Acute Theophylline Poisoning - NCBI
6
Clinical Medicine Use of l-Blockade and Hemoperfusion for Acute Theophylline Poisoning MICHAEL P. BIBERSTEIN, MD; MICHAEL G. ZIEGLER, MD, and DAVID M. WARD, MB, MRCP, San Diego Five adults were treated successfully for severe theophylline poisoning due to intentional overdosage. Clinical features included nausea, tremor, delirium, hypotension and cardiac arrhythmias, metabolic acidosis, hyperglycemia, hypokalemia and hypophosphatemia. No seizures or deaths occurred despite very high serum theophylline concentrations (between 96 and 194 ,g per ml). Extreme elevations of plasma catecholamines were documented and are implicated in the toxicity. /3-Blockade with intravenous administration of propranolol hydrochloride was the most effective therapy for theophylline-induced hypotension. All patients were treated with resin hemoperfusion, which resulted in significant clinical improvement and rapid lowering of the serum theophylline level. (Biberstein MP, Ziegler MG, Ward DM: Use of p-blockade and hemoperfusion for acute theophylline poisoning. West J Med 1984 Oct; 141:485-490) A cute theophylline poisoning due to intentional or J~ accidental ingestion of massive quantities of the drug has been reported with increasing frequency.1-'" Complications include seizure, hypotension, cardiac arrhythmia and major metabolic disturbances. Mor- tality cain be high.' Until recently, therapy has been largely limited to general supportive measures. Dur- ing the past five years, hemoperfusion techniques have been applied to the treatment of theophylline poison- ing.2'4'6 7,9,12-14 We describe our recent experience treat- ing five severely poisoned patients and outline an ap- proach to acute theophylline poisoning. In addition, we propose that adrenergic hyperactivity contributes sig- nificantly to manifestations of theophylline poisoning and we present evidence of a therapeutic role for in- travenous administration of propranolol hydrochloride in the treatment of severe theophylline-induced hypo- tension. All patients herein described* had been given pre- scriptions for sustained-release theophylline prepara- tions in conventional dosage weeks to months before admission. Compliance is unknown. Admissions were precipitated by a single deliberate ingestion of several *We thank Dennis Leahy, MD; John Lilley, MD, and Robert Steiner, MD, for access to patients under their care. grams of theophylline. In each case the clinical exami- nation showed clear lung fields. Laboratory abnormali- ties that developed are shown in Table 1. Potassium and phosphate supplementation was given intravenous- ly to all patients. Serum theophylline concentrations and measures intended to lower them are shown in Figure 1. All hemoperfusions were done using Amber- lite XAD-4 resin cartridges (Extracorporeal Medical Specialists, King of Prussia, Pa). Vascular access was by femoral vein catheterization and blood flows of 200 ml per minute were achieved regularly. Heparin was given at a 4,000-unit loading dose followed by 2,000 units per hour by continuous infusion except where explicitly stated. Reports of Cases CASE 1. The patient, a 61-year-old woman, said she attempted suicide two hours before admission by tak- ing an overdose of a preparation of theophylline anhy- drous, ephedrine hydrochloride and phenobarbital (TEP). She was alert with a blood pressure of 110/70 mm of mercury, pulse rate 120 per minute and respira- tions 28 per minute. The serum theophylline concen- tration was 88 ,ug per ml and the phenobarbital value was 3.8 mg per dl. A urine toxicology screen showed OCTOBER 1984 * 141 * 4 From the Department of Medicine, University of California Medical Center, San Diego. Submitted, revised, October 31, 1983. Reprint requests to David M. Ward, MB, Dept of Medicine, University of California Medical Center, San Diego (Mail Code, H-781-A), 225 Dickinson Street, San Diego, CA 92103. 485
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Acute Theophylline Poisoning - NCBI

Clinical Medicine
Use of l-Blockade and Hemoperfusion forAcute Theophylline PoisoningMICHAEL P. BIBERSTEIN, MD; MICHAEL G. ZIEGLER, MD, and
DAVID M. WARD, MB, MRCP, San Diego
Five adults were treated successfully for severe theophylline poisoning due to intentionaloverdosage. Clinical features included nausea, tremor, delirium, hypotension and cardiacarrhythmias, metabolic acidosis, hyperglycemia, hypokalemia and hypophosphatemia. Noseizures or deaths occurred despite very high serum theophylline concentrations (between 96and 194 ,g per ml). Extreme elevations of plasma catecholamines were documented and areimplicated in the toxicity. /3-Blockade with intravenous administration of propranololhydrochloride was the most effective therapy for theophylline-induced hypotension. Allpatients were treated with resin hemoperfusion, which resulted in significant clinicalimprovement and rapid lowering of the serum theophylline level.(Biberstein MP, Ziegler MG, Ward DM: Use of p-blockade and hemoperfusion for acutetheophylline poisoning. West J Med 1984 Oct; 141:485-490)
Acute theophylline poisoning due to intentional orJ~ accidental ingestion of massive quantities of thedrug has been reported with increasing frequency.1-'"Complications include seizure, hypotension, cardiacarrhythmia and major metabolic disturbances. Mor-tality cain be high.' Until recently, therapy has beenlargely limited to general supportive measures. Dur-ing the past five years, hemoperfusion techniques havebeen applied to the treatment of theophylline poison-ing.2'4'6 7,9,12-14 We describe our recent experience treat-ing five severely poisoned patients and outline an ap-proach to acute theophylline poisoning. In addition, wepropose that adrenergic hyperactivity contributes sig-nificantly to manifestations of theophylline poisoningand we present evidence of a therapeutic role for in-travenous administration of propranolol hydrochloridein the treatment of severe theophylline-induced hypo-tension.
