The many faces of cutaneous vasculitis
17
The Many Faces of Cutaneous Vasculitis GIUSEPPE HAUTMANN, MD GRAZIA CAMPANILE, MD TORELLO M. LOTTI, MD V asculitis is a general term that refers to seg- mental, angiocentric inflammation and damage to the blood vessel walls. 1 This term does not specify the type of inflammation, nor the size of the vessel involved in the skin, an organ that is well sup- plied with vasculature and frequently develops differ- ent manifestations of vasculitis. 2 Often, the skin appar- ently serves as the initial organ upon which vasculitis is manifest, with involvement of the small to medium- sized vessels that supply nutrients to the skin itself. Although there are times when the only recognizable organ system involved is the skin, cutaneous vasculitis represents a systemic disease process that in many cases is linked to the presence of circulating or locally formed immune complexes (CIC), or may occur through differ- ent direct vessel-based immunologic or nonimmuno- logic mechanisms. Vasculitis: The Hard Challenge for the Clinician and the Pathologist Vasculitis is not a distinct clinical syndrome but may manifest in a wide variety of clinical signs and symp- toms depending on the localization and size of the vessels involved, the nature of the inflammatory pro- cess, and the presence of an underlying or associated condition. Many investigators have attempted to clas- sify the vasculitides. Some examples are shown in Ta- bles 1 and 2. 3 Classification generally is based on the size of the involved vessels, the histopathologic and clinical findings, and the mechanisms or inciting agents supposedly underlying the disease process. For a num- ber of idiopathic vasculitides, criteria for classification have been developed by the American College of Rheu- matology (ACR) (Table 3). 4 Within the skin, vasculitis, in many cases, is his- topathologically manifest as leukocytoclastic vasculitis. The term leukocytoclastic vasculitis is used to describe a process that is recognized within a biopsy specimen. 5 The features that are observed include endothelial swelling and segmental fibrinoid necrosis of the vessel walls, with infiltration of polymorphonuclear neutro- phils (PMNs), some of which are disrupted, resulting in the presence of nuclear debris within the tissue. This pathologic process can be observed in a variety of vas- culitic syndromes, including those that have severe as- sociated systemic disease, and also in processes in the skin that are not vasculitic in their nature, such as insect bites. Furthermore, similar histopathological changes can occur in the related conditions known as “neutro- philic dermatoses” in which massive infiltration with PMNs occurs in the absence of vascular wall involve- ment. Table 4 lists many of the clinical syndromes in which leukocytoclastic vasculitis can be seen. The histologic features required to make the diagnosis, as stated, in- clude small-vessel destruction characterized by a trans- mural, inflammatory infiltrate consisting of neutrophils and nuclear fragments, endothelial swelling, fibrin dep- osition, and, often, erythrocyte extravasation. In later stages there is frequently some thrombosis of affected small vessels, as well as hyalinization and fibrosis of walls of affected vessels. In many cases, precise identi- fication of the pathogenesis of a leukocytoclastic vascu- litis is not possible. Some conditions in which leukocytoclastic vasculitis occurs, however, have additional histologic clues that may be helpful in further defining the cause of the vasculitis. In lupus erythematosus, there is frequently dermal mucin deposition, as well as an inflammatory infiltrate at the dermoepidermal junction. Thrombosis of the small dermal blood vessels is present to a much greater extent in septic vasculitis than in most other types of leukocytoclastic vasculitis, probably as a result of bacterial toxins. Vascular plugging with eosinophilic material is often seen in cryoglobulinemia. In Henoch- Schoenlein purpura, immunofluorescence characteristi- cally shows IgA deposits within vessel walls, whereas in most other types of leukocytoclastic vasculitis, IgG or IgM deposits are seen. Some conditions characterized histologically by leu- kocytoclastic vasculitis have a chronic clinical course and do not follow the standard histologic sequence as From the Department of Dermatology, University of Florence, Florence, Italy. Address correspondence to Giuseppe Hautmann, MD, Department of Dermatology, University of Florence, Via degli Alfani, 37, 50121 Florence, Italy. © 1999 by Elsevier Science Inc. All rights reserved. 0738-081X/99/$–see front matter 655 Avenue of the Americas, New York, NY 10010 PII S0738-081X(99)00059-0
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of The many faces of cutaneous vasculitis

The Many Faces of CutaneousVasculitisGIUSEPPE HAUTMANN, MDGRAZIA CAMPANILE, MDTORELLO M. LOTTI, MD
V asculitis is a general term that refers to seg-mental, angiocentric inflammation and damageto the blood vessel walls.1 This term does not
specify the type of inflammation, nor the size of thevessel involved in the skin, an organ that is well sup-plied with vasculature and frequently develops differ-ent manifestations of vasculitis.2 Often, the skin appar-ently serves as the initial organ upon which vasculitis ismanifest, with involvement of the small to medium-sized vessels that supply nutrients to the skin itself.Although there are times when the only recognizableorgan system involved is the skin, cutaneous vasculitisrepresents a systemic disease process that in many casesis linked to the presence of circulating or locally formedimmune complexes (CIC), or may occur through differ-ent direct vessel-based immunologic or nonimmuno-logic mechanisms.
Vasculitis: The Hard Challenge for theClinician and the Pathologist
Vasculitis is not a distinct clinical syndrome but maymanifest in a wide variety of clinical signs and symp-toms depending on the localization and size of thevessels involved, the nature of the inflammatory pro-cess, and the presence of an underlying or associatedcondition. Many investigators have attempted to clas-sify the vasculitides. Some examples are shown in Ta-bles 1 and 2.3 Classification generally is based on thesize of the involved vessels, the histopathologic andclinical findings, and the mechanisms or inciting agentssupposedly underlying the disease process. For a num-ber of idiopathic vasculitides, criteria for classificationhave been developed by the American College of Rheu-matology (ACR) (Table 3).4
Within the skin, vasculitis, in many cases, is his-topathologically manifest as leukocytoclastic vasculitis.The term leukocytoclastic vasculitis is used to describe aprocess that is recognized within a biopsy specimen.5
The features that are observed include endothelialswelling and segmental fibrinoid necrosis of the vesselwalls, with infiltration of polymorphonuclear neutro-phils (PMNs), some of which are disrupted, resulting inthe presence of nuclear debris within the tissue. Thispathologic process can be observed in a variety of vas-culitic syndromes, including those that have severe as-sociated systemic disease, and also in processes in theskin that are not vasculitic in their nature, such as insectbites. Furthermore, similar histopathological changescan occur in the related conditions known as “neutro-philic dermatoses” in which massive infiltration withPMNs occurs in the absence of vascular wall involve-ment.
Table 4 lists many of the clinical syndromes in whichleukocytoclastic vasculitis can be seen. The histologicfeatures required to make the diagnosis, as stated, in-clude small-vessel destruction characterized by a trans-mural, inflammatory infiltrate consisting of neutrophilsand nuclear fragments, endothelial swelling, fibrin dep-osition, and, often, erythrocyte extravasation. In laterstages there is frequently some thrombosis of affectedsmall vessels, as well as hyalinization and fibrosis ofwalls of affected vessels. In many cases, precise identi-fication of the pathogenesis of a leukocytoclastic vascu-litis is not possible.
Some conditions in which leukocytoclastic vasculitisoccurs, however, have additional histologic clues thatmay be helpful in further defining the cause of thevasculitis. In lupus erythematosus, there is frequentlydermal mucin deposition, as well as an inflammatoryinfiltrate at the dermoepidermal junction. Thrombosisof the small dermal blood vessels is present to a muchgreater extent in septic vasculitis than in most othertypes of leukocytoclastic vasculitis, probably as a resultof bacterial toxins. Vascular plugging with eosinophilicmaterial is often seen in cryoglobulinemia. In Henoch-Schoenlein purpura, immunofluorescence characteristi-cally shows IgA deposits within vessel walls, whereasin most other types of leukocytoclastic vasculitis, IgG orIgM deposits are seen.
Some conditions characterized histologically by leu-kocytoclastic vasculitis have a chronic clinical courseand do not follow the standard histologic sequence as
From the Department of Dermatology, University of Florence, Florence,Italy.
Address correspondence to Giuseppe Hautmann, MD, Department ofDermatology, University of Florence, Via degli Alfani, 37, 50121 Florence,Italy.
© 1999 by Elsevier Science Inc. All rights reserved. 0738-081X/99/$–see front matter655 Avenue of the Americas, New York, NY 10010 PII S0738-081X(99)00059-0

outlined above. It has been outlined as a temporalsequence wherein the inflammatory infiltrate seen invasculitic lesions is initially predominantly neutrophilicand gradually evolves into a predominantly lympho-cytic/mononuclear one. Granuloma faciale, erythemaelevatum diutinum, and Behcet’s syndrome, however,may be typically leukocytoclastic vasculitides, histolog-ically. This histologic picture of neutrophil predomi-nance persists for long periods of time, with no clearevolution into a mononuclear inflammatory infiltrateunless the disease states are treated or begin to regress.6
Lymphocytic vasculitis is also a histologic diagnosisthat correlates with a long list of clinical conditions(Table 5). The gross appearances of lesions of lympho-cytic vasculitis are often indistinguishable clinicallyfrom those of leukocytoclastic vasculitis, which usuallyrepresent the starting point of the pathologic process.The histologic criteria for making a diagnosis of lym-phocytic vasculitis have not been as well defined asthose of leukocytoclastic vasculitis. Most investigatorsrequire evidence for vascular wall destruction, such asendothelial cell disruption, fibrin deposition, and ex-travasation of red blood cells. In addition, the cellularinfiltrate is composed mainly of lymphocytes and mac-rophages. Caution is needed in applying these histo-logic findings, as most cutaneous diseases that involvelymphocytic reactions derive the lymphocytes via mi-gration from the blood, through the vessel walls, andinto the adjacent tissues. Diapedesis of a few erythro-cytes is rather common in a wide variety of diseases inwhich large numbers of lymphocytes migrate throughblood vessel walls. Consequently, a lymphocytic vascu-litis should involve an infiltrate selectively targeted onvessel walls, usually with necrosis in at least some areasof those vessels.6
Granulomatous vasculitis has the least well-character-ized pathogenesis of all the subcategories of vasculitis.It may occur in a range of conditions, which are listed inTable 6. In each of the entities listed, the granulomaformation can occur either within the vessel walls or inthe extravascular surrounding tissue. The histologic cri-teria upon which to make the diagnosis usually includeevidence of vascular wall destruction, with fibrin dep-osition, extravasation of erythrocytes, and an inflamma-tory infiltrate. In lymphomatoid granulomatosis, theinfiltrate is predominantly lymphocytic (CD301). Inallergic granulomatosis (Churg-Strauss syndrome),there also may be many eosinophils. In Wegener’s gran-ulomatosis, the vascular wall infiltrate may be predom-inantly neutrophilic. In each of these conditions, there isoften granuloma formation in the tissue surroundingthe affected vessels. Deep dermal vessels are frequentlyinvolved, and produce clinical lesions similar to thosealready described. In temporal arteritis and Takayasu’sarteritis, there is actual intramural granuloma forma-tion, with lymphocytes, histiocytes, and multinucleated
Table 1. Eclectic Classification of Vasculitis
Leukocytoclastic, hypersensitivity, or allergic vasculitisHenoch-Schoenlein purpuraHypocomplementemic (urticarial) vasculitisVasculitis associated with a paraproteinSpecial forms of dermal vasculitides
Vasculitis associated with the rheumatic diseasesSystemic lupus erythematosusRheumatoid arthritisSjogren’s syndromeSclerodermaDermatomyositis
Granulomatous vasculitisAllergic granulomatous angiitis of Churg-StraussLymphomatoid granulomatosisWegener’s granulomatosis
Polyarteritis nodosaClassic typeClosely related allergic granulomatosisOverlap syndrome
Large-vessel vasculitis (giant-cell arteritis)Temporal arteritisTakayasu’s diseasePolymyalgia rheumatica
Table 2. A Classification of Vasculitis Based on the Size ofVessels Involved
Small-vessel necrotizing vasculitisNecrotizing vasculitisHenoch-Schoenlein purpuraEssential mixed cryoglobulinemiaWaldenstrom’s hypergammaglobulinemic purpuraAssociated with collagen vascular diseaseUrticarial vasculitisErythema elevatum diutinumRheumatoid nodulesReactive leprosySeptic vasculitis
Larger-vessel necrotizing vasculitisPolyarteritis nodosaGranulomatous vasculitis
Wegener’s granulomatosisAllergic granulomatosisLymphomatoid granulomatosis
Giant-cell arteritisTemporal arteritisTakayasu’s disease
Larger-vessel vasculitis with collagen vascular diseaseNodular vasculitis
Table 3. 1990 American College of Rheumatology Criteria forHypersensitivity Vasculitis (Traditional format)
Age at disease onset .16 yearsMedication at disease onsetPalpable purpuraMaculopapular rashBiopsy including arteriole and venule with histologic changes
showing granulocytes in a perivascular or extravascular location
Note: At least three of five criteria must be present; the presence of three offive criteria was associated with a specificity of 83.9% and a sensitivity of 71.0%.
516 HAUTMANN ET AL. Clinics in Dermatology Y 1999;17:515–531

