ACEM - Türkiye Acil Tıp Derneği
474
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of ACEM - Türkiye Acil Tıp Derneği


CONFERENCECONFERENCE
ON EMERGENCYON EMERGENCY
MEDICINEMEDICINE
ASIANASIAN
13th
CONGRESSCONGRESS
EMERGENCYEMERGENCY
MEDICINEMEDICINE
TURKISHTURKISH
Haliç Congress Center, Istanbul / TurkeyHaliç Congress Center, Istanbul / Turkey
www.acem2017.orgwww.acem2017.org
ACEM2017october 2017
Istanbul, Turkey

COMMITTEES 1
SCIENTIFIC PROGRAM 3
SPEAKER PROCEEDINGS 36
ORAL ABSTRACTS 108
POSTER ABSTRACTS 203
INDEX 447
CONTENTS
ORGANIZATION SECRETARIAT
Koşuyolu Mah. Mahmut Yesari Cad. No:6434718 Kadıköy / İstanbul - Turkey
Phone: +90 (216) 414 11 11Fax: +90 (216) 414 65 44
Web: www.opteamist.comE-mail: [email protected]

COMMITTEES
EMERGENCY MEDICINE ASSOCIATION OF TURKEY (EMAT)EXECUTIVE COMMITTEE
PresidentYıldıray ÇETE
Vice PresidentArzu DENİZBAŞI
General SecretaryBülent ERBİL
TreasurerCem OKTAY
Board Members (*)Ersin AKSAYMurat ÇETİN
Özgür ÇEVRİMMüge GÜNALP ENEYLİ
Özlem KÖKSALHakan TOPAÇOĞLU
Özcan YAVAŞİ* Aligned in order of the surnames.
CONGRESS SCIENTIFIC SECRETARIATHakan TOPAÇOĞLU
İstanbul Training and Research Hospital - Istanbul / Turkey
Erkan GÖKSUAkdeniz University Faculty of Medicine - Antalya / Turkey
Stephan RINNERTState University of New York (SUNY) - NY / USA
Terry MULLIGANUniversity of Maryland - MD / USA
1

COMMITTEES
ABSTRACT EVALUATION JURY
Head ReviewerErkan Göksu
Reviewers
Cüneyt AyrıkFatma Sarıdoğan
Zeynep Kekeç
ORAL PRESENTATIONS AWARDING JURYAhmet Demircan
Betül GülalpBülent ErbilBülent ErdurCem Ertan
Cuma YıldırımCüneyt Ayrık
Haldun AkoğluLevent Avşaroğullları
Mehmet Ali KaracaMurat ErselMurat Orak
Müge Günalp EneyliNurettin Özgür Doğan
Özgür KarcıoğluÖzlem Yiğit
Süleyman TürediZeynep Kekeç
POSTER PRESENTATIONS AWARDING JURY
Cemil KavalcıHalil DoğanMutlu KartalNurdan Acar
2

12. Türkiye Acil Tıp Kongresi / Kurs 1
Mekanik Ventilasyon ve Non-İnvaziv Mekanik Ventilasyon Kursu
10:30 - 10:40 Açılış, kurstan beklentiler Başak Bayram
10:40 - 11:10 Non-invaziv mekanik ventilasyon Erkan Göksu
11:10 - 12:00 İnvaziv mekanik ventilasyon Başak Bayram
12:00 - 13:30 Öğle Yemeği
13:30 - 15:30 İstasyon 1 Non-invaziv mekanik ventilasyon Erkan Göksu
İstasyon 2 İnvaziv mekanik ventilasyon Başak Bayram
10 Kasım 2016, Perşembe
3

12. Türkiye Acil Tıp Kongresi / Kurs 2
Rejyonel Anestezi - Periferal Sinir Blokları Kursu
10:00 - 10:10 Açılış, kurstan beklentiler Özlem Yiğit
10:10 - 10:40 Periferal blokların temel uygulama prensipleri ve endikasyonları Özlem Yiğit
10:40 - 11:00 Kahve Molası 11:00 - 11:20 Yüzde ve ağız içinde uygulanan sinir blokları Özlem Yiğit
11:20 - 12:00 El bileği ve Ayak bileği seviyesinde uygulanan sinir blokları Özlem Yiğit
12:00 - 13:30 Öğle Yemeği
13:30 - 14:30 Ultrasonografi ile sinir bloklarında temel prensipler Üst ekstremite proksimal sinir blokları(İnterskalen, hematom bloğu…) Gürkan Türker
14:30 - 15:00 Kahve Molası
15:00 - 16:00 Alt ekstremite proksimal sinir blokları ve gövde blokları (Femoral, popliteal, siyatik, interkostal) Gürkan Türker 16:00 - 17:00 USG ile pratik uygulama Gürkan Türker
10 Kasım 2016 - Perşembe
4

10 Kasım 2016 - Perşembe12. Türkiye Acil Tıp Kongresi / Kurs 3
Videolaringoskopi ve Fiberoptik Entübasyon Kursu
10:30 - 10:40 Açılış, kurstan beklentiler Neşe Çolak Oray Volkan Arslan
10:40 - 11:00 Havayolu anatomisi Volkan Arslan
11:00 - 12:00 Supraglottik cihazlar Neşe Çolak Oray
12:00 - 13:30 Öğle Yemeği 13:30 - 14:00 Videolaringoskopi Mustafa Yazıcıoğlu
14:00 - 14:30 Fiberoptik bronkoskopi Volkan Arslan
14:30 - 15:00 Kahve Molası
15:00 - 17:00 İstasyon 1 Videolaringoskopi 1 Volkan Arslan
İstasyon 2 Videolaringoskopi 2 Erkan Göksu
İstasyon 3 Videolaringoskopi 3 Neşe Çolak Oray
İstasyon 4 Fiberoptik Bronkoskopi Mustafa Yazıcıoğlu
İstasyon 5 Supraglottik havayolu cihazları Barış Murat Ayvacı
5

5th Eurasian Congress on Emergency Medicine 10 November 2016 - Friday / 10 Kasım 2016 - Cuma / HALL 1
08:10 - 08:55 ORAL PRESENTATIONS / SÖZLÜ BİLDİRİLER - 1 Moderator: Müge Günalp Eneyli
08:10-08:17 O-001, Burnout Level and Relationship of Burnout level to Serum S100B in the Emergency Department Worker Gamze Bozkuş
08:17- 08:24 O-002, Determination of Nursing Procedures in an Emergency Unit: Results of a Pilot Study Songül Pişkin
08:24-08:31 O-003, Effectiveness of the Synthetic Cannabinoids Seminar Murat Seyit
08:31-08:38 O-004, Evaluation of the Emergency Medicine,Education and Emergency Medicine Tranier by Residents and Trainers and Mutual Expectations About Education Yunus Emre Arık
08:38-08:45 O-005, Inter-hospital Tertiary Care Transport in Rural India Sunil Kumar Choudhary
08:45-08:52 O-006, Tetanus Immunity Status Among Adult Trauma Patients In an ED Orkun Ünek
5th Eurasian Congress on Emergency Medicine 11 November 2016 - Friday / 11 Kasım 2016 - Cuma / HALL 1
6
17:00 - 18:00 OPENING CEREMONY AND OPENING CONFERENCE
17:00 - 17:20 Opening Speeches Burak Solgun - Young EMAT Board Member Hakan Topaçoğlu - Congress General Secretary Erkan Göksu - Congress General Secretary Yıldıray Çete - EMAT and Congress President
17:20 - 18:00 Opening Conference Archaeology, Mythology and Medicine Nevzat Çevik
18:00 - 19:30 OPENING COCKTAIL - Exhibition Area

09:00 - 10:30 PANEL 1: Resuscitation Moderators: John Fowler, Rıdvan Atilla Ethics in resuscitation Gregory Luke Larkin
End-of-life decisions in ED Lee Kang Hyun
Rescue therapies in resuscitation (ECMO, PCI, etc…) Cem Oktay Being a resuscitationist: A course from knowledge to insight Imad Majzoub
10:30 - 11:00 Coffee Break
11:00 - 12:10 PANEL 3: Trauma Moderators: Amin Antoine Kazzi, Müge Günalp Eneyli
PanCT in multiple trauma patients Erhan Akpınar
Restricted fluid resuscitation and blood products in trauma Levent Avşaroğulları
Decision rules in trauma: When useful? John Fowler
12:10 - 13:30 LUNCH
13:30 - 14:40 PANEL 5: Cardiac Moderators: Alan Hodgdon, Murat Ersel
Accelerated diagnostic protocols using high sensitive troponin. Useful for ruling out? Rıdvan Atilla
Subtle ECG changes in AMI Cem Ertan
Pearls from heart failure guidelines (ESC vs AHA): A slowly progressing area Mahmoud Ghanaim
7

8
14:45 - 15:45 SATELLITE SYMPOSIUM / UYDU SEMPOZYUMU - 1 ST Yükselmeli Miyokard Enfarktüsünde Alışkanlıkları Değiştirme Zamanı Moderatör: Yıldıray Çete Konuşmacı: Hakan Topaçoğlu
15:45 - 16:15 Coffee Break
16:15 - 17:45 PANEL 7: Education Moderators: Lisa Moreno-Walton, Mahir Kunt Teaching doctors - How doctors think: Critical thinking in emergency medicine Terry Mulligan
Social media as a learning tool: Benefits and disbenefits Yusuf Ali Altuncı
Measuring EM education Yasser Alaska Teamwork training: Creating calmness from chaos in the emergency department John Foggle
17:45 - 18:30 ORAL PRESENTATIONS / SÖZLÜ BİLDİRİLER - 6 Moderator: Zeynep Kekeç
17:45-17:52 O-043, Pediatric Emergency Care Applied Research Network Head Injury Prediction Rules: On the Basis of Cost and Effectiveness Fatma Dilek Gökharman
17:52-17:59 O-044, End-Tidal Carbon Dioxide Monitoring in Patients with Tachycardia Onur Tokoçin
17:59-18:06 O-045, Sight-threatening Ocular Emergencies Raşit Kılıç
18:06-18:13 O-046, A Study on the Tactical Safety of Endotracheal Intubation Under Darkness Attila Aydın
18:13-18:20 O-047, Spontaneous Hemorrhagic Infarcts in Methanol Intoxication Hüseyin Şahin
18:20-18:27 O-048, How Emergency Physician's Gender Shaped by Patients Attending Emergency Departments in Culturally Conservative Society? Mohammed Alomar

9
08:10 - 08:55 ORAL PRESENTATIONS / SÖZLÜ BİLDİRİLER - 2 Moderator: Özlem Yiğit
08:10-08:17 O-007, A Helpful Method for Emergency Service: Predicting the Ischemic Cerebrovascular Disease with Data Mining Göksu Bozdereli Berikol
08:17- 08:24 O-008, Pleth Variability Index for Volume Assessment in Spontaneously Breathing Adults Elif Dilek Çakal
08:24-08:31 O-009, The Effectiveness of Using Luer-Lok (BD Vacutainer®) ın Reducing Hemolysis Rates in Busy Emergency Departments Mustafa Keşaplı
08:31-08:38 O-010, A New Perspective to Live Saving Procedures in Battlefield Setting: Emergency Crico thyroidotomy, Needle Thoracostomy, Chest Tube Thoracostomy with Night Vision Goggles Attila Aydın
08:38-08:45 O-011, Analyses of Demographical and Injury Characteristics of Adult and Pediatric Patients Injured in Syrian Civil War Şeref Kerem Çorbacıoğlu
08:45-08:52 O-012, Influence of Obesity Surgery on Intensive Care Unit Mortality Burcu Yormaz
09:00 - 10:30 PANEL 2: Pain and ED Management Moderators: Ahmet Demircan, Marc Sabbe Opioid free analgesia in ED: Is it possible? Sergey Motov
Alternative pain management tools in ED Alan Hodgdon
Leadership in ED: Inherited or an acquired skill? Adrian Tyndall Elements of a high performing emergency department: A personal opinion Haldun Akoğlu
10:30 - 11:00 Coffee Break
5th Eurasian Congress on Emergency Medicine 11 November 2016 - Friday / 11 Kasım 2016 - Cuma / HALL 2

10
11:00 - 12:10 PANEL 4: General EM Moderators: Özgür Karcıoğlu, Terry Mulligan
Utility of biomarkers in the emergency room Salvatore Di Somma
The prevention of readmission of the geriatric patient in the ED Marc Sabbe
Bringing palliative care into the emergency department Christian Jacobus
12:10 - 13:30 LUNCH
13:30 - 14:40 PANEL 6: Pediatrics Moderator: Mohammed Almalki
Seizing child: Pathways in management Nadeem Qureshi
Head CT in children: A pandemic abuse of imaging Özge Can
Update in lower respiratory tract infections: Therapeutic approach Murat Anıl
14:45 - 15:45 SATELLITE SYMPOSIUM / UYDU SEMPOZYUMU - 2 Kameranın Gözünden Hayat; Laringoskopinin Dünü-Bugünü-Yarını Başak Bayram, Erkan Göksu
15:45 - 16:15 Coffee Break
16:15 - 17:45 PANEL 8: Airway Moderators: Amin Antonie Kazzi, Adrian Tyndall
Cutting-edge devices for a difficult airway Selim Suner
Choosing the best medication for RSI in ED Orhan Çınar
Non-invasive ventilation: When beneficial? Erkan Göksu
Delayed sequence intubation and apneic oxygenation: Worth to change the practice? Prosen Gregor

11
17:45 - 18:30 ORAL PRESENTATIONS / SÖZLÜ BİLDİRİLER - 7 Moderator: Betül Gülalp
17:45-17:52 O-049, Short-Term Consequences of Nasal Intermittent Positive Pressure Ventilation in Patients with Obesity-Hypoventilation Syndrome Who Have Underwent Bariatric Surgery Burcu Yormaz
17:52-17:59 O-050, Can Ultrasound Quantification of Anterior Neck Soft Tissue Thickness Predict Difficult Laryngoscopy? Deniz Kılıç
17:59-18:06 O-051, Confirmation of the Endotracheal Tube Placement with ETCO2 and Tracheal Ultrasonography: A Prospective, Comparative, Diagnostic Utility Study Tuğba Mamak
18:06-18:13 O-052, Comparison of Loop Drainage and Primary Incision & Drainage Techniques in Adult Patients with Cutaneous Abscess: A Preliminary, Randomized Clinical Trial İbrahim Ulaş Özturan
18:13-18:20 O-053, Analysis of Mean Platelet Volume (MPV) and Red Blood Cell Distribution Width (RDW) in Recurrent Epistaxis Emine Emektar
18:20-18:27 O-054, Characteristics of Patients Presenting to the Emergency Department with Ophthalmologic Symptoms Ayhan Sarıtaş

12
08:10 - 08:55 ORAL PRESENTATIONS / SÖZLÜ BİLDİRİLER - 3 Moderatör: Cuma Yıldırım
08:10-08:17 O-013, Acil Serviste Tam Kullanılmayan ve İmha Edilen İlaçların Değerlendirilmesi İlknur Öztekin
08:17- 08:24 O-014, Bir Üniversite Hastanesi Acil Servisine Yaşlı Grubu Hastaların Başvuru Oranı ve Acil Servis Hemşirelerinin Yaşlı Hasta Bakımındaki Rolü Nazlı Yıldız
08:24-08:31 O-015, Hastaların Gözünden Acil Servis: Eğitim Şart mı? Umut Payza
08:31-08:38 O-016, Kadın Acil Tıp Uzmanlarının Sosyal Yaşam ve Mutluluk Analizi Elif Çelikel
08:38-08:45 O-017, Yeni Bir Topikal Hemostatik Ajan: Ön Çalışma Sonuçlarımız İsmail Altıntop
08:45-08:52 O-018, Acil Serviste Radyasyon Hasarlarının Tanı ve Tedavisi Tatbikatı Serhat Karaman
09:00 - 10:30 PANEL 1: Minör Aciller Moderatörler: İsmet Parlak, Sezgin Sarıkaya En kritik göz acilleri Gökben Çetin
Ortopedik acillerde sık karşılaşılan hatalar Özgür Tatlı
KBB acillerinde girişimler Bedia Gülen Acil serviste deri döküntülerinde tanısal yaklaşım Murat Çetin
10:30 - 11:00 Kahve Molası
12. Türkiye Acil Tıp Kongresi 11 November 2016 - Friday / 11 Kasım 2016 - Cuma / SALON 3

13
11:00 - 12:10 PANEL 2: Akut Koroner Sendromların Yönetimi (Yuvarlak Masa) Moderatör: Yıldıray Çete
Panelistler: Cuma Yıldırım Başak Bayram Mutlu Kartal Özge Duman Atilla 12:10 - 13:30 Öğle Yemeği
13:30 - 14:40 PANEL 4: Sepsis (Yuvarlak Masa) Moderatör: Hakan Topaçoğlu Panelistler: Özgür Karcıoğlu Özlem Güneysel Niyazi Özüçelik Özgür Dikme
15:45 - 16:15 Kahve Molası
16:15 - 17:45 PANEL 6: Lehte ve Alehte Olan Öneriler Moderatörler: Zeynep Kekeç, Cem Ertan Kardiyak arrestte adrenalin Ayşegül Bayır - Cüneyt Ayrık
Ağrı kesici olarak ketamin Serkan Emre Eroğlu - Neşe Çolak Oray
Acil tıp eğitiminde sosyal medya Nurettin Özgür Doğan - İbrahim Türkçüer Submasif pulmoner embolide fibrinolizis Mustafa Burak Sayhan - Betül Gülalp

14
17:45 - 18:30 ORAL PRESENTATIONS / SÖZLÜ BİLDİRİLER - 8 Moderatör: Süleyman Türedi
17:45-17:52 O-055, Pulmoner Emboli Hastalarında, Pulmoner Emboli Şiddet İndeksi (PESI) ve Basitleştirilmiş Pulmoner Emboli Şiddet İndeksinin (sPESI) 30 Günlük Mortalite Tahmini Açısından Karşılaştırılması Zeynep Yüzgeç
17:52-17:59 O-056, Acil Serviste Düşürülemeyen iNR Yüksekliğinin Altında Genetik Bozukluk mu Yatıyor? Kenan Ahmet Türkdoğan
17:59-18:06 O-057, Zehirlenmiş Hastalarda Aktif Kömür Etkinliği Müge Gülen
18:06-18:13 O-058, Lityum Zehirlenmesine Bağlı Koreatetozda Diyaliz Kullanımı Emrah Çelik
18:13-18:20 O-059, Acil Servise Baş Dönmesi Şikayeti ile Başvuran Hastalarda Nörogörüntüleme Maliyeti Ali Kablan
18:20-18:27 O-060, Kardiyopulmoner Arrestte Trombolitik Abuzer Coşkun
21:00 - 22:00 YARIŞMA: Acil Servisler Yarışıyor Moderatör: Ersin Aksay Acil Tıp Bilgi Yarışması

15
08:10 - 08:55 ORAL PRESENTATIONS / SÖZLÜ BİLDİRİLER - 4 Moderatör: Cüneyt Ayrık
08:10-08:17 O-019, Acil Serviste Hasta Başı Yapılabilecek Girişimsel Radyolojik İşlemler Betül Tiryaki Baştuğ
08:17-08:24 O-020, Acil Servise Lateral Malleol Travması ile Başvuran Hastalarda Ultrasonografinin Kırık Tanısındaki Sensitivite ve Spesifitesinin Araştırılması Pınar Öztürk
08:24-08:31 O-021, Yatak Başı Ultrasound Eşliğinde Kalıcı Tünelli Port Kateteri Takılan Hastalarda Kullanılan Sedatif Ajanların Stres Hormonları ve Yüksek Duyarlı Troponin Üzerine Etkisi Yılmaz Safi
08:31-08:38 O-022, Karbonmonoksit Zehirlenmesi Olgularının Analizi Osman Mahir Okur
08:38-08:45 O-023, Acil Servis Çalışanlarının Kesici-Delici Alet Yaralanmaları İle Karşılaşma Durumları ve Alınan Önlemler Gülten Sucu Dağ
08:45-08:52 O-024, Akciğer Dışı Tüberküloz Olgusu: Tüberküloz Peritoniti Ahmet Yunus Hatip
09:00 - 10:30 UZMANINA DANIŞ Acil servis dizaynı Serpil Karataş Yıldıray Çete
10:30 - 11:00 Kahve Molası
11:00 - 12:10 İnteraktif PANEL 3: Türkiye Acil Tıp Dergisi Editörlüğü: Bilimsel Araştırmalar ve Yayınlar
Panelistler: Süleyman Türedi Arzu Denizbaşı Orhan Çınar Haldun Akoğlu Murat Pekdemir 12:10 - 13:30 Öğle Yemeği
12. Türkiye Acil Tıp Kongresi 11 November 2016 - Friday / 11 Kasım 2016 - Cuma / SALON 4

16
13:30 - 14:40 PANEL 5: Afet ve Acil Durumlar Moderatörler: Cahfer Güloğlu, Barış Murat Ayvacı Mülteciler ve kitlesel nüfus hareketlerinde acil sağlık hizmetlerinin yönetimi Ufuk Diri
Türkiye’de terörist saldırılarda alan ve acil servis yönetimi Ömer Faruk Demir
Hastane afet ve acil durum planı Mehmet Ali Karaca
15:45 - 16:15 Kahve Molası
16:15 - 17:45 Panel 7: Acil Tıp Asistan Birliği (ATAB) Oturumu Moderatör: Gültekin Kadı
17:45 - 18:30 ORAL PRESENTATIONS / SÖZLÜ BİLDİRİLER - 9 Moderatör: Nurettin Özgür Doğan
17:45-17:52 O-061, Hiponatremi Tespit Edilen Hastalarda Serum Nöron Spesifik Enolaz Düzeyleri ile Beyin Hasarı Arasındaki İlişki Ayça Açıkalın
17:52-17:59 O-062, Acil Servise Şok Tablosuyla Gelen Hastalarda 30 Günlük Mortalitenin Öngörülmesinde End-Tidal Karbondioksit (etco2) Ölçümü Kullanılması Okan Günaydın
17:59-18:06 O-063, İntraserebral Kanamalı Hastalarda MPV ve RDW Değerlerin Mortaliteyle İlişkisi Akkan Avcı
18:06-18:13 O-064, Acil Serviste Septik Şok Tanısı Alan Hastaların Mortalitesi Üzerine Etki Eden Faktörler Duygu Kara
18:13-18:20 O-065, Fizik Muayene Bulgularının, El Bileği Kırıklarını Tanımadaki Duyarlılığı ve Özgüllüğü Yeşim Eyler
18:20-18:27 O-066, Kafa Travmasında Ultrasonla Ölçülen Optik Sinir Kılıf Çapının Hasta Takibindeki Rolü Özcan Yavaşi

17
08:10 - 10:30 ORAL PRESENTATIONS / SÖZLÜ BİLDİRİLER - 5 Moderator: Levent Avşaroğulları
08:10-08:17 O-025, Utility of Chest Computed Tomography After a Chest Radiograph in Patients Presenting to the Emergency Department with Non-traumatic Causes Naciye Sinem Gezer
08:17- 08:24 O-026, The Diagnostic Value of SCUBE1 in Acute Appendicitis Ertan Sönmez
08:24-08:31 O-027, Emergency Medicine Residents Can Assess Cranial Computed Tomography Scans Consistently with Radiologists Şenol Ardıç
08:31-08:38 O-028, Diagnostic Value and Effect of Bedside Ultrasound in Acute Appendicitis in Emergency Department Faruk Güngör
08:38-08:45 O-029, Determination of The Normal Values of Vertebral and Prevertebral Soft Tissue Distances in Lateral Cervical Vertebral Computed Tomography According to Age and Gender Haldun Akoğlu
08:45-08:52 O-030, Determination of Chest Wall Thickness with a Bedside Ultrasound for Needle Thoracostomy in the Emergency Department Taylan Kılıç
08:52-08:59 O-031, Comparison of Ultrasonography with Chest X-ray in Verification of Nasogastric Tube Placement at Emergency Department Çağdaş Yıldırım
08:59-09:06 O-032, The Comparison of Radiography and Point-of-care Ultrasonography in the Diagnosis and Management of Metatarsal Fractures Mehmet Oğuzhan Ay
09:06-09:13 O-033, The Measurement of Aortic Diameter: Is There a Difference Between Computed Tomography and Ultrasound? Engin Özakın
09:13-09:20 O-034, Turn Off the Light if Unnecessary! The Evaluation of the Unnecessary Radiological Imaging Orders from the Viewpoint of Doctors Mehmet Cihat Demir
5th Eurasian Congress on Emergency Medicine 11 November 2016 - Friday / 11 Kasım 2016 - Cuma / HALL 5

18
09:20-09:27 O-035, An Unusual Cause of Upper Gastroinstestinal Obstruction: Wilkie's Syndrome Özgür Dikme
09:27-09:34 O-036, Cardiac Tamponade without Pericardial Effusion Nurfer Zehra Gören
09:34-09:41 O-037, The Comparison of Bedside Point-of-Care Ultrasound and Computed Tomography in Elbow Injuries Mustafa Avcı
09:41-09:48 O-038, Efficacy of Sonographic Diameters and Collapsibility Index of Inferior Vena Cava in Predicting the Percentage of Body Fluid Loss Arzu Emecan
09:48-09:55 O-039, Incidental CT Findings of Patients who Admitted to ER Following a Traffic Accident Yavuz Yiğit
09:55-10:02 O-040, Detecting Shunt Dysfunction with Optic Nerve Ultrasound Özge Can
10:02-10:09 O-041, Importance of Antivenom in Management of Scorpion Envenomation with Epidemiologic and Clinical Characteristics Ali Duman
10:09-10:16 O-042, Gunshot Wound Presenting with Minor Bleeding Handan Çiftçi
10:30 - 11:00 Coffee Break
11:00 - 12:10 MEET THE EXPERT Carrier in EM Lisa Moreno-Walton 12:10 - 13:30 Lunch
13:30 - 14:40 MEET THE EXPERT - Education European board examination on emergency medicine and preparation courses Cem Oktay, Prosen Gregor 15:45 - 16:15 Coffee Break
16:15 - 17:45 MEET THE EXPERT The top ten pitfalls in clinical research: Lessons for life Gregory Luke Larkin

19
08:10 - 08:55 ORAL PRESENTATIONS / SÖZLÜ BİLDİRİLER - 10 Moderator: Özgür Karcıoğlu
08:10-08:17 O-067, Fahr Syndrome Göksu Afacan
08:17-08:24 O-068, Intranasal Lidocaine in Acute Treatment of Migraine: A Randomized Controlled Trial Nurettin Özgür Doğan
08:24-08:31 O-069, Comparison of the Efficacy of Dexketoprofen, Ibuprofen and Metoclopramide in Acute Migraine Attack Treatment: A Prospective, Observational Study Erkman Sanrı
08:31-08:38 O-070, Assessment of Delirium in Patients with Malignancy Who Admitted To Emergency Department with Altered Mental Status Mustafa Boz
08:38-08:45 O-071, Prospective Examination of the Second Seizure Frequency of Seizures in Patients Presenting to the Emergency Department Funda Karbek Akarca
08:45-08:52 O-072, The Relationship of Venous Blood Lactate Levels With The Clinical Process In Ischemic And Hemorrhagic Stroke Patients: A One Year Prospective Analysis Turgay Çağlayan
09:00 - 10:30 PANEL 9: Critically Ill Patients and Sepsis Moderators: Selim Suner, Özlem Yiğit Pediatric septic shock Nadeem Qureshi
Choosing wisely: Right fluid in critically ill patient (normal saline vs balanced fluids vs albumin) Salvatore Di Somma
Evidence-based approach to vasopressor choice in critically ill patient Murat Ersel
10:30 - 11:00 Coffee Break
5th Eurasian Congress on Emergency Medicine 12 November 2016 - Saturday / 12 Kasım 2016 - Cumartesi / HALL 1

20
11:00 - 12:00 SATELLITE SYMPOSIUM / UYDU SEMPOZYUMU - 3 "BIR" Kardiyolog "BIR" Acil Tıp Uzmanı Gözüyle Akut Koroner Sendroma Yaklaşım Müge Günalp, Yusuf Atmaca
12:00 - 13:30 Lunch
13:30 - 15:00 PANEL 11: Infectious Diseases Moderators: Mahmoud Ghanaim, Betül Gülalp
CNS Infections: Critical points and unknowns Ahmed Humaid
Crimean congo hemorrhagic fever - Turkish experience Nurşah Başol
Viral or bacterial? Tools for distinguishing Ayhan Özhasanekler
Viruses threatening masses (Zika, Ebola, etc…) John Foggle
15:00 - 15:30 Coffee Break
15:30 - 17:00 PANEL 13: Toxicology Moderators: Arzu Denizbaşı, Lee Kang Hyun Toxicology in Indonesia Tri Maharani
Street drugs: A new threat in ED setting Rıdvan Atilla
Carbon monoxide toxicity Selim Suner
Rescue therapies in toxic exposures: Lipid emulsion therapy Mohammed Almalki
20:00 Gala Dinner / Gala Gecesi

21
08:10 - 08:55 ORAL PRESENTATIONS / SÖZLÜ BİLDİRİLER - 11 Moderatör: Bülent Erbil
08:10-08:17 O-073, That’s McConnell! Well, Is this an Acute Pulmonary Embolus? Betül Gülalp
08:17-08:24 O-074, Acil Servise Konvülziyon Nedeniyle Başvuran Hastaların Retrospektif Analizi Elif Öztürk
08:24-08:31 O-075, GBS Hastalarında Görülen Sendromlardan PRES, Nadir Bir Olgu Serdar Beden
08:31-08:38 O-076, Medullanın Nadir İnfarktı Medial Medullar Sendrom Oğuzhan Bol
08:38-08:45 O-077, Bilateral Talamik İnfarkt: Olgu Sunumu Mustafa Numan Erdem
08:45-08:52 O-078, Hipofiz Adenomuna Bağlı Kitle İçi Kanama Sonrası 3. Sinir Basısı Abdurrahman Şimşek
09:00 - 10:30 PANEL 10: Neurological Emergencies Moderators: Gregory Luke Larkin, Engin Özakın Reperfusion strategies in ischemic stroke: A zone of controversies Murat Arsava
Dizzy patient and dizzy physician: Any approach easing the management? Can Özen
Imaging strategies for stroke in ED (CT vs MRI) Chan Kim Poh
10:30 - 11:00 Coffee Break
11:00 - 12:00 SATELLITE SYMPOSIUM / UYDU SEMPOZYUMU - 4 Kardiyak Biyobelirteçlerin Kullanımına Olgularla Multidisipliner Yaklaşım: Acil Tıp Gözüyle NT-proBNP ve Kardiyoloji Gözüyle Yüksek Duyarlılıklı Troponin Yıldıray Çete, Adnan Abacı 12:00 - 13:30 LUNCH
5th Eurasian Congress on Emergency Medicine 12 November 2016 - Saturday / 12 Kasım 2016 - Cumartesi / HALL 2

22
13:30 - 15:00 PANEL 12: Disaster and Environmental Emergencies Moderators: Sergey Motov, Cem Oktay Challenges of conducting disaster simulations Ali Haedar
Managing emergency care in countries with poor sources Rashmi Sharma
Managing snake envenomation Tri Maharani
Bombings: Injury patterns and care Mehmet Mahir Kunt
15:00 - 15:30 Coffee Break
15:30 - 17:00 PANEL 14: EM Literature Update Moderator: Orhan Çınar Clinical guidelines on prednisolone use in the ED Lisa Moreno-Walton
Critics over current resuscitation guidelines and future expectations Sobhi Fares
Literature update in trauma: Changing myths and new approaches John Fowler
Literature update in cardiology Fatma Sarı Doğan

23
08:10 - 08:55 ORAL PRESENTATIONS / SÖZLÜ BİLDİRİLER - 12 Moderatör: Bülent Erdur
08:10-08:17 O-079, Akut Apandisit Vakalarının Demografik Analizi ve Tanıda Alvarado Skorlama Sistemi ve CRP Burak Hasgül
08:17-08:24 O-080, Ortalama Platelet Hacminin Akut Pankreatitin Ağırlığını Belirlemedeki Rolü Neşe Nur User
08:24-08:31 O-081, Yılan Isırığı Sonrası Gelişen Kompartman Sendromu Yeşim İşler
08:31-08:38 O-082, Çocuk Acil Gözlem Hastalarında Ateş Ölçümünde İnfrared Termografi Kullanımı Ve Dört Farklı Ateş Ölçüm Yöntemlerinin Karşılaştırılması Murat Anıl
08:38-08:45 O-083, Pediatrik Ateş Kontrolünde Parasetamol ve Metamizol Etkinliğinin Karşılaştırılması, Randomize Çift Kör Plasebo Kontrollü Çalışma Onur Karakayalı
08:45-08:52 O-084, Karma Aşı Sonrası Anaflaksi: Olgu sunumu Mehmet Altuntaş 09:00 - 10:30 PANEL 8: Ultrasonografi Moderatörler: Aslıhan Ünal, Funda Karbek Akarca
Acil serviste ultrason eşliğinde sinir blokları Özlem Dikme
Kardiyak ultrasonografide gerçek yaşam deneyimleri Adnan Yamanoğlu
Toraks patolojilerinde ultrasonografi uygulamaları Nurdan Acar
Ortopedik acillerde ultrasonografi Mehmet Ali Aslaner
10:30 - 11:00 Kahve Molası
12:00 - 13:30 Öğle Yemeği
12. Türkiye Acil Tıp Kongresi 12 November 2016 - Saturday / 12 Kasım 2016 - Cumartesi / SALON 3

24
13:30 - 15:00 PANEL 10: Pecha Kucha Moderatörler: Ersin Aksay, Nurettin Özgür Doğan
Omuz Çıkıkları Halil Doğan
Birinci trimesterde vajinal kanama Ayhan Aköz
Fasiyal sinir blokları Özlem Yiğit
Antikoagülanların antidotları (TDP ve faktör konsantreleri) Mehmet Ali Karaca
Acil servis hekiminin bilmesi gereken yeni ilaçlar Okhan Akdur
Geniş kompleks düzenli taşikardilerin ayrımı Mehmet Tahir Gökdemir
İnme hastalarında kan basıncı yönetimi Engin Özakın
Senkopta yüksek riskli EKG Emine Akıncı Emektar
15:00 - 15:30 Kahve Molası

08:10 - 08:55 ORAL PRESENTATIONS / SÖZLÜ BİLDİRİLER - 13 Moderatör: Murat Orak
08:10-08:17 O-085, Acil Servisimize Başvuran Pulmoner Emboli Vakalarında Mortalite Üzerine Etkili Faktörlerin İncelenmesi Cemil Kavalcı
08:17-08:24 O-086, Acil Serviste Toplum Kökenli Pnömoni Tanısı Alan Hastalarda PSI Ve CURB-65 Pnömoni Skorlama Sistemlerinin Değerlendirilmesi Zeynep Karakaya
08:24-08:31 O-087, Pnömoni Hastalarında, CRP, Prokalsitonin ve Laktat Ölçümünün Prognostik Değerinin, Sık Kullanılan Skorlama Sistemleri ile Karşılaştırılması Nimet Gülen
08:31-08:38 O-088, Relationship between Right Ventricles Dilatation and Blood Copeptin Level in Patients with Pulmonary Thromboembolism Eren Usul
08:38-08:45 O-089, Kurban Bayramının Asıl Kurbanları Gökhan Ersunan
08:45-08:52 O-090, Acil Tıp Yaşamı Belirler! Acil Tıp Hasta Bakım ve Yönetiminde Sıradan Bir ATU’dan; Daha Çok Hasta Kurtarabilmek için Daha Fazla Ne Yapılabilir? Betül Gülalp 09:00 - 10:30 Panel 9: Acil Serviste Sık Görülen Olgular Moderatörler: Şervan Gökhan, Fatma Sarı Doğan
Acil serviste asemptomatik kan basıncı yüksekliği olan hastaya yaklaşım Vermi Değerli
Mental durum değişikliği Betül Akbuğa Özel
Erişkinde nöbet ve status epileptikus Barış Murat Ayvacı
Bir acil tıp uzmanı hemolitik anemi hakkında ne bilmelidir? Zeynep Karakaya
10:30 - 11:00 Kahve Molası
12:00 - 13:30 Öğle Yemeği
25
12. Türkiye Acil Tıp Kongresi 12 November 2016 - Saturday / 12 Kasım 2016 - Cumartesi / SALON 4

13:30 - 15:00 PANEL 11: Acil Serviste Sık Görülen Olgular Moderatörler: Bülent Erdur, Özgür Çevrim
AS’de anemi hastasına yaklaşım Taylan Kılıç İmmunsupresif hasta, ateş yüksekliği ile başvurduğunda ne yapılmalıdır Onur Karakayalı Önümüzdeki 20 yıl en çok kimi tedavi edeceğiz: Yaşlı kritik hasta Serkan Doğan Acil serviste yüksek kan şekeri olan hasta Mehmet Yiğit 15:00 - 15:30 Kahve Molası
15:30 - 17:00 YARIŞMA: Genç Acilciler Yarışıyor Moderatör: Başak Bayram Acil Tıp Asistanlarının Sunum Becerileri
26

17:00 - 18:30 ORAL PRESENTATIONS / SÖZLÜ BİLDİRİLER - 18 Moderator: Mehmet Ali Karaca
17:00-17:07 O-174, Evaluating the Predictive Value of Senescence Marker Protein 30 and peroxiredoxin1 Suspected with Pulmonary Embolism Yunus Karaca
17:07-17:14 O-175, The Prognostic Value of Early Warning Score at The Emergency Department Presentation in Patients with Dyspnea Zeynep Karakaya
17:14-17:21 O-176, Is Everthing All Right After The Bariatric Surgery? Evaluation of the Quality of Life After Pulmonary Embolism by PEmb-Qol Questionnaire Burcu Yormaz
17:21-17:28 O-177, Prediction of Poor Outcome in Non-traumatic Dyspnea: Serum Cortisol Level Özlem Dikme
17:28-17:35 O-178, The Efect of Neutrofil/Lymphocyte Ratio for 1 Year Survival in Patient Diagnosed with Pulmonary Embolism Rıfat Urnal
17:35-17:42 O-179, Pulmonary Embolism Presenting with a Single Pre-syncope Episode Harun Güneş
17:42-17:49 O-180, Evaluation of the Application of Noninvasive Mechanical Ventilation in Patients with Respiratory Distress in Emergency Department Ahmet Sebe
17:49-17:56 O-181, Does Pulmonary Embolism Severity Index Correlate with Computed Tomography Severity Criteria? Çiğdem Özpolat
17:56-18:03 O-182, Prognostic and Predicting Values of Perfusion Index and Shock Index in Community-Acquired Pneumonia Patients and Their Correlation with Risk Scoring Methods (CURB-65 and CURS) Özgür Dikme
18:03-18:10 O-183, Comparing Pneumonia Severity Scores (PSI, CURB65, NEWS, NEWS-L) of Patients Diagnosed as Pneumonia in Emergency Department Aynur Ecevit Kaya
18:10-18:17 O-184, Procalcitonin Levels, Which are Measured in Emergency Department, Relation with Etiology and Short-Term Mortality Neşe Çolak Oray
18:17-18:24 O-185, Air Medical Transport Operations of Turkish Armed Forces during Operation Enduring Freedom of Afghanistan Necati Salman
27

08:10 - 10:30 ORAL PRESENTATIONS / SÖZLÜ BİLDİRİLER - 14 Moderator: Ahmet Demircan
08:10-08:17 O-091, A Heavy Smoker Man with a Completely Occluded Aorta Leyla İnce
08:17-08:24 O-092, A Comparative Study of Appendicitis Inflammatory Response (AIR)-Alvarado Scores with Ultrasound (USG) Results in Diagnosis of Acute Appendicitis Mehmet İnce
08:24-08:31 O-093, Postoperative Complications in Bariatric Patients With Undefined Obesity Hypoventilation Syndrome Undergoing Bariatric Surgery Burcu Yormaz
08:31-08:38 O-094, Predicting Critical Duration and Reversibility of Damage in Acute Mesenteric Ischemia Ayhan Aköz
08:38-08:45 O-095, The Relationship between National Early Warning Score (NEWS) and Perfusion Index (PI) in Patients 65 Years or Older Emine Gaffari
08:45-08:52 O-096, Right Lobe of the Liver May Also Tend To Place Intratoracic ! Türkan Dübüş
08:52-08:59 O-097, Neutrophil Gelatinase Associated Lipocalin (NGAL) on Acute Gastrointestinal Bleeding Disorders of The Kidney Function That May Occur Early Impact of Predictive and Prognostic Role Aydın Çoşkun
08:59-09:06 O-098, The Effect of Inflammation on Ventricular Functions Aysel Hünük
09:06-09:13 O-099, A Prospective Study Demonstrating the Ratio of Drug Related Side Effects to the Total Application Number in Complaints of Patients Presenting to the Emergency Department Selda Çakmak
09:13-09:20 O-100, Evaluation of L-Laktat, D-Dimer, IFABP Levels in the Early Diagnosis of Acute Mesenteric Ischemia in an Experimental Study Müge Günalp
09:20-09:27 O-101, Pneumothorax Due to Foreign Body in Esophagus Nurşah Başol
28
12. Türkiye Acil Tıp Kongresi 12 November 2016 - Saturday / 12 Kasım 2016 - Cumartesi / SALON 5

09:27-09:34 O-102, Tissue Adhesives to Secure Peripheral Intravenous Catheters: A Randomized Controlled Trial Uğur Özkula
09:34-09:41 O-103, The Effect of Neutrophil/Lymphocyte Ratio and Mean Platelet Volume to Reduce Negative Laporotomy Rates in Patients with Abdominal Pain in Emergency Department Eylem Kaykısız
09:41-09:48 O-104, To Determine the Level of Biochemical Parameters of the Patients Who Apply to Emergency Services With Sickle-cell Anemia Disease Ahmet Sebe
09:48-09:55 O-105, The Diagnostic Value of İschemia-Modified Albumin in Acute Mesenteric İschemia İlhan Ece
09:55-10:02 O-106, Evaluating Methyl Alcohol Toxicity in Emergency Department Sıla Şadıllıoğlu
10:02-10:09 O-107, The Elderly as Victims - Geriatric Forensic Cases Harun Güneş
10:09-10:16 O-108, Acute Abdomen Caused by Foreign Body: IUD Elnare Günal
10:16-10:23 O-109, Evaluation of The Intershift Patient Handover At Emergency Department Mustafa Burak Sayhan
10:23-10:30 O-110, Management of Hypertrigliseridemia Induced Acute Pancreatitis in Emergency Department İlhan Uz
10:30 - 11:00 Kahve Arası
12:00 - 13:30 Öğle Yemeği
29

13:30 - 15:00 ORAL PRESENTATIONS / SÖZLÜ BİLDİRİLER - 15 Moderator: Murat Ersel
13:30-13:37 O-111, Rhabdomyolysis? Elevated Creatine Kinase (CK) via Presentation of 3 Cases Mehmet Ünaldı
13:37-13:44 O-112, Oxidative Status and DNA Damage Following Analgesic Treatment in Patients with Acute Pancreatitis Bedia Gülen
13:44-13:51 O-113, Dynamic Thiol/disulfide Homeostasis in Patients with Acute Cholecystitis Yücel Yüzbaşıoğlu
13:51-13:58 O-114, Comparison of Protective Effects of High Dose NAC and Isotonic NaCl Prophylaxis for Contrast Nephropathy Eren Gökdağ
13:58-14:05 O-115, Assessment of Physical Activity in Morbid Obese Patients With COPD Following A Pulmonary Rehabilitation Procedure After Bariatric Surgery Burcu Yormaz
14:05-14:12 O-116, The Characterıstıc Features of Relatıves Accompanyıng Adult Patıents who Consulted to Emergency Servıces Selman Yeniocak
14:12-14:19 O-117, Prevalence of Psychiatric Disorders in Fast Track Area (Triage Category 3) with Prime MD Evaluation Scale: A Study from Eskisehir Osmangazi University Emergency Department Mustafa Emin Çanakçı
14:19-14:26 O-118, The Metronome Usage Improves the Cardiopulmonary Resuscitation Practice Quality: A Manikin Study Necmiye Yalçın Ocak
14:26-14:33 O-119, Evaluation of The Effect of Initial Lactate Level on Short-Term Survival Outcomes in Patients with out-of Hospital Cardiac Arrest Şeref Kerem Çorbacıoğu
14:33-14:40 O-120, Investigating of Using SCUBE 1 and S100B Proteins as an Early Prognostic Marker at Predicting Prognosis after Cardiopulmonary Resuscitation in Cardiac Arrest Patients Gürkan Altuntaş
14:40-14:47 O-121, Investigating of Using Ischemia-Modified Albumin and Neuron Specific Enolase Proteins as an Early Prognostic Marker at Predicting Prognosis after Cardiopulmonary Resuscitation in Cardiac Arrest Patients Betül Abanoz
14:47-14:54 O-122, Thrombolytic Therapy Delay is an Independent Predictor of Mortality in Acute Pulmonary Embolism in the Emergency Service Bedriye Müge Sönmez
14:54-15:01 O-123, Tar Burn Sultan Tuna Akgöl Gür
15:00 - 15:30 Kahve Arası
30

15:30 - 18:30 ORAL PRESENTATIONS / SÖZLÜ BİLDİRİLER - 16 Moderator: Haldun Akoğlu
15:30-15:37 O-124, The Evaluation of a New Marker of Transmyocardial Repolarization Parameters in Ischemic Stroke Patients; Tpeak–Tend (Tp-e), Tp-e/QTc Emine Emektar
15:37-15:44 O-125, The Relationship of High Sensitive Troponin I (hs-cTnI) to TIMI Score, Grace Score and Mortality in NSTEMI Patients in the Emergency Department Hazar Lisar
15:44-15:51 O-126, Adropin as New Biochemical Marker to Diagnose of Patients with Acute Coronary Syndrome Nurettin Dağ
15:51-15:58 O-127, Correlation between Syncope Risk Scores of the Patients Presented with Syncope to Emergency Department and Carotid Intima-Media Thickness Arzu Emecen
15:58-16:05 O-128, Diagnostic Value of Copeptin in Patients with Acute Myocardial Infarctus Mehmet Oğuzhan Ay
16:05-16:12 O-129, Diagnostic Value of Tei Index (Myocardial Perfusion Index) Calculation in Emergency Department Patients With Chest Pain Complaints for Acute Myocardial Infarct Diagnosis Aslı Bahar Uçar
16:12-16:19 O-130, Evaluation of Neutrophil/Lymphocyte Ratio in patients Referring To Emergency Department with Chest Pain Mustafa Uğur Göktaş
16:19-16:26 O-131, A High Framingham Risk Score is Associated with Increased Carotid Intima-Media Wall Area in the Patients with Acute Coronary Syndrome Ecem Deniz Kırkpantur
16:26-16:33 O-132, Copeptin as a Surrogate of Right Ventricular Dysfunction in Acute Pulmonary Embolism Özcan Yavaşi
16:33-16:40 O-133, Annual Non-Traumatic Chest Pain Evaluation in Eskisehir Osmangazi University Emergency Department Ayşe Yasemin Özgan
16:40-16:47 O-134, Correlation between New York Heart Association (NYHA) Functional Classification and Pro-BNP Levels With Number of B-Lines on Bedside Lung Ultrasound in Emergency Department: Prospective, Cross-Sectional Study Nurdan Acar
31

16:47-16:54 O-135, The Association between In Perfusion Index Changes and Clinical Improvement in Patients with Acute Heart Failure Derya Abuşka
16:54-17:01 O-136, Safely Use of Rivaroxaban for Treatment of Thromboembolic Disease Following Surgery: Interpretation of Emergency Service Admittance Burcu Yormaz
17:01-17:08 O-137, Perfusion Index Changes in Patients with Chest Pain Who Underwent Coronary Angiography Özgur Dikme
17:08-17:15 O-138, Prognostic Factors Determining Morbidity and Mortality in Organophosphate Poisoning Ayça Açıkalın
17:15-17:22 O-139, Effects of Intravenous Lipid Emulsion Therapy on Synthetic Cannabinoid İntoxication Merve Güneş
17:22-17:29 O-140, Assessment of Pretreatment Tetracycline (T), Doxycycline (D) and Minocycline (M) for the Prevention of Acute Cocaine Toxicity in a Mouse Model Atakan Yılmaz
17:29-17:36 O-141, Clinical Patterns and Outcomes of Bonsai Usage Nezih Kavak
17:36-17:43 O-142, The Arrhythmia Developed by Inorganic Flourine Intoxication Serkan Doğan
17:43-17:50 O-143, Extremely Low Frequency Pulsed Magnetic Field Inhibits Myocardial Damage and Apoptosis in Rats with Clp-Induced Sepsis: A Histopathological and Immunohistochemical Evaluation Nurşah Başol
17:50-17:57 O-144, The Prognostic Value of ETCO2 in Shock Patients in the Emergency Department Murat Ersel
17:57-18:04 O-145, The High Risk of Contrast Induced Nephropathy in Patients with Suspected Pulmonary Embolism despite Three Different Prophylaxis: A Randomized Controlled Trial Süleyman Türedi
18:04-18:11 O-146, Evaluation of The Effectiveness of Clinical Classifications in Patients Who Apply to the Emergency Department with Upper Gastrointestinal System Bleeding Serkan Bilgin
18:11-18:18 O-147, Incidence of Contrast-Induced Nephropathy (CIN) In Patients Undergoing CT in Emergency Department Ruşengül Koruk
18:18-18:25 O-148, Early Endoscopy: Is Affect Prognosis in Patients with Upper GI Bleeding Who Admitted in the ED Ebubekir Arslan
32

15:30 - 18:30 ORAL PRESENTATIONS / SÖZLÜ BİLDİRİLER - 17 Moderator: Cem Ertan
15:30-15:37 O-149, A Basic Method by Cunningham; Reduction of Anterior Shoulder Dislocation İrfan Aydın
15:37-15:44 O-150, The Diagnostic Value of Serum Pentraxin 3 Levels in Pulmonary Contusion Özgür Tatlı
15:44-15:51 O-151, Effects of Intraperitoneal and Intravenous Mesenchymal Stem Cells on Inflammatory Response and Bone, Liver Tissue Healing in Experimental Polytrauma Rat Model Ayça Koca Tanrıverdi
15:51-15:58 O-152, Effects of Spinal Immobilization at 20 Degrees on Respiratory Functions Şeref Kerem Çorbacıoğlu
15:58-16:05 O-153, Analyzing and Reducing the Pressure and Pain according to Trauma Board: Physio Mechanical Work Ali Türkeli
16:05-16:12 O-154, What Happens after the Quite Ended Emergency Surgery? Interpretation of C-Reactive Protein and Procalcitonin Outcomes as Predictive Markers of Postoperative Complications Serdar Yormaz
16:12-16:19 O-155, Correlation of Trauma Severity Scores (GAP, RTS, EMTRAS) with Short Term Mortality in Multiple Trauma Patients: An Observational Study Haldun Akoğlu
16:19-16:26 O-156, Missed Injuries in Hospitalized Trauma Patients in the Emergency Department Serhat Örün
16:26-16:33 O-157, Spontaneous Resolution of Acute Subdural Hematoma Fatih Ahmet Kahraman
16:33-16:40 O-158, Comperision of Scoring Systems in Pediatric Trauma Patients Hasan Sultanoğlu
16:40-16:47 O-159, Relation with Attention Deficit/Hyperactivity Disorder at Patients Admitting Emergency Service with Presentation of Occupational Injuries Atakan Yılmaz
33
12. Türkiye Acil Tıp Kongresi 12 November 2016 - Saturday / 12 Kasım 2016 - Cumartesi / VIP SALON - 2

16:47-16:54 O-160, Determining the Effectiveness of Ultrasonography in the Evaluation of Pneumothorax, Rib Fracture, and Hemothorax with Imaging Techniques among the Patients Presented To Emergency Department with Blunt Thorax Trauma Yücel Yüzbaşıoğlu
16:54-17:01 O-161, Body Mass Index and Risk of Postoperative Respiratory Complications in Patients with Perforated Appendicitis: An Emergency-Based Workout Burcu Yormaz
17:01-17:08 O-162, Falling From Height Eren Sert
17:08-17:15 O-163,Thoracic Trauma Patients in a Tertiary Hospital: Last Year's Experience Serhat Yalçınkaya
17:15-17:22 O-164, Acil Serviste Hiperglisemi: Stres Hiperglisemisi veya Yeni Tanı Diyabet Murat Koyuncu
17:22-17:29 O-165, Akut Apandisit Tanısında Alvarado Skoru ve C-Reaktif Proteinin Etkinliğinin Saptanması Vehbi Özaydın
17:29-17:36 O-166, Türkiye’de Yapılmış Acil Tıp Uzmanlık Tezlerinin Değerlendirilmesi ve Bilimsel Literatüre Katkıları Oğuz Eroğlu
17:36-17:43 O-167, Radyoaktif İyot Alımı Sonrası Acil Servislere Başvuran Hastaların Günlere Göre Radyoaktivite Düzeyi Serhat Koyuncu
17:43-17:50 O-168, Acil Serviste Hiponatremi Tespit Edilen Hastaların Etyolojik Değerlendirilmesi ve Hastaların Serum NGAL Düzeylerinin Prognoz Üzerine Etkileri Nezihat Rana Dişel
17:50-17:57 O-169, Acil Serviste Yazılan Reçetelerin Analizi-Retospektif 2 Yıllık Çalışma Cem Şen
17:57-18:04 O-170, Üst Gastrointestinal Sistem Kanamalarında Risk Skorlarının Prognostik Önemi Serdar Biricik
18:04-18:11 O-171, Hiperkalemiye Sekonder Gelişen Paraparezi Burak Çelik
18:11-18:18 O-172, Enjeksiyonlarda Oluşabilecek Beklenmedik Yabancı Cisim Togay Evrin
18:18-18:25 O-173, Nadir Olan Bilateral Anterior Omuz Çıkığı Sercan Bıçakçı
34

09:00 - 10:00 PANEL 15: General EM Moderators: Ali Haedar, Erkan Göksu
Mindset of ED physician: What differs from the other specialties? Amin Antoine Kazzi Ophthalmologic emergencies: What eye need to know! Davut Savaşer Reversing the effects of anticoagulants Arzu Denizbaşı10:00 - 10:20 Coffee Break10:20 - 11:50 PANEL 17: Air Medical Transport Moderators: Davut Savaşer, Serkan Şener Decision-making between plane (fixed-wing) and helicopter (rotor-wing) transport in critically ill patient: EMAT preliminary national air medical transport statement Yahya Ayhan Acar
Air ambulance system in United Kingdom and training alternatives and certification for air ambulance healthcare staff Mark Forth
Difficulties and tips in air medical transport: Perspective of a Turkish armed forces air ambulance flight doctor Onur Tezel
Future and personnel rights of air ambulance healthcare staff in Turkey Serkan Şener
11:50 - 12:00 Closing Remarks
09:00 - 10:00 PANEL 16 Moderators: Salvatore Di Somma, Özcan Yavaşi Pneumonia in ED: When to admit and discharge? Yasser Alaska Evidence based therapeutic choices in COPD Serpil Yaylacı Larkin Hemoptysis: A Disregarded or an overestimated symptom? Best evidence John Foggle10:00 - 10:20 Coffee Break
10:20 - 11:50 PANEL 12: Dahili Aciller Moderators: Özgür Söğüt, Özlem Köksal Olgularla arteriyel kan gazı analizi Kamil Tunay
ÜST GİS kanaması yönetimine güncel yaklaşım Şenol Ardıç
Tanısı konmamış şok hastasına yaklaşım Yılmaz Zengin
Akılcı ilaç kullanımı Arzu Denizbaşı
35
5th Eurasian Congress on Emergency Medicine 13 November 2016 - Sunday / 13 Kasım 2016 - Pazar / HALL 1
12. Türkiye Acil Tıp Kongresi 13 November 2016 - Sunday / 13 Kasım 2016 - Pazar/ SALON 2
5th Eurasian Congress on Emergency Medicine 13 November 2016 - Sunday / 13 Kasım 2016 - Pazar / HALL 2
5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
36
SPEAKER PROCEEDINGS

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
37
RESCUE THERAPIES IN RESUSCITATION (ECMO, PCI, ETC…)
Cem Oktay
Akdeniz University School of Medicine, Department of Emergency Medicine, Antalya, Turkey Cardiopulmonary resuscitation (CPR) is the emergency procedure that combines chest compression with ventilation in an effort to manually preserve intact brain function until further measures are taken to restore spontaneous blood circulation and breathing in a person who is in cardiopulmonary arrest. Although the mainstay of CPR is chest compressions, ventilations and defibrillation of the shockable rhythm, new methods and therapies are studied to improve the chance of survival. Extracorporeal cardiopulmonary resuscitation (ECPR) is a method of CPR that passes the patient's blood through an external device to provide oxygen. An extracorporeal membrane oxygenation (ECMO) device is used as adjunct to standard CPR. Theoretically, the application of ECPR allows for the return of cerebral perfusion in a more sustainable manner than with external compressions alone. Systematic post-cardiac arrest care can also improve the likelihood of patient survival with good quality of life. Acute coronary syndromes (ACS) are a common cause for out-of-hospital cardiac arrest in adults and also can precipitate some in-hospital cardiac arrest. Coronary angiography should be performed emergently for OHCA patients with suspected etiology of arrest and STE elevation on ECG. When there is high suspicion of AMI, local protocols for treatment of AMI and coronary reperfusion should be activated. Thrombolysis may also be considered in cardiac arrest patients with suspected massive PE or as a so-called rescue therapy after unsuccessful conventional CPR in patients with a suspected thrombotic cause of cardiac arrest. Targeted temperature management (TTM) is another intervention demonstrated to improve neurologic recovery after cardiac arrest.
The science of CPR is continuously evolving. The primary objective is to improve the likelihood of survival with good neurologic and functional outcomes. In this presentation, efficacy and applicability of rescue therapies in resuscitation will be discussed.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
38
RESTRICTED FLUID RESUSCITATION AND BLOOD PRODUCTS IN TRAUMA
Levent Avşaroğulları
Erciyes University Medical School, Department of Emergency Medicine, Kayseri, Turkey Shock can be basically defined as inadequate organ perfusion and tissue oxygenation. Hemorrhage is the most commonly encountered cause of shock in patients with trauma. The fundamental management principles in case of hemorrhagic shock are to control the bleeding definitively and replace the volume loss. The goal of the resuscitation is to restore organ perfusion and tissue oxygenation. Resuscitation fluids are used to replace lost intravascular volume. However, a very careful approach is mandatory while administering fluids to avoid some complications. Namely, infusion of large volumes of fluids can result in catastrophic consequences such as exacerbation of hypothermia, coagulopathy, and acidosis. And also, if the bood pressure is increased rapidly without definitive hemostasis, bleeding can increase. Because of the reasons explained above, fluid administration should be restricted to limit intravascular volume expansion and not to normalize blood pressure. Current literature recommends that blood pressure goals are systolic blood pressures of 80-90 mm Hg in trauma and 90-95 mmHg in head injury. Crystalloid solutions such as normal saline or lactated Ringer can be administered in initial resuscitation. The usual, initial amount is 1 to 2 liters for adult trauma cases and 20 mL/kg for pediatric trauma cases. The patient’s response is observed during the inital fluid administration and subsequent volumes of resuscitation fluids and further steps are decided in accordance with the patient’s response. The patient should be under close and continous reevaluation. ATLS 9 Manual describes the potential patterns of response to the initial fluid therapy in three groups, namely “ rapid response ”, “ transient response ” and “ minimal or no response ”. This grouping can help simplify to evaluate the patient’s response.The rationale underlying avoidance of using large volumes of fluid and rapidly increased blood pressure is to achieve and maintain a balanced value of blood pressure, thus to prevent rebleeding and other risks such as development or exacerbation of the lethal triad “ acidosis, hypothermia and coagulopathy” . A rescucitation process of this kind is only a maintenance or balancing process until definitive hemostasis. The absolute solution is definitive surgical control of bleeding. This approach, i.e. restriction in fluid administration, is expressed in various terms such as “permissive hypotension”, “hypotensive resuscitation”, “controlled resuscitation”, and “balanced resuscitation”. However, in fluid resuscitation of blunt trauma patients especially those with traumatic brain injury, hypotension should be avoided. In patients with bleeding due to penetrating injury, delaying aggressive fluid administration until definitive bleeding control may prevent additional hemorrhage. Whether blood transfusion is initiated is decided in accordance with the patient’s response to the initial therapy. For example, transient responders or nonresponders (i.e., patients with Class III or Class IV bleeding) will be administered packed red blood cells in early stages of the resuscitation. Severe trauma and bleeding can induce coagulopathy, a serious problem in trauma patients. Coagulopathy occurs due to a combination of various factors. These factors are: loss and consumption of coagulation factors, hemodilution, acidosis, and hypothermia. To evaluate coagulation status of the patients and decide use of blood and blood products (packed red blood cells, fresh frozen plasma, platelets, cryoprecipitate …), various laboratory studies can be obtained such as prothrombin time, partial prothrombin time, platelet count, INR fibrinogen levels, viscoelasticity tests with regard to the clinical Picture of the patient. A hospital should have its massive transfusion protocol, by which emergency department and the blood bank teams should be ready and coordinated for potential massive blood transfusion patients. In resuscitation with fluids, blood and blood products, special conditions related to patients such as advanced age, athleticism, pregnancy, used medications, having pacemaker and comorbid diseases should be taken into consideration. References 1.Rossaint R, Bouillon B, Cerny V, Coats TJ, Duranteau J, Fernández-Mondéjar E, Filipescu D, Hunt BJ, Komadina R, Nardi G, Neugebauer EA, Ozier Y, Riddez L, Schultz A, Vincent JL, Spahn DR. The European guideline on management of major bleeding and coagulopathy following trauma: fourth edition. Crit Care. 2016 12;20:100. doi: 10.1186/s13054-016-1265-x. 2.Cherkas D. Traumatic hemorrhagic shock: advances in fluid management. Emerg Med Pract. 2011; 13: 1-19. 3.Shock. Advanced Trauma Life Support Student Course Manual. Ninth Edition. American College of Surgeons 2012. Chicago, IL, USA. pp 62-81. 4.Hai SA. Permissive hypotensive resuscitation--an evolving concept in trauma. J Pak Med Assoc. 2004; 54: 434-6. 5. Somand DM, Ward KR. Fluid and Blood Resuscitation in Traumatic Shock. Emergency Medicine. A Comprehensive Study Guide. International Edition. Eighth edition. Eds: Tintinalli JE, Stapczynski JS, Ma OJ, Yealy DM, Meckler GD, Cline DM 2016. The McGraw Hill Companies, USA. pp 69-74.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
39
ACCELERATED DIAGNOSTIC PROTOCOLS USING HIGH SENSITIVE TROPONIN: USEFUL FOR RULING OUT?
Rıdvan Atilla
Dokuz Eylül University Faculty of Medicine, Department of Emergency Medicine, Izmir, Turkey Cardiac troponin (cTn) testing is an essential component of the diagnostic workup and management of acute coronary syndromes (ACS). The troponin–tropomyosin complex is composed of three subunits: troponins T, I and C. Troponin T anchors the troponin complex to tropomyosin on thin myofibril filaments. Troponin I inhibits the binding of myosin with actin and Troponin C binds calcium ions released from the sarcoplasmic reticulum. Assays for cTn, namely cTnI and cardiac troponin T (cTnT), are the preferred diagnostic tests for ACS, in particular non–ST-segment–elevation myocardial infarction, because of the tissue-specific expression of cTnI and cTnT in the myocardium. Advances in biomarker technology leaded to redefine safe clinical thresholds. It has declared that the ideal troponin test will have a coefficient of variability (CV), of ≤ 10% at or below the 99th percentile cutoff. Therefore, the 99th percentile limit was set at the test’ limit of detection, This has further reduced the upper limit of normal to ≤ 0.010 ng/ml with the highest sensitive troponin test currently available. From 1995 to 2007, the level of detection fell from 0.5 ng/mL for cTn tests to 0.006 ng/mL and for some cTnI tests to 0.005 ng/mL. (Both below the level of normal). Contempororay High-Sensitivity Troponin (hs-Tn) tests have substantially higher analytical sensitivity than conventional tests, enabling precise quantification of low troponin concentrations. In the definition of MI by WHO, in 1979, the diagnostic criteria were based on the triad of ECG, clinical findings, and serial cardiac enzymes. After the introduction of troponins in 1990’s, these were renewed at 1995, 2003 and 2007. In 2007, it was stated that “in the presence of a clinical history suggestive of ACS, maximal concentration of cTn exceeding the 99th percentile of values CV ≤10%) is considered indicative of myocardial necrosis. The use of the 99th percentile cutoff for cTn positivity is best effective only when combined with Accelerated Diagnostic Protocols (ADS) in ED. For ruling out ACS, negative hs-Tn results are best useful when combined with ADS especially in patients with early onset of symptoms (< 3hrs). For ruling in ACS, positive hs-Tn results are best useful when combined with ADS especially in patients after ≥ 3hrs admission in ED. Serial hs-Tn tests will improve diagnostic clinical decision making. However, with hs-Tn tests, circulating cTnT or cTnI can be found in the plasma as a result of non-ischemic, inflammatory myocardial injury or even healthy individuals. Thus, elevated cTn may be detected in heart failure, cardiomyopathies, myocarditis, renal failure, tachyarrhythmias, and pulmonary embolism, and even after strenuous exercise in healthy individuals. In every myocardial cell death, hs-Tn will rise but unfortunately the reason of myocardial death (and consequently elevated levels of hs-Tn) is not always due to ischemia. This means more patients may be detected as false positive hs-Tn because of ACS. In real life, this paradoxically may contribute to potential ED crowding and unnecessarily length of stay also. References:
1. Wu AH, Bolger AF, Hollander JE. Growing pains with the use of high-sensitivity cardiac troponin assays. J Am Coll Cardiol. 2013 Oct 1;62(14):1250-1.
2. Maznyczka A, Kaier T, Marber M. Troponins and other biomarkers in the early diagnosis of acute myocardial infarction. Postgrad Med J. 2015 Jun;91(1076):322-30
3. Jesse RL. In the relative value of an assay versus that of a test: a history of troponin for the diagnosis of myocardial infarction. J Am Coll Cardiol. 2010 May 11;55(19):2125-8.
4. Mahajan VS, Jarolim P. How to interpret elevated cardiac troponin levels. Circulation. 2011 Nov 22;124(21):2350-4. 5. Meller B, Cullen L, Parsonage WA, et al. Accelerated diagnostic protocol using high-sensitivity cardiac troponin T in
acute chest pain patients. Int J Cardiol. 2015 Apr 1;184:208-15.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
40
SUBTLE ECG CHANGES
Cem Ertan
Izmir Medicalpark Hospital, Emergency Service, Izmir, Turkey
Chest pain is one of the most common complaints in the emergency department (ED). Acute coronary syndrome (ACS) is one of the leading life threatening causes of chest pain. ACS should be vigilantly diagnosed and proper treatment should be initiated in the ED. Therefore, the emergency physician has to be well trained and informed about focused physical examination, history findings and diagnostic tools such as electrocardiography (ECG) and cardiac markers. Although most cardiac events are easily recognized by a number of significant ECG changes, some changes which are less obvious may go unnoticed. These subtle ECG changes may make the difference between malpractice and saving life. A deeper understanding of ECG is should be deemed necessary to recognize these subtle ECG changes, since the eye can not notice what the mind does not look for. • O'Connor R, Brady W, Brooks CS, Diercks D, Egan J, Ghaemmaghami C, et al, Part 10: Acute Coronary Syndromes: 2010
Americ an Hea rt Association Guidelines for Cardio Pulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2010;122 (18 Suppl 3):S787-817.
• C Ertan, Y Cete, I Kilicaslan, E Goksu, H Kanalici. The prognostic values of the admission electrocardiography, myocardial injury markers and physical examination in patients with acute myocardial infarction. Hong Kong j. emerg. med. Vol. 18(5) Sep 2011

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
41
PEARLS FROM HEART FAILURE GUIDELINES (ESC VS. AHA): A SLOWLY PROGRESSING AREA
Mahmoud Ghanaim
Dubai Hospital, Department of Emergency Medicine, Dubai, UAE There are many similarities between the most recent recommendations of the European Society of Cardiology and the American Heart Association on the management of acute heart failure (AHF). There is a consensus that the symptoms of AHF should be relieved as rapidly as possible, which requires combining oxygen, noninvasive ventilation, vasodilators, and diuretics. There is also a consensus that long-lasting oral treatments such as beta-blockers and angiotensin-converting enzyme inhibitors or angiotensin- receptor blockers should be administered to patients unless they are hemodynamically unstable. The diagnosis of AHF is based on clinical signs. However, electrocardiography and chest X-ray should be performed in all AHF patients. Natriuretic peptides should be measured in doubtful cases to either confirm or exclude the diagnosis of AHF. Cardiologists should promptly perform echocardiography. We will focus on the concept of an early initiation of appropriate therapy going along with relevant investigations in acute HF that follows the ‘time to therapy’ approach already well established in acute coronary syndrome (ACS). New algorithms for a combined diagnosis and treatment approach of acute HF based on the presence/absence of congestion/hypoperfusion will be also discussed with main differences between the American and European guidelines. Lastly will discuss the past, current and future management of acute heart failure stressing weather we are moving fast or just formulating old concepts. U.S. guidelines have tended to stay away from areas where there are no evidence-based data. To their credit, the Europeans will take on something like acute heart failure where we don’t have an adequate evidence base. Despite that, they provide guidelines, which are important because clinicians need guidance even when the evidence is not very good, when the guideline is based mostly on experience and expert consensus.
1- 2016 ACC/AHA/HFSA Focused Update on New Pharmacological Therapy for Heart Failure: An Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure- Circulation 2016.
2- 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure - doi:10.1093/eurheartj/ehw128
3- Cardiology News: Elusive evidence pervades ESC’s 2016 heart failure guideline Publish date: June 23, 2016. 4- Improving care for patients with acute heart failure: before, during and after hospitalization- ESC Heart Failure:
Volume 1, Issue 2- December 2014 -Pages 110–145. 5- Mebazaa et al. Acute heart failure and cardiogenic shock: a multidisciplinary practical guidance. Intensive Care
Medicine, Review; Volume 42, Issue 2 / February 2016, Pages 147 – 163.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
42
SOCIAL MEDIA AS A LEARNING TOOL: BENEFITS AND DISBENEFITS
Yusuf Ali Altuncı
Ege University Faculty of Medicine, Department of Emergency Medicine, Izmir, Turkey
• If you want to know how we practised medicine 5 years ago, read a textbook. • If you want to know how we practised medicine 2 years ago, read a journal. • If you want to know how we practise medicine now, go to a (good) conference. • If you want to know how we will practise medicine in the future, listen in the hallways and use FOAM.
Joe Lex 2012 Social media (SM) tools have the potential to build on the interactivity of e-learning with additional features that are more learner-generated, collaborative, and engaging. However, use of SM by physicians and medical trainees has given rise to concerns about patient privacy and online professionalism. There is an urgent need for a synthesis of the evidence on SM use in medical education to inform educators and researchers of any demonstrated benefits that would justify the potential risks of incorporating SM tools into educational interventions (2013 & 88(6):893-901.). Most important aspects of this new tool are its capacity to bring together geographically separate groups to a common platform. It is stated in a systematic review that the use of SM in education enhances knowledge, student attendance, feedback, professional development, and cooperation. SM use is not only a social communication tool but also a free-of-charge and freely accessible resource contributing to training and professional development (Cevik AA). Residency programs are using SM increasingly for recruiting, communication, and education. Many programs report higher learner satisfaction, improved peer collaboration, increased communication, and benefits of asynchronous learning opportunities. Despite their potential benefits, SM pose substantial potential legal, ethical, personal, and professional risks. Disclosures of private health information and breaches of professionalism issues leading to termination have been reported. Residency programs have been advised to provide education regarding SM use (Pearson D et al. Evaluation of Social Media Use by Emergency Medicine Residents and Faculty. West J Emerg Med. 2015;16(5):715-20.). One of the studies suggested that they posit that using SM can
• help to promote event awareness and attendance, • increase attendee interaction and engagement, • enhance learning and knowledge sharing, • help to build a lasting community, • provide tools to measure attendee involvement and identify future speakers.
But they have little hard evidence of the validity and effectiveness of such tools (Paton C et al. Experience in the use of social media in medical and health education. Contribution of the IMIA Social Media Working Group. Yearb Med Inform. 2011;6:21-9.). Asynchronous learning allows trainees to educate themselves using resources that suit their needs when the time is right for them. This model is also suited to trainees who are isolated or in remote locations, distant from specialist clinical teachers. FOAM resources being misunderstood by learners if they do not have sufficient base knowledge or clinical experience to appreciate the nuances and ramifications. No single technology or educational resource can replace bedside mentoring by an expert clinician educator, but adjunctive, asynchronous learning combined with a flipped classroom gives learners the best of both worlds. It is a challenge to define the value, validity, utility and return-on-investment of FOAM resources. It is easy to get involved and, as emergency physicians, we have a moral imperative to take part in the ongoing battle for the hearts and minds of health professionals, patients and the wider community in a sea of misinformation (Nickson CP, Cadogan MD. Free Open Access Medical education (FOAM) for the emergency physician. Emerg Med Australas. 2014;26(1):76-83.). References 1. 2013, Cheston CC et al. Social media use in medical education: a systematic review. Acad Med. ve 88(6):893-901. 2. Cevik AA, et al., Social media, FOAMed in medical education and knowledge sharing: Local experiences with international perspective, Turkish Journal of Emergency Medicine (2016), http://dx.doi.org/10.1016/j.tjem.2016.07.001. 3. Pearson D et al. Evaluation of Social Media Use by Emergency Medicine Residents and Faculty. West J Emerg Med. 2015;16(5):715-20. 4. Paton C et al. Experience in the use of social media in medical and health education. Contribution of the IMIA Social Media Working Group. Yearb Med Inform. 2011;6:21-9. 5. Nickson CP, Cadogan MD. Free Open Access Medical education (FOAM) for the emergency physician. Emerg Med Australas. 2014;26(1):76-83.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
43
TEAMWORK TRAINING: CREATING CALMNESS FROM CHAOS IN THE EMERGENCY DEPARTMENT
John L. Foggle
Brown University, Warren Alpert School of Medicine, Department of Emergency Medicine, RI, USA Emergency Departments can be chaotic environments. Too many patients, not enough staff, nonstop interruptions, and dealing with critically ill patients where there may be limited data and significant time constraints. It is not surprising that Emergency Departments were identified as one of the highest risk areas in the 1999 U.S. Institute of Medicine (IOM) report entitled “To Err is Human: Building a Safer Health System”. The conclusions were shocking: between 44,000 to 98,000 people were dying each year in U.S. hospitals as a result of preventable medical errors. This lecture will focus on skills that we did not learn in medical school or in residency. Non-technical skills that improve teamwork and communication are of prime importance in creating a safe and calm environment for our patients and our staff. Key concepts and definitions with examples that will be discussed include: patient satisfaction, team roles, situational awareness, CRM, call-outs and check-backs, shared mental model, and SBAR. These can be taught, modeled, and role-played with simulation. Studies have shown that these non-technical skills allow healthcare professionals to improve their ability to monitor critically ill patients, make quick and appropriate decisions, take leadership roles as needed, and efficiently coordinate their actions within a team in order to improve patient outcomes. REFERENCES: • Miller D, et. al., “Improving Teamwork and Communication in Trauma Care Through In Situ Simulations”, Academic
Emergency Medicine Vol 19: No. (5), 608-612, May 2012. • Ford K, et. al., “Leadership and Teamwork in Trauma and Resuscitation”, West J Emerg Med. 2016 Sep; 17(5 • Capella J, et. al., “Teamwork Training Improves the Clinical Care of Trauma Patients”, J of Surgical Education, Vol 67, No. 6,
Nov/Dec 2010, 439-43. • Inge Verbeek-van Noord I, et. al., “More explicit communication after classroom-based crew resource management training:
results of a pragmatic trial”, Journal of Evaluation in Clinical Practice, Volume 21, Issue 1, February 2015, 137–144. • Lowe DJ, et. al., “Exploring situational awareness in emergency medicine: developing a shared mental model to enhance
training and assessment”, Postgrad Med J 2016;92:653–658.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
44
DO WE HAVE ALTERNATIVES TO OPIOIDS IN THE ED?
Sergey Motov
Maimonides Medical Center, Department of Emergency Medicine, Brooklyn, New York, USA
Over the past 10 years significant advances have been made to improve our understanding of neurobiological aspect of pain with a shift from symptom-based approach to a mechanistic approach. This approach has led to development of the channels/enzymes/receptors targeted analgesia (CERTA) concept that focuses on patient-specific, pain syndrome-targeted analgesia in the ED. More importantly, this approach allows for broader utilization of combinations of non-opioid analgesics and more refined and judicious use of opioids. These synergistic combinations of different classes of analgesics acting on different target sites will result in greater analgesia, reduced dose of each individual medication that may lead to fewer side effects and shorter length of stay. The ultimate goal of CERTA is to arm ED providers with variety of analgesic modalities and to promote patient-specific, pain syndrome targeted analgesia. An example of this concept would include a combination of COX enzymes inhibitor (ketorolac, apap) with a sodium channel blocking agent (IV lidocaine) for patients with renal colic. Another examples would include a combination of NMDA-receptor antagonist (ketamine) with sodium channel blockade (lidocaine via ultrasound guided nerve blocks) for acute traumatic musculoskeletal pain; combination of COX enzymes inhibitor ( Ibuprofen) with calcium channel blocking agents( either gabapentin or pregabalin) and sodium channel blocking agent ( Lidocaine patch) for neuropathic pain; and combination of antidopaminergic agents ( metoclopramide, prochlorperazine) with COX enzymes inhibitor ( ketorolac) and/or sodium channel blockade ( lidocaine/bupivacaine for paracervical blocks) for patients with various types of headache. This lecture will review the literature supporting the use of non-opioid analgesia in the ED for renal colic, traumatic and non-traumatic musculo-skeletal pain, neuropathic pain, and pain related to vaso-occlusive crisis of sickle cell disease.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
45
ALTERNATE PAIN MANAGEMENT TOOLS IN THE ED
Alan Hodgdon
University of Pittsburgh School of Medicine, Department of Emergency Medicine, PA, USA The abuse of and addiction to opioids such as heroin, morphine, and prescription pain relievers is a serious global problem that affects the health, social, and economic welfare of our societies. It is estimated that between 26 and 36 million people abuse opioids worldwide, with an estimated 2.1 million people in the United States suffering from substance use disorders related to prescription opioid pain relievers and an estimated 467,000 addicted to heroin. The number of unintentional overdose deaths from prescription pain relievers has soared in the United States, more than quadrupling since 1999. There is also growing evidence to suggest a relationship between increased non-medical use of opioid analgesics and heroin abuse in the United States. Because of these alarming numbers, there is continuous pressure now to reduce the spiraling number of prescriptions written for opioids and to generally reduce their use. The number of prescriptions for opioids (like hydrocodone and oxycodone products) have escalated from around 76 million in 1991 to nearly 207 million in 2013, with the United States their biggest consumer globally, accounting for almost 100 percent of the world total for hydrocodone (e.g., Vicodin) and 81 percent for oxycodone (e.g., Percocet). In this lecture, we will discuss alternate pain management tools, such as adjunctive agents and the use of non-traditional pain methods in an effort to expand your practice to reduce opioid use in the emergency setting. The following will be discussed: Non opioid analgesics, Nitrous Oxide, Antiemetics, Skeletal Muscle Relaxants, Ketamine, Guided Imagery, Hypnosis, Music, Nerve blocks, Acupuncture, Biofeedback. References: 1. Senate Caucus on International Narcotics Control hearing America’s Addiction to Opioids: Heroin and Prescription Drug Abuse (United States Senate Caucus on International Narcotics Control) 2. UNODC, World Drug Report 2015 3. Mack, K.A. Drug-induced deaths - United States, 1999-2010. MMWR Surveill Summ. 2013 Nov 22;62 Suppl 3:161-3. CDC

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
46
ELEMENTS OF A HIGH PERFORMING EMERGENCY DEPARTMENT: A PERSONAL OPINION
Haldun Akoğlu
Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey What is high performance emergency medicine? It is a new paradigm for the central role the emergency department (ED) plays in the healthcare system and the set of operational and management changes necessary to bring transformative change to the ED, leading to organizational and operational improvements, downstream costs savings, and more efficient patient care. But why do we need a high-performing ER? Why EDs become the centre of healthcare? In this talk, I will guide you through the unending list of demanding tasks (System-wide changes, management and policies that clearly define the scope of ED care, Improved access and processes surrounding resources, Improved medical decision-making ability, clear role definition, Standardization of patient management, Optimization of ED processes with lean initiatives, staffing models, education and training programs, team-training, EDIS and whole capacity protocols) to visualize the Vicious Cycle of ED Overcrowding to find the ultimate Element of a high-performing emergency department. We will try to find what has changed since the perfect days where everything seemed fine and in-order when we were in medical school, and I will share with you the name of the secret “change” that we have to establish.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
47
BIOMARKERS UTILITY IN EMERGENCY ROOM
Salvatore Di Somma
University Sapienza Rome, Department of Emergency Medicine, Italy High mortality, morbility and hospitalization as a result of acute diseses sucha s Acute Heart Failure ,Sepsis and Acute Kidney Injury represents an increasing public health dilemma. A prompt and appropriate therapeutic approach in the management of These diseases has been demonstrated to be of great importance in reducing patient mortality and in-hospital length of stay. As consequence, at the moment of patient presentation, it is of great importance to make a fast and accurate diagnosis and risk stratification. Although a global clinical evaluation is mandatory, in some cases the signs and instrumental findings are not sufficient for a complete patient’s diagnosis and risk stratifications. Multiple studies demonstrated that biomarkers assessment plus clinical judgement provide additional diagnostic and prognostic value in These patients patients. Moreover, data from the literature demonstrated the utility of a multimarkers approach in patients with heart failure, Sepsis or AQcute Kidney injury,in order to ameliorate diagnostic and prognostic accuracy. This talk is dedicated to addressing the actual state of the art on the utility in the management of acute patients using the following biomarkers: natriuretic peptides, procalcitonin, MRproADM, copeptine, neutrophil gelatinase associated lipocalin ,galectin 3,ST2 ,PenKid and BioADM. References Biomarkers and low risk in heart failure. Data from COACH and TRIUMPH. Meijers WC, de Boer RA, van Veldhuisen DJ, Jaarsma T, Hillege HL, Maisel AS, Di Somma S, Voors AA, Peacock WF. Eur J Heart Fail. 2015 Dec;17(12):1271-82. doi: 10.1002/ejhf.407. Epub 2015 Oct 14. ST2 and multimarker testing in acute decompensated heart failure. Mebazaa A, Di Somma S, Maisel AS, Bayes-Genis A. Am J Cardiol. 2015 Apr 2;115(7 Suppl):38B-43B. doi: 10.1016/j.amjcard.2015.01.039. Epub 2015 Jan 23. Review. Diagnostic and short-term prognostic utility of plasma pro-enkephalin (pro-ENK) for acute kidney injury in patients admitted with sepsis in the emergency department. Marino R, Struck J, Hartmann O, Maisel AS, Rehfeldt M, Magrini L, Melander O, Bergmann A, Di Somma S. J Nephrol. 2015 Dec;28(6):717-24. doi: 10.1007/s40620-014-0163-z. Epub 2014 Dec 9. Predictive value for death and rehospitalization of 30-day postdischarge B-type natriuretic peptide (BNP) in elderly patients with heart failure. Sub-analysis of Italian RED Study. Di Somma S, Marino R, Zampini G, Magrini L, Ferri E, Shah K, Clopton P, Maisel AS. Clin Chem Lab Med. 2015 Feb;53(3):507-13. doi: 10.1515/cclm-2013-0927. Opinion paper on utility of point-of-care biomarkers in the emergency department pathways decision making. Di Somma S, Zampini G, Vetrone F, Soto-Ruiz KM, Magrini L, Cardelli P, Ronco C, Maisel A, Peacock FW. Clin Chem Lab Med. 2014 Oct;52(10):1401-7. doi: 10.1515/cclm-2014-0267. Atrial fibrillation impairs the diagnostic performance of cardiac natriuretic peptides in dyspneic patients: results from the BACH Study (Biomarkers in ACute Heart Failure). Richards M, Di Somma S, Mueller C, Nowak R, Peacock WF, Ponikowski P, Mockel M, Hogan C, Wu AH, Clopton P, Filippatos GS, Anand I, Ng L, Daniels LB, Neath SX, Shah K, Christenson R, Hartmann O, Anker SD, Maisel A. JACC Heart Fail. 2013 Jun;1(3):192-9. doi: 10.1016/j.jchf.2013.02.004. Epub 2013 Jun 3.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
48
THE PREVENTION OF READMISSION OF THE GERIATRIC PATIENT IN THE ED
Marc Sabbe
Catholic University of Leuven, University Hospital, Department of Emergency Medicine, Leuven, Belgium Demography is our destiny in the ED. The number of frail elderly admitted to the ED is increasing and those not admitted to the hospital are often readmitted to the ED in a short time. Previous research revealed up to 34 % with one month after the initial admission. A system with home care and a specific case manager was set up to reduce the readmission rate. The results of this ongoing project will be presented and other options will be discussed.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
49
BRINGING PALLIATIVE CARE INTO THE EMERGENCY DEPARTMENT
Christian Jacobus
Bridge Home Health and Hospice, Palliative Medicine, Findlay, Ohio, USA Hospice and Palliative Medicine is the newest subspecialty of Emergency Medicine in the United States. The goal of Palliative Care is to improve the quality of life for a seriously ill patient and their loved ones. This is done by managing symptoms, addressing social, psychological, and spiritual concerns, and assisting in medical decision making. Emergency physicians can bring Palliative Care skills into the Emergency Department (ED) in many ways. In this lecture I will discuss two of them: caring for the dying patient in the ED and discussing a patient’s resuscitation preferences. While we, as emergency practitioners, excel in resuscitation, we often fall short in providing patients the opportunity to have a peaceful and comfortable death in the ED. Simple acts such as providing a quiet space, minimizing medical interventions, and allowing family to be present are very important. Comfort-based pharmacologic care of the dying patient focuses primarily on the use of an opioid and a benzodiazepine, with an antipsychotic agent and an anticholinergic drug being helpful as well. While many practitioners are wary of speeding a patient’s death by providing sedating medications like opioids and benzodiazepines, the literature is quite clear that their use does not shorten life and does provide comfort. While the ethics and legality of orders not to resuscitate a patient vary from country to country, one thing is clear: patients believe that cardiopulmonary resuscitation (CPR) is more effective than it truly is. Evidence shows that patients in the following three categories are extremely unlikely to benefit from an attempted resuscitation: age greater than 75; presence of a hematologic or metastatic solid malignancy; or dependence on others for the majority of activities of daily living. The Good Outcomes Following Attempted Resuscitation (GO-FAR) score can provide more prediction of a patient’s likelihood of benefiting from an attempted resuscitation. This information can help guide the discussion and decision. References Diem SJ, et al. Cardiopulmonary Resuscitation on Television: Miracles and Misinformation. NEJM 1996; 334 (24): 1578 – 1582. Ebell MH and Afonso AM. “Pre-arrest predictors of failure to survive after in-hospital cardiopulmonary resuscitation: a meta-analysis.” Family Practice 2011; 28(5): 505 – 515. Ebell MH, et al. Development and Validation of the Good Outcome Following Attempted Resuscitation (GO-FAR) Score to Predict Neurologically Intact Survival After In-Hospital Cardiopulmonary Resuscitation. JAMA 2013; 173(20). Edwards MJ. Opioids and benzodiazepines appear paradoxically to delay inevitable death after ventilator withdrawal. Journal of Palliative Care 2005; 21: 299 – 302.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
50
UPDATE IN LOWER RESPIRATORY TRACT INFECTIONS: THERAPEUTIC APPROACH
Murat Anıl
Tepecik Teaching and Research Hospital, Department of Pediatrics, Izmir, Turkey BRONCHIOLITIS Bronchiolitis is a clinical syndrome that occurs in children <2 years of age and is characterized by upper respiratory symptoms leading to lower respiratory infection with inflammation, which results wheezing and or crackles.
• Infants and children with nonsevere bronchiolitis usually can be managed in the outpatient setting, unless there are concerns about the caregivers' ability to care for them at home. Supportive care (maintenance of adequate hydration, relief of nasal congestion/obstruction, monitoring disease progression) and anticipatory guidance are the mainstays of management. Pharmacologic interventions (eg, bronchodilators, glucocorticoids) or nebulized hypertonic saline are not recommended in the management of children with nonsevere bronchiolitis.
• Infants and children with severe bronchiolitis usually require treatment in the emergency department or inpatient setting. Supportive care (maintenance of adequate hydration, provision of oxygen and respiratory support as necessary, monitoring disease progression) and anticipatory guidance are the mainstays of management of severe bronchiolitis.
• Inhaled bronchodilators (albuterol or epinephrine) are not recommended routinely. However, a one-time trial of inhaled bronchodilators may be warranted for infants and children with bronchiolitis and severe disease. The bronchodilator response should be objectively assessed before and up to one hour after treatment. If there is a clinical response, aerosolized bronchodilator therapy can be administered every four to six hours as needed (based on clinical status) and discontinued when the signs and symptoms of respiratory distress improve.
• Systemic glucocorticoids are not recommended routinely in the treatment of previously healthy infants hospitalized with a first episode of bronchiolitis.
• Nebulized hypertonic saline or heliox is not recommended routinely in the treatment of bronchiolitis in infants and children.
• Infants and children with bronchiolitis and arterial or capillary carbon dioxide tension > 55 mmHg, hypoxemia despite oxygen supplementation, and/ or apnea may require mechanical ventilation. Noninvasive strategies that may be effective in reducing work of breathing, improving gas exchange, and avoiding the need for endotracheal intubation include heated humidified high-flow nasal cannula therapy and continuous positive pressure ventilation.
PNEUMONIA Community-acquired pneumonia (CAP) is defined as signs and symptoms of an acute infection of the pulmonary parenchyma in an individual who acquired the infection in the community. Supportive care for children hospitalized with pneumonia includes provision of adequate respiratory support, hydration, antipyresis, and analgesia. Decisions regarding empiric antimicrobial therapy for CAP in children are usually based upon age unless there are other overriding epidemiologic or clinical factors to suggest a specific etiologic agent. The empiric antibiotic therapy for presumed bacterial pneumonia in hospitalized children include coverage for Streptococcus pneumoniae Oral therapy typically is initiated when the patient has been afebrile for 24 to 48 hours and can tolerate oral intake. The total duration of antibiotic therapy is usually 7 to 10 days for uncomplicated CAP and up to four weeks in complicated CAP. The respiratory status of children receiving appropriate therapy for CAP should improve within 48 to 72 hours. Children who fail to improve as anticipated may be receiving inadequate antibiotic therapy, have developed complications, or have an alternative or coincident diagnosis.
References 1. Ralston SL, Lieberthal AS, Meissner HC, Alverson BK, Baley JE, Gadomski AM, Johnson DW, Light MJ, Maraqa NF, Mendonca EA, Phelan KJ, Zorc JJ, Stanko-Lopp D, Brown MA, Nathanson I, Rosenblum E, Sayles S 3rd, Hernandez-Cancio S; American Academy of Pediatrics. Clinical practice guideline: the diagnosis, management, and prevention of bronchiolitis. Pediatrics. 2014;134(5):1474-502. 2. Harris M, Clark J, Coote N, Fletcher P, Harnden A, McKean M, Thomson A; British Thoracic Society Standards of Care Committee. British Thoracic Society guidelines for the management of community acquired pneumonia in children: update 2011. Thorax. 2011;66 Suppl 2:

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
51
CUTTING EDGE DEVICES FOR A DIFFICULT AIRWAY
Selim Suner
Brown University, Alpert Medical School in Providence, RI, USA Assessing for a patent airway is one of the first actions taken with every patient encounter. If an adequate airway is not present or in danger of compromise immediate measures are taken to obtain and maintain an artificial airway. This can be accomplished by placement of a tube through the nose or mouth or by creation of an opening in the trachea. In the majority of patients requiring an artificial airway, the preferred route is oro-tracheal and in the vast majority of these patients the procedure of intubation is performed without difficulty. There are cases which present a challenge in obtaining an airway due to a variety of causes such as: trauma, body habitus, foreign body, bleeding, vomiting, both congenital and acquired anatomical anomalies. The safest technique for obtaining an airway involves visualization of the tracheal opening through the vocal cords and visually assuring passage of the endotracheal tube through this opening. This requires alignment of the clinician’s line of sight through the mouth and in the same plane as the vocal cords. This requires manipulation of the patient’s head, neck, torso and the elevation of the stretches as well as the clinician’s head. In less than ideal conditions this may not be optimal or possible at all, leading to blind intubation attempts. Failed or delayed intubation may lead to increased mortality or morbidity. Over the past few decades, there has been developments in technological insertions into the domain of airway management which have improved the ability to visualize the airway. Cameras, often involving fiberoptic and LED technology allow the clinician to visualize the airway without manipulation. The use of these devices and are now standard teaching in emergency medicine training programs. However, there is currently not sufficient scientific evidence supporting superiority of these devices when compared to standard techniques. In this lecture, I will explore the use some of these devices and present case scenarios of patients with difficult airways.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
52
NON-INVASIVE VENTILATION: WHEN BENEFICAL?
Erkan Göksu
Akdeniz University Faculty of Medicine, Department of Emergency Medicine, Antalya, Turkey Soon after the introduction of endotracheal intubation, many complications of positive pressure ventilation were identified. Laryngeal or tracheal injury, cardiac arrest following endotracheal intubation and baro and volutrauma are well known complications of endotracheal intubation. Endotracheal tube bypasses the barrier of the upper airway and may cause ventilator associated pneumonia. Non-invasive ventilation (NIV) may be an appropriate medical intervention for suitable patients. NIV not only protects patients from complications of endotracheal intubation but also decrease the need for sedation and catheters such as urinary, nasogastric tube, central IV lines. In this lecture author will discuss how to select an appropriate patient, the right modes of delivery, correct amount of positive pressure, interfaces and appropriate methods to monitor the patient. In this lecture audience will be able to find evidence based approach to use of NIV in certain diseases such as COPD, CHF, chest trauma and immunocompromised patient population.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
53
DELAYED SEQUENCE INTUBATION AND APNEIC OXYGENATION: WORTH TO CHANGE THE PRACTICE?
Gregor Prosen
Center for Emergency Medicine Maribor, Maribor, Slovenia RSI (Rapid Sequence Intubation) is established and accepted concept of endotracheal intubation in critical care/EM. RSI is traditionally broken down in 7 steps. It is well understood, that actual act of endotracheal tube placement is in majority of cases “least difficult”. RSI carries 1-19% desaturation rate and hemodynamic and/or respiratory instability is major reason for peri-/post-intubation decompensation. Most important steps of RSI are systematic preparation and pre-oxygenation, of which later can be severely hindered if patient can/will not cooperate with. This is especially true, if cause of patient's altered mental state is respiratory failure, where desaturation can follow after even brief period of apnea (minutes). In order to make pre-oxygenation more efficient, Weingart et al. proposed “DSI”; Delayed Sequence Intubation, where the main difference/addition is pre-oxygenation be done as “procedural sedation” with ketamine in anaesthetic dose. Since ketamine (in slow push) generally does not cause respiratory depression and maintains excellent hemodynamic profile, it is agent of choice for this DSI. Dexmetomidine can also be used. After ketamine takes effect (less then a minute), patient doesn’t “fight the mask” anymore and more successful pre-oxygenation can be achieved. Weingart et al. propose pre-oxygenation with NIV or even gentle BVM ventilation if SpO2 levels are below 90% (very high risk for de-saturation during laryngoscopy attempt). Other proposed concept by same authors is “apneic oxygenation”. Due to constant gradient towards alveoli (and contrary to common belief), there is slight passive oxygenation possible from bronchi, through alveolo-capillary membrane into blood even if passive oxygen inflation. This rate is estimated to 250ml O2/min, enough to prolong apnea time, thus giving clinicians additional time for successful tube placement. Although SpO2 levels fall less steeply, CO2 levels of course rise. Apneic oxygenation is easily done with nasal cannula at 15L/min oxygen flow. There are no untoward side effects to such high oxygen flows and nasal cannula are left on patient’s face during laryngoscopy, only removed after successful tube placement. In real-life practice, both proposed concepts are easily adopted; author’s group has fully incorporated both in their RSI protocol; every RSI attempt starts with clear indication and preparation commences; All patients have non-rebreather mask (NRM) with min. 15L/min and nasal cannula with 15L/min oxygen applied. If baseline SpO2 is <95%, pre-ventilation with NIV or BVM (with nasal cannula underneath) are considered. If patient is not tolerant of any of this pre-oxygenation attempts, ketamine 1mg/kg IV slow push is applied as 2nd step of “DSI”. After such successful (pre)oxygenation, sometimes mechanical intubation is not even needed anymore! During “double” pre-oxygenation (with or without ketamine) other equipment for RSI is prepared. After sedative and paralytic is pushed, NRM is of course removed, but high-flow nasal cannula remains on face during laryngoscopy attempt, only removed after successful airway placement. We find adoption of DSI and apneic oxygenation in our daily practice as simple, easy, logical and beneficial, requiring no additional (mental) or material resources! References 1. Weingart SD. Preoxygenation, reoxygenation, and delayed sequence intubation in the emergency department. J Emerg
Med. 2011;40:661-667. 2. Weingart SD, Levitan RM. Preoxygenation and prevention of desaturation during emergency airway management. Ann
Emerg Med. 2012;59:165-175.e1. 3. Hayes-Bradley et al. Effect of Nasal Cannula Oxygen as Preoxygenation Adjunct. Ann Emerg Med. 2015; 11:1-7 4. Brainard et al. Subject Tolerance and Adverse Effects of Higher- vs Lower-Flow Nasal Oxygen. [Ann Emerg Med.
2015;65:356-361 5. Weingart et al. Delayed Sequence Intubation: A Prospective Observational Study. Ann Emerg Med. 2014;9;25:1-8.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
54
EN KRİTİK GÖZ ACİLLERİ
N. Gökben Beceren
Süleyman Demirel Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Isparta
En kritik göz acilleri görme kaybına, hayatı tehdit eden durumlara neden olan hastalıları kapsamaktadır. Görme keskinliği muayenesinin şart olduğu durumları üç başlık altında inceleyeceğiz; Enfektif Göz Acilleri Özellikle paranazal sinüziti olanlarda; periorbital dokuları tutan, görmenin korunduğu, eritem, ısı artışı ve palpasyonla hassasiyet olan Preseptal Sellülit ile orbital dokuları tutan, ileri dönemde görmede azalmaya neden olan, göz hareketleri ile ağrı ve ateş ile presente olan ve hayatı tehdit eden Kavernöz Sinüs trombozuna ilerleyebilen Postseptal Sellülit. Her iki durumda da acil serviste antibiyoterapinin başlanması gerekmektedir. Yine acil servislerde sık gördüğümüz yanma, batma, kaşıntı, sulanma, çapaklanmayla giden konjuktivitlerden bulaşıcılığı en fazla olan Viral Konjuktivitler olup, şüphe durumunda mutlaka muayene sırasında eldiven ile bireysel korumamızı yapmamız gerekirken; Herpes Simplex ve Zoster şüphesinde erken dönem Asiklovir tedavisi aklımızda bulunmalıdır Bulanık veya puslu görüş, gözde kızarıklık, kaşıntı,e akıntı, fotofobi , şiddetli göz ağrısı ile gelen, kornea üzerinde beyaz leke olan; tedavisiz şiddetli olgularda nadiren kısmi görme kaybına, körlüğe neden olabilen Kornea Ülserinde kapamadan kaçınmalı, antibiyo terapiyi hızla başlamalı, oftalmoloji görüşü alınmalıdır. Kırmızı göz, görmede azalma, fotofobi ve konsensual ağrı olan İritis için ve sıklıkla travma sonrası ağrı, görme kaybı ile gelen göz küresinde derin dokuların enfeksiyonu olan Endoftalmi için oftalmoloji konsültasyonu yapılmalıdır. Travmatik Göz Acilleri Görme muayenesi için topikal anastezik gerekebilen şiddetli ağrı, fotofobi ve sulanma ile gelen özellikle de travma veya lens kullanımı olanlarda Korneal Abrazyon tanısında fluorosein ile boyanarak epitelin kalktığı alan gözlenmelidir. Korneal yabancı cisimlerde erken dönemde ağrı, batma, sulanma, fotofobi, görmenin bulanması söz konusudur. Metalik YC’lerde YC etrafındaki pas halkası da gecikmeden tamamen çıkarılmalıdır. Tam kat laserasyonlar, lakrimal kese yada kanalı içeren, göz kapağının iç yüzeyini içeren, tarsal plak ve kas tutulumu olan laserasyon oftalmalog tarafından onarılmalıdır. Künt travmalarda göze basınç uygulamaktan kaçınmalı, anormal ön kamera derinliği, düzensiz pupil ve körlük durumunda acil oftalmoloji görüşü alınmalıdır. Göz içi basınç artışında görme kaybı riski olan ön kameradaki kanamalarda –Hifema-, beta-blokerler ve karbonik anhidraz inhibitörleri akılda tutulmalıdır. Orbital yapıların sinüse doğru yer değiştirdiği, yukarı bakışta diplopi olan Blowout Kırıklarında oftalmoloji görüşü alınmalıdır Ciddi subkonjunktival kanama, ön kamera derinliğinin kaybolması, iris prolapsusu, hifema, pupillanın şekil ve yer değişikliği, göz yaşı şeklinde pupil, hareket kısıtlılığı, görmede azalma ile karakterize penetran travmalarda palpasyonda aşırı hipotoni görülür Görme muyenesinin atlanarak tedaviye geçilen tek durum Kimyasal Yaralanmalar olup, alkaliler çok daha fazla zarar verirler. Ani Görme Kaybı Gözde ağrı, baş ağrısı, korneada bulanıklaşma, ışıkların etrafında renkli haloların olduğu Akut Açı Kapanması Glokomunda pupiller middilatedir, iridokorneal açıyı kapatarak humor aköz emilimin azaltır,GİB yükselir, tedavide amaç humor aköz yapımını azaltmaktır Optik sinirin inflamasyonun neden olduğu Optik Nöritde renkli görmede belirgin azalma ile birlikte akut görme kaybı söz konusudur; tedavide IV steroid düşünülmelidir. Ani, ağrısız, tek gözde görme kaybı Retinal Arter Trombozundansa , göz masajına başlanması gerekirken; optik disk ödemi olan Retinal Ven Trombozunde GİB ölçülmelidir. Görme alanında ani koyu renkli perde inmesi ise Retina Dekolmanını düşündürür acil Oftalmoloji konsültasyonu yapılmalıdır. Ağrısız iskemik optik nöropati,Temporal Arterit de; Görmede değişim, baş ağrısı, çene kladikasyosu, kafa derisi ve temporal arterde hassasiyet olup bilateral görme kaybı nedeniyle şüphe varsa steroid başlanmalıdır. Kaynakça:
1. Tintinalli Acil Tıp Kapsamlı Bir çalışma Kalvuzu cilt 2, 1517-1550 2. emedicine.medscape.com 3. http://www.kadircankeskinbora.com/goz-cukurunun-orbita-blow-out-travmasi-ve-kirigi/ 4. http://www.fulyaretina.com/retinadamartikanikligi.asp

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
55
ORTOPEDİK ACİLLERDE SIK KARŞILAŞILAN HATALAR
Özgür Tatlı
Karadeniz Teknik Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Trabzon Acil servisler başta olmak üzere hemen her travma merkezinde atlanmış ortopedik yaralanmalarla sıklıkla karşılaşılmaktadır. Hekimin yorgun ve dikkatinin dağınık olması, hastadan iyi öykü alınmaması, yetersiz muayene yapılması, doğru bölgenin doğru açıdan görüntülenmemesi, gerekli grafilerin istenmemesi ya da çekilen grafilerde patolojinin tespit edilememesi ve yanlış yorumlanması sonucunda hekim ve hasta çeşitli medikolegal problemlerle karşılaşabilmektedir. Acil serviste tanısal hataları değerlendiren bir çalışmada , hatalı tanıların %80’ini atlanmış kırıkların oluşturduğu bildirilmiştir (1). En sık kırık atlanan bölgeler; Ayak (%7.6); Diz (%6.3); Dirsek (%6); El (%5.4); El bileği (%4.1); Kalça (%3.9); Ayak bileği (%2.8) (2). Tanı konulmamaış ortopedik patolojiler, kötü ve yetersiz uygulama (malpraktis) iddialarının en önemli sebeplerinden biridir. Acil servis hekimlerinin ceza ile sonuçlanan malpraktis davalarında kırıklar (%6) ile 1. Sıradadır (3). Bu sebeplerden dolayı acil servislerde ortopedik yaralanmalarda sıkça yapılan hataların neler olduğunu bilmek ve hasta yönetimini bu özellikli durumlara göre yapabilmek hekim ve hasta açısından çok önemlidir. Referanslar 1.Guly HR. Diagnostic errors in an accident and emergency department. Emerg. Med. J. 2001; 18: 263–269. 2. Wei C-J, et al. Systematic analysis of missed extremity fractures in emergency radiology. Acta Radiol. 2006; 47: 710–717. 3. Brown TW, et al. An Epidemiologic Study of Closed Emergency Department Malpractice Claims in a National Database of Physician Malpractice Insurers. Acad Emerg Med.2010 May;17(5):553-60

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
56
KULAK BURUN BOĞAZ ACİLLERİNDE GİRİŞİMLER
Bedia Gülen
Bezmialem Vakıf Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, İstanbul Kulak burun boğaz acilleri ciddi patolojilerdir. Ancak yoğun acil tıp programı içinde sıkça değinilemeyen minör aciller başlığı altında toparlanan konulardır. Hava yolu obstrüksiyonu, epistaksis, maksillofasial travmalar, yabancı cisimler, penetren ya da künt boyun travmaları, ani işitme kayıpları, birçok nedenle ortaya çıkabilen fasial paraliziler, enfeksiyonlar gibi değişik nedenlere bağlı olarak oluşabilmektedir. Erken tanı ve tedavileri uygulanmadığı takdirde yüksek morbidite ve mortalite oranlarına sahip olabilmektedirler. Hayati önemi olan hava yolu tıkanıklığına yaklaşımda tam tıkanıklık oluşmadan teşhisin konulması ve gerekli müdahalelerin yapılması hayat kurtarıcıdır. Kuşkulanılan olgular için ilk önlemler alınmalı ve müdahaleye hazır olunmalıdır. Hava yolu tıkanıklığı oluşturan sebeplerin araştırılması bazen tedavi anlamına da gelebilir. Örneğin bir yabancı cismin görülmesi ve çıkartılması hem teşhis hem de tedavi özelliği taşır. Çocuklarda hava yolu tıkanıklıkları ani olduğunda, her zaman kuşkulanılması gereken durum hava yolu yabancı cisimleridir. Epistaksis acil servislerde sıkça karşılaşılan bir durumdur. Acil servise başvuran epistaksisi olan hastada kanama kontrolü ve hastanın hemodinamik stabilizasyonu sağlanmalıdır. Bir diğer önemli kulak burun boğaz acili travmalardır. Yüze gelen travmalarda en sık zarar gören bölge burundur. Kırığa sebep olan travmalara sıklıkla epistaksis eşlik eder. Burunda eksternal deformite gelişmesi, palpasyonla nazal kemikte krepitasyon olması ve direkt lateral grafilerde fissür hattının görülmesi ile tanı konulur. Müdahale için en uygun zaman ödem gelişmeden, travmadan sonraki ilk bir-iki saattir. Fakat bazen farklı bir hasta tek taraflı kanama ve birkaç gündür olan pürülan burun akıntısı ile acil servise başvurabilir. Akılda bulundurulması gereken acil bir durum olan burunda yabancı cisim genellikle çocuklarda ve mental retarde kişilerde görülür. Koopere hastalarda acil serviste çıkartılması gerekir. Yukarıda kısaca giriş yapıldığı gibi kulak burun boğaz acillerinde girişimler başlığı altındaki dersimizde acil serviste karşılacabileceğiz kulak burun boğaz acil durumları ve tedavileri anlatılacaktır. Kaynaklar; 1. Minor Emergencies, 3rd Ed; Buttaravoli P, Leffler SM, 2012. 2. Tintinalli’s Emergency Medicine A Comprehensive Study Guide 8th Edition

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
57
ACİL SERVİSTE DERİ DÖKÜNTÜLERİNDE TANISAL YAKLAŞIM
Murat Çetin
Tekirdağ Devlet Hastanesi, Acil Tıp Kliniği, Tekirdağ
Dermatolojik aciller, tüm acil servis başvurularının %5’ini oluşturmaktadır(1). Bazı durumlarda yaşamı tehdit eden hastalıkların işaretleri derinin altında olabilir. Deri, tanısal ipuçları ne kadar önemli ise, bir o kadar etkilenen birincil organdır. Acil serviste dermatolojik semptomların uygun tanı ve tedavisi için erken dönemde tanınması genellikle hastanın prognozu ve yaşam-ölüm arasındaki farkı tek bir kararla değiştirmek mümkündür.Deri döküntüleri; şiddetli ilaç reaksiyonları, enfeksiyonlar, otoimmün alevlenmeler, yanıklar ve çocuk istismarı gibi çevresel etkenlere inflamatuar yanıtlar arasında olabilir(2).Döküntülerin tanısında, klinisyenin bilgisi, becerisi ve fizik muayene bulguları, laboratuvar değerlendirmeden çok daha ağır basmaktadır.Hastanın dikkatli öyküsü almak, döküntünün başlangıç yeri, Bağışıklık durumu ve yeni ilaçlar kullanımı olması, bizim yön bulamamızı sağlayabilir.Sonuçta görüntü tanıma genellikle doğru tanı koymak için çok önemlidir.Sürekli söylenen “bilinmeyen deri döküntüsü” efsanesi için acil tıp uzmanın klinik becerilerini kullanarak, hızla potansiyel olan ölümcül koşulları tanımak ve meningokoksemi gibi nedenlerde ampirik tedaviye, TEN ve TSS gibi diğer nedenler için destekleyici agresif bakım gerektirdiğini bilmesi önemlidir.Başta anjiyonörotik ödem ve pemfigus vulgaris gibi immünolojik hastalıklar, nekrotizan erizipel ve nekrotizan fasiit, stafilotoksik ve streptotoksik toksik şok sendromu gibi bakteriyel, toksik epidermal nekrolizis, yılan ısırmaları gibi toksik olaylar ve benzeri pek çok tıbbi durumu kapsamaktadır. (3)Ayrıca bazı dermatozlar acil cerrahi girişim gerektirdiği gibi bazı estetik veya onkolojik cerrahi girişimlerden sonra kanama, enfeksiyon ve flept nekrozu gibi acil dermatolojik durumlar da gelÖşebÖlÖr.LÖteratürde acÖl servÖse başvuran dermatolojÖk hastalıkların dağılımına yönelÖk çok az sayıda çalışma bulunmaktadır. Bu konuda yapılan çalışmaların çoğunluğu dermatolojÖ servÖslerÖnden ÖstenÖlen acÖl konsültasyonları kapsamaktadır. Genel hastalıklar ÖçÖnde derÖ hastalıkları oranı farklı klÖnÖklere göre %17-54 olarak bÖldÖrÖlmektedÖr(4).SymvoulakÖs ve ark. referans bÖr hastanede yaptıkları çalışmalarında 3715 hastada dermatÖtler, Ölaç döküntüsü, ürtÖker, erÖtema nodozum, erÖtema multÖformeden oluşan alerjÖk ve döküntülü hastalıklar grubunu %38,4 oranında, enfeksÖyon hastalıklarını %26,1 ve böcek ısırıklarını %10,2 oranında rapor etmÖşlerdÖr. Bu çalışmada hastaların hastaneye yatış oranı %4,8 olarak belÖrtÖlmÖştÖr(5).NadÖr görülmelerÖne rağmen, letal sonuçları nedenÖyle, bu hastalıkların erken tanı ve tedavÖsÖ önemlÖdÖr. AcÖl servÖs hekÖmlerÖnÖn görevÖ tanının erken konulup, tedavÖnÖn başlatılması ve ÖlgÖlÖ konsültasyonların gerçekleştÖrÖlmesÖdÖr.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
58
KARDİYAK ARRESTTE ADRENALİN ( LEHTE GÖRÜŞ)
Ayşegül Bayır
Selçuk Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Konya
Epinefrinin kardiyak arrest sırasında kullanılması yıllardır savunulmakta ve ileri yaşam desteği kılavuzlarında tüm ritimlerde kullanılması gereken ilaç olarak önerilmektedir. İnsanlar üzerinde yapılan az sayıda çalışmaya ait kanıtlar yetersiz olmakla birlikte, hayvanlarda yapılan çalışmaların sonuçları ile kardiyak arrest sırasında etkinliği desteklenmektedir. Epinefrin etkisini α ve β adrenerjik reseptörler üzerinden gösterir. Nonsellektif α ve β adrenerjik reseptör agonistidir. α1 reseptörler üzerinden arteriyollerde vazokonstrüksiyona, pozitif inotrop ve kronotrop etkiye sebep olur, koroner vazokonstrüksiyon meydana getirebilir. α2 reseptörler aracılığı ile venokonstrüksiyon meydana getirir. Böylece sistolik ve diastolik kan basıncını, koroner ve serebral perfüzyon basıncını arttırır. β1 ve β2 reseptörler üzerinden pozitik inotrop ve kronotrop etkiye ve yine, koronerlerde vazodilatasyona sebep olur. Kalp hızını ve miyokardın kontraksiyonunu arttırır. Bronkodilatasyon yapar ve histaminin etkisini antagonize eder. Başarılı bir resussitasyonun anahtarı olarak kabul edilen, koroner perfüzyon basıncını (sağ atriyal diastolik basıncını) arttırması kardiyak arrest sırasındaki en önemli etkisidir. Hem insan, hem de hayvan çalışmalarında kardiyopulmoner resusitasyon (KPR) sırasında epinefrin uygulanması sonrası, koroner perfüzyon basıncının 15 mmHg üzerinde tutulması ile artmış spontan dolaşıma geri dönme oranı arasında ilişki olduğu ve hayvanlarda hayatta kalma oranının arttığı bulunmuştur. Kardiyak arrest sırasında kullanılan adrenalinin, kaba yavaş VF’yi hızlı ve ince VF’ye dönüştürdüğünü tespit edilmiştir. Loomba ve ark. tarafından yapılan bir sistematik review’de hastane öncesi kardiyak arrest geçiren ve hastaneye ulaşmadan epinefrin verilen toplam 655 853 hastayı kapsayan 14 çalışma incelenmiştir. Bu çalışmanın sonucunda hastane öncesi kardiyak arrestlerde epinefrin uygulanması ile hastane öncesi spontan dolaşımın geri dönmesi arasında anlamlı ilişki olduğu bulunmuştur. Deakin ve ark. tarafından yapılan bir başka çalışmada ise hastanede gerçekleşen kardiyak arrest hastalarında epinefrin uygulanmadan önce ve sonraki serebral oksijenasyon araştırılmıştır. Çalışmanın sonucunda KPR sırasında uygulanan 1 mg adrenalinin serebral oksijenasyonu arttırdığı bildirilmiştir. Olasveengen ve ark. tarafından hastane dışında nontravmatik kardiyak arrest geçiren hastalarda yapılan bir çalışmada, KPR sırasında intravenöz ilaç tedavisi verilen ve verilmeyen grup olarak hastalar ikiye ayrılmışlardır. Çalışmaya tüm arrest ritimlerinden toplam 851 hasta alınmıştır. Bu çalışmada hastane dışı kardiyak arrest geçiren hastalarda özellikle şoklanamaz ritimlerde (nabızsız VT ve VF) spontan dolaşımın deri dönmesi oranının ilaç tedavisi verilmeyen gruptan anlamlı yüksek olduğu bulunmuştur. Ayrıca KPR sırasında intravenöz ilaç tedavisi verilen grupta kısa dönem hayatta kalma, hastaneye kabul ve yoğun bakım ünitesine yatış oranlarının daha yüksek olduğu tespit edilmiştir. Hastane içi kardiyak arrest geçiren şoklanamaz ritimli çocuklarda, epinefrin uygulanmasının gecikmesi ile spontan dolaşımın geri dönmesi, 24 saatlik sağ kalım, hastaneden taburcu olma ve iyi nörolojik sonuç oranlarının azaldığı da bazı çalışmalarla kanıtlanmıştır. Kardiyak arrest sırasında uygulanan epinefrin; 1. Koroner perfüzyon basıncını ve spontan dolaşımın geri dönmesi ihtimalini arttırır. 2. Aortik relaksasyon basıncını, koroner ve serebral perfüzyon basıncını arttırır. 3. Serebral oksijenasyon üzerine iyileştirici etki gösterir. 4. Uygun zaman ve uygun dozda kullanılan adrenalin spontan dolaşımın erken dönmesini, spontan dolaşım döndükten sonra, postresusitasyon erken dönemde kan basıncı ve kalp hızı üzerine olumlu etkilere sahiptir. Sonuç olarak; şimdiye kadar yapılan deneysel ve klinik çalışmaların sonuçları değerlendirildiğinde, kardiyak arrest sırasında kullanılabilecek, adrenalin dışında etkinliği kanıtlanmış bir ilaç henüz yoktur. Adrenalinin kardiyak arrest sırasında etkinliği uygun dozda ve zamanda kullanılmasına bağlıdır. Kaynaklar; 1. Ewy GA, Bobrow BJ, Chikani V, Sanders AB, Otto CW, Spaite DW, Kern KB. The time dependent association of adrenaline administration and survival from out-of-hospital cardiac arrest. Resuscitation. 2015;96:180-185. 2. Loomba RS, Nijhawan K, Aggarwal S, Arora RR. Increased return of spontaneous circulation at the expense of neurologic outcomes: Is prehospital epinephrine for out-of-hospital cardiac arrest really worth it? J Crit Care. 2015 Dec;30(6):1376-81 3. Deakin CD, Yang J, Nguyen R, Zhu J, Brett SJ, Nolan JP, Perkins GD, Pogson DG, Parnia S. Effects of epinephrine on cerebral oxygenation during cardiopulmonary resuscitation: A prospective cohort study. Resuscitation. 2016. pii: S0300-9572(16)30444-0. 4. Olasveengen TM, Sunde K, Brunborg C, Thowsen J, Steen PA, Wik L. Intravenous drug administration during out-of-hospital cardiac arrest: a randomized trial. JAMA 2009; 302: 2222–2229. 5. Andersen LW, Berg KM, Saindon BZ, Massaro JM, Raymond TT, Berg RA, Nadkarni VM, Donnino MW. Time to Epinephrine and Survival After Pediatric In-Hospital Cardiac Arrest. JAMA. 2015;314(8):802-810.
5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
59
KARDİYAK ARRESTE EPİNEFRİN
Cüneyt Ayrık, Güllü A. Dündar
Mersin Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Mersin
Epinefrin hastane dışında kardiyak arrest (HDKA) hastalarında iyi nörolojik sonuçlar ile birlikte sağkalım oranını artırıyor mu? Bu soru 10 yıl önce Ottawa Hastane Öncesi İleri Yaşam Desteği (OPALS) çalışmasında cevaplanmıştır. Kısaca bakacak olursak:
OPALS prospektif bir çalışmaydı. HDKA verilerini İKYD öncesi dönemde 12 ay boyunca (paramedikler yalnızca CPR ve
defibrilasyon yaptılar) ve İKYD adaptasyonu sonrasındaki 36 ay boyunca topladılar. ROSC (return of spontaneous circulation - spontan sirkülasyonun geri dönmesi) oranında anlamlı bir artış gördüler fakat sağkalım/taburculuk oranlarında anlamlı bir artış görmediler. Buna ek olarak, İKYD grubunda taburculuk sırasındaki nörolojik sonuçlar daha kötüydü. Sonuç olarak bu çalışma ile İKYD uygulamasının bazı zararlarının olduğu gösterilmiştir.
Epinefrin karşıtı bulgular nelerdir?
1. Arrest hastasında beta-adrenerjik (taşikardi, taşidisritmi ve artmış miyokardiyal oksijen) etkiler istenmeyebilir. 2. Trombogenez ve platelet aksivasyonu artabilir 3. Koroner perfüzyon basıncını artırmasına rağmen, miyokardiyal fonksiyonu bozmaktadır (hayvan çalışmaları) 4. Mikrovasküler perfüzyonu azalmaktadır (özellikle beyin perfüzyonu). Eğer beyin ölecekse kalbi yaşatmanın ne faydası var?
Bu konudaki bazı çalışmalara bakalım. İyi nörolojik sağkalım oranında artış olmaksızın, ROSC artışının varlığı, bazı
gözlemsel çalışmalarda gösterilmiştir. Hagihara A et al. Prehospital Epinephrine Use and Survival among Patients with OHCA. JAMA 2012; 307(11): 1161-68 http://www.ncbi.nlm.nih.gov/pubmed/22436956
● Gözlemsel bir çalışma. 4 yıl boyunca tüm kardiyak arrestler (415,000) dahil edildi. 15,000 vakada epinefrin kullanılırken, diğerlerinde kullanılmamış.
● ROSC oranında artış görülmüş (OR = 3.75) ● Bir aylık sağkalım oranında artış 5.4% vs. 4.7% (OR 1.15) ● İyi nörolojik sonuç anlamlı derecede daha az 1.4% vs. 2.2%
Nakahara S et al. Evaluation of pre-hospital administration of adrenaline (epinephrine) by emergency medical services for patients with out of hospital cardiac arrest in Japan: controlled propensity matched retrospective cohort study. BMJ December 2013 http://www.bmj.com/content/347/bmj.f6829 VF/VT Arest
● Genel sağkalım: %17 vs. %13.4 (Epinefrin grubunda daha yüksek) ● Nörolojik intakt sağkalım: %6.6 vs. %6.6
Non-VF/VT Arest ● Genel sağkalım: %4.0 vs. %2.4 (Epinefrin grubunda daha yüksek) ● Nörolojik intakt sağkalım: %0.7 vs. %0.4
Olasveengen TM, Sunde K, Brunborg C, et al. Intravenous drug administration during out-of-hospital cardiac arrest: a randomized trial. JAMA 2009;302:2222–2229.http://www.ncbi.nlm.nih.gov/pubmed/19934423 Randomize kontrollü (kör değil) bir çalışmaydı ve epinefrin kullanımının HDKA’te sonuçları iyileştirip iyileştirmediği araştırılmıştır.
● ROSC %40 (IV ilaçlar) vs %25 ● ROSC ve yatış %32 (IV ilaçlar) vs. %21 (p<0.001) ● Taburculuğa kadar sağkalım %10.5 (IV ilaçlar) vs. %9.2 (ilaç yok) (p = 0.61) ● İyi nörolojik sonuçlar ile birlikte sağkalım %10 vs. %8 (p = .53)
Jacobs IG, Finn JC, Jelinek GA, et al. Effect of adrenaline on survival in out-of hospital cardiac arrest: a randomised double-blind placebo-controlled trial. Resuscitation 2011; 82:1138–1143.http://www.ncbi.nlm.nih.gov/pubmed/21745533 Placebo grubu içeren randomize kontrollü bir çalışmadır. 600 hastadan toplam 534 veri çalışmaya dahil edilebilmiştir.
● ROSC %23.5 (epinefrin) vs. %8.4 OR = 3.4 ● Hastaneden sağ taburculuk: %4.0 (epinefin) vs. %1.9 – istatistiksel olarak anlamlı değil

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
60
Sonuç: Epinefrin ve diğer ACLS ilaçları HDKA sonrası ROSC oranlarını artırmaktadır fakat iyi nörolojik sonucun görüldüğü hasta sayısını artıramamaktadır. İKYD’nde yer alan epinefrin kullanım tavsiyesi ilginçtir. “yetişkin bireylerde kardiyak arrest durumunda her 3-5 dakikada bir 1 mg IV/IO epinefrin uygulaması uygundur.” denilmektedir. Bu tavsiyeye göre hekim uygun görmezse epinefrini kullanmayabilmektedir. OPALS çalışması oldukça güçlü bir çalışmadır ve son 10 yılda oldukça az şey değişmiştir. Epinefrin kullanımı tavsiyesinin yeniden değerlendirilmesinin vakti gelmiştir. Kaynaklar 1.Hagihara A et al. Prehospital Epinephrine Use and Survival Among Patients with OHCA. JAMA 2012; 307(11): 1161-68. 2.Olasveengen TM, Sunde K, Brunborg C, et al. Intravenous drug administration during out-of-hospital cardiac arrest: a randomized trial. JAMA 2009; 302:2222–2229. 3.Jacobs IG, Finn JC, Jelinek GA, et al. Effect of adrenaline on survival in out-of hospital cardiac arrest: a randomised double-blind placebo-controlled trial. Resuscitation 2011; 82:1138–1143. 4.Nakahara S et al. Evaluation of pre-hospital administration of adrenaline (epinephrine) by emergency medical services for patients with out of hospital cardiac arrest in Japan: controlled propensity matched retrospective cohort study. BMJ December 2013. 5.Callaway CW. Questioning the use of epinephrine to treat cardiac arrest. JAMA 2012; 307(11): 1198-1200.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
61
PANEL 6: LEHTE VE ALEHTE OLAN ÖNERİLER AĞRI KESİCİ OLARAK KETAMİN
Serkan Emre Eroğlu
Sağlık Bilimleri Üniversitesi, Ümraniye Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Günümüz Acil servislerinde sıklıkla tercih edilen ajan olan Ketamin, 1962 yılında geliştirilmiştir. Fensiklidin derivesi
olan molekül, kan beyin bariyerini aşabilme özelliğine sahip olup, sitokrom p450 enzimi aracılığı ile metabolize edilmektedir. 30 yılı aşkın bir süredir genel anestezik olarak kullanılan ajan, saniyeler içinde başlayan etkisini N-metil-D-aspartat
(NMDA) reseptörleri antagonizması üzerinden gösterir. Aynı antagonizma sayesinde; NMDA reseptörlerinin aktivasyonu ile ilişkili olan kronik ağrı, zorlu kanser ağrıları ve nöropatik ağrı yönetiminde de kullanılabileceği varsayılsa da, bazı randomize kontrollü çalışma raporlarının da belirttiği üzere etkin tedavi doz ve zamanlaması konularında tam bir konsensüs sağlanmış değildir.
Ketamin, kullanıldığı endikasyonlar itibari ile; sıklıkla morfin, hidromorfon ya da fentanil’ in yerine düşünülmesine karşın, optimal etki için bu ajanlarla kombine kullanım önerilmektedir. Bununla birlikte, genel anestezi etkisini ortaya çıkaran yüksek dozların aksine, çok daha düşük dozlar yeterli olabilmektedir. Subanestezik bu dozlar, belirgin analjezi oluştururken hastanın uyanık kalmasına da imkan tanımaktadır. Literatürde, minimal yan etkiye sahip önerilen dozun 0.2 mg/kg/h olduğuna dair raporlamalar mevcuttur. Afsharimani ve ark. larının 2015 yılında yayınlanan çalışmalarında analjezinin sağlanmasında intravenöz yolun yanı sıra intratekal kullanımın da etkin olduğu belirtilmektedir. Bununla birlikte, Bu iki yolun haricinde Javarinia ve ark. larının geçtiğimiz aylarda yayınlanan çalışmalarında oral formu ile diklofenak karşılaştırılmış olup, günde 3 kez 50 mg alınan Ketamin ile kronik ağrı şikayeti bulunanlarda depresyon semptomlarının gelişimine karşı etkinlik saptandığı da bildirilmektedir.
Sonuç olarak, Literatür incelemelerinde de belirttiği üzere; Onlarca yıldır kronik ağrı tedavisinde kullanılan Ketamin, kritik bakı hastalarına yönelik sedoanaljezi de dahil, pek çok ağrının yönetiminde giderek artan sıklıkta tercih edilmektedir. Ajanın, subanestezik olan düşük dozlarında dahi yan etki profilinin düşük olması önemli bir avantajdır. Geleceğine dair daha çok çalışma yapıldığı takdirde konumunu güçlendirebilme şansına sahip olabilecektir.
Kaynaklar;
1. Bell RF, Eccleston C, Kalso EA. Ketamine as an adjuvant to opioids for cancer pain (Review). Cochrane Database of Systematic Reviews 2012, Issue 11. Art. No.: CD003351. DOI: 10.1002/14651858.CD003351.pub2.
2. Loveday BA, Sındt J. Ketamine Protocol for Palliative Care in Cancer Patients With Refractory Pain. J Adv Pract Oncol 2015;6:555–61.
3. Jafarinia M, Afarideh M, Tafakhori A, et al. Efficacy and safety of oral ketamine versus diclofenac to alleviate mild to moderate depression in chronic pain patients: A double-blind, randomized, controlled trial. Journal of Affective Disorders 204 (2016) 1–8.
4. Martinez V, Derivaux B, Beloeil H, et al. Ketamine for pain management in France, an observational survey. Anaesth Crit Care Pain Med 34 (2015) 357–61.
5. Erstad BL, Patanwala AE. Ketamine for analgosedation in critically ill patients. Journal of Critical Care 35 (2016) 145–49.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
62
AĞRI KESİCİ OLARAK KETAMİN
Neşe Çolak Oray
Dokuz Eylül Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, İzmir
Ketamin hipnotik, amnezik ve analjezik etkileri olan anestezik bir ajandır. Kortikal ve limbik sistemde dissosiyasyon yaratarak oluşturduğu duruma ‘dissosiyatif anestezi’ denir. Halüsinojenik etkileri nedeni ile suistimal edilme riski yüksektir. Etki süresi 15-45 dakika kadar kısadır. Acil tıp pratiğinde girişimsel sedasyon analjezi ve hızlı seri entübasyonda sedasyon amaçlı kullanılmaktadır. Son yıllarda sedatif etkisinin dışında, analjezik etkisinin yeterliliğinden bahseden çalışmalar yapılmıştır. Ancak günümüz rutininde analjezik amaçla tek başına kullanılmamaktadır. Lehte- alehte sunumunda bu konudaki literatürü tarayarak Ketamin’in analjezik etkinliğinin yeterliliği tartışılacaktır.
Kaynaklar:
1- Vadivelu N, Schermer E, Kodumudi V, Belani K, Urman RD, Kaye AD. Role of ketamine for analgesia in adults and children. J Anaesthesiol Clin Pharmacol. 2016 Jul-Sep;32(3):298-306. doi: 10.4103/0970-9185.168149. Review.
2- Sassano-Higgins S, Baron D, Juarez G, Esmaili N, Gold M. A revıew of ketamıne abuse and dıversıon. Depress Anxiety. 2016 Aug;33(8):718-27. doi: 10.1002/da.22536. Epub 2016 Jun 22. Review.
3- Kator S, Correll DJ, Ou JY, Levinson R, Noronha GN, Adams CD. Assessment of low-dose i.v. ketamine infusions for adjunctive analgesia. Am J Health Syst Pharm. 2016 Mar 1;73(5 Suppl 1):S22-9. doi: 10.2146/ajhp150367.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
63
PANEL 6: LEHTE VE ALEHTE OLAN ÖNERİLER “ACİL TIP EĞİTİMİNDE SOSYAL MEDYA”
Nurettin Özgür Doğan
Kocaeli Üniversitesi Tıp Fakültesi Acil Tıp Anabilim Dalı
(EN) Free open-access medical education (FOAM) is an educational concept involving electronic learning (e-learning) strategies to access accurate and reliable resources in medicine. The FOAM trend and social media tools paved the way for allowing today's educators and students to have rapid access to information anywhere in the world. FOAM is about sharing knowledge, interacting with other people and staying up to date in our rapidly changing medical environment. Emergency medicine is a progressively growing and dynamic speciality in medical community, thus this trend may aid sharing and disseminating the knowledge in various developing settings. (TR) Serbest, açık erÖşÖmlÖ tıp eğÖtÖmÖ (FOAM); tıp alanında doğru ve güvenÖlÖr kaynaklara ulaşmak ÖçÖn elektronÖk öğrenme (e-öğrenme) stratejilerinin kullanılmasını amaçlayan bir eğitimsel konsepttir. FOAM trendi ve sosyal medya araçları, günümüzün eğitmenlerÖ ve öğrencÖlerÖnÖn, bÖlgÖye dünyanın her yerÖnden ulaşabÖlmesÖnÖn yollarını açar. FOAM, hızla değÖşen tıp dünyasında bÖlgÖyÖ paylaşmak, dÖğer Önsanlarla etkÖleşÖme gÖrmek ve güncel kalmakla ÖlgÖlÖdÖr. AcÖl tıp, tıp dünyasında hızla büyüyen ve dinamik bir uzmanlık dalıdır, bu nedenle bu trend acil tıbbın gelişmekte olduğu merkezlerde bilginin paylaşılmasına ve yayılmasına yardım edebilir. Referanslar; 1. Doğan NÖ. Serbest, açık erişimli tıp eğitimi: FOAM. Tıp Eğitimi Dünyası 2016;15(45):5-11. 2. Akoğlu H. Bir İnternet Devrimi: Serbest, Açık Erişimli, Tıp Eğitimi (FOAM). Turk J Emerg Med 2013;13(1):1-4. 3. Cevik AA, Aksel G, Akoglu H, Eroglu SE, Dogan NO, Altunci YA. Social media, FOAMed in medical education and knowledge sharing: Local experiences with international perspective. Turk J Emerg Med 2016 [In Press] DOI: 10.1016/j.tjem.2016.07.001

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
64
SUBMASİF PULMONER TROMBOEMBOLİZMDE TROMBOLİTİK TEDAVİ
Mustafa Burak Sayhan
Trakya Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Edirne Pulmoner tromboembolizm (PE) olgularında trombüsü aktif olarak eriten trombolitik ilaçlar, pulmoner perfüzyonu, hemodinamik bozukluğu, gaz değişimini ve sağ ventrikül fonksiyonlarını hızla düzeltmektedir. Masif (Yüksek Risk) PE grup hastalarda trombolitik tedavi mutlak yapılmalıdır. Submasif PE’li hastalarda ise trombolitik tedavi uygulanması tartışmalıdır. Ancak bu grupta prognozu kötü olup, trombolitik verilmesi gereken grubun belirlenmesi amacıyla, ileri risk değerlendirmesi yapılmalıdır. Bu değerlendirmede submasif (orta riskli) olgular, yüksek riskli submasif (orta-yüksek riskli grup) ve düşük riskli submasif (orta-düşük riskli grup) PE olguları olarak yeniden tanımlanmıştır. Bu sunuda; PE ileri risk değerlendirilmesinde kullanılan; klinik skorlamalar, sağ ventrikül disfonksiyon ve miyokard hasarı belirteçlerini kullanarak kötü prognozlu submasif PE olguları saptanma metotları kısaca gözden geçirildikten sonra, tarafımdan submasif PE’li hastalarda trombolitik tedavinin uygulanması konusunda lehte konuşma gerçekleştirilecektir.
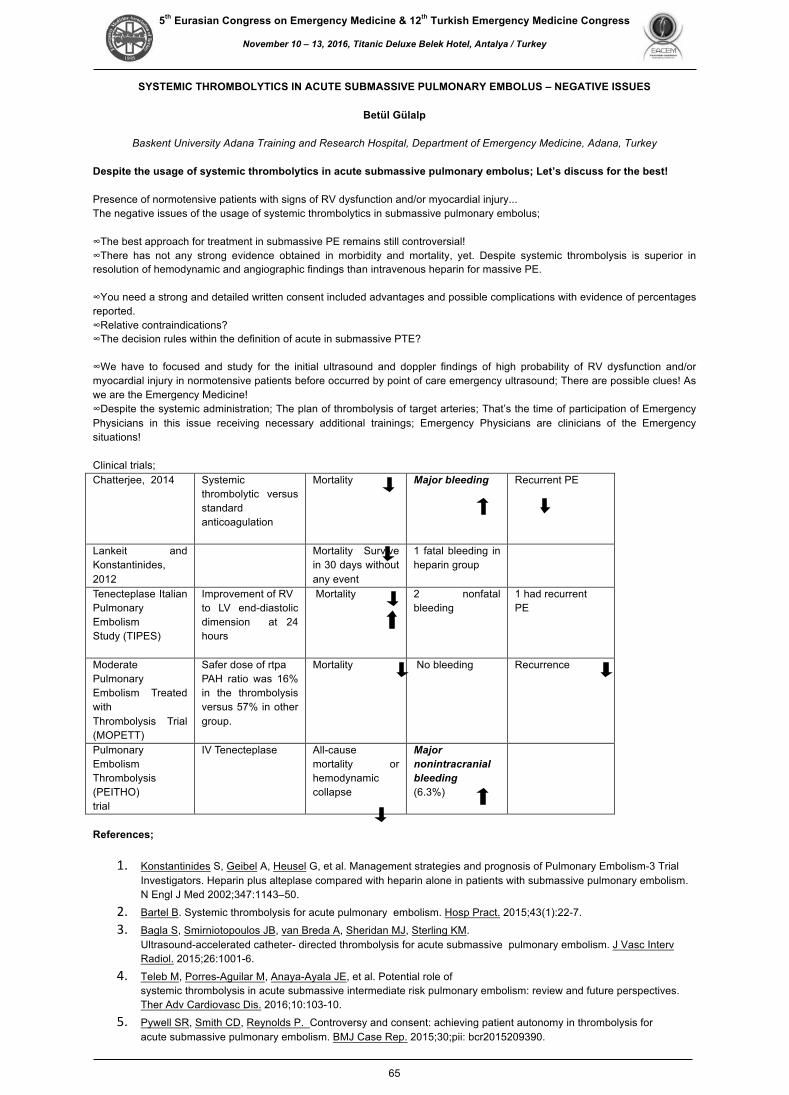
5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
65
SYSTEMIC THROMBOLYTICS IN ACUTE SUBMASSIVE PULMONARY EMBOLUS – NEGATIVE ISSUES
Betül Gülalp
Baskent University Adana Training and Research Hospital, Department of Emergency Medicine, Adana, Turkey Despite the usage of systemic thrombolytics in acute submassive pulmonary embolus; Let’s discuss for the best! Presence of normotensive patients with signs of RV dysfunction and/or myocardial injury... The negative issues of the usage of systemic thrombolytics in submassive pulmonary embolus; ∞The best approach for treatment in submassive PE remains still controversial! ∞There has not any strong evidence obtained in morbidity and mortality, yet. Despite systemic thrombolysis is superior in resolution of hemodynamic and angiographic findings than intravenous heparin for massive PE.
∞You need a strong and detailed written consent included advantages and possible complications with evidence of percentages reported. ∞Relative contraindications? ∞The decision rules within the definition of acute in submassive PTE?
∞We have to focused and study for the initial ultrasound and doppler findings of high probability of RV dysfunction and/or myocardial injury in normotensive patients before occurred by point of care emergency ultrasound; There are possible clues! As we are the Emergency Medicine! ∞Despite the systemic administration; The plan of thrombolysis of target arteries; That’s the time of participation of Emergency Physicians in this issue receiving necessary additional trainings; Emergency Physicians are clinicians of the Emergency situations! Clinical trials; Chatterjee, 2014 SystemÖc
thrombolytÖc versus standard antÖcoagulatÖon
MortalÖty Major bleedFng Recurrent PE
LankeÖt and KonstantÖnÖdes, 2012
MortalÖty SurvÖve Ön 30 days wÖthout any event
1 fatal bleedÖng Ön heparÖn group
Tenecteplase ItalÖan Pulmonary EmbolÖsm Study (TIPES)
Improvement of RV to LV end-dÖastolÖc dÖmensÖon at 24 hours
MortalÖty
2 nonfatal bleedÖng
1 had recurrent PE
Moderate Pulmonary EmbolÖsm Treated wÖth ThrombolysÖs TrÖal (MOPETT)
Safer dose of rtpa PAH ratÖo was 16% Ön the thrombolysÖs versus 57% Ön other group.
MortalÖty
No bleedÖng Recurrence
Pulmonary EmbolÖsm ThrombolysÖs (PEITHO) trÖal
IV Tenecteplase All-cause mortalÖty or hemodynamÖc collapse
Major nonFntracranFal bleedFng (6.3%)
References;
1. Konstantinides S, Geibel A, Heusel G, et al. Management strategies and prognosis of Pulmonary Embolism-3 Trial Investigators. Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolism. N Engl J Med 2002;347:1143–50.
2. Bartel B. Systemic thrombolysis for acute pulmonary embolism. Hosp Pract. 2015;43(1):22-7. 3. Bagla S, Smirniotopoulos JB, van Breda A, Sheridan MJ, Sterling KM.
Ultrasound-accelerated catheter- directed thrombolysis for acute submassive pulmonary embolism. J Vasc Interv Radiol. 2015;26:1001-6.
4. Teleb M, Porres-Aguilar M, Anaya-Ayala JE, et al. Potential role of systemic thrombolysis in acute submassive intermediate risk pulmonary embolism: review and future perspectives. Ther Adv Cardiovasc Dis. 2016;10:103-10.
5. Pywell SR, Smith CD, Reynolds P. Controversy and consent: achieving patient autonomy in thrombolysis for acute submassive pulmonary embolism. BMJ Case Rep. 2015;30;pii: bcr2015209390.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
66
HASTANE AFET VE ACİL DURUM PLANI
Mehmet Ali Karaca
Hacettepe Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Ankara Ülkemizde kayıtlara geçen ilk afet ve afet yönetimi ile ilgili bilgiler 14 Eylül 1509 yılında gerçekleşen İstanbul Depremi ile ilgilidir. İstanbul depreminde 13.000 kişi ölmüş, 1047 bina yıkılmıştır. Padişah II. Beyazıt tarafından çıkarılan ferman ile evlerin yeniden yapılabilmesi için hane başına 20 altın verilmiştir. Cumhuriyet tarihinde afetle ilgili çıkarılan ilk yasa 1939 yılında gerçekleşen Erzin Depremi sonrası 17 Ocak 1940 yılında çıkarılan 3773 sayılı “ Erzincan Depreminden Müteessir Olan Mıntıkalarda Zarar Görenlere Yapılacak Yapılar Hakkında Kanun”dur ve bu kanunla evleri yıkılanlar ayni ve nakdi yardım yapılmıştır. Günümüze kadar ülkemizde çok sayıda afet gerçekleşmiş, ülkemizin afet yanıtını tek merkezden koordine edebilmek amacıyla 2009 yılında 5902 sayılı kanunla Afet ve Acil Durum Yönetimi Başkanlığı (AFAD) kurulmuştur. Dünyada özellikte ABD’de ülke olarak koordine yanıt verilmesi 1979 yılında FEMA (Federal Emergency Management Agency)’nın kurulması ile başlamaktadır. Bu tarihten sonra başta ABD olmak üzere Afet Tıbbı hızla gelişmiş ve afetlerden elde edilen deneyimlerle toplumu afetin olumsuz etkilerinden daha az etkilenir kılmak için düzenlemeler getirmiştir. ABD’de bu düzenlemelerin merkezini Ulusal Afet Sorumluluk Ağı oluşturmaktadır. Ülkemizde de bu kurumun karşılığını ülke düzeyinde AFAD oluşturmakta ve il düzeyinde hazırlıklar ise İl Sağlık Afet ve Acil Durum (İL-SAP) Yönergesine göre yapılmaktadır ve Hastane Afet Planları bu hazırlıkların temellerinden birini oluşturmaktadır. 2 Kasım 2011 tarihinde yayınlanan 663 sayılı KHK ile Sağlık Bakanlığı’na acil durum ve afet hallerinde sağlık hizmetlerini planlama ve yürütme yetkisi verilmiş, 20 Mart 2015 tarihinde de Hastane Afet ve Acil Durum (HAP) Uygulama Yönetmeliği yayınlanmıştır. Bu yönetmelikle ülkemizde faaliyet gösteren tüm sağlık kurumlarına HAP hazırlama zorunluluğu getirilmiştir. ABD’de ilk olarak hastane afet planlarının oluşturulmaya başlanması FEMA’nın kuruluş dönemlerine dayanmaktadır ve 1980’lerde organize olarak HEICS (Hospital Emergency Incident Command System) adı altında ve 5815 hastanenin katılımıyla yayınlanmıştır. Hastane afet planları ile ilgili son güncelleme HICS (Hospital Incident Command System) adı altında 2014 yılında 4.revizyon olarak gerçekleştirilmiştir. Hastane afet planları, afet anlarında hastane yanıtı yardım etmek için hazırlanmış, hastane temelli tüm tehlikeli olaylara karşı standardize edilmiş organizasyon yapısını içeren bir acil durum yönetim sistemidir. HAP 3 ana bileşenden oluşmaktadır:
1- Önleme/zarar azaltma ve hazırlık aşamalarını içeren faaliyetler 2- Afet meydana geldiğinde olayın etkilerini azaltma veya gidermek için gerçekleştirilecek müdahaleler ve 3- Rehabilitasyon ve iyileşme aşamasında yapılacak faaliyetleri içermektedir.
HAP hazırlığının temelini hastane ve hastanenin bulunduğu bölgenin tanınması, risklerin ve tehlikelerin belirlenmesi oluşturmaktadır. Bununla birlikte hastanenin güçlü, zayıf ve geliştirilmesi gereken özellikler tespit edilmeli, etkin risk analizi yapılarak risk ve tehlikeleri azaltıcı önlemler geliştirilmeli ve uygulanmalıdır. HAP Müdahale aşamasında HAP görev alan görevliler ve görevler ile organizasyon şeması ve olay yönetim araçlarının kullanımı bulunmaktadır. Bu amaçla hastane afet planlarında HAP yönetimini sağlayacak Olay Yönetim Ekibi (OYE) üyeleri ve Olay Yönetim Merkezinin (OYM) kuruluşu ve işleyişi belirtilmektedir. Bunlara bağlı olarak müdahale aşamalarının ana rehberlerini oluşturan Olay yönetim araçları (Standart operasyon prosedürleri, İş akış talimatları, departman/servis/birim müdahale prosedürleri ve olay eylem planları) bulunmaktadır ve hepsi Acil Müdahale Planını oluşturmaktadır. Hastane afet planında Olay Yönetim Ekibi; HAP başkanı, olay yönetim merkezinde görev alan İş Güvenliği Sorumlusu, Kurumlar Arası Koordinasyon Sorumlusu, Halkla İlişkiler Sorumlusu, HAP Sekreteryası, Tıbbi Teknik Danışma Kurulu ile Operasyon Şefi, Planlama Şefi, Lojistik Şefi ve Finans Şefi’nden oluşmaktadır. Organizasyon şemasında bu ana birimlere bağlı görev alan görevliler ve görevleri belirtilmiştir.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
67
CAREERS IN EM
Lisa Moreno-Walton
Louisiana State University, Health Sciences Center, Department of Emergency Medicine, LA, USA
Professor Moreno graduated from residency training in 2004, and in less than 10 years, she had been promoted to the rank of full Professor. We consider the goals that should be set at each level of career development: Resident/ Registrar and Junior Faculty (Instructor and Assistant Professor), Mid-Career (Associate Professor), and Senior Faculty (Professor/ Chair/ Deanship). Dr. Moreno will discuss the habits and values that support academic achievement, success and promotion, and how to apply them for the development of your own satisfying and productive career in Emergency Medicine. References; 1. Oshimura JM, Bauer BD, Shah N, et al. Current Roles and Perceived Needs of Pediatrics Hospital Medicine Fellowship Graduates. Hosp Pediatr. 2016 Sep 23. Pii: hpeds. 2016-0031. http://dx.doi.org/10.1542/hpeds.2016-0031 2. Law M, Wright S, Mylopoulos M. Exploring community faculty members’ engagement in educational scholarship. Canadian Family Physician. 2016;62(9):e524-e530. 3. R. Micheal Siatkowski. Excellence in Ophthalmology: continuous certification. Volume 123, Issue 9, Supplement, September 2016, Pages S25-S29. DOI:http://dx.doi.org/10.1016/j.ophtha.2016.06.014 4. Ashley M. Strobel, Rose M. Chasm, Dale P. Woolridge. A Survey of Graduates of Combined Emergency Medicine Programs: An Update. The Journal of Emergency Medicine. August 2016. doi:10.1016/j.jemermed.2016.03.038. 5. Cumbler E, Herzke C, Smalligan R, Glasheen JJ, O`Mally c, Pierce JR. (2016), Visiting professorship in hospital medicine: An innovative twist for growing specialty. J. Hosp. Med. Doi:10.1002/jhm.2625.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
68
EVIDENCE-BASED APPROACH TO VASOPRESSOR CHOICE IN CRITICALLY ILL PATIENT
Murat Ersel
Ege University Medical Faculty, Department of Emergency Medicine, Izmir, Turkey Critically ill patients needs rapid evaluation and all efforts should be given to stabilize those patients hemodinamic status as soon as possible. Vasopressor are widely used in conditions such as cardiogenic, septic and neurogenic shock, acute decompansated heart failure, anaphylaxis and also postcardiopulmonary arrest.(1) Vasopressors are powerful class of drugs to elevate mean arterial pressure (MAP) through inducing vasoconstruction. Vasopressors differ from inotropes, which increase cardiac contractility; however, many drugs have both vasopressor and inotropic effects. (2) Mostly shock is a cardinal situation in critically ill patients. Shock is the final pre-terminal event in many diseases.(3) If shock is not managed as promptly, severe systemic deterioration in tissue perfusion will lead to multipl organ dysfunction. When shock is not reversed promptly with fluid therapy to restore adequate cardiac filling pressures, vasoactive agents can increase MAP and/or CO to restore tissue perfusion. Vasopressors should be titrated to achieve an adequate systemic blood pressure which is a a systolic BP 90 mm Hg and/or a MAP 65 to 70 mm Hg.(4) Clinically, this is achieved by improving blood pressure and CO through the optimization of preload, augmentation of SVR, and the increase of cardiac contractility. To achieve these goals, the physician can use a number of vasoactive agents. (5) The selection of these vaso- or inopressor agents should be decided according the status and shock type of the patient. Vasoactive medications are classified according their effects on the heart and vascular tonus. in three main categories: Vasopressors with pure vasopressor effects on vascular structures (phenylephrine and vasopressin), inoconstructors, drugs that are highly effective vasopressors and stimulate myocardial contractility (epinephrine, norepinephrine and dopamine) and inodilators, increase SV and CO through direct stimulation of myocardial contractility coupled with reduced afterload from systemic vasodilation.(4) Norepinephrine is the first-line vasopressor for all forms of shock with severe hypotension, including undifferentiated shock, vasodilatory/septic shock, and cardiogenic shock. Dopamine is often used as a second-line alternative to norepinephrine in patients with absolute or relative bradycardia and a low risk of tachyarrhythmias, because its variety of effects depending upon its administered dose in cardiogenic shock. (3) Also recent guidelines recommend the combination of norepinephrine and dobutamine for cardiogenic shock instead of dopamine. (4) Dobutamine is most frequently used in severe, medically refractory heart failure and cardiogenic shock, it should’nt routinely used in sepsis because of the risk of hypotension.(2,4) In patients with hyperdynamic septic shock (low vascular resistance and high cardiac index - warm sepsis), vasopressors such as norepinephrine and phenylephrine with alpha vasoconstrictor effects may be more effective, especially phenylephrine may be useful when patients have also tachycardia or dysrythmias precluding use of beta-adrenergic agents. In cold septic shock, characterized by low systemic vascular resistance and low cardiac index, norepinephrine is a reasonable first choice because of its beta-1 (inotropic) and alpha-1 (vasocontuctive) effects. Typically, in cases of septic shock patients with persistent hypotension, dobutamine and epinephrine becomes an alternative. Epinephrine is the preferred agent in anaphylactic shock.(2) References:
1. Kanter J, DeBlieux P. Pressors and Inotropes. Emerg Med Clin N Am 32 (2014) 823–834. 2. Manaker S. Use of vasopressors and inotropes. http://www.uptodate.com/contents/use-of-vasopressors-and-inotropes 3. Gamper G, Havel C, Arrich J, Losert H, Pace NL, Müllner M, Herkner H. Vasopressors for hypotensive shock. Cochrane Database Syst Rev. 2016 15;2:CD003709. 4. Jentzer JC, Coons JC, Link CB, Schmidhofer M. Pharmacotherapy update on the use of vasopressors and inotropes in the intensive care unit. J Cardiovasc Pharmacol Ther. 2015 May;20(3):249-60. 5. Ellender TJ, Skinner JC. The Use of Vasopressors and Inotropes in the Emergency Medical Treatment of Shock Timothy J. Emerg Med Clin N Am. 26 (2008) 759–786

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
69
CRIMEAN-CONGO HAEMORRHAGIC FEVER: TURKISH EXPERIENCE
Nurşah Başol
Gaziosmanpaşa University Medical Center, Department of Emergency Medicine, Tokat, Turkey
Crimean-Congo haemorrhagic fever (CCHF) is a fatal viral disease with haemorrhagic symptoms. The viral agent is CCHF virus, a member of the Bunyaviridae family, Nairovirus group, and is a single helical RNA virus. The disease is primarily transmitted by tick bite; however it can be transmitted by removing or smashing ticks with bare hands, or contacting body fluids like blood of infected people, or handling of tissue, blood or other body fluids of infected animals unprotected. The disease is endemic to Eastern Europe, Asia, Africa, and the Middle East, including Turkey. In Turkey, most CCHF cases are observed in the Tokat province of the Black Sea region. Our hospital is located in Tokat and nearly 280 CCHF cases have been seen in a year. An early diagnosis of CCHF, which has a high mortality rate, is important for emergency medicine physicians, especially in endemic areas. The mortality rate from CCHF is 3-30%. According to data from the Turkish Ministry of Health, a total of 4453 CCHF cases were reported between the years 2002-2009, among whom 218 (4.9%) fatal ones were accounted. In this lecture, I will present pathogenesis, clinical and laboratory findings, emergency approach and treatment of CCHF with our experiences in Tokat. References:
1- Başol N, Duygu F, Ayan M. (2013). Detailed evaluation of patients admitted to emergency department with a tick bite complaint. Medicina (Kaunas). 2013;49(8):367-71.
2- Başol N, Duygu F, Gokbakan MA & Alatlı T. (2014). Anxiety Experienced in the fear of Disease: Tick Bite and Crimean-Congo Hemorrhagic Fever. Acta Medica Mediterranea, 2014, 30: 691-696.
3- Akinci E, Bodur H, Sunbul M, Leblebicioglu H. (2016). Prognostic factors, pathophysiology and novel biomarkers in Crimean-Congo hemorrhagic fever. Antiviral Res. 2016 Aug;132:233-43.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
70
VIRAL OR BACTERIAL? TOOLS FOR DISTINGUISHING
Ayhan Özhasenekler
Yıldırım Beyazıt University Faculty of Medicine, Department of Emergency Medicine, Ankara
A major challenge underlying effective management of febrile ED patients is the difficulty in clinically distinguishing between bacterial and viral etiologies. On the other hand the early initation of antibiotic therapy has a major impact on the clinical outcome of critically ill patients. This clinical uncertanity causes antibiotics misuse, underuse and overuse. For the patient, that causes detrimental ramifications, antibiotics resistance ang high costs1. Several laboratory diagnostic tests are used for establishing an etiologic diagnosis. Rapid tests that provide additional insight in the bacterial or viral etiology of infection may guide appropriate use of antibiotics anda re urgently needed. However, the specificity of single biomarkers in terms of etiologic distiction between bacterial or viral infections may not be enough. In a study, so biomarkers were used in combination (i.e.; CRP, CRP+LBP, CRP+PCT, CRP+IL-6, CRP+IL-18 vs). But this combinations were not superiority than CRP2. In other study’s results strongly support the use of the PCT serum level as a routine biomarker of bacterial infection. Furthermore, some of the novel potential biomarkers (i.e., heparin-binding protein, [IL-6], cortisol , IFN-c, and IL-8) demonstrated interesting differences based on the etiology and localization of bacterial infections, suggesting potential for their future clinical use. In addition, leukocytes and neutrophils levels increase in the bacterial infections, on the other hand lymphocytes levels increase in the viral infections3. References
1. Eden E, Srugo I, Gottlieb T, Navon R, Boico O, Cohen A, Bamberger E, Klein A, Oved K. Diagnostic accuracy of a TRAIL, IP-10 and CRP combination for discriminating bacterial and viral etiologies at the Emergency Department. J Infect. 2016 Aug;73(2):177-80. doi: 10.1016/j.jinf.2016.05.002.
2. ten Oever J, Tromp M, Bleeker-Rovers CP, Joosten LA, Netea MG, Pickkers P, van de Veerdonk FL. Combination of biomarkers for the discrimination between bacterial and viral lower respiratory tract infections. J Infect. 2012 Dec;65(6):490-5. doi: 10.1016/j.jinf.2012.08.004.
3. Chalupa P, Beran O, Herwald H, Kaspříková N, Holub M. Evaluation of potential biomarkers for the discrimination of bacterial and viral infections. Infection. 2011 Oct;39(5):411-7. doi: 10.1007/s15010-011-0126-4.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
71
Z'BOLA: VIRUSES THREATENING MASSES
John L. Foggle
Brown University, Warren Alpert School of Medicine, Department of Emergency Medicine, RI, USA Once there was smallpox, then yellow fever, followed by the Spanish influenza pandemic which killed as many as 50 million people in 1918-19. The scourge of viruses have afflicted mankind since ancient history, and there now appears to be an acceleration in the evolution, frequency, and geographic distribution of these diseases. The second half of the 20th century saw an upsurge in emerging viruses around the world with easier spread due to new “vectors” like air transport. We have seen HIV, avian flu, West Nile virus, SARS, Chikungunya, deadly outbreaks of hemorrhagic diseases like Ebola, and we are now facing the spread of Zika virus around the globe. Mass media and the Internet have complicated the response to these emerging diseases by spreading incomplete information and sowing the most deadly virus of all: fear. Are we prepared for a mega virus, one with the ease of spread of the flu or Zika combined with the deadliness of Ebola? This lecture will attempt to highlight where we have come from and how we can be better prepared to manage what some experts say is inevitable. REFERENCES: • Krauthammer C, “AIDS Hysteria”, The New Republic, October 5, 1987. • Friedman E, “Health Care Hysteria: The Case of Ebola Fever”, Hospitals and Health Networks, February 3, 2015. • Donnelly C and Dye C., “Ebola Virus Disease in West Africa -- The First 9 Months of the Epidemic and Forward Projections”,
N Engl J Med, October 16, 2014, vol. 371 no. 16. • Petersen L, et. al., “Zika Virus”, Review Article, N Engl J Med, March 30, 2016; 374:1552-63. • OSHA, United States Department of Labor, “Pandemic Influenza Preparedness and Response Guidance for Healthcare
Workers and Healthcare Employers”, 2007, pp: 1-63.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
72
STREET DRUGS: A NEW THREAT IN ED SETTING
Ridvan Atilla
Dokuz Eylül University Faculty of Medicine, Department of Emergency Medicine, Izmir Substance dependence is described as the abuse of the substances without the prescription of a clinician to achieve stimulation, depression, hallucination, or similar effects on central nervous system. Variety of abused substances has been described in the literature. Abuse of drugs for substance dependence is a common problem throughout the world and these drugs are generally named as street drugs. Street drug usage has become an insidious danger for Turkish population especially among young generation in recent years. During the past decade, more forensic and medical cases had been visited to EDs due to side effects of these drugs. The most important reason for the increasing amount of their usage could be being underestimated. By means of the most comprehensive report about the substance abuse among the primary school students in Turkey has been published last year. In these lecture, I aimed to review some well-known street drugs, and their clinical effects with their clinical managements in ED setting. Although I have described some street drugs that have not been currently found in Turkey, some informative critics will further help clinicians. The main dominating effects were grouped into three: stimulating, depressants and hallucinogens. Roughly the synthetic agents are more dangerous than natural sources; so that clinical importance is highlighted mainly on synthetic agents. Synthetic cannabinoids and synthetic cathinones are described as well as the other synthetic stimulants and depressants. References:
1. Ögel K, Tamar D, Evren C, Çakmak D. Lise Gençleri Arasında Sigara, Alkol ve Madde Kullanım Yaygınlığı. Türk Psikiyatri Dergisi 2001; 12(1): 47-52
2. The European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) web site. http://www.emcdda.europa.eu/ 3. Batem Bağımlılık Tanı Ve Tedavi Merkezi web site. www.batem.info.tr 4. Yeşilay web site. www.yesilay.org.tr. 5. Balseven A, Özdemir Ç, Tuğ A., Hancı H, Doğan Y B. Madde Kullanımı, Bağımlılıktan Korunma ve Medya. Sted
2002; 11(3):91

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
73
CARBON MONOXIDE TOXICITY
Selim Suner
Brown University, Alpert Medical School in Providence, RI, USA
Carbon monoxide (CO) toxicity is a common cause of death by poisoning. Most cases of CO poisoning result from fires and suicide attempts. CO is produced by incomplete combustion of fossil fuels, therefore; coal and wood burning, oil heaters, kerosene burners and gasoline fires can all lead to CO emission. Use of motorized vehicles utilizing fossil fuel indoors such as warehouses, sports arenas and convention centers may set the stage for CO poisoning. Although most cases of CO poisoning is sporadic and isolated, clusters of cases occur more often in the winter when indoor burning of fossil fuel is prevalent. Neurological or psychiatric sequelae occur in up to 2/3 of patients who survive CO intoxication1. Neuropsychiatric syndromes resulting from CO toxicity can occur immediately, days, weeks or in some cases months after exposure and encompass a wide spectrum of clinical findings ranging from apraxia to coma. Although the exact mechanisms of CO toxicity have not yet been elucidated, it has been known for over a century that a contributing mechanism for toxicity from CO is hypoxia from carboxyhemoglobin (COHb) formation at the expense of oxyhemoglobin2. Other mechanisms of CO toxicity involving cellular processes have also been postulated. Most of the current research evaluating the mechanisms of CO toxicity is centered around the central nervous system effects of CO; however, other organ systems, such as the cardiovascular system, are also adversely effected by exposure to CO. The presence of the patient in an environment containing products of combustion coupled with constitutional, GI, neurological or cardiovascular signs and symptoms and an elevated COHb level form the basis for the diagnosis of CO toxicity. Since CO is eliminated by breathing, delayed presentation of a patient with an exposure history yet normal COHb should not preclude the diagnosis. CO exposure produces a spectrum of toxicity. In order to determine the mode of therapy, the degree of toxicity is arbitrarily categorized as mild, moderate and severe. In cases of mild CO toxicity, the patient presents with constitutional symptoms such as headache, dizziness, lightheadedness, nausea and vomiting but has not lost consciousness. In moderate toxicity, there is transient loss of consciousness or neuropsychiatric abnormalities. With severe CO intoxication, the patient remains comatose, manifests gross neurological deficits, displays cardiovascular symptoms (i.e: coronary ischemia seen on electrocardiography, acute myocardial infarction, persistent hypotension or congestive heart failure), pulmonary edema or profound metabolic acidosis. COHb levels have been shown to correlate well with severity of CO toxicity. COHb should only be used to confirm CO exposure. Pregnant women and children under the age of 10, except for the most trivial of exposures, even with mild or no symptoms, should be placed in the severe toxicity group if their COHb level is elevated above l0%. The special treatment of pregnant women originates from various case reports showing fetal demise with maternal CO exposure 3. Perhaps the greatest controversy in the topic of CO poisoning is the mode of therapy used once toxicity has been determined. There are, it seems, two major groups at each end of the controversy: those that advocate the use of HBO therapy and those that prefer NBO. Even within each pole there is division. Proponents of HBO treatment cannot agree on how high to tum the pressure and for how long. On the other hand, those who oppose HBO therapy have not determined the ideal dose of normobaric oxygen. References; 1- Tibbles PM, Perrotta PL: Treatment of carbon monoxide poisoning: a critical review of human outcome studies comparing normobaric oxygen with hyperbaric oxygen. Ann Emerg Med l 994;24:269-76. 2- Ginsburg MD: Carbon monoxide intoxication: clinical features, neuropathology and mechanisms of injury. Clin Toxicol l 985;23:281-88. 4- Cramer CR: Featl death due to accidental maternal CO poisoning. J Toxicol Clin Toxicol. 1982; 19:297-30 l.
5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
74
INTRAVENOUS LIPID EMULSION
Mohammed Almalki
King Saud Medical City, Department of Internal Medicine, Riyadh, Kingdom of Saudi Arabia
Background: The use of intravenous lipid emulsion (ILE) therapy for the treatment of lipophilic drug toxicity is increasing. Despite this, the evidence for its effect in non-local anesthetic toxicity remains sparse. Intravenous lipid emulsion (ILE) therapy involves the administration of a large amount of fat for the purposes of treating drug toxicity due to fat-soluble drugs. The most prevalent of several theories describing the purported mechanism of ILE is the “lipid sink” theory. According to this theory, the administration of lipid reduces the volume of distribution of the drug in question by pulling lipid soluble drugs out of the periphery and into the vascular compartment Mechanism
o Modulation of intracellular metabolism: addition of excess FAs may overcome blocked/inhibited enaymes by mass actionàenergy to “starved heartàreversal of toxicity
o Modulation of intracellular metabolism: addition of excess FAs may overcome blocked/inhibited enaymes by mass actionàenergy to “starved heartàreversal of toxicity
o Activation of ion channels: FAs directly activate cardiac Ca2+ channelsàdose-dependent increase in Ca2+ current
§ Oleic, linoleic, and linolenic acids act directly on Ca2_ channel No direct evidence supporting this mechanism
Conclusion
The Clinical Toxicology’s lipid emulsion collaborative workgroup was created to review all appropriate evidence pertaining to the use of ILE in clinical toxicology. This manuscript summarizes the findings of ILE as it relates to non-local anesthetic substance toxicity. Despite use of ILE for multiple substances in medical toxicology, the effect of ILE in various non-local anesthetic poisonings is heterogenous and the quality of evidence remains low to very low.
The currently available published evidence concerning the effect of ILE in severe LA toxicity is limited to very low quality studies such as small animal experiments and human and animal case reports or series. It is possible that ILE may be effective for reversal of cardiovascular or neurological features in some cases of LA toxicity. However, there is currently no consistent evidence that ILE is more effective than vasopressors. The available evidence is insufficient to judge the combined effects of ILE and vasopressors and to determine whether one drug should precede the other in treating severe LA toxicity. References: Systematic review of the effect of intravenous lipid emulsion therapy for non-local anesthetics toxicity. Levine M1, Hoffman RS2, Lavergne V3, Stork CM4, Graudins A5, Chuang R6, Stellpflug SJ7, Morris M8, Miller-Nesbitt A8, Gosselin S9; Lipid Emulsion Workgroup. Systematic review of the effect of intravenous lipid emulsion therapy for non-local anesthetics toxicity. Levine M1, Hoffman RS2, Lavergne V3, Stork CM4, Graudins A5, Chuang R6, Stellpflug SJ7, Morris M8, Miller-Nesbitt A8, Gosselin S9; Lipid Emulsion Workgroup. Goldfrank's Toxicologic Emergencies 10th

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
75
DIZZY PATIENT AND DIZZY PHYSICIAN: ANY APPROACH EASING THE MANAGEMENT?
Can Özen
Ümraniye Research and Education Hospital, Emergency Medicine Clinic, Istanbul Cases of dizziness in emergency department (ED) are common. Studies suggest %3.5 to %11 which means about 35 – 100 cases a day in a busy ED in Turkey. ED physicians may benefit from having a systematic approach to these patients and use some red flags for more serious conditions to help distinguish between central and peripheral causes. Over 60 conditions lead to dizziness are described, over 90% of those can be grouped in 7 main etiological groups: Peripheral vestibular disorders, hyperventilation, multisensory dizziness, psychiatric disorders, brainstem stroke, neurological disorders and cardiovascular disorders. Feeling of dizziness is categorized into 4 groups; vertigo, presyncopy, disequilibrium and light headedness. Vertigo implies a motion of self or the environment in space. Presyncopy is a feeling of impending faint or loss of conscioussness. Disequilibrium simply means impaired gait. Lightheadedness is a vague sensation often used to categorize non specific causes which don’t belong in previous 3 groups. In ED perspective, life threatening etiologies should be distinguished. Vital signs, both normal and ortostatic, are needed for differentiating these entities. ECG and glucose should be monitered. If these are abnormal treatment should start immediately. Patient history may suggest other serious conditions. If severe headache and/or neck pain accompanies dizziness subarachnoid hemorrhage, Hemorrhagic stroke, Vertebral artery dissection are potential diagnosis. Chest pain and shotness of breath lead us to coronary diseases or pulmanory embolism. Palpitations suggest arrythmia. Focal neurological deficits point out stroke. Triggers, onset and duration of symptoms may help narrowing our diagnosis. Second line of more serious conditions include hypovolemia, poor oral intake or GI fluid loss, vasovagal episodes, electrolyte disturbences, infections and medications. After all dangerous conditions are excluded, otological causes of dizziness which are about 1/3 of all ED cases can be considered. These include benign positional vertigo, vestibular neuritis, Meniere’s disease. A detailed physical exam would help diagnosing benign conditions. HiNTS exam(head impluse, nystagmus, test for skew) is described in 2009 and is specific for central pathologies. Head impulse or head thrust test is an important component in bedside evaluation. Vestibuloocular reflex is tested on each side. This reflex triggers eye movements when stimulated. A positive test with unilateral horizontal nystagmus suggest vestibular neuritis. Dix Hallpike test is used as a positional testing and Epley maeuver for particle repositioning in vestibular canal. Meniere’s disease have recurrent episodes of dizzines and is typically accompanied with tinnitus and sometimes with unilateral loss of hearing. Head thrust tests are usually normal. Symptomatic treatment includes fluid resuscitation for nausea and vomiting and drug therapy for relieving the symptoms. Vestibular supressents like antihistamines, benzodiazepines and anticolinergic agents are generally sufficient but a combination weith an antiemetic may be necessary. In emergency settings, causes of dizziness should be well investigated and life threatening conditions should be distinguished. Physicians should not overrely a normal head CT and patients’ description of thier symptoms. A detailed patients history, a thorough neurological examination and knowing your differentials are keys for successful management of patients with dizziness. References:
• Crespi, V. (2004). "Dizziness and vertigo: an epidemiological survey and patient management in the emergency room." Neurol Sci 25 Suppl 1: S24-25.
• Lammers, W., et al. (2011). "Demographic analysis of emergency department patients at the ruijin hospital, shanghai." Emerg Med Int 2011: 748274.
• Newman-Toker, D. E., et al. (2008). "Spectrum of dizziness visits to US emergency departments: cross-sectional analysis from a nationally representative sample." Mayo Clin Proc 83(7): 765-775.
• Newman-Toker, D. E., et al. (2007). "Imprecision in patient reports of dizziness symptom quality: a cross-sectional study conducted in an acute care setting." Mayo Clin Proc 82(11): 1329-1340.
• Navi BB, et al. (2012). “Rate and predictors of serious neurologic causes of dizziness in the emergency department.” Mayo Clin Proc 87(11):1080-8.
• Edlow J, et al. (2016). “Using the physical examination to diagnose patients with acute dizziness and vertigo”. Journ Emerg Med. in press: http://dx.doi.org/10.1016/j.jemermed.2015.10.040.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
76
IMAGING STRATEGIES IN STROKE IN ED (CT VS MRI)
Chan Kim Poh
Sengkang Health Alexandra Hospital, Department of Emergency Medicine, Singapore Though non-contrast computed tomography (NCCT) has always been considered as the initial imaging modality of choice for patients who present with acute stroke symptoms, recent promising results from acute stroke endovascular clinical trials confirm the value of treatment-related acute imaging target (TRAIT) selection and enrichment for endovascular reperfusion strategies. These trials demonstrated that patient recruitment limited to an imaging-defined subset of stroke led to positive trials with smaller samples completed within reasonable periods of time. So the imaging modality of choice (i.e. CT or MRI) has generated much debate, not to mention the advances in diagnostic imaging of stroke which include multimodal techniques such as noninvasive angiography and perfusion imaging. The aim of this session is to review the neuroimaging recommendation derived from the various clinical studies, during the acute phase of an ischemic stroke. References:
1. Jamary Oliveira Filho. Neuroimaging of acute ischemic stroke. UpToDate. Apr 04, 2016. 2. Steven J. Warach, Marie Luby, Gregory W. Albers, Roland Bammer, Andrew Bivard, Bruce C.V. Campbell et al. Acute
Stroke Imaging Research Roadmap III Imaging Selection and Outcomes in Acute Stroke Reperfusion Clinical Trials: Consensus Recommendations and Further Research Priorities. Stroke. 2016;47:1389-1398. doi: 10.1161/STROKEAHA.115.012364.
3. Kloska SP, Nabavi DG, Gaus C, Nam EM, Klotz E, Ringelstein EB et al. Acute stroke assessment with CT: do we need
multimodal evaluation?. Radiology. 233(1):79-86, 2004 Oct. 4. Wintermark M, Rowley HA, Lev MH. Acute stroke triage to intravenous thrombolysis and other therapies with advanced
CT or MR imaging: pro CT. Radiology. 251(3):619-26, 2009 Jun.
Pexman JH, Barber PA, Hill MD, Sevick RJ, Demchuk AM, Hudon ME et all. Use of the Alberta Stroke Program Early CT Score (ASPECTS) for assessing CT scans in patients with acute stroke. American Journal of Neuroradiology. 22(8):1534-42, 2001 Sep.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
77
CHALLENGES IN CONDUCTING DISASTER SIMULATIONS
Ali Haedar
Universitas Brawijaya, Saiful Anwar General Hospital, Department of Emergency Medicine, Indonesia
The purposes of disaster simulation are to prepare and coordinate a multiple-jurisdictional integrated response to a national catastrophic event, test plans and critical response & recovery functions, to challenge our systems and procedures, to identify gaps and shortfalls. The emergency management could include Preparation & Protection, Mitigation Respond, and Recovery. Objectives of each emergency management simulation are to assess and validate our capabilities and role in the communications, critical resource logistics and distribution, mass care (sheltering, feeding and related services), medical surge, citizen evacuation and shelter-in-place, emergency public information and warning, emergency operations center (EOC) management, and long term recovery. The 3 important challenges in conducting disaster simulation are triage, prerequisite skills, and documentation. Triage in the field is not simple as it is a complex, comprehensive, and controversial procedure. It needs should be immediate and timely, adequate and accurate assessment, decided based on assessment, intervened according to acuity condition, matched with patient satisfaction, complete in documentations. First Responder team should have prerequisite skills to control airway-breathing-circulation, to control external bleeding, to treat shock, to treat wounds, and to splint injuries to stabilize extremities. Documentation should record initial condition of patient, patient’s description of injury or illness, initial and later vital signs, treatment given, personnel who took over care, and any other pertinent information. Good planning and exercising ED triage system in daily practice can help maintain hospital disaster preparedness & critical functions. “START” triage system should be feasible to be implemented during disaster. A written guideline is required to ensure all staff to understand. We need to build capacities Basic Life Support Curse, First Responder Course, Triage Officer Course, and Ambulance Protocol Course.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
78
MANAGING EMERGENCY CARE IN COUNTRIES WITH POOR SOURCES
Rashmi Sharma
Brown University, Division of Disaster Medicine and Emergency Preparedness, RI, USA My name is Rashmi Sharma, and I am a physician from Nepal. Currently, I am doing a fellow in disaster medicine and emergency preparedness in Brown university. Since my graduation from medical school, I’ve worked with several charities and aid groups that provide access to health care and medical services in remote areas. The practice of medicine and the circumstances in these overlooked communities are challenging. Working under such situations, I have learnt a great deal of things that I value most about practicing medicine: for eg, being compassionate, and an appreciation and love for working with a multiethnic patient population with complex psycho-social and medical needs. Nepal, my home country, is struggling to overcome the legacy of a decade long Maoist insurrection. The probability of dying between birth and age 5 is 83% - one of the highest in the world. Lack of adequate infrastructure, financial resources, proper equipments, supplies, trained people, reliable electricity, transportation, proper roads and water supplies, as well as various insurgent activities have continued to hinder development, expansion, and implementation of basic health services. Many Nepalese go abroad in search of employment and a better life which has not only resulted in a massive resource migration, but has also contributed to the massive influx of infections such as HIV and tuberculosis in the country. And this is a similar pattern I have witnessed repeatedly - wherever I have been involved clinically - be it Haiti, Kenya or most recently South Sudan. I have been working on and off on field missions with msf as a clinician for the past 3 years. Hence, as I grow more personally and professionally, I am learning how to be most effective in working for vulnerable population during times of conflict and catastrophe and applying them globally. I feel I understand the expertise and skills needed to improve medical care and attendant services in challenging circumstances. Hence, I would like to discuss about the challenges faced by humanitarian organisations working actively in the field to prepare, and respond to health threats, while working with a multi-ethnic team in a volatile enviroment.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
79
BOMBING INJURY PATTERNS AND CARE
Mehmet Mahir Kunt
Hacettepe University Faculty of Medicine, Department of Emergency Medicine, Ankara The explosives will continue to be one of the instrument used by terrorists in the future. Approximately 17 bomb attacks occurred and 298 people were killed and nearly a thousand people were injured during last year in Turkey. It is not forgotten, half of all initial casualties to seek medical care may admit to the hospital that in first one-hour period. The most severely injured victims arrive after the less injured, who bypass Emergency Medical System’s triage and go directly to the closest hospitals. Triage and lifesaving procedures should never be delayed in the possibility of radioactive contamination of the victim; the risk of exposure to caregivers is small. Universal precautions effectively protect against radiological secondary contamination of first responders and first receivers. Blast Injuries are classified as:
♦ Primary: Injury from over-pressurization force (blast wave) impacting the body surface o Tympanic membrane rupture, pulmonary damage and air embolization, hollow viscus injury
♦ Secondary: Injury from projectiles (bomb fragments, flying debris) o Penetrating trauma, fragmentation injuries, blunt trauma
♦ Tertiary: Injuries from displacement of victim by the blast wind o Blunt/penetrating trauma, fractures, and traumatic amputations
♦ Quaternary: All other injuries from the blast o Crush injuries, burns, asphyxia, toxic exposures, exacerbations of chronic illness
No definitive guidelines for observation, admission, or discharge. Most of the injuries are more complex and multidimensional than seen in daily trauma practice. So innovative and multidisciplinary approach is needed. References:
1. https://www.acep.org/blastinjury/ 2. https://emergency.cdc.gov/masscasualties/blastinjury-mobile-app.asp 3. http://www2c.cdc.gov/podcasts/player.asp?f=10224

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
80
CLINICAL GUIDELINES ON PREDNISONE USE IN THE ED
Lisa Moreno-Walton
Louisiana State University, Health Sciences Center, Department of Emergency Medicine, LA, USA
Prednisone is one of the 10 most commonly prescribed drugs, yet most of the common uses are off-label uses. We will examine the clinical guidelines established by specialty colleges and societies for the use of prednisone to treat asthma, COPD, Bell’s Palsy, Crohn’s Disease and ulcerative colitis, gout, and other diseases (as presentation time allows). We will review the meaning of categories of evidence and strength of recommendation, and will apply these standards to the recommendations made by specialty societies. We will assess risks and benefits of steroid use for each disease and indication reviewed, concluding with firm evidence based recommendations for your EM practice. References
1.Sherwin RL, Garcia AJ, Bilkovski R. Do low-dose corticosteroids improve mortality or shock reversal in patients with septic shock? A systematic review and position statement prepared for the American Academy of Emergency Medicine. J Emerg Med. 2012 Jul;43(1):7-12. doi: 10.1016/j.jemermed.2011.08.015. Epub 2012 Jan 4. doi: 10.1016/j.jemermed.2011.08.015 2.Xin-Ming Su, Na Yu, Ling-Fei Kong & Jian Kang (2014). Effectiveness of inhaled corticosteroids in the treatment of acute asthma in children in the emergency department: A meta-analysis. Annals of Medicine. 46:1, 24-30. doi: 10.3109/07853890.2013.859855. 3.Cormac McCarthy, John R Brennan, Lindsay Brown, Deirdre Donaghy, et al. Use of a care bundle in the emergency department for acute exacerbations of chronic obstructive pulmonary disease: a feasibility study. Int J Chron Obstruct Pulmon Dis. 2013; 8: 605–611. doi: 10.2147/COPD.S52883. 4.Brian E. Grunau, Matthew O. Wiens, Brian H. Rowe, Rachel McKay. Emergency Department Corticosteroid Use for Allergy or Anaphylaxis Is Not Associated With Decreased Relapses. Annals of Emergency Medicine Volume 66, Issue 4, October 2015, Pages 381–389. doi:10.1016/j.annemergmed.2015.03.003. 5.Hirotaka Chikuda, Hideo Yasunaga, Katsushi Takeshita, Hiromasa Horiguchi. Mortality and morbidity after high-dose methylprednisolone treatment in patients with acute cervical spinal cord injury: a propensity-matched analysis using a nationwide administrative database. Emerg Med J. 2014 Mar; 31(3): 201–206. doi: 10.1136/emermed-2012-202058.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
81
LITERATURE UPDATE IN CARDIOLOGY
Fatma Sarı Doğan
Kartal Dr. Lütfi Kırdar Education and Research Hospital, Emergency Medicine Clinic, Kartal, Istanbul, Turkey
Cardiovascular diseases are the leading causes of death worldwide. Early diagnosis and the most apppropriate management are necessary to prevent mortality and morbidity . New methods and guidelines are being developed constantly for this purpose. In this presentation; results of the research about approach to chest pain, myocardial ınfarction (MI) , acute heart failure (AHF), pulmonary embolism (PE) and arrhythmia will be discussed with some current issues. References:
1- Mueller C, Giannitsis E, Christ M, Ordóñez-Llanos J, deFilippi C, McCord J, Body R, Panteghini M, Jernberg T, Plebani M, Verschuren F, French J, Christenson R, Weiser S, Bendig G, Dilba P, Lindahl B; TRAPID-AMI Investigators. Multicenter Evaluation of a 0-Hour/1-Hour Algorithm in the Diagnosis of Myocardial Infarction With High-Sensitivity Cardiac Troponin T. Ann Emerg Med. 2016 Jul;68(1):76-87.e4. doi: 10.1016/j.annemergmed.2015.11.013.
2- Weekes AJ, Thacker G, Troha D, Johnson AK, Chanler-Berat J, Norton HJ, Runyon M. Diagnostic Accuracy of Right Ventricular Dysfunction Markers in Normotensive Emergency Department Patients With Acute Pulmonary Embolism. Ann Emerg Med. 2016 Sep;68(3):277-91.doi:10.1016/j.annemergmed.2016.01.027.
3- Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, Castella M, Diener HC, Heidbuchel H, Hendriks J, Hindricks G, Manolis AS, Oldgren J, Popescu BA, Schotten U, Van Putte B, Vardas P; Authors/Task Force Members.; Document Reviewers:.. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS European Heart Journal doi:10.1093/eurheartj/ehw210.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
82
ACİL SERVİSTE ULTRASON EŞLİĞİNDE SİNİR BLOKLARI
Özlem Dikme
Koç Üniversitesi Hastanesi, Acil Servis, İstanbul
Acil serviste periferik sinir blokları akut ekstremite ağrısının yönetiminde ve prosedürel anestezide kullanılmaktadır. Deneyimli kişilerce seçilmiş olgularda ultrasonografi eşliğinde sinir bloğu uygulaması acil hasta yönetiminde birçok potansiyel yarara sahiptir. Analjezi spesik bir bölgeyi hedefleyerek uygulandığında genel anestezi hali oluşmayacağından dolayı seçili hasta gruplarında (kafa travması, bilinci bozuk hasta) hastanın ek problemlerine yönelik acil servisteki değerlendirme ve takip sürecine herhangi bir etkisi olmayarak ekstremitenin saatler süren analjezisi sağlanabilir. Yine çok miktarda lokal anestezik kullanımı gerektiren işlemlerde (tek dermatom üzerindeki çoklu kesilerde) hastayı yüksek dozda lokal anestezik kullanımından korur. Ek olarak hastanın girişim sonrası izlem süresi azaltılarak acil serviste kalış süresinin azalması sağlanır. Lokal anestetik alerjisi olanlarda, enjeksiyon bölgesinde enfeksiyon varlığında, kompartman sendromuna yol açabilecek yaralanma varlığında, kooperasyonun kurulamadığı hastalarda, uygulanacak ekstremitede yaralanmaya ait nörolojik defisit varlığında, ciddi obezite nedeni ile görüntülemenin sağlanamayacağı olgularda ve relatif olarak antikoagülasyon altındaki hastalarda kullanımı kontrendikedir.
Yaralanmanın yerine ve hastanın özelliğine göre seçilerek üst ekstremite için interskalen pleksus, supraklaviküler
pleksus, infraklaviküler pleksus, aksiller pleksus, median sinir, radial sinir ve ulnar sinir blokları uygulanabilirken alt ekstremite için ise femoral, popliteal, tibial, derin peroneal, safen ve sural sinir blokları uygulanabilir. Uygulama için yüksek frekanslı lineer prob kullanılmalı ve öncelikle periferik sinirlerin normal sonoanatomisi öğrenilmelidir. Periferik sinirler çevrelerindeki dokulara bağlı olarak birçok farklı ekojenik şekilde karşımıza çıkabilir. Klasik olarak sinir lifi etrafı hipoekoik kollajenöz doku içerisinde gömülü hiperekojenite veren perinöryum ve endonöryum olarak görüntülenir. Grup halinde olduklarında transvers düzlemde bakıldığında tipik “bal peteği” görüntüsü vardır. Sinirin distal veya kısa segmenter bölgelerinde myelinli aksonlar tendon ile karışabilir. Sinirler uzanımları boyunca oval, yuvarlak ya da üçgen şekillerde karşımıza çıkabilir. Uygulama yapılacak sinirin distalini belirleyerek proksimale doğru takip etmek girişim bölgesini belirlemede yardımcı olacaktır. Yine sinirler damarlar ile birlikte seyrettiği için ayrımında kompresyon ve doppler kullanılarak girişim yapılacak bölgeden emin olunduktan sonra işlem başlatılmalıdır. İşlem öncesinde hastanın ve uygulama yapılacak odanın hazırlığında ışığın azaltılması görüntü kalitesini arttır. Karanlık bir odada işlem yapılacak alana aydınlatma kullanılması tercih edilmelidir. Hasta lokal anesteziklerin yan etkileri nedeni ile monitörize ve damar yolu açık olmalı ve ileri hava yolu ekipmanları odada hazır bulundurulmalıdır. İşlem öncesinde değerlendirilmesi gereken bir diğer konuysa anestezik madde seçimidir. Lokal anestezik olarak lidokain, mepivakain, bupivakain seçilebilir. Anestezi süresini uzatmak amacıyla epinefrin eklenebilir. İğne seçiminde 22g genişlikte 50-100mm iğneler tercih edilmelidir. Yaklaşım, iğne oryantasyonu ve iğnenin genişliği ile ilgili olarak komplikasyonlar görülebilir. Blok süresince komplikasyonları azaltabilmek için iğne ucu doku içerisinde görüntülenebilir halde olmalıdır. Uç görüntülenmeden anesteziye başlanmamalı, görüntülenemiyorsa prob iğneye doğru oynatılarak uç aranmalı, bulunamıyorsa iğne oynatılarak doku içerisinde bıraktığı efekt gözlenmeli ya da 1ml lokal anestezik enjekte edilerek ucun etrafında oluşan anekoik görüntü ile yeri doğrulanmalıdır. Eğer bu yöntemler ile iğne yeri doğrulanamıyorsa başka bir iğne yada girişim yeri seçilerek işlem tekrarlanmalıdır. Yaklaşımda iki yöntem düzlemsel (in-plane) yada düzlem dışı (out-of-plane) yaklaşım kullanılabilir. Düzlemsel yaklaşımda iğne deriye probun olduğu noktadan giriş yapar, transvers şekilde tüm görüntüyü kat eder ve hedefe ulaşır. Düzlem dışı yaklaşımda ise iğne probdan uzak bir noktadan deriye giriş yapar sadece iğne ucu görüntüye dahil olur. Düzlemsel yaklaşımda iğne artefaktı nedeniyle giriş yolunun izlenmesi daha kolay sağlanabilir. Kaynaklar
1. Tsui B, Hadzic A. Chapter 17. Equipment for Peripheral Nerve Block. In Hadzic A (ed). NYSORA Textbook of Regional Anesthesia and Acute Pain Management, 1e. McGraw-Hill, 2007.
2. Shariat AN, Horan PM, Gratenstein K, McCally C, Frulla AP. Chapter 3. Equipment for Peripheral Nerve Blocks. In Hadzic A (ed). Hadzic's Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia, 2e. McGraw-Hill, 2012.
3. Lehmann LJ. Chapter 68. Peripheral Nerve Blocks. In Warfield CA, Bajwa ZH (eds). Principles & Practice of Pain Medicine, 2e. McGraw-Hill, 2004.
4. Spence BC, Parra MC. Chapter 49. Peripheral Nerve Blocks. In Longnecker DE, Brown DL, Newman MF, Zapol WM (eds). Anesthesiology, 2e. McGraw-Hill, 2012.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
83
KARDİYAK ULTROSONOGRAFİDE GERÇEK HAYAT DENEYİMLERİ
Adnan Yamanoğlu
Haseki Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Tanı ve tedavisinde Ekokardiyografinin etkin kullanıldıldığı dört ayrı vaka sunulmuştur;
´ Birinci olguda 25 yaşında nefes darlığı ve kanlı balgam şikayetiyle başvuran lohusa genç bayan hasta sunulmuştur. Yapılan temel tetkiklerde pulmoner emboli ve kalp yetmezliği ve pnomoni ayırıcı tanısına ihtiyaç duyan hastanın yapılan ekokardiyografik incelenmesi neticesinde klnik bulgularla korele edilerek Peripartum Kardiyopati tanısıyla tedavi altına alınmıştır.
´ İkinci olguda 55 yaşında ciddi nefes darlığı şikayetiyle başvuran erkek hasta sunulmuştur. Daha önceden bilinen kalp yetmezliği ve koraner arter hastalığı olmayan hastanın yapılan ekokardiyografik incelemesi hikayesiyle birleştirildiğinde hastanın dört gün önce myokart enfaktüsü geçirdiği ve son gün buna bağlı gelişen kalp yetmezliği pulmoner ödem ile başvurduğu anlaşılmıştır. Hastanın tedavisinde koroner girşim ön plana alınarak tedavisi düzenlenmiştir.
´ Üçüncü olguda ciddi nefes darlığı ve bayılma şikayetiyle acil servise getirilen 67 yaşında erkek hasta sunulmuştur. Gelişinde üçüncü dakikasında entübe edilmek zorunda kalan hastanın 1 ay önce Tip 1 aort diseksiyonu operasyonu geçirdiği öğrenilmesi üzerine yapılan ekokardiyografik incelemede tekrar diseksiyon gerçekleştiği saptanan hasta ikinci operasyona alınmıştır.
´ Dördüncü olguda 1 aydır olan nefes darlığı şikayetine sol taraf göğüste 2 gündür şiddeti giderek artan, devamlı vasıflı batıcı göğüs ağrısı eşlik eden 35 yaşında bayan hasta sunuldu. Özgeçmişinde derin ven trombozu geçirme öyküsü olması üzerine yapılan ekokardiyografide pulmoner emboliyi destekleyen sağyüklenme bulguları saptanan hastanın çekilen pulmoner anjiografi ile tanı kesinleştilerek tedavi altına alınmıştır.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
84
ORTOPEDİK ACİLLERDE ULTRASONOGRAFİ
Mehmet Ali Aslaner
Nevşehir Devlet Hastanesi, Acil Servis Birimi, Nevşehir Kas iskelet sisteminde tanımamız gereken temel yapılar; kas, tendon, kemik ve eklem yapılarıdır. Bu yapıları tanımak aradığımız patolojiyi nerede bakacağımıza veya gördüğümüz patolojinin nerede olduğunu anlamamızda gerekli olacaktır.
• Kemik yapıları tanımada sıklıkla korteksi tanımak yeterlidir. Düzgün yapılı hiperekojen hat bu alanda belirteçtir, arkasında ise ses dalgaları geçmediği için görüntü oluşmayacaktır.
• Kas dokusu için; kasılma/gevşeme ile kayma hareketi göstermesi ve içeriğinin daha heterojen-çizgili olması yol göstericidir.
• Tendon yapıları; kasa göre, daha homojen düzgün sınırları olan ve kalınlaşma / incelme göstermeyen yapılar olması, tanısaldır.
• Eklem yapıları; tipine göre, sabit veya oynar eklem olarak farklı görüntü sergileyebilmektedir.
Olgu 1: 20 yaş erkek hasta, düşme sonrası sağ el bilek düzeyinde şişlik ve ağrı ile başvuruyor. İlk bakıda, ön kol distalinde deformite nedeniyle kırık ön tanısı ile radyografi isteniyor. Distal Radius kırığı saptanan hastada (Smith kırığı) yaklaşımımız ne olurdu? 1,2 Hangi analjezi yöntemi ? Redüksiyon yönetimi ? Olgu 2: Düşme sonrası dizde şişlik ve morarma ile başvuran 50 yaşında bayan hasta. Radyografide kırık izlenmiyor. Hematom şüphesi ile ultrasonografi yapılıyor. Cilt altı hematom? Hemartroz? Olgu 3: Futbol oyunu sırasında uyluk kısmında şiddetli bir ağrı duyan hasta, acil servise başvuruyor. Dışarıdan sadece şişlik saptanan hastaya yatak başı ultrasonografi yapılıyor. Rektus femoris rüptürü Olgu 4: 45 yaşında bayan hasta düşme sonrası omzunda hareket kısıtlılığı ve ağrı ile başvuruyor. Nörovaskuler muayenesi normal saptanıyor. Radyografide kırık saptanmıyor fakat eklem aralığının arttığı fark ediliyor. Tanıyı netleştirmek için ultrasonografi yapılıyor. Posterior disloke omuz çıkığı Olgu 5:21 yaşında hafif mental retarde erkek hasta. Babası tarafından ayak bileğinde şişlik ve kızarıklık ile getiriliyor. Öyküde, yabancı cisme maruziyet şüphesi hasta yakınları tarafından belirtiliyor. Radyografide patoloji saptanmıyor. Ultrasonografi görüntüsünde yabancı cisim görülüyor ve başarılı bir şekilde çıkarılıyor. 3 Referanslar 1.Fathi M, Moezzi M, Abbasi S, Farsi D, Zare MA, Hafezimoghadam P. Ultrasound-guided hematoma block in distal radial fracture reduction: a randomised clinical trial. Emergency medicine journal : EMJ 2015;32:474-7. 2.Sabzghabaei A, Shojaee M, Arhami Dolatabadi A, Manouchehrifar M, Asadi M. Ultrasound-Guided Reduction of Distal Radius Fractures. Emerg (Tehran) 2016;4:132-5. 3.Mohammadi A, Ghasemi-Rad M, Khodabakhsh M. Non-opaque soft tissue foreign body: sonographic findings. BMC Med Imaging 2011;11:9.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
85
ANTİKOAGÜLANLARIN ANTİDOTLARI (TDP VE FAKTÖR KONSANTRELERİ)
Mehmet Ali Karaca
Hacettepe Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Ankara Primer ve sekonder embolik olayların önlenmesinde kullanılan warfarin dünyada en yaygın olarak tercih edilen oral antikoagülandır. K vitaminine bağımlı faktörler II, VII, IX ve X’un sentezini inhibe eder. Son yıllarda kullanımları giderek yaygınlaşan yeni nesil oral antikogülanlardan Dabigatran aktive Trombin; Rivoraxaban ve Apixaban ise aktive Faktör X üzerinde etkilerini gösterir. Oral antikoagülanlara bağlı gelişen kanama komlikasyonları minör kanamadan majör kanamaya kadar geniş bir spektrumda görülmektedir. En sık gastrointestinal (%60) olmak üzere üriner (%15) sistemde kanamalar gelişmektedir. Oral antikoagülan kullananlarda yıllık kanama görülme olasılığı %6,3’tür ve her 10 kanamadan birisi ölümle sonuçlanmaktadır. Özellikle kanama riskleri oral antikoagülan başlanmasından sonraki ilk 3 ayda en yüksektir. Kanama riski INR yüksekliği ile doğru orantılı olarak artmaktadır. Örneğin: INR düzeyleri 2.0-2,9’dan 3.0-4.4 düzeylerine yükseldiğinde kanama riski 2 kat; INR düzey 4,5-6 düzeyine ulaştığında ise bu oran 4 kat artmaktadır. INR düzeyinde her 0,5 birimlik yükselme kanama riskin 1,43 oranında artırır. Oral antikoagülan kullanımına bağlı gelişen kanamalar ölümcül, majör ve minör olarak sınıflanabilir. İntrakraniyal, gastrointestinal ve retroperiton kanamalar majör kanamalar olarak kabul edilir. Oral antikoagülanlara bağlı en sık gastrointestinal kanamalar görüldüğünden hastalar sıklıkla melena ve hematokezya yakınmaları ile acil servislere başvurmaktadır. Oral antikoagülanlara bağlı gelişen kanama komlikasyonlarında INR düzeyleri hızlı ve etkin şekilde normal düzeylere döndürülmelidir. Bu konuda çok sayıda öneri olmakla beraber en yaygın Avustralya ve Fransız Klavuzları kullanılmaktadır. Bu klavuzlara göre ciddi olmayan kanamalarda (INR ≥ 2) warfarin tedavisi kesilmeli, vitamin K1 5-10 mg intravenöz olarak verilmeli ve protrombin kompleks konsantreleri (PCC) 35-50 IU/kg dozunda başlanmalıdır. PCC yokluğunda ise Taze Donmuş Plazma (15 ml/kg) kullanılmalıdır. Ciddi kanamalarda ise hedef en kısa sürede INR düzeyini 1,5 ve altına indirmektir ve bu amaçla PCC 25-50 IU/kg dozunda hızla verilmelidir. Buna benzer olarak da İngiliz Hematoloji Standartları Kalvuzunda ciddi kanamalarda 4 faktörlü PCC ve Vitamin K 5 mg İV verilmesi önerilmekte PCC yokluğunda TDP tercih edilmesi gerektiği belirtilmektedir. Ülkemizde yaygın olarak kullanılan 4 faktörlü PCC formunda standart olarak her 10 ml’de 250 IU Faktör IX bulundurmaktadır. Oral antikoagülanlara bağlı majör kanamalar dışında PCC’ler hemofili A, hemofili B ve konjenital faktör eksikliklerinde de kullanılmaktadır. Son yıllarda yapılan çalışmalar travma sonrası masif transfüzyon planlamasında TDP yerine PCC kullanımını önermektedir. PCC doz hesaplamasında gerekli doz klavuzlarda 25-50 IU/kg olarak belirtilmiş olsa da en yararlı doz rejimi hastanın INR ve vücut ağırlığının da göz önüne alındığı formülasyondur. Bu formül ile gerekli PCC dozu; Gerekli olan birim= vücut ağırlığı (kg) X gerekli olan faktör X artışı (IU/ml) X60 ve PCC verilme hızı 2 ml/dk olmalıdır.
PCC’nin TDP’ye olan başlıca üstünlükleri; sabit oranda faktör içermesi, hızlı uygulanabilmesi, etkisinin hızlı başlaması, volüm yüklenmesine neden olmaması, virüs inaktivasyonu ve kan grubu uygunluğu gerektirmemesi olarak belirtilebilir. Son yıllarda yeni nesil oral antikoagülanların (dabigatran, rivaroxaban ve apixaban) etkilerinin geri döndürülmesinde PCC’nin kullanımı ile ilgili çalışmalar yapılmaya başlanmıştır ve bu çalışmalar ilerleyen dönemde bu yeni ilaçların etkinliklerinin geri döndürülmesinde PCC’lerin de etkin bir alternatif olabileceğini göstermektedir.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
86
ACİL SERVİSTE ASEMPTOMATİK KAN BASINCI YÜKSEKLİĞİ OLAN HASTAYA YAKLAŞIM
Vermi Değerli
Bozyaka Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İzmir
Erişkinlerde (>18 yaş), sistolik KB ≥140 mmHg ve/veya diyastolik KB ≥90 mmHg olması HT (yüksek KB) olarak tanımlanmaktadır (Tablo I). “Hipertansif emergency = hipertansif acil” belirgin kan basıncı yüksekliği ile birlikte akut hedef organ hasarının olduğu klinik durumdur. Bu grup hastaların acil servis yönetimi literatürde net olarak tanımlanmıştır. “Hipertansif urgency = hipertansif ivedi durum” ise belirgin kan basıncı yüksekliği olmasına rağmen akut hedef organ hasarının olmadığı durumdur, acil serviste net bir yönetimi tanımlanmamıştır. Joint National Committee (JNC) 7 asemptomatik hipertansiyona yaklaşım ile ilgili algoritmalar hazırlasa da, bu algoritmalar hastaları uzun dönem takip eden birinci basamak hekimlerine yöneliktir. Asemptomatik HT ve hipertansif urgency sıklıkla HT tanısı olsun/olmasın akut hedef organ hasarı olmaksızın belirgin yükselmiş kan basıncını ifade etmek için kullanılan terimlerdir. Literatürde belirgin olarak yükselmiş kan basıncının evrensel bir tanımı bulunmamakla birlikte bu kılavuz, 2003 yılında, JNC 7’de evre 2 HT olarak kabul edilen SKB ≥160 mm Hg veya DKB ≥100 mm Hg değerlerini almıştır. American College of Emergency Physicians (ACEP) tarafından 2013 yılında güncellenen “Asemptomatik Yüksek Kan Basıncı Olan Hastaların Acil Serviste Yönetimi” konusunda, literatür taranarak ve kanıta dayalı tıp verileri incelenerek klinisyenlere faydası olacağına inanılan iki soruya yanıt aranmıştır.
1- Asemptomatik yüksek kan basıncı olan acil servis hastalarında hedef organ hasarı varlığını araştırmak istenmeyen etki oranlarını düşürür mü? Düzey A ve B öneri bulunmamaktadır. Düzey C öneriler;
• Acil servislerde asemptomatik belirgin yüksek kan basıncı olan hastalara rutin olarak hedef organ hasarı araştırması (serum kreatinin değeri, idrar tetkiki, EKG gibi) gerekmemektedir.
• Seçilmiş vakalarda (hastane takibi zor) serum kreatinin değerinin ölçülmesi böbrek hasarını belirleyebilir ve taburculuk kararını (hastaneye yatış gibi) değiştirebilir.
2- Belirgin yüksek kan basıncı olan asemptomatik hastaların kan basıncına acil serviste müdahale etmek istenmeyen etki oranlarını düşürür mü? Düzey A ve B öneri bulunmamaktadır. Düzey C öneriler;
• Acil servislerde asemptomatik belirgin yüksek kan basıncı olan hastalara rutin olarak tıbbi müdahale ile kan basıncını düşürmek gerekmemektedir.
• Seçilmiş vakalarda (kötü poliklinik takibi gibi) acil tıp hekimleri kan basıncına ilaçla müdahale edilebilir ve/veya uzun süreli kan basıncı kontrolü tedavisine başlayabilir (konsensus önerisi).
• Asemptomatik yüksek kan basıncı olan hastalar taburculuk sonrası poliklinik takibine yönlendirilmelidir (konsensus önerisi).
Klinik bulgular ve hasta yönetimi ile ilgili öneri düzeyleri aşağıdaki kriterlere göre derecelendirilmiştir: Düzey A öneriler: Klinik olarak yüksek kesinlik derecesine sahip öneriler (Sınıf I çalışmalarca desteklenen veya Sınıf II çalışmalarca yüksek kanıt düzeyinde bulunmuş öneriler). Düzey B öneriler: Klinik olarak orta derecede değerli verilere sahip öneriler (Sınıf II çalışmalarca desteklenen veya Sınıf III çalışmalarca ciddi ortak görüşe sahip öneriler). Düzey C öneriler: Sınıf III çalışmalarca desteklenen veya literatür yokluğunda ACEP panelinde oluşturulan öneriler. Asemptomatik hastalarda belirgin yüksek kan basıncının hızlı olarak düşürülmesinin potansiyel olarak zararlı olduğu kabul edilir. Ancak bazı sosyal veya klinik durumlarda (kötü takip, yaşlı hasta, tedaviye ulaşımda kısıtlılıklar, vb) acil tıp hekimlerinin belirgin yüksek kan basıncı olan asemptomatik hastalarda taburculuk öncesi kan basıncını düşürebileceği ve/veya uzun süreli kontrolü sağlamak için tedaviye başlayabileceği belirtilmiştir. Asemptomatik hipertansif hastaların önemli bir bölümünün kan basıncı acil servisteki ilk ölçümden sonra 60-90 dk içerisinde herhangi bir müdahale olmaksızın spontan olarak düşmektedir. Tablo I. JNC 7’ye göre kan basıncının sınıflaması
Normal: < 120/80 mmHg PrehÖpertansÖyon: 120-139/80-89 mmHg Evre 1: 140-159/90-99 mmHg Evre 2: ≥160/100 mmHg
Kaynaklar:
1. Goldberg EM. An evidence-based approach to managing asymptomatic elevated blood pressure in the emergency department. Emergency medicine practice February 2015 volume 17, number 2.
2. Wolf SJ, Lo B, Shih RD, et al. Clinical Policy: Critical issues in the evaluation and management of adults patients in the emergency department with asymptomatic elevated blood pressure. Ann Emerg Med. 2013;62(1):59-68.
3. JNC VII: http://www.nhlbi.nih.gov/guidelines/hypertension/jnc7full.pdf 4. http://www.uptodate.com/contents/what-is-goal-blood-pressure-in-the-treatment-of-hypertension/abstract/2 5. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in
adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014;311:507

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
87
MENTAL DURUM DEĞİŞİKLİĞİ
Betül Akbuğa Özel
Başkent Üniversitesi Tıp Fakültesi , Acil Tıp Anabilim Dalı, Ankara Mental durum değişikliği; genel anlamda beyin fonksiyonlarındaki; konfüzyon, letarji, amnezi, farkındalık kaybı, oryantasyonun kaybı, düşünce ve yargı kusurları, alışılmadık ve garip davranışlar, algı, psikomotor beceriler ve davranışlarda aksamalar ve koma gibi değişiklikleri ifade eder. Psikiyatrik tanıların tetiklediği mental durum değişiklikleri karakteristik olmakla beraber diğer nedenlere göre daha az görülmektedir. Medikal durumlar (özellikle enfeksiyonlar), beyin hasarına neden olan yaralanmalar, ilaç overdozları, geri çekilme sendromları mental durum değişikliklerine neden olabilen diğer nedenler arasında sayılabilir. Mental durum değişikliğinin zengin etyolojisi universal olarak AEIOUTIPS mnemoniği ile kodlanır. AEIOTIPS içindeki etyolojik durumlardan biriyle tetiklenmiş olan hastaların kliniğini tanımlamak içinse deliryum, demans, ensefalopati ve organik beyin sendromu gibi terimler kullanılmaktadır. Deliryum akut mental değişikliklerine, demans ise kronik mental durum değişkiliklerine işaret eder. Demans daha stabil ve progresif seyrederken AEIOUTIPS ile alevlenebilir. Deliryum ise AEIOUTIPS ile ortaya çıkar ve daha gürültülü ve iniş çıkışlı bir kliniğe sahip olma eğilimindedir. Ancak acil servise başvuran demans hastalarının akut alevlenmesi ile yeni gelişen deliryum tabloları klinik olarak birbiriyle karışabilecek benzerlikler gösterir. Acil servis primer başvuru nedeni mental durum değişikliği olan hasta oranının %4-10 olduğu ve acil servise başvuran >65 yaş hasta grubunun %30’unda mental durum değişikliği bulunduğu bildirilmektedir (1,2). Deliryumla başvuran hastaların mortalitesi de %10-26 oranlarındadır(3). Deliryum varlığının, uzamış hastane kalım süreleriyle, artmış komplikasyonlarla, artmış hastane maliyetleriyle ve uzun süreli yetersizlikle korele olduğu bulunmuştur (3). Mental durum değişikliğini değerlendirmek için yatak başı kullanılan birçok araç üretilmiştir. Bilinç seviyesini değerlendirmek için, AVPU ve GKS; ajitasyon ve sedasyon seviyesini değerlendirmek için, Richmond Ajitasyon ve Sedasyon Skalası; bilişsel durumu değerlendirmek için, Mini Mental Durum Değerlendirmesi, Ottowa 3DY, Altı Madde Eleme; konfüzyonu değerlendirmek için, Konfüzyon Değerlendirme Metodu mevcuttur (4). Deliryumun hiperaktif subtipi daha kolay farkedilir ve prognozu en iyi olandır (5). Buna karşın hipoaktif ve mikt tip deliryum zor farkedilir. Mikst tip deliryum prognozu en kötü olan deliryum tipidir (5). Acil servislerde, mortal seyredebilen mental durum değişiklikleri için uygun klinik yaklaşım becerisi sergilemek elzemdir. Bu nedenle, tıp eğitimi literatüründe, bu elzem becerisinin kazandırılması için klasik derslerle yüksek gerçeklikli simülasyon bazlı eğitimlerin kombine edilmesi önerilmektedir (6). Mental durum değişikliklerinin spektrumunu tanıyabilmek, bu spektrumun hayatı tehdit edici etyolojik nedenlerini değerlendirebilmek, etyolojik nedene ve klinik görünüme uygun şekilde hastayı yönetebilmek ve Acil Tıp öğrenenlerine, öğretim çıktılarıyla uyumlu eğitimlerle bu akademik becerileri edindirmek Acil Tıp uzmanlarının önündeki görevler olarak durmaktadır. Kaynaklar
1. Wolfe RE, Brown DFM. Coma and depressed level of consciousness. JA Marx, RS Hockberger, RM Walls, et al (eds.). Rosen's Emergency Medicine: Concepts and Clinical Practice (ed 5). Mosby, St Louis, MO (2002), pp. 137–144.
2. McCusker J, Cole M, Abrahamowicz M, Primeau F, Belzile E. Delirium predicts 12-month mortality. Arch Intern Med. 2002;162(4):457-63.
3. Wilber ST, Ondrejka JE. Altered Mental Status and Delirium. Emerg Med Clin North Am. 2016;34(3):649-65. 4. Stagno D, Gibson C, Breitbart W. The delirium subtypes: a review of prevalence, phenomenology, pathophysiology,
and treatment response. Palliat Support Care. 2004;2(2):171-9. 5. Sperling JD, Clark S, Kang Y. Teaching medical students a clinical approach to altered mental status: simulation
enhances traditional curriculum. Med. Educ. Online. 2013; 18:19975- http://dx.doi.org/10.3402/meo.v18i0.19775.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
88
ERİŞKİNDE NÖBET VE STATUS EPİLEPTİKUS
Barış Murat Ayvacı
Okmeydanı Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Nöbet, beyin disfonksiyonu sonucu oluşan ani bir davranış değişikliği olarak tanımlanmaktadır. Nöbetler ilaç veya alkol
çekilmeleri gibi metabolik bozukluklardan kaynaklanabileceği gibi inme veya ensefalit gibi akut nörolojik bozukluklardan da kaynaklanabilirler. Epilepsi ise tanımı nitelik arzeden, serebral korteksteki nöronal ağların elektriksel hipersenkronizasyonu sonucu oluşmaktadır.
Epileptik Nöbet Nedenleri (1)
• Kafa travması • Beyin tümörleri • İnme • İntrakraniyal enfeksiyon • Serebral dejenerasyon • Konjenital beyin malformasyonları
Nöbete Neden Olan Metabolik Bozukluklar
• Alkol ve ilaç çekilmesi • İlaç intoksikasyonu • Hiponatremi, hipernatremi • Hipomagnezemi • Hipokalsemi • Hipoglisemi • Non ketotik hiperglisemi • Üremi • Hipoksi • Hipertroidizm • Porfiri • Diyaliz disequilibrium sendromu
Bu sebeplerle nöbet oluşumda altta yatan metabolik bozukluğun ciddiyetinden ziyade oluşum hızı ön plana çıkmaktadır. (2,3)
Adolesan ve Genç Erişkinlerde Epilepsiyi Taklit Eden Durumlar
• Senkop • Psikolojik bozukluklar • Uyku bozuklukları • Migren
Çoğu nöbet iki dakika içinde kendiliğinden sonlanır. Bu nedenle hızlı bir benzodiazepin uygulamasının gereği yoktur ancak yine de nöbetin daha da uzun seyretmesi durumunda ilaçların uygulanabilmesi için intravenöz yol mutlaka sağlanmalıdır. Tedavi nöbeti oluşturan altta yatan nedene bağlı olmalıdır. Nöbet önleyici ilaç seçimi hastanın mevcut komorbiditelerine, kullandığı diğer ilaçlara, nöbetinin tipine, yaş ve cinsiyetine ve maliyete göre karar verilmelidir. Yatış uzayan postiktal durumun veya tam olmayan düzelmenin eşlik ettiği ilk nöbet hastalarında düşünülmelidir.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
89
STATUS EPİLEPTİKUS Status epileptikusu tanımlamak için kullanılan devam eden nöbet aktivite süresi zaman içinde farklılık göstermiştir.
Tarihte International League Against Epilepsy (ILAE) status epileptikusu 30 dakikadan uzun süren tek bir epileptik nöbet veya 30 dakikalık bir süre zarfında iktal dönemler arsında fonksiyonun sağlanamadığı tekrarlayan epileptik nöbetler olarak tanımlamıştır(4). Ancak 30 dakikalık bir süre generalize konvulzif status epileptikus tedavisi yönetiminde klinik pratik için uygun değildir ki birkaç dakikadan uzun süren nöbetlerde gecikme olmaksızın tedavi başlanılmalıdır.
2015 yılında ILAE status epileptikus için iki süreyi içeren bir tanımlama yayınladı :
• Status epileptikus nöbet sonlanımından sorumlu mekanizmaların yetersizliği veya anormal olarak uzayan nöbetlere yol açan mekanizmaların başlatılması sonucu oluşan bir durumdur (zaman noktası t1 sonrası ).
• Status epileptikus nöbetlerin süre ve tipine bağlı olarak nöronal ölüm, nöronal yaralanma ve nöronal ağlarda bozulmayı da içeren uzun dönem sonuçlara sahip bir durumdur (zaman noktası t2 sonrası ).
Generalize konvulzif status epileptikus için ILAE t1:5 t2:30 dakika olarak tanımlamaktadır(5). Fokal ve absans status epileptikuslar için bu süreler farklıdır. Tedavi iv benzodiazepinler ve rekürrens için benzodiazepin olmayan bir nöbet ilacının tedaviye eklenmesi ile sağlanmalıdır.
KAYNAKLAR
1. Schachter SC. Iatrogenic seizures. Neurol Clin 1998; 16:157. 2. Beghi E, Carpio A, Forsgren L, et al. Recommendation for a definition of acute symptomatic seizure. Epilepsia 2010;
51:671. 3. Riggs JE. Neurologic manifestations of electrolyte disturbances. Neurol Clin 2002; 20:227. 4. Guidelines for epidemiologic studies on epilepsy. Commission on Epidemiology and Prognosis, International League
Against Epilepsy. Epilepsia 1993; 34:592. 5. Trinka E, Cock H, Hesdorffer D, et al. A definition and classification of status epilepticus--Report of the ILAE Task
Force on Classification of Status Epilepticus. Epilepsia 2015; 56:1515.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
90
BİR ACİL TIP UZMANI HEMOLİTİK ANEMİ HAKKINDA NE BİLMELİDİR?
Zeynep Karakaya
İzmir Katip Çelebi Üniversitesi, Atatürk Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İzmir HEMOLİTİK ANEMİLER Normal şartlarda kırmızı kan hücrelerinin (RBC) ömrü 120 gündür ve mononükleer fagositik sistem aracılığı ile yıkılır(1). Hemolitik anemiler RBC lerin erken yıkımı olarak tanımlanır(2). Acil tıp hekimi için en önemli kaygı Hayatı tehdit eden komplikasyonlara hızla yol açabilen akut hemolitik anemileri tanımaktır(3). Anamnez ve periferik yayma hemolizi tanımada anahtar rol oynar. Hemolitik anemiler konjenital ve edinilmiş olarak ve RBC lerin yıkım yerine göre ise; extravasküler ve intravasküler olarak ikiye ayrılır. İntravasküler hemoliz hem daha akut hem de daha yıkıcı bir seyir gösterir(4,5). A.Extravasküler Hemoliz Extravasküler hemoliz olabilmesi için eritrosit membranına bağlı antikorun olması veya eritrosit deformabilitesini etkileyen bazı fiziksel faktörlerin olması gerekir. Laboratuar: Eritrositler esas olarak dalak ve/veya Karaciğerde bulunan Makrofajlar’lar tarafından fagosite edilirler ve parçalanırlar. Haptoglobulin düşer, hemoglobinüri ve hemosiderinüri beklenmez. Serum LDH ve İndirek Bilüribin yüksektir. Klinik: Sarılık,Splenomegali, Hemolitik-aplastik krizler,Kolelitiazis, Bacak ülserleri, Kemik anormallikleri olabilir. B. İntravasküler Hemoliz Eritrositlerin travmayla( prostetik kapak), eritrositlere kompleman bağlanması (immün hemolitik anemi ve ortamda bulunan ekzojen toksik faktörlerin (bakteri toksini) saldırısına uğraması sonucu oluşur. Acil Serviste Kaçırılmaması Gereken Hemolitik Anemiler
1. Mikroanjiopatik Hemolitik Anemiler(MAHA) a. DIC, HELLP b. TTP c. HÜS d. Malign Hipertansiyona bağlı hemoliz
2. Otoimmün Hemolitik Anemiler(OİHA) a. Sıcak aracılı (IgG ) OİHA b. Soğuk aracılı(IgM) OİHA
1.Mikroanjiopatik Hemolitik Anemiler(MAHA) 1a. Dzssemzne İnravasküler Koagülasyon DÖssemÖne Önravasküler koagülasyon , tromboz ve kanamalarla seyreden sÖstemÖk bÖr olaydır. KlÖnÖk bulguların çoğu beklenmeyen aşırı trombÖn oluşumu nedenÖyledÖr.
DÖssemÖne Öntravasküler koagülasyonda ana tedavÖ prensÖbÖ; trombÖn jenerasyonunu arttıran ve alta yatan nedenÖ bulmaya odaklanma şeklÖnde olmalıdır. Ancak, altta yatan nedenÖ kolayca bulup ortaya çıkarmak her zaman mümkün olamadığından veya bu süreç uzun zaman alacağın- dan, kanama ve tromboz döngüsünü de hemen kırma zorunluluğu vardır.
1b.Trombotik Trombositipenik Purpura
MAHA, Trombositopeni, Üremi, Nörolojik bulgular, Ateş klasik pentadını oluşturur. İntravasküler hemolÖzÖn laboratuar bulgularına eşlÖk eden trombosÖtopenÖ ve çevresel kanda parçalanmış erÖtrosÖt varlığı (şÖstosÖt) aksi kanıtlanana kadar TTP kabul edilmelidir. ADAMTS13 aktivitesinin belirlenmesi tedavi kararını vermek için gereklÖ değÖldÖr. TTP’de prognoza etkÖsÖ gösterÖlen başlıca tedavÖ yöntemÖ plazma değÖşÖmÖdÖr (PD). KortÖkosteroÖd tedavÖsÖnÖn gereklÖlÖğÖne karar verÖrken hastalığın şÖddetÖ dÖkkate alınmalıdır TrombosÖt transfüzyonu sadece hayatı tehdÖt eden kanama varlığında endÖkedÖr. 1c. Hemolitik Üremik Sendrom MAHA,Üremi, Trombositopeni klasik tiradıdır. <10 y çocuklarda ABY nin en sık nedenlerindendir. Diare ile ilişkili tipik HÜS de shiga toxin %90 sebeptir. İshalde antibiyotik kullanımı ve antiperistaltik ilaçlar kontrendikedir. Atipik HÜS nedenleri arasında Strep. Pnömonia, genetik hastalıklar, malignensiler saayılabilir. %90 akut fazda iyileşir, böbrek fonksiyonları düzelir. Atipik HÜS seyri daha yıkıcıdır. Atipik HÜS de plazmaferez ve eculizumab kullanılabilir. 1d. Malign Hipertansiyona bağlı Hemolitik Anemi Kan Basıncı yüksekliği, Trombositopeni, mikroanjiopatik hemolitik anemi, Papill ödemi ensefalopati ve böbrek yetmezliği ile karekterizedir. Tedavisinde tansiyon regülasyonu esastır.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
91
2. Otoimmun Hemolitik Anemi Hastanın kendi eritrosit antijenlerine karşı antikor üretmesi ve bunun sonucunda eritrositlerin yıkılmasıdır. IgG ve IgM tipinde iki grup antikor tarafından oluşturulabilir. 2a. Sıcak Aracılı Hemolitik Anemi Ig G bağımlıdır. Bu tür, OİHA’nin en sık türü olup (%70-80), eritrositler dalakta sekestre olmaktadır. Hemoliz ekstravasküler alanda gerçekleşir. Spenomegalinin(%80) yanısıra HM(%45) ve LAP’da(%35) saptanabilir. Sarılık, solukluk, abdominal ağrı ve ateş görülür. Tedavide RBC transfüzyonu hayatı tehdit eden anemi ve/veya iskemi varsa düşünülebilir. Kortikosteroid hemen başlanmalıdır. Sonuç Acil tıp hekiminin amacı, çok hızlı ve mortal bir şekilde klinisyenin karşısına çıkabilen Hemolitik anemileri tanımak ve doğru yönetimini sağlamaktır. Kaynaklar
1. Bunn HF, Rosse W. Harrison’s Internal Medicine. 16th Ed. New York: McGraw Hill; c2005. Hemolytic anemias and acute blood loss; p. 607-617.
2. Ucar K. Clinical presentation and management of hemolytic anemias. Oncology 2002; 16 (9, Suppl 10): 163-70. 3. Hamilton GC, Janz TG. Anemia, polycythemia, and white blood cell disorders. 5th ed. Saint Louis: Elsevier Mosby,
c2002. P. 1665-87. (Marx JA, editor-in-chief. Rosen’s Emergency Medicine; vol. 2.) 4. Gehrs BC, Friedberg RC. Autoimmune hemolytic anemia. Am J Hematol 2002; 69: 258-71. 5. Wada H, Matsumoto T, Yamashita Y. Diagnosis and treatment of disseminated intravascular coagulation (DIC)
according to four DIC guidelines. J Intensive Care 2014;2:15. 6. Ulusal TedavÖ RehberÖ 2011 Trombotı̇k Trombosı̇topenı̇k Purpura Tanı Ve Tedavı̇ Kılavuzu

