
RANDOMISED PROSPECTIVE COMPARATIVE STUDY ON ...
107
1 RANDOMISED PROSPECTIVE COMPARATIVE STUDY ON THE EFFICACY OF SHARMA JHAWER’S OPERATION WITH LORD’S PLICATION AND JABOULEY’S OPERATION IN THE TREATMENT OF PRIMARY VAGINAL HYDROCELE Dissertation submitted to THE TAMILNADU DR. M.G.R. MEDICAL UNIVERSITY CHENNAI – 600032 M.S. GENERAL SURGERY (BRANCH - I) DEPARTMENT OF GENERAL SURGERY MADURAI MEDICAL COLLEGE AND GOVERNMENT RAJAJI HOSPITAL, MADURAI – 625020 MAY – 2019
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of RANDOMISED PROSPECTIVE COMPARATIVE STUDY ON ...

1
RANDOMISED PROSPECTIVE COMPARATIVE STUDY
ON THE EFFICACY OF SHARMA JHAWER’S
OPERATION WITH LORD’S PLICATION AND
JABOULEY’S OPERATION IN THE TREATMENT OF
PRIMARY VAGINAL HYDROCELE
Dissertation submitted to
THE TAMILNADU DR. M.G.R. MEDICAL UNIVERSITY
CHENNAI – 600032
M.S. GENERAL SURGERY (BRANCH - I)
DEPARTMENT OF GENERAL SURGERY MADURAI MEDICAL COLLEGE AND GOVERNMENT RAJAJI
HOSPITAL, MADURAI – 625020
MAY – 2019

2
CONTENTS
1. Certificate
2. Declaration by the candidate
3. Acknowledgement
4. Bonafide certificates
5. Introduction
6. Review of Literature
7. Aim & objectives
8. Design of study
9. Compartments of the study
10. Statistical analysis
11. Study population
12. Eligibility criteria
13. Types of operations to be studied
14. End point
15. Results
16. Conclusion
17. Bibliography
18. Annexures
3
CHARTS (COMPARTMENT I)
SHARMA JHAWER(SJ) Vs LORD’S PLICATION(LP)
1. Age distribution in I compartment (SJ Vs LP)
2. Distribution of occupation in I compartment
3. Distribution of socio-economic status in I compartment
4. Distribution of occupation in both procedures
5. Distribution of socioeconomic status among both procedures
6. Side distribution in I compartment
7. Side distribution among SJ v LP procedures
8. Distribution of symptoms in I compartment
9. Symptoms within each procedure
10. Distribution of duration of illness in I compartment
11. Duration of illness among both the procedures
12. Percentage of hematoma in both procedures
13. Percentage of scrotal edema in both procedures
14. Percentage of pain in both the procedures
15. Percentage of fever in both the procedures
16. Complications in both procedures

4
CHARTS (COMPARTMENT II)
SHARMA JHAWER(SJ) Vs JABOULEY’S OPERATION(JAB)
17. Age distribution in II compartment (SJ Vs JAB)
18. Distribution of occupation in II compartment
19. Distribution of socio-economic status in II compartment
20. Distribution of occupation in both procedures
21. Distribution of socioeconomic status among both procedures
22. Side distribution in II compartment
23. Side distribution among SJ v LP procedures
24. Distribution of symptoms in II compartment
25. Symptoms within each procedure
26. Distribution of duration of illness in II compartment
27. Duration of illness among both the procedures
28. Percentage of hematoma in both procedures
29. Percentage of scrotal edema in both procedures
30. Percentage of pain in both the procedures
31. Percentage of fever in both the procedures
32. Complications in both procedures

5
TABLES
1. Distribution of socio-demographic variables SJ v LP procedures
2. Clinical profile among patients in both the procedures (SJ vs LP)
3. Complications in I compartment
4. Outcome measures in I compartment
5. Distribution of socio-demographic variables SJ v JAB procedures
6. Clinical profile among patients in both the procedures (SJ vs JAB)
7. Complications in II compartment
8. Outcome measures in II compartment

6
CERTIFICATE
This is to certify that this Dissertation titled “RANDOMISED
PROSPECTIVE COMPARATIVE STUDY ON THE EFFICACY OF
SHARMA JHAWER’S OPERATION WITH LORD’S PLICATION
AND JABOULEY’S OPERATION IN THE TREATMENT OF
PRIMARY VAGINAL HYDROCELE” submitted by Dr. M. JOYNER
ABRAHAM to the faculty of general surgery, The Tamilnadu Dr.M.G.R
Medical University, Chennai in partial fulfilment of the requirement for the
award of MS Degree (Branch I) General Surgery, is a bonafide research work
carried out by him under our direct supervision and guidance from June 2016
to May 2018.
.
Prof.Dr. K. G. Subangi., M.S., D.G.O Prof. Dr.S.R.Dhamodharan., M.S Professor of General Surgery Professor & Head of the Department
Department of General Surgery Department of General Surgery
Madurai Medical College, Madurai. Madurai Medical College, Madurai

7
DECLARATION BY THE CANDIDATE
I Dr. M. JOYNER ABRAHAM, hereby solemnly declare that this
Dissertation entitled “RANDOMISED PROSPECTIVE COMPARATIVE
STUDY ON THE EFFICACY OF SHARMA JHAWER’S OPERATION
WITH LORD’S PLICATION AND JABOULEY’S OPERATION IN
THE TREATMENT OF PRIMARY VAGINAL HYDROCELE” is a
bonafide and genuine research work carried out by me.
This is submitted to The Tamil Nadu Dr. M.G.R. Medical
University, Chennai, in partial fulfilment of the regulations for the award
of M.S Degree (Branch I) in General Surgery.
Place: Madurai
Date : 10-2018 (Dr. M. JOYNER ABRAHAM)

8
ACKNOWLEDGEMENT
It is my honour and privilege to thank Prof. Dr. K.G. SUBANGI
M.S.,DGO Professor of General Surgery, who helped me in choosing the
subject for this study and guided me at every stage. Her valuable suggestions
and timely advice were of immense help to me throughout all phases of this
study.
I express my gratitude towards Prof. Dr. S.R. DHAMODHARAN.,
M.S., Head of the Department of General Surgery, Madurai Medical College,
Madurai, for his valuable suggestions, support and guidance.
I thank Dr..G.Saravanakumar,M.S.,D.A., Dr.K.S.Gokulnath
Premchand, M.S., D.ortho., Dr.R.Rani M.S.,DDVL., for their
encouragement and guidance.
I am very thankful to my colleagues who helped me in preparing
this dissertation. My ‘sincere thanks’ to all the patients without whose
co-operation this study would have not been possible and last but not the
least, I wish to express my gratitude to my family & friends also, without
them, this study would have not been possible.
Date: 10-2018 (Dr. M. JOYNER ABRAHAM)

9
BONAFIDE CERTIFICATE FROM THE GUIDE
This is to certify that this dissertation entitled “RANDOMISED
PROSPECTIVE COMPARATIVE STUDY ON THE EFFICACY OF
SHARMA JHAWER’S OPERATION WITH LORD’S PLICATION
AND JABOULEY’S OPERATION IN THE TREATMENT OF
PRIMARY VAGINAL HYDROCELE” is the bonafide work of
Dr. M. JOYNER ABRAHAM in partial fulfilment of the university
regulations of the Tamil Nadu Dr.M.G.R.Medical University, Chennai, for
M.S.General Surgery Branch I examination to be held in May 2019.
Prof.Dr.K. G. SUBANGI., M.S.,DGO., Professor of Surgery,
Department of General Surgery
Madurai Medical College, Madurai.

10
BONAFIDE CERTIFICATE FROM THE HOD
This is to certify that this dissertation entitled “RANDOMISED
PROSPECTIVE COMPARATIVE STUDY ON THE EFFICACY OF
SHARMA JHAWER’S OPERATION WITH LORD’S PLICATION
AND JABOULEY’S OPERATION IN THE TREATMENT OF
PRIMARY VAGINAL HYDROCELE” is the bonafide work of
Dr. M. JOYNER ABRAHAM in partial fulfilment of the university
regulations of the Tamil Nadu Dr.M.G.R.Medical University, Chennai, for
M.S.General Surgery Branch I examination to be held in May 2019.
Prof. Dr.S.R.Dhamodharan., M.S Professor & Head of the Department
Department of General Surgery
Madurai Medical College, Madurai

11
BONAFIDE CERTIFICATE FROM THE DEAN
This is to certify that this dissertation entitled “RANDOMISED
PROSPECTIVE COMPARATIVE STUDY ON THE EFFICACY OF
SHARMA JHAWER’S OPERATION WITH LORD’S PLICATION
AND JABOULEY’S OPERATION IN THE TREATMENT OF
PRIMARY VAGINAL HYDROCELE” is the bonafide work of
Dr. M. JOYNER ABRAHAM in partial fulfilment of the university
regulations of the Tamil Nadu Dr.M.G.R.Medical University, Chennai, for
M.S.General Surgery Branch I examination to be held in May 2019.
Dr. D. MARUTHUPANDIAN, M.S, FICS, FIAS.,
DEAN
Madurai Medical College, Madurai.

12
INTRODUCTION
Hydrocele is known to occur in man since time immemorial. Indian
surgeons have reported it as early as 5th century BC.
Hydrocele has been described in ancient Indian surgery by Sushrutha
(6th century BC), who stated that any swelling in the body is due to
thridhosha (three faults), viz. vatha, pitta and kaffa. Sushrutha, the
father of Indian surgery had written the details regarding hydrocele in
his book “Sushrutha Samhitha” about 2,500 years ago.
According to Charaka the causes of diseases are:
✓ The excessive, deficient or wrongful administration of drugs.
✓ The climatic characteristics of heat and cold.
✓ The misuse of intelligence.
Celsus in 53 B.C. – 17 A.D. distinguished hydrocele from hernia by
translucency. Arvelius Cornelius Celsus, a roman encyclopaedist of the first
century A.D. who dealt very extensively with hernia, was the most important

13
single figure in the long history of this subject for more than a millennium.
He described hydrocele, varicocele and tumor.
Sauncuoglu, an ancient surgeon (1385-1470) defined hydrocele as “a fluid
collection between the white fascia beneath the skin (tunica vaginalis
parietalis) and fascia surrounding the testis (tunica vaginalis visceralis),
resembling a natural capsule” .He cautioned that if the sac was not excised
appropriately, hydrocele might recur. He also listed the complications
Edward Gibbon, 1737 - 93, the English historian, who is best known for
history of the decline and fall of the Roman empire, was greatly embarrassed
by a large hydrocele. The second time this was tapped, the hydrocele became
infected and Gibbon died a few days after the operation. The hydrocele was
associated with a large scrotal hernia, probably was punctured.
Dupeutyran, 1834 and later Lister, 1858 did some work on hydrocele
especially on abdomino scrotal hydrocele.

