
Who Benefits Most From Adjuvant Interferon Treatment for Melanoma?
Upload
irsp-ouidahCategory
view
2download
0
Contemporary Clinical Trials 36 (2013) 531–543
Contents lists available at ScienceDirect
Contemporary Clinical Trials
j ourna l homepage: www.e lsev ie r .com/ locate /conc l in t r ia l
Adapted physical activity and diet (APAD) during adjuvantbreast cancer therapy: Design and implementation of aprospective randomized controlled trial
Marion Carayol a,b,⁎, Gilles Romieu c, Jean-Pierre Bleuse c, Pierre Senesse c,Sophie Gourgou-Bourgade c, Chakib Sari c, William Jacot c, Hélène Sancho-Garnier c,Chloé Janiszewski c, Silène Launay c, Florence Cousson-Gélie a,c, Grégory Ninot a
a Laboratory Epsylon, EA 4556 Dynamics of Human Abilities & Health Behaviors, University of Montpellier, 4 boulevard Henri IV, F-34000 Montpellier, Franceb INSERM UMR 1027, Paul Sabatier University, 37 allées Jules Guesde, F-31000 Toulouse, Francec Val d'Aurelle Montpellier Cancer Institute (ICM), Parc Euromédecine, 34298 Montpellier cedex, France
a r t i c l e i n f o
⁎ Corresponding author at: INSERM UMR 1027 (TeaSabatier, 37 allées Jules Guesde, F-31000 Toulouse, Fra56 47; fax: +33 5 62 26 42 40.
E-mail addresses: [email protected] (M. [email protected] (G. Romieu),[email protected] (J.-P. Bleuse),[email protected] (P. Senesse),[email protected] (S. [email protected] (C. Sari), William.Jacot@(W. Jacot), [email protected] ([email protected] (C. Janiszewski),[email protected] (S. Launay),[email protected] (F. [email protected] (G. Ninot).
1551-7144/$ – see front matter © 2013 Elsevier Inc. Ahttp://dx.doi.org/10.1016/j.cct.2013.09.016
a b s t r a c t
Article history:Received 30 May 2013Revised 6 September 2013Accepted 24 September 2013Available online 4 October 2013
Exercise practice and appropriate nutrition have been advanced as non pharmacological supportivecare to reduce side effects related to cancer and its treatment, but large sample-sized randomizedcontrolled trials are needed to confirm such results. The Adapted Physical Activity and Dietcounseling (APAD) study is a prospective randomized controlled trial designed to evaluate theeffectiveness of a 26-week hospital- and home-based lifestyle intervention on cancer-related fatigueinwomen receiving breast cancer adjuvant treatment (chemotherapy and radiotherapy). The aimofthis paper is to describe the APAD study protocol. Study recruitment goal is 264 adult breast cancerwomen with newly, histologically proven, incident and non metastatic breast cancer scheduled for6 cycles of adjuvant chemotherapy followed by radiotherapy. Patients are randomized either in theexperimental armwith tailored exercise training and diet counseling program or in the control armwithout any lifestyle intervention (usual care). Outcome measures are collected at baseline, and at15 weeks (i.e., mid-intervention), 26 weeks (i.e., immediately post-intervention), and at 12-monthand 18-month of follow-up. Intervention effect is assessed on fatigue (emotional, cognitive,physical), quality-of-life, anxiety, depression, body weight and composition. In addition, levels ofphysical activity, dietary intakes and adjuvant therapy observance are measured and a cost–utilityanalysiswill be performed. If improvements in fatigue, quality-of-life and a betterweight control areobserved, the APAD study could demonstrate the feasibility and the effectiveness of such exerciseand nutrition supportive care with limited additional cost in patients receiving adjuvant breastcancer therapy.
© 2013 Elsevier Inc. All rights reserved.
Keywords:Breast cancerPhysical activityDietRandomized controlled trialFatigueQuality-of-life
m 5), Université Paulnce, Tel.: +33 5 61 14
ayol),
de),icm.unicancer.frH. Sancho-Garnier),
Gélie),
ll rights reserved.
1. Introduction
With over one million cases per year, breast cancer is themost common cancer affecting women in the world [1]. InFrance, the incidence rate (world age-standardized) has almostdoubled, passing from 56.8 in 1980 to 101.5 in 2005 [2]. Earlierdiagnosis and more effective treatments have led to decreasedmortality (−1.4% per year) since 2000, however an increasingnumber of women receive cancer adjuvant therapy followingsurgery and have to deal with severe side effects related tochemotherapy and radiotherapy [3,4]. With a prevalence of

532 M. Carayol et al. / Contemporary Clinical Trials 36 (2013) 531–543
70–100%, cancer-related fatigue is perceived by patients beingtreated for cancer, as themost distressing symptom, evenmorethan pain, nausea and vomiting, which, for most patients, cangenerally be managed by medications [5–7]. Cancer-relatedfatigue has been defined by the National ComprehensiveCancer Network as “a distressing, persistent, subjectivesense of physical, emotional and/or cognitive tiredness orexhaustion related to cancer or cancer treatment that isnot proportional to recent activity and interferes with usualfunctioning” [5]. The multidimensional nature of the cancerrelated-fatigue symptom has been primarily explored throughself-reported questionnaires including several constructs aboutphysical, emotional and cognitive dimensions [8], but most ofthe experimental studies did not use objective measures ofcognitive and physical dimensions.
Descriptive studies have shown that fatigue commonlyoccurs within a symptom cluster [9–13] including anxiety,depression, pain, sleep disturbance, reduced activity level,nutritional changes, comorbidities, etc., resulting in impairedquality-of-life (QoL).1 To alleviate fatigue, physical activityenhancement and nutritional consultations have been indi-cated [5,14], however, to our knowledge, none randomizedcontrolled trial (RCT) has investigated to date the impact ofan intervention involving both exercise practice and nutritioncounseling on fatigue in breast cancer patients undergoingadjuvant therapy. Only one feasibility RCT tested a diet/exerciseintervention to prevent adverse body composition changes, butdid not assess fatigue [15]. Meta-analyses of exercise-based RCTsreported significant decrease of fatigue in experimental patientscompared to controls among all cancer patients [16] and morespecifically, in those receiving adjuvant therapy for breastcancer [17]. However, subsequent analyses have pointed outthat the highest effect sizes of exercise on fatigue decreasewere reported by studies with methodological limitations(no use of intent-to-treat analyses, sample size b40 experi-mental patients) [18]. The guidelines of the American Collegeof Sports Medicine also suggest that further high quality andwell-dimensioned studies are needed to test the impact ofexercise on fatigue in patients undergoing adjuvant therapy, bygrading evidence level B implying that “reviewed RCTs weresmall and reported inconsistent findings” [19].
Therefore, in such context, evidence is needed from awell-dimensioned RCT investigating the effect of an interven-tion involving adapted physical activity and diet counseling(APAD) on comprehensive cancer related-fatigue during adju-vant therapy in breast cancer patients. Compared to previoussimilar RCTs that mostly focused on self-declared subjectivefatigue [16,17], the APAD study intend to assess the threedimensions of cancer related-fatigue i.e., physical, emotional andcognitive including both subjective and objective measures anda wide range of secondary outcomes taking part of the fatiguesymptom cluster. The aim of this paper is to describe theprotocol of the prospective and interventional APAD study.
1 QoL: quality-of-life; RCT: randomized controlled trial; APAD: adaptedphysical activity and diet; QALY: quality-adjusted life year; CRA: clinicalresearch assistant; WCRF: world cancer research fund; MFI: Multidimen-sional Fatigue Inventory; BMI: body mass index; BMR: basal metabolic rate.
2. Methods, design, population and material
The protocol was approved by all local institutional reviewboards andwas accepted by the independent ethics committeeof Montpellier and registered with ClinicalTrials.gov, numberNCT01495650.
2.1. Experimental design
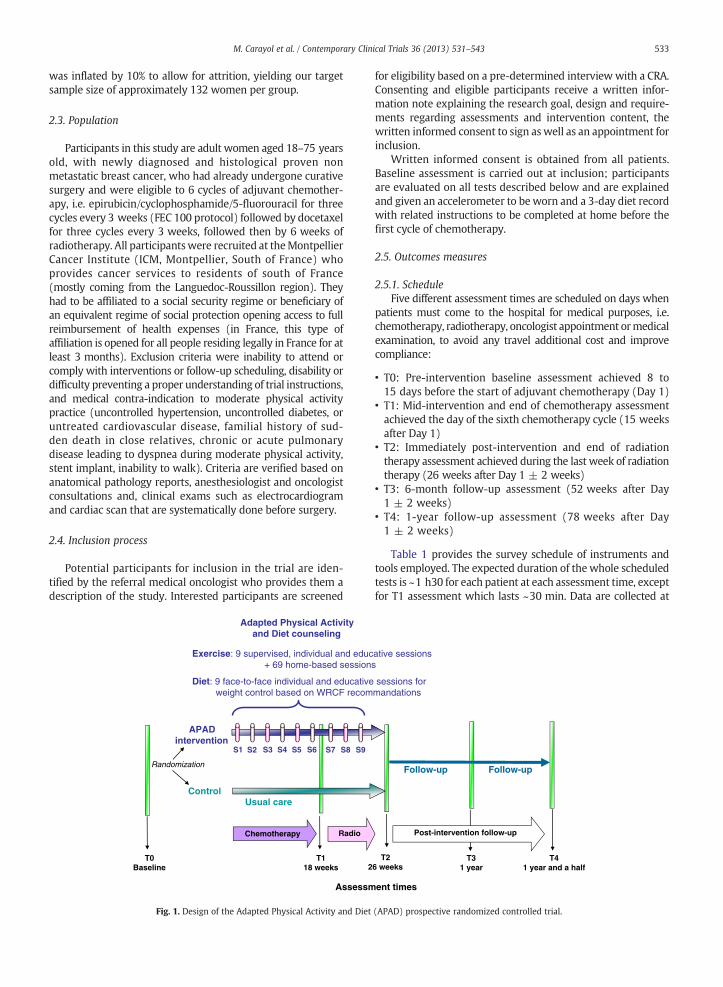
The objectives of the study are to evaluate the effects ofa 26-week lifestyle intervention designed to be easilyimplemented by women receiving breast cancer adjuvanttherapy (chemotherapy and radiotherapy), on several dimen-sions of cancer related-fatigue (emotional, physical and cogni-tive), QoL, anxiety and depression symptoms, body weight andcomposition as well as time to return to work. In addition,intervention effect will be assessed on lifestyle behaviorsregarding physical activity, sedentary, nutrition and adju-vant treatment observance. Finally, economic efficiency ofthe intervention for the enhancement of health-related QoLwill be estimated by the quality-adjusted life years (QALYs)gained. To reach such objectives, patients are randomizedwith equal allocation to one of the two study arms: 1) theAPAD experimental arm receiving tailored exercise trainingand diet counseling program both hospital- and home-basedduring the 26 weeks of adjuvant therapy (chemotherapy andradiotherapy); 2) the control arm with usual adjuvant breastcancer care, without any specific lifestyle counseling (see Fig. 1).
