Vascularised Scaffolds for Cutaneous Wound Reconstruction ...

An Evidence-based Staging System forCutaneous Melanoma1
Charles M. Balch, MD; Seng-Jaw Soong, PhD; Michael B. Atkins, MD;Antonio C. Buzaid, MD; Natale Cascinelli, MD; Daniel G. Coit, MD; Irvin D. Fleming, MD;Jeffrey E. Gershenwald, MD; Alan Houghton, Jr., MD; John M. Kirkwood, MD;Kelly M. McMasters, MD; Martin F. Mihm, MD; Donald L. Morton, MD;Douglas S. Reintgen, MD; Merrick I. Ross, MD; Arthur Sober, MD;John A. Thompson, MD; John F. Thompson, MD
ABSTRACT A completely revised staging system for cutaneous melanoma was implemented
in 2003. The changes were validated with a prognostic factors analysis involving 17,600 mel-
anoma patients from prospective databases. This major collaborative study of predicting mel-
anoma outcome was conducted specifically for this project, and the results were used to finalize
the criteria for this evidence-based staging system. In fact, this was the largest prognostic
factors analysis of prospectively followed melanoma patients ever conducted. Important results
that shaped the staging criteria involved both the tumor-node-metastasis (TNM) criteria and
stage grouping for all four stages of melanoma. Major changes in the staging include: (1)
melanoma thickness and ulceration are the dominant predictors of survival in patients with
localized melanoma (Stages I and II); deeper level of invasion (ie, IV and V) was independently
associated with reduced survival only in patients with thin or T1 melanomas. (2) The number of
metastatic lymph nodes and the tumor burden were the most dominant predictors of survival in
patients with Stage III melanoma; patients with metastatic nodes detected by palpation had a
shorter survival compared with patients whose nodal metastases were first detected by sentinel
node excision of clinically occult or “microscopic” metastases. (3) The site of distant metastases
(nonvisceral versus lung versus all other visceral metastatic sites) and the presence of elevated
serum lactate dehydrogenase (LDH) were the dominant predictors of outcome in patients with
Stage IV or distant metastases. (4) An upstaging was implemented for all patients with Stage I,
II, and III disease when a primary melanoma is ulcerated by histopathological criteria. (5) Satellite
metastases around a primary melanoma and in-transit metastases were merged into a single
staging entity that is grouped into Stage III disease. (6) A new convention was implemented for defining clinical and pathological
staging so as to take into account the new staging information gained from lymphatic mapping and sentinel node biopsy. (CA Cancer
J Clin 2004;54:131–149.) © American Cancer Society, 2004.
INTRODUCTION
It is estimated that 55,100 cases of invasive melanoma will be diagnosed in the United States in 2004 (4% of allcancer cases) and that 7,910 patients will die of the disease (1% to 2% of all cancer deaths). Melanoma is estimatedto be the fifth and seventh most common cancers in men and women, respectively, among new cases of cancer in
1Three meetings held by the AJCC Melanoma Staging Committee were partially supported by an unrestricted educational grant from Schering Pharmaceutical,Kenilworth, NJ.
Dr. Balch is Executive Vice-President and CEO, American Soci-ety of Clinical Oncology, Alexandria,VA and Professor, Surgery and On-cology, Johns Hopkins MedicalCenter, Baltimore, MD.
Dr. Soong is Professor, Departmentsof Medicine and Biostatistics, and Di-rector, Biostatistics and BioinformaticsUnit, University of Alabama Compre-hensive Cancer Center, Birming-ham, AL.
Dr. Atkins is Director, BiologicTherapy and Cutaneous OncologyPrograms; Associate Director, Clin-ical Research; and Professor, De-partment of Medicine, Beth IsraelDeaconess Medical Center, Bos-ton, MA.
Dr. Buzaid is Executive Director,Oncology Center, Hospital Sirio Li-banes, São Paulo, Brazil.
Dr. Cascinelli is Scientific Director,Italian National Cancer Institute, andPresident, WHO Melanoma Pro-gram, Milan, Italy.
Dr. Coit is Co-leader, MSKCC Mel-anoma Disease Management Team,Memorial Sloan-Kettering CancerCenter, New York, NY.
Dr. Fleming is Professor, Departmentof Surgery, University of Tennesseefor the Health Sciences, Memphis, TN.
Dr. Gershenwald is Associate Pro-fessor, Departments of Surgery andCancer Biology, University of TexasMD Anderson Cancer Center, Hous-ton, TX.
CA Cancer J Clin 2004;54:131–149
Volume 54 Y Number 3 Y May/June 2004 131

the United States in 2004.1 Forthese reasons, physicians involvedin diagnosing and treating cancerwill need to know about the stagingof this common cancer.
The staging of melanoma, as withother cancers, is important to clini-cians and researchers because itprovides: (1) a nomenclature of con-sistent terms and definitions based onprognosis; (2) compartmentalizationof patients into definable risk groupswith regard to metastatic risk and sur-vival rates; (3) criteria for stratificationand reporting results of melanomaclinical trials; (4) a critical componentfor comparisons of treatment resultsamong different centers; and (5) avaluable tool for clinical decisionmaking. The melanoma staging sys-tem was selected as the first topic in aseries of articles for this Journal fromthe American Joint Committee onCancer (AJCC). It is representative ofa new approach incorporating prog-nostic factors analyses of large cancerdatabases as an evidence-based meth-od to create and/or validate AJCCstaging criteria.2
The Melanoma Staging Commit-tee of the AJCC was formed in 1998with experts from all relevant medicalspecialties, including the leadership ofmost of the major melanoma centersand cooperative groups from NorthAmerica, Europe, and Australia, andit convened in March 1999.3 Mem-bers of the Melanoma Staging Com-mittee and additional consultantsagreed to an unprecedented collabo-ration to share prospectively accumu-lated melanoma outcome data, and atthat time they established the AJCCMelanoma Staging Database.2 This isa single large database involving mel-anoma patients from 13 cancer cen-ters and cooperative groups createdfor the purpose of validating the pro-
posed revisions to the melanoma staging system.The data were merged from prospective databases
of patients who did not receive any adjuvantsystemic therapy and for whom all had qualitycontrol measures in place regarding data entry,pathology, and surgery. Details about the datacollection, statistical methodologies, and resultshave been published.2 The resultant collaborativeresearch project is the largest prognostic factorsanalysis of melanoma ever conducted. Resultsfrom the prognostic factors analyses, as well asinput from melanoma clinicians, were used bythe AJCC Melanoma Staging Committee to cre-ate an evidence-based melanoma staging systemthat was published in 2001.4 This staging systembecame official with publication of the sixth edi-tion of the AJCC Cancer Staging Manual.5 Inaddition, these melanoma staging criteria havebeen approved and adopted by the InternationalUnion Against Cancer/Union Internationale Contre le Cancer (IUAC/UICC) TNM Committee, by the World HealthOrganization Melanoma Program, and by theEuropean Organization for Research and Treat-ment of Cancer Melanoma Group.
This educational article draws substantiallyfrom the original scientific publications onthe melanoma staging and prognostic factorsanalysis as well as from the melanoma stagingchapter in the sixth edition of the AJCCCancer Staging Manual.2–5 The staging criteriadeveloped in this AJCC prognostic factorsanalysis have been independently confirmedby results from melanoma referral cen-ters.6 –10
Selection by the AJCC Melanoma StagingCommittee of independent prognostic featuresof melanoma to be used in the revised mela-noma tumor-node-metastasis (TNM) classifi-cation and the stage groupings was guided byfive principles:1. The staging system must be reproducible
and applicable to the practical needs of di-verse medical disciplines.
2. The criteria must reflect the biology ofmelanoma based on consistent outcomesof patients treated at multiple institutionsfrom multiple countries.
3. The criteria used must be evidence-basedand reflect the dominant prognostic factors
Dr. Houghton is Chief, Clinical Im-munology Service; Head, MelanomaDisease Management Team; andChairman, Immunology Program atMemorial Sloan-Kettering CancerCenter, New York, NY.
Dr. Kirkwood is Professor andVice-Chairman, Clinical Research,Department of Medicine, and Direc-tor, Melanoma Center, University ofPittsburgh Medical Center, Pitts-burgh, PA.
Dr. McMasters is Professor andDirector, Division of Surgical Oncol-ogy, University of Louisville MedicalCenter, Louisville, KY.
Dr. Mihm is Clinical Professor, De-partment of Pathology, Massachu-setts General Hospital, HarvardMedical School, Boston, MA.
Dr. Morton is Medical Director andSurgeon-in-Chief, John WayneCancer Institute, Saint John’s HealthCenter, Santa Monica, CA.
Dr. Reintgen is Director, LakelandRegional Cancer Center, Lake-land, FL.
Dr. Ross is Professor, Departmentof Surgery, and Chief, MelanomaSection, Department of Surgical On-cology, University of Texas MDAnderson Cancer Center, Hous-ton, TX.
Dr. Sober is Professor, Departmentof Dermatology, Harvard MedicalSchool, and Associate Chief, De-partment of Dermatology, Massa-chusetts General Hospital, Bos-ton, MA.
Dr. JA Thompson is AssociateProfessor, Department of Medicine,University of Washington, and Co-director, Melanoma Clinic, Univer-sity of Washington Medical Center,Seattle, WA.
Dr. JF Thompson is Professor,Department of Surgery (Melanomaand Surgical Oncology), Universityof Sydney, and Executive Director,Sydney Melanoma Unit, RoyalPrince Alfred Hospital, Sydney,NSW, Australia.
The article is available online at:http://CAonline.AmCancerSoc.org
An Evidence-based Staging System
132 CA A Cancer Journal for Clinicians