giant cells within the vessel walls.1,6 These last condi-tions involve large arteries, and only rarely, if ever,affect the dermis.
The clinicians stole the exact diagnosis of vasculitisfrom the pathologists. Vasculitis really refers to focalmicroscopic damage or inflammatory change in theblood vessels. But the clinician has become so adept atrecognizing the gross effects of such vasculitis that he orshe uses the term in daily practice. The lesions thatpermit the clinician to anticipate the histopathologicchanges of vasculitis are the following:
Y Purpura, petechiae, (as in Henoch-Schoenlein syn-drome)
Y Palpable purpuraY Urticarial lesions persisting for more than a dayY Vesicular, bullous, or pustular lesions with a pur-
puric base
Y Livedo reticularisY Painful retiform maculesY NecrosisY Infarct scars, as in atrophie blanche or Degos’ disease
(malignant atrophic papulosis).
Sams and co-workers5 documented their observationthat the lesions of cutaneous vasculitis are dynamic.The lesions are often polymorphic, yet at some stagethey become purpuric and palpable. The early stages ofdevelopment may be characterized by wheals followedby macular purpura, whereas older lesions can becomenodular, vesiculobullous, necrotic, or ulcerative. Otherinvestigators have suggested that palpable purpuraand/or vesiculobullous lesions are representative ofsmall-vessel involvement, whereas nodules, ulcers, andinfarctive lesions occur as a reflection of involvement ofthe medium-sized vessels.7 The classic and most typical
Table 4. Main Clinical Forms and Differential Diagnosis of Leukocytoclastic Vasculitis (LCV) and Associated Conditions
Entities manifested by palpable purpura and LCV histopathologicallyIdiopathic
Henoch-Schoenlein purpura (IgA-related LCV)Acute hemorrhagic edema in infancy
Infectious: any infection can be associated; thefollowing are perhaps more common:
Hepatitis B Human immunodeficiency virusInfluenza MeningococcemiaMononucleosis Otitis mediaGonoccemia Streptococcus
Systemic disease:Chronic active hepatitis ParaproteinemiaCystic fibrosis Rheumatoid arthritisDermatomyositis SclerodermaInflammatory bowel disease Sjogren’s syndromeLupus erythematosus Wegener’s granulomatosis
Malignancy (“paraneoplastic vasculitis”)Hodgkin’s diseaseLeukemia and lymphomaMultiple myelomaSolid tumors
Drugs and chemicals: any drug can beassociated; the following are perhaps morecommon:
Allopurinol PropylthiouracilFood additives QuinidinePenicillin Sulfonamides
Entities that demonstrate LCV histopathologically but may not exhibit palpable purpuraHypocomplementemic (urticarial) vasculitisDegos’s diseaseErythema elevatum diutinum
Entities that may demonstrate palpable purpura but are not LCV histopathologicallyAntiphospholipid syndromeAtheroemboliAtrophie blanche (livedoid vasculitis)Bacterial endocarditisCholesterol emboliCoumarin necrosisCryofibrinogenemiaDisseminated intravascular coagulopathyEmbolic phenomenonLeft atrial myxomaPurpura fulminans
Clinics in Dermatology Y 1999;17:515–531 MANY FACES OF VASCULITIS 517

cutaneous lesion observed in patients with leukocyto-clastic vasculitis is palpable purpura. This lesion variesfrom bright red to purple, and in contrast to lesionsrepresentative of thrombocytopenia or of capillaritis,the lesion of vasculitis is papular rather than macular.The size varies from 1 mm to plaques that are severalcentimetres in diameter. The lesions are often distrib-uted on dependent surfaces such as the legs or the back,with symmetry almost always present. As the lesionsresolve, an ecchymotic appearance often remains, butscar formation is rare. In general, the lesions of leuko-cytoclastic vasculitis are asymptomatic or, rarely, itch-ing/burning, but if they ulcerate or form nodules, painmay be present. Resolution of the lesions of palpablepurpura rarely results in scar formation, and usuallythere is no visible or palpable residual. Piette and Stone8
have suggested that adult patients with palpable pur-pura who are found to have IgA on immunofluores-cence microscopy have a distinctive appearance to theirlesions, with multifocal areas of hemorrhage or super-ficial necrosis within the lesion and a livedoid or reti-form background.
Urticaria-like lesions may be a manifestation of leuko-cytoclastic vasculitis. The patient with this type of le-sion generally presents a chronic course, and the lesionsare clinically different from those of nonvasculitic urti-caria.9 Urticarial vasculitic lesions tend to be of longerduration than those of nonvasculitic urticaria. This canbe measured by asking the patient to encircle one ormore lesions of recent onset and then note the time toresolution. In patients with urticarial vasculitis, the le-sions tend to last for more than 6 hours and are oftenpresent for .24 hours, while those of nonvasculiticurticaria are of short duration, lasting ,4 hours. Fur-thermore, the lesions of urticarial vasculitis frequentlyresolve with a residual ecchymosis or pigmentation,whereas with nonvasculitic urticaria there is no residualevidence of the lesion’s location. Urticarial vasculitic
lesions are also said to be less pruritic, with the patientoften complaining of a burning sensation or pain. Fi-nally, patients with vasculitic urticaria often havesymptoms of accompanying diseases or systemic organinvolvement.
Vesicles and bullae can be seen in patients with moresevere inflammation of the vessels of the skin. Thevesicular lesions tend to arise on purpuric skin and thusare often hemorrhagic. In patients with bullous lesions,the separation is generally found at the dermal-epider-mal junction, but the exact level of the split has not beencharacterized. The mechanism of the blister formationis believed to be tissue ischemia. The presence of thistype of lesion is seemingly not indicative of the type ofassociation nor correlated with the size of the vesselsinvolved. Resolution of the lesions results in erosions,and thus scarring is not residual.
Necrosis and/or ulceration may also occur in patientswith cutaneous vasculitis. Usually the necrosis occursin relation to the intensity of the inflammatory reactionwithin the vessels, which produces vascular compro-mise due to interruption of the normal blood flow.Although ulceration and necrosis can occur in patientswith involvement of the small dermal vessels, its pres-ence often follows the involvement of larger vessels. Inparticular, when nodules are present along with a li-vedo reticularis and ulcerations, the vessel involved isoften the medium-sized arteriole in the deep dermis orat the subcutaneous-dermal margin. Another patternthat might occur in patients with vasculitis involvessmall purpuric lesions, livedo reticularis, and small ul-cerations that heal with stellate ivory white scars. Thispattern has been termed atrophie blanche, livedoid vas-culitis, or segmental hyalinizing vasculitis. Althoughsome patients with this pattern have demonstrable leu-kocytoclastic vasculitis, others do not, simply exhibitingvascular thrombosis. These lesions are probably at theend-stage of the vasculitic process and thus owing tothe timing of the sampling, a vasculitic histopathologymay not be evident.
Vasculitis can involve vessels of any size and anylocation. As a result, the clinical change may range fromthe petechiae of capillaritis to the gangrene of arteritis.
Vasculitis can be leukocytoclastic, lymphocytic,granulomatous, or, in some cases, obliterative, the le-
Table 5. Main Clinical Forms and Differential Diagnosis ofLymphocytic Vasculitis
Urticarial vasculitis*Erythema multiformePityriasis lichenoide and varioliformis acutaDrug reactionErythema perstansGranuloma annulareNodular scabiesInsect bitesNecrobiosis lipoidica diabeticorumViral infectionsRickettsial infectionsSpirochetal infections**Pigmented purpuric eruptionsLymphomatoid granulomatosis**Lymphomatoid papulosis
* See also leukocytoclastic vasculitis.** See also granulomatous vasculitis.
Table 6. Main Clinical Forms and Differential Diagnosis ofGranulomatous Vasculitis
Wegener’s granulomatosis*Allergic granulomatosis*Lymphomatoid granulomatosis**SyphilisTemporal arteritisTakayasu’s disease
* See also leukocytoclastic vasculitis.** See also lymphocytic vasculitis.
518 HAUTMANN ET AL. Clinics in Dermatology Y 1999;17:515–531

