
Synthesis and Characterization of Novel Polyurethanes and ...

Biomaterials 22 (2001) 2683–2693
Bisphosphonate derivatized polyurethanes resist calcification
Ivan Alferieva, Narendra Vyavaharea, Cunxian Songa, Jeanne Connollya, John TravisHinsona, Zhibin Lua, Sruthi Tallapragadaa, Richard Biancob, Robert Levya,*
aDivision of Cardiology, The Children’s Hospital of Philadelphia, Abramson Research Bldg., 3516 Civic Center Blvd, Philadelphia, PA 19104, USAbThe Department of Surgery, The University of Minnesota, Minneapolis, MN 55455, USA
Received 6 September 2000; received in revised form 2 January 2001; accepted 8 January 2001
Abstract
Calcification of polyurethane cardiovascular implants is an important disease process that has the potential to compromise the
long-term function of devices such as polymer heart valves and ventricular assist systems. In this study we report the successfulformulation and characterization of bisphosphonate-derivatized polyurethanes, hypothesized to resist implant calcification based onthe pharmacologic activity of the immobilized bisphosphonate. Fully polymerized polyurethanes (a polyurea–polyurethane and a
polycarbonate polyurethane) were modified (post-polymerization) with bromoalkylation of the hard segments followed byattachment of a bisphosphonate group at the bromine site. These bisphosphonate-polyurethanes resisted calcification in rat 60 daysubdermal implants compared to nonmodified control polyurethane implants, that calcify. Bisphosphonates-modified polyurethanes
were also studied in circulatory implants using a pulmonary valve cusp replacement model in sheep. Polyurethane cusps modifiedwith bisphosphonate did not calcify in 90 day implants, compared to control polyurethane cusps implants, that demonstratednodular surface oriented calcific deposits. It is concluded that bisphosphonate modified polyurethanes resist calcification both insubdermal implants and in the circulation. This novel biomaterial approach offers great promise for long-term blood stream
implantation with calcification resistance. # 2001 Elsevier Science Ltd. All rights reserved.
Keywords: Heart valves; Prostheses; Mineralization; Biomaterials
1. Introduction
Polymeric heart valve prostheses have been used inboth experimental [1–6] and clinical studies [7–11].These constructs, which have been fabricated frompolyurethane and other elastomers, have all failed dueto either thrombosis or calcification or both [1–11].However, the attraction of the potential desirablefeatures of a polymer heart valve remains. Heart valvesfabricated from elastomers such as polyurethane, canhypothetically be designed with tri-leaflet functionality,and anatomic and fluid dynamic characteristics identicalto human heart valves. Furthermore, there are a largenumber of candidate polymers with appropriate me-chanical and durability characteristics. Despite this,there has been no clinical success with polymeric heartvalves.
Bisphosphonates are well-established pharmaceuticalsthat have potent effects modulating mineralization [12–20]. Bisphosphonates are now widely used for prevent-ing, and promoting the regression of osteoporosis[12,13]. These agents also have potent activity inpreventing pathologic calcification, with a significantrisk of associated osteomalacia due to unwanted bone-targeted side-effects [14]. Prior work by our group hasdemonstrated inhibition of glutaraldehyde fixed bio-prosthetic heart valve leaflet calcification with systemicbisphosphonate administration, but with significantbone toxicity [13]. However, local administration ofbisphosphonates in this same model system usingpolymeric controlled release completely prevented calci-fication without adverse effects [15–17]. This concept oflocal efficacy led to our recent investigations concerningsynthetic modifications of polyurethane.Previous research from our laboratory has investi-
gated bisphosphonate modified polyeurethanes, inwhich ethane hydroxy bisphosphonate was covalentlylinked to polyurethane through an epoxy derivatization[19]. Although these materials appeared promising in rat
*Corresponding author. Tel.: +1-215-590-6119; fax: +1-215-590-
5454.
E-mail address: [email protected] (R. Levy).
0142-9612/01/$ - see front matter # 2001 Elsevier Science Ltd. All rights reserved.
