Urinary melatonin levels in human breast cancer patients
14
[. Neura~ Tran~misskgrr 52, 281-294 {1981) ./ourno/of lg~ ~.a.sm/ss/on by Springer-Verlag 1981 Urinary Melatonin Levels in Human Breast Cancer Patients ~" C. Bartsch 1' **' ***, Hella Bartsch 1' **' ***, A. K.Jain 2, K. R. Laumas 2' 3, and L, Wetterberg 4 1 Department of Biochemistry, All India Institute of Medical Sciences, New Delhi, India 2 Department of Reproductive Biology, All India Institute of Medical Sciences, New Delhi, India 3 At present Instituto de Ciencias Biomedicas, Universidad Autonoma de CD Juarez, CD Juarez, Mexico 4 Karolinska Institute, Department of Psychiatry, St. G6ran's Hospital, Stockholm, Sweden With 2 Figures Received June 20, 1981 Summary Urinary melatonin levels were measured in 10 postmenopausal Indian women suffering from advanced stages of breast cancer and in 9 well- matched women with non-endocrine complaints, mostly uterovaginal prolapse. Urines of each patient were collected over a period of 2-3 days in four 4-hourly intervals from 6 a.m. to 10p.m. and one 8-hourly interval from 10 p.m. to 6 a.m. * Part of this work was presented at the second colloquium of the European Pineal Study Group, Gietgen, July 1-5, 1981. ** This work was carried out by us as scholars of the Society of Servants of God, India, under the "Cancer Research" programme of the Society. Throughout this study we received guidance and directions from Dr. Dinshah K. Mehta, who is the Chair- man of the Society of Servants of God and the All India Nature Cure Foundation Trust, founded by Mahatma Gandhi. Dr. D. K. Mehta, among other things, is the Founder of modern Naturopathy in India. He was also personal physician to Mahatma Gandhi. *~ At present: Physiologisch-chemisches Institut, Universit~it Tiibingen, Tfibingen, Federal Republic of Germany. 0300-9564/81/0052/0281/$ 02.80
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Urinary melatonin levels in human breast cancer patients

[. Neura~ Tran~misskgrr 52, 281-294 {1981) ./ourno/of l g ~ ~.a.sm/ss/on �9 by Springer-Verlag 1981
Urinary Melatonin Levels in Human Breast Cancer Patients ~"
C. B a r t s c h 1' **' ***, Hella Bartsch 1' **' ***, A. K . J a i n 2, K. R. L a u m a s 2' 3, and L, Wetterberg 4
1 Department of Biochemistry, All India Institute of Medical Sciences, New Delhi, India
2 Department of Reproductive Biology, All India Institute of Medical Sciences, New Delhi, India
3 At present Instituto de Ciencias Biomedicas, Universidad Autonoma de CD Juarez, CD Juarez, Mexico
4 Karolinska Institute, Department of Psychiatry, St. G6ran's Hospital, Stockholm, Sweden
With 2 Figures
Received June 20, 1981
S u m m a r y
Urinary melatonin levels were measured in 10 postmenopausal Indian women suffering from advanced stages o f breast cancer and in 9 well- matched women with non-endocrine complaints, mostly uterovaginal prolapse.
Urines o f each patient were collected over a period o f 2 - 3 days in four 4-hourly intervals from 6 a.m. to 10p.m. and one 8-hourly interval from 10 p.m. to 6 a.m.
* Part of this work was presented at the second colloquium of the European Pineal Study Group, Gietgen, July 1-5, 1981.
** This work was carried out by us as scholars of the Society of Servants of God, India, under the "Cancer Research" programme of the Society. Throughout this study we received guidance and directions from Dr. Dinshah K. Mehta, who is the Chair- man of the Society of Servants of God and the All India Nature Cure Foundation Trust, founded by Mahatma Gandhi. Dr. D. K. Mehta, among other things, is the Founder of modern Naturopathy in India. He was also personal physician to Mahatma Gandhi.
*~ At present: Physiologisch-chemisches Institut, Universit~it Tiibingen, Tfibingen, Federal Republic of Germany.
0300 -9564 /81 /0052 /0281 /$ 02.80

282 C. Bartsch, Hella Bartsch, A.K.Jain, K. R. Laumas, and L. Wetterberg:
Serum LH, FSH, prolactin, estradiol and cortisol levels at 11a.m. were determined as well as estrogen and progesterone receptors of the breast tumors.
It was found that 24 hour urinary melatonin excretion in cancer patients was on the average 31% decreased as compared to the controls. This change was accompanied by a 33% increase in serum cortisol levels in the cancer patients, The melatonin excretion patterns of the cancer patients were not synchronized as compared to synchronized patterns of the controls. The number of tumors tested for steroid receptors does not yet allow to conclude if melatonin is different in patients with or without hormone-dependent tumors.
The data suggest that pineal melatonin secretion may be modified in quantity as well as rhythmicity in breast cancer patients.
Introduction
A number of publications deals with the treatment of human (Hofitdtter, 1959; Lenti et al., 1954; Starr, 1970) and experimental cancers (Engel, 1935; Engel and Bergmann, 1952; Engd and Fischl, 1954; Buswell, 1975; El-Domeiri and Das Gupta, 1973; Anisimov et al., 1973) with pineal substances and extracts. The functional relationship be- tween the pineal gland and cancer is well summarized in the review article of Lapin (1976), while many more data have since been obtained (Dilman et al., 1979; Lapin and Ebds, 1981).
