Applicability of ultrasonic tissue characterization for longitudinal assessment and differentiation...
8
88 JACC Vol. 4, No.1 July 1984:88-95 Applicability of Ultrasonic Tissue Characterization for Longitudinal Assessment and Differentiation of Calcification and Fibrosis in Cardiomyopathy JULIO E. PEREZ, MD, BENICO BARZILAI, MD, ERIC 1. MADARAS, PHD, ROBERT M. GLUECK, MD, JEFFREY E. SAFFITZ, MD, PATRICK JOHNSTON, MA, JAMES G. MILLER, PHD, BURTON E. SOBEL, MD, FACC St. Louis, Missouri Progress in tissue characterization of myocardium with ultrasound suggests that quantitative recognition of isch- emic or scarred tissue will be achieved. Despite the in- creasing recognition and importanceofcardiomyopathy, its diagnosis generally requires invasive procedures such as cardiac catheterization and biopsy. To investigate methods that permit the characterization of longitudinal cardiomyopathic changes that might ultimately be ex- tended for noninvasive studies in patients, quantitative ultrasonic methods were utilized for in vitro tissue char- acterization of hearts from Syrian hamsters of selected age of either 2 to 3 or 5 to 7 months. Normal hamsters were used as controls. Myocardial sites (n = 600) from the young Syrian hamsters exhibited values (± standard error) of inte- grated ultrasonic backscatter averaging - 53.87 ± 0.26 The diagnosis of cardiomyopathy is generally made by ex- cluding other causes of ventricular dysfunction on clinical or laboratory grounds. In the case of either hypertrophic, congestive or restrictive cardiomyopathy, the diagnosis is suggested on the basis of hemodynamic findings. Only rarely is it based on analysis of characteristics of the actual myo- cardium by means of myocardial biopsy (1). Thus, it would be desirable to develop noninvasive methods for detection of salient histopathologic features of cardiomyopathies that would permit their longitudinal characterization. From the Cardiovascular Division, Biomedical Computer Laboratory, and Department of Physics, Washington University, SI. Louis, Missouri. This work was supported in part by Grants HL-17646 (SCOR in Ischemic Heart Disease), HL-28998, RR00396 and RR01362 from the National Institutes of Health, Bethesda, Maryland and the Ella L. Buder and Ida Marie Peters Cardiovascular Research Scholar Award of the 51. Louis Heart Association (Dr. Perez). Address for reprints: Julio E. Perez, MD, Cardiovascular Division, Box 8086, Washington University School of Medicine, 660 South Euclid Avenue, SI. Louis, Missouri 63110. © 1984by the American College of Cardiology dB, which were significantly different from values (n = 500) in age-matched control hamsters (- 58.07 ± 0.08 dB; P < 0.001). Cardiomyopathic hearts from older an- imals exhibited backscatter values (n = 500 sites) av- eraging - 50.87 ± 0.22 dB, again significantly different from values (n = 300 sites) in age-matched control ham- sters (-55.91 ± o.n dB; P < 0.001). In addition, ul- trasonic attenuation was significantly different for hearts from the control and cardiomyopathic hamsters of both age ranges. The results correlated with sequential calcification and fibrosis characteristics assessed histopathologically. This study indicates that quantitative characterization of myocardium with ultrasound may permit longitudinal assessment of cardiomyopathic changes in diverse dis- ease entities and their response to therapy. Previous studies from our laboratory (2-5) demonstrated that quantitative ultrasonic variables permit differentiation of normal from ischemic and fibrotic canine myocardium in vitro and in vivo. Diffuse myocardial fibrosis resulting from exposure to doxorubicin was also identified (6). The use of integrated backscatter, obtained with reflected as opposed to transmitted ultrasound, represents an approach to applications in vivo because it has the potential to be interfaced with conventional echocardiography, which is also based on reflected ultrasound. The present study was undertaken to: I) lay a foundation for the development of techniques of quantitative ultrasonic tissue characterization potentially applicable in vivo for analysis of diffuse pathologic changes in myocardium by assessment of multiple regions to obtain quantitative ultra- sonic variables indicative of the physical properties of each region; and 2) test the method developed in an experimental animal preparation with a well defined natural history of cardiomyopathic change that includes both calcification and 0735-1097/84/$3.00
Transcript of Applicability of ultrasonic tissue characterization for longitudinal assessment and differentiation...

88 JACC Vol. 4, No.1July 1984:88-95
Applicability of Ultrasonic Tissue Characterization for LongitudinalAssessment and Differentiation of Calcification and Fibrosisin Cardiomyopathy
JULIO E. PEREZ, MD, BENICO BARZILAI, MD, ERIC 1. MADARAS, PHD,
ROBERT M. GLUECK, MD, JEFFREY E. SAFFITZ, MD, PATRICK JOHNSTON, MA,
JAMES G. MILLER, PHD, BURTON E. SOBEL, MD, FACC
St. Louis, Missouri
Progress in tissue characterization of myocardium withultrasound suggests that quantitative recognition of ischemic or scarred tissue will be achieved. Despite the increasing recognition and importance of cardiomyopathy,its diagnosis generally requires invasive procedures suchas cardiac catheterization and biopsy. To investigatemethods that permit the characterization of longitudinalcardiomyopathic changes that might ultimately be extended for noninvasive studies in patients, quantitativeultrasonic methods were utilized for in vitro tissue characterization of hearts from Syrian hamsters of selectedage of either 2 to 3 or 5 to 7 months. Normal hamsterswere used as controls.
