
Cycling injuries and epidemiology - PNZ
28
www.pnz.org.nz ISSN 1179-7967 (Print) ISSN 1179-7975 (Online) THE LATEST NEWS & VIEWS FROM PHYSIOTHERAPY NEW ZEALAND MARCH 2017 PHYSIO MATTERS Cycling injuries and epidemiology Also in this issue: • Effective communication • Professor Pernilla Åsenlöf • ACC integrity services
-
Upload
khangminh22 -
Category
Documents
-
view
5 -
download
0
Transcript of Cycling injuries and epidemiology - PNZ
www.pnz.org.nzISSN 1179-7967 (Print)
ISSN 1179-7975 (Online)
THE LATEST NEWS & VIEWS FROM
PHYSIOTHERAPY NEW ZEALAND MARCH 2017
PHYSIOMATTERS
Cycling injuries and epidemiology
Also in this issue: • Effective communication• Professor Pernilla Åsenlöf• ACC integrity services
cOnTEnTS
2 | PHYSIO MATTERS MARCH 2017
www.pnz.org.nz
Editorial and Advertising
• SendeditorialitemstotheEditor,[email protected]
• LetterstotheEditorarelimitedto250wordsandmaybeedited.
• SendadvertisementsandcourseinformationtoClaireAnglisspnz@physiotherapy.org.nz
• Advertisingratesandspecificationsareonourwebsite.
• Deadlineforeditorialandadvertisingbookingisno later than 20th of the month, two months before the issue is published.Ifthisdatefallsonaweekendoraholiday,pleasesupplybytheclosestworkingdaybefore.
• MembersmayreadPhysioMattersonourwebsiteandfollowworkablelinks.
The Editor reserves the right to edit material for space and clarity, and to withhold material from publication. Individual views expressed in this publication are not necessarily those of Physiotherapy New Zealand. Inclusion of product or service information or of links to external websites does not imply PNZ endorsement of the product, service or website unless specifically stated. Advertising in Physio Matters does not constitute endorsement of a product and no advertiser may use publication of an advertisement in the magazine to support the marketing of every product. While every endeavour is made to ensure the accuracy of information, no responsibility is accepted for inaccurate information.
Booking deadlines
Issue Booking deadline
February2017 12December2016
March2017 20January
April2017 19February
May2017 18March
June2017 20April
July2017 22May
August2017 20June
September2017 20July
October2017 21August
November2017 20September
December2017 20October
Physiotherapy New Zealand
POBox27386,MarionSquareWellington6141Level6,342LambtonQuay,Wellington6011,NewZealand
Phone:+6448016500|Fax:+6448015571
March 2017
PRESIDENT’S COLUMN 3
NATIONAL OFFICE 4
FEATURE: CYCLING AND EPIDEMIOLOGY 5
ACC: WHERE FRAUD STOPS AND WASTE STARTS 9
LEARNING & RESEARCH 10
SCHOLARSHIP 11
ETHICS Q & A COLUMN 12
INTERVIEW WITH PERNILLA ÅSENLöF 14
SIG 16
WEBSITE 18
NEWS IN PICTURES 19
CLAIMS TO ACC OVER THE SUMMER PERIOD 20
TAE ORA TINANA 22
MEMBER STORY: FROM PHYSIOTHERAPIST TO AUTHOR 23
GENERAL NOTICES 24
PROFESSIONAL DEVELOPMENT – CALENDAR 25
CONTACT DETAILS 27

PRESIdEnTS cOluMn
PHYSIO MATTERS MARCH 2017 | 3
Booking deadlines
Issue Booking deadline
February2017 12December2016
March2017 20January
April2017 19February
May2017 18March
June2017 20April
July2017 22May
August2017 20June
September2017 20July
October2017 21August
November2017 20September
December2017 20October
Physiotherapy New Zealand
POBox27386,MarionSquareWellington6141Level6,342LambtonQuay,Wellington6011,NewZealand
Phone:+6448016500|Fax:+6448015571
Presidents Column
LIZ BINNS
PRESIDENTPHYSIOTHERAPY NEW ZEALAND
March is the month that universities are back in full force (and in Auckland the traffic that comes with it!) so I would like to extend a warm welcome to all the undergraduate students who are embarking on their physiotherapy degrees. PNZ was recently involved with the Otago Physiotherapy Students Association camp for incoming second year students. Staff from National office visited the camp to promote PNZ and assist students joining. They also put on a lunch for the students (which was apparently a nice change from sausages and baked beans).
Welcome to the profession and the family of physiotherapists. Although you are not yet qualified or have an annual practicing certificate, you are the junior members of our profession, the bright lights of our future (no pressure!).
Building a Stronger Future
Work is continuing on the Building A Stronger Future proposal for change project. Following the Leadership
Day in March, a number of attendees volunteered to be part of the smaller co-design working group. The first meeting of the group having took place on February 24th. The start point for this group was the key 4 themes that were identified at the November 2016 Leadership day of Liability & Risk (legal & financial); Identity & voice; Asset ownership; Resourcing (during and after the change process). Underlying these 4 themes are much more specific points that need to be considered.
The members of the group are:
•DerekTimmins
•DuncanReid
•KellyDavison
•RebeccaWashbourn
Welcome to the profession and the family
of physiotherapists. Although you are not yet qualified or have an annual practicing
certificate, you are the junior members of our profession, the bright
lights of our future (no pressure!).
•MarkShirley
•LouiseCoughlan
• JeanetteKing
•LeeGardiner
•HamishAshton
•ChrissieRussell
•WendyHill
•KurtThomas
•LizBinns
The size of the group is small to keep discussions manageable so it isnotrepresentativeofeverySIGand Branch, however a larger group which includes a representative from eachSIGandBranchisinvolvedwiththe review process and is actively providing feedback to the smaller working group.
The next co-design meeting is on 24th March. The expectation is that after this meeting, a model of the future structure of PNZ will have been produced and this will then be circulated for wider discussion. The May 2017 Leadership Day will be a key day when representatives ofalltheSIGsandBrancheswillbeable to discuss the proposed model in a face-to-face forum, after which a paper will be circulated to all members.
Liz

nATIOnAl OFFIcE
4 | PHYSIO MATTERS MARCH 2017
You have told us that you want us to have a strong working relationship with ACC and that this is key. It is promising to see this has been reciprocated by
ACC to date.
Inputting to ACC’s Consumer Outlook Group
jOE ASGHAR
CHIefexeCuTIveoffICeRPHYSIOTHERAPY NEW ZEALAND
Well, here we are at the beginning of another year with lots of activity for PNZ on the horizon. I am sure that last year was as flat out for you as it was for the National Office, and I’d like to give a warm welcome to the almost 3000 members to date.As you may know, I have continued tospendtimeworkingwithACCacross a variety of activities that help us remain connected, understand the changing landscape and provide an opportunity to input into plans and projects at an early stage. You have told us that you want us to have a strongworkingrelationshipwithACCand that this is key. It is promising to seethishasbeenreciprocatedbyACCto date. We have already worked with ACCtoprovidememberfeedbackona number of relevant issues and this is something we will continue to do. We are looking to increase our participation and contribution to relevant working groups by bringing physiotherapists with insight and expertise into the mix at an early stage.
For this piece, I thought it might be useful for me to share some insight into the workings and activity of the
voiceoftheCustomer–ConsumeroutlookGroup(CoG).Thegroupis an interesting mix of professional associations (including Occupational Therapy, Orthopaedic Association, TheRoyalCollegeofGPsetc.)andconsumergroupssuchasAgeConcernAssociationforSpinalConcerns,DisabledPersonsAssembly,CarersNZ, Auckland Pacific People and a medical centre. Meetings are roughly every two months and go for a full day with a mix of working sessions and presentations - by the end your head can really hurt! Typically there are 20–30projects/programmesonthego at any one time with timescales for delivery between 12 months and two years.
Making sure contributions and discussion are from the client (not provider) perspective is always a challenge. This is why we come to you, our members, for the feedback clients give to you. The flip side is that the patient groups provide a different but complementary perspective. The real advantage in being there is that we have the opportunity to shape policy and projects as they unfold. We are given insight into the working machine thatisACCandareabletopositivelycontribute.
The most recent meeting was as mixed and diverse as our summer! We kicked offwiththeChiefCustomerofficer(Mike Tully) outlining the strategic directionfortheGroupasitlinkstotheoverall Transformation Programme. We then had a working session user testing ACC’sfirstcutofthenewevolvingwebsitefromavisualdesign/contentlayout perspective. The expectation is thesitewillgolivefromJulythisyear(but you can start to see some changes now at acc.co.nz).
Next up was a presentation and workshoponestablishinganACCledNational Advocacy Service, following the recommendation from a recent review of disputes processes.
The session following this focused on communityinsightsintoACC,withdiscussions from a client perspective about current activities in community settings,whoACCwereseentobeworking with, what appeared to be working/makingadifference,andwhatcould be done.
We ended the day with a working session on the Nursing Service Review that’s in early stages of development. Our job was to test the consumer needsidentifiedbyACCanddevelophypotheses and implications from these. The review team will then go and work up the next step to collect evidence from service clients to form some of the evidence that will inform the review. This work will continue through to March 2018.
Sothereyouhaveit–youmightfindthis fascinating (or as dull as dishwater) but in my view every opportunity to workalongsideACCaddsvaluetoourclients, you as members, and for the profession.
Wishing you all a fantastic and successful 2017.

FEATuRE
PHYSIO MATTERS MARCH 2017 | 5
Cycling and Epidemiology Cyclingisfastbecomingapopularwayofexercisingandgettingaround.With so many people hopping on a bike these days, the specialist knowledge needed to ensure cyclists are looked after is more important than ever.
FEATuRE
FEATuRE
6 | PHYSIO MATTERS MARCH 2017
Cycling and Epidemiology
Recent increases in the proportion of New Zealand adults cycling recreationally and to work, coupled with a growth in the absolute numbers of cyclists, means the increase in associated injuries is keeping physiotherapists busy. That’s without even taking into account competitive cycling.
According to the Accident CompensationCorporation(ACC),bikeinjuries from road cycling and mountain biking are on the increase. This is a reflection of the boom of biking with more opportunities to ride, due to more cycle ways, trails and bike parks.
are ex-runners and rugby players, so even though their joints are worn, they can ride. Add in the development of the country’s cycle trails, as well as the popularity of mountain biking and iron man, and suddenly you’ve got a huge and diverse amount of people getting into cycling.”
Although most bike shops will now offer some form of set-up, this service ismostlyaboutup-selling,Kirstysays.Despite these retailers claiming a scientific basis to their fitting, much of it is marketing hype that wouldn’t make it into any peer-reviewed journal.
Therefore, she sees many patients who were worse off following a “professional fit” at a bike shop. At the end of the day, it is more beneficial and cost-effective for a rider to consult a specialised physio first before spending $300 plus for a fit at the shop, she says.
Kirsty’sexpertiseoncyclingcomesfrom personal as well as professional experience.Kirstyrodeprofessionallyin Europe, competed in five world championships and the 2002 ManchesterCommonwealthGames.ShethenworkedforbothCyclingNZand HPSNZ and was a physio for Bike at London Olympics 2012.