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
92
ANEMİYE YAKLAŞIM
Taylan Kılıç
Antalya Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Antalya
Anemi kan hemoglobin düzeyinin yaş, cinsiyet ve ırklara göre belirlenen standart değerlerin altında olmasıdır. Anemiye yaklaşım ve anemi ayırıcı tanısı için kullanılan en sık algoritma morfolojik yaklaşım algoritması olup çoğunlukla altta yatan primer anemi tanısının aydınlatılması için kullanılmaktadır. Fakat hasta yoğunluğu, ileri yaş, multiple ilaç kullanımı ve komorbid durumlar ile GİS kanama gibi hayatı tehdit eden birçok farklı klinik durumun aynı anda bulunması gibi hasta özellikleri nedeniyle bu yaklaşımın acil servislerde kullanılması pek pratik değildir. Bu hastalarda öncelikli olarak altta yatan bir kanamanın varlığı, acil serviste kan transfüzyonu gerekliliği ve hastaneye yatırılarak acil tedavi gerektiren kritik hastaların belirlenmesi acil servislerde cevaplanması gereken sorulardır. Bu sunum ile anemi etiyolojisi ve patofizyolojisinin anlaşılması, anemi ayırıcı tanısının yapılabilmesi, kanaması olan hastaların saptanabilmesi ve kanama ipuçları, acil serviste transfüzyon gerektiren hastaların belirlenmesi ve transfüzyon eşikleri ile acil tedavi gerektiren ve hastaneye yatırılması gereken hastaların belirlenmesi amaçlanmaktadır. Kaynaklar:
1. Tintinalli JE, Stapczynski JS, Ma OJM, Yealy DM, Mekler GD, Cline DM. Emergency Medicine: A Comprehensive Study Guide. 8th ed. USA: The McGraw-Hill Companies; 2016.p.1483-6.
2. Schrier SL, Mentzer WC, Tirnauer JS. 2016. Approach to the adult patient with anemia. [ONLINE] Available at: http://www.uptodate.com/contents/approach-to-the-adult-patient-with-anemia. [Accessed 22 September 2016].
3. Carson JL, Kleinman S, Silvergleid AJ, Tirnauer JS. 2016. Indications and hemoglobin thresholds for red blood cell transfusion in the adult. [ONLINE] Available at: http://www.uptodate.com/contents/indications-and-hemoglobin-thresholds-for-red-blood-cell-transfusion-in-the-adult. [Accessed 22 September 2016].
4. Janz TG, Johnson RL, Rubenstein SD. Anemia In The Emergency Department: Evaluation And Treatment. Emerg Med Pract. 2013:15(11);1-15.
5. Holst LB, Petersen MW, Haase N, Perner A, Wetterslev J. Restrictive versus liberal transfusion strategy for red blood cell transfusion: systematic review of randomised trials with meta-analysis and trial sequential analysis. BMJ. 2015;350:h1354.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
93
İMMUNSUPRESİF ATEŞLİ HASTAYA YAKLAŞIM
Onur Karakayalı
Kocaeli Derince Eğitim Ve Araştırma Hastanesi, Acil Tıp Kliniği, Kocaeli
Bir birey kendisine veya çevresine ait birtakım faktörlerin etkisiyle enfeksiyonlara açık bir konak haline geçebilir. Özellikle son ÖkÖ dekatta tıp alanındakÖ gelÖşmelerÖn paralelÖnde bÖrçok hastalığın tedavÖsÖnde Ölerlemeler kaydedÖlmÖş ve hastaların yaşam süresÖ uzatılmış, ancak bu hastaların tıbbÖ tedavÖ uygulamaları nedenÖyle vücut savunmaları bozulduğundan, enfeksÖyonlara yatkın hale gelmÖşlerdÖr.İmmünsüpresÖf konak olarak tanımladığımız hasta grupları; nötropenÖ, transplantasyon (solÖd organ transplatasyonu, kemÖk ÖlÖğÖ transplantasyonu, perÖferÖk kök hücre transplantasyonu), AIDS, uç yaşlar (yenÖdoğan dönemÖ, yaşlılık dönemÖ), travma, yanık, dÖyabet, alkolÖzm, sÖroz, splenektomÖ, IV uyuşturucu kullanımı ve kronÖk böbrek yetmezlÖğÖ olanlardan oluşmaktadır.(1)TarÖhsel olarak ÖmmunsupresÖf hasta gruplarında en sık gram (-) bakteriler (E.coli,Klebsiella pneumoniae,pseudomonas aureginosa) etken olarak olarak görünsede günümüzde sefalosporin ve penisilin grubu antibiyotiklere hızlı direnç kazanan enterobakteriler ve gram (+) bakterilere sekonder enfeksiyon sıklıklarında artış görünmektedir.(2) Uzamış nötropeni süresi,KT kür sayısında artIş ve önceki antibiyotik kullanım varlığında yüksek riskli hastalarda fungal enfeksiyon riski artmaktadır.
İmmunsupresif hasta yönetiminde lokal protokol ve algoritm yokluğu,klinisyenlerin farkındalığının azlığı,uygun ve izole alanların yokluğu,ilk doz antibiyotik uygulamalarındaki gecikmeler,kılavuz dışı antibiyotik kullanımı karşılaşılan kurumsal ve klinik sorunlardır. Klinik bakıda en sık karşılaşılan kemoterapi sonrasında nötropenik ateş ile başvuran hasta grubudur. Bu hasta gruplarında ateş sadece enfeksiyonun tek bulgusu olabilir.İmmunsupresif hasta gruplarında enfeksiyon progresif ve hayatı tehdit edici düzeyde olduğu için tüm klinisyenler tarafından hasta yönetimi kılavuzlar ışığında hızlı ve etkin biçimde yapılmalıdır.
İmmunsupresif ateşli hasta acil servis yönetiminin temel basamakları erken tanı,erken resusitasyon,tanı ile eş zamanlı hızlı ampirik antibiyoyerapi ve kılavuz uyumlu bakımdır. Anamnezde organ spesifik semptomlar,antimikrobiyal profilaksi öyküsü,risk sınıflaması için komorbiteler ve enfeksiyon dışı ateş nedenleri (kan transfüzyon,pulmoner emboli) sorgulanmalıdır. Kapsamlı fizik muayene yapılmalı,özellikle primer tümörün olduğu sistem ayrıntılı değerlendirilmelidir.Rektal tuşe mukozal iritasyon nedeniyle yeni enfeksiyon odağı olabileceğinden önerilmemektedir. (3) (IDSA) Ateş özellikle nötropenik hasta grubunda tek seferde >38.3°C (101°F) yada 1 saatin üzerinde >38.0°C (100.4°F) olarak ölçülmesidir. Aynı kılavuzda risk skorlaması için hastalardan CBC,kan üre,kreatin,serum elektrolit,hepatik transaminaz ve total bilurubin düzeyleri istenmeli (A-III) en az iki set kan kültürü ve idrar kültürü (A-III) önerilmektedir. (4) Hospitalizasyon yada ayaktan tedavi kararı,antibiyoterapinin süresinin ve uygulama yolunun belirlenmesi amaçlı risk skorlamaları yapılmalıdır. ESMO,IDSA ve ASCO tarafından risk skoru olarak MASSC skorunun kullanılması önerilmektedir. (4,5,6) MASSC skoru 21 ve üstü olan hastalar düşük risk, 21’in altında puan alanlar yüksek risk kabul edilmektedir.IDSA kılavuzuna göre nötropenik hastalarda 7 günden uzun nötropeni süresi,derin
nötropeni (ANC<100 h/ mm3) (4) , ve/veya medikal komorbidite (hipotansiyon,pnomoni,yeni başlangıçlı karın ağrısı yada nörolojik değişiklikler) varlığını yüksek risk olarak kabul etmektedir. Tedavinin en önemli basamağı erken dönem ampirik antibiyotik başlanılmasıdır. Kılavuzlarda başvuru anından itibaren ilk 60 dakika içerisinde antibiyotik tedavisi önerilmekte (7) iken bazı araştırmacılar ilk 30 dk içerisinde uygulanmasını önermektedir. (8). 2014;58(7):3799 Ortak düşünce mümkün olduğu en kısa sürede verilmesidir. Nötropeni varlığında kılavuz IDSA kılavuzu tarafından cefepime,karbapenem,piperasilin tazobactam önerilmektedir.(A-I)Antimikrobial direnç şüphesi yada komplikasyon (hipotansiyon ve pnomoni) varlığında aminoglikosid,florokinolon ve/veya vankomisin tercih edilebilinir. Vankomisin febril nötropeni varlığında ilk basamak tedavide önerilmemektedir. (A-I) Düşük riskli hastalarda oral tedavide siprofiloksasin ve amoksisilin-klavulonat kombinasyonu önerilmektedir.(A-I) Florokinolon profilaksi alan hastalarda tedavide florokinolon önerilmemektedir. (A-III) Antibiyoterapiye ANC>
500 cells/mm3 olana kadar devam edilmelidir. (B-III) Standart tedaviye Granulosit koloni stimule edici faktör eklenmesinde total mortalite farkı bulunmamakta ancak daha kısa hospitalizasyon,nötropeni süresi ve daha az antibiyotik kullanımı sonuçlarına varılmıştır. ASCO düşük riskli hastaların ilk doz antibiyotik sonrasında 4 saatlik gözlem ile taburcu edilebileceğini önerirken ESMO 24 saat gözlem sonrası taburculuk önermektedir. Yüksek riskli hastalar, sosyal bakımı iyi olmayan,evde takibi ile ilgili klinik şüphe durumunda yatarak tedavi önerilmektedir. (5,6)
Referanslar;
1) Özsüt H, Karadeniz H. (2007). What is the immunosupresive host. İmmunsupreif Hastalarda Enfeksiyon Özel sayısı,3.Cilt, Sy 1-20. 2016, Türkiye Klinikleri.
2) John r Wingard, MD. (2016) Treatment of neutropenic fever syndromes in adults with hematologic malignancies and hematopoietic cell transplant recipients (high-risk patients), (2016) www.uptodate.com
3) John R Wingard, MD (2015). Diagnostic approach to the adult presenting with neutropenic fever (2016) www.uptodate.com 4) Alison G. Freifeld, Eric J. Bow, Kent A. Sepkowitz, et all. Clinical Practice Guideline for the Use of Antimicrobial Agents in
Neutropenic Patients with Cancer: 2010 Update by the Infectious Diseases Society of America. CID 2011:52 5) J. Klastersky, J. de Naurois, K. Rolston, B. Rapoport, G. Maschmeyer, M. Aapro and J. Herrstedt. Management of Febrile
Neutropaenia: ESMO Clinical Practice Guidelines. Ann Oncol (2016) 27 (suppl 5): v111-v118 6) Christopher R. Flowers, Jerome Seidenfeld, Eric J. Bow, et all. Antimicrobial Prophylaxis and Outpatient Management of
Fever and Neutropenia in Adults Treated for Malignancy: American Society of Clinical Oncology Clinical Practice Guideline. American Society of Clinical Oncology. 2013
7) Bell MS, Scullen P, McParlan D, et al. Neutropenic sepsis guidelines. Northern Ireland Cancer Network, Belfast 2010. p. 1-11
8) Rosa RG, Goldani LZ. Cohort study of the impact of time to antibiotic administration on mortality in patients with febrile neutropenia, Antimicrob Agents Chemother. 2014 Jul;58(7):3799-803. doi: 10.1128/AAC.02561-14. Epub 2014 Apr 21

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
94
ÖNÜMÜZDEKİ 20 YIL EN ÇOK KİMİ TEDAVİ EDECEĞİZ: YAŞLI KRİTİK HASTA
Serkan Doğan
Kanuni Sultan Süleyman Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Dünya sağlık örgütü yaşlı bireyleri yaş sınırları ile gruplandırmıştır. Buna göre 45-64 yaş aralığını orta yaş, 65-74 yaş aralığını erken yaşlılık, 75-84 yaş aralığını orta yaşlılık ve 85 yaş üzerini ileri yaşlılık(ihtiyarlık) olarak sınıflamıştır. Özet olarak yaşlı hasta 65 ve üzeri yaştaki hastalardır. Hem ülkemizde hem de dünyada yaşlı nüfusun artışı ile birlikte tüm acil servis başvurularının içinde yaşlı popülasyon payı artmaktadır. Dünyadaki yaşlı bireylerin sayısı dünya sağlık örgütüne göre 1998 de 580 milyon iken 2050 yılında 1.97 milyara ulaşacağı veya başka bir deyişle 2015 ve 2050 yılları arasında yaşlı nüfus oranının %12 den %22 ye çıkacağı öngörülmektedir(1). Ülkemizde ise yaşlı nüfus oranı TUİK verilerine göre 2008 yılında %6.8 iken 2015 de %8.2 olup 2025 de %9 ları geçeceği öngörülmektedir(2). Yaşlılık döneminde organ sistemlerinde önemli fizyolojik değişiklikler meydana gelir. Fonksiyonel kapasitede azalmalar görülür. Günlük yaşam faaliyetlerinde azalmalar ve kısıtlılıklar sıktır. Hastalıklar normal seyrinden farklı olarak sık ve atipik şekilde görülür. Özellikle yaşlı hastalarda çoklu patoloji ve polifarmasi vardır. Bir başka açıdan bakıldığında ise yaşlılık dönemi psikolojik, sosyoekonomik, ailesel ve toplum sağlığı açısından farklı ve sorunlu olabilecek bir yaş grubudur(3). Yaşlı hastaların acil servisleri kullanım sıklığına baktığımızda gençlere oranla ambulans hizmetlerinden ve acil servislerinden daha fazla yararlandıkları, acil servislerde daha uzun süre kaldıkları ve yoğun bakım yatışlarının daha fazla olduğu gözlenmektedir. Acil servisler yaşlı hastaların gelişmiş bakımlarında önemli bir rol oynamaktadır. Yaşlı hastaların acil servislere başvuru nedenleri incelendiğinde ise dünyada en sık ilk 3 neden serebrovasküler, kanser ve kardiyak sorunlar oluşturmaktadır(4). Ülkemizde ise ilk 3 neden metabolik/sistemik hastalıklar, kardiovasküler ve serebrovasküler sorunlar oluşturur. Acil servislere başvuran yaşlı hastaların değerlendirilmeleri kapsamlı bir yaklaşım gerektirir. Amaç yaşlı hastaların fonksiyonlarını korumak ve daha iyi bir yaşam kalitesi ile beraber mümkün olan en üst sağlık düzeyine onları ulaştırabilmektir. Yaşlılardaki hastalıkların çeşitliliği ve atipik seyri her zaman göz ününde bulundurulmalıdır. Muayenede mental durum değişiklikleri, fonksiyonel kapasiteleri, travma, infeksiyonlar ve sistemik tüm hastalıklar irdelenmelidir. Yaşlı hastaların değerlendirmesi dikkat ve sabır isteyen bir süreçtir. Yaşa bağlı fizyolojik değişiklikler değerlendirmeyi zorlaştırabilir ve dikkate alınması gerekir. Polifarmasi mutlaka sorgulanmalıdır(5). Sonuç olarak yaşlı nüfus arttıkça acil servislerde tedavi edilen yaşlıların oranı artar. Yaşlı kritik hastalara acil servislerde verilen hizmetlerin doğal olarak olumsuz yanları da vardır. Yaşlı hastaların acil servislerde daha uzun kalışlara, daha fazla tetkik ve tedaviye, tekrarlayan acil servis başvurularına ve aşırı kalabalığa neden olacağı açıktır. Palyatif bakım merkezlerinin açılması ile bu önlenebilir. Son olarak; yaşlılık asla bir hastalık olmayıp hepimizin yaşayacağı yaşamın bir dönemidir. Kaynaklar:
1. World Health Organization: WHO/Ageing And Health september 2015. http://www.who.int/mediacentre/factsheets/fs404/en/.
2. TUİK. Türkiye İstatistik Kurumu, istatistiklerle yaşlılar, 2015. www.tuik.gov.tr. 3. B Yıldırım, S Özkahraman, S Ersoy. Yaşlılıkta Görülen Fizyolojik Değişiklikler ve Hemşirelik Bakımı. Düzce
Üniversitesi Sağlık Bilimleri Enstitüsü Dergisi 2012; 2 (2): 19-23 4. Hu SC, Yen D, Yu YC, Kao WF, Wang LM. Elderly use of the ED in an Asian metropolis. Am J Emerg Med
1999;17:95-99. 5. Geriatric Emergency Department Guidelines. Annals of Emergency Medicine, 2014.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
95
ACİL SERVİSTE YÜKSEK KAN ŞEKERİ OLAN HASTA
Mehmet Yiğit
Sağlık Bilimleri Üniversitesi, Haseki Eğitim ve Araştırma Hastanesi, Acil Tıp Anabilim Dalı, İstanbul
Diabetes Mellitus (DM), insülin eksikliği, insülin salgılanması ya da insülin etkisindeki defektler nedeniyle organizmanın karbonhidrat, yağ ve proteinlerden yeterince yararlanamadığı, sürekli tıbbi bakım gerektiren, hiperglisemi ile karakterize kronik, metabolik bir hastalık grubudur. Dünyada görülme sıklığı yetişkinlerde %8.8’dir. Ülkemizde de bu oran benzer olmakla birlikte 40 yaşın üzerinde % 10’nun üzerine çıkmaktadır. Hastanede yatan hastalarda DM sıklığı %12,4-25 arasındadır. Acil servis başvurularında da DM ve DM’ye bağlı sağlık sorunları ilk sıralarda yer almaktadır. DM komplikasyonlarından sorumlu ana faktör hiperglisemidir. DM komplikasyonları hayatı tehdit eden akut komplikasyonlar veya kronik komplikasyonlar olarak karşımıza çıkabilirler. DM’ye bağlı gelişen akut ve kronik komplikasyonlar önemli mortalite ve morbiditeye yol açarlar. Tüm tedavi yaklaşımları bu nedenle kan glukoz kontrolü üzerine odaklanmıştır. Acil servise kan şekeri yüksekliği ile başvuran ya da acil serviste kan şekeri yüksekliği saptanan hastalar basitçe iki grupta incelenebilir:
1) Hiperglisemik Aciller; DM’nin hiperglisemik acil durumları üç ana başlık altında incelenebilir. A. Diyabetik ketoasidoz (DKA). B. Hiperozmolar hiperglisemik durum (HHD). C. Laktik asidoz. Diyabetik ketoasidoz ve HHD, insülin eksikliği ve ağır hiperglisemi sonucu ortaya çıkan, patogenez ve tedavisi büyük
ölçüde benzeşen, iki önemli metabolik bozukluktur. DKA’da ön plandaki sorun insülin eksikliği iken HHD’de ise dehidratasyondur. Aslında DKA ve HHD, patogenez olarak aynı klinik tablonun iki farklı ucunu oluşturur. Oluşum mekanizması hemen hemen aynıdır. DKA’da mutlak insülin eksikliği nedeniyle lipoliz baskılanamaz, ketonemi ve ketonüri olur. Halbuki, HHD’de az miktarda insülinin bulunması lipolizi baskılamak için yeterli olduğundan, keton cisimlerinin oluşumu gerçekleşmez.
Laktik asidoz, ise daha seyrek görülen, ancak özellikle DM’ye eşlik eden diğer ciddi (kardiyak, renal, serebral vb) sağlık sorunları nedeniyle mortalitesi oldukça yüksek olan bir tablodur. Laktik asidoz kanda laktat konsantrasyonunun arttığı durumlarda görülen anyon açıklı bir asidoz durumudur. Genellikle altta yatan ciddi bir hastalığı bulunanlarda görülen ve dokulara oksijen dağılımı ve kullanımının yetersizliğinden kaynaklanan ağır bir metabolik asidoz biçimidir. Laktik asit birikimi laktat yapımı ile kullanımı arasındaki dengenin bozulduğuna işaret eder.
2) Acil Servise Anormal Yüksek Glukoz Değeri ile Başvuran Hastalar: A. Yeni başlangıçlı hiperglisemi/Tanı konulmamış DM. B. Önceden tanı almış DM. C. Şiddetli hiperglisemi. D. Glikokortikoid-ilişkili DM. E. Pankreatit. F. Pankreatik kanser.
G. Hipertiroidizm.
H. İlaçlar. I. Stres. İ. Hayatı tehdit eden hastalıklar (Miyokard enfarktüsü, inme). J. Yanlış kapiller glukoz yüksekliği.
Acil servise kan şekeri yüksekliği ile başvuran ya da acil serviste kan şekeri yüksekliği saptanan hastalar hiperglisemik aciller açısından acil tıp hekimince dikkatlice muayene edilmelidirler. Tanı, takip ve tedavideki tüm gelişmelere rağmen hiperglisemik aciller ciddi morbidite ve mortaliteye (%2-42) neden olabilmektedirler. Ayrıca acil tıp hekimleri acil servise anormal yüksek glukoz değeri ile başvuran hastaya, maksimum özen göstererek bu hastanın potansiyel bir hiperglisemik acil adayı olabileceğini unutmamalıdırlar.
Kaynaklar 1. Tintinalli JE, Stapczynski JS, Ma OJ, Cline DM, Cydulka RK, Meckler GD, Tintinalli Acil Tıp, Kapsamlı Bir Çalışma Kılavuzu, 7. Baskı , Y. Çete, A. Denizbaşı, AA. Çevik, C. Oktay, R. Atilla (Editörler), Kısım 17, Endokrin Aciller, Bölüm 218, Tip 1 Diabetes Mellitus, ss. 1415-9. (Çevirmen, A. Yürüktümen), Nobel matbaacılık, İstanbul (2013) 2. Abrahamson M, Barzilay JI, Blonde L, et al. AACE/ACE Comprehensive Diabetes Management Algorithm 2015. Endocr Pract 2015;21:e1-e10. 3. American Diabetes Association. Position Statement. Hyperglycemic crises in diabetes. Diabetes Care 2004;27(Suppl.1):S94-S102. 4. American Diabetes Association. Position Statement. Diagnosis and classification of diabetes mellitus. Diabetes Care 2014;37(Suppl. 1): S81-S90. 5. Diabetes Mellitus Çalışma ve Eğitim Grubu. Diabetes mellitus ve komplikasyonlarının tanı, tedavi ve izlem kılavuzu-2016, ss. 15-203 (2016). Türkiye Endokrinoloji ve Metabolizma Derneği İktisadi İşletmesi -2016. ISBN: 978-605-66410-0-8.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
96
REVERSING THE EFFECTS OF ANTICOAGULANTS
Arzu Denizbaşı
Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey
Emergency Department visits may frequently be as a result of the patients with adverse effects of anticoagulant. The mainstay of the anticoagulant therapy is to decrease the potential risk of the morbidity and mortality in cardiovascular patients. As a result; traditional drugs, namely Warfarin, and new generation direct oral anticoagulant drugs are widely used all over the world to decrease the cardiovascular risks in patients. Since death due to the cardiovascular risk factors is the leading concern, we assume that these drugs will be in our practice with our without their adverse effects. The patients present to the emergency services either after ingestion of these tablets for suicidal purposes or as a result of the everyday drug usage. In each of these circumstances, the therapy algorythyms are similar, and the main scheme is to control fatal bleeding episodes. Overview of the supportive management: If a patient presents with a serious bleeding or with a clinical indication that such a bleeding will soon occur; then he should be managed in a critical care unit where he can have an appropriate hemodynamic support. With closing monitoring such patients may survive the anticoagulant state they are in. Laboratory tests are helpful in monitoring the patients and abnormal coagulation testing is consistent with the presence of continued anticoagulant effect. However; normal testing does not necessarily eliminate the possibility of clinically important concentrations of these new agents. Therefore, the results of coagulation tests do not meaningfully inform reversal of direct oral anticoagulant associated bleeding.Supportive therapy consists of close clinical observation; decontamination of the drug; removal of the drug with activated charcoal; elimination with hemodialysis or hemoperfusion ; and active interventions by using antifibrinolytic agents or prothrombotic clotting factor products. Team approach of appropriate specialists is vital for definitive interventions for the bleeding patients. This may be especially significant when reversing the anticoagulant therapy in patients with high risks of thromboembolism. If the patient has a gastrointestinal bleeding, consulting endoscopist should be considered immediately. Overview of reversal therapy: Reversal of anticoagulation is generally thought to be desirable in a patient with serious or life-threatening bleeding who remains actively anticoagulated, although randomized trial data to support this practice are lacking. In the traditional Warfarin overdose therapy, Vitamin K analogues is still the best antidote to be used. There are many references supporting the usage and the dosage of Vitamin K analogues. However, in the new generation anticoagulants, a reversal agent is available only for dagibatran, namely Idarucizumab. Idarucizumab is only used for the reversal of dagibatran, and the anticoagulant effect of oral direct factor Xa inhibitors cannot be reversed by any specific drug. Remaining strategies after decontamination for reversing the anticoagulant effect of direct oral anticoagulant agents include pro-hemostatic therapies such as antifibrinolytic agents and DDAVP; Prothrombin complex concentrates which is a controversial technique considering the patient risks. These agents are only used for life threatening bleeding conditions because the efficacy of prothrombin complex concentrates has not been validated in prospective clinical trials. Available data consist largely of non-bleeding volunteers, case reports, and preclinical models .Since there is no data to support the use of these products, recombinant activated factor VII (rFVIIa), Fresh Frozen Plasma (FFP), or cryoprecipitate are not used in direct oral anticoagulant associated bleeding. FFP is used to treat comorbidity such as coagulopathy. References
1. Barnes GD, Ageno W, Ansell J, et al. Recommendation on the nomenclature for oral anticoagulants: communication from the SSC of the ISTH. J Thromb Haemost 2015; 13:1154. 2. Chai-Adisaksopha C, Hillis C, Isayama T, et al. Mortality outcomes in patients receiving direct oral anticoagulants: a systematic review and meta-analysis of randomized controlled trials. J Thromb Haemost 2015; 13:2012. 3. Kakkos SK, Kirkilesis GI, Tsolakis IA. Editor's Choice - efficacy and safety of the new oral anticoagulants dabigatran, rivaroxaban, apixaban, and edoxaban in the treatment and secondary prevention of venous thromboembolism: a systematic review and meta-analysis of phase III trials. Eur J Vasc Endovasc Surg 2014; 48:565. 4. Majeed A, Hwang HG, Connolly SJ, et al. Management and outcomes of major bleeding during treatment with dabigatran or warfarin. Circulation 2013; 128:2325.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
97
DECISION-MAKING BETWEEN PLANE (FIXED-WING) AND HELICOPTER (ROTOR-WING) TRANSPORT IN CRITICALLY ILL PATIENT: EMAT PRELIMINARY NATIONAL AIR MEDICAL TRANSPORT STATEMENT
Yahya Ayhan Acar
Gulhane Training and Research Hospital, Department of Emergency Medicine, Ankara, Turkey
Critically ill patient transports are mainly interfacility transports rather than scene to facility. Major adverse events can happen during interfacility transfer of critically ill and mechanically ventilated patients by air ambulance due to different environmental conditions. Emergency physicians have important role in the management of the patients in all phaes including inter-facility transport. However, they are very experienced in the ground transport of the patients, air transport can be challenging. Medical considerations for air medical transport are hypobarism, cold environment, vibration, night conditions, motion sickness, distance, limited space, strict aviation rules, and difficulties in adequate monitoring. They are associated for both fixed and rotor wing transports, but in planning phase of the air medical transport, primary physician must be avare of pros and cons for aircrafts. Besides medical considerations, air medical transport has specific official and economic concerns. Modern air medical transport system in Turkey include both rotor and fixed wing aircrafts and showed a great progress in the last decade. However, in the selection of transport mode, according to current legislation, main determinant is the time and current legislation seems to be needed improvement. To form standards for national system in the light of scientific information and update the current official regulations worth the effort. In this regard, Air Medical Transport Study Group was founded within the scope of EMAT to contribute Turkish air medical transport system by means of introducing new projects, conducting scientific researchs, giving speeches and seminars, and offering legal arrangements. In this talk, we will discuss especially major concerns about air transport of critically ill patients. Additionally, we will analyze strengths and weaknesses of national air medical transport system. Finally, as the EMAT Air Medical Transport Study Group, we will introduce preliminary national air medical transport statement.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
98
AIR AMBULANCE SYSTEM IN UK, TRAINING ALTERNATIVES AND CERTIFICATION FOR AIR AMBULANCE HEALTHCARE STAFF
Mark Forth
Anaesthetics and Intensive Care Registrar Level Doctor and current Flight Doctor, Capital Air Ambulance Ltd., UK
According to recorded history, the very first British aeromedical evacuation actually took place in Turkey during the first world war. A wounded soldier was transferred to a nearby hospital in a de Havilland DH.9 aircraft saving a very long land journey which would have likely cost the soldier his life. The British aeromedical world has come a long way since those times, from both the medical and aviation perspectives. In fact it is hard to know which of those fields has changed more with the advent of revolutionary technological advances transforming both aviation and medical practise. However, the fundamental vision remains – the safe and prompt movement of a patient, whether it be for emergency, life-saving medical intervention or simply to bring them home. During my brief lecture, I would like to illustrate the current structure and capability of aeromedical services within the United Kingdom, from first response helicopter work to the movement of patients internationally using large fixed wing aircraft. I would also like to explain our system of recruitment and training within these services, service standards, and importantly some of the limitations to our practise. In short, one could perhaps divide the aeromedical industry in the UK into distinct ‘front line’ services and commercial repatriation companies, although with the nature of the work there is often some crossover. The former is the domain of a large number of helicopter based, emergency air ambulance services (known as HEMS). These organisations support local ambulance services on the ground and are generally charitably funded, at least in England and Wales. At the time of writing there are 24 such organisations in operation. The UK has far fewer commercial repatriation companies, which is perhaps surprising given the undoubted growth of this industry over the past several years. This is a reflection of how difficult it can be to make such a service commercially viable given the huge costs and expertise needed for such an enterprise. The largest private UK provider of aeromedical services is Capital Air Ambulance, based on the South coast of England in the city of Exeter. They fly around 700 air ambulance missions per year with patients requiring anything from simple nursing care to level 3 intensive care support. Their model is a successful one, and is also one with which I am personally most familiar given that I am currently a full time employee! The routes of entry and training for personnel in the aeromedical sphere in the UK are perhaps less well defined and regulated than one might imagine for a field that requires a large degree of specific knowledge and expertise. However, training courses and qualifications in this area do exist and further training is completed ‘in-house’. My knowledge of the aeromedical industry in Turkey is sadly somewhat limited. However, I hope that my contribution will throw up some interesting similarities and also differences in how our countries solve this fascinating problem of aeromedical repatriation. References: Dr Terry Martin Consultant Intensive Care and Aerospace Medicine Medical Director at Capital Air Ambulance Email: [email protected] Tel: 01392 350020 Mr Malcolm Humphries Managing Director and Chief pilot at Capital Air Ambulance Email: [email protected] Tel: 01392 350020 Mrs Lisa Humphries Accountable Manager and Sales Director at Capital Air Ambulance Email: [email protected] Tel: 01392 350020 Dr Simon Rang Anaesthetics Consultant at QEQM Hospital, Margate, UK Email: [email protected]
Tel: Available via QEQM Hospital switchboard (01843 225544)
Dr Rini Poddar Anaesthetics Consultant at QEQM Hospital, Margate, UK Email: [email protected]
Tel: Available via QEQM Hospital switchboard (01843 225544)

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
99
DIFFICULTIES AND TIPS IN AIR MEDICAL TRANSPORT: PERSPECTIVE OF A TURKISH ARMED FORCES AIR AMBULANCE FLIGHT DOCTOR
Onur Tezel
Gulhane Training and Research Hospital, Department of Emergency Medicine, Ankara, Turkey
Aeromedical medical transport (AMT) can be defined as transportation of the patients with and arcraft and specialized personnel. AMT has been considered as the best option for the transportation of the patients especillay for long distances. AMT includes both evacuation of patients from the scene to the medical facility and from one medical facility to another. AMT can be elective or urgent. Urgent AMT refers to the air transportation of a potentially unstable patient to save life or limb. Lack of appropriate equipment and/or personnel in local resources is the main indication for AMTs. The management of patients who become unstable during flight is difficult because several factors hinder the ability to detect changes in the patients’ conditions. Noise and dark enviroment is the main factors. These factors making difficult to perform the critical actions such as obtaining vascular access, airway management, and teamwork approach. Another important restrictor is limited space in aircraft. Classical flight stressors (barometric pressure changes, temperature, vibration, decreased humudity, acceleration) have negative impact on patients and the crew too. All of these factors make AMT challenging but currently AMT has not any alternative for specific indications In this talk we will discuss the general impact of the classic flight stressors on patient physiology and medical care. We will try to understand the altitude physiology combined with disease – or injury-specific considerations to anticipate and respond to potential problems.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
100
FUTURE AND PERSONNEL RIGHTS OF AIR AMBULANCE HEALTHCARE STAFF IN TURKEY
Serkan Şener
Acıbadem Ankara Hastanesi, Acil Servis, Ankara
Air medical transport industry has been growing increasingly every year both in government and private side for nearly 10 years. It not questionable that the main determinants of this system is the flight and medical crew. Medical flight crew working conditions and opportunities are going to be discussed in this presentation with the highlights below.
• Workplace Opportunities and Safety
Medical Flight Crew Configuration Medical Flight Crew Working Hours Sallary and Compensation Differentials
• Medical Flight Crew Insurance • Crew Resource Management Training for Medical Staff • Future of the air medical transport medical staff
Emergency Medicine Association of Turkey (EMAT) Air Medical Transport Study Group (AMTSG) was established in 2014 targeting to be a bridge between air medical transport healthcare workers, industry leaders and government.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
101
HEMOPTYSIS: A DISREGARDED OR AN OVERESTIMATED SYMPTOM?
John L. Foggle
Brown University, Warren Alpert School of Medicine, Department of Emergency Medicine, RI, USA What are the causes of hemoptysis, and how does geography affect the differential diagnosis? How does one differentiate between hemoptysis and hematemesis? How reliable are measurements of the amount of hemoptysis? How much has changed regarding management since the middle of the last century. This talk is based on an extensive review of the most recent literature, as well as some older sources, in order to determine best practices for recognizing and treating the relatively uncommon complaint of massive hemoptysis. History and physical exam clues, appropriate labs and imaging, as well as old and new techniques for managing it will be explored. The accurate identification of the cause and early proper management in the Emergency Department may be critical to the survival of the patient. References: • Khalil A, et. al., “Severe hemoptysis: From diagnosis to embolization”, Diagnostic and Interventional Imaging, July–August
2015, Volume 96, Issues 7–8: 775–788. • Souders C and Smith A, “The Clinical Significance of Hemoptysis”, NEJM, Nov. 20, 1952, Vol 247: 790-793. • Jean-Baptiste E, “Clinical Assessment and Management of Massive Hemoptysis”, Crit Care Med 2000; 28: 1642. • Morell F, et. al., “Intentional Occlusion of the Right Upper Lobe Bronchial Orifice to Tamponade Life-threatening
Hemoptysis”, Anesthesiology, June 1995, Vol.82: 1529-1531. • Lee BR, “Analysis of Patients with Hemoptysis in a Tertiary Referral Hospital”, Tuberc Respir Dis 2012, Aug: 73(2): 107-114.
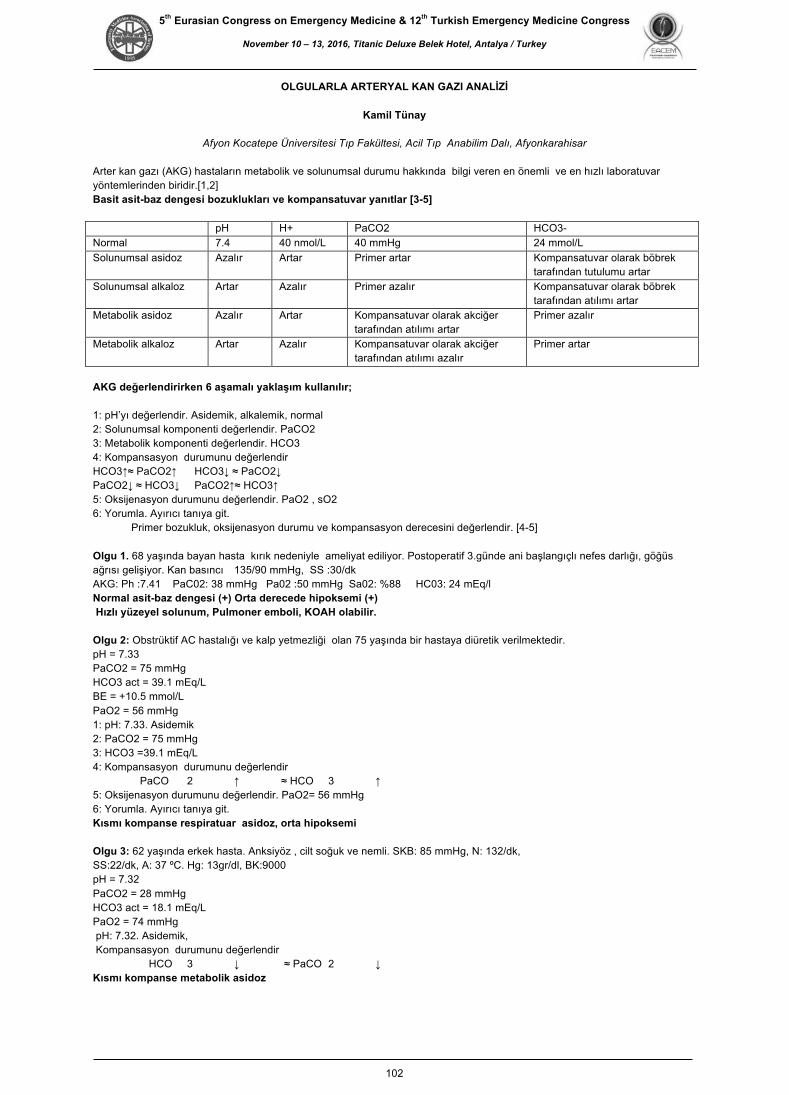
5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
102
OLGULARLA ARTERYAL KAN GAZI ANALİZİ
Kamil Tünay
Afyon Kocatepe Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Afyonkarahisar
Arter kan gazı (AKG) hastaların metabolik ve solunumsal durumu hakkında bilgi veren en önemli ve en hızlı laboratuvar yöntemlerinden biridir.[1,2] Basit asit-baz dengesi bozuklukları ve kompansatuvar yanıtlar [3-5] pH H+ PaCO2 HCO3- Normal 7.4 40 nmol/L 40 mmHg 24 mmol/L Solunumsal asÖdoz Azalır Artar PrÖmer artar Kompansatuvar olarak böbrek
tarafından tutulumu artar Solunumsal alkaloz Artar Azalır PrÖmer azalır Kompansatuvar olarak böbrek
tarafından atılımı artar MetabolÖk asÖdoz Azalır Artar Kompansatuvar olarak akcÖğer
tarafından atılımı artar PrÖmer azalır
MetabolÖk alkaloz Artar Azalır Kompansatuvar olarak akcÖğer tarafından atılımı azalır
PrÖmer artar
AKG değerlendirirken 6 aşamalı yaklaşım kullanılır; 1: pH’yı değerlendir. Asidemik, alkalemik, normal 2: Solunumsal komponenti değerlendir. PaCO2 3: Metabolik komponenti değerlendir. HCO3 4: Kompansasyon durumunu değerlendir HCO3↑≈ PaCO2↑ HCO3↓ ≈ PaCO2↓ PaCO2↓ ≈ HCO3↓ PaCO2↑≈ HCO3↑ 5: Oksijenasyon durumunu değerlendir. PaO2 , sO2 6: Yorumla. Ayırıcı tanıya git. Primer bozukluk, oksijenasyon durumu ve kompansasyon derecesini değerlendir. [4-5] Olgu 1. 68 yaşında bayan hasta kırık nedeniyle ameliyat ediliyor. Postoperatif 3.günde ani başlangıçlı nefes darlığı, göğüs ağrısı gelişiyor. Kan basıncı 135/90 mmHg, SS :30/dk AKG: Ph :7.41 PaC02: 38 mmHg Pa02 :50 mmHg Sa02: %88 HC03: 24 mEq/l Normal asit-baz dengesi (+) Orta derecede hipoksemi (+) Hızlı yüzeyel solunum, Pulmoner emboli, KOAH olabilir. Olgu 2: Obstrüktif AC hastalığı ve kalp yetmezliği olan 75 yaşında bir hastaya diüretik verilmektedir. pH = 7.33 PaCO2 = 75 mmHg HCO3 act = 39.1 mEq/L BE = +10.5 mmol/L PaO2 = 56 mmHg 1: pH: 7.33. Asidemik 2: PaCO2 = 75 mmHg 3: HCO3 =39.1 mEq/L 4: Kompansasyon durumunu değerlendir PaCO 2 ↑ ≈ HCO 3 ↑ 5: Oksijenasyon durumunu değerlendir. PaO2= 56 mmHg 6: Yorumla. Ayırıcı tanıya git. Kısmı kompanse respiratuar asidoz, orta hipoksemi Olgu 3: 62 yaşında erkek hasta. Anksiyöz , cilt soğuk ve nemli. SKB: 85 mmHg, N: 132/dk, SS:22/dk, A: 37 ºC. Hg: 13gr/dl, BK:9000 pH = 7.32 PaCO2 = 28 mmHg HCO3 act = 18.1 mEq/L PaO2 = 74 mmHg pH: 7.32. Asidemik, Kompansasyon durumunu değerlendir HCO 3 ↓ ≈ PaCO 2 ↓ Kısmı kompanse metabolik asidoz

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
103
Olgu 4: 49 yaşında postop 2.günde A:39 °C, KB:150/90 mmHg, N:110/dk, SS:24/dk. Alt zonlarda solunum sesleri alınmıyor. pH = 7.52 PaCO2 = 29 mmHg HCO3 = 24 mEq/L BE = -1 mmol/L PaO2 = 52 mmHg pH: 7.52. Alkaloz, Kompansasyon durumunu değerlendir PaCO 2 ↓ ≈ HCO 3 N Respiratuar alkaloz, orta hipoksemi Olgu 5: 54 KKY hastası , halsizlik uyku hali, kas krampları ile geliyor. Diüretik ve digital kull pH = 7.52 PaCO2 = 48 mmHg HCO3 = 40 mEq/L PaO2 = 91 mmHg FiO2 = 0.21 pH: 7.54. Alkaloz, Kompansasyon durumunu değerlendir HCO 3 ↑ ≈ PaCO 2 ↑ Kısmı kompanse metabolik alkaloz 1. Börekçi Ş, Umut S. Arter kan gazı analizi, alma tekniği ve yorumlanması. Türk Toraks Dergisi 2011;12(Ek 1):5 9. 2. Acıcan T. Arter kan gazları. Yoğun Bakım Dergisi 2003;3:160-75. 3. Saryal S. Arter kan gazları. İçinde: Numanoglu N, editor. Solunum sistemi ve hastalıkları. Ankara: Antıp AŞ; 1997. s.201-17. 4. Kaufman DA. Interpretation of arterial blood gases (ABGs). Available at: http://www.thoracic.org/clinical/critical-care/clinical-education/abgs.php. Accessed: February 10, 2014. 5. Williams AJ. ABC of oxygen: assessing and interpreting arterial blood gases and acid-base balance. BMJ 1998;317:1213-6

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
104
ÜST GİS KANAMASI YÖNETİMİNE GÜNCEL YAKLAŞIM
Şenol Ardıç
Sağlık Bilimleri Üniversitesi, Trabzon Kanuni Eğitim ve Araştırma Hastanesi Acil Tıp Kliniği, Trabzon Tanım/ Giriş
• Treitz ligamanının proksimalinden kaynaklanan GİS kanamaları olarak tanımlanır. • Hayatı tehdit edici ve önemli hastane yatış nedenlerindendir. • Treitz ligamanının proksimalinden kaynaklanan GİS kanamaları olarak tanımlanır. • Hayatı tehdit edici ve önemli hastane yatış nedenlerindendir. • % 6-10 mortalite
Semptom/ Bulgular • Hematemez • Melena • Hematokezya • Senkop/ Presenkop • Dispepsi • Epigastrik ağrı • Göğüste yanma • Yaygın karın ağrısı • Disfaji • Kilo kaybı • Sarılık
Tanı • Ortostastik kan basıncı • Tam kan sayımı • Hgb düzeyi • Kan gurubu ve crossmatch kan • Temel metabolik profil, üre/ kreatinin, koagulasyon profili • Ca düzeyi • Gastrin düzeyi • Endoskopi • PA akciğer grafisi • N/ G lavaj • Anjiografi ( kanama dirençli ve endoskopik görünüm yeterli değilse) • CT yada USG ?
Ne zaman CT yada USG istenmeli? • KC hastalığı ve siroz birlikteliği • Kolesistit ve kanama birlikteliği • Pankreatit ve pesudokist-kanama birlikteliği • Aortoenterik fistül
Genel Yönetim • Havayolu korunmalı, • Bilateral periferik en az 16 gauge luk üst ekstremite damar yolu açılması, • Her mililitre kan kaybı için 3 ml kristalloid sıvı, • Şiddetli ölümcül ek hastalık varlığı var ise hemodinamik monitörizasyon için pulmoner kateter, • Üriner çıkışın takibi için Foley idrar sondası, • Endoskopik kanama durdurucu tedavi (kanayan ülser ve varis) • Perforasyon mevcut ise cerrahi, • Yüksek riskli peptik ülser hastaları için yüksek doz PPI gerekir.
Peptik ülser kanaması olan hastada ne zaman cerrahi?
• Şiddetli, hayatı tehdit eden, resüsitatif yaklaşımlara yanıtsız hemoraji var ise, • Medikal tedavi ve endoskopik kanama durdurucu tedavinin tekrarlayan dirençli kanamada yetersizliği mevcut ise, • Perforasyon, obstrüksiyon ve malignansi gibi ölümcül ek neden var ise, • Uzamış kanama, hastanının kan volümünün % 50’sinden fazla kan kaybı var ise cerrahi uygulanır.
Prognoz • 60 yaş üstü • Şiddetli komorbidite • Aktif kanama (NG ile aktif gelen, RT de yumuşak kanama vb) • Hipotansiyon • 6 ve üzeri ünite kan tx • Hastanede yatış esnasında gelişen kanama • Şiddetli koagulopati
&Artmış mortalite, tekrarlayan kanama, endoskopik kanama durdurcu ihtiyacı ve cerrahi ile ilişkili *.. • Hemorajik şok ile başvurusu olan hastanın mortalitesi ise % 30’un üzerindedir.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
105
Risk Sınıflamaları • Hastaların yönetiminde gerekli parametreleri, hastanede de yatarak tedavi edilecek hastaları ve yapılacak
endoskopinin zamanını belirlemek amacıyla hekimlere yardımcı olabilmek için skorlamalar geliştirilmiştir. • Özellikle yüksek ve düşük risk grubundaki hastaları belirleyen, acil müdahale gerektiren ve ayaktan acil servisten
hastanın taburcu edilebilmesinin belirlenmesinde etkindirler. • Rockall (hastanın yaşı, hemodinamik durum ve eşlik eden komorbit hastalık varlığı) • Glasgow-Blatchford skoru (kalp hız, hemoglobin değeri, BUN değeri, sistolik kan basıncı, melena varlığı, senkop,
hepatik hastalık ya da kalp yetmezliği) • AIMS65 • T-skor gibi sınıflamalarda geliştirilmiştir
Referanslar:
1. Lam KL, Wong JC, Lau JY. Pharmacological treatment in upper gastrointestinal bleeding. Curr Treat Options Gastroenterol. 2015 Dec. 13 (4):369-76
2. Fujishiro M, Iguchi M, Kakushima N, et al. Guidelines for endoscopic managements of non-variceal upper gastrointestinal bleeding. Dig Endosc. 2016 Feb 22
3. Transfusion Strategies for Acute Upper Gastrointestinal Bleeding. N Engl J Med. 2013 May 16.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
106
TANISI KONMAMIŞ ŞOK HASTASINA YAKLAŞIM
Yılmaz Zengin
Dicle Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Diyarbakır Amaçlar Patofizyolojinin öğrenilmesi, tanısal yaklaşım geliştirmek, önceliklerin belirlenmesi ve tedavi hedeflerinin öğrenilmesidir Şok Kan dolaşımı ve doku perfüzyonunun azalması sonucu, oksijen ve diğer hayati maddelerin sağlanamadığı, metabolik atıkların temizlenemediği, akut ve hayati tehlike oluşturan bir durumdur. Şok Patofizyolojisi: Vücutta sunum ihtiyacı karşılayamaz hale gelirse; ilk kompansatuar yanıt olarak kardiyak output artışı meydana gelir. Yetersizlik uzun süre devam ederse, hemoglobinden dokulara daha fazla oksijen molekülü verilir. Miks venöz oksijen saturasyonu düşer. Şok-Tanı Şok tanısı dolaşımın değerlendirilmesi ile tespit edilir. Dolaşım değerlendirilmesi, kalp hızı kan basıncı, nabız sayısı ve dolgunluğu, cilt rengi, bilinç düzeyi ve idrar miktarı ile yapılır. Kan basıncı değerlendirilmesi yaş gruplarına göre yapılmalıdır. Azalmış cilt dolaşımı şokun erken belirtisi olabilir. Kötü cilt dolaşımının göstergeleri; alacalı, soluk cilt, gecikmiş kapiller geri doluş zamanı (>2 sn) ve çevresel siyanozdur. Bilinç Düzeyi Glasgow koma skalası veya AVPU ile yapılabilir. İdrar miktarı normalde 1-2ml/kg/saat olmalıdır. Şok İndeksi: Kalp hızının sistolik kan basıncına oranıdır. Normal değeri: 0.5-0.7’ dir. Vital bulguları normal olan hastalarda şok indeksi > 0.9 ise şok açısından dikkat edilmelidir. Şokun odağının saptanmasında en önemli basamak öncelikle şokun varlığının farkına varmaktır. Şokun kompansatuar dönemde tanımak önemlidir. Şok Sınıflaması Hipovolemik Şok: En sık hemorajik tipi görülür, kanama durdurulur ve transfüzyon yapılarak tedavi edilir. İleus, pankreatit vb gibi, ekstravasküler alana intravasküler sıvının göçü sonucu gelişen durumlarda sıvı resüsitasyonu gerekir. Diare, kusma, yanık, aşırı diüertik kullanımı gibi sıvı yapıları nedeniyle gelişen durumlarda yine sıvı replasmanı yapılır. Altta yatan nedenin tedavisi unutulmamalıdır Dağılımsal Şok: İntravasküler volüm veya kardiyak fonksiyon bozukluğu yoktur. Problem kan ve oksijen dağılımındadır. Anaflaktik, nörojenik ve septik şok dağılımsal şok tipleridir. Kardiyojenik Şok: Pompa disfonsiyonu sonucu meydana gelir. Etkin kontraktilite kaybı veya kan akımında mekanik bozulmalar sonucu oluşur. Obstrüktif Şok: Obstrüksiyon nedeniyle boyun venöz dolgunluğu saptanır. Örneğin, tansiyon pnömotoraks , kardiyak tamponad ve pulmoner emboli. Tanısı Konmamış Şok Hastasının Yönetimi Aşağıdaki soruların cevaplanması tanısı konulmamış hasta yönetiminin esaslarını oluşturmaktadır: 1)Tanısı konmamış şok hasta değerlendirilmesinde öykünün anahtar bileşenleri nelerdir? 2) Şok tipinin belirlenmesinde önemli fizik muayene bulguları nelerdir? 3) Şok sebebinin belirlenmesinde ek labaratuvar ve görüntüleme çalışmaları nelerdir? 4) Değişik şok nedenlerinde önemli tedavi prensipleri nelerdir? Kaynaklar; 1. Vincent JL, De Backer D. Circulatory shock. N Engl J Med 2013; 369:1726. 2. Seymour CW, Liu VX, Iwashyna TJ, et al. Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis3). JAMA 2016; 315:762. 3. CardenasGarcia J, Schaub KF, Belchikov YG, et al. Safety of peripheral intravenous administration of vasoactive medication. J Hosp Med 2015; 10:581. 4. Perera P, Mailhot T, Riley D, Mandavia D. The RUSH exam: Rapid Ultrasound in SHock in the evaluation of the critically lll. Emerg Med Clin North Am 2010; 28:29. 5. Volpicelli G, Lamorte A, Tullio M, et al. Pointofcare multiorgan ultrasonography for the evaluation of undifferentiated hypotension in the emergency department. Intensive Care Med 2013; 39:1290.

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
107
KRİTİK HASTALARDA AKILCI İLAÇ SEÇİM KRİTERLERİ
Arzu Denizbaşı
Marmara Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, İstanbul
Kritik hastada doğru ilaç tedavisi verilmesi için ilk şart ilaçların farmakokinetiği ve farmakodinamiğini anlamak önemlidir ancak bu süreçler normal insandan çok farklı gelişir. Kritik hastada fizyolojik değişiklikler iki fazda gelişir.
1. Hipodinamik Faz
Sepsis, travma, major cerrahi girişimler, mezenter iskemisi, ARDS, pankreatit ve zehirlenme gibi kritik hastalarda SIRS gelişir. SIRS: Taşikardi, arteryel vaskuler tonusta azalma, vaskuler membran permeabilitesinde artış olur. Eğer sıvı yeterli miktarda verilmezse intravaskuler hacim ve preload azalır, kardiyak atım düşer. Böbrek ve karaciğer gibi ilaç metabolizmasında önemli organlarda kan akımı azalır. İlaç klerensi azaldığından dokuda birikir.
2. Hiperdinamik Faz
Sıvı resusitasyonu başlayınca preolad düzelir ve kardiyak atım artar.Kalp hızı arttığı ve sistemik direnç düşük olduğu için bu aşamada hiperdinamik fizyolojik duruma geçilir. Organlara kan akımı normalden de fazla olduğu için ilaç klerensi de normalden fazla olur. Yani verdiğimiz ilaç bu devrede daha fazla metabolize ediliyordur. Bu hiperdinamik faz yüzünden hastalarda normal dozlarda verilse bile hastaların serum düzeyleri düşük olabilir; SIRS hastalarında sıvı tedavisi yapılırken ilacın dağılım hacmi de etkilenmektedir. Sepsiste erken hedefe yönelik tedavi protokolunde hastalara ortalama 10 L kadar sıvı da eklenir. Travma hastaları ve ARDS hastalarında da Vd değişmektedir. SIRS hastalarında kapiler permeabilite değişiklikleri eğer ilaç hidrofilik özellikte ise Vd üzerinde etki eder. Aminoglikosidlerde hastalık durumlarında Vd çok değişkendir. Vd iki katına dek artabilir, o zaman da serum ilaç konsantrayonu yarı yarıya azalır (Lineer kinetik). İlacın yarı ömrünü belirleyen iki parametre vardır: Klerens ve Vd. Vd artarsa ilacın yarılanma ömrü de uzar. Akut Faz Cevabında proteine bağlanma oranı değişkendir. Akut fazda Albumin azalırken AAG artmaktadır (ters orantı). Protein oranında değişiklik olunca bağlanan ilaç miktarı değişir.
1. Serbest ilaç miktarı değişir. 2. Serbest ilaç oranı artınca dokulara geçip etki eden ilaç miktarı artar, Vd artar, vücuttan klerensi olan ilaç
oranı artar. 3. İlacın serumdeki konsantrasyonu azalır. 4. Serbest konsantrasyon/ total konsantrasyon oranı sabit kalır
Serbest/ total ilaç miktarında önemli bir farmakolojik değişikliğe neden olmaz. Yüksek oranda proteine bağlanan ilaçlarda çoğunlukla bu sonuç beklenir. Bazı ilaçların yüksek ekstraksiyon oranı ve düşük terapötik indeksi vardır. Bu ilaçlar GİS den emildikten sonra portal kanla karaciğerden ilk geçişte pre- sistemik metabolizma edilirler. Bu ilaçların verilen dozu daha sistemik kana ulaşmadan azalmakta ve biyoyararlanımları düşmektedir. Kodekslerde bilgilere ulaşmak mümkündür ancak genel eğilim Acil Servislerde ilk dozların standart olarak verilmesi ve sonra nefroloji ile konsulte ederek idamenin sağlanmasıdır. Antibiyotik seçimi Kritik bakım hastalarında hayati önem taşır Seçimde MIC kullanışlı, pratik ama bazen de anlamsız bir parametredir. MIC in vitro etkiyi gösterir, canlı organizmada yani insanda MIC değerinin üzerinde doku konsantrasyonu hedeflenmelidir. Bir diğer hedef de MIC değerinin ne kadar uzun süreli ulaşılmasının belirlenmesidir. Antibiyotiğin farmakodinamik profili iki faktörle belirlenir:
1. Etkinin konsantrasyon düzeyine bağlı olması 2. Etkinin dozlardan sonra devamlılığı
Aminoglikozidler ve florokinolonlarda gibi hücre içine girerek etki eden olduğu gibi bazı antibiyotiklerde konsantrasyon arttıkça ilacın bakterisit etkisinin hem gücü hem de hızı artmaktadır. β-lactam antibiyotiklerde ise bu etki gözlenmez, yani doz arttıkça bakterisit etkileri artmaz. Çünkü hedef yeri bakteri hücre duvarındaki PBP dir. Referanslar: Czosnowski QA, Mianno TA. Principal of drug dosing in critically ill patients. Parillo, Chapter 20: Critical Care Procedures, Monitoring, Pharmacology. 272- 295, 2014

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
108
ORAL ABSTRACTS

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
109
O 001 BURNOUT LEVEL AND RELATIONSHIP OF BURNOUT LEVEL TO SERUM S100B IN THE EMERGENCY DEPARTMENT WORKER
Gamze Bozkus, Bedia Gulen, Ertan Sonmez Bezmialem Vakıf University, Department of Emergency Medicine, Istanbul, Turkey Background: Burnout syndrome includes physical, emotional and mental signs and symptoms. It characterizes physical fatigue and tiredness, helplessness and hopelessness, negative self-concept, and negative attitudes towards work and environment. In our study the relationship of S100B protein to the diagnosis of burnout and depression was investigated in the emergency department (ED) workers. Methods: This study was done in Bezmialem Vakif University Medical Faculty department of emergency medicine where paramedics and nurses were enrolled. Rate of depression and burnout levels were determined using Beck Depression Inventory (BDI) and the Maslach Burnout Inventory (MBI) before the shift. Blood samples were drawn for S100B level before and after the shift. These results were compared with S100B level. Statistical analysis was performed using SPSS. Results: Study population includes 29 nurses (65.9%) and 15 paramedics (34.1%). This study demonstrates emotional exhaustion (mean=30.0 ± 6.4, median (IQ) = 28.5(25.0-35.8)), depersonalization (mean=30.0 ± 6.4, median (IQ) = 28.5(25.0-35.8)), lack of personal accomplishment (mean=30.0 ± 6.4, median (IQ) = 28.5(25.0-35.8)), and BDI (mean=34.4 ± 8.0, median (IQ) = 33.5 (29.0-36.8)). Before the shift S100B level is 21.8 ± 77.0 (median (IQR) = 72.4 (66.4- 80.6). After the shift S100B level is 113.0 ± 129.6 (median (IQR) = 72.5 (65.7 to 87.8). Before and after the shift S100B levels were statistically significant (p = 0.046). A significant relation was not found between Serum S100B level after the shift and emotional exhaustion, depersonalization, lack of personal success, and BDI score (p ˃ 0.05). Conclusions: There were significant changes in S100B levels after and before the shift. Although a significant correlation was not found between S100B level and BDI/MBI score. S100B level cannot predict burnout and depression in the long-term in the emergency room workers. But this study suggests S100B level can be used to effectively determine the night shift time. Keywords: Burnout, S100B, Beck, Maslach, paramedic O 002 DETERMINATION OF NURSING PROCEDURES IN AN EMERGENCY UNIT: RESULTS OF A PILOT STUDY Gulten Sucu Dağ1, Songül Pişkin2, Meral Karabıyık Gözkaya2
1Eastern Mediterranean University Faculty of Health Sciences, Department of Nursing, Famagusta, Northern Cyprus 2Akdeniz University Hospital, Emergency Department, Antalya, Turkey Introduction: Planning patient care and evaluating patient outcomes are an important part of nursing roles. There have not been any studies determining nursing procedures in emergency units in Turkey. This study was directed towards revealing interventions performed by nurses in an emergency unit. Aim: This study aimed to identify the procedures performed by emergency nurses and the frequency of their practice. Methods: The study had a descriptive and cross-sectional design. The population comprised of 139 emergency nurses working in a state hospital in Turkey. Ninety-two nurses who agreed to participate in the study formed the study sample. A response rate of 66% was achieved. Written informed consent was received from the nurses and a written permission was obtained from the hospital administration. Approval to undertake the study was obtained from the University Ethics Board. Data were gathered by using "The Form of Demographic Characteristics of Nurses" developed by the researchers and "Emergency Nursing Procedures Questionnaire" composed of three sections to reveal nursing procedures performed in the emergency department. Results: The procedure most frequently performed by nurses was "participating in making medical diagnosis and in implementing treatment plan" (3.37 ±0.23), followed by " management and organizational procedures" (3.29 ±0.46). The least frequently performed procedure was "nursing care" (3.09±0.25). Emergency procedures most frequently performed by the participants were "administration of pain medication and assessment of patient responses” " and “administration of emergency drugs" (3.97). "Assessment of the patient's nutritional status" (1.79) and "reporting forensic cases” (1.85) were among the least frequently performed procedures. ��
Conclusion: In view of the results of the study, it is clear that the emergency nurses carry out nursing care procedures least frequently and take part most frequently in procedures related to medical diagnosis and treatment. Therefore, it is necessary to increase education programs about nursing care practices. Keywords: Nursing procedures, emergency nursing, emergency care setting, nursing care

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
110
O 003 EFFECTIVENESS OF THE SYNTHETIC CANNABINOIDS SEMINAR Murat Seyit1, Mert Özen2, Alten Oskay2, Emine Kadioglu1
1Dumlupınar University, Evliya Çelebi Training and Research Hospital, Kütahya, Turkey 2Denizli State Hospital, Denizli, Turkey Objectives: Synthetic cannabinoid or “Bonzai” use is a public health issue as its use has increased in Turkey as well as all over the world. The aim of this study is to evaluate the effectiveness of the “Synthetic Cannabinoids Seminar” that was provided to physicians who work in emergency services, using multiple choice questionnaires before and after the seminar as a tool for evaluation.��
Material-Method: Synthetic cannabinoids seminars were provided to physicians who work in emergency services in two different cities, with the participation of 20 physicians in each scheduled seminar. The seminars were instructed by emergency medicine specialists and psychiatrists who were certified as an instructor by the Turkish Ministry of Health, after receiving an instructor course in synthetic cannabinoids. In order to measure basal knowledge levels of the participants, a pretest was performed for all participants before the seminar. After the seminar, a posttest was performed using the same questions in the pretest. The number of correct answers in both tests was then compared. Results: In total, 85 individuals attended the seminars; 29 individuals from Dumlupınar University Evliya Çelebi Training and Research Hospital constituted first group, and 56 individuals from Denizli State Hospital constituted second group. In both groups, the ratios of correct answers in the posttest were determined to be higher when compared to the pretest. Keywords: Cannabinoids, Education, Emergency, Evaluation studies O 004 EVALUATION OF THE EMERGENCY MEDICINE, EDUCATION AND EMERGENCY MEDICINE TRANIER BY RESIDENTS AND TRAINERS AND MUTUAL EXPECTATIONS ABOUT EDUCATION Yunus Emre Arık1, Ayhan Özhasenekler2, Fatih Tanrıverdi2, Gülhan Kurtoğlu Çelik1, Mehmet Ergin2, Şervan Gökhan2
1Atatürk Training and Research Hospital, Clinic of Emergency Medicine, Ankara, Turkey�2Yıldırım Beyazıt University, Medicine School, Clinic of Emergency Medicine, Ankara, Turkey Introduction and Aim: Emergency medicine is a different specialties that is new and has different dynamics. Although many studies on emergency medicine training, limits are not clearly known. In this study we aimed to evaluate emergency medicine training by residents and trainers for defining better education needs based on mutual expectations. Materials-Methods: This descriptive and cross-sectional study performed by filling questionnaire to emergency residents and trainers in Turkey via e-mail. The survey created from 50 questions that include following headings, demographic characteristics, clinical training facilities, trainers educational skills and qualifications, personal and social characteristics of trainers and mutual expectations. Results: A total of 384 individuals participated in the study, 291 (75,8%) of them were residents, 93 (24,2%) were trainers. 91,4% of respondents (n = 351) had standard clinical education program, 79,4% (n = 305) indicated that assistant exam conducted. There was all statistically differences between residents and trainers answers in following headings; clinical training facilities, trainers educational skills and qualifications, personal and social characteristics of trainers. When participants were assessed according to the institutions they work in, the residents who work in research hospitals and trainers who work in medical school were more positive. When residents most popular expectation from trainers was “education should come before service delivery” in ratio 17,1% (n=18), trainers most popular expectations from residents were “be enthusiastic and willing” and “tracking and reading literature” both in ratio 38,2% (n=18).��
Conclusion: Our study showed that there was a difference of opinion among teachers and assistants in emergency medicine education in almost every issue. Although trainers feel themselves enough in education, residents have high expectations. Taken into account the results by the emergency medical educators and administrators make an opportunity for a better emergency medicine education and training more high quality emergency medicine professionals. Keywords: Emergency medical education, emergency medical assistance, emergency medicine trainer

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
111
O 005 INTER-HOSPITAL TERTIARY CARE TRANSPORT IN RURAL INDIA Sunil Kumar Choudhary Medica Superspeciality Hospital, Accident & Emergency Department, Ranchi, Jharkhand, India Objectives: Study the utilization of an emergency resident (EMR)-based ACLS ambulance service for inter-hospital transfers. Materials-Methods: A retrospective review of inter-hospital transfers by EMR-ACLS ambulance to a tertiary care hospital in Durgapur, India. The study was conducted from January 2011 to December 2013. Patients aged 18 and older, with a triage score of 1 (highest severity) were included. Data was obtained from a transfer registry, that included patient age, gender, diagnosis, duration of transport, interventions performed, and drugs administered. Descriptive statistics were used to evaluate these variables. Results: 1298 patients were transported, 449 of whom were over 18 years and assigned a triage priority score of 1. 257 (57.2%) were males and 192 were females. Three patients expired during transfer. Travel times ranged from 30 minutes to 2,520 minutes (42 hours), (mean of 176 minutes). Resuscitative efforts included intubation in 58 patients (12.9%), managing patients on a ventilator 41 patients (9.1%), administering inotropes and vasopressors 131 patients (29.2%)and transcutaneous pacing in 6 patients (1.3%). Conclusion: An organized EMS system might ensure that patients initially routed to the appropriate centers, reduce the number of transfers. Keywords: EMS services, critical patients, lifesaving intervention
O 006 TETANUS IMMUNITY STATUS AMONG ADULT TRAUMA PATIENTS IN AN ED İbrahim Toker1, Şükran Köse2, Turgay Yılmaz Kılıç1, Orkun Ünek1, Murat Yeşilaras1, Feriyde Çalışkan1, Özge Duman Atilla1, Çağrı Kokkoz3, Serkan Hacar1
1Tepecik Training and Education Hospital, Department of Emergency Medicine, İzmir, Turkey�2Tepecik Training and Education Hospital, Department of Infectious Diseases and Clinical Microbiology, İzmir, Turkey�3Celal Bayar University Faculty of Medicine, Department of Emergency Medicine, Manisa, Turkey, Turkey Background: Tetanus is is a vaccine-preventable infectious disease and caused by Clostridium tetani. The aim of this study was to investigate the tetanus immunity among adult trauma patients. Methods: This study was performed on 267 trauma patients admitted to the emergency department of Tepecik Research and Training hospital in Izmir City, Turkey during 6 month period. After obtaining a written informed consent from the patients, a questionnaire consisted of demographic information and tetanus vaccination history was completed by the physician. The tetanus antibody levels equal or more than 0.1 IU/mL were considered protective. Results: From a total of 267 patients, 75 cases (28.1%) were females and 192 (71.9%) were males. The average age of the patients was 39 (IQR=24, min: 18, max: 95). 75.3% of the patients (n=201) had the protective rate of immunity to tetanus. There was statistically significant difference in the rate of immunity between females (64%) and males (79.7%) (p = 0.007). There was statistically significant difference in the rate of immunity among age groups (p < 0.001). There was no statistically significant difference in the rate of immunity among educational levels (p > 0.05). There was no significant difference in protective antibody rate between the patients who known and unknown history of tetanus vaccination (p = 0.144). Conclusions: In our study, protective tetanus immunity rate decreased with age and this rate was significantly lower in adults aged >=65 years. Keywords: Tetanus immunity, adult trauma patients, emergency medicine

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
112
O 007 A HELPFUL METHOD FOR EMERGENCY SERVICE: PREDICTING THE ISCHEMIC CEREBROVASCULAR DISEASE WITH DATA MINING
Göksu Bozdereli Berikol1, Gürkan Berikol2
1Karaman Public Hospital, Clinic of Emergency Medicine, Karaman, Turkey 2Karaman Public Hospital, Clinic of Neurosurgery, Karaman, Turkey Diagnosing fast and accurate in emergency departments is a matter of all emergency physicians. Data mining is a computational science which enables analysis of a specific data compile, understands and predicts an outcome. Recently there are studies about data mining techniques which helps physicians in emergency services without advanced imaging technologies. Some techniques of data mining are decision trees, Naive bayes method, K nearest neighbour(Knn), genetic algorithms, artificial neural networks, clustering analysis and support vector machines. This study aims to define the accuracy of predicting ischemic cerebrovascular diseases with data mining techniques as Knn, Naive Bayes and decision trees. Chronic ischemia, cerebral atrophy and WBC, MCV, RDW, PLT, MPV, PCT, PDWvalues of thirty four patients recorded and analysed with Knn, decision tree and Naive Bayes algorithms via MATLAB R2012r. The accuracy of methods were calculated. Decision tree algorithms has the lowest accuracy of 66%. Knn and Naive Bayes has a success rate of 83,3% and 88,2%. In the literature, there are studies which defines the correlation of MPV, PDW, RDW, PLT values and ischemic cerebrovascular disease. In our study, we determined Knn and Naive Bayes methods are succesful over 80% about predicting the ischemic cerebrovascular disease using those parameters. Success of the computer via machine learning can help emergency physicians to support their diagnosis especially in insufficient equipped emergency services. Keywords: Artificial intelligence, data mining, ischemic cerebrovascular disease O 008 PLETH VARIABILITY INDEX FOR VOLUME ASSESSMENT IN SPONTANEOUSLY BREATHING ADULTS Elif Dilek Cakal, Murat Ersel, Funda Karbek Akarca Ege University Medical School, Department of Emergency Medicine, Izmir, Turkey Objective: Pleth Variability Index (PVI), a recently designed noninvasive method of volume management, is shown to be useful in predicting fluid responsiveness in mechanically ventilated patients. PVI has been tested in limited groups of spontaneously breathing adult volunteers. We studied the ability of PVI to predict fluid responsiveness in larger groups. Materials - Methods: This study, which is prospective, cross-sectional and analytical, took place in Hospital of Medical School of Ege University, Emergency Department and Blood Donation Center. Patients were parted in two groups by procedure: Volume Replacement and Volume Displacement. Exclusion criteria were age younger than 18, pregnancy, instability, congestive heart failure and chronic renal failure. The vitals, shock index (SI) and modified shock index (MSI), cardiac output (CO) measured by left ventricular outflow tract velocity time integral (LVOT VTI) method, inferior vena cava (IVC) collapsibility index, perfusion index (PI) and PVI were recorded before and after procedures. All data are given as mean ± SD. All the results were analyzed by Statistical Package for Social Sciences (SPSS) version 20.0 software. Student's t-test and Pearson's chi-square test were used to evaluate the level of significance. Results: Volume replacement induced significant changes in pulse rate, VTI, stroke volume (SV), CO, IVC diameters and collapsibility. Volume displacement induced significant changes in systolic arterial pressure (SAP), diastolic arterial pressure (DAP), Mean Arterial Pressure (MAP), SI, MSI, PVI, VTI, SV, IVC minimum and maximum diameters. In this group, the correlations between PVI and SI (r=-0.306; P<0.05), MSI (r=-0.291; P<0.05) were significant but weak. Overall, PVI sensed fluid replacement and displacement but had no significant correlation with CO. Conclusion: Our study confirms that, in spontaneously breathing volunteers, PVI changes significantly with fluid replacement and displacement. However, PVI is not correlated with CO. Keywords: Pleth Variability Index, cardiac output, ivc collapsibility index, spontaneously breathing adults, emergency department

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
113
O 009 THE EFFECTIVENESS OF USING LUER-LOK (BD VACUTAINER®) IN REDUCING HEMOLYSIS RATES IN BUSY EMERGENCY DEPARTMENTS
Mustafa Keşaplı, Faruk Güngör, Güzin Aykal, Ahu Göğebakan, Taylan Kılıç, Mehmet Akçimen, Can Akyol Antalya Research and Training Hospital, Antalya, Turkey Introduction: In busy emergency departments, mistakes made during the pre-analytical phase can cause delayed diagnosis and treatment, and prolonged follow-up periods. The most common error in the pre-analytical phase is hemolysis in blood samples. In this study, we aimed to assess the effectiveness of the Luer-Lok (BD Vacutainer®) method of taking samples in avoiding hemolysis. Materials and Methods: The study was conducted at the emergency department of a tertiary healthcare facility on patients that register at level 1 or 2 of the Emergency Severity Index triage algorithm. Three sets of prospective observations were made, each lasting for five days. In the first period, hemolysis rates were determined. Following a training course on appropriate blood sampling techniques during the second period, hemolysis rates were determined again while Luer-Lok (BD Vacutainer®) was being used. Taking and processing of samples were carried out by the same personnel throughout the study. Assessment of hemolysis was performed by those that were blind to sampling. All the samples were analyzed at the laboratory located inside the emergency department. Results: In total, 2,027 blood samples were sent to the emergency laboratory for analysis. The hemolysis rate was 8.1% in the first period, 5.5% in the second and 1.4% in the third. The difference in rates between the first and second periods was not statistically significant (p=0.0793). The hemolysis rate in the third period was significantly lower compared to the other two periods (p=0.0001). Conclusion: Using Luer-Lok (BD Vacutainer®) may be effective in reducing hemolysis rates in busy emergency departments. Keywords: Busy emergency department, hemolysis, pre-analytical phase O 010 A NEW PERSPECTIVE TO LIVE SAVING PROCEDURES IN BATTLEFIELD SETTING: EMERGENCY CRICOTHYROIDOTOMY, NEEDLE THORACOSTOMY, CHEST TUBE THORACOSTOMY WITH NIGHT VISION GOGGLES Attila Aydın1, Sedat Bilge1, Meltem Bilge2, Cemile Aydın3, Erdem Cevik4, Mehmet Eryılmaz1
1Gulhane Research and Training Hospital, Department of Emergency Medicine, Ankara, Turkey 2Dışkapı Research and Training Hospital, Clinic of Anesthesia and Resuscitation, Ankara, Turkey 3Etimesgut State Hospital, Clinic of Internal Medicine, Ankara, Turkey 4Haydarpaşa Research and Training Hospital, Clinic of Emergency Medicine, İstanbul, Turkey Background: In the patients with multiple and serious trauma, early applications of life saving procedures are related with improved survival. We tried to determine experimentally the feasibility of life-saving interventions that are applied with the aid of night vision goggles (NVG) in nighttime combat scenario. Methods: Chest tube thoracostomy (CTT), emergency cricothyroidotomy (EC) and needle thoracostomy (NT) interventions were administered by 10 combatant medical staff. The success and duration of interventions were explored in the study. Procedures were applied on the formerly prepared manikins/models in a bright room and were applied in a dark room with the aid of NVG. Operators graded the ease of interventions. Results: All interventions were found successful. Operators rated the CTT interventions in dark were more difficult compared to in daytime and EC interventions were more difficult compared to in daytime (p <0.05). There was no significant difference in the difficulty in the NT groups. When compared regarding completion times of interventions, there was no significant difference between in daytime and in dark scenario. Conclusions: The operators who use NVGs have to be aware of that they can perform their tactic and medical activities without taking off the NVGs, and without the requirement of an extra light source. Keywords: Chest tube thoracostomy, needle thoracostomy, emergency cricothyroidotomy, live saving procedures
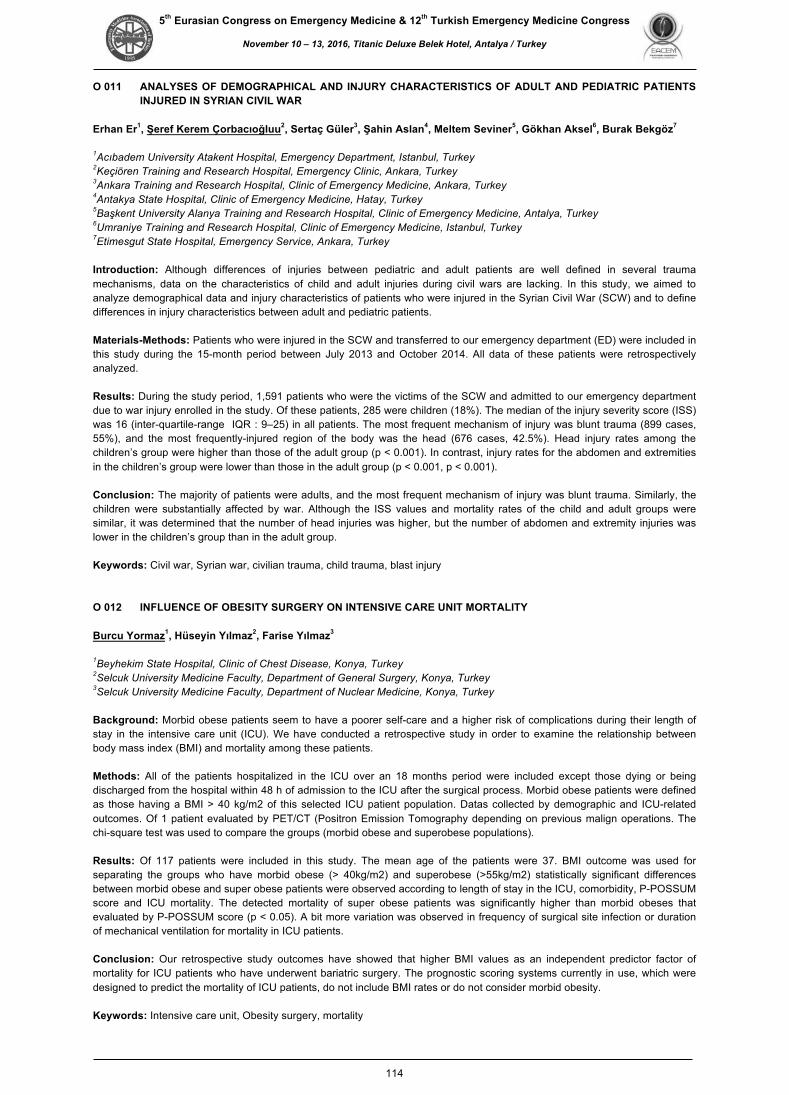
5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
114
O 011 ANALYSES OF DEMOGRAPHICAL AND INJURY CHARACTERISTICS OF ADULT AND PEDIATRIC PATIENTS INJURED IN SYRIAN CIVIL WAR
Erhan Er1, Şeref Kerem Çorbacıoğluu2, Sertaç Güler3, Şahin Aslan4, Meltem Seviner5, Gökhan Aksel6, Burak Bekgöz7
1Acıbadem University Atakent Hospital, Emergency Department, Istanbul, Turkey 2Keçiören Training and Research Hospital, Emergency Clinic, Ankara, Turkey�3Ankara Training and Research Hospital, Clinic of Emergency Medicine, Ankara, Turkey 4Antakya State Hospital, Clinic of Emergency Medicine, Hatay, Turkey 5Başkent University Alanya Training and Research Hospital, Clinic of Emergency Medicine, Antalya, Turkey�6Umraniye Training and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey 7Etimesgut State Hospital, Emergency Service, Ankara, Turkey Introduction: Although differences of injuries between pediatric and adult patients are well defined in several trauma mechanisms, data on the characteristics of child and adult injuries during civil wars are lacking. In this study, we aimed to analyze demographical data and injury characteristics of patients who were injured in the Syrian Civil War (SCW) and to define differences in injury characteristics between adult and pediatric patients. Materials-Methods: Patients who were injured in the SCW and transferred to our emergency department (ED) were included in this study during the 15-month period between July 2013 and October 2014. All data of these patients were retrospectively analyzed. Results: During the study period, 1,591 patients who were the victims of the SCW and admitted to our emergency department due to war injury enrolled in the study. Of these patients, 285 were children (18%). The median of the injury severity score (ISS) was 16 (inter-quartile-range IQR : 9–25) in all patients. The most frequent mechanism of injury was blunt trauma (899 cases, 55%), and the most frequently-injured region of the body was the head (676 cases, 42.5%). Head injury rates among the children’s group were higher than those of the adult group (p < 0.001). In contrast, injury rates for the abdomen and extremities in the children’s group were lower than those in the adult group (p < 0.001, p < 0.001). Conclusion: The majority of patients were adults, and the most frequent mechanism of injury was blunt trauma. Similarly, the children were substantially affected by war. Although the ISS values and mortality rates of the child and adult groups were similar, it was determined that the number of head injuries was higher, but the number of abdomen and extremity injuries was lower in the children’s group than in the adult group. Keywords: Civil war, Syrian war, civilian trauma, child trauma, blast injury O 012 INFLUENCE OF OBESITY SURGERY ON INTENSIVE CARE UNIT MORTALITY Burcu Yormaz1, Hüseyin Yılmaz2, Farise Yılmaz3
1Beyhekim State Hospital, Clinic of Chest Disease, Konya, Turkey 2Selcuk University Medicine Faculty, Department of General Surgery, Konya, Turkey 3Selcuk University Medicine Faculty, Department of Nuclear Medicine, Konya, Turkey Background: Morbid obese patients seem to have a poorer self-care and a higher risk of complications during their length of stay in the intensive care unit (ICU). We have conducted a retrospective study in order to examine the relationship between body mass index (BMI) and mortality among these patients. Methods: All of the patients hospitalized in the ICU over an 18 months period were included except those dying or being discharged from the hospital within 48 h of admission to the ICU after the surgical process. Morbid obese patients were defined as those having a BMI > 40 kg/m2 of this selected ICU patient population. Datas collected by demographic and ICU-related outcomes. Of 1 patient evaluated by PET/CT (Positron Emission Tomography depending on previous malign operations. The chi-square test was used to compare the groups (morbid obese and superobese populations). Results: Of 117 patients were included in this study. The mean age of the patients were 37. BMI outcome was used for separating the groups who have morbid obese (> 40kg/m2) and superobese (>55kg/m2) statistically significant differences between morbid obese and super obese patients were observed according to length of stay in the ICU, comorbidity, P-POSSUM score and ICU mortality. The detected mortality of super obese patients was significantly higher than morbid obeses that evaluated by P-POSSUM score (p < 0.05). A bit more variation was observed in frequency of surgical site infection or duration of mechanical ventilation for mortality in ICU patients. Conclusion: Our retrospective study outcomes have showed that higher BMI values as an independent predictor factor of mortality for ICU patients who have underwent bariatric surgery. The prognostic scoring systems currently in use, which were designed to predict the mortality of ICU patients, do not include BMI rates or do not consider morbid obesity. Keywords: Intensive care unit, Obesity surgery, mortality

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
115
O 013 ACİL SERVİSTE TAM KULLANILMAYAN VE İMHA EDİLEN İLAÇLARIN DEĞERLENDİRİLMESİ İlknur Öztekin, Merve Bahadır, Hakan Topaçoğlu İstanbul Eğitim ve Araştırma Hastanesi, İstanbul Amaç: Acil serviste başvuran hastalarda genellikle sedasyon veya analjezi nedeniyle kontrol altında uygulanan ilaçların uygun kullanımı açısından bazı raporlar bulunmaktadır. Özellikle opiat grubu ilaçların hastalara tamamen uygulanmaması atık olarak işlem görmesine ve mali kayıplara neden olabilmektedir. Bu çalışmanın amacı acil serviste imha edilen ilaçların bedel etkinlik değerlendirilmesidir. Metot: Çalışma retrospektif, kesitsel tek merkezli olarak düzenlendi. Çalışmada acil serviste bir yıl içerisinde hastalara uygulanan ancak artık olarak kalan veya açılarak kullanılmamış olan opiat, sedatif-hipnotik, resusitatif ilaç miktarı ve ilaç oranları hesaplandı. Aynı zamanda imha edilen ilaçların kurum açısından ekonomik maliyet hesabı yapıldı.��
Bulgular: Acil servise bir yıl içerisinde 221.954 hastanın başvurduğu ve bu hastalara tam olarak uygulanmayan ve imha edilen ilaç sayısı 3726 olarak saptandı. Acil servise başvuran bu hastalar arasından tedavi için 2275 hastaya fentanil (%100 imha sayısı, %70,3 imha oranı, 5341,7 TL kayıp), 71 hastaya morfin (%100 imha sayısı, %72,7 imha oranı, 29,1 TL kayıp) İV olarak uygulandığı tespit edilmiştir. Sedatif ilaç grubuna bakıldığında ise 1915 hastaya midazolam (%62 imha oranı, 183,7 TL kayıp), 455 hastaya diazepam (%29 imha sayısı, %50 imha oranı 44,22 TL kayıp), 129 hastaya ketamin (%46 imha sayısı, %80 imha oranı, 438,7 TL kayıp), 480 hastaya etomidate uygulandığı (%0,4 imha sayısı) ve imha edildiği tespit edildi. ��
Sonuç: Acil serviste kullanılan ve imha edilmesi gereken ilaçlar için imha nedeninin; eksik doz uygulanması, hastada gelişen komplikasyon ve hekimin karar değiştirmesi gibi nedenlerden kaynaklandığı söylenebilir. Ancak özellikle opiat grubu ilaçlarda üretilen ampul formlarının bedel etkinlik açısından uygun şekilde üretilmediği düşünülebilir. Sebep ne olursa olsun bu ilaçların kullanımı için özel bir ekip kurulması etkin tedavi ve olası ekonomik kayıplar açısından etkili olabilecektir. Anahtar Kelimeler: Atık ilaç, acil servis, opiat O 014 BİR ÜNİVERSİTE HASTANESİ ACİL SERVİSİNE YAŞLI GRUBU HASTALARIN BAŞVURU ORANI VE ACİL SERVİS HEMŞİRELERİNİN YAŞLI HASTA BAKIMINDAKİ ROLÜ
Hülya Karabulut, Nazlı Yıldız, Müge Günalp Eneyli Ankara Üniversitesi Tıp Fakültesi İbn-i Sina Hastanesi, Acil Tıp Anabilim Dalı, Ankara Giriş-Amaç: Yaşam süresinin uzaması, toplumun eğitim seviyesinin yükselmesi kronik hastalıkların yönetimi, sağlık hizmetlerinin ulaşılabilirliğinin artması ile birlikte sağlık hizmetlerinin yaşlılar tarafından kullanım oranı artmıştır. Bu artışa bağlı olarak ta sağlık çalışanları yaşlı birey ile daha sık karşılaşmaktadır. Çalışma, yaşlı hastaların acil servise başvuru oranını belirleyerek, hemşirelerin, yaşlılık ve yaşlanma konusuna dikkat çekmek, bu konuda farkındalıklarını arttırmak ve yaşlı hasta bakım kalitesini yükselmek için yapılmıştır. ��
Metaryal - Metot: Avicenna hastane bilgi yönetim sisteminden geriye dönük tarama yapılıp 2014 yılı, acil servise olan toplam hasta başvuru sayılarına ulaşılmış olup 65 yaş üstü hasta başvuruları değerlendirilmiştir. ��
Sonuç: Yaşlı grubun acil servise başvuru oranına baktığımızda 2014 yılı toplam 39950 hasta başvurusu içinde 8285(%20) hastanın 65 yaş üstü(yaşlı) olduğu tespit edilmiştir. Bu bağlamda yaşlı hastalar/hasta yakınları için taburculuk sonrası broşürler hazırlanmaya başlanmıştır. Acil servis hemşire oryantasyon programlarına ve acil servis hizmet içi eğitim programlarına da yaşlı hasta bakımı konusunun ayrıntılı şekilde ele alınması planlanmıştır. Anahtar Kelimeler: Yaşlı hasta, hemşire, acil servis

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
116
O 015 HASTALARIN GÖZÜNDEN ACİL SERVİS: EĞİTİM ŞART MI? Umut Payza, Zeynep Karakaya, Fatih Esad Topal, Pınar Yeşim Akyol, Serkan Bilgin, Gözde Canan Yavaş İzmir Katip Çelebi Üniversitesi Atatürk Eğitim Araştırma Hastanesi, Acil Tıp Anabilim Dalı, İzmir Amaç: Acil servislere olan başvurular sürekli bir artış göstermektedir. Aciliyet algısı açısından bir standardın olmaması acil servis yoğunluğunun çözülmesi zorlaştırmaktadır. Çalışmamızda acil servisimize başvuran ve yeşil alana yönlendirilen hastaların acil servisi tercih sebeplerini sorgulayarak, acil servis kalabalığını azaltabilecek nedenleri tespit etmeyi amaçladık.��
Gereç ve Yöntemler: Çalışma 3 aylık süre içinde Katip Çelebi Üniversitesi Atatürk Eğitim Araştırma Hastanesi Acil Servisi’ne müracaat eden ve triaj sonrası yeşil alan hastası olarak değerlendirilen 1000 hasta ile yapıldı. Hastalara demografik özellikleri, eğitim durumları şikayetlerinin başlama süresi, kendilerince şikayetlerinin gerçekten acil olup olmadığı, acil servise başvuru amaçları, hastaneye ulaşım yolu ve kendilerine göre acil servislerin tanımının sorulduğu bir anket cevaplatıldı. ��
Bulgular: Hastalarımızın %40,1’i acil servisi ’’tetkiklerin hızlı yapıldığı yer’’ tanımlamışlardır. %24,3’ü 24 saat her türlü hizmetin verildiği yer, %18,2’si durumu acil olanların bakıldığı yer ve geri kalan hasta grubu da acil servisi acil hasta olan ya da olmayan herkesin bakılması gereken yer olarak tanımladı. Bu tanımlama için eğitim seviyeleri arasında anlamlı fark bulunmadı. Hastaların%60’ı şikayetleri başladıktan1 saat içerisinde, %12’si ise yıllardır olan şikayetleri için acil servisi seçmişti. Hastalarımızın %38.2’sine göre şikayetleri acil değildi. Acil servislere mesai dışı gelme nedenleri sorulduğunda,% 29.4’ünün kendileri ya da refakatçileri çalıştığı için mesai saatleri içinde hastaneye başvuramadıkları, % 27.4 ’ü polikliniklerin çok yoğun olması nedeniyle acil servisi tercih ettikleri öğrenildi. Çalışmaya alınan hastaların %11,9’unun acil müdahale gereği olmadığı halde hastaneye ulaşım için 112 sağlık hizmetlerini kullandığını tespit edildi. Eğitim seviyeleri arasında da 112 sağlık hizmetlerinin kullanımı konusunda anlamlı bir fark saptanmadı.��
Sonuç: Acil servis ve 112 gibi acil hizmetler toplumun her kesimince amacı dışında kullanılmaktadır. Eğitim seviyesine olursa olsun, bu yanlış algının düzelmediği görülmektedir. Eğitim seviyesinin yüksek olması acil servis ve acil hizmetlere bakış açısını değiştirmemekte olup, acil hizmetlerin doğru kullanımı için toplumun her kesiminde bu algı yeniden oluşturulmalıdır.�Anahtar kelimeler: Acil Servis, Acil servis kullanım amaçları, acil servis kalabalığı Anahtar Kelimeler: Acil servis, acil servis kullanım amaçları, acil servis kalabalığı O 016 KADIN ACİL TIP UZMANLARININ SOSYAL YAŞAM VE MUTLULUK ANALİZİ Elif Çelikel1, Afsin Emre Kayipmaz2, Betül Akbuga Özel2, Cemil Kavalci2, Ümmügülsüm Kocalar2
1Ankara Numune Eğitim ve Araştırma Hastanesi, Ankara�2Baskent Üniversitesi Ankara Hastanesi, Ankara Acil Tıp, ülkemizde 1993 yılından beri uzmanlık eğitimi verilen bir anabilim dalıdır. Bu anabilim dalında eğitim veren kliniklerin ve bu kliniklerin yetiştirdiği acil tıp uzmanlarının sayısı giderek artmaktadır. Acil tıp vaat ettiği mesleki tatmin ve nispeten yeni bir dal olmanın getirdiği avantajlar sebebiyle kadın hekimlerin de tercihi olmaya devam etmektedir. Kadın acil tıp uzmanları tıpkı erkek meslektaşları gibi beklenmeyen kritik vakalar, toplumun kendisinden yüksek profesyonellik beklentisi, kendini mesleki anlamda sürekli geliştirme gerekliliği gibi stres faktörleriyle karşı karşıya kalmaktadır. Bu da onların sosyal yaşamlarını ve mutluluklarını etkileyebilir. Bu nedenle kadın acil tıp uzmanlarının çalıştığı stresli ortamın sosyal yaşamlarına ve mutluluk düzeylerine etkisini ortaya koyacak çalışmalara ihtiyaç vardır. Biz de bu çalışmada kadın acil tıp uzmanlarının ev içi desteklerini, sosyal aktivitelerini, iş tatmini düzeylerini ve subjektif mutluluk ölçeği sonuçlarını analiz etmeyi amaçladık. Anahtar Kelimeler: Acil tıp, kadın, uzman doktor

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
117
O 017 YENİ BİR TOPİKAL HEMOSTATİK AJAN: ÖN ÇALIŞMA SONUÇLARIMIZ İsmail Altıntop1, İbrahim Özcan2, Çiğdem Karakükçü3, Yasemin Ay Altıntop4, Mehmet Tatlı1
1Kayseri Eğitim Araştırma Hastanesi, Acil Tıp Kliniği, Kayseri�2Kayseri Eğitim Araştırma Hastanesi, Kulak Burun Boğaz Kliniği, Kayseri�3Kayseri Eğitim Araştırma Hastanesi, Tıbbi Biyokimya Bölümü, Kayseri�4Kayseri Eğitim Araştırma Hastanesi, Tıbbi Mikrobiyoloji Bölümü, Kayseri Amaç: Kanamalar; travmaya bağlı yaralanma, savaş ve afet yaralanmaları, kesici delici alet yaralanmaları, burun kanamaları, yanık sonrası kanamalar, gastrointestinal sistem kanamaları olarak karşımıza çıkmaktadır. Boyutu, nedeni ve şekli ne olursa olsun kanamaların erken durdurulması önemlidir. Kanama durdurucu ajanlar acil servislerde, ambulanslarda ve modern cerrahide yaygın olarak kullanılmaktadır. Ülkemizde kanama durdurucu ürünler ithalat yoluyla elde edildiğinden maliyetleri yüksek olmaktadır. Ulusal olarak başarılı olacak, yerli üretim ilaç modelleri yapılabilmesi için çalışmamız planlanmıştır.� Materyal Metod:Kayseri Eğitim Araştırma hastanesi Acil Servis, Tıbbi Mikrobiyoloji, Tıbbi Biyokimya, Kulak Burun Boğaz ünitelerinde Eylül 2016-Ekim 2016 tarihleri arasında onam alınan hastalardan alınan kan numuneleri ile çalışma yapılmıştır. Çalışmamız prospektif, deneysel, tanımlayıcı, kesitsel olarak planlanmıştır. İşlenmiş diatomit (ID) ile yapılan in vitro çalışmalar devam etmektedir. Ön sonuçların başarılı olması üzerine in vivo çalışma planlanmıştır. ��
Bulgular: Çalışmada kullanılması planlanan diatomit bileşiminde bulunan bileşiklerin özelliklerini araştırmak amacıyla iki ayrı bölgeden elde edilen diatomit bileşikleri X-Ray Floresan (XRF) ile incelenerek ön sonuçları tabloda verilmiştir (Tablo 1). İncelenen diatomitler elde edildikleri bölgelere göre nispeten bileşen oranları farklı olduğu için diatomit-1 ve diatomit-2 olarak gösterilmiştir. Ön çalışmalarımızda diatomit-1 bileşenlerine yüzey alanı ölçümleri yapılmıştır. BET sonuçlarına göre 16.0385 m²/g yüzey alanı bulunmuştur.��
Sonuç��Sitratlı tüpe alınan kan örneklerine 0.05 gr kadar toz ID eklendikten sonra yapılan PT, INR ve aPTT ölçümlerinde (özellikle yüksek değerlerde), PT ve INR sonuçlarında %40-50'ye varan oranlarda azalma gözlenirken, aPTT sürelerinde belirgin artış (%30-40) kaydedildi. ID’in trombosit fonksiyonu üzerine olan etkileri ile ilgili ön çalışmamızda, in vitro kanama zamanında herhangi bir değişiklik gözlenmemiştir. Anahtar Kelimeler: Modifiye diatomit, kanama durdurucu, kanama zamanı, koagülasyon O 018 ACİL SERVİSTE RADYASYON HASARLARININ TANI VE TEDAVİSİ TATBİKATI
Serdar Savaş Gül1, Serhat Karaman2, Serhat Koyuncu2
1Gaziosmanpaşa Üniversitesi Tıp Fakültesi, Nükleer Tıp Anabilim Dalı, Tokat�2Gaziosmanpaşa Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Tokat Radyoaktif maddelerin tıp, araştırma ve endüstri alanında kullanımı giderek yaygınlaşmaktadır. Önlemlere rağmen, her ne kadar seyrekte olsa, radyasyon kaynaklarıyla ilgili kazalar meydana gelmektedir. Ülkemizde 1989 yılında İkitelli’de bir hurdalıkta bulunan Kobalt-60 radyoaktif kaynağı yüzünden 18 kişi hastane acil servisine kaldırılmıştır. Ülkemiz, komşularımızda bulunan nükleer reaktörlerden kaynaklanabilecek kaza riskleri ile karşı karşıya bulunmaktadır. Radyasyon kazası sonucunda hastalar ilk olarak acil servise getirileceklerdir. Acil çalışanları yüksek doz radyasyona maruz kalacaktır. Bu çalışmadaki amacımız; radyasyon hasarlarının tanı ve tedavisi tatbikatını uygulamak, acil serviste radyasyon güvenlik önlemlerini almak ve acil servis çalışanlarında radyasyon farkındalığı oluşturmaktır.��
Radyasyon tatbikatı senaryosunda; nükleer tıp bölümünde 200mCi İyot-131 ile ablasyon tedavisi alan hasta, yatışının 1. Gününde miyokard enfarktüsü tanısı ile acil servise getirileceği haber verilir. Acil serviste “Radyasyon Güvenliği Yönetmeliği” uygulamaya konulur: Tüm acil servis çalışanlarına bilgi verilir, radyasyon koruyucu önlemler başlatılır. Hastaya müdahale edecek ekip radyasyon koruyucu giysilerini giyer. Hastanın yatacağı oda etrafındaki diğer hastalar uzak odalara nakledilir. Hasta getirildikten sonra birinci ekip hastaya tıbbi müdahale ederken, ikinci ekip radyasyon güvenlik önlemlerini alır. Hastanın bulunduğu alanın radyoaktivite yüzey ölçüm cihazı ile radyasyon ölçümleri yapılır: 0.2mR radyasyon ölçüm değeri olacak şekilde radyasyon güvenlik alanı belirlenir. Bu alan içerisine görevli olmayan kişilerin girmesi engellenir. Hasta tetkik ve tedavi sırasında kusar. Radyoaktif madde bulaşı gerçekleşir. Radyoaktivite yüzey ölçüm cihazı ile radyoaktivite miktarı belirlenir. Dekontaminasyon solüsyonları ile zemin radyoaktiviteden temizlenir. Hastanın tedavisinin tamamlanmasının ardından nükleer tıp bölümünde bulunan radyoaktif hasta odasına sevki yapılır. �İkitellideki radyasyon kazası Türkiye’de meydana gelen, bilinen ilk büyük radyolojik kazadır. Bu olay sonucunda 18 kişi hastaneye yatırılmış ve 10 kişi akut radyasyon sendromu nedeniyle tedavi görmüştür. Acil servis çalışanları bu tür kazalar sonrasında bilerek ya da bilmeyerek external ya da internal radyasyona maruz kalabilir. Radyasyon kazaları sonrası oluşabilecek semptomlar ve bulgular açısından acil servis çalışanların farkındalık düzeyinin artırılması için radyasyon hasarlarının tanı ve tedavisi tatbikatı gerekli olduğu düşünülmüştür. Anahtar Kelimeler: Acil servis, radyasyon kazası, radyoaktivite

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
118
O 019 ACİL SERVİSTE HASTA BAŞI YAPILABİLECEK GİRİŞİMSEL RADYOLOJİK İŞLEMLER Betül Tiryaki Baştuğ Eskişehir Osmangazi Üniversitesi Tıp Fakültesi, Radyoloji Anabilim Dalı, Eskişehir Amaç: Girişimsel radyoloji, radyolojinin tedavi edici bölümü olup hızla ilerlemektedir. Görüntüleme kılavuzluğunda minimal invaziv yöntemlerle ciltten girilerek tedavi yapılmaktadır. İlk girişimsel radyolojik işlemler 60’lı yıllarda denenmiş olup işlemlerin çeşitliliği giderek çok artmıştır. Bu şekilde çok geniş bir spektrumdaki işlemler ve teknikler geliştirilmiş olup artık hasta başında dahi cok kısa zamanda bile çoğu klinik duruma yardım sağlanabilmektedir.��
Gereç-Yöntem: Radyologlar önceden elde edilmiş görüntüler üzerinde gerçekleştireceği işlemi planlar. Daha sonra kateterleri damarlardan veya perkütan olarak, görüntüleme kılavuzluğunda (Dijital Substraksiyon Anjiografi, Floroskopi, Ultrason, Bilgisayarlı Tomografi) yönlendirirler. Bu işlemler lokal veya gereğinde nadiren genel anestezi altında gerçekleştirilir. ��
Bulgular: Girişimsel radyolojik işlemler vasküler ve nonvasküler olarak iki büyük gruba ayrılır. Vasküler girişimler anjiyografik teknikleri kullanarak yapılan tedavi edici işlemlerdir. Bu grup sıklıkla Dijital Substraksiyon Anjiografi ve Floroskopi klavuzluğunda yapılan işlemlerdir. Acilde hasta başı uygulama bu nedenlerle kısıtlıdır. Non Vasküler girişimsel işlemlerin büyük çoğunluğu ise;acil serviste hasta başında lokal anestezi ile ultrasonografi eşliğinde yapılabilinir: kolesistit ve hidropik keselerde kolesistostomiler, hidronefroz durumlarında acil nefrostomiler, primer veya sekonder nedenli abse-hematom drenajları, plevral ve peritoneal sıvı örneklemeleri ve drenajları hasta başında uygulanabilecek prosedürlerden bazılarıdır.��
Sonuç: Girişimsel radyolojik işlemler; cerrahi uygulamalara kıyasla çok daha az invaziv olup genellikle bu işlemlerde hasta tolerabilitesi daha yüksektir: geniş kesiler yoktur, daha az ağrı, risk ve daha kısa iyileşme zamanı ile işlemler tamamlanır. Acil serviste hasta başında hızlı bir şekilde uygulanabilecek böylece hasta kliniğinin hızlı bir şekilde toparlanmasını sağlayacak tedaviyi yönlendirebilecek tolerabilitesi yüksek pek çok girişimsel radyolojik prosedür bulunmaktadır. Anahtar Kelimeler: Acil servis, girişimsel radyoloji, hasta başı uygulamalar O 020 ACİL SERVİSE LATERAL MALLEOL TRAVMASI İLE BAŞVURAN HASTALARDA ULTRASONOGRAFİNİN KIRIK TANISINDAKİ SENSİTİVİTE VE SPESİFİTESİNİN ARAŞTIRILMASI Pınar Öztürk1, Ersin Aksay1, Neşe Çolak Oray1, Başak Bayram1, Duygu Tokgöz1, Onur Başçı2
1Dokuz Eylül Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, İzmir�2Dokuz Eylül Üniversitesi Tıp Fakültesi, Ortopedi ve Travmatoloji Anabilim Dalı, İzmir Giriş-Amaç: Kırık tanısında standart yöntem direkt grafi olmasına rağmen, ultrasonografi kullanımı giderek yaygınlaşmaktadır. Bizim çalışmamamızın amacı erişkinlerde lateral malleol kırıklarının tanısında ultrasonografik incelemenin tanısal değerini araştırmaktır.� Gereç-Yöntem: Acil servise lateral malleol travması sebebiyle başvuran 18 yaş ve üstü hastaların alındığı ileri yönelik kesitsel bir çalışmadır. Hastalara acil servis hekimi tarafından ultrasonografik inceleme yapıldıktan sonra anteroposterior ve lateral direkt grafi çekildi. Direkt grafi ve ultrasonografi arasında uyumsuzluk olması durumunda hastalara bilgisayarlı tomografi çekildi. Direkt grafi ve varsa bilgisayarlı tomografi görüntüleri ultrasonografik bulgularından ve hastanın klinik bulgularından habersiz bir ortopedi uzmanı tarafından yorumlandı. Ortopedi uzmanının kararı altın standart kabul edildi. İstatiksel analiz için SPSS 15.0 Windows ve vassarstats programı kullanıldı.��
Bulgular: Çalışmaya alınan 120 hastanın 42’sinde kırık olduğu tespit edildi (toplam kırık prevelansı %35). Ultrasonografik incelemede 47 hastada lateral malleol kırığı görüldü. Ultrasonografi lateral malleol kırıklarının tümünü tespit ederken, beş olguda yanlış pozitif sonuç verdi. Ultrasonografinin lateral malleol kırıklarının tanısında sensitivitesi %100, spesifitesi %93, pozitif likelihood ratio (LR) değerleri 8.4, negatif LR değerleri none saptandı. Direkt grafinin lateral malleol kırıklarının tanısında sensitivitesi sırasıyla ise %92.8, spesifitesi %100, pozitif LR değerleri ∞, negatif LR 0.03 saptandı. ��
Sonuç: Ultrasonografinin, lateral malleol kırıkları tanısındaki duyarlılığı, direkt grafiden yüksektir. Acil servis hekimleri lateral malleol kırıklarının tanısında yatak başı ultrasonografik incelemeyi efektif bir tanı aracı olarak kullanabilirler. Anahtar Kelimeler: Acil servis, acil servis hekimleri, yatak başı ultrasonografi, lateral malleol kırıkları

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
119
O 021 YATAK BAŞI ULTRASOUND EŞLİĞİNDE KALICI TÜNELLİ PORT KATETERİ TAKILAN HASTALARDA KULLANILAN SEDATİF AJANLARIN STRES HORMONLARI VE YÜKSEK DUYARLI TROPONİN ÜZERİNE
ETKİSİ Yılmaz Safi, Cuma Yıldırım, Cem Şen, Mustafa Sabak, Süleyman Nogay, Suat Zengin Gaziantep Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Gaziantep Amaç: Bu çalışmada acil serviste santral venöz kateter takılan hastalarda uygulanan sedasyon ve analjezi kombinasyonlarının, ağrı skalaları, anksiyete, ACTH, Kortizol ve Yüksek duyarlı Troponin üzerine olan etkilerini araştırdık.��
Materyal-Metod: Bu çalışma prospektif olarak, 01 Mart 2015-01 Eylül 2015 tarihleri arasında Gaziantep Üniversitesi Tıp Fakültesi Acil Tıp Anabilim Dalı’na Hematoloji ve Onkoloji tarafından Port kateteri takılma endikasyonu konulan 90 hasta üzerinde yapıldı. Hastalar; Midazolam-Ketamine kombinasyonu, Midazolam-Fentanil kombinasyonu ve Propofol uygulanan 30’ar kişilik 3 gruba ayrıldı. Hastaların kan basıncı, nabız değerleri ve yatak başı Doppler ultrasonografi (USG) bulguları değerlendirildi. Visuel Analog Skala(VAS) kullanılarak ölçeklendirilen ağrı düzeyleri, Beck Anksiyete Ölçeği kullanılarak anksiyete düzeyi ile kan numunesi alınarak ACTH, Kortizol ve Yüksek duyarlı Troponin değerleri Port takılma işlemi öncesi (0.dakika) ve sonrası (30.dakika) olmak üzere kaydedildi. Bu değerler kıyaslandı. İstatistiksel değerlendirme için, Windows için SPSS 18.0 (SPSS Inc, Chicago, Illinois, ABD) paket programı kullanıldı ve tüm karşılaştırmalarda p <0.05 istatistiksel anlamlı kabul edildi. Bulgular: Gruplar arasında cinsiyet ve yaş açısından anlamlı istatistiksel bir fark yoktu (p=0,836 ve p=0,182). Her üç sedasyon grubundaki hastalarda anlamlı anksiyete azalması oldu. Midazolam-Fentanil ile Propofol yapılan hastalarda ağrı düzeyindeki azalma anlamlı bulundu. Midazolam-Fentanil ile Propofol grubunda sistolik ve diastolik kan basıncında anlamlı bir düşüş ooldu. Her üç sedasyon grubundaki hastalarda anlamlı SPO2 azalması olmadı. Midazolam-ketamin grubu ile Midazolam-Fentanil grubundaki hastaların nabız sayılarındaki anlamlı artış oldu. Midazolam-Ketamin ile Propofol grubundaki hastalarında kan ACTH düzeylerindeki anlamlı artış bulundu. Her üç sedasyon grubundaki hastalarda anlamlı Kortizol değişikliği bulunmadı. Her üç sedasyon grubundaki hastalarda anlamlı Yüksek duyarlı Troponin I bulundu ve gruplar arası anlamlı fark yoktu��
Tartışma ve Sonuçlar: Santral Venöz Kateter gibi minör cerrahi girişimlerde sedatif ajanlar acil servisteki etkin, güvenli ve kolay uygulanabilirler. Acil servislerde invaziv işlem uygulanacak hastalara anksiyolitik ve sedatif ilaçlara ek olarak analjezik ilaçların da eklenmesini önermekteyiz Anahtar Kelimeler: Port kateter, sedasyon, anksiyete, troponin O 022 KARBONMONOKSİT ZEHİRLENMESİ OLGULARININ ANALİZİ Abuzer Coşkun1, Afşin Emre Kayıpmaz2, Sedat Özbay1, Osman Mahir Okur1, Şevki Hakan Eren3, Cemil Kavalcı2
1Sivas Numune Hastanesi, Acil Servis, Sivas 2Başkent Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Ankara�3Gaziantep Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Gaziantep Giriş: Karbon monoksit zehirlenmesi dünya çapında ölüme sebep olan başlıca zehirlenmelerden birisi olmasına rağmen, kesin insidansı henüz tespit edilememiştir. Karbon monoksit hemoglobine ve hücresel oksidatif enzimlere oksijenden daha yüksek bir affiniteyle bağlanarak doku hipoksisine neden olan renksiz ve kokusuz bir gazdır. Kalp ve sinir sinir sistemi hücrelerindeki hipoksi ise onun nöropsikiyatrik ve kardiyolojik belirtileriyle bulgularının oluşmasına yol açar. Bu çalışmada karbon monoksit zehirlenmesi nedeniyle acil servise başvuran olguların demografik özelliklerini araştırmayı amaçladık. Ayrıca bu olguların klinik özelliklerini ve bu olgularda mortaliteyi etkileyen faktörleri ortaya koymayı hedefledik. Gereç ve Yöntem: Erişkin acil servisimize 2 yıllık bir sure zarfında başvurup karbon monoksit zehirlenmesi tanısı alan 1013 hastanın demografik ve klinik özelliklerini retrospektif olarak gözden geçirdik. Hastaların yaş, cinsiyet, başvuru mevsimi, hastane yatış oranı, zehirlenmenin kaynağı, başvuru belirtileri, mortalite oranı, karboksi hemoglobinle troponin I seviyeleriyle ilgili bilgileri kayıt ve analiz ettik. ��
Bulgular: Çalışma popülâsyonunun ortalama yaşı 36,2±16,2’ydi. Hastaların %70,5’i kış mevsiminde başvuru yapmıştı. Hastaların %66,1’inin zehirlenme kaynağı sıcak su ısıtıcısı-gazla çalışan sobalardı. En sık bulgular bulantı, baş ağrısı ve sersemlik hissiydi. Multilojistik regresyon analizinde ölüm hızı, yaş ve troponin I düzeyiyle anlamlı oranda koreleydi. Sonuç: Çalışmamızın sonuçları, karbon monoksit zehirlenmesinin zorlu kış koşullarının hâkim olduğu bölgelerde halen önemli bir halk sağlığı problemi olduğunu ortaya koydu. Toplumun eğitimi ve zehirlenme kaynaklarının etkin kontrolü için gösterilen çabaların yoğunlaştırılmasının, karbon monoksit zehirlenmesinin önüne geçilmesinde en önemli basamaklar olduğunu düşünmekteyiz. Anahtar Kelimeler: Epidemiyoloji, karbonmonoksit, zehirlenme

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
120
O 023 ACİL SERVİS ÇALIŞANLARININ KESİCİ-DELİCİ ALET YARALANMALARI İLE KARŞILAŞMA DURUMLARI VE ALINAN ÖNLEMLER
Gulten Sucu Dağ1, Meral Dölek2
1Doğu Akdeniz Üniversitesi, Sağlık Bilimleri Fakültesi, Hemşirelik Bölümü, Gazimağusa, KKTC�2Katip Çelebi Üniversitesi, Sağlık Bilimleri Fakültesi, Hemşirelik Bölümü, İzmir Giriş ve Amaç: Kesici-delici alet yaralanmaları, acil servis çalışanlarının maruz kaldığı mesleki riskler arasında ilk sıralarda yer almaktadır. Bu çalışmanın amacı, acil servis çalışanlarının kesici-delici alet yaralanmaları ile karşılaşma durumları, yaralanma nedenleri ve alınan önlemleri belirlemektir. Yöntem: Araştırma tanımlayıcı kesitsel araştırmadır. Veri toplamada Acil Hemşireleri Derneği web sayfasına anket formu eklenmiş ve tüm üyeler araştırmaya davet edilmiştir. Araştırma katılmayı kabul eden üyeler araştırmanın örneklemini oluşturmuştur. Araştırma, Dernek web sitesinden, online veri toplama yöntemi ile, araştırmaya katılmayı kabul eden 159 dernek üyesi ile yürütülmüştür. Veri toplamada araştırmacılar tarafından literatürden yararlanarak hazırlanan, sosyO demografik veriler ile kesici-delici alet yaralanmalarını ve alınan önlemleri sorgulayan 27 sorudan oluşan anket formu kullanılmıştır. Anket formu uygulanmadan önce üç uzmandan görüş alınmıştır. Veriler sayı ve yüzde dağılımları ile değerlendirilmiştir. ��
Bulgular: Acil servis çalışanlarının %67.3’ünün kesici delici alet yaralanmasına maruz kaldığı, %52.2’inin ilk kesici-delici alet yaralanmasını mesleğe başladıktan sonraki 1-5 yıl arasında olduğu, %95’inin iğne batmasına maruz kaldığı, %29.6’nın iğne ucu kapatma sırasında yaralanmaya maruz kaldığı saptanmıştır. %36.5’inin meslek süresince birden fazla yaralanmaya maruz kaldığı, %58.9’unun meslek süresince 2 kez kesici delici alet yaralanmasına maruz kaldığı, belirlenmiştir. Katılımcıların %64.8’nin kesici delici alet yaralanmasından sonra bildirimde bulunmadığı, %52.2’inin HBV-HCV-HİV için takibe alındığı, %54.2’inin kaynağını bildiği, %43.5’nin yaralanma sonrası eğitim aldığı saptanmıştır. Kesici delici alet yaralanması sonrası hastanede önlem alındığını bildirenlerin oranı %47.5’tir. Araştırmaya katılanların %63.5’i sadece korumalı branülün alınan önlemler arasında olduğunu belirtmişlerdir. ��
Sonuç: Araştırmaya katılan acil servis çalışanlarının yarısından fazlasının iğne batma yaralanmasından dolayı, iğne ucunu kapatma nedeniyle kesici delici alet yaralanmasına maruz kaldıkları saptanmıştır. Koruyucu önlemlerinde yetersiz olduğu belirlenmiştir. Acil servis çalışanlarının kesici delici alet yaralanmalarını en aza indirmek ve koruyucu önlemleri artırmak için hizmet içi uygulamalı eğitim programlarının düzenlenmesi ve belli aralıklarla tekrarlanması önerilmektedir. Anahtar Kelimeler: Acil servis, kesici-delici yaralanma, önlem O 024 AKCİĞER DIŞI TÜBERKÜLOZ OLGUSU: TÜBERKÜLOZ PERİTONİTİ Hamit Hakan Armağan, Ahmet Yunus Hatip, Furkan Çağrı Oğuzlar, Göker Çoskun, Makpere Delikanlı, Önder Tomruk, Nesrin Gökben Beceren Süleyman Demirel Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Isparta Giriş: Akciğer dışı tüberküloz, tüberküloz basilinin tüm organ ve sistemleri tutabilme yeteneğine bağlı gelişir. Vücutta saç ve tırnaklar dışında her bölgede görülebilir. Özellikle tüberkülozun endemik olduğu bölgelerde tüm sistemlerin enfeksiyonlarında ayırıcı tanıda düşünülmelidir. Tüberküloz peritonitte akut batını taklit eden karın ağrısı ve ateş görülebilir. Alternatif olarak karın ağrısı, şişlik, gece terlemesi ve kilo kaybı gibi bulgularla sinsi bir tablo da olabilir. Burada tüberküloz peritoniti tanısı almış bir olgu sunarak özellikle tüberkülozun endemik olduğu bölgelerdeki karın ağrısı ile başvuran hastalarda tüberküloz tanısına dikkati çekmek istenmiştir.��
Olgu: 29 yaşında erkek hasta yaklaşık 15 gündür olan karın ağrısı ve karında şişlik şikayetiyle acil servise başvurdu. Hastanın başvurusunda genel durumu orta-iyi tespit edilmiş olup başvuru vital bulgularında ateş tespit edilmiştir. Hastanın fizik muayenesinde batın distansiyonu ve yaygın hassasiyet izlenmiş olup, defans-rebaund izlenmemiştir. Hastanın hikâyesinde son 1 ay içerisinde 15 kg kilo kaybı mevcuttur. Hastanın yapılan laboratuar incelemelerinde lökopeni görülmüş ve CRP değeri artmış olarak izlenmektedir. Hastanın çekilen abdomen tomografisinde yaygın asit izlenmektedir. Hastanın yapılan periton sıvısı örneklemesinde transuda vasfında aside saptanmıştır. Hasta merkezimiz gastroenteroloji servisine yatırılmıştır. Merkezimizde laparotomi ile yapılan periton biyopsisinde kazifikasyon nekrozu ve granülamatöz değişiklikler saptanmış, yapılan kültürler neticesinde mycobacterium tuberculosis izole edilmiştir. Yapılan antibiyogram sonrası izoniazid, rifampisin, etambutol, streptomisin duyarlı tespit edilmiş olup hastanın tedavisine başlanmıştır.� Sonuç: Tüberküloz halen ülkemizde önemli bir sağlık sorunu olarak varlığını sürdürmektedir. Bu yüzden bir çok enfeksiyon araştırmasında ayırıcı tanıda aklımıza gelmesi gerekmektedir. Anahtar Kelimeler: Karın ağrısı, peritonit, tüberküloz

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
121
O 025 UTILITY OF CHEST COMPUTED TOMOGRAPHY AFTER A CHEST RADIOGRAPH IN PATIENTS PRESENTING TO THE EMERGENCY DEPARTMENT WITH NON-TRAUMATIC CAUSES
Naciye Sinem Gezer1, Pınar Balcı1, Kemal Çağlar Tuna1, Işıl Başara Akın1, Mustafa Mahmut Barış1, Neşe Çolak Oray2
1Dokuz Eylul University Faculty of Medicine, Department of Radiology, Izmir, Turkey 2Dokuz Eylul University Faculty of Medicine, Department of Emergency Medicine, Izmir, Turkey Introduction: Chest radiography is the initial choice of modality in thoracic imaging. However, wide availability of computed tomography (CT) have led to substantial increase in its use at the emergency department (ED). Purpose: To evaluate the utility of chest CT after a chest radiograph in patients presenting to the ED with non-traumatic thoracic emergencies and to determine how physicians' diagnoses and management decision are affected by the results of CT. Materials-Methods: 500 consecutive patients (age range: 18 –97) with both chest radiography and CT who presented to the ER with non-traumatic causes were included in this study. Chest radiographs and CT images obtained at the same day were evaluated for emergent pathologic findings including pulmonary edema, pneumonic infiltration, pleural effusion, atelectasia, pneumothorax and fractures. Concordance of the detection of these findings by chest radiography compared with CT, sensitivity and specificity of radiography compared with CT were assessed. Impact of chest CT after a chest radiograph on diagnosis and management at the ED was evaluated. Results: Radiographic findings were concordant in 49.2% of 500 patients and this finding was negatively correlated with the patient age (p=0.025, r=-0.1). The leading diagnosis and management decisions according to the chest radiography changed after CT in 35.4% of the study group and this finding was also correlated with age (p=0.002, r=0.138). In 55% of 205 patients, pneumonic infiltration was undiagnosed with radiography. Pulmonary edema was the most specific (93.3%) and sensitive (85.4%) finding of radiography. Posterioranterior chest radiography taken in upright position had higher concordance and impact on diagnosis and management than anteriorposterior radiography taken in supine position. Conclusions: Chest CT would be an appropriate choice of thoracic imaging in patients presenting to the ED with non-traumatic causes, especially in elderly and when the radiography is taken in supine position. Keywords: Chest, computed tomography, emergency department, non-traumatic, radiograph O 026 THE DIAGNOSTIC VALUE OF SCUBE1 IN ACUTE APPENDICITIS Ertan Sönmez1, Dursun Akbay1, Bedia Gülen1, Hüseyin Metin1, Ömer Faruk Özer2
1Bezmialem Vakıf University Medical Faculty, Department of Emergency Medicine, Istanbul, Turkey 2Bezmialem Vakıf University Medical Faculty, Department of Biochemistry, Istanbul, Turkey Background: SCUBE1 has recently studied as a diagnostic biomarker for acute coronary syndrome, ischemic stroke and acute mesenteric ischemia. The aim of this study is to evaluate the value of SCUBE1 and routine parameters used in patients diagnosed with acute appendicitis. Methods: Of the 150 patients admitted to the emergency department whose initial diagnosis were acute appendicitis (AA), 103 patients were excluded from the study for various reasons. Forty-seven patients with a definitive diagnose of AA and 43 volunteers were enrolled in the study. SCUBE1, Alvarado scoring (ASK), C-reactive protein (CRP) and routine tests were compared between the two groups. Results: SCUBE1 was not statistically significant between the patient and the control groups (p=0.209). SCUBE1 was significantly higher in the CRP (+) group (p=0.048). Both the diameter of the appendix on computerized tomography (CT) and SCUBE1 levels increased proportionally (p=0.043). CRP was significantly higher in the perforated appendicitis (PA) compared to non-perforated appendicitis (NPA) (p=0.007). White blood cell (WBC) count was not differential for perforation (p=0.06). Conclusions: Although SCUBE1 was significantly higher in CRP (+) patients, it was not a diagnostic biomarker for AA. There was a positive correlation between SCUBE1 values and the diameter of appendix measured on CT. Keywords: SCUBE1, acute appendicitis, Alvarado scoring, USG, CT

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
122
O 027 EMERGENCY MEDICINE RESIDENTS CAN ASSESS CRANIAL COMPUTED TOMOGRAPHY SCANS CONSISTENTLY WITH RADIOLOGISTS
Şenol Ardıç1, Özlem Güneysel2
1Health Sciences University, Trabzon Kanuni Training and Research Hospital, Clinic of Emergency Medicine, Trabzon, Turkey 2Health Sciences University, İstanbul Kartal Dr.Lütfi Kırdar Training and Research Hospital, Clinic of Emergency Medicine, İstanbul Purpose/Aim: The aim of this study was to determine competence of emergency medicine residents in the assessment of cranial computed tomography (CT) scans and to evaluate the level of consistency with radiologists. Methods: A total of 525 cases were included in the study. Cranial CT scans obtained from patients who presented to Dr Lutfi Kirdar Kartal Education and Research Hospital Department of Emergency Medicine, between January 1st and July 1st 2012, were assessed by an emergency medicine resident who ordered the scan after physical examination and by a radiologist within 2 days after CT order. CT scans were interpreted within 2 days using the Picture Archiving and Communication System by two different radiologists with emergency medicine experience. Radiologists were blinded to the assessment of the emergency medicine resident and the other radiologist. Results: The noncoincidental consistency was 82.3% between cranial CT scan interpretations by radiologists and emergency medicine residents. The sensitivity, specificity, positive predictive value, and negative predictive value of statistical accuracy between interpretations by emergency medicine residents and radiologists were 92.55%, 94.9%, 79.81%, and 98.32%, respectively. Conclusion: Emergency medicine residents can assess cranial CT scans consistently with radiologists. Keywords: Cranial computed tomography, emergency medicine resident, radiologist O 028 DIAGNOSTIC VALUE AND EFFECT OF BEDSIDE ULTRASOUND IN ACUTE APPENDICITIS IN EMERGENCY DEPARTMENT Faruk Güngör, Taylan Kılıç, Can Akyol, Gizem Ayaz, Umut Çakır, Akçimen Mehmet, Eken Cenker Antalya Training and Research Hospital, Clinic of Emergency Medicine, Antalya, Turkey Objective: Early and accurate diagnosis of acute appendicitis (AA) with ultrasound can minimize the morbidity and mortality of the patients. In this regard, ultrasound can help to the emergency physicians (EPs) in the diagnosing process and clinical decision making for AA. Therefore, we aimed to evaluate the effectiveness of point of care ultrasound (POCUS) in the diagnosis and clinical decision making for AA in the emergency department (ED). Methods: The study sample consisted of patients over the age of 18 years that presented to the ED with an abdominal pain and underwent diagnostic evaluation for AA. All patients were examined initially with point of care ultrasound (POCUS) by EPs and then with radiology performed ultrasound (RADUS) by radiologists. Pre- and post-POCUS median diagnostic certainty values (MDCVs) for AA were determined with visual analogue scale (VAS) scores (0 not present, 100 certainly present) by POCUS performers. Definitive diagnoses were determined by surgery, pathologic evaluation of appendectomy specimens, or clinical follow results. The sensitivity, specificity, positive likelihood ratio (PLR), and negative likelihood ratio (NLR) for POCUS and RADUS along with pre- and post-POCUS VAS scores of MDCVs were compared. Results: A total of 264 patients were included into the final analysis and 169 (64%) of them were diagnosed with AA. Sensitivity, specificity, PLR, and NLR of ultrasound examinations were 92.3% (95% CI; 87.2-95.8%), 95.8% (95% CI; 89.5-98.8%), 21.9 (95% CI; 8.4-57.2) and 0.08 (95% CI; 0.05-0.1) for POCUS, and 76.9% (95% CI; 69.8-83%), 97.8% (95% CI; 84.9-99.7%), 36.4 (95% CI; 9.25-144.3) and 0.24 (95% CI; 0.18-0.31) for RADUS, respectively. Pre-POCUS and post-POCUS VAS scores of MDCVs were 60 (IQR: 50-65) and 95 (IQR: 20-98), respectively (p=0.000). Conclusion: POCUS, performed in ED for diagnosis of AA, has high sensitivity and specificity, and had a positive impact on the clinical decision making of EPs. Keywords: Appendicitis, point of care, ultrasound, emergency department
5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
123
O 029 DETERMINATION OF THE NORMAL VALUES OF VERTEBRAL AND PREVERTEBRAL SOFT TISSUE DISTANCES IN LATERAL CERVICAL VERTEBRAL COMPUTED TOMOGRAPHY ACCORDING TO AGE AND
GENDER Serhad Omercikoglu, Erhan Altunbas, Haldun Akoglu, Ozge Onur, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Goal: Trauma of the spine and spinal cord may lead to potentially debilitating injuries with serious complications. Different imaging modalities can be used for the examination of spinal trauma and accurate evaluation of the spinal axis and vertebra. The thickness of prevertebral soft tissue (TOPST) in lateral cervical radiographic examination is reported to be a useful indicator and an indirect sign of underlying cervical spine injury. Today, cervical computed tomography (CT) is the main and the first scanning method for cervical injuries. However, upper normal values of predental, and basion-dental distances as well as the TOPST were not determined for CT imaging. In this retrospective study, we aimed to validate the normal reference values of the TOPST by cervical CT scans and report normal reference values according to gender and age groups, for the first time in the literature, to the best of our knowledge. Materials-Methods: Five hundred adult trauma patients admitted to our ED in whom a cervical CT was performed at the time of admission were retrospectively selected. All distances were measured by two researchers who were blinded to eachother, patients and radiology reports. Results: 488 c-spine CTs were normal. Mean predental, basion-dental, C1, C2, C6 and C7 prevertebral distances were found to be statistically significantly wider in males. In females, predental and basion-dental distances were significantly narrower with the increase in age. In males, only predental distance was significantly narrower, and TOPST of C6 and C7 vertebra were significantly wider with the increase in age. All measurements were reference values are depicted in Figures for different age groups. Discussion: In our study, upper normal ranges of predental, basion-dental distances and TOPST for CT were determined for the first time, to the best of our knowledge. We hope these ranges helps physicians to interpret cervical CT findings. Keywords: Cervical CT, distance, trauma O 030 DETERMINATION OF CHEST WALL THICKNESS WITH A BEDSIDE ULTRASOUND FOR NEEDLE THORACOSTOMY IN THE EMERGENCY DEPARTMENT Faruk Güngör1, Taylan Kılıç1, Havva Neslihan Korkmaz Sayraç1, Dilek Soydam Güven1, Abdullah Şükün2, Erkan Göksu3
1Antalya Training and Research Hospital, Clinic of Emergency Medicine, Antalya, Turkey 2Antalya Training and Research Hospital, Clinic of Radiology, Antalya, Turkey 3Akdeniz University School of Medicine, Department of Emergency Medicine, Antalya, Turkey Introduction: Tension pneumothorax is a life threatening condition and requires emergent decompression with needle thoracostomy (NT). But the catheter length can be short to reach intra-pleural space. Therefore, we aimed to measure chest wall thickness (CWT) with a bedside ultrasound (BUS) to determine the adequacy of catheters used for NT. Method: Patients who were over 18 years and underwent a chest CT scan in the radiology department included in the study. Patients with any chest wall deformity or surgical history of thorax excluded from the study. Body mass indices (BMIs) of patients were calculated. CWT was measured bilaterally at the second intercostal space midclavicular line (2ICSML) and fourth intercostal space anterior axillary line (4ICSAAL), with a BUS by emergency physicians in the emergency department (ED). Each measurement was compared with chest CT results. Results: Two hundred and seventeen patients, 115 (53%) male and 102 (47%) female, were included in the study. Mean age was 55 (19-87) years old. Overall mean BMI was 28.6 kg/m2 (95% CI, 26.8- 31.8): 28.1 kg/m2 (95% CI, 25-34.5) for men and 29.3 kg/m2 (95% CI, 28.2-30.4) for women. Mean CWT of the patients at 2ICPML and 4ICSAAL were 47.4 mm (±15.6) and 40 mm (±13) for left side, and 47.5 mm (±16) and 40.2 mm (±13.2) for right side, respectively. All bedside US measurements was statistically and significantly correlated with chest CT results (p:0.000). Conclusion: CWT for NT can be properly and real-timely measured with a BUS, and then, a catheter with a proper length can be chosen to increase procedure success. Keywords: Tension pneumothorax, ultrasound, needle thoracostomy

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
124
O 031 COMPARISON OF ULTRASONOGRAPHY WITH CHEST X-RAY IN VERIFICATION OF NASOGASTRIC TUBE PLACEMENT AT EMERGENCY DEPARTMENT
Çağdaş Yıldırım1, Selçuk Çoşkun1, Şervan Gökhan2, Gül Pamukçu Günaydın1, Ayhan Özhasenekler2
1Atatürk Training and Research Hospital, Clinic of Emergency Medicine, Ankara, Turkey 2Yıldırım Beyazıt University Medicine School, Department of Emergency Medicine, Ankara, Turkey Introduction: Rapid and sequence insertion of nasogastric (NG) tube is one of the most common procedures in emergency department(ED). Misplacement of tube can cause rare but serious complications. Gold standard method for verification is chest X-ray (CXR). The aim of this study is to show the effectiveness of ultrasonography (USG) and compare with CXR in patients who have NG tube placement indication. Material-Methods: This study includes 49 patients with over 18 years of age, who admitted to our hospitals ED with NG tube placement indication between February 1, 2016 - June 10, 2016. NG tubes were inserted by the patients emergency medicine resident. After the tube inserted auscultation, USG and CXR was performed respectively. USG was performed to neck and subxiphoid area by single emergency medicine resident who certified in emergency ultrasonography. CXR has been interpreted by another emergency medicine specialist who did not conduct the ultrasonography. CXR was considered the gold standard. Results: Our study consists of 49 patients with indications for nasogastric tube insertion. The average age of our patients was 58.3 ± 22.7 years. 55.1% of our patients were male, 44.9% were female. NG tube insertion indications were; ileus (51.0%), medication (30.6%), gastric lavage (10.2%), gastrointestinal bleeding (6.1%) and perforation (2.0%). 2 patient’s NG tube was curled in pharynx and the tube was not detected by USG and CXR. USG has confirmed the location of NG tube in 45 patients and was significantly consistent with chest radiography (κ: 0.647).The sensitivity of USG was 95.74%. When auscultation used in conjunction with ultrasound, kappa value was 0.790, was found to be significantly consistent with CXR and sensitivity is 97.87%. � Conclusion: USG can be used effectively for the nasogastric tube placement verification. We think unnecessary and repeat CXRs can be avoided with ultrasonography. It should be verified with the participation of more and larger patient groups. Keywords: Ultrasonography, nasogastric tube placement, emergency department O 032 THE COMPARISON OF RADIOGRAPHY AND POINT-OF-CARE ULTRASONOGRAPHY IN THE DIAGNOSIS AND MANAGEMENT OF METATARSAL FRACTURES Nalan Kozaci1, Mehmet Oguzhan Ay2, Mustafa Avci1, Inan Beydilli1, Sadullah Turhan3, Eda Donertas1, Ertan Ararat1
1Antalya Training and Research Hospital, Clinic of Emergency Medicine, Antalya, Turkey 2Hitit University, Çorum Training and Research Hospital, Department of Emergency Medicine, Çorum, Turkey�3Antalya Training and Research Hospital, Clinic of Orthopedics and Traumatology, Antalya, Turkey Objective: It was aimed to compare the efficacy of point-of-care ultrasonography (POCUS) with radiography in the diagnosis and management of metatarsal fracture (MTF). Methods: Patients aged 5-55 years admitted to emergency room due to low-energy, simple extremity trauma and had a suspected MTF, were included in this prospective study. Patients were evaluated by two different physicians in the emergency room. The first physician performed POCUS examination. Second physician evaluated the radiography images. The obtained results were compared. Results: Seventy-two patients were enrolled in the study. Fracture was detected in 40% by radiography and in 44% of patients by POCUS. Multiple MTFs were identified in 5% of patients. Compared with radiography, POCUS had a sensitivity of 93%, specificity of 89%, positive predictive value of 84% and a negative predictive value of 95% (95% CI, 83-98%) in the detection of fractures. While soft tissue edema was seen in 61% of patients by POCUS, soft tissue edema with hematoma was detected in 14%. Compared with radiography, the sensitivity and specificity of POCUS in the decision for surgery were 100% and 98% (95% CI, 97-100%), respectively, whereas its sensitivity and specificity were both 100% in the decision for reduction. Conclusion: In our study, we demonstrated that POCUS could be applied with success in the diagnosis and treatment of MTF in low-energy injuries. POCUS can be used as an alternative to radiography in the emergency rooms due to being easy to learn and practice and availability of soft tissue examination along with bone tissue examination. Keywords: Metatarsal, fracture, radiography, ultrasonography, diagnosis

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
125
O 033 THE MEASUREMENT OF AORTIC DIAMETER: IS THERE A DIFFERENCE BETWEEN COMPUTED TOMOGRAPHY AND ULTRASOUND?
Engin Özakın1, Ruşengül Koruk1, Nilgün Işıksalan Özbülbül2, Muzaffer Bilgin3, Mustafa Emin Çanakçı1, Nurdan Acar1, Filiz Baloğlu Kaya1
1Eskişehir Osmangazi University, Department of Emergency Medicine, Eskişehir, Turkey�2Eskişehir Osmangazi University, Department of Radiology, Eskişehir, Turkey�3Eskişehir Osmangazi University, Department of Biostatistics, Eskişehir, Turkey Methods: A number of 45 patients admitted to the ESOGU emergency service between the dates 05.09.2016-18.09.2016 was included in the study. Measurements were performed on patients before the scheduled thoracoabdominal CT from 4 different locations, which are 1 cm distal to the aortic outlet, suprasternal, suprarenal and infrarenal, by the 3rd and 4th year medical emergency physicians. The measurements from the same point after the CT scan were recorded by the radiologist, who is unaware of ultrasound results. The comparisons of all the measurements were performed using the paired Wilcoxon test analysis. Results: 51% of patients were men and the mean age of the patients included in the study was 49 respectively. The average of the measurements assessed by ultrasound was found to be for aortic outlet: 2.73±0,4593 mm, for suprasternal 2.22±0.4194 mm, for suprarenal: 1.69±0.37179 mm and for infrarenal: 1.42±0.27240 mm. The average of the measurements assessed by CT was found to be for aortic outlet: 2.82±0.45788 mm, for suprasternal: 2.46±0.3823 mm, for suprarenal: 1.72±0.30061 mm, and for infrarenal: 1.54±0.27208 mm, respectively. Differences were detected on the suprasternal (p<0.001) and infrarenal (p<0.001) localisations in the comparison of the ultrasound and CT values and these differences were considered as statistically significant. There were no significant differences in the aortic outlet (p=0.137) and suprarenal (p=0.160) localisations. Conclusion: The aortic diameter especially aortic outlet and suprarenal localisations, measured by emergency medicine physicians with USG is very valuable. EM physicians should be more careful with the US in the examinations on the suprasternal and infrarenal localisations due to mismeasurement when compared with CT in terms of the results of our study. Keywords: Aortic diameter measurements, ultrasound, CT, emergency medicine O 034 TURN OFF THE LIGHT IF UNNECESSARY! THE EVALUATION OF THE UNNECESSARY RADIOLOGICAL IMAGING ORDERS FROM THE VIEWPOINT OF DOCTORS Mehmet Cihat Demir, Damlanur Kucur, İlter Ağaçkıran, Yasemin Özdamar, Nalan Metin Aksu, Meltem Akkaş Hacettepe University Medicine of Faculty, Department of Emergency Medicine, Ankara, Turkey Objective: Due to the development and proliferation of radiological equipment in recent times, overutilization and unnecessary use of radiological imaging has come into question. In this study, the unnecessary imaging orders will be evaluated from the viewpoint of the doctors who request the tests. Again, while examining the reasons behind these unnecessary orders, we aimed to detect the causes and any variation according to the departments. Methods: The study is made in 2015.The doctors were divided into 5 groups as emergency medicine, medical sciences, surgical sciences, radiology departments or general practitioners (GP).140 doctors who have at least working experience of three years were present in each groups, and a total of 700 doctors answered questionnaire via e-mail about radiological imaging p<0.05 were considered statistically significant. Findings: In this study, we revealed ultrasonography (US), magnetic resonance imaging (MRI), radiography and computed tomography (CT) were found as unnecessary requests by 55%, 65.9%, 70.9%and 88% of doctors, respectively. The main causes of unnecessary requests for all radiological imaging are overcrowding/time limitation, patient satisfaction, lack of knowledge, lack of history and avoiding malpractice. For unnecessary radiography examinations, the lack of information, poor history and medical habits were stated as primary causes compared to the other divisions by radiologists while in emergency medicine department the consultant physician claim was stated the most important cause compared to the other departments(p<0.001).Lack of information is the main cause of unnecessary CT orders in radiology department compared to the other departments(p<0.001).The lack of information, being less harmful than CT, diagnostic difficulties, patient satisfaction, institutional expectations were the primary causes of unnecessary MRI orders, requested by radiologists compared to the other divisions(p<0.001). Conclusion: Most of the radiological imaging are considered unnecessary requests from the viewpoint of doctors. In order to reduce these unnecessary requests, training of doctors about radiological imaging and increasing awareness is required. The development and implementation of appropriateness criteria for radiological imaging will be effective in reducing unnecessary orders and also ensure a common approach among the doctors from each divisions. Keywords: Radiological imaging, overutilization, appropriateness criteria

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
126
O 035 AN UNUSUAL CAUSE OF UPPER GASTROINTESTINAL OBSTRUCTION: WILKIE'S SYNDROME Özgür Dikme Istanbul Training and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey Superior mesenteric artery syndrome (SMAS) (known as Wilkie's syndrome, cast syndrome, mesenteric root syndrome, chronic duodenal ileus and intermittent arterio mesenteric occlusion) is one of the rarest but potentially life-threatening cause of upper gastrointestinal obstruction. The third or transverse portion of the duodenum was compressed between the aorta and the superior mesenteric artery. A 30-year-old female presented with abdominal pain, epigastric fullness, nausea, intermittent vomiting and 13 kg weight loss over three months. There was no history of hematemesis and melena. Her vital parameters were within normal limits. Abdominal examination revealed a distended abdomen, mild epigastric tenderness, hyperactive bowel sounds and normal digital rectal examination. On work-up, laboratory findings were: Urea 98 mg/dl and creatinin 3.01 mg/dl with normal serum electrolytes and liver function tests. Bedside ultrasonography was performed by emergency physician and showed dilated duodenum. Gastric and duodenal decompression was performed via nasogastric tube. Computed tomography of the abdomen showed grossly distended stomach and duodenum up to D3 without any mass lesion. She was transferred to surgery ward. Her symptoms improved after three days with conservative management and she was discharged home. SMAS is an unusual cause of upper gastrointestinal obstruction, and the diagnosis of SMAS is often delayed. SMAS should be kept in mind in the differential diagnosis of the patients who admitted with non specific symptoms like persistent nausea, vomiting and significant weight loss to the emergency room. Keywords: Abdominal pain, arterio mesenteric occlusion, Wilkie's Syndrome O 036 CARDIAC TAMPONADE WITHOUT PERICARDIAL EFFUSION Nurfer Zehra Gören, Başak Bayram Dokuz Eylül University Faculty of Medicine, Department of Emergency Medicine, Izmir, Turkey Introduction: Cardiac tamponade is a rare complication of blunt chest trauma. Clinically; mediastinal hematoma is one of the reason that can mimick cardiac tamponade. This case report is about a mediastinal hematoma after blunt chest trauma. Case: A 28 years old male was transported to our ED after a motor-vehicle collision. On initial evaluation the patient was alert and oriented. Vital signs on arrival were BP 133/78 mmHg, PR 76/min and O2 saturation %99. He had tenderness of anterior chest and deformity of left wrist. The breath sounds were clear bilaterally. Bedside FAST revealed no pericardial effusion, no pleural and intraperitoneal fluid. Pan scan CT was planned because of the high energy trauma. The patient suddenly developed signs of shock after tomography. He was cold, pale and clammy and juguler venous distension has developed. At the same time his vital signs were BP 82/44 mmHg, PR 132/min. 1000 mL bolus of saline was given to the patient and treatment followed by 2 units of type O packed RBCs infusion. FAST exam was repeated. There was no detected free abdominal fluid or pericardial effusion but we detected left ventriculer filling defect without pericardial effusion. Therefore cardiac ultrasound was performed which discovered a huge mediastinal hematoma compresses left ventricule. Thoracic CT showed fracture of inferior sternum, bilateral hemothorax and anterior mediastinal hematoma with extravasation of contrast medium. Than patient was transferred to the operating room. After performing sternotomy, there was active bleeding in the left internal mammary artery (LIMA) and its branch; LIMA repaired and bleeding controlled. The patient was discharged five days after the operation without sequel. Conclusion: Anterior mediastinal hematoma should be considered if a patient have classic findings of cardiac tamponade but no pericardial effusion is identified with ultrasound and parasternal long-axis view should be added to the traditional FAST. Keywords: Mediastinal hematoma, cardiac tamponade, traumatic extrapericardial tamponade

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
127
O 037 THE COMPARISON OF BEDSIDE POINT-OF-CARE ULTRASOUND AND COMPUTED TOMOGRAPHY IN ELBOW INJURIES
Mustafa Avcı1, Nalan Kozacı1, İnan Beydilli1, Fevzi Yılmaz1, Arif Onur Eden2, Sadullah Turhan3
1Antalya Education and Research Hospital; Clinic of Emergency Medicine, Antalya/Turkey 2Erzincan University Mengucek Gazi Training and Research Hospital, Department of Emergency Medicine, Erzincan, Turkey 3Antalya Training and Research Hospital, Clinic of Orthopedics and Traumatology, Antalya, Turkey Objective: The objective of the study was to compare the efficacy of point-of-care ultrasound (POCUS) and computed tomography (CT) in the diagnosis of the fracture of the bones that form the elbow joint and the determination of treatment method in elbow injuries. Methods: Forty-nine patients aged 5-65 years, who were admitted with low-energy elbow injuries, had at least one fracture of the elbow joint bones and underwent CT scanning, were included in this study. Before the initiation of the study, orthopedic surgeons and emergency physicians determined a common treatment based on the fracture characteristics. Patients were first evaluated with direct radiography (DR), and then with POCUS by trained emergency physicians. Emergency physicians made treatment decisions based on the ultrasonography results. Then computed tomography scans were performed. CT images were interpreted by radiologists. Orthopedic surgeons made treatment decisions based on the CT interpretations. Results: Forty-nine patients with elbow injury were included in the study. Eighteen (37%) patients were female and 31 (63%) were male. The mean age was 21 ± 15 years. Compared with CT, sensitivity, specificity, positive predictive value and negative predictive value of POCUS in fracture detection was 97%, 88%, 94% and 93%, respectively. While the sensitivity and specificity of POCUS in the decision for reduction was 95% and 100%, respectively, it was 93% and 100% in the decision for surgery. Conclusion: In conclusion, POCUS was shown to be successfully applied in the diagnosis and management of elbow injuries in which DR was inefficient and CT scans were required. Keywords: Ultrasound, elbow injuries, diagnosis O 038 EFFICACY OF SONOGRAPHIC DIAMETERS AND COLLAPSIBILITY INDEX OF INFERIOR VENA CAVA IN PREDICTING THE PERCENTAGE OF BODY FLUID LOSS Yalman Eyinç1, Arzu Emecan1, Burak Nakış2, Cansu Arslan1, Özge Ecmel Onur1
1Fatih Sultan Mehmet Education and Research Hospital, Istanbul, Turkey 2Kahta State Hospital, Adıyaman, Turkey The aim of our study is to use the changes in vital parameters and ultrasonographic measurements before-after hemodialysis and deciding the sufficiency of fluid responsiveness. Our prospective and observational study has been performed in the hemodialysis unit of Fatih Sultan Mehmet Education and Research Hospital. The cases were evaluated by their vital signs and ultrasonographic measurements of inferior vena cava (IVC). Inferior Vena Cava diameters in inspirium/expirium (IVCi, IVCe) were measured and ultrafiltration (UF) amount was noted. For all the cases ultrafiltration ratios (UF amount / Total body fluid x 100) and inferior vena cava collapsibility indexes were calculated based on the suitable formulas before hemodialysis and compared with those after hemodialysis. Body weight, diastolic blood pressure, mean arterial pressure and pulse rate were compared before and after hemodialysis and statistically significant difference was found. While all ultrasonographic metrics have decreased after hemodialysis the collapsibility index increased which also supports the efficacy of hemodialysis session. The uniqueness of our study is that we did not only compared the change in vitals and diameters as increase or decrease but also aimed to find a rational correlation between them. According to the results of our study, IVCe diameters before-after hemodialysis and UF ratios showed statistically significant correlation, which in turn makes it a useful parameter for monitoring the patients for fluid loss or replacement. In order to establish this technique as an assessment to volume status and fluid responsiveness in emergency ward, more studies in larger groups performed by different researchers are need to be performed. Keywords: Correlation, emergency medicine, fluid responsiveness, IVC, ultrasound

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
128
O 039 INCIDENTAL CT FINDINGS OF PATIENTS WHO ADMITTED TO ER FOLLOWING A TRAFFIC ACCIDENT Yavuz Yiğit1, Harun Ayhan2
1Derince Education and Research Hospital, Clinic of Emergency Medicine, Kocaeli, Turkey 2Haydarpasa Numune Education and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey Objective: The aim of this study was to investigate and analyze incidental CT findings of traffic injury patients discharged from the ER, and to determine overall notification rates. Methods: All traffic injury-related patient records between 01.06.2013-01.03.2013 were obtained from Derince Training and Research Hospital Emergency Service using patient files and the hospital database. Brain, thorax and/or abdominal CT images of 340 patients aged between 0 to 84 years were included in the study. ER observation forms were investigated for the patients who had incidental findings on CT scanning and overall notification rates were recorded. Results: Mean age of the 363 cases was 31.2 (SD 17.9, min 0, max 84) and 35.5% of patients were female (n=129) and 64.5% were male (n=234). A total of 537 CT scans were performed on 363 patients. 147, 319 and 71 CT scans were performed on the thorax, brain and abdominal, respectively. 27.3% (n=99) of scan results showed the presence of a coincidental pathology. The most common disease on scans were bone lesions (8%, n=29), followed by sinus abnormalities (7.7%, n=28). Incidental findings ratio in patients aged over 60 was 60.8%, while under 60 was 24.8%. It was found that seven patients (7.1%) were informed about the imaging results. Conclusion: Most of the incidental findings were found to be benign; however, 16.5% of them were considered to require in-depth investigation. Further investigations are needed to understand the clinical relevance of these findings and their effects on patients. Keywords: Incidental findings, tomography, emergency O 040 DETECTING SHUNT DYSFUNCTION WITH OPTIC NERVE ULTRASOUND Özge Can1, Sercan Yalçınlı1, Ali Akay2, Funda Karbek Akarca1
1Ege University Faculty of Medicine, Department of Emergency Medicine, İzmir, Turkey�2Ege University Faculty of Medicine, Department of Neurosurgery, İzmir, Turkey Introduction: Intracranial shunt is the choice of treatment of hydrocephalus in children and adults. Shunt obstruction and infection is frequent references to the emergency department. Similarly, we have presented to the emergency service four patient with suspect of interventricular shunt dysfunction. Optic nerve sheath diameter (ONSD) was measured to determine the shunt dysfunction. And we want to share this experiences. Case: Four patients with ventriculoperitoneal shunt were admitted to the emergency department with complaints of headache, blurred vision, nausea and vomiting. Only one patient was 50 years old and shunt implanted due to tumor. Vital signs are stable in patients with no any signs of new neurological deficit. Behind 3 mm posterior of glob all patients optic nerve sheath diameter was measured transverse with 7 mHz linear probe. The traditional method shunt series, cranial tomography and abdominal ultrasound was performed. Neurosurgery was consulted. ONSD was measured in order to 0,44-0,48-0,47-0,53 mm. After consultation only one patient was accepted shunt dysfunction and underwent revision. Intracranial pressure was measured during operation. Patient who has 0.53mm of ONSD, ICP was measured above 20 mmHg. Disscusion: Interventricular shunt dysfunction is difficult to diagnose. No abnormal examination, subjective symptom and no sign gets more difficult to diagnose. Diagnostic tests is needed to be performed easier, fast ad nonionize. In the literature there are studies measures ONSD on children determination of hydrocephalus and on adults detect increased intracranial pressure after trauma or hypertension. The idea of us measurement of ONSD can be shown shunt dysfunction. In this four case only one patient ONSD was above 5 mm (according to literature normal range <5 mm) and intracranial pressure was measured high (above 20 mmHg) Conclusion: ONSD may a good diagnostic tool on shunt dysfunction. Keywords: Hydrocephalus, interventricular shunt dysfunction, optic nerve sheath diameter, ultrasound in emergency medicine

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
129
O 041 IMPORTANCE OF ANTIVENOM IN MANAGEMENT OF SCORPION ENVENOMATION WITH EPIDEMIOLOGIC AND CLINICAL CHARACTERISTICS
Ali Duman, Bekir Dagli, Ayhan Akoz, Mucahit Avcil, Serhat Orun, Kenan Ahmet Turkdogan Adnan Menderes University, Department of Emergency Medicine, Aydın, Turkey Objective: Especially including antivenom treatment, the management of scorpion stings remains a subject of controversy. The purpose of this study was to offer the epidemiologic and clinical characteristics of patients with scorpion sting and to determine the efficacy of antivenom treatment in the management of these patients. Methods: A total of 106 adult patients presented for scorpion sting to our ED, between January 2013 and December 2015 and 98 patients were included in the study. The clinical severity and treatment of each case was evaluated using Abroug’s classification. � Results: According to Abroug’s classification, there were 75 (76.5%), 15 (15.3%), and eight (8.2%) patients in grade I, II, and III, respectively. Length of stay of the Abroug grade II patients who did not receive scorpion antiserum was longer then grade II patients who received scorpion antiserum. But Length of stay of the grade III patients who did not receive scorpion antiserum was shorter then grade III patients who received scorpion antiserum. Conclusion: We observed that; even though scorpion antiserum can have serious side effects, the administration of a low dose of antivenom relieved severe pain that was not relieved by symptomatic treatment or narcotic analgesics, and the Abroug’s classification grades of the cases and not requiring antivenom treatment at the beginning can change or require antivenom in the following period, patients with local symptoms to be followed up for 6-12 hours or to be referred to centers performing this follow up. Keywords: Antivenom treatment, scorpion sting, Abroug’s classification, local symptoms, systemic symptoms O 042 GUNSHOT WOUND PRESENTING WITH MINOR BLEEDING Handan Çiftçi1, Elnare Günal1, Gülşen Çığşar1, Zeynep Bilgi2, Murat Özdemir1
1Kafkas University Faculty of Medicine, Department of Emergency Medicine, Kars, Turkey 2Harakani State Hospital, Department of Emergency Medicine, Kars, Turkey Introduction: Thorax trauma comprises approximately 30% of all trauma cases and is a very important cause of Emergency Room visits. 30% of all thorax trauma is penetrant injury. Penetrating thorax trauma can have high morbidity and mortality in proportion to damage to vital organs. Rarely, a thoracal gunshot wound may present as a simple injury. Case: 72 year old male patient presented to ER after noticing a small open wound on his back. Physical examination revealed a 1 cm wound with irregular borders on the midscapular line, at the 9th-10th intercostal level. Further examination showed that the depth of the wound is 6-7 cm further than subcutaneous tissue and that there is a palpable mass on the contralateral side (right midscapular line, at the 9th-10th intercostal levels). Patient also recalled a day old episode which involved a sudden burning sensation, presyncope and quick recovery. Patient’s wife noticed blood on his back at that time. Thorax CT showed hyperdense tissue plans at posterior chest wall, T9-10-11 levels, subcutaneous emphsema, 12 mm foreign body with metallic artefact at the right side. Patient was discharged after removal of the foreign body (gun pellet) under local anesthesia. Conclusion: Even patients presenting to ER with minor complaints, a complete history and thorough physical examination are of utmost importance. Keywords: Gunshot, minor bleeding, thorax trauma

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
130
O 043 PEDIATRIC EMERGENCY CARE APPLIED RESEARCH NETWORK HEAD INJURY PREDICTION RULES: ON THE BASIS OF COST AND EFFECTIVENESS
Fatma Dilek Gökharman, Sonay Aydın, Erdem Fatihoğlu, Pınar Nercis Koşar Ankara Training and Research Hospital, Radiology Department, Ankara, Turkey Introduction: Head injuries have still been one of the most common reasons for children to apply to the emergency department and tend to increase in the last decade. A non contrast enhanced cranial CT is the method of choice for detecting a possible TBI. Concerns about ionizing radiation exposure and body movements make the evaluation of children with minor head trauma via CT more challenging. Pediatric Emergency Care Applied Research Network (PECARN) stated age-based TBI clinical prediction rules can differentiate children who need a CT scan from those who may avoid it. In the current study we intended to evaluate the effectiveness of PECARN rules for predicting a ciTBI and find the amount of medical resource waste, unnecessary radiation exposure. Material-Method: This retrospective study included 1041 pediatric patients with minor blunt head trauma presenting to ED between September 2015 and July 2016. The patients are divided into subgroups of “appropriate for cranial CT”, “not appropriate for cranial CT” and “cranial CT / following the patient, both are appropriate”. To detect effectiveness of PECARN rules, data were analyzed according to the presence of pathological findings on CT images. Results: PECARN is an independent predictor for pathology presence. PECARN is able to predict pathology presence with a sensitivity of 74,8% and specificity of 91,7%. An “appropriate for cranial CT” result can predict pathology presence 118,056 fold in contrast with “not appropriate for cranial CT” result. Having a “cranial CT / following the patient, both are appropriate” result predict pathology presence 11,457 fold in contrast with “not appropriate for cranial CT” result.��
Conclusion: PECARN rules can predict pathology presence successfully in pediatric TBI. PECARN recommendation also can predict the severity of the present pathology and approximate time of hospitalization. Using PECARN can decrease both resource waste and exposure to ionizing radiation. Keywords: PECARN, cost, effectiveness, CT O 044 END-TIDAL CARBON DIOXIDE MONITORING IN PATIENTS WITH TACHYCARDIA Abdullah İlhan, Onur Tokocin, Hakan Topacoglu Istanbul Training and Research Hospital, Emergency Department, Istanbul, Turkey Objective: The aim of the study was to evaluate the changes in non-invasive measured ETCO2 levels in patients with tachycardia in the emergency room (ER). Materials-Methods: The study was conducted as a prospective, single centered cohort study over two months. All consecutive patients who had heart rate over 100 bpm were included the study. Their vital signs and ETCO2 levels were measured by using sidestream method. The correlation between ETCO2 levels and the changes in heart rates of the patients with tachycardia were analyzed. Results: A total of 108 patients were included in the study. Of these patients, 57 (52,8%) were women, 51(47,2%) were male. Median age was 63 years. ETCO2 levels had negative correlation with heart rate, respiration rate and age (respectively p=0.010, p=0.022, p=0.007). There was a positive correlation between ETCO2 levels versus systolic blood pressure, mean arterial pressure and oxygen saturation (respectively p<0.001, p=0.002, p=0.013). At discharge from ER the study group revealed a statistically significant difference in average ETCO2 levels (p=0.005). ETCO2 average of the patients admitted to intensive care unit was significantly lower than discharged patients (p=0.007). Conclusion: As a result of this study, it can be deduced that ETCO2 levels, have significant negative correlation with age, tachycardia and respiratory rate. In addition, patients that were admitted to ICU and the hospital exhibited a meaningful difference as compared to those discharged. In conclusion, ETCO2 measurement can be used as a vital parameter to predict their hospitalization in patients with tachycardia. Keywords: Emergency department, capnography, tachycardia, end tidal carbondioxide

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
131
O 045 SIGHT-THREATENING OCULAR EMERGENCIES Raşit Kılıç Ahi Evran University Faculty of Medicine, Department of Ophthalmology, Kırşehir, Turkey Aim: Critical eye emergencies are not common in emergency clinics, however, they are required immediate treatment. Prompt diagnosis and proper treatment of ocular emergencies are essential when the visual prognosis may depend on timely management. Careful ophthalmic examination with simple tests can help emergency physicians for make decisions about appropriate treatment and consultation. The aim of this review was to update the current approaches of ocular emergencies. Methods: Current literature was searched and the disorders were categorized as mechanical globe injuries, chemical injuries, retinal disorders, acute glaucoma attack and neurO ophthalmic emergencies. Visual acuity test, pupillary examination, ocular movements test, confrontation visual field examination, and direct ophthalmoscopy of both eyes should be performed for the first evaluation in emergency clinics. Results: Globe perforation requires eye shielding and consultation for surgical evaluation. It’s indicators are moderate to severe pain, decreased vision, hyphema, and deviation of pupil toward the laceration. The patients often suffer of moderate to severe pain, blepharospasm, photophobia, blurred vision, and foreign body sensation after chemical injury. Central retinal artery occlusion rapidly causes ocular stroke, which can lead to severe vision loss. Patients’ history includes painless and sudden vision loss in one eye. Acute glaucoma attack patients often present with blurred vision, eye redness, severe eye pain, frontal headache, discomfort, nausea, and vomiting. If it is not treated immediately and properly, optic nerve damage and permanent vision loss can occur within hours. NeurO ophthalmic emergencies can be life-threatening or sight-threatening and include findings of diplopia, abnormal pupillary light reflex and eye movements. Conclusions: In this review, practical approaches and clinical indicators were presented for quick recognition and prompt intervention to avoid vision loss in emercency clinics. Keywords: Acute glaucoma attack, central retinal artery occlusion, ocular emergencies O 046 A STUDY ON THE TACTICAL SAFETY OF ENDOTRACHEAL INTUBATION UNDER DARKNESS Attila Aydın1, Sedat Bilge1, Meltem Bilge2, Cemile Aydın3, Erdem Cevik4, Mehmet Eryılmaz1
1Gulhane Research and Training Hospital, Department of Emergency Medicine, Ankara, Turkey 2Dışkapı Research and Training Hospital, Clinic of Anesthesia and Resuscitation, Ankara, Turkey�3Etimesgut State Hospital, Clinic of Internal Medicine, Ankara, Turkey 4Haydarpaşa Research and Training Hospital, Clinic of Emergency Medicine, Istanbul, Turkey Strict blackout discipline is extremely important for all military units. To be able to effectively determine wound characteristics and perform the necessary interventions at nighttime, vision and light restrictions can be mitigated through the use of tactical Night Vision Goggles (NVGs). In this study, we developed a modified laryngoscope (ML) model by changing the standard lamp on a classical laryngoscope (CL) with an infrared light-emitting diode (IR-LED) lamp, in order to obtain a tool which can be used to perform endotracheal intubation (ETI) under night conditions in combination with NVGs. We first evaluated the safety of ETI procedures in pre-hospital conditions under darkness by using both the CL and the ML we designed for our study, and then researched the procedures and methods by which ETI could be performed in in the dark under tactically safe conditions. In addition, to better ensure light discipline in the field of combat, we also researched the benefits, from a light discipline standpoint, of using the poncho liner and of taking advantage of the oropharyngeal region during ETIs performed by opening the laryngoscope blades directly in the mouth and using a cover. During the ETI procedures performed on the field, two experienced combatant staff (ECS) simulated the enemy by determining whether the light from the two different types of laryngoscope could be seen, and the distance from which these light sources could be seen in case they were visible. On the field, the ETI procedures were applied either with the naked eye by using the CL blade, or with an NVG by using the ML blade using. We believe that findings of our study are rather unique. The findings of our study are likely to shed light on the tactical safety of ETI performed with NVGs under darkness. Keywords: Modified laryngoscope, tactical, endotracheal intubation, dark conditions

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
132
O 047 SPONTANEOUS HEMORRHAGIC INFARCTS IN METHANOL INTOXICATION Hüseyin Şahin1, Hilal Horozoğlu2, Mustafa Numan Erdem1
1Namık Kemal University Faculty of Medicine, Department of Emergency Medicine, Tekirdağ, Turkey�2Tekirdag State Hospital, Clinic of Neurology, Tekirdağ, Turkey Introduction: Methanol poisoning is rare, can occur when someone drinks industrial solvents, cologne, cleaning and antifreeze liquids or also adulterated wine. It is oxidized to formaldehyde in the liver and eventually turns into formic acid. Formic acid is six times more toxic than methanol. Case: A 45-year-old man with a history of chronic alcoholism was referred to the emergency department with ambulance. The patient was in comatose state and intubated. His Glasgow Coma Scala (GCS) score was 4 in that time. Electrocardiography, laboratory tests levels were normal. On admission, he presented unilateral mydriasis but fundoscopic examination did’nt show papilledema. Cranial CT was normal. Diffusion MR scan of brain showed bilateral external capsule ischemia. And than he was taken intensive care unit (ICU). Fundoscopic examination on the third day is detected papill and optic nerve edema and also hyperemia. MR imaging performed on the 7th day revealed haemorrhagic infarcts in both basal ganglia, thalamus and capsule interna. In the intensive care unit, until the 20th day of discharge with minimal sequelae, patients were followed by CT Discussion: The clinical presentation of methanol intoxication can vary greatly from patient to patient. Acute methanol poisoning can cause permanent neurologic dysfunction, and death. We report a case of 45-year-old man with methanol poisoning via drinking cologne. Although Acute intracranial haemorrhage is quite rare, lethal complication can be seen as well. Intracranial necrosis and haemorrhage probably result from the direct toxic effects of methanol metabolites and metabolic acidosis in the basal ganglia. In the same cases that come with unconsciousness, we should consider intracranial haemorrhage. If the patient comes with comatose state,we should immediately perform CT scan and MR imaging for detect infarcts and haemorrhage. We wanted to explain with this case that one of the rare complications methanol intoxication to you. Keywords: Methanol, poisoning, intracranial haemorragia O 048 HOW EMERGENCY PHYSICIAN'S GENDER SHAPED BY PATIENTS ATTENDING EMERGENCY DEPARTMENTS IN CULTURALLY CONSERVATIVE SOCIETY? Mohammed Alomar, Ali Almajed, Fatimah Alkandari, Ranya Aboshanb, Abdelmoneim Eldali King Faisal Specialist Hospital and Research Centre, Riyadh, Saudi Arabia Objectives: Patient reassurance and trust is an important aspect of communication in emergency situations. Culturally conservative patients may feel uncomfortable when examined by opposite sex of EP (emergency physician). With the dominance of the male and the scarcity of female EP this descriptive study determines the preference of EP gender among ED (emergency department) patients and investigates the characteristics affecting those choices. Materials and Methods: Randomly selected patients attended four major EDs answered a structured questionnaire detailing sociO demographic, religious commitment, preferred EP gender in critical and non-critical presentations and the diverse characteristics of EP. Categorical variables were summarized as frequencies, percentages and compared by Chi-square test. Univariate and multivariate logistic regression was used to assess the impact of important variables over gender preference. The level of statistical significance was set at p< 0.05. Results: The interviewed 407 patients (56% females) reflected a wide range of age, educational level, marital status and occupation. In a non-critical conditions, 41% of female patients preferred female EP which was statistically significant (p<0.004). In critical conditions 27% of female patients preferred female EP. Experience, concerning, trustfulness and making the patient comfortable were the major characteristic features among EP. With using univariate logistic regression in non-critical conditions for female EP preference; the significant factors are: origin (p=0.02), gender (p<0.0001), age (p=0.006), and occupation (p=0.01). Using multivariate logistic regression only gender and age was found to be significant (p<0.0001), (p=0.01) respectively. With using univariate logistic regression in critical conditions for female EP preference; the significant factors are: gender (p<0.0001), occupation (p<0.0001), and religion commitment (p=0.03). Using multivariate logistic regression only gender and occupation were found to be significant (p<0.0001), (p=0.004) respectively. Conclusion: Both genders of EP are needed. However, More females EP are needed for the delivery of high quality care in a gender sensitive community. Keywords: Emergency, physician, department, female, gender

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
133
O 049 SHORT-TERM CONSEQUENCES OF NASAL INTERMITTENT POSITIVE PRESSURE VENTILATION IN PATIENTS WITH OBESITY-HYPOVENTILATION SYNDROME WHO HAVE UNDERWENT BARIATRIC SURGERY
Burcu Yormaz1, Ilhan Ece2, Serdar Yormaz2
1Beyhekim State Hospital, Clinic Of Chest Diseases, Konya, Turkey 2Selcuk University Faculty of Medicine, Department Of General Surgery, Konya, Turkey Background: The incidence of obesity, defined as a body mass index (BMI) of > 40 kg/m2, is increasing dramatically in all over the growing world. As obesity progresses, hypoventilation may develop in some individuals, leading to respiratory failure and mortality. Obesity-hypoventilation syndrome (OHS) is a clinical entity that is characterized by the coexistence of morbid obesity and hypercapnia during wakefulness. Noninvasive positive-pressure ventilation (NIPPV) has been successfully used in patients in which the patient presents with hypercapnia.The aim of Our study is to evaluate the outcome of patients with obesity-hypoventilation syndrome (OHS) who were underwent bariatric surgery and treated with nasal intermittent positive-pressure ventilation (NIPPV). Methods: Of 28 patients between the years of May 2015 to june 2016, OHS was diagnosed. three patients (10.7%) refused to be treated with NIPPV and 25 patients were started on NIPPV therapy electively. We were taken daytime arterial blood gas values and overnight pulse oximetry results to detect the initial NIPPV modes and settings. Results: Among the 25 study patients,of 18 (72%) female,7(28%) were male, the mean age was 41 ± 8 years. The mean BMI was 47 ± 3.4 kg/m2. At presentation, 14 (56 %) of the 25 patients have experienced an acute hypercapnic situation (pH < 7.34). Twenty one patients required supplemental oxygen. At the end of the follow-up period (mean period, 6 months), PaO2 had increased by 24 mm Hg from baseline (95% confidence interval CI ) and PaCO2 had decreased by 17 mm Hg (95% CI ). NIPPV therapy and bariatric surgery procedure decreased dyspnea in all patients due to lose weight and enhances physical capacity. None of the patient died. Conclusions: NIPPV therapy is more effective in the treatment of patients with OHS after the bariatric surgery, providing a significant improvement in clinical status and oxygen saturation. Keywords: Intermittent positive pressure ventilation, obesity-hypoventilation, bariatric O 050 CAN ULTRASOUND QUANTIFICATION OF ANTERIOR NECK SOFT TISSUE THICKNESS PREDICT DIFFICULT LARYNGOSCOPY? Deniz Kılıç, Erkan Göksu Akdeniz University Faculty of Medicine, Department of Emergency Medicine, Antalya, Turkey Prediction of difficult laryngoscopy in the ED (Emergency Department) is an important issue. Although ‘LEMON’ mnemonic is suggested for possible difficult laryngoscopy in ED, it has some limitations. Ultrasound has many applications in ED. The aim of the study is to compare the ultrasound quantification of anterior soft tissue thickness of neck in easy and difficult laryngoscopy patients. This was a prospective, cross-sectional study performed in the emergency department of a tertiary care facility with 90,000 annual patient visits to the emergency department. The study was approved by the institutional review board. Demographic properties (age, gender, Body mass index), thyromental distance, sternomental distance, soft tissue thickness measured from the point of vocal cords (zone 1) and thyroid isthmus (zone 2) with linear US probe and Cormack-Lehane (CL) grades were recorded. Intubation difficulty score and visual analog scale (VAS) to predict intubation difficulty was recorded. Patients were grouped as easy (CL 1 and 2) and difficult (CL 3 and 4) laryngoscopy. Fifty-one patients participated in this study. Mean age of the study population was 64±19 SD and 58.8 % of population was male. Mean thyromental and sternomental distance and interincisor gap was not statistically significant among the laryngoscopy groups. Intubation difficulty score and VAS measured for to predict intubation difficulty was statistically significant between the groups according to CL grading. Zone 1 measured from the skin to vocal cords or zone 2 measured from the skin to thyroid isthmus was not statistically significant according to CL grading. The presence of abnormal incisor teeth was detected only one participant in difficult intubation group. The neck mobility was limited in 3 cases in the easy laryngoscopy group. Laryngeal manipulation was needed in 4 patients (BURP) in easy laryngoscopy group and 3 patients in difficult laryngoscopy (1 cricoid pressure and 2 BURP) group. Keywords: Difficult intubation, neck, obesity, ultrasound

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
134
O 051 CONFIRMATION OF THE ENDOTRACHEAL TUBE PLACEMENT WITH ETCO2 AND TRACHEAL ULTRASONOGRAPHY: A PROSPECTIVE, COMPARATIVE, DIAGNOSTIC UTILITY STUDY
Tugba Mamak, Okkes Yilmaz Cinar, Erkman Sanri, Haldun Akoglu, Ozge Onur, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Introduction: Verification of endotracheal tube (ETT) placement is the most important process of airway management. End-tidal carbon dioxide pressure (ETCO2) measurement is offered to be a valuable tool for confirmation. However, technical problems and measurement errors hinder its utility. The use of tracheal ultrasound (TU) is a promising new approach and it doesn’t have the biases of ETCO2 measurements. Therefore, we aimed to calculate the diagnostic utility of ETCO2 and TU of EPs for the confirmation of the ETT placement compared to boroscopic visualization as a gold standard. Method: This is a prospective, diagnostic utility study. All adult (>18) patients who were decided to be intubated in the ED for any purpose were enrolled. Patients with any serious traumatic or anatomical disturbance hindering sonographic imaging of the neck were excluded. During the intubation process intubating physicians confirmed the placement of ETT by usual methods. ETCO2 values were recorded by capnography at the same time. Blinded investigators performed TU and boroscopy. Results: 287 patients were included. There were no failed intubations. 46(16%) patients were intubated during an arrest state. In 286(%99.65) of intubated patients, intubation success was confirmed by boroscopy. In 1 patient, visualization with the boroscope could not be performed. TU was successful in all patients and confirmed all intubations. Measurement of the ETCO2 could not be performed in 5 patients. Correlation of ETCO2 with arterial pCO2 was poor(r=0.31). ETCO2 measurements were observed to be unreliable during an arrest state. Only 16/46(34.8%) of the patients with an arrest state had an ETCO2 value of less than 10 mmHg. In 24/282(8.5%) patients, ETCO2 was below 10 mmHg despite successful intubations. Conclusion: TU may be a reliable method for the confirmation of ET placement, at least comparable to boroscopy. However, serious measurement errors hinder the utility of ETCO2 on the bedside for confirmation. Keywords: Boroscopy, endotracheal intubation, confirmation O 052 COMPARISON OF LOOP DRAINAGE AND PRIMARY INCISION & DRAINAGE TECHNIQUES IN ADULT PATIENTS WITH CUTANEOUS ABSCESS: A PRELIMINARY, RANDOMIZED CLINICAL TRIAL Ibrahim Ulaş Özturan1, Nurettin Özgür Doğan1, Onur Karakayalı2, Asım Enes Özbek2, Serkan Yılmaz1, Elif Yaka1, Murat Pekdemir1, Selim Süner3
1Kocaeli University Faculty of Medicine, Department of Emergency Medicine, Kocaeli, Turkey 2Derince Training and Research Hospital, Clinic of Emergency Medicine, Kocaeli, Turkey 3Brown University, Rhode Island Hospital, Clinic of Emergency Medicine, Rhode Island, USA Objectives: The aim of the present study is to compare efficacy of loop drainage and primary incision & drainage techniques in adult patients with cutaneous abscess in the emergency department. Methods: This study is an interventional, two centered, parallel group, randomized clinical trial. Adult patients with cutaneous abscess were randomized into loop drainage and standard incision & drainage (ID) groups. ID group received standard care with drainage of abscess, whereas two small incisions were made on each side of abscess in the loop drainage group. Also in this group, a sterile, non-powder, non-latex surgical glove cuff was inserted through in one incision and brought out through the other side and two tips of cuff were tied loosely. The primary outcome was defined as change in diameter of abscess and cellulitis after 7 days of admission. Secondary outcome measures were pain intensity and procedure time at the end of the procedure. Also patient satisfaction, need for antibiotherapy and repetitive drainage need were investigated. Results: A total of 46 patients were included to randomization. Both groups were similar regarding to demographic characteristics and baseline abscess features. According to change in abscess diameter, loop drainage group showed –0.6 cm (95% CI: –1.5 - 0.3) difference in reduction comparing with ID group. Also this difference was similar in cellulitis diameter (–0.6 cm, 95% CI: –2.3 - 1.1). No statistically significant difference was found between groups regarding to patient satisfaction, need for antibiotherapy and need for repetitive drainage.��
Conclusion: This preliminary study revealed that, loop drainage technique was not superior to ID technique regarding to abscess resolution and complication reduction. Keywords: Cutaneous abscess, loop drainage, emergency department

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
135
O 053 ANALYSIS OF MEAN PLATELET VOLUME (MPV) AND RED BLOOD CELL DISTRIBUTION WIDTH (RDW) IN RECURRENT EPISTAXIS
Ali Ekber Karabulut, Yunsur Çevik, Emine Emektar, Şeref Kerem Çorbacıoğlu, Seda Dağar, Oğuz Yardım Keçiören Training and Research Hospital, Department of Emergency Medicine, Ankara, Turkey Aim: In our study, we aimed at determining the effect of mean platelet volume (MPV) and red blood cell distribution width (RDW) levels which are parameters in complete blood count, on epistaxis in patients with recurrent epistaxis. Material and Method: Patients with recurrent epistaxis, presented to Emergency Department of Keçiören Training and Research Hospital, were included in the study. The bleeding of the patients who had admitted to hospital with epistaxis at least twice since the previous year, was considered as recurrent epistaxis. Demographic data of these patients, their vital findings and the results of their complete blood counts were recorded. The patients who had clinical conditions that might affect the levels of MPV or RDW, were excluded. SPSS for Windows 15.0 program was used for statistical analysis. Results: A total of 136 patients and 170 control cases were included in the study. The median age was 38.5 (IQR%25-75: 23.0-51.0) in the study group and 35 (IQR%25-75: 27.0-46.2) in the control group. The median level of MPV was 7.6 fL (IQR%25-75: 7.1-8.4) in the study group and 8.2 fL (IQR%25-75: 7.8-8.9) in the control group (p=0.000). The median levels of RDW were found for study and control groups in order %15.4 (IQR%25-75: 14.5-15.4) and %14.3 (IQR%25-75: 13.4-15.4) (p=0.000). Systolic blood pressure, leukocyte count, age, sex, RDW and MPV levels that were variables with p levels<0.2, were included in the multivariate analyses. It was determined that high RDW levels increased epistaxis (p=0.000; OR:1.89 95% CI:1.53-2.33 ) and high MPV levels decrased epistaxis (p=0.000; OR:0.54 95% CI:0.39-0.72 ). Conclusion: We observed that in patients with recurrent epistaxis, low MPV and high RDW levels caused an increased bleeding tendency. Although exact mechanism is not known, referring those patients for the assessment of etiologic causes would be proper. Keywords: Recurrent epistaxis, MPV, RDW, emergency department O 054 CHARACTERISTICS OF PATIENTS PRESENTING TO THE EMERGENCY DEPARTMENT WITH OPHTHALMOLOGIC SYMPTOMS Kuddusi Teberik1, Ayhan Saritas2
1Düzce University School of Medicine, Department of Ophthalmology, Düzce, Turkey�2Düzce University School of Medicine, Department of Emergency Medicine, Düzce, Turkey Aim: To investigate the patients presenting to the emergency department of our hospital with ophthalmologic symptoms. Material-Method: Out of 141613 patients who presented to the emergency department between August 2014 and September 2014, 2509 had ophthalmologic symptoms. The records of the patients were evaluated retrospectively. Age, gender, etiologic factors and diagnoses of the cases were recorded and detailed eye examinations were investigated. The patients were divided into three groups as simple cornea-conjunctiva pathologies, traumatic injuries and serious emergencies. Results: 30.2% of the patients were female while 69.8% were male. The mean age of the patients was 39.4 years old (range 0-93). The patients were investigated dividing them into groups of simple cornea-conjunctiva pathologies (n= 1730), traumatic injuries (n=439) and serious emergencies (n=340). 19.1% of 439 trauma cases were female. 1730 patients had simple cornea-conjunctiva pathologies and 530 of them (30.6%) were diagnosed with conjunctivitis. The most frequent pathology turned out to be conjunctival cut (21.2%) in patients who were consulted as serious emergency. Conclusion: Considering the gender distribution of the cases suffering from trauma, males have dominance. Conjunctivitis is a problem that increases the burden and workload of emergency departments. It is thought that a lot of eye injuries can be prevented through simple measures at workplaces, at home and in the traffic. Keywords: Eye diseases, emergency, ophthalmology

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
136
O 055 PULMONER EMBOLİ HASTALARINDA, PULMONER EMBOLİ ŞİDDET İNDEKSİ (PESI) VE BASİTLEŞTİRİLMİŞ PULMONER EMBOLİ ŞİDDET İNDEKSİNİN (SPESI) 30 GÜNLÜK MORTALİTE TAHMİNİ AÇISINDAN
KARŞILAŞTIRILMASI Zeynep Yüzgeç, Ayfer Keleş, Ahmet Demircan, Fikret Bildik, Alev Duygu Süre Pirhan, Ayşe Keçecioğlu Gazi Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Ankara Amaç: Pulmoner emboli nonspesifik semptom ve bulguları nedeniyle tanı koymanın zor olduğu ciddi bir hastalıktır. Hemodinamik durum, kardiyak enzimler, ve görüntüleme bazlı risk sınıflamaları pulmoner emboli hastalarını değerlendirmek için sıkça kullanılır. Bu çalışmada pulmoner emboli şiddet indeksi (PESI) ve basitleştirilmiş pulmoner emboli şiddet indeksinin (sPESI) 30 günlük mortalite tahmini açısından karşılaştırılması amaçlanmıştır. ��
Yöntem-Gereçler: Bu çalışma, prospektif gözlemsel bir klinik çalışma olarak düzenlenmiş olup, Gazi Üniversitesi Tıp Fakültesi Acil Tıp Anabilim Dalı Erişkin Acil Servisinde 01.07.2015 - 31.03.2016 tarihleri arasında yapılmıştır. Veriler SPSS 22.0 programı kullanılarak bilgisayar ortamina aktarılıp değerlendirilmiştir. PESI ve sPESI arasındaki uyum Kappa Uyumluluk Testi ile değerlendirildi. PESI ve sPESI'nin 30 günlük mortalite durumunu öngörmede tanısal karar verdirici özelliği ROC eğrisi analizi ile incelendi. Risk düzeylerinin sensitivite, spesifisite, pozitif ve negatif prediktif değerleri hesaplandı. ��
Bulgular: Gazi Üniversitesi Hastanesi Acil Servisinde toraks bilgisayarlı tomografi anjiyografi (BTA) ile pulmoner tromboemboli tanısı almış 87 hasta çalışmaya dahil edildi (yaş ortalaması 62,64±16,17, %54,0’ı erkek). 30 günlük mortalite %13,8 idi. Orjinal PESI, basitleştirilmiş PESI'ye göre daha fazla oranda hastayı düşük riskli olarak sınıflandırmıştır (%26,4 ve %12,6). Her iki indeksin de 30 günlük mortalite için sensitivitesi ve negatif prediktif değeri %100 idi. ROC eğrisi altında kalan alanlara bakıldığında; PESI’nin tanısal karar verdirici özelliğinin, sPESİ'den yüksek olduğu görüldü (AUC=0,848 (%95 CI:07,23-0,972); p<0,001 vs AUC=0,782 (%95 CI:0,661-0,902); p=0,002). Sonuçlar: Sonuç olarak, hem PESİ’nin hem de sPESİ'nin benzer olduğu, sPESI'nin kullanımının daha kolay olduğu ve PESI'nin sPESI'ye göre 30 günlük mortaliteyi öngörmede tanısal karar verdirici özelliğinin daha fazla olduğu görüldü. Anahtar Kelimeler: Pulmoner emboli, pulmoner emboli şiddet indeksi, basitleştirilmiş pulmoner emboli şiddet indeksi O 056 ACİL SERVİSTE DÜŞÜRÜLEMEYEN İNR YÜKSEKLİĞİNİN ALTINDA GENETİK BOZUKLUK MU YATIYOR? Kenan Ahmet Turkdogan1, Ali Duman1, Gökay Bozkurt2, Mücahit Avcil1, Selçuk Eren Çanakçı1, Bekir Dağlı1
1Adnan Menderes Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Aydın�2Adnan Menderes Üniversitesi Tıp Fakültesi, Tıbbi Genetik Anabilim Dalı, Aydın Arteriyel ve venöz trombozların önlenmesinde oral antikoagülan tedavi oldukça önemlidir. Varfarin, günümüzde en sık kullanılan oral antikoagülan ajan olup terapötik aralığı oldukça dardır ve ilaç doz ayarlanması bireylere göre değişebilmektedir. Yetersiz doz tromboembolik olaya ve aşırı doz ise kanama riskini arttırabilir. Diyet ve ilaç gibi çevresel faktörlerin yanında genetik faktörler de varfarinin farmakokinetik ve farmakodinamik özelliklerini etkileyebilmektedir. Bu durum varfarin tedavisi doz ayarlamasını zorlaştırmakta ve varfarine bağlı kanama riskini artırmaktadır. ��
37 yaşında, daha önce 2 kez suicidal girişim öyküsü ve bipolar tanılı kadın hasta 7 gün önce ve 3 gün önce fare zehiri içerek dış merkeze halsizlik şikayeti ile başvurdu. Hb düşük ölçüldü (6.3), batında yaygın hassasiyet ve hematüri mevcuttu. Batın içi serbest sıvı, over kist rüptürü ve INR yüksekliği mevcut olan hastaya konakion (k vit) ve TDP replasman tedavisi başlandı. Tedaviye rağmen 15 gün yoğun bakım, 20 gün acil yataklı servisinde takibinin ardından dahiliye bölümüne devri yapılmıştır. 4 gün dhiliye servisinde takip edilen hasta kendi isteği ile taburcu edilmiştir.� Olgunun CYP2C9 geni analizi yapıldığında CYP2C9*1*3 genotipini taşıdığı saptanmıştır. Literatürde CYP2C9*3 allelini heterozigot taşıyan bireyler için yaklaşık %15-49 daha düşük varfarin dozu uygulaması önerilmiştir. Hastamızın CYP2C9 geninde saptanan bu polimorfizm suisid girişiminden sonra K vitamini ve TDP verilmesine rağmen INR yüksekliğini kısmen açıklamakla birlikte, VKORC1 geninde görülebilecek ve aynı tabloya sebep olabilecek olan VKORC1*2 polimorfizminin hastada bulunma olasılığı, VKORC1 geni çalışması yapılamadan hasta ex olduğu için dışlanamamıştır. ��
Genetik polimorfizmler bireyin farmakolojik ajanlara cevabını etkilerler. Sitokrom P450 CYP2C9 polimorfizmi ve son yıllarda vitamin K epoksitredüktaz kompleks subunit 1 (VKORC1) gen mutasyonunun varfarin kullanan hastalarda sabit doz aralığına ulaşılmasını zorlaştırdığı ve kanama komplikasyonlarını artırdığı gösterilmiştir.��
Biz bu sunumda suisid girişimde bulunmuş olan bir hastada gelişen varfarin toksisitesinin sebebinin genetik mutasyonlara bağlı olabileceğini sunmaya çalıştık. Anahtar Kelimeler: Warfarin intoksikasyonu, CYP2C19, VCORC1

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
137
O 057 ZEHİRLENMİŞ HASTALARDA AKTİF KÖMÜR ETKİNLİĞİ Erdem Aksay1, Müge Gülen2, Akkan Avci2, Salim Satar2
1Mersin Toros Devlet Hastanesi, Mersin 2Adana Numune Eğitim ve Araştırma Hastanesi, Adana Amaç: Bu çalışmanın amacı bir eğitim araştırma hastanesi acil tıp kliniğine ilaç zehirlenmesi nedeniyle başvuran ve sağlık bakanlığınca aktif kömür temin edilememesi nedeniyle aktif kömür verilemeyen hastalar ile daha sonra aktif kömür temini ile birlikte aktif kömürün verilebildiği hastalar arasında karşılaştırma yaparak aktif kömürün etkinliğini göstermektir.��
Gereç-Yöntem: Bu çalışmaya 01.05.2011-22.05.2012 tarihlerinde ilaç zehirlenmesi nedeniyle başvuran ve aktif kömür verilemeyen hastalarla 01.08.2014-31.08.2015 tarihleri arasında başvuran aktif kömür verilebilen vakalar dahil edildi. Hastalar yaşları, cinsiyetleri, başvuru anına kadar geçen süre, başvuru tarihi, ne şekilde zehirlendikleri, zehirlenmeye yol açan etken, acil serviste kullanılan antidot tedavi, acil servise başvuru anındaki bilinç düzeyleri, hasta takip süresi ve hastanın sonlanımı açısından değerlendirildi. ��
Bulgular: Çalışmadaki 2159 olgunun 625’i erkek (% 28.9 ) 1534’ ü kadındı (% 71.1). Hastaların yaş ortalaması aktif kömür verilemeyen grupta (1. grup) 28,2 ±9,6 iken, verilebilen grupta (2. grup) 30,2 ±10,9 idi. 1. grupta 1167 hasta (%94,9) 2. grupta 883 hasta (%95) intihar amaçlı ilaç almıştı. 1. grupta 63 (%5,1) 2.grupta ise 46 hasta (%5,0) kazara ilaç almıştı. 1. Grupta 371 ve 2. Grupta 298 hasta ile en sık neden çoklu ilaç alımı idi. 1. gruptan 257 hastada (% 20.9), 2. grupta 177 hastada (%19.1) ilaca ait bulgu gözlendi. 1. gruptan 454 (%36.9) hastada, 2. grupta 341 (%36.7) hastada antidot kullanımı gereksinimi oldu. Çalışmaya dahil olan hastalardan sadece biri eksitus (2. grupta). 1. grupta 683 (% 55.5), 2. grupta 550 hasta (% 59.2) 8 saat gözlem sonrası taburcu edildi. 1. grupta yatış süresi ortalama 15.3 ± 9.9 saat iken, 2. grupta ortalama 15.5 ± 13.2 saatti. ��
Sonuç: Aktif kömür kullanımı hasta yatış süresini ve sonlanımını etkilememektedir. Konu ile ilgili daha detaylı çalışmalara ihtiyaç vardır. Anahtar Kelimeler: Acil, zehirlenme, aktif kömür, antidot, yatış süresi O 058 LİTYUM ZEHİRLENMESİNE BAĞLI KOREATETOZDA DİYALİZ KULLANIMI Emrah Çelik, Aylin Erkek Kocaeli Derince Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Kocaeli Giriş: Lityum bipolar affektif bozukluk tedavisinde yaygın olarak kullanılan terapotik indeksi dar bir ajandır. Birçok klinisyen tarafından teorikte toksisite bulguları kan düzeyi ile ilişkili olduğu düşünülmektedir. Bu düşüncelerin aksine lityum toksisite klinik semptomlarının kan konsantrasyonundan bağımsız olarak ortaya çıkan, koreatatoik hareketlerle başvuran ve hemodializ ile klinik tam düzelme sağlanan olgumuzu paylaşmayı amaçladık.��
Olgu: 53 yaşında kadın hasta uyku hali, istemsiz hareketler, titreme şikayetleriyle acil servise getirildi. 5 gün önce psikiyatri tarafından bipolar bozukluk nedeniyle kullandığı lityum dozunun 2X300mg dan 2x600 mg çıkarıldığı, lorazepam 1mg 1x1,ketiapin 25 mg 1x1 başlandığı öğrenildi. Özgeçmişinde 30 yıldır bipolar bozukluk nedeniyle lityum kullanımı, diyabet, hipertansiyon, karaciğer sirozu tanıları mevcuttu. Fizik muayenede vital bulguları stabil, üst extremite ve tüm vücudu içine alan koreatetoik hareketler gözlenmiş olup, diğer sistem muayeneleri doğaldı. Laboratuarda Lityum seviyesi 2,05mmol/L dışında anormal bulgu yoktu. Beyin tomografide akut patoloji saptanmadı. Mevcut endikasyon ile acil diyalize alınan hastanın diyaliz sonrası kan lityum seviyesi:0,797mmol/l’a geriledi, istemsiz hareketleri tamamen düzeldi. Yoğun bakım ve servis takibi sonrasında hasta şifa ile taburcu edildi. Tartışma: Lityum toksisitesi olan hastalarda erken dönemde gastrointestinal semptomlar takibinde SSS sistemi bulguları görülebilir. Lityum toksisitesinde tanı, serum lityum seviyesindeki yükseklik ile konulur, ancak serum lityum seviyesi ile klinik bulguların her zaman örtüşmeyeceği akılda tutulmalıdır. Bu vakada olduğu gibi Lityumla birlikte diğer antipsikotik ilaçların kullanımı ile toksisite belirtilerinin ortaya çıkabileceği bilinmektedir. Bu hastada gözlenen sürekli aşırı ve istemsiz düzensiz hareketler koreatetoz olarak tanımlanmıştır. Olgunun tıbbi öyküsü laboratuar sonuçları ve görüntüleme tetkikleri ile koreyi açıklayacak lityum dışında başka etiyolojik neden saptanamamıştır. Olguda lityum seviyesinin azalması ile birlikte semptomlar ortadan kalkmıştır. Lityumun spesifik antidotu yoktur. Destek tedavisi verilmelidir. Tedavide verilecek olan yüksek miktardaki sodyum ve sıvı ile lityum atılımı artar. Bu nedenle lityum zehirlenmesi tedavisinde en önemli nokta uygun sıvı tedavisinin sağlanması, sıvı tedavisi yetersiz ve toksisite bulguları ağırsa diyaliz uygulanmasıdır. ��
Sonuç: Lityum intoksikasyonlarında kliniğin ilaç düzeyinden bağımsız olabileceği ve diğer ilaçların lityum düzeyini etkileyebileceği akılda tutulmalıdır. Anahtar Kelimeler: Lityum intoksikasyonu, dializ, koreatetoz

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
138
O 059 ACİL SERVİSE BAŞ DÖNMESİ ŞİKAYETİ İLE BAŞVURAN HASTALARDA NÖROGÖRÜNTÜLEME MALİYETİ Ali Kablan1, Serhat Karaman2, Nurşah Başol2
1Mardin Devlet Hastanesi, Acil Servis, Mardin 2Gaziosmanpaşa Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Tokat Baş dönmesi acil servislere sık başvuru nedenlerinden birisidir. Pek çok hastalığın baş dönmesi belirtisi vermesi ve bunlardan bazılarının hayatı tehdit edici nitelikte oluşu acil servislerde baş dönmesi yönetiminin başlıca zorluklarındandır. Acil serviste baş dönmesi ile başvuran hastalarda nörogörüntüleme maliyetlerinin giderek artması göz önünde bulundurularak, çalışmamızda hastaların, anamnez, fizik muayene bulguları ve yapılan tetkikler doğrultusunda semptomatolojik ve etyolojik alt gruplarının belirlenmesi ve özellikle nörogörüntüleme maliyetlerinin ortaya konarak bu verilerin literatürle kıyaslanması amaçlanmıştır. �Çalışma hastanemiz Acil Tıp Kliniğine 01.01.2013-31.12.2013 tarihleri arasında baş dönmesi şikayeti gelen hastaların dosyalarının retrospektif incelenmesi ile yürütüldü. Tanıları santral nedenli baş dönmesi, periferik nedenli baş dönmesi, kardiak ve tansiyon nedenli baş dönmesi, dahili nedenlere bağlı baş dönmesi, psikojenik nedenli baş dönmesi ve diğer nedenler olmak üzere altı grupta sınıflandırıldı. �Hastaların %59.8’i kadın(n:228), %40.2’si erkek(n:153) olup yaş ortalamaları 46,12+18,92 idi. Tanılarına göre gruplandırıldığında santral nedenli baş dönmesi grubunda 31 (%8.1), periferik grupta 175 (%45.9), kardiyak veya tansiyon nedenli grupta 43 (%11.2), dahili nedenli grupta 18 (%4.7), psikojenik grupta 6 (%1.5) ve diğer nedenli grupta 108 (%28.3) hasta yer aldı. Hastaların 72’sine (%18.8) BT, 35’ine (%9.1) MRG çekildiği gözlendi. En fazla santral nedenli gruba nörogörüntüleme yapıldığı görüldü (BT%41.9, MRG%32.2). Nörogörüntüleme maliyetinin en yüksek olduğu grup, periferik vertigo grubunda idi. Ancak hasta başı maliyet hesap edildiğinde, bir hastanın maliyetinin en az olduğu grup periferik vertigo grubuydu. Baş dönmesi şikayeti olan hastaların maliyetinin, kliniğimizin toplam yıllık maliyetinin %1.2 ‘sini, nörogörüntüleme maliyeti ise toplam yıllık maliyetin %0.1’ini oluşturmaktaydı.�Baş dönmesi şikayetiyle acil başvuruların yıl geçtikçe artması ve hekimlerin önemli bir patolojiyi atlamak istememesi nedeniyle baş dönmeli hastaların maliyetinin giderek artırdığı görülmüştür. Çalışmamızda literatüre göre maliyetin daha düşük olması kliniğimiz adına pozitif bir bulgu olmakla birlikte, tüm acil servisler bağlamında bunun bir sorun olduğu gerçeği yadsınmamalıdır. Gereksiz maliyetleri kontrol etmek geliştirilecek olan algoritmalarla birlikte, acil serviste iyi ve doğru bir hasta yönetimi ile mümkündür. Anahtar Kelimeler: Baş dönmesi, vertigo, acil servis, nörogörüntüleme maliyeti O 060 KARDİYOPULMONER ARRESTTE TROMBOLİTİK Abuzer Coşkun1, Osman Mahir Okur1, Sedat Özbay1, Şevki Hakan Eren2
1Sivas Numune Hastanesi, Acil Servis, Sivas 2Gaziantep Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Gaziantep 73 yaşında bayan hasta acilimize solunum sıkıntısı şikayeti ile başvurdu. Yaklaşık 3 ay önce femur boyun kırığı nedeniyle opere olmuş. Son 3-4 gündür giderek artan solunum sıkıntısı mevcut olup, daha önceden şikayeti ve ilaç kullanımı öyküsü yokmuş.�Hasta acilde tansiyon arteriayali 70/40mmHg, nabız 117/dk, solunum32/dk’dı. Akciğerler dinlemekle bazallerde ince ral, kalp taşiaritmikti. Cilt soluk, soğuk ve terliydi. Pulse oksimetrede saturasyon %67’di. Pulmoner emboli düşünüldü. Hastada gerekli tetkikler istendi. Hastaya tomografi çekildikten hemen sonra kardiyopulmoner arrest gelişti. Acil resüsitasyon odasında hasta entübe edilip mekanik ventilatöre(MV) bağlandı. Eş zamanlı kardiyopulmoner resusitasyona(CPR) başlandıı ve her 3-5/dk da 1mg adrenalin intravenöz yapıldı. Tansiyon arteriyal için dopamin hidroklorür 40mg/ml’lik ampulden 10mcg/kg/dk’ dan infüzyon verildi. CPR sırasında hastada aralıklı ventriküler fibrilasyon (VF) geliştiği için 3-4 kez defibrilasyon yapılarak rekürrens VF ataklarını sonlandırmak için Cordarone(Amiodaron HCI) 150mg/ml ampulden 300mg 20sn de puşe verildi. CPR’ın 37. dakikasında yanıt alındı. Hastanın tomografisi; sağda daha fazla olmak üzere ana pulmoner arterlerde masif emboli ile uyumluydu. Arter kan gazında; respiratuvar alkaloz, hipokapni ve hipoksemi vardı. EKG de sağ dal bloğu, sağ atriayal ve ventriküler yüklenme bulguları ile taşikardikti. D-Dimer; 10457ng/ml, troponin I; 0,93ng/ml’di. Biyokimyada; kan şekeri;178mg/dl, üre;108 mg/dl, BUN;42 mg/dl, Krea;1.57 mg/dl, ALT;168U/L, AST;153U/L, ALP; 341U/L’di. Hemogram; WBC; 19200U/L, Platelet; 204000U/L, Neutrofil; 13,4.10³/UL, Lmyphosit; 4,9.10³UL’di.�Kardiyoloji, göğüs hastalıkları ve yoğun bakım ünitesinden konsültasyon istendi. Kardiyoloji ve göğüs hastalıkları, hasta mekanikte olduğundan takip edemeyecekleri, yoğun bakımda da yer olmadığı gerekçesiyle hastayı kabul etmediler. Hasta yakınlarına geniş bilgi verildi. Yer olmadığı söylendi. Acil servis ekibi olarak hastaya Alteplase (rt-PA) verilmesine karar verildi. Hasta yakınlarından imzalı onam alındı. Acil resusitasyon odasında rt-PA 100mg 2 saatte infüzyon verildi. Hasta Acil Servis Gözlem Ünitesine mekanik ventilatör ile yatırıldı. Hasta 9. günde extübe edildi. 8 gün Coumadin (Varfarin sodyum) doz ayarı yapıldı. Hasta 17. gününde 2.3 international normalized ratio (INR) ile şifayla taburcu edildi. Anahtar Kelimeler: Resusitasyon, masif pulmoner emboli, trombolitik

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
139
O 061 HİPONATREMİ TESPİT EDİLEN HASTALARDA SERUM NÖRON SPESİFİK ENOLAZ DÜZEYLERİ İLE BEYİN HASARI ARASINDAKİ İLİŞKİ
Selçuk Matyar1, Ayça Açıkalın2, Nezihat Rana Dişel2, Özlem Görüroğlu Öztürk1, Gülçin Dağlıoğlu1, Onur Akpınar3
1Çukurova Üniversitesi Tıp Fakültesi, Merkez Laboratuvarı, Adana�2Çukurova Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Adana�3Yakın Doğu Üniversitesi Tıp Fakültesi, Kardiyoloji Anabilim Dalı, K.K.T.C. Amaç: Hiponatremi klinikte en sık karşılaşılan elektrolit denge bozukluğudur. Hiponatremiye ikincil gelişen santral sinir sistemi (SSS) bulguları ve ödeme bağlı nöron dejenerasyonu görülür. Son yıllarda sıklıkla kullanılan Nöron-Spesifik Enolaz (NSE), nöronların fonksiyonel hasarını direkt olarak değerlendiren önemli bir belirteç olarak kabul edilmektedir. Hiponatremili hastalarda SSS hasarının belirginleştiği sodyum değerlerinin bilinmesi tedavi protokolleri için oldukça önemlidir. Klinik pratikte serum sodyumun 125mEq/L ve altı değerler ağır hiponatremi kabul edilir ve agresif düzeltme önerilir. Bu çalışmada amacımız, serum sodyum seviyesi ile NSE düzeyleri arasındaki ilişkiyi araştırarak, nöronlardaki yoğun hasarın geliştiği serum sodyum ve NSE düzeylerini saptamaktır. Materyal-Metod: Çalışmamıza çeşitli nedenlerle acil servise başvuran, serum sodyum düzeyi 135mEq/L altında olan toplam 181 (87 erkek, 94 kadın) hasta alındı. Hiponatremi ile beraber SSS bozukluğu olan hastalar (SSS enfeksiyonu, Akut iskemikinme, Travmatik beyin hasarı, subaraknoid ve intrakranial kanama, Menenjit, Alzheimer, Epilepsi ve intrakranial tümör) NSE düzeylerini yanlış yükseltebileceği için çalışma dışı bırakıldı. Tüm hastaların klinik bulguları, kullandığı ilaçlar, yandaş hastalıkları, kan sayım sonuçları, biyokimyasal test sonuçları, serum NSE düzeyleri ve sonlanım şekilleri kaydedildi.� Bulgular: Hastaların ortalama yaşı 59.4 ± 17.0 yıl idi. Ortalama serum sodyum düzeyi 126.5 ± 4.8mEq/L ve NSE düzeyi 25.3 ± 18.0 ng/mL olarak saptandı. Hastaların serum sodyum düzeyi ile NSE arasındaki ilişki değerlendirildiğinde, serum sodyum düzeyi 122 - 130mEq/L arasında olan hastaların NSE düzeyinin belirgin yüksek olduğu tespit edilmiştir (Şekil 1).��
Sonuç: Serum sodyum düzeyi 122 - 130mEq/L değerleri arasında NSE değerlerinin yüksek olması, bu düzeylerde nöron hasarının daha fazla olduğunu düşündürmektedir. Serum sodyum düzeyi 125-130mEq/L değerleri arasında serum NSE düzeylerinin yüksek olması, klinik olarak bu hastalar daha erken dönemde agresif tedavi edilmeli mi sorusunu akla getirmektedir. Bu değerlerin altındaki serum sodyum değerlerinde azalan nöron hasarı, agresif tedavinin daha erken düşünülmesi açısından, daha ileri çalışmaların yapılması gerektiği kanaatine varılmıştır. Anahtar Kelimeler: Beyin hasarı, hiponatremi, nöron-spesifik enolaz O 062 ACİL SERVİSE ŞOK TABLOSUYLA GELEN HASTALARDA 30 GÜNLÜK MORTALİTENİN ÖNGÖRÜLMESİNDE END- TİDAL KARBONDİOKSİT (ETCO2) ÖLÇÜMÜ KULLANILMASI Okan Günaydın, Ayfer Keleş, Fikret Bildik, Uğur Gülöksüz, Hüseyin Avni Demir Gazi Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Ankara Giriş: Hipotansif şok, acil servise gelen birçok hastalığın ana başvuru bulgusudur. Gelişen şok tedavi ve yönetimlerine rağmen mortalitesi yüksek olmaya devam etmektedir. Acil hekimleri erken aşamada şoku tanımak için yeni yöntemler bulmaya çalışmaktadır. Kardiyak outputun azaldığı volüm ilişkili hipotansif durumlarda ETCO2 değerlerinin de düştüğü gösterilmiştir.��
Amaç: Çalışmanın birincil amacı, acil servise hipotansif şok ile başvuran hastalarda 30 günlük mortalitenin öngörülmesinde end- tidal karbondioksit ölçümü kullanımının değerlendirilmesidir. Çalışmanın ikincil amacı, ETCO2 ile geleneksel vital bulgular ve laboratuvar bulguları arasındaki ilişkiyi belirlemek ve erken bakılan ETCO2 değeri ile şok hastalarının prognozu arasındaki ilişkiyi göstermektir.��
Gereç-Yöntem: Bu çalışmaya SKB < 90 mm/hg veya MAP < 60 mm/hg olan şok klinik bulgularıyla acil servise başvuran toplam 58 hasta dahil edildi. Hastaların başvurusunun 0. ve 120. dakikalardaki ateş, nabız, solunum sayısı, kan basınca, oksijen saturasyonunu içeren vital bulguları ve sidestream olarak hasta başı mönitor cihazıyla(Petaş KMA®900 hastabaşı mönitörü) tek kullanımlık CO2 maske veya entübe hasta kitiyle hastaya en uygun yöntemle ETCO2 değerleri ölçüldü. Kan gazı ve laktat düzeyleri hastaların gelişinde bakıldı. Tüm hastalar standart protokoller ve tedavi rejimine göre tedavi edildi. Hastaneye başvurudan itibaren 30 gün sonraki hasta sağkalımı kaydedildi. ��
Bulgular: İncelenen hastaların %46,6’sı (n=27) başvurudan sonraki ilk 30 gün içinde eksitus olurken geriye kalan %53,4’ü (n=31) sağdı. Eksitus olan hastaların 0. ve 120. dakikalardaki ETCO2 değerleri sağ kalanlara göre anlamlı olarak düşüktü (p<0,001). 0. dakikadaki ETCO2 değerinin mortalite durumunu öngörmede tanısal karar verdirici özelliği olduğu görülmüştür. Mortalite durumu için 23,5 mmHg ve 24,5 mmHg olmak üzere iki ETCO2 cut-off değeri belirlenmiştir. Eksitus olan hastaların pH, bikarbonat düzeyi ve baz eksisi, sağ kalanlardan anlamlı olarak düşükken kan laktat düzeyi anlamlı olarak yüksekti(p<0,05).� Sonuç: ETCO2 ölçümü şoklu hastalarda mortaliteyi öngörmede kullanılabilecek kullanışlı bir yöntemdir. ��
Anahtar Kelimeler: End-tidal karbondioksit, mortalite, şok

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
140
O 063 İNTRASEREBRAL KANAMALI HASTALARDA MPV VE RDW DEĞERLERİN MORTALİTEYLE İLİŞKİSİ Özkan Kömürcü, Akkan Avci, Salim Satar, Müge Gülen Adana Numune Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Adana Giriş-Amaç: İnme, iskemik ve hemorajik kaynaklı olabilen, morbidite ve mortalitesi yüksek, ciddi komplikasyonları olan, erken tanı ve tedavi gerektiren önemli bir nöroloji acilidir. Çalışmamızda hemorajik inme tanısı alan hastaların yapılan tam kan sayımlarındaki ortalama trombosit hacmi, eritrosit dağılım hacmi değeri ve bilgisayarlı beyin tomografisinde saptanan kanamanın hacmi hesaplanarak aralarındaki ilişki olup olmadığı belirlenmesi amaçlandı.��
Materyal-Metot: Araştırmamıza 1 Haziran 2014 ve 30 Haziran 2016 tarihleri arasında Adana Numune Eğitim ve Araştırma Hastanesi Acil Tıp Kliniği’ne başvuran ve hemorajik inme tanısı alan ve verilerine ulaşılabilen 18 yaş üzerindeki tüm hastalar dahil edildi. ��
Bulgular: Toplam 86 hemorajik inme tanılı vaka retrospektif olarak incelenmiştir. 86 vakanın % 58,1’i (n=50) erkek hasta,% 41,9’u (n=36) kadın hastadır. Tüm hastaların yaş ortalaması 60,4±16,5 idi. Hastaların % 60,5’inin (n=52) en sık ani bilinç bulanıklığı şikâyetiyle acil servisimize getirildiği saptandı. Ani bilinç bulanıklığı şikâyetiyle getirilen hastaların % 79,5’i eksitus oldu. Eksitus olan hasta grubunda eritrosit dağılım hacmi değeri eksitus olmayan hasta grubundan anlamlı (p<0,05) olarak daha yüksekti. Hastaların % 55,8’inde (n=48) olduğu gibi en sık parankimal kanama görüldü. Kanama hacmi yüksek olanlarda mortalite oranı daha yüksek saptandı. Eksitus olan ve eksitus olmayan hastaların öngörüsünde kanama hacminin anlamlı etkisi gözlendi.� Sonuç: Bilinç bozukluğu, hipertansiyon varlığı, eritrosit dağılım hacmi yüksekliği ve kanama hacminin mortaliteyi etkileyen bağımsız değişkenler olduğu gösterilmiştir. Anahtar Kelimeler: Kanama, MPW, RDW, mortalite O 064 ACİL SERVİSTE SEPTİK ŞOK TANISI ALAN HASTALARIN MORTALİTESİ ÜZERİNE ETKİ EDEN FAKTÖRLER Duygu Kara, Dilek Toprak, Özgür Çevrim Şişli Hamidiye Etfal Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Amaç: Septik şok tanısı alan hastaların komorbiditeleri ve SOFA skorları, biyokimyasal takip parametreleri, acil serviste kalış süreleri ile mortaliteleri arasındaki ilişkiyi incelemek, ünitemizin verilerini paylaşmaktır.��
Yöntem-Gereçler: Çalışma Ocak 2015 ile Aralık 2015 tarihleri arasında acil servise başvuran septik şok tanısıyla yoğun bakıma yatmış toplam 325 hastanın dosyalarının incelenmesiyle yapılmıştır. Hastalarda trombosit, MPV, laktat, SOFA skoru, acilde kalış süreleri süreleri ile 24. Saat ve 30. Gün mortaliteleri arasında ilişki araştırılmıştır.��
Bulgular: Ortalama yaş 74.72 ± 14.07’dir. Hastaların 261’i 65 yaş üstü, 153’ü kadın, 172’si erkektir. 24 saatlik mortalite % 17, 30. gün mortalitesi % 70’dir. Vakaların % 81 (n=262)’i dış merkez yoğun bakımlara sevk edilmiştir. Acil servise en sık üç başvuru sebebi solunum sistemi enfeksyonları (% 82), üriner sistem enfeksiyonları (% 14) ve yumuşak doku enfeksiyonlarıdır (% 2). En sık yandaş hastalıklar hipertansiyon (% 28), malignite (% 26) ve serebrovasküler hastalıklar (% 19)’dır. Vakaların % 63 (n=204)’ünde mekanik ventilasyon ihtiyacı olmuştur. Laktat değerleri % 77 (n=252) vakada 2 mmol/L’nin üzerindedir. MPV değerlerinin % 97 (n=314)’si normal sınırlardadır. 24 saatlik mortalite malignitesi olan hastalarda % 27 (n=22) ve DM olan hastalarda % 26 (n=15) olup; 30 günlük mortaliteye bakıldığında malignite % 84 (n=70), diğer hastalıklar % 76 (n=31) olarak bulunmuştur. 24 saatlik mortalite yumuşak doku enfeksiyonlarında % 44 (n=4) iken üriner sistem enfeksiyonlarında % 11 (n=5) iken; 30 günlük mortalite yumuşak doku enfeksiyonları % 78 (n=7) ve üriner sistem enfeksiyonlarında % 76 (n=34) olarak bulunmuştur. 24 saatlik mortalite trombosit 150.000/mm3’ün üzerinde olan hastalarda % 14 iken 20.000/mm3 altında % 67 bulunmuştur. 30 günlük mortaliteye bakıldığında 150000/mm3’ün üzerinde % 69, 20000/mm3 altında % 100 bulunmuştur.��
Sonuç: Hastaların yaşı, cinsiyeti, laktat düzeyi, prokalsitonin düzeyi, acil serviste kalış süreleriyle mortalite arasında bir ilişki bulunamamışken, düşük trombosit sayısı, artmış SOFA skoru, yüksek birirubin düzeyi ve mekanik ventilasyon ile mortalite arasında ilişki bulunmuştur. Anahtar Kelimeler: Mortalite, septik şok, SOFA skoru, trombosit

