
Focal hand dystonia in musicians: phenomenology, etiology, and psychological trigger factors
Upload
independentCategory
view
0download
0
Herpes zoster: etiology, clinical features and treatmentoptions, and case reportShrikant Mali
Herpes zoster is a painful vesicular rash resulting
from reactivation of the virus that also causes
chickenpox – Varicella zoster virus. Typically, the rash
runs its course in a matter of 4–5 weeks. The pain,
however, may persist months, even years, after the
skin heals. This phenomenon is known as postherpetic
neuralgia. Conventional therapies include prescription
antivirals, corticosteroids, and analgesics, both oral
and topical. Here I present a case report of post
herpetic neuralgia patient with discussion about
etiology, pathology and treatment options. Egypt J Oral
Maxillofac Surg 3:91–100 �c 2012 The Egyptian
Association of Oral & Maxillofacial Surgeons.
Egyptian Journal of Oral & Maxillofacial Surgery 2012, 3:91–100
Keywords: acyclovir, herpes zoster, neuralgia, postherpetic neuralgia, shingles
Oral and Maxillofacial Surgery, CSMSS Dental College, Aurangabad,Maharashtra, India
Correspondence to Shrikant Mali, MDS, Oral and Maxillofacial Surgery,CSMSS Dental College, Aurangabad, Maharashtra, IndiaE-mail: [email protected]
Received 30 January 2012 accepted 3 May 2012
IntroductionHerpes zoster (HZ) is the reactivated form of the
varicella zoster virus (VZV), the same virus responsible
for chickenpox. HZ is more commonly known as shingles,
from the Latin cingulum for ‘girdle’. This is because a
common presentation of HZ involves a unilateral rash
that can wrap around the waist or torso like a girdle.
Similarly, the name zoster is derived from classical Greek,
referring to a belt-like binding (known as a zoster) used
by warriors to secure armor [1].
Case reportA 60-year-old male patient reported to the department of
oral and maxillofacial surgery, CSMSS Dental College and
Hospital, Aurangabad, with a chief complaint of pain and
rashes on the right side of his face. On examination,
multiple vesicles and rashes were found on the lower lip,
angle of the mandible region, in front of the ear, lateral to
the eye, and intraorally on the lateral border of the tongue
and the floor of the mouth.
The patient reported prodromal signs of fever and
malaise 3–4 days before the appearance of rashes. These
rashes then became pustules, which formed crusts. The
patient reported unilateral pain along the distribution of
the trigeminal nerve of the right side. He also reported
lack of sleep because of pain. Because of unilateral pain
and rashes along the nerve distribution, coupled with
prodromal signs, a diagnosis of HZ was made.
Treatment with acyclovir 800 mg five times a day was
started. Combiflam was also started to combat pain.
Antiviral treatment was carried out for 7 days. The
patient responded well to acyclovir and the rashes
disappeared after 7–10 days. However, he developed
severe neuralgic pain along the course of the trigeminal
nerve on the right side. Trigger zones were the cheek, the
skin below the infraorbital ridge, and the intraoral buccal
mucosa. The patient did not shave for fear of activating
trigger zones. On the basis of the clinical findings and
history of HZ, a diagnosis of postherpetic neuralgia
(PHN) was made as a complication of HZ.
Treatment with carbamazapine 200 mg three times a day
was started to control neuralgic pain. The patient
responded well and pain was relieved. This treatment
was continued for 1 month. On completion of 1 month,
carbamazapine tables were discontinued and the patient
was fine.
DiscussionThere is no way to predict who will develop HZ, when
the latent virus may reactivate, or what may trigger its
reactivation. However, the elderly and those with
compromised immunity – such as those who have
undergone organ transplantation or recent chemotherapy
for cancer, or individuals with HIV/AIDS – are at a greater
risk for developing HZ. Between 10 and 20% of normal
(immunocompetent) adults will get shingles during their
lifetime. This figure increases markedly to 50% for those
older than 85 years of age [1].
Spontaneous pain, pain induced by trivial stimuli, and
altered sensation accompany HZ and may continue long
after its characteristic rash has healed – a condition
known as PHN. Many approaches have been proposed to
treat the pain of acute zoster, to avert its progression to
PHN, and to alleviate PHN. Few of these approaches
have been shown to be beneficial, and PHN remains a
source of frustration for both patients and physicians [2].
Etiology and pathology [1–4]
VZV is one of eight known herpes viruses that infect
humans. Its structure is characterized by an icosahedral
nucleocapsid surrounded by a lipid envelope. Double-
stranded DNA is located at its center. The virus is
B150–200 nm in diameter and has a molecular weight of
B80 million.
During its viremic phase, cell-associated VZV gains access
to epidermal cells, causing the typical varicella rash. The
virus then enters the sensory nerves in mucocutaneous
sites and travels by retrograde axonal transport to the
sensory dorsal-root ganglia adjacent to the spinal cord,
where the virus establishes permanent latency in
Case report 91
2090-097X �c 2012 The Egyptian Association of Oral & Maxillofacial Surgeons DOI: 10.1097/01.OMX.0000418695.06506.6c
Copyright © The Egyptian Association of Oral and Maxillofacial Surgeons. Unauthorized reproduction of this article is prohibited.

neuronal cell bodies. Latent VZV is present in B1–7% of
sensory ganglion neurons, with less than 10 genomic
copies per infected cell. Seeding of the dorsal-root ganglia
might also occur during viremia. The magnitude of
viremia, the number of skin lesions, and the burden of
VZV that establishes latency during primary varicella
infection might be linked. As with other members of the
herpes virus family, VZV is noninfectious in its latent
form, but can reactivate at a later time to form intact
virions in the involved sensory neurons. These virions
then migrate to the skin through axons, spread from cell
to cell, and penetrate the epidermis. In its full clinical
expression, zoster causes pain, which is followed by a
vesicular rash distributed across closely overlapping
dermatomes of the involved sensory nerve roots.
The triggers for the reactivation of VZV have not been
identified and probably involve multiple factors. However,
specific components of cell-mediated immunity (CMI)
play an important role in controlling the development of
zoster by preventing reactivation within the neuron or the
full clinical expression of reactivated VZV as zoster. The
effectiveness of these protective components of CMI is
well maintained in immunocompetent individuals during
childhood and early adulthood. These CMI components are
believed to be partially or substantially maintained by
periodic immunologic boosting. ‘Endogenous boosting’
might occur in response to the subclinical reactivation of
latent VZV or to the development of zoster itself, and
‘exogenous boosting’ might occur in response to exposure
to VZV circulating in the population as chickenpox.
