Epidemiology of burns in Malaga, Spain
10
ELSEVIER Burns Vol. 23, No. 4, pp. 323-332, 1997 0 1997 Elsevier Science Ltd for ISBI. AII rights reserved Printed in Great Britain 0~5~179/97 $17.00 + 0.00 PII: SO305-4179(96)00136-2 Epidemiology of burns in Maiaga, Spain E. FernBndez-Morales, L. Gklvez-Alcaraz, J. Fernrindez-Crehuet-Navajas, E. Gbmez-Gracia and J. M. Sagas-Ma~nez Preventive Medicine Department, Universitary Hospital, Malaga, Spain The incid~ce of burns in the province of Malaga, Spain, was defe~ined by mans of a desc~~tive, cross-sectional, ~u~fion- based study, and the individual, social and environmenfal condi- tions of the patients were analysed. Five hundred families(1846 persons), selected by a three-stage, stratified sampling, were inter- viewed in their homes. Five hundred and six burnswere found in 406 persons (2.25 burns/person); 89.5 per cent of these were in an urbanen~ironmenf and 10.5per cenf in a rural en~ironmenf. Eighfeen and a hatf per cent of the sample had burnt f~rn~lves only once and 4.7 per cent morethan once.The burnsaffected 23.3 per cent of the population, althoughthe majority were of little clinicalimportance. Therisk of burnsisgreater in the urban enuironment than in the rural environment, with burns occur- ring most often in the home (65.8 per cent),and es~cially in the kitchen.Themost ~~uenf burnsinvotvehot fiquids wifh special riskfrom cooking oil. Theother burns(in the strict sense of the word, proper burns or true burns), were primarily caused by contact. The incidence washigher in women (33.0 vs. 21.1 per cent), with burns occurringmostly on the hands. Only 21.9 per cenf of the burnsreceived the correct first aid after the a~cidenf. 0 2997 Etsevier Science Ltd fir IS El. Key words: Epidemiology, burns,Spain, population-based study, incidence. Burns, Vol. 23, No. 4,323-332,1997 Introduction Burns are currently a health problem the importance of which is determined by its magnitude, its indivi- dual significance, its particular risk factors, vulnera- biiity’*2 and its cost both socially and to the individual and family. Consequently, prevention is equally the best treatment for slight burns as weIl as serious burns because both constitute a health-care problem, some by their seriousness, others by their sheer numbe?. The absence of adequate recording systems implies a loss of information which may be signifi- cant for research in this field. Most of the available data concern patients who request medical attentian (out-patients or in-pati- ents), but most accidents are slight and require no more than self-care. Therefore unless medical assist- ance is requested, the accidents escape our statistics. Friction burns are an example5, since many are treated in other departments (orthopaedics, etc.) this, added to the codification problem, causes them to be underestimated. The importance of such information for the establishment of preventive measures has been demonstrated by many author@. Most of the data that are published lack common denominators and there exists a scarcity of such data, both nationally and internationally. In the same way that the true frequency of burns in our environment is not known, neither are the personal, family, social and env~onmental conditions of the persons who suffer them, essential knowledge for the control of every illness and the starting point necessary for the introduction of any preventative regime”‘. The present study was carried out with the objectives of quantifying the magnitude of the problem in our environment, estab~hing the epidemiologic al variables of person, place and time, determining the most important aetiological types, places and agents, and evaluating first aid therapy for burns. Patients and methods As working material, a total of 1746 persons of the province of Malaga were used, which allowed us to study 500 families, of which 421 were urban and 79 rural. They were interviewed in their houses using family surveys. The survey was directed at the housewife as being the most available {more time at home) and the person who was, perhaps, better able to remember family accidents. The scope of our survey refers to the population of the province of Malaga who reside in family dwellings and which comprises 1166891 inhabitants9. Those lacking a family home (5 per cent of the population) were excluded from the sample, and we do not believe that this influenced final results. Following the most accepted criteria for this kind of survey, we used a three-stage, stratified sampling “‘-12. In the first stage the primary units were the municipalities, divided into two strata denomi-
Transcript of Epidemiology of burns in Malaga, Spain
ELSEVIER
Burns Vol. 23, No. 4, pp. 323-332, 1997 0 1997 Elsevier Science Ltd for ISBI. AII rights reserved
Printed in Great Britain 0~5~179/97 $17.00 + 0.00
PII: SO305-4179(96)00136-2
Epidemiology of burns in Maiaga, Spain
E. FernBndez-Morales, L. Gklvez-Alcaraz, J. Fernrindez-Crehuet-Navajas, E. Gbmez-Gracia and J. M. Sagas-Ma~nez Preventive Medicine Department, Universitary Hospital, Malaga, Spain
The incid~ce of burns in the province of Malaga, Spain, was defe~ined by mans of a desc~~tive, cross-sectional, ~u~fion- based study, and the individual, social and environmenfal condi- tions of the patients were analysed. Five hundred families (1846 persons), selected by a three-stage, stratified sampling, were inter- viewed in their homes. Five hundred and six burns were found in 406 persons (2.25 burns/person); 89.5 per cent of these were in an urban en~ironmenf and 10.5 per cenf in a rural en~ironmenf. Eighfeen and a hatf per cent of the sample had burnt f~rn~lves only once and 4.7 per cent more than once. The burns affected 23.3 per cent of the population, although the majority were of little clinical importance. The risk of burns is greater in the urban enuironment than in the rural environment, with burns occur- ring most often in the home (65.8 per cent), and es~cially in the kitchen. The most ~~uenf burns invotve hot fiquids wifh special risk from cooking oil. The other burns (in the strict sense of the word, proper burns or true burns), were primarily caused by contact. The incidence was higher in women (33.0 vs. 21.1 per cent), with burns occurring mostly on the hands. Only 21.9 per cenf of the burns received the correct first aid after the a~cidenf. 0 2997 Etsevier Science Ltd fir IS El.
Key words: Epidemiology, burns, Spain, population-based study, incidence.
Burns, Vol. 23, No. 4,323-332,1997
Introduction Burns are currently a health problem the importance of which is determined by its magnitude, its indivi- dual significance, its particular risk factors, vulnera- biiity’*2 and its cost both socially and to the individual and family. Consequently, prevention is equally the best treatment for slight burns as weIl as serious burns because both constitute a health-care problem, some by their seriousness, others by their sheer numbe?.
The absence of adequate recording systems implies a loss of information which may be signifi- cant for research in this field.
Most of the available data concern patients who request medical attentian (out-patients or in-pati- ents), but most accidents are slight and require no
more than self-care. Therefore unless medical assist- ance is requested, the accidents escape our statistics. Friction burns are an example5, since many are treated in other departments (orthopaedics, etc.) this, added to the codification problem, causes them to be underestimated. The importance of such information for the establishment of preventive measures has been demonstrated by many author@.