consistently identified in Cox multivariateregression analyses.
4. The criteria must be relevant to currentclinical practice and regularly incorporatedin clinical trials.
5. The required data in medical records mustbe easily identifiable by tumor registrarswho code staging information.The 2003 versions of the TNM categories
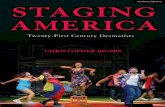
and stage groupings are defined in Tables 1and 2, respectively. Figure 1 shows 15-yearsurvival rates for patients with Stage I to IVmelanoma. The major differences betweenthe new (2003) and the previous (1997) ver-sions of the melanoma staging system aresummarized in Table 3. For example, the2003 version retains the anatomic compart-mentalization that categorizes patients withlocalized melanoma (ie, without any evi-dence of metastases) to Stages I and II, thosewith regional metastases to Stage III, andthose with distant metastases to Stage IV.The 1997 version assigned patients withthick melanomas (�4.0 mm in thickness orT4NOMO) to Stage III, whereas in the newversion these patients are grouped to Stage II.
RULES FOR CLASSIFICATION
The primary difference in the definitions ofclinical versus pathological stage grouping iswhether the regional lymph nodes are stagedby clinical/radiologic examination or bypathologic examination (after partial or com-plete lymphadenectomy).
Clinical Staging
Clinical Stages I and II are confined to thosepatients who have no evidence of metastases,either at regional or distant sites, based on clin-ical, radiologic, and/or laboratory evaluation.Stage III melanoma patients are those withclinical or radiologic evidence of regional me-tastases, either in the regional lymph nodes orintralymphatic metastases manifesting as eithersatellite or in-transit metastases. Clinical StageIII groupings rely on clinical and/or radiologicassessment of the regional lymph nodes, which
is inherently difficult, especially with respect toassessing both the presence and the number ofmetastatic nodes. The Melanoma StagingCommittee therefore made no subgroup defi-nitions of clinically staged patients with nodalor intralymphatic regional metastases. They areall categorized within the group of clinicalStage III disease (Table 2). Clinical Stage IVmelanoma patients have metastases at some dis-tant site and are not substaged.
Pathological Staging
In contrast to clinical staging, there is greateraccuracy (both qualitatively and quantitatively)in defining distinctive prognostic subgroupswhen combining pathological informationabout both the primary melanoma and theresults of pathological examination of the re-gional lymph nodes after sentinel or completelymphadenectomy.
Pathological Stages I and II melanoma com-prise those patients who have no evidence ofregional or distant metastases, based on absenceof nodal metastases after careful pathologicalexamination of the regional lymph nodes, andabsence of distant metastases based on routineclinical and radiologic examination. Patholog-ical Stage III melanoma patients have patho-logical evidence of regional metastases, eitherin the regional lymph nodes or intralymphaticsites. The quantitative classification for patho-logical nodal status requires that pathologistsperform a careful examination of the surgicallyresected nodal basin and report on the actualnumber of lymph nodes examined and thenumber of nodal metastases identified. Patho-logical Stage IV melanoma patients have histo-logic documentation of metastases at one ormore distant sites.
The ability to stage melanoma patients moreaccurately with sentinel node technology hasmarkedly changed our understanding of thenatural history of melanoma.11,12 This power-ful new staging technology has caused a signif-icant stage migration that is now accounted forin this version of melanoma staging. With thewidespread use of sentinel node lymphadenec-tomy, it is clear that there is considerable stage
CA Cancer J Clin 2004;54:131–149
Volume 54 Y Number 3 Y May/June 2004 133

migration of patients previously staged as“node negative,” but who, in fact, had unde-tected nodal metastases. These previously un-derstaged Stage III patients have revealed anextraordinary heterogeneity of metastatic riskfor Stage III melanoma. Thus, the range ofsurvival rates among various subgroups ofpathological Stage III patients is quite large,ranging from 9% to 63% 10-year survival.2
Clinical Versus Pathological Staging
The AJCC Melanoma Staging Committee ad-dressed the issue of staging information after sen-tinel lymphadenectomy or elective lymph nodedissection through the definition of clinical and
pathological staging. By convention, clinical stag-ing should be performed after complete excisionof the primary melanoma (including microstag-ing) with clinical assessment of regional lymphnodes. Pathological staging will use informationgained from both microstaging of the primarymelanoma and pathological evaluation of thenodal status after partial (ie, sentinel) or completelymphadenectomy (ie, after elective or therapeu-tic lymph node dissection).
Significant differences were identified whensurvival rates for melanoma patients who wereclinically staged were compared with those pa-tients whose nodal disease was staged patholog-ically (Table 4). These survival differencesbetween clinically and pathologically staged pa-
TABLE 1 Melanoma TNM Classification
T Classification
Thickness Ulceration Status
T1 �1.0 mm a: without ulceration and level II/IIIb: with ulceration or level IV/V
T2 1.01 to 2.0 mm a: without ulcerationb: with ulceration
T3 2.01 to 4.0 mm a: without ulcerationb: with ulceration
T4 �4.0 mm a: without ulcerationb: with ulceration
N Classification
No. of Metastatic Nodes Nodal Metastatic Mass
N1 One node a: micrometastasis*b: macrometastasis†
N2 Two to three nodes a: micrometastasis*b: macrometastasis†c: in-transit metastases/satellite(s)
without metastatic nodes
N3Four or more metastatic nodes, or matted nodes, or in-transit
metastases/satellite(s) with metastatic node(s)
M Classification
Site Serum LDH‡
M1a Distant skin, subcutaneous tissue, or nodal metastases NormalM1b Lung metastases NormalM1c All other visceral metastases Normal
Any distant metastasis Elevated
*Micrometastases are diagnosed after sentinel or elective lymphadenectomy.†Macrometastases are defined as clinically detectable nodal metastases confirmed by therapeuticlymphadenectomy or when nodal metastasis exhibits gross extracapsular extension.‡LDH � Lactate dehydrogenase.Adapted from Balch CM, Buzaid AC, Soong SJ, et al.4 with permission from the American Society ofClinical Oncology.
An Evidence-based Staging System
134 CA A Cancer Journal for Clinicians

