The value of varicella vaccination in healthy children: cost–benefit analysis of the situation in...
10
The value of varicella vaccination in healthy children: cost– benefit analysis of the situation in France Laurent Coudeville *, Franc ° ois Paree, The´re`se Lebrun, Jean-claude Sailly Centre de Recherches Economiques, Sociologiques et de Gestion (CRESGE-LABORES, URA-CNRS 362), 1 rue Norbert SEGARD, BP 109, 59016 Lille Cedex, France Received 14 October 1997; received in revised form 6 April 1998; accepted 28 April 1998 Abstract The purpose of the cost–benefit analysis described in this article is to determine the economic value of vaccination of healthy children against varicella in France. It is based on the results of two specific investigations — an epidemiological model and a prospective observational study (1832 cases studied) of the socio-economic consequences of varicella. This cost–benefit analysis was conducted from the viewpoint of the society and that of the patient, for vaccination coverage rates ranging from 10 to 90%. This analysis demonstrates the value of varicella vaccination when associated with measles–mumps–rubella (MMR) vaccination: if varicella and MMR vaccines are co-administered, the vaccination of 80% of the children against varicella leads to a reduction in medical costs associated with varicella including that of vaccination, ranging from 10 to 77% according to the values adopted for vaccination costs, varicella treatment costs, discount rate and vaccine ecacy. The results of this study also underline the benefits of a vaccination policy that aims to achieve a high rate of coverage, thereby reaping the highest benefit from vaccination, and also avoiding potential negative consequences. # 1998 Elsevier Science Ltd. All rights reserved. Keywords: Varicella; Vaccination; Cost–benefit analysis; Child; Prevention 1. Introduction The varicella vaccine, developed in Japan at the start of the 1970s [1], is a live attenuated vaccine specific for VZV (varicella-zoster-virus, the virus re- sponsible for varicella and zona); this vaccine was for a long time reserved exclusively for subjects particu- larly at risk for serious forms of the disease (mainly immunodeficient children) [2]. Following Japan and South Korea, the United States and Germany have recently authorized the use of this vaccine in healthy subjects. In many other countries, such as France, the debate over targeted vaccination versus mass vacci- nation remains open. In order to allow proper discus- sion, it is necessary to assess the medico-economic value of a vaccination programme, thus implying measurement of the medical impact, as well as the socio-economic consequences of vaccination. As regards the medical aspects, the following three points should be considered: . first, reduction in the incidence of varicella in vacci- nated subjects, but also in non-vaccinated subjects, for whom there is a decreased risk of exposure; . second, a decrease in the number of complications associated with varicella. A complication is reported in 2% of the cases seen in 1996 by the general prac- titioners involved in the French epidemiologic sur- veillance network sentinel [3]. This rate is similar to the one observed by Chow et al. [4] (2.0%) with US data. Yawn et al. [5], also in the US case, recently reported a higher rate for varicella complications (3.7%). If most of these complications are mild, var- icella complications may be severe (encephalitis and Reye’s Syndrome: between 1 and 2/100 000 cases of varicella [6]), and even fatal (2/100 000 cases of vari- cella in non-immunodeficient subjects [6]). . finally, the possible reoccurrence of cases of varicella in adults, who are reputed to be at greater risk. Vaccine 17 (1999) 142–151 0264-410X/98/$19.00 # 1998 Elsevier Science Ltd. All rights reserved. PII: S0264-410X(98)00161-3 PERGAMON * Corresponding author. Tel.: +33-320-134060; fax: +33-320- 134070.
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of The value of varicella vaccination in healthy children: cost–benefit analysis of the situation in...
The value of varicella vaccination in healthy children: cost±bene®t analysis of the situation in France
Laurent Coudeville *, Franc° ois Paree, The reÁ se Lebrun, Jean-claude Sailly
Centre de Recherches Economiques, Sociologiques et de Gestion (CRESGE-LABORES, URA-CNRS 362), 1 rue Norbert SEGARD, BP 109,
59016 Lille Cedex, France
Received 14 October 1997; received in revised form 6 April 1998; accepted 28 April 1998
Abstract
The purpose of the cost±bene®t analysis described in this article is to determine the economic value of vaccination of healthy
children against varicella in France. It is based on the results of two speci®c investigations Ð an epidemiological model and aprospective observational study (1832 cases studied) of the socio-economic consequences of varicella. This cost±bene®t analysiswas conducted from the viewpoint of the society and that of the patient, for vaccination coverage rates ranging from 10 to 90%.This analysis demonstrates the value of varicella vaccination when associated with measles±mumps±rubella (MMR) vaccination:
if varicella and MMR vaccines are co-administered, the vaccination of 80% of the children against varicella leads to a reductionin medical costs associated with varicella including that of vaccination, ranging from 10 to 77% according to the values adoptedfor vaccination costs, varicella treatment costs, discount rate and vaccine e�cacy. The results of this study also underline the
bene®ts of a vaccination policy that aims to achieve a high rate of coverage, thereby reaping the highest bene®t fromvaccination, and also avoiding potential negative consequences. # 1998 Elsevier Science Ltd. All rights reserved.
Keywords: Varicella; Vaccination; Cost±bene®t analysis; Child; Prevention
1. Introduction
The varicella vaccine, developed in Japan at thestart of the 1970s [1], is a live attenuated vaccinespeci®c for VZV (varicella-zoster-virus, the virus re-sponsible for varicella and zona); this vaccine was fora long time reserved exclusively for subjects particu-larly at risk for serious forms of the disease (mainlyimmunode®cient children) [2]. Following Japan andSouth Korea, the United States and Germany haverecently authorized the use of this vaccine in healthysubjects. In many other countries, such as France, thedebate over targeted vaccination versus mass vacci-nation remains open. In order to allow proper discus-sion, it is necessary to assess the medico-economicvalue of a vaccination programme, thus implyingmeasurement of the medical impact, as well as thesocio-economic consequences of vaccination.
As regards the medical aspects, the following threepoints should be considered:
. ®rst, reduction in the incidence of varicella in vacci-nated subjects, but also in non-vaccinated subjects,for whom there is a decreased risk of exposure;
. second, a decrease in the number of complicationsassociated with varicella. A complication is reportedin 2% of the cases seen in 1996 by the general prac-titioners involved in the French epidemiologic sur-veillance network sentinel [3]. This rate is similar tothe one observed by Chow et al. [4] (2.0%) with USdata. Yawn et al. [5], also in the US case, recentlyreported a higher rate for varicella complications(3.7%). If most of these complications are mild, var-icella complications may be severe (encephalitis andReye's Syndrome: between 1 and 2/100 000 cases ofvaricella [6]), and even fatal (2/100 000 cases of vari-cella in non-immunode®cient subjects [6]).
. ®nally, the possible reoccurrence of cases of varicellain adults, who are reputed to be at greater risk.