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
141
O 065 FİZİK MUAYENE BULGULARININ, EL BİLEĞİ KIRIKLARINI TANIMADAKİ DUYARLILIĞI VE ÖZGÜLLÜĞÜ Yeşim Eyler, Ersin Aksay, Mustafa Sever, Murat Yeşilaras, Ali Turgut, Necmiye Yalçın Tepecik Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İzmir Amaç: Akut el bileği travması hastalarında, fizik muayene bulgularının el bileği kırıklarını tanımadaki duyarlılığının ve özgüllüğünün araştırılmasıdır.��
Yöntem: Çalışmamız, 3. basamak akademik bir acil tıp kliniğinde, ileri dönük kesitsel olarak gerçekleştirildi. Altı ay süresince, acil servise el bileği travması nedeniyle başvuran 14 yaş üstü tüm hastalar ardışık olarak çalışmaya dâhil edildi. Her hasta için el bileğine özel 18 farklı fizik muayene bulgusu değerlendirildi ve kayıt edildi. Tüm hastalara anterO posterior ve lateral el bileği X-Ray grafileri çekildi. Fizik muayene bulguları ile kırık düşünülen ancak grafide kırık saptanmayan hastalara ayrıca bilgisayarlı tomografi çekildi. Tüm radyografik görüntülemeler hastanın klinik bilgisine kör bir ortopedi öğretim üyesi tarafından tekrar değerlendirildi. Ortopedi hekiminin kararı kırık tanısı için altın standart olarak kabul edildi.��
Bulgular: İki yüz yedi hasta değerlendirildi. 70 (%34) hastada kırık tespit edildi. En sık distal radius kırığı (%30) tespit edildi. Çalışmamızda el bileğine özel 18 muayene bulgusunun prevalans, el bileği kırıklarını tanımadaki duyarlılık, özgüllük, negatif öngörü ve pozitif öngörü değerleri ayrı ayrı hesaplandı. En yüksek duyarlılığa sahip üç fizik muayene bulgusu; dorsal fleksiyonda ağrı (%94), palmar fleksiyonda ağrı (%93) ve distal radiusta hassasiyet (%90) olarak tespit edildi. En yüksek özgüllüğe sahip üç fizik muayene bulgusu ise ekimoz (%98), krepitasyon (%97) ve deformite (%96) olarak bulundu. Tek bir fizik muayene bulgusunun el bileği kırıklarını tanımadaki duyarlılık ve özgüllüğünün yetersiz olması nedeniyle bulgular 3’lü kombinasyonlar şeklinde tekrar değerlendirildi. Distal radius ve distal ulnada hassasiyet ile beraber el bileği dorsifleksiyonunda ağrı kombinasyonunun el bileği kırıklarını tanımadaki duyarlılığı %100, özgüllüğü %11 olarak saptandı.��
Sonuç: Akut el bileği travması olan hastalarda, fizik muayenede, distal radius ve distal ulnada hassasiyet ile beraber el bileğinin dorsifleksiyonunda ağrı olmasının, kırığı yüksek hassasiyetle öngördüğü saptandı. Anahtar Kelimeler: El bileği travması, distal radius, distal ulna, dorsal fkelsiyon, duyarlılık O 066 KAFA TRAVMASINDA ULTRASONLA ÖLÇÜLEN OPTİK SİNİR KILIF ÇAPININ HASTA TAKİBİNDEKİ ROLÜ Erhan Uğraş1-2, Özcan Yavaşi1, Kamil Kayayurt1-3, Özlem Bilir1, Vaner Köksal4, Gökhan Ersunan1, Mehmet Altuntaş1, Bülent Özdemir4
1Recep Tayyip Erdoğan Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Rize�2Ordu Üniversite Hastanesi, Ordu�3Acıbadem Üniversitesi Maslak Hastanesi, İstanbul 4Recep Tayyip Erdoğan Üniversitesi Tıp Fakültesi Nöroşirürji Anabilim Dalı, Rize Giriş ve Amaç: Bu çalışmadaki amacımız, kafa travması (KT) ile acil servise başvuran erişkin hastalarda optik sinir kılıf çapının (OSKÇ) hasta takibindeki ve kontrol beyin bilgisayarlı tomografi (BBT) ihtiyacını belirleyebilmedeki rolü ve hasta takibindeki prognostik önemini ortaya koymaktır. Materyal ve Metod: Acil servisine başvuran kafa travmalı hastaların stabilizasyon sonrası 7.5 MHz transduser ile OSKÇ’ları ölçüldü sonra BBT çekildi. Acil servisten taburculuk kararı verilen hastalara takipleri sonunda ikinci bir ölçüm yapıldı. Yatırılmış hastalarda ise beyin cerrahı tarafından hastanın kliniğinde değişiklik olup olmamasına göre kontrol BBT çekilmesine karar verildiyse, çekim öncesi ikinci bir ultrason ölçümü yapıldı. İstatistiksel analizler SPSS v.23.0 paket programı aracılığıyla yapıldı. P < 0.05 istatistiksel olarak anlamlı kabul edildi. ��
Bulgular: Çalışmaya 65 hasta alındı. Bunların 5 tanesi ağır hafif, 11 tanesi orta ve 49 tanesi hafif KT idi. Hafif KT olan hastaların ortalama OSKÇ değeri 4.7±0.29, orta ve ağır KT olan hastalarınki ise 5.5 ±0.57 idi (p=0.001). OSKÇ nin orta ve ağır KT olan hastaları ayırabilecek eşik değerini 4.95mm (%93.8 duyarlılık, %83.7 özgüllük) olarak bulundu. BBT’de kafa içi basınç artışı (KİBA) bulgusu olan hastalarla olmayanların ölçülen OSKÇ değerleri ortalaması 5.7±0.52 mm ve 4.7±0.27 mm olarak ölçüldü (p = 0.001). 30 gün içinde ölen hastalar ile sağ kalan 4 hastanın OSKÇ değerleri ortalaması 6.2±0.68 mm ve 4.86±0.40 mm olarak hesaplandı (p = 0.001). 49 hafif KT hastasının ilk OSKÇ değeri ortalaması 4.72±0.29 mm, kontrol 2. değeri ise 4.73 ±0.29 idi (p = 0.938). Orta ve ağır HKT olan hastaların ilk OSKÇ değerleri ile klinik durumunda değişiklik olmasından dolayı istenen kontrol BBT’den hemen önce ölçülen ikinci OSKÇ değerleri otalaması 5.5 ± 0.57 mm ve 5.7 ± 0.79 olup ikinci OSKÇ lehine istatistiksel olarak artış saptandı (p = 0,002).��
Sonuç: Travma hastalarında OSKÇ kontrol BBT ihtiyacını belirlemede yardımcı bir tanı testi olarak kullanılabilir. Anahtar Kelimeler: Kafa içi basınç artışı, kafa travması, optik sinir kılıf çapı, ultrasonografi

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
142
O 067 FAHR SYNDROME Göksu Afacan, Orhan Delice Erzurum Regional Training and Research Hospital, Emergency Service, Erzurum, Turkey Introduction: Fahr’s Disease (Bilateral Striopallidodentate Calcinosis) characterized by symmetric calcifications at thalamus, nucleus dentatus, cerebral white substance and basal ganglia is a rare condition. Calcifications may be shown by computerized tomography provided for another reason. The clinic manifestations of the disease are variable but commonly progressive mental disorder, tremor, ataxia, disartria, convulsion, Parkinson-like symptoms and neurO psychological disorders may be seen. The related conditions which may cause to Fahr’s Disease are anoxia, radiation, systemic disorders, toxins, disorders of calcium metabolism and encephalitis.��
Case: 63-year-old female patient presented to our clinic with "worst headache of her lifetime". Her neurological examination was fine, vital signs were stable and there was no neck stiffness but revealed brain tomography was seemed like excessive subarachnoid heamorrhagia. her pain was relieved after analgesic treatment and she was discharged with suggestions. Conclusion: Fahr is a syndrome that is defined many years ago, althoug it is overlooked because it is not frequently encountered in the clinic. Keywords: Fahr syndrome, subarachnoid hemorrhagia, brain computerized tomography O 068 INTRANASAL LIDOCAINE IN ACUTE TREATMENT OF MIGRAINE: A RANDOMIZED CONTROLLED TRIAL Nazire Avcu1, Nurettin Özgür Doğan1, Murat Pekdemir1, Elif Yaka1, Serkan Yılmaz1, Cansu Alyeşil1, Latif Erdem Akalın2
1Kocaeli University Faculty of Medicine, Department of Emergency Medicine, Kocaeli, Turkey 2Bandırma State Hospital, Clinic of Emergency Medicine, Balıkesir, Turkey Objective: The study aim was to evaluate the efficacy and safety of intranasal lidocaine administration for migraine treatment. Methods: This single-center, double-blind, randomized controlled trial was conducted in a tertiary-care emergency department (ED). Patient enrolment followed the migraine criteria of the International Headache Society. Patients were randomized to intranasal lidocaine and saline groups and all participants received 10 mg intravenous metoclopramide. Patient pain intensity was assessed with an 11-point numeric rating scale (NRS) score. The primary outcome measure was the change in pain scores at 15 and 30 minutes; secondary outcomes were changes in pain intensity after pain onset and rescue medication need. Also a short meta-analysis was conducted together with the results of present study. Results: Patients (n=162) were randomized into two groups with similar baseline migraine characteristics and NRS scores. The median reduction in NRS score at 15 minutes was 3 (IQR:2–5) for the lidocaine and 2 (IQR:1–4) for the saline group median difference=1.0 (95%Cl: –0.1 to 2.1) . The reduction in pain score at 30 minutes was 4 (IQR:3–7) for the lidocaine and 5 (IQR:2–7) for the saline group median difference=–1.0 (95%Cl: –2.1 to 0.1) . Patients presenting earlier after headache onset and receiving lidocaine showed similar pain reduction. Rescue medication need did not differ between the groups, and local irritation was the most common adverse event in the lidocaine group. The results of the meta-analysis revealed that intranasal lidocaine was effective in acute migraine headaches regarding the results of three trials (Odds ratio: 2.51, 95% CI: 1.48 to 4.27). Conclusion: Although intranasal lidocaine was found no more efficacious than normal saline in our study, the results of the meta-analysis suggested using this drug in patients with acute migraine attacks. Keywords: Migraine, headache, lidocaine, intranasal administration, emergency medicine

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
143
O 069 COMPARISON OF THE EFFICACY OF DEXKETOPROFEN, IBUPROFEN AND METOCLOPRAMIDE IN ACUTE MIGRAINE ATTACK TREATMENT: A PROSPECTIVE, OBSERVATIONAL STUDY
Sinan Karacabey1, Erkman Sanri2, Sercan Yalcinli1, Haldun Akoglu2
1Bozok University Faculty of Medicine, Department of Emergency Medicine, Yozgat, Turkey 2Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Introduction: Migraine is a common and often debilitating neurological disorder. The unified theory suggests that vascular tone, inflammation, and serotonin are involved in the genesis of migraine syndromes. In the treatment of migraine serotonin agonists and dopamine antagonists were using including sumatriptan, metoclopramide and prochlorperazine. Also nonsteroidal anti-inflammatory drugs such as dexketoprofen or ibuprofen (NSAIDs), or simple analgesics like paracetamol or aspirin can be used for attack treatment. The aim of this study was to compare the degree of pain relief among 3 groups of patients who had dexketoprofen, metoclopramide or ibuprofen in emergency department. Materials-Methods: This prospective, observational study conducted in a tertiary care emergency department. Primary outcome of this study was the change in the severity of the perceived pain, and it was measured at the beginning, 15th and 30th minutes by a Visual Analogue Scale (VAS). Results: 54 patients were included in the final analysis. Mean (SD) age of the study subjects was 38.3 years (9.0) years and 83% (n=45) were women. Median (IQR) pain improvement at 30 minutes was 7.5 (7 -8) with dexketoprofen, 5 (4.75-7.00) with Ibuprofen and 7 (6.00-7.25) with Metoclopramide, and the differences between all groups were statistically significant (p<0.001). No adverse events were observed. Conclusions: We found dexketoprofen as the best treatment option in this observational study. Keywords: Dexketoprofen, ibuprofen, metoclopramide, migraine, pain O 070 ASSESSMENT OF DELIRIUM IN PATIENTS WITH MALIGNANCY WHO ADMITTED TO EMERGENCY DEPARTMENT WITH ALTERED MENTAL STATUS Mustafa Boz, Ali Batur, Elif Öztürk, Mehmet Mahir Kunt, Nalan Metin Aksu Hacettepe University Faculty of Medicine, Department of Emergency Medicine, Ankara, Turkey Delirium is a common and life-threatining neuropsychiatric syndrome. Diagnosis of delirium can be difficult, which increase morbidity and mortality rates also health care costs. In our study we aimed to asses delirium in patients with malignancy complaining of altered mental status admitted to emergency department, to compare delirium screening tests bCAM, MMT and NDRS. Between November 15, 2015 – May 31, 2016, 195 patients with malignancy admitted to Hacettepe University Faculty of Medicine Emergency Department complaining of altered mental status. Twenty-six patients (13,3%) were diagnosed with delirium based on criteria DSM-IV. In 117 patients (60%) delirium can not be determined and 52 patients (26,7%) testing could not be performed. Thirteen patients (50%) with delirium are men, there is no statistically significant difference by gender (p=0,353). Mean age of the patients with delirium 68,04±12,49; the average age of patients without delirium 66,53±11,38 there is no statistically significant difference by age (p=0,548). Delirium is most frequently seen in patients with colon tumor (19,2%), however, due to the small number of patient (5 patients), it was unable to obtain statistically reliable data. The most common diagnosis was hepatic encephalopathy in patient with delirium, however, due to the small number of patient (7patients), it was unable to obtain statistically reliable data. The mortality rate was significantly higher in patients with delirium (15,4% to 26,9%). Concordance between delirium screening tests bCAM, MMT and NDRS was found statistically significant (Eta=0,70 and Eta=0,95). bCAM was the test administered shortly with an average of 46,92±6,16 seconds. bCAM come forward at the end of our study by being a more detailed cognitive test, by being performed in a short time and by being easier to use. In conclusion, each department should choose appropriate test to diagnose delirium and should use it in routine. Keywords: Altered mental status, bCAM, delirium, emergency department, malignancy

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
144
O 071 PROSPECTIVE EXAMINATION OF THE SECOND SEIZURE FREQUENCY OF SEIZURES IN PATIENTS PRESENTING TO THE EMERGENCY DEPARTMENT
Gizem Söyler1, Funda Karbek Akarca1, Ayşe Güler2, Yusuf Ali Altuncı1, Murat Ersel1 1Ege University School of Medicine, Department of Emergency Medicine, Izmir, Turkey 2Ege University School of Medicine, Department of Neurology, Izmir, Turkey Introduction: In this study, patients admitted to the emergency room with seizures, aims to evaluate the frequency of seizures during follow again Method: The patients over the age 18 admitted the university hospital with seizures between March 2014 - February 2016. The study planned as a prospective analitic examination. Who first traumatic seizure and arrest of emergency that followed were not included. 450 patients confirming the volunteer form were included to the study. This complaint with the seizure of 450 patients in the emergency department patients with repeated admissions are also available. The second admission in the next thirty day period were not included; but over a period of thirty days between the two admissions it was included the study. Results: 439 patients were included in evaluation. The average age of patients was 46 ± 20 years (18-94), respectively. The 35,1's% of patients(n = 154) patients had a seizure for the first time in his life. Comparison to seizures of property 48.5% of patients (n = 213), seizures, 51.5% (n: 266) were found to be symptomatic seizures. 31.9%(n = 140) of patients suffered a seizure at least once during the follow in emergency. When patients first seizure median follow-up time of the distribution range of 2.0 (1- 40) were the interquartile range 1,0- 4,0. 39.3% of seizures in patients with observation (n = 55) were assessed as status epilepticus. Discussion: The presence of neurological deficits and low GCS score of application, detection of hypoxia and hyperthermia has been found to increase the risk of seizures in the ER observation. CT, EEG and other tests (ammonia, blood drug levels, lactate, MRI, LP) has no effect in determining the risk of seizures in ER follow up. However, clinicians were found to increase the risk of seizures if he wishes to follow any of these tests. Keywords: Seizure, emergency follow up, recurrence O 072 THE RELATIONSHIP OF VENOUS BLOOD LACTATE LEVELS WITH THE CLINICAL PROCESS IN ISCHEMIC AND HEMORRHAGIC STROKE PATIENTS: A ONE YEAR PROSPECTIVE ANALYSIS Turgay Çağlayan1, Engin Özakın1, Atilla Özcan Özdemir2, Mustafa Emin Çanakçı1, Nurdan Acar1, Filiz Baloğlu Kaya1, Ebubekir Arslan1, Hakan Dolgun1, Yasemin Dinç2, Muzaffer Bilgin3
1Eskişehir Osmangazi University, Department of Emergency Medicine, Eskişehir, Turkey�2Eskişehir Osmangazi University, Department of Neurology, Eskişehir, Turkey�3Eskişehir Osmangazi University, Department of Biostatistics, Eskişehir, Turkey Objective: The aim of our study is to investigate the relationship between venous blood lactate levels (VBLL) and clinical process in stroke patients. Methods: The stroke patients over 18 years of age admitted to the ESOGU ED, and with the diagnosis <12 hours before admission between 01.12.2014-30.11.2015 were included. The demographic features, the VBLL and NIHSS at admission, following 24 and 72h, the CT findings, the mRs at admission and following 3 months were recorded and the relationships between them were evaluated. Findings: Totally 88 patients, of whom 51(58%) were male and 72(81.8%) were diagnosed with ischemic, 16(18.2%) and hemorrhagic stroke, were included. The infarct size was evaluated on CT; in 56(63.6%) patients <1/3 of the MCA territory, in 9(10.2%) patients between 1/3-2/3 of the MCA territory, in 7(8%) patients >2/3of the MCA territory. Also 12 (13.6%) patients with intraparenchymal hemorrhage and 4(4.5%) patients with subarachnoid hemorrhage, were diagnosed with hemorrhagic stroke on CT. The VBLL were 1.98 ± 1,36mg/dl, 1.63 ± 0,77mg/dl and 1.41 ± 0,56mg/dl at admission, following 24 and 72h, respevtively. It was detected that VBLL decreases with time as statistically significant (p=0.019 between 0-24h and p<0.001 between 0-72h). The VBLL at admission in patients with ischemic stroke were detected higher in the patients with the infarct size >2/3 of the MCA territory than the patients with the infarct size <1/3 of the MCA territory (p=0.018). The admission VBLL in hemorrhagic stroke were detected higher in the subarachnoid hemorrhage than the intraparenchymal hemorrhage (p=0.047). No significant correlation could be detected between the VBLL at admission, following 24 and 72h with NIHSS and mRs. Conclusion: VBLL measurement, which's correlation can not be found with NIHSS and mRs, but can help emergency physicians in determining the type of bleeding, ischemic infarct size and management of stroke. Keywords: Stroke, lactate, NIHSS, mRs

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
145
O 073 THAT’S MCCONNELL! WELL, IS THIS AN ACUTE PULMONARY EMBOLUS? Betül Gülalp1, Özlem Karagün1, Tansel Erol2
1Başkent University Adana Medical and Research Center, Department of Emergency Medicine, Adana, Turkey�2Başkent University Adana Medical and Research Center, Department of Cardiology, Adana, Turkey Introduction: McConnell’s sign is defined as medial and inferior free wall hypokinesis/akinesis despite an apical part protected within contraction of right ventricle. There are many reports associated in acute pulmonary embolus. Besides, it can be related in chronic corpulmonale and even in miyocard infarct. Case: A 53 year old man presented to the emergency department with pain on chest and bilateral arms. An electrocardiogram revealed sinus tachycardia and left ventricle hypertrophy with nonspesific st and t wave changes. He had a right coronary artery stent and hypertension in history. On physical examination, his heart rate was 154 beats/min, blood pressure was 190/120 mm Hg, and oxygen saturation was 97% on room air. There were not any abnormal finding on sytemic physical examination. A point of care emergency ultrasound revealed hypokinesis of the RV free wall with protected normal contraction in the apical four chamber view obtained with a phased-array transducer of Philips Envisor by Emergency Physician (Figure 1-2 and Video 1). Medical treatment were administered for hypertension and acute coronary syndrome. The patient was admitted to the coronary angiography unit followed cardiology consultation without waiting the blood examination results. The only abnormality in blood tests was the Troponin; 0.59 ng/Ml (0.02-0.06). Percutaneous transluminal coronary angioplasty demonstrated 90% occlusion in left anterior descending artery. Stent and balloon were applied and discharged from hospital on third day. Result: McConnell sign defines the increased pressure in right ventricle related in acute corpulmonale as reported in 68%, chronic corpulmonale or cardiac infarcts. The normal contraction function in apical part of right ventricle occurs with contribution of the left ventricle. The distinction is the pulmonary arterial pressure for corpulmonale. Coronary infarcts are considered in differential diagnosis. Keywords: Emergency medicine, McConnell sign, point of care emergency ultrasound O 074 ACİL SERVİSE KONVÜLZİYON NEDENİYLE BAŞVURAN HASTALARIN RETROSPEKTİF ANALİZİ Elif Öztürk, Aslı Bilge İpek, Mustafa Boz, Bülent Erbil, Mehmet Ali Karaca Hacettepe Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Ankara Türkiye ve dünyada epileptik nöbet önemli bir halk sağlığı sorunudur. Acil servislere yapılan tüm başvuruların %1 - 2’sini oluşturduğundan ve tanı almış epilepsi hastalarının dışında her yıl 150,000 hasta genellikle acil serviste tanı aldığından, sık karşılaşılan önemli bir problemdir. Çalışmamızda Hacettepe Erişkin Acil Servisi’e konvülziyon nedeniyle başvuran hastaların genel özelliklerinin tanımlanması ve konvülzyon tanısında acil servisdeki izleminde yapılan EEG inceleme, nörogörüntüleme sonuçlarını ve acil servisteki izlem süreleri yönetiminde katkısı olup olmadığını göstermeyi amaçladık. 2010-2014 yılları arasında acil serviste nöbet nedeniyle başvurup çalışma kriterlerini sağlayan 209 başvuru incelendi. Hastaların yaş ortalaması 43.8 19.3 olarak ve yaş grubuna göre 18-29 yaş arası ağırlıkta bulundu. Özgeçmişinde hastaların %39.7’sinde malignite olduğu saptandı. İntrakraniyel malignitesi olan hastalar %20.5 olarak bulunurken en sık Glioblastoma Multiforma (%7.7) tanısı izlendi. Nöbet etiyolojisine göre %37.4’ünde primer nöbet, %62.6’sında sekonder nöbet saptandı. Sekonder nöbetlerle ilgili en sık karşılaşılan etiyolojik faktörlerin %21.5 oranında yapısal SSS anormalisi ve metabolik bozukluklar (%8.1) olduğu görüldü. Sekonder nöbet tipi için yaş ortalaması 48.4 (19.5) bulunmuş olup primer nöbetle kıyaslandığında istatistiksel olarak anlamlı daha yüksekti. Sekonder nöbetle gelen hastalarda acilde kalış süre ortalaması 40.5 (85.1), hastanede kalış süresi ortalaması 78,9,(158.1) saat olup anlamlı olarak primer nöbete göre daha uzun bulundu. EEG raporunda aktif epileptiform değişiklik saptanan hastaların %33.3’ünde izlemde nöbet izlendi. Başvuruda hiperglisemisi saptanan hastalarda izlemde nöbet riskinin anlamlı şekilde arttığı saptandı. İzlemde nöbeti olan hastaların başvurudaki GKS ortalaması (12.48) daha düşük olduğu tespit edildi. Acil servise nöbet nedeniyle başvuran ileri yaş grubunda provakatif nedenlerin araştırılması, hipoglisemi kadar hipergliseminin de nöbet etiyolojisinde ve nöbet rekürrensinde rol oynayabileceği, bu nedenle yakın kan şekeri takibi yapılması ve gelişinde GKS düşük saptanan hastaların izlemde nöbet riskinin daha yüksek olduğu göz önünde bulundurulmalıdır. Acil serviste optimum izlem süresi ile ilgili öneri ve tekrarlayan nöbetle ilgili risk faktörlerinin belirlenmesi için prospektif çalışmalara ihtiyaç duyulmaktadır. Anahtar Kelimeler: Acil servis, EEG, epilepsi, nöbet, nörogörüntüleme

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
146
O 075 GBS HASTALARINDA GÖRÜLEN SENDROMLARDAN PRES, NADİR BİR OLGU Vefa Açıkgözlü, Serhat Akay, Caner Sağlam, Serdar Beden, Bahadır Çağlar, Gökhan Yılmaz, Saylav Ejder Bora, Nesli Belen, İsmet Parlak İzmir Bozkaya Eğitim Araştırma Hastanesi, Acil Tıp Kliniği, İzmir Guillain Barre Sendromu (GBS), akut gelişen progresif olarak distalden proksimale ilerleyen motor ve sensorial fonksiyon kaybı ile karakterize bir durumdur. Hastalar genelde viral olan üst solunum yolu enfeksiyonu veya gastroenterit tablosundan sonra prezente olurlar. Olgumuz olan 43 yaşında bayan hastada 5 gündür olan ishal şikayeti sonrası başlayan yürüme zorluğu nedeniyle acil servisimize başvurdu. Gelişte hipertansif ve taşikardik olan hastanın nörolojik muayenesinde bilateral alt ekstremitelerde distalde daha belirgin 3/5 kuvvet kaybı ve hipoestezi, sol santral santral fasial paralizi ile arefleksi mevcuttu. GBS öntanısıyla yapılan lomber ponksiyonunda beyin omurilik sıvısında artmış protein (100.4 mg/ml) ve hücre görülmemesi sonucunda tanı kesinleşti. Bulber tutulumlu GBS düşünülen hastada tedavi olarak acil serviste intravenöz immunoglobin başlanan hasta izlem amaçlı nöroloji servisine yatırıldı. Solunum sıkıntısının artması nedeniyle entübe edilen, görüntülemede nozokomiyal pnomoni saptanan hastaya antibiyoterapi başlanarak yoğun bakıma transferi yapıldı. Tekrarlayan nöbetler nedeniyle levetirasetam başlandı. İzlemde ekstübe edilmesi üzerine tekrar servise alınan hastada ani gelişen bilinç bozulması sonrası yapılan muayenede Glasgow Koma Skalası 3, sözel ve ağrılı uyaranlara cevap vermemesi üzerine tekrar entübe edilen hastanın magnetik rezonansında bilateral serebellar, oksipital ve parasagittal bölgelerde yaygın difüzyon kısıtlılığı, t2 flair görüntülemede hiperintens görünüm ve t1 de posterior bölgelerde sulkuslarda hiperintensite saptanması üzerine posterior reversibl ensefalopati (PRES) tanısı konuldu. Yoğun bakımda izlenen hasta kardiyak arrest gelişmesi ve resusitasyona cevap vermemesi üzerine kaybedildi. Nadir olarak saptanan GBS hastalarında PRES insidansı bilinmemektedir. Otonomik disfonksiyonun sık olduğu GBS hastalarında görme bozukluğu, nöbet, bilinç bozukluğu bulguları saptandığında PRES akla gelmelidir. Anahtar Kelimeler: Guillan barre, posterior reversible ensefalopati, arefleksi, gastroenterit O 076 MEDULLANIN NADİR İNFARKTI MEDİAL MEDULLAR SENDROM Oğuzhan Bol, Sercan Bıçakçı, Hüseyin Şahin, Rahime Merve Yanıker Namık Kemal Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Tekirdağ Giriş: Medial medullar infarktlar tüm infarktlar içinde % 1’den daha az görülmektedir. Medial medüller sendrom medullayı etkileyen iki temel iskemik inme tipinden nadir olanıdır. İpsilateral dil zaafı, derin duyu kusuru, yüzün kurtulduğu kontralateral hemipareziden oluşan klasik triadı vardır. Bizim size farklı bulgularla karşılaştığımız iki medial medullar infarkt olgusunu anlatacağız.� Olgu 1: 70 yaşında erkek hasta 2 gün önce başlayan yüzde uyuşma, ağızda kayma ve sağ tarafta güç kaybı şikayetiyle acil servise başvurdu. Öyküsünde 4 gün önce kafa travması mevcut. Başka bilinen bir özellik ve kronik hastalık öyküsü yok. �Hastanın muayenesinde vital bulgular normal, sağ hemiparezi ve sağ fasial hemipleji dışında nörolojik muayene normaldi. Yapılan laboratuar tetkiklerinde herhangi bir patoloji görülmedi.� Kafa travması sonrası kanama düşünülen hastada Beyin BT’lerde kanama ve fraktür görülmedi. Difüzyon MR’ında sol medulla oblangatada medial infarkt görüldü. Hastaya antitrombotik tedavi başlanarak nöroloji servisine yatışı yapıldı��
Olgu 2: 63 yaşında erkek hasta 1-2 saat önce başlayan yüzün sol yarısında uyuşma ve konuşma bozukluğu ile hastanemize başvurdu. Hastanın bilinen bir kronik hastalık öyküsü yoktu.�Sol santral fasial hemipleji saptanan hastada dil sağa deviye olması dışında nörolojik muayene normaldi. Hastanın ilerleyen saatlerde sağ üst ekstremitede hemiparezisi gelişti.�Beyin BT ve tetkiklerde akut patoloji saptanmadı. Difüzyon MR'ında sol medulla oblangatada medial infarkt görüldü. Hasta antitrombolitik tedavi başlanrak nöroloji servisine yatırıldı.��
Tartışma: İpsilateral hipoglossal sinir paralizisi, kontralateral hemiparezi ve kontralateral proprioseptif duyu kaybından oluşan klinik triat ile karakterizedir. Dil ve arka kordonun tutulmadığı saf motor hemiparezi ile seyreden formları da vardır. Bilateral olduğunda hastada kuadriparezi görülür. Sonuç: Heterojen kliniğe sahip olan medial meduller infarktlar klinik olarak diğer prognozu daha kötü olan infarktlara benzese de MR’da oldukça küçük alanda olmaları nedeniyle atlanabilmektedir. Biz birinci vakamızda hem MCA infarktı ayırıcı tanısına girmesi ve her iki vakamızda da görüldüğü üzere farklı semptomlarla karşılaşılabilir olması ve MR da kolay atlanabilmesi dolayısıyla medial meduller infarktı sizlere hatırlatmak istedik. Anahtar Kelimeler: Medullar, infarkt, hemiparezi

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
147
O 077 BİLATERAL TALAMİK İNFARKT: OLGU SUNUMU Mustafa Numan Erdem1, Nurcan Bıçakçı2, Oğuzhan Bol1
1Namık Kemal Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Tekirdağ�2Tekirdağ Devlet Hastanesi, Acil Tıp Kliniği, Tekirdağ Giriş: Bilateral talamik infarktlar arteriyel veya venöz kaynaklı olabilir, tüm serebral infarktlar içinde %0,6 oranında görülür. Basiller arter tepe veya sıklıkla Percheron arteri olarak isimlendirilen arterin oklüzyonu arteriyel iskemiden sorumludur.��
Olgu: 78 yaşında kadın hasta, ani gelişen uykuya meyil/bilinç bulanıklığı nedeniyle acil servise başvurdu. Nörolojik muayenesinde lateralizan bulgusu yoktu.�Rutin kan tetkiklerinde üre 96 mg/dL, kreatinin 1.14 mg/dL, AST 168 U/L, ALT 166 U/L, troponin 0,28 ng/mL, CRP 23 mg/L olması dışında patoloji saptanmadı.�Beyin tomografisinde serebral atrofi ile uyumlu görünüm mevcuttu, kanama izlenmedi. Diffüzyon MR'da bilateral talamik bölgelerde diffüzyon kısıtlılığı ve ADC haritalamasında tanımlanan bölgelerde hipointensite izlendi.�Talamus kortikal fonksiyonların düzenlenmesinde rol alan pek çok nukleus içerir ve ayrıca serebral korteks ile beyin sapı arasında iletişimi sağlar. Talamus ayrıca uyanıklık, uyku ve dikkatin düzenlenmesinden sorumludur. Talamik infarktlarda vertikal bakış parezisi, hafıza kaybı, konfüzyon ve koma izlenebilir.�Bilateral talamik arteriyel infarktlarda en sık etiyolojik neden kardiyoembolismdir. Straight sinüse drene olan posterior grup talamik ven trombozu da venöz etiyolojiden sorumludur.� Beyin MR'da bilateral talamik infarkt düşündürebilecek diğer durumlar Wernicke ensefalopatisi, ekstrapontin miyelinolizis, Wilson hastalığı, Creutzfeldt-Jacob hastalığı ve bilateral talamik gliomlardır.� Olgumuzda klinik tablonun ani gelişmesi, MR görüntülerinde izlenen lezyonun talamusta sınırlı kalması, diffüzyon ağırlıklı görüntülerde hiper, ADC karşılığında hipointens izlenmesi iskemi lehine bulgulardır.�Acil servise bilinç bulanıklığı ile başvuran hastalarda bilateral talamik infarkt, nadir rastlanan, ancak ayırıcı tanıda gözönünde bulundurulması gereken bir durumdur. Anahtar Kelimeler: Bilateral, talamik, infarkt O 078 HİPOFİZ ADENOMUNA BAĞLI KİTLE İÇİ KANAMA SONRASI 3. SİNİR BASISI Hamit Hakan Armağan, Abdurrahman Şimşek, Furkan Çağrı Oğuzlar, Berker Şahin Süleyman Demirel Üniversitesi Tıp Fakültesi Hastanesi, Acil Tıp Anabilim Dalı, Isparta Giriş: Hipofiz, internal karotid arterlerin kavernöz segmentlerinin arasında, optik sinirlerin ve kiazmanın altında yer alır. Hipofiz adenomları, primer beyin tümörlerinin % 10-15’ini oluştururlar ve 3-5. dekatta ve kadınlarda daha sık görülür. Baş ağrısı ve görme bulguları (bitemporal hemianopsi %67) en sık görülen bulgulardır. Tümör içerisinde %2.9 oranında hematom oluştuğu ve bunların genelde cerrahi sonrasında görüldüğü saptanmıştır. Olgu: Yirmi iki yaşında erkek hastaya 5 gündür olan baş ağrısı şikayeti ile başvurduğu hastanede sinüzit reçetesi düzenlenmiştir. Acil servisimize sabah başlayan diplopi ve tek taraflı pitozis şikayetiyle başvurdu. Başvuru vitalleri; TA: 130/82 mmHg, Nb: 70/dk, Ateş:36.5 C SPO2: %97 idi. Fizik muayenesinde; sol göz dışa bakış kısıtlılığı ve pitozis dışında patolojik muayene bulgusu yoktu. Yapılan laboratuar tetkiklerinde; Na: 128 mmol/L (normali:136-145 mmol/L) ve CRP: 45mg/L (normali (0-3 mg/L) dışında anormal sonuç yoktu. Hastanın BBT'si normaldi. Klinik bulgularının devan etmesi dolayısıyla çekilen Kontrastlı beyin MR'ında; Hipofiz 14 mm(hipofiz adenomu?), sfenoid sinüse indentasyon göstermekte olup, adenom komsulugunda T1a'da hiperintens T2a serilerde hipointens (hemoraji) alan saptandı. Hemorajik alanın sol kavernöz sinüste asimetrik daralmaya (3. ve 4. kranial sinir basısı) sebep olduğu gözlendi ve pituiter apopleksi lehine değerlendirildi. Hasta beyin cerrahi konsültasyonu sonrası hipofiz cerrahisi yapılabilecek bir merkeze sevk edildi.��
Sonuç: Pitüiter apopleksi, hipofiz glandındaki akut hemoraji veya infarkt sonucu gelişen, yüksek morbidite ve mortalite ile seyreden ve nadir görülen klinik bir tablodur. Ani başlayan başağrısı ile birlikte görme kaybı ve değişik derecelerde hipofiz hormon yetersizliği klinik tabloyu oluşturur. Acil servise gelen ani başlangıçlı başağrısı, bulantı, kusma, bilinç değişiklikleri ve ateş gibi semptomlar varlığında veya oftalmik semptomlarda hipofiz adenomları düşünülmelidir. Anahtar Kelimeler: Hipofiz adenomu, pituiter apopleksi, pitozis

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
148
O 079 AKUT APANDİSİT VAKALARININ DEMOGRAFİK ANALİZİ VE TANIDA ALVARADO SKORLAMA SİSTEMİ VE CRP
Burak Hasgül, Serhat Karaman, Nurşah Başol Gaziosmanpaşa Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Tokat Akut apandisit (AA); tüm yaş gruplarında akut karın olarak karşılaşılan, acil cerrahi gerektiren ve halen teşhis edilmesinde güçlükler olan durumlardan biridir. Erken teşhis edilmesiyle mortalite ve morbidite oranı oldukça düşüktür. Şikayetlerin ve bulguların diğer karın ağrısına neden olabilecek hastalıklarla karışabilmesi tanıda hatalara sebep olabilir. Alvarado Skoru (AS) ve CRP’nin klinisyenlere hasta yönetiminde ne kadar yol gösterici olabileceğini ve güvenilirliğini araştırmayı hedefledik. �Bu çalışma prospektif olarak planlandı. Acil servis kliniğine karın ağrısı ile başvuran toplam 150 hastadan histopatolojik sonucu AA olarak sonuçlanan 73 hasta grubunun ve yapılan incelemeler sonrası akut apandisit çıkmayan 77 kontrol grubunun verileri incelendi. �AA grubundaki 73 hastanın 37’si (% 50.6) kadın iken, 36’sı (%49.4) erkekti (kadın/erkek: 1.02/1). Ortalama yaş hasta grupta; 30.6 iken, erkeklerde 30.5, kadınlarda 30.8 idi. AA düşünülüp operasyona alınan 86 hastanın 13’ ünde (% 15.1) apandisit harici farklı bir patoloji ile karşılaşıldı (negatif apendektomi). Hasta grubun patoloji sonuçlarına göre akut apandisite en sık yol açan sebep % 84.9 ile fekaloidler olduğu görüldü. Hastaların % 85’ inde basit apandisit saptanırken, % 8.2’ sinde perforasyon tespit edildi. AA vakalarının fizik muayenesinde en sık sağ alt kadran hassasiyeti (%95.8) görülürken, en sık görülen semptom bulantı ve kusma (%67.1) idi. AS parametrelerinden biri olan ateş ise %12.4 oranında görülerek en nadir gözlenen bulgu oldu. AS laboratuar parametrelerinden lökositozun sensitivitesi hasta grup üzerinde % 79.4 iken nötrofili % 75.3 olarak bulundu. Çalışmamızda AS ve lökosit arasındaki ilişki ki-kare testi ile analiz edildi ve hem hasta 5 grubunda hem kontrol grubunda bu iki değer birbiriyle uyumlu bulundu. AS ve CRP arasındaki ilişkiye bakıldığında hasta grubunda bu iki değer birbiriyle uyumsuz bulunurken, kontrol grubunda uyumlu bulundu. AS ile AA arasındaki ilişki ki-kare testi ile incelendi. Karın ağrısı şikayeti ile başvuran hastaların AA açısından ayrımında AS sisteminin tek başına yeterli olmadığı görüldü. Laboratuar testleri veya görüntüleme yöntemleri ile tanının desteklenmesi gerekmektedir. Anahtar Kelimeler: Akut apandisit, CRP, alvarado skorlama sistemi O 080 ORTALAMA PLATELET HACMİNİN AKUT PANKREATİTİN AĞIRLIĞINI BELİRLEMEDEKİ ROLÜ Neşe Nur User1, Burcu Çoker1, Emel Gökalp1, Sezgin Yılmaz2
1Afyon Kocatepe Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Afyonkarahisar�2Afyon Kocatepe Üniversitesi Tıp Fakültesi, Genel Cerrahi Anabilim Dalı, Afyonkarahisar Giriş-Amaç: Akut pankreatitin prognozunu tahmin edebilmek için çeşitli klinik ve radyolojik kriterler kullanılmaktadır. Ortalama platelet hacmi (MPV), akut inflamasyonu belirlemek için son yıllarda kullanılan bir belirteçtir. Bu çalışmada akut pankreatitli hastalarda Acil Servis başvurusundaki MPV değerinin hastalığın ağırlığını belirlemedeki değeri araştırıldı.��
Materyal-Metod: AKÜTF Acil Servisine 01.01.2014-30.09.2016 tarihleri arasında başvuran akut pankretitli hastalar retrospektif olarak değerlendirilerek MPV değerlerinde; hastaların yaşı, cinsiyeti, hastalığın klinik ağırlığı, biliyer veya nonbiliyer olması, görüntüleme bulguları, yatış süresine göre istatistik anlamlı fark olup olmadığı istatistik olarak incelendi. Sonuç: Akut pankreatitli hastalarda MPV’nin tanısal ve prognostik değeri güncel bir araştırma konusudur. MPV değeri, akut pankreatitin erken döneminde tanısal veya prognostik olarak değerli olmayabilir. Anahtar Kelimeler: Akut biliyer pankreatit, akut nonbiliyer pankreatit, MPV

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
149
O 081 YILAN ISIRIĞI SONRASI GELİŞEN KOMPARTMAN SENDROMU Yeşim İşler1, Şükrü İşler2, Halil Kaya1, Suna Eraybar1
1Bursa Yüksek İhtisas Eğitim ve Araştırma Hastanesi, Acil Tıp Anabilim Dalı, Bursa�2Bursa Yüksek İhtisas Eğitim ve Araştırma Hastanesi, Plastik Rekonstruktif ve Estetik Cerrahi Kliniği, Bursa Giriş: Yılan zehiri birçok toksik protein ve enzimin bir araya gelmesinden oluşan karmaşık bir yapıya sahiptir. Toksinin şiddetine göre hastada lokal ve sistemik belirtiler gözlenir. Isırılan bölgede ağrı, ısı artışı, hemorajik ödem, ekimoz, lenfanjit ve doku nekrozu gibi lokal bulguların yanında, ateş, bulantı, kusma, dolaşım kollapsı, sarılık, delirium, konvülziyon ve koma gibi sistemik komplikasyonlar ortaya çıkabilir. Olgu: 61 yaşındaki bayan hasta sol el bileğinden yılan ısırması sonrası kolunda şişmenin artması nedeniyle tarafımıza sevkedildi. Hastanın genel durumu orta- iyi, bilinci açık,oryante koopereydi. Vitalleri stabildi. Yara yerinde 30 x 8 cm'lik alanda ekimoz, ödem ve axiller bölgeye kadar uzanan ağrısı mevcuttu. 80 mg prednizolon, 20 mg Pheniramine hydrogen maleate, 100 mg ulcuran ve tetanoz proflaksisi uygulandı. GKS: 15, kan basıncı 120/70 mmHg, kalp atım hızı 95 dk ve düzenliydi. Solunum sayısı 18 dk ateşi 36.5 C olarak kaydedildi. Olgunun özgeçmişinde diabetes mellitus ve hipertansiyon mevcuttu.. Arteriyel kan gazı analizi normal olarak değerlendirildi. Elektrokardiyografisinde herhangi bir patolojiye rastlanmadı. Tedavisinde 2 L dk oksijen verildi. Profilaktik olarak sulbaktam-ampisilin antibiyoterapisi ve serum fizyolojik başlandı. Mide koruyucu tedavi olarak Famotidine, ağrı ve inflamasyon için Diklofenac sodyum başlandı. Extremite elevasyonu yapıldı. Yılan ısırmasından yaklaşık 2 saat sonra antivenom 20 ml iv infüzyon uygulandı. Hastanın tedavisinin 2. saatinde sol el bölgesinde solukluk, soğukluk, nabızlarının zayıflaması nedeniyle klinik olarak periferik dolaşım bozukluğu saptandı. Olgunun ekimozlarında ve ödeminde artma olması nedeniyle orta düzey yılan ısırması olarak değerlendirildi ve 30 mL antivenom iv infüzyon uygulandı. Kompartman sendromu gelişen hastaya plastik cerrahi konsultasyonu istendi ve acil fasiyotomi için operasyona alındı. Sol el dolaşımı sağlanan hastanın yatışının 5. gününde sağlıklı bir şekilde taburcu edildi. ��
Sonuç: Yılan ısırıkları acil olgular olarak kabul edilip tedavisi; sıvı- elektrolit tedavisi, antibiyotik, antihistaminikler, tetanoz profilaksisi yapılmalı, antivenom tedavisi klinik bulgulara göre belirlenmelidir. Yılanın ısırdığı bölge kompartman sendromu açısından yakın takibe alınmalı,erken fasiyotominin önemi unutulmamalıdır. Anahtar Kelimeler: Kompartman, nekroz, toksin O 082 ÇOCUK ACİL GÖZLEM HASTALARINDA ATEŞ ÖLÇÜMÜNDE İNFRARED TERMOGRAFİ KULLANIMI VE DÖRT FARKLI ATEŞ ÖLÇÜM YÖNTEMLERİNİN KARŞILAŞTIRILMASI Emel Berksoy, Murat Anıl, Yüksel Bıcılıoğlu, Gamze Gökalp, Alkan Bal, Didem İlhan, Tuğçe Akgün Sağlık Bilimleri Üniversitesi, Tepecik Eğitim ve Araştırma Hastanesi, Çocuk Acil Kliniği, İzmir Giriş: Son zamanlarda çocuk acil servislerde vücut sıcaklığı ölçümünde pratik, hızlı, konforlu oluşları nedeniyle timpanik ve infrared termografi (IFR) yöntemleri kullanılmaktadır.��
Amaç: Bu çalışmanın amacı, çocuk acil gözlem biriminde izlenen hastaların rektal, aksiller digital( ADT), IFR - timpanik (IFR-T), IFR- alın ( IFR-F), IFR- boyun ( IFR- N), IFR- gövde (IFR-B) ile yapılan vücut sıcaklığı ölçümlerini karşılaştırmak, ‘altın standart’ rektal ateş ölçüm değerine göre diğer ölçüm değerlerinin ateşi öngörme yeteneğini belirlemektir. ��
Yöntem: Çalışmaya 09- 11 saatleri arasında acil gözlem birimine izlem için kabul edilen yenidoğan dönemi hariç 4 yaşa kadar olan 65 hasta alındı. Aynı hemşire tarafından digital elektronik termometre ile rektal (n: 139) ölçümler alındı. Eş zamanlı olarak diğer hemşire tarafından her hastadan ortalama 3 kez ADT, IFR timpanik sol (LAT), IFR timpanik sağ ( RAT), IFR- F, IFR- N, IFR- B ölçümleri alınıp kaydedildi. Rektal >= 38 °C ateş olarak kabul edildi. Yedi ayrı vücut bölgesinden dört farklı teknikle yapılan ölçümler istatistiksel olarak karşılaştırıldı.��
Sonuçlar: Total 139 rektal ateş ölçümü referans alındığında; rektal vücut sıcaklığı, 37.6 ± 1.7 ° C, ADT 37.0 ± 1.6° C; RAT 37.0 ±1.3° C; LAT 37.0 ±1.4 °C,IFR-F 36.8 ±1.4 °C; IFR-N 37.1±1.7 °C; IFR-B 37.1±1.4° C ( median± IQR) olarak bulundu. �Bland Altman analizi ile rektal ölçüm ile diğer altı farklı ölçüm değerlerinin birbiriyle uyumlu olduğu saptandı. ROC analizi kullanıldığında; rektal ateş >= 38 ° C için en yüksek AUC değerleri sırasıyla; ADT AUC 0.942 ( %95 CI 0.906 – 0.979), RAT AUC 0.882 ( %95 CI 0.817- 0.948); en düşük IFR-F AUC 0.745 ( %95 CI 0.656- 0.834 ) olarak bulundu. ( p <0.001)� Sonuç: Çalışma grubumuzda ADT ve IFR- timpanik termometre en iyi rektal ateş prediktörü olarak bulunmuştur. Anahtar Kelimeler: Ateş ölçümü, çocuk acil, infrared termografi

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
150
O 083 PEDİATRİK ATEŞ KONTROLÜNDE PARASETAMOL VE METAMİZOL ETKİNLİĞİNİN KARŞILAŞTIRILMASI, RANDOMİZE ÇİFT KÖR PLASEBO KONTROLLÜ ÇALIŞMA
Onur Karakayali, Serkan Yılmaz, Ahmet Akdoğan, Yavuz Yiğit, Hüseyin Cahit Halhallı Kocaeli Derince Eğitim ve Araştırma Hastanesi, Acil Tıp Anabilim Dalı, Kocaeli Giriş-Amaç: Bu randomize çift kör placebo kontrollü çalışmada acil kliniğine ateş ile başvuran pediatri vakalarında tek doz intravenöz antipiretiklerin etkinliği, yan etki, tolerabilitesisinin karşılaştırılması ile hızlı, güvenli antipiretik ajanın tespiti amaçlanmıştır.� Materyal-Metot: Randomize çift kör çalışmaya acil servise 1-18 yaş arasında ateş ile başvuran hastalar dahil edildi. Hastalar bilgisayar programı ile randomize edildi. Katılımcılar parasetamol, metamizol ve plasebo 3 grup olarak randomize edildi. Hastaların demografik verileri ve vital bulguları kayıt altına alındı. Başvuru anında ve 10.günde tüm hastalardan agrunolositozis açısından hemogram tetkikleri alındı. Hastalar 21 C soğutulmuş standart müşahede odasına alınarak tanı ve tedavide yer almayan 3.araştırmacı tarafından körlük sağlanarak kapalı zarflarda uygun dozda 1. Gruba ıv parasetamol, 2. Gruba metamizol ıv, 3. Gruba iv SF verildi. İstatistiksel analizler SPSS versiyon 21 yazılımı kullanılarak yapıldı.��
Sonuçlar: Hastaların demografik verileri, ateş takipleri (0’, 30’,60’,90’,120’), ortalama arter basınçları (0’,90’) tablo 1 ve tablo 2 de verilmiştir. Demografik özellikler tedavi grupları arasında benzerdi. Hedef ölçüm süresi olan 90. dk sonunda PS ve NV grubunda düşüş birbirine benzer olarak bulundu (PS: -1.37 ± 0.84 (%95 GA:-1.21 to – 1.52), NV:-1.38 ± 0.80 C (%95 GA-1.23 to -1.52)).Her 3 tedavi grubunda da başvuru değerine göre ateş değerindeki düşüş istatistiksel anlamlıydı (p<0.001). Tedavi gruplarının 90 dk.da ateşi hedef ölçüm değerine düşürme başarısı anlamlı olarak birbirlerinden farklıydı (p<0.001). 60.dk.da en belirgin düşüş PS grubunda elde edildi (-1.17 ± 0.85 C (%95 CI -1.02 to -1.33). 120. dk. sonunda PS ve NV grubunda düşüş birbirine benzerdi. (PS: -1.68 ± 0.86 (%95 GA:-1.53 to – 1.84), NV:-1.60 ± 0.76 C (%95 GA-1.46 to -1.74)). Agrunolositoz açısından 3 grup arasında istatistksel olarak anlamlı fark bulunmadı. OAB açısından metamizol grubunda diğer gruplara göre daha fazla düşüş gözlendi ancak klinik olarak anlamlı hipotansiyon saptanmadı.��
Tartışma: Pediatrik ateş kontrolünde her iki grupta ateş kontrolü ve yan etki açısından güvenilirdir. Birçok ülkede agrunulositoz açısından yasaklı madde olarak görülen metamizol grubunda yan etki profili açısından güvenilirdir. Anahtar Kelimeler: Pediatric fever treatment, antipiretics, metamizole O 084 KARMA AŞI SONRASI ANAFLAKSİ: OLGU SUNUMU Mehmet Altuntaş, Mehmet Oktay Recep Tayyip Erdoğan Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Rize Giriş: Aşılar, aşıyla önlenebilir hastalıkların kontrolü için kullanılan temel halk sağlığı araçlardan biridir. Etkin bir bağışıklama programıyla çeşitli enfeksiyon hastalıklarına bağlı ölüm ve morbidite azaltılabilir. Ancak aşılara karşı alerjik reaksiyonlar çok nadiren de olsa ortaya çıkabilmekte ve hayatı tehdit edici olabilmektedir. Bu reaksiyonlar genellikle jelatin veya yumurta ve nadiren maya ya da lateks olarak imalat işleminde kullanılan artan protein bileşenlerine bağlıdır. Aşı reaksiyonlarının çoğu enjeksiyon yerinde lokalize, ancak bazı durumlarda, şiddetli anafilaktik reaksiyonlar şeklinde oluşabilir. Bir çocuğun aşıya karşı alerjik bir reaksiyon geliştiği için etiketlenmesi, sonraki aşılar için muhtemel riskler nedeniyle aşılama programını tamamlayamamasına neden olacaktır. Bu nedenle karar verirken dikkatli davranılmalıdır. Anafilaksi tanısı bir alerjenin alınmasından dakikalar veya saatler sonra aniden ortaya çıkan yaygın ürtiker, kaşıntı veya kızarıklık; dudaklarda uvulada şişmeye ek olarak solunum sistemi tutulumu(dispne, bronkospazm, stridor, hipoksemi), kan basıncında düşme veya uç organ fonksiyonlarında bozulma belirtilerinden (şok, senkop ) en az birinin olmasıyla konulabilir. Olgu: Acil servise huzursuzluk, vücudunda kızarıklık şikayetleriyle 6 aylık bebek hasta getirildi. Şikayetleri başlamadan yaklaşık 2 saat önce aşılama programı dahilinde Hepatit B aşısı, Beşli Karma aşı (DaBT-İPA-Hib), Konjuge Pnomokak aşısı ve Oral Polio aşısı yapıldığı öğrenildi. Fizik muayenesinde Nb: 170 atım/dk, TA: 80/60 mmHg, ateş: 37 C, genel durumu orta-iyi, huzursuz, saçlı deride ve yer yer tüm vücudunda yüzeyden kabarık, eritemli farklı boyutlarda ürtikeryal deri döküntüleri mevcuttu. Uvula ödemi ve stridoru mevcuttu. Tam monitorize edilen hastada aşıya bağlı anaflaktik reaksiyon düşünülerek 0,01 mg/kg adrenalin intramüsküler yolla uygulandı. 10 ml/kg’dan serum fizyolojik 10 dakika bolus, metilprednizolon 2 mg/kg intravenöz (IV) yavaş infüzyon, ranitidin 1mg/kg IV uygulandı. Bronkospazm bulguları olan çocuğa 5 mg salbutamol nebülizer ile verildi. Deri bulguları adrenalin uygulamasının 10. dakikasında düzelmeye başladı. Bronkospazmı gerileyen hasta takip amaçlı pediatri servisine yatırıldı. Sonuç: Aşıya bağlı anaflaksi kararı vermek çocuğun aşı programını bozabilir ancak anafilaksi tedavi edilmezse yaşamı tehdit eden bir reaksiyondur. Anahtar Kelimeler: Anaflaksi, aşı, pediatri

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
151
O 085 ACİL SERVİSİMİZE BAŞVURAN PULMONER EMBOLİ VAKALARINDA MORTALİTE ÜZERİNE ETKİLİ FAKTÖRLERİN İNCELENMESİ
Meliha Fındık, Cemil Kavalci, Afşin Emre Kayıpmaz, Murat Muratoğlu, Elif Kılıçlı Başkent Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Ankara Pulmoner emboli sık karşılaşılan kardiyovasküler acillerden biridir. PE özgül bir klinik tablo ile ortaya çıkmadığı için tanısının konulması güçtür ve gözden kaçabilir(1). Tüm dünyada olduğu gibi Türkiye’de de yaşlı nüfus hızla artmaktadır, bunun sonucu olarak da acil servislerde PE ve venöz tromboemboli daha sık görülmektedir. Aynı zamanda son yıllarda, tanı yöntemlerindeki gelişmeler de PE tanı sıklığını arttırmıştır. PE geçiren ve tanı konulamayan hastalarda mortalite oranı %30’lara ulaşmaktadır, tanı konup uygun tedavi yapıldığında bu oran %3’lere düşebilmektedir(3,5). Olguların büyük bölümünde trombüs kaynağı alt ekstremitelerin derin venleri özellikle de ana femoral, süperfisal femoral, pelvik ve popliteal venlerdir. Pulmoner anjiyografi tanıda halen altın standarttır (8).�Pulmoner tromboemboli yaşlı nüfusun artması ile birlikte acil tıp doktorlarının sık karşılaşabileceği mortalite ve morbiditesi yüksek bir tanı haline gelmektedir. Bu nedenle risk faktörlerinin belirlenmesi ve bu risk faktörlerinin mortaliteye katkısının belirlenmesi; tanı ve önlenebilir risk faktörlerinin saptanması açısından önem taşımaktadır.�Bu çalışmada Başkent Üniversitesi Ankara Hastanesi Erişkin Acil Servisinde Ocak 2011-Aralık 2015 tarihleri arasında pulmoner emboli tanısı alan hastalar retrospektif olarak incelendi. Tüm olgularda öykü, fizik muayene bulguları, laboratuar bulguları, arter kan gazı, akciğer grafileri, risk faktörleri, bilgisayarlı tomografi ve yapılabilen olgularda ekokardiografi, alt ekstremite venöz doppler incelendi ve bu değişkenler ile mortalite arasındaki korelasyon bakıldı. Çalışma kapsamına toplamda 146 hasta dâhil edildi. İlk 30 gün gerçekleşen ölümleri erken ölüm olarak kabul edildi. %13,7’sinde (20 hasta) erken mortalite gerçekleştiği saptandı. Hastaların %90’ı 65 yaş ve üzerinde; kalan %10’uysa 45-64 yaş arasındaydı. %55’ini erkek, %45’ ini ise kadın hastalar oluşturmaktaydı.�Acil serviste PE tanısı konan hastaların yaş, cinsiyet, d-dimer, kreatinin, lenfosit, pH ve vücut sıcaklığı ile erken mortalite arasında ilişki saptandı. Geçirilmiş cerrahi, malignite, kardiyolojik hastalık öyküsü, nörolojik hastalık öyküsü ve immobil olan hastalarda pulmoner emboli olasılığının daha fazla olduğu görüldü. Anahtar Kelimeler: Acil servis, pulmoner emboli, erken mortalite O 086 ACİL SERVİSTE TOPLUM KÖKENLİ PNÖMONİ TANISI ALAN HASTALARDA PSI VE CURB-65 PNÖMONİ SKORLAMA SİSTEMLERİNİN DEĞERLENDİRİLMESİ Güzin Toygar İlhan1, Zeynep Karakaya2, Pınar Yeşim Akyol2, Fatih Esad Topal2, Umut Payza2, Serkan Bilgin2, Gözde Canan Tan2
1Erzurum Bölge Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Erzurum�2İzmir Katip Çelebi Üniversitesi Atatürk Eğitim ve Araştırma Hastanesi, Acil Tıp Anabilim Dalı, İzmir Amaç: Hastanemiz acil servisine başvuran toplum kökenli pnömoni tanılı hastalarda, pnömoni ciddi-yet indeksi (PSI) ve CURB-65 pnömoni skorlama sistemlerinin hastaneye yatış ya da taburculuk açısından uygunluklarının karşılaştırılmasıdır. ��
Gereç ve Yöntemler: Bu retrospektif çalışmaya Haziran 2013-Haziran 2014 tarihleri arasında acil servise başvuran ve pnömoni tanısı alan 150 olgu dahil edildi. Olguların demografik özellikleri, klinik, radyolojik ve laboratuar bulguları kayıt edildi. Tüm olgular PSI ve CURB-65 skorlamasına göre grup-landırıldı ve hastaneye yatış ya da taburculuk açısından uygunlukları incelendi.��
Bulgular: Çalışmaya yaş ortalamaları 69.15 ± 13.34 (min: 19; max: 92) olan 47 (%31.3) kadın, 103 (%68.7) erkek, toplam 150 olgu dahil edildi. Toplam 109 olguda CURB-65 ile PSI arasında yatarak tedavi gerekliliği açısından uyumluluk mevcuttu (κ=0,602, p<0,001). Yoğun bakım yatış olasılığı ele alındığında, PSI, CURB-65’e göre daha anlamlı bulundu (p=0,011, p=0,045, p<0, 05).��
Sonuçlar: Güncel pratikte kullanılmakta olan iki pnömoni ağırlık gruplamasının (CURB- 65, PSI) has-taneye yatarak tedavi endikasyonunu değerlendirmek açısından birbirleri ile korele olduğu görüldü. CURB-65, değerlendirme kriterlerinin az olması ve bunların birinci basamak merkezlerde dahi kolaylıkla uygulanabilecek kriterler olması nedeni ile pnömoni olgularında yatarak tedavi gerekliliğini değerlendirmede tercih edilecek yöntem olabilir. Anahtar Kelimeler: Toplum kökenli pnömoni, PSİ, CURB-65, acil servis

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
152
O 087 PNÖMONİ HASTALARINDA, CRP, PROKALSİTONİN VE LAKTAT ÖLÇÜMÜNÜN PROGNOSTİK DEĞERİNİN, SIK KULLANILAN SKORLAMA SİSTEMLERİ İLE KARŞILAŞTIRILMASI
Nimet Gülen1, Müge Günalp Eneyli1, Onur Polat1, Selda Çakmak1, Nalan Metin Aksu2
1Ankara Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Ankara�2Hacettepe Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Ankara Pnömoni hastalarında hastalığın ciddiyetini ve prognozu belirlemek amacıyla oluşturulmuş, farklı skorlama sistemleri mevcuttur. Ancak hiçbir skorlama sisteminin sensitivite ve spesivitesi yeterince yüksek değildir. Bu çalışmada amaçlanan, farklı demografik özellikler, etyolojiler ve ko morbiditelere göre, CRP, laktat ve prokalsitonin değerlerinin, prognozu saptamada sık kullanılan skorlama sistemlerine göre etkinliklerini belirlemek ve hastaların tedavisini düzenlemedeki faydasını saptamaktır. �Ankara Üniversitesi Tıp Fakültesi Hastanesi Acil Servisi'ne 1 Aralık 2015 ile 31 Mayıs 2016 tarihleri arasında başvuran, pnömoni tanısı alan 144 hastanın vital bulguları, kan tetkikleri ve kan gazı analizinin sonuçları değerlendirmeye alınmıştır. Hastaların tedavileri kılavuzların önerdiği şekilde düzenlenmiştir. Çalışma kapsamında, hastaların tanı ve tedavisini yönlendirilecek herhangi bir müdahalede bulunulmamıştır. Çalışmanın sonlanım noktaları hastane ve yoğun bakım ünitesine yatış ihtiyacı ile 28 günlük mortalite olarak belirlenmiştir. �Çalışmaya dahil edilen hastaların kadın-erkek dağılımı dengelidir ve yaş ortalaması 71±20 olarak saptanmıştır. Hastaların başvuru anında konfüzyonu bulunması mortalite ile ilişkili bulunmuştur. Hastaların CRP, prokalsitonin, laktat ve WBC değerleri arasında mortalite ile istatistiksel olarak anlamlı ilişki saptanmazken, hipoalbuminemi (p=0,092) ve üremi (0,018) değerlerinde korelasyon saptanmıştır. Skorlama sistemlerine bakıldığında; en sık kullanılan CURB-65’in ayaktan takip olacak hastaları ayırt etme gücü yetersiz kalırken (p=0,179); PSI’ın ayaktan takip edilecek hastaları saptamada (p=0,009), SMART-COP’un ise yoğun bakım ihtiyacı olabilecek hastaları saptamada (p=0,007) oldukça başarılı olduğu görülmüştür. Araştırılan tüm parametreler ve skorlar arasında hem ayaktan takip olacak hastaları hem de yoğun bakım ihtiyacı olacak hastaları saptamada, klinisyenin öngörüsü, en güvenilir sonucu vermektedir. (p<0,001)�Çalışmamızda hasta sayısı yetersizliği sebebiyle, çoklu analizler yapılamamış olup, bu en önemli kısıtlılığı oluşturmaktadır. İlerde yapılacak yüksek hasta sayılı araştırmalar ışığında, biyokimyasal belirteçlerin farklı demografik gruplardaki tanısal ve prognostik değeri daha net ortaya konabilir ve biyokimyasal belirteçler ile birlikte yorumlanarak daha güçlü skorlama sistemleri oluşturulabilir. Anahtar Kelimeler: CRP, laktat, pnömoni, prognoz, prokalsitonin O 088 RELATIONSHIP BETWEEN RIGHT VENTRICLES DILATATION AND BLOOD COPEPTIN LEVEL IN PATIENTS WITH PULMONARY THROMBOEMBOLISM Eren Usul1, Seda Özkan1, Aynur Ecevit Kaya1, Fatma Uçar2, Tolga Çimen3
1Dışkapı Yıldırım Beyazıt Training and Research Hospital, Emergency Medicine Clinic, Ankara, Turkey 2Dışkapı Yıldırım Beyazıt Training and Research Hospital, Biochemistry Clinic, Ankara, Turkey�3Dışkapı Yıldırım Beyazıt Training and Research Hospital, Cardiology Clinic, Ankara, Turkey Introduction: Pulmonary Embolism (PE) is a life-threatening cardiopulmonary emergency that occurs with arterial occlusion by a venous clot. Despite the difficulty in diagnosis, early treatment is very effective; early diagnose and appropriate treatment is important on progress of disease. Nowadays, there is an increase in surveys on purpose of evaluating disease severity and prognosis by working with various blood markers in PE patients. In this study, we wanted to find if we can use copeptin for determining right ventricles dilatation, and evaluation of disease severity and prognosis on diagnosis of PE. Material-Method: In this prospective study, we included 100 patients over 18 years old which is diagnosed as PTE in Department of Emergency Medicine of Dışkapı Training and Research Hospital. Complaints of patients at admission, curriculum vitae, symptoms and physical examination findings, electrocardiography findings, the echocardiography (ECHO) findings, computed tomography findings, labaratory results and the treatment they received were written on pre-established forms. We recorded the pulmonary artery pressure (PAP)right ventricles dilatation from the ECHO reports which done to patients for diagnose or after 24 hours of diagnose. Results: The 51% of the patients were women. The mean age was 68.03±15.31. Copeptin levels of Acute PE patients were significantly higher than healty individuals. Copeptin levels of the patients have right ventricles dilatation on the ECHO were significantly higher than the patients do not have right ventricle dilatation and healty individuals. Determining of right ventricles dilatation by copeptin’s AUC degree;0.82, specifity: %83.3, sensitivity was%69.9. Copeptin levels were significantly higher in Patients with increased PAP. In ROC analysis which made for Copeptin’s ability of determining PAP increase, AUC; 0.78, specifity: %72.5, sensitivity was %80. Conclusion: As a result, copeptin could be a new biomarker in the detection of right ventricular dilatation and PE diagnosis and evaluation of disease severity and prognosis. Anahtar Kelimeler: Copeptın, PAB, EKO

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
153
O 089 KURBAN BAYRAMININ ASIL KURBANLARI Gökhan Ersunan, Özlem Bilir, Mehmet Altuntaş, Ensar Topaloğlu Recep Tayyip Erdoğan Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Rize Giriş: Tüm islam düyasında her yıl hicri takvime göre zilhice ayının 10. Gününden itibaren 4 gün boyunca kurban bayramı kutlanır. Bu bayram boyunca binlerce büyükbaş ve küçükbaş hayvan kurban edilir. Gerek hayvanın kesimi, gerekse etin işlenmesi sırasında çok sayıda çeşitte yaralanmalar meydana gelmektedir. Bu çalışmanın amacı kurban bayramı süresince doğu Karadeniz bölgesinde bir eğitim araştırma hastanesine, hayvan kesimi ile ilişkili yaralanma sonucu başvuran hastaların, demografik özelliklerini, yaralanma tiplerini saptamaktır.��
Gereç-Yöntem: 12-15 Eylül 2016 tarihleri arasında Recep Tayyip Erdoğan Üniversitesi Eğitim ve Araştırma Hastanesi Acil Servisine hayvan kesimi ve et işlenmesi ile ilişkili yaralanma şikayetiyle başvuran ve çalışmaya katılmayı kabul eden 17 yaş üstü erişkin 55 hasta çalışmaya alınmıştır. Yaş, cinsiyet, travma şekli, oluşan lezyonun türü, uygulanan tedavi şeklinin frekans değerleri hesaplanmıştır. Bulgular: Hastaların yaş ortalaması 46,38±15,15 ve 49’u (%89,1) erkekti. Hastaların 50’si (%90,1) bayramın ilk günü başvurdu. Yaralanmaların 41’nin (%74,5) kesici alete bağlı, 14’dü ise (%25,5) düşme, boynuzlanma veya tekmelenme ile gerçekleştiği tespit edildi. 36 vakada (%60) primer sütürle düzeltilebilen cilt ciltaltını içeren kesi gözlenmiş. 8 vakada (%14,5) tendon kesisi, 2 vaka’da (% 3,6) künt travma sonucu oluşan kafa travması ve abdominal travma nedeni ile hastaneye yatış verilmiştir. 3 vakada ise(% 5,5) künt extremite travması sonucu atele alınmıştır. 8 vaka (%14,5) ise künt kafa, toraks, abdomen travması nedeni ile acil serviste takip edilmiştir. 1 vaka (%1,8) ise takibi kabul etmeyip acil servisi kendi isteği ile terk etmiştir. ��
Sonuç: Belediyeler tarafından kurban kesimi için uygun koşullar hazırlanmalı, profesyonel kişilerce kesimlerin yapılması sağlanmalı. Özellikle kurban bayramının ilk günlerinde acil servisler el cerrahisi açısından takviye edilmelidir. Anahtar Kelimeler: Kurban bayramı, travma, kurban kazaları O 090 ACİL TIP YAŞAMI BELİRLER! ACİL TIP HASTA BAKIM VE YÖNETİMİNDE SIRADAN BİR ATU’DAN; DAHA ÇOK HASTA KURTARABİLMEK İÇİN DAHA FAZLA NE YAPILABİLİR?
Betül Gülalp Başkent Üniversitesi Adana Uygulama ve Araştırma Merkezi, Acil Tıp Anabilim Dalı, Adana Acil Tıp, zamana karşı gerçekleştirilen yaşamsal ayırıcı tanı ve tedavi yönetimini sağlayan bilim dalıdır. Ülkemizde hızla gelişmekte ve örnek olacak şekilde bilimin ve azmin ışığında yükselmektedir. Branşımız adına hastalarımıza sunulan bu hizmet hep kendini yenileyen, süregen, bilimsel kanıt ve kılavuzları uygulayan, yönetsel destek ve vizyonun gerektiği yöntemleri içerir. �Bu amaçla;�1. Yaşamsal ve gerçek acil hastanın hastabaşında gerçekleştirilebilen, yaşamda kalımını, kanıta dayalı, erken ve doğru yönetimini, doğru tedavi ve doğru konsültasyon ve doğru yatışı zamana karşı yapabilmesini sağlayan, destekleyen ve kanıtlanan, onlarca yıldır uluslar arası kılavuzlarda yer alan, Acil Tıp Uzmanının ihtisasında ve ihtisas sonrası eğitimlerinde de yer alan Bakı Noktasında Acil Yaşamsal Ultrason amaçlı 3 problu yüksek rezolüsyonlu ultrason cihazlarının günlük kayıt, ve otomatik arşivli olarak Acil Tıp Uzmanı olan tüm Acil servislerde hasta hakları, hastane kalite ve hizmet kriteri olarak düzenlenebilmesi ve süreklilik önlemleri, �2. Acil durum ve hastalıklara ait güncel acil hasta yazılı süreçlerinin oluşturulabilmesi ve tüm hastane acil servislerinde uygulanımını düzenleyebilmek,�3. Acil Tıp Uzmanlarının hasta yatış kararlarında ve hastane yönetiminde aktif yer alabilmesini artırabilmek,�4. Halktan ilkyardım uygulayıcı kurslarında otomatik eksternal kalp şok cihazının aktif olarak yer alabilmesi,�5. Toplu yaşam alanlarında, stadyumlarda, spor yapılan tüm alanlarda, okullarda alan ölçüsüne uyumlu sayıda kanıtlanmış garantili şok cihazlarının sağlanabilmesi ile �Acil Tıp Ailesi ve Acil Tıp Hizmetleri olarak hep gurur ve özveri ile bilimin ışığında bir adım daha ilerleyecek. Anahtar Kelimeler: Acil hasta ve yönetimi, acil tıp, yeni öneriler

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
154
O 091 A HEAVY SMOKER MAN WITH A COMPLETELY OCCLUDED AORTA Leyla İnce1, Mehmet İnce2, Eyüp Duran2, Nail Ersöz2
1Abdurrahman Yurtaslan Oncology Training and Research Hospital, Oncology Service, Ankara, Turkey 2Gulhane Military Medical Academy, Clinics of General Surgery, Ankara, Turkey Chronic abdominal aortic occlusion (CAAO) is rare and potentially chancy and can cause severe ischemic manifestations in the lower extremities, spinal cord, intestine or kidneys. However, the diagnosis may refrain detection because of collateral vasculature can maintain a basal perfusion and prevent the expression of acute ischemic phenomena for a long time. We present a case with chronic severe CAAO disease, which was referred to us late, only after complete left renal artery-aortic occlusion had caused diffuse abdominal pain. A 69-year-old man was referred to our department with acute abdominal pain that had started 15 days before admission. Remarkable in his medical history were cigarette smoking over the last 50 years, leg claudication over the last 2 years and sudden occurrence of uncontrolled arterial hypertension over the last 2 months. There was tenderness for all quadrant of the abdomen on the physical examination. He was diagnosed as mesenteric ischemia with other laboratory findings. However, the abdominal computed tomography showed that left renal artery and-aortic occlusion including superior and inferior mesenteric artery on the abdominal aorta. After consultation of cardiovascular surgery, he was discharged with drugs treatment which including 100mg acid-salicylic- acid, pentoksifilin, and LMWH. Aortic occlusive disease causing ischaemic nephropathy should be suspected in patients who suddenly manifest uncontrollable arterial hypertension or renal function deterioration and the diagnosis can be confused with acute abdominal symptoms. Keywords: Aortic, occlusion, acute, abdominal pain O 092 A COMPARATIVE STUDY OF APPENDICITIS INFLAMMATORY RESPONSE (AIR)-ALVARADO SCORES WITH ULTRASOUND (USG) RESULTS IN DIAGNOSIS OF ACUTE APPENDICITIS Anar Aslanov, Mehmet İnce, Nail Ersöz, Orhan Kozak Gulhane Military Medical Academy, Department of General Surgery, Ankara, Turkey Introduction: Differential diagnosis of acute appendicitis is important due to the multiplicity of causes of acute abdomen. In this study, AIR and Alvarado scores were compared with ultrasound (USG) results. Methods: All parameters for scoring systems were taken prospectively from patients admitted to our clinic between April-September 2015. For the making diagnose alongside both scoring methods we compared USG results. The sensitivity and specificity of groups were compared. Results: 50 patients(8 female, 42 male) with pre-diagnosed acute appendicitis were included. The 5 pathology results of these patients were evaluated as negative. While positively pathology results evaluated patients’ average Alvarado and AIR score were 7.5 and 6.8; negatively pathology results evaluated patients’ average Alvarado score were 5.6, AIR score were 4.4. Although there is a high correlation (.821) between the Alvarado and AIR scores, AIR score diagnostic value according to the pathologic results is higher (ROC Curve). The USG, Alvarado and AIR sensitivity and specificity were 77.8%-80%, 73.3%-80% and 20%-100%, respectively. According to the congruity with pathology result Kappa value of USG, Alvarado score and AIR score were.321, 270 and 048, respectively. Conclusion: Although the specificities of both scores are higher in acute appendicitis, USG should be used pre-diagnosed patients due to non side effects and being able to verify the diagnosis as early as possible. Keywords: Appendicitis, inflammatory-response, Alvarado score

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
155
O 093 POSTOPERATIVE COMPLICATIONS IN BARIATRIC PATIENTS WITH UNDEFINED OBESITY HYPOVENTILATION SYNDROME UNDERGOING BARIATRIC SURGERY
Burcu Yormaz1, Ilhan Ece2, Serdar Yormaz2
1Beyhekim State Hospital, Clinic of Chest Diseases, Konya, Turkey 2Selcuk University Medical Faculty, Department of General Surgery, Konya, Turkey Objective: Among patients who have obstructive sleep apnea (OSA), a higher number of medical morbidities are known to be associated with those who have obesity hypoventilation syndrome (OHS) compared with OSA alone. OHS can pose a higher risk of postoperative complications after bariatric surgery (BS)in superobeses (BMI>50) and often is unrecognized at the time of surgery. The aim of this study was to assess retrospectively identify patients with OHS and compare their postoperative outcomes with those of patients with OSA alone. Methods: Patients meeting criteria for OHS were identified within a large cohort with OSA who underwent BS at a tertiary university care center. We identified postoperative outcomes associated with OSA and OHS as well as the clinical findings of OHS (BMI, apnea-hypopnea index AHI ). Multivariable models were used for outcomes, respectively. Diagnostic parameters have used according to novel indexes and criterias which wa designed by WORLD Health Organization (WHO). Results: Patients with hypercapnia from definite or possible are more likely to experience postoperative respiratory failure ( P <.0001), postoperative heart failure ( P =.002), prolonged intubation ( P = 0,02), postoperative ICU transfer ( P <.0001), and longer ICU (P = 0.09) and hospital ( P = 0.08) lengths of stay compared with patients with OSA. All of the pursuit parameters have changed according to the patients undercontrolled morbidity number and steady treatment procedures. Superobesity ‘s complication rates increases due to preoperative evaluations of smoke pack year, copd disease treatment period and compliance to medical doctor’s advice. Among the clinical determinants of OHS, neither BMI nor AHI showed associations with any postoperative outcomes in multivariable regression. Conclusion: More significance emphasis is needed on preoperative recognition of hypercapnia among patients with OSA undergoing BS. Further studies should be needed among morbid obese patients who would underwent bariatric surgery in respiratory etiology. Keywords: Obese, hypoventilation, complication O 094 PREDICTING CRITICAL DURATION AND REVERSIBILITY OF DAMAGE IN ACUTE MESENTERIC ISCHEMIA Ayhan Aköz1, Kenan Ahmet Turkdogan1, Nesibe Kahraman Çetin2, Selen Kum3, Ali Duman1, Mevlüt Türe4
1Adnan Menderes University Faculty of Medicine, Department of Emergency Medicine, Aydın, Turkey�2Adnan Menderes University Faculty of Medicine, Department of Pathology, Aydın, Turkey�3Adnan Menderes University Faculty of Medicine, Department of Histology and Embryology, Aydın, Turkey�4Adnan Menderes University Faculty of Medicine, Department of Biostatistics, Aydın, Turkey Objective: There is not any recognized laboratory predictor for detecting acute mesenteric ischemia. In current study we aimed to investigate recent ischemic biomarkers endothelial cell-specific molecule-1 (ENDOCAN) and signal peptide-CUB-EGF domain-containing protein 1 (SCUBE-1) in acute mesenteric ischemia. Method: An experimental mesenteric ischemia reperfusion model was designed with 54 rats. Nine groups were created as; Three control groups Groups I (30th min), IV (2nd h), and VII (6th h) which blood and tissue specimens were sampled only; three ischemia groups Groups II (30th min), V (2nd h), and VIII (6th h) which blood and tissue specimens were sampled after ligation of superior mesenteric artery (SMA); and three reperfusion groups Groups III(30th min), VI (2nd h), and IX (6th h) which blood and tissue specimens were sampled after declamping of SMA and reperfusion was induced for 1 hour. SCUBE-1 and ENDOCAN studied from blood samples and tissue samples were examined histopathologically. Results: SCUBE-1 levels are higher in ischemia groups when compare with controls (p<0.05) while ENDOCAN markedly different at the late ischemia (6th h) group. When groups were compared for irreversible mesenteric damage in according to histopathologic examination, the specificity and sensitivity of ENDOCAN was found to be as 94.7%, 76.5%, (AUC:0.870, 95% CI:0.775-0.965) with a cut-off value of <2.18 and the specificity and sensitivity of SCUBE-1 was found to be as %89.5, %79.4 (AUC:0.870, 95% CI:0.775-0.965) with a cut-off value of <1.48. Conclusion: Alone elevation of SCUBE-1 seems to be significant for predicting early mesenteric ischemia. However, combination of SCUBE-1 and ENDOCAN can useful for detecting irreversible intestinal damage. Keywords: Scube 1, endocan, acute mesenteric ischemia, irreversibility

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
156
O 095 THE RELATIONSHIP BETWEEN NATIONAL EARLY WARNING SCORE (NEWS) AND PERFUSION INDEX (PI) IN PATIENTS 65 YEARS OR OLDER
Mehmet Özel, Emine Gaffari, Hakan Topaçoğlu Istanbul Training and Research Hospital, Department of Emergency Medicine, Istanbul, Turkey Objective: The main purpose of the study was to investigate the relationship between National Early Warning Score (NEWS) and Perfusion Index (PI) in patients 65 years or older admitted to emergency room. Furthermore, this study evaluated patient outcomes with regards to NEWS and PI. Method: The study was conducted as a single-centered, prospective and cohort study. Randomly selected 967 patients 65 years or older were included in the study during two months period in ER. The vital parameters including NEWS criteria and the perfusion index of the patients were measured. Results: A total of 967 patients of which 533 (%55,1) female and 434 (%44,9) male were included into the study. The mean age of the patients were 74,8±6,9 (Median: 74 years, interval 65-97 years ). The initial NEWS scores of the patients had a significantly strong negative correlation with the observed PI values (p<0,001). NEWS scores of the hospitalised patients were higher than the discharged patients (p<0,001). In addition, the patients who were admitted to intensive care unit had significantly higher scores than those patients who were transferred to other clinical units (p<0,001). The mean PI value of the hospitalised patients were lower than those who were discharged (p<0,001). The patients who were admitted to ICU had a significantly lower PI average than the patients that were admitted to other clinical units (p<0,001). Conclusion: The study shows that there is a correlation between NEWS scores and PI values. Moreover, for the patients 65 years or older, PI and NEWS scores have predictive effects on admission to hospital or ICU. PI is non-invasive, cheap and fast method that can be used in conjunction with NEWS or other parameter measurments that can enhance the accuracy and the reliability of early warning scoring systems in patients 65 years or older. Keywords: NEWS, perfusion index, older patients O 096 RIGHT LOBE OF THE LIVER MAY ALSO TEND TO PLACE INTRATORACIC ! Turkan Dubus1, Soykan Arikan2, Ozgür Dikme3, Baki Dogan2
1Istanbul Training and Research Hospital, Thoracic Surgery Clinic, Istanbul, Turkey 2Istanbul Training and Research Hospital, General Surgery Clinic, Istanbul, Turkey 3Istanbul Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey Introduction: In this article, a delayed diaphragmatic hernia case diagnosed about 37 years after right iatrogenic diaphragmatic was injured is presented. Case: 37-year-old female patient with complaints about shortness of breath was admitted to our department. Abdominal surgery due to an unknown reasons is available in her case history. In (PA) lung graph acquired, a condensed lesion, in which an air-fluid level was monitored, was detected in lower lobe of the right lung. It was thought as possible diaphragmatic defects, aspects of etiology that having been taken in the chest-abdominal CT scan, right lobe of the liver into the thoracic had been substituted. She was decided to operate. It was found with right laparascopic exploration that somehow, the lobe of the liver, have entered the thorax from a diaphragmatic defect which is about 10 cm in diameter on the right. Bowel loops, part of the mesenteric adipose tissue were taken out of the abdomen but part of bowel loops and the right lobe of the liver were turned to the right thoracotomy due to obliteration- duplication and adhesions in the same session. The right lobe of the liver rotated 180 degrees, bowel loops were pushed into the abdomen from the right diaphragmatic defect in a proper way to the anatomy. Right diaphragmatic defect was repaired by using both side non-stick -dual mesh. The patient whose general condition was stable was discharged on the seventh day. Result: It is very difficult to establish a right diaphragmatic defect diagnosis. In our case, we therefore aim to present that the right lobe of the liver placed in the thoracic without symptoms for many years and not showing any strangulation as well as anatomically being placed into the abdomen again is a rare case. Keywords: Diaphragmatic rupture, liver dislocation, surgical treatment

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
157
O 097 NEUTROPHIL GELATINASE ASSOCIATED LIPOCALIN (NGAL) ON ACUTE GASTROINTESTINAL BLEEDING DISORDERS OF THE KIDNEY FUNCTION THAT MAY OCCUR EARLY IMPACT OF PREDICTIVE AND
PROGNOSTIC ROLE Aydın Çoşkun1, Özlem Bilir1, Gökhan Ersunan1, Özcan Yavaşi1, Mehmet Altuntaş1, Ekrem Kara2
1Recep Tayyip Erdoğan University Faculty of Medicine, Department of Emergency Medicine, Rize, Turkey 2Recep Tayyip Erdoğan University Faculty of Medicine, Department of Nephrology, Rize, Turkey Objective: To predict early stages of renal dysfunction and to determine the prognostic importance of NGAL in the patients who resort with gastrointestinal bleeding to Hospital Emergency Clinic. Materials-Methods: Prospectively and consecutively 50 patients who resorts to emergency service with bloody vomiting, bloody or black stools presenting with symptoms or after application who was diagnosis gastrointestinal bleeding. Patients admitted to the emergency service, their blood group, blood count, biochemistry, coagulation profile, venous blood gases were studied; remaining serum was stored for NGAL. As a control group with no history of any disease than ever before, the positive physical examination findings undetected 50 healthy volunteers were included in the study. The values obtained were statistically compared by analysis of biochemical processes and then making another. Results: The patients beginning average value of NGAL is 94,27 ± 37,64 ng/mL and the control group average value of NGAL is 83,67 ± 28.11 ng/mL, The difference between the two groups was not statistically significant. When the patients were evaluated in terms of their internal bleeding etiology of 0 and 24 hours value of NGAL, it was found to be statistically significant differences between groups. Conclusion: In the Emergency service patients resort with gastrointestinal bleeding NGAL may be useful for determining the etiology, the presence of bleeding and endoscopy and how many days hospitalized in the intensive care unit could be used as a biochemical parameters help in tracking decisions. Patients' NGAL value were not significantly high compared to healthy people. Gastrointestinal bleeding in patients as a predictor of mortality was determined that not enough information for NGAL. Bleeding in the gastrointestinal tract in patients with ARF it can be used as markers. In patients with diabetes, bleeding in the gastrointestinal tract can provide information about NGAL diabetic nephropathy. Keywords: GI Bleeding, ARF, NGAL O 098 THE EFFECT OF INFLAMMATION ON VENTRICULAR FUNCTIONS Aysel Hünük, Ebru Ünal Akoğlu, Merve Manap, Arzu Emecen, Tevfik Patan Fatih Sultan Mehmet Training and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey Recent research shows a negative relationship between the level of inflammatory markers and right ventricular (RV) functions. Reducing the overall inflammatory burden and risk are proven to improve survival in patients with critical diseases such as end-stage heart failure and coronary artery disease. Therefore, we aimed to investigate this phenomenon in a healthy, young adult population. Among adult patients who were admitted to our emergency department with symptoms of upper respiratory tract infection (URTI) without any past history of cardiovascular/systemic disease, patients who had a CRP level of 3 mg/dl or more were included in our study. Subjects with complete bundle branch blocks on ECG, non-sinus rhythms and any pathologic abnormality on cardiac examination and TTE were excluded from the study. Transthoracical echocardiography (TTE) was performed in all patients to evaluate LV and RV systolic and diastolic parameters. Subjects were invited for a follow-up exam after the 10th day of the resolution of URTI symptoms. During the follow-up TTE was performed again in subjects with a CRP level of 3 mg/dl or less. This study was concluded with 16 female (30%) and 37 male (70%) patients. All mean inflammatory marker levels were found to be significantly lower in the follow-up exam compared to primary exam and were as follows: Temperature (37.7±0.7°C vs 36.5±0.4°C, p<0.01), Neutrophil to lymphocyte ratio (NLR) (6.37±3.58 vs 1.89±1.27, p<0.01), CRP (8.9± 4.9 mg/dL vs 0.4±0.6 mg/dL, p<0.01). A statistically significant association was observed between RV TTE parameters and the levels of inflammatory markers. We were able to demonstrate a clinically subtle, however significant functional cardiac deterioration with URTI in healthy young adults. Cardiac functions, particularly right heart, seems to be acutely affected by the acute inflammatory states and a relationship might be observed regarding the effect of inflammatory markers on RV functions. Keywords: Inflammation, ventricular functions, Crp, Upper respiratory tract infection

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
158
O 099 A PROSPECTIVE STUDY DEMONSTRATING THE RATIO OF DRUG RELATED SIDE EFFECTS TO THE TOTAL APPLICATION NUMBER IN COMPLAINTS OF PATIENTS PRESENTING TO THE EMERGENCY DEPARTMENT
Selda Çakmak, Onur Polat, Hakan Ergün, Müge Günalp Eneyli, Serdar Gürler, Sinan Genç Ankara University Faculty of Medicine, İbni Sina Hospital, Department of Emergency Medicine, Ankara, Turkey Objective: In our study, we investigated the frequency of presenting to the to the Ankara University İbni Sina Hospital Emergency Department due to adverse drug reaction (ADR) as a guiding data on rational drug use. Method: In our prospective, descriptive, observational study we enrolled all patients at least 18 years of age and older who met the inclusion criteria and presented to the Ankara University İbni Sina Hospital Emergency Department between June 2016- August 2016�within the shift of the physician who conducted the study. Age, sex, presenting complaint,�medical history, final diagnosis of patients and the medications and herbal products used were recorded. The ADR causality classification are made as 'ineffectiveness, unknown, unlikely, possible, likely, certain' according to World Health Organization- Upsala Monitoring Center (WHO UMC). Results: The number of patients who used drugs was 556 (34.6%) and who did not use drugs was 1052 (65.4%) among the total of 1608 patients enrolled to the study. The number of patients who had a drug related ADR was 279 (17.3%) and who had no drug related ADR was 279 (82.7%) among the patients who used drugs. The average age across the patients who had an ADR was 56.2 and who had no ADR was 63.9. There was no difference in sex between the patients who had an ADR and had no ADR (p=0.579). Thirty-seven percent of patients who had an ADR was 65 years and older. The most common ADR causing drugs consisted of group C drugs (29%) according to the ATC classification. This was followed by Group A (17%) and Group B (14%) drugs. Conclusion: In compliance with international literatures, drug related adverse effect was determined in 17.3% of patients presented to Ankara University İbni Sina Hospital�Emergency Department representing the adult patient population. Keywords: Adverse, drug, reaction O 100 EVALUATION OF L-LAKTAT, D-DIMER, IFABP LEVELS IN THE EARLY DIAGNOSIS OF ACUTE MESENTERIC ISCHEMIA IN AN EXPERIMENTAL STUDY Emre Öner1, Müge Günalp1, Oya Evirgen2, Emine Nazlı Hayırlı2, Arda Demirkan3, Onur Polat1, Serdar Gürler1, İlker Yeşilkaya1
1Ankara University School of Medicine, Department of Emergency Medicine, Ankara, Turkey 2Ankara University School of Medicine, Department of Histology and Embryology, Ankara, Turkey 3Ankara University School of Medicine, Department of General Surgery, Ankara, Turkey Introduction: Mesenteric ischemia which has nonspecific laboratory values and the low clinical suspicion lead to late diagnosis and undesirable outcomes. Early diagnosis to begin treatment is vital, therefore, new strategies are needed. In recent years some markers have been investigated for their diagnostic value in early diagnosis in acute mesenteric ischemia (AMI). After AMI, ischemia symptoms initiate in mucosal layers where ideal biomarkers should be detected. Materials-Methods: Sixtythree female 250-300 gr Wistar albino rats were used in this randomized, controlled study. Rats were divided into 9 groups as control, sham and ischemia and each group was divided into 30th, 60th and 180th minutes subgroups. Anaesthesia was applied in the control group as well as other groups additionally laparotomy performed in the sham groups, and the superior mesenteric artery was ligated followed by laparatomy in the ischemia groups. Jejunum and ileum tissue specimens were processed by histological methods, stained with Hematoxylin and Eosin. Results: The histological assessment of sections prepared from the ileum and jejunum of control rats revealed the healthy structure of the mucosa. Mild to moderate ischemia injury scores were observed in sham groups.Ischemia groups were possessed higher ischemia injury scores in comparison with other groups. Compared to control and sham groups, ischemia group revealed a significant rise in L-Laktat levels at the 30th minute (p<0.002, p<0.001). The rise in IFABP values in ischemia group at 30th minute was significantly high compared to control group(p<0.004).However, in the sham groups IFABP levels were higher than control group in all time points. Ddimer was negative in all ischemia groups. Conclusions: L-laktat levels can be helpful in the early diagnosis of acute mesenteric ischemia. IFABP levels may increase in the case of laparotomy as well as ischemic conditions and relative duration, therefore it needs to be further insvestigated. D-dimer assessed as an insufficient biomarker in the non trombotic mesenteric ischemia. Keywords: Acute mesenteric ischemia, IFABP, jejunum, ileum

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
159
O 101 PNEUMOTHORAX DUE TO FOREIGN BODY IN ESOPHAGUS Mehmet Esen, Nurşah Başol Gaziosmanpaşa University School of Medicine, Department of Emergency Department, Tokat, Turkey Introduction: Foreign bodies in esophagus (EFB) are emergencies that can be encountered in all ages, being more common in childhood era. About 28-68% of gastrointestinal foreign bodies are located in esophagus. Sharp pointed objects can be caught in esophagus and can lead to life threatening complications. We report a case here who applied to our emergency department with dyspnea and difficulty swallowing and had aspiration of the foreign body that caused pneumothorax through esophagus perforation. Case: Sixty years old male patient presented with the complaints of globus sensation and breath shortness. Following vital findings were measured: arterial tension: 150/80 mm/Hg; fever: 36.70 °C; pulse: 117/minute; SPO2: 68. He had dyspnea and respiratory sounds were markedly diminished in pulmonary auscultation of left lung. Plain radiography did not show any pathology. In thorax computerized tomography(CT), an irregularly contoured mass of 15 mm diameter was observed in proximal and middle part of esophagus, and partial pneumothorax was determined in left side. Discussion: Morbidity and mortality risk of EFB are higher in older ages. Ten to twenty percent of EFB cases need non-operative intervention and only 1% or less need surgical intervention. At the first stage of EFB cases, plain radiographies(front-back and lateral) are suggested(only 64% of EFB are radiopaque), but in cases where findings of anamnesis and physical examinations were not confirmed through positive radiographies, CT or magnetic resonance imaging(MRI) is suggested at the second stage. Perforation, aspiration and aortoesophageal fistula risks are positively associated with the time passed. Complication rates could go up to 35% when sharp pointed objects or batteries are not urgently removed. Conclusion: EFB may not be seen in plain radiographies as in our case. Diagnosis should be fast since esophageal foreign bodies can lead to serious complications such as perforation and pneumothorax and may require emergency surgical intervention. Keywords: Esophagus, foreign bodies, perforation, pneumothorax O 102 TISSUE ADHESIVES TO SECURE PERIPHERAL INTRAVENOUS CATHETERS: A RANDOMIZED CONTROLLED TRIAL Uğur Özkula1, Gülhan Kurtoğlu Çelik1, Ayhan Özhasenekler2, Mehmet Ergin2, Fatih Tanrıverdi2, Şervan Gökhan2
1Atatürk Training and Research Hospital, Department of Emergency Medicine, Ankara, Turkey 2Yıldırım Beyazıt University Medical School, Department of Emergency Medicine, Ankara, Turkey Introduction: Peripheral venous catheterization is the most used medical procedure in hospitals on worldwide. Recent researches on literature signified that using intravascular devices is a risk factor for both local and systemic complications. We aimed that addition of tissue adhesive to the insertion site of peripheral intravenous catheters in the emergency department (ED) would reduce the device failure rate during at first 6 hours and 24 hours. Methods: We designed a single-site, 2-arm, single-blinded, randomized, controlled trial of 80 peripheral intravenous catheters inserted into 80 adult patients. To rule out patient related factors as much as possible, patients were eligible for enrollment if they were aged 65 years or older without chronic renal insufficiency diagnosis and history of chemotherapeutic drug insertion, had a patient upper limb peripheral intravenous catheter inserted through healthy intact skin by an ED nurse, and gave written informed constent. Results: Peripheral intravenous catheter device failure was 15,4% in the tissue adhesive group vs. 25,6% with standard care. There was not statistically difference between two groups (p>0,05). In addition to this the study showed us; in the tissue adhesive group female patients had less frequent peripheral catheter failures with 22 G catheters (5,1%) versus standard care (10,2%) (p<0,05). Conclusion: Tissue adhesive administration may be reasonable in use of small sized peripheral venous catheters in female patients to protect from related complications. In this study, contrary to the literature; the routine use of tissue adhesive in addition to standard care to reduce peripheral intravenous catheter failure for adult ED patients admitted to hospital are not supported. Keywords: Tissue adhesive, peripheral intravenous catheter, emergency department

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
160
O 103 THE EFFECT OF NEUTROPHIL/LYMPHOCYTE RATIO AND MEAN PLATELET VOLUME TO REDUCE NEGATIVE LAPOROTOMY RATES IN PATIENTS WITH ABDOMINAL PAIN IN EMERGENCY DEPARTMENT
Eylem Kaykısız1, Pınar Yeşim Akyol2, Zeynep Karakaya2, Umut Payza2, Serkan Bilgin2, Gözde Canan Yavaş2, Fatih Esad Topal2
1Bitlis Public Hospital, Emergency Clinic, Bitlis, Turkey 2Izmir Katip Çelebi University Atatürk Research and Training Hospital, Department of Emergency Medicine, Izmir, Turkey Introduction: Acute appendicitis is one of the most common cause of abdominal pain which often offering insufficient symptoms and may interfere many diseases and appendectomy is the most performed intraabdominal operation in the world. Despite of the use of advanced technology diagnostic methods, it is not shown a decrease in perforation and negative appendectomy rates. The aim of this study is to identify the effect of obtained neutrophil, lymphocyt, neutrophyl/lymphocyt ratio and mean platelet volume with right lower quadrant pain in reducing the negative appendectomy. Materials-Methods: 341 patients who have operated with initial diagnosis of acute appendicitis between 01.01.2014 and 31.12.2014 were included in this study. The patients who had taking antibiotics before admission, trauma history, cancer history, pregnancy and under age of 17 were exclueded. Histopathologic reports of 318 patients who met criterias were evaluated retrospectively and the patients divided into 3 groups in terms of histopathologic reports as non-acute appendicitis (group 1), acute appendicitis ( group 2) and complicated appendicitis (group 3). Neutrophil/lymphocyt ratio and mean platelet volume values were compared between groups. Results: %15,7 (n=50) of the patients were in non-acute appendicitis group however %79,2(n=252) of the patients had the diagnosis of acute appendicitis and %5 (n=16) of the patients had the diagnosis of complicated appendicitis. Cut-off value of obtained neutrophil/lymphocyt ratio determined 4,659; sensivity of %69 and spesifity of %70 in predicting acute appendicitis and neutrophil/lymphocyt ratio was statistically significant to differentiate non-acute appendicitis from acute appendicitis but there was no statistically significance to differentiate acute appendicitis from complicated appendicitis. Finally it is concluded that mean platelet volume had no statistically significant to diagnose acute appendicitis. Conclusion: We found out that preoperative neutrophil/lymphocyt ratio is a valuable data for this purpose. We hope that our study may contribute to developing new protocols for definitive diagnosis in emergency department. Keywords: Acute appendicitis, neutrophyl/lymphocyt ratio, mean platelet volume, negative appendectomy O 104 TO DETERMINE THE LEVEL OF BIOCHEMICAL PARAMETERS OF THE PATIENTS WHO APPLY TO EMERGENCY SERVICES WITH SICKLE-CELL ANEMIA DISEASE Ahmet Sebe, Özgür Şahan, Ayça Açıkalın Akpınar, Nezihat Rana Dişel Çukurova University Faculty of Medicine, Department of Emergency Medicine, Adana, Turkey Aim: In this study we aimed to show the relation between complete blood count, sedimentation rate, lactate level, blood gas values, symptoms and outpatient treatment time of the patients who come to emergency services with severe pain crisis. Methods and Procedures: In this study 40 patients, combination of 21 male and 19 female, are included. Patients are told to mark the level of pain on a scale after they are questioned about their symptoms. Then patients’ complete blood count, sedimentation rate, lactate level, and blood gas values are examined. Patients’ outpatient treatment time are recorded. Symptoms, pain scale levels, blood biochemical levels and outpatient treatment time are statistically compared.��
Result: Patients age average and standard deviation is 28,65±6,841. Most observed symptoms are pains at joints of 35 patients ((%87,5) and chest area of 24 patients (%60). Patients pain level and their standard deviation on visual analog scale (VAS) 7,84±1,408; numerical pain scale (SAS) 7,95±1,449; Wong Baker face scale 4,08±0,616. Biochemical parameters average and Standard deviation: pH:7,39±0,041, pO2:45,69±11,02, pCO2:39,52±6,68, HCO3:23,94±3,15, leucocyte:16,59±6,73, hemoglobin:8,31±1,03, hematocrit:24,35±3,50, trombocyt:456±216,03, laktat:1,43±1,10, sedimentation:5±4,86. Treatment Time and it’s Standard Deviation of 22 outpatient was 5,23±2,65 hours while it was 6,27±4,50 days for the 18 patients treated in the hospital. Outpatients were mostly treated for 2 hours (%15) and 4 hours (%15). Longest outpatient treatment time was 12 hours (%2,5) in the emergency service. When patients biochemical parameters and their outpatient treatment time were compared there was no meaningful result (p value˃0,05). Conclusion: No interrelation was found between the level of biochemical parameters of the patients who apply to emergency services and their outpatient treatment time. Keywords: Sickle-cell anemia disease, biochemical parameters, outpatient treatment time, pain level scale

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
161
O 105 THE DIAGNOSTIC VALUE OF ISCHEMIA-MODIFIED ALBUMIN IN ACUTE MESENTERIC ISCHEMIA İlhan Ece Selçuk University Faculty of Medicine, Department of Surgery, Konya, Turkey Objective: Acute mesenteric ischemia (AMI), an abdominal emergency that have high mortality rate, although diagnostic methods have advanced in recent years. The most important step in success of treatment is early diagnosis. Ischemia-modified albumin (IMA) has emerged as sensitive biomarker in the evaluation of acute coronary syndromes, and was used in many other ischemic conditions. The aim of this study was to evaluate the value of IMA in early diagnosis of acute mesenteric ischemia. Methods: In total of 50 patients were enrolled to the study that were diagnosed as acute mesenteric ischemia with the first evaluation of physical examination. Blood samples were taken for measurement of IMA in all patients. Complete blood count, biochemical parameters, arterial blood gases, abdominal computed tomography scan were also examined. All patients were consulted with general surgery. All blood samples were analyzed for serum IMA and then the data of patients who were diagnosed as acute mesenteric ischemia during surgery (Group I) were compared with the other patients datas that treated medically (Group II). Results: In the study; 22 of 50 patients were operated due to acute mesenteric ischemia. Acute mesenteric ischemia was identified in 20 patients during surgery. One spontaneous intramural bleeding and a Crohn's disease was detected in 2 patients. Segmenter small bowel resection and end to end bowel anastomosis were performed to 17 of patients, and 3 of patients were treated with segmenter bowel resection and ileostomi. Demographics and characteristics of the patients were similar in each groups. IMA levels in the Group I was significantly higher than Group II. Conclusion: IMA can be used as a biochemical marker in the diagnosis of acute mesenteric ischemia; however, it has a poor diagnostic value. Although the findings of our study confirm the hypothesis that IMA is a sensitive biomarker in the evaluation of ischemia-based conditions, further research is needed. Keywords: Ischemia modified albumin, acute mesenteric ischemia, surgery, emergency O 106 EVALUATING METHYL ALCOHOL TOXICITY IN EMERGENCY DEPARTMENT Sila Sadillioglu, Incifer Kanbur, Behlul Bas, Hakan Topacoglu Istanbul Training and Research Hospital, Department of Emergency Medicine, Istanbul, Turkey Objective: Methyl alcohol (MA) is used in illegal alcohol production because it is cheap which may result in multiple simultaneous poisoning cases. Although the toxic effects of MA commonly appear after 12-24 hours in acute poisoning cases, it may take longer when ethyl alcohol is consumed concomitantly. The aim of this study was to investigate the factors influencing the survival of patients with methanol poisoning. Method: All charts of MA toxicity patients treated in emergency room over a two year period were reviewed retrospectively. The age, sex, initial complaints, state of consciousness, blood-gas analysis, blood glucose, sodium and anion gap levels and death rates of the patients were analyzed. Results: A total of 18 patients (mean age 51 years; %100 male) with MA toxicity were included in the study. The median GCS score of the patients at time of arrival was 11 (range 3-15). Seventy-two percent of the patients had blurred vision, 55.6% had dyspnea and 16.7% had gastrointestinal complaints. In the blood-gas analysis of the patients, the mean pH and HCO3 levels were 7.1±3 (range 6.55-7.43), 11.5±9 (range 3.4-26.7), respectively. In the biochemical parameters of patients mean blood glucose level was 150.1±61.9 mg/dL. However, hypokalemia in 16.6% of the patients and anion gap deficit (AG) (average 26.3) in 94.4% were observed. All the patients were treated with dialysis and mortality rate was 22.2%. The mean pH (CI:-2,38/-7,54), GCS (CI:-1,61/-12,17) and HCO3 (CI:-4,02/-14,73) values were statistically lower while mean AG (CI:13.3/18.0) was higher (for all p<0.05) in mortality group as compared to the survival group. Conclusion: The delay of MA poisoning cases admission to the hospital increases mortality and morbidity. Metabolic acidosis is strong predictor for poor prognosis in MA toxicity. In addition, the anion gap deficit of the patients may be associated with mortality Keywords: Methyl, alcohol, toxicity

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
162
O 107 THE ELDERLY AS VICTIMS - GERIATRIC FORENSIC CASES Feruza Turan Sönmez, Harun Güneş, Ayhan Sarıtaş Duzce University School of Medicine, Department of Emergency Medicine, Düzce, Turkey Introduction: National Institute on Aging (USA) predict that 50 million people will fall into geriatric age range by the year 2020, one-half of whom will be over age 75(1). More and more older adults take place in active life. Aging of community-dwelling persons inevitably leads to increase of geriatric patients among medicolegal cases. The elderly are vulnerable category of patients, and the best we can do for comprehensive assessment of geriatric forensic cases is to characterize and evaluate them first. Methods: We retrospectively investigate a 1-year –period hospital records of medicolegal cases and elected the geriatric admissions. Sixty five-year-old and above all patients with all sorts of trauma, injury, neglect, abuse and drug abuse were included��
Results: Data of 83 patients with mean age of 74.3 (min, 65, max. 93) years was evaluated. Men number dominated (53 male, 30 female). While there was no significant difference in seasonal distribution; event time and hospital admission time differed (most cases admitted to emergency during day time, between 8:00-18:00, n= 66 and n=56 respectively). Priority of the cases were falls (n=28) and traffic accidents; car accidents and pedestrian accidents (n=21, n= 7 respectively). One of the cases died, it was fatal carbon monoxide intoxication, and 36 patients needed hospitalization. Conclusion: In almost every developed country, the proportion of people over 65 years of age is growing faster than any other age group, As a result, more elderly individuals are presenting to emergency departments following trauma. No doubt, quality of life is as important as prolongation of lifespan. Comprehensive assessment of geriatric injuries and better knowledge of management of them lead to lower rate of misdiagnoses and morbidity. Keywords: Elderly, geriatric cases, forensic cases, emergency O 108 ACUTE ABDOMEN CAUSED BY FOREIGN BODY: IUD Elnare Günal1, Handan Çiftçi1, Gülşen Çığşar1, Şahin Kahramanca2, Murat Özdemir1
1Kafkas University Faculty of Medicine, Department of Emergency Medicine, Kars, Turkey 2Harakani State Hospital, Clinic of Emergency Medicine, Kars, Turkey Introduction: 5-10% of the admissions to emergency department are because of abdominal pain. 15-40% of abdominal pain is surgical. There are many diseases in the etiology of surgical abdominal pain such as appendicitis, ileus, perforation and diverticulitis. Although it is rare but foreign body in the bowels could be a cause of acute abdomen too. We aimed to present the patient that admitted to emergency department with severe abdominal pain, and was found foreign body in her sigmoid colon. Case: 34 year old female patient admitted to emergency department with sudden onset abdominal pain, nausea and burning sensation during urination. There was acute abdomen on her physical examination and radiological examinations and blood tests were requested. There wasn't any surgical operation in her medical history. Although an intrauterine device (IUD) was inserted 3 years ago and the patient got pregnant while having IUD. There was an IUD image at her abdominal radiogram but the device was located above intrauterine cavity and placed transversely. There was a foreign body image at her contrast enhanced abdominal computerized tomography (CT) that was located in her sigmoid colon and penetrated through colon wall. The IUD was taken off and the perforated colon wall was repaired by general surgeons. Conclusion: Foreign bodies must be considered in the differential diagnosis of the patients that admitted to emergency department with abdominal pain and especially have acute abdomen findings. Also keeping genital tract in mind during taking detailed medical history and physical examination will help to diagnose and prevent misdiagnose. Keywords: Acute abdomen, intrauterine device (IUD), foreign body

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
163
O 109 EVALUATION OF THE INTERSHIFT PATIENT HANDOVER AT EMERGENCY DEPARTMENT Metin Akpınar, Ömer Salt, Mustafa Burak Sayhan Trakya University Medical Faculty, Department of Emergency Medicine, Edirne, Turkey Patient handover is defined as; the transfer of patient information care to another physician from the responsibility and authority. Especially in industries working on shifts, patient handover such as emergency medicine, but is a process applied in all branches of medicine is of much more importance. Emergency medicine can cause not fully aware of another doctor transferred or not followed and will continue to be treated by the doctor in the diagnosis and treatment of some unwanted disruptions have implemented the shift system and the patients of the transaction. Lack of communication between the transferor and transferee or doctors during the handover disorder causes an increased incidence of adverse events and medical errors. Although it developed standardized procedures for the handover of the work in professions related to the delivery of standardized patients, though turnover in the medical disciplinary procedure has not been developed can. Oral delivery of the first things to be done to ensure a patient transfer standardization in this field is to be carried out in accordance with certain rules. The use of existing technological capabilities delivered during the second important point speed is. Keywords: Emergency department, intershift, patient handover O 110 MANAGEMENT OF HYPERTRIGLISERIDEMIA INDUCED ACUTE PANCREATITIS IN EMERGENCY DEPARTMENT İlhan Uz, Enver Özçete, Meltem Songür Kodik, Yasemin Delice, Murat Ersel, Güçlü Selahattin Kıyan Ege University Faculty of Medicine, Department of Emergency Medicine, Izmir, Turkey Introduction: Seriously high triglyceride levels, is an important risk factor for development non biliary acute pancreatitis. In hypertrigliceridemia induced acute pancreatitis (HTGiAP), for prevention of complications and treatment of pancreatitis, the lowering of triglyceride level is important. Despite present publications about treatment modalities such as apheresis, insulin and heparin; there is no randomized study representing the superiority of apheresis to insulin or heparin treatment. On the other hand there is no published guide for treatment HTG- induced acute pancreatitis (HTGiAP). In this study the authors aimed to share their experience on the treatment of HTGiAP. Results: During study period of one year, 142.482 patients were admitted to our emergency department. 370 patients were diagnosed as acute pancreatitis (AP). Among these 10 patients diagnosed as HTGiAP. The mean age at admission was 36.2 ± 19.8 years and there was a female predominance (60%). Of the patients there was a history of hyperlipidemia in 7 (70 %), in 6 diabetes mellitus (60 %), in 2 (20 %) hypothyroid and 6 (60 %) had a prior AP attack. In ED, after a diagnosis of HTGiAP, insulin infusion treatment was started to all of the patients. Two of those patients had apheresis treatment. Average stay of these patients in emergency department is one day, and after 24 hour of follow up, clinical signs and levels of triglyceride, amylase, and lipase were regressed. Conclusion: In emergency department in case of acute pancreatitis, HTG in etiology should be kept in mind. In patients diagnosed HTGiAP to decrease the complications, early treatment may be started in ED. Whereas insulin infusion treatment compared to apheresis is more practical and easy to follow, may be preferred as the first choice of treatment in such cases. Keywords: Acute pancreatitis, emergency department, hypertrigliceridemia, insulin treatment

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
164
O 111 RHABDOMYOLYSIS? ELEVATED CREATINE KINASE (CK) VIA PRESENTATION OF 3 CASES Mehmet Ünaldı1, Soner Işık1, Ümit Ölmez1, Cihan Büyüksütcü1, Ersen Gündüz1, Meltem Çöllü1, Tuçe Düzkel1, Didem Ay1, Hatice Eryiğit2
1Medeniyet University Goztepe Training and Research Hospital, Department of Emergency Medicine, Istanbul, Turkey 2Dr. Lütfi Kırdar Kartal Training and Research Hospital, Thorax Surgery Department, Istanbul, Turkey An elevated serum CK level is the most sensitive and reliable indicator of muscle injury. The degree of CK elevation correlates with the amount of muscle injury and the severity of illness. We present to 3 different caused cases with abnormal elevated serum CK and aim to important of possibility of rhabdomyolysis. Case 1: 19-year-old adult presented to the ED with complaints of fever, weakness and sore throat. In physical examination we detected bilateral cryptic tonsilllitis. Laboratory findings revealed high level of creatine kinase (CK:31862 U/L), AST(345 U/L), ALT (130 U/L), LDH (1030 U/L) and CRP (14,2 mg/dl) respectively. Case 2: 29-year-old male patient presented to ER with delirium. Vital signs of him were stable but he was agitated and orientation and cooperation were poor.In history we detected he used syntetic cannobinoid. CK evaluated; 6634 U/L. The second value was 4638 U/L after about 4 hours. Case 3: 41 year-old male patient admitted to the ED with widespread myalgia. Vital signs of him were normal. In medical history he had no comorbidity and had used Silodosin 8 mg, an alpha blocker, treating the signs and symptoms of enlarged prostate (BPH) a year. Laboratory signs revealed serum CK:15868, 15368 U/L, AST:299,298 U/L, ALT:137,141 U/L. After iv 3000 cc rehydration, serum CK:20000 U/L. Rhabdomyolysis is a syndrome characterized by injury to skeletal muscle with subsequent effects from the release of intracellular contents included CK, myoglobin, aldolase, LDH, AST and potassium. The most common causes appear to be alcohol and drugs of abuse, followed by medications, muscle diseases, trauma, NMS, seizures, infection, strenuous physical activity. It must be considered a fivehold or greater increase above the upper threshold of normal in serum CK level, in the absence of cardiac or brain injury, as the requirement for the diagnosis of rhabdomyolysis. Keywords: Creatine kinase, elevated, rhabdomyolysis O 112 OXIDATIVE STATUS AND DNA DAMAGE FOLLOWING ANALGESIC TREATMENT IN PATIENTS WITH ACUTE PANCREATITIS Bedia Gülen1, Abdurrahim Kocyigit2
1Bezmialem Vakıf University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey�2Bezmialem Vakif University Faculty of Medicine, Department of Biochemistry, Istanbul, Turkey Background: This study is designed to investigate the effect of three different analgesics used to treat pain in AP on oxidative stress, DNA damage in mononuclear leukocytes and on oxidative status. Methods: This parallel design randomized controlled trial is composed of three treatment arms, intravenous paracetamol, intravenous dexketoprofen and intravenous tramadol. Results: A total of 107 patients were diagnosed with acute pancreatitis within the study period in the ED. Seventy-seven of them were included for the study; 26 patients for the paracetamol group, 24 patients for the dexketoprofen group and 27 patients for the tramadol group. The mean age of study subjects was 52.73 ± 15.38 and 66% (n = 51) of them were men. At the beginning of the study (before treatment) mean levels of DNA damage, TOS and OSI levels significantly higher and TAS was significantly lower in the acute pancreatitis groups than in the control group. DNA damage and OSI in HAPS-positive patients were found to be significantly greater than HAPS-negative patients (p = 0.046). DNA damage and oxidative stress were compared between the three groups. There were no differences between the groups in terms of DNA damage (p = 0.42) and also for the oxidatif stress parameters (OSI,TAS,TOS respectively p = 0.26, p = 0.78, p = 0.35) Conclusions: There is no difference between the effects of paracetamol, dexketoprofen and tramadol which are commonly used to manage acute pain in AP on DNA damage in human T-lymphocytes and on serine parameters of oxidative status. Keywords: Acute pancreatitis, treatment, pain, paracetamol, tramadol
5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
165
O 113 DYNAMIC THIOL/DISULFIDE HOMEOSTASIS IN PATIENTS WITH ACUTE CHOLECYSTITIS Yücel Yüzbaşıoğlu1, Güllü Ercan Haydar1, Selcuk Çoskun1, Gül Pamukcu Günaydın1, Yavuz Otal1, Çağdaş Yıldırım1, Murat Alışık2, Özcan Erel2
1Yıldırım Beyazıt University Atatürk Training and Research Hospital, Department of Emergency Medicine, Ankara, Turkey�2Yıldırım Beyazıt University Atatürk Training and Research Hospital Biochemistry Department, Ankara, Turkey Aim: Thiols, which are sulfhydryl (-SH) group-containing organic compounds, capable to react against free radicals for resist cell damage caused by reactive oxygen species. So, the aim of this study is to evaluate the changes of this new oxidative stress markers (the balance of the thiol-disulfide) in patients who diagnosed with acute cholecystitis. Material-Method: Eighteen patients and 20 controls who admitted to the emergency room of our hospital between November 2015- September 2016 were included. The diagnosis of acute cholecystitis was made according to the Tokyo protocol by using clinical, laboratory and imaging results. Serum thiol-disulfide levels were measured by this newly automatic method, developed by Erel&Neselioglu, in blood samples of patients diagnosed with acute cholecystitis. Serum thiol-disulfide results in the patient and control groups were statistically evaluated. Results: There was no significant difference in terms of age and gender between patient and control groups. Native thiol levels were not significantly different in both groups. Disulfide levels in the patient group (19.29 ± 8.22) were lower than the control group (24.41 ± 22.58) appeared statistically significant (p <0.05). Total disulfide levels of the patient group (429.39 ± 72.64) was statistically significantly lower (p <0.05) than the control group (441.44 ± 25.20). ��
Conclusion: Disulfide levels showed a statistically significant decrease in acute cholecystitis patients compared with the control group. This may be related to increased free radicals due to inflammation in acute cholecystitis. Additional studies are needed on this topic. Keywords: Thiol-disulfide balance, acute cholecystitis, oxidative stress, acute abdomen O 114 COMPARISON OF PROTECTIVE EFFECTS OF HIGH DOSE NAC AND ISOTONIC NACL PROPHYLAXIS FOR CONTRAST NEPHROPATHY Ömerul Faruk Aydın, Eren Gökdağ, Özlem Güneysel Kartal Dr. Lütfi Kırdar Training and Research Hospital, Istanbul, Turkey Aim: NAC (N-Acetil Cysteine) was compared with serum physiologic in terms of efficacy for the prevention of contrast-induced nephropathy on emergency patients in this study. Patients with mild renal function loss were studied. Matherial and Methods: Patients were randomly divided into two groups; “High dose NAC” and “Salin (NaCl)”. In first group (NAC), 150 mg/kg NAC (Asist©, Nacosel©) was administered intravenously in 30–60 minutes with 2–4 mL/kg/hr – 0.9% NaCl immediately before contrast agent application. After contrast (Omnipque© 300mg/100ml) imaging 50 mg/kg NAC was administered in 2–4 hours with 1-2 mL/kg/hour – 0.9% NaCl intravenously. In second group (salin) 6-8 mL/kg/h 0.9% NaCl was administered intravenously in 60–120 minutes immediately before contrast agent application. After contrast imaging 3 – 4 mL/kg/h 0.9% NaCl (up to 2000 cc) was administered intravenously in 4–6 hours. Serum kreatin levels checked immediately before and after 24 and 72 hours contrast agent application. Increase of creatinin value %25 or more than 0,5 mg/dL compared with value on addmission to emergency department was considered to be development of contrast-induced nephropathy. The creatinin levels checked on emergency department admission (Before contrast agent application), 24th and 72nd hours after contrast agent application. Results dvided into three groups according to changes on their creatinin levels; “Decrease on creatinin levels %25 or more”, “no change on creatinin leves” and “Increase on creatinin levels %25 or more than 0,5 mg/dL”. ��
Results: None of the patients in the first group were observed nephropathy. Furthermore, the creatinin levels were in normal range on 72nd hours after contrast agent application in high dose NAC group whose first creatinin levels were 1,2–1,8.��
Conclusion: The result of study, for preventing of contrast inducing nephropathy; high dose NAC application is more effective and usable than isotonic NaCl, in patients with mildly impaired renal function on emergency department. Keywords: Contrast agent, nephropathy, NAC, prophylaxis

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
166
O 115 ASSESSMENT OF PHYSICAL ACTIVITY IN MORBID OBESE PATIENTS WITH COPD FOLLOWING A PULMONARY REHABILITATION PROCEDURE AFTER BARIATRIC SURGERY
Burcu Yormaz1, Ilhan Ece2, Serdar Yormaz2, Bayram Çolak2
1Beyhekim State Hospital, Clinic of Chest Diseases, Konya, Turkey 2Selcuk University Medicine Faculty, Department of General Surgery, Konya, Turkey Background: In morbid obese patients with COPD, physical stagnation and laziness is believed to play a vital role in the development of comorbidities (such as skeletal muscle weakness, osteoporosis, depression, cardiovascular disease). Increasing physical activity has become a patient-centered goal for the treatment of patients with COPD. This study investigated the effect of physical activity outcomes after pulmonary rehabilitation in morbid obese patients who were underwent metabolic surgery. Methods: Physical activity was observed in 37 patients with morbid obese COPD (mean age, 46 ± 5years) before and after 3 months of pulmonary rehabilitation after the surgical process. Physical activity was measured before and immediately after surgery for 7 consecutive days with the smartphone, which detects wearing time directly by nonskin contact. The option of outcome (number of steps in day NSD , time spent in at least moderate physical activity TSA , and activity time ACT ), number of days of assessment of duration in daylight time (DT) were investigated. Results: The NSD and ACT were the most sensitive outcomes. Excluding weekends decreased the sample size for NSD (83 vs 56) and TSA (160 vs 148) Using 4 weekdays (NSD and TSA) rendered the lowest sample size. Promoting physical activity has become an increasingly important part of the treatment of morbid obese patients with COPD. Therefore the measurement of physical activity is indisputable clinical importance. We suggest that our way of analysis can be generalized to other validated activity monitoring devices. Conclusions: Changes in physical activity following pulmonary rehabilitation are best measured for 4 weekdays, including only days with at least 8 h of wearing time (during waking hours). These findings have implications for trial design and data processing and would potentially be cost saving for researchers. We trust that novel methods could detect the physical measurements and added features in later years. Keywords: Physical activity, COPD, pulmonary rehabilitation O 116 THE CHARACTERISTIC FEATURES OF RELATIVES ACCOMPANYING ADULT PATIENTS WHO CONSULTED TO EMERGENCY SERVICES Selman Yeniocak1, Hakan Topaçoğlu2
1University of Health Sciences, Haseki Training and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey 2Istanbul Training and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey Objective: The objective of this study is to analyze number, and characteristic features of the relatives accompanying their intimate patients who applied to the emergency service. Method: The patients who applied to the clinics of emergency medicine were questioned about their means of transportation to the emergency service, number of their applications to the ER, and their level of education. However their attendant relatives were subjected to the same questions in addition to the number of patients’ intimates, the degree of their intimacy, the place where they came from, and their thoughts about the severity of the patient’s disease. Then responses to all of these questions were recorded. Results: A total of 5046 patients (male, n=2950; 58.5 %, and female, n=2096; 41.5 %) were included in the study. Mean age of the patients was 38.4±17.4 years. The patients included in the study were accompanied by at least one relative (5046/3690; 73.1%), while 1356 (26.9%) patients were not attended by any intimates. Most of the female (n=1811; 86.4 %), and only 63.7 % (n=1879) of the male patients were attended by a relative. (p<0.001). Mean number of accompanists per male, and female patients were 1.48±0.749, and 1.51±0.759 individuals, respectively. A total of 3690 patients were accompanied by at least one, and at most 8 individuals, and on an average each patient were accompanied by 1.5 persons. The patients who applied to the emergency services were accompanied most frequently by one (2336 patients; 46.3%) person. Conclusion: Unneeded patient accompaniment leads to patients’ intimates leaving the workplace with or without giving any notice and keeps them away from services, and productivity they will provide with resultant increase in the work load of the other employees still working at the workplace. Keywords: Relatıves, accompanyıng, patıents, emergency services

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
167
O 117 PREVALENCE OF PSYCHIATRIC DISORDERS IN FAST TRACK AREA (TRIAGE CATEGORY 3) WITH PRIME MD EVALUATION SCALE: A STUDY FROM ESKISEHIR OSMANGAZI UNIVERSITY EMERGENCY
DEPARTMENT Mustafa Emin Çanakçı1, Nurdan Acar1, Çınar Yenilmez2, Engin Özakın1, Filiz Baloğlu Kaya1, Ebubekir Arslan1, Turgay Çağlayan1, Hakan Dolgun1
1Eskişehir Osmangazi University School of Medicine, Department of Emergency Medicine, Eskişehir, Turkey�2Eskişehir Osmangazi University School of Medicine, Department of Psychiatry, Eskişehir, Turkey Objective: The aim of the study is to define the prevalence of psychiatric disorders in the patients without active psychiatric illness admitted to our fast track area. Method: The study was planned as a randomized and prospective design. Older than 17 yo and patients without active psychiatric illness admitted to fast track area of emergency department(ED) between Oct 1st –Dec 31st, 2015 were assessed by Prime MD questionnaire after their consent. The residents were trained about the scale before the study. After the patient's ED process completed and before discharge, forms were applied by residents who has not involved in patient’s medical care.��
Results: 14800 patients were admitted in fast track and 4320 of them included. 54.1% of patients was female and 45.9% was male. The mean age was 30.03 ± 11.7. 39.5% was a university degree. 84.3% no chronic illness. At least one psychiatric disorder on the scale was 44.1%. The most frequent diagnoses were minor depression (24.7%), major depression (12.2%). Mood disorders, anxiety disorders and somatoform disorders were found significantly higher in women compared to men (p<0.05). The presence of chronic medical state was found as a cause of increased psychiatric disorders significantly in all modules except alcohol abuse. When the final diagnoses were evaluated, less psychiatric morbidity was found in patients with orthopedic injuries. Conclusions: Using Prime MD, at least one psychiatric disorder with a substantial degree was detected in category 3 patients. Neurotic disorders were observed more in women than men. In general, medical staff thinks these patients make a crowded and fatigue in ED do not have enough time for real emergencies. On the other side, patients with psychiatric illnesses think themselves urgent and in a serious pathological condition. This visit is not a trip but shouting for help! Keywords: Category 3 patient group, emergency medicine, prime MD O 118 THE METRONOME USAGE IMPROVES THE CARDIOPULMONARY RESUSCITATION PRACTICE QUALITY: A MANIKIN STUDY Necmiye Yalçın Ocak, Mustafa Sever, İbrahim Toker, Orkun Ünek, Emirhan Erdem İzmir Tepecik Training and Research Hospital, Clinic of Emergency Medine, İzmir, Turkey Objective: Clinical studies have been reported that removing the negative performer factor is important for high quality Cardiopulmonary Resuscitation (CPR). There aren’t enough recommendations have been reported about metronome usage on CPR quality. This study is aimed to investigate the effect of metronome usage on quality of CPR. Methods: 30 volunteer emergency physicians were attended. Participants were divided in to 15 groups. Firstly, each participant performed conventional CPR on manikin, and then performed metronome guided CPR after a short brief. The all parameters which affect the quality of CPR were evaluated based on recommendations and limits as reported in 2016 Advanced Cardiac Life Support guideline were compared. Also participants fatigue levels were evaluated with Borg Fatigue Index. Results: Metronome guided CPR was significantly improved the average chest compression count (mean; 129.1±13.9 compression/m vs. 110.3±1.8 compression/m in 95%CI, p<0.001), deep compression count (81±44.1 compression/m vs. 30.6±23.3 compression/m in 95%CI, p<0.001), proper compression count (34.2±35.3 compression/m vs. 13.1±15.1 compression/m in 95%CI, p<0.05), ventilation count (13.6±6.6 ventilation/m vs. 9.7±0.37 ventilation/m in 95%CI, p<0.05), ventilation with low volume count (13.6±6.6 ventilation/m vs. 0.6±1.27 ventilation/m in 95%CI, p<0.001), ventilation volume (13.6±7.67 l/m vs. 9.1±5.2 l/m in 95%CI, p<0.05) and rescuer fatigue (3.0±1.3 vs. 1.9±1.0, in 95%CI, p<0.05) were detected.��
Conclusions: Our study showed that metronome is a useful device for provide to reach effective CPR parameter levels and metronome guidance may improve quality of CPR. This study results should confirm with the studies that investigate the effect of metronome guided CPR practices on survival. Keywords: Cardiopulmonary resuscitation, metronome, manikin study

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
168
O 119 EVALUATION OF THE EFFECT OF INITIAL LACTATE LEVEL ON SHORT-TERM SURVIVAL OUTCOMES IN PATIENTS WITH OUT-OF HOSPITAL CARDIAC ARREST
Tuba Sarıaydın, Şeref Kerem Çorbacıoğu, Yunsur Çevik, Emine Akıncı Keçiören Training and Research Hospital, Ankara, Turkey Purpose: In this study, we purposed to evaluate whether serum lactate levels (SLE) on admission in patients with CA can use for prediction of success of ROSC or short-term survival, within especially first 24-hours or cannot. Material-Method: This prospective-observational study was conducted in the emergency department (ED) of a training and Research Hospital fromApril 2015 through February 2016. During the study period, all older than 18 years patients who presented to ED with non-traumatic OHCA were included to this study. In this study, two end points were determined; whether achieve ROSC or not and whether achieve short-term survival or not. ROSC was defined as presence of spontaneous circulation for first hour after CPR. The survival was defined as survived for a minimum of 24 hours after ROSC. Results: A total of 140 patients who was admitted to ED with OHCA were included to this study during the study period. ROSC was supplied in 55 patients (39.3%) and survival for 24-hour after following CA was supplied 42 patients (30%). It was detected that means of SLE in ROSC (+) and ROSC (-) groups were 9.1±3.2 and 9.8±2.9, respectively. And means of SLE in survivor and non-survivor groups were 8.6±2.9 and 10±3.1, respectively. These differences were not significant statistically (p=0.1). When created multivariate regression model to assess the factors predicting both ROSC and 24h survival, it was calculated that odds ratio (OR) of initially SLE were 1.3 (95%CI: 1.05 – 1.6,) and 1.1 (95%CI: 0.9 – 1.3), respectively. Conclusion: This study has showed that in OHCA patients, measured serum lactate levels on admission were not associated with gained ROSC or 24h survival. Keywords: Cardiac arrest, OHCA, resuscitation, serum lactate level, emergency medicine O 120 INVESTIGATING OF USING SCUBE 1 AND S100B PROTEINS AS AN EARLY PROGNOSTIC MARKER AT PREDICTING PROGNOSIS AFTER CARDIOPULMONARY RESUSCITATION IN CARDIAC ARREST PATIENTS Gürkan Altuntaş1, Faruk Özşahin2, Selim Demir3, Betül Abanoz1, Ahmet Ali Top1, Şenol Ardıç1, Özgür Tatlı4, Ahmet Menteşe5, Süleyman Türedi1
1Kanuni Research and Training Hospital, Clinic of Emergency Medicine, Trabzon, Turkey 2Giresun Dr. İlhan Özdemir State Hospital, Clinic of Emergency Medicine, Giresun, Turkey�3Karadeniz Technical University Faculty of Health Sciences, Department of Nutrition and Dietetics, Trabzon, Turkey 4Karadeniz Technical University Faculty of Medicine, Department of Emergency Medicine, Trabzon, Turkey 5Karadeniz Technical University Vocational School of Health Sciences, Program of Medical Laboratory Techniques, Trabzon, Turkey Objective: The aim of this study is to evaluate usability of early prognostic marker of SCUBE 1 and S100B proteins for survival of the patients performed CPR after cardiac arrest, for the success of resuscitation and for good neurological outcome. Material-Method: After approval by the local ethics committee, non-traumatic cardiac patients admitted to the emergency department of a tertiary hospital in the range of six months. Blood samples were obtained from patients to evaluate the S100 and SCUBE 1 levels at the initiation of CPR. The post-resuscitative care for the patients provided ROSC or sustained ROSC were received at related services or intensive care units by the respect of AHA 2010 guideline (without applying of therapeutic hypothermia). The levels of SCUBE and S100B obtained at the initiation of CPR were compared and evaluated the usability of determination for the patients who provided sustained ROSC and the patients who had a good prognosis at the end of three months according to Glasgow Outcome Scale (GOS). Results: During the study period, 17 of 82 cardiac arrest patients were excluded from the study because of having minimum one exclusion criteria and 65 non-traumatic cardiac arrest patients were included to this study. 26 (40%) of 65 patients were provided sustained ROSC and 5 (7,7%) patients ended in a good neurological prognosis. The level of S100B and SCUBE 1 proteins were not found as a determinant for providing sustained ROSC and also these were not found as determinant for providing good or poor neurological conditions. However, the level of SCUBE 1 proteins were twO times higher in the group of poor neurological condition than good neurological condition group. Conclusion: The level of S100B and SCUBE 1 proteins evaluated at the initiation of CPR were not useful to determine survival and good neurological conditions after CPR. Keywords: Advanced cardiac life support, cardiopulmonary resuscitation, S100B, SCUBE 1

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
169
O 121 INVESTIGATING OF USING ISCHEMIA-MODIFIED ALBUMIN AND NEURON SPECIFIC ENOLASE PROTEINS AS AN EARLY PROGNOSTIC MARKER AT PREDICTING PROGNOSIS AFTER CARDIOPULMONARY
RESUSCITATION IN CARDIAC ARREST PATIENTS Betül Abanoz1, Şenol Ardıç1, Gürkan Altuntaş1, Süleyman Türedi1, Bestami Köse1, Ahmet Menteşe2, Selim Demir3
1Trabzon Kanuni Training Research Hospital, Emergency Medical Clinic, Trabzon, Turkey 2Karadeniz Technical University Faculty of Medicine, Department of Biochemistry, Trabzon, Turkey 3 Karadeniz Technical University Faculty of Health Sciences, Department of Nutrition and Dietetics, Trabzon, Turkey Introduction: The aim of the present study was to investigate the value of ischemia-modified albumin (IMA) and neuron specific enolase (NSE) levels at initiation of cardiopulmonary resuscitation (CPR) in patients of cardiac arrest in determining sustained return of spontaneous circulation (ROSC), 3-month survival and neurological outcome after cardiac arrest. Methods: This study was performed prospectively with in- or out- of hospital cardiac arrest patients admitted to emergency department of a tertiary hospital between July 2014 and March 2015. IMA and NSE levels were measured in blood samples obtained at initiation of CPR. Patients were divided into two groups as sustained ROSC and non-sustained ROSCin terms of CPR success. For 3-month survival and neorological outcome, patients were grouped as good and poor outcome groups according to Glasgow Outcome Scale (GOS) and levels of IMA and NSE were compared between the groups. Results: Sustained ROSC was achieved 40% of 65 cardiac arrest patients. 3-month survival was 10.7% and survival with good neurological outcome 7.7%. The median IMA and NSE levels did not differ from the patients with sustained ROSC to those without. The median IMA and NSE levels were not statistically significant difference between the good outcome group and the poor outcome group. Conclusion: IMA and NSE levels at initiation of CPR are not sufficient to be used to predetermine sustained ROSC, survival and neurological outcome after cardiac arrest. Keywords: Cardiopulmonary resuscitation, IMA, neurological outcome, NSE, prognosis O 122 THROMBOLYTIC THERAPY DELAY IS AN INDEPENDENT PREDICTOR OF MORTALITY IN ACUTE PULMONARY EMBOLISM IN THE EMERGENCY SERVICE İnan Beydilli1, Fevzi Yılmaz1, Bedriye Müge Sönmez2, Nalan Kozacı1, Akar Yılmaz3, İbrahim Halil Toksul1, Ramazan Güven4
1Antalya Training and Research Hospital, Clinic of Emergency Medicine, Antalya, Turkey 2Ankara Numune Training and Research Hospital, Clinic of Emergency Medicine, Ankara, Turkey 3İzmir University Faculty of Medicine, Department of Cardiology, İzmir, Turkey�4Bitlis State Hospital, Clinic of Emergency Medicine, Bitlis, Turkey Background: Acute pulmonary embolism carries a high risk of morbidity and mortality. Delays in diagnosis or therapy may result in sudden, fatal deterioration; therefore, rapid diagnosis and an appropriate therapeutic approach are needed. We aimed to investigate the effect of delaying thrombolytic administration on the mortality rate in a suspected PE. Methods: We retrospectively analyzed 49 consecutive patients who were 18 years or older and received thrombolysis for a high-risk PE without a major contraindication. All patients were classified according to the time of onset of the thrombolytic therapy. Patients experiencing cardiopulmonary arrest were analyzed from the time of admission to thrombolytic administration with 10-min cut-off values. Data were analyzed by a regression and a receiver operating characteristic (ROC) analysis for significant and independent associated risk factors and in-hospital mortality. Results: Mortality was seen in 17 of the 49 cases. Thirteen of these had received thrombolytic therapy 1 h after their emergency department (ED) admission. Among all cases, the mortality rate was 35%. The ROC analysis indicated that a >97-s delayed thrombolytic administration time was associated with mortality with 53% sensitivity and 91% specificity (Area Under the Curve (AUC): 0.803, 95% confidence interval CI 0.668–0.938). In the logistic regression, a 5 min delay in thrombolytic therapy (beta = 1.342, 95% CI 1.818–2.231, p = 0.001 was associated with in- hospital mortality in the multivariable model. No major bleeding complications were seen in PE survivors. ��
Conclusions: We conclude that early-onset thrombolytic therapy in the ED for high-risk and hemodynamically worsening patients appears safe and life-saving. Keywords: Acute pulmonary embolism, core pulmonale, thrombolytic therapy

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
170
O 123 TAR BURN Sultan Tuna Akgöl Gür, Göksu Afacan Erzurum Regional Training and Research Hospital, Emergency Service, Erzurum, Turkey Introduction: Tar is petroleum based hydrocarbon compound that used in road construction, roof and vehicle isolation. Tissue damage by tar is serious and treatment is difficult due to its chemical structure, usage in high temperatures and its sticky favor. Tar burns are more common in man and usually seen as a work accident. Tar burns are unusual and we aimed to remind its treatment options. Case: 42-year-old male patient, who works in road construction, presented in our clinic with tar burns due to asphalt explosion. On physical examination, general situation was mean, full conscious and it was found that vital signs and hemodynamics were stable. There was tar on his right arm, left hand and around his belly. We scrubbed the tar out of patients body with the help of olive oil which we procure from hospital's kitchen. Patient was admitted to the burn center. Conclusion: Regardless of the name, treatment agent should be selected for the properties of being fast, effective, painless and not increasing irritation and tissue damage. Keywords: Burn, olive oil, tar O 124 THE EVALUATION OF A NEW MARKER OF TRANSMYOCARDIAL REPOLARIZATION PARAMETERS IN ISCHEMIC STROKE PATIENTS; TPEAK–TEND (TP-E), TP-E/QTC Emine Emektar1, Şeref Kerem Çorbacıoğlu1, Osman Korucu2, Selma Ramadan3, Yunsur Çevik1, Hüseyin
Uzunosmanoğlu1, Eda Kan1
1Keçiören Training and Research Hospital, Clinic of Emergency Medicine, Ankara, Turkey�2Keçiören Training and Research Hospital, Clinic of Neurology, Ankara, Turkey�3Keçiören Training and Research Hospital, Clinic of Radiology, Ankara, Turkey Introduction: This study aimed to investigate the changes transmyocardial repolarization parameters, in ischemic stroke patients. Material and Method: The study is a prospective, blind, controlled clinic study. The patients, who applied to the emergency department within the first 6 hours after stroke symptoms started, without cardiac disease, who received ischemic stroke diagnosis were included. Electrocardiography (ECG) was received from the patients in the first hour and 72 hours. The P, QT, Tp-e, Tp-e dispersion, and the Tp-e/QT ratio were calculated. Results: All dispersion values and Tp-e/QTc ratio in patients group were higher than those of control group (p<0.05 for all values). When evaluated between ECGs’ on first and third days, it was found that decreasing on all dispersion values and Tp-e/QTc ratio in ECGs on third day than ECGs on first day (p<0.05 for all values). QT, QTc, and Tp-e dispersions values in patients who have insular lobe involvement were higher than those of patients who do not have insular lobe involvement (p<0.001 for all values). Conclusion: In this study, we showed that acute stroke increases that Pd, QTd, OTcd and new repolarization markers Tp-e and Tp-e/QTc, during first 24 and 72 hours in acute stroke patients without cardiovascular disease compared with the control group. The physicians should be awake about ventricular dysrhythmias in patients with ischemic stroke and these patients closely observed with cardiac monitoring, especially within first 24-hour and especially patients with insular lobe involvement. Keywords: Stroke, P, QT, Tpe, Tpe dispersion

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
171
O 125 THE RELATIONSHIP OF HIGH SENSITIVE TROPONIN I (HS-CTNI) TO TIMI SCORE, GRACE SCORE AND MORTALITY IN NSTEMI PATIENTS IN THE EMERGENCY DEPARTMENT
Hazar Lisar, Bedia Gulen, Ertan Sonmez Bezmialem Vakıf University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Background: Nowadays, Coronary Heart Diseases (CHD) are the most important cause of mortality and morbidity. Non ST Segment Myocardial Infarctions (NSTEMI) is responsible for 25% of acute coronary syndromes (ACS). In this study we looked for the effect of hs-cTn I upon patients with newly diagnosed NSTEMI in the emergency room settings in terms of prognosis and 6 month-mortality. Methods: This retrospective study was done in Bezmialem Vakif University Medical Faculty Department of Emergency Medicine where 864 patients per day apply. 100 patients were enrolled to this study. While the causes of death who died in the hospital were recorded by investigating archival records; the causes of death who died at the outside hospital were confirmed by phone encounters. Study data was saved and analyzed by utilizing SPSS. Results: Study population includes 16 patients (16%) who died (Mortality +) and 84 patients (84%) who were alive (mortality -) in the first 6 months of the study. HsTnI mean value (Mean ±SS: 8981.81±6183.49 Median (IQR): 9350 (2533.25-12675)) of the mortality (+) group is showed statistically significance (p=0.001) than this (Mean±SS: 4333.58±8653.62 Median (IQR): 857 (574.25-3674.25)) of the mortality (-) group. In our study hs Tn I value indicated sensitivity of 75%, specificity of 82.14%, positive predictive value of %44.40, the negative predictive value of %94.50, likelihood ratio LH (+) value of 4.20 and predictive value of 6754>= for NSTEMI. A significant relation was not found between hs-cTn I value and TIMI/GRACE scores, respectively (p=0.068, p=0.068) Conclusions: In our study, hs-cTnI value with regard to 6 months mortality is showed statistically significance. This result indicates hs-cTnI can be used as a prognostic marker in patients with newly diagnosed NSTEMI in the ER settings. However, there is need for more extensive and randomized controlled trials. Keywords: NSTEMI, GRACE, TIMI, hs-cTnI, mortality O 126 ADROPIN AS NEW BIOCHEMICAL MARKER TO DIAGNOSE OF PATIENTS WITH ACUTE CORONARY SYNDROME Nurettin Dag, Bedia Gulen, Ertan Sonmez Bezmialem Vakıf University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Background: In our study, effectiveness of adropin (ADR) which was discovered in recent years and consists 76 amino acids was investigated to diagnose of acute coronary syndrome (ACS) in patients presenting with chest pain in emergency department (ED). Methods: 198 patients who presented with chest pain and suspected ACS in the ED were enrolled to this study. Patients were classified into three groups which include unstable angina (USAP), non-ST elevation myocardial infarction (NSTEMI) and ST segment elevation myocardial infarction (STEMI) according to American Heart Association (AHA) guidelines. Troponin level was recorded at least 6 hours after the onset of chest pain in patients with suspected ACS. 5 cc of blood in a biochemistry tube was drawn immediately after hospital admission to measure the ADR level. Blood samples were centrifuged and kept at - 80 degrees until the runtime. Then ADR level was compared with the ECG, the troponin level, and final diagnosis of patients and sensitivity, specificity, and cut-off values of ADR were calculated in patients with acute myocardial infarction (AMI). Results: In our study, ADR level in the STEMI and NSTEMI groups was significantly lower in the USAP group (p=0.000). The ADR level in the STEMI group was significantly lower than in the USAP group GA 95% 0872 (0811-0932) (p = 0.000) . The highest ADR value was 400 ng / dL in the area under the curve differentiation USAP group with STEMI group GA 95% 0.810 (0732-0888) (p = 0.000). Sensitivity of 82%, positive predictive value of 69.5%, specificity of 80%, and negative predictive value of 88.9% are found. Conclusions: ADR can be used as a new biomarker in patients presenting with chest pain in the ED. Keywords: Adropin, USAP, NSTEMI, STEMI

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
172
O 127 CORRELATION BETWEEN SYNCOPE RISK SCORES OF THE PATIENTS PRESENTED WITH SYNCOPE TO EMERGENCY DEPARTMENT AND CAROTID INTIMA-MEDIA THICKNESS
Burak Nakış, Arzu Emecen, Cansu Arslan Turan, Tuba Cimilli Öztürk, Özge Ecmel Onur Fatih Sultan Mehmet Training and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey Objective: The purpose of the study is to determine the correlation between San Francisco Syncope Rules, OESIL Syncope Rules, Anatolian Syncope Rules, EGSYS Syncope Rules, which determine the mortality and morbidity risks of the patients presented with syncope to Fatih Sultan Mehmet Training and Research Hospital Emergency Department during the study, and carotid intima-media thickness and if available to determine the limits of significance. The secondary purpose is to determine the demographic features of the patients presented with syncope to our hospital. Materials-Methods: The prospective and observing study was carried out at Fatih Sultan Mehmet Training and Research Hospital Emergency Department between 01.11.2015 – 30.06.2016. All the adult patients presented with syncope to the emergency department between the dates mentioned were evaluated in accordance with the study criteria and the ones complying with the criteria were included. USG was performed for the carotid intima-media thicknesses of the patients. The risk scores of all patients were calculated in accordance with SFRS, OESIL, ASR and EGSYS scoring systems. Following that the relation between CIMT values and risk scores were evaluated and compared. Results: In CIMT measurement, the cut-off value > 0,9 mm was recognized significant. As the patients with the cut-off value below 0,9 mm were evaluated with the risk scores, there was significant relation observed ( p <0,05 ). Likewise the patients with the cut-off value above 0,9 mm had the significant relations with the risk scores (p<0,05). Conclusion: As the risk scoring systems and CIMT values of the patients presented with syncope to our emergency department are correlated, it could be used as a determiner/indicator. This study reminds that the further, multi-centered studies with the higher number of patients whose outcomes are determined are required. Keywords: Syncope, carotid intima-media thickness, syncope scoring systems O 128 DIAGNOSTIC VALUE OF COPEPTIN IN PATIENTS WITH ACUTE MYOCARDIAL INFARCTUS Mehmet Oguzhan Ay1, Ali Kemal Erenler1, Ramazan Kocabas2, Tolga Dogan3, Mucahit Yetim3
1Hitit University Çorum Training and Research Hospital, Department of Emergency Medicine, Çorum, Turkey�2Hitit University Çorum Training and Research Hospital, Department of Biochemistry, Çorum, Turkey�3Hitit University Çorum Training and Research Hospital, Department of Cardiology, Çorum, Turkey Objective: In this study, it was aimed to reveal the usefullness of copeptin in the early diagnosis of acute myocardial infarction (AMI) and to compare the diagnostic efficacy of copeptin with other cardiac markers. Methods: A total of 160 cases in both gender, over 18 years, who were consisted of 54 non-ST elevation MI (NSTEMI), 54 ST segment elevation MI (STEMI) and 52 healthy subjects (control) were enrolled. Patients who had the value of creatinine >1.5 mg/dL, who had normal levels of cardiac troponin tests during follow-up were excluded from the study. Troponin-I, CK-MB mass, Copeptin and CRP levels were measured in serum samples of of the cases, and they were compared statistically with each other. Results: Median serum levels of Copeptin (ng / mL) in Control, NSTEMI and STEMI groups were 2.22 (2.18-2.35), 2.50 (2.34-2.72) and 2.94 (2.85-3.24), respectively. Copeptin levels of STEMI group were found to be significantly higher than both control and NSTEMI group (p <0.001). There was also low level of statistically significant difference between NSTEMI and control group (p = 0.042). Spearman correlation analysis show significant positive correlation between the level of Copeptin and the presence of AMI (r=0.285, p< 0.001), CK-MB mass (r=0.246, p=0.002), Troponin-I (r=0.199, p=0.012). Sensitivity, specificity and AUC values of the tests according to ROC analysis performed for the diagnosis of AMI; Troponin-I >0.1 ng/mL (71.0%, 100.0% and 0.855); CK-MB mass >3.59 ng/mL (77.8%, 92.3% and 0.911); CRP >6.37 mg/L (53.7%, 88.5% and 0.769); Copeptin >2.47 ng/mL (66.7%, 75.0% and 0.676), respectively (p<0.001). Conclusion: For the diagnostic evaluation of AMI, cardiac Troponin remains the gold standard biomarker. Copeptin alone should not be considered as a single diagnostic marker in patients with suspected AMI. This study was supported by the Hitit University Research Projects Unit (Project Code: TIP19002.16.003). Keywords: Acute myocardial infarction, Copeptin, Troponin-I, CK-MB, CRP

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
173
O 129 DIAGNOSTIC VALUE OF TEI INDEX (MYOCARDIAL PERFUSION INDEX) CALCULATION IN EMERGENCY DEPARTMENT PATIENTS WITH CHEST PAIN COMPLAINTS FOR ACUTE MYOCARDIAL INFARCT DIAGNOSIS
Aslı Bahar Uçar, Özge Ecmel Onur, Ebru Ünal Akoğlu, Tuba Cimilli Öztürk, Hasan Demir, Abdullah Taşçı Fatih Sultan Mehmet Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey Introduction: Acute myocardial infarction (AMI) is the most common cause of mortality in developed countries. High sensitive troponin (Hs-troponin) in AMI patients usually become positive 3 hours from the onset of symptoms. Tei index is a parameter measured by echocardiography that ventricular systolic and diastolic function can be assessed together. Tei index measurement in emergency department (ED) as an early diagnosis of AMI and the correlation of Tei index and Hs-troponin were investigated. Methods: Our study was conducted prospectively and patients were evaluated with Hs-troponin levels, ECG and echocardiography findings. They were divided into two groups according to their final diagnosis "which considered AMI and not considered as AMI". Hs-troponin levels at admission and at 3rd hour were compared with Tei index values. Results: 200 patients presenting to ED with ischemic chest pain complaints were evaluated. 46 not meeting inclusion criteria were excluded. 109 patients were diagnosed as AMI; the rest had a final diagnosis other than AMI. Tei indexes were detected positive 88.1% of AMI patients and 48.9% of non-AMI patients on admission. Because STEMI patients were referred to a PCI centre, control Hs-troponin and Tei index values could not be obtained. All NSTEMI patients (84) had positive Hs-troponin and Tei index values (100%) at 3rd hour controls. In AMI patients there was %53,5 of correlation between Tei index and Hs-troponin on admission and 100% correlation at the 3rd hour. Conclusion: Our study shows that the use of Tei index values with Hs-troponin levels would not be a useful parameter in the early and effective diagnosis for acute myocardial infarction. The disruption of Tei index appearing before 3rd hour becomes more valuable determining absence of AMI then Hs-troponin (sensitivity Tei. 88%; Hs-trop: 48.6%). Hs-troponin is more powerfull diagnosing AMI then Tei index (specifity Tei: 51%; Hs-troponin 80%). Keywords: Acute coronary syndrome, acute myocardial infarction, Hs-troponin, Tei index O 130 EVALUATION OF NEUTROPHIL/LYMPHOCYTE RATIO IN PATIENTS REFERRING TO EMERGENCY DEPARTMENT WITH CHEST PAIN Mustafa Uğur Göktaş1, Pınar Yeşim Akyol2, Zeynep Karakaya2, Umut Payza2, Serkan Bilgin2, Gözde Canan Yavaş2, Fatih Esad Topal2
1Haseki Research and Training Hospital, Clinic of Emergency Medicine, Istanbul, Turkey 2Izmir Katip Çelebi University Atatürk Research and Training Hospital, Department of Emergency Medicine, Izmir, Turkey Introduction: Acute coronary syndrome(ACS) is one of the most important causes of mortality. Inflammatory reaction,which causes tissue damage in ACS, is leading the dire course. White cell and NLR relations with ACS in patients with chest pain is evaluated in this study. Material-Methods: Patients reffering to ER with chest pain examined within 3 months time, retrospectively. 100 patients are involved.Patients' white blood cell (WBC) count, NLR and WBC values average distribution; gender, Troponin-I and CK-MB positivity, history of coronary heart disease(CHD) and additonal diseases are examined according to final diagnosis. In-hospital and after discharge mortality and morbidities are examined. Data's statistical analysis is processed with IBM SPSS Statics V22 software package. Results: After patients' WBC values average distribution, gender, Troponin-I and CK-MB positivity, history of CHD and additonal diseases are examined according to final diagnosis are examined; WBC values in patients with positive Troponin-I are found statistically higher than patients with negative Troponin-I (p<0,05). In STEMI group, WBC values are statistically higher than USAP group(p<0,0083). When patients' N/L ratio average distribution is examined; Troponin-I and CK-MB positive patients' NLR is statistically higher than Troponin-I and CK-MB negative ones(p<0,05). In NSTEMI group, WBC values are statistically higher than USAP group(p<0,0083). Conclusion: To define the role of inflammation in CHD will help us to develop new and effective ways of protection from this disease, which is prominent causes of mortality in our country like rest of the world. Keywords: Acute coronary syndrome, neutrophil/lymphocyte Ratio, emergency department

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
174
O 131 A HIGH FRAMINGHAM RISK SCORE IS ASSOCIATED WITH INCREASED CAROTID INTIMA-MEDIA WALL AREA IN THE PATIENTS WITH ACUTE CORONARY SYNDROME
Ecem Deniz Kırkpantur1, Damla Selma Özalp1, Tuba Cimilli Öztürk1, Hasan Demir1, Özge Ecmel Onur2
1Fatih Sultan Mehmet Training and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey 2Marmara University Pendik Training and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey Introduction: Acute Coronary Syndromes (ACS) have very high rates of mortality in the world. Atherosclerotic coronary artery disease is the major cause of ACS. Carotid artery system has almost excellent properties for the assessment of peripheral artery system. Framingham Risk Score (FRS) is used to predict the risk of major cardiac events. In this study, we aimed to evaluate the association of the carotid intima-media wall area (CIMA) and FRS in the patients with acute coronary syndrome. Method: This study constitutes 88 patients with Acute Coronary Syndrome. Carotid intima-media thickness (CIMT) was measured from a 10 mm long, plaque free section of the far wall of the proximal part of the bifurcation of carotid artery. CIMA was calculated from the recorded videographic data of the CIMT. Results: Mean CIMA was 0,08±0,02 cm2 (Range: 0,045 and 0,155 cm2), and mean FRS was 19,62±13,00% (Range: 0 and 59%). FRS was 10% and more in 68 (77%), and less than 10% in 20 (23%) patients. Mean CIMA of the patients with FRS >= 10% was significantly higher than those of the patients with FRS <10% (p:0,040). A positive but weak correlation was found between FRS measurements and CIMA (r=0,224;p:0,036). CIMA was statistically significantly higher in the patients with HT or DM than the patients with no HT or DM history (p:0,038 and p:0,035). Discussion: In conclusion, statistically significant but weak correlation was found between the increased values of CIMA and higher FRS values of the patients. Moreover, it was observed that CIMA values were higher in the patients with HT and DM. Our study reveals that the patients with high values of carotid intima-media wall area may be under acute MI risk. Keywords: Myocardial infarction, carotid intima media thickness, Framingham Risk Score O 132 COPEPTIN AS A SURROGATE OF RIGHT VENTRICULAR DYSFUNCTION IN ACUTE PULMONARY EMBOLISM Ozcan Yavasi1, Kamil Kayayurt1-2, Songul Özyurt3, Özlem Bilir1, Gökhan Ersunan1, Asım Kalkan1-4, Mehmet Altuntaş1, Erhan Uğraş1
1Recep Tayyip Erdogan University Faculty of Medicine, Department of Emergency Medicine, Rize, Turkey 2Acıbadem University, Maslak Hospital, Istanbul, Turkey�3Recep Tayyip Erdogan University Faculty of Medicine, Department of Chest Diseases, Rize, Turkey 4Haseki Research and Training Hospital, Istanbul, Turkey Objective: We aimed to compare copeptin with N-terminal pro brain natriuretic peptide (NT-proBNP) and cardiac troponin I in the acute stage of pulmonary embolism (PE) for predicting right ventricular dysfunction (RVD) and the severity of acute PE. Material-Methods: Two tubes of blood samples, one for troponin and one for NT-proBNP and copeptin were derived from the patients who were confirmed to have acute PE via computed tomography (CT) angiography within six hours of diagnostic work-up. Within one hour, all patients underwent transthoracic echocardiography in the ED for the assessment of RVD by a cardiologist. Results: Forty-five of the 77 patients patients had RVD on echocardiography. The patients with RVD had higher concentrations of troponin I, NT-proBNP and copeptin (p = 0.014, p < 0.001, and p < 0.001, respectively). Fifty-nine PESI intermediate-high risk patients had higher NT-proBNP and copeptin levels but not troponin I compared to 18 PESI low risk patients (p = 0.040, p = 0.037, and p = 0.86, respectively). Receiver operating characteristic (ROC) analysis yielded an area under the curve (AUC) of 0.82 (0.72–0.89) for NT-proBNP and AUC of 0.73 (0.62–0.83) for copeptin. A cut-off value of 376 ng/L (sensitivity, 84% and specificity, 75%) for NT-proBNP, and 6.63 ng/mL (sensitivity 55% and specificity 90%) for copeptin were associated with the best prognostic performance. There was not a statistical difference between the both ROC curves (p = 0.184). There was a strong correlation between copeptin and NT-proBNP (r = 0.55, P < 0.001). Conclusion: Copeptin, a non-cardiac marker is as accurate as NT-proBNP to diagnose RVD in acute PE when echocardiography is not available. Keywords: Acute pulmonary embolism, copeptin, N-terminal probrain natriuretic peptide, right ventricular dysfunction

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
175
O 133 ANNUAL NON-TRAUMATIC CHEST PAIN EVALUATION IN ESKISEHIR OSMANGAZI UNIVERSITY EMERGENCY DEPARTMENT
Nurdan Acar, Mustafa Emin Canakci, Ayse Yasemin Ozgan, Engin Ozakin, Ezgi Akcaci Baran, Emre Catal Eskişehir Osmangazi University School of Medicine, Department of Emergency Medicine, Eskişehir, Turkey Objective: Patients who presented with nontraumatic chest pain were evaluated annually in our Emergency Department (ED). Methods: Patients older than 17 yo and had non-traumatic chest pain complaints were evaluated retrospectively between July 1st, 2015 and June 30th, 2016 patients in our ED. Tests, diagnosis, localization and duration of hospitalization were assessed. Results: In this period of time 2549 patients got included in this study. 1548 (60.7%) were male, 1001 (39.3%) were female. The mean age of all patients was 50.7±18.61 (min: 18-max:93).Mean age of male and female patients were similar 50.2±16.49 (min:18-max:93) and 51.3±17.31(min:18-max:91) respectively . 465 (18.2%) of the patients hospitalized into coronary intensive care unit (ICU) and 160 (6.3%) to cardiology clinic. 18 (0.7%) into pulmonary clinic and 21 (0.8%) into other departments. Mean age of hospitalized patients according to departments were: coronary ICU 62.69±13.68 (min: 24-maks:93), cardiology clinic 62.09±14.80 (min:20-max:88), pulmonary clinic 58.82±18.53 (min:27-maks:85) and the others 66.14±15.97 (min:24-max:93). Duration of stay in coronary ICU, cardiology clinic, pulmonary clinic and the others were respectively 4.72±4.17 (min: 0-maks:61) day, 4.10±4.68 (min:0-maks:53) day, 7.88±3.77 (min:3-maks:15) day, 9.38±9.64 (min:0-maks:41) day. 5 patients (%0.2) died in ED. CPR was applied to 7 patients, electrical cardioversion was applied to 7 patients and 7 patients were endotracheally intubated. 2959 high sensitive troponin-T test were used for 1879 patients. Bedside emergency ultrasound was performed 1552 times. D-Dimer was worked up 123 times. 51 patients were imaged with thorax CT. 36 patients died in departments where hospitalized. Conclusion: One four of patients admitted to emergency department with nontraumatic chest pain have been hospitalizing to coronary ICU and cardiology clinic. Emergency physicians have to use ECG ve cardiac biomarkers selective and carefully. In spite of there are wide spectrum differentials, good history and complete physical exam help accurate management. Keywords: Chest pain management, emergency, non-traumatic chest pain O 134 CORRELATION BETWEEN NEW YORK HEART ASSOCIATION (NYHA) FUNCTIONAL CLASSIFICATION AND PRO BNP LEVELS WITH NUMBER OF B-LINES ON BEDSIDE LUNG ULTRASOUND IN EMERGENCY DEPARTMENT: PROSPECTIVE, CROSS-SECTIONAL STUDY Hakan Dolgun, Nurdan Acar, Engin Özakın, Filiz Baloğlu Kaya, Mustafa Emin Çanakçı, Ebubekir Arslan, Turgay Çağlayan
Eskişehir Osmangazi University School of Medicine, Department of Emergency Medicine, Eskişehir, Turkey Aim: Aim of this study is to determine the correlation between New York Heart Association (NYHA) Functional Classification and pro BNP levels with number of B-lines on bedside lung ultrasound. Method: This study has a prospective and cross-sectional design. We studied patients from April 2015 to July 2016 in Eskisehir Osmangazi University Emergency Department. Patients older than 17 yo with shortness of breath and heart failure diagnosis in past medical history were included. Younger than 18 yo, pregnants and patients unwilling to give a consent were excluded. Power analysis was 0.95 for 138 patients. Kruskal-Wallis H test was used for comparing NYHA classification (I-IV) and pro BNP levels with the number of B-lines. In determining the direction and magnitude of the relationship between the calculations Spearman correlation coefficients were used. Ultrasonographic application of patients was performed after the physical exam and before starting treatment. All ultrasound applications performed by emergency physicians using Vivid E machine and 4C convex probe. As defined by Blue protocol 8 views were recorded. Results: Total of 143 patients were included. 92 of them (64.3%) were male and 51 (35.7%) were female. NYHA classification and number of B lines on the upper right, lower right, lateral right, posterior right, upper left, lower left, lateral left, and posterior left were highly correlated (r=0.910, r=0.905, r=0.881, r=0.908, r=0.882, r=0.892, r=0.881 and r=0.895 respectively) (p<0.001). prO BNP values were also highly correlated with B-lines (r=0.796, r=0.764, r=0.747, r=0.791, r=0.727, r=0.746, r=0.773 and r=0.784 respectively) (p<0.001). When the number of B-lines with NYHA classes are analyzed, the nu mber of B-lines were significantly different for each class (p<0.001). Conclusion: Pro BNP levels and NYHA classification, was found to be strongly correlated with B-line numbers on lung ultrasound. Bedside lung ultrasound provides a strong prediction about the clinical severity of the patient's heart failure. Keywords: Emergency department, heart failure, lung ultrasound

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
176
O 135 THE ASSOCIATION BETWEEN IN PERFUSION INDEX CHANGES AND CLINICAL IMPROVEMENT IN PATIENTS WITH ACUTE HEART FAILURE
Ekin Dumanlı, Derya Abuşka, Hakan Topaçoğlu Istanbul Training and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey Objective: There are no clear reports that the association between perfusion index (PI) and clinical improvement parameters of the patients with acute heart failure (AHF). The objective this study was to evaluate of changes in the perfusion index during the treatment period in patients with AHF and was investigated affecting factors. Materials-Methods: A prospective, cross-sectional, observational, cohort study was conducted in emergency department (ED) during 3-month period. In the study, patients with dyspnea presented to ED whose numerical rating scale (NRS) values for dyspnea were over 4 (0=no shortness of breath, 10=worst shortness of breath), were enrolled. Echocardiography was performed all patients and those with non-cardiac dyspnea were excluded. PI, NRS, respiratory rate (RR), blood pressures, inferior vena cava (IVC) diameter and oxygen saturation of the patients were measured simultaneously at the time of admission and 10-minute intervals and analyzed for changes. Results: The study included a total of 42 patients; with 19 (45.2%) females and median age was 73 years (range 45-88 years). Factors affecting the PI values of the patients at admission times were found to be age (p=0.020), oxygen saturation (p=0.034) and IVC diameter (p=0.032). (Linear Regression Analysis, Enter and Backward Method). PI values of the patients increased significantly with the resolution of symptoms of cardiac decompensation. PI means that measured at the time of relieve of dyspnea (RR<20 breath pm, NRS value for dyspnea <=4) were statistically higher than PI values at admission time. Whereas, PI values did not predict to determine their hospitalizations, admit to ICU or mortality. Conclusion: PI value in patients with AHF have been found to be effective in showing clinical follow-up and can be used in clinical improvement, but there was no correlation with the outcomes of the patients. Keywords: Acute heart failure, perfusion index, dyspne scale O 136 SAFELY USE OF RIVAROXABAN FOR TREATMENT OF THROMBOEMBOLIC DISEASE FOLLOWING SURGERY: INTERPRETATION OF EMERGENCY SERVICE ADMITTANCE Burcu Yormaz1, Ilhan Ece2
1Beyhekim State Hospital, Clinic of Chest Diseases, Konya, Turkey 2Selcuk University Medicine Faculty, Department of General Surgery, Konya, Turkey Background: Low-molecular weight heparin (LMWH) has been the standard of care for treatment of venous thromboembolism (VTE) in morbid obese patients with cardiopulmonary diseases. However Rivaroxaban is a novel molecule among anticoagulans for the treatment of pulmonary embolism (PE) and thrombosis (DVT), but no studies have proved the efficacy and the safety of rivaroxaban for diseases.The aim of this study was to assess the admittance to emergency service due to rivaroxaban following bariatric surgery. Methods: Of 21 patients who have underwent bariatric surgery and taken rivaroxaban pills due to cardiopulmonary disease were evaluated in this study between the years of august 2015 to april 2016. Of 14 patients were female and 7 were male. We included patients who had received up to 3 days of a parenteral anticoagulant as initial treatment prior to change to rivaroxaban. Recurrent VTE, major bleeding and death from any cause were considered competing risks for the purpose of the analysis of study. Results: The consisted patients of the study, of whom 13 had sustained a PE (with or without DVT) and 8 had experienced a symptomatic, proximal lower extremity DVT. Of 17 patients had a comorbidity disease. No patient was lost to follow up. In the first 6 months of treatment, there were four cases of recurrent VTE, one case of major bleeding on the other hand two cases of discontinuation in rivaroxaban and no deaths detected when admittance to the emergency service. Conclusions: This study also provides some guidance for possible threatening situations that arise morbidity setting, including uncontrolled changing dose, thrombocytopenia. Further, our decision to dose-reduce in the elderly was associated with comparable bleeding rates with the overall obese population. Further support for the clinical resolutions will require expansion of the number of patients operated under these situations. Keywords: Rivaroxaban, surgery, emergency

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
177
O 137 PERFUSION INDEX CHANGES IN PATIENTS WITH CHEST PAIN WHO UNDERWENT CORONARY ANGIOGRAPHY
Ali Can Midik1, Ozgur Dikme2, Ozlem Dikme3, Hakan Topacoglu2
1Çanakkale State Hospital, Emergency Clinic, Çanakkale, Turkey�2Istanbul Training and Research Hospital, Emergency Clinic, Istanbul, Turkey 3Koc University Hospital, Department of Emergency Medicine, Istanbul, Turkey Objective: Chest pain is one of the most popular admission to EDs. Millions of people around the world are admitted to EDs annually for workup of acute coronary syndromes (ACSs). The aim of the study was that determinate the perfusion index (PI) changes in the course of coronary angiography (CAG) and reveal the factors that affect it. Method: This prospective cross-sectional study enrolled on 116 patients with chest pain who admitted to Cardiology ward from ED or Cardiology Outpatient Clinic and planned CAG. Twenty-eight of 116 patient was presented to the ED with chest pain and then admitted to the Cardiology ward with diagnosis of ACS. The remaining 88 was presented to the Cardiology Outpatient Clinic with chest pain and then admitted there with diagnosis of Stable Angina Pectoris (SAP). PI values were measured with Masimo Rainbow Root Radical-7-oximeter before, during and after CAG. Mann-Whitney-U and Student-T test were used to test for differences between and within groups. Results: Of the 116 patients enrolled, 69 (59.5%) were male, mean age was 58.3±11.1, 6% were STEMI, 5.2% were NSTEMI, 12.9% were USAP and totally 24.1% were ACS. Stent rate on CAG was found as 23.3%. When the patients were evaluated about admission ECGs, 88 of them (75.9%) had normal sinus rhythm. When the all chest pain patients were evaluated interms of the presence of ACS, the need for stents, and after the CAG to ensure normal coronary flow (TIMI3), there was no significant statistically and clinically difference in any subgroup (ACS: p=0.256, p=0.420, p=0.372; Stent: p=0.256, p=0.420, p=0.372; TIMI3: p=0.369, p=0.546, p=0.377; Mann Whitney U-test). Conclusion: Although, the PI changes in patients presenting with chest pain to the ED is projected to be meaningful, it is not clinically and statistically significant in patients who underwent coronary angiography. Further researchs needed. Keywords: Perfusion index, acute coronary syndrome, coronary angiography, coronary flow O 138 PROGNOSTIC FACTORS DETERMINING MORBIDITY AND MORTALITY IN ORGANOPHOSPHATE POISONING Ayça Açıkalın1, Nezihat Rana Dişel1, Selçuk Matyar2, Ahmet Sebe1, Zeynep Kekeç1, Yüksel Gökel1, Emre Karakoç3
1Çukurova University Faculty of Medicine, Department of Emergency Medicine, Adana, Turkey 2Çukurova University Faculty of Medicine, Central Laboratory, Adana, Turkey �3Çukurova University Faculty of Medicine, Internal Medicine Intensive Care Unit, Adana, Turkey Introduction and Aim: Our aim in this retrospective study was to determine the factors affecting poor prognosis and mortality of organophosphate (OP) poisoning by reviewing patient data. We also reviewed present knowledge to make conclusions on certain longstanding debates in light of the literature. Results: A total of 80 patients were included in the study. The mean age of the study patients was 32.4±15.0 (13-94). Forty-nine (61.2%) patients were female. Twenty-two (27.5%) of the patients were seriously poisoned and needed mechanical ventilation (MV) support. Low pseudocholinesterase (PChE), high creatinine (Cr), low Glasgow Coma Scale (GCS) scores and long hospitalization durations were all found to be poor prognostics in MV patients. Low PChE and high Cr levels were found to be independent predictors of the hospitalization duration and high Cr was found to be an independent predictor of the intubation duration of MV patients in regression analyses. Ten (45.5%) of the MV patients were unresponsive to medical treatment, and plasmapheresis was performed. Seven patients were discharged healthy. Three patients with low PChE levels and comorbidities died. Persistent low PChE levels 48 hours after admission and comorbidities were found to be relevant to fatalities. Conclusions: Persistant respiratory depression, low PChE levels at the 48th hour of admission and comorbidities are all found to be indicators of mortality. Utilizing plasmapheresis in OP poisoning patients under MV support with low GCS scores and ongoing low PChE levels should be kept in mind before the occurrence of complications due to long hospitalization duration. Keywords: Poisoning, organophosphates, plasmapheresis, mortality

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
178
O 139 EFFECTS OF INTRAVENOUS LIPID EMULSION THERAPY ON SYNTHETIC CANNABINOID INTOXICATION Merve Gunes1, Ozlem Guneysel1, Fatma Sari Dogan1, Vehbi Ozaydin2
1Dr.Lutfi Kirdar Kartal Training and Research Hospital, Istanbul, Turkey 2Istanbul Medeniyet University Goztepe Training and Research Hospital, Istanbul, Turkey Objectives: Synthetic cannabinoids started to use in early 2000s in Europe but synthetic additives were defined in 2009 by Auwärter. ‘Spice’, ‘K2’ are the most common names and in Turkey named as ‘Bonzai’. Definition and recognition of synthetic cannabinoids are more important in emergency department. Treatment and management of synthetic cannabinoid is all supportive and specific treatment is not described. Intravenous Lipid Emulsion (ILE) therapy first started to use for local anesthetic toxicity then followed to use for lipophilic drug overdoses according to lipid silk theory. We aimed to detect effect of Intravenous lipid emulsion therapy on synthetic cannabinoid intoxication who presented in emergency department. Methods: This is a retrospective observational study; enrolment period was 2015-2016 for a year period. Patients, who presented in our emergency department (E.D) after use of Bonsai, were all included. Patient’s initial Glasgow Coma Scale (GCS), situation (intubated/non-intubated) and treatment (symptomatic/ ILE) was recorded. Patient’s carbon dioxide value (CO2), GCS differences were compared between the treatments of ILE and symptomatic. ��
Results: 77 patients were included; initial GCS median was 10 (3-15), initial CO2 was 59 (35-109) mmHg. Forty patients were treated with ILE. The number of patient who had endotracheal intubation indications was 43 and the number of intubated patients was 9. ILE treatment had significant effect on C02 and GCS difference. ILE treatment made no difference between intubated or non-intubated patients who had endotracheal intubation indication. Conclusion: Synthetic cannabinoid intoxication could present with hypercapnia and low GCS and treatment is symptomatic likewise; intravenous fluids, benzodiazepines, oxygen administration. In this study we found that ILE therapy helped to decrease CO2 retention and improve GCS. But ILE therapy is not enough to prevent from intubation. Keywords: Intravenous Lipid Emulsion Therapy, synthetic cannabinoid intoxication, bonsai O 140 ASSESSMENT OF PRETREATMENT TETRACYCLINE (T), DOXYCYCLINE (D) AND MINOCYCLINE (M) FOR THE PREVENTION OF ACUTE COCAINE TOXICITY IN A MOUSE MODEL Tarık Bektaş1, Bülent Erdur2, Atakan Yılmaz2, Aykut Yüksel3, Hasan Avcı4, İbrahim Türkçüer2, Mert Özen5, Murat Seyit6
1Yunus Emre State Hospital, Eskisehir, Turkey 2Pamukkale University School of Medicine, Department of Emergency Medicine, Denizli, Turkey 3Istanbul Medeniyet University Göztepe Training and Research Hospital, Department of Emergency Medicine, Istanbul, Turkey 4Afyonkarahisar State Hospital, Afyon, Turkey 5Denizli State Hospital, Denizli, Turkey 6Dumlupınar University Evliya Celebi Training and Research Hospital, Kutahya, Turkey Study Objective: In this study we aimed to evaluate the efficacies of pretreatment Tetracycline, Doxycycline and Minocycline in a mouse model for acute cocaine toxicity. Methods: One hundred twenty male (25-30gr) balb-c mice were randomized to 4 groups in this experimental study.Then all animals received intraperitoneal injections of tetracycline (255mg/kg),D(157mg/kg),M(170 mg/kg) or C (saline only) as a pretreatment. Ten minutes later,all animals intraperitoneally were received 93mg/kg cocaine (an estimated lethal dose to 50%).All of the animals in each group were observed for the seizures (popcorn jumping, tonic-clonic activity,or a loss of the righting reflex) and lethality over the following 30 minutes by a blinded observer. Results: While there were significant differences between D and M group in terms of prevention of seizure compared with placebo,T group was ineffective.There were significant differences between M group in terms of death compared with placebo (p<0.001). However D and T group proportionally reduced the death D group was statistically ineffective (p=0.139) and T group was statistically borderline significant (p=0.055).There were no significant differences among T,D,M groups in terms of seizure, however significant differences among M vs. T in terms of mortality was observed (p=0.030).Seizure rate was observed least in M(73,3%) and D(73,3%) groups and mortality rate was observed least in M(23,3%) compared with the control group (death 73.3%,seizure 93.3% ).The least death was observed in M group and the least seizure was observed in M and D group compared with placebo. Conclusion: According to the results M and D were effective for the prevention of cocaine induced seizure. Although D and T reduced the death rate, they were not as effective as M in terms of prevention of death. As a result we determined that M can be an effective agent in the prevention of cocaine induced seizure and death. Keywords: Cocaine toxicity, doxycycline, minocycline, tetracycline

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
179
O 141 CLINICAL PATTERNS AND OUTCOMES OF BONSAI USAGE Nezih Kavak1, Umut Yücel Çavuş1, R. Pelin Kavak2, Hasan Sultanoğlu1
1Ankara Dışkapı Yıldırım Beyazıt Training and Research Hospital, Department of Emergency Medicine, Ankara, Turkey�2Ankara Numune Training and Research Hospital, Clinic of Radiology, Ankara, Turkey Objective: In our report we aimed to identify the clinical pattern and outcomes of synthetic cannabinoids, namely “Bonsai”. Patients and Methods: Our study has been established in Dışkapı Yıldırım Beyazıt Training and Research Hospital during 01.01.2013-31.12.2015. Including isolated bonsai users retrospectively. The study included 149 patients parameters were age, gender, tension arterial, heart rate, respiratory rate, temperature, Glasgow coma scale, symptoms, primary diagnosis, follow-up durations in emergency room, ICU or ward, need for mechanical ventilation, antidote administration, the effects of antidote administrations, results of cranial computerized tomographies, laboratory results, withdrawal symptoms, toxicity, mortality and morbidity. Data analyses were performed by SPSS for Windows v.18. Results: The correlation between intoxication and age, gender, administration modality, usage frequency, usage duration were insignificant. Agitation, confusion and speech disorders were significantly higher in intoxicated patients while restlessness, headache, sweating and deprival symptoms were significantly higher in non-intoxicated patients(p<0,05). No significant correlation was detected between intoxication and vital parameters, GCS, glucose, BUN, ALT, AST and CK levels (p> 0.05) but CKMB and Creatinine levels were significantly higher (p<0,05). All the patients whom need mechanical ventilation, antidote administration or hospitalization was intoxicated. Duration in hospital was statistically higher intoxicated patients. Patients whom died or required sick leave report was all intoxicated but there was not any correlation between these parameters. Conclusion: As a result, synthetic cannabinoids with their ever changing chemical structure and content may have complex clinical consequences. Despite having difficulties to develop standard treatment and management methods due to continuously changing quality of the drug, more investigations should be performed and guidelines should be established. Keywords: Bonsai, emergency room, synthetic cannabinoids O 142 THE ARRHYTHMIA DEVELOPED BY INORGANIC FLOURINE INTOXICATION Serkan Doğan, Alp Yılmaz, Utku Murat Kalafat, Ali Saglık, Bensu Bulut, Tarik Ocak Istanbul Kanuni Sultan Suleyman Training and Research Hospital, Clinic of Emergency Medicine, İstanbul, Turkey Introduction: Fluorine is one of the essential elements for human body. The fluorine is used in insecticides for agricultural contention. Therefore, the importance of fluorine has been raised in the context of toxicology. Most of the disorders including hypocalcaemia and cellular hypoxia are caused acute fluorine intoxications. The most important side effect that might be mortal is: loosing ability of contraction in heart muscle, arrhythmia, systolic and diastolic function disorders which caused by hypocalcaemia. In this case report, we want to take consider the case hypocalcaemia secondary deathly cardiac arrhythmia caused by mistakenly drinking chemical fluid that contains inorganic fluorine. Case: The patient is 31 years old female who came to emergency service after taking a swig of rust dissolvent Stain-Ex A (contains 15-30 percent inorganic fluorine). Vomiting, short breath, and sore throat were the main complaints of the patient. The general situation of the patient was normal and her vital signs were stable. Patient's physical examination was normal. It was seen in laboratory results that the patient was metabolic acidosis and hypocalcaemia (4.4 mg/dl). During the calcium replacement therapy, it was observed a ventricular tachycardia in the patient. It was given 50 joule for cardioversion. Patient's rhythm turned into normal. During the observation two times ventricular fibrillations (VF) was developed in the patient, so the defibrillation was applied in each VF. Patient was consulted cardiology and internal medicine because of arrhythmia and hypocalcaemia. During the observation the patient hasn't developed arrhythmia, and the calcium level was 7.1 mg/dl following calcium replacement. Patient was transferred to intensive care unit in another hospital Result: As seen also in this case it is important to be aware that the patient be exposed chemical agents requires close follow up and treatment to avoid unwanted complications that might be even mortal. Keywords: Inorganic flourine, intoxication, arrhythmia

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
180
O 143 EXTREMELY LOW FREQUENCY PULSED MAGNETIC FIELD INHIBITS MYOCARDIAL DAMAGE AND APOPTOSIS IN RATS WITH CLP-INDUCED SEPSIS: A HISTOPATHOLOGICAL AND IMMUNOHISTOCHEMICAL
EVALUATION Serkan Gurgul1, Nursah Basol2, Can Demirel3, Fikret Gevrek4, Serkan Yelli4
1Gaziosmanpasa University Faculty of Medicine, Department of Biophysics, Tokat, Turkey 2Gaziosmanpasa University Faculty of Medicine, Department of Emergency Medicine, Tokat, Turkey 3Gaziantep University Faculty of Medicine, Department of Biophysics, Gaziantep, Turkey 4Gaziosmanpasa University Faculty of Medicine, Department of Histology and Embryology, Tokat, Turkey Background&Aim: Sepsis is the most common causes of death in patients with critical illness. It causes myocardial damage (MD) which is one of the main reasons of myocardial-dysfunction. Apoptosis is closely associated with MD and is involved in sepsis-induced myocardial-dysfunction. The potential preventive effects of PMF on SIMD have not been yet investigated. We aimed to investigate whether extremely low frequency (1 mT) may have preventive effects on MD and apoptosis in rats with sepsis. Methods: A total of twenty-eight Wistar-Albino rats were used. Cecal ligation and puncture (CLP) model was used to induce sepsis. The rats were divided equally into four groups as follows: Sham: sham-operated and sham-exposed; CLP: CLP-operated and untreated group; LFPMF: CLP-operated and low frequency (LF; 7.5 Hz) PMF-exposed; HFPMF: CLP-operated and high frequency (HF; 15 Hz) PMF-exposed. The tissue expression levels of Bax, Bcl-2, Caspase-3, and cardiac troponin-I were measured immunohistochemically. Myocardial damage was evaluated histopathologically using myocardial fiber organization system. Results: The increased tissue levels of Caspase-3, Bax and Bax/Bcl-2 ratio and decreased levels of Bcl-2 and cTnI were detected in CLP when compared to those of the Sham group (P<0.05 for all comparisons). On the other hand, the levels of Caspase-3, Bcl-2, Bax, cTnI, and Bax/Bcl-2 ratio in LFPMF and HFPMF were found similar to those of the Sham group (P>0.05). In histopathological evaluation, sham group had normal morphologic view; however, there were widespread degenerative changes in integrity of myofibrils and in organization of myocardial fibers in CLP group. Inflammatory cell infiltrations were also evident in this group. Although a great amount of myocardial cells in LFPMF and HFPMF groups had normal morphological features, myofibrillar degenerations and disorganized fibers were observed in some myocardial cells. Conclusion: This study has demonstrated that ELF-PMF may prevent SIMD and apoptosis via regulating expression of apoptotic proteins. Keywords: Extremely low frequency, pulsed magnetic fields, sepsis, myocardial damage, apoptosis O 144 THE PROGNOSTIC VALUE OF ETCO2 IN SHOCK PATIENTS IN THE EMERGENCY DEPARTMENT
Şadiye Mıdık1, Murat Ersel1, Funda Karbek Akarca1, Özge Can1, Gizem Altınsoy1, İlhan Uz1, Gül Kitapçıoğlu2 1Ege University School of Medicine, Department of Emergency Medicine, Izmir, Turkey 2Ege University School of Medicine, Department of Biostatistics, Izmir, Turkey Objectives: ETCO2 is a noninvasive quickly and easily measurable vital finding. The objective of this study was to determine theprognostic value of EtCO2 and to compare with ABG and other vital signs, in patients treated for shock in the emergency department. Methods: Prospective cross-sectional study was designed to include patients diagnosed as shock in Ege University Department of Emergency Medicine. Vital signs and EtCO2 levels, blood gas analysis outputs and laboratory values on admission were recorded. Those parameters were measured again on the 2nd hour after admission of the patient. SOFA scores were calculated for each patient. First day mortality, internation or externation status were recorded. Results: 300 patients were included in the study. Mean age was 68±16. 46.3% were male. Mortality in the first 24 hours was 16.7%, mortality in the first 30 days was 56.7%. In the patient group who died in the first 24 hours, mean EtCO2 was 17.2 (95% CI:18.4-20.5), while in the patient group who survived, mean EtCO2 was 22.3 (95% CI:23.4-25.2). The difference between these two groups, were considered to be statistically significant (p<0.001). When monitor parameters were compared with ROC analysis by means of predicting 1st day mortality, AUC was largest for EtCO2 (AUC:0.76; %95 GA:0.66-0.84; p<0.001). AUC for 2nd hour control EtCO2 measurements was even larger (AUC:0.81; %95 CI:0.73-0.90; p<0.001). For prediction of 30 day mortality, EtCO2 levels were statistically significant (p<0.001) and AUC was similar to that of 1st day mortality. Cut-off value for EtCO2 was determined as 21mmHg, using the ROC analysis and 50% percentile. For patients with EtCO2 levels<= 21mmHg, sensitivity was 78%, specificity was 52.8% and NPV was 92.3%. Conclusion: EtCO2 may be used to predict mortality in patients with shock. Monitoring EtCO2 in patients with capnography may reveal better clinical results by means of predicting mortality. Keywords: ETCO2, shock, emergency department, mortality, prognostic value

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
181
O 145 THE HIGH RISK OF CONTRAST INDUCED NEPHROPATHY IN PATIENTS WITH SUSPECTED PULMONARY EMBOLISM DESPITE THREE DIFFERENT PROPHYLAXIS: A RANDOMIZED CONTROLLED TRIAL
Suleyman Turedi, Erkan Erdem, Yunus Karaca, Ozgur Tatli, Aynur Sahin, Suha Turkmen, Abdulkadir Gunduz Karadeniz Technical University Faculty of Medicine, Department of Emergency Medicine, Trabzon, Turkey Study Objective: To compare the protective effects of NAC plus normal saline (NS), NaHCO3 plus NS and NS alone in the prevention of contrast-induced nephropathy (CIN) after CTPA. Materials-Methods: This study was planned as a randomized, controlled clinical research. Patients undergoing CTPA on suspicion of PE in the ED and with at least one risk factor for development of CIN were included in one of three different prophylaxis groups. The groups received 3 ml/kg IV NAC+NS or NaHCO3+NS solution or NS alone 1 h before CTPA and 1 ml/kg IV per hour for a minimum of 6 h after CTPA. CIN was evaluated as the primary outcome and moderate or severe renal insufficiency, and in-hospital mortality as secondary outcomes. Results: A total of 257 patients were enrolled in the study. The total level of CIN development was 23.7% (61/257), the level of moderate and severe renal failure was 12.5% (32/257) and the in-hospital mortality rate was 12.8% (33/257). Rates of CIN development in the drug groups were 23.5% in the NAC group (20/85), 21.2% (18/85) in the NaHCO3 group and 26.4% in the NS group (23/87). Rates of development of moderate or severe renal insufficiency were 9.4% in the NAC group (8/85), 10.6% in the NaHCO3 group (9/85) and 17.2% in the NS group (15/87). In-hospital mortality rates were 12.9% in the NAC group (11/85), 11.8% in the NaHCO3 group (10/85) and 13.8% in the NS group (12/87). No difference was determined between the drug groups in terms of CIN, moderate or severe renal injury or hospital mortality. Conclusion: there is a high risk of CIN in patients with suspected PE despite three different types of prophylaxis being administered, and no statistically differences were observed among prophylactic NAC, NaHCO3 and NS in prevention of CIN following contrast-enhanced CTPA. Keywords: Contrast agent, contrast-enhanced computed tomography pulmonary angiography, contrast induced nephropathy, N-acetylcysteine, sodium bicarbonate O 146 EVALUATION OF THE EFFECTIVENESS OF CLINICAL CLASSIFICATIONS IN PATIENTS WHO APPLY TO THE EMERGENCY DEPARTMENT WITH UPPER GASTROINTESTINAL SYSTEM BLEEDING Ahmet Kayalı1, Zeynep Karakaya2, Pınar Yeşim Akyol2, Fatih Esad Topal2, Umut Payza2, Firdes Topal3, Serkan Bilgin2
1Cizre State Hospital, Clinic of Emergency Medicine, Şırnak, Turkey�2izmir Katip Çelebi University Atatürk Training and Research Hospital, Department of Emergency Medicine, İzmir, Turkey�3izmir Katip Çelebi University Atatürk Training and Research Hospital, Department of Gastroenterology, İzmir, Turkey Objective: The study was planned to determine the suitability of using Rockalland Blatchford scoring systems in emergency departments by evaluating their success in estimating the need for endoscopy and hospitalization along with mortality possibilities in upper GIS bleedings. Materials-Methods: Hematemesis, melena, gastrointestinal hemorrhage, hemoptysis, nausea and vomiting, syncope ICD 10 diagnosis codes were entered during the application to the emergency department and 644 patients subject to endoscopy were scanned with 644 patient protocol numbers, 188 patients were included in the study. Rockalland Data about Blatchford scores, patient mortality, hospitalization and discharge were entered into the system. The calculated scores were compared. Results: The general age average was 65,16±16.61.Rockallscore average was calculated as 2.75±1.88, Blatchford score average was calculated as 9.72±3.84. Based on the Rockallscores, 86 (45.7%) of 188 patients were low risk, 102(54.3%) were high risk; whereas based on the Blatchford scores, 9 (4.8%) of the 188 patients were low risk and 179 (95.2%) were high risk. When the reliabilities of the scores were evaluated, it was determined for the Rockall score that the sensitivity value was 73.9% and the specificity value was 45.6%, whereas sensitivity for the Blatchford score was 96.1%and specificity was 10%. Conclusions: In conclusion, risk evaluations carried out using laboratory and clinical findings (Rockall, Blatchford) may be used to generate prediction models for defining the hemorrhage risk that is life threatening in patients with upperGIS bleeding. Early and effective evaluation of the patients along withproper medical and support treatment are very important for the prevention of advanced morbidity and mortality that might occur as a result of upper GIS bleeding. Keywords: Upper GIS bleeding, Rockall scoring, Blatchford scoring, emergency department

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
182
O 147 INCIDENCE OF CONTRAST-INDUCED NEPHROPATHY (CIN) IN PATIENTS UNDERGOING CT IN EMERGENCY DEPARTMENT
Ruşengül Koruk1, Engin Özakın1, Gökhan Temiz2, Nurdan Acar1, Filiz Baloğlu Kaya1, Muzaffer Bilgin3
1Eskişehir Osmangazi University Faculty of Medicine, Department of Emergency Medicine, Eskişehir, Turkey�2Eskişehir Osmangazi University Faculty of Medicine, Department of Nephrology, Eskişehir, Turkey 3Eskişehir Osmangazi University Faculty of Medicine, Department of Biostatistics, Eskişehir, Turkey Objective: The aim of the study is to investigate CIN in patients admitted to the ED who underwent CT contrast. Method: The patients above the age of 18, who admitted to the ED of ESOGU between the dates of 01.11.2015-01.03.2016, and had contrast CT were included prospectively. The demographic data of patients, creatinine values at admission, 24 and 48 hours were recorded. The duration of hospitalization, the discharge, inpatient or intensive care hospitalization, and in which situations they develop nephropathy were evaluated. The 25% enhancement in creatinine value was considered as CIN. Results: 106 patients were enrolled, of whom 52% was male. The mean age was 61.4. While 92 patients were admitted to the hospital, 14 of them were discharged. 5 of 45 patients hospitalized in the service and, 12 of 47 patients hospitalized in ICU were identified as having nephropathy. In none of the discharged patients nephropathy was detected. The mean age of 17 patients, in whom nephropathy developed, was 70.35±14.59 and, the mean age of those, in whom nephropathy did not develop, was 60.06±19.35. In terms of nephropathy development the age difference between the two groups (p=0.04) and between inpatients and ICU hospitalized patients for nephropathy (p=0.036)was found statistically significant. From the perspective of developing nephropathy the rate of underlying risk for the patients hospitalized in ICU was 2,743 in comparison with the hospitalized inpatients(OR=2.743,1.137-8.556 95%CI). When 54 patients, who had the risk of nephropathy as subgroup and were hospitalized and taking hydration before and after contrast, were examined, the development of nephropathy risk was detected as increased 9.857 times in patients hospitalized in ICU in comparison to inpatients (OR=9.857, 1.149 -84.538 95%CI). Conclusion: Age and intensive care unit admission increase the risk for the development of nephropathy itself in patients applying to ED and underwent CT. Keywords: Contrast CT, nephropathy, emergency O 148 EARLY ENDOSCOPY: IS AFFECT PROGNOSIS IN PATIENTS WITH UPPER GI BLEEDING WHO ADMITTED IN THE ED Ebubekir Arslan1, Engin Özakın1, Tuncer Temel2, Aysegul Harmancı Özakyol2, Nurdan Acar1, Filiz Baloğlu Kaya1 1Eskişehir Osmangazi University Faculty of Medicine, Department of Emergency Medicine, Eskişehir, Turkey�2Eskişehir Osmangazi University Faculty of Medicine, Department of Gastroenterology, Eskişehir, Turkey Objective: The purpose of our study is to determine the benefit of endoscopy in early stage and the epidemiological characteristics of patients with non-variceal acute upper gastrointestinal bleeding in the ED. Methods: Patients above the age of 18 with upper gastrointestinal bleeding and being applied endoscopy in the ED between 01.01.2015-31.12.2015 were included. Results: 57.7% of the 104 patients was male and the average age was 58.63. Average arterial pressure was 84,76 mmHg and 96.2% of the patients was hemodynamically stable. 69.2% of patients had additional diseases, 43.3% of them was using NSAIDs. The symptoms at admission were fatigue (81.7%) and syncope (4.8%), respectively. The physical examination signs were hematemesis (64.4%), melena (67.3%) and hematochezia (4.8%). There were not any differences in terms of endoscopic procedure time between mortality, rebleeding, the need for transfusion and surgery intervention. However, the relationship between the patients applied endoscopy in early period with hospitalisation days (p=0.011) and the cost of treatment (p=0.030) was found as significant. We compared the prognosis of 60 patients undergoing high-risk group in terms of the duration of endoscopy according to Glasgow Blatcfhord risk score. The duration of hospitalisation of the patients applied endoscopy in late period was found to be significantly higher (p = 0.033). However, there were no significant differences in transfusion requirement and the rates of rebleeding and treatment costs (p = 1.000, p = 0.077, p = 0.330). There was no need for surgical intervention and mortality did not occur in any patients. Conclusion: In patients with acute gastrointestinal bleeding admitted to the ED, early therapeutic endoscopic procedure is an essential method for accurate diagnosis and successful treatment results. In particular, the endoscopic therapeutic procedures applied in high-risk patients have more positive effect on patient length of stay hospital. Keywords: Gastrointestinal bleeding, early endoscopy, mortality, transfusion needs

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
183
O 149 A BASIC METHOD BY CUNNINGHAM; REDUCTION OF ANTERIOR SHOULDER DISLOCATION İrfan Aydın1, Mehmet Kaan Poyraz1, Abdullah Algın1, İsmail Ağır2, İbrahim Halil Cebe1
1Adıyaman University Training and Research Hospital, Department of Emergency Medicine, Adıyaman, Turkey�2Adıyaman University Training and Research Hospital, Department of Orthopedics, Adıyaman, Turkey This method is developed for the reduction of anterior shoulder dislocation by Neil J Cunningham in 2005. We have done successful shoulder reduction on several patients in our emergency department. We believe that this method should be preferred for anterior shoulder dislocations as a priority because of being a non-invasive, painless and easy method that can be applied by all emergency physicians. Introduction: The most common dislocation occurs in the shoulder joint and the major type is the anterior dislocation. There are many methods for anterior shoulder dislocation reduction. The method which has to be applied with a massage on the shoulder joint developed by Neil J Cunningham in 2005(1, 2), we used on our patients who applied to our emergency service and we have achieved successful results. As the objective of our study, whole emergency services could apply this method successfully on the anterior shoulder dislocation. Cases: Three male patients which are 63, 22 and 27 years old have applied to our emergency department with shoulder pain and limitation caused by trauma. Anterior shoulder dislocation was diagnosed with clinical examination and radiography. The patients were performed shoulder reduction by Cunningham method. Clinical and radiological improvement provided in three patients were discharged with the recommendations (shown on the video). Conclusion: As a result, we claim that using this method has less chance to damage bones and soft tissues (Labrum, Rotator cuf, other ligaments) and axillary nerve. It is a useful and easily applicable method for all emergency services. References 1. Cunningham, Neil J. "Techniques for reduction of anteroinferior shoulder dislocation." Emergency Medicine Australasia 17.5-6 (2005): 463-471. 2. Tintinalli Judith E, “Omuz ve Humerus Yaranmaları”, Tintinalli Acil Tıp Kapsamlı Bir Çalışma Klavuzu, Çeviri Editörü; Yıldıray Çete,2013 Nobel Tıp Kitabevleri. Bölüm 268 sf:1834 Keywords: Cunningham, shoulder, dislocation O 150 THE DIAGNOSTIC VALUE OF SERUM PENTRAXIN 3 LEVELS IN PULMONARY CONTUSION Özgür Tatlı1, Nur Banu Keha Kurt1, Yunus Karaca1, Aynur Sahin1, Ali Aygün2, Elif Sahin3, Burak Katipoglu4, Umut Eryigit1, Suha Turkmen5
1Karadeniz Technical University Faculty of Medicine, Department of Emergency Medicine, Trabzon, Turkey 2Ordu University Training and Research Hospital, Department of Emergency Medicine, Ordu, Turkey 3Karadeniz Technical University Faculty of Medicine, Department of Medical Biochemistry, Trabzon, Turkey 4Ankara Training and Research Hospital, Department of Emergency Medicine, Ankara, Turkey 5Acıbadem University Faculty of Medicine, Department of Emergency Medicine, Istanbul,Turkey Purpose: To investigate the difference in pentraxin 3 (PTX 3) levels between patients with pulmonary contusion and healthy volunteers. Materials and Methods: This study was conducted with a group of 20 trauma patients diagnosed with pulmonary contusion and 30 healthy individuals enrolled as a control group in a tertiary university hospital. Results: Median PTX 3 levels were 7.05 (3.29-13.1), ng/ml in the contusion group and 1.03 (0.7-1.58) ng/ml in the control group. PTX 3 titers were significantly higher in patients with pulmonary contusion compared to those of the control group (p < 0.001). Conclusion: PTX 3 levels in pulmonary contusion increased significantly compared to the healthy control group. If supported by wider series, PTX 3 may be expected to be capable of use as a marker in pulmonary contusion. Keywords: Pulmonary contusion, pentraxin 3, inflammation

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
184
O 151 EFFECTS OF INTRAPERITONEAL AND INTRAVENOUS MESENCHYMAL STEM CELLS ON INFLAMMATORY RESPONSE AND BONE, LIVER TISSUE HEALING IN EXPERIMENTAL POLYTRAUMA RAT MODEL
Ayça Koca Tanriverdi1, Onur Polat1, Yaşar Murat Elçin2, Ayşe Eser Elçin2, Günhan Gürman3, Müge Günalp Eneyli1, Serdar Gürler1, Sinan Genç1
1Ankara University School of Medicine, Department of Emergency Medicine, Ankara, Turkey 2Ankara University Stem Cell Institute, Ankara, Turkey 3Ankara University School of Medicine, Department of Hematology, Ankara, Turkey Objective: Trauma is the most common cause of death of young people in the world. In our study, we aimed to create the closest polytrauma experimental model and investigate the effect of mesenchymal stem cells on liver and bone tissue healing by considering trauma secondary endocrine, metabolic, and inflammatory responses. Materials - Methods: Mesenchymal stem cells were obtained from 20 female donor rats femurs and tibias. 56 male Wistar albino rats weighing 250-300 g were used for the experimental study. After general anesthesia, rats were divided into two groups, polytrauma (liver and bone) (n = 28), and liver trauma group (n = 28). At 36 hours and 5th day after surgey, both rats with polytrauma and with isolated liver injury were injected intravenous mesenchymal stem cells and intraperitoneal mesenchymal stem cells (1.106 cells / kg). Control groups received intravenous and intraperitoneal saline injections. Results: The rats were monitored throughout the study in individually ventilated cages. At day 21 after surgery, after cardiac ponction for laboratory studies, the rats were sacrificed by exsanguination, and liver, tibia and fibula were excised. Whole blood count (white blood cells, hemoglobin and platelets), C-reactive protein (CRP), glucose, alanine aminotransferase (ALT), aspartate aminotransferase (AST), albumin, from blood gas analysis and trauma markers interleukin-1B (IL-1B ), interleukin-6 (IL-6), tumor necrosis factor alpha (TNF alpha) was carried out. Histopathologic examination of liver and bone tissue were evaluated. Conclusion: It was found that ALT, CRP, albumin and İL-1B levels were significantly lower in rats who received MSC (p<0,001). Inflammation of the liver and bone tissue in rats given MSCs were significantly lower than the control group. Keywords: Experimental liver injury, experimental bone fractures, metabolic response, mesenchymal stem cells, polytrauma O 152 EFFECTS OF SPINAL IMMOBILIZATION AT 20 DEGREES ON RESPIRATORY FUNCTIONS Şaban Akkuş1, Şeref Kerem Çorbacıoğlu2, Yunsur Çevik2, Emine Akıncı2, Hüseyin Uzunosmanoğlu2
1Başakşehir State Hospital, Istanbul, Turkey�2Keçiören Training and Research Hospital, Ankara, Turkey Purpose: The present study aimed to investigate whether spinal immobilization with a long backboard (LBB) and semi-rigid cervical collar (CC) at 20 degrees instead of 0 degrees conserves pulmonary functions, including FEV1, FVC, and FEV1/FVC ratio. Material-Method: The study included 56 healthy, adult, non-smoking volunteers who had no acute or chronic diseases. Volunteers were randomly divided into two groups, and those in the first group (Group 1) had LBBs and CCs applied at 0 degrees (n = 30), while volunteers in the second group (Group 2) had LBBs and CCs applied at 20 degrees (n = 26). All volunteers were given pulmonary function tests, which included FEV1 and FVC levels and FEV1/FVC ratios, while in the sitting position. Measurements were repeated at 0, 5, and 30 minutes. Results: Results showed significant decreases in FEV1 and FVC values and FEV1/FVC ratios in group-1 and significant decreases in FEV1 values and FEV1/FVC ratios in group-2 (p<0.001). However, FVC values were not decreased in group-2 when compared to basal levels taken while in a sitting position (p = 0.45). In addition, the study evaluated the amounts of decrease in the FEV1 and FVC levels and the FEV1/FVC ratios (ΔFEV1, ΔFVC, and ΔFEV1/FVC ratio). Results showed that ΔFEV1 values compared to basal levels and levels at 0, 5, and 30 minutes were all lower in Group 2 than in Group 1. However, ΔFEV1/FVC ratios were similar in both groups.��
Conclusion: In trauma patients, especially those suffering from multiple traumas, the oxygen demands of the tissues are increased. Thus, such patients should be prevented from experiencing conditions that cause decreased respiratory function. The results of this and previous studies have shown that traditional spinal immobilization decreases respiratory function, while using spinal immobilization at 20 degrees can reduce this decrease in function. Keywords: Spinal immobilization, long backboard, cervical collar, FEV1, FVC

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
185
O 153 ANALYZING AND REDUCING THE PRESSURE AND PAIN ACCORDING TO TRAUMA BOARD: PHYSIO MECHANICAL WORK
Ali Türkeli1, Onur Polat1, Aydın Öztoprak2, Evren Yaşar3, Müge Günalp Eneyli1, Serdar Gürler1, Sinan Genç1
1Ankara University School of Medicine, Department of Emergency Medicine, Ankara, Turkey 2TOBB University of Economics and Technology, Ankara, Turkey 3Gülhane Training and Research Hospital, Department of Physical Medicine and Rehabilitation, Ankara, Turkey Objective: Spinal backboard is routinely used in all major trauma cases. In this study, we aim to reduce discomfort and pressure pain, via enhancing the spinal backboard with viscoelastic support. Materials-Method: 20volunteers that were asked to lie in the supine position on standard backboards with and without viscoelastic support for 5 minutes each. Occipital, scapular and sacral pressures were measured via pressure gauge matt (XSensor ®) as mm/Hg, in order to compare pressures per minute of both surface area of supported and supportless backboards. The second phase was composed of two periods of 60 minutes during while the volunteers lied supine on standard and viscoelastic supported backboard. The first 10 minutes of each periods took place in a moving ambulance, the volunteers stayed lying in the same supine position for the next 50 minutes. For evaluation of pain 10, 15, 30, 45 and 60 minutes VAS was used. Results: VAS comparison of subjects' visco elastic supported and unsupported trauma board in all interrogation minutes was statistically significant for general pain (p <0.001), occipital region (p <0.001), scapular region (p <0.001) and sacral region (p <0.001). Capillary refill pressure in the occipital region (p = 0.086), and in the scapular region (0,100) in comparison to the remaining surface of the entire surface under pressure were not significant in statistical evaluations in both visco elastic supported and unsupported trauma board groups, but the sacral region statistical evaluation was significant (p <0.001). Conclusion: Viscoelastic support is an important tool for reducing pressure pains over the course of transport and follow up, especially when imaging times is prolonged. It is shown that patient comfort can be enhanced for a low cost and overall pain of trauma patients. Future studies should investigate viscoelastic support backboards role in pediatric trauma patients. Keywords: Backboard, pain, pressure, transport, trauma O 154 WHAT HAPPENS AFTER THE QUITE ENDED EMERGENCY SURGERY ? INTERPRETATION OF C-REACTIVE PROTEIN AND PROCALCITONIN OUTCOMES AS PREDICTIVE MARKERS OF POSTOPERATIVE COMPLICATIONS Serdar Yormaz
Selcuk University Medical Faculty, Department of General Surgery, Konya, Turkey Background: The search for a preoperative marker defining patients at risk for postoperative complications is of great clinical interest. These patients may benefit from intensified monitoring or prophylactic therapies. The aim of this study was to evaluate the role of the C-reactive protein (CRP) and procalcitonin (PCT) in the postoperative course of group in newly diagnosed emergence colorectal diseases retrospectively. Methods: Hundred seventeen colorectal resections with primary anastomosis for emergence newly diagnosed tumors and perforations were evaluated for infectious postoperative complications. Body mass temperature (BMT),WBC, CRP and PCT serum levels were measured on postoperative (PO) 1, 3 and 7. Days.Patients were followed for postoperative all-type of infectious state (IC) and surgical site infections (SSI).Diagnostic accuracy of values was analyzed by de receiver operating characteristics (ROC) curve for each marker. Results: 18 patients had IC (15%), and in 21 cases (18%) SSI were seen. We have found statistically significant differences in BMT on PO3 (p<0.05), neutrophils on PO3 (p<0.05) and PO7 (p<0.05), CRP level on PO1 (p<0.05), PO3 (p<0.05), and PCT level on PO1, PO3 (p<0.05) and PO7 (p>0.05). We have also found statistically significant differences in PCT on PO7 in IC (p<0.05) and SSI (p<0,05) groups. In the ROC analysis, PCT cutoff value of 0.2 ng/ml on PO1 yielded 84% sensitivity(SS) and 52% specificity(SP) (p<0.05), also 0.11 on PO7, 81%SS and 47%SP (p<0.05). In the logistic regression model, the combination of CRP and PCT levels on PO3and PO7 was the best for prediction of postoperative complications. Conclusion: As a result of this CRP and PCT were seemed to be a more sensitive than the other parameters.Also these patients require special attention and probably further diagnostic tests to detect potential inflammatory processes for life-threatening complications. Further prospective trials have needed to test the early diagnostic actions after emergence colorectal surgery. Keywords: Emergency surgery, predictive markers, complications

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
186
O 155 CORRELATION OF TRAUMA SEVERITY SCORES (GAP, RTS, EMTRAS) WITH SHORT TERM MORTALITY IN MULTIPLE TRAUMA PATIENTS: AN OBSERVATIONAL STUDY
Melis Efeoglu Sacak, Haldun Akoglu, Ozge Onur, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Aim: With the increase in the number of admissions to emergency departments, accurate medical triage to sort the severe patients who acquire immediate and intense medical care has become more crucial. Several severity scores have been developed and suggested for this purpose. In this study, correlation between trauma severity scores (GAP, RTS, EMTRAS) and short term mortality in the multiple trauma patient population is assessed and compared with the data in the literature. Method: This study was performed at the Emergency Department of Marmara University Pendik Research and Training Hospital between November 2013 and November 2015. Data was obtained prospectively or through the patient charts retrospectively regarding the principal author was either on duty or off, respectively. Patients with multi-trauma, aged 16 or over, and with informed consents were included. Demographic data, Glasgow Coma Scale score and data acquired for severity score assessments were recorded. Correlation between 30-day mortality rates and trauma scores was assessed. Results: 184 patients with multiple trauma were included. Median age was 38 years (interquartile range: 29,50 – 50,0). 160 patients were male (87%) and 24 were female (13%). RTS and GAP scores of all 184 patients and EMTRAS scores of 144 patients were measured. In accordance with the ROC curve values, GAP and EMTRAS were found to be the most accurate of severity scores to indicate 30-day mortality (AUC for GAP, RTS, EMTRAS were 0,947 ± 0,021 %95 CI, 0,904-0,975 , 0,898 ± 0,038 %95 CI, 0,844-0,938 , 0,957 ± 0,016 %95 CI, 0,910-0,984 , respectively (p<0,0001)).��
Conclusion: Data obtained in this study suggests that routine application of EMTRAS and GAP scores in emergency departments may ensure distinguishing severe trauma from less severe for providing more rapid and better health care. Keywords: Multiple trauma, GAP, EMTRAS, RTS, mortality O 156 MISSED INJURIES IN HOSPITALIZED TRAUMA PATIENTS IN THE EMERGENCY DEPARTMENT Serhat Örün1, Ayhan Aköz2, Ali Duman2
1Iğdır State Hospital, Emergency Clinic, Iğdır, Turkey�2Adnan Menderes University Faculty of Medicine, Department of Emergency Medicine, Aydın, Turkey Objective: Intensive emergency department bring along to medical errors with trauma care for unstabil patients. The aim of our study; determine the extent of missed injuries, causes, clinical adverse consequences in hospitalized patients with trauma in a Turkish Level 3 emergency department and provide recommendations to emergency service workers and supervisors to reduce them. Materials-Methods: In the study; patients who are admitted to the emergency room with trauma, were examined by a emergency physician and if necessary by a consultant. Injuries that detected were recorded to case forms. Hospitalized patients were discharged from hospital when their treatment was completed. Their files have been reviewed and investigated new injuries that was different from recorded in the case form. Results: Total 515 trauma patients who were hospitalized included in our study. There were 20(3,9%) patients who have missed injury. 65% of missed diagnosis were about the musculoskeletal system. There were insufficient clinical evaluation 95% of the patients who have missed diagnosis and in 70% of missed diagnosed cases radiology reports were delayed or incorrect reporting. Missed diagnosed patients were consulted 2(1-2,75), non-missed diagnosed patients were consulted 1(1-2). When compared the two groups of the number of consultation there were statistically significant difference. The 40% of missed diagnosed patients were not consulted to the relevant departments but 60% of missed diagnosed patients were consulted to the relevant departments. Conclusion: As a result of missed diagnoses increse if the trauma patients don't examined by the experienced trauma team, and if consultant physician don't have enough knowledge and experience. We believe that missed diagnosis rate can be reduced in trauma patients with fast and reliable radiological support, secondary and tertiary examination and the intervention of a multidisciplinary trauma team Keywords: Emergency department, missed diagnoses, trauma

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
187
O 157 SPONTANEOUS RESOLUTION OF ACUTE SUBDURAL HEMATOMA Sinan Karacabey1, İskender Samet Daltaban2, Hakan Ak2, Fatih Ahmet Kahraman1
1Bozok University Faculty of Medicine, Department of Emergency Medicine, Yozgat, Turkey 2Bozok University Faculty of Medicine, Department of Neurosurgery, Yozgat, Turkey Introduction: Acute subdural hematoma (ASDH) is a severe insult with a mortality rate of 60%-80%. Most cases undergo surgical removal of ASDH or external decompression except for inoperable patients with irreversible brain stem injuries or poor general condition. Case: A 19 month-old girl presented to Emergency Department after fall from 1 meter height. She vomited three times before presentation. On admission pupils were isochoric and reacted normally to light. No motor weakness was noted. CT 1 hour after injury disclosed a subdural hematoma with a thickness of approximately 0.55 cm in the left frontotemporoparietal region without midline shift. She was consulted to Neurosurgery and admitted to hospital. No treatment was given to the patient. Additional findings, such as cerebral contusion and cerebral swelling, were not recognized. CT was obtained …… hours after injury showing that the hematoma and midline shift had almost totally disappeared. An operation and medical treatment was not done because of the disappearance of the hematoma.��
Discussion: There have been several reports describing mechanisms of spontaneous ASDH resolution. Polman et al. indicated that although CT showed the hematoma had completely disappeared, MRI demonstrated redistribution rather than disappearance of the blood in the subdural space. Kuroiwa et al. reported that the volume of the interhemispheric subdural hematoma increased as the size of ASDH decreased, which suggested redistribution of the blood. Makiyama et al. speculated that ASDH was obliterated by pressure induced by acute cerebral swelling in their cases and emphasized that cerebral swelling was necessary. On the other hand, Nagao et al. speculated that a pediatric case, the hematoma was exposed, diluted, and washed out by participation of the CSF secondary to tearing of the arachnoid membrane. Keywords: Acute subdural, spontaneous resolution, trauma O 158 COMPARISON OF SCORING SYSTEMS IN PEDIATRIC TRAUMA PATIENTS Hasan Sultanoğlu1, Seda Özkan1, Tuba Erdem Sultanoğlu2, Nezih Kavak1
1Dışkapı Yıldırım Beyazıt Training and Research Hospital, Emergency Health Care Department, Ankara, Turkey 2Kazan State Hospital, Clinic of Physical Therapy and Rehabilitation, Ankara, Turkey Objective: in our research we aimed to evaluate and compare the performans of BIG score (Baz deficite, INR, GCS), pediatric trauma score (PTS), revised trauma score (RTS), injury severity score (ISS), new injury severity score (NISS) in mortality and stay intensive care unit. Patients and Methods: Patients under 18 age admitted to Dışkapı Yıldırım Beyazıt Education and Research Hospital with multiple trauma between 1 July 2012- 1 July 2016. Were included in the research which is retrospective. Demographic data, vital in the emergency department, trauma location, injurity severity indexes (BIG, PS14, PTS, RTS, ISS, NISS, GCS) and follow up of patients were examined. Data was evaluated with SPSS 17. Results: 1510 patient were included, %40.5 (n=612) were female and %59.5 (n=898) were male. Mean age was 7.81±4.847 mortality was %4.2. The best score to evoluate mortality was PS14 (AUC; 0.994, sensitivity %96.51, specifity %99.64) following in order was NISS, ISS, GCS, BIG, RTS and PTS. The best score to forsec the stay in ICU was found as NISS (AUC; 0.936). The most sensitivite system was NISS and PS14 (%94.88) and the most specific was NISS (86.69). PS14 was the first to evoluate the survival. In our research %94.3 of patient had blunt trauma and %5.7 had penetrating trauma. For blunt traumas PS14 was found the best score to determine survival and mortality. Conclusion: For penetrating traumas PS14 is the first score and the others are very close to this. For pediatric trauma patients PS14 is the best score to evaluate mortality and survival, for see to need NISS is and also all scores are close to each other. Especially new PS14 can be used as a stronge scoring system in all pediatric trauma patients regardless penetrating or blunt. Keywords: Pediatric trauma, trauma scores, mortality, morbidity