tients were statistically significant among all Tsubstages except for T4b (Table 4). The differ-ences were most striking in patients with clin-ical T2bN0M0, T3aN0M0, T3bN0M0, andT4aN0M0 disease, where 10-year survival ratesfor the same category of clinically versus patho-logically staged patients varied significantly,with clinically staged patients having an abso-
lute survival rate that was 20% to 29% lower incomparison with pathologically staged patientsof equivalent T categories (Table 4). Theseresults highlight the compelling prognosticvalue of knowing the nodal status as identifiedby lymphatic mapping and sentinel lymphade-nectomy in those situations where accuratestaging is important.
TNM CLASSIFICATION
Primary Tumor (T)
Primary tumors are classified according tothe categories below:Y Tx: Primary tumor cannot be assessed (eg,
shave biopsy or regressed melanoma).Y T0: No evidence of primary tumor.Y Tis: Melanoma in situ.Y T1: Melanomas �1.0 mm in thickness.Y T2: Melanomas 1.01 to 2.0 mm.Y T3: Melanomas 2.01 to 4.0 mm.Y T4: Melanomas �4.0 mm.
Ten-year survival rates for each of the Tcategories in clinically staged patients areshown in Figure 2.
Melanoma Thickness
The T category of melanoma is classified pri-marily by measuring the thickness of the mela-noma. In the 1997 version of the melanomastaging system, the threshold of a T1/T2 mela-noma was defined as 0.75 mm, as empiricallyrecommended by Dr. Alexander Breslow in1970.13,14 The 2003 version defines the T cate-gory thresholds of melanoma thickness in evenintegers (ie, at 1.0, 2.0, and 4.0 mm), becausethey represent both a statistical “best fit” and aremost compatible with current thresholds in mak-ing clinical decisions and classifying prognosticgroups of node-negative (N0) melanoma pa-tients.
Melanoma Ulceration
The secondary criterion for T staging is thepresence or absence of ulceration above the pri-mary melanoma based on a histopathological ex-amination. Melanoma ulceration is definedhistologically as the absence of an intact epidermis
TABLE 2 Stage Groupings for CutaneousMelanoma
Clinical Staging*
0 Tis N0 M0IA T1a N0 M0IB T1b N0 M0
T2a N0 M0IIA T2b N0 M0
T3a N0 M0IIB T3b N0 M0
T4a N0 M0IIC T4b N0 M0III Any T Any N M0IV Any T Any N Any M
Pathologic Staging†
0 Tis N0 M0IA T1a N0 M0IB T1b N0 M0
T2a N0 M0IIA T2b N0 M0
T3a N0 M0IIB T3b N0 M0
T4a N0 M0IIC T4b N0 M0IIIA T1–4a N1a M0
T1–4a N2a M0IIIB T1–4b N1a M0
T1–4b N2a M0T1–4a N1b M0T1–4a N2b M0T1–4a N2c M0T1–4b N2c M0
IIIC T1–4b N1b M0T1–4b N2b M0Any T N3 M0
IV Any T Any N Any M
*Clinical staging includes microstaging of the primarymelanoma and clinical/radiologic evaluation for metasta-ses. By convention, it should be used after complete ex-cision of the primary melanoma with clinical assessmentfor regional and distant metastases.†Pathologic staging includes microstaging of the primarymelanoma and pathological information about the regionallymph nodes after partial or complete lymphadenectomy.Pathologic Stage 0 or Stage IA patients are the exception;they do not require pathologic evaluation of their lymphnodes.Adapted from Balch CM, Buzaid AC, Soong SJ, et al.4 withpermission from the American Society of Clinical Oncology.
CA Cancer J Clin 2004;54:131–149
Volume 54 Y Number 3 Y May/June 2004 135

overlying a significant portion of the primarylesion.2,15,16 Survival rates for patients with anulcerated melanoma are lower than those of pa-tients with a nonulcerated melanoma of equiva-lent T category but are remarkably similar tothose of patients with a nonulcerated melanomaof the next highest T category (Figure 2 andTable 5).
Melanoma Level of Invasion
A third criterion, the level of invasion(with regard to the papillary dermis, reticulardermis, and subcutis) as defined by Dr. Wal-lace Clark,17 is used when defining subcate-gories of T1 melanomas but not for thickermelanomas (ie, T2, T3, or T4). The level ofinvasion does not reflect prognosis as accu-rately as tumor thickness for reasons thathave been discussed in previous publica-tions.3,15,18,19 Nevertheless, level of invasiondoes provide additional prognostic discrimi-
nation in the specific subgroup of thin (ie,T1; �1.0 mm) melanomas.2,20,21
DEFINING T1 MELANOMAS
In this cohort of T1 melanomas, the as-signment of T1a is restricted to patients sat-isfying three criteria: (1) �1.0 mm thick; (2)absence of ulceration; and (3) depth of inva-sion limited to level II or III. T1b melanomasare defined as those with a thickness of �1.0mm and with the more aggressive features oflevel IV or V, or those with ulceration (re-gardless of level). Both conditions are asso-ciated with a significant reduction in survivalrates in patients with T1 melanomas.20,22–24
About three fourths of patients with T1 mel-anomas are T1a and have a 95% five-yearsurvival, while the remaining T1 patientshave T1b lesions and experience a somewhatlower 91% five-year survival (Figure 2 andTable 5).
FIGURE 1 Fifteen-year Survival Curves for the Melanoma Staging System Comparing Localized Melanoma (Stages Iand II), Regional Metastases (Stage III), and Distant Metastases (Stage IV).The numbers in parentheses are the numbers of patients from the AJCC melanoma staging database used to calculatethe survival rates. The differences between the curves are highly significant (P � 0.0001).Adapted from Balch CM, Soong SJ, Gershenwald J, et al.4 with permission from the American Society of ClinicalOncology.
An Evidence-based Staging System
136 CA A Cancer Journal for Clinicians

TABLE 3 Differences Between the Previous Version (1997) and the Present Version (2002) of theMelanoma Staging System
Factor Previous Version Present Version Comments
Thickness Secondary prognostic factor;thresholds of 0.75, 1.50, 4.0mm
Primary determinant of Tstaging; thresholds of 1.0,2.0, 4.0 mm
Correlation of metastatic risk is acontinuous variable
Level of invasion Primary determinant of T staging Used only for defining T1melanomas
Correlation only significant forthin lesions; variability ininterpretation
Ulceration Not included Included as a seconddeterminant of T and Nstaging
Signifies a locally advancedlesion; dominant prognosticfactor for grouping Stage I, II,and III
Satellite metastases In T category In N category Merged with in-transit lesionsThick melanomas(�4.0 mm)
Stage III Stage IIC
Dimensions of nodalmetastases
Dominant determinant of Nstaging
Not used No evidence of significantprognostic correlation
Number of nodalmetastases
Not included Dominant determinant of Nstaging
Thresholds of 1 versus 2 to 3versus �4 nodes
Metastatic “volume� Not included Included as a seconddeterminant of N staging
Clinically occult (microscopic)versus clinically apparent(macroscopic) nodal volume
Lung metastases Merged with all other visceralmetastases
Separate category as M1b Has a somewhat betterprognosis than other visceralmetastases
Elevated serum LDH* Not included Included as a seconddeterminant of M staging
Included as a seconddeterminant of M staging
Clinical versuspathologic staging
Did not account for sentinel nodetechnology
Sentinel node resultsincorporated into definition ofpathologic staging
Large variability in outcomebetween clinical andpathologic staging; pathologicstaging encouraged prior toclinical trials
*LDH � Lactate dehydrogenase.
TABLE 4 Five- and 10-year Survival Rates for 5,346 Patients with Clinically Negative Nodal MetastasesReceiving Regional Lymph Node Dissection or Sentinel Lymphadenectomy
T StagePath Nodes
(N)Five-year Survival
% � SE*10-year Survival
% � SE* P Value
T1a N � (n � 379) 94 � 2.0 86 � 4.0 0.0035N � (n � 15) 64 � 17.7 64 � 17.7
T1b N � (n � 319) 90 � 2.5 84 � 3.5 0.0039N � (n � 18) 76 � 14.9 76 � 14.9
T2a N � (n � 1480) 94 � 0.8 86 � 1.6 �0.0001N � (n � 150) 73 � 5.6 73 � 5.6
T2b N � (n � 408) 83 � 2.3 68 � 3.7 �0.0001N � (n � 62) 56 � 8.8 43 � 9.7
T3a N � (n � 808) 86 � 1.6 73 � 2.4 �0.0001N � (n � 177) 59 � 6.0 53 � 5.1
T3b N � (n � 639) 72 � 2.1 61 � 2.6 �0.0001N � (n � 176) 49 � 4.5 32 � 6.1
T4a N � (n � 203) 75 � 3.9 63 � 6.1 0.0116N � (n � 66) 61 � 7.4 41 � 11.4
T4b N � (n � 330) 53 � 3.1 41 � 3.5 0.2403N � (n � 116) 44 � 5.5 37 � 5.9
*SE � Standard error.The presence of ulceration (histopathologically) of a primary melanoma (designated Tb) causes upstagingby one substage compared with a nonulcerated melanoma (designated Ta).Adapted from Balch CM, Buzaid AC, Soong SJ, et al.4 with permission from the American Society of Clinical Oncology.
CA Cancer J Clin 2004;54:131–149
Volume 54 Y Number 3 Y May/June 2004 137