Hamilton based physio and bike mechanicMattClarknotesthatinaddition to poor set-up, incorrectly sized bikes and poor training advice (e.g. amateur riders encouraged to do too much too soon), are also contributing to the increase in injuries.
Physio Matters spoke to physios who have cycled in highly competitive environments and have first-hand experience in dealing with cycle related injuries. They’ve seen things from both sides of the bike.
Men in tights
RotoruaphysioKirstyWalkerhasaninteresting theory on the popularity of cycling and why physios are now having to deal with so many cycling injuries.
Kirstysayscyclingisthe“newgolf”,hence the term MAMILS (Middle Aged Men In Lycra). “Many of these men
Cyclingasamodeoftransport,exerciseandsportisbeneficialforNewZealander’shealth - not to mention reducing the number of cars on our roads. Malcolm Aitken looks at the challenges and opportunities working with cyclists presents.
Kirsty Walker

PHYSIO MATTERS MARCH 2017 | 7
After graduating from physio school (now known as AUT) in 1992, Matt headed off on an extended OE working inboththeuSanduK.Heworkedinanumber of hospitals and sports clinics, treating kids through to older adults. Returning to New Zealand in 1996, he settled in Hamilton and undertook acupuncture training through the Physiotherapy Acupuncture Association of New Zealand. After a four year stint
in Australia, he returned to Hamilton where he is based at a Sports Med Clinic,treatingweekendwarriorsthrough to elite athletes.
When Matt’s not at work, he can be found out on his mountain bike, and even doing the odd race now and again”. He says the longer the race the better, as there is nothing quite like pedalling a bike round and round in circles for 12 or 24 hours!
So many injuries
The most common bike injuries, like with most sports and recreation, involves the knees and the shoulders. With mountain biking specifically, shoulders are the number one injury site.
Kirstyalsoseeswhatshecallsanumber of “grumpy” Achilles heels, necks and lower backs. She believes poor bike set-up and inadequate post-accident physiotherapy have a lot to answer for.
Matt adds that he often sees many nerve compressions and trauma in hands.
Incidentally, head injuries are not as common,butareseriousandACCisactively campaigning to raise awareness of head injuries, including concussion.
Can we fix it? Yes we can!
Matt emphasises that when rehabilitating cyclists, it is important to build up their routine, make sure everything is well set up and not do too much too soon.
Like any training programme, you can increase the workload by 10 percent or you make a number of small changes in their set-up so they can keep their training volume unchanged. Some people tolerate change, and others don’t, he adds.
Trish Wisbey-Roth has very specific ideas on rehabilitation priorities.
A physio with over 20 years’ experience, Trish is well-known for her work around musculo-skeletal problems. Now in New Plymouth, after spending most of her career in Australia, she has completed both a Sports Physiotherapy Masters at theAISCanberraandPostgraduateManipulative Therapy training. She has been an Olympic Physiotherapist
Matt Clark
FEATuRE
8 | PHYSIO MATTERS MARCH 2017
since 1996. Trish also worked closely with the Australian National and NSW cycling squads, having toured withAustralianCyclingfor10yearsnationally, internationally and at Olympic events.
She says rehabilitating stiffness in the hips, thoracic and lumbar spine is important to ensure the lumbar spine can be relatively flat and not held in flexion while cycling. Rehabilitation with tendon specific exercise protocols for any tendinopathy around the hip is crucial, including glut, hamstring or hip
flexor tendinopathy to retrain maximal power performance from the hip.
Trish notes it’s important to remember that in the functional position, the gluteus maximus and medius is generally in a lengthened or outer range position in cyclists, so exercises are needed to work the muscle in that area.
Evidence shows that cyclists have a greater risk of developing osteoporosis due to long hours exercising with no actualimpactoccurring.Gettingcyclistsinto the gym is great for enhancing
overall performance, as well as benefiting the bones.
More than the bike
So, what exercises should cyclists do apart from cycling to maintain their fitness?
Kirstysayshipflexorandquadstretching exercise is of great use, as well as scapular mechanics and thoracic extension mobility.
CorestabilityisvitalforMatt.Herecommends Pilates, stretching or yoga. Additionally he sees value in a conditioning programme aimed at correcting any deficit found during the assessment, probably in the gluteals.
Trishrecommendseccentric/concentricgluteal activity (from hip flexion towards hip extension) as an important exercise to gain maximal power from the gluteals when cycling. After that, she recommends retraining and strengthening of the hamstrings and calves. Thoracic mobility work and eccentric calf strength activity is also worthwhile.
The right start
Bike set-ups are a specialist area within a specialist area. However, this step was considered key by all the physios we spoke to, if one wants to ensure safe and successful cycling of any type.
Kirstyemphasisedthebiomechanicsof the knee, and all three agreed the importance of seat height and correcting the fore and aft positions of the seat was crucial. The handlebar drop was another factor.
There’s a lot physios can learn and do as professionals to reduce the physical risks that go with cycling, and support what is a positive life style choice with a multitude of benefits for both the rider and our society.
Trish Wisbey-Roth
Acc
PHYSIO MATTERS MARCH 2017 | 9
Where fraud stops and waste starts
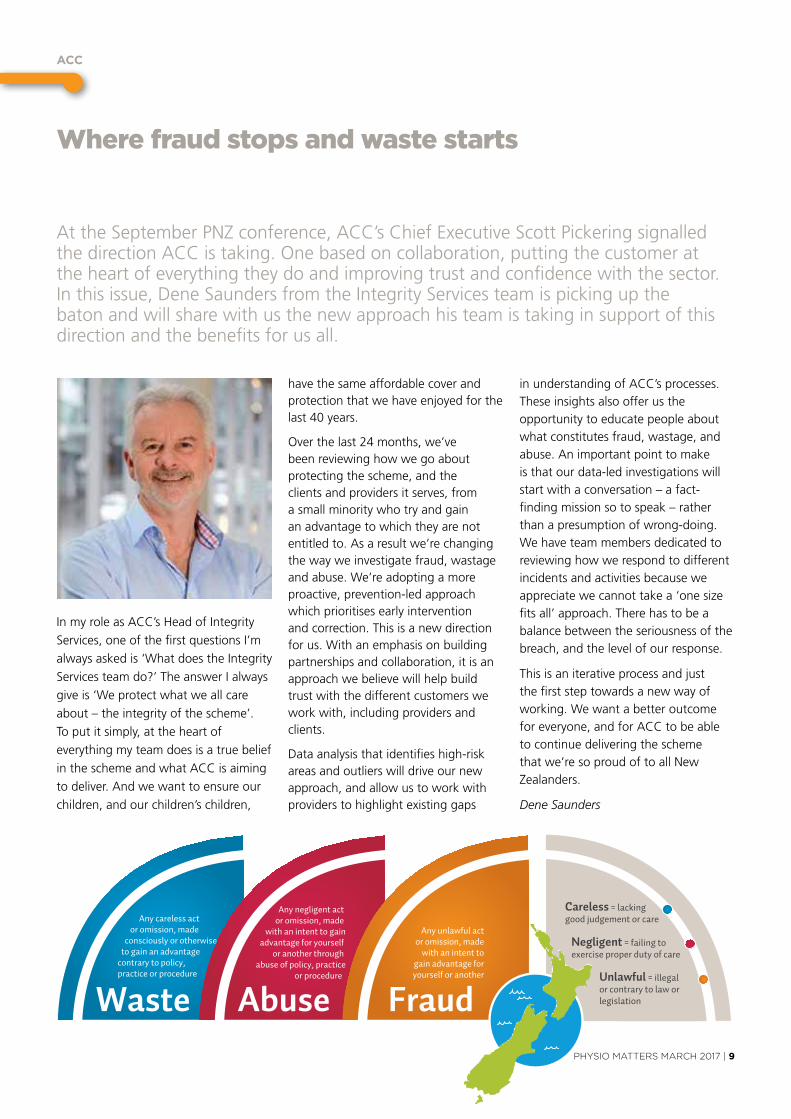
AttheSeptemberPNZconference,ACC’sChiefexecutiveScottPickeringsignalledthedirectionACCistaking.onebasedoncollaboration,puttingthecustomeratthe heart of everything they do and improving trust and confidence with the sector. In this issue, Dene Saunders from the Integrity Services team is picking up the baton and will share with us the new approach his team is taking in support of this direction and the benefits for us all.
InmyroleasACC’sHeadofIntegrityServices, one of the first questions I’m always asked is ‘What does the Integrity Services team do?’ The answer I always give is ‘We protect what we all care about–theintegrityofthescheme’.To put it simply, at the heart of everything my team does is a true belief intheschemeandwhatACCisaimingto deliver. And we want to ensure our children, and our children’s children,
have the same affordable cover and protection that we have enjoyed for the last 40 years.
Over the last 24 months, we’ve been reviewing how we go about protecting the scheme, and the clients and providers it serves, from a small minority who try and gain an advantage to which they are not entitled to. As a result we’re changing the way we investigate fraud, wastage and abuse. We’re adopting a more proactive, prevention-led approach which prioritises early intervention and correction. This is a new direction for us. With an emphasis on building partnerships and collaboration, it is an approach we believe will help build trust with the different customers we work with, including providers and clients.
Data analysis that identifies high-risk areas and outliers will drive our new approach, and allow us to work with providers to highlight existing gaps
inunderstandingofACC’sprocesses.These insights also offer us the opportunity to educate people about what constitutes fraud, wastage, and abuse. An important point to make is that our data-led investigations will startwithaconversation–afact-findingmissionsotospeak–ratherthan a presumption of wrong-doing. We have team members dedicated to reviewing how we respond to different incidents and activities because we appreciate we cannot take a ‘one size fits all’ approach. There has to be a balance between the seriousness of the breach, and the level of our response.
This is an iterative process and just the first step towards a new way of working. We want a better outcome foreveryone,andforACCtobeableto continue delivering the scheme that we’re so proud of to all New Zealanders.
Dene Saunders
ACC physio matters pop out graphic_DCv4D
Totally new layout
Any negligent act or omission, made
with an intent to gainadvantage for yourself
or another through abuse of policy, practice
or procedure
AbuseUnlawful = illegal or contrary to law or legislation
Careless = lacking good judgement or care
Negligent = failing toexercise proper duty of care
FraudWaste
Any unlawful actor omission, made
with an intent togain advantage foryourself or another
Any careless act or omission, made consciously or otherwise to gain an advantage contrary to policy, practice or procedure
lEARnIng And RESEARcH
10 | PHYSIO MATTERS MARCH 2017
The expert opinion: Cases of negligence in cervical spine manual therapy and the updated New Zealand guidelines
In New Zealand there have been cases recently where manual therapy and or manipulation has been involved in the treatment of neck pain where there may have been a relationship with an adverse event such as a stroke according to Professor Duncan Reid from AUT. It is every clinicians’ worst nightmare to undertake a treatment procedure that inadvertently causes permanent harm, or death, to a patient. Unfortunately, adverse events in healthcare do occur. It is a scenario which is devastating for both the patient and the physiotherapist involved in the care.