Vaccine 17 (1999) 142±151
0264-410X/98/$19.00 # 1998 Elsevier Science Ltd. All rights reserved.
PII: S0264-410X(98 )00161 -3
PERGAMON
* Corresponding author. Tel.: +33-320-134060; fax: +33-320-
134070.
Various socio-economic aspects must also be con-sidered.
. ®rst, the cost of the vaccination programme. The co-administration of the varicella vaccine with theMMR vaccine may however decrease this cost.
. second, reduction in the economic costs related tothe illness (cost of treatment for all cases of vari-cella, management of complications, working dayslost...).
The purpose of the present article is to provide acost±bene®t analysis regarding the potential advan-tages of varicella vaccination in healthy children builton a thorough examination of these di�erent elements.
2. Materials and methods
This cost±bene®t analysis, involving successiveexamination of the viewpoint of the society and thatof the patient, is based on comparison of costs of apreventive strategy (vaccination programme for thechildren aged less than 6 years and medical treatmentof residual cases of varicella) and of a curative strategy(no vaccination and medical treatment of individualpatients presenting with varicella). Since only thoseconsequences evaluative in ®nancial terms were con-sidered in the analysis, this is a cost±bene®t analysis inthe strict sense of the word [7].
We considered in this analysis the usefulness of avaricella vaccine di�used in the same conditions thatvaccines against measles, mumps and rubella, namely arecommended vaccine for the children aged between9 months and 6 years. We then focused our analysis onthe co-administration of the varicella vaccine with theMMR vaccine to children aged between 9 months and6 years. The vaccine coverage analysed in the basecase, 80% of 6 year-old children, is close to the oneobserved for measles, mumps, rubella in France (re-spectively 81, 77 and 80% in 1993 [8]). Other scen-arios, with vaccine coverage ranging from 10 to 90%,are also studied. Within the same scenario, the vaccinecoverage is identical for all cohorts involved in vacci-nation.
In order to ensure proper analysis, information wasrequired in three areas:
. the epidemiological outcome of vaccination (changesin the number and age-related distribution of casesof varicella and complications thereof) evaluated bymeans of modelling;
. the socio-economic consequences of varicella asdetermined by a speci®c survey;
. ®nally, the costs associated with vaccination asdetermined by comparison of several sources of in-formation.
2.1. Collection of data required for the cost±bene®tanalysis
2.1.1. Modelling of the epidemiological consequences ofvaccination against varicella
Modelling of the epidemiological consequences ofvaccination against varicella are based on a modeldeveloped by Halloran et al. [9]. This model, whichtakes account of heterogeneity in the risk of trans-mission and contraction of infection according to theindividual's age group, allows simulation for an entirepopulation of the changes in number of cases of vari-cella and age-related distribution as a result of vacci-nation. This type of deterministic model, based on theprinciple of mass action and de®ned by a system ofnon-linear di�erential equations, is known as the RASmodel (realistic-age-structured model) [10].
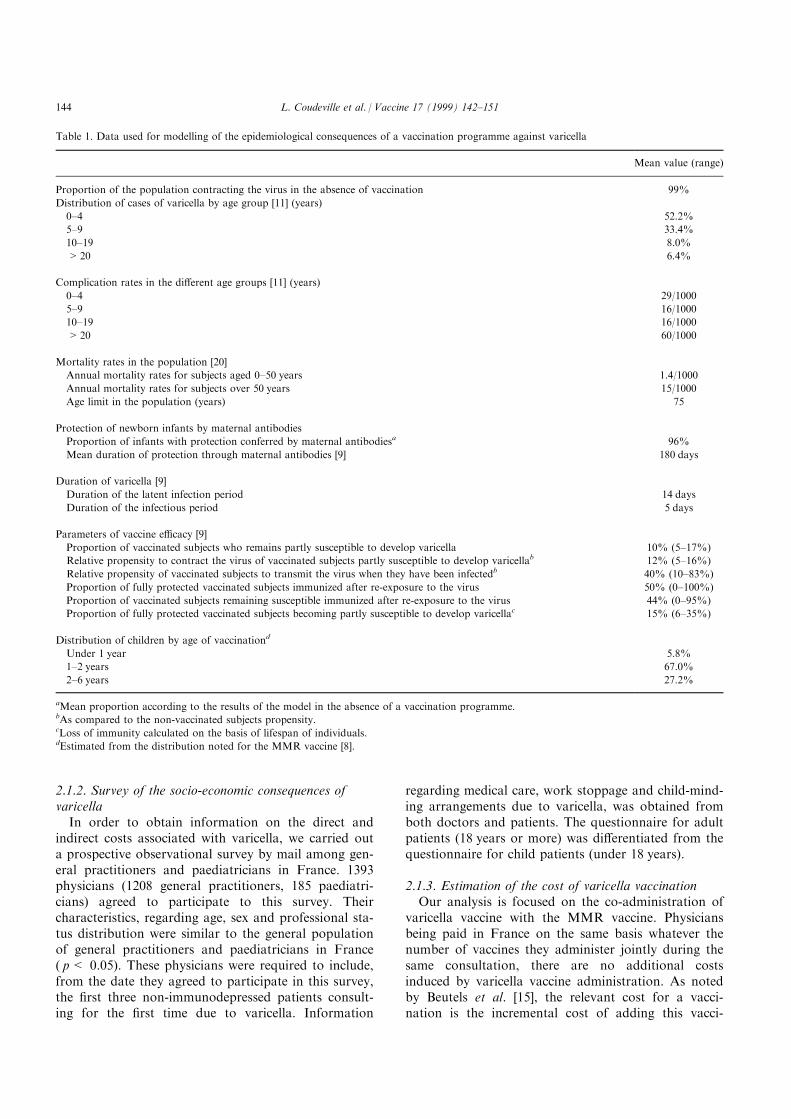
Simulations were performed for a population withcharacteristics similar to those of the French popu-lation. The simulated population was thus divided into75 cohorts of 700 000 individuals at birth. The size ofthe cohort falls regularly as a function of mortalityrates, up to the age limit for individual subjects. Oldpeople having practically no role in the spread of thevirus, the age limit is set at 75 years. The data used inthe model are shown in Table 1.
It has to be noted that the data used for age-speci®crate of complications, based on the results of epide-miologic surveillance achieved by Sentinel networkfrom 1991 to 1994 [11], are the same whatever varicellaoccurs in vaccinated or non-vaccinated persons.Considering that varicella in vaccinated persons isalmost exclusively mild [12], this assumption is conser-vative. In the same way, following previously pub-lished studies on the usefulness of varicella vaccinationin the USA [13, 14] or Germany [15], the e�ects of var-icella vaccination on zoster were not taken intoaccount in this analysis. As it has been shown that var-icella vaccination results in a reduced risk of zoster forchildren with leukemia [16] and in reductions of boththe incidence and the severity of zoster for healthyindividuals [17], this assumption is also conservative.