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
188
O 159 RELATION WITH ATTENTION DEFICIT/HYPERACTIVITY DISORDER AT PATIENTS ADMITTING EMERGENCY SERVICE WITH PRESENTATION OF OCCUPATIONAL INJURIES
Sadık Oğuz Doğanlı1, Bülent Erdur2, Atakan Yılmaz2, İbrahim Türkçüer2, Mert Özen3
1Ardahan State Hospital, Ardahan, Turkey 2Pamukkale University School of Medicine, Department of Emergency Medicine, Denizli, Turkey 3Denizli State Hospital, Denizli, Turkey Study Objective: Adult attention deficit/ hyperactivity disorder(AADHD), we think it is one of the essential problems of social health and health service for it’s adverse effects on patient’s social, work and academic life and a major cause of occupational injuires. That’s why taking precautions reducing risks related to attention deficit/hyperactivity disorderbefore occupational injuries is taken place is extremely important.In this study, patients who admitted to Pamukkale university hospital adult emergency service with the presentation of occupational injury are evaluated for AADHD. Method: Then Number Series Test, Stroop Test and Prof Dr Atilla Turgay‘s Test’s second chapter which searchs the hyperactivity dominant type of AADHD are performed. These three tests used for scanning AADHD and gives a result of significant or insignificant(140 patient). Also same three tests used for scanning AADHD performed on 140 patients in control group. Data gathered from study and control groups are analyzed with SPSS ‘Statiscal Package for Social Scienses’ for Windows 17 programme. ��
Findings: According to tests we used in our study (Number Series Test, Stroop Test and second chapter of Prof Dr Atilla Turgay’s Test) occupational injury cases which are positive for AADHD, gender and age are not related factors with occupational injury. When age, gender and number series test are added to model and it is evaluated with logistic regression analysis, it shows positive number series test cases are 7.3 times more likely to have an occupational injury. Our study shows as education level of patients presented with occupational injury decreases, AADHD frequency becomes more common according to Stroop Test and Number Series Test. Our findings show experience of work reduce the risk of occupational injury. Conclusion: This study shows positive number series test cases are 7.3 times more likely to have an occupational injury. Keywords: Occupation injury, adult, attention deficit, hyperactivity disorder O 160 DETERMINING THE EFFECTIVENESS OF ULTRASONOGRAPHY IN THE EVALUATION OF PNEUMOTHORAX, RIB FRACTURE, AND HEMOTHORAX WITH IMAGING TECHNIQUES AMONG THE PATIENTS PRESENTED TO EMERGENCY DEPARTMENT WITH BLUNT THORAX TRAUMA Halil Çetinkaya1, Yücel Yüzbaşıoğlu2, Mehmet Akif Karamercan3, Yavuz Katırcı4, Figen Coskun5
1Samsun Gazi State Hospital, Clinic of Emergency Medicine, Samsun, Turkey 2Ataturk Training and Research Hospital, Clinic of Emergency Medicine, Ankara, Turkey 3Gazi University Faculty of Medicine, Clinic of Emergency Medicine, Ankara, Turkey 4Ankara Keçiören Training and Research Hospital, Clinic of Emergency Medicine, Ankara, Turkey�5Kırıkkale University Faculty of Medicine, Department of Emergency Medicine, Kırıkkale, Turkey Aim: This study is designed to determine the efficacy of ultrasonography (USG) in the diagnosis of pneumothorax, rib fracture, and hemothorax among the patients presented to emergency department with blunt thorax trauma, and appropriateness of USG for emergency room usage for his purpose. Material-Method: This study was prospectively performed in patients who were over 16 years old and presented to Ankara Training and Research Hospital Emergency Department with blunt thorax trauma between 15 January 2011 – 15 July 2011. Patients were evaluated initially with bedside USG and results were recorded. After that supin antero posterior chest radiography (SAPCR) and thorax computerized tomography were performed. The results were analized statistically. Results: One hundred (%80.6) male and twenty four (%19.4) female, totally 124 patients were included in this study. For pneumotorax USG sensitivity, specificity, positive and negative predictive values were 84.2%, 100%, 100% and 93.5%; and SAPCR sensitivity, specificity, positive and negative predictive values were 57.9%, 100%, 100% and 83.31% respectively. For hemothorax USG sensitivity, specificity, positive and negative predictive values were 92.6%, 100%, 100% and 98%; and SAPCR sensitivity, specificity, positive and negative predictive values were 25.9%, 100%, 100% and 82% respectively. For rib fractures USG sensitivity, specificity, positive and negative predictive values were 89.8%, 96.9%, 96.4% and 91.3%; and SAPCR sensitivity, specificity, positive and negative predictive values were 54.2%, 98.5%, 98.5% and 70.3% respectively. Conclusion: Our study demonstrates superior sensitivity and less diagnostic time of bedside USG, compared to SAPCR, for identification of pneumothorax and hemothorax in adults suffering blunt thorax trauma. Although bedside USG is more sensitive than SAPCR in diagnosis of rib fractures due to longer application time it has limited usage in the emergency room. Keywords: Ultrosonography, pneumothorax, hemothorax, rib fractures

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
189
O 161 BODY MASS INDEX AND RISK OF POSTOPERATIVE RESPIRATORY COMPLICATIONS IN PATIENTS WITH PERFORATED APPENDICITIS: AN EMERGENCY-BASED WORKOUT
Burcu Yormaz1, Ilhan Ece2, Serdar Yormaz2
1Beyhekim State Hospital, Clinic of Chest Diseases, Konya, Turkey 2Selcuk University Medical Faculty, Department of General Surgery, Konya, Turkey Background: Morbid obese patients are thought to be at higher risk of postoperative pulmonary complications. We have determined whether body mass index (BMI) is associated with postoperative complications following perforated appendicitis. Methods: We were conducted a patient-based study between the years of March 2015 to May 2016. BMI was categorized as normal (18.5-24.9 kg/m2), overweight (25.0-29.9 kg/m2), obese (> or = 30 kg/m2) and morbid obese (>40 kg/m2). Postoperative pulmonary complications were assessed. Complication rates were estimated for each BMI category and overall rates were assessed using logistic regression modeling. Results: There were 84 (35%) normal, 64 (27%) overweight, 57 (23.5%) obese, and 35 (14.5%) morbid obese appendectomy (mean age, 32,6 +/- 11,3 years; 60% female, 40% male ). After adjustment, the risk of developing an inpatient pulmonary complication for each BMI category, compared to normal BMI, was: overweight (P = 0.247), obese (P = 0.012) and morbid obese (P = 0.007). Analysis demonstrated that history of chronic obstructive pulmonary disease (COPD) or asthma (P = 0.02), older age (P < 0.01) contributed to an increased risk of developing a postoperative pulmonary complication. Morbid obese patients had higher mortality rates in length of stay in hospital than normal BMI patients (P = 0.012). Conclusion: BMI has more significant effect on postoperative pulmonary complications in appendectomy patients. These results reduce that morbid obese, overweight appendectomy patients have higher pulmonary risk at postoperative period. Keywords: Emergency, pulmonary, BMI O 162 FALLING FROM HEIGHT Eren Sert, Alp Yılmaz, Serkan Dogan, Rabia Birsen Tapkan, Tarik Ocak Istanbul Kanuni Sultan Süleyman Training and Research Hospital, Clinic of Emergency Medicine, İstanbul, Turkey Object: Trauma is one of the common cases in emergency clinics and this patients can be seen with different clinical presentations from simple soft tissue injuries to life threating conditions. With this study, we wanted to share a nightmarish case of falling from height. Case: Forty-two years old male patient was brought by 112 teams with declaration of to fall from the 6th floor. The patient was taken to the resuscitation room. The patient's vital signs were stable. The patient had been monitorized close. Necessary laboratory and imaging tests had been ordered. Two rebars were observed, one of them had been entered from anterolateral and exited from anteromedial of the bottom of the right thigh. The other one had been entered from inferior of right angulus mandibula and exited from right parietal area. Both of the shoulders were deformed. On the CT scan, it was observed fractures of mandibula, right maxillar sinus medial and lateral wall, sella,right ethmoidal and frontal sinus, right orbita walls and deformation of righ tbulbus oculi. Metalic material had been continued its way in the frontal and parietal lobe and caused to fractures of right temporal and frontal bones. Also its observed pulmonary contusion, free fluid in the pelvis, fracture of humerus, 12th right costa, lomber vertebras, right ramus pubis, right acetabulum and sacrum. After the consultation of relevant clinics, the patient had been referred to a further center in terms of the necessary materials to cut the iron bars and for the operation by at least three relevant clinics. Conclusion: A wide angle, multidisciplinary aproach is essential to gross traumas in an emergency center of a third grade hospital as seen in our case. And we think that an urgent interruption can decrease mortality and morbidity. Keywords: Falling, trauma, iron bar

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
190
O 163 THORACIC TRAUMA PATIENTS IN A TERTIARY HOSPITAL: LAST YEAR'S EXPERIENCE Serhat Yalçınkaya1, Emine Kadıoğlu2, Zeki Tahsin Yapakçı3, Mehmet Suat Patlakoğlu3
1Dumlupınar University Medical School, Department of Thoracic Surgery, Kütahya, Turkey�2Dumlupınar University Medical School, Department of Emergency Medicine, Kütahya, Turkey�3Evliya Çelebi Hospital, Clinic of Thoracic Surgery, Kütahya, Turkey Aim: Thoracic trauma is a frequent cause of emergency rooms administration. It may be accompanied with head, bone and abdominal injuries. We work at the only tertiary hospital localized in Kutahya and are the first and the last step of medical treatment for such trauma patients. We would like to share our experience with thoracic trauma patients we treated within the last year. Materials-Methods: Following the institutional board approval, the files of the patients administered to our emergency department between 01 January 2015 and 31 December 2015 were reviewed. Age, gender, type of trauma, site of trauma, diagnosis, treatment modality, length of hospital stay, and outcome were noted. The patients with multiple system trauma and needed intensive care were excluded. Results: Between the aforementioned period 1408 patients referred to our emergency department due to various types of trauma. Of these patients, 103 were consulted to Thoracic Surgery Department and only 12 patients had pure thoracic trauma. There were 10 (83%) male and 2 female patients with a median age of 51 years (range 29-79 years). Eight patients (67%) were administered due to car accidents. Three patients had isolated rib fractures, 3 had traumatic pneumothorax, 2 had rib fractures and traumatic pneumothorax, 2 had sternal body fracture, 1 had rib and sternal body fracture, and 1 had rib and sternal body fracture with traumatic hemothorax. The injuries were on the right side in 5, left side in 4, and bilateral in 1 patient. Average length of hospital stay was 5.3 ± 3.3 days (range 3-12 days). ��
Conclusion: Thoracic trauma is a frequent cause of emergency department administration. Of the patients consulted for thoracic trauma, only less than 10 % have pure thoracic trauma. The remaining 90 % have multiple system trauma and mostly are administered to intensive care units. Keywords: Rib fracture, sternal body fracture, thoracic trauma, traumatic pneumothorax, traumatic hemothorax

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
191
O 164 ACİL SERVİSTE HİPERGLİSEMİ: STRES HİPERGLİSEMİSİ VEYA YENİ TANI DİYABET Murat Koyuncu1, Sümeyra Koyuncu2, Serap Biberoğlu1, Ali Ramazan Benli3, Serhat Koyuncu4, Bahri Atlı5, Şenol Kadir Köstekçi5, Duygu Yılmaz6, Güleser Akpınar7
1Karabük Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Karabük�2Tokat Devlet Hastanesi, İç Hastalıkları Servisi, Tokat�3Karabük Üniversitesi Tıp Fakültesi, Aile Hekimliği Anabilim Dalı, Karabük�4Gaziosmanpaşa Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Tokat�5KBÜ Karabük Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Karabük�6Hitit Üniversitesi Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Çorum�7Şişli Hamidiye Etfal Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Giriş: Tüm dünyada morbidite ve mortalitenin en önemli nedenlerinden biri olan Diabetes Mellitus (DM), sıklığı, yaşlı nüfus ve obezite ile birlikte gittikçe artmaktadır. Stres hiperglisemisi (SHG) tanımı ilk olarak 1877’de Claude Bernard tarafından ortaya koyulmuş ve acil serviste sık karşılaşılan klinik durumlardan biridir. Özellikle hastalıkların akut dönemlerinde ve travma sonrası hastalarda gelişen SHG diyabetik olmayan ve diyabetik bir çok acil servis hastasında görülmektedir. �Bu çalışma ile Acil Servise çeşitli nedenlerle başvuran ve kan glukoz düzeyi 200mg/dL ve üzeri çıkan hastalar da diabetes mellitus gelişme insidansını tespit ederek, DM öyküsü olmayan, kan şekeri yüksek çıkan hastalarda DM yönünden ileri tetkik gerekip gerekmeyeceği tartışmak amaçlandı.��
Gereç-Yöntem: Bu çalışma için etik kurul onayı alındı. Acil servisine çeşitli nedenlerle başvurmuş ve Kan Glukoz düzeyi yüksek tespit edilen hastaların dosyaları retrospektif olarak incelendi. Hastaların demografik verileri, kan şekeri düzeyi, acil servise geliş öncesi ve sonrası diyabet tanısı alıp almadığı, acil servise başvuru harici başvurusu olup olmadığı, birden fazla başvurularda acil servis başvurusu sonrası tetkik yapılıp yapılmadığı, acil servis başvurusu sonrası tetkik yapılmış ise kan şekeri düzeyi incelendi.� Tartışma: DM hastalarının %46’sı tanı konmadan yaşamaktadır. Hastanede yatan hastalarda katabolik hormonların ve hepatik glukoneogenezin artması, ayrıca periferal ve hepatik insülin direnci nedeniyle hiperglisemi görülebilmektedir. Aşırı dekstroz verilmesi de hiperglisemiyi artırabilmektedir. Diyabete bağlı hiperglisemi ile karşılaştırıldığında SHG nin mortaliteyi daha fazla artırdığını gösteren çalışmalar mevcuttur. Akut hastalık geçtikten sonra SHG sıklıkla düzelmektedir. Ancak, hastaneye kabulde yeni hiperglisemi saptanan hastaların %60'ına bir yıl içinde diyabet tanısı konması nedeniyle hastalar takip edilmelidir. �Çalışmamızda, kan şekeri tekrar başvurularında yüksek çıkan, ancak herhangi bir tanı ve tedavi almayan hastaları içeren Gurup 3 te ise %29,2 gibi azımsanamayacak bir oran bulunmaktadır. Tanı konmamış hastaların mortalite ve morbidite oranı yüksek olan komplikasyonlarla başvurabileceği bilinmektedir. Bu nedenle DM riski olan hastaların tespit edilerek tedaviye ve DM konusunda eğitime alınması gerektiğini düşünmekteyiz. Anahtar Kelimeler: Diabetes mellitus, stres hiperglisemisi, kan glukoz düzeyi

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
192
O 165 AKUT APANDİSİT TANISINDA ALVARADO SKORU VE C-REAKTİF PROTEİNİN ETKİNLİĞİNİN SAPTANMASI Vehbi Özaydın1, Fatma Sarı Doğan2, Merve Güneş2, İsmail Fırat Arslan3
1İstanbul Medeniyet Üniversitesi Göztepe Eğitim ve Araştırma Hastanesi, İstanbul �2Sağlık Bilimleri Üniversitesi Kartal Dr. Lütfi Kırdar Kartal Eğitim ve Araştırma Hastanesi, İstanbul�3İstanbul Esenyurt Devlet Hastanesi, İstanbul Giriş: Apandisit, abdominal acillerin en sık sebebi olup hayat boyu apandisit ile karşılaşma oranı %7 civarındadır ve en sık 15 ile 30 yaş arasında görülür. Apandisit; vermiform apendiksin tıkanıklığı sonucu gelişir. Akut apandisitte klinik tanı ön plandayken, diğer taraftan negatif laparatomi oranın azaltmak için skorlama sistemleri, akut faz reaktanları ve görüntüleme kullanılmaktadır.�Alvarado skorlama sistemi, apandisit tanısı için en sık kullanılan skorlama olup; üç semptom(iştahsızlık, sağ alt kadrana yayılan ağrı, bulantı-kusma), üç belirti(sağ alt kadran hassasiyeti, sağ alt kadranda rebound, ateş) ve iki labaratuvar bulgusu (lökositoz, sola kayma) kullanılmaktadır. Çalışmanın amacı acil servise karın ağrısıyla başvuran hastalarda Alvarado skorlamasının tanı için yeterliğini araştırmak, akut apandisit için C-Reaktif Proteinin (CRP) tanı koymadaki yeri ve cut off değerini saptamaktır.��
Metot: Prospektif gözlemsel olarak planlanmış olan çalışmaya, bir yıl süre ile acil servise karın ağrısı ile gelen akut apandisit ön tanısı alan hastalar dahil edilmiştir. Hastaların Alvarado skorları ve CRP değerleri kaydedilip, taburcu olanların telefon ile izlemi, cerrahi tedavi yapılanlarda ise histopatolojik tanı pozitifliği karşılaştırılmıştır.��
Bulgular: Çalışmaya 212 hasta katılmış olup, hastaların %59 apandisit tanısı almıştır. Alvarado skor belirteçlerinden ateş, lökositoz ve sola kayma istatistiksel olarak anlamlı saptanmıştır. Reciever Operating Charactheristics (ROC) analizinde Alvarado skoru AUC 0,714 (%95CI 0,648-0.774), CRP AUC 0,658 (%95CI 0,590-0,722) saptamıştır. Apandisit patolojik tanısı pozitif olan hastalarda, Alvarado skoru ortanca değeri 7 saptanmış olup, cut off > 7 spesifitesi %80,4 ve CRP’ nin ortanca değeri 2,1 olup, cut off > 2,1 spesifitesi %71,2 saptanmıştır. Lojistik regresyon analizinde ise CRP anlamlı saptanmayıp modelden dışlanmıştır.� Sonuç: Alvarado skoru, düşük skorlarda apandisit dışlama için yeterli olmayıp, skoru > 7 olanlar içinse kesin cerrahi kararı verdirmez. CRP ise, apandisit tanısı için anlamlı olsa bile, skorlama içinde anlamlı olmayıp tek başına dışlama ve tanı koyma kriterine sahip değildir. Anahtar Kelimeler: Alvarado skoru, apandisit, c- reaktif protein, acil servis O 166 TÜRKİYE’DE YAPILMIŞ ACİL TIP UZMANLIK TEZLERİNİN DEĞERLENDİRİLMESİ VE BİLİMSEL LİTERATÜRE KATKILARI Mustafa Köksal, Oğuz Eroğlu, Figen Coşkun Kırıkkale Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Kırıkkale Giriş: Ülkemizde toplam 86 klinikte Acil Tıp Uzmanlık (ATU) eğitimi verilmektedir. Çalışmamızın tamamlandığı Ocak 2015 tarihine kadar 1144 hekim, ATU olmuştur. Çalışmamızda Türkiye’de yapılan ATU tezlerinin demografik özellikleri ve bilimsel literatürdeki yeri değerlendirilmiştir.��
Gereç-Yöntem: YÖK Ulusal Tez Merkezinden ve Eğitim Araştırma Hastanesi (EAH) arşivinden elde edilen ATU tezleri incelendi. Tezlerin yayınlanma durumu, tez yazarının ve/veya tezin ismiyle Google Akademik, TR Dizin, PubMed, Web of Science’de araştırıldı. Tezlere ait konu başlıkları, araştırma yöntemleri, tez danışmanı, seçilen hasta ve/veya hastalık grupları, yayınlanma düzeyleri ayrı ayrı değerlendirildi. Elde edilen veriler SPSS 21.0 programı kullanılarak analiz edildi.��
Bulgular: Çalışma kapsamındaki 782 ATU tezinin %85’i devlet üniversitelerinde, %10.7’si EAH’de, %3.3’ü GATA’da, %1’i özel üniversitelerde yapılmıştır. Tezlerin %44’üne doçent, %35’ine yardımcı doçent, %17’sine profesör doktorlar danışmanlık yapmıştır. Tez danışmanlarının %75’i ATU, %25’i diğer uzmanlık dallarında görevlidir. Tez konusu dağılımı incelendiğinde ilk sırada “Kardiyovasküler sistem acilleri” (%14.2) ve ikinci sırada “Travma” (%13.2) gelmektedir. Yapılan tezlerin %76’sı prospektif, %24’ü retrospektif olarak planlanmış; %50’sinde gözlemsel, %28’inde metodolojik, %22’sinde deneysel araştırma yöntemi kullanılmıştır. İncelenen tezlerin %37’si daha sonra makale olarak yayınlanmış, tüm tezlerin %18’i; makale olarak yayınlananların ise %48.6’sı SCI’da dizinlenmiştir. Üniversite, EAH ve GATA’da yapılmış tezlerin yayınlanma oranları arasında istatistiksel farklılık saptanmış olup, en çok üniversitelerde (%38.8) yapılan tezler yayın haline getirilmiştir. Ancak SCI’da dizinlenme oranına bakıldığında GATA’da (%86) yapılan tezlerin SCI dergilerde yayınlanma oranı daha fazladır (p<0.05). Profesör ve yardımcı doçentlerin danışmanlık yaptığı tezlerin (sırasıyla %42; %40) yayınlanma oranı daha fazla olduğu tespit edilmiştir. ATU’nın danışmanlığını yürüttüğü tezlerde yayınlanma oranı %33 iken, ATU dışındaki uzmanların danışmanlığını yürüttüğü tezlerde yayınlanma oranı %48’dir (p<0,05). Prospektif planlanan tezlerin genel yayınlanma oranları %38.9 ve SCI dergilerde yayınlanma oranı %52.2’dir.��
Sonuç: Prospektif planlanan, profesör danışmanlığında, üniversitelerde yürütülen çalışmaların yayınlanma oranlarının daha yüksek olduğu saptanmıştır. Genel ve SCI dergilerde yayınlanma oranı, Türkiye ortalamasına göre yüksek olup; uluslararası literatüre bakıldığında başarılı kabul edilebilir. Anahtar Kelimeler: Acil tıp, bilimsel yayın, bilimsel indeksler, tez, Türkiye

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
193
O 167 RADYOAKTİF İYOT ALIMI SONRASI ACİL SERVİSLERE BAŞVURAN HASTALARIN GÜNLERE GÖRE RADYOAKTİVİTE DÜZEYİ
Serhat Koyuncu1, Serdar Savaş Gül2, Serhat Karaman1
1Gaziosmanpaşa Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Tokat�2Gaziosmanpaşa Üniversitesi Tıp Fakültesi, Nükleer Tıp Anabilim Dalı, Tokat Tiroid dokusunun radyoaktif iyot ile ablasyonu nükleer tıp pratiğinde tiroid kanserinde cerrahi sonrası sıklıkla başvurulan bir tedavi yöntemidir. Radyoaktif iyot alımı sonrası hastaların gelişebilecek komplikasyon ve diğer nedenlerle acil başvuruları görülmektedir. Hastaların acil başvuru esnasında radyoaktivite miktarının bilinmezliği, acil servis personelinin ve diğer hastaların sağlığı açısından risk taşıyabilmektedir. Bu çalışmadaki amacımız radyoaktif madde verilen hastaların günlük radyoaktivitesini belirlemek ve bu sayede acil servise kabulü sırasında alınacak önlemlerin seviyesini belirlemektir.��
Yüksek doz I-131 tedavisi uygulanan 38 hasta (29K, 9E, Yaş ortalaması 50,2±15,6) çalışmaya dahil edildi. Hastalara yüksek doz I-131 tedavisi verilmesinin ardından radyoaktif tedavi odasında kalışları süresince Geiger Müller tipi radyasyon ölçüm cihazı ile 1m uzaklıktan mR/h olarak radyoaktivite ölçümleri yapıldı. ��
Tedavi verilen 35 hastada Papiller Tiroid kanseri ve 3 hastada ise Folliküler Tiroid Kanseri tanısı mevcuttu. 25 hastaya 100 mCi, 9 hastaya 150 mCi, 4 hastaya 200 mCi I-131 ile ablasyon tedavisi uygulandı. Hastaların I-131 verilmesinden sonra, 1., 2. ve 3. günlerdeki radyoaktivite ölçümleri yapıldı. Birinci gün içerisinde radyoaktivite miktarında önemli bir azalma olduğu (r= %96), diğer günlerde ise daha yavaş bir azalma olduğu görüldü (r= %39). İlginç olarak hastalara verilen radyoaktif iyot miktarı ne olursa olsun 2. ve 3. günde hastaların radyoaktivite miktarlarının birbirine yakın olduğu saptandı. ��
Tiroid kanseri ve hipertiroidi tedavisi amacıyla verilen radyoaktif iyot uygulaması gittikçe yaygınlaşmaktadır. Radyoaktif iyot alan hastalar ilk 3 gün 3mR/h değeri üzerinde radyoaktivite bulunduğundan acil servise başvurularında radyasyon güvenlik önlemlerinin alınması gerekli olduğu görülmüştür. Özellikle radyoaktif iyot alan hastalar 3. günden sonra radyoaktivite düzeylerinin 3mR/h değeri altına düştüğü görülmüştür. Radyoaktivite açısından taburculuk sınırı olarak görülen 3mR/h değeri altında olsa da hastalar bebek ve hamilelerden izole edilmelidir. Anahtar Kelimeler: Radyoaktif iyot, acil servis, radyasyon güvenliği O 168 ACİL SERVİSTE HİPONATREMİ TESPİT EDİLEN HASTALARIN ETYOLOJİK DEĞERLENDİRİLMESİ VE HASTALARIN SERUM NGAL DÜZEYLERİNİN PROGNOZ ÜZERİNE ETKİLERİ
Nezihat Rana Dişel1, Selçuk Matyar2, Saime Paydaş3, Ayça Açıkalın1, Ebru Çil Direk1, İlker Ünal4, Ahmet Sebe1
1Çukurova Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Adana�2Çukurova Üniversitesi Tıp Fakültesi, Merkez Laboratuvarı, Adana�3Çukurova Üniversitesi Tıp Fakültesi, Dahiliye Nefroloji Bilim Dalı, Adana�4Çukurova Üniversitesi Tıp Fakültesi, Biyoistatistik Anabilim Dalı, Adana Giriş-Amaç: Hiponatremi neden ya da sonuç olarak (siroz, kalp yetmezliği, böbrek yetmezliği, hipotroidi, sürrenal hastalıklar, uygunsuz ADH sendromu, ilaçlara bağlı vs.) böbrek yetmezliğine sıkça eşlik eder. Nötrofil jelatinaz ilişkili lipokalin (NGAL) akut böbrek hasarlanmasında (ABH) kan ve idrarda yüksek bulunan bir belirteçtir. Bu çalışma acil servise başvuran ve hiponatremi tespit edilen hastalarda hiponatreminin etyolojisinin değerlendirilmesi ve böbrek yetmezliği kaynaklığı olup olmadığını anlamak amacıyla planlanmıştır. Hiponatremili hastalarda serumda NGAL düzeyinin değerlendirilmesi, NGAL'ın prognostik değeri ve Cr normal olan hiponatremili hastalarda ABH’nın erken tanısında NGAL kullanılabilir mi gösterilmesi amaçlanmıştır. ��
Materyal-Metod: Çukurova Üniversitesi Bilimsel Araştırma Projeleri Birimi tarafından TSA-2015-4748 no’lu proje ile desteklenen çalışma, etik kurul onayıyla Çukurova Üniversitesi Tıp Fakültesi Acil Tıp Anabilim Dalı'nda 16 Eylül 2015-1 Ocak 2016 tarihleri arasında gerçekleştirilmiştir. Hastalar dört gruba ayrılarak (serum sodyum; <120 mmol/L, 121-125 mmol/L, 126-130 mmol/L ve >130 mmol/L) bu gruplar ile yaş, cinsiyet, kronik hastalıklar ve geliş şikayetleri, NGAL düzeyleri, Cr değerleri, NGAL/Cr oranı, nt-proBNP değerleri, vena cava inferior çapları ve ilk 30 günlük mortalite arasındaki ilişkilere bakılmıştır. �
Bulgular: Çalışmaya alınan 147 hastanın 70’i (%47,6) erkektir. Hastaların cinsiyet, Cr değerleri ve Na değerleri arasında anlamlı fark bulunmazken, sodyumu 121-125 mmol/L arası olanların, NGAL değerinin ve mortalitesinin en yüksek olduğu, kadın cinsiyet ve Cr yüksekliği olanların da mortalitesinin yüksek olduğu görüldü. Tüm hastalarda NGAL/Cr oranı azaldıkça mortalitenin arttığı görüldü. �
Tartışma ve Sonuç: Kan sodyum düzeyi 121-125 mmol/L olan hastaların NGAL seviyeleri daha yüksek olduğundan bu aralıktaki hastalarda böbrek hasarlanması tanı ve takibi açısından daha dikkatli olunmalıdır. Serum NGAL seviyesi yüksek olan hiponatremili hastalarda ABH’nın erken tanı ve tedavisi amacıyla hasta başı ya da otomatik ölçüm yapan NGAL kitlerinin kullanımı faydalı olabilir. Böbrek hasarlanmasına neden olan böbrek dışı kronik hastalıklara sahip daha geniş hasta popülasyonunda ileri çalışmalar gerekmektedir. Anahtar Kelimeler: Acil servis, akut böbrek hasarlanması, hiponatremi, prognoz, serum NGAL

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
194
O 169 ACİL SERVİSTE YAZILAN REÇETELERİN ANALİZİ-RETOSPEKTİF 2 YILLIK ÇALIŞMA Cem Şen1, Cuma Yıldırım1, Yılmaz Safi1, Mustafa Sabak1, İrem Akın Şen2, Suat Zengin1
1Gaziantep Üniversitesi, Gaziantep�2Gaziantep Ersin Aslan Eğitim ve Araştırma Hastanesi, Gaziantep Amaç: Bu çalışmanın amacı; acil servise başvuran hastalara reçete edilen ilaçların analizini yapmaktır. Gereç-Yöntem: 01.06.2013-01.06.2015 tarihleri arasındaki iki yıllık süre içinde Gaziantep Üniversitesi Şahinbey Araştırma ve Uygulama Hastanesi Acil Servisine başvuran ve reçete yazılan hastaların yaş, cinsiyet, ICD tanı kodları, geliş zamanları ve yazılan ilaçlar incelendi. İstatistiksel analiz için SPSS 22.0 paket programı kullanıldı. ��
Bulgular: 01.06.2013-01.06.2015 tarihleri arasında Gaziantep Üniversitesi Şahinbey Araştırma ve Uygulama Hastanesi Acil Servisine başvuran hasta sayısı 358.437’dir. Bunun 189.437'si erkek, 169.336'sı kadın hastadır. Bunlardan 40.875 hasta herhangi bir servise yatış verilmiştir. 1010 hasta eks olmuştur. 39.867 hasta ise ya başka kuruma sevk edilmiş ya da reçete yazılmadan taburcu olmuştur. 276.685 hastaya reçete yazılmıştır. Reçete yazılan 140.573 hasta (%50,8) erkek, 136.112 hasta ise (%49,2) kadındır. Yaş sınıflamasına baktığımızda en çok başvuru 16-35 yaş aralığında olup 151994 (%54,9) hastadır.�ICD-10 tanı kodlama sistemine göre en çok başvurunun J tanı koduyla solunum sistemi hastalıkları olduğu görülmüştür. En çok başvuru yapılan günlere bakıldığında hafta sonu ve hafta içi günler arasında anlamlı bir fark görülmemiştir. Cuma, Cumartesi, Pazar günleri kadın hasta başvurularının daha fazla olduğu tespit edilmiştir. Saatlere göre başvuru sıklığı incelendiğinde en çok başvurunun 20.00-21.00 saatleri arasında, en az başvurunun ise 03.00-06.00 saatleri arasında olduğu görülmektedir. Yazılan ilaçlar incelendiğinde toplam 310.404 kutu ilaç yazıldığı ve bunun 97.682 (%31,6) kutusunun antibiyotik olduğu tespit edilmiştir. Antibiyotikleri 84.667 (%27,6) kutu ile ağrı kesici ilaçlar takip etmektedir.��
Sonuç: Acil servisler her türlü hastanın 24 saat direk başvurabildiği sağlık tesisleridir. Sevk zincirinin olmadığı ülkemizde birçok hasta acil olmayan sağlık problemlerini de acil servislerde çözmeyi tercih etmektedir. Bu nedenle acil servisten en çok reçete edilen ilaçlar antibiyotik ve analjezik grubu ilaçlar olmuştur. En çok başvurunun diğer sağlık tesislerinin kapalı olduğu mesai saatleri dışında olması da bunun en önemli göstergesidir. Anahtar Kelimeler: Acil servis, triaj, reçete yazımı, akıllı ilaç kullanımı, ICD10 O 170 ÜST GASTROİNTESTİNAL SİSTEM KANAMALARINDA RİSK SKORLARININ PROGNOSTİK ÖNEMİ Yasin Uysal1, Seyran Bozkurt Babuş1, Ataman Köse1, Serdar Biricik1, Semra Erdoğan2, Fehmi Ateş3, Cüneyt Ayrık1
1Mersin Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Mersin�2Mersin Üniversitesi Tıp Fakültesi, Biyoistatistik ve Tıbbi Bilişim Anabilim Dalı, Mersin�3Mersin Üniversitesi Tıp Fakültesi, Gastroenteroloji Bilim Dalı, Mersin Giriş-Amaç: Akut üst gastrointestinal sistem (GİS) kanamalar sık karşılaşılan mortalite ve morbidite nedenlerindendir. Mortalite ve tekrar kanama riski yüksek olan hastaların erken teşhisi ve doğru risk sınıflaması, hastaların bakım verimliliğinin artmasına ve sonlanma kararı için acil servis doktoruna yardımcı olabilir. Üst GİS kanaması ile başvuran hastalarda takipte kanama, endoskopik tedavi ihtiyacı, transfüzyon ihtiyacı ve ölümü tahmin etmede Preendrockal (PERS), Fullrockal (FRS), Glaskow Blatchford Skoru (GBS), Preendbaylor (PEBS) ve Fullbaylor (FB) skorlarının değerliliğine bakıldı. Gereç-Yöntem: Bu çalışma 01 Ocak 2010 – 31 Aralık 2014 tarihleri arasında acil servise başvuran üst GİS kanama tanısı alan hastalarda retrospektif olarak gerçekleştirilmiştir. Hastaların demografik ve klinik özellikleri kaydedildi. Bu skorların hastanedeki sonlanma durumu, takipte kanama, endoskopik tedavi, transfüzyon ihtiyacı ve ölüm parametreler ile ilişkisi değerlendirildi.� Bulgular: Yatırılan hastaların skorlarının ortanca değerleri taburcu olanlara göre, yoğun bakıma yatırılan hastaların skorlarının ortanca değeride servise yatırılanlara göre yüksek bulundu. PERS ve GBS’nin ölüm gözlenen olguların ortanca değerlerinin yatış yapılan hastalara göre daha yüksek olduğu bulundu. (sırasıyla p değerleri; 0.029 ve 0.027). PERS için >3, FRS için >4, GBS için >9, PEBS için >5, FB için >8 olan hastaların transfüzyon ihtiyacı olduğu gözlendi (p değerleri; <0.0001). Endoskopik tedavi ihtiyacı açısından GBS, PEBS ve PERS arasında sadece PERS’in (>3 değerleri için) tahmin etme yeteneğinin anlamlı olduğu bulundu (p=0.0102). PERS için >1, FRS için >5, GBS için >9, PEBS için >3, FB için >8 olan hastalarda takipte kanama olacağı saptandı (sırasıyla p değerleri; <0.0001, <0.0001, <0.0001, 0.0046 ve <0.0001). PERS için >3, FRS için >5, GBS için >13, PEBS için >6, FB için >10 olan hastalarda ölüm olabileceği tespit edildi (p değerleri; <0.0001). Ölümü tahmin etme açısından FRS’nin negatif prediktif değeri (%99.09) diğer skorlara göre yüksekti. ��
Sonuç: Takipte kanama, endoskopik tedavi, transfüzyon ihtiyacı, ölümü tahmin etme, hasta bakım seviyesinin (servis veya yoğun bakım) ihtiyacını belirleme konusunda skorlar yararlı bilgiler sunabilir. Anahtar Kelimeler: Acil servis, gastrointestinal sistem kanama, prognoz, skorlar

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
195
O 171 HİPERKALEMİYE SEKONDER GELİŞEN PARAPAREZİ Burak Çelik, Hüseyin Narcı, Güllü A Dündar, Cüneyt Ayrık Mersin Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Mersin Amaç: Hiperkalemiye sekonder akut paraparezi çok nadir ve ciddi bir klinik tablo olmasına rağmen geri döndürülebilir acil bir durumdur.Ciddi hiperkalemide nörolojik semptomlar kardiyak semptomlara oranla daha nadir tanımlanmıştır. Bunun nedeni kardiyak semptomların daha erken bulgu vermesi ve hekimler tarafından daha iyi biliniyor olması olabilir. Sekonder hiperkalemik paraparezi ile prezente olan bir olguyu tartışmayı amaçladık. ��
Olgu: 67 yaşında diabet ve kronik börek yetmezliği olan bayan hasta ani başlayan bilateral alt exremitede simetrik güçsüzlük ile acil servise başvurdu. Hastanın vital bulguları stabil, şuuru açık kopere idi. Nörolojik muayenede bılateral 3/5 kas gücü defisiti, mevcut, kraniyal sinir ve duyu muayenesi normaldi. Yapılan ileri radyolojik görüntülemede acil patoloji saptanmadı. Laboratuvar tetkiklerinde glukoz: 382 mg/dl, Üre: 69.8 mg/dl, kreatinin:1.58 mg/dl, potasyum: 8.78 mEq/L bulundu. Hastanın kan gazı analizi; pH:7.26, HCO3: 16 mEq/L. Hastada KBY ye sekonder hiperpotasemi düşünülerek, kalsiyum glukonat, insülin dekstroz ve beta-2 agonist tedavisine başlandı. Kontrol potasyumu 8.45 mg/dl olan hasta acil diyalize alındı. Diyaliz sonrası potasyum 5.7 mg/dl olan hastanın alt ekstremite güçsüzlüğün düzeldiği görüldü. Hasta yatışının 3. gününde şifa ile taburcu edildi.��
Sonuç: Serum potasyum düzeyinin akut artışı ölümcül ritim bozukluklarına, paralizilere, solunum kaslarının tutulumuna ve kardiyak arreste neden olabilir. Sekonder hiperkalemik parezi potansiyel olarak ölümcül bir klinik durumdur. Tanının erken koyulup tedaviye erken başlanması hayat kurtarıcı olabilir. Anahtar Kelimeler: Hiperpotasemi, paraparezi, acil tedavi O 172 ENJEKSİYONLARDA OLUŞABİLECEK BEKLENMEDİK YABANCI CİSİM Leyla Öztürk Sönmez1, Giray Sönmez2, Togay Evrin1, Mehmet Ergin3, Kemal Zamir Ertürk1
1Ufuk University Medical Faculty, Department of Emergency Medicine, Ankara, Turkey 2Necmettin Erbakan University Medical Faculty, Department of Urology, Konya, Turkey 3Yıldırım Beyazıt Medical Faculty, Department of Emergency Medicine, Ankara, Turkey Wren İngiltere’ de ilk defa 1656’ da köpeklerde opioid enjeksiyonu için şırınga kullanımını rapor etmiştir. Şırınganın bir iğne ile yapılanması yaklaşık 100 yıllık bir zaman almıştır. Günümüzde enjektör; plastikten yapılmış tek kullanımlık bir malzemedir. Hazne, ajutaj ve piston denilen parçalardan oluşur. İğne iç çapı Gauge birimi ile ölçülmektedir. Birçok parenteral ilaç uygulamasında kullanılmakla beraber, 20 ml’ lik enjektörler "genellikle" 18 G(pembe) iğne ile alınmaktadır. Epidural analjezi/ anestezi uygulamaları, yoğun bakımlarda perfüzörlerle yapılan ilaç infüzyonları, feriferal bloklarda yüksek volümlü anestezik ilaç kullanımı ve benzeri pek çok tıbbi girişimde 20 ml’ lik enjektörler tercih edilmekte, dolayısıyla “genellikle” paketten çıkan 18G(pembe) iğne ucu ile ilaç hazırlanmaktadır. Bazı ilaçların flakonlarında şişenin üzerinde kauçuk membran bulunmaktadır. Bu kauçuk membrana keskin uçlu 18 G iğne ile girildiğinde, aspirasyon ile uygulanan negatif basınç ve vakum etkisi, kauçuk membrandan kopan parçanın da ilaçla beraber enjektör içine girmesine neden olmaktadır. Kliniğimizde ilaç hazırlama sırasında enjektörün içinde kauçuk membran parçası olduğu fark edildiğinde deneysel amaçlı 10 adet citanest ve 10 adet marcain ve 1 adet %2 propofol flakondan 20 ml’lik enjektöre 18G iğne ile ilaç çekilmiş, sonuçta 21 enjektörün 17’ sinde gözle görülebilir kauçuk parçaya rastlanmıştır. Bu parçanın ilgili enjeksiyon alanına kaçması halinde yabancı cisim reaksiyonu, enfeksiyon ve içinde bulunan lateks nedeniyle alerji riski bulunmaktadır. Yazımızın amacı kauçuk tıpaya sahip flakonlardan ilaç çekimi sırasında kauçuk parçanın giriş esnasında kopması sonrası enjektörün içine kaçabileceğine dikkat çekmektir. Enjeksiyon sırasında da intravenöz, periferik blok bölgesi, epidural aralık ve benzeri ilaç enjekte edilen alanlarda bu kopan parça; x- ray ile tespit edilemeyen yabancı cisim reaksiyonuna ve ayrıca epidural aralıkta ise epidural fibrosis ya da yabancı maddenin tipine göre silikonoma gibi beklenmedik sonuçlara da neden olma olasılığını beraberinde getirmektedir. Bu nedenle ilaç hazırlanması sırasında pembe uçlu enjektör iğnelerinin kullanılmamasına ya da yüksek volümlü ilaç hazırlanması gerektiğinde filtreli iğnelerin kullanılmasına dikkat edilmesi gerekmektedir. Anahtar Kelimeler: Yabancı cisim reaksiyonu, 18 gauge iğne, point of technique

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
196
O 173 NADİR OLAN BİLATERAL ANTERİOR OMUZ ÇIKIĞI Sercan Bıçakçı, Rahime Merve Yanıker, Hüseyin Şahin Namık Kemal Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Tekirdağ Giriş: Acil servise başvuran eklem çıkığı olguları içinde omuz çıkıkları ilk sırayı almaktadır. Bu çıkıklar geliştiği yöne göre; anterior, posterior ve inferior (luxatio erecta) şeklinde sınıflandırılır. En sık görüleni anterior yönde olanıdır ve %95 oranında gözlenir. Fakat çift taraflı omuz çıkıkları oldukça az görülür ve çoğunlukla posteior çıkık şeklindedir. Biletarel anterior omuz çıkıları ile ilgili literatürde sadece 80 kadar olgu bildirilmiştir.��
Olgu: 61 yaşında erkek hasta, traktörden düşme sonucu her iki omuz ekleminde ağrı ve hareket kısıtlılığı ile tarafımıza başvurdu. Hastanın yapılan fizik muayenesinde her iki kolunun abduksiyon ve dış rotasyon konumunda olduğu görüldü. Fizik muayenesinde, her iki tarafta da akromionun uç kısmının altında omuz eklemlerinde düzleşme belirlendi. Her iki üst ekstremitede nörolojik olarak motor ve duysal defisite rastlanmadı, nabızlar palpabl idi. Klinik olarak bilateral omuz çıkığı düşünülen hastaya her iki omuz AP radyografileri çekilerek bilateral anterior omuz çıkığı tanısı konuldu. Her iki omuz sedO analjezi altında kapalı redüksüyonla yerine oturtularak velpau bandajına alındı��
Tartışma: Omuz çıkıkları tüm çıkıkların %45’ini oluşturur ve bunların %96’sı öne, %3'ü arkaya, %0,5'i aşağı omuz çıkığıdır. Kolun dışa rotasyon, abduksiyon ve ekstansiyonda zorlanmasıyla anterior omuz çıkıkları oluşur. Glenohumeral çıkıkların çoğu genç erkeklerde ve travma sonucu meydana gelir. Eş zamanlı iki taraflı omuz çıkıkları ise oldukça nadir meydana gelmekte ve güçlü internal rotator kaslara oranla nispeten daha zayıf olan dış rotator kaslar nedeniyle çıkıklar çoğunlukla arkaya yönlü olmaktadır. Bilateral anterior omuz çıkıklarında tek taraflı anterior çıkılarda olduğu gibi etyolojik neden genellikle travmadır.�Bizim olgumuzda da yüksekten düşme sonrasında aynı anda iki taraflı omuz çıkığı, literatürde belirtildiği gibi el üzerine dirsek ekstansiyondayken düşme sonucu ile oluşmuştur��
Sonuç: Omuz çıkıkları nadir olarak çift taraflı görülebilmektedir. Değişik nedenlerle meydana gelen yaygın konvülziyonlar, ani nöbetlerden ve her iki kolu kapsayan travmadan sonra her iki omuzda ağrı ve hareket kısıtlılığı olan hastalarda, bilateral omuz çıkığı olabileceği düşünülmeli ve radyolojik değerlendirme mutlaka yapılmalıdır. Anahtar Kelimeler: Bilateral anterior, omuz, çıkık O 174 EVALUATING THE PREDICTIVE VALUE OF SENESCENCE MARKER PROTEIN 30 AND PEROXIREDOXIN1
SUSPECTED WITH PULMONARY EMBOLISM Yunus Karaca1, Nurbanu Keha Kurt1, Suha Turkmen2, Ozgur Tatli1, Aynur Sahin1, Diler Us Altay4, Elif Sahin5, Ozgen Gonenc Cekic6, Suleyman Turedi3
1Karadeniz Technical University Faculty of Medicine, Department of Emergency Medicine, Trabzon, Turkey 2Acıbadem University Taksim Hospital, Department of Emergency Service, Istanbul, Turkey�3Kanuni Training and Research Hospital, Clinic of Emergency Medicine, Trabzon, Turkey 4Ordu University Ulubey Vocational School, Department of Chemical and Chemical Processing Technology, Ordu, Turkey 5Karadeniz Technical University, Faculty of Medicine, Department of Medical Biochemistry, Trabzon, Turkey, 6Fatih State Hospital, Clinic of Emergency Service, Trabzon, Turkey Aim: Pulmonary thromboembolism (PTE) cannot be easy diagnosed because of nonspecific symptoms and signs of patients applying to emergency departments. In this study, the predictive value of senescence marker protein 30 (SMP30) and peroxiredoxin 1 (PRDX1) in the suspicion of pulmonary embolism has been evaluated. Materials-Methods: Sixty-one pulmonary embolism suspected patients who got spiral computerized tomographic pulmonary angiography were included in the study. Patients who were diagnosed as PTE were in PTE group (n=26) and patient who were not diagnosed as PTE were accepted as control (n=35) group. From both groups serum samples were taken to measure serum PRDX1 and SMP30 levels. Results: PRDX1 levels were significantly higher in the patients with PTE (p=0,001), but, for SMP30 levels, there were no statistical significance between these two groups (p=0,37). Conclusion: In this study PRDX1 values in this patients with PTE were found to be significantly higher, whereas there were no statistical significance between these two groups for SMP30 levels. This suggests that measurement of serum PRDX1 may be distinctive marker for the diagnosis of PTE, but, for SMP30 this cannot be suggested. Further studies involving larger case series and also clinical studies are needed to collaborate these findings. Keywords: Pulmonary embolism, biomarker, PRDX1, SMP30

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
197
O 175 THE PROGNOSTIC VALUE OF EARLY WARNING SCORE AT THE EMERGENCY DEPARTMENT PRESENTATION İN PATIENTS WITH DYSPNEA
Zeynep Karakaya1, Şerife Özdinç2, Fatih Esad Topal1, Erden Erol Ünlüer1, Güler Korol3, Umut Payza1
1İzmir Katip Çelebi University Atatürk Training and Research Hospital, Department of Emergency Medicine, Izmir, Turkey�2Afyon Kocatepe University, Department of Emergency Medicine, Afyon, Turkey 3İstanbul Bahçelievler State Hospital, Department of Clinic Medicine, Istanbul, Turkey Introduction: Clinical deterioration and death among patients with dyspnea are often preceded by detri-mental changes in physiological parameters. The objective of this study was to investigate whether the aggregate weighted track and trigger system Early warning score (EWS) can be used as a simple observational tool to identify patients at risk and predict treatment success in a population of patients with dyspnea. Methods: Adult patients who applied to the emergency service with dyspnea complaints and who were taken in for monitoring were included in this prospective and empirical study. Pulse, systolic blood pressure, temperature, respiratory rate, oxygen saturation and neurologi-cal status at the time of arrival, 15minutes later and 30 minutes later were used for EWS cal-culation. Patients were divided into four score categories based on their EWS. The patients were compared with regard to hospitalization, discharge and response to the treatment. Results: 91 patients were included in the study. The EWS values of dyspnea patients calculated for the 15th and 30th minutes were observed to be statistically significant as a result of an evaluation with regard to hospitalization and discharge ( p=0.015, p=0.001). It was determined that the oxygen saturation values measured on the 15th and 30th minutes were important for giving the hospitalization decision (p=0.048, p=0.009). Improvement in the physiological parameters measured at the time of arrival, 15minu- tes later and 30 minutes later were determined to be significant for the evaluation of the response to the treatment. Conclusions: In this study, it was put forth that the difference between the EWS value at the time of arrival, 15minutes later and 30 minutes later is an early indicator for the result and success of the treatment. This can ease making clinical decisions and shorten the time that patients stay at the emergency service by prioritizing risky patients. Keywords: Dyspnea, emergency service, early warning score O 176 IS EVERTHING ALL RIGHT AFTER THE BARIATRIC SURGERY ? EVALUATION OF THE QUALITY OF LIFE AFTER PULMONARY EMBOLISM BY PEMB-QOL QUESTIONNAIRE Burcu Yormaz1, Ilhan Ece2, Serdar Yormaz2, Bayram Çolak2
1Beyhekim State Hospital, Clinic Of Chest Disease, Konya, Turkey 2Selcuk University Medical Faculty, Department of General Surgery, Konya, Turkey Background: The evaluating the clinical outcome of acute pulmonary embolism (APE) involves short-term mortality, higher recurrence rate and more complications. The studies which were evaluated by the PEmb-QoL questionnaire(Pulmonary Embolism Quality of Life) in morbid obese patients who were underwent bariatric surgery with a history of acute pulmonary embolism (APE) are not common available, although PEmb -QoL is a key outcome component of medical care and a predictor of disease-specific prognosis. We want to evaluate the outcomes after surgical process and embolism in this study. Methods: We identified consecutive patients average age 34 to 65 years with an acute, objectively confirmed PE admitted at the intensive care unit n tertiary clinic, from marc 2014 to june 2016. The confirmation of APE was based on a high-sensitive computed tomography scan. PEmb-QoL was presented to consecutive patients who have underwent obesity surgery and survived of acute PE. It covers six dimensions: frequency of complaints, activities of daily living limitations, work-related problems, social limitations, intensity of complaints and emotional complaints. We used standard psychometric tests and criteria to evaluate the acceptability and validity of the PEmb-QoL Results: The PEmb-QoL was enrolled to 26 morbid obese patients (BMI>40kg/m2) in this study overall in operated 521 patients.of 17 (65%) patients were female and 9 (35%) were male in group. The six dimensions of the PEmb-QoL were originally defined clinically and assuming to provide unique information to the treating physician. Awareness of illness, coping mechanisms, and self-management behavior might be additional important indicators of QoL in our study population. Conclusion: We have identified several PE-related determinants of QoL in morbid patients with a history of acute PE, which is impaired compared with sex- and age-adjusted population norms. PEmb -QoL after acute PE should be studied more extensively and added as a standard measure to outcome studies. Keywords: Bariatric, questionnaire, embolism

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
198
O 177 PREDICTION OF POOR OUTCOME IN NON-TRAUMATIC DYSPNEA: SERUM CORTISOL LEVEL Ozlem Dikme1, Ozgur Dikme2
1Koc University Hospital, Department of Emergency Medicine, Istanbul, Turkey 2Istanbul Training and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey Objectives: Elevated cortisol levels have been described in stressful conditions but it is unclear if these are associated with adverse outcomes. The hypothesis for this study was that elevated serum cortisol levels in dyspneic patients would be associated with poor outcome as intubation in the ED, admission to the ICU, and in-hospital mortality. Methods: This prospective cross-sectional study enrolled consecutive patients presenting to the ED with non-traumatic dyspnea. Serum cortisol levels were measured at the ED presentation and compared between those with and without poor outcome which are intubated in the ED, admission to the ICU and in-hospital mortality. Mann-Whitney U test and Kruskal-Wallis test were used to test for differences between and within groups and ROC curve analyses performed. Results: Of the 87 patients enrolled, 44 (50.6%) were female and 33 (37.9%) were diagnosed as heart failure. Twenty-four (27.6%) patients had poor outcome. Six (6.9%) patients were intubated at the ED, 19 (21.8%) patients admitted to the ICU, and 8 (9.2%) patients died in-hospital. All patients’ median serum cortisol level was found as 26.7 μg/dL (IQR: 14.9 to 34.1 μg/dL). Patients who had poor outcome had higher mean cortisol levels than those with non-poor outcome (34.3μg/dL vs 23.8μg/dL, p<0.001). Additionally, when evaluating each poor outcome criteria separately, patients who intubated in the ED or admitted to the ICU or died in-hospital had higher mean cortisol levels than others (respectively, 54.2μg/dL vs 25.7μg/dL, 38.7μg/dL vs 24μg/dL, 50μg/dL vs 24.3μg/dL, p<0.001). Also, a ROC curve analyze was performed to determine the accuracy of serum cortisol in predicting poor outcome, and the AUC was calculated as 0.76 (95% CI, 0.65- 0.84).��
Conclusions: Serum cortisol levels may predict poor outcome in non-traumatic dyspneic adult ED patients on arrival. Further research into serum cortisol levels as a prognostic tool in non-traumatic dyspnea is warranted. Keywords: Dyspnea, cortisol, emergency department O 178 THE EFECT OF NEUTROFIL/LYMPHOCYTE RATIO FOR 1 YEAR SURVIVAL IN PATIENT DIAGNOSED WITH PULMONARY EMBOLISM Rıfat Urnal, Pınar Yeşim Akyol, Zeynep Karakaya, Umut Payza, Serkan Bilgin, Gözde Canan Yavaş, Fatih Esad Topal Izmir Katip Çelebi University Atatürk Research and Training Hospital, Department of Emergency Medicine, Izmir, Turkey Objective: Pulmonary embolism (PE) is a common and potentially lethal condition. In this study, clinical variables and the neutrophil-lymphocyte ratio (NLR) rates of the patients who diagnosed with PE are used to investigate the effect on mortality and prognosis. Materials-Methods: A total of 66 patients which consists of 43 female and 23 male who were admitted to emergency medicine service and diagnosed PE in a year and interpretated as PE according to their CT pulmonary angiography (CTPA) imaging results are included in the study. The patients are excluded who have active infection, sepsis, chronic heart disease, chronic obstructive pulmonary disease, diabetes mellitus, hypertension, serious hepatic and renal failure, using anticoagulant, leukemia, myeloproliferative disease, trauma history, splenectomy, pregnancy, megaloblastic anemia, massive bleeding, under age 18 and not found data collections, exitus not diagnosed before CTPA imaging. Results: 66 patients are gathered in our study. The number of the study is recorded as 23(35,84%) male and 43 (65,15%) female patients. The percentage of death rate in a year is %33,33 (n=6) in males and %66.67 (n=12) in females. It is revealed that the N/L relation is not significiant statistically, lymphocyte rates are lower in ex patients and neutrophile/lymphocyte rates are higher as well. By grouping N/L rates, it is found that N/L rates and to survive are related significiantly (p<0,05). When N/L rates are investigated, the rates of N/L are higher in ex patients (%61,1). Conclusion: NLR can be used as a sign of a-year-mortality in pulmonary emboli cases. NLR should be investigated in future prospective randomized trials regarding prognostic value in acute PE. Keywords: Pulmonary embolism, neutrophil-lymphocyte ratio, emergency department

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
199
O 179 PULMONARY EMBOLISM PRESENTING WITH A SINGLE PRE-SYNCOPE EPISODE Harun Gunes, Feruza Turan Sonmez, Ayhan Saritas Düzce University School of Medicine, Emergency Department, Düzce, Turkey Syncope is a recognized presenting symptom of pulmonary embolism (PE), and pre-syncope, which shares the same pathophysiologic mechanisms with syncope but does not lead to loss of consciousness, also may be the sole presenting symptom in PE. However, it is very much rarer. Recurrent pre-syncope episodes were also reported in a patient with PE. A case of PE presenting with a single pre-syncope episode was presented here. A 69-year-old man who had experienced a pre-syncope attack in the morning was brought to our emergency department. He had generalized weakness, dizziness and fatigue. He had been operated for brain tumor 6 months previously. Blood pressure was 111/84 mmHg, pulse rate was 108 beats/minute, and peripheral oxygen saturation (SpO2) was 98%. He was able move all extremities but a generalized weakness was prominent. He had been experiencing difficulty on standing upright and walking but he was still able to do since he had been operated for the brain tumor. No lateralizing sign was found on neurological examination. His SpO2 was changing between 90-98% though he denied having dyspnea. His respiratory system examination was normal except labile SpO2 levels. Pathologic S waves in the lead I, and pathologic Q waves and ST segment depression in the lead III were seen on the electrocardiogram. Posterior-anterior chest X-Ray showed a radiO opaque region in the right lower zone. Intravenous contrast-enhanced computed tomography scan of the chest showed bilateral emboli in the main pulmonary arteries and their branches. The patient was given 8000 IU enoxaparin sodium intravenously. He was consulted with the Pulmonology Department and hospitalized by the same department. In conclusion, PE should be included in the differential diagnosis of pre-syncope, and even a single pre-syncope episode should raise the suspicion of PE especially when the clinical picture does not point out another significant diagnosis. Keywords: Pulmonary embolism, pre-syncope, peripheral oxygen saturation O 180 EVALUATION OF THE APPLICATION OF NONINVASIVE MECHANICAL VENTILATION IN PATIENTS WITH RESPIRATORY DISTRESS IN EMERGENCY DEPARMENT Ahmet Sebe, Ibrahim Akça, Ayça Açıkalın Akpınar, Nezihat Rana Dişel Çukurova University Faculty of Medicine, Department of Emergency Medicine, Adana, Turkey Purpose: Respiratory distress and effectiveness of non -invasive mechanical ventilation in patients admitted to the emergency room hypercapnic respiratory failure will be investigated. The study gender differences in disease regardless of whether consciousness is open and patients older than 18 years, closed consciousness and patients under age 18 will be excluded from the study. Material-Methods: Studies with prospective method Ç.Ü.TF Emergency Medicine US sex admitted with respiratory distress, disease without differentiating consciousness is open and 18 years of age will be great hypercapnic patients with respiratory failure. This non-invasive mechanical ventilation to patients and the effectiveness of the method to be applied will be investigated. Non- invasive ventilation, according to the invasive more comfortable, easier and less costly applicable method. With this method, the need for hospitalization and stay in intensive care in hospital time is markedly shortened. Findings: In this study Admitted with respiratory distress and arterial blood gases in the emergency work hypercapnic respiratory failure received a total of 51 cases detected. PCO 2 values ranged from 45.8 to 91.7 in the advent of the average of the PCO 2 values were 63.69 ± 11.13. After NIV average ranged from 35.9 to 87.7 after the PCO 2 values were 53.75 ± 10.58. Length of stay in hospital ranged from 0-18 days with a mean of 4.18 ± 4.80. At the end of the arterial PCO 2 levels it was observed patients and the intensive care unit stay and hospital stay were significantly shorter. Result: Non-invasive mechanical ventilation applications with emergency admitted with respiratory distress, consciousness that is open in the hypercapnic respiratory failure possible to shorten the length of stay and hospital mortality. Keywords: Emergency department, hypercapnic respiratory failure, non- invasive mechanical ventilation

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
200
O 181 DOES PULMONARY EMBOLISM SEVERITY INDEX CORRELATE WITH COMPUTED TOMOGRAPHY SEVERITY CRITERIA?
Cigdem Ozpolat, Ozge Onur, Haldun Akoglu, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Introduction: Many reports have shown the usefulness of pulmonary CT angiography in the diagnosis of acute pulmonary embolism (PE). Evaluation of the degree of pulmonary arterial obstruction which may be relevant for patient treatment, remains under investigated. Pulmonary embolism severity index (PESI) score is the most validated score in the prognostic assessment of the patients with acute PE. The aim of our study was to investigate whether the severity of acute PE assessed with spiral CT angiography can be used to predict severity of the disease. Method: We searched our hospital's database retrospectively for patients who underwent to pulmonary CT angiography and diagnosed as acute PE. PESI scores of the patients were calculated using the data obtained from the electronic database and PESI class I and II were regarded as low risk PESI scores. The percentage of vascular obstruction was calculated to score vascular obstruction as ∑ (n. d) (n, value of the proximal clot site, equal to the number of segmental branches arising distally; d, degree of obstruction scored as partial obstruction value of 1 or total obstruction value of 2 ) Result: A total of 176 patients were included in the study. Medians (IQR) of CT obstruction indexes of low and high risk PESI classes was 40 (25-50) and 35 (25-56) respectively. There were not any significant differences between low and high risk PESI score groups in the terms of CT obstruction index (p: 0.88). Discussion: The degree of arterial obstruction in pulmonary embolism may be quantified by CT obstruction index but it does not correlate with PESI which is used for risk stratification of patients with acute PE. Keywords: PESI, pulmonary embolism, obstruction rate O 182 PROGNOSTIC AND PREDICTING VALUES OF PERFUSION INDEX AND SHOCK INDEX IN COMMUNITY- ACQUIRED PNEUMONIA PATIENTS AND THEIR CORRELATION WITH RISK SCORING METHODS (CURB-65 AND CURS) Ozan Sahin1, Ozgur Dikme2, Ozlem Dikme3, Hakan Topacoglu2
1Bayrampasa State Hospital, Emergency Clinic, Istanbul, Turkey 2Istanbul Training and Research Hospital, Emergency Clinic, Istanbul, Turkey 3Koc University Hospital, Department of Emergency Medicine, Istanbul, Turkey Objective: The aim of the study was to evaluate the correlation between perfusion index (PI), shock index (SI) and risk scoring methods (CURB-65 and CURS) in patients who were diagnosed with community-acquired pneumonia (CAP) in emergency department (ED). In addition, predictive performance of PI on short-term mortality, re-admission rate and intensive care unit admission of patients were investigated. Materials-Methods: The study was conducted as prospective, double center cohort study over a month period. All consecutive adult patients with pneumonia presenting to ED were enrolled in this study. PI and SI values of the patients were measured at presenting time and compared with the measured values of CURB-65 and CURS. Results: A total of 135 patients with CAP included the study. Eighty-four patients (62,2%) were male, with median age of 62. Sixty-four patients were older than 65 years. The mean PI of the patients was 5,2±4,6, while average of SI was 0,9±0,2. Out of 135 patients, 93 were admitted to the hospital of which 3 of them were admitted to ICU. Whereas re-admission rate of the patients to hospital was 23%, 18 of patients (13,3%) died within 30 day. It was observed that there was no statistically significant correlation between risk scores of CAP versus PI and SI values of the patients. Conclusion: PI values did not indicate accuracy in predicting short-term mortality, 30-day readmission rate or ICU admission of the patients with CAP. PI may not be useful to classify severity risk in CAP patients Keywords: Perfusion index, community-acquired pneumonia, CURB-65, CURS

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
201
O 183 COMPARING PNEUMONIA SEVERITY SCORES (PSI, CURB65, NEWS, NEWS-L) OF PATIENTS DIAGNOSED AS PNEUMONIA IN EMERGENCY DEPARTMENT
Aynur Ecevit Kaya, Seda Özkan, Eren Usul Dışkapı Yıldırım Beyazıt Training and Research Hospital, Clinic of Emergency Medicine, Ankara, Turkey Objective: We aimed to compare pneumonia severity scores (PSI, CURB65, NEWS, NEWS-L) for patients diagnosed as pneumonia in emergency department and to investigate the usability at new scores. Methods: Patients diagnosed as pneumonia in emergency department between 11.01.2015-05.01.2016 were included. We used laboratory and scanning results; CURB65, PSI, NEWS, NEWS-L scores and hospitalizations transfer and discharge situations after diagnose besides demographic data. Final data was evaluated with SPSS 17 and Med Calc. Results: 250 patients were included. The best score to foresee the mortality was found as NEWS-L (AUC: 0.96). In order NEWS (0.91), CURB65 (AUC: 0.86), PSI (AUC: 0.71) followed NEWS-L. The best score to foresee treatment need in ICU was found as NEWS-L (AUC: 0.72) and NEWS (AUC: 0.72). In order CURB65 (AUC: 0.69) and PSI (AUC: 0.64) followed this. The best score to foresee hospitalization was found as NEWS-L (AUC: 0.72). In order NEWS (AUC: 0.71) CURB65 (AUC: 0.69) and PSI (AUC: 0.64) followed NEWS-L. Between all scores for living and died patients was found as significant (p<0.05). Between all scores for patients stay in service and ICU was found as significant (p< 0.05). Conclusion: The new scores, NEWS and NEWS-L were found stronger than CURB65 and PSI to determine the pneumonia severity. We think that NEWS and NEWS-L can be used successfully to determine the mortality hospitalization and prognoses of pneumonia patients. Keywords: Emergency department, pneumonia, pneumonia severity scores O 184 PROCALCITONIN LEVELS, WHICH ARE MEASURED IN EMERGENCY DEPARTMENT, RELATION WITH ETIOLOGY AND SHORT-TERM MORTALITY Onur Baris Cehreli, Basak Bayram, Duygu Tokgoz, Nese Colak Oray Dokuz Eylül University Faculty of Medicine, Department of Emergency Medicine, Izmir, Turkey Objective: According to the final diagnosis of the patients who visited the Dokuz Eylul University Hospital Emergency Department and was sent procalcitonin levels, we planned to investigate the relationship between procalictonin levels with seven day mortality. Materials-Methods: This retrospective analytic study was made between 01.01.2016 and 31.03.2016. 499 patients from who were sent procalcitonin levels took place in this study. Patients’ blood tests, etiologies and the situations were scanned. We compared parameters in two groups (died, living). Results: The patients mean age was 70.9± 15.3 and woman’s rate was 46.1%. the most common ICD was with 41.6% respiratory disease and 22.3% infectious disease. In seven days outcome 249 patients were discharged. 112 of the patients were in service, 66 patients were still in intensive care unit and 72 patients were dead. The patients in the death group, compared to living group SKB, DKB and oxygen saturation was low (p for each <0.001); pulse rate, respiratory counts, white blood cell, neutrophil precentage, lactate, base deficit and procalcitonin values (p for each <0.001) was high. Procalcitonin level categorized as <0.5 ngr/mL, 0.05-0.5 ngr/mL, 0.5-2.0 ngr/mL, 2.0-10.0 ngr/mL and >10.0 ngr/mL. Seven days follow up which was finished as death was in %60 (0.05-0.5 ngr/mL), following with %20.7 (0.5-2.0 ngr/mL), %12 (2.0-10.0 ngr/mL) and %5 (>10.0 ngr/mL). According to the procalcitonin category, we found more deaths in sepsis (9, %34.6). In infectious disease, procalcitonin level in 0.93 ngr/mL was %89 sensitive and %72 specific. In respiratory disease 0.15 ngr/mL was %89 sensitive and %21 specific. Conclusion: Measured procalcitonin levels in the emergency service were high in deceased patients than living patients. The mortality increases as the procalcitonin levels increase. In 2.0-10.0 ngr/mL and >10.0 ngr/mL the mortality rate was higher than the other procalcitonin categories. Keywords: Emergency service, etiology, mortality, procalcitonin

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
202
O 185 AIR MEDICAL TRANSPORT OPERATIONS OF TURKISH ARMED FORCES DURING OPERATION ENDURING FREEDOM OF AFGHANISTAN
Necati Salman1, Yahya Ayhan Acar1, Onur Tezel1, Serkan Şener2, Etem Düzok3
1Ankara Gülhane Training and Research Hospital, Department of Emergency Medicine, Ankara, Turkey�2Acıbadem University School of Medicine, Department of Emergency Medicine, Istanbul, Turkey 3Güven Hospital, Clinic of Emergency Medicine, Ankara, Turkey Objectives: We aimed to present our experiences with fixed-wing AMT operations of TAF during OEF. Material-Methods: We performed a retrospective observational study by collecting the data of TAF AMT cases between 2003 and 2014. Data include date (month/year), flight medical team (physician, nurse, anesthesiology technician), patient gender, age, status (Afghan civilian, NATO soldier), transferred clinic, mental status (Glasgow Coma Scale), medical state (undetermined/good/fair/serious/critical/dead), endotracheal intubation (+/-), in-flight medications, type of injury (trauma +/-) and pre-flight surgical intervention (+/-). Results: During 12-year period, 18 patients were transported by TAF flight medical team at 10 operations from Kabul (KAIA) to Ankara Etimesgut Air Base (LTAD). Eight patients (44%) were civilians and 10 (56%) were soldiers. Physicians reported that 8 patients (44%) had life threatening conditions and five (28%) were intubated and connected to the mechanical ventilator at the handover procedures. Conclusion: AMT facilities had an integral role at both military medical activities and humanitarian care facilities in operation enduring freedom of Afghanistan. Role 3 military medical facility evaluation is an important stage of AMT operations, and provides patients a tertiary triage decision before a long distance air transport. We conclude that all experiences of military medical care systems at conflict areas, even in limited numbers, should be accepted as a valuable source for patient care. Keywords: Air medical transport, Afghanistan, humanitarian care

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
203
POSTER ABSTRACTS

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
204
P 001 THE USE OF PROPOFOL FOR PROCEDURAL SEDATION FOR TRAUMA PATIENTS IN THE EMERGENCY DEPARTMENT
Danielle Meels, Luc De Geyter Belgium Propofol has been set only to be used by anesthesists. However it has become increasingly popular because the easy use for quick sedation and quick recovery, by non-anesthesists, even in pre-hospital setting. We try to establish evidence that it can be safely used by emergency room doctors for the management of minor trauma with little risk for the patient. We will compare propofol with ketamine, etomidate and midazolam for the same procedures. Keywords: Propofol sedation, minor trauma, emergency room physician P 002 YAN AĞRISININ NADİR BİR NEDENİ: RENAL İNFARKT Yeşim Eyler, Mustafa Sever, Necmiye Yalçın Ocak, Didem Avcı Dönmez Tepecik Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İzmir Giriş: Renal infarkt, yan ağrısının nadir nedenlerinden biri olup insidansı 0.004- 0.007% arasındadır. (1)(2) Atrial fibrilasyon, iskemik kalp hastalığı, kardiyomiyopati, mitral kapak hastalığı ve travma risk faktörleri arasında gösterilir. (3),(4) Yan ağrısı, bulantı ve kusma gibi silik semptomlar göstermesi nedeniyle tanı koyabilmek için klinik şüphe gerekir. Olgu: 54 yaşında erkek hasta; sabah başlayan bulantı, kusma ve sağ yan ağrısı şikayetleri ile acil servisimize başvurdu. Başvurusunda kan basıncı: 151/66 mmHg, kalp hızı: 90/dk ve ritmik, solunum sayısı 16/dk ve ateş: 36.5 C° olarak tespit edildi. Özgeçmişinde bilinen bir hastalığı yoktu. Sağ paravertebral alanda kostavertebral açı hassasiyeti dışında tüm fizik muayene bulguları normaldi. Hasta öncelikle renal kolik olarak değerlendirildi. Laboratuvar incelemelerinde renal fonksiyon testleri, tam kan sayımı ve idrar analizi normaldi. Kontrassız abdominal bilgisayarlı tomografi (BT) sonucu da normal olarak değerlendirildi. Hastaya tedavi olarak intravasküler skopolamid butil bromür ve intramuskuler diklofenak sodyum uygulandı. Hastanın ağrısı analjezik tedavilere yanıt vermedi. Hastaya renal infark şüphesiyle kontrastlı abdominal BT çekildi ve sonucu, sağ renal arter trombozu ve sağ renal infarkt olarak yorumlandı. Kardiyovasküler cerrahi, nefroloji ve üroloji klinikleriyle konsülte edilen hastaya oral warfarin tedavisi başlandı. Hasta olası komplikasyonların takibi için ilgili polikliniklere kontrole çağırılarak taburcu edildi. Sonuç: Yan ağrısı ile acil servise başvuran hastalarda ayırıcı tanılar arasında renal infarkt da düşünülmelidir. Renal infarkt tanısını koymada renal anjiografinin sensitivitesi %100 dür. Acil servislerde renal infarkt tanısını koymak için en uygun strateji ise kontrassız spiral abdominal BT ile nefrolitiazis tanısını dışladıktan sonra kontrastlı abdominal BT tercih etmek olacaktır. (5) Hastaların tedavisinde antikoagulanlar tercih edilir. Trombolitik uygulama ya da cerrahi revaskülarizasyonda diğer tedavi seçenekleri arasındadır. Mortalite, böbrek fonksiyon bozukluğundan çok tekrarlayan embolik olaylarla ilişkilidir. (4) (5) Sunduğumuz bu olgu ile acil servislerde tanısı kolayca atlanabilecek ancak mortalite ve morbiditesi yüksek bu tanıya dikkat çekmek istedik. Anahtar Kelimeler: Kontrastlı abdominal bilgisayarlı tomografi, renal infarkt, yan ağrısı

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
205
P 003 TOTAL PARENTERAL BESLENMEYE BAĞLI GELİŞEN WERNİCKE ENSEFALOPATİSİ Doğukan Akçay1, Mehmet İnce1, Leyla İnce2, Tahir Özer1
1Gülhane Askeri Tıp Akademisi, Genel Cerrahi Anabilim Dalı, Ankara 2Abdurrahman Yurtaslan Onkoloji Hastanesi, Radyoloji Bölümü, Ankara Wernicke ensefalopatisi(WE) erken tanı konulup uygun şekilde tedavi edilmediği takdirde ölümcül seyredebilen nörolojik acil bir durumdur. Biz burada, rektum kanserine sekonder gelişen mekanik barsak tıkanıklığı nedeniyle total parenteral nütrisyon(TPN) alırken WE gelişen bir olgumuzu sunmak istiyoruz. Olgu: 54 yaşında erkek hasta bulantı, kusma, iştahsızlık ve zihin karışıklığı(konfüzyon) şikayetleri ile yakınları tarafından hastanemize getirildi. Hastaya, 2014 yılında perfore rektum karsinomu tanısıyla acil şartlarda Hartman prosedürü ameliyatı uygulanmış. Sonrasında kolostomi revizyonu yapılan ve takiben inkomplet intestinal tıkanıklığı ve enterokutan fistül tanısı konan hastaya iki ay boyunca parenteral beslenme verilmiş. Fizik muayenede; baş dönmesi, bulanık görme ve dengesiz yürüyüşü olan hastanın hipotansif ve taşikardik olduğu görüldü. Hasta yatırıldı, iki günlük medikal takip ve tedavisinde genel durumun kötüleştiği ve arteriyel kan basıncının 80/45mmHg ya kadar düştüğü görüldü. Hastaya acil serebral MR incelemesi yapıldı. Üçüncü ventrikül, thalamus mediali ve orta beyin etrafında, T2WI ve FLAIR görüntülemede simetrik hiperintens alanlar izlendi. TPN alan ve serebral MR incelemede izlenen tipik görüntüler bize, hastada tiamin eksikliğine bağlı WE si olabileceğini düşündürdü. Vakit geçirmeden hastaya intravenöz yoldan tiamin infüzyonu yapıldı. Tedavi sonrası hastanın dramatik bir şekilde düzeldiği görüldü. Ertesi gün hastanın bilinç durumu düzeldi, vazoaktif ilaç kullanımına gerek kalmadan hastanın kan basıncı ve kalp hızı normale döndü. Bir haftalık tiamin tedavisi sonrası hastanın tüm klinik semptomları kayboldu. Biz bu olgu sunumuyla; TPN alan hasta popülasyonunda WE gelişme riskine karşı tiamin ve diğer vitaminlerin beslenme desteğine eklenmesi gerektiğini, WE düşünülen hastalara serebral MR inceleme ile erken tanı konularak biran evvel tedaviye başlanmasının akıldan çıkarılmamasını önermekteyiz. Anahtar Kelimeler: Wernicke, ensefalopatisi, total parenteral beslenme P 004 A CASE OF MASSIVE HEMOLYSIS IN A PATIENT WITH LIVER ABSCESS CAUSED BY KLEBSIELLA PNEUMONIAE Gun Bea Kim Ilsan Hospital, National Health Insurance, South Korea Klepsiella pneumoniae (K. pneumoniae) has been most common cause of liver abscess in Asia. Prognosis of K. pneumoniae liver abscess is relatively good, although there are some fatal outcomes with massive hemolysis caused by Clostridium perfringens in liver abscess. In our knowledge, it is very rare to take rapid course of fatal outcome in patient with K. pneumoniae liver abscess due to massive hemolysis. A 56-year-old man came to our emergency room because of low back pain and general weakness. Past medical and surgical histories were unremarkable and he was not a alcoholic. He was alert, but appeared acute-ill looking. His body was febrile, 38.7 ℃. Oral bleeding was observed without definite bleeding source, and gross hematuria was seen after foley catheterization. No laboratory tests could be performed because of a repeated massive hemolysis and only arterial blood gas analysis(ABGa) showed metabolic acidosis, pH 7.343; PaCO2 18.2 mmHg; PaO2 81.2 mmHg; base excess –14.5; HCO3- 9.7 mmol/L. We intubated him because he deteriorated suddenly and his ABGa showed mixed respiratory and metabolic acidosis. He had no urine output. So continuous renal replacement therapy was started. The blood smear revealed spherocytosis. Computer tomography demonstrated a ruptured gas-forming liver abscess. We started on massive inotropes and broad-spectrum antibiotics. Repeated blood samples showed massive hemolysis with no possibility of chemical or hematologic testing. The patient died within 8 hours. After a patient died, blood samples cultured a Klesbiella pneumoniae. Patient cremated without autopsy.We recommend that PB smear can be helpful to diagnosis of massive hemolysis patients with no laboratory results. If infection is suspected, first impression is not only Clostridium perfringens septicemia, Gram-positive rods but also Klebsiella pneumonia septicemia, Gram negative rods. Fast broad spectrum antibiotics administration is necessary. If abscess formation is found, surgical debridement or drainage is also needed. Keywords: Massive hemolysis, liver abscess, Klebsiella pneumoniae

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
206
P 005 ERİŞKİNDE MİNÖR TRAVMA İLE OLUŞAN DİRSEK ÇIKIĞI Göksu Afacan, Orhan Delice Erzurum Bölge Eğitim ve Araştırma Hastanesi, Acil Servis, Erzurum Giriş: Basit dirsek çıkığı yalnız yumuşak doku yaralanması ya da eklem dışı kopma kırıklarıyla birlikte olan dirsek çıkıklarını içermektedir; çıkığın yönü ya da süresine göre sınıflandırılmaktadır. Etiyolojik olarak birinci sırada, eli açık yere düşme gelmektedir. Fizyopatolojisinde, ön kolun patolojik dış rotasyonunun dirsek çıkığına neden olduğu ileri sürülmektedir. Vücudun ağırlığıyla oluşan aksiyel yüklenmeyle birlikte dirseğe gelen valgus ya da varus yüklenmeleri, yaralanma şiddetini ve dokuların yaralanma sırasını belirlemektedir. Basit dirsek çıkığı tanısı klinik ve radyografik tetkik ile konur. Özellikle adolesan dönemde, mediyal ve lateral epikondil kopma kırıklarının teşhisi için sağlam tarafla karşılaştırmalı grafiler çekilmelidir. Kopma kırıkları ve eklem içi osteokondral kırık parçalarını araştırmaya yönelik olarak her hastaya bilgisayarlı tomografi (BT) ve üç boyutlu bilgisayarlı tomografi (3D-BT) yapılmalıdır. Stabil olmayan çıkıklarda ise yumuşak doku yaralanmasının boyutlarını görmek amacıyla manyetik rezonans (MR) görüntüleme tercih edilir. Basit dirsek çıkıklarının tedavisinde, kapalı redüksiyon sonrası stabil olanlarda 10 günü geçmeyen tespit ve hemen hareket, stabil olmayanlarda pronasyonda breys, pronasyonda ekstansiyon bloklu breys ya da cerrahi tedavi uygulanır. Dirsek çıkığı sonrası görülen komplikasyonlar; dirsek ekleminde kontraktür, heterotopik kemikleşme, nörovasküler yaralanma, Essex-Lopresti yaralanması ve rezidüel instabilitedir. Olgu: 38 yaş erkek hasta, ayağı takılması sonrası yere düştüğünü ve daha sonrasında kolunu kıpırdatamadığını söylemekte. Fizik muayeneyi reddeden hastanındış bakı ile etkilenmiş olduğunu söylediği kolun dirsek bölgesinde şişlik olduğu görülmüş olup çekilen karşılaştırmalı grafik sonrası dirsek çıkığı saptanmıştır. Ortopedi yardımı ile yerine oturtulan dirsek, takiplerinde sekelsiz iyileşmiş ve hareket kusuru kalmamıştır. Sonuç: Fizik muayeneye uyumsuz hastalarda dahi kendisini eklem yüzeyinde şişlik ile belirtebilecek dirsek çıkığı genellikle çocuk yaşlarda görülüp; erişkinlikte nadirdir. Ancak atlandığında daha kötü sonuçlara yol açabilmektedir. Anahtar Kelimeler: Dirsek çıkığı, erişkin, minör travma, uyumsuz hasta P 006 ÜLKE İÇİN NADİR, ERZURUM İÇİN SIRADAN Sultan Tuna Akgöl Gür, Göksu Afacan Erzurum Bölge Eğitim ve Araştırma Hastanesi, Acil Servis, Erzurum Gazeteciliğin yüzyıllık klişesidir; köpek adamı ısırırsa haber olmaz. Adam köpeği ısırırsa haber olur. Aynı şekilde araba bir ata çarparsa olgu sunumu olmaz ancak; at bir arabaya çarparsa durum değişir. Olgu: 50 ve 23 yaşlarında erkek hastalar (baba ve oğul), babanın kullandığı araç ile Erzurum şehir merkezinde seyahat halinde iken caddede karşıdan karşıya geçmeye çalışan (!) atın araçlarına çarpmak sureti ile aracın içine girmesi sonucu oluşan trafik kazası ile servisimize 112 tarafınca interne edildi. Geldiklerinde bilinç açık, oryente, koopere ve vital bulgularında herhangi bir anormallik yoktu. 23 yaşındaki hastada fizik muayenede herhangi bir anormallik veya vücudunun herhangi bir bölgesinde abrazyon saptanmamasına rağmen; 50 yaşındaki hastada frontal bölgede primer sütürasyon ile kapatılan minimal kesi bulunmaktaydı. 50 yaşındaki hastanın Beyin BT'sinde frontal bölgede lineer fraktür ve minimal serebral kontüzyon tespit edildi. Takiplerinde uykuya meyil de gelişen hasta Beyin ve Sinir Cerrahisi Yoğun Bakımına yatırıldı. 23 yaşındaki hasta ise önerilerle taburcu edildi. Sonuç: Ülkemizde trafik kazaları her dönem acil servisleri meşgul eden önemli problemler arasında yer almıştır, ancak sunduğumuz olgudaki gibi durumlar -şanslıyız ki- nadir yaşanmaktadır. Anahtar Kelimeler: At, araba, trafik kazası

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
207
P 007 İŞ KAZALARI: ELEKTRİK ÇARPMASINA BAĞLI YÜKSEKTEN DÜŞMELER Göksu Afacan Erzurum Bölge Eğitim ve Araştırma Hastanesi, Acil Servis, Erzurum Yüksekten düşme, trafik kazalarından sonra en sık travma sebebi olarak karşımıza çıkarken; çocukluk yaş grubundaki düşmeler, en sık travma sebebi olarak izlenir. Tüm teknolojik gelişme ve uygulamalara karşın dikkatsizlik nedeniyle veya insan hayatı için geliştirilmiş emniyet tedbirlerini almadan çalışan birçok insan hayatını kaybetmekte, sakat kalmakta ya da ciddi şekilde yaralanmaktadır. Travma vakaları; hem hızlı hem de doğru teşhislerin konulmasının aynı anda en önemli olduğu tıbbi vakalardır. OLGULAR Olgu 1: 35 yaş erkek hasta, servisimize elektrik çarpmasına bağlı yüksekten düşme şikayeti ile başvurdu. Hastada oksipital bölgede hemorajik kontüzyon, sağ hemotoraks, T10-11 seviyesinde tam kat ayrışma ve kardiyak etkilenme mevcuttu. Yoğun Bakım şartlarında takip edilen hasta kardiyak arrest sonrasında kaybedildi. Olgu 2: 30 yaş erkek hasta, servisimize elektrik çarpmasına bağlı duvardan düşme şikayeti ile başvurdu. Hastanın sol omzunda ve belinde ağrı şikayeti mevcuttu. Hasta Kardiyoloji konsültasyonu sonrası yanık ünitesinde takibe alındı. Olgu 3: 37 yaş erkek hasta, servisimize elektrik çarpmasına bağlı direkten düşme şikayeti ile başvurdu. Hasta elektriğin giriş yerinin elleri olduğunu belirtmekte ve oksipital ölgesinde ağrısı olduğundan yakınmakta. Hastanın kardiyak etkilenmesi olduğundan dolayı Kardiyoloji konsültasyonundan sonra SAK takibi amaçlı yoğun bakımda gözlem altına alındı. Sonuç: Yüksekten düşme ve iş kazaları tüm dünyada ve ülkemizde önemli bir halk sağlığı sorunudur. Anahtar Kelimeler: Elektrik çarpması, yüksekten düşme, iş kazası P 008 NEEDLE INGESTİON Göksu Afacan1, Sultan Tuna Akgöl Gür1, Serdar Can2, Serhat Örün2
1Erzurum Regional Training and Research Hospital, Emergency Service, Erzurum 2Iğdır State Hospital, Emergency Service, Iğdır Swallowing of foreign body is one of the common reason for application of emergency patients to the hospitals. It is more common in children than adults. It is mainly seen between 4 months - 4 years children. In adults it is usually associated with mental or psychiatric failure. In terms of incidence and demographic features, there is no statistically significant research about foreign body swallowing. However there is a significant increase in the patients who suffer from foreign body swallowing. One of the main cause of foreign body swallowing in our country is swallowing of pin during putting on veil in religious women. Most common foreign bodies are; metallic coins, toy components, watch batteries, needles, fish bone and chicken bones. Case: 34-year-old, veil wearing female patient, presented to our clinic assuming that she ingested a needle. We perform chest X-ray but there was nothing to be shown. After X-ray patient said that she had a severe dyspnea, but in the auscultation there was nothing to be heard. Patient insisted on that she had swallown a needle so we perform thorax BT. As a result; there is a needle which is lying on her left lung. After the Thoracic Surgery consultation patient was discharged from hospital. In our case; we want to imply about the importance of the complications of foreign body swallowing and be more careful while treating these patients. Keywords: BT, foreign body, ingestion, needle

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
208
P 009 DÜŞÜK ENERJİLİ TRAVMA İLE OLUŞAN ÖNKOL FRAKTÜRÜ Göksu Afacan1, Serdar Can2
1Erzurum Bölge Eğitim ve Araştırma Hastanesi, Acil Servis, Erzurum 2Iğdır Devlet Hastanesi, Iğdır Suprakondiler humerus kırıkları klasik olarak distal humeral kondillerin proksimalinde olekranon fossadan geçen kırıklar olarak tarif edilir. Bu kırıklar çocuk dirsek kırıklarının yaklaşık olarak %50’sini ve cerrahi gerektiren kırıkların%85’ini oluşturur. Genellikle 3-10 yaşlarında ve erkeklerde daha sık görülür. Suprakondiler humerus kırıklarında yaralanma mekanizması %98-99 açık el üzerine düşme veya %1-2 oranında da fleksiyonda ki dirsek üzerine düşme şeklindedir. Dirsek kırığı olan çocuk hastanın değerlendirilmesine fizik muayene ile başlanmalıdır. Bu muayene özellikle küçük çocuklarda ağrı ve hastanın anksiyetesi nedeniyle zor olabilir. Yaralanma olan eksteremitenin muayenesine inspeksiyonla başlanır. İnspeksiyonla, ayrılmış suprakondiler humerus kırıklarında belirgin deformite ve şişlik, kubital fossada brakialis kasında yırtık olup olmadığını gösteren çadırlaşma tespit edilebilir. Kompartman sendromu açısından aşırı ağrı, pasif hareketle parmaklarda ağrı olması ve kompartman gerginliği kontrol edilmelidir. Nörovasküler muayene çok önemlidir. Birçok çocukta motor muayeneyi tamamlamak zordur. ancak bunun için yeterli çaba harcanmalıdır. Özellikle anterior interosseoz sinir yaralanmasını değerlendirmek için parmak fleksiyonuna ameliyatöncesi bakılmalıdır. Median, ulnar ve radial sinirlerinduyu muayenesi de yapılmalıdır. Vasküler muayene için radial nabız bakılabilir ancak kapiller dolum daha önemlidir. Çünkü ayrılmış suprakondiler humerus kırığı olan çocukların çoğunda radial nabzı palpe etmek mümkün olmayabilir. Nabızlar genelde kapalı redüksiyonu takiben geri döner. Hastanın eli soğuk, soluk ve kapiller dolumu yetersizse acil cerrahi müdahale için hasta ameliyathaneye alınmalıdır. Olgu: 6 yaş kız çocuğu, parkta kaydıraktan kayarken dirseğinin üzerine düşmüş; aile travmanın şiddetini minimal olarak tarif etmekte. Hastanın yapılan ilk muayenesi dirsek çıkığı ile uyumlu ancak hastanın dirseğinde ailenin de başvuru sebebi olan şişlik mevcut. Redüksiyon manevrası yapılmaya çalışılmadan önce -hastanın yaş itibariyle de muayeneye uyumsuz olması sebebiyle- hastadan direkt grafi istenmesi sonucu hastada humerus alt uç kırığı tespit edilmiş olup cerrahi müdahale amaçlı Ortopedi Servisine yatışı sağlanmıştır. Sonuç: Minimal travma sonrası acil servise başvuran çocuk hastalarda sonuçlar katastrofik olabileceğinden daha dikkatli olunmalıdır. Anahtar Kelimeler: Kaydırak, çocuk parkı, humerus alt uç kırığı P 010 RECTUM AND BLADDER RUPTURE DUE TO ANIMAL ATTACK Göksu Afacan Erzurum Regional Training and Research Hospital, Emergency Service, Erzurum Animal related trauma is a major medical problem due to its potential for serious morbidity and mortality. Since livestock breeding still remains important source of income in Turkey, the risk for this problem increases. There is a very little data in the literature related to the trauma caused by the attack of the ox. In this case report we aimed to present a livesock breeders' rectum and bladder rupture after the ox attack. Case: 54-year-old male livestock breeder admitted to hospital with serious back pain and minimal hematuria. After the physical examination he seemed to be fully oriented and cooperated and have minimal pain on both lower quadrants. After the full anamnesis patient said that the ox hit on him via his rectum, fter the rectal examination we found that there is a rectum rupture and which urine comes out from there. Our diagnosis was confirmed by cystouretherogram. Patient was immediately sent to operating room for emergency surgery which is performed by both Urologists and General Surgeons. In our country -especially in the countryside- many people earn money from living animals. Both domestic and wild animals are the major cause of traumatic injury so we especially keep in mind katastrophic scenarios. Keywords: Bladder, rectum, trauma

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
209
P 011 KENDİ KENDİNE TRAVMA: KAYA İLE BİRLİKTE YUVARLANMA Göksu Afacan, Sultan Tuna Akgöl Gür Erzurum Bölge Eğitim ve Araştırma Hastanesi, Acil Servis, Erzurum Yüksekten düşme, trafik kazalarından sonra en sık travma sebebi olarak karşımıza çıkarken; çocukluk yaş grubundaki düşmeler, en sık travma sebebi olarak izlenir. Tüm teknolojik gelişme ve uygulamalara karşın dikkatsizlik nedeniyle veya insan hayatı için geliştirilmiş emniyet tedbirlerini almadan çalışan birçok insan hayatını kaybetmekte, sakat kalmakta ya da ciddi şekilde yaralanmaktadır. Travma vakaları; hem hızlı hem de doğru teşhislerin konulmasının aynı anda en önemli olduğu tıbbi vakalardır. Olgu: 61 yaş erkek hasta, köyde tarlasına giderken ayağı kayması sonrası hafif eğimli yaklaşık beş metre yüksekliği olan bir yerden düşmeye başlamış, ancak düşerken hastanın kendi deyimiyle can havliyle bir kayaya sarılmış ve düşerken de onu bırakmamış. Hasta acil servisimize başvurduğunda, bilinç açık, oryente, koopere, vitalleri stabil idi ve stabil seyretti. hastanın durmak amaçlı sarıldığı kaya parçası da hasta ile birlikte yuvarlandığından hastanın vücudunda multipl abrazyonlar, minimal kesiler, sağ ön kolda fraktür ve frontal kemikte linner fraktür tespit edildi. Hasta takip ve tedavisinin devamı için Beyin ve Sinir Cerrahisi Servisine yatırıldı. Sonuç: Yüksekten düşme bazen minimal sonuçlar doğurabilse de bazen de sunduğumuz olgudaki gibi insan faktörü ile birlikte katastrofik sonuçlara yol açabilmektedir. Anahtar Kelimeler: Yüksekten düşme, kafa travması, kaya P 012 İLEUSA NEDEN OLAN NÜKS SPİEGEL VE EPİGATRİK HERNİLER: OLGU SUNUMU
Mehmet İnce1, Leyla Ince2, Ümit Alakuş1, Nail Ersöz1
1Gülhane Askeri Tıp Akademisi, Genel Cerrahi Anabilim Dalı, Ankara 2Abdurrahman Yurtaslan Onkoloji Hastanesi, Radyoloji Bölümü, Ankara Spiegel hernisi çok nadir (tüm hernilerin %1–2) görülen karın ağrısı nedenlerinden birisidir. Karında şişlik ve ağrı şikayetleri ile acil servise başvuran bu hastaların yaklaşık %20’sinde inkarsere fıtık ve buna sekonder ileus ile karşılaşılabilinmektedir. Nüks inkarsere Spigel ve epigastrik herni tanısı ile acil olarak opere edilen olgumuzu sunmayı amaçladık. Kırk dört yaşında kadın üç gündür devam eden karın ağrısı, karında şişlik, bulantı ve kusma şikâyetleri ile acil servise başvurdu. Özgeçmişinde diabetus mellitus sol meme kanser tanıları mevcut olan hastanın yapılan fizik muayenesinde; 4 yıl önce geçirmiş olduğu epigastrik ve Spigel hernilerine sekonder göbek üstü ve sağ alt kadranda insizyon skarları ve skarların altında şişlik saptandı. Ayrıca sağ alt kadrandaki şişliğin içinde ince barsak anslarının olduğu ve redükte olmadığı görüldü. Lökosit sayımı olan hastanın ayakta direk batın grafisinde hava-sıvı seviyeleri görülemsi üzerine çekilen kontrastlı batın BT‘de epigatrik bölgede nüks herni ve sağ alt kadranda Spigel hattına uyan bölgede sfak defekti olduğu ve defentten çıkan ince barsak anslarının cilt altına doğru yerleştiği görüldü (Resim 1). Hasta gerekli hazırlıklar yapıldıktan sonra acil şartlarda opere edildi. Yapılan ekplorasyonda epigatrik bçlgede nüks herniye sekonder fıtık kesesi ve içinde omentum olduğu görüldü. Sağ alt kadrakdaki defektten çıkan ince barsak anslarının ise herni kesesine ve cilt altına yapışıklıklar gösterdiği görüldü (Resim 2). Postopertaif dönemde komplikasyon gelişmeyen hasta postopertatif 4.günde taburcu edildi. İleus ön tanısı ile başvuran hastalara yapılacak fizik muayene ve tetkiklerle nadir görülen Spigel herni tanısı kolaylıkla konularak geç kalmadan opere edilerek komplikasyonsuz olarak iyileşme sağlanabilir. Anahtar Kelimeler: Spigel hernisi, ileus, cerrahi tedavi

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
210
P 013 THE EMERGENCY ROOM OVERCROWDING: WHY THE EMERGENCY ROOM INSTEAD OF A GENERAL PRACTITIONER AND HOW TO MANAGE IT
Anouk Etienne, Thierry Preseau Free University of Brussels, CHU Brugmann, Emergency Room, Brussels, Belgium Objective: Since many years, we have to deal with a growing problem: the ER (emergency room) overcrowding. There are many reasons to that, in particular there are patients appealing to the ER for a non-urgent pathology. We tried to understand why patients go to the ER instead of another first line care center. Materials - Methods: A questionnaire was handed to each patient at the ER of CHU Brugmann, Brussels to find out the reason of coming to the ER instead of another first line care facility and to investigate about their knowledge concerning first line care structures. A second questionnaire was filled by the doctor and nurse who had taken the patient in charge. The purpose was to determine triage level, treatment and destination of the patient. Results: 528 questionnaires were handed and 374 patients answered them. 51% of them had a general practitioner but came straight to the ER mostly because of the possibility to have immediate test (119) or due to the too long waiting time for an appointment with a general practitioner (60). 49% didn’t have a family doctor mostly because they are never sick (36). We also pointed out that the knowledge in first line care structures was really poor. Finally, we fund there was a little correlation when comparing nurse’s triage and doctor’s conclusion or nurse’s triage and hospitalization. Nurses tend to consider a patient more urgent than he really is. Conclusion: One of the reason for ER overcrowding is the misuse of this structure, mostly because patients want « everything immediately ». We have to inform patients on first line care facility especially since screening and prevention remain a major factor in public health. Keywords: ED overcrow, ED design, triage system, first line care structures P 014 SUDDEN HEARING LOSS AND CONVULSION Mehmet Ünaldı1, Soner Işık1, Didem Ay1, Ersen Gündüz1, Cihan Büyüksütcü1, Hatice Eryiğit2
1Medeniyet University Göztepe Training and Research Hospital, Department of Emergency Medicine, Istanbul, Turkey 2Kartal Training and Research Hospital, Thorax Surgery Clinic, Istanbul, Turkey Sudden hearing loss is hearing loss occurring over 3 days or less. The incidence increases with increasing age. Most cases of sudden hearing loss are idiopathic, others include vascular causes, trauma, infection, metabolic disorders and drugs. In this case we present to a patient with convulsion, admitted to the ED with complaint of sudden hearing loss. Case: 61 year-old male patient admitted to the ED with sudden hearing loss in right ear and numbness in right arm. In vital signs tension 160/80 mm-Hg, pulse 88/min and others were stable. He had no comorbid disease in history. Neurologic examination of his was normal. In radyologic scanning brain CT showed suspected hypodens area on left temporal lobe. During follow-up he had generalize tonic-clonic convulsion 3 min period. We applied Diazepam and Fenitoin in order to avoid. The obtained MRI scanning confirmed 28*21 mm as coronal and about 21 mm as axial focal pathologic focus in left medial temporal area. He was interned to neurosurgery clinic. The evaluation of sudden hearing loss must begin with a comlplete history and physical examination. Systemic ilnesses also should be considered as in this case. Keywords: Convulsion, hearing loss, sudden

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
211
P 015 PERICARDIAL FLUID MAY BE CAUSED OF RHEUMATIC DISEASE Mehmet Ünaldı1, Soner Işık1, Didem Ay1, Cihan Büyüksütcü1, Ersen Gündüz1, Ümit Ölmez1, Hatice Eryiğit2
1Medeniyet University Göztepe Training and Research Hospital, Department of Emergency Medicine, Istanbul, Turkey 2Kartal Training and Research Hospital, Thorax Surgery Clinic, Istanbul, Turkey Systemic rheumatic diseases are chronic, inflammatory, autoimmune disorders. ED patients with systemic rheumatic diseases have complex clinical and pharmacologic histories, and multiorgan system pathology. We present to a case with diagnosed rheumatic disorder, admitted to the ED with chest pain. Case: 60 year-old female patient was presented to the ED with chest pain about 15 days period. Vital signs of her were stable. Laboratory sampling demonstrated Hb:9,2 g/dl, Hct:27 %, sedimentation: 94 mm/h, LDH:354 U/L and ALP:143 U/L. In radiologic scanning, Thorax BT showed plevral effusion on both right (20 mm) and left (21 mm) hemitorax and about 19 mm pericardial effusion. She was interned to internal medicine clinic with prediagnosed rheumatic disease. Many of extra-articular manifestations of rheumatic diseases can result in serious morbidity and mortality if not recognized and properly managed. One of clinical signs and symptoms associated with systemic rheumatic diseases is cardiovascular manifestations including chest pain, hypertension, pericarditis, valvular diseases etc. So rheumatic disease should be considered in differential diagnosis. Keywords: Fluid, pericardial, rheumatic disease
P 016 TWO CASES OF A DAY: SPONTANEOUS SUBARACHNOID HEMORRHAGE Mehmet Ünaldı1, Soner Işık1, Didem Ay1, Ersen Gündüz1, Onur Incealtın1, Hatice Eryiğit2
1Medeniyet University Göztepe Training and Research Hospital, Department of Emergency Medicine, Istanbul, Turkey 2Kartal Training and Research Hospital, Thorax Surgery Clinic, Istanbul, Turkey Nontraumatic subarachnoid hemorrhage accounts for a relatively small portion of ED visits but a missed diagnosis can produce devastating results. In this study we present to two cases (elder patient and young patient) of spontaneous subarachnoid hemorrhage a day in ED. Case 1: 28 year-old male patient admitted to the ED with the most severe headache until that day. Brain BT showed subarachnoid hemorrhage on anterior interhemisferic, suprasellar sistern and both of sylvian fissur. Case 2: 60 year-old male patient presented with headache that persists for several days. Brain BT angiograhy demonstrated 4 mm saccular aneursymal dilatation on left Anterior Cerebral Arteria (ACA). Both of them were interned neurosurgery clinic and were discharged in good health.The potentially devastating results of a missed or delayed diagnosis of subarachnoid hemorrhage mandate that any patient for whom the diagnosis of subarachnoid hemorrhage is considered receives an aggressive evaluation. Keywords: Hemorrhage, spontaneous, subarachnoid

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
212
P 017 A RETROSPECTIVE STUDY OF CARBON MONOXIDE POISONING CASES IN ÜMRANIYE TRAİNİNG AND RESEARCH HOSPİTAL PEDIATRIC EMERGENCY DEPARTMENT
Mustafa Özgür Toklucu1, Caner Araz2, Mehmet Nizamoğlu2, Emin Pala2, Sevgi Akova1, Burcu Karakayalı1, Şirin Güven1
1Sağlık Bilimleri University, Ümraniye Training and Research Hospital, Department of Pediatrics, İstanbul, Turkey 2Sağlık Bilimleri University Ümraniye Training and Research Hospital, Department of Family Medicine, İstanbul, Turkey The epidemiological and clinical characteristics of the carbon monoxide poisoning cases (n=167); aged between 8 months to 15 years (std deviation: 6,38±4,32), who had applied to Ümraniye Training and Research Hospital Pediatric Emergency Unit, between the dates of 1st January 2010 - 01 July 2012; were evaluated retrospectively. Childhood poisoning cases constituted 0,07% of the total pediatric emergency visits. 87 of the cases (52,1%) were female and 80 (47,9%) were male. According to age groups, respectively, 13 months-4 age group were 25,1% of all cases, the ages 8-11 were more frequent generating 24%. All the poisoning cases were accidental and occurred mostly in winter (%46,7 n=78). Carboxyhemoglobine levels measured at first visit, most frequently ranged between 0 and9,99 (n=57, 34,1%), and 20 and 29,9 (n=48, 28,7%). The average pH values measured during the application of blood gases were 7,36 (± 0.,52 ). It was observed that most of the cases (45,51%, n=76) were asymptomatic initially. Nausea and vomiting (32,9%, n=55), headache (16,1%, n=27) and dizziness (15,51%, n=27) were the most frequent symptoms and signs. Three cases were transferred to the critical care units, while six patients were referred for hyperbaric oxygen therapy. No mortality was reported during the treatment in our hospital. We hope our study will help determine strategies for preventive measures of carbon monoxide poisoning in Ümraniye and İstanbul. Keywords: Carbon monoxide poisoning, childhood, epidemiology P 018 MİNÖR KÜNT KAFA TRAVMALI ÇOCUKLARDA PECARN VE CATCH KLİNİK KARAR VERME KURALLARI
ETKİNLİKLERİNİN KARŞILAŞTIRILMASI Öner Bozan, Gökhan Aksel, Hande Akbal Kahraman, Özlem Giritli, Serkan Emre Eroğlu Sağlık Bilimleri Üniversitesi Ümraniye Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Bu çalışmada minör künt kafa travmalı çocuklarda bilgisayarlı tomografi çekiminde PECARN ve CATCH kurallarının klinik anlamlı intrakranialpatoloji saptamadaki etkinliklerinin karşılaştırılması amaçlanmıştır. Acil servise GKS 14-15 olan minor künt kafa travması ile başvuran 18 yaş altı pediyatrik hastaların çekilen beyin tomografileri sonuçları kayıt altına alınmıştır. 18 yaş ve üstü ve GKS:14 altı olan hastalar, çalışmaya katılmayı reddeden hastalar, hasta takibinde verileri kaybolan hastalar çalışma dışı bırakıldı. Çalışmada asıl karşılaştırılacak olan intrakranial patolojilerin saptanmasında PECARN ve CATCH’in karşılaştırılmasına ek olarak prognoz göstergeleri olarak taburculuk, servise yatış, operasyon, yoğun bakım ünitesine yatış ve ölüm olmak üzere 4 ayrı sonuç dikkate alınmıştır. Bu çalışma prospektif olarak 01.01.2016- 30.04.2016 tarihleri arasında gerçekleştirilmiştir. Yapılan çalışmada PECARN testinin sensivitesi %95 spesifitesi %53 olarak hesaplanmış olup pozitif prediktif değeri %14, negatif prediktif değeri %99 olarak hesaplanmıştır. Yine bu testin pozif likelihood ratio değeri 2, negatif likelihood ratio değeri 0,1 olarak hesaplanmıştır. CATCH testinin sensivitesi %48, spesifitesi %83 olarak hesaplanmış olup pozitif prediktif değeri %19, negatif prediktif değeri %95 olarak hesaplanmıştır. Yine bu testin pozif likelihood ratio değeri 2.95, negatif likelihood ratio değeri 0,63 olarak hesaplanmıştır. Yaptığımız çalışmada PECARN bir hastayı atlamış olup hastanın çekilen BBT’sinde hastada kafa tabanı kırığı ve lineer fraktür saptanmış hastaya beyin cerrahisi servisine yatış verilmiştir. İki gün beyin cerrahi servisinde takip edilmiş opere edilmeksizin taburcu edilmiştir. Aynı hastayı CATCH’te yakalayamamıştır. Subdural hematomu olan 1 hastayı, kontüzyosu olan 2 hastayı, epidural hematomu olan 3 hastayı, lineer fraktürü olan 3 hastayı CATCH atlamasına rağmen PECARN yakalamıştır. Gerek PECARN gerekse CATCH klinik karar verme kurallarının minör künt kafa travması ile başvuran çocuk hastalarda BBT çekme kararı vermede etkili kurallar olduğunu tespit etmekle birlikte, PECARN’ın daha yüksek sensitiviteye sahip olması sebebiyle acil servislerde daha kullanışlı bir kural olduğunu düşünmekteyiz. Özellikle GKS<15 olan, nonfrontal hematomu olan küçük çocuklarda BBT çekilmesinindoğru bir yaklaşım olduğunu düşünmekteyiz. Anahtar Kelimeler: PECARN, CATCH, minör künt kafa travmalı çocuklar

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
213
P 019 LIDOCAINE-INDUCED CARDIAC ARREST WITHIN THERAPEUTIC DOSES TREATED WITH INTRAVENOUS LIPID EMULSION
Yunus Emre Özlüer, Alev Peker Seçim, Burçak Kantekin, Duygu Ege Adnan Menderes University, Aydın, Turkey Lidocaine has a worldwide use for treatment of ventricular arrhythmias such as ventricular tachycardia and fibrillation and also it is a choice of drug in pretreatment phase of rapid sequence intubation. In an overdose, lidocaine can cause sinus slowing, asystole, hypotension, and shock. However, little is known about proarrhythmic effect of lidocaine. An 80-year-old male who has been diagnosed as sepsis had tachypnea, dyspnea and respiratory acidosis unresponsive to noninvasive mechanical ventilation during his stay in our intensive care unit. As a matter of course, a rapid sequence intubation was planned. After proper and adequate preoxygenation, a 1.5 mg/kg of lidocaine of 2% has been administered as a pretreatment agent. Subsequently, patient had a brief episode of ventricular fibrillation and then asystole. Alongside with the initiation of cardiopulmonary resuscitation a bolus of 1.5 ml/kg of intravenous lipid emulsion has been administered. After a cardiopulmonary resuscitation effort of 15 minutes, the patient had return of spontaneous circulation with a rhythm of first degree atrioventricular block with sinus arrhythmia. As the hypotension and the arrhytyhmia persisted in despite of proper treatment with inotropic drugs such as norepinephrine and epinephrine, another bolus of 1.5 ml/kg of intravenous lipid emulsion has been administered. Following the bolus of intravenous lipid emulsion sinus rhythm has been achieved alongside with the improvement of arterial blood pressure. Although lidocaine is used for treatment of ventricular arrhythmias, clinicians should always keep in mind that drugs can cause toxicity even in their therapeutic dose ranges. Thus, according to the general rule, drugs should be administered with titrating in their lowest doses as possible. Keywords: Cardiac arrest, intravenous lipid emulsion, lidocaine-induced, ventricular fibrillation P 020 DIFFUSION-WEIGHTED MAGNETIC RESONANCE IMAGES THAT MIMIC ISCHEMIC STROKE Gamze Çopuroğlu, Hüseyin Çetin Arslan, Murat Yeşilaras Tepecik Training and Research Hospital, Emergency Medicine Clinic, Izmir, Turkey Introduction: Diffusion-Weighted Magnetic Resonance Imaging (DW-MRI) is used for acute ischemic stroke. The image on DW-MRI is obtained by Brownian movement of water molecules. Lesions are being evaluated together with apparent diffusion coefficient (ADC). Ischemia is seen hyperintense on DW-MRI and hypointense on ADCs. Case: We present the case of a 27 year-old male patient who refers to Emergency Department (ED) with complaints of headache and dizziness three times. He had chronic suppurative otitis on the right ear and was given medical treatment 7 days ago. His vital signs were normal. He had no fever, no lateralized motor deficits in neurological examination, his pupils were isochoric, light reflex were bilaterally positive. Babinski reflex was negative bilaterally. He had confusion attacks that he could be awaken with verbal stimulus and did not have vertigo and ataxia. White Blood Cells: 24000/uL Procalcitonin: 0.41ng/mL C-Reactive Protein:273mg/L. Brain Computed Tomography was regarded as normal (Figure 1).The DW-MRI was interpreted as ischemia in the first evaluation and the patient had admitted to the neurology service. He was intubated soon because of worsening awareness and admitted to intensive care unit. DW-MRI was interpreted; right cerebellopontine corner subdural empyema (arrow), left paracentral localization of subdural abscess collection neighbors of posterior cerebellar vermis and abscess formation reaching toward the anterior temporal lobe. (Figure 2) He was operated immediately but a few days later he was dead. Discussion: DWI is an imaging tool often used in ED; although the assessment is easy, emergency physician and neurologists can make mistakes. However it should be kept in mind; that DWI-MRI may give false negative and positive results for stroke patients.Table 1 shows pathologies other than stroke which seen hyperintensity on DWI-MRI and hypointensity on ADC images. Keywords: Diffusion-Weighted Magnetic Resonance Imaging, stroke mimic, diagnoses

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
214
P 021 DIFFUSE IDIOPATHIC SKELETAL HYPEROSTOSIS: AN INCIDENTAL DIAGNOSIS DUE TO TRAUMA – A CASE REPORT
Yasin Yıldız, Mine Kayacı Yıldız, Serkan Emre Eroğlu University of Health Sciences Ümraniye Training and Research Hospital, Department of Emergency Medicine, Istanbul, Turkey Introduction: Diffuse idiopathic skeletal hyperostosis (DISH) is an ossification of the vertebral body's anterior and lateral side.Most of patients are asymptomatic, dysphagia is the most common symptom due to compression of esophageus. Cervical subaxial pain, stiffness and decreasing range of motion of the cervical spine are the other complains. Case: A 72-year-old male presented to our emergency department with backache and neck pain. He was fall down due to a traffic accident while standing in a bus. He had type II diabetes.There was a mild tenderness on palpation of cervical vertebras.There was no focal neurological deficit on central nervous system examination.Cervical computed tomography (CT) revealed bony ankylosis from C2 to C7. And there was a suspected fracture on C3.Axial images showed syndesmophytes at C3 to C7.The patient was referred to the neurosurgery clinic, and they offered out-patient follow up with a soft cervical coller. The patient treated with nonsteroidal anti-inflammatory drugs (NSAIDs). Discussion: DISH is a clinically common pathological condition but usually unrecognized and misdiagnosed by clinicians.This rare entity is diagnosed incidentally cause of usually been asymptomatic. The most common symptoms of DISH are pain and stiffness, dysphagia and decreased range of motion.Lumbar spine is the most commonly affected vertebrae and cervical spine is less involved. Rarely, dysphagia and dysphonia are seen when cervical spines are affected.Diagnostic methods include X-ray, CT, MRI (magnetic resonance imaging), videofluoroscopy, and endoscopy.The management is mostly conservative as NSAID and steroid therapy. In patients with severe and progressive symptoms, surgery could be an appropriate choice. Conclusion: DISH, even though rare, should be kept in mind in the differential diagnosis for the patients, especially who have diabetes, with a complaint of neck pain or dysphagia. It is important that emergency physicians are familiar with the diagnosis and treatment of the cervical manifestations of this disorder. Keywords: Cervical trauma, diffuse idiopathic skeletal hyperostosis, DISH syndrome P 022 AN OVERLOOKED DIAGNOSIS OF HEAD TRAUMA: INTRAOCULAR LENS DISLOCATION Ozlem Dikme, Elif Degirmenci, Eda Ars, Can Aktas Koc University Hospital, Department of Emergency Medicine, Istanbul, Turkey Lens dislocation is completely losing its normal anatomic position of the lens while the lens subluxation is a partial disruption of anatomical position. It can be seen in association with some hereditary systemic diseases or may develop aftermath of ocular surgery or trauma. A 92-year-old woman has bilaterally prior cataract surgery two years ago presented to the ED with head trauma due to fall down. She had not any loss of consciousness after trauma. When the ecchymosis appeared around her right eye her son decided to bring her to the ED. On admission her vital signs were normal. There was right periorbitally ecchymosis and conjunctival hemorrhage. Eye examination revealed no visual acuity. Ocular motility examination was normal. The pupil was in normal shape and reactive on bilaterally. Head and neck exams were otherwise unremarkable. Her neurological exam was normal. When evaluated her age, trauma mechanism and physical findings together, brain CT was planned and it was normal about skull fracture, facial fracture, or intracranial abnormality. It only showed suspected right lens dislocation. When the emergency physician examined her with bedside ocular US, indicating a freely floating lens inside the eye globe with reverberation artifacts. She consultated with Ophtalmologiest. Initial intraocular pressure was measured as 18 mm Hg and there wasn’t any retinal complication. Medical follow-up decision was taken and she was discharged to follow in outpatient clinic to the intraocular pressure measurement. Point-of-care US has been widely used by emergency physicians particularly in trauma cases. Ocular US is a part of it and should be the first line imaging in the ED. It has several advantages, first of all it is a readily available tool in the ED and does not radiation expose. Secondly it can quickly establish the diagnosis and prompt ophthalmology consultation. Keywords: Ocular trauma, ultrasound, emergency

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
215
P 023 SYMPTOMATIC HYPONATREMIA ASSOCIATED WITH PSYCHOGENIC POLIDIPSIA Zeynep Karakaya, Eylem Kuday Kaykisiz, Pinar Yeşim Akyol, Umut Payza, Fatih Esad TOPAL Katip Çelebi University Atatürk Training and Research Hospital, Department of Emergency Medicine, Izmir, Turkey Introduction: Primary or psychogenic polidipsia characterized by excessive thirst and compulsive water drinking is a prevelant problem among psychiatric patients, affecting 6% to 20% of them. Excessive oral fluids consumption over a short time period may lead to hyponatremia, which can causes confusion and seizures.This is a frequent condition in chronic psychiatric population. Case: A 33 year old male patient was referred to the emergency unit of our hospital with loss of consciousness. He was admitted to intensive care unit. His physical examination revealed with normal vital signs in spite of his agitation. In his labaratory tests showed that he had hyponatremia 104 mmol /L. His blood urea nitrogen was 4 mg/dL, Serum K+ level was 3 mEq/l, Creatin Kinase was 620 U/L. No abnormalities was found in cranial pathology with computed tomography. Medical testing ruled out all medical condition known to be etiologically related to hyponatremia. In his psychiatric assesment, he was diagnosed with psychogenic polidipsia. He was supplemented with saline intravenously infused at 60 ml/h and his serum concentration returned to 133 mmol/L on the third day. He was discharged with his psychiatric drugs that used for schizophrenia. Discussion: Water intoxication usually happens in patients with psychiatric problem who are subject to compulsive water ingestion. Our patient also had schizophrenia. Water intoxication causes headache, blurred vision, muscle cramps, confusion, letargy, delirium, seizure and coma. Since it may cause brain edema and coma, it can be mortal. When Na concentration gets lower than 125 mmol /L hipernatremic encephalopathy and neurological symptoms begin. It is important to consider water intoxication as a cause of hyponatremia in a patient without signs of dehydration but one should rule out all medical conditions known to be related to hyponatremia Keywords: Polidipsia, hyponatremia, emergency department P 024 NON-TRAUMATIC PUBIC DIASTASE Bulut Demirel Ankara Atatürk Training and Research Hospital, Clinic of Emergency Medicine, Ankara, Turkey Introduction: Symphysis pubis is the middle line cartilaginous joint which unites superior rami of the both pubic bones. Symphysis pubic diastase can be seen after a trauma or after delivery in females. In this study, the event of a non-traumatic diastase in a 36-year-old male patient was presented. Case Report: A 36 year-old male patient presented to the ED with the complaint of lumbar pain. Physical examination of the patient and the inspection was normal. Any sign of trauma was observed in the patient. In the examination of the patient’s pelvic bone, a disorder was recognized in the region of symphysis pubic. In the direct pelvis graphy, the abnormal extension of symphysis pubis was observed. The pubic diastase of the patient was thought by a prior trauma, past pelvic trauma story was questioned. However, it was indicated that there wasn’t any such kind of trauma in the patient’s past medical history. Thus, additional examination and treatment weren’t done. Discussion: Symphysis pubis diastase is a rarely seen kind of injury occurring with anterior compression force. At the same time, symphysis pubis disintegration events which occur after vaginal delivery are seen. In our study, the patient is male and in his past medical history there is no medical trauma. Congenital large symphysis pubis events and urogenital pathology which are seen in those patients are present in the literature. In the treatment, posterior stabilization of internal fixation is recommended. Symphsis pubis diastase except from delivery and trauma can also be watched in osteitis pubis, osteomyelitis and osteolytic metastasis and in rare syndromes such as Prune Belly, Sjögren-Larson and Wolf. In our case, symphysis pubic diastase was wanted to be evaluated but it wasn’t accepted by the patient. Consequently, pubic diastase generally can be seen after either delivery or trauma. It should be kept in mind that it can be seen in non-traumatic situations, as well. Keywords: Emergency, non-traumatic, pubic diastase

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
216
P 025 KOUNIS SYNDROME: REPORT OF TWO CASES Maruf Beğenen, Özlem Köksal Uludağ University School of Medicine, Department of Emergency Medicine, Bursa, Turkey Introduction: Allergy is one of the most frequent causes of the emergency department(ED) admissions. A wide spectrum of etiologic causes including foods, inhalation, insect bites and contacts are responsible for this situation. Allergic Myocardial Infarction also named as Kounis Syndrome is one of these reasons. Here, we report two different case of Kounis Syndrome that admitted to our ED same day. Case 1: A male patient aged 48 admitted to the ED with the complaint of bee sting 1 hour ago.He had no prior illness, he was so agitated and hardly stated that he had bee sting on his left arm nearly an hour ago while he was working on the field.He hasn’t got any additional complaint including chest pain.His initial ECG was normal.Coronary angiography revealed a 90% stenosis in the RCA and stent successfully placed. The patient's situation were regarded as Kounis Syndrome following bee sting. Case 2: A male patient aged 49 admitted to the ED with the complaint of syncope 15 minutes ago.He stated that he had bee sting on his nearly two hours ago.His initial ECG revealed 1 mm ST elevation in D2-3 and aVF derivations and had no resiprocal changes.He was regarded as ST elevated myocardial infarction and coronary angiography was planned.Coronary angiography revealed a 90% stenosis in the LAD, stent successfully placed.The patient's situation were regarded as Kounis Syndrome following bee sting. Conclusion: Kounis syndrome is a group of symptoms that manifests as unstable vasospastic or nonvasospastic angina and even as acute myocardial infarction and is triggered by the release of inflammatory mediators following an allergic insult. Medical acute coronary syndrome management and supressing the allergic reaction were the basic principles in the management of Kounis Syndrome. Also coronary angiography must be performed, vasospasm should be dissolved by direct intracoronary drugs and angioplasty should be performed if it is necessary. Keywords: Kounis syndrome, emergency department, allergic reaction P 026 LATERALİZAN BULGU OLMAKSIZIN İNTRAKRANİYAL KANAMA VAKASI Kıvanç Karaman Şanlıurfa Mehmet Akif İnan Eğitim Araştırma Hastanesi, Acil Servis, Şanlıurfa İntrakranial hematomlar, serebrovasküler hastalıkların en sık görülen nedenidir. Etyolojisinde sıklıkla hipertansiyon, vasküler patolojiler, antikoagülan kullanımı, ilaç ve alkol bağımlılığı, intrakranial tümörler ve travma vardır. Tanı beyin tomografisi ve kranial MRG ile konur. Cerrahi kararı; hasta yaşı, nörolojik skoru, hematom yerleşim yeri ve hacmine göre değişiklik gösterir. Bu olgu sunumunda acil servise baş ağrısı şikayeti ile başvuran genç erkek hastada saptanan ve patolojik fizik muayene bulgusu olmayan intraparankimal hematom bulgusu paylaşılmıştır. Daha önce bilinen hastalığı olmayan 24 yaşında erkek hasta baş ağrısı şikayeti acil servisimize ayaktan başvurdu. Hasta son iki gündür bu şikayet ile acil servise başvurmuş, uygulanmış ve taburcu edilmiş. Genel durumu iyi, vital bulguları stabil olan hastanın bilinci açık, oryante koopere, pupilleri izokorik, IR +/+, Glaskow Koma Skoru 15 saptandı. Nörolojik muayenede lateralizan bulgu yoktu. Hastaya intramusküler analjezik tedavisi uygulandı ancak şikayetinin gerilememesi üzerine hastaya bilgisayarlı beyin tomografi (BBT) çekildi. BBT’ de sağ temporal lobda lokalize 49x35 mm boyutlarında hematom saptanan hasta beyin cerrahiye konsulte edildi. Hasta beyin cerrahi tarafından servise yatırıldı ve intravenöz 2x500 mg sodyum valproat, 4x100 cc %20 mannitol ve 4x8 mg deksametazon tedavileri başlandı. Servis takibinde hastaya MR anjiografi çekildi; vasküler patoloji saptanmadı. Bir hafta serviste takip edilen hastanın kontrol BBT’ de hematom boyutunun değişmemesi ve klinik durumunun stabil olması üzerine DSA yapılabilen bir merkeze başvurması önerilerek taburcu edildi. Hastaya levatirasetam 2x500 mg PO reçete edildi. Hastanın taburculuktan 15 gün sonra çekilen BBT’de hematomun 40x25 mm’ ye gerilediği görüldü. Hastaya ek öneride bulunulmadı. İntrakraniyal kanamalar sıklıkla ileri yaşta, hipertansif bireylerde görülmekte ve klinik olarak ciddi nörolojik defisite sebebiyet vermektedir. Fakat bahsettiğimiz olguda görüldüğü gibi, yerleşim yeri ve kanama hacmi ciddi miktarda olmasına rağmen bazı hastalarda hafif klinik bulgular ile prezente olabilmektedir. Acil servis hekimleri özellikle tedaviye rağmen şikayetleri gerilemeyen hastalarda görüntüleme yöntemlerine başvurmakta çekinmemeleri uygun görünmektedir. Anahtar Kelimeler: Acil servis, baş ağrısı, intrakraniyal kanama

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
217
P 027 TOMOGRAFİDE SAK MR VENOGRAFİDE SİNÜS VEN TROMBOZU Kıvanç Karaman Şanlıurfa Mehmet Akif İnan Eğitim Araştırma Hastanesi, Acil Servis, Şanlıurfa Baş ağrısı, bulantı, kusma özellikle yaz aylarında acil servise en sık başvuru sebepleri arasındadır. Acil servis hekimleri açısından bu semptomlarla başvuran hastalarda en büyük problem intrakraniyal patolojilerin ekarte edilmesidir. Biz de bu yazıda baş ağrısı, bulantı, kusma gibi nonspesifik semptomlarla başvuran genç hastada saptanan sinüs ven trombozu olgusunu paylaştık. Yirmi bir yaşındaki genç bayan hasta baş ağrısı, bulantı, kusma şikayeti ile ilçe devlet hastanesine başvuruyor. Diş absesi nedeniyle 3 gündür antibiyotik tedavisi aldığını belirtiyor. Hastaya analjezik tedavi uygulanıyor ve taburcu ediliyor. Hasta ertesi gün şikayetlerinin geçmemesi ve ellerde kasılmalarının başlaması üzerine tekrar aynı hastaneye başvuruyor. Yapılan tedavi ile şikayetlerinin gerilememesi üzerine tarafımıza sevk ediliyor. Hastanın başvurusunda bilinç açık, ajite, pupiller izokorik, IR+/+, her iki elde istemsiz kasılmalar mevcuttu. Hastanın rutin kan tetkiklerinde patoloji saptanmadı. Hastaya bilgisayarlı beyin tomografisi çekildi. Tomografi çekimi sonrası hastada gözlerin sağa deviye olduğu jeneralize tonik nöbet gelişti. Hastanın nöbetine intravenöz midazolam ile müdahale edildi. Hastanın tomografisi sağ parietooksipital bölgede Subaraknoid Kanama(SAK) ile uyumlu görünüm şeklinde raporlandı. Beyin cerrahi bölümüne konsulte edilen hastada kliniğin SAK ile uyumlu olmadığı düşünülerek kontrastlı beyin MR ve MR venografi çekilmesine karar verildi. Çekilen MR venografide sol transvers sinüs trombozu saptandı. Bunun üzerine tomografi görüntüsünün tromboze vende göllenen kana bağlı olduğu düşünüldü. Nöroloji konsültasyonu istenen hastaya Clexane 0,6 cc flk SC yapıldı. Nöroloji tarafından değerlendirilen hasta sol transvers sinüs ven trombozu tanısıyla yoğun bakıma yatırıldı. İntrakraniyal patolojilerin semptomları benzer olmasına rağmen oluşum mekanizmaları ve tedavileri birbirlerinden çok büyük farklılıklar içerir. Bizim olgumuzda da hasta başta klinik ve tomografi görüntüsü ile değerlendirildiğinde SAK olarak düşünülmüş fakat MR venografi tetkiki ile hastaya kesin tanı konulabilmiştir. Acil servis hekimlerinin intrakraniyal patoloji düşündükleri hastalarda tanıyı netleştirmeden önce ayrıntılı muayene ve tetkik yapmaktan kaçınmamaları uygun olacaktır. Anahtar Kelimeler: Acil servis, SAK, sinüs ven trombozu P 028 EVALUATION OF MORBID OBESE PATIENTS WHO HAVE UNDERGONE BARIATRIC SURGERY WITH STOP BANG QUESTIONNAIRE REFERRED FOR SUSPECTED OBSTRUCTIVE SLEEP APNEA Burcu Yormaz1, Ilhan Ece2, Serdar Yormaz2
1Beyhekim State Hospital, Department of Chest Diseases, Konya, Turkey 2Selçuk University Medical Faculty, Department of General Surgery, Konya, Turkey Objective: There were different types of questionnaire and indexus used for people whom have obstructive sleep apnea (OSA).The STOP-BANG is a simple obstructive sleep apnea (OSA) screening tool, part questionnaire (STOP) and part demographic or physical measures (BANG), developed for use in surgical clinics preoperatively. This study aimed to perform validation tests of obstructive sleep apnoea screening (OSA) tests STOP-Bang and its short version STOP in obese people who were undergone laparoscopic sleeve gastrectomy (LSG). Methods: In 58 adult patients who were admitted to the obesity clinic for LSG with an initial diagnosis of obstructive sleep apnoea, the STOP-Bang questionnaire was used to calculate the sensitivity, specificity, negative predictive value, positive predictive value and likelihood ratios. Adults were completed the STOP questions and answered yes/no questions (BANG self-reported) about their body mass index (weight and height), age and gender in preoperatively and postoperatively period. Results: In the study, statistically significant difference was detected between two periods (pre and postoperative) for the presence of risk of obstructive sleep apnoea (p<0.05). When apnoea-hypopnoea index (AHI) <=5 patients and AHI >5 patients were compared, no significant differences were found in the values of age, sex and body mass index (p>0.05). Mean AHI value was 3.4 in AHI >5 patients, while it was 21.8 in AHI >5 patients in various severities of OSA (AHI >5, AHI >15 and AHI >30), their specificities were found to be low. As the severity of BMI (body mass index) increases, the positive predictive values of of both periods were decreased, while the negative predictivevalues were increased. Conclusions: STOP-BANG in which all information is self-reported may be as effective as the original version bedside screening test for OSA, and has potential to facilitate research or community screening where good negative predictive value is required for an effective screening tool Keywords: Sleep apnea, bariatric, obese

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
218
P 029 ASSESSMENT OF COPD PATIENTS WHO WERE UNDERWENT BARIATRIC SURGERY WITH EQ-5D VAS QUESTIONNAIRE
Burcu Yormaz1, Ilhan Ece2, Serdar Yormaz2
1Beyhekim State Hospital, Clinic of Chest Diseases, Konya, Turkey 2Selçuk University Medical Faculty, Department of General Surgery, Konya, Turkey Aim: Obesity prevalence in COPD was increased in the last decades. Obesity could be expected to exaggerate the ventilatory demand that characterized COPD. The combination of multi deficits in obese patients with COPD could increase the activity limitation and also this was caused to more oxygen uptake (air hunger), heart rate, and ventilation per minute. The objective of this study was to assess the results of EQ-5D VAS questionnaire during hospitalization period. Method: Sixty two patients among those admitted to the tertiary hospital, were recruited during a 10-month period (may 2015 to march 2016). Eight patients were excluded, The demographic knowledges, clinical results, biochemical findings, the duration period in hospital and treatment were collected for hospital records. Clinical datas were compared between each obese groups. Results: The final sample was composed of 54 patients. The sample was composed of 70,3% (n = 38) women and 29,7% (n = 16) men. Age values were similar between intervention (42.31 ± 6.71) and control groups (43.5 ± 8.18), p = 0.627. The groups were statistically equivalent on the clinical measures and importantly on the length of hospital stay. EQ-5D VAS questionnaire scores were similar between operation groups and statistically significant than control group. The dyspnea values showed a significant improvement in both groups (2.20 ± 2.6; p < 0.05 in the LSG vs. 3.6 ± 2.21; p < 0.05 in the LGB) with no between group differences (p = 0.785). Between-groups comparisons showed significant differences in the EQ-5D VAS self-care, usual activities, anxiety and depression sub scores with higher improvements in the LSG (p < 0.05). Conclusion: Life quality evaluation score has a beneficial effect hospitalized obese COPD patients who were underwent LSG and LGB process. Furthermore new researchs would contribute to other modalities of physical therapy in obese COPD subjects. Keywords: COPD, questionnaire, surgery P 030 APPRAISAL OF EXACERBATION INCIDENCE OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE WITH PROCALCITONIN AFTER LAPAROSCOPIC SLEEVE GASTRECTOMY IN MORBID OBESE PATIENTS Burcu Yormaz1, Ilhan Ece2, Serdar Yormaz2
1Beyhekim State Hospital, Clinic of Chest Diseases, Konya, Turkey 2Selçuk University Medical Faculty, Department of General Surgery, Konya, Turkey Aim: Procalcitonin (PCT) is a prognostic marker in obese patients (BMI>40) with exacerbation of chronic obstructive pulmonary disease (COPD). Our study was detected whether PCT measured on intensive care unit (ICU) admission is predictive of 7-day mortality in obese patients who have undergone Laparoscopic sleeve gastrectomy (LSG) with COPD retrospectively. Methods: A total of 38 obese patients with COPD admitted to the ICU in a tertiary university hospital, during a 10-month period between January 2015 and December 2015, were assessed. Patients with nontreated by any drugs were excluded. Results: The median age was 48 year (range, 29-66), and 58.3% of the patients were female,41,7% were male. 23 patients required exclusively non-invasive ventilation, 11 required exclusively invasive ventilation, 2 required both non-invasive and invasive ventilation, and 12 required only oxygen therapy. The median level of PCT on ICU admission was 0.30ng/mL (range,0.02- 32.00ng/mL; IQR, 0.0-0,5ng/mL), and the median SAPS –II score was 42 (range, 24-98). The 10-day mortality rate was 0,46%. In prediction of 7-day mortality, the area under the curve for PCT inLSG was in confidence interval. Conclusion: The length of stay in hospital less than 7-day showed significantly decreased levels of PCT compared with more than 7 day on ICU admission. PCT on ICU admission might be predictive for 7-day mortality in patients with exacerbated COPD. Moreover, combining PCT with SAPS II score added little additional power in predicting 7-day mortality in our study. Keywords: Pulmonary disease, sleeve gastrectomy, obese

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
219
P 031 COMPARISON OF OBSTRUCTIVE SLEEP APNEA IN OBESE AND SUPEROBESE PATIENTS WITH LOG TRANSFORMED LAP INDEX IN HEPATIC STEATOSIS
Burcu Yormaz1, Ilhan Ece2, Serdar Yormaz2
1Beyhekim State Hospital, Clinic of Chest Diseases, Konya, Turkey 2Selçuk University Medical Faculty, Department of General Surgery, Konya, Turkey Objective: The relationship between obstructive sleep apnea (OSA) in morbid obese patients and nonalcoholic fatty liver disease (NALD) is gaining increased attention. The aim of our study was to determine the effect of morbid obesity added OSA on hepatic steatosis defined by elevated log-transformed LAP (LnLAP) index. Methods: A total of 70(54,2%) morbid obese patients of 38 (45,8%) patients have BMI>40 and 32 have BMI>50 who underwent standard polysomnography were enrolled to this study. Blood samples took from all patients for biochemical measurements, and demographic data were collected. LnLAP was calculated using waist circumference and serum triglycerides levels for each patient. Results: Patients with higher BMI >50 and LnLAP scores were significantly lower O2 saturation (Sao2,73 vs. 83%,), higher apnea-hypopnea index (40 vs. 18, p<0.05), higher oxygen desaturation index (39 vs. 11, p<0.05) and higher percentage of sleep time spent with SpO2<90% (5 vs. 1%, p<0.05) compared with those with BMI >40. Conclusion: Our findings suggested that the occurrence of morbid obesity and super obesity added OSA was associated with hepatic steatosis defined by elevated LnLAP. Further studies were needed to assess the impact of OSA treatment in the future Keywords: Sleep apnea, hepatic steatosis, superobese P 032 THE EFFECTS OF LAPAROSCOPIC SLEEVE GASTRECTOMY FOR MORBID OBESITY ON QUALITY OF LIFE INDEX IN OBSTRUCTIVE SLEEP APNEA SYNDROME Burcu Yormaz1, Ilhan Ece2, Serdar Yormaz2
1Beyhekim State Hospital, Clinic of Chest Diseases, Konya, Turkey 2Selçuk University Medical Faculty, Department of General Surgery, Konya, Turkey Objective: Obesity has become a serious problem for the developed countries. At the same time dyspnea which triggered by morbid obesity has common prevalence and contributes to physical activity limitation in today’s World. Weight loss due to bariatric surgery in obese individuals has been shown to decrease dyspnea attacks and improved functional lung capacity. The aim of this study was to understood and evaluate the postoperative additive effects of bariatric surgery in obstructive sleep apnea syndrome (OSAS). Material-Method: World Health Organization Quality of Life-BREF (WHOQOLBREF) questionnaire, oxygen saturation (SaO2), heart rate (HR) and breathing frequency (fR) were compared in 26 super obese (BMI >50 kg/m2) patients, of 18 female, 8 male were adults, mean aged 34.2 ± 8.1 years. Parameters evaluated before (preoperatively) and 6-months period after laparoscopic sleeve gastrectomy (LSG) (postoperatively), which decreased body mass index (BMI) approximately BMI by ~10 kg/m2 between May 2015 and February 2016. Results: Compared to preoperative period, bariatric surgery was associated with an increase in WHOQOLBREF scores and oxygen saturation (SaO2). Mean values of HR, fR and dyspnea were reduced in postoperative versus preoperative period. The ratios of inspiratory reserve volume and inspiratory capacity to vital capacity were reduced at rest during exercise in postoperative period. Conclusion: Excess weight loss after LSG was associated with improved functional capacity and decreased dyspnea attacks. Attenuated dyspnea attacks following LSG could be explained by decreased BMI and increased excess weight loss. Bariatric procedures would bring about more additive gains and should investigated by multidisciplinary branches. Keywords: Life index, obstructive sleep apnea, sleeve gastrectomy

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
220
P 033 SLEEP QUALITY DETERMINATION IN MORBID OBESE PATIENTS AND THE FACTORS THAT AFFECT IT Burcu Yormaz1, Ilhan Ece2, Serdar Yormaz2
1Beyhekim State Hospital, Clinic of Chest Diseases, Konya, Turkey 2Selçuk University Medical Faculty, Department of General Surgery, Konya, Turkey Objective: This study was aimed to determine the sleep quality in morbid obese patients who were undergone bariatric surgery and the factors that affect it. Material-Method: The study has done by surveying the 126 operated morbıd obese patients. We have used Pittsburg Sleep Quality Index (PUKI) and Epworth Sleepiness Scale (EUÖ) in the research between the years of January 2015 to October 2015. Results: The average age of the patients were 35,2±6,4 (range 20 to58 years). The average total PUKI is 8,42±3,5 preoperatively and 3.51± 1.2 postoperatively. The rate of the ones whose sleep quality is bad is 69,2 % preoperatively. The average point of the Epworth sleepiness scale is 4,61±3,87, and the 18 % of the adolescents have suffered from sleepiness during the day. The sleep quality was found to be 76,3 % in those who have sleep problem while studying, 34% in those who drink too much coffee and tea, 53,1% in the smokers, 52,3% in those having social-familial problems, 43,2% in those having physical and psychological problems, 87,3% in the ones with GIS disorder. In the analysis of demographic datas, social and familial problems the formerly experienced sleep disorders and the consuming of big appetite are the determining factors responsible for the decrease in the sleep quality. Conclusions: The sleep quality of morbid obese patients were low. It is considerably important to raise awareness of the effects of sleep quality in obeses on the social happiness and workplace success by eliminating the controllable factors and applying the bariatric surgery. Keywords: Sleep quality, obese, surgery P 034 RELATIONSHIP BETWEEN OSAS PATIENTS WHO WERE UNDERGONE BARIATRIC SURGERY VERSUS NONE OPERATED WITH BECK DEPRESSION INVENTORY POINTS Burcu Yormaz1, Ilhan Ece2, Serdar Yormaz2
1Beyhekim State Hospital, Clinic of Chest Diseases, Konya, Turkey 2Selçuk University Medical Faculty, Department of General Surgery, Konya, Turkey Objective: Obstructive Sleep Apnea Syndrome (OSAS) is characterized as narrowing in the upper bronchial tube repetitively or partially during sleep and reduction in the saturation of oxygen in the blood, obesity is one of the caused reason for this disease. Its causes were related to multi-variant parameters such as genetic, respiratoral, endocrinal, nutritional, psychological factors, gender and physical hypo-activity. Morbid Obesity is also related with depression and antisocialism. In our study, the relationship between obesity, asthma and Beck Depression Inventory (BDI) points is aimed to explore. Material-Methods: In our study, we wanted to evaluate the relation between operated and non-operated patients obesity and depression 32 male and 23 female subjects between the age of 25-54 are included in the survey. It is evaluated as BMI (body mass index)> 40 kg/m2. According to these criteria for obesity, all of the subjects were overweight; and for blood pressure values 17 subjects were normal and 38 subjects were hypertensive in 55 totally. Results: According to values of BMI, BDI points and the blood pressure values are found higher in non-operated than operated subjects. These results are also found statistically meaningful (p<0,01 and p<0,05 respectively) compared to operated subjects. Bariatric surgery is so feasible and effective method for decreasing the excess weight and morbidity. Conclusion: Bariatric surgery and its modalities is an efficient way to be a appropriate person for the society and work place and need to be performed more studies in this field. Keywords: OSAS, bariatric, Beck Depression Inventory

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
221
P 035 THE DIFFERENT PERSPECTIVES AND PREVENTING METHODS OF VENOUS THROMBOEMBOLISM IN MORBID OBESE COPD PATIENTS
Burcu Yormaz1, Ilhan Ece2, Serdar Yormaz2
1Beyhekim State Hospital, Clinic of Chest Diseases, Konya, Turkey 2Selçuk University Medical Faculty, Department of General Surgery, Konya, Turkey Objective: Venous thromboembolism (VTE) is a known and mortal complication of obesity surgery. Therefore, morbid obesity has been accepted as a high risk factor and justification for chemoprophylaxis for VTE. We aimed to review the prevalence and effects of venous thromboembolism treatment (VTT) among our patients and evaluate the incidence rates of VTE among operated and non-operated patients. Methods: We were evaluated 148 patients who have undergone elective bariatric surgery (BMI(body mass index) > 40) by experienced surgeons worked in tertiary hospital from March 2013 to November 2015.The patient demographics analyzed included age, gender, body mass index, excess weight loss and the additive comorbid diseases. Results: Venous thromboembolism treatment (VTT) procedure (enoxaparin) and pneumatic tape were used before and after the surgical procedure. All of the patients mobilized after the postoperative 6 th hour of surgery. The incidence of VTE of 0.27% in our patients (5 patients of 148). Three of five patients (60%) who developed DVT and PE belonged to superobese group (BMI>55). The frequency of VTE in superobese patients was 0.60% and 0.40% in the obese patients. There were no significant differences in age, number of comorbidities, and a history of COPD (chronic obstructive pulmonary disease) between those who developed DVT and PE and those who did not. Conclusion: With the low prevalence of VTE among our patient population, including patients with morbid obesity, advanced age, multiple comorbidities or COPD, the practice of routine chemoprophylaxis should be reviewed and new researchs needed to be studied in the future. Keywords: Thromboembolism, COPD, obese P 036 LERICHE SYNDROME WITH UNUSUAL PRESENTATION Emine Gaffari, Aziz Vatan, Özgür Karcıoğlu
Istanbul Training and Research Hospital, Clinic of Emergency Medicine Istanbul, Turkey Background: Leriche Syndrome is a highly mortal clinical manifestation due to thrombotic occlusion of the infrarenal abdominal aorta or both iliac arteries. Prevalence of the disease 1/7500 of the population and 2% are due to trauma. Prevelance in men is higher than in women. The entity presents with a classical triad of lower limb claudication, absent or decreased femoral pulses and erectile dysfunction. Below is a report of a patient presented with abdominal pain, shortness of breath and poor clinical condition who was eventually diagnosed with Leriche Syndrome. Case: A 84-year-old male patient presented with generalized abdominal pain, shortness of breath, tachypnea and poor clinical condition was admitted to emergency department (ED). His medical history included prostatic carcinoma (operated on) with pulmonary metastasis and he had been discharged two days ago from intensive care unit (ICU) after being treated for pneumonia. His vital signs were blood pressure 100/60 mmHg, pulse: 54 bpm, respiratory rate 20 bpm, and SpO2: 98%. His pulses in the femoral, popliteal and ankle arteries were non-palpable bilaterally without any ischemic signs. His chest x-ray showed bilateral pulmonary effusion. Medical history did not reveal claudication or erectile dysfunction. His labarotory results were prothrombin time: 21,5 s; activated partial thromboplastin time: 59,1 s, International Normalized Ratio: 2,0. His abdominal CT-angiography imaging showed occlusion of infrarenal abdominal aorta and both iliac arteries. Both iliac arteries had minimal distal circulation due to collaterals. Non-surgical approach was planned due to sufficient circulation supported with collateral vascularisation. The patient was admitted to ICU due to his comorbid illnesses. After the treatment he was discharged from ICU in eight days. Conclusion: Leriche syndrome can be mortal if not treated expediently in the ED. It should be kept in mind for elderly patients with abdominal pain and poor condition. Keywords: Leriche syndrome, aortailiac occlusion, peripheral artery disease

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
222
P 037 A RARE COMPLICATION AFTER MINOR TRAUMA: FOURNIER’S GANGRENE Emine Gaffari, Burcu Gülşen, Özgür Karcıoğlu Istanbul Training and Research Hospital, Clinic of Emergency Medicine Istanbul, Turkey Background: Fournier’s Gangrene is the life-threatening acute necrotizing infection of genitourinary system, which spreads quickly should there be any delay in the diagnosis and treatment. The infection site is painful, sensitive and swollen; crepitation, inflammation and soft tissue necrosis develops in the clinical course. Genitourinary system infection, diabetes mellitus, chronic alcohol consumption, renal failure, obesity, cirrhosis, malignancies, vasculopathies and trauma play role in development of Fournier’s gangrene. Case: 36 years old male patient presents in the emergency department with pain in testis and anus. The patient has a history of closed coccyx fracture caused by falling on a hard surface five days ago. On physical examination, bilateral sensitivity in testicles -especially in the left testicle-, hyperemia starting from perianal area covering both scrotal and pubic areas were noted. Body temperature was 37.7 C and leukocyte count was 15700/mm3. In the ultrasonographic examination, the air image was seen extensively in the perianal and scrotal areas. The patient was administered Ampicillin 2 g qid, ciprofloxacin 400 mg bid and metronidazol 500 mg qid intravenously and is admitted to the general surgery ward to proceed with emergent surgical intervention. Conclusion: Fournier’s Gangrene is a rare disease but requires emergent examination and treatment. This progressive necrotizing disease of genitourinary system should be included in the differential diagnosis since it can be encountered as a result of local and minor injury patterns. Keywords: Fournier’s Gangrene, trauma, coccyx fracture, emergency department P 038 FOURNIER'S GANGRENE: A RARE COMPLICATION OF RECTAL CANCER Emine Gaffari, Burcu Gülşen, Özgür Karcıoğlu Istanbul Training and Research Hospital, Clinic of Emergency Medicine Istanbul, Turkey Introduction: Fournier's gangrene is an acute necrotic infection of scrotum, penis or perineum. It is characterized by scrotal pain, edema and hyperemia with rapid progression to gangrene of tissue. Fournier's gangrene was also encountered as a rare complication of rectal cancer. We report a patient with rectal cancer presented with perineal necrotizing fasciitis. Case: A 62-year-old male patient who had been diagnosed of metastatic adenocarcinoma of rectum was admitted to the emergency department with a painful swelling of the perineum and poor condition. On presentation he had altered mental status, low blood pressure (60/40 mmHg) and digital rectal examination revealed fluctuation and enduration on the anal margin. and perineum He had suprapubic pain and tenderness. He had no fever, Abdominal and pelvic CT scan disclosed a perforation in the posterior rectum (4 cm in size) with a massive infiltration of the perineum including air bubbles. despite 30ml /kg fluid replacement, the hypotension resisted. So we started with inotropic support. Antibiotics were administered Broad-spectrum antibiotics in form of meropenem and fluconazole were started and the patient was admitted to hospital for emergency surgery. He died two days later. Conclusion: Fournier's gangrene is a true emergency in which diagnosis can be delayed in the emergency setting. The treatment of the entity should include rigorous resuscitation and antibiotics along with surgical intervention. Errors in diagnosis and treatment can cause rapid deterioration. Emergency physicians must be aware of Fournier's gangrene in patients with rectal cancer and poor general condition. Keywords: Fournier's gangrene, rectum cancer, emergency department

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
223
P 039 BAŞKENT ÜNİVERSİTESİ ANKARA HASTANESİ ACİL SERVİSİ’NE İŞ KAZASI NEDENİYLE BAŞVURAN HASTALARIN ÖZELLİKLERİ VE MALİYET ANALİZİ
Hayati Artuk, Cemil Kavalci, Dilek Suveren Artuk Başkent Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Ankara Çalışmamızda; hastanemiz acil servisine başvuran iş kazaları olgularının özellikleri ve maliyeti analizinin tespiti amaçlandı. Başkent Üniversitesi AS’de 1 Ocak 2013 - 31 Aralık 2014 tarihleri arasında, iş kazası sebebiyle başvuran 469 hasta ile retrospektif olarak yapıldı. Hastalarımızın yaş, cinsiyet, hizmet sektörü, başvuru saat, gün, ay ve yılı, başvuru şikayeti, travma bölgesi, prognoz, maliyet ve travma şiddetleri değerlendildi. Kategorik değişkenlerin analizinde Kİ-Kare testi, nonparametrik verilerin analizinde Mann Whitney U ve Kruskall Wallis testleri kullanıldı. Sonuçlar p<0,05 düzeyinde anlamlı kabul edildi. Hastalarımızın yaş ortalaması 34,18±11,4 yıldı ve hastaların %73,1’i erkekti. Hastalar en sık hizmet sektöründe (%44,8) çalışmaktaydı. Başvuruların en sık günün 0900-1600 saatleri arasında, pazartesi günleri ve ağustos ayında gerçekleştiği saptandı. İş kazalarının 2013 yılında, 2014 yılına göre fazla olduğu saptandı. En sık başvuru sebebi kesici/delici alet yaralanması (%30,5) olup, ensık yaralanan bölge üst ekstremite (%45,4) idi. Hastaların %92,1’inin ayaktan tedavi edilerek taburcu edildiği saptandı. Cinsiyet ile; yaş, travmanın olduğu gün, kaza yılı, travma alınan bölge ve hasta prognozları arasında anlamlı bir ilişki saptanmadı (p>0,05). Cinsiyet ile; başvuru sebebi, sektör ve başvuru ayları arasında anlamlı ilişki vardı (p<0,05). Maliyet ortancası 77,14 (IQR:75,75) TL idi. İş kazalarında maliyet ile; cinsiyet, travmanın olduğu ay ve yıl arasında anlamlı bir ilişkiye rastlanmadı. Maliyet başvuru sebebi ve sektör arasında anlamlı ilişki vardı (p<0,05). RTS ortancası 7,84 (0,0000) idi. RTS’nin; cinsiyet, yaş, başvurma sebebi ve çalışılan sektör ile istatistiksel olarak anlamlı bir ilişkisi saptanmadı (p>0,05). Sonuç olarak; iş kazaları daha çok genç erkeklerde görülür. Genel olarak tek lokalizasyonda gelişen patolojilerdir. Anahtar Kelimeler: İş kazası, RTS, maliyet P 040 COMPARISON OF CHEST COMPRESSIONS WITH THE LIFELINE ARM DEVICE AND THOSE PERFORMED MANUALLY DURING SIMULATED RESUSCITATION IN A HOSPITAL BED Lukasz Szarpak1, Zenon Truszewski1, Jacek Smereka2, Sebastian Aleksandrowicz3, Jerzy R Ladny4, Krzysztof J Filipiak5
1University of Warsaw, Department of Emergency Medicine, Medical Warsaw, Poland 2Wroclaw Medical University, Department of Emergency Medical Service, Wroclaw, Poland 3International Institute of Rescue Research and Education, Warsaw, Poland 4Medical University Bialystok, Department of Emergency Medicine and Disaster, Bialystok, Poland 5Medical University of Warsaw, Department of Cardiology, Warsaw, Poland Background: The aim of the study was to compare the quality of CCs performed with and without a Lifeline ARM device (ARM; Defibtech, Guilford, USA) in the course of simulated CPR performed by nurses. Methods: The study involved 34 nurses working in emergency units or anesthesiology and intensive care units. Before the study, all the participants received a 60-minute training in advanced life support, extended by the usage of mechanical CC systems, including the ARM. Then the nurses took part in a 30-minute practical training in ARM application, which allowed to assure that they were familiar with the proper usage of the device. CCs were performed in a Resusci Anne manikin (Laerdal, Stavanger, Norway). Participants were randomized to perform a 2-minute session of uninterrupted CCs with and without the ARM. The CCs were implemented in 2 scenarios: with the patient located on the floor (scenario A), and with the patient lying in a standard intensive care bed adapted to CPR application (scenario B). Results: The effectiveness of CCs with the use of the ARM and of those applied manually varied and amounted to 99%vs.36% for scenario A (p<.001), and 99%vs.33% for scenario B, respectively (p<.001). The correct CC depth was achieved by 98% with the ARM vs. 53% of those not using the ARM for scenario A, and 99%vs.41%, respectively, for scenario B. The correct CC rate with ARM was achieved by 100% in both A and B scenarios, whereas in the case of manual CCs the results were 65% for scenario A and 72% for scenario B. Conclusions: CCs with the use of ARM are more effective than those performed manually in patients located on the floor, as well as in patients in a standard intensive care bed adapted to conduct CPR, with better CC depth and compression rate. Keywords: Cardiopulmonary resuscitation, chest compression, quality, simulation

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
224
P 041 COMPARISON OF TRUVIEW EVO2 AND ETVIEW SL WITH THE MACINTOSH 3 BLADE FOR INTUBATION WITH MANUAL IN-LINE STABILIZATION PERFORMED BY NOVICE PHYSICIANS
Lukasz Szarpak1, Jacek Smereka2, Zenon Truszewski1, Sebastian Aleksandrowicz3, Togay Evrin4, Kurt Ruetzler5
1Medical University of Warsaw, Department of Emergency Medicine, Warsaw, Poland 2Wroclaw Medical University, Department of Emergency Medical Service, Wroclaw, Poland 3International Institute of Rescue Research and Education, Warsaw, Poland 4Ufuk University Medical Faculty, Department of Emergency Medicine, Ankara, Turkey 5Cleveland Clinic, Departments of Outcomes Research and General Anesthesiology, Cleveland, USA Objective: Endotracheal intubation (ETI) is considered a gold standard for airway secure in many emergency situations, such as cardiopulmonary resuscitation or trauma. The aim of the study was to compare the time and success rate of 3 different intubation methods applied in emergency intubation with manually immobilized cervical spine in a standardized manikin model. Material: The total of 50 novice physicians (mean age, 26.7 ± 1.5 years) participated in the randomized crossover manikin trial. Method: The participants performed ETI in an Adult Airway Management Trainer (Simulaids, Inc., Saugerties, NY, USA) with manual in-line cervical spine stabilization. We compared the time to successful intubation and the overall intubation success rate when using Trueview EVO2 (EVO2), ETView SL (ETView), and Macintosh (MAC) laryngoscopes in a randomized order. Results: The time to successful intubation was significantly shorter with the ETView as compared with EVO2 (49 [interquartile range, IQR, 45–54.5] seconds; p <.001) and with MAC (41.5 [IQR, 36–44.5] seconds; p <.001), although the overall success rate of applying the ETView (100%) compared with the EVO2 (86%) and with MAC (92%) did not reach the statistical significance (p =.065 and p =.055, respectively). Conclusion: The ETView performed better than EVO2 and MAC for intubation in the conditions of manual in-line cervical spine stabilization. Keywords: Endotracheal intubation, physician, difficult airway, stabilization P 042 A NON-INVASIVE HEMOGLOBINOMETER: CAN WE USE IT OR IS IT TOO EARLY? Eren Gökdağ, Özlem Güneysel, Ömerul Faruk Aydın, Fatma Sarı Doğan Istanbul Kartal Dr. Lütfi Kırdar Training and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey Introduction: Point of care devices are fast and easy to use but their true potential is still waiting to come up. TensorTip MTX is a non-invasive medical device can measure various bioparameters, including hemoglobin. Purpose of this study is to measure the correlation between TensorTip MTX and our routine laboratory analysis of hemoglobin and to see that device is useable in emergency department settings for situations like gastrointestinal bleeding and acute traumatic hemorrhages. Methods: In the month after the ethical board approval, we conduct our study in 147 patients. Their hemoglobin levels were already measured while their course of emergency department visit. To gather accurate data of hemoglobin measurement of TensorTip MTX, device put on the ring finger of the patients and wait at least 45 seconds for measurement. All measurement documented and recorded by researcher. Measurements from blood samples and TensorTip MTX device are compared with Intraclass Correlation Coefficient and Pearson Correlation Coefficient. Results: In 147 patients; %61.2 (n=90) were male, %38.8 (n=57) were female and ages are between 18 and 89. Mean age is 55.72±20.30 years; %23.1 (n=34) of them is under 35 years old, %76.9 (n=113) over 35 years. Statistically, correlation between hemoglobin levels of reference measurement and TensorTip measurement is found %42.4 significantly compatible (p=0,001; p<0,01) (Intraclass Correlation Coefficient: 0.424; %95 CI: 0.281-0.548). Correlation between hematocrit level measurements is %46.9 significantly compatible (p=0,001; p<0,01) (Intraclass Correlation Coefficient: 0.429; %95 CI: 0.333-0.586). Conclusion: Our study showed that correlation between reference measurement and TensorTip MTX device is fair (ICC:0.424 for hemoglobin and 0.429 for hematocrit). Further studies needed to determine that this device is suitable or not to identify the need of blood transfusion and management of patients with acute hemorrhages for now. Keywords: Hemoglobin, hemoglobinometer, non-invasive

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
225
P 043 THE ROLE OF COUNT OF BLOOD CELLS PARAMETERS FOR DIAGNOSIS AND DETERMINATION OF THE SEVERITY OF ACUTE ISCHEMIC STROKE AND TRANSIENT ISCHEMIC ATTACK
Ömür Aşık1, Murat Ersel1, Ayşe Güler2, Gul Kitapçıoğlu3, Funda Karbek Akarca1
1Ege University School of Medicine, Department of Emergency Medicine, Izmir, Turkey 2Ege University School of Medicine, Department of Neurology, Izmir, Turkey 3Ege University School of Medicine, Department of Biostatistics, Izmir, Turkey Introduction: There are few studies investigate the relationship between blood hemogram parameters and illness severity in patients with acute ischemic stroke. The aim of this study is to investigate the relationship between blood hemogram parameters and the severity of the disease mortality and imaging findings in patients presenting ischemic stroke and transient ischemic attack clinics to the emergency department. Methods: This prospective cross-sectional study were conducted between 1 July 20015 and 31 March 2016 in patients admitted to the emergency department consecutively with findings of acute ischemic stroke and TIA. Patients diagnosed as any other pathology such as hemorrhagic stroke, intracranial mass and Todd’s paralysis and also whoes data were lacked were excluded from the study. Patients demographic data, vital findings, GCS, blood hemogram parameters, NIHSS and Modified Rankin Scores were recorded. NLR, neutrophil / leukocyte ratio were calculated by division of neutrophyls to leukocytes. Results: Three hundred and eighty one of the 431 patients were included to the study, 261 of those were ischemic stroke and 120 transient ischemic attack patients. Patients with ischemic stroke who have lower Glasgow Coma Scores had statistically significant RDW (p<0,001) and NLR (p:0,043) results. The patients with high scores of NIHSS has significantly higher RDW values (p=0,008). Means of NLR were found to be higher in high NIHSS score group (NIHSS<9= 3,70 – NIHSS >16 = 5,93), an also for RDW (NIHSS<9= 14,2 – NIHSS >16 = 14,9). Patient who died in 30 days has significantly higher NLR (3,62–6,46:p<0,001) and RDW (14,1–15,5;p <0,001) means in comparision with who survive. Conclusion: Blood count parameters are easily obtained and useful in the emergency department for prediction of ischemic stroke patients mortality and mobidity. Especially NLR values have to be found the highest prediction for mortality and mobidity in patients with acute ischemic stroke. Keywords: RDW, MPV, neutrophil-lymphocyte ratio, ischemic stroke, transient ischemic attack P 044 FOCAL MYOCARDITIS MIMICKING SUBENDOCARDIAL ISCHAEMIA: A CASE REPORT
Fikret Bildik1, Hüseyin Avni Demir2, Gültekin Kadı1
1Gazi University Faculty of Medicine, Department of Emergency Medicine, Ankara, Turkey 2Mehmet Akif İnan Training and Research Hospital, Emergency Clinic, Şanlıurfa, Turkey Myocarditis is an uncommon, potentially life-threatening, and inflammatory disease of the myocardium with a wide range of clinical presentations, often caused by infectious agent. Patients with myocarditis usually have clinical history of acute decompensation of heart failure and present with disproportionate dyspnea on exertion, mild symptoms of chest pain, arrhythmias and sudden death. The diagnosis of acute myocarditis is usually difficult and presumptive due to the heterogeneity of clinical presentations. The diagnosis of acute myocarditis may be based on clinical presentation, physical examination, laboratory testing, the course of electrocardiographic changes, and the lack of epicardial coronary disease revealed by cardiac angiography. Endomyocardial biopsy (EMB) is the gold standard tool for diagnosis, but is used infrequently. We present the case of a young patient presenting with angina-like chest pain who had electrocardiographic changes and cardiac enzyme levels suggesting acute myocardial ischaemia of which the diagnosis of acute myocarditis was confirmed using cardiac magnetic resonance imaging. Keywords: Chest pain, coronary angiography, electrocardiography, magnetic resonance imaging, myocarditis

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
226
P 045 HEY DOC! I’M PREGNANT AND I HAVE ABDOMINAL PAIN Hüseyin Avni Demir1, İsa Kılıçaslan2, Gültekin Kadı2
1Mehmet Akif İnan Training and Research Hospital, Emergency Clinic, Şanlıurfa, Turkey 2Gazi University Faculty of Medicine, Department of Emergency Medicine, Ankara, Turkey Despite developments in diagnosis and treatment, maternal death is still a serious public health problem. Pre-eclampsia is an important disease affecting maternal and fetal health worldwide. Hemolysis, Elevated Liver enzymes, Low Platelet (HELLP) syndrome is considered a more severe form of pre-eclampsia. In obstetric pathologies, pre-eclampsia, eclampsia, and HELLP syndrome are the most common reasons for intensive care unit (ICU) admission, followed by hemorrhage and disseminated intravascular coagulation (DIC). These diagnoses are confirmed to be associated with increased maternal morbidity and mortality. Here, we present a pregnant patient admitted to emergency department with abdominal pain and diagnosed HELLP syndrome and DIC. After termination, she was discharged without any sequelae or complaint. Keywords: Abdominal pain, emergency, HELLP syndrome, preeclampsia, pregnancy P 046 NEKROTİZAN FASİİT: OLGU SUNUMU Şule Yakar1, Yusuf Kantar2, Necmi Baykan3
1Şırnak Devlet Hastanesi, Acil Servis, Şırnak 2Erciyes Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Kayseri 3Nevşehir Devlet Hastanesi, Acil Servis, Nevşehir Giriş: Nekrotizan fasit; travma sonrası gelişebilen, deri ve yumuşak dokuların enfeksiyonu ile karakterize, progresif ilerleyen kritik bir hastalıktır. Olgu: Acil servise genel durum bozukluğu ve şuur değişikliği şikayetleri ile getirilen, 4 ay önce travma öyküsü olan ve nekrotizan fasiit tanısı alan bir olgu sunulmuştur. Sonuç: Nekrotizan fasit tanısının koyulmasında bilgisayarlı tomografinin önemli bir yeri vardır. Tanı alan hastaların tedavisi; geniş spektrumlu antibiyoterapi ve erken cerrahi debridmandan oluşmaktadır. Anahtar Kelimeler: Nekrotizan fasiit, Acil servis, bilgisayarlı tomografi

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
227
P 047 DİZ ÜSTÜNDE ŞİŞLİK VE AĞRI ŞİKAYETİ İLE ACİLE BAŞVURAN HASTADA NADİR BİR PATOLOJİ: FEMORAL ANEVRİZMA
Şenol Ardıç1, Süha Türkmen2, Sertaç Yılmaz1, İbrahim Altun1, Bestami Köse1
1Sağlık Bilimleri Üniversitesi Trabzon Kanuni Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Trabzon 2İstanbul Acıbadem Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı Taksim Yerleşkesi, İstanbul Giriş: Hastaların travma dışı nedenlerlere bağlı diz etrafında ağrı ve şişlik ile acil servislere başvurusu sık değildir. Acil hekimi hastada ciddi komplikasyonlara sebep olabilecek vasküler orijinli nedenleri tanıması ve yönetmesi gerekir. Amaç: Acil servislerde torakal ve abdominal aort anevrizmaları sıkça tanımlanmaktadır. Perferik arter anevrizmalar ise nadirdir. Bu olgumuzda; diz etrafında arter orijinli anevrizmaların başka tanılarla karışabilecek kadar klinik bulgu verebileceğini, acil hekiminin fizik muayene ve/veya USG kullanımıyla tanıya gidebileceğini göstermeyi amaçladık. Olgu: 80 yaşında kadın hasta acil servise sol diz üstünde ani gelişen şişlik (Resim 1) ve ağrı nedeniyle getirildi. Bilinen hipertansiyon ve abdominal aort anevrizma (AAA) nedeniyle operasyon öyküsü olduğu öğrenildi. Vital bulgular; TA: 160/ 90 mmHg (sağ/sol farkı yok), KTA 90atım/ dk, 37.8 C ateş, Sa02 % 98 idi. Fizik muayenede; sağ diz normal görünümde iken sol diz medial taraf üzerinde belirgin ele gelen, pulsatil ve nispi ısı artışı olan şişlik mevcut idi. Bilateral üst/ alt ekstremite nabızlar eşit alınıyordu. Diğer sistem muayeneleri ise normal olarak değerlendirildi. Hemogram tahlilinde lökositoz, biyokimya panelinde CRP 3.5 dışında normal sınırlarda idi. Ayırıcı tanıda apse, hematom, baker kisti ve anevrizma düşünüldü. Acilimizde sıkça kullandığımız USG (Resim 2) ile yaptığımız yüzeysel B-mod vertikal bakıda sınırları düzgün hipoekoik sıvı kolleksiyonu, horizontal bakıda ise pulsatil damar trasesi olması nedeniyle anevrizma tespit ettik. Hasta kalp damar cerrahisine sevk edildi. Kalp damar cerrahisi tarafından anjiosu yapılıp, bypass grefti ile rekonstrüksiyon cerrahi modalitesi uygulanıldığı öğrenildi. Sonuç: Olgumuzdaki gibi durumlarda lezyonun pulsatil olması ve takipte çap ölçümü yönlendirici olabilir. Hastaların hikayesi ve özgeçmişi kliniğin belirginleşmesinden önce daha dikkatli alınmalı, gelişen FM bulguları da doğru değerlendirilmelidir. Acil hekimi USG kullanmayı bilmelidir ve bu tür şikayetler de klinik basit nedenleri akla getirse de vasküler yapılar için yüzeysel B-mod USG kullanılması ciddi durumların gözden kaçmasını engelleyebilir. Anahtar Kelimeler: Diz etrafında ağrı, femoral anevrizma, pulsatil P 048 OUTCOMES OF SUPEROBESE PATIENTS WHO WERE UNDERWENT BARIATRIC SURGERY RECEIVING NONINVASIVE MECHANICAL VENTILATION: A TERTIARY CARE EXPERIENCE Burcu Yormaz1, Ilhan Ece2, Serdar Yormaz2
1Beyhekim State Hospital, Clinic of Chest Diseases, Konya, Turkey 2Selçuk University Medical Faculty, Department of General Surgery, Konya, Turkey Objective: Super obesity is a growing epidemic condition in all over the world especially in growing countries, with a current prevalence estimated to be about 40% in all genders and populations, respectively. Super obese patients (BMI >= 55 kg/m2) are at more highly risk of respiratory failure requiring noninvasive mechanical ventilation (NIMV). It has so multivariant factors in etiology about super obese patients who are undergone bariatric surgery. Because of limited cardiopulmonary reserve, they may have poor and mortal outcomes. However, literature about this population was too limited. Methods: We were used the Inpatient Sample form to examine the outcomes of super obese people receiving NIMV and compared them to morbid obese people who have lower BMI (BMI<55kg/m2) than superobeses. Primary outcomes were detected in ICU mortality, percentages of prolonged non-invasive mechanical ventilation (>= 48h). We also examined outcomes stratified by number of organs failingin MODS (multiorgan disease syndrome). Results: Of all operated and ICU required super obese people, 3.6% were underwent NIMV. Mean age, severity of illness and comorbidity scores were lower in morbidly obese people. The exact rate of mortality in superobeses were significantly different than morbidly obese people. When stratified the diseases of super obese population, there was quietly increase in risk for mortality among super obese relative to morbid obese people not only respiratory failure but also cardiac failures. Percentages of prolonged non-invasive mechanical ventilation were significantly higher in patients who were super obese. Conclusions: Super obese population who were underwent NIMV have highly risk for death than morbid obese people if only respiratory failure is present. When more organs failure happens, super obese people have two fold increased risk for mortality compared with morbid obese people Keywords: Non-invasive mechanical ventilation, superobese, bariatric

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
228
P 049 USE OF NITHINOL PLATE AND SURGICAL RESULTS IN PATIENTS WITH MULTIPLE DISPLACED RIB FRACTURES AND STERNAL DEHISCENCE
Turkan Dubus1, Bektaş Akpolat2, Derya Abuşka3, Hakan Topacoglu3, Ozgür Karcioglu3
1Istanbul Training and Research Hospital, Thoracic Surgery Clinic, Istanbul, Turkey 2Taksim GOP Training and Research Hospital, Thoracic Surgery Clinic, Istanbul, Turkey 3Istanbul Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey Background: Multiple rib fractures due to blunt thorax trauma result in serious respiratory problems. Numerous cases indicate surgery which require stabilization of the chest wall. We detected obvious clinical improvement following chest wall stabilization using heat sensitive and MRI compatible nithinol plates in our series of 12 patients. Our aims of surgery by choosing this system were to improve life quality of patients, to prevent possible complications, to treat the thoracal organs more effectively with a much easily applicable stabilization material which does not restrict radiologic studies. Material-Method: Eight of the patients had multiple rib fractures and 4 of them had postoperative late term sternal dehiscence. The indications of operation were severe respiratory distress, flail chest, serious pain and admission to intensive care unit. Nine of the patients were male. The mean age of the patients were 54 (ranging from 38 to 66) years. Six of the patients were in-car-accidents, 2 of them were falls from height, 4 of them were detachment of sternal fixation wires in the late postoperative period of cardiac surgery. All of the patients had at least 4 (ranging from 4 to 8) comminuted and displaced rib fractures. All of the patients were operated under general anesthesia. The plates were applied in extrathoracic fashion during the operations. No complications occurred. The patients were followed up in the inpatient room and were discharged on an average of 4th postoperative days (ranging from 2 to 6). No problems were found in the outpatient follow up. Results: Heat sensitive and MRI compatible nithinol plates are extremely useful materials for treatment of multiple displaced rib fractures and sternal dehiscences as late term complication of any type of operations, in terms of providing thorax integrity and normal respiratory functions of the patients. Keywords: Trauma, rib fractures, nithinol fixing plate, sternum dehiscence P 050 THE OUTCOMES OF VENTILATION/PERFUSION DISTRIBUTIONS COMPARED WITH SUPEROBESE AND MORBID OBESE İNDIVIDUALS BEFORE AND AFTER THE BARIATRIC SURGICAL PROCESS Burcu Yormaz1, Ilhan Ece2, Serdar Yormaz2
1Beyhekim State Hospital, Clinic of Chest Diseases, Konya, Turkey 2Selçuk University Medical Faculty, Department of General Surgery, Konya, Turkey Objective: Morbid obesity has become a worlwide and rising public health problem which influenced millions of people. Current estimates indicate that > 6% of the world population is morbid obese. Bariatric surgery (BS) call forth a significant and continuous reduction of BMI, with minor morbidity and mortality, in morbidly obese subjects. According to our knowledge, the effects of morbid obesity and BS on ventilation/perfusion (V. A/Q) ratio were definitely increased after the surgical process. The aim of our study was to evaluate the ventilation/perfusion (V. A/Q) rates after bariatric surgery procedure. Methods: Of all patients who were underwent bariatric surgery compared by respiratory (V. A/Q.) Ratio distributions. Of 14 (56%) female of 11(44%) male patients (BMI>55 kg/m2,group A) and Of 42 (30%) female,18 (30%) male patients (BMI<55 kg/m2,group B), were evaluated according to their ventilation/perfusion (V. A/Q) ratios before and after the process. Results: When we compared the periods between preoperative and postoperative 6 months results of ventilation perfusion ratios. We have detected that before the surgical process group A population individuals had reduced arterial PO2 (72 ± 4 mm Hg) and an increased alveolar-arterial PO2 difference (29 ± 3 mm Hg) on the other hand group B population’s arterial PO2 (75 ± 6 mm Hg)and a bit less alveolar-arterial PO2 difference detected before the surgical process. After BS period, body mass index was reduced significantly in both groups, and pulmonary gas exchange abnormalities were decreased especially in first group due to more weight loss and increase in pulmonary capacity. Conclusions: This study shows that even in the absence of major lung volume alterations, morbidly obese individuals have abnormal.V. A/Q. distributions that are reduced after BS especially in superobese group.further more novel studies and methods should be encouraged and evaluated. Keywords: Ventilation/perfusion distributions, bariatric, pulmonary

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
229
P 051 THE EVALUATIONS OF CARDIORESPIRATORY FITNESS TEST OUTCOMES BETWEEN MORBID OBESE AND NONOBESE PATIENTS
Burcu Yormaz1, Ilhan Ece2, Serdar Yormaz2
1Beyhekim State Hospital, Clinic of Chest Diseases, Konya, Turkey 2Selçuk University Medical Faculty, Department of General Surgery, Konya, Turkey Background: The applicability and effective commentary of cardiorespiratory fitness test (CRFT) in obesity is important for enough evaluating cardiovascular conditioning, underlying comorbidities and disease risk. We were retrospectively compared peak oxygen uptake (V O2peak) in absolute terms, and relative terms (% predicted) using three currently suggested prediction equations. Methods: This was a retrospective study using patients who took part in projects related to exercise and morbid obesity in our tertiary clinic. All details of the experiments were explained to patients. Patients were instructed to avoid exercise 24 hour before the study and food and caffeine for at least 2 hour before testing. Of 58 patients were evaluated by this programme of 21(36%) were nonobese and of 37 (64%) were obese (BMI>40kg/m2) individuals. Patients characteristics were analyzed by Chi-square test and % predicted V O2peak by kruskal wallis test. Results: V˙O2peak (L/min) was not different between nonobese and morbid obese adults. V˙ O2peak was higher according to lower body mass index in both group. Cardiorespiratory fitness test evaluated as % predicted was different in the nonobese and obese (93% ± 14% predicted vs 82% ± 11% predicted) however this different was closing according to values of BMI. We observed a decrease in relative V˙O2peak (L/min) in the obese, although this approach was not an adequate representation of CRF in morbid obese patients. We have also observed that V˙ O2peak adjusted for BMI was still significantly lower in the morbid obese compared with the nonobese individuals Conclusions: Conventional methods of reporting V˙O2peak has not allow enough evaluating the CRFT in obese adults. Predicted V O2peak has allow a standardized assessment of CRFT in population. On the other hand healthy morbid obese has not fit as is commonly believed, although CRFT may be slightly higher in nonobese subjects depending on the uniqueness of the prediction values. Keywords: Cardiorespiratory, obese, patients P 052 RISKS OF VENOUS THROMBOEMBOLISM AFTER BARIATRIC SURGERY OPERATIONS:AN EXPERIENCED CLINIC RESULTS Burcu Yormaz1, Ilhan Ece2, Serdar Yormaz2
1Beyhekim State Hospital, Clinic of Chest Diseases, Konya, Turkey 2Selçuk University Medical Faculty, Department of General Surgery, Konya, Turkey Background: Bariatric surgery (BS) operations for morbid obesity are believed to be associated with greater risks of VTE (Venous Thromboembolism) in postoperative period. Our aim was to systematically review the evidence on this association and on the absolute risk of VTE following BS. Methods: We were searched our bariatric surgery results of 114 morbid obese patients who were BMI>40kg/m2 between may 2015 to june 2016 for reports on the associations of delivery methods with postoperative VTE and on the incidence of VTE following BS. Studies on thrombophilia or recurrent VTE were excluded. A logistic regression analysis controlling for demographic and comorbidity variables was utilized to determine the independent effect of morbid obesity on complication rates after BS. Results: Of 72 patients were female and 42 patients were male patients,female ratio was %63.4 and mean age of all patients were 34 (range 22 to 64). The median length of hospital stay was 6 (3 to 17) days in postoperative period. Morbid obese patients morbidity ratio were gradually increasedthan nonobeses according to their BMI (body mass index) scores respectively. low molecular weight heparin (LMWH ) was injected to all of the patients who were underwent BS after the surgical process for 5 days when they exactly mobilize and started to feed by liquids.Of 3 patients have VTE disease despite applying the LMWH in postoperative 48 hours. Treatment doses were twofold increased to these people,all three patients were quietly healed by this procedure. Conclusions: Morbid obese patients (BMI >40 kg/m2) have higher rates of postoperative complications after BS than nonobese patients. Morbid obesity is an independent risk factor for increased rates of most postoperative complications including the need for early revision BS.Furthermore new treatment procedures and drugs should be researched and innovated in recent years. Keywords: Venous thromboembolism, bariatric, treatment

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
230
P 053 LIGHTNING STRIKE-INDUCED ACUTE LUNG INJURY Melahat Uzel Şener1, Ali Demir2, Alp Şener3
1Ankara Atatürk Chest Diseases and Chest Surgery Training and Research Hospital, Department of Chest Disease, Ankara, Turkey 2Van Training and Research Hospital, Department of Anesthesiology, Van, Turkey 3Ankara Atatürk Training and Research Hospital, Department of Emergency Medicine, Ankara, Turkey Objective: Electrical injuries constitute between 2 and 5% of admissions to burn centers. Lightning strike is an environmental electrical injury with high rates of mortality. We want to present to the literature a rare case of lung injury due to direct effect of lightning strike. Case: A 19-year-old male patient was admitted to the emergency department with complaints of severe abdominal pain, shortness of breath, signs of hypoxia and history of amnesia as a result of a very close lightning strike within the previous 24 hours. His vital signs upon admission were 80/50 mmHg blood pressure, 110/min heart rate, 18/min respiratory rate, 85% partial O2 saturation. Breath sounds were diminished. Computed tomography (CT) of the thorax revealed bilateral pleural effusion that was 1.2cm on the right and 0.8cm on the left and bilateral diffuse ground glass areas that were significant at the apex of the lung parenchyma (Figure 1). The patient was discharged from the intensive care unit with clinical improvement on the tenth day, where he was treated with supplemental oxygen, intravenous hydration, and invasive cardiac monitoring. There were no pathological findings on his chest CT on the 20th day after treatment (Figure 2). Conclusion: Lightning is a rare cause of emergency department visits. Also pulmonary involvement is rare. In addition, in cases of lightning-induced primary lung damage, there is a possibility for various mechanisms of trauma to the thorax or secondary effects due to cardiac damage, and all of these should be taken into consideration. We interpret this case as a lung contusion directly connected to the damage from lightning which is a rare mechanism. Lightning strike cases should be handled as high-energy trauma. However, as in this case, mostly a conservative approach and support are sufficient. Keywords: Electrical injuries, lightning strike, direct effect, lung injury, high-energy trauma P 054 THE POTENCY OF PULMONARY REHABILITATION PROGRAMMES FOR MORBID OBESE PATIENTS WHO HAVE CHRONIC OBSTRUCTIVE PULMONARY DISEASE Burcu Yormaz1, Ilhan Ece2, Serdar Yormaz2
1Beyhekim State Hospital, Clinic of Chest Diseases, Konya, Turkey 2Selçuk University Medical Faculty, Department of General Surgery, Konya, Turkey Background: Chronic obstructive pulmonary disease (COPD) is a global systemic disease that is often associated with cardiovascular and metabolic comorbidities. The assertive effects of pulmonary rehabilitation (PR) in COPD patients are well known. The purpose of our study is to evaluate the comorbidities frequently associated in morbid obese patients with COPD. Methods: Of 38 morbid obese patients hospitalized with stable COPD, GOLD stages II, III and IV, aged between 41 and 63 years, recorded in the PR program that were divided into two groups according to their BMI (body mass index) results. Of 32 (74%)(group1) were morbid obese and 6 (16%)(group 2) were super obese patients. The efficacy of the PR programs results (dyspnea, exercise capacity, body mass index (BMI), quality of life) was shown using the BODE Index, the 6-minute walk tests (6MWT) and the dyspnea scales (mMRC), the COPD Assessment Test (CAT). Results: Most patients had at least one chronic comorbidity. Of these, the cardiovascular ones widespread, hypertension being the most commonly reported comorbidity (71.0%), followed by metabolic diseases (65.7%) and other respiratory disorders (55.2%).28 of the 38 patients (73.6%) experienced a clinically significant improvement in distance in the 6MWT. 68.4%, 16.6%of the patients have reductions in the BMI respectively, the scores of the CAT, breathlessness and depression, parameters that correlated well with the improvement in the walking distance in the first than second group of patients. Analysis reports showed that respiratory failure adversely affect the health status of morbid obese patients. Conclusıons: PR is equally effective in super and morbid obese patients with COPD and chronic comorbidities however its effectiveness being influenced by the BMI decreasing rates. The outcomes of our study suggest that also morbid obese patients with COPD and comorbidities have to be included in PR programs for specific training. Keywords: Pulmonary rehabilitation, chronic obstructive pulmonary disease, obese

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
231
P 055 SHOULD ACUTE APPENDICITIS ALWAYS BE IMMEDIATELY OPERATED? Anouk Etienne Free University of Brussel, CHU Brugmann, Emergency Room, Belgium Introduction: With this work we tried to determine: (i) If there are clinical or para-clinical criteria to determine, in the emergency room (ER), the level of gravity of an acute appendicitis. (ii) If any delay between first symptoms apparition and surgery had an impact on complications occurrence or length of hospital stay. (iii) If there are clearly defined situations where recommendations could come to an agreement between the ER practitioner and the surgeon. Method: This work is a retrospective study of 317 cases of appendicitis on a two years period. After exclusion, the results of 175 adults were analyzed. Results: This work studied the influence of different delay on the level of gravity, based on the anatomopathology report. There was a linear augmentation of gravity in relation with a longer delay between first apparition of symptoms and arrival in the ER. But there was no difference in the stage of gravity when looking at the delay between arrival in the ER and surgery. We also defined clinical and para-clinical criteria that helps to determine the level of severity in appendicitis, criteria such as the disappearing of Mc Burney sign, the raising of the C reactive protein, the lowering of eosinophilia, or the presence of liquid in the Douglas when performing an ultrasound. This study also showed a longer need for antibiotics, a longer hospital stay and more complications in advanced stages of appendicitis. Conclusion: If it’s obvious that complicated appendicitis need immediate surgery, it seems reasonable to believe that surgery in a simple appendicitis can be postponed. This is why it’s important to develop clinical and para-clinical criteria to determine, in the ER, the severity of an appendicitis. Keywords: Appendicitis, abdominal surgery, ED delay P 056 WE USE OFTEN, BUT DO WE KNOW? THE SELF-EVALUATION OF LEVEL OF RADIOLOGICAL KNOWLEDGE MADE BY DOCTORS AND THE CONDITIONS TAKEN INTO CONSIDERATION WHILE ORDERING RADIOLOGICAL IMAGING. Mehmet Cihat Demir, Damlanur Kucur, İlter Ağaçkıran, Yasemin Özdamar, Nalan Metin Aksu, Meltem Akkaş Hacettepe University Faculty of Medicine, Department of Emergency Medicine, Ankara, Turkey Objective: Diagnostic imaging plays an important role in today's medical practice. In this study, it is asked doctors to evaluate their levels of knowledge associated with radiological imaging, and sources of radiological knowledge that they have. In addition, we planned to detect what they pay attention to while ordering radiological imaging. Methods: The study is made in 2015.The doctors were divided into 5 groups as emergency medicine, medical sciences, surgical sciences, radiology departments or general practitioners(GP).140 doctors who have at least working experience of three years were present in each groups, a total of 700 doctors answered questionnaire via e-mail about radiological imaging. p<0.05 were considered statistically significant. Findings: Nearly 20.7% of radiologists,46.4% of emergency medicine physicians(EMP),and over 50% of other physicians self-evaluated their radiological knowledge level as insufficient (very low, l ow, medium).Compared to other departments, self-evaluated knowledge levels of radiologists, a combined group of radiologists and EMP, and GP were found “very high”, ”high”, and "very low”, respectively (p<0.001).As for the source of information obtained about radiological examinations; medical school (83.9%),residency training (65.3%),individual interests (57.1%),radiological courses(39.9%) and congresses(32%) have been determined. Among departments, radiologists and EMP reported residency training and individual efforts more as a way of learning while radiologists also adding radiological courses to the list (p<0.001).When the doctors are asked what they pay attention risk-wise while ordering radiological imaging; 16.7% in CT, 22.1% in radiography, 31.6% in MRI,76% in ultrasonography “I do not care/I cannot afford to ”answer is received. In all investigations, informed consent was the least considered condition. Conclusion: Most doctors even the radiologists in this study see their knowledge as insufficient. Another result confirms this assessment; pregnancy, radiation exposure, contrast nephropathy, contrast allergy, and presence of MRI-incompatible devices were not questioned enough. The results showed that training of doctors about imaging modalities which become more widely used every passing day is not enough. Radiological training should be supported in medical school and residency training, afterwards the courses, seminar, symposiums and congresses should be used to support the training. Adequate training will raise awareness about the risks. Keywords: Imaging, knowledge level, radiological training

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
232
P 057 HEMORRHAGIC LESIONS DUE TO RAMIPRIL/HYDROCHLOROTHIAZIDE AND CARVEDILOL: A RARE SIDE EFFECT
Elif Çelikel1, Betül Akbuga Özel2, Irem Güngör1, Miray Özlem1, Irfan Kala1, Sercan Hastürkoglu1, Oktay Hakbilir1
1Ankara Numune Training and Research Hospital, Ankara, Turkey 2Başkent University Ankara Hospital, Ankara, Turkey A 73-year-old male patient was admitted to emergency department with hemorrhagic lesions on the buccal mucosa and throughout his body. He was started on Delix (ramipril/hydrochlorothiazide), Decalin (furosemide), and Arlec (carvedilol) on a different health care center several days prior to the visit. The initial blood test results revealed a platelet count of 5000 µL. Series of other tests, including gastrointestinal endoscopy, thyroid fine needle aspiration biopsy, and bone marrow biopsy were conducted in the ward, however no significant cause of thrombocytopenia was detected. His condition was attributed to rare side effects of ramipril/hydrochlorothiazide and carvedilol. Keywords: Hemorrhagic lesions, ramipril/hydrochlorothiazide, carvedilol P 058 PNEUMOMEDIASTINUM AND RETROPERITONEAL AIR Elif Çelikel, Irfan Gökcek, Murat Dogan Iscanlı, Esra Çıvgın, Ugur Bal, Tamer Durdu, Serkan Muhittin Yılmaz, Müge Bedriye Sönmez, Evvah Muhammed Karakılıç Ankara Numune Training and Research Hospital, Ankara, Turkey Seventy eight years old women came to emergency with hematemesis. İn first examination with found common emphysema at abdomen. She had got lung cancer and multiple metastasis She took radiotherapy to abdomen last week. We think that she could be organ perforation due to ischemic colitis. Bu we diagnosis that after she made very hard valsalva maneuver, spontaneous pneumomediastinum occurred and air passaged to the retroperitoneal area and abdomen. We met spontaneous pneumomediastinum and different air passaged. Keywords: Emphysema, retroperitoneal air, pneumomediastinum

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
233
P 059 SPONTAN RETROPERITONEAL HEMATOM Mümin Murat Yazıcı1, Ensar Topaloğlu1, Aydın Çoşkun1, Özlem Bilir1, Süleyman Kalcan2
1Recep Tayyip Erdoğan Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Rize 2Recep Tayyip Erdoğan Üniversitesi Eğitim ve Araştırma Hastanesi, Genel Cerrahi Kliniği, Rize Giriş: Retroperitoneal hematom, sıklıkla travma, vasküler lezyonlar, tümörler, cerrahi girişim ve antikoagülan tedaviye bağlı olarak retroperitoneal alana olan kanamalar sonucunda meydana gelmektedir. Spontan olarak karşımıza çıkabilmekle birlikte nadir görülen bir durumdur. Patolojinin normal olan retroperitoneal damarlardan kaynakladığı düşünülmekle birlikte çoğu zaman patolojik sebep ortaya koyulamamaktadır. Semptom ve bulgular hematomun kendinden ziyade yaralanan organa ait bulgular şeklindedir. Karın ağrısı ve batında ekimotik lezyonlarla acil servise başvuran spontan retroperitoneal hematom’lu olguda acil servis takip-tedavi sonuçlarını tartışmayı amaçladık. Olgu: 77 yaşında erkek hasta 24 saat önce başlayan karın üzerinde olan morluk ve kuşak tarzı karın ağrısı şikayetiyle acil servise başvurdu. Hastanın soy geçmişinde ve öz geçmişinde herhangi bir özellik mevcut değildi. Yapılan fizik muayenede; vital bulguları TA:130/65 mmHg, Nabız:74/dk Solunum Sayısı:15/dk Ateş:36.70C olarak tespit edilirken, batın muayenesinde tüm kadranlarda hassasiyet ve sağ alt kadranda defans mevcuttu. Hastanın çalışılan laboratuar tetkiklerinde ve Ayakta Direkt Batın Grafisinde herhangi bir patolojik bulguya rastlanılmadı. Hastanın çekilen Batın Bilgisiyarlı Tomografisinde, retroperitoneal alanda psoas kasında hematom tespit edilmesi üzerine Genel Cerrahi konsültan hekimi tarafından değerlendirilerek takip amacıyla ilgili kliniğe yatırıldı. Sonuç: Spontan retroperitoneal hematom, herhangi bir travma öyküsü olmayan ve antikoagülan ilaç kullanmayan hastalarda hematomun nedeninin açıklanamadığı durumdur. Fizik muayenede retroperitoneal hematomu ilgilendiren sisteme yönelik bulgular yanısıra, laboratuar ve görüntüleme yöntemleri tanıda yardımcı olmaktadır. Bilgisayarlı tomografi öne çıkan görüntüleme yöntemidir. Tedavi operasyonel ve non-operasyonel olarak hastanın klinik, etkilenen organ veya sistemlerine göre tercih edilmektedir. Hastada retroperitoneal hematoma sebep olacak etyolojik neden saptanamaması nedeniyle Spontan retroperitonel hematom olarak değerlendirildi. Acil servise cilt lezyonları ve karın ağrısı şikayetiyle başvuran non-tarvmatik olgularda spontan retroperitoneal hematom akılda olması gereken tanılar arasında yer almalıdır. Anahtar Kelimeler: Karın ağrısı, retroperitenael hematom, spontan P 060 SOL DAL BLOĞU VE MYOKARD INFAKTÜSÜ Mümin Murat Yazıcı1, Mehmet Oktay1, Ensar Topaloğlu1, Özlem Bilir1, Ece Hastas2
1Recep Tayyip Erdoğan Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Rize 2Recep Tayyip Erdoğan Üniversitesi Tıp Fakültesi, Kardiyoloji Anabilim Dalı, Rize Göğüs ağrısı acil servis başvuruları içerisinde en sık nedenler arasında yer almakla birlikte ayırıcı tanıda ölümcül olabilecek tanılar ilk olarak dışlanması gerekmektedir. Başvuru sonrası hastada anemnezle birlikte Elektrokardiyografi (EKG) çekilerek en kısa sürede değerlendirilmelidir. Ancak değerlendirmede sırasında, özellikle sol dal bloğunu(LBBB) içeren EKG’lerin infarkt lehine yorumlanması sırasında acil servis hekimlerini arada bırakmaktadır. LBBB içeren EKG’lerde ST segment ve T dalgaları diskordan olma eğilimindedir bu özellikten dolayı infarkı EKG’de tespit etmek maskelene bilinir veya taklit edilebilir hale gelmektedir. Bu tanı zorluğundan dolayı seri EKG kaydı almak ST değişikliklerini tespit etmede bize yardımcı olmaktadır. Özellikle LBBB içeren EKG’lerde infarkt tanısı koymada Sgarbossa Kriterleri MI tanısı için %90 özgüllüğe sahiptir. Burada göğüs ağrısıyla acil servise başvuran hastada, çekilen seri EKG kayıtlarında; LBBB ve iskemik ST değişiklerine bağlı olarak MI tanısı ile perkütan koroner girişim planlanan bir olguyu sunmayı amaçladık. Acil servise göğüs ağrısı, sersemlik, bulantı şikayetleriyle başvuran 71 yaşında erkek hastanın öz geçmişinde hipertansiyon öyküsü mevcutken soy geçmişinde ise hipertansiyon ve koroner arter hastalığı olduğu öğrenildi. Yapılan fizik muayenesinde vital bulguları; TA:140/90 mmHg, Nabız:70/dk, Ateş:36.7 C, Solunum sayısı:15/dk SO2:%98 olup sistem muayenelerinde patolojik bulguya rastlanılmadı. Çekilen EKG’de LBBB tespit edilen hasta monitörize edilerek seri EKG kayıtları alındı. Çalışılan laboratuar tetkiklerinde kardiyak belirteçler dahil olmak üzere herhangi bir patolojiye rastlanılmadı. Ancak seri EKG kayıtlarında dinamik EKG değişikliklerinin göğüs ağrısıyla birlikte olması nedeniyle kardiyolog tarafından değerlendirilerek perkütan koroner anjiografi planlandı. Atherosklerotik değişiklikler dışında özellik gözlemlenmeyen hasta şifayla taburcu edildi. Acil servise göğüs ağrısı ile başvuran hastalarda akut koroner hastalığı tanısını koymak veya dışlamak için ilk istenmesi gereken tetkik EKG olmalıdır. Seri EKG kayıtları iskemik değişiklerin tespitinde ve özellikle LBBB içeren EKG’lerde infarkt tanısını sırasında Sgarbossa kriterleri yol gösterici olmaktadır. Acil servise göğüs ağrısı ile başvuran olgularda EKG’nin değerlendirilmesini zorlaştıran LBBB varlığında Sgarbossa Kriterleri ve seri EKG kayıtları MI tanısını koymada aklımızda mutlak bulunmalıdır. Anahtar Kelimeler: EKG, sol dal bloğu, MI

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
234
P 061 ACCESSORY RENAL ARTERY INJURY SECONDARY TO THE GUNSHOT WOUND Selçuk Parlak1, Esra Çıvgın1, Elif Çelikel2, Perihan Polattaş1, Hamza Özer1
1Numune Training and Research Hospital, Clinic of Radiology, Ankara, Turkey 2Numune Training and Research Hospital, Clinic of Emergency Medicine, Ankara, Turkey Urinary tract (UT) is frequently affected in abdominal traumas. UT injury accounts for 8–10% of trauma patients, with blunt injury representing 80–95% of cases. The most common affected organ is the kidney. Traumatic renal injuries are consist of subcapsular hematoma, renal laceration, renal contusion and renal vascular injury. Renal vascular injury is more rare but serious concern in patients suffering blunt trauma. Computed tomography (CT) is the preferred method of investigation in the setting of acute renal trauma. It can help in the evaluation of the severity of parenchymal injury, the presence of urinary extravasation and determine the status of the renal vascular pedicle. We present a 40-year-old male patient who was taken to the emergency room after gunshot wound and detected left accessory renal artery (ARA) injury after multidetector CT evaluation. Contrast-media extravasation, avascularity in renal parenchyme and concomitant duodenal injury were also detected. Keywords: Trauma, renal artery, multidetector computed tomography P 062 THE INTERPRETATION OF RELATIONSHIP BETWEEN BODY MASS INDEX AND INTENSIVE CARE UNIT RESULTS IN ACUTE LUNG DISEASE IN MORBID OBESE PATIENTS Burcu Yormaz1, Ilhan Ece2, Serdar Yormaz2, Bayram Çolak2
1Beyhekim State Hospital, Clinic of Chest Diseases, Konya, Turkey 2Selçuk University Medical Faculty, Department of General Surgery, Konya, Turkey Background: The association between body mass index (BMI), excess weight loss (EWL) after the metabolic surgery procedure and outcomes of critically ill patients is unclear. Our objective was to detect the relative between BMI, EWL and outcomes in morbid obese patients with acute lung disease (ALD). Methods: In a retrospective study of all ICU (intensive care unit) patients in tertiary clinic, 0f 74 patients have a BMI recorded who were higher BMI than nonoobese population. Patients in the morbid obese BMI groups (>40kg/m2) were compared to nonobese patients in the following sites: length of stay in hospital (LOSH), ICU LOS, period of invasivemechanical ventilation, mortality, and discharge situation. Results: There was only one mortality detected in morbid obese BMI group compared to non-obese patients. Seriously morbid obese patients have longer stay in hospital than non-obese patients (mean day increase, 12.3 days; 95% average interval [AI], 5.1 to 18.4 days; p < 0.05); this was emphasized when analysis was restricted to survivors (mean increase, 15.7 days; 95% AI, 8.3 to 23.7 days; p < 0.05). ICU LOS and duration of mechanical ventilation were also longer in the morbid obese group. Morbid obese patients were more likely to be discharged to a rehabilitation programme before returning to their social life. Conclusions: BMI which is higher than >40kg/m2 in is interrelated with mortality in morbid obese patients who have sick of ALD, on the other hand this global disease is also associated with increased morbidity and long discharge period in hospital. So the scientist have stil researching novel methods to prevent th obesity all over the world, because this illness has been the disease of our age. Keywords: Acute lung disease, obese, intensive care

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
235
P 063 THE EFFICACY OF BODY MASS INDEX ON LUNG VOLUMES IN MORBID OBESE PATIENTS WITH AIRWAY OBSTRUCTION
Burcu Yormaz1, Ilhan Ece2, Serdar Yormaz2, Bayram Çolak2
1Beyhekim State Hospital, Clinic of Chest Diseases, Konya, Turkey 2Selçuk University Medical Faculty, Department of General Surgery, Konya, Turkey Background: The prevalence of morbid obesity is increasing seriously throughout the world. It is well founded that obesity can result increased respiratory symptoms, even in individuals without airway obstruction. The main effects of morbid obesity include reduced respiratory system compliance, increased work and oxygen cost of breathing. Therefore, the aim of this study was to examine the relationship between BMI (>40kg/m2) and lung volumes in morbid obese patients with airway obstruction of various severity. Methods: We have studied the impact of higher body mass index (BMI >40kg/m2) in morbid obeses on static lung volumes and airway function of 64 patients (of 45 (70,3%) who were 42 to 64 years of age and met GOLD (Global Initiative for Chronic Obstructive Lung Disease) spirometric criteria for COPD between the years may 2014 to june 2016. We have also evaluated the severity of airway obstruction on these relationships. Results: Higher values of BMI in the morbid obese patient group as a whole, functional residual capacity, residual volume, expiratory reserve volume decreased exponentially (P < 0.05); total lung capacity (TLC) decreased hard acceleration (P < 0.05); and inspiratory capacity (IC) and IC/TLC increased hard acceleration (P < 0.05).The effects of higher BMI on FEV1/FVC was biggest in GOLD stage III/IV (P < 0.05), whereas higher BMI has greater effects on IC in GOLD stage II (P < 0.05). Conclusions: The relationship between higher BMI ( > 40 kg/m2) and lung volumes, capacities in patients with airflow obstruction has potentially important effects for the accurate interpretation of pulmonary function tests. Volume-derived equations or ratios such as the FEV1/FVC is strongly influenced by the lung volume-reducing effects of higher BMI levels in morbid obese patients with COPD. Based on the results of this study, future studies should ideally account for the influence of higher BMI values. Keywords: Airway obstruction, lung, obese P 064 DISTRIBUTIVE SHOCK IN THE ED: SEPSIS, ANAPHYLAXIS OR CAPILLARY LEAK SYNDROME? Cansu Alyeşil, Nurettin Özgür Doğan, Ibrahim Ulaş Özturan, Seda Güney
Kocaeli University Faculty of Medicine, Department of Emergency Medicine, Kocaeli, Turkey Distributive shock is a hyperdynamic process, resulting from excessive vasodilation. Impaired blood flow causes inadequate tissue perfusion and consequently it may lead to end organ damage. Although the most common etiology is septic shock; anaphylactic and other etiologies should be taken into consideration. We report a thirty years old female patient presented to emergency department with nonspecific symptoms and hypotension after a viral upper respiratory infection. Her physical examination revealed mild edema, rebound in right upper and lower quadrants; also hypotension concomitant with hypoperfusion symptoms, which manifested by loss of consciousness in the following hour after presentation. The hypotensive state was refractory to large amount of crystalloid infusion and a series of investigations were carried out to find out shock etiology including ECG, echocardiography and thoracoabdominal computed tomography (CT). No etiologic agent or drug were defined by her at the presentation, which may cause to anaphylaxis; however later she concluded that she took propolis extract one day ago. After the investigations, CT images showed pneumonic infiltrates in the lower zone of right lung, enlarged liver, thickened gallbladder wall and extensive amount of free fluid in perihepatic and retroperitoneal area. Although this changes was considered as a secondary effect to water shift, septic shock cannot be excluded. Her laboratory findings revealed hypoalbuminemia and a transient increase in liver function tests. She took either a broad spectrum antibiotic and norepinephrin infusion in the following days. After third day of her presentation, her hypotension improved, abdominal tenderness disappeared and discharged healthy. This case report puts different forms of distributive shock forward which may be seen rarely concomitant. When the treatment fails to resolve clinical signs and symptoms, alternative diagnoses should be considered. Keywords: Shock, anaphylaxis, propolis, capillary leak syndrome, emergency department

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
236
P 065 SUBCUTANEUS INJECTION OF AN ORGANOPHOSPHATE COMPOUND Bulut Demirel1, Mücadiye Demirel2
1Ankara Atatürk Training and Research Hospital, Clinic of Emergency Medicine, Ankara, Turkey 2Ankara Ufuk University Dr. Rıdvan Ege Hospital, Department of Emergency Medicine, Ankara, Turkey Introduction: Organophosphat compounds are in common household use in countries where the economy is based on agriculture. The following is a presentation and a discussion of a 26 years-old patient who subcutaneously injected herself organophosphate compound for suicidal purposes. Case Report: 26 year-old female patient presented to the ED with the complaint of pain and swelling in the left anticubital area. Upon questioning, she explained that she injected herself 2.5ml of an agricultural product Diazonin. The patient vitals was normal. In patient’s left antecubital region, a hyperemic area was visible. Pseudocholinesterase levels in the blood sample studied, the patient was discharged after 24 hours of follow-up without any symptoms or complications. The patient was followed up on daily basis. On the second day, upon observing cellulite around the area of injection, a treatment of amoxicilline clavunate of 1gr, 12 hrs was begun. The swelling which was observed to be going down on daily checks was completely healed at the end of one week. Discussion: Acetylcholine is a neurotransmitter which acts on both sympathetic and parasympathetic system. When acetylcholinesterase, which catalyzes the breakdown of acetylcholine, is inhibited, acetylcholine accumulation starts in synapses. Chemicals in organophosphat group irreversibly inhibit cholinesterase. Consequently, muscaranic and nicotinic effects are observed together. According to the route of administration, various local complications manifest themselves. Hemorrhage and gastrointestinal ulcers are observed in cases where organophosphat intake is through gastrointestinal pat whereas local abscess and cellulite can be observed in parenteral routes. In our patient, cellulite was observed in the area of injection and therefore she was given amoxicilline clavunate treatment. To conclude, following subcutaneous organophosphate injection, if no problem was observed in short period ED follow, patient may be put on outpatient status and during outpatient treatment if cellulite is observed, as it did in our case, oral antibiotic treatment will be adequate. If medically indicated, atropine and pralidoxime should be used. Keywords: Cellulite, injection, organophosphate P 066 A RARE CAUSE OF ABDOMINAL PAIN; FASCIOLA HEPATICA INFESTATION Bulut Demirel
Ankara Atatürk Training and Research Hospital, Clinic of Emergency Medicine, Ankara, Turkey Introduction: Fasciola Hepatica is an endemic infestation reason in Turkey. General reasons for patients’ presenting to the EDs are abdominal pains, and the diagnosis of those pains is quite hard. In this study, we will present a Fasciola Hepatica case which was diagnosed at the ED. Case report: A 25 year-old young woman presented to the emergency department with the complaint of abdominal pain lasting for a week and restlessness. The vitals of the patient were stabile. In her physics examination, apart from epigastric sensitivity, any kind of pathology wasn’t seen. In laboratory tests any pathology wasn’t observed. However, linear ehcogenicity which was moving towards upright in lumen in the gall bladder was monitored in US examination. Primarily, infestation was thought. With the pre-diagnosis of Fasciola Hepatica, serum sample was taken from the patient. While the treatment of the patient was continuing, in her serum sample 1/160 in titre fasciola hepatica was measured as positive by means of ELISA method. After 14-days treatment of the patient, in her ultrasonography there wasn’t seen any pathology. Discussion: Fasciola Hepatica which usually appears with the infestation of the farm animals such as sheep and cattle, even if it is rare, chooses human body as a dwelling. The dwelling of fasciola hepatica in the body is the liver and the gall bladder. In our case, the clinic of fasciola hepatica which may rarely cause obstructive jaundice hasn’t developed yet. In the literature even though bithionol and triclabendazole are recommended as the basic cure, the treatment as being metronidazole 1.5mg/per day was begun because of its easy accessibility and cost-effectiveness in our country. The patient was totally healed after a 14 -day treatment. Consequently, in our country parasitic infestations are present as endemically. Primarily in abdominal pain cases, every patient should also be evaluated in terms of parasitic infestations and those diseases should have differential diagnosis. Keywords: Emergency, infection, fasciola hepatica, ultrasonography

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
237
P 067 PHANTOM PAIN; A NEW SYMPTOM OF CEREBRALLY HEMORRHAGE Bulut Demirel1, Sema Avcı2, Gözde Çavumirza3
1Ankara Atatürk Training and Research Hospital, Clinic of Emergency Medicine, Ankara, Turkey 2Kars Harakani State Hospital, Clinic of Emergency Medicine, Kars, Turkey 3Ankara Dışkapı Yıldırım Beyazıt Training and Research Hospital, Clinic of Emergency Medicine, Ankara, Turkey Introduction: Intracerebral bleedings have a rank of high mortality and morbidity. Non-traumatic bleedings in the cerebellum are called as spontaneous cerebrally hematomas. Spontaneous cerebrally hematomas primarily resulting from hypertension. As much as we know, among the symptoms of spontaneous cerebrally hematomas, there is no phantom pain. In our study, a case of spontaneous cerebrally hematom with the type of phantom having been applied to the emergency department was presented. Case report: A 64 year-old male patient presented to the emergency department with the complaint of toothache. The patient had hyperlipidemia and surgery of prostate in his medical background. At his physical examination, it was seen that the patient was edentulous and he was wearing denture. The patient was observed to have speech disorders and slow articulation but the examination findings of his other systems were normal. At brain CT a hyper dense area was observed and compatible with cerebrally hematom was monitored. The patient was transferred to the neurology department. Discussion: Pain is one of the most primary reasons for presenting to the emergency department. The location, intensity, changes in the course of time and the beginning period of pain may inform us about the pathology underlying the pain. In the patients who present to the emergency with a complaint of pain, apart from the examination being compatible with the possible pathology, the examination of other systems may help hidden pathologic cases to be come out. Phantom type of pain is a phenomenon which demonstrates itself within amputee organs and unpleasant senses such as irritancy and itchiness. It should be remembered that there may be an underlying acute neurologic pathology in phantom pains. Consequently, it should be kept in mind that a patient presenting to the emergence service with a complaint of a phantom type of headache may have neurologic pathology. Thus, detailed neurologic examinations and suitable diagnostic methods where necessary should be applied. Keywords: Cerebellary hemorrhage, emergency department, Phantom pain P 068 A RARE COMPLICATION OF NEURAL THERAPY: PNEUMOTHORAX Bulut Demirel1, İzzettin Hür2, Yıldız Yıldırımer2, Ömer Faruk Demir2
1Ankara Atatürk Training and Research Hospital, Clinic of Emergency Medicine, Ankara, Turkey 2Ankara Dışkapı Yıldırım Beyazıt Training and Research Hospital, Clinic of Emergency Medicine, Ankara, Turkey Introduction: Neural therapy is a kind of intervention which is used in alternative medicine and attempts to treat chronic pain and illnesses by which local anesthetic is injected into certain locations of the body. However, the effects of neural therapy haven’t been proved, yet and it has some risks. We will present you a case in which pneumothorax developed after neural therapy. Case report: 46 year-old female patient applied to the emergency department with the complaint of pain which was located in her back and under her left scapula. The patient didn’t have any certain illnesses apart from bruxism. The patient was also learnt to have attended to neural therapy center for the pain in her jaw caused by bruxism. When questioned, the patient told that during the neural therapy she had felt acute pain just after the injection. In her respiratory system examination, the lung sounds were inaudible on the left. The patient was hospitalized after she was administered thorax tube treatment. She was healed without any complication after five days’ treatment. Discussion: Alternative medicine which is increasingly requested both in our country and in the world is a form of techniques used to treat an illness. Neural therapy is an approach which claims to treat pain and diseases by injecting local anesthetics into nerves, scar tissues, glands and certain examination points. In this method, novocaine and procain are indicated to be generally used. Among its complications, there may be bleedings, infections and side effects caused by local anesthetics medicine. In the literature, there isn’t any data about the occurrence of pneumothorax development during neural therapy. In our case pneumothorax, which is a more hazardous complication caused by the injection was developed. The patient benefitted from the administration of tube of thoracostomy and she was healed. To conclude it should be known that pneumothorax may develop during neural therapy. Keywords: Alternative medicine, neural therapy, pneumothorax

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
238
P 069 PENETRATING HEAD TRAUMA ADMITTED 24-HOUR AFTER THE EXPLOSION AND BY FOOT Bulut Demirel Ankara Atatürk Training and Research Hospital, Clinic of Emergency Medicine, Ankara, Turkey Introduction: Penetrating skull injuries and cerebral damage are among the injuries which have bad prognosis. The form of the injury, the starting time of treatment, the size of the cerebral damage and the existence of infection are among the factors which affect the prognosis. In our case, a young male patient with head trauma was recognized to have penetrating injury and intracranial extraneous substance one day after the trauma. Case Report: 21-year-old male patient presented to the ED with the complaint of headache. He told that a day before he had witnessed an explosion. The patient had gone to a small medical clinic for his excoriations and had suture on his forehead. The vitals of the patient were normal and he didn’t have any pathologic findings except that he had a sutured cut on his glabella. Considering the trauma history and the headache of the patient, the brain CT was taken, by which anterior and posterior fracture in the frontal sinus, an appearance of metallic extraneous substance both in the left frontal brain lobe and in the left lateral parenchyma and, extensive pneumocephalus were monitored. Therefore, he was conveyed to neurosurgery intensive care unit. Discussion: Considering the examination findings of head trauma patients, the necessity of the computerized tomography scan should be decided. In penetrating head traumas, for skin integrity is damaged, even if the patient has the conscious and GCS score as 15, brain CT should be done. In our case, since the patient had normal examination findings and also didn’t have any complaint, computerized tomography scan didn’t need to be taken. However, a day after the incident, the patient presented to ED with the complaint of severe headache, and an extraneous substance was noticed in his head. To conclude, it is extremely crucial the indications be regarded for the necessity of a head trauma patient’s having computerized tomography scan in terms of both the patient himself and the physician, as well. Keywords: Emergency department, late admission, penetrating head trauma P 070 A RARE CAUSE OF TRACHEAL COMPRESSION: THYROID HEMOTAMA Bulut Demirel Ankara Atatürk Training and Research Hospital, Clinic of Emergency Medicine, Ankara, Turkey Introduction: Securing respiratory tract is an emergency. Hematomas and abscess may pressurize trachea. Those effects should be disposed of as soon as possible and respiratory tract should be secured with invasive operations when necessary. Case report: 43 year-old female patient presented to ED with the complaint of labored breathing. The patient who didn’t have a certain disease told that she had been feeling a bulginess on her throat for two weeks and from then her labored breathing had been gradually soaring. The other system examination findings of the patient were normal excluding her neck examination. In her neck examination a palpable bulk was recognized in her thyroid. An encysted hematoma in the thyroid was observed in the ultrasonography. In order to decide the borders of the hematoma neck CT was planned. In the CT a 5cm-sized cystic nodule was monitored in the right lobe of her thyroid. With a purpose of reducing the patient’s labored breathing US asissted derinage performed and almost 35 cc liquid was drained. The samples taken from the patient were in hemorrhagic character. Discussion: Almost all of the patients with thyroid hematoma present to ED with the complaint of bulginess and pain in the throat. Arterial hematomas may be massive in a very short time. If they are threatening the vital organs such as trachea by pressuring, they should be drained. In our case, there was an obvious tracheal pressure. Therefore, the hematoma was drained and the patient was hospitalized for it highly poses risks of reoccurring. To conclude, thyroid hematomas and abscess may result in labored breathing in patients because of tracheal pressure. It is significant to reduce the pressure in both of those cases by drainage. At the same time, as it is in other hematoma cases, drainage with company of ultrasonography is more comfortable and safe in thyroid hematomas. Keywords: Drainage, thyroid haematoma, ultrasonography

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
239
P 071 MAGNESIUM DEFICIENCY; A RARE CAUSE OF STATUS EPILEPTICUS DIAGNOSED BY DATABASE SEARCH Bulut Demirel1, Yasemin Yılmaz Aydın2, Ayça Özel Sönmez2, Sema Avcı3
1Ankara Atatürk Training and Research Hospital, Clinic of Emergency Medicine, Ankara, Turkey 2Ankara Dışkapı Yıldırım Beyazıt Training and Research Hospital, Clinic of Emergency Medicine, Ankara, Turkey 3Kars Harakani State Hospital, Clinic of Emergency Medicine, Kars, Turkey Introduction: Deficiency of electrolytes may cause seizures. It can be difficult to obtain a medical history from a patient and to inform the doctor of a complete list of the medications used by the patient during the time when the patient is having a seizure. Reliable and national database can be of great value for physicians. In our case, we will present a status epilepticus of which etiology we were able to ascertain by help of the database. Case Report: A 62 year-old female patient presented to the emergency department with loss of consciousness after a seizure. The patient was said to have had a seizure in the street and only an ID was found on her. Because patient cooperation was compromised, and relatives were absent, no detailed information was obtained. She had no cooperation and there was no other neurological abnormality. As the patient was followed, seizures ranging between 3-5 minutes were observed. The patient was diagnosed as status epilepticus and intubated. Hospital records revealed that the patient had presented to infectious diseases and had a history of hypoparathyroidism. We found out that she had taken 0.5 mg rocaltrole twice a day for hypoparathyroidism and she had hypomagnesemia which suggested the cause of status epilepticus be hypomagnesemia and consequently replacement treatment were given. At the end of the third day, the patient was extubated. Discussion: Our information on patient’s electrolyte imbalance and infection has been a guide to our treatment. Effective use of developing database has helped solve the problem. In cases where a patient is unable to give an account of their medical history as was the case in our situation, effective use of databases has enabled an early diagnosis and treatment. As a conclusion, it poses a challenge to take medical history of patients with neurological findings. Therefore, it is imperative that databases be developed and be actively made use of. Keywords: Database, hypomagnesemia, seizure P 072 KÜNT TRAVMA OLDUĞU ZANNEDİLEN PENETRAN BİR GÖĞÜS TRAVMASI Bulut Demirel Ankara Atatürk Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Ankara Giriş: Travmaların yönetiminde travmanın oluş zamanı, enfekte olup olmaması, oluş şekli ve penetran veya künt olma durumu da önemlidir. Bir travma hastanın künt veya penetran yaralanma durumuna göre hem tanı hem de tedavi şekli değişebilmektedir. Travmada öykü ve muayene ile tanı genellikle belirlenebilmesine rağmen olayın oluş şeklinin tam anlaşılamadığı durumda görüntüleme yöntemleri gibi tetkikler bize tanıda yardımcı olabilmektedir. Bu vakamızda künt travma düşünülen bir hastanın tetkik sonucunda penetran bir yaralanmanın da eşlik ettiği görülmektedir. Vaka takdimi: 67 yaşında erkek hasta acil servise üzerine demir kapı düşme şikayeti ile başvurdu. hastanın acil servise başvurusu esnasında vital değerleri normal sınırlarda idi. Yapılan fizik muayenede sağ skapula altında 4 cm’ lik cilt kesisi izlendi, sağ akciğer sesleri azalmıştı, sağ hemitoraks bazalde matite mevcuttu. Bunlar dışında patolojik bir bulgu saptanmadı. Yapılan muayene sonucunda hastada hemotoraks veya pnömotoraks olabileceği düşünülerek yapılan toraks bilgisayarlı tomografide de sağ akciğer içerisinde 2*6 cm’ lik düzenli sınırlı hiperdens yabancı cisim varlığı ile uyumlu görüntü ve hemotoraks izlendi. Hastanın detaylı sorgulamasında düşen kapının camının kırıldığı öğrenildi. Hasta göğüs cerrahisi tarafından operasyona alındı. Çıkarılan yabancı cismin kapının üstündeki camın bir parçası olduğu belirlendi. Tartışma: Travmaların yönetiminde olabildiğince detaylı öykü alınması tetkik ve tedavinin doğru yönlendirilmesi için elzemdir. Travmaya maruz kalan kişilerden doğru ve detaylı bilgi alınması doğası itibariyle zordur. Bu yüzden alınan öykü ve muayenenin olabildiğince detaylandırılması gereklidir. Bizim vakamızda alınan anamnez bize künt travmaya yönlendirmesine rağmen muayenede penetran yaralanma tespit edilmiştir. Ve bakılan bilgisayarlı tomografi sonucunda künt travma ile birlikte penetran bir travmanın eşlik ettiği gözlenmiştir. Sonuç: Travma hastalarından olabildiğince detaylı anamnez alınması ve tam sistemik muayene yapılması hem hasta hem de hekim açısından faydalıdır. Detaylı anamnez ve muayene ile ileri tetkik ve tedaviler daha uygun planlanabilir. Anahtar Kelimeler: Anamnez, göğüs travması, künt, penetran

