
Shenmai injection as an adjuvant treatment for chronic cor ...
Upload
independentCategory
view
0download
0
Adjuvant Targeted Therapy in EarlyBreast CancerJohn Mackey, MD1, Deanna McLeod, BSc2, Joseph Ragaz, MD3, Karen Gelmon, MD4, Sunil Verma, MD5,
Kathleen Pritchard, MD5, Kara Laing, MD6, Louise Provencher, MD7,
and Lauren F. Charbonneau, RPh, BSc(Pharm)5
For this review, the authors appraised the evidence for adjuvant trastuzumab therapy in early breast can-
cer. There was level 1 evidence to support the routine use of 1 year of adjuvant trastuzumab in conjunction
with chemotherapy for women with human epidermal growth factor receptor 2 (HER-2)-positive early
breast cancer. The relative benefits of concurrent versus sequential administration remained unclear; how-
ever concurrent administration permitted the earliest possible intervention with trastuzumab with possible
superiority. There was evidence to support the use of trastuzumab in both lymph node-positive and high-
risk lymph node-negative patients, and preliminary data suggested that all patient subgroups that were eli-
gible for the trials benefit equally from trastuzumab. Adjuvant trastuzumab was associated with a risk of
cardiotoxicity, the long-term impact of which remains largely unknown. Routine cardiac risk assessment
considering left ventricular ejection fraction, age, and prior history of cardiac events is recommended along
with the selection of trastuzumab-based regimens that minimize cardiotoxicity. Trastuzumab acquisition
costs for 1 year of therapy were the largest component of treatment costs. Cancer 2009;115:1154–68.
VC 2009 American Cancer Society.
KEY WORDS: breast neoplasms, drug therapy, trastuzumab, therapeutic use, monoclonal antibodies,
adjuvant chemotherapy, erbB-2 receptor, antineoplastic agents, humans.
Increased knowledge of the biologic diversity of breast cancer has been accompanied by increasedefforts to individualize breast cancer treatment based on the underlying molecular features of each tumor.Approximately 15% to 20% of early breast cancers have amplification of the human epidermal receptor-2(HER-2) gene, with resultant overexpression of the HER-2 protein.1-3 HER-2 belongs to a family of 4transmembrane receptor tyrosine kinases that mediate the growth, differentiation, and survival of cells.4-6
Tumors that over express this protein are imbued with more aggressive qualities, including enhancedgrowth and proliferation, increased invasive and metastatic capability, and stimulation of angiogenesis.4,6
Individual trials, population-based studies, and retrospective analyses also have shown that HER-2 overex-pression is associated with poorly differentiated, high-grade tumors and lymph node involvement.4,6 Until
Received: June 24, 2008; Revised: September 12, 2008; Accepted: September 19, 2008
Published online: January 21, 2009, VC 2009 American Cancer Society
DOI: 10.1002/cncr.24114, www.interscience.wiley.com
Corresponding author: John Mackey, MD, Cross Cancer Centre, 11560 University Avenue, Edmonton, Alberta, T6G 1Z2, Canada; Fax: (780)
432-8221; [email protected]
1Cross Cancer Center, Edmonton. Alberta, Canada; 2Kaleidoscope Strategic, Toronto, Ontario, Canada; 3McGill University, Montreal, Quebec, Canada;4British Columbia Cancer Agency, British Columbia, Canada; 5Sunnybrook Odette Cancer Center, Toronto, Ontario, Canada; 6Cancer Care Program,
Dr. H. Bliss Murphy Cancer Center, St. John’s, Newfoundland, Canada; 7Deschenes-Fabia Center for Breast Disease, Quebec, Canada
We thank Kaleidoscope Strategic Inc., for the information management services required for developing this review.
1154 Cancer March 15, 2009
Review Article

recently, patients who had breast cancer with HER-2overexpression (HER-2-positive breast cancer) faced amarkedly poorer prognosis than patients who had breastcancer without HER-2 overexpression (HER-2 negativebreast cancer).4,6 A promising recent addition to the adju-vant treatment arsenal is trastuzumab (Herceptin; Genen-tech, South San Francisco, Calif), a new agent biologicallytargeted against the HER-2 protein that has demonstratedthe ability to mitigate the prognostic disadvantage ofHER-2 expression.
Trastuzumab is a humanized monoclonal antibody
that targets the extracellular domain of the HER-2 pro-
tein. Trastuzumab activates antibody-dependent, cell-
mediated cytotoxicity and disrupts the signal transduction
process through interference with receptor dimerization,
downstream effectors, and receptor internalization and
degradation.5 Trastuzumab was tested formally in combi-
nation with chemotherapy for the first-line treatment of
metastatic breast cancer and demonstrated both improved
response rate and improved survival compared with
chemotherapy alone in patients with HER-2-positive
breast cancer.7 Although the risk of cardiotoxicity
increased with the addition of trastuzumab to chemother-
apy, otherwise, trastuzumab was well tolerated. These
results triggered several prospective clinical trials to test
the efficacy of adjuvant trastuzumab in early breast cancer.
In the current review, we have appraised the evidence for
adjuvant trastuzumab therapy in early breast cancer,
considered treatment costs, and reviewed select quality-
of-life factors as a means of navigating the landscape of
available and emerging treatment options.
Search Strategy and Study Overview
Published clinical trials of for early breast cancer were
identified in a search of the PubMed database through to
April 2007 using the terms ‘adjuvant or postoperative,’
‘trastuzumab,’ and ‘breast cancer.’ In addition, conference
proceedings from the American Society of Clinical
Oncology (ASCO) (2003-2007), the San Antonio Breast
Cancer Symposium (2003-2007), and the European
Society of Clinical Oncology (2004-2006) were searched
manually for studies that met the eligibility criteria.
Results presented at symposia were considered an impor-
tant source of current clinical information, and, whenever
available, data from presentations were used to supple-
ment published abstract information. Studies were eligi-
ble for inclusion if they reported efficacy results from
prospective, randomized controlled trials; if they were
published in the English language, and if they investigated
the use of adjuvant trastuzumab therapy in patients with
early breast cancer. Six prospective clinical trials met the
eligibility criteria of this review.
Study Findings
Efficacy
The largest of the adjuvant trastuzumab trials is the
Herceptin Adjuvant (HERA) trial,8,9 which an interna-
tional randomized study investigating the use of trastuzu-
mab in HER-2-positive patients who have completed
locoregional therapy and a minimum of 4 courses of
chemotherapy. In total, 5102 women with HER-2-posi-
tive breast cancer were assigned randomly within 6 weeks
of completing primary therapy to 1 of 3 groups: 1)
women who underwent observation alone; 2) women
who were treated with adjuvant trastuzumab (8 mg/kg
load followed by 6 mg/kg every 3 weeks) for 1 year; and 3)
women who were treated with adjuvant trastuzumab at
the same dose and schedule for 2 years. The baseline char-
acteristics of the patients in the HERA trial are summar-
ized in Table 1. It is noteworthy that just over half (57%)
of the women in this trial had lymph node-positive
disease, less than one-third (26%) had received prior
adjuvant anthracycline and taxane therapy, and an
additional 11% received neoadjuvant chemotherapy.