Myocardial sites (n = 600) from the young Syrianhamsters exhibited values (± standard error) of integrated ultrasonic backscatter averaging - 53.87 ± 0.26
The diagnosis of cardiomyopathy is generally made by excluding other causes of ventricular dysfunction on clinicalor laboratory grounds. In the case of either hypertrophic,congestive or restrictive cardiomyopathy, the diagnosis issuggested on the basis of hemodynamic findings. Only rarelyis it based on analysis of characteristics of the actual myocardium by means of myocardial biopsy (1). Thus, it wouldbe desirable to develop noninvasive methods for detectionof salient histopathologic features of cardiomyopathies thatwould permit their longitudinal characterization.
From the Cardiovascular Division, Biomedical Computer Laboratory,and Department of Physics, Washington University, SI. Louis, Missouri.This work was supported in part by Grants HL-17646 (SCOR in IschemicHeart Disease), HL-28998, RR00396 and RR01362 from the NationalInstitutes of Health, Bethesda, Maryland and the Ella L. Buder and IdaMarie Peters Cardiovascular Research Scholar Award of the 51. LouisHeart Association (Dr. Perez).
Address for reprints: Julio E. Perez, MD, Cardiovascular Division,Box 8086, Washington University School of Medicine, 660 South EuclidAvenue, SI. Louis, Missouri 63110.
© 1984by the American College of Cardiology
dB, which were significantly different from values (n =500) in age-matched control hamsters ( - 58.07 ± 0.08dB; P < 0.001). Cardiomyopathic hearts from older animals exhibited backscatter values (n = 500 sites) averaging - 50.87 ± 0.22 dB, again significantly differentfrom values (n = 300 sites) in age-matched control hamsters (-55.91 ± o.n dB; P < 0.001). In addition, ultrasonic attenuation was significantly different for heartsfrom the control and cardiomyopathic hamsters of bothage ranges.
The results correlated with sequential calcificationand fibrosis characteristics assessed histopathologically.This study indicates that quantitative characterizationof myocardium with ultrasound may permit longitudinalassessment of cardiomyopathic changes in diverse disease entities and their response to therapy.
Previous studies from our laboratory (2-5) demonstratedthat quantitative ultrasonic variables permit differentiationof normal from ischemic and fibrotic canine myocardiumin vitro and in vivo. Diffuse myocardial fibrosis resultingfrom exposure to doxorubicin was also identified (6). Theuse of integrated backscatter, obtained with reflected asopposed to transmitted ultrasound, represents an approachto applications in vivo because it has the potential to beinterfaced with conventional echocardiography, which isalso based on reflected ultrasound.
The present study was undertaken to: I) lay a foundationfor the development of techniques of quantitative ultrasonictissue characterization potentially applicable in vivo foranalysis of diffuse pathologic changes in myocardium byassessment of multiple regions to obtain quantitative ultrasonic variables indicative of the physical properties of eachregion; and 2) test the method developed in an experimentalanimal preparation with a well defined natural history ofcardiomyopathic change that includes both calcification and
0735-1097/84/$3.00
JACC v«. 4, No. IJuly 1984 ~8-95
PEREZ ET AL.QUANTITATIVE ULTRASOUND AND CARDIOMYOPATHY
89
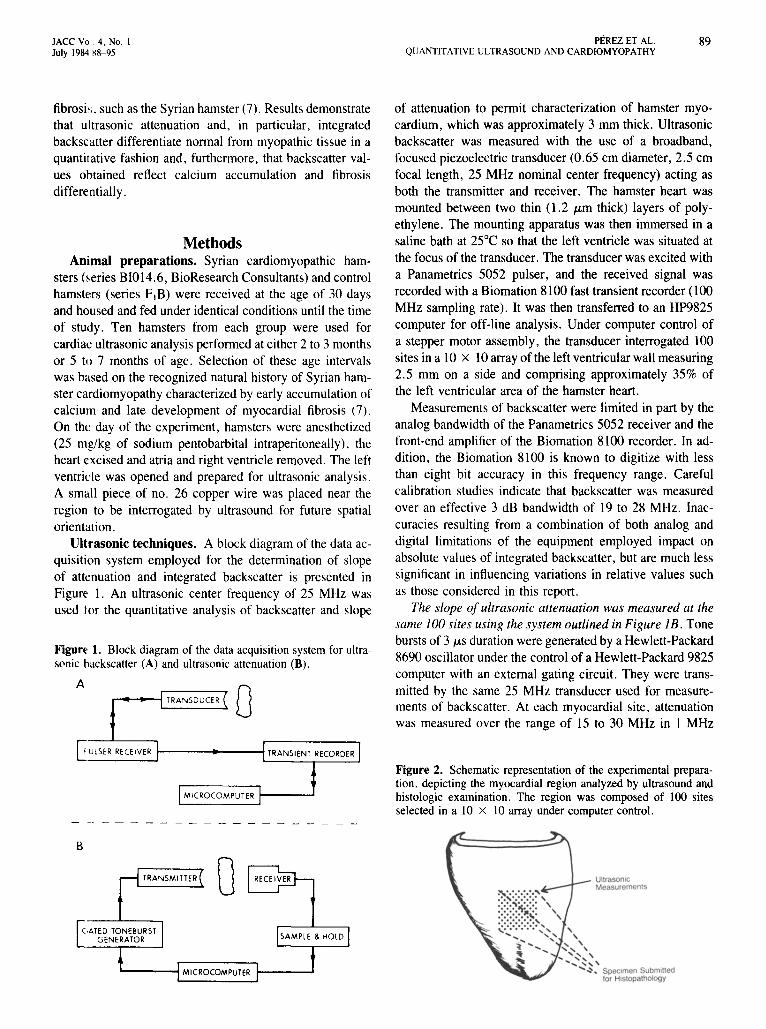
Figure 1. Block diagram of the data acquisition system for ultrasonic backscatter (A) and ultrasonic attenuation (B).