Most of the data that are published lack common denominators and there exists a scarcity of such data, both nationally and internationally. In the same way that the true frequency of burns in our environment is not known, neither are the personal, family, social and env~onmental conditions of the persons who suffer them, essential knowledge for the control of every illness and the starting point necessary for the introduction of any preventative regime”‘. The present study was carried out with the objectives of quantifying the magnitude of the problem in our environment, estab~hing the epidemiologic al variables of person, place and time, determining the most important aetiological types, places and agents, and evaluating first aid therapy for burns.
Patients and methods As working material, a total of 1746 persons of the province of Malaga were used, which allowed us to study 500 families, of which 421 were urban and 79 rural. They were interviewed in their houses using family surveys.
The survey was directed at the housewife as being the most available {more time at home) and the person who was, perhaps, better able to remember family accidents.
The scope of our survey refers to the population of the province of Malaga who reside in family dwellings and which comprises 1166891 inhabitants9. Those lacking a family home (5 per cent of the population) were excluded from the sample, and we do not believe that this influenced final results.
Following the most accepted criteria for this kind of survey, we used a three-stage, stratified sampling “‘-12. In the first stage the primary units were the municipalities, divided into two strata denomi-
3% Bums: Vol. 23, No. 4# 1997
nated urban and rural. The variable in the stratifica- tion was the number of inhabitants per municipality, those with less than 10000 inhabitants being considered rural, and those with more than that number considered urban.
In the second stage we selected sections from the census whose size and shape gave them homogeneity of families in residence; at the same time they were easier for the interviewer to visit.
Finally, in the third stage, the houses were selected as basic units; all the persons resident in the house being taken together as a unit of analysis, thus not introducing any subsample. This decision was based on two considerations: on the one hand the methodological difficulties which confine surveys directed at individual elements, in which it is difficult to avoid losing the more mobile population groups, this becomes translated into the appearance of signi- !$cant slants or biases on the estimations; on the other hand, economic factors.
In this way the possible loss of precision due to the existence of interfamily correlation has been amply compensated for by the greater sampling dimension granted by this design10~12.
The sampling size (1746 persons, 500 families) was calculated for P=O.l (obtained from a previous study, performed with a similar methodology), alpha = 0.05 and error or accuracy, 0.01413.
The affixing procedure, i.e. distribution of the sampling size between the two strata, determined that subsamplings were obtained from 421 families of the urban stratum and 79 families of the rural stratum.
Inside each stratum, the muni~pa~ties that formed part of the sample were random selections, with probab~ities proportional to the number of inhabitants of each municipality at the last census. Equally, the census sections of each municipality were selected randomly with probabilities propor- tional to the number of inhabitants. In this way, self- balanced estimations1o,‘2 were obtained for each of the two strata, without the need to use elevation coefficients to obtain the corresponding estimations.
Inside each section a mixed method was used to select the dwellings or households. In those cases where we had access to the municipal electoral or census rolls, the households were selected by a systematic sampling procedure with a random starting point or base, and a period of the inverse fraction of the sampling. In those cases where, for different reasons, the census was not available, we proceded to select the households by the procedure of random rounds (or visits inside the section).
There are no statistically significant differences between the characteristics of the sample and those of the population they came from (Table I).
A family interview-survey, typical of the social sciences, was applied, in which data were collected about the person, the household, family appearance, risk factors related to burns and the location and extent of the burn. These data were collected by two interviewers, trained for this objective.
Table I. Sociodemographic characteristics
Variable
Gender Male Female
Age o-5 6-15 16-29 30-64 >64
Education Hliterate School High school University
Marital status Single Married Widowed Others
General population Sample lper cent) lper cent)
47 47 53 53
8.8 5.3 18.1 14.0 25.4 28.0 38.4 40.5
9.8 12.2
7.1 9.0 55.1 63.1 11.8 19.1
5.4 8.7
49.2 46.8 44.3 43.9
5.3 8.1 1.0 1.2
Personal info~ation has been classified in accord- ance with that of the population census, except profession, for which we used the two-digit list of the National Occupations Classification of the National Institute of Statistics.
For burn definition we followed KirschbaumX4. For burn classification we used Hildanus’s classic first- second- and third-degree burns, since it was easier for the housewife to determine if the bum produced a reddening of the skin, a blister or the destruction of tissue, whereas other classifications require profes- sional judgement.
The presence of signs and/or s~ptoms connected with the act of burning oneself was considered as a case.
The question was formulated in the following manner: “Between September of last year and August of this year, did you or any member of your family burn yourself with . . .?“, then suggesting a list of possible causes to the housewife.
The epidemiological-statistical analysis of the urban and rural populations was carried out by means of the descriptive statistical analysis of person, place and time. In the case of quantitative variables we used the Student’s t-test, or the Mann-Whitney U test if there was no homogenei~ of variance. In the case of discrete or qualitative variables, we used the Chi-squared test with the Yates correction, or the Fisher exact test.
The SAS information package of statistical and epidemiological applications was used for this study’?
We established a period of reference of 1 year from I September 1991 to 31 August 1992, but gave consideration to the influence of possible variables (sampling errors and memory).
Results The total number or burns that occurred in our sample during 1 year was 506. Of these, 453 occurred
Fernindez-Morales et al.: Epidemiology of burns in Malaga, Spain 325
Table II. Individual and family data
Interviewed families Burn families Studied people Burn persons Burns
Urban Rural Total
421 79 500 92 16 108
1487 259 1746 358 48 406 453 53 506
in an urban environment (28.6 per cent of that population) and 53 in a rural environment (20.1 per cent). There were significant frequency differences in municipal, urban and rural environments (P < 0.0004) (Table II).
The 506 burns were in 406 persons, thus the number of burns per person burned is 1.25. Eighteen and a half per cent of the population surveyed had burned themselves only once (79.6 per cent of the burnt persons) and 4.8 per cent had burned themselves more than once (20.4 per cent of burnt persons) (P < 0.0001). These differences were main- tained for the strata considered (P < 0.003).
It is more usual to find more than two burns in a family than one or two (kO.003) (Table 111).
More mothers burned themselves (36.8 per cent) than other members of the family (23.8 per cent) (P<O.OOOl). Besides this, more mothers in the urban environment burned themselves than in the rural environment (P < 0.0006).
The greatest frequency of burns was found in the adult population aged 16-64 years, with significant differences with respect to ages greater than 64 years (P<O.OOOl), and to infants and juveniles up to 15 years of age (P <O.OOOl). These differences were maintained in the urban (P <O.OOOl) and the rural (P ~0.05) populations (Table IV).