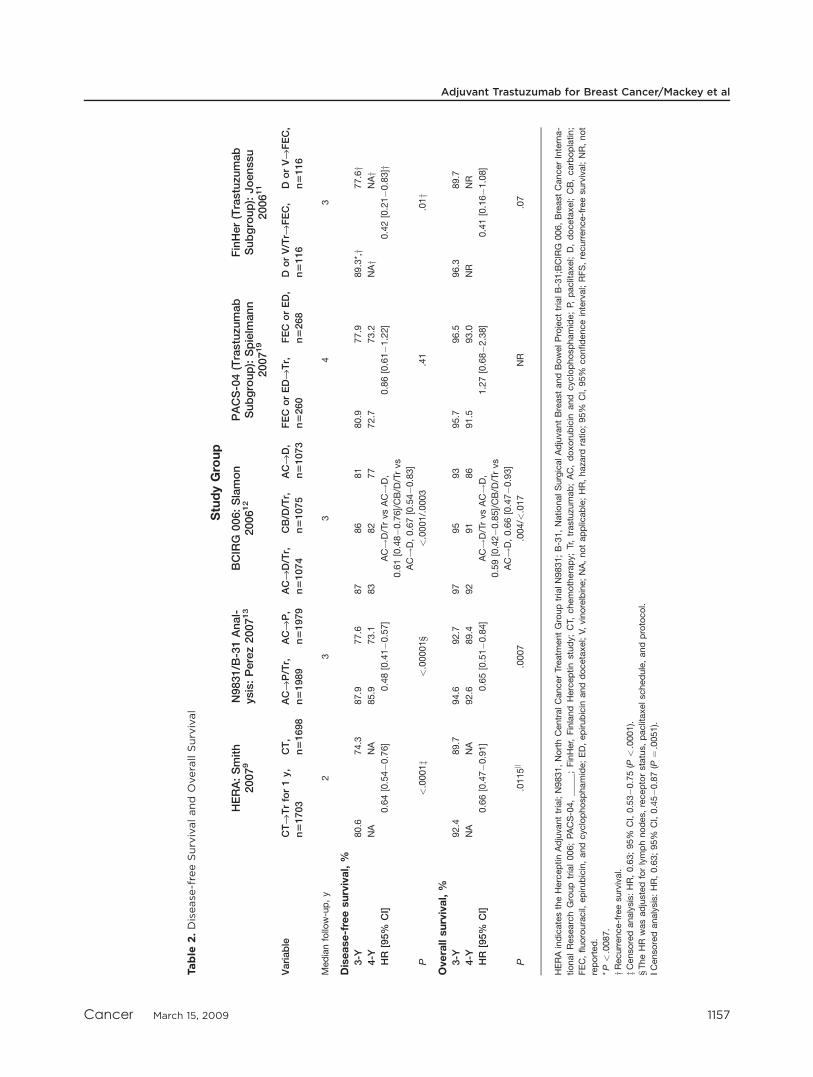
At a median follow-up of 23.5 months, 1 year of
trastuzumab therapy resulted in significant reductions in
the risk of recurrence (hazards ratio [HR], 0.64; 95% con-
fidence interval [95% CI], 0.54�0.76 [P < .0001]) and,
despite a 51% crossover rate, the risk of death was signifi-
cantly reduced (HR, 0.66; 95% CI, 0.47�0.91 [P ¼.0115]) (Table 2) compared with observation.9 When
considering the clinical application of sequentially admin-
istering trastuzumab after chemotherapy as in the HERA
trial (chemo-trastuzumab sequences), it is important to
consider the following: 1) a potential further benefit may
exist from the concurrent administration of chemotherapy
and trastuzumab10-14 that was not explored in the trial; 2)
significant losses in patient follow-up (5.7% experimental
arm and 3.4% observation arm) and a high rate of patient
Adjuvant Trastuzumab for Breast Cancer/Mackey et al
Cancer March 15, 2009 1155

Table
1.PatientCharacteristics,T
umorCharacteristics,andPriorChemoth
erapy
StudyGroup
HERA:Piccart-
Gebhart
2005,8
Smith20079
N9831/B
-31
Analysis:Perez
200713
BCIRG
006:Slamon200612
PACS-04(Trastuzu
mab
Subgroup):Spielm
ann
200719
FinHer(Trastuzu
mab
Subgroup):
Joenssu200611
Variable
CTfiTrfor
1y,n51703
CT,
n51698
ACfiP/Tr,
n51989
ACfiP,
n51979
ACfiD/Tr,
n51074
CB/D
/Tr,
n51075
ACfiD,
n51073
FEC
orEDfiTr,
n5260
FEC
orED,
n5268
DorV/Trfi
FEC,
n5116
DorVfiFEC,
n5116
AdjuvantATtherapy,
%26
26
100
100
100
0100
50
50
50
50
Horm
onetherapy:ER/PgR-positive
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Age<50y,
%52
52
51
50
52
54
52
48(M
ed)
49(M
ed)
51(M
ed)
50(M
ed)
Horm
one-receptorpositive,%
50
50
50
50
54
54
54
58
61
50(ERþ)/
39(PgRþ)
44(ERþ)/
29(PgRþ)
Lymphnodestatus,%
NeoadjuvantCT
11
10
NA
NA
NA
NA
NA
NA
NA
NA
NA
High-risklymphnodenegative
32
33
77
29
29
29
00
10
22
No.ofpositivelymphnodes
1-3
29
29
53
52
38
39
38
60
56
55
50
‡428
28
40
40
33
33
33
40
44
34
28
Tumorsize,%
£2cm
39
40
38
40
38
40
41
30(<
2cm)
35(<
2cm)
40
30
2.125cm
45
43
52
51
55
54
53
70(�
2cm)
65(�
2cm)
59(>
2cm)
71(>
2cm)
>5cm
46
97
76
6
Trastuzu
mabinitiatedbasedon
norm
alcardiacfunction
Atcompletionof
RTandCT
Atcompletion
ofAC
AtcompletionofAC
forAC!
Dandafter
surgery
forCB/D
/Tr
AtcompletionofRTandCT
Aftersurgery
HERA
indicatestheHerceptinAdjuvanttrial;N9831,NorthCentralCancerTreatm
entGrouptrialN9831;B-31,NationalSurgicalAdjuvantBreastandBowelProjecttrialB-31;BCIRG
006,BreastCancerInter-
nationalResearchGrouptrial006;PACS-04,Protocole
Adjuvantdansle
CancerduSein;FinHer,FinlandHerceptinstudy;CT,
chemotherapy;Tr,trastuzu
mab;AC,doxorubicin
andcyclophosphamide;P,
pacli-
taxel;D,docetaxel;CB,carboplatin;FEC,fluorouracil,
epirubicin,and
cyclophosphamide;ED,epirubicin
and
docetaxel;V,
vinorelbine;AT,
anthracyclin
e-taxane;ER,estrogen
receptor;
PgR,progesterone
receptor;Med,median;þ,positive;NA,notapplicable;RT,
radiotherapy.
Review Article
1156 Cancer March 15, 2009
Table
2.Disease-freeSurvivalandOverallSurvival
StudyGroup
HERA:Smith
20079
N9831/B
-31Anal-
ysis:Perez200713
BCIRG
006:Slamon
200612
PACS-04(Trastuzu
mab
Subgroup):Spielm
ann
200719
FinHer(Trastuzu
mab
Subgroup):Joenssu
200611
Variable
CTfiTrfor1y,
n51703
CT,
n51698
ACfiP/Tr,
n51989
ACfiP,
n51979
ACfiD/Tr,
n51074
CB/D
/Tr,
n51075
ACfiD,
n51073
FEC
orEDfiTr,
n5260
FEC
orED,
n5268
DorV/Trfi
FEC,
n5116
DorVfiFEC,
n5116
Medianfollo
w-up,y
23
34
3
Disease-freesurvival,%
3-Y
80.6
74.3
87.9
77.6
87
86
81
80.9
77.9
89.3*,y
77.6y
4-Y
NA
NA
85.9
73.1
83
82
77
72.7
73.2
NAy
NAy
HR
[95%
CI]
0.64[0.54�0.76]
0.48[0.41�0.57]
AC!D/TrvsAC!D,
0.61[0.48�0.76]/CB/D
/Trvs
AC!D,0.67[0.54�0.83]
0.86[0.61�1.22]
0.42[0.21�0.83]y
P<.0001z
<.00001§
<.0001/.0003
.41
.01y
Overallsurvival,%
3-Y
92.4
89.7
94.6
92.7
97
95
93
95.7
96.5
96.3
89.7
4-Y
NA
NA
92.6
89.4
92
91
86
91.5
93.0
NR
NR
HR
[95%
CI]
0.66[0.47�0.91]
0.65[0.51�0.84]
AC!D/TrvsAC!D,
0.59[0.42�0.85]/CB/D
/Trvs
AC!D,0.66[0.47�0.93]
1.27[0.68�2.38]
0.41[0.16�1.08]
P.0115k
.0007
.004/<
.017
NR
.07
HERAindicatestheHerceptinAdjuvanttrial;N9831,NorthCentralCancerTreatm
entGrouptrialN9831;B-31,NationalSurgicalAdjuvantBreastandBowelProjecttrialB-31;BCIRG
006,BreastCancerInterna-
tionalResearchGroup
trial006;PACS-04,_____;FinHer,Finland
Herceptinstudy;CT,
chemotherapy;Tr,trastuzu
mab;AC,doxorubicin
and
cyclophosphamide;P,
paclitaxel;D,docetaxel;CB,carboplatin;
FEC,fluorouracil,
epirubicin,andcyclophosphamide;ED,epirubicin
anddocetaxel;V,
vinorelbine;NA,notapplicable;HR,haza
rdratio;95%
CI,95%
confidenceinterval;RFS,recurrence-freesurvival;NR,not
reported.
*P<.0087.
yRecurrence-freesurvival.
zCensoredanalysis:HR,0.63;95%
CI,0.53�0.75(P
<.0001).
§TheHR
wasadjustedforlymphnodes,receptorstatus,paclitaxelschedule,andprotocol.
||Censoredanalysis:HR,0.63;95%
CI,0.45�0.87(P
¼.0051).
Adjuvant Trastuzumab for Breast Cancer/Mackey et al
Cancer March 15, 2009 1157

crossover (51%) may affect outcomes, particularly overall
survival; and 3) the prior chemotherapy in this trial may
be considered suboptimal. In addition, women were
randomized after they completed chemotherapy, which
may have resulted in a more favorable cohort, because
those with early recurrences were omitted and were not el-
igible for enrollment.
The 5 subsequent adjuvant trastuzumab trials investi-
gated the administration of trastuzumab in conjunction
with prescribed chemotherapy, whereby trastuzumab was
administered either as a chemo-trastuzumab sequence or
concurrently with the taxane component of the prescribed
regimen (concurrent trastuzumab-taxane regimens) in
women with HER-2-positive tumors. The North Central
Cancer Treatment Group trial (N9831)10,13,15 and the
National Surgical Adjuvant Breast and Bowel Project trial
(B-31)10 are multicenter, open-label, randomized controlled
trials that were designed to explore the benefits of adding
trastuzumab to an adjuvant combination of doxorubicin
and cyclophosphamide (AC) followed by paclitaxel.
In the N9831 trial,10 women with lymph node-posi-
tive and high-risk lymph node-negative breast cancer were
assigned randomly to 1 of 3 arms: 1) women who received
AC then weekly paclitaxel (AC!P), 2) women who
received the same AC!P with weekly trastuzumab (4
mg/kg load followed by 2 mg/kg per week) administered
concurrently beginning with the first dose of paclitaxel
and continuing for 1 year (AC!P/Tr), 3) and women
who received the same AC!P followed sequentially, after
the completion of paclitaxel, by 1 year of weekly trastuzu-
mab therapy at the same dose and schedule as the other 2
arms (AC!P!Tr).
