
A spatial approach using imprecise soil data for modelling crop yields over vast areas
Upload
independentCategory
view
1download
0
Acute undifferentiated fever in Binh Thuan province, Vietnam:
imprecise clinical diagnosis and irrational pharmaco-therapy
Hoang L. Phuong1,2, Peter J. de Vries1, Nico Nagelkerke3, Phan T. Giao2, Le Q. Hung2, Tran Q. Binh2,
Tran. T. Thanh Nga1,4, Nguyen V. Nam5 and Piet A. Kager1
1 Division of Infectious Diseases, Tropical Medicine and AIDS, Academic Medical Center, Amsterdam, The Netherlands2 Department of Tropical Diseases, Cho Ray Hospital, Ho Chi Minh City, Vietnam3 Department of Community Medicine, United Arab Emirates University, Al Ain, United Arab Emirates4 Department of Microbiology, Cho Ray Hospital, Ho Chi Minh City, Vietnam5 Binh Thuan Malaria and Goiter Control Center, Phan Thiet, Vietnam
Summary objectives To describe the characteristics of patients consulting commune primary healthcare posts
for acute undifferentiated fever not being malaria (AUF), and to explore the diagnostic and therapeutic
responses of the healthcare workers.
methods All patients presenting with AUF at 12 commune health posts and one clinic at the provincial
malaria station, Binh Thuan, a dengue endemic province in southern Vietnam, were included. Record
forms were used to fill in patient and diseases characteristics, pre-referral treatment, signs and symptoms,
provisional diagnosis and installed treatment, referral and final outcome.
results Two thousand ninety-six patients were included from April 2001 to March 2002. The median
delay to attend the health posts was, 0.87 day for >5, 1.15 days for children aged 5–15 years and
1.41 days for adults (P < 0.001). Sixty-five per cent of patients took some measures before consulting
the health post, of whom 82% applied self-medication and 69% took antibiotics. Pre-referral medica-
tion with antibiotics increased with age (RR 1.012 per year of age; 95% CI: 1.004–1.019). The diag-
nostic and therapeutic response of healthcare workers was very unspecific. The tourniquet test was
inappropriately used as general discriminating test, not only for detecting dengue haemorrhagic fever.
Empiric antibiotic therapy was installed in 77.2% of cases.
conclusions Management of uncomplicated fever, not being malaria, at the primary healthcare level
in Vietnam is non-specific, dominated by searching signs of hemorrhagic dengue and empiric antibiotic
treatment. This can probably be improved by better education.
keywords fever, clinical diagnosis, treatment, Vietnam
Introduction
Vietnam has been highly successful in bringing malaria
under control during the last decade (Ettling 2002).
Despite the rapid decline of malaria (Ettling 2002; Hung
et al. 2002; Nam et al. 2005), fever remains a common
reason for seeking help at communal health posts. Unlike
malaria, for which microscopic confirmation has become
standard practice at many health posts, laboratory diag-
nosis of other infectious diseases is lacking, and diagnosis
and treatment are generally only based on signs and
symptoms.
Self-medication has become very common among febrile
subjects in Vietnam and many other developing countries,
similar to what was observed for malaria before the large-
scale introduction of early diagnosis and treatment of
malaria (EDTM) (Boonstra et al. 2002; Deressa et al.
2003). Unguided use of antibiotics has many disadvanta-
ges, such as selection of drug resistant micro-organisms,
adverse drug effects, drug interactions and increased health
expenditure (Larsson et al. 2000; Okumura et al. 2002).
In the case of malaria, we recently showed that
improving the public knowledge and offering early diag-
nosis and effective treatment diverted patients from self-
treatment towards professional help (Giao et al. 2005). We
wondered if this can be achieved for other fevers as well.
This requires further study into the interaction between
health-seeking behaviour and the provided care. Health-
seeking behaviour is frequently investigated by techniques,
which are common in social sciences or marketing research
Tropical Medicine and International Health doi:10.1111/j.1365-3156.2006.01636.x
volume 11 no 6 pp 869–879 june 2006
ª 2006 Blackwell Publishing Ltd 869
(Font et al. 2001; Giao et al. 2005). The response of the
healthcare provider is less well studied (Halfvarsson et al.
2000; Guyatt & Snow 2004).
Here we describe the characteristics of patients with
acute fever, not being malaria, who present to a public
primary health post and explore patterns in the healthcare
workers’ diagnostic and therapeutic response.
Methods
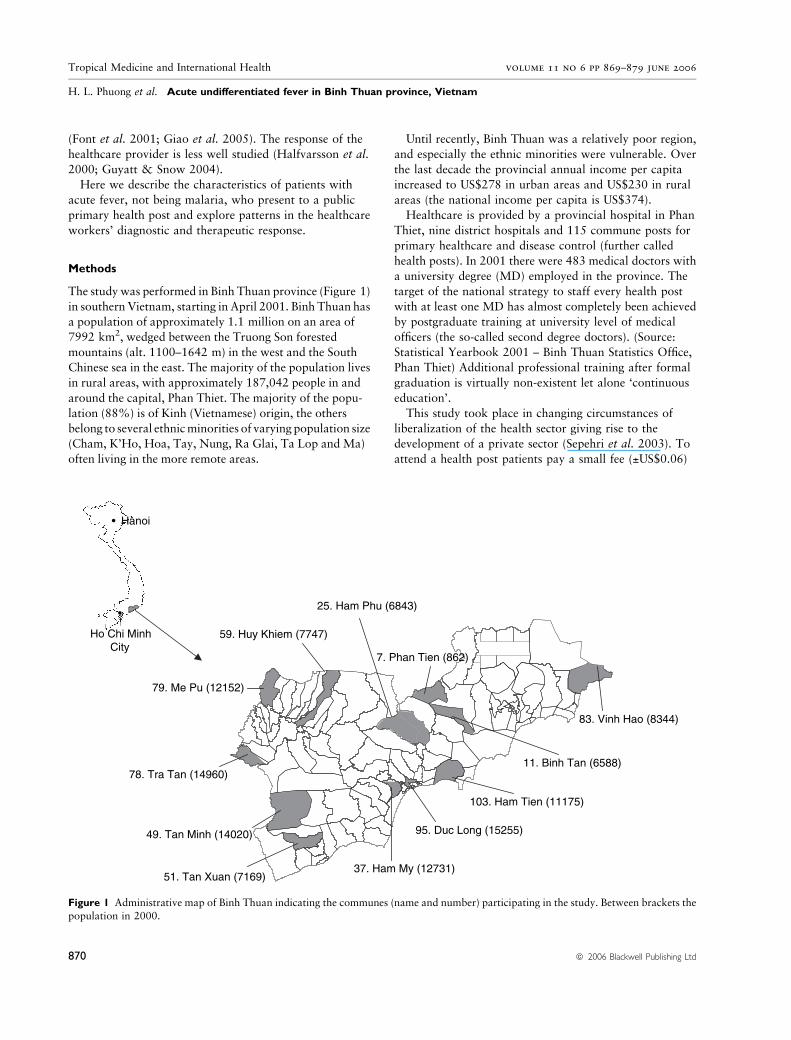
The study was performed in Binh Thuan province (Figure 1)
in southern Vietnam, starting in April 2001. Binh Thuan has
a population of approximately 1.1 million on an area of
7992 km2, wedged between the Truong Son forested
mountains (alt. 1100–1642 m) in the west and the South
Chinese sea in the east. The majority of the population lives
in rural areas, with approximately 187,042 people in and
around the capital, Phan Thiet. The majority of the popu-
lation (88%) is of Kinh (Vietnamese) origin, the others
belong to several ethnicminorities of varying population size
(Cham, K’Ho, Hoa, Tay, Nung, Ra Glai, Ta Lop and Ma)
often living in the more remote areas.