After the completion of baseline testing, patients arerandomly assigned to each group in a 1:1 ratio by thebiostatistics unit of Montpellier Cancer Institute, using arandomization block method based on computer generatednumbers. The allocation assignment was concealed fromthe project directors and the allocation result was faxed tothe clinical research assistant (CRA) dedicated to the study.Assignments are consecutively made, in the order in whichparticipants completed the baseline testing. Included partici-pants are informed about randomization result by the CRAsphoning them during the week after inclusion.
2.2. Sample size and power considerations
The research hypotheses of the APAD study are: first,participants of the APAD group will experience significantlyless subjective fatigue, and will have significantly greaterattentional and strength performances compared with partic-ipants of the control group; second, participants of the APADgroup will have significantly greater QoL with less anxiety anddepression symptoms andwill present betterweight control aswell asmore favorable leanmass/fatmass ratio, comparedwithparticipants of the control group.
Sample size calculations were based on the primaryoutcome, cancer related-fatigue, as measured by the Multidi-mensional Fatigue Inventory (MFI) questionnaire [20]. A meangeneral fatigue score of 16 points ± 8 units for standarddeviation has been measured in cancer patients receivingradiotherapy [20]. To detect a difference in general fatiguesubscale between the 2 groups of 4 points, with 90% power and5% type I error (two sided), taking into account a 4-timerepeated analysis [21], 120womenper groupwere required. Assimilar studies reported 9 to 20% attrition [15,22], sample size
533M. Carayol et al. / Contemporary Clinical Trials 36 (2013) 531–543
was inflated by 10% to allow for attrition, yielding our targetsample size of approximately 132 women per group.
2.3. Population
Participants in this study are adult women aged 18–75 yearsold, with newly diagnosed and histological proven nonmetastatic breast cancer, who had already undergone curativesurgery and were eligible to 6 cycles of adjuvant chemother-apy, i.e. epirubicin/cyclophosphamide/5-fluorouracil for threecycles every 3 weeks (FEC 100 protocol) followed by docetaxelfor three cycles every 3 weeks, followed then by 6 weeks ofradiotherapy. All participantswere recruited at theMontpellierCancer Institute (ICM, Montpellier, South of France) whoprovides cancer services to residents of south of France(mostly coming from the Languedoc-Roussillon region). Theyhad to be affiliated to a social security regime or beneficiary ofan equivalent regime of social protection opening access to fullreimbursement of health expenses (in France, this type ofaffiliation is opened for all people residing legally in France for atleast 3 months). Exclusion criteria were inability to attend orcomply with interventions or follow-up scheduling, disability ordifficulty preventing a proper understanding of trial instructions,and medical contra-indication to moderate physical activitypractice (uncontrolled hypertension, uncontrolled diabetes, oruntreated cardiovascular disease, familial history of sud-den death in close relatives, chronic or acute pulmonarydisease leading to dyspnea during moderate physical activity,stent implant, inability to walk). Criteria are verified based onanatomical pathology reports, anesthesiologist and oncologistconsultations and, clinical exams such as electrocardiogramand cardiac scan that are systematically done before surgery.
2.4. Inclusion process
Potential participants for inclusion in the trial are iden-tified by the referral medical oncologist who provides them adescription of the study. Interested participants are screened
Randomization
Chemotherapy Radio
APAD intervention
Control
Adapted Physical Activity and Diet counseling
Usual care
T118 weeks
T0 Baseline 2
Exercise: 9 supervised, individual and educ+ 69 home-based session
Diet: 9 face-to-face individual and educativeweight control based on WRCF recom
S1 S2 S3 S4 S5 S6 S7 S8 S9
Assessm
Fig. 1. Design of the Adapted Physical Activity and Diet
for eligibility based on a pre-determined interview with a CRA.Consenting and eligible participants receive a written infor-mation note explaining the research goal, design and require-ments regarding assessments and intervention content, thewritten informed consent to sign aswell as an appointment forinclusion.
Written informed consent is obtained from all patients.Baseline assessment is carried out at inclusion; participantsare evaluated on all tests described below and are explainedand given an accelerometer to be worn and a 3-day diet recordwith related instructions to be completed at home before thefirst cycle of chemotherapy.
2.5. Outcomes measures
2.5.1. ScheduleFive different assessment times are scheduled on days when
patients must come to the hospital for medical purposes, i.e.chemotherapy, radiotherapy, oncologist appointment ormedicalexamination, to avoid any travel additional cost and improvecompliance:
• T0: Pre-intervention baseline assessment achieved 8 to15 days before the start of adjuvant chemotherapy (Day 1)
• T1: Mid-intervention and end of chemotherapy assessmentachieved the day of the sixth chemotherapy cycle (15 weeksafter Day 1)
• T2: Immediately post-intervention and end of radiationtherapy assessment achieved during the last week of radiationtherapy (26 weeks after Day 1 ± 2 weeks)
• T3: 6-month follow-up assessment (52 weeks after Day1 ± 2 weeks)
• T4: 1-year follow-up assessment (78 weeks after Day1 ± 2 weeks)
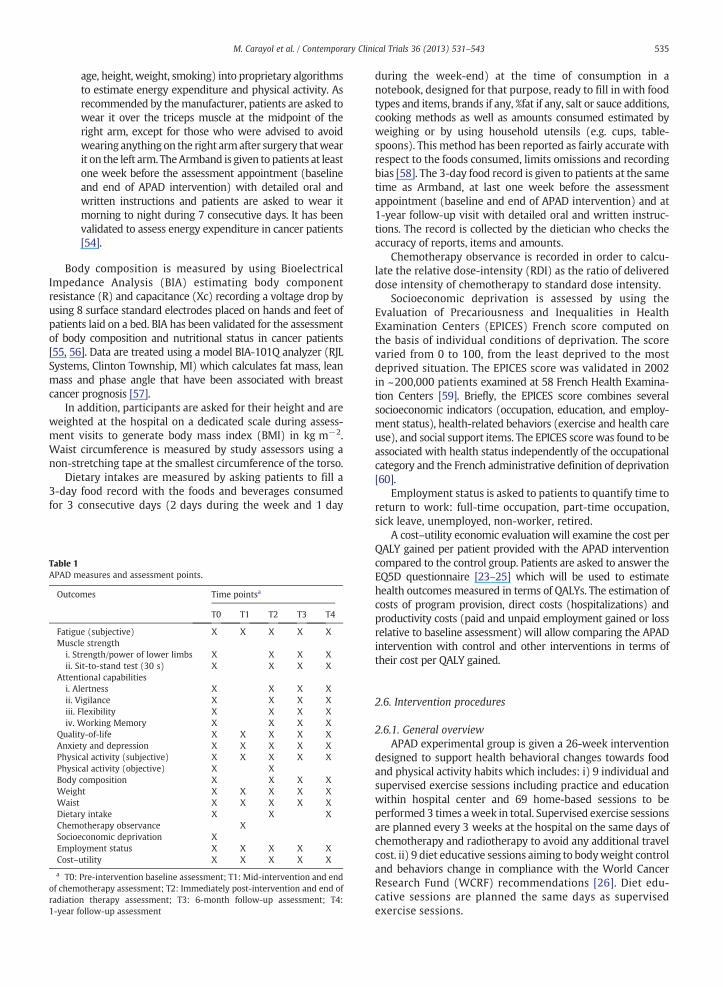
Table 1 provides the survey schedule of instruments andtools employed. The expected duration of the whole scheduledtests is ~1 h30 for each patient at each assessment time, exceptfor T1 assessment which lasts ~30 min. Data are collected at
T31 year
Follow-up
Post-intervention follow-up
T41 year and a half
Follow-up
T26 weeks
ative sessionss
sessions formandations
ent times
(APAD) prospective randomized controlled trial.
534 M. Carayol et al. / Contemporary Clinical Trials 36 (2013) 531–543
the hospital in a dedicated office involving standardized andsafe conditions via clinical assessment under the supervisionof an assessor who distributes questionnaires and ensures thecompletion of all undermentioned participant- and interviewer-administered surveys and tests. For T0 and T2 assessments, thestudy staff provides the accelerometer and diet record to theparticipants along with instructions. Participants are instructedto complete the assessments at home and return themoneweeklater.
2.5.2. InstrumentsQuestionnaires and scales used are all validated and available
in French. Outcome measures include fatigue (emotional,cognitive, and physical), QoL, psychological symptoms, bodyweight and composition, adjuvant therapy observance, employ-ment status, assessment for cost–utility analysis. In addition,physical activity and dietary intakes measures are performed inorder to evaluate behavior changes.
The cancer related-fatigue primary outcome is assessedwith the Multidimensional Fatigue Inventory (MFI), a 20-itemself-administered instrument designed to measure perceivedfatigue. It has been initially validated in English in a general andclinical population including patients with cancer [16] andtranslated in French [40]. It includes five dimensions: GeneralFatigue, Physical Fatigue, Mental Fatigue, Reduced Motivationand Reduced Activity.