14
It was MATHEW JABOULAY (1860-1913) who contributed the
operation of partial excision with eversion of the sac in the treatment of
hydrocele.
In 1907, Andrews described the bottle operation for treatment of
Hydrocele.
Dupuytren described hydrocele en bissac in 1834 and the name
abdomino scrotal hydrocele was proposed by Bickle in 1919.
In 1955, salomon described the extrusion operation for hydrocele.
Ozdilek 1957 and Rinker and Allen, 1951 gave some theoretical evidence
that an imbalance in the secretion and absorption in responsible for the
collection of the fluid.
In 1960 Wallace found that, the hydrocele is due to the result of lymphatic
obstruction, either due to the low grade inflammation of epididymis or due to
trauma to the scrotum.

15
Peter Lord (1964) described the plication operation for hydrocele. In
1970, he described a blood less operation for spermatocele and
epididymal cyst.
In 1975, Moloney reported good results with sclerotherapy. It is
performed as an outpatient procedure and thus, it is cost effective.
In 1979 SHARMA – JHAWER described a technique which involved
lesser complications as compared to other procedures.
In 1995, study done by Gunaydin G et al, indicated that fluids within
spermatoceles and epididymal cysts do not become infected under
normal circumstances.
However, still the surgery for hydrocele has a significant morbidity
rate. The common complications include
➢ Bleeding
➢ Haematoma
➢ Scrotal Edema

16
➢ Testicular pain
➢ Infection
➢ Injury to the cord structures and epididymis
➢ Torsion of the testis
in the order of decreasing frequency.
Commonest among these is post-operative haematoma which is due to
oozing from small vessels. Unless meticulous haemostasis is secured oozing
from small vessels may continue into the layers of the loose scrotal tissue
giving rise to a haematoma. It is apt to say that a patient comes for surgery of
a tennis ball and goes back with a cricket ball, considering the size and
weight.
To study which among all these procedures has the least morbidity, in
our study we have compared the popularly used Lord’s plication for small
and Jaboulay’s operation for medium sized uncomplicated primary vaginal
hydroceles with Sharma and Jhawer’s minimal dissection technique in two
separate compartments.

17
REVIEW OF LITERATURE
ANATOMICAL CONSIDERATIONS
SCROTUM
The scrotum is a cutaneous bag containing the right and left testes, the
epididymis and the lower parts of the spermatic cords. Externally, the
scrotum is divided into right and left parts by a ridge or raphe which is
continued forwards on to the under surface of the penis and backwards along
the middle of the perineum to the anus. The left half of the scrotum hangs a
little lower than the right, in correspondence with the greater length of the
left spermatic cord. Under the influence of cold, and in young and robust
persons, the scrotum is short, corrugated and closely applied to the testis.
This is due to contraction of the subcutaneous muscle of scrotum, called the
dartos. However, under the influence of warmth, and in old and debilitated
persons, the scrotum is elongated and flaccid due to relaxation of dartos.
From this it appears that the dartos muscle helps in regulation of temperature
within the scrotum.

18
Layers of the Scrotum
The scrotum is made up of the following layers from outside to inside
1. Skin.
2. Dartos muscle which replaces the superficial fascia.
3. The external spermatic fascia.
4. The cremasteric muscle and fascia.
5. The internal spermatic fascia.
The dartos muscle is prolonged into a median vertical septum between
the two halves of the scrotum.
Blood Supply
The scrotum is supplied by the following arteries:
• Superficial external pudendal
• Deep external pudendal

19
• Scrotal branches of internal pudendal
• Cremasteric branch of inferior epigastric.
Nerve Supply
The anterior one-third of the scrotum is supplied by
• Segment LI of the spinal cord through the ilioinguinal nerve.
• Genital branch of the genitofemoral nerve.
The posterior two-thirds of the scrotum are supplied by
• Segment S3 of the spinal cord through the posterior scrotal branches of
the pudendal nerve.
• Perineal branch of the posterior cutaneous nerve of the thigh.
The areas supplied by segments LI and S3 are separated by the ventral
axial line.
The dartos muscle is supplied by the
• genital branch of the genitofemoral nerve.
TESTIS
The testis is the male gonad. It is homologous with the ovary of the
female. It is suspended in the scrotum by the spermatic cord. It lies obliquely,
so that its upper pole is tilted forwards and medially. The left testis is slightly
lower than the right. The testis is oval in shape, and is compressed from side
20
to side. It is 3.75 cm long, 2.5 cm broad from before backwards, and 1.8 cm
thick from side to side. An adult testis weighs about 10 to 15 g.
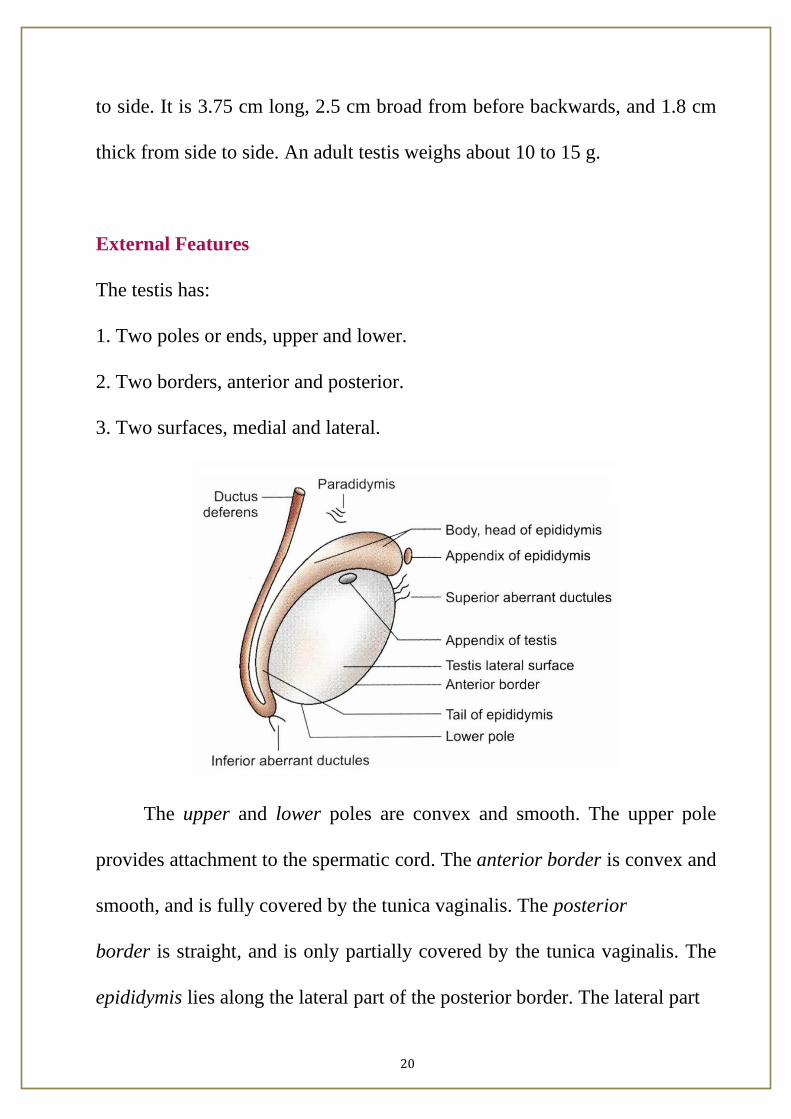
External Features
The testis has:
1. Two poles or ends, upper and lower.
2. Two borders, anterior and posterior.
3. Two surfaces, medial and lateral.
The upper and lower poles are convex and smooth. The upper pole
provides attachment to the spermatic cord. The anterior border is convex and
smooth, and is fully covered by the tunica vaginalis. The posterior
border is straight, and is only partially covered by the tunica vaginalis. The
epididymis lies along the lateral part of the posterior border. The lateral part

21
of the epididymis is separated from the testis by an extension of the cavity of
the tunica vaginalis. This extension is called the sinus of epididymis. The
medial and lateral surfaces are convex and smooth. Attached to the upper
pole of the testis, there is a small oval body called the appendix of the testis.
It is a remnant of the paramesonephric duct.
Coverings of the Testis
The testis is covered by three coats. From outside inwards, these are
the tunica vaginalis, the tunica albuginea and the tunica vasculosa. The
tunica vaginalis represents the lower persistent portion of the processus
vaginalis. It is invaginated by the testis from behind and, therefore, has a
parietal and a visceral layer with a cavity in between. It covers the whole
testis, except for its posterior border. The tunica albuginea is a dense, white
22
fibrous coat covering the testis all around. It is covered by the visceral layer
of the tunica vaginalis, except posteriorly where the testicular vessels and
nerves enter the gland. Albuginea is thickened to form an incomplete vertical
septum, called the mediastinum testis, which is wider above than below.
Numerous septa extend from the mediastinum to the inner surface of the
tunica albuginea. They incompletely divide the testis into 200 to 300 lobules.
The tunica vasculosa is the innermost, vascular coat of the testis lining its
lobules.
Structure of the Testis
The glandular part of the testis consists of 200 to 300 lobules. Each
lobule contains two to three seminiferous tubules. Each tubule is highly
coiled on itself. When stretched out, each tubule measures about 60 cm in
length, and is about 0.2 mm in diameter. The tubules are lined by cells which
represent stages in the formation of spermatozoa. The seminiferous tubules
join together at the apices of the lobules to form 20 to 30 straight tubules
which enter the mediastinum. Here they anastomose with each other to form
a network of tubules, called the rete testis. In its turn, the rete testis gives rise
to 12 to 30 efferent ductules which emerge near the upper pole of the testis
and enter the epididymis. Here each tubule becomes highly coiled and forms