sions’ clinical signs ranging from papules to nodulesand ulcers. With such disparate manifestations, it issmall wonder that the clinician casts the diagnosis ofvasculitis as a wide net. But what may this net catchthat looks like vasculitis but isn’t? The catch of non-vasculitis lesions includes those of the “blue toes” ofatheroembolism, as well as the purpuric lesions ofscurvy, macroglobulinemia, blood dyscrasias, and fac-titial dermatitis. Thus, the biopsy is always the arbiterof authenticity. There are several issues that are impor-tant about the histopathological findings in patientswith cutaneous vasculitis.
First, what is the histopathological correlate of thecutaneous disease? Second, is it always necessary toconfirm the diagnosis of vasculitis by tissue examina-tion? Third, is the process, as viewed under the micro-scope, dynamic? As stated, the term vasculitis simplymeans segmental/angiocentric inflammation. It is notspecific regarding the nature of the infiltrate. The use ofthis general term can lead to confusion as there is ahistopathological entity known as reactive “perivascu-litis,” which is also not representative of a specificclinical process, but is represented by a perivascularcuffing with a sparse lymphohistiocytic infiltrate. Thisdoes not represent vasculitis.
Histopathologically, typical leukocytoclastic vasculi-tis classically demonstrates endothelial swelling of thepostcapillary venules, eosinophilic fibrin depositionwithin and around the vessels walls, fibrinoid necrosis,neutrophilic infiltration of the vessel walls, extravasa-tion of erythrocytes (hemorrhage), and fragmentationof neutrophils (leukocytoclasis or nuclear dust).10,11
Several investigators have studied the nature of theinflammatory infiltrate in patients with cutaneous vas-culitis. From these investigations two theories haveevolved. One suggests that the process is dynamic,changing with time from a neutrophil-predominantprocess to a mononuclear-predominant process.12 Theother theory suggests that two distinct clinical-patho-logical entities represent inflammatory vascular disease(vasculitis), one in which the neutrophil is the predom-inant cell invading the vessel wall (these cases havebeen defined as those in which there are .5% neutro-phils present), and the other in which mononuclearcells predominate.13,14
Another issue relates to whether or not there is aneed for pathological documentation of the vasculiticprocess. It is our opinion that documentation of thehistopathology is usually necessary. There are manyconditions that can simulate vasculitis of the skinand/or internal organs, but in which the pathologicalprocess is not that of an inflammatory angiocentricvasculopathy. The diagnosis of embolic phenomenasuch as artheromatous emboli, cholesterol emboli, orleft atrial myxoma can be suggested on examination ofbiopsy specimens. Similarly, patients with cryoglobu-
linemia, cryofibrinogenemia, and antiphospholipidsyndrome have a noninflammatory vasculopathy char-acterized by amorphous proteinaceous material withinthe vessels. There are also instances when the patholo-gist returns a report with a diagnosis of vasculitis, in acase in which the clinician did not suspect it. In thisinstance it is necessary to reexamine the patient prior toestablishing the final clinical diagnosis, as there aremany diseases in which inflammation surroundingblood vessels (perivasculitis) may occur, but which donot represent vasculitis with or without clinical evi-dence of vasculitis.
Besides processing tissue for light microscopy, directimmunofluorescence of tissue specimens is sometimeshelpful. This may show a predominance of IgA de-posits in Henoch-Schoenlein purpura and other con-ditions, or immune deposits in other forms of im-mune-complex-mediated small-vessel vasculitis. Inaddition, typical patterns of immune deposits may beseen at the dermal-epidermal junction in patientswith lupus erythematosus.
When granulomatous vasculitis is suspected and ear-nose-throat examination shows signs of inflammation,biopsy specimens should be obtained. These will fre-quently show nonspecific necrotizing inflammation butmay also reveal granuloma formation and/or necrotiz-ing vasculitis. When laboratory studies suggest thepresence of renal involvement, a renal biopsy is helpfulin many patients. The biopsy specimen should be pro-cessed at least for light microscopy and direct immu-nofluorescence. It may show characteristic staining forIgA as in Henoch-Schoenlein purpura and IgA ne-phropathy, or pauci immune necrotizing glomerulone-phritis with or without crescent formation in cases ofWegener’s granulomatosis or microscopic polyangiitis.
Generally, histopathologic confirmation of a diagno-sis of vasculitis should always be sought. In this respect,biopsies from the sural nerve in cases of suspectedmononeuritis or even “blind” biopsies of muscle ortestis in patients suspected of polyarteritis nodosa maybe helpful.
Thus, we stole the diagnosis of vasculitis from thepathologist. But we always have to go back to thepathologist and ask whether we stole the real thing.
Clinical Aspects of Cutaneous Vasculitides
Hypersensitivity Vasculitis
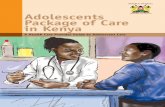
Hypersensitivity vasculitis (synonyms: allergic angiitis,leukocytoclastic vasculitis, small-vessel vasculitis, cuta-neous necrotizing vasculitis) (Fig 1) is a term that wasintroduced by Pearl M. Zeek, a pathologist, in the late1940s. Zeek and her co-workers were struggling withthe many overlapping features they observed in pa-tients with vasculitis.15 Their work provided the firstclassification system and started the separation of hy-
Clinics in Dermatology Y 1999;17:515–531 MANY FACES OF VASCULITIS 519

persensitivity vasculitis (angiitis) from rheumatic vas-culitis, polyarteritis (periarteritis) nodosa, granuloma-tous vasculitis, and large-vessel vasculitis, amodification of which we present in Table 1. The defi-nition of hypersensitivity vasculitis in general refers toa clinico-pathological process that is manifest as leuko-cytoclastic vasculitis of the postcapillary venule andoften includes the observation that the condition wasprecipitated by a drug or other substance. This term hasalso been used to describe those patients in whom thedisease is an idiopathic, small-vessel, cutaneous leuko-cytoclastic vasculitis.16 As such, some investigatorshave used this term to include patients with palpablepurpura associated with abnormal proteins (eg, cryo-globulinemia, hyperglobulinemia, etc), with a variety ofinfections, with a variety of “autoimmune” disorders,or with malignancy (paraneoplastic vasculitis).
The rationale for hypersensitivity vasculitis being adistinct entity is based on the observation that there arepatients in whom the disease follows the administrationof a drug or other substances (serum sickness in the1940s). Table 7 lists some of the more common drugsand other agents that have been implicated as causes ofhypersensitivity vasculitis. Foods, food additives, andinhalants should be considered in addition to drugs aspotential causes of hypersensitivity vasculitis in se-lected patients.17–22 Although the early reports of hy-persensitivity vasculitis stressed the cutaneous diseaseand the usual benign course, recent studies have clearlydocumented the potential for systemic involve-ment,23–25 as well as the risk of death.26
The concept of hypersensitivity vasculitis as a spe-
cific entity has generally endured and is probably clin-ically useful because it defines a relatively benign sub-set of vasculitis. Therefore, the authors of the 1990American College of Rheumatology (ACR) criteriaelected to include this entity among seven other clinicalentities.27 Unfortunately, 15 of the 21 criteria they se-lected for examination related to the histopathologicalchanges found on the biopsy. This approach wouldmost likely not take into account the dynamic nature ofthe infiltrate. Furthermore, one of the criteria was theage of the patient (.16 years for hypersensitivity vas-culitis versus ,16 years for Henoch-Schoenlein purpu-ra). In subsequent studies of the same individuals usedto create the criteria for hypersensitivity vasculitis andHenoch-Schoenlein purpura, the only clear difference isthe age of onset.28
Figure 1. The typical picture of cutaneous necrotizing vasculitis.
Table 7. More Common Drugs and Other Agents Implicated asCause of Hypersensitivity Vasculitis
AllopurinolAntibiotics: penicillins, sulfonamides, tetracycline, erythromycin,
gentamicin, zovirudineDiphenylhydantoinFoods and food additives (tartrazine)HerbicidesInhalantsInsecticidesNonsteroidal anti-inflammatory drugs: aspirin, naproxen,
phenylbutazonePhenothiazinesPotassium iodidePropylthiouracilThiazidesVaccines
520 HAUTMANN ET AL. Clinics in Dermatology Y 1999;17:515–531

Despite the shortcomings of the ACR’s criteria, theconcept of hypersensitivity vasculitis as a distinct entityremains somewhat reasonable; however, patients clas-sified as having hypersensitivity vasculitis still requirecareful assessment to establish that the cutaneous vas-culitis is not part of a systemic process (Table 4). Usingthe ACR criteria, it is evident that most of the patientswe diagnosed with cutaneous leukocytoclastic vasculi-tis can be correctly classified as hypersensitivity vascu-litis; however, patients with polyarteritis nodosa orgranulomatous vasculitis who have palpable purpuraand leukocytoclastic vasculitis on skin biopsy will bemisclassified; furthermore, patients with nonvessel-based neutrophilic inflammatory dermatoses, such asSweet’s syndrome, may also be misclassified. Presumedhypersensitivity vasculitis must still be differentiatedfrom other forms of vasculitis and from other dermato-ses, and the practitioner must consider a variety ofpotential etiological agents or associated conditionsother than drugs, serum, or other ingestants (Table 4).
Hypersensitivity vasculitis is generally manifest bythe appearance of palpable purpura, most commonlyon the lower extremities below the knees. The disease isusually symmetrical and may be exacerbated by pro-longed dependency of the legs. In addition, patientswho are confined to bed will manifest their lesions ondependent surfaces such as the buttocks and back. Le-sions may also occur in areas of trauma (pathergy) orunder tight-fitting clothing. Intertriginous areas may bespared, perhaps due to the warmer environment. Whilethe lesions are most frequent on dependent surfaces, attimes the disease may be generalized and even involvethe mucosal surfaces. The eruption can be acute, sub-acute, chronic or recurrent. In the acute forms, hemor-rhagic, purpuric, and necrotic lesions predominate andmay be extensive and severe, with the legs chiefly in-volved; the arms, buttocks, and thighs, commonly. Ves-icles, hemorrhagic bullae, and necrotic areas arise sud-denly, and subside within 2 to 3 weeks; crops may recurover a prolonged period.
In the subacute form, purpura, maculo-erythematouslesions, and urticaria with papules predominate; nod-ules and small necrotic lesions also occur. Confluence ofpapules may give rise to plaques resembling erythemaelevatum diutinum. It is common a combination ofnodules and purpura or urticaria. The group of chronicforms is represented by the mild forms of “trysymp-tome” and its extension and by many syndromes de-scribed under the title of cutaneous vasculitis. Intermit-tent cropping of new lesions may persist for months oryears. Erythematous macules, nodules, papules, andpurpuric and urticarial lesions predominate. The patientdoes not feel ill and suffers little inconvenience from theeruption, although a mild degree of malaise and constitu-tional disturbance may precede exacerbations.
The lesions of hypersensitivity vasculitis are usually
asymptomatic, but occasionally patients may sufferburning or itching. The lesions tend to occur in cropsand often begin as a macular erythema, macular pur-pura, or urticarial papules that progress over hours topalpable purpura. Sams et al.5 suggested that the de-velopment of the clinical lesion is dynamic, often be-ginning as nonpalpable purpura that eventually be-comes palpable. Further, they suggested that in “laterstages, some lesions become nodular, bullous, infarctiveand ulcerative.”5 Most often, the patient has only onetype of lesion, which fades as reparative processes be-gin. There are patients who have nodules, bullae, ul-cers, necrosis and/or livedo reticularis in combinationwith palpable purpura or as a sole manifestation ofsmall-vessel vasculitis. Most patients with these addi-tional findings will be classified with another vasculiticsyndrome despite finding leukocytoclastic vasculitis onhistopathological examination.
Systemic involvement in patients with hypersensitiv-ity vasculitis is not uncommon, but its frequency hasnot been clearly determined. In a review by Liss andWolverton reported by Callen29 of 58 patients withhypersensitivity vasculitis, 19/44 (43%) had renal in-volvement as defined by an abnormal urinary sediment(renal failure was not documented in this group ofpatients), 13/44 (32%) had arthralgias, but only 9% hadliver or lung involvement, 5% had gastrointestinal in-volvement, and only 2% had central nervous system orcardiac involvement. Further, constitutional symptomssuch as fever or myalgias were present in 20% and 11%,respectively. Moreover, constitutional upset, arthralgiaand gastrointestinal symptoms may frequently occurbefore the attack or during its course. Even mild,chronic or recurrent episodes may be preceded byheadache and malaise. Rechallenge resulted in confir-mation that a drug was involved in 13 of these patients.
The course of hypersensitivity vasculitis is highlyvariable. The disease duration has ranged from 1 day toup to 10 months. The duration of the disease is usuallyshort (,1 month) in patients in whom the skin is thesole clinical manifestation of the disease process, and inwhom there is an easily identified and removable anti-gen. In patients in whom the source of the antigen is notknown or cannot be altered, the disease may be pro-longed. In the setting of systemic involvement, wide-spread cutaneous disease is more common, the courseis often prolonged, and death may occur in up to one-third of the patients.30 In fact, this has been the reason todifferentiate skin-limited leukocytoclastic vasculitisfrom leukocytoclastic vasculitis with systemic disease.31
Cutaneous necrotizing vasculitis must be differenti-ated from the lesions of subacute bacterial endocarditisor meningococcal septicemia: this differential diagnosisis important because of the disastrous effects of steroidsin subacute bacterial endocarditis. Purely pustularforms resemble pustular bacterid.
Clinics in Dermatology Y 1999;17:515–531 MANY FACES OF VASCULITIS 521

