
5. Vergara, Epidemiology of varicella JCV 2012
7
Journal of Clinical Virology 55 (2012) 51–57 Contents lists available at SciVerse ScienceDirect Journal of Clinical Virology j ourna l ho mepage: www.elsevier.com/locate/jcv Epidemiology of varicella in Mexico Arely Vergara-Casta ˜ neda a , Alejandro Escobar-Gutiérrez b , Karina Ruiz-Tovar b , Julio Sotelo c , Graciela Ordo ˜ nez c , Mayra Yolanda Cruz-Rivera a , Salvador Fonseca-Coronado a , Armando Martinez-Guarneros b , Juan C. Carpio-Pedroza b , Gilberto Vaughan b,∗ a Universidad Nacional Autónoma de México, México City, Mexico b Instituto de Diagnóstico y Referencia Epidemiológicos, Secretaría de Salud, México City, Mexico c Unidad de Neuroinmunología, Instituto Nacional de Neurología y Neurocirugía de México, México City, Mexico a r t i c l e i n f o Article history: Received 4 February 2012 Received in revised form 8 June 2012 Accepted 11 June 2012 Keywords: Varicella Mexico Epidemiology a b s t r a c t Background: The epidemiological patterns of varicella-zoster virus (VZV) infection, which are strongly associated with climate, are characterized by more frequent infections occurring among children in tem- perate regions than in the tropics. In temperate regions, varicella exhibits a seasonal cyclic behavior in which the number of cases increases significantly during the winter and spring seasons, further sup- porting the role of environmental factors in disease transmission. However, the underlying mechanisms responsible for this distinctive behavior are not fully understood. In Mexico, information regarding the epidemiology of varicella is scarce, and the distribution of VZV infection has not been analyzed. Objectives: In this article we investigate the epidemiological patterns of varicella in Mexico and their relationship with different environmental and demographic factors. Study design: A retrospective study was conducted using the data reported by the National Center of Epidemiological Surveillance and Disease Control. The overall varicella incidence was calculated and associated with temperature, overcrowding, age, gender and population density. Results: The epidemiology of varicella showed an intriguing pattern, in which warmer regions were characterized by higher incidences than in temperate regions. Young children were the most affected age group. There was no correlation between varicella incidence and overcrowding or population density. Conclusions: The epidemiology of varicella in Mexico significantly departs from the characteristic patterns observed in other tropical latitudes, with some features resembling those commonly associated with temperate regions. Published by Elsevier B.V. 1. Background Varicella (chickenpox) is caused by varicella-zoster virus (VZV), also known as human herpesvirus 3, an alphaherpesvirus of the Herpesviridae family. This is a highly contagious disease character- ized by a generalized exanthematous rash that is usually benign in children but in some cases it may result in complications such as pneumonia and bacterial superinfection. 1 The binomial nature of this infection leads to two distinctive clinical presentations, chick- enpox and herpes zoster, commonly known as shingles. 2 After the Abbreviations: VZV, varicella-zoster virus; CENAVECE, National Center of Epi- demiological Surveillance and Disease Control. ∗ Corresponding author at: Departamento de Investigaciones Inmunológicas, Instituto de Diagnóstico y Referencia Epidemiológicos, Carpio 470, México City 11340, Mexico. Tel.: +52 55 5342 7563; fax: +52 55 5341 3264. E-mail address: [email protected] (G. Vaughan). primary infection, the virus becomes latent in cranial nerve ganglia, dorsal root ganglia and autonomic ganglia along the entire neuraxis. Subsequently, later in life, and as specific cell-mediated immunity to the virus declines with age or immunosuppression, VZV reacti- vates to cause shingles, often followed by postherpetic neuralgia, vasculopathy, myelopathy, retinal necrosis and cerebellitis. 3 The epidemiology of varicella exhibits significant differences in temperate and tropical regions. 4 In temperate locations, varicella primarily affects children 5 ; however, in tropical areas, varicella tends to occur at a later age, during adolescence and adulthood, with an increased risk of developing a more severe disease. 6 The mechanisms responsible for these differences are not completely understood. Diverse environmental and social factors have been proposed to play a role in the epidemiology of different diseases. 7 Temperature has been suggested to affect viral transmission due to viral inactivation. 7,8 Additionally, household size has been shown to be critical for VZV transmission in tropical latitudes. 9 In addition, adult susceptibility in tropical rural areas has been proposed to be 1386-6532/$ – see front matter. Published by Elsevier B.V. http://dx.doi.org/10.1016/j.jcv.2012.06.004
-
Upload
indresecretariadesaludmexico -
Category
Documents
-
view
0 -
download
0
Transcript of 5. Vergara, Epidemiology of varicella JCV 2012

E
AGAa
b
c
a
ARRA
KVME
1
aHicpte
d
I1
1h
Journal of Clinical Virology 55 (2012) 51– 57
Contents lists available at SciVerse ScienceDirect
Journal of Clinical Virology
j ourna l ho mepage: www.elsev ier .com/ locate / j cv
pidemiology of varicella in Mexico
rely Vergara-Castanedaa, Alejandro Escobar-Gutiérrezb, Karina Ruiz-Tovarb, Julio Soteloc,raciela Ordonezc, Mayra Yolanda Cruz-Riveraa, Salvador Fonseca-Coronadoa,rmando Martinez-Guarnerosb, Juan C. Carpio-Pedrozab, Gilberto Vaughanb,∗
Universidad Nacional Autónoma de México, México City, MexicoInstituto de Diagnóstico y Referencia Epidemiológicos, Secretaría de Salud, México City, MexicoUnidad de Neuroinmunología, Instituto Nacional de Neurología y Neurocirugía de México, México City, Mexico
r t i c l e i n f o
rticle history:eceived 4 February 2012eceived in revised form 8 June 2012ccepted 11 June 2012
eywords:aricellaexico
pidemiology
a b s t r a c t
Background: The epidemiological patterns of varicella-zoster virus (VZV) infection, which are stronglyassociated with climate, are characterized by more frequent infections occurring among children in tem-perate regions than in the tropics. In temperate regions, varicella exhibits a seasonal cyclic behavior inwhich the number of cases increases significantly during the winter and spring seasons, further sup-porting the role of environmental factors in disease transmission. However, the underlying mechanismsresponsible for this distinctive behavior are not fully understood. In Mexico, information regarding theepidemiology of varicella is scarce, and the distribution of VZV infection has not been analyzed.Objectives: In this article we investigate the epidemiological patterns of varicella in Mexico and theirrelationship with different environmental and demographic factors.Study design: A retrospective study was conducted using the data reported by the National Center ofEpidemiological Surveillance and Disease Control. The overall varicella incidence was calculated andassociated with temperature, overcrowding, age, gender and population density.