Duncan provides an expert opinion forACCintreatmentinjuryclaimsagainst physiotherapists related to manual therapy of the neck. As past vice-president of the International Federation of Orthopaedic Manual Therapists (IFOMT) and co-ordination of the musculoskeletal physiotherapy at AUT, Duncan is conscious that improving professional education is a pre-requisite to ensure physiotherapists maintain competence in the management of patients with cervical disorders. This is particularly necessary for clinicians working in areas of increased risk suchasacupunctureandmanual/manipulative therapy.
Duncan points out where therapists involved in negligence cases might have gone wrong.
“Therapists were sometimes missing the new information related to
subjectively identifying the bigger health risk,” explains Duncan.
He notes that investigating the patient’s symptoms, alongside sustained rotation tests of the cervical spine, were the traditional standard, however these are no longer sufficient to evaluate risks of manual therapy to the neck.
Duncan and others have been involved in the development and dissemination of the updated Code of Practice for Cervical Spine Management, which was released by the New Zealand Manipulation Association (NZMPA) in 2016. The new framework has a greater emphasis on investigating a patient’s vascular health.
“Looking at blood pressure, lipids, cholesterol are important, as well as the ability to identify pre-eminent features to a stroke, including alterations to cranial nerve function.”
These subjective and objective markers, alongside features that don’t fit with mechanical neck pain, should raise the clinical index of suspicion of more serious pathology, and influence management of patients with cervical spine pain.
In response to the risks of adverse events with cervical manual therapy, physiotherapy teaching institutions have moved away from the old ‘end of range’ forcible thrusts previously taught, to gentler mid-range physiological techniques. Some therapists may have even moved away from delivering manual therapy to the cervical spine altogether due to the perceived risks. However, Duncan does not want to discount the positive benefits of manual and manipulative therapy to the neck.
“Cervicalmanipulationisausefultool,in
the right patient, on the right day. Lots of things we do as physiotherapists have risk and you just have to manage it.”
When asked for advice about what physiotherapists could do to limit their risk of being involved in a negligence claim, Duncan’s suggestions are to stay current and keep abreast of the literature. AUT and the University of Otago and NZMPA provide postgraduate courses in musculoskeletal physiotherapy.
Reading the new NZMPA Code of Practice for Cervical Spine Management may be a good start to inform decisions around when manual therapy may or may not be appropriate for cervical spine pain. Duncan advises that all physiotherapists should pay special attention to the new code of practice as the Physiotherapy Board have substantiated this document in a Position Statement.
New Zealand is renowned internationally for producing high quality, competent manual therapists. However, manual therapies have been getting increasing challengingpressintheuKandothercountries about their efficacy, particularly around spinal pain, due to the passive nature of the treatment causing disempowerment and dependency.
To listen to an interesting debate held atIfoMT,Glasgow2016ontheefficacyof manual therapy in spinal pain, pleaseseethefollowinglink:http://www.physio-pedia.com/conferences/ifompt/tag/duncan-reid/.Ifyouusemanual therapy within your treatment toolbox for cervical spine pain, reading this document may be vital for you to maintain safe and effective physiotherapy practice.
Written by Nick Clode

ScHOlARSHIP
PHYSIO MATTERS MARCH 2017 | 11
Scholarship Trust Recipients
CongratulationstothefollowingsuccessfulapplicantsoftheScholarshipTrustfund:
Daniel Cury Ribeiro
The efficacy of tailored rehabilitation for patients with shoulder pain: a feasibility randomised controlled trial.
Dr David Rice
Resistance training for hand osteoarthritis: A randomised controlled trial comparing two different forms of training.
Miranda Buhler
Understanding the impact of thumb base osteoarthritis (and the perceptions about interventions such as splints).
Natalie Parlane
Muscle endurance of quadriceps and hamstrings and repeated lower limb function before and after arthroscopic meniscal surgery: a case controlled inter-limb comparison.
Catherine Smith
Developing an intervention to promote physical activity engagement for people with multiple sclerosis living in rural settings: a feasibility study.
CatherineSmithdescribesherresearchproject below:
There is strong evidence for the health and wellbeing benefits of regular physical activity (PA) for people with multiple sclerosis (MS). However, in a previous stakeholder consultation process, we heard that people with MS living in rural communities struggle to engage in PA primarily because of limited PA choices in rural areas.
Our study will combine two different interventions for people with MS living in rural areas: Web-based Physio
(WBP) and Blue Prescription. We want to see if these two interventions complement each other and, whether it is feasible and acceptable to deliver both online. Web-based Physio is an online library of exercises with video demonstrations. It was developed by Dr Lorna Paul and colleagues (Glasgowuniversity)specificallyforpeople with MS. Following an initial face-to-face consultation, programmes can be tailored and modified by the physiotherapist at a distance. Participants can also record exercise experiences in a daily online diary which is monitored by the physiotherapist. In previous studies, we found that although exercise programmes can be tedious, a short tailored programme can help to give people a little more confidence in their ability to exercise (especially when starting out).
After 12 weeks of WBP, the physiotherapist visits the participant face-to-face for a second time
to deliver the Blue Prescription intervention. This involves a collaborative discussion between physiotherapist and participant about ‘physical activity beyond the home exercise programme’. The physiotherapist uses behaviour change tools (including motivational interviewing,goalsettingandif/thenquestionnaires) to elicit discussion from the participant about desired physical activities and how to go about initiating and maintaining these activities.
The Blue Prescription approach was developed by researchers at the School of Physiotherapy and Department of Psychology at the University of Otago. In earlier feasibility studies, we identified that the Blue Prescription approach might be more useful for people who are more confident in their ability to start and maintain new physical activities.
Following face-to-face meetings at the beginning of each study phase, the physiotherapist will stay in touch with participants via Zoom (similar to Skype), online WBP diary, text, email and telephone. We will evaluate the acceptability of the combined intervention through qualitative analysis of interview data with both participants and research physiotherapists. Additional data on quality of life, physical activity levels, anxiety and depression, fatigue, exercise self-efficacy and readiness for physical activity behaviour change will contribute towards our feasibility and acceptability analysis.
Catherine Smith
Catherine Smith
FOcuS On ETHIcS
12 | PHYSIO MATTERS MARCH 2017
Ethics Q & A Column – Effective communication with patients and other service providers
ThismonththeProfessionalStandardsandethicsCommitteeanswersomememberquestions about communication with patients and other service providers.
What are the physiotherapist’s duties to ensure effective communication?
The rights of consumers and the duties of providers under the Code of Health and Disability Services Consumers’ Rights are as follows:
Right 5 – Right to effective communication
1. Every consumer has the right to effective communication in a form, language, and manner that enables the consumer to understand the information provided. Where necessary and reasonably practicable, this includes the right to a competent interpreter. A member of the family is not ideal, and this is examined in greater detail in the Informed Consentarticleintheresourcessection on the PNZ website.
2. Every consumer has the right to an environment that enables both consumer and provider to communicate openly, honestly, and effectively.
Principle 10 of the Aotearoa New Zealand Physiotherapy Code of Ethics and Professional Conduct requires physiotherapists to communicate effectively and cooperate with colleagues, other health professionals and agencies, for the benefit of theirpatients/clientsandthewidercommunity.
Physiotherapists must:
8.1 engage in effective communication and cooperate with colleagues, other health professionals and agencies to achieve optimal outcomesforthepatient/client
once informed consent has been gained
8.2 referpatients/clientsinatimelyfashion when their needs fall outside the physiotherapist’s scope of practice or skill level
8.3 collaborate with other service providers for the benefit of the patient/client,keepingreferringcolleagues informed of the outcomes of assessment and treatment
8.4 behave respectfully in communication to and about colleagues or other health professionals
What is the best approach to communicating with patients?
Physiotherapists should communicate openly and honestly with patients. In some circumstances, for example a rehabilitation programme or terminal care, an approach to communication may need to be agreed within the team.
The physiotherapist should use active listening skills, providing opportunities for the patient to communicate effectively.Careshould be taken with non-verbal communication that could affect the interaction.
What are the patient’s rights to an interpreter?
In some circumstances an interpreter may be required to assist in communication between the physiotherapist and patient. This is the patient’s right under Right 5(1) of the Code of Health and Disability Services Consumers’ Rights.
How can I make sure that the patient comprehends what I am communicating with them?
It is up to the physiotherapist to assess the patient’s understanding of the information given. Physiotherapists must always give a clear explanation to the patient of what they will be doing and why, and gain consent (see the Code of Health and Disability Services Consumers’ Rights: Right 6 Right to be Fully Informed; Right 7 Right to Make anInformedChoiceandGiveInformedConsent).Thisalsominimisestheriskthat an examination or treatment procedure is misconstrued by the patient.
Jargonandabbreviationsshould not be used when communicating with patients. The physiotherapist needs to adapt their method of communication to meet the requirements of the patient such as providing patient information in written or diagrammatic form. Have a copy of PNZ Rights and Responsibilities brochures on hand to give to your patient, so they understand their rights.
When can physiotherapists communicate using technical language?
Technical language may be used when communicating with other physiotherapists, physiotherapy colleagues and other members of the health care team as well as funders of physiotherapy services. You may also use technical language with referrers when keeping them informed of the patient’s progress, including a discharge summary or other service providers.

PHYSIO MATTERS MARCH 2017 | 13
For more information please refer to the Physiotherapy New Zealand Standards of Practice, the Code of Health and Disability Services Consumers’ Rights and the Aotearoa New Zealand Physiotherapy Code of Ethics and Professional Conduct.
If you have any questions regarding this article, please contact Sue Doesburg – [email protected]
Do you have a Q&A request for the Professional Standards and Ethics Committee? If so, please email it to [email protected]
Are social media sites acceptable in communicating with patients?
Physiotherapists need to maintain professional boundaries when using social networking sites. Social media sites can put physiotherapists at risk. There is a danger that the patient will be identifiable, and patient confidentiality may be inadvertently breached. Physiotherapists must be particularly careful when discussing any aspect of clinical practice online. The physiotherapist should inform the patient and get consent if the physiotherapist wishes to post identifiable patient information to an online site.
Some social networking sites allow public access to information. Physiotherapists should be aware of the public persona they want to display and avoid making comments about other professionals or institutions that could be interpreted as defamatory or inappropriate. Physiotherapists should not compromise the dignity of the profession.
SeetheProfessionalStandardsandethicsCommittee’spaperon Examining our profile in social media. This resource is available on the PNZ website, under the Resource section. Also available in the Resource section is downloadable ebook: Social Media for Physios - a complete how-to guide for harnessing the power of social media.