Until recently, Binh Thuan was a relatively poor region,
and especially the ethnic minorities were vulnerable. Over
the last decade the provincial annual income per capita
increased to US$278 in urban areas and US$230 in rural
areas (the national income per capita is US$374).
Healthcare is provided by a provincial hospital in Phan
Thiet, nine district hospitals and 115 commune posts for
primary healthcare and disease control (further called
health posts). In 2001 there were 483 medical doctors with
a university degree (MD) employed in the province. The
target of the national strategy to staff every health post
with at least one MD has almost completely been achieved
by postgraduate training at university level of medical
officers (the so-called second degree doctors). (Source:
Statistical Yearbook 2001 – Binh Thuan Statistics Office,
Phan Thiet) Additional professional training after formal
graduation is virtually non-existent let alone ‘continuous
education’.
This study took place in changing circumstances of
liberalization of the health sector giving rise to the
development of a private sector (Sepehri et al. 2003). To
attend a health post patients pay a small fee (±US$0.06)
37. Ham My (12731)
95. Duc Long (15255)
103. Ham Tien (11175)
11. Binh Tan (6588)
83. Vinh Hao (8344)
51. Tan Xuan (7169)
49. Tan Minh (14020)
78. Tra Tan (14960)
79. Me Pu (12152)
59. Huy Khiem (7747)
25. Ham Phu (6843)
7. Phan Tien (862)
• Hanoi
•
Ho Chi MinhCity
Figure 1 Administrative map of Binh Thuan indicating the communes (name and number) participating in the study. Between brackets the
population in 2000.
Tropical Medicine and International Health volume 11 no 6 pp 869–879 june 2006
H. L. Phuong et al. Acute undifferentiated fever in Binh Thuan province, Vietnam
870 ª 2006 Blackwell Publishing Ltd
and patients have to pay for examinations and drugs. Poor
subjects, including members of the ethnic minority groups,
are exempted from payment. The motives why patients
choose the public or private sector are largely unknown.
Twelve, not adjacent, health posts and one clinic at the
provincial malaria station, where febrile patients, suspect-
ing malaria, come for diagnosis and treatment, were
selected in a manner that would ensure a representative
selection of rural and (semi-)urban, lowland and highland
communes, and the province’s ethnic population structure.
The staff of the participating health posts were composed
of MDs and second degree doctors.
All patients presenting with acute undifferentiated fever
(AUF) were included in this study. AUF was defined as any
febrile illness of duration less than 14 days, confirmed by
an axillary temperature ‡38.0 �C, without any indication
for either severe systemic or organ specific disease. Malaria
was excluded by microscopic examination of a thick blood
smear.
Data collection
Record forms were filled in for all AUF patients recording
patient identifiers (age, sex, occupation and address),
history of recent exposure factors such as occupation, fresh
water contact, visiting forests, duration of disease and
invalidation, treatment taken, signs and symptoms at
presentation, provisional diagnosis and prescribed treat-
ment, referral and final outcome. Diagnoses such as ‘acute
fever’ and ‘viral infection’ were all reclassified to ‘undif-
ferentiated fever’.
Blood samples were collected for sero-diagnosis, results
of which will be presented elsewhere. All included subjects
were asked to come back after 2–4 weeks for re-assessment
and collection of a second blood sample.
Data were entered by the attending healthcare worker at
the first presentation of the patient. All health posts were
monitored at monthly visits by the research team from Cho
Ray Hospital, Ho Chi Minh City.
The study was approved by the Review Board of the Cho
Ray Hospital. The study was explained and discussed in
meetings with provincial authorities and staff of the health
posts. All patients (or, for children, the parents or
guardian) gave written informed consent.
Data analysis
Statistical analysis was done using SPSS (Version 11.5,
SPSS Inc., Ill.) and S-Plus 2000 (release 2, Mathsoft Inc,
MA). Frequencies and means or medians were calculated
to describe background variables. The chi-square test and
the median test were applied to assess the relation of
variables such as time of presentation at primary health
posts and age groups, time of presentation at primary
health posts and previous treatment, and season and
presumptive diagnosis. A logistic regression model was
used to explore the variables that related to antibiotic
use. Associations between the different indicators were
sought with explorative techniques such as correspon-
dence analysis, an explorative cluster analysis technique
and classification trees (Benzecri 1992; Venables &
Ripley 1999).
Results
From April 2001 until April 2002, 2096 patients with
undifferentiated fever (867 females and 1229 males,
female/male ¼ 1/1.3) were included. The median age was
18 years (range from 1 to 82). Their main occupation was
farming (820 adults, 39%) and school attendance (768
children, 37%). Other occupations included construction
and industrial labour (n ¼ 153; 7%), civil officer (n ¼ 39;
2%), child at home (n ¼ 163; 8%) and retirement (n ¼ 41;
2%).
Patients were divided into three age groups: adults
>15 years (n ¼ 1198; 57.2%), children from 5 to 15 years
(n ¼ 730; 34.8%) and >5 (n ¼ 166; 7.9%). The age
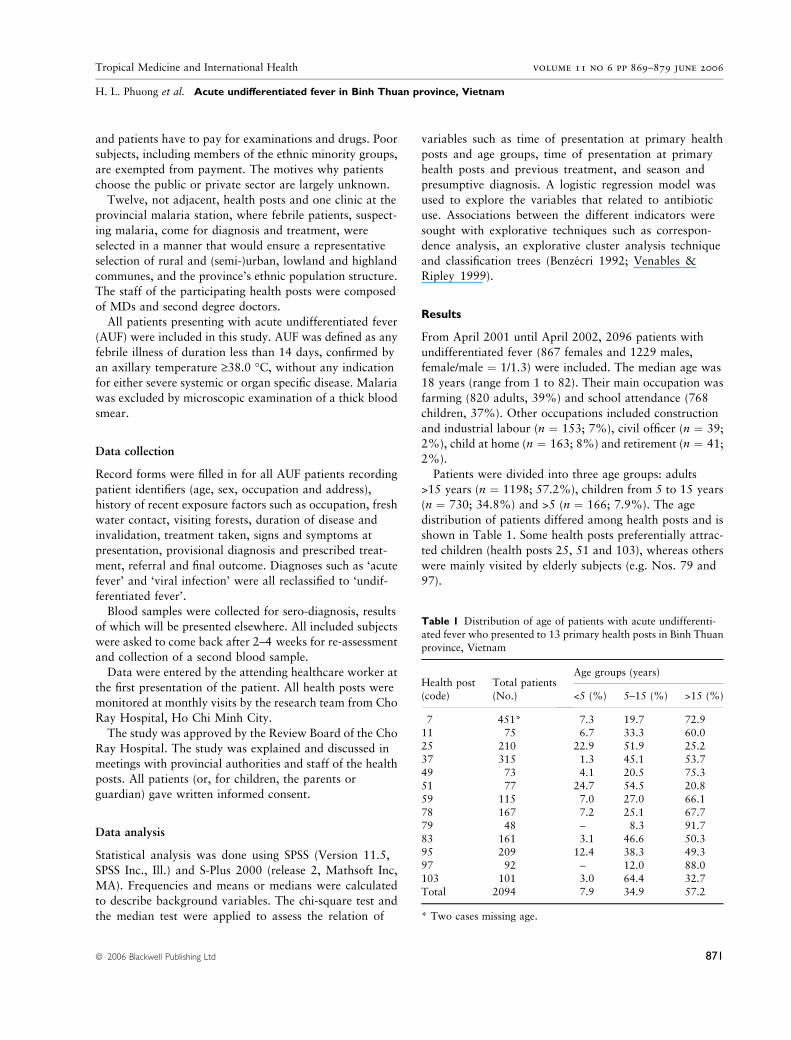
distribution of patients differed among health posts and is
shown in Table 1. Some health posts preferentially attrac-
ted children (health posts 25, 51 and 103), whereas others
were mainly visited by elderly subjects (e.g. Nos. 79 and
97).