Results: The epidemiology of varicella showed an intriguing pattern, in which warmer regions werecharacterized by higher incidences than in temperate regions. Young children were the most affected agegroup. There was no correlation between varicella incidence and overcrowding or population density.Conclusions: The epidemiology of varicella in Mexico significantly departs from the characteristic patternsobserved in other tropical latitudes, with some features resembling those commonly associated withtemperate regions.Published by Elsevier B.V.
. Background
Varicella (chickenpox) is caused by varicella-zoster virus (VZV),lso known as human herpesvirus 3, an alphaherpesvirus of theerpesviridae family. This is a highly contagious disease character-
zed by a generalized exanthematous rash that is usually benign inhildren but in some cases it may result in complications such as
neumonia and bacterial superinfection.1 The binomial nature ofhis infection leads to two distinctive clinical presentations, chick-npox and herpes zoster, commonly known as shingles.2 After theAbbreviations: VZV, varicella-zoster virus; CENAVECE, National Center of Epi-emiological Surveillance and Disease Control.∗ Corresponding author at: Departamento de Investigaciones Inmunológicas,
nstituto de Diagnóstico y Referencia Epidemiológicos, Carpio 470, México City1340, Mexico. Tel.: +52 55 5342 7563; fax: +52 55 5341 3264.
E-mail address: [email protected] (G. Vaughan).
386-6532/$ – see front matter. Published by Elsevier B.V.ttp://dx.doi.org/10.1016/j.jcv.2012.06.004
primary infection, the virus becomes latent in cranial nerve ganglia,dorsal root ganglia and autonomic ganglia along the entire neuraxis.Subsequently, later in life, and as specific cell-mediated immunityto the virus declines with age or immunosuppression, VZV reacti-vates to cause shingles, often followed by postherpetic neuralgia,vasculopathy, myelopathy, retinal necrosis and cerebellitis.3
The epidemiology of varicella exhibits significant differences intemperate and tropical regions.4 In temperate locations, varicellaprimarily affects children5; however, in tropical areas, varicellatends to occur at a later age, during adolescence and adulthood,with an increased risk of developing a more severe disease.6 Themechanisms responsible for these differences are not completelyunderstood. Diverse environmental and social factors have beenproposed to play a role in the epidemiology of different diseases.7
Temperature has been suggested to affect viral transmission due toviral inactivation.7,8 Additionally, household size has been shownto be critical for VZV transmission in tropical latitudes.9 In addition,adult susceptibility in tropical rural areas has been proposed to be
52 A. Vergara-Castaneda et al. / Journal of Clinical Virology 55 (2012) 51– 57
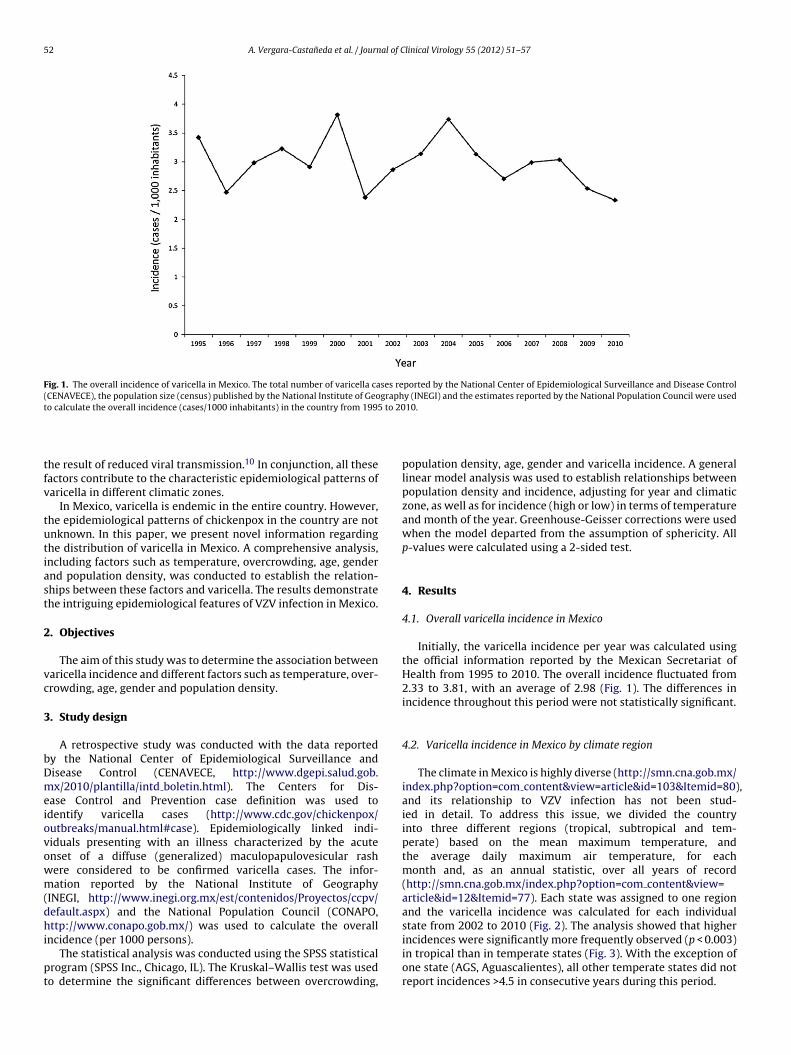
Fig. 1. The overall incidence of varicella in Mexico. The total number of varicella cases reported by the National Center of Epidemiological Surveillance and Disease Control(CENAVECE), the population size (census) published by the National Institute of Geography (INEGI) and the estimates reported by the National Population Council were usedt to 20
tfv
tutiast
2
vc
3
bDmeiovowm(dhi
pt
,
and the varicella incidence was calculated for each individualstate from 2002 to 2010 (Fig. 2). The analysis showed that higher
o calculate the overall incidence (cases/1000 inhabitants) in the country from 1995