23
a lobe of the head of the epididymis. The tubules end in a single duct which
is coiled on itself to form the body and tail of the epididymis. It is continuous
with the ductus deferens.
Arterial Supply
The testicular artery is a branch of the abdominal aorta given off at the
level of vertebra L2. It descends on the posterior abdominal wall to reach the
deep inguinal ring where it enters the spermatic cord. At the posterior border
of the testis, it divides into branches. Some small branches enter the posterior
border, while larger branches; medial and lateral, pierce the tunica albuginea
and run on the surface of the testis to ramify in the tunica vasculosa.
Venous Drainage
The veins emerging from the testis form the pampiniform plexus
(pampiniform = like a vine). The anterior part of the plexus is arranged
around the testicular artery, the middle part around the ductus deferens and
its artery, and the posterior part is isolated. The plexus condenses into four
veins at the superficial inguinal ring, and into two veins at the deep inguinal
ring. These veins accompany the testicular artery. Ultimately one vein is

24
formed which drains into the inferior vena cava on the right side, and into
the left renal vein on the left side.
Lymphatic Drainage
The lymphatics from the testis ascend along the testicular vessels and
drain into the preaortic and paraaortic groups of lymph nodes at the level of
second lumbar vertebra.
25
Nerve Supply
The testis is supplied by sympathetic nerves arising from segment T10
of the spinal cord. They pass through the renal and aortic plexuses. The
nerves are both afferent for testicular sensation and efferent to the blood
vessels (vasomotor).
DEVELOPMENT OF TESTIS
Testis: It is comprised of spermatogenic cells, cells of Sertoli and
Leydig’s cells. Spermatogenic series of cells are derived from endoderm of
dorsocaudal part of yolk sac, i.e. endoderm. Cells of Sertoli are derived from
epithelial cells, i.e. coelomic epithelium. Leydig’s cells: Mesoderm.
Descent of the Testis
The testes develop in relation to the developing mesonephros, at the
level of segments T10 to T12. Subsequently, they descend to reach the
scrotum. Each testis begins to descend during the second month of
intrauterine life. It reaches the iliac fossa by the 3rd month, rests at the deep
inguinal ring from the 4th to the 6th month, traverses the inguinal canal
during the 7th month, reaches the superficial inguinal ring by the 8th month

26
and the bottom of the scrotum by the 9th month. An extension of peritoneal
cavity called the processus vaginalis precedes the descent of testis into the
scrotum, into which the testis invaginates. The processus vaginalis closes
above the testis. Descent does not occur after one year of age. The causes of
descent are not well known. The following factors may help in the process.
1. Hormones including the male sex hormone produced by the testis, and
maternal gonadotropins.
2. Differential growth of the body wall.
3. Formation of the gubernaculum: This is a band of loose tissue extending
from the lower pole of the testis to the scrotum. It was earlier thought that
contraction of this tissue was responsible for descent of the testis, but it is
now known that this tissue is not contractile.
4. Intra-abdominal temperature and intraabdominal pressure may have
something to do with descent of the testis.

27
HYDROCELE
It is the collection of fluid between the two layers of tunica vaginalis of
testis.
Types
• Congenital
• Acquired
• Primary
• Secondary
Aetiology
✓ Defective absorption of fluid by the tunica vaginalis, probably due to
damage to the endothelial wall by low-grade infection.
✓ Excessive production of fluid as in secondary hydrocele.
✓ Interference with drainage of fluid by lymphatic vessels of the cord.
✓ Communication with the peritoneal cavity.

28
Hydrocele fluid is amber-coloured with specific gravity of 1.022 to 1.024.
It contains water, salts, albumin, fibrinogen. Per se, hydrocele fluid does not
clot, but if it comes in contact with the blood, fibrinogen gets activated and
clots firmly. Often fluid contains cholesterol and tyrosine crystals.
(a) communicating hydrocele, (b) non-communicating or scrotal hydrocele, (c)
funicular hydrocele, (d) encysted hydrocele or spermatic cord cyst, (e)
inguinoscrotal hydrocele and (f) abdominoscrotal hydrocele.
PRIMARY VAGINAL HYDROCELE
Occurs in middle-aged, common in tropical countries. Testis is not
palpable as it usually attains a large size (unlike secondary hydroceles which
are small, except in filarial hydrocele). Fluctuant (elicited by, fixing the
hydrocele with hand and feeling for the fluid movement using fingers placed
in two perpendicular directions). Can get above the swelling (you can feel
only cord structures and nothing else at the root of the scrotum, unlike in

29
hernia). Testicular sensation can be elicited in vaginal hydrocele by
transmitting the pressure sensation through the fluid.
Infantile Hydrocele
Here tunica and processus vaginalis (hydrocele) are distended up to
internal ring, but sac has no connection with the general peritoneal cavity.
Congenital Hydrocele
Processus vaginalis communicates with the peritoneal cavity. As this
communicating orifice is too small, bowel does not descend and so hernia
usually will not develop. While lying down, fluid disappears gradually and
while standing fluid recollects. Hydrocele cannot be emptied by digital
pressure as it causes “inverted ink bottle” effect. Ascites, tuberculous
peritonitis are the aetiologies for the same.
Encysted Hydrocele of the Cord
It is the fluid collection in a portion of patent funicular process part of
the tunica vaginalis; but closed above and below; located in
inguinal/inguinoscrotal/scrotal part which is fluctuant and transilluminant.

30
On gentle traction to the testis, the swelling becomes less mobile (traction
test).
Hydrocele-en-bisac (Bilocular Hydrocele)
Hydrocele has got two intercommunicating sacs, one above and one
below the neck of the scrotum. Upper one lies superficial or in the inguinal
canal or may insinuate itself between the muscle layers—cross-fluctuant.
Hydrocele of the Canal of the Nuck
It occurs in females, in relation to the round ligament, always in the
inguinal canal.
Hydrocele of the Hernial Sac
It is due to adhesions of the content of hernial sac. Fluid secreted
collects in the hernial sac and forms hydrocele of the hernial sac.

31
SECONDARY HYDROCELE
Causes
• Infection: Filariasis
• Tuberculosis of epididymis
• Syphilis
• Injury: Trauma, postherniorrhaphy hydrocele
• Malignancy
Secondary hydrocele rarely attains large size. It is usually small, lax and
testis is usually palpable (unlike primary hydrocele). Exception is, secondary
hydrocele due to filariasis. It can be very large.
Post herniorrhaphy Hydrocele
It is a secondary hydrocele occurring after the surgery for inguinal hernia. It
is due to the damage to lymphatic vessels of the tunica vaginalis and is 0.2%
common. It is treated like any hydrocele but usually after about 6 months

32
Filarial Hydrocele and Chylocele
Occurs commonly in coastal region, and in and around the equator. Usually
occurs after repeated attacks of filarial epididymitis. Hydrocele is usually of
large size and the sac is thickened. Fluid contains fat, rich in cholesterol, and
is derived from ruptured lymph varix into the tunica. It is often difficult to
differentiate from primary hydrocele.
Complications of hydrocele
✓ Infection
✓ Pyocele
✓ Haematocele
✓ Atrophy of testis, hernia of hydrocele (rare)
✓ Infertility
✓ Hernia of hydrocele sac (rare)
Differential diagnosis
➢ Inguinal hernia
➢ Epididymal cyst
➢ Spermatocele
➢ Testicular tumour
➢ Scrotal oedema

33
Role of Scrotal Ultrasound
Ultrasound of the scrotum can detect intra scrotal masses with a sensitivity
of nearly 100%. It plays a major role in the evaluation of scrotal masses
because of its accuracy of 98% to 100% in differentiating intra testicular and
extra testicular pathology. This distinction is important in patient
management because most extra testicular masses are malignant. All intra
testicular masses should be considered potentially malignant until
proven otherwise.
A direct contact scan is most commonly performed, but a water
bath approach may also be employed. The patient is examined in supine
position and 7.5 MHZ or 10 MHZ transuducer is commonly used
because it provides increased resolution of the scrotal contents.

34
Sonographically the normal testis has homogenous granular echotexture
composed of uniformly distributed medium level echoes. The tunica
albuginea is not usually visualized as separate structure. The septum of
testis may be seen as linear echogenic or hypoechoic structure. The
epididymis is normally iso echogenic or slightly more echogenic than
the testis.
Intra testicular cysts have sonographic characteristics of benign
simple cysts occurring in other organs. They are well defined, anechoic
lesions with thin, smooth walls and posterior acoustic enhancement.
Epidermoid cysts are generally well defined, solid hypoechoic masses.
The mass typically has an echogenic capsule. Testicular abscess
demonstrates, an enlarged testicle containing a predominantly fluid
filled mass with hypoechoic or mixed echogenic areas. Sonography
plays an important role in the evaluation of hydroceles. They are
characteristically anechoic collections with good sound to transmission
surrounding the anterolateral aspects of the testis. The fluid provides an
excellent acoustic window for imaging the testis, however to medium
level echoes from fibrin bodies or cholesterol crystals may occasionally

35
be visualized moving freely within a hydrocele. Both haematoceles and
pyoceles contain internal septations and loculations.
Treatment for Hydrocele
Surgery
✓ Tapping
✓ Lord’s plication
✓ Sub-total excision
✓ Partial excision and eversion (Jaboulay’s operation)
✓ Evacuation and eversion
✓ Sharma and Jhawer’s technique
✓ Total excision of sac
Procedure
Under G/A or spinal or L/A, after cleaning and draping, vertical
incision of about 6-8 cm in length is made over the scrotum, anteriorly 1 cm
lateral to the median raphe. Skin, dartos, external spermatic fascia, internal
spermatic fascia are incised. Bluish hydrocele sac is identified, i.e. parietal
layer of the tunica vaginalis of testis. Fluid is evacuated using trocar and
cannula. Sac is opened.

36
If the sac is small, thin and contains clear fluid, either Lord’s plication,
i.e. tunica is bunched into a “ruff” by placing series of multiple interrupted
chromic catgut sutures so as to make the sac to form fibrous tissue (It is
relatively avascular and so haematoma will not occur).
Or evacuation and eversion of the sac behind the testis (after eversion,
everted sac is sutured with chromic catgut by continuous sutures) is done.
If the sac is thick, in large hydrocele and chylocele, subtotal excision of
the sac is done (as tunica vaginalis is reflected on to the cord structures and
epididymis posteriorly, total excision leads to orchidectomy with division of
cord).
Often the sac is excised partially and then eversion is done, which is
called as Jabouley’s operation.
After evacuation, the sac with the testis is placed in a newly created
pocket between the fascial layers of the scrotum (Sharma and Jhawer’s
technique).