In the B-31 trial,10 only lymph node-positive
patients were eligible. Enrolled women were assigned to 1
of 2 arms: 1) AC followed by paclitaxel administered ev-
ery 3 weeks (AC!P), and 2) the same AC!P with
weekly trastuzumab administered concurrently beginning
with the first cycle of paclitaxel and continuing for 1 year
(AC!P/Tr). Because the N9831 and B-31 trials had
somewhat similar control and treatment arms, a joint
analysis (N9831/B-31 Analysis) comparing the concur-
rent trastuzumab-taxane arms (AC!P/Tr) with the con-
trol arms (AC!P) of the 2 trials was conducted. The
primary endpoint of the N9831/B-31 Analysis was dis-
ease-free survival (DFS). A subset of 3968 women quali-
fied for inclusion in the joint analysis, of whom 93% had
lymph node-positive disease (Table 1) and approximately
57% had received weekly paclitaxel.13
At a median follow-up of 2.9 years, despite a 21%
crossover rate,13 AC!P/Tr produced significant reduc-
tions in the risk of both recurrence (HR, 0.48; 95% CI,
0.41�0.57 [P< .00001]) and death (HR, 0.65; 95% CI,
0.51�0.84 [P ¼ .0007]) compared with AC!P (Table
2).13 These data confirm the findings of the HERA trial.
When considering these findings, it is important to
remember the following: 1) the joint analysis of 2 distinct
trials with different treatment and statistical approaches is
unorthodox; 2) the standards for validation and source
verification used in these trials were less rigorous than
those used in the HERA trial and the Breast Cancer Inter-
national Research Group 006 (BCIRG 006) trial; 3) a
small percentage of patients who were treated on the study
were identified as HER-2 negative at central review13,16;
and 4) AC!P may be considered suboptimal adjuvant
therapy.3,17
The BCIRG 006 trial is an international, multicen-
ter, open-label, randomized controlled study12,18 that was
designed to assess the benefits of adding trastuzumab to an
anthracycline/docetaxel-based or a nonanthracycline, doce-
taxel, and carboplatin-based adjuvant chemotherapy regi-
men in patients with HER-2-positive breast cancer. In
total, 3222 women were assigned randomly to 1 of 3 treat-
ment arms: 1) women who received a combination of AC
followed by docetaxel administered every 3 weeks
(AC!D); 2) women who received AC!D with concur-
rent, weekly trastuzumab beginning with docetaxel (4 mg/
kg load followed by 2 mg/kg weekly) for the duration of
chemotherapy followed by trastuzumab administered every
3 weeks for a total therapy duration of 1 year (AC!D/Tr);
and 3) women who received a combination of carboplatin,
docetaxel, and weekly trastuzumab followed by trastuzu-
mab administered every 3 weeks for a total therapy dura-
tion of 1 year (CB/D/Tr). Patient characteristics were well
balanced across study arms, and approximately 71% of
patients had lymph node-positive disease (Table 1).12
At a median follow-up of 36 months, both the
AC!D/Tr regimen and the CB/D/Tr regimen, com-
pared with AC!D, produced significant reductions in
the risk of both recurrence (HR, 0.61; 95% CI,
0.48�0.76 [P < .0001]; and HR, 0.67; 95% CI,
0.54�0.83 [P ¼ .0003], respectively) and death (HR,
0.59; 95% CI, 0.42�0.85 [P ¼ .004]; and HR, 0.66;
Review Article
1158 Cancer March 15, 2009

95%CI, 0.47�0.93 [P¼ .017], respectively) (Table 2).12
When considering these study results, it is important to
note that: 1) the results of the BCIRG 006 trial have not
yet been published or peer reviewed, and 2) the nonan-
thracycline CB/D regimen is not an established adjuvant
regimen for breast cancer.
The Protocole Adjuvant dans le Cancer du Sein
(PACS) 04 study is a multicenter, open-label, random-
ized controlled trial.19 It is the first study designed to
evaluate the benefits of a chemo-trastuzumab sequence
following a prescribed escalated-dose epirubicin or epi-
rubicin-taxane regimen. In total, 3010 women with axil-
lary lymph node-positive breast cancer were assigned
randomly to 1 of 2 arms: 1) a combination of epirubicin
and docetaxel (ED), or 2) a combination of escalated-
dose epirubicin, fluorouracil and cyclophosphamide
(FEC100). Once their HER-2 status was determined,
women with HER-2-positive tumors (n ¼ 528) imme-
diately underwent a second randomization to 1 year of
trastuzumab administered every 3 weeks (8 mg/kg load
followed by 6 mg/kg every 3 weeks) or observation. As
in the HERA trial, trastuzumab therapy was initiated af-
ter the completion of both chemotherapy and radiother-
apy. Baseline characteristics of the patients with HER-
2-positive disease were well balanced (Table 1).19
At a median follow-up of 4 years, the PACS-04
study has the longest follow-up of trastuzumab trials
reported to date. Results from the first randomization
comparing concomitant ED with FEC100 have yet to be
reported; however results of the second randomization
failed to demonstrate a significant reduction in the risk of
recurrence (HR, 0.86; 95% CI, 0.61�1.22 [P ¼ .41]) or
death (HR, 1.27; 95% CI, 0.68�2.38 [P value not
reported]) for chemo-trastuzumab sequences compared
with observation (Table 2). When considering these find-
ings, it is important to note that: 1) the study may have
been underpowered because of the small sample size; 2) as
in the HERA trial, the sequential approach may have pre-
cluded a potential benefit from the concurrent adminis-
tration of chemotherapy and trastuzumab10-14; 3) in
contrast to the HERA trial population, a large proportion
of patients in the PACS-04 trial received optimal chemo-
therapy, which may explain the reduced incremental ben-
efit of trastuzumab observed in the PACS-04 relative to
the HERA trial; and 4) the PACS-04 results have not
been published or peer reviewed.
The Finland Herceptin (FinHer) study is a multi-
center, open-label, randomized controlled trial11 that was
designed to assess the benefits of docetaxel administered
every 3 weeks (D) or weekly vinorelbine (V) followed by
fluorouracil, epirubicin, and cyclophosphamide (FEC) in
1010 women with axillary lymph node-positive or high-
risk, lymph node-negative breast cancer. The study also
assigned 232 women with HER-2-positive tumors to
receive 9 cycles of weekly trastuzumab (4 mg/kg load fol-
lowed by 2 mg/kg weekly) administered concurrently
with either docetaxel, or vinorelbine, or no further treat-
ment. Baseline characteristics of the patients were bal-
anced with the exception of axillary lymph node
metastases, which were somewhat more frequent in the
trastuzumab group than in the observation group (89% vs
78%, respectively) (Table 1).11
At a median follow-up of 3 years, as in the 4 larger
trastuzumab trials, fewer events of recurrence were evident
for women who received trastuzumab (HR, 0.42; 95%
CI, 0.21�0.83 [P ¼ .01]) compared with women who
did not (Table 2), although overall survival reached only
borderline significance, most likely because of the small
sample size (HR, 0.41; 95% CI, 0.16�1.08 [P ¼ .07])
(Table 2).11 Although the short 9-week course of trastuzu-
mab therapy (short-course trastuzumab therapy) proved
beneficial, caution should be used when interpreting these
findings, because: 1) the sample size of the HER-2-posi-
tive patient population was small; 2) the study prescribed
lower than standard doses of both anthracyclines and tax-
anes; and 3) although there was a trend toward improved
overall survival with the addition of trastuzumab, the
findings were not statistically significant.
Safety
Noncardiac adverse events
Trastuzumab is associated with few grade 3 or 4
adverse effects. Small but significant increases in severe
adverse events were reported with trastuzumab compared
with observation (11% vs 6%; P < .0001) in the HERA
trial.9 However, the addition of trastuzumab to chemo-
therapy did not result in clinically significant increases
in the incidence of adverse events compared with controls
in the FinHer trial,11 the N9831/B-31 Analysis,10 or the
AC!D/Tr arm of the BCIRG 006 trial.12 The CB/D/Tr
regimen was the only treatment that produced less severe
toxicity compared with controls.12
Adjuvant Trastuzumab for Breast Cancer/Mackey et al
Cancer March 15, 2009 1159

Cardiotoxicity
Because both anthracyclines and trastuzumab are
cardiotoxic,20-22 significant measures were undertaken to
mitigate cardiac risk in all trials. These include appropri-
ate eligibility criteria, cardiac screening and monitoring,
and strict criteria for the initiation and discontinuation
of trastuzumab therapy.8-12,19
Chemo-trastuzumab sequences were explored in 3
of the 6 trials: the HERA trial, the sequential arm of the
N9831 trial, and the PACS-04 trial. The reported car-
diac data captured differing components of therapy
across trials. Because patients in the HERA and PACS-
04 trials were randomized after the completion of chem-
otherapy, the reported cardiotoxicity data from these
trials reflects trastuzumab-induced cardiotoxicity exclu-
sively, because patients with compromised cardiac
capacity after chemotherapy were excluded from the
trastuzumab portion of the trial. In the N9831 trial,
although patients were randomized before they received
chemotherapy, the trial reports cumulative post-AC car-
diotoxicity, which may not fully capture the anthracy-
cline-induced cardiotoxicity of the AC portion of
chemotherapy.
Furthermore, the rigor of cardiac screening in the 3
trials differed considerably: Patients in the HERA trial
had a more favorable cardiac profile (left ventricular
ejection fraction [LVEF] >55% after chemotherapy and
locoregional therapy) relative to patients in both the
PACS-04 trial (LVEF �55% or between 50% and 55%
with cardiologist approval) and the N9831 trial (LVEF
>50%).