It has been maintained that this gland exerts fundamental control over the endocrine system (Mess et al., 1979) as well as the immune (Rella and Lapin, 1976) and the nervous system (Romijn, 1978). Reciprocally, the pineal gland is affected by both, exogenous factors, particularly light (Reiter, 1978), and a number of endogenous factors, namely several hormones (Cardinali and Vacas, 1976) and sympathetic nervous inputs (Ueck, 1979). We concluded that the pineal gland is also likely to affect development and growth of malig- nant tumors. We regard a malignant tumor as a disintegrative process that went out of the control of the central nervous, endocrine and immune system. This process is antagonistic to the integrative func- tion of the pineal gland.
After having formulated this hypothesis we designed experi- ments to investigate the link between the pineal gland and cancer, both from the therapeutic and the analytical angle. For our initial studies we started working with melatonin since this is the best docu- mented hormone of the pineal, although others are under investiga- tion, such as arginine vasotocin (Pavel, 1978), certain pteridines (Ebds, 1980) and gonad-inhibiting substances (Reiter, 1977).

Urinary Melatonin Levels in Human Breast Canter Patients 283
In our therapeutic approach we found that melatonin can show a stimulating as well as an inhibiting effect on experimental tumors, depending on the time of administration (H. and C. Bartsch, submit- ted for publication).
In the analytical approach we initially determined the urinary melatonin levels in 2 female cancer patients (cancer of breast and gall bladder) and 2 healthy controls by the method described by LyncJ~ et al. (1975), using the antibody of Levine and Riceberg (1975), generously provided to us. In this study we found normal day/night urinary melatonin rhythms in the healthy women, whereas melatonin could not be detected in the 2 cancer patients (C. and H. Bartsch, unpub- lished results).
We then determined the urinary melatonin levels in a greater number of patients suffering from breast cancer and non-malignant complaints as described in the present paper. Breast cancer was chosen because of its high frequency in many parts of the world and because the mechanisms involved in its growth are relatively well- known (Namer and Lalanne, 1976). In order to examine whether melatonin is involved in the control of either hormone-dependent or independent tumors or both, melatonin along with pituitary and ovarian hormone levels as well as those of sex-steroid receptors in the malignant breast tissue were determined.
In 1978, Cohen et al. published a hypothesis about the role of melatonin in the aetiology of breast cancer, which was based upon statistical material showing that increased pineal calcification is accompanied by a high incidence of breast cancer. They concluded that calcification leads to decreased pineal function, which causes an increased pituitary-mediated ovarian steroid production stimulating malignant growth in the breast. In the subsequent discussion, oppos- ing views were expressed stating that breast cancer may be stimulated by increased prolactin secretion due to pineal hyperactivity (Tapp, 1978). This view was supported by a study on DMBA-induced mammary tumors in rats stating that melatonin administration leads to a higher yield of malignant tumors (Hamilton, 1969). However, according to Reiter (1977), pineal calcification may not at all indicate malfunctioning of the pineal gland, but rather be a measure for past pineal activity.
Wetterberg et al. (1979 a) reported higher levels of urinary mela- tonin in healthy American women than in Japanese women, indicat- ing that the high incidence of breast cancer in American women may be related to high melatonin levels as compared to Japanese women showing a low breast cancer incidence.
In relation to other pineal substances, Russian authors reported

284 C. Bartsch, Hella Bartsch, A.K.Jain, K.R. Laumas, and L. Wetterberg:
decreased urinary excret ion o f a pineal gonad-inhibi t ing substance in breast cancer patients, indicating a decreased pineal activity (Ostrou- mova, 1972).
We hope that this study may help in elucidating the role o fme la - ton in in human breast cancer.
Materials and Methods
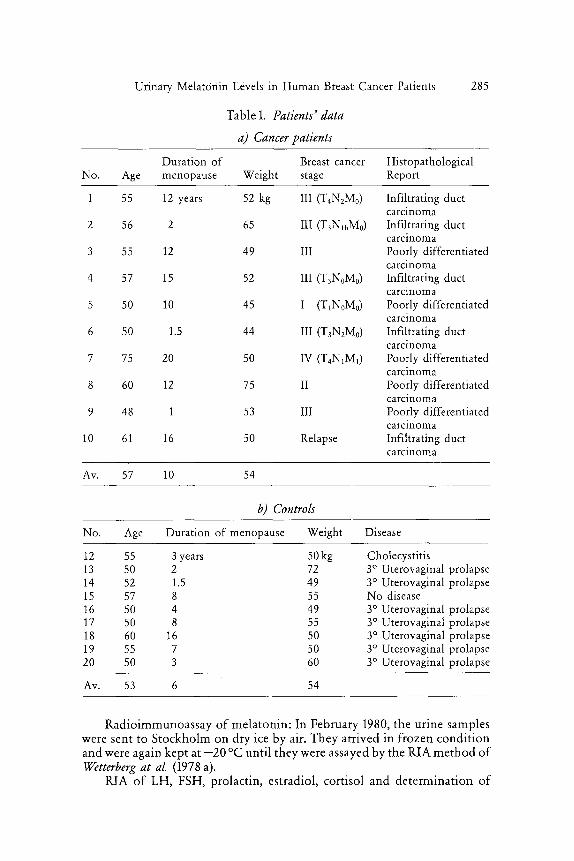
Cancer patients and controls were hospitalized at either the All India Institute of Medical Sciences (AIIMS) or Safdarjang Hospital, New Delhi, India. They came from different parts of Northern India and had all reached menopause. This age-group was selected to avoid changes in melatonin due to different phases of the menstrual cycle (Wetterber& eta[., 1976). All women were vegetarians. Their diets mainly consisted of rice and/or wheat, pulses, vegetables, fruits, milk and milk products, and eggs in some cases. Nine out of the ten cancer patients were fresh cases awaiting treatment. One patient (no. 10) had a relapse after her tumor had been removed and she had received chemo- and radiotherapy 6-12 months ago. The presence of a malignant tumor was always confirmed by biopsy. The clinical stages were assessed by the treating doctors. The data of the cancer patients are given in Table 1 a. The controls were awaiting surgical treatment for uterovaginal prolapse in 7 cases and removal of the gall bladder due to chotecystitic complaints in one case. Patient 15 was not hospitalized for medical reasons but attended to her mother, patient 7, and was staying with her in the ward throughout the study. Data of the controls are given in Table lb.