Muscle strength is measured to assess physical fatigue by2 different tests:
(i) The Myotest® accelerometer system [41,42] is used tomeasure strength and power of vertical jumps [43].After an initial warm-up, patients are asked to flextheir knees in a 90° angle and at the signal, to perform10 successive vertical jumps allowing a 10-secondinterval in between. The ratio of the last three to thefirst three jumps represents the percentage of force/power maintained during the task, considered as anindicator of muscular fatigue in healthy individualsand athletes [44–46].
(ii) The sit-to-stand test (30 s) consists in performing themaximum flexion–extension during a 30-second peri-od; it has been used to assess lower limbs' strength inthe elderly [47] and cancer patients [48]. Patientsbegin seated on a chair adjusted to set a 90° leg/thighangle and are asked to perform the maximum sit-and-stand during 30 s. The number of repetitions isrecorded at 15 s and 30s.
Assessment of cognitive fatigue through attentionalcapabilities is performed using the 4 following sub-testsof the Test of Attentional Performance (TAP 2.2. software)[49]:
(i) Alertness refers to the condition of general wakefulnessthat enables a person to respond quickly and appropri-ately to any given demand. In this test, reaction time ismeasured under two conditions: first, simple measure-ment, in which a cross appears on the monitor atrandomly varying intervals (intrinsic alertness); second,response to a critical stimulus preceded by a cue stimuluspresented as warning tone. An increase in reaction timethroughout the test signals lack of attention.
(ii) Vigilance (square—10 min) consists in the detectionof rare critical events that are difficult to discrimi-nate. It assesses sustained attention in which theattentional focus is maintained by exerting mentaleffort over a longer period of time (10 min). Theeffect of monotony is an essential aspect for the levelof performance under vigilance conditions. Numberof errors, number of omissions, and reaction time aremeasured.
(iii) Flexibility sub-test assesses the ability to changeattentional focus in order to apprehend and adapt todifferent situations. This procedure is a “set shifting”task. A letter and a number are simultaneously presentedto the right and left of themonitor screenwith alternatingtypes of target stimuli (i.e. letter–number–letter–number…). The patient's task is to press the left orright key according to whether the target stimulus(e.g. letter or number) appears to the left or the rightof the center of the monitor. A performance-index iscalculated using the median score of the reaction timeand the number of errors. A negative value indicates aperformance below the average (high number of errorsand/or slow reactions).
(iv) Working memory (level 2) examines the control ofinformation flow and the capability to update infor-mation in working memory. A 5-min sequence ofnumbers is presented to the patient on the monitor.The patient is required to determine whether eachnumber corresponds with the second last numberbefore. Number of omissions, errors, and reactiontime are recorded.
QoL is evaluated by the EORTC QLQ-C30, 30-item self-administered questionnaire designed tomeasure cancer-relatedQoL [50]. It presents 9 multi-item scales: 5 functional scales(physical, role, cognitive, emotional, and social); 3 symptomscales (fatigue, pain, and nausea/vomiting); and a globalhealth and QoL scale.
Anxiety and depression symptoms are recorded by theHospital Anxiety Depression Scale (HADS), a 14-item self-administered questionnaire validated in French [51] designedto assess anxiety and depression symptoms by calculating 2sub-scores.
Physical activity is assessed by both subjective andobjectives instruments:
(i) The Global Physical Activity Questionnaire (GPAQ)contains 16 items designed to quantify declarativephysical activity within the week before completioncompleted by face-to-face interview. Intensity of physicalactivity is expressed in the Metabolic Equivalent of theTask (METs; low, moderate, high levels), which entailsthe energetic cost of physical activities. Reliability andvalidity were established in nine countries includingFrance [52] and has been used in patients with breastcancer [53].
(ii) The SenseWear Pro Armband™ (version 3.0) analyzesmovement in order to objectively quantify the level ofphysical activity very precisely by incorporating a varietyof measured parameters (two-axis accelerometer, heatflux, galvanic skin response, skin temperature, near-bodytemperature) and demographic characteristics (gender,
535M. Carayol et al. / Contemporary Clinical Trials 36 (2013) 531–543
age, height, weight, smoking) into proprietary algorithmsto estimate energy expenditure and physical activity. Asrecommended by themanufacturer, patients are asked towear it over the triceps muscle at the midpoint of theright arm, except for those who were advised to avoidwearing anything on the right armafter surgery thatwearit on the left arm. TheArmband is given to patients at leastone week before the assessment appointment (baselineand end of APAD intervention) with detailed oral andwritten instructions and patients are asked to wear itmorning to night during 7 consecutive days. It has beenvalidated to assess energy expenditure in cancer patients[54].
Body composition is measured by using BioelectricalImpedance Analysis (BIA) estimating body componentresistance (R) and capacitance (Xc) recording a voltage drop byusing 8 surface standard electrodes placed on hands and feet ofpatients laid on a bed. BIA has been validated for the assessmentof body composition and nutritional status in cancer patients[55, 56]. Data are treated using a model BIA-101Q analyzer (RJLSystems, Clinton Township, MI) which calculates fat mass, leanmass and phase angle that have been associated with breastcancer prognosis [57].
In addition, participants are asked for their height and areweighted at the hospital on a dedicated scale during assess-ment visits to generate body mass index (BMI) in kg m−2.Waist circumference is measured by study assessors using anon-stretching tape at the smallest circumference of the torso.
Dietary intakes are measured by asking patients to fill a3-day food record with the foods and beverages consumedfor 3 consecutive days (2 days during the week and 1 day
Table 1APAD measures and assessment points.
Outcomes Time pointsa
T0 T1 T2 T3 T4
Fatigue (subjective) X X X X XMuscle strength
i. Strength/power of lower limbs X X X Xii. Sit-to-stand test (30 s) X X X X
Attentional capabilitiesi. Alertness X X X Xii. Vigilance X X X Xiii. Flexibility X X X Xiv. Working Memory X X X X
Quality-of-life X X X X XAnxiety and depression X X X X XPhysical activity (subjective) X X X X XPhysical activity (objective) X XBody composition X X X XWeight X X X X XWaist X X X X XDietary intake X X XChemotherapy observance XSocioeconomic deprivation XEmployment status X X X X XCost–utility X X X X X
a T0: Pre-intervention baseline assessment; T1: Mid-intervention and endof chemotherapy assessment; T2: Immediately post-intervention and end ofradiation therapy assessment; T3: 6-month follow-up assessment; T4:1-year follow-up assessment
during the week-end) at the time of consumption in anotebook, designed for that purpose, ready to fill in with foodtypes and items, brands if any, %fat if any, salt or sauce additions,cooking methods as well as amounts consumed estimated byweighing or by using household utensils (e.g. cups, table-spoons). This method has been reported as fairly accurate withrespect to the foods consumed, limits omissions and recordingbias [58]. The 3-day food record is given to patients at the sametime as Armband, at last one week before the assessmentappointment (baseline and end of APAD intervention) and at1-year follow-up visit with detailed oral and written instruc-tions. The record is collected by the dietician who checks theaccuracy of reports, items and amounts.
Chemotherapy observance is recorded in order to calcu-late the relative dose-intensity (RDI) as the ratio of delivereddose intensity of chemotherapy to standard dose intensity.
Socioeconomic deprivation is assessed by using theEvaluation of Precariousness and Inequalities in HealthExamination Centers (EPICES) French score computed onthe basis of individual conditions of deprivation. The scorevaried from 0 to 100, from the least deprived to the mostdeprived situation. The EPICES score was validated in 2002in ~200,000 patients examined at 58 French Health Examina-tion Centers [59]. Briefly, the EPICES score combines severalsocioeconomic indicators (occupation, education, and employ-ment status), health-related behaviors (exercise and health careuse), and social support items. The EPICES score was found to beassociated with health status independently of the occupationalcategory and the French administrative definition of deprivation[60].
Employment status is asked to patients to quantify time toreturn to work: full-time occupation, part-time occupation,sick leave, unemployed, non-worker, retired.
A cost–utility economic evaluation will examine the cost perQALY gained per patient provided with the APAD interventioncompared to the control group. Patients are asked to answer theEQ5D questionnaire [23–25] which will be used to estimatehealth outcomes measured in terms of QALYs. The estimation ofcosts of program provision, direct costs (hospitalizations) andproductivity costs (paid and unpaid employment gained or lossrelative to baseline assessment) will allow comparing the APADintervention with control and other interventions in terms oftheir cost per QALY gained.
2.6. Intervention procedures
2.6.1. General overviewAPAD experimental group is given a 26-week intervention
designed to support health behavioral changes towards foodand physical activity habits which includes: i) 9 individual andsupervised exercise sessions including practice and educationwithin hospital center and 69 home-based sessions to beperformed 3 times aweek in total. Supervised exercise sessionsare planned every 3 weeks at the hospital on the same days ofchemotherapy and radiotherapy to avoid any additional travelcost. ii) 9 diet educative sessions aiming to bodyweight controland behaviors change in compliance with the World CancerResearch Fund (WCRF) recommendations [26]. Diet edu-cative sessions are planned the same days as supervisedexercise sessions.

