found the expressionlevel of PD-L1 to be closely correlated with tumorcell proliferation. A previous study also reporteda strong positive link between PD-L1 expressionand the cell proliferative Ki-67 marker in patientswith breast cancer.22 Fujii et al4 reported that nostatistically significant difference was presentbetween the prognosis and Ki-67 labeling indexof 30patientswithCA,which correspondswith ourresults indicating Ki-67 was not identified as aprognostic predictor. Although the Ki-67 indexclosely correlates with the expression level ofPD-L1, it remains unclear why the expressionlevel of Ki-67 was not significantly associated withthe prognosis of patients with CA. The small sam-ple size may have biased our results. Furtherinvestigation is required to confirm whether the
relationship between prognostic significance andKi-67 labeling index exists in CA.
Angiosarcoma is a rare disease and no effectivechemotherapeutic regimen has been established.Surgical resection or radiation therapy has beenconventionally recommended. Panel et al23 havedescribed that paclitaxel is an effective and well-tolerated regimen for patients with unresectableangiosarcoma, yielding an overall response ofapproximately 18% and median survival time of8 months. Moreover, Nagano et al24 reported thatsix of nine patients treated with docetaxel revealedgood response: complete responses in two pa-tients and partial response in four patients. Thus,docetaxel has been accepted as an effective che-motherapeutic agent against CA. In patients withadvanced CA, taxane-based agents have beenchosen for treatment. In our study, 26 patientswere treated with taxane regimens, includingdocetaxel (n =25) andpaclitaxel (n =1). However,we foundno significant difference in the prognosisafter systemic chemotherapy with respect to theexpression level of PD-L1. Further investigation isnecessary to understand the relationship betweenthe PD-L1 expression and the clinical effective-ness of chemotherapeutic agents.
One limitation of our study was a small samplesize. However, CA is an extremely rare sarcomaamong the Japanese and its frequency seems tobe different among races.25,26 We could not find asignificant difference in OS between patients withpositive and negative PD-L1 expression among the29 patients treated with chemotherapy. Of these29 patients, 21 had clinical stage I disease andeight had clinical stage III disease. Heterogenousgroups of different clinical stagesmay have biasedthe results of our survival data. Second, PD-L1antibodies were not same as those used in pre-vious immunohistochemical studies. We checkedseveral commercially available PD-L1 antibodiesto obtain clear staining. Finally, we have not car-ried out the experimental study using any inhib-itors targeting PD-L1. The inhibitors of PD-1/PD-L1 have been widely used for treating lungcancer, malignant melanoma, and other cancers,and these agents show a favorable survival out-come compared with the cytotoxic agents.27,28
Further studies to investigate the antitumor effectof PD-1/PD-L1 in vivo using the animal model ofCA would expand our understanding of PD-L1expression in angiosarcoma.
In conclusion, high expression levels of PD-L1in CA were identified as a significant predictorfor poor prognosis, especially in patients of the
Fig 2. Kaplan-Meiercurves for the patients witha positive or negativeexpression of programmeddeath ligand-1 (PD-L1). Asignificant difference in the(A) overall survival (OS) and(B) progression-freesurvival (PFS) wasrecognized with respectwith the expression of PD-L1 in all patients (N = 52).(C) In patients with clinicalstage I disease (n = 39),a significant difference inthe OS was observedbetween positive andnegative expression of PD-L1 and (D) between highand low numbers of CD8+TILs, (E) but not betweenhigh and low numbers ofCD4+ TILs. (F) Nostatistically significantdifference in the OS wasobserved between high andlow expression of Ki-67. (G)OS according to scoring ofPD-L1 expression.
366 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

clinical stage I disease, and could be an im-portant clinicopathological marker for choiceof treatments. Moreover, we confirmed highlevels of CD8+ TILs could also be a significantbiomarker for favorable outcome, as previously
described.4 The inhibition of PD-L1 functioncould be a novel therapeutic target for CA withhigh PD-L1 expression.
DOI: https://doi.org/10.1200/JGO.2016.005843Published online on jgo.org on October 5, 2016.
AUTHOR CONTRIBUTIONS
Conception anddesign:Akira Shimizu,Kyoichi Kaira, TakayukiAsao, Masahiko Nishiyama, Osamu Ishikawa
Financial support:Takayuki Asao,MasahikoNishiyama, KenzoTakahashi
Administrative support:AkiraShimizu,KyoichiKaira,MasahitoYasuda, Kenzo Takahashi, Osamu Ishikawa
Provision of study materials or patients: Yuko Okubo, DaisukeUtsumi, Kenzo Takahashi, Osamu Ishikawa
Collection and assembly of data:Akira Shimizu, Kyoichi Kaira, YukoOkubo, Daisuke Utsumi, Masahito Yasuda, Kenzo Takahashi
Data analysis and interpretation: Akira Shimizu, Kyoichi Kaira,Yuko Okubo, Osamu IshikawaManuscript writing: All authors
Final approval of manuscript: All authorsAccountable for all aspects of the work: All authors
AUTHORS’ DISCLOSURES OFPOTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided byauthors of this manuscript. All relationships are consideredcompensated. Relationships are self-held unless noted. I =Immediate Family Member, Inst = My Institution. Relation-ships may not relate to the subject matter of this manuscript.For more information about ASCO’s conflict of interest policy,please refer to www.asco.org/rwc or ascopubs.org/jco/site/ifc.
Akira ShimizuNo relationship to disclose
Table 4. Univariate and Multivariate Survival Analysis in Patients With Clinical Stage I Disease
Variable
Overall Survival Progression-Free Survival
Univariate Multivariate Univariate Multivariate
MST (days) P HR 95% CI P MST P HR 95% CI P
Age (years) .831 .571
< 75 335 161
. 75 617 355
Sex .315 0.725 0.450 to 1.096 .131 .011 0.457 0.255 to 0.742 , .001
Male 351 187
Female 618 1,141
Primary site .129 .705
Parietal 367 267
Nonparietal 610 352
Tumor size (mm) .675 .924
< 45 581 331
. 45 564 187
PD-L1 , .001 2.456 1.467 to 4.337 , .001 .013 1.758 1.123 to 2.805 .014
Positive 263 124
Negative 676 436
Ki-67 .265 .451
High 3,712 278
Low 618 361
CD4 .717 .395
High 448 321
Low 652 335
CD8 .043 1.511 1.019 to 2.327 .039 .024 1.632 1.064 to 2.607 .024
High 1,239 502
Low 387 200
Abbreviation: HR, hazard ratio; MST, median survival time; PD-L1, programmed death ligand-1.
367 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Kyoichi KairaNo relationship to disclose
Yuko OkuboNo relationship to disclose
Daisuke UtsumiNo relationship to disclose
Masahito YasudaNo relationship to disclose
Takayuki AsaoNo relationship to disclose
Masahiko NishiyamaResearch Funding: Yakult Honsha
Kenzo TakahashiNo relationship to disclose
Osamu IshikawaNo relationship to disclose
ACKNOWLEDGMENTWe thank Yuka Matsui (Gunma University), and AyakoNakamura and Ritsuko Tokumon (University of the Ryukyus)for their technical assistance during the manuscriptpreparation.Wealso thankTomokoOkada (GunmaUniversity)for her help in data collection and technical assistance, andDrs. Ryoko Awazawa, Takuya Miyagi, and Sayaka Yamaguchi(University of the Ryukyus) for their helpful guidance andassistance in data collection.
REFERENCES1. Goldblum JR, Folpe AL, Weiss SW: Malignant vascular tumors, in Weiss SW, Goldblum JR (eds), Enzinger andWeiss’s
Soft Tissue Tumors. Philadelphia, PA, Mosby Elsevier, 2008, pp 703-732.
2. Mendenhall WM, Mendenhall CM, Werning JW, et al: Cutaneous angiosarcoma. Am J Clin Oncol 29:524-528, 2006
3. Guadagnolo BA, Zagars GK, Araujo D, et al: Outcomes after definitive treatment for cutaneous angiosarcoma of theface and scalp. Head Neck 33:661-667, 2011
4. Fujii H, Arakawa A, Utsumi D, et al: CD8⁺ tumor-infiltrating lymphocytes at primary sites as a possible prognostic factorof cutaneous angiosarcoma. Int J Cancer 134:2393-2402, 2014
5. Maddox JC, Evans HL: Angiosarcoma of skin and soft tissue: A study of forty-four cases. Cancer 48:1907-1921, 1981
6. Zietz C, Rumpler U, Sturzl M, et al: Inverse relation of Fas-ligand and tumor-infiltrating lymphocytes in angiosarcoma:Indications of apoptotic tumor counterattack. Am J Pathol 159:963-970, 2001
7. Carter L, Fouser LA, Jussif J, et al: PD-1:PD-L inhibitory pathway affects both CD4(+) and CD8(+) T cells and isovercome by IL-2. Eur J Immunol 32:634-643, 2002
8. Liang SC, Latchman YE, Buhlmann JE, et al: Regulation of PD-1, PD-L1, and PD-L2 expression during normal andautoimmune responses. Eur J Immunol 33:2706-2716, 2003
9. Nishimura H, Honjo T: PD-1: An inhibitory immunoreceptor involved in peripheral tolerance. Trends Immunol 22:265-268, 2001
10. Kim JR, Moon YJ, Kwon KS, et al: Tumor infiltrating PD1-positive lymphocytes and the expression of PD-L1 predictpoor prognosis of soft tissue sarcomas. PLoS One 8:e82870, 2013
11. Shen JK, Cote GM, Choy E, et al: Programmed cell death ligand 1 expression in osteosarcoma. Cancer Immunol Res2:690-698, 2014
12. Kaira K, Endo M, Abe M, et al: Biologic correlation of 2-[18F]-fluoro-2-deoxy-D-glucose uptake on positron emissiontomography in thymic epithelial tumors. J Clin Oncol 28:3746-3753, 2010
13. Ghebeh H, Mohammed S, Al-Omair A, et al: The B7-H1 (PD-L1) T lymphocyte-inhibitory molecule is expressed inbreast cancer patients with infiltrating ductal carcinoma: Correlation with important high-risk prognostic factors.Neoplasia 8:190-198, 2006
14. Ohigashi Y, Sho M, Yamada Y, et al: Clinical significance of programmed death-1 ligand-1 and programmed death-1ligand-2 expression in human esophageal cancer. Clin Cancer Res 11:2947-2953, 2005
15. Nomi T, Sho M, Akahori T, et al: Clinical significance and therapeutic potential of the programmed death-1 ligand/programmed death-1 pathway in human pancreatic cancer. Clin Cancer Res 13:2151-2157, 2007
16. Wu C, Zhu Y, Jiang J, et al: Immunohistochemical localization of programmed death-1 ligand-1 (PD-L1) in gastriccarcinoma and its clinical significance. Acta Histochem 108:19-24, 2006
17. Nakanishi J, Wada Y, Matsumoto K, et al: Overexpression of B7-H1 (PD-L1) significantly associates with tumor gradeand postoperative prognosis in human urothelial cancers. Cancer Immunol Immunother 56:1173-1182, 2007
18. Thompson RH, Gillett MD, Cheville JC, et al: Costimulatory molecule B7-H1 in primary and metastatic clear cell renalcell carcinoma. Cancer 104:2084-2091, 2005
19. D’Angelo SP, Shoushtari AN, Agaram NP, et al: Prevalence of tumor-infiltrating lymphocytes and PD-L1 expression inthe soft tissue sarcoma microenvironment. Hum Pathol 46:357-365, 2015
20. Homet Moreno B, Ribas A: Anti-programmed cell death protein-1/ligand-1 therapy in different cancers. Br J Cancer112:1421-1427, 2015
368 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

21. Sznol M, Chen L: Antagonist antibodies to PD-1 and B7-H1 (PD-L1) in the treatment of advanced human cancer. ClinCancer Res 19:1021-1034, 2013
22. Ghebeh H, Tulbah A, Mohammed S, et al: Expression of B7-H1 in breast cancer patients is strongly associated withhigh proliferative Ki-67-expressing tumor cells. Int J Cancer 121:751-758, 2007
23. Panel N, Bui BH, Bay JO, et al: Phase II trial of weekly paclitaxel for unresectable angiosarcoma: The ANGIOTAX study.J Clin Oncol 26:269-272, 2008
24. Nagano T, Yamada Y, Ikeda T, et al: Docetaxel: A therapeutic option in the treatment of cutaneous angiosarcoma:Report of 9 patients. Cancer 110:648-651, 2007
25. Luke JJ, Keohan ML: Advances in the systemic treatment of cutaneous sarcomas. Semin Oncol 39:173-183, 2012
26. Sturgis EM, Potter BO: Sarcomas of the head and neck region. Curr Opin Oncol 15:239-252, 2003
27. Brahmer J, Reckamp KL, Baas P, et al: Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lungcancer. N Engl J Med 373:123-135, 2015
28. Wolchok JD, Kluger H, Callahan MK, et al: Nivolumab plus ipilimumab in advanced melanoma. N Engl J Med 369:122-133, 2013
369 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

originalreport
Comparison of Symptom Score andBronchoscopy-Based AssessmentWith Conventional ComputedTomography–Based Assessment ofResponse to Chemotherapy in LungCancer
abstract
Purpose There is a paucity of literature on symptom score (SS) plus fiberoptic bronchoscopy (FOB) –basedresponse evaluation (RE) to chemotherapy for lung cancer. This study aimed to compare the reliability of REby SS, chest radiograph (CXR), and FOB with computed tomography (CT) –based assessment (ResponseEvaluation Criteria in Solid Tumors (RECIST) and WHO criteria) for lung cancer chemotherapy.Methods This was a prospective observational study involving treatment-naıve patients with lung cancerplanned for chemotherapy, with one or more lesions on FOB and CT. Patients underwent assessment twiceby SS, CXR, FOB, and CT (at baseline and after chemotherapy). Six symptoms (dyspnea, cough, chest pain,hemoptysis, anorexia, and weight loss) were noted on visual analog scale. Respiratory symptom burden(RSB)and total symptomburden (TSB)werecalculated from the first four andall six symptoms, respectively,as the mean of individual SS. Bronchoscopic findings were recorded as per European Respiratory Societyclassification for tracheobronchial stenosis. Responseswereclassified as complete response (CR), partialresponse (PR), stable disease (SD), or progressive disease (PD) by each method. For FOB and SS, im-provement or worsening by ‡ 20% was taken as PR or PD, respectively, whereas < 20% change wasconsidered SD. Agreements were tested using Cohen’s k statistic.Results All individual SS, RSB, and TSB scores, and the number and distribution of FOB lesions improvedsignificantly after chemotherapy. Individually, CXR and SS had no or minimal agreement with FOB-basedand CT-based responses. RECIST andWHO criteria had strong agreement overall (Cohen’s k = 0.872) andperfect agreement for PD (Cohen’sk=1.000). Cohen’skvalues for FOB-basedassessmentwith RECISTandWHOwere0.324and0.349, respectively foroverall RE, and0.462and0.501 for differentiating responders(CRandPR) fromnonresponders (SDandPD), respectively. Cohen’skvalues for PDwere0.629 (FOBalone),0.672 (FOB and RSB), 0.739 (FOB and TSB), and 0.764 (FOB and CXR).Conclusion CT-based assessment should remain the reference for objective RE of chemotherapy in lungcancer. A combination of FOB and CXR may be used as a surrogate to diagnose PD if CT is not feasible.J Glob Oncol 3. © 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
INTRODUCTION
Computed tomography (CT) measurementsof primary tumor and/or metastatic sites arecommonly used for objective assessment ofresponse to chemotherapy by RECIST and/orWHO criteria.1,2 In clinical practice, symptomcontrol is also often an important considerationwhen making decisions regarding the contin-uation or discontinuation of chemotherapy.3
There is a paucity of published literature onsymptom- plus bronchoscopy-based decisionmaking for lung cancer. This study aimed tocompare the reliability of response evaluationby symptom, chest radiograph (CXR), andfiberoptic bronchoscopy (FOB) –based assess-ment with conventional CT-based assessmentfor patients with lung cancer undergoing chemo-therapy who had bronchoscopically-visible tumors.
Lakshimikant BaburaoYenge
Digambar Behera
Mandeep Garg
Ashutosh Nath Aggarwal
Navneet Singh
All authors: PostgraduateInstitute of MedicalEducation and Research,Chandigarh, India.
Corresponding author:Navneet Singh, MD, DM,Department of PulmonaryMedicine, PostgraduateInstitute of MedicalEducation and Research,Chandigarh-160012,India; e-mail:[email protected].
370 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
© 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License

METHODS
Patient Population and Treatment Details
Treatment-naıve patients with lung cancer whohad at least one evaluable lesion each on FOBandCT and who were planned for initiation of chemo-therapy were prospectively enrolled over a 1-yearperiod (January 2013 to January 2014) at theauthors’ institute—a tertiary care referral centerthat caters to the population of several states innorthern India. Informed consent was obtainedfrom all patients, and the study was approved bythe institutional ethics committee. At the authors’institute, all patients with lung cancer (after histo-logic and/or cytologic confirmation of diagnosis)are registered in the Lung Cancer Clinic. In thisspecial clinic, managed by the faculty (DB, ANA,NS) and residents of theDepartment of PulmonaryMedicine, patients receive medical oncologictreatment (including chemotherapy and/or tar-geted therapy) as indicated and are followed upsubsequent to treatment completion. The chemo-therapy regimens and normal management pro-tocols used at our center have been previouslydescribed in detail.4-8 In general, the standardchemotherapy regimen was a histology-guidedplatinum doublet with pemetrexed, docetaxel,and irinotecan being preferred nonplatinumagents for nonsquamous non–small-cell lungcancer, squamous cell carcinoma (SqCC), andsmall-cell lung cancer (SCLC) histologic types,respectively.
Tumors were classified histologically on the ba-sis of morphology and relevant immunochem-istry, as deemed appropriate, according to the
International Association for the Study of LungCancer, the American Thoracic Society, and theEuropean Respiratory Society classification of lungtumors.9 The seventh edition of the TNM classifi-cation,which is basedon tumor size andextension,lymph nodal involvement, and presence of distantmetastasis, was used for staging.10 Before chemo-therapy initiation, demographic characteristics,including age, sex, and Karnofsky and EasternCooperative Oncology Group performance status,histology, disease stage, and smoking status, werenoted for all patients.
Symptom and Response Assessment
Enrolled patients underwent assessment with SS,CXR, FOB, and CT scan of the thorax/upper ab-domen at baseline and reassessment by all ofthese modalities after the third cycle of chemo-therapy. Six symptoms (dyspnea, cough, chestpain, hemoptysis, anorexia, and weight loss) on avisual analog scale (VAS; 0 to 100 mm) werenoted. Respiratory symptom burden (RSB) andtotal symptomburden (TSB) were calculated fromthe first four and all six symptoms, respectively, asthe mean of individual SSs. The first author (LBY)was responsible for getting patients to record SSs,and he was blinded to the bronchoscopic andradiologic findings. Flexible bronchoscopy wasperformed under local anesthesia in the depart-ment of pulmonary medicine as per protocol de-scribed previously.11 Bronchoscopic findingswere recorded as per European Respiratory Soci-ety classification for tracheobronchial stenosis,from 0 (no stenosis) to 5 (. 90% obstruction).12
Video recordings of all bronchoscopies were
Underwentbronchoscopy for suspected
lung cancer (N = 317)
Excluded (n = 230)
No abnormalityon bronchoscopy (n = 56)
Did not complete diagnostic evaluation (n = 70)
Alternative diagnosis established (n = 12)
Baseline bronchoscopy video recording not available (n = 39)
Poor PS, unfit forchemotherapy (n = 53)
Completed baselineevaluation and consented
for participation in study (n = 87)
Did not completethree cycles ofchemotherapy (n = 34)
Died (n = 11)
Withdrewconsent (n = 4)
Lost tofollow-up (n = 9)
Poor PS (n = 12)Patients completed three
or more cycles of chemotherapy,and investigations for responseevaluation were included for
final analysis (n = 53)
Fig 1. Flow diagram asper Strengthening theReporting of ObservationalStudies in Epidemiology(STROBE) guidelinesillustrating the enrolment ofpatients in this study. PS,performance status.
371 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

preserved for objective review and graded inde-pendently by two authors (NSandANA),whowereblinded to SSs and radiologic findings, and anydisagreement was resolved subsequently by mu-tual discussion. In caseswithmore thanone lesionon bronchoscopy, the lesion with the highest de-gree of severity was used for scoring the severity oftracheobronchial stenosis. CXR responses wereassessed asperWHOcriteria.2 CT responseswereassessedusingbothWHOcriteria andRECIST1.1,1
with the latter being taken as reference standard.Patients were classified as having complete re-sponse (CR), partial response (PR), stable disease(SD), or progressive disease (PD) for each of thepreviouslymentionedmethods. In thecase of FOBfindings and SSs, an improvement and worseningby > 20% was arbitrarily taken as PR and PD,respectively, whereas a change of , 20% wasconsidered SD.
Statistical Analysis
DatawereanalyzedusingSPSSstatistical softwareversion 22.0 (SPSS, Chicago, IL). Descriptive dataare presented as mean (standard deviation), me-dian (interquartile range [IQR]), or percentages.Agreements between symptom, bronchoscopy,CXR, and CT response assessments were testedusing Cohen’s k statistics.13 Wilcoxon signed ranktest was used to compare changes in mean SSs(six individual symptoms, as well as RSB andTSB). Overall survival (OS) was calculated in daysfrom date of initiation of chemotherapy to date ofdeath or last follow-up, as applicable. Survivalprobability and median OS were calculated bythe Kaplan-Meier method, and group differenceswere analyzed using the log-rank test.
RESULTS
Of 87 patients enrolled, 53 completed three ormore cycles and were included for final analysis.Patient flow is depicted in Figure 1. The demo-graphic profile of the 53 patients who enrolled inthe study population is represented in Table 1.Mean (standard deviation) age was 55.4 (9.3)years; the majority (81.1%) were men and hadadvanced/metastatic disease (stage IV, 56.6%;stage IIIB, 37.7%) and an Eastern CooperativeOncology Group performance status of 0 to 1(52.8%) or 2 (32.1%). SqCC (50.9%) and SCLC(35.8%)were themost commonhistologic types. Aprimary bronchoscopic lesion was most commonin the left (34.0%) or the right (24.5%) main bron-chus, followed by the lower one third of the trachea(15.1%)and the lobar/segmental bronchi (26.4%);its degree of mucosal obstruction/stenosis was as
Table 1. Characteristics, Histology, and Disease Stage Profile of the Study Population(n = 53)
Baseline Characteristic Study Population
Age, years, mean (standard deviation) 55.4 (9.3)
Male 43 (81.1)
Current or former smoker 46 (86.8)
Karnofsky performance status, %
100 05 (09.4)
90 12 (22.6)
80 18 (34.0)
70 13 (24.5)
< 60 05 (09.4)
ECOG performance status
0 06 (11.3)
1 22 (41.5)
2 17 (32.1)
3 08 (15.1)
Histology
Squamous cell carcinoma 27 (50.9)
Adenocarcinoma 04 (07.5)
NSCLC-undiff 03 (05.7)
Small cell 19 (35.8)
T group
T2 05 (09.4)
T3 06 (11.3)
T4 42 (79.2)
N group
N0 03 (05.7)
N1 03 (05.7)
N2 26 (49.1)
N3 21 (39.6)
M stage
M0 23 (43.4)
M1a 12 (22.6)
M1b 18 (34.0)
Stage
IIIA 03 (05.7)
IIIB 20 (37.7)
IV 30 (56.6)
Extrathoracic metastasis 20 (37.7)
Small-cell lung cancer (n = 19)
Disease stage
Limited 08 (42.1)
Extensive 11 (57.9)
NOTE. Data are presented as No. (%) unless specified otherwise.Abbreviations: ECOG, Eastern Cooperative Oncology Group;M, presence of distant metastasis; N, lymphnodal involvement;NSCLC-undiff, undifferentiatednon–small-cell lung cancer;NSCLC-NOS,NSCLCnototherwise specified; T, tumor size and extension.
372 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
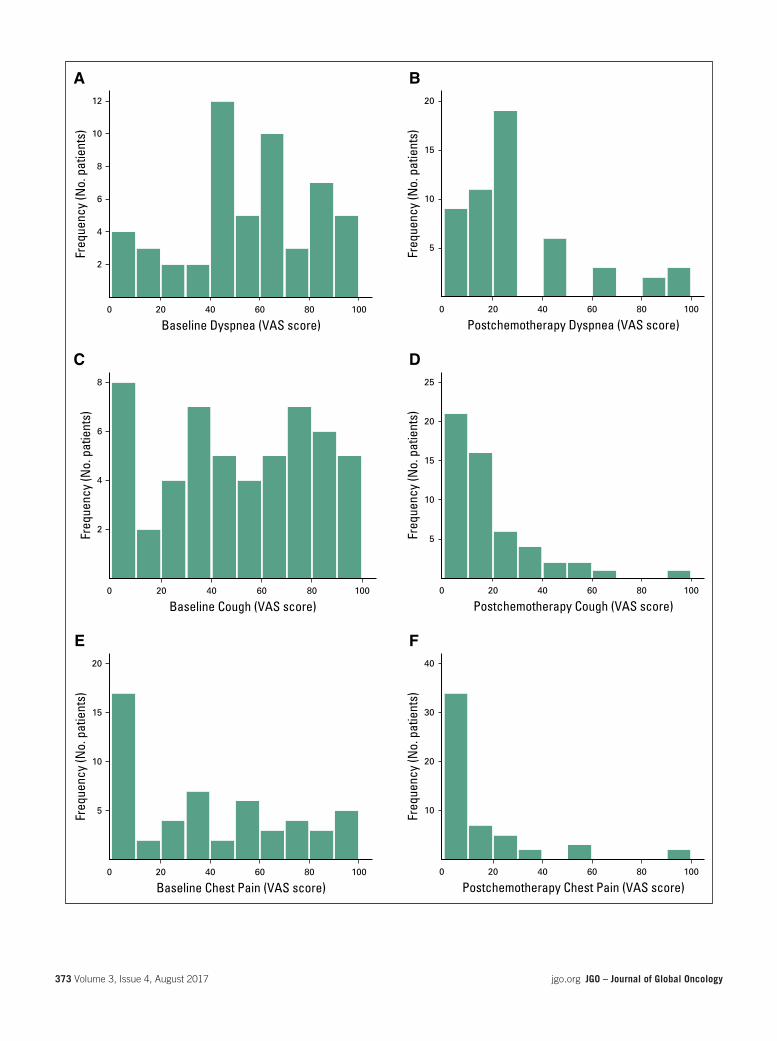
Baseline Dyspnea (VAS score)10080604020
Freq
uenc
y (N
o. p
atie
nts)
12
10
8
6
4
2
A
Baseline Cough (VAS score)10080604020
Freq
uenc
y (N
o. p
atie
nts)
8
6
4
2
C
Baseline Chest Pain (VAS score)100806040200
Freq
uenc
y (N
o. p
atie
nts)
20
15
10
5
E
Postchemotherapy Dyspnea (VAS score)1008060402000
0
Freq
uenc
y (N
o. p
atie
nts)
20
15
10
5
B
Postchemotherapy Cough (VAS score)100806040200
Freq
uenc
y (N
o. p
atie
nts)
25
20
15
10
5
D
Postchemotherapy Chest Pain (VAS score)100806040200
Freq
uenc
y (N
o. p
atie
nts)
40
30
20
10
F
373 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Baseline Hemoptysis (VAS score)100806040200
Freq
uenc
y (N
o. p
atie
nts)
30
20
10
G
Baseline Anorexia (VAS score)10080604020
Freq
uenc
y (N
o. p
atie
nts)
10
8
6
4
2
0
I
Baseline Fatigue (VAS score)10080604020
Freq
uenc
y (N
o. p
atie
nts)
10
8
6
4
2
0
K
Postchemotherapy Hemoptysis (VAS score)100806040200
Freq
uenc
y (N
o. p
atie
nts)
50
40
30
20
10
H
Postchemotherapy Anorexia (VAS score)10080604020
Freq
uenc
y (N
o. p
atie
nts)
20
15
10
5
0
J
Postchemotherapy Fatigue (VAS score)100806040200
Freq
uenc
y (N
o. p
atie
nts)
10
8
6
4
2
L
374 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