• Become a certified APPI Pilates Instructor in 2017• Therapeutic Yoga Training for Health Professionals • Full Matwork Certification Series Available• Online CPD Courses
2017 COURSE DATES Clinical Pilates Training
Book Online / unitehealth.com.au / [email protected] / +61 3 9525 0080
AUCKLANDAPPI Matwork CertificationAPPI Matwork Level 1 1-2 AprilAPPI Matwork Level 2 9-10 SepAPPI Matwork Level 3 18-19 Nov
APPI Equipment APPI Equipment Level 1 17-18 Jun
CPD Pilates CoursesAPPI Pilates for Runners 21 Oct APPI Pilates for Cyclists 22 Oct
Therapeutic YogaTherapeutic Yoga Training Level 1 15-16 Jul

InTERnATIOnAl
14 | PHYSIO MATTERS MAY 2016
Interview with Pernilla Åsenlöf
Professor Pernilla Åsenlöf from Uppsala University in Sweden recently visited New Zealand after the Otago and Southland Physiotherapy Trust sponsored a visit for her to run a workshop entitled; “The application of learning theory and behavioural change techniques in physiotherapy”.
Professor Åsenlöf has a background working as a physiotherapist in primary care, where she developed an interest in pain management. She later undertook a PhD entitled; Individually Tailored Treatment in the Management of Musculoskeletal Pain: Development and Evaluation of a Behavioural Medicine Intervention in Primary Health Care. Professor Åsenlöf has since published widely in the area of behavioural intervention in patients’ with persistent pain, and currently works across Uppsala University and the pain centre at Uppsala University Hospital.
Physio Matters managed to catch up with Professor Åsenlöf to ask her some topical questions on creating behavioural changes in patients’ with persistent pain:
What are the challenges with creating behavioural changes in people with persistent pain?
Professor Åsenlöf felt that whilst physiotherapists were more aware of psychosocial approaches to management of pain, they still possess too great a biomedical focus on treatment and need to place a greater emphasis on behavioural models within patient management; “We tend to focus on pain intensity… as the patient often comes with reductions of pain the main focus. One of the main challenges is to shift the patient’s focus from pain intensity to the consequences of pain. When you shift that focus research has shown us you are much more successful helping people”.
“To really change from a pain perspective to a behavioural perspective, the challenge is that we need to learn behavioural theory”. Professor Åsenlöf believes physiotherapists need an understanding of psychological theory in how behaviour develops and is maintained over time. She feels that physiotherapists need to know how to integrate behavioural skills training, maintenance and relapse prevention into practice.
Commentinginanarticleshewrotefor Eular Rheumatology Newsletter, Professor Åsenlöf suggests;
•firstly,physiotherapistsneedtobeskilled in discussing and setting behavioural goals for daily living activity (rather than goals), including pain reduction.
•Secondly,physiotherapistsshouldnotstay with pain diagnostics but move forward to establish relationships between patient-specific context, explanatory biopsychosocial variables, activity behaviours and consequences ofbehaviour–thatisestablishfunctional behavioural analysis on key behaviours for goal attainment for each particular person.
•Thirdly,ifapatienthasunconsciouslylearned a new way to move, or even worse, not to move, and is staying sedentary due to pain, behavioural skills training is needed to re-learn how to move.
Are there any resources you recommend to physiotherapists in this area?
Professor Åsenlöf would recommend reading text books in health psychology and behavioural psychology and notes there are a number of courses for physiotherapists at university level that helps them to better understand behavioural theory.
In addition, she points out that the universityCollegeofLondonhasrecentlydevelopedanappcalledBCTTaxonomy which includes a taxonomy of behavioural change techniques. Professor Åsenlöf believes this app is useful to provide an overview of different techniques, and how they can be applied to patients.
When asked if there were any other app’s to support physiotherapy practice, Professor Åsenlöf says there are many apps that track activity behaviours,
PHYSIO MATTERS MARCH 2017 | 15
sleep and diet, but little evidence that these can be helpful in changing behaviour. Her research team at Uppsala University are working on developing an evidence based app which encourages the adoption and maintenance of physical activity over the lifespan, targeting patients with rheumatoid arthritis. One challenge she notes is that “physiotherapists often want to be involved in the monitoring of activity behaviours”, however she feels that research should be more focused around technology that allows healthcare professionals to “let go” of patients and empowers them to self-manage their own health.
You led a 10 year longitudinal study that looked at using behavioural techniques to improve pain related disability: what were the findings?
It was a randomised controlled trial of 122 patients with a 10 year follow-up which started in 2003, and compared a tailored behavioural intervention with best evidence based treatment. Preliminary findings suggested pain related disability and pain intensity reduced in the short-term in both groups and significantly more in the behavioural intervention compared to control group. This improvement was maintained at 2 years. However, by the 10 year follow-up there were no differences between groups and participants in both groups still had their pain conditions, so they weren’tcured.Conclusionsofthestudywerethattailoredbehavioural intervention (which which were in accordance with patient’s values, preferences and goals) were effective to reduce pain related disability and pain intensity in the short term.
Are there any nuggets of advice you can provide to physiotherapist about facilitating behavioural changes with patients?
Physiotherapists need to be careful not to over-simplify their thinking and take a linear approach to pain and behaviour; that the intensity of pain relates to the level of disability; and discount the behavioural aspects of pain. We need to understand the behavioural components of the patients’ presentation and account for these within our reasoning.
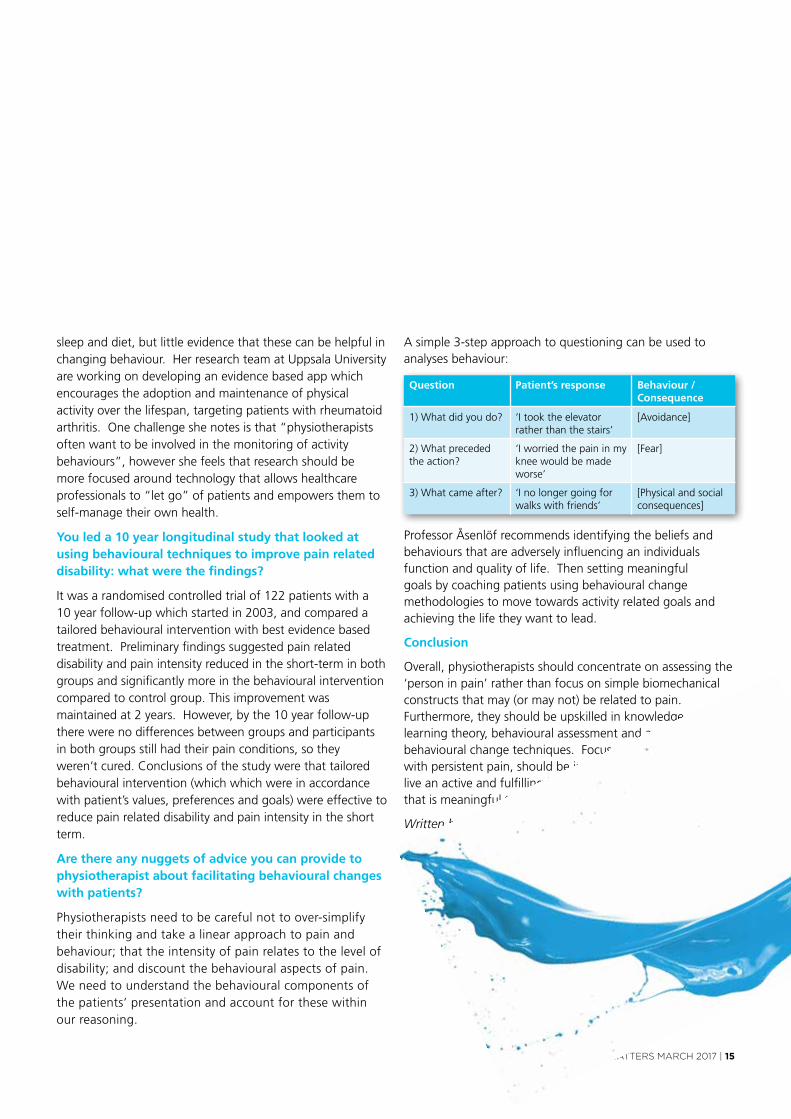
A simple 3-step approach to questioning can be used to analyses behaviour:
Question Patient’s response Behaviour / Consequence
1) What did you do? ‘I took the elevator rather than the stairs’
[Avoidance]
2) What preceded the action?
‘I worried the pain in my knee would be made worse’
[Fear]
3) What came after? ‘I no longer going for walks with friends’
[Physical and social consequences]
Professor Åsenlöf recommends identifying the beliefs and behaviours that are adversely influencing an individuals function and quality of life. Then setting meaningful goals by coaching patients using behavioural change methodologies to move towards activity related goals and achieving the life they want to lead.
Conclusion
Overall, physiotherapists should concentrate on assessing the ‘person in pain’ rather than focus on simple biomechanical constructs that may (or may not) be related to pain. Furthermore, they should be upskilled in knowledge of learning theory, behavioural assessment and application of behavioural change techniques. Focus of therapy, in patients with persistent pain, should be in supporting individuals to live an active and fulfilling life despite their pain, in a way that is meaningful to the given individual.
Written by Nick Clode
SIg
16 | PHYSIO MATTERS MARCH 2017
Pelvic, Women’s & Men’s Health Physiotherapy SIG (PWMH)
Exciting news for believers in ‘prevention rather than cure’: the multi-centre PRevPoLstudypublishedinTheLancet(Dec2016)showsbenefitofpelvicfloormuscle exercise for those with early signs of prolapse post-childbirth.
The treatment group received five one-to-one pelvic floor muscle training consultations over 16 weeks, including tailored lifestyle advice, pilates based exercisesandahomeexerciseDvD.The non-treatment group received a prolapse lifestyle advice leaflet. Two years later, 14.4% of the non-treatment group had required further prolapse treatment compared to 6% intheinterventiongroup.Co-authorProf Don Wilson says, “these (pelvic floor exercises) can prevent prolapse symptoms developing in the future”.