Chemo-trastuzumab sequences were associated with
increases in cardiotoxicity in all 3 trials. Patients in the
HERA trial experienced a small but significantly greater
degree of cardiotoxicity with trastuzumab compared with
observation, including a confirmed, significant decrease
in LVEF (3.04% vs 0.53%; P < .0001), symptomatic
congestive heart failure (CHF) (2.15% vs 0.12%; P <
.0001), and severe CHF (0.60% vs 0%; P< .0001); thus,
4.3% of patients were unable to complete trastuzumab
therapy for cardiac reasons.9,23 Patients in the PACS-04
trial also experienced increased cardiotoxicity with the
addition of trastuzumab, resulting in increases in severe
CHF (1.7% vs 0.4%) and a higher rate of discontinuation
due to cardiotoxicity (17.9%) (Table 3).19 Finally, when
sequential trastuzumab was added to the AC!P arm of
the N9831 trial, increases in cardiac events once again
were apparent (2.8% vs 0.3%).24
Concurrent trastuzumab-taxane regimens were
explored in 3 of the 6 trials.10,12,15 In all 3 studies, only
patients who had an LVEF>50% after the completion of
AC therapy were eligible for trastuzumab therapy, result-
ing in a small proportion of enrolled patients in all 3 trials
being denied trastuzumab therapy (N9831/B31 Analysis,
6.7% of patients; BCIRG 006 trial, 2% of patients). Car-
diotoxicity was evident in all 3 trials. The addition of tras-
tuzumab to paclitaxel after the completion of AC resulted
in an increase in cumulative cardiac events (either events
from cardiac causes or New York Heart Association
[NYHA] class III or IV CHF) compared with controls in
both the N9831 and B31 trials (3-year cumulative cardiac
events [N9831], 3.3% vs 0.3%; 5-year cumulative cardiac
events [B31], 3.8% vs 0.9%).24,25 Furthermore, 15% of
patients in the N9831 trial and 19% of patients in the
B31 trial were unable to complete trastuzumab therapy
for cardiac reasons.26,27 Increased cardiotoxicity also was
apparent in the AC!D/Tr arm of the BCIRG 006 com-
pared with controls (>10% relative LVEF decline; 18.1%
vs 10.1%, respectively; P < .0001; NYHA grade 3 or 4
CHF, 1.9% vs 0.4%, respectively)12; and, similar to the
other concurrent trastuzumab-taxane trials, 8.3% of
patients who received AC!D/Tr were unable to com-
plete therapy because of trastuzumab-mediated cardiotox-
icity (unpublished data).
The nonanthracycline-containing, concurrent tras-
tuzumab-taxane regimen (CB/D/Tr) of the BCIRG 006
trial and the short-course trastuzumab regimen of the
FinHer trial were the least cardiotoxic. At 3 years, no
increase in cardiotoxicity was apparent for CB/D/Tr com-
pared with controls (>10% relative LVEF decline, 8.6%
vs 10.1%; grade 3/4 CHF, 0.4% vs 0.4%) in the BCIRG
006 trial (Table 3),12 and none of the 4 patients who
experienced cardiac infarction or failure in the FinHer
trial had received trastuzumab (Table 3).11
DISCUSSION
There is overwhelming evidence to support the overall
benefits of adding adjuvant trastuzumab to chemotherapy
in women with HER-2-positive cancer despite the risk of
developing clinically significant cardiac toxicity. Although
the benefit of adjuvant trastuzumab is clear, many
Review Article
1160 Cancer March 15, 2009

Table
3.Card
iacSafety
StudyGroup
N9831/B
-31Analysis:Perez2008,24Rastogi
2007,25Perez2005,26Tan-C
hiu
200527
HERA:Suter200723
ACfiP/Tr
ACfiP
BCIRG
006:Slamon200512*
PACS04:
Spielm
ann200719
FinHer:Joensuu
200611
Variable
CTfiTr
CTfi
Observation
N9831
B-31
N9831
B-31
ACfiD/Tr
CB/
D/Tr
Control
FEC
orEDfiTr
FEC
orED
Dor
V/Trfi
FEC
Dor
VfiFEC
Sample
size,no.ofpatients
1678
1708
579y
947
670z
898
1068
1056
1050
260
268
115
116
Trastuzumabdiscontinuedbecauseofcardiacproblems
Percentageofpatients
4.3
NA
15.4
26
1927
NA
NA
8.3*
3.6*
NA
17.9
NA
NR
NA
Medianfollo
w-up,y
23
Decreasesin
LVEF�15%
points
from
baseline
Percentageofpatients
7.0§
2.1§
17.3
26|
NR
6.7
26|
NR
18.1
12¶
8.6
12¶
10.1
12¶
NR
NR
3.5#
6.0
zz
P<.0001
.5
Medianfollo
w-up,y
22
33
33
33
Severe
CHF
Percentageofpatients
(no.)
0.6
0.0
3.3
24**
3.8
(n¼35)25yy
0.3
24**
0.9
(n¼6)25yy
1.9
(n¼20)zz
12
0.4
(n¼4)zz
12
0.4
(n¼4)zz
12
1.7
(n¼4)
0.4
(n¼1)
0.0
(n¼0)§§
NR
Medianfollo
w-up,y
22
3.75
53.75
53
33
44
3
Cardiacdeath
Percentageofpatients
(no.)
0.0
(n¼0)
0.06(n¼1)
0.2
(n¼1)25
0.0
(n¼0)25
0.2
(n¼1)24
0.1
(n¼1)25
0.0
(n¼0)12
0.0
(n¼0)12
0.0
(n¼0)12
0.0
(n¼0)
0.0
(n¼0)
0.0
(n¼0)
0.0
(n¼0)
Medianfollo
w-up,y
22
3.75
53.75
53
33
44
33
HERA
indicatestheHerceptinAdjuvanttrial;N9831,NorthCentralCancerTreatm
entGrouptrialN9831;B-31,NationalSurgicalAdjuvantBreastandBowelProjecttrialB-31;BCIRG
006,BreastCancerInternationalResearchGroup
trial006;PACS-04,Protocole
Adjuvantdansle
CancerduSein;FinHer,FinlandHerceptinstudy;CT,
chemotherapy;Tr,trastuzu
mab;AC,doxorubicin
andcyclophosphamide;P,
paclitaxel;D,docetaxel;CB,carboplatin;FEC,fluoroura-
cil,
epirubicin,andcyclophosphamide;ED,epirubicin
anddocetaxel;V,
vinorelbine;NA,notapplicable;LV
EF,
leftventricularejectionfraction;NR,notreported;CHF,
congestiveheartfailure.
*Unpublisheddata.
yAt3.75years,n¼570.
At3.75years,n¼664.
§Adecreasein
LVEF�10%
from
baselineto
anLV
EF<50%
atanytime.
|Thegreatestchangein
LVEF�15%
comparedwiththepre-A
Clevelatanytimepointin
thestudy.
¶Definedasa>10%
relativeLV
EFdecline.
#Definedas�1measurement(s)ofLV
EF<15%
ofthebaselinevalue.
**The3-yearcumulativeincidenceofcardiacevents.Acardiaceventwasdefinedasdeath
from
cardiaccausesorNew
York
HeartAssociationclassIIIorIV
CHF.
yyThe5-yearcumulativeincidenceofcardiacevents.A
cardiaceventwasdefined
asdeath
from
cardiaccauses,orNationalHeart
AssociationclassIIIorIV
CHF,
andanabsolute
dropin
LVEFonamutigated
acquisitionscanor
echocardiogram
of>10%
points
tobelow
55%
or>5%
andbelow
thelowerlim
itofnorm
alin
subpopulationsofpatients
elig
ible
fortrastuzu
mabtherapy.
zzGrade3or4CHF,
excludingarrhythmias.
§§Definedascardiacfailure
orcardiacinfarction.

questions remain related to the clinical application of
these findings.
Are There Patient Groups That Benefit
More or Less From Trastuzumab Therapy?
In light of the risks and costs associated with trastuzumab
therapy, the accurate identification of patients with HER-
2-positive tumors who preferentially may benefit from tras-
tuzumab therapy is imperative. Both fluorescent in situ
hybridization (FISH) and chromogenic in situ hybridiza-
tion, as well as immunohistochemistry testing with or with-
out FISH confirmation, have been used in the adjuvant
setting to assess HER-2 status.9-12 Central confirmation of
HER-2 status before enrolment was required in all studies
with the exception of an initial cohort of the N9831 trial
and all patients in the B-31 trials, which relied on testing in
approved local laboratories. Differences between local and
central HER-2 assessment and between immunohisto-
chemistry and FISH testing have been reported in the
N9831 and B-31 trials, revealing a proportion of patients
in both trials withHER-2-negative tumors at central review
(8.8% and 9.7, respectively).13,28 Unexpectedly, in addi-
tion to the benefits of trastuzumab among HER-2-positive
patients, exploratory subgroup analyses from both the
N9831 trial and the B-31 trial revealed a potential benefit
for trastuzumab among patients who tested negative for
HER-2 at central review.13,28 Discordance in HER-2 test-
ing and the possibility of heterogeneity in relative treatment
effect underscore the importance of continued research
into optimal HER-2 testing and the use of standardized
HER-2 testing in clinical practice.
