
Herpes zoster: etiology, clinical features and treatment options, and case report
Upload
independentCategory
view
12download
0
Acute varicella zoster encephalitis without evidence of primary
vasculopathy in a case-series of 20 patients
T. De Broucker1, A. Mailles2, S. Chabrier3, P. Morand4, J.-P. Stahl5 on behalf of the steering committee and investigators
group*
1) Neurology, Hospital Delafontaine, Saint Denis, 2) French Institute for Public Health Surveillance, Saint Maurice, 3) Paediatric Intensive Care Unit,
University Hospital, Saint-Etienne, 4) Department of Virology and 5) Department of Infectious Diseases, University Hospital and University Joseph Fourier,
Grenoble, France
Abstract
Varicella zoster virus (VZV) is a leading cause of acute viral encephalitis but little is known about its clinical, biological and imaging fea-
tures. Furthermore, the most favourable treatment regimen has not been determined. We studied a prospective cohort of 20 HIV-neg-
ative patients presenting with acute VZV encephalitis caused by primary infection or reactivation. VZV was identified in 16 of 20 cases
by PCR detection of the DNA in the cerebrospinal fluid. The four remaining cases occurred during or soon after a VZV rash. The med-
ian age of the 17 adults was 76 (19–86) years; the three other patients were children (0.5–5 years). Three patients were immunocom-
promised. Nine adult patients presented with a rash. Eighteen patients presented with fever and an acute encephalitic syndrome: diffuse
brain dysfunction, focal neurological signs, seizures and cranial nerve palsies. Three patients presented with either ventricular or sub-
dural haemorrhage, one with myelitis, and one with asymptomatic stenosis of the middle cerebral artery. The imaging was either normal
or revealed non-specific abnormalities such as cortical atrophy but no evidence of stroke. All patients were given acyclovir at various
dosages and durations but the case fatality rate remained high (15%) and sequelae were frequently observed either at discharge or at
follow-up 3 years later.
Keywords: Encephalitis, imaging, varicella zoster virus, vasculopathy
Original Submission: 16 August 2011; Revised Submission: 13 October 2011; Accepted: 17 October 2011
Editor: L. Kaiser
Article published online: 22 October 2011
Clin Microbiol Infect 2012; 18: 808–819
10.1111/j.1469-0691.2011.03705.x
Corresponding author: A. Mailles, Institut de veille sanitaire
(French Institute for Public Health Surveillance), 12 rue du Val
d’Osne, 94415 Saint-Maurice Cedex, France
E-mail: [email protected]
*Members of the Steering committee and Investigators are listed in
Appendix.
Introduction
Varicella zoster virus (VZV) is a virus of the Alphaherpesviri-
nae subfamily, responsible for human infections with various
clinical presentations. Primary infection occurs most fre-
quently during childhood and presents as varicella; it is fol-
lowed by long-lasting viral latency in the spinal and cranial
ganglia [1,2]. This infection is common, affecting almost all
non-vaccinated children. Infection reactivation occurs mainly
in immunocompromised or elderly patients. The most fre-
quent presentation in adults is herpes zoster (shingles), with
an estimated annual incidence of 1.2–5.2 cases/1000 [2].
Post-herpetic neuralgia is a frequent complication in elderly
patients [3].
Neurological complications caused by varicella can involve
peripheral or central nervous system. They include cerebelli-
tis, meningitis, myelitis, optic neuritis, polyneuropathy, acute
encephalitis and vasculopathy [2,4]. Some neurological pre-
sentations can also appear with, precede, or follow herpes
zoster: sensory or motor peripheral paralysis, isolated and
multiple cranial nerve palsies including ophthalmoplegia and
the Ramsay Hunt syndrome, myelitis, encephalitis, vasculopa-
thy and cerebellar ataxia [5]. Neurological symptoms caused
by VZV infection can also occur without any cutaneous rash
(zoster sine herpete) and the detection of DNA or specific
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases
ORIGINAL ARTICLE VIROLOGY

VZV antibodies in the cerebrospinal fluid (CSF) is here the
only proof of VZV involvement [5].
Several mechanisms explain the occurrence of neurological
signs after VZV infection: parenchymatous encephalitis (with
or without demyelination), microglial influx, granulomatous
and large vessel vasculopathy inducing strokes (grossly tran-
sient cerebral arteriopathy in children and delayed contralat-
eral hemiparesis of zoster ophthalmicus in the elderly),
meningitis or necrotizing myelitis [6,7]. Subacute or chronic
VZV encephalitis are encountered in immunocompromised
patients as the result of small vessel vasculopathy and glial
infection inducing leukoencephalitis. Myelitis, large vessel
involvement and ventriculitis have also been reported [7,8].
Acute ataxia in children and vasculopathies in adults are the
most frequently cited neurological complications of VZV
infection [5,9,10]. In contrast, acute encephalitis sensu stricto
has rarely been reported [11–14] and even fewer reports
have been published describing the clinical features and fol-
low-up of these patients [15–18]. The importance of VZV in
the epidemiology of acute encephalitis in the general popula-
tion has been highlighted in multicentre prospective studies
[11–13].
We report the clinical features of patients with VZV
encephalitis enrolled in a prospective multicentre study in
France, in 2007.
Methods
A case-patient with acute encephalitis was a patient 28 days
of age or older hospitalized in mainland France in 2007, with
(i) an acute onset of illness; (ii) at least one abnormality of
CSF (white blood cell count ‡4 cells/mm3 or protein level
‡40 mg/dL); (iii) fever or recent history of fever ‡38�C; and
(iv) decreased consciousness, or seizures, or altered mental
status, or focal neurological signs. HIV infection was an
exclusion criterion. Aetiological investigation of enrolled
patients was described previously [11].
A confirmed case of VZV encephalitis was a case-patient
with VZV DNA detected in the CSF by PCR. A possible
case of VZV encephalitis was a case-patient with encephali-
tis occurring simultaneously or shortly after varicella or
herpes zoster without biological confirmation of VZV infec-
tion, and with other possible aetiologies of encephalitis
excluded by the investigation. Clinical and biological data
were collected using a standardized questionnaire and the
results of electroencephalography examinations were
recorded. A single expert (TdB) reviewed all available mag-
netic resonance and computed tomography images to assess
brain lesions.
The outcome of VZV patients was assessed 3 years after
discharge using the Glasgow outcome scale [19].
Informed written consent was obtained from all patients
or from their parents for children aged <18 years. The study
was approved by the ethics committee of Grenoble (No.
172003).
Results
Demography
Twenty of 253 (8%) case-patients enrolled in the initial study
were VZV patients [11]. Sixteen were confirmed cases and
four were possible cases (Table 1). Two possible cases were
5-year-old boys with negative VZV CSF PCR on admission
and no further CSF testing. They presented with varicella,
respectively, 1 day and 1 week before the onset of neurolog-
ical symptoms. The two other possible cases were adults (76
and 78 years of age) presenting with radicular zoster (one
spinal, one ophthalmicus) 3 days and 3 weeks, respectively,
before the onset of neurological symptoms.
The male to female ratio was 3. Three patients were chil-
dren (the two 5-year-old boys mentioned above and a 6-
month old boy). The distribution of age among adult patients
was bimodal with three young adults (19, 20 and 26 years
old) and 11 people ‡75 years old (median 76 years old,
range 19–86 years). None of the VZV patients had ever been
vaccinated against VZV.
Clinical features
Ten (50%) patients (nine adults and one child) had comorbid-
ities, three of which could be considered immunosuppressive
conditions: osteosarcoma, recent heart–lung transplant and
systemic lupus erythematosus with long-term corticosteroid
treatment (Table 1).
Eleven VZV patients (55%) had a rash before hospitaliza-
tion: zoster in eight adults and varicella in three children, of
whom two (a child and an adult) no longer had cutaneous
signs on admission.
The symptoms of the VZV patients on admission are pre-
sented by frequency in Table 2. Six patients (30%) required
admission to intensive care units, four were mechanically
ventilated. The most frequent neurological symptoms were
disorientation and confusion (70%), meningeal signs (60%),
focal neurological signs (55%) and apathy (50%). Cranial
nerve palsy was present in eight patients (40%), namely cen-
tral facial nerve paralysis in seven cases and oculomotor
nerve paralysis in one case.