All T2, T3, and T4 melanomas are de-fined using thickness and ulceration criteriaas described above, but not the level of in-vasion.
Melanoma In Situ, Indeterminate Melanomas,Multiple Primary Melamonas
Patients with indeterminate melanoma presen-tations and those who cannot be microstagedshould be categorized as Tx. Two examples ofindeterminate staging of melanoma would be adiagnosis with a shave or a curettage biopsy thattransected the base of the melanoma or when anunknown primary melanoma presents with re-
gional or distant metastases. Patients with mela-noma in situ are categorized as Tis. For patientswith multiple primary melanomas, the T cate-gory staging is based on the primary lesion withthe worst prognostic features.
Melanoma Growth Patterns
Most of the data used to derive the TNMcategories are from cases of melanoma withsuperficial spreading and nodular growth pat-terns. There is some evidence that lentigo ma-ligna melanoma, acral lentiginous melanoma,and desmoplastic melanoma may have a differ-ent etiology and natural history, with the
TABLE 5 Five-year Survival Rates of Pathologically Staged Patients*
IA IB IIA IIB IIC IIIA IIIB IIIC
Ta: T1 T2 T3 T4 N1a N1b N3Nonulcerated N2a N2b
95% 89% 79% 67% 67% 54% 28%
Tb: T1 T2 T3 T4 N1a N1b, N2bUlcerated N2a N3
91% 77% 63% 45% 52% 24%
*Survival rates appear in bold.Adapted from Balch CM, Buzaid AC, Soong SJ, et al.4 with permission from the American Society of Clinical Oncology.
FIGURE 2 Ten-year Survival Rates from the AJCC Melanoma Staging Database Comparing the Different T Categoriesand the Stage Groupings for Stages I and II Melanoma.Note that the stage groupings involve upstaging to account for melanoma ulceration, where thinner melanomas with ul-ceration are grouped with the next greatest T substage for nonulcerated melanomas.Adapted from Balch CM, Soong SJ, Gershenwald J, et al.4 with permission from the American Society of ClinicalOncology.
An Evidence-based Staging System
138 CA A Cancer Journal for Clinicians

former having a more favorable prognosis andthe latter two having a less favorable progno-sis.24 Nonetheless, the same staging criteriashould be used for melanomas with any ofthese growth patterns, even though their prog-noses may differ somewhat.
Regional Lymph Nodes (N)
Regional lymph nodes are classified accord-ing to the categories below:Y N0: No regional metastases detected.Y Nx: Patients in whom the regional nodes
cannot be assessed (ie, previously removed).Y N1 to N3: Regional metastases based on
the number of metastatic nodes and pres-ence or absence of intralymphatic metasta-ses (in-transit or satellite metastases).
Number of Metastatic Nodes
This factor is the primary criterion for de-fining the N category, because the number ofmetastatic nodes is most strongly associatedwith 10-year survival compared with all otherprognostic factors.2 Thus, patients with onemetastatic node were categorized as N1, thosewith two to three metastatic nodes as N2, andthose with four or more metastatic nodes as N3
(Table 1). Survival rates for these N subgroupsare shown in Figures 3 and 4.
Micrometastases Versus Macrometastases
The second most significant prognosticfeature for patients with lymph node metas-tases is the tumor burden of nodal metastases.Patients without clinical or radiologic evi-dence of lymph node metastases but whohave pathologically documented nodal me-tastases are defined by convention as having“microscopic” or “clinically occult” nodalmetastases. Although such nodal metastasesmay vary in size (especially for deep-seatednodes or in obese patients), this delineationcan be identified in the medical record, basedon the preoperative clinical examination andthe operative notation about the intent of thelymphadenectomy (ie, whether it is an elec-tive, sentinel, or therapeutic lymphadenec-tomy). In contrast, patients with both clinicalevidence of nodal metastases and pathologi-cal examination documenting the num-ber of lymph nodes containing melanomametastases (after therapeutic lymphadenec-tomy) are defined as having “macroscopic”or “clinically apparent” nodal metastases.Survival rates for these two patient groups
FIGURE 3 Five-year Survival Rates from the AJCC Melanoma Staging Database Comparing the Different N Catego-ries and the Stage Groupings for Stage III Melanoma.The survival results are significantly different when the primary melanoma is ulcerated compared with equivalent N cate-gory of patients without ulceration. See Tables 1 and 2 for definitions.Adapted from Balch CM, Soong SJ, Gershenwald J, et al.4 with permission from the American Society of ClinicalOncology.
CA Cancer J Clin 2004;54:131–149
Volume 54 Y Number 3 Y May/June 2004 139

differ significantly.2,25,26 Although previousmelanoma staging systems used maximummeasured dimensions of lymph node metas-tases (�5 cm in the 1987 version and �3 cmin the 1992 and 1997 versions), the Mela-noma Staging Committee found no compel-ling evidence in the literature that themeasured size of nodal metastases had anyindependent prognostic value.18,27
Intralymphatic Metastases
The third criterion for defining the Ncategory is the presence or absence of satel-lites or in-transit metastases, regardless of thenumber of lesions. Clinical or microscopicsatellite lesions around a primary melanomaand in-transit metastases between the pri-mary melanoma and regional lymph nodesrepresent intralymphatic metastases.18,28,29
The available data show that these two ana-tomically defined entities are associated withequally poor survival outcomes.18 Both sat-
ellites and in-transit metastases are, in theabsence of synchronous nodal metastases, as-signed to a separate N2c classification be-cause both have a prognosis equivalent tomultiple nodal metastases (Table 1). Theavailable data also demonstrate that patientswith a combination of satellites/in-transitmetastases plus nodal metastases have a worseoutcome than patients with either eventalone, so that these patients were assigned toan N3 classification regardless of the numberof synchronous nodal metastases (Table 1).
Contiguous or Multiple Nodal Basinsand Staging
By convention, regional nodal metastases re-fer to disease confined to one nodal basin ortwo contiguous nodal basins. For example,nodal metastases in combinations of femoral/iliac, axillary/supraclavicular, cervical/supra-clavicular, axillary/femoral, bilateral axillary, orbilateral femoral lymph nodes are considered as
FIGURE 4 Fifteen-year Survival Curves for the Stage Groupings of Patients with Regional Metastatic Melanoma(Stage III).See Table 2 for the stage grouping definitions. Numbers of patients from the AJCC Melanoma Staging Database areshown in parentheses. The differences between the survival curves are highly significant (P � 0.0001).Adapted from Balch CM, Soong SJ, Gershenwald J, et al.4 with permission from the American Society of ClinicalOncology.
An Evidence-based Staging System
140 CA A Cancer Journal for Clinicians