We simulated the implementation of a vaccinationprogramme for children aged under 6 years.Distribution of children according to age of vacci-nation was calculated using data for the MMRvaccine [8]. This distribution remains stable in thedi�erent simulations, whatever the coverage rate.
L. Coudeville et al. / Vaccine 17 (1999) 142±151 143
2.1.2. Survey of the socio-economic consequences ofvaricella
In order to obtain information on the direct andindirect costs associated with varicella, we carried outa prospective observational survey by mail among gen-eral practitioners and paediatricians in France. 1393physicians (1208 general practitioners, 185 paediatri-cians) agreed to participate to this survey. Theircharacteristics, regarding age, sex and professional sta-tus distribution were similar to the general populationof general practitioners and paediatricians in France( p< 0.05). These physicians were required to include,from the date they agreed to participate in this survey,the ®rst three non-immunodepressed patients consult-ing for the ®rst time due to varicella. Information
regarding medical care, work stoppage and child-mind-ing arrangements due to varicella, was obtained fromboth doctors and patients. The questionnaire for adultpatients (18 years or more) was di�erentiated from thequestionnaire for child patients (under 18 years).
2.1.3. Estimation of the cost of varicella vaccinationOur analysis is focused on the co-administration of
varicella vaccine with the MMR vaccine. Physiciansbeing paid in France on the same basis whatever thenumber of vaccines they administer jointly during thesame consultation, there are no additional costsinduced by varicella vaccine administration. As notedby Beutels et al. [15], the relevant cost for a vacci-nation is the incremental cost of adding this vacci-
Table 1. Data used for modelling of the epidemiological consequences of a vaccination programme against varicella
Mean value (range)
Proportion of the population contracting the virus in the absence of vaccination 99%
Distribution of cases of varicella by age group [11] (years)
0±4 52.2%
5±9 33.4%
10±19 8.0%
>20 6.4%
Complication rates in the di�erent age groups [11] (years)
0±4 29/1000
5±9 16/1000
10±19 16/1000
>20 60/1000
Mortality rates in the population [20]
Annual mortality rates for subjects aged 0±50 years 1.4/1000
Annual mortality rates for subjects over 50 years 15/1000
Age limit in the population (years) 75
Protection of newborn infants by maternal antibodies
Proportion of infants with protection conferred by maternal antibodiesa 96%
Mean duration of protection through maternal antibodies [9] 180 days
Duration of varicella [9]
Duration of the latent infection period 14 days
Duration of the infectious period 5 days
Parameters of vaccine e�cacy [9]
Proportion of vaccinated subjects who remains partly susceptible to develop varicella 10% (5±17%)
Relative propensity to contract the virus of vaccinated subjects partly susceptible to develop varicellab 12% (5±16%)
Relative propensity of vaccinated subjects to transmit the virus when they have been infectedb 40% (10±83%)
Proportion of fully protected vaccinated subjects immunized after re-exposure to the virus 50% (0±100%)
Proportion of vaccinated subjects remaining susceptible immunized after re-exposure to the virus 44% (0±95%)
Proportion of fully protected vaccinated subjects becoming partly susceptible to develop varicellac 15% (6±35%)
Distribution of children by age of vaccinationd
Under 1 year 5.8%
1±2 years 67.0%
2±6 years 27.2%
aMean proportion according to the results of the model in the absence of a vaccination programme.bAs compared to the non-vaccinated subjects propensity.cLoss of immunity calculated on the basis of lifespan of individuals.dEstimated from the distribution noted for the MMR vaccine [8].
L. Coudeville et al. / Vaccine 17 (1999) 142±151144

nation to an existing immunization program. We canthen use, in the base case, a null cost for the adminis-tration of the varicella vaccine. In a sensitivity analy-sis, we also considered a case in which half of thevaricella vaccinations were achieved separately fromMMR vaccination. In this case, the cost of the admin-istration of the vaccine had been determined by usingthe national tari� for the consultation of a generalpractitioner in France (FF110).
The price of varicella vaccine (FF 100 in the basecase, ranging from FF50 to 150 in sensitivity analyses)was determined using as a reference the price of thisvaccine in countries in which it is widely used (UnitedStates, Japan, South Korea). Following Lieu et al. [13]and Huse et al. [14], we postulated that from 0.31 and2% of vaccinations (1% in the base case), result in aconsultation due to side e�ects. We therefore ®xed thecost of varicella vaccination, borne at 35% by thepatients, at FF101.2 in the base case, varying fromFF50.4 to 207.4 in sensitivity analysis.
2.2. Calculation of cost±bene®t ratio
2.2.1. Viewpoint of societyIn this viewpoint, comparison is made between all
direct and indirect costs of varicella for a ®xed dur-ation of 30 years. Regarding methodological problemsraise by their addition [7], the indirect costs were sep-arated in the analysis of direct costs and were not eval-uated in monetary terms.
Comparison of direct costs made by means of theactualized net bene®t (ANB) calculation, which is asfollows:
ANB �Xt0�30t�t0
C 0t�1� r�tÿt0 ÿ
Xt0�30t�t0
Ct � Vt
�1� r�tÿt0
The ANB is the di�erence, updated for rate r, betweenannual cost of treatment for varicella (C 0t) without avaccination program, and annual cost of treatment ofvaricella (Ct) where there is a varicella vaccination pro-gramme (Vt) at t0.
Comparison of the indirect costs for each of thesestrategies is based on the number of days of absencefrom work avoided due to the vaccination programme(AA) calculated as follows:
AA � Xt0�30
t�t0A 0t ÿ
Xt0�30t�t0
At
!=30
This indicator is based on the di�erence between theannual number of days of work stoppage (A 0t) wherethere is no vaccination programme and the annualnumber of days of work days lost due to varicella (At)where there is a vaccination programme at t0.
2.2.2. Patient viewpointThe actualized cost of varicella (ACV) either for
vaccinated and non-vaccinated subjects may be calcu-lated as follows:
ACV �XLa�0
Ca � Va
�1� r�a
The ACV is the mean total spending, actualized at arate r, by individual patients, (Ca) and of vaccination(Va) during their lifetime (a represents the age of theindividual patients, and L represents the age limit ofthe population). Comparison of ACVs for vaccinatedand non-vaccinated subjects can be used to determinethe group for whom a vaccination programme is ®nan-cially advantageous. It has to be noted that the costsconsidered as supported by patients are those whichare not supported by the national Social Security sys-tem. Additional private reimbursement schemes havenot been taken into account.