he result of reduced viral transmission.10 In conjunction, all theseactors contribute to the characteristic epidemiological patterns ofaricella in different climatic zones.
In Mexico, varicella is endemic in the entire country. However,he epidemiological patterns of chickenpox in the country are notnknown. In this paper, we present novel information regardinghe distribution of varicella in Mexico. A comprehensive analysis,ncluding factors such as temperature, overcrowding, age, gendernd population density, was conducted to establish the relation-hips between these factors and varicella. The results demonstratehe intriguing epidemiological features of VZV infection in Mexico.
. Objectives
The aim of this study was to determine the association betweenaricella incidence and different factors such as temperature, over-rowding, age, gender and population density.
. Study design
A retrospective study was conducted with the data reportedy the National Center of Epidemiological Surveillance andisease Control (CENAVECE, http://www.dgepi.salud.gob.x/2010/plantilla/intd boletin.html). The Centers for Dis-
ase Control and Prevention case definition was used todentify varicella cases (http://www.cdc.gov/chickenpox/utbreaks/manual.html#case). Epidemiologically linked indi-iduals presenting with an illness characterized by the acutenset of a diffuse (generalized) maculopapulovesicular rashere considered to be confirmed varicella cases. The infor-ation reported by the National Institute of Geography
INEGI, http://www.inegi.org.mx/est/contenidos/Proyectos/ccpv/efault.aspx) and the National Population Council (CONAPO,ttp://www.conapo.gob.mx/) was used to calculate the overall
ncidence (per 1000 persons).The statistical analysis was conducted using the SPSS statistical
rogram (SPSS Inc., Chicago, IL). The Kruskal–Wallis test was usedo determine the significant differences between overcrowding,
10.
population density, age, gender and varicella incidence. A generallinear model analysis was used to establish relationships betweenpopulation density and incidence, adjusting for year and climaticzone, as well as for incidence (high or low) in terms of temperatureand month of the year. Greenhouse-Geisser corrections were usedwhen the model departed from the assumption of sphericity. Allp-values were calculated using a 2-sided test.
4. Results
4.1. Overall varicella incidence in Mexico
Initially, the varicella incidence per year was calculated usingthe official information reported by the Mexican Secretariat ofHealth from 1995 to 2010. The overall incidence fluctuated from2.33 to 3.81, with an average of 2.98 (Fig. 1). The differences inincidence throughout this period were not statistically significant.
4.2. Varicella incidence in Mexico by climate region
The climate in Mexico is highly diverse (http://smn.cna.gob.mx/index.php?option=com content&view=article&id=103&Itemid=80)and its relationship to VZV infection has not been stud-ied in detail. To address this issue, we divided the countryinto three different regions (tropical, subtropical and tem-perate) based on the mean maximum temperature, andthe average daily maximum air temperature, for eachmonth and, as an annual statistic, over all years of record(http://smn.cna.gob.mx/index.php?option=com content&view=article&id=12&Itemid=77). Each state was assigned to one region
incidences were significantly more frequently observed (p < 0.003)in tropical than in temperate states (Fig. 3). With the exception ofone state (AGS, Aguascalientes), all other temperate states did notreport incidences >4.5 in consecutive years during this period.