Burns were more frequent in women than in men (P <O.OOOl), and more women in the urban environ- ment burned themselves than in the rural environ- ment (P-cO.001) (Table IV).
Married persons burned themselves more (33.2 per cent) than the rest of the population (P<O.OOOl).
Table III. Burn frequency by burn family
Urban Rural
1 33 5 2 19 6 >2 40 5 Total 92 16
Total
38 25 45
108
Table IV. Age and gender distribution
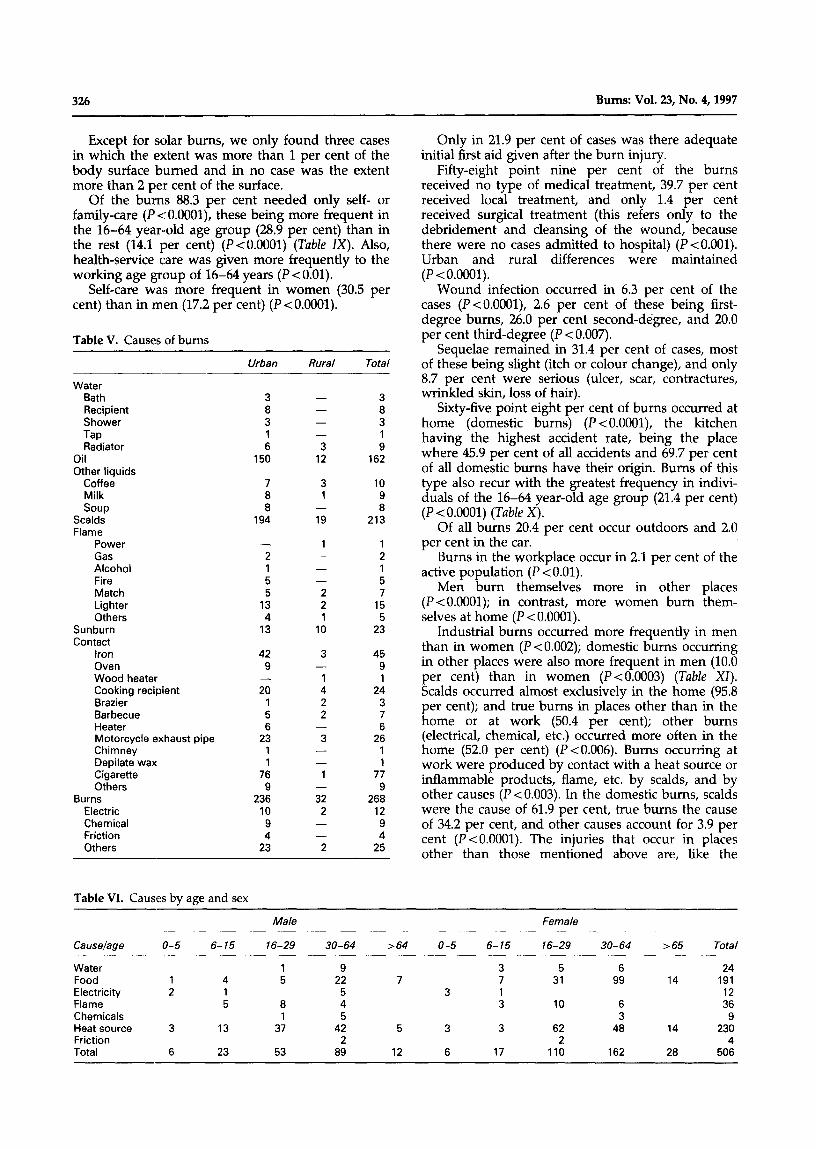
We found that the frequency of true burns (53.0 per cent) was greater than that of scalds (42.1 per cent) and other burns (4.9 per cent) (P < 0.007), with a similar distribution in the urban (P-K 0.03) and rural environments (Table V).
The most frequent aetiological agent in burns involving hot liquids was cooking oil, which was responsible for 76.1 per cent of these (P< 0.0001). Next in frequency were other liquids (12.7 per cent) and hot water (11.3 per cent). Cooking oil alone was the cause of 32.0 per cent of all the burns encoun- tered in our study.
Among the other burns, the most frequent cause was contact with a heat source (78.0 per cent), followed by cases involving inflammable products and flame (13.4 per cent) and then solar burns (8.6 per cent) (P<O.OOOl). In patients younger than 16 years of age, burns predominated (57.7 per cent) over scalds (28.9 per cent) (PcO.003) and over other types of burns (P<O.OOOl). The domestic smoothing iron was responsible for 16.8 per cent of cases, motorcycle exhaust pipes for 9.7 per cent and cooking recep- tacles for 9.0 per cent (Table VI).
In the 16-64 year-old age group, true burns also predominated (52.4 per cent) over scalds (43.3 per cent) (P<O.O08) and over other causes (4.4 per cent) (P <0.0001).
From ages 16-29 years, burns predominated whilst in the remainder of the working age groups (30-64 years) scalds were more frequent.
In men, true burns (63.9 per cent) were more frequent than scalds (27.3 per cent) (P<O.OOOl) and other types of burns (8.7 per cent).
There was a predominance of scalds in females over males (16.9 vs. 5.8 per cent) (P <O.OOOl).
Eighty-five point five per cent of the scalds and 85.6 per cent of the burns which befell women occurred in the 16-64 year-old age group (P<O.OOOl).
The type of burn which requires most medical attention is that of ‘other burns’ (40.0 per cent of cases), followed by scalds (12.1 per cent) and then true burns (8.6 per cent) (P <O.OOl).