follows:.90%(24.5%);76%to90%(18.9%);51%to 75% (11.3%); 26% to 50% (18.9%); < 25%(15.1%); and 0 (11.3%). The mean (standard de-viation) number of FOB lesions at baseline was1.7 (0.9), with 24, 11, and two patients havingtwo, three, and four lesions, respectively.
The mean scores of all six individual symptoms,RSB, and TSB (Figs 2 and 3) showed statisticallysignificant improvement after chemotherapy. Themean change in VAS scores after chemotherapywas 24.7 mm for dyspnea; 31.4 mm for cough;25.5 mm for chest pain; 22.5 mm for hemoptysis;25.4 mm for anorexia; 15.9 for weight loss;25.7 mm for RSB; and 24.2 mm for TSB, with aP value , .001 for each comparison. The meannumber, as well as the distribution, of FOB lesionsdecreased significantly after chemotherapy (Fig4). CXR response had poor agreement with bothFOB-based (Cohen’s k = 0.069; P = .476) andCT-based (Cohen’s k = 0.208; P = .018) re-sponses. Changes in the RSB and TSB categorieshad no/minimal agreement with either FOB- orCT-based responses. On the basis of RECIST, CRand PR were observed in two and 38 patients,respectively, whereas five and eight patients hadSD and PD, respectively. RECIST and WHO cri-teria had strong agreement with each other foroverall response assessment (Cohen’s k=0.872;P, .001). Bronchoscopic assessment had min-imal agreement with assessment based onRECIST(Cohen’sk=0.324;P, .001) andWHO(Cohen’sk = 0.349; P , .001). For differentiating re-sponders (CR and PR) from nonresponders(SD and PD), FOB-based assessment had weakagreementwith assessment based onbothRECIST(Cohen’s k = 0.462; P = .001) and WHO criteria(Cohen’s k = 0.501; P , .001). For differentiatingdisease control (CRandPRandSD) fromPD,WHOcriteria-based CT response had perfect agreement(Cohen’s k = 1.000; P , .001), whereas FOB-based assessment had moderate agreement(Cohen’s k = 0.629; P, .001) in comparison withRECIST. Combinations of FOB-based assessmentwith symptom-based assessment and/or CXR re-sponse also showed only moderate agreement(FOB and RSB, Cohen’s k = 0.672; FOB andTSB, Cohen’s k = 0.739; FOB and CXR, Cohen’sk = 0.764; P , .001 for each of the three) withCT-based assessment for detecting PD. MedianOSwas 372 days (95%CI, 284 to 460 days) and itdiffered significantly between responders andnonresponders (469 v 225 days; log-rank P ,.01) on the basis of RECIST-, WHO-, and FOB-based assessments, but not on the basis ofchanges in RSB or TSB categories.
DISCUSSION
This study was an attempt to assess whether SS-,CXR-, and FOB-based assessment, singly or incombination, could serve reliably as an alterna-tive to conventional CT-based assessment for re-sponse to chemotherapy in patients with lungcancer and bronchoscopically visible lesions. Itis important to determine tumor responses be-cause, as per current guidelines, two to threeadditional cycles (maximum, six) of the first-line chemotherapy regimen may be given to re-sponders (CR and PR), whereas there are con-cerns about increasing toxicity without substantialbenefit to nonresponders (SD and PD).14,15 Inaddition, those with PD may warrant a changein chemotherapy regimen (second-line drugs)and/or alternative treatment plans on the basisof histology, stage, and performance status. Thepresence of SqCC and SCLC (approximately 51%and 36%, respectively) as the most frequent his-tologic types is consistent with the enrolmentcriteria for this study because both are predomi-nantly central in location, as compared with ade-nocarcinoma,which tends to bemoreperipherallylocated. Themean age anddemographic profileof our patient population is also similar to thatobserved in previous epidemiologic studies atour center.16-19
We wish to point out that, although FOB is aninvasive modality, a repeat assessment, as wasperformed in this study, typically has a shortprocedural time with a minimal complication ratebecause no tissue specimens are taken. Making adecision on obtaining a repeat CT scan for assess-ment of chemotherapy responsemaybedifficult attimes because of the presence of preexisting renaldisease, contrast hypersensitivity, cisplatin-inducedrenal dysfunction (during chemotherapy), or the riskof developing contrast-related renal disorders (espe-cially in elderly patients and in those with long-standing diabetes mellitus/hypertension). In addi-tion, there are several logistic limitations in resource-constrained settings such as ours; waiting times forgetting a repeat CT scan are often much longer andthecostmuchhigher than those for a repeat FOB.4,5
In this study, changes in SSs aswell as FOB-basedassessment correlated poorly with CT responses,although symptomatic improvement after chemo-therapy was observed in the majority of patients.The choice of using VAS for graded symptomassessment was based on another recent studyin which baseline symptoms were observed to beprognostic in nature for predicting both OS andradiologic responses.20 One explanation for poor
Fig 2. Histogramsillustrating the distributionof baseline andpostchemotherapysymptom scores in thepatient population asassessed by visual analogscale (VAS) for respiratorysymptoms: (A and B)dyspnea, (C and D) cough,(E and F) chest pain, and(G and H) hemoptysis.Baseline andpostchemotherapysymptom scores in thepatient population asassessed by VAS forconstitutional symptoms: (Iand J) anorexia, and (K andL) fatigue. The horizontalaxes represent the absolutevalue on the VAS from 0 to100 mm, and vertical axesrepresent the number ofpatients with each value.
375 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

agreement between FOB- and CT-based evalua-tions is that the former primarily assesses theintraluminal extent of tumor, whereas CT primarilyassesses its extraluminal extent. Similarly, it islikely that patients experienced symptomatic ben-efit from chemotherapy but that the change (re-duction) in size of measurable (target) lesions wasnot enough to fulfill the criteria for objective radio-logic response.
The major limitations of this study were the smallnumber of patients and the fact that the resultsmay be applicable only to patients with centraltumors that are visible bronchoscopically. More-over, the inclusion criteria of bronchoscopicallyvisible tumors led to a higher percentage of en-rolled patients having SCLC histology (approxi-mately 36%) as compared with the histologicdistribution (approximately 18% to 20% SCLC)seen among patients with lung cancer as awhole.16,18 The fact that SCLC is more chemo-sensitive than other histologic types also ledto a higher proportion of this study cohort havingobjective response rates. The nonavailability of
baseline video recordings because of technicalreasons led to a few patents being excluded fromenrollment; this may also have been a potentialsource of inadvertent selection bias in the study.Another limitation is that although both the au-thors who graded tracheobronchial stenosis werehighly experienced in performing and interpret-ing bronchoscopic findings, the degree of agree-ment between the two observers was not formallyrecorded. Finally, this study only assessed the roleof FOB and not that of newer bronchoscopic pro-cedures suchas endobronchial ultrasound,whichhas emerged as an important tool for both diag-nosis and staging. These limitations notwithstand-ing, there are two important observations that mayhave applications for routine clinical practice.First, both CT-based criteria (WHO and RECIST)showed good agreement with each other andtherefore, either/both may be used. Second, thecombination of bronchoscopic and CXR progres-sion may be used as a surrogate for disease pro-gression if CT assessment is not feasible. Giventhe increasing role of targeted therapies in thetreatment of advanced/metastatic nonsquamous
Baseline Respiratory Symptom Burden (VAS score)806040200
Freq
uenc
y (N
o. p
atie
nts)
6
4
2
A
0
Baseline Total Symptom Burden (VAS score)80604020
Freq
uenc
y (N
o. p
atie
nts)
8
6
4
2
C
Postchemotherapy Respiratory Symptom Burden(VAS score)
100806040200
Freq
uenc
y (N
o. p
atie
nts)
30
20
10
B
Postchemotherapy Total Symptom Burden (VAS score)806040200
Freq
uenc
y (N
o. p
atie
nts)
20
15
10
5
D
Fig 3. Histogramsillustrating the distributionin the patient populationof (A) baseline and(B) postchemotherapyrespiratory symptomburden,and (C) baseline totalsymptom burden and(D) postchemotherapytotal symptom burden.Respiratory symptomburden and total symptomburden were calculated fromfour respiratory symptoms(dyspnea, cough, chest pain,andhemoptysis) and fromallsix symptoms (dyspnea,cough, chest pain,hemoptysis, anorexia, andfatigue), respectively, as themean of individual symptomscores assessedby the visualanalog scale. Horizontal axesrepresent the absolute valueon the visual analog scalefrom 0 to 100 mm, andvertical axes represent thenumber of patientswith eachvalue. VAS, visual analogscale.
376 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

non–small-cell lung cancer and consequently,the emphasis on obtaining a repeat biopsy at PDboth to rule out a change in histologic type and totest for actionable targets including those asso-ciated with the development of resistance to theinitial agent, it could be argued that FOBcould becomplementary toCT for documentingPDaswellas performing rebiopsy.21-23
Previous studies comparing FOB- and CT-basedassessments of response to chemotherapy were inthe era before RECIST and found poor correlation(Cohen’s k = 0.271 to 0.335), with none havingexamined a composite of FOB, symptoms, andCXR.24,25 Ours is probably the first study to compare
FOB-, CXR-, and SS-based assessments, as well astheir combinations, with CT-based assessment ofresponse to chemotherapy in patients with lungcancer.
Although not a primary aim of this study anddespite the small number of patients, preliminarysurvival data indicated that OS was significantlybetter for responders (CR and PR) compared withnonresponders, and this difference was apparentfor assessmentsmadeon thebasis ofRECIST-andWHO-based CT criteria, as well as FOB-basedevaluation. This also indicates that the role ofFOB both to aid decision making regarding con-tinuing or stopping chemotherapy and as a
A
Location of Primary BronchoscopicLesion at Baseline
Segm
enta
l
LULB
RULBLM
B
Lower
3rd
trach
ea
0
No.
of P
atie
nts
(%)
40
30
20
10
RMB
RIB
C
Location of Primary BronchoscopicLesion after Chemotherapy
Segm
enta
l
LULB
RULBLM
BNo0
No.
of P
atie
nts
(%)
60
30
20
10
Lower
3rd
trach
ea RMB
RIB
40
50
B
Severity of Primary BronchoscopicLesion at Baseline (%)
25-50 75-9050-75 > 9000
No.
of P
atie
nts
(%)
25
20
10
< 25
5
15
D
Severity of Primary BronchoscopicLesion after Chemotherapy (%)
25-50 75-9050-75 > 9000
No.
of P
atie
nts
(%)
40
20
< 25
60
Fig 4. (A) Location and(B) severity of primarybronchoscopic lesion atbaseline. (C) Location and(D) severity showedsignificant improvement onrepeat bronchoscopicassessment afterchemotherapy. LMB, leftmain bronchus; LULB, leftupper lobe bronchus; RIB,right bronchusintermedius; RMB, rightmain bronchus; RULB,right upper lobe bronchus.
377 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

prognostic indicator for OS deserves to be assessedfurther in prospective randomized trialswith a great-er number of patients.
In summary, the results of this prospectivestudy indicate that CT scan–based assessmentby RECIST/WHO criteria remains the refer-ence standard for objective evaluation of pa-tient response to chemotherapy in lung cancer.
Repeat FOB assessment for patient responseto chemotherapy is not routinely indicated andshould be reserved only for cases in which arepeat CT scan is not feasible and in patientsin whom disease progression is suspectedon CXR.
DOI: https://doi.org/10.1200/JGO.2016.006593Published online on jgo.org on November 16, 2016.
AUTHOR CONTRIBUTIONS
Conception and design: Digambar Behera, Ashutosh NathAggarwal, Navneet Singh
Collection and assembly of data: Lakshimikant Baburao Yenge,Mandeep Garg
Data analysis and interpretation:Lakshimikant Baburao Yenge,Mandeep Garg, Ashutosh Nath Aggarwal, Navneet SinghManuscript writing: All authorsFinal approval of manuscript: All authorsAccountable for all aspects of the work: All authors
AUTHORS’ DISCLOSURES OFPOTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided byauthors of this manuscript. All relationships are consideredcompensated. Relationships are self-held unless noted. I =
Immediate Family Member, Inst = My Institution. Relation-ships may not relate to the subject matter of this manuscript.For more information about ASCO’s conflict of interest policy,please refer to www.asco.org/rwc or ascopubs.org/jco/site/ifc.
Lakshimikant Baburao YengeNo relationship to disclose
Digambar BeheraNo relationship to disclose
Mandeep GargNo relationship to disclose
Ashutosh Nath AggarwalNo relationship to disclose
Navneet SinghNo relationship to disclose
REFERENCES1. Eisenhauer EA, Therasse P, Bogaerts J, et al: New response evaluation criteria in solid tumours: Revised RECIST
guideline (version 1.1). Eur J Cancer 45:228-247, 2009
2. Miller AB, Hoogstraten B, Staquet M, et al: Reporting results of cancer treatment. Cancer 47:207-214, 1981
3. Singh N, Aggarwal AN: Quality of life as an endpoint of treatment efficacy in malignant lung tumours. Lancet Oncol9:820-821, author reply 821-822, 2008
4. Singh N, Aggarwal AN, Behera D: Management of advanced lung cancer in resource-constrained settings: A per-spective from India. Expert Rev Anticancer Ther 12:1479-1495, 2012
5. SinghN, Aggarwal AN, BeheraD, et al: Intercycle delays during chemotherapy of non-small cell lung cancer in a healthcare resource-constrained setting and their effect on overall survival. J Thorac Oncol 5:236-239, 2010
6. Singh N, Mootha VK, Madan K, et al: Tumor cavitation among lung cancer patients receiving first-line chemotherapyat a tertiary care centre in India: Association with histology and overall survival. Med Oncol 30:602, 2013
7. Singh N, Aggarwal AN, Kaur J, et al: Association of graded folic acid supplementation and total plasma homocysteinelevels with hematological toxicity during first-line treatment of non-squamous NSCLC patients with pemetrexed basedchemotherapy. Am J Clin Oncol 10.1097/COC.0000000000000111 [epub ahead of print on August 7, 2014]
8. Singh N, Singh PS, Aggarwal AN, et al: Comorbidity assessment using Charlson Comorbidity Index and SimplifiedComorbidity Score and its association with clinical outcomes during first-line chemotherapy for lung cancer. Clin LungCancer 2016;17:205-213.e1
9. Travis WD, Brambilla E, Noguchi M, et al: International Association for the Study of Lung Cancer/American ThoracicSociety/European Respiratory Society international multidisciplinary classification of lung adenocarcinoma. J ThoracOncol 6:244-285, 2011
10. International Association for the Study of Lung Cancer: Staging Manual in Thoracic Oncology (ed 1). Orange Park, FL,Editorial Rx Press, 2009
11. Gupta AA, Sehgal IS, Dhooria S, et al: Indications for performing flexible bronchoscopy: Trends over 34 years at atertiary care hospital. Lung India 32:211-215, 2015
12. Freitag L, Ernst A, Unger M, et al: A proposed classification system of central airway stenosis. Eur Respir J 30:7-12, 2007
13. McHugh ML: Interrater reliability: The kappa statistic. Biochem Med (Zagreb) 22:276-282, 2012
14. Azzoli CG, Baker S, Jr., Temin S, et al: American Society of Clinical Oncology Clinical Practice Guideline update onchemotherapy for stage IV non-small-cell lung cancer. J Clin Oncol 27:6251-6266, 2009
378 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

15. Azzoli CG, Temin S, Aliff T, et al: 2011 focused update of 2009 American Society of Clinical Oncology Clinical PracticeGuideline Update on Chemotherapy for Stage IV Non-Small-Cell Lung Cancer. J Clin Oncol 29:3825-3831, 2011
16. Singh N, Aggarwal AN, Gupta D, et al: Unchanging clinico-epidemiological profile of lung cancer in North India overthree decades. Cancer Epidemiol 34:101-104, 2010
17. Singh N, Aggarwal AN, Gupta D, et al: Prevalence of low body mass index among newly diagnosed lung cancerpatients in North India and its association with smoking status. Thorac Cancer 2:27-31, 2011
18. Singh N, Aggarwal AN, Gupta D, et al: Quantified smoking status and non-small cell lung cancer stage at presentation:Analysis of a North Indian cohort and a systematic review of literature. J Thorac Dis 4:474-484, 2012
19. SinghN, BeheraD: Lung cancer epidemiology and clinical profile in North India: Similarities and differenceswith othergeographical regions of India. Indian J Cancer 50:291, 2013
20. Singh PS, Aggarwal AN, Behera D, et al: Simplified graded baseline symptom assessment in lung cancer patientsundergoing first-line chemotherapy: Correlations and prognostic role in a resource constrained setting. J Glob Oncol3:54-63, 2017
21. Singh N, Vishwanath G, Aggarwal AN, et al: Clinical experience on use of oral EGFR-TKIs as first-line treatment ofadvanced NSCLC from a tertiary care centre in North India and implications of skin rash. Indian J Chest Dis Allied Sci56:149-152, 2014
22. SinghN, Jindal A, Behera D: Erlotinib usage after prior treatment with gefitinib in advanced non-small cell lung cancer:A clinical perspective and review of published literature. World J Clin Oncol 5:858-864, 2014
23. Maturu VN, Singh N, Bal A, et al: Relationship of epidermal growth factor receptor activating mutations with histologicsubtyping according to International Association for the Study of Lung Cancer/American Thoracic Society/EuropeanRespiratory Society 2011 adenocarcinoma classification and their impact on overall survival. Lung India 33:257-266,2016
24. Parrat E, Pujol JL, Gautier V, et al: Chest tumor response during lung cancer chemotherapy. Computed tomography vsfiberoptic bronchoscopy. Chest 103:1495-1501, 1993
25. Pujol JL, Parrat E, Lehmann M, et al: Lung cancer chemotherapy. Response-survival relationship depends on themethod of chest tumor response evaluation. Am J Respir Crit Care Med 153:243-249, 1996
379 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

originalreport
Identifying and Prioritizing Gaps inNeuroendocrine Tumor Research: AModified Delphi Process With Patientsand Health Care Providers to Set theResearch Action Plan for the NewlyFormed Commonwealth NeuroendocrineTumor Collaboration
abstract
Purpose Neuroendocrine tumors (NETs) are a diverse group ofmalignancies that pose challenges commonto all rare tumors. The Commonwealth Neuroendocrine Tumor Collaboration (CommNETS) was establishedin 2015 to enhance outcomes for patients with NETs in Canada, Australia, and New Zealand. A modifiedDelphi process was undertaken involving patients, clinicians, and researchers to identify gaps in NETsresearch to produce a comprehensive and defensible research action plan.
Methods A three-round modified Delphi process was undertaken with larger representation than usual formedical consensus processes. Patient/advocate and health care provider/researcher expert panels un-dertook Round 1, which canvassed 17 research priorities and 42 potential topics; in Round 2, thesepriorities were ranked. Round 3 comprised a face-to-face meeting to generate final consensus rankingsand formulate the research action plan.
Results The Delphi groups consisted of 203 participants in Round 1 (64% health care providers/researchers, 36% patient/advocates; 52% Canadian, 32% Australian, and 17% New Zealander), ofwhom 132 participated in Round 2. The top eight priorities were biomarker development; peptide receptorradionuclide therapy optimization; trials of new agents in advanced NETs; functional imaging; sequencingtherapies for metastatic NETs, including development of validated surrogate end points for studies;pathologic classification; early diagnosis; interventional therapeutics; and curative surgery. Two majorareas were ranked significantly higher by patients/advocates: early diagnosis and curative surgery. SixCommNETS working parties were established.
Conclusion This modified Delphi process resulted in a well-founded set of research priorities for the newlyformed CommNETS collaboration by involving a large, diverse group of stakeholders. This approach tosetting a research agenda for a new collaborative group should be adopted to ensure that research plansreflect unmet needs and priorities in the field.
J Glob Oncol 3. © 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
INTRODUCTION
Neuroendocrine tumors (NETs) are a diverse, un-common group of malignancies important becauseof their increasing incidence and prevalence, partlyas a result of increased detection with advancesin imaging technology.1 NETs are extremely
heterogeneous, with a prognosis ranging frommonths inaggressivedisease todecades for indolentdisease. Multiple new diagnostic and treatment mo-dalities have become available in the past 10 years.
The treatmentofpatientswithNETsposesall of thechallenges common to other rare tumors for both
Eva Segelov
David Chan
Ben Lawrence
Nick Pavlakis
Hagen F. Kennecke
Christopher Jackson
Calvin Law
Simron Singh
Author affiliations appear atthe end of this article.
Written on behalf of theCommNETScollaborators.Corresponding author: EvaSegelov, 438 Victoria St,Darlinghurst NSW 2010,Australia;e-mail:[email protected].
380 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
© 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License

patients and clinicians, including delays in diag-nosis; low levels of nonexpert clinician under-standing of the disease; limited evidence basefor treatment options, including a paucity of clin-ical trials2-4; difficulty in obtaining research fund-ing; small patient numbers over large geographicalareas; and limited advocacy for improved patientcare.5,6 International research consortia havebeen identified as a key strategy for integratingmultidisciplinary expertise, enhancing the evi-dence base, and improving management of rarecancers.3,7
The CommonwealthNeuroendocrine Tumor Group(CommNETS) is a new collaboration among pa-tients with NETs, clinicians, and researchers inCanada, Australia, and New Zealand. The groupformed in 2015, with the mission of improvingoutcomes for patients with NETs, recognizing sim-ilarities of care provision in the three countries:high-performing universal health care with cen-tralized processes for introduction of newmedicalprocedures and treatments.6,8 In addition, thethree countries confronted the challenge of geo-graphically dispersed populations.
CommNETS was established explicitly to facilitatecollaboration in areas of need in NET researchandcare common tomember countries, includinggreater power to recruit to clinical trials, sharedregistry information, and interchange of clinicalexpertise. Although it shares similarities with otherinternationalNETsocieties, including theEuropeanNeuroendocrine Tumor Society and the NorthAmerican Neuroendocrine Tumor Society, a dis-tinguishing feature is the deliberate embedding ofpatients and advocates as full members of thegroup, with the shared vision of CommNETS asthe actual vehicle to conduct high-quality clinicaltrial and translational research. This maximizesopportunity and productivity over what can beachieved as individual centers or countries. De-velopment of a research agenda that was mean-ingful to patients and health care providers wasan essential first step.
To establish an a priori robust and defensible re-search agenda, an evaluation of gaps in NET re-search from the perspectives of patients/advocatesand health care providers/researchers was under-taken using a modified Delphi process. The Delphimethodology of developing consensus about futureplanning and identifying emerging trends and is-sues is well established in fields as diverse as healthcare, infrastructure planning, and defense.9-11 It isbased on the principle that structured decisionprocesses drawing on a wide range of expertise
result in better decisions and prioritization thanunstructured ones.12 Delphi processes are mostrelevant in circumstanceswhere there is insufficientempirical evidence to guide clinical practice anddecision making alone.13,14 This method usuallyinvolves a panel of 15 to 20 topic experts who rateagreement with a series of statements in an iterativefashion, typically with three rounds of ranking.15-18
One shortfall of an expert group, however, is that itmay represent a homogeneous and incompleteview of the topic.12,19 Modification of the Delphiprocess is well accepted for both the priorityquestion development process and the panelcomposition, the latter to achieve inclusion of amore heterogeneous population, which may besplit into multiple panels to broaden demographicand other desired representations.15-17 The mod-ifiedDelphi process has beenused successfully toset various health care priorities over the last 15years.15,20-23 The benefit of an increased numberof participants needs to be weighed against thechallenge of ensuring continuity of participation.
It has been established that exposing health careprofessionals to the views of patients may influ-ence the prioritization of outcomes.20 This is par-ticularly relevant in the field of NETs because of itsheterogeneity with a variety of clinical interactions,treatments, and outcomes experienced by pa-tients; the involvement of a broad range of multi-disciplinaryhealthcareprofessionals; and the lackof well-defined outcome end points to measureoutcomes in clinical studies. In setting priorities forthe new CommNETS collaboration, we selected amodified Delphi methodology to ensure a scien-tifically valid and rigorous set of strategic prioritiesthat harnessed the views of all stakeholders.
METHODS
A three-round modified Delphi process was un-dertaken over a 6-month period, collecting theviews of two expert panels to identify gaps inNET research and then developing a consensusranking of research priorities.12,24 The Patient/Advocate Panel included patients, caregivers, pa-tient advocates, support societies, and health careconsumer representatives, whereas the HealthCare Provider/Researcher Panel consisted ofmul-tidisciplinary health care professionals, includingmedical, nursing, and allied health practitionersand basic and translational researchers. Thepanel participants were recruited through e-mailinvitations circulated through NET patient advo-cacy groups and support societies and clinicaland research groups and networks in Canada,Australia, and New Zealand. The rationale for
381 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

separating the panels was to allow the questions tobe presented using appropriate descriptors (lay vmedical terminology) or targeted when relevant toone panel only.
Round1.Thepurposeof theRound1online surveywas to identify gaps in current research and pro-pose relevant NET research priorities or topics. Asystematic review of current NET clinical trials wasundertaken to identify areas under active investi-gation to underpin the survey topics. A 70-questionsurvey, framed as a series of statements, was de-vised by a multidisciplinary project steering com-mittee to be deliberately overinclusive of potentialresearch topics and priorities. This was presentedas a two-part electronic survey (Data Supplement)during an 18-day response window. The first partrequired both panels to rate 17 research priorities(proposed areas of research) on a five-point scalefrom high (1) to low (5), presented in four cate-gories: the conduct of trials and research, trials/research that did not involve investigating efficacyof therapies, trials of systemic therapies, and trialsof local therapies. The second part, sent only tothe Health Care Provider/Researcher Panel, ratedagreement with 52 specific research topics (state-ments outlining the specific methodology for theresearch question). Agreement was set at. 80%of participants, consistent with the consensus thresh-old set for other Delphi processes.15,25,26
Round 2. This online survey was open to allRound 1 participants. Comparative ranking ofthe Round 1 research priorities was undertakenby both panels within the conserved four cate-gories. TheHealthCareProvider/Researcher Panelalso ranked the specific and detailed researchtopics that had reached 80% agreement inRound 1.
Round 3. This comprised a face–to-face workshopconducted among a subset of panel members, allof whom had participated in the previous rounds.Participant numbers were limited because of lo-gistics andcost; however, all who applied to attendwere accommodated. Detailed deliberation onthe 10 top research priorities and topics emergingfrom Round 2 was undertaken through a full dayof group work, exploring the following aspects ofeach topic: importance and significance, feasibil-ity, and relevance for the CommNETS tri-nationcontext and the specific consumer perspectives.The consumer perspective was specifically dis-cussed in detail as representation of this panelat the workshop was proportionally reduced. Eachparticipant then assigned three votes among thenine research priorities (two had been merged
during workshop deliberations) and three voteswithin each of the four categories of research topics,for five voting rounds. Votes could be distributedacross separate research priorities/topics or allassigned to a single entity; this approach is basedon voting methods used for multicriteria decisionanalysis.27,28
Statistical Analysis
Descriptive statistics were used to analyze re-sponses in Rounds 1 and 2 (means and standarddeviations). The ranking of research statementsand topics was based on the mean score acrossthe two panels and was compared using theMann-Whitney U test.
RESULTS
Two hundred three participants undertook Round1 (Patient/Advocate and Health Care Provider/Researcher Panels, 36% and 64%, respectively),of whom 132 participated in Round 2 (32% and68%, respectively) and 49 in Round 3 (6% and49%, respectively). There were 17 research pri-orities and 42 research topics presented inRound 1, which was reduced to 10 prioritiesand 26 topics for Round 2.
Panel Composition
Representation by country was similar across allrounds (Canada, Australia, and New Zealand av-erage, 45%, 34%, and 21%, respectively). Threepatients (one from the Carcinoid-NeuroendocrineTumour Society Canada; one each from the Uni-corn Foundation Australia and Unicorn Foun-dation New Zealand) represented the Patient/Advocate Panel in Round 3; in addition, onemember of the Health Care Provider/ResearcherPanel had a personal history of NET and anotherspecifically represented indigenous cultural as-pects of care and research. The following spe-cialties were represented on the Health CareProvider/Researcher Panel: nursing, medicalphysics, medical oncology, endocrinology, ana-tomic pathology, nuclear medicine, endocrinesurgery, upper GI surgery, diagnostic radiology,and interventional radiology. Research exper-tise covered the fields of translational, labora-tory, health services, and psychosocial research, aswell as the conduct of clinical trials.
Rounds 1 and 2
All 17 initial research priorities were confirmed tobe important in Round 1; however, 16 of 52 pro-posed research topics did not reach the consen-sus threshold (Data Supplement). In Round 2, all
382 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