PII: S 0 1 4 2 - 9 6 1 2 ( 0 1 ) 0 0 0 1 0 - 2

subdermal studies, this formulation was not suitable forcirculatory implants.In the present series of experiments, we report the
formulation, characterization, and successful in vivo useof a new family of polyurethanes, based on hardsegment activation with bromo-alkyl derivatization.These bromo-alkyl activated polyurethanes have beencovalently derivatized with bisphosphonates. The goalsof the present study were as follows.
(1) To formulate bisphosphonate derivatized polyur-ethanes based on hard segment alkylation chemis-try.
(2) To characterize these new polymers in terms of theirbisphosphonate content, stability of bisphospho-nate binding, and water absorption properties.
(3) To evaluate their efficacy for calcification resistancewith in vivo studies using both rat subdermalimplants, and sheep circulatory implants.
2. Methods
2.1. Materials
The following candidate polyurethanes were investi-gated for their calcification properties and bispho-sphonate derivatization. A polyurea polyurethane(Biospan, Polymer Technology Group Medical LLC,Berkeley, CA) and a polycarbonate polyurethane(Bionate 80A, from the same manufacturer) werestudied. Vinylidene-bisphosphonic acid (VBP) tetraso-dium salt was obtained from Albright & Wilson UKLtd. (England). The salt was transformed into the freeacid using cation exchange with Dowex-50.
2.2. Polyurethane modifications and characterization
The derivatization of polymers with bisphosphonategroups was carried out in dimethylacetamide solutions
in two steps (Scheme 1) as previously published[20]. First, auxiliary 6-bromohexyl groups were attachedto the urethane nitrogens of polymers hard segmentsvia base-induced alkylation with 1,6-dibromohexaneat low temperature (�5 to 08C) using the followingprocedure. The polyurethanes dissolved in N,N-dimethylacetamide (DMA) were mixed with a largeexcess of 1,6-dibromobutane, cooled to �5 to �88C, andthe polyanions (with the negative charges localized onthe urethane nitrogens) were generated by addition oflithium diisopropylamide solutions. After 2 h at 08C, thereactions were complete. The polyurethanes containingpendant 6-bromohexyl groups were precipitated withcold methanol, purified by washing, and dried. Thebromoalkylated polymers were then reacted with thiol-containing bisphosphonate in the form of a tetrabuty-lammonium salt (containing 1.5 Bu4N-cations for eachbisphosphonate group) to ensure the solubility in DMA.The reaction conditions were as follows. The bro-moalkylated polyurethanes were dissolved in DMA,mixed with DMA-solutions of thiol-bisphosphonate (ina 10-fold excess), and the thiol groups were activatedtowards the nucleophilic substitution of Br by additionof tetrabutylammonium tetraborate. After 1 h at 08C thereactions were complete. The thiol-bisphosphonate wasprepared by reacting VBP with a large excess of 1,3-propanedithiol at 1208C (Scheme 2) as describedpreviously [20]. The values of polyurethanes’ bispho-sphonate modifications were determined using phos-phorus analysis combined with 31P NMR (BrukerAvance DMX 400, 101.97MHz), which indicated
Scheme 1. Hard segment alkylation, with subsequent covalent binding of a thiol-bisphosphonate.
Scheme 2. Thiol-bisphosphonate synthesis.
I. Alferiev et al. / Biomaterials 22 (2001) 2683–26932684
uniform phosphorus peaks at ca. 19 ppm characteristicof 2,2-diphosphonoethylthio groups [20].Water absorption by unmodified and bisphosphonate
polyurethanes was studied using the following metho-dology: Polymer films (0.15mm thick, weighing from 30to 100mg) were soaked in water for 1–2 days, wipedfree of droplets of water, weighed and dried in vacuo.Water absorption was calculated from the differencebetween the wet and dry weights. The stability ofcovalently bound bisphosphonate was assessed byincubating films of bisphosphonate-modified polyur-ethanes at pH 7.4 (0.05m HEPES) and 378C for 9months, followed by decomposition with boiling H2SO4containing small amounts of HNO3 and analyses forphosphorus according to established procedures [21].Infrared spectra (Fourier transform, FTIR) of unim-planted polyurethane films, and explants, both rat
subdermal and sheep circulatory, were obtainedusing a prot!eeg!ee 460 ESP FT-IR spectrometer withInspect IR-FT-IR micro sampling and imaging acces-sory supported by OMNIC software for spectralanalysis including subtraction and deconvolution (Nico-let, Madison, WI).