All patients herein described* had been given pre-scriptions for sustained-release theophylline prepara-tions in conventional dosage weeks to months beforeadmission. Compliance is unknown. Admissions wereprecipitated by a single deliberate ingestion of several
*We thank Dennis Leahy, MD; John Lilley, MD, and Robert Steiner,MD, for access to patients under their care.
grams of theophylline. In each case the clinical exami-nation showed clear lung fields. Laboratory abnormali-ties that developed are shown in Table 1. Potassiumand phosphate supplementation was given intravenous-ly to all patients. Serum theophylline concentrationsand measures intended to lower them are shown inFigure 1. All hemoperfusions were done using Amber-lite XAD-4 resin cartridges (Extracorporeal MedicalSpecialists, King of Prussia, Pa). Vascular access wasby femoral vein catheterization and blood flows of200 ml per minute were achieved regularly. Heparinwas given at a 4,000-unit loading dose followed by2,000 units per hour by continuous infusion exceptwhere explicitly stated.
Reports of CasesCASE 1. The patient, a 61-year-old woman, said she
attempted suicide two hours before admission by tak-ing an overdose of a preparation of theophylline anhy-drous, ephedrine hydrochloride and phenobarbital(TEP). She was alert with a blood pressure of 110/70mm of mercury, pulse rate 120 per minute and respira-tions 28 per minute. The serum theophylline concen-tration was 88 ,ug per ml and the phenobarbital valuewas 3.8 mg per dl. A urine toxicology screen showed
OCTOBER 1984 * 141 * 4
From the Department of Medicine, University of California Medical Center, San Diego.Submitted, revised, October 31, 1983.Reprint requests to David M. Ward, MB, Dept of Medicine, University of California Medical Center, San Diego (Mail Code, H-781-A), 225 Dickinson
Street, San Diego, CA 92103.
485
ACUTE THEOPHYLLINE POISONING
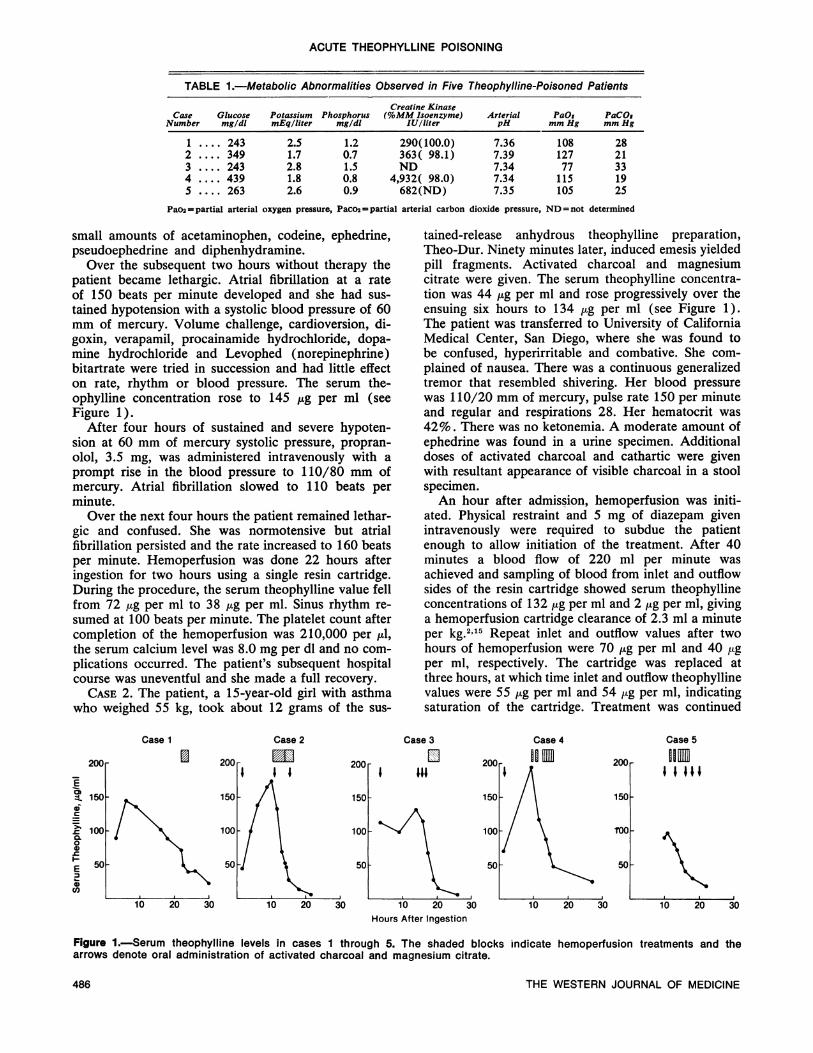
TABLE 1.-Metabolic Abnormalities Observed in Five Theophylline-Poisoned Patients
Creatine KinaseCase Glucose Potassium Phosphorus (%MM Isoenzyme) Arterial PaOs PaCOs
Number mg/dl mEqlliter mg/dl lU/liter pH mm Hg mm Hg
2.5 1.2 290(100.0)1.7 0.7 363( 98.1)2.8 1.5 ND1.8 0.8 4,932( 98.0)2.6 0.9 682(ND)
Pao2 - partial arterial oxygen pressure, Paco2= partial arterial carbon dioxide pressure, ND = not determined
small amounts of acetaminophen, codeine, ephedrine,pseudoephedrine and diphenhydramine.