involvement of two contiguous nodal basins.All such patients would be categorized as hav-ing Stage III melanoma.
Distant Metastatic Melanoma (M)
Distant metastatic melanomas are classifiedaccording to the categories below:Y M0: No detectable evidence of distant me-
tastases.Y Mx: Presence or absence of metastases
cannot be assessed.Y M1: Metastases to skin, subcutaneous tis-
sue, or distant lymph nodes.Y M2: Metastases to lung.Y M3: Metastases to all other visceral sites.
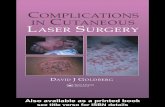
In patients with distant metastases, the site(s)of metastases and elevated serum levels of lac-tate dehydrogenase (LDH) are used to delineatethe M categories into three groups: M1a, M1b,and M1c, with one-year survival rates rangingfrom 40% to 60% (Figure 5).
Site(s) of Distant Metastases
Patients with distant cutaneous, subcutane-ous, or distant lymph node metastasis are cate-gorized as M1a; they have a better prognosis
compared with those patients with metastaseslocated in any other anatomic site.2,30 Patientswith metastasis to the lung are categorized asM1b and have an intermediate prognosis whencomparing one-year survival rates. Those pa-tients with metastases to any other visceral siteshave a relatively worse prognosis and are des-ignated as M1c.
Elevated Serum Lactate Dehydrogenase
Although it is uncommon in staging classi-fications to include serum factors, an exceptionwas made for elevated levels of serum LDH.This factor was among the most predictiveindependent factors of diminished survival inmultivariate analysis of all published studies,even after accounting for site and number ofmetastases.31–34 Therefore, when the serumLDH is elevated above the upper limits ofnormal at the time of staging, such patientswith distant metastases are assigned to M1cregardless of the site of their distant metastases.An elevated serum LDH should be used instaging only when there are two or more de-terminations obtained more than 24 hoursapart, because an elevated serum LDH on asingle determination can be falsely positive due
FIGURE 5 One-year Survival Rates from the AJCC Melanoma Staging Database Comparing the Different M Catego-ries.See Table 1 for definitions. There is a significant difference comparing skin, subcutaneous tissue, and lung metastasesto all other sites (P � 0.0001).Adapted from Balch CM, Soong SJ, Gershenwald J, et al.4 with permission from the American Society of ClinicalOncology.
CA Cancer J Clin 2004;54:131–149
Volume 54 Y Number 3 Y May/June 2004 141

to hemolysis or other factors unrelated to mel-anoma metastases.
Number of Metastases
The number of distant metastases has previ-ously been documented as an important prog-nostic factor.30 However, this feature was notincorporated into this version of the stagingsystem because of the significant variability inuse of imaging tests to comprehensively searchfor distant metastases. These may range from achest x-ray in some centers to positron emis-sion tomography (PET) scanning in others,with obvious implications for sensitivity of thisevaluation. Until the indications for variousdiagnostic imaging modalities are better stan-dardized, the number of metastases cannot re-liably be used for staging purposes.
Stage Groupings
Localized Melanoma (Stages I and II)
Patients with primary melanomas whohave no evidence of regional or distant me-tastases (either clinically or pathologically)are divided into two stages: Stage I for pa-tients at low risk for metastases andmelanoma-specific mortality or Stage II forthose with intermediate risk for metastasesand melanoma-specific mortality. The pres-ence of melanoma ulceration portends a highrisk for metastases and “upstages” the prog-nosis of patients with this finding relative topatients with nonulcerated melanomas ofequivalent thickness. For this reason, twosubgroups of Stage I patients are defined: (1)Stage IA for T1 melanomas without ulcer-ation or level IV or V depth of invasion(T1aN0M0 melanomas); and (2) Stage IB foreither T1 melanomas with histopathologicalevidence of level IV/V depth of inva-sion or with surface ulceration (T1bN0M0)or those T2 melanomas without ulceration(T2aN0M0). There are three subgroups ofStage II patients: (1) Stage IIA are T2 mela-nomas with ulceration (T2bN0M0) or T3melanomas without ulceration (T3aN0M0);(2) Stage IIB are either T3 melanomas with
ulceration (T3bN0M0) or T4 melanomaswithout ulceration (T4aN0M0); and (3)Stage IIC are T4 melanomas with ulceration(T4bN0M0). Survival rates for these stagegroupings are shown in Figure 2.
Patients with T4bN0M0 melanomas are atparticularly high risk for harboring both re-gional and distant metastases. Mortality rates forpatients with these thick, ulcerated melanomasare the same or even higher than mortality ratesfor some groups of patients with nodal metas-tases (Figure 2 and Table 5). Based on their riskfor melanoma-specific mortality, the 1997 ver-sion of the melanoma staging grouped suchpatients as Stage II. In developing the 2003version, the Melanoma Staging Committeeconcluded that such a categorization would addsignificant complexity to the new stage group-ings. To stay within the conventional anatomicdefinitions, the 2003 system assigns T4 mela-nomas to Stage II. This includes T4b melano-mas that would still be grouped with otherlocalized melanomas but are designated sepa-rately as Stage IIC because of their high risk forclinically occult nodal and systemic metastases.The 10-year survival rate for patients with clin-ical Stage IIC melanoma is 32% (Table 5 andFigure 2).
Regional Metastases (Stage III)
There are no substages for Clinical Stage IIImelanoma.
There are four major determinants of out-come for pathological Stage III melanoma:(1) the number of metastatic lymph nodes;(2) whether the tumor burden is microscopic(ie, clinically occult and detected pathologi-cally by sentinel or elective lymphadenec-tomy) or macroscopic (ie, clinically apparentphysical or radiologic examination and veri-fied pathologically); (3) the presence or ab-sence of ulceration of the primary melanoma;and (4) the presence or absence of satellite orin-transit metastases. The five-year survivalrates for patients in each of the N categoriessubgrouped by presence or absence of pri-mary melanoma ulceration are shown in Fig-ure 3 and Table 5.
An Evidence-based Staging System
142 CA A Cancer Journal for Clinicians