536 M. Carayol et al. / Contemporary Clinical Trials 36 (2013) 531–543
2.6.2. Exercise interventionAPAD exercise intervention combines aerobic exercise
with muscle-strength exercise according to establishedrecommendations about exercise to decrease fatigue forpatients with cancer [19,27,28]. A recent meta-analysis thatfocused on patients receiving adjuvant therapy for breastcancer, found that interventions targeting lower dosesreported better improvements of fatigue as compared to highprescribed exercise doses [17]; a prescription of 90–120 min perweek of moderate intensity physical activity was suggested.APAD patients from the experimental group are prescribed 3exercise sessions per week combining one muscular strengthsession and 2 aerobic sessions, each session lasting 30 to 45 min.The intervention goals are to gradually increase partici-pants practice to 120 weekly minutes of moderate intensityphysical activity and to maintain this amount of practice allover chemotherapy and radiotherapy periods. As someparticipants may try to exercise excessively, they areinstructed not to exercise beyond the upper limit of 150weekly minutes because higher prescribed exercise doseswere not generally associated with fatigue decrease [17,18]and also, to prevent adverse events related to cardio-toxiceffects of chemotherapy. The exercise starting parameters andrate of progression towards the 120 min weekly goal wereindividualized accounting for the participant's baseline physicalability, exercise preferences and history, and the severity oftreatment-related side-effects. The CRA informs the exercisespecialist with patient's medical problems collected atpre-screening interview that could affect physical exerciseability to practice. The specialist who has expertise inexercise physiology will then favor aerobic activities orstrength exercises that are suitable with patient's medicaldifficulties. Hospital-based exercise sessions systematicallystart with an individual patient interview; at the first session,the exercise specialist asks the patient exercise backgroundand its preferences upon nature of activities and modalities ofpractice (group, individual, inside, outside, etc.), that hewill tryto implement in the prescription of exercise home-basedsessions as long as it is compatible with the protocol require-ments. The exercise specialist will then ask patients aboutthe severity of treatment-related side-effects and their interac-tions with exercise practice in every following session, to helppatients finding ways to maintain exercise practice through-out the intervention (e.g. schedule management, other exercisemodalities). The pattern of fatigue has been showed to evolvethrough chemotherapy cycles, presenting a fatigue peaklevel 5 days approximately after chemotherapy adminis-tration [29,30]. Considering fatigue management require-ments, patients were suggested the possibility to postponeone planned exercise session from the first week to the thirdweek of each chemotherapy cycle. According to the hospitalorganization, supervised exercise sessions are scheduled afterthe oncologist visit and before the chemotherapy infusionresulting in individual sessions, as time of sessions depends onhospital appointment schedule.
2.6.2.1. Supervised sessions. Nine supervised exercise sessionsare scheduled with a frequency of one session every 3 weeks,6 during chemotherapy followed by 3 during radiotherapy.Face-to-face exercise sessions are carried out by an exercisespecialist who is certified in adapted physical activity by the
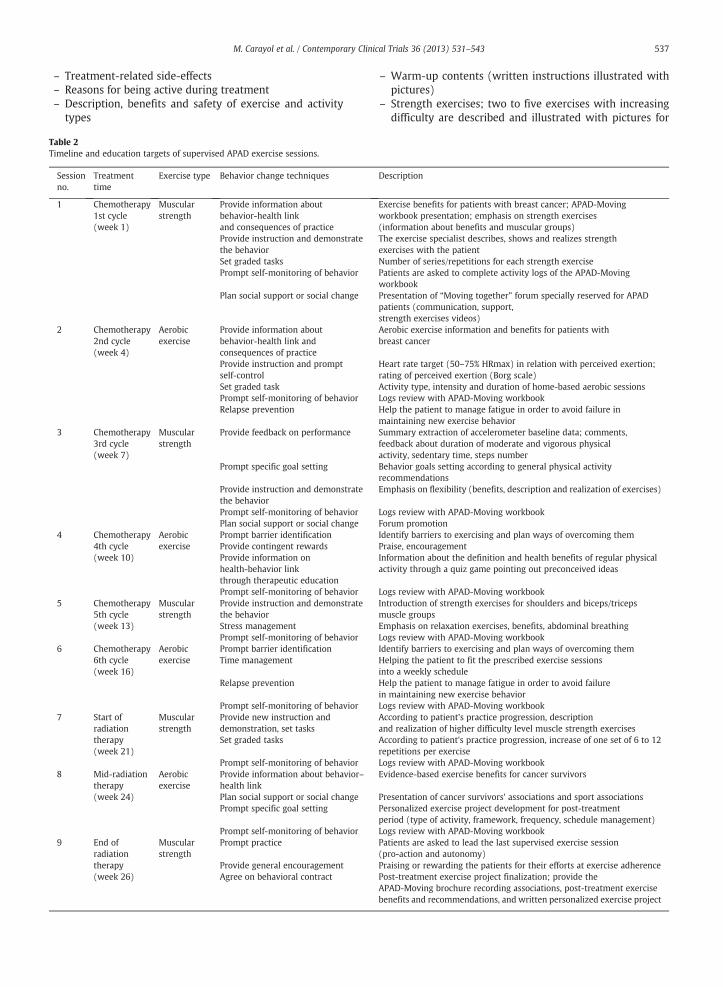
French University of Sports Sciences and Physical Activity (or iscertification eligible), use a structured appointment form, andlast about 1 h. Strength sessions consist in achieving 6 differenttasks that correspond to 6mainmuscle groups of the trunk andlower limbs (hamstrings, quadriceps, buttocks, abdominal,back, shoulders/arms), each task is performed 2 to 5 sets of 6 to12 repetitions. According to patient's physical condition, theexercise specialist proposes a 2-repetition or 1-set increaseevery 6 weeks. Depending on muscle group, 2 to 5 exerciseswith increasing difficulty were available for each group; atsession 7 (beginning of radiation therapy), higher levelexercises are proposed to patients. Aerobic exercise sessionsare performed at moderate intensity on a cycloergometer andadapted to individuals on the basis of 50–75% of themaximumheart rate. Patients wear heart rate monitors throughout theexercise sessions and heart rate is assessed at regular intervals.Every supervised session begins with warm-up (body move-ments followed by aerobic fitness, 10 min) and ends withcool-down and flexibility exercises (10 min). At the end ofevery session, patients are asked to rate their perceivedexertion on a 10-point scale. In addition, physical activityeducation is provided at each session by the exercise specialistaccording to the education program presented in Table 2.Supervised exercise sessions intend to provide the patientswith adequate instructions to increase autonomy and to allowreproducibility at home. In addition, exercise specialists aim toimprove patient's adherence and behavioral change usingvarious techniques (e.g. self-efficacy, problem-solving barriers,social support) [31].
A few patients who receive radiotherapy in anotherhospital, are only asked to attend one supervised sessioninstead of 3 scheduled sessions during radiotherapy (to avoidtravel expenses). As compensation for the 2 exempted sessions,the exercise specialist made 2 phone calls to assess adherenceregarding home-based program in the last three weeks, toencourage the patient attending exercise goal and to delivereducation targets and content of the supervised exemptedsession.
2.6.2.2. Home-based sessions and exercise intervention material.Home-based muscular strength sessions repeat the exercisescarried out with the exercise specialist at the hospital. Inaccordance with the recommendations of Biddle et al. [32],patients are proposed a range of aerobic exercise modalities(e.g. walking, cycling, jogging, swimming, dancing/fitness) topromote enjoyment and to aid compliance to the program.Patients are encouraged to use their preferred exercisemode tostrengthen the maintenance of a physically active lifestyleduring and after completion of the program. Home-basedsessions are supported by precise written instructions includedin theAPAD-Movingworkbookwhich is given and explained topatients at the first supervised session. This educational andpersonable workbook (available on request, French language)has been developed by the study investigators team withexpertise in adapted physical activity and behavioral medicine,and is used to inform patients about expected benefits ofexercise intervention, to serve as a link between hospital-and home-based sessions conducing patients to independentpractice and to enable patients logging home-based exercisepractice. The APAD-Movingworkbook contains information ona range of topics, including:
537M. Carayol et al. / Contemporary Clinical Trials 36 (2013) 531–543
– Treatment-related side-effects– Reasons for being active during treatment– Description, benefits and safety of exercise and activity
types
Table 2Timeline and education targets of supervised APAD exercise sessions.
Sessionno.
