Treating snow sport injuries - PNZ
32
www.pnz.org.nz ISSN 1179-7967 (Print) ISSN 1179-7975 (Online) THE LATEST NEWS & VIEWS FROM PHYSIOTHERAPY NEW ZEALAND AUGUST 2017 PHYSIO MATTERS Treating snow sport injuries Also in this issue: • Health literacy • Transforming clinical practice • Advertising your services – what’s the standard?
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Treating snow sport injuries - PNZ

www.pnz.org.nzISSN 1179-7967 (Print)
ISSN 1179-7975 (Online)
THE LATEST NEWS & VIEWS FROM
PHYSIOTHERAPY NEW ZEALAND AUGUST 2017
PHYSIOMATTERS
Treating snow sport injuries
Also in this issue: •Healthliteracy
•Transformingclinicalpractice
•Advertisingyourservices–what’sthestandard?

cOnTEnTS
2 |PHYSIO MATTERS AUGUST 2017
www.pnz.org.nz
Editorial and Advertising
• SendeditorialitemstotheEditor,[email protected]
• LetterstotheEditorarelimitedto250wordsandmaybeedited.
• Advertisingratesandspecificationsareonourwebsite.
• Deadlineforeditorialandadvertisingbookingisno later than 20th of the month, two months before the issue is published.Ifthisdatefallsonaweekendoraholiday,pleasesupplybytheclosestworkingdaybefore.
• MembersmayreadPhysioMattersonourwebsiteandfollowworkablelinks.
The Editor reserves the right to edit material for space and clarity, and to withhold material from publication. Individual views expressed in this publication are not necessarily those of Physiotherapy New Zealand. Inclusion of product or service information or of links to external websites does not imply PNZ endorsement of the product, service or website unless specifically stated. Advertising in Physio Matters does not constitute endorsement of a product and no advertiser may use publication of an advertisement in the magazine to support the marketing of every product. While every endeavour is made to ensure the accuracy of information, no responsibility is accepted for inaccurate information.
Booking deadlines
Issue Booking deadline
February2017 12December2016
March2017 20January
April2017 19February
May2017 18March
June2017 20April
July2017 22May
August2017 20June
September2017 20July
October2017 21August
November2017 20September
December2017 20October
Physiotherapy New Zealand
POBox27386,MarionSquareWellington6141Level6,342LambtonQuay,Wellington6011,NewZealand
Phone:+6448016500|Fax:+6448015571
AUGUST 2017
PRESIDENT’S COLUMN 3
NATIONAL OFFICE 4
FEATURE: Snow Sport Injuries and How To Treat Them 6
ACC: Reducing Treatment Injuries 10
POLICY & PRACTICE: Health Literacy 12
MEMBERSHIP BENEFITS: EBSCOhost Database 14
PHYSIOTHERAPY BOARD: Advertising Your Services 17
SIG: Transforming Clinical Practice with a Whole Person-Centred Approach 18
TOMORROW’S PROFESSION: Physiotherapy Students Have Much To Learn From the Humanities 20
SCHOLARSHIP TRUST: Understanding Obesity from an Indigenous Angle 23
STUDENT: Experiences of a Final Year Physiotherapy Student 24
RESOURCES: NZ Rehabilitation Research Review 26
GENERAL NOTICES 28
PROFESSIONAL DEVELOPMENT CALENDAR 29
CONTACT DETAILS 31
Cover image © iStock

PRESIdEnT’S cOluMn
PHYSIO MATTERS AUGUST 2017 | 3
Booking deadlines
Issue Booking deadline
February2017 12December2016
March2017 20January
April2017 19February
May2017 18March
June2017 20April
July2017 22May
August2017 20June
September2017 20July
October2017 21August
November2017 20September
December2017 20October
Physiotherapy New Zealand
POBox27386,MarionSquareWellington6141Level6,342LambtonQuay,Wellington6011,NewZealand
Phone:+6448016500|Fax:+6448015571
Updates from the President
LIZ BINNS
PRESIDENTPHYSIOTHERAPY NEW ZEALAND
I often write my monthly columns two to three weeks before the issue arrives to you all, so when it comes to discussing significant events and goings-on within the PNZ community, often I am writing about events that are yet to happen. What I do know this month however, is that by the time you read this column, our vote of YES to build a stronger future for PNZ will have taken place, with the result to be shortly known.
Therefore, I would like to start this column by once again thanking everyone for voting and contributing to the stable future of PNZ.
As some of you may have heard, I represented PNZ at the two day general meeting of the World Confederation for Physical Therapy Asia Western Pacific region in Bangkok, Thailand last month. One thing is for sure – our region is incredibly diverse! Having the opportunity to meet with representatives from Nepal, Bangladesh, Fiji, Malaysia and other
countries in the region really brought home to me that we are part of a global family, and how fortunate we are coming from the country we do.
While I was thankful we had recently successfully recruited Sandra Kirby as our CEO, concerns held by my peers from other countries were quite serious. For example, during one discussion with a rep from one of these countries I learned how amputation secondary to diabetes was a big problem and they had no access artificial limbs; another country was short 1,000 physiotherapists. Sobering to say the least. But despite this, all of us in the room shared the exact same passion for the profession, the belief in tomorrow being a better day and the energy to make things happen. For
By the time you read this column, our vote of YES
to build a stronger future for PNZ will have taken place, with the result to
be shortly known.
a full list of countries in our region, have a look at this website www.wcpt.org/awp
National Executive members Ricky Bell and Melissa Davidson represented PNZ at the WCPT Congress in South Africa last month. Once again, it was a great opportunity for like-minded and passionate people to come together for the benefit of the profession. Ricky Bell (pictured with below with Melissa) was an invited speaker for the first ever discussion session on the topic of Indigenous issues and he did us proud. Check out this link to learn more about the session: www.wcpt.org/news/Indigenous-people-July17
It is so important for New Zealand to be involved in these international discussions from day one, and it was an honour for us to represent PNZ at these two global events.
Liz Binns President
Melissa and Ricky in Cape Town

nATIOnAl OFFIcE
4 | PHYSIO MATTERS AUGUST 2017
World Physiotherapy Day is on Friday
8th September and it’s a day where
physiotherapists all over the world come
together to raise awareness about the profession in creative and innovative ways.
Updates from the National Office
PETER CHRISTIE
INTERIM CHIEF EXECUTIVE OFFICERPHYSIOTHERAPY NEW ZEALAND
It’s hard to believe that we are in August already! Here in National Office, we have many things on the go. Preparing for annual Business Symposium and AGM 2017
As we mentioned briefly a couple of issues ago, we are currently organising the inaugural 2017 PNZ Business Symposium and Annual General Meeting, which is due to be held in Auckland on Saturday 28th October. We are at the stage of finalising the speakers for the day and look forward to sharing these details with you as soon as we have them set in stone. So for now, lock in the date and we look forward to seeing you all there.
World Physiotherapy Day 2017
It’s that time of year again! World Physiotherapy Day is on Friday 8th September and it’s a day where physiotherapists all over the world come together to raise awareness about the profession in creative and innovative ways. The message this year is “physical activity for life”, highlighting the important role physiotherapy plays in healthy ageing. Following the success of last year’s photo competition, the National Office marketing team will once
again be running an online Facebook competition in the lead up to the day. So keep an eye out on our website and Facebook page for the competition details as well as downloadable resources you can print out and use to celebrate the day.
Allied Health Aotearoa New Zealand (AHANZ) update
Earlier in the year, AHANZ embarked on the project of developing an Allied Health Best Practice Guide for Telehealth. PNZ has a representative on the working group and a draft document is almost ready for dissemination to stakeholders to invite feedback. The guide provides a definition, discusses benefits, challenges, risks, and considerations for providing best practice care along with links to relevant documents and where to get advice.
Another AHANZ initiative is the opportunity for members to hear from a political panel comprising of representatives from Labour, the Greens and the Opportunities Party discussing Health Manifestos and their vision for the future. PNZ reps from National Office will attend the forum, which finishes with a presentation/discussion from the current Minister of Health. September’s issue of Physio Matters will
feature an article detailing various Party views on physiotherapy and health in the lead up to the September 23rd election.
National Office staff
After a year and a half with us here at PNZ, our Membership Administrator Claire Angliss finished up at the National Office at the end of July. Claire is leaving us to go travelling with her partner. We wish Claire the safest of travels and all the best for her future endeavours – she will be missed!
The Annual Hawkes Bay Symposium
Dynamic Wellness Embracing the Four Pillars of Healthfor Allied Health Professionals
Join us for a jam-packed day in The Bay listening to a diverse range of speakers who will share their expertise in creating dynamic wellness for clients by embracing the Four Pillars of Health.
HAWKES BAY PHYSIOTHERAPY BRANCH presents
DATE: Saturday September 16th
VENUE: The Education Centre at Hastings Memorial Hospital, Canning Road, Hastings.
TIME: 8.30am – 5.30pm (9 CPD hours)
Key Note Speaker: Warren Bernard - “Psychology and the Body”
Warren works as a clinical psychologist in the cancer, renal and chronic pain service at the HBDHB.
More information about Warren is available on his website: www.wiseandshine.co.nz
Our topics throughout the day will include issues such as:
• Mental Health• Community Services• Chronic Pain• Pain Management.
Book now for the Early Bird Price (Book before August 20th)
$150Regular price
$175Closing date: Friday September 8thRegistrations available online through PNZ website.For further information contact [email protected]
On that note, we’d like to extend a very warm welcome to Bridgette O’Connor, who joins us as our new Membership Support Coordinator. I’m sure you’ll all make her feel very welcome and we are very pleased to have her as part of the team.
Peter Christie Interim Chief Executive
Bridgette O’Connor

The Annual Hawkes Bay Symposium
Dynamic Wellness Embracing the Four Pillars of Healthfor Allied Health Professionals
Join us for a jam-packed day in The Bay listening to a diverse range of speakers who will share their expertise in creating dynamic wellness for clients by embracing the Four Pillars of Health.
HAWKES BAY PHYSIOTHERAPY BRANCH presents
DATE: Saturday September 16th
VENUE: The Education Centre at Hastings Memorial Hospital, Canning Road, Hastings.
TIME: 8.30am – 5.30pm (9 CPD hours)
Key Note Speaker: Warren Bernard - “Psychology and the Body”
Warren works as a clinical psychologist in the cancer, renal and chronic pain service at the HBDHB.
More information about Warren is available on his website: www.wiseandshine.co.nz
Our topics throughout the day will include issues such as:
• Mental Health• Community Services• Chronic Pain• Pain Management.
Book now for the Early Bird Price (Book before August 20th)
$150Regular price
$175Closing date: Friday September 8thRegistrations available online through PNZ website.For further information contact [email protected]

FEATuRE
6 | PHYSIO MATTERS AUGUST 2017
Snow sport injuries and how to treat them
Skiing and snowboarding are popular winter sports in New Zealand and come with their fair share of associated injuries. Esther Bullen uncovers what the most common injuries are and what treatment methods are available to physiotherapists.
FEATuRE
© iStock