Over the subsequent two hours without therapy thepatient became lethargic. Atrial fibrillation at a rateof 150 beats per minute developed and she had sus-tained hypotension with a systolic blood pressure of 60mm of mercury. Volume challenge, cardioversion, di-goxin, verapamil, procainamide hydrochloride, dopa-mine hydrochloride and Levophed (norepinephrine)bitartrate were tried in succession and had little effecton rate, rhythm or blood pressure. The serum the-ophylline concentration rose to 145 jig per ml (seeFigure 1).
After four hours of sustained and severe hypoten-sion at 60 mm of mercury systolic pressure, propran-olol, 3.5 mg, was administered intravenously with aprompt rise in the blood pressure to 110/80 mm ofmercury. Atrial fibrillation slowed to 110 beats perminute.
Over the next four hours the patient remained lethar-gic and confused. She was normotensive but atrialfibrillation persisted and the rate increased to 160 beatsper minute. Hemoperfusion was done 22 hours afteringestion for two hours using a single resin cartridge.During the procedure, the serum theophylline value fellfrom 72 jug per ml to 38 jug per ml. Sinus rhythm re-sumed at 100 beats per minute. The platelet count aftercompletion of the hemoperfusion was 210,000 per MuI,the serum calcium level was 8.0 mg per dl and no com-plications occurred. The patient's subsequent hospitalcourse was uneventful and she made a full recovery.
CASE 2. The patient, a 15-year-old girl with asthmawho weighed 55 kg, took about 12 grams of the sus-
tained-release anhydrous theophylline preparation,Theo-Dur. Ninety minutes later, induced emesis yieldedpill fragments. Activated charcoal and magnesiumcitrate were given. The serum theophylline concentra-tion was 44 jug per ml and rose progressively over theensuing six hours to 134 jug per ml (see Figure 1).The patient was transferred to University of CaliforniaMedical Center, San Diego, where she was found tobe confused, hyperirritable and combative. She com-plained of nausea. There was a continuous generalizedtremor that resembled shivering. Her blood pressurewas 110/20 mm of mercury, pulse rate 150 per minuteand regular and respirations 28. Her hematocrit was42%. There was no ketonemia. A moderate amount ofephedrine was found in a urine specimen. Additionaldoses of activated charcoal and cathartic were givenwith resultant appearance of visible charcoal in a stoolspecimen.An hour after admission, hemoperfusion was initi-