Treatmenttime
Exercise type Behavior change techniques
1 Chemotherapy1st cycle(week 1)
Muscularstrength
Provide information aboutbehavior-health linkand consequences of practiceProvide instruction and demonstratethe behaviorSet graded tasksPrompt self-monitoring of behavior
Plan social support or social change
2 Chemotherapy2nd cycle(week 4)
Aerobicexercise
Provide information aboutbehavior-health link andconsequences of practiceProvide instruction and promptself-controlSet graded taskPrompt self-monitoring of behaviorRelapse prevention
3 Chemotherapy3rd cycle(week 7)
Muscularstrength
Provide feedback on performance
Prompt specific goal setting
Provide instruction and demonstratethe behaviorPrompt self-monitoring of behaviorPlan social support or social change
4 Chemotherapy4th cycle(week 10)
Aerobicexercise
Prompt barrier identificationProvide contingent rewardsProvide information onhealth-behavior linkthrough therapeutic educationPrompt self-monitoring of behavior
5 Chemotherapy5th cycle(week 13)
Muscularstrength
Provide instruction and demonstratethe behaviorStress managementPrompt self-monitoring of behavior
6 Chemotherapy6th cycle(week 16)
Aerobicexercise
Prompt barrier identificationTime management
Relapse prevention
Prompt self-monitoring of behavior7 Start of
radiationtherapy(week 21)
Muscularstrength
Provide new instruction anddemonstration, set tasksSet graded tasks
Prompt self-monitoring of behavior8 Mid-radiation
therapy(week 24)
Aerobicexercise
Provide information about behavior–health linkPlan social support or social changePrompt specific goal setting
Prompt self-monitoring of behavior9 End of
radiationtherapy(week 26)
Muscularstrength
Prompt practice
Provide general encouragementAgree on behavioral contract
– Warm-up contents (written instructions illustrated withpictures)
– Strength exercises; two to five exercises with increasingdifficulty are described and illustrated with pictures for
Description
Exercise benefits for patients with breast cancer; APAD-Movingworkbook presentation; emphasis on strength exercises(information about benefits and muscular groups)The exercise specialist describes, shows and realizes strengthexercises with the patientNumber of series/repetitions for each strength exercisePatients are asked to complete activity logs of the APAD-MovingworkbookPresentation of “Moving together” forum specially reserved for APADpatients (communication, support,strength exercises videos)Aerobic exercise information and benefits for patients withbreast cancer
Heart rate target (50–75% HRmax) in relation with perceived exertion;rating of perceived exertion (Borg scale)Activity type, intensity and duration of home-based aerobic sessionsLogs review with APAD-Moving workbookHelp the patient to manage fatigue in order to avoid failure inmaintaining new exercise behaviorSummary extraction of accelerometer baseline data; comments,feedback about duration of moderate and vigorous physicalactivity, sedentary time, steps numberBehavior goals setting according to general physical activityrecommendationsEmphasis on flexibility (benefits, description and realization of exercises)
Logs review with APAD-Moving workbookForum promotionIdentify barriers to exercising and plan ways of overcoming themPraise, encouragementInformation about the definition and health benefits of regular physicalactivity through a quiz game pointing out preconceived ideas
Logs review with APAD-Moving workbookIntroduction of strength exercises for shoulders and biceps/tricepsmuscle groupsEmphasis on relaxation exercises, benefits, abdominal breathingLogs review with APAD-Moving workbookIdentify barriers to exercising and plan ways of overcoming themHelping the patient to fit the prescribed exercise sessionsinto a weekly scheduleHelp the patient to manage fatigue in order to avoid failurein maintaining new exercise behaviorLogs review with APAD-Moving workbookAccording to patient's practice progression, descriptionand realization of higher difficulty level muscle strength exercisesAccording to patient's practice progression, increase of one set of 6 to 12repetitions per exerciseLogs review with APAD-Moving workbookEvidence-based exercise benefits for cancer survivors
Presentation of cancer survivors' associations and sport associationsPersonalized exercise project development for post-treatmentperiod (type of activity, framework, frequency, schedule management)Logs review with APAD-Moving workbookPatients are asked to lead the last supervised exercise session(pro-action and autonomy)Praising or rewarding the patients for their efforts at exercise adherencePost-treatment exercise project finalization; provide theAPAD-Moving brochure recording associations, post-treatment exercisebenefits and recommendations, and written personalized exercise project
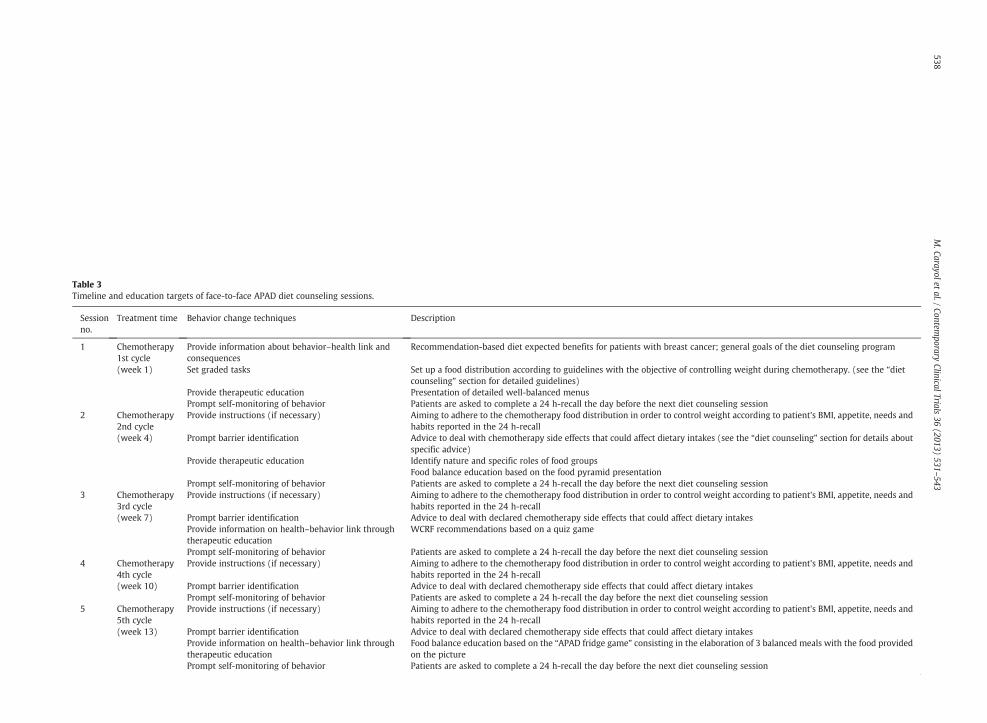
Table 3Timeline and education targets of face-to-face APAD diet counseling sessions.
Sessionno.
Treatment time Behavior change techniques Description
1 Chemotherapy1st cycle(week 1)
Provide information about behavior–health link andconsequences
Recommendation-based diet expected benefits for patients with breast cancer; general goals of the diet counseling program
Set graded tasks Set up a food distribution according to guidelines with the objective of controlling weight during chemotherapy. (see the “dietcounseling” section for detailed guidelines)
Provide therapeutic education Presentation of detailed well-balanced menusPrompt self-monitoring of behavior Patients are asked to complete a 24 h-recall the day before the next diet counseling session
2 Chemotherapy2nd cycle(week 4)
Provide instructions (if necessary) Aiming to adhere to the chemotherapy food distribution in order to control weight according to patient's BMI, appetite, needs andhabits reported in the 24 h-recall
Prompt barrier identification Advice to deal with chemotherapy side effects that could affect dietary intakes (see the “diet counseling” section for details aboutspecific advice)
Provide therapeutic education Identify nature and specific roles of food groupsFood balance education based on the food pyramid presentation
Prompt self-monitoring of behavior Patients are asked to complete a 24 h-recall the day before the next diet counseling session3 Chemotherapy
3rd cycle(week 7)
Provide instructions (if necessary) Aiming to adhere to the chemotherapy food distribution in order to control weight according to patient's BMI, appetite, needs andhabits reported in the 24 h-recall
Prompt barrier identification Advice to deal with declared chemotherapy side effects that could affect dietary intakesProvide information on health–behavior link throughtherapeutic education
WCRF recommendations based on a quiz game
Prompt self-monitoring of behavior Patients are asked to complete a 24 h-recall the day before the next diet counseling session4 Chemotherapy
4th cycle(week 10)
Provide instructions (if necessary) Aiming to adhere to the chemotherapy food distribution in order to control weight according to patient's BMI, appetite, needs andhabits reported in the 24 h-recall
Prompt barrier identification Advice to deal with declared chemotherapy side effects that could affect dietary intakesPrompt self-monitoring of behavior Patients are asked to complete a 24 h-recall the day before the next diet counseling session
5 Chemotherapy5th cycle(week 13)
Provide instructions (if necessary) Aiming to adhere to the chemotherapy food distribution in order to control weight according to patient's BMI, appetite, needs andhabits reported in the 24 h-recall
Prompt barrier identification Advice to deal with declared chemotherapy side effects that could affect dietary intakesProvide information on health–behavior link throughtherapeutic education
Food balance education based on the “APAD fridge game” consisting in the elaboration of 3 balanced meals with the food providedon the picture
Prompt self-monitoring of behavior Patients are asked to complete a 24 h-recall the day before the next diet counseling session
538M.Carayolet
al./Contem
poraryClinicalTrials
36(2013)
531–543
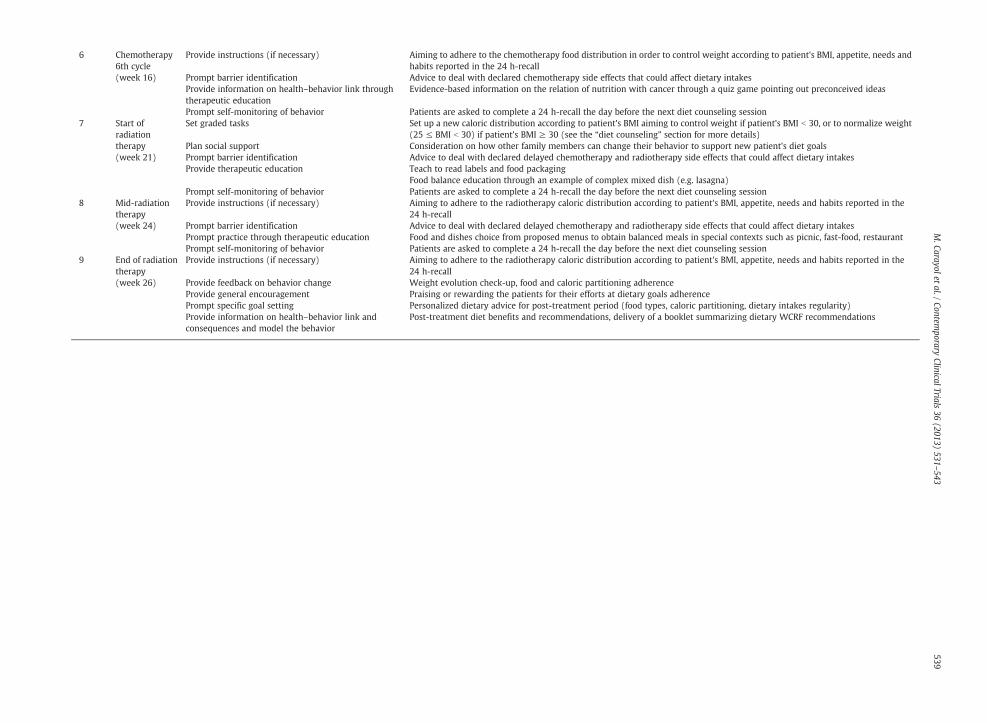
Session no.