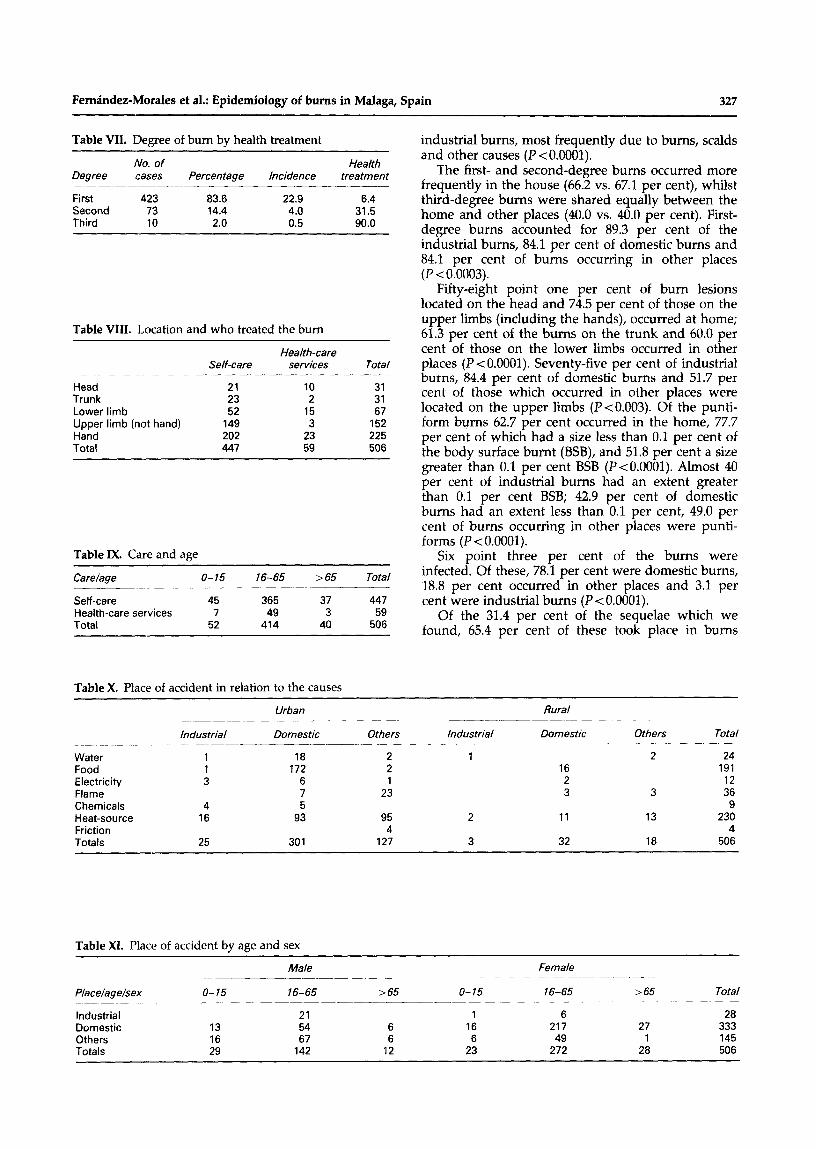
Eighty-three point six per cent of the bums were first-degree, 14.4 per cent second-degree, and 2.0 per cent third-degree (P < 0.0001) (Table VII).
Accidents occurred more frequently to the hands and fingers (44.7 per cent) than to the rest of the body areas considered (P~O.001) (Table VIII). Of all the burns, the greatest frequency corresponded to the lesions which we denominated puntiform (41.9 per cent), like those that occur through the splash of a drop of liquid or the sparks from a lighted cigarette.
Male Female Total
o- 15 16-64 >64
Urban Rural Urban Rural Urban Rural Total __- ~-__
26 3 120 22 IO 2 183 21 2 250 22
31 2 323
47 5 370 44 4 506
326 Bums: Vol. 23, No. 4,197
Except for solar burns, we only found three cases in which the extent was more than 1 per cent of the body surface burned and in no case was the extent more than 2 per cent of the surface.
Of the bums 88.3 per cent needed only self- or family-care (P < O.OOOl), these being more frequent in the 16-64 year-old age group (28.9 per cent) than in the rest (14.1 per cent) (P<O.OOOl) (Table IX). Also, health-service care was given more frequently to the working age group of 16-64 years (P < 0.01).
Self-care was more frequent in women (30.5 per cent) than in men (17.2 per cent) (P<O.OOOl).
Table V. Causes of bums
Water Bath Recipient Shower
Tap Radiator
Oil Other liquids
Coffee Milk soup
Scalds Flame
Power Gas Alcohol Fire Match Lighter Others
Sunburn Contact
Iron Oven Wood heater Cooking recipient Brazier Barbecue Heater Motorcycle exhaust pipe Chimney Depilate wax Cigarette Others
Burns Electric Chemical Friction Others
Urban Rural Total
3 8 3 1 6
150
- - - 3 12
3 1 9
162
7 3 10 8 1 9 8 - 8
194 19 213
- 1 1 2 - 2 1 - 1 5 - 5 5 2 7
13 2 15 4 1 5
13 10 23
42 9
-
20 1 5 6
23 1 1
76 9
236 10
9 4
23
3 -
1 4 2 2
-
3 - -
1 -
32 2
- -
2
45 9 1
24 3 7 6
26 1 1
77 9
268 12
9 4
25
Table VI. Causes by age and sex
Only in 21.9 per cent of cases was there adequate initial first aid given after the burn injury.
Fifty-eight point nine per cent of the burns received no type of medical treatment, 39.7 per cent received local treatment, and only 1.4 per cent received surgical treatment (this refers only to the debridement and cleansing of the wound, because there were no cases admitted to hospital) (RO.001). Urban and rural differences were maintained (P < 0.0001).
Wound infection occurred in 6.3 per cent of the cases (P <O.OOOl), 2.6 per cent of these being first- degree bums, 26.0 per cent second-degree, and 20.0 per cent third-degree (P < 0.007).
Sequelae remained in 31.4 per cent of cases, most of these being slight (itch or colour change), and only 8.7 per cent were serious (ulcer, scar, contractures, wrinkled skin, loss of hair).
Sixty-five point eight per cent of bums occurred at home (domestic burns) (P<O.OOOl), the kitchen having the highest accident rate, being the place where 45.9 per cent of all accidents and 69.7 per cent of all domestic burns have their origin. Burns of this type also recur with the greatest frequency in indivi- duals of the 16-64 year-old age group (21.4 per cent) (P < 0.0001) (Table X).
Of all burns 20.4 per cent occur outdoors and 2.0 per cent in the car.
Burns in the workplace occur in 2.1 per cent of the active population (P < 0.01).
Men burn themselves more in other places (P <O.OOOl); in contrast, more women burn them- selves at home (P-cO.0001).
Industrial bums occurred more frequently in men than in women (P<O.O02); domestic bums occurring in other places were also more frequent in men (10.0 per cent) than in women (P<O.O003) (Table XI). Scalds occurred almost exclusively in the home (95.8 per cent); and true burns in places other than in the home or at work (50.4 per cent); other burns (electrical, chemical, etc.) occurred more often in the home (52.0 per cent) (P ~0.006). Bums occurring at work were produced by contact with a heat source or inflammable products, flame, etc. by scalds, and by other causes (P < 0.003). In the domestic burns, scalds were the cause of 61.9 per cent, true burns the cause of 34.2 per cent, and other causes account for 3.9 per cent (P <O.OOOl). The injuries that occur in places other than those mentioned above are, like the
Causelage
Water Food Electricity Flame Chemicals Heat source Friction Total
Male Female
o-5 6-15 16-29
1 1 4 5 2 1
5 8 1
3 13 37
30-64 >64 o-5 6- 15 16-29 30-64 >65 Total
9 3 5 6 24 22 7 7 31 99 14 191
5 3 1 12 4 3 10 6 36 5 3 9
42 5 3 3 62 48 14 230 2 2 4
89 12 6 17 110 162 28 506 6 23 53
Femhdez-Morales et al.: Epidemiology of bums in Malaga, Spain 327
Table VII. Degree of burn by health treatment
Degree
First Second Third
No. of cases
423 73 10
Percentage Incidence
83.6 22.9 14.4 4.0 2.0 0.5
Health treatment
3% 90.0
Table VIII. Location and who treated the burn
Self-care Health-care
services Total
Head 21 IO 31 Trunk 23 2 31 Lower limb 52 15 67 Upper limb (not hand) 149 3 152 Hand 202 23 225 Total 447 59 506
Table IX. Care and age
Car e/age o-15 16-65 >65 Total
Self-care 45 365 37 447 Health-care services 7 49 3 59 Total 52 414 40 506
Table X. Place of accident in relation to the causes
industrial burns, most frequently due to burns, scalds and other causes (P <O.OOOl).