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
240
P 073 INTRAMURAL AORTIC HEMATOMA MIMICKING RENAL COLIC IN A PATIENT WITH KIDNEY STONE DISEASE Emine Gaffari, Fulya Temizsoy Korkmaz, Hakan Topaçoğlu, Özgür Karcıoğlu Istanbul Training and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey Introduction: Intramural aortic hematoma is a rare condition with a high mortality rate. It is a variation of aortic dissection which has no intimal laceration. The false lumen results from ruptured vaso vasorum located in media layer of the aortic wall. The entity is usually associated with long-standing hypertension and is also seen iatrogenically or following trauma. Two mechanisms of rupture have been described: spontaneous or induced by a penetrating atherosclerotic ulcer. Intramural aortic hematoma can be treated with conservative procedure in uncomplicated stable patients. Below is a report of a patient presented with flank pain, diagnosed with spontaneous intramural aortic hematoma with renal hypoplasia and staghorn renal calculi. Case: 55-year old male patient presented with nausea, vomiting, exhaustion and pain in the left flank area to the emergency department. His medical history included hypertension, diabetes mellitus and coronary artery disease. His vital signs were heart rate 108 bpm, body temperature 37.50C. On physical examination, guarding and rebound tenderness were noted as negative while tenderness in costovertebral angle was absent. Mural thrombus was detected in aortic arch and descending aorta with the thoracoabdominal computed tomography scan with angiography. Moreover, atrophy in left renal artery and staghorn shaped calculi in left kidney were found. No sign of dissection and aneurysm was encountered. Medical treatment was administered and the patient was discharged after uneventful clinical course. Conclusion: Intramural aortic hematoma should be kept in mind for patients presented with acute-onset flank pain. Uncomplicated and stable patients can be followed up with medical treatment. Keywords: Intramural aortic hematoma, renal colic, kidney stone P 074 EARLY TREATMENT IN ORGANOPHOSPHATE POISONING AT ER Onur Tokocin, Tolgahan Güleç, Hakan Topacoglu Istanbul Training and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey The typical toxidrome in organophosphate (OP) poisoning comprises of the Salivation, Lacrimation, Urination, Defecation, Gastric cramps, Emesis (SLUDGE) symptoms (1). In treatment of organophosphate poisoning, uses atropine and oxime treatment (pralidoksim) (2). Patients with OP early and effective treatment is important to prevent possible deaths. We reported a case which organophosphate poisoning early admitted to ER. 24 year old male patient was came with taking insecticide which contains organophosphate 90 minutes ago by paramedics. In first examination; Glasgow Coma Scale: 15/15, Orientated, Cooperated, Blood Pressure: 121/89 mmHg, Pulse: 91/dk, Fever:36 C sO2:%97. Also patient was agitated and had hypersalivation, lacrimation, myozis, muscle fasciculations, smell like organophosphate and vomiting. In ER was started eyes and skin decontamination, oxygenation, 1 mg atropine IV and monitored. Applied 1 gr pralidoxime as a loading dose. Agitation and muscle fasciculations were removed after treatment but salivation were continuing. Patient admitted to ICU. In ER was applied 68 mg atropine IV every 5 minutes. After patient’s follow-up observed any arrhythmia, seizure, paralysis, neurotoxicity. Patient wasn’t intubated because of he wasn’t hypoxic and hadn’t bronchosecration. Only cholinergic symptoms was observed and late findings of OP (intermediate syndrome, late neuropathy) wasn’t observed. Patient was discharged with health on psychiatric control. Keywords: Organophosphate, emergency, early treatment

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
241
P 075 ADULT TYPE STILL DISEASE AT ER Onur Tokocin, Yusuf Cankat Bozkurt, Hakan Topacoglu Istanbul Training and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey Adult type still disease is an inflammatory disease which characterized with fever, arthratis and disappearing rashes in young adults(1). It can associate with some viruses and mycoplasma pneumonia, yersinia enterocolitica pathogens. We are reporting a patient came to ER with swelling at right foot and after diagnosed as Still disease.32 years old, Afghan, male patient admitted to ER with swelling at foot, intermittent fever, rush, weakness. He was cooperated, orientated. Vitales: blood pressure: 130/67 mmHg, pulse: 96/min, respiratory rate: 17/min, sO2: %95, fever: 37,7 C. Respiratory and cardiovascular examination were normal. There weren’t hepatomegaly or lymphadenopathy. At patient’s right ankle had rash, limitation of movement, and arthritis like symptoms. Right lower extremity motor strength was 3/5. At CBC: WBC 20,94 10^6/mm3, and there was any other anomaly. Biochemical markers were normal. Transthoracic echocardiography showed no findings about endocarditis, pericarditis, myocarditis and acute coronary syndrome. Cranial CT were normal.Venous Doppler at right lower extremity showed no deep venous thrombosis. There weren’t transmission delay in lower extremity at EMG. Cardiac, neurologic, vascular pathologies excluded and couldn’t find any infective cause. Patient with fever, leukocytosis with neutrophil dominance, arthritis, rash admitted to hospital pre-diagnose as systemic rheumatic diseases. During hospital follow-ups determined that without positive blood cultures and erythrocyte sedimentation rate was 105 mm/h, ASO 614 IU/ ml, CRP 26,309 mg/dl. Patient diagnosed as Adult Type Still Disease and started steroid treatment. He was discharged on the decline in complaints. Young patients presenting to ER with skin rash, fever, arthritis if other infective, vascular and neurological disease if not detected Adult Type Still Disease should be considered. Keywords: Adult, still disease, ER P 076 A CASE: DIAGNOSIS OF PRIMARY SPINAL CORD TUMOR PRESENTING WITH WEAKNESS IN LOWER EXTREMITIES Onur Tokocin, Pinar Akhanlı, Osman Aydemir, Hakan Topacoglu Istanbul Training and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey Primary spinal tumors are rare diseases. Extramedullary tumors are more common and include meningiomas, schwannomas, extramedullary ependymomas, haemangioblastomas. The most frequently used therapeutic modalities for spinal cord compressions are surgery, corticotherapy and radiotherapy. We describe a case of 57-year-old female patient who developed acute paraplegia as a result of spinal meningiom. 57 year-old woman presented to ED with complaint of urinary and bowel incontinence and bilateral lower extremities weakness for 10 days. She had not chronical disease. Respiratory and abdominal examination was normal. No significant finding was found in biochemical parameters and lab tests. On admission, he was conscious, fully cooperated and oriented, his Glascow Coma Scale (GCS) was 15/15, direct/indirect pupillary reflex to light was bilaterally positive, cranial nerves examination was intact. Neurological examination revealed flaccid paraplegia, total sensory loss below the level of second thoracic vertebra (T2). Spinal magnetic resonance imaging (MRI) with intravenous contrast revealed the mass at T2 level causing spinal cord compression. The dexamethasone was started until the patient taken to the surgery. Immediate surgical decompression was performed. Surgeons considered tumor was primary meningioma during the surgery. His neurologic function, including motor strength, bowel and bladder function improved in the postoperative period. Spinal cord compression is an oncologic emergency which, unless diagnosed early and treated promptly, can lead to permanent neurologic impairment and can seriously affect a patient’s quality of life (2). Keywords: Spinal cord compression, lower extremities weakness, ER
5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
242
P 077 KÜNT TRAVMA SONRASI GELİŞEN MULTİ ODAKLI VENA CAVA RÜPTÜRÜ Umut Payza, Zeynep Karakaya, Pınar Yeşim Akyol, Fatih Esad Topal, Gözde Canan Yavaş, Serkan Bilgin İzmir Katip Çelebi Üniversitesi Atatürk Eğitim Araştırma Hastanesi, Acil Tıp Anabilim Dalı, İzmir Amaç: İnferior vena cava (VCİ) yaralanmaları venöz sistemin bir parçası olmasına rağmen oldukça ölümcül yaralanmalardır. Bu yaralanmaların büyük bir kısmını penetran yaralanmalar oluşturur, künt travma nedenli vasküler yaralanmalar daha nadirdir. Şok tablosu ile acil servise getirilen künt travmalı hastada operatif şartlarda konulmuş organ yaralanması olmaksızın çift odaklı infrarenal vena cava rüptürü olgusunu sunarak, bu çok nadir görülen vasküler yaralanmaya dikkat çekmeyi amaçladık. Olgu: 65 yaş erkek hasta araç dışı trafik kazası ile acil servisimize getirildi. Hastanın ölçülen TA: 80/60 mmHg ve nabzı 125 atım/dk idi. Hastanın fizik muayenesinde pelvik bölgede ve sağ flank bölgede hassasiyet tespit edildi. Hemorajik şok için dengeli sıvı ve kan resusitasyonuna başlandı. Yapılan odaklanmış travma ultrasonunda hepatorenal fossada ve douglas poşunda serbest sıvı görüldü. Gelişinde şuuru açık olan hastada muayene esnasında konfüzyon gelişmesi üzerine entübe edildi. IV kontrastlı bilgisayarlı batın tomografisinde pelvik kemiklerde yaygın fraktür mevcut olduğu ve retroperitonel alanda hematom, sağ üreter üst polde hemoraji, sağ renal arter segmenter dallarında şüpheli yaralanma olduğu raporlandı. Batın içi solid organ hasarı ve ana vasküler yapılarda yaralanma bulgularına rastlanmadığı bildirildi. Hasta renal arter yaralanması şüphesi nedeniyle operasyona alındı. Laporotomi esnasında VCİ’un infrarenal seviyeden 0,5 cm genişliğinde rupture olduğu tespit edildi. Kanama odağı onarıldıktan sonra da batın içine kanamanın devam ettiği gözlendi. VCİ yukarıya doğru tarandığında yaklaşık 1 cm genişliğinde ikinci bir rupture tespit edildi ve onarıldı. Ancak operasyon esnasında hastada kardiyopulmoner arrest gelişti. Müdahaleye yanıt alınamayan hasta exitus kabul edildi. Sonuç: Tüm dünyada 45 yaş altı ölümlerin en sık nedeni travmalardır. Ölümlerin yaklaşık %25’i major vasküler yaralanmalara bağlı kanamalardan kaynaklanmaktadır. Künt travmalara bağlı vasküler yaralanma insidansı %1.6 gibi küçük bir oranda gözlense de künt abdominopelvik travmalı hastalarda hemorojik şok tablosu geliştiğinde vasküler yaralanmalar klinisyenlerin aklına erken dönemde gelmelidir. Tanısal ve tedavi amaçlı cerrahide vasküler yaralanmanın çok odaklı olabileceği de göz ardı edilmemelidir. Anahtar Kelimeler: Acil Servis, vena cava inferior, künt travma, çok odaklı rüptür P 078 MOTOSİKLET KAZASI SONRASI İZOLE HYOİD KEMİK KIRIĞI İbrahim Toker, Turgay Yılmaz Kılıç, Emirhan Erdem, Gamze Çopuroğlu, Nur Zafer, Yeşim Eyler, Necmiye Yalçın Ocak
Tepecik Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İzmir İzole hiyoid kemik kırığı, hiyoid kemiğin yerleşimine bağlı olarak nadir görülen bir durumdur. Bu olgu sunumunda, motosiklet kazası sonrası izole hyoid kemik kırığı gelişen kask takmayan 27 yaşında erkek bir hasta sunduk. Hastaya tanı çekilen servikal tomografi ile kondu. Sonrasında yatak başı yapılan ultrasonografide herhangi bir patolojiye rastlanmadı. Kulak burun boğaz hastalıkları hekimi tarafınca yapılan laringoskopi normal sınırlarda idi. Takip sonrası komplikasyon gözlenmeyen hasta konservatif tedavi ile taburcu edildi. Anahtar Kelimeler: Künt boyun travması, hyoid kemiği, motosiklet

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
243
P 079 NE YAPTIYSAM GEÇMEDİ DOKTOR BEY!! Ali Göksu, Azizcan Kılıç, Tevfik Patan Fatih Sultan Mehmet Eğitim Ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Serebral sinüslerin trombozu(SVT) nadir, ancak tanısı atlanan veya geç konan önemli bir serebro-vasküler hastalıktır. Her yaş grubunda görülmekle birlikte, daha çok genç ve orta yaşlardaki bireyleri ve çoğunluklada kadınları etkiler (1). Klinik prezentasyonları değişken ve sıklıkla dramatiktir. Genellikle intrakranial hipertansiyona bağlı başağrıları, fokal defisit ve nöbetler veya konfüzyonel durum ve letarji tablolarının birisiyle akut olarak başlamaktadırlar (1-3). Olgumuzda 68 yaşında bayan hasta, 1 haftadır hafif hafif başlayan, son 2 gündür şiddetli hissettiği, tüm başında olan ağrı şikayeti mevcut. Bulantı-kusma eşlik etmiş, şu anda yokmuş. Bir gün önce bu şikayetle başka bir merkeze başvurmuş, analjezik yapılmış hiç geçmemiş. Orada çekilen kranyal BT CD'si var; akut lezyon yok. Ağrısının geçmemesi üzerinde acil polikliniğimize başvurmuş. Acile geliş tansiyonu 133/74. Ateş öyküsü yok. Kafa travması olmamış. Gençliğinde migrenöz ağrıları olurmuş ancak yıllardır olmuyormuş. SVT geniş nonspesifik semptom spekturumuyla akut olarak prezente olurlar. Sıklıkla genç ve orta yaşlardaki bireyleri ve çoğunlukla da kadınları etkiler (1). Baş ağrıları en sık (%75-90) görülen başlangıç semptomudur (3). Tutulan yapılara bağlı olarak belirti ve bulgular değişmekle birlikte sıklıkla fokal nörolojik defisitler, epileptik nöbet, konfüzyon, letarji, koma gelişebilir ve hatta ölümle sonuçlanabilir. Mortalite %5–30 olarak bildirilmektedir (1, 5). Pek çok olgu komplet bir düzelme gösterir. Yaklaşık %20’sinde rezidüel nörolojik defisitler ve %5’inde epileptik nöbetler sekel olarak kalır (1, 5, 6). BBT hemorajik veya iskemik değişiklikler ve bazı olgularda kontrastlı görüntüler sagittal sinüs trombozunda boş delta bulgusunu gösterebilir. Ancak SVT tanısında MRİ ve MR venogram SVT tanısında daha sensitiftir (7). Nihayet olgumuzda da MR venogramla tanı konulabildi. Ayrıca ağır dehidratasyon, protein S veya C eksikliği, otit ve infeksiyonlar ve septisemi, malignansi, kafa travması, hematolojik hastalıklar ve OKS kullanımı majör risk faktörleri olarak bildirilmiştir (1,4,5,6). %30’u idiopatiktir (1). Sonuç olarak atipik persistan başağrılı olgularda ve hiperkoagülabilite durumlarında SVT’da düşünülmelidir. Tanıda MR venogram yol gösterici olabilir. Bu olgular antikoagülan tedaviden faydalanabilir. Anahtar Kelimeler: Baş ağrısı, sinüs ven trombozu, serebral ven trombozu P 080 ABUSING DRUGS FOR SMOKING CESSATION Ali Batur, Orhan Delice Erzurum Regional Training and Research Hospital, Emergency Medicine Clinic, Erzurum, Turkey Introduction: Bupropion is a monocyclic antidepressant structurally related to amphetamine. Zyban is sustained released formulation of bupropion hydrochloride which is used for smoking cassetion. In the early studies buprapion did not produce any psycho-stimulant effects. However clinical experiences and increasing number of case reports show that Zyban is going to be an abusing drug for the last years. The common side effects of bupropion overdose are lethargy, vomiting, tachycardia, drowsiness, seizures. Case: In the last two months 3 patients admitted to ED for Zyban overdose. Although they all started for stopping smoking, they abused Zyban. The three patients were male and their ages were between 25–34 years. They took between 10-16 pills. All of them admitted to ED with altered mental status, their GCS were between 11-13. All of them monitorized and had full supporting therapy. The two of them had generalized tonic clonic seizures and it lasted with two repeated doses of benzodiazepine. The third patient had seizures in the first hour and treated with 3 repeated doses of benzodiazepine and after treating propofol it was stopped. During monitoring the patient had supraventriculer tachycardia (160/min). One dose of adenosine stopped it and reverted to SAN rhythm. After following 24 hours their GCS were 15, had no any complaints and discharged. Conclusion: At therapeutic doses bupropion is well tolerated. And it can be easily taken from doctors for smoking cessation aid. Bupropion lowers the seizures threshold even at therapeutic doses. Acute overdose can be seen with seizures in a few hours. The median doses associated with seizures is about 4,4 g. Zyban can cause cardio-toxicity which goes with tachycardia, prolonged QTc interval and cardiogenic shock. The potential side effects should be considered to the patients before using as smoking cessation aid. Keywords: Bupropion overdose, seizure, smoking

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
244
P 081 A RARE CASE: ISOLATED DISTAL RADIO-ULNAR JOINT (DRUJ) DISLOCATION Ali Batur Erzurum Regional Training and Research Hospital, Emergency Medicine Clinic, Erzurum, Turkey Introduction: Isolated distal radioulnar joint (DRUJ) dislocations are rare and are more commonly part of complex forearm fracture-dislocations. Isolated dislocations are difficult to diagnose and are initially missed in up 50 % of cases. The mechanism of injury is commonly force to the elbow with a direct dorsal trauma. The common complaints are pain, swelling and deformity. The patient will unable to supinate or pronate the forearm. In the DRUJ subluxation the %50 of articulate surface is displaced. There are simple and complex types of DRUJ dislocation. In the simple type dislocation can reduces spontaneously. Surgical treatment should be needed in the complex one. Case: 16-year-old male admitted to the ED, after falling down from bicycle, with pain on her wrist and could not make pronation. The pain was located at the level of the distal radioulnar joint and there was no swelling. There was deformity and instability on the DRUJ. The patient admitted 2 other hospital before and had no diagnosis about her pain. In her X-Ray distal ulna was superposed with triquetrum and displaced from articulate surface. The diagnosis is isolated DRUJ subluxation. Orthopedic consultation was done and after replacement a wrist splint was done. The patient discharged with appointment of orthopedics control. Conclusion: Partial dislocation of the distal radioulnar joint (DRUJ) without a fracture is known as distal radioulnar joint subluxation. DRUJ is not easy to perceive on initial presentation as there is no visible appearance of positional deformity. The complex form of DRUJ dislocations should be evaluated with CT and MRI for the rupture of ligaments and ulnar styloid fracture. And must be careful about DRUJ dislocations in the ED. Keywords: Distal radioulnar joint dislocation, DRUJ, subluxation P 082 DON’T FORGET TO EVALUATE TALUS… Ali Batur, Orhan Delice Erzurum Regional Training and Research Hospital, Emergency Medicine Clinic, Erzurum, Turkey Introduction: The talus is the second largest tarsal bone and has no muscular attachments. The blood supply to the talus is from a vascular ring. Because of the tenuous nature of these vessels avascular necrosis can be occur with talar fractures. Talar neck fractures account for 50 % of major talar injuries. Common mechanism of fractures are extreme dorsiflexion force in falls and motor vehicle collisions. Common complaints of talar fractures are dorsal swelling, tenderness and painful hindfoot on eversion and inversion. Talar neck fractures are classified by Hawkins into 3 groups. Case: 40-year-old male was admitted to ED for ankle pain and swelling after falling down from 3 meters. On the physical examination he had pain on eversion. The X-ray showed a suspected fracture line on the talus. To diagnose talar fracture we performed CT. Talar neck fracture Hawkins type 2 was diagnosed. Orthopedic consultation and surgical treatment was performed in an hour to prevent possible avasculer necrosis. Conclusion: The talus is hidden by its anatomic location and clinicians are failing to put diagnosis on talar fracture. Frequently CT and MRI are needed to diagnose talar fracture. Talar neck or head fractures require surgical intervention and immediate orthopedic consultation should be performed. The risk of avascular necrosis increases with increasing talar displacement, ranging from 10 % for type 1 and 70 % or more for type 3. Keywords: Talus, talar fracture, Hawkins type 2

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
245
P 083 RETROSPECTIVE EVALUATION THE CONCORDANCE OF IMAGING MODALITIES IN PATIENTS ADMITTED TO THE EMERGENCY DEPARTMENT WITH ABDOMINAL PAIN
Cihat Aygün, Emine Emektar, Şeref Kerem Çorbacıoğlu, Hüseyin Uzunosmanoğlu, Yunsur Cevik Keçiören Training and Research Hospital, Clinic of Emergency Medicine, Ankara, Turkey Aim: In our study, we aimed to evaluation concordance of imaging modalities of patients admitted to the emergency department (ED) with abdominal pain. Material method: The study was conducted between the dates 01.06.2014-31.05.2015 after the local ethical committee approval. Patients admitted to the ED, with abdominal pain, whose multiple imaging were done (abdominal ultrasonography and computed tomography) were screened for 1 year retrospectively. Data analysis was performed using SPSS 15.0. Results: The study included a total of 413 patients of which 242 (58.6%) of women. The final diagnosis of the patients, 133 (32.2%) patients had nonspecific abdominal pain, the most commonly seen surgical diagnosis was acute appendicitis. When USG and CT sensitivity evaluated according to the final diagnosis; for acute appendicitis; USG was 38.9%, CT 86.1%, for acute pancreatitis; USG 0%, CT 30.4%, for ovarian pathology; USG 65.4% CT 98.1%, for acute cholecystitis; USG 94.9%, CT 87.2% sensitive. There was detected concordance in 63.2% between USG and CT. While this rate was 61.7% among recent diagnosis with USG, for CT recent diagnoses it was found as 87.7%. Conclusion: In conclusion, when final diagnoses are compared with imaging methods in patients with abdominal pain, CT seems superior to USG. Especially in clinics where USG cannot be performed for 24 hours like in our clinic, CT may be preferred as the first imaging method. Keywords: Abdominal pain, ultrasonography, computed tomography, emergency department P 084 ACİL SERVİS’DE NADİR GÖRÜLEN BİR OLGU: “TETANOZ” Ayşegül Aktaş, Özlem Köksal Uludağ Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Bursa Giriş: Tetanoz gram pozitif anaerob bir basil olan Clostridium tetani’nin etken olduğu, çizgili kaslarda uzun süreli sertleşme ve kasılmayla süregelen, toksik ve mortal bir enfeksiyon hastalığıdır. Etken mikroorganizmanın derideki bir yara aracılığı ile vücuda girdikten sonra 2-12 gün süren kuluçka döneminin ardından, önce çene kaslarında görülen sonra tüm vücuda yayılan ağrılı kas spazmları ile prezente olur. Olgu: 71 yaşında erkek, 3 ay önce Akciğer kanseri tanısı almış tedavisiz takipte olan hasta; 10 gün önce odun keserken sağ eline odun kıymığı batmış ve 3 gün sonra hastaneye başvurup tetanoz aşısı yaptırmış. Son 3-4 gündür çenede progresif kasılmaları olması üzerine Acil Servise başvurdu. Genel durumu iyi, oryante koopere, dört ekstremite hareketli mobil olan hastanın vital bulguları; Tansiyonu:160/90 mmHg, NDS:80/dk, ateş:36,8 idi. Sağ el dorsal yüzde ciltte 2 cm çaplı hiperemik ödemli üzerinde noktasal giriş deliği olan, sınırları belirsiz lezyon mevcuttu. Nörolojik muayenede özellik yoktu. Acil servisteki takibinde progresif olarak artan çenede, boyunda, kollarda kasılmaları mevcut olan hasta enfeksiyon hastalıkları tarafından değerlendirildi. Tetanoz immünoglobulin yapıldı ve enfekte yarası için pansuman yapıldı. Takibinde yaygın kas kasılmaları minimal uyarı ile irkilmeleri gelişen ve solunum sıkıntısı olan hasta entübe edildi. Reanimasyon yoğun bakım ünitesine yatırıldı. Hasta yatışının 9. gününde exitus oldu. Tartışma ve Sonuç: Tetanoz Clostridium tetani toksinlerinin neden olduğu kas spazmlarıyla karakterize bir santral sinir sistemi hastalığıdır. Tetanoz aşısı rutin uygulama programlarının gelişmesiyle birlikte görülme sıklığı oldukça nadir olmasına rağmen, gelişmekte olan ülkelerde aşısız insanların çokluğu nedeniyle hala büyük bir tehdit olmaya devam etmektedir. Anahtar Kelimeler: Tetanoz, acil servis, kas spazmları

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
246
P 085 SAĞ ALT KADRAN AĞRISINDA NADİR GÖRÜLEN BİR PATOLOJİ: AKUT DİVERTİKÜLİT Cem Keskin1, Şenol Ardıç1, Doğukan Atabay2, Davut Sadoğlu1, Süleyman Türedi1, Murat Aydın1
1Sağlık Bilimleri Üniversitesi Trabzon Kanuni Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Trabzon 2Sağlık Bilimleri Üniversitesi Trabzon Kanuni Eğitim ve Araştırma Hastanesi, Radyoloji Bölümü, Trabzon Giriş: Acil servis başvurularında karın ağrısı önemli bir yer tutar. Sağ alt kadran ağrısı yapan nedenler içinde akut apandisit en çok düşünülen patolojidir. Ancak soliter çekal divertikülit ise nadir görülen bir durumdur ¹. Amaç: Sağ alt kadran ağrısı yapabilen önemli bir nedenin divertikülit olabileceğini göstermeyi amaçladık. Olgu: 44 yaşında erkek hasta acil servisimize, karın ağrısı şikayeti ile ayaktan başvurduğunda genel durumu iyi bilinci açık oryante ve koopereydi. Anamnezinde bir gün önceden başlayan giderek şiddetlenen, sağ alt kadranda lokalize karın ağrısı olduğunu ve aynı ağrıyı 10 yıl önce yaşamış olduğunu belirtmekteydi. Vital bulgular; TA: 130/ 80 mmhg, nabız 80 atım/ dak, SS 16/ dak ve ateş 37.8 idi. Yapılan fizik muayenesinde her iki akciğer solunuma eşit katılmakta, Ral(-), ronküs(-) ve wheezing(-)’ti. Batın muayenesinde hassasiyet(+), sağ alt kadranda defans(+) ve rebound (+) ti. Diğer sistem muayeneleri normal olarak değerlendirildi. Hemogram’da 13.000 lokosit değeri ve biyokimya panelinde CRP 13 idi. Diğer labratuvar değerleri normal idi. Hastanın çekilen kontrastlı batın BT’sinde (Resim 1) çekumda divertikülit saptandı ve apendiks normal olarak yorumlandı. Hasta genel cerrahi servisine yatırıldı. Herhangi bir komplikasyon gelişmeyen hasta 4 gün antibiyoterapi ve hidrasyon tedavi sonrası şifa ile taburcu edildi. Sonuç: Divertikülit hastaları genellikle sol alt kadran ağrısı ile acil servise başvurmaktadır ². Kontrastlı batın tomografisi benzer kliniğe neden olan farklı patolojilerin ayrımı için önemli bir görüntüleme yöntemidir. Referans: ¹ Karatepe O, Gulcicek OB, Adas G, et al. Cecal diverticulitis mimicking acute appendicitis: a report of 4 cases. World J Emerg Surg. 2008 Apr 21. 3:16. ² [Guideline] Miller FH, Bree RL, Rosen MP, et al. Expert Panel on Gastrointestinal Imaging. ACR Appropriateness Criteria left lower quadrant pain. [online publication]. Reston (VA): American College of Radiology (ACR); 2008. Anahtar Kelimeler: Divertikülit, sağ alt kadran ağrısı, kontrastlı batın BT P 086 IS IT POSSIBLE? ANURIA DUE TO BILATERAL UROLITHIASIS… Ali Batur, Orhan Delice Erzurum Regional Training and Research Hospital, Emergency Medicine Clinic, Erzurum, Turkey Introduction: Urolithiasis is a common clinical problem seen commonly in young adults and middle aged men in ED. 70 % of all ureteral calculi occurring between the ages of 20 and 50 years. The patients admit ED with a crescendo pain on the flank area. The pain can extends laterally around the abdomen and sometimes testicles and labia majora. Urolithiasis can present with rebound (29%), defense (61%), rigidity (8%) and hematuria (85%). Case: 34-year-old male admitted to ED with bilateral flank, lower quadrant pain and anuria for about 24 hours. In physical examination there was bilateral costovertebral angle tenderness. Also sonographic evaluation findings not detected the globe vesicale. In laboratory tests creatine: 1,43 mg/dL BUN:16 mg/dL and he was able to give scant urine test that revealed 22 leukocytes and 0 (zero) erythrocyte. Non-contrast-enhanced helical CT was performed. Bilaterally urolithiasis and hydro uretero nephrosis were detected. After consultation of urology and hospital admission, lithotripsy was performed. The patient discharged without any complaint. Conclusion: Urolithiasis is one of a postrenal reasons of acute kidney injury (AKI) and may present with anuria. Bilateral urolithiasis that cause anuria is a rare condition. Non-contrast-enhanced helical CT is the standard imagining modality which has 97 % sensitivity and 96 % specificity. Although 85 % of urolithiasis presents with hematuria, 24% of renal colic patients have no significant radiological findings of urolithiasis. With rapid diagnosis, surgical decompression can applied quickly. Studies have shown that timely relief of obstruction is needed and that recovery of renal function depends on the degree and duration of the obstruction. Keywords: Bilateral urolithiasis, renal colic, anuria

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
247
P 087 DELİRYUM AYIRICI TANISI: DATURA STRAMONİUM ZEHİRLENMESİ Ali Karakuş1, Türkan Parlar1, Ali Bucak1, Zeynep Kekeç2
1Mustafa Kemal Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Hatay 2Çukurova Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Adana Deliryum, acil servislerde sıkça görülebilen, tanısı zor konulan bir durumdur. Etyolojide birçok neden suçlanmaktadır. Bu yazıda literatürde az rastlanan bir neden olan datura stramonium ile zehirlenme olgusu sunularak toksikasyonların önemi vurgulanmak istenmiştir. Olgu Sunumu: 61 yaşında erkek hasta şuur bozukluğu ve bayılma şikayetiyle acil servise getirildi. Hikayesinde 1 saat önce adını bilmediği bitkinin tohumlarından bir çay kaşığı içme sonrası bayıldığı belirtildi. Hastanın genel durumu orta, ajite, anlamsız sesler çıkarmakta ve halusinasyonları mevcut idi. Glaskow koma skalası 12, tansiyon arteryel 160/90 mmHg, nabzı 136/dk, solunumu 22/dk, pupiller dilate idi. Elektrokardiyografisinde (EKG) sinüs taşikardisi olan hastanın düzeltilmiş QT uzunluğu 0.50 sn (0.36-0.44sn) uzamış ve QRS kompleksi 0.12 sn genişlemiş olarak değerlendirildi. Hastanın hemogram, biyokimya ve kangazında anormallik saptanmadı. Hastaya mide lavajı, tekrarlı aktif kömür (6 saat ara ile 2 doz) 1gr/kg, sıvı tedavisi, midazolam ampul 5mg, diazepam ampul 10mg, magnezyum ampul 3gr (2 ampul 100 cc mediflex içinde de 30 dk.da ), NaHCO3 5 ampul puşe, 6 saat sonra tekrar 5 ampul puşe ve 5 ampul NaHCO3 500cc serum fizyolojik içine konularak 100cc/saatten 5 saatte gönderildi. Hastaya fizostigmin planlandı ancak bulunamadığı için yapılamadı. Hastanın 12 saat sonra ajitasyonları azaldı. Kontrol EKG’sinde normal sinüs ritmi tespit edildi. Şuuru açılan hasta acil gözlemdeki 24 saatlik takibinin ardından önerilerle şifa ile taburcu edildi. Deliryum tablosuyla acil servise getirilen hasta anamnezi dikkatlice alınmalı ve fizik muayene ile değerlendirilmelidir. İleri tetkiklere gerek duyulmadan toksikasyon düşünülen olgularda antidot mevcut ise gecikmeden verilmelidir. Toplumun bilinçsiz ilaç kullanımı veya bitkisel tedavi yöntemleri açısından bilgilendirilmesi gerekmektedir. Anahtar Kelimeler: Deliryum, Datura, antikolinerjikler P 088 ATRIAL FIBRILATION (USE RINAVESS IN CARDIOVERSION) Vuk Nikovic1, Anton Laggner2, Hans Domanovits2, Ranka Bulajic3, Dušan Milenkovic4
1Institut for Emergency Medical Care Montenegro, Podgorica Unit, Podgorica, Montenegro 2AKH Hospital Vienna University, Clinic for Emergency Medicine, Vienna, Austria 3General Hospital Toronto, Toronto, Canada 4Institut for Emergency Medical Care Niš, Niš, Serbia Introduction: The current estimate of the prevalence of atrial fibrillation (AF) in the developed world is approximately 1.5-2% the general population, with the average age of patients this conditional steadily rising, such that it now averages between 75 and 85 years. The arrhythmia is associated with a five-fold risk of stroke and a three-fold incidence of congestive heart failure and higher mortality. Hospitalization of patients with AF also is very common. Brinavess is a concentrate that is made up into a solution of infusion (drip into a vein). Case outline: 47y/o man felt discomfort and palpitations in this chest after stenourous work (lifting haevy objects). He called emergency responece who transferred patient to the hospital. Upon taking more detail history it was established patient had diagnosis of paroxysmal atraial fibrillation for which he was on Concor 1.25 mg and Simvastatin 40 mg. In ER ECG was done which showed atrial fibrillation with RVR of 135 bpm with no any ST – T changes. Laboratory analisis showed: pro BNP 89.1 pg/ml,CK 3.8,venosus ABG unremarkable. ECHO was done which was unremarkable and the patient is appropriately anticoagulated with Heparine and Enoxaprin in order to reaceive Vernakalant.In ER he was treated with Vernakalant 3mg/kg i.v. After 10 minutes repeated ECG was normal with sinus rhythm at 75 bpm. The patient was discharged home in stable condition. Conclusion: Vernakalant was successful in converting recent onset atrial fibrilation to sinus rhythm in the emergency department. Keywords: Heart rhythm, vernakalant, atrial fibrilation, successful cardioversion

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
248
P 089 SAĞLIKLI GENÇ ERİŞKİNLERDE İNFLAMASYONUN SAĞ VE SOL VENTRİKÜL ÜZERİNE ETKİSİ Aysel Hünük, Ebru Ünal Akoğlu, Merve Manap, Arzu Emecen, Tevfik Patan Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Son çalışmalar, inflamatuvar belirteç düzeyleri ile özellikle sağ ventrikül fonsksiyonları arasında negatif bir ilişki olduğunu göstermektedir. Son dönem kalp yetmezliği ve koroner arter hastalığı gibi kritik patolojilere sahip hastalarda toplam inflamasyon yükünü ve riskini azaltmanın sağkalım üzerinde olumlu etkileri olduğu gösterilmiştir. Bizim bu çalışmadaki amacımız, sağlıklı genç erişkinlerde inflamasyonun kardiyak fonksiyonlar üzerindeki etkisini araştırmaktır. Acil servisimize üst solunum yolu enfeksiyonu (ÜSYE) şikayetleri ile başvuran erişkin hastalardan, kardiyovasküler veya sistemik herhangi bir hastalık öyküsü olmayan ve CRP değeri 3 mg/dl’nin üstünde olan vakalar çalışmamıza dahil edildi. Fizik muayenesinde ya da transtorasik ekokardiyografi (TTE)’de herhangi bir kardiyak patoloji saptanan, EKG’de tam dal bloğu ya da sinüs dışı ritimler görülen vakalar çalışmaya dahil edilmedi. Çalışmaya dahil olan hastalara başvuru muayenelerinin ardından sol ventrikül (LV) ve sağ ventrikül (RV) sistolik ve diyastolik fonksiyonlarını incelemek için transtorasik ekokardiyografi (TTE) uygulandı. Hastalar, akut üst solunum yolu semptomları geriledikten yaklaşık 10 gün sonra kontrole gelmek üzere taburcu edildi. Kontrol muayenelerinde CRP değeri 3 mg/dL altına düşen hastalarda ilk muayene esnasında gönderilen kan parametreleri ve TTE işlemi tekrarlandı. Çalışmamız 16’sı (%30) kadın ve 37’si (%70) erkek toplam 53 olgu ile tamamlandı. Olguların ortalama geliş ve kontrol inflamatuvar parametreleri karşılaştırıldığında; ateş (37,7±0,7°C; 36,5±0,4°C; p<0,01), nötrofil lenfosit oranı (NLR) (6,37±3,58; 1,89±1,27; p<0,01), CRP (8,9±4,9 mg/dL; 0,4±0,6 mg/dL; p<0,01) istatistiksel olarak anlamlı saptandı. Bulgularımızda CRP ve NLR tersil değerleri de (<25, 25-75 and >75 persentil) incelendi. İnflamatuvar belirteç düzeyleri ile RV TTE parametreleri arasında istatistiksel olarak anlamlı bir ilişki saptandı. LV TTE parametreleri ile inflamatuvar belirteçler arasında ise böyle bir ilişki saptanmadı. Çalışmamızda sağlıklı genç erişkinlerde ÜSYE’nin klinik olarak hafif ama anlamlı bir kardiyak fonksiyonel bozulma ile beraber gittiği gözlendi. Özellikle sağ kalp fonksiyonları inflamatuvar olaylardan akut olarak etkilenebilir ve sağ ventrikül ile ateş ve CRP gibi inflamatuvar belirteçler arasında bir ilişki vardır. Anahtar Kelimeler: İnflamasyon, ventrikül fonksiyonları, CRP, Üst solunum yolu enfeksiyonu P 090 A FOLEY PROBE FIXING PROJECT: ELASTICATED RUBBER Taygun Baykal, Tanju Biçer, Muharrem Doğan, Demet Doğan, Abdullah Taşcı Istanbul Fatıh Sultan Mehmet Training and Research Hospital, Istanbul, Turkey Foley probe is a common used instrument to help urinary drenage and monitorize urine output. İt is cheap and easy to use, but it should be remembered that it’s still an invasive procedure and have some complications. Patients who have foley probe needed to hide or fixing the probe, and this efforts can be cause extereme situations.In our case 76-year-old man was admitted to our emergency department because of wounds on the waist with history of benign prostate hyperplasia. 4 months ago a foley probe inserted because of this condition. At that time the patient fixed the probe around her waist with the aid of a elasticated rubber and never moved again. Recently he was suffering some psychological problems. Because of this condition his mobility reduced he was closed in and reckless. The relatives had no idea about probe or fixing. They just saw the wounds and decided to bring him our service by the force. Initial vital signs were: temperature:38,3°C, blood pressure:86/55 mmHg, pulse:161 bpm, sp02:%96. Physical examination revealed –unlike the simple complaint- massive infected wounds that fistulised to subcutaneous area. It was roundabout the waist and goes through under the scrotum. The probe was infected and inactive. Central venous pressure was calculated as 0-5 cmH2O. In his laboratory wbc:15.8, neu:13.8, crp:21.7, kre:4.13, bun:85, inr:1.58, urinary sample test turned out nitrin:+, leu:+++. So elasticated rubber and inactive foley probe removed, cystostomy, antibiotherapy and fluid rescucitation performed. After the consultations of releated departments, the patient interned with the diagnosis of urosepsis and foreign body releated dermo-infection. Some patients approach to emergency department with seemingly simple complaints but it should be remembered there can be more serious underlying problems. A complete physical examination and vital sign evaluation and Fast effective and across-the-board treatment should be performed Keywords: Foley probe, urosepsis, elasticated rubber

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
249
P 091 YOUNG MAN WITH FEVER Süleyman İbze, Erkan Göksu, Deniz Kılıç, Hanife Yenigün Akdeniz University Faculty of Medicine, Department of Emergency Medicine, Antalya, Turkey Endocarditis can have profound and devastating neurologic consequences. The incidence of central nervous system (CNS) complications in infective endocarditis is approximately 30%, and these manifestations are often the first sign of illness (47% of the time in one series). A 37-year-old man presented to the Emergency Department (ED) complaining of fever, inability to ambulate and agitation. The patient had a history of intravenous drug abuse and infective endocarditis, in which S. aureus were growing in his blood culture. On initial evaluation, his vital signs were as follows: blood pressure 119/81 mmHg; pulse 126 beats/minute; respiratory rate of 26 breaths/min; oxygen saturation 100% on room air, and; temperature 38.1˚C. Clinical examination revealed tachycardia on cardiac auscultation and non-focal neurological examination findings due to patient agitation. The ECG revealed sinus tachycardia without any ST-T segment change. In this case, bedside ultrasound (US) was performed to reveal the source of fever and a possible explanation for non-focal neurologic deficits because of his past medical history. Bedside US revealed pedunculated vegetation adhered to the ventricular portion of the mitral valve. Non-contrast computed tomography (NCCT) and a diffusion weighted MRI was ordered. Diffusion weighted MRI of the brain revealed multiple hyper-intense lesions, suggesting multiple embolic infarcts. The reported sensitivity of transthoracic echocardiography to detect vegetation is 60% to 70%. The signs and symptoms of IE are mostly associated with the valve(s) involved and the responsible organism. Patients may present to the ED with a variety of clinical presentations; neurologic abnormalities are seen in 30-40% of the cases. Complications, such as cerebrovascular accidents (occurring in 15% to 20% of patients), are caused by emboli or ruptured mycotic aneurysms. Vegetations may be echogenic or isoechoic, and have an irregular appearance. Vegetation may be seen on any leaflet as laminated or pedunculated attachments. Keywords: Drug abuse, infective endocarditis, neurologic complications, staphylococcus species, ultrasound P 092 VERNAKALANT USE IN CARDIOVERSION OF RECENT-ONSET ATRIAL FIBRILLATION Vuk Nikovic1, Anton Laggner2, Hans Domanovits2, Ranka Bulajic3, Dusan Milenkovic4
1Institute for Emergency Medical Care Montenegro, Podgorica, Montenegro 2AKH Hospital Vienna University Clinic for Emergency Medicine, Vienna, Austria 3General Hospital Toronto, Toronto, Canada 4Institute for Emergency Medical Care Niš, Niš, Serbia Introduction: The current estimate of the prevalence of atrial fibrillation (AF) in the developed world is approximately 1.5-2% in general population, with the average age of patients with this condition steadily rising to between 75 and 85 years. The arrhythmia is associated with a five-fold risk of stroke and a three-fold incidence of congestive heart failure and higher mortality rate. Hospitalization of patients with AF is also very common. Vernakalant (Brinavess®) is a concentrate that is made up into a solution of infusion (drip into a vein). In recent years vernakalant has emerged as a novel agent for termination of AF. Case outline: 47y/o man felt chest discomfort and palpitations after strenuous work (lifting heavy objects). After calling the EMS, patient was transferred to the hospital. When more detail history was taken, it was established that patient had diagnosis of paroxysmal atrial fibrillation for which he was taking Concor 1.25 mg q.d. and Simvastatin 40 mg q.d. ECG was done in the ER which revealed atrial fibrillation with RVR of 135 bpm with no ST–T changes. Laboratory analysis showed: pro BNP 89.1 pg/ml, CK 3.8, venous ABG unremarkable. Cardiac US was done which was unremarkable and the patient was properly anticoagulated with heparin and enoxaparin in order to receive vernakalant. He was treated with vernakalant 3mg/kg i.v. in the ER. Ten minutes afterwards a repeated ECG was done revealing normal with sinus rhythm at 75 bpm. The patient was discharged home in stable condition. Conclusion: Vernakalant was successful in converting recent onset atrial fibrillation to sinus rhythm in the emergency department. Keywords: Heart rhythm, vernakalant, atrial fibrillation, successful cardioversion

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
250
P 093 ESOPHAGIAL PERFORATION DUE TO CHICKEN BONE: MULTIDETECTOR CT FINDINGS Selcuk Parlak1, Esra Çıvgın1, Elif Çelikel2, Hamza Özer1, Perihan Polattaş1
1Numune Training and Research Hospital, Clinic of Radiology, Ankara, Turkey 2Numune Training and Research Hospital, Clinic of Emergency Medicine, Ankara, Turkey Esophageal perforation due to foreign body (FB) impaction is rare and requires prompt treatment. The most common esophageal FB diseases in adults are due to impacted meat or other food. Fish bone is the most common cause in many countries. Spontaneous and iatrogenic ruptures may also be seen. Approximately 80-90% of ingested FBs are passed spontaneously without complications, while 10-20% of FBs in the alimentary tract require endoscopic removal and approximately 1% require surgical intervention. The common symptoms are sore throat, dysphagia, and vomiting. But in the presence of perforation mediastinitis and other complications can occur. Both computed tomography and endoscopy are necessary for diagnosis and treatment. A 52-year-old man who was admitted to the emergency room with a 6-day history of sore throat and dysphagia after eating chicken. Computed tomography (CT) of the thorax revealed a Y shaped FB representing wishbone of the chicken. Mediastinal air secondary to esophagial perforation and findings of mediastinitis were also detected on multidetector CT. Upper gastrointestinal endoscopy confirmed the diagnosis and the fish bone was removed with a snare. A right toracotomy was performed and mediastinal cavity was cleaned. We aim to present the multiformatted CT images of this interesting and rare case. Keywords: Foreign body, esophagus, mediastinitis, multidetector computed tomography P 094 SEREBRAL VENÖZ TROMBOZ: OLGU SUNUMU
İbrahim Toker1, Turgay Yılmaz Kılıç1, Ezgi Şeker Eren2, Olcay Gürsoy1, Hüseyin Çetin Arslan1, Özge Duman Atilla1, Gamze Çopuroğlu1
1Tepecik Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İzmir 2Yıldırım Beyazıt Üniversitesi Atatürk Eğitim ve Araştırma Hastanesi, Acil Tıp Anabilim Dalı, Ankara Serebral sinüslerin trombozu inmenin aksine, çoğu zaman genç yetişkinleri ve çocukları etkileyen, semptom ve klinik tablosu çok değişken bir serebrovasküler hastalıktır. Erişkin hastaların büyük çoğunluğu kadınlardır. Gelişen nörogörüntülemeler ve tedaviler sayesinde tanı konulma zamanları ve prognozları düzelmektedir. Bu olguda, acil servise sinirlenme sonrası baş ağrısı ile başvuran hikayesinde oral kontraseptif kullanım olan ve tetkikleri sonrası serebral sinüs ven trombozu ve hemorajik venöz infarkt tanısı konan 31 yaşında bayan hastayı sunduk. Anahtar Kelimeler: Serebral venöz tromboz, inme, oral kontraseptifler

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
251
P 095 THE EVALUATION OF ECG FINDINGS WHO NEEDS PHENYTOIN INFUSION IN EMERGENCY ROOM Mazlum Kılıç, Rohat Ak, Onur Yeşil, Tuba Cimilli Öztürk, Özge Ecmel Onur, Arzu Emecan Fatih Sultan Mehmet Training and Research Hospital, Istanbul, Turkey Objective: Phenytoin is an anticonvulsant medication used for the treatment of epilepsy. It is also group 1B antiarrhythmic. Phenytoin infusion treatment is generally applied in the emergency department and it may cause serious cardiac side effects. The purpose of the study is to determine whether the patients presented to the emergency department with the need of phenytoin infusion need the cardiac monitoring. Materials-Methods: The observational study was carried out on 82 patients at Fatih Sultan Mehmet Training and Research Hospital Emergency Department between 01.05.2016 and 01.08.2016. The patients were given 18 mg/kg phenytoin with 25 mg/min infusion rate. The patients were monitored during the treatment and the vital findings were followed through ECG taken before, mid and at the end of the treatment. Results: The average of ages of 82 patients included in the study is 49,59 + 21,79; and 43,9% of them is female and 56.1% is male. During the treatment, 4 patients had hypotension, 15 of them had nystagmus and 10 patients had ataxia; whereas apnea or arrhythmia was not seen. The ECG’s was obtained and PR, QRS and qTC intervals have been analyzed. There was no significant difference. Conclusion: Phenytoin with 25mg/min infusion rate is a medication safely used in the treatment; it is not required to have cardiac monitoring during the use of medication. Keywords: Phenytoin, neurological emergencies, emergency medicine P 096 EVALUATION OF ECHOCARDIOGRAPHIC FINDINGS WHO NEEDS DILTIAZEM OR METOPROLOL IN THE MANAGEMENT OF ATRIAL FIBRILLATION WITH RAPID VENTRICULAR RATE IN THE EMERGENCY DEPARTMENT Mehmet Barış Memiş1, Rohat Ak2, Onur Yeşil2, Tuba Cimilli Öztürk2, Özge Ecmel Onur2, Arzu Emecan2
1Kartal Lütfi Kırdar Training and Research Hospital, Istanbul, Turkey 2Fatih Sultan Mehmet Training and Research Hospital, Istanbul, Turkey Objective: Atrial Fibrillation (AF) is the most commonly observed rhythm problem in clinical practices. AF increases significantly the morbidity and mortality rates due to all causes especially the cardiovascular diseases. Sudden cardiac death risk, heart failure, thromboembolic complications, prolonged hospitalizations, increased costs and decreased life quality are well known end results related with AF. Even if the cardiovascular diseases eliminated, AF remains as one of the major risk factor for death. Although the majority of the cases related with organic heart diseases (coronary artery diseases, valvular heart diseases, congestive heart failure and hypertension), in 31% of cases there is not any kind of underlying heart disease. In order to control the rapid ventricular rate in AF, beta blockers and dihydropyridin calcium channel blockers are recommended. However the superiority of the two drugs against each other is not well known. Materials-Methods: In our study we have aimed to investigate the effectivity of the diltiazem and metoprolol in the rate control of AF patients in emergency department. Besides the demographic and laboratory findings, transthoracic echocardiographic measurements were evaluated after the rate control. Fifty patients were treated with diltiazem and 50 patients were treated with metoprolol with the doses suggested in the AF Management Guidelines. Dose responses and transthoracic echocardiographic findings were compared. Results: The rate of incidence for the total response in the patients having diltiazem was (92%) and higher than the patients having metoprolol (52%). In order to maintain the normal ventricular rate in patients with AF, diltiazem would be a better choice. Similarly in patients with valvular heart disease diltiazem is better than metoprolol in the rate control. Conclusion: Particularly to ensure the AF rate control in patients with valvular heart disease, choosing diltiazem would be reasonable. Keywords: Atrial fibrillation, diltiazem, metoprolol, rate control

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
252
P 097 ÇOCUKLARDA PENETRAN BATIN TRAVMASI VE KOLON PEFORASYONU Ferhat Yıldız, Demet Devrimsel Doğan, Ebru Ünal Akoğlu, Abdullah Taşçı, İzzet Ustaalioğlu Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, Acil Anabilim Dalı, İstanbul Giriş: Çocuklarda abdominal travma, travmaya bağlı ölümler arasında üçüncü sıradadır. Neden arasında % 85’ini künt travma, %15’ini penetran travmalar oluşturur. Yüksek mortaliteli bu yaralanmalarda acil tanı, tedavi ve takip önemlidir. Tanısal olarak direk batın grafisi, iv kontrastlı abdomen bilgisayarlı tomografi (BT) ve endoskopik tetkiklerden faydalanabiliriz. Biz bu vakamızda sol iliak kemik komşuluğunda yabancı cisim batması nedeniyle başvuran bir hastamızda şüpheli kolon perforasyonundan bahsedeceğiz. Olgu: Bilinen hastalık öyküsü olmayan 5 yaşında erkek hasta acil servise düşme sonrası sol alt falank bölgede yabancı cisim batması nedeniyle getirildi. Hastanın vitallerinde TA: 90/60mmHg, Nb: 102atım/dk, Ateş: 36.4C ve sat: %98 olarak saptandı. Fizik muayenede sol iliak kemik orta hatta fikse yabancı cisim görüldü. Hastanın ayakta direk batın grafisinde yabancı cismin sol iliak kemiğe penetre olma ihtimali ve komşuluğundan dolayı kolon yaralanmasından şüphe edildi. Hastaya iv kontrastlı batın BT görüntülemesi yapıldı. BT sonucunda perforasyon bulgusuna rastlanmayan ve kemiğe nafiz yabancı cisim görülen hasta çocuk cerrahisi ve ortopedi ile konsülte edildi. Hasta takip ve tedavi amaçlı çocuk cerrahisi servisine interne edildi. Tartışma: Kolon perforasyonunun en sık nedenleri; ülser, bağırsak obstrüksiyonu, kesici-delici alet yaralanması, ateşli silah yaralanmaları, travmalar ve kanserlerdir. Kesici-delici alet yaralanmalarına bağlı gelişen perforasyon yaşamı tehdit edici peritonite neden olabilirken; genellikle acil tedavi gerektirir. Tanıda, batın BT veya düz grafide diafram altı yoğun serbest hava görünmesi ile konur. Hemen her hastada bölgesel ve yaygın peritonit bulguları gelişebilirken; ateş ve lökositoz her zaman bulunmayabilir. Sonuç: Kesici-delici alet yaralanmalarına bağlı kolon perforasyonu tanısında düz garfi veya batın BT çekmek hem tanıyı koymada hem de erken cerrahi girişim kararında önemli role sahiptir. Anahtar Kelimeler: Batın, perforasyon, yabancı cisim P 098 ACİL SERVİSE TRAVMA NEDENİYLE BAŞVURAN OKUL ÇAĞI ÇOCUKLARIN DEMOGRAFİK DEĞERLENDİRİLMESİ Feride Sinem Akgün1, Cem Ertan2, Özlem Güneysel3
1Maltepe Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, İstanbul 2İzmir Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, İzmir 3Kartal Dr. Lütfi Kırdar Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Amaç: Çalışmanın amacı, Özel Üniversite Hastanesi Acil Servisine travma nedeniyle başvuran okul çağı çocuk hastaların demografik, epidemiyolojik özelliklerini ve tedavi sonuçlarını saptamak, ulusal verilerimize katkıda bulunmaktır. Gereç-Yöntem: Hastanemiz Acil Servisine 1 Ocak 2013- 31 Aralık 2014 tarihleri arasında travma nedeniyle başvuran 6-12 yaş çocuk hastaların dosyaları ve hastane kayıt defteri retrospektif olarak incelendi. Yaş, cinsiyet, ay, yaralanma yeri (okulda veya okul dışında), travma sebepleri (düşme, trafik kazası, yabancı cisimle kesi, yanık), vücutta yaralanma bölgeleri (kafa, toraks, abdomen, alt ve üst extremite, çoklu), konsültasyonlar, acil serviste yapılan işlemler, yatış, taburculuk ve mortalite oranları gibi özellikleri kaydedildi. İstatistiksel analizleri yapıldı. Bulgular: Çalışmaya alınan 500 hastanın çoğu erkekti (n=287;%57,4) ve Nisan- Mayıs aylarında başvuru sayısı yüksekti (%11,8; 12). Okul dışında yaralanma oranı (n=284; % 56,8) okuldaki yaralanmalara (n=216; % 43,2) göre daha fazla idi. Oluş şekli incelendiğinde düşme (%96,6) ve trafik kazası olgularının (%2,4) daha sık olduğu gözlendi. En çok ekstremite yaralanması (%63,6) tespit edilirken kafa yaralanmaları (%31,6) ikinci sıklıktaydı. Çalışmaya dahil edilen hastaların 485’i acil serviste takip ve tedavisi yapıldıktan sonra taburcu edilirken, 14’ü hastaneye yatırıldı. 1 hastamız da ex oldu. Sonuç: Travma çocuk yaş grubunda en önemli mortalite ve morbidite nedeni olmasına rağmen bunların büyük bir kısmı önlenebilir niteliktedir. Güvenli bir çevre oluşturulması, ailelere ve okul çalışanlarına sürekli koruyucu sağlık eğitimi verilmesi yaralanma kontrolünde etkili olacaktır. Anahtar Kelimeler: Acil servis, çocuk, okul çağı, travma

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
253
P 099 THE COMPARISON OF STATIC DIAGNOSTIC METHOD IN MORBID OBESE AND SÜPER OBESE PATIENTS WITH OSAS AFTER METABOLIC SURGERY
Burcu Yormaz1, Ilhan Ece2, Serdar Yormaz2, Bayram Çolak2
1Beyhekim State Hospital, Department of Chest Diseases, Konya, Turkey 2Selçuk University Medical Faculty, Department of General Surgery, Konya, Turkey Background: Obstructive sleep apnea syndrome (OSAS) is a serious and potentially life-threatening disease which is common in morbid obese population. Body mass index (BMI) influences the cephalometric measurements which is one of the static diagnostic method. The aim of this study was to compare the cephalometric features of operated morbid obese and süper obese patients with obstructive sleep apnea syndrome (OSAS). Methods: The study population consisted of 70 (54,2%) morbid obese patients with OSAS, They were classified into two subgroups according to BMI of 38 (45,8%) patients have BMI>40 and 32 have BMI>50 were listed. lateral cephalometries (left to right view) were performed on all of the morbid obese patients preoperatively and postoperative 3 months. Results: The morbid obese patients with OSAS in both subgroups showed significant cephalometric outcomes compared with super obeses postoperatively. Soft-tissue enlargements including anteriorly positioned hyoid bone, a longer tongue and narrowed PAS (The distance between pharyngeal wall and back of the tongue) pharyngeal were found in the super obese patients. A significant regression model for super obese OSAS patients using cephalometric measurement could not be obtained as morbid obese patients. However, morbid obese patients have shorter ANS-PNS (The facial A-P distance at the maxilla levels) than super obese patient in postoperative period. Conclusion: Characteristics of the craniofacial bony structure such as narrowing of the nasopharynx and oropharynx and expansion of the soft tissue in the upper airway may be important risk factors for the development of OSAS in morbid obese patients than super obeses in surgical period. In super obeses, the accumulation of adipose tissue in the upper airway may aggravate the severity of OSAS however these accumulation decreased after the bariatric surgery process in both group especially in morbid obese group according to shorter follow up period. Keywords: Cephalometry, OSAS, obese P 100 PATIENTS WITH FEVER IN EMERGENCY DEPARTMENT: CLINICAL DIFFERENCES BETWEEN SEPSIS AND BACTEREMIA Veysel Avci1, Mehmet Tahir Gökdemir2, Ramazan Giden1, Ömer Kaçmaz2, Hadi Bahadur2
1Harran University School of Medicine, Department of Emergency Medicine, Şanlıurfa, Turkey 2Gazi Yaşargil Training and Research Hospital, Clinic of Emergency Medicine, Diyarbakır, Turkey Aim: In this study, it is aimed at management of diagnosis and treatment for the bacteremia and sepsis patients that emerged with high fever, retrospective examination of factors that play a role on mortality and revealing differences between bacteremia and sepsis in terms of the treatment and prognosis. Materials-Methods: Electronic data of totally 200 patients admitted to our emergency service in between December 2015 and January 2013 with high fever and diagnosed with sespsis (60) and bacteremia are analyzed retrospectively. Statistical analyses are performed using SPSS Windows –version#20. Chi-square test (2) is utilized for categorical variables and Student t test is used for continuous variables of the study. Significances evaluated at the rate of p <0.05. Results: Sixty patients (30 %) are diagnosed to be sepsis and the rest, 140 (70%),are bacteremia. Sepsis patients are observed to have lower fever compared to those with bacteremia and it was statistically meaningful (p<0.001). Duration of hospitalization in patients with sepsis was higher than the patients’ with bacteremia(p<0.001), however, their average systolic and diastolic blood pressures were lower(respectively, p<0.001;p=0.005). The following values were lower in sepsis disease case; GCS (p = 0.010), glucose (p = 0.004), albumin (p = 0.002), calcium (p = 0.007) and PCT (p = 0.034). Conclusions: Sepsis patients have longer hospital stay. sepsis patients seem to be more unstable than bacteremia in terms of hemodynamic and laboratory conditions. Sepsis patients should be treated in intensive care. Keywords: High fever, sepsis, bacteremia, emergency department

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
254
P 101 ACUTE INFERIOR MYOCARDIAL INFARCTION; IS IT SAFE TO USE ENERGY DRINK? İsmail Erkan Aydın1, Hakan Süygün2, Yavuz Otal3, Ayhan Özhasenekler1, Şervan Gökhan1
1Yıldırım Beyazıt University Hospital, Department of Emergency Medicine, Ankara, Turkey 2Yıldırım Beyazıt University Hospital, Department of Cardiology, Ankara, Turkey 3Ataturk Training and Research Hospital, Emergency Medicine Clinic, Ankara, Turkey The main active constituents of energy drinks (EDs) include varying amounts of caffeine, guarana extract, taurine and ginseng. The cardiovascular effects of caffeine are perhaps the best defined. This report describes a case of an acute inferior ST elevation myocardial infarction (STEMI) and established coronary artery disease in a young patient with no clear risk factors beyond smoking history and energy drink usage. A 25-year-old male patient presented to our emergency department with severe chest pain. He had been feeling his pain characterized crashed on retrosternal area with radiating to left arm and neck. He has no history of chronic diseases or drug use. The patient reported excessive consumption (i.e. three to four 250 mL drinks per day) of energy drinks, in the week preceding the admission. Physical examination was unremarkable. The admission electrocardiography (ECG) showed 1 mm ST segment elevation in leads II, III, aVF, V2 to V5. Coronary angiography (CAG) was performed immediately by cardiologist. There were irregulary edged %20 stenoses consecutively on right coronary artery (RCA Consecutive measurements of cardiac enzymes elevated. Other laboratory findings were unremarkable. He was transferred to coronary care unit with diagnosis of acute inferior STEMI. Transthoracic echocardiography was normal. Patient’s follow-up ECGs were consistent with MI progression. The patient was pain free during the 4-day observation period and was discharged home. He had been prescribed acetylsalicylic acid, clopidogrel, statin and a β-blocker, all to continue on discharge. Although a causal relationship between large consumption of EDs and myocardial ischemia cannot be definitely established so far, the considerable number of published case reports and the plausible biological abnormalities suggest that the concerns raised about the health risks of excessive consumption of these beverages may be in part justified. We believe that there may be an association between excessive consumption of EDs and myocardial infarction. Keywords: Acute coronary syndrome, energy drink, myocardial infarction, myocardial ischemia P 102 DELİ BAL VE SİNÜS BRADİKARDİSİ Ahmet Aykut, Abide Merve Manap, Ecem Deniz Kırkpantur Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, İstanbul MÖ 401 yılında ilk defa Atinalı Xenephon tarafından tanımlanan Rhododendron ailesine ait bitkilerle beslenen arıların ürettikleri balın tüketilmesi sonucu ortaya çıkan tabloya deli bal zehirlenmesi denmektedir. Rhododendron familyasına ait bitkilerin Türkiye, İspanya, Portekiz, Japonya, Brezilya, Amerika Birleşik Devletleri, Nepal ve İngiliz Kolombiyası gibi birçok ülkede 750’den fazla türü bulunmaktadır. Fakat buna karşın zehirlenmeye sebep olan GTX bu bitkinin çok az türünde mevcuttur. Yaklaşık 18 adet GTX tipi tanımlanmış olup kardiyak etkilerden sorumlu olan GTX I’dir.⁽⁶⁾⁽⁷⁾ GTX hücre zarında sodyum kanallarına bağlanarak sodyum kanallarının blokajına sebep olur. Hücre zarında sodyum geçirgenliğinin artmasıyla repolarizasyon inhibe olur ve hücre membranı depolarizasyon süresi uzar. Sürekli depolarizasyon hali aksiyon potansiyelini azaltır ve sinüs nodu disfonksiyonuna yol açar. Deli bal zehirlenmesi ile başvuran hastalarda gastrointestinal, kardiyak ve nörolojik semptomlar görülebilmektedir.Balın hangi miktarda alındığında intoksikasyona yol açtığı net olarak bilinmemekle birlikte yapılan çalışmalarda 15-60 gr balın yenilmesinin semptomlara sebep olabileceği bildirilmiştir. Bal alımında sonra belirtilerin başlama zamanı değişik çalışmalarda değerlendirilmiş ve ortalama 1 saat ile 3 saat arasında olduğu saptanmıştır. Deli bal zehirlenmesi ile takip edilen hastaların hastanede ne kadar süre gözlem altında kalması gerektiğine dair net bir fikir birliği sağlanamamıştır. Acil servise özellikle bradikardi ve hipotansiyon ile gelen ve hız kısıtlayıcı ilaç kullanımı olmayan hastalarda bal yeme öyküsü sorgulanmalıdır. Bu yazıda deli bal yedikten 45 dakika sonra başlayan kusma ve göğüs ağrısı şikâyeti ile Acil Servisimize başvuran bir olgu üzerinden deli bal intoksikasyonu anlatılmıştır. Anahtar Kelimeler: Deli bal, acil servis, sinüs bradikardisi

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
255
P 103 MANAGEMENT OF PEDIATRIC PATIENTS WITH MILD HEAD TRAUMA: IS IT IMPORTANT LEVEL OF THIOL DISULFIDE?
Ramazan Giden1, Mehmet Tahir Gökdemir2, Veysel Avcı1, Ömer Kaçmaz2, Hamza Karabağ3, Özcan Erel4
1Harran University School of Medicine, Department of Emergency medicine, Şanlıurfa, Turkey 2Gazi Yaşargil Training and Research Hospital, Clinic of Emergency Medicine, Diyarbakır, Turkey 3Harran University School of Medicine, Department of Neurosurgery, Şanlıurfa, Turkey 4Yıldırım Beyazıt University School of Medicine, Department of Biochemistry, Ankara, Turkey Aim: in this study, we aim to investigate a relationship between the level of Thiol Disulfide and the level of trauma for isolated pediatric head injury patients. Methods: 85 patients and 58 healthy controls were included to study. Statistical analyses were conducted with SPSS for Windows 20,0. A P-value < 0.05 was considered statistically significant. Results: In the patients’ group, the level of Native Thiol (SH) and the ratio of %SH/TT were found statistically to be at significantly higher (p =0,009; p<0,001). The values of Disulfide (SS), the ratios of %SS/SH and % SS/TT were statistically determined to be significantly higher (p<0,001). The regarding SS level of the patients with linear fractures and additional pathology was lower than the case of the patients without any pathology but head trauma complaint and statistically it was at meaningful rate (p=0,02). In another study in which computed brain topographies of 60 patients’ group without any pathology but head trauma complaint and 58 control group is compared, the following findings are obtained (The levels of patients’ group are compared to the control group); SH and TT values are determined to be significantly higher and statistically meaningful (p=0,003;p=0,021). The regarding SS level is significantly lower (p=0,001). It was also noticed that the SS level of 60 isolated pediatric head injury patients’ group without linear fractures and additional pathology was statictically at lower level compared to the control group (p=0,001). The SS level of 25 isolated pediatric head injury patients’ group with linear fractures and additional pathology was significantly lower and statistically at meaningful value (p<0,001). Conclusion: In our study, for patients with mild isolated head trauma, but, no pathology detected in computed brain tomography, it was statistically found that the balance in Thiol/Disulfide homeostasis was not shifted toward SS. Keywords: Isolated pediatric head trauma, Thiol/Disulfide homeostasis, Glasgow coma scale, and emergency department P 104 CONSERVATIVE MANAGEMENT OF TRACHEAL RUPTURE DUE TO BLUNT TRAUMA IN A CHILDREN
Mehmet Tahir Gökdemir1, Ramazan Giden2, Ömer Kaçmaz1, Veysel Avcı2
, 1Gazi Yaşargil Training and Research Hospital, Diyarbakır, Turkey 2Harran University Faculty of medicine, Department of Emergency Medicine, Şanlıurfa, Turkey Tracheobronchial injury can cause problems ranging from difficulty breathing to respiratory collapse and even death by airway obstruction. Tracheal injuries from blunt trauma causes are rare, but due to their severity and sequelae they should have a more definitive treatment regimen. Early detection of these injuries is critical to improving outcomes. The most common presenting signs and symptoms of tracheobronchial injuries are subcutaneous emphysema, respiratory distress, pneumothorax, and pneumomediastinum. Radiological studies such as plain films and computerized tomography can help confirm the diagnosis. Although surgery has traditionally been considered the treatment of choice for these injuries, recent reports show that conservative treatment can be effective in selected patients. A case history of tracheal laceration due to blunt trauma in a child is presented to our Emergency department. The laceration was small and was managed conservatively (Figure 1). The resolution of signs and symptoms was rapid, and the patient was discharged after 7 days of hospitalization. Keywords: Conservative management, tracheal rupture, blunt trauma

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
256
P 105 AORT DUVARINDA HAVA İMAJI İLE SEYREDEN NADİR BİR DURUM: CLOSTRİDİUM SEPTİCUM AORTİT VAKASI
Abide Merve Manap1, Ahmet Aykut1, Ebru Ünal Akoğlu1, Tevfik Patan1, Özge Ecmel Onur2
1Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, Acil Tıp Anabilim Dalı, İstanbul 2Marmara Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, İstanbul Giriş: Ülkemizde her gün acil servislere sırt ağrısı ve nefes darlığı şikayeti ile onlarca hasta başvurmaktadır. Yüksek mortalite ve morbidite ile seyreden çok nadir bir hastalık olan enfeksiyöz aortit tablosunda da başlangıç semptomları non-spesifik ve değişkendir. Biz olgumuzda sırt ağrısı ve dispne şikayeti ile acil servise başvuran ve clostridium septicum aortiti tanısı alan bir hastadan bahsedeceğiz. Olgu: Bilinen hipertansiyon dışında kronik hastalığı olmayan 91 yaşında bayan hasta acil servise 1 saat önce başlayan şiddetli, bıçak saplanır tarzda sırt ağrısı ve eşlik eden nefes darlığı şikayeti ile başvurdu. Hasta öyküsünde göğüs ağrısı, ateş, bulantı veya kusma gibi ek şikayetlerden bahsetmedi. Vital bulgularında anormal bulguya rastlanmadı. Fizik muayenesinde batında yaygın hassasiyet ve defans mevcuttu. Yapılan tetkiklerinde beyaz küre sayısı 28.400 K/uL, CRP 26.38, hemoglobin değeri 8.7 mg/dl ve troponin düzeyi 3.8 pg/ml (0-13.8) olarak saptandı. Hastanın çekilen iv-oral kontrastlı abdomen ve toraks bilgisayarlı tomografisinde aortik bifurkasyo düzeyinde 8-10 mm çaplı sakküler anevrizmatik genişleme ve kraniokaudalde yaklaşık 7-8 cm boyunca aortik duvarda kalınlaşma ve hava imajı saptandı. Acil serviste ampirik antibiyotik tedavisi sonrasında kardiyovasküler cerrahi yoğun bakım ünitesine sevkedildi. Hastanın takibinde bakılan kan kültürlerinde clostridium septicum üremesi olduğu saptandı. Tartışma: Literatürde aortite neden olan en bakteriler arasında ilk sırada stafilokosus aureus ve salmonella türleri sayılırken; clostridium türlerinin neden olduğu 26 vaka bildirilmiştir. Tipik prezentasyon bulguları karın veya sırt ağrısına eşlik eden ateş ve lökositozdur. Kesin tanı kan kültürü ile konulurken, tedavide tutulan kısmın cerrahi debritmanı ve uzun süreli antibiyotik kullanımı önemli rol oynar. Uygun tedavi başlanmadığında yüksek mortalite ile seyreden bir durumdur. Anahtar Kelimeler: Aortit, clostridium, enfeksiyöz, septicum P 106 THE OSBORN WAVES AND ATRIAL FIBRILLATION WHICH IS RELATED TO HYPOTHERMIA AFTER SYNTHETIC CANNABIS (BONSAI) ABUSE Hatice Topcu, Banu Karakuş Yılmaz Şişli Hamidiye Etfal Training and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey Osborn wave can be observed in ECG as a late delta wave, seen at the end of the QRS complex in hypothermic people. In this case, an 18-year-old boy with bonsai abuse was found unconscious and hypothermic. After rewarming and supportive management the Osborn Waves and atrial fibrillation was disappeared within hours. Starting to support treatment as fast as in emergency department leads to normalization of the patient's ECG. Keywords: Bonsai, hypothermia, Osborn waves

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
257
P 107 A PEDIATRIC PATIENT AFTER MINOR EYE INJURIE WITH BLOW-OUT TRAPDOOR TYPE FRACTURE Hatice Topcu, Necmettin Sutaşır Şişli Hamidiye Etfal Training and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey After a blunt trauma, by a sudden increase in intraocular pressure orbital wall fracture results with fractures in the thin walls. In children, the most common type of blow-out fracture is seen trapdoor. Blow out fracture occurs most often in the inferior (maxillary) and medial (ethmoid) wall. In the inferior wall fracture limitation glance up, enophtalmus, ptosis, pain at the cheek on the same side and diplopia occur because of inferior rectus muscle tightness. 12-year-old girl was brought to emergency department with the left eye and facial injuries after facial trauma, and then for diplopia and limitation of upgaze maxillofacial CT was performed that have trapdoor orbital floor fracture. After medical treatment with patients trauma at an early stage being operated on the third day guided surgery. This case is presented to emphasize the importance of sending surgery in the early stages and not be overlooked in this type of fracture. Keywords: Blow-out, trapdoor, trauma P 108 SEREBROVASKÜLER HASTALIKLARDA KONTROL MR'IN YERİ İzzet Ustaalioğlu, Abide Merve Manap, Rohat Ak, Ebru Ünal Akoğlu, Özge Ecmel Onur, Ferhat Yıldız, Öncü Sancak Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, İstanbul Giriş: Serebrovasküler hastalıklar (SVH) beynin bir bölgesinin geçici veya kalıcı olarak, iskemi veya kanama nedeniyle etkilendiği, beyni besleyen damarların patolojik bir süreç ile doğrudan tutulduğu durumları kapsar. SVH tanısının konmasında hastanın kliniği ve muayenesi önemli bir paya sahipken; kesin tanı için Bilgisayarlı Tomografi (BT) ve/veya Manyetik Rezonans Görüntüleme (MR) kullanılmaktadır. Olgu: 85 yaşında bayan hasta acil servise 112 ekipleri tarafından ani gelişen bilinç bulanıklığı nedeni ile getirildi. Bilinen demans ve Parkinson tanıları olan hastanın Madopar, Ebixa ve Exelon kullandığı öğrenildi. Hastanın yakınlarından alınan anamnezde 1 aydır konuşmasında azalma olduğu, son 1 saat içinde bilincinde değişiklik ve uykuya meyil geliştiği öğrenildi. Hastanın öyküsünde ateş, nöbet, travma veya aspirasyon durumu saptanmadı. Hastanın vitallerinde anormal bulguya rastlanmadı. Parmak ucu kan şekeri 175mg/dl olarak saptandı. Nörolojik muayenesinde GKS:8 (e2m5v1) gözler hafif sağa deviye, sol telem silik, dil ve uvula orta hatta, ağrılı uyarana her dört ekstremite ekstansiyon yanıtlı, pupiller izokorik ışık refleksleri bilateral mevcut, taban cildi rekleksi bilateral lakayt saptandı. Hastanın EKG’sinde 120 atım/dk hızında atriyal fibrilasyon ritmi gözlendi. Hastaya beyin BT planlandı. BBT de akut hemoraji saptanmayan hastaya iskemik SVH ön tanısı ile difüzyon MR tetkiki planlandı. Difüzyon MR sonucunda iskemi ile uyumlu olabilecek tutulum saptanmadı. Hastanın klinik durumundaki değişiklikler SVH ile uyumlu olmasından dolayı hasta nöroloji ile konsülte edildi. Hastaya kontrol difüzyon MR planlandı. 4 saat sonraki difüzyon MR’ında sol serebellum ve serebellopontin pedinkülde akut infarkt ile uyumlu görünüm saptandı. GKS’si gerileyen hasta entübe edilerek yoğun bakım ünitesine devredildi. Sonuç: Çalışmalarda İlk 6 saatte BT ve konvansiyonel MR’ın enfarktı saptamadaki duyarlılığı %50’nin altında saptanmıştır. Difüzyon MR’da ise bu oran %88-100 arasında değişmektedir. Erken dönemde iskemik SVH hastalarında klinik oturmasına rağmen görüntüleme tetkiklerinde iskemi ile uyumlu bulgu saptanamayabilir. Kliniği ve nörolojik muayenesi iskemi ile uyumlu olan hastaların ilk görüntüleme sonuçlarımız negatif olsa da kesin tanı için kontrol difüzyon MR planlanabilir. Anahtar Kelimeler: Serebrovasküler hastalık, nörolojik aciller, acil servis

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
258
P 109 KUMADİNİZE HASTADA MEKANİK İLEUS Ali Şahiner, Rohat Ak, Özden Özlük, Özge Ecmel Onur, Abdullah Taşcı, Ecem Deniz Kirkpantur Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, İstanbul Giriş: İnce barsak obstrüksiyonu; mekanik obstrüksiyon ya da adinamik ileusa sekonder olarak gelişen gıda ve barsak içeriğinin düzenli geçişinin olmamasıdır. En sık sebebi geçirilmiş abdominal cerrahi, inkarsere kasık fıtığı, obtrator ve femoral fıtıklardır. Hastaların klinik prezentasyonu karın ağrısı bulantı kusma şeklinde olabileceği gibi; akut batın veya sepsis tablosu şeklinde de olabilir. Biz bu olgu sunumu ile acil servise bulantı kusma ile başvuran ve ileus tanısı alan hastalarda ileusun GİS kanamasına bağlı da gelişebileceğine dikkat çekmeyi amaçladık. Olgu: 61 yaşında erkek hasta bir gündür devam eden karın ağrısı şikâyeti ile başvurdu. Bulantısı olan fakat kusması olmayan hastanın bir gündür gaz ve gayta çıkışı olmamış. Başvurusunda vital parametreleri; ateş: 36,4, nabız:96/dk, TA: 164/96 mmHg, sO2: 97 olarak ölçüldü. Alınan anamnezde özgeçmişinde AF ve kapak replasmanı sebebiyle yaklaşık 10 yıldır coumadin kullandığı öğrenildi. Fizik muayenede batında yaygın hassasiyeti ve distansiyonu vardı yapılan rektal tuşede hematokezya mevcuttu. Laboratuar tetkikleri; lökosit: 14,2 K/uL, Hb:13,2 g/DL, INR: 7,49 olarak ölçüldü. Bilgisayarlı batın tomografisinde ince barsak duvarlarında hematom ve hematomların proksimalinde hava sıvı seviyeleri olduğu görüldü. Hasta için ES ve TDP istemleri yapıldı. Hasta ileus ve GİS kanama ön tanılarıyla genel cerrrahi servisine yatışı yapıldı. Hasta yaklaşık 2 gün genel cerrahi servisinde takip edilerek girişim yapılmadan taburcu edildi. Sonuç: Kumadinize hastalarda gis kanama gibi komplikasyonlar sık olarak görülmektedir, ancak bu durumda barsaklarda oluşacak hematoma bağlı ileus görülebileceği de unutulmamalıdır. Anahtar Kelimeler: Coumadin, ileus, cerrahi aciller P 110 RISPERIDONE INOXICATION AND TARDIVE DYSKINESIA Ecem Deniz Kırkpantur, Rohat Ak, Özge Ecmel Onur Fatih Sultan Mehmet Clinic of Emergency Medicine, Istanbul, Turkey Introduction: Tardivedyskinesia (chorea, dystonia, sterotypes and akathisia) is a movement disorder that is generally caused by levodopa drugs, used for parkinsonism, or with dopamine receptor blocking drugs which are used for psychiatric or gastrointestinal disorders. Risperidone is a second generation antipsychotic drug that is used for treatment of schizophrenia and bipolar disorder. Comparing to other conventional antipsychotic drugs it causes tardive dyskinesia less. Cases of unequivocal risperidone-induced tardive dyskinesia have been described afterlong-term exposure. Here we report a case of risperidone intoxication presented with tardive dyskinesia. Case: A 15 years old girl presented to emergency room with risperidone intoxication in a suicidal attempt. She had taken totally 9 mg of Risperdal orally. After the drug ingestion she had fallen asleep. When she woke up, she had felt swelling of her tongue and referred to our emergency room. Her vitals were normal, in her physical examination there was no uvula edema, no swelling of tongue or no any other abnormalities. During her follow-ups, patient represented- repetitive jaw movements, tongue protrusion, lip-smacking- tardive dyskinesia like symptoms. She was started on biperiden treatment and her symptoms disappeared. Discussion: Tardive syndromes refer to abnormal movements caused by dopamin ereceptor blocking agents, with the risk thought to be higher with typical antipsychotics but present even with the use of atypical neuroleptic agents. In literature tardivedyskinesia is treated with tetrabenazine, amantadine, clonazepam, piracetam, levatiracetam, electroconvulsive therapy or with botulinum toxin. Also Biperiden like anticholinergic agents can be used for resolving of symptoms. Keywords: Tardive dyskinesia, risperidone, biperiden

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
259
P 111 ACİL SERVİSTE ŞOK HASTASININ DEĞERLENDİRİLMESİNDE ULTRASONOGRAFİ: RUSH PROTOKOLÜ Oğuz Eroğlu, Mustafa Köksal, Barış Yılmaz, Figen Coşkun Kırıkkale Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Kırıkkale Giriş: Acil serviste yatak başı ultrasonografi (USG) kullanımı tanı koydurucu ve hayat kurtarıcıdır. Ultrasonografi sırasında FAST, EFAST, RUSH, RADIUS gibi farklı; ancak birbiriyle ilişkili protokoller uygulanabilir. RUSH (Rapid Ultrasound for Shock and Hypotension) protokolü, şok sebebi ile başvuran hastalarda farklı organ ve sistemlerin ultrasonografi ile değerlendirmesini içerir. Olgu: On dokuz yaşında bayan hasta acil servise bilinç değişikliği ve karın ağrısı sebebiyle getirildi. Aileden alınan bilgiye göre suicid girişimi veya GİS kanamaya yol açabilecek herhangi bir ilaç kullanımı öyküsü bulunmamaktaydı. Fizik muayenesinde genel durum kötü, oryantasyon ve kooperasyon kurulamıyor, IR: +/+, pupiller izokorik, TA: 50/- mmHg, Nabız: 178 vuru/dk, A:37.2 C, Solunum: 32/dk, SatO2: 88 idi. Yapılan RUSH protokolü değerlendirmesinde kalbin kasılması normal, LV fonksiyonu normal, sağ boşluklar normal genişlikte, EF %65, perikardial mayi izlenmemekteydi. Toraks USG’sinde pnömotoraks veya sıvı birikimi izlenmedi. Abdominal USG’de ise Morrison poşunda serbest sıvı bulunmamakta, ancak karaciğerde rüptüre olmuş ince septalı intrahepatik kist görünümü izlendi. İnferior Vena Cava (İVC) çapı 1.4 cm ve %50’den fazla kollabe olmaktaydı. Sol üst kadran, aort ve pelvis değerlendirmesi normaldi. Alt ekstremite USG'de DVT izlenmedi. Çekilen Beyin BT normal iken; kontrastlı Abdomen BT'de karaciğer segment 8 hizasında 68x63 mm ebadında içerisinde ince septalar bulunan ve orta hepatik vene yakın olacak şekilde rüptüre olmuş kist hidatik izlendi. Hasta genel cerrahiye danışılarak acil operasyona alındı. Sonuç: Ultrasonografide RUSH protokolü uygulaması üç aşamada yapılır. Bu aşamalar “The Pump”, “The Tank”, “The pipes” olarak da isimlendirilir. “The Pump” aşamasında kardiak ultrasonografi, “The Tank” aşamasında tüm abdomen, İVC ve Akciğerlerin ultrasonografisi, “The pipes” aşamasında ise aort ve ekstremite venlerinin ultrasonografisi değerlendirilir. Karaciğer kist hidatiğinde rüptür riski %1.7-8.6 arasındadır. İntraperitoneal alana rüptür gelişen olgularda anafilaksi ve ani ölüm oranı %25 olarak bildirilmiştir. Acil serviste yatak başı ultrasonografi kullanımı hayatı tehdit edici şok tablosu ile başvuran hastaların tanı ve tedavi yönetimi için vazgeçilmezdir. Anahtar Kelimeler: Acil servis, RUSH protokolü, şok, ultrasonografi P 112 ACİLDE SİNÜS TAŞİKARDİSİ AYIRICI TANISI: PULMONER EMBOLİ Ali Karakuş1, Güven Kuvandık1, Zeynep Kekeç2
1Mustafa Kemal Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Hatay 2Çukurova Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Adana Sinüs taşikardisi acil servislerde en sık görülen aritmilerdendir. Ayırıcı tanıda ateş, hipovolemi, anemi ve hipertroidi ilk akla gelecek tanılar içerisindedir. Bu yazıda bir olgu üzerinden sinüs taşikardisi olan ve pulmoner emboli düşünülen olgu vurgulandı. Olgu: 24 yaşında bayan hasta acil servise yaklaşık 15 gündür devam eden nefes darlığı şikâyeti ile başvurdu. Hasta 2 gün önce dâhiliye servisinde orak hücre anemisi araştırılmak üzere yatırılıp 2 ünite eritrosit süspansiyonu verilmiş ve 10 gün sonra hematoloji poliklinik kontrolü önerilerek taburcu edilmiş. Hastanın acil servise geldiğinde genel durumu orta, şuuru açık, tansiyon arteryel:120/70mmHg, nabzı: 145/dk, oksijen saturasyonu: %87, akciğer sesleri doğal, kalp sesleri ritmik taşikardik, batın muayenesi gebelikle uyumlu idi. Hastanın hemogram, biyokimya ve EKG si istendi, monitörize edildi. Damar yolu açılıp sıvı ve oksijen tedavisine başlandı. Hasta sonuçları değerlendirilmek üzere acil servisde takibe alındı. Hastada pulmoner emboli olabileceği düşünülerek kangazı ve D-Dimer tetkiki istendi. Kangazında pH 7,36, pCO2 19, pO2 55, SpO2 %86 tespit edildi. Yapılan ekokardiyografide sağ boşlukları dilate ve septum paradoks olarak tespit edildi. Hastaya düşük molekül ağırlıklı heparin 0.6 cc subkutan yapıldı. Kardiyoloji, kadın doğum ve göğüs konsultasyonu istendi. Takipler sırasında genel durumu kötüleşti ve kardiyopulmoner arrest gelişti ve resusitasyon uygulandı. Resusitasyona cevap veren hasta yoğun bakıma 34 haftalık gebelik+ pulmoner emboli? + akut chest sendromu?+ kardiyopulmoner arrest+ orak hücre anemisi taşıyıcılığı ön tanılarıyla yatırıldı. Kadın doğum tarafından yoğun bakımda in utero ex fetüs tespit edilmesi üzerine sezeryan yapıldı. Tekrar kardiak arrest olan ve resüsitasyona cevap vermeyen hasta eksitus kabul edildi. Pulmoner emboli, klinikte ayırıcı tanıda düşünülmez ise tanısı zor konulan hastalık grubundadır. Ani solunum sıkıntılı, sinüs taşikardili ve altta yatan risk faktörlerini( gebelik, oral kontraseptif kullanımı, geçirilmiş operasyon ve immobilizasyon gibi..) taşıyan hastalarda ayırıcı tanıda düşünülerek acil tedavisi zaman geçirmeden başlanmalıdır. Anahtar Kelimeler: Sinüs taşikardisi, pulmoner emboli, acil servis

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
260
P 113 SPİNAL ANESTEZİ SONRASI ÜRİNER RETANSİYON OLGUSU Dilşat Erümit Balcı1, Şenol Ardıç1, Süleyman Türedi1, Gürkan Altuntaş2, Seda Öztaş Menteşe1, Hülya Gençbay1, Şennur Ekici Yılmaz1
1Sağlık Bilimleri Üniversitesi Trabzon Kanuni Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Trabzon 2Sağlık Bilimleri Üniversitesi Recep Tayyip Erdoğan Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Rize Giriş: Spinal anestezi ile ameliyat edilen hastalar, yapılan prosedürel işlem ve tekniğine bağlı olarak bazı şikayetlerle acil servise başvurmaktadır. Genellikle baş ağrısı, sırt ağrısı, hipotansiyon ve enfeksiyon gibi sık görülen komplikasyonlar bulunurken, nadir de olsa üriner retansiyon, epidural apse ve hematom, menenjit ve araknoiditler görülebilir. Amaç: İdrar yapamama ile acil servise başvuran hastalarda etyolojide yakın zamanda geçirdiği spinal anestezi nedeniyle gelişen bir üriner retansiyon olabileceğini göstermeyi amaçladık. Olgu: 27 yaşında erkek hasta acil servisimize, spinal anestezi ile hemoroidektomi olduktan sonra 1 hafta süresince sık idrara çıkma hissi olduğu, 1 gündür de idrara çıkamama nedeniyle ayaktan başvurmuştur. Vital Bulgular: genel durumu iyi, bilinci açık, oryante koopere, TA: 110/ 70 mmHg, nabız 70 atım/ dak, SaO2: 98% ve Ateş 37 C idi. Solunum, KVS, SSS muayenesi normal olarak değerlendirildi. Batın muayenesinde defans ( - ), rebound (-), hassasiyet (-), organomegali yok, CVAH -/- ve suprapubik muayenede glob vesikale tespit edildi. Nörolojik muayenede kas gücü normal ve defisit yoktu. Börek fonksiyon testleri ve idrar tahlili normal sınırlarda idi. İşlemi yapan anestezi uzmanı ile hasta konsülte edildi. Acil serviste 16 foley idrar sondası takılarak glob boşaltıldı. Sıcak kompresyon önerisiyle taburcu edildi. 1 hafta sonra şikayetlerinin kendiliğinden geçtiği öğrenildi. Sonuç: S2-S4 köklerinin lokal anestezikle blokajı mesane tonusunu azaltır ve miksiyon refleksini inhibe eder. Bu etkiler erkek hastalarda daha belirgindir. Postoperatif kateter kullanılmamışsa hasta miksiyon açısından yakından takip edilmelidir. Devam eden mesane disfonksiyonu ise ciddi nörolojik hasarlanmanın belirtisi olabilir (1). Spinal anestezi sonrası üriner retansiyon insidansı % 0 ile % 69 arasında değişen rakamlarla bildirilmektedir.(2,3,4). Eğer cerrahi girişim sırasında mesane travmatize edilmemiş ise kateter uygulanmalıdır. Spontan idrar atılımı, perineye sıcak tatbiki veya hastanın hareketi ile artırılabilir. Eğer mesane travmatize edilmiş ise ilk olarak mesane ek bir travmadan korunmalı ve rezidüel idrar önlenmelidir. Bu amaçla 4-6 gün süreyle kalıcı bir kateter konulmalıdır (1). Anahtar Kelimeler: Spinal anestezi, üriner retansiyon, üriner kateter P 114 BİR BIÇAK DELİĞİ, BİLATERAL PNÖMOTORAKS: OLGU SUNUMU Oğuz Eroğlu1, Nesimi Günal2, Ertan Cömertpay1, Hatice Algan Kaya1
1Kırıkkale Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Kırıkkale 2Kırıkkale Üniversitesi Tıp Fakültesi, Göğüs Cerahisi Anabilim Dalı, Kırıkkale Giriş: Travmatik pnömotoraks, penetran yaralanmalarda kesici delici aletin veya merminin direk etkisine bağlı doğrudan ortaya çıkarken; künt travmalarda ise sıklıkla kot fraktürü, nadiren de barotravma sonucu gelişebilir. Olgu: Yirmi yaşında erkek hasta bıçaklanma ve darp edilme sebebiyle acil servise getirildi. Geldiğinde genel durum kötü, bilinç açık, oryantasyon ve kooperasyon normal, TA: 85/45 mmHg, Nabız:142/dk, Solunum: 32/dk, SatO2:78 idi. Fizik muayenede sol beşinci kaburga ile sternumun birleşme yerinde bıçaklanmaya ait yaklaşık 3 cm genişliğinde cilt kesisi ve etraf dokuda kanama; buna ek olarak sol koltuk altında minimal cilt kesileri mevcuttu. Hastanın yapılan EFAST ultrasonografisinde kalbin etrafında serbest sıvı bulunmamakta, EF % 65, görülebildiği kadarıyla kalp duvarları ve damarsal yapılar normaldi. Sol hemitoraksta ise pnömotoraks izlendi ve 32 gauge toraks tüpü takılarak su altı drenaja alındı. Takibinde hemodinamisi düzelmeye başlayan hastada (TA: 135/80 mmHg, SatO2:83 (Oksijen altında)) kardiovasküler yaralanmayı netleştirmek amacıyla angio protokolünde kontrastlı Toraks BT çekildi. Kardiovasküler yaralanma izlenmeyen hastanın tomografik değerlendirmesinde, EFAST’ta izlenen sol pnömotoraksına (kalınlığı 9 mm) ek olarak, sağ tarafta en kalın yerinde 12 mm’ye ulaşan pnömotoraksı ve yine sağ tarafta 6 mm kalınlığında pnömomediastinumu olduğu, herhangi bir kot fraktürü olmadığı görüldü. Hastanın tekrarlanan fizik muayenesinde sağ hemitoraksta herhangi bir kesici delici alet yaralanmasına, dermabrazyon veya ekimoza rastlanılmadı. Göğüs cerrahisine yatırılan hasta, takibinin altıncı gününde şifa ile taburcu edildi. Sonuç: Penetran yaralanmalarda travma alanındaki hasar miktarı çıplak gözle görülebildiği için tanı ve tedavi yönetimi daha kolay organize edilir. Künt travmalarda ise, travmanın şiddetini gösterecek bir bulgunun varlığı her zaman izlenmediğinden tanı ve tedavi yönetimi daha zordur. Travma olgularında acil hekimi, her zaman gözlerinin görebildiğinden daha fazlası için hazırlıklı olmalıdır. Anahtar Kelimeler: Acil servis, bıçaklanma, pnömotoraks

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
261
P 115 SPINAL EPIDURAL HEMATOMA AFTER A MINOR INJURY Ramazan Sivil, Erkan Goksu, Salahi Engin, Deniz Kilic Akdeniz University School of Medicine, Department of Emergency Medicine, Antalya, Turkey A spinal epidural hematoma (SEH) is a rare condition that occurs due to rupture of the posterior epidural venous plexus. Epidural hematoma accounts for less than 1% among all spinal space-occupying lesions. In this poster, we discuss a 73 year-old male patient who present with head trauma after falling from ground level. Patient's chief complaint was neck pain and right arm weakness. Patient's physical examination was remarkable for c7-c8 vertebral tenderness, right upper extremity hemiparesis. CT showed an epidural hematoma from c5 to t2 with fractures of c7 vertebra. Patient was consulted and admitted to Neurosurgery for surgical treatment. Keywords: Epidural, hematoma, spinal, trauma P 116 ATİPİK PREZENTASYON İLE ACİLE BAŞVURAN SÜPERİOR MEZENTER ARTER TROMBOZU Davut Sadoğlu1, Şenol Ardıç1, Bestami Köse1, Süleyman Türedi1, Gamze Tüten1, Zakire Uslu1, Çiğdem Önal1, Gürbüz Meral1, Gürkan Altuntaş2, Melih İmamoğlu3
1Sağlık Bilimleri Üniversitesi Trabzon Kanuni Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Trabzon 2Sağlık Bilimleri Üniversitesi Recep Tayyip Erdoğan Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Rize 3Trabzon Fatih Devlet Hastanesi, Acil Servis, Trabzon Giriş: Hastalar acil serviste sıkça akut apandisit tanısı almaktadır. Sağ alt kadran ağrısında ayırıcı tanıda birçok hastalık söz konusudur. Günümüzde görüntüleme yöntemlerinden ayırıcı tanı için sıkça faydalanılmaktadır. Süperior mezenter arter (SMA) trombozu nedenli sağ alt kadran ağrısı nadir görülen bir durumdur. Kontrastı batın BT vasküler orijinli bu tür patolojiler için tanı koydurucudur ¹. Vaka: 50 yaşında kadın hasta, acil servise karın ağrısı, iştahsızlık ve bulantı kusma ile dış merkez hastaneden akut apandisit ön tanısı ile 112 ile getirildi. Karın ağrısı göbek çevresinde başlayıp 6 saat sonra sağ alt kadrana yayılım gösterdiği öğrenildi. Ek hastalık öyküsü olmayan hastanın vital bulguları; genel durumu iyi, bilinci açık, oryante koopere, TA: 130/ 70 mmHg, ateş 37 C, nabız 76 atım/ dak ve Sa02 % 98 idi. Yapılan fizik bakısında SS, KVS, SSS muayenesi normal olarak değerlendirildi. Karın muayenesinde sağ alt kadranda hassasiyet +, defans+, rebound+, organomegali yok ve CVAH -/- idi. Bilateral üst/ alt ekstremite nabızları açık ve eşit idi. NM normal olarak değerlendirildi. Ekg NSR idi. Labratuvar panelinde Crp 19.9 mg/ dl ve tam idrar tahlilinde eritrosit 50 U/L idi. BUN/ Kreatinin, KCFT, elektrolit değerleri normal düzeylerde idi. Yapılan kontrastlı batın BT’de Süperior mezenterik arterde orjin düzeyinden yaklaşık 4 cm lik segment sonrasında yaklaşık 1-1,5 cm lik segmentte lümeni büyük oranda dolduran parsiyel dolum defektine neden olan trombüs izlendi. Hasta girişimsel radyoloji ünitesi olan KTÜ Tıp Fakültesi’ne sevk edildi. SMA orta kesiminde % 70-80 darlık için stent takıldı ve 24 saat yatak istirahati ile taburcu edildiği öğrenildi. Sonuç: SMA trombozu olan hastaların tedavisinde gecikme olması halinde bağırsak nekrozu gelişebileceğinden cerrahi gereksinim olabilir ². Olgumuza ifade ettiğimiz klinikte ise girişimsel yöntem önceliklidir. Anahtar Kelimeler: Süperior mezenter arter, Sağ alt kadran ağrısı, Girişimsel radyoloji

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
262
P 117 NADİR BİR İNTİHAR YÖNTEMİ: ÇAKMAK YUTMA Mehmet Altuntaş, Ozcan Yavası, Ensar Durmus Recep Tayyip Erdoğan Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Rize Giriş: Yutulan yabancı cisimler genellikle sindirim sisteminde komplikasyon oluşturmadan spontan olarak atılır. İntihar amacıyla yutulan cisimler çok sayıda ve çeşitte olabilir. Tanıda gecikme komplikasyon oranında artma ile sonuçlanır. Büyük ve sert cisimler pilordan geçmeyerek; obstrüksiyon, ülser, kanama ve perforasyon oluşturabilir. Olgu: Karın ağrısı nedeniyle acil servise başvuran 41 yaşında erkek hastanın yapılan fiziksel incelemesinde karında minimal hassasiyeti vardı. Çekilen ayakta direkt karın grafisinde karında çok sayıda radyoopak cisim saptandı. Tekrar sorgulandığında hastanın bir gün önce intihar amaçlı 8 adet çakmak yuttuğu öğrenildi. Obstrüksiyon bulgusu olmayan hasta takip amaçlı genel cerrahi servisine yatırıldı. Bir ay sonra hastanın acil servise tekrar farklı bir sebepten başvurusunda herhangi bir girişimi kabul etmediği, psikiyatrik destek aldığı çakmaklardan dördünü defekasyonla çıkardığı öğrenildi. İkinci başvurunda çekilen grafisinde 4 adet çakmağın mide seviyesinde olduğu görüldü. Sonuç: Bu olgu sunumu ile intihar amaçlı yabancı cisim yutma nedeniyle acil servise başvuran psikiyatrik hastalarda karşılaşılan zorluklar irdelenmeye çalışılmıştır. Anahtar Kelimeler: Çakmak, intihar, yabancı cisim P 118 PİKA HASTALIĞI: OLGU SUNUMU Mehmet Altuntaş, Özlem Bilir, Ensar Topaloğlu
Recep Tayyip Erdoğan Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Rize Giriş: Pika hastalığı, en az 1 ay boyunca besleyici değeri olmayan maddelerin ısrarcı şekilde yenmesi olarak tanımlanır. Çocukluk yaş grubunda daha fazla olmak üzere, tüm toplumlarda ve yaş gruplarında görülebilir. Hastalığın tanısının konulabilmesi için çocuğun minimum 2 yaşında olması gerekmektedir. iki yaş altı çocuklarda ağza uygunsuz maddeleri atma ve yemeye çalışma davranışı sık görülmektedir. Pika hastalığının demir, çinko gibi mineral eksikliklerine bağlı olduğu düşünülse ruhsal problemlerin de etken olduğu gösterilmiştir. Pika hastalığında tüketilen maddelerden en yaygın olanları kum, toprak, plastik, bez, kireç ve kağıttır. Olgu: Acil servise kusma şikayeti ile ailesi tarafından getirilen 3 yaşındaki hastanın ayakta direkt karın muayenesinde en büyüğü 23 mm 15 adet radyoopak yabancı cisim tespit edildi. Hasta takip amaçlı cerrahi servisine yatırıldı. Takibinde obstrüksiyon gelişmeyen hastanın yuttuğu yabancı cisimlerin çakıl taşı olduğu anlaşıldı. Bir yıl sonra aynı çocuk karın ağrısı, kusma şikayeti ile getirildi. Ailesinden çocuğun çakıl taşı yutmaya devam ettiği 1 yıl boyunca seksene yakın defekasyonla çıkardığı, mineral eksikliği açısından araştırıldığı ancak mineral eksikliği tespit edilmediği çocuk psikiyatsine yönlendirildiği öğrenildi. Sonuç: Sadece çakıl taşı yuttuğu anlaşılan, mineral eksikliği tespit edilmeyen bu yaş grubu çocuklarda pika ayırıcı tanısında mental ve ruhsal patolojilerde araştırılmalıdır. Anahtar Kelimeler: Pediatri, Pika hastalığı, taş

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
263
P 119 AORTIC DISSECTION: A CASE REPORT ‘’EXPLODED FLAME BALL IN MY CHEST’’ Mehmet Ünaldı1, Soner Işık1, Didem Ay1, Ersen Gündüz1, Ümit Ölmez1, Hatice Eryiğit2, Onur Incealtın1, Kurtuluş Açıksarı1
1Medeniyet University Goztepe Training and Research Hospital, Department of Emergency Medicine, Istanbul, Turkey 2Kartal Training and Research Hospital, Thorax Surgery Clinic, Istanbul, Turkey Acute aortic dissection is one of life-threatening aortic emergencies and occurs in the setting of chronic hypertension and other factors that lead to degeneration of the media of the aortic wall. All mechanisms involve weakening of the medial layer that leads to higher intimal wall stress. In this study we present to a case of type A dissection. Case: 41-year-old male patient was presented to the ED with abdominal pain, chest pain and severe back pain. In history he had diabetes mellitus and hypertension. He described to pain as ‘’ exploded flame ball in my chest and beginned back pain’’. Vital signs revealed Tension: 200/110 mm-Hg (right), 150/90 mm-Hg (left), pulse:98/min, O2 saturation:97%. Thorax CT angiography showed that false lumen and true lumen were in the ascending aorta and descending aorta. He was interned to cardiovascular surgery clinic with diagnosed aortic dissection. Aortic dissection occurs after a violation of the intima allows blood the enter the media and dissect between the intimal and adventitial layers. It has a bimodal age distribution. The group accounting for the first peak consists of younger patients with specific predisposing conditions. The larger group accounting for the second peak is comprised of those aged> 50 years with chronic hypertension. Keywords: Aort, dissection, explode flame ball P 120 IS THORACIC TRAUMA ALWAYS BAD?
Mehmet Ünaldı1, Hatice Eryiğit2, Soner Işık1, Didem Ay1, Ersen Gündüz1, Onur Incealtın1, Kurtuluş Açıksarı1
1Medeniyet University Goztepe Training and Research Hospital, Department of Emergency Medicine, Istanbul, Turkey 2Kartal Training and Research Hospital, Thorax Surgery Clinic, Istanbul, Turkey Blunt chest trauma often occurs during motor vehicle accidents. Otherwise it consists reasons such as work accidents, high falls and sports injuries. We present two geriatric cases with simple falling in home in this study. Case 1: 83 year-old female patient was presented tothe ED as a result of simple falling. Clinical signs were good. Radiologic evaluation revealed 2nd, 3th, 4th and 5th rib fractures in right hemithorax and scapular fracture. She was observed in the ED and discharged with good clinical condition. Case 2: 71 year-old male patient admitted to the ED with same reason. Vital signs were tension:120/74, pulse: 92/min, O2 saturation:96%. In radiologic assessment we detected pneumothorax on left side. We implemented tube thoracostomy and he was interned to thorax surgery clinic. Blunt thoracic injuries account for up to one fourth of all injury deaths. In most cases of thoracic trauma, the mechanism of injury predicts the clinical course and outcome. In some cases ınjury may occur despite minor trauma as in these cases. Keywords: Blunt, thorax, trauma

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
264
P 121 BETA BLOKÖR KULLANIMINA BAĞLI WENCKEBACH FENOMENİ Gizem Gülcan, Rohat Ak, Ecem Deniz Kırkpantur, Tuba Cimilli Öztürk, Özge Ecmel Onur Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, İstanbul Wenckebach fenomeni, elektrokardiyografide (EKG) pr mesafesinde uzama sonucu iletilmeyen bir p dalgası ile sonuçlanan durumdur. Genellikle atrioventriküler düğüm seviyesindeki geri dönüşümlü iletim bloğuna bağlıdır. Nedenleri arasında beta blokör, kalsiyum kanal blokörü gibi ilaçların kullanımı, inferior mı,miyokardit sayılabilir. Olgumuzda acil servise çarpıntı şikayeti ile başvurup EKG'sinde Wenkebach fenomeni saptadığımız bir hastanın bisoprolol kullanımını kestikten sonra bu EKG paterninin düzeldiğini ve bu durumun benign bir neden olduğunu sunmayı amaçladık. 60 yaşında kadın hasta acil servisimize 10 gündür devam eden çarpıntı halsizlik şikayetiyle başvurdu. Başvuru anındaki vitalleri; ateş: 36,2 °C, tansiyon: 136/65 mmHg, nabız: 67 vuru/dk, sp02: %98 idi. Göğüs ağrısının hafif baskı şeklinde olduğunu belirten hastanın özgeçmişinde hipertansiyon ve koroner arter hastalığı öyküsü mevcuttu. Bir hafta önce kardiyoloji polikliniğine aynı şikayetlerle başvuran hastanın orada çekilen EKG’sinde normal sinüs ritmi ve ara ara olan ventriküler ekstra sistolleri olması nedeniyle hastaya bisoprolol başlanmış. Acil serviste çekilen EKG’de Wenckebach fenomeni izlendi. Rutin laboratuvar tetikleri ve kardiyak paneli normaldi. Takiplerinde şikayetlerinin düzelmesi üzere beta blokör kesilerek hasta taburcu edildi. Wenckebach fenomeni digoksin intoksikasyonu miyokardit inferior mı gibi durumlarda görülmekle beraber en sık beta blokör, kalsiyum kanal blokörleri kullanımı sonrası görülebileceği unutulmamalıdır. Ayırıcı tanılar göz önünde bulundurulmalıdır. Asemptomatik hastalarda tedavi gerekmezken 3.derece av bloğa ilerleyebileceği nadiren kardiyak pace gerektireceği akılda tutulmalıdır. Anahtar Kelimeler: Wenckebach fenomeni, beta blokör, aritmi P 122 SPONTANEOUSLY REDUCED INTERNAL HERNIA: MULTIDETECTOR CT FINDINGS
Selcuk Parlak1, Esra Çıvgın1, Elif Çelikel2, Hamza Özer1, Perihan Polattaş1
1Numune Training and Research Hospital, Radiology Clinic, Ankara, Turkey 2Numune Training and Research Hospital, Emergency Medicine Clinic, Ankara, Turkey Internal hernias (IH) are protrusion of the gut through the peritoneum, mesentery, or omentum into a compartment in the abdominal cavity. The hernia orifice is usually a preexisting foramen, recess, and fossa but can be caused by surgery, ischemia, and trauma. Preoperative diagnosis is difficult because clinical symptoms may range from intermittent and mild digestive complaints to acute-onset intestinal obstruction. Internal hernias are clinically apparent only when incarcerated therefore, a delay in diagnosis may lead to strangulation and an increased risk of serious complications. It is important for radiologists to be familiar with and to understand the various types of internal hernias and their imaging features so that prompt and accurate diagnosis of these conditions can be made. In the literature, there are few reports about spontaneously reduced internal hernias. A 39-year-old man was admitted to emergency room with the complaints of abdominal pain, nausea, and vomiting. Abdominal computed tomography (CT) showed cluster of dilated ileal loops with features suggestive of strangulation in left lower quadrant. Mural thickening, engorged and displaced mesenteric vascular pedicle, mesenteric stranding were also seen. The diagnosis of internal hernia was suggested by CT. On control CT, it was clear that internal hernia was reduced spontaneously, as the herniated ileal loops were detected on their normal anatomic locations in right side. Due to the persistence on the clinical course, the patient was operated, and ischemic ileal loops were resected. Keywords: Internal hernia, bowel obstruction, computed tomography

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
265
P 123 JOB EXPERIENCE IS NOT ENOUGH FOR PREVENTION FROM WORK ACCIDENT Ömer Engin1, Erkan Güvenç2, Burcu Tanay Demirdöven2, Hilmi Güngör1
1Buca Seyfi Demirsoy State Hospital, Surgery Clinic, Izmir, Turkey 2Buca Seyfi Demirsoy State Hospital, Emergency Department Clinic, Izmir, Turkey Aim: Our case is a butcher for 32 years. He was working in a butcher shop as an employee. He has knowledge about prevention from work accident. For example he known that protective aprons must be worn if meat is sliced with a butcher knife, but he relied on himself and he had not worn any protective apron. When he sliced the meat on the bone, the knife in his hand injured his abdominal wall. Case: The case is 57 years old male. He applied to emergency department for stabbing to his abdominal wall. Vital signs were stabil. Abdominal CT (computerized tomography) was taken with contrast medium. The contrast medium was given intravenous route and into abdominal wall laceration. Any organ laceration or intraabdominal free air and liquid were not found on CT. Intralesional given contrast medium was not passed to intraperitoneal cavity, it is only seen in intramuscular and subcutaneous layers. The case was discharged without any complication. Results: Work accidents may be occur every time. Job experience is not enough for prevention from work accidents as in our case. So rules must always be observed. If the employee do not observe the rules, employers must ensure compliance with the rules. Another important point in our case is that CT with contrast medium (intravenous and intralesional route) is very important for diagnosis of intraperitoneal penetration and any organ injury. Keywords: Job, accident, CT, organ laceration, stabbing P 124 DIEULAFOY'S LESION: A RARE LOCATION FOR GASTROINTESTINAL HEMORRHAGE Cansu Alyeşil, İbrahim Ulaş Özturan, Nurettin Özgür Doğan Kocaeli University Faculty of Medicine, Department of Emergency Medicine, Kocaeli, Turkey Dieulafoy’s lesion is a rare and potentially life-threatening cause of gastrointestinal bleeding. These lesions are arteries of the gastrointestinal tract that protrude through the submucosa. The lesion is mostly located in the lesser curvature of the stomach, however it could be found anywhere in the GI tract. Here, we report a case of Dieulafoy’s lesion located in esophageal diverticulum which is a very rare location for this condition. Keywords: Dieulafoy’s lesion, gastrointestinal hemorrhage, emergency department

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
266
P 125 ACİL SERVİSTE TÜP TORAKOSTOMİ SONRASI KOMPLİKASYON GELİŞEN PNÖMOTORAKS OLGUSU Gizem Gizli, Özlem Köksal Uludağ Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Bursa Giriş: Spontan pnömotoraksın, amfizem benzeri değişikliklerle ilgili subplevral büllerin rüptürü sonucu geliştiği düşünülmektedir. Sigara kullanımı bleb oluşumunu tetikleyebilir ve büller rüptüre olarak pnömotoraksa yol açar. Klinik pnömotoraksın büyüklüğü, gelişme hızı ve altta yatan nedene bağlıdır. Tedavide tüp torakostomi uygulanarak, plevral aralıktaki havanın drenajı sağlanır. Uzamış hava kaçağı olan hastalar heimlich valf mekanizmasına bağlanabilir. Tüp torakostomi sonrası nadir de olsa bazı komplikasyonlar gelişebilir. Olgu: 32 yaş erkek hasta göğüs ağrısı, nefes alırken batma şikayeti ile Acil Servise başvurdu. Genel durumu iyi, vital bulguları stabil olan hastanın dinlemekle akciğer sesleri solda alınmıyordu ve sO2: %94 idi. Çekilen PA akciğer grafisinde sol tarafta totale yakın pnömotorax mevcuttu. Tüp torakostomi sonrası kliniği düzelen hastanın çekilen kontrol akciğer grafisinde akciğerin ekspanse olduğu gözlendi. İstenen göğüs cerrahisi konsültasyonunda heimlich valfi uygulanan hasta birkaç saatlik gözlem sonrası toraks tomografisi sonucu ile poliklinik kontrolüne çağrıldı. Çekilen toraks tomografisinde hemotoraks tespit edilmesi üzerine göğüs cerrahisi tarafından operasyon amaçlı yatırıldı. Operasyonda 500 cc hematom aspire edildi, kanama odağı olarak akciğer apikalde göğüs duvarında pnömotorakstan kopmuş bir yapışıklık izlendi ve koterize edilerek kanama kontrolü sağlandı. Akciğer apikaldeki yapışıklığa neden olan büllöz alan rezeke edildi. Hasta, yatışının 10. gününde taburcu edildi. Sonuç: Tüp torakostomi yöntemi hayat kurtarıcı bir yöntem olmakla beraber, nadir de olsa komplikasyonlara yol açabilir. Komplikasyonları arasında; kanama, akciğer parenkim hasarı, göğüs ön duvarında yanma, ağrı, yara yeri enfeksiyonu, dren malpozisyonu ve reekspansiyona bağlı akciğer ödemi yer almaktadır. Tüp torakostomi uygulanan hastaların taburculuk öncesinde komplikasyonların gelişimi açısından bir süre yakın takip edilmesi uygun olacaktır. Anahtar Kelimeler: Spontan pnömotoraks, tüp torakostomi, komplikasyon P 126 BİR OLGU SUNUMU: "İNTESTİNAL OBSTRÜKSİYONA BAĞLI ÇEKUM PERFORASYONU" Ziya Uzun, Özlem Köksal Uludağ Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Bursa Giriş: İntestinal obstrüksiyon intestinal içeriğin gastrointestinal sistem içinde distale doğru olan geçişinin parsiyel ya da tam olarak engellenmesidir. Mekanik intestinal obstrüksiyona, yetersiz barsak motilitesine ve psödo-obstrüksiyona bağlı olarak gelişebilir. Obstrüksiyona bağlı olarak intestinal içeriğin absorbsiyonu bozulur, kusma gelişir ve oral alım bozulur. Mekanik obstrüksiyonda barsak distansiyonu gelişir. İleoçekal valve çalışıyorsa kolon obstrüksiyonu kapalı loop obstruksiyonuna neden olur. Bu durumda perforasyon riski çekumda en yüksektir. Olgu: 34 yaş bayan hasta, karın ağrısı şikâyetleri ile başvurduğu dış merkezde kolelithiazis tanısı ile 10 gün önce laparoskopik kolesistektomi yapılmış. Hasta 3 gündür devam eden karın ağrısı ve gaz-gaita yapamama şikâyetiyle başvurdu. Fizik bakıda batın sağ alt kadranda hassasiyeti, defans ve reboundu olan hastada palpasyonda sağ alt kadranda ele gelen kitle mevcuttu. Laboratuar tetkiklerinde lökositozu saptanan hastanın, ayakta direkt batın grafisinde sağ tarafta içinde küçük hava-sıvı seviyeleri olan sınırları seçilebilen yaklaşık 7- 8 cm lik barsak ansı mevcuttu. Hastaya çekilen kontrastlı abdominal tomografide; hepatik fleksura düzeyinde obstrüktif kitle saptandı. Dilate çekum etrafında sıvı görünümü, yağ planlarında kirlilik ve yer yer lenf nodları mevcuttu. Çekum postero-anterior çapı 9 cm ve transvers çapı 10 cm'di ve kapalı valf obstrüksiyonu gelişmişti. Nazogastrik tüp ile drenajı sağlanan hastadan Genel Cerrahi konsültasyonu istendi ve operasyona alındı. Operasyonda çekum perforasyonu saptanan hastaya sağ hemikolektomi yapıldı ve kolostomi açıldı. Tartışma ve Sonuç: Mekanik kolon obstrüksiyonlarının en sık nedeni gelişmiş batı ülkelerinde kolon kanseri iken, gelişmekte olan ülkelerde kolonik volvuluslardır. Kolonik obstrüksiyonların semptomları konstipasyon, karın ağrısı, karında distansiyon ve hastalığın terminal döneminde görülen kusmadır. Tanı genellikle fizik muayene ve görüntüleme ile konulur. Öncelikle hastanın sıvı elektrolit dengesi düzeltilir ve nazogastrik ile dekompresyon uygulanır. Tanının erken konularak acil laparotomi ile obstrüksiyonun giderilmesi hayat kurtarıcıdır. Anahtar Kelimeler: İntestinal obstrüksiyon, perforasyon, akut batın

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
267
P 127 İŞ KAZASI NEDENİYLE ACİL SERVİSE BAŞVURAN HASTALARIN DEMOGRAFİK ANALİZİ Emine Kadıoğlu1, Serhat Karaman2, Özlem Arık3
1Dumlupınar Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Kütahya 2Gaziosmanpaşa Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Tokat 3Dumlupınar Üniversitesi Tıp Fakültesi, Biyoistatistik Anabilim Dalı, Kütahya İş kazaları sonrası kazazedelerin ilk müdahalesi çoğunlukla acil servislerde yapılmaktadır. Acil servis başvuruların da iş kazası olarak bildirimi zorunlu olan bu hasta gurubu adli vakaların önemli bir kısmını oluşturmaktadır. İş kazaları çalışanı, aileleri, işvereni, sosyal güvenlik kurumları, sağlık sistemini etkilemektedir. Bir eğitim araştırma hastanesinde acil tıp kliniğine başvuran iş kazalarının mortalite, morbidite ve demografik özelliklerini değerlendirmeyi planladık. Çalışma 1 Ocak 2015 – 31 Aralık 2015 tarihleri arasında acil servise başvuran iş kazalarının geriye yönelik kayıtları incelenerek yapıldı. Veriler kategorik ölçümler sayı ve yüzde olarak, sayısal ölçümler ise ortalama ve standart sapma olarak özetlendi ve SPSS 16 paket programı ile analiz edildi. 1044 vakanın %36, 2 si 20-29, %33’ü 30-39 yaş aralığında olmakla, 70-79 yaş arasında olan bireylerin sayısı oldukça azdı. Vakaların %89,3`ü erkekti. Kazazedelerin %93,1`i ayaktan tedavi, %5,4`ü hospitalize, %1,1`i sevk edilmiştir. Vakaların %0,5`i acil serviste ex olmuştur. Kazazedeler en çok (%2,6) ortopedi servisine yatırılmıştır. Beyin ve plastik cerrahi servislerine de 8`er hastanın yatışı yapılmıştır yani 1044 vaka içerisinde her ikisi de ayrı ayrı %0,8 olmak üzere en çok yatış yapılan ikinci servislerdir. Başvuruların mevsimsel dağılımında; %11, 9 ile en çok Ağustos, %10, 2 ile Haziran ve Temmuz ayları ikinci sıradadır. %4,3 ile en az vaka ise Aralık ayında başvurmuştur. Yaz aylarında vaka sayılarında artış görülmüştür. Haftanın günleri açısından %17,3 ile vaka sayısı en çok Perşembe günündedir, %15,6 ile Salı günü ikinci sıradadır. %15 ile Cuma ve Cumartesi günleri üçüncü sırada iken en az vaka Pazar günüdür. Başvuru zamanlarına bakıldığında %55,3 ile en çok 08-16 saat dilimindedir. Acil müdahale gerektiren 1044 vakanın oluş şekilleri incelendiğinde batın travması, elektrik çarpması, gözde yabancı cisim, intox, travma, yanık ve zehirlenmedir. Vakaların %96, 4’ü travma ile meydana gelmiştir. İş kazaları sonrası acil başvuruları içeren çalışmaların, iş sağlığı ve güvenliği konusunda farkındalığı artıracağını, acil müdahale için gelen hasta profilinin belirlenmesi ve iş kazalarının önlenmesine katkı sağlayacağı düşüncesindeyiz. Anahtar Kelimeler: İş kazaları, acil tıp, iş sağlığı ve güvenliği P 128 SERUM LACTATE AND BASE DEFICIT AS PREDICTORS OF MORTALITY AND MORBIDITY IN TRAUMA PATIENTS Engin Özakın1, Pakize Gözde Gök1, Mustafa Emin Çanakçı1, Muzaffer Bilgin2, Nurdan Acar1, Filiz Baloğlu Kaya1, Arif Alper Cevik3
1Eskişehir Osmangazi University, Department of Emergency Medicine, Eskişehir, Turkey 2Eskişehir Osmangazi University, Department of Biostatistics, Eskişehir, Turkey 3United Arab Emirates University, Medical College and Health Sciences, Al Ain, United Arab Emirates Objective: Lactate and base deficit (BD) affect the mortality and morbidity associated with the severity of trauma in trauma patients during the first admission to the hospital, theoretically. The aim of this study is to evaluate the relationship of arterial lactate concentration and BD with the duration of hospitalization, use of blood products, intubation, operation and mortality. Methods: A total of 50 patients over 18 years of age admitted to the ESOGU ED between 01.09.2015-01.09.2016 due to traffic accident and whose blood gas parameters were ready during admission, were investigated, retrospectively. The demographic characteristics of the patients, vital signs, blood product usage, intubation operation, the number of hospitalization days and the mortality were evaluated. Findings: 82% of the patients were female and the average age was 48.42±19.78(min:19,max:90), respectively. Average blood pressure was 86.86±28.43mm/hg, pulse average was 96.92±36.04/min, lactate levels were 3.38±3,06 mg/dl (min:0.7,max:18), mean BD was -5.4±4.59 mEq/L (min:-21.3,max:2.7). The relationship was found as significant between lactate levels and shock index (p=0,041), hospitalization days in discharged patients (p<0,001), intubation (p=0,001), operation (p= 0,027) and mortality (p= 0,002), however this was not valid for blood product use (p=0,061). The relationship of BD with the blood product use (p=0,031), intubation (p=0.001) and mortality (p=0,001) was found as significant, however this was not valid for the shock index (p=0,150), the duration of hospitalization in discharged patients (p= 0,610), and operation (p= 0,224). When lactate levels were examined, the sensivity and the specificity was measured as 80%,68% in terms of mortality for > 2,6 mg/dl; When BD were examined, the sensivity and the specificity was measured as 80%,74% in terms of mortality for levels <=-5mEq/L Conclusion: Decreased BD and increased lactate levels in trauma patients admitted to the ED can help at the early stage in terms of determining emergency management Keywords: Base deficit, lactate, trauma, mortality

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
268
P 129 RAMADAN FASTING AND ITS INFLUENCE ON SERUM OSMOLALITY IN EMERGENCY PATIENTS Ozlem Dikme1, Ozgur Dikme2
1Koc University Hospital, Department of Emergency Medicine, Istanbul, Turkey 2Istanbul Training and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey Introduction: Ramadan is the ninth month of the Islamic calendar and Muslims fasting during this month. The effect of Ramadan fasting has been studied in various studies which are conducted on normal healthy individuals worldwide, but the changes of serum osmolality during Ramadan fasting are not known well. We aimed to investigate clinical worthiness of serum osmolality on fasting patients at Emergency Department (ED). Methods: This prospective, cross-sectional, case-control study was conducted on 62 fasting patients and 62 age- and sex- matched non-fasting controls in a tertiary training and research hospital ED. We obtained demographic, clinical and laboratory data including serum sodium, glucose, blood urea nitrogen, systolic and diastolic blood pressure, pulse rate and ED outcomes including discharge and hospitalization status in study and control patients. All analyses were performed using SPSS version 15.0 for Windows. Results: A total of 124 patients enrolled into the study. When the subjects evaluated about their diagnosis there was statistically significant difference between the study and control group (p< 0.001). The most common diagnosis was related with neurological and gastrointestinal systems in the study group and was related with gastrointestinal and cardiovascular systems in the control group. The median serum osmolality averages of the study and control group were found as 300 mosm/kg (IQR = 295-304) and 299 mosm/kg (IQR = 296-305), respectively (p = 0.990). In the study group, statistically significant positive correlation was observed between serum osmolality and duration of hunger, age, urea, creatinine, sodium levels (p= 0.007, p< 0.001, p< 0.001, p= 0.002, p< 0.001). Conclusion: This study has shown that serum osmolality isn’t affected by Ramadan fasting on ED patients. Nonetheless, further prospective larger studies are needed to assess the relationship between serum osmolality and Ramadan fasting. Keywords: Serum osmolality, fasting, ramadan, emergency department P 130 NIGHT SHIFT IS A NIGHTMARE? AFFECTING FACTORS OF THE RESIDENT DOCTORS DEPRESSION LEVELS Mehmet Bunyamin Gucuyener1, Hakan Topacoglu2, Ozlem Dikme3, Ozgur Dikme2
1Okmeydanı Training and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey 2Istanbul Training and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey 3Koc University Hospital, Department of Emergency Medicine, Istanbul, Turkey Objective: Residency training can cause to the emergence of depressive condition that might lead to possible academic and professional consequences. We aimed to determine the depression levels of the residency medical doctors (RMDs) and evaluation of the affecting factors. Methods: This cross-sectional questionnaire study performed on the RMDs working at a tertiary research hospital in Istanbul. Participation in the study was on voluntary basis. A questionnaire form was distributed among the RMDs participating in the study and the Beck Depression Inventory-II (BDI-II) was used for measurement of the depression levels. Results: A total of 161 RMDs were included in the study (Participation rate: 68.8%), mean age was determined as 28.2±2.7 years (interval 24-45 years), 35.4% were females and 42.9% were married. The general mean of the BDI-II was 12.4±9.0 (interval 0-57) which classifies as minimal depression, the lowest category of depression on the BDI-II. Considering the BDI-II cut-off points as >=20, 28 (17.4%) was moderate/severe depressed. An exploratory analysis of possible risk factors showed that night shift works, duration on residency and which residency department in worked were factors for the development of depressive symptoms (respectively independent T-Test, p= 0.030, Pearson Correlation coefficient -0.160 p= 0.043, ANOVA, p= 0.03). There was no relationship to determine between the BDI-II scores and age, gender, marital status, number of children, living alone, losing a loved one recently, presence of a chronic disease, having been diagnosed with depression and using antidepressant medication. Conclusion: There is a high prevalence towards depressive symptoms among the RMDs, particularly night workers and less experience times in their residency. The active assessment of these RMDs in evaluating their depressive symptoms is important. Preventive policies and educational programs towards improvement of working conditions must be reviewed again. Keywords: Resident medical doctors, depression, Beck depression inventory

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
269
P 131 A RARE CASE: URACHAL ABSCESS Hande Candemir, Ezgi Ceylan, Halil Ibrahim Atalay, Erkman Sanri, Haldun Akoglu, Ozge Ecmel Onur, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Introduction: Urachus is a cord between the bladder and umbilicus and urachal abscess is the infection of the residue of fetal urachus. It is more common in children. There are four types of abnormalities: urachal cyst; in which both side of the cord closed but there is an opening in the middle, patent urachus; in which there is a connection between bladder and umblicus, vesicourachal diverticulum urachus; in which the connection with bladder stays patent, and urachal sinus; if there is a persistent tissue with umblicus. Case: A 21-year-old man, who has no history of chronical diseases, presented with an abdominal pain of 3 days and fever for a day. He was weak and had no appetite. GCS was 15. His vital signs were as follows: BP, 140/88 mmHg, HR, 70 bpm, SpO2 98% Temp, 37 C and RR 16/min. No pathological findings were observed on physical examination except a subtle tenderness in the abdomen. Laboratory examinatioan of the patient revelaed a WBC of 20.400/µL, Hg 14.1 g/dL, PLT: 256.000/µL and CRP of 193 mg/L. CT of the abdomen revealed an abscess with a volume of approximately 210 cm3 between the urachus and bladder. Diagnosis of an urachal abscess was confirmed. The patient was admitted and started on IV antibiotics. Discussion: Clinical signs and symptoms are not specific for urachal abscess, it can be abdominal pain, umblical excudation, fever or weakness. Ultrasound and CT are gold standard for the diagnosis. The treatment of urachal abscess is similar to other abscess using antibiotics, percutaneous drainage, and finally surgical excision because, there is always the risk of recurrences. Urachal abscess is rare for adults but should be considered in the differential of abdominal pain. Keywords: Urachus, abscess, abdominal pain P 132 ANXIETY LEVELS AND INFLUENCING FACTORS IN EMERGENCY DEPARTMENT PATIENTS’ RELATIVES Secgin Bahar Sezgin1, Hakan Topacoglu2, Ozlem Dikme3, Ozgur Dikme2, Sıla Sadıllıoglu2, Sennaz K. Hussein4 1Umraniye Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey 2Istanbul Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey 3Koç University Hospital, Department of Emergency Medicine, Istanbul, Turkey 4Buyukcekmece State Hospital, Emergency Medicine Clinic, Istanbul, Turkey Objective: Anxiety is an abnormal, groundless state of restlessness characterized by over-stimulation of autonomic nervous system accompanied by concern, fear and obsession. The aim of study was to measure anxiety levels in relatives of emergency department (ED) patients upon arrival to ED and determination of the factors affecting it. Methods: 687 patient relatives aged 18 and older who came to the ED in the 24-hour period in seven days were included in the prospective, cross-sectional survey study. Data was obtained on demographic and personally identifying information of the patient relatives participating in the study. For the purpose, State-Trait Anxiety Inventory State Anxiety (STAI-S) and Trait Anxiety (STAI-T) surveys were conducted. Results: For the patient relatives participating in the study, STAI-S average was 46.1±7.8 while their STAI-T average was 45.4±8.0 (STAI-S range=22-70, STAI-T range=24-64) (t-test, p= 0.020). Patients that had been hospitalized before, there was no statistically significant differences in STAI-S while significantly higher STAI-T values were observed (t-test, p = 0.018). It was found out that degree of kinship of patient relatives, previous history of hospitalization, having history of surgery, escorting patients previously during hospitalization and confidence in hospitals all have effect on STAI values. According to STAI scale, 42 was taken as the boundary value. Base on this boundary value mean scores of the patients were found high. Conclusion: In this study societal anxiety level was determined to be high. Reasons for patients anxiety and their expectations can help to plan the measures that will reduce their anxiety and contribute to the patients management. Keywords: Anxiety levels, emergency department, patient's relatives

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
270
P 133 BILATERAL SUBDURAL HEMATOMA PRESENTING WITH STATUS EPILEPTICUS Hande Candemir, Ezgi Ceylan, Halil Ibrahim Atalay, Erkman Sanri, Haldun Akoglu, Ozge Ecmel Onur, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Introduction: Bleeding between the dura and the arachnoid membranes is called subdural hematoma (SH). Subdural hematomas are usually caused by trauma but they can also be spontaneous or caused by a procedure. It may present in various ways and in this case it was status epilepticus. Case: A 77-year-old female patient with history of Alzheimer’s disease and hypertension attended to ER with partial seizure. She denied any history of seizure then. History of trauma, headache or any other neurological problem was not present. The initial treatment with midazolam was not successful. Her relatives stated that she was seizing for more than 30 minutes, so it was accepted as a status epilepticus. Patient was intubated to protect the airway. Her brain computed tomography revealed bilateral chronic SHs and she was transferred to OR. Discussion: There are three types of SH; acute SH is diagnosed within 72 hours and is denser than the brain paranchyma on CT. Subacute SH diagnosed within 3-20 days and is isodense or denser than the brain paranchma. Chronic SH is diagnosed after 21 days of the bleeding and is hypodense. However, a subdural hematoma may contain all three types of bleedings at the same time. Treatment of a subdural hematoma is surgery or close monitorization of the patient until resolution. Clinical presentation of chronic subdural hematoma is often insidious with symptoms like; decreased level of consciousness, headache, change of personality, loss of cognitive function and memory, motor deficits and seizures. Causes of chronic subdural hematoma include; head trauma, acute subdural hematoma. Prognosis may depend on the volume of hematoma, amount of the midline shift, compression of the brainstem or basal cisterns and having other traumatic intraparenchymal lesions. Conclusion: In patients of first seizure, subdural hematoma should be excluded if the seizure is persistent and unresponsive to treatment. Keywords: Seizure, subdural hematoma, CT P 134 STERNOCLAVICULAR DISLOCATION Tanju Tasyurek, Halil Ibrahim Atalay, Atanur Ince, Erkman Sanri, Haldun Akoglu, Ozge Onur, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Introduction: Sternoclavicular dislocations (SD) supervenes upon high-energy trauma directly to medial clavicle, shoulder belt or medial compression of shoulder belt. We intended to discuss the management of SD via a case. Case: A 43-years-old male patient was brought to the ER after a car accident. During the accident, the driver (patient) hit his chest to the vehicle's dashboard. GCS: 15, vital signs; TA: 114/78 mmHg HR: 112 beats/min SpO2: 99% Temp: 36.3 C RR: 15 / min. There were no pathological physical examination findings except the increased sensitivity to palpation spreading from right shoulder to the sternum, and ROM was limited at the right shoulder. It was determined from the images of the patient that right sternoclavicular joint (SCJ) was dislocated, the head of the right clavicle displaced to posterior of sternum. Reduction of the joint was performed with appropriate sedo-analgesia by Cunningham technique. Control imaging showed that clavicle was successfully replaced to its anatomical position. Discussion: SCJ dislocations can be anterior or posterior. Although posterior SCJ dislocations are rare, they can cause significant vascular injury. Posterior displacement of the clavicle can cause breathing difficulty from tracheal compression, lacerate or occlude the subclavian or brachiocephalic vessels, damage the lung parenchyma causing a pneumothorax, or injure the laryngeal nerve. Examination may reveal a prominence at the SCJ with anterior dislocation, but a corresponding depression may be difficult to detect with a posterior dislocation. It is important to check pulses in the effected extremity. Plain radiographies are not sensitive for detecting SC dislocation. It is best to obtain a contrast-enhanced CT of the chest if there is any suspicion for posterior dislocation or internal injury. A true anterior dislocation should be reduced within 12 to 24 hours. Posterior SC dislocations become increasingly difficult to reduce after 24 hours. Keywords: Dislocation, CT, sternoclavicular

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
271
P 135 ÇAKMAK GAZI KULLANIMINA BAĞLI GELİŞEN NADİR BİR ÖLÜM NEDENİ; DİFFÜZ ALVEOLAR HEMORAJİ Serdar Can1, Serhat Örün1, Göksu Afacan2, Ayhan Aköz3, Ali Duman3
1Iğdır Devlet Hastanesi, Acil Servis Birimi, Iğdır 2Erzurum Bölge Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Erzurum 3Adnan Menderes Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Aydın Amaç: Çakmak gazı olarak da bilinen bütan gazının inhalasyonu hafif sarhoşluktan aşırı neşe ve halüsinasyon görmeye kadar değişen belirtilere neden olur. Bazı durumlarda ise ölüme neden olmaktadır. Bizim vakamızda bütan gazı alımına bağlı alveolalar hemoraji gelişmiştir. Bu vakayı sunmaktaki amacımız bütan gazı alımına bağlı oluşan alveolar hemoraji sonucu yaşamını yitiren olguyla ilgili tecrübelerimizi paylaşmaktır. Olgu: On beş yaşında erkek hasta evinde baygın bulunarak 112 ambulans hizmeti ile acil servisimize getirildi. Bilinci kapalı olan hastanın spontan kardiyak atımı ve solunumu yoktu, glaskow koma skoru 3 idi. hastaya kardiyopulmoner resüsitasyon(CPR) işlemi başlandı. İşlem sırasında hızlı-seri entübe edilen hastanın entübasyon tüpünden masif hemorajisinin olduğu tespit edildi. Taze donmuş plazma ve eritrosit süspansiyonu replasmanı planlanan hastanın Hg:14,3 g/dl, INR:1,34, Pt:16,8 tespit edildi. Hasta yakınlarından alınan anamnezde hastanın çakmak gazı kullanma alışkanlığının olduğu öğrenildi,gün içinde bütan gazını poşete doldurarak inhale eden hastanın daha sonra çakmak gazı tüpünü ağzına yüksek miktarda sıkarak kullandığı öğrenildi. 80 dakika CPR uygulana hasta spontan solunum ve kardiyak atımı olmaması nedeniyle exitus kabul edildi. Sonuç: Bütan gazı alımı sonucu hipoksi, pnomoni, kalp yetmezliği, kardiyak arrest ve kusmaya bağı aspirasyon nedeniyle ölümler oluşabilmektedir. Fakat nadiren alveolar hemoraji gelişmektedir. Diffüz alveolar hemoraji etyolojisi geniş ve mortalitesi yüksek bir hastalıktır. Özellikle acil servislerde çakmak gazı kullanımı öyküsü olan hastalarda akılda tutulmalı ve hızla tedaviye başlanmalıdır. Anahtar Kelimeler: Bütan gazı, çakmak gazı, diffüz alveolar hemoraji P 136 HYPOKALEMIC PARALYSIS DUE TO METHYLPREDNISOLONE TREATMENT Zuhal Kalyon, Okkes Yilmaz Cinar, Ezgi Ceylan, Erkman Sanri, Haldun Akoglu, Ozge Ecmel Onur, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Introduction: Hypokalemia is defined as the serum potassium level of <3.5 mEq/L. Symptoms of hypokalemia is determined by the depth of hypokalemia, the cell or the organ type to be affected, and the general health of the patient. Symptoms can be non-specific, including palpitations, skeletal muscle weakness, easy fatigability, muscle pain and depression, or may range from myalgia to life-threating paralysis and dysrhythmias. Corticosteroids effect Na-K-ATPaz pump and may cause hypokalemia. We present a case of hypokalemic paralysis due to methylprednisolone. Case: 35-year-old man admitted to ER suffering from muscle weakness starting from legs and ascending to his trunk and arms. The patient was on methylprednisolone for sinusitis. Physical examination revealed a GCS of 15, quadrilateral weakness due to lower motor neuron involvement, and diminished deep tendon reflexes. No other pathological findings were present. No acute pathologies were present on the brain CT and DW-MRI. Initial laboratory tests revealed a significant hypokalemia of 2.2 mEq/L. The complete blood count, electrolytes and coagulation parameters were in normal ranges. Venous blood gas examination revealed a pH of 7.34, bicarbonate of 25.5 mmol/L, PCO2 of 48 mmHg, lactate of 2.6 mg/L, and a base deficit of -0.3 mEq/L. Patient was diagnosed with hypokalemic paralysis according to clinical and laboratory findings. Potassium was replaced with 40 mEq/L of solution. After the treatment, serum level was increased to 3.8 mEq/L and motor weakness of the patient was resolved. Conclusion: Alterations in potassium concentration will have broad effects on muscle, cardiac, and gastrointestinal systems. Skeletal muscle cells are the first to be affected. When serum potassium level is less than 2.5 mEg/L paresthesias, depressed deep tendon reflexes, fasciculations, muscle weakness and confusion may occur. When evaluating a patient suffering from muscle weakness in the ER, hypokalemic paralysis should always be considered in the differential diagnosis. Keywords: Hypokalemic paralysis, corticosteroid, weakness

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
272
P 137 A RARE CASE: ACUTE BILATERAL RENAL INFARCTION Hande Candemir, Ezgi Ceylan, Erkman Sanri, Haldun Akoglu, Ozge Onur, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Introduction: Renal infarction (RI) is the hypoperfusion of the kidney, mostly caused from cardiological pathologies such as atrial fibrillation, injury of the renal arteries and coagulation disorders. RI is a rare disease with the incidence of 1.4%. Infarction of both kidneys at the same time is much rarer. Most common symptoms are abdominal pain, back pain or flank pain, which are similar to nephrolithiasis or pyelonephritis. We would like to present a case of bilateral renal infarction due to the exceptionally uncommon nature of this disease. Case: A 53-year-old man admitted to ER with severe abdominal pain which started a week ago. There were no other symptoms. He had a history of hypertension and diabetes mellitus. He denied any recent travel, or use of any NSAIDs. Vital signs were as follows: GCS:15, BP: 220/108 mmHg, HR: 78 bpm, SpO2 98%, Temp: 36.8 C and RR: 16 /min. There were no pathological physical examination findings except a subtle tenderness of abdomen. Laboratory examination revealed that, WBC:10.600/µL, Hg:14.1 g/dL, plt: 256.000/µL and INR:1.09. CT of the abdomen revealed partial renal infarction of both kidneys. Patient was admitted, and started on enoxaparin and acetylsalicylic acid. Discussion: Acute renal infarction is exceptionally uncommon to diagnose in the ER. Diagnosis is usually delayed or missed, because of the nonspecific nature of the symptoms. Lactate dehydrogenase level is a sensitive marker and computed tomography is gold standard for renal infarction. Hematuria and proteinuria are also seen in urine samples. Anticoagulation with warfarin or heparin is the standard treatment. Thrombectomy or angioplasty can also be performed. This diagnosis should be considered in patient with abdominal pain and history of atrial fibrillation, embolism, valvular or ischemic heart diseases. Keywords: Renal, infarct, pain P 138 NADİR GÖRÜLEN ÜST HAVAYOLU TIKANIKLIĞI NEDENİ Ufuk Akday, Sultan Özselçuk, Zeynep Kekeç Çukurova Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Adana Dil kanlanması iyi bir organdır. Kişinin kendi dilini ısırması nadir görülen bir durum olup, sıklıkla mental retardasyon ve nörolojik hastalıklar sonucu görülür. Bu yazıda; psikoz tanısı ile takip edilen ve tekrarlayan ısırmalar sonucu dilinde hematom ve ödem oluşturarak üst hava yolu tıkanıklığı ve solunum sıkıntısı oluşumuna neden olan bir olgusu tartışılmıştır. Olgu: Otuz üç yaşında, on iki yıldır psikoz tanısı ile tedavi edilen erkek hasta üç gün içinde ilerleyen solunum sıkıntısı,dilde ödem ve hematom nedeniyle acil servise başvurdu. Acilde yapılan fizik muayenesinde; genel durumu orta, kooperasyonu zayıf ve oldukça ajite idi. (GKS:9). Kulak burun boğaz muayenesinde: ağız açıklığı kısıtlı, anterior rinoskopide bilateral nasal kavite doğal idi. Orofarenks muayenesinde dilde ileri derecede ödem ve hematom mevcut idi. Acilde hastaya havayolu, solunum ve dolaşım güvenliğine yönelik değerlendirme yapıldı.buna yönelik antiödem tedavi olarak mannitol ve steroid ile uygun antibiyoterapi verildi. Olgunun kontrastlı maxillofasiyal tomografisinde dil ileri derece büyük ve ödemli olarak raporlandırılmıştır. Acil takipleri sırasında solunum sıkıntısı artan hastaya kulak burun boğaz bölümü görüşü sonucu yakınlarınında onamı alınarak trakeostomi açıldı. Sonrasında hasta reanimasyon ünitesine yatırıldı. On gün reanimasyon ünitesinde yatan hastanın dilindeki ödeminin gerilemesi üzerine kulak burun boğaz konsültasyonu istenerek trakeostomisi kapatıldı. Takiplerinde solunum sıkıntısı olmayan, kliniğinde belirgin düzelme saptanan hasta taburcu edildi. Sonuç olarak Psikoz tanılı hastalarda hava yolu açıklığını etkileyen, solunum sıkıntısına neden olabilecek dil ısırmaları konusunda uyanık olunmalı ve Nöropsikiatrik durumun düzeltilmesine yönelik gerekli tedavilerin yapılması yanında koruyucu önlemler alınarak dilinin ısırması engellenmelidir. Anahtar Kelimeler: Havayolu tıkanıklığı, dilde ısırma, hematom

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
273
P 139 A CASE OF LUDWIG’S ANGINA Halil Ibrahim Atalay, Murat Doganay, Hande Candemir, Oguzhan Demir, Erkman Sanri, Musa Adanc, Haldun Akoglu, Ozge Onur, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Introduction: Ludwig’s Angina (LA) is a cellulite which starts and penetrates rapidly and aggressively in submandibular space without any lymphadenopathy. It needs to be observed closely as it may cause airway obstruction. In this case, we discussed a patient who admitted to ER with submandibular space infection causing dyspnea. Case: A 51-year-old man admitted to the ER with the complaint of swelling which spread from the bottom of the chin through the neck, with severe pain and fever. He was on amoxicilin-clavulanate for 5 days for his tooth abscess without any improvement. On the contrary, he stated to feel an “obstruction” in his throat and shortness of breath. Vital signs were as follows: GCS:15, BP:107/67mmHg, HR:136bpm, SpO2:94%, Fever: 39,6 RR: 24/min. On physical examination, he had stridor, oropharynx was hyperemic and tonsils were hypertrophic. Left lower molar teeth and the gingiva that surrounds it were abscetic. A swelling of 5-cm was present beneath the mandibula, which created a mass effect. There were no other pathological findings. WBC was 19800/mcL, CRP:235mg/dL, procalcitonin:5.45ng/mL, lactate:4.3mmol/L. All other laboratory tests were normal. Contrast-enhanced-CT revealed multiple abscess formations extending from the left submandibular area to trachea, deviating it to the right and posterior. Diagnosis of Ludwig’s Angina was considered and empiric antibiotics, iv fluids and antipyretics were started. He was taken to the OR, and drainage of the abscess was performed. Discussion: The most common symptoms of LA are fever, malaise, the leak of saliva, dysphagia and neck pain. CT is the gold standard imagining. In the ER, primary goal is to protection of the airway. Empiric antibiotic therapy has a vital importance. Ampicillin or clindamycin together with metronidazole is recommended. If the swelling on the neck starts to fluctuate or an abscess is formed, needle aspiration and drainage of the abscess should be performed. Keywords: Ludwig's angina, fever, swelling P 140 COLD INDUCED KOUNIS SYNDROME Okkes Yilmaz Cinar, Halil Ibrahim Atalay, Bulent Taskin, Cigdem Ozpolat, Haldun Akoglu, Ozge Onur, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Introduction: Kounis syndrome (KS) is a coronary hypersensitivity disorder induced by environmental exposures, drugs, and coronary stents which may manifest as coronary spasm, acute myocardial infarction and stent thrombosis. KS is related to mast cell degranulation resulting from inflammatory mediators. We report a case of cold-induced urticaria complicated as Kounis syndrome admitted to our ED on a cold night. Case: A 32-years-old male was brought to ED with the complaints of chest discomfort, shortness of breath, rashes and cold sweating. His vital signs were as follows: HR:134bpm, BP:80/50mm/Hg, and T:35°C. His electrocardiogram revealed sinus tachycardia without ischemic signs. On examination, his body was covered with generalized erythematous rashes and he was cold. He was treated with adrenaline, difenhydramine, and prednisone. His control BP was 105/65 mmHg, and HR was 105bpm. The first high sensitivity cardiac troponin level was 0.01 (normal values 0.00–0.04), and control troponin level was 0.6. His symptoms resolved gradually and he was transferred to a CCU as NSTEMI. His coronary angiography was normal. The patient was diagnosed as kounis syndrome (KS) variant 1. He was advised to avoid cold weather and to use prophylactic antihistamines and corticosteroids. Discussion: Three types of KS have been previously described. Variant I is caused by coronary artery spasm. In Variant II, allergic events induce plaque rupture. Variant III is observed with coronary stent hypersensitivity. Variant I has the best prognosis. This syndrome has been observed in every race, age and geographic location. It seems to be a common but infrequently reported and recognized in clinical practice. A high index of suspicion should ensue in patients with systemic allergic reactions associated with clinical, electrocardiographic and laboratory findings of acute myocardial ischemia. Keywords: Kounis syndrome, urticaria, cold

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
274
P 141 VOCAL CORD HEMATOMA DUE TO BLUNT NECK TRAUMA Mehmet Fatih Korcak, Halil Ibrahim Atalay, Cigdem Ozpolat, Haldun Akoglu, Ozge Onur, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Introduction: Larynx and adjacent anatomical structures have complicated physiological functions and mechanical features. In the management of laryngeal trauma, maintenance of airway patency has the utmost priority. Hemorrhage of the vocal cords secondary to blunt neck trauma can lead to compromised airway even in patients with minimal clinical findings. We reported a 20-year-old male patient who had a blunt anterior neck trauma with unilateral hematoma of a vocal cord. Case: A 20-year-old man presented to our ED with the gradual increase in the complaints of hoarseness, dysphagia and mild shortness of breath. He stated to receive punches to his anterior neck the day before. He was speaking in a high-pitched whisper and had inspiratory stridor. His vital signs were normal despite a respiration rate of 33/minute. On physical examination, a 2-cm area of ecchymosis over the thyroid cartilage with an intact skin was detected with no crepitus or deformity. The trachea was in the midline, and examination of the oral cavity was normal. The CT of the neck revealed a laryngeal hematoma. Otolaryngological evaluation, including laryngoscopy, revealed a hematoma on the right vocal cord. Patient was observed in the ward for a day and discharged to home since he was stabile then. Discussion: Isolated hemorrhage of the vocal cords secondary to blunt neck trauma is a rare but clinically important disorder since it may transform the condition to a life-threatening event with the development of upper airway obstruction. So, the main priority is to secure the airway of the patient. Even in the absence of signs of significant soft-tissue injury, dysphonia or stridor, a true airway emergency may still occur. All patients with blunt trauma of the neck should undergo laryngoscopy for assessment and monitorization of their airway. Keywords: Vocal cord, hematoma, neck trauma P 142 UNILATERAL OCCLUSION OF THE VERTEBRAL ARTERY PRESENTING WITH CONFOUNDING SYMPTOMS Halil Ibrahim Atalay, Mehmet Fatih Korcak, Tugba Mamak, Erkman Sanri, Cigdem Ozpolat, Haldun Akoglu, Ozge Onur, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Introduction: Ischemic stroke is a major cause for paralysis and paresthesia. The atherosclerotic narrowing and development of thrombus is the major cause of ischemic stroke, which are mostly seen in common carotis, middle cerebral, basilary and vertebral arteries. We present a case of vertebral artery (VA) occlusion with an atypical clinical presentation. Case: 46-years-old male with no history of diseases admitted to ER with dysphagia, numbness at the left half of his face and left lower extremity without any weakness. His vital signs were as follows: GCS 15, BP:100/71 mmHg, HR:85bpm, SpO2:98%, Fever:36,6C. On physical examination, paresthesia of the left half of the face and left lower extremity, decreased gag and deep tendon reflexes on the left, bilateral flexor babinski reflexes, ataxic cerebellar examination without dysmetry or dysdiadochokinesia was found. EKG was sinus rhythm. Lab exam revelaed WBC:12000/mcL, and lactate:1,1 mmol/L. Liver and kidney function tests and electrolytes were normal. No acute pathological findings were imminent in Cranial CT, CT Angiogram and Diffusion MRI. In cervical angiogram, right vertebral artery was narrower beginning from the level of C7 vertebra to C4, and no flow was present at the level of C4. VA dissection or VA occlusion were considered. In saturated-MRI no dissection was present, however, a thrombus at the distal VA at the level of C4 vertebra was observed and diagnosis of VA occlusion was performed. Patient was hospitalized and started on acetylsalicylic acid. Seven days after the hospitalization he was discharged with minimal sequela. Discussion: Major symptoms of VA occlusion are headache, dizziness, tinnitus, ataxia, paralysis and paresthesia. CT and MRI angiogram may help to diagnose VA dissection and occlusion. Patients should be treated with anticoagulant, antiplatelet, antidiabetic, antihypertensive and anticholesterol agents. Keywords: Vertebral artery, occlusion, ataxia

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
275
P 143 DIAGNOSTIC VALUES OF IRISIN, AND VISFATIN IN EXPERIMENTAL TESTICULAR TORSION Fatma Saraç1, Selman Yeniocak2, Sevgi Büyükbeşe Sarsu3, Esma Yücetaş4, Vakur Olgaç5, Mehmet Toptaş6, Macit Koldaş4 1University of Health Sciences, Haseki Training and Research Hospital, Department of Pediatric Surgery. Istanbul, Turkey 2University of Health Sciences, Haseki Training and Research Hospital, Department of Emergency Medicine. Istanbul, Turkey 3Cengiz Gökcek Obstetrics and Children’s Hospital, Department of Pediatric Surgery. Gaziantep, Turkey 4University of Health Sciences, Haseki Training and Research Hospital, Department of Biochemistry. Istanbul, Turkey 5Istanbul University, Institute of Oncology, Department of Pathology. Istanbul, Turkey 6University of Health Sciences, Haseki Training and Research Hospital, Department of Anesthesia and Reanimation, Istanbul, Turkey Objective: Testicular torsion is one of the most important causes of acute scrotum in children, and young men. If not diagnosed, and treated in due time, it may result in loss of the affected testis, so early diagnosis has utmost importance. Very scarce number of serum laboratory parametres might be used in the early diagnosis of the patients with testicular torsion. We planned this study in consideration of the possible significance of the changes in serum irisin, and visfatin levels in the diagnosis of testicular torsion. Method: In our study we used a total of 28 Wistar-Hannover strain rats in torsion, and control groups. In the control groups at 2., and 4. hours after resection of gubernaculum, and exposure of the testis, blood samples, and specimens of testicular tissue were retrieved. In the torsion groups, left testis was torsioned, and at 2., and 4. hours blood samples, and specimens of testicular tissue were retrieved for analysis. At the end of the study all animals were sacrificed. Results: A statistically significant difference was not detected in rats with testicular torsion regarding mean irisin, and visfatin levels at 2., and 4. hours when compared with the control group. (p=0.559, p=0.125, p=0.631, and p=0.435, respectively ). A statistically significant change was not detected between the testicular torsion, and control groups as for mean 4., and 2. hour-measurements. (p=0.735, p=0.939, p=0.398, and p=0.555, respectively). Mean differences in irisin, and visfatin levels were not statistically significant different between groups (p=0.655,and p=0.611, respectively). Conclusion: In our experimental testicular torsion method, we couldn’t find a statistically significant difference between serum levels of irisin, and visfatin. We think that additional studies are needed on this issue Keywords: Testicular torsion, experimental, irisin, visfatin P 144 POLYCYSTIC KIDNEY DISEASE AS A SERIOUS CAUSE OF HEMORRHAGE Cemalettin Sakal1, Abdullah Taşcı1, Özge Onur2
1Fatih Sultan Mehmet Training and Research Hospital, Istanbul, Turkey 2Marmara University Hospital, Istanbul, Turkey Introduction: Polycystic kidney disease (PKD) is a systemic disorder mainly involving the kidney. Early hypertension and progressive renal failure due to massive enlargement of cysts and fibrosis are hallmarks of the disease. Complications in PKD usually result from kidney involvement and include cyst bleeding and cyst infection. Most patients admit to emergency room with back pain, abdominal pain or blood in urine. If left alone, hemorrhagic cyst may cause infection, sepsis or other life-threatening complications easily. So early detection and effective therapy is necessary. Case: A 59-year-old man was admitted to our emergency department because of abdominal pain and distention with history of hypertension, chronic renal failure and coronary artery bypass greft. Vital signs were normal. Physical examination revealed general abdominal tenderness and distention, costovertebral angle tenderness on left side. In his rectal digital examination, there was no evidence of gastrointestinal hemorrhage. Electrocardiography was normal. Laboratory tests were normal except blood urea nitrogen 73mg/ dL (normal 8.9-20.6 mg/dL), creatine 5,58 mg/dL(normal 0.72-1.25 mg/dL) and hemoglobin 6,3 (normal 14.1 - 18.1 mg/dL ). CT scan of the abdomen revealed no evidence of obstruction or intraperitoneal free air. Both kidneys are bigger than normal and include hemorrhagic multiple cortical cysts( autosomal dominant polycystic kidney disease). So renal cystic hemorrhage was diagnosed and admitted to hospital. Discussion: Renal cystic hemorrhage especially in PKD is a rare but life- threating entity. So emergency physicians should be aware of this serious condition. Keywords: Polycystic Kidney disease, renal hemorrhage, urological emergency

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
276
P 145 DON’T SAY THAT IT’S JUST AT THE LEFT UPPER QUADRANT Tanju Tasyurek, Halil Ibrahim Atalay, Atanur Ince, Erkman Sanri, Haldun Akoglu, Ozge Onur, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Introduction: Most of the time, the cause of abdominal pain is non-specific and benign. Critical thinking is needed to determine if observation or further evaluation should be considered. We present a case of adrenal hematoma presenting with subtle abdominal pain. Case: 64-year-old male patient with known malign melanoma admitted to the ER with abdominal pain and nausea. He indicated metastases to the lungs and received chemotherapy 15 days ago. His vital signs were as follows: GCS:15, BP:142/75 mmHg, HR:76 bpm, SpO2:96%, T: 36C. No pathological findings were present on physical examination except a subtle tenderness at the left upper quadrant of the abdomen. Laboratory test (CBC, kidney function, liver function and urinalysis) did not reveal any abnormalities. A 60x50 mm hematoma of the left adrenal gland was determined with contrast-enhanced abdominal CT. No indication for operation was found and the patient was discharged from hospital with planned outpatient follow-up. Discussion: The localization, duration, type and presence of underlying disease should address the cause of non-traumatic abdominal pain. Dividing abdomen into quadrants to diagnose or to rule out prominent serious causes of pathology is a widely used approach. In patients with acute localized abdominal pain, the differential diagnosis can be considered in terms of "symptom clusters" in order to guide further management. There is limited literature on the usefulness of laboratory and radiologic imaging in evaluation of acute left upper quadrant abdominal pain, and clinical features should guide testing. US and CT imaging may be used when there is high clinical suspicion for an acute abdominal process, particularly in the elderly, immunosuppressed, or trauma patient. In our case, although acute causes of possible diagnosis were excluded with physical examination and laboratory results, due to advanced age and underlying immunosuppressed state, a CT scan was performed and adrenal hematoma was diagnosed. Keywords: Adrenal, hematoma, pain P 146 ACİL SERVİSTE DİKKAT EDİLMESİ GEREKEN BİR TANI: DOKSİSİKLİNE BAĞLI ÖZEFAJİT Serhat Karaman1, Burak Hasgül1, Serhat Koyuncu1, Nurşah Başol1, Abdullah Özgür Yeniova2
1Gaziosmanpaşa Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Tokat 2Gaziosmanpaşa Üniversitesi Tıp Fakültesi, Gastroenteroloji Anabilim Dalı, Tokat İlaç kullanımı sonrası özofajit nadir görülen, kliniği değişebilen bir durumdur. 650’den fazla ilaca bağlı özofajit vakası ve 30’un üzerinde sorumlu ilaç bilinmektedir. Literatürde ilaca bağlı özefajitlerin yaklaşık %50’sini tetrasiklin, doksisiklin ve klindamisinin oluşturduğu bildirilmektedir. İlaçların kapsül formları, tablet formlarına kıyasla daha sık özefagus yaralanmasına neden olur. Kapsül formundaki ilaçların özofageal yüzeye yapışmasının daha kolay olması sebep olarak gösterilmektedir. İlacın özofagusta temas süresini uzatan ve yapışmasına neden olan faktör olarak; ilaçla beraber az su ile alımı ile ilaç alımı akabinde yatma gibi sebepler gösterilmiştir. 50 yaşında kadın hasta acil servise göğsünde şiddetli bir yanma hissi ve mide ağrısı şikayeti ile başvurdu. Şikayetinin dört gündür olduğunu ve her gün bu şikayetle acil servise başvurduğunu, verilen ilaçlarla kısmi rahatlama olduğu ve sonrasında aynı şikayetlerinin tekrar ettiğini ifade etti. Öyküsünde bir haftadır genital enfeksiyon nedeniyle doksisiklin kapsül kullandığı öğrenildi. İlaçları bol su ile almadığını ifade eden hastanın fizik muayenesinde; TA: 130/80 mm/Hg, ateş 36 ° idi. EKG’ sinde iskemi açısından anlamlıbir bulgu izlenmedi. Akciğer ve ayakta direkt batın grafisinde acil patoloji olmayan hastanın acilde yapılan laboratuar değerleri de normal aralıkdaydı. Hastaya acil serviste iv. sıvı desteği yanında proton pompa inhibitörü, H2 reseptör blokeri ve anti-asit tedavi verilmesine rağmen şikayetlerinde tam bir gerileme olmaması üzerine endoskopi amaçlı gastroenteroloji kliniğine konsulte edildi. Hastanın yapılan endoskopisinde; özofagus distalinde tüm lümeni çepeçevre saran üzeri eksudalı ülsere görünüm ve midede pangastrit tespit edildi. Hasta iki hafta sonra tedavisi düzenlenerek şifa ile taburcu edildi. Acil serviste reflü ve dispeptik şikayetlerle gelen hastaları değerlendirirken; özellikle tetrasiklin grubu antibiyotiklerin kullanımının özofajit, özofageal ülserasyon ve perforasyon gibi durumlara neden olabileceğini hatırlamak gerekir. Olgumuzda genital enfeksiyon nedeniyle doksisiklin kullanımına bağlı özofajit ve pangastrit geliştiğini tespit ettik. Anahtar Kelimeler: Özefajit, doksisiklin, acil servis

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
277
P 147 A RARE CASE: DUODENAL INTRAMURAL HEMATOMA INDUCED BY THROMBOCYTOPENIA Halil Ibrahim Atalay, Okkes Yilmaz Cinar, Atanur Ince, Erkman Sanri, Haldun Akoglu, Ozge Onur, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Introduction: Ileus is partial or total obstruction of the intestines or bowel. One of the unexpected causes of the ileus is duodenal intramural hematomas (DIH). Trauma, anticoagulant drug use, coagulation disorders, interventions such as gastroscopy or ERCP are most common causes of DIH. In this case we present a case of DIH secondary to suspected thrombocytopenia. Case: 20-years-old male patient who suffered from autism and epilepsy admitted to ER with vomiting for 3 days and syncope attacks after each vomiting. Vitals were as follows: fever:36.5, HR:85bpm, BP:131/79mmHg, GCS:12/12. There were no pathological physical examination findings except tenderness and distension in his epigastrium. Laboratory results were as follows: wbc:15200µL, Hg: 11.2 g/dL, plt: 45.000/µL. All other laboratory tests were normal. Intravenous and oral contrast-enhanced abdominal CT revealed obstruction in the distal part of the duodenum. In the OR, a giant DIH was found in the second part of the duodenum, which was believed to be occur secondary to thrombocytopenia. Gastrojejunostomy was performed. After two days of hospitalization the patient was discharged. Discussion: Most common symptom of ileus is abdominal pain. The other common symptoms are nausea, vomiting and distention of the abdomen. CT which shows bowel wall thickening, intramural hyperdensity and obstruction, is helpful in diagnosis. Gastroscopy is also helpful in patients who present with GI bleeding. In the differential diagnosis, inflammatory bowel diseases, infections, neoplasms and ischemic bowel diseases should be considered. Nasogastric feeding tube insertion, bowel resting, discontinuation of the anticoagulant agents and reversal of the anticoagulation are suggested. If all these treatments fail, surgery is inevitable. In this case our patient had a big DIH which obstructed the passage totally. Conservative treatment was insufficient, so surgery was performed. Keywords: Duodenal, intramural, hematoma P 148 OUTPATIENT MANAGEMENT OF FEBRILE NEUTROPENIA AND THE UTILITY OF MASCC SCORE Emre Ciran, Halil Ibrahim Atalay, Atanur Ince, Erkman Sanri, Haldun Akoglu, Ozge Onur, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Inroduction: Febrile neutropenia(FN) is defined as total neutrophil count below 500/mm3 or presumed to be under 500/mm3 in 48 hours, body temperature over 38,3⁰C or over 38⁰C at least 1 hour. Despite prophylaxis and broad spectrum of antibiotics, patients have high morbidity and mortality. Determination of the MASCC risk-index score which integrates several clinical parameters that can be readily assessed at the bedside is a good risk predictor of complications. Case Presentation: A 58-years-old male chronic myeloid leukemia patient referred to our ED with watery diarrhea, nausea, fever, and fatigue. He was diagnosed 4 months ago and last chemotherapy was 2 weeks ago. He was alert with a fever of 38.4⁰C, BP 118/74 mmHg, and HR 122bpm. Physical examination was normal except his hyperemia in oropharynx. Lab results were normal except a WBC of 1200/mcL, Neuthrophil count of 300/mcL. MASCC score was calculated as 23 and outpatient treatment was considered. Empiric ampicillin-sulbactam and ciprofloxacin were started. After his vital signs were stabilized with IV hydration and antipyretics patient was discharged to home. Discussion and Result: In the evaluation of patients with fever and neutropenia, determination of the risk status with MASCC scoring system is recommended. A MASCC score of >= 21 suggests a low risk for severe complications. Proper empiric antibiotics should be given in less than 60 minutes. While low risk patients should take ampicillin-sulbactam and ciprofloxacin, high risk patients should be given cefephime, meropenem, imipenem or piperacillin-tazobactam. Keywords: MASCC, neutropenia, fever

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
278
P 149 ACİL SERVİSTE KARIN AĞRISININ NADİR NEDENLERİNDEN BİRİ: RENAL İNFARKT Erdem Kurt, Rohat Ak, Şebnem Zeynep Eke, Tuba Cimilli Öztürk, Özge Ecmel Onur, Arzu Emecan Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, İstanbul Renal infarkt akut karın ve yan ağrısının nadir bir nedeni olup, tanısı güç olabilir. Renal infarktın en yaygın nedenlerÖ kardÖyak hastalığa sekonder gelÖşen embolÖ, travma, pıhtılaşma bozuklukları ve konnektÖf bağ dokusu hastalıklarıdır. NadÖren ÖdÖopatik de olabilmektedir. Olgumuzda acil servise karın ağrısı şikayeti ile başvurup renal infarkt tanısı konan bir hastayı sunmayı amaçladık. 53 yaşında kadın hasta dün başlayan karın ağrısı nedenÖyle acÖl servÖse başvurdu. AnamnezÖnde bulantı-kusmasının olduğu, gaz gaÖta çıkışının Öse normal olduğu öğrenÖldÖ. MuayenesÖnde vÖtal bulguları stabÖl ÖdÖ. Tüm batında yaygın hassasÖyetÖ mevcu olup, özellÖkle batın sol kadranlarda defans ve reboundu mevcuttu. ÖzgeçmÖşÖnde geçÖrÖlmÖş derÖn ven trombozu ve pulmoner tromboemboli nedeniyle kumadinize olduğu ancak son 2 aydır ilacı kestiği öğrenildi. Laboratuar tetkiklerinde lökositoz saptandı. BÖyokÖmya değerlerÖ normaldÖ. Yapılan batın ultrasonografÖsÖnde patolojÖ saptanmaması üzerÖne kontrastlı batın tomografÖsÖ (BT) planlandı. TomografÖde Önen aorttan başlayıp sol renal artere uzanım gösteren trombüs ve böbrekte totale yakın Önfarkt alanı izlendi. Hasta üroloji kliniğine yatırıldı. Heparin infüzyonu başlanan hastaya sol nefrektomi yapılıp oral antikoagülan ile taburcu edildi. AcÖl servÖslerde daha önce tromboza eğÖlÖmÖ olup akut karın tablosu Öle başvuran hastalarda renal arter trombüsüne bağlı renal infarkt olasılığı akılda tutulmalıdır. Anahtar Kelimeler: Renal infarkt, antikoagülan, ürolojik aciller P 150 ACİL SERVİSTE KARIN AĞRISININ NADİR NEDENLERİNDEN BİRİ: OMENTUM İNFARKTI
Şebnem Zeynep Eke, Rohat Ak, Erdem Kurt, Tuba Cimilli Öztürk, Özge Ecmel Onur, Arzu Emecan Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, İstanbul Omental Önfarkt, omentum majusun kan dolaşımının bozulması sonucu gelÖşmekte, bÖr çok akut karın nedenÖnÖ taklÖt edebilmektedir. Hastaların % 90’ı sağ karın ağrısı Öle acÖl servÖslere başvurur. Olgumuzda karın ağrısı şÖkayetÖ Öle acÖl servÖsÖmÖze başvurup omentum infarktı tanısı alan bir hastayı sunmayı amaçladık. 36 yaşında erkek hasta, karın sağ tarafında ağrı, bulantı-kusma, nedeniyle acil servÖse başvurdu. Batın muayenesÖnde sağ üst ve orta kadranlarda hassasÖyet, rebaund mevcuttu. Kan tetkÖklerÖ normaldÖ. UltrasonografÖsÖnde mezenter yağ dokusunda ödem, barsak segmentlerÖ arasında mÖnÖmal serbest sıvı tespÖt edÖldÖ. Omentum Önfarktı şüphesÖ nedenÖyle BT Öle değerlendÖrÖldÖ. BT “MezenterÖk yağ doku dansÖtesÖnde artışın ÖzlendÖğÖ omental Önfarkta aÖt olduğu düşünülen görünüm, sağ parakolÖk ve pelvÖste serbest sıvı ÖzlendÖ” şeklÖnde rapor edÖldÖ. Hasta takÖbe alındı. KlÖnÖğÖnÖn kötüleşmesi üzerine laparoskopik segmental omentum rezeksiyonu uygulandı ve postoperatif ikinci günde taburcu edildi. GenellÖkle acÖl servÖslerde tanısı koyularak operasyona verÖlen akut karınlı hastaların yaklaşık % 0.1’ÖnÖ omentum Önfarktı oluşturur. Sıklıkla 4. ve 5. dekatlarda görülür. Erkeklerde 2 kat daha fazla görülür. Omentumun daha çok sağ tarafı tutulur. BÖr çok akut karın nedenÖyle karışabÖlÖr. KlÖnÖk genellÖkle nonspesÖfÖktÖr. Ağrı anÖ başlangıçlı, sağ alt kadrana veya paraumblikal bölgeye lokalizedir. Bulantı, kusma, Öştahsızlık gÖbÖ semptomlar çoğunlukla yoktur. HafÖf ya da yaygın perÖtonÖt bulgularına rastlanabÖlÖr. HafÖf lökosÖtoz ve ateş sık olmamakla bÖrlÖkte görülebÖlÖr. Hastamızda da lökosÖt ve ateş normaldÖ. Omentum Önfarktı kendi kendini sınırlayabÖlen ve cerrahÖ gerektÖrmeyebÖlen benÖgn seyÖrlÖ bÖr hastalıktır. KlÖnÖk ve radyolojÖk bulgular gereksÖz cerrahÖ gÖrÖşÖmlerÖ önlemede yol gösterÖcÖdÖr. İzlem yapılan hastaların yaklaşık %16’sında cerrahÖ tedavÖ gerekebÖlmektedÖr. Akut batın nedenlerÖnÖn büyük kısmı cerrahÖ gerektÖrÖrken, tanımlanmış tÖpÖk BT bulguları sayesÖnde kesÖn tanı alan omentum infarktlı olgular konservatif olarak tedavi edilebilme şansına sahiptir. Anahtar Kelimeler: Omentum infarktı, cerrahi aciller, karın ağrısı

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
279
P 151 GEBELİKTE KIRMIZI BAYRAK: BAŞ AĞRISI Burcu Poyraz, Ali Kaan Ataman, Emre Şancı, Neşe Çolak Oray Dokuz Eylül Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, İzmir 40 yaşındaki kadın hasta, acil servise bilinç kapalı halde getirildi. Öyküsünde 28 haftalık ikiz gebelik olduğu (parite:2, gravite:3), bilinen komorbid hastalığı olmadığı, sabah saatlerinde düşme nedeniyle kafa travması olduğu, dış merkez nöroloji polikliniğine baş ağrısı nedeniyle başvurduğu, MRG çekildikten sonra taburcu edildiği öğrenildi. Akşam saatlerinde baş ağrısının artması ve 4 kez kusma sonrası bilincinde kötüleşme ve nöbet geçirme nedeniyle ilçe devlet hastanesine başvuran hasta sonrasında hastanemize sevk edildi. Başvuruda tansiyon 160/82mmHg, nabız 90/dk, solunum sayısı 30/dk, pulseO2 %96, genel durumu kötü, bilinç kapalı, GKS: E1M3V1, pupiller anizokorik (sağ dilate) ve IR sağda negatif, sağda üst ve alt ekstremite motor güç 1/5 ve babinsky pozitif tespit edildi. Diğer fizik muayenesi gebelik hastasıyla uyumlu görünüm dışında normal idi. Hastaya hızlıca 1mg/kg dozda İV mannitol başlandı, Hızlı seri entübasyon prokololü ile entübe edildi. Hasta yakınının getirdiği dış merkez MRG raporunda subaraknoid kanama (SAK) ile uyumlu görünüm rapor edildiği öğrenildi. Acil servisimizde çekilen Beyin BT’sinde sağ temporoparietalde 50*25mm anevrizmatik görüntü ve ventikülleri dolduran yaygın SAK, ödem ve 8mm shift tespit edildi. Diğer biyokimyasal parametreleri normal saptandı. Acil nöroşirurji ve obstertri konsültasyonu yapıldı. Nöroşirurji acil operasyon düşünmedi, medikal takip önerdi. Obstetri, NST ‘de bebek kalp atımlarının yavaşlaması üzerine hastayı acil sezeryana aldı. 1500 ve 1599 gr doğan çocuklar prematüre yoğun bakıma alındı. Post op yoğun bakıma alınan hasta halen yoğun bakımda entübe halde izlenmeye devam etmektedir. Gebelikte anevrizmatik SAK nadir görülmekle birlikte önemli bir mortalite nedenidir. İlerleyen gebelik haftaları SAK riskini arttırır. En sık semptom baş ağrısıdır. Hastamızda erken dönem düşme ve baş ağrısı semptomları mevcuttu. Ancak poliklinikten istenen MRG’ sonucu yeterli değerlendirilemediğinden yada hastanın klinik durumunun iyi olması nedeniyle subaraknoid kanama raporlanmasına rağmen hasta taburcu edildi. Bizim hastamızda olduğu gibi, riskli ve özellikli hasta gruplarında ileri incelemelerin daha dikkatli değerlendirilmesi, klinik semptom varlığında taburcu edilmeden yatırılarak gözlenmesi, morbidite ve mortaliteyi önleme açısından önemlidir. Anahtar Kelimeler: Subaraknoid kanama, gebelik, baş ağrısı P 152 KUMADİNİZE HASTADA KARIN AĞRISI Azizcan Kılıç, Rohat Ak, Ebru Ünal Akoğlu, Tuba Cimilli Öztürk, Özge Ecmel Onur, Arzu Emecan Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, İstanbul Dalak rüptürü genellikle künt karın travmaları sonrası görülen ve hayatı tehdit edebilecek bir durumdur. Ayrıca, nadir olarak travma olmadan spontan dalak rüptürleri de bildirilmiştir. Spontan dalak rüptürü etyolojisi ise altı ayrı kategoride incelenir. Bunlar enfeksiyöz nedenler, neoplastik nedenler, inflamatuar nedenler, konjenital veya yapısal nedenler, iatrojenik nedenler ve idyopatik nedenlerdir. Bu sunumda warfarin sodyum kullanımı olan ve hemodiyaliz sonrası karın ağrısı, bulantı ve kusma şikayetleri ile acil servisimize başvuran bir spontan (atravmatik) dalak rüptürü olgusu sunulmuştur. Elli bir yaşında erkek hasta acil servise hemodiyaliz sonrasında başlayan karın ağrısı, bulantı, kusma şikayetleri ile başvurdu. Kronik böbrek yetmezliği nedeniyle haftada üç gün hemodiyalize giren hastanın öyküsünde sekiz ay önce geçirdiği aort ve mitral kapak replasmanı nedeniyle Warfarin sodyum (Coumadin 5 mg) kullanımı mevcuttu. Hastanın genel durumu orta, soluk görünümde, bilinci açık, oryante ve koopere idi. Vital bulguları; ateş 36,7°C, arteryel kan basıncı 86/61 mmHg, nabız 131/dk, solunum sayısı 18/ dk, oksijen satürasyonu %96 olarak ölçüldü. Fizik muayenesinde, sol üst kadran ve sol kostavertebral hassasiyeti olan hastanın defans ve reboundu yoktu. Laboratuvar incelemesinde; hemoglobin: 9,2 gr/dL, hematokrit: %29,9, lökosit: 21.000/mm3, trombosit: 326.000/mm3, CRP: 11,18, PT: 42,7 sn(11,5-15,5), INR: 4,47(0.75-1,27), kreatinin: 5,95 mg/dl, BUN: 29 mg/dl, LDH: 449U/L(125-220), ALP:179U/L(40-150), GGT:158 U/L(12-64) olarak ölçüldü. Hastanın diğer kan biyokimyasal parametreleri normal sınırlarda saptandı. Hastanın IV kontrast madde verilerek yapılan alt ve üst batın bilgisayarlı tomografisinde ‘Dalak alt polde 8 cm çaplı heterojen hipodens subkapsüller lezyon(hematom)’ izlendi. Hastaya IV 10 mg K vit, iki ünite taze donmuş plazma, iki ünite eritrosit süspansiyonu verildi. Kontrol INR: 1,7, hemoglobin: 7,8, hematokrit: %26 ölçülen hasta genel cerrahi servisine yatırıldı. Spontan dalak rüptürü oldukça nadir görülen ve tanıda yüksek şüphe gerektiren zor bir tanıdır. Travma öyküsü olmasa da hastalarda dalak rüptürü gelişebileceği unutulmamalıdır. Hızlı tanı, agresif resüsitasyon ve erken cerrahi mortalitenin önlenmesi açısından önem taşımaktadır. Anahtar Kelimeler: Dalak rüptürü, antikoagülan, cerrahi aciller

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
280
P 153 DİZ ÇIKIĞI VE POPLİTEAL ARTER YARALANMASI OLAN BİR OLGU: POPLİTEAL ARTER TROMBOZU Ramazan Özel1, İbrahim Altun2, Şenol Ardıç1, Ayşegül Gümrükçü1, Bestami Köse1, Gökhan Peker2, Süleyman Türedi1
1Sağlık Bilimleri Üniversitesi Trabzon Kanuni Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Trabzon 2Sağlık Bilimleri Üniversitesi Trabzon Kanuni Eğitim ve Araştırma Hastanesi, Ortopedi Bölümü, Trabzon Giriş: Tüm travmaların yaklaşık % 2-3’ünü vasküler travmalar, bunların % 19’unu da popliteal vasküler yaralanmalar oluşturmaktadır(1). Acil servis başvurularında diz çıkıkları ve/veya beraberinde popliteal damar yaralanması ise nadir görülen durumlardır. Künt diz travmaları acil servislerde çoğunlukla atel yapılarak taburcu edilmektedir. Hastaların bu tür klinik durumlarda acil servsilerde takip sürelerinin uzun tutulması yada yatırılarak takip edilmesi gerekebileceğini olgumuzla göstermeyi amaçladık. Olgu: 21y bayan hasta, araç içi trafik kazası nedeniyle acil servise 112 tarafından getirildi. Özgeçmişinde kronik hastalık öyküsü olmadığı öğrenilen hasta bilinci açık, oryante ve koopereydi.Vital bulgular; TA 140/ 70 mmHg, nabız 70 atım/ dak, ateş 37.2 C ve Sa02 % 96 idi. Glaskow koma skoru 15 olan hastanın fizik muayenesinde kafa travması yok, SS, KVS, SSS ve gastrointestinal muayenesi normal olarak değerlendirildi. Bilateral üst ekstremite muayenesinde nabızlar açık ve eşit, travma izi yoktu. Alt ekstremite muayenesinde ise sol dizde subluksasyon, ödem ve hareketle hassasiyet mevcut, palpasyonla patella morfolojisi normal ve aktif quadriceps çekme testi negatif olarak değerlendirildi. Bilateral alt ekstremite nabızlar açık ve eşit idi. Yapılan FAST USG’de batın içi serbest mai tespit edilmedi. Bakılan Hb takibinde ilk Hb:13.2 takibinde ise Hb:13.0 idi. PLT:300.000, APTT:23.1, INR:0.98 olarak geldi. Çekilen direkt grafi ve tomografisinde sol diz tibia proksimali anteriorunda minimal nondeplase kırık mevcut idi (Resim 1). Unstabil diz eklemi olarak değerlendirilen hasta takip amaçlı ortopedi tarafından atel yapılarak interne edildi. Yatışının ikinci gününde ağrı ve ödem artışı, sol dorsalis pedis nabzı alınamaması nedeniyle sol alt ekstremite anjio BT çekildi. Anjio BT’de popliteal arter trombozu (Resim 2) tespit edildi. Kalp damar cerrahisi tarafından embolektomi yapıldı ve sonrasında yatışının üçüncü gününde fasyotomi (Resim 3), plastik cerrahi ile takip edilerek yara yerine flep (Resim4) yapıldı. Yatışının 36.gününde şifa ile taburcu edildi. Sonuç: Popliteal arter yaralanmaları multidisipliner yaklaşım gösteren klinik durumlardır. Acil hekimi ilk muayene bulgularına güvenmemeli ve bu tür durumlarda klinik takibi önemsemelidir. Anahtar Kelimeler: Popliteal arter trombozu, diz çıkığı, embolektomi, fasyotomi P 154 ANALYSIS OF HOMELESS PATIENTS BROUGHT INTO THE EMERGENCY SERVICE BY AMBULANCE Selman Yeniocak1, Asım Kalkan1, Özgür Söğüt1, Gökçe Akgül Karadana2, Mehmet Toptaş3
1University of Health Sciences, Haseki Training and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey 2Koc University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey 3University of Health Sciences, Haseki Training and Research Hospital, Clinic of Anesthesiology and Reanimation, Istanbul, Turkey Objective: Since homeless individuals have a higher risk of encountering health problems relative to the population in general, indications, and frequencies of referrals to the emergency services demonstrate variations. Our aim in this study is to analyse medical problems, and the issues to be heeded by emergency service physicians who will get contact with homeless patients by means of evaluation of demographic, and clinical characteristics of these patients. Materials and Methods: The medical files of homeless adult patients who were brought into the Clinics of Emergency Medicine by 112 Ambulance Team between January 2014, and December 2014.were retrospectively analyzed. Results: A total of 167 patients were included in the study. The homeles patients included in the study were referred to the hospital with traumatic (n=36;21.56%), and non-traumatic (n=131; 78.44 %) indications. The study population consisted of 137 male (82.4 %), and 30 female (17.96 %) patients. The mean ages of the patients who consulted with traumatic, and non-traumatic indications were 36.9±14.4, and 47.3±15.2 years, respectively. The patients with non-traumatic indications who consulted to our emergency department had clouded consciousness (n=39, 23.35 %), followed by deterioration in general health state (n=26, 15.57%), shortness of breath (n=25;14.97 %), and abdominal pain (n=21; 12.57%). The patients who were brought into emergency service because of a traumatic event had most frequently experienced traffic accident (n=13; 7.78%), followed by penetrating stab wounds (n=9; 5.39%). Four (2.4 %) homeless patients exited in the emergency service, while 3 (1.8%) patients were discharged from the emergency service, and the remaining 160 (95.8 %) patients were hospitalized. Conclusion: In this study we have concluded that rates of hospital stay among homeless patients were similar to those of geriatric patients, but much higher in comparison with normal population. Anahtar Kelimeler: Homelessness, homeless patient, emergency department visit, hospital stay rates

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
281
P 155 CASE REPORT: A CASE OF SIGMOID VOLVULUS PRESENTING NAUSEA AND ABDOMINAL PAIN IN EMERGENCY MEDICINE
Selin Bulut, Vermi Değerli, Serdar Beden Bozyaka Training and Research Hospital, Clinic of Emergency Medicine, Izmir, Turkey Introduction: Volvulus refers to torsion of a segment of the alimentary tract, which often leads to bowel obstruction. The most common sites of volvulus are the sigmoid colon and cecum. The majority of patients with sigmoid volvulus present with the insidious onset of slowly progressive abdominal pain, nausea, abdominal distension and constipation. Sigmoid volvulus is an important emergency which requires rapid detorsion of the affected bowel. Emergency diagnosis is crucial. Case Presentation: 88 year old female, with hypertansion and cerebrovascular disease history presented to the emergency department with nausea and abdominal pain for 2 days. There was no associated trauma, fever, diarrhoea, recent travel or any surgical history. On examination the patient was dehydrated, with normal vital signs. Breath sounds were clear bilaterally and heart sounds were as a regulary rate without murmurs. The abdomen was distended with tympanic percussion tones in all quadrants. Digital rectal examination revealed an empty rectum.The patient’s laboratory results were all normal. Her chest and abdominal x-rays strongly suggested a sigmoid volvulus due to the presence of a distended bowel loop arising from the pelvis which projected over the epigastrium, the “coffee bean sign”, scarcity of gas in the distal sigmoid and rectum. Computed tomography (CT) images were read by the staff radiologist as sigmoid volvulus with severe dilation of the colon. A nasogastric tube and foley catheter were placed. Surgical consultation were requested. The patient was taken to the operating room for exploratory laparotomy. No intraoperative complications were noted, and patient was transferred to the surgical ICU. The abdominal distension resolved, stools were passed and she was discharged after 8 days of hospitalization. Discussion: Sigmoid volvulus is a surgical emergency which requires prompt diagnosis, resuscitation and management. Urgent detorsion and assessment of the bowel mucosa must be performed. Keywords: Volvulus, sigmoid colon, abdominal distension, nausea P 156 AKUT BÖBREK YETMEZLİĞİ İLE PREZENTE OLAN WEGENER GRANÜLOMATOZİSİ Elçin Ömercikoğlu1, Muharrem Doğan1, Abide Merve Manap1, Onur Yeşil1, Özge Ecmel Onur2
1 Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul 2Marmara Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, İstanbul Amaç ve Giriş: Wegener granülomatozisi (WG) solunum yollarının tutulumuyla karakterize, vaskülit ve glomerülonefritin eşlik ettiği bir hastalıktır. Küçük arter ve venüllerin sistemik tutulumuyla karakterizedir. Sınırlı ve generalize formu bulunmaktadır. Generalize WG’de solunum yolları, böbrek ve yaygın sistemik vaskuler tutulum vardır. Sınırlı WG’de böbrek tutulumu yoktur ve hastalık yavaş seyirlidir. Bu vakada, akut böbrek yetmezliği tablosu (ABY) ile gelen bir hastanın tanı süreci anlatılmıştır. Olgu: 30 yaşında kadın hasta nefes darlığı, halsizlik ve döküntü şikayetleriyle başvurdu. 2 ay önce solunum yolu enfeksiyonu nedeniyle antibiyotik kullanımı, sonrasında ABY gelişmesi üzerine hemodiyaliz aldığı öğrenildi. Vitalleri stabil. Muayenesinde bibaziler krepitan ralleri ve ciltte yaygın peteşileri mevcuttu. Tetkiklerinde pH:6.9, pO2:66, pCO2:15, wbc:20.000, Hb:11, Plt:253.000, Kreatinin:12, CRP:15, Na:126, K:1.7 olarak görüldü. Dahiliyeyle konsülte edilerek yoğun bakımda diyalize alınarak takibinde WG tanısı almıştır. Tartışma: WG; akciğerler ve diğer sistemleri tutan nekrotizan granülomlar ve vaskülit ile karakterizedir. Her yaşta görülebilir. Prezentasyonlar çeşitli olmakla birlikte genellikle solunum yollarına ait semptomlar sık görülmektedir. Vakaların %95’inde pulmoner tutulum vardır. Ateş, halsizlik, iştahsızlık, kilo kaybı, eklem ağrıları ve cilt lezyonları, öksürük, nefes darlığı, hemoptizi, atelektazi, pnömoni ve bunlara bağlı manifestasyonlar görülebilir. Böbrek tutulumu genellikle asemptomatiktir. Eritrosit sedimentasyon hızı hastalığın aktivitesine bağlı normal yada yüksek bulunabilir. Tedavinin takibi açısından değerlidir. Böbrek tutulumunu değerlendirmede idrar tahlili, üre, kreatinin değerleri yardımcıdır. Eritrositüri ve proteinüri hastalık için tipiktir. WG’nin tanısında rutine giren c-ANCA, nötrofillerin sitoplazmik komponentine karşı gelişmiş IgG antikorlarıdır. WG için oldukça spesifiktir. Aktif hastalıkta c-ANCA pozitifliği %90-95’i geçer. Bu nedenle remisyon ve nüks takibinde güvenilirdir. Günümüzde WG’nin tedavi seçeneklerini siklofosfamid ve kortikosteroidler oluşturmaktadır. Son zamanlarda trimetoprim-sulfametoksazol tedavisinin yararları bildirilmektedir. Ağır olgularda gamaglobulin tedavisi verilebilmektedir. Sonuç: WG multisistemik bir hastalıktır. Çeşitli prezentasyonlarla başvurular olabilmektedir. Böbrek tutulumu asemptomatik olabilmekle birlikte son derece mortal seyredebilmektedir. Bu sebeple solunum yolları semptomlarıyla birlikte böbrek yetmezliği tablosu bulunan hastalarda WG akılda bulundurulması gereken tanılar arasında yer almalı ve ekarte edilmelidir. Anahtar Kelimeler: Akut böbrek yetmezliği, Wegener granülamatozis, vaskülit

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
282
P 157 İSHAL ŞİKAYETİYLE GELEN HASTADA AKUT ABDOMİNAL AORT OKLÜZYONU Selim Yurtsever1, Gökhan Ersunan1, Gürkan Altuntaş1, Aydın Coşkun1, Mehmet Oktay1, Ensar Durmuş1, Eda Beykoz Çetin2
1Recep Tayyip Erdoğan Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Rize 2Recep Tayyip Erdoğan Üniversitesi Tıp Fakültesi, Radyoloji Anabilim Dalı, Rize Giriş: Abdominal aortun oklüzyonları akut ve kronik olabilmekle beraber bu iki formun klinikleri birbirinden çok farklı şekilde ortaya çıkabilir. Akut aort oklüzyonu çok nadir görülmekle birlikte acil cerrahi müdahale edilmezse ölüm kaçınılmaz hale gelir. Bu olgu ile acil servise yürüyerek gelen ve ishal şikayeti tarifleyen, akut abdominal aort oklüzyonu tanısı alan hasta sunulmuştur. Olgu: 65 yaş erkek hasta acil servise ayaktan başvuru yaptı. Karın ağrısı, ishal ve bulantı kusma şikayeti mevcuttu. Muayenesinde barsak sesleri artmış batında yaygın hassasiyet vardı defans ve rebound yoktu. özgeçmişinde Leriche sendromu ve periferik arter embolisi olan hastanın takibinde alt ekstremitelerde bilateral uyuşma ve ağrı gelişmesi üzerine hastaya BT anjiografi çekildi. Abdominal aortta infrarenal seviyeden her iki ana iliak artere uzanım gösteren stent vardı ve stent içi akım yoktu. Çölyak trunkus orjininde akut trombus izlendi. Splenik arter, ana hepatik arter ve sol gastrik arterde akım izlenmedi. Superior mezenter arter ve sağ renal arter orjininde akut trombüs izlendi. Hasta kalp damar cerrahisi tarafından acil ameliyata alındı. Hasta ameliyat esnasında ex oldu. Sonuç: İshalli hastalar sıklıkla acil servise başvururlar ve acil hekimleri tarafından genellikle hızla taburcu edilmek istenirler. Abdominal aort oklüzyonu, mezenter arter trombüsü gibi acil vakalarda ishal, dispepsi, kusma gibi şikayetlerle acil servise başvurabilmekte olup risk faktörü olan hastalarda mutlaka titizlikle irdelenmelidir Anahtar Kelimeler: Aort oklüzyonu, Leriche sendromu, mezenter arter trombozu P 158 SU TENDON KESER Mİ? BİR OTO YIKAMA KAZASI: EKSTANSÖR HALLUSİS LONGUS TENDON KESİSİ İbrahim Altun1, Şenol Ardıç2, Gökhan Peker1, Süleyman Türedi2, Davut Sadoğlu2
1Sağlık Bilimleri Üniversitesi Trabzon Kanuni Eğitim ve Araştırma Hastanesi, Ortopedi Bölümü, Trabzon 2Sağlık Bilimleri Üniversitesi Trabzon Kanuni Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Trabzon Giriş: Acil servise travma nedeniyle sıkça tendon kesisi vakaları başvurmaktadır. Ayak tendon yaralanmaları ise nispeten az görülmektedir. Ayak baş parmağına ekstansiyon hareketini sağlayan majör kas olan ekstansör hallusis longus ayak başparmağında distal falanksın bazisinin dorsaline yapışarak tendonunu oluşturur. Bu tendon direkt yada indirek olarak rüptüre olabilir. Olgumuzda oto yıkama basınçlı su püskütrme makinasının atipik ayak yaralanmasına neden olabileceğini göstermeyi amaçladık. Olgu: 21y erkek hasta, acil servisimize ayak baş parmakta düşüklük (Resim 1) şikayetiyle başvurdu. Hastanın hikayesinde 1 hafta önce otomobil temizliği için basınçlı su püskürtme makinasını (Resim 2) kullanırken kaza sonucu ayağına su değdirdiği ve ayak baş parmak hizasında kesi oluştuğu öğrenildi. Başlangıçta kısmen olan düşüklük giderek artmış. Hastanın vital bulgular stabil, yapılan fizik muayenesinde sağ ayak baş parmak metatarsofalangeal eklemin dorsal kısmının 2 cm proksimalinde 3 cmlik kabuklanması olan horizontal düzgün kenarlı cilt kesisi ile birlikte dorsifleksiyonda kısıtlılık tespit edildi. Diğer sistem muayeneleri ise doğal idi. Hastada ekstansör hallusis longus tendonu kesisi (Resim 3) düşünülerek ortopedi uzmanı ile konsülte edildi. Vakanın 1 hafta sonra opere edildiği, 3 hafta süre ile atel uygulandığı ve kısa süreli fizik tedavi sonrası tam iyileşme (Resim 4) ile düzeldiği öğrenildi. Sonuç: Basınçlı su ile yıkama yapan makinelerin güvenlik problemleri yeterince bilinmemektedir. Literatürde ekstansör hallusis longus tendon rüptürleri case report yada case serisi şeklinde bildirilmektedir (1) ancak vakamız, bu şekilde yaralanma ile ilk kez bildirilmektedir. Referans 1)Extensor hallucis longus tendon injury: an in-depth analysis and treatment protocol.Kass JC, Palumbo F, Mehl S, Camarinos N.J Foot Ankle Surg. 1997 Jan-Feb;36(1):24-7; discussion 80. Review Anahtar Kelimeler: Su, ekstansör tendon kesisi, iş kazası

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
283
P 159 A RARE COMPLICATION OF BLUNT THORAX TRAUMA: ACUTE MYOCARDIAL INFARCTION Mehmet Umut Akbulut, Su Izel Sesigur, Ali Celik, Mehmet Fatih Korcak, Cigdem Ozpolat, Haldun Akoglu, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Introduction: Cardiac complications due to blunt thorax trauma is common with a variety of disturbances. The most frequent one is cardiac contusion and it is hard to identify because of lack of a standard diagnostic method. However, acute myocardial infarction (MI) due to chest trauma is a rare complication. We report a case of a patient presenting with acute myocardial infarction secondary to blunt chest trauma. Case: 57-year-old male has presented to ED with blunt thorax trauma due to a hard kick and jab to his anterior chest-wall and face. His chief complaint was chest pain and he was hemodynamically stable. His physical examination revealed tenderness with palpation on chest-wall, ecchymosis of the face with no crepitation or stepping sign. In past medical history, he had a PCI 8 months ago. EKG has shown ST segment elevation on inferior leads (D2-3- and aVF) and ST segment depressions on high lateral leads as reciprocal changes. After medical treatment and stabilization patient has referred to coronary angiography laboratory and right coronary artery occlusion was diagnosed. 8 days later he was discharged without complications. Discussion: Myocardial infarction (MI) secondary to blunt chest trauma is rare since the ensuing cardiac pain is commonly attributed to contused myocardium or the traumatic injuries in the local chest wall. Although, on the pathophysiological view, there are many underlying mechanisms like intimal injuries, plaque ruptures and vasospasms, dissection of the coronary artery with subsequent thrombus formation. Since it may be fatal, it has utmost importance to be diagnosed in the ED. Keywords: AMI, blunt trauma, thorax P 160 ASPIRED GASOLINE THROUGH SIPHONAGE: CHEMICAL PNEUMONIA Okkes Yilmaz Cinar, Zuhal Kalyon, Cigdem Ozpolat, Haldun Akoglu, Ozge Onur, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Introduction: Hydrocarbons constitute a heterogenous group of organic substances such as gasoline, motor oil, lamb oil, lighter fluid and kerosene. Aspiration of hydrocarbons cause respiratory pathologies from simple symptoms to critical result. We would like to present a case of gasoline aspiration. Case: 32-years-old man admitted to ED with the complaints of chest discomfort and cough. He declared to aspirate gasoline 24 hours-ago, examined in a hospital and discharged after the normal chest radiogram at the first hour of aspiration. His RR was 25/minute, other vitals and physical exam were all normal. On laboratory examination WBC count was 20000/µL, CRP was 195 mg/L, PCT was 1,04 ng/L. Serum electrolytes, hepatic and renal function tests were normal. Chest radiograph showed bilateral basilar consolidation. The patient was admitted to hospital with chemical pneumonia and bacterial superinfection. Blood cultures were taken and antibiotheraphy was initiated. On the second day of the admission, patient has desaturated and developed tachypnea. Thorax CT revealed bilateral diffuse infiltration. He was admitted to ICU as ARDS and NIMV was started. On the 14th day he was discharged from hospital without any sequela. Discussion: Hydrocarbon pneumonitis, resulting from aspiration of diesel/petrol or other hydrocarbons can present as acute onset breathlessness. The entity may be more common than reported, as the practice of diesel/petrol siphoning is quite common. Hydrocarbons are related to lung injury by direct destruction of alveolar septal pulmonary capillaries. Volatility, surface tension and viscosity affects destruction level. Pulmonary manifestations occur in 30 minutes to 2 days. Corticosteroids are first line treatment on chemical pneumonia. Prophylactic antibiotic use is not recommended unless bacterial superinfection develops. Early recognition of the condition and timely supportive treatment may be beneficial and lifesaving. Keywords: Chemical pneumonia, gasoline, ARDS

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
284
P 161 BUCKSHOT IN THE BRAIN Adnan Karadaş, Olcay Yeşil, İbrahim Ulaş Özturan Kocaeli University Medical Faculty, Department of Emergency Medicine, Kocaeli, Turkey Introduction: Eye and brain injuries caused by buckshot are severe, life threating injuries which may cause high morbidity and mortality. Many survivors live with significant disabilities, resulting in major socioeconomic burden. In our case report, we present a patient who have buckshots in his eye and brain came to the emergency department (ED) by walking. Case: Thirty three years old male came to the ED by walking, complaining of being shot by a firearm. He was shot ten hours ago far about ten meters. Physical examination revealed two input of buckshot at left frontal and left perietal area of the head. His vital signs were normal. He was alert and orientated. He stated that he could not see with his right eye. We noticed perforation in the right eye at side of seven o’clock. Direct and indirect light reflection could not be noticed. Brain and orbital computed tomography revealed two hyperdense foreign body in the left parietal area and one foreign body in the left parietal area under the skin. A foreign body was noticed posterior side of orbita, near the optic nerve. Another foreign body was found in the right temporal lobe. After initial evalution and treatment, the patient had consulted neurosurgery and ophtalmology departments. Because of the patient’s good state and the risks of the surgery, neurosurgery department suggested to leave the foreign body in the brain and the patient admitted to ophtalmology department. Discussion: Head injuries by gunshots are very serious and require elaborated evaluation. Most of the cases are operated by neurosurgeons to remove the foreign body if the foreign body is one piece and lead contained. Regarding our case, despite the patient had a foreign body in his brain, he was able to walk and admit to the ED, 10 hours later after being shot. Keywords: Buckshot, emergency department, traumatic brain injury P 162 MARCIHAFAVA-BIGNAMI DISEASE: AN UNCOMMON CAUSE OF NEUROLOGIC DEFICIT Nurseli Bayram, Merter Gumusel, Tugba Mamak, Cigdem Ozpolat, Haldun Akoglu, Ozge Onur, Haldun Akoglu Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Introduction: Marcihafava-Bignami Disease (MBD) is an uncommon neurological disease mostly seen in middle-aged males who are addicted to alcohol. Etiology is still unknown. Demyelinization or hyperintense lesions on corpus callosum due to necrosis on MRI are characteristic signs for diagnosis of the disease. The clinical presentation includes a large variety of presentations, with no specific or pathognomonic clinical features and it can develop as acute, subacute or chronic. Mostly the prognosis is bad but with early diagnosis and proper treatment, totally cured patients exist. We present a case of an MBD. Case: A 38 years old female patient admitted to ER with complaints of unable to walk, blurry speech, tingling sensations on hands and feet which are started 10 days ago and increased gradually. Patient had an obesity surgery 3 months ago and she doesn’t use alcohol. She was suffering from oral intolerance because of nausea after surgery. On physical examination; bilaterally lower extremity muscle strength was 3/5, gloves like hypoesthesia on hands and feet, nystagmus (both vertically and horizontally) and dysarthria were detected. On cranial MRI on corpus callosum periventricular hyperintense lesions were observed. MBD was thought in differential diagnosis based on history of malnutrition and MRI findings. After IV thiamin treatment for 15 days, patient was discharged with oral treatment. After 3 months, bilaterally lower extremity strength was 4/5, she could walk with tripod. Also there were no lesions left on MRI. Conclusion: Today, etiology of MBD is unknown. As most patients reported are alcohol addicts, it is considered as chronic alcohol consumption and malnutrition are the leading cause. Early diagnosis and proper treatment with parenteral thiamine may lead to total cure. ER doctors are in major role for early diagnosis. Patients with a history of malnutrition and neurological symptoms should suggest MBD on differential diagnosis. Keywords: Marcihafava-Bignami disease, demyelinization, weakness

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
285
P 163 NAR SUYU VE WARFARIN ETKİLEŞİMİ Rohat Ak, Fatih Doğanay, Ali Şahiner, Tuba Cimilli Öztürk, Özge Ecmel Onur, Arzu Emecan, Mazlum Kılıç Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, İstanbul Warfarin, antikoagülasyon amacıyla sık kullanılan bir ilaç olup vücutta sitokrom p450 enzimleri ile metabolize edilir. Bu enzimlerin aktivitelerini arttıran veya azaltan çeşitli ilaçlar ve besinler mevcuttur. Olgumuzda warfarin kullanan bir hastada nar suyu kullanımına bağlı uluslararası düzeltme oranında (INR) görülen yüksekliği sunmayı amaçladık. 63 yaşında erkek hasta atriyal fibrilasyon tedavisi için warfarin kullandığı ve INR kontrolünü yaptırmak için acil servisimize başvurdu. Herhangi bir şikayeti olmayan hastanın bakılan INR değeri 10,8 (normali; 0,8-1,2) olarak saptandı. Öyküsü derinleştiğinde her gün bir su bardağı kadar nar suyu içtiği, bunun dışında warfarin ile etkileşebilecek başka bir ilaç veya besin tüketmediği öğrenildi. Hastaya warfarin ve ilaç-besin etkileşimleri hakkında bilgi verildi. Nar suyu ve warfarin kulanımı kesilen hastanın takiplerinde INR terapotik aralığa ulaştı. Ülkemizde warfarin sık kullanılan bir ilaç olup acil servislere INR kontrolü için başvuran birçok hasta mevcuttu. Acil servis hekimleri INR yüksekliği saptadıkları hastalarda warfarin metabolizmasını etkileyecek tüm ilaç ve besinleri akılda bulundurmalıdır. Anahtar Kelimeler: Warfarin, nar suyu, ilaç etkileşimi P 164 TODD PARALİZİSİ Rohat Ak, Fatih Doğanay, Ali Şahiner, Tuba Cimilli Öztürk, Özge Ecmel Onur, Arzu Emecan, Mazlum Kılıç
Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, İstanbul Epilepsi, acil servislerde sık görülen bir durum olup hastalar tek bir konvulzif nöbetten status haline kadar farklı klinik tablolarla gelebilir. Olgumuzda sıklıkla fokal nöbetler sonrası görülen ve ayırıcı tanısının mutlaka yapılması gereken Todd paralizisi durumunu sunmayı amaçladık. 28 yaşında erkek hasta nöbet geçirme sonrası sağ kolda güçsüzlük şikayeti ile acil servisimize başvurdu. Özgeçmişinde yaklaşık 6 yıldır epilepsi tanılı olduğu ve valproik asit kullandığı öğrenildi. Son zamanlarda ilaçlarını düzenli kullanmadığı için nöbet geçirme sıklığında artış olduğu ve acil servisimize başvurmadan yaklaşık 2 saat önce birkaç dakika süren nöbet geçirdiği ve sonrasında sağ kolunda güçsüzlük yakınmasının başladığı öğrenildi. Başvuru anındaki vitalleri stabil olan hastaya yapılan nörolojik muayenede sağ kolda 3/5 kuvveti olduğu ve bunun haricindeki nörolojik muayenesinin normal olduğu görüldü. Laboratuar tetkikleri ve kranyal nöro-görüntülemesi normal olan hastanın sağ kolundaki kuvvet kaybının nöbet sonrası gelişebilecek Todd paralizisi olduğu düşünülerek nöroloji servisine yatışı gerçekleştirildi. Takiplerinde yatışının 10. Saatinde şikayetlerinin tamamen düzeldiği öğrenildi. Epileptik nöbetler sonucu ortaya çıkan nörolojik belirtiler tipik olarak saniyeler-dakikalar veya saatler içinde geçer. Todd paralizisi fokal nöbeti izleyen monoparezi veya hemiparezi olarak tanımlanır. Kas güçsüzlüğünün nöbeti takiben ilk 24 saat içinde geçmesi beklenir. Ayırıcı tanısını serebrovasküler hastalıklar, enfeksiyöz hastalıklar ve santral sisteminin yer kaplayıcı lezyonları ile yapmak gerekir. Anahtar Kelimeler: Todd paralizisi, epilepsi, nörolojik aciller

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
286
P 165 DELİ BAL TÜKETİMİNE BAĞLI AKUT BÖBREK YETMEZLİĞİ Rohat Ak, Fatih Doğanay, Ali Şahiner, Tuba Cimilli Öztürk, Özge Ecmel Onur, Arzu Emecan, Mazlum Kılıç Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, İstanbul Deli bal zehirlenmesi, Rhododendron çiçeklerinden üretilen ve grayanotoksin içeren balın tüketilmesiyle ortaya çıkar. İnsanda zehirlenme belirtileri doza bağlıdır ve birkaç dakika ile iki veya daha fazla saat süren latent bir periyoddan sonra ortaya çıkar. İlk belirtÖler, tükürük sekresyonunda artış, kusma, ağız çevresÖ ve ekstremÖtelerde parestezÖdÖr. TÖpÖk zehÖrlenme tablosu; hayatı tehdÖt edebÖlen bradÖkardÖ ve hÖpotansÖyon Öle karakterÖze Öken, nadÖr de olsa sÖndÖrÖm sÖstemÖ ÖrrÖtasyon bulgularına bağlı olarak akut böbrek yetmezliğine yol açabilir. 38 yaşında erkek hasta göz kararması, bayılma hÖssÖ ve bulantı-kusma şÖkayetlerÖ Öle acÖl servÖsÖmÖze başvurdu. Sabah bal tüketÖmÖ olduğunu Öfade eden hastanın yapılan fÖzÖk muayenesÖnde; genel durumu ÖyÖ, şuur açık, koopere, oryante, TA: 95/60 mmHg, Nbz: 43 vuru/dk, ateş:36.2 C°, satO2: %99, solunum sayısı: 21/dk ÖdÖ. ÇekÖlen elektrokardiografide sinüs bradikardisi izlenmesi üzere intravenöz hidrasyon başlanan hastanın takiplerinde şikayetlerinde gerileme izlendÖ. RutÖn bÖyokÖmyasal testlerde; kreatÖnÖn: 3,16 mg/dL, üre:73 mg/dL, Na:138 mmol/L, K: 4.2 mmol/L olarak ÖzlendÖ ve delÖ bal zehÖrlenmesÖne bağlı akut böbrek yetmezlÖğÖ nedenÖ Öle dahÖlÖye servisine yatışı gerçekleştirildi. Deli bal intoksikasyonu olguları hÖpereksÖtabÖlÖte, düşük dozlarda, kalpte kolÖnerjÖk etkÖlerle bradÖkardÖ ve hÖpotansÖyon, yüksek dozlarda sürrenal medulladan epÖnefrÖn salgılatarak taşÖkardÖ ve hÖpertansÖyon ve ayrıca dÖgoksÖn zehÖrlenmesÖne benzer her tür rÖtm bozukluğu oluşturabilir. Gastrointestinal bulguları ön planda olan hastalarda nadirde olsa akut böbrek yetmezliği görülebilir. Acil servis hekimlerinin daha çok bradikardi ve hipotansiyon ile hatırladıkları deli balın akut böbrek yetmezliğine neden olabileceği de unutulmamalıdır. Anahtar Kelimeler: Deli bal, akut böbrek yetmezliği, toksikoloji P 166 A RARE INFECTION: SPINAL EPIDURAL ABSCESS AND OSTEOMYELITIS Tugba Mamak, Nurseli Bayram, Halil Ibrahim Atalay, Erkman Sanri, Cigdem Ozpolat, Haldun Akoglu, Ozge Onur, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul Introduction: Spinal epidural abscess (SEA) is mostly characterized by the fluid collection and inflammatory process on the surrounding dura and adipose tissue. The incidence of SEA is reported to be 1/100.000, whereas some other studies have reported higher rates. In our case we want to emphasize on consideration of the postoperative complications during the evaluation of back pain and neurological deficit in emergency department (ED). Case: 61-years-old female patient was admitted to ED with the complaints of urinary incontinence, loss of strength in right leg and a discharge around lower back. She declared to have lumbar disc herniation operation a month ago. Her vital parameters were stable. Her physical examination was normal except serous discharge on the operation site and 2/5 of muscle strength on the right lower extremity. Laboratory findings were as follows: WBC:17000/mL, CRP:35 mg/L, kidney function tests and urinanalysis were normal. MRI and spinal CT revealed the presence of SEA and osteomyelitis in 3rd lumbar vertebra. A surgical debridement was performed by neurosurgery department and IV antibiotics treatment was started. 10 days after the operation she was discharged to home with oral antibiotics. Conclusion: Postoperative wound infections in spinal surgery remain an important complication to diagnose and treat. In most cases of deep infection, even with instrumentation, aggressive soft-tissue debridement followed by intravenous antibiotics is sufficient as in our case. Primary SEAs result from hematogenous spread of pathogens from a distant focus to the epidural space, while secondary SEAs occur after spinal trauma, injections, surgery or direct inoculation of a pathogen into the epidural space. So it is important to diagnose post-op complications of a spinal surgery. Keywords: Spinal epidural abscess, osteomyelitis, lumbar

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
287
P 167 SENTETİK KANNABİNOİD KULLANIMINA BAĞLI AKUT BÖBREK YETMEZLİĞİ VE RABDOMİYOLİZ Rohat Ak, Fatih Doğanay, Ali Şahiner, Tuba Cimilli Öztürk, Özge Ecmel Onur, Arzu Emecan, Mazlum Kılıç Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, İstanbul Sentetik kannabinoidler sın yıllarda özellikle ülkemizin büyük metropollerinde kullanımı artan, bağımlılık oluşturan bir grup uyuşturucu maddedir. Kannabinoidler beyinde bulunan kannabinoid reseptörlerini uyararak etkilerini gösterirler. Olgumuzda bonsai kullanımı sonucu akut böbrek yetmezliği ve rabdomiyoliz gelişen bir vakayı sunmayı amaçladık. 23 yaşında erkek hasta acil servisimize sokakta baygın bulunduğu için getirildi. Başvuru anındaki vitalleri; ateş: 36,7 °C, tansiyon: 124/76 mmHg, nabız: 84 vuru/dk, sp02: %97 idi. Glaskow Koma Skalası 15 olan hastanın bilinci açık, oryantasyonu ve kooperasyonu tamdı. Anamnezinde madde kullanım öyküsü mevcuttu. Yapılan fizik muayenesinde cilt turgoru azalmış ve dehidrate görünüm mevcuttu. Idrar sondası takılan hastanın anürik olarak izlenmesi üzere hastaya intravenöz hidrasyon başlandı. Bakılan biyokimyasal testlerde; kreatin:3,24, LDH: 6703, ALT: 672 U/L, AST:2344 U/L, potasyum 5.6 tespit edildi. Bu bulgular ışığında hastada ön tanı olarak rabdomiyoliz ve buna bağlı akut böbrek yetmezliği ön tanısı konularak dahiliye servisine yatışı gerçekleştirildi. İskelet kas liflerinin akut nekrozu ve hücre içeriğinin dolaşıma karışmasıyla seyreden rabdomiyoliz yetişkinlerde en sık alkol ve keyif verici maddelerin kötüye kullanımı sonrası görülmektedir. Rabdomiyoliz olaylarında madde kullanımı mutlaka sorgulanmalıdır. Anahtar Kelimeler: Sentetik kannabinoid, rabdomiyoliz, akut böbrek yetmezliği P 168 A CASE OF RHABDOMYOLYSIS ASSOCIATED WITH ALCOHOL AND DRUGS
Su Izel Sesigur, Melis Efeoglu, Oguzhan Demir, Musa Adanc, Haldun Akoglu, Ozge Onur, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Introduction: Rhabdomyolysis is a clinical syndrome of acute necrosis of the skeletal muscle fibers and the release of intracellular muscle constituents into the circulation. Muscular traumas are the most common cause of rhabdomyolysis. Muscle enzyme defects, electrolyte imbalances, infections, drugs, toxins and endocrinopathies are the other common causes. Although the classical triad is muscle pain, weakness and dark urine, approximately half the patients lack these symptoms. In this report we present a case of rhabdomyolysis, who was found lying on the road and was brought to our ED by EMS with the suspicion of assault and trauma. Case Presentation: A 28-years-old man was brought to ED by EMS after being found lying unconsciously. At admittance patient had a fair medical status, GCS of 12, HR was 132 bpm and other vitals were normal. Initial ECG revealed sinus tachycardia. Blood glucose level was 104 mg/dL. Physical exam was within normal limits except the alcohol smell on patient's breath. Lab results revealed a CK level of 24847 which led to the diagnosis of rhabdomyolysis. IV fluid treatment was started with an initial 2000 cc IV bolus and maintenance of 500 cc/h with NS titrated depending on the urinary output. Discussion: Although commonly rhabdomyolysis is due to muscle damage after trauma, drugs and alcohol are within the countless etiologies. Within drugs antipsychotics (quetiapine, aripiprazole) and statins are first in line. In a study of ARF due to rhabdomyolysis from substance misuse, alcohol is the most commonly misused substance (%54 of cases).At our case patient’s usage of alcohol and quetiapine was confirmed by the patient’s relatives, and both physical exam and laboratory tests did not show a sign of compartment syndrome or trauma. Keywords: Rhabdomyolysis, alcohol, ketiapin