PHYSIO MATTERS AUGUST 2017 | 7
We’re a nation of snow seekers – when the ski fields open, we flock there in droves. On average over one million people take to the ski fields in New Zealand every winter. And on the international stage, the New Zealand skiing and snowboarding team have high hopes for winning medals at next year’s Winter Olympics.
Snow sports are exhilarating and fun, but as physiotherapists know only too well, they come with a safety warning: injuries can happen. A recent study titled New Zealand Snow Sports Injury Trends Over Five Winter Seasons 2010–2014 found that over a five-year period, more than 18,000 skiers and snowboarders suffered injuries on the slopes. Falls accounted for 74.3% of all injuries, followed by collisions (9.6%), jumps (7.3%), man-made terrain features (5.3%) and lifts (2%). The most common injuries were to the knee (36%), followed by the back (18%), wrist (14%), head (11.2%), shoulder (11%), lower leg (6.4%), and collar bone (3.4%).
The study’s lead researcher, Brenda Costa-Scorse, senior lecturer in paramedicine at the Auckland University of Technology, is quick to point out that the figures need to be kept in perspective. “Skiing and snowboarding can often be pitched
by the media as really dangerous, but if you look at the proportion of the recreational skiing and snowboarding population that aren’t injured, that doesn’t necessarily ring true. Many people go skiing and snowboarding, and come away uninjured having had a really great time. However, there is definitely latitude to increase injury-free fun with injury preventive actions.”
Reducing the injury rate
Brenda is also the primary author of the New Zealand Snow Sports Injury Prevention Strategy 2015-2020, which was written in collaboration with Ski Areas Association New Zealand. The strategy aims to reduce the injury rate by 10% over a five-year period. A key initiative of the strategy is a new New Zealand Snow Safety Code, which was launched by the association and ACC last year. “We need to promote the code and encourage people to get fit to ski or board – not just generally fit to run around the streets of their hometown. I think physios, particularly those doing work with Pilates, have a huge opportunity to reduce the odds of re-injury and push the injury prevention message”, says Brenda.
In terms of equipment, Brenda advises recreational skiers to get their skis serviced annually, including torque testing ski bindings to ensure that the spring and lever system is functioning at the correct release setting. She says skiers and snowboarders should wear helmets, and snowboarders with less than 30 days boarding experience should wear wrist guards. Skiers and snowboarders also need to understand the mountain environment – how changing snow conditions and visibility can affect their ability to ski or snowboard safely.
Picking up the pieces
Keen snowboarder and physiotherapist Deborah Torrington sees hundreds of knee injuries, mostly from skiing, through her Queenstown Physiotherapy clinic every season. “They’re typically ligament injuries, so they’re sprains, most commonly MCLs,” she explains. “They tend to be twisting-type injuries, where the knee becomes the pivot point. Skiers can also have more serious knee injuries such as ACLs, and again, that’s when their ski doesn’t release from their boot.” Another injury specific to skiers is “skier’s thumb” – when skiers fall and the pole forces their thumb backwards injuring the ligament.
Snowboarders, on the other hand, come to the clinic with mostly upper limb injuries because both their feet are attached to the board, so they don’t have that same twisting force to the lower limbs. These injuries are commonly fractured wrists or collarbones, or shoulder and elbow dislocations. However, snowboarders can also rupture their ACL following Brenda Costa-Scorse
Deborah Torrington

FEATuRE
8 | PHYSIO MATTERS AUGUST 2017
a “big air, flat landing”, where they overshoot a jump and miss the angled slope, and land on the flat with their quad muscles absorbing the full force of the landing. Then there’s “snowboarder’s ankle” or a talus fracture, also from landing hard after a jump. This injury has become more common since snowboarding increased in popularity.
What’s to blame?
Injuries are usually the result of the force of a fall, but sometimes, says Deborah, it is purely bad luck and the way the person happens to fall. However, clients often blame fatigue. Deborah’s advice? “We always say, don’t call last run.” As the name implies, “last run” is the last run before heading to lunch or home for the day, and this can often be when an injury occurs. She says that “weekend warriors” like herself are most at risk from fatigue-related injuries. These are people who work Monday to Friday and go to the mountain only on weekends. “We’re likely to think we’ve only got the weekend, and then we go too hard and too fast.”
Another common cause of injury is people exceeding their technical ability. Deborah says people go too fast for their skill level, use the chairlift before they can get off safely, or progress to the more challenging slopes or the terrain park – where the jumps and other man-made obstacles are – before they are ready.
There are other factors that can play a part, such as poor gear setup, particularly if the boot binding is too tight and doesn’t release; and icy conditions, which make falling injuries more severe. “That’s when we see whiplash and concussion, which we see in both skiers and snowboarders. And we see quite a lot of that. Or it can be breaks and fractures which, as physios, we don’t tend to see straight away.”
Mitigating the risk of injury
There are ways to mitigate the risk of injury, and Deborah’s advice to clients is
simple and easy to follow: “Obviously the stronger and fitter you are, the less likely fatigue will play a part in any injury. But I always tell my clients to walk from the car park and not to take the shuttle, because the walk is a nice, gentle warmup, especially for lower limbs. And then to ease into it on the slopes, start gently.”
Deborah recommends protective gear, including helmets for everyone and wrist guards for snowboarders, particularly for beginners and those progressing to the terrain park where there’s further to fall and, therefore, more force in the landing. After a day on the slopes, Deborah would encourage stretching, particularly the lower limbs – quads, hamstring, glutes and hips. For pre-season preparation, Deborah prescribes squats, particularly done on an uneven surface to challenge balance as well as build strength.
Rehabilitation
The most common question Deborah gets asked is: “When can I get back on the snow?” For clients on holiday from Australia, the question becomes more loaded. “In the more serious injuries, that’s really easy to answer: they won’t be back. But in a grade one sprain in any ligament – and the majority is knees – it can be a bit more challenging because they’ve got a limited time and a small injury, and they don’t want it to affect their whole holiday.”
Deborah stresses the need to respect healing timeframes, but knows that this can fall on deaf ears. “Often, I recommend that they don’t ski, but I know that a lot of them will. I explain to my patients that they won’t ski to their full ability if they’ve got a little niggle, and that puts them at risk of other injuries.”
When assessing whether a client is fit for return to the ski field, Deborah uses a checklist to assess strength, ability and balance. For an injured knee, she will get clients to hop, jump and lunge. “With a hop, I’m looking more at their
power up. When they’re jumping, I’d look at how they land comparing left and right. And with skiers, you need that sideways agility so that’s the lunging or jumping out on one leg to the side.”
Enjoy the snow!
In Deborah’s opinion, the risk of injury is small and shouldn’t stop people enjoying the snow. She has worked in a first aid clinic on Coronet Peak and says the statistics tell the story: “On a busy day, we might see 30 patients, but there would be 3,000 or 4,000 people up the mountain. Obviously, some come straight down the mountain, but overall injuries are a very small proportion of the number of people up there having a great time.”
Professional skiers and snowboarders
For professional skiers and snowboarders, it is a whole different story. This is a high-risk sport, says Wanaka physiotherapist Ginny Rutledge, who is contracted to High Performance Sports New Zealand (HPSNZ) to work with the Olympic park and pipe ski and snowboard athletes. She is also physiotherapist for the USA Men’s Alpine Ski Racing Team, where for the past five years she has worked with the current Olympic Gold medallist and three-time world champion in the giant slalom event.
Ginny Rutledge
PHYSIO MATTERS AUGUST 2017 | 9
the weather like? Were they up to doing the trick? What did the landing look like? We try to be on top of every single athlete when an injury happens.”
Strength and conditioning is a big factor in injury prevention, which requires gym-based work. Ginny says attitudes have changed in the last 10 years, and now park and pipe athletes see the benefits of such programmes. “My role with High Performance Sports is largely involved with supporting strength and conditioning to keep these athletes uninjured, because we have real medal prospects for the next Olympic Games.”
Written by Esther Bullen
Last year, the 15 park and pipe athletes lost 840 days of training and competition to injury. Injuries commonly occur to the knee, back, shoulders, ankles and hips, and can include concussion. “The sport has high injury rates internationally so we are not an exception,” explains Ginny. In alpine ski racing, injuries are predominantly to the knee, but there is currently an increasing number of lumbar spine disc-related injuries.
Injury prevention for the professionals
Injury prevention is the focus of the HPSNZ snow sports support team. “If we think they’re at risk or not, all our athletes have a strong injury prevention programme,” says Ginny. Each athlete has a regular risk analysis, known as a rocket ship profile. Athletes are scored on a range of categories, such as strength, neuromuscular control, landing patterns and technical ability. This helps the support team identify the areas that need to be improved before the athlete can progress.
Every injury is analysed. “We sit around as a group and reflect on issues, such as their current acute and longer-term load management. We also ask: Were they tired? Were they fatigued? What were the snow conditions like? What was
World Class Education
Professional Instructors
Face to Face Learning
Ongoing Clinical Support
Money Back Guarantee
Treatment techniques combining the IMS and Trigger Point Models maximising clinical outcomes.
REGISTER ONLINE @ www.gemtinfo.com.au
CAA Accredited Courses Osteopathy Australia Endorsed Courses
EARLY
BIRD RATES
APPLY!
For more information, visit our website, call +61 3 9585 8100 or email [email protected]
2017 COURSE LOCATIONS: AUCKLAND, CHRISTCHURCH, MELBOURNE, SYDNEY, KUALA LUMPUR & MORE!
These courses will change the way you view the human body!
TRIGGER POINT DRY NEEDLING COURSES 2017Applications for Pain Management & Sports Injuries