Lumbar puncture was performed before day 2 of hospi-
talization in 80% of cases and before day 4 in 95%. The
CMI De Broucker et al. Varicella zoster encephalitis in France in 2007 809
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases, CMI, 18, 808–819

TA
BL
E1.C
hara
cte
rist
ics
of
20
pati
en
tsw
ith
vari
cella
zo
ster
vir
us
en
cep
haliti
s,F
ran
ce
2007
Co
nfi
rmed
/P
oss
ible
Age
(years
)S
ex
Co
mo
rbid
itie
sV
ZV
rash
Clin
ical
sign
sG
CS
ao
nad
mis
sio
n
WB
Cco
un
t(/
mm
3)
CS
Fp
rote
ins
(g/L
)C
Tsc
an
MR
IO
utc
om
e
Pat
ients
with
bra
inva
sculo
pat
hy
C0.5
MN
one
Var
icella
Feve
r,vo
mitin
g,fo
nta
nelle
bulg
ing,
dow
nw
ard
gaze
devi
atio
n,ap
athy
10
400
0.8
D0:V
entr
icula
rhyd
roce
phal
y,ve
ntr
icula
rble
edin
gD
8:exte
rnal
hyd
roce
phal
y
D1:exte
rnal
hyd
roce
phal
yR
eco
very
,C
SFder
ivat
ion
still
inpla
ce3
year
sla
ter
C20
MN
one
None
Feve
r,head
ache,
inco
here
nt
speech
,ap
has
ia,fa
cial
par
alys
is,hem
ipar
esi
s,
–350
0.8
D0:fo
calst
enosi
sof
the
left
mid
dle
cere
bra
lar
tery
Full
reco
very
C79
MC
ardia
cin
suffi
ciency
Shin
gles
Dis
ori
enta
tion,in
cohere
nt
speech
,m
enin
geal
syndro
me,
faci
alpar
alys
is,se
vere
sepsi
s
14
66
1.1
D4
and
D22:norm
alJ2
7:ve
ntr
icula
rble
edin
g,th
alam
ican
dte
mpora
lhae
mat
om
a,bra
inhern
iation
D1:le
ftexte
rnal
capsu
lela
cunar
sequela
eD
ied
on
D34
of
hosp
ital
stay
C34
MLungs
and
hear
ttr
ansp
lant,
Renal
insu
ffici
ency
,D
iabet
es
melli
tus
Ster
oid
s
None
Feve
r,fo
und
unco
nsc
ious
athom
e,se
izure
s,decr
eas
ed
consc
iousn
ess
,bra
inst
em
defici
ts,te
trap
aresi
s
3100
5N
orm
alD
0:bila
tera
lm
illim
etr
ichig
hsi
gnal
T2
lesi
ons
of
inte
rnal
capsu
les,
pons
and
spin
alco
rdat
T7–T
8le
vel
D12
:bila
tera
lsu
bdura
lhyd
rom
asD
16
:norm
alD
45
:ventr
icula
rble
edin
gan
dhyd
roce
phal
y
Dis
char
ged
tore
hab
ilita
tion
faci
lity,
still
par
aple
gic
3ye
ars
late
r
Pat
ients
with
par
ench
ymal
non
vasc
ula
rle
sions
C75
MH
isto
ryof
renal
carc
inom
aN
one
Feve
r,ag
gres
sive
ness
,id
eo-m
oto
rap
raxia
,re
petitive
speech
,dis
ori
enta
tion,
seiz
ure
s
–40
0.8
D0:bila
tera
lte
mpora
lhyp
odensi
ties
–Fu
llre
cove
ry
C55
MN
one
None
Feve
r,bra
inst
em
defici
ts,
tinnitus,
atax
ia15
48
0.8
–H
ypers
ignal
sin
bra
inst
eman
dupper
medulla
Still
suffers
from
tinnitus,
atax
iaan
dap
has
ia3
year
sla
ter
P5
MA
dre
nal
insu
ffici
ency
Ster
oid
s,Fa
ilure
toth
rive
Var
icella
bFe
ver,
dis
ori
enta
tion,ag
itat
ion,
seiz
ure
s,fa
cial
par
alys
is,
hem
ipar
esi
s,hem
ianopia
7930
0.2
–H
ypers
ignal
inte
mpora
l,par
ieta
l,an
docc
ipital
lobes
on
T2
weig
hte
dM
RI
Bac
kto
pre
vious
medic
alco
nditio
n
Pat
ients
with
non-s
pec
ific
lesi
ons
on
imag
ing
C86
FC
ardia
cin
suffi
ciency
Dem
entia
Shin
gles
Feve
r,m
ore
dis
ori
enta
ted
and
inco
here
nt,
decr
eas
ed
consc
iousn
ess
,defici
tof
righ
tle
g
830
1C
ort
ical
atro
phy
–D
ied
with
acute
com
a2
month
saf
ter
dis
char
ge
C77
FR
esp
irat
ory
insu
ffici
ency
,O
steosa
rcom
a,bila
tera
lnephre
ctom
y
Shin
gles
Feve
r,ag
itat
ion,in
cohere
nt
speech
,fa
cial
par
alys
is,at
axia
,ra
dic
ulit
is
15
16
0.4
–C
ort
ical
atro
phy
Die
dof
cance
r2
year
saf
ter
dis
char
ge
C85
MC
ardia
cin
suffi
ciency
,Par
apar
esi
sfo
llow
ing
dis
calhern
iation
None
Feve
r,dis
ori
enta
tion,ap
athy,
inco
here
nt
speech
14
200
1.9
–Leukoar
aiosi
s,bila
tera
lbas
alga
ngl
iala
cunar
sequela
e
Consi
dere
dcu
red
on
dis
char
ged,deaf
and
bedri
dden
3ye
ars
late
r
810 Clinical Microbiology and Infection, Volume 18 Number 8, August 2012 CMI
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases, CMI, 18, 808–819
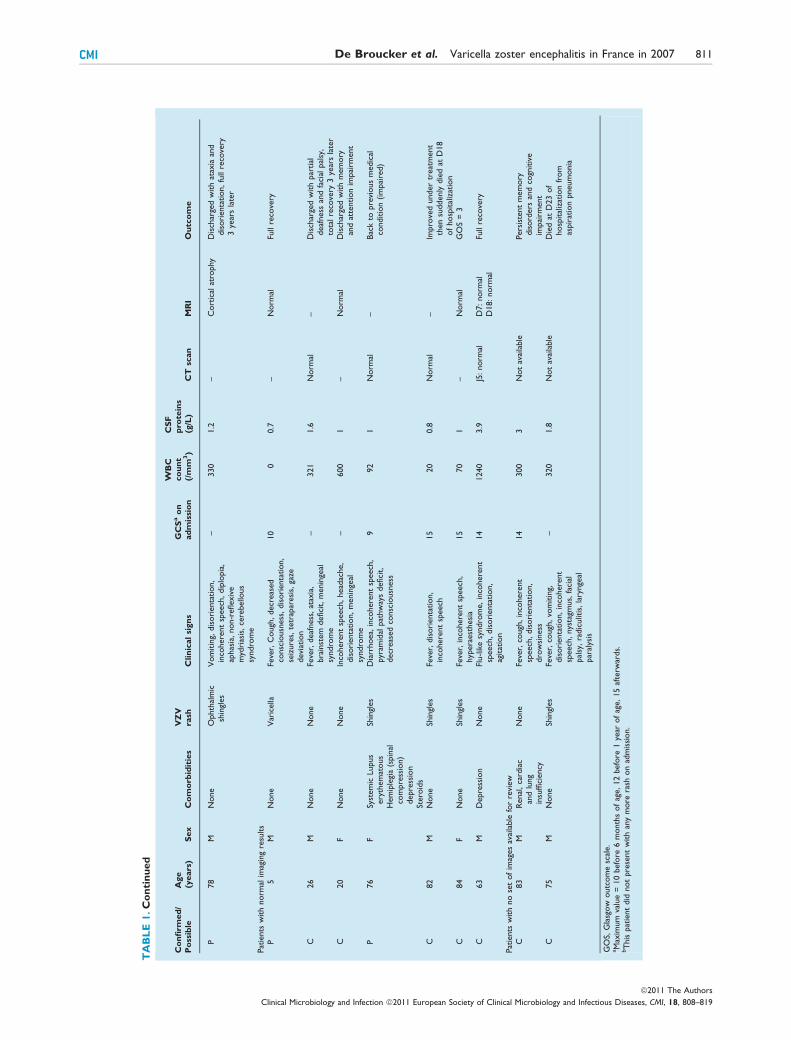
TA
BL
E1.C
on
tin
ued
Co
nfi
rmed
/P
oss
ible
Age
(years
)S
ex
Co
mo
rbid
itie
sV
ZV
rash
Clin
ical
sign
sG
CS
ao
nad
mis
sio
n
WB
Cco
un
t(/
mm
3)
CS
Fp
rote
ins
(g/L
)C
Tsc
an
MR
IO
utc
om
e
P78
MN
one
Ophth
alm
icsh
ingl
es
Vom
itin
g,dis
ori
enta
tion,
inco
here
nt
speech
,dip
lopia
,ap
has
ia,non-r
eflexiv
em
ydri
asis
,ce
rebello
us
syndro
me
–330
1.2
–C
ort
ical
atro
phy
Dis
char
ged
with
atax
iaan
ddis
ori
enta
tion,fu
llre
cove
ry3
year
sla
ter
Pat
ients
with
norm
alim
agin
gre
sults
P5
MN
one
Var
icella
Feve
r,C
ough
,decr
eas
ed
consc
iousn
ess
,dis
ori
enta
tion,
seiz
ure
s,te
trap
aresi
s,ga
zedevi
atio
n
10
00.7
–N
orm
alFu
llre
cove
ry
C26
MN
one
None
Feve
r,deaf
ness
,at
axia
,bra
inst
em
defici
t,m
enin
geal
syndro
me
–321
1.6
Norm
al–
Dis
char
ged
with
par
tial
deaf
ness
and
faci
alpal
sy,
tota
lre
cove
ry3
year
sla
ter
C20
FN
one
None
Inco
here
nt
speech
,head
ache,
dis
ori
enta
tion,m
enin
geal
syndro
me
–600
1–
Norm
alD
isch
arge
dw
ith
mem
ory
and
atte
ntion
impai
rment
P76
FSy
stem
icLupus
ery
them
atous
Hem
iple
gia
(spin
alco
mpre
ssio
n)
depre
ssio
nSt
ero
ids
Shin
gles
Dia
rrhoea,
inco
here
nt
speech
,pyr
amid
alpat
hw
ays
defici
t,decr
eas
ed
consc
iousn
ess
992
1N
orm
al–
Bac
kto
pre
vious
medic
alco
nditio
n(im
pai
red)
C82
MN
one
Shin
gles
Feve
r,dis
ori
enta
tion,
inco
here
nt
speech
15
20
0.8
Norm
al–
Impro
ved
under
treat
ment
then
suddenly
die
dat
D18
of
hosp
ital
izat
ion
C84
FN
one
Shin
gles
Feve
r,in
cohere
nt
speech
,hyp
era
est
hesi
a15
70
1–
Norm
alG
OS
=3
C63
MD
epre
ssio
nN
one
Flu-lik
esy
ndro
me,in
cohere
nt
speech
,dis
ori
enta
tion,
agitat
ion
14
1240
3.9
J5:norm
alD
7:norm
alD
18:norm
alFu
llre
cove
ry
Pat
ients
with
no
set
of
imag
es
avai
lable
for
revi
ew
C83
MR
enal
,ca
rdia
can
dlu
ng
insu
ffici
ency
None
Feve
r,co
ugh
,in
cohere
nt
speech
,dis
ori
enta
tion,
dro
wsi
nes
s
14
300
3N
ot
avai
lable
Pers
iste
nt
mem
ory
dis
ord
ers
and
cogn
itiv
eim
pai
rment
C75
MN
one
Shin
gles
Feve
r,co
ugh
,vo
mitin
g,dis
ori
enta
tion,in
cohere
nt
speech
,nys
tagm
us,
faci
alpal
sy,ra
dic
ulit
is,la
rynge
alpar
alys
is
–320
1.8
Not
avai
lable
Die
dat
D23
of
hosp
ital
izat
ion
from
aspir
atio
npneum
onia
GO
S,G
lasg
ow
outc
om
esc
ale.