but two research priorities received broadly similarrankings between the panels. Early diagnosis ofNETs was ranked top priority by the Patient/Advocate Panel but only ninth by the Health CareProvider/Researcher Panel (mean ranking, 4.0 v9.6; P, .001; Data Supplement). Curative surgeryfor NETs was also rated significantly higher by thePatient/Advocate Panel (mean ranking, 7.2 v 9.9;P = .008). Other statistically significant differenceswere noted in the ranking of sequencing of ther-apies for metastatic disease (8.9 v 6.3;P = .01) andpeptide receptor radionuclide therapy (8.8 v 6.6;P = .045). The Health Care Provider/ResearcherPanel ranked 26 topics to be taken forward intoRound 3 (Data Supplement).
Round 3
After extensive discussion, workshop participantsvoted on the final research priorities (Table 1) andtopics (Table 2). Seven working groups were thenformed to develop action plans (Table 3).
DISCUSSION
As a new research collaboration for neuroen-docrine cancer, defining research priorities in astructured way from the outset was consideredvital. Traditionally, many health-related societieshave been established without formal processesto interrogate and document capabilities and con-stituent priorities. Furthermore, stakeholder en-gagement with patients and advocates, althoughoften sought, is frequently subsequent to the de-velopment process and limited to feedback on anadvancedset of proposals. Thechallenge inestab-lishing CommNETS as a tri-nation multidisciplin-ary collaboration with the mission of improvingoutcomes for patients with NETs was to define fromthe outset a robust and defensible set of stream-lined research topics prioritized through broadconsultation. Recognition of current research
in the field was required to avoid duplication.Understanding the differences in health systems,funding models, and patterns of care among thethree countries was also important to achieve aworkable model for collaborative activities and torecognize issues that may be restricted to partic-ular sites or settings.
The modified Delphi methodology allowed inclu-sion of a much larger number of patients andclinicians/researchers than many health-relatedDelphi consensus activities, including those re-cently performed in theNET field.29,30 These havetypically involved a small number of experts withbroadly similar experience, which is ideal for acomplex discussion of specific treatment guide-lines or other expert statements. Because ouraims were different, we facilitated a blue-sky ap-proach while adopting a formal process to gathera wide range of perspectives. Consequently, theprimary strength of this study is that the rankingsof research priorities and topics robustly reflectsthe needs of patients/advocates and clinicians/researchers across our member countries.
Fromadiverseandcomprehensivebase,73%of theresearch questions floated in Round 1 were takenforward. These included the study of the utility ofvarious old and new end points in trials, selection ofpatient populations for trials, and the need for trialsof both systemic and nonsystemic therapies. Thosenot prioritized centered on the feasibility of includingdifferent subtypes of NETs in the same trial; imagingfor trials (likely related to the different availability ofimaging modalities across the three countries); anddevelopment of clinical trials, particularly those re-lated to surgery. The lack of consensus regardingsurgical trials was in part due to concerns aboutthe difficulty of balancing robust trial design withadequate accrual in this rare cancer.
The modified Delphi process identified two mainareas of difference in priorities between the twopanels: early diagnosis of NET and curative re-section. This was explored in Round 3, in whichdeliberations revealed that the Health CareProvider/Researcher Panel had ranked theselower not because they were considered unim-portant but, rather, they were considered to betoo difficult to study. This was attributed to thelack of an obvious research path to approachthese topics, as well as the lack of obvious craftgroup ownership. This was acknowledged as asalient lesson and stimulated discussion regard-ing the process of harnessing research exper-tise and familiarity to devise projects with novel
Table 1. Final Research Priorities
1. Biomarkers (prognostic and predictive)2
2. Peptide receptor radionuclide therapy
3. New investigational drugs/trials for advanced NETs
4. Functional imaging
5. Sequencing of therapies for metastatic disease
6. Pathologic classification of NETs
7. Early diagnosis of NETs
8. Interventional radiology/liver-directed therapy
9. Curative surgery for NETs
Abbreviation: NETs, neuroendocrine tumors.
383 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
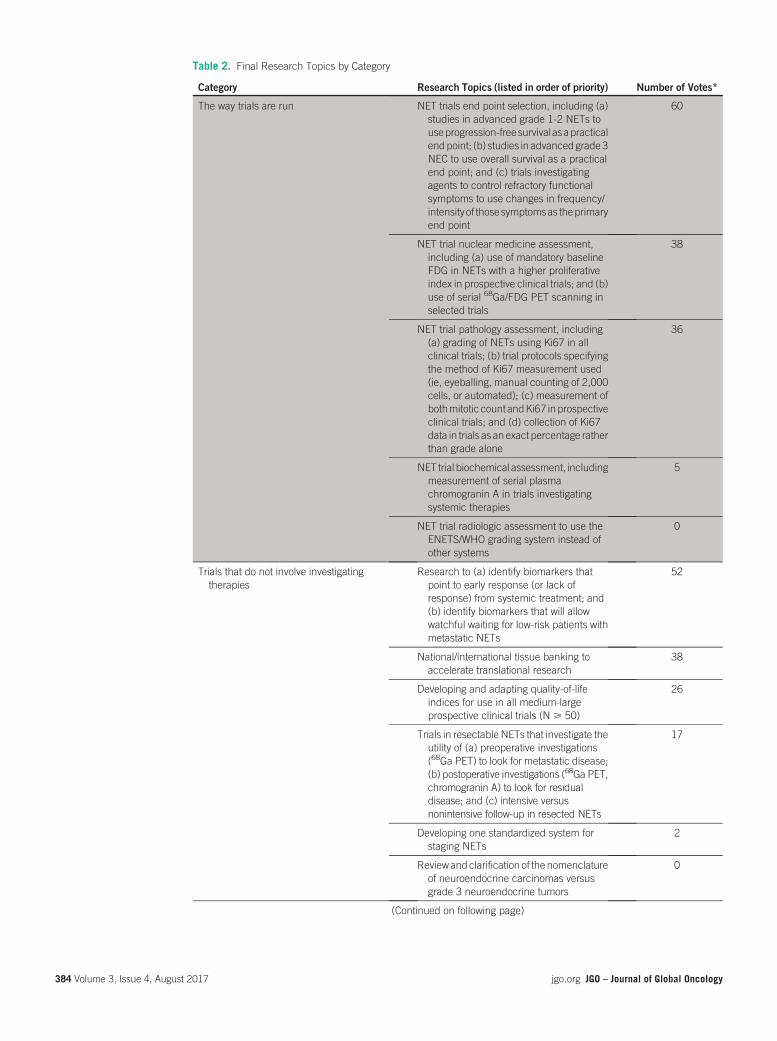
Table 2. Final Research Topics by Category
Category Research Topics (listed in order of priority) Number of Votes*
The way trials are run NET trials end point selection, including (a)studies in advanced grade 1-2 NETs touseprogression-freesurvivalasapracticalendpoint; (b) studies in advancedgrade3NEC to use overall survival as a practicalend point; and (c) trials investigatingagents to control refractory functionalsymptoms to use changes in frequency/intensity of thosesymptomsas theprimaryend point
60
NET trial nuclear medicine assessment,including (a) use of mandatory baselineFDG in NETs with a higher proliferativeindex in prospective clinical trials; and (b)use of serial 68Ga/FDG PET scanning inselected trials
38
NET trial pathology assessment, including(a) grading of NETs using Ki67 in allclinical trials; (b) trial protocols specifyingthe method of Ki67 measurement used(ie, eyeballing, manual counting of 2,000cells, or automated); (c) measurement ofbothmitotic count andKi67 inprospectiveclinical trials; and (d) collection of Ki67data in trials as an exact percentage ratherthan grade alone
36
NET trial biochemical assessment, includingmeasurement of serial plasmachromogranin A in trials investigatingsystemic therapies
5
NET trial radiologic assessment to use theENETS/WHO grading system instead ofother systems
0
Trials that do not involve investigatingtherapies
Research to (a) identify biomarkers thatpoint to early response (or lack ofresponse) from systemic treatment; and(b) identify biomarkers that will allowwatchful waiting for low-risk patients withmetastatic NETs
52
National/international tissue banking toaccelerate translational research
38
Developing and adapting quality-of-lifeindices for use in all medium-largeprospective clinical trials (N > 50)
26
Trials in resectable NETs that investigate theutility of (a) preoperative investigations(68Ga PET) to look for metastatic disease;(b) postoperative investigations (68Ga PET,chromogranin A) to look for residualdisease; and (c) intensive versusnonintensive follow-up in resected NETs
17
Developing one standardized system forstaging NETs
2
Reviewandclarification of the nomenclatureof neuroendocrine carcinomas versusgrade 3 neuroendocrine tumors
0
(Continued on following page)
384 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

approaches to tackle difficult but importantareas.
One limitation of this study is the relatively smallnumber of patients and advocates present forRound 3. We used an online methodology forRounds 1 and 2 to specifically allow for increasedpatient input; however, for Round 3, the logisticand financial constraints of attending an overseasmeeting affected more participants on the Patient/Advocate Panel. Although there is broad and en-thusiastic acceptance of consumers in disease-related societies across the health community,
funding remains amajor challenge. The strategy ofspecifically considering the consumer perspectiveseems to have been a successful surrogate.
In conclusion, CommNETS, as a new internationalNET organization, has developed a comprehen-sive set of prioritized consensus research topicsthrough broad stakeholder engagement thatuniquely included the patient voice from incep-tion. The modified Delphi project demonstratesthat formal processes can bring patient and ad-vocate voices together with clinicians and re-searchers to formulate a plan for collaborative
Table 2. Final Research Topics by Category (Continued)
Category Research Topics (listed in order of priority) Number of Votes*
Trials of systemic therapies Trials of novel agents in metastatic NETs 25
Further trials comparingPRRTwithstandardsystemic therapy
25
Trials of drugs that target actionablemutations found in each patient’s tumor,given the heterogeneity in NETs
24
Trials investigating control of refractoryfunctional symptoms (diarrhea, flushing,fatigue) are warranted
18
Trials investigating optimal sequencing ofagents in metastatic NETs are warranted
15
Trials of radiosensitizing therapy (eg,capecitabine, CAPTEM) with PRRTcompared with PRRT alone
12
Trials investigating therapies after resectionof NETs (ie, adjuvant therapies)
7
Trials to repurpose existing agents inmetastatic NETs
7
Trials investigating optimal dosing of PRRT(number of cycles, frequency, dose percycle)
6
Trials comparing different chemotherapyregimens in grade 3 NEC
4
Trials of nonchemotherapy systemic therapy(eg, antiangiogenic agents) in grade 3NEC
1
Trials comparing chemotherapy with othersystemic therapies
0
Trials of local therapies Trials investigating the relative efficacy andtoxicity of different liver-directed therapies(TAE, TACE, radioembolization, SIRT)
74
Trials to determine whether gross resectionof oligometastatic disease improvesoutcomes are warranted
27
Surgical trials investigating pancreatic,midgut, and bronchial NETs separately
17
Abbreviations: CAPTEM, capecitabine plus temozolomide; ENETS, European Neuroendocrine Tumor Society; FDG, 18F-labeled fluoro-deoxyglucose; NEC, neuroendocrine carcinoma; NET, neuroendocrine tumor; PET, positron emission tomography; PRRT, peptide receptorradionuclide therapy; SIRT, selective internal radiotherapy; TAE, transarterial embolization; TACE, transarterial chemoembolization.*Forty-nine participants could assign up to three votes within each category.
385 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

research on the basis of priorities addressingunmet needs. CommNETS will now undertakeresearch activities on the basis of the rankedpriorities and topics matched to perceived gapsin NET research and care across Canada, Aus-tralia, and New Zealand. Research prioritization
and goal setting by collaborative groups should beundertaken through formal processes to ensurethat subsequent resource utilization has a com-prehensive and strategic basis.
DOI: https://doi.org/10.1200/JGO.2016.006916Published online on jgo.org on October 12, 2016.
AUTHOR CONTRIBUTIONS
Conception and design: Eva Segelov, David Chan, NickPavlakis, Simron SinghCollection and assembly of data: Eva Segelov, David Chan,Simron SinghData analysis and interpretation: All authorsManuscript writing: All authorsFinal approval of manuscript: All authorsAccountable for all aspects of the work: All authors
AUTHORS’ DISCLOSURES OFPOTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided byauthors of this manuscript. All relationships are consideredcompensated. Relationships are self-held unless noted. I =Immediate Family Member, Inst = My Institution. Relation-ships may not relate to the subject matter of this manuscript.For more information about ASCO’s conflict of interest policy,please refer to www.asco.org/rwc or ascopubs.org/jco/site/ifc.
Eva SegelovConsulting or Advisory Role: Roche, Bayer, Ipsen, PfizerResearch Funding: Merck Serono (Inst), Ipsen (Inst)Travel, Accommodations, Expenses: Ipsen, Roche
David ChanHonoraria: IpsenTravel, Accommodations, Expenses: Novartis
Ben LawrenceHonoraria: NovartisTravel, Accommodations, Expenses: Novartis
Nick PavlakisHonoraria: Pfizer, Merck Serono, Amgen, AstraZeneca,Boehringer IngelheimConsulting or Advisory Role: Boehringer Ingelheim,AstraZeneca, Ipsen, Bayer, Novartis, Amgen, Merck, PfizerTravel, Accommodations, Expenses: Ipsen, BoehringerIngelheim
Hagen F. KenneckeHonoraria: Ipsen, Novartis, AmgenTravel, Accommodations, Expenses: Amgen
Christopher JacksonResearch Funding: Athenex PharmaceuticalsPatents, Royalties, Other Intellectual Property: AthenexPharmaceuticalsTravel, Accommodations, Expenses: Athenex Pharmaceuticals
Table 3. Planned Activities on the Basis of Research Priorities
Working Group Planned Activities 2015-2016
Biomarkers (prognostic and predictive) Identify genomics research capacity across countries involved
Investigate scope for tissue sharing across countries involved
Identify common data set fields that could be used in a future registry
Peptide receptor radionuclide therapy Survey PRRT practices, protocols, and trials across countries involved
Develop a consensus on protocol development
New investigational drugs/trials foradvanced NETs
Identify and enhance communication mechanisms for sharinginformation about trials
End points Define consistent, achievable surrogate end points
Work with consumers to identify patient-centered end points
Pathologic classification of NETs Share synoptic reporting format
Refine pathologic classification of rectal, thymic, and gastric NETs
Early diagnosis of NETs Further analyze the International Neuroendocrine Cancer Allianceinternational surveydata for specific insights relevant toCommNETScountries
Survey patients about the symptoms they experienced that were notdiagnosed/addressed
Interventional radiology Identify interventions for comparative trials/studies
Increase overall numbers through multicenter trials
Abbreviations: CommNETS, Commonwealth Neuroendocrine Tumor Group; NETs, neuroendocrine tumors; PRRT, peptide receptorradionuclide therapy.
386 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Calvin LawConsulting or Advisory Role: Ipsen, Novartis, Baxalta, Amgen
Travel, Accommodations, Expenses: Novartis
Simron SinghEmployment: Novartis (I)Honoraria: Novartis, IpsenTravel, Accommodations, Expenses: Novartis, Ipsen, Pfizer
ACKNOWLEDGMENTSupported by an unrestricted educational grant to the Aus-tralian Gastrointestinal Trials Group from Ipsen Pty Ltd. Therewas no input from IpsenPty Ltd into any aspect of studydesignor conduct.
Affiliations
Eva Segelov, University of New South Wales; David Chan and Nick Pavlakis, Royal North Shore Hospital, Sydney, Australia; BenLawrence, University of Auckland, Auckland; Christopher Jackson, University of Otago, Dunedin, New Zealand;Hagen F. Kennecke,University of British Columbia, Vancouver; and Calvin Law and Simron Singh, Odette Cancer Centre, Toronto, Canada.
REFERENCES1. Hallet J, Law CHL, Cukier M, et al: Exploring the rising incidence of neuroendocrine tumors: A population-based
analysis of epidemiology, metastatic presentation, and outcomes. Cancer 121:589-597, 2015
2. Oberg K, Modlin IM, De Herder W, et al: Consensus on biomarkers for neuroendocrine tumour disease. Lancet Oncol16:e435-e446, 2015
3. Chan DL, Goldstein D, Zalcberg JR: Neuroendocrine tumours - models for rare tumour management. Cancer Forum39:13-16, 2015
4. van Essen M, Sundin A, Krenning EP, et al: Neuroendocrine tumours: The role of imaging for diagnosis and therapy.Nat Rev Endocrinol 10:102-114, 2014
5. BillinghamL,Malottki K, StevenN: Researchmethods to change clinical practice for patients with rare cancers. LancetOncol 17:e70-e80, 2016
6. Schoen C, Osborn R, Doty MM, et al: Toward higher-performance health systems: Adults’ health care experiences inseven countries, 2007. Health Aff (Millwood) 26:w717-w734, 2007
7. Blay J-Y, Coindre J-M, Ducimetiere F, et al: The value of research collaborations and consortia in rare cancers. LancetOncol 17:e62-e69, 2016
8. Morgan SG, McMahon M, Mitton C, et al: Centralized drug review processes in Australia, Canada, New Zealand, andthe United Kingdom. Health Aff (Millwood) 25:337-347, 2006
9. Bishop P, Hines A: Thinking About the Future: Guidelines for Strategic Foresight. Sydney, Australia, Hinesight, 2013
10. Rowe G, Wright G: The Delphi technique as a forecasting tool: Issues and analysis. Int J Forecast 15:353-375, 1999
11. Fitch K, Bernstein SJ, Aguilar MD, et al: The RAND/UCLA appropriateness method user’s manual. https://www.rand.org/content/dam/rand/pubs/monograph_reports/2011/MR1269.pdf
12. Adler M, Ziglio E: Gazing into the oracle: The Delphi method and its application to social policy and public health.London, United Kingdom, Jessica Kingsley Publishers, 1996
13. Okoli C, Pawlowski SD: The Delphimethod as a research tool: An example, design considerations and applications. InfManage 42:15-29, 2004
14. Landeta J: Current validity of the Delphi method in social sciences. Technol Forecast Soc Change 73:467-482, 2006
15. Reavley NJ, Ross AM, Killackey E, et al: Development of guidelines for tertiary education institutions to assist them insupporting students with a mental illness: A Delphi consensus study with Australian professionals and consumers.PeerJ 1:e43, 2013
16. Martin JS, Chaney LH: Determination of content for a collegiate course in intercultural business communication bythree Delphi panels. Int J Business Commun 29:267-283, 1992
17. Preble JF: The selection of Delphi panels for strategic planning purposes. Strateg Manage J 5:157-170, 1984
18. Jones J, Hunter D: Consensus methods for medical and health services research. BMJ 311:376-380, 1995
19. Fletcher AJ, Marchildon GP: Using the Delphi method for qualitative, participatory action research in health lead-ership. Int J Qual Methods 13:1-18, 2014
20. Macefield R, BlencoweN,Brookes S, et al: Core outcome set development: The effect of Delphi panel composition andfeedback on prioritisation of outcomes. Trials 14:P77, 2013 (suppl 1)
21. Langlands RL, Jorm AF, Kelly CM, et al: First aid for depression: A Delphi consensus study with consumers, carers andclinicians. J Affect Disord 105:157-165, 2008
387 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

22. Elwyn G, O’Connor A, Stacey D, et al: Developing a quality criteria framework for patient decision aids: Online in-ternational Delphi consensus process. BMJ 333:417, 2006
23. Deane K, Ellis-Hill C, Dekker K, et al: A Delphi survey of best practice occupational therapy for Parkinson’s disease inthe United Kingdom. Br J Occup Ther 66:247-254, 2003
24. Tiernan J, Cook A, Geh I, et al: Use of a modified Delphi approach to develop research priorities for the association ofcoloproctology of Great Britain and Ireland. Colorectal Dis 16:965-970, 2014
25. Pinnock H, Østrem A, Rodrıguez MR, et al: Prioritising the respiratory research needs of primary care: The In-ternational Primary Care Respiratory Group (IPCRG) e-Delphi exercise. Prim Care Respir J 21:19-27, 2012
26. Snape D, Kirkham J, Preston J, et al: Exploring areas of consensus and conflict around values underpinning publicinvolvement in health and social care research: A modified Delphi study. BMJ Open 4:e004217, 2014
27. Mendoza GA, Macoun P, Prabhu R, et al: Guidelines for applying multi-criteria analysis to the assessment of criteriaand indicators. http://www.cifor.org/livesinforests/publications/pdf_files/toolbox-9c.pdf
28. Mendoza GA, Martins H: Multi-criteria decision analysis in natural resourcemanagement: A critical review of methodsand new modelling paradigms. For Ecol Manage 230:1-22, 2006
29. Kocha W, Maroun J, Kennecke H, et al: Consensus recommendations for the diagnosis and management of well-differentiated gastroenterohepatic neuroendocrine tumours: A revised statement from a Canadian national expertgroup. Curr Oncol 17:49-64, 2010
30. Singh S, Dey C, Kennecke H, et al: Consensus recommendations for the diagnosis and management of pancreaticneuroendocrine tumors: Guidelines from a Canadian national expert group. Ann Surg Oncol 22:2685-2699, 2015
388 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

originalreport
Presentation, Treatment, and Outcomesof Haitian Women With Breast Cancer inMiami and Haiti: Disparities in BreastCancer—A Retrospective Cohort Study
abstract
Purpose We compared a cohort of Haitian immigrants with residents in Haiti with breast cancer (BC) toevaluate the effects of location on presentation, treatment, and outcomes.
Patients and Methods Participants were Haitian women with BC living in Miami who presented to theUniversity of Miami/Jackson Memorial Hospital and women with BC living in Haiti who presented to theInnovating Health International Women’s Cancer Center. The primary outcome was the relationship be-tween location, cancer characteristics, and survival. The secondary objective was to compare our resultswith data extracted from the SEER database. Cox regression was used to compare survival.
Results Onehundred twopatients fromUniversity ofMiami/JacksonMemorial Hospital and94patients fromInnovating Health International were included. The patients in Haiti, compared with the patients in Miami,were younger (mean age, 50.2 v 53.7 years, respectively; P = .042), presented after a longer duration ofsymptoms (median, 20 v3months, respectively;P< .001), hadmore advanced stage (44.7% v25.5%withstage III and27.6%v18.6%withstage IVBC, respectively), andhadmoreestrogen receptor (ER)–negativetumors (44.9% v 26.5%, respectively; P = .024). The percentage of women who died was 31.9% in Haitidied comparedwith 17.6% inMiami.Median survival timewas53.7months forwomen inHaiti andwas notreached inMiami. The risk of deathwas higher for women in Haiti versuswomen inMiami (adjusted hazardratio, 3.09; P = .0024).
Conclusion Women with BC in Haiti experience a significantly worse outcome than immigrants in Miami,which seems to be related to a more advanced stage and younger age at diagnosis, more ER-negativetumors, and lack of timely effective treatments. The differences in age and ER status are not a resultof access to care and are unexplained.
J Glob Oncol 3. © 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
INTRODUCTION
In the past 20 years, breast cancer (BC) diagnosisand death has risen in low- and middle-incomecountries (LMICs), and BC is the most frequentcauseof cancer death inwomen inmost regions.1-3
Disparities in BC outcomes have been reported fordifferent races and ethnicities and income levelswithin a country despite adjusting for known con-founders.4 These differences aremultifactorial andare related to differences not only in tumor biologybut also in screening practices, access to care, andoverall socioeconomic status. However, accurateregistries are missing for many regions, and char-acterization of how migration status influences BCcharacteristics and survival in different populationshas not yet been demonstrated.
The Haitian population constitutes 1.5% of immi-grants in theUnited States and is the fourth largestgroup from the Caribbean after Cuba, the DominicanRepublic, and Jamaica.5 Many Afro-Caribbean im-migrants live in south Florida. In this study, wecompared Haitian immigrants with residents inHaiti diagnosed with BC to evaluate the effects ofgeographic location on presentation, treatment, andoutcomes.
PATIENTS AND METHODS
Study Design and Study Population
This was a retrospective cohort study. The studypopulation included Haitian women, living inMiami, who presented to the University of Miami(UM)/Jackson Memorial Hospital (JMH) between
Alexandra Gomez
Vincent DeGennaro
Sophia H.L. George
Isildinha M. Reis
Estefania Santamaria
Gustavo FigueiredoWestin
Dieudina Gabriel
Judith Hurley
Author affiliations appear atthe end of this article.
Supported by a grant fromSusan G. Komen for theCure and funded in part byGatorade Trust,Department of Medicine,University of FloridaCollege of Medicine andInnovating HealthInternational.Presented inpart at the8thAnnual AmericanAssociation for CancerResearch Conference ofthe Science of CancerHealth Disparities inRacial/Ethnic Minoritiesand the MedicallyUnderserved, Atlanta, GA,November 13-15, 2015.
Corresponding author:Judith Hurley, MD,Division of Hematologyand Oncology, Universityof Miami/JacksonMemorial Hospital, 1550NW 10th Ave, Fox 300,Miami, FL 33136, e-mail:[email protected].
389 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
© 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License