Acc
10 | PHYSIO MATTERS AUGUST 2017
Reducing treatment injuries
ACC has recently published information on treatment injury claims for New Zealand public hospitals – cases where patients are inadvertently harmed during the course of their treatment. The number of treatment injury claims has grown steadily since ACC cover for injuries arising from treatment was expanded in 2005.
In 2016 more than 1.1 million people were discharged from public hospitals and during that time ACC accepted 5,034 claims for people harmed during the course of public hospital treatment. ACC plans to publish treatment injury information on a regular schedule to support improvements in patient safety. In future the information will be expanded to include private hospitals, primary care, and other health settings. The report is available at www.acc.co.nz/for-providers/treatment-safety/index.htm
The costs to ACC provide some indication of the impact of those injuries on patients. The actual and predicted future costs for treatment injuries last year was $418 million. ACC’s liability for the future costs of all treatment injuries to date is $5.1 billion.
A range of treatment injury prevention programmes are underway including initiatives for safer surgery, pressure injuries, infections after surgical procedures, and brain injuries at birth.
What is a treatment injury?
A treatment injury is a physical injury caused by treatment from a registered health professional — but some exclusions apply. There is no requirement to find fault, although in some cases the cause of the injury will be treatment that is inappropriate in the circumstances.
Both the underlying disease that led to treatment and other pre-existing diseases are not covered, although a significant worsening of disease caused by treatment may be covered.
Also excluded are:
•anecessarypartofthetreatment(forexample an incision is a necessary part of surgery);
• theordinaryconsequencesoftreatment (for example hair loss following chemotherapy or radiotherapy burns are unlikely to be covered);
• injurycausedsolelybydecisionsabout allocating health resources (such as waiting list delays for joint replacement surgery);
• injurycausedbecauseapatientunreasonably delayed or refused to give consent for treatment;
• treatmentthatdoesnotachievethe desired result is not a treatment injury, for example if a physiotherapy programme that includes specific exercises fails to improve muscle weakness and balance following a stroke.
Injuries from physiotherapy
Between 1 January 2012 and 31 December 2016 ACC made decisions on 734 claims where the injury was caused by physiotherapy treatment. Of those 287 (39%) were declined. The main treatments that resulted in an accepted claim include manual therapy, joint mobilisation, spinal manipulation, strapping, and acupuncture. The most common primary injuries are strain/sprain, mainly affecting the lower back / spine, chest, shoulder and knee; followed by allergic reactions (95% caused by the use of strapping / tape / bandage) and burns from heat
treatment, which together comprise over 50% of accepted treatment injury claims from physiotherapy.
Reporting of harm
ACC is required to assess claims information and report ‘risk of harm to the public’ for both accepted and declined claims. Notifications to a health professional registration authority are made if ACC reasonably believes there is a risk of harm related to an individual professional. In most cases the decision to notify a risk of harm is based on advice regarding the appropriateness of care from an external clinical advisor.
Of the 13,825 decided claims in 2015/16 financial year, 509 claims were notified for serious risk of harm and 78 were notified for sentinel risk of harm. No claims from physiotherapy injuries resulted in notifications during this period. Between 1 January 2012 and 31 December 2016, five physiotherapy related treatment injury claims were notified for risk of harm.
Nick Kendall and Peter Jansen Injury Prevention Team ACC

PHYSIO MATTERS AUGUST 2017 | 11
Southern Physiotherapy Symposium 8
The philosophy of the Southern Physiotherapy Symposium is to combine clinically-relevant, evidence-based content with a weekend of fun and social activities. The programme will include a dynamic mix of both nationally and internationally recognised speakers addressing the diversity of contemporary clinical practice.
Date Venue
3-5 November 2017 Heritage Hotel, Queenstown
Symposium (Saturday 4 and Sunday 5 November)
Category Before 29.09.17 After 29.09.17
A. Otago-Southland PNZ members
$250 $300
B. Other PNZ members $380 $420
C. Non-members $480 $520
Pre-conference Workshops (Friday 3 November)
Category Workshop I:
Professor Bill Vicenzino9am-5pm,
Lateral epicondylalgia:
a pragmatic evidence informed approach
Workshop II:
Professor Lorna Paul
9am-12noon, Technology supported
rehabilitation
Workshop III:
Dr Bronwyn Thompson1pm-5pm,
Persistent pain management: “how to use those darned psychometric
questionnaires”.
D: Otago-Southland PNZ members (code OTAGOSOUTH8)
$150 $50 $75
E. Other PNZ members
$180 $60 $90
F. Non-members $225 $75 $112.50
Workshops only open to NZ Registered Physiotherapists. Conference attendace is mandatory for workshop attendance.
Programme now available at www.pnz.org.nz
Keynote Speakers:
• Professor Lorna PaulTopics: Multiple Sclerosis & quality of life after lower limb amputation.
• Professor Anne HollandTopics: The future is now: transforming pulmonary rehabilitation to improve uptake and outcomes. New guidelines for pulmonary rehabilitation in Australia and New Zealand – how will they impact on practice?
• Professor Bill Vicenzino Topics: Managing common mid-life tendinopathies like tennis elbow and gluteal tendinopathy: a pragmatic evidence informed approach. Proximal or distal approach to managing patellofemoral pain: which one and why?
Invited Speakers:
• Dr Bronwyn ThompsonTopics: How well do physiotherapists integrate a biopsychosocial perspective in clinical reasoning?
• Associate Professor Nicola KayesTopics: Co-creating health: optimising what happens at the point of care for better outcome.
• Katrina BryantTopics: Perspectives of disability and wellness of hau-a M -aori.
MSK UNIVERSITY OF OTAGO SPONSORED SPEAKERS:
Seven researchers from the School of Physiotherapy, University of Otago will give a brief (5 minute) synopsis of their research area or one aspect of it, with relevance to practicing clinicians. The session will include an interactive component for questions & discussion with attendees.
Dr Steve Tumilty
Dr Ramakrishnan Mani
Dr Daniel Cury Ribeiro
Dr Ewan Kennedy
Dr Meredith Perry
Dr Cathy Chapple
Dr Prasath Jayakaran
Registration Fees (GST not applicable)
Registration link via www.pnz.org.nz
Early-bird rates apply to all registrations received before Friday 29 September 2017. Registrations close Friday 20 October 2017. If booking accommodation at the Heritage Hotel please state that you are attending the SPS8. For further terms and conditions see www.pnz.org.nz

POlIcY & PRAcTIcE
12 | PHYSIO MATTERS AUGUST 2017
Health literacy
It’s a common occurrence for patients to volunteer that they have not been told anything or very little about their condition, medicines or treatment plan. However, in reality it’s more likely that health professionals have spent time discussing information that’s relevant to their condition and circumstances, but for a variety of reasons the information was not clear to or retained by the patient.
The concept of ‘health literacy’ came from the USA in the mid-1970’s where people with low health literacy were regarded as “risks”. Health organisations worried about being sued if informed consent was not provided or instructions followed. Initially responsibility was placed on the individuals with low health literacy, however over time health systems have focused on improving health provider communication and developing the health literacy skills of individuals.
New Zealand’s health literacy statistics come from the Adult Literacy and Life (ALL) Skills Survey (2006) which tested the literacy, numeracy and problem-solving skills of a large sample of New Zealanders aged 16-65 years.
Health literacy in New Zealand is broadly similar to other OECD countries including Australia, Canada and the United States with over half of all New Zealanders (56.2%) having poor health literacy skills. Maori have much poorer health literacy skills compared with non-Maori (regardless of gender), and almost 90% of Pacific men and women have poor health literacy.
Limited health literacy is associated with higher health system costs. There is minimal New Zealand data about specific costs per individual, however Canadian data shows that people with lower health literacy can have an increased spend between $143 and $7,798 per person per year compared to people with adequate health literacy.
Lower levels of health literacy are associated with:
• increasedratesofhospitalisationandgreater use of emergency care
•poorerabilitytotakemedicationsproperly and interpret labels
•pooreroverallhealthstatusandahigher risk of death among older people
In New Zealand, health literacy has been defined as ‘the degree to which individuals have the capacity to obtain, process and understand basic health information and services in order to make informed and appropriate health decisions’.
As motivated health professionals we have a responsibility to present information in accessible ways, but also to engage with individuals to make sure they can access, understand and act on the information they receive.
How can health literacy be improved?
A ‘universal precautions’ approach based on the concept that “you can’t tell by looking” is recommended as the best way. This means assuming that anyone could have poor health literacy, finding out what is actually known, then assisting the person to build their knowledge and skills as needed.
People with high general literacy can still experience poor health literacy and it can vary over time. When patients are sick or anxious, their ability to take in, recall and use health information can
be compromised which in turn affects their ability to manage their health.
Every interaction with a patient or their family and whanau provides an opportunity to develop people’s health literacy. The provision of good, clear communication (both written and spoken) to all patients and their family and whanau is important. This approach maintains the mana of the patient and their family and whanau. The Health Quality Safety Commission (HQSC) has developed a resource titled Three steps to better health literacy – a guide for health professionals.
Hints for helping people increase their health knowledge
Hopefully you’re able to build the kind of relationship with your patients where they feel comfortable enough with you to volunteer that they haven’t understood the information or instructions, despite your efforts. If and when this happens then an apology like; “I’m sorry I wasn’t clear. Let’s go over that again – what would work better for you?” can go a long way.
At times you may come across people who have incorrect knowledge or beliefs about their health condition. Before providing the correct information, you will have to deal with the incorrect knowledge in a way that recognises the person may have held those beliefs for a long time and that there are valid reasons for those beliefs.
Try to link all new information back to what the person knows already
PHYSIO MATTERS AUGUST 2017 | 13
by using the words the person used and building on these words. Tone used is important – aim for conversational and friendly. Putting “tell me” in front of any questions you ask can provide an informal opening to your information gathering and encourage people to open up.
When it comes to delivering information, people are more likely to remember it if it’s been relayed in a logical sequence – but they can only take in so much information before there’s short term memory overload, so it’s better not overwhelm someone with too much information. The best approach is to try and limit what you are discussing to 3-5 pieces of information. If it’s complex information, check that you have been clear after each chunk before going on to the next chunk.
Visuals and diagrams are helpful for reinforcing new info – the saying ‘a picture is worth a thousand words’ is very relevant in health situations. Don’t speak too quickly – especially if English is not their first language, and the use of an interpreter may be necessary if there is limited proficiency in English. Most importantly encourage people to ask you questions – “What questions do you have for me?” is more engaging than, “Do you have any questions?”
Remember: never make assumptions!
A letter to the Editor published in the New Zealand Medical Journal a few years ago told the story of David, who had had a radical prostatectomy and “was told to do pelvic floor exercises to reform and strengthen the muscles that control the bladder”. David outlined that he had carefully listened
to instructions and read the written material provided by the health professionals, but no one had actually explained to him that the exercises did not have to be done while sitting on the floor. In fact, he was not aware that the pelvic floor muscles were a group of muscles at the base of the abdomen. So for 15 months David endured pain as he got down on the ‘floor’ to exercise his ‘pelvis’, and this in turn affected his compliance and progress. In his letter, David pointed out that he was well-educated (two postgraduate degrees) but as a bachelor he had never been privy to any conversations about pelvic floor muscles or exercises prior to his operation. He eventually received a pamphlet from ACC that clearly explained what pelvic floor exercises were in a way that made sense to him and he was able to make progress.
Perhaps David could have been spared some frustration and discomfort if a health professional had asked; “I just want to check I have been clear – what exercise are you going to do to strengthen your pelvic floor when you get home?”
Sue Doesburg Professional Advisor – Policy & Practice
NEW ZEALAND BOBATH ASSOCIATION (NZBA) Inc. PO Box 74432 - Market Road, Auckland, New Zealand
BASICBOBATHCOURSEVENUE:MIDDLEMOREHOSPITALDATES:13TH-24THNOVEMBER(10DAYS)5TH-9THMARCH(5DAYS)COST:$3450FORMOREINFORMATIONPLEASEEMAIL:[email protected]
ThiscourseaimstohelpdevelopyourabilitytousethecurrentBobathConceptintheassessmentandtreatmentofpatientswithneurologicaldysfunction.Expandyourclinicalreasoningandproblemsolvingskills.Developyourskillsofobservation,analysisandfacilitationofmovement.
BOBATHWORKSHOPTheBobathConceptistheLearningofThePatient:CompensationvsRecoveryofImpairment
VENUE:TAURANGADATES:11TH-12THNOVEMBERCOST:TBAFORMOREINFORMATIONPLEASEEMAIL:[email protected] course is aimed at those therapists (Physiotherapists and Occupational Therapists) who have completed a 3 week Basic Bobath Course (Adults)
A three-step model for better health literacy
Step 1
Find out what people know
Step 2
Build health literacy skills
and knowledge
Step 3
Check you were clear (and,ifnot,gobacktostep2)