ated. Physical restraint and 5 mg of diazepam givenintravenously were required to subdue the patientenough to allow initiation of the treatment. After 40minutes a blood flow of 220 ml per minute wasachieved and sampling of blood from inlet and outflowsides of the resin cartridge showed serum theophyllineconcentrations of 132 ,ug per ml and 2 jug per ml, givinga hemoperfusion cartridge clearance of 2.3 ml a minuteper kg.2' 5 Repeat inlet and outflow values after twohours of hemoperfusion were 70 Mig per ml and 40 4tgper ml, respectively. The cartridge was replaced atthree hours, at which time inlet and outflow theophyllinevalues were 55 Mg per ml and 54 MAg per ml, indicatingsaturation of the cartridge. Treatment was continued
Case 1
150o
10 20 30
Case 2 Case 3
! 2O~200[ El
Case 4
IIUfI
1501
200r
Case 5
DDnI I III
1501
T0ool
501
10 20 30 10 20 30Hours After Ingestion
Figure 1.-Serum theophylline levels in cases 1 through 5. The shaded blocks indicate hemoperfusion treatments and thearrows denote oral administration of activated charcoal and magnesium citrate.
THE WESTERN JOURNAL OF MEDICINE
I1.... 2432 .... 3493 .... 2434 .... 4395 .... 263
7.367.397.347.347.35
108 28127 2177 33115 19105 25
E
cI-6
E0c0
1001
50-
20or 200r
486
ACUTE THEOPHYLLINE POISONING
- = = -~20t*.-
150 - -140-- X -I -
l r_______ - - 130--l ----.-3
-- --=--2110---- -
--- - - - -~~so -
--- - - - -~~50 '--- - - - - -~~40----
-30 - -
-20----10 - - -
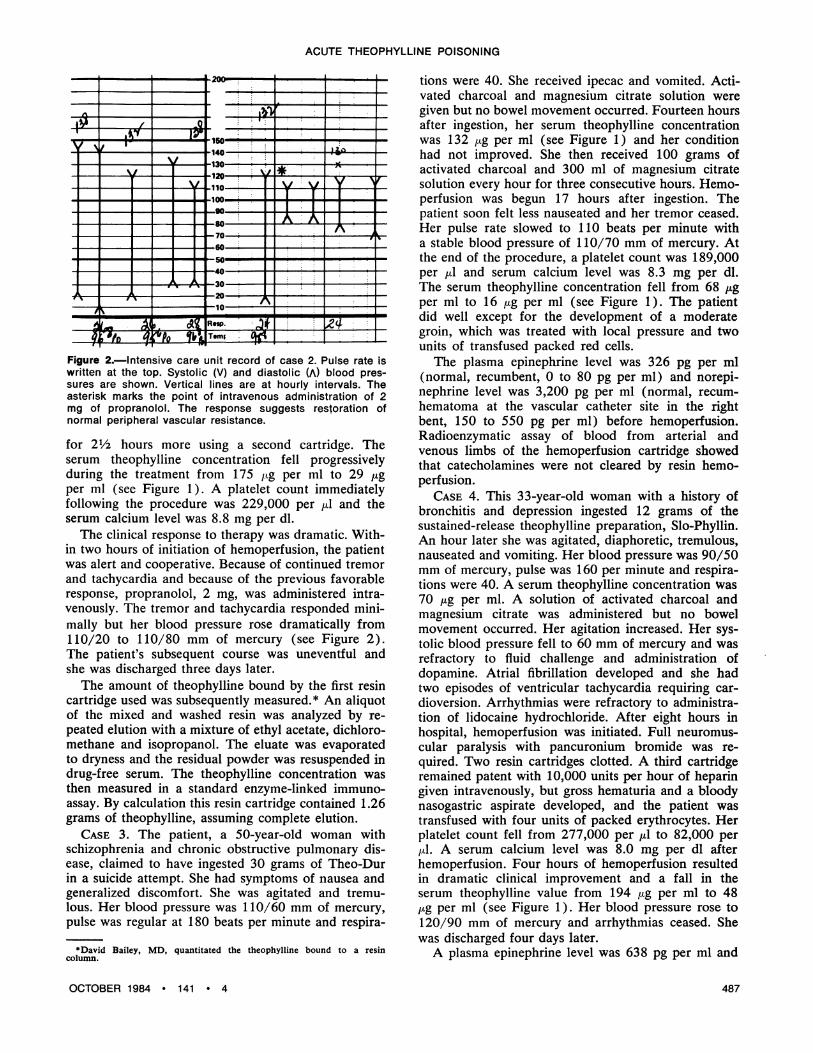
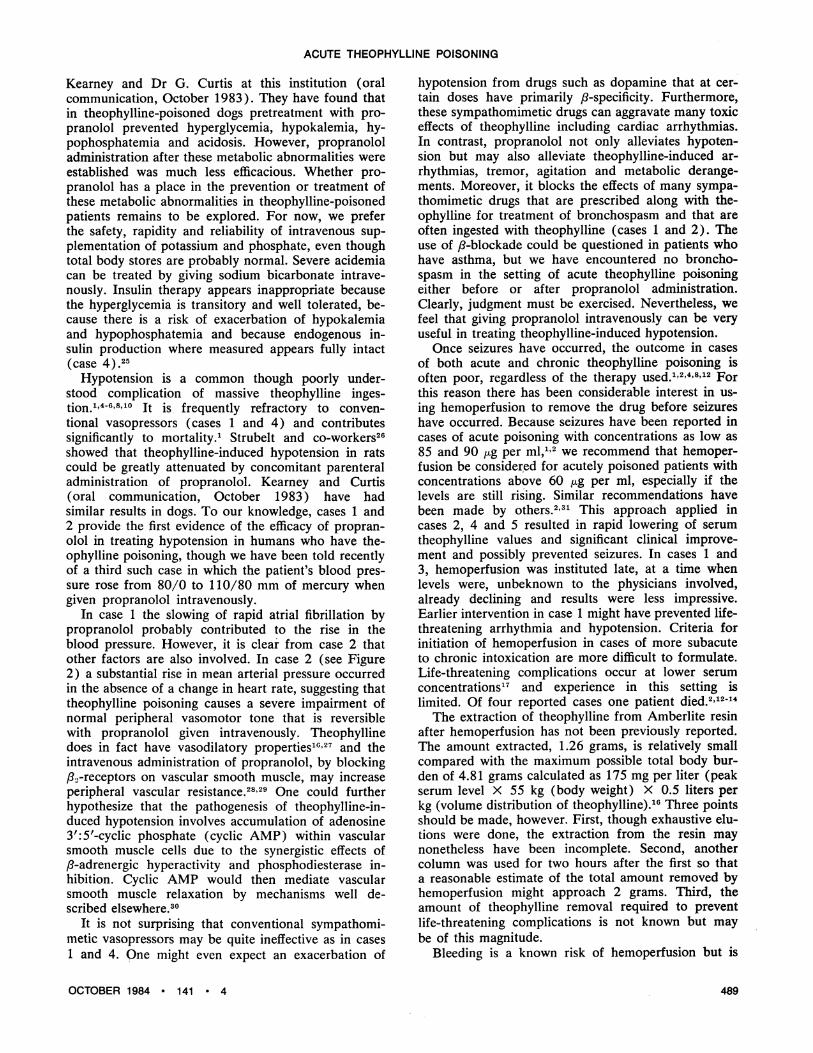
Figure 2.-Intensive care unit record of case 2. Pulse rate iswritten at the top. Systolic (V) and diastolic (A) blood pres-sures are shown. Vertical lines are at hourly intervals. Theasterisk marks the point of intravenous administration of 2mg of propranolol. The response suggests restoration ofnormal peripheral vascular resistance.
for 21/2 hours more using a second cartridge. Theserum theophylline concentration fell progressivelyduring the treatment from 175 ,Lg per ml to 29 jugper ml (see Figure 1). A platelet count immediatelyfollowing the procedure was 229,000 per Adl and theserum calcium level was 8.8 mg per dl.The clinical response to therapy was dramatic. With-
in two hours of initiation of hemoperfusion, the patientwas alert and cooperative. Because of continued tremorand tachycardia and because of the previous favorableresponse, propranolol, 2 mg, was administered intra-venously. The tremor and tachycardia responded mini-mally but her blood pressure rose dramatically from110/20 to 110/80 mm of mercury (see Figure 2).The patient's subsequent course was uneventful andshe was discharged three days later.