A. Vergara-Castaneda et al. / Journal of Clinical Virology 55 (2012) 51– 57 53
Fig. 2. The climatic zones in Mexico. Mexico has a wide range of climate zones including deserts, steppes, and tropical rain forests. The country was divided into threedifferent regions (tropical, subtropical and temperate) according to the average maximum annual temperature to better define the influence of temperature on varicellaincidence. Climatic regions are color-coded; pink, tropical; orange, subtropical and yellow temperate.
Fig. 3. The climatic zones and varicella incidence in Mexico. Each state was assigned to a climatic zone based on the maximum average annual temperature. The criterion toassign a state to a particular climatic zone was based on the number of inhabitants living in each region. Thus, if the vast majority of the population resided in the tropicalregion of a given state, the entire state was assigned to the tropical category. The annual incidence was calculated, as described for Fig. 1, for each state from 2002 to 2010.The color map represents the incidence per year in each state and in each climatic zone. The incidence is color-coded; warmer colors depict high and colder colors representl
4p
cdpofI
ow incidence rates.
.3. Tropical regions of Mexico follow the characteristic cyclicatterns observed in temperate regions
It has been reported that VZV infection in Mexico follows theharacteristic winter–spring pattern.11 To this pattern in moreetail, the varicella incidence from 2002 to 2010 was calculated
er month in each state. The analysis showed that the numberf cases generally increased in February, reaching a maximumrom March to May, and declined rapidly around June (Fig. 4a).nterestingly, a second peak was commonly observed in August.Thus, the number of infections increases during the late winter,peaks during the spring and plummets in the early summer. Thischaracteristic seasonal profile has not seen significant changesfor almost a decade. Furthermore, when the states were sep-arated into two groups, high (>3) and low (<3) incidence, thestates with high incidences were significantly warmer (p < 0.001)
than the states with low incidences (Fig. 4b). Interestingly, vari-cella incidence and temperature profiles followed very similarpatterns. A second peak in the incidence profile, occurring inAugust, was also observed in the temperature pattern. Overall,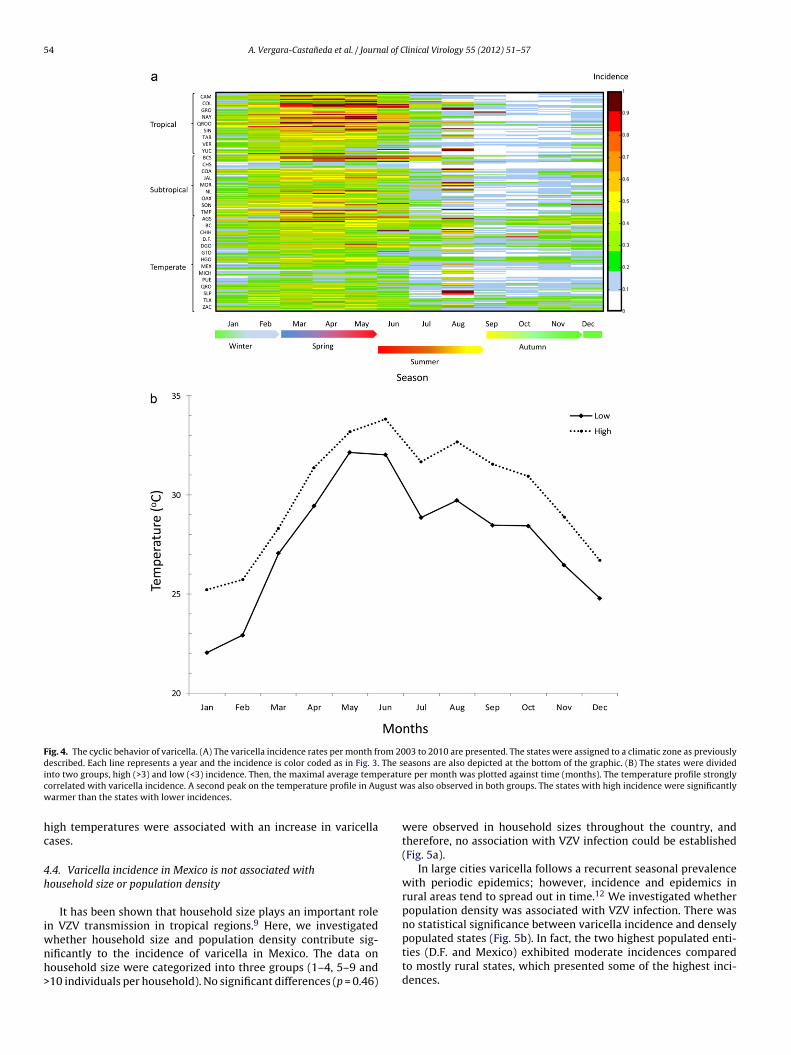
54 A. Vergara-Castaneda et al. / Journal of Clinical Virology 55 (2012) 51– 57
Fig. 4. The cyclic behavior of varicella. (A) The varicella incidence rates per month from 2003 to 2010 are presented. The states were assigned to a climatic zone as previouslydescribed. Each line represents a year and the incidence is color coded as in Fig. 3. The seasons are also depicted at the bottom of the graphic. (B) The states were dividedi eratuc gust ww
hc
4h
iwnh>
nto two groups, high (>3) and low (<3) incidence. Then, the maximal average temporrelated with varicella incidence. A second peak on the temperature profile in Auarmer than the states with lower incidences.
igh temperatures were associated with an increase in varicellaases.