Primary infection is clinically identified as varicella or
chickenpox. VZV is ubiquitous and highly contagious,
with initial exposure typically occurring during childhood.
The virus enters the host through the respiratory system,
replicates at an undefined site (presumably the naso-
pharynx), infiltrates the reticuloendothelial system, and
eventually makes its way into the bloodstream. Evidence
of viremia is manifested by the scattered nature of the
telltale skin lesions on the body.
The usual incubation period for varicella is 14–16 days,
with communicability ranging from 10 to 21 days after
initial exposure. An individual can no longer transmit VZV
once the final skin lesions have crusted. Indirect
transmission (through an immune third person) is not
believed to occur.
Once the initial outbreak has subsided, VZV then retreats
into the dorsal-root ganglia, where it can remain dormant
for years until some excitatory factor triggers reactivation.
Fig. 1
Crusted healed lesions on the chin along with erythematous lesionsafter acyclovir therapy.
Fig. 2
Erhythomatous maculopapular unilateral rashes seen on the cheek,temple, and angle of the mandible area.
92 Egyptian Journal of Oral & Maxillofacial Surgery 2012, Vol 3 No 2
Copyright © The Egyptian Association of Oral and Maxillofacial Surgeons. Unauthorized reproduction of this article is prohibited.

The associated outbreak is then clinically identified as HZ
or shingles. Microscopic examination of select dorsal-root
ganglia tissue during active HZ shows the presence of
hemorrhage, edema, and lymphocytic infiltration. Figure 1
shows the typical progression of VZV from varicella to
zoster [3–5].
Reduced cellular immunity places an individual at risk for
HZ, hence the susceptibility of immunocompromised
individuals and the elderly. It has been proposed that one
reason why VZV may not recur as frequently as other herpes
viruses, such as Herpes simplex virus, type 1 (HSV-1),
or Herpes simplex virus, type 2 (HSV-2), is that genes
involved in the reactivation of HSV are missing in VZV.
Signs and symptoms [1–5]
The classic presentation of HZ starts with a prodrome of
mild-to-moderate burning or tingling (or in some cases
numbness) in or under the skin of a given dermatome, often
accompanied by fever, chills, headache, stomach upset, and
general malaise. Within 48–72 h from the prodrome, an
erythematous, maculopapular rash forms unilaterally along
the dermatome and rapidly develops into vesicular lesions
reminiscent of the original chickenpox outbreak. The pain
associated with shingles varies in intensity from mild to
severe, such that even the slightest touch or breeze can
elicit excruciating spasms. The lesions usually begin to dry
and scab 3–5 days after appearing Figs 2–4.
Prodromal stage – sensations such as burning, tingling,
etching, boring, prickly, and knife like occurring along the
nerve distribution.
Active stage – rash forms after a few hours to several days,
with malaise, low-grade fever, and headache.
Rash changes from papules and edema to vesicles in
12–24 h and to pustules in 1–7 days.
Pustules dry and form crusts that fall off in 14–21 days
and leave erythematous lesions leading to hypopigmenta-
tion or hyperpigmentation.
Intraoral lesions appear after cutaneous lesions.
Pain and dysasthesia are minimal during the active stage.
However, during crusting, it returns.
Chronic stage PHN – constant deep pain, sharp shock
like a tic.
Radiating dysasthesia with trigger zones.
Differential diagnosis – trigeminal neuralgia, maxillary
sinusitis, periodic migrainous neuralgia, atypical facial pain.
HZ typically erupts within one or two adjacent derma-
tomes, with thoracic, cervical, and ophthalmic involve-
ment being the most common.
Most patients report a deep aching or burning pain,
altered sensitivity to touch (paresthesia) that may be
Fig. 3
Vesicular lesion on the ventral surface of the tongue, ulcerative lesionseen near the tonsillar area.
Fig. 4
Erythematous and vesicular lesions bluish black in color on the lateralsurface of the tongue.
Herpes zoster Mali 93
Copyright © The Egyptian Association of Oral and Maxillofacial Surgeons. Unauthorized reproduction of this article is prohibited.

painful (dysesthesia), exaggerated responses to stimuli
(hyperesthesia), or electric shock-like pain.
Pain induced by otherwise trivial stimuli (allodynia),
unbearable itching, and escalating pain in response to
repeated stimulation (windup pain) are also reported.
These abnormal sensations resolve or persist unpredic-
tably, making it difficult to draw absolute distinctions
between pain associated with zoster and PHN. Pain-
induced disruption of sleep, mood, and work contributes
toward the impact of zoster on the quality of life, in both
the short and the long term.
Zoster rash is typically unilateral and does not cross the
mid-line, erupting in one or two adjacent dermatomes.
The frequency of zoster occurrence in different derma-
tomes has been evaluated in certain studies. In general,
thoracic, cervical, and ophthalmic involvements are most
common. Small numbers of lesions can occur outside the
primary or adjacent dermatome.
A common and potentially debilitating consequence of
zoster is PHN, a persistent pain after resolution of the
rash. Pathologic observations believed to distinguish PHN
from uncomplicated zoster include axonal and cell body
degeneration, atrophy of the spinal cord dorsal horn,
scarring of the dorsal-root ganglion, and loss of epidermal
innervation of the affected area. Some experts believe that
this neuronal damage might be caused by ongoing viral
replication. In addition, consensus is lacking on the criteria
required to distinguish the quality, duration, or underlying
pathophysiology of pain occurring with zoster versus PHN.
Therefore, the duration of pain used to define PHN has
been inconsistent, ranging from any duration after resolu-
tion of the rash to periods from greater than 30 days to
greater than 6 months after the onset of rash.
The nature of PHN pain varies from mild to excruciating
in severity, constant, intermittent, or triggered by trivial
stimuli. Approximately half of patients with zoster or
PHN describe their pain as ‘horrible’ or ‘excruciating’,
ranging in duration from a few minutes to constant on a
daily or an almost daily basis. The pain can disrupt sleep,
mood, work, and activities of daily living, adversely
impacting the quality of life, and leading to social
withdrawal and depression. Anecdotes of suicide among
patients with PHN have been reported. Among patients
experiencing zoster, predictors of PHN include the
occurrence and severity of pain both before and after
the onset of the rash, the extent of the rash, trigeminal or
ophthalmic distribution, and the occurrence of viremia.