Adjuvant trastuzumab trials enrolled significant pro-
portions of patients with lymph node-positive and high-
risk, lymph node-negative disease. Although low numbers
of very small T1a and T1b tumors were included in the
high-risk, lymph node-negative cohorts,9,12 nevertheless,
it is reasonable to consider the use of the aforementioned
trastuzumab regimens in all patients who have lymph
node-negative, HER-2-positive disease with a high-risk of
recurrence.
None of the trials that we reviewed were powered to
detect the effect of trastuzumab in patient subgroups at
the time of their interim analyses. However, an early look
at the forest plots of HRs for DFS in the HERA trial,9 the
BCIRG 006 trial,12 and the N9831/B-31 Analysis10,13
suggest that all eligible patient subgroups, regardless of
age, lymph node status, menopausal status, or hormone
status, benefited equally from trastuzumab.
BothHER-2/neu amplification and topoisomerase IIa
(Topo IIa) amplification are associated with a relative ben-
efit from anthracycline-containing regimens compared
with nonanthracycline-containing regimens.29-34 It has
been postulated that this benefit may relate to the physical
proximity on chromosome 17q of the HER-2 and Topo
IIa gene, because topoisomerase II is involved integrally in
the mechanism of action of the anthracyclines. Data from
the BCIRG 006 trial demonstrated that CB/D/Tr is
equivalent to AC!D/Tr in patients overall; however, in
the 35% of women with HER2-positive early breast can-
cer in whom the Topo IIa and HER-2 genes are coampli-
fied, CB/D/Tr and AC!D/Tr are equivalent to
AC!D.12 These data suggest that anthracycline-contain-
ing chemotherapy may not be required in HER-2-overex-
pressing women and/or that trastuzumab may not be
required in addition to an anthracycline-containing
regimen in women with HER-2/Topo IIa coamplified
tumors.
A meta-analysis of studies comparing higher dose
anthracycline-containing regimens with standard-dose
anthracycline-containing regimens suggested that women
with HER-2-positive tumors benefited from higher dose
chemotherapy compared with standard-dose chemother-
apy, whereas women with HER-2-negative tumors did
not.35 Similarly, a significant interaction between HER-2
status and taxane-containing versus nontaxane-containing
regimens have been reported.36,37 In Cancer and Leuke-
mia Group B trial 9344 trial, both women with HER-2-
positive tumors and women with HER-2-negative tumors
benefited from the addition of taxanes; however, those
with HER-2-positive tumors did so to a greater degree.
An analysis of the PACS-04 and BCIRG 006 clinical trial
populations designed to assess the benefits of HER-2 and
Topo IIa as predictors of response to trastuzumab cur-
rently is underway.
Should Trastuzumab Be Administered
Concurrently or Sequentially With
Chemotherapy?
Annualized DFS hazards rates for patients with HER-2-
positive early breast cancer who have not received
Review Article
1162 Cancer March 15, 2009

trastuzumab indicate an increased risk of recurrence
within 1 to 2 years, providing a rationale for the earliest
possible intervention with trastuzumab.9,13 Concurrent
trastuzumab-taxane regimens10-12 minimize postsurgery
trastuzuamb treatment delays (1�4 months), whereas
chemo-trastuzumab sequences administered in the HERA
trial (8 months) and the PACS-04 trial9,19 tend to incur
greater trastuzumab delays. At 3 years, all 4 concurrent
trastuzumab-taxane regimens10,12 resulted in improved
DFS compared with controls, and 2-year results from the
HERA trial demonstrated a similar improvement in DFS
for chemo-trastuzumab sequences compared with obser-
vation. However, at 4 years, outcomes for the PACS-04
trial did not indicate a benefit for aggressive anthracy-
cline-based regimens or anthracycline-taxane regimens
compared with controls (HR, 0.86; 95% CI, 0.61�1.22
[P ¼ .41]) despite a trend toward improved DFS during
the first 18 months (HR, 0.57; 95% CI, 0.30�1.09
[P value not reached]).19 This suggests a potential attenu-
ation of the benefit of trastuzumab with delayed
administration, which may indicate a cytostatic effect for
sequential trastuzumab administration, whereas concur-
rent use may result in a cytotoxic effect.
The N9831 trial is the only adjuvant trastuzumab
trial that was designed to directly compare the sequential
versus concurrent approaches.15 Although a sufficient
number of events are currently unavailable to complete
this analysis, initial data suggest that sequential trastuzu-
mab administration may result in inferior efficacy (DFS:
HR, 0.64; 95% CI, 0.46�0.91 [P ¼ .0114]) compared
with concurrent administration.15,24 Until the final
results of this analysis are available, the benefits of concur-
rent versus sequential administration remain unclear.
What Is the Optimal Duration of
Trastuzumab-based Therapy?
The balance of available evidence supports the use of
1-year of adjuvant trastuzumab therapy.8-10,12,13 The
HERA trial, which was designed to evaluate duration of
therapy, assessed the benefits of 2 years of therapy com-
pared with 1 year.9 Results from that trial, anticipated in
the fall of 2008, will provide insight into the risk-benefit
ratio for extended trastuzumab exposure; however, even
longer follow-up will be required to confirm the safety of
this treatment approach.
The use of short-course trastuzumab therapy has
clinical appeal because of the enhanced safety profile,
reduced cost, and improved quality of life of this
approach compared with 1 year of trastuzumab therapy.
The significant reductions in the risk of recurrence
observed with short-course trastuzumab therapy com-
pared with controls in the FinHer trial11 and the nonin-
feriority of short-course trastuzumab therapy relative
to 1 year of therapy in the randomized phase 2 E2198
pilot trial,38 although not powered to assess therapy
duration, support this approach. Nevertheless, evidence
from larger randomized clinical trials, such as the Syn-
ergism or Long Duration (SOLD) study and the Proto-
col of Herceptin Adjuvant with Reduced Exposure
(PHARE) trial, directly comparing short versus longer
durations of trastuzumab therapy is needed to establish
the noninferiority of this approach. Until mature study
findings from these trials are available, short-course
trastuzumab therapy should be reserved for instances in
which institutional budgetary restraints or patient
preference limit the administration of a full year of
trastuzumab therapy.
What Are the Implications of
Trastuzumab-related Cardiotoxicity?
Unlike anthracycline-mediated cardiotoxicity, some
degree of cardiac recovery appears to be possible with tras-
tuzumab-mediated cardiotoxicity. In the HERA trial,
heart failure treatment was recommended for all patients
with severe CHF. At a median follow-up of 1 year, of the
10 patients who had severe CHF at the last scheduled
assessment, 8 patients (80%) were asymptomatic, and 6
patients (60%) had an LVEF �55%.23 In the N9831
trial, at a median follow-up of 2 years, the majority of
patients who developed CHF improved on medical treat-
ment, and LVEFs>50% were observed in approximately
50% of patients who received sequential therapy and in
61% of patients who received concurrent therapy at 2
years.26 Finally, in the B-31 trial, with 5 years follow-up,
women who had confirmed CHF and at least 6 months of
follow-up usually were asymptomatic (85%). Although a
large proportion required medication (61%), approxi-
mately 66% of patients had an LVEF >50% on a follow-
up multigated acquisition (MUGA) scan.25
Adjuvant Trastuzumab for Breast Cancer/Mackey et al
Cancer March 15, 2009 1163

Which Patients Are at a Greater Risk
of Cardiotoxicity?
The ability to reliably predict a patient’s risk of developing
CHF is of great clinical importance. The HERA, N9831,
and B-31 trials conducted analyses to identify factors that
were correlated with an increased risk of cardiotoxicity
with adjuvant trastuzumab therapy. Lower screening
LVEFs,23-25 lower post-AC LVEFs,25 and age24,25 were
associated with significant increases in cardiotoxicity.
Other factors that were associated with increased cardio-
toxicity included higher doses of anthracyclines,23
increased body mass index,23 and the requirement for
hypertensive medications.24,25 Although the analyses of
potential risk factors are exploratory and were based on
small numbers, routine cardiac risk assessment is recom-
mended for all trastuzumab candidates, especially those at
an increased risk for cardiotoxicity.
Should Trastuzumab-based Therapy Be
Given Concurrently With Radiotherapy?
Preclinical data indicate that trastuzumab may exert a
radiosensitizing effect on HER-2-positive breast cancer
cells, although it is uncertain whether it has a similar effect
on normal cells.39,40 In the adjuvant studies that we
reviewed, trastuzumab was administered either concur-
rently with radiotherapy after the completion of chemo-
therapy10 or after the completion of both chemotherapy
and radiotherapy.9,19 When trastuzumab was adminis-
tered concurrently, left-sided tumors and radiation
therapy were not identified as cardiac risk factors,25 radio-
therapy was not observed to increase cardiac events or
radiation-related adverse events, and internal mammary
radiotherapy appeared to be feasible when the cardiac
dose was limited.39 These study findings support the con-
tinued practice of concurrent trastuzumab and radiother-
apy administration after the completion of chemotherapy
in conjunction with continued cardiac follow-up.
Should Trastuzumab-based Therapy Be
Given Concurrently With Endocrine
Therapy?
There is a strong rationale for the concurrent, early
administration of endocrine therapy and trastuzumab in
HER-2-positive and hormone receptor-positive breast
cancer because of preclinical evidence of cross talk
between HER-2 and estrogen receptor signaling path-
ways. Recent evidence from the first-line metastatic
breast cancer setting provides further support for this
approach.41 Women who received concurrent endocrine
therapy had a benefit from trastuzumab similar to the
benefit experienced by those who did not receive
endocrine therapy with no increase in toxicity.8,10-12,19
These findings support the continued practice of concur-
rent endocrine and trastuzumab administration after the
completion of chemotherapy in HER-2-positive and hor-
mone receptor-positive patients.