After accounting for these prognostic fea-tures in pathological Stage III melanoma,there are three definable subgroups with sta-tistically significant differences in survival:Stages IIIA, IIIB, and IIIC (Figure 4). Pa-tients with pathological Stage IIIA are de-fined as those who have one to threemicroscopic lymph node metastases (detectedby sentinel or elective lymphadenectomy)and whose primary melanoma is not ulcer-ated (T1 to 4aN1aM0 or T1 to 4aN2aM0).Five-year and 10-year survival rates for suchpatients are 67% and 60%, respectively (Fig-ures 3 and 4, Table 5). Patients with patho-logical Stage IIIB are those with one to threemacroscopic lymph node metastases and anonulcerated primary melanoma (ie, T1 to4aN1bM0 or T1 to 4aN2bM0), those withone to three microscopic lymph node metas-tases and an ulcerated primary melanoma (T1to 4bN1bM0 or T1 to 4bN2aM0), and thosewith in-transit or satellite metastases withoutnodal metastases, regardless of ulceration orT category (T1 to 4bN2cM0) (Figures 3 and4, Table 5).4 The estimated five-year survivalfor Stage IIIB patients is 53% (Figure 3,Table 5). Stage IIIC melanoma comprisesthose patients with a one to three macro-scopic lymph node metastases and an ulcer-ated primary melanoma (T1 to 4bN1bM0 orT1 to 4bN2bM0) or any patient with N3disease regardless of T status, including pa-tients with four or more nodal metastases ormatted nodes or satellites or in-transit metas-tases along with and nodal metastases (Fig-ures 3 and 4, Table 5). The estimated five-year survival rate for pathological Stage IIICpatients is 26%.4
Distant Metastases (Stage IV)
Because the survival differences between theM categories are small, there are no subgroupsof Stage IV melanoma.
Prognostic Factors Analysis
Thirteen institutions and cooperative studygroups agreed to contribute prospectively ac-
cumulated melanoma patient data to validatethe proposed staging system. The AJCC Mel-anoma Database consisted of a total of 30,450melanoma patients, of which 17,600 patients(59%) had information available for all of thefactors required for the proposed TNM classi-fication and stage grouping.2
In a multivariate analysis of 13,581 patientswith localized melanoma (either clinically orpathologically), the two most powerful inde-pendent characteristics of the primary mela-noma were tumor thickness and ulceration(Table 6). Indeed, no other feature of the mel-anoma or the patient with localized melanomahad the predictive capability of these two fac-tors. Other statistically significant prognosticfactors were patient age, site of the primarymelanoma, level of invasion, and gender (Table6). To determine the relative predictivestrength of these prognostic features within co-horts of tumor thickness, the Cox regressionanalysis was performed within each of the ma-jor thickness subgroups used in the melanomaT categories (Table 7). When comparing levelof invasion and ulceration within thicknesssubgroups, there was a pattern of predictivecapability for thin melanomas (�1.0 mm) thatwas different from all other thickness groups.Thus, for this specific subgroup of patients,level of invasion was more predictive of sur-vival outcome than tumor ulceration. The op-posite was true for all melanomas thicker than1.0 mm, where ulceration was clearly the mostpredictive, and level of invasion ranked belowthat of patient age and anatomic site of theprimary melanoma (Table 7).
Complete clinical and histopathologic datawere available for 1,151 patients with lymphnode metastases. A Cox multivariate analysisdemonstrated that three factors were mostsignificant (P � 0.0001): (1) the number ofmetastatic nodes; (2) the tumor burden at thetime of staging (ie, microscopic versus mac-roscopic); and 3) the presence or absence ofulceration of the primary melanoma (Table8). Melanoma-specific survival (calculatedfrom the onset of primary melanoma diag-nosis) decreased significantly with increasingnodal involvement (P � 0.0001; Figure 6).The best grouping for the number of meta-
CA Cancer J Clin 2004;54:131–149
Volume 54 Y Number 3 Y May/June 2004 143

static nodes that correlated with five-yearsurvival was one versus two to three versusfour or more metastatic nodes.
There was a significantly lower survival(calculated from the onset of primary mela-noma diagnosis) for those patients who pre-
sented with macroscopic (ie, palpable) nodalmetastases compared with those with micro-scopic (ie, nonpalpable) nodal metastases,even after accounting for lead-time bias (P �0.0001; Figure 7). Diminishing five-year sur-vival with increasing tumor burden based on
TABLE 6 Cox Regression Analysis for 13,581 Melanoma Patients Without Evidence of Nodal or DistantMetastases
VariableChi-square
Value (Wald) P Value Risk Ratio 95% CL*
Thickness 244.3 �0.00001 1.558 1.473-1.647Ulceration 189.5 �0.00001 1.901 1.735-2.083Age 45.6 �0.00001 1.101 1.071-1.132Site 41.0 �0.00001 1.338 1.224-1.463Level 32.7 �0.00001 1.214 1.136-1.297Gender 15.1 0.001 0.836 0.764-0.915
*CL � Confidence level. Only patients with no missing data in all covariates were included in this multivariate study.Adapted from Balch CM, Soong SJ, Gershenwald J, et al.2 with permission from the American Society of Clinical Oncology.
TABLE 7 Cox Regression Analysis by Tumor Thickness Category for Stages I and II Primary Melanoma
VariableChi-square
Value (Wald) P Value Risk Ratio 95% CL*
Thickness <1.00 (n � 5,299)
Level 24.778 �0.00001 1.451 1.253-1.680Ulceration 17.239 �0.00001 2.073 1.469-2.924Age 12.563 0.0004 1.156 1.067-1.253Site 6.940 0.0084 1.394 1.089-1.784Gender 5.506 0.0189 0.744 0.581-0.952
Thickness 1.01 to 2.00 mm (n � 3,943)
Ulceration 57.215 �0.00001 1.965 1.650-2.341Site 24.085 �0.00001 1.567 1.310-1.876Age 11.613 0.0007 1.101 1.042-1.164Level 6.656 0.0099 1.211 1.047-1.400Gender 2.668 0.1024 0.861 0.719-1.030
Thickness 2.01 to 4.00 mm (n � 2,959)
Ulceration 62.291 �0.00001 1.766 1.634-2.034Age 12.529 0.0004 1.087 1.038-1.138Site 12.342 0.0004 1.306 1.125-1.516Level 4.451 0.0349 1.143 1.010-1.294Gender 3.165 0.0752 0.872 0.750-1.014
Thickness >4.00 mm (n � 1,380)
Ulceration 47.246 �0.00001 1.932 1.601-2.331Age 8.745 0.0031 1.087 1.028-1.148Level 4.065 0.0438 1.139 1.004-1.293Gender 2.875 0.0951 0.858 0.716-1.027Site 2.547 0.1106 1.154 0.968-1.376
*CL � Confidence level. Only patients with no missing data in all covariates were included in this multivariate analysis.Adapted from Balch CM, Soong SJ, Gershenwald J, et al.2 with permission from the American Society of Clinical Oncology.
An Evidence-based Staging System
144 CA A Cancer Journal for Clinicians

increasing number of metastatic nodespresent was observed for all subgroups (P �0.0001; Table 9).
Ulceration of a primary melanoma was theonly primary tumor feature that still predictedan adverse outcome in Stage III disease (Table8). This was true even within each of the StageIII subgroups examined, including a two-waysurvival analysis correlating presence or absenceof ulceration with the number of metastatic
lymph nodes (P � 0.0001), or a three-wayanalysis that integrated subgroups according toall three of the most important prognostic fac-tors: ulceration of the primary melanoma,nodal tumor burden, and the number of met-astatic nodes (Table 9).
The prognostic influence of different dis-tant metastatic sites was analyzed in 1,158Stage IV patients using various combinationsof sites of metastases. The most significant
TABLE 8 Cox Regression Analysis for 1,151 Stage III (Nodal Metastases) Patients
VariableChi-square
Value (Wald) P Value Risk Ratio 95% CL*
No. of metastatic nodes 57.616 �0.00001 1.257 1.185-1.334Tumor burden 40.301 �0.00001 1.792 1.497-2.146Ulceration 23.282 �0.00001 1.582 1.313-1.906Site 17.843 0.0001 1.461 1.225-1.746Age 13.369 0.0003 1.118 1.053-1.187Thickness 1.964 0.1611 1.091 0.966-1.233Level 0.219 0.6396 1.033 0.901-1.186Gender 0.006 0.9407 1.007 0.836-1.213
*CL � Confidence level. Only patients with no missing data in all covariates were included in this multivariate analysis.Adapted from Balch CM, Soong SJ, Gershenwald J, et al.2 with permission from the American Society of Clinical Oncology.
FIGURE 6 Survival Curves of 1,528 Melanoma Patients with Lymph Node Metastases Subgrouped by the ActualNumber of Metastatic Nodes.The correlation is highly significant (P � 0.0001).Adapted from Balch CM, Soong SJ, Gershenwald J, et al.2 with permission from the American Society of ClinicalOncology.
CA Cancer J Clin 2004;54:131–149
Volume 54 Y Number 3 Y May/June 2004 145