Table 1 Distribution of age of patients with acute undifferenti-
ated fever who presented to 13 primary health posts in Binh Thuan
province, Vietnam
Health post(code)
Total patients(No.)
Age groups (years)
<5 (%) 5–15 (%) >15 (%)
7 451* 7.3 19.7 72.911 75 6.7 33.3 60.0
25 210 22.9 51.9 25.2
37 315 1.3 45.1 53.7
49 73 4.1 20.5 75.351 77 24.7 54.5 20.8
59 115 7.0 27.0 66.1
78 167 7.2 25.1 67.7
79 48 – 8.3 91.783 161 3.1 46.6 50.3
95 209 12.4 38.3 49.3
97 92 – 12.0 88.0103 101 3.0 64.4 32.7
Total 2094 7.9 34.9 57.2
* Two cases missing age.
Tropical Medicine and International Health volume 11 no 6 pp 869–879 june 2006
H. L. Phuong et al. Acute undifferentiated fever in Binh Thuan province, Vietnam
ª 2006 Blackwell Publishing Ltd 871
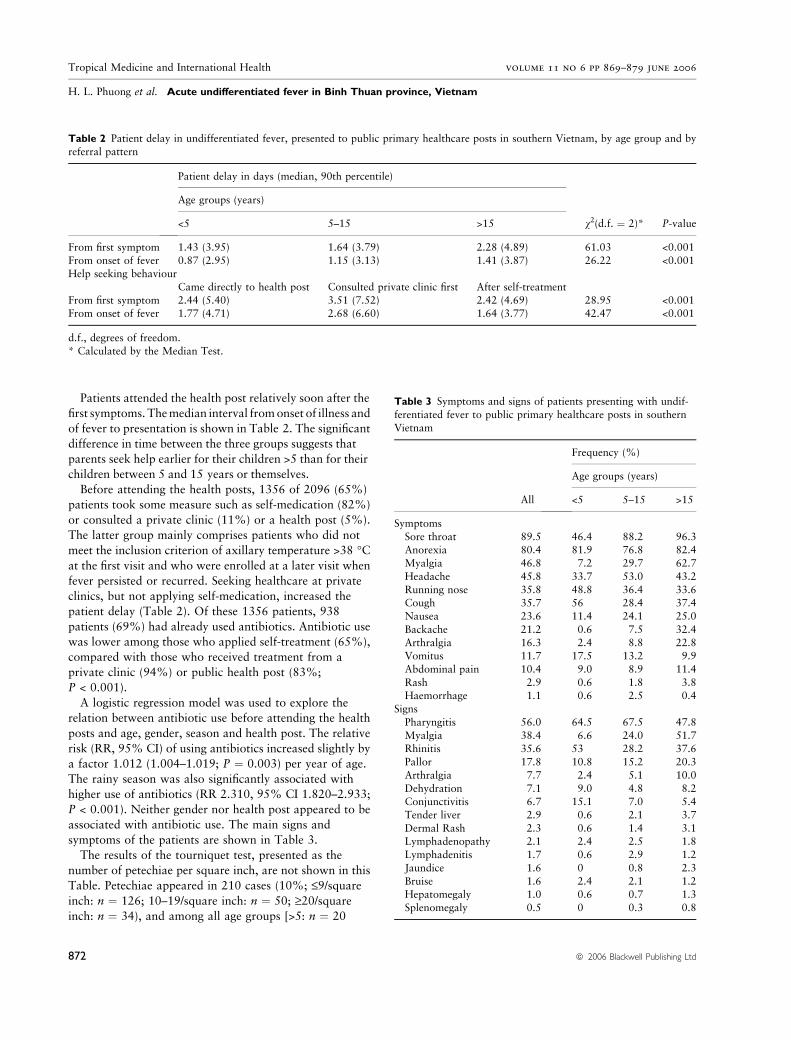
Patients attended the health post relatively soon after the
first symptoms. Themedian interval fromonset of illness and
of fever to presentation is shown in Table 2. The significant
difference in time between the three groups suggests that
parents seek help earlier for their children >5 than for their
children between 5 and 15 years or themselves.
Before attending the health posts, 1356 of 2096 (65%)
patients took some measure such as self-medication (82%)
or consulted a private clinic (11%) or a health post (5%).
The latter group mainly comprises patients who did not
meet the inclusion criterion of axillary temperature >38 �Cat the first visit and who were enrolled at a later visit when
fever persisted or recurred. Seeking healthcare at private
clinics, but not applying self-medication, increased the
patient delay (Table 2). Of these 1356 patients, 938
patients (69%) had already used antibiotics. Antibiotic use
was lower among those who applied self-treatment (65%),
compared with those who received treatment from a
private clinic (94%) or public health post (83%;
P < 0.001).
A logistic regression model was used to explore the
relation between antibiotic use before attending the health
posts and age, gender, season and health post. The relative
risk (RR, 95% CI) of using antibiotics increased slightly by
a factor 1.012 (1.004–1.019; P ¼ 0.003) per year of age.
The rainy season was also significantly associated with
higher use of antibiotics (RR 2.310, 95% CI 1.820–2.933;
P < 0.001). Neither gender nor health post appeared to be
associated with antibiotic use. The main signs and
symptoms of the patients are shown in Table 3.
The results of the tourniquet test, presented as the
number of petechiae per square inch, are not shown in this
Table. Petechiae appeared in 210 cases (10%; £9/squareinch: n ¼ 126; 10–19/square inch: n ¼ 50; ‡20/squareinch: n ¼ 34), and among all age groups [>5: n ¼ 20
Table 2 Patient delay in undifferentiated fever, presented to public primary healthcare posts in southern Vietnam, by age group and by
referral pattern
Patient delay in days (median, 90th percentile)
v2(d.f. ¼ 2)* P-value
Age groups (years)
<5 5–15 >15
From first symptom 1.43 (3.95) 1.64 (3.79) 2.28 (4.89) 61.03 <0.001
From onset of fever 0.87 (2.95) 1.15 (3.13) 1.41 (3.87) 26.22 <0.001Help seeking behaviour
Came directly to health post Consulted private clinic first After self-treatment
From first symptom 2.44 (5.40) 3.51 (7.52) 2.42 (4.69) 28.95 <0.001From onset of fever 1.77 (4.71) 2.68 (6.60) 1.64 (3.77) 42.47 <0.001
d.f., degrees of freedom.
* Calculated by the Median Test.
Table 3 Symptoms and signs of patients presenting with undif-
ferentiated fever to public primary healthcare posts in southern
Vietnam
All
Frequency (%)
Age groups (years)
<5 5–15 >15
Symptoms
Sore throat 89.5 46.4 88.2 96.3Anorexia 80.4 81.9 76.8 82.4
Myalgia 46.8 7.2 29.7 62.7
Headache 45.8 33.7 53.0 43.2
Running nose 35.8 48.8 36.4 33.6Cough 35.7 56 28.4 37.4
Nausea 23.6 11.4 24.1 25.0
Backache 21.2 0.6 7.5 32.4
Arthralgia 16.3 2.4 8.8 22.8Vomitus 11.7 17.5 13.2 9.9
Abdominal pain 10.4 9.0 8.9 11.4
Rash 2.9 0.6 1.8 3.8Haemorrhage 1.1 0.6 2.5 0.4
Signs
Pharyngitis 56.0 64.5 67.5 47.8
Myalgia 38.4 6.6 24.0 51.7Rhinitis 35.6 53 28.2 37.6
Pallor 17.8 10.8 15.2 20.3
Arthralgia 7.7 2.4 5.1 10.0
Dehydration 7.1 9.0 4.8 8.2Conjunctivitis 6.7 15.1 7.0 5.4
Tender liver 2.9 0.6 2.1 3.7
Dermal Rash 2.3 0.6 1.4 3.1Lymphadenopathy 2.1 2.4 2.5 1.8
Lymphadenitis 1.7 0.6 2.9 1.2
Jaundice 1.6 0 0.8 2.3
Bruise 1.6 2.4 2.1 1.2Hepatomegaly 1.0 0.6 0.7 1.3
Splenomegaly 0.5 0 0.3 0.8
Tropical Medicine and International Health volume 11 no 6 pp 869–879 june 2006
H. L. Phuong et al. Acute undifferentiated fever in Binh Thuan province, Vietnam
872 ª 2006 Blackwell Publishing Ltd
(9.5%), 5–15 years: n ¼ 127 (60.5%) and >15 years:
n ¼ 63 (30%)].