How Do Trastuzumab-based Regimens
Compare in Terms of Cost?
The administration of adjuvant trastuzumab therapy is
associated with considerable expense. In addition to the
cost of diagnostic testing, significant treatment costs
include acquisition costs, administration costs (nursing
and pharmacy time), and the costs of clinical cardiac mon-
itoring. Numerous cost-effectiveness studies suggest that
costs are comparable to other accepted and standard uses
of healthcare dollars42-46; nevertheless, factoring in treat-
ment costs when selecting from among safe and effective
treatment options improves the overall cost-benefit ratio
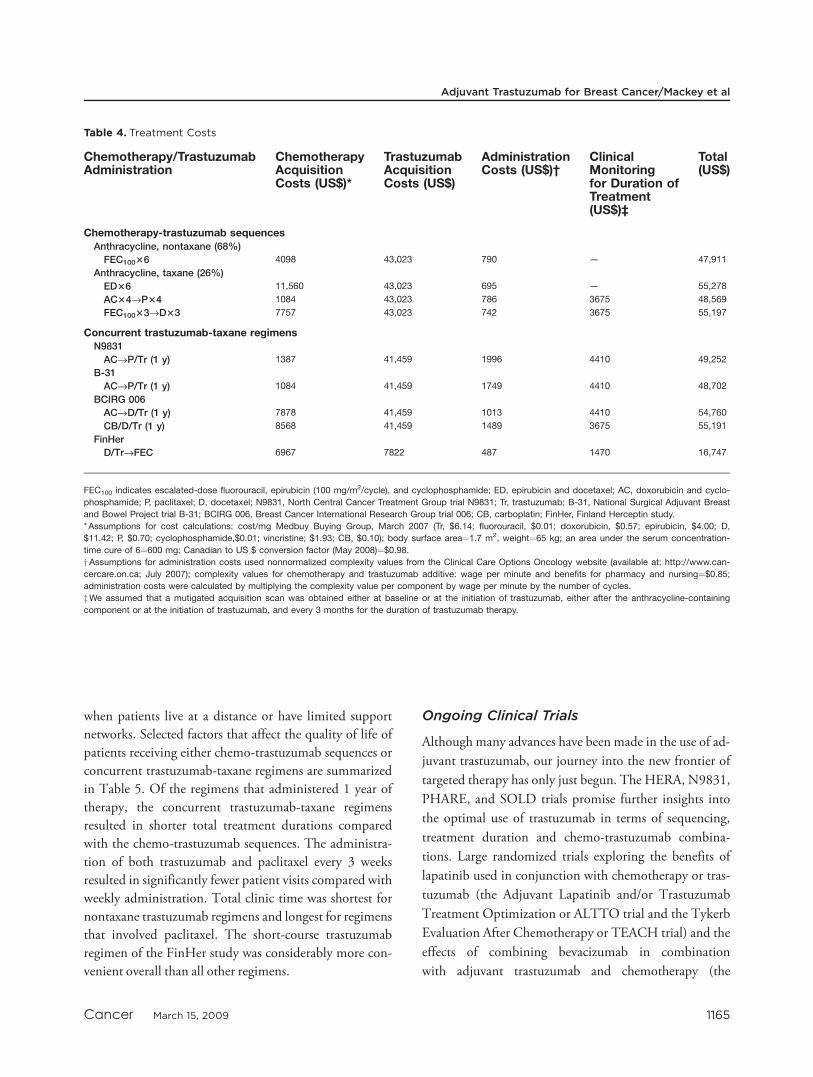
of the intervention. Selected treatment costs for chemo-
trastuzumab sequences and concurrent trastuzumab-tax-
ane regimens are summarized in Table 4.
Trastuzumab acquisition costs for 1 year of therapy
were the single greatest factor contributing to total treat-
ment costs (in U.S. dollars, between $41,459 and $43,023),
followed by cardiac monitoring by MUGA scan (between
$3675 and $4410). The administration costs associated
with 1 year of trastuzumab therapy administered every 3
weeks were significantly less than those associated with
weekly administration ($510 vs $1473). The inclusion of
taxanes increased total treatment costs. The short-course
trastuzumab regimen from the FinHer trial ($16,747) was
associated with the lowest total treatment cost.
Which Trastuzumab-based Regimen Is Most
Convenient for Patients?
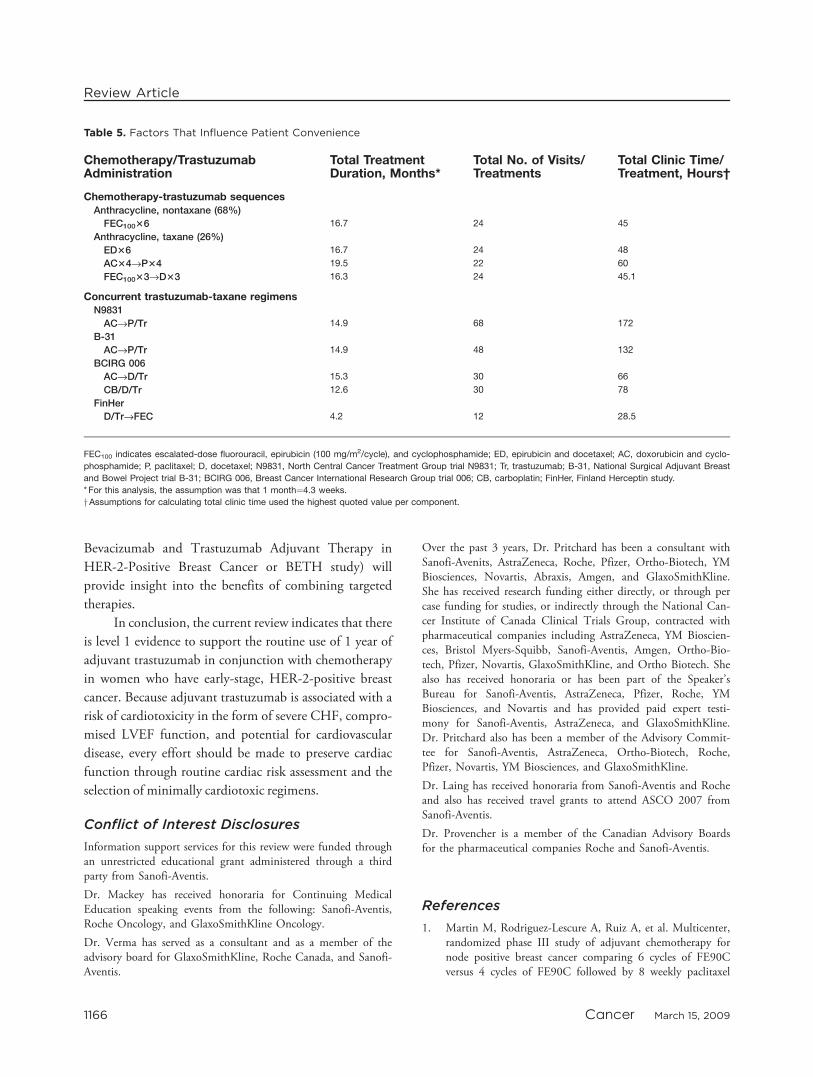
The patient-related convenience of a regimen can have a
significant impact on a patient’s quality of life, especially
Review Article
1164 Cancer March 15, 2009
when patients live at a distance or have limited support
networks. Selected factors that affect the quality of life of
patients receiving either chemo-trastuzumab sequences or
concurrent trastuzumab-taxane regimens are summarized
in Table 5. Of the regimens that administered 1 year of
therapy, the concurrent trastuzumab-taxane regimens
resulted in shorter total treatment durations compared
with the chemo-trastuzumab sequences. The administra-
tion of both trastuzumab and paclitaxel every 3 weeks
resulted in significantly fewer patient visits compared with
weekly administration. Total clinic time was shortest for
nontaxane trastuzumab regimens and longest for regimens
that involved paclitaxel. The short-course trastuzumab
regimen of the FinHer study was considerably more con-
venient overall than all other regimens.
Ongoing Clinical Trials
Although many advances have been made in the use of ad-
juvant trastuzumab, our journey into the new frontier of
targeted therapy has only just begun. The HERA, N9831,
PHARE, and SOLD trials promise further insights into
the optimal use of trastuzumab in terms of sequencing,
treatment duration and chemo-trastuzumab combina-
tions. Large randomized trials exploring the benefits of
lapatinib used in conjunction with chemotherapy or tras-
tuzumab (the Adjuvant Lapatinib and/or Trastuzumab
Treatment Optimization or ALTTO trial and the Tykerb
Evaluation After Chemotherapy or TEACH trial) and the
effects of combining bevacizumab in combination
with adjuvant trastuzumab and chemotherapy (the
Table 4. Treatment Costs
Chemotherapy/TrastuzumabAdministration
ChemotherapyAcquisitionCosts (US$)*
TrastuzumabAcquisitionCosts (US$)
AdministrationCosts (US$)†
ClinicalMonitoringfor Duration ofTreatment(US$)‡
Total(US$)
Chemotherapy-trastuzumab sequencesAnthracycline, nontaxane (68%)
FEC10036 4098 43,023 790 — 47,911
Anthracycline, taxane (26%)
ED36 11,560 43,023 695 — 55,278
AC34fiP34 1084 43,023 786 3675 48,569
FEC10033fiD33 7757 43,023 742 3675 55,197
Concurrent trastuzumab-taxane regimensN9831
ACfiP/Tr (1 y) 1387 41,459 1996 4410 49,252
B-31
ACfiP/Tr (1 y) 1084 41,459 1749 4410 48,702
BCIRG 006
ACfiD/Tr (1 y) 7878 41,459 1013 4410 54,760
CB/D/Tr (1 y) 8568 41,459 1489 3675 55,191
FinHer
D/TrfiFEC 6967 7822 487 1470 16,747
FEC100 indicates escalated-dose fluorouracil, epirubicin (100 mg/m2/cycle), and cyclophosphamide; ED, epirubicin and docetaxel; AC, doxorubicin and cyclo-
phosphamide; P, paclitaxel; D, docetaxel; N9831, North Central Cancer Treatment Group trial N9831; Tr, trastuzumab; B-31, National Surgical Adjuvant Breast
and Bowel Project trial B-31; BCIRG 006, Breast Cancer International Research Group trial 006; CB, carboplatin; FinHer, Finland Herceptin study.