.4. Varicella incidence in Mexico is not associated withousehold size or population density
It has been shown that household size plays an important rolen VZV transmission in tropical regions.9 Here, we investigated
hether household size and population density contribute sig-ificantly to the incidence of varicella in Mexico. The data onousehold size were categorized into three groups (1–4, 5–9 and10 individuals per household). No significant differences (p = 0.46)
re per month was plotted against time (months). The temperature profile stronglyas also observed in both groups. The states with high incidence were significantly
were observed in household sizes throughout the country, andtherefore, no association with VZV infection could be established(Fig. 5a).
In large cities varicella follows a recurrent seasonal prevalencewith periodic epidemics; however, incidence and epidemics inrural areas tend to spread out in time.12 We investigated whetherpopulation density was associated with VZV infection. There wasno statistical significance between varicella incidence and densely
populated states (Fig. 5b). In fact, the two highest populated enti-ties (D.F. and Mexico) exhibited moderate incidences comparedto mostly rural states, which presented some of the highest inci-dences.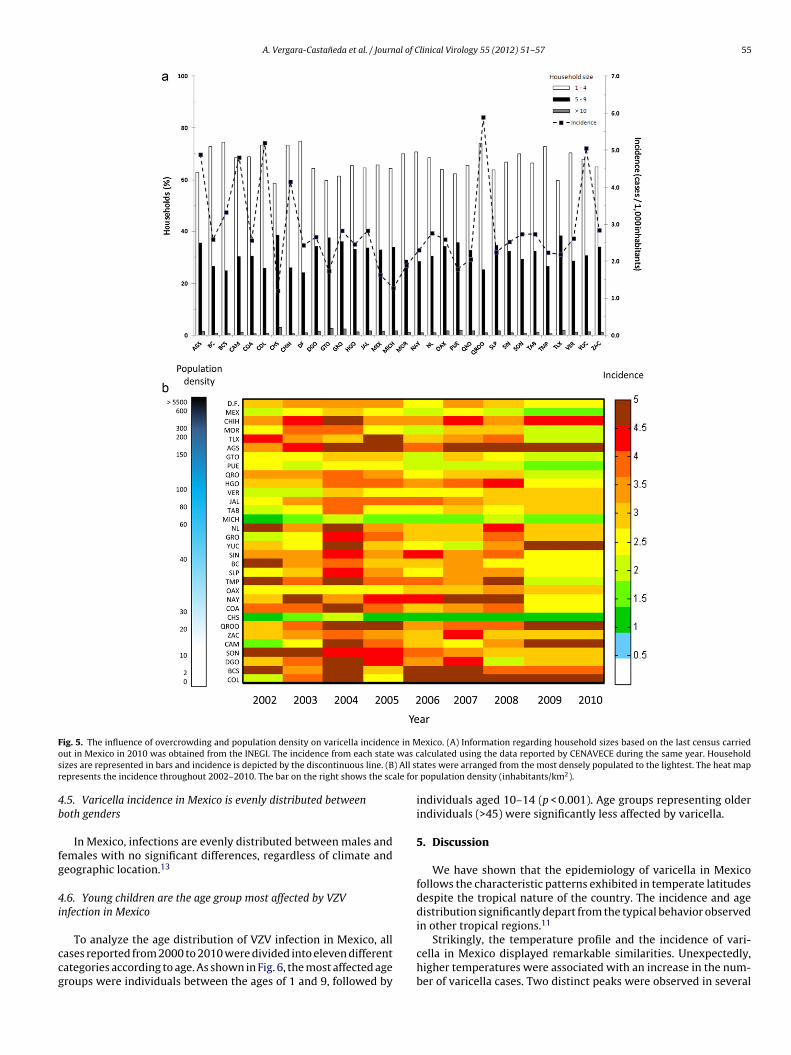
A. Vergara-Castaneda et al. / Journal of Clinical Virology 55 (2012) 51– 57 55
F e in Mo was cs ) All sr ale for
4b
fg
4i
ccg
ig. 5. The influence of overcrowding and population density on varicella incidencut in Mexico in 2010 was obtained from the INEGI. The incidence from each stateizes are represented in bars and incidence is depicted by the discontinuous line. (Bepresents the incidence throughout 2002–2010. The bar on the right shows the sc
.5. Varicella incidence in Mexico is evenly distributed betweenoth genders
In Mexico, infections are evenly distributed between males andemales with no significant differences, regardless of climate andeographic location.13
.6. Young children are the age group most affected by VZVnfection in Mexico
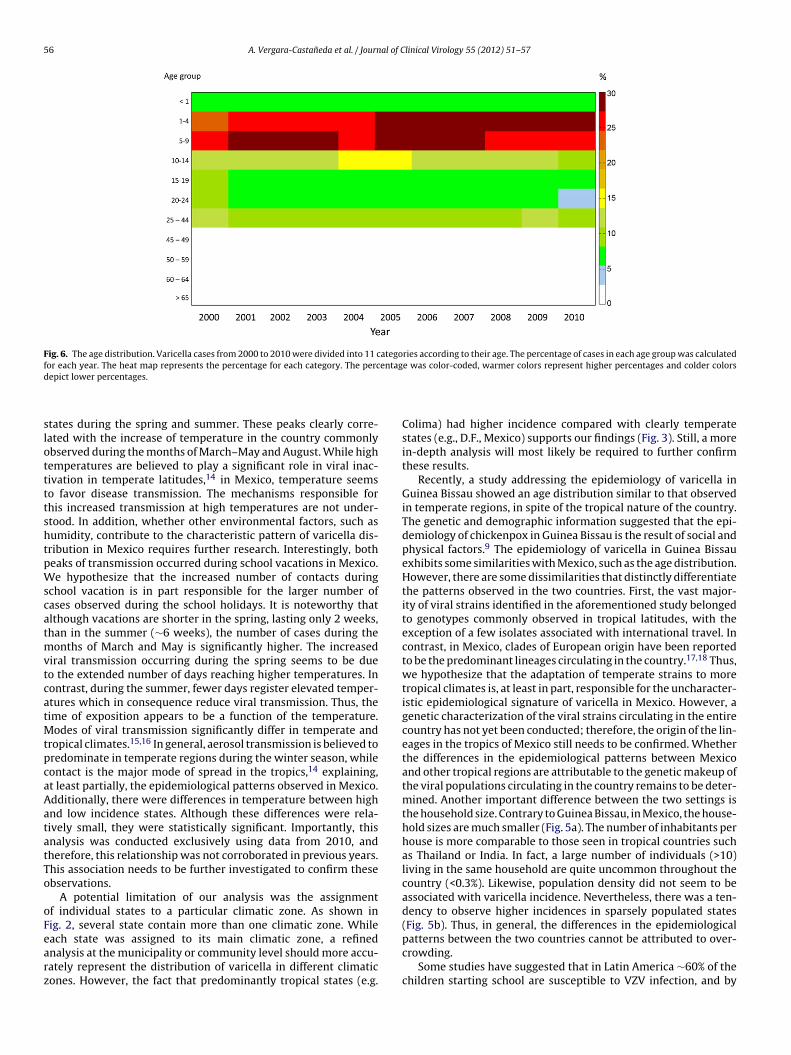
To analyze the age distribution of VZV infection in Mexico, allases reported from 2000 to 2010 were divided into eleven differentategories according to age. As shown in Fig. 6, the most affected ageroups were individuals between the ages of 1 and 9, followed by
exico. (A) Information regarding household sizes based on the last census carriedalculated using the data reported by CENAVECE during the same year. Household
tates were arranged from the most densely populated to the lightest. The heat map population density (inhabitants/km2).
individuals aged 10–14 (p < 0.001). Age groups representing olderindividuals (>45) were significantly less affected by varicella.
5. Discussion