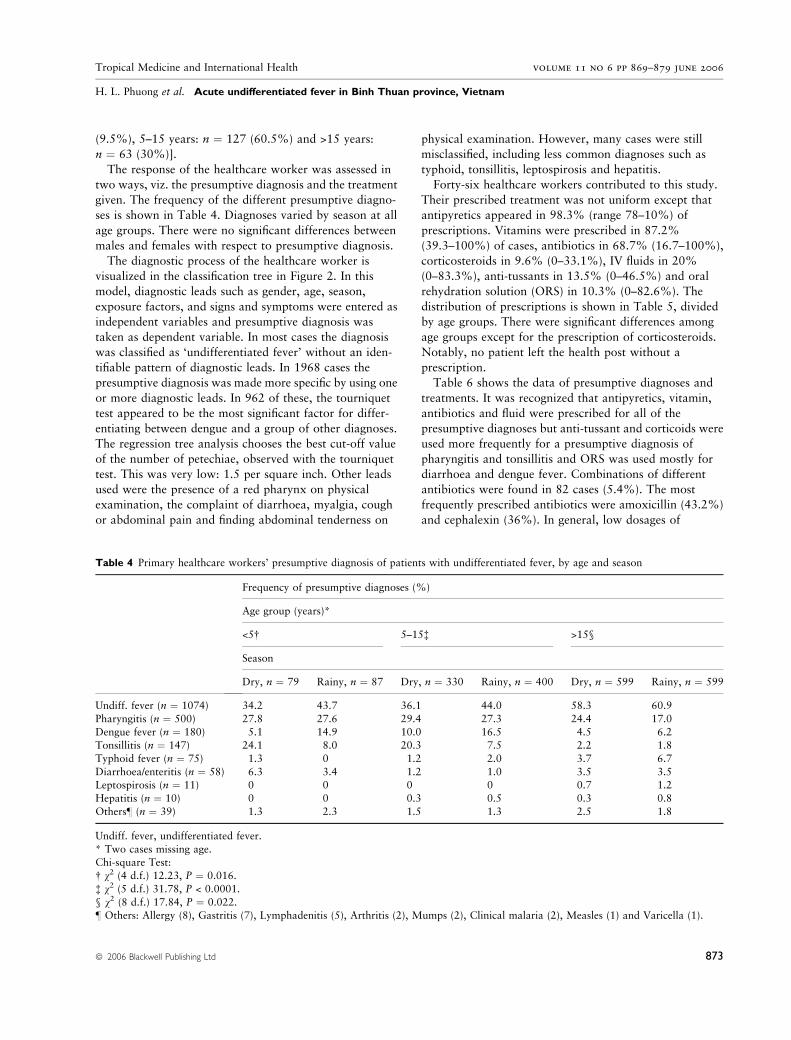
The response of the healthcare worker was assessed in
two ways, viz. the presumptive diagnosis and the treatment
given. The frequency of the different presumptive diagno-
ses is shown in Table 4. Diagnoses varied by season at all
age groups. There were no significant differences between
males and females with respect to presumptive diagnosis.
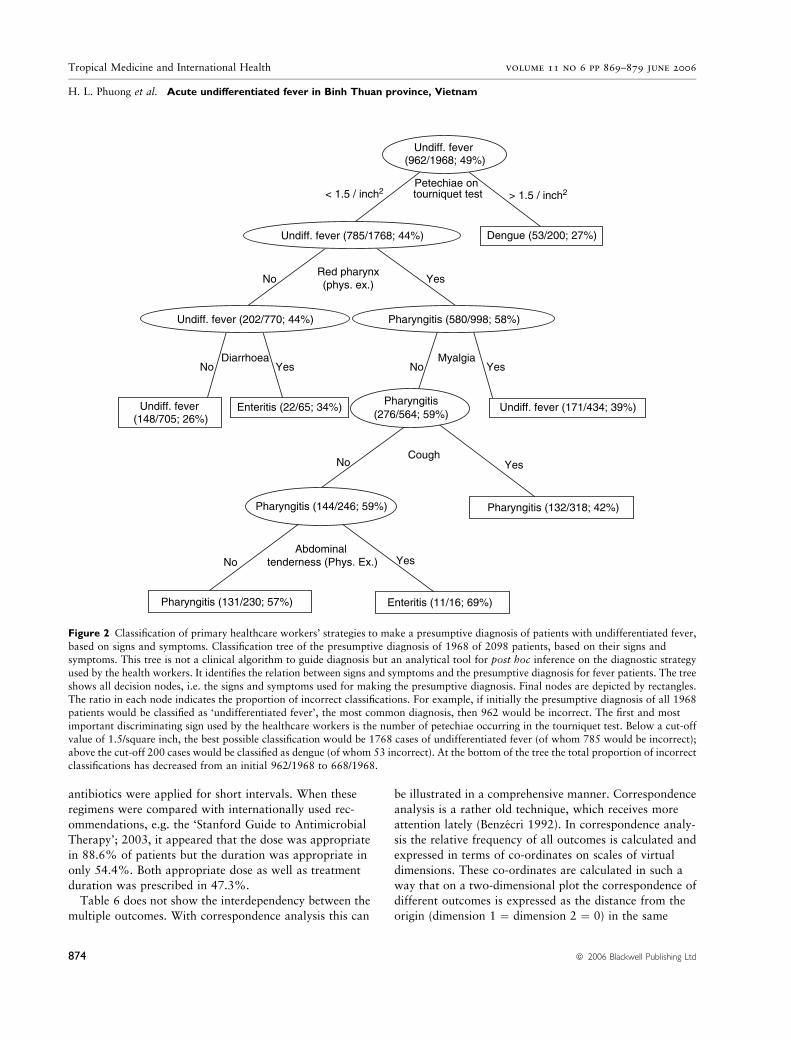
The diagnostic process of the healthcare worker is
visualized in the classification tree in Figure 2. In this
model, diagnostic leads such as gender, age, season,
exposure factors, and signs and symptoms were entered as
independent variables and presumptive diagnosis was
taken as dependent variable. In most cases the diagnosis
was classified as ‘undifferentiated fever’ without an iden-
tifiable pattern of diagnostic leads. In 1968 cases the
presumptive diagnosis was made more specific by using one
or more diagnostic leads. In 962 of these, the tourniquet
test appeared to be the most significant factor for differ-
entiating between dengue and a group of other diagnoses.
The regression tree analysis chooses the best cut-off value
of the number of petechiae, observed with the tourniquet
test. This was very low: 1.5 per square inch. Other leads
used were the presence of a red pharynx on physical
examination, the complaint of diarrhoea, myalgia, cough
or abdominal pain and finding abdominal tenderness on
physical examination. However, many cases were still
misclassified, including less common diagnoses such as
typhoid, tonsillitis, leptospirosis and hepatitis.
Forty-six healthcare workers contributed to this study.