37
Aspiration must be avoided as much as possible as it is only a
temporary measure (recurrence occurs very early) and chances of
haematocele, infection are higher.
A drain is placed near the root of the scrotum on the lateral aspect
because it becomes the most dependent portion, when scrotal support is
given. Scrotal support is given to reduce the scrotal oedema. Wound is closed
in layers. Drain is removed in 48 hours.
Complications of surgery
➢ Reactionary haemorrhage
➢ Oedema
➢ Pain
➢ Infection
➢ Pyocele
➢ Sinus formation
➢ Recurrent hydrocele

38
AIM & OBJECTIVES
➢ To study the various clinical presentations of primary vaginal
hydrocele.
➢ To compare the efficacy of Sharma & Jhawer’s surgery Vs Lord’s
plication for small sized uncomplicated primary vaginal hydrocele
(<7cms)
➢ To compare the efficacy of Sharma & Jhawer’s surgery Vs Jaboulay’s
for medium sized uncomplicated primary vaginal hydrocele (>7cms
and <14cms)
➢ To assess postoperative complications, morbidity associated with the
above surgical procedures.
➢ To analyze the simplicity, expenditure & effectiveness of the three
procedures.

39
DESIGN OF STUDY
➢ Randomized prospective comparative Study
➢ Simple Randomization
➢ Sample Size
➢ Epi info software
➢ Time taken to revert back to normal taken as mean
➢ SD 1.7 and 1.36 for respective procedure
➢ Confidence interval 95% and Power 80%
➢ 23 rounder off to in each group
➢ Duration
➢ 2 Years (June 2016 to May 2018)

40
COMPARTMENTS OF THE STUDY
• The study was done in two compartments to assess the efficacy of
Sharma and Jhawer’s for both small and medium sized primary vaginal
hydrocele.
• Hydrocele size < 7cm diameter are considered as small sized hydrocele
and are included in compartment I.
• In compartment I, Sharma & Jhawer’s technique was compared with
the Lord’s Plication procedure for small sized hydrocele.
• Hydrocele size >7 cm and <14 cm diameter are considered as medium
sized hydrocele and are included in compartment II.
• In compartment II Sharma & Jhawer’s technique was compared with
Jaboulay’s procedure for medium sized hydrocele.
• Size measured using Vernier’s Caliper.

41
STATISTICAL ANALYSIS
• Data entered into Microsoft Excel (Windows 7; Version 2007)
• Analysis done using the Statistical Package for Social Sciences (SPSS)
for Windows software (trial version 22.0; SPSS Inc, Chicago)
• Descriptive statistics
– Mean and Standard Deviation (SD) for continuous variables
– Frequencies and percentages will be calculated for categorical
variable
• Comparison between groups analyzed using
– Chi square test of independence and Fischer’s test for
categorical variables
– Unpaired T test for quantitative variables
• Bar charts and Pie charts for visual representation of analysed data
• Level of significance set at 0.05

42
STUDY POPULATION
• All patients with primary vaginal hydrocele satisfying eligibility
criteria admitted for surgery in the surgical ward of Government Rajaji
hospital / Madurai Medical College during the study period of June
2016 to May 2018.

43
ELIGIBILITY CRITERIA
INCLUSION CRITERIA
✓ Solitary swelling in the scrotum incorporating the testis.
✓ The swelling should be positive for trans-illumination.
✓ It should be possible to get above the swelling at the root of scrotum.
✓ Hydrocele size < 7cm diameter are considered as small sized hydrocele
and are included in compartment I.
✓ Hydrocele size between 7 to 14 cm diameter are considered as medium
sized hydrocele and are included in compartment II.
✓ In a patient with bilateral hydrocele each hydrocele will be considered
as a separate case in this study.

44
ELIGIBILITY CRITERIA
EXCLUSION CRITERIA
✓ Swelling arising from the skin of scrotum.
✓ Solitary swelling in the scrotum which is separate from the testis.
✓ Diffuse swelling in the scrotum incorporating the testis but negative on
trans-illumination. (All secondary long standing complicated hydrocele
are ruled out of the study).
✓ Swelling in which there is associated impulse on coughing and
reducibility.

45
TYPES OF OPERATIONS TO BE STUDIED
• Lord’s Plication
• Jaboulay’s procedure
• Sharma and Jhawer’s technique

46
LORD’S PLICATION
Peter Herent Lord, FRCS, surgeon, High Wycombe, England and
Karger Verlaz, Basel, Switzerland evolved an operation in which there is
no direct mobilization of the tunica vaginalis. The hydrocele is entered
directly and plication is performed
An incision of one and half inches is made on the anterior aspect of
the scrotum avoiding the superficial vessels. The incision is extended
through the skin and dartos but not through the tunica vaginalis.
Hemostasis is secured through diathermy or by ligation. To further
control the oozing, the wound edges including all the tissues to the
tunica are grasped by Allis forceps. The hydrocele is then emptied by
incising the sac.
The testis is evaginated through the scrotal incision which results
in turning the sac inside out. Since the sac is not dissected from the
scrotal covering, the maneuver is bloodless. Using ‘00’ chromic catgut
with an atraumatic needle interrupted gathering or plication sutures
small bites being taken at 1cm intervals are inserted from the cut edges
of the sac to the junction of the epididymis and testis. Depending upon
the size of the hydrocele 8-10 such sutures are inserted in series. This

47
step pleats the sac obliterating the subcutaneous tissue between the
scrotal incision and opening in the tunica vaginalis.
Fig: Plication of tunica vaginalis.
JABOULAY’S OPERATION
In Jaboulay’s operation, we grasp scrotum firmly in one hand to stretch
scrotal skin. 6-10 cm incision made on anterior surface of scrotum over most
prominent part of hydrocoele, well away from testicle which lies postero
inferior.
Skin, dartos and thin cremasteric fascia are incised and reflected
together as a single layer from the underlying parietal layer of the tunica
vaginalis which is the outer wall of the hydrocoele.
When hydrocoele is well separated laterally and medially from overlying
layers, it is grasped with 2 Allis forceps and a trocar is inserted to aspirate the

48
fluid. With one finger inside the sac, we dissect it free from the overlying
scrotum so that spermatic cord and testicle with attached hydrocoele lie free
in operative field.
Hydrocele sac is then opened completely. Testicle is then carefully
inspected and palpated. Redundant wall sac is trimmed leaving a margin of
2cm. Great care must be taken with haemostasis. Sac is then everted behind
testis with interrupted suture.
Fig: Excision & Eversion of tunica vaginalis
49
SHARMA JHAWER’S TECHNIQUE
It has been quoted that tissue handling and dissection during
hydrocele operation proportionately increase oozing of blood from the
scrotal coverings with resultant tissue edema and hematoma formation.
Hence the minimal dissection was devised
STEPS:
The scrotum is scrubbed well and painted with spirit & betadine.
Incision:
The scrotum is held with its skin stretched by the assistant, 4cm
incision made avoiding subcutaneous vessels.
Evacuation of the sac:
The sac with all the fascial layers together is picked up with two
tissue forceps and emptied with a trocar and cannula. The same holes are
then extended on either side avoiding visible blood vessels. Through the
opening polar delivery of testis is done.

50
Creation of space in the scrotum:
To lodge the testis, with its sac back into the scrotum, a testis size
space is created between the scrotal subcutaneous layers outside and the
testicular fascial layers on the inside. This is easily done by introducing
the two index fingers to do blunt separation of tissues and make room
just enough to allow a tight fit of testis when reloaded in the scrotum.
Reloading of testis:
The testis with its everted sac is put back into the new space in the
scrotum very carefully.
Wound closed in layers:
After achieving complete haemostasis, wound is closed in layers with
3’0 chromic catgut.
Complications like hematoma and sepsis are remarkably low, sutures
are not used inside the scrotum thus saving on operation time and reducing
an infection factor hence reducing hospital stay.

51
Incision
Evacuation of Sac

52
Delivering the testis out
Creation of Sub dartos pouch

53
Reloading of testis in newly created pouch
Wound closed in layers

54
3rd Postoperative Day
5th Postoperative Day

55
POST OPERATIVE COMPLICATIONS
Mostly operations are successful and the patients recover soon and go
home. In certain number of instances, however complications develop.
The complication will prolong the stay in hospital. The complications
associated with these procedures are:
Pain: As the effect of the anaesthetic passes off the patient begins to
feel the post-operative pain of the operation. Faulty reposition of the testis
(torsion of testis) will cause agonizing pain. If the pain is persisting re-
exploration is indicated and the testis should be repositioned. If the testis
is totally infarcted it should be removed. Pain will also be present in
massive haematoma and in infected wound usually after 3 days. In a scale
of 0 to 10 in Visual Analog Scale, >5 is considered pain in our study.
Fever: The temperature is often 1 or 2 degrees, even after clean
surgery up to 3 days, this is aseptic traumatic fever. >99O F is considered
as fever in our study.

56
Haematoma: This is a common postoperative complication because of
following factors.
• Inadequate / imperfect haemostasis
• Oozing from small vessels
• In heavy spinal anaesthesia blood pressure falls. Hence bleeding
points are few. Though haemostasis is secured with care, after
the effect of anaesthesia is worn off, the blood vessels of the
testis which arise from the aorta directly, bleed profusely and
cause haematoma along with its complications.
• Testis is covered by loose scrotal layers
It is usually manifested with a sensation of pressure or pain in the
scrotum (Shortly after the anaesthetic affect wears off). Scrotum will be big
in size and firm in consistency. The haematoma can be prevented by
meticulous haemostasis and scrotal support. Drain can be used if tissue
dissection has been extensive. It will eventually be absorbed. Persisting
haematoma is treated with evacuation of the clot.

57
Skin Oedema:
It is due to abnormal increase in interstitial fluid following tissue
dissection and disruption of scrotal lymphatics, can be prevented by
careful dissection and gentle handling of tissues. Treatment consists of
scrotal support and anti-inflammatory drugs.
Infection:
Infection is a major cause of postoperative morbidity. The hallmark of
developing infection is fever usually associated with leucocytosis. An
increase in the pulse-rate occurs. The local signs of wound infection
consist of pain, swelling erythema and soaking of the dressing.
Stitch abscess: This is usually seen after 6th or 7th postoperative days.
It is localized suppuration in relation to one of the stitches, localised
blister will be formed. If the stitch is thick blood stained pus will come
out.