In addition to PHN, zoster is associated with a variety of
other complications. Among patients with zoster, 10–25%
have eye involvement, called herpes zoster ophthalmicus
(HZO). HZO can occur when reactivation involves the
nasociliary branch of the trigeminal nerve, sometimes
preceded by the presence of zoster vesicles on the nose
(Hutchinson sign). Keratitis occurs in approximately two-
thirds of patients with HZO, often causing corneal
ulceration. Other complications include conjunctivitis,
uveitis, episcleritis and scleritis, retinitis, choroiditis,
optic neuritis, lid retraction, ptosis, and glaucoma.
Extraocular muscle palsies also occur. Prolonged or
permanent sequelae of HZO include pain, facial scarring,
and loss of vision.
An uncommon complication of zoster is Ramsay Hunt
syndrome, a peripheral facial nerve palsy accompanied by
zoster vesicles on the ear, hard palate, or tongue. The
pathophysiology of this complication involves the reacti-
vation of VZV in the geniculate ganglion of the facial
nerve. Additional signs and symptoms of Ramsey Hunt
syndrome can include pain, vertigo, hearing loss, sensi-
tivity to sound, tinnitus, and loss of taste. Many patients
do not recover completely. Idiopathic facial palsy (Bell’s
palsy) might be caused by inapparent VZV reactivation.
Occasionally, zoster can cause motor weakness in
noncranial nerve distributions, called zoster paresis. The
mechanism has not been determined. The weakness
develops abruptly within 2–3 weeks after onset of the
rash and can involve the upper or the lower extremities.
Diaphragmatic paralysis has also been described. The
prognosis of zoster paresis is good. Zoster can also result
in autonomic dysfunction, causing urinary retention and
colon pseudo-obstruction.
Rarely, patients will experience acute focal neurologic
deficits weeks to months after resolution of the zoster
rash, involving the trigeminal distribution contralateral to
the initial rash. This ischemic stroke syndrome, termed
granulomatous angiitis, is believed to be caused by the
direct extension of VZV from the trigeminal ganglion to
the internal carotid artery or its branches, resulting in
inflammation. Mortality from this syndrome is substan-
tial. Other rare neurologic complications of zoster include
myelitis, aseptic meningitis, and meningoencephalitis.
The prognosis for these conditions is good, although
encephalomyelitis can be life threatening. Guillain–Barre
syndrome has also been reported in association with
zoster.
In immunocompromised individuals, zoster initially
might present typically. However, the rash tends to be
more severe and its duration may be prolonged. One
specific risk for patients with some immunosuppressive
conditions is dissemination of the zoster rash. True
cutaneous dissemination generally occurs only among
immunocompromised patients, occurring in up to 37% of
zoster cases in the absence of antiviral treatment.
Dissemination usually begins with a dermatomal rash;
however, the rash sometimes begins with no primary
dermatomal involvement.
The risk for neurologic zoster complications is generally
increased in immunocompromised individuals. These
complications, which can be aggressive and even fatal,
include myelitis, chronic encephalitis, ventriculitis, me-
ningoencephalitis, and cranial palsies. However, the risk
for PHN is not appreciably increased among immuno-
compromised patients who develop zoster.
Diagnosis [1–5]
The diagnosis of zoster might not be possible in the
absence of rash (e.g. before rash or in cases of zoster sine
herpete). Patients with localized pain or altered skin
94 Egyptian Journal of Oral & Maxillofacial Surgery 2012, Vol 3 No 2
Copyright © The Egyptian Association of Oral and Maxillofacial Surgeons. Unauthorized reproduction of this article is prohibited.

sensations might undergo evaluation for kidney stones,
gallstones, or coronary artery disease until the zoster rash
appears and the correct diagnosis is made. In its classical
manifestation, the signs and symptoms of zoster are
usually distinctive enough to make an accurate clinical
diagnosis once the rash has appeared. Occasionally, zoster
might be confused with impetigo, contact dermatitis,
folliculitis, scabies, insect bites, papularurticaria, candidal
infection, dermatitis herpetiformis, or drug eruptions.
More frequently, zoster is confused with the rash of the
HSV, including eczema herpeticum. The accuracy of
diagnosis is lower for children and younger adults in
whom the incidence of zoster is lower and its symptoms
are less often classic.
In some cases, particularly in immunosuppressed indivi-
duals, the location of rash appearance might be atypical or
a neurologic complication might occur well after resolu-
tion of the rash. In these instances, laboratory testing
might clarify the diagnosis. Tzanck smears are inexpen-
sive and can be used at the bedside to detect multi-
nucleated giant cells in lesion specimens, but they do not
distinguish between infections with VZV and HSV. VZV
obtained from lesions can be identified using tissue
culture, but this can take several days and false-negative
results occur because viable virus is difficult to recover
from cutaneous lesions. Direct fluorescent antibody
staining of VZV-infected cells in a scraping of cells from
the base of the lesion is rapid and sensitive. Direct
fluorescent antibody and other antigen-detection meth-
ods can also be used on biopsy material, and eosinophilic
nuclear inclusions (Cowdry type A) are observed on
histopathology. PCR techniques performed in an experi-
enced laboratory can also be used to detect VZV DNA
rapidly and sensitively in properly collected lesion
material, although VZV PCR testing is not available in
all settings. A modification of PCR diagnostic techniques
has been used at a few laboratories to distinguish wild-
type VZV from the Oka/Merck strain used in the licensed
varicella and zoster vaccines.
In immunocompromised individuals, even when VZV is
detected by laboratory methods in lesion specimens,
differentiation of chickenpox from disseminated zoster
might not be possible by physical examination or
serologically. In these instances, a history of VZV exposure,
a history that the rash began with a dermatomal pattern,
and the results of VZV antibody testing at or before the
time of rash onset might help guide the diagnosis.
Zoster transmission [1–5]
Zoster lesions contain high concentrations of VZV that
can be spread, presumably by the airborne route, and
cause primary varicella in exposed susceptible individuals.
Localized zoster is only contagious after the rash erupts
and until the lesions crust. Zoster is less contagious than
varicella.
Pain
The pain associated with acute zoster and PHN is
neuropathic and results from injury of the peripheral
nerves and altered central nervous system signal processing.
After the injury, peripheral neurons discharge sponta-
neously, have lower activation thresholds, and show
exaggerated responses to stimuli. Axonal regrowth after
the injury produces nerve sprouts that are also prone to
unprovoked discharge.
The excessive peripheral activity is believed to lead to
hyperexcitability of the dorsal horn, resulting in exagger-
ated central nervous system responses to all input.