The treatment of all patients consisted of multivitamin and iron tablets. In a few cases low doses of antibiotics were given.
Samples were collected within the period of one month, lasting from mid-December to mid-January 1979/1980, to avoid seasonal variations in melatonin secretion (drendt et al., 1977). The sun rose around 7 a.m. and set around 6 p.m. The patients were lying in shaded rooms. Lights were turned offbetween 10 p.m. and 6 a.m., thus the light/dark cycle was 16/8 hours. The environmental temperature was 15-20 ~
Urine was collected in dark wide-mouth bottles without adding any preservative during the day at four 4-hourly intervals between 6 a.m. and 10 p.m. and during the night from 10 p.m. to 6 a.m. at one 8-hourly interval. Immediately at the end of each collection the sample was taken to the laboratory, measured and 4 ml were filled into a screw cap bottle, which was code-labelled and frozen at - 2 0 ~ The remaining urine was kept in a cold room and was later pooled with the other samples for 24 hours creatinine determination. Urine was collected overa period of 2 -3 days before opera- tion.
Blood was usually collected on the second day of urine collection around 11a.m. The serum was stored at --70 ~ till RIAs were carried out.
Tumor tissues were collected during the operation in an ice-containing cooling-box and immediately taken to the laboratory for steroid receptor assay.
Urinary Melatonin Levels in Human Breast Cancer Patients
Table 1. Patients" data
a) Cancer patients
285
Duration of Breast cancer Histopathological No. Age menopause Weight stage Report
1 55 12 years 52 kg III (T4N2M0)
2 56 2 65 III (T3NlbM0)
3 55 12 49 III
4 57 15 52 III (T3NoM0)
5 50 10 45 I (TxNoM0)
6 50 1.5 44 III (T3N2M0)
7 75 20 50 IV (TaNxM1)
8 6O 12 75 II
9 48 1 53 III
10 61 16 50 Relapse
Infiltrating duct carcinoma Infiltrating duct carcinoma Poorly differentiated carcinoma Infiltrating duct carcinoma Poorly differentiated carcinoma Infiltrating duct carcinoma Poorly differentiated carcinoma Poorly differentiated carcinoma Poorly differentiated carcinoma Infiltrating duct carcinoma
Av. 57 10 54
b) Controls
No. Age Duration of menopause Weight Disease
12 55 3 years 50 kg Cholecystitis 13 50 2 72 3 ~ Uterovaginal prolapse 14 52 1.5 49 3 ~ Uterovaginal prolapse 15 57 8 55 No disease 16 50 4 49 3 ~ Uterovaginal prolapse 17 50 8 55 3 ~ Uterovaginal prolapse 18 60 16 50 3 ~ Uterovaginal prolapse 19 55 7 50 3 ~ Uterovaginal prolapse 20 50 3 60 3 ~ Uterovaginal prolapse
Av. 53 6 54
Radioimmunoassay of melatonin: In February 1980, the urine samples were sent to Stockholm on dry ice by air. They arrived in frozen condit ion and were again kept at - 2 0 ~ unti l they were assayed by the RIA method of Wetterberg at al. (1978 a).
RIA of LH, FSH, prolactin, estradiol, cortisol and determinat ion of
286 C. Bartsch, Hella Bartsch, A.K.Jain, K.R. Laumas, and L.Wetterberg:
estrogen and progesterone receptor levels in the malignant breast tissues were carried out in the Department of Reproductive Biology, AIIMS, according to the methods established in this department Orba et al., 1978; Singb et al., 1978; Verma et al., 1978).