Their prescribed treatment was not uniform except that
antipyretics appeared in 98.3% (range 78–10%) of
prescriptions. Vitamins were prescribed in 87.2%
(39.3–100%) of cases, antibiotics in 68.7% (16.7–100%),
corticosteroids in 9.6% (0–33.1%), IV fluids in 20%
(0–83.3%), anti-tussants in 13.5% (0–46.5%) and oral
rehydration solution (ORS) in 10.3% (0–82.6%). The
distribution of prescriptions is shown in Table 5, divided
by age groups. There were significant differences among
age groups except for the prescription of corticosteroids.
Notably, no patient left the health post without a
prescription.
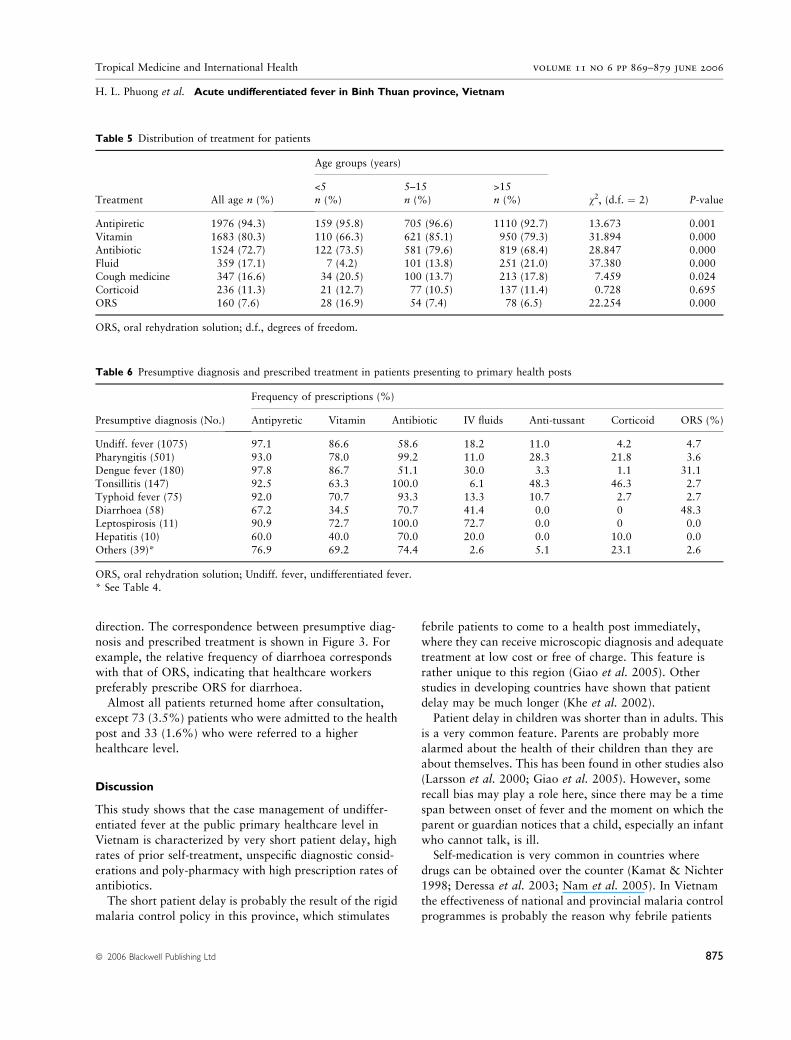
Table 6 shows the data of presumptive diagnoses and
treatments. It was recognized that antipyretics, vitamin,
antibiotics and fluid were prescribed for all of the
presumptive diagnoses but anti-tussant and corticoids were
used more frequently for a presumptive diagnosis of
pharyngitis and tonsillitis and ORS was used mostly for
diarrhoea and dengue fever. Combinations of different
antibiotics were found in 82 cases (5.4%). The most
frequently prescribed antibiotics were amoxicillin (43.2%)
and cephalexin (36%). In general, low dosages of
Table 4 Primary healthcare workers’ presumptive diagnosis of patients with undifferentiated fever, by age and season
Frequency of presumptive diagnoses (%)
Age group (years)*
<5� 5–15� >15§
Season
Dry, n ¼ 79 Rainy, n ¼ 87 Dry, n ¼ 330 Rainy, n ¼ 400 Dry, n ¼ 599 Rainy, n ¼ 599
Undiff. fever (n ¼ 1074) 34.2 43.7 36.1 44.0 58.3 60.9
Pharyngitis (n ¼ 500) 27.8 27.6 29.4 27.3 24.4 17.0Dengue fever (n ¼ 180) 5.1 14.9 10.0 16.5 4.5 6.2
Tonsillitis (n ¼ 147) 24.1 8.0 20.3 7.5 2.2 1.8
Typhoid fever (n ¼ 75) 1.3 0 1.2 2.0 3.7 6.7
Diarrhoea/enteritis (n ¼ 58) 6.3 3.4 1.2 1.0 3.5 3.5Leptospirosis (n ¼ 11) 0 0 0 0 0.7 1.2
Hepatitis (n ¼ 10) 0 0 0.3 0.5 0.3 0.8
Others– (n ¼ 39) 1.3 2.3 1.5 1.3 2.5 1.8
Undiff. fever, undifferentiated fever.
* Two cases missing age.Chi-square Test:
� v2 (4 d.f.) 12.23, P ¼ 0.016.
� v2 (5 d.f.) 31.78, P < 0.0001.
§ v2 (8 d.f.) 17.84, P ¼ 0.022.– Others: Allergy (8), Gastritis (7), Lymphadenitis (5), Arthritis (2), Mumps (2), Clinical malaria (2), Measles (1) and Varicella (1).
Tropical Medicine and International Health volume 11 no 6 pp 869–879 june 2006
H. L. Phuong et al. Acute undifferentiated fever in Binh Thuan province, Vietnam
ª 2006 Blackwell Publishing Ltd 873
antibiotics were applied for short intervals. When these
regimens were compared with internationally used rec-
ommendations, e.g. the ‘Stanford Guide to Antimicrobial
Therapy’; 2003, it appeared that the dose was appropriate
in 88.6% of patients but the duration was appropriate in
only 54.4%. Both appropriate dose as well as treatment
duration was prescribed in 47.3%.