fibrosis. such as the Syrian hamster (7). Results demonstratethat ultrasonic attenuation and, in particular, integratedbackscatter differentiate normal from myopathic tissue in aquantitative fashion and, furthermore, that backscatter values ohtained reflect calcium accumulation and fibrosisdifferentially.
MethodsAnimal preparations. Syrian cardiomyopathic ham
sters (series BI014.6, BioResearch Consultants) and controlhamsters (series FIB) were received at the age of 30 daysand housed and fed under identical conditions until the timeof study. Ten hamsters from each group were used forcardiac ultrasonic analysis performed at either 2 to 3 monthsor 5 to 7 months of age. Selection of these age intervalswas based on the recognized natural history of Syrian hamster cardiomyopathy characterized by early accumulation ofcalcium and late development of myocardial fibrosis (7).On the day of the experiment, hamsters were anesthetized(25 rug/kg of sodium pentobarbital intraperitoneally), theheart excised and atria and right ventricle removed. The leftventricle was opened and prepared for ultrasonic analysis.A small piece of no. 26 copper wire was placed near theregion to be interrogated by ultrasound for future spatialorientation.
Ultrasonic techniques. A block diagram of the data acquisition system employed for the determination of slopeof attenuation and integrated backscatter is presented inFigure 1. An ultrasonic center frequency of 25 MHz wasused lor the quantitative analysis of backscatter and slope
ATRANSDUCER 0
of attenuation to permit characterization of hamster myocardium, which was approximately 3 mm thick. Ultrasonicbackscatter was measured with the use of a broadband,focused piezoelectric transducer (0.65 em diameter, 2.5 emfocal length, 25 MHz nominal center frequency) acting asboth the transmitter and receiver. The hamster heart wasmounted between two thin (1.2 ILm thick) layers of polyethylene. The mounting apparatus was then immersed in asaline bath at 25°C so that the left ventricle was situated atthe focus of the transducer. The transducer was excited witha Panametrics 5052 pulser, and the received signal wasrecorded with a Biomation 8100 fast transient recorder (l00MHz sampling rate). It was then transferred to an HP9825computer for off-line analysis. Under computer control ofa stepper motor assembly, the transducer interrogated 100sites in a lOx 10 array of the left ventricular wall measuring2.5 mm on a side and comprising approximately 35% ofthe left ventricular area of the hamster heart.
Measurements of backscatter were limited in part by theanalog bandwidth of the Panametrics 5052 receiver and thefront-end amplifier of the Biomation 8100 recorder. In addition, the Biomation 8100 is known to digitize with lessthan eight bit accuracy in this frequency range. Carefulcalibration studies indicate that backscatter was measuredover an effective 3 dB bandwidth of 19 to 28 MHz. Inaccuracies resulting from a combination of both analog anddigital limitations of the equipment employed impact onabsolute values of integrated backscatter, but are much lesssignificant in influencing variations in relative values suchas those considered in this report.
The slope of ultrasonic attenuation was measured at thesame 100 sites using the system outlined in Figure lB. Tonebursts of 3 ILS duration were generated by a Hewlett-Packard8690 oscillator under the control of a Hewlett-Packard 9825computer with an external gating circuit. They were transmitted by the same 25 MHz transducer used for measurements of backscatter. At each myocardial site, attenuationwas measured over the range of 15 to 30 MHz in 1 MHz
~UlSER RECEIVER f--------1'-----r-----l
MICROCOMPUTER t--_..J
Figure 2. Schematic representation of the experimental preparation, depicting the myocardial region analyzed by ultrasound andhistologic examination. The region was composed of 100 sitesselected in a 10 x 10 array under computer control.
UltrasonicMeasurementso
B
1.-__--1 MICROCOMPUTER t--_.....
90 PEREZ ET AL.QUANTITATIVE ULTRASOUND AND CARDIOMYOPATHY
JACC Vol. 4, No.1July 1984:88-95
steps. The signal transmitted through the tissue was detectedby an acoustoelectric receiver (0.5 x 1.0 em aperture)placed directly behind the sample (8,9). The signal receivedwas recorded for off-line analysis. Operating characteristiccurves describing the combined response as a function offrequency of the transmitting electronics and transducer andthe receiving transducer and electronics were measured in1dB increments over the full dynamic range employed. Thefrequency-dependent system transfer function thus obtainedwas deconvolved from the measured data, so that the valuesof attenuation reported are entirely independent of instrumental operating characteristic curves.