2008 and 2014 with a new diagnosis of BC andwomen in Haiti who presented to the InnovatingHealth InternationalWomen’s Cancer Center (IHI-WCC) in Port-au-Prince from 2013 to 2015 forcare. Patients were identified by a review of theUM/JMHBC clinic patient roster and the IHI-WCCprogram database. All patients were confirmed bychart review. The institutional review board at UMand the Haitian National Bioethics Committeeapproved the study, data collection, transmissionmethods, and storage protocols.
JMH is a university-based, tertiary, safety nethospital inMiami, Florida. It is estimated thatmorethan 40%ofHaitians in Florida live inMiami-DadeCounty6 and that 8% of the patients attending theJMHBCclinicareHaitian.Haiti hasapopulationof11 million and no fellowship-trained oncologists.This clinical and research program in Haiti issupported through a collaboration of the US-based nonprofit IHI and the University of FloridaCollege of Medicine. IHI-WCC, working with theHaitianMinistry of Health, partners in a public andprivate hospital that serves as an urban tertiarycenter and is the second largest BCprogram in thecountry.
Definitions and End Points
Data were collected on patient demographics,disease and treatment characteristics, and clin-ical outcome. Slightly more than half of biopsiesfrom Haiti (52%) were sent to the United Statesfor pathology and immunohistochemistry, butnot all of those had human epidermal growthfactor receptor 2 (HER2) expression performedbecause it does not affect treatment decisionsin Haiti as a result of the lack of trastuzumab.Those biopsies performed in Haiti reported his-topathologic diagnosis but not estrogen recep-tor (ER), progesterone receptor (PR), or HER2statuses.
Follow-up was defined as time in months from BCdiagnosis to date of death or last date of follow-up.Progression-free survival (PFS) was defined as thetime from cancer diagnosis to relapse, diseaseprogression, new contralateral BC, or death fromany cause; patients who were alive and progres-sion free were censored at the date of last docu-mented progression-free status. Overall survival(OS) was defined as the time from cancer diag-nosis to death from any cause; follow-up for alivepatients was censored at date of last contact.Death was confirmed by clinical records and theSocial Security Death Index for patients in Miamiand by direct contact with family members forpatients in Haiti.
Historical Comparison Data
We extracted data from the SEER-18 registriesresearch database. We selected women diag-nosedwith BC from2008 to 2012 (American JointCommittee on Cancer, sixth edition, stage 0 to IV),with an age at diagnosis > 18 years and race orethnicity of non-Hispanic white (NHW) or non-Hispanicblack (NHB).These race/ethnicity groupswere derived from the SEER variables race recode(RAC_RECY) and the North American Associationof Central Cancer Registries Hispanic/Latino Iden-tification Algorithm recode of Hispanic origin. Weselected patients on the basis of ER and PR status,who were then classified as both ER and PR neg-ativeorasERorPRpositive.Theseselectioncriteriayielded a case listing of 35,285 NHB and 232,072NHW women to compare with our two cohorts ofHaitian women. In this selected SEER data set, wederived triple-negative status. Note that ERBB2status (formerly HER2 or HER2/neu) is availablein SEER for cases diagnosed in 2010 and later.
Statistical Analysis
Data were analyzed by complete case analysis.Patient-related and cancer-related variableswere described as categorical, discrete, or con-tinuous variables using the corresponding de-scriptive statistics such as absolute and relativefrequencies, mean, median, range, interquartilerange, and standard deviation (SD); 95% CIs orSEs were reported as appropriate. Comparisonsbetween the cohorts were performed using thet test or the nonparametric Mann-Whitney-Wilcoxontest for continuous variables and the Fisher’s exacttest or the x2 test for categorical variables.
OS curves were estimated using the Kaplan-Meier method. The 95% CIs for time-specificrates and median OS were estimated using thelog-log transform method and the Greenwood’svariance. The log-rank test and Cox proportionalhazards regression analysis were used to com-pare OS between women in Haiti and in Miami.The method by Fine and Gray was used to esti-mate the effect of study cohort on the risk of deathfrom BC, taking into account death from othercauses as the competing risk.7 Statistical ana-lyses were performed using SAS 9.4 (SAS In-stitute, Cary, NC).
RESULTS
Baseline Patient Characteristics
One hundred two patients were included in theMiami cohort, and 98 patients were included inthe Haiti cohort. Demographic, cancer-related,and treatment characteristics are listed in Table 1.
390 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Table 1. Demographic and Breast Cancer–Related Characteristics of Study Cohorts
Characteristic
Haitians in Haiti Haitians in Miami
PNo. (n = 94) % No. (n = 102) %
Age at diagnosis, years
, 40 21 22.3 8 7.8 .024
40-49 27 28.7 27 26.5
50-59 27 28.7 40 39.2
> 60 19 20.2 27 26.5
, 50 48 51.1 35 34.3 .018
> 50 46 48.9 67 65.7
Mean 50.2 53.7 .042
SD 12.9 11.1
Median 48.5 54
Range 27-89 27-88
BMI, kg/m2 86 99 , .001
, 25 41 47.7 18 18.2
25-29.99 29 33.7 33 33.4
> 30 16 18.6 48 48.5
Mean 25.9 30.0 , .001
SD 5.1 5.4
Symptoms before presentation
Yes 87 92.6 82 80.4 .014
No/NA 7 7.4 20 19.6
Time with symptoms, months 62 82 , .001
Mean 26.6 6
SD 24.3 7.7
Median 20 3
Range 1-120 0.5-48
Cancer stage
0 (DCIS) 1 1.1 14 13.7 , .001
I 2 2.1 15 14.7
II 23 24.5 28 27.5
III 42 44.7 26 25.5
IV 26 27.6 19 18.6
0/I/II 26 27.7 57 55.9 , .001
III 42 44.7 26 25.5
IV 26 27.6 19 18.6
Receptor status
ER 49 .024
Negative 22 44.9 27 26.5
Positive 27 55.1 75 73.5
PR 34 .013
Negative 22 64.7 41 40.2
Positive 12 35.3 61 59.8
(Continued on following page)
391 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
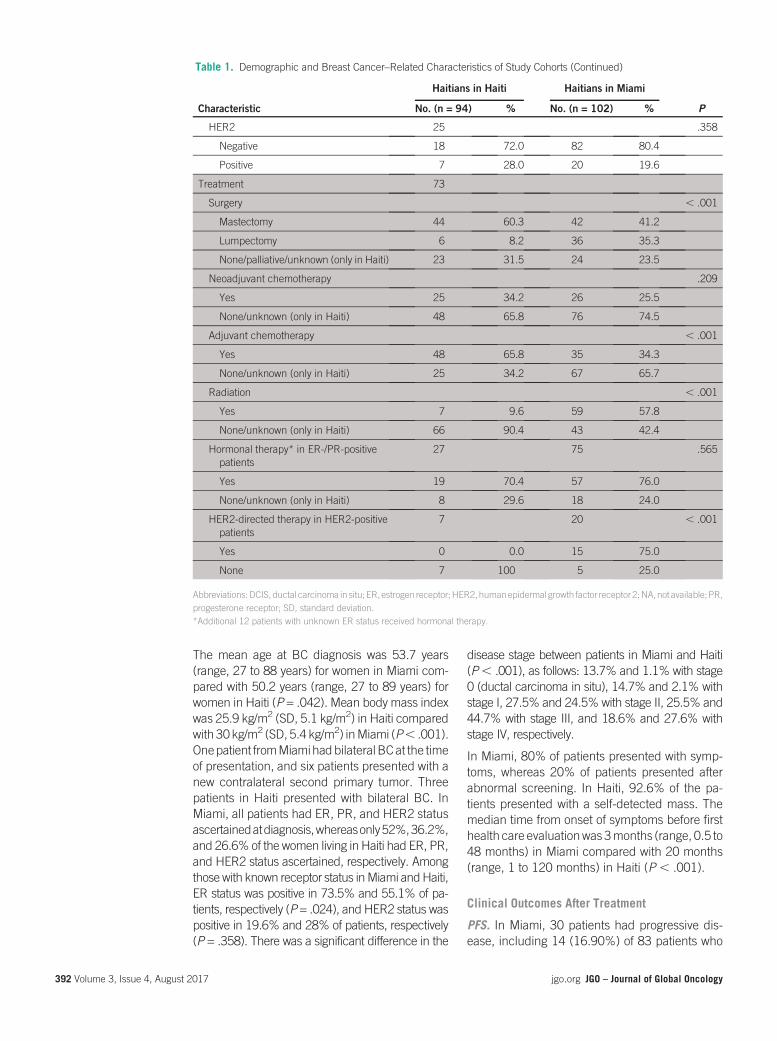
The mean age at BC diagnosis was 53.7 years(range, 27 to 88 years) for women in Miami com-pared with 50.2 years (range, 27 to 89 years) forwomen in Haiti (P = .042). Mean body mass indexwas 25.9 kg/m2 (SD, 5.1 kg/m2) in Haiti comparedwith 30 kg/m2 (SD, 5.4 kg/m2) inMiami (P, .001).Onepatient fromMiamihadbilateral BCat the timeof presentation, and six patients presented with anew contralateral second primary tumor. Threepatients in Haiti presented with bilateral BC. InMiami, all patients had ER, PR, and HER2 statusascertainedatdiagnosis,whereasonly52%,36.2%,and 26.6% of the women living in Haiti had ER, PR,and HER2 status ascertained, respectively. Amongthosewith known receptor status inMiami andHaiti,ER status was positive in 73.5% and 55.1% of pa-tients, respectively (P = .024), and HER2 status waspositive in 19.6% and 28% of patients, respectively(P = .358). There was a significant difference in the
disease stage between patients in Miami and Haiti(P, .001), as follows: 13.7% and 1.1% with stage0 (ductal carcinoma in situ), 14.7% and 2.1% withstage I, 27.5% and 24.5% with stage II, 25.5% and44.7% with stage III, and 18.6% and 27.6% withstage IV, respectively.
In Miami, 80% of patients presented with symp-toms, whereas 20% of patients presented afterabnormal screening. In Haiti, 92.6% of the pa-tients presented with a self-detected mass. Themedian time from onset of symptoms before firsthealth care evaluationwas 3months (range, 0.5 to48 months) in Miami compared with 20 months(range, 1 to 120 months) in Haiti (P , .001).
Clinical Outcomes After Treatment
PFS. In Miami, 30 patients had progressive dis-ease, including 14 (16.90%) of 83 patients who
Table 1. Demographic and Breast Cancer–Related Characteristics of Study Cohorts (Continued)
Characteristic
Haitians in Haiti Haitians in Miami
PNo. (n = 94) % No. (n = 102) %
HER2 25 .358
Negative 18 72.0 82 80.4
Positive 7 28.0 20 19.6
Treatment 73
Surgery , .001
Mastectomy 44 60.3 42 41.2
Lumpectomy 6 8.2 36 35.3
None/palliative/unknown (only in Haiti) 23 31.5 24 23.5
Neoadjuvant chemotherapy .209
Yes 25 34.2 26 25.5
None/unknown (only in Haiti) 48 65.8 76 74.5
Adjuvant chemotherapy , .001
Yes 48 65.8 35 34.3
None/unknown (only in Haiti) 25 34.2 67 65.7
Radiation , .001
Yes 7 9.6 59 57.8
None/unknown (only in Haiti) 66 90.4 43 42.4
Hormonal therapy* in ER-/PR-positivepatients
27 75 .565
Yes 19 70.4 57 76.0
None/unknown (only in Haiti) 8 29.6 18 24.0
HER2-directed therapy in HER2-positivepatients
7 20 , .001
Yes 0 0.0 15 75.0
None 7 100 5 25.0
Abbreviations:DCIS, ductal carcinoma in situ; ER, estrogen receptor;HER2,humanepidermal growth factor receptor 2;NA,not available; PR,progesterone receptor; SD, standard deviation.*Additional 12 patients with unknown ER status received hormonal therapy.
392 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
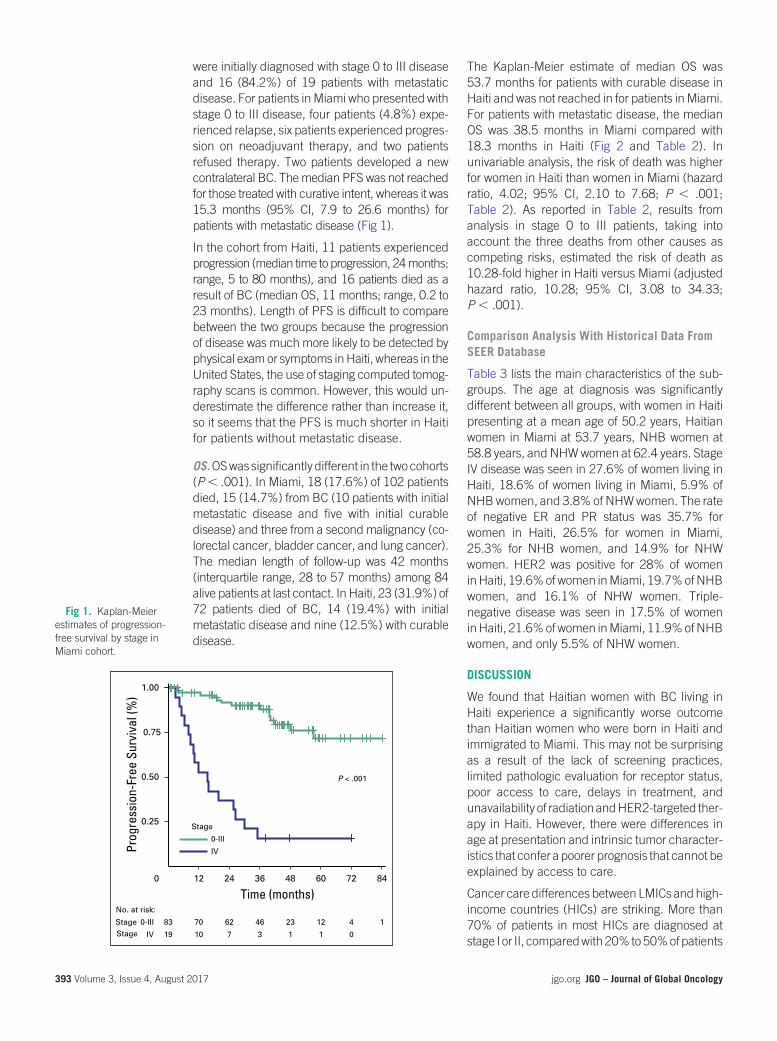
were initially diagnosed with stage 0 to III diseaseand 16 (84.2%) of 19 patients with metastaticdisease. For patients inMiami who presented withstage 0 to III disease, four patients (4.8%) expe-rienced relapse, six patients experienced progres-sion on neoadjuvant therapy, and two patientsrefused therapy. Two patients developed a newcontralateral BC. Themedian PFS was not reachedfor those treated with curative intent, whereas it was15.3 months (95% CI, 7.9 to 26.6 months) forpatients with metastatic disease (Fig 1).
In the cohort from Haiti, 11 patients experiencedprogression (median time to progression, 24months;range, 5 to 80 months), and 16 patients died as aresult of BC (median OS, 11 months; range, 0.2 to23 months). Length of PFS is difficult to comparebetween the two groups because the progressionof disease was much more likely to be detected byphysical exam or symptoms inHaiti, whereas in theUnited States, the use of staging computed tomog-raphy scans is common. However, this would un-derestimate the difference rather than increase it,so it seems that the PFS is much shorter in Haitifor patients without metastatic disease.
OS.OSwas significantly different in the twocohorts(P, .001). In Miami, 18 (17.6%) of 102 patientsdied, 15 (14.7%) from BC (10 patients with initialmetastatic disease and five with initial curabledisease) and three from a second malignancy (co-lorectal cancer, bladder cancer, and lung cancer).The median length of follow-up was 42 months(interquartile range, 28 to 57 months) among 84alive patients at last contact. In Haiti, 23 (31.9%) of72 patients died of BC, 14 (19.4%) with initialmetastatic disease and nine (12.5%) with curabledisease.
The Kaplan-Meier estimate of median OS was53.7 months for patients with curable disease inHaiti and was not reached in for patients inMiami.For patients with metastatic disease, the medianOS was 38.5 months in Miami compared with18.3 months in Haiti (Fig 2 and Table 2). Inunivariable analysis, the risk of death was higherfor women in Haiti than women in Miami (hazardratio, 4.02; 95% CI, 2.10 to 7.68; P , .001;Table 2). As reported in Table 2, results fromanalysis in stage 0 to III patients, taking intoaccount the three deaths from other causes ascompeting risks, estimated the risk of death as10.28-fold higher in Haiti versus Miami (adjustedhazard ratio, 10.28; 95% CI, 3.08 to 34.33;P , .001).
Comparison Analysis With Historical Data FromSEER Database
Table 3 lists the main characteristics of the sub-groups. The age at diagnosis was significantlydifferent between all groups, with women in Haitipresenting at a mean age of 50.2 years, Haitianwomen in Miami at 53.7 years, NHB women at58.8 years, and NHWwomen at 62.4 years. StageIV disease was seen in 27.6% of women living inHaiti, 18.6% of women living in Miami, 5.9% ofNHBwomen, and 3.8% of NHWwomen. The rateof negative ER and PR status was 35.7% forwomen in Haiti, 26.5% for women in Miami,25.3% for NHB women, and 14.9% for NHWwomen. HER2 was positive for 28% of womeninHaiti, 19.6%ofwomen inMiami, 19.7%ofNHBwomen, and 16.1% of NHW women. Triple-negative disease was seen in 17.5% of womeninHaiti, 21.6%ofwomen inMiami, 11.9%ofNHBwomen, and only 5.5% of NHW women.
DISCUSSION
We found that Haitian women with BC living inHaiti experience a significantly worse outcomethan Haitian women who were born in Haiti andimmigrated to Miami. This may not be surprisingas a result of the lack of screening practices,limited pathologic evaluation for receptor status,poor access to care, delays in treatment, andunavailability of radiationandHER2-targeted ther-apy in Haiti. However, there were differences inage at presentation and intrinsic tumor character-istics that confer a poorer prognosis that cannot beexplained by access to care.
Cancer care differences between LMICs andhigh-income countries (HICs) are striking. More than70% of patients in most HICs are diagnosed atstage I or II, comparedwith20%to50%ofpatients
0 12 24 36 48 60 72 84
Time (months)
0.25
0.50
0.75
1.00
183 70 62 46 23 12 40-III
19 10 7 3 1 1 0IV
No. at risk:
IV
0-III
Stage
P < .001
Prog
ress
ion-
Free
Sur
viva
l (%
)
StageStage
Fig 1. Kaplan-Meierestimates of progression-free survival by stage inMiami cohort.
393 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

in the majority of LMICs.8 Stage at presentation inHaiti was skewed to stage III and IV, with only27.7% of women presenting with stage 0 to II. ForHaitians living inMiami, thispercentagewasbetter(55.9%), but was still lower than for NHB women(80.7%) and NHW women (87.1%). Delays indiagnosis have been associated with more ad-vanced stage and worse prognosis.9-14 In a reviewof delays comparing HICs with LMICs, where BCtotal delay is defined as more than 3 months be-tween symptom discovery and the beginning oftreatment, it was found that among HICs, themedian range of symptom duration before treat-ment was 30 to 48 days and more than 60% ofpatients began treatment less than 3months aftersymptom discovery. In comparison, the mediantime of symptom duration before treatment forLMICs was 5.5 to 8 months, and less than30% of patients started treatment in less than
3 months.8 Women in Haiti had extreme delays indiagnosis even by LMIC standards, with a mediantime from onset of symptoms before first healthcare evaluation of 20months. Although living in anHIC, Haitian women living in Miami still experi-enced both patient delays (median time betweensymptomonset andpresentation of 3months) andprovider delay (median time from the initial healthcareencounter to treatmentof72days).Only18.6%of patients started treatment within 4 months ofsymptom discovery, and this remains outside ofthe average for HICs.
Access and quality of care deficiencies are mul-tifactorial. Patients in Haiti have no access toscreening, but even after they moved to an HIC,their utilization rates remained suboptimal. Arecent report documents that only 58% of Hai-tian women living in the United States whoshould undergo screening actually do so.15 This
0 12 24 36 48 60 72 84 0 12 24 36 48 60 72 84
Time (months)
P < .001
Time (months)
P < .001
Miami
Haiti
Miami
Haiti0.25
0.50
0.75
1.00
OS (%
)
0.25
0.50
0.75
1.00
No. at risk: No. at risk:
72 50 13 8 5 3 1 0Haiti
102 88 78 59 31 16 5 1Miami
49 37 8 5 3 1 1 0Haiti
83 72 65 49 28 14 5 1Miami
OS (%
)
A
0 12 24 36 48 60 72 84
Time (months)
Miami
Haiti
P = .0757
0.25
0.50
0.75
1.00
19 16 13 10 3 2 0
No. at risk:
23 13 5 3 2 2 0Haiti
Miami
OS (%
)
C
BFig 2. Kaplan-Meier
estimates of overall survival(OS) by study cohort in (A)all patients, (B) patientswith stage 0 to III disease,and (C) patients with stageIV disease at presentation.The median OS time was53.7 months for patientswith curable breast cancer(stage 0 to III) in Haiti andwasnot reached forpatientsin Miami. For metastaticdisease (stage IV), themedian OS times were18.3 months for patientsin Haiti compared with38.5 months for patientsin Miami.
394 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Table2.
Summaryof
Death
Even
ts,O
S,an
dDea
thFrom
BreastC
ance
rBetwee
ntheTw
oStud
yCoh
orts,O
verallan
dby
Stageat
Disea
sePresentation
Survival
AllPatients
Stage
0-IIIPatients
Stage
IVPatients
Haiti
Miami
Haiti
Miami
Haiti
Miami
No.
ofpa
tients
7210
249
8323
19
No.
ofde
aths
2318
*9
8*14
10
OS M
edianOS,
mon
ths(95%
CI)
53.7
(23.1to
65.6)
NE
53.7
(23.1to
NE)
NE
18.3
(11.7to
38.5)
38.5
(15.4to
NE)
4-year
OS,
%(95%
CI)
50.1
(28.6to
68.2)
80.8
(69.7to
88.2)
70.6
(45.5to
85.8)
91.9
(81.5to
96.6)
22.6
(4.2
to49
.6)
39.2
(15.1to
62.8)
P†,
.001
,.001
.075
7
Una
djustedHR(95%
CI)
4.02
(2.10to
7.68
)Ref
5.26
(1.91to
14.52)
Ref
2.10
(0.91to
4.82
)Ref
P‡,
.001
.001
3.080
7
AdjustedHR§(95%
CI)
3.09
(1.49to
6.40
)Ref
7.24
(2.15to
24.34)
Ref
2.10
(0.83to
5.31
)Ref
P‡
.002
4.001
20.11
8
Survivalfrom
brea
stca
ncer
Una
djustedHR(95%
CI)
4.83
(2.51to
9.28
)Ref
8.19
(2.96to
22.67)
Ref
P§,
.001
,.001
AdjustedHR¶(95%
CI)
3.46
(1.65to
7.24
)Ref
10.28(3.08to
34.33)
Ref
P§.001
,.001
NOTE
.Inallpatients,pa
tientswith
stage0toIIIdisease,an
dpa
tientswith
stageIV
disease,un
ivariablemod
elswereba
sedon
174,
132,
and42
patients,respectively,an
dmultivariablemod
elswereba
sedon
163,
124,
and42
,patients,
respectively,
asaresultof
missing
data.
Abb
reviations:H
R,h
azardratio;N
E,no
tevaluab
le;O
S,overallsurvival;Ref,referen
ce.
*Three
deaths
occu
rred
from
othe
rcauses
atthefollowingtim
esfrom
diagno
sis:16
.1mon
ths(stage
II,53
yearsold),4
9.3mon
ths(stage
0,73
yearsold),a
nd59
.2mon
ths(stage
I,72
yearsold).
†Pvaluefrom
log-rank
testcompa
ringthetwocoho
rtOScu
rves
estim
ated
bytheKap
lan-Meier
metho
d.‡Pvaluefrom
Waldtestforsign
ificanc
eof
theHRcompa
ringHaitiversus
Miami(Ref)de
rived
from
Cox
regression
mod
els.
§Pvaluefrom
Waldtestforsign
ificanc
eof
theHRde
rived
from
Fine
andGrayregression
mod
elstaking
into
accoun
tdeath
from
othe
rcauses
asco
mpe
tingrisk.
¶AdjustedHRcompa
ringHaitiversus
Miami(Ref),from
multivariablemod
elsinclud
ingage(>
v,50
years)an
dbo
dymassinde
x(>
v,30
kg/m
2).Inthean
alysisofallpatients,wealso
includ
edstageatdiseasepresen
tation(IVv0-III).
395 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

rate is low compared with national averages,which were reported to be 66.8% for NHWand 67.1% for NHB in 2013.16 Barriers forhealth care utilization cited for this cohort in-cluded lack of health insurance coverage, lackof health education, communication and lan-guage barriers, and concerns about immigration
status.15,17,18 Other factors that have been de-scribed for BC total delay include low socioeco-nomic factors, ethnic minorities, travel time tohospital, long waiting times to get medical ap-pointments, and consulting three or more dif-ferent health services before arrival to a cancercenter.8
Table 3. Age, Disease Stage, andReceptor Status at Diagnosis of Our Study Cohorts ComparedWithData Extracted From the SEERDatabase From2008 to2012 for Non-Hispanic Black and Non-Hispanic White Women
Characteristic
Percentage of Patients
Haitians in Haiti(n = 94)
Haitians in Miami(n = 102)
Non-Hispanic Black Women(n = 35,285)
Non-Hispanic White Women(n = 232,072)
Age at diagnosis, years
, 40 22.3 7.8 6.5 3.3
40-49 28.7 26.5 19.2 14.9
50-59 28.7 39.2 27.8 23.8
> 60 20.2 26.5 46.5 57.9
, 50 51.1 34.3 25.7 18.3
> 50 48.9 65.7 74.3 81.7
Mean (SD) 50.2 (12.9) 53.7 (11.1) 58.8 (13.2) 62.4 (13.3)
Median 48.5 54 58 62
Interquartile range 41-58 47-60 49-58 52-72
Range 27-89 27-88 18-108 18-114
Cancer stage
0 (DCIS) 1.1 13.7 18.4 17.2
I 2.1 14.7 31.2 42.9
II 24.5 27.5 31.1 27.0
III 44.7 25.5 13.3 9.0
IV 27.6 18.6 5.9 3.8
Receptor status
ER, No. 49 35,278 232,029
Negative 44.9 26.5 26.9 15.7
Positive 55.1 73.5 73.1 84.3
PR, No. 34 34,930 229,161
Negative 64.7 40.2 38.8 27.1
Positive 35.3 59.8 61.2 72.9
ER/PR, No. 42
Both negative 35.7 26.5 25.3 14.9
Either one or both positive* 64.3 73.5 74.7 85.1
HER2,† No. 25 17,988 116,992
Negative 72.0 80.4 80.3 83.9
Positive* 28.0 19.6 19.7 16.1
Triple-negative status, No. 40 31,147 214,439
Yes 17.5 21.6 11.9 5.5
No 82.5 78.4 88.1 94.5
Abbreviations: DCIS, ductal carcinoma in situ; ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; PR, progesterone receptor; SD, standard deviation.*Positive includes borderline.†HER2 status available in SEER for patients diagnosed in 2010 and later.
396 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

It is unclear why the native Haitians in our studypresentedwithmoreER-negative disease than theimmigrantHaitianwomen. The triple-negative rateinnativeHaitianwomenwith known receptor statuswas 44.9% compared with 26.5% in Haitians inMiami. The rate of triple-negative BC was similarbetween Haiti immigrants and African Americanwomen (26.5% v28.4%, respectively). These ratesremain significantly elevated compared with the15.2% rate of triple-negative BC reported in NHWwomen. All ER and HER2 testing was performed inthe United States, so the testing was consistent andaccurate, although there may be some effect fromstorage or preservation of the Haitian samples thatinfluenced the rate of positive ER tests.
There are distinct differences in the age of BCpresentation in the four cohorts. Thewomen in ourstudy who lived in Haiti had symptoms for almost2 years before presentation, which argues that theage of onset is actually younger than stated andthat the age difference is greater than what wedocument. One explanation is that the life expec-tancy inHaiti is 61years,whichmeans thatwomendie of competing causes of mortality before theyreach ages where BC incidence increases. Theaverage age of a Haitian immigrant is 45 years,which is younger than the average age of BC onsetin Haiti. Thus, it seems that women immigratebefore the average age of BC onset. According toinstitutional data, 96% of Haitian women seekingcare at JMH immigrated within 5 years.15 Re-search shows that environmental and behavioralfactors in Westernized countries, such as smok-ing, nutrition, physical inactivity, and fertility fac-tors, increase the incidence of hereditary andsporadic BC in immigrants over a prolonged pe-riod.19-21 Short-term effects of immigration on BCdevelopment have never been documented.
Our study suggests that Afro-Caribbean womenfrom Haiti have different age of onset and tumorcharacteristics than NHB women reported inSEER data. Recently, members of our researchgroup found that other Afro-Caribbean womendevelop BC at an earlier age than either EuropeanAmerican or African American women.22 Taioliet al23 found that Caribbean women living inBrooklyn are diagnosed at an older age thanwomen from the Caribbean territories. The Afro-Caribbean population has extremely diverse an-cestry, with populations with deep genetic rootsin West Africa, northern Europe, the Indian sub-continent, China, the Middle East, and southernEurope and native Caribbean populations. Thedifferent ethnicities within African descents aredistinct in terms of beliefs, behaviors, risk fac-tors, and disease experience, which have animpact on the accurate use of this term forepidemiologic and public health research.24-26
Our data raise the question about whether dis-parities exist within subgroups of women ofAfrican origin.
In conclusion, Haitians diagnosed with BC in Haitiexperience a significantly worse outcome thanHaitian immigrants in Miami, which seems to berelated to amore advanced stage and younger ageatdiagnosis,moreER-negative tumors, and lackoftimely effective treatments. In addition, thereare differences in the age of presentation andER-positive status that raise the question ofwhether there are disparities within subgroupsof women of African origin who have BC. Con-founding epigenetic-related variables and otherenvironmental factors might impact survivaland need further exploration.
DOI: https://doi.org/10.1200/JGO.2016.005975Published online on jgo.org on November 2, 2016.
AUTHOR CONTRIBUTIONS
Conception and design: Alexandra Gomez, Judith HurleyAdministrative support: Vincent DeGennaro, Judith Hurley
Provision of study materials or patients: Vincent DeGennaro,Judith Hurley
Collection and assembly of data: Alexandra Gomez, VincentDeGennaro, Estefania Santamaria, Gustavo FigueiredoWestin, Dieudina Gabriel, Judith HurleyData analysis and interpretation: Alexandra Gomez, VincentDeGennaro, Sophia H.L. George, Isildinha M. Reis, JudithHurleyManuscript writing: All authors
Final approval of manuscript: All authorsAccountable for all aspects of the work: All authors
AUTHORS’ DISCLOSURES OFPOTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided byauthors of this manuscript. All relationships are consideredcompensated. Relationships are self-held unless noted. I =Immediate Family Member, Inst = My Institution. Relation-ships may not relate to the subject matter of this manuscript.For more information about ASCO’s conflict of interest policy,please refer to www.asco.org/rwc or ascopubs.org/jco/site/ifc.
397 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Alexandra GomezNo relationship to disclose
Vincent DeGennaroNo relationship to disclose
Sophia H.L. GeorgeNo relationship to disclose
Isildinha M. ReisNo relationship to disclose
Estefania SantamariaNo relationship to disclose
Gustavo Figueiredo WestinNo relationship to disclose
Dieudina GabrielNo relationship to disclose
Judith HurleyNo relationship to disclose
Affiliations
Alexandra Gomez, Gustavo Figueiredo Westin, and Judith Hurley, University of Miami/Jackson Memorial Hospital; Sophia H.L.George, SylvesterComprehensiveCancerCenter,University ofMiami; IsildinhaM.Reis, SylvesterBiostatistics andBioinformaticsCore Resource, University of Miami, Miami; Vincent DeGennaro and Estefania Santamaria, University of Florida College ofMedicine, Gainesville, FL; and Vincent DeGennaro and Dieudina Gabriel, Innovating Health International, Port-au-Prince, Haiti.
REFERENCES1. Ferlay J, Soerjomataram I, Ervik M, et al: GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC
CancerBase No. 11, 2013 ed. Lyon, France, International Agency for Research on Cancer, 2013. http://globocan.iarc.fr
2. Ferlay J, Soerjomataram I, Dikshit R, et al: Cancer incidence and mortality worldwide: Sources, methods and majorpatterns in GLOBOCAN 2012. Int J Cancer 136:E359-E386, 2015
3. Torre LA, Siegel RL, Ward EM, et al: Global cancer incidence and mortality rates and trends: An update. CancerEpidemiol Biomarkers Prev 25:16-27, 2016
4. Ward E, Jemal A, Cokkinides V, et al: Cancer disparities by race/ethnicity and socioeconomic status. CA Cancer J Clin54:78-93, 2004
5. Department of Homeland Security, Office of Immigration Statistics: U.S. Yearbook of Immigration Statistics: 2013.Washington, DC, Department of Homeland Security, Office of Immigration Statistics, 2014
6. SohmerR: TheHaitian Community inMiami Dade. Growing theMiddle Class: Connecting All Miami-DadeResidents toEconomic Opportunity. Washington, DC, The Brookings Institution Metropolitan Policy Program, 2010
7. Fine JP, Gray RJ: A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc 94:496-509, 1999
8. Unger-Salda~na K: Challenges to the early diagnosis and treatment of breast cancer in developing countries. World JClin Oncol 5:465-477, 2014
9. Kothari A, Fentiman IS: 22. Diagnostic delays in breast cancer and impact on survival. Int J Clin Pract 57:200-203,2003
10. Arndt V, Sturmer T, Stegmaier C, et al: Patient delay and stage of diagnosis among breast cancer patients in Germany:A population based study. Br J Cancer 86:1034-1040, 2002
11. Richards MA, Smith P, Ramirez AJ, et al: The influence on survival of delay in the presentation and treatment ofsymptomatic breast cancer. Br J Cancer 79:858-864, 1999
12. Gorin SS, Heck JE, Cheng B, et al: Delays in breast cancer diagnosis and treatment by racial/ethnic group. Arch InternMed 166:2244-2252, 2006
13. Balasubramanian BA, Demissie K, Crabtree BF, et al: Black Medicaid beneficiaries experience breast cancertreatment delays more frequently than whites. Ethn Dis 22:288-294, 2012
14. McGee SA, Durham DD, Tse CK, et al: Determinants of breast cancer treatment delay differ for African American andwhite women. Cancer Epidemiol Biomarkers Prev 22:1227-1238, 2013
15. Seay JS, Carrasquillo O, Campos NG, et al: Cancer screening utilization among immigrant women in Miami, Florida.Prog Community Health Partnersh 9:11-20, 2015 (suppl)
16. Centers for Disease Control and Prevention, National Center for Health Statistics: Health, United States, 2014: Withspecial feature on adults aged 55–64. http://www.cdc.gov/nchs/data/hus/hus14.pdf#076
17. Sambamoorthi U, McAlpine DD: Racial, ethnic, socioeconomic, and access disparities in the use of preventiveservices among women. Prev Med 37:475-484, 2003
18. Kobetz E, Menard J, Diem J, et al: Community-based participatory research in Little Haiti: Challenges and lessonslearned. Prog Community Health Partnersh 3:133-137, 2009
398 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