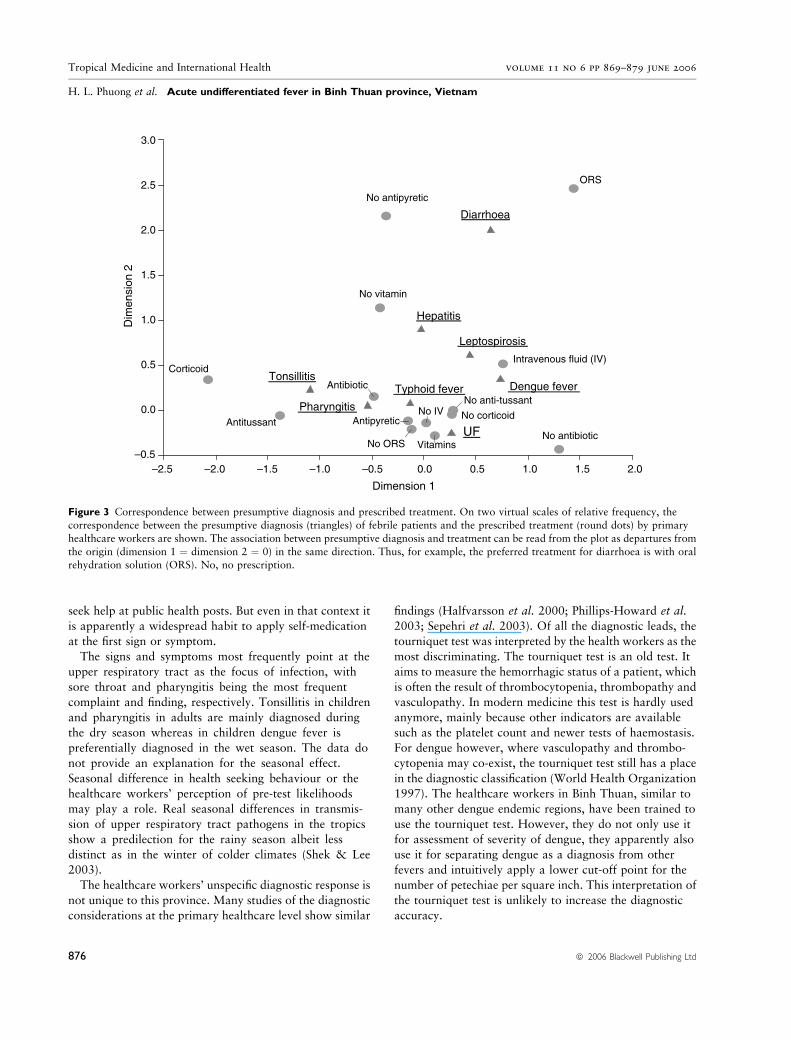
Table 6 does not show the interdependency between the
multiple outcomes. With correspondence analysis this can
be illustrated in a comprehensive manner. Correspondence
analysis is a rather old technique, which receives more
attention lately (Benzecri 1992). In correspondence analy-
sis the relative frequency of all outcomes is calculated and
expressed in terms of co-ordinates on scales of virtual
dimensions. These co-ordinates are calculated in such a
way that on a two-dimensional plot the correspondence of
different outcomes is expressed as the distance from the
origin (dimension 1 ¼ dimension 2 ¼ 0) in the same
Undiff. fever (962/1968; 49%)
Enteritis (22/65; 34%)
Enteritis (11/16; 69%)
Pharyngitis (132/318; 42%)
Pharyngitis (131/230; 57%)
Undiff. fever (171/434; 39%)
< 1.5 / inch2
No Yes
Dengue (53/200; 27%)
Undiff. fever (148/705; 26%)
No YesNo Yes
No Yes
> 1.5 / inch2Petechiae on tourniquet test
Diarrhoea
Red pharynx(phys. ex.)
Myalgia
CoughNo Yes
Abdominal tenderness (Phys. Ex.)
Undiff. fever (785/1768; 44%)
Undiff. fever (202/770; 44%)
Pharyngitis(276/564; 59%)
Pharyngitis (580/998; 58%)
Pharyngitis (144/246; 59%)
Figure 2 Classification of primary healthcare workers’ strategies to make a presumptive diagnosis of patients with undifferentiated fever,
based on signs and symptoms. Classification tree of the presumptive diagnosis of 1968 of 2098 patients, based on their signs andsymptoms. This tree is not a clinical algorithm to guide diagnosis but an analytical tool for post hoc inference on the diagnostic strategy
used by the health workers. It identifies the relation between signs and symptoms and the presumptive diagnosis for fever patients. The tree
shows all decision nodes, i.e. the signs and symptoms used for making the presumptive diagnosis. Final nodes are depicted by rectangles.
The ratio in each node indicates the proportion of incorrect classifications. For example, if initially the presumptive diagnosis of all 1968patients would be classified as ‘undifferentiated fever’, the most common diagnosis, then 962 would be incorrect. The first and most
important discriminating sign used by the healthcare workers is the number of petechiae occurring in the tourniquet test. Below a cut-off
value of 1.5/square inch, the best possible classification would be 1768 cases of undifferentiated fever (of whom 785 would be incorrect);above the cut-off 200 cases would be classified as dengue (of whom 53 incorrect). At the bottom of the tree the total proportion of incorrect
classifications has decreased from an initial 962/1968 to 668/1968.
Tropical Medicine and International Health volume 11 no 6 pp 869–879 june 2006
H. L. Phuong et al. Acute undifferentiated fever in Binh Thuan province, Vietnam
874 ª 2006 Blackwell Publishing Ltd
direction. The correspondence between presumptive diag-
nosis and prescribed treatment is shown in Figure 3. For
example, the relative frequency of diarrhoea corresponds
with that of ORS, indicating that healthcare workers
preferably prescribe ORS for diarrhoea.
Almost all patients returned home after consultation,
except 73 (3.5%) patients who were admitted to the health
post and 33 (1.6%) who were referred to a higher
healthcare level.
Discussion
This study shows that the case management of undiffer-
entiated fever at the public primary healthcare level in
Vietnam is characterized by very short patient delay, high
rates of prior self-treatment, unspecific diagnostic consid-
erations and poly-pharmacy with high prescription rates of
antibiotics.
The short patient delay is probably the result of the rigid
malaria control policy in this province, which stimulates
febrile patients to come to a health post immediately,
where they can receive microscopic diagnosis and adequate
treatment at low cost or free of charge. This feature is
rather unique to this region (Giao et al. 2005). Other
studies in developing countries have shown that patient
delay may be much longer (Khe et al. 2002).
Patient delay in children was shorter than in adults. This
is a very common feature. Parents are probably more
alarmed about the health of their children than they are
about themselves. This has been found in other studies also
(Larsson et al. 2000; Giao et al. 2005). However, some
recall bias may play a role here, since there may be a time
span between onset of fever and the moment on which the
parent or guardian notices that a child, especially an infant
who cannot talk, is ill.
Self-medication is very common in countries where
drugs can be obtained over the counter (Kamat & Nichter
1998; Deressa et al. 2003; Nam et al. 2005). In Vietnam
the effectiveness of national and provincial malaria control
programmes is probably the reason why febrile patients
Table 5 Distribution of treatment for patients
Treatment All age n (%)
Age groups (years)
v2, (d.f. ¼ 2) P-value<5 5–15 >15n (%) n (%) n (%)
Antipiretic 1976 (94.3) 159 (95.8) 705 (96.6) 1110 (92.7) 13.673 0.001Vitamin 1683 (80.3) 110 (66.3) 621 (85.1) 950 (79.3) 31.894 0.000
Antibiotic 1524 (72.7) 122 (73.5) 581 (79.6) 819 (68.4) 28.847 0.000
Fluid 359 (17.1) 7 (4.2) 101 (13.8) 251 (21.0) 37.380 0.000Cough medicine 347 (16.6) 34 (20.5) 100 (13.7) 213 (17.8) 7.459 0.024
Corticoid 236 (11.3) 21 (12.7) 77 (10.5) 137 (11.4) 0.728 0.695
ORS 160 (7.6) 28 (16.9) 54 (7.4) 78 (6.5) 22.254 0.000
ORS, oral rehydration solution; d.f., degrees of freedom.
Table 6 Presumptive diagnosis and prescribed treatment in patients presenting to primary health posts
Presumptive diagnosis (No.)
Frequency of prescriptions (%)
Antipyretic Vitamin Antibiotic IV fluids Anti-tussant Corticoid ORS (%)
Undiff. fever (1075) 97.1 86.6 58.6 18.2 11.0 4.2 4.7
Pharyngitis (501) 93.0 78.0 99.2 11.0 28.3 21.8 3.6Dengue fever (180) 97.8 86.7 51.1 30.0 3.3 1.1 31.1
Tonsillitis (147) 92.5 63.3 100.0 6.1 48.3 46.3 2.7
Typhoid fever (75) 92.0 70.7 93.3 13.3 10.7 2.7 2.7
Diarrhoea (58) 67.2 34.5 70.7 41.4 0.0 0 48.3Leptospirosis (11) 90.9 72.7 100.0 72.7 0.0 0 0.0
Hepatitis (10) 60.0 40.0 70.0 20.0 0.0 10.0 0.0
Others (39)* 76.9 69.2 74.4 2.6 5.1 23.1 2.6
ORS, oral rehydration solution; Undiff. fever, undifferentiated fever.* See Table 4.