Ultrasonic data analysis. The integrated backscatteranalysis involved a 1.28 IJ-S portion (representing a volumeof approximately I mm long x the beam area) of the digitized data corresponding to the central region of the intramural myocardium at each site selected so as to be independent of the biologic variability in wall thickness. Integratedbackscatter was calculated by summing the squares of theamplitude of the radiofrequency data and expressed in unitsof decibels below the level of backscatter obtained from anearly perfect reflector (a stainless steel plate) at the focusof the transducer. The frequency averaging properies ofintegrated backscatter serve to minimize the effects of phasecancellation, a major instrumentation artifact associated withthe use of piezoelectric receiving transducers (8,9). Atten-
125 A
100 mean' -55.91SD '1.87SE '0.11
III 75 n '300sites.~Vl
UJ 50UZUJ 25C£C£:::JUU0
125 BL.L.
0>- 100 mean' -50.87U SD :4.90Z SE '0.22UJ:::J 75 n : 500 sitesCUJC£
50L.L.
25
-65 -60 -55 -50 -45 -40 -35INTEGRATED BACKSCATTER (dB)
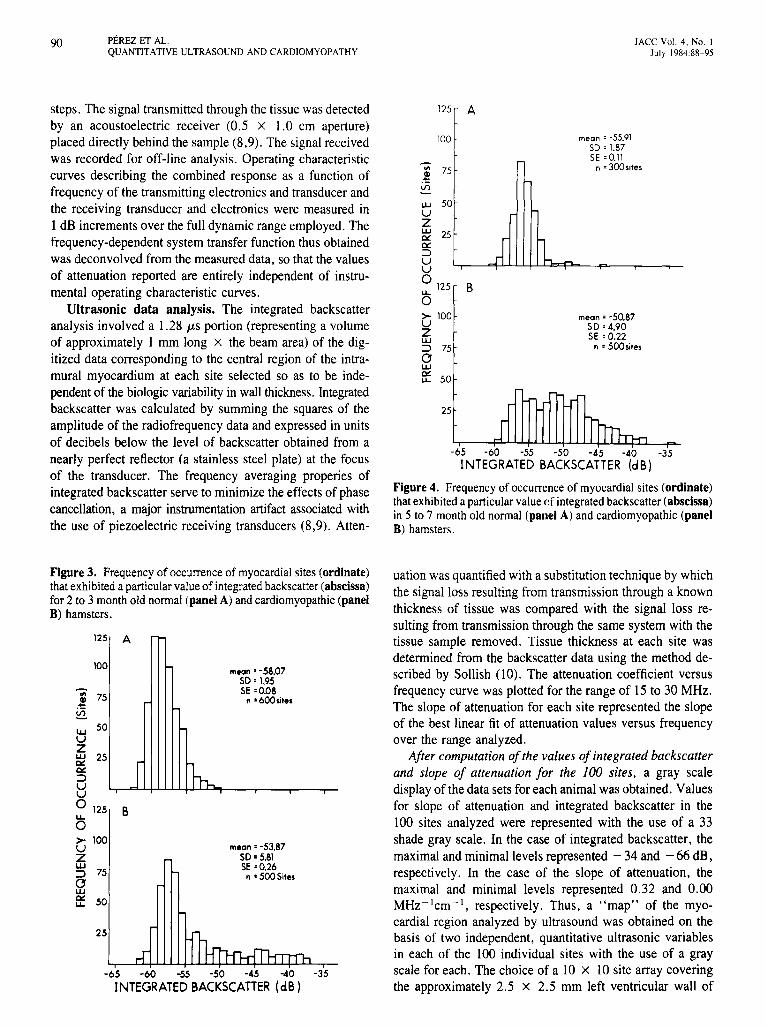
Figure 4. Frequency of occurrenceof myocardial sites (ordinate)thatexhibiteda particularvalueof integrated backscatter(abscissa)in 5 to 7 monthold normal (pane) A) and cardiomyopathic (panelB) hamsters.
-65 -60 -55 -50 -45 -40 -35
INTEGRATED BACKSCATTER (dB)
Figure 3. Frequencyof occurrenceof myocardial sites (ordinate)that exhibiteda particularvalueof integratedbackscatter(abscissa)for 2 to 3 monthold normal(panel A) and cardiomyopathic (panelB) hamsters.
125
100
.! 75
~w 50UZ~ 25Cll::::J
~o 125LA-
O>- 100UZUJ:::J 75se: 50
25
A
B
mean' -58.07SD'1.95SE:0.08
n • 6oo.;le.
m.an : -53.87SD' 5.81SE :0.26n • 500Sil••
uation was quantified with a substitution technique by whichthe signal loss resulting from transmission through a knownthickness of tissue was compared with the signal loss resulting from transmission through the same system with thetissue sample removed. Tissue thickness at each site wasdetermined from the backscatter data using the method described by Sollish (10). The attenuation coefficient versusfrequency curve was plotted for the range of 15 to 30 MHz.The slope of attenuation for each site represented the slopeof the best linear fit of attenuation values versus frequencyover the range analyzed.