19. Nodora JN, Gallo L, Cooper R, et al: Reproductive and hormonal risk profile according to language acculturation andcountry of residence in the Ella Binational Breast Cancer Study. J Womens Health (Larchmt) 23:532-540, 2014
20. John EM, Phipps AI, Davis A, et al: Migration history, acculturation, and breast cancer risk in Hispanic women. CancerEpidemiol Biomarkers Prev 14:2905-2913, 2005
21. Andreeva VA, Unger JB, Pentz MA: Breast cancer among immigrants: A systematic review and new research di-rections. J Immigr Minor Health 9:307-322, 2007
22. George SA, Donenberg T, Albari M, et al: Breast cancer in the Caribbean: A six-country cohort. 8th American As-sociation for Cancer Research Conference of the Science of Cancer Health Disparities in Racial/Ethnic Minorities andthe Medically Underserved, Atlanta, GA, November 12-16, 2015
23. Taioli E, Attong-Rogers A, Layne P, et al: Breast cancer survival in women of African descent living in the US and in theCaribbean: Effect of place of birth. Breast Cancer Res Treat 122:515-520, 2010
24. Agyemang C, Bhopal R, Bruijnzeels M: Negro, black, black African, African Caribbean, African American or what?Labelling African origin populations in the health arena in the 21st century. J Epidemiol Community Health 59:1014-1018, 2005
25. Aspinall PJ: The categorization of African descent populations in Europe and the USA: Should lexicons of recom-mended terminology be evidence-based? Public Health 122:61-69, 2008
26. Oppenheimer GM: Paradigm lost: Race, ethnicity, and the search for a new population taxonomy. Am J Public Health91:1049-1055, 2001
399 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

reviewarticle
Cervical Precancer Treatment inLow- and Middle-Income Countries:A Technology Overview
abstract
Cervical cancer is the fourth leadingcauseof cancer-relateddeath inwomenworldwide,with90%ofcasesoccurring in low- and middle-income countries (LMICs). There has been a global effort to increase accessto affordable screening in these settings; however, a corresponding increase in availability of effective andinexpensive treatmentmodalities for ablating or excising precancerous lesions is also needed to decreasemortality. Thisarticle reviews thecurrent landscapeof availableanddeveloping technologies for treatmentof cervical precancer in LMICs. At present, the standard treatment ofmost precancerous lesions in LMICs isgas-based cryotherapy. This low-cost, effective technology is an expedient treatment in many areas;however, obtaining and transporting gas is often difficult, and unwieldy gas tanks are not conducive tomobile health campaigns. There are several promising ablative technologies in development that aregasless or require less gas than conventional cryotherapy. Although further evaluation of the efficacy andcost-effectiveness is needed, several of these technologiesare safeandcannowbe implemented in LMICs.Nonsurgical therapies, such as therapeutic vaccines, antivirals, and topical applications, are alsopromising, but most remain in early-stage trials. The establishment of evidence-based standardizedprotocols for available treatments and the development and introduction of novel technologies arenecessary steps in overcoming barriers to treatment in LMICs and decreasing the global burden of cervicalcancer. Guidance from WHO on emerging treatment technologies is also needed.
J Glob Oncol 3. © 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
INTRODUCTION
Inmost high-income countries, the incidence andmortality of cervical cancer have decreased by75% over the past 50 years due to the develop-ment of screening tests and the ability to detectand treat patients with lesions that have not pro-gressed to invasive cancer.1 Yet, cervical cancerremains the third most common cancer in womenworldwide, with nearly 90%of new cases diagnosedin low- andmiddle-income countries (LMICs).2 Lowpopulation coverage, poor-quality cytology, incom-plete follow-up of screen-positive women, and bar-riers to effective treatment all contribute to the lowsuccess of cervical cancer prevention programs inLMICs. Because cervical cancer predominantly af-fectswomenof reproductiveage, thesocietal impactand years of life lost attributable to the disease aresubstantially greater than for other female cancers.3
Prophylactic vaccinesagainsthumanpapillomavi-rus (HPV) have been developed and can be ex-pected to prevent 70% to 90% of invasive cancercases in unexposed women.4-9 Given the large
numberofwomenexposedand lowratesof vaccineuptake in LMICs, screening and treatment will beneeded for the foreseeable future.10
TheWHOendorses screeningwith cytology, visualinspection with acetic acid, or primary high-riskHPV testing. Although many countries have cytol-ogy programs, effectiveness is limited by a lack ofaffordable treatment.11-14 In somecountries, up to80%of women diagnosedwith cervical precancernever receive the recommended treatment.15Cur-rent treatment methods are often expensive anddifficult to implement at scale. Low-cost, durable,user-friendly treatment options in LMICs areneeded. The purpose of this review is to discusscurrent and emerging technologies (Table 1) forprecancer treatment, with a focus on utility in low-resource settings.
AVAILABLE TECHNOLOGIES
Loop Electrosurgical Excision Procedure
Brief history of the device. In the 1900s, loopconization procedures were performed to remove
Mauricio Maza
Celina M. Schocken
Katherine L. Bergman
Thomas C. Randall
Miriam L. Cremer
MauricioMaza,Katherine L.Bergman, and Miriam L.Cremer, Basic HealthInternational, New York,NY; Celina M. Schocken,Pink Ribbon Red Ribbon,Washington, DC; ThomasC. Randall, NationalCancer Institute,Massachusetts GeneralHospital, Boston, MA; andMiriam L. Cremer,Cleveland Clinic,Cleveland, OH.Corresponding author:Miriam L. Cremer, MD,MPH, Cleveland ClinicLerner College ofMedicine9500 Euclid Ave A81,Cleveland OH; e-mail:[email protected].
400 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
© 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License

grossly visible tumors. Electrosurgical excision ofcervical intraepithelial neoplasia (CIN) with wireloop electrodes, commonly known as loop elec-trosurgical excision procedure (LEEP), grew inpopularity in the last decades of the twentiethcentury, particularly in high-resource countries.Prendiville et al16 demonstrated in 1986 that a finewire loop can be used to excise the transformationzone in unanesthetized patients, a significant ad-vance in the management of CIN. LEEP can beperformed in outpatient settings under local anes-thesia. It is currently the standard of care for high-grade lesions in developed countries.
Descriptionof thedevice.ThefirstcommercialLEEPmachine was introduced by CooperSurgical (Trum-bull, CT) in 1991. LEEP equipment includes anelectrosurgical unit that generates power, a smokeevacuator with tubing, disposable loop electrodes,andaspeculumcoatedwithanticonductivematerial.
How it works. LEEP uses wire loop electrodes toremove precancerous lesions and the entire cer-vical transformation zone, excising and coagulat-ing simultaneously.
Cure rates.ACochrane review reported a cure rateof 91% to 98% for CIN grade 3 with LEEP.17
Advantages. LEEP is considered the standard ofcare for cervical precancer treatment. It is highlyeffective and has a low complication rate. InLMICs, LEEP is necessary if any of the followingcontraindications for cryotherapy are present:
·the lesion is not fully visible on the trans-formation zone or its borders are not distinct
·the lesion continues into the endocervix/os
·the patient is postmenopausal
·the lesion covers more than 75% of the cervix
Tissue collected during LEEP can be biopsied andpathologically examined to ensure that no invasivecancer goes undiagnosed.
Disadvantages/challenges. LEEP needs to be per-formed by an experienced clinician, generally anobstetrician/gynecologist. This requirement, inaddition to the need for electricity, local anesthe-sia, and resources for managing rare but seriousadverse events such as hemorrhage, limit the useof LEEP as a first-line treatment in LMICs.
Complications. Complications of LEEP includeintraoperative bleeding (3.4%), infection (4.9%),and postoperative bleeding (5.3%).18 Less than1% of women have cervical stenosis post-LEEP,
Table 1. Overview of Available and Developing Ablative Technologies
Attribute
Available Technologies Technologies in Development
CryotherapyThermal
CoagulatorLMIC-Adapted
CryoPen CryoPopUpdated Thermal
Coagulator
Device powersource
N2O or CO2 gas Electricity Electricity or battery CO2 gas (1/10 ofcryotherapy)
Electricity or battery
Portability Gas tanks can be heavy Portable Portable (device is20 lb)
Portable (gas tank is 5 lb) Portable
Pain/discomfort Minor Minor Minor Minor Minor
Time 15 min (double freeze) Approximately1 min
15 min (double freeze) 15 min (double freeze) Approximately 1 min
Cost(approximate)
Machine, $2,000; gas,$13-$38 per Tx (+ costof gas transport)
Machine, $2,000;probes, $600 each
Machine, $4,000;ethanol (cost isnegligible)
Machine, $800-$1,200;gas, $2-$4 per T
Approximately $2,500
Effectivenessrange
77%-93% 87%-97% Clinical trials inprogress
Clinical trials inprogress
Device indevelopment
Benefits Only ablative Txrecommended byWHO; simple tooperate
Does not require gas;simple to operate
Does not require gas;simple to operate
Requires 1/10 of gas oftraditional cryotherapy;inexpensive; simple tooperate
Does not requiregas; simple to operate
Limitations Challenges with gasprocurement
Need updated dataon effectiveness,protocol uniformity;pain
Ethanol needed formaintenance; durabilityof device unknown
Challenges withgas procurement
Need updated data oneffectiveness, protocoluniformity; pain
Abbreviations: LMIC, low- and middle-income country; Tx, treatment.
401 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

and in 2% of women, there is inadequate visu-alization of the squamocolumnar junction.19 Al-though there was significant heterogeneity, ameta-analysis of studies on fertility and preg-nancy outcomes after treatment of cervical pre-cancer revealed that there is no evidence tosupport that treatment adversely affects theseoutcomes; the overall pregnancy rate was higherfor women who received treatment comparedwith women who were untreated.20
Sterilization. LEEP requires an individual dispos-able probe for each procedure. No sterilization isrequired.
Costs. The LEEP device, including the electro-surgical unit and smoke evacuator, generallycosts approximately$3,500 and is made by sev-eral companies. Disposable probes cost approx-imately $20 apiece; a box of five probes costs$110. An insulated speculum costs approxi-mately $200.
Approval by regulatory agencies. The CooperSur-gical LEEP device was approved by the Food andDrug Administration (FDA) in 1991 for the treat-ment of cervical precancer, including CIN 1 to 3.
WHO recommendations. The WHO recommendsLEEP for treatment of CIN 2+ and recognizes thepotential benefit of LEEP over cryotherapy. TheWHO states that either LEEP or cryotherapy maybe used, as available.21
Cryotherapy
Brief history of the device. Cryotherapy has beenused since 3000 BC, when ancient Egyptiansused the technique to cure inflammation and asan analgesic. It has been used to treat chroniccervicitis since 1883 and to treat cervical neo-plasia since 1964.22
Description of the device. There are several com-mercially available cryotherapy devices that aresimilar in design, consisting of a probe that isattached to a tank of gas that cools the probe.Cryotherapy devices must reach 250°C to beeffective.23 Gas-based cryotherapy uses nitrousoxide (N2O), medical-grade carbon dioxide (CO2),or industrial (beverage-grade) CO2. N2O is con-sidered the standard gas for the procedure, be-cause it is colder than CO2 (freezing at 289°Ccompared with 278°C for CO2) and achieves agreater depth of tissue necrosis than CO2.
24
How it works. The goal of ablative treatment is tofreeze or heat the transformation zone, causing
cellular necrosis. The transformation zone is theonly area in which squamous cervical precancercan arise. To ablate precancer cells, it is importantto reach a target depth of necrosis (DON). A DONof 3.5 mm is needed to treat 95% of CIN 1 to 3lesions, and a depth of 4.8 mm is needed to treat99% of all patients.25
Cure rates.According to theCochrane review, curerates for CIN 3 following cryotherapy range from77% to 93%.17 There is conflicting evidence onwhetherHIV-positivewomenhave lower cure ratesthan HIV-negative women after treatment withcryotherapy. Although cryotherapy is normally77% to 93% effective, recent evidence suggeststhat this is lower in HIV-positive women. Omengeet al26 found that the cure rate was only 37% at6 months, using N2O.$
Advantages. Traditional cryotherapy has many ad-vantages. It is effective, relatively low cost, and lowmaintenance. It is also safe. Major bleeding andinfection are less common in cryotherapy com-pared with cold-knife conization and LEEP.27
Disadvantages/challenges. There are many chal-lenges with the use of gas-based cryotherapy inlow-resource settings, including difficulty in pro-curing high-quality gas. Industrial CO2 is readilyavailable, but impurities in the gas may lead toinconsistent temperatures and device block-ages.28 A trained technician is required to removesome blockages, but simple techniques—eitherwiping thenozzlewithalcohol or placing thenozzlein water while the gas is on—can remove mostclogs. The potentially high cost of obtaining andreplenishing gas can be a barrier for use in LMICs.The cumbersomeequipment canalso prove prob-lematic in field settings. Cryotherapy is typicallyperformed using a tank weighing 50 to 70 lb, with20 lb of compressed gas, that can treat two to 20patients.29 A smaller tank can be used, but fewerpatients can be treated. In addition, continual usereduces the pressure at the cryoprobe tip,29 whichcan prevent the device from reaching its lowesttemperature.
Complications. Complication rates are generallylow. In a review by the WHO,30 risks of spontane-ous abortion and infertility were not higher thanthat of the general population.
Sterilization. Cryotherapy instruments generallyhave tips that are removable and can be auto-claved or sterilized using high-level disinfection(HLD) between patients. HLD recommended bytheWHOuses chlorine bleach solution andcanbe
402 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

completed in 20 to 30 min.31 The probe, whichenters the vaginal canal but does not come intocontact with mucous membranes, can be disin-fected with alcohol between patients.
Costs. The most widely used cryotherapy deviceshave an estimated cost between $1,700 and$2,000, with additional tips costing approxi-mately $200 each. These prices may increasesignificantly because of distribution costs andtaxes, specific to each country. Cheaper devices($250) are available, but decreased cost may beassociated with decreased quality. In addition tothe cost of the machine, the required gas andrelated costs can range from $13 to $38 pertreatment.32 To perform high-throughput cryo-therapy, multiple tips must be available, whichcan increase cost.
Approval by regulatory agencies. The WallachLLl00 (Wallach Surgical, Trumbell, CT) receivedFDA approval for treatment of CIN 1 to 3 in 1981.Similar cryotherapy devices have received FDAapproval by demonstrating equivalency to thisdevice.
WHO recommendations. Use of CO2 over N2O isrecommended in settings where both gasesare available, because N2O is not as widelyavailable in LMICs and CO2 is significantlycheaper.21 The WHO recommends a double-freeze technique—a 3-min freeze followed by a5-min thaw and a 3-min freeze—which is moreeffective than the single-freeze technique.21
The Cochrane review also recommended thedouble-freeze approach.17 Cremer et al24
found that the DON resulting from a singlefreeze using N2O was noninferior to DONresulting from a double freeze using N2O; ne-crosis with CO2-based cryotherapy was 1-mmless deep. Most devices come with various tipsizes and shapes, including flat and conicalshapes ranging from16 to 21mm in diameter. Asmall diameter tip with a flat shape may notadequately cover the lesion, resulting in treat-ment failures. WHO guidelines suggest that atip should be 19 6 2 mm in diameter.29
WHO recommendations: Special cases to consider.Pregnant patients. Only women with invasive cervi-cal cancer should be treated during pregnancy, andthis should be at a referral facility. Pregnant womenwith preinvasive lesions should be asked to return 6to 12 weeks postpartum for evaluation.33
HIV-positive women.HIV-positive patients have anincreased risk of cervical precancers, and these
progress faster to invasive cancer than in HIV-negative women. Therefore, HIV-positive womenneed to be screened more frequently, and theirlesions should be treated immediately. Follow-upevaluations of HIV-positive women should be per-formed within 12 months of treatment.33 In addi-tion, HIV-positive women need to be screenedearlier than do HIV-negative women. Thesewomen should be screened within 1 year ofthe onset of sexual activity, but starting no laterthan 21 years of age.34
Postmenopausal women. Postmenopausal womenshould be treated using an excisional, rather thanan ablative, technique if the transformation zone isnot visible.33
Repeat patients. Patients who are treated for pre-cancerous lesions should be reevaluated after12months. Patients with CIN 1 and CIN 2 lesionswho are free of lesions at 12months can return tothe normal screening timeline. Patients with CIN3 lesions should be screened yearly for 3 years,even if they are lesion free at 12 months. Ifpatients have lesions at 12 months, they shouldbe referred for treatment with LEEP or cold-knifeconization.33
Thermocoagulation (Cold Coagulation)
Brief history. Thermocoagulation was used fordecades to treat noninvasive cervical conditionsprimarily in the United Kingdom, but its applica-tion diminished after the introduction of excisionprocedures in the 1980s.
Description of the device. The current commercialdevice, the WiSAP Cold-Coagulator (WiSAP,Brunnthal, Germany) is a simple box with a tem-perature dial and probes attached by cables. Thedevice runs on either electricity or an automotivebattery.
WiSAP is in the process of overhauling the ther-mocoagulator for the first time since 1966, with afocus on increasing ease of use and optimizing thedevice for low-resource settings with probe tipsthat require only HLD.
How it works. Thermocoagulation uses heat todestroy cervical tissue: the superficial epitheliumsloughs off after treatment, and the underlyingstroma and glandular crypts are destroyed bydesiccation.35 Expert interviews reveal no consen-sus on treatment regimens, with preference forboth single-burn and multiple-burn techniquesand with treatment durations ranging from 30 to60 seconds.
403 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Cure rates. In 2014, Dolman et al36 published ameta-analysis on thermocoagulation, which is themost comprehensive review of the therapy (13studies, with 4,569patients). They concluded thatit had cure rates similar to other ablative therapies,that it was safe and effective, and that it heldparticular promise for low-resource settings.36
They estimated an overall cure rate of 94% forCIN 1 to 3.36
A study of 1,628 women with CIN 3 treatedwith overlapping, 20-second, 100°C applicationsfound a primary success rate of 95%at 1 year.37 Astudy of 725womenwith CIN1, 2, and 3 treated at120°C for 30 to 40 seconds found that 87.2% ofwomen had normal cytology after treatment andlong-term negative follow-up.38 More rigorous tri-alsneed tobecompleted to standardize treatment.
Advantages. Thermocoagulation is easy to admin-ister, requiring only the small device and electric-ity. Theupdatedmodel includes only one tipwith alarger diameter that will prevent the need forchanging tips to accommodate different lesionsizes. The probe tip can be disinfected rather thansterilized.
Disadvantages/challenges. Reliance on electricityas a power source is a limitation of thermocoagu-lation. The optimal temperature and applicationtiming have not yet been determined, and con-sensus is lacking on the DON needed with ther-mocoagulation. A study of 80 patients found thatthe mean depth of tissue destruction after a sin-gle application of a flat tip ranged from 2.6 mm(100°C for 20 seconds) to 3.5 mm (120°C for 30seconds).39
Pain during thermocoagulation procedures isalso a concern. Studies are needed to establishthe optimal treatment parameters and ensure atolerablepatient experience. Themeta-analysis byDolman et al36 noted that at least one study foundthat 19% of women experienced pain, suggestinganalgesia would improve acceptance of the pro-cedure. Although DON increases with higher tem-peratureand longerdurationof exposure,39,40 andlarger (20-mm) tips allow full coverage of lesions,these factors may contribute to increased pain.
Complications. Dolman et al36 concluded thatthermocoagulation treatment has no effect onfertility, noting that 94% of women were pregnantwithin 2 years of treatment.
Sterilization. The thermocoagulation device hastwo components—only the probe (with attachedtip) is in contact with the patient. The probe in the
original devicemust be autoclaved after each use,whereas the probe in the updated device requiresonly HLD.
Costs. The original WiSAP Cold-Coagulator devicecosts approximately $3,000: the electrical unitcosts approximately $2,000, the instrument cableattaching theprobe to theunit costs approximately$370, and one probe costs approximately $700.Theupdateddevicecustomized foruse inLMICs isprojected to cost approximately $2,500 and offerscost-saving benefits by requiring HLD rather thanautoclave sterilization of the probe.
Regulatory approval and indications. The WiSAPCold-Coagulator is CE Mark–certified and indi-cated for CIN 1 to 3.
WHO recommendations. Thermocoagulation wasnot included in the WHO 2013 cervical cancerguidelines. However, use of thermocoagulation isgaining popularity in LMICs, where ablative ther-apy is still common. Many countries in Africa andAsia have active thermocoagulation projects, andeaseofusemakesacceptability of thisdevicehigh.There remains a need for formal WHO guidelinesand standardization of the procedure.
LMIC-Adapted CryoPen
Brief history. The CryoPen is a nongas–basedablation method that destroys tissue throughapplying a cooled single pen core (cryoprobe) tothe cervix. CryoPen was originally founded to pro-vide cryotherapy for dermatologic lesions butwas modified for gynecologic use. The originalgynecologic-adapted CryoPen was best usedin a controlled office setting and required chang-ing the cold core during the procedure. A newLMIC-adapted device has been designed andoptimized for use in low-resource settings, be-cause the device is more portable, durable, andcost-effective than the standard model.
Description of the device. The LMIC-adapted Cryo-Pen consists of a cooling device built into a toolbox,with an adjoining probe. The system is portable, isequipped with a handle, weighs 20 lb, and can treatapproximately 24 women per 8-hour day.
How it works. The machine cools by using a Stirlingcooler, with helium as the refrigerant. The singlepen core (cryoprobe) is inserted into a sheathwith a 20-mm tip. The probe remains cold longenough to complete either a single, 5-min freezeor to follow the double-freeze method. It can useeither electricity or batteries. Ethanol is needed toprevent the core from freezing to the device.
404 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Cure rates. The LMIC-adapted CryoPen is cur-rently being developed and studied by MiriamCremer, MD, supported by National Institutes ofHealth grant No. 5UH2CA189883. The purposeof the grant is to compare the LMIC-adaptedCryoPen with conventional cryotherapy. A pilotstudy (n = 5) was performed in women undergo-ing hysterectomy for indications unrelated tocervical pathology. In these women, the averageDON was 4.12 mm. A larger DON trial is underway, and a trial is planned to determine curerates.
Advantages. The LMIC-adapted CryoPen does notdepend on gas and can be operated on electricityor a car battery. It is lighter andmore portable thanconventional cryotherapy. Midlevel providers arecurrently using the device in Haiti and have hadpositive experiences.
Disadvantages/challenges. Reliance on electricityas a power source is a limitation of the LMIC-adapted CryoPen, although it can be chargedwith a car battery, if necessary. The device alsorequires small amounts of ethanol to keep theprobe from freezing to the well.
Complications.Complications have not been stud-ied but are projected to be low and similar tocryotherapy.
Sterilization. The LMIC-adapted CryoPen probedoes not come into contact with the vaginal tissue.The LMIC-adapted CryoPen tips and the sheathcan be cleaned using HLD methods.
Costs. The LMIC-adapted CryoPen model isprojected to cost approximately $4,000, whichis more expensive than a gas-based system($2,000). However, both the long-term costand the cost per patient will be less than thatfor gas-based cryotherapy because there is noneed to procure and distribute gas.
Regulatory approval and indications. The CryoPenis approved by the FDA to treat CIN 1 to 3.
WHO recommendations. To date, theWHO has notevaluated the device.
CryoPop
Brief history of the device. The idea of the CryoPopwas conceived in a class at the Center for Bio-engineering Innovation and Design at Johns Hop-kins University in 2011. Three graduate studentsin Biomedical Education worked with the non-profit organization Jhpiego, anaffiliate of the Johns
Hopkins University, to come up with creative low-cost solutions for precancer treatment.
Description of the device.CryoPop is anadaptationof cryotherapy technology that is designed to useless CO2 than existing equipment.
How it works. The CryoPop consists of an ergo-nomic hand-held device and a detachable appli-cator with an anodized metal tip. The detachableapplicator is connected to the gas tank to collectCO2 in the form of dry ice. It is then removed fromthe gas tank, clipped onto the CryoPop handle,and the anodized metal tip is placed against thecervix.
Cure rates. The cure rates are unknown at thistime. There is a current clinical trial under way atJohns Hopkins University, with Jean Anderson,MD, as the principal investigator on the study.The current trial (1UH2CA189923-01) is takingplace in the Philippines, where the CryoPop isbeing compared with standard cryotherapyequipment. The current chamber holds enoughdry ice for a single freeze, thus requiring a refill toperform a double freeze. In vitro studies usingballistic gelatin have documented tip tempera-tures comparable to or lower than existing cryo-therapy devices.
Advantages. The device is durable, easily repair-able in the field, and inexpensive. It runs on anygrade of CO2 gas, including industrial and foodgrade, and uses only a tenth as much gas pertreatment as do existing cryotherapy devices.Mid-level providers found it easy to use during hands-on simulation exercises.
Disadvantages/challenges. The CryoPop uses sig-nificantly less gas than standard cryotherapyequipment; however, the device still requiresgas, which can be challenging to obtain in somesettings.
Complications. Complications are likely to be lowand similar to conventional cryotherapy.
Sterilization. The tips will require HLD or auto-claving. The applicator, which enters the vaginabut does not come in contact with mucous mem-branes, can be disinfected with alcohol.
Costs. The device is expected to cost approxi-mately $800 to $1,200, in addition to lower per-patient costsbecauseof the reducedgas required.Jhpiego expects to get 15 to 20 treatments out ofone 5-lb tank of gas or 150 to 200 treatmentsfrom a 56-lb tank.
405 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Regulatory approval and indications. The CryoPopreceived FDA approval in the Philippines beforethe clinical trial in January 2016.
WHO recommendations. To date, theWHO has notreviewed the device.
TREATMENTS OF THE FUTURE
Current treatment methods are invasive and atleast somewhat uncomfortable to the patient.They can also be expensive, both in terms ofdevice and commodity costs and health workertime. There are some promising new technolo-gies in development, including therapeutic vac-cines, antivirals, and topical applications.WHO isalready studying therapeutic vaccines and anti-virals, and has a working group between thecervical cancer and immunology teams. The In-ternational Agency for Research on Cancer isconducting several studies, as is the NationalCancer Institute.
Therapeutic Vaccines
There are several therapeutic vaccines to cureHPV indevelopment, several of which are enteringphase III clinical trials. The goal of a therapeuticvaccine would be to elicit an immune responsetargeting E6 and E7 antigens; thus, these treat-ments can be thought of as a form of immuno-therapy.41 An excellent summary of potentialmethods for therapeutic vaccines can be foundin the article by Khallouf et al,42 “TherapeuticVaccine Strategies Against Human Papillomavi-rus.” The most advanced therapeutic vaccinecandidates include ADXS11-001 by Advaxis Im-munotherapies’ (Princeton, NJ), GTL001 (Pro-Cervix) by Genticel (Labege, France), and VGX-3100 by Inovio Pharmaceuticals (PlymouthMeeting, PA).43-45 The vaccine candidates allfocus on cancers caused by HPV 16, or 16/18,which is responsible for approximately 70% of allcancers. Limitations to the vaccine are that it willstill require multiple doses and only targets the16/18 virus, missing 30% of oncogenic HPVtypes, although there is evidence of cross-reactivity.
Antivirals
Several groups are studying the use of antivi-ral drugs to target HPV, although these are
early studies. Early-stage trials are underway for ranpirnase,46 HTI-1968, and otherantivirals.47
Adoptive T-cell therapy is also being studied. In anearly trial reported in 2014, two women with ad-vanced invasive cervical cancer experiencedcomplete recovery for 18 and 21 months at thetime of reporting. One patient had a partial re-sponse, andsix continued toprogress.48 Critics ofantiviral solutions note that so far, none haveadvanced to phase III clinical trials, and theyhave not shown significant effectiveness againstHPV.
Artesunate
Artesunate is a semisynthetic analog of artemi-sinin that is used to treatmalaria and is thought tohave strong antineoplastic activity. A phase I trialof intravaginal artesunate is under way to eval-uate its potential to treat precancerous cervicallesions.49
In conclusion, as low-resource settings beginto implement and improve cervical cancerscreening programs, there is a greater needfor effective and affordable treatment modali-ties for precancerous lesions. In LMICs, thecurrent primary methods of gas-based cryo-therapy and thermocoagulation are simple, ef-fective, and widely accepted; however, thereare clear gaps in evidence and consensus onproper implementation of these technologies,despite decades of use. Insufficient resourcesand infrastructure in LMICs further impede gas-based cryotherapy, because securing reliablegas supply chains is often difficult and expen-sive. Thus, the continued development of low-cost, effective treatment methods optimized forlow-resource settings is necessary. Devicesin development that require no or reducedamounts of gas are promising, as are nonsur-gical therapies. Standardized, evidence-basedprotocols for current treatment modalities andthe continued development of novel treatmentmethods are necessary to serve the increasingnumber of diagnosed women and decrease theworldwide burden of cervical cancer.
DOI: https://doi.org/10.1200/JGO.2016.003731Published online on jgo.org on August 17, 2016.
AUTHOR CONTRIBUTIONS
Conception and design: All authorsCollection and assembly of data: All authorsData analysis and interpretation: All authors
Manuscript writing: All authorsFinal approval of manuscript: All authorsAccountable for all aspects of the work: All authors
406 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