Treatment time Behavior change techniques Description
6 Chemotherapy6th cycle(week 16)
Provide instructions (if necessary) Aiming to adhere to the chemotherapy food distribution in order to control weight according to patient's BMI, appetite, needs andhabits reported in the 24 h-recall
Prompt barrier identification Advice to deal with declared chemotherapy side effects that could affect dietary intakesProvide information on health–behavior link throughtherapeutic education
Evidence-based information on the relation of nutrition with cancer through a quiz game pointing out preconceived ideas
Prompt self-monitoring of behavior Patients are asked to complete a 24 h-recall the day before the next diet counseling session7 Start of
radiationtherapy(week 21)
Set graded tasks Set up a new caloric distribution according to patient's BMI aiming to control weight if patient's BMI b 30, or to normalize weight(25 ≤ BMI b 30) if patient's BMI ≥ 30 (see the “diet counseling” section for more details)
Plan social support Consideration on how other family members can change their behavior to support new patient's diet goalsPrompt barrier identification Advice to deal with declared delayed chemotherapy and radiotherapy side effects that could affect dietary intakesProvide therapeutic education Teach to read labels and food packaging
Food balance education through an example of complex mixed dish (e.g. lasagna)Prompt self-monitoring of behavior Patients are asked to complete a 24 h-recall the day before the next diet counseling session
8 Mid-radiationtherapy(week 24)
Provide instructions (if necessary) Aiming to adhere to the radiotherapy caloric distribution according to patient's BMI, appetite, needs and habits reported in the24 h-recall
Prompt barrier identification Advice to deal with declared delayed chemotherapy and radiotherapy side effects that could affect dietary intakesPrompt practice through therapeutic education Food and dishes choice from proposed menus to obtain balanced meals in special contexts such as picnic, fast-food, restaurantPrompt self-monitoring of behavior Patients are asked to complete a 24 h-recall the day before the next diet counseling session
9 End of radiationtherapy(week 26)
Provide instructions (if necessary) Aiming to adhere to the radiotherapy caloric distribution according to patient's BMI, appetite, needs and habits reported in the24 h-recall
Provide feedback on behavior change Weight evolution check-up, food and caloric partitioning adherenceProvide general encouragement Praising or rewarding the patients for their efforts at dietary goals adherencePrompt specific goal setting Personalized dietary advice for post-treatment period (food types, caloric partitioning, dietary intakes regularity)Provide information on health–behavior link andconsequences and model the behavior
Post-treatment diet benefits and recommendations, delivery of a booklet summarizing dietary WCRF recommendations
539M.Carayolet
al./Contem
poraryClinicalTrials
36(2013)
531–543

540 M. Carayol et al. / Contemporary Clinical Trials 36 (2013) 531–543
each muscular group so that, according to patient'sexpertise and condition, the exercise specialist can choosethe best adapted one for each muscular group; next toeach exercise, a space enables the exercise specialist torecord realized number of sets and repetitions.
– Flexibility contents (written instructions illustrated withpictures)
– Aerobic home-based activity: chosen activity type andgoal setting (time and intensity)
– A list of all planned exercise sessions for the 26-weekintervention period is provided and patients are asked torecord whether planned sessions were achieved or not,number of achieved muscular exercises or type of aerobicactivity, duration of session, rating of perceived exertion(on scale of 1 to 10), reason for missed session and anycommentary that they would like to discuss with theexercise specialist at the next supervised session.
2.6.3. Diet counselingAPAD patients benefit from nine face-to-face individual
sessions of diet education performed by a dietician who iscertified by a French University and Technological Institute ofbiology and dietetic (or is certification eligible). Each sessionincludes nutritional status assessment followed by nutritioncare tailored to the patient's caloric requirements and nutritionadvice according to potential treatment-related toxicities, aswell as therapeutic nutritional education. During chemo-therapy, 6 diet sessions are planned (i) to achieve balanceddietary intakes advising patients in controlling their weightand (ii) to help patients managing with chemotherapyside-effects and potential toxicities. In patients with BMI b30,the goal of weight control is pursued for 3more sessions duringradiotherapy; in patients with BMI ≥30, the normalization ofweight is targeted during radiotherapy, aiming to reduce BMIto meet the range of 25 to 30 by the end of adjuvant therapy.
At each session, nutritional status is assessed according tothe criteria defined by the French National Authority forHealth taking into account the current weight, the usualweight, the weight measured one and six months prior tostudy enrolment. The dietician determines the patient's dailycalories requirement based on the estimation of the basalmetabolic rate (BMR) by the corrected formula of Harris andBenedict [33]: in women, BMR = 447.593 + (9.247 × weightin kg) + (3.098 × height in cm) − (4.330 × age). The BMR issystematically multiplied by 1.3 to allow for calorie require-ments needed for daily living activities, and a final increase by1.2 is optionally applied when patients follow the exerciseprescription. The dietician ensures that the patient is able to eatand assesses dietary intake by a food survey (3-day food recordat first and last sessions, and a 24 h-recall at the other sessions)as well as appetite through a 10-point visual analogue scale.Data about dietary intakes are entered on a nutritional analysissoftware [34] which converts foods in calories and nutrients.The dietician checks the patient's intakes to be in accordancewith the following guidelines: (i) daily calories intakeis compared to the estimated daily calories requirement,(ii) dietary intakes are advised to be regularly distributed,as breakfast, lunch and dinner with an optional snack in theafternoon, (iii) macronutrient distribution is compared to theFrench dietary reference intakes for balanced diet i.e. 50–55%of carbohydrates, 10–15% of proteins and 30–35% of lipids
[35] and, (iv) food groups intake are advised to meet WCRFrecommendations [26] i.e. avoid sugary drinks, limit consump-tion of energy-dense foods; eat more of a variety of vegetables,fruits, whole grains and legumes such as beans; limit consump-tion of red meats (such as beef, pork and lamb) and avoidprocessedmeats; if consumed at all, limit alcoholic drinks to 1 forwomen a day; limit consumption of salty foods and foodsprocessedwith salt (sodium); do not use supplements to protectagainst cancer. If either patient's habits are not in accordancewith these guidelines, or daily calories intake differs from morethan 10% of the estimated daily calories requirement, thedietician proposes adjustments regardingmeals, foods, nutrientsand calories distribution, e.g. taking breakfast and reducing lunchand dinner intakes, switching excessive meat consumption forlegumes, replacing sugary foods with fruits, eliminating theconsumption of alcohol and processed meat, increasing satietyby consuming some starchy food at every meal. When patient'sBMI exceed 30 by the end of chemotherapy, a new range of dailycalories requirement is calculated based on a new weight goaldefined by reducing the patient's BMI within the range of 25to 30. To reach this goal, the dietician proposes a daily caloricdistribution close to the new calories requirement whilefollowing the guidelines regarding foods groups balanceand WRCF recommendations, by giving to patients a printedexample of food groups and servings they should eat at everymeal on a whole day.
At every next session, the dietician assesses again thepatient's intakes to check that the advice was likely to beimplemented. She also asks patients about the severity oftreatment-related side-effects and their interactions withdietary intakes, to help patients finding ways to follow theguidelines throughout the intervention. In case of nausea orvomiting, patients are advised to consume foods at roomtemperature or cold, to avoid fatty, sugary and highly flavoredfoods, to consume dry foods (toasted or crisp bread), steamedvegetables, fresh dishes (yogurts, sorbet, fresh fruits), to drinklittle amounts of cool drinks outside meals, to remove excitingdrinks (coffee, tea, alcohol). In case of mucositis, patients arerecommended to avoid spicy and acid foods (lemon,vinegar, mustard…), to favor cooked and smooth foods atroom temperature and to keep their month wet by drinkingfrequently. In case of taste disorders, the dietician adviceto reinforce or reduce dishes seasoning (spices, herbs, salt,sugar…) depending on patient's tasting; when patients feel ametallic taste, they are told to favor starchy foods (e.g. pasta,rice, potatoes), white or béchamel saucewith green vegetables,and white meat, fish or eggs rather than red meat, andalso, to start meals by drinking acid beverages or acid fruits(e.g. grapefruit, pineapple).
The dietician also pay particular attention to the diettherapeutic education in order to make patients feelingconcerned with the way they eat. Through practical appli-cations and educational games, diet therapeutic educationteaches patients the principles of healthy and well balanceddiet, key information about how to read industrial food productspackaging, WCRF recommendations and aim to develop dietculture and to fight against preconceived ideas. Content of dieteducation sessions is detailed in Table 3. During the lastconsultation (end of intervention and treatments), the patientsfrom the experimental group are given a booklet summarizingdietary WCRF recommendations [26].

541M. Carayol et al. / Contemporary Clinical Trials 36 (2013) 531–543
2.6.4. Missed sessionsAs patients only come to the hospital once every three
weeks during chemotherapy, missed supervised exercise ordiet counseling sessions are not possible to be repeated. Aphone call will then be made to the patient by the exerciseand/or dietician specialists. It aims to discuss reasons for notattending the session and adherence regarding home-basedprogram in the last three weeks, to encourage the patientattending future exercise or diet counseling sessions takinginto account its difficulties and to deliver education targetsand content of these missed session.
As most of the patients come to the hospital everyweekday during radiation therapy, if a supervised session ismissed, a make-up session is scheduled as soon as possible.
For the few patients who receive their radiotherapy inanother hospital, the samemissed session procedure is appliedduring radiotherapy as during chemotherapy.
2.7. Usual care
The patients allocated to the usual care group (normalpractice) participated in all data collection assessments (asdescribed below) but did not receive any APAD-interventionrelated material until study completion. They may havereceived ad hoc information related to exercise or nutritionfrom breast cancer associations or other sources. To controlfor dilution of treatment effect, usual care patients wereasked for dietician consultations and membership of sportiveor other type of associations at T2 and T4 assessments.
2.8. Statistical analysis
Computerized data capture and management are per-formed at the Montpellier Cancer Institute biostatistical unitby individuals blinded to the participant's group allocation.After quality control of database, statistical analysis will beperformed.
Baseline comparisons between arms will be performedusing univariate analysis of variance for continuous variablesand χ2 test for categorical variables. Missing data will beimputed under the missing at random assumption of themixed-model analysis. An intent-to-treat analysiswill be done. Ifdisproportionate numbers of participants are lost to follow-upbetween the two study groups, data will be analyzed with andwithout the imputed missing data with results compared fordiscrepancies suggesting potential bias.
Cancer related-fatigue scores of the intervention groupwill be compared to those of the control group by usingmixed-model analysis which allows assessing changes overtime between groups within a repeated measures designwith the determination of time effect (T0, T1, T2, T3 and T4),group effect (APAD, control) and, the interaction effectbetween time and group. Group, time and group-by-timeinteraction will be treated as fixed effects, and participantswill be treated as random. In the sameway, all other continuousoutcome measures collected at two, three, or four time pointswill be analyzed using mixed-model by comparing the differ-ences across groups and changes over time. Unadjusted andadjusted analyses controlling for baseline values of outcomesand other identified confounders will be performed.