The results of the cost±bene®t analysis are expressedin 1995 French Francs. They underwent sensitivityanalysis based on values for the most favourable andleast favourable parameters for vaccination. The indi-cators used were adapted to the size of the Frenchpopulation. The actualization rate used in the centralhypothesis was ®xed at 5%, and was 0% for the mostfavourable hypothesis for vaccination and 10% for theleast favourable hypothesis for vaccination.
3. Results
3.1. Epidemiological consequences of the establishmentof a varicella vaccination programme
Figure 1 shows changes over time in the incidence ofvaricella following a vaccination programme. It showsthat over the ®rst years, the vaccination programme isaccompanied by wider changes in the incidence of vari-cella, but this situation subsequently stabilizes.Consequently, isolated consideration of the ®rst yearsfollowing a vaccination programme would lead to biasin the analysis of the consequences of vaccination.
Table 2 and Fig. 2 show that, although vaccinationappears bene®cial in all cases for the population, thesituation di�ers depending on whether one considersthe group of vaccinated subjects or that of non-vacci-nated subjects:
. Vaccinated subjects bene®t both from the protectionacquired through vaccination and from the indirecte�ects of vaccination (reduction of the risk to con-tract the disease due to the decrease of the numberof infectious subjects in the population). When 80%of the children born after the di�usion of the vac-
L. Coudeville et al. / Vaccine 17 (1999) 142±151 145
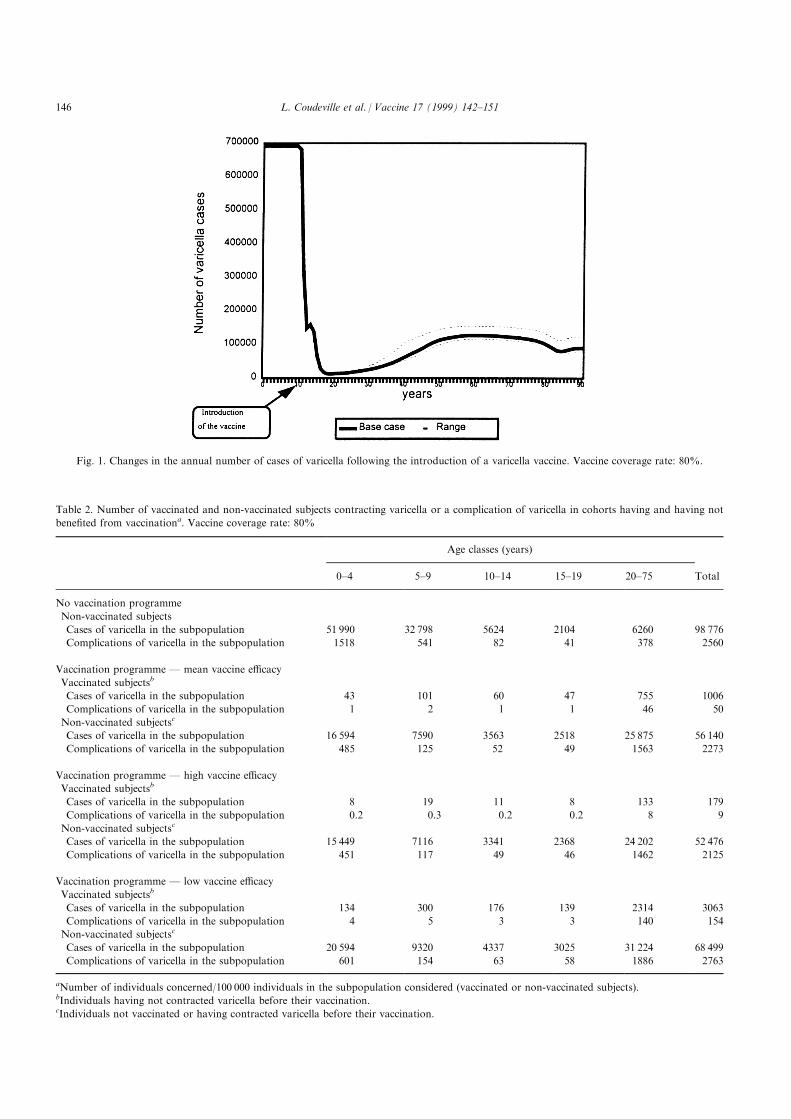
Fig. 1. Changes in the annual number of cases of varicella following the introduction of a varicella vaccine. Vaccine coverage rate: 80%.
Table 2. Number of vaccinated and non-vaccinated subjects contracting varicella or a complication of varicella in cohorts having and having not
bene®ted from vaccinationa. Vaccine coverage rate: 80%
Age classes (years)
0±4 5±9 10±14 15±19 20±75 Total
No vaccination programme
Non-vaccinated subjects
Cases of varicella in the subpopulation 51 990 32 798 5624 2104 6260 98 776
Complications of varicella in the subpopulation 1518 541 82 41 378 2560
Vaccination programme Ð mean vaccine e�cacy
Vaccinated subjectsb
Cases of varicella in the subpopulation 43 101 60 47 755 1006
Complications of varicella in the subpopulation 1 2 1 1 46 50
Non-vaccinated subjectsc
Cases of varicella in the subpopulation 16 594 7590 3563 2518 25 875 56 140
Complications of varicella in the subpopulation 485 125 52 49 1563 2273
Vaccination programme Ð high vaccine e�cacy
Vaccinated subjectsb
Cases of varicella in the subpopulation 8 19 11 8 133 179
Complications of varicella in the subpopulation 0.2 0.3 0.2 0.2 8 9
Non-vaccinated subjectsc
Cases of varicella in the subpopulation 15 449 7116 3341 2368 24 202 52 476
Complications of varicella in the subpopulation 451 117 49 46 1462 2125
Vaccination programme Ð low vaccine e�cacy
Vaccinated subjectsb
Cases of varicella in the subpopulation 134 300 176 139 2314 3063
Complications of varicella in the subpopulation 4 5 3 3 140 154
Non-vaccinated subjectsc
Cases of varicella in the subpopulation 20 594 9320 4337 3025 31 224 68 499
Complications of varicella in the subpopulation 601 154 63 58 1886 2763
aNumber of individuals concerned/100 000 individuals in the subpopulation considered (vaccinated or non-vaccinated subjects).bIndividuals having not contracted varicella before their vaccination.cIndividuals not vaccinated or having contracted varicella before their vaccination.
L. Coudeville et al. / Vaccine 17 (1999) 142±151146
cine receive vaccination, from 0.2 to 3.0% of thevaccinated children contract varicella according tothe values adopted for vaccine e�cacy. The residualrisk of complication is then very low among vacci-nated subjects (always less than 0.1%) even if, asdone here, one considers that the risk of compli-cations is the same for vaccinated persons than fornon-vaccinated persons. Vaccination is thus pro®t-able in all cases for this population.