Certain forms of cutaneous vasculitis may resemblescurvy, as described in the following case reported byWarshauer.32 “A 54-year-old woman was referred forevaluation of leukocytoclastic vasculitis. For the pastmonth she had had painful petechiae and palpable pur-pura. These skin lesions had been accompanied by mal-aise, myalgias, and arthralgias. The dietary history wassignificant. Because of dyspepsia, she had lived foryears on peanut butter sandwiches, and black decaf-feinated coffee. She took no vitamins. On examination,the backs of the hands and feet as well as the soles wereecchymotic. The lower legs showed multiple palpableperifollicular petechiae as well as follicular hyperkera-tosis. Of special note were corkscrew hairs in theseareas. All laboratory studies, including coagulograms,were normal with the exception of a hemoglobin valueof 10 g/dl. The serum vitamin C level was at the low endof normal at 0.2 mg/dl (normal 0.2 to 2 mg/dl). A skinbiopsy failed to show any vasculitis. A diagnosis ofscurvy was made. This was promptly confirmed by therapid clearing of all skin lesions as well as dramaticinvolvement of the myalgias and arthralgias within aweek of starting vitamin C therapy (500 mg/day). In-deed, the vitamin C level climbed fivefold after thepatient’s first hospital meal.”
Henoch-Schoenlein Purpura
This disease (synonyms: anaphylactoid purpura, pur-pura urticans) was first described by Schoenlein33 in1837 and then by Henoch34 in 1868. Henoch-Schoenleinpurpura was defined as a syndrome that combines thetetrad of palpable purpura, arthritis, gastrointestinalinvolvement, and nephritis.35 It is recognized that notall patients will manifest involvement of all four of theorgan systems. Also, it appears that Henoch-Schoenleinpurpura is much more common in childhood, but canoccur during adulthood.36 During recent years it hasalso been recognized that these patients, whether adultsor children, frequently have IgA immune complexes inthe circulation and/or deposited within the skin orkidneys.37 Depending on the definition used, however,it may not be necessary for these immune complexesto be present in order to diagnose Henoch-Schoenleinpurpura.
The disease is usually acute in its onset and oftenfollows an upper respiratory tract infection, particularlystreptococcal pharyngitis, with a latency period of 1 to2 weeks. By definition, children are more frequentlyaffected than are adults, and men more than women.Also, the disease appears to follow a seasonal variation,with a peak during the winter. The incidence of He-noch-Schoenlein purpura in the 2-to-14-year-old popu-lation has been estimated to be 14 cases per 100,000 peryear.38 It starts with fatigue, headache, mild fever, ab-dominal pains, and rheumatic joint pains. In fact, pro-dromal symptoms of headache, anorexia, and fever
may precede an acute onset of arthralgia, abdominalpain, and rash. These may occur together or in succes-sive waves and all three may not be present in any onepatient.
Skin lesions are one of the defining features of He-noch-Schoenlein purpura. The rash may begin as asymmetrical, macular erythema or urticaria, but over avery short time period the eruption becomes purpuric,with pin-head to coin-sized inflammatory petechialhemorrhages that pass through the characteristic colorchange of blood-pigment degradation with progressionof the disease. The lower extremities and buttocks arethe most common sites for skin lesions, with the exter-nal aspects of the limbs as the site of predilection;occasionally, the face is involved. Sometimes, purpuramay be the only symptom, and the diagnosis must besuspected whenever this occurs in children with a nor-mal platelet count. It is the urticarial component of thegeneral picture that is characteristic, however. The pur-puric lesions of vasculitis are characterized by smooth,discrete papules with relatively uniform lesional hem-orrhage.
Piette and Stone8 attempted to distinguish IgA-re-lated palpable purpura from other forms of leukocyto-clastic vasculitis. They described a distinct pattern ofIgA-associated cutaneous vasculitis in which the lesionswere superficial purpuric plaques with multifocal areasof hemorrhage and necrosis arranged in a retiform pat-tern. The importance of recognizing this form of cuta-neous small-vessel vasculitis is because of the associa-tion of IgA cutaneous vasculitis with IgA nephropathy.Unfortunately, the work of Piette and Stone has not yetbeen reconfirmed.
Gastrointestinal involvement occurs in about 50%–70% of the patients. The most common symptom iscolicky abdominal pain, which may be accompanied byvomiting. Bloody diarrhea or melena occur in about50% of affected individuals. In some patients the symp-toms are so severe that they mimic an acute abdomen.Bowel involvement may be complicated by perforationor intussusception. The involvement of the bowel isdue to a vasculitis of the small vessels in the submu-cosa with resultant edema and hemorrhage of thebowel wall.
Renal involvement in Henoch-Schoenlein purpuraoccurs in 20%–100% of patients and is the most seriousfeature of the disease and the one that should receivethe most careful attention because of its prognosticsignificance. The manifestations of renal involvementinclude hematuria, proteinuria, hypertension, and im-paired renal function. The involvement can be eithertransient and minor, or can result in progressive renalinsufficiency. In Henoch-Schoenlein purpura, notablyin adults, the entire clinical spectrum of glomerulone-phritis can be found. The histopathological patterns canvary from minor abnormalities to severe lesions. In
522 HAUTMANN ET AL. Clinics in Dermatology Y 1999;17:515–531

mild cases, there is only mesangial proliferation. Inmore severe cases, focal and segmental intracapillaryand extracapillary proliferation with adhesions andsmall crescents will be seen. The most severe lesion ischaracterized by diffuse proliferation with influx ofpolymorphonuclear leukocytes and crescents and inter-stitial infiltration.39
The histopathology of renal involvement in Henoch-Schoenlein purpura may be identical to that in IgAnephropathy or Berger’s disease,40 a condition thatprobably can be considered a form of Henoch-Schoen-lein purpura limited to the kidney. The IgA nephropa-thy can be subdivided into forms with minor changes,diffuse mesangial proliferative glomerulonephritis, fo-cal and segmental proliferative glomerulonephritis, andfocal glomerulosclerosis.41 The immunohistology in IgAnephropathy and Henoch-Schoenlein purpura revealsIgA1 as the predominant subclass.42 Despite completeresolution of the acute process in most of the cases ofHenoch-Schoenlein purpura, long-term follow-up stud-ies have demonstrated that subsequent pregnancies aremore frequently complicated by hypertension, and thatthe frequency of hypertension or renal insufficiency ishigher than that for the general population.43
The joints are involved in 60% to 90% of patientswith Henoch-Schoenlein purpura. Joint involvementmay be less frequent in adults than in children. Arthritisand/or arthralgias occur most often in the knees andankles, but the wrists and elbows may also be involved.The joints of the pelvis and shoulder girdle and thesmall joints of the hands and feet are rarely affected.Physical examination of the joints reveals periarticularedema. Joint effusions, warmth, and tenderness are notusually found. With resolution of the process, there isno permanent damage to the affected joints.
Manifestations of Henoch-Schoenlein purpura mayalso occur in other organ systems. Individual reports ofassociated asthma, hemoptysis, myocarditis, hepato-megaly, seizures, hemiparesis, subarachnoid hemor-rhage, parotitis, orchitis, adrenal necrosis with resultantAddison’s disease, and pancreatitis have appeared inthe literature.44
Henoch-Schoenlein purpura must be differentiatedfrom other vasculitic syndromes. In adults the distinc-tion from hypersensitivity vasculitis may be impossiblein the absence of immunofluorescence microscopy.45 Inchildren, other causes such as systemic lupus erythem-atosus or polyarteritis nodosa should be considered.When the disease is manifest first by colicky abdominalpain, appendicitis must be considered.
In the typical case of Henoch-Schoenlein purpura,the only laboratory tests that need to be routinely per-formed are those which assess the presence of renalinvolvement. In cases in which the diagnosis is indoubt, histologic confirmation of a small-vessel vascu-litis can be easily accomplished by a skin biopsy. In
adults with presumed Henoch-Schoenlein purpura, thedemonstration of IgA deposition in around the cutane-ous vessels is diagnostic. Increases in serum levels ofIgA occur in some patients with Henoch-Schoenleinpurpura, and Saulsbury demonstrated that the increasewas due to IgA1.46 Other vasculitic syndromes, menin-gococcemia, bacterial endocarditis, and Rocky Moun-tain spotted fever should be included in the differentialdiagnosis.
Acute Hemorrhagic Edema of Infancy
This rare form of leukocytoclastic vasculitis occurs ininfants under 2 years of age.47,48 It has an acute onset,often following an upper respiratory tract infectionand/or drug ingestion. The rash begins as urticarialplaques, but rapidly becomes intensely purpuric, withfever and generalized edema as common features. Thisdisorder may simulate purpura fulminans or dissemi-nated intravascular coagulopathy. Acute hemorrhagicedema of infancy has been distinguished from Henoch-Schoenlein purpura on the basis of both clinical andimmunological grounds. Patients with the former dem-onstrate IgM within the dermal vessels rather than IgA,which is observed in the latter. The process of acutehemorrhagic edema of infancy is benign and self-lim-ited without residua.
Urticarial Vasculitis
This disease is characterized clinically by urticarial le-sions and histopathologically by leukocytoclastic vas-culitis. This disorder was perhaps first clearly distin-guished as an entity by researchers,49 who reported“four patients with recurrent attacks of erythematousurticarial and hemorrhagic skin lesions associated withsynovitis and sometimes abdominal distress.” Two oftheir four patients also had glomerulonephritis, and allfour had hypocomplementemia. For this entity theycoined the term “hypocomplementemic urticarial vas-culitis.” Since the original description, it has been rec-ognized that (1) some patients with urticaria have vas-culitis in the absence of hypocomplementemia; (2)about one-fifth of the patients with urticarial vasculitiswill have significant pulmonary disease;50 (3) whenurticaria occurs in patients with collagen vascular dis-eases, leukocytoclastic vasculitis is the usual his-topathological correlate, and the urticarial vasculiticlesions usually correlate with active systemic inflamma-tory disease;51,52 (4) urticarial vasculitis may also occurin patients with hepatitis-associated vasculitis, paraneo-plastic vasculitis, and paraprotein-associated vasculi-tis;53 and (5) almost all of the patients have long-stand-ing chronic urticaria.
Clinically, urticarial vasculitis is distinguished fromroutine urticaria by lesions that are painful or burningrather than pruritic, by lesions that last more than 24hours, and by lesions that resolve with purpura, scaling
Clinics in Dermatology Y 1999;17:515–531 MANY FACES OF VASCULITIS 523