Tropical Medicine and International Health volume 11 no 6 pp 869–879 june 2006
H. L. Phuong et al. Acute undifferentiated fever in Binh Thuan province, Vietnam
ª 2006 Blackwell Publishing Ltd 875
seek help at public health posts. But even in that context it
is apparently a widespread habit to apply self-medication
at the first sign or symptom.
The signs and symptoms most frequently point at the
upper respiratory tract as the focus of infection, with
sore throat and pharyngitis being the most frequent
complaint and finding, respectively. Tonsillitis in children
and pharyngitis in adults are mainly diagnosed during
the dry season whereas in children dengue fever is
preferentially diagnosed in the wet season. The data do
not provide an explanation for the seasonal effect.
Seasonal difference in health seeking behaviour or the
healthcare workers’ perception of pre-test likelihoods
may play a role. Real seasonal differences in transmis-
sion of upper respiratory tract pathogens in the tropics
show a predilection for the rainy season albeit less
distinct as in the winter of colder climates (Shek & Lee
2003).
The healthcare workers’ unspecific diagnostic response is
not unique to this province. Many studies of the diagnostic
considerations at the primary healthcare level show similar
findings (Halfvarsson et al. 2000; Phillips-Howard et al.
2003; Sepehri et al. 2003). Of all the diagnostic leads, the
tourniquet test was interpreted by the health workers as the
most discriminating. The tourniquet test is an old test. It
aims to measure the hemorrhagic status of a patient, which
is often the result of thrombocytopenia, thrombopathy and
vasculopathy. In modern medicine this test is hardly used
anymore, mainly because other indicators are available
such as the platelet count and newer tests of haemostasis.
For dengue however, where vasculopathy and thrombo-
cytopenia may co-exist, the tourniquet test still has a place
in the diagnostic classification (World Health Organization
1997). The healthcare workers in Binh Thuan, similar to
many other dengue endemic regions, have been trained to
use the tourniquet test. However, they do not only use it
for assessment of severity of dengue, they apparently also
use it for separating dengue as a diagnosis from other
fevers and intuitively apply a lower cut-off point for the
number of petechiae per square inch. This interpretation of
the tourniquet test is unlikely to increase the diagnostic
accuracy.
Dimension 1
2.01.51.00.50.0–0.5–1.0–1.5–2.0–2.5
Dim
ensi
on 2
3.0
2.5
2.0
1.5
1.0
0.5
0.0
–0.5No ORS
ORS
No anti-tussant
AntitussantNo IV
Intravenous fluid (IV)
No vitamin
Vitamins
No corticoid
Corticoid
No antipyretic
Antipyretic
No antibiotic
Antibiotic Typhoid feverTonsillitis
Pharyngitis
Leptospirosis
Hepatitis
Diarrhoea
Dengue fever
UF
Figure 3 Correspondence between presumptive diagnosis and prescribed treatment. On two virtual scales of relative frequency, the
correspondence between the presumptive diagnosis (triangles) of febrile patients and the prescribed treatment (round dots) by primary
healthcare workers are shown. The association between presumptive diagnosis and treatment can be read from the plot as departures from
the origin (dimension 1 ¼ dimension 2 ¼ 0) in the same direction. Thus, for example, the preferred treatment for diarrhoea is with oralrehydration solution (ORS). No, no prescription.
Tropical Medicine and International Health volume 11 no 6 pp 869–879 june 2006
H. L. Phuong et al. Acute undifferentiated fever in Binh Thuan province, Vietnam
876 ª 2006 Blackwell Publishing Ltd

The therapeutic response of the healthcare workers, i.e.
prescribing drugs for all and antibiotics for most patients,
is extreme but not unique (Sepehri et al. 2003; Yanagisawa
et al. 2004). Although the diagnosis ‘undifferentiated fever’
might exclude bacterial infections, this apparently was no
reason to withhold antibiotics. Especially the use of
corticosteroids seems an inadequate response to a short-
lived fever. However, it is common knowledge that the
patient’s subjective improvement after the use of cortico-
steroids is impressive, and that for a healthcare worker, not
restrained by much knowledge of evidence-based medicine,
it is a logical step to improve the patients well-being as
soon as possible.
This study indicates some potential points for
improvement in the management of undifferentiated
fever. First, febrile patients or parents of febrile patients
seek help shortly after onset of symptoms. The patient
delay may be even too short as most of the diseases are
self-limiting by nature. The low threshold for early
detection of malaria is probably one of the main reasons
for this short patient delay and high consumption of
healthcare. In order to reduce the workload of the public
primary healthcare service, a two-step policy, with
screening for malaria for all, but further consultation
only for severe cases, based on carefully defined criteria,
can be considered. However, the patients’ perceptions of
fever and disease and economic incentives should be
taken into consideration. For example, a high workload
can also mean a high income for a healthcare worker.
Second, the presumptive diagnosis of the healthcare
worker can be improved. The most rational approach
would be to upgrade the educational level of all
healthcare workers. As mentioned previously, such an
approach is currently being carried out by the Vietnam-
ese government. In addition, at every health post the
epidemiology of the locally prevalent infectious diseases
should also be known. These data are often available,
but not used as a way to increase the prior likelihood of
the presumptive diagnosis. This should be part of,
ongoing, postgraduate training. Another way of improv-
ing the diagnosis, by providing rapid confirmatory tests,
is a point for further study.
Last, improved, rational, pharmacotherapy may do
much benefit. The drawbacks of unguided drug use are
evident: high costs, potential side effects, selection of
resistant micro-organisms and so on. This requires extra-
education, including postgraduate training, of the
healthcare workers. It definitely also needs some re-
education of the population, to redress its hunger for
drugs.
In conclusion, management of uncomplicated fever at
the primary healthcare level in Vietnam can be improved
by better specification of the diagnosis, better knowledge
of local diseases and more rational pharmacotherapy.
These objectives can be achieved by better, postgraduate,
education.
Acknowledgements
The study was supported by the Dutch Foundation for the
Advancement of Tropical Research (WOTRO). We grate-
fully acknowledge the contributions of the healthcare
workers at 13 studied sites. We would like to thank Prof.
Truong Van Viet, MD, PhD, the director of Cho Ray
Hospital, HCMC and the authorities of Binh Thuan
province for their cooperation.
References
Benzecri J-P (1992) Correspondence Analysis Handbook. Marcel
Dekker Inc., New York.
Boonstra E, Lindbaek M, Khulumani P, Ngome E & Fugelli P
(2002) Adherence to treatment guidelines in primary health care
facilities in Botswana. Tropical Medicine and International
Health 7, 178–186.
Deressa W, Ali A & Enqusellassie F (2003) Self-treatment of
malaria in rural communities, Butajira, southern Ethiopia.
Bulletin of the World Health Organization 81, 261–
268.
Ettling MB (2002) The control of Malaria in Vietnam from 1980
to 2000: what went right? 2002. Report of Consultancy for
World Health Organization Regional Office for Western Pacific,
Manila.
Font F, Alonso GM, Nathan R et al. (2001) Diagnostic accuracy
and case management of clinical malaria in the primary health
services of a rural area in south-eastern Tanzania. Tropical
Medicine and International Health 6, 423–428.
Giao PT, de Vries PJ, Hung LQ et al. (2005) Early diagnosis and
treatment of uncomplicated malaria in Vietnam and patterns of
health seeking. Tropical Medicine and International Health 10,
919–925.
Guyatt HL & Snow RW (2004) The management of fevers in
Kenyan children and adults in an area of seasonal malaria
transmission. Transactions of the Royal Society of Tropical
Medicine and Hygiene 98, 111–115.