MEMBER BEnEFITS
14 |PHYSIO MATTERS AUGUST 2017
Refresher on using the EBSCOhost database to access articles and journals
As a member of PNZ, you are given special access to the EBSCOhost database – an online research catalogue where you can source industry-specific full text articles and journals (like our very own New Zealand Journal of Physiotherapy).
Over 3000 full-text journals can be found in EBSCO including:
•PhysiotherapyResearchInternational
•PhysicalTherapy
•PhysiotherapyTheoryandPractice
•SpinalCord
•TopicsinStrokeRehabilitation
•ClinicalRehabilitation
•DiabetesCare
•GeriatricsandGerontologyInternational
You can access the database from your dashboard on the PNZ members’ website (pnz.org.nz) – the EBSCO link can be found under ‘News, Publications and Resources’.
Conducting a basic search on EBSCOhost
Begin by entering your search terms in the search box. Click the Search button to view results or click Search Options to apply limiters and expanders.
the Detailed Record. To print, email, save, cite or export multiple results, add them to the folder, then click the appropriate icon inside the folder. Folder contents can be permanently saved by clicking on the Sign In link, and then creating a free personalized My EBSCOhost folder account.
Browsing publications in EBSCOhost
The Publications Authority File lists the titles included in the database by publication name.
You can browse the list of publications or perform a search on one or more publications within a specific database.
To browse a Publications Authority File:
1. Click the Publications link (or Hierarchical Journal link) at the top of the screen.
Search Options allow you to limit or expand your search results before viewing the result list. Choose one of the available Search Modes and depending upon the databases you are searching, you may see the ability to limit results by Full Text articles, Scholarly (Peer Reviewed) Journals, or a particular publication. After applying limiters and expanders, click Search.
You can refine your results using the options in the Refine Results column. Results can be filtered by source types, such as Academic Journals, Magazines, or Newspapers, by clicking the checkboxes next to the desired source type. Click an article title to view the Detailed Record, or click a full text link to read an article.
You can print, email, save, cite or export a single result from
2. The Publications Authority File appears, with the beginning of the list displayed. (If you are searching multiple databases, several Publication files may be available. They will appear in the drop-down list under the Hierarchical Journal link.)
3. On the Publications Screen, enter your search terms in the Browse field. You can enter all or part of a publication name, for example, “New Zealand Journal of Physiotherapy”.
PHYSIO MATTERS AUGUST 2017 | 15
4. Select a search type by clicking the radio button next to:
•Alphabetical–Thissearchtypefindsjournalsbeginningwith the letters entered. Results are displayed in alphabetical order.
•BySubject&Description–Thissearchtypeallowsyoutosimultaneously search the subject, description and title fields of a journal.
•MatchAnyWords–Thissearchtypefindspublicationscontaining one or more of your terms. Results are displayed in order of relevance.
5. Click Browse to view your terms as they appear in the Publications Authority File. A Publication Title List is displayed.
For a description of the journal or publication, click the hyperlinked Publication Name. The information found in the Publication Details may include: the title, ISSN, publisher information (name, address, publisher URL), title history, bibliographic record and full text coverage, publication type, the subject and/or a description of the journal, and whether the journal is peer reviewed.
Marking items for search
You can use the Mark Items for Search feature to search several publications at the same time, or to combine publication names with other search terms.
To search for several publications at the same time:
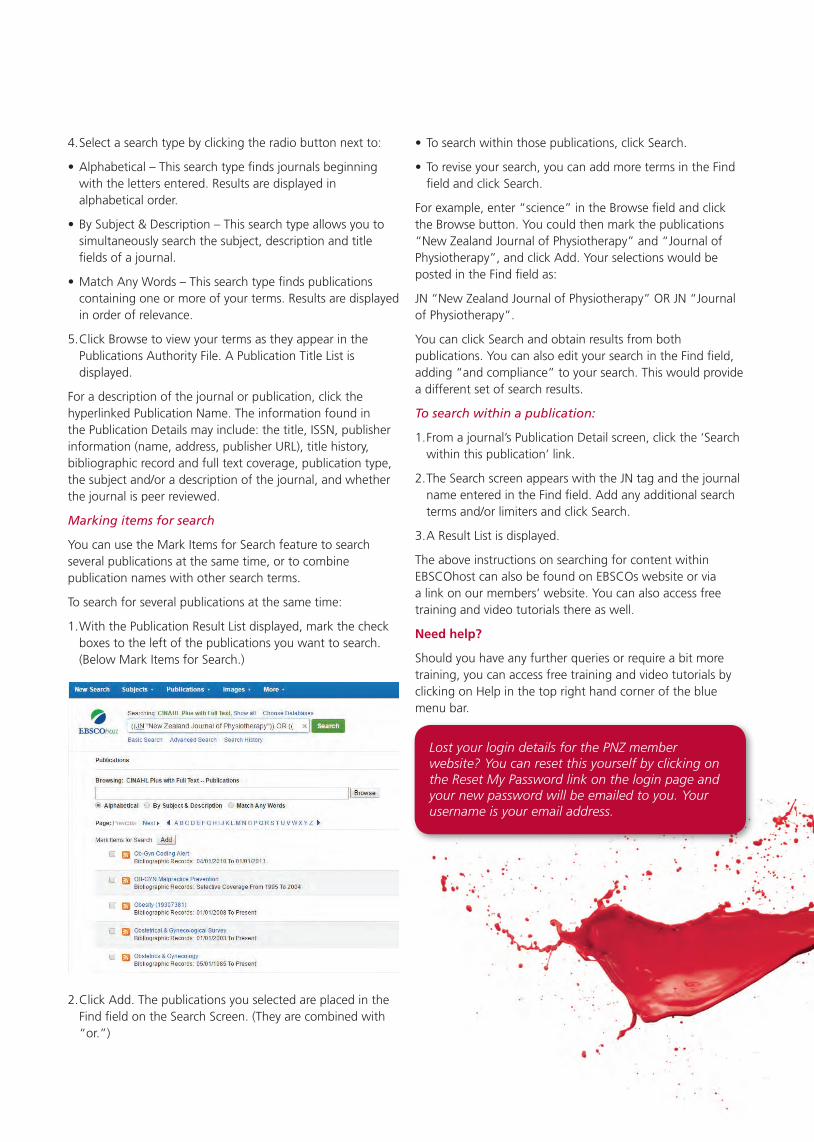
1. With the Publication Result List displayed, mark the check boxes to the left of the publications you want to search. (Below Mark Items for Search.)
•Tosearchwithinthosepublications,clickSearch.
•Toreviseyoursearch,youcanaddmoretermsintheFindfield and click Search.
For example, enter “science” in the Browse field and click the Browse button. You could then mark the publications “New Zealand Journal of Physiotherapy” and “Journal of Physiotherapy”, and click Add. Your selections would be posted in the Find field as:
JN “New Zealand Journal of Physiotherapy” OR JN “Journal of Physiotherapy”.
You can click Search and obtain results from both publications. You can also edit your search in the Find field, adding “and compliance” to your search. This would provide a different set of search results.
To search within a publication:
1. From a journal’s Publication Detail screen, click the ‘Search within this publication’ link.
2. The Search screen appears with the JN tag and the journal name entered in the Find field. Add any additional search terms and/or limiters and click Search.
3. A Result List is displayed.
The above instructions on searching for content within EBSCOhost can also be found on EBSCOs website or via a link on our members’ website. You can also access free training and video tutorials there as well.
Need help?
Should you have any further queries or require a bit more training, you can access free training and video tutorials by clicking on Help in the top right hand corner of the blue menu bar.
2. Click Add. The publications you selected are placed in the Find field on the Search Screen. (They are combined with “or.”)
Lost your login details for the PNZ member website? You can reset this yourself by clicking on the Reset My Password link on the login page and your new password will be emailed to you. Your username is your email address.

Plan your 2018 Musculoskeletal CPD now!
Online learning and courses
Clinical doctorate level educational program in 4Modules. Intensive self-directed online learning and 3Seminar days that may be spread over years. Upskill indiagnostics and 'diagnosis by subtraction' methodologyfor the lumbopelvic region, in readiness for musculoskeletal specialization. Comprehensive cover of
Dist inguish between
• different discogenic pains• nerve root syndromes• facet joint pain• sacroiliac joint pain• central/foramenal stenosis
Ident i f y confounders• central sensitization• psychosocial factors
common and rare conditions in a user friendly onlineenvironment with active interaction with Mark Laslett oncurrent case studies and clinical problems.
Start Module 1 in September 2017!
Shoulder Course Series Dr Angela Cadogan. PhD, NZRPS, Dip.MT, Physiotherapy Specialist (Musculoskeletal)
On l ine modu les inc lude between 6 -12 study hours cons ist ing o f :
1. Pre-reading articles2. Video presentation3. Additional resources and links for extended learning4. Module Quiz
The course cons ists o f f i ve on l ine l earn ing modu les that can be purchased ind iv idua l l y or as a package . The f i ve modu les cover :
1. Differential Diagnosis2. The “Stiff” Shoulder3. The “Unstable” Shoulder4. Subacromial Conditions5. Clavicular Conditions (AC and SC joint)
Completion of the online learning module is a pre-requisite for attendance at the optional courseweekends. Course weekends focus on practical assessment, diagnostic and clinical reasoning cases with real-time patient assessments and an orthopaedic surgeon will present relevant surgical techniques and post-operative rehabilitation considerations.
The Shoulder Course Series provides a comprehensive learning experience with a focus onclinical applications to help fulfill your 2018 CPD requirements.
To receive notifications when registration is available, "Like" us on Facebook or visit our website for more course information.
SOUTHERN MUSCULOSKELETAL SEMINARS
[email protected] | musculoskeletal.courses | @southernmskseminars | @SMS_Courses
NZ Registered Musculoskeletal Physiotherapy Specialists Drs Mark Laslett & Angela Cadogan collectively have over 40 publications on the diagnostic validity of the clinical examination for lower back and shoulder pain.
Follow a series of online lectures, readings, videos and quizzes covering the diagnosis and management of lower back and shoulder conditions. Audio enhanced lectures and a library of case study videos are all online for you to pause,rewind and playback. Practical seminar days are used for practice of physical tests and skills, logical diagnostic andtherapeutic clinical reasoning, problem solving including interpretation of imaging & live case demonstrations. Online quizzes and assignments allow you to self-assess your understandingand augment your retention of lectures, readings and patient videos.
Clinical Diagnosis of Persistent Back & Referred Leg Pain Dr Mark Laslett, PhD, NZRPS, FNZCP, Dip.MT, Dip.MDT
Shoulder online courses available now. See website for 2018 course dates.
Online learning modules providing a systems approach to diagnosis, rehabilitation and management of all common shoulder conditions. Suitable for all levels of experience including new or recent graduates or those looking for a musculoskeletal career pathway towards advanced practitioner or specialisation. Study at home, in your own time using a variety of interactive learning tools.