or bruising.54 Histopathologically, the lesions show leu-kocytoclastic vasculitis with fibrinoid necrosis. Thesechanges should be distinguished from the nonvasculiticprocesses of neutrophilic urticaria and urticaria withdiffuse dermal neutrophilia. Both of these conditionshave been described55 and do not seem to be associatedwith the risk of systemic disease or hypocomple-mentemia that may occur in some patients with urticar-ial vasculitis; however, it is not clear from these studieswhether repeated biopsies were taken, nor is it statedhow old the lesions were that were biopsied. Thus, it ispossible that these entities are benign variants of urti-carial vasculitis.
Laboratory evaluation other than an increased eryth-rocyte sedimentation rate and abnormal complementlevels is usually unremarkable with the exception ofabnormalities that would be found with an associateddisease process, such as a positive antinuclear antibodytest in patients with lupus erythematosus. In the anal-ysis of 72 patients with urticarial vasculitis, research-ers56 found that only 23 of the 68 patients tested had anelevated sedimentation rate. Thus, while an elevatedsedimentation rate is more often present in patientswith urticaria who have vasculitis, a normal rate doesnot rule out the presence of vasculitis. Likewise, only 23of 65 patients had a depressed total hemolytic comple-ment (CH50), only 18 had a decreased C3 level, andonly 6 had a decreased C4 level. Abnormal urinarysediment correlated with the presence of nephritis, usu-ally associated with an accompanying disease such aslupus erythematosus. Tests of lung function reveal ab-normalities in those with associated chronic obstructivepulmonary disease.
Mehregan et al.56 also analyzed the clinical differ-ences between those patients with hypocomple-mentemia and those with normocomplementemia.They found that those with hypocomplementemia hada significantly higher frequency of residual purpura,arthralgias, abdominal pain, chronic obstructive pulmo-nary disease, and deposition of immunoglobulin or C3in blood vessels or the basement membrane zone. Al-though pulmonary disease is relatively common in pa-tients with hypocomplementemic urticarial vasculitis,renal involvement is an uncommon complication.
Erythema Elevatum Diutinum
Erythema elevatum diutinum is an unusual form ofcutaneous vasculitis characterized by persistent ery-thematous, violaceous and/or yellow papules, plaquesand nodules.57 The lesions are persistent, symmetrical,red or rust-colored and purple plaques affecting thebacks of the hands and other extensor surfaces overly-ing joints. Smaller annular lesions on the extensor as-pects of the hands and arms have been described. Thelesions often occur over bony prominences. The lesionsstart as papules or nodules on the backs of the hands
and less frequently the extensor surface of the knee andelbows, around the wrists and ankles or on the but-tocks. Plaques form that are often voluminous and al-ways infiltrated; they may be irregular in shape but aresometimes gyrate or annular. At first the lesions are softbut become hard as fibrosis supervenes. They eventu-ally heal without scarring, leaving hyperpigmentation.
Perilesional bullous and vesicular lesions have alsobeen reported. Ulceration may precede disappearanceof the lesions. Occasionally, the patients may have ar-thralgias, but other systemic manifestations of vasculitisare virtually absent. The disease is of unknown origin,but some of the patients with erythema elevatum diuti-num have a paraprotein, usually IgA, or, occasionally,IgM. Erythema elevatum diutinum can be regarded as achronic, low-grade form of leukocytoclastic vasculitiswith a slow fibrotic healing phase. This particular vas-culitic disease appears to respond poorly to all thera-pies other than oral dapsone or equivalent agents.
Pustular Vasculitis
Jorizzo coined the term pustular vasculitis to describe theneutrophilic lesions that occur in patients with bowelbypass surgery, inflammatory bowel disease, blind loopsyndromes, and Behcet’s disease.58 These patients man-ifest similar cutaneous and systemic abnormalities,which include pustular lesions, erythematous plaquesthat simulate acute febrile neutrophilic dermatosis(Sweet’s syndrome), erythema nodosum-like lesions, orpyoderma gangrenosum-like lesions, in conjunctionwith polyarthritis, fever, and myalgias. Although theinitial reports described a leukocytoclastic vasculitis, ithas become evident that this process is not one in whichthe vessel walls are clearly destroyed. Thus, it might bebest to consider this entity under the lesions that sim-ulate vasculitis.
Cutaneous Vasculitis May Also Represent aManifestation of Another Rheumatic Disease Process
Inflammatory vasculopathy is a relatively frequent pro-cess associated with the group of disorders often re-ferred to as “collagen-vascular diseases.”59 Amongthese diseases, vasculitis may be a common occurrencein patients with rheumatoid arthritis (RA), systemiclupus erythematosus, and Sjogren’s syndrome; it occursin some patients with mixed connective tissue disease,scleroderma and relapsing polychondritis, and is rareamong patients with inflammatory myopathy.
Several vascular complications occur in patients withRA from the more benign capillaritis to severe, life-threatening systemic vasculitis.60,61 The rheumatoid nod-ule, which is histopathologically a palisading necrobi-otic granuloma, may well start as an inflammatoryvasculitis. In addition, researchers have described acondition they term rheumatoid papules,62 characterizedby small erythematous papules; on histological exami-
524 HAUTMANN ET AL. Clinics in Dermatology Y 1999;17:515–531

nation a palisading granuloma and leukocytoclasticvasculitis are revealed. The nomenclature associatedwith the inflammatory vasculopathy that occurs in pa-tients with RA is controversial and often confusing.Some investigators will diagnose rheumatoid vasculitisin RA patients with small-vessel vasculitis, whereasothers reserve this term for patients with “serious”vasculitis that involves the small arteries of the digits,nerves, and mesentery.
Vollertsen and Conn have divided the vasculopa-thies associated with RA into three categories: (1) vas-cular involvement as part of the pathogenesis of RA, (2)isolated digital vasculitis, and (3) the syndrome of clin-ical rheumatoid vasculitis.63 The last include those pa-tients who demonstrate systemic rheumatoid vasculitisand those with vasculitis localized primarily to the skin.The patient with “serious” vasculitis frequently has anactive arthritis with rheumatoid nodules and high lev-els of rheumatoid factor. These patients will have dig-ital infarcts, leg ulcers, and/or palpable purpura. In-volvement of the mesenteric vessels or coronary arteriescan be associated with the more severe and life-threat-ening consequences.
In contrast, there are patients with RA whose inflam-matory vessel disease involves only the small cutane-ous vessels. It has not been clearly delineated howmany of these patients have secondary Sjogren’s syn-drome, a condition that would be expected to be asso-ciated with vasculitis of the small vessels. These pa-tients generally have highly elevated levels ofrheumatoid factor, but they often suffer a more pro-tracted course of the vasculitis, which is usually notcomplicated by arteritis of the viscera.
Lupus erythematosus (LE) is a disease with proteanmanifestations. Systemic LE is usually associated withthe presence of immune complexes in the circulation. Ithas been presumed that the LE-associated vasculitis is amanifestation of these circulating immune complexes(CIC); however, while many of the patients with LEhave CIC, only some will have vasculitis. The types ofvasculitic disease manifest in LE are similar to thoseseen in RA, in that vessels of any size may be affected.In patients with large-vessel disease, serious and poten-tially life-threatening consequences can occur, whereasthose patients who have small-vessel vasculitis experi-ence a milder process. Also, secondary Sjogren’s syn-drome can complicate LE. Few (if any) of the studies ofLE-associated vasculitis have checked for the presenceof Sjogren’s syndrome.
In addition, urticarial lesions can complicate LE andoften represent vasculitis.64 The presence of clinicallyrecognizable vasculitis in patients with LE, regardlessof the size of the vessel involved, suggests active dis-ease and has been associated with a poorer prognosis.The most severe prognosis is associated with involve-ment of the larger vessels and with digital gangrene
and nailfold infarcts. Another correlated issue in LE isthe presence of antiphospholipid antibodies. Thoughthese antibodies are associated with a vasculopathy,there is no evidence to suggest that it is an inflamma-tory lesion; rather, the vasculopathy is seemingly athrombotic process.
Sjogren’s syndrome can be either a primary diseaseprocess or a corollary to another connective tissue dis-ease such as RA or LE. It is characterized by keratocon-junctivitis sicca and xerostomia. It has been suggested13
that there are two distinct patterns to the vasculopathyassociated with Sjogren’s syndrome, and that these pat-terns correlate with hypocomplementemia, and the riskof central nervous system involvement. The two pat-terns that have been suggested include the one which isrich in neutrophils and the one in which there is mono-nuclear-related destruction of the vessel wall. This con-cept of two distinct patterns has been challenged by theobservation that the character of the infiltrate changeswith time in patients who are serially biopsied. Never-theless, the vasculitic lesions occurring in Sjogren’s syn-drome most often involve the skin and are manifest asa palpable purpura or, occasionally, as urticarial le-sions. In many reports, it appears that the vasculopathyis a marker of more serious internal disease not neces-sarily vasculitic in its nature. However, there are a fewreports in which patients with Sjogren’s-associated vas-culitis had serious systemic vasculitic complications.65
Cutaneous Vasculitis as a Manifestation ofParaproteinemia
Abnormal immunoglobulins either arising from mono-clonal proliferation (eg, paraprotein and cryoglobuline-mia type I or II) or from polyclonal proliferation, as inhyperglobulinemic purpura and cryoglobulinemia typeIII, may be associated with vasculitis. Regardless of thetype of abnormal immunoglobulin, there is a commongroup of associated diseases that include lymphoprolif-erative disorders, collagen-vascular diseases, and infec-tious diseases.66 The skin disease found with these ab-normal proteins is commonly characterized by palpablepurpura, livedo reticularis, urticaria, and/or ulceration.Histopathological evaluation of skin biopsy specimensfrom patients with abnormal proteins most commonlyreveals either a vasculitis or a noninflammatory hyalinethrombosis within the vessel.
Cryoglobulins are serum immunoglobulins that pre-cipitate when the serum is cooled. There are three majortypes of cryoglobulinemia. Type I is a monoclonal im-munoglobulin usually occurring in patients with amonoclonal gammopathy (lymphoproliferative dis-ease—in particular, multiple myeloma) and Walden-strom macroglobulinemia; type II is a mixed cryoglob-ulin consisting of both monoclonal and polyclonalelements occurring in association with Sjogren’s syn-drome, lymphoproliferative disorders, and macroglob-
Clinics in Dermatology Y 1999;17:515–531 MANY FACES OF VASCULITIS 525