2.3. Animal implant studies
Rat subdermal implants were carried out using ourestablished calciphylaxis model [19]. In brief, dihydro-tachysterol (DHT, 1mg in 1ml of corn oil) wasadministered with an oral-gastric tube to Sprague–Dawley rats (males, 150 g in weight) 24 h prior to sub-dermal implant surgery. Polyurethane samples (100 mmin thickness, and 1� 1 cm) were implanted in subdermalpouches over the ventral abdominal wall. Animals were
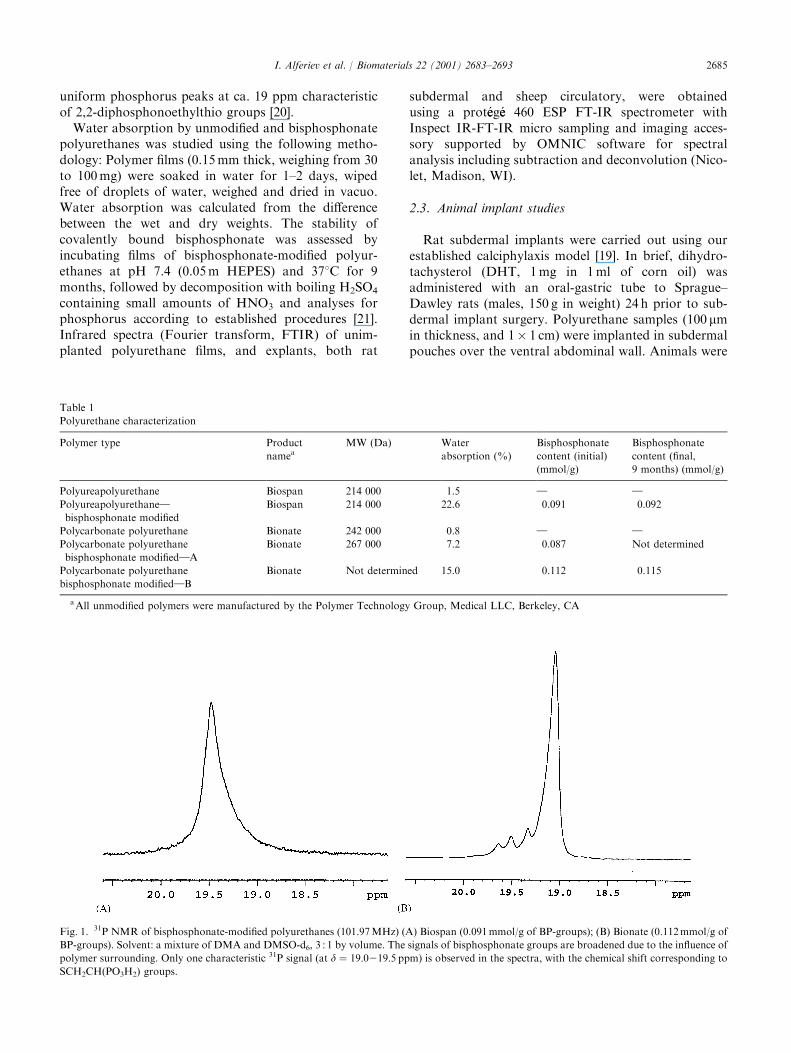
Fig. 1. 31P NMR of bisphosphonate-modified polyurethanes (101.97MHz) (A) Biospan (0.091mmol/g of BP-groups); (B) Bionate (0.112mmol/g of
BP-groups). Solvent: a mixture of DMA and DMSO-d6, 3 : 1 by volume. The signals of bisphosphonate groups are broadened due to the influence of
polymer surrounding. Only one characteristic 31P signal (at d ¼ 19:0219:5 ppm) is observed in the spectra, with the chemical shift corresponding toSCH2CH(PO3H2) groups.