58
Superficial infection: The wound becomes red, swollen and the stiches
are buried in the oedematous skin. Treatment includes regular dressing of
wound and antibiotics.
Deep infection or disruption of wound: This is severe type of
infection involving all the layers of scrotum. The wound is gaped and the
testis is seen.
Treatment includes regular dressing of wound, debridement, antibiotics
and secondary suturing.
Infection can be prevented by shaving the scrotum and cleansing it
with savlon preoperatively and use of antibiotics.
59
END POINT
• The primary end point was once the testis returned back to normal size
• The secondary end points were hematoma, infection and wound
disruption.
• So the follow up period was different for every patient which varied
from 8 to 28 days

60
RESULTS OF I COMPARTMENT
• A total of 40 patients were included in the study COMPARTMENT I
with 20 in each surgical procedure.
• The follow up period ranged from 7 to 28 days
• There was no difference in baseline characteristics among the two
groups.
• The age of the study population ranged between 18-59 with a mean of
38.75 and standard deviation of 13.14.
• None of the cases had wound disruption .

61
15-25 26-35 36-45 46-55 >55
30%
5%
25%32.5%
7.5%
CHART 1: AGE DISTRIBUTION IN I COMPARTMENT (SJVLP)
AgricultureLaborers
Coolie Others
57.5%27.5%
15%
CHART 2: DISTRIBUTION OF OCCUPATION IN I COMPARTMENT

62
TABLE 1: DISTRIBUTION OF SOCIO-DEMOGRAPHIC
VARIABLES SJ V LP PROCEDURES
SOCIO-
DEMOGRAPHIC
VARIABLES
SHARMA
AND
JHAWAR
LORD’S
PLICATION
P VALUE
AGE (MEAN) 43.4 39.5 0.314
OCCUPATION
Agriculture
laborers
Coolie
Others
12(52.2%)
5(45.5%)
3(50%)
11(47.8%)
6(54.5%)
3(50%)
0.935
SOCIO-
ECONOMIC
STATUS
II
III
IV
V
3(43%)
3(43%)
8(57%)
6(50%)
4(57%)
4(57%)
7(43%)
6(50%)
0.903
II III IV V
17.5% 17.5%
35% 30%
CHART 3: DISTRIBUTION OF SOCIO-ECONOMIC STATUS IN I COMPARTMENT

63
Sharma andJhawar
Lord's Plication
60% 55%
25% 30%15% 15%
CHART 4: DISTRIBUTION OF OCCUPATION WITHIN PROCEDURES IN COMPARTMENT I
Agriculture Laborers Coolie Others
Sharma andJhawar
Lord's Plication
15% 20%15% 20%40% 30%
30% 30%
CHART 5: DISTRIBUTION OF SOCIOECONOMIC STATUS WITHIN PROCEDURES IN COMPARTMENT I
II III IV V

64
47%53%
CHART 6: SIDE DISTRIBUTION IN COMPARTMENT I
Right Left
Right Left
47.4% 52.6%
52.4% 47.6%
CHART 7: SIDE DISTRIBUTION WITHIN PROCEDURES IN COMPARTMENT I
Sharma and Jhawar Lord's Plication

65
Only swelling Only Pain Pain andSwelling
70%
17.5% 12.5%
CHART 8: DISTRIBUTION OF SYMPTOMS IN I COMPARTMENT
Sharma and Jhawar Lord's Plication
75% 65%
15% 10%10% 15%
CHART 9: SYMPTOMS WITHIN EACH PROCEDURE IN COMPARTMENT I
Only swelling Only Pain Pain and Swelling

66
0-6months
6m - 1year
1-3years
3-5years
5-10years
>10years
10%22.5%
35%
12.5%2.5%
17.5%
CHART 10: DISTRIBUTION OF DURATION OF ILLNESS IN I COMPARTMENT
Sharma andJhawar
Lord's Plication
75% 60%
5% 25%20% 15%
CHART 11: DURATION OF ILLNESS WITHIN PROCEDURES IN COMPARTMENT I
0-3 years 3-10 years >10 years

67
TABLE 2: CLINICAL PROFILE AMONG PATIENTS IN BOTH THE
PROCEDURES (SJ VS LP)
CLINICAL
PROFILE
SHARMA
AND
JHAWAR
LORD’S
PLICATION
P VALUE
SIDE
RIGHT
LEFT
9(47.4%)
11(52.4%)
10(50%)
10(50%)
0.752
SYMPTOMS
ONLY
SWELLING
ONLY PAIN
SWELLING AND
PAIN
15(53.6%)
3(43%)
2(40%)
13(46.4%)
4(57%)
3(60%)
0.784
DURATION OF
ILLNESS
6MONTHS –
3YEARS
4YR – 6YR
>6YR
15(55.6%)
1(16.7%)
4(57%)
12(44.4%)
5(83.3%)
3(43%)
0.208

68
Sharma andJhawar
Lord's Plication
0%
15%
CHART 12: PERCENTAGE OF HAEMATOMA IN BOTH PROCEDURES IN COMPARTMENT I
Sharma andJhawar
Lord's Plication
0%
20%
CHART 13: PERCENTAGE OF SCROTAL EDEMA IN BOTH PROCEDURES IN COMPARTMENT I

69
Sharma andJhawar
Lord's Plication
10%20%
CHART 14: PERCENTAGE OF PAIN IN BOTH THE PROCEDURES IN COMPARTMENT I
Sharma andJhawar
Lord's Plication
5%10%
CHART 15: PERCENTAGE OF FEVER IN BOTH THE PROCEDURES IN COMPARTMENT I

70
TABLE 3: COMPLICATIONS IN I COMPARTMENT
COMPLICATIONS SHARMA
AND
JHAWAR
LORD’S
PLICATION
P VALUE
HAEMATOMA
PRESENT
ABSENT
0(0%)
20(55.6%)
4(100%)
16(44.4%)
0.035
SCROTAL
EDEMA
PRESENT
ABSENT
0(0%)
20(55.6%)
4(100%)
16(44.4%)
0.035
PAIN
PRESENT
ABSENT
2(33.3%)
18(53%)
4(66.7%)
16(47%)
0.376
FEVER
PRESENT
ABSENT
1(33.3%)
19(51.4%)
2(66.7%)
18(48.6%)
0.548
Haematoma Scrotaledema
Pain Fever
0% 0%
10%5%
15%20% 20%
10%
CHART 16: COMPLICATIONS IN BOTH PROCEDURES IN COMPARTMENT I
Sharma and Jhawar Lord's Plication

71
TABLE 4: OUTCOME MEASURES IN I
COMPARTMENT
OUTCOME
MEASURES
SHARMA AND
JHAWAR
MEAN(SD)
LORD’S
PLICATION
MEAN(SD)
P VALUE
TIME TAKEN
FOR
SCROTUM TO
REVERT TO
NORMAL (IN
DAYS)
3.8(0.89)
6.25(1.68)
<0.001
DURATION OF
SURGERY
19.25(1.55) 25.2(1.15) <0.001

72
RESULTS II COMPARTMENT
• Sharma Jhawer’s Vs Jaboulay’s (II compartment).
• A total of 40 patients were included in the study compartment-II with
20 in each surgical procedure.
• The follow up period ranged from 7 to 28 days.
• There was no difference in baseline characteristics among the two
groups (SJ vs Jab).
• The age of the study population ranged between 18-58 with a mean of
39.38 and standard deviation of 9.6.
• None of the cases had wound disruption.

73
15-25 26-35 36-45 46-55 >55
10%20%
42.5%
22.5%5%
CHART 17: AGE DISTRIBUTION IN II COMPARTMENT (SJ VS JAB)
Agriculturelaborers
Coolie Others
55%27.5% 17.5%
CHART 18: OCCUPATION DISTRIBUTION IN II COMPARTMENT (SJ VS JAB)

74
II III IV V
10%22.50%
40%27.50%
CHART 19:SOCIOECONOMIC STATUS DISTRIBUTION IN II COMPARTMENT (SJ VS JAB)
Sharma and Jhawar Jaboulays
60% 50%
25% 30%
15% 20%
CHART 20: OCCUPATION DISTRIBUTION WITHIN PROCEDURES IN II COMPARTMENT
Agriculture laborers Coolie Others
75
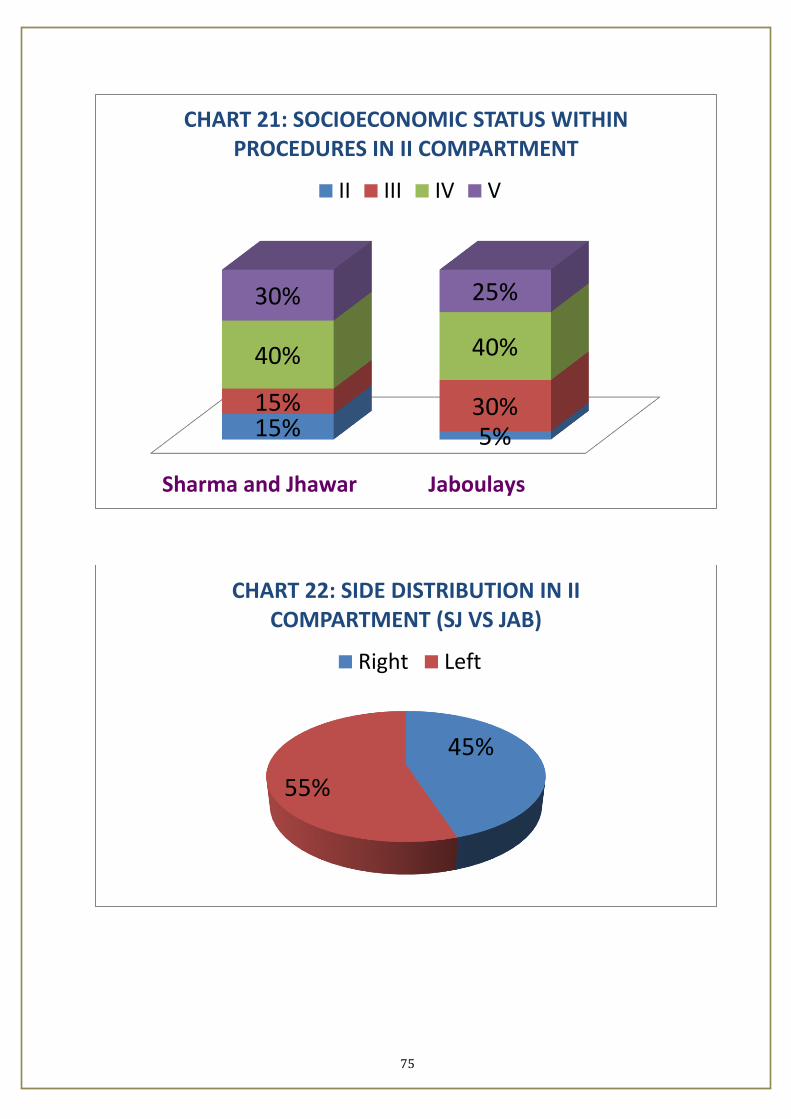
Sharma and Jhawar Jaboulays
15% 5%
15% 30%
40% 40%
30% 25%
CHART 21: SOCIOECONOMIC STATUS WITHIN PROCEDURES IN II COMPARTMENT
II III IV V
45%
55%
CHART 22: SIDE DISTRIBUTION IN II COMPARTMENT (SJ VS JAB)
Right Left