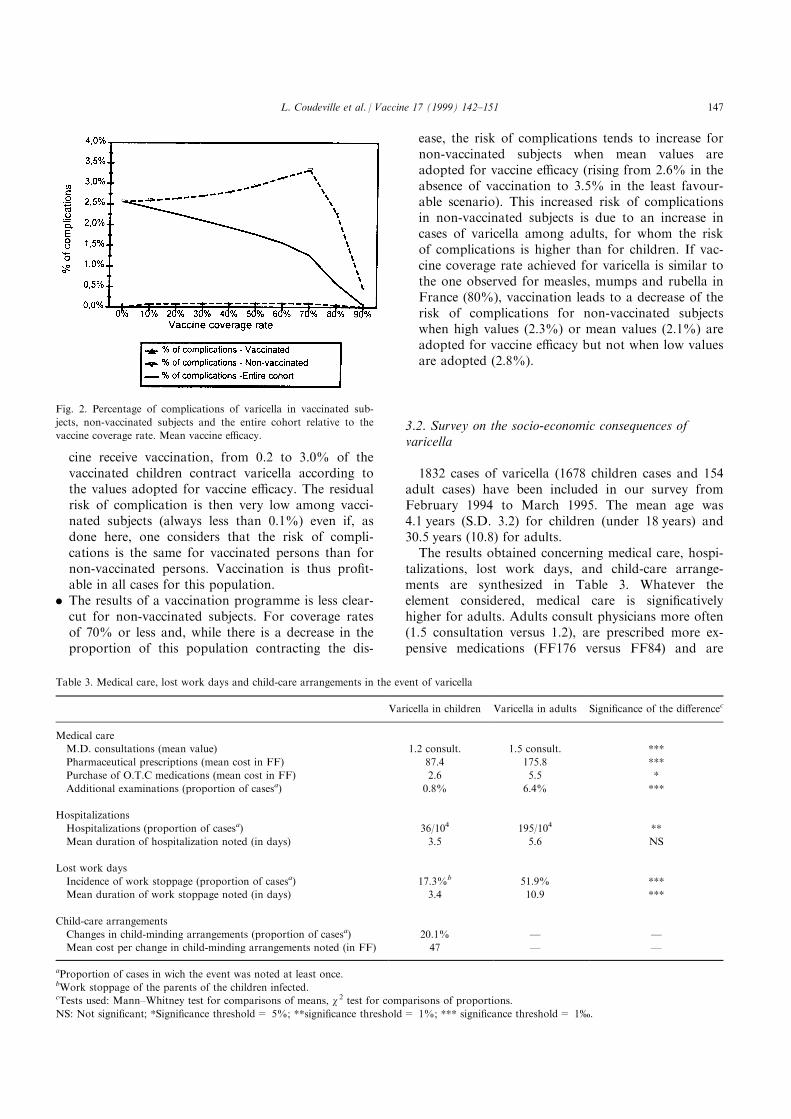
. The results of a vaccination programme is less clear-cut for non-vaccinated subjects. For coverage ratesof 70% or less and, while there is a decrease in theproportion of this population contracting the dis-
ease, the risk of complications tends to increase fornon-vaccinated subjects when mean values areadopted for vaccine e�cacy (rising from 2.6% in theabsence of vaccination to 3.5% in the least favour-able scenario). This increased risk of complicationsin non-vaccinated subjects is due to an increase incases of varicella among adults, for whom the riskof complications is higher than for children. If vac-cine coverage rate achieved for varicella is similar tothe one observed for measles, mumps and rubella inFrance (80%), vaccination leads to a decrease of therisk of complications for non-vaccinated subjectswhen high values (2.3%) or mean values (2.1%) areadopted for vaccine e�cacy but not when low valuesare adopted (2.8%).
3.2. Survey on the socio-economic consequences ofvaricella
1832 cases of varicella (1678 children cases and 154adult cases) have been included in our survey fromFebruary 1994 to March 1995. The mean age was4.1 years (S.D. 3.2) for children (under 18 years) and30.5 years (10.8) for adults.
The results obtained concerning medical care, hospi-talizations, lost work days, and child-care arrange-ments are synthesized in Table 3. Whatever theelement considered, medical care is signi®cativelyhigher for adults. Adults consult physicians more often(1.5 consultation versus 1.2), are prescribed more ex-pensive medications (FF176 versus FF84) and are
Fig. 2. Percentage of complications of varicella in vaccinated sub-
jects, non-vaccinated subjects and the entire cohort relative to the
vaccine coverage rate. Mean vaccine e�cacy.
Table 3. Medical care, lost work days and child-care arrangements in the event of varicella
Varicella in children Varicella in adults Signi®cance of the di�erencec
Medical care
M.D. consultations (mean value) 1.2 consult. 1.5 consult. ***
Pharmaceutical prescriptions (mean cost in FF) 87.4 175.8 ***
Purchase of O.T.C medications (mean cost in FF) 2.6 5.5 *
Additional examinations (proportion of casesa) 0.8% 6.4% ***
Hospitalizations
Hospitalizations (proportion of casesa) 36/104 195/104 **
Mean duration of hospitalization noted (in days) 3.5 5.6 NS
Lost work days
Incidence of work stoppage (proportion of casesa) 17.3%b 51.9% ***
Mean duration of work stoppage noted (in days) 3.4 10.9 ***
Child-care arrangements
Changes in child-minding arrangements (proportion of casesa) 20.1% Ð Ð
Mean cost per change in child-minding arrangements noted (in FF) 47 Ð Ð
aProportion of cases in wich the event was noted at least once.bWork stoppage of the parents of the children infected.cTests used: Mann±Whitney test for comparisons of means, w 2 test for comparisons of proportions.
NS: Not signi®cant; *Signi®cance threshold= 5%; **signi®cance threshold= 1%; *** signi®cance threshold= 1-.
L. Coudeville et al. / Vaccine 17 (1999) 142±151 147
more often concerned by additional examinations(6.4% versus 0.8%). Nine cases of hospitalizations (6children and 3 adults) have been observed through thissurvey. These hospitalizations are notably related tohigh fever, cutaneous or ORL complications for chil-dren and pulmonary complications for adults.
Overall, the mean medical cost for a varicella case,including expenses related to complications, wasFF274 (con®dence interval: 240±308) for children, andFF637 (328±945) for adults. About 65% of these medi-cal costs were ®nanced throughout the French Social
Security System. The mean cost associated to workstoppage borne by an adult having varicella wasFF279 (158±399). Finally, the parents of a child hav-ing varicella supported on average, FF62 (43±81)owing to work stoppage and child-care arrangements.Mean values and con®dence interval bounds presentedabove are used respectively to determine cost±bene®tresults in the base case and in sensitivity analysis.