PHYSIOTHERAPY BOARd OF nEw ZEAlAnd
PHYSIO MATTERS AUGUST 2017 | 17
Advertising your services – what’s the standard?
The Physiotherapy Board is drafting new standards for the profession. These are the minimum quality standards for physiotherapists. They also provide information in regards to the public’s expectations of physiotherapy.
That’s why it’s important that physiotherapists like you have your say on them before they’re set.
Over the next few months, we’ll be consulting via email, online presentations, and local meetings. But we’ll also be highlighting some of the draft standards here.
We’d like to work with you to get it right in terms of the content, but also the style and the wording – it’s important that these standards are clear and easy to understand.
How we market what we do, what we can and can’t say is important
to preserving the reputation of the profession and protecting the public from false or confusing claims.
The full draft standard can be downloaded at physioboard.org.nz/advertising, but the key points to think about are:
•Anyinformationprovidedinanadvertisement should be reliable and useful to consumers.
•TheAdvertisingStandardsAuthorityprevents patient testimonials. This is to ensure the public is informed objectively, rather than subjectively, which is appropriate for responsible
science-based health professions.
•Althoughtherearewebsitesthatsolicit feedback and testimonials from patients, it’s the responsibility of the physiotherapist not to solicit or publish/post these. If other people/organisations do and this is not endorsed or supported, the individual therapist is not responsible.
You can provide feedback on this standard and others or ask us questions anytime – just visit physioboard.org.nz/your-say-on-standards or our Facebook page: facebook.com/physioboard.
SIG
18 | PHYSIO MATTERS AUGUST 2017
Transforming clinical practice with a whole person-centred approach
When it comes to treating clients and patients, the practice of employing a whole person-centred approach can have many benefits – both for the client and for the physiotherapist. Susan Lugton from Physiotherapy in Mental Health SIG explains the benefits from her own experience.
I became a physiotherapist both because of a conviction that touch was healing and a desire to care and connect with people, through the body, in a way that was meaningful to them.
My training taught competency in anatomy, physiology and pathology, observation of the “objective body” and movement patterns. But, as I trained harder (to become better) in my chosen musculoskeletal arena, my original desire to know the whole person and touch intuitively was stifled, and I found myself more focused on clinical reasoning, diagnosis and evidence-based exercise and outcome measures. It felt like the person had to be pushed aside in order to treat the “broken bit”. I felt disheartened and exhausted.
Everybody is a story
Whole person healthcare is about being treated as a whole person rather than being separated into parts to be fixed. This approach recognises that everybody is a story and deliberately invites the person’s story into the clinical encounter together with the routine physical and diagnostic examination. Story is personal life events, significant experiences, feelings and emotions, relationships, relationship issues, family history, and much more (Broom, 2007). Although there are common themes to patient stories, such as unresolved feelings, loss, or isolation, they are always individual and uniquely meaningful. The story aspect is integrated with their physical dimensions to treat the whole person (Broom, 2013).
Being relational
Inviting story into our clinical encounter requires a special kind of practitioner. They need to be fully present, caring enough to understand and deeply listening for story (Broom, 2007, Charon, 2001). Your professionalism is based on ‘being in relationship’. The clinician values and notices how the patient feels when listening to their patient’s story and wonders or imagines what might be the meaning, relationship or significance between the patient’s symptoms and their experiences (Broom, 2000). This is not an easy task. As physiotherapists we have been taught to be directive in our assessments, ask questions that give us the answers we want, and hope that the patient doesn’t go “off on their story in the subjective examination.” Ironically, the spontaneous language expressed by the patient is often highly significant and connected to the whole story and the presenting physical symptoms (Lakoff & Johnson, 1999, Broom, 2007).
How to invite story into the room
In my initial consultation I say something like, “I have a whole person approach to healthcare which might be different to the way you have been treated in the past. I don’t see a separation between your physical body and all the subjective elements that are unique to you, such as personal life events, experiences, relationships and feelings. I value all of these things, rather than merely focusing down on parts, such as your painful neck or sprained ankle. Are you comfortable with that approach?” The patient often says something like, “Oh, that how’s I see things too. Everything
is connected, isn’t it?” If you begin this way, it is less likely that they will feel that you think (and often that they think) their symptoms are less “legitimate” if they begin to realise that their symptoms are more connected to their story than to mere physicality (personal communication, Broom, 2016). This integration creates a trust, curiosity and spaciousness within the physiotherapy sessions for “story” to emerge.
A story
I met a patient with right-sided gluteal pain that began after gardening. It seemed to be somatic lumbar dysfunction with L1/2 and L4/5 stiffness, overactive gluteals and weak abdominals, but I sensed there was more. The story emerged during the treatment. Spontaneously, the patient expressed difficulty with a family member, describing them as a “right pain in the butt”. The symptoms disappeared within hours of that session, where her feelings were explored and acknowledged around this difficulty. The pain persisted until the story emerged. This is symbolic language, known as somatic metaphor (Broom, 2002) where the patient’s language “right pain in the butt” is very congruent with their experience or suffering (Lakoff & Johnson, 1999). It is not always this clear, but if the clinician is genuinely interested in the person’s story, the story telling in itself can create healing (Broom, 2000, Charon, 2001).
Symbolic language
I met with a young woman suffering eight months of debilitating abdominal and back pain and nausea, threatening
PHYSIO MATTERS AUGUST 2017 | 19
References available upon request.
her university studies and destroying her life. She sat holding her breath and body. There was palpable anxiety. We respectfully observed her body’s movements and breathing pattern, felt her spinal joints and muscles through gentle touch, always sensitive to the nausea being provoked. Through creating a space of safety, warmth and genuine interest for her personhood, the story eventually emerged.
She was “sick to the stomach” whenever she even thought about visiting a certain family member who had been very volatile and unpredictable during her childhood. Very similar feelings of “it makes me sick” occurred when she heard a friend say, “behind my back” that “my pain is not as bad as I say it is”. Her experience of “undiagnosed abdominal pains” is distressing to her. It feeds the invalidation that she receives from her family and most of the health professionals she has encountered. Through gentle touch, breathing, encouraging healthy movements and exploring story with compassion and validation, her abdominal, back and nausea symptoms subsided.
Summary
When asked if I would write an article about my whole person-centred approach, there was excitement for the opportunity to reveal the expansive way I treat since embarking on the AUT Mindbody Healthcare papers in 2010. The Mindbody Trust led by Dr Brian Broom has recently created an excellent website that describes whole person
healthcare in more detail: www.wholeperson.healthcare
Practicing with a whole person-centred approach has undoubtedly challenged me and stimulated a much deeper and meaningful practice as a physiotherapist. Physiotherapists are in a privileged position, for we have a licence to touch. It is much easier to seek help for physical pain than it is emotional pain. I do not see a separation between story and body. I have a strong trust that when we bring both aspects of the person together in the same room at the same time, something special frequently happens. Make no mistake. Touching heals. This does not mean discarding my clinical tests, diagnoses, observations and exercise prescription but equally valuing the role a person’s story has in the manifestation of symptoms or disease. Getting caught up in the norms of evidence-based practice and following patient outcome measures, rather than your heart, may render the person invisible. Be relational, invite the person’s story to emerge as well as your skilful exercise prescription, touch, advice and education, and be prepared to witness transformations.
Written by Susan Lugton
The whole story often lies underneath. ©iStock
NB: All courses held in Wellington. Both Part A & B courses have an online component requiring successful completion prior to attending the 3 day course. This is approximately 7 hours work. Registration can now be completed online at: www mckenzieinstitute.org/nz
2017 Education Programme
For further info, please contact: Kay Morgon, Branch Manager. Ph: 04 299 6645 or Email: [email protected]
Credentialled Update Day 4 August 2017
Seminar Day 5 August 2017
Part A The Lumbar Spine (3 days) 15-17 Sep 2017
Part C Advanced Lumbar Spine & Extremities – Lower Limb (4 days)
16-19 Nov 2017
Part A The Cervical and Thoracic Spine (3 days)
16-18 Mar 2018

TOMORROw’S PROFESSIOn
20 |PHYSIO MATTERS AUGUST 2017
Physiotherapy students have much to learn from the humanities
Many medical disciplines have started encouraging their students to embrace lessons from the arts and humanities. Physiotherapy is lagging behind, says Senior Lecturer in Physiotherapy Michael Rowe from South Africa’s University of the Western Cape.
Undergraduate physiotherapy students spend most of their time learning about the basic and clinical sciences. This has a certain pragmatic appeal, but a person is more than an assemblage of body parts. Our students learn anatomy and biomechanics – the idea of bodies as machines – and then explore what can be done to those bodies in order to “fix” them. Universities pay lip service to the idea that patients require holistic management. But not much in
and their patients.
In addition, a relationship between emotion and learning has been well established, with findings from multiple domains supporting the idea that emotion is intimately intertwined with cognition, serving to guide learning, behaviour and decision making. This suggests that introducing concepts from the humanities when educating health professionals can do two important things: develop
the curriculum signals to students that it really matters.
Research has confirmed what seems intuitively true to many: empathy is critical in developing medical students’ professionalism. The humanities, and particularly literature, are considered effective tools for increasing students’ empathy. There is also some evidence that health professionals who are trained in the humanities and liberal arts are better at caring for themselves
A photograph taken by a fourth-year student in the author’s professional ethics module. ©Sarah Manig