76
Only swelling Only pain Pain andSwelling
72.50%
17.50% 10%
CHART 23: SYMPTOMS AMONG THE PATIENTS IN II COMPARTMENT (SJ VS JAB)
0-6months
6m-1year
1-3years
3-6years
6-10years
>10years
5% 2.50%12.5%
32.5%40%
7.5%
CHART 24: DURATION OF ILLNESS IN II COMPARTMENT

77
TABLE 5 : CLINICAL PROFILE AMONG PATIENTS IN
BOTH THE PROCEDURES (SJ VS JAB)
CLINICAL
PROFILE
SHARMA AND
JHAWAR
JABOULAYS P VALUE
SIDE
Right
Left
11(55%)
9(45%)
11(55%)
9(45%)
1.000
SYMPTOMS
Only Swelling
Only Pain
Swelling And
Pain
15(75%)
3(15%)
2(10%)
14(70%)
4(20%)
2(10%)
0.915
DURATION OF
ILLNESS
6months – 3years
4yr – 6yr
>6yr
5(62.5%)
12(41.4%)
3(100%)
3(37.5%)
17(58.6%)
0(0.0%)
0.113

78
Sharma andJhawar
Jaboulays
55% 55%
45% 45%
CHART 25: SIDE DISTRIBUTION WITHIN PROCEDURES IN II COMPARTMENT
Right Left
Sharma and Jhawar Jaboulays
75% 70%
15% 20%10% 10%
CHART 26: SYMPTOMS WITHIN PROCEDURES IN II COMPARTMENT
Only swelling Only pain Pain and Swelling

79
Sharma andJhawar
Jaboulays
25% 15%
60% 85%15% 0%
CHART 27: DURATION OF ILLNESS WITHIN PROCEDURES IN II COMPARTMENT
0-3 years 3-10 years >10 years
Sharma andJhawar
Jaboulays
0%
20%
CHART 28: PERCENTAGE OF HAEMATOMA IN BOTH PROCEDURES (SJ VS JAB)

80
Sharma and Jhawar Jaboulays
0%
25%
CHART 29: PERCENTAGE OF SCROTAL EDEMA IN BOTH PROCEDURES (SJ VS JAB)
Sharma andJhawar
Jaboulays
15%30%
CHART 30: PERCENTAGE OF PAIN IN BOTH PROCEDURES (SJ VS JAB)
81
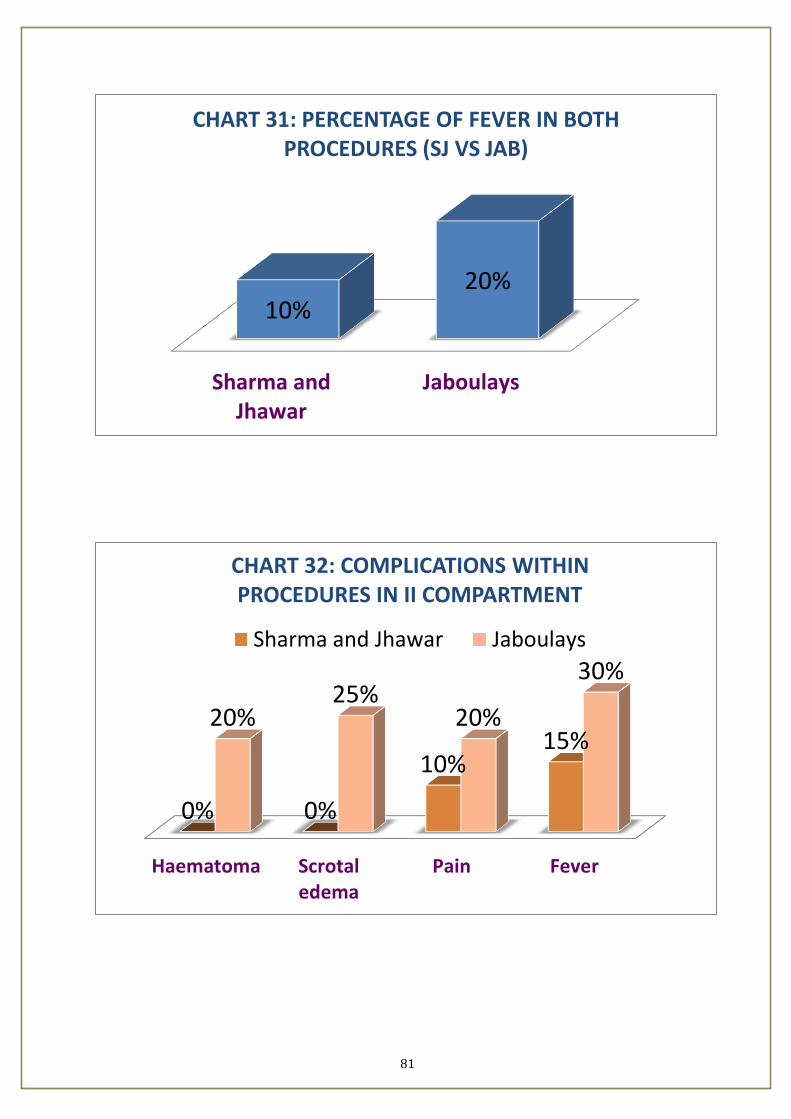
Sharma andJhawar
Jaboulays
10%20%
CHART 31: PERCENTAGE OF FEVER IN BOTH PROCEDURES (SJ VS JAB)
Haematoma Scrotaledema
Pain Fever
0% 0%
10%15%
20%25%
20%
30%
CHART 32: COMPLICATIONS WITHIN PROCEDURES IN II COMPARTMENT
Sharma and Jhawar Jaboulays

82
TABLE 6: COMPLICATIONS IN II COMPARTMENT
COMPLICATIONS SHARMA AND
JHAWAR
JABOULAYS P VALUE
HAEMATOMA
PRESENT
ABSENT
0
20(55.6%)
4(100%)
16(44.4%)
0.035
SCROTAL
EDEMA
PRESENT
ABSENT
0(0%)
20(57%)
5(100%)
15(43%)
0.017
PAIN
PRESENT
ABSENT
3(33.3%)
17(55%)
6(66.7%)
14(45%)
0.256
FEVER
PRESENT
ABSENT
2(33.3%)
18(53%)
4(66.7%)
16(47%)
0.376

83
TABLE 7: OUTCOME MEASURES IN II
COMPARTMENT
OUTCOME
MEASURES
SHARMA AND
JHAWAR
JABOULAYS P VALUE
TIME TAKEN
FOR
SCROTUM TO
REVERT TO
NORMAL (IN
DAYS)
3.8(0.89)
11.1(2.1)
<0.001
DURATION
OF SURGERY
19.2(1.55) 31.1(1.34) <0.001

84
DISCUSSION
To study which among the surgical procedures available for primary
vaginal hydrocele has the least morbidity and most beneficial for the patient,
in our study we have compared the popularly used Lord’s plication with
Sharma Jhawer’s operation for small sized uncomplicated primary vaginal
hydrocele and Jaboulay’s operation with Sharma Jhawer’s operation for
medium sized uncomplicated primary vaginal hydroceles in two separate
compartments.
The study was done in two compartments in the patients satisfying the
eligibility criteria to assess the efficacy of Sharma and Jhawer’s for both
small and medium sized hydrocele. Hydrocele size < 7cms diameter are
considered as small sized hydrocele and are included in compartment I. In
compartment I Sharma & Jhawer’s technique was compared with the Lord’s
Plication procedure for small sized hydrocele. Hydrocele size between 7 to
14 cms diameter are considered as medium sized hydrocele and are included
in compartment II. In compartment II Sharma & Jhawer’s technique was
compared with Jaboulay’s procedure for medium sized hydrocele. Size
measured using Vernier’s Caliper.

85
In both compartments patients were allocated in either of the two arms
in each compartment by simple randomization technique and were surgically
intervened after prior consent, pre-op evaluation and anaesthesia assessment.
Patients were followed up for post-operative complications and return
of testis to normal size. The primary end point was once the testis returned
back to normal size. The secondary end points were hematoma, infection and
wound disruption. So, the follow up period was different for every patient. It
varied from 8 to 28 days in both compartments.
In compartment I, 40 patients who satisfied the eligibility criteria with
swelling less than 7cm in size were included. Of which 20 were included in
the Sharma and Jhawer’s(SJ) arm and another 20 were included in the Lord’s
plication(LP) arm.
On analysing the socio demographic variables in compartment I,
(Table: 1, Chart:1,2,3,4,5) mean age of patients in SJ arm is 43.4 and LP arm
is 39.5. 57.5% of patients in compartment I were agricultural laborers, 27.5%
coolies and 15% other occupation. 65% of patients in compartment I

86
belonged to lower and lower middle class. In compartment I there was no
significant difference in the base line characteristics in the two arms.
On analysing the clinical profile in compartment I, (Table: 2, Chart:
6,7,8,9,10,11), 53% had swelling pain the right side, 47% in the left side.
70% of the patients had complaints of only swelling, 17.5% had only pain,
12.5% had both pain and swelling. 80% patients had complaints less than 5
years’ duration.
On analysing the mean time taken for duration of surgery in
compartment I (Table: 4), it took 19.25 minutes in SJ arm and 25.2 minutes
in LP arm. Time taken for Sharma and Jhawer’s procedure is less than the
time taken for Lord’s plication which was statistically significant.
On analysing the post-operative complications in compartment I
(Table: 3, Chart: 12,13,14,15,16) the SJ arm had less post-operative
haematoma and oedema than the LP arm which was again statistically
significant (p value < 0.05). SJ arm also had less pain and fever though it was
not statistically significant (p value >0.05).