aM
axim
um
valu
e=
10
befo
re6
month
sof
age,12
befo
re1
year
of
age,15
afte
rwar
ds.
bT
his
pat
ient
did
not
pre
sent
with
any
more
rash
on
adm
issi
on.
CMI De Broucker et al. Varicella zoster encephalitis in France in 2007 811
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases, CMI, 18, 808–819

median CSF white blood cell count was 150 cells/mm3
(range 0–1240). Lymphocytes were predominant in CSF
(median rate: 81.5% of white blood cells) in all but two
VZV patients. The median protein level in CSF was 0.99 g/L
(0.22–5 g/L). The glucose CSF/serum ratio was >0.40 in 16
patients (80%).
Thirteen of 14 (92%) encephalography recordings showed
abnormalities and all such abnormalities were consistent with
diffuse brain lesions. Focal temporal slow waves were identi-
fied in four cases, and subclinical seizures in two cases.
Imaging
All patients underwent computed tomography scan (n = 10),
magnetic resonance imaging (n = 2), or both (n = 8) on
admission. Eighteen sets of images were available for review-
ing (14 confirmed cases and four possible cases). Four (20%)
patients demonstrated vascular lesions on computed tomog-
raphy of magnetic resonance imaging:
• stenosis of the left middle cerebral artery M1 segment
was observed using magnetic resonance angiography in a
20-year-old patient without stroke (Fig. 1);
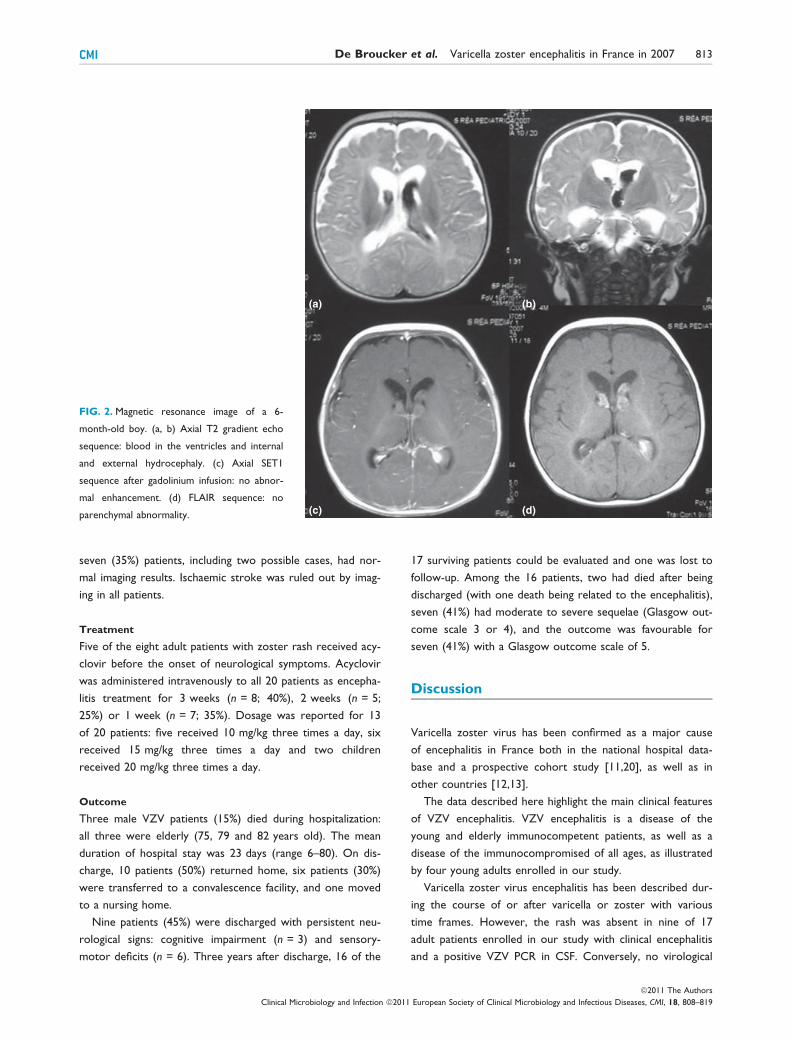
• a 6-month-old boy presented with diffuse bleeding and
dilatation of the ventricles on admission and still had a
dilatation of the subarachnoid area with normal ventricu-
lar size on follow-up imaging (Fig. 2);
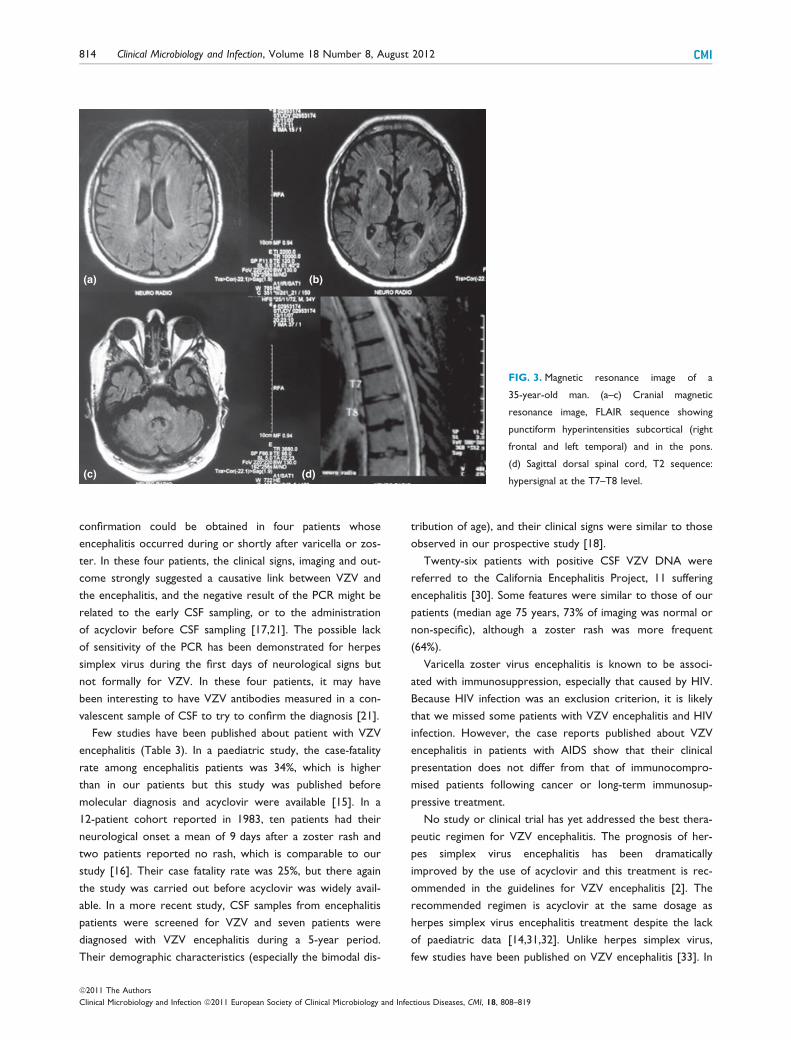
• thoracic myelitis was observed on admission in a 34-
year-old man with paraplegia, who developed at day 45 a
bilateral subdural haematoma and massive ventricular
bleeding (Fig. 3);
• a 79-year-old patient with cortical atrophy on early
images later demonstrated a haematoma in the thalamic
area with fatal ventricular bleeding at day 23.