* Assumptions for cost calculations: cost/mg Medbuy Buying Group, March 2007 (Tr, $6.14; fluorouracil, $0.01; doxorubicin, $0.57; epirubicin, $4.00; D,
$11.42; P, $0.70; cyclophosphamide,$0.01; vincristine; $1.93; CB, $0.10); body surface area¼1.7 m2, weight¼65 kg; an area under the serum concentration-
time cure of 6¼600 mg; Canadian to US $ conversion factor (May 2008)¼$0.98.
yAssumptions for administration costs used nonnormalized complexity values from the Clinical Care Options Oncology website (available at: http://www.can-
cercare.on.ca; July 2007); complexity values for chemotherapy and trastuzumab additive: wage per minute and benefits for pharmacy and nursing¼$0.85;
administration costs were calculated by multiplying the complexity value per component by wage per minute by the number of cycles.
zWe assumed that a mutigated acquisition scan was obtained either at baseline or at the initiation of trastuzumab, either after the anthracycline-containing
component or at the initiation of trastuzumab, and every 3 months for the duration of trastuzumab therapy.
Adjuvant Trastuzumab for Breast Cancer/Mackey et al
Cancer March 15, 2009 1165
Bevacizumab and Trastuzumab Adjuvant Therapy in
HER-2-Positive Breast Cancer or BETH study) will
provide insight into the benefits of combining targeted
therapies.
In conclusion, the current review indicates that there
is level 1 evidence to support the routine use of 1 year of
adjuvant trastuzumab in conjunction with chemotherapy
in women who have early-stage, HER-2-positive breast
cancer. Because adjuvant trastuzumab is associated with a
risk of cardiotoxicity in the form of severe CHF, compro-
mised LVEF function, and potential for cardiovascular
disease, every effort should be made to preserve cardiac
function through routine cardiac risk assessment and the
selection of minimally cardiotoxic regimens.
Conflict of Interest Disclosures
Information support services for this review were funded throughan unrestricted educational grant administered through a thirdparty from Sanofi-Aventis.
Dr. Mackey has received honoraria for Continuing MedicalEducation speaking events from the following: Sanofi-Aventis,Roche Oncology, and GlaxoSmithKline Oncology.
Dr. Verma has served as a consultant and as a member of theadvisory board for GlaxoSmithKline, Roche Canada, and Sanofi-Aventis.
Over the past 3 years, Dr. Pritchard has been a consultant withSanofi-Avenits, AstraZeneca, Roche, Pfizer, Ortho-Biotech, YMBiosciences, Novartis, Abraxis, Amgen, and GlaxoSmithKline.She has received research funding either directly, or through percase funding for studies, or indirectly through the National Can-cer Institute of Canada Clinical Trials Group, contracted withpharmaceutical companies including AstraZeneca, YM Bioscien-ces, Bristol Myers-Squibb, Sanofi-Aventis, Amgen, Ortho-Bio-tech, Pfizer, Novartis, GlaxoSmithKline, and Ortho Biotech. Shealso has received honoraria or has been part of the Speaker’sBureau for Sanofi-Aventis, AstraZeneca, Pfizer, Roche, YMBiosciences, and Novartis and has provided paid expert testi-mony for Sanofi-Aventis, AstraZeneca, and GlaxoSmithKline.Dr. Pritchard also has been a member of the Advisory Commit-tee for Sanofi-Aventis, AstraZeneca, Ortho-Biotech, Roche,Pfizer, Novartis, YM Biosciences, and GlaxoSmithKline.
Dr. Laing has received honoraria from Sanofi-Aventis and Rocheand also has received travel grants to attend ASCO 2007 fromSanofi-Aventis.
Dr. Provencher is a member of the Canadian Advisory Boardsfor the pharmaceutical companies Roche and Sanofi-Aventis.
References
1. Martin M, Rodriguez-Lescure A, Ruiz A, et al. Multicenter,randomized phase III study of adjuvant chemotherapy fornode positive breast cancer comparing 6 cycles of FE90Cversus 4 cycles of FE90C followed by 8 weekly paclitaxel
Table 5. Factors That Influence Patient Convenience
Chemotherapy/TrastuzumabAdministration
Total TreatmentDuration, Months*
Total No. of Visits/Treatments
Total Clinic Time/Treatment, Hours†
Chemotherapy-trastuzumab sequencesAnthracycline, nontaxane (68%)
FEC10036 16.7 24 45
Anthracycline, taxane (26%)
ED36 16.7 24 48
AC34fiP34 19.5 22 60
FEC10033fiD33 16.3 24 45.1
Concurrent trastuzumab-taxane regimensN9831
ACfiP/Tr 14.9 68 172
B-31
ACfiP/Tr 14.9 48 132
BCIRG 006
ACfiD/Tr 15.3 30 66
CB/D/Tr 12.6 30 78
FinHer
D/TrfiFEC 4.2 12 28.5
FEC100 indicates escalated-dose fluorouracil, epirubicin (100 mg/m2/cycle), and cyclophosphamide; ED, epirubicin and docetaxel; AC, doxorubicin and cyclo-
phosphamide; P, paclitaxel; D, docetaxel; N9831, North Central Cancer Treatment Group trial N9831; Tr, trastuzumab; B-31, National Surgical Adjuvant Breast
and Bowel Project trial B-31; BCIRG 006, Breast Cancer International Research Group trial 006; CB, carboplatin; FinHer, Finland Herceptin study.
* For this analysis, the assumption was that 1 month¼4.3 weeks.
yAssumptions for calculating total clinic time used the highest quoted value per component.
Review Article
1166 Cancer March 15, 2009

administrations: interim efficacy analysis of GEICAM 9906trial [abstract]. Breast Cancer Res Treat. 2005;94(suppl1):S20. Abstract 39.
2. Martin M, Pienkowski T, Mackey J, et al. Adjuvant doce-taxel for node-positive breast cancer. N Engl J Med.2005;352:2302-2313.
3. Sparano JA, Wang M, Martino S, et al. Phase III study ofdoxorubicin-cyclophosphamide followed by paclitaxel ordocetaxel given every 3 weeks or weekly in operable breastcancer: results of Intergroup Trial E1199 [abstract]. 2007ASCO Annual Meeting Proceedings, Part I (June 20 Sup-plement). J Clin Oncol. 2007;25(18S):516.
4. Yarden Y, Sliwkowski MX. Untangling the ErbB signalingnetwork. Nat Rev Mol Cell Biol. 2001;2:127-137.
5. Menard S, Pupa SM, Campiglio M, Tagliabue E. Biologicand therapeutic role of HER2 in cancer. Oncogene. 2003;22:6570-6578.
6. Gschwind A, Fischer OM, Ullrich A. The discovery of re-ceptor tyrosine kinases: targets for cancer therapy. Nat RevCancer. 2004;4:361-370.
7. Slamon DJ, Leyland-Jones B, Shak S, et al. Use of chemo-therapy plus a monoclonal antibody against HER2 for met-astatic breast cancer that overexpresses HER2. N Engl JMed. 2001;344:783-792.
8. Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al.Trastuzumab after adjuvant chemotherapy in HER2-posi-tive breast cancer. N Engl J Med. 2005;353:1659-1672.
9. Smith I, Procter M, Gelber RD, et al. Two-year follow-upof trastuzumab after adjuvant chemotherapy in HER2-posi-tive breast cancer: a randomised controlled trial. Lancet.2007;369:29-36.
10. Romond EH, Perez EA, Bryant J, et al. Trastuzumab plusadjuvant chemotherapy for operable HER2-positive breastcancer. N Engl J Med. 2005;353:1673-1684.
11. Joensuu H, Kellokumpu-Lehtinen PL, Bono P, et al. Adju-vant docetaxel or vinorelbine with or without trastuzumabfor breast cancer. N Engl J Med. 2006;354:809-820.
12. Slamon D, Eiermann W, Robert N, et al. BCIRG 006:2nd interim analysis phase III randomized trial comparingdoxorubicin and cyclophosphamide followed by docetaxel(ACT) with doxorubicin and cyclophosphamide followedby docetaxel and trastuzumab (ACTH) with docetaxel, car-boplatin and trastuzumab (TCH) in Her2neu positive earlybreast cancer patients [abstract]. Breast Cancer Res Treat.2006;100(suppl 1):S90. Abstract 52.
13. Perez EA, Romond EH, Suman VJ, et al. Updated resultsof the combined analysis of NCCTG N9831 and NSABPB-31 adjuvant chemotherapy with/without trastuzumab inpatients with HER2-positive breast cancer [abstract]. 2007ASCO Annual Meeting Proceedings, Part I (June 20 Sup-plement). J Clin Oncol. 2007;25(18S):6s. Abstract 512.