87
On analysing the time taken for scrotum to revert to normal size in
compartment I (Table: 4), mean time for SJ arm was 3.8 days and mean time
for LP arm was 6.25 days. Hence SJ arm had less time for scrotum to revert
to normal size when compared with LP arm which again was statistically
significant (p value < 0.05).
In compartment II, 40 patients who satisfied the eligibility criteria with
swelling more than 7cm and less than 14 cm in size were included. Of which
20 were included in the Sharma and Jhawer’s(SJ) arm and another 20 were
included in the Jaboulay’s procedure(Jab) arm.
On analysing the socio demographic variables in compartment II,
(Chart:17,18,19,20,21,22) mean age of patients in SJ arm is 43.6 and Jab arm
is 40.8. 55% of patients in compartment II were agricultural laborers, 27.5%
coolies and 17.5% other occupation. 67.5% of patients in compartment II
belonged to lower and lower middle class. In compartment II there was no
significant difference in the base line characteristics in the two arms.
On analysing the clinical profile in compartment II, (Table: 5, Chart:
22,23,24,25,26,27), 55% had swelling pain the right side, 45% in the left

88
side. 72.5% of the patients had complaints of only swelling, 17.5% had only
pain, 10% had both pain and swelling. 52.5% patients had complaints less
than 5 years duration.
On analysing the mean time taken for duration of surgery in
compartment II (Table: 4), it took 19.2 minutes in SJ arm and 31.1 minutes in
Jab arm. Time taken for Sharma and Jhawer’s procedure is less than the time
taken for Jaboulay’s procedure which was statistically significant. (p value <
0.05)
On analysing the post-operative complications in compartment II
(Table: 6, Chart: 28,29,30,31,32) the SJ arm had less post-operative
haematoma and oedema than the Jab arm which was again statistically
significant (p value < 0.05). SJ arm also had less pain and fever though it was
not statistically significant (p value >0.05).
On analysing the time taken for scrotum to revert to normal size in
compartment II (Table: 7), mean time for SJ arm was 3.8 days and mean time
for Jab arm was 11 days. Hence SJ arm had less time for scrotum to revert to

89
normal size when compared with Jab arm which again was statistically
significant (p value < 0.05).
Analysing the results of compartment I, we conclude that in treating
small uncomplicated primary vaginal hydrocele (hydrocele size < 7cms)
Sharma and Jhawer’s minimal dissection technique has statistically
significant less operative time and statistically significant less post-operative
complications (haematoma and oedema) and also has less time for scrotum to
revert to normal size which is again statistically significant when compared
with Lord’s plication.
Analysing the results of compartment II, we conclude that in treating
medium sized uncomplicated primary vaginal hydrocele (hydrocele size
>7cms and <14 cms) Sharma and Jhawer’s minimal dissection technique has
statistically significant less operative time and statistically significant less
post-operative complications (haematoma and oedema) and also has less time
for scrotum to revert to normal size which is again statistically significant
when compared with Jaboulay’s procedure.

90
CONCLUSION
➢ Between the three procedures analyzed, in our setting Sharma and
Jhawer’s minimal dissection technique had statistically significant
✓ lesser complications
✓ lesser time to revert back to normal and
✓ cost effective
than Lord’s plication for small sized primary vaginal hydrocele
and Jaboulay’s operation for medium sized primary vaginal
hydrocele.
➢ Hence Sharma Jhawer’s is the most beneficial for the patient and
with least complications for treating small and medium sized
primary vaginal hydrocele.
➢ Further multi centric randomized trials and meta-analysis are
needed to emphasize the significance of the results in our study.

91
BIBLIOGRAPHY
[1] Ku JH, et al. The excisional placation and internal drainage
techniques: A comparison of results for idiopathic hydrocele. BJU Ent
2001; 87(1): 82-84.
[2] Albercht W, Hohl. The best operation for hydrocele? Br. J Urol
1991;68(2):187-9.
[3] Shah PA, et al. Ambulatory hydrocele surgery – a review of 50 cases.
Jr Coll Surg Edinb 1992; 37(6): 385-6.
[4] Dunaeuskii Iaz, Gorokhov. A comparative evaluation of surgical
methods for treating hydrocele. Urol (Mosk) 1990; 1: 59-62.
[5] Singh DR, Gupta SK, Gupta S, Lord‟s procedure a curative outpatient
operation for primary hydrocele. J Indian Med. Assoc 1996; 94(4):141-2
[6] Sharma LS, Jhawar PK. Surgery of hydrocele (A simplified minimal
dissection technique). Ind J Surg 1979; 41: 700-704.

92
[7] Chalasani V, Woo HH. Why not use a small incision to treat large
hydroceles. ANZ Surg 2002; 72(8): 594-5.
[8] Christopher G Fowler. Hydrocele, Bailey and Love, short practice of
surgery 25th ed, India: Edward Arnold ltd; 2008. p.1381-1382.
[9] Parviz K. Kavoussi, Raymond A. Costabile. Hydrocelectomy,
Campbell walsh urology 10th ed,. United States of America: Elsevier
Saunders; 2012.p.1009-1010. 105
[10] Margaret Farquharson, Brenden Moran. Farquharson‟s textbook of
operative general surgery. 9th ed, India: Edward Arnold; 2005.p. 474.
[11] Tanga et al., 1973, "Abdomino scrotal hydrocele-Shoffhotes of Rare
of obscure Cases, British Journal Surgery. 60: 834-836.
[12] Andrews E.W., 1907, "The bottle operation method for the radical
cure of hydrocele", Annals of Surgery. 46: 915
[13] Solomon A.A., 1955, "The extrusion operation for Hydrocele", N.Y,
State Journal of Medicine. 55: 1885.

93
[14] Lord P.H., 1970, "A bloodless operation for spermatocele or cyst of
the epididymis", British Journal of Surgery. 57(9): 641-544.
[15] Singh DR, Gupta SK, Gupta Saroj, Lord's procedure - A curative
outpatients operation for primary hydrocele, J.Indian Med. Association
1996, April, Vol. 94, NO. 4, 141-2.
[16] Lord H Peter. "A bloodless operation for the radical cure of
Idiopathichydrocele", British Journal of Surgery, 1964 Dec, Vol. 51,NO.
12: 914-16
[17] Johstone J.M.S, Hargreave T.B, "Male Urethra and Genital
organs", Edited by R.F. Rintoul. Farquharson's Text Book of
Operative Surgery, Churchill Living stone 8th Edn. 1995; 672-683.
[18]Guyton, Arthur C, "The lymphatic system, interstitial fluid
dynamics edema and pulmonary fluid" Chapter 31 in Textbook of
Medical Physiology, Philadelphia, 1986, 366-7.

94
[19]Role of filariasis in the etiology of Idiopathic Hydrocele, I.J.S 44,
161- 66, March 1982.
[20]Hamilton Bailey & McNeil Love, Arnold Publishers’ Short
Practice of Surgery, 24th
edition, 1407-9.
[21]H. Kimleyeryl, David C. Sabiston, W.B. Sounders publication
Sabiston Text Book of Surgery, 16th edition, 1499-1500.
[22]Wendy Cowler Hurser, Seymour L. Schwartz, Flanc Spencer, G.
Tom Shires, McGraw-Hill Publishers’ Schwartz Principles of
Surgery, 7th edition, 1761.
[23]Park John Evert, "Lympahtic filariasis", Ch. 5 in Parks Textbook
of preventive and social medicine, Calcutta, 2000: 199-203.
[24]Belokar W.K. et.al. : A simple eversion operation for radical cure of
large scrotal hydrocele; I.J.S., July 1979; Vol. 41, 414-17.
[25]Jhawar P.K. & Sharma L.S. : Surgery of Hydrocele- A Simplified
minimal dissection technique, I.J.S., Dec. 1979; Vol. 41, 700-4.
95
PROFORMA(ANNEXURE I)
A) PARTICULARS OF THE PATIENT:
Name : IP No.:
Age : D.O.A:
Sex : D.O.S:
Occupation: D.O.D:
Religion :
Address :
B) PRESENTING SYMPTOMS:
a) Swelling Duration Uni/Bilateral
b) Mode of Onset Right/Left
c) Trauma
d) Fever
e) Pain
f) Progress
g) Difficulty in micturition

96
h) Other Symptoms
C) PAST HISTORY
a. Any operative procedures
b. Co morbidities
c. Urinary tract infection
d. Suggestive of T.B:
e. STD
D) FAMILY HISTORY
a. Married/Single
b. Children
c. Any other members with similar complaints
E) PERSONAL HISTORY
a. Food Habits
b. Micturition
c. Bowel Habits
d. Sleep
e. Smoking
f. Alcohol
g. Tobacco

97
F) SOCIO ECONOMIC STATUS
G) GENERAL AND PHYSICAL EXAMINATION
a. Pulse
b. BP
c. Anaemia
d. Oedema
e. Lymphadenopathy
f. Cyanosis
g. Others
H) LOCAL EXAMINATION
a. Scrotal Swelling
b. Side
c. Size
d. Skin
e. Impulse on coughing
f. Consistency
g. Fluctuation
h. Get above the swelling
i. Trans illumination

98
j. Testis and cord structures
k. Lymph nodes PR:
I) SYSTEMIC EXAMINATION
a. CVS
b. RS
c. CNS
d. P/A
J) INVESTIGATIONS
a. Routine Blood Investigations
b. B G & T
c. BT & CT
d. Urine Investigations
e. USG Scrotum
K) DIAGNOSIS\
L) ANAESTHESIA ASSESMENT
M) OPERATION DONE
a) Sharma & Jhawer’s
b) Lord’s Plication

99
c) Jaboulay’s Operation
N) INTRA OPERATIVE TIME
O) COMPLICATIONS
a) Fever
b) Pain
c) Oedema
d) Haematoma
e) Wound Infection
P) FOLLOW UP
Q) TIME FOR SCROTUM TO REVERT BACK TO NORMAL SIZE