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
288
P 169 KICKED LIKE A STEER, BLED LIKE A HUMAN Ayse Demir, Mehmet Fatih Korcak, Musa Adanc, Haldun Akoglu, Ozge Onur, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Introduction: Traumatic subarachnoid hemorrhage (TSH) is a serious causes of morbidity and functional impairment in head trauma. Probably versatile mechanism plays a role in the formation of TSH. TSH may occur from the bleeding of intracranial arteries or bridging veins. It was reported more frequently in the middle-aged men. MVAs are the most common cause of TSH. However, we present a different and rare mechanism for the trauma resulting in TSH: a kick of a steer! Case: 58 year-old female patient admitted to our ED with a 3-5 min lenght of loss of consciousness after a kick by a steer. Patient had an amnesia of the event. After gaining consciousness, he declared to vomit for 3 times. Her GCS was 15. Physical examination was normal except dermal abrasions on her head. A pan-CT was performed. A TSH was diagnosed around the right parietal lobe with frontal cerebral contusion. She was observed in the ED for 48 hours. After 2 days a control CT was performed. A significant reduction of the contused area and subarachnoid hemorrhage was observed. Discussion: TSH is one of the most common pathologies after head trauma, especially after MVA. Kick by a steer at the head is an extremely rare event, with an incidence similar to shark bite. A pan-CT may be warranted for all patients after a trauma by such a strong animal. Keywords: Bull, steer, kick P 170 SUBARAKNOİD KANAMA VE SEREBRAL VEN TROMBOZU BİRLİKTELİĞİ
Tanju Biçer, Taygun Baykal, Muharrem Doğan, Demet Devrimsel Doğan, Rohat Ak, Tevfik Patan, Abdullah Taşçı Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, İstanbul Giriş: Serebral venöz tromboz (SVT) ile subaraknoid kanama (SAK) ilişkisi nadirdir. Klinik bulguların çeşitliliği nedeniyle SVT tanısı zordur. Akut SAK kliniği ile başvuran SVT’li hastalarda ise tanı koymak daha zordur. Spontan SAK’ ın %85’i anevrizma rüptürüne bağlı, %10’u nonanevrizmatik perimezansefalik hemoraji, %5’i ise diğer sebeplerden kaynaklanır. SVT de kortikal SAK’ın sebepleri arasındadır. SVT ile ilişkili SAK’ın kesin nedeni bilinmemektedir. Vaka: 68 yaşında kronik hastalık öyküsü olmayan kadın hasta baş ağrısı ve bilinç değişikliği şikayetiyle hastanemize başvurdu. Nörolojik muayenesinde gks 15 bilinç konfüze olarak tespit edildi. Hastanın diğer muayene bulgularında patolojik bulgusu yoktu. Çekilen bilgisayarlı beyin tomografisinde (BBT) sol temporooksipital lob posteromedialinde 28x12 mm. boyutlarında akut parankimal hematom ve subaraknoid kanama izlendi. Kraniyal MRG ve MR venografi çekildi. MRV'de hipoplazik görünüm izlendi. Hasta SVT ve SAK birlikteliği nedeni ile nöroloji servisine yatırıldı. Hastaya DSA yapıldı ve tüm sinüslerde tromboze görünüm izlendi. Hastaya clexane, coumadin ve fenitoin tedavisi başlandı.SVT etyolojisine yönelik istenen tetkikleri (Protein C, Protein S, ATIII, antifosfolipit antikor, MTHFR gen mutasyonu ) normaldi. Hastanın takiplerinde baş ağrısı ve bilinç bulanıklığı tama yakın düzeldi, şifa ile taburcu edildi. Tartışma: SVT’ye bağlı kortikal SAK’ın mekanizması bilinmemektedir. Baş ağrısı, fokal nörolojik defisit ve nöbetler SVT’de bildirilen nonspesifik semptomlardır. Bizim olgumuzda da başlangıç semptomu baş ağrısı olup bu baş ağrısı tromboza bağlı artmış intrakraniyal basınç artışı ile açıklanabilir. İntrakraniyal enfeksiyon, inflamatuvar hastalıklar, kalıtsal trombofili, oral kontraseptif kullanımı, gebelik, steroid tedavisi, nefrotik sendrom, antifosfolipit antikorlar ve kafa travması gibi hiperkoagülabilite ile ilişkili predispozan faktörler tanıda önemlidir. Bunun yanında %25 olguda bizim hastamızda olduğu gibi neden belirlenemez. SVT’ye bağlı kortikal SAK tanısı tanısı kesinleşince antikoagülan tedavinin yararlı olduğu gösterilmiştir. Biz de SAK’a rağmen olgumuza antikoagülan tedavi başladık ve şikayetleri gerileyen hastayı şifa ile taburcu ettik. Bu olgu kortikal SAK saptanan olgularda nörolojik muayene ve anemnez ile SVT birlikteliğinin akılda bulundurulması gerektiğini göstermektedir. Anahtar Kelimeler: Antikoagülan, Serebral Ven Trombozu, Subaraknoid Kanama
5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
289
P 171 METOKLOPRAMİDE BAĞLI DİSTONİ Rohat Ak, Fatih Doğanay, Ali Şahiner, Tuba Cimilli Öztürk, Özge Ecmel Onur, Arzu Emecan, Mazlum Kılıç Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, İstanbul Metoklopramid, dopamine reseptör antagonisti olup acil servislerde bulantı-kusma, migren gibi hastalıkların tedavisinde kullanılır. En önemli yan etkisi distoni gibi ekstrapiramidal semptomlardır. Olgumuzda akut gastroenterite bağlı kusma şikayeti olan bir hastaya metklopramid enjeksiyonu uygulanması sonucu gelişen distoni durumunu sunmayı amaçladık. 28 yaşında erkek hasta acil servise boyunda istemsiz hareketler şikayeti ile başvurdu. Anamnezinde bir gün önce tavuk ve pilav yediği, sonrasında kusma, ishal şikayetlerinin geliştiği,bu nedenle başvurduğu acil serviste 10 mg iv (intravenöz) metklopramid uygulandığı öğrenildi. Hastaya 5 mg biperiden im (intramuskuler) uygulandıktan sonra şikayetleri düzeldi. Metoklopramid, periferik ve santral etkileri olan selektif dopamine reseptör antagonistidir. Farmakolojik etki başlangıcı iv uygulamada 1-3 dk (dakika), im uygulamada 10-15 dk, oral kullanımda 30-60 dk olup etki süresi 1-2 saat sürmektedir. En sık görülen yan etkisi halsizlik ve huzursuzluk iken en ciddi yan etkisi distoni gibi ekstrapiramidal semptomlardır. Bu etkiler günde 30-40 mg ile tedavi edilen hastaların yaklaşık % 0,2’sinde görülür. Anormal postür ve sürekli tekrarlayan istemsiz hareketlerle karekterize bir hiperkinetik hareket bozukluğu olan akut distonik reaksiyonun tedavisinde biperiden (5 mg), prometazin (25-50 mg) ve difenhidramin (1 mg/kg oral,iv veya im) kullanılabilir. Acil servis hekimleri sık kullanılan metklopramidin bu yan etkisini ve tedavisini bilmelidir. Anahtar Kelimeler: Metoklopramid, distoni, nörolojik aciller P 172 ABDOMİNAL EPİLEPSİ Rohat Ak, Fatih Doğanay, Ali Şahiner, Tuba Cimilli Öztürk, Özge Ecmel Onur, Arzu Emecan, Mazlum Kılıç Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, İstanbul Abdominal epilepsi, karın ağrısı, bulantı-kusma gibi gastrointestinal semptomlarla birlikte letarji, konvülziyon gibi nörolojik bulguların beraber görüldüğü bir hastalıktır. Genellikle çocukluk yaş grubunda görülmekle birlikte erişkinlerde de görülebilir. Olgumuzda karın ağrısı ve bilinç değişikliği ile acil servise başvurup abdominal epilepsi tanısı alan bir hastayı sunmayı amaçladık. 19 yaşında erkek hasta acil servisimize bilinç değişikliği şikayeti ile getirildi. hastanın genel durumu orta, şuuru konfüze, glaskow koma skalası: 12 idi. Başvuru anındaki vitalleri; ateş: 36,4 °C, tansiyon: 130/80 mmHg, nabız: 76 vuru/dk, sp02: %99 olup parmak ucu kan şekeri 136 mg/dl idi. Yakınlarından alınan anamnezde uzun zamandır ara ara karın ağrısının olduğu, karın ağrısına bulantı-kusmanın eşlik ettiği ve zaman zaman bu şekilde bilinç değişikliği yaşadığı da öğrenildi. Bakılan hemogram, biyokimya, tam idrar tetkiki parametreleri normal olan hastaya çekilen beyin ve kontrastlı batın tomografisinde patolojik bir durum izlenmedi. Takipleri sırasında bilinci tamamen düzelen hastaya çekilen elektroensefalografide (EEG) patolojik dalgaların görülmesi üzere nöroloji servisine yatışı gerçekleştirildi. Acil servis hekimleri bilinç değişikliğine eşlik eden karın ağrısı durumlarında nadir görülen abdominal epilepsiyi ayırıcı tanıları arasında bulundurmalıdırlar. Anahtar Kelimeler: Karın ağrısı, abdominal epilepsi, nörolojik aciller

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
290
P 173 BURIED BUMPER SYNDROME Rohat Ak, Fatih Doğanay, Ahmet Aykut, Abide Merve Manap, Özge Ecmel Onur, Tuba Cimilli Öztürk, Ali Şahiner Fatih Sultan Mehmet Training and Research Hospital, Istanbul Buried bumper syndrome (BBS) is an uncommon complication of percutaneous endoscopic gastrostomy (PEG) tube placement. This unusual phenomenon occurs when the internal bumper of a PEG tube erodes and migrates through the gastric wall and becomes lodged anywhere between the gastric wall and the skin. A 91-year-old woman presented to the emergency department (ED) because of pain and drainage at her PEG tube site and inability to instill fluid. Three months prior, she had PEG performed. Three hours prior to arrival, she noticed peritubal leakage and localized discomfort with attempts to flush the tube. She denied prior complications with the tube. On examination, the patient had normal vital signs and appeared comfortable. Her head, chest, and extremity exams were normal. Her abdomen was soft with no appreciable tenderness. There was no evidence of distention or palpable masses. The patient’s PEG site was not indurated and showed no erythema or drainage. The external bolster was approximately 1 centimeter from the skin surface. The tube was not mobile within the stoma. A tube study was performed. Based on this study, a computed tomography (CT) was performed to determine the exact location of the PEG tube as well as any secondary complications resulting from its misplacement. General surgery was consulted for the malfunctioning PEG tube. The patient was admitted to the hospital for intravenous (IV) antibiotics and fluid hydration. Her PEG tube was removed operatively and was not replaced. Complications of PEG tubes are commonly encountered by the emergency physician. Although most complications are minor, BBS is a potentially life-threatening process that may mimic more benign conditions. Early diagnosis and surgical consultation for the management of BBS may help avoid repeated ED visits and more serious complications. Keywords: Buried bumper syndrome, percutaneous endoscopic gastrostomy, emergency department P 174 AN ATYPICAL LOCALIZATION OF ACUTE APPENDICITIS Rohat Ak, Fatih Doğanay, Ali Şahiner, Tuba Cimilli Öztürk, Özge Ecmel Onur, Arzu Emecan, Mazlum Kılıç Fatih Sultan Mehmet Training and Research Hospital, Istanbul Acute appendicitis is one of the most common causes of acute abdomen. Symptoms are most frequently right lower quadrant pain, nausea, vomiting and decreased appetite. Appendicitis can be situated at different localizations although rare. Among the causes of this condition are congenital small bowel malrotation, situs inversus totalis, very long appendix and mobile cecum. We aimed to present a case of an acute appendicitis in a different localization due to mobile cecum. A 24 year-old female patient presented to the emergency service with abdominal pain which had started one day earlier and nausea, vomiting and decreased appetite. Physical examination of the case revealed signs of peritoneal irritation at the suprapubic region and left lower quadrant. His WBC was 17500/ mm3. Contrast enhanced computed abdominal tomography disclosed that cecum was located at the middle and to the left lower quadrant and the appendix was extended to the left lower quadrant. He underwent surgery which revealed that the appendix was in a different location compatible with the tomography images and an appendectomy was performed. In acute appendicitis, atypical abdominal pain or variable symptomatology may affect morbidity inevitably. Sigmoid diverticulitis, dissection of abdominal aortic aneurysm, renal colic, epididymitis, incarcerated hernia, bowel obstruction and psoas abscess are considered in the differential diagnosis of left lower quadrant abdominal pain; however, acute appendicitis should also be taken into account. Keywords: Acute appendicitis, atypical localization, abdominal pain

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
291
P 175 THE IMPORTANCE OF TEAM APPROACH IN THE PROCESS OF ASSESSING THE EMERGENCY PSYCHIATRIC CASES
Zümra Ülker Dörttepe1, İlkay Keser2
1Uşak University Vocational School of Health Services, Emergency and First Aid Program, Uşak, Turkey 2Akdeniz University, Faculty of Nursing, Department of Psychiatric Nursing, Antalya, Turkey Introduction and Purpose: This review study was carried out to emphasize the importance of the team approach in the process of assessing the emergency psychiatric cases admitted to the emergency service. Material and Method: The literature review was performed using the words of “psychiatric emergency, emergency team approach, emergency psychiatric assessment” from up-to-date databases. The studies were selected and analyzed especially in the process of assessing the emergency psychiatric patients admitted to the emergency service by revising the articles. Findings: In the studies carried out, it is stated that emergency psychiatric cases should be assessed quickly and effectively and the assessment and intervention could vary depending on the type of the psychiatric disorder by emphasizing the necessity of prioritizing the safety of patients and their relatives. During the assesment process there are some requirements like performing triage appropriately, identifying the emergency psychiatric crisis, determining the risks, applying emergency interventions, ensuring patient's stabilization, the possibility that the situation may be associated with the legal situation. Besides, the medical team consisting of different professions should make contribution to the assessment of the cases in accordance with their role definitions. Conclusion: In emergency psychiatry, it is important for the members of health care team to fulfill their roles in offering an effective approach to the individual. It's considered that the absence of a triage system for emergency psychiatric cases in Turkey and the fact that the emergency team is not fully-equipped for these cases negatively affect the assessment process. It is suggested to increase information and equipment, raise the awareness of the occupational groups on their roles and responsibilities and make arrangements to enable them to understand the importance of teamwork to make an accurate diagnosis, plan the treatment and perform an appropriate intervention. Keywords: Emergency psychiatry, emergency psychiatric assesment, emergency medical team, team approach P 176 A RARE FATAL SYNDROME DIAGNOSIS WITH ECG: BRUGADA SYNDROME Fatih Doğanay, Rohat Ak, Hasan Demir, Abdullah Taşcı, Özge Ecmel Onur, Ali Şahiner
Fatih Sultan Mehmet Training and Research Hospital, Istanbul, Turkey Brugada syndrome is a disorder characterized by sudden death associated with one of several ECG patterns characterized by incomplete right bundle-branch block and ST-segment elevations in the anterior precordial leads ECG changes can be transient with Brugada syndrome and can also be unmasked or augmented by multiple factors, such as; fever, ischaemia, sodium channel blockers eg: flecainide, propafenone, calcium channel blockers, alpha agonists, Beta blockers, nitrates, cholinergic stimulation, cocaine, alcohol, hypokalaemia, hypothermia, post DC cardioversion. We reported a case, resorted the ED with syncope, had Brugada syndrome. A previously healthy 27-year-old man presented to emergency department (ED) with syncope. He had vomiting and epigastric pain during sleep than he waked up and blacked out. His Glascow Coma Scale (GCS) was 15;blood pressure was 110/75 mmHg, pulse rate was 84 bpm, oxygen saturation 98%. In his physical exam, there was no pathology. İn his Electrocardiography there was a coved-type ST segment and an inverted T wave in lead V1, grater than 2 mm saddleback shaped ST elevation in lead V2 (Brugada type 2). Bed-side echocardiography revealed a normal-sized heart and didn’t visualise any patology. There were no abnormalities in routine blood tests. The symtoms and findings were supporting Brugada syndrome. He was transported coronary care unite for provocation tests and treatment with implantable cardiac defibrillator (ICD). The case represents a diagnostic ecg finding about the fatal syncope reasons. Brugada Syndrome is an important cause of Sudden Unexplained Nocturnal Death Syndrome (SUNDS). It is easy to diagnose if the ecg findings was known. The only treatment that has proven effective in treating ventricular tachycardia and fibrillation and preventing sudden death in patients with Brugada syndrome is implantation of an automatic ICD. ED doctor should think Brugada Syndrome in differential diagnosis of syncope. Keywords: ECG, Brugada syndrome, cardiovascular emergencies

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
292
P 177 MAGIC WAND FOR SYNTHETIC CANNABINOID TOXICITY Fatih Doğanay, Rohat Ak, Ecem Deniz Kırkpantur, Tuba Cimilli Öztürk, Özge Ecmel Onur, Ali Şahiner Fatih Sultan Mehmet Training and Research Hospital, Istanbul, Turkey Synthetic cannabinoids have been popular since 2004 in Europe, and were first reported in the U.S. in December 2008. Acute intoxication with synthetic cannabinoids is a clinical diagnosis. Synthetic cannabinoids have serious neuropsychiatric toxicity potential, like hallucinations, delirium, psychosis, agitation and seizures. Intravenous lipid emulsion therapy (IV Lipid) has been used for nutrition support in the past. Since 1998, İv lipid has also been used as a resuscitative agent for cardiac and/or neurologic toxicity of xenobiotics. This case illustrates resolving neurologic toxicity of Synthetic cannabinoids with only iv Lipid. A 30-year-old man presented to the emergency department (ED) with altered mental status after using a Synthetic cannabinoid named as Bonzai. There was no remarkable past medication history. His blood pressure was 120/80 mmHg, pulse rate was 102 bpm, body temperature was 37,1°C, oxygen saturation was 92% and his Electrocardiography was normal. He had a Glascow Coma Scale (GCS) score of 4. In his physical exam, there was no pathology except low GCS score. We decided to give only IV Lipid and 6 lt/dk O2 with mask. No other medications were given. 1.25 mL/kg bolus of %20 lipid and followed with infusion of 0.50 mL/kg/minute for 40 minutes. After IV Lipid infusion, his GCS score improved to 10 in forty minutes, and 15 after four hours. His laboratory results were normal. The patient did not have any symptoms of Synthetic cannabinoids toxicity in his follow-ups for 24 hours in the ED. There is no specific antidote for intoxication with synthetic cannabinoids. IV Lipid available for the patients with cardiac and/or neurologic toxicity of SC intoxication. Keywords: Synthetic cannabinoids, lipid emulsion therapy, toxicology P 178 NEUROLEPTIC MALIGNANT SYNDROME Fatih Doğanay, Rohat Ak, Azizcan Kılıç, Tuba Cimilli Öztürk, Özge Ecmel Onur, Ali Şahiner Fatih Sultan Mehmet Training and Research Hospital, Istanbul, Turkey Neuroleptic malignant syndrome (NMS) is a life-threatening neurological disorder most often caused by an adverse reaction to neuroleptic or antipsychotic drugs. NMS typically consists of muscle rigidity, fever, autonomic instability, and cognitive changes such as delirium, and is associated with elevated plasma creatine phosphokinase (CPK) We reported a case of NMS presents to Emergency Department (ED) with altered mental status and fever. A 28-year-old man presented to ED with altered mental status and fever. In his medical history, he followed up for psychosis related drug abuse and yesterday he took his first quetiapine pill. His Glascow Coma Scale (GCS) was 7, blood pressure was 188/120 mmHg, pulse rate was 147 bpm, respiration rate was 45 bpm, oxygen saturation 87%, and body temperature 38,3˚C. All extremities were rigid. In his laboratory results Hb: 15,8 gr/dL, Wbc: 34000 k/μl, Plt: 269000 k/μl, BUN: 25 mg/dL, creatinine: 2,43 mg/dL INR: 1,80, CPK:31200 mg/dL, ALT: 72 mg/dL, AST:523 mg/dL. After endotracheal intubation, the patient sent to intensive care unit for further therapy and follow-up. In DSM-IV to diagnose for NMS, there will be both of the major criteria (muscle rigidity and fever) or at least two of the minor criteria; sweating, dysphagia, shivering, incontinence, altered mental status, mutism, tachycardia, high or variable blood pressure, leukocytosis, and laboratory findings indicative of muscle injury such as CPK elevation. NMS is an important clinical condition that develops as a result of antipsychotic therapy. Past history and use of certain drugs should be thoroughly questioned for its diagnosis. ED doctors be aware for NMS in patients who take antipsychotic drugs and present with fever, altered mental status, muscle rigidity, and CPK elevation. Keywords: Neuroleptic malignant syndrome, emergency department, toxicology

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
293
P 179 BİTKİLERLE ALTERNATİF TEDAVİ: PITRAK KULLANIMINA BAĞLI KİMYASAL YANIK Handan Çiftçi, Elnare Günal, Gülşen Çığşar, Murat Özdemir Kafkas Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Kars Giriş: Modern tıbbın tüm gelişmelerine rağmen, alternatif uygulamalara eğilim her popülasyonda görülebilir. Bitkilerle tedavi alternatif yöntemlerden birisi olup avantajları tartışmalıdır ve beklenmeyen sonuçlara neden olabilir(1).Asteraceae ailesinden Xanthium (pıtrak otu) cinsinin dünya çapında 25 türü vardır ve geçmişten günümüze bitkisel ilaçlar olarak kullanılmaktadır(2). Türkiye'de çayır ve meralarda bulunan Xanthium spinozum türü; alkaloit ve glikozit özelliklere sahip olup cilt yaralarında ve romatizmal eklem ağrılarında kullanılabilmektedir(3). Bizde bitki ve köklerini lapa haline getirerek alternatif tedavi yöntemi olarak uygulayan iki vakayı sunduk. Olgu 1: 65 yaşındaki bayan hasta 2 gün önce ayak tabanında çıkan yarayı pıtrak otunun kökleri ile sardığı ve 24 saat sonra sargıyı açtığında ayağının şiştiğini ve yanık oluştuğunu görmüş, ayağındaki yanık bülünün artması üzerine 2. gün acil servise başvurmuştu. Bilinen bir hastalığı ya da düzenli aldığı bir ilacı yoktu. Fizik muayenesinde nabızları açık, sağ ayak tabanında yaklaşık 10 cm çapında 2. derece yanık mevcuttu. Ayak ödemli ve hiperemikti. Tetkiklerinde anormal bulgusu olmayan hastaya yanık pansumanı ve tetanoz aşısı yapılıp taburcu edildi. Olgu 2: 50 yaşında bayan hasta iki gün önce dizlerindeki ağrı sebebi ile çevreden topladığı pıtrak otunun yapraklarını ezerek dizlerine sardığı ve yaklaşık iki gün sonra sargıyı açtığında dizlerinde şişlik, kızarıklık ve su dolu keseler oluştuğunu tarifleyerek acil kliniğine başvurdu. Özgeçmişinde herhangi bir özellik yoktu fakat dizlerindeki ağrılar nedeniyle sürekli analjezik-antienflamatuar aldığını belirtiyordu. Fizik muayenesinde her iki alt ekstremite nabızları açık, her iki dizde yaygın ödem, sirkülere yakın hiperemi ve medial yüzlerde yaklaşık 10 cm çapında bülleri mevcuttu. Hareket kısıtlılığı yoktu. Tetkiklerinde anormal bulgusu olmayan hastaya yanık pansumanı ve tetanoz aşısı yapılıp taburcu edildi. Sonuç: Alternatif tedavi yöntemlerinde kullanılan bitkiler saf olmadığı ve içerikleri tam olarak bilinmediği için bilinçsizce kullanımlarda faydadan çok zarar vermektedir. Tedavide kullanılan maddelerin, kimyasal içeriklerini bilen ve kullanma dozlarını öneren kişilere danışarak uygulanması yan etki potansiyelini azaltacaktır. Anahtar Kelimeler: Alternatif tedavi, pıtrak otu, kimyasal yanık P 180 HYPOKALEMIC PERIODIC PARALYSIS Fatih Doğanay, Rohat Ak, Abide Merve Manap, Tuba Cimilli Öztürk, Özge Ecmel Onur, Ali Şahiner Fatih Sultan Mehmet Training and Research Hospital, Istanbul, Turkey Hypokalemic periodic paralysis (hypoKPP) is a rare, autosomal dominant channelopathy characterized by muscle weakness or paralysis with a matching fall in potassium levels in the blood (primarily due to defect in a voltage-gated calcium channel). hypoKPP is a condition in which affected individuals may experience paralytic episodes with concomitant hypokalemia (<2.5 mmol/L), and occasionally may develop late-onset proximal myopathy. We reported a case, resorted the Emergency Department (ED) with weakness, had hypoKPP. A 42 year-old male with no significant past medical history presented to ED with sudden onset paralysis. The weakness was bilateral and involved all extremities equally. He had no respiratory or swallowing difficulty and was able to move his neck and facial muscles. He did not take any medications and denied use of alcohol or drugs, or significant changes in diet or activity levels. His Glascow Coma Scale (GCS) was 14;blood pressure was 140/85 mmHg, pulse rate was 104 bpm, oxygen saturation 96%. On physical exam, there was pathology except weakness. His upper and lower extremity pulses were normal and equal. Neurologic exam revealed flaccid paralysis of all extremities. Sensation was intact but deep tendon reflexes was 3/4. There was no patology in his cranial CT and brain diffusion MRI. The laboratuary tests were normal except potassium levels of 2.1 mmol/L. Two hours after initiation of intravenous potassium replacement, the patient's neurologic symptoms had completely resolved. Periodic Paralysis is important to consider when seeing a patient with sudden onset weakness or paralysis, especially those with no history or evidence of other diseases and no significant risk factors for stroke. Failure to properly diagnose and treat Periodic Paralysis can be fatal, but rapid correction of potassium abnormalities can resolve the symptoms quickly and completely. Keywords: Hypokalemia, paralysis, emergency department

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
294
P 181 ACUTE PANCREATITIS WITH NORMAL LIPASE LEVEL Fatih Doğanay, Rohat Ak, Abdullah Taşcı, Tuba Cimilli Öztürk, Özge Ecmel Onur, Ali Şahiner Fatih Sultan Mehmet Training and Research Hospital, Istanbul, Turkey Serum lipase is a very sensitive marker of Acute pancreatitis (AP), with sensitivity in the range of 85%-100%. Normal serum lipase in the setting of AP is thus a rare phenomenon. It is thought that typically, acute inflammation and auto-digestion of the pancreas leads to the release of both amylase and lipase, leading to elevated levels in the blood. For this reason, normal serum amylase and lipase levels in a patient with acute abdominal pain would typically rule out acute pancreatitis in favor of another diagnosis. Here we present a case of acute pancreatitis with normal lipase level and the diagnose was confirmed with abdominal CT scan. 44 year old male patient who was admitted to emergency department with abdominal pain and nausea. There was epigastric tenderness in his physical exam. Laboratory tests including lipase were normal. In abdominal CT scan, there was thickness increase in the pancreatic head sections and slightly heterogeneous pancreatic parenchyma. Findings were coherent with acute pancreatitis. Epigastric pain is an important sign for AP. If there is a doubt for AP even if lipase level was normal, ED physician must confirm the diagnosis with CT. The laboratory tests should be accompanied with abdominal CT scan with IV contrast, so no diagnosis of pancreatitis is missed. Keywords: Acute pancreatitis, lipase, emergency department P 182 BEHÇET HASTALIĞINA BAĞLI AKUT BATIN BULGULARI: TERMİNAL İLEİT
Elnare Günal1, Handan Çiftçi1, Gülşen Çığşar1, Murat Özdemir1, Ali Cihat Yıldırım2
1Kafkas Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Kars 2Harakani Devlet Hastanesi, Genel Cerrahi Kliniği, Kars Giriş: Behçet Hastalığı ilk defa 1937 yılında Hulusi Behçet tarafından tanımlanmıştır. Etyolojisi bilinmeyen, kronik, multisistemik, vaskülitle seyreden bir hastalıktır. Küçük- orta- büyük arter ve venleri tutabilir. Rekürren aftöz ülserler, genital ülserler, iridosiklitis/üveitis, kutanöz püstüle vaskülitis ve artritis ile karakterizedir. Klinikopatolojik bulgular nörolojik, gastrointestinal(Gİ), mukokütanöz ve genitoüriner sistemi içeren geniş bir yelpazede gözlenir. Bazen abdominal ağrı, diare, Gİ kanamalar gibi semptomlarla ve bazen de ince bağırsak perforasyonu ile gelebilirler. Gİ sistemdeki en sık lezyonu ülserasyon olup en sık terminal ileum ve çekumda bulunmaktadır. Gİ ülserler gibi gastrit, duodenit, özefajit veya kolit gibi Gİ belirtiler saptanabilir ve nadiren intestinal perforasyon, peritonitle ilişkilidir. Bizde Behçet hastalığı olan ve akut batın şikayetleri ile acil servisimize gelen hastayı sunduk. Olgu: 40 yaşında erkek hasta iki gündür olan karın ağrısı şikayeti ile acil servisimize başvurdu. Özgeçmişinde Behçet hastalığının olduğu ve iki yıldır Kolşisin aldığı öğrenildi. Fizik muayenesinde sağ alt kadranda hassasiyeti, istemsiz defansı ve rebound vardı. Hasta tahta karın durumundaydı ve hareketle ağrıları arttığı için hareketsiz kalıyordu, bağırsak sesleri normaldi. Diğer sistem muayeneleri doğaldı. Batın ultrasonografisinde apendiks lojunda minimal serbest sıvı izlendi ancak apendiks vizualize edilemedi. Kontrastlı batın tomografisinde; batın sağ yarıda orta kadranda terminal ileum anslarında bağırsak duvarında diffüz hafif kalınlaşma izlenmekte olup bu bölgedeki mezenterde yer yer kalın çizgisel dansite artışları dikkati çekmiştir (terminal ileit?). Genel cerrahi konsültasyonu istenen hastaya akut batın olması nedeniyle genel cerrahi tarafından yatış önerildi ancak acil operasyon önerilmedi. Genel cerrahi servisinde takiplerinde enterit gelişen hasta klinik ve radyolojik bulguları beraber değerlendirilip Behçet Hastalığına bağlı ileit tanısı ile tedavisi düzenlendi. Sonuç: Behçet hastalığı vaskülite bağlı klinik semptomlar ile seyreden bir hastalıktır. Nadir görülmesine rağmen Gİ sistem bulguları da saptanabilir. Özgeçmişinde Behçet hastalığı olan ve akut batın bulguları ile acil servise başvuran hastalarda öncelikle bu bulguların Behçet hastalığına bağlı olabileceği düşünülüp genel cerrahi konsültasyonu istenirken daha spesifik olunmalıdır. Anahtar Kelimeler: Behçet Hastalığı, akut batın, terminal ileit

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
295
P 183 ÜST GASTROİNTESTİNAL SİSTEM KANAMASINDA NADİR BİR SEBEP Muharrem Doğan1, Demet Devrimsel Doğan1, Tanju Biçer1, Taygun Baykal1, Abdullah Taşcı1, Özge Ecmel Onur2
1Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul 2Marmara Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, İstanbul Giriş: Gastrointestinal hemorajiler acil servise sık başvuru sebeplerinden olup erken tanı ve tedavisi sağlanmadığı durumlarda ve devam eden aktif kanamalarda yaşamı tehdit edici seviyelerde ulaşabilir. Vakamızda daha önce de 4 kere sebebi bulunamayan gis kanama öyküsü olan ve yine koyu renkli dışkılama ve kusma yakınması ile acil servisimize başvuran 68 yaşındaki erkek hastadadan bahsedeceğiz. Vaka: 68 yaşında erkek hasta acil servisimize koyu renkli, cıvık dışkılama ve kahve telvesi renginde kusma yakınması ile başvurdu. Daha önce de 4 kere benzer yakınması olmuş ve gastrointestinal kanama tanısı ile takip edilmiş ve odak saptanamamış. Başvurusunda ateş: 37,2C nabız: 125atım/dk so2: %96 ta: 85/45 rektal tuşede melena saptanan hastaya nazogastrik sonda takıldı ve koyu kahve telvesi renginde geleni görüldü. Hemoglobin seviyesi 6,3mg/dl saptanan hastaya eritrosit transfüzyonu yapıldı. Gastroskoposinde aktif yada eski gastrointestinal kanamayı gösterecek bulguya rastlanmadı. Servis takiplerinde yapılan kolonoskopisinde kanama odağı yada eski kanama bölgesi gözlenmedi. Hastaya yapılan çölyak arter, SMA ve IMA anjiyografisinde SMA distalinde jejenum seviyesinde ekstravazasyon saptandı ve embolizasyon uygulandı. Hastanın takiplerinde hemoglobin düşüşü gözlenmedi. Tartışma: Üst gastrointestinal sistem kanamalarında en sık peptik ülser kanaması saptansa da endoskopik yöntemlerle kanama odağı saptanamayan olgularda nadir görülen diğer etyolojiler açısından ileri görüntüleme yöntemlerine başvurmak gerekmektedir. Kanamanın erken farkedilmesi ve gerekli replasmanların erken başlanması devam eden kanama durumlarında hayat kurtarıcıdır. Anahtar Kelimeler: Gastrointestinal, anjiyografi, embolizasyon P 184 BİR TOKSİKASYON KLASİĞİ: TCA Demet Devrimsel Doğan1, Muharrem Doğan1, Taygun Baykal1, Tanju Biçer1, Azizcan Kılıç1, Özge Ecmel Onur2
1Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul 2Marmara Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, İstanbul Giriş: İlaç intoksikasyonları bilinç değişikliği ile başvuran her hastada akılda bulundurulması gereken bir durumdur. Antidepresanlar ilaca bağlı ölümlerde en sık 3. etken olmakla birlikte bunlar arasında ölümlerde trisiklik antidepresanlar ilk sıradadır. Amitriptilin için 1gr üzerinde alımlarda hayatı tehdit edici ciddi kardiyovasküler ve nörolojik etkiler beklense de daha düşük dozlarda da benzer etkiler görülebilir. Vakamızda 1gr amitriptilin alımı sonrası bilinç bulanıklığı ve nöbet ile acil servisimize başvuran 24 yaşında kadın hastadan bahsedeceğiz. Vaka: 24 yaşında günlük 25mg amitriptilin kullanan kadın hasta başvurusundan yaklaşık 2 saat önce yaklaşık 1gr amitriptilin alımı sonrası gelişen bilinç bulanıklığı yakınması ile yakınları tarafından acil servisimize başvurdu. Başvurusunda ateş: 36,4C nabız: 115atım/dk so2: %97 ta: 95/45mmHg GKS: 14 hastanın EKG sinde TCA intoksikasyonu ile uyumlu sinüs taşikardisi, aVR’de pozitif R dalgası D1de negatif S dalgası ve QRS genişlemesi mevcuttu. Kan gazında pH: 7,25 Bikarbonat: 16 saptanan hastanın takipleri sırasında JTK nöbeti oldu. Hastaya antiepileptik tedavisi verildi, sistemik alkalizasyon ve destek tedavisi verildi. Hasta orotrakeal entübe edilerek yoğun bakım ünitesinde takibe alındı. Yoğun bakım takibi sonrası hastanın iyilik hali sağlandı ve psikiyatri takibi ile taburcu edildi. Tartışma: Trisiklik antidepresanlar ile olan toksikasyonlarda ciddi kardiyovasküler ve nörolojik etkiler görülebilmektedir. Ölüm olan olgular genelde ilk birkaç saat içerisinde hastaneye ulaşmadan olmaktadır. Hastaneye ulaşan olgular erken tanı ve uygun tedavi ile yüksek oranda iyileşmektedir. Bu nedenle bilinç değişikliği, kardiyovasküler yada nörolojik bulguları olan uygun yada güvenilir anamnez alınamayan her hastada toksikasyonlar mutlak akılda bulundurulmalıdır. Anahtar Kelimeler: TCA, toksikasyon, nöbet

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
296
P 185 ÇEVRESEL BİR ACİL: YILDIRIM ÇARPMASI Handan Çiftçi1, Gülşen Çığşar1, Elnare Günal1, Murat Özdemir1, Şahin Kahramanca2
1Kafkas Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Kars 2Harakani Devlet Hastanesi, Genel Cerrahi Kliniği, Kars Giriş: Çevresel acillerden olan yıldırım çarpmasının insidansı bilinmemektedir. Özellikle şantiye ve çiftlikler gibi açık alanda çalışanlar yıldırım çarpmalarına karşı savunmasızdır. Bizde Açık arazide çalışırken yıldırım çarpmasıyla yaralanan üç vakayı sunduk. Olgu 1: 20 yaşında erkek hasta yıldırım çarpmasıyla acil servisimize 112 ambulansıyla getirildi. Hastanın şuuru açık, oryante-koopereydi, vitalleri stabildi. Elektrokardiyogramı(EKG) normal sinüs ritmindeydi. Muayenesinde boynundan başlayıp göğsüne doğru uzanan eğrelti otu biçiminde ağrısız eritematöz dallanmalar gösteren cilt lezyonları mevcuttu(Lichtenberg figürü).Serum kreatin-kinaz, troponinI ve elektrolitleri normaldi.24 saat takip edilen hasta, cilt bulgularının gerilemesi üzerine taburcu edildi. Olgu 2: 32 yaşında erkek hasta yıldırım çarpması sonrası acil servisimize 112 ambulansıyla getirildi. Genel durumu kötü, şuuru açık, oryante-koopereydi. Hastanın TA:120/90, Nb:128,solunum sayısı:24, ateş:35°C,SO2:%60, EKG:sinüs taşikardisi olup hemoptizisi mevcuttu. Parkland kanununa göre vücudunun %70'inde (boyun ön yüzü, toraks ve batın ön yüzü, penil bölgesi, her iki alt ekstremite ön yüzlerinde ve ellerde) çoğunluğu 2.derece olan 1 ve 2.derece yanık mevcuttu. Kaşlarının, kirpiklerinin, burun kıllarının da yandığı saptandı.Her iki hemitoraks solunuma eşit katılıyor ancak solunum sesleri azalmış, ralleri mevcuttu. Toraks tomografisinde sol hemitoraksta kalınlığı 12mm’ye ulaşan hemotoraksla uyumlu plevral efüzyon, sol hemitoraksta belirgin olmak üzere bilateral hemorajik kontüzyon saptandı, beyin tomografisindeyse bilateral nazal kemiklerde medialde deplase fraktür saptandı. Yanık tedavisine başlandıktan sonra solunum sıkıntısının ve hemoptizinin artması üzerine hasta entübe edildi, toraks tüpü takılıp yoğun bakıma yatırıldı. Olgu 3: 22 yaşında erkek hasta yıldırım çarpması sonrası göğüs ağrısıyla acil servise getirildi. Genel durumu iyi,şuuru açık, oryante-koopereydi. Fizik muayenesi normal,vitalleri stabildi. EKG sinüs ritminde olup inkomplet sağ dal bloğu tespit edildi. Monitörlü takibe alınıp ve iv-hidrasyon başlandı. Kan tetkiklerinde TropI:0.03,CK:402,CKMB:22.8 olan hastanın dördüncü saat tetkiklerinde TropI:0,12,CK:340,CKMB:20,3'dü.Onikinci saatteki değerleri düşme eğilimindeydi.24 saat takip edilen hasta şikayetlerinin gerilemesi, EKG değişikliğinin olmaması ve kadiyak enzim değerlerinde gerileme olması üzerine önerilerle taburcu edildi. SONUÇ: Birçok sistemi etkileyebilen yıldırım çarpması ciltte yoğun elektron akışının, dielektrik bozunmaya ve kırmızı kan hücrelerinin kapillerlerden yüzeyel cilt tabakalarına sızmasına sebep olarak Lichtenberg figürünü oluşturduğu düşünülmektedir. En sık ölüm sebebi asistoliye bağlı kardiyopulmoner arresttir. Bu nedenle yıldırım çarpması ile acil servise başvuran hastalar multisistemik olarak değerlendirilmelidir. Anahtar Kelimeler: Yıldırım çarpması, Lightenberg figürü, yanık

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
297
P 186 POSTTRAUMATIC ANOSMIA AS A CONSEQUENCE OF MILD HEAD INJURY Ozcan Yavasi1, Yavuz Metin2, Bülent Özdemir3, Erhan Uğraş1
1Recep Tayyip Erdoğan University, Department of Emergency Medicine, Rize, Turkey 2Recep Tayyip Erdoğan University, Department of Radiology, Rize, Turkey 3Recep Tayyip Erdoğan University, Department Neurology, Rize, Turkey Introduction: Depending on the severity of the head trauma, approximately 12.8 % of the cases suffer from anosmia. Possible mechanisms of posttraumatic olfactory dysfunction are: direct injury to the sinonasal tract or olfactory epithelium, shearing effect on olfactory fibers at the cribriform plate, focal trauma to the olfactory bulb, diffuse injury to primary or secondary olfactory cortex, or injury to the connections between central olfactory structures. Although spontaneous recovery of olfactory function has been observed in approximately one-third of patients with posttraumatic olfactory loss, such patients usually have irreversible dysfunct ion and a poor prognosis. The level of recovery from post-traumatic olfactory loss remains around 10%. There is no standard treatment for patients with posttraumatic olfactory loss. Oral steroids are beneficial to some degree. Case: A 21-year-old boy hit the back of his head to the door of a wardrobe. About 20 minutes following the event,he noticed that he had anosmia and loss of taste sensation. His Glasgow Coma Scale score was 15. Her systemic and neurological examination was almost normal except loss of smell and taste sensations bilaterally. His oropharyngeal and nasal examination revealed no obvious sign of trauma. He underwent cranial computed tomography scanning of 5 mm-thickness, that was normal. As he had ungoing complaints he underwent magnetic resonance imaging (MRI) that revealed contusion of the ophtalmic bulbi. He was consulted with neurosurgeon and ordered 250 mg intravenous prednisolon as antiedemic therapy. The patient was discharged for outpatient follow-up with prescription of oral steroid with tapering dose. On his one-year follow-up visit, his taste sensation was recovered but smelling was partially recovered. Conclusion: Impairment of smell may ocur following injury to any portion of the olfactory tract, from nasal cavity to brain. MRI should be the choice of imaging. Keywords: Anosmia, olfactory dysfunction, mild head trauma P 187 FALLOPIAN TUBE TORSION IN AN ADOLESCENT: DIAGNOSTIC ROLE OF MAGNETIC RESONANCE IMAGING Yavuz Metin1, Nurgül Orhan Metin1, Ozcan Yavasi2, Yeşim Bayoğlu Tekin3
1Recep Tayyip Erdoğan University Faculty of Medicine, Department of Radiology, Rize, Turkey 2Recep Tayyip Erdoğan University Faculty of Medicine, Department of Emergency Medicine, Rize, Turkey 3Recep Tayyip Erdoğan University Faculty of Medicine, Department of Obstetrics and Gynecology, Rize, Turkey Introduction: Isolated torsion of the fallopian tube is uncommon. It is usually difficult to evaluate clinically and surgical exploration is often necessary to establish the diagnosis. We present a case of isolated left tubal torsion and discuss the role of magnetic resonance imaging (MRI) in diagnosis. Case: A 14-year-old, previously healthy, adolescent girl presented with acute left lower quadrant pain, nausea and vomiting since 3 days. On abdominal examination she had tenderness at left lower quadrant and costophrenic angle with voluntary guarding. Her white blood cell count was 12.4 103/uL and neutrphil count was 9.15 103/uL. Urinanalysis and β-hcG were normal. Pelvic ultrasound showed a left adnexal septated cystic mass measuring 90 x 76 mm. Left ovary could not be visualized. Right adnexial structures were visualized. Patient underwent pelvic MRI and diffusion-weighted MRI that confirmed the diagnosis of left tubal torsion. The patient underwent left salpingectomy with the preservation of left ovary. Conclusion: Isolated torsion of the fallopian tube should be considered in the differential diagnosis of acute lower abdominal or pelvic pain in the female patients. MRI plays a major role in the diagnosis. Keywords: Acute pelvic pain, fallopian tube, magnetic resonance imaging, sonography, torsion

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
298
P 188 AN INTERESTING RELATION: ACUTE ISCHEMIK STROKE DRAINING CHRONIC SUBDURAL HEMATOM Ozcan Yavasi1, Ömer Lütfi Gündoğdu2, Vaner Köksal3
1Recep Tayyip Erdoğan University Faculty of Medicine, Department of Emergency Medicine, Rize, Turkey 2Recep Tayyip Erdoğan University Faculty of Medicine, Department of Neurology, Rize, Turkey 3Recep Tayyip Erdoğan University Faculty of Medicine, Department of Neurosurgery, Rize, Turkey Introduction: A subdural hematoma (SDH) is a collection of blood below the inner layer of the dura but external to the brain and arachnoid membrane through the bridging veins which connect the brain surface with the dura mater. A SDH may cause local ischemia by compressing adjacent cortical blood vessels. Although surgical evacuation is the choice of treatment in symptomatic patients, rarely spontaneous resolution may be observed. The mechanism of spontaneous resolution is usually the compression of the hematoma by acute brain swelling followed by redistribution. We present an interesting case in which, chronic SDH partially contributed to development of ischemic stroke, which then drained chronic SDH by compression. Case: 83-year-old female patient presented with complaints of sudden onset loss of onsciousness, and right sided hemiparesis. She has been on follow-up for chronic subdural hematome since one-year. She had no chronic systemic disease. She was lethargic and non-cooperated, had facial asymmetry, right hemiplegic and positive right-sided Babinsky reflex. Tension arterial was 140/80 mmHg; pulse rate was 90 bpm. Finger-tip blood glucose was 122 g/dL. Electrocardiogram showed atrial fibrillation. Non-contrast cranial computed tomography (CT) to exclude hemorrhage revealed left chronic subdural hematoma (13 mm in thickness), left dens middle cerebral artery (MCA) sign, effacement of grey-white matter differentiation on left hemisphere, and 5 mm midline shift. Diffusion-weighted magnetic resonance imaging showed total acute left MCA infarction. He was hospitalized in neurology intensive care unit. Carotid Doppler ultrasonography revealed total occlusion of left internal carotid artery. Serial cranial CTs showed edema in left hemisphere and resolution of subdural hematoma. She was discharged for home-care at day 21. Conclusion: Any type of edema may cause resolution of chronic SDH by compression. Keywords: Subdural hematoma, spontaneous resolution, cerebral edema, ischemic stroke P 189 TEMPORARY HEPATODIAPHRAGMATIC INTERPOSITION OF THE COLON Ozcan Yavasi1, Ali Özdemir2, Mehmet Oktay1, Murat Yazıcı1
1Recep Tayyip Erdoğan University Faculty of Medicine, Department of Emergency Medicine, Rize, Turkey 2Recep Tayyip Erdoğan University Faculty of Medicine, Department of Surgery, Rize, Turkey Introduction: Chilaiditi’s sign is the asymptomatic interposition of the intestine between the liver and diaphragm, whereas Chilaiditi’s syndrome refers to clinical symptoms such as abdominal bloating, pain or anorexia developing from this phenomenon. The interposition may appear only when the patient is in the erect position and resolve in the supine position. Conservative management for the syndrome includes bed rest and bowel decompression with rectal or nasogastric tube; surgical treatment may be required in cases of persistent pain, refractory ileus, colonic volvulus or bowel ischemia. We report herein a case of temporary hepatodiaphragmatic interposition of the colon that was treated conservatively. Case: A 45-year-old, previously healthy man presented with complaints of abdominal pain, nausea and vomiting. Abdominal examination showed distended abdomen, epigastric tenderness, rebound tenderness and increased bowel sounds. Posteroanterior chest and plain abdominal radiography showed right subdiaphragmatic colonic air. To differentiate free air, a nasogastric catheter was applied. Repeat radiography did not reveal free abdominal airHis complete blood count and routine biochemistry were non-specific.. The patient had ongoing symptoms. He was consulted to general surgeon and intravenous contrast-enhanced computed tomography (CT) was ordered. CT revealed colonic segments between liver, diaphragm and anterior abdominal wall. He was considered to have hepatodiaphragmatic interposition of the colon (Chilaiditi’s syndrome). He was treated symptomatic and conservatively with intravenous fluid and medication, nasogastric decompression and barium enema. After a follow-up period of approximately 12 hours, the symptoms were completely resolved. Repeat plain radiogrphy showed the inappearence of the colonic gas. Conclusion: Although most patients with Chilaiditi’s sign have persistent interposition especially in the erect position, it may occur temporarily without recurrence as a result of transient distention of the bowel. Keywords: Chilaiditi’s sign, Chilaiditi’s syndrome, colon, hepatodiaphragmatic interposition
5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
299
P 190 FAMILIAL MEDITERRANEAN FEVER IN THE EMERGENCY DEPARTMENT Seçil Kapar Yavasi1, Ozcan Yavasi2
1Rize State Hospital, Clinic of Physical Medicine and Rehabilitation, Rize, Turkey 2Recep Tayyip Erdoğan University Faculty of Medicine, Department of Emergency Medicine, Rize, Turkey Introduction: Familial Mediterranean fever (FMF) is a hereditary autoinflammatory disorder characterized by recurrent bouts of fever and serosal inflammation. Ninety-five percent of patients with FMF have episodic abdominal pain, therefore can be mistaken for an acute surgical abdomen. Case: A 18-year-old male patient presented to the emergency department with complaints of abrupt onset of fever, abdominal and back pain that had started almost 24 hours ago. She applied to an emergency department at previous night where he was followed for acute abdomen. After exclusion of acute abdomen he was discharged. On his second presentation, he also had right leg pain. Vital signs were: Tension arterial, 120/60 mmHg; heart rate, 100 bpm; respiratory rate, 16 breaths/min; temperature, 39 °C. He had generalized abdominal guarding with normal bowel sounds. His thighs were in anteflexion and he had antalgic gait. Active and passive right hip movements were severely painful. Pathologic findings at routine laboratory examination were: WBC, 19.54 K7uL; neutrophil, 15.38 K/uL; total bilirubin 1.93 mg/dL; direct bilirubin 0.53 mg/dL; LDH 386 U/L; CPK, 278 U/L; Ca, 10.78 mg/dL; CRP, 0.57 mg/dL. Urinanalysis and abdominal sonography were normal. His symptoms were partially resolved. He stated that he had a same episode a month ago that lasted 4 days. He aroused the suspicion of Familial Mediterranean Fever. After exclusion of acute abdomen by general surgery he was hospitalized for further investigation. On the following day, eryhrocyte sedimentation rate, C-reactive protein, and fibrinogen were 24 mm/h, 4.90 mg/dL, and 430 mg/dL, respectively. He was given tenoxicam 20 mg 2X1 im, colchicine 0.5 mg 2x2 po and paracetamol 1mg 2 x 1 iv. He was discharged at day 5 with oral colchicine. During 1-year he did not have another attack. Conclusion: Emergency physicians should be aware of FMF which can mimic acute abdomen. Keywords: Acute abdomen, colchicine, Familial Mediterranean fever P 191 AZOTİOPRİN İLİŞKİLİ AKUT PANKREATİT Arzu Emecen, Ayşe Çağla Özmert Toplu, Burak Nakış, Rohat Ak, Özge Ecmel Onur Sağlık Bilimleri Üniversitesi Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Giriş: Akut pankreatit bazen fatal sonuçlar doğuran ve etyolojisinde ağırlıklı olarak alkolizm ve biliyer patolojinin olduğu bir sağlık sorunudur. İlaçlarla tetiklenen akut pankreatitte ilk bildiriler kortizon (1955) ve thiazidler (1959) kullanıma bağlıdır. Bir immünmodülatörolan azatioprin, immün sistem yanıtını baskılama aşamasında bağ doku hastalıklarında kullanılan etkili bir ajandır. Azatioprinmaruziyetindeki hastalarda yaklaşık akut pankreatit riski %0.4-1.6’dır. Olgu Sunumu: 47 yaşında kadın hasta, 30 dakika önce başlayan baskı tarzında epigastrik ağrı şikayetiyle acil servisimize başvurdu. Bilinen hipertansiyon ve skleroderması mevcuttu. 3 gün önce azotiopirin kullanmaya başlanmıştı. Vital bulguları TA: 120/72 mmHg spo2: %98 nabız:74/dk. Fizik muayenesinde epigastriumda hassasiyet dışında bulgu izlenmedi. Takibi esnasında bir kez kusması oldu. Tetkiklerinde Wbc: 7600 Hb: 13 mg/dl Hct: 38.2 Plt: 315000Amilaz:6155 Lipaz: 464’tü. Çekilen kontrastlı batın BT’de pankreas çevresinde serbest mayi izlendi. Azatiopirin tedavisi kesilerek dahiliye servisine interne edildi. Tartışma: İlaç ilişkili akut pankreatit araştırmalarında LAREB'in 1977 ve 1998 yılları arası yaptığı çalışmada azatioprin, simetidin, interferon-alpha, metildopa, metronidazol kullanımının akut pankreatit ile ilişkili olduğu bildirilmiştir (1). Almanya’dan 45 merkezin katıldığı 12 aylık bir çalışmada 1.613 hasta akut pankreatit ile değerlendirilmiş, hastaların 22’sinde (%1.4) etken ilaç olmuştur. Toplum bazlı çalışmalarda azatioprin kullanımında 8 kat artmış akut pankreatit riski olduğu bildirilmektedir. Azatioprin, ilaç-ilişkili akut pankreatit ile ilgili çalışmalarda kesin bir akut pankreatit nedeni olarak sunulmaktadır(2). Azatioprin ilişkili pankreatitin genellikle hafif seyirli olup, idiyosenkratik ve doz-bağımlı geliştiği öngörülmektedir. Sonuç: Azatioprin kullanım öyküsü olup bulantı,kusma,karın ağrısı gibi semptomlarla başvuran hastalarda ilaç ilişkili akut pankreatit göz önünde bulundurulmalıdır. Referanslar 1. Eland IA, van Puijenbroek EP, Sturkenboom MJ, Wilson JH, Stricker BH. Drug-associated acute pancreatitis: twenty-one years of spontaneous reporting in The Netherlands. Am J Gastroenterol. 1999;94(9):2417-22. 2. Herrlinger KR, Stange EF. The pancreas and inflammatory bowel diseases. Int J Pancreatol. 2000;27(3):171-9. Anahtar Kelimeler: Akut pankreatit, azotioprin, skleroderma

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
300
P 192 METOKLOPRAMİDE KULLANAN GEBEDE AKUT DİSTONİK REAKSİYON Necmiye Yalçın Ocak, Özge Dağtekin, Yeşim Eyler, Ufuk Taşcı İzmir Tepecik Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İzmir Giriş: Gebelikte; gebelik öncesi kilonun % 5’inin kaybına kadar varan şiddetli bulantı-kusma hiperemezis gravidarum olarak tanımlanır ve %0.5-2 oranında görülür. Tablonun şiddetine göre tedavi düzenlenir. Bu populasyonda yeterli randomize kontrollü çalışma olmamasına rağmen metoclopromide gibi dopamin antagonistleri sık reçete edilir. Metoklopromide kullanımına bağlı akatizi ve akut distonik reaksiyon görülebilir. Akut distonik reaksiyon, özellikle yüz, boyun ve sırt kaslarında kontraksiyonlar, opistotonus, tortikollis, okulerjik kriz, dizartri ve trismus ile kendini gösterir. Olgu: Onsekiz yaşında, Suriyeli, 10 haftalık gebeliği olan kadın hasta; boyun ağrısı, boyunda kasılma şikayeti ile hastanemiz acil servisine başvurdu. Başvuruda kan basıncı 110/70mmHg, nabız 89/dk, ateş 36.6°C, solunum sayısı 20/dk idi. Fizik muayenede hasta pasif boyun hareketlerini yapamıyor ve boyun sola aksiyal rotasyonda, baş hiperekstansiyonda, çene sola deviyeydi. Boyun sol lateral kasları spazmotikti. Hastadan hemogram, biyokimyasal parametreler ve elektrolit düzeyleri istendi. Kullandığı ilaçlar sorgulandığında aşırı bulantı ve kusmaları olması nedeniyle eczaneden metpamid tablet alıp kullandığı öğrenildi. Hastada metoklopramide kullanımına bağlı akut distoni geliştiği düşünüldü. Hastaya difenhidramin 20mg intravenöz yoldan uygulandıktan yaklaşık 10 dk sonra hasta şikayetlerinin gerilediğini belirtti. Uygulamadan 30 dk sonra hiçbir şikayeti kalmadı ve semptomları tamamen geriledi. 1 saat semptomsuz izlemi sonrasında bu grup ilaçlardan bir daha kullanmaması gerektiği anlatılıp kadın doğum poliklinik kontrolü önerilerek taburcu edildi. Tartışma: Metoklopramid, dopamin reseptör antagonisti olarak bulantı ve kusma şikayetlerinin giderilmesinde kullanılmaktadır. Kan-beyin bariyerini kolayca aşar ve ekstrapiramidal sisteme ait hareket bozuklukları (özel¬likle çocuklarda akut distonik reaksiyonlar) gibi yan etkiler oluşturabilir. Gebelikte ektrapiramidal semptomların görülmesi nadir bir durum olduğu için bu hastalarda ilaç kullanımı ve uygulanan tedaviler iyi sorgulanmalı ve metoklopramid kullanımına bağlı distoni gelişmiş olabileceği unutulmamalıdır. Böyle bir durumla karşılaşıldığında metoklopramid kullanımı sonlandırılıp antikolinerjik ilaçlar yardımı ile tedavi edilmelidir. Anahtar Kelimeler: Gebelik, distonik reaksiyon, metoklopramide P 193 CAUDA EQUINA SYNDROME Necmiye Yalçın Ocak, Serkan Hacar, Ufuk Taşcı, Özlem Susur İzmir Tepecik Training and Research Hospital, Clinic of Emergency Medicine, İzmir Case: A 44 years old male patient with unknown history of chronic disease, presented to the emergency room and complained of being unable to urinate. On arrival his status was as follows; blood pressure 154/92 mmHg; heart rate: 91/min, body temp: 36.7°C, respiration rate: 21/min. His anamnesis revealed that the patient presented to the neurosurgery department with complaints of lower back and right leg pain and was given an appointment for a lumbar MRG. The patient has been having numbness in the groin for 2 days. He had no urine output for 16 hours, urgency was present however he was unable to void. In the performed neurological examination; he was conscious, orientated, cooperative, no drop-foot was present, babinski bilaterally negative, normal rectal tonus and saddle-type sense defect was present. The urinary bladder was observed to be in the globe during the USG performed on the bedside. A foley catheter was applied and 1800cc of urine discharge was observed. A lumbar MRG was performed on the patient. As a result of the imaging; a right centrolateral herniation that is distinctively narrowing both neural foramina of the L4-L5 disk and causing significant pressure on the right dural sac. The patient was taken into an operation by the neurosurgery team on duty emergently, as soon as right L5 nerve root compression is determined. Discussion: The cauda equina syndrome is a rare condition. It has to be considered that centrally located disc hernia in the lumbosacral area only affect the lower sacral fibres and therefore causes a clinical condition without motor deficit or reflex changes in the lower extremities, but is accompanied by sensorineural defects and sphincter dysfunctions. Keywords: Cauda equina syndrome, urinary retention, low back pain

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
301
P 194 SEFOPERAZONE -SULBACTAM MEDICATION CAUSING ISOLATED INR ABNORMALITY IN A SEPTIC PATIENT
Halil Yıldırım1, Duygua Albayrak1, Fulya Yılmaz Duran1, Vermi Değerli2
1Bozyaka Training and Research Hospital, Clinic of Anesthesiology and Reanimation, İzmir, Turkey 2Bozyaka Training and Research Hospital, Clinic of Emergency Medicine, Izmir, Turkey Introduction: Cefoperazone-sulbactam, a combination of wide spectrum antibiotics including gram-negative and gram-positive activity. Cefoperazone has plasma half-life of 1.5-2 hours and eliminated by the kidney 15-25% and 70% in bile. Dose arrangement is not required in renal failure. Cefoperazone causes hipoprotrombinemia by inhibiting vitamin K-dependent carboxylation, as a result bleeding complications might occur. Case: 65 years old female patient who underwent surgical fixation with a plate for her humeral fractures. She was admitted ICU for her unconsciousness and respiratory failure due to severe anemia with haemoglobin levels of 5 gr/dl on fifth day postoperatively. On 10th day postoperatively a hematoma evolved on the operation site and was drained surgicaly. On follow up; in ventilatory treatment patient’s overall medical condition worsened and was diagnosed as klebsiella pnomonia sepsis according to tracheal aspirat and blood culture results. Patient was primarily treated with colistin. Within the first week of treatment acute renal faikure developed and antibiotherapy was replaced with cefoperazone sulbactam 2 * 1 g intravenous. Since the start of antibiotherapy INR values increased from normal values up to 10.3 in 48 hours without any evidence of bleeding. On laboratory examination; liver enzyms, bilurubin levels and other coagulation parameters were all within normal limits. According to all these findings patient was diagnosed as having isolated INR irregularity due to hepatic toxicity of sefoperazone- sulbactam. INR values dropped to normal level and did not rise again with therapeutic fresh frozen plasma. Conclusion: Preparations containing Cefoperazone sulbactam frequently used in the treatment of infectious diseases occuring due to sensitive micro-organisms. We believe that the cefoperazone sulbactam treatment which was given recently can lead to bleeding disorders, detailed antibiotherapy should be asked while taking medical history of patients coming to the emergency room and these patients should be viewed primarily with coagulation tests. Keywords: Sefoperazone, sulbactam, INR abnormality P 195 ACUTE INTERHEMISPHERIC SUBDURAL HEMATOMA PRESENTING AS FALX SYNDROME Ozcan Yavasi1, Selim Kayacı2, Mecit Çokluk1, Murat Yazıcı1
1Recep Tayyip Erdoğan University Faculty of Medicine, Department of Emergency Medicine, Rize, Turkey 2Recep Tayyip Erdoğan University Faculty of Medicine, Department of Neurosurgery, Rize, Turkey Introduction: Acute interhemispheric subdural hematoma (ISDH) is a rare form of posttraumatic intracranial hemorrhage and reported to account for about 6% of all traumatic subdural hematomas. It usually manifests itself with signs of Falx Syndrome (contralateral monoparesis of lower extremity or contralateral hemiparesis with lower limb weakness predominating). Several etiologies of acute ISDH have been described, including trauma, coagulopathies, anticoagulation therapy, and aneurysmal rupture. It may sometimes causes diagnostic challenge because of its’ location. Computed tomography (CT) shows a band of increased attenuation along the falx and remote from the sagittal sinus. We present a case of acute ISDH with its characteristic appearance on CT. Case: A 86-year-old female presented with weakness on right side. She had 2-3 syncope attacks in the previous week. She was cooperated and oriented. Glasgow Coma Scale score was 15. Vital signs were: Tension arterial, 150/110 mmHg; heart rate, 100 bpm; respiratory rate, 18/min; oxygen saturation, 98%. She was under antihypertensive treatment. She had 2/5 motor deficit and hypoestesia on right lower extremity, 4/5 motor deficit on right upper extremity. Electrocardiogram showed atrial fibrillation. Non-contrast cranial CT yielded hyperdensity along the superior saggital sinus. She was thought to have subdural hematoma. Diffusion-weighted magnetic resonance imaging to exclude ischemic stroke was normal. She was hospitalized by the neurosurgery clinic with the diagnosis of ISDH. The patient died due to cardiovascular complications at day 9. Conclusion: Although ISDH is a rare clinical entity, symptoms can be severe and clinical course can be devastating. Therefore, clinicians should be aware of this condition. Keywords: Interhemispheric subdural hematoma, computed tomography, falx cerebri, hemiparesis

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
302
P 196 SUBİLEUSLU GERİATRİK OLGUDA SPİNAL BLOK SONRASI GAİTA DEŞARJINA BAĞLI ERTELENEN TOTAL KALÇA PROTEZİ
Fulya Yılmaz Duran1, Kubilay Gülenç1, Zeki Tuncel Tekgül1, Vermi Değerli2
1Bozyaka Eğitim ve Araştırma Hastanesi, Anesteziyoloji ve Reanimasyon Kliniği, İzmir 2Bozyaka Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İzmir Giriş: Geriatrik popülasyonda görülen kalça kırıkları, günümüzde karşılaşılan önemli sağlık sorunlarından birisidir. İleri yaş grubundaki ameliyatlar perioperatif mortalite ve morbidite yönünden yüksek riski beraberinde getirdiği için rejyonel anestezi tekniklerine yönelme gereği duyulmaktadır. Olgu: 83 yaşında bayan olguya, sağ femur fraktürü nedeniyle operasyon planlanıyor. Özgeçmişinde 15 yıldır DM hikayesi mevcut ve oral antidiabetik kullanıyor. 2 yıl önce sol femur fraktürü nedeniyle rejyonal anestezi ile opere olmuş. Servisteki izlemi sırasında genel durumu kötüleşen, akut böbrek yetmezliği ve batın distansiyonu gelişen olgunun laboratuar sonuçları: Hb: 9.6 mg/dL, Na: 133, K: 3.3, Glukoz:200 mg/dL. Genel cerrahi tarafından subileus olarak değerlendiriliyor ve takibe alınıyor; akut böbrek yetmezliği için nefroloji hekimi tarafından takip ediliyor. 10 günlük takip sonrası genel durumu düzelen olgu spinal anestezi ile operasyona alındı. Spinal blok sonrası gaita deşarjı olan olgunun operasyonu ortopedi ekibi tarafından olası protez enfeksiyonu riski nedeniyle ertelendi. 5 gün sonra aynı olgu tekrar spinal anestezi ile operasyona alındı ve spinal blok sonrası tekrar gaita deşarjı gerçekleşti. Genel cerrahi hekimi tarafından rektal tahliye seti takıldı ve ancak yine olası protez enfeksiyonu riski nedeniyle ortopedi ekibi tarafından operasyon tekrar ertelendi. Bundan 5 gün sonra hasta elektif koşullarda barsak temizliği yapıldıktan sonra spinal anestezi ile operasyona alındı ve protez uygulandı. Sonuç: Nöroaksiyel blok uygulanması sonrası parasempatik sistem hakimiyeti artar. Subileus tanısyla izlenmiş olan olguda da parasempatik sistem hakimiyetinin oluşturduğu sorunla karşılaşılmıştır. Nöroaksiyel blok ile cerrahi planlanan geriatrik subileuslu olgularda preoperatif dönemde hazırlık aşamasında barsak temizliğinin de yapılması olası cerrahinin ertelenmesi, enfeksiyon riskinin ve maliyetin azaltılması, hastanede kalış süresinin kısalması açısından önem taşımaktadır. Anahtar Kelimeler: Subileus, geriatri, spinal blok P 197 USING INTRAVENOUS LIPID THERAPHY FOR OLANZAPINE OVERDOSE Begüm Öktem, Hüseyin Avni Demir, Ahmet Demircan Gazi University Faculty of Medicine, Department of Emergency Medicine, Ankara, Turkey Olanzapine is an atypical antipsychotic, which is commonly used in for treatment of schizophrenia and bipolar disorder. Symptoms of olanzapine overdose are mostly due to depression of central nervous system; varying from agitation to coma. We are presenting a 53-year-old male patient, reported to take 28 pills of olanzapine 10 mg, intentionally, about 3 hours ago. He has a heart rate of 111/min and blood pressure of 113/81 mmHg. He was unresponsive, his GCS was 3, pupils were miyotic, and has gasping breaths. He was intubated, and intravenous lipid therapy was given from a central venous catheter. After 12 hours, he was extubated. His GCS was 15, he was fully awake, and has no neurologic deficit. His physcial examination of other organ systems was normal as well. He was consulted to phsychiatry deparment, and hospitalized for management of schizophrenia. İntravenous lipid therapy is mostly studied on local anesthetic toxicity, although it can be used for other lipid soluable drugs as well. There are no certain criterias about when to use lipid emulsion therapy, due to its uncertainity of beneficial effects. A statement published by American College of Medical Toxicology(ACMT) suggests that the decision should be made by treating physician, due to patients clinical state, and it can be combined with other therapies as the patients’ medical condition needs. ACMT offers a dosing scheme, as we followed in our patient’s therapy. Reported side effects of the therapy are mostly lipemia and hyperamylasia, and pulmonary complications, as well as a case report of a patient with clogged renal replacement therapy filter due to intravenous lipid therapy. Low-rate infusion seems relatively safe, and lipid emulsion can be used as a treating method in oral overdoses of lipid soluable drugs, as a supportive of standart care protocols. Keywords: Toxicology, antipsychotic overdose, Lipid emulsion therapy

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
303
P 198 TOXIC EPIDERMAL NECROLYSIS FOLLOWING ALLOPURINOL INTAKE: CASE REPORT Derya Abuşka, Onur Karabay, Özgür Karcıoğlu Istanbul Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey Background: Toxic epidermal necrolysis (TEN) is a potentially life-threatening disorder characterized by widespread erythema, necrosis and bullous detachment of the epidermis and mucuosmembranes, resulting in exfoliation and possible sepsis. TEN is most commonly induced by drug ingestion. The average annual incidence is 1 cases per million population. Age, extent of epidermal involvement and serum urea level are the most important prognostic factors. Below is a report of patient presented with fever, decreased oral intake, canker in the mouth and poor clinical condition diagnosed with TEN. Case: A 83-year old female patient presented with fever, canker in the mouth, swallowing difficulties, weakness, decreased oral intake and poor clinical condition was admitted to emergency department (ED). Her medical history included hypertension, diabetes mellitus, chronic renal failure. Her vital signs were blood pressure 135/75mmHg, pulse 72bpm, respiratory rate 20bpm, body temperature 38,50C and SpO2:92%. On physical examination, pulmonary bilateral crepitant rales, diffuse maculopapular rash on the torso and peri-oral crusting with ulceration of the buccal mucosa were noted. Skin tenderness and Nikolsky’s sign were positive. She was learned to have been started on allopurinol a week ago. She was diagnosed with TEN on the basis of history and clinical findings. The patient was hospitalized in Intensive Care Unit (ICU). All drugs were withdrawn, vitals were monitored and treated symptomatically, concurrent with supportive treatment. Antibiotics and corticosteroids were also administered. On the 8th day of ICU admission the patient died. Conclusion: TEN is rare, life-threatening drug reaction. Eldery patients have a poor prognosis. It should be kept in mind for patient presented to ED with widespread skin rash. Keywords: Toxic epidermal necrolysis, skin rash, Nikolsky’s sign P 199 TRAUMA WITH FAHR'S SYNDROME Yeliz Simsek1, Gonca Koksaldi Sahin1, Ozan Demir1, Selin Bulut2
1Numune Training and Research Hospital, Emergency Medicine Clinic, Adana, Turkey 2Bozkaya Training and Research Hospital, Emergency Medicine Clinic, Izmir, Turkey Introduction: In the emergency department, computed tomography (CT) in patients presenting with head trauma is used especially to recognize hemorrhagic complications. In our case, we want to emphasize the Fahr's disease which is a rare etiology of calcifications. Case: Our case is a 17 years old female patient. She was admitted to emergency department because of motor vehicle accident. She had post traumatic amnesia and there wasn’t another symptom. In physical examination; her vital signs were stabil and glascow coma score was 15. Other physical examination findings were normal. We took cranial CT for his post traumatic amnesia. There was bilateral thalamic hypodense lesion compatible with calcification. Typical image and localization of lesions were suggestive of Fahr's disease. For Fahr's disease, there wasn't any symptoms in her history and her family history was normal. Patient was admitted 24 hour for minor head trauma and then she was discharged. Discussion: Fahr’s disease, also known familial idiopathic basal ganglia calcification (IBGC), or strio-pallidodentate calcinosis, is characterised by bilateral basal ganglia calcification. Diagnosis is made by clinic, radiology and excluding the other intracranial calcification etiology (Parathyroid disorders, Vascular lesion, Mitochondrial Disorders, Adult-Onset Neurodegenerative Conditions, Infectious disease like toxoplasmosis, syphilis and Inflammatory illness such as systemic lupus erythematosus). Fahr’s disease has been associated with a variety of neurological, cognitive and psychiatric abnormalities. Sporadic and familial types have been documented in the literature. CT is useful for identifying these calcifications. The cause of hyperdense image on CT is bleeding or calcifications. Each pathology are distinguished by density measurement. The absence of family history, the absence of any previous symptom and admitted with head trauma are remarkable for our case Keywords: Fahr’s syndrome, tomography, trauma

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
304
P 200 A CASE OF AN UNUSUAL GASTRIC FOREIGN BODY: RAZOR BLADE Harun Gunes, Feruza Turan Sonmez, Ayhan Saritas Düzce University School of Medicine, Department of Emergency Medicine, Düzce, Turkey Foreign body ingestion may be seen un-intentionally in children and adults. It also commonly occurs in psychiatric patients and prison inmates intentionally. Although the swallowed objects are generally harmless, those having a high potential to cause serious injury like the ones with sharp edges may also be swallowed. Therapeutic approach for ingested foreign bodies depends on the type and location of the foreign body in gastrointestinal tract. We present the case of a 29-year-old man who was brought from a prison after making cuts on his neck and right arm. There were a few superficial cuts on his neck and multiple horizontal cuts, some of which are deeper, on his right arm and limited extension in his 3rd right finger. Thus, he was consulted to the Plastic and Reconstructive Surgery Department, and decided to be hospitalized by that department for repair of his lesions however he, later, stated he swallowed a razor blade. Then, plain radiographs of the chest and abdomen were taken but no radio-opaque foreign body could be visualized so thoracic-abdominal computed tomography scan was performed, and a hyper-dense foreign body was detected in the stomach. Hence, he was consulted with the General Surgery Department. They performed upper gastro-intestinal endoscopy but could not find the foreign body. Afterwards, the patient was transferred to the Plastic and Reconstructive Surgery Department and discharged after repair of his lesions. No complications developed during his out-patient follow-up by the related departments. Foreign bodies even those with sharp edges can be passed through gastrointestinal tract however they may also cause some serious complications like perforation and obstruction depending on the type of the object. Thus, emergency physicians should be vigilant of this subject and confirm or exclude the diagnosis quickly, and consult the patient with the related department when the diagnosis is confirmed. Keywords: Gastric foreign body, razor blade, prison inmate P 201 THE RELATIONSHIP BETWEEN BLOOD LACTATE LEVELS IN PATIENTS APPLYING TO THE EMERGENCY SERVICE WITH UPPER GASTROINTESTINAL BLEEDING Ebubekir Arslan1, Engin Özakın1, Tuncer Temel2, Aysegul Harmancı Ozakyol2, Nurdan Acar1, Filiz Baloglu Kaya1
1Eskişehir Osmangazi University Faculty of Medicine, Department of Emergency Medicine, Eskişehir, Turkey 2Eskisehir Osmangazi University Faculty of Medicine, Department of Gastroenterology, Eskişehir, Turkey Objective: The aim of our study is to evaluate the relationship of the lactate level during admission with the hemodynamic parameters, the need and the amount for blood products replacement and the mortality. Methods: The patients over 18 years of age who applied to the ED during the year of 2016 with upper gastrointestinal bleeding have been investigated retrospectively. The demographic characteristics of the patients, their vital signs, symptoms, blood parameters within the course of admission following 12, 24 and 48 hours, lactate levels, Rockall risk scores, need and quantity for blood transfusion were recorded. Findings: 57% of the 104 patients was male and the mean age was 66.27. MAP was an average of 84.76. Hematemesis (64.4%), melena (67.3%) and hematochezia (4.8%) were detected in the physical examination. The relationship of the lactate levels within the course of admission with the MAP (p=0.02), the Hb at admission (p=0.01), hemoglobin values following 12 hours (p=0.013), 24 hours (p=0.084) and 48 hours (p=0.061), the need for transfusion of blood products (p=0.040), the amount of blood product transfusions (p=0.02), and Rockall score (p=0.001) was determined. 51% of endoscopic procedures was lesions without signs of recent hemorrhage or fibrin-covered clean ulcer base (Forrest 3), 21% was flat pigmented haematin on ulcer base (Forrest 2c), 19.2% was adherent clot (Forrest 2b), 5.8% was visible vessel (Forrest 2a), and 2.9% was oozing hemorrhage (Forrest 1b) patients. Spurting hemorrhage (Forrest 1A), was not detected in any of our patients. Their relationship between lactate levels was detected according to Forrest classification (p=0.016). No deaths occurred in any of our patients. Result: At their first admission to the ED the lactate levels of the patients with acute UGI bleeding the measurement of lactate levels may be useful in determining the blood transfusion and morbidity. Keywords: Blood lactate level, hematemesis, melena, hematochezia, blood transfusion

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
305
P 202 AN ANALYSIS OF INTOXICATED PATIENTS ADMITTED TO THE EMERGENCY DEPARTMENT Ahmet Sebe, Yücel Cansu Ünaldı, Ayça Açıkalın Akpınar, Nezihat Rana Dişel Çukurova University Faculty of Medicine, Department of Emergency Medicine, Adana, Turkey Objective: In this study, we aimed to analyse the demographic features, toxic material or medicines and mortality rates of the patients admitted to the emergency department and diagnosed as intoxication. Material-Methods: One thousand and eight patients; admitted to Çukurova University Faculty of Medicine Emergency Department and diagnosed as intoxication during January 1, 2013 and September 1, 2015 were included in this study. Patients evaluated retrospectively from the emergency department registration forms and admission files. The specialities including age, sex, admittance time, medical history, reason of poisoning, duration of hospitalization, consciousness state, administration route in emergency department and mortality rates were evaluated. Results: Of the 1008 patients, %56,3 were female. Most of the cases were in 24-40 year of age group (%44,9). Patients were admitted mostly in summer. They were mostly intoxicated with multidrugs and mostly suicidal (%69,7). The mostly used intoxication route was orally (%78,4). %87,8 of patients were discharged after evaluation and observation from the emergency department. Conclusion: For decreasing the intoxication rate, education of society and families, prevention of medicine sales without prescription and usage of farming chemicals with ignorance and keeping cleaning materials and insectisides in safe boxes are necessary. Key Words: Emergency department, drug, intoxication P 203 İMMOBİL HASTADA GENEL DURUM BOZUKLUĞU; AYIRICI TANIDA NELER DÜŞÜNELİM? Mümin Murat Yazıcı1, Ensar Topaloğlu1, Ercan Nalbant1, Gürkan Altuntaş1, Özcan Yavaşi1, Ahmet Pergel2
1Recep Tayyip Erdoğan Üniversitesi Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Rize 2Recep Tayyip Erdoğan Üniversitesi Eğitim ve Araştırma Hastanesi, Genel Cerrahi Kliniği, Rize Yaşlanma ile birlikte, kronik hastalıkların artması ve kronik hastalıklarla ilişkili veya ilişkisiz olarak akut hastalıkların ortaya çıkması acil servislere başvuruların önemli nedenlerini oluşturmaktadır. Akut mezenter arter iskemisi, ölümcül vasküler aciller içerisinde olup mortalitesi %50- %80 arasında değişmektedir. Klinik olarak ani başlayan, ciddi, yaygın karın ağrısı, bulantı, kusma, kanlı ishal gibi gastrointesitnal şikayetlerle acil servise başvurular olabileceği gibi, bilinç değişikliği, genel durum bozukluğu gibi spesifik olmayan şekillerde de acil servise başvurular olmaktadır. Bizim vakamızda ise; 82 yaşında erkek hasta, bir gündür olan solunum sıkıntısı ve genel durumunda kötüleşme şikayetleriyle acil servise getirilmiştir. Hastanın özgeçmişinde, hipertansiyon ve 3 ay öncesinde geçirilmiş hemorajik serobravasküler hastalık(SVH) öyküsü vardı. Geçirmiş olduğu hemorajik SVH’a bağlı olarak son 3 aydır immobildi. Hastanın yapılan ayrıntılı tetkik ve tedavileri sonucunda Akut mezenter arter iskemisi tanısı konulmuştur. Genel durum bozukluğu ve solunum sıkıntısı şikayetleriyle acil servise getirilen hastalarda vasküler patolojilerin akılda bulundurulması gerektiği unutulmamalıdır. Anahtar Kelimeler: Acil servis, genel durum bozukluğu, superior mezenter arter iskemisi

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
306
P 204 ALIŞILMAMIŞ ORGANOFOSFAT KÖTÜYE KULLANMA YÖNTEMİ: İNTRAVENÖZ UYGULAMA Ali Duman, Ayhan Akoz, Selçuk Eren Çanakçı, Burçak Kantekin, Mucahit Avcil, Kenan Ahmet Turkdogan Adnan Menderes Universitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Aydın, Türkiye Giriş: Organofosfat özellikle gelişmekte olan ülkelerde intihar girişiminde sık kullanılan bileşiktir. İntramusküler ve intravenöz yol kullanımı nadirdir. Organafosfat zehirlenmesinde tedavide dekontaminasyon, emilimin azaltılması, genel destek tedavisi ve antidot tedavisidir. Zehirlenmelerde güncel çoklu tedavi yöntemleri; spesifik antidot ve antikor, lipid emülsiyon tedavisi ve plazma değişimi tedavilerinden oluşmaktadır. Bizde literatürde nadir görülen intravenöz yolla intihar amaçlı 2 ml monocrotophos uygulayan erkek hastayı ve uyguladığımız tedavi yöntemlerini sunmak istedik. Olgu: 18 yaşına erkek hasta intihar amaçlı 2 ml monocrotophos (Hukron) intravenöz uygulama sonrası 2. saatte acil servisimize kabul edildi. Hastanın acil servis kabulünde GKS:15, tansiyon 130/110 mmHg, nabız 80/dakika, solunum sayısı 23/dakika idi. Hastada aşırı terleme, hipersalivasyon ve pupillerde miyozis vardı. Hastanın serum kolinesteraz düzeyi 344 units idi. Tedavide 12 mg/saat atropin infüzyonu başlandı ve klinik bulgularına göre titre edildi. Pralidoksim 500 mg yükleme ve 500 mg/saat infüzyon tedavisi başlandı. Lipid 75 ml yükleme, 80 ml/saat idame infüzyon tedaviye eklendi. 10. saat lipid tedavisi sonlandırıldı. 6. ve 17. saatte hematolojiye danışılarak plazmaferez tedavisini aldı. 4. gün hastanın klinik bulguların gerilemesi ve kolinesteraz düzeyinin 1045 units olması sonrasında atropin ve pralidoksim tedavisi stoplandı. Takibinin 7. günü hasta acil gözleme alındı ve 14. günde kolinesteraz düzeyinin 6448 units olan hasta psikiyatri konsultasyonu sonrasında taburcu edildi. Sonuç: Organofosfat zehirlenmede genel destek tedavisine ek olarak atropin ve pralidoksimden oluşur. Pandit ve arkadaşlarının olgusunda solunum yetmezliğine bağlı 12 gün ventilatör ihtiyacı olmuştur. Bande ve arkadaşları olgusunda solunum yetmezliğine bağlı 10 gün ventilatör ihtiyacı olmuştur. Bizim olgumuzda da geleneksel tedaviye ek olarak uygulanan İV lipid ve plasmaferez tedavisi sonrasında hastanın ventilatör ihtiyacı olmamış, 7. gün acil gözleme alınmış ve 14. günde şifa ile taburcu edilmiştir. Biz olgumuzda da olduğu gibi organofosfat zehirlenmelerinde hızlı genel destek ve antidot tedavisine ek olarak lipid emülsiyon tedavisi ve plasmaferez gibi tedaviler ile hastaların yoğun bakım ihtiyacı ve hastanede yatış sürelerinin azaltılabileceğini düşünmekteyiz. Anahtar Kelimeler: Zehirlenme, organofosfat, intravenöz uygulama, lipid emilsyon, plasmaferez P 205 CAN PUPILLOMETRIC EVALUATION OF BLUNT OCULAR TRAUMA PATIENTS HELP PHYSICIANS AS A COUNTATIVE MEASUREMENT TOOL? Necati Salman1, Salih Uzun2, Yahya Ayhan Acar1, Onur Tezel1, Fatih Çakır Gündoğan3, Ömer Faruk Şahin2
1Ankara Gülhane Training and Research Hospital, Department of Emergency Medicine,Ankara, Turkey 2Etimesgut Military Hospital, Ophthalmology Clinic, Ankara, Turkey 3Ankara Gulhane Training and Research Hospital, Department of Ophthalmology, Ankara, Turkey Objective: Pupillometry is a physiological measurement method of pupil diameters currently used in ophthalmology, anesthesiology, and psychology procedures, and assesses both sympathetic and parasympathetic pathways. Aim of this study was to evaluate the pupillary light reflex responses of blunt ocular trauma patients with pupillometry in order to investigate the diagnostic value of this method. Material-Methods: This was a retrospective observational study. Emergency department and ophthalmology policlinic admissions of patients with blunt ocular trauma patients were enrolled to the study. We compared 11 pupillometric parameters (initial diameter, amplitude of contraction, latency of contraction, duration of contraction, velocity of contraction, latency of dilatation, duration of dilatation, velocity of dilatation, maximum diameter, minimum diameter, average diameter) of traumatic and non-traumatic eyes of patients. SPSS 15.0 program was used for statistical analyses. Results: During a 15-month period a total of 32 patients admitted to our emergency service and ophthalmology policlinic with complaint of blunt orbital trauma. All the patients had trauma at one side. We observed that five of the patients didn’t have pupillometry evaluation (2: under 18 years old, 2: generalized orbital lip edema, 1: technical problem). All of the patients were male and mean age of them was 21.74 years (min:21, max:31 years). Patients’ mean post-trauma period at admission time was 24.67 hours (min: 30 minute, max: 120 hours). Our data analysis presented that initial diameter of traumatic eye was significantly shorter compared with the initial pupil diameter of the patients’ non-traumatic eyes (p<0.01). There was not any statistical significant difference at the comparison of other pupillometry variables. Conclusion: In addition to physical examination, clinicians can use pupillometry for the assessment and follow-up of blunt ocular trauma as a quantitative measurement tool. Keywords: Pupillometry, blunt ocular trauma, emergency department
5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
307
P 206 A CHALLENGING DIAGNOSIS FOR EMERGENCY PHYSICIANS: THREE CASES OF MUCORMYCOSIS Sinan Genç, Ayça Koca Tanrıverdi, Müge Günalp Eneyli, Fatma Candan Aydın, Onur Polat, Serdar Gürler Ankara University School of Medicine, Department of Emergency Medicine, Ankara, Turkey Mucormycosis is a rare but emerging fungal infection with a high mortality rate. The most important conditions predisposing to mucormycosis are malignant hematological disease, severe neutropenia, poorly controlled diabetes mellitus (DM), iron overload, major trauma, prolonged use of corticosteroids, illicit intravenous drug use, neonatal prematurity. Based on clinical presentation and anatomic site, mucormycosis is classified as rhinocerebral, pulmonary, cutaneous, gastrointestinal, disseminated and uncommon rare forms. Management of mucormycosis includes prompt diagnosis, early treatment with antifungal agents, control of predisposing factors and surgical debridement if necessary. Case 1: A 64-year-old male patient presented to emergency department with fever, weakness and redness at right eye. He has an undiagnosed type-2 DM. Rhinoorbital mucormycosis was diagnosed and amphotericin B treatment was initiated. Patient was discharged unventfully few weeks later. Case 2: A 63-year-old male patient presented to emergency department with left fascial pain and periorbital swelling. He has idiopathic thrombocytopenic purpura and steroid induced DM. Rhinoorbital mucormycosis was diagnosed and liposomal amphotericin B treatment initiated. Surgical debridement and left orbital exanteration, subtotal maxillectomy and ethmoidectomy was performed. A frontotemporal brain abscess has been found patient’s follow up. Patient was died 2 months after admission. Case 3: A 51-year-old female patient with DM presented to emergency department with left hemiparesis and right fascial pain. She was on antibiotic treatment for dental abscess for 10 days. Rhinoorbitocerebral mucormycosis was diagnosed and liposomal amphotericin B treatment initiated. She was died at 6th day of admission. The pleiotropic clinical manifestations and elusive presentation of mucormycosis often delay diagnosis, with resultant poor outcomes. A high index of suspicion for mucormycosis based on appropriate risk stratification and improved laboratory diagnosis are important for improving the natural history of this devastating infection. Keywords: Emergency medicine, mucormycosis, orbital cellulitis P 207 THE DIAGNOSTIC ROLE OF ISCHEMIA MODIFIED ALBUMIN (IMA) IN PATIENTS WITH ACUTE ABDOMINAL PAIN AND ITS ROLE IN THE DIFFERENTIATION OF ACUTE ABDOMEN Selman Yeniocak1, Fatma Saraç2, Mustafa Yazıcıoğlu3, Nadiye Karabulut4, Ünal Akın5, Esma Yücetaş6, Macit Koldaş6
1University of Health Sciences, Haseki Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey 2University of Health Sciences, Haseki Training and Research Hospital, Pediatric Surgery Clinic, Istanbul, Turkey 3University of Health Sciences, Bakırköy Sadi Konuk Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey 4University of Health Sciences, Haseki Training and Research Hospital, Family Medicine Clinic, Istanbul, Turkey 5University of Health Sciences, Haseki Training and Research Hospital, General Surgery Clinic, Istanbul, Turkey 6University of Health Sciences, Haseki Training and Research Hospital, Biochemistry Clinic, Istanbul, Turkey Objective: Differential diagnosis of a patient presenting with abdominal pain poses various difficulties to the emergency physician. Laboratory tests in addition to the patient’s history and physical examination facilitate diagnosis. This study assessed the diagnostic value and potential use of ischemia modified albumin (IMA) in the differentiation of acute surgical abdomen in patients presenting to the emergency department (ED) with acute abdominal pain. Method: Following approval from the institutional ethical committee 334 patients aged over 18 presenting to the ED with non-traumatic abdominal in the preceding week, definitely diagnosed and either hospitalized in a specific department or planned for discharge and agreeing to take part were enrolled in this prospective study. Results: Three hundred thirty-four cases were included in the study, 194 subjects in the patient group and 140 in the control group. The patient group consisted of 100 (51.5%) males and 94 (48.5%) females. Shortest time from onset of pain to presentation to the emergency department was 3 hours and the longest 72 hours, with a mean time of 21.4 ± 14.9 hours. The mean IMA value of the patients diagnosed with acute appendicitis was statistically significantly higher compared to that of the control group (p<0.001). Mean IMA value in the discharged patients was 687.9 ± 478.3 ng/ml, and this differed statistically significantly from the mean IMA value in the hospitalized patients (p=0.037). The mean IMA value in the cases determined as necrotizing acute appendicitis based on pathology results was 1539.9±610.8 ng/ml, statistically significantly higher than the mean IMA value in the cases of non-necrotizing appendicitis, 735.1 ± 109.0 ng/ml (p=0.001). Conclusion: Serum IMA levels might be useful in the differential diagnosis of abdominal pain, and particularly acute appendicitis, in patients presenting to abdominal pain with suspected acute abdomen the emergency department. Keywords: Abdominal pain, acute abdomen, ischemia modified albumin, acute appendicitis

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
308
P 208 BİR ÜNİVERSİTE HASTANESİNİN ACİL SERVİSİNDE KURBAN BAYRAMI Selahattin Gürü1, Sezer Eşfer2, Gültekin Kadı2, Begüm Öktem2, Onur Çakmak2, Mehmet Akif Karamercan2
1Ankara Atatürk Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Ankara 2Gazi Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Ankara Giriş: Müslüman ülkelerde her yıl kurban bayramının ilk 3 gününde çok sayıda hayvan kesilip yoksul insanlara dağıtılır. Gerek hayvanların kesimi ve parçalanması, gerekse canlı hayvanlarla olan temaslar sırasında insanlar çeşitli künt ve delici travmalara uğrarlar. Bu araştırmada bir üniversite hastanesine 4 yıl süresince kurban bayramında acil servise başvuran hastaların özellikleri ve akıbetleri değerlendirilmiştir. Materyal & Metot: Araştırma kapsamında; 2012 ile 2015 yılları arasındaki üst üste 4 kurban bayramı süresince kurban kesimi ve parçalanması sırasında meydana gelen delici ve künt travmalar sebebiyle, Ankara Gazi Üniversitesi Tıp Fakültesi Hastanesi Acil Servisi’ne başvuran 18 yaşını doldurmuş hastalar prospektif olarak gözlendi. Araştırmaya katılmayı kabul eden hastaların yaşları ve cinsiyetlerinin yanı sıra; yaralanmanın mekanizması, yaralanma sonucu acil serviste koyulan tanı, varsa uygulanan tedavi ve hastanın acil servisten çıkış şekli kayıt altına alındı. Bulgular: Araştırma kapsamında 78 hasta değerlendirildi. 63 hasta bayramın ilk gününde başvurdu. Hastaların yaş ortalaması 41,52 idi. Hastaların 10’u (%12,8) kadın, 68’i (%87,2 )ise erkekti. Başvuruların 63’ü (%80,7) bayramın ilk gününde gerçekleşti. Yaralanmaların 67’si (%85,9) kesici-delici yaralanmalarken, 11’i (%14,1) künt travmaya bağlı yaralanmalardı. Hastaların 23’ü (%29,4) cerrahi branşlara konsulte edildi ve 12’si (%15,3) hastaneye yatırıldı. 3 hasta (%3,8) geciken konsültasyon sebebi ile kendi isteği ile hastaneyi terk etti. 55’ine (%70,5) sütürasyon uygulanan 63 hasta (%80,7) acil servisten taburcu edildi. Ölen hasta olmadı. Tartışma: Kurban bayramlarında acil servislerde, kurban kesimi ve parçalanması ile ilişkili yaralanmalar belirgin bir iş yükü oluştururlar. Bu iş yükü ağırlıklı olarak bayramın ilk gününde gerçekleşir. Çoğu kesici-delici olan yaralanmaların cerrahi tedavileri ise yine çoğunlukla acil serviste yapılır. Gerek acil servisler gerekse konsulte edilen cerrahi bölümler kurban bayramlarına, hem çalışan sayısı hem de ekipman olarak hazırlanmalıdır. Anahtar Kelimeler: Kurban kesimi, kurban bayramı, acil servis P 209 EVANS SENDROMLU ÇOCUKTA GENEL VÜCUT TRAVMASI: OLGU SUNUMU Mehmet Altuntaş, Gökhan Ersunan, Aydın Coşkun Recep Tayyip Erdoğan Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Rize Giriş: Evans sendromu; altta yatan bilinen bir etyoloji olmaksızın eş zamanlı veya ardışık olarak otoimmün hemolitik anemi (OIHA), immün trombositopeni (ITP) ve bazen immün nötropeninin kombinasyonu olarak tanımlanır. Nadir görülen bir hastalıktır. Tüm etnik gruplarda ve her yaş grubunda görülebilir. İmmün regulasyonda bozukluk olduğu bilinmekle birlikte patofizyolojisi net değildir. Olgular kliniğe solukluk, sarılık, letarji, kalp yetmezliği, peteşi, ekimoz, mukokutanöz kanama gibi nedenlerle başvururlar. Fizik incelemede lenfadenopati, hepatomegali ve splenomegali saptanabilir. Tedavide kortikosteroidler ve/veya IVIG en sık kullanılan ilk seçenek ilaçlardır. Bunun dışında immünsupresif ajanlar, monoklonal antikorlar, vinkristin, siklofosfamid, azathioprin, 6-thioguanin, tacrolimus, plazmaferez, splenektomi, kemik iliği transplantasyonu Evans sendromu tedavisinde nadir olarak kullanılmaktadır. Olgu: Araç içi trafik kazası sonrası acil servise getirilen 10 yaşında çocuk hastanın başvuru anında fizik muayenesinde bilinci açık, oryente, koopere, GKS: 15, TA:110/70 mmHg, nabız: 88 atım/dk, SPO2: %100, batın normal bombelikte hassasiyet yoktu, toraks muayenesi normal, sağ temporal bölgede yüzeyel abrazyon, sol dış kulak yolunda laserasyon, sol gözde periorbital ekimoz, nazal faktür ve epistaksisi mevcuttu. Ekstremite muayenesinde her iki dizde ekimoz ve abrazyonu mevcuttu. Başvuru laboratuar değerleri WBC:15.3 K/uL, Hb: 9,0 g/dL, Plt: 55 K/uL idi. Beyin tomografisinde sağ oksipitalde lineer fraktür tespit edildi. Beyin parankimi normaldi. Akciğer ve batın görüntülemesinde patoloji tespit edilmedi. Hastanın acil serviste takibi sırasında 2 saat sonraki Hb:7,7 g/dL, Plt:59 K/dL tespit edildi. Hastaya çocuk hematolojisinin öneriyle random trombosit, 30 mg/kg metilprednizolon ve 1gr/kg'dan IVIG infüzyonu önerildi. hasta takip amaçlı cerrahi yoğun bakıma yatırıldı. Hastanın yoğun bakım takibinde Hb:6,5 g/dl'ye düştüğü cross uygun kan bulunamadığı için hastanın hava ambulansı ile daha ileri merkeze sevk edildiği öğrenildi. Sonuç: Travmaya maruz kalmış Evans sendromlu çocuk hastanın yönetiminde karşılaşılan zorluklar irdelenmeye çalışılmıştır. Anahtar Kelimeler: Evans sendromu, travma, kanama

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
309
P 210 KAFA TRAVMASI SONRASI İZOLE 3. KRANİAL SİNİR FELCİ: OLGU SUNUMU Mehmet Altuntaş, Özlem Bilir, Murat Yazıcı Recep Tayyip Erdoğan Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Rize Giriş: Okülomotor sinir paralizisinde aynı tarafta m. rectus medialis, m. rectus inferior, m. obliguus inferior, m.rectus superior ve m. levator palpebrae superior paralizisi görülür. Bunun sonucunda, m. rectus lateralis ve m. obliquus superior'un aktivitelerine bağlı olarak, ipsilateral göz dışa ve aşağıya bakar. Aynı gözde pitozis görülür. Ayrıca aynı taraftaki gözde direkt ve indirekt ışık refleksi ile akomodasyon refleksi kaybolur; pupil dilate durumda (midriazis) kalır. Okülomotor sinir paralizisinin etiyolojik ayırıcı tanısı vasküler (anevrizma, karotis arter diseksiyonu, karotikokavernöz fistül, kavernöz sinüs trombozu), diyabete bağlı mikrovasküler infarkt, neoplastik (primer parasellar tümörler, lokal ve uzak metastazlar), inflamatuvar tablolar (orbitaltümör, sarkoidoz, Tolosa-Hunt sendromu), enfeksiyonlar ve diğer nedenler (oftalmoplejik migren, travma, dev hücreli arterit) gibi oldukça geniştir. En sık etiyolojik neden iskemidir. İskemik tutuluşta neredeyse daima pupil korunmuştur. Bunun nedeni, parasempatik liflerin, sinirin periferik kısmında seyretmesi ve iskeminin sinirin periferik kısımlarını daha az etkilemesidir. Pupil tutulumu olan okulomotor sinir paralizisinin en sık ve en acil nedenlerinden biri posterior kommunikan arter anevrizmasıdır. Daha nadir olarak hipofiz makroadenomları ve pituiter apopleksinin bir belirtisi olarak görülür. Olgu: Bölgemizde çay taşımak için kullanılan teleferikten düşme sonrası acil servise getirilen 45 yaşında bayan hastanın fizik muayenesinde bilinci açık oryente, koopere, GKS: 15'di. Travma sonrası gelişen sağ gözde pitozis, içe bakış kısıtlılığı ve midriazis tespit edildi. Vital bulguları ve diğer sistem muayeneleri normaldi. Beyin tomografisinde ve MR görüntülemelerinde fraktür hattı, kanama ve yer kaplayan lezyon tespit edilmedi. Hasta takip amaçlı beyin cerrahisi servisine yatırıldı. Sonuç: Ani gelişen izole okülomotor sinir paralizisinde travma akılda tutulması gereken etiyolojik ayırıcı tanılardandır. Anahtar Kelimeler: Okülomotor sinir, pitozis, travma P 211 SPONTANEOUS SUBDURAL BLEEDING: UNKNOWN ETIOLOGY? Incifer Kanbur, Sila Sadillioglu, Hakan Topacoglu Istanbul Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey Subdural hematoma is the most commonly seen traumatic intracranial tumor lesion. Besides severe trauma patients, subdural hematoma can develop in elderly patients due to minor trauma or use of anticoagulants. About 25% of all subdural bleedings are spontaneous. In this article we look at a case in which spontaneous hemorrhaging developed and no etiology was identified. A 19-year-old male patient was admitted to emergency department with a severe headache lasting 5 days. He had no history of disease, medical procedures or recent head trauma. He denied any use of recreational drugs. Following a physical examination it was determined that he was stable, conscious, cooperative and oriented. His Glasgow Coma Scale score was determined to be 15/15. His respiration and cardiovascular examinations were ordinary. His vital parameters were: fever of 36.6 °C, pulse of 75/min, blood pressure of 110/70 mmHg and a respiration rate of 16/min. His blood test results and coagulation factors were normal. No motor or sensory disorders were identified during the neurological examination. His cranial computed tomography scan (CT) revealed a subdural hematoma in the left frontoparietal area, its widest part reaching 15 mm. No tumor or aneurysmal rupture were found. The patient underwent a decompressive operation by neurosurgeons and was discharged after 4 days with no neurological comprimise. We suggest that even if spontaneous subdural hematoma is rare in young patients without head trauma, the possibility of intracranial bleeding should be eliminated by cranial CT if they are reporting a severe headache. It should also be kept in mind that recreational drug users may deny this fact during questioning. Keywords: Intracranial, spontaneous, subdural hematoma

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
310
P 212 DELAYED SPLENIC RUPTURE IN ED Pınar Yeşim Akyol, Yusuf Şahin, Ecem Ermete, Zeynep Karakaya, Fatih Esad Topal, Umut Payza Izmir Katip Çelebi University Atatürk Training and Research Hospital, Department of Emergency Medicine, Izmir, Turkey Introduction: Splenic rupture can occur immediately or it can be delayed up to 14 days following injury. Delayed splenic rupture (DSR) is a scene of blunt splenic injury in the form of significant hemorrhage from a ruptured spleen more than 48 h after injury A case report is presented involving a patient who sustained a ruptured spleen four days following an altercation. Case: A 39-year-old man presented with abdominal pain which had localised left upper quadrant admitted in emergency department. Examination findings revealed abdomen with tenderness and ecchymoses. İn history he had a blunt trauma before 4 days. Vital signs are normal. CT scan was performed and grade 3 splenıc rupture was described. The patient was admitted to general surgery department. Conclusion: DSR after blunt splenic injury is an entity that has been described in the literature but it is still seen relatively infrequently in clinical practice. When a patient presents with a blunt abdominal trauma, awareness of the problem of splenic rupture and active diagnostic approach may help reduce the morbidity and mortality associated with splenic hemorrhage, either immediate or delayed. Keywords: Splenic rupture, abdominal pain, emergency department P 213 HASTANELERDE KBRN YAPILANMASI VE DEKONTAMINASYONUN ÖNEMI Aynur Geyik, Mehmet Nur Geyik, Mahmut Taş, Evin Çim Sağlık Bilimleri Üniversitesi, Gazi Yaşargil Eğitim ve Araştırma Hastanesi, Diyarbakır Kimyasal, biyolojik, radyolojik ve nükleer olayların, toplum sağlığı için oluşturdukları bilinmesine ve eski tarihlerden bu yana savaş aracı olarak kullanılmalarına rağmen, tıp çevrelerinin ve kamuoyunun ilgisini çekmeleri yakın tarihte olmuştur. Nitekim 1995 yılında Tokyo metrosunda bir tarikatın militanlarının sarin gazı ve şarbon ile gerçekleştirdiği saldırılardan sonra 2001 yılında Amerika Birleşik Devletleri’nde şarbon taşıyan mektuplarla yapılan saldırılar farkındalığı arttırmıştır. Biyolojik-kimyasal ajanlar her ne kadar terörizm sayesinde popüler hale gelmişse de, biyolojik-kimyasal, radyolojik-nükleer gibi zararlı maddelerle temas insanoğlunun endüstriyel faaliyetlerinin bir sonucu olarak sürekli yaşanmaktadır. Genel olarak ajanlara maruz kalmış kişilere hastanede bakım veren personelin ajandan etkilenme oranı düşüktür. Herhangi bir ajan maruziyeti durumunda, tüm maruz kalan kişiler ve maruz kalmış olma ihtimali olanlar mutlaka dekontaminasyon işlemine tabi tutulmalı ve işlemi yapacak sağlık personeli uygun kişisel koruyucu ekipman kullanan ve eğitimli biri olmalıdır. Hastanenin hemen giriş kısmında ayrı bir yerde dekontaminasyon alanı oluşturulmalıdır. Bu alan Sağlık Bakanlığı'nın belirlediği kriterlere uygun olarak yeterince geniş olmalı, birbirinden perdelerle ayrılmış duşlar içermelidir. Kapalı ortamlarda kullanılmak üzere tasarlanmış dört tarafı perdelerle kapalı altta atık suyu depolayan haznesi olan üniteler olmalıdır. Günümüzün koşullarını düşünecek olursak hastanelerin KBRN olaylarına karşı mutlaka hazırlıklı olması gereklidir. Olayların tanımlanması, hastaların ve sağlık çalışanlarının korunması, etkin ve hızlı dekontaminasyon olay anında hızla hayata geçirilmelidir. Anahtar Kelimeler: KBRN, dekontaminasyon, şarbon saldırıları, arındırma üniteleri

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
311
P 214 DİŞ ÇEKİMİ SONRASI GELİŞEN MAKSİLLOFASİYAL CİLT ALTI AMFİZEM Emin Uysal, Süleyman Solak, Mustafa Furkan Özel Bağcılar Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Giriş: Maksillofasiyal cilt altı amfizem rutin diş çekimlerinden sonra görülen oldukça nadir bir komplikasyondur. Yaşamı tehdit etme potansiyeli olan bir durum olsa da olguların büyük çoğunluğunda kendini sınırlar ve tehlike oluşturmaz. Biz bu bildiride, alt orta kesici diş çekimi sonrasında sağ maksillofasiyal cilt altı amfizemi gelişen bir olguyu sunduk. Olgu: 26 yaşındaki kadın hasta acil servise sağ yüz ve göz kapağında şişlik şikâyeti ile başvurdu. Hastanın hikâyesinden yaklaşık 14 saat önce sağ alt orta kesici dişinin çekildiği ve 6 saat öncesinde sağ yüzde başlayan hızla göze ve yüze yayılan şişliğin olduğu öğrenildi. Fizik muayenesinde; nabız 88/dk, kan basıncı 110/70 mm/Hg, solunum sayısı 18/dk, ateş 36,6 °C ve oksijen satürasyonu %92'idi. Nefes darlığı tariflemeyen hastanın fizik muayenesinde palpasyonla sağ orbita etrafında, yüzünün sağ tarafında cilt altında krepitasyonlar alınıyordu. Etyolojik neden için çekilen maksillofasiyal tomografisinde sağ orbita, sağ yanak, sağ temporal fossada kas planları arasında yaygın hava dansiteleri izlendi (Figür 1). Boyun ve dişte ağrı tariflemesi üzerine analjezik tedavi ile servis izlemine alınan hastanın 6 saat takip sonrası, aktif şikâyeti olmaması üzerine önerilerle taburcu edildi. Tartışma: Maksillofasiyal cilt altı amfizemin hafif formlarında az miktarda hava lokal doku içine geçer. Bunun sonucunda hafif şişlik, hafif rahatsızlık ve palpasyonda hafif krepitasyona neden olabilir. Oysa büyük miktarda hava doku içine geçerse ağrı belirgin olarak artar, şişlik daha fazla olur ve daha fazla krepitasyon alınır. Hava miktarının fazla olması normal fonksiyonları bozabilir. Hava yoluna baskı yapabilir veya disfajiye neden olabilir. Orbital amfizem sonrasında görme kaybı olabileceği bildirilmiştir. Çoğu olguda fizik muayene bulgularının destekleyici tedavinin 2. ve 3. günlerinden sonra azalmaya başladığı görülmüş ve artakalan şişliğin ise 7-10. günden sonra minimale indiği gözlenmiştir. Sonuç: Diş hekimleri ve acil hekimleri dental işlem sonrası allerjik reaksiyonu taklit eden cilt altı amfizemine bağlı maksillofasiyal bölgede yumuşak dokuda şişme olabileceği konusunda dikkatli olmalıdırlar. Anahtar Kelimeler: Acil servis, maksillofasiyal, cilt altı amfizem P 215 A RARE CAUSE OF SYNCOPE: RENAL ANGIOMYOLIPOMA Ozan Emre Torun, Havva Yigit, Ahmet Ak, Aysegul Bayir, Hasan Kara Selcuk University Faculty of Medicine, Department of Emergency Medicine, Konya, Turkey Renal angiomyolipomas are (AML) hamartomatous lesions consisting of vascular, smooth muscle and adipose tissues and are associated with syndromes such as tuberous sclerosis by 20%. Although often asymptomatic, they may be presented with pain, mass, gross hematuria and massive hemorrhage. They most commonly originate from the kidney, but to a lesser extent they can occur in the liver, lymph nodes, spleen, lung and retroperitoneal space. In this case report, a renal AML detected incidentally in a 29-year-old male patient admitted to our clinic with syncope has been presented by reviewing the literature. Keywords: Case report, syncope, renal angiomyolipoma

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
312
P 216 AN ELEVATED SERUM CK LEVEL: A RARE CAUSE Mehmet Ünaldı1, Meltem Çöllü1, Ferdi Kala1, Cihan Büyüksütcü1, Vehbi Özaydın1, Didem Ay1, Hatice Eryiğit2
1Medeniyet University Goztepe Training and Research Hospital, Department of Emergency Medicine, Istanbul, Turkey 2Dr. Lutfi Kirdar Kartal Training and Research Hospital, Thorax Surgery Clinic, Istanbul, Turkey An elevated serum creatine kinase (CK) level is the most sensitive and reliable indicator of muscle injury. The degree of CK elevation correlates with the amount of mucle injury. In this study we present to a case with abnormal elevated CK caused using an alpha blocker agent. Case: 41 year-old male patient admitted to the ED with widespread myalgia. Vital signs of him were normal. In medical history he had no comorbidity and had used Silodosin 8 mg, an alpha blocker, treating the signs and symptoms of enlarged prostate (BPH) a year. Laboratory signs revealed serum CK:15868, 15368 U/L, AST:299,298 U/L, ALT:137,141 U/L. We performed iv rehydration total 3000 cc.Later we identified serum CK:20000 U/L. He was interned to internal medicine clinic for follow-up and suspicion of rhabdomyolysis. Serum CK elevation not correlate the development of renal failure and other morbidity. The requirement for the diagnosis of rhabdomyolysis should be considered a fivefold or greater increase above the upper threshold of normal in serum CK level in the absence of cardiac or brain injury. Keywords: Elevated, rhabdomyolysis, serum CK P 217 THIOL DISULPHIDE HOMEOSTASIS IN PATIENTS WITH ACUT MYOCARDIAL İNFARCTION
Havva Şahin Kavaklı1, Ozcan Erel2, Ahmet Ali Sezer1, Hdır Yılmaz1, Pınar Koptur1, Filiz Banu Ethemoğlu3, Ülkü Arslan1, Cem Akman1, Cemile Koca2, Mustafa Karakuş1, Betül Özbek2, Cenk Fırat Uncugil4
1Yıldırım Beyazıt University, Yenimahalle Training and Research Hospital, Department of Emergency Medicine, Ankara, Turkey.� 2Atatürk Training and Research Hospital, Biochemistry Clinic, Ankara, Turkey.� 3Yıldırım Beyazıt University Yenimahalle Training and Research Hospital, Department of Anesthesiology and Reanimation, Ankara, Turkey� 4Yıldırım Beyazıt University Yenimahalle Training and Research Hospital, Department of Biochemistry, Ankara, Turkey Background: The aim of this study was to investigate a novel oxidative stress marker (thiol disulphide homeostasis) in patients with acute myocardial infarction (AMI), and compare the results with healthy controls. Methods: A total of 128 including 43 patients with STEMI, 35 patients with NSTEMI, 20 patients with nonspesific chest pain and 30 healthy individuals were included in the study. Troponin levels, native thiol, total thiol, and disulphide were compared between the groups. Results: Levels of native thiol and total thiol are lower in the MI group (STEMI and NSTEMI) with respect to control group and nonspesific group. Disulphide levels are lower in the MI group compared to control and nonspesific group. There were significant negative correlations between troponin I level and native thiol, total thiol and disulphide levels. (p<0.05). Conclusion: Native thiol and total thiol levels may be used as a novel oxidative stres marker in patients with AMI. Since these tests are easy, cheap, automated and optionally manual spectrophotometric assay, can be applied easily. Keywords: Acute myocardial infarction, oxidative stress, native thiol, total thiol, disulphide

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
313
P 218 PHANTOM TUMOR: IS FLUID OR MASS? Mehmet Ünaldı1, Hatice Eryiğit2, Ümit Ölmez1, Ersen Gündüz1, Didem Ay1, Vehbi Özaydın1, Soner Işık1
1Medeniyet University Goztepe Training and Research Hospital, Department of Emergency Medicine, Istanbul, Turkey 2Dr. Lutfi Kirdar Kartal Training and Research Hospital, Thorax Surgery Clinic, Istanbul, Turkey Phantom tumor or vanishing tumor is the name given to the temporary pleural effusion in the interlobar fissure generally occurring due to congestive heart failure. Since its radiologic image appears like malignancy, it may cause confusion in diagnosis. In this study we offer a case of phantom tumor in ED presented with weakness and dyspnea Case: 94-year-old female patient admittted to the ED with weakness and dyspnea.In physical examination decreased breath sounds and efor dyspnea were seen. Chest X-Ray showed the quite properly limited spherical mass in the minor fissure traces in the middle zone of the right lung. So thorax CT was performed with suspect of malignancy, ıt showed that in both lung lower lobe to be more pronounced the appearance of pleural effusion as focal areas in right lung upper lobe was available and widespread patchy ground-glass opacities in all segments. She was diagnosed as phantom tumor and consultated with cardiology clinic. These radiological findings of congestive heart failure is encountered less frequently but should be well because informed as this form of pleural effusion, differential diagnosis of lung mass detected on X-Ray can be diagnosed more accurately Keywords: Fluid, phantom, tumor P 219 ACUTE FLACCID PARALYSIS DUE TO CONN’S SYNDROME: A CASE REPORT OF HYPOKALEMIC PERIODIC
PARALYSIS İbrahim Ulaş Özturan, Cansu Alyesil, Serkan Yilmaz, Nurettin Ozgur Dogan Kocaeli University Medical Faculty, Department of Emergency Medicine, Kocaeli, Turkey Background: Acute onset weakness is one of the common alarming symptom in the emergency department (ED). Strokes, myopathies, spinal disorders, electrolyte disturbances and snake bites are common and potentially dangerous conditions which requires immediate attention. Case: We report thirty-five years old female patient who was referred to our ED with suspected Guillain-Barre Syndrome by a neurologist from a rural hospital. She had one-day history of acute onset bilateral lower and unilateral upper extremity weakness. Also she stated having flu-like symptoms for a week. Detailed history revealed mild similar symptoms in the past. In addition to EKG findings, laboratory results confirmed the severe hypokalemia. Since she had past medical history of hypertension, we considered hypokalemic paralysis due to primary hyperaldosteronism. Right sided surrenal adenoma was identified by abdominal MRI and confirmed with ultrasound. Because of the patient was resistant to medical treatment, she was admitted to endocrinology department. Conclusion: Hypokalemic periodic paralysis is rare disorder which is difficult to diagnose in the ED. Despite the differential diagnoses are vary, definitive diagnosis can be recognizable with taking elaborated history and stepwise approach. Keywords: peridodic hypokalemic paralysis, primary hyperaldosteronism, emergency department
5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
314
P 220 ACİL SERVİSE GELEN FARKLI BİR OLGU SUNUMU: “TRAKONYA BALIĞI ISIRIĞI" Vahide Aslıhan Durak1, Özden Cerit1, Gökhan Akdur1, Nezahat Kahriman2, Özlem Köksal2
1Kırklareli Devlet Hastanesi, Acil Servis, Kırklareli 2Uludağ Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Bursa Giriş: Trakonya denizlerimizde yaşayan en zehirli balıklardandır. Kumlu çamurlu zeminlerde kendilerini zemine gömerek yaşarlar. Genel olarak yazın sığ yerlere, kışınsa derinlere çekilirler. Hareketsiz bir balıktır, fakat deniz dibinde avlarına karşı çok süratlidir. Zehirleri bir insanı sakat bırakabilir. Denizden çıktıktan, hatta öldükten sonra dahi zehirliliği devam eder. Aynı zamanda “çarpan balığı” olarak adlandırılan trakonya, küçük balık ve kabuklularla beslenir. Olgu: 60 yaşında erkek hasta, acil servise balık avlarken elinde aniden meydana gelen çok şiddetli ağrı, kızarıklık ve şişlik ile başvurdu.Hastanın ilk müdahelesi ilçe hastanesinde yapıldıktan sonra tarafımıza sevk edilmişti. Geldiğinde hastanın kan basıncı 90/60 mmHg, nabzı 110/dk ve vücut ısısı ise 37.0 dereceydi. Fizik muayenesinde el sırtından ön kol ½’lik kısmın kadar uzanan endurasyon ve kızarıklık saptandı. Hastanın çok şiddetli ağrıya bağlı anksiyetesi mevcut olup, fizik muayenesinde ek bulgu saptanmadı ve tetkikleri de normaldi. Eline sıcak kompres uygulandı ve elevasyona alındı. Ağrı kesici olarak ilk önce NSAİİ türevi uygulandı, ancak şikayeti gerilemeyen hastaya narkotik analjezik yapıldı. Hasta 24 saat boyunca acil serviste kompartman sendromu gelişimi açısından takip edildi. Şikayetleri gerileyen hasta antibiotik ve analjezik reçete edilerek taburcu edildi. Tartışma ve Sonuç: Trakonya çoğunlukla kum ya da çamura tamamen gömülü olarak yatar. Bu tip balıkların yayılım gösterdiği plajlarda dolaşan insanlar için en büyük tehlike, balıkların üzerine basmaktır. Bu nedenle plajlarda yürürken ayağı zeminde sürümek balıkların ürküp kaçmasını sağlayacak ve tehlikeyi kısmen uzaklaştıracaktır. Zehirli balıkların oluşturduğu bir diğer tehlike de, bu balıkların olta veya ağlarla yakalanması sırasında ortaya çıkar. Balık sudan dışarıya çıkarılırken, korunma içgüdüsüyle dikenlerini, solungaç kapaklarını açar. Bu yüzden zehirlenmeler olgumuzda olduğu gibi, genellikle dikkatsizce elleme nedeniyle balık ağdan ya da oltadan çıkarılırken ortaya çıkar. Tedavide; etkilenen bölgeyi sıcak su içinde bekletmek, dikeni hızla çıkartmak, yara bölgesini sabunlu su ile yıkamak ilk etapta yapılması gerekenlerdir. Takipte hidrokortizon içeren kremler ve oral antibiotikler de uygulanabilmektedir. Ağrı için asetaminofen veya ibuprofen kullanılabilir. Anahtar Kelimeler: Trakonya, acil servis, yönetim P 221 FARKLI BİR YEME BOZUKLUĞU; DİABULİMİA VAKASI Bulut Demirel Ankara Atatürk Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Ankara Giriş: Yeme bozuklukları kişinin dış görünüşü, kilosu ve yiyeceklere aşırı takıntısı sonucunda ortaya çıkmaktadır. Yeme bozuklukları anoreksiya nervoza, bulimiya nervoza ve yeni tanımlanan tıkınırcasına yeme bozukluğu alt guruplarında toplanmaktadır. Yeme bozuklukları her ne kadar dışsal bir problem gibi görünse bile altında yatan derin içsel kargaşaya dışsal bir çözüm getirmeye çalışmaktır. Bu yüzden uzun süreli psikiyatrik tedavi gerektirmektedir. Yeme bozuklukları karşımıza farklı biçimlerde çıkabilmektedir. Bu vakamız ise nadir izlenen tip 1 diyabetlilerin bir yeme bozukluğu olan diabulimia görülmektedir. Vaka Takdimi: 24 yaşında kadın hasta acil servise karın ağrısı şikayeti ile başvurmuştur. Bilinen tip 1 diyabeti olan vitalleri normaldi. Parmaktan ölçülen kan şekeri ise 440 mg/dl olarak ölçüldü. Batını rahat olan hastanın, batında defans ve rebound bulguları izlenmedi. Diğer sistem muayeneleri de doğal olan hastanın laboratuvar tahlillerinde idrar ketonu pozitif olarak izlendi. Kan gazı örneklemesinde ise asidozu bulunmamaktaydı.Hastanın son 6 ayda 2 defa hastane yatışı olduğu ve 9 defa acil servise başvurduğu ve her başvurusunda kan şekeri yüksekliği hastane kayıtlarından izlendi. Hastanın detaylı sorgulamasında hastanın bilerek insülin dozlarını azalttığı ve bunu kilo vermek için yaptığını belirtti.Son bir seneden bu yana kilo vermek için spor ve diyet yaptığını belirten hasta, altı ay önce internet aramalarında insülin dozunun azaltılması ile kilo verilebileceğini öğrendiğini belirtti ve giderek artan dozda azaltma eğiliminde olduğu öğrenildi.Hasta bunun üzerine yeme bozukluğu değerlendirildikten sonra hasta psikiyatri gözetimine devredildi. Tartışma: Diabulimia bilimsel bir ifade olmamasına rağmen artık literatürde de sıkça karşımıza çıkan bir durumu kolayca ifade etmemizi sağlamaktadır. Yeme bozukluklarından bulimiaya benzer şekilde davranışlar gösteren bu hastalar tip 1 diyabetlidir ve insülin dozlarını azaltarak kilo vermeyi hedeflerler. Kan şekeri düzenlenemediği için ölümcül sonuçlar doğurabilecek diabulima hastaları için endokrinolog, psikolog, psikiyatrist ve diyetisyenin de için bulunduğu bir ekibin tedavide uyumlu şekilde hareket etmeleri gerekmektedir. Sonuç: Yeme bozuklukları çok farklı şekilde acil servise başvurabilmektedir. Erken tanı ve tedavi için hastalardan detaylı anamnez alınmalıdır. Anahtar Kelimeler: Acil servis, bulimia nervosa, diabulimia, yeme bozuklukları

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
315
P 222 BİLGİSAYARLI TOMOGRAFİNİN NORMAL OLDUĞU SUBDURAL AMPİYEM OLGUSU Göksu Bozdereli Berikol1, Gürkan Berikol2, Mehmet Serkan Yurdakul1, Tuğrul Önge1, Attila Beştemir1 1Karaman Devlet Hastanesi, Acil Servis, Karaman 2Karaman Devlet Hastanesi, Beyin ve Sinir Cerrahisi, Karaman Geriatrik ve bakım hastalarının acil servis ziyaretlerinin büyük bir bölümünü enfeksiyonlar oluşturmaktadır. Özellikle bilinç durumunun tam değerlendirilemediği hastalarda enfeksiyon odağını saptamak klinisyenleri zorlamaktadır. Seksen altı yaşında erkek hasta yakınları tarafından genel durum bozukluğu nedeni ile getirildi. Hastanın bilinen Diyabetes mellitus tanıları mevcut. Hastanın son zamanlarda gelişen halusinasyon, ateş ve idrar kaçırma olduğu hasta yakınları tarafından belirtildi. Laboratuar tetkiklerinde lökositoz ve CRP yüksekliği mevcuttu. Hastanın çekilen beyin tomografisinde akut nörolojik bir patoloji saptanmamakla birlikte sağ mastoid dokuda heterojen görünüm, hava boşluklari izlenmediği saptandı. Hastanın kulak muayenesinde sağ kulakta otitis media saptanmasi üzerine hastaya ensefalit ve abse ön tanilarıyla MR çekildi. MR sonucunda subdural ampiyem saptanan hasta vankomisin ve meronem tedavisi altında yoğun bakım ünitesine yatırıldı. Genel durum bozukluğu ve oral alım bozukluğuna neden olan ek bir şikayet ya da belirti sıklıkla hasta ve yakınları tarafından saptanamamaktadır. Hasta ve yakınlarının tam tanımlayamadığı kulak enfeksiyonu bulguları dikkatli incelenmediği takdirde atlanabilmektedir. Hastanın otitis media komplikasyonu olan mastoidit beyin tomografisinde saptansa da beyin tomografisinin subdural ampiyem icin yanlış negatifliği göz önünde tutulmalı ve subdural ampiyemin bu hastalarda MR ile saptanabileceği akılda bulundurulmalıdır. Anahtar Kelimeler: Bilgisayarli tomografi, manyetik rezonans, subdural ampiyem P 223 YILAN ISIRMASI ANTİVENOM REAKSİYONU VE OSMOTİK DİÜRETİKLER Ali Karakuş1, Zeynep Kekeç2
1Mustafa Kemal Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Hatay 2Çukurova Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Adana Yılan ısırması sonrası verilen antivenoma karşı anaflaktik reaksiyon gelişme oranı %20-75 arasında değişmekte olup yapılan bir seride %1.6 olarak belirtilmiştir.1 Bu yazıda nadir olarak anaflaksi gelişen, antivenom verilemeyen ve osmotik diüretikle ödemi gerileyip şifa ile taburcu edilen olgu sunuldu. Olgu: 53 yaşında erkek hasta sağ el bileğinden 6 saat önce yılan ısırması nedeniyle getirildi. hastanın genel durumu iyi, şuuru açık koopere, vital bulguları stabildi. Hastaya dış merkezde yılan antiserumu başlanmış ancak ürtikeryal döküntüler geliştiği için verilememişti. Hastanın kolu eleve edilip kısa kol ateline alındı. Ekimoz ve ödem takibine alındı. Yapılan hemogram ve kanama diyatezi değerleri normaldi. Hastaya antivenom verilemediğinden ödemi çözmek amaçlı %20’lik mannitolden 1gr/kg dan 3 doz verildi. 48 saat takip edilen hastanın ödeminde gerileme oldu. Kontrol laboratuar değerlerinde anormallik saptanmayan hasta önerilerle taburcu edildi. Antivenom tedavisi yılan ısırması olgularına, evrelere göre ayrılarak endikasyonu varsa verilmelidir. Sistemik tutulumu olan, vital bulguları bozuk, trombositopenisi olan veya kanama diyatezi değerleri uzayan ileri evre hastalarda uygulanmalıdır. Antivenom reaksiyonu gelişen hastalara ödemi çözmek amaçlı ekstremite elevasyonu, atel ve osmotik diüretikler başlanabilir. 1 Anahtar Kelimeler: Yılan ısırması, antivenom reaksiyonu, osmotik diüretikler

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
316
P 224 ACİL SERVİSTE TANDIRA BAĞLI YANIK VAKALARINA MÜDAHALEDE UNUTULMAMASI GEREKEN BİR DURUM: İNHALASYON YANIKLARI
Serhat Örün1, Göksu Afacan2, Serdar Can1, Ayhan Aköz3, Ali Duman3
1Iğdır Devlet Hastanesi, Acil Servis Birimi, Iğdır 2Erzurum Bölge Eğitim ve Araştırma Hastanesi, Acil Tıp Anabilim Dalı, Erzurum 3Adnan Menderes Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Aydın Amaç: Tandır Doğu ve Güneydoğu Anadolu bölgesinde yemek pişirme amaçlı kullanılan merkezindeki sıcaklığı 200 ile 400 C arasında olan bir çeşit fırındır. Küçük ve yüzeysel yanıklardan ciddi mortalite ve morbiditesi olan yanıklara kadar farklı tiplerde yaralanmalara neden olabilmektedir. Bu vakaları sunmaktaki amacımız tandıra bağlı gelişen farklı tip ve lokalizasyonlardaki yanık olgularının resüsitasyonu ile edindiğimiz tecrübeyi paylaşmak ve inhalasyon yanıklarının önemini vurgulamaktır. Olgu 1: Üç yaşında erkek hasta kaza sonucu tandıra düşme sonrası 112 ambulans servisi ile acilimize getirildi. Hastanın, getirildiği sıradaki Glaskow koma skalası değeri 15 idi. Hipotansif ve taşikardik olan hastanın vücudunun %50' ye yakın bir bölümünde 1. ve 2. dereceden yanıklar mevcuttu. Hemoptizisi de başlayan hastaya 2 adet damar yolu açıldı parkland formülü ile hesaplanan sıvı replasmanı başlandı, debritmanı ve pansumanı yapılan hasta 3. basamak bir yanık merkezine sevk edildi. Sevk sırasında nöbet geçiren hastanın sevk edildiği yere ulaşamadan exitus olduğu öğrenildi. Olgu 2: Onsekiz aylık kız bebek tandıra düşme nedeniyle acil servisimize getirildi. Sağ alt ekstremitede, sırt bölgesinde ve gluteal bölgede olmak üzere vücut yüzey alanının %20'sinde 2.ve 3. derece yanıklar mevcuttu. Parkland formülüne uygun sıvı resüsitasyonu başlanan hasta 3. basamak bir yanık merkezine sevk edildi. Tedavi altına alınan hasta 15 gün sonra şifa ile taburcu edildi. Olgu 3: Seksen yaşında kadın hasta tandır yanığı sonucu acil servisimize başvurdu. Hastanın her iki avuç içinde 2. derece 3. ve 4. parmağında ise 3. derece yanıklar mevcuttu. Tetanoz profilaksisi, yara debritmenı ve sıvı resüsitasyonu yapılan hasta ileri tetkik ve tedavi amacıyla 3. basamak bir yanık merkezine sevk edildi. Sonuç: Acil servislerde yüzeysel yanıklardan ciddi mortalite ve morbiditesi olan yanıklara kadar farklı tiplerde yaralanmalarla karşılaşılmaktadır. İnhalasyon yanıkları da yaşamı tehdit eden yanık vakaları arasındadır. Özellikle tandıra bağlı yanık vakalarına müdahale ederken inhalasyon yanıkları mutlaka akılda tutulması gereken bir durumdur. Anahtar Kelimeler: Acil servis, tandır, inhalasyon yanığı P 225 RUHA İNEN EN BÜYÜK DARBE: TERÖR TRAVMASI Emin Uysal, Süleyman Solak, Ahmet Kutur Bağcılar Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Giriş: Travma kavramının çok geniş bir tanımı olmakla birlikte toplumsal şiddeti, terörizmi, ülkelerarası savaşı, iç savaşı, ulaşım kazalarını ve doğal afetleri de içermektedir. Terörizm, kitleler üzerinde en yüksek psikolojik etkiye neden olabilecek şekilde tasarlanmış bir savaş biçimidir. Ülkemizde de terör gündemden hiç inmeyen, herkesin hayatını bir yönüyle etkileyen bir olgu olarak yıllardır varlığını sürdürmektedir. Yazımızda terör saldırısı sırasında yaralanan ve daha sonra hayatını kaybeden 3 yaşındaki çocuğu ve terörizmin özellikle toplumlarda ve bireylerde yarattığı negatif psikososyal etkilerin altını çizmek amaçlandı. Olgu: 28 Haziran 2016’da İstanbul'un Bakırköy ilçesindeki Atatürk Havalimanı'nda gerçekleştirilen silahlı ve bombalı terör saldırısı sonucu acil servisimize getirilen yaralılardan en küçüğü 3 yaşında bir erkek çocuktu. Fizik muayenesinde genel durumu kötü şuuru kapalı GKS:4, nabız 108/dk, kan basıncı 90/60 mm/Hg, solunum sayısı 18/dk, ateş 36,7°C ve oksijen satürasyonu %88'idi. Oksipital bölgeden bir şarapnel parçası giriş deliği mevcuttu, çıkışı yoktu. Hasta hemen entübe edildi ve destek tedaviye başlandı. Çekilen bilgisayarlı beyin tomografisinde oksipitalden giren frontal bölgede kalan yabancı cisim, yaygın travmatik SAK ve ödem mevcuttu (Şekil 1). Hasta beyin cerrahisi ile konsülte edildi ve yoğun bakıma yatırıldı. Tedavisinin 2. gününde exitus oldu. Tartışma: Terörizm, planlı ve organize bir şiddet içermesi, gizliliği, sadece düşmanı değil masum sivilleri de bilinçli şekilde hedef alması, şiddeti bir siyasal eylem ve propaganda aracı olarak kullanması, ideolojik bir amaca yönelmesi gibi yönleriyle diğer şiddet türlerinden ayrılmaktadır. İlk müdahaleyi gerçekleştiren polis memurları, acil tıp uzmanları, kriz danışmanları gibi profesyonellerin, şok, inanmama, şaşkınlık, fiziksel acı, titreme, ağlama, öfke ve suçluluk gibi ilk tepkileri göz önünde bulundurması gerekmektedir. Teröre doğrudan veya dolaylı olarak maruz kalan bireylerin ve toplumların günlük yaşantılarında, düşünce sistemlerinde, geleceğe ilişkin beklenti ve umutlarında kalıcı hasarlar oluşabilmektedir. Sonuç: Fiziksel, sosyal ve siyasi koşullara göre şekli, amacı, yöntemleri ve etkileri değişse de terörün insan hayatına olan etkisi çoğunlukla travmatik olmaktadır. Anahtar Kelimeler: Acil servis, terör, travma

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
317
P 226 IDENTIFICATION OF INTERNAL JUGULAR VEIN THROMBUS BY POINT OF CARE ULTRASONOGRAPHY Betül Gülalp Başkent University Adana Training and Research Center, Department of Emergency Medicine, Adana, Turkey Introduction: Local swelling is a possible complaint in patients as a finding of complication due to inserted central cathether. Thrombus is the major reason to differentiate in this group of patients and a life-threaten risk. Case: A 58-year-old woman presented to the Emergency Department (ED) with pain and swelling of the neck and right arm for 2 days on the same side of the internal jugular central catheter inserted for hemodialysis. Chronical renal disease, diabetes mellitus and atrial fibrillation were the comorbidities. Initial vital signs were the following: Blood pressure 130/80 mmHg, pulse 96 beats per minute, respiratory rate 18, SatO2 97%. She was morbid obesity. On physical examination, she had moderate swelling and tenderness on the right side of the neck and partially right arm. Bedside ultrasonography performed by the emergency physician identified findings of internal juguler vein thrombus (Figure 1). Anticoagulation therapy was initiated and immobilization of the extremity was provided. Result: Central hemodyalysis catheters are used temporarily for hemodyalysis. However this method is a risk for thrombus formation. Point of care ultrasonography performed by Emergency Physician is the current management in differential diagnosis in ED. Uncompressibility and/or limited compression of the affected vein are the clues of deep vein thrombus. Limited compression reported in a sensitivity and specificity 91% and 97%, respectively. It is not needed to show the thrombus for the diagnosis. Although, limited compressibility alone is a finding with a high probability of DVT, there was a thrombus appeared obviously filled the internal jugulary vein (IJV) around the central catheter. Besides color Doppler and pulse wave doppler are helpful in confirmation of diagnosis with the characters of wall and flow of the vein, however these are not generally necessary in the emergent patient. Keywords: Emergency medicine, point of care emergency ultrasound, thrombus P 227 A RARE AND DELAYED COMPLICATION OF APPENDECTOMY: STUMP APPENDICITIS Özgür Dikme, Behlül Bas, Özgür Karcıoglu Istanbul Training and Research Hospital, Department of Emergency Medicine, Istanbul, Turkey Acute appendicitis is one of the most common reason of acute abdomen and surgical intervention. Stump appendicitis is acute inflammation of the residual part of the appendix and a rare and delayed complication of incomplete appendectomy 1/50000 the rate seen. In 1945, Rose was the first to describe stump appendicitis in patients who had previously undergone an appendectomy for appendicitis. 29 year old male was admitted with acute right lower quadrant abdominal pain and nausea to the emergency department. He has an appendectomy scar on lower right quadrant and history of open appendectomy15 years ago. His workup in the emergency department revealed a white blood cell count of 16,00 cells/mm3. A abdomino-pelvic ultrasonography scan of his abdomen/pelvis revealed an inflamed remnant whose wall was thickened, dilated, fluid filled and measuring 8mm in diameter. There was pericecal/periappendiceal stranding suggestive of acute appendicitis. Computed tomography of abdomen showed an inflamed stump and measuring 12mm in diameter and 25mm in lenght in ileocaecal area. An uncomplicated open appendectomy was performed. The pathological examination revealed acute appendicitis. Our patient had no post operative complications and was discharged home on post operative day 2. The stump appendicitis is a rare and delayed complication. The perforation rate of stump appendicitis was reported high as 68% and patients’ length of stay in hospital is longer than patients with acute appendicitis. Therefore, incomplete appendectomy should be considered as a differential diagnosis of acute abdomen in patients with medical history of appendectomy. Keywords: Acute abdomen, appendectomy, stump appendicitis

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
318
P 228 MİYOKART ENFARKTÜSÜ GİZLEYEN AKUT APPENDİSİT Umut Payza, Gözde Canan Yavaş, Zeynep Karakaya, Fatih Esad Topal, Serkan Bilgin, Pınar Yeşim Akyol İzmir Katip Çelebi Üniversitesi Atatürk Eğitim ve Araştırma Hastanesi, Acil Tıp Anabilim Dalı, izmir Amaç: Dünyada en sık ölüm sebebi başta miyokard enfarktüsü olmak üzere kardiyak nedenlerdir. Her 5 ani ölümün birinin de nedenidir. Miyokard enfarküsü, gerek yaş gerekse komorbid hastalıklar sebebiyle alışkın olduğumuz klinik semptomların dışında bulgularla da karşımıza çıkmaktadır. Başka bir akut bir tablo ile birliktelikte gösterebilir ve bu durum oldukça ölümcül olabilecek tanının gözden kaçmasına neden olabilir. Olgu: 65 yaş bayan hasta iki gün önce başlayan göbek etrafında ağrı, göğüste ve midede yanma şikayeti ile başvurduğu dış merkezden acil servisimize sevk edildi. Orada yapılan tüm batın ultrasonografi ve çekilen kontraslı abdominal bilgisayarlı tomografisinde akut apandisit tanısı aldığı öğrenildi. Hastanın alınan anamnezinde göğüsteki yanma hissinin devam ettiği ve ağrının sağ alt kadrana yerleştiği öğrenildi. Hastanın yapılan fizik muayenesinde kalp ve solunum sistem muayeneleri olağandı. Hastanın batın muayenesinde barsak sesleri normoaktif, her iki alt kadranda da hassasiyet mevcuttu. Sağ alt kadranda defans ve reboundu vardı. Vital parametreleri: tansiyon:140/80 mmHg, nabız: 85 atım/dakika, saturasyon:%96 ateş:37.2 C idi. Çekilen elektrokardiyografisinde inferolateral st segmen depresyonları tesbit edildi. Laboratuar sonuçları; glu:298mg/dl cre:1.48mg/dl bun:32mg/dl ck:196u/l wbc:21.05k/ul nöt:18.57k/ul hb:10.4 mg/dl plt:265k/ul trop ı:3.166ng/ml(0-0.06) ck-mb:12.78ng/ml(0-5) ınr:1.54 geldi. Yapılan transtorasik ekokardiyografiyle de nonstemi tanı netleştirildi. Kardiyoloji ve genel cerrahi ile ortak olarak değerlendirilen hastaya akut apandisit ve miyokart enfarktüsü tanısı konarak yatışı yapıldı. Sonuç: Atipik semptomları da olması nedeniyle kardiyak hastalıklara tanı koymak zorlu bir süreçtir. Bu süreç kardiyak semptomları gizleyen durumlar nedeniyle daha da zorlu bir hale gelmektedir. Akut apandisit her yaşta karşılaşılabilen bir tablodur. Her yıl ABD ‘de 200.000-300.000, Avrupada 700.000 kadar apendektomi ile sonuçlanır. Kimi zaman ortak semptom olan karın ağrısı klinisyeni kardiyak nedenlerden uzaklaştırabilir. Acil servislere başvuran hastalarda anamnez her yönüyle iyi değerlendirilmeli, fizik muayene eksiksiz tamamlanmalı ve nadir de olsa aynı anda birden fazla hastalık olabileceği göz önünde bulundurulmalıdır. Anahtar Kelimeler: Appandisit, miyokart enfarktüs, acil servis P 229 VERTEBRAL ARTERY DISSECTION SECONDARY TO A NECK MASSAGE TOOL Oguzhan Demir, Bülent Taskin, Ali Celik, Haldun Akoglu, Ozge Onur, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey
Introduction: Cervical artery dissection (CAD) involves carotid or vertebral arteries and is a common cause of stroke in young patients. CAD presents as headache, vision disorders, stroke or death. Various etiological factors such as genetic factors, vascular structure and trauma are responsible from this clinical entity. MRI imaging, CT angiography, conventional angiography and ultrasonography (US) are used as diagnostic modalities for CAD. Wewould like to describe a young adult with vertebral artery dissection due to usage of a massage tool on neck. Case: A 28-year-old woman presented with dizziness and nausea. She declared that her symptoms started 2 hours ago while driving car after a sudden neck movement to look back. She had no past relevant medical or surgical history, and no previous use of medications or previous infectious symptoms. Her Glasgow Coma Scale (GCS) was 15, and motor and sensory neurological examinations were normal. However, cerebellar examination was positive with severe ataxia, and she could not walk without help. Acute infarction of the left cerebellum was diagnosed by unenhanced brain computed tomography (CT) and diffusion magnetic resonance imaging (DWI-MRI) studies. A computed tomography angiogram (CTA) revealed a left vertebral artery dissection (VAD). When the history was deepened use of a neck massage tool for 3 days was learned. Patient was admitted to neurology ward and started on acetylsalicylic acid. Discussion: Cervical artery dissections are rare but mortal cause of young stroke based on risk factors as genetic or vascular tendency and trauma. A late or missed diagnosis of vertebral artery dissection can result in devastating neurological sequelae, so emergency clinicians must be alert to diagnose quickly and begin treatment as soon as possible. Treatment should be aimed at preventing additional complications, including recurrent stroke or transient ischemic attack, with antiplatelets, anticoagulants, and endovascular or surgical therapy. Keywords: Vertebral artery dissection, massage, young adult

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
319
P 230 AHOY! HAWSER MOORED TO WRONG BERTH: ENTANGLED TO A NECK Tugba Mamak, Halil Ibrahim Atalay, Nurseli Bayram, Erkman Sanri, Cigdem Ozpolat, Kerem Kabaroglu, Haldun Akoglu, Ozge Onur, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Introduction: Pneumomediastinum is defined as the presence of air in the mediastinum. It has also been described as mediastinal emphysema (1-2). Subcutaneous emphysema is defined as the presence of air in the subcutaneous tissue. Emergency physicians should know and recognize these two situations since they both can be indicators of serious injuries. We tried to bring attention to this matter via a case of pneumomediastinum and cervical subcutaneous emphysema due to tracheabronchial injury after blunt neck trauma in emergency department. Case: A 29-year-old male labor in a ship company was brought to ER with the complaint of dyspnea. According declared that complaints started after a ship rope coiled around his neck. Vital signs were as follows; BP:103/54mmHg, HR:120/min, RR:30bpm, O2sat:%89, Arterial blood gas analysis were as follows; pH: 7.29, PCO2: 56 mmHg, PO2: 35 mmHg, HCO3: 25.9 mmol/L. In physical examination stridor was present, and abrasion and subcutaneous emphysema was present on the anterior neck region (Figure 1). No other pathological physical examination findings were present. The patient was intubated due to his compromised airway. There were no pathological findings in the FAST USG and CT scans except pneumomediastinum, tracheabronchial injury and cervical subcutaneous emphysema (Figure 2,3). The patient was transferred to ICU for further management. Results: The hospital admittance rate of pneumomediastinum is %0.13-%1.4(3). There are 2 types of pneumomediastinum; spontaneus and secondary. Mechanism of spontaneus pneumomediastinum is unclear. Secondary pneumomediastium usually develops due to chronic diseases and traumatic events. EPs should always be alert for subcutaneuos emphysema to raise suspicion for tracheal, bronchial, esophageal and/or thoracic injury. Keywords: Hawser, berth, entangle, pneumomediastinum P 231 ACUTE ISCHEMIC STROKE IN A PREGNANT PATIENT Mehmet Umut Akbulut, Emir Unal, Erkman Sanri, Cigdem Ozpolat, Ozge Onur, Haldun Akoglu, Arzu Denizbasi Marmara University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey Introduction: The incidence of stroke is 11-34/100.000 among pregnant patients. The risk factors are pregnancy induced HT, smoking, arterial and cardiac diseases, thrombophilia, infarction, paradoxal embolism, hyperalbuminemia, multiple gestation, postpartum infections, postpartum cerebral angiopathy, substance abuse and sickle cell anemia. We would like to present a case of stroke in pregnancy since it is an uncommon entity. Case: Patient in her 20th week of pregnancy (G:4,A:1,P:3) admitted to ER with weakness on the right side of her body, diminished right nasolabial sulcus and nausea. She had no known disease or medications. All vital parameters were normal. there were no pathological physical examination findings except the weakness on her right limbs (4/5,4/5), diminished right nasolabial sulcus and extensor response in Babinski reflex. There were no abnormal laboratory findings. Acute left middle cerebral artery infarction was revealed in diffusion MRI and the patient admitted to neurology service for further treatment. Results: Heparins are used for most pregnant women because they do not cross the placenta and do not result in fetal anticoagulation. LMWH is recommended rather than unfractionated heparin for all pregnant patients but the ones in the final weeks of the pregnancy. Early aspirin therapy is recommended in pregnant patients with acute ischemic stroke who are not receiving tPA or anticoagulants. Warfarin is potentially teratogenic between 6.- 9. weeks and 2. 3. trimester, and can lead to central nerve system abnormalities. So emergency physicians should be alert when a pregnant patient presents with neurological deficits such as motor weakness, nausea, speech abnormalities and facial asymmetries. Keywords: Stroke, pregnancy, acute

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
320
P 232 GEÇİCİ 3. DERCE AV BLOK VAKASI Mehmet Oktay1, Osman Sezer Çinaroğlu1, Enes Suman1, Turan Erdoğan2
1Recep Tayyip Erdoğan Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Rize 2Recep Tayyip Erdoğan Üniversitesi Tıp Fakültesi, Kardiyoloji Anabilim Dalı, Rize 3.derece av blok kalbin iletim sisteminde gelişen bozukluklar sonucu atrium ve ventrikül arasındaki iletinin kesilmesi yada gecikmesine bağlı olarak gelişen bir ritm bozukluğudur. Bu vakada geçici olarak 3. derece av bloğa girip çıkan bir hasta ele alınacaktır. 75 yaş erkek hasta kahvaltıda 2sn süren baygınlık hissi ile acil servise başvurdu. Anamnezde ve çekilen ekg sinde anlamlı değişiklik yoktu. Yatak başı monitörizasyonda baygınlık hissi geldiği sırada monitörde QRS dalgaları görülemeyince sinüs pause şüphesiyle defibrilatöre alınarak ritmin ekg de yakalanması amaçlandı. Takipte aralıklı olarak antiroventriküler tam bloğa girip çıktığı görüldü. Koroner yb ünitesine takip amaçlı yatışı yapıldı. Bu vakamızda yatak başı monitörizasyon ve yakın takibin kardiyak sebepli pre-senkopla gelen hastaların yakalanmasındaki önemi vurgulanmak amaçlanmıştır. Anahtar Kelimeler: AV blok, geçici 3. derece av blok, pre-senkop P 233 NON-STEROİD KULLANIMI SONRASI TOKSİK EPİDERMAL NEKROLİZİS Serhat Karaman, Serhat Koyuncu, Burak Hasgül, Nurşah Başol, Hülya Güney Gaziosmanpaşa Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Tokat Toksik epidermal nekrolizis(TEN) tüm yaş gruplarında karşılaşılabilen, kadın/erkek eşit oranda görülen şiddetli sistemik inflamatuar bir deri hastalığıdır. Bu tablodan ilaçlar, kimyasallar, infeksiyonlar ve immünolojik faktörler sorumlu tutulmuştur. Deri bulguları eritrodermiden yaygın büllerle ve erozyonlarla karakterize olabilmektedir. Mukozal lezyonlar ve sistemik toksisite sıkça eşlik eder. TEN %25-35 hastada mortal seyreder. Tanı klinik özellikler ve deri biyosisi ile konulur. Ayırıcı tanıda eritema marginatum majör, Stevens-Johnson sendromu, eksfolyatif eritrodermi, primer büllü hastalıklar, Kawasaki hastalığı ve toksik enfeksiyöz eritem düşünülmelidir. TEN kritik bakım üniteleri veya yanık ünitelerinde takip edilmelidir. Tedavide; sıvı ve elektrolit replasmanının yanı sıra kardiyopulmoner resüstasyon ve sepsis tedavisi gerekebilmektedir. 17 yaşında kadın hasta acil servise boğazında karıncalanma hissi, nefes darlığı ve tüm vücudunda yaygın döküntü şikayeti ile başvurdu. Alınan öyküsünde üç gündür üst solunum yolu tedavisi gördüğü ve ağrıları olması üzerine ağrı kesici kullandığı ve şikayetlerinin ilaç alımından sonra başladığı öğrenildi. Özgeçmişinde özellik olmayan hastanın yapılan fizik muayenesinde; TA: 110/70 mm/Hg, ateş:36 °, SPO2: % 98 idi. Bilinç açık, uvula ödemi yoktu. Dinlemekle akciğerlerinde bilateral minimal ronküsleri mevcut idi. Tüm vücutta yaygın ürtikeryal, yer yer eritematöz ve büllü lezyonları mevcut idi. Yüz bölgesinde ve ekstremitelerinde ayrıca ülsere ve eksfolyatif lezyonlar görüldü. Hastaya antihistaminik ve prednizolon tedavisi intravenöz başlandı. Serum fizyolojik ile hidrasyon başlandı. İnhale albuterol ve budenosid verildi. Hastada ilaca bağlı toksik epidermal nekrolizis düşünüldü ve acil yanık merkezine nakli sağlandı. TEN acil servislerde nadir görülen etyolojide ilaç, kimyasallar ve enfeksiyonlar gibi çeşitli faktörler suçlanan hızlı progresyon gösteren mortalitesi yüksek bir inflamatuar deri hastalığıdır. Tanı sonrası hastanın hızlıca sıvı ve gerekiyorsa elektrolit replasmanı başlanmalı, gelişebilecek kardiyopulmoner arrest ve septik şok açısından dikkatli olunmalıdır. Hastalar kritik bakım ünitelerinde veya yanık ünitelerinde takip edilmelidir. Üst solunum yolu enfeksiyonu nedeniyle naproksen sodyum kullanımı sonrası ilaca bağlı TEN gelişen vakamızı paylaşmak istedik. Anahtar Kelimeler: Toksik epidermal nekrolizis, nonsteroid kullanımı, acil tıp

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
321
P 234 CEREBRAL VENOUS SINUS THROMBOSIS DUE TO USE OF ORAL CONTRASEPTIVE İncifer Kanbur, Sila Sadillioglu, Hakan Topacoglu Istanbul Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey Venous sinus thrombosis is a disease more often found in female patients; a rare cause of stroke. However, if untreated it has a high mortality and morbidity rate. A 37-year-old female was referred to emergency department by neurologist with a day-long compressive headache on the right side, a 10-minute paresthesia in her left leg and a prediagnosis of transient ischemic attack. She had a history of tension-type headaches and had been using oral contraceptives for the past 6 months. Her neurological examination revealed a Glasgow Coma Scale score of 15/15 and hemihypoasthesia on the left side of her face. Her blood-cell count, biochemical parameters, and coagulation factors were normal. She had no history of coagulation factor diseases. Her vital parameters were normal, and no pathology was found in her cardiovascular examination. Her cranial computed tomography (CT) revealed hyperdensity from the superior sagittal sinus to the cortical veins. Hyperdensity was the most significant in the right transverse sinus. Her diffusion weighted magnetic resonance imaging (DWI) showed increased density in the right transverse sinus, the superior sagittal sinus and the right sigmoid sinus indicating venous thrombus. She was diagnosed with venous sinus thrombosis and admitted to hospital. The magnetic resonance angiography showed no flow in the right transverse sinus, the sigmoid sinus or the superior sagittal sinus on the proximal side of the internal jugular vein. Nadroparin and warfarin treatments were applied, and the patient was discharged in healthy condition after 14 days. It should be noted that venous sinus thrombosis has a high mortality rate and may imitate stroke syndromes. In order to determine if there is a predisposition, the patient must be questioned about the use of oral contraceptives as well. For diagnosis, the most efficient scanning methods must be employed. Keywords: Sinus, thrombosis, stroke P 235 UZUN SÜREN İSHAL SONRASI GELİŞEN HİPOTANSİYON: PULMONER EMBOLİ OLGU SUNUMU Merve Akpancar, Mehmet Esen, Serhat Koyuncu, Burak Hasgül, Gülten Yılmaz Gaziosmanpaşa Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Tokat Giriş: Akut pumoner emboli(APE); pulmoner arter ve dallarının herhangi bir nedenle tıkanması sonucu oluşur. Yüksek mortaliteye sahiptir, ancak erken tanı ve tedavi ile sağkalım oranı hızla yükselir. Acil servisler için önlenebilir ölüm nedenleri arasında önemli yer tutar. APE Pollack ve arkadaşlarının(2011) belirttiği gibi birçok semptomla başvurabilir. Biz burada uzun süren ishal sonrası acil servise hipotansiyonla gelen hastada saptanan pulmoner emboli olgusunu sizlerle paylaşacağız. Olgu: 61 yaşında bayan hasta dış merkezden dahiliye polikliniğine uzun süreli(30 gün) ishal sonrası elektrolit imbalansı nedeni ile sevkedilmiş. Poliklinikte hipotansiyon saptanması üzerine acil servise yönlendirilmiş. Özgeçmişinde bilinen hastalığı yok. Vital bulguları; tansiyonu: 60/40 mmHg, nabız: 84 atım/dk, ateş:36.6 0C, SO2:94 saptandı. Çekilen EKG normal sinüs ritmi idi. Hastadan alınan kan gazında, metabolik asidoz(pH:7.24, HCO3:11mmol/l, BE: -18 mmol/l), hipokarbi (pCO2:17 mmHg) ve hipoksisi (PO2:58mmHg) mevcuttu. Laktat düzeyi normaldi. Na+:127 mmol/l, K+:2.7 mmol/l, albumin:1.4g/dl’ydi ve idrarda proteinürisi mevcuttu. Üre, kreatin değerleri normaldi. Hasta dehidrate ve kaşektik görünümdeydi. Sıvı resüsitasyonuna cevap vermeyen inatçı hipotansiyon etiyolojisini araştırmak amacıyla yapılan EKO’sunda sağ yapılarda dilatasyon ve PAB:60mmHg saptanması üzerine pulmoner BT anjiografi çekildi. Sağ pulmoner arter proksimalinde tama yakın lümeni oklude eden trombüs saptandı. Tartışma ve Sonuç: APE’de erken tanı ve tedavi çok önemlidir. Çünkü hastaların %50’si ilk yarım saatte, % 70’i ilk bir saatte, %85’i ilk 6 saatte ölmektedir. Tedavinin başlanması ile mortalite riski hızla azalmaktadır. Bu nedenle çoğu zaman şüphe tanı anlamındadır. APE için birçok skorlama sistemi geliştirilmiştir. Ancak hastalar atipik prezentasyonla başvurabilir. Hastanın PE şiddet indeksi(PESI): 30(Class I <65 puan) ve revize Geneva skoru 3 (düşük risk), Wells skoru sonucuna göre düşük riskli idi. Dehidratasyonun tromboemboliyi tetikleyebileceği, inflamatuar barsak hastalıklarının APE için orta risk grubunda yer aldıkları bilinmektedir. Akut pulmoner embolide tek başına hipotansiyon veya şok bulguları 2014 ESC klavuzuna göre yüksek riskli kabul edilmektedir. Bu nedenle hipotansiyon ile gelen tüm hastalarda, APE ayırıcı tanıda akla getirilmelidir Anahtar Kelimeler: Hipotansiyon, ishal, pulmoner emboli

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
322
P 236 Uvula Ödemi ile Başvuran Bir Olgu: Ecballium elaterium Ahmet Aykut, Abdullah Taşçı, Arzu Emecen Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, Acil Tıp Anabilim Dalı, İstanbul Bilimsel adı Ecballium elaterium L. olan ve halk arasında cırtatan, acı dülek, eşek hıyarı, şeytan keleği, yabani kavun olarak da bilinen acı kavun, Cucurbitaceae ailesine mensup bir bitki türüdür. Ecballium elaterium L. bitkisinin kökleri çok eski zamanlardan bu yana, hemoroidin tedavisinde ve ağrı kesici olarak; meyveleri de, sinüzit, sarılık, noktüri, bel ağrısı ve kulak ağrısı gibi hastalıkların tedavisinde kullanılmıştır. Ecballium elaterium, içeriğindeki aktif madde elaterin aracılığıyla etki gösteren bir bitkidir. Elaterin, muköz membranlarda su geçirgenliğinde yaptığı değişiklikler nedeniyle akciğer ödemi ve assit tedavisinde de kullanılmıştır. Bunun yanı sıra literatürde boğaz ağrısı, irritasyon, salgı artışı, burun, ağız ve solunum yollarında ödem ve nekroza ilerleyen yan etkileriyle birlikte, hayatı tehdit eden anafilaktik reaksiyonlar, kanlı ishal ve hipovolemik şoka neden olduğu bildirilmiştir. Ecballium elaterium’a bağlı ciddi renal ve kardiyak toksisite belirtilerinin gösterildiği yayınlar da mevcuttur. Bu bitkinin özellikle allerji hikâyesi olan bireylerde kullanılmasının daha ciddi yan etkiler meydana getireceği söylenmektedir.Tedavide intravenöz steroid, antihistaminikler ve semptomların şiddetine bağlı olarak adrenlin kullanılmaktadır. Biz acil servisimize burun tıkanıklığı sebebiyle burnuna acı kavun suyu damlattığını ve ardından başlayan boğazda şişlik ve nefes almada güçlük şikâyeti olan bir vakayı sunmayı ve bitkisel tedavilere karşı oluşabilecek yan etkilere karşı dikkat çekmeyi planladık. Anahtar Kelimeler: Ecballium elaterium, uvula ödemi, acil tıp P 237 OCCUPATIONAL VERTEBRAL ARTERY DISSECTION Sila Sadillioglu, Incifer Kanbur, Hakan Topacoglu Istanbul Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey Vertebral artery dissection (VAD) is a major cause of stroke in young people. Signs and symptoms may vary. In the literature it has been reported in connective tissue diseases such as Ehlers-Danlos Syndrome, Marfan Syndrome, fibromuscular fibroplasia, in minor neck traumas, nose blowing, painting, as a result of sport activities such as yoga and sailing, and as an occupational consequence, in one professional jockey. Initial symptoms may delay until 3 days after trauma. We reported a case of VAD due to repetetitive work activity. A 25-year-old male patient was admitted to Emergency Department with a sudden-onset severe headache and weakness on the left side. His neurologic examination showed that he had left hemiparesis, left facial weakness, and dysarthria and loss of the left nasolabial fold. His vital parameters and laboratory studies including blood-cell count, biochemical parameters and coagulation factors were normal. His respiratory and cardiovascular examinations were normal. He denied any blunt trauma. As a textile-factory worker, the patient was in the habit of lifting heavy weights; he reported that the day before, he had swung 30-40 kilograms of weight on to his shoulder. The cranial computed tomography indicated no pathology. The diffusion weighted magnetic resonance imaging (DWI) revealed restriction on the right side of the pons and of the cerebellum, and the computed tomography angiography showed dissection on the left vertebral artery. The patient was treated by endovascular intervention and was admitted to hospital. When the young patients diagnosed as stroke in emergency department, physicians should consider the possibility of VAD. For this reason, a careful history should be taken. Morever, they keep in mind that the cause might be work-related minor trauma, and not only a sport-related injury. Keywords: Vertebral, artery, dissection, occupational

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
323
P 238 INSUFFICENT IMMUNIZATION: A CASE OF TETANUS İncifer Kanbur1, Burcu Gulsen2, Sila Sadillioglu3
Istanbul Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey Tetanus is an infectious disease caused by clostridium tetani, a strict anaerobic Gram-positive bacterium. It affects the central nervous system and causes severe neurological impairment. It may occur despite passive and/or active immunizations. A 39-year-old male patient presented to the emergency department with paresthesia between the chest and neck regions and mouth spasms. His vital parameters were stable and his respiratory and cardiovascular examinations were normal. During the neurological examination, the patient was conscious, cooperative and oriented. His pupils were isochoric with a positive light reflex response. Motor and cerebellar system examinations were normal. The patient was suffering from trismus and profuse sweating from the upper torso and the head. Ten days before he had stepped on a nail puncturing his skin. He indicated that, when he went to the hospital, the physian there told him that there was no need tetanus shot as he had one three years ago. On our inspection, we found the lesion on his foot to be clean, with no hypo- or hyperasthesia. In the cranial computed tomography (CT) and the magnetic resonance imaging (MRI) there were no signs of pathology. During his stay at the ED, the patient began to exhibit signs of risus sardonicus. After diagnosing him with tetanus, we administered tetanus immunoglobuline, and the patient was transferred to the intensive care unit. Due to sepsis, he died on his tenth day at the hospital. It has been suggested that immunoglobuline should be administered together with a tetanus vaccine in cases where the patient’s primary immunization was not complete or where no tetanus vaccine had been received for over ten years. This treatment should also be applied to any case where one cannot completely rule out the possibility of tetanus infection. In all of these situations, this treatment could prove life-saving. Keywords: Tetanus, immunization, insufficient P 239 THE SUCCESS OF ENDOTRACHEAL INTUBATION WITH A LARYNGOSCOPE MODIFIED WITH INFRARED LIGHT EMITTED DIODE LAMP USING NIGHT VISION GOGGLES Sedat Bilge1, Attila Aydın1, Meltem Bilge2, Cemile Aydın3, Erdem Cevik4, Mehmet Eryılmaz1
1Gülhane Training and Research Hospital, Department of Emergency Medicine, Ankara, Turkey 2Dışkapı Training and Research Hospital, Clinic of Anesthesia and Resuscitation, Ankara, Turkey 3Etimesgut State Hospital, Internal Medicine Clinic, Ankara, Turkey 4Haydarpaşa Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey Airway obstruction, life-threatening hemorrhages, and tension pneumothorax are preventable causes of death in the combat area. With the naked eye, the light of the classical laryngoscope (CL) can be viewed; however, infrared (IR) light cannot be visualized, unless observed with the NVG. There is still ongoing debate regarding the technical equipment which should be used while performing ETI in the dark environment of a combat area to prevent the visibility of the CL and ensure safety. In the present study, by replacing the CL bulb with an infrared Light Emitting Diode bulb, we created a modified laryngoscope model (ML) to be used with NVG, while performing ETI in a dark environment. In this environment, we compared the efficacy and safety of ML versus CL in performing pre-hospital ETI. Two ETI methods were used, by engaging and locking the blade on the handle either in the mouth or outside of it. The methods were performed in an illuminated area using CL with the naked eye and in a dark, isolated area using ML with NVG.The success and duration of ETI were explored in the study. No more than an attempt was permitted for the insertion of the endotracheal tube, after which the procedure was considered to be failed. All ETI procedures were found to be successful (100%).For the comparison of the completion times of the interventions, there were statistically significant differences between bright and dark room. Based on the evidences from several healthcare disciplines, simulation can improve the knowledge and skill performance. Combat medics should have at their disposal IR-LED laryngoscope bulbs such as the ML designed in the present study, and keep them at a location that will be readily accessible for all personnel, when required. Keywords: Endotracheal intubation, night vision goggles, battlefield, combat

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
324
P 240 ACUTE CHOROID PLEXUS CYST (CPC) INFARCTION: A RARE ENTITY Taygun Baykal1, Tanju Biçer1, Muharrem Doğan1, Demet Devrimsel Doğan1, Ecem Deniz Kırkpantur1, Özge Onur2
1Fatih Sultan Mehmet Training and Research Hospital, Istanbul, Turkey 2Marmara University Training and Research Hospital, Istanbul, Turkey Introduction: The choroid plexus plays an important role in the regulation of cerebrospinal fluid (CSF), determining permeability of the blood-CSF barrier. The cyst forms when fluid becomes trapped inside and forms a blister. Symptomatic lesions are rare since the atria typically enlarge to accommodate the cyst.Infarction of the choroid plexus may result from ischemia in the distribution of the medial posterior choroidal artery. Here, we describe an unusual case of infarction of the choroid plexus cyst. Case: A 41-year-old female patient presented to the emergency department with the complaint of headache, dizziness and nausea. She has a history of periferal arterial disease and use of acetylsalicylic acid. Her vital signs were normal. The physical and neurologic examination was totally normal. The ECG showed a normal sinus rhythm. She was suffering an insistent headache and neuroimaging was made. In her cranial CT there was no pathological finding. In diffusion-weighted (DW) imaging, there was a CPC in the right lateral ventricle and there was an infarction of the CPC. Discussion: Increasingly routine use of DW image for stroke will likely reveal various clinically silent infarct patterns that may invoke an underlying stroke or vascular mechanism. Unusual stroke syndromes such as medial posterior choroidal artery infarction may be readily apparent on DW images, leading the clinician to search for relatively subtle aspects of stroke origin. Choroidal infarction as demonstrated by DW imaging may have limited clinical significance yet may provide further insight into the pathophysiology of this complex structure. Keywords: Choroid plexus cyst, diffusion-weighted imaging, neurologic emergency P 241 VERTEBRAL ARTERY ANEURYSM: A DIAGNOSTIC CHALLENGE Taygun Baykal1, Tanju Biçer1, Demet Devrimsel Doğan1, Muharrem Doğan1, Abide Merve Manap1, Özge Onur2
1Fatih Sultan Mehmet Training and Research Hospital, Istanbul, Turkey 2Marmara University Training and Research Hospital, Istanbul, Turkey Introduction: Intracranial arteries in the subarachnoid space may compress the brain parenchyma and cranial nerves. Most arterial compressive lesions have been attributed to dolichoectasia in the vertebral-basilar system, and prior reports have concentrated on the pressure effects of basilar artery ectasia. Much less is known about vertebral artery compression of the medulla. Aneurysms of the vertebral artery are rare and can provide a diagnostic and therapeutic challenge. Here we report a symptomatic patient with vertebral artery aneurysm near medulla oblangata. Case: A 80-year-old woman with hypertension and diabetes presented to emergency service with complaint of severe neck pain, dizziness, nausea and vomiting. Her vitals were normal except a blood pressure of 164/70 mmHg. On neurologic examination, no abnormalities were apparent. In cranial computed tomography, there was a hyperdense lesion on the right side of medulla oblangata. Diffusion-weighted MR imaging revealed a compressing vascular lesion to medulla oblangata. Cranial MRI and MR anjiography were performed and revealed a lesion that focally enlarged and indentated to medulla from right side (partially trombosed aneurysm). So a vertebral artery aneursym diagnosis was made and the patient directed to a neurosurgeon after symptomatic relief. Discussion: Vertebral artery aneurysms are rare and represent less than 0.5% of all reported aneurysms. Medullary compression by the vertebral artery is a little-known clinical entity in the medical literature. The major findings were as follows: patients can present with transient symptoms or permanent deficits, motor and vestibular or cerebellar features are the most common clinical presentations, there is a poor correlation between radiographic features and symptoms. They have an increased bleeding risk so should be treated as early as possible. Catheter angiography (DSA) remains the “gold standard”, however, the increasing sophistication of non-invasive techniques has improved the reliance on magnetic resonance (MR) imaging, MR angiography (MRA), and computed tomography angiography CTA). Keywords: Aneursym, neurologic emergency, vertebral artery

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
325
P 242 GASTROİNTESTİNAL SİSTEM KANAMALARINDA KONTRAST MADDE EKSTRAVASYONU
Duygu Tokgöz, Ersin Aksay, Neşe Çolak Oray, Başak Bayram
Dokuz Eylül Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, İzmir Hemodinamik anstabil bulgularla başvuran senkop hastalarında, etiyolojinin araştırılmasında torakoabdominal BT(bilgisayarlı tomografi) anjiografi kullanışlı bir tetkiktir. Masif pulmoner emboli, aortik diseksiyon, intraabdominal kanama ve mezenter iskemi gibi etyolojileri ortaya koyabilir. Biz acil servise senkop nedeniyle başvuran ve izlemi sırasında hipotansif seyreden bir hastaya yukarıda belirtilen ayırıcı tanıların araştırılması için BT anjiografi tetkiki istenilen ve sürpriz bir şekilde masif üst gastrointestinal sistem kanaması tanısı konulan bir hastayı özetlemek istedik. 60 yaşında erkek, acil servise senkop nedeniyle başvurdu. Hastanın başvurudaki kan basıncı 100/58 mmHg, nabız 112/dk, solunum sayısı 16/dk olarak kaydedildi. Hastanın bilinci açık, koopere oryante görünümdeydi. Rektal tuşesinde normal gayta bulaşı vardı. Tekrarlayan ölçümlerde hastanın kan basıncı: 70/40 mmHg nabız 132/dk, solunum sayısı:18/dk, olarak ölçüldü. Arteriyel kan gazı analizinde laktat değerinde yükseklik, baz açığı düşük olarak saptandı. Hemoglobin değeri 9.6 g/dl idi. Hastaya mevcut klinik, laboratuar testleri sonrasında şok ön tanısı ile torakoabdominal BT anjiografi çekilmesine karar verildi. BT anjiografide aort diseksiyonu, perikardiyal tamponat, batın içi kanama ve abdominal sepsise yol açabilecek batın içi perforasyon gibi şok nedenleri ekarte edildi. Ancak duedonum içinde kontrast madde ekstravazasyonu dikkat çekti. Hastanın öyküsünde koyu renk dışkılama, kan içeriği şeklinde kusma olmaması ve muayenenin ise normal gaita bulaşı olması nedeniyle gastrointestinal sistem kanamasından şüphe edilmemişti. BT görüntülemesinden hemen sonra hastada defekasyon ihtiyacı ile birlikte yoğun bir melena çıkışı oldu. Hastaya masif üst gastrointestinal kanama düşünülerek hızlı şekilde kan transfüzyonu başlandı. Hastanın izlemi sırasında yoğun miktarda kanlı kusması nedeniyle üst hava yolunu güvence altına almak için hızlı ardışık entübasyon uygulandı. Daha sonra yapılan endoskopisinde antrumda pilor komşuluğunda forrest 1B kanama saptandı. Hasta ilerleyen süre içinde acil serviste ekstübe edildi ve gastroenteroloji servisine yatırıldı ve 9 gün sonra servisten taburcu edildi. Hemodinamik anstabil hastalarda etyolojiye yönelik çekilen BT anjiografi gastrointestinal sistem kanaması açısından yol gösterici olabilmektedir. Anahtar Kelimeler: Gastrointesitinal kanamalar, görüntüleme, kontrast madde ekstravasyonu
P 243 RADIOLOGIC AND CLINICAL CORRELATION MILLARD-GUBLER SYNDROME
Nezih Kavak1, R.Pelin Kavak2, Hasan Sultanoğlu1
1Ankara Dışkapı Yıldırım Beyazıt Training and Research Hospital, Emergency Medicine Clinic, Ankara, Turkey 2Ankara Numune Training and Research Hospital, Department of Radiology, Ankara, Turkey Introduction: We describe a patient with Millard-Gubler syndrome caused by an ischemic stroke in the left pons and confirmation was obtained by magnetic resonance (MR). Our report compares the clinical findings with the radiologic correlation. Case: A 55 -year-old man in presented with sudden weakness of the left arm and leg and slurred speech. He had a history of essential hypertension. On examination he was oriented with slight dysarthria. There was a peripheral right facial palsy and flaccid left hemiparesis. Ocular movements were normal. Deep tendon reflexes were brisk on the left side, and plantar responses were extensor on the left. The other remainder of the physical and neurologic examination was normal. Brain CT scan was normal. MRI of the brain of difussion imaging showed a well-defined area in the right anteromedial pons. Discussion: Varieties of classical syndromes have been described in literature which involve various combinations of brainstem lesions. Millard Gubler syndrome, known as ventral pontine syndrome, is one of the crossed paralysis syndromes, which are characterised by cranial nerves VI and VII palsies with contralateral body motor and or sensory disturbances. This syndrome is easier to diagnose identified based on the symptoms described above and the technical advances in brain imaging. Keywords: Diffussion imaging, Millard-Gubler syndrome, ventral pontine syndrome

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
326
P 244 HERPES SIMPLEX VIRUS ENCEPHALITIS
Nezih Kavak1, R.Pelin Kavak2, Burcu Doğan1, Hasan Sultanoğlu1
1Ankara Dışkapı Yıldırım Beyazıt Training and Research Hospital, Department of Emergency Medicine, Ankara, Turkey 2Ankara Numune Training and Research Hospital, Department of Radiology, Ankara, Turkey Introduction: Herpes simplex (HSV) encephalitis is the most common cause of fatal sporadic fulminant viral encephalitis which has characteristic imaging findings. HSV have variable clinical presentation making fast and accurate diagnosis difficult but of critical importance. Case: A 40 years old female patient presented to emergency room with complaints of fever, headache, vomiting, memory loss and confusion. On clinical examination, she was lethargic, disoriented, febrile with a pulse of 120/min, regular in rhythm. Blood pressure was 135/75 mm of Hg. Cardiovascular examination revealed tachycardia. Respiratory system and abdomen examination was within normal limits. CNS examination revealed Glassgow Coma Scale (GCS) 14/15, no neck rigidity, all reflexes intact, normal tone and power, left plantar extensor and right flexor, pupils normal sized & bilaterally reacting to light. Fundus examination revealed papilloedema. CT Scan Brain revealed no significant abnormality. MRI Brain study revealed swelling of bilatheral medial temporal lobe, parahippocampal gyrus, insular cortex with restricted diffusion in bilateral medial temporal lobes, insular cortices, cingulated gyri. Discussion: Herpes simplex encephalitis (HSE) is an acute or subacute illness that causes both general and focal signs of cerebral dysfunction. Patients the most common symptoms: Fever, headache, focal neurological deficits, mental status changes, vomiting, seizures, memory loss, Symptoms vary in intensity early in the disease, but tend to progress rapidly. There are no pathognomonic clinical findings associated with HSE. MRI is more sensitive than CT scan and plays an important role in determining the diagnosis and extent of the disease. MRI showing abnormalities in one temporal lobe of the brain, which spread to the other temporal lobe. T1 may show general oedema, T2 weighted imagines hyperintensity of affected white matter and cortex, diffusion weighted imagines shows restricted diffusion in the affected region. The gold standard for the diagnosis relies primarily on Cerebrospinal Fluid PCR analysis. Keywords: Herpes simplex encephalitis, memory loss, confusion, MRI
P 245 AN INTERESTING CASE: ADULT TYPE DIAFRAGMA HERNIA
Pınar Koptur, Havva Şahin Kavaklı, Hıdır Yılmaz, Ahmet Ali Sezer, Cem Akman, Ülkü Arslan, Mustafa Karakuş Yıldırım Beyazıt University, Yenimahalle Training and Research Hospital, Emergency Medicine Clinic, Ankara, Turkey Background: Congenital diaphragmatic hernia is usually seen early in infants. That seen in adults in diaphragmatic hernia is the most common cause of trauma. It is rare in mediastinal shift. In our case, there was no history of trauma and mediastina shift was present. Case: A: Forty-five-year-old male patient was admitted to the emergency service with chest pain with pressure style. Physical examination demonstrated no evidence of trauma in the chest area or surgery. Listen to the patient's lung sounds bilaterally equal, heart rate was in the right lower end of 4th intercostal breast. ECG findings were right axis deviation, a positive QRS complex in AVR. We had no abnormalities except for the elevation of the left diaphragm in patient’s chest X-ray. Biochemical, complete blood count and serum troponin blood test results were normal. He was referred to the cardiology department with a preliminary diagnosis of type 2 dextrocardia. The patient had minimal pericardial, there was no vascular abnormalities. In thoracic computed tomography, Filled on the left chest of the patient liver, bowel loops and mediastinal shift was detected. The heart was replaced on the right side. He was hospitalized with a diagnosis of diaphragmatic hernia, thoracic surgery department. Result: Chest pain is one of the most common reasons for an emergency. We must research all of the reason every time. Keywords: Chest pain, chest radiography, diaphragmatic hernia, troponin

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
327
P 246 BRAIN ABSCESS IN YOUNG PATIENT
İncifer Kanbur, Mehmet Can Girgin, Hakan Topacoglu Istanbul Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey Cerebral abscess is the most common cause of autogenous intracranial complications after meningitis. It may occur as a complication of acute or chronic otitis media. Mortality rates range between 7 % and 61 % in the literature. A 29-year-old male patient was brought to the Emergency Department (ED) by ambulance with altered mental status. He recently had otitis media and had been treated with antibiotics, which he did not use at regular intervals. His relatives denied any use of recreational drugs. At admission time, he was unconscious and had a Glasgow Coma Scale score of 6 (E2 M2 V2). His vital signs were; a temperature of 37.8 0C, heart rate of 85 bpm, blood pressure of 143/73 mmHg, oxygen saturation of 99% and respiration rate of 16 breaths per minute. His blood glucose level was 165 mg/dL. He had purulent discharge in the right external auditory canal and nuchal rigidity. He required endotracheal intubation due to depressed mental status and for airway control. Cranial computed tomography (CT) revealed heterogeneous hypodense space-occupying lesion with a diameter of 32 mm in the right temporal lobe. The mass effect with surrounding edema caused effacement of the adjacent sulcus and partial effacement of the adjacent lateral ventricle, as well as an 11-mm leftward midline shift. The contrast enhanced CT showed a ring-enhancing lesion with edema. The patient was transferred to the intensive care unit and died on his tenth day at the hospital. In patients with loss of consciousness who have symptoms or a history of otitis media, intracranial abscess should be considered as a differential diagnosis; an early diagnosis and adequate antibiotic treatment can significantly decrease mortality rates. Keywords: Brain abcess, young, patient
P 247 A CASE OF UNTREATED PNEUMOTHORAX
Sila Sadillioglu, Incifer Kanbur, Hakan Topacoglu Istanbul Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey In cases of pneumothorax treated with tube thoracostomy, it is necessary to have certain conditions before removing the chest tube. Here, we report a patient who had removed himself the drainage device from his chest tube for about a week without the consent of the physician. A 56-year-old homeless patient has admitted to the Emergency Department (ED) requesting the removal of his chest tube. In his history, he had recently been treated of assault induced maxillofacial trauma and left sided pneumothorax in ED a week ago. Although he had been treated with chest tube drainage, which had resulted in complete lung expansion, he had intentionally disconnected the drainage device with water seal from his chest tube and had run away from the ED. He did not seek treatment at another facility and the end of the chest tube was open during that time. He was hemodynamically stable with oxygen saturation level of 96% at time of admission. Chest X-ray showed left-sided pneumothorax and complete left lung collapse without mediastinal shift. The old tube was removed and a new one was inserted in the 4th intercostal space. Although serous fluid of about 400 ml was immediately drained from chest cavity after the chest tube drainage, lung expansion was not observed when checked with chest X-ray. Because of a risk of empyema, intravenous antibiotic was administered. During his treatment at the ED, he refused admission to hospital and left the hospital. The patient’s psychiatric evaluation could not be completed. In cases of pneumothorax with a totally collapsed lung, the formation of serous fluid is an expected finding. But in cases of disconnected drainage system, the timing of the complication is unpredictable. Keywords: Untreated, pneumothorax, tube removal

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
328
P 248 HYPOXIC ISCHEMIC ENCEPHALOPATHY
Nezih Kavak1, R.pelin Kavak2, Hasan Sultanoğlu1, Burcu Doğan1
1Ankara Dışkapı Yıldırım Beyazıt Training and Research Hospital, Emergency Medicine Clinic, Ankara, Turkey 2Ankara Numune Training and Research Hospital, Department of Radiology, Ankara, Turkey Introduction: Hypoxic ıschemic encephalopathy (HIE) is often seen in emergency departments and the causes are myocardial infarction, cardiac arrest, shock, asphyxia, respiratory paralysis and carbon monoxide poisoning. Case: A 43-year-old man developed cardiac arrest after anaphylactic shock caused by insect bite. After cardiopulmonary resuscitation, the patient lapsed into a deep coma. His brain CT Scan revealed no significant abnormality. Diffusion-weighted MRI images show high signal intensity cerebral cortex, basal ganglia and thalami. Discussion: The brain is our most essential organ but also the most sensitive to oxygen deprivation. HIE insults develop in varying regions of the brain depending on the severity and duration of hypoperfusion or hypo-oxygenation. Patients typically present to emergency department following an acute event (near-drowning, asphyxia, cardiac/respiratory arrest). They are usually intubated and have a history of prolonged resuscitation. Computed tomography (CT) scan has limited sensitivity to diagnose. It is well known that diffusion-weighted MR imaging is the earliest imaging modality to become positive in acute phase, usually within the first few hours after a hypoxic-ischemic event. Diffusion-weighted images show high signal intensity cerebral cortex, basal ganglia and thalami. Keywords: Cardiac arrest, diffusion-weighted MRI, hypoxic ıschemic encephalopathy
P 249 MYOCARDIAL INFARCTION AND SUBARACHNOID HEMORRHAGE
Pınar Koptur, Hıdır Yılmaz, Havva Şahin Kavaklı, Ahmet Ali Sezer, Cem Akman, Ülkü Arslan, Mustafa Karakuş Yıldırım Beyazıt University Yenimahalle Training and Research Hospital, Department of Emergency Medicine, Ankara, Turkey Background: Electrocardiographic changes can occur in non-cardiac-induced state. Stroke, subarachnoid hemorrhage, acute pancreatitis are a few of them. The cause of detected electrocardiographic changes in patients with subarachnoid hemorrhage is a sympatho-adrenal effect. Tachycardia, baradycardia, ST segment elevation, ST depression, T inversion, U wave can be seen. Case: Fifty-six-year-old female patient came to the emergency department with 112 due to a sudden loss of consciousness. The patient's arterial blood pressure 190/110 mmHg, 97% O2 saturation, pulse 114 / min, glaskov scale was 1o points. Patient's left arm and leg weakness neck stiffness was present in the examination. There was ST elevation of inferior leads in the electrocardiography. Brain computed tomography examination revealed a subarachnoid hemorrhage image. In the analysis of the blood glucose 154 mg / dL, urea 54 mg / dL, creatinine of 0.74 mg / dL, hemoglobin 12, platelets 223, troponin 12 IU / l. Patient was transferred to the intensive care unit. Result: Electrocardiographic changes may cause non-cardiac. It is important because it contains two patterns, both the neurological and the cardiac. For that reason this case is important. Keywords: subarachnoid hemorrhage, electrocardiographic changes, ST segment elevation

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
329
P 250 PENİL FRAKTÜR
Oğuzhan Bol, Sercan Bıçakçı, Hüseyin Şahin, Numan Erdem, Merve Yanıker Namık Kemal Üniversitesi Tıp Fakültesi, Acil Anabilim Dalı, Tekirdağ Penil fraktür tunika albuginea’nın travmatik rüptürüdür. Genellikle cinsel ilişki sırasında, mastürbasyon yaparken veya o bölgenin travması neticesinde oluşur. Hastalar genellikle peniste ani kırılma sesine benzer bir ses sonrası şiddetli ağrı, hematom ve şekil bozukluğundan yakınırlar. Tedavisi acil cerrahi müdahale ile fasianın onarımıdır. Bizim vakamızda hasta mastürbasyon sırasında ayağının kayması sonucunda penise olan travma sonrası benzer kliniğin oluşması ile hastaneye başvurdu. Muayene sırasında ağrı tariflemeyen hastada penis üzerinde hematom, ekimoz ve deviasyon gözlendi. Üroloji konsültasyonu sonrası hasta acil operasyona alındı. Literatür araştırmamızda cinsel ilişki sırasında düşmeye bağlı penil fraktür vakalarından bahsedilse de mastürbasyon sırasında travmaya bağlı olgu örneklerine rastlamadık. Her ne kadar bu durumdaki hastaların bu rahatsızlıklarına dair ayrıntılı ve net bir anamnez vermediklerini düşünsekte vakanın oluşu açısından ilginç bir örnek olarak değerlendirdik. Anahtar Kelimeler: Penil fraktür, travma, mastürbasyon
P 251 HER DİFFÜZYON KISITLAMASI ENFAKT ALANI MIDIR?
Nezih Kavak1, R.Pelin Kavak2 1Ankara Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Ankara 2Ankara Numune Eğitim ve Araştırma Hastanesi, Ankara Amaç: Her diffüzyon kısıtlamasının enfakt alanı olmadığını olgularla değerlendirmek. Yöntem-gereç: Diffüzyon ağırlıklı incelemede görülen kısıtlama alanlarının sadece akut enfakt alanında izlenmediği; enfektif, ensefalopatik, iskemik, demiyelizan, vaskülitik, tümöral, metastatik hastalıklar da izlenebileceğini, olgularımızla incelemek ve ayrıcı tanılarında kullanılan klinik ve radyolojik tetkikleri tartışmak. Bulgular: Posterior iskemik ensefalopati(PRESS), beyin metastazı, yüksek gradeli beyin tümörü, primer beyin lenfoması, medulloblastom, akut dissemine ensefalopati (ADEM), hipoksik iskemik ensefalopati(HIE), nörobehçet, Creutzfeldt–Jakobs ve herpes ensefalitli olguların difüzyon inceleme bulguları değerlendirilecektir. Sonuç: Diffüzyon MRG akut arteryel iskemik inmede doğru ve hızlı tanı sağladığı bilinen ve acil servislerimizde çok sık kullanılan bir radyolojik teshiş yöntemidir. Difüzyon kısıtlamasının değerlendirilmesi literatür bulguları eşliğinde olgularımızla tartışmak istedik. Anahtar Kelimeler: Akut enfakt, diffüzyon ağırlıklı inceleme, diffüzyon kısıtlaması

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
330
P 252 CEREBROSPINAL FLUID (CSF) ANALYSIS IN MENINGITIS: IS AFFECT THE HOSPITAL LENGTH OF STAY?
Engin Özakın, Eşref Genç, Mustafa Emin Çanakçı, Nazlı Özcan, Nurdan Acar, Filiz Baloğlu Kaya
Eskişehir Osmangazi University Faculty of Medicine, Department of Emergency Medicine, Eskişehir, Turkey Objective: The aim of our study is to evaluate the symptoms and signs and relationship of the laboratory findings with hospitalization of meningitis patients admitted to the ED. Methods: The patients older than 18 years old who admitted to the ESOGU ED between 2012-2016 diagnosed with meningitis were retrospectively evaluated. Results: 66.7% of the 45 patients was male and the mean age was 44.20. The symptoms at ED admission were: fever in 35(77.8%), headache in 30(66.7%), altered consciousness in 22(48.9%), and seizures in 2(4.4%) patients. Average vitals on admission; SBP was 125 mmHg, pulse rate was 88/min, and mean temperature was 37.4°C. On physical examination; there were neck stiffness in 34(75.6%), Kernig sign in 6(13.3%), Brudzinski sign in 7(15.6%), neurological symptoms in 5(11.1%). No significant difference in frequency of symptoms between genders was detected. In the laboratory investigations, the average WBC value was detected as 13700/IU. The average values on CSF examination were: 2280/IU for WBC, 220.45 mg/dl for protein, 41.70 mg/dL for glucose. There was no significant relationship between the CSF WBC amount and the duration of hospitalization. There was no significant difference in duration of hospitalization of patients with CSF glucose level. There was significant difference in duration of hospitalization of patients with high CSF protein levels (p<0.01) (mean duration of hospitalization was 13.63 days for CSF protein>=45 mg/dL, and 6.66 days for CSF protein<45mg/dL). 43 patients were admitted to the in-patient clinics and 2 patients were admitted to the neurological intensive care unit. The mean duration of hospitalization was 17.5 days in intensive care unit, 12.8 days (min:4-max:31/day) in in-patient clinics. Conclusion: The sensitivity and specificity of clinical signs and symptoms are low. Our study showed that the high CSF protein affect the affect the hospital length of stay. Keywords: Meningitis, CSF, hospital length of stay
P 253 DRUGS TAKEN FROM INTERNET ARE NOT INNOCENT AS THEY APPEAR
Sevil Kuşku Kıyak1, Burçak Ekinci2, Cüneyt Örük3, Güliz Yılmaz3
1Yeni Yüzyıl University Faculty of Medicine, Department of Emergency Medicine, Istanbul, Turkey 2Yeni Yüzyıl University Faculty of Medicine, Department of Neurology, Istanbul, Turkey 3Yeni Yüzyıl University Faculty of Medicine, Department of Radiology, Istanbul, Turkey Objective: Various drugs that give strength and improve sexual performance are sold in internet. Most of these drugs contain sildenafil citrate. We present a 38 year-old-man who had an ischemic stroke 24 hours after ingesting a chocolate which contain sildenafil. Case: A 38-year-old man presented with dizziness, right hemiparesis, vomiting. His Glasgow coma scale was 15/15 and physical examination was normal. His neurological assessment revealed dysarthric speech, dysphagia, right facial weakness, 4/5 strength in his right lower extremity, hypoesthesia on the left side and evident horizontal nystagmus. His systemic blood pressure was: 170/100, pulse rate: 90/min, oxygen saturation: %98. Acute multiple infarctions in right serebellar hemisphere and medulla oblangata, also a small infarct in left occipital lobe are confirmed on brain diffusion-weighted MR imaging. Brain CT angiography revealed an occlusion in right vertebral artery. He had no previous history of hypertension, cardiac disease or stroke and smoked 20 cigarettes per day during last 10 years. Electrocardiography, echocardiography and laboratory studies including hypercoagulation disorders were normal. Acetyl salicylic acid 300 mg, low molecular weighted heparin 0.6 cc and pirasetam infusion started. He had physical therapy sections and could walk with help of one person. He was discharged from hospital after 40 days. Conclusion: Drugs sold in internet are not safe and can cause serious harm, because the amount of sildenafil is not standard. The vasodilating property lowers blood pressure in clinical trials by 8-10 mm Hg over the initial 24 hours after ingestion. Hypotension might be responsible for vascular insufficiency and stasis leading to stroke. Our case report suggests that an ischemic stroke is a rare adverse reaction of sildenafil, however other drug interactions, unknown genetic factors could also be implicated. The potential users should be warned about various risks of these drugs sold in internet. Keywords: Stroke, internet, sildenafil

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
331
P 254 SAFRA TAŞI İLEUSU: OLGU SUNUMU
Feride Fulya Coşkun, Emre Şancı
Dokuz Eylül Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, İzmir Giriş: Safra taşı ileusu ince barsak obstrüksiyonlarının nadir bir sebebidir. Tüm intestinal obstrüksiyonların sadece %1-4’ünde rastlanır. İleri yaş, yandaş hastalıklar, sıvı-elektrolit dengesizliği ve tanıda gecikme nedeniyle %12-18 mortal seyreder. İntestinal obstrüksiyon; taş 2.5 cm ve üzerinde ise izlenir. Olgu: 87 Yaşında kadın hasta; Mayıs 2014 tarihinde şiddetli sağ üst kadran ağrısı nedeni ile merkezimizde yapılan incelemelerinde safra kesesinde 33.2 mm çaplı safra taşı olduğu görülmüş ve uzamış biliyer kolik olarak değerlendirilen hastaya medikal tedavi başlanarak elektif kolesistektomi önerilmiş ancak hasta ve yakınları istememiş. 18 Haziran 2016'da şiddetli kusma ve karın ağrısı şikayetiyle hastanemize başvurdu. Gelişinde vital bulguları normal sınırlarda olan hastanın fizik muayenesinde epigastrik hassasiyet saptandı. Batında defans ve rebound yoktu. Çekilen batın tomografisinde: kese lümeninde ve intrahepatik safra yollarında aerobilia, jejunal segmentlerde 37.3 mm çapındaki safra taşının oluşturduğu obstrüksiyon ve ileus ile uyumlu dilatasyon izlendi. Genel Cerrahi ile konsülte edilen hastaya acil operasyon önerildi ancak hasta ve yakınları operasyonu ve hastaneye yatmayı kabul etmeyerek hastanemizden ayrıldılar. 19 Haziran 2016'da 112 ambulansı ile solunum arresti nedeniyle entübe edilerek acil servisimize getirilen hasta izlemde hipotansif seyretmesi nedeniyle iv hidrasyon ve noradrenalin desteği verildi. İdrar çıkışı sağlanamayan, yapılan tetkiklerinde asidozu ve böbrek fonksiyon bozukluğu saptanan hasta hemodiyaliz hazırlıkları yapılırken arrest oldu. Kardiyopulmoner resüsitasyona yanıt alınamadı. Tartışma: Olguda anemnez safra taşı varlığını gösteriyordu. Hastaya kolelitiyazis nedeniyle operasyon önerilmesi ancak kabul etmemesi, daha sonra da ileus bulgularıyla başvurması safra taşı ileusunu düşündürmektedir. Radyolojik olarak yapılan tetkiklerinde taşa ait görüntü izlenebilmiştir. Fistülün yeri gösterilememiş ancak fistül varlığını bildiren safra yollarında hava bulgusu görülmüştür. Safra taşı ileusunda radyolojik olarak ince barsakta ektopik safra taşı, ileus ve aerobilia izlenebilir. Safra taşı ileusunda obstrüksiyonun giderilmesi tedavinin esasını oluşturur. Sonuç olarak; safra taşı ileusunun morbidite ve mortalitesinin oldukça yüksek seyredebilmesi nedeniyle ileus etiyolojisi araştırılırken akılda tutulması gerektiğini vurgulamak istiyoruz. Anahtar Kelimeler: Safra taşı ileusu, aerobilia, ileus
P 255 BROKEN HEART SYNDROME; BE CAREFUL WHEN WORRY ABOUT SOMETHING
Iremgül Güngör, Elif Çelikel, Pınar Uysal, Binnur Eşfer, İrfan Kala, İsmail Ağı, Muhammed Evvah Karakılıç, Muhittin Serkan Yılmaz
Ankara Numune Training and Research Hospital, Emergency Medicine Clinic, Ankara, Turkey A 60-year-old female admitted emergency department with typical cardiac chest pain and dispnea for last few minutes. She was companion of her sick daughter and she had been staying in hospital to help her. She had no history of disease, smoking or drug use. Her vital signs was temperature of 36.4°C, blood pressure of 147/91 mmHg, respiratory rate of 18/min, heart rate of 87/min and pulse oximetry reading of 94 % on room air. ECG was taken and it showed normal sinus rithym and non-specific ST segment elevation. At physical examination the patient was conscious, oriented, neurological examination was normal. Cardiac auscultation was also normal and rithymic. Pulmoner auscultation also was normal. There was no rales or ronchus. The other system examination was normal. Routine blood tests were studied. In results cardiac enzymes increased. Troponin I:0,22 (>0,15 is meaning). Other results were normal. Against the possibility of laboratory error blood tests were repeated, but the results were nearly same as before. Her chest X-Ray was normal. Patient were consulted to cardiology department and she was taken catheter laboratory. Coronary angiography was also normal. Our diagnosis in this patient is Takotsubo cardiomyopathy. The patient revealed that she had recently experienced severe emotional stress due to her sick daughter. We aim to share with you this rare case in this presentation. Keywords: Chest pain, emotional stress, Takotsubo syndrome

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
332
P 256 PURPLE URINE BAG SYNDROME
Fatih Doğanay, Rohat Ak, Ali Şahiner, Tuba Cimilli Öztürk, Özge Ecmel Onur, Burcu Azapoğlu Kaymak, Abide Merve Manap
Fatih Sultan Mehmet Training and Research Hospital, Istanbul, Turkey Purple urine bag syndrome (PUBS) is a medical syndrome where purple discoloration of urine occurs in people with urinary catheters and co-existent urinary tract infection. Bacteria in the urine produce the enzyme indoxyl phosphatase. This converts indoxyl sulfate in the urine into the red and blue colored compoundsindirubin and indigo. The most commonly implicated bacteria are Providencia stuartii, Providencia rettgeri, Klebsiella pneumoniae, Proteus mirabilis, Escherichia coli, Morganella morganii, and Pseudomonas aeruginosa. Here we report a case of PUBS, Escherichia coli isolated in urine culture. A 85-years-old man with a history of benign prostatic hypertrophy and had urinary catheter presented to the emergency department with 2 days of “dark” urine, suprapubic pain, and decreased oral intake. The patient’s physical examination revealed mild suprapubic tenderness and a discolored foley catheter bag. Serum laboratory test results were unremarkable. His urinalysis revealed a specific gravity of 1.014, many WBCs, 3 to 5 RBCs, many bacteria, and a pH of 7,8. Escherichia coli isolated in urine culture. Discoloration of urine is not uncommonly encountered in clinical practice and may indicate a significant pathology. However, the majority of instances are benign and occur as the result of trauma to the urological system during procedures or ingestions of substances such as medication or food. Purple discoloration of a urinary catheter bag is rare and can be alarming to both patients and healthcare workers. Keywords: Purple urine bag syndrome, foley catheter, escherichia coli
P 257 ABDOMINAL PAIN CONTINUED 20 DAYS; RECTUM PERFORATION
Iremgül Güngör, Elif Çelikel, Bilge Karaca, Merve Alyamaç, Uğur Bal, Erinç Müderris, Bedriye Müge Sönmez, Oktay Hakbilir
Ankara Numune Training and Research Hospital, Emergency Medicine Clinic, Ankara, Turkey
A 40 years old female patient was admitted to our department with the abdominal pain which started suddenly before 20 days ago. There was no nausea, vomiting, diarrhea or constipation concomitant. She had no history of disease, smoking or drug use. Her vital signs was temperature of 37.4°C, blood pressure of 135/73 mmHg, respiratory rate of 23/min, heart rate of 97/min and pulse oximetry reading of 98 % on room air. At physical examination the patient was conscious, oriented. The abdomen was tender on deep palpation especially in the left iliac fossa. The other system examination was normal. The rectal digital examination was normal. Routine blood tests were studied, results were unremarkable. Her chest X-Ray showed a normal sized heart and there was subdiaphragmatic free gas. Patient was taken to the operation for laparotomy and found rectum anterior wall rupture due to malignancy. We aim to share with you this rare case in this presentation. Keywords: Abdominal pain, malignancy, rectum perforation

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
333
P 258 MILLER FISHER SYNDROME
Fatih Doğanay, Rohat Ak, Ali Şahiner, Tuba Cimilli Öztürk, Özge Ecmel Onur, Öncü Sancak, Abdullah Taşcı
Fatih Sultan Mehmet Training and Research Hospital, Istanbul, Turkey
Guillain–Barré syndrome (GBS) is a post infectious disease characterized by rapid-onset symmetrical muscle weakness caused by the immune system damaging the peripheral nervous system. Miller Fisher syndrome (MFS) is an uncommon variant of GBS that can be diagnosed by tests for its characteristic triad of conditions: areflexia, ataxia, and ophthalmoplegia. Here we report the clinical features of a patient who initially presented with ataxia, areflexia and ophthalmoplegia. A 67-years-old man presented to Emergency Department (ED) with general weakness, diplopia and ataxia for two days duration. He had several risk factors for stroke including atrial fibrillation, essential hypertension and hyperlipidemia. His Glascow Coma Scale (GCS) was 15, his vital parameters were all normal. On his cranial nerve examination he has lateral, medial and upward gaze. Rests of the cranial nerves were normal. On Deep tendon reflexes at the lower limbs were absent. Power of extremities was normal initially. On sensory examination, all modalities of sensations were preserved. Romberg’s test was positive. He had wide based ataxic gait with tendency to fall on either side. Examinations of other systems were normal. On admission, the laboratory blood tests were all normal. In CSF study there was albuminocytological dissociation. There was no pathological findings on brain CT scan. MRI scan of the brain was normal. As the patient clinically had ataxia, areflexia, ophthalmoparesis, weakness and albuminocytological dissociation in CSF, he was diagnosed to Miller Fisher syndrome. Miller Fisher syndrome is an uncommon variant of GBS that can be diagnosed by tests for its characteristic triad of conditions: areflexia, ataxia, and ophthalmoplegia.The present case demonstrates that physicians need to be aware of symptoms and examination findings consistent with MFS so as not to confuse them with those of such ischemic events as stroke and transient ischemic attack. Keywords: Miller fisher syndrome, Guillain–Barre syndrome, neurological emergencies
P 259 ACUTE ISCHEMIC SVO, ASSOCIATED WITH DRUGS
Iremgül Güngör1, Elif Çelikel1, Selim İnan2, Murat Ongar2, Funda Gök1, İrfan Gökçek1, Nurullah Tarhan1, Tamer Durdu1
1Ankara Numune Training and Research Hospital, Emergency Medicine Clinic, Ankara, Turkey 2Ankara Training and Research Hospital, Emergency Medicine Clinic, Ankara, Turkey A 34-year-old male patient was admitted to emergency department with weakness in the right upper and lower limbs. He had no history of disease, smoking or drug use. His father said that he was substance user. His vital signs was temperature of 36.4°C, blood pressure of 169/91 mmHg, respiratory rate of 19/min, heart rate of 103/min and pulse oximetry reading of 96 % on room air. ECG was taken and it showed sinus tachycardia. At physical examination the patient was consciousness confused, neurological examination was right hemiplegia. The other system examination was normal. Routine blood tests were studied, results were normal. In the urine, cannabis metabolites and opioid were detected, both known to be associated with stroke events. This report highlights the role of cannabis and opioid abuse that induce ischemic strokes. Keywords: Drugs, ischemic SVO, younger adults

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
334
P 260 GUILLAIN–BARRE SYNDROME
Fatih Doğanay, Rohat Ak, Ali Şahiner, Tuba Cimilli Öztürk, Özge Ecmel Onur, Ecem Deniz Kırkpantur
Fatih Sultan Mehmet Training and Research Hospital, Istanbul, Turkey
Guillain–Barré syndrome (GBS) is a post infectious disease characterized by rapid-onset symmetrical muscle weakness caused by the immune system damaging the peripheral nervous system. The initial symptoms are typically changes in sensation or pain along with muscle weakness, beginning in the feet and hands. This often spreads to the arms and upper body with both sides being involved. The symptoms develop over hours to a few weeks. About 25% of patients develop respiratory insufficiency and many show signs of autonomic dysfunction. A 22 years-old woman, admitted to emergency service with tingling sensation and numbness in her feet symmetrically. Her symptoms began slowly following an acute gastroenteritis infection that she had about 14 days prior. No history of trauma was reported nor had she ever complained of the current symptoms. She had no other complaints. Her vital signs were normal generalized weakness of the lower extremities was noted when testing the quadriceps, hamstrings and the gastrocnemius-soleus muscle groups. Sensory loss was variable in his feet. Deep tendon reflexes of her lower extremities were absent. Respiratory and cardiac function was within normal limits. The laboratory blood tests were all normal. There was no pathological findings on brain CT scan. MRI scan of the brain was normal. In CSF study there was albuminocytological dissociation. Electrophysiological studies demonstrating demyelination. Guillain-Barré syndrome (GBS) is generally diagnosed on clinical grounds. Basic laboratory studies, such as complete blood counts (CBCs) and metabolic panels, are normal and of limited value in the workup. They are often ordered, however, to exclude other diagnoses and to better assess functional status and prognosis. The ordering of specific tests should be guided by the patient's history and presentation. Keywords: Guillain–Barre Syndrome, neurological emergencies, emergency medicine
P 261 PROLONGED QTc ASSOCIATED WITH DULOXETINE OVERDOSE
Fatih Doğanay, Rohat Ak, Ali Şahiner, Tuba Cimilli Öztürk, Özge Ecmel Onur, Arzu Emecan Fatih Sultan Mehmet Training and Research Hospital, Istanbul, Turkey Duloxetine is an SNRI. It is mostly prescribed for major depressive disorder, generalized anxiety disorder. Death has been reported of duloxetine doses as low as 1000 mg. In premarketing clinical trials, four patients recovered following acute ingestions of 300 to 1400 mg of duloxetine. Somnolence, coma, serotonin syndrome, seizures, syncope, tachycardia, hypotension, hypertension, and vomiting have been reported in patients taking duloxetine doses as low as 1000 mg. In healthy young adults, duloxetine is rarely capable of prolonging the QT interval. We report a duloxetine overdose which has a prolonged QTc and treated successfully with IV 0.9% saline and NaHCO3. A 32 years old woman presented to emergency department with ingestion 1200 mg dose of duloxetine before 30 minutes. Vital signs were as follows: 36,5°C, blood pressure: 130/80 mmHg, pulse:109, sp02:%98. Physical examination revealed an alert woman in no distress with clear lungs, a soft abdomen, and a non-focal neurologic examination. Cardiac exam revealed tachycardia with a regular rhythm. Fifty grams of activated charcoal was administered orally. The laboratory tests was normal. The ECG revealed sinus tachycardia with no ischemic changes and a prolonged QTc (544 msec). The patient was given IV 30 ml/kg 0.9% saline bolus and 80 mEq NaHCO3. After treatment ECG revealed sinus rhythm with normal QTc (440 msec). She was admitted to the intensive care unit for further monitoring and supportive treatment. Usually, duloxetine is considered to be a well-tolerated drug at therapeutic doses, but its pharmaco-toxicological profile is still not completely known. This case suggests that clinicians should be alerted to toxic effects of duloxetine. Treatment for prolonged QTc associated duloxetine overdose, 0.9% saline and NaHCO3 have been found effective in our case. Keywords: Duloxetine, QTc, toxicology

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
335
P 262 BRUGADA-LIKE ECG PATTERN INDUCED BY HYPERKALEMIA
Fatih Doğanay, Rohat Ak, Ali Şahiner, Tuba Cimilli Öztürk, Özge Ecmel Onur, Abide Merve Manap
Fatih Sultan Mehmet Training and Research Hospital, Istanbul, Turkey To date Brugada syndrome (BrS) is considered a primary electrical heart disease and the diagnosis is based on precise clinical and electrocardiographic features. Many other diseases and conditions can lead to a Brugada like ECG pattern but the vast majority of patients with BrS possess a structurally normal heart, which is consistent with the notion that this is a primary electrical heart disease.We report a case of 63-year-old man with hyperkalaemia and had Brugada phenocopy on ECG. A 63-year-old man presented to Emergency Department (ED) with vomiting and prostration. He had terminal stages lung cancer and multiple metastasis on liver. His Glascow Coma Scale (GCS) was 15;blood pressure was 120/75 mmHg, pulse rate was 104 bpm, oxygen saturation 95%. In his physical exam, there was no pathology. The initial ECG in the emergency department showed normal sinus rhythm, rightward axis, and coved-type down sloping ST-segment elevation in leads V1 and V2 with Brugada type 1 pattern. The patient denied any history of syncope, or a family history of syncope or sudden cardiac death. Blood analysis confirmed severe hyperkalaemia (K+ 6,8 mmol/L) because of tumor lysis and acute renal failure (serum creatinine 2,2 mg/dL). Troponin I was normal. His initial ECG showed Brugada type 1 pattern resolved after several hours of observation and treatment of hyperkalemia. The ECG pattern in Brugada phenocopy resolves once underlying condition is treated or resolved; and family history of syncope or sudden cardiac death is typically negative. The causes of Brugada phenocopy include metabolic conditions as hyperkalaemia, ischemia, mechanical compression, and myocardial and pericardial disease. List of agents that cause Brugada phenocopy is growing consistently. The physicians must be alert for ECG findings of hyperkalemia like Brugada phenocopy at ED. Keywords: Brugada, ECG, Hyperkalemia
P 263 TORTIONED BOWEL LOOP; TWIST BRID AROUND
Iremgül Güngör, Elif Çelikel, Esma Kır, Uğur Bilgay Kaya, Hilmi Gökhan Ulubay, Bengisu Özer, Murat Doğan İşcanlı, Muhittin Serkan Yılmaz Ankara Numune Training and Research Hospital, Emergency Medicine Clinic, Ankara, Turkey A 31 years old female was admitted emergency department with the abdominal pain which started suddenly before 3 days ago. There was no nausea, vomiting, diarrhea or constipation concomitant. She had no history of disease, smoking or drug use. She had surgery ovarian cyst rupture before 8 years ago. Her vital signs was temperature of 36.2°C, blood pressure of 119/74 mmHg, respiratory rate of 16/min, heart rate of 68/min and pulse oximetry reading of 99 % on room air. At physical examination the patient was conscious, oriented. The abdomen was tender on deep palpation especially in the right mid and lower region. The other system examination was normal. The rectal digital examination was also normal. Routine blood tests were studied. In the results; there was leukocytosis, other results were normal. Her chest and abdominal X-Ray were normal. Abdominal Computerized tomography (CT) was taken with oral and intravenous contrast agent. There was dilatation at jejenal and proximal ileal segments at ct reports. Terminal ileum was normal calibration. And it was revealed ileal bowel loop adhesions and tortioned bowel loop. Patient were consulted to general surgery and patient was taken to the operation for laparotomy and tortioned bowel loops were also seen at operation. That tortioned segment was detortioned in operation. We aim to share with you this rare case in this presentation. Keywords: Abdominal pain, brid ileus, tortioned bowel loop

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
336
P 264 NARGİLE- KOVA YÖNTEMİ İLE BONZAİ ALIMI, SONUÇ; ARDS
Adnan Yamanoğlu1, Sümeyye Çakmak1, Nalan Gökçe Çelebi Yamanoğlu2, Özgür Süğüt1
1Haseki Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul 2Beykoz Devlet Hastanesi, İstanbul Giriş: ARDS, her iki akciğeri de içine alabilen nonkardiyojenik özellikteki diffüz infiltrasyonla karakterize, oksijen tedavisine cevap vermeyen akut solunum yetmezliği sendromudur. Bu yazıda Bonzai inhalasyonu sonrasında bilincinde kapanma üzerine acil servise başvuran 19 yaşında bir olgu sunulmuştur. Olgu: Bilinen ek hastalık öyküsü olmayan 19 yaşındaki erkek hasta, inhaler olarak suda süzülmüş nargile benzeri hazırlanan düzenekle bonzai alma (kova yapma yöntemi ile) sonrası bilincinde kapanma üzerine acil servisimize getirildi. Hastanın gelişinde bilinç kapalı, GKS 4, agonal solunum 4-5/dk olması üzerine entübe edildi. Geliş vitalleri TA 80/60 mmHg KTA 102 olan hastanın saturasyonu entübe edilmesine rağmen %85 idi. Geliş Kan gazında PH:7.0, HCO3:25 PaCO2: 100 idi. Entubasyon sonrası surcentle soluyulan hasta PEEP değeri 40cm/su değerine kadar öıkarılmasına rağmen parmak ucu saturasyon%85 arter kan gazında %96 değeri elde edilebildi. ARDS kriterlerini; "PaO2/FiO2 <200 mmHg olması, akciğer grafisinde bilateral diffüz infiltratların görülmesi ve bu tablonun sol kalp yetmezliğine bağlı olmaması " kriterlerini karşılayan hasta bonzai alımına bağlı ARDS tanısıyla tedavi altına alındı. Sonuç: Bonzai denen ve keyif verici olarak kullanılan madde içinde onlarca farklı madde içerir. Sentetik olarak elde edilmiş bu son zamanlarda ucuz olması nedeniyle sık tercih edilmekte ve içerdiği yabancı cisimlerin birçoğunun etkisi henüz aydınlatılamamıştır. Bu vaka göstermektedir ki içeriğindeki bir veya birkaç madde inhaler olarak alınırsa ARDS’ye neden olabilmektedir. Anahtar Kelimeler: Bonzai, ARDS, Akut Solunum Yetmezliği Sendromu
P 265 İDRAR RETANSİYONUNA HASTA ÇÖZÜMÜ: ÜRETERDE YABANCI CİSİM
Metin Yadigaroğlu1, Melih İmamoğlu2, Ayhan Arslan3, Yasin Erol1, Vildan Özer1, Yunus Karaca1
1Karadeniz Teknik Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Trabzon 2Fatih Devlet Hastanesi, Acil Servis, Trabzon 3Karadeniz Teknik Üniversitesi Tıp Fakültesi, Üroloji Anabilim Dalı, Trabzon Giriş: Üretral yabancı cisimler nadir görülen ancak acil müdahale gerektiren vakalardır. Birçok vakada zeminde ciddi psikiyatrik problemlerin olduğu görülmekle birlikte; üretral kaşıntı, üriner retansiyon gibi nedenlerle de hastaların üretralarına yabancı cisimler yerleştirdikleri görülmüştür. Biz bu yazıda idrar yapamama nedeni ile üretrasına kancalı metal bir yabancı cisim yerleştiren, çıkarmak için de kancalı saç tokası kullanan ancak her ikisini de çıkaramayınca acil servise başvuran bir olgudan bahsettik. Olgu Sunumu: 49 yaşında erkek hasta acil servise bir süredir devam eden idrar yapamama şikayetlerinin olması nedeniyle bu şikayetlerini gidermek amacıyla üretrasına kancalı bir metal demir parçası sokması ve sonrasında bu yabancı cismi çıkaramaması nedeniyle başvurdu. Fizik muayenede üretra eksternal açıklığındaki yabancı cisimler ve kanama alanı gözlemlenmekteydi. Basit yöntemlerin başarısız olması nedeniyle üroloji ile konsulte edilen hastanın üretrasındaki yabancı cisimler acil operasyonla ameliyathanede çıkarıldı. Tartışma: Üretral yabancı cisimler nadir karşılaşılan olgulardır ve literatürde sıklıkla olgu sunumları şeklinde yer bulurlar. Hastaların çoğu sosyal çekingenlikten dolayı doktora geç dönemde başvururlar ve kendileri yabancı cismi çıkarmak için farklı müdahalelerde bulunurlar. Bu müdahaleler daha ciddi yaralanmalara ve yabancı cismin mesaneye ilerlemesine neden olabilir. Yabancı cismin tam şekil ve boyutunun net tespiti yapılmadan kateterizasyon işlemi ya da çıkarma girişiminde bulunmak önerilmemektedir. Yabancı cismin belirlenmesinde direk grafiler ilk seçenek olarak kullanılabilir. Ancak radyoopak olmayan cisimlerin belirlenmesinde ultrasonografi ve kontrastsız bilgisayarlı tomografiler de tanıda yardımcı olur. Sistoüretreskopi, hem tanıda hem de tedavide kullanılabilecek bir yöntemdir. Yabancı cismin çıkarımında açık ve kapalı cerrahi operasyonlar yapılabilmektedir. Üriner sistemdeki yabancı cisimlere bağlı üriner sistem enfeksiyonları, striktür gibi geç dönem komplikasyonlar da akılda tutulmalı ve tedavinin şeklinde belirleyici olmalıdır. Acil servise üriner sistem şikayetleri ile başvuran özellikle psikiyatrik bozukluğu olan hastalarda üretral yabancı cisimlerin olabileceği ürolojik aciller açısından akılda bulundurulmalıdır. Anahtar Kelimeler: Acil, üriner retansiyon, yabancı cisim

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
337
P 266 UÇUŞA BAĞLI NADİR BİR KOMPLİKASYON: FRONTAL SİNUS BAROTRAVMASI
Esra Ersöz Genç, Metin Yadigaroğlu, Olgun Aşık, Sinan Paslı, Damla Aydın Altay, Özgür Tatlı Karadeniz Teknik Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Trabzon Giriş: Uzun mesafelerdeki ulaşımın kolaylıkla sağlanması açısından havayolu seyahatleri dünya genelinde oldukça yaygın yapılmaktadır. Kilometrelerce yüksek irtifa gerektiren uçuşlar gerek yükselirken gerekse de alçalırken kısa zamanda ortaya çıkan ani basınç farklılıkları nedeniyle insanlarda birtakım komplikasyonlara neden olmaktadır. Bu vakada tarafımıza uçuş esnasında şiddetli baş ağrısı gelişip acil servise başvuran hasta anlatılmıştır. Olgu sunumu: 30 yaşında erkek hasta acil servise uçuş sırasında gelişen şiddetli baş ağrısı sebebi ile başvurdu. Alınan öyküde hastanın uçağın inişe geçmesinden sonra özellikle sol kaşının üst kesiminde olmak üzere göze de vuran hayatında daha önce hiç yaşamadığı şekilde bir ağrısı olduğu öğrenildi. Bilinen bir hastalık öyküsü olmayan ve yeni gelişen herhangi bir görme problemi olmayan hastanın fizik muayenesinde bir patolojiye rastlanmadı. Hastanın çekilen kontrastsız beyin tomografisinde sol frontal sinüste 13x4 mm boyutunda hiperdens hemoraji tespit edildi. Hastanın klinik öyküsü ve elde olunan beyin tomografisi sonucuyla hastada barotravmaya sekonder submukozal hematom (sinüs barotravması) düşünüldü. Konservatif tedavi olarak dekonjestan ve analjezik tedavi ile semptomlarda gerileme sağlandı. Sonuç: Ani basınç değişikliğine maruziyet çoğunlukla dalgıçlarda ve uçakla yolculuk yapanlarda izlenir. Uçuş esnasında olan hastamızdaki gibi frontal ve retroorbital şiddetli baş ağrısı ilk kez 2004 yılında bir vaka olarak tanımlanmıştır. Bunu takiben birçok benzer vaka literatürde yerini almış ve ilk kez Mainardi tarafından 2007 yılında özgün tanı kriterleri şeklinde listelenmiştir. Uçuşla ilişkili sinüs barotravması tanısı için öncelikle klinik şüphenin yanında diğer ciddi baş ağrısı sebeplerini dışlamak gereklidir. Tanısında beyin ya da paranazal bilgisayarlı tomografi görüntüsü çoğunlukla yeterli olmaktadır. Tedavisi semptomlara yönelik olarak dekonjestan ve analjezik tedavi kombinasyonu içermektedir. Acil servislerde çalışan hekimlerin kuvvetle, sinüzit belirtileri ve yakın zamanda uçuş öyküsü olan hastalarda nadir görülen bir durum olan uçuşla ilişkili sinüs barotravması tanısını göz önünde bulundurmaları gerekmektedir. Anahtar Kelimeler: Acil, barotravma, baş ağrısı, uçuş
P 267 KOUNIS SYNDROME INDUCED BY CEPHALOSPORIN
Yasin Metiner, Rohat Ak, Ali Şahiner, Tuba Cimilli Öztürk, Özge Ecmel Onur, Arzu Emecan Fatih Sultan Mehmet Training and Research Hospital Kounis syndrome (KS) is defined as the concurrence of acute coronary syndrome (ACS) with conditions associated with mast cell activation relating to hypersensitivity. Multiple agents have been described to trigger KS including drugs, contrast media, stent material, insect stings, food, environmental exposures and medical conditions like asthma. Here we report a case presented with features of anaphylactic reaction after cefazolin injection. A 23-year-old woman with no conventional coronary risk factors was treated elsewhere for fever, cough with expectoration and diarrhea with antibiotic (Inj. Cefazolin 1 gm as an infusion) and analgesics. He experienced generalized itching 5 minutes after cefotaxime infusion along with sweating, headache, chest pain and facial swelling for which he was brought to our hospital. On examination he was afebrile, mildly tachycardic and tachypneic with a blood pressure of 80/60 mmHg. Her initial ECG revealed ST elevation in V1-4 derivations and had no resiprocal changes. In laboratory tests; CK: 218 IU/L, CK-MB: 12 IU/L and Troponin-I was valued as 0.006 ng/ml however there was not anything spesific tests either. He was initiated feniramine maleat and metil prednisolone due to allergic reactions also acetylsalicylic acid and nitrate infusion were given regarding to acute coronary syndrome. She was regarded as ST elevated myocardial infarction as she had no ECG changes during follow-ups in addition to her decreasing symptoms. After that she was consulted to cardiology department and coronary angiography was planned. No patologic findings were observed during the operation and the patient’s situation were regarded as Kounis Syndrome following cephalosporin injection. Kounis syndrome is a clinical feature difficult to diagnose, but is important that a possibility of KS as a cause of acute coronary syndrome be considered when patients present with features suggestive of anaphylactic reaction and ACS. Keywords: Kounis syndrome, cephalosporin, acute coronary syndrome

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
338
P 268 A PATHOLOGIC LUCENCY DEMOSTRATING PARTIAL ACHILLES TENDON RUPTURE: FAT PAD SIGN AT DISTAL POSTERIOR CRURIS
Necati Salman1, Alptuğ Özen2, Serkan Şener3, Onur Tezel1, Yahya Ayhan Acar1 1Ankara Gülhane Training and Research Hospital, Department of Emergency Medicine,Ankara, Turkey 2Ankara Gülhane Training and Research Hospital, Department of Radiology, Ankara, Turkey 3Acıbadem University School of Medicine, Department of Emergency Medicine, Istanbul, Turkey Introduction: Complete or partial anatomical defect of the strongest tendon of the human body, the Achilles tendon rupture, occurs with the incidence of 7 per 100.000 in the general population. Activities involving eccentric force loading to hind foot are usually the main reason of these pathologies. We can diagnose the complete form of tendon ruptures with only physical findings at initial examination. However, diagnosis of the partial ruptures usually requires imaging studies including roentgenograms, ultrasonography, and magnetic resonance imaging. Case: A 55 year old man admitted to our emergency department with the complaint of pain localized at the distal posterior part of the right cruris. He described his pain as a sharp, increasing with walking and first occurred with the sudden running move of the right cruris. He had pain with palpation at the upper side of the right heel but other physical examination findings were normal. We obtained a fat pad sign at the lateral cruris roentgenogram at lesion localization (Figure 1). Soft tissue ultrasound confirmed the partial rupture of the Achilles tendon (Figure 2) and intra muscular hemorrhage (Figure 3). Patient consulted to orthopedics department. He was applied a lower leg splint and recovered after a four week follow-up period. Conclusion: A fat pad sign, visualization of the lucency on a true lateral radiograph of an elbow flexed at 90° is an indicator of occult elbow fracture. We assess that local hematoma and soft tissue edema localized around the Achilles tendon may represent the complete or partial rupture. Keywords: Achilles tendon rupture, fat pad sign, emergency department
P 269 BACAKTA ŞİŞLİK: DVT Mİ?
Emel Korkmaz, Hamza Çıldır, Başak Bayram, Ersin Aksay Dokuz Eylül Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, İzmir Giriş: Derin ven trombozu (DVT) için test öncesi olasılığı yüksek olan hastalarda, DVT dışında sürpriz tanılar ortaya çıkabilir. Biz DVT için Wells skoru yüksek bir hastaya yaptığımız yatak başı ultrasonografide tanınan gastroknemius hematomu olgusunu sunuyoruz. Olgu: 42 yaşında erkek hasta sol bacakta şişlik yakınması ile acil servise başvurdu. Hasta kronik böbrek yetmezliği nedeniyle hemodiyaliz programında izlenmekte ve geçirilmiş kaza nedeni ile paraplejik ve yatağa bağımlı. Kan basıncı 118/68 mmHg, kalp hızı 73/dk, solunum sayısı 16/dk, vücut ısısı 36,2 °C, oksijen saturasyonu % 97 saptandı. Muayenede sol bacakta çap farkı ve ısı artışı mevcuttu. Hasta yakın zamanlı bir travma öyküsü tarif etmiyordu. Hastanın DVT için Wells skoru 5 olarak hesaplandı. Hastaya doppler ultrasonografisi yapıldı ve gastroknemius kası içerisinde hipoekoik görünümde kas hematomu fark edildi. Derin venöz yapılarında akım saptandı ve kompresyona yanıt alındı. Ortopedi ile konsülte edildi. Elevasyon ve buz kompresyonu önerilerek uygun analjezi ile taburcu edildi. Tartışma: Bacakta şişlik yakınması ile acil servise başvuran hastalar DVT için Wells skoru ile değerlendirilmelidir. Buna rağmen test öncesi olasılığı yüksek olan hastalarda bile DVT saptanma oranı %42’dir. Bacak ağrısı ve şişliğinin varlığı durumunda ayırıcı tanıda travma ilişkili durumlar, enfeksiyon, enflamasyon, kistik lezyonlar, vasküler lezyonlar, neoplaziler akla getirilmelidir. Çalışmalarda DVT ön tanısı ile ileri inceleme yapılan hastalarda, DVT dışında en sık konulan tanıların egzersiz sonucu kas incinmesi, bacak burkulması, paralize bacakta bacak şişliği, venöz yetmezlik, kas yırtığı, baker kisti ve sellülit olduğu gösterilmiştir. Cilt, cilt altı ve kas tabakaları genellikle yüksek frekanslı lineer prob ile değerlendirilir. Kas lifleri fibroadipoz dokusu, perimysium ve septalarla ayrılmış fasiküller halinde gruplandırılmıştır. İntermusküler septalar ve perimysium oblik paralel olarak, parlak ekojenik görünür. Kas hematomu ise akut durumda izoekoik görünürken, daha sonra hiperekoik, 2-3 gün sonra ise hipoekoik görülmektedir. Sonuç: Acil servise başvuran ve DVT için yüksek klinik şüphesi bulunan olgularda gastroknemius hematomu akla getirilmelidir. Anahtar Kelimeler: Gastroknemius hematomu, derin ven trombozu, ultrasonografi