We have shown that the epidemiology of varicella in Mexicofollows the characteristic patterns exhibited in temperate latitudesdespite the tropical nature of the country. The incidence and agedistribution significantly depart from the typical behavior observedin other tropical regions.11
Strikingly, the temperature profile and the incidence of vari-cella in Mexico displayed remarkable similarities. Unexpectedly,higher temperatures were associated with an increase in the num-ber of varicella cases. Two distinct peaks were observed in several
56 A. Vergara-Castaneda et al. / Journal of Clinical Virology 55 (2012) 51– 57
Fig. 6. The age distribution. Varicella cases from 2000 to 2010 were divided into 11 categories according to their age. The percentage of cases in each age group was calculatedf entagd
slottttshtpWscatmvtcatMtpcaAatatTo
oFearz
or each year. The heat map represents the percentage for each category. The percepict lower percentages.
tates during the spring and summer. These peaks clearly corre-ated with the increase of temperature in the country commonlybserved during the months of March–May and August. While highemperatures are believed to play a significant role in viral inac-ivation in temperate latitudes,14 in Mexico, temperature seemso favor disease transmission. The mechanisms responsible forhis increased transmission at high temperatures are not under-tood. In addition, whether other environmental factors, such asumidity, contribute to the characteristic pattern of varicella dis-ribution in Mexico requires further research. Interestingly, botheaks of transmission occurred during school vacations in Mexico.e hypothesize that the increased number of contacts during
chool vacation is in part responsible for the larger number ofases observed during the school holidays. It is noteworthy thatlthough vacations are shorter in the spring, lasting only 2 weeks,han in the summer (∼6 weeks), the number of cases during the
onths of March and May is significantly higher. The increasediral transmission occurring during the spring seems to be dueo the extended number of days reaching higher temperatures. Inontrast, during the summer, fewer days register elevated temper-tures which in consequence reduce viral transmission. Thus, theime of exposition appears to be a function of the temperature.
odes of viral transmission significantly differ in temperate andropical climates.15,16 In general, aerosol transmission is believed toredominate in temperate regions during the winter season, whileontact is the major mode of spread in the tropics,14 explaining,t least partially, the epidemiological patterns observed in Mexico.dditionally, there were differences in temperature between highnd low incidence states. Although these differences were rela-ively small, they were statistically significant. Importantly, thisnalysis was conducted exclusively using data from 2010, andherefore, this relationship was not corroborated in previous years.his association needs to be further investigated to confirm thesebservations.