Results
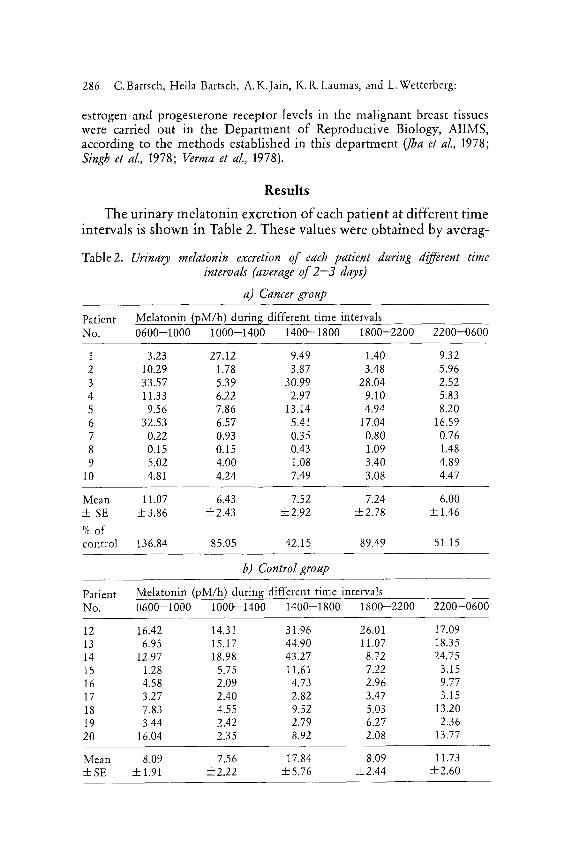
The u r i na ry m e l a t o n i n exc re t ion o f each p a t i e n t at d i f f e ren t t ime in terva ls is s h o w n in Table 2. These va lues were o b t a i n e d by averag-
Table2. Urinary melatonin excretion of each patient during different time intervals (average of 2--3 days)
a) Cancer group
Patient Melatonin (pM/h) during different time intervals No. 0600-1000 1000-1400 1400--1800 1800-2200 2200-0600
1 3.23 27.12 9.49 1.40 9.32 2 10.29 1.78 3.87 3.48 5.96 3 33.57 5.39 30.99 28.04 2.52 4 11.33 6.22 2.97 9.10 5.83 5 9.56 7.86 13.14 4.94 8.20 6 32.53 6.57 5.41 17.04 16.59 7 0.22 0.93 0.35 0.80 0.76 8 0.15 0.15 0.43 1.09 1.48 9 5.02 4.00 1.08 3.40 4.89
10 4.81 4.24 7.49 3.08 4.47
Mean 11.07 6.43 7.52 7.24 6.00 + SE 4-3.86 4-2.43 4-2.92 4-2.78 4-1.46
% of control 136.84 85,05 42.15 8%49 51.15
b) Control group
Patient Melatonin (pM/h) during different time intervals No. 0600-1000 1000-1400 i400-1800 1800-2200 2200--0600
12 16.42 14.31 31.96 26.01 17.09 13 6.95 15.17 44.90 11.07 18.35 14 12.97 18.98 43.27 8.72 24.75 15 1.28 5.75 11.61 7.22 3.15 16 4.58 2.09 4.73 2.96 9.77 17 3.27 2.40 2.82 3.47 3.15 18 7.83 4.55 9.52 5.03 13.20 19 3.44 2.42 2.79 6.27 2.36 20 16.04 2.35 8.92 2.08 13.77
Mean 8.09 7.56 17.84 8.09 11.73 • +1.91 4-2.22 4-5.76 _-/-2.44 _4-2.60
Urinary M e l a t o n i n Levels in H u m a n Breast Cancer Patients &
, / / :.~1 ,,,/
!1 :
lt .. ' Z-" i
8
o •
, , i~J
~ . . . "'~-... ~,.. A II t'~ '~- .... ~ " - ~ , ~ ' ~ i/~-"-:
g
/ - - - " - - - - - - . . "~ . . /~ ' , ' ; / ' , ~; / ) i
, : ' r""~'-~ ('~. ~ t '~:~.~.._. %, F' 'I
, $ g o
v
K
~8
287
288 C. Bartsch, Hella Bartsch, A.K.Jain, K.R. Laumas, and L. Wetterberg:
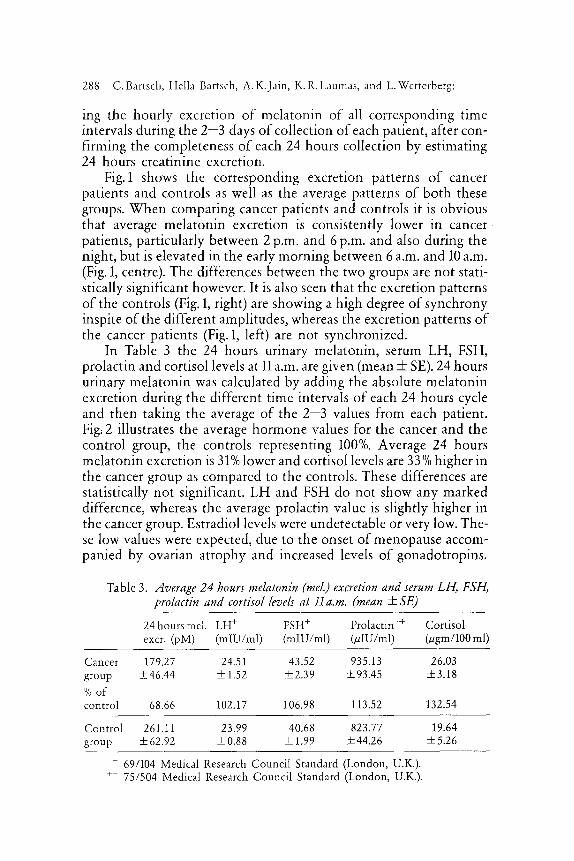
ing the hourly excretion of melatonin of all corresponding time intervals during the 2 -3 days of collection of each patient, after con- firming the completeness of each 24 hours collection by estimating 24 hours creatinine excretion.