These changes may be so complex that no single
therapeutic approach will ameliorate all the abnormalities.
Histopathological features [2,3]
In acute zoster, the skin is inflamed and already partially
denervated, and the dorsal-root ganglion shows inflam-
mation, hemorrhagic necrosis, and neuronal loss.
Inflammation in the peripheral nerves may persist for
weeks to months and usually leads to demyelination,
wallerian degeneration, and sclerosis.
Ultimately, there may be scarring of the skin, peripheral
nerves, and dorsal-root ganglia.
Pathologic changes are also evident in the central nervous
system during zoster. They include acute degeneration of
the dorsal horn of the spinal cord, unilateral segmental
myelitis and leptomeningitis, and the involvement of
spinal cord segments at levels adjacent to the affected
skin. In patients who have had zoster, atrophy of the
dorsal horn has been found at autopsy in those with PHN,
but not in those without PHN.
Complication
Neurologic Guillian–Barre syndrome, encephalitis, mye-
litis, ramsay hunt syndrome, horner’s syndrome.
The four main domains of complications (excluding
PHN) identified in patients with acute HZ.
Antiviral agents [2–8]
The first line of treatment and the most widely used agents
for zoster infection are antiviral agents. As nucleoside
analogs, they block viral replication. Antiviral agents
accelerate healing in the acute phase of illness by reducing
the duration of viral shedding as well as time to crusting
and scabbing. In addition, they prevent the formation of
new lesions. Pharmacotherapy with antiviral agents must be
initiated within 72 h of symptom onset (i.e. rash) for
maximum effectiveness. Any delay in administration may
result in neuronal destruction – leading to the derange-
ments of the central nervous system that are responsible for
the neuropathic pain syndrome associated with PHN.
However, a course of therapy with an antiviral agent is
recommended beyond the 72-h window, especially in
immunosuppressed patients as well as those with ophthal-
mic zoster. Administration of an antiviral agent is
recommended for 7–10 days – although it is acceptable to
extend treatment to up to 15 days, especially for individuals
who are immunosuppressed.
Ideally, antivirals should be administered until no new
lesions have been observed for about 2 days. Acyclovir,
Herpes zoster Mali 95
Copyright © The Egyptian Association of Oral and Maxillofacial Surgeons. Unauthorized reproduction of this article is prohibited.

valacyclovir, and famciclovir are available antiviral agents.
Valacyclovir is the prodrug of acyclovir; famciclovir is the
prodrug of penciclovir.
Acyclovir
Oral acyclovir is used for the management of acute HZ. It is
also commonly used in immunosuppressed patients or those
with central nervous system disease. Intravenous acyclovir
may be administered to immunosuppressed patients 72 h
after rash onset. Acyclovir is initially phosphorylated by only
the viral thymidine kinase; therefore, it is active only within
cells infected with the VZV. Cellular kinases metabolize the
monophosphate to the triphosphate form, which acts as
a competitive inhibitor of viral DNA polymerase.
Placebo-controlled trials four to six have shown that oral
acyclovir shortens the duration of viral shedding, halts the
formation of new lesions, and accelerates the rate of
healing, reducing the severity of acute pain.
Malaise was the most frequent adverse effect with both
acyclovir (11.5%) and placebo (11.1%). Adverse effects
associated with intravenous acyclovirare are local pro-
blems such as phlebitis or inflammation. Transient
elevations in serum creatinine may also be observed.
Oral acyclovir has a limited oral bioavailability of 10–30%,
which necessitates frequent dosing. The recommended dosing
for oral acyclovir is 800 mg five times a day for 7–10 days.
Valacyclovir
Valacyclovir is the L-valyl ester of acyclovir. It is rapidly
converted into acyclovir after oral administration and, in
humans, results in three to five times greater bioavail-
ability than that of acyclovir. The recommended dose of
this medication is 1 g three times daily for 7 days, with
each gram of valacyclovir yielding B700 mg acyclovir and
300 mg of the essential amino acid valine.
Famciclovir
Famciclovir is the diacetyl, 6-deoxy ester of penciclovir,
which is a guanosine nucleoside analog. Metabolism of
the prodrug to penciclovir begins with uptake by
intestinal cells and is completed by the liver.
The current recommended dose is 500 mg three times
daily. Famciclovir has been shown to accelerate zoster
lesion healing and viral shedding. Famciclovir at 250 mg
three times daily for 7 days was as effective as – and had a
more favorable safety profile than – acyclovir at a dosage
of 800 mg five times daily for 7 days. Moreover,
famciclovir at a dose of either 750 mg once daily or
500 mg twice daily plus 250 mg once daily is as effective
as acyclovir 850 mg five times daily. Thus, famciclovir is as
effective as acyclovir when administered only once a day,
a regimen that leads to better patient compliance.
Limitations of antiviral agents
As reported previously, therapy must be initiated within
72 h of rash onset for maximal effectiveness. Finally,
although they may reduce the duration of PHN, they do
not function prophylactically.
Oral corticosteroids [2,5–7]
As an adjuvant option in the treatment of patients with
acute zoster infection, oral corticosteroids have been
shown to ameliorate the inflammatory characteristics of
this condition, cosmetically improving the rash. Moreover,
oral corticosteroids have been shown to reduce acute pain
but not the chronic pain associated with PHN.
Finally, corticosteroids are associated with upper gastro-
intestinal adverse events such as dyspepsia, and they have
been shown to exacerbate diabetes, hypertension, and
osteoporosis. These adverse effects are especially un-
desirable among older patients, the majority of indivi-
duals in whom zoster infection is diagnosed.
Pharmacotherapeutic options for postherpetic
neuralgia [2,4–8]
Treatment goals include alleviating the pain associated
with PHN and improving the quality of life, allowing the
patients to maintain sleep, physical activity, and nutri-
tion. Tricyclic antidepressants(TCAs), anticonvulsants,
opioid analgesics, and topical agents are recommended
first-line therapies for PHN.
Neuroactive agents [2,4–8]
TCAs are important components of therapy for PHN.
Because of their ability to block the reuptake of
norepinephrine and serotonin, these drugs may relieve
pain by increasing the inhibition of spinal neurons
involved in pain perception.
Amitriptyline decreases neuronal reuptake of both
norepinephrine and serotonin. In one trial, desipramine,
a selective inhibitor of norepinephrine reuptake, also
significantly reduced pain at 3 and 6 weeks.
Serotonin-selective drugs are of little value in the
treatment of PHN.