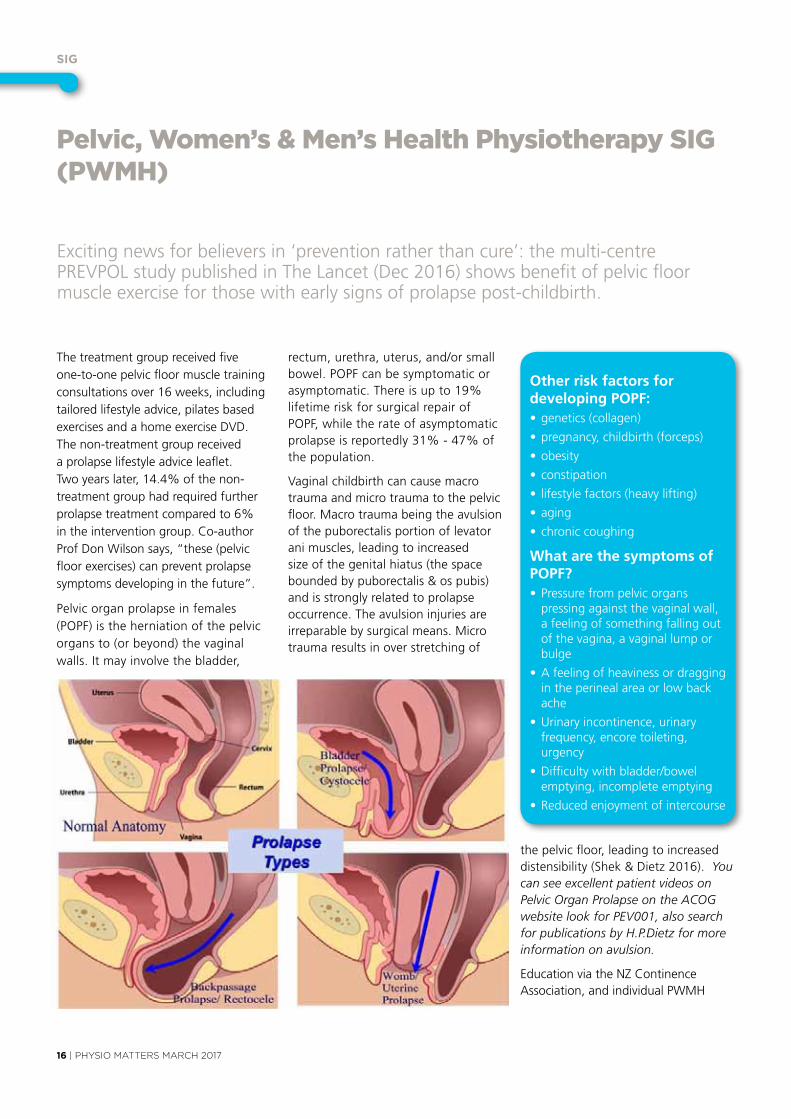
Pelvic organ prolapse in females (POPF) is the herniation of the pelvic organs to (or beyond) the vaginal walls. It may involve the bladder,
rectum,urethra,uterus,and/orsmallbowel. POPF can be symptomatic or asymptomatic. There is up to 19% lifetime risk for surgical repair of POPF, while the rate of asymptomatic prolapse is reportedly 31% - 47% of the population.
vaginalchildbirthcancausemacrotrauma and micro trauma to the pelvic floor. Macro trauma being the avulsion of the puborectalis portion of levator ani muscles, leading to increased size of the genital hiatus (the space bounded by puborectalis & os pubis) and is strongly related to prolapse occurrence. The avulsion injuries are irreparable by surgical means. Micro trauma results in over stretching of
Other risk factors for developing POPF:•genetics(collagen)
•pregnancy,childbirth(forceps)
•obesity
•constipation
• lifestylefactors(heavylifting)
•aging
•chroniccoughing
What are the symptoms of POPF?•Pressurefrompelvicorgans
pressing against the vaginal wall, a feeling of something falling out of the vagina, a vaginal lump or bulge
•Afeelingofheavinessordraggingin the perineal area or low back ache
•urinaryincontinence,urinaryfrequency, encore toileting, urgency
•Difficultywithbladder/bowelemptying, incomplete emptying
•Reducedenjoymentofintercourse
the pelvic floor, leading to increased distensibility (Shek & Dietz 2016). You can see excellent patient videos on Pelvic Organ Prolapse on the ACOG website look for PEV001, also search for publications by H.P.Dietz for more information on avulsion.
educationviatheNZContinenceAssociation, and individual PWMH
PHYSIO MATTERS MARCH 2017 | 17
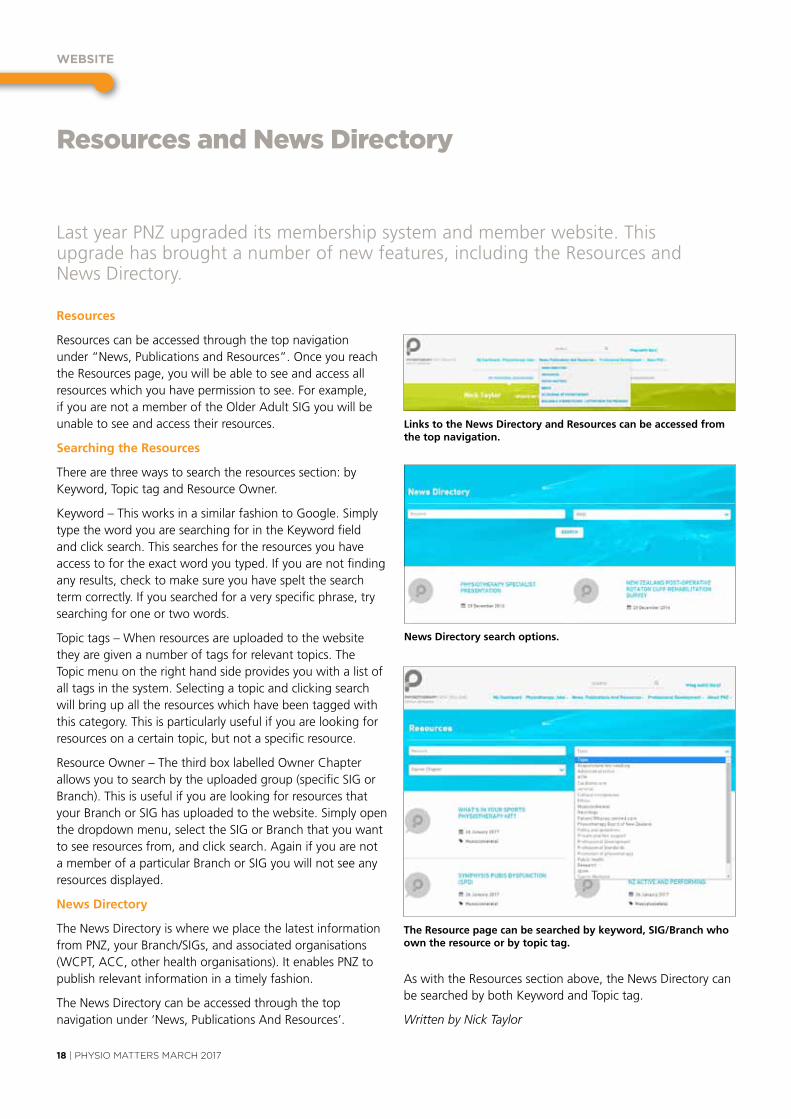
The Best Performance BikeIn The World
The Wattbike offers a unique insight for the rehabilitation professional. It not only allows a data driven recovery programme that is accurate and user friendly on the smoothest riding static bike in the marketplace, but in the case of leg injury or operation rehab, also allows left leg and right leg comparisons. This offers a unique insight over a series of sessions into how the patient is recovering.
Contact us now to discuss hiring or buying your Wa bike Call 07 552 5833 or email info@wa bike.co.nz
©Continence Foundation of Australia 2011.
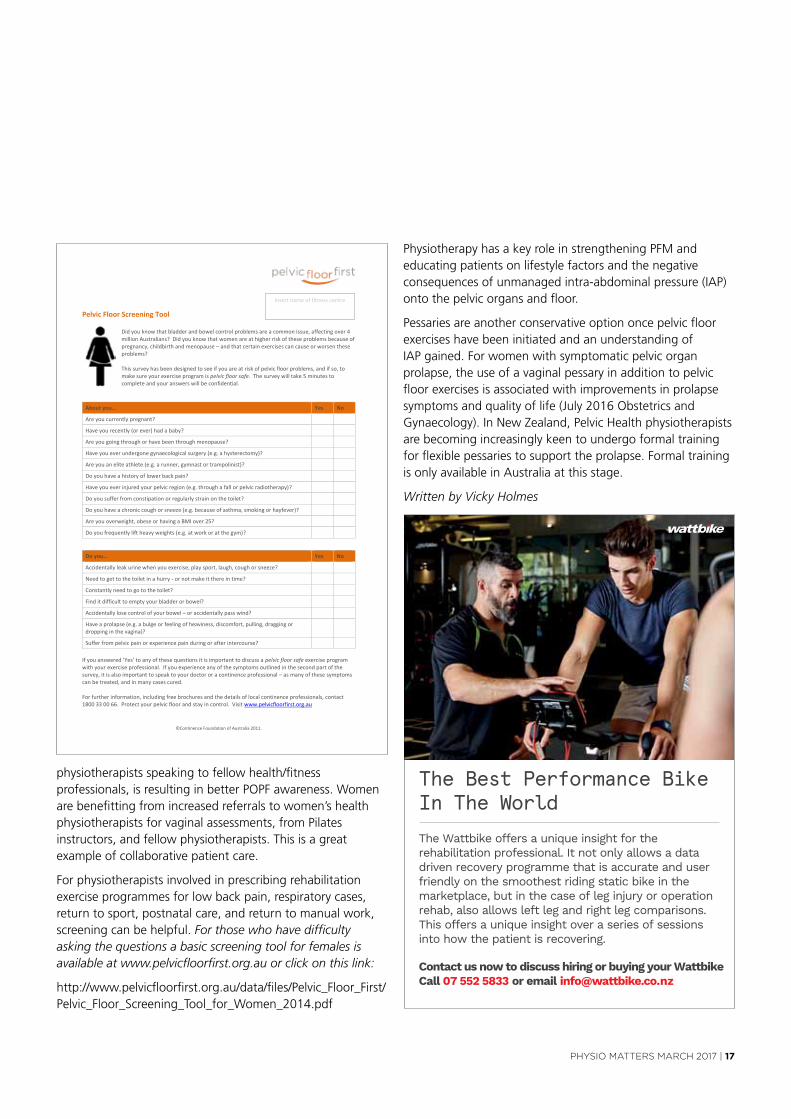
Pelvic Floor Screening Tool
Did you know that bladder and bowel control problems are a common issue, affecting over 4 million Australians? Did you know that women are at higher risk of these problems because of pregnancy, childbirth and menopause – and that certain exercises can cause or worsen these problems? This survey has been designed to see if you are at risk of pelvic floor problems, and if so, to make sure your exercise program is pelvic floor safe. The survey will take 5 minutes to complete and your answers will be confidential.
About you… Yes No
Are you currently pregnant?
Have you recently (or ever) had a baby?
Are you going through or have been through menopause?
Have you ever undergone gynaecological surgery (e.g. a hysterectomy)?
Are you an elite athlete (e.g. a runner, gymnast or trampolinist)?
Do you have a history of lower back pain?
Have you ever injured your pelvic region (e.g. through a fall or pelvic radiotherapy)?
Do you suffer from constipation or regularly strain on the toilet?
Do you have a chronic cough or sneeze (e.g. because of asthma, smoking or hayfever)?
Are you overweight, obese or having a BMI over 25?
Do you frequently lift heavy weights (e.g. at work or at the gym)?
Do you… Yes No
Accidentally leak urine when you exercise, play sport, laugh, cough or sneeze?
Need to get to the toilet in a hurry - or not make it there in time?
Constantly need to go to the toilet?
Find it difficult to empty your bladder or bowel?
Accidentally lose control of your bowel – or accidentally pass wind?
Have a prolapse (e.g. a bulge or feeling of heaviness, discomfort, pulling, dragging or dropping in the vagina)?
Suffer from pelvic pain or experience pain during or after intercourse? If you answered ‘Yes’ to any of these questions it is important to discuss a pelvic floor safe exercise program with your exercise professional. If you experience any of the symptoms outlined in the second part of the survey, it is also important to speak to your doctor or a continence professional – as many of these symptoms can be treated, and in many cases cured. For further information, including free brochures and the details of local continence professionals, contact 1800 33 00 66. Protect your pelvic floor and stay in control. Visit www.pelvicfloorfirst.org.au
Insert name of fitness centre
physiotherapistsspeakingtofellowhealth/fitnessprofessionals, is resulting in better POPF awareness. Women are benefitting from increased referrals to women’s health physiotherapists for vaginal assessments, from Pilates instructors, and fellow physiotherapists. This is a great example of collaborative patient care.