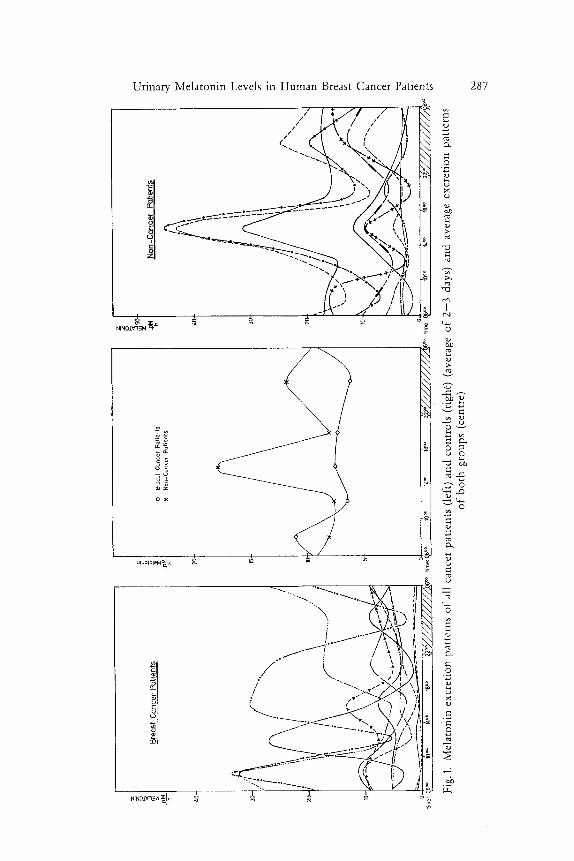
Fig. 1 shows the corresponding excretion patterns of cancer patients and controls as well as the average patterns of both these groups. When comparing cancer patients and controls it is obvious that average melatonin excretion is consistently lower in cancer patients, particularly between 2 p.m. and 6 p.m. and also during the night, but is elevated in the early morning between 6 a.m. and 10 a.m. (Fig. 1, centre). The differences between the two groups are not stati- stically significant however. It is also seen that the excretion patterns of the controls (Fig. 1, right) are showing a high degree of synchrony inspire of the different amplitudes, whereas the excretion patterns of the cancer patients (Fig. 1, left) are not synchronized.
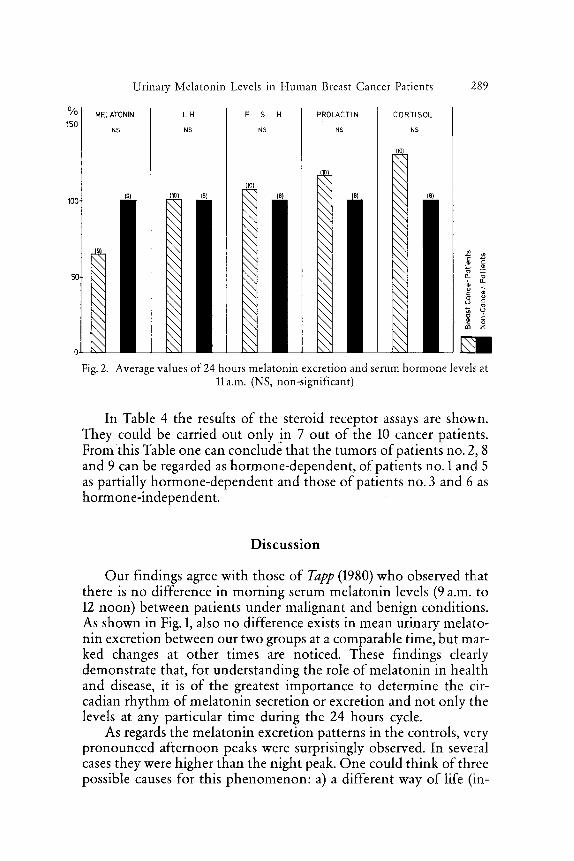
In Table 3 the 24 hours urinary melatonin, serum LH, FSH, prolactin and cortisol levels at 11 a.m. are given (mean + SE). 24 hours urinary melatonin was calculated by adding the absolute melatonin excretion during the different time intervals of each 24 hours cycle and then taking the average of the 2 -3 values from each patient. Fig: 2 illustrates the average hormone values for the cancer and the control group, the controls representing 100%. Average 24 hours melatonin excretion is 31% lower and cortisol levels are 33% higher in the cancer group as compared to the controls. These differences are statistically not significant. LH and FSH do not show any marked difference, whereas the average prolactin value is slightly higher in the cancer group. Estradiol levels were undetectable or very low. The- se low values were expected, due to the onset of menopause accom- panied by ovarian atrophy and increased levels of gonadotropins.