Table 1
Polyurethane characterization
Polymer type Product
nameaMW (Da) Water
absorption (%)
Bisphosphonate
content (initial)
(mmol/g)
Bisphosphonate
content (final,
9 months) (mmol/g)
Polyureapolyurethane Biospan 214 000 1.5 } }
Polyureapolyurethane}
bisphosphonate modified
Biospan 214 000 22.6 0.091 0.092
Polycarbonate polyurethane Bionate 242 000 0.8 } }
Polycarbonate polyurethane
bisphosphonate modified}A
Bionate 267 000 7.2 0.087 Not determined
Polycarbonate polyurethane
bisphosphonate modified}B
Bionate Not determined 15.0 0.112 0.115
aAll unmodified polymers were manufactured by the Polymer Technology Group, Medical LLC, Berkeley, CA
I. Alferiev et al. / Biomaterials 22 (2001) 2683–2693 2685

under general anesthesia using ketamine and xylazine aspreviously published [18,19]. The implant duration was60 days, and implants were retrieved following eutha-nasia using a carbon dioxide overdose.
A sheep model of polyurethane-pulmonary cuspreplacement to study blood material interactions wasused, in which under general anesthesia, and cardiopul-monary bypass, the right anterior pulmonary leaflet of
Fig. 2. Infrared surface scans of polyurethane films demonstrating Fourier transform infrared spectra (FTIR) spectra before and after derivatization
and rat subdermal implantation for polyurea–polyureathane (Biospan) and polycarbonate–polyurethane (Bionate). Results demonstrating unique
spectra for the parent polyurethanes without bulk changes following either derivatization or implantation. (A) Biospan spectra: (a) bisphosphonate
modified and unimplanted, (b) bisphosphonate modified, rat subdermal explant, (c) non-modified, unimplanted, (d) non-modified, rat subdermal
explant (B) Bionate spectra: (a) bisphosphonate modified and unimplanted, (b) bisphosphonate modified, rat subdermal explant, (c) non-modified,
unimplanted, (d) non-modified, rat subdermal explant.
I. Alferiev et al. / Biomaterials 22 (2001) 2683–26932686

the sheep pulmonary valve apparatus was removed, andreplaced with a 1.5� 1.5 cm polyurethane flap sewn in,as a replacement valve cusp. Animals were recovered,and after 90 days were subjected to euthanasia with anoverdose of barbiturates, followed by retrieval of thepulmonary outflow track, for explant analyses.
2.4. Explant evaluation
Polyurethane samples were subjected to calciumanalyses using atomic absorption spectroscopy toevaluate calcium levels in acid hydrolysates [18,19].Phosphorous content was determined using molybdatecomplexation spectroscopy on samples of the same acidhydrolysates [18,19]. Scanning electron microscopy[18,19] was performed on mounted, carbon-sputteredexplants using a JEOL model 330 scanning electronmicroscope (JEOL, Tokyo, Japan). Elemental analysescarried out with the same instrument using backscatterX-ray methodology (EDAX) with X-ray microanalysissoftware (Quantex V, Smyrna, GA). Microscopicstudies were carried out on neutral buffered formalinfixed specimens of the explanted polyurethane materials.Hematoxylin and eosin stains were used to determinemorphology characteristics, and calcification-specificstaining used the von Kossa method.
2.5. Statistical methods
Data were calculated as means� standard error (SE).The significance of differences was examined withStudent’s t-test. Statistical significance was noted withp40:05.