For physiotherapists involved in prescribing rehabilitation exercise programmes for low back pain, respiratory cases, return to sport, postnatal care, and return to manual work, screening can be helpful. For those who have difficulty asking the questions a basic screening tool for females is available at www.pelvicfloorfirst.org.au or click on this link:
http://www.pelvicfloorfirst.org.au/data/files/Pelvic_floor_first/Pelvic_floor_Screening_Tool_for_Women_2014.pdf
Physiotherapy has a key role in strengthening PFM and educating patients on lifestyle factors and the negative consequences of unmanaged intra-abdominal pressure (IAP) onto the pelvic organs and floor.
Pessaries are another conservative option once pelvic floor exercises have been initiated and an understanding of IAP gained. For women with symptomatic pelvic organ prolapse, the use of a vaginal pessary in addition to pelvic floor exercises is associated with improvements in prolapse symptomsandqualityoflife(July2016obstetricsandGynaecology).InNewZealand,PelvicHealthphysiotherapistsare becoming increasingly keen to undergo formal training for flexible pessaries to support the prolapse. Formal training is only available in Australia at this stage.
Written by Vicky Holmes
wEbSITE
18 | PHYSIO MATTERS MARCH 2017
Resources and News Directory
Resources
Resources can be accessed through the top navigation under “News, Publications and Resources”. Once you reach the Resources page, you will be able to see and access all resources which you have permission to see. For example, ifyouarenotamemberoftheolderAdultSIGyouwillbeunable to see and access their resources.
Searching the Resources
There are three ways to search the resources section: by Keyword,TopictagandResourceowner.
Keyword–ThisworksinasimilarfashiontoGoogle.SimplytypethewordyouaresearchingforintheKeywordfieldand click search. This searches for the resources you have access to for the exact word you typed. If you are not finding any results, check to make sure you have spelt the search term correctly. If you searched for a very specific phrase, try searching for one or two words.
Topictags–Whenresourcesareuploadedtothewebsitethey are given a number of tags for relevant topics. The Topic menu on the right hand side provides you with a list of all tags in the system. Selecting a topic and clicking search will bring up all the resources which have been tagged with this category. This is particularly useful if you are looking for resources on a certain topic, but not a specific resource.
Resourceowner–ThethirdboxlabelledownerChapterallowsyoutosearchbytheuploadedgroup(specificSIGorBranch). This is useful if you are looking for resources that yourBranchorSIGhasuploadedtothewebsite.Simplyopenthedropdownmenu,selecttheSIGorBranchthatyouwantto see resources from, and click search. Again if you are not amemberofaparticularBranchorSIGyouwillnotseeanyresources displayed.
News Directory
The News Directory is where we place the latest information fromPNZ,yourBranch/SIGs,andassociatedorganisations(WCPT,ACC,otherhealthorganisations).ItenablesPNZtopublish relevant information in a timely fashion.
The News Directory can be accessed through the top navigation under ‘News, Publications And Resources’.
Links to the News Directory and Resources can be accessed from the top navigation.
News Directory search options.
The Resource page can be searched by keyword, SIG/Branch who own the resource or by topic tag.
Last year PNZ upgraded its membership system and member website. This upgrade has brought a number of new features, including the Resources and News Directory.
As with the Resources section above, the News Directory can besearchedbybothKeywordandTopictag.
Written by Nick Taylor
nEwS In PIcTuRES
PHYSIO MATTERS MARCH 2017 | 19
News in pictures
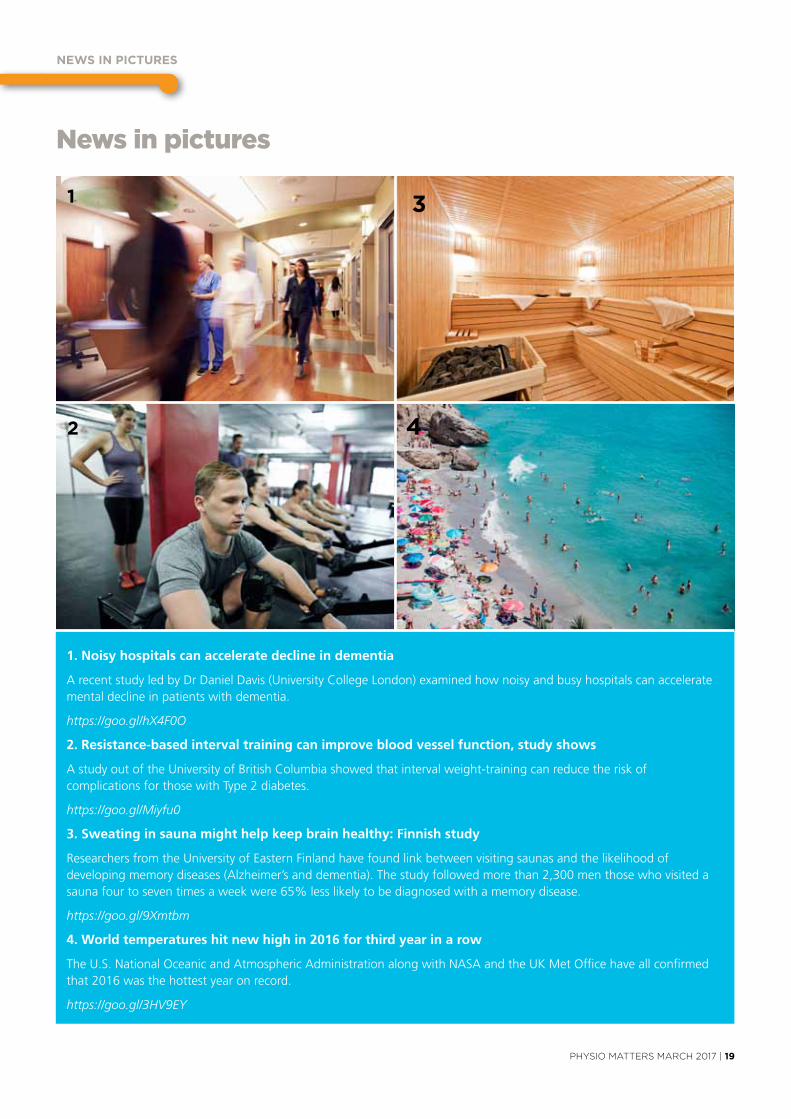
1. Noisy hospitals can accelerate decline in dementia
ArecentstudyledbyDrDanielDavis(universityCollegeLondon)examinedhownoisyandbusyhospitalscanacceleratemental decline in patients with dementia.
https://goo.gl/hX4F0O
2. Resistance-based interval training can improve blood vessel function, study shows
AstudyoutoftheuniversityofBritishColumbiashowedthatintervalweight-trainingcanreducetheriskofcomplications for those with Type 2 diabetes.
https://goo.gl/Miyfu0
3. Sweating in sauna might help keep brain healthy: Finnish study
Researchers from the University of Eastern Finland have found link between visiting saunas and the likelihood of developing memory diseases (Alzheimer’s and dementia). The study followed more than 2,300 men those who visited a sauna four to seven times a week were 65% less likely to be diagnosed with a memory disease.
https://goo.gl/9Xmtbm
4. World temperatures hit new high in 2016 for third year in a row
Theu.S.NationaloceanicandAtmosphericAdministrationalongwithNASAandtheuKMetofficehaveallconfirmedthat 2016 was the hottest year on record.
https://goo.gl/3HV9EY
1 3
42

Claims to ACC over the summer month period
In New Zealand we love our beaches, outdoor activities, barbeques, jandals and backyard cricket. ACC had a number of claims, over the December 2015 to February 2016 period, from us Kiwis just being, well, Kiwis!
5,653
278
2,626
1,940
1,661
2,324
Tramping – 1,940 claimsAccidents included falls from climbing, losing balance on steep slopes and tripping over rocks.
Swimming – 5,653 claimsAccidents included slipping on tiles around pools, to diving and chipping a tooth.
Diving – 278 claimsAccidents included diving in shallow water, burst eardrums and standing on rocks.
Surfing – 2,626 claimsAccidents included colliding with other surfers, cutting feet on surfboard fins, or falling off in shallow water.
Boating – 1,661 claimsInjuries involved boats capsizing or being hit by waves, and injuries sustained from getting in and out of boats.
Horse riding – 2,324 claimsInjuries from falling off horses or being kicked by horses.
553
88
4,655
72
538
388
1,466
31
Backyard cricket – 72 claimsAccidents included being hit by the ball, and arm, shoulder and back injuries from bowling and batting.
Jandals – 553 claimsMishaps included glass entering through the jandal and piercing the foot, and slips and trips while wearing jandals.
Deck chair – 88 claimsMishaps involving legs and fingers getting caught and injuries from collapsing deckchairs.
Beach – 4,655 claimsAccidents included sand in the eyes, tripping on items on the beach and standing on rocks in the water.
Barbeques – 538 claimsInjuries included burns or dropping objects on feet, to strains from lifting or moving barbeques.
Jet ski – 388 claimsInjuries from coming off a jet ski and hurting back and shoulders.
Camping – 1,466 claims
Injuries from tripping over campsite objects, putting up tents and burns from campfire cooking.
Sunburn – 31 claimsBad sunburn forming blisters.

553
88
4,655
72
538
388
1,466
31
Backyard cricket – 72 claimsAccidents included being hit by the ball, and arm, shoulder and back injuries from bowling and batting.
Jandals – 553 claimsMishaps included glass entering through the jandal and piercing the foot, and slips and trips while wearing jandals.
Deck chair – 88 claimsMishaps involving legs and fingers getting caught and injuries from collapsing deckchairs.
Beach – 4,655 claimsAccidents included sand in the eyes, tripping on items on the beach and standing on rocks in the water.
Barbeques – 538 claimsInjuries included burns or dropping objects on feet, to strains from lifting or moving barbeques.
Jet ski – 388 claimsInjuries from coming off a jet ski and hurting back and shoulders.
Camping – 1,466 claims
Injuries from tripping over campsite objects, putting up tents and burns from campfire cooking.
Sunburn – 31 claimsBad sunburn forming blisters.
TAE ORA TInAnA
22 | PHYSIO MATTERS MARCH 2017
Tae Ora Tinana Student Prize
Each year Tae Ora Tinana presents a prize to an exceptional student from either AUT or Otago. 2016 recipient Witana Roy Petley tells us about what motivates him.
KoWitanaPetleyTakulngoa
KoNg-ati Porou me Ng-ai Te Rangi. ng-a lwi
KoPirir-akau me Te Wh-anau a T-uwhakairiora ng-a Hap
-u
KoHinemaureameopureorang-a Marae
KoTuwhakairiorameTuwhiwhiawhareTupuna
KoHikirangimeMauaong-a Maunga
KoHoroutameTaakitimung-a Waka I hoea
KoWaipahuteAwa
KoTaurangatemoana
T-en-a koutou katoa
I have been heavily involved with the promotion of M-aoritanga Hauora M-aori and the values of Tae Ora Tinana after enrolling in the School of Physiotherapy in 2014.