The amount of theophylline bound by the first resincartridge used was subsequently measured.* An aliquotof the mixed and washed resin was analyzed by re-peated elution with a mixture of ethyl acetate, dichloro-methane and isopropanol. The eluate was evaporatedto dryness and the residual powder was resuspended indrug-free serum. The theophylline concentration wasthen measured in a standard enzyme-linked immuno-assay. By calculation this resin cartridge contained 1.26grams of theophylline, assuming complete elution.
CASE 3. The patient, a 50-year-old woman withschizophrenia and chronic obstructive pulmonary dis-ease, claimed to have ingested 30 grams of Theo-Durin a suicide attempt. She had symptoms of nausea andgeneralized discomfort. She was agitated and tremu-lous. Her blood pressure was 110/60 mm of mercury,pulse was regular at 180 beats per minute and respira-
*David Bailey, MD, quantitated the theophylline bound to a resincolumn.
tions were 40. She received ipecac and vomited. Acti-vated charcoal and magnesium citrate solution weregiven but no bowel movement occurred. Fourteen hoursafter ingestion, her serum theophylline concentrationwas 132 /Ag per ml (see Figure 1) and her conditionhad not improved. She then received 100 grams ofactivated charcoal and 300 ml of magnesium citratesolution every hour for three consecutive hours. Hemo-perfusion was begun 17 hours after ingestion. Thepatient soon felt less nauseated and her tremor ceased.Her pulse rate slowed to 110 beats per minute witha stable blood pressure of 110/70 mm of mercury. Atthe end of the procedure, a platelet count was 189,000per ,ul and serum calcium level was 8.3 mg per dl.The serum theophylline concentration fell from 68 jugper ml to 16 ,tg per ml (see Figure 1). The patientdid well except for the development of a moderategroin, which was treated with local pressure and twounits of transfused packed red cells.
The plasma epinephrine level was 326 pg per ml(normal, recumbent, 0 to 80 pg per ml) and norepi-nephrine level was 3,200 pg per ml (normal, recum-hematoma at the vascular catheter site in the rightbent, 150 to 550 pg per ml) before hemoperfusion.Radioenzymatic assay of blood from arterial andvenous limbs of the hemoperfusion cartridge showedthat catecholamines were not cleared by resin hemo-perfusion.
CASE 4. This 33-year-old woman with a history ofbronchitis and depression ingested 12 grams of thesustained-release theophylline preparation, Slo-Phyllin.An hour later she was agitated, diaphoretic, tremulous,nauseated and vomiting. Her blood pressure was 90/50mm of mercury, pulse was 160 per minute and respira-tions were 40. A serum theophylline concentration was70 jig per ml. A solution of activated charcoal andmagnesium citrate was administered but no bowelmovement occurred. Her agitation increased. Her sys-tolic blood pressure fell to 60 mm of mercury and wasrefractory to fluid challenge and administration ofdopamine. Atrial fibrillation developed and she hadtwo episodes of ventricular tachycardia requiring car-dioversion. Arrhythmias were refractory to administra-tion of lidocaine hydrochloride. After eight hours inhospital, hemoperfusion was initiated. Full neuromus-cular paralysis with pancuronium bromide was re-quired. Two resin cartridges clotted. A third cartridgeremained patent with 10,000 units per hour of heparingiven intravenously, but gross hematuria and a bloodynasogastric aspirate developed, and the patient wastransfused with four units of packed erythrocytes. Herplatelet count fell from 277,000 per ul to 82,000 perfil. A serum calcium level was 8.0 mg per dl afterhemoperfusion. Four hours of hemoperfusion resultedin dramatic clinical improvement and a fall in theserum theophylline value from 194 ,ug per ml to 48,ug per ml (see Figure 1 ). Her blood pressure rose to120/90 mm of mercury and arrhythmias ceased. Shewas discharged four days later.A plasma epinephrine level was 638 pg per ml and
OCTOBER 1984 * 141 * 4 487

ACUTE THEOPHYLLINE POISONING
norepinephrine was 5,966 pg per ml before hemoper-fusion. A plasma insulin level by radioimmunoassay was279 MuU per ml (normal fasting, 4 to 24 MuU per ml).
CASE 5. The patient, a 24-year-old man with schizo-phrenia, came into the emergency room eight hoursafter having taken 6 grams of Theo-Dur in an attempt,he said, to improve his breathing. He had nausea,vomiting and abdominal pain and was anxious, hyper-irritable and tremulous. His blood pressure was re-corded as 140/0 mm of mercury, pulse rate 120 perminute and respirations 36. The serum theophyllineconcentration was 90 ,Lg per ml. Serum lactate level was80 mg per dl. The patient was given multiple doses ofactivated charcoal and magnesium citrate by nasogas-tric tube (Figure 1). Diazepam was given to controlagitation and combativeness. Hemoperfusion was initi-ated four hours after admission but two cartridgesclotted. It was successful using a third cartridge andgiving 4,000 units per hour of heparin by continuousinfusion. His tremor, agitation and tachycardia abated.The serum theophylline value fell from 96 to 35 Mug perml (see Figure 1). At the end of the procedure, theserum calcium level was 9.8 mg per dl but the plateletcount had fallen from 283,000 per Mul to 19,000 per Mul.A partial thromboplastin time was greater than 200seconds. A femoral artery blood specimen drawn 30minutes after the completion of hemoperfusion resultedin a large hematoma requiring transfusion of two unitsof packed erythrocy-tes. The patient recovered fullyfrom the inigestion. Psychiatric consultants found himto be psychotic and actively suicidal.