After computation ofthe values of integrated backscatterand slope of attenuation for the 100 sites. a gray scaledisplay of the data sets for each animal was obtained. Valuesfor slope of attenuation and integrated backscatter in the100 sites analyzed were represented with the use of a 33shade gray scale. In the case of integrated backscatter, themaximal and minimal levels represented - 34 and - 66 dB,respectively. In the case of the slope of attenuation, themaximal and minimal levels represented 0.32 and 0.00MHz-1cm- 1, respectively. Thus, a "map" of the myocardial region analyzed by ultrasound was obtained on thebasis of two independent, quantitative ultrasonic variablesin each of the 100 individual sites with the use of a grayscale for each. The choice of a 10 x 10 site array coveringthe approximately 2.5 x 2.5 mm left ventricular wall of

JACC v.: 4, No. IJuly 198A :~8-95
PEREZET AL.QUANTITATIVE ULTRASOUND AND CARDIOMYOPATHY
91
the hamster heart was made on the basis of the followingconsiderations. The average 3 dB full beam width in thefocal zone of the transducer was 0.26 mm at 25 MHz.Measurements spaced by one-half the beam width have beenshown to represent statistically independent measurements(11). Thus, measurements spaced at 0.25 mm provided 100independent measurements that served to characterize thespatial distribution of the diffusely inhomogeneous myopathy.
Histology. Immediately after ultrasonic analysis. thehamster heart was removed from the tissue holder and theregions interrogated by ultrasound were analyzed microscopically , Appropriate regions were identified with reference to the copper wire located at the left upper portion ofthe 10 x 10 area previously analyzed by ultrasound (Fig.2). The tissue was immersed in formalin and subsequentlycut and evaluated with hematoxylin-eosin, Von Kossa andMasson staining techniques.
Statistical analysis. Comparison among ultrasonic variables (integrated backscatter and slope of ultrasonic attenuation) between control and Syrian hamsters was performedwith the use of Student's t test for unpaired samples. Furtheranalysis to ascertain whether data obtained from normal andcardiomyopathic hamster hearts conformed to different distributi ems was performed with the use of the Kolmogorov-
~igure 5. Gray scale frequency distribution of 100 myocardialsites based on ultrasonic integrated backscatter from representativen~rmal (Ie~) and 3 (middle) and 6 month old cardiomyopathic(right) Synan hamsters. The horizontal bar on the top illustratesthe levcis of backscatter from - 66 to - 34 dB. Syrian hamsterhearts n~t only exhibited higher backscatter values when averagedfor all Sites, but also their distribution revealed marked heterogeneity consistent with the histologic pattern.
-66dB
Smimov test (12). Probability (p) values, obtained from bothtests, less than 0.05 were considered significant.
Results
Ultrasonic AnalysisBackscatter variables. Values of integrated backscatter
clearly differentiated cardiomyopathic from age-matchedcontrol hamster heart tissue (at both 2 to 3 and 5 to 7 monthsof age). Two to 3 month control and cardiomyopathic hamster hearts had integrated backscatter values averaging - 58.07± 0.08 dB (± SE) and - 53.87 ± 0.26 dB, respectively(p < 0.001). To elucidate the nature of the differentiation,histograms were constructed on the basis of distribution ofmyocardial sites exhibiting a particular backscatter value intissue from animals at each age. Two to 3 month old controlhamsters displayed a relatively narrow distribution of backscatter values clustered around - 58 dB (Fig. 3A). In contrast, values obtained from myopathic hamster hearts exhibited a broad numerical distribution, with values from sitesas high as - 38 dB (Fig. 3B). A similar analysis was performed with backscatter values from tissue of 6 month control and myopathic hearts. The results were similar, withcontrol hamster hearts exhibiting a narrow distribution ofsites with backscatter values around - 57 dB in contrast tocardiomyopathic hearts exhibiting a broad range of valuesfrom - 60 to - 34 dB (Fig. 4A and B). Statistical analysisof the distribution of backscatter values between control andcardiomyopathic tissue confirmed that the distributions weresignificantly different in both age groups (KolmogorovSmimov test, p < 0.05).
Among control hamsters, younger animals (2 to 3 months)
-34dB
Normal Hamster3 Months
(11I55)
Cardiomyopathic Hamster3 Months
(11I53)
Cardiomyopathic Hamster6 Months
(Ill70)

92 PEREZ ET AL.QUANTITATIVE ULTRASOUND AND CARDIOMYOPATHY
JACC Vol. 4. No. J
July 1984:88- 95
exhibited lower values of integrated backscatter comparedwith 6 month old hamsters (- 58.07 ± 0.08 dB versus- 55.91 ± 0.11 dB; p < 0.05). These results suggest thatultrasonic tissue characterization may permit assessment ofthe aging processes, which is known to be associated withgradually increased deposition and cross-linking of collagen(13).
Slope of ultrasonic attenuation. Mean values of slopeof ultrasonic attenuation differed significantly in controlcompared with cardiomyopathic hamster s of either 2 to 3months (0.099 ± 0.001 MHz - 1cm- I versus 0.108 ± 0.001MHz -lcm - l ; p < 0.00l) or 5 to 7 months of age (0.108± 0.001 MHz -1cm- 1 versus 0.118 ± 0.001 MHz-lcm - l;
p < 0 .001). Despite the relatively small shifts in meanvalues , the differences were significant because of the largenumber of sites measured. The Kolmogorov-Smirnov testprovide s a more revealing approach for distinguishing cardiomyopathic from normal tissue on the basis of the distributions . When the distribution of myocardial sites exhibitingparticular values of the slope of attenuation was evaluatedwith the Kolmogorov-Smirnov test , control and cardiomyopath ic hearts were distinctly separated for either 3 or 6month old hamsters . The character of the distribution of
both backscatter and attenuat ion values for each hamsterusually permitted appropriate segregation into control orcardiomyopathic categories by simple inspection .