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
339
P 270 DOKUZ YAŞINDA BİR VAN NECK-ODELBERG SENDROMU
Vildan Özer, Ogün Küpçük, Kadir Çoban, Elif Özgenç, Esma Kızılay, Aynur Şahin, Yunus Karaca Karadeniz Teknik Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Trabzon Giriş: Bu yazıda, koşarken kalçası üzerine düşme sonrası acil servise başvuran ve yapılan tetkikler sonrası Van Neck-Odelberg Sendromu tanısı alan bir olgu sunulmaktadır. Olgu Sunumu: 9 yaşında erkek hasta başvurudan yaklaşık 2 saat önce koşarken düşme sonrası başlayan sol kalçada ağrı şikayeti ile acil servise getirildi. Hastaneye yürüyerek gelen hastanın yapılan fizik muayenesinde sol kalça eklemi trokanter major üzerinde palpasyon ile hassasiyet dışında bir özellik yoktu. Bütün vital bulguları normaldi. Özgeçmişinde herhangi bir hastalık olmayan hastanın çekilen Pelvis Anteroposterior (AP) grafisinde sol inferior ischiopubic ramusun epifizi üzerinde genişlemiş düzensiz radyolüsen alan saptandı, sağ inferior ramus tamamen normaldi. Hastanın bilgisayarlı tomografi (BT) görüntülemesinde ise sol inferior ischiopubic ramus epifizi kapanmamış olup epifiz yüzeylerinde düzensizlikler ve sklerotik alanlar mevcuttu. Kan tetkikleri normal olarak saptanan hastanın öyküsü derinleştirildiğinde yaklaşık 1 yıldır sol kalçasında özellikle fiziksel aktivitelerden sonra (futbol, koşma vb) olan hafif derecede ağrıları olduğunu ifade etti. Fizik muayenede travmatik patoloji düşünülmeyen hastaya non-steroid antiinflamatuar analjezik reçete edilip yatak istirahati önerilerek taburcu edildi. Tartışma: Van Neck-Odelberg Sendromu, ilk olarak Odelberg (1923) ve Van Neck (1924) tarafından "osteochondritis ischiopubica" olarak tanımlanmıştır. Bu sendrom benign bir iskelet anomalisi olup asimetrik ischiopubic synchondrosisi ile atipik ossifikasyon paterni olarak karşımıza çıkmaktadır. Synchondrosis puberte öncesi bütün çocuklarda pubic ve ischium kemiklerin füzyonu sırasında ortaya çıkar. Normal fizyolojik gelişim sürecinin bir parçası olarak değerlendirilmesine rağmen semptomatik olan çocuklarda sendrom olarak değerlendirilmektedir ve Van Neck-Odelberg Sendromu olarak adlandırılmaktadır. Sıklıkla insidental olarak farkedilir. Klinikte kronik veya akut kalça ağrısı veya gluteal bölgede ağrı ile başvurular görülebilir. Patogenezinde mekanik stres faktörlerinin inflamasyonu indüklemesi sonucu ossifikasyon sürecini geciktirmesi suçlanmaktadır. Radyolojik incelemede direkt grafiler, BT ve manyetik rezonans kullanılmaktadır ve stres kırıkları, osteomyelit, post travmatik osteolizis, kemik tümörü gibi durumların ekarte edilmesi gerekmektedir. Laboratuar değerleri genelde normaldir Tedavide non-steriod antiinflamatuar ajanlar ve yatak istirahati önerilmektedir ve tedaviye yanıt genelde iyidir. Anahtar Kelimeler: Pelviste ağrı, travma, Van Neck-Odelberg
P 271 HEMORRHAGE AROUND DEEP VEIN THROMBUS INDUCED SEPSIS
Betül Gülalp Başkent University Adana Training and Research Hospital, Department of Emergency Medicine, Adana, Turkey Introduction: Local hemorrhage developed from the leakage of the deep vein thrombus (DVT) is a rare complication. I would present a patient according to the infected local hemorrhage occurred around the DVT. Case: A 77 year old female complained in palpitation and pain with edema on left thigh on presentation. She had a diagnosis of DVT and pulmonary embolism (PE) confirmed 20 days ago in another hospital and a usage of warfarin and enoxaparin in history. While warfarin had stopped. She was morbid obesity. Initial vital signs were the following: Blood pressure 140/90 mmHg, pulse 84 beats per minute, respiratory rate 20, SatO2 92%, temperature 37°C. Abnormal laboratory tests; Hematocrit was 28%, leukocyte 17000/mm3, Cr was 1.8 mg/dL, INR 1,38, CRP was 80 mg/L. Physical examination revealed a large area of ecchymosis, edema and crepitation on the left thigh extended to the distal with septic systemic clinical findings. Point of care emergency ultrasound showed the incompressibility of vein, even incomplete thrombus with around hemorrhage in soft tissues (Figure 1-2, Video 1). Result: Hemorrhage around DVT is a complication occurred in the late phase of PE treatment, a risk for sepsis. Point of care emergency ultrasound identifies the differential diagnosis and the treatment in patient care with evidence in Emergency Medicine. Keywords: Hemorrhage, point of care emergency ultrasound, DVT

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
340
P 272 ONE OF THE MOST COMPLEX AND TECHNICAL MEDICAL TRANSPORTATION: AIR TRANSPORT OF A PATIENT ON EXTRACORPOREAL MEMBRANE OXYGENATION (ECMO)
Onur Tezel1, Yahya Ayhan Acar1, Necati Salman1, Serkan Sener2, Etem Duzok3
1Gülhane Training and Research Hospital, Department of Emergency Medicine, Ankara, Turkey 2Acibadem University Faculty of Medicine, Department of Emergency Medicine, Ankara, Turkey 3Güven Hospital, Emergency Medicine Clinic, Ankara, Turkey Aim: In this case report, we aimed to present a patient on extracorporeal membrane oxygenation (ECMO) with fixed wing air ambulance and state specific technical issues. Method: This is a case report of a patient on ECMO transported by air ambulance and treated successfully. Results: A 35-year old patient on ECMO due to dilated cardiomyopathy was indicated cardiac transplantation and needed to be transported between hospitals located in two different cities, Trabzon and Istanbul, in Turkey. The distance of the destination was over 1000 kilometers and takes 12 hours by ground transportation. Air ambulance was the first choice and average flight time was 1 hour and 40 minutes. Rotor and fixed wing air crafts are being used in Turkish air medical transport system but as the distance is too far for rotor wing air crafts, fixed wing transportation was decided. In this phase, civilian aircrafts were the first choice but their loading space was not large enough to place the ECMO device. Because of using aircrafts with loading ramp enabling putting the ECMO equipment into the aircraft, military air ambulance was decided for the transportation. An emergency physician leaded the team and the patient was transported without any complication and any technical problem was not occurred during flight. Conclusion: Air medical transportation is a complex and expensive service and must be established nationwide under standard regulations. Air medical transportation system must be country-specific as being considered geographical aspects. Different types of aircrafts should be used for possible specific indications and establishing specific ECMO transport teams can be feasible. Keywords: Air medical transport, ECMO, cardiac transplantation
P 273 A MERCILESS POISONING: COLCHICINE
Sercan Yalçınlı, Özge Can, Yusuf Ali Altuncı Ege University Faculty of Medicine, Department of Emergency Medicine, Izmir, Turkey Introduction: Colchicine is used as an anti-inflammatory drug in the treatment of gout, amyloidosis, Behcet ‘s syndrome, familial Mediterranean fever, pericarditis, arthritis, pulmonary fibrosis, vasculitis, biliary cirrhosis, pseudogout, certain spondyloarthropathies, calcinosis, and scleroderma. Clinical manifestations of colchicine intoxication include abdominal cramps, diarrhea, and multiorgan failure including cardiovascular collapse with fatal outcome Case: A 22-year-old, female patient admitted to emergency department after 1 hour with about 500 colchicine 0.5 mg tablets intake for the purpose of suicide. She had a history of congenital adrenal hyperplasia and familial Mediterranean fever. On admission her vital signs were a Glasgow coma scale of 15, tympanic temperature 36.6 °C, respiratory rate 16 counts/min, heart rate 116 beats/min, blood pressure 105/63 mmHg and the saturation O2: 96% at the room air. There was no clinical finding on the physical examination except emesis. Orogastric lavage was performed to the patient and activated charcoal was given. Patient was observed in intensive unit by monitored. Initial laboratory studies in the emergency department were in normal limits. Gastrointestinal symptoms as nausea, emesis and diarrhea were observed at follow-up. Fluid treatment was performed because of the hypotension. Metabolic and lactic acidosis were determined on blood gas analysis. Hemodialysis was performed to patient because of the acute renal failure and decreased urine output. Despite full inotropic treatment, patient's hypotension couldn't be improved. Mechanical ventilation support was given for the respiratory distress syndrome. Despite aggressive supportive care, the patient died in ED after 61 hour. Conclusion: Because of the significant morbidity and mortality, all symptomatic patients with suspected or known overdoses of colchicine should be hospitalized. Agressive supportive treatment should be given for selected patients. Long term observation (>7 days) should be made for toxic patients. Keywords: Colchicine, poisoning, supportive treatment, death

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
341
P 274 D VİTAMİNİ İNTOKSİKASYONUNA BAĞLI HİPERKALSEMİ OLGUSU
Seyran Bozkurt Babuş1, Serdar Biricik1, Ataman Köse1, Hüseyin Narcı1, Akın Hizmetçi2
1Mersin Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Mersin 2Mersin Üniversitesi Tıp Fakültesi, İç Hastalıkları Anabilim Dalı, Mersin Amaç: D vitamini yanlış kullanımı sonrası gelişen intoksikasyon ve hiperkalsemi olgusunu sunmayı amaçladık. Olgu: 10 yıldır Multiple Skleroz (MS) tanısıyla takip edilmekte olan hasta 4-5 gündür halsizlik, bulantı, ağızda kuruma yakınmaları mevcut iken yeni başlayan yediklerini içerir tarzda kusma yakınmasıyla Acil Servise başvurdu. Hastanın 3-4 gündür idrar miktarında artış, iştahsızlık ve kabızlık yakınmaları mevcutmuş. MS nedeniyle glatiramer asetat ve memantin kullanımı mevcuttu. Fizik muayenesinde hastanın hipovolemik görünümde olduğu görüldü. Vital bulguları stabil olan hastanın bilinci açık, oryante ve koopere idi. Diğer sistem muayenesi doğaldı. Hastaya intravenöz hidrasyon başlandıktan sonra gönderilen tetkiklerinde düzeltilmiş kalsiyum değerinin 14.9 mg/dL olduğu, kreatinin değerinin 1,8 mg/dL olduğu görüldü. 10 gün önceki böbrek fonksiyonları normaldi. Diğer rutin biyokimya ve kangazı tetkiklerinde anlamlı özellik saptanmadı. Hastanın 10 gün önceki tetkiklerinde 25-OH vitamin D düzeyi 24 mg/mL görülmesi üzerine hastaya 2 ampul D vitamini (1 ampül=300,000 IU) reçete edilmiş. Çekilen EKG sinde QT kısalığı dikkati çeken hastada tekrar sorgulamasında yüksek dozda D vit kullandığı öğrenildi. Endokrinoloji’ye konsulte edilen hastaya D vitamini intoksikasyonu ön tanısıyla yatış verildi. Hastanın 25-OH d vitamini düzeyinin laboratuar cihaz okuma sınırlarının dışında olduğu öğrenildi. 2 gün dahiliye yoğun bakımda yakın kardiyak monitorizasyonla izlenen hastanın hidrasyon, diüretik ve 100 IU kalsitonin sonrası 48. Saatte serum kalsiyum düzeyinin 9,4 mg/dL’ye gerilediği görüldü. Takiplerine serviste devam edilen hastanın poliürisi düzeldikten ve böbrek fomksiyonları düzeldikten sonra hasta taburcu edildi. Sonuç: Günlük güvenli D vitamini replasmanı dozu 2000 IU olmakla birlikte daha yüksek dozların kronik alımı veya kısa sürede daha yüksek dozların alımında özellikle 25-OH vitamin D düzeyi 100 mg/mL’yi aştığında D vitamini intoksikasyonundan şüphelenmek gerekir. En ciddi bulgusu hiperkalsemi ve kısa QT sendromu olan bu durum dikkatli tedavi edilmelidir. Anahtar Kelimeler: D vitamini, hiperkalsemi, kısa QT
P 275 A FATAL METHOTREXATE INTOXICATION CASE
Sibel Senem Baş, Ömer Salt, Mustafa Burak Sayhan Trakya University Medical Faculty, Department of Emergency Medicine, Edirne, Turkey Since the early eighties, the folic antagonist methotrexate (MTX) has been used in long-term treatment of rheumatoid arthritis. As a folic acid antagonist; Methotrexate inhibits the enzyme dihydrofolate reductase, resulting in decreased levels of tetrahydrofolate in the cells. This blocks the synthesis of thymidylate, which is necessary for DNA synthesis. In low-doses it is used in the therapy of diseases of the immune system such as rheumatoid arthritis with the dose of 5–25 mg weekly. Even in low-dose therapy severe side effects can occur, leading to bone myelosuppression with pancytopenia to agranulozytosis, inflammation and necrotic changes in mucous tissues, liver cell necrosis and hepatic cirrhosis, pulmonary fibrosis, disorders of the kidney function, skin erythema and vasculitis. And the Intoxication mainly concerns the haematopoietic system leading to severe bone marrow depression with consecutive neutropenia and the risk of sepsis. We would like to present a case of life-threatening methotrexate intoxications of patients with rheumatological disease. A 68-year-old woman with rheumatoid arthritis admitted to our emergency department with diarrhaea and weakness. For the treatment of rheumatoid arthritis, she has been using MTX in the dose of 15 mg/day. On the physical examination, the patient was weaked with the heart rate of 118 beam/minute, fewer 38.6 °C, arterial blood pressure 90/60 mmHg. Laboratory examinations revealed a pancytopenia (haemoglobin 7,2 g/dL, leucocytes 0.38* 103/L, platelets 63*103/L). For the prophylaxis piperacillin – tazobactam 3*2.25 g/d and fluconasole 1*100 mg intravenously has been started. In spite of treatment with calcium folinate as well as with filgrastim, both the pancytopenia and the diarrhaea got worse and the patient died 3 days with the symptoms of septic shock. The presented cases demonstrate the severe risks of MTX treatment and the overriding importance of Emergency Physicians. Keywords: Emergency medicine, methotrexate intoxication, sepsis

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
342
P 276 ÇOCUKLARDA MİNÖR KAFA TRAVMASI KOMPLİKASYONLARINDAN SUBDURAL HEMATOM
Ömer Yüceer, Ferdi Özdemir, Ümran Gürbilek, Ali Duman Adnan Menderes Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Aydın Giriş: Subdural hematom beyin parankiminin ani sarsıntısına bağlı köprü venlerde yırtılma sonucu oluşur. Ciddi kafa travmalarından sonra yaklaşık %30 sıklıkta görülebilir. Subdural hematomlar %60’a kadar mortaliteye sebep olabilir. Travmadan sonraki ilk saatler önemlidir ancak haftalar sonra dahi ortaya çıkabilir. Özellikle çocuklarda en sık etyoloji düşmelerdir. Olgu: 3 yaş 9 aylık kız çocuğu, ailesinden alınan anamneze göre yaklaşık 50 cm yüksekten yumuşak zemine düşme sonucu kafa travması tarif ediyor. Hasta düştükten sonra gelişen şişlik nedeniyle yaklaşık 1 hafta sonra acil servise başvuruyor. Acil servisten beyin cerrahisi polikliniğine yönlendiriliyor. Sonrasında acil servisimize beyin cerrahisi polikliniğinde sıra bulamadığı için başvuruyor. Hastanın fizik muayenesinde Glaskow Koma Skorlaması:15 vitalleri Tansiyon arterial:110/70 Nabız:90 Ateş:36.3 solunum sayısı:22/dakika Oksijen Saturasyonu:%98 olup stabildi. Hastada herhangi bir semptom olmayıp nörolojik muayenesi olağandı. Hastanın sol parietotemporal bölgesinde yaklaşık 7X5cm kalınlığa ulaşan hematom dışında bulgusu yoktu. Hastanın beyin tomografisi çekildi; Sol frontoparietotemporal bölge komşuluğunda akut-geç, akut evre subdural hematom ve bası etkisi nedeniyle soldan sağa shift izlendi. Hasta beyin cerrahisine konsulte edilerek beyin cerrahisi servisine yatışı yapıldı. Sonuç: Olgumuz minör kafa travması olan çocuklarda beyin tomografisi çekilme kriterlerinden sadece hematomu kapsıyordu. Çocuklarda beyin tomografisi endikasyonu olduğunda radyasyon vermekten çekinilmemelidir. Radyasyon riski gerekli hallerde göze alınarak hayati risk taşıyan durumlar atlanmamalıdır. Ayrıca acil servislere başvuran minör kafa travması dahil tüm kafa travması olan hastalar bilgilendirilip beyin cerrahisi poliklinik kontrolü önerilmelidir. Anahtar Kelimeler: Çocuk, kafa travması, subdural hematom
P 277 OLGU SUNUMU: HİPOKALEMİK PERİODİK PARALİZİ
Özlem Bayrak, Ersin Aksay Dokuz Eylül Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, İzmir Hipokalemik periyodik paralizi (HPP), periyodik paralizinin en sık formudur. Kollarda güçsüzlük ve yürüyememe şikayetiyle acil servisimize başvuran ve hipokalemi dışında ek akut patoloji saptanmayan hastamızda nadir görülen bir hastalık olan HPP saptanması nedeni ile sunmaktayız. Hipertansiyon nedeni ile tedavi izleminde olan 42 yaşında erkek, uykusundan uyandıran vücudunda kasılma ve titreme sonrasında oluşan güçsüzlük ve yürüyememe şikayeti ile sabaha karşı acil servise getirildi. Vital bulgularında anormallik saptanmadı. Fizik muayenesinde kas gücü sol üst proksimal 3/5, distal 4/5, sağ üst 4/5, sağ alt 2/5, sol alt 1-2/5, kas tonusu olağandı. Sol üst ekstremitede derin tendon refleksi (DTR) alınamadı, diğer ekstremitelerde DTR normoaktifti.. Duyu ve serebellar muayene olağandı. Laboratuvar bulgularında kan potasyum seviyesi 2.15 mmol/l (normali 3.5-5.5) ölçüldü. EKG (elektrokardiyografi) normal sinüs ritminde 76 atım/dakika, ST-T dalga değişikliği yoktu. Beyin tomografisi, difüzyon ve servikal manyetik rezonans görüntülemesinde akut patoloji saptanmadı. Potasyum replasmanı sonrası şikayetleri tamamen gerileyen, kontrol potasyum seviyesi 4,24 mmol/l ölçülen hasta nefroloji poliklinik kontrolü önerilerek taburcu edildi. Proksimal kaslarda daha belirgin, genelde simetrik tutulumla giden HPP’de, güçsüzlük en önemli klinik yakınmadır. Erkeklerde daha sıktır, otozomal dominant geçiş gösterir ve patofizyolojisinden kas iyon kanallarındaki mutasyonlar sorumludur. Solunum ve yüz kasları nadiren tutulur. Duyusal kusurun görülmediği hastalıkta, ölüme yol açan atak çok nadirdir. DTR azalmış veya kaybolmuştur. HPP’de fazla karbonhidrat alımı, ağır egzersizler, alkol, travma, enfeksiyonlar, emosyonel stres, katekolaminler atakları tetikleyebilir. Ataklar çoğunlukla sabaha karşı olur. Bizim hastamızda da şikayetleri sabaha karşı meydana gelmişti ve hastamızın fazla miktarda karbonhidrat tüketimi olduğu öğrenilmişti. HPP ‘de tedavi semptomatik ve etiyolojiye yönelik olarak yapılır. Hastamızda potasyum replasmanı ile kas gücü defisiti kalmadı. HPP ataklarının önüne geçmek için, bu hastalara potasyumdan zengin diyet ile beslenme, karbonhidrat ve tuzlu diyetten kaçınma, yoğun egzersiz ve emosyonel stresten uzak durulması önerilmelidir. Aniden oluşan kas güçsüzlüğü ve paralizilerde nörolojik hastalıklarla beraber nadir bir hastalık olan HPP de sebep olarak düşünülmelidir. Anahtar Kelimeler: Hipokalemi, derin tendon refleksi, periyodik paralizi

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
343
P 278 HIGH PRESSURE INJECTION INJURY OF HAND WITH NITROGEN GAS
Çeral Efe Aracı1, Deniz Kılıç1, Yıldıray Çete1, Musa Küçükkapdan1, Duygu Kefal1, Taylan Kılıç2, Caner İşkorur1
1Akdeniz University Faculty of Medicine, Department of Emergency Medicine, Antalya, Turkey 2Antalya Training and Research Hospital, Clinic of Emergency Medicine, Antalya, Turkey High-pressure jets of a variety of fluids (eg, grease, water, plastics, or organic solvents) and gases are widely used in industry. Accidental penetration of the skin through a pinpoint portal of entry may result in devastating damage, even though the initial (post injection) appearance of the hand or other body part is usually and deceptively normal. The nature of the injected material is also important. There are a few cases of high pressure pneumatic tool injection injuries with gases. A 15-year-old right-handed boy presented to our ED with pain and swelling in his left arm. He had accidently injected nitrogen gas into his left thenar eminence by a high-pressure pneumatic tool when he was making confetti. He was complaining of severe pain on his left hand and forearm. On the left thenar eminence, a small entry mark was noted. There was minimal circumferential edema in the left arm up to shoulder, in comparison to right arm. There was not any neurovascular deficit on physical examination. Crepitation can be felt in the whole left arm and anterior chest wall with palpation. Anteroposterior and lateral radiographs of the left arm and chest showed subcutaneous emphysema extending from the left hand through the shoulder up to the chest without any bony fracture or pneumothorax. The left extremity was elevated, and the patient was consulted with orthopedic department. Treatment with antibiotics and analgesics together with tetanus prophylaxis was started. Then, the patient was admitted to the orthopedic department and discharged after 3 days with a full recovery. Although high pressure injection injuries with gases tends to recover with minimal intervention emergency physicians should be aware of the possibilities of deep injuries and observe these patients carefully. Keywords: Compartment syndrome, high pressure injection injury, nitrogen gas, trauma
P 279 METİL ALKOL İNTOKSİKASYONLU VAKADA GELİŞEN İATROJENİK MALİGN NÖROLEPTİK SENDROM
Gökhan Sağlamol, Zeynep Kekeç Çukurova Üniversitesi Tıp Fakültesi, Adana Nöroleptik Malign Sendrom (NMS) müsküler rijidite, yüksek ateş, otonomik disfonksiyon ve bilinç bozukluğu ile karakterize idyosenkratik bir sendromdur. Antipsikotik tedavi esnasında görülen, potansiyel olarak ölümcül bir sendromdur. Bu olguda; metil alkol intoksikasyonu nedeniyle acil servis kritik bakımında takip edilen hastanın haloperidol ve vb. sedasyon amaçlı tedavi sonrası gelişen malign nöroleptik sendrom olgusu tartışılmıştır. Olgu: 36 yaşında,16 yıldır alkol bağımlısı olduğu bilinen, sistemik hastalığı olmayan erkek hasta alkol kullanımı sonrası terleme, tansiyon yüksekliği ve titreme şikayetleri ile acil kliniğimize başvurdu. Hastanın yapılan ilk fizik muayenesinde; genel durum orta, kooperasyonu zayıf ve ajite idi.(GKS:13) Kan gazı değerlendirmesinde anyon gapi artmış metabolik asidozu olması ve alkol kullanım öyküsü olması üzerine metil alkol intoksikasyonu düşünüldü. Hastanın metabolik asidozu düzelinceye kadar hemodiyaliz uygulandı ve etil alkol tedavisi uygulandı. Bu tedavi sırasında hastanın ajitasyonları devam etmesi üzerine sedasyon amacıyla haloperidol ve diazepam uygulandı. Hastaya uygulanan metil alkol intoksikasyonu tedavisine rağmen hastada rijidite,yüksek ateş, extrapiramidal yan etkiler ortaya çıktı. Kan biyokimyasında CK düzeyleri ardışık günlerde ölçülen değerleri giderek yükseldiği ve 130000 U/L düzeylerine geldiği görüldü. Hastada bu tablo gelişmesi üzerine malign nöroleptik sendrom tanısı konularak tüm antipsikotik ajanlar kesilerek nöroloji yoğun bakımına devredildi. Nöroloji yoğun bakımda bromokriptin 3*5 mg tedavisi ve destekleyici tedavilerle hastanın semptomlarında gerileme görüldü.2. hafta sonunda semptomların tamamen kaybolduğu, CK değerinin 184 U/L'ye düştüğü görülerek hasta şifa ile taburcu edildi. Sonuç olarak acil serviste herhangi bir tabloda sedasyon amaçlı kullandığımız antipsikotiklerin kısa süre içinde malign nöroleptik sendroma neden olabileceği akılda tutulmalı, özellikle alkoliklerde ilaç etkileşimi ve merkezi sinir sistemi baskılanmasının daha kısa sürede ve daha düşük dozda ortaya çıkacağı unutulmamalı ve malign nöroleptik sendrom tanısı atlanmamalıdır. Anahtar Kelimeler: Malign nöroleptik sendrom, antipsikotik, metil alkol

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
344
P 280 AIR AMBULANCE SYSTEM IN THE UNITED KINGDOM, TRAINING OPTIONS AND CERTIFICATION FOR AIR AMBULANCE HEALTHCARE STAFF
Mark Forth Capital Air Ambulance, UK According to recorded history, the very first British aeromedical evacuation actually took place in Turkey during the first world war. A wounded soldier was transferred to a nearby hospital in a de Havilland DH.9 aircraft saving a very long land journey which would have likely cost the soldier his life. The British aeromedical world has come a long way since those times, from both the medical and aviation perspectives. In fact it is hard to know which of those fields has changed more with the advent of revolutionary technological advances transforming both aviation and medical practise. However, the fundamental vision remains – the safe and prompt movement of a patient, whether it be for emergency, life-saving medical intervention or simply to bring them home. During my brief lecture, I would like to illustrate the current structure and capability of aeromedical services within the United Kingdom, from first response helicopter work to the movement of patients internationally using large fixed wing aircraft. I would also like to explain our system of recruitment and training within these services, service standards, and importantly some of the limitations to our practice. The routes of entry and training for personnel in the aeromedical sphere in the UK are perhaps less well defined and regulated than one might imagine for a field that requires a large degree of specific knowledge and expertise. However, training courses and qualifications in this area do exist and further training is completed ‘in-house’. My knowledge of the aeromedical industry in Turkey is sadly somewhat limited. However, I hope that my contribution will throw up some interesting similarities and also differences in how our countries solve this fascinating problem of aeromedical repatriation. Keywords: Capital, aeromedical, ambulance, UK
P 281 GÖĞÜS AĞRISININ NADİR BİR NEDENİ: CİLT ALTI AMFİZEMLE BİRLİKTELİK GÖSTEREN SPONTAN PNÖMOMEDİASTİNUM
Zeynep Karakaya, Mahmut Şahin, Umut Payza, Pınar Yeşim Akyol, Serkan Bilgin, Sabri Togan İzmir Katip Çelebi Üniversitesi Atatürk Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İzmir Giriş: Spontan pnömomediastinum nadir rastlanan, daha çok gençlerde görülen ve çoğu kez kendiliğinden iyileşme eğilimi gösteren bir acildir. Spontan pnömomediastinum travma olmaksızın ortaya çıkar; ancak aşırı öksürük, yoğun egzersiz, valsalva manevrası, özofagusun aşırı zorlanması, vajinal doğum gibi durumlardan ortaya çıkabildiği bildirilmiştir. Bu yazıda, boğaz ve göğüs ağrısı ile acil servise başvuran 20 yaşındaki spontan cilt altı amfizem ve pnömomediastinum olgusu sunulmuştur. Vaka: Yirmi yaşında, 1 paket/gün sigara içen erkek, 1 gün önce boğazından başlayan ve göğsüne yayılan sıkıştırıcı tarzda ağrı ve göğüste yanma hissi ile acil servise başvurdu. Acil serviste yapılan ilk muayenesinde kan basıncı: 128/72 mmhg, Nabız: 85/dk, Ateş: 36,5 C, ve solunum sayısı 20/dk idi. Dinlemekle kalp ve solunum sesleri doğaldı. Palpasyonda hastanın boyunun kulak hizasından başlayıp sol flank bölgesine kadar uzanan cilt altı krepitasyon tespit edildi. Tetkiklerde hemogram değerleri, kardiyak enzim düzeyleri, elektrokardiyogram bulguları normaldi. Ön-arka (PA) akciğer grafisinde sol boyundan batına doğru uzanan cilt altı radyolusen hat ve sol hiller şüpheli lineer radyolüsen hat nedeniyle hastaya toraks bilgisayarlı tomografisi (TBT) çekildi. Toraksın BT’sinde mediastende yaygın hava görüntüsünün yanısıra ciltaltı amfizem bulguları saptandı. Hastanın bronkoskopi ve özofagoskopisinde pnömomediastinumu ya da cilt altı amfizemi açıklayacak herhangi bir bulguya rastlanılmadı. Tartışma: Pnömomediastinum mediasten içinde gaz veya serbest hava varlığı olarak tanımlanır. Pek çok farklı nedenden oluşsa da nadir görülen bir klinik tablodur. Sonuç olarak, pnömomediastinum prognozu etiyolojiye ve mediastene sıkışmış havaya bağlıdır. Spontan vakalarda komplikasyonların önlemesi için yatırılarak tedavi edilmelidir. SPM genellikle iyi huylu seyir gösterdiği ve ek tedavi gerektirmez; Ancak hastalar gözlem altında tutulmalıdır. Göğüs ağrısı ile başvuran hastalarda SPM ön tanılar arasında düşünülmelidir. Anahtar Kelimeler: Spontan pnömomediastenium, spontan cilt altı amfizem, acil servis

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
345
P 282 EMERGENCY BREAST DISORDERS
R.Pelin Kavak1, Hafize Aktaş1, Arzu Özsoy1, Eda Elverici1, Esra İşcanlı1, Nezih Kavak2
1Ankara Numune Training and Research Hospital, Radiology Clinic, Ankara, Turkey 2Ankara Dışkapı Yıldırım Beyazıt Training and Research Hospital, Emergency Medicine Clinic, Ankara, Turkey Introduction: A variety of breast complaints may present in the emergency setting. Case reports: This article reviews case reports of the breast emergencies as well as less urgent but more common concerns relating to the breast such, as breast pain, breast mass, trauma, nipple discharge, complications of breast cancer, infection, breast abscess, or postoperative complications. Discussion: The emergency physicians must be familiar with the pathology encountered and the associated imaging findings. While generally mammography is the most commonly and frequently used modality for breast imaging, in the emergency setting, ultrasound may be more readily available and better tolerated by the patient. Keywords: Breast disorders, breast emergencies, ultrasound
P 283 TRACHEOESOPHAGEAL FISTULA ASSOCIATED WITH POSTOPERATIVE EMPYEMA
Iremgül Güngör, Elif Çelikel, Pınar Uysal, Bilge Karaca, Merve Alyamaç, İrfan Kala, Berkin Karapınarlı, Miray Özlem Ankara Numune Training and Research Hospital, Emergency Medicine Clinic, Ankara, Turkey A 53-year-old male patient was admitted emergency department with the efflux of nutrition matter from his pesser dren. He had lung cancer and so he was operated left pneumonectomy. Postoperatively, he was empyema so that pesser dren fitted into his left hemithorax before a years ago. In the last few days, nutrition matter was came from the pesser dren. There has been no history of chronic disease excepting lung ca, smoking or drug use. His vital signs was temperature of 36°C, blood pressure of 96/72 mmHg, respiratory rate of 16/min, heart rate of 78/min and pulse oximetry reading of 96 % on room air. At physical examination the patient was conscious, oriented. Cardiac auscultation was normal and rhythmic. Right pulmonary auscultation also was normal. There was no rales or ronchus. There is no sound from his left pulmonary auscultation. The other system examination was normal. Routine blood tests were performed, results were unremarkable. His chest X-Ray showed that the right lobe of lung was normal sized and there was an appearance of air-fluid levels in left hemithorax. So that he had a chest computerized tomography (CT) scan. There was stomach, left kidney and spleen in the left hemithorax. There was an empyema cavity with a pesser dren in the upper zone of the left hemithorax. Then oral contrast agent was given him and diagnosed tracheoesophageal fistula. We aim to share with you this rare case in this presentation. Keywords: Empyema, malignancy, tracheoesophageal fistula

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
346
P 284 PENETRAN PERİANAL TRAVMA SONRASI GELİŞEN FOURNIER GANGRENİ
Sinem Raziye Ceylan, Ersin Aksay Dokuz Eylül Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, İzmir Giriş: Fournier gangreni genellikle immün baskılanmış kişilerde ortaya çıkan ve hayatı tehdit eden bir enfeksiyon acilidir. Genellikle belirgin bir travma olmaksızın diyabetik hastalarda ortaya çıkar ve hızla ilerler. Biz, 32 yaşında olan herhangi bir immün yetmezliği olmayan sağlıklı bir erişkinde delici kesici alet yaralanması sonrası ortaya çıkan fournier gangreni olgusunu sunuyoruz. Olgu: 4 gün önce sol kalçadan kesici-delici alet yaralanması nedeni ile bir acil serviste kesi onarımı yapılıp siprofloksasin reçetesiyle taburcu edilen 32 yaşında sağlıklı erkek, skrotal şişlik yakınması ile acil servisimize başvurdu. İlk değerlendirmede kan basıncı: 133/78 mmHg, nabız 76 atım/dk, oksijen saturasyonu %99 ve vücut ısısı 38 °C olarak ölçüldü. Genel durumu iyi olan hastanın, skrotum ve sağ uyluk bölgesinde şişlik, kızarıklık ve cilt altında yaygın krepitasyonu mevcuttu. (Resim 1) Laboratuvar incelemesinde WBC 22.800 mm3 (nötrofil %96,3), kreatinin 0.74 mg/dL, glukoz 101 mg/dL, CRP 324 mg/L (normali 0.2-5) ve prokalsitonin 12 ng/mL (10 ve üzeri sepsis) olarak ölçüldü. Yatak başı USG değerlendirmesinde (Resim 2) skrotumda cilt altı dokuda yaygın hava ekojeniteleri ve kalınlık artışı izlendi. Testislerin ekojeniteleri normaldi. Hastaya fournier gangreni şüphesi ile intravenöz kontrastlı abdominal bilgisayarlı tomografi (BT) çekildi. BT değerlendirilmesinde (resim 3 ve 4) karın ön duvarında, sağda retroperitoneal alanda, sağ skrotal kesede, penis kökü komşuluğunda ve sağ uyluk medialinde yaygın derin yumuşak doku amfizemi, sağ skrotal kese penis kökü ve sağ uyluk medialinde enfeksiyon ile uyumlu olabilecek loküle sıvı koleksiyonları ve bu düzeyde penetran doku travmasına sekonder yumuşak doku değişiklikleri dikkat çekti. Hasta üroloji bölümü tarafından acil olarak operasyona alındı. Hastaya abse drenajı, ve fasiatomi uygulandı, enfekte dokular temizlendi. 3 gün sonra hasta nekrotik kasların eksizyonu için tekrar opere edildi. Hasta post-operatif 20. günde sekelsiz olarak taburcu edildi. Hastanın 1 aylık izleminde ek sorunu olmadı. Sonuç: Acil servise başvuran ve yakın zamanlı genital bölge çevresinden penetre yaralanması olan genç sağlıklı bireylerde fournier gangreni akla getirilmelidir. Anahtar Kelimeler: Fournier gangreni, penetran travma, nekrozitan fasit
P 285 DEATH BY ELECTROCUTION, TWO CASE REPORTS
Mustafa Ramiz Tel, Murat Berberoğlu Mardin State Hospital, Emergency Service, Mardin Electrical injury is a relatively infrequent but causing potentially devastating multisystem injury with high morbidity and mortality, resulting 0.54 deaths per 100,000 people each year (1). Electrical shocks commonly cause widespread acute and delayed tissue damage. Cardiac arrhythmias and respiratory arrest are the most life-threatening complications in the acute phase (2). Factors influencing the severity of electrical injury include whether the current is alternating [AC] or direct [DC], voltage, and pathway of current through the patient, and the area and duration of contact. Contact with AC may cause tetanic contraction of skeletal muscle, which may prevent release from the source of electricity (1). We are presenting two case reports of death by electrocution. Both victims suffered from prolonged exposure to AC current of low voltage. First patient was 36 y.o. male who was repairing a circuit breaker. Second patient was a 17 y.o. female who was taking a shower with an instant electrical heater. Both patients received extended time of resuscitation in the emergency department, and both of them was defibrillated multiple times for persistent ventricular fibrillation. Male patient had a burn mark in his right palm and his right foot. Female patient had burn marks in both hands. Patients died in the emergency department after a long resuscitation. In both cases, muscle spasm and tetani was evident. Attending doctors thought that the defibrillator was not working due to lack of visible muscular reaction to the defibrillation. Conditions such as tetani and generalized muscle spasm can prevent visible reaction. Clinicians must not assume equipment malfunction just because there are no visible response. This can cause both medical and legal problems. References: 1) Soar J1, Perkins GD, Abbas G, et al., Resuscitation. 2010 Oct;81(10):1400-33. 2) Veneman TF, van Dijk GW, Boereboom E, Joore H, Savelkoul TJ., Intensive Care Med. 1998 Mar;24(3):255-7. Keywords: Electrical injury, defibrillation, resuscitation

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
347
P 286 TYPHILITIS: A RARE DIAGNOSIS FOR EMERGENCY DEPARTMENT
Nezih Kavak1, R. Pelin Kavak2
1Ankara Dışkapı Yıldırım Beyazıt Training and Research Hospital, Emergency Medicine Clinic, Ankara, Turkey 2Ankara Numune Training and Research Hospital, Radiology Clinic, Ankara, Turkey Introduction: Neutropenic enterocolitis or typhlitis is characterized by fever and abdominal pain. We will report a case of it. Case: The patient was a 26-year-old women diagnosed with common acute lymphoblastic leukemia. She was on remission induction phase of chemotherapy. For her fever, abdominal pain in the right lower quadrant,she came to emergeny department. She revealed a blood pressure 110/80 mmHg, heart rate 112 beats per minute, a body temperature of 38.8 0C and breathing count 17/min. On her physical examination there was not any focus on fever. Her leukocyte count was 0.6 × 109/L and absolute neutrophil count was 0.0 × 109/L. C-reactive protein (CRP) was 2.8 mg/dL. It was learned that he received the last chemotherapy ten days ago. On axial contrast enhaced CT of the abdomen and pelvis demostrates marked cecal wall thickening. According to the fever, abdominal pain, neutropenia and CT find-ings, patient was diagnosed as typhlitis and his oral intake was halted. Intravenous paranteral fluid therapy, antibiotic (tazocin), and IV analgesia therapy was started. Discussion: Enterocolitis of the ileocecal region in neutropenic patients is called typhlitis. Typhlitis is more often seen in hematologic malignancies, especially during the induction phase of chemotherapy which is encountered in increasing frequency, because of the agressive chemotherapy applications. Fever, abdominal pain especially in the right lower quadrant with or without rebound tenderness, abdominal distension, diarrhea, nausea, and vomiting in the patients with neutropenia are the main clinical findings of typhlitis. İn ultrasonography reveals a target sign encircling mural thickening as a result of mucosal edema in ileum and cecum. İn CT bowel wall thickening, dilated cecum, pericecal fluid, inflammatory changes in the soft tissue, presence of intramural edema and right lower-quadrant inflammatory mass, and inflammatory stranding in the mesenteric fat surrounding the bowel are the main abnormal findings of imaging studies. Keywords: Neutropenia, neutropenic enterocolitis, typhilitis
P 287 ACUTE ABDOMEN IS ALWAYS REALLY ACUTE ABDOMEN?
Mehmet Efe, Elif Dilek Cakal, Funda Karbek Akarca Ege University Medical School, Department of Emergency Medicine, Izmir, Turkey Introduction: Abdominal pain comprises 5-10% of emergency department (ED) visits. Widespread availability of advanced imaging modalities improved the management of abdominal diseases requiring surgery. Despite this, undifferentiated abdominal pain accounts for approximately 25% of ED discharge diagnoses and extra-abdominopelvic causes of abdominal pain remain obscure and challenging. We present a case of acute intermittent porphyria (AIP) as a rare cause of abdominal pain. Case: A 22-year-old female with a history of diabetes mellitus type 1, AIP and ileus operation admitted to ED with 4 days of diffuse and severe abdominal pain and constipation. Abdomen was distended with diffuse tenderness and no rebound tenderness. She had mild compensated metabolic acidosis, however, ketone and glucose were not high. Glucose infusion, for AIP and insulin infusion for DM were started. The patient was admitted to ICU. Discussion: AIP is an autosomal dominant disease that results from porphobilinogen deaminase enzyme defects and the most common form of the four acute porphyrias. AIP is a rare disorder with a prevalence of only 1 to 5 cases per 100,000 persons. Attacks occur 20% of patients, more often in females than males. The most common age for an attack is from the late teens to the early forties. Abdominal pain, neuropsychiatric symptoms and peripheral neuropathies are characteristic of the attacks. AIP causes no skin lesions. The "four M's" may provoke AIP attacks: medication, menstruation, malnutrition and maladies. Treatment consists of managing symptoms, preventing extremes of vitals and specific treatment. While mild attacks may be treated with glucose administration, severe attacks with neurological symptoms may require hematin administration. Conclusion: AIP is a rare but potentially life-threatening cause of abdominal pain and neuropsychiatric complaints. Emergency physician should become familiar with the disease to prevent morbidity and mortality, to guide patients and to protect them from attack provokers. Keywords: Abdominal pain mimics, acute intermittent porphyria, emergency department

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
348
P 288 SACROILIAC HYDATID CYST
Nezih Kavak1, R. Pelin Kavak2
1Ankara Dışkapı Yıldırım Beyazıt Training and Research Hospital, Emergency Medicine Clinic, Ankara, Turkey 2Ankara Numune Training and Research Hospital, Radiology Clinic, Ankara, Turkey Introduction: Hydatid cyst is a parasitary infection. Sacroiliac hydatid cyst is less than 1% of all hydatid cysts. In this study, we aimed to present radiological findings of our patient. Case: A 59-year-old woman came to emergency department increasing back pain and bilateral radiculopathy. Radiographs showed an expansive lytic lesion affecting the sacroiliac bone with destruction of the bone cortex. Laboratory analyses were performed and the patient gone to CT. CT images demonstrate multilocule cysts, bone erosion affecting sacroiliac destruction. We learned that 6 month ago her serology for echinococcus was positive. Discussion: Although hydatid disease of bone is rare in world, but not in our country, it should be included in the differential diagnosis in emergency department. Keywords: Echinococcus, hydatid cyst, sacroiliac
P 289 WHICH DRUG CAUSES VERTIGO WITH A SINGLE DOSE?
Busra Sapmaz, Elif Dilek Cakal, Funda Karbek Akarca Ege University Medical School, Department of Emergency Medicine, Izmir, Turkey Introduction: Dizziness is 5% of the emergency department (ED) visits. It is used to explain four different situations: Syncope, disequilibrium, vertigo and various syndromes. It is mostly caused by vestibular conditions but cerebrovascular incidents are seen in 6% of the cases. As a rare cause of vertigo-like symptoms, we would like to discuss drug adverse effects. Case: A 30-year old female with no known disease admitted to emergency department with dizziness. She explained that she had taken “a muscle relaxant named Lyrica” for headache and neck pain. Her symptoms started 20 minutes after taking the pill. Physical examination revealed minimal horizontal-rotatory nystagmus and no lateralizing sign, no dysmetria or dysdiadochokinesia. After hydration, dimenhydrinate and metoclopramide administration, her symptoms regressed. Discussion: Pregabaline is effective for the treatment of neuropathic pain, fibromyalgia and epilepsy; in addition, it may be useful for the reduction of postoperative pain. The most accepted mechanism is binding the alpha-2-delta subunit of the presynaptic neuron's voltage-gated calcium channels, which decreases neuroexcitatory neurotransmitters and provides a normal physiologic state in hyperexcited neurons. Most of the adverse effects caused by pregabaline are related to the central nervous system. Dizziness and nystagmus are common adverse effects which may affect more than 1 person in 100. These symptoms regress after discontinuation of medication. Another vitally important aspect of the case is the necessity of accurate drug history. Patients may misname the group of their medication as in our case. Therefore, the individual drug names should be asked. Conclusion: Our case shows that single-dose of pregabaline may cause dizziness and nystagmus. It is important to question the history of medication, and especially, the name of the drugs to prevent misstatements. Keywords: Vertigo, pregabaline, single dose, emergency department

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
349
P 290 OLGU SUNUMU: İSKEMİK SEREBROVASKULER OLAY OLGUSU: AKUT İSKEMİDE DİFÜZYON MRG NORMAL OLABİLİR Mİ?
Yasemin Uyar, Ümit Çiloğlu, Mesut Günay Çiğli Bölge Eğitim Hastanesi, Acil Tıp Kliniği, İzmir Giriş: Dünya sağlık örgütüne göre inme, vasküler nedenlere bağlı fokal serebral fonksiyon kaybına ait belirti ve bulguların hızla yerleşmesi ile karakterize klinik bir sendromdur. İnmelerin yaklaşık %80’i iskemiktir. İnme önemli halk sağlığı sorunlarından biridir. Gelişmiş toplumlardaki ölüm nedenleri arasında üçüncü ve sakatlık nedenleri arasında en sık görülenidir. İnme aynı zamanda demansın ikinci en sık, yaşlılardaki epilepsinin en sık nedeni olup, depresyonun da sık nedenleri arasındadır. Serebral iskemik inme subtipinin doğru olarak belirlenmesi tanı ve tedaviye yönelik kararların verilmesinde önemlidir. Bu kararlar hastanın prognozunu belirlediği gibi altta yatan etyolojinin rekürrensini de etkilemektedir. Difüzyon ağırlıklı manyetik rezonans görüntüleme (DAG) iskemik inme tanısında en sık kullanılan ve en önemli görüntüleme yöntemidir. Difüzyon ağırlıklı MRG’ (DAG) hiperintensite ve ‘apparent diffusion coefficient’ (ADC) haritalamasında hipointensite sitotoksik ödemi gösteren bir bulgudur. Bu değişiklikler akut iskemik serebrovasküler olay için tipiktir. Deneysel çalışmalarda iskemik hasarı izleyen birkaç dakika içerisinde tüm sekanslar normal iken ADC değerlerinde belirgin düşme olduğu saptanmıştır. İskemi başlangıcından 2 saat sonra duyarlılığın %100’e yakın olduğu bildirilmektedir. Olgu: Altmış altı yaş erkek hasta acil servise senkop, bilinç bulanıklığı nedeniyle getirildi. Başvuruda kan basıncı 160/80, nabız:55(sinüs ritmi ) SO2:96 idi. Bilinci konfüze, kooperasyon sınırlı, E3M4V1 idi. Pupiller izokorik,IR +/+, meninks irritasyon buguları negatif idi. Solda ılımlı hemiparezi saptandı. Beyin tomografisinde ve difüzyon ağırlıklı (DWI-diffusion weighted image) MRG' da (Magnetik Rezonans Görüntüleme) akut nöropatoloji saptanmadı. Hastanın aynı gün içindeki takibinde E1M3V2 IR -/- ve semptomların 21.saatinde çekilen difüzyon ağrlıklı MRG'de pons mezensefalon ve her iki talamus medialinde, sol oksipital lobta akut infarkt ile uyumlu diffüzyon kısıtlılığı izlenmiştir. Tartışma: Magnetik rezonans görüntüleme (MRG) incelemesi iskemik lezyonları görüntülemede kranyal bilgisayarlı tomografiden daha duyarlı bir yöntemdir. Difüzyon ağırlıklı görüntüleme sekansı ile iskemik lezyonlar ilk dakikalardan itibaren güvenilir bir şekilde belirlenebilir. Ancak hiperakut dönemde ilk difüzyon MRG %5,8- 9,8 negatif olarak tesbit edilmektedir. Anahtar Kelimeler: İskemi, magnetik rezonans görüntüleme, senkop, serebrovasküler olay
P 291 CLAY-SHOVELER’S FRACTURE: A CASE REPORT
Mehmet Ünaldı1, Sedanur Bağdiden1, Tuçe Düzkel1, Soner Işık1, Didem Ay1, Hatice Eryiğt2
1Medeniyet University Goztepe Training and Research Hospital, Department of Emergency Medicine, Istanbul, Turkey 2Dr. Lütfi Kirdar Kartal Training and Research Hospital, Thorax Surgery Clinic, Istanbul, Turkey Avulsion off the end of one of the lower cervical spinous processes is known as a clay-shoveler’s fracture. A clay shoveler's fracture may occur anywhere between C6-T3, with the most common level being C7. We report a case of clay shoveler’s fracture consequent to a traffic accident with CT scan showing healing the fracture. Case: A 76-year-old male presented to the ED after traffic accident. No loss of consciousness was experienced. Immediately following the accident, mild neck pain was reported. Plain film radiograph performed demonstrated nondisplaced fracture on the spinous process fragment of C7. CT was performed to further evaluate the osseous integrity of the region. The results showed no other osseous involvement. The patient was consultated with neurosurgery clinic and then was sent home with a hard servical collar. This injury is caused by intense flexion against a contracted posterior erector spinal muscle that fractures te tip of the spinous process. An isolated spinous process avulsion fracture is mechanically stable. Keywords: Clay-Shoveler's, fracture, spinous process

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
350
P 292 HYDATIDOSIS OF THE PERITONEUM
Nezih Kavak1, R. Pelin Kavak2
1Ankara Dışkapı Yıldırım Beyazıt Training and Research Hospital, Emergency Medicine Clinic, Ankara, Turkey 2Ankara Numune Training and Research Hospital, Radiology Clinic, Ankara, Turkey Introduction: One of the most important complications of hydatid disease is secondary hydatidosis of the peritoneum. We will present a case of ruptured peritoneal hydatidosis due to blunt abdominal trauma. Case: 45 years old man with lower abdominal pain was admitted to our emergency department. His complaint was started after he had been hit on the lower abdomen. Abdominal examination revealed tenderness on the upper and lower quadrants. We learned that he had been operated on for liver hydatid cyst one years ago. İn the bed side ultrasonography revealed a giant, 90 x 110mm multilobular cyst in the abdomen and free fluid in the subhepatic area and pelvic region. Computed tomography showed multilobule cystic lesions and free fluid. Emergency laparotomy was performed. Discussion: After operation of the hydatid cysts, it can become bigger in size within the peritoneum or pelvic region with time it can rupture either spontaneously or following trauma. Keywords: Echinococcus, hydatid cyst, hydatidosis
P 293 COMPARISON OF TRAUMA SCORING SYSTEMS IN MULTIPLE TRAUMA PATIENTS
Mehmet Hilmi Höke1, Seda Özkan2, Hasan Sultanoğlu2
1Sincan State Hospital, Emergency Medicine Clinic, Ankara, Turkey 2Dışkapı Yıldırım Beyazıt Training and Research Hospital, Emergency Medicine Clinic, Ankara, Turkey Objective: In our study the performances of Injury Severity Score (ISS), New Injury Severity Score (NISS), Glasgow Coma Scale (GCS), BIG score, Trauma and Injury Severity Score (TRISS) and Revised Trauma Score (RTS) in multiple trauma patients were aimed to evaluate and compare. Patients and Methods: Records of 426 multiple trauma patients who applied to S.B.Dışkapı Yıldırım Beyazıt Training and Research Hospital Emergency Clinic between January 2014 and January 2016 were analyzed retrospectively. All patients’ data; including age, gender, cause of injury, initial vital signs, injury region, trauma scores (AIS, ISS, NISS, GKS, BIG, RTS, TRISS), hospitalization time, mortality, operation data and final diagnosis, were collected and calculated. SPSS 17 and Medcalc 15 statistical software were used to analyze the collecting data. Results: 426 patients were included. Mortality rate was 8,2%. The mean age of these 426 patients included in the study was 41,1±18,4 (18-90) with %19,2(n=82) female and %80,8(n=344) male. TRISS showed the best performance for predicting mortality(AUC:0,93 sensitivity %97,1 spesifity %76,7). Than NISS, BIG, ISS, RTS followed TRISS respectively. RTS was the most specific scoring system with %91,6. For predicting need of intensive care unit; NISS was the most successful (AUC:0,81), ISS was the most sensitive (%97,7) and RTS was the most specific (%94,3) scoring system. Also TRISS took the first place for predicting survival rate (AUC:0,94) after that NISS, BIG, ISS followed respectively. There was a meaningful relationship with hospitalization time in all trauma scoring systems (p<0,005). Conclusion: TRISS was the most successful, sensitive and accuracy scoring system for predicting mortality and survival rate in multi trauma patients. Although NISS was the best for predicting need of intensive care unit. The BIG score which was improved recently, also can be used for trauma scoring as a powerful scoring system. Keywords: Trauma, trauma score, mortality, morbidity

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
351
P 294 GÖRME VE KONUŞMA BOZUKLUĞUNUN NADİR SEBEBİ: TAKAYASU ARTERİTİ
Hasan Sultanoğlu1, Tuba Erdem Sultanoğlu2, Nezih Kavak1, Seda Özkan1
1Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Ankara 2Kazan Devlet Hastanesi, Fizik Tedavi ve Rehabilitasyon Kliniği, Ankara Amaç: Takayasu arteriti büyük arterlerde stenoz, oklüzyon ve anevrizmal değişikliklere yol açan, kronik inflamatuvar bir hastalıktır. Özellikle aorta ve onun koroner, karatid, pulmoner ve renal gibi büyük dallarını etkiler. Hastalık sıklıkla 2. veya 3. dekatta ortaya çıkar ve sıklıkla kadın cinsiyeti etkiler. Bu olguda bulantı, kusma, görme ve konuşma bozukluğu ile acil servise başvuran ve Takayasu Arteriti tanısı konan hastayı sunmayı amaçladık. Olgu: 46 yaşında kadın hasta bulantı, kusma, halsizlik, eklem ağrısı, görme ve konuşma bozukluğu şikayeti ile acil servise başvurdu. Eşlik eden komorbid hastalığı ve kullandığı ilacı yoktu. Soygeçmişinde özellik yoktu. Hastanın genel durumu iyi ve bilinci açıktı, ateşi yoktu. Kollar arasında sistolik kan basıncında 20 mm Hg fark mevcuttu ve her iki kolda brakial arter nabzında azalma vardı. Fizik muayenesinde görmede bulanıklık mevcuttu. Sağ subklavian arter üzerinde oskültasyon ile duyulabilen üfürüm vardı. Motor muayenesi normal ve fasial asimetrisi yoktu. Elektrokardiyogram normal sinüs ritminde idi, patolojik değişiklik yoktu. Laboratuvar değerlendirmesinde akut faz reaktanı yüksekti, lökositoz ve trombositoz vardı. Görüntülemede beyin BT ve MRG normaldi. Torakoabdominal BT anjiografisinde çıkan aortada, subklavian arterde segmental daralma ve oklüzyon mevcuttu. Hastada mevcut bulgular ile Takayasu arteriti tanısı konuldu. Sonuç: Acil servise başvuran genç kadın hastalarda, kollar arası sistolik kan basıncı farkı ve nabızlarda azalma Takayasu arteriti tanısı için önem taşır. Anahtar Kelimeler: Takayasu arteriti, görme bozukluğu, konuşma bozukluğu
P 295 DOLUNAYDA SUİCİD ORANLARI ARTIYOR MU?
Serhat Karaman1, Emine Kadıoğlu2
1Gaziosmanpaşa Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Tokat 2Dumlupınar Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Kütahya Geçmişte olduğu gibi günümüzde de insanlara dolunay zamanları hala gizemli ve esrarengiz gelmeye devam etmektedir. Acaba gerçekten dolunay zamanlarının insanların hayatları üzerine olumlu ya da olumsuz açıdan bir etkisi var mıdır? sorusu zihinleri meşgul etmektedir. Suicid girişimi oranı toplumumuzda azımsanmayacak düzeydedir. Bu çalışmada bir yıllık süreçte acil servise başvuran 930 suicid vakasının dolunay zamanları ile olan ilişkisi ve demografik analizi sunulmuştur. Çalışma retrospektif olarak planlanıp, elde edilen veriler SPSS 16 ile istatistiksel analizi yapılmıştır. İlgili tarihlerdeki ayın döngüsü ve dolunay zamanları Ankara Üniversitesi Rasathanesi verileri esas alınarak ( ± 3 ) belirlenmiştir. Çalışma bir yıllık periyod da acil servise suicid girişimi sonrası gelen 930 hasta verileri değerlendirilerek yapılmıştır. Vakanın %33,2`si erkek, %66,8`i bayandır. Yaş skalası 16 ile 86 arasındadır ve yaş ortalaması 35`tir. 930 vakanın %89,6`sı ilaç ile intihar girişiminde bulunurken, %10,4`ü diğer yöntemleri tercih etmiş olduğu görülmektedir. Vakaların %11,7`sinin yoğun bakıma yatışının yapılmış olduğu görülmüştür. Cinsiyet ile yoğun bakıma yatış oranlarına bakıldığında erkeklerin %14,6`sının yoğun bakıma yatışı yapılmış iken, bayanların %10,3`ünün yoğun bakıma yatışının yapıldığı görülmüştür. Cinsiyet ile yoğun bakıma yatış arasında istatistiksel açıdan da anlamlı bir ilişki vardır (<0,05). 930 vakanın 270’i (%29) dolunay zamanında iken 660’ı (%71) diğer günlerdedir. Toplam vaka sayısı açısından bakıldığında dolunay zamanlarında gelen suicid vakaları diğer günlerde gelen vaka sayısından daha az olduğu gözükmekle birlikte bu açıdan bakıldığında bizi yanıltmaktadır. Vakaların değerlendirmeye alındığı periyod da toplam 84 günlük bir dolunay süresi vardır. Günlük gelen ortalama suicid sayıları değerlendirildiğinde dolunay günlerinde günde 3.2 vaka acil servise başvurmuşken, diğer 281 günde ortalama 2.3hasta acil servise getirilmiştir. Dolunay günlerinde, diğer günlere oranla yaklaşık %40 kadar daha fazla vaka geldiği hesaplanmıştır. Dolunay günlerinde başvuran suicid vaka sayısındaki artış yanında cinsiyet açısından da bakıldığında bu durumdan bayanların daha çok etkilendiği görülmüştür. Dolunay zamanlarındaki suicid oranlarındaki bu artış dolunay günlerinin gizem ve esrarengizliğini korumaya devam edeceğini göstermektedir. Anahtar Kelimeler: Dolunay, suicid, acil servis

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
352
P 296 AXILLARY BRACHIAL PLEXUS BLOCK WITH BEDSIDE ULTRASOUND FOR FOREARM FRACTURE
Attila Aydın1, Sedat Bilge1, Murtaza Kaya5, Erdem Cevik4, Meltem Bilge2, Cemile Aydın3
1Gülhane Training and Research Hospital, Department of Emergency Medicine, Ankara, Turkey 2Dışkapı Training and Research Hospital, Clinic of Anesthesia and Resuscitation, Ankara, Turkey 3Etimesgut State Hospital, Internal Medicine Clinic, Ankara, Turkey 4Haydarpaşa Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey 5Şırnak Training and Research Hospital, Emergency Medicine Clinic, Şırnak, Turkey Upper extremity fractures are one of the most frequent reasons for admission to an Emergency department (ED). In EDs, procedural sedation analgesia, hematoma block, intravenous regional anesthesia and peripheral nerve blocks are usually used for pain control in the forearm fractures. We describe eight patients, who presented to the ED with forearm fractures, and were successfully reduced using US-guided axillary approach of brachial plexus block (AABPB) performed by emergency physician. AABPB is a technique that can be applied easily in the ED by emergency physicians for forearm fractures. In this technique, the procedural success rate is high and without any complications. Keywords: Analgesia, brachial plexus, regional anesthesia, axillary
P 297 KÜLTÜR MANTARI TÜKETİMİNE BAĞLI ANAFLAKSİ; EL VE AYAK ÖDEMİ
Hasan SULTANOĞLU1, Tuba Erdem Sultanoğlu2, Nezih Kavak1 1Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Ankara 2Kazan Devlet Hastanesi, Fizik Tedavi ve Rehabilitasyon Kliniği, Ankara Amaç: Anafilaksi, genellikle daha önceden duyarlılaşmış mast hücresi ve bazofillerden, IgE aracılığı ile salınan pek çok biyolojik aktif mediatörün çeşitli organları etkilemesi ile ortaya çıkar. Anafilaksinin oluşması için duyarlılaşma peryoduna ve aynı antijenle ikinci kez karşılaşmaya gereksinim vardır. Anafilaksi sırasında kaşıntı, deride kızarıklık ve kabarıklıklar, hırıltılı solunum, nefes darlığı, bulantı, kusma, karın ağrısı, ishal gibi değişik yakınmalar oluşur. Bu olguda kültür mantarı tüketimi sonucu ellerde ve ayaklarda şişlik şikayeti ile acil servise başvuran hastayı sunmayı amaçladık. Olgu: 33 yaşında erkek hasta acil servise kültür mantarı yedikten bir saat sonra ellerde ve ayaklarda şişlik şikayeti ile başvurdu. Hastanın anamnezinde daha önce benzer yakınmalarının ve allerji öyküsünün olmadığı, mantarı tüketen diğer aile bireylerinde herhangi bir şikayet olmadığı öğrenildi. Hastanın ellerde ve ayaklarda ödeme neden olabilecek allerjen teması yoktu. Öz ve soygeçmişinde özellik yoktu. Vital bulguları normaldi. Fizik muayenesinde uvula ödemi mevcuttu, ellerde ve ayaklarda gode bırakmayan ödem vardı. Laboratuvar değerlendirmesi normaldi. Hastaya başlanan antihistaminik ve steroid tedavisi sonrası hastanın şikayetlerinde gerileme olduğu görüldü. Sonuç: Acil servislerde sıklıkla görülen anaflaksinin nadir bir nedeni olan kültür mantarına bağlı izole el ve ayak ödemi görülebileceği akılda tutulmalıdır. Anahtar Kelimeler: Anaflaksi, mantar, el ve ayak ödemi

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
353
P 298 THE EFFECTS OF COMORBIDITIES ON LENGTH OF STAY IN HOSPITAL AFTER LAPAROSCOPIC SLEEVE GASTRECTOMY: ANALYSIS OF MORBID OBESE PATIENTS WITH COPD IN AN EXPERIENCED CLINIC
Burcu Yormaz1, Hüseyin Yılmaz2
1Beyhekim State Hospital, Clinic of Chest Diseases, Konya, Turkey 2Selçuk University Medical Faculty, Department of General Surgery, Konya, Turkey Background: Morbid obesity surgery and novel variations is still improving in today’s world. Tertiary clinics in which applying bariatric procedures face several financial pressure to reduce hospitalization costs and so some clinics are called to develop short staying procedures. However short staying in hospital after the bariatric procedure is not always like this. The aim of our study is to detect morbid obese patients with COPD who have underwent surgical process required more than 1 day of hospitalization to recover; whether length of stay in hospital can be predicted by factors known before or after the operation. Methods: We have reviewed all laparoscopic sleeve gastrectomy (LSG) procedures between the years of May 2014 to June 2016. Revision and open procedures were excluded for this study. Patient characteristics, comorbidities, length of stay in hospital, and 2 weeks morbidity and mortality were reviewed. Predictors of longer stay in hospital (defined as more than 7 days) were identified by student t test. Results: Of 58 LSG operations with COPD, median length of stay was 5 days (range 3 to 21 days) and of 22 (37%) were male and of 36 (63%) were female patients. longer hospitalization rates were predicted by chronic obstructive pulmonary disease, bleeding diathesis, renal insufficiency, prolonged operating time, and resident involvement with the procedure, but not by patient age, sex, body mass index, and other co-morbidities. Conclusion: Characteristics and comorbiditive additional knowledges of patients could predict length of stay in hospital after LSG procedure. On the other hand this data can be used to identify patients, their health outcomes and could help to improve the treatment methods and intensive care unit standards following bariatric surgery procedure. Keywords: comorbidities, COPD, bariatric
P 299 YÜZDE KARINCALANMA BULGUSU İLE TESPİT EDİLEN BULBUS ENFARKTI
Nezih Kavak1, Rıdvan Sarıkaya2, Hasan Sultanoğlu1, Seda Özkan1
1Ankara Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Ankara 2Kastamonu Doktor Münif İslamoğlu Devlet Hastanesi, Kastamonu Giriş ve Amaç: Serebrovasküler hastalıklar yaşlı popülasyonda morbidite ve mortalitenin önde gelen nedenleri arasında yer almaktadır. Hastalar acil servise ani gelişen uyuşma, tek taraflı yüz kol ve bacakta güçsüzlük, afazi, konfüzyon, görsel defisit, yürüme bozukluğu, baş ağrısı, mental durum değişikliği gibi şikayetler ile başvurabilirler. Bu olgu sunumunda nörolojik muayenesi normal olan hastanın difüzyon MRG ‘da saptanan bulbusta infarktı sunmayı amaçladık. Olgu Sunumu: 63 yaşında kadın hasta acil servise sağ yüz yarısında yaklaşık dört saattir devam eden uyuşma ve karıncalanma hissi nedeniyle başvurdu. Hastanın öyküsünde hipertansiyon hastalığı mevcut olup hastanın amlodipin 10 miligram kullanımı mevcut idi. Fizik muayenede genel durum iyi, bilinç açık, koopere ve oriyente olan hastanın nörolojik muayenesinde sağ yüz yarısında karıncalanma hissi haricinde ek bulgu yoktu Laboratuar tetkiklerinde patoloji tespit edilmedi; beyin BT’ de herhangi bir patoloji saptanmadı, bunun üzerine çekilen difüzyon MRG’de bulbusta infarkt saptandı. Hastaya acil serviste oral asetylsalycilic acid 300 mg verildikten sonra hospitalize edildi. Tartışma ve Sonuç: Bulbus enfarktı görme alanı defektleri ile prezente olur. Tek taraflı baş ağrısı en sık başvuru sebeplerindendir. Şiddetli vertigo, bulantı, kusma, ataksi ve nistagmus görülür. Vertigodan yakınan hastaların hemen hepsinde nistagmus vardır. Bizim hastamızda da sadece yüzün tek tarafında karıncalanma hissi mevcuttu. Sonuç olarak acil serviste serebrevasküler hastalıklar çok çeşitli şikayet ve semptomlar ile gelebilmektedir. Yüzde karıncalanma hissi ile acil servise başvurmuş hastalarımızda bulbus enfarktı ayırıcı tanıda göz önünde tutulmalıdır. Anahtar Kelimeler: Serebrovasküler hastalıklar, Bukbus enfarktı, yüzde uyuşma

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
354
P 300 PRE-HOSPITAL AIRWAY MANAGEMENT PREFERENCES OF PARAMEDICS, ITS EFFECT ON MORTALITY AND TRANSPORT TIME
İnan Beydilli1, Mustafa Avcı1, Nalan Kozacı1, Fevzi Yılmaz1, Vedat Kırpat1, İsmail Atik2
1Antalya Training and Research Hospital, Emergency Medicine Clinic, Antalya, Turkey 2Ümraniye Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey Objectives: The success of paramedics in the pre-hospital airway management in traumatic and non-traumatic critically ill patients, especially in cardiac arrest, is very important in terms of mortality and morbidity. Materials-Methods: Patients who were admitted to the Emergency Department by pre-hospital emergency ambulance service were included in the study. Standard data registration form was created for the study. Demographic data, pre-hospital and in-hospital vital signs, GCS scores, cardiac rhythms, applied airway method, transport time and 48-hour mortality rates were recorded in the study form. Results: While the initial approach to airway management was bag-mask in 80 patients (82%), advanced airway interventions were performed in 18(18%) patients. The mean time period for the ambulance arriving at the patient was 6.52±3.064 min. and the mean time period of transport to the hospital was 11.42±9.538 min in all patients. Although there was no difference between patients managed with BM and patients managed with advanced airway interventions in terms of time period to patient access (p=0.957), there were significant differences in terms of time period to emergency service access (p=0.001) and total time period (p=0.001) Among patients with CPA, there was a significant difference between patients managed with and without advanced airway interventions in terms of 48-hour mortality (p=0.035). Discussion and Conclusion: Although the pre-hospital airway management still remains its mystery, we think that providing ventilation with BVM without losing time and transport to the hospital in patients in short distances and patients with less risk of aspiration would be more appropriate in terms of mortality and transport time. Keywords: Airway, cardiopulmonary arrest, outcome
P 301 BUPROPİYON İNTOKSİKASYONU
Nezih Kavak1, Hasan Sultanoğlu1, Rıdvan Sarıkaya2, Burcu Doğan1, Seda Özkan1
1Ankara Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Ankara 2Kastamonu Doktor Münif İslamoğlu Devlet Hastanesi, Kastamonu Giriş ve Amaç: Sigara kullanımı toplumda her türlü önleme ve zararlarının bilinmesine rağmen kullanımı artmaktadır. Sigarayı bırakma ünitelerinin yaygınlaşması ile sigarayı bırakma ilaçlarını kullanımı artmıştır. Buna bağlı olarak ta bu ilaçlara bağlı istenmeyen durumlar artmıştır. Olgu Sunumu: 25 yıldır sigara kullanım öyküsü olan 46 yaşında bayan hastanın sigara alışkanlığını bırakmada yardımcı olarak bupropiyon tedavisi başlanmış. Hasta acil servisimize intihar amaçlı yaklaşık 20-30 adet bupropiyon 150 miligram tablet alımı sonrası nöbet, titreme, tremor, solunum sıkıntısı şikayeti ile geldi. Fizik muayenede hastanın vital bulguları stabildi. Hastaya nazogastrik sonda ile mide lavajı yapıldı ve bu yol ile 50 gr aktif kömür verildi. Hastada takip sırasında jeneralize tonik klonik tarzda nöbet görülmesi üzerine 5mg iv diazepam ile müdahale edildi ve nöbet sonlandırıldı. Hastanın kan tetkikleri normal idi. Bilgisayarlı beyin tomografisi ve elektroensefalogramda herhangi bir patoloji saptanmadı. Hastanın sonrasında 24 saatlik izleminde herhangi bir semptomu olmadı ve 24 saat sonunda taburcu edildi. Tartışma ve Sonuç: Bupropionun nikotin bağımlılığı tedavisinde sigarayı bırakmaya yardımcı olarak kullanılır. Kullanımı sırasında yan etki olarak ateş, nöbet, göğüs ağrısı, dispne, asteni, taşikardi, hipertansiyon, postüral hipotansiyon, senkop, uykusuzluk, tremor, konsantrasyon bozukluğu, baş ağrısı, baş dönmesi, depresyon, halüsinasyon, ajitasyon, endişe, irritabilite, bulantı, kusma görülebilir. Bizim vakamızda nöbet, dispne ve tremor belirgin olarak görüldü. Bupropion hastalara iyi niyetle başlansa bile cok geniş yan etki profiline sahip olduğundan dikkatli kullanılması gereken bir ajandır. Anahtar Kelimeler: Sigara, bupropiyon, intihar

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
355
P 302 FAHR HASTALIĞI
Nezih Kavak1, Burcu Doğan1, Hasan Sultanoğlu1, Engin Deniz Arslan1, R.Pelin Kavak2
1Ankara Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Ankara 2Ankara Numune Eğitim ve Araştırma Hastanesi, Ankara Giriş: Fahr hastalığı(FH) bazal gangliyonlar, serebellar dentat nükleus ve sentrum semiovalede kalsifikasyonla karakterize, sporadik ve genetik geçişli vakaların da bulunduğu ender bir hastalıktır. Olgu: 16 yaşında kadın hasta, artan şiddetli baş ağrısı şikayeti nedeniyle acil servisimize başvurdu. Anamnezinde 3 gün önce kafa travması hikayesi olduğu öğrenildi. Özgeçmişinde, 10 yaşından beri aralıklarla baş ağrıları ve yüzünde istemsiz kasılmaları ve ara sıra idrar kaçırması olduğu, bunların dışında tanı konmuş lokal ya da sistemik bir hastalığının olmadığı öğrenildi. Yapılan kranial bilgisayarlı tomografisi incelemesinde; subkortikal alanda, bilateral bazal ganglionlarda, sentrum semiovalede, bilateral frontal ve oksipital loblarda yaygın simetrik kalsifikasyonlarla uyumlu hiperdens görünümler izlendi. Mevcut klinik, laboratuar ve radyolojik bulgular ışığında değerlendirilerek hastanın tablosu FH olarak kabul edildi Nöroloji kliniği ile konsülte edilen hasta, aynı tanı ile takip ve tedavi için ilgili kliniğe devredildi. Tartışma: FH uzun yıllar önce tanımlanmış bir hastalık olmasına rağmen, klinikte sık olarak karşılaşılmaması nedeniyle yanlış tanı alabilmektedir, bu nedenle bu olgunun klinik ve radyolojik bulgularının litertür bilgileri eşliğinde gözden geçirmek istedik. Anahtar Kelimeler: Bazal gangilionlar, bilateral striopallidodentat kalsinozis, Fahr hastalığı
P 303 AKREP SOKMASINA BAĞLI DİRENÇLİ BRADİKARDİ
Nezih Kavak1, Rıdvan Sarıkaya2, Hasan Sultanoğlu1, Engin Deniz Arslan1 1Ankara Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Ankara 2Kastamonu Doktor Münif İslamoğlu Devlet Hastanesi, Kastamonu Giriş ve Amaç: Akrep sokmaları halen tropikal ve subtropikal bölgelerde ciddi bir sağlık sorunudur. Akrep sokmaları en sık 20-40 yaş arası erkek cinsiyette, ayak ve bacaklarda görülür. Olguların çoğuna sıcak ve yağmurlu mevsimlerde kırsal kesimlerde rastlanmaktadır. Acil servisimize akrep ısırığı sonrası görülen dirençli bradikardi olgusu sunuldu. Olgu Sunumu: 28 yaşında erkek hasta acil servise fenalaşma hissi ve soğuk terleme şikayetiyle başvurdu. Hastanın ilaç kullanma öyküsü ek hastalığı yoktu. Hastanın anamnezinden yaklaşık 2 saat önce sağ el 2.parmak distal uçtan türü bilinmeyen bir akrep tarafından sokulduğu öğrenildi. Hastanın genel durum orta, bilinç açık olup sağ el 2. ve 3. parmaklarda eritem ve ısı artışı mevcut idi. Hastada aynı ekstremitede karıncalanma hissi ve ağrı şikayeti vardı. Hastanın vital bulgularından tansiyon arteriyel 60/40 mmHg, solunum sayısı 23/dk, nabız 35 atım/dk idi. EKG’de sinüs bradikardisi mevcuttu. Hastaya acil serviste tetanoz proflaksisi, soğuk uygulama, akrep venomu 1 ampül (5ml), 50 ml %0.9 NaCl içinde 30 dakikalık intarvenöz infüzyonla verildi. Analjezik olarak fentanyl 50 mcg intravenöz yoldan yapıldı. Hastaya 1 mg atropin intravenöz yoldan 10 defa uygulandı. Buna rağmen hastanın kalp atım hızının 35-40 atım/dakika olarak devam etmesi üzerine hasta Koroner Yoğun Bakım Ünitesi’ ne yatırıldı. Tartışma ve Sonuç: Akrep sokmlarında bölgesel olarak yanıcı ağrı, eritem, şişlik ve parestezi görülebilir.Bu bulgular bizim vakamızda mevcut idi. Sistemik bulgular hipertansiyon, hipotansiyon, taşikardi, terleme, kas güçsüzlüğü, çift görme, nistagmus, akciğer ödemi, aşırı uyarılabilirlik, kas seyirmeleri, tükrük ve ter salgısında artış, pıhtılaşma bozukluğu, konvülsiyon, kas felci ve koma olarak sıralanabilir.Bizim vakamızda hipotansiyon ve sistemik bulgulardan farklı olarak sinüs bradykardisi mevcut idi.Hayvan ısırıkları acil serviste nadiren görülen başvuru nedenlerindendir. Acil servise hayvan ısırığı nedeniyle başvuran hastalarda kalp hızı değişikliklerinin olabileceği akılda bulundurulmalıdır. Anahtar Kelimeler: Akrep sokması, Bradikardi, hipotansiyon

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
356
P 304 ABDOMINAL AORT ANEURYSM
Pınar Koptur, Ülkü Arslan, Hıdır Yımaz, Ahmet Ali Sezer, Cem Akman, Mustafa Karakuş Yıldırım Beyazıt University Yenimahalle Training and Research Hospital, Ankara, Turkey Background: Abdominal Aortic Aneurysm (AAA), is seen in about 2% of the population over 60 years old. The most important factor is the media layer of the aorta elastin and collagen degeneration. The most serious complication of AAA rupture. The risk of rupture or over 5.0 cm or fast growing than 0.5 cm per year or paınful AAA is high. İn this group patients have indication of treatment. Treatment is open surgery or endovascular surgery. Case: Seventy-eight-year-old male patient was brought to the emergency department with syncope. Patient's arterial blood pressure 120/70 mm Hg, pulse 76 / min, blood sugar 123 mg/dl, saturation O2 98 %. Urea 36 mg / dL, creatinine was 0.95 mg / dL, hemoglobin 13.4, 229 platelets, detected. The patient was neurologically intact. Upon detecting a pulsatile mass over the abdominal area during inspection, we planned abdominal and thorax tomography shots. Abdominal aorta diamater is 81 cm, bifurcation of renal artery distal and revealed aneurysmal dilatation. There was hemorrhage aneurysm in the neighborhood, especially including para-aortic retroperitoneal space, paracaval, extending to left field pararenal area hemorrhage. We started in 0.9% saline infusion to the patient. He was transferred for endovascular surgery to another hospital. Result: AAA is often called a "silent killer" because there are usually no obvious symptoms of the disease. When symptoms are present, they may include: Abdominal pain (that may be constant or come and go), Pain in the lower back that may radiate to the buttocks, groin or legs, The feeling of a "heartbeat" or pulse in the abdomen. Once the aneurysm bursts, symptoms include: Severe back or abdominal pain that begins suddenly, paleness, dry mouth/skin and excessive thirst, nausea and vomiting, signs of shock, such as shaking, dizziness, fainting, sweating, rapid heartbeat and sudden weakness. Keywords: Abdiminal Aort Aneurysm, rupture, sign of shock P 305 DULOKSETİN İLE SUİCİD GİRİŞİMİ Nezih Kavak1, Rıdvan Sarıkaya2, Hasan Sultanoğlu1, Seda Özkan1
1Ankara Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Ankara 2Kastamonu Doktor Münif İslamoğlu Devlet Hastanesi, Kastamonu Giriş ve Amaç: Serotonerjik sendrom SSRI kullanımı, MAO inhibitör kullanımı, trisiklik antidepresan kullanımı, çeşitli ilaç ve bitkisel madde kullanımı sonucu ortaya çıkmaktadır. Bu olgu sunumunda suicidal amaçla serotonin geri alım inhibitörü duloksetin alan hastada gelişen tipik serotonerjik sendrom bulgularını sunuldu ve tartışıldı. Olgu Sunumu: 24 yaşında bayan hasta acil servise 1 saat önce intihar amaçlı 30 adet duloksetin alımıyla başvurdu. Hastanın genel durum orta, bilinç uykuya meyilli, bulantı, kusma, ajitasyon, huzursuzluk, halüsinasyon görme ve yaygın vücut kasılmaları mevcuttu. Hatanın tansiyon arteriyel 200/110 mm/Hg, nabız 110 atım/dk solunum sayısı 28,ateş 39.8ºC olarak saptandı. Hastaya nazogastrik sonda ile gastrik lavaj yapıldı ve bu yoldan 50 gr aktif kömür verildi. Hastaya ateşi için i.v paracetamol 1000 mg, antihipertansif olarak iv 5 mcg/kg/dk perlinganit, ajitaston ve tremor için 5 mg iv diazepam verildi. Acil serviste 24 saat takip süresince semptomları gerileyen hastanın, takibinin son 12 saatini semptomsuz geçirmesi üzerine taburculuğu yapıldı. Tartışma ve Sonuç: Serotonerjik sendrom periferde ve santral sinir sisteminde bulunan serotonin (5-hidroksitriptamin; 5-HT) reseptörlerinin aşırı uyarılması sonucu gelişir. Klinik bulgular mentaldurum değişiklikleri, otonomik disfonksiyon ve nöromusküler uyarılmadan oluşan bir triadı içerir. Klinik olarak terleme, taşikardi, titreme, kasılma, hiperrefleksi, ateş ve rabdomiyoliz ortaya çıkmaktadır. Tedavi semptomatik olmakla beraber spesifik antidotu bulunmamaktadır.Bizim vakamızda hastanın semptomatik tedavi ile iyileştiği ve acil servisten tam sağkalım ile taburcu edildiği görülmüştür. Anahtar Kelimeler: Duloksetin, suicid, serotonerjik sendrom

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
357
P 306 MAD HONEY CASE WITH NODAL RITM
Hıdır Yılmaz, Pınar Koptur, Havva Şahin Kavaklı, Mustafa Karakuş, Ülkü Arslan, Cem Akman, Ahmet Ali Sezer Yıldırım Beyazıt University Yenimahalle Training and Research Hospital, Ankara, Turkey Background: Mad honey is the essence of rhododendron plants, it includes Grayanotoxin agent. Mad honey is produced, particularly in the Black Sea region of Turkey. Symptoms - occur a dose dependent within hours in minutes. Even when used in small amounts can cause loss of balance and hallucinations. At high doses, loss of coordination, severe and progressive muscle weakness, bundle branch block and / or electrocardiographic changes, including ST segment elevation, bradycardia, nodal rhythm, Wolff-Parkinson-White syndrome can be seen. Mad honey poisoning is rarely fatal. Medical treatment is usually not necessary. Atropine and other vasopressor agents used for symptomatic treatment. Case: Twenty-year-old man was admitted to our emergency department with 112 due to the change of consciousness. The patient had a history of eating honey immediately before the complaints. When the patient was brought to the emergency room, poor general condition, it was confused consciousness. Blood pressure 80/50 mm Hg, pulse 36 / min, blood glucose of 93 mg / dl, fever: 36 degrees, and oxygen saturation was 90%.The electrocardiogram (ECG) was also present nodal rhythm. 1 mg of intravenous atropine was made. After atropine, pulse was 80/min and blood pressure increased 110 / 70mmhg. Control ECG was sinus rhythm. Biochemical blood tests cardiac markers analysis results had normal limits. Patient hospitalized for following up. Conclusion: İt is very important to take anamnesis for diagnosis of mad honey poisoning. Mad honey intoxication should be kept in mind in the sudden arrhythmias. Keywords: Mad honey, arrhythmia, atropine
P 307 YÜRÜME BOZUKLUĞUNUN NADİR BİR NEDENİ; NÖROMYELİTİS OPTİKA
Gökhan Ersunan, Özlem Bilir, Mehmet Altuntaş, Sezer Osman Çınaroğlu, Mecit Çokluk Recep Tayyip Erdoğan Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Rize Giriş: Nöromyelitis optika (NMO) veya diğer adı ile “Devic hastalığı” genellikle optik sinirleri ve omuriliği tutan, santral sinir sisteminin inflamatuar demiyelinizan bir hastalığıdır. Omurilik tutulumu NMO’nun temel bir özelliğidir. Üç veya daha fazla vertebra segmenti boyunca uzanan, omuriliğin tüm transvers kesitini veya santral gri cevherini tutması NMO için tipik bir özelliktir. NMO’lu bazı hastaların serumunda kan beyin bariyerindeki astrositlerin ayak çıkıntılarında yerleşik olan aquaporin-4 isimli su kanallarını tanıyan otoantikorlar ayırt edilmiştir. Bu antikorların sensitivitesi %73 iken, spesifitesi % 91’dir. Testin pozitif olması tanı ve erken tedavide oldukça önemlidir. Ancak testin tek başına pozitif olması tanı koydurmaz, negatif olması NMO tanısını ekarte ettirmez. Biz burada nadir görülen diğer nörolojik kliniklerle karışabilen NMO vaksını sunmak istedik. Olgu: 18 yaşın da erkek hasta acil servise yürüme bozukluğu ve idrar yapamama şikayeti ile başvurdu. Alınan anemnezde şikayetlerin 5 gündür olduğu giderek artığı bu nedenle birkaç kere doktora başvurduğu öğrenildi. Yapılan nörolojik muayenede bilinci açık oryante koopere GKS:15 hastanın sağ veya sol taraf bulgusu yok fakat her iki alt ekstremitede 4/5 güç kaybı mevcuttu. Derin tendon refleksleri artmıştı, Serebellar testler normaldi, hastanın görme keskinliği azalmıştı. Yapılan laboratuvar testlerinde bir pataloji tespit edilmedi. Diğer sistem muayeneleri doğaldı. Çekilen beyin MRI’da Pons sol posterior kesminde pontoserebeller pedinküle uzanan 13x10 mm boyutunda düzensiz sınırlı T1’de hipo T2-FLAİR da hiperintens kontrastlanmayan lezyon tespit edilmiştir. Yine çekilen vertebra MRI’da ise servikal segmente spinal kordda uzun longuitidinal tutlum gösteren (4 den fazla vertebral seviyede), kord santralinde, kontrastlanma göstermeyen T2’ de sınırları seçilemeyen hiperintens lezyonlar tespit edilmiştir. Nöroloji kliniği ile konsulte edilen hasta hospitilize edilmiştir. Mevcut klinik ve MRI bulguları ayrıca uygulanan steroid tedavisine cevap vermesi nedeni ile NMO tanısı almıştır. Sonuç: NMO nadir görülen bir hastalık olsa da acil servise yürüme bozukluğu ve görme bozukluğunun birlikte olduğu hastalarda aklımıza gelmesi gereken tanılardan biridir. Anahtar Kelimeler: Nöromyelitis optika, ayırıcı tanı, spinal MRI

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
358
P 308 ACİL SERVİSTE KOLAY ATLANABİLEN BİR TANI: SEREBRAL VENÖZ SİNÜS TROMBOZU
Akif Yarkaç, Hüseyin Narcı, İpek Gülin Ağar, Cüneyt Ayrık Mersin Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Mersin Amaç: Serebral venöz sinüs trombozu acil servislerde nadir tanı konulan bir hastalıktır. Geniş bir yelpazede spesifik olmayan semptomlarla kendini göstermesi ve çok değişken etiyolojilere bağlı olarak ortaya çıkması, tanısında güçlüklere neden olabilmektedir. Erken tanı ve tedavi mortalite ve morbiditenin önlenmesi açısından çok önemli yer tutar. Şiddetli baş ağrısı olan tanı konulamayan bir sagittal sinüs trombozu vakasını sunmayı amaçladık. Olgu: 39 yaşında kadın hasta 3 haftadır devam eden değişken karakterde baş ağrısı, sağ kol ve bacakta yeni gelişen güçsüzlük nedeniyle acil servise başvurdu. Dış merkezde yapılan tetkiklerinde tanı konulamamış. Fizik muayenede sağ hemipleji saptanan hasta acil serviste tetkikleri devam ederken jeneralize tonik klonik karakterde nöbet geçirdi. Nörogörüntülemede superior sagittal venöz sinüs trombozu saptandı. Etiyolojiye yonelik yapılan tetkiklerde patoloji saptanmadı. Heparin infüzyonu başlanan hastaya yatış verildi. Sonuç: Serebral venöz sinüs trombozu olan hastalar acil servise çok çeşitli klinik bulgular ile başvurabilirler. Hızlı radyolojik görüntüleme ile tanı koymak ve erken tedaviye başlanması mortalite ve morbidite azaltılabilir. Anahtar Kelimeler: Sagital sinüs trombozu, acil servis, zor tanı
P 309 ETANOL VE METANOL’ÜN ENTERASAN KULLANIMI
Nezih Kavak1, Rıdvan Sarıkaya2, Hasan Sultanoğlu1, Burcu Doğan1, Engin Deniz Arslan1
1Ankara Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Ankara 2Kastamonu Doktor Münif İslamoğlu Devlet Hastanesi, Kastamonu Giriş: Toplumda alkol kullanımının artması, beraberinde daha fazla ticari kazanç elde etmek için sahte alkol üretimini de arttırmıştır. Bu durum metanol zehirlenmesi olarak kliniğe yansımaktadır. Tedavisinin etanol ile yapılabileceğinin toplum tarafından bilinmesi bir takım garip hadiselere sebep olmaktadır. Olgu Sunumu: 36 yaşında erkek hasta yerde yatar vaziyette sokakta bulunduğu belirtilen hasta 112 acil sağlık ekibi tarafından acil servise getirildi. Hastanın genel durum kötü bilinç kapalı (GKS=8, G:1,M;5,S;2), pupiller izokorik, TA:130/80 mmHg, nabız 96 atım/dk, solunum sayısı 24/dk ve ateş 36.3 ºC derece idi. Hastanın parmak ucundan kan şekeri 108 idi. Hastanın üzerindeki alkol kokusu dikkat çekti ve etonal yüksek doz alımı olabileceği düşünülerek ilk aşamada %5 dekstroz 500 cc/saat ve 500 mg intravenöz tiyamin verildi. Kan gazında pH:7.29 ml, laktat:3.08 mmol/L, anyon açığı 19.5 mmol/L etanol düzeyi 360.2 mg/dl idi. Hastanın bilinci 2 saat sonra açıldı ve bu sırada GKS 15 idi. Hastadan alınan öyküde 400 mg/dl etanol kullandığı öğrenildi. Hasta aldığı etanolün etkisini azaltmak için yaklaşık olarak 180-200 ml metanol aldığını ifade etti. Daha sonra metanolden zehirlendiğini düşünüp etanol almaya devam ettiğini ve sonrasını hatırlamadığını ifade etti. Hasta acil serviste 24 saat takip edildi.Takibinin son 12 saatini semptomsuz geçiren hasta öneriler ile acil servisten taburcu edildi. Sonuç: Etanol akut ve aşırı alımı sağlıklı düşünme yetisini bozmaktadır. Klinik olarak dizartri, öfori, nistagmus, hipotansiyon, refleks taşikardi, senkop, SSS depresyonu, koma görülebilir; ayrıca hafif derecede laktik asidoz görülebilir. Sonuç olarak acil serviste bilinç kapalı hastalarda etanol ve metanol alımı akılda tutulmalıdır. Anahtar Kelimeler: Etanol, metanol, intoksikasyon

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
359
P 310 VALUE OF HANDHELD ULTRASOUND IN HYPOTENSIVE PATIENT: “D SIGN ” PULMANARY EMBOLISM
Zamir Kemal Ertürk1, Togay Evrin1, Sinan Cem Uzunget1, Saffet Özdemir1, Leyla Öztürk Sönmez1, Erden Erol Ünlüer2
1Ufuk University Medical Faculty, Department of Emergency Medicine, Ankara, Turkey 2İzmir Katip Çelebi University Atatürk Training and Research Hospital, Emergency Medicine Clinic, Izmir, Turkey Dyspnea and hypotension are common symptom which critical patient presented to emergency department(ED). Pulmonary embolism, acute myocardial injury, trauma, pneumothorax etc. could be the reasons of these symptoms. Massive pulmonary embolism (PE) is a common consideration in unstable patients presenting to the emergency department. In this case, importance of using hand-held ultrasound in ED will be shared.60 years old female patient with a history of chronic renal disease, presented to emergency department with dyspnea. She was in shock with hypotension (60/40 mm/hg), bradycardia (30 per minute), hypoxemia (%50 on pulse oximeter). In a short time because of cardiac arrest, had started to cardiopulmonary resuscitations for fifteen minutes. After CPR, normal sinus ritm was shown in second electrocardiogram. Focused cardiac ultrasonography performed by emergency physician using handheld ultrasound (GE Healthcare, Vscan version 1.1, 1.7MHz to 3.8 MHz probe). Views of the apical 4-chamber view at the apex of the heart revealed enlarged RV, which was greater than the left ventricle (LV), hypokinetic. A views of parasternal shot axes revealed D sign which means septum lean to left ventricle. Her laboratory results were normal except some parameters. Kreatinin was 7 mg/dl (0,8-1,2 mg/dl). D-dimer level was too high (55000 mg/dl). Cardiac troponin level were normal range. Diagnosis of pulmonary embolism can be delayed by a number of problems, including difficulty obtaining intravenous access, renal impairment resulting in the inability to administer intravenous contrast, wait times for imaging, and the inability to obtain some imaging at certain times of day Hypocsemia, hypotension, high level of d-dimmer and finding focused cardiac ultrasound by using handheld ultrasound had enough to diagnosis massive pulmonary embolism. Increased experience of using ultrasound in ED makes diagnosis and treatment faster and more reliable. ED physician can use hand-held ultrasound devices for diagnosis. It can be called physician’s new stethoscope. Keywords: Hand-held ultrasound, pulmonary embolism, dispnea, D-sign
P 311 NADİR GÖRÜLEN BİR TAŞ: BİLATERAL TESTİKÜLER MİKROLİTİYAZİS
Süleyman Solak, Emin Uysal
Bağcılar Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Giriş: Testiküler mikrolitiyazis (TM) çocuklarda nadir görülen ve çoğu kez belirti vermeksizin inguino-skrotal patolojiler için yapılan ultrasonografi (USG) sırasında rastlantısal olarak izlenen testiküler parankimal kalsifikasyonlardır. Karakteristik sonografik bulgusu, diffüz, intratestiküler ve gölge vermeyen ekojenik foküslerdir. TM testiküler ve ekstratestiküler neoplaziler ile birlikte görülebilmesi nedeni ile klinik öneme sahiptir. Olgu: 11 yaşında erkek hasta, bilinen komorbid hastalığı olmayan ve testislerde son günlerde daha da artan şişlik ve dokunmakla ele gelen küçük sert cisimler olması nedeni ile ailesi tarafından acil servise getirildi. Çocuk hastanın yapılan fizik muayenesinde skrotumda bilateral hafif şişlik ve palpasyonla ele gelen ve yer değiştiren küçük sert oluşumlar hissedilmesi sonrası skrotal USG istendi. Skrotal USG incelemesinde bilateral testiste çok sayıda hiperekojen alan (mikrolitiyazis) izlenmektedir (Şekil 1). Hasta çocuk cerrahi ile konsulte edildi. Hasta ileri tetkik ve tedavisinin planlanması için polikliniğe gelmek üzere taburcu edildi. Sonuç: TM karakteristik sonografik görünümü olan ve nadir görülen asemptomatik bir antitedir. Genellikle tanımlanan karakteristik sonografik bulgular saptandığında USG ile saptanabilir. TM birlikte görülebilecek tümör gelişiminin erken tanısı için yakın takip edilmelidir. Anahtar Kelimeler: Testiküler mikrolitiyazis, çocukluk çağı, tümör

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
360
P 312 MANAGEMENT OF TRAUMATIC PATIENT WITH A HISTORY OF HEART FAILURE AND WARFARIN USAGE
Eren Sert, Cemal Zeren, Serkan Doğan, Ali Saglik, Tarik Ocak Istanbul Kanuni Sultan Süleyman Training and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey Object: Trauma is one of the common cases in emergency clinics. Comorbidities can take us to irrelevant conclusions in the trauma management. We aimed to direct attention to the difficulties of trauma patients with heart failure and warfarin usage. Case: Sixty six years old male applied to emergency service with posttraumatic pain on the left upper quadrant. In medical history, there were cardiac operation and warfarin usage. In the physical examination, respiratory sounds were normal. There was minimal tenderness on the left upper quadrant but defense and rebound. Other system examinations were normal. There was AF on the ECG. Free fluid was detected in the abdomen via abdominal USG. First laboratory results were WBC: 13.730/mcL, Hgb: 7.431g/dL, Hct: %25.81, Plt: 146.100/mcL, aPTT: 24.5sc, PTZ: 26.4sc, PT: %34.4, INR: 2.34. There was contusio pulmonalis on the basal part of left lung with chronic changes and hipodense fluid on the perihepatic, perisplenic and paracolic area in the CT (Picture1-2). There were serious clinical difficulties in the management of this case because of the continuation of pain, decreasing Hgb values, also inability to perform paracentesis and determine the source of fluid related high INRR values. It was observed that EF was %55 in the echocardiography. One unit of red cell concentrate and two units of fresh frozen plasma had been given to the patient. Patient had been discharged after 72 hours follow up. Conclusion: There is an increase number of elderly and multidrug user patients related to the easy access to modern health care. Nowadays, one of the most important problems is the increase of the trauma cases. We aimed to determine the difficulties of the diagnosis and treatment process of trauma patients with comorbidities and drug use. Keywords: Trauma, warfarin, elderly patient
P 313 A RARE CAUSE OF SEIZURE: NEUROSARCOIDOSIS
Kemal Aygün, Cansu Arslan, Burcu Azapoğlu Kaymak, Tevfik Patan Health Sciences University Istanbul Fatih Sultan Mehmet Training and Research Hospital, Istanbul, Turkey Introduction: Sarcoidosis is a multisystem inflammatory granulomatous disease of unknown etiology although current opinion favors an immune response to an as yet unknown antigen. Although the characteristic noncaseating granulomas can occur in any organ system, the lungs and the draining mediastinal lymph nodes are the most common sites of involvement. Neurosarcoidosisis thought to be much rarer occurring in less than 5% of patients with systemic sarcoidosis. It is estimated that less than 1% of patients have isolated central nervous system involvement, without systemic evidence of disease. We describe a case of epilepsy and sarcoidosis. Case: A 80-years-old woman presented to the emergency department because of new onset seizures which started 25 minutes ago. Her medical history included hypertension and sarcoidosis. Vital signs were as follows: 36,5°C, blood pressure: 140/85 mmHg, pulse:119 beats per minute, sp02:%94 and her fingerstick glucose level was 214 mg/dl. She was immediately treated with diazepam 20 mg iv and 1250 mg phenytoin with a 25 mg/min infusion rate. Hemogram, biochemistry, cardiac enzymes and coagulation panel were obtained and found within normal limits. MR brain plain with contrast revealed multiple enhancing dural based lesions in frontal, parietal, in the left temporal convexity regions. She was transported to neurology services with diagnosis of neurosarcoidosis. Discussion: Clinical symptoms of neurosarcoidosis depends on the site of granuloma involvement and are nonspecific. Facial nerve paralysis and vision loss are common symptoms, as are headaches, seizures, and signs of meningeal irritation. Seizures are estimated to occur in 5–20% of neurosarcoidosis patients. Neurologic involvement is a significant cause of mortality and morbidity in patients with sarcoidosis. However, with timely diagnosis, these can be successfully managed. Keywords: Neurosarcoidosis, seizure disorder, causes of seizure

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
361
P 314 THE EVALUATION OF CLINICAL FEATURES AND COSTS OF MULTITRAUMA PATIENTS ADMINISTERED TO EMERGENCY ROOM
Dilek Kurgun Girgin1, İbrahim Türkçüer2, Atakan Yılmaz2, Bülent Erdur2, Mert Özen1, Asiye Höbel3
1Denizli State Hospital, Denizli, Turkey 2Pamukkale University School of Medicine, Department of Emergency Medicine, Denizli, Turkey 3Tunceli State Hospital, Tunceli, Turkey Study Objective: Trauma is the most important cause of deaths in young and reproductive population. To reduce the death toll and disablements caused by trauma, in severely injured patients it’s necessary to evaluate the injury rapidly and to detect the life-threathing situation immediately. It’s important to know in reduce of deaths caused by trauma; development of pre-hospital and hospital trauma organization, public education and applying preservative precautions take place. Emergency rooms are important components of health system and the costs should be controlled without any decline in the service quality. We tried to contribute the data in our country on this matter by investigating the multitrauma patients clinical features and their effect on the treatment costs. Methods: We retrospectively analyzed the multitrauma patients who administered to Pamukkale University Medical Faculty Emergency Room between 01.01.2014-31.12.2014.Patients demographics and treatment cost were examined. Findings: 244 patients were included to our study. There were 171 (70,1%)male, 73(29,9%) female. Most frequent administration time was between 08.00-15.59 a.m.(43,9%)Traffic accidents were the most frequent cause of the trauma. 135 (55,3%)patients were discharged, 104 (42,6%) patients were hospitalized and 5 (2%) patients died in the emergency room. Mean cost per patient is 440,5+/- 185,2 TL. For the patients who were older than 65 years mean cost 529,1+/- 292,3TL. For the patients who were hospitalized and had trauma score above 16 total amount 531,2 +/- 196,5 ve 522+/- 213,7 TL. Conclusion: In conclusion to our study the factors that affect the costs in the emergency room are tests and prolonged treatments due to prolonged emergency room stay. We might suggest that to control the costs of trauma patient it is prior to take preservative precautions and education. Keywords: Clinical features, costs of multitrauma, emergency room
P 315 ACİL SERVİSTE BİR İNTİHAR OLGUSU: “ORGANOFOSFAT ZEHİRLENMESİ”
Ziya Uzun, Fatma Özdemir, Özlem Köksal Uludağ Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Bursa Giriş: Organofosfatlar endüstride, tarımda ve evlerde pestisid olarak yaygın kullanılan toksik maddelerdir. Deri yoluyla veya oral yoldan alıma bağlı olarak zehirlenmeleri olabilir. Organofosfatlar asetilkolinesteraza geri dönüşümsüz bağlanarak asetikolinesteraz inaktivasyonuna ve kolinerjik reseptör bölgelerinde aşırı asetilkolin birikimine neden olur. Aşırı asetilkolin birikimi parasempatik sinir uçlarında ve nöromusküler bileşkede kolinerjik etkiyi başlangıçta stimüle, sonrasında ise paralize eder. Olgu: 57 yaş erkek hasta, yaklaşık 3 aydır psikiyatrik bir rahatsızlık nedeniyle tedavi almaktaymış. 10 gündür içine kapanıklık hali olan hasta, son üç gündür idrar ve gaita inkontinansı, nefes alamama ve uyku hali gelişmesi üzerinde dış merkezde değerlendirilmiş ve yapılan tetkiklerinde patoloji saptanmaması üzerine taburcu edilmiş. Hasta acil servisimize ağızdan salya gelmesi, güçsüzlük, genel durum bozukluğu, şuur bulanıklığı şikâyetiyle getirildi. Yakınlarından alınan anamneze göre öncesinde de intihar girişimi olan hastanın tekrar intihar amaçlı ilaç almış olabileceği düşünüldü. Fizik bakısında ateş: 38.3 derece, tansiyonu: 110/60 mmHg, nabız: 140 atım/dk, sO2: %98, solunum sayısı: 20/dk, GKS: 9 ve miyozisi mevcuttu. Akciğer seslerinde sağ tarafta yaygın raller ve sol bazalde ralleri mevcuttu. Yoğun ağız içi sekresyonları aspire edilen, nazogastrik tüp ve mesane sondası uygulanan hastaya hidrasyon başlandı. Kolinerjik toksidrom olarak değerlendirilen hasta, organofosfat intoksikasyonu ön tanısıyla atropinize edildi. Hastanın laboratuar tetkiklerinde kolonesteraz düzeyi düşük saptandı ve pralidoksim yükleme dozu uygulandı. Entübe edilen hasta anestezi yoğun bakıma yatırıldı, ventilatöre bağlandı ve Pralidoksim infüzyonuna başlandı. Yatışının 12. gününde ekstübe edilen hasta 16. gününde ise taburcu edildi. Tartışma ve Sonuç: Organofosfat zehirlenmesi gelişmekte olan ülkelerde en sık zehirlenme nedenlerindendir. Mortalitesi genellikle gecikmiş veya uygunsuz tedaviye bağlı çok yüksektir. Zehirlenmeler genellikle tarım işçilerinde ve çocuklarda yüksektir. Kolay elde edilebildikleri için intihar amaçlı kullanımları yaygındır. Tedavide hastanın organofosfattan uzaklaştırılması, dekontaminasyonu, dolaşım ve solunumun yolu açıklığını sağlanması, semptomatik tedavi ve monitörizasyon önemlidir. Hastalarda atropin kullanılmasının mortaliteyi önemli oranda azalttığı kanıtlanmıştır. Oksim tedavisi ise inhibe olan asetikolinesterazları aktive ederek asetilkoline bağlı etkileri geri döndürmede önemli yer tutmaktadır. Anahtar Kelimeler: Acil servis, kolinerjik toksidrom, organofosfat zehirlenmesi, tedavi

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
362
P 316 MULTİVİTAMİN İLE İNTİHAR GİRİŞİMİ
Nezih Kavak1, Rıdvan Sarıkaya2, Hasan Sultanoğlu1, Engin Deniz Arslan1
1Ankara Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Ankara 2Kastamonu Doktor Münif İslamoğlu Devlet Hastanesi, Kastamonu Giriş ve Amaç: Pharmaton® günümüzde halk tarafından yaygın olarak kullanılan multivitamin desteği içeren bir gıda takviyesi olarak kullanılmaktadır.. Bu gıda takviyesinin içerisinde kalsiyum hidrojen fosfat, kolza yağı, sığır jelatini, gliserol, askorbik asit, ginseng G 115, demir sülfat, dl–alfa tokoferol asetat, niasinamid, çinko sülfat monohidrat, manganez sülfat monohidrat, bakır sülfat, A vitamini, etil vanilin, pridoksin hidroklorid, riboflavin, tiamin, kırmızı demir oksit, siyah demir oksit, folik asit, sodyum selenit, biotin, kolekalsiferol, siyanokobalamin bulunmaktadır.Bu olgu sunumu ile Pharmaton® kapsülün suicid amaçlı alımı sonucu ortaya çıkan klinik tabloyu sunmayı amaçladık. Olgu Sunumu: 19 yaşında bayan hasta acil servise baş ağrısı, ajitasyon, bulantı, kusma ve epistaksis nedeniyle baş vurdu. Hastanın yaklaşık dört saat önce suicid amaçlı 30 adet Pharmaton® kapsül aldığı belirtildi. Fizik muayenede TA 190/90 mmHg, nabız 119 atım/dk, ateş kulaktan 36.2ºC idi. Başvuru sırasında hastanın epistaksisi mevcut idi ve 30 dakika sürdü. Soğuk uygulama ve nazal tampon yapılarak epistaksis durduruldu. Hastanın başvuru sırasında yapılan laboratuvar tetkiklerinde bir anormallik saptanmadı. Hastanın tedavisinde gastrik lavaj, aktif kömür, izotonik ile sıvı desteği verildi. Hastanın 72 saatlik takibinde laboratuvar değerlerinde anormallik görülmedi, hastanın ek semptomu olmadı ve taburcu edildi. Tartışma ve Sonuç: Multivitamin ve mineral içeren gıda takviyesi ürünleri masum görünse de intihar girişimi için kullanılabilmektedir. Bizim vakamızda da görüldüğü gibi, reçetesiz temin edilebilen bu ürünler intihara meyilli kişilerde ciddi sağlık sorunları yaratabilir. Bu ürünlerin hekim tavsiyesi ile bireyin ihtiyacına göre düzenlenip kullanılması daha doğru olacaktır. Anahtar Kelimeler: Multivitamin, intihar, hipertansiyon
P 317 ANALYSIS OF THE FACTORS AFFECTING THE SATISFACTION OF PATIENTS CONSULTING PAMUKKALE UNIVERSITY FACULTY OF MEDICAL HOSPITAL EMERGENCY SERVICE
Cihan Kıray1, İbrahim Türkçüer2, Atakan Yılmaz2, Bülent Erdur2, Mert Özen1
1Denizli State Hospital, Denizli, Turkey 2Pamukkale University School of Medicine, Department of Emergency Medicine, Denizli, Turkey Introduction and Aim: The aim of this study is to evaluate the satisfaction degree of the patients who consult Pamukkale University Faculty of Medical Hospital Emergency Service, to determine the factors affecting patient satisfaction and help the planned improvements in the future. Method: This study has been performed with volunteer patients 18 and over the age of 18 who consult Pamukkale University Faculty of Medical Hospital Emergency Service. 5-star satisfaction scale has been utilized in the survey form. Ratings with 3 and below are considered unsatisfied. Collected data has been recorded by “SPSS for Windows, Version 17.0” and analyzed by utilizing chi-square test. Findings: 498 (46.4%) male, 573 (53.6%) female constituting 1071 patients have been included in the evaluation. The number of patients who are generally satisfied with the emergency service is identified as 879(82%). Patients’ age, social security, mode of transport to the emergency service, the state in the emergency service, the reason for consultation to the emergency service, the initial encounter by paramedics, the treatment in a timely manner at the emergency service, the consultation time and attitude of consultant doctor, attitude of doctors and nurses, patient briefing by doctors and nurses, the frequency of patient check (the number of times that patients are checked) by doctors and nurses, general organization, hygiene and comfort of the emergency service of patients are identified as statistically significant on the overall satisfaction (p<0.05). Overall satisfaction of patients is correlated with preferring and recommending the same hospital. Other parameters are not statistically significant on the satisfaction. Conclusion: Attitude of doctors and nurses are identified as the most important factor on patient satisfaction. Patients, who wait for too long for the initial consultation and examination, whose consultation takes longer, who are hospitalized or sent to another hospital after prolonged emergency service stay are identified unsatisfied. Keywords: Emergency service, patient satisfaction, doctor’s attitude, waiting time

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
363
P 318 FUSIDIC ACID-INDUCED THROMBOCYTOPENIA
Utku Murat Kalafat, Serkan Dogan, Rabia Birsen Tapkan, Ayse Fethiye Kalafat, Ramiz Yazıcı, Tarık Ocak Kanuni Sultan Süleyman Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey Introduction: Fusidic acid is an active agent against a wide variety of gram-positive bacteria, and it has been used in soft tissue infection. The major adverse effects are mild gastrointestinal discomfort and diarrhea. The hematological side effects such as granulocytopenia and thrombocytopenia. The published literature regarding hematological adverse effects caused by fusidic acid is an immune-mediated mechanism possibly by drug-dependent antibody. We report the case has thrombocytopenia due to fusidic acid used for two weeks. Case: The 23-years-old man patient was admitted to our emergency service due to widespread petechial rash in the right lower extremities. We learnt that he treated with fusidic acid 500 mg twice a day and etodolac 600 mg one a day for two weeks because of he had open fracture in the right lateral malleol and then the splint was applied and the lession was sutured. He has any chronic disease. Laboratory findings demonstrated that platelets count: 8.2x10 3, hgb: 14.4 g/dl, wbc: 6200 and total bilirubin: 1.9, direct bilirubin: 0.6. The patient was consult to internal medicine specialist and 16 units of trombocyte suspension were transfused to him. He was hospitalized for furthermore follow-up and treatment. Result: We recommend periodic complete blood count check in patients receiving long-term fusidic acid treatment to avoid serious hematological adverse effects. Keywords: Adverse effect, fusidic acid, thrombocytopenia
P 319 NADİR BİR İNTESTİNAL OBSTRÜKSİYON NEDENİ: ABDOMİNAL KOZA SENDROMU
Süleyman Solak, Emin Uysal Bağcılar Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Giriş: Abdominal koza, primer ya da sekonder olarak bağırsak anslarının bir kısmının veya tamamının fibrokollajenöz bir membranla sarılması sonucu akut veya subakut intestinal obstruksiyon bulguları ile karşımıza çıkan ender bir ileus nedenidir. Genelde genç adölesan kadınlarda bildirilmişse de her iki cinste ve her yaşta karşılaşılabilen bir hastalık olduğu unutulmamalıdır. Olgu: 29 yaşında erkek hasta 2-3 gündür olan bulantı-kusma, karın ağrısı ve takiben gaz-gaita yapamama yakınması ile getirildi. Öyküsünde kabızlık dışında bilinen bir hastalık olmadığını belirtiyordu. Fizik muayenede palpasyonla batında yaygın hassasiyet ve umblikal bölgede ele gelen kitle hissi mevcuttu. Laboratuvar biyokimyasal paramatreleri normaldi. Ayakta direk karın grafisinde ince bağırsak düzeylerinde yaygın hava-sıvı seviyeleri mevcuttu. Batın kontrastlı bilgisayarlı tomografi incelemesinde minör pelvis lokalizasyonunda ileal anslar ve mezenterik yağlı dokuda kümeleşme ve çevresini tamamen saran ince hat halinde kapsüle ait görünüm ve proksimalinde ileal anslarda dilatasyon ve hava-sıvı seviyeleri saptandı (Şekil 1). Genel cerrahi ile konsulte edilen hasta abdominal koza sendromu tanısıyla operasyona alındı. Sonuç: Abdominal koza sendromu, bağırsak tıkanıklığı ile gelen özellikle genç yaşlardaki hastalarda olmak üzere tanıda düşünülmesi gereken bir hastalıktır. Anahtar Kelimeler: Karın ağrısı, ileus, abdominal koza

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
364
P 320 MAN WITH NO FACE: AIRWAY MANAGEMENT OF A MAXILLOFACIAL TRAUMA PATIENT
Altuğ Kanbakan, Onur Yılmaz, Hanife Bilgili, Afşın İpekci, Yonca Senem Akdeniz Istanbul University Cerrahpaşa Medical Faculty, Department of Emergency Medicine, Istanbul, Turkey Background: Maxillofacial injuries and head traumas are common results of high-velocity traumas arising from road traffic accidents, sport injuries, falls and gunshot wounds. Lack of a seatbelt or an airbag increases the risk of facial and pan facial fractures. Airway management contains crucial steps and redflags that overlooking them may lead to grave morbidity and mortality in prehospital or hospital settings. Case: Twenty-three years old male patient was brought to our emergency service by ambulance. Trauma mechanism reported by the paramedic team indicated that patient was seated in the driver seat without his seatbelt on, and he had crushed his face to the steering wheel during the accident. After the initial examination, it was noted that patients bilateral orbitas; maxillary, zygomatic and nasal bone structures were not observed. Patient was breathing spontaneous in tripod position and he had tachypnea. On his primary survey, patients hemorrhage control was maintained with aspiration. Oxygen saturation was normal while sitting but he wasn’t able to keep his airway open in supine position. Also after stabilization of patient, urgent plastic surgery planned. Because of his severe facial fractures, surgical airway (tracheostomy) placement was performed accompanied with a otolaryngologist. Plastic and reconstructive surgery had taken the patient to operation. Discussion: The most common cause of maxillofacial fractures is traffic accidents and young male patients are more prone to maxillofacial injury. The best approach to difficult trauma airway involves planning ahead by having equipment ready for oral endotracheal intubation as well as keeping the neck prepared and cricothyrotomy kit ready. Also, tracheostomy was the best option for this patient Conclusion: Even though this patient was conscious enough to maintain breathing; his severe maxillofacial trauma was compromising his airway. In the end, even patients with 15/15 Glasgow Coma Scoring might need airway intervention. Keywords: Airway management, maxillofacial trauma, surgical airway
P 321 WILD BOAR ATTACK
Ece Soykan, İlhan Uz, Yusuf Ali Altunci Ege University Faculty of Medicine, Department of Emergency Medicine, Izmir, Turkey Introduction: Wild boar is a common name for various species of the pig of the genus Sus, part of the biological family Suidae. They have bulky, massively built suid with short and relatively thin legs. They first charge and bite, often from behind, resulting in injuries to the lower extremities, and if the assault continues and the victim is knocked to the ground, more dangerous and severe secondary lesions may occur in any anatomic location depending on the relative position of the victim and attacking animal. Case: A 48-years-old male patient was brought to our emergency department following a wild boar attack. On physical examination the patient had a 20 cm of deep laceration on the posterolateral side of his thigh. His hamstring muscles were lacerated. The wound was irrigated with 3000 cc saline and iodine solution. Bony structures were intact Tetanus and rabies immunoglobulins were infiltrated to the wound and the rest was administered to the deltoid area with rabies and tetanus vaccines. Discussion: Management of an animal bite wound should start with proper local care of the wound. The wounds should be washed vigorously and irrigated with saline solution to reduce the high inocula of the oral flora of the biting animal. Tendon, nerve, muscle and vessel structures must also be examined. Specific antibiotherapy is essential but amoxicillin and clavulanic acid can be chosen as empirical therapy. Rabies vaccine and immunoglobulin, tetanus vaccine and immunoglobulin is essential and immunoglobulins should be administered to the wound as much as possible. In conclusion, a wild boar bite is a rarely seen case in emergency departments. Proper wound care, tetanus immunization, rabies prevention, and appropriate antibiotics should be administered to the survivors of wild boar attacks. Therefore deadly interactions between humans and wild boars could be avoided. Keywords: Wild boar, bite, trauma

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
365
P 322 TAXUS BACCATA ÇEKİRDEĞİ İNTOKSİKASYONU
Leyla Öztürk Sönmez1, Lukasz Szarpak2, Mehmet Ergin3, Togay Evrin1, Zamir Kemal Ertürk1
1Ufuk Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Ankara 2Medical University of Warsaw, Department of Emergency Medicine, Warsaw, Poland 3Yıldırım Beyazıt Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Ankara Giriş: Taxus türlerinde buluna alkaloidler Na+ ve Ca++ kanallarını bloke ederek ve mikrotübül fonksiyonlarını bozarak iletim defektlerine neden olmaktadır. Ağacın çekirdeği ve yaprağının toksik olduğu bilinmektedir. Başlangıçta ve hafif olgularda bulantı, kusma, sersemlik, yaygın karın ağrısı olarak prezente olabilirken, ağır olgularda bradikardi, ventriküler taşikardi, ventriküler fibrilasyon, hipotansiyon ve şoku içeren kardiyovasküler etkileri ile fatal seyredebilmektedir. Letal dozu yapraklarında 0,3- 1,6 g/kg iken taksinlerde 3.0- 6.5 mg/kg’ dır. Olgu: 30 y Kadın Hasta acil servise porsuk ağacı meyvesi ve çekirdeğini (taxus baccata) yeme şikayeti ile oral alımının 20. Dk’ sında acil servise başvurdu. İlk değerlendirmede GKS: 15 genel durumu iyi, vital bulguları stabil(TA:136/97 HR: 85/dk ATEŞ:36, 9 SAO2:98) olan hastada sinüs aritmisi dışında patolojik bulgu saptanmadı. EKG çekildi, atrial ekstrasistol saptandı. Kardiyak, Kan basıncı, SaO2, SS monitorizasyonu ile takip edildi. 20G kateter ile iv damar yolu açıldı. CBC, BFT, KCFT, kardiyak marker, koagulasyon profili, b HCG çalışıldı. NG takıldı, 3000 cc sf ile midede partikül kalmayana kadar gastrik lavaj yapıldı. Tek doz aqua carbon tedavisi 1 mg/kg dozda verildi. Çekirdekğin bir örneği alındı, sarraf tartısında 0,10 g olarak tartıldı. Takiplerinde TA:90/45 HR:61/dk olan hasta kırmızı alana çekildi, arterline açıldı, invaziv kan basıncı monitorizasyonuna başlandı. 200cc/sa %0,9 NaCL ile hidrate edildi. Takiplerinde normotansif seyretti. İdrar sonrası takıldı girişte 400cc idrar geldi, takiplerinde 100cc/s idrarı geldi. Kan sonuçları normal geldi. Hasta Anesteziyoloji ve Reanimasyon ile konsülte edildi, hastaya ybü yatışı verildi. Atrial ekstrasistolü olan hasta Kardiyoloji ile konsülte edildi. Elektif şartlarda EKO ve Holter planlanarak poliklinik kontrolü önerdiler. Hasta yoğun bakım yatışını kabul etmedi, kendi isteği üzerine taburcu edildi. Sonuç: Hastamızda 0,10 g’ lık taxus baccata çekirdeği intoksikasyonunda erken gastrik lavaj sonrasında fatal bir komplikasyon gelişmemiştir. Ertesi gün yapılan telefon vizitinde hastada mide bulantısı dışında bir rahatsızlık gelişmemiştir. Anahtar Kelimeler: Aritmi, intoksikasyon, Taxus Baccata P 323 INTESTINE IN SCROTUM AND MORE Betül Gülalp Başkent University Adana Training and Research Hospital, Department of Emergency Medicine, Adana, Turkey Introduction: Scrotum pain is an emergency complain in especially geriatric and obese patient in Emergency Department (ED). The point of care emergency sonographic features obtained at presentation addition to the physical examination performed by Emergency Physician assesses the first patient care. Case: A 73 year old male presented with pain and edema in scrotum to the emergency department. Comorbities were diabetes mellitus, atrial fibrillation, and hypertension. Initial vital signs were the following: Blood pressure 140/70 mmHg, pulse 111 beats per minute, respiratory rate 22, SatO2 95%. On physical examination he was obese and had arryhtmic arryhtmic heart sounds with pansystolic 1st degree murmur on oscultation of mesocardiac area. He had an edema, inflamation and tenderness included the left side of scrotum extended to the pelvis with an irreductable scrotal hernia. The only abnormal result examined in CBC and biochemical tests was K, 6 mEq/L. Bedside ultrasonography was performed by emergency physician following the first systemic physical examination identified findings of intestine in scrotum with a surprised addition of air artefacts (Figure 1-3). Result: Point of care ultrasonography performed by Emergency Physician is the current management in differential diagnosis in ED. Incarcerated inguinal hernia is an irreductable one on physical examination and uncompressible with preserved peristaltism on emergency ultrasound. Air artefacts are needed to differentiate the Fournier gangrene at first or in herniated bowel in scrotum related in, also. Keywords: Air artefact, point of care emergency ultrasound, scrotal hernia

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
366
P 324 LİSFRANK KIRIKLI ÇIKIĞI Tuğba Atmaca Temrel1, Çağrı Elgörmüş1, Fatih Tanrıverdi2, Mehmet Ergin2, Şervan Gökhan2
1Atatürk Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Ankara�2Yıldırım Beyazıt Üniversitesi, Acil Tıp Anabilim Dalı, Ankara Giriş: Tarsal kemikler ile metatarsal kemikler arasındaki eklem lisfrank eklemi olarak bilinir. Bu eklemin kemiksel stabilitesini, ikinci metatarsın medial ve lateral küneiform arasındaki oluğa anahtar kilit şeklinde oturmasını sağlar. Lisfrank kırığı çok nadirdir, bütün ortopedik travmaların %1’den azında görülür. Acil serviste ilk değerlendirmede yaklaşık %20 olgu gözden kaçmaktadır. Eğer tanı konulamaz ise kronik ağrı ile birlikte hareket kaybı riski yüksektir. Biz burda nadir görülen lisfrank olgusunu sunmak istedik.��
Olgu: 58 yaşında erkek hasta acil servise yüksekten düşme sebebiyle başvurdu, ayak ve ayak bileğinde ve torakal vertebra (T11) hassasiyeti mevcuttu. Görüntülemelerinde lisfrank kırıklı çıkığı olan hasta ortopedi ile konsülte edildi. Ortopedi tarafından açık redüksiyon internal fiksasyon yapılan hasta ortopedinin takibine alındı.��
Tartışma ve Sonuç: Lisfrank kırıklarının nadir görülmesi ve akut dönemde ağrı olmasına rağmen hastanın eklemini kullanabilmesi nedeniyle gözden kaçma riski yüksektir. Muayenede ayak arkası sabitlendikten sonra ayak önü pasif pronasyon ile abduksiyona getirildiğinde ağrı ortaya çıkar.�Bu bulgu tarsometatarsal yaralanmalar için spesifiktir. Lisfrank yaralanmaları, açık redüksiyon gerektirmesi, gözden kaçması durumunda sıklıkla fonksiyon kaybı ve kronik ağrı ortaya çıkması nedeniyle akılda tutulmalıdır. Şüphelenilmesi durumunda direk grafi ile tanı konulamazsa BT ve MR yardımcı olacaktır. Anahtar Kelimeler: Lisfrank kırıklı çıkığı, acil servis, nadir olgu P 325 PNEUMOCEPHALUS FOLLOWING EYE INJURY WITH NAIL Pınar Yeşim Akyol, Yusuf Şahin, Murat Çalışkan, Zeynep Karakaya, Fatih Esad Topal Izmir Katip Çelebi University Atatürk Training and Research Hospital, Department of Emergency Medicine, Izmir, Turkey Introduction: Pneumocephalus is defined as presence of air in the cranial cavity which may be present in the subdural space, or intraventricular space. Pneumocephalus may be seen in 0.5-1.0% of head injuries, and they are the most common cause of pneumocephalus. The presenting symptom in pneumocephalus is usually headache, and other symptoms include CSF rhinorrhea, meningeal signs, hemiparesis, papilledema, and cranial nerve palsies. We report a rare case of post traumatic pneumocephalus in a man who was exposed after a penetrating eye trauma with nail. Case: A 54-year-old man was admitted to our hospital following eye injury with nail. On admission to the hospital his Glasgow Coma Score was fifteen. Pupillary response was normal. There was rhinorrhoea and 5 mm laceration on conjunctiva. His complain was headache. He was otherwise clinically stable with normal vital parameters. Imaging with computed tomography of his head revealed pneumocephalus in left orbita and intracranial compartment. Ethmoid bone was fractured. He was hospitalized in neurosurgery service for observation. Discussion: Penetrating brain injuries have a higher mortality rate than closed brain injuries. Nails, wooden, foreign bodies, Stones and umbrella tips are examples of reported objects. Pneumocephalus develops due to a cranial or facial fracture through which air enters the intracranial cavity. Other common causes are surgery, tumors and infections. Meningitis, otitis media, orbital emphysema and high pressure air applied into the orbit is also suggested as reasons to pneumocephalus without bone fracture. The air is considered to enter from tenon fascis. CT is the “gold standard” diagnostic tool for tension pneumocephalus. CT identifies the presence of air via the density differences between air, fluid, tissue, and bone. İn the presented case, there was a fracture on ethmoidal bone for this reason the patient was placed under observation 2 days in neurosurgery service. He was discharged from the hospital. Keywords: Pneumocephalus, eye injury, nail, emergency department

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
367
P 326 SAVAŞ SONRASI GÖÇMENLERDE KÖTÜ KİŞİSEL BAKIM, YARA YERİNDE MİYAZİS: OLGU SUNUMU Kerim Abatay, Ali Halıcı, Ali Şahin, Gözde Çavumirza Ergül, Seda Özkan Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Ankara Giriş-Amaç: Miyazis, sinek larvalarinin neden olduğu bir hastalıktır. İnsan miyazı, çoğunlukla kötü hijyeni olan, kırsal kesimde yaşayan, düşük sosyo ekonomik seviyeye sahip ya da zeka geriliği olan hastalarda görülmektedir. Bu kişilerde larvalara yaşam alanı hazırlayan bir takım predispozan faktörler bulunmaktadır. Bunlar arasında diabetes mellitus, immobilizasyon, düşük kişisel bakım, immünsupresyon, açık yaralar, çocuklar, mental retardasyon sayılabilir. Biz geçirilen beyin operasyonu sonrası kötü hijyenik şartları olan, bakımı iyi yapılmayan yara bölgesinde gelişen miyazis olgusu sunmaktayız.��
Olgu: 43 yaşında erkek hasta yemek yememe, saçlı deriden kötü koku gelmesi şikayetleriyle 112 acil ekipleri tarafından acil servise getirildi. Hastanın öyküsünden Suriye de savaş sırasında kafa travması sonrası beyin operasyonu geçirdiği öğrenildi. Genel durumu orta, bilinci açık olan hastanın vitalleri stabildi. Fizik muayenesinde kafada sağ temporalde 5x4 cm doku kraniotomi defekti mevcuttu. Defektin ortasında nekroz, sarı akıntı ve kurtçuklar izlendi. Yapılan parazitolojik incelemede sinek larvası şeklinde raporlandı. Hastaya pansuman yapıldı ve antibiyoterapisi acil serviste başlandı. Hasta yara debritmanı ve tedavi için beyin cerrahisi kliniğine yatırıldı.��
Sonuç: Miyazis kendini sınırlama eğiliminde olmasına rağmen, santral sinir sistemi penetrasyonu gibi ölümcül komplikasyonlara da neden olabilir. Düzenli pansuman, iyi hijyenik koşullar ve malnütrisyondan kaçınılması miyazisten korunmak için gereklidir. Anahtar Kelimeler: Miyazis, sinek larvası, yara, kötü hijyen P 327 İLEUSA BAĞLI ABDOMİNAL KOMPARTMAN SENDROMU: OLGU SUNUMU Kerim Abatay, Ali Şahin, Uğur Kahveci, Ali Halıcı, Seda Özkan Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Ankara Giriş-Amaç: Abdominal kompartman sendromu artmış intraabdominal basınç sonucu progresif intraabdominal organ disfonksiyonu ile karakterize bir klinik sendromdur. Risk faktörleri arasında intraabdominal kanama, travma, peritonit, ileus, yanık bulunmaktadır. Abdominal kompartman sendromu gelişen olgularda mortalite %40’ ın üzerindedir. İleus sonrası abdominal kompartman sendromu ve buna bağlı çoklu organ yetmezliği gelişen bu olguyu sunmadaki amacımız; ileus hastalarında mortalitesi yüksek abdominal kompartman sendromunun gelişimi açısından dikkatli olunması gerektiğini vurgulamaktır.��
Olgu: 31 yaşında kadın hasta yemek yememe ve hareketlerinde yavaşlama farkedilmesi üzerine bakıcıları tarafından acil servise getirildi. Hastanın genel durumu orta-kötü, bilinci konfüze, hipotansif ve solunumu düzensizdi. Fizik muayenede karında distansiyon mevcuttu. Hasta entübe edilip, mekanik ventilatöre bağlandı. Direk batın grafisinde yaygın gaz distansiyonu ve hava-sıvı seviyeleri mevcuttu. Hasta ileus ve invaginasyon ön tanıları ile genel cerrahi ile konsülte edildi. Hastanın acil serviste takibinde batın distansiyonu arttı, kompartman sendromu ön tanısıyla kontrastlı batın BT çekildi. Batın BT de ince barsak anslarında ve kolonik anslarda yaygın gaz ile distansiyon, dalak ve her iki böbrekte global enfarkt, abdominal aorta ve dallarında belirgin çap azalması görünümü izlendi. Hasta mevcut klinik ve bulgularla abdominal kompartman sendromu düşünülerek genel cerrahi kliniğine yatırıldı. Hasta opere edildi. Post op. birinci günde ex oldu.��
Sonuç: Abdominal kompartman sendromu; hızlı gelişen ve mortalitesi yüksek acil klinik bir durumdur. Tedavisi farklılık ve aciliyet gerektirdiğinden ileus nedeniyle takip edilen hastalarda batında gerginlik, distansiyon gelişmesi ve genel durum bozulması durumunda mutlaka göz önünde bulundurulmalı ve hızlı hareket edilmelidir. Anahtar Kelimeler: İleus, abdominal kompartman sendromu, mortalite

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
368
P 328 AN UNUSUAL CAUSE OF ACUTE ABDOMEN IN ADULTS: INVAGINATION! Ece Soykan, İlhan Uz Ege University Faculty of Medicine, Department of Emergency Medicine, Izmir, Turkey Introduction: Invagination is the infolding of one part of intestine within the following part. Intestinal invaginations mostly seen in children younger than 2 years. Herein we present an invagination case in an elderly, developed secondary to a lipoma in ileocecal valve. Case: 54-year-old female referred to our emergency room with abdominal pain. On physical examination she had pain, defence and rebound on her lower right abdominal quadrant. Blood tests were normal and there was leucocyte on urinanalysis. There were no pathology on plain graphs and USG. Patient was taken to abdominal CT with a prediagnosis of acute abdomen. CT showed short segment invagination of ileocaecal valve secondary to a 2cm lipoma in caecum (Figure 1). Patient was taken to surgery by general surgery department. Discussion: Intestinal invagination is a rare condition in adults with abdominal pain which is more common in children. In adults invagination is seen mostly secondary to benign and malignant intestinal tumors and commonly present on the 6-7. decades. Our case was an invagination secondary to a lipoma in ileocaecal valve. Abdominal mass, pain and rectal bleeding is known as invagination triad however this triad is not compatible in adults. Other symptoms are nausea, vomiting and alteration of defecation routine. There was no symptom besides abdominal pain in our case. Plain abdominal graph, USG and CT scan are helpful in diagnosis. Hence the CT scan is not golden standard on diagnosis it still has a sensitivity of %50-80. On CT scan target sign, thickened intestinal Wall and mesentary are diagnostic. The treatment is surgery in adults. Deinvagination caused mucosal injury leads to venous embolism, perforation and tumoral expansion and therefore is not suggested. In conclusion intestinal invagination in adults is not a common condition and therefore must be kept in mind for patients with acute abdomen. Keywords: Acute abdomen, invagination, lipoma, target sign P 329 KÜNT TRAVMAYA BAĞLI NADİR BİR OLGU; DİYAFRAGMA RÜPTÜRÜ Eren Usul, Kerim Abatay, Uğur Kahveci, Ahu Karsandı, Sevil Tanrıverdi, Seda Özkan Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Ankara Giriş-Amaç: Travmatik diyafragma rüptürü, penetran ya da künt travmalar sonrası nadir görülen ve kolaylıkla gözden kaçabilen önemli bir komplikasyondur. Künt travmada toraks ile karın arasında oluşan ani basınç farkı ile ya da travmanın yol açtığı yüksek kinetik enerji sonucu diyafragma yaralanması oluşur. Acil serviste sık karşılaşılan geç dönem travma vakalarının ayırıcı tanısında düşünülmesi gerekmektedir. Biz nadir görülen, künt travmaya bağlı geç dönemde ortaya çıkan bir diyaframa rüptürü olgusu sunuyoruz.��
Olgu: Otuz dokuz yaşında erkek hasta bir haftadır devam eden sol üst kadran ağrısı ve göğüste batma şikayetleri ile acil servise başvurdu. Hastanın hikayesinde bir hafta önce yaklaşık bir buçuk metre yükseklikten düştüğü öğrenildi. Vital bulguları stabil, oksijen satürasyonu normaldi. Hastanın bilinci açık, oryante ve koopereydi. Hastanın yapılan fizik muayenesinde, sol akciğer bazalde solunum seslerinde azalma mevcuttu. Diğer sistem muayeneleri normal olarak değerlendirildi. EKG si normal sinüs ritmiydi. Laboratuvar tetkiklerinde herhangi bir patoloji tespit edilmedi. Çekilen toraks bilgisayarlı tomografisinde: diyafragma 11 cm eleve olarak değerlendirildi. Karaciğer ve hepatik flexura intratorasik alana herniye olmuş, mediasten karşı tarafa itilmiş, sağda plevral sıvı mevcuttu. Hasta diyaframa rüptürü tanısıyla takip ve tedavi amaçlı genel cerrahi servisine yatırıldı.��
Sonuç: İzole diyafragma rüptürleri erken dönemde semptom vermeyebilir. Bu nedenle minör travma olgularında özellikle respiratuvar ve/veya gastrointestinal yakınmalarla birlikte, akciğer grafisinde şüpheli görünümü olan hastalarda diğer ön tanıların yanı sıra diyafragma rüptürü olasılığı da akılda tutulmalıdır. Anahtar Kelimeler: Diyafragma rüptürü, künt travma, acil servis

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
369
P 330 MCA ANEVRİZMA TROMBÜSÜ: OLGU SUNUMU Kerim Abatay, Uğur Kahveci, Ali Halıcı, Emrah Arı, Seda Özkan Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Ankara Giriş-Amaç: İntrakranial anevrizma trombüsleri genellikle dev intrakranial anevrizmaların yaklaşık %50’inde bulunmaktadır. Trombüsler lümen içinde değişik boyutta olabilirler ve stabil değillerdir. Trombüse bağlı iskemik inme veya geçici iskemik ataklar görülebilmektedir. Biz bildirimizde baş ağrısı şikayeti ile gelen genç hasta da saptanan MCA anevrizma trombüsü olgusunu sunuyoruz.��
Olgu: 32 yaş bayan hasta baş ağrısı, sağ kol ve omuz kuşağında hissizlik şikayeti ile acil servisimize başvurdu. Öyküsünde ek bir hastalık, ilaç kullanım yoktu. Fizik muayenesinde nörolojik defisit saptanmadı. Vitalleri stabildi. Laboratuvar testlerinde özellik yoktu. Hastaya beyin BT planlandı. Hastanın çekilen beyin BT’sinde sol MCA M2 segmentinde yaklaşık 15x12 mm boyutta kalsifiye tromboze anevrizma ile uyumlu nodüler lezyon saptandı. Hastaya acil serviste full sekans MR çekildi. MR raporunda sol serebral hemisferde, sol MCA anterior komşuluğunda silvian fissür içerisinde T2AG'de daha hipointens, FLAIR’da izo-hafif hipointens sinyal özelliğinde ekstraaksiyel yerleşimli IV. Gad enjeksiyonu sonrası kontrast tutulumu göstermeyen yaklaşık 14x11 mm boyutunda fokal olası benign karakterli lezyon izlenmiştir Hasta nöroloji ve beyin cerrahisi ile konsülte edildi. Beyin cerrahisine takip açısından devir edildi. ��
Sonuç: İntrakranial anevrizmalar rüptüre olmadıkça nadir klinik bulgu verirler. İntrakranial anevrizma içi trombüs ise çok nadir görülür ve iskemik olaylardan sorumludur. Bizim olgumuzda olduğu gibi iskemi oluşturmadan veya rüptüre olmadan önce teşhis edilen anevrizma trombüslerinin klinik sonuçları iyidir. Anahtar Kelimeler: MCA, trombüs, anevrizma P 331 TROMBOTİK TROMBOSİTOPENİK PURPURA SEYRİNDE İSKEMİK İNME: OLGU SUNUMU Kerim Abatay, Ali Halıcı, Uğur Kahveci, Eslem Zehir, Seda Özkan Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Ankara Giriş-Amaç: Trombotik Trombositopenik Purpura tanılı hastaların %50-%70’inde serebral iskemiye dair bulgular görmek mümkündür. Nörolojik bulgular; inme ve geçici iskemik ataktan, başağrısı, nöbetler, aralıklı konfüzyon ve komaya varan bir yelpazede değişkenlik gösterir. Bu bildirimizde TTP seyrinde iskemik SVH gelişen bir olgu sunulmaktadır. ��
Olgu: 47 yaşında kadın hasta ağız kenarında kayma, yüzde uyuşma ve baş ağrısı şikayeti ile acil servise başvurdu. Öyküsünde iki yıldır TTP tanısı ile takipli olduğu öğrenildi. Genel durumu iyi, bilinç açık, oryante koopere idi. Fizik muayenesinde fasial asimetri mevcut olup diğer sistem muayeneleri normaldi. Beyin BT’ de hemoraji saptanmadı. Laboratuvar tetkiklerinde hemogramında Plt: 39000/L (150.05-372.2 /L)’ di. Periferik yayması eritrositlerde anizositoz ve her alanda 3-4 trombosit şeklinde değerlendirildi. Acil serviste takibi sırasında dizartri gelişen hastaya çekilen MR görüntülemede diffüzyon kısıtlaması görüldü. Mevcut klinik ve bulgularla TTP seyrinde gelişen iskemik SVH tanısı ile nöroloji kliniğine yatırıldı. ��
Sonuç: Sonuç olarak, TTP farklı klinik tablolar ile karşımıza gelebilir, nadir de olsa akut iskemik SVH da bunlardan biridir. Anahtar Kelimeler: TTP, SVH, trombositopeni, tromboz

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
370
P 332 BEYİN BT’Sİ GELİŞ ANINDA VE TAKİBİNDE NORMAL OLAN HASTADA SAK Hamit Hakan Armağan, Furkan Çağrı Oğuzlar, Abdurrahman Şimşek, Nesrin Gökben Beceren, Seda Dağlı, Burak Güler, Berker Şahin Süleyman Demirel Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Isparta Giriş: SAK kanın subaraknoid boşluğa sızmasıdır. %75’i anevrizma rüptürü sonucu oluşur. SAK süphesinde kullanılacak ilk tanısal tetkik olan modern kontrastsız BT’nin sensitivitesi semptomların başlangıcından itibaren 12 saatte kadar %98 ila en yüksek seviyeye sahiptir. Yapılan çalışmalar klinisyenlerin böyle davranmadıklarını göstersede artık birçok otorite BT’nin normal olması durumunda bos incelenmesi gerektiğini belirtmektedir. Bos sıvısında ksantokromi varlığı ve kırmızı kan hücresi bulunması SAK tanısı koymada en fazla ilgilenilen iki testtir.��
Olgu: 86 yaşında bayan hasta. 3-4 gündür bilinç değişiklikleri oluyormuş. Gece kötüleşme nedeniyle acil servise getirildi. Başvuru anında TA: 180/92 Nbz: 113 Ateş: 37.5 Pulse O2: 92 Solunum Sayısı: 21 GKS: 9 oryantasyon kooperasyon kısıtlı. Yapılan fizik muayenesinde genel durum orta-kötü, ışık refleksi normal, kas gücü hastanın durumundan dolayı değerlendirilemedi. Patolojik refleks yok, DTR bilateral +/+, ense sertliği + olan hastadan beyin bt ve iskemik svo acısından difüzyon mr istendi. Hastanın hemogram doğal, BK da üre: 128,2 bun: 60 kreatin 1.81, ast: 141, alt: 73 elektrolitler doğal geldi. Görüntülemelerinde akut patoloji saptanmayan hastada menenjit? Ön tanısı ile LP yapıldı. LP sonucunda 6 tüp hemorajik (hare oluşturan) bos geldi. Direkt bakıda hücre saptanmayan ksantokromik görünüm olan hasta SAK ön tanısı ile nöroloji yoğun bakıma yatışı verildi. 1 hafta takibi sırasında bilinci düzelmeyen hastanın kontrol beyin BT’si normal geldi. Tekrar LP yapıldı. Ksantokromik görünüm devam etti. Hastanın takibinde kardiyak arrest gelişmesi sonrasında eksitus kabul edildi.��
Sonuç: Bos’da ksantokromi izleri en fazla 3 hafta pozitif kalır ve çoğunlukla da 12 saatte kadar pozitif kaldığı için tanı koymada sınırlıdır. Normal BT bulguları, ksantokromi yokluğu, kırmızı kan hücresinin olmaması veya azlığı (<5 x 106RBCs/L) SAK’ı dışlar. Genelde takip BT’lerinde kanama kendini gösterse de bu hastada BT normalken ksantokromi takibi ile SAK’ın devam ettiği gözlenmiştir. Anahtar Kelimeler: SAK, LP, beyin tomografisi, ksantokromi P 333 SOL ALT KADRANDA KİTLE GÖRÜNÜMÜ VEREN İLİAK ARTER ANEVRİZMASI; BİR OLGU SUNUMU
Kerim Abatay, Uğur Kahveci, Eren Usul, Engin Deniz Arslan Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Ankara Giriş-Amaç: İliak arter anevrizması intraabdominal anevrizmaların %2-7’sini oluşturur. Genellikle intraabdominal aort anevrizması ile birlikte bulunmaktadır. Semptomsuz bir şekilde büyüyebilir, rüptüre olabilir. Biz karın ağrısı şikayeti ile başvuran iliak arter anevrizmalı bir erkek olgu sunuyoruz. ��
Olgu: Hasta karın ağrısı ve nefes darlığı şikayetleriyle acil servise başvurdu. Hastanın hikayesinden bu şikayetlerinin yaklaşık bir aydır olduğu, son iki üç gündür arttığı öğrenildi. Hastanın vitalleri; arteriyel kan basıncı 160/100 mmHg, nabız 100 vuru/dk, solunum sayısı 20/dk, vücut ısısı 36,7o C idi. Hastanın bilinci açık, oryante ve koopere idi. Hastanın fizik muayenesinde palpasyonda karında sol alt kadranda defansı vardı. Yine sol alt kadranda sınırları net ayırt edilemeyen, ele gelen kitlesi mevcuttu. Solunum sesleri kabalaşmış, diğer sistem muayeneleri normaldi. Hastaya tanıya yönelik çekilen tüm abdomen BT’sinde solda pelvik alanda sol internal iliak arterden origin alan 7x6 cm çapında anevrizma mevcuttu.�Hastaya mevcut bulgularla izole iliak arter anevrizması düşünüldü.��
Sonuç: İliak arter anevrizmalarının tanısı güçtür ve nadir görülür. Rüptür ve ölüm riski çok fazladır. Başka nedenlere yönelik olarak yapılan görüntüleme yöntemleri esnasında tesadüfen tespit edilir. Anahtar Kelimeler: İliak arter anevrizması, intraabdominal anevrizma, karın ağrısı, sol alt kadran

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
371
P 334 GAZİ ÜNİVERSİTESİ TIP FAKÜLTESİ HASTANESİ ACİL SERVİSİNE BAŞVURAN BİR YILLIK HASTA PROFİLİ VE ACİL SERVİS KALABALIĞININ SEBEPLERİ
Gülbahar Alkaş, Ayfer Keleş, Dikmen Çalışkan, Ahmet Demircan Gazi Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Ankara Giriş: Acil servis kalabalığı günümüzde en önemli sorunlardan biridir. Hasta sayısı arttığı halde hastane yatakları sınırlı kalmakta, acil servise başvurular ve acil kalabalığı artmaktadır. Tüm dünyada olduğu gibi ülkemizde de acil servise acil olmayan hastalar başvurmakta, ayrıca hastanenin özelliklerine göre farklı hasta profilleri görülmektedir. Hastanelerin özelliklerine, bulundukları yere ve verdikleri özel hizmetlere göre hasta profili değişmektedir. Biz de bir üniversite acil servisine başvuran hastaların profilini tespit etmek için bu çalışmayı planladık.��
Metot: Çalışma Gazi Üniversitesi Tıp Fakültesi Acil Tıp Anabilim Dalında yapılmıştır. 01 Temmuz 2015-30 Haziran 2016 tarihleri arasında Erişkin Acil Servise başvuran hasta verileri toplandı. Hastane bilgi sisteminden hastaların demografik verileri, başvuru tarih ve şehirleri, başvuru ICD kodları, hastaların sosyal güvenceleri kaydedildi. SPSS 20.0 istatistik programı kullanıldı. ��
Bulgular: 01.07.2015-30.06.2016 tarihleri arasında erişkin acil servise toplam 49 149 hasta başvurmuştur. Hastaların %48.5’i kadın %51.5’i erkektir. Hastaların yaş ortalaması 41.68 ± 17.77 (ortanca 37) olarak saptanmıştır. Hastaların 17 257’si 18-30 yaş arasında (%35.1)olup 1550’si 80 yaş üzerindedir (min 18, max 104 yaş). Hastaların sosyal güvencelerine bakıldığında 27 123’ü (%55.2) SSK olarak görülmektedir. Hastaların %72.7 ‘si muayene odalarına (sarı-yeşil alan), %5 ‘i resüsitasyon odasına(kırmızı alan) alınmıştır. Hastaların %88.8’i geldiği gün acil servisten çıkmış, 4917 hasta bir gün acil serviste yatmıştır. 5 hasta 10 günden fazla acilde kalmıştır. Hastaların %93.5’i acil olarak, %2,7’ si adli, %2,8’i iş kazası ve %1 ‘i trafik kazası olarak provizyon almıştır. Hastaların 5649’u servis ve yoğun bakımlara yatmış, 126 hasta exitus kabul edilmiştir. Hastaların başvuru ICD2lerine bakıldığında en sık başvuru abdominopelvik ağrı(%6.6), akut tonsillit(%2.8), alt extremite yaralanması (%2.1), başağrısı(%3.3), başdönmesi(%2.1), belağrısı(% 2.4), boğaz ağrısı (%5.4), bulantı-kusma(%4.3), extremite ağrısı (%5.2) şikayetleriyle olmuştur.��
Sonuç: Acil serviste 24 saatten fazla kalan hasta sayısı fazla olup en çok medikal şikayetlerle başvuru olmaktadır. Orta ve ileri yaş hastalar çoğunluğu oluşturmaktadır. Tüm bunlar acil serviste yaşanan kalabalığın başlıca sebepleri olarak gösterilebilir. Anahtar Kelimeler: Acil servis, hasta profili, kalabalık P 335 YER SEVİYESİNDEN DÜŞME SONRASI GÖRÜLEN ANTERİOR KORD SENDROMU: OLGU SUNUMU
Ali Halıcı, Uğur Kahveci, Kerim Abatay, Ali Şahin, Seda Özkan Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Ankara Giriş-Amaç: Anterior kord sendromu; lezyon seviyesi altında paralizi, ağrı ve ısı duyu kaybı olan ancak dokunma, titreşim ve pozisyon duyuları sağlam olan spinal kord hasarıdır. Prognozu kötüdür. İyileşme oranı % 10-20 arasındadır. Biz bu olgumuzda düşük enerjili travma sonrası gelişen anterior kord senromunu sunmaktayız.��
Olgu: 55 yaşında kadın hasta gece uyurken yaklaşık 50 cm yükseklikten yere düşüyor. Kollar ve bacaklarda tutmama şikayeti ile acil servise başvuruyor. Yapılan muayenesinde; genel durumu iyi bilinci açık oryante koopere idi. Alt kraniyaller kabaca intakt, üst ekstremitelerde bilateral önkol ekstansiyonu 3/5, omuz abdüksiyonu ağrılı. Alt ekstremiteler paraplejik. His kusuru C7 – T1 segmenti altında mevcuttu. Vitalleri stabildi. Diğer sistem muayeneleri doğaldı. Medulla spinalis basısı düşünülerek görüntüleme yapılmaksızın Beyin Cerrahisi ile konsülte edildi. Dislokasyon, fraktür, medulla spinalis kesisi ön tanılarıyla ve lezyon yerini saptamak amaçlı Bilgisayarlı Tomografi istendi. C5-C6 seviyesinde dislokasyon saptanan hastaya sinir hasarının derecesini saptamak amacıyla acil serviste servikal MR çekildi. Medullası spinalis basısı görülen hasta operasyon amacıyla beyin cerrahisi kliniğine devredildi.��
Sonuç: Düşük enerjili travma olsa da servikal yaralanmalar göz ardı edilmemelidir. Erken müdahale nörolojik defisitin ilerlemesini önler ve hastanın yaşam kalitesini artırır. Hasta mortalite ve morbiditesini çok fazla etkileyen bu durum karşısında alert olmalıyız. Anahtar Kelimeler: Anterior Kord Sendromu, düşük enerji, travma

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
372
P 336 ANALYSIS OF FOREIGN BODY INGESTION CASES AT THE EMERGENCY DEPARTMENT: A RETROSPECTIVE STUDY
Necip Gökhan Güner, Filiz Baloğlu Kaya, Engin Özakın, Adem Köksal Eskişehir Osmangazi University School of Medicine, Department of Emergency Medicine, Eskişehir, Turkey Objective: Although foreign body (FB) ingestion is often seen in children, accidental FB ingestion in adults are also common. Early diagnosis and treatment is essential as it might cause pathologic changes in the digestive system (DS). This study aims to analyze the cases of FB ingestion at the emergency department (ED) relating to the type of the FB, where it was located, and the clinical process. Materials-Methods: The records of the patients aged 18 years or older, who came to the Eskisehir Osmangazi University Hospital’s ED with FB ingestion and feeling of something stuck in throat between 01.01.2010 and 31.12.2015, were examined retrospectively. Information about the demographic characteristics, location of the FB, type of the FB, endoscopic procedure if used, hospitalization and the development of complications were obtained from the patient records. Results: The records of 61 cases eligible for the inclusion criteria of our study were examined. The average age of the cases was 42.9 and 34 of the cases were female (55.7%). The most common ingested FB or those which causes feeling of something stuck in throat were meat pieces (26.2%), fish bone (19.7%), and pin (11.5%). FBs were often located in the esophagus (37.7%) and at the level of oropharynx (21.3%). Endoscopic procedure was used in 35 cases (57.4%), 25 of those cases (41%) were hospitalized. 36 patients (59%) were discharged from the ED. No complications were found. Conclusion: Early diagnosis and treatment of FB in the DS is essential to avoid any possible complications and to assure the comfort of the patient. In our study, we detected that the ingested FBs were often located in the upper level of the DS. Therefore, if necessary for the diagnosis and treatment, positive results will be attained when the emergency physician refer the patients for the endoscopic procedure. Keywords: Digestive system, foreign body, endoscopy P 337 DYSPNEA AS THE PRESENTING SYMPTOM OF MASSIVE SPONTANEOUS HEMOTHORAX CAUSED BY UN- DIAGNOSED LUNG CANCER Harun Gunes1, Feruza Turan Sonmez1, Elif Nisa Unlu2, Ayhan Saritas1
1Düzce University School of Medicine, Department of Emergency Medicine, Düzce, Turkey 2Düzce University School of Medicine, Department of Radiology, Düzce, Turkey Dyspnea, a common presenting symptom in emergency department, is mostly related to respiratory system problems like chronic obstructive pulmonary disease or cardiovascular problems such as acute cardiogenic pulmonary edema. The other much rarer causes of dyspnea include pneumothorax and hemothorax. Hemothorax may rarely be seen without any trauma, and is called spontaneous hemothorax. Extraction of more than 1500 cc of blood upon chest drain insertion indicates massive hemothorax. It is a severe, life-threatening condition that requires immediate medical attention. Massive spontaneous hemothorax caused by lung cancer is very much rarely reported in the literature. Here, we report an unusual case of massive spontaneous hemothorax caused by an un-diagnosed lung cancer presenting to the emergency department due to rapidly progressive dyspnea. A 56-year-old man with no past history of disease or recent trauma presented to emergency department with dyspnea, which had gradually increased in three days. His vital signs were as follows: body temperature 36.3 °C, pulse rate 108/min, blood pressure 110/77 mmHg, respiratory rate 24 breaths/min and peripheral oxygen saturation 92%. No breath sounds could be heard on the right hemithorax. Posterior-anterior chest film showed a right-sided pleural effusion reaching to the level of the anterior margin of the 3rd rib. Then, diagnostic thoracentesis was performed, and 20 ml of bloody effusion was taken. Hemoglobin concentration of the sample was found to be 5.3 g/dl, and massive spontaneous hemothorax was diagnosed. Afterwards, intravenous contrast-enhanced computed tomography scan of the chest was performed, and a mass lesion was seen around the branching point of the right pulmonary artery. Then, the patient was diagnosed with massive spontaneous hemothorax caused by an un-diagnosed lung cancer and referred to another medical facility for surgical treatment. In conclusion, emergency physicians should include massive spontaneous hemothorax in the differential diagnosis of patients with rapidly progressive dyspnea. Keywords: Dyspnea, massive spontaneous hemothorax, lung cancer

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
373
P 338 KARIN AĞRISI ŞİKAYETİ İLE GELEN PULMONER EMBOLİ OLGUSU Ali Halıcı, Kerim Abatay, Uğur Kahveci, Eren Usul, Engin Deniz Arslan Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Ankara Giriş-Amaç: Akut pulmoner tromboemboli(PTE) sık izlenen ve ölümcül bir hastalıktır. Erken teşhis ve tedavi ile bu ölümlerde azalma sağlanabilir. Yıllık insidansı 100-200/100.000’dir. Çoğunlukla derin ven trombozu(DVT) eşlik etmektedir. �Pulmoner arteriyel tıkanma sonucu; yaşamı tehdit eden akut geri dönüşümlü sağ ventikül yetmezliğine yol açabilir. Erken tanı kritik öneme sahiptir. Tedavi; pulmoner arteriyel kanlanmanın yeniden sağlanması ya da retrombüslerin önlenmesidir. Acil serviste sık karşılaşılan karın ağrısı vakalarında solid organ ve barsak kaynaklı patolojilerin dışında, vasküler patolojilerin de unutulmaması gerekliliğini vurgulamak istedik. Biz acil servise karın ağrısı şikayeti ile gelen ve PTE tanısı alan bir olgu sunuyoruz. Olgu: Otuz altı yaşında erkek hasta karın ağrısı şikayeti ile acil servise başvurdu. Hastanın vitalleri stabil oksijen satürasyonu normaldi. Fizik muayenede, Sağ alt kadranda defans ve reboundu vardı. Diğer sistem muayeneleri doğal olarak değerlendirildi. EKG si normal sinüs ritmiydi. Laboratuvar tetkiklerinde tam kanda lökositozu mevcuttu. Arter kan gazında solunumsal alkalozu vardı. Tanıya yönelik yapılan tüm batın USG(ultrasonografi)’sinde patoloji saptanmamıştı. Şikayetleri devam eden hastanın yapılan alt ekstremite venöz doppler USG sinde femoral ven ve popliteal vende subakut süreçte trombüs ile uyumlu bulunmuştu. Bunun üzerine hastaya PTE protokolü kontrastlı toraks BT görüntüleme planlandı. Toraks BT’sinde her iki ana pulmoner arter üst ve alt lobar ve segmental arterlerde emboli ile uyumlu dolum defekti şeklinde görünüm izlendi. Hastada mevcut bulgularla PTE düşünüldü, trombolitik tedavi verildi. Takip ve tedavi amaçlı göğüs hastalıkları servisine yatışı yapıldı.��
Sonuç: Pulmoner tromboembolide zamanında doğru tanı konularak erken tedavinin başlanması hayati öneme sahiptir. Tanı ve tedavi gecikmesi, mortaliteyi artıran en önemli nedenler olarak bilinmektedir. Şikayeti devam eden hasta için ayırıcı tanıları genişletip taramaya devam etmeliyiz. Anahtar Kelimeler: Karın ağrısı, pulmoner tromboemboli, derin ven trombozu P 339 EMPHYSEMATOUS PYELONEPHRITIS - CASE REPORT Necmiye Yalçın Ocak, İbrahim Toker, Rana Toktaş, Emirhan Erdem İzmir Tepecik Training and Research Hospital, Emergency Medicine Clinic, İzmir, Turkey A 72 years old, female patient who had no chronic illnesses other than DM, was admitted to the emergency department with decreased oral intake for the last 3-4 days, nausea, vomiting, blurred urination and pain in the left side. The status on her arrival was as follows; blood pressure 86/48mmHg, heart rate 76/bpm, body temp 36,4oC, SaO2 98%. The anamnesis of the patient stated that, she was hospitalized due to urinary tract infection and was discharged 1 week ago. The performed physical examination revealed, sensitivity in the upper left quadrant and the costovertebral region. Pyuria was seen after insertion of a foley catheter. The laboratory results were as follows; Urea 283 mg/dL, creatinine 4.3 mg/dL, TIT 3 red blood cells/mm3, 3 leukocytes / mm3, leukocytes 7300/mm3, procalcitonin 0,24ng/ml. Abdomen CT was performed on the patient. A 10x8 mm calculus was seen in the mid 1/3 region of the left urethra, and an 11x7 cm sized lesion with heterogeneous appearing and air densities in the superior pole of the left kidney. The patient was consulted with the urology department with a diagnosis of emphysematous pyelonephritis and was hospitalized. Discussion: The early diagnosis of emphysematous pyelonephritis is very important due to its high morbidity and mortality. Using inappropriate imaging techniques as well as the fact that symptoms are nonspecific may delay the diagnosis. It should be considered carefully in diabetic patients with indications of sepsis, impaired kidney function and blood sugar control in addition to urinary tract infection symptoms As a result, emphysematous pyelonephritis is a life-threatening, rare infection that has to be diagnosed and treated urgently. Keywords: Diabetes mellitus, emphysematous pyelonephritis, urinary tract infection

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
374
P 340 PROTHROMBIN COMPLEX CONCENTRATE USE FOR WARFARIN ASSOCIATED BLEEDING AT THE EMERGENCY DEPARTMENT: A RETROSPECTIVE STUDY
Filiz Baloğlu Kaya, Engin Özakın, Nurdan Acar, Burak Özkan Eskişehir Osmangazi University School of Medicine, Department of Emergency Medicine, Eskişehir, Turkey Introduction: Patients on warfarin might sometimes need emergency interventional procedures. The varied clinical cases might involve minor and fatal bleedings. In cases of warfarin use, prothrombin complex concentrates (PCC), which achieve the targeted INR level at the 15th minute after its application, could be used. This study aims to examine within cases of warfarin use, those of which diagnosed with bleeding and high INR levels during the emergency department (ED) visits and/or follow-ups, and involve PCC use in treatment afterwards. Material-Method: This study was conducted at the ESOGU Medical School Hospital ED between 01.01.2013 and 01.07.2016. The patients, who were younger than 18 years old, came to the ED with trauma, used additional anticoagulant or were pregnant, were excluded. Demographic data, the reasons for warfarin use, INR levels at the beginning of ED visit and after the application of PCC, the reasons for PCC use and the clinical results of the cases were examined. Results: 23 cases were included. The average age was 68. 15 patients were female. The two most common causes listed for warfarin use were AF and CAD; and the most common diagnoses in ED were intracranial and GIS hemorrhage. The average of INR was 7,58 at the beginning of the ED visit and 1,59 after the application of PCC. 4 cases were discharged from the ED. 3 cases left the ED at their own request. Within 16 hospitalized cases, 5 resulted in death during ICU follow-up. In 4 (out of 23) cases, the targeted INR was not achieved. No thromboembolic event was recorded. In all cases, 10 mg IV vitamin K was given at the ED. Conclusion: Patients with warfarin-associated fatal bleeding or bleeding risk should be treated regarding indication for use, and bleeding severity. PCC use would be beneficial to restore coagulation factors at the ED. Keywords: Anticoagulant, bleeding, prothrombin complex concentrate P 341 INTERPRETATION OF POTENTIAL DISEASES FOLLOWING BARIATRIC SURGERY: OBSERVED SHORT TERM COMPLICATIONS IN EMERGENCY SERVICE Burcu Yormaz1, Hüseyin Yılmaz2, Farise Yılmaz3
1Beyhekim State Hospital, Chest Diseases Clinic, Konya, Turkey 2Selçuk University Medical Faculty, Department of General Surgery, Konya, Turkey 3Selçuk University Medical Faculty, Department of Nuclear Medicine, Konya, Turkey Background: Barrett’s esophagus (BE) and chemical pneumonia (CP) is present in < 2 % of patients. Laparoscopic Sleeve gastrectomy (LSG) has been shown to be effective in excess weight loss for morbid obese patients, but its possible effect on gastroesophageal-reflux-disease (GERD) and AP have been contradictory. We evaluated whether GERD after LSG could predict progression to be BE and CP in a retrospective study. Methods: When we have performed gastroscopy to the patients who have underwent LSG (Group-A) and who have not underwent bariatric-procedures (Group-B). Also the group B was composed of morbid obese patients (BMI>40kg/m2). GERD-symptoms, CRP results, chest images and BMI were collected. Of 2 patient have evaluated by nuclear scintigraphy due to severe GERD problem. BE was histologically evaluated and compared between the groups. Results: Group-A was composed of 65 patients (mean follow-up 6 months, BMI at LSG 45.1 kg/m2), while Group-B by 45 patients ( BMI 46.4 kg/m2).In Group-A and Group-B GERD symptoms and CP were present in 26 % and 42 %. LA-esophagitis percentage was: LA-B 11.2%and 20.5%, LA-C 7.7%and 14,3%,in Group A and Group B respectively.CURB-65(confusion, urea, respiratory rate, blood pressure, age) scoring, results were decreased in group A than group B according to excess weight loss outcomes. Conclusion: Our results have showed that 23%of patients who were underwent LSG procedure had a mild-to severe esophagitis, not corresponding to reflux symptoms, 13.4 % of them had a histologically confirmed Barrett esophagus and 6,7% of had chemical pneumonia. Whether these results will be confirmed, LSG should be considered a reflux-inducing bariatric procedure, a very close follow-up should be performed to avoid Barrett esophagus progression and chemical pneumonia in the surgical procedure should be considered. Keywords: Pneumonia, complicatıons, surgery

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
375
P 342 POSTERİOR KORD SENDROMU Necmiye Yalçın Ocak, Yeşim Eyler, Rana Toktaş, Didem Dönmez İzmir Tepecik Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İzmir Giriş: Posterior kord sendromu insidansı %1’in altında olan nadir bir durum olup, genellikle servikal hiperekstansiyon mekanizmalı yaralanmalarda görülür. Spinal kord arka kolumn yaralanmalarında genellikle pozisyon ve vibrasyon duyusu kaybı görülürken sıcaklık ve ağrı duyusu korunur. Motor fonksiyon korunabilir(1,3).��
Olgu: Otuz yedi yaşında erkek hasta, yüksekten düşme nedeniyle 112 ambulansı ile getirildi. Başvuruda kan basıncı: 116/70 mmHg, nabız:83/dk, solunum sayısı: 22/dk, ateş:36.2°C, oksijen satürasyonu: %97 idi. Yaklaşık 2 metre yükseklikteki ağaçtan ayağı kayıp düşmüş. Bilinç kaybı olmayan, amnezi tariflemeyen hastanın her 2 kolunda ve ellerinde yanma ve batma şikayeti vardı. Yapılan fizik muayenesinde; solunum sistemi, batın ve kardiak bakısı olağandı. Nörolojik muayenesinde; bilinç açık oryante koopere, pupiller normo-izokorik, alt ve üst ekstermitelerde motor defisiti yok, servikal spinöz proçes hassasiyeti ve her iki üst ekstremitede parestezisi mevcuttu. Hastadan hemogram, biyokimya, koagülasyon, tit istendi. Beyin, servikal, thoraks ve batın tomografileri çekildi. Tetkikleri normal gelen ancak her iki üst ekstremitede yanma şeklinde parestezisi devam eden hastadan servikal MRG istendi. Multipl seviyelerde disklerde dejeneratif T2 sinyal azalımı, C4-5 düzeyinde diskte diffüz bulging, santral minimal fokal protrüzyon ve dural kese basısı,C5 düzeyinde spinal kord ödemi izlendi. Posterior kord sendromu ön tanısı ile beyin cerrahi ile konsulte edilen hastaya servis yatışı verildi. ��
Tartışma: Spinal kord yaralanmaları multidisipliner yaklaşım gerektiren klinik sendromlardır. Bunlar içinde posterior kord yaralanmaları en nadir görülen ve hakkında en az bilgi sahibi olunan sendromdur. Genellikle servikal hiperekstansiyon mekanizmalı yaralanmalarda görülür. Vibrasyon ve propriosepsiyon duyusu kaybı olurken, ağrı ve ısı duyusu korunur. Motor fonksiyonlar korunabilir. Hastanın semptomları genellikle üst ekstremitelerinde yanma, batma şeklinde olan ağrıdır. Görüntülemelerde anlamlı bulgu olmayabilir. Bu olgu sunumu ile nadir görülen bir sendroma dikkat çekmek istedik. Anahtar Kelimeler: Posterior kord sendromu, spinal kord yaralanmaları, travma P 343 A RARE INFARCTION; SEPTIC EMBOLISM
Mehmet Birkan Korgan, Özge Can, Murat Ersel Ege University School of Medicine, Department of Emergency Medicine, Izmir, Turkey Introduction: Septic emboli (SE) is rare but life-threatening condition. Most common cause is infective endocarditis. Vascular complications include central nervous system, spleen, hepatic, pulmonary, renal, musculoskeletal, mesenteric and coronary. Clinical signs changed by effected organs and systems. Our case admitted with fatigue and diagnosed cranial, splenic and renal infarct. Case: 71 years male patient admitted to emergency department with fatigue, fever, loss of walking capability. He has a chronic renal failure and hypertension on his history. Vital parameters are normal. On physical exam there was no abnormality on neurologically. Generally abdominal tenderness was assigned. Cranial and abdominal computered tomography was performed and cranial, splenic and renal infarct was determined. We started antibiotic for septic emboli. Source of embolus was examined. For infective endocarditis transthoracic echocardiography was performed and vegetation was not seen. Blood culture was taken. He transferred to ICU. Discussion: Septic embolism is a rare condition but important for different treatment from thromboemboli and has high risk of mortality. Risk factors are obesity, diabetes, chronic immunosuppression, renal failure, malignancies. SE frequently associated with Bacterial endocarditis, septic thrombophlebitis, periodontal, and central venous catheter infections. İnfarcts are involved central nervous system (CNS), spleen, hepatic, renal, musculoskeletal and mesenteric. In our case CNS, splenic and renal infarcts were established. In literature there were cases about septic emboli and cranial emboli but only two case had a renal embolism concomminant with coronary embolism that were identified postmortem. Most common cause of septic embolism is infective endocarditis. For diagnosis Duke criteria was described. In our case vegetation was not seen. Conclusion: SE is clinically similar with thromboemboli, due to antimicrobial usage in treatment and mortal survey physicians should be suspect patients who has risk factors Keywords: Septic embolism, infective endocarditis, renal infarction, splenic infarction

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
376
P 344 THE USE OF INTRAVENOUS LIPID ADMINISTRATION IN A PATIENT WITH SYNTHETIC CANNABIOID INTOXICATION
Halil Yıldırım1, Duygu Albayrak1, Fulya Yılmaz Duran1, Vermi Değerli2
1Bozyaka Training and Research Hospital, Clinic of Anaesthesiology and Reanimation,Izmir, Turkey 2Bozyaka Training and Research Hospital, Clinic of Emergency Medicine,Izmir, Turkey Introduction: Synthetic cannabinoid receptor agonists (SCRA) abuse are among the most frequent substances lately. Among the people ''bonzai 'known as’ 1-naphthalenyl of methanol", also known as JWH-18 group, the drug substance is a synthetic cannabinoid group. Synthetic cannabinoids cause nausea, vomiting, shortness of breath, tachycardia, bradycardia, hypertension, chest pain, myocardial infarction, anxiety, poisoning and sympathomimetic drugs with stimulant-like effects such as psychosis may occur. In literature, improvement in cardiac side effects observed in patients with SCRA usage, with iv lipid infusion have been reported. In this poster presentation the effectiveness of iv administered lipid infusion in a patient transferred to emergency department with sinusal bradycardia and t wave negativity in the ECG is being presented. Case: Our case was 30 years-old-male, with no known disease history. CPR was applied for 3 minutes due to cardiac arrest on arrival emergency department, GCS 9, ABG values within normal limits. Cranial MRI findings had no correlation with present condition, but toxicological evaluation revealed SCRA abuse. Routine biochemical tests were normal except a slight rise in AST, ALT values. ECG revealed sinusal bradycardia with HR 48/min and T wave negativity in anteroseptal derivations. Hemodynamically stable. Patient was scheduled for intubation and intensive care. IV 20% lipid solution of 1.5ml/kg bolus followed by a 0.25ml/kg infusion was administered in 60 minutes. EGC recordings obtained immediately after lipid bolus, at the end of infusion, 24 hours later. T wave abnormality in the chest leads were recovered partially immediately after the bolus. 24 hours after infusion, bradycardia and T wave negativity resolved completely. Conclusion: In our case, it was concluded that ECG changes due to SCRA intoxication might be resolved with IV lipid infusion. IV lipid administration may be a useful option to eliminate cardiac side effects for the treatment of SCRA patients in emergency departments. Keywords: Synthetic cannabinoid, intoxication, lipid infusion P 345 İNME İLE KARIŞAN NADİR BİR VAKA; SPONTAN SPİNAL EPİDURAL HEMATOM Mustafa Cicek1, Ozgen Gönenc Cekic2, Burcu Saglam1, Ihsan Yildiz1, Abdurrahman Ipek1, Aynur Sahin1, Ozgur Tatli1
1Karadeniz Teknik Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Trabzon�2Fatih Devlet Hastanesi, Acil Servis, Trabzon Giriş: Spontan spinal epidural hematom nadir görülen bir klinik durumdur. Konservatif tedavi veya cerrahi dekompresyon kullanılan tedavi seçenekleri arasındadır. Hastalarda tek taraflı veya bilateral nörolojik defisit bulunabilir ve ayırıcı tanıda iskemik stroke mutlaka dışlanmalıdır. ��
Olgu Sunumu: 51 yaşında erkek hasta 2 gündür olan sırt ağrısı, idrar inkontinansı, sağ el ve ayakta kuvvet kaybı olması nedeniyle acil servise başvurdu. Hastanın öyküsünde aort anevrizma cerrahisi ve aort kapak replasmanı öyküsü mevcuttu. Hasta aspirin, enoksaparin ve warfarin tedavisi almakta idi. Bilinci açık, oryante, koopere olan hastanın genel durumu orta, vital bulguları stabil idi. Yapılan nörolojik muayenede sağ üst ve alt ekstremitede 1/5 kuvvet kaybı vardı. Fasial etkilenme gözlenmedi. Yapılan değerlendirme sonrası stroke ön tanısı ile beyin tomografisi ve beyin MRG ve difüzyon MRG çekildi. Kanama veya infarkt tespit edilmedi. Hastanın aort anevrizma cerrahisi öyküsü olması nedeniyle aort diseksiyonu ön tanısı ile alınan kontrastlı toraks+batın BT’de spinal kanal içinde hematom tespit edilmesi üzerine ayrıntı değerlendirme amacıyla spinal MRG alındı. Buna göre medulla spinaliste C6-T6 arasında en kalın yerinde 8.5 mm’ye ulaşan epidural hematom tespit edildi. Hasta beyin cerrahisi ile konsülte edildi. Cerrahi dekompresyon için beyin cerrahisine yatış yapıldı.��
Sonuç: Spinal epidural hematomun etiyolojisinde birçok neden bulunmaktadır. Travmatik hadiseler, cerrahi işlemler, trombolitik tedaviler, antikoagülan kullanım öyküsü, hatta tek başına öksürmek bile buna neden olabilir. Ana klinik bulgu nörolojik defisittir. Tespit aşamasında BT kullanılabilecek bir tanı aracı olup MR görüntüleme altın standart tekniktir. Cerrahi drenaj temel tedavi yaklaşımıdır. Oral antikoagülanlar spontan spinal epidural hematomun en sık nedenidir. Böyle durumlarda oral antikoagulanların kanama arttırıcı etkilerine yönelik ilaç tedavi seçenekleri uygulanmalıdır. Anahtar Kelimeler: Spinal epidural hematom, acil, oral antikoagulan

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
377
P 346 A PATIENT ADMITTED TO THE EMERGENCY SERVICE WITH SEIZURE HISTORY: POSTERIOR REVERSIBLE ENCEPHALOPATHY SYNDROME
Mustafa Emin Çanakçı1, Engin Özakın1, Atilla Özcan Özdemir2, Necip Gökhan Güner1, Nurdan Acar1, Filiz Baloğlu Kaya1
1Eskişehir Osmangazi University School of Medicine, Department of Emergency Department, Eskişehir, Turkey 2Eskişehir Osmangazi University School of Medicine, Neurology Department, Eskişehir, Turkey Objective: Posterior reversible encephalopathy syndrome (PRES) may be presented with seizure, altered mental status and nausea. It has been reported that the disease is often observed after acute hypertensive episodes, and recovers without any neurological sequelae with early diagnosis. We would like to present you a rare PRES phenomenon admitted to our emergency department(ED). Case: A 39-year-old female patient was admitted to our ED due to two generalized tonic-clonic seizures and recurrent nausea episodes in the last seven days. She had hypertensive episodes in the last one week and used several non-steroidal anti-inflammatory agents due to flank pain in the last two months. She was conscious, cooperative, oriented and all her vital signs were detected normally at admission. Physical examination did not reveal any pathology other than horizontal left beating nystagmus. There were no additional anomalies detected except creatinine: 2 mg / dL in the laboratory examination. Brain computed tomography performed for first seizure and it was normal. Brain magnetic resonance performed and multiple hyperintense lesions was detected in the parietooccipital region in the MRI T2 Flair sections. Radiological findings observed in the Flair section of the posterior system in particular, was considered as PRES and our patient was transferred to the neurology service. There wasn’t any pathological finding observed after 3 days on the CT and MRI. who received blood pressure regulation and hydration therapy in the follow-up. The patient was discharged from the neurology service on the 7th day.��
Conclusion: ED physicians are often confronted with seizure-patients. Besides the known epileptic patients, seizure activity is also observed in patients with intracranial pathology. PRES can not be recognized in patients with traditional diagnostic and imaging methods. Emergency medicine physicians should keep in mind the possibility of PRES, which will occur in the emergency services with the widespread use of MRI. Keywords: Magnetic Resonance Imaging, posterior reversible encephalopathy syndrome, seizure P 347 BİLATERAL PULMONER ARTER EMBOLİSİ - OLGU SUNUMU Hanife Bilgili, Melek Aktepe, Yonca Senem Akdeniz, Afşın İpekci Cerrahpaşa Tıp Fakültesi, Acil Tıp Anabilim Dalı, İstanbul Giriş: Pulmoner emboli, kardiyovasküler hastalıklara bağlı ölümlerin koroner arter hastalığı ve stroktan sonra en sık 3. sebebidir. Farklı klinik manifestasyonlar, semptom ve bulguların sensitivite ve spesifitesinin zayıf olmasından dolayı; pulmoner emboli zor bir tanıdır. Hiçbir semptom pulmoner emboli için spesifik değildir. Pulmoner emboli asemptomatik olabilirse de, hastalar genellikle göğüs ağrısı, dispne, hemoptizi ile başvururlar. Risk faktörleri; herediter trombofililer, travma, immobilizasyon, malignite, gebelik ve postpartum dönem, ileri yaş, obesite, santral venöz kateterizasyon, kemoterapi ve bazı ilaçlardır.��
Olgu: 43 yaşında, KOAH ile takipli kadın hasta, ani başlayan nefes darlığı şikayetiyle Acil Servise başvurdu. Başvuruda SpO2:%75 idi, diğer vital bulgular normal sınırlarda idi. Fizik muayenede solda solunum sesleri azalmıştı. Kan gazında pH:7,41 pCO2:47 pO2:59 idi. Oksijen desteği başlanan hastaya çekilen PA akciğer grafisinde sol tarafta üst zonlara kadar uzanan opasite saptandı ve trakea sola deviye olmuştu. Hastanın inhaler tedaviler dışında kullandığı bir ilaç yoktu, immobilizasyon, cerrahi, malignite, gebelik öyküsü yoktu. Rutin kan tetkiklerinde patoloji saptanmadı. Iv kontrastlı toraks BT çekildi ve bilateral ana pulmoner arterlerde emboli saptandı. Göğüs hastalıkları konsültasyonu istenerek Enoxaparin 2x0,8 cc başlandı ve Göğüs hastalıkları servisine yatışı yapıldı.��
Sonuç: Pulmoner emboli yaşlı, immobil, malignitesi olan, herediter trombofili öyküsü olan hastalarda, gebelerde, tromboza eğilim yaratan ilaç kullanan hastalarda daha sık görülür. Fakat nadir de olsa altta yatan hastalığı, ilaç kullanım öyküsü olmayan genç hastalarda da görülebileceği akılda tutulmalı, Acil Servise nefes darlığı ile başvuran hastalarda, bu semptomlar sadece KOAH’a bağlanmamalı, Pulmoner emboli ön tanılar arasında yer almalıdır. Anahtar Kelimeler: Pulmoner emboli, risk faktörleri, tanı

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
378
P 348 NEW EXPERIENCES IN THE OLD AREA: OUR PEDIATRIC TRAUMA EXPERIENCES IN THE ESKISEHIR OSMANGAZI UNIVERSITY EMERGENCY DEPARTMENT
Nurdan Acar, Mustafa Emin Canakci, Engin Ozakin, Filiz Baloglu Kaya Eskişehir Osmangazi University School of Medicine, Department of Emergency Medicine, Eskişehir, Turkey Objective: We have started to accept pediatric trauma patients (<18 yo) on the date of May 2nd, 2016. All pediatric patients with trauma (minor, major and multiple) cared by emergency physicians by the time. We report our newly experiences for this four months period. Method: We analyzed our pediatric trauma work during May 2nd to Aug 31th, 2016 in Eskisehir Osmangazi University Emergency Department. In this period, we admitted the pediatric trauma patients, made trauma management and decided the outcome. Age, hospitalization durations and ratios analyzed. Results: Total 1895 pediatric trauma patients was evaluated in this period. Mean age was 8.31±5.04, 1199 patients were male (63.3%), 786 were female (36.7%). 110 patients had motor vehicle accidents (MVA) (5.8%). Hospitalization ratio for pediatric patients with trauma was 6%. Eight patients had sent to intensive care units (0.4%), 4 of them (50%) were male and 4 (50%) were female. 107 patients (5.6%) were hospitalized in various clinics. 71 of them (66.3%) were male and 36 (33.7%) were female. 6.1% of male patients and 4.8% of the female patients were hospitalized. The most of the hospitalizations were into orthopedia clinic (n=52, 45.2%). The mean age of patients hospitalized in clinics was 9.00±4.79, in the intensive care was 7.87±6.29.The mean duration of stay in clinic patients was 2.85±2.41 days and in the intensive care was 12.12± 9.98 days respectively. One of the patients (0.05%) died in the emergency department.��
Conclusion: The rate of hospitalization in the intensive care unit was found equally in boys and girls. The majority of hospitalized children was school-age children. The majority of pediatric trauma patients were evaluated and discharged from the emergency department. Emergency physicians can manage accurately by knowing the profile. Keywords: Pediatric trauma, hospitalization, emergency department P 349 İNTERNÜKLEER OFTALMOPLEJİ OLGUSU Neşe Nur User1, Burcu Çoker1, Zeliha Copcuoğlu1, Emel Gökalp1, Hayri Demirbaş2
1Afyon Kocatepe Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Afyonkarahisar�2Afyon Kocatepe Üniversitesi Tıp Fakültesi, Nöroloji Anabilim Dalı, Afyonkarahisar Giriş - Amaç: İnternükleer oftalmopleji (İNO), beyin sapında medial longitudinal fasikül (MLF) hasarı sonucu ortaya çıkan nadir bir durumdur (1). İNO, lezyon tarafındaki gözde adduksiyon yetersizliği ve abduksiyon yapan karşı gözde dissosiye nistagmus ile karakterizedir. Aşağı ve yukarı bakış kısıtlılığı da tabloya eklenebilir. Nistagmus her hastada gözlenmeyebilir. (2). �İnternükleer oftalmopleji genellikle vertebrobaziler inme ve genç hastalarda (<45 yaş) multiple skleroza (MS) bağlı olarak görülür. Bilateral olması MS varlığını düşündürürken, unilateral İNO genellikle MLF’in vasküler olaylara bağlı hasarlanmasına işaret eder.(3) Küçük iskemik paramedian lezyonlara bağlı İNO’da başlangıç anidir, genellikle tek taraflıdır ve her zaman MRG’de görülmeyebilir (4). Karotis ve vertebral arterin diseksiyonu özellikle genç hastalarda inmenin sıklıkla gözden kaçırılan bir nedenidir. Literatürde pek çok olgu sunumunda ve küçük vaka serilerinde izole iskemik İNO’da prognozun iyi olduğu ve birkaç ayda düzelme saptandığı bildirilmiştir.��
Olgu Sunumu: Elli yaşında kadın hasta acil servisimize çift görme sağ gözde içe bakamama ve baş ağrısı şikayeti ile başvurdu. Hastanın özgeçmişinde migren tanısı mevcuttu. Hastanın TA: 130/90 mmHg nabız: 80 atım/dk SS: 20 ateş: 36,8 C SO2:97 idi. Hastanın genel durumu iyi bilinç açık, oryante koopere idi. Fizik muayenesinde sağ gözde içe bakış kısıtlılığı mevcuttu. Abduksiyon nistagmusu yoktu. Hastanın diğer nörolojik ve sistemik muayenelerinde patoloji saptanmadı. Hastanın laboratuar tetkikleri normaldi. Yapılan beyin BT, difüzyon MRG, beyin MRG ve karotis anjiografi görüntülemeleri normal olarak değerlendirildi. Hasta İNO ön tanısıyla nöroloji kliniğe yatırıldı.� Sonuç: İnternükleer oftalmopleji beyin sapını tutan vasküler ve demiyelinizan hastalıklarda (multipl skleroz gibi) ortaya çıkan önemli bir bulgudur. İNO ile başvuran hastalarda vertebral arter diseksiyonu veya demiyalinizan hastalıklar için öncelikle tanının akla gelmesi ve buna yönelik uygun incelemenin yapılması gerektiği akılda tutulmalıdır. Anahtar Kelimeler: İnternüklear oftalmopleji, medial longitudinal fasikül, MLF, vertebrobasiler

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
379
P 350 ÖLÜMCÜL PENETRAN TORAKS YARALANMASI; İNTRATORASİK BIÇAK Yasin Erol, Mustafa Sisman, Iskender Sertbas, Fatih Beser, Mustafa Cıcek, Emre Dılaver, Ahmet Uzundurukan, Ozgur Tatli Karadeniz Teknik Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Trabzon Giriş: Toraksın penetran yaralanmaları hayatı tehdit eden bir yaralanma şeklidir. İntratorasik yabancı cisimler toraksın penetran yaralanmaları veya iatrojenik sebeplerden dolayı olabilmektedir. Bu yaralanmalar pulmoner ve vasküler yaralanmalara neden olabilmektedir.� Olgu Sunumu: Yirmi dokuz yaş bayan hasta acil servise bıçaklanma nedeniyle 112 ekibi tarafından getirildi. Göğüs sağ tarafında, sağ skapula 2 cm altında ve sol uylukta 2 cm’lik kesici-delici alet giriş delikleri ile uyumlu yaralanmalar görüldü. Gks-14 hafif uykuya meyilli olan hastanın tansiyon:80/50 nb:130 olarak görüldü. İv hidrasyonu ve kan hazırlığı planlanan hastanın alınan akciğer grafisinde orta hatta 8x1.5 cm metalik yabancı cisim ile uyumlu görüntü tespit edildi. hbg:6.5 g/dl, Htc. 20.9 g/dl, Plt: 369.000 Inr: 1.45 olarak görüldü. Hasta acilen ameliyata alındı. Göğüs ve Kalp Damar Cerrahisi tarafından yapılan operasyon sırasında sol dekübit pozisyonda sağ 4. İnterkostal aralıktan posterior torakotomi yapıldı. Eş zamanlı olarak kan transfüzyonu verildi. Bıçağın 8-9 cm lik segmentinin toraks içerisinde olduğu görüldü. Aynı seviyedeki vertebra korpusunun, paravertebral damarların ve vena cava inferiorun yaralanmış olduğu görüldü. Bu bölgeden abondan kanama olduğu tespit edildi. Kanama odağı durdurulmaya çalışıldı bu sırada sağ 9. İnterkostal aralıktan ikinci bir torakotomi yapıldı ve yabancı cisim çıkarıldı. Kanama odakları suture edilmeye çalışıldı. Kanama odakları durdurulamadı. Operasyon sırasında kardiyak arrest gelişti. Yapılan açık kalp masajına yanıt alınamadı ve hasta exitus olarak kabul edildi. operasyon sonlandırıldı.� Sonuç: Acil servise başvuran toraksa penetran yaralanmalarda hastaların cilt lezyonları toraks içerisindeki yaralanmaların ciddiyetini veya yabancı cisim olup olmadığını göstermez. Hastaları değerlendirirken bu ihtimalleri göz önünde bulundurarak hastaların değerlendirilmesi yapılmalıdır ve erken cerrahi operasyona verilmelidir. Anahtar Kelimeler: Penetran toraks yaralanması, acil, yabancı cisim P 351 PEDIATRIC EMERGENCIES FACE A CRUCIAL PROBLEM: SHORT-TERM UNSCHEDULED REVISITS TO A PEDIATRIC EMERGENCY DEPARTMENT Önder Kılıçaslan1, Feruza Turan Sönmez2, Harun Güneş2, Ramazan Cahit Temizkan1, Kenan Kocabay1, Ayhan Sarıtaş2
1Düzce University School of Medicine, Department of Pediatric Emergency Medicine, Düzce, Turkey 2Düzce University School of Medicine, Department of Emergency Medicine, Düzce, Turkey Objectives: Revision of the return visit characteristics of patients who returned within 24 hours is a very important method of determining possible problems and the sources of them. In this study we aimed to determine rate, number and demographic data of patients returning to pediatric emergency department in 24 hours at Düzce University Hospital, Turkey. Patients revisiting Pediatric Emergency Department (PED) with the same complaints within 24 hours after discharge were included. Patient age, gender, number, second visit time data was recorded by chart review. The data was analyzed with SPSS15 statistical package for windows. Methods: The present study design involves retrospective data of patients who returned to PED within 24 hours after being discharged. Data includes 6-year period and was collected from July 1, 2010 to June 30, 2016. Results: A total of 1994 patients returned to PED within 24 hours from July 1, 2010 to June 30, 2016. The most common group of revisiting patients were toddlers (age 0-2), n=1168, and the least number represented young adolescents (age 15-18), n=82. Number of patients returning to PED in 24 hours has significantly increased within years from approximately 90 patients to 720(p<0.05). This increase in number was observed in all and each age group (from 0-18) without any exception. Seasonal distribution of the patients showed no significant difference (p>0.05) for each age, but again, presented definite negative correlation with age (the older is the patient group, the less is the number of revisits). The most common time for revisits was 17-24 hours after first discharge from PED, n=1277. Conclusion: It is obvious that return visits impose additional pressure on the emergency departments. Determination of the factors influencing this number is essential; both in order to obtain more sufficient medical service for patients and to increase quality assurance of emergency departments. Keywords: Pediatric emergency department, unscheduled revisits, quality assurance

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
380
P 352 TRAVMA SONRASI GEÇ ORTAYA ÇIKAN YAĞ EMBOLİSİ: OLGU SUNUMU Fulya Yılmaz Duran1, Duygu Albayrak1, Halil Yıldırım1, Ertaç Özeroğlu1, Vermi Değerli2
1Bozyaka Eğitim ve Araştırma Hastanesi, Anesteziyoloji ve Reanimasyon Kliniği, İzmir�2Bozyaka Eğitim ve Araştırma Hastanesi, Acil Servis Kliniği, İzmir Giriş: Yağ embolisi sendromu, yağ partiküllerinin dolaşıma girmesine bağlı olarak solunum sıkıntısı, bilinç bulanıklığı ve peteşiyal döküntülerin ortaya çıktığı bir klinik durumdur. Travmatik, cerrahi ve travma dışı olayları takiben gelişebilir. En sık uzun kemik kırıklarını takiben 24-72 saat içinde gelişir. Klinik tablo hafif olabileceği gibi solunum yetmezliği ve komaya kadar değişebilir. Tanı klinik kriterlere göre konulmaktadır. Spesifik laboratuvar ve radyografik bulgusu yoktur. Tedavi kırığın erken fiksasyonu, sıvı elektrolit dengesinin sağlanması ve hipoksinin giderilmesini içeren destekleyici yaklaşımlardan oluşmaktadır. Burada travma sonrası 9. Günde ortaya çıkan yağ embolisi sendromunu sunmayı amaçladık. ��
Olgu: 36 yaşında erkek hasta araç dışı trafik kazası sonrası acil servise getirilmiş. Yapılan tetkiklerinde femur fraktürü saptanan olgu, operasyon amacıyla ortopedi servisine yatırılmış. Takibinin 9. Gününde göğüs ağrısı ve nefes darlığı gelişen olgu, Göğüs Hastalıkları uzmanı tarafından konsülte edilmiş ve Anjio BT ile pulmoner emboli tanısı almış. Yakın takip ve izlem amacıyla Anestezi Yoğun Bakım Ünitesi’ ne devralındı. Emboliye yönelik tedavisi başlatıldı. AKG: ph:7.42 pO2:40.5 pO2:46.9 SpO2:81.4. yoğun bakıma yatışının 5. Gününde genel durumu düzelen olgunun, rejyonal anestezi ile operasyonu gerçekleştirildi. Postop 1 gün yoğun bakımda takip edilen olgu önerilerle servisine gönderildi. ��
Sonuç: Acil servise gelen uzun kemik kırığı mevcut travma vakalarında nefes darlığı ve göğüs ağrısı semptomlarının bulunması yağ embolisini akla getirmelidir. Yaşamı tehdit eden Yağ Embolisi Sendromu’nda hızlı tanı konulması, erken ve uygun yoğun bakım tedavisi mortaliteyi azaltabilir. Anahtar Kelimeler: Travma, yağ embolisi, solunum sıkıntısı P 353 KALKANEUS AVULSİYON FRAKTÜRÜ AVULSİYON FRAKTÜRÜ OLGU SUNUMU Neşe Nur User1, Emel Gökalp1, Zeliha Copcuoğlu1, Burcu Çoker1, Gökhan Karamişe1, Gökhan Maralcan2
1Afyon Kocatepe Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Afyonkarahisar�2Afyon Kocatepe Üniversitesi Tıp Fakültesi, Ortopedi Anabilim Dalı, Afyonkarahisar Giriş – Amaç: Ayağın arka bölümünün taşıyıcı bileşenleri olan talus ve kalkaneusun eklem yüzeylerinin uyumu kusursuz ve ağırlık taşıyacak kuvvetlere karşı koyabilecek yapıda olması gereklidir. Kalkaneus kırıkları tüm kırıkların %2'sini oluşturur ve tarsal kemik kırıkları içinde en sık karşılaşılan kırıklardır. Tüm tarsal kemik kırıklarının %65'i kalkaneus kırıklarıdır. Ayağın yaralanma sırasındaki pozisyonu, kemik kalitesi ve uygulanan kuvvetin şiddeti kırığın anatomisini belirler. Bu kırıkların oluşmasında kompresyon, açılanma ve makaslama gibi kuvvet bileşenleri rol oynar. Bir diğer mekanizma da avulasyon tipi yaralanmalardır; anterior ve posterior prosesler kopabilir. Posterior avulasyonlarda, aksiyel zorlamaya ek olarak gastrosoleus ve aşil tendonun ani ve güçlü kasılması; anterior olanda ise ayak bileği burkulmalarında ani plantar fleksiyonun da olaya katılması sonunda “bifurcate” ligamentin ön bölümünden kalkaneusu avulse etmesi olasıdır.[1 ��
Olgu Sunumu: 43 yaşında kadın hasta acil servisimize yaklaşık 1 saat önce dengesini kaybedip kendi yüksekliğinden düşme sonucu sol ayakta ağrı şikayeti ile başvurdu. Hastanın genel durumu iyi bilinç açık, oryante koopere idi. Vital bulguları stabildi. Fizik muayenesinde sol ayak bileği posteriorunda hassasiyet, ve yaygın hematomu bulunmaktaydı. Hasta yürüyemiyordu. Hastanın kardiovasküler sistem, solunum ve batın muayeneleri olağandı. Hastaya çekilen ayak iki yönlü direkt grafide kalkaneus posteriorunda intraartiküler avulsiyon fraktürü saptandı. Hasta opere edilmek üzere ortopedi kliniğine yatırıldı.��
Sonuç: Kalkaneus fraktürünün tedavisi; kırığın paterni, hastanın yaşı, hastanın sağlık durumu, yumuşak doku hasarı ve cerrahın deneyimine göre konservatif ya da cerrahi tedavi olmak üzere ayrılır. [2 Avülsiyon tipi kalkaneus kırıkları seyrek görülmektedir. [3 �Kalkaneus tüberkülü bölgesinde kan dolaşımı zayıf ve cilt ince olduğundan, dolaşım bozulmadan ve cilt sorunları gelişmeden erken cerrahi girişim önerilir. ��
Kaynaklar [1 Türk Ortopedi ve Travmatoloji Birliği Dergisi, 2006 cilt 5 sayı 1-2 �[2 Gürkan İ, Atalar H, Kınık H, Mergen E. Kalkaneal tuberositasın avulsiyon kırığı (Olgu Sunumu). Eklem Hastalik Cerrahisi 1999;10:211-3.�[3 İltar S, Gül D, Tanoğlu O, Alemdaroğlu B, Aydoğan N Tuber Kalkanei Kopma Kırığı Olgu Sunumu TOTBİD Dergisi 2013;12(2):194-196 Anahtar Kelimeler: Kalkaneus, avülsiyon fraktürü, travma

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
381
P 354 GÖĞÜS AĞRISINDA NADİR BİR SEBEBİ; HİATAL HERNİ Sinan Paslı1, Mustafa Cıcek1, Melih Imamoglu2, Ogün Kupcuk1, Kadir Coban1, Olgun Asik1, Yunus Karaca1
1Karadeniz Teknik Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Trabzon�2Fatih Devlet Hastanesi, Acil Servis, Trabzon Giriş: Hiatal herni, toplumda çok sık görülen ve semptomatik olduğunda gastroözofajiyal reflüye neden olan bir patolojidir. Sıklıkla kayıcı tipte herniler görülürken, %1-5 hastada mide fundusu veya midenin tamamının toraks içerisine girmesi ile oluşan paraözofajiyal herniler görülebilir. Bu yazıda yaklaşık iki haftadır göğüs ve sırt ağrısı şikayeti olan bir hiatal herni olgusu sunulmuştur.� Olgu Sunumu: Elli üç yaşında kadın hasta yaklaşık iki haftadır devam eden göğüs ağrısı ve sırt ağrısı şikayetleri ile acil servise başvurdu. Ağrısının iki hafta içinde giderek arttığı ve boyun bölgesine doğru yayılım gösterdiği öğrenildi. Vital bulguları; tansiyon 110/70 mm/Hg, nabız 55/dk, solunum sayısı 18/dk, ateş 36,6 C° idi, elektrokardiyogram normaldi, epigastrik bölgede hassasiyet mevcuttu. Diğer sistem muayeneleri normaldi ve laboratuar tetkikleri normal olarak değerlendirildi.�Radyolojik incelemelerinde, akciğer grafisinde mediastende hava-sıvı seviyesi saptandı. Çekilen toraks bilgisayarlı tomografisinde mide antrumu ve gastroözefajiyal bileşkenin toraks içerisine yer değiştirdiği, özefagusun proksimalden itibaren dilate ve tortioze görünümde olduğu saptandı. Lümen içerisinde gıda artıkları izlendi. Hastanın oral alımı durduruldu ve nazogastrik sonda uygulanarak dekompresyon sağlandı. Genel cerrahi konsultasyonu istendi ve yapılan değerlendirmeler sonucunda genel cerrahi servisine yatışı uygun görüldü.��
Sonuç: Göğüs ağrısı, sırt ağrısı, epigastrik ağrı şikayeti ile başvuran olgularda kardiyak ve pulmoner nedenler ile damarsal patolojilerin yanında, gastrointestinal nedenler de göz önünde bulundurulmalıdır. Paraözefajiyal herniler bu klinik durumlardan biridir. Tanısı için klinik şüphenin yanında akciğer grafisi, baryumlu özefagus-mide duodenum pasaj grafisi, üst gastrointestinal sistem endoskopisi, bilgisayarlı tomografi, özefajiyal manometri ve pH’metri testleri kullanılmaktadır. Paraözefajial hernilerin cerrahi onarımı, komplikasyonların azaltılması amacı ile elektif şartlarda uygulanmaktadır. Hastalarda tedavisiz takip, ciddi mortalite ve morbidite oluşturan komplikasyonlara sebep olabilir. Anahtar Kelimeler: Paraözefajial herni, göğüs ağrısı, sırt ağrısı P 355 POSTTRAVMATİK AKUT SERVİKAL DİSK HERNİSİ OLGUSU Neşe Nur User, Zeliha Copcuoğlu, Emel Gökalp, Burcu Çoker, Merve Çavuşoğlu Afyon Kocatepe Üniversitesi, Acil Tıp Anabilim Dalı, Afyonkarahisar Giriş - Amaç: Servikal disk hernileri tüm disk hernileri arasında ikinci sıklıkta, genellikle 35-40 yaş erkek populasyonda görülür. En sık C5-C6, ikinci sıklıkta ise C6-C7 segmentinde görülür. Kliniğinde boyunda hareket kısıtlılığı, parezi, parestezi, baş ağrısı, baş dönmesi, tinnitus, yalancı anjina pektoris görülebilir. Ağrı genellikle travma eşlik eden akut servikal disk hernilerinde görülür. Anamnezde travma öyküsü mutlaka sorgulanmalıdır. Geçirilen kranioservikal travmaya bağlı olarak ani fleksiyon, ekstansiyon ya da bunların kombinasyonu sonucu disk mesafesinin daralması ve posterior longitudinal ligamentin gerilerek diski sıkıştırmasının etkili olduğu düşünülür.��
Olgu Sunumu: Yetmiş sekiz yaşında erkek hasta acil servise ağaçtan düşme (yaklaşık 5 m) sonrası boyunda ağrı, sol elde uyuşukluk şikayetiyle başvurdu. Hastanın tansiyon arteriel değerleri 140/90 mmHg, nabız 86 atım/dk, solunum sayısı 16/dk, ateş 36 °C idi. Yapılan fizik muayenede sol elde hipoestezi saptandı. Motor defisit yoktu. Hastada ayrıca sternum fraktürü ve akciğer kontüzyonu saptandı. Hastaya BT ve MR görüntüleme yapıldı. BT görüntülemesinde C4-C5, C5-C6, C6-C7’de osteofitik ve dejeneratif değişiklikler saptandı. Servikal MR görüntülemesinde C5-C6 da spondilodiskit, C6-C7 de fokal santral bulging saptandı. Acil nöroşirürjik patoloji saptanmayan hasta, izlem ve elektif operasyon amacıyla Nöroşirürji kliniğine yatırıldı. ��
Sonuç: Akut travmatik servikal disk hernisi gençlerde (<20 yaş) spor yaralanmalarıyla birlikte görülebilir. İleri yaşlarda hastanın mevcut dejeneratif disk patolojisi, travma nedeniyle herniasyon ve nörolojik defisitle bulgu verebilir. Travma sonrası boyun ağrısı olan BT görüntülemesi olağan olan, üst ekstremitelerinde parestezi, parezi tarifleyen hastalarda travmaya sekonder servikal disk hernisi olabileceği akılda tutulmalıdır. Anahtar Kelimeler: Akut servikal disk hernisi, hipoestezi, disk hernisi

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
382
P 356 FLUID RESUSCITATION FOR NON-OPERATIVE MANAGEMENT OF BLUNT SPLEEN TRAUMA IN CHILDREN WITH EMPHASIS ON URINARY OUTPUT
Didem Baskın Embleton1, Neşe Nur User2, Nazan Okur3, Ahmet Ali Tuncer1, Salih Çetinkurşun1
1Afyon Kocatepe University Faculty of Medicine, Department of Pediatric Surgery, Afyonkarahisar, Turkey 2Afyon Kocatepe University Faculty of Medicine, Department of Emergency Medicine, Afyonkarahisar, Turkey 3Isparta State Hospital, Clinic of Radiology, Isparta, Turkey Objective: To evaluate the results of pediatric blunt spleen trauma patients treated with a standard fluid protocol. Material-Method: Children that were treated in a university hospital for blunt spleen trauma between 2012 and 2015 were included. Age, gender, mechanism of injury, spleen injury scale, additional injuries, hemoglobin levels, thrombocytopenia and thrombocytosis, administration of blood and blood products, hospitalization time and results were evaluated. Fluid protocol after the initial resuscitation was starting the fluids calculated with Holliday-Segar equation and adjusting the fluid intake according to the urinary output which is set to 1 ml/kg/h unless there is a contraindication. Pain management and careful monitorization of the blood pressure to keep it between the limits appropriate for age were also done. Results: There were 28 children aged 3-18 years. Injury grade was G1 in 3, G2 in 12, G3 in 10, G4 in 2 and G5 in 1 patient. There were no side effects related with the fluid protocol and monitorization with urinary output was helpful. Three patients had blood transfusion. Other than the G5 patient that had immediate splenectomy, spleen was preserved in all patients. Mean hospitalization time was 5.64 days. G4 patients developed spleen hypofunction during hospitalization and one G3 patient developed re-bleeding after discharge. Re-bleeding was controlled with conservative treatment. Spleen functions returned to normal during follow-up in G4 patients. There was no mortality. Conclusion: Our management protocol was successful, spleen loss was only in a grade 5 injury. Urinary output was helpful in management of fluid resuscitation. G4 injuries may need a special management regarding the spleen functions. Keywords: Spleen, trauma, child, hyposplenism, fluid protocol P 357 GEBELİKTE STATUS EPİLEPTİCUSUN VE GÖRME KAYBININ NADİR NEDENİ; PRESS SENDROMU Onur Karakayali, Okay Albayrak Kocaeli Derince Eğitim ve Araştırma Hastanesi, Acil Tıp Anabilim Dalı, Kocaeli Posterior Reversibl Ensefalopati Sendromu (PRES), nörolojik muayene ve radyolojik görüntüleme yöntemleri ile konulabilen geçici bir klinik tablodur. Klinikte sık görülmemekle birlikte gebelik toksemisi, organ transplantasyonu, immünsüpresif tedaviler, sistemik inflamatuvar yanıt sendromu (SIRS), otoimmün hastalıklar, porfiri, kemoterapi tedavileri ve şok sonrası vakalar bildirilmiştir. Gebelik döneminde dönemde status epileptikus tablosuna giren klinik, nöroradyolojik bulguları ile PRES tanısı konulan, ancak tek bir hipertansif atak dışında da hiçbir risk faktörü olmayan bir olguyu tartışmak amaçlanmıştır. ��
Olgu: 35 yaşında 38 haftalık gebe kadın hasta dün başlayıp giderek artan görme kaybı ile kliniğimize başvurdu, gözleri etrafına lokalize olmuş baş ağrısı şikayetlerine eşlik ediyordu. Gravida:3 parite: 2 abortus öyküsü olmayan hastanın özgeçmiş ve soy geçmişte özellik yoktu. Fizik muayenesinde sol anizokorik pupili mevcut, ışık refleksleri bilateral alınamıyordu. Vitalleri doğal, TA:160/100 bilinç açık, gks 15 olan hastanın ek muayene bulgusu yoktu. Laboratuvar testlerinde özellik olmayan hasta acil servis takibinin 30. Dakikasında jeneralize tonik klonik nöbet geçirdi, diazem 5mg iv ile nöbeti sonlandı. Beyin/difüzyon MR görüntülemesinde her iki serebral hemisferde oksipital lobda daha belirgin olmak üzere kortekste multi fokal T2-FLAIR incelemelerde sinyal intensite artışı izlenen hastanın bu bölgelerde diffüzyon kısıtlanması yoktu (akut hipertansif ensefalopati). Kranial MR venografi de transvers sinüs lojunda akım sinyali alınınamıyordu. Nöroloji ve Kadın doğum konsültasyonları istenen hasta sezeryana alındı. Sezeryan operasyonu sonrası 3 gün yoğun bakımda takip edilen hastanın semptomu olmadı ve muayene bulguları geriledi, hasta 2 gün daha semptomsuz takibi sonrası taburcu edildi.��
Tartışma: Gebelik döneminde nöbet ayırıcı tanısı hızlı bir şekilde yapılmalı ve klinik tanı tedavi açısından en kısa sürede aydınlatılmalıdır. Gebelik döneminin nadir konvulsiyon nedeni olan Press sendromu baş ağrısı, konfüzyon, nöbet geçirme, görmede bulanık (normal pupiller refleks ve göz dibi bakı) ve kural olmasa da hipertansiyon ile karakterizedir. Olgumuz nöbet ve görme kaybı ile başvurmuş olup tedavi sonrası görme fonksiyonları tamamen düzelmiştir. Acil servise nöbet ve hipertansif atakla başvuran hastalarda ayırıcı tanıda PRESS sendromu göz önünde bulundurulmalıdır. Anahtar Kelimeler: Press sendromu, gebelik, görme kaybı, Status Epilepticus

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
383
P 358 WORK-RELATED INJURIES BETWEEN 2011-2015 AT ESKİŞEHİR OSMANGAZİ UNIVERSITY EMERGENCY DEPARTMENT
Emre Çatal, Mustafa Emin Çanakçı, Nurdan Acar, Engin Özakın, Ruşengül Koruk, Eşref Genç Eskişehir Osmangazi University School of Medicine, Department of Emergency Medicine, Eskişehir, Turkey Objective: We analyzed the kind of injuries, hospitalization and discharge rates of work-related injuries in our emergency department (ED) for five years. Method: We evaluated adult work-related injury patients older than 17 y.o. retrospectively between the dates of 01.01.2011-31.12.2015. We assessed kind of injuries at admission, hospitalization and discharge rates of work-related injuries. Results: A total of 2210 patients included the study. The most diagnosed injuries are 1221 (55.2%) isolated limb injuries, 272 (12.3%) fall from heights, 230 (10.4%) isolated eye injuries. 1101 (49.8%) of patients discharged from Emergency department after their diagnosis and treatment. The most seen injuries in discharged patients have isolated limb injuries (58.7%) and isolated eye injuries (15.6%). 961 (43.3%) patients are hospitalized for advanced diagnostic investigation and treatment. 47.0% of 1221 isolated extremity injuries and 23.9% of 230 isolated eye injuries were hospitalized. Of all hospitalized patients, 818 (85.1%) transferred to various clinics, 143 (14.9%) to intensive care unit. The most transfers to plastic and reconstructive surgery clinic (47.13%) and orthopedic surgery clinic (27.2%). Majority of patients in ICU [n=85, (59.4%) were fall from heights. 3 (0.14%) patients died in Emergency department and all of them fell from heights. Conclusion: Work-related injuries are a group of trauma that affect young population. Fall from heights have a high morbidity and mortality rate because of multiple trauma has seen in this patient group. Almost half of isolated extremity injuries and one four of isolated eye injuries need hospitalization. Work-related injuries affect young and productive population. Emergency Physicians should evaluate this clinical conditions accurately. Keywords: Emergency, trauma, work-related injury P 359 DİREKT GRAFİDE GÖRÜLEN SAFRA TAŞI OLGUSU Hanife Bilgili, Serpil Soyudoğru, Melek Aktepe, Yonca Senem Akdeniz İstanbul Üniversitesi Cerrahpaşa Tıp Fakültesi, Acil Tıp Anabilim Dalı, İstanbul Giriş: Safra taşları erkeklerin %6 sı, kadınların %8 inde görülen yaygın bir durumdur. Çoğu hasta yaşamları boyunca asemptomatik kalır. Akut kolesistit, kolanjit, safra taşı pankreatiti gibi komplikasyonlar geliştiğinde semptom verir. Safra kesesi kanseri, safra taşı ileusu, Mirizzi sendromu nadir komplikasyonlardır. Non-komplike safra taşı olan hastalar; biliyer kolik, normal fizik muayene bulguları ve laboratuvar sonuçları ile prezente olabilir. ��
Olgu: 97 yaşında kadın hasta, karın ağrısı bulantı kusma şikayeti ile Acil Servise başvurdu. Hastanın bilinen hastalığı yoktu, şikayetleri aynı gün içinde başlamıştı. Gaz-gayta çıkışı mevcuttu, dizüri tariflemiyordu. Vitalleri stabil ve EKG’ si normal sınırlarda idi. Fizik muayenede batın sağ üst kadranda hassasiyet mevcuttu, defans-rebound yoktu, diğer sistem muayeneleri doğaldı. Çekilen ADBG’de safra kesesi lojunda, yaklaşık 2x3 cm’lik opasite görüldü. Laboratuvar testleri normal sınırlarda saptandı. Batın USG çekildi; safra kesesinde 3 cm boyutlarında kalkül saptandı, kolesistit lehine bulgu saptanmadı. Hastaya analjezik yapılarak, Genel Cerrahi poliklinik önerisiyle taburcu edildi. Sonuç: Safra taşı toplumda sık görülmesine rağmen hastaların çoğu asemptomatik seyreder. Çoğu hastada safra taşı, transabdominal ultrasonla görüntülenir. Düz karın grafilerinde nadiren görüntülenir; çünkü safra taşlarının yalnızca % 10’u, onları radyoopak ve düz karın grafilerinde görünür kılacak kalsiyum içeriğine sahiptir. BT’ nin sensivitesi %50-80 olarak bildirilmiştir. BT’ de safra taşları kaçırılabilir, çünkü taşların çoğu safra ile izodenstir. Anahtar Kelimeler: Direkt grafi, radyoopak, safra taşı

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
384
P 360 ESWL SONRASI RENAL KOLİK VAKASI; RENAL SUBKAPSÜLLER HEMATOM Okay Albayrak, Onur Karakayalı Kocaeli Derince Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Kocaeli Giriş: Extracorporeal Shock Wave Lithotripsy (ESWL) 20 yıldan uzun süredir üriner sistem taşlarının tedavisinde kullanılan güvenli ve efektif bir tedavi yöntemidir. ESWL sonrası hastalar acil sevise karın veya yan ağrısı, bulantı, kusma ( özellikle ilk 48 saat içinde), cilt ekimozu, gross hematüri ve ateş şikayeti ile %30 oranında başvurabilirler. Neredeyse tüm abdominal organ sistemleri bu işlem sırasında hasar gördüğü raporlanmıştır, ancak en sık hasar akut renal hemorajilerdir. Subkapsuller veya perinefrik hematom ESWL’nin en sık ve ciddi komplikasyonlarıdır. Bu komplikasyonların erken tanı ve tedavisi genellikle acil serviste başlar. Bu vaka örneği ile konu hakkında farkındalık yaratmak amaçlanmıştır.��
Olgu: 51 yaş erkek, sabah ESWL yöntemi ile taş kırdırma öyküsü olan hasta (sağ böbrek), akşam saatlerinde sağ yan ağrısı ile acil servise başvurmuş. Ağrısının önceki ağrılarına benzer ancak daha şiddetliymiş, idrarda yanma, bulantı, kusma ve halsizliğin eşlik ediyormuş. Geliş vitalleri doğal ve stabil, fizik muayenede şiddetli sağ kostovertebral açı hassasiyeti olan hastanın özgeçmişinde böbrek taşı ve sağ böbrekte double J katater dışında ek hastalığı yoktu. Renal kolik ön tanısıyla müşhadeye alınan hastanın ağrısı nonsteroid antiiflamatuar ajan ve bolus serum fizyolojik tedavisine rağmen devam ediyordu. Hastanın TIT de 536 eritrosit 53 lökosit dışında laboratuar bulgusu yoktu. Batın Tomografide sağ böbrek boyutları artmış, yaygın subkapsüller hematom, perirenal çizgilenmelerde artış gözlenen hasta üroloji kliniğine yatırıldı.��
Tartışma: ESWL böbrek taşı tedavisinde cerrahiye göre devrim niteliği taşımaktadır. ESWL öncesi her hastanın bazal hematokrit, koagülasyon değerleri değerlendirilmeli, kan basıncı ve şeker monitörizasyonları yapılmalı. İlerleyen yaş ve yüksek kan basıncı ESWL sonrası artan kanama riskiyle ilişkilidir. Hipertansiyon, pıhtılaşma bozuklukları, önceki ESWL öyküsü, ileri yaş, diyabet, yaygın ateroskleroz, koroner arter hastalığı, obezite ve küçük böbrek ileri sürülen anlamlı risk faktörleridir. ESWL öncesi hastaların risk faktörü oluşturan tetkik ve takiplerinin yapılması subkapsüller hematom riskini azaltabilir, Acil serviste bu risk faktörlerini sorgulanması tanı ve tedaviye erken karar vermede yardımcı olabilir. Anahtar Kelimeler: ESWL, subkapsuler hematom, renal kolik P 361 AKCİĞERDE KİST HİDATİK OLGUSU
Birdal Güllüpınar, Tayfun Öztürk, Arif Akkaya, Özlem Ezgi Aktürk Bozyaka Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İzmir Giriş: Kist hidatik (KH), Echinococcus granulosus (E. Granulosus)’un neden olduğu bir helmint enfeksiyonudur. KH hastalığı en sık karaciğer ve akciğerde görülmekle birlikte, nadiren diğer dokuları da tutabilmektedir. Sindirim sistemi ile vücuda giren E. granulosus yumurtalarının ilk geçiş yeri olduğundan KH vakalarının yaklaşık 2/3’u karaciğer yerleşimli olmaktadır. Karaciğerden komşuluk yoluyla yakın organlara veya kan akımı ile uzak organlara yayılabilir. Bu nedenle hastalığın klasik tutulumu karaciğer olmakla birlikte, akciğer, böbrek, dalak, beyin, kemik ve kalp başta olmak üzere hemen hemen her organa yerleşim gösterebilmektedir.��
Olgu: 26 yaşında göçmen erkek hasta, nefes darlığı ve öksürük yakınması nedeniyle acil kliniğimize başvurdu. Özgeçmişi olağandı. Genel durumu iyi, şuur açık, koopere ve oryenteydi. TA:127/69 mmHg, Nb:78/dk; Ateş:37.1, SS:16/dk. olarak değerlendirildi. Hastanın fizik muayenesinde sol akciğerde solunum kabalaşması mevcut olup diğer sistem muayenesi olağandı. Biyokimyasal parametreler normal sınırlarda idi. PA Akciğer grafisi ve daha sonra çekilen toraks BT’de sol akciğer alt lob bazal segmentte 92x85x74 mm boyutlarda kalın cidarlı kistik dansitede lezyon izlenmektedir. Lezyonun ön planda ayırıcı tanısında tip 1 kisthidatik düşünüldü. Göğüs cerrahi konsültasyonu sonrası operasyon amaçlı yatırıldı. ��
Tartışma: Sonuç olarak, nefes darlığı ve öksürük yakınması ile başvuran hastalarda kist hidatiğe bağlı organ tutulumu olabileceği akılda tutulmalıdır. Anahtar Kelimeler: Acil servis, akciğer, kist hidatik