DiscussionTheophylline intoxication is a common problem that
occurs in two distinct clinical settings. In patients whohave been repeatedly administered standard doses ofthe drug, subacute or chronic intoxication may developthat is often attributable to excessive dosage or de-creased clearance due to heart failure, liver disease ordrug interactions.16-'8 Such patients may have seriouscomplications such as seizure at blood concentrationsthat are just above the therapeutic range.17 In contrastwe and others'-" report a syndrome of acute massiveingestion in which very high blood levels may be initi-ally well tolerated but that may nonetheless have afatal outcome. This distinction is critical in interpretingserum theophylline concentrations and also in formu-lating criteria for aggressive therapeutic intervention.In Table 2 findings from the present series are com-pared with those from two previously published series
of adults with acute theophylline poisoning.The standard treatment of theophylline poisoning
includes emptying the stomach and monitoring closelyfor cardiovascular and neurologic complications. Inaddition, administering activated charcoal and anosmotic cathartic to limit absorption is importantespecially when dealing with sustained-released the-ophylline preparations.19 Furthermore, it has beenshown that repeated oral dosing with activated char-coal increases the rate of elimination of theophyllinefrom the blood.20 In case 3, repeated hourly adminis-tration of charcoal and magnesium citrate until char-coal was seen in the stool resulted in a remarkable fallin the serum theophylline value to 70 M>g per ml thatoccurred before the initiation of hemoperfusion (Fig-ure 1).
Theophylline administration has recently been shownto stimulate catecholamine release."-24 Our finding ofvery high plasma levels of epinephrine and norepi-nephrine in cases of acute theophylline poisoning istherefore not altogether unexpected and very likelyrepresents a direct pharmacologic effect of the drugrather than simply a stress reaction. The effects ofthese high catecholamine levels on p-adrenergicallymediated functions may be magnified by theophylline-induced intracellular phosphodiesterase inhibition,which is likely to be substantial at the extreme the-ophylline levels found in acutely poisoned patients. Wetherefore propose that acute theophylline poisoningproduces a state of uncontrolled /8-adrenergic stimula-tion that accounts at least in part for many of the toxiceffects, including cardiac arrhythmias, hypotension,tremor, agitation and metabolic disturbances. This pro-vides a rationale for therapeutic intervention with ,B-blocking agents.
Metabolic disturbances in cases of acute theophyl-line poisoning have been reported previously and in-clude hyperglycemia," 8"0"5 hypokalemia"5-8l0"5 andmetabolic acidosis4-6'8"25 probably due to lactate ac-cumulation (case 5).2 These abnormalities were pres-ent in all of our cases (see Table 1). In addition, wereport the consistent development of severe hypophos-phatemia, a metabolic abnormality previously docu-mented in only a single case of mixed overdosage withtheophylline and a sympathomimetic.25 The creatinekinase levels were also uniformly mildly raised, ascrib-able to abnormal muscular activity or hypophosphate-mia (or both). The hypothesis that these metabolicabnormalities are due to adrenergic overdrive has nowbeen confirmed by the work of our colleagues, Dr T.
TABLE 2.-Three Studies of Acute Theophylline Poisoning in Adults*
Number Peak Theophyllineof Concentrations ptg/ml Patients
Study Patients Mean Range Hemoperfused Outcome
Helliwell and Berry, 19791 .. 8 68 25-120 0 2 deathsPark et al, 19832.5 80 71-90t 4 (charcoal) I with severe residual neurologic deficitsThis study.5 148 96-194 5 (Amberlite XAD-4) All recovered
*Pediatric and nonacute cases are excluded.tDenotes values obtained by extrapolation. Other peak levels represent highest values directly measured.
THE WESTERN JOURNAL OF MEDICINE488
ACUTE THEOPHYLLINE POISONING
Kearney and Dr G. Curtis at this institution (oralcommunication, October 1983). They have found thatin theophylline-poisoned dogs pretreatment with pro-pranolol prevented hyperglycemia, hypokalemia, hy-pophosphatemia and acidosis. However, propranololadministration after these metabolic abnormalities wereestablished was much less efficacious. Whether pro-pranolol has a place in the prevention or treatment ofthese metabolic abnormalities in theophylline-poisonedpatients remains to be explored. For now, we preferthe safety, rapidity and reliability of intravenous sup-plementation of potassium and phosphate, even thoughtotal body stores are probably normal. Severe acidemiacan be treated by giving sodium bicarbonate intrave-nously. Insulin therapy appears inappropriate becausethe hyperglycemia is transitory and well tolerated, be-cause there is a risk of exacerbation of hypokalemiaand hypophosphatemia and because endogenous in-sulin production where measured appears fully intact(case 4).25
Hypotension is a common though poorly under-stood complication of massive theophylline inges-tion." 4-6,8"10 It is frequently refractory to conven-tional vasopressors (cases 1 and 4) and contributessignificantly to mortality.' Strubelt and co-workers26showed that theophylline-induced hypotension in ratscould be greatly attenuated by concomitant parenteraladministration of propranolol. Kearney and Curtis(oral communication, October 1983) have hadsimilar results in dogs. To our knowledge, cases 1 and2 provide the first evidence of the efficacy of propran-olol in treating hypotension in humans who have the-ophylline poisoning, though we have been told recentlyof a third such case in which the patient's blood pres-sure rose from 80/0 to 110/80 mm of mercury whengiven propranolol intravenously.