PHYSIO MATTERS AUGUST 2017 | 21
students’ emotional responses and their empathy; and simultaneously improve their overall learning.
Examples from other disciplines
The medical disciplines have started to embrace the role that the humanities and the arts can play in developing empathy in their graduates. In the US, Johns Hopkins Medical School has a department of art as applied to medicine and Stanford School of Medicine has a programme for medical humanities and the arts. These are two of the world’s top medical schools. Elsewhere in the world, South Africa’s University of Cape Town’s medical school chose the theme “Medicine and the Arts” for its first ever Massive Open Online Course.
In an editorial explaining Stanford’s stance, the medical school’s dean, Lloyd B Minor, wrote:
“The specificity of scientific interventions does not account for the messiness of human life … We as physicians heal best when we listen to and communicate with our patients and seek to understand the challenges they face in their lives. The perspectives on illness, emotions and the human condition we gain from literature, religion and philosophy provide us with important contexts for fulfilling these roles and responsibilities.”
Physiotherapy lags behind
There is little evidence that physiotherapy and other health professions are following these medical schools’ innovative approaches in undergraduate education. Some physiotherapy researchers have explored how concepts from the humanities could be integrated into clinical practice. But this has tended to focus on the impact on professional practice among qualified therapists, rather than on students and their learning.
The reasons for this are unclear, though several factors may be at play. Physiotherapy is conservative
by its nature and tends to privilege positivist methods in general. It favours quantitative measurements of progress as the standard against which impact is measured. Our students are taught how to address physical impairments in a patient’s anatomy and biomechanics, using joint range of motion, strength and fitness as indicators. This is important but also tends to sideline approaches that are more interpretive in nature. For example, it’s good to know how to treat back pain from a purely physiological point of view – but it’s also important to know how to respond to a patient who believes his or her pain is the result of witchcraft.
These differences in perspective may be what limits the potential for the humanities to have much impact on curriculum change from the point of view of the clinical therapist. My own teaching experience, though, suggests that physiotherapy students benefit hugely from practices and ideas that are influenced by the humanities.
Putting theory to the test
About three years ago, as an experiment, I started applying some of these ideas in the professional ethics module I teach at a South African university. Initially the module’s emphasis was on human rights, but I started foregrounding empathy and the development of empathy instead.
Over the past few years my students have explored the humanities – art, literature, theatre, music and dance – in their assignments for this module. This has helped them to develop a sense of awareness of empathy in the context of clinical education.
Students can interpret the assignment in any way they want as long as they integrate concepts from the ethics module with their own experiences in clinical practice. They must also express their work through “creative” means: they write poems, draw pictures or cartoons, film video diaries or re-interpret popular songs. Two of my students have even filmed themselves
This article was originally published on The Conversation website. Republished with permission.
using interpretive dance to try and embody what it might be like to live with a disability. Others have completed PhotoVoice assignments (such as the image on the facing page). Here, they photograph people in community or clinical contexts, and then reflect on how those experiences and interactions informed their personal and professional development as ethical practitioners.
Students’ response
Many students were initially worried about the assignments, telling me they were “not creative” and would prefer to write an essay. I suspect that they were simply feeding off my own hesitation in the early days. Now that I provide literature to support the assignment design, give examples from previous students and am fully committed to the process, far fewer students express these concerns.
They are also starting to open up in much more interesting ways. They draw from their own very deep emotions and personal experiences, and are more willing to share and discuss their work in class.
Building empathy
Creativity does not naturally decrease over time. Instead, higher education systems place less and less emphasis on creative expression as students move through the system. If universities want to graduate physiotherapists who have an increased awareness of patient suffering, and an associated empathic response, maybe the key is to provide them with learning tasks that encourage their creative expression through humanities and the arts.
Michael Rowe Senior Lecturer in Physiotherapy University of the Western Cape Cape Town South Africa
Our 4th Biennial SPNZ Sports Physiotherapy Symposium
We would like to welcome you to attend our 4th Biennial SPNZ Sports Physiotherapy Symposium.
The 2017 Symposium will again be the top clinically based program for the year. All speakers will provide practical information that you can use in your clinic tomorrow.
Pre and post workshops will again be available. For more details on these, see our website www.spnz.org.nz
Date Venue
October 14-15th 2017 Pullman Hotel, Auckland
For further information and to register please see our website:
http://sportsphysiotherapy.org.nz/
Featuring:
• Dr Phil GlasgowPhil was the Chief Physiotherapy Officer for Team GB at the Rio 2016 Olympic Games.
Phil is particularly interested in understanding the factors that influence the development of mastery and effective performance in both sporting and professional environments.
• Chris BishopChris is the founder of The Biomechanics Lab in Adelaide.
Chris’ research has focussed on the relationship between the foot and shoe, in both how the foot moves inside the shoe and how the shoe design can be optimised to influence the biomechanical function of the foot.
• Jordan SalesaBHSc – Physiotherapy, PGD Sports Medicine, Masters Health Practice – Physiotherapy (Manipulative & Acupuncture), NZRP.
Jordan is one of the owners of Physio Rehab Group. He is also a performance physiotherapist at the National Training Centre (High Performance Sport New Zealand) where he looks after many of New Zealand’s top athletes. He is also the lead physiotherapist to Swimming New Zealand and holds roles with Rugby Sevens and gym sports.
He has extensive professional experience having been a Physiotherapist with: Manu Samoa (7s and 15s) 2000-2007, Samoan Olympic and Commonwealth Games Team – Sydney 2000, Manchester 2002, New Zealand Olympic and Commonwealth Games Team – Athens 2004, Melbourne 2006, Beijing 2008, New Delhi 2010, London 2012, Glasgow 2014, Rio 2016, and has been appointed to the Gold Coast Commonwealth Games for 2018.
• Justin Ralph(PGD HSc)
Justin is a performance physiotherapist with High Performance Sport New Zealand based in Cambridge, primarily working with Cycling New Zealand. He has previously worked with para-cycling from 2011-2016, including the London and Rio Paralympic Games. Justin has a special interest in the field of bike fitting, which continues to evolve with his new full-time role with Cycling New Zealand.
• Dr Bruce Hamilton• Rob Moran• Dr Steve Kara• And many more quality speakers
Registration Fees(early bird rate available until 21 August 2017)
Symposium
Category Before 21.08.17 After 21.08.17
A. SPNZ members* $330 $380
B. Other PNZ members $400 $450
C. Non-members $590 $590
*To receive the SPNZ member price, please use the discount code provided in the event listing on pnz.org.nz
Early-bird rates apply to all registrations received before 21 August 2017. Registration is secured by payment on a first come first served basis. For other terms and conditions see www.pnz.org.nz

ScHOlARSHIP TRuST
PHYSIO MATTERS AUGUST 2017 | 23
Understanding obesity from an indigenous perspective
New research led by Scholarship Trust recipient and Physiotherapy New Zealand (PNZ) member Ricky Bell finds increased connectedness and collective health care approaches may be the key to reducing rates of indigenous obesity. Nick Clode summarises the findings of the study.
Bell’s qualitative study titled Understanding obesity in the context of an Indigenous population was recently published in the Obesity Research and Clinical Practice journal. The study found healthcare practitioners and healthcare agencies responsible for improving public wellness would be wise to focus on strategies targeted at the
collective and those which improve an individuals’ feelings of connectedness – as opposed to focusing on providing simplistic advice around calorific restriction, exercise and diet.
The study looked at indigenous groups with a view to revealing a better understanding of how obesity effects indigenous people within their context, and identifying the complex inter-related drivers that contribute to its high prevalence in indigenous populations. The study’s authors hoped a deeper understanding of these issues could inform the development of culturally relevant approaches to increase indigenous wellbeing and therefore reduce the prevalence of indigenous obesity.
This study involved semi-structured interviews of 15 individuals recruited from indigenous tribal groups that were over 30 on the BMI scale. Results from these interviews informed the study’s main findings.
The findings were categorised into four different themes, and identified factors that may support reductions in obesity and facilitate obesogenic environments:
The importance of relationships and social connectedness, or kotahitanga, were highlighted by study participants as being central in facilitating any changes towards reducing obesity prevalence. One participant described this eloquently as, “the healthier we are collectively, the better off we are individually” (Bell et al., 2017). The importance of incorporating indigenous customs and worldviews into healthcare intervention was also paramount; “I think tikanga (indigenous custom) and health and wellbeing are actually in unison”, (Bell et al., 2017) and many participants reported being disenfranchised by a western approach to healthcare.
The study highlighted facilitators that may lead to obesogenic environments. This included use of an over simplistic biomedical model which emphasises a personal responsibility narrative of caloric restriction, diet and exercise – described as “non-relatable” to indigenous people. Contrary to the common western view of obesity, most participants did not express body image dissatisfaction, and most of the benefits of losing weight for indigenous people were around an increased ability to participate in activities with their wh-anau.
It was also found that colonisation was an intrinsic stressor for participants. The authors hypothesised this stress may have interacted with neuro-endocrine responses and epigenetics to create an obesogenic environment.
Overall, the study’s findings indicate radically different strategies are required to support reductions in this significant public health problem. These strategies need to focus on holistic health care, connectedness and approaches that are collective, rather than individual.
It is hoped that this exploratory study will lead to further work in designing new indigenous wellness programmes targeted at reducing the prevalence of obesity.
Nick Clode Learning and Research Advisor
Factors that may contribute to Indigenous wellness, and support reductions in obesity prevalence
Facilitators to obesogenic environments
Holistic healthcare supporting Indigenous customs and worldviews
Biomedical model is un-relatable and culturally insensitive
Relationships and social connectedness “kotahitanga”
Historical trauma and the effects of colonisation
All references available on request. Readers can find the original article by following this link: www.sciencedirect.com/science/article/pii/S1871403X17300285
Ricky Bell

STudEnT
24 | PHYSIO MATTERS AUGUST 2017
Experiences of a final year physiotherapy student
For some of us, our student days may be a distant memory. But for many young people currently studying physiotherapy in our universities, it is very much their reality. AUT physiotherapy student Katie Bennet and her classmates share some of their experiences during their final year clinical placement with Physio Matters.
We thought that three years of studying would be enough to at least give us a little bit of understanding of what physio life was like. After all, three years is a pretty long time to a twenty-something year-old. Oh, how we were wrong. Even after just three weeks into our first placement in our final year, there has been so much growth and learning going on that is far beyond what can be taught in a classroom. Classrooms and lecture theatres are great for teaching fundamentals and basics, but the real guts of physiotherapy comes in the doing; it is, after all, a physical therapy.
I asked my classmates for a few thoughts on these first weeks and there were some very distinct themes, as you’ll see below.
It’s completely different
“It’s completely different to uni ... you think you’ll be able to continue doing all the things you used to do … like playing sport, coaching [sports], exercising, keeping up relationships. But it’s so much harder than I could’ve imagined. At placement I’m constantly taking in new information, meeting new people and the cognitive demands are insane!”
“University-based learning can only get you so far within this career and it’s the practice and experience that make truly great physiotherapists! That’s what I’ve found in burns and hands – we aren’t taught a lot on the subject, but learning from the section head and the senior physiotherapists and the consultants has got me thinking and challenging my knowledge acquired while I was at uni”.
“Fit, young, healthy, twenty-something year-olds just can’t pretend well enough to allow another student to truly understand a given set of impairments or conditions”.
It’s exactly like they told us
“It’s great to finally be able to experience the different conditions we have been learning about over the past few years of our degree. To see and feel the impairments, of say a stroke, and the impact to a patient’s functional life. It really solidified, and gave context and true appreciation to our previous learning.”
“I knew the concepts of measuring tone and spasticity, I’d practiced the physical doing of this dutifully on my neurotypical classmates. Feeling the catch of spasticity the first time was exhilarating, it was exactly like my lecturers described. It makes so much more sense now being able to put a real experience to the theory”.
It’s overwhelming
“We have been learning about physiotherapy for the past three years but that’s nothing in comparison to learning for doing placement and having your own patients and learning from those [who are] more experienced”.
“While I know that I know stuff, I feel like there’s so much more that I don’t know. It’s overwhelming at times and I feel quite inadequate when I watch the more experienced therapists doing their thing – they just go, go, go, and never seem to stop to process any of it”.
It’s exhausting
“Many people (supervisors, past students and lecturers) warned about how tiring placement was going to be. I did take the advice, but the level of exhaustion was still more than I was prepared for.”
“One word: ‘fatigue’”.
AUT Physiotherapy students: (L-R) Kairan Govender, Hamish Donnison, Katie Bennett, Kirsty Wilson, Caitríona Denny, and Christie Whitehead.