Three (15%) other patients had non-vascular lesions: brain-
stem lesions suggesting rhombencephalitis were observed in
two patients; and right-side temporal, parietal and occipital
hypersignals were observed with magnetic resonance imaging
in a 5-year-old boy (possible case).
Four patients (20%), including one possible case, had non-
specific abnormalities (cortical atrophy) and the remaining
FIG. 1. Magnetic resonance image of a 20-year-old man. Narrowing
of the M1 segment of the middle cerebral artery.
TABLE 2. Clinical features of 20 patients presenting with varicella zoster virus encephalitis at day 0 and day 5
Day 0 Day 5
All cases(n = 20)
Confirmed cases(n = 16)
Possible cases(n = 4)
All cases(n = 20)
Confirmed cases(n = 16)
Possible cases(n = 4)
Fever 18 (90%)a 15 (94%)b 3 (75%)b NA NA NAMechanical ventilation 4 (20%) 1 (6%) 3 (75%) 3 (15%) 1 (6%) 2 (50%)Severe sepsis 1 (5%) 1 (6%) 0 0 0 0Meningism 12 (60%) 9 (56%) 3 (75%) 3 (15%) 3 (19%) 0Decreased level of consciousness 5 (25%) 3 (19%) 2 (50%) 2 (10%) 1 (6%) 1 (25%)Disorientation 14 (70%) 11 (69%) 3 (75%) 5 (25%) 5 (31%) 0Confusion 14 (70%) 12 (75%) 2 (50%) 2 (10%) 2 (13%) 0Seizures 4 (20%) 2 (13%) 2 (50%) 0 0 0Focal neurological signs 11 (55%) 7 (44%) 4 (100%) 9 (45%) 7 (44%) 2 (50%)Speech disorders 6 (30%) 5 (31%) 1 (25%) 2 (10%) 1 (6%) 1 (25%)Cranial nerve palsy 8 (40%) 6 (38%) 2 (50%) 8 (40%) 6 (38%) 2 (50%)Cerebellous syndrome 3 (15%) 2 (13%) 1 (25%) 3 (15%) 2 (13%)Sensory disorders 1 (5%) 1 (6%) 0 NA NA NAMyelitis 0 0 0 1 (5%) 1 (6%) 1 (25%)Aggressiveness 1 (5%) 1 (7%) 0 0 0 0Apathy 10 (50%) 7 (44%) 3 (75%) 3 (15%) 3 (19%) 0Agitation 6 (30%) 4 (27%) 2 (50%) 1 (5%) 1 (6%) 0Parkinsonism 0 0 0 NA NA NAMovement disorders 0 0 0 0 0 0Hallucination 0 0 0 0 0 0
NA, not available.aTwo patients were afebrile while taking antipyretic treatment but reported fever before hospitalization.bOne patient was afebrile while taking antipyretic treatment but reported fever before hospitalization.
812 Clinical Microbiology and Infection, Volume 18 Number 8, August 2012 CMI
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases, CMI, 18, 808–819
seven (35%) patients, including two possible cases, had nor-
mal imaging results. Ischaemic stroke was ruled out by imag-
ing in all patients.
Treatment
Five of the eight adult patients with zoster rash received acy-
clovir before the onset of neurological symptoms. Acyclovir
was administered intravenously to all 20 patients as encepha-
litis treatment for 3 weeks (n = 8; 40%), 2 weeks (n = 5;
25%) or 1 week (n = 7; 35%). Dosage was reported for 13
of 20 patients: five received 10 mg/kg three times a day, six
received 15 mg/kg three times a day and two children
received 20 mg/kg three times a day.
Outcome
Three male VZV patients (15%) died during hospitalization:
all three were elderly (75, 79 and 82 years old). The mean
duration of hospital stay was 23 days (range 6–80). On dis-
charge, 10 patients (50%) returned home, six patients (30%)
were transferred to a convalescence facility, and one moved
to a nursing home.
Nine patients (45%) were discharged with persistent neu-
rological signs: cognitive impairment (n = 3) and sensory-
motor deficits (n = 6). Three years after discharge, 16 of the
17 surviving patients could be evaluated and one was lost to
follow-up. Among the 16 patients, two had died after being
discharged (with one death being related to the encephalitis),
seven (41%) had moderate to severe sequelae (Glasgow out-
come scale 3 or 4), and the outcome was favourable for
seven (41%) with a Glasgow outcome scale of 5.
Discussion
Varicella zoster virus has been confirmed as a major cause
of encephalitis in France both in the national hospital data-
base and a prospective cohort study [11,20], as well as in
other countries [12,13].
The data described here highlight the main clinical features
of VZV encephalitis. VZV encephalitis is a disease of the
young and elderly immunocompetent patients, as well as a
disease of the immunocompromised of all ages, as illustrated
by four young adults enrolled in our study.
Varicella zoster virus encephalitis has been described dur-
ing the course of or after varicella or zoster with various
time frames. However, the rash was absent in nine of 17
adult patients enrolled in our study with clinical encephalitis
and a positive VZV PCR in CSF. Conversely, no virological
(a) (b)
(c) (d)
FIG. 2. Magnetic resonance image of a 6-
month-old boy. (a, b) Axial T2 gradient echo
sequence: blood in the ventricles and internal
and external hydrocephaly. (c) Axial SET1
sequence after gadolinium infusion: no abnor-
mal enhancement. (d) FLAIR sequence: no
parenchymal abnormality.
CMI De Broucker et al. Varicella zoster encephalitis in France in 2007 813
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases, CMI, 18, 808–819
confirmation could be obtained in four patients whose
encephalitis occurred during or shortly after varicella or zos-
ter. In these four patients, the clinical signs, imaging and out-
come strongly suggested a causative link between VZV and
the encephalitis, and the negative result of the PCR might be
related to the early CSF sampling, or to the administration
of acyclovir before CSF sampling [17,21]. The possible lack
of sensitivity of the PCR has been demonstrated for herpes
simplex virus during the first days of neurological signs but
not formally for VZV. In these four patients, it may have
been interesting to have VZV antibodies measured in a con-
valescent sample of CSF to try to confirm the diagnosis [21].
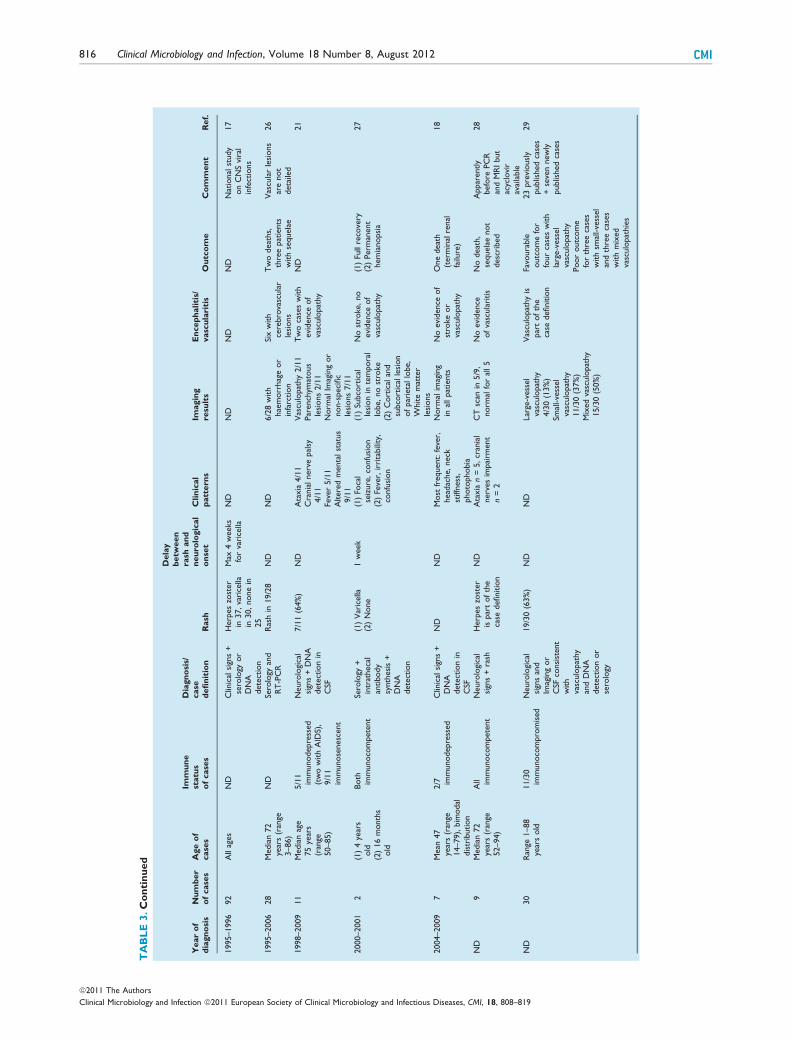
Few studies have been published about patient with VZV
encephalitis (Table 3). In a paediatric study, the case-fatality
rate among encephalitis patients was 34%, which is higher
than in our patients but this study was published before
molecular diagnosis and acyclovir were available [15]. In a
12-patient cohort reported in 1983, ten patients had their
neurological onset a mean of 9 days after a zoster rash and
two patients reported no rash, which is comparable to our
study [16]. Their case fatality rate was 25%, but there again
the study was carried out before acyclovir was widely avail-
able. In a more recent study, CSF samples from encephalitis
patients were screened for VZV and seven patients were
diagnosed with VZV encephalitis during a 5-year period.