2.9. Quality control
This trial is conducted under the supervision of theSteering Committee involving oncologists, epidemiologists,exercise physiologists, nutritionist physicians and biostatis-ticians, who meet once every 6 months in order to reviewinclusions and problems encountered. The CRAs monitorthe quality of data and complete the case report forms toallow the direct logging of information. The Steering Commit-tee will supervise inclusions, data analysis and drafting ofpublications.
Participant safety is a priority during all study activitiesand emergency response protocols are posted at study site.Participants are encouraged to call a corresponding number,provided in their workbook and cover letter, if they experienceany adverse events. Revision of electronic patient files by CRAsand follow-up surveys also question participants for possibleadverse events. Adverse events have to be reported to theinstitutional review board and a detailed written description isprovided to the Clinical Research Unit whomust ensure that allregulatory requirements were observed according to localregulations.
3. Discussion
The APAD study is the first randomized controlled trialexamining the impact of an intervention involving bothhospital- and home-based physical exercise combined withface-to-face diet counseling on cancer related-fatigue in patientsundergoing breast cancer adjuvant therapy. In previous studies,interventions involving both exercise and nutrition focusedeither on other cancer locations [36–38], cancer survivors [37,39]or other primary outcome [15]. Most of these interventionswere home-based usingwrittenmailedmaterials and telephonecounseling [15,37,38]. The originality of the APAD study isfurther supported by its assessment of several dimensions offatigue involving emotional/subjective (self-reported ques-tionnaire), physical (muscle strength) and cognitive fatigue(attentional capabilities) as well as objective physical activitymeasurement. The long-term APAD intervention (26 weeks)and follow-up (1 year post-intervention) will allow theexamination of long-term exercise and dietary guidelinesadherence and maintenance while most published studiespresented shorter intervention period or follow-up time anddid not assess such long term effects. Moreover, the APADstudy is one of the largest sample sized trial compared tosimilar ones [17]which should ensure enough statistical powerto detect changes between groups on primary outcomes.Whileinvestigations of exercise programs for women with breastcancer have found a range of benefits including improvedphysical function [22,40,41], psychological factors [17] andchemotherapy completion rates [22], the cost effectivenessof these programs needs to be investigated. The estimationof the cost per QALY gained per patient will enable toperform a cost–utility analysis. To our knowledge, cost–utility analysis of exercise intervention in women under-going adjuvant therapy of breast cancer has been conductedin only one study [42].
The implementation of the APAD study was quitechallenging for the hospital organization and the personnelinvolved. The hospital had to settle down an exercise hall and

542 M. Carayol et al. / Contemporary Clinical Trials 36 (2013) 531–543
to engage collaborations with research teams, bringingexpertise on exercise and behavioral medicine. The hospitalexpertise in the management of pharmacological clinicaltrials contributed to high quality control on the collection andthe capture of data. The accuracy of rated questionnaires wasfurther guaranteed by systematic assessor checking of filledquestionnaires during assessment sessions and CRAs moni-toring of collected data. One of the most challenging issueswas to maximize patients' compliance with the protocolintervention and assessments. All the assessments, the super-vised exercise and the diet hospital-based sessions are plannedon days when patients must come to the hospital for othermedical purposes, i.e. chemotherapy, radiotherapy, oncologistappointment or medical examination which ensures theirpresence on site, and are supervised by, respectively, anassessor, an exercise specialist and a dietician who check forthe patient attendance. This organization requires the studypersonnel to have a flexible schedule for appointments. Inaddition, patients are asked to record the achievement ofprescribed home-based exercise sessions and logs are checkedand, if needed, completed with the patient by the exercisespecialist at every supervised session, which will enable toestimate intervention adherence. The large number of testsand the duration of assessment sessions were somewhatdissuasive for a few patients; when patients did not complywith the whole range of tests, the completion of question-naires was favored (as they include the primary outcome).We anticipated this issue regarding physical activity assess-ment, by adding a declarative measure (GPAQ questionnaire),easy to collect, to the objective measure (7-day armbandwearing).
An important limitation of this study is the absence ofblinding of participants and assessors. In lifestyle interven-tion studies, blinding of participants to allocation is almostimpossible, especially when one arm receives usual care. Inaddition, as assessment sessions included a face-to-faceinterview about participant physical activity practice (GPAQquestionnaire), the blinding of assessors was unworkable.The absence of blinding could induce placebo effect in theintervention group that it would not be quantifiable apartfrom the effect of treatment. A dilution of treatment effectcould occur if patients from the usual care group undertakeexercise classes or diet consultations. The scheduled assess-ments of physical activity and dietary intakes for all partic-ipants will enable measuring this bias.
The APAD study has been designed in order to evaluatethe effectiveness of the intervention when implemented innormal practice. French cancer centers or hospitals need toassess their ability to implement such exercise and nutritionsupportive care with limited additional cost. Hence, APADintervention takes place alternatively at the hospital, on thesame days of chemotherapy and radiotherapy to avoid anyadditional travel cost, and at home with printed material.In addition, women are not selected on their exercise abilityor history and criteria are not restrictive to a particularpopulation to fit with real clinical context. Recommendedhealth behaviors are well-known to be better adopted bysocio-economically advantaged individuals as compared todisadvantaged individuals [27,43,44]. The design of the APADintervention has been done with a pragmatic attitude [45,46]to avoid increasing health inequalities by providing equal
access to nutrition counseling and exercise sessions withoutany additional cost or travel fees.
The present APAD study will firstly assess the effective-ness of the intervention in the Montpellier Cancer Institute.In order to evaluate the feasibility of implementation of theAPAD intervention in various contexts, the APAD study hasrecently been funded to be expanded to 9 supplementaryFrench care centers which will be provided specifications andgood practice guidelines according to observations and findingsfrom the present APAD study.
Acknowledgments
This research is funded by a Project Grant from thenational French Cancer League [Ligue contre le Cancer] aswell as the regional French Cancer League of Hérault andLanguedoc-Roussillon (No. 8FI10347LQOP). We would liketo acknowledge the significant contributions of the careteams of the Montpellier Cancer Institute—ICM [InstitutRégional du Cancer de Montpellier] who make this studybeing carry out and especially, medical oncologists thathave contributed to participant recruitment, includingAnna Durigova, Véronique D'Hondt, and Stéphane Pouderoux;exercise physiologists trainees, including Samuel Deaux, CamilleDeravet, and Marjorie Devais. The authors thank the ProfessorHenri Pujol for his support in finding funds. Finally, the womenwho participated in this trial also need to be acknowledged fortheir significant contributions, in particular for their willingnessto participate despite knowing theymay not be allocated to theirdesired group.
References
[1] Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CACancer J Clin 2005;55(2):74–108.
[2] Bélot A, Velten M, Grosclaude P, Bossard N, Launoy G, Remontet L, et al.French national estimation of cancer incidence and mortality ratesbetween 1980 and 2005 (Estimation nationale de l'incidence et de lamortalité par cancer en France entre 1980 et 2005). Saint-Maurice,France: Institut de veille sanitaire; 2008 [132 pp. Available at www.invs.sante.fr Accessed December 21, 2012].
[3] Partridge AH, Burstein HJ, Winer EP. Side effects of chemotherapy andcombined chemohormonal therapy in women with early-stage breastcancer. J Natl Cancer Inst Monogr 2001;30:135–42.
[4] Truong PT, Olivotto IA, Whelan TJ, Levine M. Clinical practice guidelinesfor the care and treatment of breast cancer: 16. Locoregional post-mastectomy radiotherapy. CMAJ 2004;170(8):1263–73.
[5] National Comprehensive Cancer Network. Clinical practice guidelines inoncology. Cancer-related fatigue. Version 1 2011; Available from http://www.nccn.org/professionals/physician_gls/pdf/fatigue.pdf . [AccessedAugust 21, 2013].
[6] Holley S. Cancer-related fatigue. Suffering a different fatigue. CancerPract 2000;8(2):87–95.
[7] Vogelzang NJ, Breitbart W, Cella D, Curt GA, Groopman JE, Horning SJ,et al. Patient, caregiver, and oncologist perceptions of cancer-relatedfatigue: results of a tripart assessment survey. The Fatigue Coalition.Semin Hematol 1997;34(3 Suppl. 2):4–12.
[8] Ahlberg K, Ekman T, Gaston-Johansson F, Mock V. Assessmentand management of cancer-related fatigue in adults. Lancet2003;362(9384):640–50.
[9] Borneman T, Piper BF, Koczywas M, Munevar CM, Sun V, Uman GC,et al. A qualitative analysis of cancer-related fatigue in ambulatoryoncology. Clin J Oncol Nurs 2012;16(1):E26–32.
[10] Broeckel JA, Jacobsen PB, Horton J, Balducci L, Lyman GH. Characteristicsand correlates of fatigue after adjuvant chemotherapy for breast cancer. JClin Oncol 1998;16(5):1689–96.
[11] Curt GA. Impact of fatigue on quality of life in oncology patients. SeminHematol 2000;37(4 Suppl. 6):14–7.
543M. Carayol et al. / Contemporary Clinical Trials 36 (2013) 531–543
[12] Dodd MJ, Miaskowski C, Paul SM. Symptom clusters and their effecton the functional status of patients with cancer. Oncol Nurs Forum2001;28(3):465–70.
[13] Jacobsen PB, Hann DM, Azzarello LM, Horton J, Balducci L, Lyman GH.Fatigue in women receiving adjuvant chemotherapy for breast cancer:characteristics, course, and correlates. J Pain Symptom Manage1999;18(4):233–42.
[14] Kalman D, Villani LJ. Nutritional aspects of cancer-related fatigue. J AmDiet Assoc 1997;97(6):650–4.
[15] Demark-Wahnefried W, Case LD, Blackwell K, Marcom PK, Kraus W,Aziz N, et al. Results of a diet/exercise feasibility trial to prevent adversebody composition change in breast cancer patients on adjuvantchemotherapy. Clin Breast Cancer 2008;8(1):70–9.