3. Results
3.1. Polyurethane pre-implant characteristics
Bisphosphonate derivatized polyurethanes in generalappeared physically comparable to non-derivatizedpolyurethanes. Water absorption capacity markedlyincreased with bisphosphonate derivatization, comparedto non-derivatized controls (Table 1). Bisphosphonatederivatized Biospan demonstrated the greatest waterabsorption capacity, increasing more than 15-fold frombaseline levels. Similarly, two examples of derivatizedBionate had roughly the same magnitude of changefrom control conditions. A stability study of the bindingof the bisphosphonates derivatized to each type ofpolyurethane to be used in implant studies was carriedout for a period of 9 months at 378C at pH 7.4 in 0.05mHEPES buffer (Table 1). No detectable change ofphosphorus content in either type of polyurethane wasnoted after this period. Thus, covalently linked bispho-sphonate within either type of polyurethane studied, was
stable over time with virtually no dissociation. FTIRscans of unmodified and modified polyurethanes re-vealed no spectra differences due to the covalentattachment of bisphosphonate (Figs. 1 and 2). Thus,both types of polyurethane, polyurea and polycarbo-nate, were successfully derivatized with bisphosphonate,in a stable covalent attachment that did not result in anysignificant changes in chemical bonding characteristicsas noted by FTIR.
3.2. Rat explant results
Implants of non-modified polyurea polyurethane, butnot polycarbonate polyurethane, calcified under condi-tions of DHT induced calciphylaxis. The polyureapolyurethane calcification was documented both withbulk analyses (Fig. 3), and scanning electron microscopystudies (Fig. 4). In general, the calcification was nodularin nature and completely surface-oriented. Bisphospho-nate modified polyurea polyurethane (Biospan) did notcalcify significantly, as documented both by chemicalanalyses and by scanning electron microscopy (Figs. 3and 4). Similarly, bisphosphonate derivatized polycar-bonate polyurethane (Bionate) also did not calcify in thesubdermal studies, as was true for the non-modifiedmaterial. FTIR spectra of non-calcified regions ofpolyurethane samples revealed no differences betweenmodified and non-modified, and in fact these spectra didnot differ from unimplanted samples (Fig. 2). However,calcific nodules could be scanned on the surface of thenonmodified Biospan explants, and these mineraldeposits have spectral characteristics in the IR rangeconsistent with the presence of hydroxyapatite and otherunidentified calcium phosphate mineral phases as well
Fig. 3. Calcification of polyurethanes implanted subdermally in rats
inhibited by bisphosphonate modification (Biospan Mod. & Bionate-
Mod). Results of 60 day explants. p ¼ 0:05 Biospan vs. Biospanbisphosphonate modified.
I. Alferiev et al. / Biomaterials 22 (2001) 2683–2693 2687

Fig. 4. Scanning electron micrographs demonstrating calcification of polyurea–polyurethane (Biospan) subdermal implants A(100� ) and B(2000� ) compared to an absence of calcification noted in bisphosphonate modified polyurethane C (100� ) and D (3500� ). Note calcific nodules(see arrows in A and B) confirmed as calcium phosphates by backscatter X-ray spectra (E).
I. Alferiev et al. / Biomaterials 22 (2001) 2683–26932688

Fig. 5. Scanning electron micrographs of polyurea–polyurethane (Biospan) pulmonary cusp replacements (in sheep) demonstrating calcification
A(500� ) and B (5000� ), confirmed by back scatter X-ray spectra (E). Note calcific nodules (see arrows in A and B). By comparison there was anabsence of calcification noted in bisphosphonate modified polyurethane C (500� ) and D (5000� ).
I. Alferiev et al. / Biomaterials 22 (2001) 2683–2693 2689

(Fig. 2). In addition, the bisphosphonate modifiedimplants were not associated with any deleterious effectson growth; mean rat weights (�S.E.) at the conlcusionof the implant period for the Biospan and Bionategroups were 495� 16.1 and 473� 13.0 respectively,compared to control, 473� 10.0 and 474� 12.0(p > 0:25).