Their demographic characteristics (especially the bimodal dis-
tribution of age), and their clinical signs were similar to those
observed in our prospective study [18].
Twenty-six patients with positive CSF VZV DNA were
referred to the California Encephalitis Project, 11 suffering
encephalitis [30]. Some features were similar to those of our
patients (median age 75 years, 73% of imaging was normal or
non-specific), although a zoster rash was more frequent
(64%).
Varicella zoster virus encephalitis is known to be associ-
ated with immunosuppression, especially that caused by HIV.
Because HIV infection was an exclusion criterion, it is likely
that we missed some patients with VZV encephalitis and HIV
infection. However, the case reports published about VZV
encephalitis in patients with AIDS show that their clinical
presentation does not differ from that of immunocompro-
mised patients following cancer or long-term immunosup-
pressive treatment.
No study or clinical trial has yet addressed the best thera-
peutic regimen for VZV encephalitis. The prognosis of her-
pes simplex virus encephalitis has been dramatically
improved by the use of acyclovir and this treatment is rec-
ommended in the guidelines for VZV encephalitis [2]. The
recommended regimen is acyclovir at the same dosage as
herpes simplex virus encephalitis treatment despite the lack
of paediatric data [14,31,32]. Unlike herpes simplex virus,
few studies have been published on VZV encephalitis [33]. In
(a) (b)
(c) (d)
FIG. 3. Magnetic resonance image of a
35-year-old man. (a–c) Cranial magnetic
resonance image, FLAIR sequence showing
punctiform hyperintensities subcortical (right
frontal and left temporal) and in the pons.
(d) Sagittal dorsal spinal cord, T2 sequence:
hypersignal at the T7–T8 level.
814 Clinical Microbiology and Infection, Volume 18 Number 8, August 2012 CMI
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases, CMI, 18, 808–819
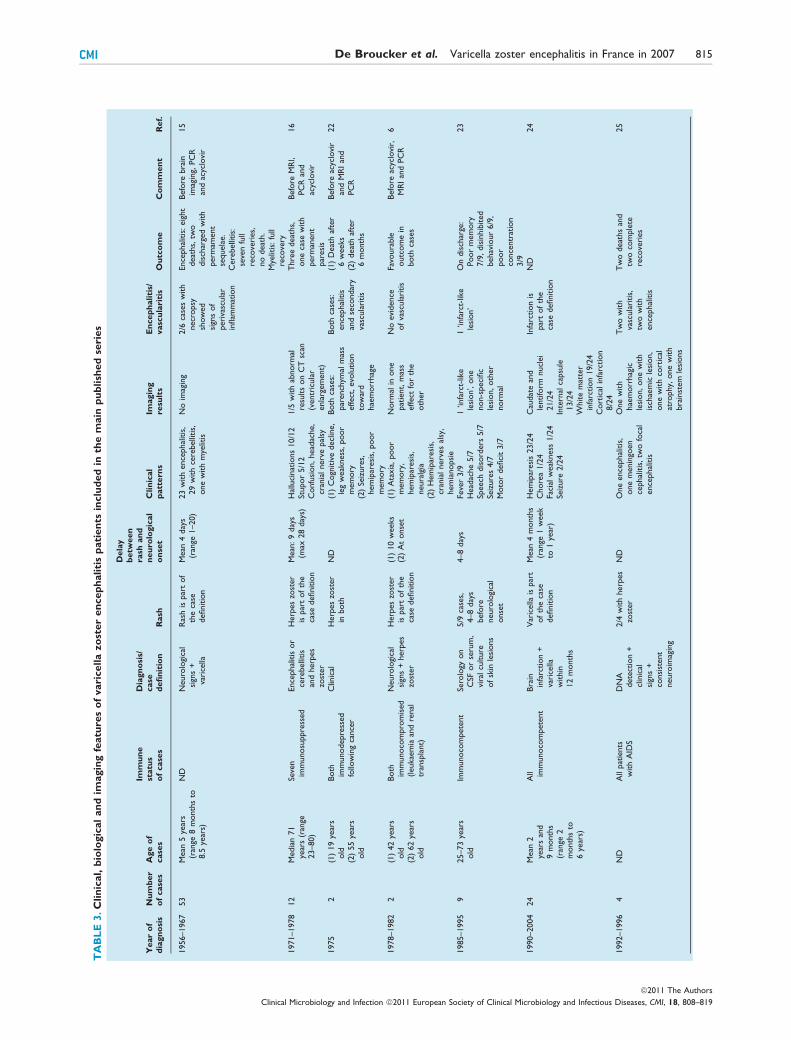
TA
BL
E3.C
lin
ical,
bio
logic
al
an
dim
agin
gfe
atu
res
of
vari
cella
zo
ster
en
cep
haliti
sp
ati
en
tsin
clu
ded
inth
em
ain
pu
blish
ed
seri
es
Year
of
dia
gn
osi
sN
um
ber
of
case
sA
ge
of
case
s
Imm
un
est
atu
so
fcase
s
Dia
gn
osi
s/case
defi
nit
ion
Rash
Dela
yb
etw
een
rash
an
dn
eu
rolo
gic
al
on
set
Clin
ical
patt
ern
sIm
agin
gre
sult
sE
ncep
haliti
s/vasc
ula
riti
sO
utc
om
eC
om
men
tR
ef.
1956–1967
53
Mean
5ye
ars
(ran
ge8
month
sto
8.5
year
s)
ND
Neuro
logi
cal
sign
s+
vari
cella
Ras
his
par
tof
the
case
definitio
n
Mean
4day
s(r
ange
1–20)
23
with
ence
phal
itis
,29
with
cere
belli
tis,
one
with
mye
litis
No
imag
ing
2/6
case
sw
ith
necr
opsy
show
ed
sign
sof
peri
vasc
ula
rin
flam
mat
ion
Ence
phal
itis
:eig
ht
deat
hs,
two
dis
char
ged
with
perm
ament
sequela
e.C
ere
belli
tis:
seve
nfu
llre
cove
ries,
no
deat
h.