3.3. Cost±bene®t analysis
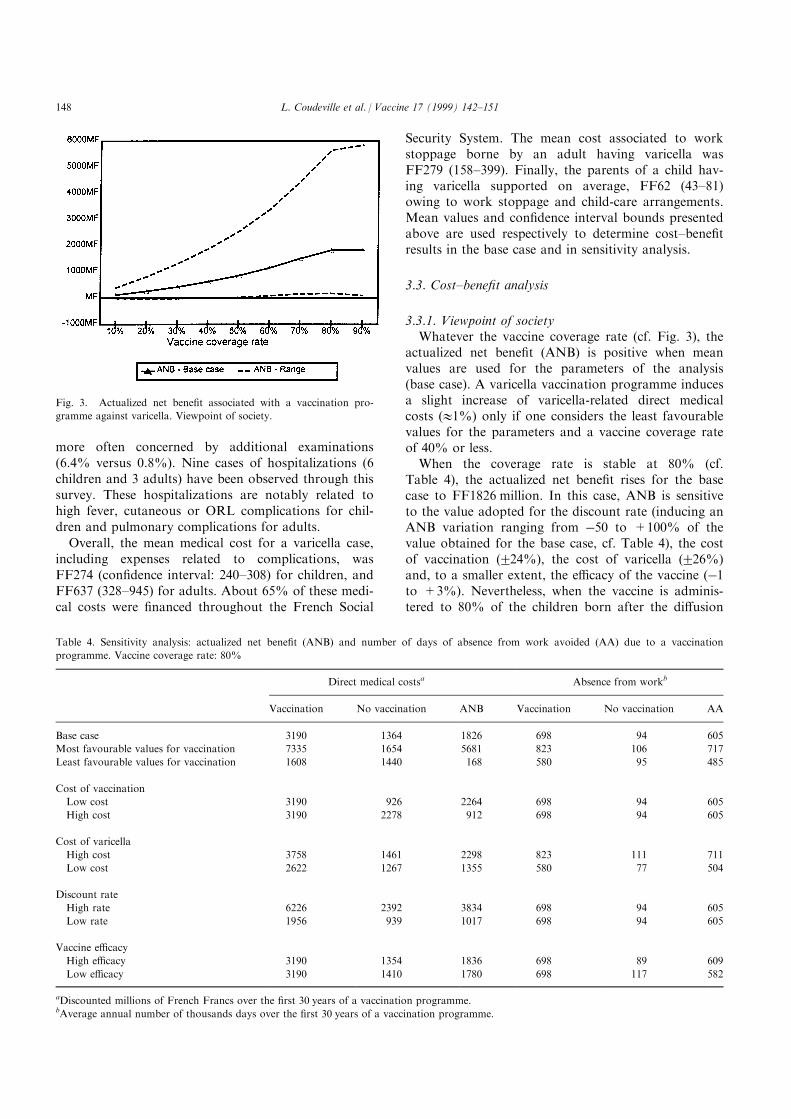
3.3.1. Viewpoint of societyWhatever the vaccine coverage rate (cf. Fig. 3), the
actualized net bene®t (ANB) is positive when meanvalues are used for the parameters of the analysis(base case). A varicella vaccination programme inducesa slight increase of varicella-related direct medicalcosts (11%) only if one considers the least favourablevalues for the parameters and a vaccine coverage rateof 40% or less.
When the coverage rate is stable at 80% (cf.Table 4), the actualized net bene®t rises for the basecase to FF1826 million. In this case, ANB is sensitiveto the value adopted for the discount rate (inducing anANB variation ranging from ÿ50 to +100% of thevalue obtained for the base case, cf. Table 4), the costof vaccination (224%), the cost of varicella (226%)and, to a smaller extent, the e�cacy of the vaccine (ÿ1to +3%). Nevertheless, when the vaccine is adminis-tered to 80% of the children born after the di�usion
Fig. 3. Actualized net bene®t associated with a vaccination pro-
gramme against varicella. Viewpoint of society.
Table 4. Sensitivity analysis: actualized net bene®t (ANB) and number of days of absence from work avoided (AA) due to a vaccination
programme. Vaccine coverage rate: 80%
Direct medical costsa Absence from workb
Vaccination No vaccination ANB Vaccination No vaccination AA
Base case 3190 1364 1826 698 94 605
Most favourable values for vaccination 7335 1654 5681 823 106 717
Least favourable values for vaccination 1608 1440 168 580 95 485
Cost of vaccination
Low cost 3190 926 2264 698 94 605
High cost 3190 2278 912 698 94 605
Cost of varicella
High cost 3758 1461 2298 823 111 711
Low cost 2622 1267 1355 580 77 504
Discount rate
High rate 6226 2392 3834 698 94 605
Low rate 1956 939 1017 698 94 605
Vaccine e�cacy
High e�cacy 3190 1354 1836 698 89 609
Low e�cacy 3190 1410 1780 698 117 582
aDiscounted millions of French Francs over the ®rst 30 years of a vaccination programme.bAverage annual number of thousands days over the ®rst 30 years of a vaccination programme.
L. Coudeville et al. / Vaccine 17 (1999) 142±151148
of the vaccine, vaccination always leads to a reductionof the medical costs associated with varicella rangingfrom 10 to 77% and rising to 57% for the base case.
The number of days of absence from work avoidedeach year through vaccination reaches 33 871 for acoverage rate of 10% and 643 831 for a coverage rateof 90% when mean values are adopted for the par-ameters of the analysis. When the most and leastfavourable values are used for each of the parameters,the mean number of days of absence from work variesby220%.