Since being accepted into the University of Otago’s School of Physiotherapy, and completing my Bachelor of Physiotherapy, I have always strived to display a high sense of Whanaungatanga. I now have various strong relationships that I developed during my time with the School of Physiotherapy, the University of Otago’s M-aori Health workforce Development Unit, Te Roopu M-aori and Te Huka M-atauraka. Through these relationships I had been able to ensure various benefits for other M-aori physiotherapy students during my third and fourth year such as tutorials and study spaces.
I am a firm believer of supporting other
students of all backgrounds to be as successful as they possibly can be. This led me to provide support as a mentor with Te Huka M-atauraka for two years, as well as two years as Residential AssistantatStudholmeCollege–myleadership role within the M-aori physiotherapy students supports my large belief in Manaakitanga.
Due to my upbringing in a small rural town where the health of M-aori is sadly in a low state, I am a large supporter of movements to support Hauroa M-aori. A highlight of my time at University of Otago was when I was accepted to become an ambassador to promote the university in my hometown of P-ut-aruru. It was a very humbling time as I was able to show younger M-aori, from a
similar background, the benefits and different pathways that are available to them and hoping they will one day be able to do the same.
I have been able to attend hui and other programmes, such as the 2015 Tae Ora Tinana hui and Tair-awhiti lnterprofessional program in 2016. These events focussed on the different aspects of Hauroa M-aori promotion. Through the information shared at these events, I have been able to use the Te Whare Tapa Wh-a model more confidently with my patients and explain the importance to other students as a topic of interest.
Ng-a Mihi, Witana Roy Petley

MEMbER STORY
PHYSIO MATTERS MARCH 2017 | 23
From Physiotherapist to Author
With over 45 years’ experience in diagnosing, teaching and treating spinal pain, Barbara Mawson can now add ‘author’toherCv,followingthe2016releaseofherbook Becoming the Shape of the Chair You Sit In.
Accessible and without the use of any medical jargon, the self-published book is very much a personal account focused on delivering basic spinal information that can be easily understood. Drawing on Barbara’s personal experience of what works when advising and getting information across to patients, Becoming the Shape of the Chair You Sit In is a practical and educational book that takes a general look at what people need to do at home and in their work places to maintain the integrity of the spine and reduce stresses.
Barbara’s career in physiotherapy has been exciting and varied. She has owned and managed her own private practices, worked in Myanmar where she helped build the skills of graduate
physiotherapists in disability resource centres, educated and supervised Otago university students, audited practice standards and served on the Physiotherapy Board during the introductionoftheHPCAA2003.
During Barbara’s career, she would often use handouts and stick figure drawings to educate and encourage her clients to work on themselves between treatments. Having all that material from her many years of practice, she had the idea to collate it into one fun and easy to read book.
“I guess creating the book was just a natural progression,” she explains. “The writing process was not difficult because I was giving the information that I provide patients every day in my clinic and have done so for years.”
Becoming the Shape of the Chair You Sit In is written from the viewpoint of successful outcomes and provides people with the information to help themselves in as many ways as possible, with minimal intervention and cost to the patient.
“Many people just need the information on what is a good chair, how to sit well, what type of pillow to buy, what to do after sitting at the computer and how to manage episodes of back and neck pain.”
The book gives the public a guide to repairs and maintenance of the spine and it works by showing how to prevent, reduce or eliminate episodes of pain, especially those experiencing mechanical back pain.
While physios can treat the symptoms of pain, Becoming the Shape of the Chair You Sit In looks at the causes of the pain. Barbara believes there is a role to play in educating the public so they don’t necessarily need to see a physiotherapist to be fixed.
“As physiotherapists we can all make people feel better in the clinic, but unless changes are made in the patient’s lifestyle the improvement is often not maintained.”
Although this message is often communicated to patients during consultation, the book reinforces the concept.
Barbara’s extensive network of physiotherapists, health professionals and past patients helped to review the book from both a clinical and readability perspective, and Barbera says feedback from both public and health professionals has been great.
“People come up to me on the street and ring me at work to tell me how much this book has changed their lives already. It is such a buzz to know the difference you’re making in people’s lives is ongoing. “
Barbara Mawson’s website has a free resource page for anyone to access, with videos on posture, pain, joint noises as well as videos on how to manage practical everyday activities, such as getting out of a chair and out of bed. visitwww.barbaramawson.com

24 | PHYSIO MATTERS MARCH 2017
DRY NEEDLINGCOURSES
AdvancedCourseSPECIAL
$329 AUD
Online Theory plus face to face Practical
VISIT www.cpdhealthcourses.com TODAY!
Auckland 2017: Intro & Advanced CoursesComplete all your Dry Needling Intro & Advanced practical training in 1 weekend. Join the Advanced course for only $329 AUD!Save time by completing all your Dry Needling theory ONLINE in your own time.Dr Wayne Mahmoud has over 30 years of clinical & teaching experience and a Masters Degree in Acupuncture.Receive course certificates, free needle starter pack, fully illustrated course manuals and review all techniques on the Video Training Site.
Intro: April 28/29 and Advanced: April 30Intro: August 25/26 and Advanced: August 27
(Intro = Fri 5-8pm & Sat 8-5pm. Advanced = Sunday 8-5pm)
"Just wanted to take this opportunity to say BIG THANKS for all your teaching & guidance overthe weekend. Your course was phenomenal. I thoroughly enjoyed it & am sure other studentsdid too. The intermix of online theory followed by practical was great set up. The contentsweren't too challenging and left enough thought provoking questions. I had a fantasticweekend. Very inspirational Wayne." Lockie N (Physiotherapist)
NB: All courses held in Wellington. Both Part A & B courses have an online component requiring successful completion prior to attending the 3 day course. This is approximately 7 hours work. Registration can now be completed online at: www mckenzieinstitute.org/nz
2017 Education Programme
For further info, please contact: Kay Morgon, Branch Manager. Ph: 04 299 6645 or Email: [email protected]
Advanced Extremities (prerequisite completion of Part D)
25-26 Feb 2017
Part A The Lumbar Spine (3 days) 17-19 Mar 2017
Part D Advanced Cervical and Thoracic Spine & Extremities – Upper Limb (4 days)
27-30 Apr 2017
Part B The Cervical and Thoracic Spine (3 days)
9-11 Jun 2017
Credentialling Examination 29 July 2017
Credentialled Update Day 4 August 2017
Seminar Day 5 August 2017
Part A The Lumbar Spine (3 days) 15-17 Sep 2017
Part C Advanced Lumbar Spine & Extremities – Lower Limb (4 days)
16-19 Nov 2017
World Class Education
Professional Instructors
Face to Face Learning
Ongoing Clinical Support
Money Back Guarantee
Treatment techniques combining the IMS and Trigger Point Models maximising clinical outcomes.
REGISTER ONLINE @ www.gemtinfo.com.au
APA, CAA Accredited Courses Osteopathy Australia Endorsed Courses
EARLY
BIRD RATES
APPLY!
For more information, visit our website, call +61 3 9585 8100 or email [email protected]
2017 COURSE LOCATIONS: AUCKLAND, CHRISTCHURCH, MELBOURNE, SYDNEY, KUALA LUMPUR, NEW DELHI & MORE!
These courses will change the way you view the human body!
TRIGGER POINT DRY NEEDLING COURSES 2017Applications for Pain Management & Sports Injuries
PROFESSIOnAl dEvElOPMEnT
PHYSIO MATTERS MARCH 2017 | 25
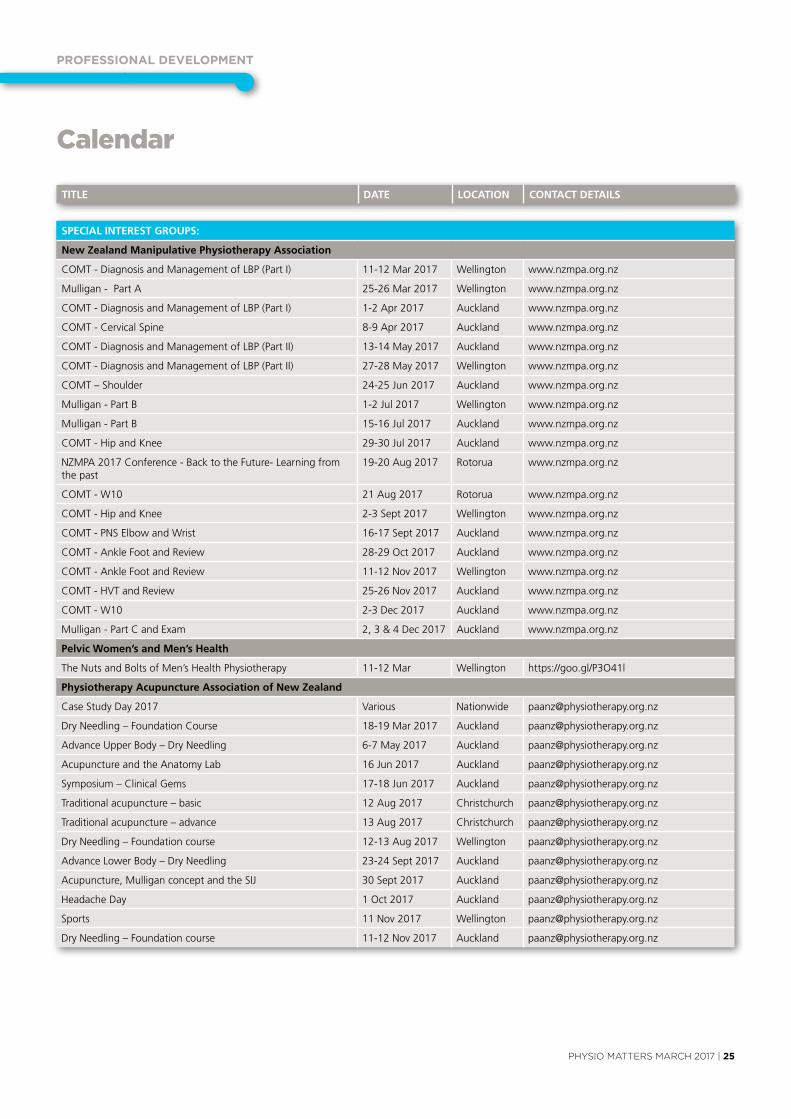
Calendar
SPECIAL INTEREST GROUPS:
New Zealand Manipulative Physiotherapy Association
CoMT-DiagnosisandManagementofLBP(PartI) 11-12 Mar 2017 Wellington www.nzmpa.org.nz
Mulligan - Part A 25-26 Mar 2017 Wellington www.nzmpa.org.nz