A potential limitation of our analysis was the assignmentf individual states to a particular climatic zone. As shown inig. 2, several state contain more than one climatic zone. While
ach state was assigned to its main climatic zone, a refinednalysis at the municipality or community level should more accu-ately represent the distribution of varicella in different climaticones. However, the fact that predominantly tropical states (e.g.e was color-coded, warmer colors represent higher percentages and colder colors
Colima) had higher incidence compared with clearly temperatestates (e.g., D.F., Mexico) supports our findings (Fig. 3). Still, a morein-depth analysis will most likely be required to further confirmthese results.
Recently, a study addressing the epidemiology of varicella inGuinea Bissau showed an age distribution similar to that observedin temperate regions, in spite of the tropical nature of the country.The genetic and demographic information suggested that the epi-demiology of chickenpox in Guinea Bissau is the result of social andphysical factors.9 The epidemiology of varicella in Guinea Bissauexhibits some similarities with Mexico, such as the age distribution.However, there are some dissimilarities that distinctly differentiatethe patterns observed in the two countries. First, the vast major-ity of viral strains identified in the aforementioned study belongedto genotypes commonly observed in tropical latitudes, with theexception of a few isolates associated with international travel. Incontrast, in Mexico, clades of European origin have been reportedto be the predominant lineages circulating in the country.17,18 Thus,we hypothesize that the adaptation of temperate strains to moretropical climates is, at least in part, responsible for the uncharacter-istic epidemiological signature of varicella in Mexico. However, agenetic characterization of the viral strains circulating in the entirecountry has not yet been conducted; therefore, the origin of the lin-eages in the tropics of Mexico still needs to be confirmed. Whetherthe differences in the epidemiological patterns between Mexicoand other tropical regions are attributable to the genetic makeup ofthe viral populations circulating in the country remains to be deter-mined. Another important difference between the two settings isthe household size. Contrary to Guinea Bissau, in Mexico, the house-hold sizes are much smaller (Fig. 5a). The number of inhabitants perhouse is more comparable to those seen in tropical countries suchas Thailand or India. In fact, a large number of individuals (>10)living in the same household are quite uncommon throughout thecountry (<0.3%). Likewise, population density did not seem to beassociated with varicella incidence. Nevertheless, there was a ten-dency to observe higher incidences in sparsely populated states(Fig. 5b). Thus, in general, the differences in the epidemiological
patterns between the two countries cannot be attributed to over-crowding.Some studies have suggested that in Latin America ∼60% of thechildren starting school are susceptible to VZV infection, and by

al of C
tItiiicyiar
ovpboitebrwtaedM
enmrbar
fiaotatc
C
F
d
C
1
1
1
1
1
1
1
1
1
1
2
2
2
2nation program: a review. J Infect Dis 2008;197(Suppl 2):S82–9.
A. Vergara-Castaneda et al. / Journ
he age of 10, a third of these individuals remain susceptible.19,20
n Mexico, studies conducted during the late 1980s have shownhat ∼18% of the individuals aged between 1–19 years, and 5.2% ofndividuals aged 25–29 years, are still susceptible to VZVnfection.21 This degree of susceptibility among older individuals ismportant because infection among adults is more likely to be asso-iated with clinical complications.20,22 As shown here, in Mexico,oung children are the age group that is primarily affected by VZVnfection, although a substantial number of individuals aged 10–14re also affected. Thus, in general, the age distribution in Mexicoesembles the profile observed in temperate regions.
A intangible parameter that may play a role in the epidemiol-gy of varicella in Mexico is the extent of vaccination. The varicellaaccine was approved in Mexico in 2000. Its use has been restrictedrimarily to medical private practices and children undergoingone-marrow-transplant. It is believed that approximately 1–2%f children born in Mexico are vaccinated against VZV, primar-ly, in large cities and by private pediatricians. Unfortunately,here are no accurate records that can be used to evaluate thextent of vaccination coverage throughout the country. Despiteeing highly effective,23 vaccination against varicella is not cur-ently included in the National Immunization Program, whichould undoubtedly help to prevent acute infection as well as
he complications associated with chickenpox.24 Vaccination is major force that dramatically shapes the epidemiology of dis-ases. In the case of varicella, vaccination must be studied in moreetail to assess its impact on the epidemiology of chickenpox inexico.Although varicella in Mexico is considered to be notifiable dis-
ase, underreporting might mask the burden of the disease inon-tropical regions.13,25 Therefore, the differences between cli-atic zones could be partially attributed to deficiencies in the
eporting system. However, the fact that the incidence rates haveeen constant for such an extended period of time (approximately
decade) supports the reliability of the data and the findingseported in this communication.
The characteristic distribution of varicella in Mexico warrantsurther investigation. Active surveillance, including molecular test-ng aimed at uncovering the architecture of the viral population,nd cost-effectiveness studies designed to assess the benefitsf vaccination, are of high priority in Mexico. This informa-ion is critical for understanding the current status of varicelland for implementing health policies and vaccination programshat will most likely reduce the incidence of the disease in theountry.
onflict of interest
The authors do not have any conflict of interest.
unding
Intramural funding, Instituto de Diagnóstico y Referencia Epi-emiológicos, SSA, México.
ompeting interest
None to be declared.
2
2
linical Virology 55 (2012) 51– 57 57
Ethical approval
Ethical review approval was granted by the Ethical Committee ofthe Mexican Institute for Epidemiological Diagnosis and Reference(InDRE).