Adverse reactions to TCAs, including confusion, urinary
retention, postural hypotension, and arrhythmias, limit
their usefulness in older patients, and plasma concentra-
tions should be monitored to ensure compliance and help
determine the optimal dose.
Lorazepam, postulated to inhibit neurotransmission in
the spinal cord and brain stem, also proved inferior to
amitriptyline in a controlled trial.
The phenothiazine chlorprothixene is of no value, but in
controlled studies, other phenothiazines combined with
TCAs resulted in the partial relief of pain.
In a double-blind, controlled study, carbamazepine reduced
lancinating pains but was ineffective for continuous pain.
The combination of clomipramine and carbamazepine led
to only partial relief in a controlled trial, and combinations
of other antidepressant and anticonvulsant drugs had some
benefit in uncontrolled trials.
Tricyclic antidepressants [2,4–8]
They block the reuptake of norepinephrine and serotonin.
Thus, they may relieve pain by increasing the inhibition of
spinal neurons involved in pain perception. Animal studies
have shown that TCAs may also work as sodium channel
96 Egyptian Journal of Oral & Maxillofacial Surgery 2012, Vol 3 No 2
Copyright © The Egyptian Association of Oral and Maxillofacial Surgeons. Unauthorized reproduction of this article is prohibited.
antagonists within the peripheral nervous system, another
mechanism that may be responsible for pain relief.
Amitriptyline was found to be superior to lorazepam, and
nortriptyline hydrochloride, a metabolite of amitriptyline,
was also found to be effective in ameliorating the pain
associated with PHN. However, physicians prefer nor-
triptyline to amitriptyline because the former has fewer
anticholinergic effects.
Adverse events associated with TCAs, which are mainly
because of anticholinergic effects, include sedation,
confusion, urinary retention, dry mouth, blurred vision,
postural hypotension, and arrhythmia. These adverse
events limit the usefulness of TCAs for the treatment of
older patients.
Anticonvulsants [2,4–8]
Two anticonvulsants are indicated for the treatment of
PHN: gabapentin and pregabalin. Anticonvulsants are
believed to work in neuropathic pain syndromes because
they are involved in membrane stabilization, which reduces
neuronal derangement. Although gabapentin’s mechanism
of action is currently unknown, it appears to be indepen-
dent of aminobutyric acid receptors. It is lipophilic and
penetrates the blood–brain barrier (Tables 1 and 2).
Adverse events that occurred more frequently in the
gabapentin group compared with those in the group
receiving placebo were somnolence, dizziness, ataxia,
peripheral edema, and infection. Pregabalin was initially
reported to be effective in alleviating neuropathic and
nociceptive pain in a variety of animal models.
Opioid analgesics [2,4–8]
The opioid analgesics morphine and methadone were
found to be as effective as the TCAs nortriptyline or
desipramine in a randomized double-blind, placebo-
controlled cross-over trial. Intravenous morphine sulfate
infusions have been shown to be effective in reducing the
pain and hyperalgesia of PHN.
Adverse events observed with opioids are minimal and
include constipation, nausea, loss of appetite, dizziness,
and drowsiness. A theoretical limitation to the use of
opioids is the potential for addiction.
Topical treatment [2,4–8]
Topical treatment is also a good therapeutic option for
patients in whom systemic treatment is contraindicated.
Topical treatment is currently divided into three groups:
combined aspirin and NSAID formulations, local analge-
sics, and capsaicin cream.
Topical nonsteroidal anti-inflammatory drugs [2,4–8]
NSAIDs applied topically are useful in the treatment of
patients with zoster during the active and early post-
herpetic phase of illness because pain symptoms are
associated with tissue trauma and inflammation as well as
an increased level of tissue prostaglandins.
NSAIDs inhibit cyclooxygenase, decreasing the synthesis
of prostaglandins. Thus, there has been a recent focus on
developing topical NSAIDs, such as powdered aspirin in
chloroform or ethyl ether, to treat patients for PHN.
Over-the-counter creams and topical indomethacin, diclofe-
nac, and benzydamine hydrochloride cream have also been
investigated for their pain-alleviating properties in PHN.
Topical aspirin has been shown to be superior to placebo in
reducing PHN, whereas other topical NSAIDs such as
indomethacin, diclofenac, and benzydamine have not.
Analgesics [2,4–8]
A topical lidocaine 5% patch is a targeted peripheral
analgesic that is indicated for the treatment of patients
with PHN. When four patches were applied for up to 24 h,
the systemic absorption of lidocaine from the patch was
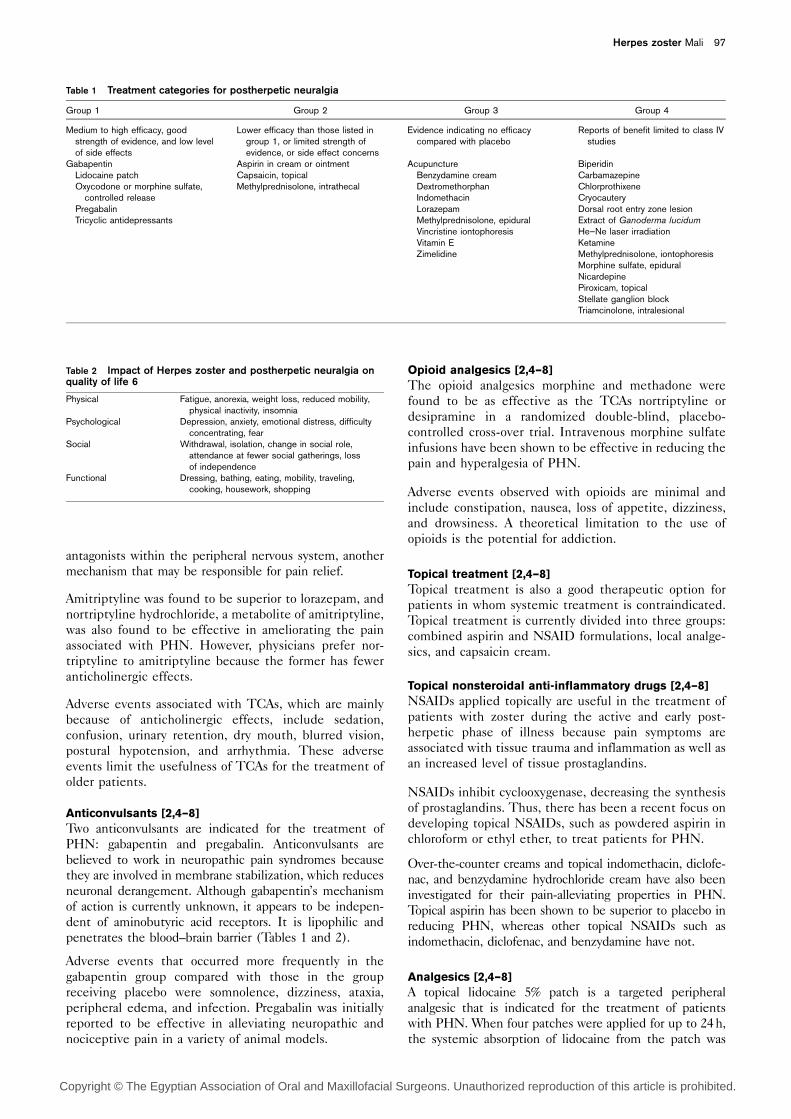
Table 1 Treatment categories for postherpetic neuralgia
Group 1 Group 2 Group 3 Group 4
Medium to high efficacy, goodstrength of evidence, and low levelof side effects
Lower efficacy than those listed ingroup 1, or limited strength ofevidence, or side effect concerns
Evidence indicating no efficacycompared with placebo
Reports of benefit limited to class IVstudies
GabapentinLidocaine patchOxycodone or morphine sulfate,
controlled releasePregabalinTricyclic antidepressants