In case 1 the slowing of rapid atrial fibrillation bypropranolol probably contributed to the rise in theblood pressure. However, it is clear from case 2 thatother factors are also involved. In case 2 (see Figure2) a substantial rise in mean arterial pressure occurredin the absence of a change in heart rate, suggesting thattheophylline poisoning causes a severe impairment ofnormal peripheral vasomotor tone that is reversiblewith propranolol given intravenously. Theophyllinedoes in fact have vasodilatory properties"'627 and theintravenous administration of propranolol, by blockingB2-receptors on vascular smooth muscle, may increaseperipheral vascular resistance.2829 One could furtherhypothesize that the pathogenesis of theophylline-in-duced hypotension involves accumulation of adenosine3':5'-cyclic phosphate (cyclic AMP) within vascularsmooth muscle cells due to the synergistic effects of,8-adrenergic hyperactivity and phosphodiesterase in-hibition. Cyclic AMP would then mediate vascularsmooth muscle relaxation by mechanisms well de-scribed elsewhere.30
It is not surprising that conventional sympathomi-metic vasopressors may be quite ineffective as in cases1 and 4. One might even expect an exacerbation of
hypotension from drugs such as dopamine that at cer-tain doses have primarily pl-specificity. Furthermore,these sympathomimetic drugs can aggravate many toxiceffects of theophylline including cardiac arrhythmias.In contrast, propranolol not only alleviates hypoten-sion but may also alleviate theophylline-induced ar-rhythmias, tremor, agitation and metabolic derange-ments. Moreover, it blocks the effects of many sympa-thomimetic drugs that are prescribed along with the-ophylline for treatment of bronchospasm and that areoften ingested with theophylline (cases 1 and 2). Theuse of 8-blockade could be questioned in patients whohave asthma, but we have encountered no broncho-spasm in the setting of acute theophylline poisoningeither before or after propranolol administration.Clearly, judgment must be exercised. Nevertheless, wefeel that giving propranolol intravenously can be veryuseful in treating theophylline-induced hypotension.
Once seizures have occurred, the outcome in casesof both acute and chronic theophylline poisoning isoften poor, regardless of the therapy used." 2'4'8"12 Forthis reason there has been considerable interest in us-ing hemoperfusion to remove the drug before seizureshave occurred. Because seizures have been reported incases of acute poisoning with concentrations as low as85 and 90 /g per ml," 2 we recommend that hemoper-fusion be considered for acutely poisoned patients withconcentrations above 60 ,tg per ml, especially if thelevels are still rising. Similar recommendations havebeen made by others.2'31 This approach applied incases 2, 4 and 5 resulted in rapid lowering of serumtheophylline values and significant clinical improve-ment and possibly prevented seizures. In cases 1 and3, hemoperfusion was instituted late, at a time whenlevels were, unbeknown to the physicians involved,already declining and results were less impressive.Earlier intervention in case 1 might have prevented life-threatening arrhythmia and hypotension. Criteria forinitiation of hemoperfusion in cases of more subacuteto chronic intoxication are more difficult to formulate.Life-threatening complications occur at lower serumconcentrations'7 and experience in this setting islimited. Of four reported cases one patient died.2'12-'4The extraction of theophylline from Amberlite resin
after hemoperfusion has not been previously reported.The amount extracted, 1.26 grams, is relatively smallcompared with the maximum possible total body bur-den of 4.81 grams calculated as 175 mg per liter (peakserum level X 55 kg (body weight) X 0.5 liters perkg (volume distribution of theophylline).16 Three pointsshould be made, however. First, though exhaustive elu-tions were done, the extraction from the resin maynonetheless have been incomplete. Second, anothercolumn was used for two hours after the first so thata reasonable estimate of the total amount removed byhemoperfusion might approach 2 grams. Third, theamount of theophylline removal required to preventlife-threatening complications is not known but maybe of this magnitude.
Bleeding is a known risk of hemoperfusion but is
OCTOBER 1984 * 141 * 4 489

ACUTE THEOPHYLLINE POISONING
said to occur uncommonly.32'33 In the present seriesbleeding complications developed in three of five pa-tients. Contributing factors included platelet depletion(cases 4 and 5), the need for larger than usual dosesof heparin (cases 4 and 5), an unnecessary arterialpuncture (case 5) and early removal of a femoral vas-cular catheter in a patient who still showed substantialheparin effect (case 3). We feel that although none ofthe patients suffered serious morbidity as a result ofbleeding, the potential definitely exists. We currentlyplace emphasis on careful monitoring of vital signs,hemoglobin and platelet count and on avoiding theaforementioned errors.
In summary, we believe that most patients with acutetheophylline intoxication can be managed in a tradi-tional manner including careful monitoring, intensivesupport and thorough evacuation of remaining drugfrom the gastrointestinal tract. Repeated doses of char-coal and an osmotic cathartic should be administeredat least until charcoal is visible in the stool. Metabolicabnormalities including hyperglycemia, hypokalemia,hypophosphatemia and acid-base disturbances shouldbe expected and treated as discussed. Intravenous ad-ministration of propranolol may be useful, especiallyfor refractory theophylline-induced hypotension. Fin-ally, there is a subset of acutely poisoned patients withlife-threatening complications or serum levels above60 /tg per ml and still rising who should be consideredfor hemoperfusion, a procedure that has the capacityto remove significant quantities of theophylline, whichcan result in dramatic clinical improvement.