The first- and second-degree burns occurred more frequently in the house (66.2 vs. 67.1 per cent), whilst third-degree burns were shared equally between the home and other places (40.0 vs. 40.0 per cent). First- degree burns accounted for 89.3 per cent of the industrial burns, 84.1 per cent of domestic burns and 84.1 per cent of burns occurring in other places (P <0.0003).
Fifty-eight point one per cent of burn lesions located on the head and 74.5 per cent of those on the upper limbs (including the hands), occurred at home; 61.3 per cent of the burns on the trunk and 60.0 per cent of those on the lower limbs occurred in other places (P-~O.0001). Seventy-five per cent of industrial burns, 84.4 per cent of domestic burns and 51.7 per cent of those which occurred in other places were located on the upper limbs (P<O.O03). Of the punti- form burns 62.7 per cent occurred in the home, 77.7 per cent of which had a size less than 0.1 per cent of the body surface burnt (BSB), and 51.8 per cent a size greater than 0.1 per cent BSB (P<O.OOOl). Almost 40 per cent of industrial burns had an extent greater than 0.1 per cent BSB; 42.9 per cent of domestic burns had an extent less than 0.1 per cent, 49.0 per cent of burns occurring in other places were punti- forms (P < 0.0001).
Six point three per cent of the burns were infected. Of these, 78.1 per cent were domestic burns, 18.8 per cent occurred in other places and 3.1 per cent were industrial burns (P < 0.0001).
Of the 31.4 per cent of the sequelae which we found, 65.4 per cent of these took place in burns
Water Food Electricity Flame Chemicals Heat-source Friction Totals
Urban Rural
Industrial Domestic
1 18 1 172 3 6
7 4 5
16 93
25 301
Others
2 1 2 16 1 2
23 3
95 4
127
Industrial Domestic
2 11
3 32
Others Total
2 24 191
12 3 36
9 13 230
4 18 506
Table XI. Place of accident by age and sex
Place/age/sex
Industrial Domestic Others Totals
o-15
13 16 29
Male _-_---.-
16-65 265
21 54 6 67 6
142 12
o-15
1 16 6
23
Female
16-65
6 217
49 272
>65
27 1
28
Total
28 333 145 506
328 Burns: Vol. 23, No. 4,1997
occurring in the home, 23.3 per cent in burns occur- ring in other places, and 11.3 per cent in those occur- ring in the work place (P c 0.0001).
Sequelae remained in 64.3 per cent of the indus- trial burns (PcO.03). No sequelae remained in 68.8 per cent of domestic burns or in 74.5 per cent of burns occurring in other places (P < 0.0001).
Discussion General frequency The health-care and social problem of burns in our community represents a subject of great epidemio- logical interest when it affects, according to our study, 23.3 per cent of the population; as there is usually no request for health-care assistance due to its limited clinical importance, there is even a great ignorance that the problem exists.
In this community of 1166 891 inhabitants, 271885 persons burn themselves each year.
This is the highest burn frequency of all those found, 10.1 per cent higher than a population study in GranadaI and much higher than the others found in the literaturelam. This is due to the fact that throughout our survey we came across burn pathology that did not receive health-care attention and thus was not included in any recording system.
Specific frequency per municipality The descriptive epidemiological analysis detected a higher risk of burn accidents in the urban environ- ment than in the rural environment, at a ratio of 1.3:1. This data agrees with that of Granada and of Salamanca. The authors of these latter studies explain it by the difference in accessibility of the health-care services2,17. Our data is in disagreement with other Andalusian findings, and with the findings of Sorensen, in whose opinion there exists little differ- ence in the incidence of burns per municipality in developed countrieP’. It is also contrary to that indicated by the American population requiring admission to hospitaP2. In that data the incidence of burns in the rural population is 1.5 times that of the urban population.
Frequency of bums requiring health-care treatment The 11.7 per cent of the total injuries that required health-care treatment is lower than that found in Granada17, 9.0 times greater than the general inci- dence for CopenhagerP and 9.3 times that of other authors for the same city, in a prospective study which collected all the burns studied during 1 year”.
The slight nature of the burns found in the present study has meant that none required hospital- ization, whereas, in other studies, between 8 and 10 per cent of the cases have required medical attention7+27.
Age In relation to age, the 16-64 year-old age group is most at risk (81.8 per cent of the burns and 2.8 per cent of the population sampled). Similar data was collected in Spain for the provinces of Granada,
Bilbao and Valencia, and also for countries like Denmark and the USA7,*7,19,2*,28,29.
The ages for which most medical attention was requested were those of the adult or worker (74.8 per cent), whereas other authors have found that this occurred most frequently at the extreme ages of life, especially in the first four years27,30,31.
Sex Sex strongly influenced the risk of injury, since the burn frequency in women was 33.0 per cent vs. 21.1 per cent in men. The study found male predomi- nance during infancy and adolescence (55.8 per cent) in agreement with several authors24,3LX, and female predominance in the rest of the age groups studied, which also coincides with other studies.
Both scalds and burns are more frequent in women than in men. Male predominance was found only in the group of other types of burns. These data coincide with that of the GranadaI population study, but are contrary to those indicated by the rest of the authors studied2,7,24,4”.
Marital status From our bibliographic review we gathered that married people are generally least affected by burn accidents; nevertheless, in our study we found a higher frequency among married people due to the slightness of the injuries and to the fact that the kitchen was the place where most accidents occurred.
Causes The accidents collected in our study show that burns predominate over scalds. This data agrees with some authors27 but differs from others who found a predominance of scalds2,“,35,s, or, at most, a similarity between both7,37,38. The frequency of burns found is greater than the 24.6 per cent described for HaberaB5 and lower than the 57.0 per cent indicated for MirabeP. With regard to, burns, the prime cause was contact with hot surfaces, which agrees with results from other researchers2,7,‘9,“.