Halfvarsson J, Heijne N, Ljungman P et al. (2000) Knowing when
but not how! – mothers’ perceptions and use of antibiotics in a
rural area of Vietnam. Tropical Doctor 30, 6–10.
Hung LQ, Vries PJ, Giao PT et al. (2002) Control of malaria: a
successful experience from Vietnam. Bulletin of the World
Health Organization 80, 660–666.
Kamat VR & Nichter M (1998) Pharmacies, self-medication and
pharmaceutical marketing in Bombay, India. Social Sciences and
Medicine 47, 779–794.
Khe ND, Toan NV, Xuan LT et al. (2002) Primary health concept
revisited: where do people seek health care in a rural area of
Vietnam? Health Policy 61, 95–109.
Tropical Medicine and International Health volume 11 no 6 pp 869–879 june 2006
H. L. Phuong et al. Acute undifferentiated fever in Binh Thuan province, Vietnam
ª 2006 Blackwell Publishing Ltd 877

Larsson M, Kronvall G, Chuc NT et al. (2000) Antibiotic medi-
cation and bacterial resistance to antibiotics: a survey of chil-
dren in a Vietnamese community. Tropical Medicine and
International Health 5, 711–721.
Nam NV, de Vries PJ, Toi LV & Nagelkerke N (2005) Malaria
control in Vietnam: the Binh Thuan experience. Tropical Med-
icine and International Health 10, 357–365.
Okumura J, Wakai S & Umenai T (2002) Drug utilisation and self-
medication in rural communities in Vietnam. Social Sciences and
Medicine 54, 1875–1886.
Phillips-Howard PA, Wannemuehler KA, ter Kuile FO et al.
(2003) Diagnostic and prescribing practices in peripheral health
facilities in rural western Kenya. American Journal of Tropical
Medicine and Hygiene 68, 44–49.
Sepehri A, Chernomas R & Akram-Lodhi AH (2003) If they get
sick, they are in trouble: health care restructuring, user charges,
and equity in Vietnam. International Journal of Health Services
33, 137–161.
Shek LP-C & Lee BW (2003) Epidemiology and seasonality of
respiratory tract virus infections in the tropics. Paediatric Re-
spiratory Reviews 4, 105–111.
Venables WN & Ripley BD (1999)Modern Applied Statistics with
S-Plus, 3rd Edn. Springer, New York.
World Health Organization (1997) Dengue Haemorrhagic Fever:
Diagnosis, Treatment, Prevention and Control, 2nd Edn. WHO,
Geneva.
Yanagisawa S, Mey V & Wakai S (2004) Comparison of
health-seeking behaviour between poor and better-off people
after health sector reform in Cambodia. Public Health 118,
21–30.
Corresponding Author Peter J. De Vries, Division of Infectious Diseases, Tropical Medicine and AIDS, Academic Medical Center,
F4-217, Meibergdreef 9, 1105 AZ Amsterdam, The Netherlands. Tel.: +31 20 5664380; Fax: +31 20 6972286; E-mail:
Fievres aigues indifferenciees dans la province de Binh Thuan au Vietnam: diagnostic cliniques imprecises et pharmacotherapie irrationnelle
objectifs Decrire les caracteristiques des patients consultant des postes communautaires de soins de sante primaire pour des fievres aigues indiffe-
renciees autres que la malaria et explorer le diagnostic et les interventions therapeutiques des agents de la sante.
methodes Tous les patients presentant une fievre aigue indifferenciee dans 12 postes communautaires de sante et une clinique ont ete inclus dans
l’etude effectuee dans la station provinciale de malaria de Binh Thuan, une province endemique pour la dengue, dans le sud du Vietnam. Les formulaires
de records ont ete utilises pour saisir les caracteristiques de la maladie du patient, le traitement avant que le patient ne soit refere, les signes et les
symptomes, le diagnostic provisionnel et le traitement instaure, le resultat au moment ou le patient a ete refere et apres.
resultats 2096 patients ont ete inclus dans l’etude entre avril 2001 et mars 2002. Les delais medians pour atteindre le poste de sante etaient de 0,87
jour pour les moins de 5 ans, 1,15 jours pour ceux ages de 5 a 15 ans et de 1,41 jours pour les adultes (p < 0,001). 65% des patients ont recouru a
d’autres mesures avant de consulter le centre de sante. Parmi ceux-ci, 82% ont eu recours a l’automedication et 69% ont pris des antibiotiques. La prise
d’antibiotiques avant que le patient ne soit refere augmentait avec l’age (RR: 1,012 par annee d’age; IC95%: 1,004–1,019). Le diagnostic et l’inter-
vention des agents de sante etaient totalement non specifiques. Le test du tourniquet etait utilise de facon inappropriee comme test de discrimination et
pas uniquement pour la detection de la fievre hemorragique de dengue. Une therapie empirique aux antibiotiques etait instauree dans 77,2% des cas.
conclusion La prise en charge des fievres non compliquees et non malariques au niveau des services de sante primaire au Vietnam est non specifique,
dominee par la recherche de signes de dengue hemorragique et par un traitement empirique par antibiotiques. Cette attitude pourrait etre amelioree par
une meilleure education.
mots cles fievre, diagnostic clinique, traitement, Vietnam
Tropical Medicine and International Health volume 11 no 6 pp 869–879 june 2006
H. L. Phuong et al. Acute undifferentiated fever in Binh Thuan province, Vietnam
878 ª 2006 Blackwell Publishing Ltd

Fiebre aguda indiferenciada en la provincia de Binh Thuan, Vietnam: Diagnostico clınico impreciso y farmacoterapia irracional
objetivos Describir las caracterısticas de pacientes que consultan puestos comunitarios de atencion primaria por fiebre aguda indiferenciada (FAI), y
explorar el diagnostico y la respuesta terapeutica de los trabajadores sanitarios.
metodos Se incluyeron todos los pacientes con FAI en doce puestos comunitarios de salud y un hospital en la estacion provincial de malaria en Binh
Thuan, provincia de Vietnam del Sur endemica para dengue. Se utilizaron las historias clınicas para completar las caracterısticas de los pacientes y la
enfermedad, la medicacion previa, los signos y sıntomas, el diagnostico provisional y el tratamiento establecido, la derivacion y la resolucion final.
resultados Se incluyeron 2096 pacientes entre Abril 2001 y Marzo 2002. La media en el retraso de atencion en los centros de salud: 0.87 para
menores de cinco anos, 1.15 para ninos entre 5–15 anos y 1.41 para adultos (p < 0.001). El 65% de los pacientes tomo las mismas medidas antes de
consultar un centro de salud, de los cuales el 82% se automedico y el 69% tomo antibioticos. La automedicacion con antibioticos aumentaba con la
edad (RR 1.012 por ano por edad; 95% CI: 1.004–1.019). El diagnostico y la respuesta terapeutica de los trabajadores sanitarios fue muy inespecıfica.
La prueba del torniquete se utilizaba de forma inapropiada, no solo para detectar dengue hemorragico sino como un teste discriminatorio general. La
terapia antibiotica empırica se dio en un 77.2% de los casos.
conclusiones El manejo de la fiebre no complicada, no debida a malaria, en los centros de atencion primaria de Vietnam es inespecıfica y esta
dominada por la busqueda de signos de dengue hemorragico y por el tratamiento empırico con antibioticos. Tal vez esta situacion podrıa mejorarse
mediante campanas de educacion.
palabras clave fiebre, diagnostico clınico, tratamiento, Vietnam
Tropical Medicine and International Health volume 11 no 6 pp 869–879 june 2006
H. L. Phuong et al. Acute undifferentiated fever in Binh Thuan province, Vietnam
ª 2006 Blackwell Publishing Ltd 879
Copyright © 2022 FDOKUMEN




