References
1. Whitley R. Varicella-zoster virus. In: Mandell GL, Bennett JE, Dolin R, editors.Principles and practice of infectious diseases, vol. 2. New York: Churchill, Living-stone; 2009. p. 1963–9.
2. Oxman MN. Clinical manifestations of herpes zoster. In: Arvin AMAAG, editor.Varicella-zoster virus: virology and clinical management. Cambridge, UK: Cam-bridge University Press; 2000. p. 246–75.
3. Gilden D, Nagel MA, Mahalingam R, Mueller NH, Brazeau EA, Pugazhenthi S, et al.Clinical and molecular aspects of varicella zoster virus infection. Future Neurol2009;4:103–17.
4. Lolekha S, Tanthiphabha W, Sornchai P, Kosuwan P, Sutra S, Warachit B, et al.Effect of climatic factors and population density on varicella zoster virus epi-demiology within a tropical country. Am J Trop Med Hyg 2001;64: 131–6.
5. Taylor-Wiedeman J, Yamashita K, Miyamura K, Yamazaki S. Varicella-zostervirus prevalence in Japan: no significant change in a decade. Jpn J Med Sci Biol1989;42:1–11.
6. Garnett GP, Cox MJ, Bundy DA, Didier JM, St Catharine J. The age of infection withvaricella-zoster virus in St. Lucia, West Indies. Epidemiol Infect 1993;110:361–72.
7. Lytle CD, Sagripanti JL. Predicted inactivation of viruses of relevance to biode-fense by solar radiation. J Virol 2005;79:14244–52.
8. Lowen AC, Steel J, Mubareka S, Palese P. High temperature (30 ◦C) blocks aerosolbut not contact transmission of influenza virus. J Virol 2008;82:5650–2.
9. Nichols RA, Averbeck KT, Poulsen AG, al Bassam MM, Cabral F, Aaby P, et al.Household size is critical to varicella-zoster virus transmission in the tropicsdespite lower viral infectivity. Epidemics 2011;3:12–8.
0. Mandal BK, Mukherjee PP, Murphy C, Mukherjee R, Naik T. Adult susceptibilityto varicella in the tropics is a rural phenomenon due to the lack of previousexposure. J Infect Dis 1998;178(Suppl 1):S52–4.
1. Vaughan G, Rodriguez-Castillo A, Cruz-Rivera MY, Ruiz-Tovar K, Ramirez-Gonzalez JE, Rivera-Osorio P, et al. Is ultra-violet radiation the main force shapingmolecular evolution of varicella-zoster virus? Virol J 2011;8:370.
2. Gordon JE, Chickenpox:. an epidemiological review. Am J Med Sci1962;244:362–89.
3. Cabrera Gaytan DA, Munoz Mendoza W, Gomez Altamirano CM. Compor-tamiento epidemiológico de la varicela en Mexico: 18 anos de estudiosy estimaciones para los proximos cinco anos. Rev Enferm Infec Pediatr2009;22:77–82.
4. Lowen A, Palese P. Transmission of influenza virus in temperate zones ispredominantly by aerosol, in the tropics by contact: a hypothesis. PLoS Curr2009;1:RRN1002.
5. Viboud C, Alonso WJ, Simonsen L. Influenza in tropical regions. PLoS Med2006;3:e89.
6. Dowell SF. Seasonal variation in host susceptibility and cycles of certain infec-tious diseases. Emerg Infect Dis 2001;7:369–74.
7. Rodriguez-Castillo A, Vaughan G, Ramirez-Gonzalez JE, Escobar-Gutierrez A.Simultaneous cocirculation of both European varicella-zoster virus genotypes(E1 and E2) in Mexico city. J Clin Microbiol 2010;48:1712–5.
8. Rodriguez-Castillo A, Vaughan G, Ramirez-Gonzalez JE, Gonzalez-Duran E,Gudino-Rosales JC, Escobar-Gutierrez A. Genetic variation of varicella-zostervirus strains circulating in Mexico City. J Clin Virol 2009;46:349–53.
9. Flisser A, Fernandez-Quintanilla G, Magos C, Tapia-Conyer R. Changing epidemi-ology of varicella. Virus Life 1997;12:212–5.
0. Flisser A, Tapia-Conyer R. Epidemiology of varicella infections. Contrib Microbiol1999;3:76–85.
1. Alvarez, Munoz MT, Torres J, Damasio-Santana L, Gomez A, Fernandez-Quintanilla G, et al. Susceptibility to varicella-zoster infection in individuals1–29 years of age in Mexico. Arch Med Res 1999;30:60–3.
2. Almuneef M, Memish ZA, Balkhy HH, Alotaibi B, Helmy M. Chickenpox compli-cations in Saudi Arabia: is it time for routine varicella vaccination? Int J InfectDis 2006;10:156–61.
3. Seward JF, Marin M, Vazquez M. Varicella vaccine effectiveness in the US vacci-
4. Takahashi M, Asano Y, Kamiya H, Baba K, Ozaki T, Otsuka T, et al. Developmentof varicella vaccine. J Infect Dis 2008;197(Suppl 2):S41–4.
5. Choo PW, Donahue JG, Manson JE, Platt R. The epidemiology of varicella and itscomplications. J Infect Dis 1995;172:706–12.




