Mye
litis
:fu
llre
cove
ry
Befo
rebra
inim
agin
g,PC
Ran
dac
yclo
vir
15
1971–1978
12
Media
n71
year
s(r
ange
23–80)
Seve
nim
munosu
ppre
ssed
Ence
phal
itis
or
cere
belli
tis
and
herp
es
zost
er
Herp
es
zost
er
ispar
tof
the
case
definitio
n
Mean
:9
day
s(m
ax28
day
s)H
allu
cinat
ions
10/1
2St
upor
5/1
2C
onfu
sion,head
ache,
cran
ialnerv
epal
sy
1/5
with
abnorm
alre
sults
on
CT
scan
(ventr
icula
renla
rgem
ent)
Thre
edeat
hs,
one
case
with
perm
anent
par
esi
s
Befo
reM
RI,
PC
Ran
dac
yclo
vir
16
1975
2(1
)19
year
sold
(2)
55
year
sold
Both
imm
unodepre
ssed
follo
win
gca
nce
r
Clin
ical
Herp
es
zost
er
inboth
ND
(1)
Cogn
itiv
edecl
ine,
leg
weak
ness
,poor
mem
ory
(2)
Seiz
ure
s,hem
ipar
esi
s,poor
mem
ory
Both
case
s:par
ench
ymal
mas
seffect
,evo
lution
tow
ard
hae
morr
hag
e
Both
case
s:ence
phal
itis
and
seco
ndar
yva
scula
ritis
(1)
Deat
haf
ter
6w
eeks
(2)
deat
haf
ter
6m
onth
s
Befo
reac
yclo
vir
and
MR
Ian
dPC
R
22
1978–1982
2(1
)42
year
sold
(2)
62
year
sold
Both
imm
unoco
mpro
mis
ed(leukae
mia
and
renal
tran
spla
nt)
Neuro
logi
cal
sign
s+
herp
es
zost
er
Herp
es
zost
er
ispar
tof
the
case
definitio
n
(1)
10
weeks
(2)
At
onse
t(1
)A
taxia
,poor
mem
ory
,hem
ipar
esi
s,neura
lgia
(2)
Hem
ipar
esi
s,cr
ania
lnerv
es
alsy
,hem
ianopsi
e
Norm
alin
one
pat
ient,
mas
seffect
for
the
oth
er
No
evi
dence
of
vasc
ula
ritis
Favo
ura
ble
outc
om
ein
both
case
s
Befo
reac
yclo
vir,
MR
Ian
dPC
R6
1985–1995
925–73
year
sold
Imm
unoco
mpete
nt
Sero
logy
on
CSF
or
seru
m,
vira
lcu
lture
of
skin
lesi
ons
5/9
case
s,4–8
day
sbefo
reneuro
logi
cal
onse
t
4–8
day
sFe
ver
3/9
Head
ache
5/7
Speech
dis
ord
ers
5/7
Seiz
ure
s4/7
Moto
rdefici
t3/7
1‘in
farc
t-lik
ele
sion’,
one
non-s
peci
fic
lesi
on,oth
er
norm
al
1‘in
farc
t-lik
ele
sion’
On
dis
char
ge:
Poor
mem
ory
7/9
,dis
inhib
ited
behav
iour
6/9
,poor
conce
ntr
atio
n3/9
23
1990–2004
24
Mean
2ye
ars
and
9m
onth
s(r
ange
2m
onth
sto
6ye
ars)
All im
munoco
mpet
ent
Bra
inin
farc
tion
+va
rice
llaw
ithin
12
month
s
Var
icella
ispar
tof
the
case
definitio
n
Mean
4m
onth
s(r
ange
1w
eek
to1
year
)
Hem
ipar
esi
s23/2
4C
hore
a1/2
4Fa
cial
weak
ness
1/2
4Se
izure
2/2
4
Cau
dat
ean
dle
ntifo
rmnucl
ei
21/2
4In
tern
alca
psu
le13/2
4W
hite
mat
ter
infa
rction
19/2
4C
ort
ical
infa
rction
8/2
4
Infa
rction
ispar
tof
the
case
definitio
n
ND
24
1992–1996
4N
DA
llpat
ients
with
AID
SD
NA
dete
ctio
n+
clin
ical
sign
s+
consi
stent
neuro
imag
ing
2/4
with
herp
es
zost
er
ND
One
ence
phal
itis
,one
menin
goen
cephal
itis
,tw
ofo
cal
ence
phal
itis
One
with
hae
morr
hag
icle
sion,one
with
isch
aem
icle
sion,
one
with
cort
ical
atro
phy,
one
with
bra
inst
em
lesi
ons
Tw
ow
ith
vasc
ula
ritis,
two
with
ence
phal
itis
Tw
odeat
hs
and
two
com
ple
tere
cove
ries
25
CMI De Broucker et al. Varicella zoster encephalitis in France in 2007 815
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases, CMI, 18, 808–819
TA
BL
E3.C
on
tin
ued
Year
of
dia
gn
osi
sN
um
ber
of
case
sA
ge
of
case
s
Imm
un
est
atu
so
fcase
s
Dia
gn
osi
s/case
defi
nit
ion
Rash
Dela
yb
etw
een
rash
an
dn
eu
rolo
gic
al
on
set
Clin
ical
patt
ern
sIm
agin
gre
sult
sE
ncep
haliti
s/vasc
ula
riti
sO
utc
om
eC
om
men
tR
ef.
1995–1996
92
All
ages
ND
Clin
ical
sign
s+
sero
logy
or
DN
Adet
ect
ion
Herp
es
zost
er
in37,va
rice
llain
30,none
in25
Max
4w
eeks
for
vari
cella
ND
ND
ND
ND
Nat
ional
study
on
CN
Svi
ral
infe
ctio
ns
17
1995–2006
28
Media
n72
year
s(r
ange
3–86)
ND
Sero
logy
and
RT
-PC
RR
ash
in19/2
8N
DN
D6/2
8w
ith
hae
morr
hag
eor
infa
rction
Six
with
cere
bro
vasc
ula
rle
sions
Tw
odeat
hs,
thre
epat
ients
with
sequela
e
Vas
cula
rle
sions
are
not
deta
iled
26
1998–2009
11
Media
nag
e75
year
s(r
ange
50–85)
5/1
1im
munodepre
ssed
(tw
ow
ith
AID
S),
9/1
1im
munose
nesc
ent
Neuro
logi
cal
sign
s+
DN
Adet
ect
ion
inC
SF
7/1
1(6
4%
)N
DA
taxia
4/1
1C
rania
lnerv
epal
sy4/1
1Fe
ver
5/1
1A
ltere
dm
enta
lst
atus
9/1
1
Vas
culo
pat
hy
2/1
1Par
ench
ymat
ous
lesi
ons
2/1
1N
orm
alIm
agin
gor
non-s
pec
ific
lesi
ons
7/1
1
Tw
oca
ses
with
evi
dence
of
vasc
ulo
pat
hy
ND
21
2000–2001
2(1
)4
year
sold
(2)
16
month
sold
Both
imm
unoco
mpete
nt
Sero
logy
+in
trat
heca
lan
tibody
synth
esi
s+
DN
Adet
ect
ion
(1)
Var
icella
(2)
None
1w
eek
(1)
Foca
lse
izure
,co
nfu
sion
(2)
Feve
r,ir
rita
bili
ty,
confu
sion
(1)
Subco
rtic
alle
sion
inte
mpora
llo
be,no
stro
ke
(2)
Cort
ical
and
subco
rtic
alle
sion
of
par
ieta
llo
be,
White
mat
ter
lesi
ons
No
stro
ke,no
evi
dence
of
vasc
ulo
pat
hy
(1)
Full
reco
very
(2)
Perm
anent
hem
ianopsi
a
27
2004–2009
7M
ean
47
year
s(r
ange
14–79),
bim
odal
dis
trib
ution
2/7 im
munodepre
ssed
Clin
ical
sign
s+
DN
Adet
ect
ion
inC
SF
ND
ND
Most
frequent:
feve
r,head
ache,
neck
stiff
nes
s,photo
phobia
Norm
alim
agin
gin
allpat
ients
No
evi
dence
of
stro
keor
vasc
ulo
pat
hy
One
deat
h(t
erm
inal
renal
failu
re)
18
ND
9M
edia
n72
year
s(r
ange
52–94)
All im
munoco
mpete
nt
Neuro
logi
cal
sign
s+
rash
Herp
es
zost
er
ispar
tof
the
case
defi
nitio
n
ND
Ata
xia
n=
5,cr
ania
lnerv
es
impai
rment
n=
2
CT
scan
in5/9
,norm
alfo
ral
l5
No
evi
dence
of
vasc
ula
ritis
No
deat
h,
sequela
enot
desc
ribed
Appar
ently
befo
rePC
Ran
dM
RI
but
acyc
lovi
rav
aila
ble
28
ND
30
Ran
ge1–88
year
sold
11/3
0im
munoco
mpro
mis
edN
euro
logi
cal
sign
san
dIm
agin
gor
CSF
consi
stent
with
vasc
ulo
pat
hy
and
DN
Adet
ect
ion
or
sero
logy
19/3
0(6
3%
)N
DN
DLar
ge-v
esse
lva
sculo
pat
hy
4/3
0(1
3%
)Sm
all-ve
ssel
vasc
ulo
pat
hy
11/3
0(3
7%
)M
ixed
vasc
ulo
pat
hy
15/3
0(5
0%
)
Vas
culo
pat
hy
ispar
tof
the
case
definitio
n
Favo
ura
ble
outc
om
efo
rfo
ur
case
sw
ith
larg
e-v
ess
el
vasc
ulo
pat
hy
Poor
outc
om
efo
rth
ree
case
sw
ith
smal
l-ve
ssel
and
thre
eca
ses
with
mix
ed
vasc
ulo
pat
hie
s
23
pre
viousl
ypublis
hed
case
s+
seve
nnew
lypublis
hed
case
s
29
816 Clinical Microbiology and Infection, Volume 18 Number 8, August 2012 CMI
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases, CMI, 18, 808–819

our study, 3 years after discharge, half of the survivors still
presented with moderate to severe sequelae. Some authors
have suggested that the combination of acyclovir and foscar-
net might improve the prognosis and also prevent a possible
antiviral failure caused by an acyclovir-resistant VZV strain,
but this hypothesis has yet to be confirmed by clinical trial
[34].