REFERENCES1. Helliwell M, Berry D: Theophylline poisoning in adults. Br Med J
1979 Nov; 2:11142. Park GD, Spector R, Roberts RJ, et al: Use of hemoperfusion for
treatment of theophylline intoxication. Am J Med 1983; 74:961-9663. Vaucher Y, Lightner ES, Watson PD: Theophylline poisoning. J
Pediatr 1977; 90:827-8304. Ehlers SM, Zaske DE, Sawchuk RJ: Massive theophylline overdose
-Rapid elimination by charcoal hemoperfusion. JAMA 1978; 240:474-4755. Rose C: Theophylline toxicity. West J Med 1979 May; 130:466-4676. Jefferys DB, Raper SM, Helliwell M, et al: Haemoperfusion for
theophylline overdose. Br Med J 1980 May; 280:11677. Chang TMS, Espinosa-Mel6ndez E, Francoeur TE, et al: Albumin-
collodion activated charcoal hemoperfusion in the treatment of severetheophylline intoxication in a 3-year-old patient. Pediatrics 1980; 65:811-814
8. Burgan THS, Gupta I, Bate CM: Fatal overdose of theophyllinesimulating acute pancreatitis. Br Med J 1982; 284:939-940
9. Connell JMC, McGeachie JF, Knepil J, et al: Self-poisoning withsustained-release aminophylline: Secondary rise in serum theophyllineccncentration after charcoal haemoperfusion. Br Med J 1982 Mar; 284:943
10. Dean LS, Brown JW: Massive theophylline overdose-Survivalwithout hemoperfusion. JAMA 1982 Oct 8; 248:1742
11. Iberti TJ, Hammond RS: Massive oral theophylline poisoning.South Med J 1978; 71 :965-966
12. Lawyer C, Aitchison J, Sutton J, et al: Treatment of theophyllineneurotoxicity with resin hemoperfusion. Ann Intern Med 1978; 88:516-517
13. Russo ME: Management of theophylline intoxication with char-ccal-column hemoperfusion. N Engl J Med 1979; 300:24-26
14. Fleetham JA, Ginsburg JC, Nakatsu K, et al: Resin hemoperfusionas treatment for theophylline-induced seizures. Chest 1979; 75:741-742
15. Pond S, Rosenberg J, Benowitz NL, et al: Pharmacokinetics ofhaemoperfusion for drug overdose. Clin Pharmacokinet 1979; 4:329-354
16. Rall TW: The xanthines, chap 25 In Gilman AG, Goodman LS,Gilman A (Eds): Goodman and Gilman's The Pharmacological Basis ofTherapeutics. New York, Macmillan Publishing, 1980, pp 592-607
17. Zwillich CW, Sutton FD, Neff TA, et al: Theophylline-inducedseizures in adults-Correlation with serum concentrations. Ann InternMed 1975; 82:784-787
18. Ogilvie RI: Clinical pharmacokinetics of theophylline. Clin Phar-macokinet 1978 Jul-Aug; 3:267-293
19. Sintek C, Hendeles L, Weinberger M: Inhibition of theophyllineabscrption by activated charcoal. J Pediatr 1979; 94:314-316
20. Berlinger WG, Spector R, Goldberg MJ, et al: Enhancement oftheophylline clearance by oral activated charcoal. Clin Pharmacol Ther1983; 33:351-354
21. Vestal RE, Eiriksson CE Jr, Musser B, et al: Effect of intravenousaminophylline on plasma levels of catecholamines and related cardio-vascular and metabolic responses in man. Circulation 1983; 67:162-171
22. Higbee MD, Manju K, Galant SP: Stimulation of endogenouscatecholamine release by theophylline: A proposed additional mechanismof action for theophylline effects. J Allergy Clin Immunol 1982; 70:377-382
23. Aunis D, Mandel P, Miras-Portugal MT, et al: Changes of humanplasma dopamine-beta-hydroxylase activity after intravenous administra-tion of theophylline. Br J Pharmacol 1975; 53:425427
24. Atuk NO, Blaydes MC, Westervelt FB, et al: Effect of amino-phylline on urinary excretion of epinephrine and norepinephrine in man.Circulation 1967; 35:745-753
25. McCleave DJ, Phillips PJ, Vedig AE: Compartmental shift ofpotassium-A result of sympathomimetic overdose. Aust NZ J Med1978; 8:180-183
26. Strubelt 0, Hoffmann A, Siegers CP, et al: On the pathogenesisof cardiac necroses induced by theophylline and caffeine. Acta PharmacolToxicol (Kbh) 1976; 39:383-392
27. Ogilvie RI, Fernandez PG, Winsberg F: Cardiovascular responseto increasing theophylline concentration. Eur J Clin Pharmacol 1977;12:409414
28. Nies AS, Evans GH, Shand DG: Regional hemodynamic effects ofbeta-adrenergic blockade with propranolol in the unanesthetized primate.,m Heart J 1973; 85:97-102
29. Ulrych M, Frolich ED, Dustan HP, et al: Immediate hemodynamiceffects of beta-adrenergic blockade with propranolol in normotensiveand hypertensive man. Circulation 1968; 37:411-416
30. Kramer GL, Hardman JG: Cyclic nucleotides and blcod vesselcontraction, In Bohr DF, Somlyo A, Sparks HV (Eds): Handbook ofPhysiology, Vol 2-The Cardiovascular System. Bethesda, Md, AmericanPhysiological Society, 1980, pp 179-199
31. Weinberger M, Hendeles L: Role of dialysis in the managementand prevention of theophylline toxicity. Dev Pharmacol Ther 1980; 1:26-30
32. Gelfand MC, Winchester JF: Hemoperfusion in drug overdosage:A technique when conservative management is not sufficient. Clin Toxicol1980; 17:583-602
33. Rosenbaum JL, Kramer MS, Raja R: Resin hemoperfusion foracute drug intoxication. Arch Intern Med 1976; 136:263-266
THE WESTERN JOURNAL OF MEDICINE490