Aspirin in cream or ointmentCapsaicin, topicalMethylprednisolone, intrathecal
AcupunctureBenzydamine creamDextromethorphanIndomethacinLorazepamMethylprednisolone, epiduralVincristine iontophoresisVitamin EZimelidine
BiperidinCarbamazepineChlorprothixeneCryocauteryDorsal root entry zone lesionExtract of Ganoderma lucidumHe–Ne laser irradiationKetamineMethylprednisolone, iontophoresisMorphine sulfate, epiduralNicardepinePiroxicam, topicalStellate ganglion blockTriamcinolone, intralesional
Table 2 Impact of Herpes zoster and postherpetic neuralgia onquality of life 6
Physical Fatigue, anorexia, weight loss, reduced mobility,physical inactivity, insomnia
Psychological Depression, anxiety, emotional distress, difficultyconcentrating, fear
Social Withdrawal, isolation, change in social role,attendance at fewer social gatherings, lossof independence
Functional Dressing, bathing, eating, mobility, traveling,cooking, housework, shopping
Herpes zoster Mali 97
Copyright © The Egyptian Association of Oral and Maxillofacial Surgeons. Unauthorized reproduction of this article is prohibited.

minimal in healthy adults and even lower among patients
with PHN, thus eliminating adverse systemic events.
Capsaicin [2,4–8]
Capsaicin cream is also indicated for the treatment of
patients with PHN. At high concentrations, capsaicin
depletes substance P, a principal peptide neurotransmitter.
This depletion first causes a burning sensation, and then
anesthetic effects. Capsaicin cream is the only drug
approved by the Food and Drug Administration for the
treatment of PHN.
Natural treatment options [1]
As with conventional protocols, the objective of natural
therapeutics in the prevention and treatment of HZ and
PHN is to aid healing of skin lesions, reduce pain, and prevent
complications. An underlying goal for the use of natural
therapies is to strengthen CMI, thereby allowing the body’s
natural defense mechanisms to control the virus and prevent
recurrence. Natural therapies can provide solutions to
effectively manage herpes viruses, prevent and treat complica-
tions, and minimize the risk of developing viral resistance.
Dietary/multiple-nutrient effects
The incidence of HZ increased considerably after the age
of 50 years. Maintaining adequate nutrition is one
contributing factor to ensuring healthy CMI.
Vitamin A [9,10]
Vitamin A functions both as a fat-soluble vitamin and as a
hormone, contributing to the visual pigment rhodopsin and
controlling gene transcription that allows for the normal
proliferation and differentiation of epithelial cells. Vitamin
A is a key immune modulator, involved in the synthesis of
lymphocytes, neutrophils, cytokines, and immunoglobulins.
Vitamin A deficiency has been associated with increased
susceptibility to numerous infectious diseases, and is of
particular concern in patients undergoing bone marrow
transplants. An observational trial on 120 bone marrow
transplant patients has shown an association between an
increased incidence of hyporetinolemia and an increased
risk of HZ infection.
Enzyme therapy [11,12]
Before the introduction of acyclovir, pancreatic enzyme
preparations were used effectively in Germany as a
treatment for HZ. The suspected mechanisms of action
for the enzyme formula included stimulating the break-
down of immune complexes and enhancing CMI.
Other nutritional considerations
Nutrients such as vitamin C, vitamin E, lysine, and zinc
have shown potential in the treatment of HSV-1 and
HSV-2. Consequently, they may also be helpful against
HZ, although evidence for this is primarily in the realm of
anecdotal reports and speculative extrapolation.
Licorice (Glycyrrhiza glabra) [13–17]
Licorice is one of the most widely used herbs in
traditional medicine, spanning many generations and
several continents. Its properties as an anti-inflammatory,
mucoprotectant, and antiviral agent may be potentially
valuable in the treatment of HZ. One constituent,
glycyrrhizin, inhibits virus growth and may also inactivate
viral particles. It has shown antiviral activity in vitroagainst various forms of herpes virus, including VZV, and
induces interferon production both in vitro and in vivo.
When glycyrrhizin is taken orally, it is converted into
glycyrrhetinic acid, with loss of its systemic antiviral
effects. However, as a topical agent, both glycyrrhizin and
licorice may provide antiviral activity, and as such may be
beneficial in cases of both HSV and HZ. Further
investigation of this application is warranted.
Madonna Lily (Lilium candidum) [18,19]
In northern Italy, traditional folk medicine identifies
L. candidum as a herbal treatment for HZ. Bulbs of
cultivated L. candidum have yielded successful results
when fried in olive oil and applied externally as a poultice
on HZ lesions. Its healing properties are believed to be a
result of the presence of eight spirostanolsaponins and
two furostanolsaponins identified in the bulb of the plant.
Reishi Mushroom (Ganoderma lucidum) [20,21]
A few small studies have examined the effect of
G. lucidum, either by itself or in combination with other
herbs, for the treatment of HZ or PHN. One case study
on two patients with HZ and two patients with PHN
showed that administration of hot-water-soluble extracts
of G. lucidum (36–72 g dry weight/day) led to a consider-
able decrease in pain.