AUTHORS’ DISCLOSURES OFPOTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided byauthors of this manuscript. All relationships are consideredcompensated. Relationships are self-held unless noted. I =Immediate Family Member, Inst = My Institution. Relation-ships may not relate to the subject matter of this manuscript.For more information about ASCO’s conflict of interest policy,please refer to www.asco.org/rwc or ascopubs.org/jco/site/ifc.
Mauricio MazaNo relationship to disclose
Celina M. SchockenStock or Other Ownership: Praakti Health, OmerosConsulting or Advisory Role: Praakti Health
Katherine L. BergmanNo relationship to disclose
Thomas C. RandallNo relationship to disclose
Miriam L. CremerHonoraria: MerckSpeakers’ Bureau: Merck
ACKNOWLEDGMENTSupported by National Institutes of Health grant No.1UH2CA189883-01 for development of the LMIC-adaptedCryoPen (M.L.C. and M.M.). M.L.C. and M.M. do not receivefinancial compensation for their work with the LMIC-adaptedCryoPen.
REFERENCES1. Ferlay J, Shin HR, Bray F, et al: Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 127:
2893-2917, 2010
2. Schottenfeld D, Fraumeni JF Jr (eds): Cancer Epidemiology and Prevention. Oxford, UK, OxfordUniversity Press, 2006doi:10.1093/acprof:oso/9780195149616.001.0001
3. Agosti JM, Goldie SJ: Introducing HPV vaccine in developing countries–key challenges and issues. N Engl J Med 356:1908-1910, 2007
4. Joura EA, Giuliano AR, Iversen OE, et al: A 9-valent HPV vaccine against infection and intraepithelial neoplasia inwomen. N Engl J Med 372:711-723, 2015
5. Moore KA II, Mehta V: The growing epidemic of HPV-positive oropharyngeal carcinoma: A clinical review for primarycare providers. J Am Board Fam Med 28:498-503, 2015
6. Kang YJ, Lewis H, Smith MA, et al: Pre-vaccination type-specific HPV prevalence in confirmed cervical high gradelesions in the M�aori and non-M�aori populations in New Zealand. BMC Infect Dis 15:365, 2015
7. Blomberg M, Dehlendorff C, Sand C, et al: Dose-related differences in effectiveness of human papillomavirusvaccination against genital warts: A nationwide study of 550,000 young girls. Clin Infect Dis 61:676-682, 2015
8. FUTURE II Study Group: Quadrivalent vaccine against human papillomavirus to prevent high-grade cervical lesions.N Engl J Med 356:1915-1927, 2007
9. HildesheimA, Herrero R,Wacholder S, et al: Effect of human papillomavirus 16/18 L1 viruslike particle vaccine amongyoung women with preexisting infection: A randomized trial. JAMA 298:743-753, 2007
10. Graham JE, Mishra A: Global challenges of implementing human papillomavirus vaccines. Int J Equity Health 10:27, 2011
11. ParhamGP,MwanahamuntuMH, Kapambwe S, et al: Population-level scale-up of cervical cancer prevention servicesin a low-resource setting: Development, implementation, and evaluation of the cervical cancer prevention program inZambia. PLoS One 10:e0122169, 2015
12. Khozaim K, Orang’o E, Christoffersen-Deb A, et al: Successes and challenges of establishing a cervical cancerscreening and treatment program in western Kenya. Int J Gynaecol Obstet 124:12-18, 2014
13. Kim YM, Lambe FM, Soetikno D, et al: Evaluation of a 5-year cervical cancer prevention project in Indonesia:Opportunities, issues, and challenges. J Obstet Gynaecol Res 39:1190-1199, 2013
14. Gaffikin L, Blumenthal PD, EmersonM, et al: Safety, acceptability, and feasibility of a single-visit approach to cervical-cancer prevention in rural Thailand: A demonstration project. Lancet 361:814-820, 2003
15. Gage JC, Ferreccio C, GonzalesM, et al: Follow-up care of women with an abnormal cytology in a low-resource setting.Cancer Detect Prev 27:466-471, 2003
16. Prendiville W, Davies R, Berry PJ: A low voltage diathermy loop for taking cervical biopsies: A qualitative comparisonwith punch biopsy forceps. Br J Obstet Gynaecol 93:773-776, 1986
17. Martin-Hirsch PPL, Paraskevaidis E, Bryant A, et al: Surgery for cervical intraepithelial neoplasia. Cochrane DatabaseSyst Rev 6:CD001318-CD001318, 2010
18. Sutthichon P, Kietpeerakool C: Perioperative complications of an outpatient loop electrosurgical excision procedure: Areview of 857 consecutive cases. Asian Pac J Cancer Prev 10:351-354, 2009
19. Pathfinder International: Loop Electrosurgical Excision Procedure (LEEP) Clinical Standards of Practice. Watertown,MA, Pathfinder International, 2013
20. Kyrgiou M, Mitra A, Arbyn M, et al: Fertility and early pregnancy outcomes after treatment for cervical intraepithelialneoplasia: Systematic review and meta-analysis. BMJ 349:g6192, 2014
407 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

21. WHO:WHOGuidelines: Use of Cryotherapy for Cervical Intraepithelial Neoplasia. Geneva, Switzerland,WHOPress, 2011
22. Cooper SM, Dawber RP: The history of cryosurgery. J R Soc Med 94:196-201, 2001
23. Gage AA, Baust J: Mechanisms of tissue injury in cryosurgery. Cryobiology 37:171-186, 1998
24. Cremer M, Ditzian L, Winkler JL, et al: Comparison of depth of necrosis using cryotherapy by gas and number of freezecycles. J Low Genit Tract Dis 19:1-6, 2015
25. Abdul-Karim FW, Fu YS, Reagan JW, et al: Morphometric study of intraepithelial neoplasia of the uterine cervix. ObstetGynecol 60:210-214, 1982
26. Omenge E, Liu T, Itsura P, et al: Visual inspection with acetic acid (VIA) agrees reasonably well with Pap smear and HRHPVtyping for follow-up after VIA/cryotherapy in HIV-infected women. www.croiconference.org/sites/default/files/posters/851.pdf
27. WHO: WHO Guidelines for Screening and Treatment of Precancerous Lesions for Cervical Cancer Prevention.Geneva, Switzerland, World Health Organization, 2013
28. Santos CL, Torres J, Sanchez J, et al: Lack of effectiveness of CO2 cryotherapy for treatment of CIN. Int J GynaecolObstet 87:44-45, 2004
29. WHO: WHO Technical Specifications: Cryosurgical Equipment for the Treatment of Precancerous Cervical Lesionsand Prevention of Cervical Cancer. Geneva, Switzerland, World Health Organization, 2012
30. WHO: WHO Guidelines: Use of Cryotherapy for Cervical Intraepithelial Neoplasia. Geneva, Switzerland, World HealthOrganization, 2011. Int J Gynaecol Obstet 118:97-102, 2012
31. Tietjen L, Bossemeyer D, McIntosh N: Infection Prevention Guidelines for Healthcare Facilities With Limited Re-sources. Baltimore, MD, Jhpiego, 2004
32. Campos NG, Tsu V, Jeronimo J, et al: When and how often to screen for cervical cancer in three low- and middle-income countries: A cost effectiveness analysis. Papillomavirus Res 1:38-58, 2015
33. WHO: Comprehensive Cervical Cancer Control: A Guide to Essential Practice. Geneva, Switzerland, World HealthOrganization, 2014
34. Panel onOpportunistic Infections in HIV-Infected Adults andAdolescents: Guidelines for the prevention and treatmentof opportunistic infections in HIV-infected adults and adolescents: Recommendations from the Centers for DiseaseControl and Prevention, the National Institutes of Health, and the HIV Medicine Association of the Infectious DiseasesSociety of America. http://aidsinfo.nih.gov/contentfiles/lvguidelines/adult_oi.pdf
35. SemmK:New apparatus for the “cold-coagulation” of benign cervical lesions. Am JObstet Gynecol 95:963-966, 1966
36. Dolman L, Sauvaget C, Muwonge R, et al: Meta-analysis of the efficacy of cold coagulation as a treatment method forcervical intraepithelial neoplasia: A systematic review. BJOG 121:929-942, 2014
37. Gordon HK, Duncan ID: Effective destruction of cervical intraepithelial neoplasia (CIN) 3 at 100 degrees C using theSemm cold coagulator: 14 years experience. Br J Obstet Gynaecol 98:14-20, 1991
38. Zawislak A, Price JH, McClelland HR, et al: Efficacy of cervical intraepithelial neoplasia (CIN) treatment by coldcoagulation. Ulster Med J 72:10-15, 2003
39. Duncan ID: Cold coagulation. Baillieres Clin Obstet Gynaecol 9:145-155, 1995
40. Haddad N, Hussein I, Blessing K, et al: Tissue destruction following cold coagulation of the cervix. J Gynecol Surg 4:23-27, 1988
41. Trimble CL: HPV infection-associated cancers: Next-generation technology for diagnosis and treatment. CancerImmunol Res 2:937-942, 2014
42. Khallouf H, Grabowska AK, Riemer AB: Therapeutic vaccine strategies against human papillomavirus. Vaccines(Basel) 2:422-462, 2014
43. Wallecha A, French C, Petit R, et al: Lm-LLO-based immunotherapies and HPV-associated disease. J Oncol 2012:542851, 2012
44. Trimble CL, Morrow MP, Kraynyak KA, et al: Safety, efficacy, and immunogenicity of VGX-3100, a therapeuticsynthetic DNA vaccine targeting human papillomavirus 16 and 18 E6 and E7 proteins for cervical intraepithelialneoplasia 2/3: A randomised, double-blind, placebo-controlled phase 2b trial. Lancet 386:2078-2088, 2015
45. Maciag PC, Radulovic S, Rothman J: The first clinical use of a live-attenuated Listeria monocytogenes vaccine: Aphase I safety study of Lm-LLO-E7 in patients with advanced carcinoma of the cervix. Vaccine 27:3975-3983, 2009
46. Harrison L: Antiviral promising in early HPV trial. http://www.medscape.com/viewarticle/841876
47. Keshevan M: Startup’s antiviral combats HPV, study shows. http://medcitynews.com/2014/08/san- diego-startups-topical-antiviral-drug-combats-hpv-new-study-shows/
48. Hinrichs C, Stevanovic S, Draper L: HPV-targeted tumor-infiltrating lymphocytes for cervical cancer. J Clin Oncol 32:5s, 2014 (suppl; abstr LBA3008)
49. Sidney Kimmel Comprehensive Cancer Center: Intravaginal artesunate for the treatment of HPV+ high grade cervicalintraepithelial neoplasia (CIN2/3). https://clinicaltrials.gov/show/NCT02354534
408 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

specialarticle
American Society of Clinical OncologyMultidisciplinary Cancer ManagementCourse: Connecting Lives, CancerCare, Education, and Compassion inZimbabwe—A Pilot for Efforts ofSustainable Benefit?
executivesum
mary
The burden of cancer in low- to middle-income countries is growing and is expected to rise dramaticallywhile resources to manage this disease remain inadequate. All authorities for the management of cancerrecommend multidisciplinary care. Educational efforts by international organizations to assist localprofessionals in caring for their patients tend to have a lasting impact because they empower localprofessionals and enhance their skills. A multidisciplinary cancer management course was designed byAmerican Society of Clinical Oncology staff and local experts to provide a roadmap for cross-specialtyinteraction and coordination of care in Zimbabwe. The outcome of the course was measured throughfeedback obtained from participants and impact on local workforce. The cancer management course wasrelevant to daily practice and fostered long-lasting partnerships and collaborations. Furthermore, itresulted in amoremotivated localworkforceand strengthenedexistingmultidisciplinary practices.Cancercare is in a critical state in low- to middle-income countries. Educational efforts and collaborativepartnerships may provide a cost-effective strategy with sustainable benefits. A multidisciplinary approachto optimize therapy is desirable. Evaluation of the course impact after a period of 6 months to 1 year isneeded to determine the sustainability and impact of such efforts.
INTRODUCTION
The burden of cancer in low- and middle-incomecountries (LMICs) is increasingly a global concern.The incidence of cancer is expected to rise dra-matically in these regions, while the resourcesto manage this disease remain inadequate.1,2
Several organizations are engaging in volunteer-ing efforts whereby physicians travel from high-income to low-income countries to assist localprofessionals in caring for their patients. Theseefforts, although well intentioned, are generallyshort lived, and their impact is often unsustain-able.3-7 Educational efforts, facilitating transferand sharing of knowledge, may have a morelasting impact, although there may be factors thatinfluence the success of such measures.8,9 Mul-tidisciplinary care has been widely adopted as thestandard of care in cancer management, withstudies showing significant changes in diagnosesand treatment plans.10-12 However, data on the
impact of multidisciplinary care in developingcountries are limited.
Zimbabwe is a country located in the sub-Saharanregion of Africa. It has a population of 13,061,239(according to the 2012 national census), with aratio of approximately 93 males to 100 females.13
The average life expectancy is approximately 58years.14 Its gross domestic product as of 2014was US$14.2 billion.15 The country has beengreatly affected by the HIV pandemic, with 15%of adults infected by the virus.16 This has also af-fected the epidemiology of cancers in Zimbabwe,with HIV-related cancers comprising 60% of newcases of cancer per year, as noted by the ZimbabweNational Cancer Registry (NCRZ).17 The majordiseases in Zimbabwe are HIV and AIDS, tuber-culosis, and malaria.18 Zimbabwe is now facingthe threat of noncommunicable diseases likecardiovascular disease, diabetes, and can-cer, particularly cervical cancer.19 The density
Sandra Ndarukwa
Anna Mary Nyakabau
Anees B. Chagpar
David Raben
Ntokozo Ndlovu
Webster Kadzatsa
Vanessa J. Eaton
Paida Mafunda
Evangelia Razis
Author affiliations appear atthe end of this article.
Corresponding author:Sandra Ndarukwa, MD,13 Mold Crescent,Kensington, Harare,Zimbabwe; e-mail:[email protected].
409 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
© 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License
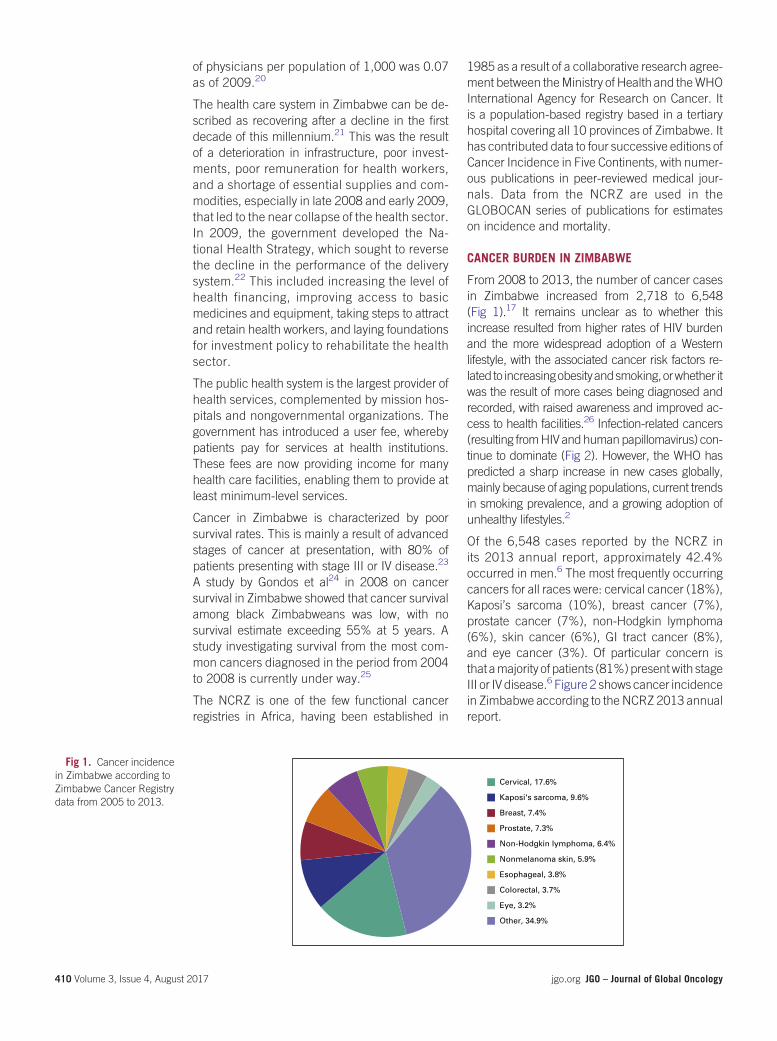
of physicians per population of 1,000 was 0.07as of 2009.20
The health care system in Zimbabwe can be de-scribed as recovering after a decline in the firstdecade of this millennium.21 This was the resultof a deterioration in infrastructure, poor invest-ments, poor remuneration for health workers,and a shortage of essential supplies and com-modities, especially in late 2008 and early 2009,that led to the near collapse of the health sector.In 2009, the government developed the Na-tional Health Strategy, which sought to reversethe decline in the performance of the deliverysystem.22 This included increasing the level ofhealth financing, improving access to basicmedicines and equipment, taking steps to attractand retain health workers, and laying foundationsfor investment policy to rehabilitate the healthsector.
The public health system is the largest provider ofhealth services, complemented by mission hos-pitals and nongovernmental organizations. Thegovernment has introduced a user fee, wherebypatients pay for services at health institutions.These fees are now providing income for manyhealth care facilities, enabling them to provide atleast minimum-level services.
Cancer in Zimbabwe is characterized by poorsurvival rates. This is mainly a result of advancedstages of cancer at presentation, with 80% ofpatients presenting with stage III or IV disease.23
A study by Gondos et al24 in 2008 on cancersurvival in Zimbabwe showed that cancer survivalamong black Zimbabweans was low, with nosurvival estimate exceeding 55% at 5 years. Astudy investigating survival from the most com-mon cancers diagnosed in the period from 2004to 2008 is currently under way.25
The NCRZ is one of the few functional cancerregistries in Africa, having been established in
1985 as a result of a collaborative research agree-ment between theMinistry of Health and theWHOInternational Agency for Research on Cancer. Itis a population-based registry based in a tertiaryhospital covering all 10 provinces of Zimbabwe. Ithas contributed data to four successive editions ofCancer Incidence in Five Continents, with numer-ous publications in peer-reviewed medical jour-nals. Data from the NCRZ are used in theGLOBOCAN series of publications for estimateson incidence and mortality.
CANCER BURDEN IN ZIMBABWE
From 2008 to 2013, the number of cancer casesin Zimbabwe increased from 2,718 to 6,548(Fig 1).17 It remains unclear as to whether thisincrease resulted from higher rates of HIV burdenand the more widespread adoption of a Westernlifestyle, with the associated cancer risk factors re-lated to increasingobesityandsmoking,orwhether itwas the result of more cases being diagnosed andrecorded, with raised awareness and improved ac-cess to health facilities.26 Infection-related cancers(resulting fromHIV andhumanpapillomavirus) con-tinue to dominate (Fig 2). However, the WHO haspredicted a sharp increase in new cases globally,mainly because of aging populations, current trendsin smoking prevalence, and a growing adoption ofunhealthy lifestyles.2
Of the 6,548 cases reported by the NCRZ inits 2013 annual report, approximately 42.4%occurred in men.6 The most frequently occurringcancers for all races were: cervical cancer (18%),Kaposi’s sarcoma (10%), breast cancer (7%),prostate cancer (7%), non-Hodgkin lymphoma(6%), skin cancer (6%), GI tract cancer (8%),and eye cancer (3%). Of particular concern isthat amajority of patients (81%)presentwith stageIII or IV disease.6 Figure 2 shows cancer incidencein Zimbabwe according to the NCRZ 2013 annualreport.
Cervical, 17.6%
Kaposi's sarcoma, 9.6%
Breast, 7.4%
Prostate, 7.3%
Non-Hodgkin lymphoma, 6.4%
Nonmelanoma skin, 5.9%
Esophageal, 3.8%
Colorectal, 3.7%
Eye, 3.2%
Other, 34.9%
Fig 1. Cancer incidencein Zimbabwe according toZimbabwe Cancer Registrydata from 2005 to 2013.
410 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

CHALLENGES IN CANCER CARE DELIVERY
There are two state-owned cancer treatment cen-ters in Zimbabwe: one at Parirenyatwa Group ofHospitals in the capital city of Harare and the otherat Mpilo Central Hospital, Bulawayo, situated inthe southwestern part of the country. At thesecenters, there are chemotherapy, radiotherapy,and nuclear medicine facilities. There are eightqualified clinical oncologists, with six working atthe main center in Harare and two in Bulawayo.There are 10 registrars at various levels of trainingin the radiotherapy and oncology masters degreeprogram at the University of Zimbabwe. The Zim-babwean model of radiotherapy and oncologytraining for physicians is based on the clinicaloncology model, where training covers both radi-ation oncology and medical oncology for a mini-mum 4-year period.
There are approximately 1,500 new patient casesseen per year at the main radiotherapy center inHarare, resulting ina ratio ofoncologists topatientsof one to 250. The Mpilo radiotherapy center seesapproximately 500 new patient cases per year.The GLOBOCAN report on human resources fortreating new cancer cases in Zimbabwe esti-mated that Harare needed eight radiation orclinical oncologists, and Bulawayo needed fouroncologists.27 These estimates are not far fromthe numbers that already exist in Zimbabwe, andthe training program will ensure these numberscontinue to increase.
Although these facilities exist, cancer care deliveryin Zimbabwe remains a challenge. Zimbabwe hasalways given priority to cancer control in its na-tional health care plan. This is guided by the 2009to 2013 National Health Strategy, which has beenexpanded to cover 2016. The main focus of thisstrategy is quality and equity in health to improvethe quality of life for Zimbabweans.22 However,becauseof theburdenof communicablediseases,especially HIV and AIDS and malaria, priority hasbeen given to combating these diseases. The re-sponse of national systems to noncommunic-able diseases is underdeveloped.19 Fundingconstraints have left noncommunicable diseaseslike cancer underfunded.
The referral system for patients is not fully func-tional, with a lack of skilled professionals at districtand provincial levels and specialized servicesavailable only at tertiary institutions. This makesit difficult for the majority of patients to accesscancer services. The cost of these services hasalso been prohibitive. All services are paid forwith either cash or medical insurance coverage. Amajority of patients who need care are unem-ployed, with most coming from the rural areas.The prohibitive cost of traveling to a center of careand receiving treatment results in most patientsfailing to access treatment.
As is the case in other low-income countries,Zimbabwe has been negatively affected by thebrain drain of skilledpersonnel, with theeducation
4,0154,175
3,349
2,718
3,519
4,520
5,553
6,107
6,548
1,74
2
1,92
2
1,44
1
1,28
6
1,61
6 2,06
4
2,13
0
2,33
7
2,45
9
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
2005 2006 2007 2008 2009 2010 2011 2012 2013
No.
of P
atie
nt C
ases
Year of Diagnosis
Zimbabwe
Harare
Zimbabwe 4,015
No. of patientcases
Harare 1,742
4,175
1,922
3,349
1,441
2,718
1,286
3,519
1,616
4,520
2,064
5,553
2,130
6,107
2,337
6,548
2,459
Fig 2. Cancer incidencein Zimbabwe according toZimbabwe Cancer Registry2013 Annual Report.17
411 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

and health sectors most affected. A study byClemens and Petterson28 found that 51% of Zim-babwean physicians and 24% of nurses wereestimated to be working elsewhere in the world.The government has responded by establishingpolicies encouraging retention of these profes-sionals. This includes providing housing andtransportation allowances for staff. The salariesand on-call allowances of critical staff have beenincreased. The government has also introducedfellowship and scholarship programs and ad-vanced training programs to improve the skills ofhealth professionals.29 A staff retention policy forgovernment-trained physicians and nurses hasbeen introduced, where staff are retained in gov-ernment service for the number of years trained.
Another challenge is inadequate resources tomaintain and improve the cancer treatment facil-ities available in the country. The two centers inHarare and Bulawayo have state-of-the-art equip-ment, including five linear accelerators, two simu-latormachines, and three brachytherapymachines;however, these need regular servicing and repair.More machines need to be acquired to meet theInternational Atomic Energy Agency (IAEA) recom-mendation of one machine per 1 million people in adeveloping country in Africa.30 Reactivation of thenuclear medicine departments, which have beennonfunctional since 2003, at both centers is alsorequired.
There is no comprehensive national cancer con-trol program in Zimbabwe.31 Efforts are under wayto address this through the strengthening of localtraining programs and the recent adoption of theNational Cancer Control Strategy, which is alignedwith theNational Health Strategy.23 Themain goalof the initiative is to coordinate cancer manage-ment from a central point to develop policies thatensure preventive treatment and palliative careservices are delivered, in an effort improve the lowcancer survival rates. The strategy was launchedin July 2013, and a task force has been estab-lished to evaluate and monitor the performanceof the program and advise the Ministry ofHealth.23
MULTIDISCIPLINARY CARE
Managing patients with cancer is becoming com-plex and requires a multidisciplinary approach.32
Multidisciplinary management of patients offersthe potential benefit of having physicians of dif-ferent specialties participating in treatment plan-ning. This may help in the establishment and useof common clinical guidelines, thus streamlin-ing care and establishing a minimum level of
quality.33,34 In turn, the streamlining of care couldresult in cost and time savings, decreasedwastageof resources, and improvement in the value ofpatient care.34 There are limited studies evaluat-ing the influence of multidisciplinary care ondecision making and patient outcomes. Single-center studies have reported significant changesin diagnosis and treatment plans.10,12 A recentmulti-institutional survey of US Veterans Affairsfound limited association between tumor boards,care, and outcomes.35
Multidisciplinary management includes multidis-ciplinary clinics, multidisciplinary team meetingsor tumor boards, and mini tumor boards.34 Theseare held regularly, often once per week, andattended by key specialists involved in cancermanagement, who discuss the diagnosis andmanagement of the patient with cancer.34 Multi-disciplinary teammeetings usually occur once perweek and are attended by a core team of oncol-ogists, surgeons, radiologists, pathologists, andother specialists, depending on the type and spe-cialty of the tumor board.36,37 Mini tumor boardstend to be smaller groups of specialists, occurringwhere there are not enough specialists, as inresource-limited countries.34,37
Global tumor boards, which are live online tele-medicine discussions of patient-based clinicalscenarios between oncologists in LMICs and can-cer experts in developed nations, are another waymultidisciplinary teams can engage. These haveassisted in situations where physicians lack thetime and resources to keep up to date on currentinternational practice guidelines or work in insti-tutions that lack key specialists.38
Data from LMICs, although limited, have shownthe effectiveness of multidisciplinary cancer care.Tumor board meetings may be important inlimited-resource settings, where specialists maybe less available, resulting in suboptimal caredelivery.34,36 Evidence has shown that limitationsin diagnosis andmanagement canbeovercome insuboptimal settings in rural or low-resource areasthrough presentation of clinical cases at multidis-ciplinary meetings or tumor boards.39 A studyexamining the use of multidisciplinary manage-ment tumor boards in Arab countries showed theimportance and usefulness of tumor board meet-ings; it also indicated that in the absence of com-plete multidisciplinary teams, mini tumor boardsare helpful.34 This study noted that in areas withlimited resources, where not all experts and sub-specialties are available, mini tumor boards en-abling radiologists, pathologists, surgeons, and
412 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

medical oncologists to meet can be appropriateand better than no boards at all. A report by theBreast Health Global Initiative on optimization ofbreast cancer management in low- and middle-resource countries identified challenges faced inthese countries, including the lack of multidisci-plinary care practice.40 A similar article by Saghiret al41 noted the relevance of this practice in low-resource countries and reported thatmost of thesecountires lacked thenecessary health care systeminfrastructure to support multidisciplinary care.41
El Saghir et al37 reported that physicians in LMICsplanning to establish tumor boards could benefitfrom the experiences of their colleagues alreadypracticing multidisciplinary tumor boards, ensur-ing they organize more efficient tumor boards.37
In Zimbabwe, the multidisciplinary cancer careapproach is slowly being adopted in an effort tobetter coordinate care and communication forpatients across different disease sites. Becauseof the challenges of patient burden and inade-quate personnel, multidisciplinary meetings andclinics are not held as regularly as they are atcenters abroad. Tumor board meetings are heldeither once per week or once per month. Estab-lished tumor board meetings include weekly gy-necology tumor boards, with general surgery andhead and neck tumor board meetings heldmonthly. The meetings tend to take the form ofmini tumor boards, because specialists represent-ing all areas of patient care are not always avail-able. Themultidisciplinary meetings tend to be forselected patients who have already received someform ofmanagement. A breastmultidisciplinary clinicis held once per week in the surgical wards. This isdone for all new patients. Surgeons and oncologistsmeet to discuss individual patient cases.
Telemedicine discussions are held regularly, withthe Parirenyatwa Group of Hospitals being a partof the Pan African e-Network project, which con-nects members with Indian experts in variousareas of medicine, including oncology, throughcontinuing medical education programs.42 TheDepartment of Radiotherapy and Oncology atParirenyatwa Hospital also holds monthly Afronetteleconference tumor board meetings, whereoncologists from various African countries pres-ent challenging patient case scenarios for discus-sion with a panel of experts from Vienna43 Thedepartment is in the process of connecting withthe Global Breast Tumor Board, organized by theGlobal Cancer Institute, which connects physi-cians around the world to discuss complex patientcases.38
As more local professionals are trained in differ-ent oncology specialties, meetings will developinto full tumor board meetings, and thus, patientswill experience the full benefits of multidisciplin-ary care. Collaborative partnerships have beenformed between the Ministry of Health and ChildCare and United Nations organizations, such asthe IAEA and the United Nations DevelopmentProgram, which provide technical and financialsupport for cancer care in Zimbabwe. The IAEA inparticular has been heavily involved in the localtraining of personnel and in the facilitation offellowship awards to oncology professionals fortraining abroad. The IAEA has also provided tech-nical and financial support toward the acquisition,installation, and maintenance of radiotherapyequipment.44
MULTIDISCIPLINARY CANCER MANAGEMENTCOURSE
The first international multidisciplinary cancermanagement course in Zimbabwe, designed toprovide a roadmap for cross-specialty interactionsandcoordinationof care, tookplace inHarare fromAugust 31, 2015, to September 4, 2015. It was acollaborative effort between the American Societyof Clinical Oncology (ASCO) and the Associa-tion of Radiation Oncologists and Radiologistsof Zimbabwe through the University of Zim-babwe College of Health Sciences. ASCO facili-tated and supported experts in breast, head andneck, and colorectal cancers to come and de-liver educational seminars and also provide ex-pert clinical advice.
Premeeting lectures delivered included a lectureon glioblastomas attended by oncologists andlocal neurosurgeons. Didactic lectures on up-to-date management of head and neck and breastcancers were given to surgical and oncology pro-fessionals. The faculty also participated in a headand neck tumor board meeting and had valuablehands-on discussions with the radiotherapy team.The visiting breast surgeon was also able to joinlocal surgeons in the operating theater, where sheassisted with surgical techniques in managingbreastmasses.Grand roundswerealsoperformedin oncology wards.
The cancer management course focused onbreast, colorectal, and head and neck cancers,inaneffort to reviewanddiscusscurrent standardsof care and the advantages of a multidisciplinaryapproach in these tumors. More than 120 healthcare professionals, mostly specialists from an arrayof disciplines, attended the course from Zimbabweand surrounding countries. Themultidisciplinary
413 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