Contact with exhaust pipes was a frequent cause of burns, and in places where the motorcycle was a common means of transport, it could reach 15.8 per cent of all the causes%. Heating appliances (braziers, heaters, barbeques), flames, ignition of liquids or gases and explosions have been named by some authors as the most frequent causes of true burns34,39, but they had little relevance in our study. Neverthe- less, cigarettes were responsible for 28.7 per cent of the (true) burns.
Solar burns were a frequent cause of out-patient treatment, but not of hospital admission. The 8.6 per cent we found was lower than the 11.0-11.7 per cent described by some researchers7,%, but much greater than the 1.0 per cent indicated by others2. There are significant geographical variations in the studies which explain the variation in the incidence of these burns.
Femhdez-Morales et al.: Epidemiology of burns in Malaga, Spain 329
In the scalds, the most frequent cause was cooking oil, data which coincide with the Granada study17, although other authors have put this cause in second place, behind hot liquids and steam (which in our study were responsible for only 24.0 per cent of scalds). This enormous incidence of cooking oil burns is much greater than that found in our review of the bibliography, owing to the enormous frequency with which this aetiological agent causes injuries which only require self-care or family care, thus escaping the accident recording systems.
Electrical burns, were the third most frequent (behind burns and scalds), coinciding with the data from Mirabetl’. In other European studies%, these burns were more frequent.
The frequency of chemical burns was 1.8 per cent (of all cases) which is lower than that found for all Spain (of 2.7 per cent)2 or that of between 5.6 per cenP and 6.2 per cenP for other European countries, and 14 per cent for the USA.
Causes by age In the under-16s, true burns predominate, which coincides with Galvez” but which disagrees with other authorP’. In young adults, 16-29 years of age, true burns also predominate, as in the Granada study17, but contrary to that indicated by other researchers27.42,43 who found a higher frequency of scalds. In the remainder of the working age group, 30-64 years of age, scalds predominate, in agreement with observations by other authors17,4M5. In patients aged over 64 years there is similarity in the frequency of scalds and true burns. Nevertheless, the slight scald predominance coincides with results from other authors’7,Z7.
Causes and health-care attention The type of burn which required most medical atten- tion was other burns (40 per cent of cases), followed by scalds (12.1 per cent) and then true burns (8.6 per cent). This contrasts with Van Rijn et al.2” who indicated that scalds absorb the greater part of medical assistance in every age group except the adult group in which contact burns predominateZO.
Degree Six point four per cent of first-degree burns required medical attention. These figures are much higher than those found in our review of the literature. The nearest are 3..3 per cenP and 1.7 per cenP. Thirty- one point five per cent of second-degree burns received medical treatment. In the Granada studyI there appeared to be 47.8 per cent of second-degree burns (4.8 per cent of the persons at risk), of which 27.9 per cent required health-care treatment. Ninety per cent of third-degree burns required medical attention. This number is lower than the 92.6 per cent recorded by Galvez17. The type of burns acci- dents which caused the greatest frequency of third- degree burns were other burns (8 per cent), with lower percentages for scalds (2.3 per cent) and burns
(1.1 per cent). These data do not coincide with those of Granada17, where nearly half of third-degree lesions occurred in true burns.
Location The hands and the rest of the upper limbs were the most frequently affected corporal parts in 74.7 per cent of cases, data with which all researchers are in agreement.
Extent In the studies based on population or hospital out-patient records, the majority of burns affect only small areas of the body. In the present study we found that 41.9 per cent of puntiform burns and 98.8 per cent of all cases did not exceed 1 per cent of the body surface, proportions higher than the 94.5 per cent and the 63 per cent described by other authors17,44. Studies based on hospital out-patient records found that 18.6 per cent of burns do not exceed 1 per cent and 52.1 per cent affect less than 2 per cent of the body surface (vs. 100 per cent in the present work)2.
Scalds were less extensive than burns, which agrees with findings of other authors17*47+8.
First therapies Appropriate first aid methods are those which attempt to eliminate the continuity of the skin contact with the damaging agent. These measures would involve application of copious amounts of cold water, application of specific neutralizers, rolling oneself around on the floor, wrapping oneself in a blanket etc., according to the type of accident being dealt withX7.
Although the majority of the burns in our environ- ment originated in the house where there is cold water readily available, only in 21.9 per cent of the cases was an adequate first aid action performed. These percentages are lower than others reported, 41.2 per cent” and 48 per centg9.
Place of accident It was observed that 65.8 per cent of accidents took place in the house. This predominance of domestic accidents is generally accepted by the community of burn workers. Inside the house, the place of maxi- mum risk was the kitchen where 69.7 per cent of domestic burns originated as well as 45.8 per cent of all burns found in this study. Only 30.3 per cent of domestic accidents take place in the rest of the house, in order of frequency these are the living room (17.4 per cent), bedroom (7.8 per cent) and bathroom (5.1 per cent). These results are very similar to those of Granada17, where the kitchen was respon- sible for 70 per cent of domestic burns and 50.3 per cent of all burns produced; the rest of the house was responsible for 30 per cent of the remaining accidents.

330 Bums: Vol. 23, No. 4,1997
Tweny-eight point seven per cent of burns were produced away from home or work; 20.4 per cent of these occurred in the street. The latter percentage is greater than the 9.8 per cenP, 15.7= and 5 per cenP found by other authors. Accidents related to motor vehicles were found in 20 per cent of all cases, a percentage lower than the 30.4 per cent also described for Spain’. The percentage involving indus- trial accidents in relation to the total number of burns found was 5.5 per cent. We found data in the litera- ture which coincided”, were superioF1 and inferior’7.2’.
Place and age Children under 16 years of age burnt themselves more often in the home. These data are lower than that of 60.8 per cent found by other authorP. In the home, children burnt themselves mainly in the kitchen (4.2 per cent of the patients at risk), which is in agreement with the majority of other publica- tions5s55. Other authors draw attention to the danger represented by the kitchen in the first years of the life of the child, emphasizing the need to establish preventive measureP.
In adults aged 16-64 years inclusive, domestic accidents were still the most frequent, these data are coincident with other authors%. The majority of these accidents in people of working age (14.9 per cent of the individuals sampled) took place in the kitchen. This fact has been underlined by some researcherP.
In patients aged over 65 years, we also found that domestic accidents predominated. Other authors have found similar percentageF7. The vast majority of burns found in patients older than 65 years of age were produced in the kitchen.