Myocardial distribution of integrated backscatter andslope of ultrasonic attenuation. Gray scale representationsof the 100 sites analyzed for either integrated backscatteror the slope of ultrasonic attenuation permitted analysis ofthe spatial distribution of both variables in the myocard ialregions interrogated . Control hamster hearts exhibited homogeneous distributions of regional backscatter values thatdid not change abruptly between contiguous areas (Fig. 5).In contrast, cardiomyopathic hearts from 2 to 3 and 5 to 7month old hamsters were characterized by a heterogeneousdistribution of regions with elevated backscatter values interposed with zones of more nearly normal values (Fig . 5).The slope of ultrasonic attenuation values, plotted in thesame fashion as backscatter values , provided maps concordant with the backscatter data (Fig. 6). A homogeneouspattern of reduced values of slope of attenuation was presentin control hamsters, whereas myopathic hamsters exhibiteda heterogeneous pattern of distribution . Furthermore, individual regions characterized by elevated values of integrated backscatter corresponded to those with elevated val-
I TEGRATED BACKSCATTER
Figure 6. Correlation of gray scalefrequency distribution of myocardialsites based on either integrated backscatter (top panels) or slope of ultrasonic attenuation (bottom panel) inthree representative Syrian hamsters.The horizontal bars illustrate the values of each ultrasonic measurementperformed separately in the same myocardial site. There was a congruenceof sites with both high backscatter andslope of attenuation values in youngand old Syrian hamster hearts.
(# 53)
-66 dB '3 4dB
(# 62) (#701
SLOPE OF ATTENUATION
CordlomyopathlC Homs'ttr3 Months
(#5 3)
( ord,ornyepolh,c Hamster6 Month s
(# 62)
Cord,omyopolhlc HomSI r6 Months
(n o )
JACC Vol. 4, No. IJuly 198H 8-95
PEREZ ET AL.QUANTITATIVE ULTRASOUND AND CARDIOMYOPATHY
93
ues of slope of attenuation, suggesting that changes in thetwo variables identify the same myocardial zones.
Histopathologic Correlates of Ultrasonic Variables
Myocardium from control hamsters was histologicallynormal. No regions of fibrosis or calcification were observed. The histologic pattern in 3 month old cardiornyopathic hamsters was characterized by discrete multifocalregions of calcified degenerated myocardium surrounded bynormal-appearing myocardium. In 6 month old cardiomyopathic hamsters, the discrete lesions were more numerousand contained both fibrous and calcified components. Myocardium surrounding the lesions appeared normal.
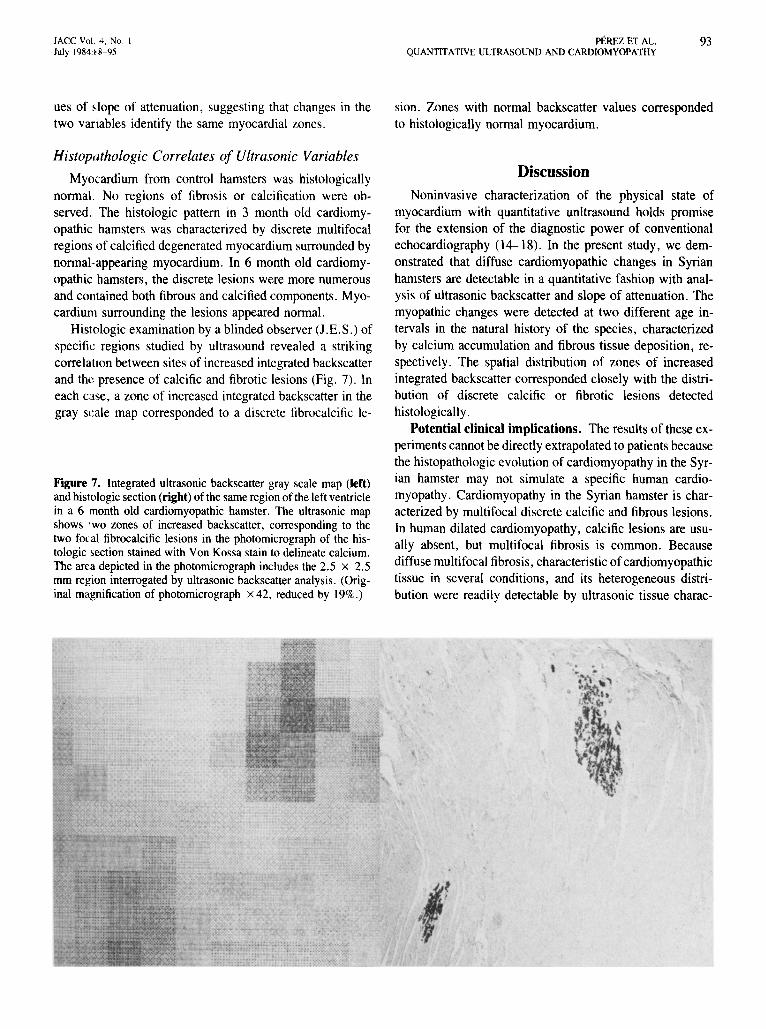
Histologic examination by a blinded observer (J.E.S.) ofspecific regions studied by ultrasound revealed a strikingcorrelation between sites of increased integrated backscatterand the presence of calcific and fibrotic lesions (Fig. 7). Ineach case, a zone of increased integrated backscatter in thegray scale map corresponded to a discrete fibrocalcific le-
Figure 7. Integrated ultrasonic backscatter gray scale map (left)and histologic section (right) ofthe same region of the left ventriclein a 6 month old cardiomyopathic hamster. The ultrasonic mapshows 'wo zones of increased backscatter, corresponding to thetwo focal fibrocalcific lesions in the photomicrograph of the histologic section stained with Von Kossa stain to delineate calcium.The area depicted in the photomicrograph includes the 2.5 x 2.5mm region interrogated by ultrasonic backscatter analysis. (Original magnification of photomicrograph x 42, reduced by 19%.)