100
CONSENT(ANNEXURE II)
I_______ Hosp No _______ in my full senses hereby give my
complete for _______________ or any other procedure deemed fit
which is a diagnostic/therapeutic/procedure/biopsy/transfusion/operation
to be performed on me/my/son/daughter/ward _________ age
_________ under any anaesthesia deemed fit. The nature and risks involved
in the procedure have been explained to me in my own language to my
satisfaction. For academic and scientific purpose, the operation/procedure be
television or photographed, or used for statistical measurements.
Date:
Signature/Thumb Impression/ of Patient/Guardian
Name:
Designation:
Guardian
Relationship
Full Address

101
ANNEXURE III

102
ANNEXURE IV
103
CERTIFICATE – II
This is to certify that this dissertation work titled
RANDOMISED PROSPECTIVE COMPARATIVE STUDY ON THE
EFFICACY OF SHARMA JHAWER’S OPERATION WITH LORD’S
PLICATION AND JABOULEY’S OPERATION IN THE TREATMENT OF
PRIMARY VAGINAL HYDROCELE of the candidate Dr. JOYNER
ABRAHAM M with registration number 221611112 for the award of
MASTER DEGREE in the branch of GENERAL SURGERY. I have personally
verified the urkund.com website for plagiarism check. I found that the uploaded
thesis file contains all from introduction to conclusion pages and result shows
ZERO percentage of plagiarism in the dissertation
Guide and Supervisor Sign with Seal

MASTER CHART SJ VS JAB
S No AGE SIDE SYMPTOMS OCCUPATION SESDURATION
OF ILLNESS
DURATION
OF ILLNESS
1 40 left only swelling agriculture laborers 4 5 0-6m
2 42 right only swelling coolie 4 7 6m-1y
3 45 left only pain agriculture laborers 3 8 5y-10y
4 36 left only swelling agriculture laborers 4 4 3y-5y
5 38 left only pain agriculture laborers 5 2 1y-3y
6 46 left only pain coolie 5 6 5y-10y
7 47 right only swelling coolie 5 12 >10y
8 50 right only swelling agriculture laborers 2 8 5y-10y
9 52 left only swelling coolie 5 14 >10y
10 28 left only swelling others 5 4 3y-5y
11 56 left only swelling others 4 3 1y-3y
12 58 left only swelling agriculture laborers 4 6 5y-10y
13 45 right both swelling and pain others 4 4 3y-5y
14 42 right both swelling and pain agriculture laborers 5 5 3y-5y
15 48 right only swelling agriculture laborers 3 11 >10y
16 51 right only swelling agriculture laborers 3 9 5y-10y
17 18 left only swelling agriculture laborers 4 5 3y-5y
18 21 right only swelling agriculture laborers 4 6 5y-10y
19 24 left only swelling agriculture laborers 2 4 0-6m
20 18 right only swelling coolie 2 5 3y-5y
21 29 right only swelling agriculture laborers 3 3 3y-5y
22 30 left only swelling agriculture laborers 4 6 5y-10y
23 31 left only swelling coolie 4 9 5y-10y
24 32 right only pain coolie 3 6 5y-10y
25 33 right only pain coolie 3 4 3y-5y
26 34 right only pain others 4 3 3y-5y
27 35 left only swelling others 5 6 3y-5y
28 36 left only swelling agriculture laborers 5 8 5y-10y
29 37 left only swelling others 5 6 5y-10y
30 38 right only swelling agriculture laborers 5 3 3y-5y
31 39 left both swelling and pain others 3 3 3y-5y
32 40 right both swelling and pain agriculture laborers 3 2 1y-3y
33 41 left only swelling agriculture laborers 4 1 1y-3y
34 42 left only swelling agriculture laborers 4 9 5y-10y
35 43 right only pain coolie 5 7 5y-10y
36 44 left only swelling agriculture laborers 4 5 5y-10y
37 45 right only swelling agriculture laborers 4 3 3y-5y
38 46 left only swelling coolie 3 8 5y-10y
39 47 left only swelling coolie 2 2 1y-3y
40 48 right only swelling agriculture laborers 4 8 5y-10y

MASTER CHART SJ VS JAB
S NoDURATION OF
SURGERYHAEMATOMA FEVER
SCROTAL
EDEMAPAIN
TIME TO
REVERT
PROCEDURE
DONE
1 21 absent absent absent absent 4 sj
2 20 absent absent absent absent 4 sj
3 20 absent absent absent absent 5 sj
4 18 absent absent absent absent 3 sj
5 17 absent absent absent absent 4 sj
6 16 absent absent absent absent 3 sj
7 20 absent absent absent absent 6 sj
8 20 absent absent absent absent 4 sj
9 21 absent absent absent absent 4 sj
10 18 absent absent absent absent 5 sj
11 19 absent absent absent absent 4 sj
12 20 absent absent absent absent 5 sj
13 20 absent absent absent absent 3 sj
14 22 absent absent absent absent 3 sj
15 20 absent absent absent absent 4 sj
16 17 absent present absent present 3 sj
17 18 absent present absent present 3 sj
18 20 absent absent absent present 3 sj
19 20 absent absent absent absent 3 sj
20 18 absent absent absent absent 3 sj
21 30 present present present present 7 jab
22 32 present present present present 12 jab
23 31 absent present present present 11 jab
24 31 present present present present 10 jab
25 32 present absent present present 10 jab
26 34 absent absent absent present 12 jab
27 30 absent absent absent absent 10 jab
28 30 absent absent absent absent 9 jab
29 30 absent absent absent absent 8 jab
30 32 absent absent absent absent 8 jab
31 33 absent absent absent absent 10 jab
32 32 absent absent absent absent 11 jab
33 31 absent absent absent absent 12 jab
34 30 absent absent absent absent 14 jab
35 30 absent absent absent absent 16 jab
36 30 absent absent absent absent 12 jab
37 31 absent absent absent absent 13 jab
38 34 absent absent absent absent 13 jab
39 30 absent absent absent absent 13 jab
40 30 absent absent absent absent 12 jab

MASTER CHART SJ VS LP
S No AGE SIDE SYMPTOMS OCCUPATION SESDURATION OF
ILLNESSDURATION OF ILLNESS
1 51 right only swelling agriculture laborers 3 11 >10y
2 18 left only swelling agriculture laborers 4 5 0-6m
3 59 right only swelling agriculture laborers 4 8 6y-10y
4 25 left only swelling agriculture laborers 2 8 6m-1y
5 18 right only swelling coolie 2 7 6m-1y
6 40 left only swelling agriculture laborers 4 11 >10y
7 42 right only swelling coolie 4 12 >10y
8 45 left only pain agriculture laborers 3 5 0-6m
9 36 left only swelling agriculture laborers 4 3 6m-1y
10 38 left only pain agriculture laborers 5 2 6m-1y
11 46 left only pain coolie 5 5 6m-1y
12 47 right only swelling coolie 5 9 6m-1y
13 50 right only swelling agriculture laborers 2 2 1y-3y
14 52 left only swelling coolie 5 2 0-6m
15 53 left only swelling others 5 3 0-6m
16 56 left only swelling others 4 2 1y-3y
17 58 left only swelling agriculture laborers 4 12 >10y
18 45 right both pain and swelling others 4 2 1y-3y
19 42 right both pain and swelling agriculture laborers 5 2 1y-3y
20 48 right only swelling agriculture laborers 3 8 6m-1y
21 46 right only swelling agriculture laborers 3 2 1y-3y
22 25 left only swelling agriculture laborers 3 1 1y-3y
23 35 left only swelling coolie 4 12 >10y
24 42 right only swelling coolie 4 4 3y-6y
25 45 left only pain coolie 5 5 3y-6y
26 52 right only pain others 5 8 6m-1y
27 55 right only pain others 5 2 1y-3y
28 48 left only swelling agriculture laborers 5 2 1y-3y
29 19 right both pain and swelling agriculture laborers 4 10 1y-3y
30 52 left only swelling others 4 3 1y-3y
31 22 left only swelling agriculture laborers 2 14 >10y
32 47 right only swelling coolie 2 2 1y-3y
33 45 left both pain and swelling coolie 4 1 1y-3y
34 22 right only swelling coolie 5 8 6m-1y
35 48 right only swelling agriculture laborers 4 1 1y-3y
36 24 left both pain and swelling agriculture laborers 5 2 1y-3y
37 25 left only swelling agriculture laborers 2 12 >10y
38 49 right only swelling agriculture laborers 3 4 3y-6y
39 36 right only swelling agriculture laborers 2 5 3y-6y
40 54 left only pain agriculture laborers 3 3 3y-6y

MASTER CHART SJ VS LP
S NoDURATION OF
SURGERYHAEMATOMA FEVER
SCROTAL
EDEMAPAIN
TIME TO
REVERT
PROCEDURE
DONE
1 17 absent absent absent present 3 sj
2 18 absent present absent present 3 sj
3 20 absent absent absent absent 3 sj
4 20 absent absent absent absent 3 sj
5 18 absent absent absent absent 3 sj
6 21 absent absent absent absent 4 sj
7 20 absent absent absent absent 4 sj
8 20 absent absent absent absent 5 sj
9 18 absent absent absent absent 3 sj
10 17 absent absent absent absent 4 sj
11 16 absent absent absent absent 3 sj
12 20 absent absent absent absent 6 sj
13 20 absent absent absent absent 4 sj
14 21 absent absent absent absent 4 sj
15 18 absent absent absent absent 5 sj
16 19 absent absent absent absent 4 sj
17 20 absent absent absent absent 5 sj
18 20 absent absent absent absent 3 sj
19 22 absent absent absent absent 3 sj
20 20 absent absent absent absent 4 sj
21 25 absent present present present 3 lp
22 26 present absent present present 8 lp
23 26 present absent absent present 6 lp
24 24 present absent present present 5 lp
25 24 present absent present absent 6 lp
26 25 absent present absent absent 5 lp
27 23 absent absent absent absent 6 lp
28 26 absent absent absent absent 8 lp
29 28 absent absent absent absent 8 lp
30 25 absent absent absent absent 3 lp
31 27 absent absent absent absent 8 lp
32 25 absent absent absent absent 7 lp
33 25 absent absent absent absent 6 lp
34 26 absent absent absent absent 7 lp
35 25 absent absent absent absent 7 lp
36 26 absent absent absent absent 8 lp
37 25 absent absent absent absent 7 lp
38 25 absent absent absent absent 7 lp
39 24 absent absent absent absent 7 lp
40 24 absent absent absent absent 3 lp




