Questions and controversies remain on the physiological
mechanisms of the neurological complications of VZV infec-
tion. These complications are different during primary infec-
tion (varicella) and after viral reactivation (zoster). The most
frequent varicella complications are cerebellitis and arterial
ischaemic strokes [15,35,36]. Usually, VZV cerebellitis or
ataxia has a favourable outcome in children and CSF analysis
is generally not performed in this context. Besides ataxia,
arterial ischaemic stroke occurs in up to 1/15 000 cases
[36]. This syndrome, now referred to as post-varicella arteri-
opathy, is defined by focal stenosis of the basal central arter-
ies in children with a history of varicella within the
12 months before the onset of neurological signs.
Varicella acute encephalopathy with fatal outcome has also
been reported following varicella in children with liver and
brain oedema and fatty macrophage infiltration as the result
of Reye’s syndrome, although this does not actually corre-
spond to a direct invasion of the central nervous system
[15].
The physiopathology of VZV encephalitis after reactivation
of the virus is still not clear. The presentations of herpes
zoster encephalitis can be divided into three main categories:
demyelinating disease, vasculopathy and acute infectious
encephalitis of undetermined pathophysiology, as reported in
this case series. The multifocal subacute demyelinating dis-
ease is mostly encountered in immunosuppressed patients,
especially those with AIDS (which was an exclusion criterion
in our study). The direct infection of glial cells and endothe-
lial vascular cells has been demonstrated in these cases [7].
The VZV-induced vasculopathy occurs in immunocompetent
elderly people or in AIDS patients (for instance, zoster oph-
thalmicus contralateral syndrome) [8,29]. Although some
authors claim that most, if not all, cases of herpes zoster
‘encephalitis’ are the result of viral vasculopathy [5,9], imag-
ing failed to demonstrate either vascular lesions or demyelin-
ating areas in 16 of 20 patients enrolled in our study, which
is in favour of direct viral parenchymatous encephalitis.
However, one patient in our series presented with both
myelitis and vasculopathy. He was under immunosuppressive
treatment following heart and lung transplant, and suffered
renal deficiency and diabetes. Myelitis has been described as
a non-vascular clinical presentation, and it has been hypothe-
sized that long-term steroids might be a risk factor for VZV
myelitis [1]. The clinical features and imaging results in this
patient suggest the simultaneous occurrence of two different
clinical presentations: first the myelitis, and second the vas-
culopathy. We can hypothesize that the immunosuppressive
condition of this patient favoured the persistence of a high
viral load in the brain arteries, leading to a massive vasculop-
athy both in subdural and ventricular areas.
Unlike herpes simplex virus, the correlation between the
presence of VZV in CSF and brain infection has not been
demonstrated. However, it has been demonstrated that the
VZV viral load in the CSF was correlated to the severity of
central nervous system symptoms in patients presenting with
encephalitis [37]. Moreover, the acyclovir-induced clearance
of VZV DNA from the CSF was associated with clinical
improvement in four cases of encephalitis [26]. These find-
ings are in favour of a direct viral encephalitis besides vascu-
laritis and demyelinating encephalitis. However, some
crossover between acute VZV encephalitis and VZV-induced
vasculopathy cannot be excluded, and both mechanisms
might exist in the same patients following reactivation of the
virus. This is suggested by the observation of a patient
enrolled in our study with a large vessel vasculopathy on
angiography and normal brain imaging excluding both a
stroke and a demyelinating process.
Conclusion
Varicella zoster virus encephalitis is the second leading cause
of acute infectious encephalitis in France, accounting for
nearly 10% of all cases. According to our results, this diagno-
sis should be considered in any case of central nervous sys-
tem acute febrile disease with lymphocytic aseptic meningitis,
especially in elderly and immunocompromised patients. The
absence of any rash, as in more than half of the cases in our
study, should not be considered as evidence excluding the
diagnosis of VZV encephalitis. Despite the low level of evi-
dence, acyclovir treatment should be prescribed to these
patients, because of its antiviral effectiveness against VZV.
The case fatality rate remains high and sequelae are frequent.
Controversies remain about its pathophysiology and further
research should be undertaken to determine the optimal
therapeutic regimen.
Contribution
TdB, AM, SB, PM and JPS contributed equally in the redac-
tion of the manuscript. AM was responsible for the analysis
of data. The members of the steering committee contributed
CMI De Broucker et al. Varicella zoster encephalitis in France in 2007 817
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases, CMI, 18, 808–819

to the critical reviewing of the manuscript. The members of
the investigators group contributed to the investigation and
management of the patients, and to the collection and inter-
pretation of data.
Transparency Declaration
The Institut de veille sanitaire (French institute for public
health surveillance), Saint Maurice, France promoted the
study and funded the salary of two data collection personnel.
Glaxo SmithKline, Roche and Biomerieux funded the setting
up and maintenance of a biobank of samples taken from the
patients. All authors have no conflict of interest to disclose.
Appendix
Steering committee
Cecile Bebear (Bordeaux), Cecile Brouard (Saint-Maurice),
Thomas De Broucker (Saint-Denis), Eric Cua (Nice), Henri
Dabernat (Toulouse), Daniel Floret (Lyon), Benoit Guery
(Lille), Marc Lecuit (Paris), Bruno Lina (Lyon), Olivier Lor-
tholary (Paris), Alexandra Mailles (Saint-Maurice), Christian
Michelet (Rennes), Patrice Morand (Grenoble), Bruno Poz-
zetto (Saint-Etienne), Jean-Paul Stahl (Grenoble), Veronique
Vaillant (Saint-Maurice), Yazdan Yazdanpanah (Tourcoing),
Herve Zeller (Lyon).
Investigators
Philippe Abboud (Rouen), Chakib Alloui (Paris), Christine Ar-
chimbaud (Clermont-Ferrand), Bruno Barroso (Pau), Louis
Bernard (Garches), Pascal Beuret (Roanne), Genevieve Bil-
laud (Lyon), Thierry Blanc (Rouen), Michele Bonnard-Gou-
geon (Clermont-Ferrand), David Boutolleau (Paris), Cedric
Bretonniere (Nantes), Celine Bressollette-Bodin (Nantes),
Fabrice Bruneel (Versailles), Marielle Buisson (Dijon), Anne
Caramella (Nice), Bernard Castan (Auch), Isabelle Cattaneo
(Bry sur Marne), Charles Cazanave (Bordeaux), Stephane
Chabrier (Saint-Etienne), Marie-Laure Chadenat (Versailles),
Martine Chambon (Clermont-Ferrand), Pascal Chavanet (Di-
jon), Mondher Chouchane (Dijon), Pierre Clavelou (Cler-
mont-Ferrand), Pierre Courant (Avignon), Eric Cua (Nice),
Fabienne de Brabant (Montelimar), Arnaud De La Blanch-
ardiere (Caen), Geoffroy De La Gastine (Caen), Henri De
Montclos (Bourg-en-Bresse), Eric Denes (Limoges), Philippe
Desprez (Strasbourg), Anny Dewilde (Lille), Aurelien Dinh
(Garches), Francois Durand (Saint-Etienne), Guillaume Emeri-
aud (Grenoble), Olivier Epaulard (Grenoble), Giovanni Fava-
retto (Avranche), Anna Ferrier (Clermont-Ferrand), Vincent
Foulongne (Montpellier), Francois Fourrier (Lille), Veronique
Gaday (Pontoise), Jacques Gaillat (Annecy), Serge Gallet
(Montlucon), Nicole Gazuy (Clermont-Ferrand), Stephanie
Gouarin (Caen), Pascale Goubin (Caen), Alain Goudeau
(Tours), Joel Gozlan (Paris), Philippe Granier (Bourg-en-
Bresse), Isabelle Gueit (Rouen), Amelie Guihot (Paris), Chris-
tine Guillermet (Besancon), Christelle Guillet-Caruba (Paris),
Yves Guimard (Bourges), Yves Hansmann (Strasbourg),
Cecile Henquell (Clermont-Ferrand), Jean-Louis Herrmann
(Garches), Jerome Honnorat (Lyon), Nadhira Houhou
(Paris), Benoit Jaulhac (Strasbourg), Olivier Join-Lambert
(Paris), Manoelle Kossorotoff (Paris), Emmanuelle Laudrault
(Montelimar), Frederic Laurent (Lyon), Jean-Jacques Lauri-
chesse (Paris), Sylvain Lavoue (Rennes), Leila Lazaro
(Bayonne), Stephane Legriel (Versailles), Olivier Lesens (Cler-
mont-Ferrand), Gerard Level (Verdun), Muriel Mace (Orle-
ans), Benedicte Maisonneuve (Montlucon), Alain Makinson
(Montpellier), Helene Marchandin (Montpellier), Laurent
Martinez-Almoyna (Saint-Denis), Patrick Marthelet (Monteli-
mar), Martin Martinot (Colmar), Bruno Massenavette (Lyon),
Laurence Maulin (Aix-en-Provence), Benoit Misset (Paris),
Catherine Neuwirth (Dijon), Florence Nicot (Toulouse),
Jerome Pacanowski (Paris), Jean-Bernard Palcoux (Clermont-
Ferrand), Patricia Pavese (Grenoble), Thomas Perpoint
(Lyon), Martine Pestel–Caron (Rouen), Robin Pouyau (Lyon),
Thierry Prazuck (Orleans), Virginie Prendki (Paris), Chris-
tophe Rapp (Saint-Mande), Christel Regagnon (Clermont-Fer-
rand), Matthieu Rigal (Auch), Nathalie Roch (Grenoble),
Olivier Rogeaux (Chambery), Sylvie Rogez (Limoges),
Charles Santre (Annecy), Anne Signori-Schmuck (Grenoble),
Fabrice Simon (Marseille), Abdelilah Taimi (Roanne), Jerome
Tayoro (Le Mans), Daniel Terral (Clermont-Ferrand), Audrey
Therby (Versailles), Francis Vuillemet (Colmar).