.:..; .~.
sion. Zones with normal backscatter values correspondedto histologically normal myocardium.
Discussion
Noninvasive characterization of the physical state ofmyocardium with quantitative unltrasound holds promisefor the extension of the diagnostic power of conventionalechocardiography (14-18). In the present study, we demonstrated that diffuse cardiomyopathic changes in Syrianhamsters are detectable in a quantitative fashion with analysis of ultrasonic backscatter and slope of attenuation. Themyopathic changes were detected at two different age intervals in the natural history of the species, characterizedby calcium accumulation and fibrous tissue deposition, respectively. The spatial distribution of zones of increasedintegrated backscatter corresponded closely with the distribution of discrete calcific or fibrotic lesions detectedhistologically.
Potential clinical implications. The results of these experiments cannot be directly extrapolated to patients becausethe histopathologic evolution of cardiomyopathy in the Syrian hamster may not simulate a specific human cardiomyopathy. Cardiomyopathy in the Syrian hamster is characterized by multifocal discrete calcific and fibrous lesions.In human dilated cardiomyopathy, calcific lesions are usually absent, but multifocal fibrosis is common. Becausediffuse multifocal fibrosis, characteristic of cardiomyopathictissue in several conditions, and its heterogeneous distribution were readily detectable by ultrasonic tissue charac-
. .... '..

94 PEREZ ET AL.QUANTITATIVE ULTRASOUND AND CARDIOMYOPATHY
JACC Vol. 4, No. IJuly 1984:88-95
terization, this method is likely to be useful for diagnosisin patients with cardiomyopathy, in whom current tissuediagnosis requires myocardial biopsy. Calcium accumulation may be a nonspecific manifestation of myocellular damage, although it is known to occur in postinfarction aneurysm and endomyocardial fibrosis (19), as well as in patientsundergoing hemodialysis (20). Therefore, its recognition byquantitative ultrasonic techniques may be useful in severalsettings.
Technical considerations. The ultrasonic techniquesemployed in this study of isolated hamster myocardiumcannot be used for investigation of the intact human heart.We elected to use a high ultrasonic frequency to interrogateintramural myocardium of thin hamster hearts. This frequency cannot be employed in the clinical setting becauseof severe limitations in penetration through the chest wall.In vitro experiments permit accurate estimation of ultrasonicattenuation, a measurement that is difficult to obtain usingclinical ultrasound which is based on reflected as opposedto transmitted energy. Also, experiments in isolated hearttissue are not subjected to motion and changes associatedwith the cardiac cycle, which influence ultrasonic signalsemanating from the regions of interest in in vivo experiments(21). Furthermore, extrapolation of the numerical values ofabsolute integrated backscatter from these measurementsobtained with an average frequency of 23.5 MHz to frequencies in the low megahertz range suitable for interrogation of the hearts of patients requires caution. Estimatesinvolve a product of three factors: the backscatter coefficientof myocardium, the attenuation coefficient of myocardiumand the properties (beam width and focal characteristics) ofthe interrogating transducer (22,23). Values for these variables over the required range of frequencies are not yetavailable.
Previous investigations (22) of normal dog myocardiumsuggest that the backscatter coefficient is proportional tofrequency to the third or fourth power. Attenuation effectscontribute a term that is approximately inversely proportional to frequency. The ultrasonic beam width in the focalzone is inversely proportional to frequency squared, butadditional geometric considerations also apply. Consequently, extrapolation of absolute values of integrated backscatter is not appropriate. Furthermore, the nature of theultrasonic scattering mechanism could be inherently different in human subjects as opposed to that in hamster myocardium. Nevertheless, the significant relative changes inbackscatter observed in these studies of hamster heart suggest that analogous investigations using frequencies and dimensions appropriate for clinical studies may yield similarrelative changes in backscatter.
Conclusions. We investigated techniques of ultrasonictissue characterization applicable to recognition of a cardiomyopathic process defined by diffuse myocellular de-
generation, calcification and fibrous proliferation. The results indicate that: I) mean integrated backscatter increasedcompared with values in control hamsters, and 2) the distribution of the values of both integrated backscatter andslope of attenuation was altered in hearts from cardiomyopathic hamsters compared with those from normal hamsters. Thus, they suggest that characterization of cardiomyopathic changes in human myocardium with extensionsof the techniques developed may prove to be a useful approach for early diagnosis and assessment of the efficacyof their treatment.