Table 3. Average 24 hours melatonin (reeL) excretion and serum LH, FSH, prolactin and cortisol levels at l l a.m. (mean + SE)
24 hours mel. LH + FSH + Prolactin ++ Cortisol excr, (pM) (mIU/mI) (mIU/ml) O~IU/ml) ~gm/100 ml)
Cancer 179.27 24.51 43,52 935.13 26.03 group ++_46.44 +1.52 _+2.39 ___93.45 ___3.18 % of control 68.66 102.17 106.98 113.52 132.54
Control 261.11 23.99 40.68 823.77 19.64 group +62.92 • +1.99 ___44.26 +5.26
+ 69/104 Medical Research Council Standard (London, U.K.). ++ 75/504 Medical Research Council Standard (London, U.K.).
% 150
100
Urinary Melatonin Levels in Human Breast Cancer Patients 289
MELATONIN
NS
\ \ \ \ \ \ \ \ \ \ \ \ \ \ \ \ \ \ \ \ \ \
(9)
LH
NS
(!e) \ \ \ \ \ - \ \ \ \ \ \ \ \ \ \ X \ \ . \ \ \ \ \ \ \ \ \ \ \ \ X \ \ \ \ \ \ \ X \
F S H
NS
x x \ x \ x x x \ \
N \
\ \
N \
\ \ N \
\ . \ r , , . , N \
b . N
PROLACTIN CORTISOL
NS NS
\ \
N \ \ \ \ \ \ \ \ \
\ \
\ \ \ \ \ \ "q \ \
x \ X X .~ ~ "-
\ \
\ \ \ \ o , \ \ \ -~ 8
m z \ \ \ \ \ \
\ \ \ N
Fig. 2. Average values of 24 hours melatonin excretion and serum hormone levels at 11a.m. (NS, non-significant)
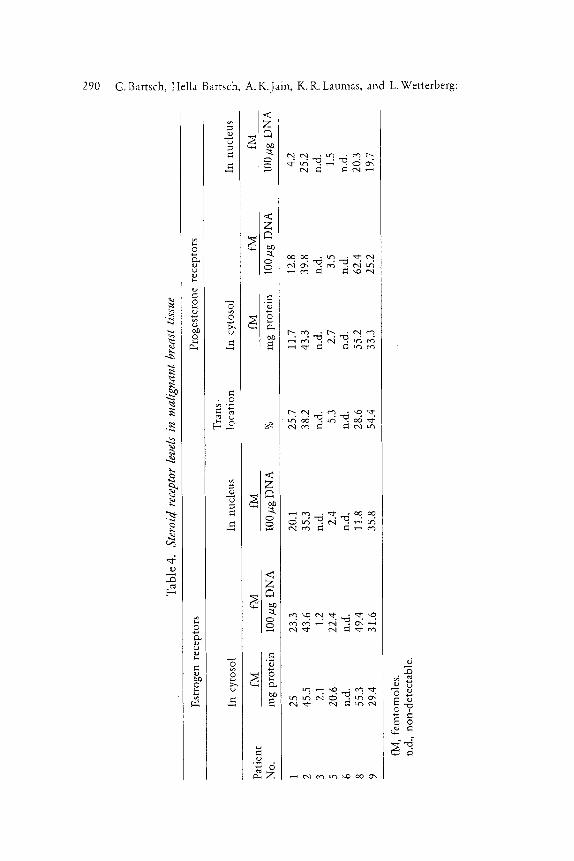
In Table 4 the results of the steroid receptor assays are shown. They could be carried out only in 7 out of the 10 cancer patients. From this Table one can conclude that the tumors of patients no. 2, 8 and 9 can be regarded as hormone-dependent, of patients no. 1 and 5 as partially hormone-dependent and those of patients no. 3 and 6 as hormone-independent.
Discuss ion
Our findings agree with those of Tapp (1980) who observed that there is no difference in morning serum melatonin levels (9 a.m. to 12 noon) between patients under malignant and benign conditions. As shown in Fig. 1, also no difference exists in mean urinary melato- nin excretion between our two groups at a comparable time, but mar- ked changes at other times are noticed. These findings clearly demonstrate that, for understanding the role of melatonin in health and disease, it is o f the greatest importance to determine the cir- cadian rhythm of melatonin secretion or excretion and not only the levels at any particular time during the 24 hours cycle.
As regards the melatonin excretion patterns in the controls, very pronounced afternoon peaks were surprisingly observed. In several cases they were higher than the night peak. One could think of three possible causes for this phenomenon: a) a different way of life (in-
290 C. Bartsch, Hella Bartsch, A.K.Jain, K.R. Laumas, and L.Wetterberg:
P,
O3
O
wa
"-d
r
"-8
~ o
e-
z
Z
N0
O
Z
c ~
t"xl ~ ~ e q ,,-.-~
Urinary Melatonin Levels in Human Breast Cancer Patients 291
cluding afternoon naps in shaded rooms, a common feature in India); b) different lighting conditions in India; and c) different ethnic groups. In studies on women from Japan, the United States and Sweden such pronounced afternoon peaks have not been report- ed (Wetterberg et al., 1978 b and 1979 a), neither in healthy males from Sweden (/]kerstedt et al., 1979), although the same assay for urinary melatonin was used in all of these studies (Wetterberg et al., 1978 a). Investigations are now in progress to find an explanation for this phenomenon.