14. Pegram MD, Pienkowski T, Northfelt DW, et al. Resultsof 2 open-label, multicenter phase II studies of docetaxel,platinum salts, and trastuzumab in HER2-positive advancedbreast cancer. J Natl Cancer Inst. 2004;96:759-769.
15. Perez EA, Suman VJ, Davidson N, et al. NCCTG N9831:May 2005 update. Presented at the 2005 Annual Meetingof the American Society of Clinical Oncology, Orlando,Florida, May 13-17, 2005.
16. Paik S, Kim C, Jeong J, et al. Benefit from adjuvant trastu-zumab may not be confined to patients with IHC 3þ and/or FISH-positive tumors: central testing results fromNSABP B-31 [abstract]. 2007 ASCO Annual MeetingProceedings, Part 1, June 20 Supplement. J Clin Oncol.2007;25(18S):5s. Abstract 511.
17. Burnell M, Levine M, Chapman JA, et al. A randomizedtrial of CEF versus dose dense EC followed by paclitaxelversus AC followed by paclitaxel in women with node posi-tive or high risk node negative breast cancer, NCIC CTGMA 21: results of an interim analysis [abstract]. Breast Can-cer Res Treat. 2007;103:117. Abstract 53.
18. Slamon D, Eiermann W, Robert N, et al. Phase IIIrandomized trial comparing doxorubicin and cyclophospha-mide followed by docetaxel (ACT) with doxorubicin andcyclophosphamide followed by docetaxel and trastuzumab(ACTH) with docetaxel, carboplatin and trastuzumab(TCH) in HER2 positive early breast cancer patients:BCIRG 006 study [abstract]. Breast Cancer Res Treat.2005;94(suppl 1):S5. Abstract 1.
19. Spielmann M, Roche H, Machiels JP, et al. 3-year follow-up of trastuzumab following adjuvant chemotherapy innode positive HER2-positive breast cancer patients: resultsof the PACS-04 trial. Breast Cancer Res Treat.2007;106(suppl 1):S19. Abstract 72.
20. Seidman A, Hudis C, Pierri MK, et al. Cardiac dysfunctionin the trastuzumab clinical trials experience. J Clin Oncol.2002;20:1215-1221.
21. Keefe DL. Trastuzumab-associated cardiotoxicity. Cancer.2002;95:1592-1600.
22. Perez EA, Suman VJ, Davidson NE, et al. Effect of doxor-ubicin plus cyclophosphamide on left ventricular ejectionfraction in patients with breast cancer in the North CentralCancer Treatment Group N9831 intergroup adjuvant trial.J Clin Oncol. 2004;22:3700-3704.
23. Suter TM, Procter M, van Veldhuisen DJ, et al. Trastuzu-mab-associated cardiac adverse effects in the herceptin adju-vant trial. J Clin Oncol. 2007;25:3859-3865.
24. Perez EA, Suman VJ, Davidson NE, et al. Cardiac safetyanalysis of doxorubicin and cyclophosphamide followed bypaclitaxel with or without trastuzumab in the North Cen-tral Cancer Treatment Group N9831 adjuvant breast can-cer trial. J Clin Oncol. 2008;26:1231-1238.
25. Rastogi P, Jeong J, Geyer CE, et al. Five year update of car-diac dysfunction on NSABP B-31, a randomized trial ofsequential doxorubicin/cyclophosphamide (AC)!paclitaxel(T) vs AC!T with trastuzumab (H) [abstract]. 20007ASCO Annual Meeting Proceedings, Part 1, June 20 Supple-ment. J Clin Oncol. 2007;25(18S):6s. Abstract LBA513.
26. Perez E, Suman V, Davidson N, et al. Exploratory analysisfrom NCCTG N9831: do clinical and laboratory
Adjuvant Trastuzumab for Breast Cancer/Mackey et al
Cancer March 15, 2009 1167
characteristics predict cardiac toxicity of trastuzumab whenadministered as a component of adjuvant therapy [abstract]?Breast Cancer Res Treat. 2005;94(suppl 1):S5.
27. Tan-Chiu E, Yothers G, Romond E, et al. Assessment of car-diac dysfunction in a randomized trial comparing doxorubicinand cyclophosphamide followed by paclitaxel, with or withouttrastuzumab as adjuvant therapy in node-positive, human epi-dermal growth factor receptor 2-overexpressing breast cancer:NSABP B-31. J Clin Oncol. 2005;23:7811-7819.
28. Paik S, Kim C, Wolmark N, Paik S, Kim C, Wolmark N.HER2 status and benefit from adjuvant trastuzumab inbreast cancer. N Engl J Med. 2008;358:1409-1411.
29. Arpino G, Ciocca DR, Weiss H, et al. Predictive value ofapoptosis, proliferation, HER-2, and topoisomerase IIalphafor anthracycline chemotherapy in locally advanced breastcancer. Breast Cancer Res Treat. 2005;92:69-75.
30. Coon JS, Marcus E, Gupta-Burt S, et al. Amplification andoverexpression of topoisomerase IIalpha predict response toanthracycline-based therapy in locally advanced breast can-cer. Clin Cancer Res. 2002;8:1061-1067.
31. Di Leo A, Gancberg D, Larsimont D, et al. HER-2 ampli-fication and topoisomerase IIalpha gene aberrations as pre-dictive markers in node-positive breast cancer patientsrandomly treated either with an anthracycline-based therapyor with cyclophosphamide, methotrexate, and 5-fluoroura-cil. Clin Cancer Res. 2002;8:1107-1116.
32. De Placido S, Perrone F, Carlomango C, et al. CMF vsalternating CMF/EV in the adjuvant treatment of operablebreast cancer. A single centre randomised clinical trial (Na-ples GUN-3 study). Br J Cancer. 1995;71:1283-1287.
33. Pritchard KI, Shepherd L, O’Malley F, et al. HER2 andresponsiveness of breast cancer to adjuvant chemotherapy.N Engl J Med. 2006;354:2103-2111.
34. Paik S, Bryant J, Park C, et al. erB-2 and response to dox-orubicin in patients with axillary lymph node-positive, hor-mone receptor-negative breast cancer. J Natl Cancer Inst.1998;90:1361-1370.
35. Pritchard KI, Messersmith H, Elavathil L, Trudeau M,O’Malley F, Dhesy-Thind B. HER-2 and topoisomerase IIas predictors of response to chemotherapy. J Clin Oncol.2008;26:736-744.
36. Hayes DF, Thor A, Dressler L, et al. HER2 predicts bene-fit from adjuvant paclitaxel after AC in node positive breastcancer: CALGB 9344 [abstract]. 2008 ASCO Annual
Meeting Proceedings, Part 1 (June 20 Supplement). J ClinOncol. 2006;24(18S):5s. Abstract 510.
37. Hayes DF, Thor A, Dressler L, et al. HER2 and responseto paclitaxel in node-positive breast cancer. N Engl J Med.2007;357:1496-1506.
38. Sledge G, O’Neill A, Thor A, Kahanic S, Zander P, David-son N. Adjuvant trastuzumab: long-term results of E2198[abstract]. Breast Cancer Res Treat. 2006;100(suppl 1):S106.Abstract 2075.
39. Halyard MY, Pisansky TM, Solin LJ, et al. Adjuvant radio-therapy (RT) and trastuzumab in stage I-IIA breast cancer:toxicity data from North Central Cancer Treatment GroupPhase III trial N9831 [abstract]. 2006 ASCO Annual Meet-ing Proceedings, Part 1 (June 20 Supplement) J Clin Oncol.2006;24(18S):8s. Abstract 523.
40. Liang K, Lu Y, Jin W, et al. Sensitization of breast cancercells to radiation by trastuzumab. Mol Cancer Ther.2003;2:1113-1120.
41. Kaufman B, Mackey J, Clemens M, et al. Trastuzumabplus anastrozole prolongs progression-free survival in post-menopausal women with HER2-positive, hormone-depend-ent metastatic breast cancer (MBC) [abstract]. Ann Oncol.2006;17(9 suppl): Page. Abstract LBA2.
42. Hillner B. Clinical and cost-effectiveness implications of theadjuvant trastuzumab in HER2þ breast cancer trials[abstract]. Breast Cancer Res Treat. 2005;94(suppl 1):S219.Abstract 5040.
43. Garrison LP Jr, Perez EA, Dueck A, Lalla D, Paton V,Lubeck D. Cost-effectiveness analysis of trastuzumab in theadjuvant setting for treatment of HER2þ breast cancer[abstract]. 2006 ASCO Annual Meeting Proceedings, Part1 (June 20 Supplement). J Clin Oncol. 2006;24(18S): Page.Abstract 6023.
44. Liberato NL, Marchetti M, Barosi G. Cost effectiveness of ad-juvant trastuzumab in human epidermal growth factor recep-tor 2-positive breast cancer. J Clin Oncol. 2007;25:625-633.
45. Kurian AW, Thompson RN, Gaw AF, Arai S, Ortiz R,Garber AM. A cost-effectiveness analysis of adjuvant trastu-zumab regimens in early HER2/neu-positive breast cancer.J Clin Oncol. 2007;25:634-641.
46. Vernaglia PR, Cunha FM, Correa M, et al. Cost-effective-ness analysis of trastuzumab therapy in patients with earlyHER-2 positive breast cancer in Brazil [abstract]. BreastCancer Res Treat. 2007;106(suppl 1):S106.
Review Article
1168 Cancer March 15, 2009
Copyright © 2022 FDOKUMEN




