nature of the faculty ensured that all aspects ofbreast, colorectal,brain,andheadandneckcancermanagement were discussed.
A so-called train the trainer course was facilitatedafter theworkshop. The purpose of the coursewasto help establish multidisciplinary care teams andguidelines in local hospital facilities. Participantswere from different regions of the country and alsofrom diverse backgrounds; they included special-ist physicians, pharmacists, and members of theCancer Association of Zimbabwe and Island Hos-pice of Zimbabwe. All participants committed toinstituting multidisciplinary teams in their hospi-tals. The lecture content was made available to allparticipants.
Course Evaluation
A postcourse evaluation was conducted by ASCOMultidisciplinary Cancer Management Course or-ganizers on site aswell as through anonline surveyshortly after the conclusion of the course; resultsare summarized in Table 1. Only 24% (29 of 120)of the attendees completed the evaluation formson day one; 10% (13 of 120) completed them onday two of the course. The feedback was quiteconsistent. The overall impression was positive,with someparticipants suggesting that the courseshould be repeated on a regular basis. A major-ity of the participants (79% of respondents)indicated a commitment to making practicechanges after the course. These changes includedadopting a multidisciplinary approach to care,improving interspecialty communication, and in-creasing the number of referrals to other special-ties. The participants listed as potential barriers tochange the lack of resources, lack of support fromother colleagues, lack of staff, and lack of time. Onaverage,80%of respondents felt they learnednewskills in diagnosis and treatment and were moreconfident in their ability to manage the cancerscovered in the course. Some participants wouldhave preferred a less technical approach, forexample, lectures at a level understandable toattendees from all specialties.
Impact of the CourseLong-lasting partnershipsand friendships were fostered at this course.The visitors appreciated the challenges faced bythe local experts and also found a lot of commonground with the local experts. One expert is work-ing with the Zimbabwean local cancer center tobuild a radiotherapy program that will providepatients with cancer rapid radiotherapy usingintensity-modulated techniques. Currently, thecancer center has advanced radiation linear ac-celerators but lacks the critical software licenses to
implement more sophisticated radiotherapy tech-niques. The local team is working with the expert toget the software. In so doing, it is hoped that state-of-the-art radiotherapy will be provided in a morecost effective manner and exposure of normaltissue to radiation damage will be minimized. Acollaborative study is also under way with oneof the experts on patients with breast cancer toassess hormone receptor status in the local com-munity, because this is currently not being per-formed at the state hospital. Monthly internationalradiotherapy medical record rounds between alocal institute and one of the expert centers arebeing established to exchange information andknowledge.
The course has resulted in a more motivatedworkforce. The existing multidisciplinary meet-ings, such as the weekly breast cancer clinic,are being attended regularly by multidisciplinaryteams. A monthly pediatric multidisciplinary teammeeting has also been established. Since thecourse was completed, there has been increasedattendance by specialists at the tumor boardmeetings and increased consultation amongspecialties.
THE FUTURE
The relationship between ASCO and the Associa-tion of Radiation Oncologists and Radiologists ofZimbabwe is ongoing. We hope to facilitate addi-tional exchanges of information and knowledgebetween high-resource countries and Zimbabwe.Thesewould include exchangeprograms, trainingprograms, and twinning programs between insti-tutions, where a local department would be pairedwith another oncology department abroad to ex-change ideas and knowledge. ASCO programs,like the International Cancer Corps, where volun-teer oncology professionals share their medicalexpertise with locals, would be of great benefit ifimplemented here in Zimbabwe.45
At this point, the main efforts are geared towardsustaining the benefits accrued through thecourse. The long-term influence of the courseneeds to be assessed, namely, whether there ispotential to build on the fostered relationships tomaintain and improve on the gained knowledgeand experience. If such courses are found to yieldsustained benefits, it may be reasonable to imple-ment them on a regular, regional basis. However,critical evaluation isneeded to identifywhat shouldbe improved on in subsequent courses or, per-haps more importantly, what previously unidenti-fied needs and opportunities were revealed by thecourse. For example, it might be beneficial to have
414 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

more onsite joint clinic visits to instruct and aid inpatient management issues, more time for inter-active discussion on specific cancer topics, or regularonline tumor-specific tumor boards or consultationsessions.
We plan to evaluate the course impact after 1 year.If a sustained impact is demonstrated, more suchcourses will need to be planned, possibly in severalcities in theregion,witha rotationscheduleandwithattendance from several different countries. Addi-tional courses will be guided by the experiencegained, with the aim of better serving local needs.
Our evaluation had some limitations. These in-clude the small number of respondents to thepostcourse assessments and the short durationof time in which measure demonstrable outcome.
In conclusion, the state of cancer care remainscritical in LMICs, with barriers to reducing theburden of cancer mostly attributed to a lack ofhealth care infrastructure, a lack of resources, andshortages in the workforce.46 Educational effortstogetherwithcollaborativepartnershipsmayproveto be themost cost-effective strategy for a sustain-able effect. Multidisciplinary care remains impor-tant in cancer care, but its impact in developingcountries needs to be evaluated. Oncology pro-fessionals in Zimbabwe are hopeful that this ex-perience of a multidisciplinary care course willhelp mitigate the challenges they face in the de-livery of state-of-the-art cancer care.
DOI: https://doi.org/10.1200/JGO.2016.003673Published online on jgo.org on September 14, 2016.
AUTHOR CONTRIBUTIONS
Manuscript writing: All authors
Final approval of manuscript: All authors
AUTHORS’ DISCLOSURES OFPOTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided byauthors of this manuscript. All relationships are consideredcompensated. Relationships are self-held unless noted.
I 5 Immediate Family Member, Inst 5 My Institution.Relationships may not relate to the subject matter of thismanuscript. For more information about ASCO’s conflict of
interest policy, please refer to www.asco.org/rwc orascopubs.org/jco/site/ifc.
Sandra NdarukwaNo relationship to disclose
Anna Mary NyakabauTravel, Accommodations, Expenses: Genentech, AstraZeneca,Novartis
Anees B. ChagparNo relationship to disclose
David RabenEmployment: AstraZenecaConsulting or Advisory Role: AstraZenecaTravel, Accommodations, Expenses: AstraZeneca
Ntokozo NdlovuNo relationship to disclose
Table 1. Post-MCMC Survey Results
MCMC Objective MCMC Zimbabwe Results All MCMC Courses
Up-to-date cancer carepractices
83% of respondents said they learned new skills in diagnosis,treatment, and multidisciplinary management of head and neckcancer
85% of all MCMC participants feel moreconfident in their ability to treat localcancer types
72% of respondents agreed they learned new skills in diagnosis,treatment, and multidisciplinary management of colorectal cancer
85% of respondents said they learned new skills in diagnosis,treatment, and multidisciplinary management of breast cancer
Multidisciplinary cancermanagement
94% of respondents said they understood better howmultidisciplinaryteams work together to provide quality care
94% of all MCMC participants report betterunderstanding of how to work inmultidisciplinary team after courseSix respondents said they planned to work in multidisciplinary team
after course
Consultation withspecialists
88% of respondents said they planned to consult with specialists todetermine best treatment approaches for their patients
86%ofallMCMCparticipantsplan toconsultwith colleagues
Supportive care 82% of respondents said they felt more comfortable in their ability toprovide supportive care to their patients
85% of all MCMC participants report feelingmore confident in their ability to providepalliative care services
NOTE. Colorectal and head and neck cancers appeared on day one form only, which was completed by 29 respondents in total; breast cancer appeared on day two formonly, which was completed by 13 respondents in total (eight people answered all four questions: four on site, four online).Abbreviation: MCMC, Multidisciplinary Cancer Management Course.
415 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Webster KadzatsaNo relationship to disclose
Vanessa J. EatonNo relationship to disclose
Paida MafundaNo relationship to disclose
Evangelia RazisHonoraria: Roche, AstraZeneca, GlaxoSmithKline, Amgen,Novartis, Zeincro, Merck, Pfizer, Bristol-Myers Squibb
Consulting or Advisory Role: Roche, Amgen, AstraZeneca,Janssen-Cilag, Astellas Pharma, Novartis, Bristol-MyersSquibb, Merck, Pfizer, ZeincroResearch Funding: Sanofi, Genentech, Novartis, AstraZeneca,Demo Pharmaceutical, Celldex, PAREXEL International
Travel, Accommodations, Expenses:Genesis Pharmaceuticals,LEO Pharma, Pfizer, Roche, GlaxoSmithKline, Sanofi,Amgen, Bristol-Myers Squibb, Genekor, Eisai, Merck, PierreFabre, Novartis
ACKNOWLEDGMENTWeacknowledge theUniversity of ZimbabweCollegeofHealthSciences,ParirenyatwaGroupofHospitals, andAssociation ofRadiologists and Radio Oncologists of Zimbabwe for facili-tating the American Society of Clinical Oncology (ASCO)Multidisciplinary Cancer Management Course. We also thankthe staff and management of the Parirenyatwa RadiotherapyCentre for their support during this course. We are grateful tothe ASCO staff, including Evangelia Razis, MD, PhD, DavidRaben, MD, Anees B. Chagpar, MD, and Vanessa J. Eaton, forall their work during the course and their continued supportafterward.
Affiliations
Sandra Ndarukwa and Anna Mary Nyakabau, Parirenyatwa Group of Hospitals; Ntokozo Ndlovu and Webster Kadzatsa, University ofZimbabwe College of Health Science, Harare; Paida Mafunda, Junior Chamber International Zimbabwe, Harare, Zimbabwe; Anees B.Chagpar, Yale University, New Haven, CT; David Raben, University of Colorado School of Medicine, Denver, CO; Vanessa J. Eaton,American Society of Clinical Oncology, Alexandria, VA; and Evangelia Razis, Hygeia Hospital, Athens, Greece.
REFERENCES
references
1. World Health Organization: Noncommunicable diseases fact sheet. http://www.who.int/mediacentre/factsheets/fs355/en/
2. Stewart BW, Wild CP (eds): World Cancer Report 2014. http://www.iarc.fr/en/publications/books/wcr/wcr-order.php
3. Snyder J, Dharamsi S, Crooks VA: Fly-by medical care: Conceptualizing the global and local social responsibilities ofmedical tourists and physician voluntourists. Global Health 7:6, 2011
4. Green T, Green H, Scandlyn J, et al: Perceptions of short-term medical volunteer work: A qualitative study inGuatemala. Global Health 5:4, 2009
5. Brinkmann JT: Providing evidence-based care in low-, middle-income countries. http://www.oandp.com/articles/2016-05_03.asp
6. DeCamp M: Scrutinizing global short-term medical outreach. Hastings Cent Rep 37:21-23, 2007
7. Perold H, Graham LA, Mavungu EM, et al: The colonial legacy of international voluntary service. Community Dev J 48:179-196, 2013
8. Philibert I: International medical education outreach: Benefits for US medical education and practice—An interviewwith Joseph Kolars, MD. J Grad Med Educ 1:162-163, 2009
9. Syed SB, Dadwal V, Rutter P, et al: Developed-developing country partnerships: Benefits to developed countries?Global Health 8:17, 2012
10. Onukwugha E, Petrelli NJ, Castro KM, et al: ReCAP: Impact of multidisciplinary care on processes of cancer care: Amulti-institutional study. J Oncol Pract 12:155-156, e157-e168, 2016
11. Abdulrahman GO Jr: The effect of multidisciplinary team care on cancer management. Pan Afr Med J 9:20, 2011
12. Wheless SA, McKinney KA, Zanation AM: A prospective study of the clinical impact of a multidisciplinary head andneck tumor board. Otolaryngol Head Neck Surg 143:650-654, 2010
13. ZimbabweNational Statistics Agency: Census 2012:National Report. http://www.zimstat.co.zw/sites/default/files/img/National_Report.pdf
14. World Health Organization: Zimbabwe country health profile. http://www.who.int/countries/zwe/en/
15. World Bank: Data: Zimbabwe. http://data.worldbank.org/country/zimbabwe
16. National AIDS Council of Zimbabwe: HIV and AIDS situation. http://www.nac.org.zw/about/hiv-aids-situation
17. Chokunonga E, Nyakabau A,Makunike-Mutasa R: ZimbabweNational Cancer Registry: 2013 Annual Report. Harare,Zimbabwe, Zimbabwe National Cancer Registry, 2015
18. World Health Organization: Global Health Observatory data: Zimbabwe country profile. http://www.who.int/gho/countries/zwe/country_profiles/en/
416 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
19. World Health Organization: Noncommunicable disease country profiles: Zimbabwe. http://www.who.int/nmh/countries/zwe_en.pdf
20. Africa Health Workforce Observatory: HRH fact sheet: Zimbabwe. http://www.hrh-observatory.afro.who.int/en/country-monitoring/93-zimbabwe.html
21. World Health Organization: Country Cooperation Strategy at a glance: Zimbabwe. http://www.who.int/countryfocus/cooperation_strategy/ccsbrief_zwe_en.pdf
22. Ministry of Health and Child Welfare: The National Health Strategy for Zimbabwe (2009-2013): A Summary—Equityand Quality in Health: A People’s Right. http://apps.who.int/medicinedocs/documents/s17996en/s17996en.pdf
23. Ministry of Health and Child Welfare: National Cancer Prevention and Control Strategy for Zimbabwe: 2013-2017.http://www.iccp-portal.org/sites/default/files/plans/CANCER%20STRATEGY%20FINAL%202013%202017.pdf
24. Gondos A, Chokunonga E, Brenner H, et al: Cancer survival in a southern African urban population. Int J Cancer 112:860-864, 2004
25. Chokunonga E, Borok MZ, Chirenje ZM, et al: Cancer Incidence in Harare: Triennial Report 2010-2012. http://afcrn.org/attachments/article/83/HARARE%20TRIENNAL%20REPORT%202010-12.pdf
26. Chokunonga E, Borok MZ, Chirenje ZM, et al: Trends in the incidence of cancer in the black population of Harare,Zimbabwe 1991-2010. Int J Cancer 133:721-729, 2013
27. National Cancer Institute Radiation Research Program: Human resources for treating new cancer cases in Zimbabwe.http://rrp.cancer.gov/programsResources/lowIncome/zimbabwe.pdf
28. Clemens MA, Pettersson G: New data on African health professionals abroad. Hum Resour Health 6:1, 2008
29. Chibango C: Zimbabwe’s medical brain drain: Impact assessment on health service delivery and examination of policyresponses—A literature review. http://www.ecsdev.org/images/V2N2/chibango%2043-58.pdf
30. International Atomic Energy Agency: Setting Up a Radiotherapy Programme: Clinical, Medical Physics, RadiationProtection and Safety Aspects. http://www-pub.iaea.org/MTCD/publications/PDF/pub1296_web.pdf
31. Nyakabau AM: Priorities for cancer prevention and control in Zimbabwe. Cancer Control, June 25, 2014. http://www.cancercontrol.info/cc2014/priorities-for-cancer-prevention-and-control-in-zimbabwe/
32. El Saghir NS, Charara RN, Kreidieh FY, et al: Global practice and efficiency of multidisciplinary tumor boards: Resultsof an American Society of Clinical Oncology international survey. J Glob Oncol 1:57-64, 2015
33. El Saghir NS, Assi HA, Khoury KE, et al: Re: Tumor boards and the quality of cancer care. J Natl Cancer Inst 105:1839-1839, 2013
34. El Saghir NS, El-Asmar N, Hajj C, et al: Survey of utilization of multidisciplinary management tumor boards in Arabcountries. Breast 20:S70-S74, 2011 (suppl 2)
35. Keating NL, LandrumMB, Lamont EB, et al: Tumor boards and the quality of cancer care. J Natl Cancer Inst 105:113-121, 2013
36. National Cancer Institute: NCI dictionary of cancer terms: Tumor board reviews. http://www.cancer.gov/publications/dictionaries/cancer-terms?cdrid5322893
37. El Saghir NS, Keating NL, Carlson RW: Tumor boards: Optimizing the structure and improving efficiency of multi-disciplinary management of patients with cancer worldwide. Am Soc Clin Oncol Educ Book. 2014:e461-e466, 2014
38. St Louis J: Global tumor boards connect doctors to improve patient care. http://globalcancerinstitute.org/health-trends/global-tumor-boards-connect-doctors/
39. El Saghir NS, Farhat RA, Charara RN, et al: Enhancing cancer care in areas of limited resources: Our next steps. FutureOncol 10:1953-1965, 2014
40. Anderson BO, Cazap E, El Saghir NS, et al: Optimisation of breast cancer management in low-resource and middle-resource countries: Executive summary of the Breast Health Global Initiative consensus, 2010. Lancet Oncol 12:387-398, 2011
41. El Saghir NS, Adebamowo CA, Anderson BO, et al: Breast cancer management in low resource countries (LRCs):Consensus statement from the Breast Health Global Initiative. Breast 20:S3-S11, 2011 (suppl 2)
42. Pan-African e-Network Project: Implementation status: At a glance. http://www.panafricanenetwork.com/Portal/ProjectDetails.jsp?projectidhide57&projectnamehide5Implementation%20Status
43. International Atomic Energy Agency: Telemedicine in Africa: Connecting professional in the fight against cancer.http://www-naweb.iaea.org/na/news-na/telemedicine-africa.html
44. International Atomic Energy Agency: IAEA Technical Cooperation in Africa. https://www.iaea.org/technicalcooperation/documents/Brochures/2013/TC-in-Africa.pdf
45. American Society of Clinical Oncology: International Cancer Corps. https://www.asco.org/international-programs/volunteer-asco-international/international-cancer-corps
46. CanTreat International: Scaling up cancer diagnosis and treatment in developing countries: What can we learn fromthe HIV/AIDS epidemic? Ann Oncol 21:680-682, 2010
417 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

casereport
Colonic Mucosa-Associated LymphoidTissue Lymphoma Presented as MultiplePolyposis at Colonoscopy in a NigerianMan: Case Report of a Rare Occurrenceand Brief Review of Literature
INTRODUCTION
Anatomically, mucosa-associated lymphoid tis-sue (MALT) is found in various parts of the body.In the colon, lymphoid tissue occurs mainly asisolated lymphoid follicles that are composedmainly of B lymphocytes.1,2 Such gastrointestinaltract MALT plays an important role in immunesurveillance and mucosal regeneration, but thecells inMALTmayoccasionally undergo abnormalproliferation and give rise to lymphoma of theMALT type.1-3 The World Health Organizationidentifies these lesions of non-Hodgkin lymphomaas being of B-cell origin and classifies them asextranodal marginal zone B-cell lymphoma of theMALT type.4,5
In 1983, Isaacson and Wright6 were the firstto describe the term MALT lymphoma. In thegastrointestinal tract, the most common site ofoccurrence is the stomach and small intestine;only rarely does MALT occur in the colon.7-9
To put its rarity in context, all colonic lympho-mas account for approximately 0.2% to 0.6%of colorectal malignant tumors and only 2.5%of all lymphomas.7-11 Among the lymphomasseen in the colon, the most common type isdiffuse large B-cell lymphoma, and MALT-typelymphoma accounts for , 20% of cases in thissubgroup.12
In the sub-Saharan region of Africa, the rarityof colonic MALT lymphoma is further high-lighted by the dearth of published reports onthe condition. Herein, we present one such rarecase.
CASE REPORT
A 55-year-old Nigerian man was referred for acolonoscopy at a private center in Lagos, Nigeria,
after a routine medical examination showed apositive fecal occult blood test. He had no familyhistory of a gastrointestinal cancer and no historyof hematochezia or dyschezia of any kind. He wasasymptomatic at presentation. The patient’s ear-lier bloodwork includednormal hemoglobin levelsalong with other normal parameters. His abdom-inal scan was also normal. The significant findingon colonoscopy was multiple polypoidal lesions ofvarying sizes scattered in isolation and in clustersacross the rectum, sigmoid, and descending co-lon. The largest was an 8-mm diameter, semi-pedunculated lesion in the rectum (Fig 1). Thesmooth surface of this rectal lesion bore multipledilated vascular structures.
Pathologic findings of the biopsy sample from therectal lesion showed sheets of dense and diffuselymphocytic infiltrate with a reactive germinal cen-ter. This extended from the submucosa and in-vaded the muscularis and mucosa glands anddestroyed the latter (lymphoepithelial lesion).The overlying mucosa was ulcerated. The ad-jacent mucosa showed diffuse and moderatemixed inflammatory cells, including lymphocytes,plasmacells, andneutrophils in the laminapropria(Fig 2). No identifiable Helicobacter-like organ-isms were found. Further immunohistochemistryfindings were markedly positive for CD20 andnegative for CD3, CD5, CD10, cyclin D1, andbcl-2 (Figs 3, 4, and 5).
A follow-up gastroscopy was normal. The onlyabnormality seen on a contrast-enhanced com-puted tomography scan of the entire abdominaland pelvic regions was localized symmetric thick-ening of the rectal wall with no evidence of localinfiltration or lymphadenopathy at any other site.Thus, the diagnosis of colonic MALT lymphomawas made. The patient was advised to have a
Aderemi Oluyemi
Nicholas Awolola
Aderemi Oluyemi, ReMayConsultancy and MedicalServices, Ikeja; andNicolas Awolola,University of Lagos, Idi-Araba, Lagos, Nigeria.Corresponding author:Aderemi Oluyemi, MD,ReMay Consultancy andMedical Services, No. 5John Olugbo St, Ikeja,Lagos, Nigeria; e-mail:[email protected].
418 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
© 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License

specialist surgical and radiotherapy oncologic re-view with a view to definitive management of hiscondition, but the referring physician reported thatthe patient declined and has not been heard fromsince.
DISCUSSION
Primary colorectal lymphoma comprises low-grade B-cell lymphoma that arises from diffuselarge B-cell, MALT, mantle cell, and T-cell lym-phomas.13 These are rare tumors that constituteonly 0.2% of all malignant tumors that arise fromthe colorectal region, with theMALT type account-ing for , 20% of cases.12,14 Thus, the novelty ofthis case report underlines that such occurrencefrom the sub-Saharan region of Africa is particu-larly rare.
Clinical presentation ranges from asymptom-atic and discovered only through routine tests(as was the case in the current patient) to pre-sentation with nonspecific abdominal com-plaints to more dramatic presentations thatinclude profuse bleeding from the rectum, in-testinal obstruction, and intussusceptions.1,15
The endoscopic appearance of these lesionsalso varies widely from protruding or ulcerativemasses that appear either singly or in clusters tomultiple widespread masses with diffuse pan-colonic involvement.10,16 The current case isan example of another type of multiple poly-poidal appearance that is restricted to thecolon.17
A critical morphologic characteristic of MALT lym-phomas is the simulation of normal MALT.18,19
The neoplastic B lymphocytes of MALT lympho-mas are found in marginal zones that adjoin re-active follicles and often in diminished rims ofmantle zone lymphocytes. Themarginal zonecellsof MALT invade not only residual reactive folliclesbut also the epithelium. Epithelial invasion withfrequent destruction by the B cells of MALT hasbeen referred to as a lymphoepithelial lesion andis a vital morphologic attribute in the diagnosis ofmany MALT-derived lymphomas.18,19 These fea-tures were clearly demonstrated in the currentpatient and prompted further elucidation withimmunohistochemistry.
The marginal zone cells of MALT share immuno-phenotypic characteristics. MALT lymphomasare B-cell derived with CD20 expression andfrequently contain numerous admixed CD3+-reactive T cells.18,19 Unlike chronic lymphocyticleukemia/small lymphocytic lymphoma andman-tle cell lymphoma, the lymphomas of MALT originusually lack CD5 and are without bcl-2 generearrangements.20 MALT lymphomas differ fromfollicular lymphomas in that they are negative forCD10 and do not exhibit bcl-2 rearrangements.20
The immunophenotypic results of the current bi-opsy samples along with the characteristic histo-logic features led to the confirmation of MALTlymphoma.
Treatment of lymphoma tends to be gratifyingbecause unlike their nodal cousins, lymphomastend to be localized at the time of diagnosis andmay be effectively treated with local therapy.However, because of the lack of an acceptedetiology and given their rarity, little consensusexists on the optimal treatment regimen of co-lonic MALT lymphomas.15,21 Antibiotic treat-ment of Helicobacter pylori is controversialbecause studies exist in support of and against
Fig 1. Image of rectalpolyp at colonoscopy.
Fig 2. Low-powerphotomicrograph thatshows sheets of denseand diffuse lymphocyticinfiltrate with reactivegerminal center (up arrow).This extended from thesubmucosa and invadedthemuscularis andmucosaglands and destroyed thelatter (lymphoepitheliallesion [right arrow]). Theoverlying mucosa wasulcerated (hematoxylin andeosin magnification, 340).
419 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

its usefulness.22-24 Various chemotherapeu-tic agents have been tried with some degreeof response, but there remains no standard-ized therapy.15 Surgical resection may be
effective when a colorectal MALT lymphomadoes not respond to H. pylori eradication ther-apy or chemotherapy and is localized withoutdissemination.15,24
Fig 3. (A) Medium-power photomicrographthat shows a positiveCD20 immunostain(3100). (B) Low-powerphotomicrograph thatshows cyclin d1 negativity(340).
Fig 4. (A) Low-powerphotomicrograph thatshows a negative CD3immunostain (340).(B) Low-powerphotomicrograph thatshows CD5 negativity(340).
Fig 5. (A) Low-powerphotomicrograph thatshows negative bcl-2(340). (B) Low-powerphotomicrograph thatshows CD10 negativity(340).
420 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