3.3. Sheep retrieval results
Since Bionate (unlike Biospan), did not calcifysubdermally, only Biospan was studied in these sheepimplants. The sheep pulmonary leaflet model was highlysuccessful, with no mortality over the 3-month implantperiod. All explanted pulmonary leaflet replacementsappeared to be mechanically functioning as semi-lunarleaflet replacements, with no significant evidence ofthrombosis. Sparse calcific nodules, as documented byscanning electron microscopy (Fig. 5), were noted in thenon-modified Biospan cusps, but not the bisphospho-nate modified explants. Calcium and phosphorus levelsin the sheep explants demonstrated lower bulk calciumlevels in the bisphosphonate modified polyurethanecusps vs. the unmodified Biospan as a control (Fig. 6),although the bulk calcium levels were low and notstatistically significant comparing bisphosphonate mod-ified to unmodified control explants. In general, FTIRscans of the retrieved polyurethane cusps revealed nosignificant spectral differences between implanted andunimplanted (Fig. 7A). However, when microminerali-zation was found, after the subtraction of Biospanabsorbances, the resultant spectra between 1100 and
900 cm�1 was typical of well crystallized hydroxy apatite(Fig. 7B) [26].
4. Discussion
This paper reports the first successful results ofcovalent modification of fully polymerized polyur-ethanes with bisphosphonate derivatization, achievedthrough the modification of the hard segment of full-length polyurethane monomers. Furthermore, ourresults show that the bisphosphonate modification ofthese polyurethanes facilitated their calcification resis-tance in rat subdermal studies. Our bisphosphonatemodified polyurethanes were also completely bloodcompatible, and calcification resistant, with excellentfunctionality based on a series of 90 day implants in asheep pulmonary leaflet replacement model.Calcification of trileaflet polyurethane valves and
comparable prostheses fabricated from other elastomershave been reported from both experimental and clinicalstudies. These polymeric calcifications have pathologicfeatures [1–10] comparable to those observed in thepresent study. Calcification of polyurethane is typicallysurface oriented with the bulk of the polymer unaffected.In the blood stream, both thrombus associated andthrombus-independent calcific deposits have been notedin clinical and experimental explants [1–11]. Althoughpolyurethanes are widely used in artificial heart andventricular assist systems, there has been little interest inthe calcification potential of polyurethanes, and vir-tually no successful formulations brought forward toresist calcification. Results of our study represent one ofthe few positive steps in this direction. Importantly, nosuccessful strategy for preventing polyurethane calcifi-cation has been reported prior to the present studies. Ingeneral, polyurethane calcification has been difficult toinvestigate experimentally. Circulatory models areexpensive and lengthy, with highly variable results.Subdermal implants in rats in general calcify very little[18,19], even with calciphylaxis provoked calcification[19]. Nevertheless, our subdermal results were definitive,showing statistically significant calcification, and inhibi-tion of mineralization, with bisphosphonate modifiedpolyurethanes.Bisphosphonates act to resist calcification through
disrupting calcium phosphate crystal growth. Thesecompounds specifically poison the crystallization ofhydroxyapatite [22–24], and other calcium phosphatemineral phases [22–24]. In addition, bisphosphonatesare known to possess some other desirable propertiesthat may facilitate calcification resistance, includinginhibition of alkaline phosphatase [25], thereby reducingthe potential for calcification of devitalized absorbedcells, or cell fragments. Our group has previouslyreported attaching a bisphosphonate (ethanehydroxybis-
Fig. 6. Calcification of polyurea–polyurethane (Biospan) implanted as
a pulmonary cusp replacement in sheep inhibited by bisphosphonate
modification (Biospan Mod). Results of 90 day explants. p ¼ 0:31Biospan Ca2+ vs. Biospan bisphosphonate modified.
I. Alferiev et al. / Biomaterials 22 (2001) 2683–26932690

phosphonate) to a polyurethane–polyepoxy–resin inter-penetrating polymer network [19]. While this derivatizedpolymer was potentially of interest for circulatoryimplants, it lacked the appropriate elastomeric char-
acteristics retained by the polyurethane derivatized inthe present studies. Furthermore, previous studies byour group have shown that localized administration ofbisphosphonates avoids the adverse effects of these
Fig. 7. Infrared surface scans of polyurethane films demonstrating FTIR spectra before and after sheep pulmonary cusp implantation for polyurea–
polyureathane (Biospan). Results demonstrating spectra typical of the parent polyurethane without bulk changes (compared to Fig. 2), following
either derivatization or implantation. (A) Bulk FTIR spectra of polyurethane surfaces: (a) bisphosphonate modified Biospan explant, (b) non-
modified explant. (B) Microscopic analysis of a calcific nodule on the polyurethane surface: (c) non-deconvoluted spectra, (d) deconvoluted peaks at
1170, 1102, 1056, and 1019, corresponding to reference peaks 1160, 1107, 1057, 1023 as published for carbonate-apatite [26].