ulinemia; and type III cryoglobulin is polyclonal andoccurs in conjunction with collagen-vascular diseasesand infections.67 One-third of the patients with types IIor III cryoglobulinemia, however, do not have an asso-ciated disorder and are thus considered as having es-sential cryoglobulinemia.68
The clinical features of patients with cryoglobuline-mia frequently occur due to inflammation or occlusionof the small vessels, following deposition of the cryo-protein in the vessel lumen or wall.69 The skin lesions inthese patients include both palpable and macular pur-pura, leg ulcers, urticaria-like lesions, livedo reticularis,acrocyanosis, and digital gangrene. Raynaud’s phe-nomenon is also a common finding. Systemic disease isfrequent and includes peripheral neuropathy, arthral-gias, renal disease (proteinuria, azotaemia and/or hy-pertension), as well as hepatic dysfunction, hepato-splenomegaly, intestinal vasculitis and coronaryvasculitis. Since many of these patients have either acollagen-vascular disease or hepatitis, the symptomsthat occur are not surprising. Furthermore, the otherareas involved and types of involvement are reminis-cent of disease observed in idiopathic forms of vascu-litis. We believe that this group of patients must bedistinguished by the others because of the potentialrecognition of an associated lymphoproliferative dis-ease and because therapy aimed at stopping the pro-duction/release of the cryoglobulin is warranted.
Waldenstrom70 first described hyperglobulinemicpurpura in 1943 as a distinct syndrome consisting ofrecurrent episodes of purpura, elevated levels ofgamma globulin, an elevated erythrocyte sedimentationrate and mild anemia. This entity may be a primaryprocess or secondary to an associated condition such asSjogren’s syndrome, LE, thyroiditis, sarcoidosis, RA,thymoma, or myeloma.71,72 The histopathology hasshown to be either a leukocytoclastic vasculitis or amononuclear perivascular infiltrate. In a patient de-scribed by researchers, repeated biopsies were per-formed, and only when the earliest lesions were sam-pled was leukocytoclastic vasculitis demonstrated.73
Thus, it seems that this entity has direct parallels withthe type of vasculopathy that occurs in patients withSjogren’s syndrome. Similar to cryoglobulin-associatedvasculitis, recognition of hyperglobulinemic purpurashould lead the physician to recognize the associatedconditions, in particular Sjogren’s syndrome.
Schnitzler’s syndrome or chronic urticaria with macro-globulinemia is another vasculitic syndrome associatedwith a paraprotein. It was first described in 1974 andwas proposed to be an entity distinct from Walden-strom’s macroglobulinemia.74–76 This is a rare syn-drome with fewer than 20 cases reported in the litera-ture. The syndrome is characterized by chronicurticaria, fever, an elevated erythrocyte sedimentationrate, a monoclonal IgM (most often K) paraprotein, and
urinary Bence-Jones protein, arthralgias, lymph nodeenlargement, hepatomegaly, and hyperostosis. Abouthalf of the patients have had bone pain and anemia, butneither myeloma nor lymphoma seemingly complicatethe course. Some patients may present an abnormalcomplement profile, rheumatoid factor, antibodies tounidentified soluble nuclear antigens, and anticytoplas-matic antibodies. Although the long-term course of thedisease is usually benign, evolution to true lymphop-lasmocytic malignancy has been reported.
Paraneoplastic Vasculitis
Neoplasia has been associated with a wide spectrum ofvasculitic syndromes, as reported in Table 8. The mostfrequent associations include polyarteritis nodosa(PAN) with hairy cell leukemia and cutaneous small-vessel vasculitis with a variety of lymphoproliferativedisorders, as well as adenocarcinomas. Occasionally,these associations are truly paraneoplastic, or in otherwords, they are recognized concurrently and follow aparallel course. Unfortunately, there are no adequatestudies documenting the frequency of neoplasia in pa-tients with vasculitis, and in one large community-based study of 82 patients, none were found to have anassociated malignancy.23 This contrasts with data fromother investigators77 who found 11 cases of paraneo-plastic vasculitis among their 222 patients with vascu-litis, and the data of still another team78 in which therewere 4 cases among 26 patients.
Hairy cell leukemia is a rare entity characterized byfatigue, fever, recurrent infections, pancytopenia, andsplenomegaly. Systemic PAN has been the primaryform of vasculitis reported in patients with hairy cellleukemia.79 However, at least one patient with a small-vessel vasculitis has been described. In general, thevasculitic syndrome appears after the diagnosis of leu-kemia, and the course is not parallel. Thus, it seems thatthe vasculitic syndrome is a complication of the leuke-mic process. The pathogenesis of the association is notknown, but theories such as an abnormal handling ofimmune complexes, the ability of the hairy cell to syn-thesize immunoglobulins, the presence of a commonantigen on the hairy cells and the endothelial cells, and
Table 8. Malignancy-Associated Vasculopathies
Cutaneous (small vessel) vasculitis and Henoch-Schoenlein purpuraPolyarteritis nodosaCryoglobulinemia (and other paraproteinemias)Digital necrosis and Raynaud’s phenomenonEmbolic phenomenon
Atrial myxomaNonbacterial thrombotic endocarditis
Thrombotic processesSuperficial migratory thrombophlebitisAntiphospholipid syndromeDeep venous thrombosis
526 HAUTMANN ET AL. Clinics in Dermatology Y 1999;17:515–531

direct tissue invasion by the hairy cells have been pro-posed. Actually, there are no data to support any one ofthese theories. Clinically, the vasculitis does not differfrom non-hairy-cell-associated PAN. One major issuerelates to the therapy for the vasculitis, as treatmentsnormally used for PAN may result in a worsening ofthe pancytopenia and/or an increase in the risk ofinfection. The prognosis in this group of patients ispoor, and death usually occurs secondary to complica-tions of leukemia rather than vasculitis.
Small-vessel vasculitis has also been noted in pa-tients with malignancy. In these patients, lymphoreticu-lar malignancies predominate, but there are numerousreports of solid tumors in patients with small-vesselvasculitis of the skin.77,80,81 In addition, multiple cases ofso-called preleukemic states in patients with small-ves-sel vasculitis have been reported.81–83 It is not clear inthese reports whether a relationship exists between themalignancy and the vasculitis, and many of these pa-tients responded to corticosteroids.
There are enough reports of the association of cuta-neous vasculitis with hematologic disorders that it seemsreasonable to assess each vasculitic patient for the pres-ence of hematologic malignancy. Therefore, the pres-ence of anemia, thrombocytopenia, leukopenia, or leu-kocytosis must be carefully evaluated. The issue of arelationship of cutaneous vasculitis and solid tumors isquestionable. Limited numbers of reports and the lackof a paraneoplastic course in all but a few patients mayobviate the need for an extensive malignancy evaluation.
Other possible relationships between vasculitic syn-dromes and neoplasia have appeared in the literature.Malignancy is a part of the disease process in lympho-matoid granulomatosis. Paraprotein-associated vasculitisis frequently complicated by neoplasia. Recently, vas-culitis was given as a complication of therapy for ma-lignancy including chemotherapeutic agents, bone mar-row transplantation with immunosuppression,84 andradiotherapy. Conversely, acute myelocytic leukemiahas been reported as a consequence of cytotoxic therapyof a patient with PAN.85
Polyarteritis Nodosa Group
This group takes into account the original classic pol-yarteritis nodosa, the closely related allergic granulo-matosis, and that difficult and most important syn-drome that overlaps the other two and does notexclusively have the distinguishing characteristics ofeither of the other two, but shares features of both,namely “overlap syndrome.”
The first two of these three subgroups have beenfirmly entrenched in the vasculitis literature, and classicpolyarteritis nodosa, as it was originally described86
and later categorized,87,88 is a necrotizing vasculitis ofsmall- and medium-sized muscular arteries. The lesionstend to be segmental with a predilection for bifurca-
tions and branchings of arteries with distal spread in-volving arterioles and, in some cases, circumferentiallyinvolving adjacent veins. Histopathologically, in theacute stages, polymorphonuclear leukocytes infiltrateall layers of the vessel wall and perivascular areas.Mononuclear cell infiltration follows as the lesions be-come subacute or chronic. Intimal proliferation, vessel-wall degeneration with fibrinoid necrosis, thrombosis,ischemia, and infarction are seen in varying degrees.Generally, the simultaneous presence of vascular le-sions is found in all stages of development. Multipleorgan systems are involved and the clinicopathologicfindings reflect the degree and location of vessel in-volvement with the resulting ischemic changes.
Table 9 outlines the salient clinicopathologic featuresof “classic” polyarteritis nodosa.87,88 Allergic historiesare uncommon, as are eosinophilia and eosinophilictissue involvement. Also, granulomata are not charac-teristically found, and lung and spleen are not charac-teristically involved. These are important distinguish-ing features and have been sources of confusion eversince Rose and Spencer88 divided polyarteritis nodosaaccording to the presence or absence of lung involve-ment and granulomata. The disease that these authorswere labeling polyarteritis nodosa with lung involve-ment and granulomata was, in essence, indistinguish-able from the allergic granulomatosis of Churg andStrauss.89 The most significant clinical sign is the pres-ence of cutaneous or subcutaneous nodules, which oc-cur in groups along the course of superficial arteries.They measure between 4 and 15 mm in diameter, andare most easily found around the knee, anterior lowerleg, and dorsum of the foot.90 They are apparently dueto local necrosis of the arterial wall at points of bifur-cation. Pulsatile aneurysms result from healing by fibrosis.Local rupture may give rise to a local intracutaneous
Table 9. Typical Clinicopathologic Features of ClassicPolyarteritis Nodosa
Allergic history uncommonArthralgias common, arthritis rareCoronary arteritis (particularly in children)Cutaneous—uncommon, usually subcutaneous nodules, livedo
reticularisEosinophilia and granulomata not characteristicGastrointestinal—infarction of visceraGenitourinary—testes, bladder, epididymis, ovaryHepatic—subclinical disease to chronic active hepatitis in patients
with hepatitis B antigenemia; liver disease related to vasculitis(up to 50%)
HypertensionLung and spleen characteristically not involvedNecrotizing vasculitis of small- and medium-sized muscular
arteriesNeurological—mononeuritis multiplexRenal involvement
Related to vasculitis (70%)Glomerulitis (30%)
Clinics in Dermatology Y 1999;17:515–531 MANY FACES OF VASCULITIS 527