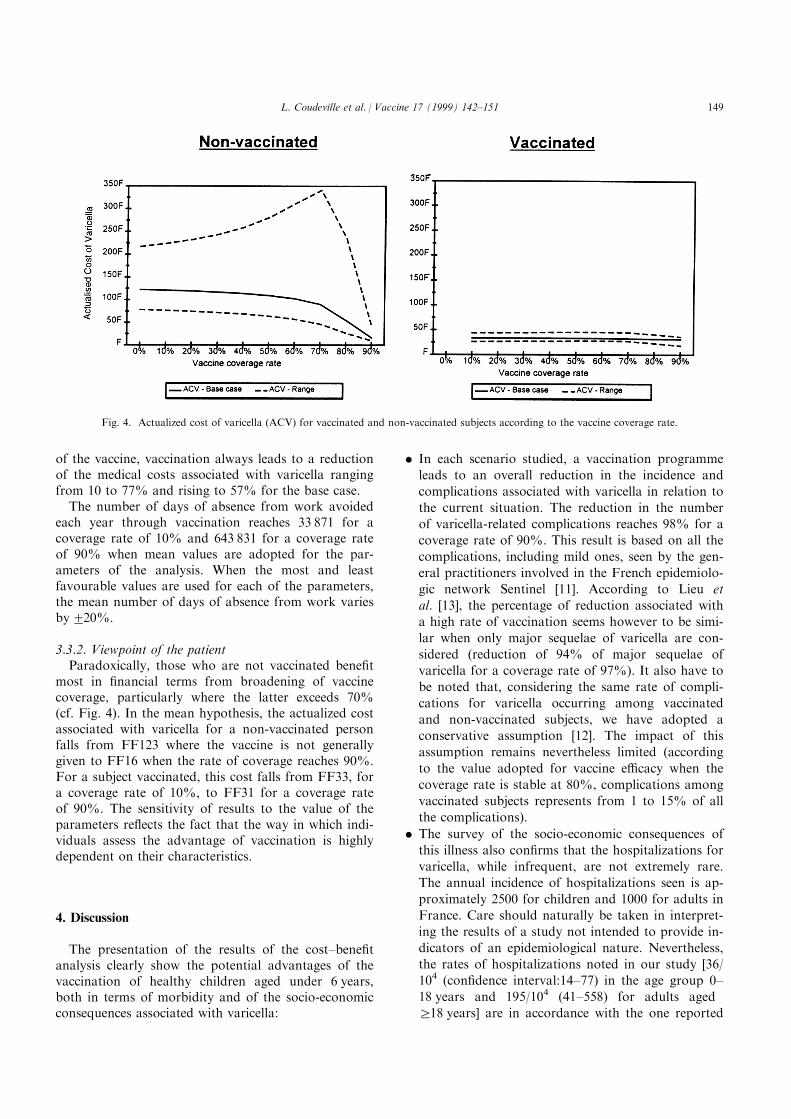
3.3.2. Viewpoint of the patientParadoxically, those who are not vaccinated bene®t
most in ®nancial terms from broadening of vaccinecoverage, particularly where the latter exceeds 70%(cf. Fig. 4). In the mean hypothesis, the actualized costassociated with varicella for a non-vaccinated personfalls from FF123 where the vaccine is not generallygiven to FF16 when the rate of coverage reaches 90%.For a subject vaccinated, this cost falls from FF33, fora coverage rate of 10%, to FF31 for a coverage rateof 90%. The sensitivity of results to the value of theparameters re¯ects the fact that the way in which indi-viduals assess the advantage of vaccination is highlydependent on their characteristics.
4. Discussion
The presentation of the results of the cost±bene®tanalysis clearly show the potential advantages of thevaccination of healthy children aged under 6 years,both in terms of morbidity and of the socio-economicconsequences associated with varicella:
. In each scenario studied, a vaccination programme
leads to an overall reduction in the incidence and
complications associated with varicella in relation to
the current situation. The reduction in the number
of varicella-related complications reaches 98% for a
coverage rate of 90%. This result is based on all the
complications, including mild ones, seen by the gen-
eral practitioners involved in the French epidemiolo-
gic network Sentinel [11]. According to Lieu et
al. [13], the percentage of reduction associated with
a high rate of vaccination seems however to be simi-
lar when only major sequelae of varicella are con-
sidered (reduction of 94% of major sequelae of
varicella for a coverage rate of 97%). It also have to
be noted that, considering the same rate of compli-
cations for varicella occurring among vaccinated
and non-vaccinated subjects, we have adopted a
conservative assumption [12]. The impact of this
assumption remains nevertheless limited (according
to the value adopted for vaccine e�cacy when the
coverage rate is stable at 80%, complications among
vaccinated subjects represents from 1 to 15% of all
the complications).
. The survey of the socio-economic consequences of
this illness also con®rms that the hospitalizations for
varicella, while infrequent, are not extremely rare.
The annual incidence of hospitalizations seen is ap-
proximately 2500 for children and 1000 for adults in
France. Care should naturally be taken in interpret-
ing the results of a study not intended to provide in-
dicators of an epidemiological nature. Nevertheless,
the rates of hospitalizations noted in our study [36/
104 (con®dence interval:14±77) in the age group 0±
18 years and 195/104 (41±558) for adults aged
r18 years] are in accordance with the one reported
Fig. 4. Actualized cost of varicella (ACV) for vaccinated and non-vaccinated subjects according to the vaccine coverage rate.
L. Coudeville et al. / Vaccine 17 (1999) 142±151 149
by Choo et al. [4] for the US case (from 20/104 to65/104 for age groups between 0 and 20 years, 125/104 for the age group of r20 years and a global rateof 43/104). Wharton et al. [18], always for the UScase, reported lower ®gures (a global rate of 27/104)but precise, as observed in our study and by Chooet al. [4], than the risk for adults is six times the oneobserved in the age group 5±9 years.
. When the vaccine coverage rate is higher than 40%,vaccination against varicella leads to a reduction indirect medical costs associated with varicella for allvalues examined for the various parameters of theanalysis. When 80% of children are vaccinated, Thesavings that can be achieved by the French SocialSecurity O�ces each year are about FF115 million.In fact, the situations in which a vaccination pro-gramme induces an increase of medical costs associ-ated to varicella are rather unlikely (least favourablevalues at the same time for vaccination costs, vari-cella treatment costs and vaccine e�cacy and a cov-erage rate of 40% or less) and, if they occur, thisincrease is limited (11%). The ®nancial bene®ts ofvaricella vaccination are then clear in the Frenchcase even if one considers, as we have done in a sen-sitivity analysis, that half of the varicella vacci-nations are achieved separately from MMRvaccination.
. When indirect costs are taken into account, the ad-vantage of vaccination is con®rmed. Widespread useof a varicella vaccine would result in a substantialreduction in work days lost due to illness: whenthere is a stable coverage rate of 80%, the annualnumber of lost work days avoided due to vacci-nation is equivalent to the annual number of workdays in a company with a sta� of more than 2700persons. It must also be noted that, if in our studywe have chosen not to evaluate absence from workin monetary terms, Lieu et al. [13] and Huse etal. [14] estimate that indirect costs represent 85% ofthe total costs associated to varicella in UnitedStates.
Widespread use of a varicella vaccine may havenegative consequences that should not be overlooked:
. In order to prevent an increase of complications inthe group of non-vaccinated subjects, a coveragerate of at least 70% must be achieved. This increasein risk of complications in the non-vaccinated popu-lation remains however slight (2.6 versus 3.5% inthe least favourable scenario) and is accompanied,in all scenarios studied, by a reduction in the absol-ute number of complications associated with the ill-ness. Moreover, our study is focused on avaccination programme for children aged under6 years and the impact of a vaccination among 12-
year-olds who have a negative history of varicellainfection (catch-up programme) has not been takeninto account. Such a catch-up programme, by limit-ing the number of persons contracting varicelladuring adulthood, is able to prevent an increasedrisk of complications for non-vaccinated observed insome scenarios analysed in our study. Lieu et al. [13]and Beutels et al. [15], underline the positive impactof a catch-up programme. Lieu et al. [13] is precise,however, in stating that its bene®ts are minimalwhen the coverage rate among 6-year-olds is high.Achieving a high coverage rate among 6-year-oldchildren clearly remains the main objective of a vari-cella vaccination programme and the best way toavoid its potential negative consequences.