The marked elevation of serum cortisol in the absence of marked changes of the mfiasured pituitary hormones in the cancer group may indicate the involvement of the adrenal cortex in breast cancer. We do not think that the cancer patients had elevated levels due to the circumstance that they were awaiting operation and therefore had developed stress, since the same did apply to the controls. We are rather of the opinion that the adrenal cortex may be actively involved in the hormonal dysregulation of an organism bearing a malignant tumor. Moreover, decreased melatonin levels have been associated with increased adrenal steroid production in mental depression (Wetterberg et al., 1979 b).
Due to the small number of tumors assayed for steroid receptors it is not yet possible to draw any definite conclusion whether melato- nin levelsare different in patients with hormone-dependent and/or hormone-independent tumors as compared to non-cancer controls.
Conclusion
This study, as part of a project on the link between the pineal gland and cancer, is an attempt to understand the role of melatonin in breast cancer. It has given some clues, underlining the possibility that modified rhythms of pineal melatonin production are involved in breast cancer. It will however be necessary to add many more data in a multi-disciplinary study, including more hormonal parameters and still more standardized conditions, preferably those present in a sleep-laboratory. The normal values of melatonin are to be well- defined under various diets, activities and lighting patterns in dif- ferent ethnic groups.
There remains much to be done to properly understand the func- tional relationship between the pineal gland and cancer, but we feel certain that the pineal, in its central role as master gland or at least as a central neuroendocrine transducer, may play an important role in cancer, although the correlations may be quite subtle and intricate as
20 Journal of Neural Transmission 52/4
292 C. Bartsch, HeRa Bartseb, A.K.Jain, K. R. [.aumas, and L. Wettcrberg:
indicated in this study. Further investigations in this area may lead to a better understanding of the canc6r problem and to its solution.
Acknowledgements
We would like to thank Prof. G. P. Talwar, Head of the Department of Biochemistry, AIIMS, New Delhi, India, for generously providing facilities and advice for this study.
We thank Dr. N. C. Madan, Associate Professor of Surgery, AIIMS, and Dr. M. Rahman, Senior Cancer Surgeon, Safdarjang Hospital, New Delhi, as well as the Departments of Gynaecology of AIIMS and Safdarjang Hospital for permitting us to collect urine and blood samples as well as tumor tissue from their patients and for providing us with the patients' data.
We are also thankful to Dr. Goel, Department of Clinical Chemistry, AIIMS, for determining urinary creatinine, and to Prof. Ramachandran, Department of Biostatistics, AIIMS, for statistical evaluation of our data.
References
•kerstedt, T., FrOberg, J. E., Friberg, Y., Wetterberg~ L.: Melatonin excretion, body temperature and subjective arousal during 64 hours of sleep deprivation. Psychoneuroendocrinol. 4, 219-225 (1979).
Anisimov, V.N., Morozov, V. G., K,~avinson, V. Kb., Dilman, V.M.: Correla- tion of anti-tumor activity of pi,aeal and hypothalamic extract, melato- nin and sygethin in mouse transplantable mammary tumors. Vopr. Onkol. 19, 99-101 (1973).
Arendt, J., Wirz-Justice, A., Bradtke, J.: Annual rhythm of serum melatonin in man. Neuroscience Letters 7, 327-330 (1977).
Bartscb, H., Bartscb, C.: Effect of melatonin on experimental tumors under different photoperiods and times of administration. J. Neural Transm. 52, 269-279 (1981).
Buswell, R. S.: The pineal and neoplasia. Lancet/, 34-35 (1975). Cardinali, D.P., Vacas, M.I.: Mechanisms underlying hormone effects on
pineal function: a model for the study of integrative neuroendocrine processes. J. Endocrinol. Invest. I, 89-96 (1976).
Cohen, M., Lippman, M., Cbabner, B.: Role of pineal gland in aetiology and treatment of breast cancer. Lancet II, 814--816 (1978).
Dilman, V. M., Anisimov, V. N., Ostroumova, M. N., Morozov, V. G., Khavin- son, V. Kh., Azarova, M.A.: Study of the anti-tumor effect of poly- peptide pineal extract. Oncology 36, 274-280 (1979).
Ebels, L: A survey of the location, isolation and identification of indoles, pteridines and some unknown active substances in sheep pineals. The possible significance of pteridines for the neuroendocrine control of neoplastic growth. J. Neural Transm. 49, 87--105 (1980).

Urinary Melatonin Levels in Human Breast Cancer Patients 293
El-Domeiri, A. /1. H., Das Gupta, T. K.: Reversal by melatonin of the effect of pinealectomy on tumor growth. Cancer Res. 33, 2830-2833 (1973).
Engel, P.: Wachstumsbeeinflussende Hormone und Tumorwachstum. Z. Krebsforsch. 4/, 488-496 (1935).
Engel, P., Bergrnann, W.: Die physiologische Funktion der Zirbeldriise und ihre therapeutische Anwendung. Z. Vitamin-, Hormon- und Ferment- forsch. 4, 564--594 (1952).
Engel, P., Fischl, S.: {3bet die Wirkung von Zirbeldriisenextrakten auf Benzo- pyrentumoren. Z. Vitamin-, Hormon- und Fermentforsch. 6, 259-268 (1954).