Bi Phaya Yaw (Clinacanthus nutans) [22]
A small shrub found in Southeast Asia, has long been used
in Thailand as a traditional medicine for snake and insect
bites and various skin ailments. Several small studies have
examined its benefit for HZ. One randomized, placebo-
controlled trial was carried out on 51 HZ patients using a
topical preparation of C. nutans extract applied five times
daily for 7–14 days until the lesions were healed. The
number of patients with lesions crusting within 3 days
and healing within 7–10 days was significantly higher in
the experimental group than in the placebo group
(P < 0.01); the pain scores were significantly reduced as
well. No side effects were reported with the medication.
Honey/propolis [23–26]
Since ancient times, bee products, specifically honey and
propolis, have been recognized in traditional medicine as
aids in wound healing. Today, their healing properties for
select herpes viruses are being confirmed in both the
laboratory and the examination room; they may prove to
be beneficial in the management of HZ.
A small, nonblinded, cross-over study comparing the
topical application of honey with acyclovir cream on
patients with HSV found a significantly shorter duration
of episodes and faster healing time when using a honey
application versus the antiviral drug. Similarly, a rando-
mized, blinded-investigator study, comparing the use
of a topical propolis ointment with acyclovir and placebo
for 90 patients with confirmed HSV, concluded that after
10 days, a significant number of patients in the propolis
98 Egyptian Journal of Oral & Maxillofacial Surgery 2012, Vol 3 No 2
Copyright © The Egyptian Association of Oral and Maxillofacial Surgeons. Unauthorized reproduction of this article is prohibited.

group (24/30) had healed, compared with those in the
acyclovir (14/30) or the placebo (12/30) group. These
findings coincide with in-vitro studies proposing the
potential antiviral property of propolis against HSV.
Sangre de Grado (Croton lechleri) [27]
Extracts of Sangre de Grado have shown activity against a
number of viruses, including influenza, parainfluenza,
hepatitis A and B, and HSV-1 and HSV-2.
Aloe (Aloe vera) [28,29]
Topical administration of A. vera has been used widely for
wound healing. Aloe emodin, an anthraquinone prepared
from A. vera, was shown in vitro to inactivate HSV-2. In
another study, acemannan (another ingredient of Aloe)
was reported to act synergistically with acyclovir against
HSV in vitro.
St John’s wort (Hypericum perforatum) [30–33]
St John’s wort is widely known in traditional medicine to
be an effective treatment for viral infections and afflictions
related to the nerves. In terms of its effect on herpes
viruses, several studies have shown promising results.
Hypericum species have been observed in vitro to show
potent antiviral activity against HSV-1. In addition, two
double-blind, placebo-controlled studies have shown the
efficacy of an orally administered H. perforatum extract
against HSV.
Other treatment options
Traditional Chinese Medicine Acupuncture has long been
considered as an effective therapy for pain management.
Preliminary studies have shown that Chinese medicine
may show promise when used in conjunction with
conventional therapies in the management of PHN. A
variety of different treatment methods are available;
these fall into the following five main categories:
(1) Treatment according to the pathogenic factor.
(2) Treatment according to the channels involved.
(3) Treatment of the local area.
(4) Use of empirical points.
(5) Ear acupuncture.
Transcutaneous electrical nerve stimulation [5,7]
The use of transcutaneous electrical nerve stimulation
therapy has been beneficial in the management of PHN.
In one review, the use of combination therapy consisting
of amitriptyline, topical capsaicin, and transcutaneous
electrical nerve stimulation was recommended for the
treatment of PHN over antiviral therapy.
Nonpharmacologic interventions [5]
Neurosurgical procedures are treatments of last resort for
intractable pain. In small studies, electrical stimulation of
the thalamus and anterolateral cordotomy to interrupt the
spinothalamic tract led to relief in patients with PHN.
Electrocoagulation of well-defined areas of the dorsal root
has been attempted, but the procedure has a substantial
risk of prolonged hemiparesis and sensory deficits, and a
recent consensus conference did not advocate its use.
A phenomenon known as ‘counterirritation’ has been
reported to relieve PHN by reintroducing normal
inhibition of the small fibers in the spinal cord.
Data from small studies suggest that ethyl chloride spray,
which evaporates rapidly and causes a freezing sensation,
and transcutaneous electrical nerve stimulation provide
partial to complete relief of pain in some patients with
PHN.
ConclusionMany options are available to the clinician for the
treatment of HZ and PHN, albeit with variable degrees
of success. Antiviral agents, such as acyclovir, valacyclovir,
and famciclovir, have been shown to reduce both the pain
and the healing time of skin lesions associated with HZ,
but have marginal success in the prevention and
treatment of PHN. Corticosteroids may be used for pain
management in HZ, but do not seem to be effective in
the prevention of PHN. Analgesics provide effective
temporary pain relief for both HZ and PHN. Nerve block
injections offer more long-term pain relief in both
conditions, provided they are administered early in the
course of the disease. TCAs may provide pain relief in
cases of PHN, but require at least 3 months for positive
effects. The potential for antiviral resistance, particularly
in immunosuppressed individuals, is of growing concern,
as this group is at a greater risk of developing HZ and
PHN. Furthermore, the increased cost of antiviral therapy
can represent a financial obstacle for at-risk individuals to
obtain conventional medication. These issues underscore
the need to investigate and identify alternative ther-
apeutic options.
Although vitamin A deficiency appears to be associated
with increased susceptibility to HZ in immunosup-
pressed individuals, further investigation is required to
determine whether a causal relationship exists. Enzyme
therapy may serve as an effective alternative to acyclovir.
The topical use of capsaicin in the management of pain
has been shown to be effective in PHN, whereas topical
applications of licorice extract, Madonna lily bulb, and
C. nutans have been used in the treatment of skin lesions
associated with HZ; further investigation is required to
determine clinical efficacy. Small case studies using hot-
water-soluble extracts of reishi mushroom by itself or in
combination with other herbs indicate potential benefit
in both HZ and PHN. As with the other herbs
mentioned, further rigorous investigation is required to
determine clinical relevance.
AcknowlegdementsConflicts of interest
There are no conflicts of interest.
References1 Roxas M. Herpes zoster and postherpetic neuralgia: diagnosis and
therapeutic considerations. Altern Med Rev 2006; 11:102–113.2 Tidwell E, Hutson B, Burkhart N, Gutmann JL, Ellis CD. Herpes zoster of the
trigeminal nerve third branch: a case report and review of the literature.Int Endod J 1999; 32:61–66.
Herpes zoster Mali 99
Copyright © The Egyptian Association of Oral and Maxillofacial Surgeons. Unauthorized reproduction of this article is prohibited.