References
1. Gilden DH, Kleinschmidt-DeMasters BK, LaGuardia JJ, Mahalingam R,
Cohrs RJ. Neurologic complications of the reactivation of varicella-
zoster virus. N Engl J Med 2000; 342: 635–645.
2. Steiner I, Kennedy PGE, Pachner AR. The neurotropic herpes viruses:
herpes simplex and varicella-zoster. Lancet Neurol 2007; 6: 1015–1028.
3. Johnson RW, McElhaney J. Postherpetic neuralgia in the elderly. Int J
Clin Pract 2009; 63: 1386–1391.
4. Gershon AA, Gershon MD, Breuer J, Levin MJ, Oaklander AL, Grif-
fiths PD. Advances in the understanding of the pathogenesis and epi-
demiology of herpes zoster. J Clin Virol 2010; 48 (suppl): S2–S7.
5. Mueller NH, Gilden DH, Cohrs RJ, Mahalingam R, Nagel MA. Vari-
cella-zoster virus infection: clinical features, molecular pathogenesis
of disease, and latency. Neurol Clin 2008; 26: 675–697, viii.
6. Reshef E, Greenberg SB, Jankovic J. Herpes zoster ophthalmicus fol-
lowed by contralateral hemiparesis: report of two cases and review
of literature. J Neurol Neurosurg Psychiatr 1985; 48: 122–127.
818 Clinical Microbiology and Infection, Volume 18 Number 8, August 2012 CMI
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases, CMI, 18, 808–819

7. Kleinschmidt-DeMasters BK, Gilden DH. Varicella-Zoster virus infec-
tions of the nervous system: clinical and pathologic correlates. Arch
Pathol Lab Med 2001; 125: 770–780.
8. de Broucker T, Verollet D, Schoindre Y et al. [Cerebral vasculitis
with aneurysms caused by varicella-zoster virus infection during
AIDS: a new clinicoangiographical syndrome]. Rev Neurol (Paris) 2008;
164: 61–71.
9. Gilden D, Cohrs RJ, Mahalingam R, Nagel MA. Varicella-zoster virus
vasculopathies: diverse clinical manifestations, laboratory features,
pathogenesis, and treatment. Lancet Neurol 2009; 8: 731–740.
10. Gilden D. Varicella-zoster virus and central nervous system syn-
dromes. Herpes 2004; 11 (suppl 2): 89A–94A.
11. Mailles A, Stahl J-P. Infectious encephalitis in France in 2007: a
national prospective study. Clin Infect Dis 2009; 49: 1838–1847.
12. Granerod J, Ambrose HE, Davies NW et al. Causes of encephalitis
and differences in their clinical presentations in England: a multicen-
tre, population-based prospective study. Lancet Infect Dis 2010; 10:
835–844.
13. Glaser CA, Honarmand S, Anderson LJ et al. Beyond viruses: clinical
profiles and etiologies associated with encephalitis. Clin Infect Dis
2006; 43: 1565–1577.
14. Tunkel AR, Glaser CA, Bloch KC et al. The management of encepha-
litis: clinical practice guidelines by the Infectious Diseases Society of
America. Clin Infect Dis 2008; 47: 303–327.
15. Johnson R, Milbourn PE. Central nervous system manifestations of
chickenpox. Can Med Assoc J 1970; 102: 831–834.
16. Jemsek J, Greenberg SB, Taber L, Harvey D, Gershon A, Couch RB.
Herpes zoster-associated encephalitis: clinicopathologic report of 12
cases and review of the literature. Medicine (Baltimore) 1983; 62: 81–97.
17. Koskiniemi M, Piiparinen H, Rantalaiho T et al. Acute central nervous
system complications in Varicella-zoster virus infections. J Clin Virol
2002; 25: 293–301.
18. Douglas A, Harris P, Francis F, Norton R. Herpes zoster meningoen-
cephalitis: not only a disease of the immunocompromised? Infection
2010; 38: 73–75.
19. Jennett B, Bond M. Assessment of outcome after severe brain dam-
age. Lancet 1975; 1: 480–484.
20. Mailles A, Vaillant V, Stahl J-P. [Infectious encephalitis in France from
2000 to 2002: the hospital database is a valuable but limited source
of information for epidemiological studies]. Med Mal Infect 2007; 37:
95–102.
21. Puchhammer-Stockl E, Popow-Kraupp T, Heinz FX, Mandl CW, Kunz
C. Detection of varicella-zoster virus DNA by polymerase chain
reaction in the cerebrospinal fluid of patients suffering from neuro-
logical complications associated with chicken pox or herpes zoster. J
Clin Microbiol 1991; 29: 1513–1516.
22. Horten B, Price RW, Jimenez D. Multifocal varicella-zoster virus leu-
koencephalitis temporally remote from herpes zoster. Ann Neurol
1981; 9: 251–266.
23. Hokkanen L, Launes J, Poutiainen E et al. Subcortical type cognitive
impairment in herpes zoster encephalitis. J Neurol 1997; 244: 239–
245.
24. Miravet E, Danchaivijitr N, Basu H, Saunders DE, Ganesan V. Clinical
and radiological features of childhood cerebral infarction following
varicella zoster virus infection. Dev Med Child Neurol 2007; 49: 417–
422.
25. Cinque P, Bossolasco S, Vago L et al. Varicella-zoster virus (VZV)
DNA in cerebrospinal fluid of patients infected with human
immunodeficiency virus: VZV disease of the central nervous system
or subclinical reactivation of VZV infection? Clin Infect Dis 1997; 25:
634–639.
26. Persson A, Bergstrom T, Lindh M, Namvar L, Studahl M. Varicella-
zoster virus CNS disease—viral load, clinical manifestations and
sequels. J Clin Virol 2009; 46: 249–253.
27. Hausler M, Schaade L, Kemeny S, Schweizer K, Schoenmackers C,
Ramaekers VT. Encephalitis related to primary varicella-zoster virus
infection in immunocompetent children. J Neurol Sci 2002; 2: 111–
116.
28. Peterslund NA. Herpes zoster associated encephalitis: clinical findings
and acyclovir treatment. Scand J Infect Dis 1988; 20: 583–592.
29. Nagel MA, Cohrs RJ, Mahalingam R et al. The Varicella-zoster virus
vasculopathies: clinical, CSF, imaging, and virologic features. Neurology
2008; 70: 853–860.
30. Pahud BA, Glaser CA, Dekker CL, Arvin AM, Schmid DS. Varicella-
zoster disease of the central nervous system: epidemiological, clinical,
and laboratory features 10 years after the introduction of the vari-
cella vaccine. J Infect Dis 2011; 203: 316–323.
31. Arvin AM. Antiviral therapy for varicella and herpes zoster. Semin
Pediatr Infect Dis 2002; 13: 12–21.
32. Dworkin RH, Johnson RW, Breuer J et al. Recommendations for the
management of herpes zoster. Clin Infect Dis 2007; 44 (suppl 1): S1–
S26.
33. Raschilas F, Wolff M, Delatour F et al. Outcome of and prognostic
factors for herpes simplex encephalitis in adult patients: results of a
multicenter study. Clin Infect Dis 2002; 35: 254–260.
34. Schmidt-Hieber M, Zweigner J, Uharek L, Blau IW, Thiel E. Central
nervous system infections in immunocompromised patients: update
on diagnostics and therapy. Leuk Lymphoma 2009; 50: 24–36.
35. Sawaishi Y, Takada G. Acute cerebellitis. Cerebellum 2002; 1: 223–
228.
36. Askalan R, Laughlin S, Mayank S et al. Chickenpox and stroke in
childhood: a study of frequency and causation. Stroke 2001; 32: 1257–
1262.
37. Aberle SW, Aberle JH, Steininger C, Puchhammer-Stockl E. Quantita-
tive real time PCR detection of Varicella-zoster virus DNA in
cerebrospinal fluid in patients with neurological disease. Med Microbiol
Immunol 2005; 194: 7–12.
CMI De Broucker et al. Varicella zoster encephalitis in France in 2007 819
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases, CMI, 18, 808–819
Copyright © 2022 FDOKUMEN












![[Herpes Zoster and its prevention in Italy. Scientific consensus statement]](https://static.fdokumen.com/doc/165x107/6332d5755f7e75f94e094855/herpes-zoster-and-its-prevention-in-italy-scientific-consensus-statement.jpg)