Place and sex Men burnt themselves more in places other than the home or workplace; women, by contrast, burnt themselves more at home than at other places and at work. In domestic accidents females predominate over males which disagrees with most of the publica- tions we viewed2y~X~4x~ho, where a greater frequency of burns was found in males. Industrial burns were more frequent in males than in females which is similar to that mentioned by other authors17,5R, and inferior to the enormous masculine predominance indicated by others5’. Males predominated over females in burns occuring in other places, which coincides with the majority of results pub- lishedl4,24.34,45,4”.“)
Place and causes Scalds and other types of burn occurred predomi- nantly in the home, true burns in other places. There is agreement between this latter result and the nearly 60 per cent of burns occurring away from the home4R,54. In domestic accidents, scalds were the cause of 61.9 per cent of cases. Similar data were found in other studiesh,“6.45,4”,h’. A type of scald to
which some authors call our attention is caused in elderly patients by hot tap wateP7. In our study we found only one case originating from hot tap water.
In industrial accidents there is a predominence of burns over the rest of causes, which agrees with some investigators17,58,62, but is in disagreement with others63, who found that scalds predominated.
Burns which occur in places other than the afore- mentioned, were caused, likewise for industrial burns, by true burns. These data are higher than that found by some researchers17,48,5*,60,~4.
Of all the accidents found in this study 1.8 per cent occurred in the street, as did 4.2 per cent of the scalds caused by hot liquids from car radiators. This typical scald, which takes place outside the home has been highlighted by some researcherPs”.
Limitations of the research Because the interview was directed at the housewife and the majority of the burns were slight, there is the possibility of respondent bias. It is easier for the housewife to remember her own wounds than those suffered by the rest of the family. The existence of this bias could exaggerate the female predominance and the higher incidence of burns in the house, especially in the kitchen.
In conclusion, the results suggest the following.
(1) The health and social problem of burns repre- sents a subject of great epidemiological interest since it affects 23.3 per cent of our population. There is even a great ignorance of the existence of these problems as there is usually no request for medical assistance.
(2) A higher risk of accidents was detected in urban areas than in rural areas, at a ratio of 1.3 : 1.
(3) The accidents collected in our study belong predominantly to scalds and true burns with predominance of the latter. Analysis of their causes showed hot cooking oil as the principal cause of scalds, and contact with a heat source as the principal cause of true burns.
(4) In relation to where the accidents happen, burns occur most frequently in the house, followed by the street and other places, then the workplace. In the home, the kitchen, followed by the dining room and the bedroom, are the areas of highest risk for accidents.
(5) Sex and age strongly influence risk, since in women the burn frequency was 33 per cent vs. 21.1 per cent in men. With relation to age, the 16-64 year- old age group is at most risk. When the two variables are related, in the age groups of 16-64 years and over 64 years, accidents to women predominate over men.
(6) The body area most affected is the hand. It is important, therefore, to establish preventive measures directed at protection of the hand and achieving the correct first aid therapy.
(7) Only a small proportion of patients made the correct initial first aid measures. It is advisable to inform the population about the benefit of such
Femindez-Morales et al.: Epidemiology of bums in Malaga, Spain 331
measures by means of preventive, informative programmes.
References 1 O’Ya H, Ohmori S. Most burns are preventable. Burns 1979;
5: 8-11.
2 Borrego Galan A, Nunez Serrano A. Estudio clinic0 epide- miolbgico de las quemaduras leves y moderadas en una consulta externa de cirugfa plastica y quemados. Rev& de Salud Pliblica de Castilla y Leo’n 1987; 2: 101-106.
3 Dulanto F. Dermatologfa mMico quirtirgica. Granada: Anel SA, 1981.
4 Sorensen B. Prevention of burns and scalds in a developed country. 1 Trauma 1976; 16: 249-258.
5 Langley 1. Description and classification of childhood burns. Burns 1984; 10: 231-235.
6 Langley J, Silva PA. Childhood accidents involving the electric jug-options for prevention. Burns 1981; 7: 286-290.
7 Glasheen WI’, Attinger EO, Anne A, Boyd DR, Ruffin W, Haynes BHiebert JT, Edlich RF. Epidemiology of minor burn injuries. Bums 1982; 8: 423-432.
8 Mackay A, Rothman KJ. The incidence and severity of burn
9
10 11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
injuries following project burn prevention. Am ] Public Health 1982; 72: 248-252. Instituto National de Estadistica. Censo de poblacidn de Espafia de 1.981. Nomenclator. Provincia de Malaga, Madrid: INE, 1984. Kirsh L. Muestreo de encuestas. Mejico: Trillas, 1982. Lininger CA, Warwick DP. La encuesta por muestreo: teoria y prrictica. Mejico: Continental, 1984. Sanchez Crespo JL. Muestreo de poblaciones fir&as aplicado al diselio de encuestas. Madrid: INE, 1973. Azorin Poch F. Curso de muestreo y aplicaciones. Madrid: Aguilar, 1972. Mirabet IV. Quemados. (Manual practice) Valencia: Quiles, 1979. SAS/STAT User’s Guide. NC: SAS Institute INC., 1990. SAS Logistic. User’s Guide. NC: SAS Institute INC., 1990. Galvez AL. Estudio epidemiologico de las quemaduras en la provincia de Granada. Thesis doctoral, Granada, Facultad de Medicina, 1989. Lyngdorf I’. Epidemiology of severe burn injuries. Burns 1986;12:491-495.
Lindblad BE, Terkelsen CJ, Christensen H. Epidemiology of domestic burns related to products. Burns 1990; 2: 89-91.
Van Rijn OJL, Grol MEC, Bouter LM, Mulder S, Kester ADM. Incidence on medically treated burns in the Nether- lands. Burns 1991;5:357-362.
Rioja LF, Alonso PE, Soria MD, Redondo A, Cruz J, Haro J. Incidence of emberburns in Andalucia (Spain). Burns 1993; 3: 220-222.
Feck G, Baptiste MS. The epidemiology of burn injury in New York. Public Health Rep 1979; 94: 312-318.
Sorensen 13, Thomsen M. Cost of burns in Denmark. Stand 1 Plast Surg 1968; 2: 32-35. Lyngdorf I’, Sorensen B, Thomsen M. The total number of bums injuries in a Scandinavian population-a prospective analysis. Burns 1986;12: 567-571.
Tejerina C, Reig A, Codina J, Safont J, Baena P, Mirabet V. An epidemiological study of burn patients hospitalized in Valencia, Spain, during 1989. Burns 1992; 1: 15-18.
Yamamoto LG, Wiebe RA, Matthews WJ. A one year
27
28
29
30
31
32
33
34
35
36
37
38
prospective cohort of pediatric burns: a proposal for stand- ardizing scald burns. Pediatr Emerg Care 1991; 2: 80-84. Mirabet Ippolito V. Quemados. Jane 1983; 572: 42-90. Bejar Abajas JM, Jul Vazquez C, Alonso Sueiro F, Fernandez Samaniego F, Gabilondo Zubizarreta FJ. Epide- miologia de las quemaduras infantiles. Gazeta Mkdica de Bilbao 1989; 1: 53-60. Tejerina C, Reig A, Codina J, Safont J, Baena P, Mirabet V. Burns in patients over 60 years old: epidemiology and mortality. Burns 1992; 2: 149-152.