hematoma or ecchymosis. Peripheral embolization ofthrombi causes infarction of the tissues, and the fingersand toes may be particularly affected by small infarcts,splinter hemorrhages, Osler’s nodes, absorption andgangrene.
A characteristic feature of this polyarteritis nodosagroup is the finding of aneurysmal dilatations up to 1cm in size in medium-sized arteries seen by angiogramin the renal, hepatic, and visceral vasculature. It isbelieved that this finding is virtually pathognomonic of“classic” polyarteritis nodosa.91,92 Multiple aneurysmsof this type, however, are seen in overlap syndromes inwhich vessels of various sizes are involved93 as well asin other disorders such as systemic lupus erythemato-sus94 and fibromuscular dysplasia.95
As previously mentioned, allergic granulomatosisstrongly resembles classic polyarteritis nodosa withsome obvious distinguishing features and is almostinvariably associated with particularly severe asthma.89
Unlike classic polyarteritis nodosa, lung involvement isa sine qua non criterion of this syndrome. Also, it ischaracterized by high levels of peripheral eosinophilia(usually higher than 1500/mm3), eosinophilic and gran-ulomatous tissue infiltration. Histopathologically, thisdisorder manifests—in addition to the fibrinoid necro-sis of small- and medium-sized muscular arteries that isthe hallmark of classic polyarteritis nodosa—a substan-tial degree of involvement of small vessels such ascapillaries and venules. Apart from these differences,the presentation, clinicopathologic manifestations, or-gan system involvement, and clinical course of thesetwo syndromes are similar.
The third disorder in this group is the “overlap syn-drome,” which manifests in the same patient featuresthat would be considered characteristic, or even patho-gnomonic, of either classic polyarteritis nodosa or aller-gic granulomatosis. It is a multisystem disease with theassociated protean clinical manifestations. Small-vessel(arterioles, capillaries, and venules), together with theclassic small- and medium-sized muscular artery in-volvement with characteristic angiographically demon-strable small aneurysms, can be seen in the same pa-tient. History of allergy, peripheral eosinophilia,eosinophilic tissue infiltration, granulomatous reac-tions, and lung involvement may or may not all to-gether be seen in the same patient.
Conclusions
Cutaneous vasculitis is often a marker of systemic dis-ease. It may represent the practically sole manifestationof the disease process or may be considered merely aminor feature of a life-threatening vasculitic syndrome.Part of the confusion is related to the classification. Forexample, when one considers patients with parapro-teinemia, it is evident that a variety of different vascu-
litic syndromes can occur in these patients, and that theparaprotein may even be a manifestation of an associ-ated collagen-vascular disease. Similarly, the patientwith hypersensitivity vasculitis may manifest the fullgamut of a systemic vasculitis, including gastrointesti-nal bleeding and nephritis. Therefore, when approach-ing the patient in whom cutaneous disease is a feature,the full array of vasculitic syndromes should be consid-ered, and further all organ systems that may be poten-tially affected should be thoroughly evaluated. It doesappear that, once present, the syndrome within whichthe patient is diagnosed remains stable. In other words,chronic cutaneous (small-vessel) vasculitis seems to in-volve nearly always only the skin, even with long-termfollow-up.
Finally, the pathogenesis of cutaneous vasculitis atleast in some part has been linked to the presence ofimmune complexes in the circulation, which under ap-propriate circumstances can become deposited in thetissues. Additional factors including endothelial abnor-malities, cytokines, neurotransmitters, and plasmino-gen activators are also potentially involved in this com-plex cascade of events.96
References
1. Callen JP. Cutaneous vasculitis: Relationship to sys-temic disease and therapy. Curr Probl Dermatol 1993;5:45– 80.
2. Churg A, Churg J, editors. Systemic vasculitis. New York:Igaku-Shoin Medical Publishers, 1991.
3. Lie JT. Vasculitis, 1815 to 1991: Classification and diag-nostic specificity. J Rheumatol 1992;19:83–89.
4. Hunder GG, Arend WP, Bloch DA, et al. The AmericanCollege of Rheumatology 1990 criteria for the classifica-tion of vasculitis. Arthritis Rheum 1990;33:1065–1136.
5. Sams WM Jr, Thorne EG, Small P, et al. Leukocytoclasticvasculitis. Arch Dermatol 1976;112:219–26.
6. Smoller BR, McNutt NS, Contreras F. The natural historyof vasculitis. Arch Dermatol 1990;126:84–89.
7. Fan PT, Davis JA, Somer T, et al. A clinical approach tosystemic vasculitis. Semin Arthritis Rheum 1980;9:248–302.
8. Piette WW, Stone MS. A cutaneous sign of IgA-associatedsmall dermal vessel leukocytoclastic vasculitis in adults(Henoch-Schoenlein purpura). Arch Dermatol 1989;125:53–56.
9. Monroe EW, Schulz CI, Maize JC, et al. Vasculitis inchronic urticaria: An immunopathologic study. J InvestDermatol 1981;76:103–7.
10. Hodge SJ, Callen JP, Ekenstam E. Cutaneous leukocyto-clastic vasculitis: Correlation of histopathological changeswith clinical severity and course. J Cutan Pathol 1987;14:279–84.
11. Sanchez NP, Van Hale HM, Su WPD. Clinical and his-topathologic spectrum of necrotizing vasculitis. Arch Der-matol 1985;121:220–24.
12. Zax RH, Hodge SJ, Callen JP. Cutaneous leukocytoclasticvasculitis: Serial histopathologic evaluation demonstrates
528 HAUTMANN ET AL. Clinics in Dermatology Y 1999;17:515–531

the dynamic nature of the infiltrate. Arch Dermatol 1990;126:69–72.
13. Alexander E, Provost TT. Sjoegren’s syndrome. Arch Der-matol 1987;123:801–10.
14. Soter NA, Mihm MC Jr, Gigli I, et al. Two distinct cellularpatterns in cutaneous necrotizing angiitis. J Invest Derma-tol 1976;66:344–50.
15. Zeek PM, Smith LC, Wector JC. Studies on perivasculitisnodosa: III. The differentiation between the vascular le-sions of periarteritis nodosa and hypersensitivity. Am JPathol 1948;24:889–917.
16. Swerlick RA, Lawley TJ. Small-vessel vasculitis and cuta-neous vasculitis. In: Churg A, Churg J, editors. Systemicvasculitis. New York: Igaku-Shoin Medical Publishers,1991:193–201.
17. Haber MM, Marboe CC, Fenoglio JJ Jr. Vasculitis in drugreactions and serum sickness. In: Churg A, Churg J, edi-tors. Systemic vasculitis. New York: Igaku-Shoin MedicalPublishers, 1991:305–13.
18. Mullick FG, McAllister HA, Wagner BM, Fenoglio JJ.Drug-related vasculitis. Hum Pathol 1979;10:313–25.
19. Michaelsson G, Pettersson L, Juhlin L. Purpura caused byfood and drug additives. Arch Dermatol 1974;109:49–52.
20. Veien NK, Krogdahl A. Cutaneous vasculitis induced byfood additives. Acta Derm Venereol 1990;71:73–74.
21. Arias JA, Santana C, Vizcaına JA, et al. Vasculitis porhipersensibilidad: Analisis de 60 pacientes. Rev Clin Esp1989;185:187–90.
22. Tencati JR, Novey HS. Hypersensitivity angiitis caused byfumes from heat-activated photocopy paper. Ann InternMed 1983;98:320–22.
23. Ekenstam E, Callen JP. Cutaneous leukocytoclastic vascu-litis. Arch Dermatol 1984;120:484–89.
24. Winkelmann RK, Ditto WB. Cutaneous and visceral syn-dromes of necrotizing or “allergic” angiitis: A study of 38cases. Medicine (Baltimore) 1964;43:59–89.
25. Handel DW, Roenigk HH Jr, Shainoff J, et al. Necrotizingvasculitis. Arch Dermatol 1975;111:847–52.
26. Yermakov VM, Hitti IF, Sutton AL. Necrotizing vasculitisassociated with diphenylhydantoin: Two fatal cases. HumPathol 1983;13:182–84.
27. Calabrese LH, Michel BA, Bloch DA, et al. The AmericanCollege of Rheumatology 1990 criteria for the classifica-tion of hypersensitivity vasculitis. Arthritis Rheum 1990;33:1108–13.
28. Michel BA, Hunder GG, Bloch DA, et al. Hypersensitivityvasculitis and Henoch-Schoenlein purpura: A comparisonbetween the 2 disorders. J Rheumatol 1992;19:721–28.
29. Callen JP, Kallenberg CGM. The vasculitides: Relation-ship of cutaneous vasculitis to systemic disease. In: KaterL, Baart de la Faille H, editors. Multi-systemic autoim-mune diseases. Amsterdam: Elsevier, 1995:267–97.
30. Savage CS, Winearls CG, Evans DJ, et al. Microscopicpolyarteritis: Presentation, pathology and prognosis. QJ Med 1985;56:467–83.
31. Jennette JC, Falk RJ, Andrassy K, et al. Nomenclature ofsystemic vasculitides: The proposal of an internationalconsensus conference. Arthritis Rheum 1993.
32. Warshauer DM, Hayes ME, Shumer SM. Scurvy: A clini-cal mimic of vasculitis. Cutis 1984;34:539–41.
33. Schoenlein JL. Allegemeine und specielle Pathologie und
Therapie. 3rd ed, Vol 2. Herisau: Germany, 1837: LiteraturComptoir, 48.
34. Henoch EH. Ueber eine eigentuemliche Form von Pur-pura. Berl Klin Wochenschr 1874;11:641–43.
35. Saulsbury E. Henoch-Schoenlein purpura. Pediatr Derma-tol 1984;1:195–201.
36. Ilan Y, Naparstek Y. Schoenlein-Henoch purpura inadults and children. Semin Arthritis Rheum1991;21:103–9.
37. Kauffmann RH, Herrmann WA, Meijer CJLM, et al. Cir-culating IgA-immune complexes in Henoch-Schoenleinpurpura. Am J Med 1980;69:859–66.
38. Farley TA, Gillespie S, Rasoulpour M, et al. Epidemiologyof a cluster of Henoch-Schoenlein purpura. AJDC 1989;143:798–803.
39. Levy M, et al. Adv Nephrol 1976;6:183–86.40. Hall RP, Stachura I, Cason J, et al. IgA-containing circu-
lating immune complexes in patients with nephropathy.Am J Med 1983;74:56–63.
41. Levy M, Beaufils H, Gubler MC, et al. Idiopathic recurrentmacroscopic hematuria and mesangial IgA-IgG depositsin children. Clin Nephrol 1973;1:63–69.
42. Conley, Cooper MD, Michael AF. Selective deposition ofimmunoglobulin A in immunoglobulin A nephropathy,anaphylactoid purpura nephritis, and systemic lupus er-ythematosus. J Clin Invest 1980;66:1432–36.
43. Goldstein AR, White RHR, Akuse R, et al. Long-termfollow-up of childhood Henoch-Schoenlein nephritis.Lancet 1992;339:280–82.
44. White RHR. Henoch-Schoenlein purpura. In: Churg A,Churg J, editors. Systemic vasculitis. New York: IgakuShein Medical Publishers, 1991;203–17.
45. Van Hale HM, Gibson LE, Schroeter AL. Henoch-Schoen-lein vasculitis: Direct immunofluorescence study of unin-volved skin. J Am Acad Dermatol 1986;15:665–70.
46. Saulsbury FT. Heavy and light chain composition of se-rum IgA and IgA rheumatoid factor in Henoch-Schoen-lein purpura. Arthritis Rheum 1992;35:1377–80.
47. Saraclar Y, Tinaztepe K, Adalioglu G, et al. Acute hemor-rhagic edema of infancy (AHEI): A variant of Henoch-Schoenlein purpura or a distinct clinical entity? J AllergyClin Immunol 1990;86:473–83.
48. Legrain V, Lejean S, Taieb A, et al. Infantile acute hemor-rhagic edema of the skin: Study of ten cases. J Am AcadDermatol 1991;24:17–22.
49. McDuffie FC, Sams WM Jr, Maldonado JE, et al. Hypo-complementemia with cutaneous vasculitis and arthritis.Mayo Clin Proc 1973;48:340–48.
50. Schwartz HR, McDuffie FC, Black LF, et al. Hypocomple-mentemic urticarial vasculitis: Association with chronicobstructive pulmonary disease. Mayo Clin Proc 1982;57:231–38.
51. Asherson RA, Sontheimer R. Urticarial vasculitis and syn-dromes in association with connective tissue diseases.Ann Rheum Dis 1991;50:743–44.
52. Asherson RA, D’Cruz D, Stephens CJM, et al. Urticarialvasculitis in a connective tissue disease clinic: Patterns,presentations and treatment. Semin Arthritis Rheum 1991;20:285–96.
53. Yasue T, Yasue A. Urticarial vasculitis with circulating
Clinics in Dermatology Y 1999;17:515–531 MANY FACES OF VASCULITIS 529