differences were noted when visceral versusnonvisceral sites (ie, skin, subcutaneous tis-sue, and distant lymph nodes) were com-pared. Although significant one-year survivaldifferences were observed when patientswith lung metastases were compared withthose patients with metastases in other vis-ceral sites (P � 0.0001), no differences were
noted when two-year survival data werecompared (Figure 8).
DISCUSSION
The results of multivariate analyses using adatabase derived from records of 17,600 pa-
TABLE 9 Five-year Survival Rates for Stage III (Nodal Metastases) Patients Stratified by Number ofMetastatic Nodes, Ulceration, and Tumor Burden
MelanomaUlceration
Microscopic% � SE*
Macroscopic% � SE*
1�Nodes
2 to 3Nodes
>3�Nodes
1�Nodes
2 to 3Nodes
>3�Nodes
Absent 69 � 3.7 63 � 5.6 27 � 9.3 59 � 4.7 46 � 5.5 27 � 4.6(n† � 252) (n � 130) (n � 57) (n � 122) (n � 93) (n � 109)
Present 52 � 4.1 50 � 5.7 37 � 8.8 29 � 5.0 25 � 4.4 13 � 3.5(n � 217) (n � 111) (n � 46) (n � 98) (n � 109) (n � 104)
*SE � Standard error.†n � Number of patients.Adapted from Balch CM, Soong SJ, Gershenwald J, et al.2 with permission from the American Society of Clinical Oncology.
FIGURE 7 Survival Curves of 1,429 Patients with Lymph Node Metastases Subgrouped by Their Presenting ClinicalStaging.There were 825 patients with clinically occult nodal metastases diagnosed pathologically after either sentinel or electivelymphadenectomy and 604 patients who presented with clinically evident nodal metastases confirmed pathologically af-ter a therapeutic lymphadenectomy. Survival rates were calculated from the onset of the primary melanoma diagnosis.The difference in survival rates is highly significant (P � 0.0001).Adapted from Balch CM, Soong SJ, Gershenwald J, et al.2 with permission from the American Society of ClinicalOncology.
An Evidence-based Staging System
146 CA A Cancer Journal for Clinicians

tients with melanoma from 13 cancer centersand cooperative groups showed: (1) tumorthickness and ulceration were the most pow-erful predictors of survival in patients with lo-calized melanoma (Stages I and II), while levelhad a significant impact only within the sub-group of thin (ie, T1; �1.0 mm) melanomas;(2) the number of metastatic nodes, the tumorburden (microscopic versus macroscopic nodalmetastases), and the presence or absence ofmelanoma ulceration and of intralymphaticmetastases (satellite or in-transit metastases)were the most powerful predictors of survivalin patients with nodal metastases (Stage III);and (3) the number and anatomic site of distantmetastases and the presence of an elevated se-rum LDH were the most significant predictorof survival in patients with distant metastases(Stage IV). Subsequent to the publication ofthe AJCC melanoma staging articles, several
institutions have independently validated theseprognostic criteria as the most predictive fromamong currently available clinical and patho-logical criteria.6–10 The major limitation of theAJCC data is that patients with early Stage Imelanoma may not have been referred to majorcancer centers or entered into clinical trials, sothat the survival rates for the Stage IA patientsin the AJCC analysis may likely have a some-what lower five- and 10-year survival ratecompared with results from a comprehensiveregional referral institution such as the SydneyMelanoma Unit, Sydney, Australia.22 In addi-tion, several studies have demonstrated thehighly significant value of mitotic rate as anindependent predictive factor,7,35 but this pa-rameter is more interpretive and would be dif-ficult to fold into a TNM criterion.
Patients with nodal metastases should notbe considered as a homogeneous group, and
FIGURE 8 Survival Curves of 1,158 Patients with Metastatic Melanomas at Distant Sites Subgrouped into Three Cate-gories or Sites: Skin, Subcutaneous Tissue, or Distant Lymph Nodes Versus Lung Versus All Other Visceral Sites.The number of patients is shown in parentheses. Note that the survival rate for patients with lung metastases is similarto that for nonvisceral sites for the first year and then approaches that of other visceral sites after two years. Survivaldifferences are significantly greater with skin, subcutaneous tissue, or distant lymph node metastases compared withlung metastases (P � 0.003) or other visceral sites of metastases (P � 0.0001).Adapted from Balch CM, Soong SJ, Gershenwald J, et al.2 with permission from the American Society of ClinicalOncology.
CA Cancer J Clin 2004;54:131–149
Volume 54 Y Number 3 Y May/June 2004 147

recommendations to enter patients into in-tensive clinical trials should take into accountthe marked diversity in the natural history ofStage III melanoma. In fact, some Stage IIIpatients actually have a good prognosis (orintermediate risk for distant metastases). Thisprognostic heterogeneity is demonstrated bymore than fivefold differences in five-yearsurvival rates for defined substages, rangingfrom 69% for patients with nonulceratedmelanomas (regardless of thickness) who hada single clinically occult nodal metastasis (de-tected by sentinel or elective lymphadenec-tomy) to 13% for patients with ulceratedmelanomas (regardless of thickness) who hadfour or more clinically apparent nodal me-tastases (detected by therapeutic lymphade-nectomy). Stage III patients are sometimesincorrectly assumed to be at uniformly highrisk for distant metastases and therefore maybe offered very intensive forms of systemictherapy (eg, biochemotherapy). Understand-ing their differences in clinical outcome willbe important not only in the design andanalysis of clinical trials but also in calibratingtherapeutic intensity to metastatic risk.
Survival rates for patients with Stage IV mel-anoma are, unfortunately, more often mea-sured more in months than in years, and only aminority of Stage IV patients survive beyondone year. None of the prognostic features inthis analysis was able to stratify Stage IV pa-tients into subgroups with median survival sep-arated by more than a few months. In general,the only Stage IV patients who live beyond oneor two years are those with limited disease whohave had a complete surgical resection of thedistant metastases.36 Whether the long-termresults reflect a more favorable biology of dis-ease or a therapeutic benefit of surgery (or acombination of the two) is a difficult issue toaddress in the absence of any randomized trials.
The prognostic factors identified by thisanalysis should be the primary stratificationcriteria and end-results reporting criteria ofmelanoma clinical trials. The AJCC Mela-noma Committee recommends that all mel-anoma patients with clinically negative
regional lymph nodes and who may be con-sidered for entry into surgical and adjuvanttherapy clinical trials should have pathologi-cal staging with sentinel lymphadenectomyto ensure prognostic homogeneity within as-signed treatment groups. In this way, inves-tigators will be better able to discern betweenthe natural history impact and the treatmentimpact being studied in melanoma clinicaltrials. Moreover, the use of a consistent set ofcriteria will facilitate the comparability ofmelanoma clinical trials and thereby acceler-ate the progress of multidisciplinary mela-noma treatment approaches.
It is evident that the next phase of stagingmelanoma will evolve as new technologyallows the clinician to reliably diagnose met-astatic melanoma at a level of tumor burdenwell below that achievable with the lightmicroscope or routine x-rays. These includemolecular diagnostic approaches, such as re-verse transcription polymerase chain reactionto detect relevant gene expression, PETscanning, use of radiolabeled antimelanomaantibodies, serum markers, and genetic/mo-lecular markers that will more accurately de-tect and stage metastatic melanoma. Some ofthese advances in molecular-based stagingwill no doubt supplant those prognostic fea-tures of melanoma now determined largelywith the light microscope.
ACKNOWLEDGMENTS
The following were members of the AJCCMelanoma Committee or were consultants to theCommittee: Charles M. Balch, MD (Chairper-son); Antonio C. Buzaid, MD; Seng-Jaw Soong,PhD; Michael B. Atkins, MD; Natale Cascinelli,MD; Daniel G. Coit, MD; Irvin D. Fleming,MD; Jeffrey E. Gershenwald, MD; Alan Hough-ton, Jr., MD; John M. Kirkwood, MD; Kelly M.McMasters, MD; Martin F. Mihm, MD; DonaldL. Morton, MD; Douglas S. Reintgen, MD;Merrick I. Ross, MD; Arthur Sober, MD; JohnA. Thompson, MD; and John F. Thompson,MD.
An Evidence-based Staging System
148 CA A Cancer Journal for Clinicians