I. Alferiev et al. / Biomaterials 22 (2001) 2683–2693 2691

agents on bone and overall somatic growth [15–17]. Thepresent study utilizing localized use of bisphosphonatescovalently bound to polyurethane, was similarly notassociated with any deleterious effects on growth of theexperimental animals studied.Future directions for our studies will include tri-leaflet
polyurethane valve prosthesis devices, with experimentalmitral valve replacements to examine the efficacy of thisapproach in an orthotopic configuration very relevant toclinical valve prosthesis replacement surgery. We willalso continue to investigate the pulmonary leaflet model,with studies extending beyond 90 days to 20 weeks, andeven 1 year.In conclusion, we have successfully derivatized poly-
urethanes with bisphosphonates, and this derivatizationresults in calcification resistance in both rat subdermaland sheep circulatory implant models. The followingpoints are of importance:
1. Bisphosphonate derivatization via activation of thepolymer hard segment of already polymerized med-ical grade polyurethanes in both polymer andpolycarbonate-urethanes has been achieved for thefirst time.
2. These derivatized polyurethanes demonstrate stableand apparently irreversible binding of bisphospho-nate through a covalent bond achieved via a strategyinvolving activating the polymer hard segment.
3. Our bisphosphonate derivatized polyurethanes resistcalcification both in rat subdermal implants, andsheep circulatory studies, without any adverse effectson growth.
Acknowledgements
The authors thank Ms. Ginger Nicholson for herefforts in preparing the manuscript. This research wassupported in part by the following grants: NIH-HL59730, The Mary W. Smith Trust, and The WilliamJ. Rashkind Endowment of The Children’s Hospital ofPhiladelphia.
References
[1] Bernacca GM, Mackay TG, Wilkinson R, Wheatley DJ.
Polyurethane heart valves: fatigue failure, calcification, and
polyurethane structure. J Biomed Mater Res 1997;34:371–9.
[2] Bernacca GM, Wheatley DJ. Surface modification of polyur-
ethane heart valves: effects on fatigue life and calcification. Int J
Artif Organs 1998;21:814–49.
[3] Billy GG, Miller CA, Pallone MN, Donachy JH, Pierce WS.
Hemolytic differences among artificial cardiac valves used in a
ventricular assist pump. Artif Organs 1995;19:339–43.
[4] Clift SE, Fisher J. Finite element stress analysis of a new design of
synthetic leaflet heart valve. Proc Inst Mech Eng [H] 1996;
210:267–72.
[5] Park Y, Ryu E, Kim H, Jeong J, Kim J, Shim J, Jeon S, Jo Y,
Kim W, Min B. Characterization of antithrombotic activity of
lumbrokinase-immobilized polyurethane valves in the total
artificial heart. Artif Organs 1999;23:210–4.
[6] Wheatley DJ, Raco L, Bernacca GM, Sim I, Belcher PR, Boyd JS.
Polyurethane: material for the next generation of heart valve
prostheses? Eur J Cardiothorac Surg 2000;17:440–8.
[7] Robin J, Martinot S, Curtil A, Vedrinne C, Tronc F, Franck M,
Champsaur G. Experimental right ventricle to pulmonary artery
discontinuity: outcome of polyurethane valved conduits. J Thorac
Cardiovasc Surg 1998;115:898–903.
[8] Braunwald NS. Performance of materials in vascular prosthetic
devices: heart valves. Bull NY Acad Med 1972;48:357–61.
[9] Braunwald NS. It will work: the first successful mitral valve
replacement. Ann Thorac Surg 1989;48:S1–3.