3 Kost RG, Straus SE. Postherpetic neuralgia – pathogenesis, treatment, andprevention. N Engl J Med 1996; 335:32–42.
4 Harpaz R, Ortega-Sanchez IR, Seward JF. Prevention of herpes zosterrecommendations of the Advisory Committee on Immunization Practices(ACIP), Vol. 57/RR-5. Division of Viral Diseases, National Center forImmunization and Respiratory Diseases.
5 Galluzzi KE. Managing herpes zoster and postherpetic neuralgia. J AmOsteopath Assoc 2009; 109 (Suppl 2):S7–S12.
6 Johnson RW, Bouhassira D, Kassianos G, Leplege A, Schmader KE, WeinkeT. The impact of herpes zoster and post-herpetic neuralgia on quality-of-life.BMC Med 2010; 8:37–49.
7 Pavan-Langston D. Herpes zoster. Antivirals and pain management.Ophthalmology 2008; 115 (Suppl.):S13–S20.
8 Dworkin RH, Schmader KE. Treatment and prevention of postherpeticneuralgia. Clin Infect Dis 2003; 36:877–882.
9 Semba RD. The role of vitamin A and related retinoids in immune function.Nutr Rev 1998; 56 (1 II):S38–S48.
10 Semba RD. Vitamin A and immunity to viral, bacterial and protozoaninfections. Proc Nutr Soc 1999; 58:719–727.
11 Murray M. Encyclopedia of nutritional supplements. Rocklin, CA: PrimaPublishing; 1996; p. 398.
12 Billigmann P. Enzyme therapy – an alternative form of treatment for herpeszoster. A controlled study involving 192 patients. Fortschr Med 1995;113:43–48.
13 Pompei R, Flore O, Marccialis MA. Glycyrrhizic acid inhibits virus growth andinactivates virus particles. Nature 1979; 281:689–690.
14 Pompei R, Pani A, Flore O. Antiviral activity of glycyrrhizic acid. Experientia1980; 36:304.
15 Baba M, Shigeta S. Antiviral activity of glycyrrhizin against varicella-zostervirus in vitro. Antiviral Res 1987; 7:99–107.
16 Abe N, Ebina T, Ishida N. Interferon induction by glycyrrhizin andglycyrrhetinic acid in mice. Microbiol Immunol 1982; 26:535–539.
17 Bone K, Mills S. Principles and practice of phytotherapy. Edinburgh, UK:Churchill Livingstone; 2000; p. 470.
18 Pieroni A. Medicinal plants and food medicines in the folk traditions of theupper Lucca Province, Italy. J Ethnopharmacol 2000; 70:235–273.
19 Mimaki Y, Satou T, Kuroda M, Sashida Y, Hatakeyama Y. New steroidalconstituents from the bulbs of Lilium candidum. Chem Pharm Bull 1998;46:1829–1832.
20 Hijikata Y, Yamada S. Effect of ganoderma lucidum on postherpetic
neuralgia. Am J Chin Med 1998; 26:375–381.21 Hijikata Y, Yasuhara A, Sahashi Y. Effect of an herbal formula containing
Ganoderma lucidum on reduction of herpes zoster pain: a pilot clinical trial.Am J Chin Med 2005; 33:517–523.
22 Sangkitporn S, Chaiwat S, Balachandra K, Dechatiwongse Na-Ayudhaya T,
Bunjob M, Jayavasu C. Treatment of herpes zoster with Clinacanthusnutans (Bi Phaya Yaw) extract. J Med Assoc Thai 1995; 78:624–627.
23 Al-Waili NS. Topical honey application vs. acyclovir for the treatment of
recurrent herpes simplex lesions. Med Sci Monit 2004; 10:MT94–MT98.
24 Vynograd N, Vynograd I, Sosnowski Z. A comparative multi-centre study of
the efficacy of propolis, acyclovir and placebo in the treatment of genitalherpes (HSV). Phytomedicine 2000; 7:1–6.
25 Amoros M, Lurton E, Boustie J, Girre L, Sauvager F, Cormier M. Comparison
of the anti-herpes simplex virus activities of propolis and 3-methyl-but-2-enylcaffeate. J Nat Prod 1994; 57:644–647.
26 Debiaggi M, Tateo F, Pagani L, Luini M, Romero E. Effects of propolis flavonoids
on virus infectivity and replication. Microbiologica 1990; 13:207–213.27 Williams JE. Review of antiviral and immunomodulating properties of plants
of the peruvian rainforest with a particular emphasis on una de gato andsangre de grado. Altern Med Rev 2001; 6:567–579.
28 Sydiskis RJ, Owen DG, Lohr JL, Rosler K-HA, Blomster RN. Inactivation of
enveloped viruses by anthraquinones extracted from plants. AntimicrobAgents Chemother 1991; 35:2463–2466.
29 Kahlon JB, Kemp MC, Yawei N, Carpenter RH, Shannon WM, McAnalley BH.
In vitro evaluation of the synergistic antiviral effects of acemannan incombination with azidothymidine and acyclovir. Mol Biother 1991; 3:214–223.
30 Vijayan P, Raghu C, Ashok G, Dhanaraj SA, Suresh B. Antiviral activity of
medicinal plants of Nilgiris. Indian J Med Res 2004; 120:24–29.31 Sokmen A, Jones BM, Erturk M. Antimicrobial activity of extracts from the cell
cultures of some Turkish medicinal plants. Phytother Res 1999; 13:355–357.32 Taylor RSL, Manandhar NP, Hudson JB, Towers GHN. Antiviral activities of
Nepalese medicinal plants. J Ethnopharmacol 1996; 52:157–163.33 Koytchev R, Alken R-G, Dundarov S. Hypericum-extract LI 160 for the therapy
of herpes simplex genitalis and labialis: results of two placebo-controlled,randomised, double-blind clinical trials. Z Phytotherapie 1999; 20:92.
100 Egyptian Journal of Oral & Maxillofacial Surgery 2012, Vol 3 No 2
Copyright © The Egyptian Association of Oral and Maxillofacial Surgeons. Unauthorized reproduction of this article is prohibited.
Copyright © 2022 FDOKUMEN



















![[Herpes Zoster and its prevention in Italy. Scientific consensus statement]](https://static.fdokumen.com/doc/165x107/6332d5755f7e75f94e094855/herpes-zoster-and-its-prevention-in-italy-scientific-consensus-statement.jpg)