REFERENCES
1. Jemal A, Tiwari RC, Murray T, et al. Cancerstatistics, 2004. CA Cancer J Clin 2004;54:8–29.
2. Balch CM, Soong SJ, Gershenwald J, et al.Prognostic factors analysis of 17,600 melanomapatients: validation of the AJCC melanomastaging system. J Clin Oncol 2001;19:3622–3634.
3. Balch CM, Buzaid AC, Atkins MB, et al. Anew American Joint Committee on Cancer stag-ing system for cutaneous melanoma. Cancer2000;88:1484–1491.
4. Balch CM, Buzaid AC, Soong SJ, et al. Finalversion of the American Joint Committee onCancer staging system for cutaneous melanoma.J Clin Oncol 2001;19:3635–3648.
5. Balch CM. Cutaneous Melanoma, in GreeneFL, Page DL, Fleming ID, et al. (eds). AJCCCancer Staging Manual. 6th ed. New York, NY:Springer Verlag; 2002:209–217.
6. Merkel S, Meyer T, Papadopoulos T, et al.Testing a new staging system for cutaneous mel-anoma proposed by the American Joint Commit-tee on Cancer. Eur J Cancer 2002;38:517–526.
7. Retsas S, Henry K, Mohammed MQ, Mac-Rae K. Prognostic factors of cutaneous melanomaand a new staging system proposed by the Amer-ican Joint Committee on Cancer (AJCC): valida-tion in a cohort of 1284 patients. Eur J Cancer2002;38:511–516.
8. Kashani-Sabet M, Shaikh L, Miller JR III, etal. NF-kappa B in the vascular progression ofmelanoma. J Clin Oncol 2004;22:617–623.
9. Garbe C, Ellwanger U, Tronnier M, et al. TheNew American Joint Committee on Cancer stag-ing system for cutaneous melanoma: a criticalanalysis based on data of the German CentralMalignant Melanoma Registry. Cancer2002;94:2305–2307.
10. Averbook BJ, Fu P, Rao JS, Mansour EG. Along-term analysis of 1018 patients with melanomaby classic Cox regression and tree-structured sur-vival analysis at a major referral center: implicationson the future of cancer staging. Surgery 2002;132:589–602; discussion 602–604.
11. Essner R, Conforti A, Kelley MC, et al. Effi-cacy of lymphatic mapping, sentinel lymphadenec-tomy, and selective complete lymph node dissectionas a therapeutic procedure for early-stage mela-noma. Ann Surg Oncol 1999;6:442–449.
12. Morton DL, Wen DR, Wong JH, et al.Technical details of intraoperative lymphaticmapping for early stage melanoma. Arch Surg1992;127:392–399.
13. Breslow A. Problems in the measurement of
tumor thickness and level of invasion in cutane-ous melanoma. Hum Pathol 1977;8:1–2.
14. Breslow A. Thickness, cross-sectional areasand depth of invasion in the prognosis of cutane-ous melanoma. Ann Surg 1970;172:902–908.
15. Balch CM, Murad TM, Soong SJ, et al. Amultifactorial analysis of melanoma: prognostichistopathological features comparing Clark’s andBreslow’s staging methods. Ann Surg 1978;188:732–742.
16. Balch CM, Wilkerson JA, Murad TM, et al.The prognostic significance of ulceration of cu-taneous melanoma. Cancer 1980;45:3012–3017.
17. Clark WH Jr, From L, Bernardino EA,Mihm MC. The histogenesis and biologic behav-ior of primary human malignant melanomas ofthe skin. Cancer Res 1969;29:705–727.
18. Buzaid AC, Ross MI, Balch CM, et al. Crit-ical analysis of the current American Joint Com-mittee on Cancer staging system for cutaneousmelanoma and proposal of a new staging system�see comments. J Clin Oncol 1997;15:1039–1051.
19. Lock-Andersen J, Hou-Jensen K, Hansen JP,et al. Observer variation in histological classifica-tion of cutaneous malignant melanoma. Scand JPlast Reconstr Surg Hand Surg 1995;29:141–148.
20. Morton DL, Davtyan DG, Wanek LA, et al.Multivariate analysis of the relationship betweensurvival and the microstage of primary melanomaby Clark level and Breslow thickness. Cancer1993;71:3737–3743.
21. Marghoob AA, Koenig K, Bittencourt FV, etal. Breslow thickness and Clark level in mela-noma: support for including level in pathologyreports and in American Joint Committee onCancer Staging �see comments. Cancer 2000;88:589–595.
22. McKinnon J, Yu XQ, McCarthy WH,Thompson JF. Prognosis for patients with thincutaneous melanoma: long-term survival datafrom New South Wales Central Cancer Registryand the Sydney Melanoma Unit. Cancer2003;98:1223–1231.
23. Gershenwald JE, Balch CM, Soong SJ,Thompson JF. Prognostic Factors and Natural His-tory, in Balch CM, Houghton AN, Sober AJ, et al.(eds). Cutaneous Melanoma. 4th ed. St. Louis, MO:Quality Medical Publishing; 2003:25–54.
24. Balch CM, Gershenwald JE, Buzaid AC, etal. Staging and Classification, in Balch CM,Houghton AN, Sober AJ, et al. (eds). CutaneousMelanoma. 4th ed. St. Louis, MO: Quality Med-ical Publishing; 2003:55–92.
25. Balch CM, Soong S, Ross MI, et al. Long-term results of a multi-institutional randomizedtrial comparing prognostic factors and surgicalresults for intermediate thickness melanomas (1.0to 4.0 mm). Intergroup Melanoma Surgical Trial.Ann Surg Oncol 2000;7:87–97.
26. Cascinelli N, Belli F, Santinami M, et al.Sentinel lymph node biopsy in cutaneous mela-noma: the WHO Melanoma Program experi-ence. Ann Surg Oncol 2000;7:469–474.
27. Buzaid AC, Tinoco LA, Jendiroba D, et al.Prognostic value of size of lymph node metastasesin patients with cutaneous melanoma. J Clin On-col 1995;13:2361–2368.
28. Cascinelli N, Bufalino R, Marolda R, et al.Regional non-nodal metastases of cutaneous mel-anoma. Eur J Surg Oncol 1986;12:175–180.
29. Harrist TJ, Rigel DS, Day CL Jr, et al. “Mi-croscopic satellites” are more highly associatedwith regional lymph node metastases than withprimary melanoma thickness. Cancer 1984;53:2183–2187.
30. Barth A, Wanek LA, Morton DL. Prog-nostic factors in 1,521 melanoma patients withdistant metastases. J Am Coll Surg 1995;181:193–201.
31. Deichmann M, Benner A, Bock M, et al.S100-Beta, melanoma-inhibiting activity, andlactate dehydrogenase discriminate progressivefrom nonprogressive American Joint Committeeon Cancer stage IV melanoma. J Clin Oncol1999;17:1891–1896.
32. Eton O, Legha SS, Moon TE, et al. Prog-nostic factors for survival of patients treated sys-temically for disseminated melanoma. J ClinOncol 1998;16:1103–1111.
33. Keilholz U, Conradt C, Legha SS, et al.Results of interleukin-2-based treatment in ad-vanced melanoma: a case record-based analysisof 631 patients. J Clin Oncol 1998;16:2921–2929.
34. Sirott MN, Bajorin DF, Wong GY, et al.Prognostic factors in patients with metastatic ma-lignant melanoma. A multivariate analysis.Cancer 1993;72:3091–3098.
35. Azzola M, Shaw HM, Thompson JF, et al.Tumor mitotic rate is a more powerful prog-nostic indicator than ulceration in patients withprimary cutaneous melanoma. An analysis of3661 patients from a single center. Cancer2003;97:1488 –1498.
36. Morton D, Essner R, Balch CM. SurgicalExcision of Distant Metastases, in Balch CM,Houghton AN, Sober AJ, et al. (eds). CutaneousMelanoma. 4th ed. St. Louis, MO: Quality Med-ical Publishing; 2003:547–572.
CA Cancer J Clin 2004;54:131–149
Volume 54 Y Number 3 Y May/June 2004 149
Copyright © 2022 FDOKUMEN