[10] Fishbein MC, Roberts WC, Golden A, Hufnagel CA. Cardiac
pathology after aortic valve replacement using Hufnagel trileaflet
prostheses: a study of 20 necropsy patients. Am Heart J
1975;89:443–8.
[11] Kay EB. Early years in artificial valve development. Ann Thorac
Surg 1989;48:S24–5.
[12] Bone HG, Adami S, Rizzoli R, Favus M, Ross PD, Santora A,
Prahalada S, Daifotis A, Orloff J, Yates J. Weekly administration
of alendronate: rationale and plan for clinical assessment. Clin
Ther 2000;22:15–28.
[13] Downs Jr RW, Bell NH, Ettinger MP, Walsh BW, Favus MJ,
Mako B, Wang L, Smith ME, Gormley GJ, Melton ME.
Comparison of alendronate and intranasal calcitonin for treat-
ment of osteoporosis in postmenopausal women. J Clin En-
docrinol Metab 2000;85:1783–8.
[14] Levy RJ, Schoen FJ, Lund SA, Smith MS. Prevention of
leaflet calcification of bioprosthetic heart valves with dipho-
sphonate injection therapy. Experimental studies of optimal
dosages and therapeutic durations. J Thorac Cardiovasc Surg
1987;94:551–7.
[15] Levy RJ, Wolfrum J, Schoen FJ, Hawley MA, Lund SA, Langer
R. Inhibition of calcification of bioprosthetic heart valves by local
controlled-release diphosphonate. Science 1985;228:190–2.
[16] Golomb G, Langer R, Schoen FJ, Smith MS, Choi YM, Levy RJ.
Controlled release of diphosphonate to inhibit bioprosthetic heart
valve calcification: dose-response and mechanistic studies. J Cont
Rel 1986;4:181–94.
[17] Golomb G, Dixon M, Smith MS, Schoen FJ, Levy RJ. Controlled
release drug delivery of diphosphonates to inhibit bioprosthetic
heart valve calcification: release rate modulation with silicone
matrices via drug solubility and membrane coating. J Pharm Sci
1987;76:271–6.
[18] Joshi RR, Frautschi JR, Phillips Jr RE, Levy RJ. Phosphonated
polyurethanes that resist calcification. J Appl Biomat 1994;5:
65–77.
[19] Joshi RR, Underwood T, Frautschi JR, Phillips Jr RE, Schoen
FJ, Levy RJ. Calcification of polyurethanes implanted subder-
mally in rats is enhanced by calciphylaxis. J Biomed Mater Res
1996;31:201–7.
[20] Alferiev IS, Vyavahare N, Song CX, Levy RJ. Elastomeric
polyurethanes modified with geminal bisphosphonate groups.
J Polymer Sci 2001;39:105–16.
[21] Chen PS, Toribara TY, Warner H. Microdetermination of
phosphorus. Anal Chem 1956;28:1756–8.
[22] Fleisch H. Experimental basis for the use of bisphosphonates in
Paget’s disease of bone. Clin Orthop 1987;72–8.
[23] Fleisch H. Bisphosphonates}history, experimental basis. Bone
1987;8(Suppl 1):S23–8.
[24] Fleisch H. Bisphosphonates: a new class of drugs in diseases of
bone and calcium metabolism. Recent Results Cancer Res
1989;116:1–28.
I. Alferiev et al. / Biomaterials 22 (2001) 2683–26932692

[25] Hirsch D, Schoen FJ, Levy RJ. Effects of metallic ions and
diphosphonates on inhibition of pericardial bioprosthetic tissue
calcification and associated alkaline phosphatase activity. Bioma-
terials 1993;14:371–7.
[26] Boskey AL, Pleshko N, Doty SB, Mendelsohn R. Applications
of fourier transform infrared (FT-IR) microscopy to the study
of mineralization in bone and cartilage. Cells Mat 1992;2:
209–20.
I. Alferiev et al. / Biomaterials 22 (2001) 2683–2693 2693
Copyright © 2022 FDOKUMEN




