Van Rijn OJ, LBouter LM, Kester ADM, Knipschild PC, Meertens RM. Aetiology of burn injuries among children aged O-4 years: results of a case-control study. Burns 1991;
3:213-219.
Mclouglin E, Mcguire A. The causes, cost and prevention of childhood burn injuries. AIDC 1990; 144: 677-683. Lindblad BE, Terkelsen CJ. Domestic burns among children. Burns 1990; 4: 254-256. Cheng JCY, Leung KS, Lam ZCL, Leung PC. An analysis of 1704 burn injuries in Hong Kong children. Burns 1990; 3: 182-184. Sanchez Muros J, Delgado V. Acute thermal dermatitis: an
epidemiology study. J Dermatol Surg Oncol 1980; 6: 821.
Haberal M, Oner Z, Bayraktar U, Bilgin N. Epidemiology of adults and childrens burns in a Turkish burn center. Burns 1987;13:136-140.
Sarto Piccolo N, Sarto Piccolo Lobo M, Sarto Piccolo Daher MT. Two years in burns care, an analysis of 12423 cases. Burns 1991;6:490-494.
Artz CP, Moncrief JA, Pruitt BA. Burns: A Team Approach. Philadelphia: WB Saunders, 1979. Panayotou I’, Alexakis D, Striglis Ch, Ioannovich J. Epi- demiological data on burn injuries in Greece: a statistical evaluation. Burns 1991; 1: 47-49.
39 Lambruschini Ferri N, Ramos Corbella ME, Ortola Casteus ME. Accidentes domesticos en la infancia. Medicina integral 1986; 7: 399-406.
40 Bradshaw C, Hawskins J, Leach M, Robins J, Valiance K, Verboom K. A study of childhood scalds. Burns 1988; 14: 21-24.
41 Larsen J, Gurumurthy, Ghali MT, Hall KV. Admissions to a new burn unit in Gizan, Saudi Arabia. Burns 1987; 13:
286-289.
42 Pegg SP, Mcdonald GP, Tracey-Patte CE, Mayze TD. Epide- miology of burns attending a casualty department in Brisbane. Burns 1983;9:416-421.
43 Delgado Florencio V, Jimenez Aguirre D, Macias Jimenez JP, Pereda Hernandez J, Turegano Fuentes P, Sanchez Muros J. Quemaduras: estudio epidemioldgico 1956-82. Actualidad MMica 1984; 70: 42-48.
44 Auchincloss JM. Survey and retrospective analysis of outpatient burns. Br J Clin Pratt 1975; 29: 251-253.
45 Jay KM, Bartlett RH, Danet R, Allyn PA. Burns epi- demiology: A basis for burn prevention. I Trauma 1977; 17:
943-947.
46 Onuba 0, Udoidiok E. The problems and prevention of burns in developing countries. Burns 1987; 13: 382-385.
47 Agha RB, Benhamala A. Epidemiology of burns in Algiers. Burns 1979; 5: 204-205.
48 Savage JP, Leitch JOW. Childhood burns, A sociological survey and inquiry into causation. Med 1 Aust 1972; 1: 1337-1342.
332 Bums: Vol. 23, No. 4,1997
49 Herd AN, W~ddowson P, Tanner NSB. Scalds in the very young: prevention or cure? Burns 1986; 12: 246-249.
50 Davies JWL. The problems of burns in India. Burns, Suppl 1, 1990.
51 Renz BM, Sherman R. The burn unit experience at Grady Memorial Hospital. ] Burn Care Rehabill992; 13: 426-436.
52 Gupta M, Gupta OK, Goil I’. Paediatric burns in Jaipur, India: an epidemiological study. Burns 1992; 18: 63-67.
53 Lari ARA, Bang RL, Ebrahim MKH, Dashti H. An analysis of childhood burns in Kuwait. Burns 1992; 18: 224-227.
54 Joseph TP, Douglas BS. Childhood burns in South Australia: a socio-economic and aetiological study. Burns 1979; 5: 335-342.
55 Palumbo L, Budin WC. A descriptive summa~ of New Jersey’s 1985 burn population. I Burn Cure Rehub~l 1990; 11: 565-572.
56 Pegg SP, Gregory JJ, Hogan PG, Mottarelly JN, Walker LF. Epidemiological pattern of adult bum injuries. Burns 1979; 5: 326-334.
57 Z&h G, Meissl G, Bayer S, Kyral E. Reduction of the mortality rate in aged burn patients. Burns 1992; 18: 153-156.
58 Lyngdorf F. Occupational burn injuries. Burns 1987; 13: 294-297.
59 Pegg SP, Miller RM, Stricklen EJ, Storie WJ. Epidemiolo~ of industrial burns in Brisbane. Burns 1986; 12: 484-490,
60 Mackay A, Halpern JP, Maclou~~n E, Locke J, Crawford JD. A comparison of age-specific burn injury rates in five Massachusetts communities. Am J Public ~ea~fh 1979; 69: 1146-1150.
61 Green AR, Fairclough J, Sykes PJ. Epidemiology of burns in childhood. Burns 1984; 10: 368-371.
62 Instituto National de Estadistlca. Encuesta de propuestas familiares. Metodologia y resultados. Madrid: INE, 1975.
63 Ross&no1 AM, Locke JA, Burke JF. Employment status and the frequency and causes of burn injuries in New England. J Occ Med 1989; 9: 751-757.
64 Kirkham S. A social survey of thermal injuries in South Australian children. Burns 1979; 5: 199-201.
65 Al-Baker AA, Attalla ME, El-Ekiabi SA, Al-Ghoul A. Car radiator bums: a report on 72 cases. Burns 1989; 15: 265-267.
66 Benmeir I’, Rosenberg L, Sagi A, Ben Yakar Y. Radiator scald burns: a preventable hazard. Burns 1990; 18: 135-136.
Paper accepted 4 November 1996.
Correspondence should be addressed to: Em&a Femhndez- Morales, Paseo de Sancha, no 60, B-3” A, 29016 Malaga, Spain.
Advances in the Therapy of Burned Children
3-4 July 1997
Graz, Austria
For further information, contact:
Marija Trop, Department of Pediatrics, Children’s Burns Unit, Auenbruggerplatz 30, A-8036 Graz, Austria
Tel: -t-43 (0)3X 385 2632 or 2643; Fax: +43 (0)3X 385 3785; e-mail: ma~ja.~op~~uni~az.ac.at