We thank Barbara Donnelly and Joyce Kalayeh for preparation of themanuscript and Delbert McGraw for skillful technical assistance.
ReferencesI. Mason JW, Billingham ME. Myocardial biopsy. In: Yu PN, Goodwin
JF, eds. Progress in Cardiology. Philadelphia:Lea & Febiger, 1980:13346.
2. Mimbs JW, Yuhas DE, Miller 10, Weiss AN, Sobel BE. Detectionof myocardial infarction in vitro based on altered attenuation of ultrasound. Circ Res 1977;41:192-8.
3. Mimbs JW, O'Donnell M, Miller 10, Sobel BE. Changes in ultrasonicattenuation indicative of early myocardial ischemic injury. Am J Physiol I979;236:H340-4.
4. Mimbs JW, Bauwens D, Cohen RD, O'Donnell M, Miller 10, SobelBE. Effects of myocardial ischemia on quantitative ultrasonic backscatter and identification of responsible determinants. Circ Res1981;49:89-96.
5. Cohen RD, Mottley 10, Miller 10, Kurnik PB, Sobel BE. Detectionof ischemic myocardium in vivo through the chest wall by quantitativeultrasonic tissue characterization. Am J Cardiol 1982;50:838-43.
6. Mimbs JW, O'Donnell M, Miller JG, Sobel BE. Detection of cardiomyopathic changes induced by doxorubicin based on quantitativeanalysis of ultrasonic backscatter. Am J Cardiol 1981;47:1056-60.
7. Jasmin G, Proschek L. Hereditary polymyopathy and cardiomyopathyin the Syrian hamster. I. Progression of heart and skeletal musclelesions in the UM-X7.1 line. Muscle Nerve 1982;5:20-5.
8. Busse LJ, Miller 10, Yuhas DF, Mimbs JW, Weiss AN, Sobel BE.Phase cancellation effects: a source of attenuation artifact eliminatedby a CdS acoustoelectric receiver. In: White D, ed. Ultrasound inMedicine. New York: Plenum Press, 1977:1519-35.
9. Busse LJ. Miller JG. Detection of spatially nonuniform ultrasonicradiation with phase sensitive (piezoelectric) and phase insensitive(acoustoelectric) receivers. J Acoust Soc Am 1981;70:1377-86.
10. Sollish BD. A device for measuring ultrasonic propagation velocityin tissue. In: Linzer M, ed. Ultrasonic Tissue Characterization. II.Washington, D.C.: U.S. Government Printing Office, 1979:125 (National Bureau of Standards Special Publications no. 525).
I I. Kuc R. Schwartz M, Darr II FW, Aisenberg R. Spatial correlationproperties of the acoustic attenuation slope for in vitro liver samples.IEEE Ultrasonics 1978;78:335-8.
12. Dietrich CF. Uncertainty, Calibration and Probability. The Statisticsof Scientific and Industrial Measurements. New York: John Wiley &Sons, 1973:371-4.
13. Shapiro BL, Lam LFH. Calcium and age in fibroblasts from controlsubjects and patients with cystic fibrosis. Science 1982;216:417-9.
14. Green SE, Joynt LF, Fitzgerald PJ, Rubenson DS, Popp RL. In vivoultrasonic tissue characterization of human intracardiac masses. AmJ Cardiol 1983:51:231-6.

JACC Vol 4, No.July 1984:~8-95
PEREZ ET AL.QUANTITATIVE ULTRASOUND AND CARDIOMYOPATHY
95
15. Parisi AF, Nieminen M, O'Boyle PF, et aJ. Enhanced detection ofthe evolution of tissue changes after acute myocardial infarction usingcolor-encoded two-dimensional echocardiography. Circulation1982:66:764-70.
16. Skorton DJ, Melton HE, Pandian NG, et aJ. Detection of acute myocard.al infarction in closed-chest dogs by analysis of regional twodimensional echocardiographic gray level distributions. Circ Res198:;:52:36-44.
17. Skorton DJ, Collins SM, Nichols J, Pandian NG, Bean JA, KerberRE. Quantitative texture analysis in two-dimensional echocardiography: application to the diagnosis of experimental myocardial contusion. Circulation 1983;68:217-23.
18. Miller JG, Sobel BE. Cardiac ultrasonic tissue characterization. HospPrac 1982;17:143-51.
19. Koestner AW, Bush CA, Baba N. Endomyocardial fibrosis with calcification of the myocardium. Arch Patho1 Lab Med 1978;102:4069.
20. Terman DS, Alfrey AC, Hammond WS. Cardiac calcification in uremia. Am J Med 1971;50:744-55.
21. Madaras EI, Barzilai B, Perez JE, Sobel BE, Miller JG. Changes inmyocardial backscatter throughout the cardiac cycle. Ultrasonic Imaging 1983;5:229-39.
22. O'Donnell M, Mimbs JW, Miller JG. The relationship between collagen and ultrasonic backscatter in myocardial tissue. J Acoust SocAm 1981;69:580-8.
23. Shung KK, Reid JM. Ultrasonic scattering from tissue. IEEE Ultrasonics 1977;77:230-3.