PHYSIO MATTERS AUGUST 2017 | 25
“I’ve worked forty plus hour weeks before but managing the mental demands and cognitive fatigue of placement, on top of part-time paid work, and still trying to exercise to stay sane, and only briefly see my family and friends, I feel like a shell of my usual person”.
“I’m so tired I told my supervisor the cuboid was a bone in the wrist”.
It’s complex
“It’s harder than I ever thought it would be”.
“It’s challenging. Putting all the bits together at the same time makes my brain work in overdrive, – but it’s definitely an enjoyable challenge, one that makes me want to work harder to figure it all out”.
“I don’t know about everywhere else but where I’m placed there
© August 2017 BIM Management Services.
Like to know more?Download our 40-page Franchise Prospectus from motionhealth.co.nz/prospectus
Or contact Andy Ross on 021 767 752 | [email protected]
Like to increase your revenue by 300%? We can show you how we’ve done it for others.
With less risk, less stress and all the business support you need to achieve your business dreams.
MHG01615_06Y17 - Physio Matters_Half page.indd 1 26/06/2017 2:46:06 PM
is so much more of an emotional, behavioural, and cognitive component to everything. People really open up, pour their hearts out, break down on you sometimes, and on the contrary you see or hear of some people who are very, very eager to tell you to jog along”.
It’s definitely what I want to be doing
“I think I’ve found my vocation. I love it”.
“My supervisor is pretty much me in ten years’ time, it’s crazy”.
It’s exciting and so much more than I ever thought
“I love it – every day so far has been different; challenging, exhausting, confronting, and exciting. I can’t wait to go back for more”.
At the end of the day, the placements
that we are on are all so incredibly
different, yet so much the same.
We’re all seeing different conditions,
in different contexts, in different
locations, with different people, who all
have different backgrounds, different
medical histories, and are at different
stages within the lifespan.
Yet, we’re all doing the same thing
– communicating with the person,
hearing their story, how their different
conditions impact their lives, assessing
functional and physiological aspects,
and working within an evidence-
informed practice to help them the best
that we can … even if we’re not very
good at it yet.
Written by Katie Bennett
AUT BHSc (Physio) student

RESOuRcES
26 | PHYSIO MATTERS AUGUST 2017
New Zealand Rehabilitation Research Review
The New Zealand Rehabilitation Research Review is an independent clinical update that features key medical articles from global rehabilitation journals with commentary from Associate Professor Nicola Kayes. Physio Matters got in touch with Associate Professor Kayes and asked her some questions about the Review and what benefits accessing the Review can have for physiotherapists in New Zealand.
Now in its eighth year, the Review covers a range of topics such as cardiac rehabilitation, stroke rehabilitation, pulmonary rehabilitation, physiotherapy, brain injury, cancer, geriatrics and orthopaedics. The Review currently has over 4,300 health professional subscribers throughout New Zealand who work in the area of rehabilitation and use the Review to keep up to date with new research.
Associate Professor Kayes and other specialists scan over 30 papers and pick the top ten that are most relevant to local practice in New Zealand for each issue.
The Review often features contributions from guest commentators, who contribute their opinions on select papers. Past contributors have included:
•DrFelicityBright,SeniorLecturerin Rehabilitation and Case Management.
•DrWilliamLevack,AssociateDeanof Research for the Wellington campus of the University of Otago, and a Senior Lecturer with the Rehabilitation Teaching and Research Unit.
•DrDavidRice,SeniorLecturerintheSchool of Clinical Sciences and a Senior Research Officer in the Health and Rehabilitation Research Institute at AUT University.
We asked Associate Professor Kayes a few questions about the Review and what motivated her to start the initiative.
What is your background?
I have a background in health psychology and my research predominantly explores the intersection between health psychology and rehabilitation. I am interested in exploring the role of the rehabilitation practitioner and their way of working as an influencing factor in rehabilitation and whether shifting practice and the way we work with people can optimise rehabilitation outcomes. I actively contribute to undergraduate and postgraduate teaching in rehabilitation at the School of Clinical Sciences at Auckland University of Technology.
Where did the idea for putting together the New Zealand Rehab Research Review come from?
Keeping up to date with research published in global journals is really time consuming. Particularly trawling through the papers relevant for New Zealand practice. Research Review follows an easy model of using an expert like myself to search through 30-40 papers each time and pick out my top ten papers that New Zealand practitioners should know about. It is an easy way to follow key research with independent expert opinion.
What benefit will accessing the Review have for physiotherapists?
We cover many hot topics and ground breaking studies in the Review that are important for physiotherapists’ practice. The Review will make physiotherapists aware of new studies they may not of heard about and the importance of them to their everyday practice. It is easy to digest – ten studies, four pages and it only takes 15 minutes to read.
What clinical areas does the Review cover?
The Review covers a broad range of clinical areas relevant to physiotherapy including cardiac, neuro, pulmonary, respiratory, cancer, musculoskeletal, orthopaedic and sports rehabilitation. We also cover topics relevant to transdisciplinary rehabilitation processes such as goal planning,
Nicola Kayes

PHYSIO MATTERS AUGUST 2017 | 27
discharge planning, therapeutic relationship, outcome measurement, and community integration.
How do you choose what to include in each Review?
The research review team identify papers published recently in key international rehabilitation journals and so I primarily select papers from that list. I tend to go for things that are particularly relevant to the NZ context at the time, or which are consistent with a ground swell of research on a particular topic. I also try to achieve some variation in terms of topic, population, rehabilitation context and methodology.
Every so often I include a paper that I have read recently which I have found particularly insightful or challenging. In the last couple of issues I have also identified a guest reviewer to focus a section of the review (five papers) on a particular topic so that readers can get a sense of the state of evidence in specific area of rehabilitation practice. This also means you get to hear from someone else instead of only getting my lens on everything!
NZ Rehabilitation Research Review is delivered by email as a PDF attachment every 3 months. Subscribe online at www.researchreview.co.nz.To get in touch with Associate Professor Kayes and her team, email [email protected].
For external use only. Avoid contact with eyes. Do not use on open wounds or infected areas of the skin. Not recommended for use during pregnancy.
P Pure magnesium with essential oils
P Relaxes muscle tension and tightness
P Supports physical performance before and after intense exercise
P Fast acting
Soothe stiff muscles and joints with Good Health Magnesium Cream
To place an order call Brandfolio Customer Service 0800 897 969 or email: [email protected]
www.goodhealth.co.nzGood Health Magnesium Cream is distributed by Brandfolio, Auckland.
Massage onto aching, tired, sore or stressed muscles to soothe & relax.
For those interested in subscribing, how can they do this?
There is no cost to subscribe to Rehabilitation Research Review. You can do so online at www.researchreview.co.nz or by emailing [email protected]. It is delivered by email as a PDF attachment bi-monthly.
We are keen to support physiotherapists’ ongoing education. If there any particular topics you would like us to cover, please get in touch.
Written by Erica George
28 | PHYSIO MATTERS AUGUST 2017
• Become a certified APPI Pilates Instructor in 2017• Full Matwork & Equipment Certification Series available • Online CPD courses
Clinical PilatesTraining
BOOK ONLINE | unitehealth.co.nz | +64 9 8896594
2017 Business Symposium and Annual General Meeting
GEnERAl nOTIcES
The inaugural Physiotherapy New Zealand 2017 Business Symposium and Annual General Meeting will be held at the Novotel at Auckland Airport on Saturday 28th October.
The whole-day event will host a range of expert speakers brought in especially to give you the latest knowledge and skills to improve your physiotherapy practice.
They key dates to make note of in the lead up to the AGM are as follows:
•NoticesofMotion–close5:00pmonFriday 8 September 2017
•PNZAGM–commences4:00pmon28th October 2017
Registrations for the Business Symposium and AGM will be available on pnz.org.nz from Monday 7 August 2017.
For the relevant nomination forms and more information, please visit pnz.org.nz
If any voting is required for Notices of Motion or National Executive vacancies, this will be done electronically.
We look forward to seeing you all there!
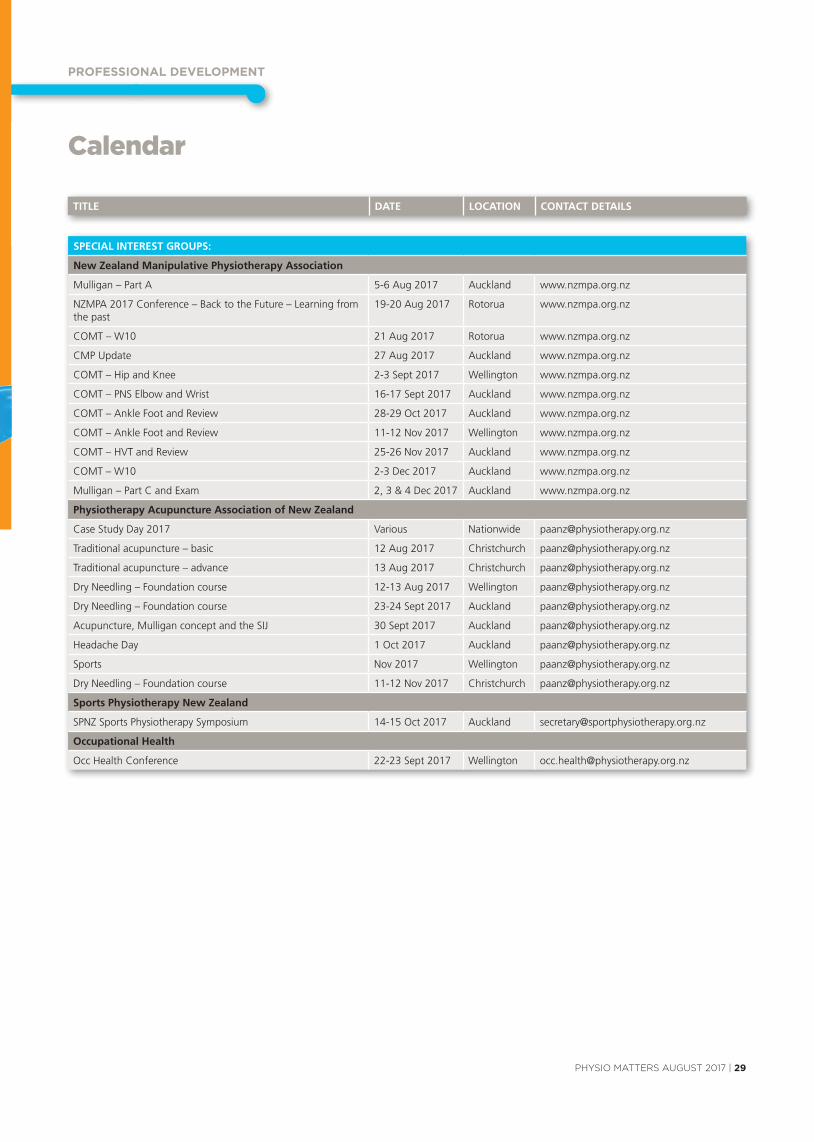
PROFESSIOnAl dEvElOPMEnT
PHYSIO MATTERS AUGUST 2017 | 29
Calendar
SPECIAL INTEREST GROUPS:
New Zealand Manipulative Physiotherapy Association
Mulligan – Part A 5-6 Aug 2017 Auckland www.nzmpa.org.nz
NZMPA 2017 Conference – Back to the Future – Learning fromthe past
19-20 Aug 2017 Rotorua www.nzmpa.org.nz
COMT – W10 21 Aug 2017 Rotorua www.nzmpa.org.nz
CMP Update 27 Aug 2017 Auckland www.nzmpa.org.nz
COMT – Hip and Knee 2-3 Sept 2017 Wellington www.nzmpa.org.nz
COMT – PNS Elbow and Wrist 16-17 Sept 2017 Auckland www.nzmpa.org.nz
COMT – Ankle Foot and Review 28-29 Oct 2017 Auckland www.nzmpa.org.nz
COMT – Ankle Foot and Review 11-12 Nov 2017 Wellington www.nzmpa.org.nz
COMT – HVT and Review 25-26 Nov 2017 Auckland www.nzmpa.org.nz
COMT – W10 2-3 Dec 2017 Auckland www.nzmpa.org.nz
Mulligan – Part C and Exam 2, 3 & 4 Dec 2017 Auckland www.nzmpa.org.nz
Physiotherapy Acupuncture Association of New Zealand
Case Study Day 2017 Various Nationwide [email protected]
Traditional acupuncture – basic 12 Aug 2017 Christchurch [email protected]
Traditional acupuncture – advance 13 Aug 2017 Christchurch [email protected]
Dry Needling – Foundation course 12-13 Aug 2017 Wellington [email protected]
Dry Needling – Foundation course 23-24 Sept 2017 Auckland [email protected]
Acupuncture, Mulligan concept and the SIJ 30 Sept 2017 Auckland [email protected]
Headache Day 1 Oct 2017 Auckland [email protected]
Sports Nov 2017 Wellington [email protected]
Dry Needling – Foundation course 11-12 Nov 2017 Christchurch [email protected]
Sports Physiotherapy New Zealand
SPNZ Sports Physiotherapy Symposium 14-15 Oct 2017 Auckland [email protected]
Occupational Health
Occ Health Conference 22-23 Sept 2017 Wellington [email protected]
TITLE DATE LOCATION CONTACT DETAILS