. Analysis from the patient's viewpoint underlines thefact that the attitude of individuals may in factimpede achievement of high coverage rates. It isthus seen that an increase in the overall coveragerate decreases the relative value of vaccination forindividual subjects, since their own risk of contract-ing the disease decreases without their having to bevaccinated. Similarly, the results of sensitivity ana-lyses show that because of the di�erence in status,individuals do not stand to gain exactly the sameadvantages from vaccination. The di�erence betweenprivate and public interest of vaccination, which hasbeen studied on a theoretical basis by Geo�ard andPhilipson [19], has to be connected to the di�cultyin France in achieving a rate of vaccine coverage ofmore than 80% against measles, mumps andrubella [8]. The relevance of a comparison, based onan actualized cost, to interpretation of the attitudeof individual subjects towards vaccination, is natu-rally open to question. Moreover, we have not takeninto account that some of the patients bene®t froman additional private reimbursement scheme.However, considering patient viewpoint has, essen-tially, an illustrative interest. The mechanismsdemonstrated by this means may be readily trans-posed to a decision by the individual depending onhis perception of the risks of serious forms of the ill-ness and his perception of the inconvenience of vac-cination.
These issues should not lead one to reject the idea ofvaccination, the bene®ts of which are, on the whole,positive. It should also be noted that the long-termpossibility of eradicating the illness, such as the poss-ible positive impact of varicella vaccination on zoster,have not been taken into account in the assessmentpresented in this article. However, the results of thisanalysis con®rm the advantages, in the context of avaccination programme, of a policy aimed at achieve-ment of high coverage rates, both in order to avoidany negative consequences of vaccination, and to de-
L. Coudeville et al. / Vaccine 17 (1999) 142±151150

rive maximum bene®t from the vaccination pro-gramme. Such a policy could in fact be an extension ofthat recommended by the WHO and carried out inFrance by the Public Health Authorities in the case ofvaccination against rubella, mumps and measles.
5. Conclusion
This cost±bene®t analysis demonstrates the value ofvaricella vaccination when associated with MMR vac-cination. This association actually presents two advan-tages: by reducing the cost of vaccine administration itmakes sure, on one hand, that varicella vaccinationleads to a decrease in the total medical costs associatedwith varicella and it allows, on the other hand, vari-cella vaccination to bene®t from high coverage ratesachieved by vaccination against MMR. Regarding po-tential negative consequences of a low coverage rate,this second advantage is a major one.
Acknowledgements
This research project, which was selected by theScienti®c Committee for Tenders of the Department of`Economic Evaluation of preventive, Diagnostic andTherapeutic Strategies' of the French Ministry ofResearch and Space, was supported by PasteurMe rieux MSD.
References
[1] Takahashi M, Otsuka T, Ikuno Y, Asano Y, Yazaki T,
Isomura M. Live vaccine used to prevent the spread of varicella
in children in hospital. Lancet 1974;II:1288±90.
[2] Weller TH. Varicella-Herpes Zoster Virus in Viral Infections of
Humans. Epidemiology and Control, 3rd edn, Ch. 25. Plenum
Medical Book Company, New York, 1991.
[3] Flahaut A, Dreau H, Farran N et al. Epide miologie des mala-
dies transmissibles en me decine libe rale: bilan du re seau senti-
nelles en 1996. BEH, 1997, 33.
[4] Choo PW, Donahue JG, Manson JE. The epidemiology of vari-
cella and its complications. Journal of Infectious Diseases
1995;172:706±12.
[5] Yawn B, Yawn R, Lydick E. Community impact of childhood
varicella infections. Journal of Pediatrics 1997;130:759±65.
[6] Preblud SR. Varicella: complications and costs. Pediatrics
1986;78(Suppl):728±35.
[7] Lily Moto, Sante et multidisciplinariteÂ: choix et deÂcisions.
Editions HermeÁ s, 1995.
[8] Guignon N. Evaluation de la couverture vaccinale rougeole-
oreillons-rube ole aÁ 6 ans pour les enfants ne s en 1987 (Enqueà te
en milieu scolaire.). BEH, 1996, 4.
[9] Halloran ME, Cochi SL, Lieu TA, Wharton M, Fehrs L.
Theoretical epidemiologic and morbidity e�ects of routine vari-
cella immunization of preschool children in the United States.
American Journal of Epidemiology 1994;140:81±103.
[10] Bolker BM, Grenfell BT. Chaos and biological complexity in
measles dynamics. Proceedings of the Royal Society London B
1993;251:75±81.
[11] Reseau National de Telesurveillance des Maladies
Transmissibles, Base de donne es des re sultats de la surveillance
e pide miologique de la varicelle par les me decins sentinelles en
France entre 1990 et 1994. RNTMT, 1995.
[12] Watson BM, Piercy SA, Plotkin SA, Starr SE. Modi®ed chick-
enpox in children immunized with Oka/Merck varicella vaccine.
Pediatrics 1993;91:17±22.
[13] Lieu TA, Cochi SL, Black SB et al. Cost-e�ectiveness of a rou-
tine varicella vaccination programme for US children. JAMA
1994;271:375±81.
[14] Huse DM, Meissner HC, Lacey MJ, Oster G. Childhood vacci-
nation against chickenpox: an analysis of bene®ts and costs.
Journal of Pediatrics 1994;124:869±74.
[15] Beutels P, Clara R, Tormans G, Van Doorslaer E. Costs and
bene®ts of routine varicella vaccination in german children.
Journal of Infectious Diseases 1996;174(Suppl 3):S335±2341.
[16] Hardy I, Gershon AA, Steinberg SP et al. The incidence of zos-
ter after immunization with live attenuated varicella vaccine: a
study in children with leukemia. New England Journal of
Medicine 1991;325:1545±50.
[17] Gershon AA, Steinberg SP et al. Live attenuated varicella vac-
cine: protection in healthy adults compared with leukemic chil-
dren. Journal of Infectious Diseases 1990;161:661±6.
[18] Wharton M, Fehrs LJ, Cochi SL, Stroup, NE. Health impact of
varicella in the 1980s. Paper presented at the 30th Interscience
Conference on Antimicrobial Agents and Chemotherapy.
Atlanta, 24 October 1994.
[19] Geo�ard PY, Philipson T. Disease eradication: private versus
public vaccination. American Economic Review 1997;87:222±30.
[20] INSEE, La situation de mographique en 1992. INSEE Re sultats
1995, Se rie De mographie et Socie te s. No 42±43.
L. Coudeville et al. / Vaccine 17 (1999) 142±151 151