Hamilton, T.: Influence of environmental light and melatonin upon mammary tumor induction. Brit. J. Surg. 56, 764-766 (1969).
Hofitdtter, R.: Versuche der postoperativen Krebsbehandlung mit Zirbelstof- fen. Krebsarzt I4, 307-316 (1959).
Jha, p.,Jain, /i. K., Rahman, S./1., Dugwekar, Y. G., Laumas, K. R.: Serum LH, FSH, progesterone and estradiol-17fl levels of normally menstruating Indian women. Indian J. Med. Res. 67, 57-65 (1978).
Lapin, V.: Pineal gland and malignancy. Z. Onkologie 3, 51-60 (1976). Lapin, V., Ebels, L: The role of the pineal gland in the neuroendocrine control
mechanisms of neoplastic growth.J. Neural Transm. 50, 275-282 (1981). Lenti, G., Molinatti, G.M., Pizzini, A., Beccaria, G. B.: Clinical, biochemical
and hormonal studies on actions of pineal body extract in patients with neoplasms. Minerva Med. 45, 1-8 (1954).
Levine, L,, Riceberg, L.J.: Radioimmunoassay for melatonin. Res. Comm. Chem. Path. Pharm. 10, 693-702 (1975).
Lynch, H. f , Wurtman, R.J., Moskowitz, M. /1., Archer, M. C., Ho, M. K.: Daily rhythm in human urinary melatonin. Science 187, 169-171 (1975).
Mess, B., Trentini, G. P., Ruzsas, C., De Gaetani, C. E: Some endocrine effects of the pineal gland and melatonin with special reference to reproduc- tion. Prog. Brain Res. 52, 329-340 (1979).
Namer, M., Lalanne, C.M. (eds.): Hormones and breast cancer. (INSERM, Colloque 55.) 1976.
Ostroumova, M.N.: Decreased excretion of antigonadotropic factor in patients with cancer of the uterus and breast. Vopr. Onkol. I& 38--42 (1972).
Pavel, S.: Arginine vasotocin as pineal hormone.J. Neural Transm., Suppl. 13, 135-155. Wien-New York: Springer. 1978.
Reiter, R. f : Mini review: Pineal antigonadotropic substances: polypeptides and indoles. Life Sci. 21, 159-172 (1977).
Reiter, R.J.: Interaction of photoperiod, pineal and seasonal reproduction as exemplified by findings in the hamster. Prog. Reprod. Biol. 4, 169-190 (1978).
Rella, W., Lapin, V..: Immunocompetence of pinealectomized and simulta- neously pinealectomized and thymectomized rats. Oncology 33, 3--6 (1976).
Romijn, H.J.: Minireview: The pineal, a tranquillizing organ? Life Sci. 23, 2257--2274 (1978).
Singh, P., Chattopadhyay, T., Kapur, M.M., Laumas, K.R.: Cytosol and
20*

294 C. Bartsch et al.: Urinary Melatonin Levels in Human Breast
nuclear estradiol receptors in normal and cancerous breast tissue of women. Indian J. Med. Res. 68, 97-106 (1978).
Starr, K. W.: Growth and new growth: environmental carcinogens in the process of human ontogeny. Prog. Clin. Cancer, 1-29 (1970).
Tad)p, E.: Role of pineal gland in aetiology and treatment of breast cancer. Lancet I], 1001--1002 (1978).
Tapp, E., Skinner, R.G., Phillips, V.: Radioimmunoassay for melatonin. J. Neural Transm. 48, 137-141 (1980).
Ueck, M.: Innervation of the vertebrate pineal. Prog. Brain Res. 52, 45-88 (1979).
Verma, U., Kapur, M.M., Laumas, K.R.: Characterization of progesterone receptors and metabolism of progesterone in the normal and cancerous human mammary gland. J. Steroid Biochem. 9, 569-577 (1978).
Wetterber~ L., Arendt, J., Paunier, L,, Sizonenko, 19. C., van Donselaar, W., Heyden, T.: Human serum melatonin changes during the menstrual cycle. J. Clin. Endocr. Metab. 42, 185-188 (1976).
Wetterberg, L., Eriksson, 0., Friberg, Y., Vangbo, B.: A simplified radio- immunoassay for melatonin and its application to biological fluids. Preliminary observations on the half-life of plasma melatonin in man. Clin. Chim. Acta 86, 169--177 (1978 a).
Wetterberg, L.: Melatonin in humans. Physiological and clinical studies. J. Neural Transm., Suppl. 13, pp.289-310. Wien-New York: Springer. 1978 b.
Wetterber~ L., Halber~ E, Tarquini, B., Cagnoni, M., Haus, E., Gri~th, K., Kawasaki, T., Wallach, k. A., Ueno, 114., Uezo, K., Matsuoka, M., Kuzd, M., Halberg, E., Omae, T.: Circadian variation in urinary melatonin in clini- cally healthy women in Japan and the United States of America. Ex- perientia 3s 416-418 (1979 a).
Wetterberg~ L., Beck-Friis; J., Aperia, B., Petterson, U.: Melatonin/cortisol ratio in depression. Lancet I/, 1361 (1979 b).
Authors' address: C Bartsch, Fichtenweg 6/110, D-7400 Tiibingen 1, Federal Republic of Germany.