Important insight to gain from this report is thatthe absence of structured colorectal screen-ing programs in sub-Saharan Africa has costus the ability to detect more of such findingsin the asymptomatic population. Thus, this has
denied patients the benefit of early detectionand intervention in more amenable neoplasticlesions.
DOI: https://doi.org/10.1200/JGO.2016.005124Published online on jgo.org on June 15, 2016.
AUTHOR CONTRIBUTIONS
Manuscript writing: All authorsFinal approval of manuscript: All authors
AUTHORS’ DISCLOSURES OFPOTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided byauthors of this manuscript. All relationships are consideredcompensated. Relationships are self-held unless noted. I =Immediate Family Member, Inst = My Institution.
Relationships may not relate to the subject matter of thismanuscript. For more information about ASCO’s conflictof interest policy, please refer to www.asco.org/rwc orascopubs.org/jco/site/ifc.
Aderemi OluyemiNo relationship to disclose
Nicholas AwololaNo relationship to disclose
REFERENCES1. Akasaka R, Chiba T, Dutta AK, et al: Colonic mucosa-associated lymphoid tissue lymphoma. Case Rep Gastroenterol
6:569-575, 2012
2. Sipos F, Muzes G: Isolated lymphoid follicles in colon: Switch points between inflammation and colorectal cancer.World J Gastroenterol 17:1666-1673, 2011
3. Thieblemont C, Bastion Y, Berger F, et al: Mucosa-associated lymphoid tissue gastrointestinal and nongastrointestinallymphoma behavior: Analysis of 108 patients. J Clin Oncol 15:1624-1630, 1997
4. Jaffe ES, Harris NL, SteinH, et al: Classification of lymphoid neoplasms: Themicroscope as a tool for disease discovery.Blood 112:4384-4399, 2008
5. Swerdlow SH, Campo E, Harris NL, et al: WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues.Lyon, France, IARC Press, 2008
6. Isaacson P, Wright DH: Malignant lymphoma of mucosa-associated lymphoid tissue. A distinctive type of B-celllymphoma. Cancer 52:1410-1416, 1983
7. Mendelson RM, Fermoyle S: Primary gastrointestinal lymphomas: A radiological-pathological review. Part 1: Stomach,oesophagus and colon. Australas Radiol 49:353-364, 2005
8. Koch P, del Valle F, Berdel WE, et al: Primary gastrointestinal non-Hodgkin’s lymphoma: I. Anatomic and histologicdistribution, clinical features, and survival data of 371 patients registered in the GermanMulticenter StudyGITNHL01/92. J Clin Oncol 19:3861-3873, 2001
9. Radaszkiewicz T, Dragosics B, Bauer P: Gastrointestinal malignant lymphomas of the mucosa-associated lymphoidtissue: Factors relevant to prognosis. Gastroenterology 102:1628-1638, 1992
10. Gezen C, KementM, OncelM, et al: Mucosa associated lymphoid tissue lymphoma of the colon: A case report. Cases J2:9316, 2009
11. Esteban JM, Gutierrez del Olmo A, Baki W, et al: Colonicmucosa-associated lymphoid tissue lymphoma presenting asmultiple polyposis. Gastrointest Endosc 61:928-930, 2005
12. Howell JM, Auer-Grzesiak I, Zhang J, et al: Increasing incidence rates, distribution and histological characteristics ofprimary gastrointestinal non-Hodgkin lymphoma in a North American population. Can J Gastroenterol 26:452-456,2012
13. Ghimire P, Wu GY, Zhu L: Primary gastrointestinal lymphoma. World J Gastroenterol 17:697-707, 2011
14. Dionigi G, Annoni M, Rovera F, et al: Primary colorectal lymphomas: Review of the literature. Surg Oncol 16:S169-S171, 2007 (suppl 1) doi:10.1016/j.suronc.2007.10.021
15. Kim MH, Jung JT, Kim EJ, et al: A case of mucosa-associated lymphoid tissue lymphoma of the sigmoid colonpresenting as a semipedunculated polyp. Clin Endosc 47:192-196, 2014
16. Schmid C, Vazquez JJ, Diss TC, et al: Primary B-cell mucosa-associated lymphoid tissue lymphoma presenting as asolitary colorectal polyp. Histopathology 24:357-362, 1994
17. Chim CS, Shek TW, Chung LP, et al: Unusual abdominal tumors: Case 3. Multiple lymphomatous polyposis inlymphoma of colon. J Clin Oncol 21:953-955, 2003
18. Burke JS: Lymphoproliferative disorders of the gastrointestinal tract. A review and pragmatic guide to diagnosis. ArchPathol Lab Med 135:1283-1297, 2011
421 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

19. Isaacson PG, Spencer J: Malignant lymphoma of mucosa-associated lymphoid tissue. Histopathology 11:445-462,1987
20. Isaacson PG, DuMQ: Gastrointestinal lymphoma:Wheremorphologymeetsmolecular biology. J Pathol 205:255-274,2005
21. Ghadir MR, Bakhshipour AR, Kolahdoozan SH: MALT lymphoma of the rectum: Report of a case treated withchemotherapy. Govaresh 14:127-130, 2009
22. Raderer M, Pfeffel F, Pohl G, et al: Regression of colonic low grade B cell lymphoma of the mucosa associatedlymphoid tissue type after eradication of Helicobacter pylori. Gut 46:133-135, 2000
23. Song EK, Lee NR, Yim CY: Regression of extensive colonic extranodal marginal zone B cell lymphoma after treatmentwith rituximab. Korean J Hematol 41:66-71, 2006
24. Matsuo S, Mizuta Y, Hayashi T, et al: Mucosa-associated lymphoid tissue lymphoma of the transverse colon: A casereport. World J Gastroenterol 12:5573-5576, 2006
422 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

casereport
DNA Repair Defect and RAS Mutationin Two Patients With Schistosomamansoni–Associated ColorectalCancer: Carcinogenesis Steps orMere Coincidence?
INTRODUCTION
Schistosomiasis is caused by nematode worms ofthe Schistosoma genus, including Schistosomamansoni, Schistosoma japonicum, and Schisto-soma haematobium as the main species. It is anendemic disease in tropical and subtropical re-gions.1 At least 230 million people worldwide areinfested with Schistosoma species.2 In Brazil,approximately 25 million people live in areas atrisk for S mansoni.3
Schistosoma eggs accumulate in the submu-cosa of the colon and induce inflammation, whichtriggers a severe granulomatous reaction that iscomplicated by microabscesses, ulceration, nod-ules, polyps, and hyperplasia.4 Along with hyper-plasia, it has been observed thatS japonicum eggsinduce colorectal carcinoma (CRC).5,6
Besides CRC, S japonicum has also been impli-cated in liver cancer development.4 In addition, anassociation between S haematobium and blad-der cancer has also been described.7 However,the association between S mansoni and CRC isscarce in the literature. InpatientswithSmansoni–associated CRC, patients are younger, their tu-mors are multicentric and present with mucinoushistology, and there is a greater risk of lymph nodemetastasis and microsatellite instability (MSI).8
We report two patients with concurrent diagnosisof CRC and intestinal schistosomiasis and thepotentially implicated carcinogenesis steps.
CASE REPORTS
The first patient was a 45-year-old woman whopresented with abdominal pain, weight loss, anddiarrhea. She underwent a colonoscopy in Octo-ber 2014, which revealed a 3-cm tumor in hercecum. A right colectomy was performed in
January 2015, and awell-differentiatedmucinousadenocarcinoma of 2.53 1.53 1.5 cm invadinginto the muscularis propria was identified. Noperineural or lymphovascular invasion was ob-served, but a mild tumor inflammatory infiltratewas present. Margins were free, andmetastasis toone of 24 lymph nodes was documented. Ilealschistosomiasis was found in the specimen. MSIwas confirmed by immunohistochemistry (loss ofMLH1 and PMS2). All RAS mutations were neg-ative. She received 6-month adjuvant capecita-bine- and oxaliplatin-based chemotherapy. Lastfollow-up visit was on June 13, 2016.
Thesecondpatientwasa47-year-oldmanwhohadapersonal history of hepatosplenic schistosomiasis.In 2012, he underwent a right hemicolectomy asa result of complications of appendicitis. In March2014, splenectomy and an esophageal varicesclampwere performed as a result of GI hemorrhage.In November 2014, he presented with diarrhea,and colonoscopy showed a 2-cm tumor next to theileum–transverse colon anastomosis. In March2015, the specimen analyzed from a segmentalcolectomy showed a 3.53 1.8 cm mucinous mod-erately differentiated adenocarcinoma infiltratingsubserosa, with free margins, presence of lympho-vascular invasion, no perineural infiltration, and amild lymphocytic infiltrateobserved.No lymphnodeswere identified in thespecimen,butagranulomatousreaction in response toSchistosomaeggs inhis ileumand colonic mucosa and Merkel diverticula weredescribed by the pathologist. MSI was negative byimmunohistochemistry, but exon 2 KRAS mutation(c.38G.A:p.G13D) was identified. Because of hiscomorbidities, he did not receive adjuvant chemo-therapy. Last follow-up visit was on June 13, 2016.
GustavoFernandesGodoyAlmeida
Filipe Wanick Sarinho
Paula Carvalho de Abreue Lima
Joao Bosco Oliveira Filho
Maxwell Alex de LimaMoura
Lais Neares BarbosaRibeiro
Bruno Rolim de Brito
Mariana Montenegrode Melo Lira
Marcelo do Rego MacielSouto Maior
Ana Lucia CoutinhoDomingues
Author affiliations appear atthe end of this article.
Corresponding author:Gustavo Fernandes GodoyAlmeida, MD, PhD,Hospital das ClinicasFederal University ofPernambuco, Av ProfMoraes Rego, 1235Cidade Universitaria,Recife, Pernambuco50670-901, Brazil;Twitter: @godoy_onco;e-mail: [email protected].
423 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
© 2016 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License

In both patients, KRAS/NRAS exons 2, 3, and 4were amplified by polymerase chain reaction, andsecond-generation sequencing was performed us-ing MiSeq (Illumina, San Diego, CA). The patientswere tested for MSI using the immunohistochem-istry antibodies MLH1, MSH2, MSH6, and PMS2.
DISCUSSION
Whether Schistosoma induces carcinogenesisand its steps is not clear yet. Hanahan and Wein-berg10 have proposed six hallmarks of cancer thatthey define as “distinctive and complementarycapabilities that enable tumor growth and meta-static dissemination.” These include sustainedproliferative signaling, evading growth suppres-sors, resisting cell death, enabling replicative im-mortality, inducing angiogenesis, and activatinginvasion and metastasis. In addition to these sixhallmarks, Hanahan and Weinberg10 outline twoemerging hallmarks and two enabling character-istics that make it possible for tumor cells toacquire the core hallmarks. The two emerginghallmarks are deregulating cellular energeticsand avoiding immune destruction. The two en-abling characteristics are properties of cancercells that facilitate the acquisition of the hallmarks.
The first of these characteristics is genomic in-stability, which enables the acquisition of themultiple mutations required for multistep tumor-igenesis. The second enabling characteristic istumor-promoting inflammation, which reflectsthe rapidly advancing concept that inflammatoryresponses can actually facilitate tumor initiationand progression in some contexts.10 According tothese hallmarks, we found in the literature someevidence of the carcinogenesis steps involvingschistosomiasis (Table 1).
In conclusion, the age of the patients and theirmucinous subtype were in accordance with theliterature.8RASmutation, alongwith the presenceofMSI,may be implicated in the carcinogenesis ofS mansoni–associated CRC or represent coinci-dental events. If the first is correct, it would de-termine treatment and prognosis implicationsamong patients infested with Smansoni. BecauseSchistosoma may be associated with colorectalcarcinogenesis, it is necessary to create a specificprotocol for screening of CRC in Schistosoma-endemic areas.18
DOI: https://doi.org/10.1200/JGO.2016.006254Published online on jgo.org on August 24, 2016.
AUTHOR CONTRIBUTIONS
Administrative support: Gustavo Fernandes Godoy Almeida,Maxwell Alex de Lima Moura, Lais Neares Barbosa Ribeiro,Bruno Rolim de Brito, Ana Lucia Coutinho DominguesProvision of study materials or patients: Gustavo FernandesGodoy Almeida, Paula Carvalho de Abreu e Lima, Joao BoscoOliveira Filho, Mariana Montenegro de Melo Lira, Marcelo doRego Maciel Souto Maior, Ana Lucia Coutinho Domingues
Manuscript writing: All authorsFinal approval of manuscript: All authors
AUTHORS’ DISCLOSURES OFPOTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided byauthors of this manuscript. All relationships are consideredcompensated. Relationships are self-held unless noted.
Table 1. Potential Implicated Schistosoma Species Colorectal Carcinogenesis Steps
Study Hallmark Schistosoma Species Findings
Almeida et al9 Proliferative Mansoni RAS mutation
El-Awady et al11 Proliferative Haematobium Induced proliferation of urothelial cell lines
Zhang et al12 Evading growth suppressors Japonica p53 gene mutations
Zalata et al13 Resisting cell death Mansoni Bcl-2 overexpression
Shao et al14 Immortality Mansoni Decreased apoptotic cell death (Fas/Fasligand system)
Paiva et al15 Angiogenesis Mansoni and japonica Transforming growth factor-b–inducedvascular endothelial growth factorproduction
Tang et al16 Avoiding immune destruction Japonica Reductions of worm burden and eggproduction in worm groups treated withanti-CD25 or anti-CTLA-4 monoclonalantibodies
Almeida et al9 Genomic instability Mansoni Mismatch repair gene mutations
Trottein et al17 Inflammation Mansoni Enhanced synthesis of chemokines IP-10and MIP-1
424 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

I = Immediate Family Member, Inst = My Institution.Relationships may not relate to the subject matter of thismanuscript. For more information about ASCO’s conflictof interest policy, please refer to www.asco.org/rwc orascopubs.org/jco/site/ifc.
Gustavo Fernandes Godoy AlmeidaSpeakers’ Bureau: Mundipharma
Travel, Accommodations, Expenses: Mundipharma
Filipe Wanick SarinhoNo relationship to disclose
Paula Carvalho de Abreu e LimaNo relationship to disclose
Joao Bosco Oliveira FilhoHonoraria: Merck, AstraZeneca, NovartisConsulting or Advisory Role: AstraZeneca, NovartisResearch Funding: Novartis
Maxwell Alex de Lima MouraNo relationship to disclose
Lais Neares Barbosa RibeiroNo relationship to disclose
Bruno Rolim de BritoNo relationship to disclose
Mariana Montenegro de Melo LiraNo relationship to disclose
Marcelo do Rego Maciel Souto MaiorNo relationship to disclose
Ana Lucia Coutinho DominguesNo relationship to disclose
Affiliations
Gustavo Fernandes Godoy Almeida, Filipe Wanick Sarinho, Bruno Rolim de Brito,Mariana Montenegro de Melo Lira,Marcelo do RegoMaciel SoutoMaior, andAnaLuciaCoutinhoDomingues,Hospital dasClinicasFederalUniversity ofPernambuco;PaulaCarvalhodeAbreu e Lima, Laboratorio de Patologia Adonis Carvalho; Joao Bosco Oliveira Filho, Genomika Diagnosticos; and Maxwell Alex deLima Moura and Lais Neares Barbosa Ribeiro, Federal University of Pernambuco, Recife, Brazil.
REFERENCES1. Hosho K, Ikebuchi Y, Ueki M, et al: Schistosomiasis japonica identified by laparoscopy and colonoscopy. Dig Endosc
22:133-136, 2010
2. Colley DG, Bustinduy AL, Secor WE, et al: Human schistosomiasis. Lancet 383:2253-2264, 2014
3. Ministerio da Saude, Secretaria de Vigilancia em Saude: Guia de Vigilancia Epidemiologica (ed 7). Brasilia, Brazil,Ministerio da Saude, 2012
4. Gray DJ, Ross AG, Li YS, et al: Diagnosis and management of schistosomiasis. BMJ 342:d2651, 2011
5. MatsudaK,Masaki T, Ishii S, et al: Possible associations of rectal carcinomawith Schistosoma japonicum infection andmembranous nephropathy: A case report with a review. Jpn J Clin Oncol 29:576-581, 1999
6. Liu W, Zeng HZ, Wang QM, et al: Schistosomiasis combined with colorectal carcinoma diagnosed based on en-doscopic findings and clinicopathological characteristics: A report on 32 cases. Asian Pac J Cancer Prev 14:4839-4842, 2013
7. MostafaMH, Sheweita SA, O’Connor PJ: Relationship between schistosomiasis and bladder cancer. ClinMicrobiol Rev12:97-111, 1999
8. Salim OEH, Hamid HKS, Mekki SO, et al: Colorectal carcinoma associated with schistosomiasis: A possible causalrelationship. World J Surg Oncol 8:68, 2010
9. AlmeidaGFG,Mattos LAR Jr, Brito BR, et al: DNA repair defect andRASmutation in Schistosomamansoni–associatedcolorectal cancer patients: Carcinogenesis steps or mere coincidence? J Clin Oncol 34, 2016 (abstr e23279)
10. Hanahan D, Weinberg RA: Hallmarks of cancer: The next generation. Cell 144:646-674, 2011
11. El-Awady MK, Gad YZ, Wen Y, et al: Schistosoma haematobium soluble egg antigens induce proliferation of urothelialand endothelial cells. World J Urol 19:263-266, 2001
12. Zhang R, Takahashi S, Orita S, et al: p53 gene mutations in rectal cancer associated with schistosomiasis japonica inChinese patients. Cancer Lett 131:215-221, 1998
13. Zalata KR, Nasif WA, Ming SC, et al: p53, Bcl-2 and C-Myc expressions in colorectal carcinoma associated withschistosomiasis in Egypt. Cell Oncol 27:245-253, 2005
14. Shao Q, Tohma Y, Ohgaki H, et al: Altered expression of Fas (APO-1, CD95) and Fas ligand in the liver of mice infectedwith Schistosoma japonicum and Schistosoma mansoni: Implications for liver carcinogenesis. Asian Pac J CancerPrev 3:361-366, 2002
15. Paiva LA, Coelho KA, Luna-Gomes T, et al: Schistosome infection-derived hepatic stellate cells are cellular source ofprostaglandin D₂: Role in TGF-b-stimulated VEGF production. Prostaglandins Leukot Essent Fatty Acids 95:57-62,2015
425 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology

16. Tang CL, Lei JH, Guan F, et al: Effect of cytotoxic T-lymphocyte-associated protein 4 on CD4(+)CD25(+) regulatoryT cells in murine schistosomiasis japonica. Exp Parasitol 136:74-78, 2014
17. Trottein F, Pavelka N, Vizzardelli C, et al: A type I IFN-dependent pathway induced by Schistosoma mansoni eggs inmouse myeloid dendritic cells generates an inflammatory signature. J Immunol 172:3011-3017, 2004
18. Konishi T, Watanabe T, Shibahara J, et al: Surveillance colonoscopy should be conducted in patients with colorectalschistosomiasis even after successful treatment of the disease. Int J Immunopathol Pharmacol 19:245-246, 2006
426 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
correspondence
Call for Breast Cancer Risk FactorEducation in Countries With LimitedHealth Care Resources
TO THE EDITOR:
The recent article by Kennedy et al1 highlights theimportance of opportunistic breast cancer educa-tion and increasing use of screening services inrural Honduras. Breast education programs thatlead to increased awareness have an impact onreducing breast cancer–related mortality and isan inexpensive and important strategy,2 regard-less of the availability of mammography and ad-juvant therapy. We believe that in addition toeducation about self- and clinical breast exami-nation, emphasis should be focused on the im-portance of reducing modifiable risk factors and,more importantly, the education of health careproviders. This is particularly important as low-and middle-income countries increasingly adopta Western lifestyle, which increases the risk ofbreast cancer.3 Inaddition, community-level healthcare providers should be a reliable source of breasthealth education in any setting.
As in Latin America, breast cancer is the mostprevalent cancer in African women, and likeHonduras, Tanzania has limited access to can-cer education, screening, and treatment.4 Tobetter understand breast cancer awareness andknowledge of risk factors in the general popula-tion, we surveyed 98 individuals in Arusha, Tan-zania. The participants were patients, visitors,and nurses present in a general outpatient wait-ing room at a private general hospital. The surveywas written in both English and Swahili (the locallanguage) and asked dichotomous questionsabout whether patients were aware of breastcancer and whether they believed that it couldbe treated if diagnosed early. Breast cancer riskfactor knowledge was assessed by a multiple-choice question that listed both true risk factorsand known common regional misconceptions.Most of the participants were female (62.2%),themedian age was35years (interquartile range,
28 to 48), 69% had a secondary education orhigher, and 85.7% reported being employed or astudent (Table 1).
Almost all surveyed had heard of breast cancer(96%), and most were aware it could be treated ifdetected early (93%). However, in the multiple-choice question, a notable 65% chose keepingmoney under the brassiere as a risk factor forbreast cancer, including 77% of nine nurses
Table 1. Participant Demographic Characteristics
Characteristic No. (%)
Age, years
18-37 45 (45.9)
38-57 25 (25.5)
58-65 8 (8.1)
Missing 20 (20.4)
Total 98 (100)
Sex
Female 61 (62.2)
Male 37 (37.8)
Missing 0 (0)
Total 98 (100)
Education
None 5 (5.1)
Primary 20 (20.4)
Secondary 31 (31.6)
Postsecondary 37 (37.8)
Missing 5 (5.1)
Total 98 (100)
Employment
Employed 72 (73.5)
Unemployed 4 (4.1)
Student 12 (12.2)
Missing 10 (10.2)
Total 98 (100)
Tara J. Rick
Judith J. Merinyo
Tara J. Rick, St CatherineUniversity, St Paul, MN;Judith J. Merinyo, ArushaLutheran Medical Centre,Arusha, Tanzania
Corresponding author:Tara J. Rick, PA-C, StCatherine University,Henrietta Schmoll Schoolof Health, Whitby Hall,Mail Stop 4227, 2004Randolph Ave, St Paul,MN 55105; e-mail:[email protected].
427 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
© 2017 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License

surveyed (Table 2). Fifty percent of participantscorrectly identified family history as a risk factor,followed by alcohol consumption (38%), diet
(38%), and increasing age (27%). Of note, severalparticipants also believed that scratching thebreast (20%), wearing a brassiere (19%), andbeing bitten by a child during breast-feeding(17%) are risk factors.
On the basis of the survey findings, we extendedthe risk factor questions to 44 medical staffmembers in the community, including physi-cians, clinical officers, assistant medical officers,and nurses. We found that 76% identified keep-ing money under the brassiere as a risk factor forbreast cancer, which was consistent with thebelief of the general population. We then pro-vided an educational session to health care pro-viderswith a focus on risk factors andearly signs ofcancer.
Similarly to Kennedy et al,1 our study highlightsthe emergent need for breast cancer educa-tion of the general population in countries withlimited health care resources. The study alsoemphasizes the need for cancer-related riskfactor education for community-level health careproviders because providers are key in educatingpatients about prevention and early detection ofbreast cancer, especially in areas with limitedscreening and adjuvant treatment capabilities.
DOI: https://doi.org/10.1200/JGO.2016.007781Published online on jgo.org on January 11, 2017.
AUTHORS’ DISCLOSURES OFPOTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided byauthors of this manuscript. All relationships are consideredcompensated. Relationships are self-held unless noted. I 5Immediate Family Member, Inst 5 My Institution. Relation-ships may not relate to the subject matter of this manuscript. Formore information about ASCO’s conflict of interest policy, pleaserefer to www.asco.org/rwc or ascopubs.org/jco/site/ifc.
Tara J. RickNo relationship to disclose
Judith J. MerinyoNo relationship to disclose
ACKNOWLEDGMENTPartially supported by a2015Physician Assistant FoundationRobert K. Pederson Global Outreach Grant.
REFERENCES1. Kennedy LS, Bejarano SA, Onega TL, et al: Opportunistic breast cancer education and screening in
rural Honduras. J Glob Oncol 2:174-180, 2016
2. Shulman LN, Willett W, Sievers A, et al: Breast cancer in developing countries: Opportunities forimproved survival. J Oncol 2010:595167, 2010
3. Porter P: “Westernizing” women’s risks? Breast cancer in lower-income countries. N Engl J Med358:213-216, 2008
4. Morse EP, Maegga B, Joseph G, et al: Breast cancer knowledge, beliefs, and screening practicesamong women seeking care at district hospitals in Dar es Salaam, Tanzania. Breast Cancer (Auckl)8:73-79, 2014
Table 2. Beliefs and Knowledge of Breast Cancer Risk Factors in the General Population
Variable Affirmative Response, No. (%)
No. of participants 98
Belief
Keeping money under brassiere 64 (65)
Scratching the breast 20 (20)
Wearing a brassiere 19 (19)
Bite during breast-feeding 17 (17)
A curse 9 (9)
Large breasts 8 (8)
Breast-feeding for . 2 years 6 (6)
Small breasts 6 (6)
Knowledge
Family history 49 (50)
Alcohol 37 (38)
Diet 37 (38)
Age 26 (27)
Not breast-feeding 26 (27)
Obesity 18 (18)
Early menarche 14 (14)
Late menopause 14 (14)
428 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
correspondence
High Epidermal Growth Factor ReceptorMutation Rates in Peruvian Patients WithNon–Small-Cell Lung Cancer: Is It aMatter of Asian Ancestry?
In a recent article, Lopez-Chavez et al1 reported ahigh mutational rate of epidermal growth factorreceptor (EGFR) in Peruvian patients (37%) that ishigher than inother LatinAmericancountries suchas Mexico, Bolivia, Venezuela, and in a mixture ofLatinos in theUnited States. Highmutational ratesof theEGFRgene inPeruvianpatientswerereportedpreviously in independent cohorts. Mas et al2 re-ported a frequency of 39.3% (n5 122), andArrietaet al3 reported a frequency of 51.1% (n 5 393).Although the frequency ofEGFRmutations in Peru-vianpatients ishigher thanother reports, these ratescould be explained by environmental factors.
However, ancestrycouldalsoplayan important roleinexplaining this fact.Wewould like to point out twoevents that could lead to a gene flow explaining thehigh prevalence of EGFRmutations in Peruvian pa-tients. Population of the Americas in the late Pleis-tocene epoch by migrants from Asia through theBering land bridge shaped the genetic pool of NativeAmericans. The second event occurred after slaverywasabolished inPeruandamassivewaveofChineseworkers reached the Peruvian coast (approximately100,000 between 1849 and 1880), with a Peruvianpopulation estimated at 2 million in 1850.4,5
Although there are not many projects that areevaluating Asian ancestry markers in Latin Amer-ican countries, data for ancestry admixture pro-portions for Mexico, Colombia, and Peru (0.012,0.021, and 0.035, respectively) suggest a corre-lation between ancestry proportion and rate ofEGFR mutations (Fig 1).1,6-8
On the other hand, the Helicobacter pylori bac-terium accompanied humans in the migrationwaves. These bacteria are not only a chronic path-ogen in humans, but also coevolve with their hostsand have been used to trace human migrationroutes.9 Work by Devi et al10 with Peruvian strainsof H. pylori found considerable homology withAsian strains. Another interesting fact is the highprevalence of human T-cell lymphotropic virus,ranging from 7% to 25%, in several Peruviancities. This pattern is typical of some Asian coun-tries such as Japan.
High rates of EGFRmutations in Peruvian patientswith non–small-cell lung cancer could be a signa-ture of Asian ancestry in the Peruvian population.
DOI: https://doi.org/10.1200/JGO.2016.008201Published online on jgo.org on January 18, 2017.
AUTHOR CONTRIBUTIONS
Manuscript writing: All authorsFinal approval of manuscript: All authors
AUTHORS’ DISCLOSURES OFPOTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided byauthors of this manuscript. All relationships are consideredcompensated. Relationships are self-held unless noted. I 5Immediate Family Member, Inst 5 My Institution. Relation-ships may not relate to the subject matter of this manuscript.
For more information about ASCO’s conflict ofinterest policy, please refer to www.asco.org/rwc orascopubs.org/jco/site/ifc.
Joseph A. PintoNo relationship to disclose
Luis A. MasNo relationship to disclose
Henry L. GomezNo relationship to disclose
Joseph A. Pinto
Luis A. Mas
Henry L. Gomez
JosephA. Pinto, Luis A.Mas,and Henry L. GomezOncosalud-AUNA, SanBorja; Luis A. Mas andHenry L. Gomez, InstitutoNacional deEnfermedadesNeoplasicas, Lima, PeruCorresponding author:Henry L. Gomez,Department of MedicalOncology, Oncosalud-AUNA, Av. Guardia Civil571, San Borja, Peru;e-mail: [email protected].
429 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology
© 2017 by American Society of Clinical Oncology Licensed under the Creative Commons Attribution 4.0 License

REFERENCES1. Lopez-Chavez A, Thomas A, Evbuomwan MO, et al: EGFR mutations in Latinos from the United
States and Latin America. J Glob Oncol 2:259-267, 2016
2. Mas L, Gomez de la Torre JC, Barletta C: Estado mutacional de los exones 19 y 21 de EGFR enadenocarcinoma de pulmon: Estudio en 122 pacientes peruanos y revision de la evidencia deeficacia del inhibidor tirosina kinasa erlotinib. Carcinos 2:52-61, 2011
3. Arrieta O, Cardona AF, Martın C, et al: Updated frequency of EGFR and KRAS mutations innonsmall-cell lung cancer in Latin America: The Latin-American Consortium for the Investigation ofLung Cancer (CLICaP). J Thorac Oncol 10:838-843, 2015
4. La Torre Silva R: La inmigracion China en el Peru (1850-1890). Boletın de la Sociedad Peruana deMedicina Interna 5: 1992 http://sisbib.unmsm.edu.pe/BvRevistas/spmi/v05n3/Inmigraci%C3%B3n.htm
5. Gootenberg P: Poblacion y etnicidad en el Peru republicano (siglo XIX): Algunas revisiones. Lima.1995 http://repositorio.iep.org.pe/handle/IEP/318
6. Silva-Zolezzi I, Hidalgo-Miranda A, Estrada-Gil J, et al: Analysis of genomic diversity in MexicanMestizo populations to develop genomic medicine in Mexico. Proc Natl Acad Sci USA 106:8611-8616, 2009
7. Sandoval JR, Salazar-Granara A, Acosta O, et al: Tracing the genomic ancestry of Peruviansreveals a major legacy of pre-Columbian ancestors. J Hum Genet 58:627-634, 2013
8. Rishishwar L, Conley AB, Wigington CH, et al: Ancestry, admixture and fitness in Colombiangenomes. Sci Rep 5:12376, 2015
9. Falush D, Wirth T, Linz B, et al: Traces of human migrations in Helicobacter pylori populations.Science 299:1582-1585, 2003
10. Devi SM, Ahmed I, Khan AA, et al: Genomes of Helicobacter pylori from native Peruvians suggestadmixture of ancestral and modern lineages and reveal a Western type cag-pathogenicity island.BMC Genomics 7:191, 2006
Peru
Mexico
Colombia
0
0.005
0.01
0.015
0.02
0.025
0.03
0.035
0.04
0.1 0.2 0.3 0.4
Asia
n An
cest
ry (p
ropo
rtion
)
EGFR Mutated (proportion)
Country
Linear (Country)
Fig 1. Graph showinga correlation betweenthe proportion of Asianancestry in Latin Americancountries and rates ofEGFRmutations in non–small-celllung cancer. EGFR,epidermal growth factorreceptor.
430 Volume 3, Issue 4, August 2017 jgo.org JGO – Journal of Global Oncology