CoMT-DiagnosisandManagementofLBP(PartI) 1-2 Apr 2017 Auckland www.nzmpa.org.nz
CoMT-CervicalSpine 8-9 Apr 2017 Auckland www.nzmpa.org.nz
CoMT-DiagnosisandManagementofLBP(PartII) 13-14 May 2017 Auckland www.nzmpa.org.nz
CoMT-DiagnosisandManagementofLBP(PartII) 27-28 May 2017 Wellington www.nzmpa.org.nz
CoMT–Shoulder 24-25Jun2017 Auckland www.nzmpa.org.nz
Mulligan - Part B 1-2Jul2017 Wellington www.nzmpa.org.nz
Mulligan - Part B 15-16Jul2017 Auckland www.nzmpa.org.nz
CoMT-HipandKnee 29-30Jul2017 Auckland www.nzmpa.org.nz
NZMPA2017Conference-Backtothefuture-Learningfromthe past
19-20 Aug 2017 Rotorua www.nzmpa.org.nz
CoMT-W10 21 Aug 2017 Rotorua www.nzmpa.org.nz
CoMT-HipandKnee 2-3 Sept 2017 Wellington www.nzmpa.org.nz
CoMT-PNSelbowandWrist 16-17 Sept 2017 Auckland www.nzmpa.org.nz
CoMT-AnklefootandReview 28-29 Oct 2017 Auckland www.nzmpa.org.nz
CoMT-AnklefootandReview 11-12 Nov 2017 Wellington www.nzmpa.org.nz
CoMT-HvTandReview 25-26 Nov 2017 Auckland www.nzmpa.org.nz
CoMT-W10 2-3 Dec 2017 Auckland www.nzmpa.org.nz
Mulligan-PartCandexam 2, 3 & 4 Dec 2017 Auckland www.nzmpa.org.nz
Pelvic Women’s and Men’s Health
The Nuts and Bolts of Men’s Health Physiotherapy 11-12 Mar Wellington https://goo.gl/P3o41l
Physiotherapy Acupuncture Association of New Zealand
CaseStudyDay2017 various Nationwide [email protected]
DryNeedling–foundationCourse 18-19 Mar 2017 Auckland [email protected]
AdvanceupperBody–DryNeedling 6-7 May 2017 Auckland [email protected]
Acupuncture and the Anatomy Lab 16Jun2017 Auckland [email protected]
Symposium–ClinicalGems 17-18Jun2017 Auckland [email protected]
Traditionalacupuncture–basic 12 Aug 2017 Christchurch [email protected]
Traditionalacupuncture–advance 13 Aug 2017 Christchurch [email protected]
DryNeedling–foundationcourse 12-13 Aug 2017 Wellington [email protected]
AdvanceLowerBody–DryNeedling 23-24 Sept 2017 Auckland [email protected]
Acupuncture,MulliganconceptandtheSIJ 30 Sept 2017 Auckland [email protected]
Headache Day 1 Oct 2017 Auckland [email protected]
Sports 11 Nov 2017 Wellington [email protected]
DryNeedling–foundationcourse 11-12 Nov 2017 Auckland [email protected]
TITLE DATE LOCATION CONTACT DETAILS

PROFESSIOnAl dEvElOPMEnT
26 | PHYSIO MATTERS MARCH 2017
TITLE DATE LOCATION CONTACT DETAILS
ExTERNAL PROVIDERS/ORGANISATIONS
AlliedHealth'ConnectingforIntegratedCare'roadshow 9 Mar 2017 Christchurch [email protected]
MyofascialReleaseCourse-Thefundamentals 10-11 Mar 2017 Tauranga www.mfrworkshops.com
visceralManipulation1:Abdomen1(vM1) 16-19 Mar 2017 Christchurch https://goo.gl/xWYbeW
McKenzieInstituteNewZealand–PartA:TheLumbarSpine 17-19 Mar 2017 Wellington www.mckenzieinstitute.org/nz
Moving and Handling 24-23 Mar 2017 Hamilton [email protected]
MyofascialReleaseCourse-Thefundamentals 24-25 Mar 2017 Christchurch www.mfrworkshops.com
RemarkableBusinessCourses-RemarkablePractice2017 1 Apr 2017 Auckland www.redsok.com/PBA
APPI Pilates Matwork Training for Physiotherapists 1-2 Apr 2017 Auckland unitehealth.com.au
The Milicich Method 1-2 Apr 2017 Hamilton [email protected]
MyofascialReleaseCourse-Thefundamentals 1-2 Apr 2017 Dunedin www.mfrworkshops.com
ClinicalDiagnosisofPersistentBackandReferredLegPain-6month course
22 Apr - 14 Oct 2017
www.musculoskeletal.courses
MyofascialReleaseCourse-Thefundamentals 21-22 Apr 2017 Nelson www.mfrworkshops.com
McKenzieInstituteNewZealand-PartD:AdvanceCervicalandThoracic Spine & Extremities - Upper Limb
27-30 Apr 2017 Wellington www.mckenzieinstitute.org/nz
CPDHealthCourses:DryNeedlingIntroductory&AdvancedCourses
28-30 Apr 2017 Auckland cpdhealthcourses.com
vestibularRehabilitation-AnAdvancedCourse 20-21 May 2017 Wellington [email protected]
McKenzieInstituteNewZealand-PartB–TheCervicalandThoracic Spine
9-11Jun2017 Wellington www.mckenzieinstitute.org/nz
McKenzieInstituteNewZealand-PartB–TheCervicalandThoracic Spine
9-11Jun2017 Wellington www.mckenzieinstitute.org/nz
vestibularRehabilitation-AnIntroductoryCourse 17-18Jun2017 Wellington [email protected]
Wintec’s Master of Professional Practice 28Jul2017 Hamilton http://www.wintec.ac.nz/postgraduate
McKenzieInstituteNewZealand-CredentialedupdateDay 4 Aug 2017 Wellington www.mckenzieinstitute.org/nz
McKenzieInstituteNewZealand-SeminarDay 5 Aug 2017 Wellington www.mckenzieinstitute.org/nz
MyofascialReleaseCourse-Thefundamentals 18-19 Aug 2017 Auckland www.mfrworkshops.com
MyofascialReleaseCourse-Thefundamentals 25-26 Aug 2017 Tauranga www.mfrworkshops.com
MyofascialReleaseCourse-Thefundamentals 8-9 Sept 2017 Nelson www.mfrworkshops.com
McKenzieInstituteNewZealand-PartA-TheLumbarSpine (3 days)
15-17 Sept 2017 Wellington www.mckenzieinstitute.org/nz
NationalCommunityPhysiotherapyConference2017 21-22 Sept 2017 Tauranga [email protected]
MyofascialReleaseCourse-Thefundamentals 22-23 Sept 2017 Christchurch www.mfrworkshops.com
MyofascialReleaseCourse-Thefundamantals 29-30 Sept 2017 Dunedin www.mfrworkshops.com
TheSportsThorax-ConnectTherapy™&theThoracicRingAp-proach™withDr.Linda-JoyLee
15-18 Nov 2017 Auckland https://goo.gl/laea3b
For all event listings, please visit pnz.org.nz
Calendar
BRANCHES
Hawkes Bay
Hawkes Bay Symposium: for Allied Health Professionals 16 Sep 2017 Hastings https://goo.gl/xewsI8
North Shore
May Branch Meeting 8 May 2017 Auckland [email protected]
NorthShoreBranchPNZCPRupdate 5Jul2017 Auckland [email protected]
NovemberBranchMeetingandAGM 13 Nov 2017 Auckland [email protected]

cOnTAcT dETAIlS
PHYSIO MATTERS MARCH 2017 | 27
www.pnz.org.nz
Branch Contacts
Northland
KimberleyPow [email protected]
North Shore
Lilian van den Bergh [email protected]
Auckland
Tony Westwood [email protected]
Waikato / Bay of Plenty
Rob Neish [email protected]
Hawke’s Bay
Raewyn Newcomb [email protected]
Middle Districts
BridieGreen [email protected]
Wellington
DarraghKenny [email protected]
Nelson / Marlborough
Sheryl Wilson nelsonmarlborough@physiotherapy. org.nz
Canterbury
JessieSnowdon [email protected]
Otago
Becky Wilson [email protected]
Southland
Fiona Morse [email protected]
Special Interest Groups
Cardiothoracic
Brigitte Eastwood [email protected]
Pelvic, Women’s and Men’s Health
Shelley Solomon [email protected]
District Health Board Leaders
Barbara Saipe [email protected]
Hand Therapists
Marlene Pouri-Lane Ph: 07 854 8949 [email protected]
Neurology
Bridget Dickson Bridget.Dickson@southerndhb. govt.nz
NZ Manipulative Physiotherapists Association (NZMPA)
Ingrid du Toit Ph: 09 476 5353 0800 646 000 [email protected] www.nzmpa.org.nz
Occupational Health
Angela Trotter (Administrator) PO Box 27386 Wellington 6141 Ph: 04 894 1685 [email protected]
Paediatrics
CatherineCoull Ph: 027 204 8069 [email protected]
The Physiotherapy Acupuncture Association (PAANZ)
Angela Trotter (Administrator) PO Box 27386 Wellington 6141 Ph: 04 894 1685 [email protected]
Physiotherapy in Mental Health
JokevanStavern [email protected]
Physiotherapy for the Older Adult
ChrissieRussell [email protected]
Sports Physiotherapy New Zealand
Michael Borich Ph: 021 717 303 [email protected] www.sportsphysiotherapy.org.nz
Chairpersons Standing Committees
ContactNationaloffice
Tae Ora Tinana
SandraKettle
Professional Standards and Ethics Committee
Ben Hinchcliff Fy Dunford
Finance Committee
Sheila Mann
Professional Development Committee
GillStotter
National Executive Committee
President
Liz Binns PO Box 27386 Wellington 6141 Ph: 04 801 6500 (National Office) [email protected]
Executive Members
Ricky Bell Melissa Davidson JessRadovanovich KurtThomas
National Office
Office Hours 8.30am - 5.00pm
L6, 342 Lambton Quay PO Box 27 386, Wellington Ph: 04 801 6500 [email protected]
CEO
MN(Joe)Asghar [email protected]
Operational and Business Services Manager
PeterChristie [email protected] DD: 04 894 1683
Marketing Manager
Nick Taylor [email protected] DD: 04 894 1686
Professional Advisor
Sue Doesburg [email protected] DD: 04 894 1684
Learning And Research Advisor
NickClode [email protected] DD: 04 894 1689
Communications and Events Advisor
ericaGeorge [email protected] DD: 04 894 1687
Professional Development Project Officer
Anna Williams [email protected] DD: 04 894 1680
Membership Administrator
ClaireAngliss [email protected] Ph: 04 801 6500
Accountant
emmaGillard [email protected] DD: 04 894 1682
Physiotherapy Business Support
Check us out on Facebook, YouTube and Twitter
www.facebook.com/PhysiotherapyNZ www.youtube.com/nzsp1 www.twitter.com/physionz

The World Confederation for Physical Therapy (WCPT)represents the physical therapy profession worldwide
www.wcpt.org/congress
C NGRESS 2017Cape Town
2-4 July 2017
Hosted by:
Where the world of physical therapy meets
Register nowAdvance rate deadline 31 May 2017




