immune complexes and mixed cryoglobulins: Studies ofpathogenesis. J Dermatol 1987;14:597–603.
54. Callen JP, Kalbfleisch S. Urticarial vasculitis: A report ofnine cases and review of the literature. Br J Dermatol1982;107:87–94.
55. Winkelmann RK, Wilson-Jones E, Smith NP, et al. Neu-trophilic urticaria. Acta Dermatol Venereol 1988;68:129–33.
56. Mehregan DR, Hall MJ, Gibson LE. Urticarial vasculitis: Ahistopathologic and clinical review of 72 cases. J Am AcadDermatol 1992;26:441–48.
57. Katz SI, Gallin JI, Hertz KC, et al. Erythema elevatumdiutinum: Skin and systemic manifestations, immuno-logic studies, and successful treatment with dapsone.Medicine (Baltimore) 1977;56:443–55.
58. Jorizzo JL, Solomon AR, Zanolli MD, et al. Neutrophilicvascular reactions. J Am Acad Dermatol 1988;19:983–1005.
59. Lakhanpal S, Conn DL, Lie JT. Clinical and prognosticsignificance of vasculitis as an early manifestation of con-nective tissue disease syndromes. Ann Intern Med 1984;101:743–48.
60. Jorizzo JL, Gonzalez EB, Apisarthanarax P, et al. Pig-mented purpuric eruption in a patient with rheumatoidarthritis. Arch Intern Med 1982;14:2184–85.
61. Scott DGI, Bacon PA, Tribe CR. Systemic rheumatoid: Aclinical and laboratory study of 50 cases. Medicine (Balti-more) 1981;60:288–97.
62. Smith ML, Jorizzo JL, Semble E, et al. Rheumatoid lesionsshowing features of vasculitis and palisading granuloma.J Am Acad Dermatol 1989;20:348–52.
63. Vollertsen RS, Conn DL. Vasculitis associated withrheumatoid arthritis. Rheum Dis Clin North Am 1990;16:445– 61.
64. O’Loughlin S, Schroeter AL, Jordon RE. Chronic urticaria-like lesions in systemic lupus erythematosus. Arch Der-matol 1978;114:879–83.
65. Aizawa Y, Zawadzki ZA, Micolonghi TS, et al. Vasculitisand Sjoegren’s syndrome with IgA-IgG cryoglobulinemiaterminating in immunoblastic sarcoma. Am J Med 1979;67:160–65.
66. Churg J. Cryoglobulinemic vasculitis. In: Churg A, ChurgJ, editors. Systemic vasculitis. New York: Igaku ShoinMedical Publishers, 1991;293–304.
67. Lawley TJ, Gorevic PD, Hamburger MI, et al. Multipletypes of immune complexes in patients with mixed cryo-globulinemia. J Invest Dermatol 1980;75:297–301.
68. Gorevic PD, Kassab HJ, Kohn R, et al. Mixed cryoglobu-linemia: Clinical aspects and long-term follow-up of 40patients. Am J Med 1980;69:287–308.
69. Cohen SJ, Pittelkow MR, Su WPD. Cutaneous manifesta-tions of cryoglobulinemia: Clinical and histopathologicstudy of seventy-two patients. J Am Acad Dermatol 1991;25:21–27.
70. Waldenstrom J. Clinical methods for the detection of hy-perproteinemia and their practical, diagnostic value.Nord Med 1943;20:2288–95.
71. Finder KA, McCollough ML, Dixon SL, et al. Hypergam-maglobulinemic purpura of Waldenstrom. J Am AcadDermatol 1990;23:669–76.
72. Ferreiro JE, Pasarin G, Quesada R, et al. Benign hyper-gammaglobulinemic purpura of Waldenstrom associatedwith Sjoegren’s syndrome. Am J Med 1986;81:734–40.
73. Hudson CI, Callen JP. Cutaneous leukocytoclastic vascu-litis with hyperglobulinemia and splenomegaly. ArchDermatol 1984;120:1224–26.
74. Schnitzler L, Schubert B, Boasson M, et al. Urticairechronique, lesions osseuses, macroglobulinemie IgM:maladie de Waldenstroem? Bull Soc Fr Dermatol Syphil1974;81:363.
75. Campanile G, Lotti T. Clinical aspects of cutaneous necro-tizing vasculitis. Int Angiol 1995;14:151–61.
76. Hautmann G, Lotti T. The role of regulatory peptides inthe pathogenesis of cutaneous necrotizing vasculitis. IntAngiol 1995;14:138–50.
77. Sanchez-Guerrero J, Gutierrez-Urena S, Vidaller A, et al.Vasculitis as a paraneoplastic syndrome: Report of 11cases and review of the literature. J Rheumatol 1990;17:1458–62.
78. Schroeter AL, Copeman PWM, Jordon RE, et al. Immuno-fluorescence of cutaneous vasculitis associated with sys-temic disease. Arch Dermatol 1971;104:254–59.
79. Komadina KH, Houk RW. Polyarteritis nodosa present-ing as recurrent pneumonia following splenectomy forhairy-cell leukemia. Semin Arthritis Rheum 1989;18:252–57.
80. Beylot J, Malou M, Doutre MS, et al. Vascularites leuco-cytoclasiques et hemopathies malignes. Rev Med Interne1989;10:509–14.
81. Castro M, Conn DL, Su WPD, et al. Rheumatic manifes-tations in myelodysplastic syndromes. J Rheumatol 1991;18:721–27.
82. Pagliuca A, Higgins E, Samson D, et al. Prodromal cuta-neous vasculitis in myelodysplastic syndromes. Br JHaematol 1990;74:444–46.
83. Lewis JE. Urticarial vasculitis occurring in associationwith visceral malignancy. Acta Derm Venereol 1990;70:345–47.
84. Seiden MV, O’Donnell WJ, Weinblatt M, et al. Vasculitiswith recurrent pulmonary hemorrhage in a long-termsurvivor after autologous bone marrow transplantation.Bone Marrow Transplant 1990;6:345–47.
85. Escalante A, Kaufman RL, Beardmore TD. Acute myelo-cytic leukemia after the use of cyclophosphamide in thetreatment of polyarteritis nodosa. J Rheumatol 1989;16:1147–49.
86. Kussmaul A, Maier K. Uber eine bischer nicht beschre-ibene eigenthuemliche Arterinerkrankung (periarteritisnodosa), die mit Morbus Brightii und rapid fortschre-itender allgemeiner Muskellaehmung einhergeht. DtschArch Klin Med 1866;1:484–517.
87. Zeek PM. Periarteritis nodosa and other forms of necro-tizing angiitis. N Engl J Med 1953;18:764–72.
88. Rose GA, Spencer H. Polyarteritis nodosa. Q J Med 1957;26:43–81.
89. Churg J, Straus L. Allergic granulomatosis, allergic angi-itis and periarteritis nodosa. Am J Pathol 1951;27:277–301.
90. Fisher I, Orkin M. Cutaneous form of periarteritis nodosa:an entity? Arch Dermatol 1964;89:180–89.
91. Fleming RJ, Stern LZ. Multiple intraparenchymal renalaneurysms in polyarteritis nodosa. Radiology1965;84:100–3.
92. Dornfeld L, Lecky LW, Peter JB. Polyarteritis and intrare-nal renal artery aneursyms. JAMA 1971;215:1950–52.
530 HAUTMANN ET AL. Clinics in Dermatology Y 1999;17:515–531

93. Deshazo RD, Levinson AI, Lawless OJ, et al. Systemicvasculitis with coexistent large and small vessel involve-ment: A classification dilemma. JAMA 1977;238:1940–42.
94. Longstreth PL, Lorobkin M, Palubinskas AJ. Renal mi-croaneursysms in a patient with systemic lupus erythe-mathosus. Radiology 1974;113:65–66.
95. Meyers DS, Grim CE, Kertzer WF. Fibromuscular dys-plasia of the renal artery with medial dissection: A casesimulating polyarteritis nodosa. Am J Med 1974;56:412–16.
96. Lotti T, Ghersetich I, Comacchi C, et al. Cutaneous small-vessel vasculitis. J Am Acad Dermatol 1998;39:667–87.
Clinics in Dermatology Y 1999;17:515–531 MANY FACES OF VASCULITIS 531