30 | PHYSIO MATTERS AUGUST 2017
TITLE DATE LOCATION CONTACT DETAILS
ExTERNAL PROVIDERS/ORGANISATIONS
The Shoulder - theory and practice 2-3 Aug 2017 Auckland https://goo.gl/8OkRwk
McKenzie Institute New Zealand – Credentialed Update Day 4 Aug 2017 Wellington www.mckenzieinstitute.org/nz
McKenzie Institute New Zealand – Seminar Day 5 Aug 2017 Wellington www.mckenzieinstitute.org/nz
Certificate in Spinal Manual Therapy 5-13 Aug 2017 Indonesia www.manualconcepts.com
Diagnosis and Management of Subacromial Conditions 5-6 Aug 2017 Christchurch www.musculoskeletal.courses/courses/shoulder
APPI Pilates Matwork 1, The Foundation 5-6 Aug 2017 Auckland unitehealth.co.nz
Rehabilitation for the Breast Cancer Patient 17-18 Aug 2017 Christchurch YourCorePT.com
Lymphoedema Therapists Hui: Elements of Care 19-20 Aug 2017 Christchurch [email protected]
APPI Pilates Equipment 1, Lumbo Pelvic Stabilisation 19 Aug 2017 Auckland unitehealth.co.nz
Myofascial Release Course – The Fundamentals 25-26 Aug 2017 Tauranga www.mfrworkshops.com
CPD Helath Courses: Dry Needling Introductory & Advanced Courses
25-27 Aug 2017 Auckland cpdhealthcourses.com
BradCliff® Breathing Method – Level 2 26-27 Aug 2017 Auckland [email protected]
Myofascial Release Course - The Fundamentals 1-2 Sept 2017 Auckland www.mfrworkshops.com
Dry Needling Advanced Lower Limb Course 2-3 Sept 2017 Queenstown https://goo/gl/Zh1qJg
Myofascial Release Course – The Fundamentals 8-9 Sept 2017 Nelson www.mfrworkshops.com
8th National Colorectal Pelvic Floor & Anorectal Disorders Course
8-9 Sept 2017 Auckland www.fhms.auckland.ac.nz/acsc
McKenzie Institute New Zealand – Part A – The Lumbar Spine 15-17 Sept 2017 Wellington www.mckenzieinstitute.org/nz
Pain - A Multidimensional Phenomenon (online course) 18-22 Sept 2017 https://goo.gl/BjsuAw
National Community Physiotherapy Conference 2017 21-22 Sept 2017 Tauranga [email protected]
Myofascial Release Course – The Fundamentals 22-23 Sept 2017 Christchurch www.mfrworkshops.com
APPI Pilates Equipment 2, Scapulo Thoracic Stabilisation 23-24 Sept 2017 Auckland unitehealth.co.nz
Myofascial Release Course – The Fundamantals 29-30 Sept 2017 Dunedin www.mfrworkshops.com
APPI Pilates Equipment 3, Spinal Articulation & Stretching 28-29 Oct 2017 Auckland unitehealth.co.nz
Mulligan Concept functional treatment of the pelvis 4-5 Nov 2017 Invercargill [email protected]
The Sports Thorax – ConnectTherapy™ & the Thoracic Ring Approach™ with Dr. Linda-Joy Lee
15-18 Nov 2017 Auckland https://goo.gl/laea3b
For all event listings, please visit pnz.org.nz
Calendar
BRANCHES
Hawkes Bay
Hawkes Bay Symposium: for Allied Health Professionals 16 Sep 2017 Hastings https://goo.gl/XewsI8
North Shore
September Branch Meeting 4 Sept 2017 Auckland [email protected]
November Branch Meeting and AGM 13 Nov 2017 Auckland [email protected]
Otago
Branch Meeting 4 Sept 2017 Dunedin [email protected]
Southern Physiotherapy Symposium 8 3-5 Nov 2017 Queenstown https://goo.gl/f1dnNE
Southern Physiotherapy Symposium 8 Workshop I: Professor Bill Vicenzino
3 Nov 2017 Queenstown https://goo.gl/Tx4Ibp
Southern Physiotherapy Symposium 8 Workshop II: Professor Lorna Paul
3 Nov 2017 Queenstown https://goo.gl/GxKweG
Southern Physiotherapy Symposium 8 Workshop III: Professor Dr Bronwyn Thompson
3 Nov 2017 Queenstown https://goo.gl/M9yKD9
PROFESSIOnAl dEvElOPMEnT

cOnTAcT dETAIlS
PHYSIO MATTERS AUGUST 2017 | 31
www.pnz.org.nz
Branch Contacts
Northland
Kimberley Pow [email protected]
North Shore
Lilian van den Bergh [email protected]
Auckland
Tony Westwood [email protected]
Waikato / Bay of Plenty
Rob Neish [email protected]
Hawke’s Bay
Raewyn Newcomb [email protected]
Middle Districts
Bridie Green [email protected]
Wellington
Darragh Kenny [email protected]
Nelson / Marlborough
Hilary Exton nelsonmarlborough@physiotherapy. org.nz
Canterbury
Jessie Snowdon [email protected]
Otago
Becky Wilson [email protected]
Southland
Fiona Morse [email protected]
Special Interest Groups
Cardiothoracic
Brigitte Eastwood [email protected]
Pelvic, Women’s and Men’s Health
Shelley Solomon [email protected]
District Health Board Leaders
Barbara Saipe [email protected]
Hand Therapists
Marlene Pouri-Lane Ph: 07 854 8949 [email protected]
Neurology
Bridget Dickson [email protected]
NZ Manipulative Physiotherapists Association (NZMPA)
Ingrid du Toit Ph: 09 476 5353 0800 646 000 [email protected] www.nzmpa.org.nz
Occupational Health
Angela Trotter (Administrator) PO Box 27386 Wellington 6141 Ph: 04 894 1685 [email protected]
Paediatrics
Merryn Robertson [email protected]
The Physiotherapy Acupuncture Association (PAANZ)
Angela Trotter (Administrator) PO Box 27386 Wellington 6141 Ph: 04 894 1685 [email protected]
Physiotherapy in Mental Health
Joke Van Stavern [email protected]
Physiotherapy for the Older Adult
Chrissie Russell [email protected]
Sports Physiotherapy New Zealand
Michael Borich Ph: 021 717 303 [email protected] www.sportsphysiotherapy.org.nz
Chairpersons Standing Committees
Contact National Office
Tae Ora Tinana
Sandra Kettle
Professional Standards and Ethics Committee
Ben Hinchcliff Fy Dunford
Finance Committee
Sheila Mann
Professional Development Committee
Gill Stotter
National Executive Committee
President
Liz Binns PO Box 27386 Wellington 6141 Ph: 04 801 6500 (National Office) [email protected]
Executive Members
Ricky Bell Melissa Davidson Jess Radovanovich Kurt Thomas Greg Knight
National Office
Office Hours 8.30am - 5.00pm
L6, 342 Lambton Quay PO Box 27 386, Wellington Ph: 04 801 6500 [email protected]
Interim CEO
Peter Christie [email protected]
Operations and Business Services Manager
Peter Christie [email protected] DD: 04 894 1683
Marketing Manager
Nick Taylor [email protected] DD: 04 894 1686
Professional Advisor
Sue Doesburg [email protected] DD: 04 894 1684
Learning And Research Advisor
Nick Clode [email protected] DD: 04 894 1689
Communications and Events Advisor
Erica George [email protected] DD: 04 894 1687
Professional Development Project Officer
Anna Williams [email protected] DD: 04 894 1680
Member Support Coordinator
Bridgette O’Connor [email protected] Ph: 04 801 6500
Accountant
Emma Gillard [email protected] DD: 04 894 1682
Physiotherapy Business Support
Check us out on Facebook, YouTube and Twitter
www.facebook.com/PhysiotherapyNZ www.youtube.com/nzsp1 www.twitter.com/physionz
With over 50,000 physiotherapists in 1,500+ cities prescribing Physiotec exercise videos to their patients, it’s no wonder we are the leader in the field of home exercise programs.
We are Physiotec and we help over 5 million patients lead a healthier, more normal life.
1,500ACTIVE IN OVER
CITIES AROUND THE WORLD
physiotec.net.au(+64) 0800 445 951