[16] Cramp F, Byron-Daniel J. Exercise for the management of cancer-related fatigue in adults. Cochrane Database Syst Rev 2012;11:CD006145.
[17] Carayol M, Bernard P, Boiche J, Riou F, Mercier B, Cousson-Gelie F, et al.Psychological effect of exercise in women with breast cancer receivingadjuvant therapy: what is the optimal dose needed? Ann Oncol2013;24(2):291–300.
[18] Carayol M, Delpierre C, Ninot G. A meta-analysis on the interestof exercise in adjuvant breast cancer patients: are the guidelinesbased on evidence? Support Care Cancer 2013;21(Suppl. 1):S187.
[19] Schmitz KH, Courneya KS, Matthews C, Demark-Wahnefried W, GalvaoDA, Pinto BM, et al. American College of Sports Medicine roundtableon exercise guidelines for cancer survivors. Med Sci Sports Exerc2010;42(7):1409–26.
[20] Smets EM, Garssen B, Bonke B, De Haes JC. The MultidimensionalFatigue Inventory (MFI) psychometric qualities of an instrument toassess fatigue. J Psychosom Res 1995;39(3):315–25.
[21] Boutitie F, Bellissant E, Blanchard J, Boissel JP, Cauquil J, Chauvin F, et al.Monitoring of clinical-trials and interim analyses—2-Statistical methods.Therapie 1992;47(4):351–5.
[22] Courneya KS, Segal RJ, Mackey JR, Gelmon K, Reid RD, Friedenreich CM,et al. Effects of aerobic and resistance exercise in breast cancer patientsreceiving adjuvant chemotherapy: a multicenter randomized controlledtrial. J Clin Oncol 2007;25(28):4396–404.
[23] Rabin R, de Charro F. EQ-5D: a measure of health status from theEuroQol Group. Ann Med 2001;33(5):337–43.
[24] Conner-Spady B, Cumming C, Nabholtz JM, Jacobs P, Stewart D.Responsiveness of the EuroQol in breast cancer patients undergoinghigh dose chemotherapy. Qual Life Res 2001;10(6):479–86.
[25] Chevalier J, de Pouvourville G. Valuing EQ-5D using time trade-off inFrance. Eur J Health Econ 2013;14(1):57–66.
[26] World Cancer Research Fund/American Institute for Cancer Research.Policy and action for cancer prevention. Food, nutrition, and physicalactivity: a global perspective. Washington DC: AICR; 2009 [Available atwww.wcrf.org Accessed August 21, 2013].
[27] INSERM Group Expertise. Physical activity: context and health impact(Activité physique: Contextes et effets sur la santé). Paris: Les EditionsInserm; 2008.
[28] Courneya KS, Mackey JR, McKenzie DC. Exercise for breast cancersurvivors: research evidence and clinical guidelines. Phys Sportsmed2002;30(8):33–42.
[29] de Jong N, Kester AD, Schouten HC, Abu-Saad HH, Courtens AM. Courseof fatigue between two cycles of adjuvant chemotherapy in breastcancer patients. Cancer Nurs 2006;29(6):467–77.
[30] Miller M, Maguire R, Kearney N. Patterns of fatigue during a course ofchemotherapy: results from a multi-centre study. Eur J Oncol Nurs2007;11(2):126–32.
[31] Abraham C, Michie S. A taxonomy of behavior change techniques usedin interventions. Health Psychol 2008;27(3):379–87.
[32] Biddle SJH, Fox K, Boutcher SH, Faulkner G. The way forward forphysical activity and the promotion of psychological well-being.In: Biddle SJH, Fox K, Boutcher SH, Faulkner G, editors. Physicalactivity and psychological well-being. London: Routledge; 2000.p. 154–68.
[33] Roza AM, Shizgal HM. The Harris Benedict equation reevaluated: restingenergy requirements and the body cell mass. Am J Clin Nutr1984;40(1):168–82.
[34] GENI: Nutritional Analysis Software, release 8. , 6Villiers-les-Nancy:MICRO;2007.
[35] Coord Martin A. Dietary reference intake for the French population(Apports nutritionnels conseillés pour la population française). In: Tecet Doc, editor. 3rd ed. France: CNERNA-CNRS, AFSSA; 2001 [Paris].
[36] von Gruenigen VE, Courneya KS, Gibbons HE, Kavanagh MB, WaggonerSE, Lerner E. Feasibility and effectiveness of a lifestyle interventionprogram in obese endometrial cancer patients: a randomized trial.Gynecol Oncol 2008;109(1):19–26.
[37] Morey MC, Snyder DC, Sloane R, Cohen HJ, Peterson B, Hartman TJ, et al.Effects of home-based diet and exercise on functional outcomes amongolder, overweight long-term cancer survivors: RENEW: a randomizedcontrolled trial. JAMA 2009;301(18):1883–91.
[38] Campbell MK, Carr C, Devellis B, Switzer B, Biddle A, Amamoo MA, et al.A randomized trial of tailoring and motivational interviewing topromote fruit and vegetable consumption for cancer prevention andcontrol. Ann Behav Med 2009;38(2):71–85.
[39] Bloom JR, Stewart SL, D'Onofrio CN, Luce J, Banks PJ. Addressing theneeds of young breast cancer survivors at the 5 year milestone: can ashort-term, low intensity intervention produce change? J Cancer Surviv2008;2(3):190–204.
[40] Markes M, Brockow T, Resch KL. Exercise for women receivingadjuvant therapy for breast cancer. Cochrane Database Syst Rev 2006;4:CD005001.
[41] McNeelyML, Campbell KL, Rowe BH, Klassen TP, Mackey JR, Courneya KS.Effects of exercise on breast cancer patients and survivors: a systematicreview and meta-analysis. CMAJ 2006;175(1):34–41.
[42] Haines TP, Sinnamon P, Wetzig NG, Lehman M, Walpole E, Pratt T, et al.Multimodal exercise improves quality of life of women being treatedfor breast cancer, but at what cost? Randomized trial with economicevaluation. Breast Cancer Res Treat 2010;124(1):163–75.
[43] Giles-Corti B, Donovan RJ. Socioeconomic status differences in recrea-tional physical activity levels and real and perceived access to asupportive physical environment. Prev Med 2002;35(6):601–11.
[44] Giles-Corti B, Donovan RJ. The relative influence of individual, socialand physical environment determinants of physical activity. Soc SciMed 2002;54(12):1793–812.
[45] Thorpe KE, Zwarenstein M, Oxman AD, Treweek S, Furberg CD, AltmanDG, et al. A pragmatic-explanatory continuum indicator summary(PRECIS): a tool to help trial designers. CMAJ 2009;180(10):E47–57.
[46] Zwarenstein M, Treweek S, Gagnier JJ, Altman DG, Tunis S, Haynes B,et al. Improving the reporting of pragmatic trials: an extension of theCONSORT statement. BMJ 2008;337:a2390.
[47] Jones CJ, Rikli RE, Beam WC. A 30-s chair-stand test as a measure oflower body strength in community-residing older adults. Res Q ExercSport 1999;70(2):113–9.
[48] Winters-Stone KM, Bennett JA, Nail L, Schwartz A. Strength, physicalactivity, and age predict fatigue in older breast cancer survivors. OncolNurs Forum 2008;35(5):815–21.
[49] Test for attentional performance (TAP). P Zimmermann, B Fimm -PsyTest, Herzogenrath 1995.
[50] Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ,et al. The European Organization for Research and Treatment of CancerQLQ-C30: a quality-of-life instrument for use in international clinicaltrials in oncology. J Natl Cancer Inst 1993;85(5):365–76.
[51] Razavi D, Delvaux N, Farvacques C, Robaye E. Screening for adjustmentdisorders and major depressive disorders in cancer in-patients. Br JPsychiatry 1990;156:79–83.
[52] Bull FC, Maslin TS, Armstrong T. Global physical activity questionnaire(GPAQ): nine country reliability and validity study. J Phys Act Health2009;6(6):790–804.
[53] Yaw YH, Shariff ZM, Kandiah M, Mun CY, Yusof RM, Othman Z, et al.Weight changes and lifestyle behaviors in women after breast cancerdiagnosis: a cross-sectional study. BMC Public Health 2011;11:309.
[54] Cereda E, Turrini M, Ciapanna D, Marbello L, Pietrobelli A, Corradi E.Assessing energy expenditure in cancer patients: a pilot validation of anew wearable device. JPEN J Parenter Enteral Nutr 2007;31(6):502–7.
[55] Fredrix EW, Saris WH, Soeters PB, Wouters EF, Kester AD, vonMeyenfeldt MF, et al. Estimation of body composition by bioelectricalimpedance in cancer patients. Eur J Clin Nutr 1990;44(10):749–52.
[56] Sarhill N, Mahmoud FA, Christie R, Tahir A. Assessment of nutritionalstatus and fluid deficits in advanced cancer. Am J Hosp Palliat Care2003;20(6):465–73.
[57] Gupta D, Lammersfeld CA, Vashi PG, King J, Dahlk SL, Grutsch JF, et al.Bioelectrical impedance phase angle as a prognostic indicator in breastcancer. BMC Cancer 2008;8:249.
[58] Biro G, Hulshof KF, Ovesen L, Amorim Cruz JA. Selection of methodologyto assess food intake. Eur J Clin Nutr 2002;56(Suppl 2):S25–32.
[59] Sass C, Dupre C, Dauphinot V, et al. The EPICES score: an individualindex of material and social deprivation related to health status. Part 2:evaluation in a population of 197 389 subjects [article online] 2005Available from http://www.cetaf.asso.fr/protocoles/precarite/protocoles_epices.htm#publis.
[60] Sass C, Gueguen R, Moulin JJ, Abric L, Dauphinot V, Dupre C, et al.Comparison of the individual deprivation index of the French HealthExamination Centres and the administrative definition of deprivation.Sante Publique 2006;18(4):513–22.
Copyright © 2022 FDOKUMEN




