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
385
P 362 BİLATERAL RENAL ENFARKTÜS OLGUSU Birdal Güllüpınar, Serhat Akay, Vermi Değerli, Tayfun Öztürk, Özlem Ezgi Aktürk, Umut Öztürk Bozyaka Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İzmir Giriş: Renal enfarktüs, tüm acil servis başvurularında oldukça nadir bir tanıdır. Renal enfarktüse ait özel klinik bulgu ve belirtinin olmaması, daha sık olarak görülen üriner sistem taş hastalığı, lumbago veya diğer karın içi patolojilerle karışması ve dolayısıyla klinik olarak ayırıcı tanıda ilk sıralara konulmaması düşük insidansın nedenleri olabilir. Atriyal fibrilasyon ise sistemik olarak aralarında böbreğin de bulunduğu birçok organda arteriyel embolizmin nedenlerinden biridir. Yazımızda, kronik atriyal fibrilasyon zemininde bilateral renal enfarktüs ve akut böbrek yetmezliği geliştiren bir hasta sunulmaktadır.��
Olgu: 59 yaşında erkek hasta, yaklaşık 15 gündür var olan ve giderek artan her iki böğür ağrısı yakınması nedeniyle acil kliniğimize başvurdu. Özgeçmişinde hipertansiyon, koroner arter hastalığı, koroner arter by-pass greftleme cerrahisi ve post-operatif erken dönemden bu yana atriyal fibrilasyonu olduğu öğrenildi. Varfarin kullandığını, ancak başvuru tarihinden 15 gün kadar önce dispeptik yakınmaları nedeniyle hem enterik kaplı asetil salisilik asit hem de varfarin tedavisini doktorlarından habersiz kestiğini belirtti. Başvuruda genel durumu iyi, şuur açık, koopere ve oryenteydi. TA:153/91 mmHg, Nb:98/dk; Ateş:37.7, SS:16/dk. olarak değerlendirildi. Hastanın fizik muayenede tüm karında yaygın hassasiyet ve bilateral CVAH pozitifliği vardı. Bunun dışında diğer sistem muayenesi olağandı. PA Akciğer grafisi, Direkt Üriner Sistem Grafisi olağan olup ve EKG’de aritmi mevcuttu. Laboratuvar incelemesinde tam kan sayımında lökositoz (16.3 x 103/mL) mevcuttu, Protrombin zamanı (International normalized ratio: INR) 1,10 olarak saptandı. İdrar tetkikinde her büyük büyütme sahasında 10-15 eritrosit tespit edildi. Diğer biyokimyasal parametreler normal sınırlarda idi. Acil serviste çalışılan laboratuvar testlerinin sonuçlarında, hematüri dışında şiddetli bilateral yan ağrısını açıklayacak anlamlı bir patoloji yoktu ve batın bilgisayarlı tomografi (BT) çekilmesine karar verildi. Batın BT’sinde, bilateral renal enfarkt ile uyumlu hipodens bir alan tespit edildi. Üroloji konsültasyonu sonrası yatışı yapıldı.��
Tartışma: Sonuç olarak, yan ağrısı ve hematüri ile başvuran hastalarda, risk faktörleri olsun veya olmasın, renal enfarktüsün pyelonefrit ve nefrolitiyazis kadar akılda tutulması gereken bir hastalık olduğunu düşünmekteyiz. Anahtar Kelimeler: Bilateral infarktüs, emboli ve tromboz, yan ağrısı P 363 FAHR SENDROMU
Birdal Güllüpınar, Huriye Akay, Özgür Duran, Vermi Değerli, Emrah Yılmaz Bozyaka Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İzmir Giriş: Fahr sendromu (FS); bazal ganglion, talamus, serebellar dentat nükleus ve serebral beyaz cevherde simetrik kalsifikasyonlar ile karakterize nadir görülen bir durumdur. Kalsifikasyonlar genellikle başka nedenlerle çekilen bilgisayarlı beyin tomografisinde dikkat çeker. Hastalığın klinik özellikleri değişken olmasına rağmen; ilerleyici mental hasar, tremor, kore, ataksi, disartri, parkinson benzeri klinik tablo, nöro-psikiyatrik davranış değişiklikleri ve zihinsel işlev bozuklukları sıklıkla görülen klinik bulgulardır. Burada şiddetli baş ağrısı ile gelen ve rastlantısal olarak FS teşhisi konulan vakayı sunuyoruz. ��
Olgu: 34 yaşında kadın hasta, son 2 gündür artan şiddetli baş ağrısı ve dengesizlik şikayeti ile gittiği başka bir sağlık merkezinden kliniğimize sevk edildi. Özgeçmişinde herhangi bir patoloji yoktu. Başvuruda genel durumu iyi, şuur açık, iletişim kurulabiliyor, yer-zaman-kişi farkındalığı tamdı. TA:120/80mmHg, Nb:88/dk; Ateş:36.7, SS:20/dk. olarak değerlendirildi. Hastanın sistemik ve nörolojik muayenesinde; sol uç bakışta horizontal nistagmus ve hafif dizartri dışında belirgin patolojik bulguya rastlanmadı. Laboratuar incelemesinde tam kan sayımı, biyokimyasal parametreler normal sınırlarda idi. Yine PA akciğer grafisi ve EKG’de özellik yoktu. Hastanın baş ağrısı ve dengesizlik yakınması ön planda olması nedeniyle bilgisayarlı beyin tomografisi (BBT) çekildi. BBT’de subkortikal alanda, bazal ganglionlarda, serebellar hemisferlerde belirgin, simetrik kalsifikasyonlarla uyumlu görünümler izlendi. İzlemde aktif yakınması kalmayan hasta mevcut klinik, laboratuar ve radyolojik bulgular, literatür bilgileri ışığında değerlendirilerek hastanın tablosu FS olarak kabul edildi. Tartışma: Özellikle serebellumda, bazal ganglionlarda ve supratentoryal mesafede kranial BTve MRI ile saptanan ve herhangi bir nedene bağlanamayan kalsifikasyonların varlığında FS ayırıcı tanıda düşünülmelidir. Anahtar Kelimeler: Acil servis, Fahr sendromu, idiyopatik bazal ganglion kalsifikasyonu

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
386
P 364 KİST HİDATİK OLGUSU Birdal Güllüpınar, Caner Sağlam, Tayfun Öztürk, Mustafa Silcan Bozyaka Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İzmir Giriş: Kist hidatik (KH), Echinococcus granulosus (E. Granulosus)’un neden olduğu bir helmint enfeksiyonudur. KH hastalığı en sık karaciğer ve akciğerde görülmekle birlikte, nadiren diğer dokuları da tutabilmektedir. Sindirim sistemi ile vücuda giren E. granulosus yumurtalarının ilk geçiş yeri olduğundan KH vakalarının yaklaşık 2/3’u karaciğer yerleşimli olmaktadır. Karaciğerden komşuluk yoluyla yakın organlara veya kan akımı ile uzak organlara yayılabilir. Bu nedenle hastalığın klasik tutulumu karaciğer olmakla birlikte, akciğer, böbrek, dalak, beyin, kemik ve kalp başta olmak üzere hemen hemen her organa yerleşim gösterebilmektedir.��
Olgu: 66 yaşında bayan hasta, yaklaşık iki aydır var olan ve giderek artan epigastrik ağrı yakınması nedeniyle acil kliniğimize başvurdu. Özgeçmişinde hipertansiyon, koroner arter hastalığı, diabet öyküsü mevcuttu. Başvuruda genel durumu iyi, şuur açık, koopere ve oryenteydi. TA:157/79 mmHg, Nb:78/dk; Ateş:37.7, SS:16/dk. olarak değerlendirildi. Hastanın fizik muayenede tüm karında yaygın hassasiyet ve özellikle epigastrik ve sağ üst kadranda defans mevcuttu. Bunun dışında diğer sistem muayenesi olağandı. PA Akciğer grafisi olağan olup ve EKG’de sinüs ritmi mevcuttu. Laboratuar incelemesinde tam kan sayımında lökositoz (13.3 x 103/mL) dışında diğer biyokimyasal parametreler normal sınırlarda idi. Yapılan USG sonrası KC sağ lob posterior bölümünü dolduran 90x80 mm boyutlarda kistik kitle lezyonu mevcuttur. Kistik lezyon hepatik venlere, porta hepatise ve koledoka bası oluşturmaktaydı. Batın BT’sinde, karaciğer sağ lobunu dolduran yaklaşık 10x15x11 cm lik lobüle konturlu, ince duvar yapısı seçilebilen ve solid komponenti olmayan kist izlenmiş olup ön planda evre 1 kist hidatik ile uyumlu olabileceği düşünülmüştür. Genel cerrahi konsültasyonu sonrası perkütan drenaj açısından girişimsel radyolojinin bulunduğu bir merkeze başvurusu önerildi. ��
Tartışma: Sonuç olarak, karın ağrısı ile başvuran hastalarda kist hidatiğe bağlı organ tutulumu olabileceği akılda tutulmalıdır. Anahtar Kelimeler: Acil servis, kist hidatik, karaciğer P 365 MESENTER İSKEMİ OLGUSU
Birdal Güllüpınar, Serhat Akay, Özgür Duran, Vermi Değerli, Selin Bulut Bozyaka Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İzmir Giriş: Akut mezenterik iskemi (AMİ) erken tanı ve tedavi gerektiren hayatı tehdit edici bir vasküler acildir. Günümüzde hala yüksek mortalite ve morbidite ile seyretmekte olan bu hastalığın önlenmesi erken klinik şüphe ve zamanında müdahaleye bağlıdır. Klinik semptomlar nonspesifik olup genellikle şiddetli karın ağrısına rağmen fizik muayene bulguları minimal olabilir. Günümüzde hala spesifitesi ve sensitivitesi yeterince yüksek bir tanı testi bulunamamıştır.��
Olgu: Altmış yedi yaşında bayan hasta yaklaşık iki aydır devam eden ve son 3 gündür giderek artan, göbek etrafında ağrı, iştahsızlık, bulantı ve kusma yakınması ile başvurdu. Özgeçmişinde hipertansiyon ve diyabet dışında herhangi bir patoloji yoktu. Başvuruda genel durumu iyi, şuur açık, koopere ve oryenteydi. TA:163/89 mmHg, Nb:108/dk; Ateş:36.7, SS:20/dk. olarak değerlendirildi. Hastanın fizik muayenede tüm karında yaygın hassasiyet ve rebound vardı ve ayrıca bağırsak sesleri hipoaktifti. Bunun dışında diğer sistem muayenesi olağandı. PA akciğer grafisi ve EKG’de özellik yoktu. Laboratuvar incelemesinde tam kan sayımında lökositoz (22.1 x 103/mL) mevcuttu, biyokimyasal parametreler normal sınırlarda idi. Hastanın abdominal bilgisayarlı tomografisinde SMA orijin ve proksimal 2 cm’lik segmentte oklüzyon mevcuttu. Genel cerrahi konsültasyonu sonrası acil operasyona alındı.��
Tartışma: Mezenter iskemi erken tanının çok önemli olduğu halen yüksek mortalite oranları taşıyan, özellikle kardiyak patolojisi olan karın ağrılı hastalarda ayırıcı tanıda mutlaka düşünülmesi gerekli bir hastalıktır. Anahtar Kelimeler: Mezenter iskemi, mortalite, karın ağrısı

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
387
P 366 UNUSUAL CAUSE OF ILEUS: GASTRIC LIPOMA Mehmet Efe, Sercan Yalçınlı, Funda Karbek Akarca Ege University Medical School, Department of Emergency Medicine, Izmir, Turkey Introduction: Gastric lipoma is a rare tumor, accounting for %2-3 of all benign gastric tumors. It usually originates from submucosa but rarely from subserosa. It usually asymptomatic and detected incidentally. It may cause abdominal pain, dyspeptic symptoms, obstruction, invagination and bleeding. Case: A 54 years old male admitted to Emergency Department (ED) with nausea and vomiting for 2 days. He had no diagnosed chronic diseases and he hadn’t defecated for 3 days. In physical examination epigastric tenderness was detected but there was no defense or rebound on abdominal region. In his lab results; urea:82 creatinin: 1,58 crp: 4,88 were detected. Other laboratory parameters were in normal limits. Air-fluid levels were detected in plain abdominal x-ray. Nasogastric tube was inserted and the patient was consulted with general surgery for suspicion of ileus. In abdominal CT, a gastric lipom detected and patient admitted to general surgery. Conclusion: It should be kept in mind that in patients with ileus symptoms, obstruction may occur by an intra-abdominal mass and CT is an important tool for preoperative diagnose. Keywords: Gastric lipoma, ileus, computed tomography P 367 METANOL ZEHİRLENMESİ OLGUSU Birdal Güllüpınar, Arif Akkaya, Caner Sağlam, Tayfun Öztürk, Mustafa Silcan, Arife Erdoğan
Bozyaka Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İzmir Giriş: Metanol zehirlenmesi şiddetli hastalık ve ölüme sebep olabilen bir acil başvuru nedenidir. Her ne kadar metanolün kendisi çok toksik değilse de metabolitleri çok toksiktir. Metanol zehirlenmesi santral sinir sistemi (SSS) depresyonu, görme bozuklukları, karın ağrısı, bulantı, kusma şikayetleri ile acil servise başvurabilir. Bu hastalarda ve artmış anyon gap’li metabolik asidoz, konfüzyon ve ciddi olgularda koma görülebilir. Görme bozuklukları hastaların yaklaşık %50’sinde ortaya çıkar. Diplopi, bulanık görme, görme keskinliğinin azalması, fotofobi, görme alanının daralması ve körlüğü içeren görme bozuklukları gelişebilir. Hipotansiyon ve bradikardi geç bulgudur ve kötü prognoz işaretidir. Zehirlenme sıklıkla oral alımdan sonra olur, an¬cak akciğerler ve deri yoluyla da zehirlenme olabilir��
Olgu: Kırk altı yaşında erkek hasta acil servisimize parkta bulunmuş halde 112 tarafından getirildi. Öyküsün¬den önceki akşam sarhoş olmak amacı ile 200-300 ml kadar kolonya içtiği öğrenildi. Fizik muayenesinde genel durumu orta-kötü, bilinç konfüze idi. Kan basıncı 50/20 mmHg, nabız 32/dakika, solunum sayısı: 14/dakika idi. Hasta monitörize edildi. Damar yolu açılarak 1 mg. Atropin verildi. %5 dextroz ve Tiamin 25 mg verildi. Hastanemizde çalışılmadığı için kan metanol düzeyi bakılamadı. Laboratuvar değerlendirmesinde; Arteryel Kan Gazında (AKG) pH: 6.79, pO2: 37.2mmHg, pCO2: 20.5mmHg, HCO3: 4.7mEq/dL, BE: -25 idi. Biyokimyada: Üre:44 mg/dl, kreatinin:3.7 mg/dl, sodyum 136 mg/dl, klor: 82 mg/dl ve beyaz küre sayısı 16.700/mm3 idi. Diğer laboratuar değerleri normaldi. Anyon gapı 50 olarak hesaplandı. Hasta metanol zehirlenme¬si olarak kabul edildi. %10’luk 10 ml/kg etanol yükleme dozu intravenöz (IV) olarak verildikten sonra, 1,5 ml/kg/saat’den IV infüzyon tedavisi uygulandı. Derin asidozu olan hastaya 1 mEq/kg’dan NaHCO3 verildi. Ayrıca 15 mg/kg Fomepizol yükleme dozunu takiben, 12 saatte bir 10 mg/kg’dan idame dozu başlandı. Ayrıca tek seans hemodializ uygulandı.��
Tartışma: Metanol zehirlenmesi uygun tedavi edilmediği zaman ölümcül olabilen bir zehirlenme türüdür. Acil hekimleri iyi an¬amnez alınamayan, bilinç değişikliği olan, artmış anyon açığı olan hastalarda metanol zehirlenmesi olasılığını düşünmeli ve uygun şekilde tedaviye başlamalıdır. Anahtar Kelimeler: Acil servis, zehirlenme, metanol

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
388
P 368 RENAL ENFARKTÜS OLGUSU Birdal Güllüpınar, Serhat Akay, Vermi Değerli, Özgür Duran, Emre Sevim Bozyaka Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İzmir Giriş: Renal enfarktüs, tüm acil servis başvurularında oldukça nadir görülen bir ürolojik acildir. Renal enfarktüse ait özel klinik bulgu ve belirtinin olmaması, daha sık olarak görülen üriner sistem taş hastalığı, lumbago veya diğer karın içi patolojilerle karışması ve dolayısıyla klinik olarak ayırıcı tanıda ilk sıralara konulmaması düşük insidansın nedenleri olabilir. Atriyal fibrilasyon ise iskemik olarak aralarında böbreğin de bulunduğu birçok organda arteriyel embolizmin nedenlerinden biridir. Yazımızda, kronik atriyal fibrilasyon zemininde sol renal enfarktüs saptanan bir hasta sunulmaktadır.��
Olgu: 52 yaşında erkek hasta, yaklaşık 15 gündür var olan ve giderek artan sol böğür ağrısı yakınması nedeniyle acil kliniğimize başvurdu. Özgeçmişinde hipertansiyon, koroner arter hastalığı, koroner arter by-pass greftleme cerrahisi ve post-operatif erken dönemden bu yana atriyal fibrilasyonu olduğu öğrenildi. Varfarin kullandığını, ancak başvuru tarihinden 15 gün kadar önce dispeptik yakınmaları nedeniyle hem enterik kaplı asetil salisilik asit hem de varfarin tedavisini doktorlarından habersiz kestiğini belirtti. Başvuruda genel durumu iyi, şuur açık, koopere ve oryenteydi. TA:153/91 mmHg, Nb:98/dk; Ateş:37.7, SS:16/dk. olarak değerlendirildi. Hastanın fizik muayenede tüm karında yaygın hassasiyet ve sol CVAH pozitifliği vardı. Bunun dışında diğer sistem muayenesi olağandı. PA Akciğer grafisi, Direkt Üriner Sistem Grafisi olağan olup ve EKG’de aritmi mevcuttu. Laboratuar incelemesinde tam kan sayımında lökositoz (16.3 x 103/mL) mevcuttu, Protrombin zamanı (International normalized ratio: INR) 1,10 olarak saptandı. İdrar tetkikinde her büyük büyütme sahasında 10-15 eritrosit tespit edildi. Diğer biyokimyasal parametreler normal sınırlarda idi. Acil serviste çalışılan laboratuar testlerinin sonuçlarında, hematüri dışında şiddetli sol yan ağrısını açıklayacak anlamlı bir patoloji yoktu ve batın bilgisayarlı tomografi (BT) çekilmesine karar verildi. Batın BT’sinde, sol renal parankimin orta kısmında, infarkt ile uyumlu hipodens bir alan tespit edildi. Üroloji konsültasyonu sonrası yatışı yapıldı.��
Tartışma: Sonuç olarak, yan ağrısı ve hematüri ile başvuran hastalarda, risk faktörleri olsun veya olmasın, renal infarktüsün pyelonefrit ve nefrolitiyazis kadar akılda tutulması gereken bir hastalık olduğunu düşünmekteyiz. Anahtar Kelimeler: Enfarktüs, emboli ve tromboz, yan ağrısı P 369 ANKSİYETE SEMPTOMLARI OLAN PERİFERİK FASİAL PARALİZİDEN MULTİPLE SKLEROZA Ali Yusuf Uyanık, Serkan Yılmaz, Asım Enes Özbek, Yavuz Yiğit Kocaeli Derince Eğitim Araştırma Hastanesi, Kocaeli Acil servise 2 gündür olan üzüntü emosyonel stres vücudun sol tarafında olan uyuşukluk, istemsiz hareketler ile başvuran 22 yaşında kadın hasta vital bulgular, TA: 120/70, Nabız:82, Ateş 36,8, SS: 16 /dk, dış merkeze daha önce başvuruşunda anksiyolitik yapılıp taburcu edilen hastanın ameliyat ilaç kronik hastalık öyküsü yok. Fizik muayenede tüm sistem muayeneleri doğal olup hasta takip amaçlı damar yolu açılıp müşahedeye alındı. Damar yolu açık kalacak şekilde serum fizyolojik verildi. Rutin tetkikleri normal olan hastanın seri kontrol muayenelerinde sol gözde pitozis, sol dudak sulkusunda düzleşme gözlendi. Santral patoloji açısından beyin bt çekilen hastanın sonucunda akut patoloji gözlenmedi. Gözlemlerinde vücudunun sol tarafında uyuşukluklarının artığını tarifleyen hastaya kontrasyon kranial mr ve difüzyon mr planlandı. Difüzyon mr sonucunda, sol lateral ventrikül korpusu komşuluğunda 1,5 cm ve sol serebeller pedinkül düzeyinde 1 cm çaplarında hafif difüzyon kısıtlanması oluşturan lezyonlar mevcut olup aktif demiyelizan plak ile uyumlu olduğu görüldü. Kontraslı kranial mr sonucunda, sol serebeller pedinkülde 1 cm, sol koroner radiyatada ve sentrum semovalede periventrükler beyaz cemherde en büyüğü 1,5 cm çapında olan multiple T2 ve FLAIR sekanslarda nodüler intensiteler mevcut olup demiyelizan hastalık ile uyumlu olduğu raporlanmıştır. Hasta multiple skleroz ön tanısıyla nöroloji servisine yatırıldı. Anahtar Kelimeler: Anksiyete, multiple skleroz, periferik fasial paralizi

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
389
P 370 SPLENİK ENFARKTÜS OLGUSU Birdal Güllüpınar, Caner Sağlam, Arif Akkaya, Özgür Duran, Tayfun Öztürk Bozyaka Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İzmir Giriş: Splenik infarkt dalak damar tıkanıklığı sonrası gelişen parankimal iskemi ve doku nekrozunu ifade eder. Splenik infarkt nadir görülen bir antitedir. Etiyolojisinde en sık hematolojik hastalıklar, ikinci sıklıkta tromboembolik durumlar, daha nadir olarak da vasküler hastalıklar, anatomik bozukluklar ve kollagen doku hastalıkları bulunmaktadır. Karın ağrısı, bulantı, kusma ve ateş şikayetleri mevcut olup fizik muayenesinde ani başlayabilen karın sol üst kadran ağrısı ile başvurur.��
Olgu: 69 yaşında bayan hasta, sol üst kadranda ani gelişen şiddetli karın ağrısı, bulantı, kusma yakınmaları ile acil servise başvurdu. Özgeçmişinde hipertansiyon ve atriyal fibrilasyonu olduğu ve AF nedeniyle beta bloker (metoprolol 50 mg) ve antiagregan kullandığı öğrenildi. Başvuruda genel durumu orta ve soluk görünümde, şuur açık, koopere ve oryenteydi. TA:193/97 mmHg, Nb:113/dk; Ateş:37.7, SS:16/dk. olarak değerlendirildi. Hastanın fizik muayenede tüm karında yaygın hassasiyet olmak üzere sol üst kadranda defans ve reabaund mevcuttu. Bunun dışında diğer sistem muayenesi olağandı. PA Akciğer grafisi, olağan olup ve EKG’de taşiaritmi ve hızlı ventrikül yanıtlı AF izlendi. Tüm laboratuar değerleri olağandı. Batın ultrasonografisinde (USG) patolojik bulguya rastlanmadı. Bu bulgularla hasta izleme alındı. Batın tomografisinde (BT) dalak anterosüperior ve inferior polünde hipodens değişiklikler görülerek, bulgular dalak infarktı ile uyumlu saptandı. Genel cerrahi konsültasyonu sonrası yatışı yapıldı.��
Tartışma: Karın ağrısının nadir nedenlerinden biri olması ve etyolojik faktör olarak atrial fibrilasyon dışında patoloji saptanmaması nedeni ile karın ağrısı şikayeti ile başvuran hastalarda splenik infark olabileceği akılda tutulmalıdır. Anahtar Kelimeler: Atriyal fibrilasyon, karın ağrısı, splenik infarkt P 371 TRAVMATİK TİP 1 ODONTOİD KIRIĞI Birdal Güllüpınar, Serhat Akay, Özgür Duran, Vermi Değerli, Caner Sağlam, Pınar Barut Bozyaka Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İzmir Giriş: Spinal kord travmaları, hayat boyu süren sakatlıklara neden olabileceği için büyük önem taşımaktadır. Travmatik C2 kırıkları üst servikal yaralanmalarda nadir değildir. Bu kırıklar üç grupta sınıflandırılmıştır; Odontoid kırıkları, pars interartikülarisin bilateral travmatik spondilolistezisi (Hangman fraktürleri) ve C2 korpus kırıklarıdır. Odontoid ile ilgili üç tip kırık ayırt edilebilir. Tip I odontoid uç kırığıdır ve çoğunlukla stabildir. Tip II: Odontoid bazisinde oluşur ve genellikle anstabildir. Tip III: Omur cismine uzanan odontoid kırığıdır. Odontoid kırıklarında olgular genellikle boynun arkasında lokalize olan hafif bir ağrı, paravertebral kas spazmı, boyun devinimlerinin azalmasından yakınırlar. Nörolojik bulgular tetraplejiden, oksipital sinir irritasyonuna bağlı nevraljiye kadar değişebilir. Tip 1 kırık saptanan olgular semirijid boyunluk ile tedavi edilebilir.��
Olgu: Seksen dört yaşında bayan hasta, yüksekten düşme sonrası acil polikliniğe getirildi. Hastanın özgeçmişinde hipertansiyon, koroner arter hastalığı, atriyal fibrilasyon mevcut olup antihipertansif ilaç ve warfarin kullanmaktaydı. Fizik muayenesinde; kan basıncı 170 / 90 mm Hg, nabız 77 / dakika, solunum sayısı 26 / dakika, oksijen satürasyonu % 92 olup, şuuru açık oryante ve koopere idi. Yapılan fizik muayenesinde sağ occipital bölgede cilt laserasyonu ve komşuluğunda cilt altı hematomu izlendi. Boyun bölgesinde hafif ağrı tarifliyordu. Travma ve diğer sistem muayeneleri olağandı. Hastanın nörolojik muayenesi normaldi. Yapılan tetkiklerinde servikal direkt grafide tespit edilemeyen ancak servikal bilgisayarlı tomografi sonrası görülen Tip I odontoid fraktürü görüldü. Beyin cerrahi konsültasyonu istendi. Servikal coller uygulaması ve beyin cerrahi poliklinik kontrolü önerildi. ��
Tartışma: Rutin grafilerde odontoid fraktürlerinin tespiti çok güç olabilir. Olgulara vertebral kolonun orta hatta olduğu anteroposterior, ağız açık odontoid ve lateral grafiler çekilmeli, ayırıcı tanı için bilgisayarlı tomografi ve spinal manyetik rezonans görüntüleme incelemeleri yapılmalıdır. Anahtar Kelimeler: Acil servis, odontoid fraktürü, travma

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
390
P 372 İNVAJİNASYON Birdal Güllüpınar, Caner Sağlam, Tayfun Öztürk, Arif Akkaya, Özlem Ezgi Aktürk Bozyaka Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İzmir Giriş: İnvajinasyon; gastrointestinal traktın bir bölümünün daha distalde yer alan bir barsak segmentin lümeni içine geçmesi olarak tanımlanır. İntestinal invajinasyon çocuklarda intestinal obstrüksiyonun temel sebebiyken, tüm invajinasyonların %5’i erişkinlerde görülür. Bu olgu sunumunda, karın ağrısı ve gaytasında kan görme şikayetiyle hastanemize başvuran bayan hastada teşhis ettiğimiz ileoçekal invajinasyon olgusunu sunduk.��
Olgu: 48 yaşında bayan hasta, karın ağrısı ve gaytasında kan görme yakınması nedeniyle acil kliniğimize başvurdu. Özgeçmişinde kolesistektomi ve apandektomi öyküsü mevcuttu. Genel durumu iyi, şuur açık, koopere ve oryenteydi. TA:147/69 mmHg, Nb:72/dk; Ateş:37.1, SS:16/dk. olarak değerlendirildi. Hastanın fizik muayenesinde sağ alt kadranda belirgin olmak üzere tüm kadranlarda hassasiyet mevcuttu. Sağ alt kadranda rebound ve istemli defans pozitifti. Rektal tuşesinde kanlı ve mukuslu bulaş görüldü. Biyokimyasal parametreler normal sınırlarda idi. Abdominal tomografisinde ise ileoçekal valv düzeyinde ileokolik invajinasyon tespit edildi. Genel cerrahi ile konsültasyon sonrası yatırıldı ��
Tartışma: Sonuç olarak, karın ağrısı yakınması ile başvuran hastalarda, ayırıcı tanı olarak erişkinlerde nadir de olsa invajinasyon düşünülmelidir. Anahtar Kelimeler: Acil servis, karın ağrısı, invajinasyon P 373 CEREBRAL VENOUS SINUS THROMBOSIS Yılmaz Uzun, Rohat Ak, Fatih Doğanay, Erdem Kurt, Emre Onur Tosun, Tuba Cimilli Öztürk, Özge Ecmel Onur, Abdullah Taşcı Fatih Sultan Mehmet Training and Research Hospital, Istanbul, Turkey Cerebral venous sinus thrombosis involves thrombosis of the dural sinus and/or cerebral veins. Patients generally present with a headache or focal neurological deficit but less frequently may present as acute neurological deterioration which may be fatal. A 45-year-old man presented with headache for two days. He described the quality of headache as throbbing, and it was unilateral. There was no history of fever, vomiting, blurred vision, ear discharge or trauma, no relevant past medical or drug history and no family history of note. On examination, he was afebrile with pulse 76/min, regular, blood pressure of 130/80mmHg. His pupils and speech appeared normal. There were no papilledema, sensory deficit, focal neurological deficit or signs of meningeal irritation. Hyperdensity of right transverse sinus and superior sagittal sinus was identified on unenhanced computed tomography (CT). Magnetic resonance venography (MRV) demonstrated lack of flow in right transverse sinus and superior sagittal sinus. Cerebral venous sinus thrombosis (CVST) is a rare condition. According to the International Study on Cerebral Vein and Dural Sinus Thrombosis, the most commonly affected site is the transverse sinus, followed by superior sagittal sinus and straight sinus. Predisposing risk factors may include the following: sinusitis, medications, malignancy, dehydration, prothrombotic conditions, head injury and inflammatory diseases. Neuroimaging modalities of choice in CVST are CT and magnetic resonance imaging (MRI) with MRV. CT may be normal in 15–30% cases, but MRI with MRV is almost 100% diagnostic.�According to the guidelines of the European Federation of Neurological Societies, the first-line treatment for CVST is antithrombolysis. Our patient was given anticoagulant therapy for six months, after which he had recovered fully. Keywords: Cerebral venous sinus thrombosis, magnetic resonance venography, neurological emergencies P 374 AN UNUSUAL CAUSE OF A BLOW OUT FRACTURE WITH SUBCUTANEUS EMPHYSEMA Tuğba Atmaca Temrel1, Selda Kıdak1, Çağdaş Yıldırım2, Gül Pamukçu Günaydın2, Uğur Özkula2, Fatih Tanrıverdi1, Şervan Gökhan1
1Yıldırım Beyazıt University Faculty of Medicine, Ankara, Turkey 2Ankara Atatürk Training and Research Hospital, Ankara, Turkey A 52-year-old man admitted to our emergency medicine department with the complaint of sudden swelling of his right eyelid. He hit his face to a truck’s door. He has no complaints or symptoms after hitting the door. At same day’s evening after he blew his nose for ritual washing, his right eyelid swelled. His eye movements was normal. A maxillofacial CT was taken. There was a fracture at lamina papyrecea (Figure 1,2.), right orbital medial wall. Infraorbital adipose tissue herniated through ethmoid cellaes. The swelling of his eyelid went down in hours. And he discharged from emergency medicine department. Keywords: Fork, swallow, surgery

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
391
P 375 RARE CAUSE OF FATIGUE: PRIMARY ADRENAL INSUFFICIENCY Mehmet Efe, Sercan Yalçınlı Ege University Faculty of Medicine, Department of Emergency Medicine, Izmir, Turkey Introduction: Adrenal insufficiency is a condition in which the adrenal glands cannot produce adequate amounts of hormones from adrenal gland’s cortex. The annual incidence is about 1-4 in 100.000 people. Primary adrenal insufficiency or Addison Disease is related to adrenal gland dysfunction. Production of aldosterone and cortisol decreases. The diagnosis and treatment of this disease is vital and it is hard to diagnose in Emergency Department (ED) because of it’s nonspecific symptoms and findings.��
Case: A 66 years old male admitted to ED with fatigue, vomiting and weight loss. His blood pressure was 62/41 mmHg. Other vital signs were normal. Physical examination was normal except hyperpigmentation in his face, hands and tongue. Urea: 107, Creatinine: 2,12, Na: 118, K:6,3 and Cl: 86 was detected in his lab results as abnormal. After through examination we learned that his fatigue existed for one year. With the suspicion of adrenal insufficiency, ACTH and Cortisol tests were performed. ACTH:1250, Cortisol: 0,54 detected and the patient admitted to internal medicine service with primary adrenal insufficiency diagnosis. Conclusion: ED physicians should suspect from primary adrenal insufficiency with the patients who admits to ED with fatigue, weight loss, hypotension and hyperpigmentation. Appropriate treatment should be started these patients to prevent them from acute adrenal insufficiency that occur in stress related conditions as infection, trauma, etc. Keywords: Chronic fatigue, diagnosis, primary adrenal insufficiency P 376 AXILLADA AKSESUAR MEME DOKUSU Hamza Çıldır, Emel Korkmaz, Başak Bayram
Dokuz Eylül Üniversitesi Tıp Fakültesi, Acil Anabilim Dalı, İzmir Giriş: Solid axiller kitle ile başvuran hastalarda lipom, lenfadenit, hidradenitis süppürativa, malignensi, seböze kistik lezyonlar olabilir. Biz daha nadir bir neden olan aksesuar meme dokusunun ultrasonografi ile saptanmasını sunuyoruz.��
Olgu: 32 yaşında kadın hasta acil servise koltuk altında şişlik yakınması ile başvurdu. 4 aydan beri mevcut olan şişlik yakınması, 10 gün önce yapmış olduğu doğumdan sonra daha belirgin hale gelmiş. Sağ memesinden süt gelmemesi, sağ meme ve koltuk altında şişlik ile birlikte ağrı olması nedeni ile başvurdu. Kan basıncı 123/71 mmHg, kalp hızı 69/dk, solunum sayısı 16/dk, vücut ısısı 36 °C, Oksijen satürasyonu %97 saptandı. Muayenede sağ meme ödemli, sağ koltuk altında 5*3 cm’lik şişlik mevcuttu. Sol meme altında meme ucu mevcuttu.�Hastanın koltuk altına yönelik yapılan ultrasonografisinde yaklaşık 5*2 cm boyutunda meme dokusu ile aynı ekojenitede fibroglandüler doku görüldü, doppler bakısında ise vaskülaritesi izlendi. Hasta takip amaçlı genel cerrahi poliklinik kontrolü önerilerek taburcu edildi. Tartışma: Polimasti; ikiden fazla meme dokusu olarak bilinmektedir. Genellikle axillar, parasternal, subclavicular, scapular, vulval ve göğüs duvarından kaynaklansa da en sık axilla yerleşimlidir. Axilla yerleşimli olan meme dokusu genellikle bilateral olmakla birlikte sıklıkla areola ve meme ucu eşlik etmez. Aksesuar meme dokusu hormon bağımlı olup genellikle gebelik ve laktasyon döneminde artış gösterirler.� Embriyolojik gelişim yönünden bakıldığında; 6. haftada meme süt çizgileri axiller bölgeden başlayıp kasığa kadar ilerlemekte olup normal gelişimde pektoral bölge dışındakiler geriler ve pektoral bölgedekiler 2 adet meme dokusunu oluşturmaktadır.�Ektopik meme dokuları malignensi gelişimi açısından riskli olduğu belirtildiği gibi axiller meme dokusundan fibroadenom saptanan vakalar mevcuttur. Kozmetik durumlarda ve semptomatik olduğunda cerrahi tedavi önerilse de; kesin tanı ince iğne aspirasyon biyopsisi ile konulmakta olup; laktasyon döneminde ilerleyen axiller meme dokusunun emzirme ile semptomların gerilediği bildirilmiştir. ��
Sonuç: Axiller kitle ile başvuran hastalarda lipom, lenfadenit, hidradenitis süppürativa, malignensi, seböze kistik lezyonlar ile birlikte aksesuar meme dokusu da akla getirilmelidir. Anahtar Kelimeler: Aksesuar meme dokusu, Aksiller bölge kitle, ultrasonografide meme dokusu

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
392
P 377 UNUSUAL SWALLOWED FOREIGN BODY: A FORK Selda Kıdak1, Çağdaş Yıldırım2, Alp Şener2, Mehmet Ergin1, Şervan Gökhan1
1Yıldırım Beyazıt University Faculty of Medicine, Ankara, Turkey 2Ankara Atatürk Training and Research Hospital, Ankara, Turkey A 16-year-old woman admitted our emergency department with the compliant of swallowing a fork. She swallowed a metal fork while she was trying to pull out a stuck fishbone to her pharynx. She hasn’t any diseases or drug use in her past medical history. Her white blood cell count was 11,2 K/uL. An abdominal X-ray was taken (Figure 1). The fork seen in her stomach. Gastroenterology and surgery consultations were requested. Endoscopy was contraindicated because of the sharp ends of the fork. Patient underwent to open surgery Keywords: Fork, swallow, surgery P 378 ACİL SERVİSTE NADİR BİR VAKA: PEDİATRİK İNME Emre Onur Tosun1, Yılmaz Uzun1, Rohat Ak1, Ebru Ünal Akoğlu1, Tuba Cimilli Öztürk1, Özge Ecmel Onur2
1Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul�2Marmara Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, İstanbul Giriş: İnme, serebral arter ve venlerdeki ani tıkanma veya rüptür sonucunda ortaya çıkan fokal serebral hasardır. Tıkanma arteriyel veya venöz olabilir. İnme, çocuklarda kronik morbidite ve mortaliteye yol açması nedeniyle önemli bir sağlık sorunudur. Çocukluk çağında görülme riski 8–10.7/100 000 çocuk/yıldır. İnmenin erişkinlerdeki en önemli sebebi arteroskleroz olmasına karşın çocukluk çağında inme sebepleri çok sayıdadır ve değişkendir. Olası nedenlerin geniş listesine rağmen inmeli çocukların %50’sinde primer bir bozukluk bulunamamaktadır. Olgu: 3 yaşında kız hasta acil servisimize 2 gündür uyku hali ve sabah başlayan konuşma bozukluğu, kuvvetsizlik ve yürüyememe şikayetleri ile başvurdu. Özgeçmişde hastalık hikayesi ilaç kullanımı hikayesi yok. Ailede akraba evliliği erken ölüm, svo veya mı öyküsü yok. Ta: 95/65 spo2: 98 nabız: 96 ateş: 36,7 pukş: 85. Fizik muayene bulguları gks: 15 Sol santral fasiyal paralizi mevcut. Işık refleksi bilateral doğal. Kuvvet muayenesi; Sol taraf ekstremitlerde 4/5 sağ taraf ekstremiteler 5/5. Meningeal irratasyon bulguları yok. Babinski bilateral fleksor, klonus bilateral negatif. Ataksi mevcut. Nörolojik bulgular dışında fizik muayene doğal. Hastaya diffüzyon mr çekildi. Mr neticesinde sağ kaudal nukleus, koronaradiata ve putamen lokalizasyonunda diffüzyon seansında hiperintens ADC haritasında akut infarkt izlenmektedir. Dispril 150 mg ve clexane 0.15 sc uygulandı. Dış merkez çocuk servisine yatışı yapıldı clexane devam edilmiş. Trombofili paneli gönderilmiş. Takiplerinde nörolojik muayenesindeki bulguları gerilemekte olan hastaya fizyoterapi önerilerek ve kontrole çağrılarak taburcu edilmiş.��
Tartışma: İskemik inmenin erken tanısında magnetik rezonans görüntüleme (MRG) BBT’den daha üstündür ve tercih edilen görüntüleme yöntemidir. Erişkinlerdekinin aksine çocuklarda Akut İskemi İnme(aii) ve Sinüs Ven Trombosunda antikoagülan kullanımı ile ilgili geniş çalışmalar yoktur. Çocuklarda düşük molekül ağırlıklı heparin akut antikoagülan tedavisinde ilk seçenek haline gelmiştir. Aİİ’de tekrarlama oranı %6-30’dur. Rekürensler genelde ilk 6 ay içinde görülmesine karşın ilk olaydan birkaç yıl sonra da rekürens bildirilmiştir. Çocuklarda Kanada verilerine göre Aİİ’ye bağlı ölüm %10, nörolojik defisit oranı da %56 olarak bildirilmiştir Anahtar Kelimeler: Akut iskemik inme, çocuklarda inme, santral fasiyal paralizi

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
393
P 379 HİDROKSİZİNE BAĞLI DİZARTRİ Nezih Kavak1, Hasan Sultanoğlu1, Rıdvan Sarıkaya2, Seda Özkan1
1Ankara Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Ankara 2Kastamonu Doktor Münif İslamoğlu Devlet Hastanesi, Kastamonu Giriş: Allerjik ürtiker sentetik ürünlere maruziyetin arttığı günümüzde, acil servise sık başvuru nedenlerindendir Antihistaminikler bu durumda tedavi için ilk tercih edilen farmakolojik ajanlardır. Bu durum acil serviste sık ve nadir görülen yan etkiler ile karşılaşmamıza neden olmaktadır. En sık yan etkiler; sedasyon, ağız kuruluğu, bulanık görme, taşikardi, idrar, retansiyonu, kabızlık, sinirlilik şeklindedir. En sık ve bilinen klasik yan etkilerinin dışında nadir yan etkilerde görülür.��
Olgu Sunumu: 27 yaşında bayan hasta acil servise konuşmada zorlanma, konuşmasında bozulma şikayetiyle başvurdu. Hastanın ilk bakıda dizartrik konuşması olduğu görüldü. Hastanın alınan anamnezinde alerjik ürtiker için tedavi başlandığı ve hidroksizin 25 mg etken maddesini içeren ajanı ilk defa aldıktan sonra dizartrisinin başladığı öğrenildi. Hastanın vitalleri normal idi. Hastanın nörolojik muayenesi normal idi. Hastanın laboratuvar tetkikleri normal idi. Hastanın akut dizartrisine sebep olacak durumları ekarte etmek amacıyla beyin tomografisi, kraniyal manyetik rezonans ve diffüzyon manyetik rezonans çekildi. İncelemelerde herhangi bir patolojik görünüm olmadığı saptandı. Hasta gözlem altına alındı. Hastaya yakın vital takibi yapıldı, bu takiplerinde patolojik bir değer saptanmadı. Hastanın acil serviste 12 saatlik takibi sonucunda klinik durumunun düzelmesi üzerine, hasta önerilerle taburcu edildi.��
Sonuç: Antihistaminikler alerjik hastalıklar, anaflaksi, ürtiker, anjionörotik ödem, böcek sokmaları, taşıt tutması, vertigo, saman nezlesi gibi durumlar da en sık kullanılan ajanlardır. Bundan dolayı nadir görülen yan etkiler bakımından acil servis hekimlerinin dikkatli olması gerekmektedir. Anahtar Kelimeler: Hidroksizin, antihistaminik, dizartri P 380 TRAUMA INDUCED HERPES ZOSTER OPHTHALMICUS Emre Şancı, Sedat Yanturalı, Feride Fulya Coşkun
Dokuz Eylül University Hospital, Department of Emergency Medicine, Izmir, Turkey Introduction: Herpes zoster is an acute, cutaneous viral infection caused by the reactivation of varicella-zoster-virus. It classicly presents itself with erythematous papules, which quickly evolve into grouped vesicles or bullae. Herpes zoster manifests in many ways; such as herpes zoster ophthalmicus, herpes zoster oticus. Individuals older than 70years and immunocompromised persons have a higher incidence of infection. Viral reactivation is relevant to smoking, trauma, antiviral therapy and stress. Case Presentation: A 31 year old male presented to emergency department for evaluation of vesculopapuler rashes on his forehead. His only complaints were headache and rashes on his forehead. He did not had prior medical history and his vital signs were normal. Patient had a head trauma history which had been 7 days before admitting to hospital and skin lesions started 6 days after trauma. In his physycal examination, He had a vesıculopapuler rashes(pic.1), the pupils were regular, light reflexes were preserved and he had no limitation of ocular movements or diplopia. He had eyelid edema and pytergyum on nasal side of left eye.(Pic.2) After initial evaluation patient at emergency department he is admitted to hospital for 7 days and during his admission also diagnosed with diabetes, after complete recovery discharged and called for weekly follow-up. Discussion: Even though trauma is a well-known predisposant factor of herpes virus reactivation, trauma induced opthalmic herpes zoster is rare. It has serious complications such as post-herpetic neuralgia, chronic ocular inflammation or even loss of sight. The treatment consists corticosteroids combination with antiviral and nonsteroidal anti-inflammatory agents. Because there is an increased risk of disseminated infection with corticosteroids, steroids should not be initiated without ophthalmologic consultation. Early diagnosis and promp treatment is important in herpes zoster due to its association with the risk of dissemination. A meticulous injury inspection is important with any patient with trauma Keywords: Herpes zoster, herpes zoster ophthalmicus, trauma

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
394
P 381 AN UNUSUAL CAUSE OF PULMONARY EDEMA: AORTIC COARCTATION BY PASS GRAFT THROMBOSIS Çağdaş Yıldırım1, Yunus Emre Arık1, Fatih Tanrıverdi2, Gülhan Kurtoğlu Çelik1, Şervan Gökhan2
1Ankara Atatürk Training and Research Hospital, Ankara, Turkey 2Yıldırım Beyazıt University Faculty of Medicine, Ankara, Turkey A 43-year-old man admitted to our emergency medicine department with the complaint of shortness of breath, back pain and hemopytisia. Also relatives of patient stated that he has had paresis on his legs at same day. He has a past surgical history of aortic coarctation by pass graft repair 15 years ago. His right radial and femoral pulses are weaker than left radial pulse. He has rales on entire lungs. Blood pressure measured from both arms. Left arm blood pressure was 200/100 mmHg and right arm was 140/90 mmHg. His heart rate was 154 beats/ min and it was normal sinus rhytm. Pulmonary edema treatment was administered. A thorax CT angiography was performed. There wasn’t any stream at by pass graft (figure 1) and there was aortic coarctation between grafts. Patient transferred to coronary care unit. Then balloon angioplasty and stent placement was successfully performed. Patient died from multiple organ failure next day. Keywords: Aortic coarctation, bypass graft, pulmonary edema
P 382 PNÖMONİ İLE KOMPLİKE MYOPERİKARDİT OLGUSU
Tuğçe Köksal, Onur Karakayalı, Sırmagül Topuk, Emrah Çelik, Kübra Selçok, Ramis Ufuk Akkoyunlu Kocaeli Derince Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Kocaeli Giriş-Amaç: Miyoperikardit, perikardın ve altındaki miyokardiyal dokunun hücresel hasarı ve inflamasyonu ile karakterize hastalıktır. Semptom ve bulguları belirsiz ve hastalığa özgü olmadığı için, genellikle klinik olarak miyoperikardit tanısı koymak güçtür. Miyoperikardit’in en sık nedeni viral enfeksiyonlardır; ancak nadir de olsa bakteriyel enfeksiyonlar sırasında da miyoperikardit görülebilir. Solunum yolu hastalıkları semptom ve bulguları ile acil servise başvuran pnomoni tanısı alan EKG bulguları normal olmasına rağmen ileri tetkik sonrasında komplike miyoperikardit tanısı alan vakamızı tartışmayı amaçladık. Olgu: On yedi yaşında erkek hasta ateş, öksürük, batıcı vasıfta göğüs ağrısı, sırt ağrısı ve bir gün önce başlayan yaklaşık bir dakika süren sol kolda uyuşma hissi yakınmaları ile acil servise başvurmuştur. Yapılan solunum sistemi muayenesinde sol akciğer bazalinde ral mevcut olup kardiyovasküler muayenesinde patoloji saptanmadı. Laboratuvar incelemelerinde WBC:9.2, C-reaktif protein 60,troponin 20.970, CK-MB 39.35 olan hastanın posterio-anterior akciğer grafisinde akciğer sol orta lobda lokalize pnömonik infiltrasyon izlendi. EKG de normal sinüs ritmi mevcuttu. Kardiyak enzim yüksekliği nedeniyle yapılan EKO bulguları miyoperikardit ile uyumlu saptandı. İleri tetkikler sonrasında hastaya pnömoni ile komplike miyoperikardit ön tanısı ile kardiyoloji kliniğine yatış verildi. Tartışma: Bakteriyel miyoperikardit primer veya başka bir bölgedeki enfeksiyonun (pnömoni, septik artrit, menenjit) yayılımına sekonder oluşabilir ve en sık etkeni Streptococcus pneumoniae’dır. Tipik bakteriyel pnömoni bulguları olan hastalarda eşlik eden göğüs ağrısı varsa hastanın öncellikle EKG ile değerlendirilmesi, gerekirse ileri kardiyak incelemeleri yapılması, eşlik edebilecek perikardit ve/veya miyokarditin saptanmasını sağlar. Böylece enfeksiyon tedavisine ek olarak gerekli destek tedavisi uygulanabilir. Sonuç: Acil servise tipik solunum yolu enfeksiyonu bulguları ile başvuran hastalarda göğüs ağrısı eşlik etmesi durumunda miyoperikardit ayırıcı tanı olarak düşünülmelidir ve ileri tetkik ile değerlendirilmelidir. Anahtar Kelimeler: Pnomoni, miyokardit, perikardit, solunum sistemi

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
395
P 383 PRES SENDROMUNA BAĞLI BİLATERAL GÖRME KAYBI
Nezih Kavak1, Hasan Sultanoğlu1, Burcu Doğan1, R.Pelin Kavak2
1Ankara Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Ankara 2Ankara Numune Eğitim ve Araştırma Hastanesi, Ankara Giriş: Posterior reversible ensefalopati(PRES) günümüzde artık sık rastlanan, farklı etiyolojilere bağlı olarak çıkan, genellikle geri dönüşümlü olan bir sendromdur. Manyetik rezonans(MRG) inceleme bulgularının tipik olması nedeniyle bu olguyu literatür bulguları eşliğinde sunmak istedik. Olgu: Daha önceden var olan böbrek taşı olan hasta, ağrısının şiddetlenmesi nedeniyle acil servise başvurdu. 49 yaşındaki bayan hastaya intramusküler diklofenak sodyum yapıldı ve bu enjeksiyondan yaklaşık 5 dakika sonra görme bozukluğu ve baş ağrısı şikayeti oldu. Hastanın ölçülen kan basıncı 230/160 mmHg idi. Pupilleri izokorik, direkt ve indirekt ışık refleksi normal, motor ve duyu muayenesi doğaldı. Hastanın hipertansiyonu için parenteral nitroprussid (0.5 mcg/ kg/dakika) infüzyon başlandı. Yaklaşık 15 dakika sonra hastanın yaygın vücut kasılmaları oldu. Laboratuvar değerleri ve çekilen kranial bilgisayarlı tomografisinde patolojik bulgu saptanmadı. Hastanın MRG incelemesinde FLAİR ve T2 ağırlıklı görüntülerde parietal ve oksipital loblarda kortikal ve subkortikal alanlarda bilateral, simetrik hiperintens sinyal değişiklikleri izlendi. Hastanın kliniği de göz önüne alındığında PRES sendromu lehine değerlendirildi. Şonuç: PRES hızlı tanı ve tedavi yapıldığı durumlarda hastalar birkaç hafta içinde tamamen iyileşir. Aksi halde klinik durum iskemi, masif infarkt hatta ölüme kadar ilerleyebilir. Sendromun kliniğinde spesifik olmayan bulgular olmasına rağmen, MRG bulgularının çarpıcı ve tipik olması nedeniyle sunmak istedik. Anahtar Kelimeler: Diklofenak sodyum, MRG, posterior reversible ensefalopati, PRES
P 384 COMPARISON OF PSI, CURB-65 AND CIRS-G SCALES IN ELDERLY PATIENTS
Elif Burcu Garda1, Özge Ecmel Onur2, Tuba Cimilli Öztürk1, Onur Yeşil1, Arzu Emecan1
1Fatih Sultan Mehmet Training and Research Hospital, Emergency Medicine Clinic, İstanbul, Turkey 2Marmara University, Pendik Training and Research Hospital, Department of Emergency Medicine, Istanbul, Turkey Introduction: Pneumonia; especially in elderly patients, taking place at the top among the causes of death and therefore the leading causes of hospitalizations worldwide. Therefore, various disease rating indices are used for the most appropriate evaluation, hospitalization decision and prediction of mortality. Our objective in this research is to find out the correlation between the CURB-65 (Confusion, Urea, Respiratory Rate, Blood Pressure, 65 years), PSI (Pneumonia Severity Index) and CIRS-G (Cumulative Illness Rating Scale for Geriatrics), to predict the mortality and the hospitalization rates of elderly patients. Methods: Our study was a prospective and observational study. Patients were classified according to CURB-65, PSI and CIRS-G. They were called back after 1 month and 3 months after their applications and questioned about their survey, hospitalization and admission to intensive care units. Results: 168 patients were included in our study. Comparisons of CURB-65, PSI and CIRS-G showed that CIRS-G’s worthiness was less than CURB-65 and PSI at the prediction of one-month survey and there was no statistically significant difference between CURB-65 and PSI. Also, PSI’s worthiness was higher than CURB-65 and CIRS-G at the prediction of hospitalization and there wasn’t statistically significant difference between CURB-65 and CIRS-G. Also we found out that PSI is the most valued scale at the prediction of mortality. Conclusion: In our study, it was found that all of these three scales could be used to predict the mortality, hospitalization and one-month survey rates. But, CIRS-G wasn’t as valuable as CURB-65 and PSI at the prediction of one-month survey. Also, PSI was more valuable than CURB-65 and CIRS-G at the prediction of hospitalization. When we evaluated the CIRS-G and CURB-65 together, results were closer to PSI’s value than CIRS-G’s, but still wasn’t as valuable as PSI and CURB-65. Keywords: CIRS-G, CURB-65, geriatrics, pneumonia, PSI

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
396
P 385 SSS ENFEKSİYON VE KOMPLİKASYONLARININ RADYOLOJİK BULGULARI
R.Pelin Kavak1, Nezih Kavak2
1Ankara Numune Eğitim ve Araştırma Hastanesi, Ankara 2Ankara Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Ankara Giriş: Santral sinir sistemi enfeksiyonlarının ve komplikasyonlarının görüntüleme bulgularını acil servis doktorlarına sunmak amacımızdır. Olgu sunumları: Çeşitli bakteriyel ve viral nedenlerle meydana gelen santral sinir sistemi enfeksiyonlarının ve komplikasyonlarının(menenjit, ensefalit, beyin apsesi, subdural apse, sinus tromboflebiti) radyolojik bulgularını değerlendirmek. Sonuç: Acil servise sık başvuru nedenlerinden biri olan ateşin etiyolojisi arasında yer alan santral sinir sistemi enfeksiyonları ve komplikasyonlarının radyolojik bulgularını literatür eşliğinde değerlendirmek istedik. Anahtar Kelimeler: Diffüzyon inceleme, santral sinir sistemi enfeksiyonları, MRG
P 386 PROBLEM: CHEST PAIN, SOLUTION: CARDIAC ULTRASOUND
Funda Karbek Akarca, Sercan Yalçınlı
Ege University Faculty of Medicine, Department of Emergency Medicine, Izmir, Turkey Introduction: Mc Connell’s sign is described as hypo- or akinesis of the right ventricular free wall with preservation of the apex. This sign is associated with acute pulmonary embolism (PE). We presented a patient who have unclear signs, but have typical cardiac ultrasound finding for PE diagnosis. Case: A 66 years old woman patient admitted to Emergency Department (ED) with chest pain, fatigue and palpitation. On admission her vital signs were a Glasgow coma scale of 15, tympanic temperature 36,4 °C, respiratory rate 21 counts/min, heart rate 88 beats/min, blood pressure 108/59 mmHg and the saturation O2: 95% at the room air. On physical examination, she had a left leg cast related with malleolus fracture before 10 days. She had hypertension as a chronic disease on history. Initial laboratory studies showed that troponin T: 96 ng/L, D-dimer >4236.4 µg/L. There was no abnormal findings on electrocardiography. Point of care focused cardiac ultrasound was performed for patient for prediction of possible diseases because of abnormal D-dimer and troponin levels and chest pain. On cardiac ultrasound; right ventricular (RV) and inferior vena cava dilatation, 3rd degree tricuspid regurgitation and 1st degree aortic regurgitation were found. RV ejection fraction (EF) was 55%. Left ventricular EF was normally. Although preserved apex contractility, free wall hypokinesis of right ventricular was determined. Computed tomography was performed for patient considering PE. At the end of the analysis patient was hospitalized for PE. Conclusion: Patients who have atypical complaints for pulmonary embolism can be scanned at bedside with cardiac ultrasound. Mc Conell’s Sign may be helped as an indicator of acute pulmonary embolism for emergency physicians. Keywords: Cardiac ultrasound, Mc Connell’s sign, pulmonary embolism

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
397
P 387 DİPİRİDAMOL İLE İNTİHAR
Nezih Kavak1, Rıdvan Sarıkaya2, Hasan Sultanoğlu1, Burcu Doğan1, Seda Özkan1
1Ankara Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Ankara 2Kastamonu Doktor Münif İslamoğlu Devlet Hastanesi, Kastamonu Giriş ve Amaç: İntihar ciddi bir sosyal sorun teşkil etmektedir. Tedavi amaçlı kullanılan ilaçlar ile intihar sık karşılaşılan bir durum olup hayati tehlikeye sebebiyet vermektedir. Olgu Sunumu: 19 yaşında bayan hasta acil servise ajitasyon, bulantı kusma, baş dönmesi, bilinç bulanıklığı şikayetiyle getirildi. Hastanın yakınlarından alınan anamnezinde 3 saat önce intihar amaçlı dipiridamol 75 mg içeren antitrombotik ajandan 90 adet aldığı öğrenildi. Hastanın vitalleri TA:140/90 nabız 74 atım/dk SS 22,ateş 36,2 idi. Hastanın fizik muayenesinde, ataksik yürüyüş, nistagmus, intansiyonel tremor mevcut idi. Hastaya mide lavajı yapıldı aktif kömür verildi. Hastanın laboratuvar sonuçları normal idi. Hastanın mevcut klinik durumunun gerilememesi ve bilinç bulanıklığının devam etmesi üzerine hastaya beyin tomografisi çekildi. Çekilen beyin tomografisinde sağ serebellar hematom saptandı. Hastaya antiödem tedavi olarak mannitol 1 mg/kg intravenöz olarak başlandı. Antiepileptik olarak fenitoin 3x100 mg intravenöz olarak başlandı. Hasta yoğun bakım ünitesine yatırıldı. Sonuç: İnraserebellar hematom etiyolojisinde, hipertansiyon,v asküler anomaliler, vaskülitler, serebral amiloid anjiopati, hematolojik bozukluklar, tümörler, ilaçlar mevcuttur. Bu vakada olduğu gibi ilaca bağlı intraserebellar hematom nadir görülen ve hayatı tehdit eden bir durumdur. Acil servise intihar amaçlı ilaç alımı sık başvuru nedenleri arasında olup dikkatlice incelenmesi gereken bir durumdur. Anahtar Kelimeler: Dipiridamol, intihar, serebellar hematom
P 388 PERİPARTUM DİSPNE MASUM MUDUR?
Melih Çamcı, Cahit Teke, İsmail Erkan Aydın, Mehmet Ergin, Ayhan Özhasenekler Yıldırım Beyazıt Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Ankara Giriş-Amaç: Peripartum kardiyomiyopati (PPKM), gebeliğin potansiyel olarak hayati tehlike arz eden komplikasyonlarından olarak bir dilate kardiyomiyopati formudur. Altta yatan kesin neden belli olmamakla birlikte enfeksiyonlar, myokardit, immünolojik faktörler, prolaktinin neden olduğu oksidatif stres gibi birçok neden suçlanmaktadır. Peripartum kardiyomiyopati, gebeliğin son 4 haftası ve postpartum 5. aylar arasında görülmektedir. Yüksek anne ve bebek mortalitesi ile ilişkilidir (%25 ile %50 arasında). Olgu sunumumuzda postpartum gelişen PPKM olgusunun acil servis yönetimini tartışmayı amaçladık. Olgu: 29 yaşında kadın hasta, acil servisimize son 10 gündür olan nefes darlığı, bacaklarda ve ayaklarda şişlik, göğüs ağrısı şikayeti ile başvurdu. Hikayesinde 3 yıllık evli, gravida 2, parite 2 olduğu öğrenildi. Hasta acil servise başvurusundan 4 gün önce spontan vajinal yolla doğum yapmış. Fizik muayenesinde solunum sisteminde bilateral alt zonlarda akciğer sesleri azalmış ve ralleri tespit edildi. Bilateral gode bırakan 3+ pretibial ödemi vardı. Vital bulgularında, KB:135/75mmHg, Nb: 76/dk, SaO2: %94 Solunum sayısı:22/dk olarak saptandı. EKG normal sinüs ritmindeydi. Laboratuar sonuçları arasında Hgb:10.7 mg/dL, pH:7.40, PCO2:38.3mmHg, pO2:85 mmHg, HCO3: 22 mmol/L, D-dimer: 2946.2 ng/ml idi. Alt ekstremite venöz Doppler USG’de derin ven trombozu yoktu. Hasta için dispne ayırıcı tanısında pulmoner emboli ve peripartum kardiyomiyopati ön tanıları düşünüldü. Yapılan ekokardiyografisinde sol ventrikül global hafif hipokinetik, EF:%40-45, MY: 1 TY: Eser PAB: 25mmHg ve sağ boşluklar normal olarak raporlandı. Peripartum kardiyomiyopati tanısı ile takip ve tedavi amacıyla koroner yoğun bakım ünitesine yatırıldı. Tartışma-Sonuç: Gebelik, kardiyovasküler sistem üzerine ek yük getiren fizyolojik bir durum olmasına rağmen buna ilave olacak bir kardiyak hastalık, sorunların ağırlaşmasına sebep olabilmektedir. Klinisyenin dikkatli ve kuşkucu, hastalığa ise aşina olması hızlı tanı ve doğru tedavi olasılığını arttırır ve prognozu en iyi hale getirir. Amaç, erken dönemde tanı koyarak kalp yetmezliği semptomlarının iyileştirilmesi ve mortalitenin azaltılmasıdır. Tedaviye erken başlanan olgularda prognoz daha iyidir. Anahtar Kelimeler: Dispne, gebelik komplikasyonları, kardiyomiyopati

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
398
P 389 NADİR GÖRÜLEN MORTALİTE NEDENİ: GAZLI GANGREN
Eren Usul, Kerim Abatay, Uğur Kahveci, Seda Özkan Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Ankara Giriş-Amaç: İnsanları etkileyen en ağır seyirli nekrotizan enfeksiyon şüphesiz gazlı gangrendir. Clostridium ailesine ait invaziv enfeksiyon oluşturan 30 tür arasında en sık (%90) gazlı gangren sebebi Clostridium perfringens’tir. Toprakta, kanalizasyon sisteminde, insanların ve birçok hayvanın gastrointestinal ve genitoüriner sistem mikrofloralarında bulunabilir. Genellikle travma ve cerrahi ile ilişkilidir. Acil serviste özellikle travma sonrası yara değerlendirilmesinde düşünülmesi gerekmektedir. Vakamızda nadir görülen bir gazlı gangren sunduk. Olgu: Elli dokuz yaşında erkek hasta acil servise bir gün önce sağ el dorsumundan başlayıp dirseğe doğru yayılan şişlik, morluk ve ağrı şikayetleri ile acil servise başvurdu. Acil servise başvurusunda arteriyel kan basıncı 140/80 mmHg, nabız 90 vuru/dk, solunum sayısı 13/dk, vücut ısısı 38,20C idi. Fizik muayenede; hastanın bilinci açık, koopere ve oryante idi. Hastanın sağ dirseğine kadar morluk, ödem ve cilt altı amfizem mevcuttu. Diğer sistem muayeneleri normal olarak değerlendirildi. Hastanın özgeçmişinde DM(+) ve lösemi olduğu; yaklaşık 1 hafta önce motorlu araç kazası geçirdiği ve sağ elinden kesici yaralanması olup toprakla teması olduğu öğrenildi. Enfeksiyon hastalıkları ve ortopedi ile konsülte edilen hastaya geniş spektrumlu antibiyotik tedavisi başlanıp ampütasyon için cerrahi hazırlıklara başlandı. Laboratuvar bulgularında; hemoglobin 12,2 g/dL, hematokrit %36,0, lökosit 58,500/mm³ (%86 PMNL, %14 lenfosit), trombosit 5,000/mm³ tespit edildi. Hastanın ameliyat öncesi hazırlıkları sırasında genel durumu bozuldu ve hasta entübe edildi. Takiplerinde arrest olan hasta gereken müdahalelere rağmen eks oldu. Sonuç: Gazlı gangren acil tanı konulması ve süratle tedavi edilmesi gereken nadir görülen bir enfeksiyondur. Özellikle diyabet, malignite gibi yatkınlığı artıran faktörlere sahip hastalarda, çok ender karşılaşılmasına rağmen yaşamı tehdit edecek şekilde ağır seyreden bir hastalıktır. Erken tanı, antibiyotik tedavisi ve özellikle de cerrahi müdahale ile tedavide başarı elde edilebilmektedir ve mortalite azalmaktadır. Anahtar Kelimeler: Gangren, sepsis, mortalite P 390 SIGNIFICANT DILATATION OF DISTAL COLON, OGYLVIE SYNDROME Ayça Çalbay, Abdullah Osman Koçak, Alparslan Ünlü, Fatma Tortum Atatürk University Faculty of Medicine, Department of Emergency Medicine, Erzurum, Turkey Introduction: Ogylvie syndrome is a gastrointestinal system disease which is characterized with significant dilatation of distal colon in the absence of mechanical obstruction. Most popular mechanisms in the pathogenesis is the sympathetic-parasympathetic imbalance of neurostimulators specially on the sacral 2-4 and N. Vagus. Case: A 17 year old young man came to our emergency department with altered mental status after a car accident ten days before. The patients vital signs as following: TA: 129/77mmHg, Pulse: 99/min, Fewer: 37,5ºC, O2 sat: 100% (intubated). His Glasgow coma scale was 6 and he was intubated. Except the leukocytosis the laboratory tests were in normal range. He had diffuse erythematous eruption on his chest, neck and extensor sides of four extremities. We had to brain, chest, abdomen and vertebra computerized tomography with contrast and x-ray scans because of high energy trauma. Colonic dilatation with full of contrast and hemorrhagic brain contusion seen on tomography scans. Patient consulted with general and brain surgery physicians. The general surgery physicians performed to paracentesis to him. The paracentesis content was hemorrhagic so they took him to surgery room for exploration for the suspicion of intraabdominal haemorrhgy and perforation. Just pseudo obstruction and reactionary mai seen on the exploration. After the hospitalization on anesthesia service for four days the patient transferred to brain surgery service. Klebsiella pneumonia increased on throat culture during his hospitalization time. He was evaluated as Ogylvie syndrome. He took a week health service on anesthesia and brain surgery services and discharged with healthy. Result: Ogylvie syndrome having no specific clinic and laboratory criteria. İt can be misdiagnosed easily if not preoperatively presumed. Surgeon should be aware of this diagnosis when he faces with acute large bowel obstruction in emergency services. Early diagnosis and therapy decreases the incidence of mortality and morbidity Keywords: Colonic aobstruction, Ogylvie syndrome, dilatation

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
399
P 391 ACİL SERVİSTE NADİR GÖRÜLEN BEL AĞRISI NEDENİ: KAUDA EKUNİA SENDROMU
Eren Usul, Ali Halıcı, Ali Şahin, Seda Özkan Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Ankara Giriş-Amaç: Acile başvuran bel ağrılı hastalar göz önüne alındığında kauda ekuina sendromu, lomber disk herniyasyonunun nadir görülen ciddi bir klinik tablosudur. Tanıda esas olan idrar ve/veya anal sfinkter fonksiyon bozukluğunun mevcudiyetidir Acil serviste sık karşılaşılan bel ağrısının ayırıcı tanısında düşünülmesi gerekmektedir. Vakamızda nadir görülen bir kauda ekuina sendromu sunduk. Olgu: Elli iki yaşında erkek hasta 4 aydır bel ve sol bacakta siyataljik tarzda ağrı yakınması mevcutmuş. Acil servise sabah başlayan anüsün sol yaninda ve skrotumda uyusukluk hissetmesi, idrar ve gaita inkontinansı, ardından perianal bölge ve skrotumda his kaybı şikayetleri ile acil servise başvurdu. Acil servise başvurusunda arteriyel kan basıncı 120/70 mmHg, nabız 80 vuru/dk, solunum sayısı 12/dk, vücut ısısı 37,2 0C idi. Fizik muayenede, hastanın bilinci açık, koopere ve oryante idi. Öz ve soy geçmişinde; 4 yıldır LDH nedeni ile ara ara fizik tedavi ve rehabilitasyon uygulanmış. Sistem muayeneleri doğal olarak değerlendirildi. Nörolojik muayenede kas gücü tam, tendon refleksleri normoaktif, S2, S3 ve S4 dermatomal hipoestezi var, anal sfinkter tonusu azalmış olarak değerlendirildi. Lomber magnetik rezonans incelemesinde, L5-S1 düzeyinde anterior epidural mesafeyi oblitere eden her iki nöral forameni daraltan disk herniasyonu görüldü. Hasta acilen nöroşirurji ile konsülte edilip operasyona alındı. Hasta sonrasında sekelsiz taburcu edildi. Sonuç: Lomber disk hernisi nedeni ile ortaya çıkan kauda equina sendromu. Acil tanı konulması ve süratle tedavi edilmesi gereken nadir görülen bir klinik tablodur. Acil cerrahi tedavi için en erken sürenin hastanın semptomlarının düzelmesi, dolayısıyla kaliteli yaşamı ile doğrudan ilişkilidir. Kuvvet kaybı ve bilateral siyatalji olmaksızın sadece duyu kusuru ve sifinkter fonksiyon bozukluğu ile gelen bilinen lomber disk hernisi olan hastalarda akılda tutulmalıdır. Anahtar Kelimeler: Kauda ekuina, bel ağrısı, lomber herni

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
400
P 392 MADDE KULLANIMINA BAĞLI RABDOMİYOLİZ GELİŞİMİ İLE İLİŞKİLİ AKUT BÖBREK YETMEZLİĞİ
Hasan Sultanoğlu1, Tuba Erdem Sultanoğlu2, Seda Özkan1
1Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Ankara 2Kazan Devlet Hastanesi, Fizik Tedavi ve Rehabilitasyon Kliniği, Ankara Amaç: Rabdomyoliz; travmatik veya nontravmatik nedenlere bağlı olarak çizgili kas hücrelerinin hasara uğraması ile oluşan klinik tablodur. Klinik seyir asemptomatik tablodan, hayatı tehdit eden hipovolemik şok, kardiyak aritmiler ve akut böbrek yetmezliğine kadar değişkenlik gösterebilir. Rabdomiyoliz nedenleri arasında ilaçlar, toksinler, enfeksiyonlar, kas travması, konvülsif nöbetler, hipertermi, elektrolit dengesizlikleri, kas enzim defektleri, kokain ve alkol kullanımı sayılabilir. Bu nedenler asidoz ve iskemiye neden olarak hücre yıkımına sebep olmaktadır. Beraberinde böbrek damarlarında kasılma, tübüler silendir oluşumu ve miyoglobinin yol açtığı toksisite radomiyolizin neden olduğu akut böbrek yetmezliğinden sorumludur. Bu yazıda ciddi klinik sonuçlara yol açabilmesi nedeniyle, madde kullanımı sonrası yaygın kas ağrısı, bulantı, kusma yakınmasıyla ile başvuran, öyküsü ve laboratuvar bulguları ile rabdomiyoliz tanısı konan ABY olgusunu sunmayı amaçladık. Olgu: 22 yaşında erkek hasta acil servise bir gün önce başlayan yaygın kas ağrısı ve sonrasında başlayan bulantı kusma şikayeti ile başvurdu. Hastanın anamnezinde bir yıldır aralıklı olarak eroin kullandığı ve bu şikayetler başlamadan bir gün önce eroin kullanımı olduğu öğrenildi. Öz ve soygeçmişinde özellik yoktu. Vital bulgularında A: 36 ºC, TA: 112/74 mmHg, Nb: 111/ dk sO2: 92 idi. Fizik muayenesinde patolojik bulgu yoktu. İdrar çıkışı mevcuttu. Laboratuvar değerlendirmesinde Üre: 103 mg/dl, Cre: 1.9 mg/dl, AST: 212 U/L, ALT: 80 U/L, CK: 8314 U/L, CK-MB: 197 U/L, K.: 4.9 mEq/lt, pH: 7.30 idi. Hastanın mevcut klinik ve laboratuvar bulguları sonucunda madde kullanımına bağlı rabdomiyoliz gelişimiyle lişkili akut böbrek yetmezliği tanısı konuldu. İntravenöz hidrasyon sonucunda hastanın klinik ve laboratuvar değerlerinde belirgin gerileme izlendi. Sonuç: Madde kullanımın giderek yaygınlaştığı günümüzde, potansiyel ve ölümcül olabilen rabdomyoliz gelişimi ile ilişkili ABY'nin bir nedeni olarak madde kullanımı akılda tutulmalıdır. Anahtar Kelimeler: Rabdomyoliz, ABY, madde kullanımı P 393 SPONDYLODISCITIS RELATED TO APPENDECTOMY Mevlana Ömeroğlu, Atıf Bayramoğlu, Fatma Tortum, Ayşe Şenyurt Atatürk University Faculty of Medicine, Department of Emergency Medicine, Erzurum, Turkey Spondylodiscitis refers to inflammation of vertebral corpus an intervertebral disc. Vertebral osteomyelitis and discitis are often used same meaning. Infections can reach this area by three way as hematogenous, direct inoculation from trauma, spinal procedures, spinal surgery and contiguous from adjacent soft tissue infections. The most common cause is hematogenous one and pathogen is S.Aureus. Other causes are enteric gram-negative bacilli, Pseudomonas and Candida, tuberculous infection and brucellosis. Diagnosing includes cultures, serology, imaging, and biopsy. Treatment should be administered with an antimicrobial regimen with activity against the common causes of vertebral osteomyelitis. 26-year-old man patient referred to our service with back pain. This complaint had started at fifth day of appendectomy operation one year ago. İnitial examination, whole system examination was normal. Only he had back pain which is exacerbated by physical activity or percussion. On neurologic examination, he had no new neurologic symptoms (paresthesia or paralysis). His vital signs were normal. Blood cultures are sterile and the CBC was normal. Biochemical investigations were unremarkable except positive C- reactive protein as 34 mg/dL. X-Ray graphy was not demonstrative. We performed MRI, it revealed high intensity edematous inflammatory appearance in vertebral corpus and end plates compatible with spondylodiscitis. Serologic studies did not suggested brucellosis, tuberculosis and spondyloarthropathies. İn our case, we presented a postoperative spondylodiscitis related to appendectomy. Postoperative spondylodiscitis had defined after lomber surgery, but we did not read any case at post appendectomy. The patient was late for the presentation about one year by the reason of the average diagnose time is 2-4 months. Because of delayed application, we found sterile culture. Brucellosis, tuberculosis and rheumatologic test were negative suggested our diagnosis as postoperative spondylodiscitis. Light of this information, clinicians should be keep in mind that recurrent back pain can be spondylodiscitis due to distant focus operation such as appendectomy. Keywords: Spondylodiscitis, appendectomy, postoperative spondylodiscitis

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
401
P 394 ACİL SERVİSTE ENDER BİR TANI: SİPROFLOKSASİN KULLANIMI SONRASI KOUNİS SENDROMU
Muharrem Doğan1, Demet Devrimsel Doğan1, Tanju Biçer1, Taygun Baykal1, Abdullah Taşcı1, Burcu Azapoğlu Kaymak1, Özge Ecmel Onur2
1Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul 2Marmara Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, İstanbul Giriş: Kounis sendromu, mast hücrelerinin etkileşmesi ile seyreden alerji, hipersensitivite, anaflaksi yada anaflaktoid reaksiyonlarla ilişkili olarak akut koroner sendrom gelişmesi durumudur. İlaçlar, böcek sokmaları, yiyecekler, çevresel etkenler ve intrakoroner stent yerleştirilmesi alerjik reaksiyonu tetikleyen neden olabilir. Hipersensitivite reaksiyonları basit ürtikerde şiddetli anjioödeme kadar değişen klinik tablolara sebep olabilir. Koroner vazospazm ve akut miyokard infarktüsü bu tablolardan biridir. Biz bu sunumda FMF dışında bilinen kronik hastalık öyküsü olmayan 45 yaşında erkek hastada siprofloksasin kullanımı sonrası gelişen akut miyokard infarktüsü-kounis sendromundan bahsedeceğiz. Vaka: 45 yaşında erkek hasta acil servisimize yaklaşım 2 saat önce başlayan baskı tarzında göğüs ağrısı ile başvurdu. FMF dışında bilinen kronik hastalık öyküsü yok ve kolşisin 0,5mg 3*1 dozunda kullanmakta. Acil servisimize başvurusundan yaklaşık 4 saat önce idrar yolu enfeksiyonu nedeniyle siprofloksasin 500mg tb alım öyküsü mevcut. Aynı ilacı daha önce hiç kullanmamış. Başvurusunda ateş: 37,1C nabız: 88atım/dk TA: 178/93mmHg sO2: %98 çekilen EKG’de anterior derivasyonlarda ST elevasyonu mevcuttu. Hastaya STEMI tanısı ile ASA, Klopidofrel, heparin ve nitrogliserin tedavileri uygun dozlarda başlandı. Nitrogliserin infüzyonu sonrası göğüs ağrısı gerileyen hasta invazif koroner girişim yapılabilecek merkeze sevk edildi. Koroner anjiografisinde koroner arterler normal olarak gözlendi. Sonuç: Kounis sendromu ile kez 1991 yılında tanımlanmıştır ve koroner arterlerde öncesinde aterom plağı olup olmamasına göre 2 tipe ayrılmaktadır. FMF geni olan E148Q ile olan ilişkisine dair literatürde yayınlar mevcuttur. Alerjenin alımından kısa süre sonra ortaya çıkan alerjik angina sendromu ani kardiyak ölüme kadar değişen klinik sendromlarla karşımıza çıkabilir. Bu nedenle böcek ısırığı yada herhangi bir alerjen maruziyeti sonrası gelişen göğüs ağrısı durumlarında kounis sendromu akılda bulundurulmalıdır. Anahtar Kelimeler: Kounis, hipersensitivite, AKS P 395 İLAÇ KULLANIMINA BAĞLI AŞİL TENDON RÜPTÜRÜ Hasan Sultanoğlu1, Tuba Erdem Sultanoğlu2
1Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Ankara 2Kazan Devlet Hastanesi, Fizik Tedavi ve Rehabilitasyon Kliniği, Ankara Giriş: Aşil tendonu insan vücudundaki en geniş ve en güçlü tendondur. Aşil tendon rüptürleri genellikle travmatiktir, spontan aşil tendon rüptürü ise oldukça nadirdir. Tendondaki yenileyen peritendinitis, tendinozis gibi dejeneratif değişiklikler, kronik steroid tedavisi, florokinolon grubu antibiyotik kullanımı rüptür için zemin hazırlar. Bu olguda antikoagülan kullanımına bağlı gelişen spontan aşil tendon rüptürünü sunmayı amaçladık. Olgu: 70 yaşında kadın hasta; sol topukta ağrı, şişlik ve ayağının üzerine kalkamama şikayetleri ile acil servise başvurdu. Hikayesinde travma olmadan, antikoagülan tedavi kullanımı sonrasında sol ayak bileği dorsalinde şişlik olduğu ve aniden sol bacağına keskin bir ağrının geldiği, ayağının üzerine yük vermede zorlandığı öğrenildi. Özgeçmişinde 20 yıldır kronik obstruktif akciğer hastalığı ve hipertansiyon, yeni tanı atrial fibrilasyon; 5 yıl önce koroner arter bypass girişimi mevcuttu. Komorbiditeleri için teofilin, inhaler steroid, anjiotensin dönüştürücü enzim inhibitörü, beta bloker, anti trombolitik kullanmaktaydı. Soygeçmişinde özellik yoktu. Fizik muayenesinde aşil tendonu üzerinde ekimoz mevcuttu. Palpasyonla tendonun bu bölgesinde hassasiyet ve gode bırakmayan şişlik tespit edildi. Hasta parmak ucunun üzerine yüklenip topuğunu yerden kaldıramıyordu. Laboratuvar değerlendirmesinde özellik yoktu. Hastanın ayak, ayak bileği direkt grafisi normal olarak değerlendirildi. Ultrasonografide aşil tendon bölgesinde hematom olduğu görüldü. Magnetik rezonans görüntülemede aşil tendonunun parsiyel yırtık olduğu belirlendi. Hastada antikoagülan kullanımına bağlı gelişen hematomun baskısı ile aşil tendonunda parsiyel rüptür tanısı konuldu. Hasta Fizik tedavi polikliniğine yönlendirildi. Sonuç: Aşil tendon rüptürü ile gelen hastalarda özellikle nontravmatik veya minör travmalar sonrası gelişenlerde ilaç kullanım öyküsü sorgulanmalıdır. Anahtar Kelimeler: Aşil tendonu, antikoagülan, nontravmatik rüptür

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
402
P 396 NADİR BİR BİLİNÇ DEĞİŞİKLİĞİ NEDENİ: NÖROLEPTİK MALİGN SENDROM
Muharrem Doğan1, Demet Devrimsel Doğan1, Taygun Baykal1, Tanju Biçer1, Azizcan Kılıç1, Özge Ecmel Onur2
1Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul 2Marmara Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, İstanbul Giriş: Nöroleptik malign sendrom; nöroleptik ilaçların kullanılmasıyla ilişkisi olan, santral nörotransmitterlerin inbalansıyla karakterize, dopaminerjik bloğun geliştiği düşünülen bir sendromdur. Nöroleptik ilaçların yanı sıra antidepresan, antikonvülzan, antiemetik ve antiparkinson ilaçların kullanımıyla da görülebilir. Yeni ilaç, düzensiz ilaç kullanımı ya yüksek doz kullanım ile tetiklenebilir. Yüksek ateş, kas rijiditesi, mental durum değişikliği, otonomik disfonksiyon ve yüksek CK seviyeleri ile karakterizedir. Vakamızda acil servise ateş ve bilinç bozukluğu ile başvurup haloperidol kullanımına bağlı nöroleptik malign sendrom tanısı konulan hastadan bahsedeceğiz. Vaka: 52 yaşında erkek hasta acil servisimize 2 gün önce başlayan yüksek ateş, bilinç değişikliği ve kollarında katılık yakınması ile başvurdu. 5 sene önce geçirilmiş iskemik SVO nedeniyle yatağa bağımlı olan hastaya 15 gün önce ajitasyonları nedeniyle 5mg/gün haloperidol başlanmış. Başvurusunda ateş: 38,9C nabız: 134/dk TA: 166/76 sO2: %97 genel durumu orta-kötü, bilinç uykuya meyilli, kooperasyonu kısıtlı ve verbal çıkışı yoktu. Laboratuar tetkiklerinde WBC: 18900/mm3, CK: 6700U/L kreatinin 2,4 saptandı. Kranial görüntülemesinde patoloji saptanmadı. Hasta nöroleptik malign sendrom ön tanısı ile yoğun bakım ünitesinde yatırıldı. Sonuç: Antipsikotik tedavideki doz değişiklikleri ve ilaçların aniden kesilmesi en önemli etyolojik faktörlerdir. Dehidratasyon, malnütrisyon, parenteral nöroleptik uygulanması, organik beyin hasarı varlığı, ileri yaş, erkek cinsiyet, demir eksikliği, minör enfeksiyonlar yatkınlaştırıcı faktörlerdir. DSM-IV ve Nierenberg nöroleptik malign sendrom tanı kriterleri tanı için en sık kullanılan kriterlerdir. Nöroleptik malign sendrom nadir görülmesine rağmen hayatı tehdit edici bir durumdur, bu nedenle erken tanı ve tedavisi büyük önem arz etmektedir. Anahtar Kelimeler: Nöroletpik, haloperidol, ateş P 397 DISLOCATION OF C4-C5 VERTEBRA IN MOTOR VEHICLE ACCIDENT VICTIM Utku Murat Kalafat, Serkan Dogan, Eren Sert, Rabia Birsen Tapkan, Elif Kececi, Tarık Ocak Kanuni Sultan Süleyman Training and Research Hospital, Department of Emergency Medicine, Istanbul, Turkey Introduction: Most fatal C-spine injuries occur in upper cervical levels, at either craniocervical junction C1 or C2. The most common site of cervical dislocation is between C5 and C6. There is very limited muscular support around C-spine area. It supports the weight of head, placing it at higher risk of sudden movements and whiplash injuries, which can cause damage to bones, ligaments, arteries, and more seriously to the cervical cord and the exiting nerve roots. Injuries to the C-spine cause neurological deficit in approximately 40% patients; 10% traumatic spinal cord injuries have no obvious roentgen graphic evidence of vertebral injury. We reported case of C4-C5 dislocation with none neurologic findings. Case: 26 years-old-man patient was brought to our emergency service due to motor vehicle accident. His vital signs and neurologic examinations were normal. He suffered from mild neck pain. His lateral cervical x-ray demonstrated cervical vertebra dislocation on C4-C5. His computerized tomography of cervical vertebra revealed that fractures of the left lamina of C3 and C4 vertebra and the left pedincule of C3 vertebra, and dislocation to anterior of C4 vertebra. The patient was transferred to further center for operation. Result: We want to emphasize that it should be high importance of the physical examination and apply to diagnostic imaging techniques in trauma patients. Keywords: Cervical vertebra, diagnostic techniques, dislocation

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
403
P 398 ATYPICAL LOCALIZATION OF ACUTE APPENDICITIS
Serkan Dogan, Rabia Birsen Tapkan, Utku Murat Kalafat, Ekim Saglam Gurmen, Ramiz Yazıcı, Tarik Ocak Istanbul Kanuni Sultan Süleyman Training and Research Hospital, Clinic of Emergency, İstanbul, Turkey Introduction: Abdominal pain is one of the most common symptoms that brings the patients to emergency services. Most of acute appendicitis besides abdominal pain requires a surgery. The defense and rebound during the physical examination at the lower quadrant are the signs of acute appendicitis. Different diagnosis can be considered other than appendicitis if the patient’s abdominal pain is not localized right lower quadrant. Therefore, it is possible to misdiagnose up to 30% of these patients. However, as in our case suprapubic pain can be a result of atypical localization of appendix, with this information the right diagnosis can be accessed. Case: The patient is 28 years old male who came to clinic with abdominal pain. The pain has been continuously repeated for three days. Overall, the patient’s vital signs are stable. The patient stated that the UTI has been diagnosed and treated in the past. During the patient’s physical examination it was seen that the patient was suprapubic sensitive, thus required laboratory examination and diagnostic imaging have been ordered to eliminate the other abdominal pathologies. Ultrasonography results indicated that in addition to minimal free fluids in the bowel loops; a rigid aperistaltic tubular image was detected. Furthermore, leukocytosis and high levels of CRP were observed in laboratory results. A surgery consultation and advanced imagining were requested to avoid any misdiagnosis. According to abdominal computerized tomography scanning a 7 mm variable appendix that was medial and superior from caecum was detected. Moreover, the wall of appendix was oedematous. The incidence of atypical clinical presentation of appendicitis also consulted with a general surgery and the patient took into operation. Result: Emergency physicians should take into account the incidence of atypical clinical presentation of appendicitis especially among the recurrent patients to avoid any misdiagnosis and possible complications. Keywords: Atypical localization, acute appendicitis, abdominal pain P 399 SUPRAVENTRİKÜLER Mİ? VENTRİKÜLER Mİ? Ali Karakuş1, Zeynep Kekeç2
1Mustafa Kemal Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Hatay 2Çukurova Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Adana Acil servislerde çarpıntı şikâyetiyle getirilen hastalarda taşikardi ayırıcı tanısı kısa zamanda doğru şekilde yapılıp acil tedavi planlanmalıdır. P dalgasının olmadığı yüksek ventrikül yanıtlı atrial fibrilasyonlar(AF), supraventriküler taşikardiler(SVT) ve ventriküler taşikardiler(VT) ayırıcı tanıda düşünülmelidir. Bu yazıda çarpıntı şikayetiyle acil servise getirilen SVT olarak kabul edilip tedavisi planlanan ancak prognozu kötüleşen hasta sunuldu. Olgu: 65 yaşında erkek hasta çarpıntı, bulantı, kusma genel durum bozukluğu nedeniyle acil servise götürülmüş. Hastaya SVT tanısı konmuş tedavisi verilmiş ancak düzelme olmayınca diğer bir hastaneye sevk edilmiş. Hasta acil servise getirildiğinde genel durumu orta, şuuru açık koopere. Tansiyonu alınamıyor, nabzı 180/dk idi. EKG sinde P dalgası yok, taşikardik, QRS dalgası 0.12 sn idi. Hasta VT olarak kabul edildi. Medikal tedaviye cevap vermeyen ve hemodinamisi bozuk olan hastaya sedasyon uygulanmasının ardından 1joule/kg dan kardiyoversion yapıldı. Kardiyoversiyon sonrası sinüs ritmine dönen ve vitalleri normal olan hastanın koroner yoğun bakımda takibine devam edildi. Düzenli ritmler olan SVT ve VT arasında ki fark QRS dalgasının SVT de dar(0.12 sn nin altında), VT de geniş(0.12 sn ve üzeri) olmasıdır. Arada kalınan olgularda VT olarak kabul edilip tedavi planlanmalıdır. Anahtar Kelimeler: Ventriküler taşikardi, QRS, kardiyoversiyon

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
404
P 400 EMPHYSEMATOUS PYELONEPHRITIS
Rohat Ak, Fatih Doğanay, Ali Şahiner, Tuba Cimilli Öztürk, Özge Ecmel Onur, Abide Merve Manap Fatih Sultan Mehmet Training and Research Hospital, Istanbul, Turkey Emphysematous pyelonephritis (EP) is a rare clinical condition characterized by the presence of gas in the renal system, most often in the parenchyma, but also extending to surrounding perinephric tissues. It is caused by gas-forming organisms, most commonly Escherichia coli (E. coli), in addition to Klebsiella, Clostridium, Candida, Aspergillus, Cryptococcus, and Amoeba. We presented a case of emphysematous pyelonephritis diagnosed on computerized tomography (CT). A 57 year old woman presented to the emergency department with right flank pain. She had had history of diabetes mellitus and hypertension. On admission, her vital signs were stable. Physical examination revealed costovertebral angle tenderness without rebound and guarding. The initial laboratory test showed a leukocytosis of 12.000/ul, hemoglobin of 11.3 g/dl, serum glucose of 254 mg/dl, urea of 18 mg/ dl, and creatinine of 0.69. Urinalysis showed 3+ erythrocyte, 3+ leukocyte and 3+ glycosuria. Non-contrasted CT of abdomen revealed right ureteral dilatation, gas within the right parenchymal and pelvicalyceal system. Also, there were appearances of the air-fluid in the urinary bladder. The patient was admitted to the hospital with diagnosis of EP. Intravenous antibiotic was started on the same day and a left JJ stent was inserted. Urine culture yielded E. coli. The diagnosis of EP must be highly suspected in diabetes mellitus. Medical management including parenteral antibiotics plus percutaneous catheter drainage or nephrectomy must be performed immediately according to the risk factors by the high morbidity and mortality associated with this disease. Keywords: Emphysematous pyelonephritis, diabetes mellitus, E.coli P 401 LİTYUM İNTOKSİKASYONU VE LİTERATÜRÜN GÖZDEN GEÇİRİLMESİ
Enver Özçete, İlhan Uz, Meltem Songür Kodik Ege Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, İzmir Lityum bipolar hastaların tedavisinde kullanılmaktadır. Terapotik aralığı dar olması nedeniyle kan düzeyi yakın takip edilmelidir. Kliniğimizde Lityum intoksikasyonu tespit edilen 10 vaka değerlendirildi. Hastaların yaş ortalaması 58,5 olup 6’sı kadın 4’ü erkekti. Hastaların başvuru şikayetleri Bilinç değişikliği(6) ve titreme(2) olarak belirlendi. 1 hasta da suisidal alım mevcuttu. Hastaların hepsi Lityum tedavisi almaktaydı. Hastaların Kranial BT leri normal olarak tespit edildi ve hiçbirinde Hipoglisemi saptanmadı. Kan lityum düzeyi en düşük 1,6-en yüksek 3,9mEq/L idi. Hastalar incelendiğinde; 5 tanesinde Üre-Kreatinin yüksekliği, 1 hastada metabolik asidoz saptandı. Hastaların hiçbirinde elektrolit anormalliği saptanmadı. Hastaların 5 tanesi diyalize alındı. Sonuç olarak hastaların 4 tanesi acil servisten taburcu, 3 tanesi yatırıldı ve 3 tanesi de sevk edildi. Lityum zehirlenmesi lityum kullanan olgular içerisinde yaklaşık %10-15 civarında görülür. Günümüzde en çok kabul gören Oakley ve arkadaşlarının zehirlenmeyi nedenine göre ayırt eden sınıflamasıdır. Bu sınıflamaya göre lityum zehirlenmeleri; akut, kronik zeminde akut ve kronik zehirlenmeler olarak gruplara ayrılırlar. Lityum zehirlenmesine bağlı gastro intestinal sistem belirtileri; iştahsızlık, ağız kuruluğu, bulantı, kusma, ishal bazen de kabızlık olmak üzere her şekilde karşımıza çıkabilir. Her türde nörolojik belirti izlenebilir. En sık görülen belirtiler; tremor, bilinç bulanıklığı, dizartri ve ataksidir. Lityum zehirlenmesinin tedavisi, lityum alımının kesilmesinin ardından sıvı elektrolit dengesinin düzenlenmesi ve destekleyici tedavi gereken ilk zorunlu adımdır. Tum barsak irrigasyonu emilimi azaltan yöntemlerin başında gelir. Aktif kömür, lityumu tutmadığından bir yararı yoktur. Bugüne dek yapılan yayınlar gözden geçirildiğinde gastrik lavajın da lityum doz aşımında, tek başına bir yararının olmadığı belirtilmektedir. Sodyum polistiren sulfonat resin adlı madde lityumu bağlamakta ve birlikte atılmaktadır. Ancak hipokalemi riski kullanımını kısıtlamaktadır. Ağır zehirlenmelerde en etkili yöntem hemodiyalizdir. Hemodiyaliz serum lityum düzeyi 1 mEq/l'nin altına düşünceye kadar ya da klinik belirti ve bulgular gerileyinceye kadar sürdürülmelidir. Anahtar Kelimeler: Acil servis, intoksikasyon, lityum

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
405
P 402 SPINAL ARTERIOVENOUS MALFORMATION: A RARE CASE IN THE EMERGENCY DEPARTMENT
Çağlar Kuas1, Mustafa Emin Çanakçı1, Nurdan Acar1, Muhammet Ali Polat2, Engin Özakın1, Didem Oktar1
1Eskişehir Osmangazi University School of Medicine, Department of Emergency Medicine, Eskişehir, Turkey 2Eskişehir Osmangazi University School of Medicine, Department of Radiology, Eskişehir, Turkey Objective: The vascular malformations of the spinal cord are a heterogeneous group of vascular disease [spinal arteriovenous malformations (SAVM), dural arteriovenous fistulas, spinal hemangioma, cavernous angiomas and aneurysms] and rare conditions. They are young population’s condition, which suggests that it is congenital. However, the etiology is undetermined yet. The spinal cord can be affected directly or indirectly. Myelopathy can be reversible if accurate and early diagnosis and treatment were made. Magnetic resonance imaging (MRI) is the choice of modality for the diagnosis. We present a patient admitted to the emergency department with paraplegia and inability to urinate with SAVM detected on the MRI. Case: A 24-year-old male patient was admitted to the emergency department with a sudden inability to walk and urinate. He did not suggest similar complaints previously. The patient was paraplegic and had suprapubic tenderness on the physical exam. Globe vesicale on bedside ultrasound imaging. Decreased anal sphincter tone determined. There were no pathological findings in the labs. Too much varicose and dilated venous structures in intradural perimedullary area were observed on spinal MRI images at all levels. Appearance was assessed as SAVM. The patient was hospitalized into neurosurgery clinic. Conclusion: SAVM is one of differential diagnosis of patients with motor and sensory defects in lower extremity presenting to the emergency department. It is important to be fast and accurate in the diagnosis of other life-threatening clinical conditions. MRI is the gold standard in the diagnosis of these patients. Keywords: Arteriovenous malformation, paraplegia, spinal magnetic resonance imaging P 403 BİLATERAL TALAMİK İNFARKT Behnan Gülünay1, Mehmet Aslanyavrusu2, Şimşek Çelik1
1Sivas Numune Hastanesi, Acil Servis, Sivas 2Sivas Numune Hastanesi, Nöroloji Servisi, Sivas Giriş: Bilateral talamik infarkt (BTİ)’lar nadir görülür. Etyolojisi değişken olup başlıca nedeni aterosklerotik küçük damar hastalığıdır. Bu yazıda uykuya meyli olan, kişi oryantasyonu bozuk olan ve acil servisimize konversif bozukluk öntanısı ile getirilen 63 yaşındaki erkek bilateral talamik infarkt olgusu sunulmuştur. Olgu: 63 yaşında, erkek hasta yaklaşık 12 saattir olan uykuya meyil, etrafındakileri algıyamama nedeni ile acile getirildi. Hikayesinde 40 yıldır 1 paket/gün sigara içtiği ve hipertansiyon nedeniyle düzensiz antihipertansif ilaçlar ve aspirin tablet kullandığı öğrenildi. Hastanın yapılan nörolojik muayenesinde bilinci somnole, kooperasyon kısıtlı, pupiller izokorik, yukarı bakış bilateral kısıtlı, motor defisit yok, taban cildi refleksi bilateral fleksör olarak belirlendi. Çekilen beyin BT de patolojik bulgu izlenmedi. Diffüzyon MR da bilateral talamik bölgeye uyan bölgede hiperintens lezyon izlendi. Bilateral talamik infarkt tanısı ile nöroloji kliniğine yatırılan hastanın takibinde kontrol kranial MR çekildi. T2 ve flair görüntülerde bilateral talamus median kısmında hiperintens lezyon izlenirken aynı bölgede T1 görüntülerde hipointens görüntü izlendi. Takibinde hastanın bilinci belirgin olarak düzeldi. Ancak 1. haftada vertikal bakış kısıtlılığının devam ettiği gözlendi. Tartışma: BTİ’da sıklıkla bilinç durum değişikliği, uyanıklıkta azalma, hafıza problemleri, kognitif problemler ve vertikal bakış paralizisi gözlenmektedir. İskemik inmeler içinde sıklık açısından oldukça az görülmelerine rağmen tipik klinik bulgularının olması ve konversif bozukluk gibi psikiyatrik durumlarla karıştırılma potansiyeline sahip olmalarından dolayı son derece önemlidirler ve acil servis hekimleri tarafından nöropsikiyatrik hastalıkların ayırıcı tanısında akılda tutulmalıdırlar. Anahtar Kelimeler: Konversiyon, paralizi, talamik infarkt

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
406
P 404 EFFECTS OF ADMINISTRATING NON-INVASIVE MECHANICAL VENTILATION ON PERFUSION INDEX AND PULSE PRESSURE IN PATIENTS WITH ACUTE RESPIRATORY FAILURE
Sukru Kockan1, Sila Sadillioglu2, Hakan Topacoglu3
Istanbul Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey Objective: Effect of administrating NIMV treatment of patients with hypoxia has been reported in literature, however its effect on peripheral perfusion is not well known. The aim of the study was to evaluate the changes in perfusion index and pulse pressure in acute respiratory failure patients treated with NIMV in the emergency department. Materials-Methods: The study was conducted as prospective and cross-sectional study. It was performed on 33 patients (63,6% acute respiratory failure due to COPD and 36,4% acute pulmonary edema) administered NIMV treatment over a period of two months in emergency department. Perfusion indexes, blood pressures, pulses and oxygen saturation of the patients were measured simultaneously before and during the NIMV treatment (10 min intervals). The relationship between perfusion index and NIMV treatment was analyzed. Results: A total of 33 patients (median age 69 years) 18 females (54,5%) were included the study. A statistically significant improvement in oxygen saturation (p<0,001), while decrease in average pulse of patients after NIMV treatment were observed (p=0,023). However, there was no statistically significant difference in blood pressure, pulse pressure, perfusion index of the patients during NIMV treatment (for all p>0,05). Conclusion: NIMV treatment applied to patients with acute respiratory failure exhibited a positive effect on hypoxia, but no observable change on pulse pressure and peripheral perfusion were observed. Keywords: Perfusion index, non-invasive mechanical ventilation, respiratory failure P 405 EVALUATION OF POSSIBLE EVENTS LIKE AS RESPIRATORY TROUBLES FOLLOWING URGENT HIATAL HERNIA REPAIR Burcu Yormaz1, Fahrettin Acar2
1Beyhekim State Hospital, Chest Diseases Clinic, Konya, Turkey 2Selçuk University Medical Faculty, Department of General Surgery, Konya, Turkey Background: Hiatal hernia (HH) is common in the morbid obese population. Its presence imposes various degrees of difficulty in performing. Patients who were underwent urgent hiatal hernia repair (HHR) have worse postoperative outcomes. Because they are usually comorbid patients, so this situation incline them to potential risks. Nowadays hernia repairs applied by experienced tertiary clinics. However, this surgical process is associated with a bit more morbidity and mortality, even when performed in emergency. Our study is aimed to determine respiratory troubles whether urgent HHR is associated with differential postoperative outcome compared to electives. Methods: We have evaluated 52 patients who were underwent hiatal hernia repair. Of 14(26%) patiens operated urgently and of 38 (74%) were electively between the years of February 2014 to May 2016.We were assessed the association between clinical predictor markers, demographics, comorbidity and length of stay in hospital (especially in intensive care unit) (LOSH) regarding with mortality and morbidity. Results: Urgent conditions of surgical process was a significant predictor of mortality (elective 0,7 %, nonelective 6,4%) and morbidity (elective 13% to nonelective 34%). The most common adverse outcomes were pulmonary complications ( 21,1%,of 11 patients). The outcomes of emergence operated patient’s Charlson comorbidity indexes (congestive heart failure and pulmonary disease) were higher than elective operated patients. Also respiratory problems is worsen in first group. Conclusıons: Patients presenting with acute symptoms related to HH have required open repair, which is associated with significant morbidity and mortality risks. The acute group was older and sicker than our elective HHR patients and had more adverse events resulting in a longer LOSH, even when compared with comorbidity-matched elective patients. However, the LOSH remained shorter than urgent group and there was no mortality. The lung treatment rates in all groups were low, comparable to elective repairs according to higher ventilator dependent rates. Keywords: Hiatal hernia, urgent, respiratory

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
407
P 406 AKSİYEL YÜKLENMELİ TRAVMALARDA BEKLENMEDİK BİR YARALANMA: QUADRİCEPS TENDON RÜPTÜRÜ
Şebnem Şakar, Ersin Aksay, Özlem Bayrak Dokuz Eylül Üniversitesi, Acil tıp Anabilim Dalı, İzmir Quadriseps tendon rüptürü genelde 50 yaş altı hastalarda, nadir görülen bir yaralanmadır. Biz yüksekten atlama sonrası sol bacakta ağrı şikayeti ile acil servisimize başvuran ve yaptığımız sonografik incelemeyle quadriseps tendon rüptürü tanısı koyduğumuz bir hastayı sunuyoruz. 32 yaşında erkek, 3 metreden ayaklarının üstüne atlama sonrası sol dizde ağrıyla başvurdu. Vital bulguları normaldi. Muayenede sol dizde şişlik, hassasiyet, suprapatellar gap ve diz ekstansiyonunda kısıtlılık mevcuttu. Diğer muayene bulguları olağandı. Direkt grafi ve bilgisayarlı tomografiside kırık görülmedi, bununla beraber prepateller yumuşak dokuda inflamatuar görünüm dikkat çekmekteydi. Yüzeysel ultrasonografide quadriceps tendonu içinde parsiyel yırtık, tendon içinde hematom ve hemotom içinde yüzen fibriler yapı görüldü ve parsiyel quadriceprs tendon rüptürü tanısı konuldu. Hasta uzun bacak ateline alınarak polikliniğe yönlendirildi. Quadriseps tendonu, vücudun en güçlü tendonlarındandır. Sağlıklı bir quadriseps tendonu spontan rüptüre olması güçtür. Quadriseps tendon rüptürleri bu nedenle ileri yaşla orantılı olarak kollajenöz dejenarasyonla veya sistemik bir hastalığa bağlı olarak oluşur. Rüptürler genelde 50 yaşın üstünde görülmekle birlikte, bu yaşın altında görülen rüptürlerin bizim hastamızda da olduğu gibi travmatik bir sebebe bağlı olabilir. Palpe edilebilir suprapatellar defekt, dizde belirgin şişlik, kasılabilir durumda bir quadriseps kası varlığına rağmen bacağı düz olarak kaldıramama quadriseps tendon rüptürünün fizik muayene bulgularıdır. Quadriseps tendon rüptürünün tanısı klinik olarak konur ancak tendon rüptürünün kesin tanısı tam veya parsiyel rüptür olup olmadığının anlaşılabilmesi için görüntüleme tetkikleri gereklidir. Acil servis hekimlerinin yatak başında yaptıkları ultrasonografi tendon rüptürlerin tanısında yüksek duyarlılığa sahiptir. Tendon rüptürlerinin klasik ultrasonongrafik görünümü normal fibriler tendon yapısında bozulma, tendon içi hipoekoik hematom görünümüdür. Ancak bizim olgumuzda daha tanısal olacak şekilde hematom içinde yüzen fibriler yapı, tendon rüptürünü daha kolay bir şekilde tanınmamıza neden olmuştur. Hematomun alt ve üst bölümünde tendon yapısının düzenli şekilde devam etmesi, tendon rüptürünün parsiyel olduğunu düşündürmüştür. Diz ekstansiyon kısıtlılığı olan travma hastalarında acil servis hekimlerinin yapacağı yatak başı ultrasonografi ile quadriseps tendon rüptürü tanısı konulabilir. Anahtar Kelimeler: Diz travması, quadriseps, tendon rüptürü P 407 TRAKONYA ISIRMASINA BAĞLI ACİL SERVİS YÖNETİMİ Bilen Çetin, Onur Karakayalı, Asim Enes Özbek, Emrah Çetin, Ramis Ufuk Akkoyunlu, Serkan Yilmaz Kocaeli Derince Eğitim ve Araştırma Hastanesi, Acil Tıp Anabilim Dalı, Kocaeli Giriş: Yaz döneminde çevresel acillerden en önemli grubu zehirli balık sokmasına bağlı tedaviler oluşturmaktadır. Ülkemizin üç tarafı denizlerle çevrili olduğu düşünüldüğünde zehirli balık sokmalarında acil yönetimi tüm acil personeli tarafından bilinmesi gerekmektedir. Bu vakamızda trakonya ısırmasına bağlı lokal yumuşak doku şişliği ve ciddi ağrı şikayeti ile gelen hastayı sunarak vaka yönetimi üzerinde tartışmayı amaçladık. Olgu: 50 yaş erkek hasta acil servisimize denizde yüzme esnasında trakonya olarak adlandırılan bir balığın yüzgecindeki iğnenin sağ el 3.parmağına batma sonrasında etkilenen parmakta şişlik ve ağrı şikayeti ile acil servisimize başvurdu. Sistem sorgusun, özgeçmiş ve soy geçmişinde özellik yoktu. Vital bulgular stabildi. Fizik muayenede sağ el 3.parmak ta lokalize yumuşak doku şişliği, kızarıklık dışında ek muayene bulgusu yoktu. Etkilenen bölgede yabancı cisim tespit edilmedi. Visuel ağrı skoru 10 olarak tespit edilen hastaya intravenöz nonsteroidal antiinflamatuar tedavi verildi. Ağrı skoru değişmeyen hastaya dayanabileceği ısıda sıcak su ile etkilenen parmak bir kap içerisinde 5-10 dakika kadar bekletildi. Ağrı skoru 3 e düşen ve yumuşak doku şişliği ve kızarıklığı azalan hasta önerilerle acil servisten taburcu edildi. Tartışma: Trakonyalar genel olarak adlandırılan çarpan balıkları, ülkemizin en zehirli balık grubunu oluşturur. Kumlu çamurlu zeminlerde kendilerini zemine gömerek yaşarlar. Literatürde komadan lokal ağrıya kadar farklı klinik başvurular bildirilmektedir. Vakamızda olduğu gibi hastalar sıklıkla ısırılan bölgede lokal yumuşak doku şişliği ve analjeziklere yanıt vermeyen ağrı şikayeti ile başvurmaktadır. Tedavinin temel basamağı hastanın dayanabileceği ısıda sıcak su ile lokal müdahaledir. Ağrı kontrolünde Alginat bazlı bezlerin yarada kalmış zehri emmesi için yaranın üzerine 8-10 gün sarılabileceğinden bahsedilmektedir. Ülkemizde diş hekimliği fakültelerinde kalıp amaçlı kullanılan bu maddeye acil şartlarda erişim çoğunlukla mümkün olmamaktadır. Etkilenen bölgede balığın dikenine ait olan yabancı cisim kontrolü yapılmalıdır. Lokal ağrı kontrolü sağlanan ve sistemik bulguları olmayan hastalar müdahale sonrasında acilden güvenle taburcu edilebilirler. Çevresel acillerin yönetimi acil serviste etkin ve hızlı bir şekilde deneyimli personel tarafından yapılmalı ve personelin zehirli balık sokmalarına bağlı acil yönetim eğitiminin verilmesi gerekmektedir. Anahtar Kelimeler: Trakonya ısırması, çevresel aciller, acil servis

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
408
P 408 A CASE WITH COMA PROTOCOL
Ali Karakuş1, Zeynep Kekeç2
1Mustafa Kemal University Faculty of Medicine, Department of Emergency Medicine, Hatay, Turkey 2Cukurova University Faculty of Medicine, Department of Emergency Medicine, Adana, Turkey The etiology are metabolic 85% and central 15% to coma patients brought to the emergency room. The tomography indicated the presence of neurological findings. Metabolic disorders when should be considered based on laboratory results. However, these results may improve clinical protocol without wasting time waiting for treatment to be given to patients with coma. This article was presented do not apply the expected protocol patients who more tests applied. Case: 75-year-old female patient was brought to the emergency room because of mental confusion. General condition of the patient moderate, confused consciousness, Glasgow Coma Scale was 10.Arterial blood pressure 100-170 mmHg, pulse: 80 beats / min, fever: 37.5 C other physical and neurological examinations were normal. There was no history of chronic disease and a history of drug use. Patients were asked to routine inspection by opening a vascular lab and underwent brain CT. CT and laboratory values normal. Blood glucose 45 mg / dL in patient. The patient was given 30% dextrose solution 1 g / kg dose, 200 ml. Follow the general state of consciousness opened in improved patient was discharged with the recommendations. Coma protocol is the recommended treatment protocol who with loss of consciousness in patients in emergency department. Although not recommended in recent guidelines dextrose 1g / kg, thiamine 1 mg / kg naloxone 2 mg, 0.2 mg flumazenil applicable for all unconsciousness patients. In this way, unnecessary tests requested and prevents waste of time. Keywords: Coma protocol, unnecessary tests, a waste of time P 409 GUILLAIN-BARRÉ SYNDROME VERSUS MYASTHENIA GRAVIS
Mehmet Birkan Korgan1, Elif Dilek Cakal1, Funda Karbek Akarca1, Ayşe Güler2
1Ege University Medical School, Department of Emergency Medicine, Izmir, Turkey 2Ege University Medical School, Department of Neurology, Izmir, Turkey Introduction: Patients use weakness to describe conditions like fatigue, dyspnea or true loss of strength. Emergency physician must carefully distinguish between neurological and non-neurological conditions such as dehydration, anemia, shock, metabolic and infectious diseases or intoxications. We present a case of acute motor axonal neuropathy presenting like myasthenia gravis (MG). Case: A previously healthy 44-year-old female presented to emergency department with a four-day history of weakness, drooping of the upper eyelids and hoarseness of the voice, all intensifying in the evenings. She denied any preceding history of flu-like symptoms or gastrointestinal infection. She had bilateral ptosis, orbicularis oculi and oris weakness, dysphonia and dysphagia. Neck flexion and extension were weak. Motor examination revealed grade 3/5 strength in upper extremities and grade 4/5 strength in lower extremities. Sensory examination and deep tendon reflexes (DTR) were normal. No pathological reflexes were present. Intravenous immunoglobulin was started. Though acute presentation implied Guillain-Barré syndrome (GBS), prominent ocular symptoms and obtainable DTR indicating MG required electromyography, which resulted consistent with demyelination suggesting GBS. Cerebrospinal fluid analysis and brain computed tomography were normal. The patient developed respiratory acidosis and was admitted to neuro-ICU receiving noninvasive mechanical ventilation. She is currently intubated. Discussion: MG, an autoimmune disease caused by antibodies against neuromuscular junction muscle membrane components, is characterized by muscle weakness and abnormal fatigability. MG generally begins with ocular symptoms and extends to other muscles in 80% of cases. Weakness is usually proximal and symmetric. Sensory examination and deep tendon reflexes are normal. GBS presents 2-4 weeks after a respiratory or gastrointestinal infection in two thirds of the cases. Classically, weakness is ascending and symmetrical. Reflexes are absent or reduced. Both may cause respiratory failure. Conclusion: GBS is generally diagnosed on clinical grounds. In this unusual case, clinical features are inadequate, auxiliary tests are key to diagnosis. Keywords: Guillain-Barré syndrome, myasthenia gravis, muscle weakness, emergency department

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
409
P 410 LONG SHOT
Bilgen İlküplü, Sercan Yalcınlı Ege University Medical School, Department of Emergency Medicine, Izmir, Turkey Introduction: Cardiac wounds are fatal injuries accounting for penetrating and non-penetrating causes. Penetrating injuries caused by weapon and knife and 30% of all cardiac injuries. Our case was admitted to emergency department due to gunshot injuries, determined pellet in pericardium cavity Case: A 29 year-old male patient was admitted to emergency department after gunshot injury. There was an insertion site for pellet in the right axillary and humerus medial and there was an ecchymotic area. Upon determination of lesion compatible with hyperechogenic foreign substance in mediastinum in lung X-ray taken during follow-up, physical examination was repeated and no insertion or exit site was identified on the thorax. In his CT, pellet material was established in the right anterior lateral and right ventricle level in the pericardium. In the echo; no pericardial fluid, wall pathology, foreign substance in ventricle was established. Pellet was thought to reach pericardium with a leap from the bone. The patient was discharged with no intervention after the follow-up. Disscusion:47% of the cardiac wounds are in the right ventricle owing to anterior placement; progress deadly since it leads to myocardial rupture, contusion, laceration, coronary and valve damage. Pellets composed of tiny particles can be stuck in myocardium and pericardium in gunshot wounds and they can settle into pericardial sac and cardiac cavity. The early determination of cardiac tamponade will be the most important to prevent life-threatening injuries. CT can be beneficial for stabile patients followed with close monitorization in diagnosis and also CT can determine the shape and direction of the pellet. Conclusion: Thorough examination of whole body must be first priority in gunshot wounds and although no insertion-exit lesion is established, it should be kept in mind that there may have been fatal damages like cardiac injury. Because the pellet can fall to pieces, scatter and it can be stuck in heart Keywords: Cardiac, injury, pellet P 411 DOES BARIATRIC SURGERY DECREASES THE ADMISSION TO EMERGENCY SERVICE FOR ASTHMA ATTACK? EFFECTS OF WEIGHT LOSS ON AIRWAY RESPONSIVENESS IN MORBID OBESE PATIENTS WITH ASTHMA Burcu Yormaz1, Ilhan Ece2, Serdar Yormaz2
1Beyhekim State Hospital, Chest Diseases Clinic, Konya, Turkey 2Selçuk University Medical Faculty, Department of General Surgery, Konya, Turkey Background: The growing epidemics of morbid obesity and asthma are major public health concerns. Asthma-morbid obesity links are widely studied however the effects of weight loss on asthma attacks severity measured by airway hyper responsiveness (AH) have received limited importance. The aim of our study was to examine whether weight reduction reduces asthma attacks (AA) in applying to emergency service. Methods: We have followed 25 obese participants with asthma aged 28 to 46 years with a BMI >= 40 kg/m2 in retrospectively between the years of aril 2015 to march 2016. Of 16 (64%) patients followed after bariatric surgery (Group S) and of 9 attend to behavioral weight reduction program (group P) for 3 months. The primary outcome was change in AH over 3 months. Changes in lung function, asthma control, and quality of life were secondary outcomes. Results: In our study, patients mean age was 37 ± 9 years, 80% were women, and mean BMI was 45.6 ± 4.7 kg/m2. Three months later, mean weight loss was 11.5 ± 5.7 kg in the surgery group, and the group P had a mean weight gain of 1.6 ± 0.3 kg. There were significant improvements in, FEV1, FVC (P <0.05), asthma control (P < 0.05), and asthma quality of life (P < 0.05) in the surgery group, but these parameters remained unchanged in group P. Emergency service admission is decreased significantly in the surgery group but not in the behavioral weight reduction program group. Conclusıons: Excess weight loss in morbid obese adults with asthma can improve asthma severity, AH, asthma control, lung function, and quality of life. These findings support the need to actively pursue healthy weight-loss measures by bariatric surgery in all over the world Keywords: Bariatric, asthma attacks, emergency service

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
410
P 412 İNTERNAL JUGULER VEN VE BRAKİOSEFALİK VEN, İNFERİYOR VENA KAVAYA ALTERNATİF OLABİLİR Mİ?
Yasin Metiner1, Mehmet Ali Kuseyri2, Rohat Ak1, Hasan Demir1, Tuba Cimilli Öztürk1, Özge Ecmel Onur1, Hakkı Muammer Karakaş2, Arzu Emecen1
1Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul 2Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, Radyoloji Kliniği, İstanbul Amaç: Santral venöz basınç ve kan volüm durumunun değerlendirilmesinde ultrasonografik olarak inferiyor vena kava (İVK) çapı görüntülemesi son zamanlarda en çok tercih edilen yöntemlerden birisidir. Biz bu çalışmamızda, internal juguler ven (İJV) ve brakiosefalik ven (BSV) doppler görüntülemelerinin, İVK çapı ile ilişkisini araştırmayı amaçladık. Santral venöz basınç ve volüm durumunu değerlendirmek için alternatif olarak bu Doppler parametrelerini kullanabileceğimiz hipotezini kurduk. Materyal-Metot: Çalışmamız, hastanemiz Klinik Araştırmalar Etik Kurulu’ndan onay alındıktan sonra 01.02.2015/01.08.2015 tarihleri arasında 20-60 yıl yaş arasındaki sağlıklı gönüllüler üzerinde yapılmıştır. Çalışmayı biri Acil Tıp asistanı, biri de Radyoloji asistanı olmak üzere iki operatör yürütmüştür. Her iki operatör, kör bir şekilde, gönüllü katılımcıların İVK, İJV ve BSV ultrasonografi ve Doppler parametrelerinin solunumsal değişkenliklerini değerlendirmişlerdir. Bulgular: Çalışmaya; yaşları, minimum 22 yıl, maksimum 54 yıl, ortalaması 33,73±8,72 yıl olan 30 sağlıklı gönüllü katılmıştır. Her iki operatör tarafından, katılımcıların İVK çapı ve solunumsal değişkenliği ölçülmüş ve bu ölçümler İJV çap ve akım hızları, BSV akım hızları ile korelasyon açısından analiz edilmiştir. Acil Tıp operatörünün yapmış olduğu ölçümlerde, İVK çapı ile diğer santral ven ölçümleri arasında ilişki saptanmamıştır. Radyoloji operatörünün yapmış olduğu ölçümlerde ise, İVK çapı ile diğer santral ven ölçümleri arasında zayıf derecede ilişki saptanmıştır. Sonuç: İnferiyor vena kava çapının solunumsal değişkenliği ile İJV ve BSV Doppler akım hızları arasında ilişki olmadığı sonucuna varılmıştır. Anahtar Kelimeler: Acil tıp, inferiyor vena kava, santral venöz basınç, juguler ven, brakiosefalik ven P 413 HIV İLİŞKİLİ TOKSOPLAZMA ENSEFALİTİ: OLGU SUNUMU İbrahim Sarbay, Halil Doğan, Dogac Niyazi Özucelik, Sezgi Sarıkaya, Onur Tosun Bakırköy Dr. Sadi Konuk Training and Research Hospital, Clinic of Emergency Medicine, Istanbul, Turkey Toksoplazmoz, AIDS hastalarında en sık görülen oportunistik merkezi sinir sistemi enfeksiyonudur. Özellikle CD4+ hücre sayısı 200’ün altında olan hastalarda daha sık görülmektedir. HIV pozitif olan hastalarda serebral toksoplazmozun en sık prezantasyonu baş ağrıları, nörolojik defisitler ve nöbetlerdir. Toksoplazma bütün beyin hücrelerini tutabildiğinden toksoplazma ensefalitinin klinik prezantasyonu vakalar arasında değişiklikler göstermektedir. 25 yaşında, kadın hasta. Baş ağrısı ve 1 haftadır sağ bacağında hissizlik şikayeti ile acil servise başvurdu. Baş ağrıları 6 aydır devam ediyormuş. Özgeçmişinde; bilinen hastalığı, ilaç kullanımı, sigara – alkol, uyuşturucu/uyarıcı madde kullanımı yok, evcil hayvan beslemiyor. Fizik muayenesinde; bilinci açık, oryante, koopere, hafif uykuya eğilimli. Yer - zaman oryantasyonu var. Dizartrik konuşması mevcut. Pupiller anizokorik, çift taraflı ışık refleksinin alınamadığı görüldü. Sağ üst ekstremitede 3/5 kuvvet kaybı mevcut. Desteksiz ayağa kalkamadığı ve yürüyemediği, sağa ataksik olduğu görüldü. Kontrastlı Kraniyal MRİ’de; serebellum her iki yarımında, mezensefalonda, sağ talamusta, solda sentrum semiovale düzeyinde postkontrast incelemelerde rim tarzında tutulumlar gösteren çok sayıda kitlesel lezyonlar izlendiği, lezyon komşuluklarında yaygın ödematöz sinyal intensite değişiklikleri görüldüğü raporlandı. Çalışılan ELİSA tetkiklerinde Anti-HIV pozitifliği saptanan hastanın, lezyonlarının ön planda Toksoplazma ile uyumlu olduğu değerlendirdi. Tetkiklerinde HIV RNA düzeyi 2.307.778 kopya, CD4 hücresi sayısı 16 hücre/µl olarak saptanan hastaya Trimetoprim/sulfametoksazol ve Steroid tedavisi başlandı. Toxo IgG pozitifliği saptandı. Tedaviye Raltegravir ve Tenofovir/Emtrisitabin eklendi. Takiplerinde sol gözde pitozisi ve içe bakış kısıtlılığı azalan, konuşma bozukluğu düzelen, kendi kendine yürüyebilmeye başlayan hasta, yatışının 22. gününde taburcu edildi. Dünyada ve ülkemizde insidansının giderek arttığı bildirilen AİDS ve buna sekonder gelişen toksoplasma ansefalitine dikkat çekerek baş ağrısı ve kuvvet kaybı ile acil servis başvuran hastalarda toksoplazma enfeksiyonunun düşünülmesi gerektiğine vurguladık. Anahtar Kelimeler: HIV, AIDS, toksoplazma, ensefalit

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
411
P 414 HİPONATREMİNİN NADİR BİR NEDENİ TRANSÜRETRAL PROSTAT REZEKSİYONU SENDROMU: OLGU SUNUMU
Eren Demir1, Halil Doğan2, Mehmet Toptaş1
1Haseki Eğitim ve Araştırma Hastanesi, Anesteziyoloji ve Reanimasyon Kliniği, İstanbul 2Bakırköy Dr. Sadi Konuk Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Transüretral prostat rezeksiyonu sendromu (TUR-P), prostatın transüretral rezeksiyonu sırasında kullanılan irrigasyon sıvısının emilimine bağlı gelişen hipervolemik hiponatremi, ajitasyon, konfüzyon, akciğer ödemi, aritmiler ve hipertansiyondan kardiyovasküler kollapsa kadar gidebilen semptomlardan oluşan bir sendromdur. Bu sunumda spinal anestezi altında gelişen TUR-P sendromunda erken tanı ve tedavinin önemini vurgulamayı amaçladık. 60 yaşında erkek hastaya benign prostat hipertrofisi nedeniyle TUR-P operasyonu planlandı. Bilinen ek hastalık öyküsü olmayan olgu preoperatif anestezi muayenesinde mallampati 1, ASA 1 olarak değerlendirildi ve elektif operasyon için ameliyathaneye alındı. Laboratuar tetkiklerinde kreatinin 1.4 mg/dl olması (0.67-1.17 mg/dl) dışında bir anormallik saptanmadı, sodyum (Na) 141 mEq/l (136-145 mEq/L) idi. Hasta masaya geldiğinde bilinç açık oryante koopere, spontan solunumda, noninvaziv arteryel kan basıncı(TA) 128/83mmHg, kalp tepe atımı(KTA) 62/dk idi. Preoperatif hastaya 500ml %0.9 NaCl infüzyonu yapıldı ve premedikasyon amaçlı 2mg midazolam intravenöz uygulandı. Hastaya spinal anestezi ile operasyona alindi, İdame sıvı olarak da yine %0.9 NaCl intravenöz uygulandı. Cerrahi ekip tarafından irrigasyon sıvısı olarak ameliyat masasından yaklaşık 80-90 cm yükseklikte asılan 3000ml'lik %0.9 NaCl kullanıldı. Operasyonun 110. dakikasında TA:167/98mmhg olarak ölçüldü, elektrokardiyografisi sinüs ritminde 69/dk, periferik oksijen saturasyonu (spO2) 98% idi. Hastada ajitasyon, şuur bulanıklığı gelişmesi üzerine arteryel kan gazı(AKG) örneği alındı. Alınan AKG de Na: 107 mEq/l gelmesi üzerine cerrahi ekibe kanama kontrolü yaparak operasyonu hızlıca sonlandırması gerektiği belirtildi. Dinlemekle solunum seslerinde azalma, bilateral bazallerde raller olması üzerine 20mg furosemid iv uygulandı. Yoğun bakımdaki ilk bakılan biyokimya örneğinde Na: 101 mEq/l gelmesi üzerine %3NaCl hipertonik sıvı 100ml/sa hızından 3 saat boyunca iv replase edildi, diüretik tedavisi başlandı. Takipleri sırasında 1.gün Na:120mEq/L ve 2.gün Na:133mEq/L geldi. Hemodinamisi stabilleşen ve glaskow koma skalası 15 olan hasta externe edildi. Sonuç olarak TUR hastalarına yıkama sıvısının 2000ml'yi aştığı olgularda sistemik emilime bağlı olarak gelişen hiponatremi, başağrısı, bulantı, kusma, konvulziyon, dispne, taşiaritmi, hipertansiyon gibi klinik bulguların varlığında TUR-P sendromundan şüphelenilmelidir. Anahtar Kelimeler: TUR-P sendromu, hyponatremia, spinal anestezi P 415 AN EXAMPLE TO INFECTIOUS COMPLICATIONS OF AN INFECTIVE ENDOCARDITIS IN INJECTION DRUG USERS: PSOAS ABSCESS Meltem Songür Kodik, Murat Ersel, Selahattin Kıyan
Ege University Faculty of Medicine, Department of Emergency Medicine, Izmir, Turkey Introduction: Injection drug users (IDUs) are likely to face very specific and well-defined issues that are inherently social and medical: addiction and related crimes, overdose, withdrawal, and infections as a consequence of drug injections. We would like to share the infectious incident of an infective endocarditis (IE) in IDUs. Case: 26 year old woman was being treated for a year due to her drug addiction. A month ago she complained that she had rubor, temperature rise, swelling, and pain in her right knee. Besides pain and limited joint mobility in her right knee that started a week before she appealed our ED. For a year, she had night sweat that causes her to change clothes 2-3 times in a night. In the transesophageal echocardiography report, it was detected that in the alignment of ascending aorta sinus of valsalva, there was 9x4 mm echogenicity in the vicinity of aorta wall and 1st degree aortic insufficiency. As a result of the radiograms due to the pain in the right hip, in the CT it is detected that collections concordant with the 10x5 cm size abscess involving air densities that starts from right iliacus muscle and continues through right iliopsoas muscle. The patient is hospitalized in the general surgery in order to have abscess drainage that is planned by interventional radiologist. Discussion and Summary: Primary psoas abscess may arise from hematogenous or lymphatic seeding from a site far away. Among the risk factors; diabetes, IDU, HIV infection, renal failure, and other forms of immunosuppression can be listed IDUs are in danger for the complications associated to the agents they inject, and also for the conditions associated mainly to transmission of infectious agents. All emergency physicians ought to be capable of identifying and handling the major bacterial infections complicating IDU. Keywords: Infective endocarditis, injection drug users, psoas abscess

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
412
P 416 PREGNANCY AND CEREBRAL VENOUS THROMBOSIS: CASE REPORT
Hasan Sultanoğlu1, Tuba Erdem Sultanoğlu2, Seda Özkan1
1Dışkapı Yıldırım Beyazıt Training and Research Hospital, Emergency Health Care Department, Ankara, Turkey 2Kazan State Hospital, Physical Therapy and Rehabilitation Clinic, Ankara, Turkey Objective: The most common reasons of Cerebral Venous Thrombosis (CVT) are pregnancy, puerperium, and oral contraceptive use. This rare, severe disease is clinically characterized by headache, papilledema, seizures, focal deficits, coma, and death. Thrombosis of the cerebral venous sinuses, particularly of the superior sagittal or lateral sinus and the tributary cortical and deep veins, gives rise to a number of important neurological syndromes. The introduction and widespread use of cerebral angiography, computerized tomography of the brain, and more recently magnetic resonance imaging have allowed early diagnosis of CVT. In this case, we aim to submit that after the eight weeks of pregnancy developing severe headache and confusion with a diagnosis of SVT admitted to the emergency service. Case: 22-year-old female patient admitted to the emergency services with severe headache, nausea, vomiting and loss of consciousness after the complaint. These symptoms began a week ago. The patient's medical history in that eight weeks of pregnancy, when she had an upper respiratory tract infection a week before it had begun to complain. Biography and family history was unremarkable. On clinical examination she was nonfebril, a pulse of 65/min, respiratory rate 20/min, blood pressure was 106/61 mm of Hg. Physical examination was with in normal limits. CNS examination conscious, cooperation and orientation was weak, no neck rigidity, all reflexes intact, normal tone and power, pupils normal sized and bilaterally reacting to light, papilloedema was not detected. Laboratory evaluation of the WBC: 12800, in the CSF didn't evaluate the impact of leukocytes, CSF glucose a protein was 50 and 41.8. MRI venography study revealed both lateral sinus thrombosis. The patient was diagnosed with cerebral venous thrombosis, anticoagulant therapy was started and was transferred to the neurology clinic. Result: SVT can be seen in pregnancy and puerperium period should be kept in mind in confusion and headache. Keywords: Cerebral venous thrombosis, pregnancy, headache P 417 TRAVMATİK TORAKAL SPONDİLOPİTOZİ: OLGU SUNUMU Emine Cabioglu, Halil Doğan, Saltuk Cabioglu, Dogac Niyazi Özucelik, Sezgin Sarıkaya Bakırköy Dr. Sadi Konuk Eğitim ve Araştırma Hastanesi,Acil Tıp Kliniği, İstanbul Giriş: Spinal travmalar, motorlu taşıt kazaları, toplumsal şiddet, eğlence etkinlikleri ve iş kazaları sonucu görülebilmekte olup yıllık milyonda 15 ila 40 vaka insidansı bildirilmiştir. Şiddetli travma nedeniyle gelişen spondilopitozis üst-orta torakal bölgenin çok nadir görülen spinal yaralanma tipidir. Vertebranın komşu vertebra üzerinde patolojik bir durum sonucunda tamamen yer değiştirmesine spondilopitozis denir. Bu olgu ile hemorajik, sapinal ve norojenik şokun goruldugu spondilopitozis vakasina yaklaşimi literatur esliginde tartistik. Olgu: 66 yaşında erkek hasta, araç dışı trafik kazası beyanı ile 112 ekipleri tarafından acil servisimize getirildi. Servikal kolor takılı halde travma tahtasında stabilize edilmiş olan hastanın bilinçli, oryante koopere olduğu gözlendi. Kan basıncı 121/67 mmHg, nabzı 90 atım/dakika, solunum sayısı 20/dakika, oksijen saturasyonu %94 idi, hastanın her iki meme ucu altından başlayan duyu ve motor fonksiyon kaybı olduğu saptandı. Çekilen bilgisayarlı tomografisinde, T4-T5 seviyesinde vertebral ayrışma(spondilopitozis), sağ akciğerde pnömotoraks ve bilateral hemotoraks izlendi. Hastaya 4 ünite eritrosit süspansiyonu, 4 ünite taze donmuş plazma infüzyonu planlandı. Takibinde hastanın kan basıncı 65/45 mmHg, nabız:110atım/dakika, solunum sayısı 22/dakika olarak izlendi. Hastaya hemopnömotoraks nedenli sağ ve sol hemitorakstan acil olarak tüp torakostomi uygulandı. 750cc hemorajik karakterde drenaj gözlendi. Sıvı, kan desteğine rağmen kan basıncı 55/45 mmHg olarak seyreden hastada nörojenik şok açisindan introp desteği başlandı. Takibinde endotrakeal entübasyon ve acil torakotomi uygulanan, akciğer onarımı ve kanama kontrolü yapıldı. Hastaya torakotomi sırasında 4 ünite eritrosit süspansiyonu, 4 ünite taze donmuş plazma, 5 ünite trombosit replasmanı yapıldı. Dopamin, Noradrenalin, Adrenalin infüzyonu devam eden hastanın kan basıncı 40/25 mmHg olarak izlendi. Nabız alınamayan hastada kardiyopulmoner resüsitasyona başlandı fakat yanıt alınamadı. Nadir görülen travmatik spondilopitozis, büyük oranda komplet spinal kord hasarı ile birliktedir. Komplet spinal kord hasarı, spinal ve nörojenik şok ile birlikte görülebilir. Bu üçü, birbirinin devamı niteliğinde ortaya çıkar. Multiptravma hastalarında nörolojik muayene atlanmamalı, spinal kord hasarını düşündüren muayene bulgusu varlığında nörojenik şok açısından dikkatli olunmalıdır. Anahtar Kelimeler: Spondilopitozis, travma, vertebra, şok

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
413
P 418 THE DIFFERENTIAL DIAGNOSIS OF NECK STIFFNESS: TETANUS
Ali Karakuş1, Zeynep Kekeç2
1Mustafa Kemal University Faculty of Medicine, Department of Emergency Medicine, Hatay, Turkey 2Cukurova University Faculty of Medicine, Department of Emergency Medicine, Adana, Turkey Tetanus, meningitis, subarachnoid hemorrhage and degenerative arthritis may be considered the differential diagnosis of neck stiffness in the emergency department. This article presented was of tetanus cases with a history of sinking nails in the emergency department. Case: 50-year-old male patient was brought to the emergency department with complaints of inability to move the jaw, which has 3 days. Patients' relatives have taken to the health center patients with these complaints. However undiagnosed. The general condition of the patient when it comes to good, clear consciousness was cooperative. There was no evidence except for a stiff neck on physical examination. It was learned that when the history of the deepening 10 days ago nail down. There were no abnormalities in the patient's laboratory values were made. Tetanus patients diagnosed with infectious diseases were admitted to the intensive care unit. Tetanus is rare in the emergency room. It should be considered in the differential diagnosis of neck stiffness. In terms of possible complications it must be treated early. Keywords: Tetanus, neck stiffness, early intervention P 419 APPENDICITIS LOOKS LIKE CHOLECYSTITIS - A CASE REPORT Hayrullah Yönak, Mine Kayacı Yıldız, Yasin Yıldız, Gökhan Aksel, Serkan Emre Eroğlu
University of Health Sciences, Ümraniye Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey Introduction: Acute appendicitis is a common cause of surgical operations. That is usually managed with early surgery and associated with low mortality. However, some patients apply with different symptoms. Atypical symptoms and examination findings may lead to a delay in diagnosis and complications. Sometimes atypical positions of appendix causes atypical symptoms. At this case we report a subhepatic appendicitis who presented with acute right upper abdominal pain. Case presentation: A 25 years old male presented with abdominal pain, loss of appetite and cause that developed one day before hospital admission. On physical examination, temperature was 37.8, heart rate was 98 bpm, blood pressure was 110/74 mmHg. His abdomen was soft, not distended, showing tenderness in the right upper quadrant. Considering the symptoms and signs, a clinical diagnosis of acute cholecytitis was made. Blood tests showed leukocitosis and high level of CRP. He had normal liver, renal functions, electrolytes, amilase and lipase. An ultrasound was done which revealed a deep located acutely inflamed subhepatic appendix at the right middle-lower quadrant. Our patient underwent laparoscopic appendectomy. Operating findings included suppurative subhepatic appendicitis and adhesiolysis. Discussion: Appendix can be variable located with in the abdominal cavity; retrocaecal (65.28%), pelvic (31%), subcaecal (2.26%), preilial (1%) and also post ileal (0.4%). Subhepatic position is a rarely reported varient that leads to delayed diagnosis and misdiagnosed such as acute cholecistits, diverticulitis, acute gastroenteritis, ureter colic, acute pyelonephritis, colon cancer and irritable bowel syndrome. Although ultrasound is the first primary screening choise for patients with abdominal pain, pregnant and young children, it requires operators experience. It has a 76% sensivity and 88-95% specificity. On the other hand computiresed tomography is required for suspected diagnosis with 88-100 % sensivity and 92-98 % specificity. Conclusion: It is important that emergency physicians are familiar with the atypical locations of appendix. Keywords: Abdominal pain, subhepatic appendicitis, ultrasounds

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
414
P 420 SPONTANEOUS HEMATOMA AFTER SNEEZING AND COUGHING IN TWO PATIENTS USING WARFARIN: REPORT OF TWO CASES
Zeynep Konyar, Bilge Ercan, Fatma Sarı Doğan, Özlem Güneysel Istanbul Dr. Lütfi Kırdar Kartal Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey Subcutaneous hematoma, a collection of blood vessels as a result of trauma. Subcutaneous hematoma among the causes of the sneezing, moderate one of the trigger. Patient using oral anticoagulants are more sensitive to external influences and is open to complications. Warfarin is the most commonly used oral anticoagulant agent today and therapeutic range is narrow. The most serious complication of warfarin therapy is bleeding. Bleeding complications usually appear on the genitourinary, gastrointestinal, spinal, intracranial system and skin. In our two cases of two patient using low-dose warfarin, without trauma, hematoma was described with reference to the emergency department after sneezing and coughing. Keywords: Hematoma, sneezing, warfarin P 421 MODAFİNİL İNTOKSİKASYONUNA BAĞLI AKUT PSİKOZ OLGUSU İsmail Altıntop, Mehmet Tatlı Kayseri Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Kayseri Amaç: Modafinil geç saatlere kadar çalışmak, uzun süre dikkat ve konsantrasyonunu devam ettirmek ve duygu durumunu canlandırmak isteyen bireyler tarafından sıklıkla kullanılmaktadır. Amfetaminden farklı nörokimyasal ve davranışsal özellikleri olan psikostimulan bir ilaçtır. Modafinilin dopaminerjik, histaminerjik, noradrenerjik, glutamaterjik, GABAerjik ve serotoninerjik etkileşimleri vardır. Psikiyatrik hastalık öyküsü olup ilaçlarına ek olarak modafinil kullanımına bağlı psikoz gelişen vakalar olmaktadır. Literatürdeki olgularda 200-400 mg/gün veya daha yüksek dozlarda psikoz veya mani geliştiği bildirilmektedir. Bu yazıda sunulan olguda tıbbi ve psikiyatrik hastalık öyküsü olmaksızın ders çalışma performansını arttırmak için kullanılan 100 mg/gün modafinil kullanan hastanın ilacı bir gün içerisinde 2700/gün alması ile psikoz gelişmiştir. Bu vakada acil servisimize anksiyete, ajitasyon, saldırganlık nedeniyle başvurun ek hastalığı olmayan modafinil intoksikasyonu ile ilgili deneyimimizin paylaşılması amaçlanmıştır. Vaka sunumu: Yirmi bir yaşında üniversite öğrencisi erkek hasta dikkatini sürdürememe ve ders çalışma performansı artırmak için kullandığı, ilaçtan toplam 2700mg/gün aldığını söyleyerek acil servisimize başvurdu. İlacın olası komplikasyonları anlatıldı. Hastada anksiyete, ajitasyon vardı. Hastanın psikotik semptomlarının devam etmesi üzerine hastaya 5 mg haloperidol ve 2 mg biperiden im enjeksiyon yapıldı. Modafinilin tetiklediği psikotik atak ve ilaç intoksikasyonu tanısıyla yoğun bakım servisine yatışının üçüncü gününde şifa ile taburcu edildi. Sonuç: Modafinil uzun bir süre dikkat korumak, uzun saatler çalışmak isteyen kişiler tarafından yaygın olarak kullanılmaktadır. Özellikle öğrenciler arasında sınavlar için uzun süre ayakta kalmak için ve rekabetçi spor başarılarını artırmak isteyen öğrenciler yaygın olarak kullanmaktadır. Bu konuda acil hekimleri modafinil etki mekanizmaları açısından ve olası psikotik etkileri açısından bilgili olmalıdır. Bu tür vakalarda hastaların ruhsal durum muayenesi normal, bilinci açık ve yer, zaman, kişi oryantasyonu olduğundan tedaviye ikna olurlar. Düşük doz modafinil kullanımlarında bile hastalarda psikotik semptomlar olabilir. Literatürde az görülen yüksek doz zehirlenmelerde hastalar gözlem altına alınmalıdır. Modafinil kullananlar ailelerine bildirilmeli, adli olarak takip edilmelidir. Bu tür ilaçlar reçete edilirken doz ve uygulama hakkında ayrıntılı bilgi verilmelidir. Anahtar Kelimeler: Modafinil, intoksikasyon, psikoz

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
415
P 422 INCOMING ANURIA COMPLAINT WITH A RARE CASE OF EMERGENCY SERVICES; RUPTURED ISOLATED ILIAC ARTERY ANEURYSM
İlhan Uz, Enver Özçete Ege University Faculty of Medicine, Department of Emergency Medicine, Izmir, Turkey Introduction: Isolated from the iliac artery aneurysms are rare and account for less than 2% of all aneurysmal disease. These aneurysms often found in association with abdominal aortic aneurysms, and is typically seen in older men. Case: Inability to urinate and abdominal pain that comes with the 74-year-old male patient. Hypotensive and anuria which made the patient bedside emergency ultrasound of the bladder distension, pelvic cystic lesions and showed minimal free fluid. Etiology of the patient in order to computed tomography (CT) angiography; the medial wall of the left internal iliac artery aneurysm rupture, reaching approximately 8 cm in diameter, and it was found secondary to intra-abdominal hemorrhage. Discussion and Results: It is not uncommon that iliac artery aneurysms are associated with abdominal aortic aneurysms, as approximately 10% to 20% of cases are found. However, isolated iliac artery aneurysms are extremely rare and generates 0.4% to 1.9% of aneurysmal disease. The incidence of this disease is estimated in 0.03% in population. Iliac aneurysms are typically seen in older men as in our case. 7: 1 ratio of male sex has dominance and has the highest incidence in the 7th, 8th decade. As a result, iliac artery aneurysm, is one of the rare diagnosis, which can present with symptoms such as bladder distension, anuria and abdominal pain in such as prostatic hypertrophy, which is seen too often in older men and in the emergency room. Differential diagnosis, bedside ultrasonography is a diagnostic tool that should be used in unstable patients. The gold standard imagination is CT angiography for the diagnosis of rupture and to determine the location of of aneurysm. Keywords: Anuria, isolated iliac artery aneurysm, ruptured aneurysm P 423 PNÖMOTORAKS OLMAKSIZIN PNÖMOMEDİASTİNUM VE DERİALTI AMFİZEMİ: OLGU SUNUMU İsmail Altıntop, Mehmet Tatlı Kayseri Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Kayseri Amaç: Acil servisimize boyunda şişlik nedeniyle başvuran takiplerinde pnömomediastinum ve derialtı amfizemi tespit edilen vakamız ile ilgili deneyimimizin paylaşılması amaçlanmıştır. Vaka sunumu: Yirmi yaşında erkek hasta, aniden ortaya çıkan şiddetli boyun ağrısı ve boyunda şişlik yakınmaları ile acil servisimize başvurdu. Hikayesinde bir gün önce yüzdüğünü, yüzdükten sonra hafif boyun ağrısı olduğunu söyledi. Ek hastalığı olmayan hastanın fizik muayenesinde her iki boyunda şişlik, her iki boyun ve aksiller bölgelerde krepitasyon vardı. Fizik bakıda, KB: 110/80 mmHg, Nb: 92/dak, Ateş: 36.5 °C, Solunum sayısı: 22/dak, SpO2: % 96 saptandı. Sol ve sağ hemitoraks ön yüzde aksiller bölgeye sırta, boyuna ve toraks alt bölümlerine yayılan derialtı amfizemi bulguları vardı. Hemogram değerleri ve EKG bulguları normal idi. Akciğer grafisinde belirgin her iki servikal bölgede aksiller hattan başlayıp boyun üst kısımlarına ilerleyen hastaya çekilen toraks bilgisayarlı tomografisinde ilginç olarak pnömotoraks veya hemotoraks olmaksızın, pnömomediastinum ve yaygın cilt altı amfizem izlendi. Pnömomediastinum ve derialtı amfizemi için konservatif tedavi uygulandı. Ayaktan takiple bir hafta sonra kontrole gelen hastada derialtı amfizeminin kaybolduğu izlendi. Akciğer grafisinde ek bir patoloji saptanmadı. Hastanın bir ay sonra yapılan solunum fonksiyon testleri ve grafileri normaldi. Sonuç: Pnömotoraks olmaksızın gelişen pnömomediastinum, derialtı amfizemi acil servislerde nadir görülen durumlardır. Boyunda şişlik sonrası yapılan muayene cilt altı amfizemi belirlemede önemlidir. Hastalara ilk olarak akciğer grafisi çekilmelidir. Olası diğer bulgular açışından tomografi planlanmalıdır. Yüzme sonrası bu tür komplikasyonlar görülebilmektedir. Sporcular bu konuda bilgilendirilmelidir. Anahtar Kelimeler: Pnömomediastinum, amfizem, boyunda şişlik

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
416
P 424 AKUT ÇİNKO FOSFİD ZEHİRLENMESİNDE BAŞARILI TEDAVİ: SIZMA ZEYTİN YAĞININ OLASI YARARI
İsmail Altıntop, Mehmet Tatlı Kayseri Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Kayseri Amaç: Çinko fosfid, depolanmış tahıllara zarar veren haşere ve böceklere rodendisit amaçlı kullanılan tarım ilacıdır. Direk zehirlenme oral yolla alınmasıyla veya kaza ile inhalasyon yoluyla fosfin gazı salınımına bağlı olabilir. Özel bir antidotu yoktur ve mortalitesi yüksektir. Acil servisimize 15 gr çinko fosfatı süisit amaçlı alındıktan 90 sonra getirilen; takiplerinde metabolik asidoz ve hipotansiyonları olan; intravenöz destek tedavisi, oral aktif kömür, oral sodyum bikarbonat ve absorbsiyonun engellenmesi için erken dönemde sızma zeytinyağı verildi. Acil servis ve yoğun bakım takipleri sonucunda şifa ile taburcu olan hastamızda sızma zeytinyağı tedavide etkili olmuş olabilir. Vaka sunumu: On yedi yaşında erkek hasta 1500 mg çinko fosfid toz alımı sonucu intihar girişimi tanısı ile hastanemize sevk edildi. Hastanın tablet alımından yaklaşık 90 dakika saat sonra hastanemizde yapılan fizik muayenesinde Glasgow koma skoru: 14 ve uykuya meyilliydi. Hastada baş ağrısı, baş dönmesi ve halsizlik mevcuttu. Yaşamsal parametreleri; TA: 95/56 mmHg, KTA: 88/dk, SpO2: %94, Ateş: 36,40 C olarak ölçüldü. Hastaya nasogastrik sonda takıldı. Hastaya mide lavajı uygulandı. Hastaya aktif kömür verildi. Aynı zamanda hastaya toplam oral 100 mg sodyum bikarbonat verildi. Hindistan cevizi yağı olmaması üzerine literatürde muadil olabilecek sızma zeytinyağı toplam 400 ml uygulandı. Zeytinyağı 100 ml olarak dört sefer 30 dk ara ile uygulandı. İlk uygulamada hasta mide içeriğini kustu. Takiplerinde hastanın vital bulguları stabil seyretti. Yoğun bakımda üç gün gözlendikten sonra şifa ile taburcu edildi. Sonuç: Çinko fosfid zehirlenmesindeki yüksek mortalitenin önlenmesinde öncelikle etkenin vücuttan uzaklaştırılması fosfin gazı oluşunun engellenmesi önemlidir. Erken dönemde kusturma veya irrigasyon sonucu etkenin vücuttan uzaklaştırılmasının mortaliteyi önemli oranda azalttığı kanaatindeyiz. Hastamızın sızma zeytinyağının ilk doz uygulamasında kusması ve devamında verilen yağın emilimi engellemesinin tedavide önemli katkısı olduğu kanaatindeyiz. Yinede tedavinin devamında metabolik asidoz, aritmi, ARDS ve şoka yönelik tedbirlerin alınması ve erken dönemde hemodiyaliz uygulanması önemlidir. Anahtar Kelimeler: Çinko fosfid, intoksikasyon, sızma zeytinyağı P 425 POLİSİTEMİA VERA OLGUSUNDA SPONTAN İNTRAABDOMİNAL HEMORAJİ Hanife Bilgili, Melek Aktepe, Yonca Senem Akdeniz, Afşın İpekci İstanbul Üniversitesi Cerrahpaşa Tıp Fakültesi, Acil Tıp Anabilim Dalı, İstanbul Giriş: Polisitemia vera(PV), eritrosit kitlesinde mutlak artış ile karakterize, sıklıkla granülosit ve trombositlerin aşırı üretiminin ve splenomegalinin eşlik ettiği bir miyeloproliferatif neoplazidir. JAK2V617F mutasyonu, PV tanılı olguların %95’inden fazlasında görülmektedir. Kemik iliği incelemesinde eritroid, miyeloid ve megakaryositik seride proliferasyon görülür. Spontan batın içi kanama travma olmadan periton boşluğunda kan olmasıdır. Nadir görülen bu durumda hastalarda karın ağrısı ile birlikte kanama miktarına göre abdominal distansiyon, hematokritte düşme ve hipovolemik şok bulguları olabilir. Olgu: 55 yaşında kadın hasta, PV ile takipli, karın ağrısı şikayeti ile başvurdu. Başvuruda vitalleri stabil olan hastanın fizik muayenesinde batın sağ üst kadranda hassasiyet mevcuttu, defans rebound yoktu. Kan tetkiklerinde WBC:45.400 Hb:12.6 PLT:1.036.000 saptandı, biyokimya normal sınırlarda ve CRP negatifti. Hastanın takiplerinde Hb:7,3 e düştü, batın sağ üst kadranda defans gelişti. Çekilen USG ‘de subhepatik alanda yaklaşık 11x8x7 cm boyutlu heterojen ekolu alan saptandı. Hastaya kontrastlı Batın BT çekildi; subhepatik alanda 10x8 cm boyutunda hematom izlendi, batın içi parankimatöz organlarda patoloji izlenmedi. Hastaya kan hazırlığı yapıldı ve Genel Cerrahi Servisine transfer edildi. Sonuç: Trombotik ve hemorajik olaylar, PV’nın en sık ve en ciddi komplikasyonlarıdır. PV’li hastaların %49’unda başvuru bulgusu trombozdur. Kanama insidansı, trombozdan düşüktür ve hastaların yaklaşık %20’sinde ortaya çıkar. Sıklıkla gastrointestinal sistem veya santral sinir sistemi kanamaları görülmektedir. Spontan batın içi kanamalı hastalarla acil serviste nadir karşılaşılır fakat bu hastalarda her zaman hayati tehlike vardır. Tanısı USG, CT ve MR ile konulabilir. Tedavisinde operatif ve non-operatif yöntemler tercih edilebilmektedir. Stabil hastalarda non-operatif yöntemin tercih edilmesi son derece önemlidir. Çünkü cerrahi yaklaşım kanamayı arttırabilir ayrıca cerrahiye bağlı komplikasyonlar görülebilir. Anahtar Kelimeler: İntraabdominal kanama, polistemia vera, spontan kanama

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
417
P 426 LOBER PNÖMONİ- RABDOMYOLİZ BİRLİKTELİĞİ
Hanife Bilgili, Melek Aktepe, Yonca Senem Akdeniz, Afşın İpekci İstanbul Üniversitesi Cerrahpaşa Tıp Fakültesi, Acil Tıp Anabilim Dalı, İstanbul Giriş: Rabdomiyoliz iskelet kası hücrelerinin akut nekrozu sonucu, kas hücre içeriğinin dolaşıma katılmasıyla gelişen klinik ve biyokimyasal bir sendromdur. Başlıca nedenleri; ilaçlar, toksinler, enfeksiyonlar, kas travması, hipertermi, elektrolit dengesizlikleri, kas enzim defektleri, alkol ve kokain kullanımıdır. En sık neden çocuklarda viral myosit, erişkinlerde batı ülkelerinde ilaçlar, gelişmekte olan ülkelerde ise travmalardır. Erişkinlerde enfeksiyonlara bağlı rabdomyoliz nadirdir. Olgu: 73 yaşında erkek hasta, göğüs ağrısı ve halsizlik şikayeti ile Acil Servise başvurdu. Kronik hastalık, ilaç kullanımı, travma ve madde kullanım öyküsü yoktu. Vital bulguları TA: 160/80 Nb: 95 Ateş: 38,9 Spo2:%90 olarak ölçüldü. Fizik muayenesinde sol orta-bazalde krepitan raller duyuldu, diğer sistem muayeneleri doğaldı. EKG’si normal sınırlarda olan hastanın çekilen PA Akciğer grafisinde sol orta lobda infiltrasyon saptandı. Kan gazında pH:7,53 pO2:54 pCO2:26 idi. WBC:14.600 Ure:43 Krea:1,1 AST:51 LDH:260 K:3,5 CK:3066 CK-MB:26 Troponin T:0,22 D-dimer:1,5 olarak sonuçlandı. Troponin kontrollerinde anlamlı artış saptanmadı. Toraks BT’de sol akciğer üst lob ve lingulada hava bronkogramı izlenen geniş konsolide alan izlendi, pulmoner emboli lehine dolum defekti izlenmedi. Hastaya O2 desteği, antipiretik ve antibiyotik başlandı. Rabdomyoliz için hidrasyon ve idrar alkalizasyonu sağlandı. Sonuç: Rabdomyoliz; asemptomatik kas enzim yüksekliğinden, myoglobinin renal tübülleri tıkamasına bağlı oluşan akut böbrek yetmezliğine kadar değişkenlik gösteren klinik bir durumdur. Tanısı biyokimyasal olarak serum kreatin kinaz (CK) değerinin yüksek (x5) olduğu vakalarda serebral infarktüs veya myokard infarktüsünün bulunmaması ile konulmaktadır. CPK, LDH ve AST gibi iskelet kası enzimlerinin ve potasyum, fosfor gibi elektrolitlerin serumda anormal artışı ile ya da pigmentüri saptanabilir. Akut böbrek yetmezliği en ciddi komplikasyondur. Renal fonksiyonları korumak için myoglobinin dolaşımdan uzaklaştırılması gerekir. Anahtar Kelimeler: CK yüksekliği, lober pnömoni, rabdomyoliz P 427 TROPONON YÜKSEKLİĞİ OLAN KARBONMONOKSİT ZEHİRLENMESİ: OLGU SUNUMU Caner Çelik1, Halil Doğan2, Sinem Çelik2, Dogac Niyazi Ozucelik2
1Bağcılar Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul 2Bakırköy Dr Sadi Konuk Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Karbonmonoksit (CO) zehirlenmesi, ülkemizde sıkça karşılaşılan ve acil servislere spesifik olmayan bulgular ile başvuruların önemli sebeplerindendir. Karbon monoksit (CO), karbon esaslı malzemelerin eksik yanması ile üretilen renksiz, kokusuz, tatsız ve irritan olmayan bir gazdır. CO zehirlenmelerinde Troponin I’ nın yüksekliği bu olgu ile literatürler eşliğinde tartışıldı. Olgu: 26 yaşında kadın hasta, baş dönmesi, dizziness, senkop ve bulantı şikayetiyle acil servisimize başvurdu. Anamnezinde, ailecek benzer şikayetler ile hastaneye getirildiği ve şikayetlerinin yaklaşık 1 saat önce başladığı öğrenildi. Hastanın geliş muayenesinde; kan basıncı: 110/70 mmHg, kalp tepe atımı: 88 atım/dk, ateş: 36 derece, solunum sayısı: 20/dk, SpO2: % 98 olarak ölçüldü. Hastanın fizik muayenesi doğaldı, herhangi patolojik bir bulgu tespit edilmedi. Hastanın EKG’si normal sinüs ritminde idi. Yapılan tetkiklerinde; kan pH:7.39, pCO2: 40.9mmHg, pO2: 23.4 mmHg, HCO3: 24.4 mmol/L, COHb: % 15.8, kan şekeri: 111 mg/dl, Troponin T: 0.045 ölçüldü. 6 lt/dk maske ile O2 ile takip edilen hastanın Troponin T’nin 0.176 olarak ölçülmesi nedeniyle akut koroner sendrom ön tanısı ile acil koroner anjiografi planlandı. Koroner anjiografide; herhangi bir koroner patoloji görülmedi. Hastanın yapılan takiplerinde komplikasyon gelişmedi. Hastanın taburculuk öncesi yapılan Ekokardiyografisinde Ejeksiyon Fraksiyonu: % 60 idi, duvar hareket kusuru görülmedi. Hasta, Metoprolol 50 mg, Aspirin 100 mg reçete edilip, poliklinik kontrolü önerisi ile taburcu edildi. Sonuç: CO belirti ve bulgular spesifik olmaması ve sık tanınmayan olması dolayısıyla, gerçek insidansı bilinmemektedir. Mortalite oranları % 1 ve% 31 arasında değişmektedir (5).Bu nedenle acil servislere özellikle kış aylarında spesifik olmayan şikayetlerle başvuran hastalarda CO zehirlenmesi mutlaka akılda bulundurulmalı, kardiak etkileniminin olabileceği ve troponin yüksekliği olsada korner anatominin normal olabileceği unutulmamalıdır. Anahtar Kelimeler: Karbonmonoksit, troponin, koroner sendrom, anjiografi

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
418
P 428 THE EFFECTS OF SMOKING AND MORBID OBESITY ON OBSTRUCTIVE SLEEP APNEA AMONG PATIENTS FOLLOWING EMERGENCY SURGERY
Burcu Yormaz1, Hüseyin Yılmaz2
1Beyhekim State Hospital, Chest Diseases Clinic, Konya, Turkey 2Selçuk University Medical Faculty, Department of General Surgery, Konya, Turkey Background: Obstructive sleep apnea syndrome (OSAS) is a chronic sleep respiratory disease with nocturnal hypoxemia and continuous hypercapnia. Obstructive sleep apnea is a common category of sleep breathing disorders among patients with associated metabolic and cardiovascular diseases. The determinants of hypercapnia in OSAS are still unclear. Also smoking and morbid obesity supports life and health conditions negatively. The aim of our study is to evaluate the patients with sleep breathing disorders who were underwent emergency surgery. Methods: Medical history, demographic parameters and body mass indexes (BMI) were determined, as well as smoking use. Metabolic and cardiovascular diseases were evaluated. Patients were grouped in smokers (SO) and nonsmokers (NSO) morbid obeses. Inactivity, stressful life was correlated with smoking. Two categories of morbid obeses with and without anxiety were defined. Results: Of 24 patients were identified smoking and Of 32 were not declared. Body mass index (BMI) was higher among smokers (SO) (42 ± 2.1 kg/m2) versus nonsmokers (47.5 ± 4.1 kg/m2) also diabetes mellitus and morbid obesity were more frequent in nonsmokers (NSO 12.5% versus SO= 4.16%; respectively), as well as medical history of cardiac disease. Smokers who were consumed more than one pack a day have a greater risk of severe OSA than nonsmokers. Conclusıons: Morbid obesity appears as a risk factor for diabetes and cardiovascular diseases among nonsmokers with sleep breathing disorders. Morbid obese smokers with obstructive sleep apnea syndrome who were admitted to emergency service and operated urgently are higher risk for mortality and morbidity. Keywords: Emergency surgery, sleep apnea, obesity P 429 SANTRAL RETİNAL ARTER TIKANIKLIĞINDA HİPERBARİK OKSİJEN TEDAVİSİ Onur Karakayali, Sırmagül Topuk Kocaeli Derince Eğitim ve Araştırma Hastanesi, Acil Tıp Anabilim Dalı, Kocaeli Giriş: Ani görme kaybı acil kliniklere sık başvuru nedenidir. Ayırıcı tanıda birçok neden bulunmakla acil şartlarda etyoloji aydınlatılması zor olmaktadır. Santral retinal arter tıkanıkları sıklıkla tek taraflı olup bilateral etkilenim nadirdir. Bu vakamızda kliniğimize total görme kaybı ile başvuran santral retinal arter tıkanıklığını tespit edilen hastayı sunarak klinisyenler tarafından ayırıcı tanı ve hızlı,etkin tedavi ile geri döndürülebilir nedenleri tartışmayı amaçladık Olgu: 60 yaşında bayan hasta acil kliniğimize 2 saat önce başlayan ağrısız her iki gözde görme kaybı şikayeti ile başvurdu. Sol gözde tama yakın sağ gözde ise kısmi görme kaybı mevcuttu. Hastanın ek şikayeti mevcut değildi. Özgeçmişinde kalp yetmezliği, diyabet öyküsü mevcut olup digoksin ve oral antidiyabetik kullanımı mevcuttu. Vital bulguları stabil fizik muayenede sağ gözde total görme kaybı sol gözde 1 metreden kısmi görme mevcut, diğer sistem bulguları normaldi. Laboratuarda anormal bulgu yok, digoksin düzeyi normaldi. Santral görme kaybı ayırıcı tanısında diffüzyon ve kontrastlı beyin MR’da akut patoloji yoktu. Acil oküler usg’de vitröz hemorajı saptanmadı. Oftalmik muayenede göz dibi beyaz renkte fovea çevresinde kırmızı alan tespit edildi. Göz muayenesi sonrasında hastaya santral retinal arter tıkanıklığı tespit edildi.Hastaya mannitol 1mg/kg yükleme ve hiperbarik tedavi uygulandı.Ayaktan hiperbarik tedavi verilen hastanın 3.seanstan sonrasında görme kaybı düzeldi. Tartışma: Santral retinal arter tıkanıklıkları klinikte sık görülmemekle birlikte acil müdahele ile geri dönüşümlü olabilmektedir. Tedavide göz içi basıncı azaltmak amacıyla mannitol tedavisi önerilmektedir. Retinal vasküler hastalıklarda meydana gelen ani görme kayıplarında Hiperbarik Oksijen Tedavisi uygulanmaktadır. Hiperbarik Oksijen Tedavisinin amacı örneğin santral retinal arter tıkanıklıklarında olduğu gibi retinanın 2/3 ünü sulayan bu arter tıkanmış olsa bile koriokapillaris yolu ile retina oksijenizasyonunu devam ettirmektir. 20 seansa kadar uzayabilen Hiperbarik Oksijen Tedavisi uygulanması sırasında kanın 02 içeriği ve ayrıca basınç yüksekliği ile orantılı olarak oksijenin difüzyonu da artacağı için retinanın canlılığını ve fonksiyonlarını korumak mümkümdür. Sonuç: Santral retinal arter, dal, retinal ven tıkanıklıklarında ve retina iskemisi ve makuler ödem ile buna bağlı göz hipoksisinin söz konusu olduğu durumlarda Hiperbarik Oksijen Tedavisi uygulanmalıdır. Anahtar Kelimeler: Santral retinal arter tıkanıklığı, acil servis, hiperbarik oksijen tedavisi

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
419
P 430 THE UTILITY OF PROCALCITONIN AS AN EARLY MARKER OF THE NEED FOR URGENT INVASIVE RESPIRATORY AID IN PATIENTS WITH COPD WHO HAVE UNDERWENT EMERGENCY SURGERY
Burcu Yormaz1, Mehmet Ertugrul Kafalı2
1Beyhekim State Hospital, Chest Diseases Clinic, Konya, Turkey 2Selçuk University Medical Faculty, Department of General Surgery, Konya, Turkey Background: Procalcitonin (PCT) is an helpful marker for detecting possible respiratory aid among adults with chronic obstructive pulmonary disease (COPD) remains challenging. The aim of this study is to evaluate the utility of PCT in the diagnosis of urgent respiratory aid (URA) in patients admitted to the intensive care unit (ICU) following emergency surgery. Methods: We have evaluated the effect of serum procalcitonin (PCT) concentration at ICU with the need for urgent invasive respiratory aid (URA). We also evaluated whether the addition of PCT changed the performance of established severity URA requirement, including the SAPS II scores. Results: Of 106 enrolled patients, 8 required URA (6.5%). PCT concentration has a strong association with URA risk. Undetectable PCT (< 0.05 ng/mL) was associated with a 4% risk of URA. For concentrations < 10 ng/mL, PCT had an approximate linear association with URA risk: for each 1 ng/mL increase in PCT, there was a 2% to 5% absolute increase in the risk of URA. With a PCT concentration of >10 ng/mL, the risk of URA was 31.7%. When added to each SAPS II score, PCT contributed significant additional risk information for the prediction of URA following emergency surgery. Conclusions: Serum PCT concentration was strongly associated with the risk of requiring URA among adults hospitalized with COPD and is potentially useful for guiding decisions about ICU admission following emergency surgery.Thus further studies are needed to define the clinical benefit of PCT testing in ICU patients after emergency surgery. Keywords: COPD, emergency, procalcitonin P 431 STEVENS-JOHNSON SYNDROME DUE TO USE ANTIBIOTICS Büşra Sapmaz, Meltem Songür Kodik, Murat Ersel Ege University Medical School, Department of Emergency Medicine, Izmir, Turkey Introduction: Dermatological problems are 4 to 10 % of the emergency department visits. While most are benign in course, some require admission as true dermatological emergencies. Stevens Johnson Syndrome/toxic epidermal necrosis (SJS/TEN) is one of the possibly life-threatening dermatological problems that emergency physicians cannot afford to miss. We present our drug-related SJS case as a rare dermatological diagnosis. Case: A 76-year old male with hypertension admitted to emergency department with erythema and fever 38.2 oC. He explained that his lesions had started on his face and spreated to thorax, back and arms after he used cefuroxime and clarithromycin, prescribed for flu, for three times. Physical examination revealed coalescing erthematous macules with purpuric centers and his lesions were tender to the touch. He, also, had oral and genital mucosal hemorrhagic erosions with positive Nikolsky sign and he had conjunctivitis with a purulent discharge. Patient medication was discontinued and started hydration. He admitted to dermatology ward. Discussion: SJS and TEN are severe mucocutaneus reactions characterized by persistent fever and most commonly triggered by medications. The literature suggests that SJS and TEN ocur in approximately 2 to 3 people per million/year in Europe and the USA and SJS’s fatality in 5% of cases. Although numerous drugs have been noted as responsible sulfonamide class of antibiotics, allopurinol, NSAI’s the most frequently reported causative ones. Results: In our case, the antibiotics were prescribed for patients flu-like symptoms. Unnecessary antibiotic use on viral infections should be reduced in order to avoid adverse drug reactions. Keywords: Cefuroxime, claritromycin, emergency department, Stevens-Johnson syndrome

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
420
P 432 AKUT PERMETRİN ZEHİRLENMESİ: OLGU SUNUMU
Selim Genç, Kemal Aydın, Esra Özer Ünal, Izzettin Hür, Ömer Faruk Demir, Macit Aydın S.B. Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Ankara Giriş: Permetrin yeryüzünde yaygın olarak kullanılan, etkisini sodyum kanallarıyla etkileşime girerek periferal ve merkezi sinir sistemini paralize ederek gösteren sentetik piretroid grubu bir insektisittir. Yüksek miktarda alındığında organoklor benzeri etki gösterebilen ve geniş toksik spektruma sahip olabilen bir ilaçtır. Her ne kadar memeliler üzerine toksik etkileri zayıf olduğu iddia edilse de gün geçtikçe sindirim sistemi toksisitesi, hematolojik etkiler, sitotoksik, nörotoksik, kardiyotoksik, hepatotoksik etkileri üzerine olan bilgiler artmaktadır. Biz bu çalışmada yüksek doz permetrin alan bir olguyu literatür eşliğinde tartışmayı hedefledik. Olgu: 45 yaşında erkek hasta bilinç bozukluğu yakınması ile acil servise getirildi. Öyküsünden yakınları tarafından acımsı ve gözleri yaşartan bir kokunun farkedilmesi ile apatman boşluğunda bulunduğu öğrenildi. Başvuruda pupilleri miyotik, sekresyonları artmış, bilinç uykuya eğilimli, kooperasyonu ve oryantasyonu ileri derecede bozulmuştu. Diğer fizik muayene ve vital bulguları normaldi. Laboratuvar incelemesinde hiperkalsemisi mevcuttu. Olay yerinde boş ilaç kutusunun bulunması ve eşlik eden fizik muayene bulguların desteği ile hastaya akut permetrin zehirlenmesi tanısı konarak kritik hasta bakım odasına alındı. Sabunlu su ile cildi yıkandı, mide irigasyonu ardından 2gr/kg aktif kömür verildi. İntravenöz mayi desteği, B vitamini, C vitamini ve furasemid başlandı. Takibinin 12. saatinde bilinç bozukluğu, kooperasyonu ve ortantasyonu düzeldi. Takibinin 2. gününde takibe alınarak taburcu edildi. Sonuç: Acil serviste akut permetrin zehirlenmesi tanısı konan hastalar kritik bakım odalarında takip edilmeli ve bu hastalar gelişebilecek sistemik toksisiteler için taburculuk sonrası izleme alınmalıdır. Anahtar Kelimeler: Permetrin, toksisite, acil servis P 433 ACİL YATAKBAŞI USG İLE BELİRLENEN DAMAR İÇİ MADDE KULLANIM SONRASI FEMORAL ARTER PSÖDOANEVRİZMASI Yesim Uz, Abdullah Taşcı Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, İstanbul Olgu: 24 yaşında erkek hasta, sağ kasıkta şişlik, ağrı, akıntı ve kanama şikayeti ile acil servise başvurdu. Hastanın gelişinde vitalleri; Ateş:36.4C, Nb: 112/dk, TA: 107/67mm/Hg, Sat:%96 olarak ölçüldü. Hastanın özgeçmişinde madde bağımlılığı öyküsü dışında özellik saptanmadı. Fizik muayenesinde GKS: 15, oryante, kooperasyon kısıtlı olarak değerlendirildi. Batın sağ alt kadran ve sağ inguinal bölgede kötü kokulu, kanlı, pürülan akıntılı, palpasyonla hassas 3x3 cm sınırlarında kitle saptandı. Diğer sistem muayenelerinde anormallik saptanmadı. Laboratuvar tetkiklerinde WBC:19.9/mm3, Hgb: 11.9 g/dL, Htc: %33.6, Kr:0.76 mg/dl, BUN:19 mg/dl, INR:1.25, PTZ:15.9/sn, CK:2091U/L dışında anormallik saptanmadı. Acilde yapılan yüzeysel yatak başı USG’de sağ eksternal iliak arter ve ven komşuluğunda sağ psoas kası içerisinde yaklaşık 30mm büyüklüğüne ulaşan hematom, çevre dokularda ödem ve ileal anslara komşu hafif derecede efüzyon görüldü. Hastaya çekilen iv kontrastlı alt batın BT’de sağ inguinal kanal içersinde femoral arter komşuluğunda psödoanevrizma ile uyumlu dansite alanı ve bu alana komşu yaygın inflamasyon bulguları izlendi. Hasta Kalp-Damar cerrahisi ile konsülte edildi. Kalp damar cerrahisi hastaya elektif olarak eksplorasyon planladı. Tartışma: Psödoanevrizma arteryal duvardaki bütünlüğün bozulması ile meydana gelir. Alt ekstremite damarlarının anevrizmaları nispeten daha sıktır. Femoral arter anevrizması daha çok iyatrojenik nedenlerle anjiyo ve katater girişimleri sonrasında görülür. Enfekte femoral arter psödoanevrizması madde bağımlılarında intra-arteryal injenksiyona sekonder geliştiği bilinen bir durumdur. Klinik olarak pürülan akıntı, kan ve pulsatil kasık kitlesi triadı tipiktir. Tanıda en yararlı ve hızlı tetkik Doppler Ultrason’dur. Femoral psödoanevrizmalar tedavi edilmezse rüptür, damar trombozu ve distal emboli ile sonuçlanabilir. Etyolojik faktörden bağımsız olarak 2cm ve üstü ekstremite psödoanevrizmaları, semptomatik ve zamanla genişliyor ise tedavi edilmelidir. Ufak psödoanevrizmaları öncelikle takip edilmelidir. Sonuç: Damar içi madde kullanımına bağlı gelişen vasküler komplikasyonların görülme sıklığı giderek artmaktadır. Acil serviste yapılan yatak başı USG’nin acil servis için önemi ve gerekliliği yadsınamaz. Anahtar Kelimeler: Madde, psödoanevrizma, USG

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
421
P 434 COOKING OILS ARE NOT FOR ONLY SALADS
Bilgen İlküplü, Sercan Yalcinli, İlhan Uz, Funda Karbek Akarca Ege University School of Medicine, Department of Emergency Medicine, Izmir, Turkey Introduction: Hydrocarbon derivatives are used in paving and roofing industry and manufacturing products such as tyres. Exposure to hot tar, a hydrocarbon derivative, causes burns. Tar burns induce extreme pain and result in dermal injuries unless immediately removed. Case A: 19 year old male admitted to emergency department with tyre explosion while his friends and he burnt a tyre for fun. His scalp from frontal to occipital area including his nose, lips, right side of his face and right ear and skin from axilla to forearm in median side were covered with tar. After removal of tar using olive oil, first and second degree burns revealed. Case B: 61 years male was brought emergency service. Patient had bilateral burn lesions on his hands and his right foot. It was done by tar at his workplace. Lesions on his hands were patch-like and they were second and third degree. Lesions on his right foot were %90 circumferential second and third degree. Lesions cleaned by olive oil. Discussion: Tar causes significant burns because of its high temperature and stickiness. In the literature, it is reported that job-related burns constitute 10-45% of all burn events whereas; tar burns account for 60.3 of all chemical burns. Like in all burn events agent should be moved away. Immediate removal of tar is important to prevent the progression of injury and secondary infections. There is still no specified appropriate agent for removal of tar. Manual debridement and organic substances were abandoned because of their detrimental effects on skin injury. Recent studies recommend oily substances such as sunflower oil, mayonnaise and butter. Skin must be also cleansed of the nonsterile oily substances because of increased infection risk. Regular and careful use of daily antibiotics and wound care are the other milestones of burn treatment. Keywords: Burns, olive oil, tar P 435 SKULL BASE OSTEOMYELITIS IN A NON-IMMUNCOMPROMISED, MIDDLE AGED PATIENT WITH A HISTORY OF MASTOIDECTOMY Ece Soykan, Özge Can, Selahattin Kıyan Ege University Faculty of Medicine, Department of Emergency Medicine, Izmir, Turkey Introduction: Osteomyelitis of the skull base is a rare and life-threatening condition commonly seen in elderly, diabetic and immunocompromised patients. The typical onset of the symptoms are otorrhea, otalgia, cranial nerve dysfunction and mostly documented as an extension of malignant otitis externa. We describe a case with skull base osteomyelitis presented with right hemiparesia and otalgia. Case: The case described is of a 50-year-old non-diabetic, non-immuncompromised male with a history of mastoidectomy 30 years ago. Presented with otalgia, otorrhea, headache, right hemiparesis. On physical examination external auditory meatus was narrowed, prior mastoid operation zone was swelled. Bilateral eye movements were impaired and exoftalmus was present. Blood tests showed elevated infectious markers. Cranial CT showed destruction of bony walls of the left carotis tunnel and no signs of intracranial bleeding. He had bilaterally chemosis and orbital CT showed thromboflebitis. Cranial MRI showed infection of the tympanic cavity, petrous bone and thrombosis of the cavernous sinuses and superior ophthalmic veins bilaterally. External auditory canal swap specimen showed P. Aeruginosa. The patient treated with antibioterapy and LMWH for his osteomyelitis and thrombosis. Discussion: Skull base osteomyelitis is a life-threatening condition which can be hard to diagnose. According to literature central or atypical presentations, headaches and cranial nerve palsies were common symptoms. Disease is mostly seen as a complication of masteidectomy and malign external otitis. Risk factors are diabetes mellitus and immunocompromised status. Elder and middle aged males are most frequently effected. In our case he has a history of masteidectomy 30 years ago. P.aeruginosa is main causing microorganism which is identified in specimen. Cranial CT or MRI are diagnostic tools. The infectious Disease Society of America suggests antibiotic therapy. Conclusion: It’s important to keep in mind especially in elderly and immunocompromised patients with cranial nerve palsy. Keywords: Mastoidectomy, skull base osteomyelitis, P. aeruginosa

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
422
P 436 ACUTE PSYCHOTIC DISORDER DUE TO ICD IMPLANTATION
Ayça Çalbay, Mert Vural, Nazım Onur Can, Sibel Güçlü Atatürk University Faculty of Medicine, Department of Emergency Medicine, Erzurum, Turkey İntroduction: The incidence of Hypertrophic cardiomyopathy (HCM) is 1 in 500 adults on the world. Although the patients with HCM are asymptomatic, the risk of sudden cardiac death (SCD) probability should be keep in mind in all patients. Most of the death reason is ventricular arrhythmias. Implantable cardioverter-defibrillators (ICDs) are much effective at ventricular arrhythmias. Case: A 25 year old man came to emergency service with history of icd implantation in 17 days ago. He engaged in violence to his family members. He had auditory hallucinations. ‘People knows my new pacemaker have not a trademark, because of this they humiliate me’ was the patient’s repeated sentence. He had been asking for marriage with a girl who is twelve year old and he has obsessions about this idea. The first mental instability of the patient began while he was resting in coronary intensive care unit. He had been examined by the psychiatrist during these days and evaluated as acute psychotic disorder. The psychiatrist recommended invega (antipsychotics) therapy to the patient on these days but he didn’t use his medication. The vital signs of the patient was in normal range. There was not any pathologic sign on his neurologic and systemic examination and also the laboratory tests were normal. The patient was evaluated by the psychiatrist in emergency department and admitted to psychiatry service for antipsychotic therapy with the diagnoses as acute psychotic disorder. Result: Psychotic disorders are serious mental disorders which cause unusual opinion and sensations. With treatment by the antipsychotics, many people can increase their life comfort. As our patient who has icd implantation history should examine detailed as systemic, neurological and psychological. The emergency physician keep in mind independent risk factors as age, low weight, chronic diseases, medical history and admission complaint to emergency service. Keywords: icd, acute psychotic disorder, antipsychotics P 437 DISSIMILAR DON JUAN Atıf Bayramoğlu1, Ayça Çalbay1, Nazım Onur Can1, Sinan Yılar2
1Atatürk University Faculty of Medicine, Department of Emergency Medicine, Erzurum, Turkey 2Atatürk University Faculty of Medicine, Department of Orthopedics and Traumatology, Erzurum, Turkey Introduction: Lover’s fracture is an intra articular fracture due to axial loading force by falling from height usually (called as “Don Juan” fracture commanly). The same axial trauma effect the spine and may cause burst fractures of the lumbar or thoracic vertebras with 10% of patient who has calcaneus fracture. Most common coexisting shown at thoraco-lumbar junction at L1,L2,T11 and T12. Case: A 32 year old woman came to emergency service with 2 day history of motor vehicle accident. The vital signs were in normal range. She complained lomber pain. There were not neurologic deficits, deformity seen on right ankle on the physical examination. Other systemic examination was unremarkable. Because of high-energy multiple trauma and examination findings, x-ray graphies obtained with thorax, vertebra, abdomen and brain computarize tomography (CT) scans. İntra articular calcaneus fracture has been showned on right foot x-ray with thoracal 12 vertebra burst fracture on CT scans. Patient was hospitalized in to neurosurgery service for the spinal surgery after the stabilization of the right ankle. Result: DJ fractures are typically produced after jumping from a height with person dropping on heels. Several cases occurred due to fall from height have been reported in the literature. Our case is unique from this perspective. İn patients admitted to emergency service with motor vehicle accident have a wide range of clinic from simple injury to death. Physician should keep in mind this simple and mortal coexisting in this special group of patient. Keywords: Don Juan, lover's fracture, vertebra fractures

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
423
P 438 TRAUMA DUE TO CEREBELLAR INFARCTION
Ayça Çalbay, Mert Vural, Fatma Tortum, Ayşe Şenyurt Atatürk University Faculty of Medicine, Department of Emergency Medicine, Erzurum, Turkey İntroduction: Cerebellar infarct is an uncommon situation with very nonspecific clinical presents. The diagnosis of cerebellar infarction (CBI) is often challenging due to non-specific or subtle presenting symptoms and signs. Case: A 58 year old woman came to emergency service with 3 day history of dizziness and 1 hour history of syncope with head trauma. She had been brought to emergency room(ER) with 112 health service. Her Glasgow coma scale was 11 during the first presentation of ER. The vital signs were as following: TA: 180/95mmHg, pulse: 120, O2 sat:85% and fewer was 36’C. There was not any pathologic sign on her systemic examination. The babinsky sign was positive on right foot and there was not stiff neck on the neurologic examination. Her ECG and biochemical lab tests were in normal range. Because of trauma and altered mental status cranial computerized tomography taken to the patient and cerebellar ischemia showned on the left part of the cerebellum. The patient consulted with the neurology clinic and hospitalized on there. Result: All neurologic infarctions have a wide range of symptom like headache to coma. The clinic of the patients with ischemia can progress slowly or aggressive depends on size of ischemia. Because of this common and uncommon signs, patients with dizziness, headache or altered mental status should examine carefully and emergency physician should keep in mind to santral ischemia with this special population. Keywords: Trauma, serebellar infarction, dizziness P 439 IS ENDOLEAK OVERLOOKED IN THE EMERGENCY MEDICINE LITERATURE?
Nihat Bulandere, İlhan Uz Ege University School of Medicine, Department of Emergency Medicine, Izmir, Turkey Introduction: Abdominal aortic aneurysm (AAA) is a deadly condition, particularly with rupture. Endovascular aortic repair (EVAR) has become the gold standard for treatment of AAA. Endoleak is a common phenomenon after EVAR. An endoleak is defined by vascular flow outside of the graft, but the management of Endoleak is not well discussed in the emergency medicine literature. Case: A 57 year old male, who came to emergency department for lower abdominal pain and palpabl abdominal mass. His vital parameters were stable and mental status was normal. He had EVAR history 2 years ago. A bedside ultrasound showed hyperechogenic object near abdominal aorta. CT scan of the abdomen showed 10x8 cm pseudoaneurism originate from endoleak on abdominal aorta. It was type 5 endoleak. Discussion and Conclusions: Although many complications may arise after AAA repair, the most common include aortoenteric fistula, endoleak, limb ischemia, and graft infection. All potential complications should receive vascular surgery consultation and hemodynamic resuscitation. There are 5 types of endoleaks, each with different causes and treatment options. Type 1 endoleak seen proximal (a) and distal (b) operation areas. Type 2 endoleak seen with blood flow back to the aneurysm sac from collateral vessels. Type 3 endoleac is made with tears from stent/greft. Type 4 endoleac is made of porpus greft wall structure. Type 5 endoleac is expansion of aneurizm bladder without leakage due to endotansion (2). With the growing use of EVAR, emergency physician exposure to complications of this procedure is increasing. Knowledge of the complication presentations, diagnoses, and management can play an integral role patient care. Emergency physicians must maintain vigilance and take extra caution in patients with indwelling vascular grafts. Keywords: Abdominal aortic repair, endoleac, pseudoaneurism

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
424
P 440 HOW DO NURSES INTERPRET LOW VOLTAGE VENTRICULAR FIBRILLATION DURING SIMULATED CARDIOPULMONARY RESUSCITATION? ARE THEY AS GOOD AS WE THINK?
Lukasz Szarpak1, Zenon Truszewski1, Jacek Smereka2, Togay Evrin3, Jerzy Radny4, Krzysztof J Filipiak5
1Medical University of Warsaw, Department of Emergency Medicine, Warsaw, Poland 2Wroclaw Medical University, Department of Emergency Medical Services, Wroclaw, Poland 3UfuK University Medical Faculty, Department of Emergency Medicine, Ankara, Turkey 4Medical University Bialystok, Department of Emergency Medicine and Disaster, Bialystok, Poland 5Medical University of Warsaw, Department of Cardiology, Warsaw, Poland Objective: The ability to interpret electrocardiographic (ECG) rhythms associated with cardiac arrest is a necessary skill, having a direct impact on the quality of advanced life support (ALS) and the patient survival. The aim of the study was to evaluate the ability to recognize low voltage ventricular fibrillation (LvVF) during simulated cardiopulmonary resuscitation (CPR) performed by nurses. Material: The study, conducted during ALS workshops, involved 42 nurses working in emergency units or anesthesiology and intensive care units. The nurses performed CPR according to the European Resuscitation Council (ERC) guidelines. During the exercise resuscitation, the team consisted of 2 independent instructors and a nurse acting as team leader. The resuscitation team leader was required to interpret the ECG rhythm and administer the appropriate treatment, including drugs and defibrillation. CPR was applied in a MegaCode Kelly manikin (Laerdal, Stavanger, Norway) with the use of a LIFEPAK 15 manual defibrillator (Physio-Control, the Netherlands). During the 10-minute scenario, the ECG rhythms were randomly altered, always including the occurrence of LvVF. Results: The median age of the participants was 32.5 (interquartile range, IQR, 27–41.5) years, and work experience – 5.5 (IQR, 3.5–7) years. LvVF was recognized only by 16 nurses (38.1%). In the case of LvVF occurrence, only 33.3% participants increased the ECG amplitude and changed the ECG lead. Among the 16 nurses who recognized LvVF, 12 performed defibrillation, and 4 followed the guidelines for non-shockable rhythms. Conclusions: There is a need to introduce compulsory periodic training for the nursing staff to focus on recognizing rhythms associated with cardiac arrest and implementing procedures based on the 2015 ERC guidelines. Keywords: Resuscitation, electrocardiography, interpretation, rhythm P 441 ACİL SERVİSTE NADİR BİR ETYOLOJİ İLE DİSTONİK REAKSİYON VAKASI
Tufan Alatlı1, Halil İbrahim Akdoğan2
1Turhal Kazova Devlet Hastanesi, Acil Servis, Tokat 2Gaziosmanpaşa Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Tokat Giriş: Akut Distonik Reaksiyon; çoğunlukla antiemetik, antipsikotik ve antidepresan ilaç kullanımına bağlı ortalama bir hafta içerisinde gelişebilen anormal kas spazmlarıdır. Ancak etyolojide histamin H2 reseptör blokerleri, bazı antimalaryan ilaçlar, antihistaminikler, lityum, fensiklidin gibi ajanlar da az da olsa yer almaktadır. Olgu: 28 yaşında bayan hasta anemi nedenli hospitalize iken intravenöz demir tedavisi başlanmış. İntravenöz demir tedavisi sırasında hastada yan etki gelişmesi üzerine hastaya antihistaminik uygulanmış ve şikayetleri gerilemiştir. Bunun üzerine taburcu edilen hasta bir gün sonra sağ üst ve alt ekstremitelerde istemsiz kasılmalar ile acil servisimize başvurdu. Hastanın bilinci açık, koopere, oryanteydi. Sağ üst ekstremitede daha yoğun ve güçlü olmak üzere sağ alt ekstremitede de istemsiz kasılmaları mevcuttu. Nörolojik muayenesinde sağda hemihipoaljezi mevcuttu. Laboratuvar tetkiklerinde Hb: 8,2 gr/dL, Hct: %27,1, RDW: % 21,3, Plt:302.000, Glc: 89 mg/dL, BUN: 11,8mg/dL, Cr: 0,45 mg/dL, CRP: 0,09 mg/L, Na: 138 mmol/L, K: 4,65 mmol/L, Ca:8,6 mg/dL, pH:7,36, Laktat: 0,8 mmol/L saptandı. Hastadan kranial görüntüleme olarak beyin tomografisi ve diffüzyon MR(manyetik rezonans) istendi. Her ikisinde de acil patoloji gözlenmedi. Göz dibi muayenesinde Kayser - Fleischer halkası saptanmadı. Akut romatizmal ateş ayırıcı tanısı için ekokardiografik görüntülemede normal sınırlar içerisinde bulgular elde edildi. Hastanın distonisi çok gerilememesi üzerine ileri tetkik ve tedavi için hasta hospitalize edildi. Sonuç: Acil servise birçok hasta farklı ilaç yan etkileri ile başvurmaktadır. Hasta ve hasta yakınları için akut distoni dramatik bir tablodur. Nadir nedenlerinden olsa da antihistaminiklerin de akut distoniye yol açabileceği akıldan çıkarılmamalıdır. Anahtar Kelimeler: Antihistaminik, distoni, yan etki

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
425
P 442 LATE DIAGNOSED PNEUMOTHORAX
Soner Işık1, Mehmet Ünaldı1, Vehbi Özaydın1, Didem Ay1, Kurtuluş Açıksarı1, Hatice Eryiğit2
1Medeniyet University Göztepe Training and Research Hospital, Department of Emergency Medicine, Istanbul, Turkey 2Dr. Lütfi Kirdar Kartal Training and Research Hospital, Thorax Surgery Clinic, Istanbul, Turkey Pneumothorax occurs when air enters the potential space between the visceral and parietal pleura as a consequence of blunt trauma, penetrating trauma, or spontaneous occurrence. We present to the case suffered trauma three weeks ago. Case: 50-year-old male patient admitted to the ED with complaints of shortness of breath, uncomfortable breathing and chest pain. Vital signs of him were normal. In history he had suffered blunt trauma about 20 days before and presented to another ED. Comparison of old and new radiologic scanning, we detected pneumothorax on right side of chest. Not requiring tube thoracostomy placement he was recommended follow-up thorax surgery clinic.Pneumothorax is an important differential diagnosis to consider in patients with chest pain. It should be mind pneumothorax may be occurred later despite normal initial radiologic evaluation as in this case. Keywords: Chest pain, diagnosed, pneumothorax P 443 WHAT CAN BE DONE IN TREATMENT RESISTANT PATIENTS IN ACE INHIBITOR INDUCED-ANGIOEDEMA? Funda Karbek Akarca1, Şadiye Mıdık2, Sercan Yalçınlı1
1Ege University School of Medicine, Department of Emergency Medicine, Izmir, Turkey 2Gaziemir State Hospital, Emergency Medicine Clinic, Izmir, Turkey İntroduction: ACE inhibitors are the most cause of drug-induced angioedema. ACE inhibitors induce angioedema in 0.1 to 0.7 percent of recipients. The clinical features of ACE inhibitor angioedema are related to elevated levels of bradykinin. In most cases, the episode of angioedema resolves without complications and response standard treatment with adrenaline, antihistamines and steroids in 24-72 hours. However, endotracheal intubation or emergent tracheostomy may be necessary for angioedema obstructing the airway. We brought this cases to deliver additional therapies for treatment resistant patients. Case 1: 74-year-old woman was admitted emergency department for swelling tongue when she woke up. She has hypertension and uses lisinopril and amlodipine. She had edema in the right side of tongue and uvula. 20 mg diphenhydramine, 50 mg ranitidine, 80 mg methylprednisolone was administered with nebulized epinephrine. The edema of the tongue progressed over and 2u FFP was replaced, but not respond.C1 esterase inhibitor concentrate (Cetor) 1000 IU was administered and clinical improvement was observed. After 24 hours of observation in emergency department were discharged. Case 2: 64 years old woman presented with swelling in the tongue. The edema of tongue was filled mouth completely. She used captopril for hypertension. Epinephrine, antihistamines and steroids were given immediately. Also tracheostomy preparation was made. Upon deterioration of the edema; the patient was treated with C1 inhibitor concentrate (1500u). Rapid clinical responses received and the patient was discharged after observation for 36 hours. Conclusion: ACE inhibitor induced-angioedema may not respond to standard treatment. Additional therapies should be considered if the swelling is threatening the patient's airway and intubation seems imminent. Additional therapies include; İkatiband, FFP and C1 esterase inhibitor concentrate. C1 esterase inhibitor acts by inhibition of kallikrein in patients. C1 inhibitor concentrate should be kept in mind with patients ACE inhibitor-induced angioedema. Keywords: Angioedema, ACE inhibitor; lisinopril, C1 esterase inhibitor

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
426
P 444 INTERPRETATION OF PNEUMOTHORAX ON EMERGENCY DEPARTMENT CHEST RADIOGRAPHS BY EMERGENCY MEDICINE PHYSICIANS AND RESIDENTS
Burcu Azapoğlu Kaymak1, Didem Ay2, Vehbi Özaydın2, Halil Tözüm3
1University of Health Sciences, Fatih Sultan Mehmet Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey 2 Medeniyet University Göztepe Training and Research Hospital, Department of Emergency Medicine, Istanbul, Turkey 3 Medeniyet University Göztepe Training and Research Hospital, Department of Thoracic Surgery, Istanbul, Turkey Objective: Pneumothorax is defined as the entry of air into the pleural space, and may cause mortal complications when diagnose and treatment delay. The diagnosis is made on an erect posteroanterior chest x-ray which shows an edge caused by visceral pleura and absence of lung markings beyond this edge. These chest radiographs are initially interpreted by an emergency physician and decisions are made on the basis of this initial interpretation. Methods: The chest radiographs of 100 patients were collected from PACS archive.50 of these radiographs were reported as normal and 50 of them were pneumothorax. Emergency staff participating in the study included four emergency medicine physician, three final year residents, four intermediate year residents and four first year residents. Each physician interpreted 100 radiograph. Effects of interobserver variability and degree of pneumothorax on diagnosing pneumothorax on chest x-rays were investigated. Chest radiographs were re-interpreted 2 weeks later to search intraobserver variability. Results: The accuracy of the emergency department physicians and residents on diagnosing total pneumothorax were 100 %, intermediate pneumothorax were 95.1%, small pneumothorax were 49.7%. Final year residents correctly diagnosed 83.3%, intermediate year residents 75.5%, first year residents 62.5%. Conclusion: Increase in the volume of pneumothorax made it easier to diagnose on chest radiograph. Residency year is associated with correct diagnose of pneumothorax especially in small pneumothorax cases. Keywords: Pneumothorax, chest radiograph, emergency medicine physicians, emergency medicine residents, interpreting radiograph P 445 ANKARA ÜNİVERSİTESİ İBN-İ SİNA HASTANESİ ACİL TIP ANABİLİM DALI HEMŞİRELERİNİN, BASI YARASI GELİŞİMİNİN ÖNLENMESİ VE BAKIMINDAKİ ROLÜ Hülya Karabulut, Nazlı Yıldız, Müge Günalp Eneyli Ankara Üniversitesi Tıp Fakültesi İbn-i Sina Hastanesi, Acil Tıp Anabilim Dalı, Ankara Giriş-Amaç: Basınç yaraları; morbidite ve mortalitede artış nedeniyle ile hem sağlık açısından hem de ekonomik açıdan oldukça önemli bir sorundur. Basınç yarası oluşumunda yatağa bağımlı olma en önemli faktörlerden biridir. Ayrıca basınç yarası oranı hemşirelik bakımının kalite göstergeleri arasında sayılmaktadır. Acil servislerde akut gelişen primer nedenlerle acil servise başvuran hastalarda bası yarasının varlığı ya da akut bir rahatsızlık ile başvuru yapan bir hastada bası yarası açılabildiği görülmektedir. Bu çalışma hemşirenin acile başvuran hastaların primer nedenlerine yönelik bakımının yanı sıra, bası yarası risk faktörlerinin belirlenmesi ve bası yarası bakımının önemi konusunda farkındalık yaratmak için yapılmıştır. Materyal ve Metot: Acil servise başvuru yapan yatağa bağımlı hastaların hepsine waterlow yara bakım skalası kullanılarak risk değerlendirmeleri yapılmakta olup riske göre önleyici faaliyetler yapılmaktadır. Ayrıca bası yarası ile gelen ya da acil serviste gelişen bası yaralarının günlük bakımı yapılıp, yaranın derecesi, yaranın çapı, kokusu rengi, yeri günlük değerlendirilip yara formuna kayıt edilmektedir. Ayrıca Acil Tıp Anabilim Dalı hizmet içi eğitim programlarına ve oryantasyon eğitimine yara bakımı konusu eklenmiştir. Tartışma: Acil servisler, acil problemi olan hastaların ilk müdahalelerin yapılıp taburculuk ya da ilgili kliniğe gönderilmeleri ile sonlandırılsa da hastalar 48 saatten uzun süre kalabilmektedir. Ayrıca hastaların acil serviste kaldığı süre boyunca sedye üzerinde takip edilmesi, immobil hastanın pozisyon değişimini güçleştirmesi açısından basınç yarası açılmasında önemli bir faktördür. Bunun için yatağa bağımlı hastaların klinik ve/veya yoğun bakıma yatışlarının hızlandırılması önemlidir. Anahtar Kelimeler: Bası yarası, hemşire, acil servis

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
427
P 446 ATROPİN KULLANIMI SONRASI DELİRYUM: SANTRAL ANTİKOLİNERJİK SENDROM
İpek Gülin Ağar, Hüseyin Narcı, Güllü A Dündar, Refika Şendağ, Cüneyt Ayrık Mersin Üniversitesi Tıp Fakültesi, Acil Tıp Anabilim Dalı, Mersin Amaç: Acil servis pratiğinde sıklıkla kullanılan atropin; taşikardi, ajitasyon, deliryum, dilate pupil, kuru cilt, hipertermi, idrar yapma güçlüğü gibi santral ve periferik bulgulara neden olabilir. Bu olguda atropin uygulanması sonrası gelişen deliryum tablosunu sunmayı amaçladık. Olgu: 80 yaşında Alzheimer tanılı kadın hasta acil servise oral alım bozukluğu, baş ağrısı şikâyetleri ile başvurdu. Kan basıncı:100/40 mgHg, nabız:39/dk olan hastanın EKG ‘sinde yavaş ventrikül yanıtlı atriyal fibrilasyon saptandı. Semptomatik bradikardisi olan hastaya 1 mg intravenöz atropin uygulandı. Atropin sonrası deliryum tablosu gözlenen hastada santral antikolinerjik sendrom düşünüldü. Hastaya acil servis takiplerinde midazolam ve propofol tedavisi uygulandı. Takip süresince kliniği düzelen hasta medikasyonu düzenlenerek önerilerle taburcu edildi. Sonuç: Deliryuma sebep olan mekanizma nöronal veya nörotransmiter fonksiyon bozukluğuyla oluşan karmaşık bir durumdur. Alzheimer hastalığı tanısı konan kişilerde ve daha az derecede olmakla birlikte diğer yaşlı kişilerde kolinerjik nöronal iletide azalma, deliryum riskini artıran önemli bir etmendir. İlaçlar, santral sinir sistemi hastalıkları, toksinler ve sistemik hastalıklara bağlı santral sinir sistemi bozuklukları deliryuma neden olabilir. Atropin santral antikolinerjik etkileriyle deliryuma yol açabilir. Sendrom; santral sinir sistemi depresyon veya aktivasyon bulgularıyla ortaya çıkabilir. Santral antikolinerjik sendrom kesin tanısı fizostigmine pozitif yanıt alınmasıyla konur. Olgumuzda atropin sonrası deliryum tablosunu santral antikolinerjik sendrom olarak değerlendirdik. Özellikle yaşlı hastalarda atropin tedavisi sonrası görülen taşikardi, ajitasyon ve deliryum gibi bulguların varlığında düşük doz uygulanmış olsa bile atropine bağlı santral antikolinerjik sendrom tanısı akla gelmelidir. Anahtar Kelimeler: Atropin, deliryum, acil servis P 447 CLAY SHOVELER KIRIĞI: HEP C7 FRAKTÜRÜ MÜ? Ayşe Dilara Öztermeli, Azizcan Kılıç, Burcu Azapoğlu, Özge Ecmel Onur Fatih Sultan Mehmet Eğitim ve Araştırma Hastanesi, Acil Tıp Anabilim Dalı, İstanbul Giriş: Clay-shoveler genel olarak C7 spinöz çıkıntı kırığı olarak bilinir. Kuvvetli fleksiyon esnasında spinöz çıkıntının ucunun kırılmasıyla oluşur ve C6 seviyesi de fraktürün görülebileceği seviyelerden biridir. Mekanik olarak stabildir, ancak bu tip kırıklar daha ciddi omurga yaralanmalarının uyarıcısı olabilirler. Biz bu olgu sunumunda, AİTK ile başvuran ve izole C6 spinöz çıkıntı kırığı saptanan hastayı sunuyoruz. Olgu Sunumu: AİTK sonrası Acil servise getirilen 49 yaşında erkek hasta bariyerlere çarpmış. Yapılan fizik muayenesinde burun dorsumunda hassasiyet, sağ torakal midclaviculer hatta hassasiyet ve boyunda alt servikal vertebralar hizası orta hatta palpasyonla hafif hassasiyet saptandı. Nörolojik muayenesi doğaldı. Yapılan BT incelemelerinde C6 vertebra spinöz prosesinde kopma şeklinde izole fraktür izlendi. Ayrıca 5-6. kostasternal bileşkede fraktür hattı ve nazal kemikte kırık hattı tespit edildi. Hasta Beyin cerrahisi bölümüne konsülte edildi, nöroşirürjikal girişim gerektirir patoloji saptanmadı. Tartışma: Servikotorakal bölgenin ani ve sert fleksiyon travmaları sonucu, kasların ters yönde uyguladıkları kuvvetler spinöz proses fraktürlerine neden olabilmektedir. Çoğunlukla trafik kazaları sonrası görülmektedir. En sık semptomu ağrıdır. Nörolojik defisit saptanması halinde ek spinal yaralanmalar akla gelmelidir. Clay-shoveler fraktürleri instabilite yaratmazlar. Tedavide, 4-6 hafta boyunluğa ek olarak analjezik ve antienflamatuvar tedavi verilmesi çoğunlukla ağrı kontrolü için gereklidir. Anahtar Kelimeler: Clay Shoveler, travma, trafik kazası, fraktür

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
428
P 448 SPONTAN MESANA PERFORASYONU: OLGU SUNUMU
Emine Cabioglu, Halil Doğan, Saltuk Cabioglu, Dogac Niyazi Ozucelik, Sezgin Sarikaya Bakırköy Dr. Sadi Konuk Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey Giriş: Mesane rüptürü sıklıkla künt veya penetran travmalar, ya da iyatrojenik yaralanmalar sebebiyle olup spontan intraperitoneal perforasyonu oldukça nadir görülmektedir. Daha nadir olarak foley kateter erozyonu, inflamasyon, dev mesane taşları, intraarteriyel kemoterapi yada aterosklerotik emboli sonrasında perforasyon görülebilir Genellikle altta yatan inflamatuar, malign ya da obstrüktif patolojilerin yaptığı mesane duvarındaki zayıflama sebebiyle oluşurlar. Olgu: 79 yaş erkek hasta 4gündür kanlı idrar yapma ve idrar miktarında azalma şikayeti ile acil servise getirildi. Bilinen Benign Prostat Hipertrofisi ve Parkinson dışı hastalığı olmadığı öğrenilen hastanın evde yatağa bağımlı olarak yaşadığı ve iki aydır devamlı olarak genitoüriner sondalı olduğu öğrenildi. Fizik muayenede bilinç açık, kan basıncı:85/55mmHg, nabzı:120 atım/ dakika, solunum:22/dakika, ateşi:38,8 C. Batın muayenesinde yaygın hassasiyet rebound ve defans ve rebound mevcuttu. Sıvı resüsitasyonu, antibiyoterapi ve antipiretik tedavisi başlanan hastanın kan tetkiklerinde kreatin 2,8 mg/dL, üre 135 mg/dL, CRP:33,9 mg/dL, beyaz küre 13600 /mm3; TİT’de eritrosit ++, lökosit +++ saptandı. Yapılan batın ultrasonunda batın alt kadranlarda serbest sıvı görüldü. Batın tomografisinde perivezikal alanda mezenter kirli ve enflame olarak gözlendi. Tanısal laparotomide mesane perforasyonu saptandı; primer tamir yapıldı. Yatışının 39.gününde haliyle taburcu edildi. Sonuç: Foley katetere bağlı mesane perforasyonu nadir olmakla birlikte, yaşlı hastalarda akut batın nedeni olarak mesane perforasyonu olabileceği unutulmamalıdır. Anahtar Kelimeler: Mesane perforasyonu, foley kateter, akut batın P 449 A PATIENT WITH CORONARY THROMBOSIS, TAMPONADE AND PERICARDIOCENTESIS Ali Karakuş1, Güven Kuvandık1, Mustafa Şahan1, Zeynep Kekeç2
1Mustafa Kemal University Faculty of Medicine, Department of Emergency Medicine, Hatay, Turkey 2Çukurova University Faculty of Medicine, Department of Emergency Medicine, Adana, Turkey Coronary thrombosis is a common and tamponade rare among the causes are reversible condition seen in resuscitation. This article presented cardiac tamponade due to inferior myocardial infarction patients who underwent pericardiocentesis and in the emergency department. Case: 70-year-old female patient was brought emergency after the resuscitation by 112 teams due to consciousness. General condition of the patient is poor. Unconscious, Glasgow Coma Scale: 7 no spontaneous respiration, arterial blood pressure was cannot be retrieved and intubated. The patient was connected to a mechanical ventilator. Positive inotropic support for dopamine 20 micrograms / kg was started. The ECG have inferior acute myocardial infarction (MI). Post MI patients were consulted with cardiologists thought that it had cardiac arrest. Echocardiography was detected fluid around the heart. Mai evacuated, accompanied ecocardiography with pericardiocentesis. The patient was admitted to monitoring and treatment in coronary intensive care. Tamponade pericardiocentesis is the presence of life-saving treatment. Sudden cardiac arrest is post-MI should be considered in cases of rupture of the walls may develop tamponade. Emergency pericardiocentesis should be planned at an early stage. Keywords: Thrombosis, tamponade, pericardiocentesis

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
429
P 450 A PATIENT WITH JAUNDICE HAD THE FINAL DIAGNOSE; ACUTE APPANDICITIS: CASE REPORT
Hasan Sultanoğlu, Ayça Özel Sönmez, Seda Özkan Dışkapı Yıldırım Beyazıt Training and Research Hospital, Emergency Medicine Clinic, Ankara, Turkey Introduction: Jaundice and diffuse abdominal pain are rare findings in patients with acute appendicitis in Emergency Room, generally due to complicated late term of appendicitis such as perforated/gangrenous appendicitis. In recent years the studies have showed the relationship between isolated hyperbilirubinemia and appendicitis. It is assumed that in perforated appendicitis excessive amount of bacteria and burden of toxins in the liver causes increased kuppfer cell function which leads to hepatocyte injury. The acute phase reactants like IL-6, TNF are released as a result of this hepatocyte injury that establishes a reduction in bilirubin catabolism in the liver. Our aim is to represent a case who was applied to our hospital with jaundice, abdominal pain and diagnosed as perforated appendicitis. Case: A 19-years-old male was admitted to emergency room with abdominal pain, diarrhea, jaundice which had lasted for 3 days. He was diagnosed as acute gastroenteritis 3 days ago when he presented with the periumbilical abdominal pain and diarrhea. He reapplied to the hospital due to his jaundice and abdominal pain that had recently established. There was no significance in his medical history. On physical examination of the patient; he had jaundice and diffuse abdominal irritation signs. There were no abnormal vital signs. Laboratory findings showed that WBC: 15600, T.Bilirubin:6.61 mg/dl, D.Bilirubin: 0.55 mg/dl, AST:21 U/L, ALT:7 U/L, K:5.56 mEq/L, Na:133 mEq/L. The hepatobiliary USG showed no abnormality as expected while the USG which examined appendix showed an inflamated appendix which is 8mm in diameter with unclear ending and a peripheral intraabdominal free fluid (3cm in depth) in the right-lower quadrant of abdomen. General surgery consultation had performed. The patient who undergone appendectomy surgery was diagnosed as perforated appendicitis. Conclusion: Perforated appendicitis diagnose should be kept in mind in the patients who admits to the ER with abdominal pain and jaundice. Keywords: Hyperbilirubinemia, abdominal pain, perforated appendicitis, male patient P 451 ATROPA BELLADONNA; UNUTMA! Bulut Demirel, Özcan Sağlam, Eyüp Karaoğlu, Güllü Ercan Haydar, Gül Pamukçu Günaydın, Neslihan Özkök Koz Ankara Atatürk Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Ankara Giriş: İnsanlık tarihinin gelişmesi ile birlikte avcı-toplayıcı olan beslenme sistemi gerilemiştir fakat gerek kültürel gerek geleneksel yapıdan kaynaklı doğadan toplanan gıdaların tüketilmesi tüm dünyada devam etmektedir. Toplanılan bitkiler hem gıda amaçlı hem de bazı geleneksel ilaçların yapılması amacıyla kullanılmaktadır. Bu gıdaların ve ilaçların kullanılması sağlık problemlerine neden olabilmektedir. Hem toplanan bitkilerden zehirli olanların birbirine benzeyenlerin yanlışlıkla tüketilmesi hem de bu bitkilerden elde edilen genellikle ilaç amaçlı kullanılan özütlerindeki etken maddenin dozunun bilinmemesinden kaynaklı zehirlenmeler görülebilmektedir. Bu vakamızda mantar zehirlenmesi olarak tarafımıza takip amaçlı sevk edilen Atropa Belladona zehirlenmesini sunacağız. Vaka Takdimi: 76 yaşında erkek hasta bilinç bulanıklığı ve baş dönmesi nedeniyle başka bir hastanenin acil servisine başvurmuş. Bilinen bir hastalığı olmayan hasta gün içerisinde eşiyle ormana mantar toplamaya gittiği ve geldikten sonra bilinç bulanıklığı ve baş dönmesi geliştiği gözlenmiş. Hasta mantar zehirlenmesi öntanısıyla ileri takip amacıyla tarafımıza gönderilmiştir. Hastanın gelişinde arteriyel tansiyon; 130/80, oksijen satürasyonu 95, nabız 87 ve ateş 37.3C idi. EKG’sinde belirgin patoloji saptanmamış olan hastanın muayenesinde bilinç bulanıktı, idrar retansiyonu mevcuttu ve gözleri midriyatikti. Diğer sistem muayenesi normal olan hastada antikolinerjik semptomlar baskın olarak izlendi. Hastanın yakınları tekrar sorgulandığında mantar yemediği fakat siyah küçük bir meyveden yediği öğrenildi. Bu bilgi üzerine Atropa Belladonna bitkisinin meyvesinin resmi gösterildi ve teyit edildi. Hastanın Atropa Belladona zehirlenmesi anlaşıldıktan sonra Fizostigmin uygulandı. 48 saat takip edilen hastanın laboratuvar değerlerinde ve muayenesinde belirgin bir patoloji olmaması üzerine taburcu edildi. Tartışma: Toplanılan bitkilerin kendisinin veya özütlerinin tüketilmesi ile zehirlenmeler sıklıkla görülmektedir. Bu bitkiler bölgeden bölgeye değişebilmekle birlikte kendisinin veya özütlerinin tüketilmesine bağlı farklı düzeyde ve farklı şekillerde zehirlenmeler görülebilmektedir. Çalışılan bölgede yetişen bitkilerin ve bunlara bağlı zehirlenmelerin bilinmesi ve gerekli antidotların hazır bulunması önemlidir. Hastamızda tükettiği iddia edilen mantar bulgularından daha ziyade antikolinerjik semptomlar görülmesi üzerine Atropa Belladonna zehirlenmesi olduğu görüldü ve fizostigmin tedavisi başlandı. Sonuç: Çalışılan bölgede tüketilebilecek bitkilerin zehirlenme bulguları bilinmesi ve gerekli antidotlar hazır bulundurulmalıdır. Anahtar Kelimeler: Atropa Belladona, atropin, fizostigmin, zehirlenme

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
430
P 452 RENAL ARTERY DISSECTION AND THROMBOSIS AFTER BLUNT ABDOMINAL TRAUMA
Nihat Bulandere, İlhan Uz Ege University School of Medicine, Department of Emergency Medicine, Izmir, Turkey Introduction: Renal artery dissection is uncommon complication of blunt abdominal trauma. Renal vascular injury is reported 3% to 14% of cases of renal trauma which may result in renal artery avulsion or intimal tear with dissection and stenosis. Case: We present a case of a 52 year-old-man who came to emergency department by a big stone fell on his in the building construction. Abdominal computed tomography showed left main renal arter long segment dissection/thrombosis, decreased renal perfusion and part of kidney had infarct. In the operation surgeries decided that it is unable to surgical intervention because of long segment dissection. He was died in the intensive care unit two days later because of kidney failure. Discussion &Conclusion: Renal injuries represent a relatively common event, involving 8–10 % of the patients admitted to an emergency department because of abdominal trauma. In 80–95 % of the cases renal injuries occur in the setting of blunt trauma.According to American Association for the Surgery of Trauma(AAST) classification of renal trauma; thrombosis of the main renal artery or vein, grade IV injury with a poorest prognosis. Arterial thrombosis is usually secondary to traumatic dissection of the main renal artery and the resulting occlusion may be complete or partial; consequently, the kidney may appear completely devascularized or hypovascularised. Management of renal artery dissection, surgical and endovascular revascularization treatment option should be determined according to the center’s experience. Anyway, in case of complete arterial occlusion the 2 hours time limit for revascularization must be considered: indeed, after 2 hours of complete renal ischemia also a good technical result will bring a poor functional outcome. Nephrectomy is always recommended if conservative treatments fail. Early diagnose and treatment are important because of mortality like our case. Therefore emergency physician keep in mind renal artery dissection in blund abdomen trauma. Keywords: Abdomen blunt trauma, renal artery dissection, renal infarct P 453 İZOLE PNÖMOMEDİASTİNUM VAKASI: GERÇEKTEN KORKMALI MIYIZ? Selma Atay, Can Özen, Serkan Emre Eroğlu Sağlık Bilimleri Üniversitesi Ümraniye Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Pnömomediastinum mediastende serbest hava veya gaz bulunması anlamına gelir. Acil serviste çok sık rastlanmayan bir tanı olmakla birlikte trakeobronşiyal ağaç, larenks ve özefagus yaralanmalarına bağlı olabileceğinden özellikle izole künt göğüs travmasında ve çoklu travma hastalarında akılda tutulmalıdır. Genellikle diğer toraks yaralanmalarına eşlik eder. Tanısı bilgisayarlı tomografi ile koyulur. Endoskopik incelemeler de kullanılabilir. Boyuna yayılan göğüs ağrısı, cilt altı amfizem, prekordiyal sistolik çıtırtı sesi (Hamman belirtisi), dispne ve disfaji bulgularındandır. Bu sunumda çoklu travma sonrasında tespit edilen izole pnömomediastinum vakasının konservatif yönetimine değinilmiştir. 28 yaşında erkek hasta acil servise 1 metre yüksekten düştükten sonra göğüs ağrısı şikayeti olması nedeniyle başvurdu. Vital bulguları ve fizik muayenesi tamamen normal olan hastanın çoklu travma protokolüne göre çekilen tomografilerinde mediastende serbest hava görüldü. Antibiyoterapi ve ağrı kontrolü sağlanan hasta 24 saat takibinin ardından önerilerle taburcu edildi. 1 hafta sonraki kontrollerinde havanın rezorbe olma eğiliminde olduğu görüldü. Pnömomediastinum spontan veya travmaya sekonder olarak gelişebilir. Spontan pnömomediastinum astım, amfizem gibi akciğer patolojilerine sekonder gelişir ve komplikasyon ve mortalitesinin travmatik pnömomediastinumdan (TPM) daha az olduğu kabul edilir. Bu nedenle TPM acil serviste korkulan bir tanıdır. TPM'nin izole olması durumuna sık rastlanmaz. Kot kırıkları, akciğer kontüzyonu ve pnömotoraks en sık eşlik eden yaralanmalardır. Steril bir alan olan mediastenin bronş veya gastrointestinal sistem florasıyla karşılaşması ölümcül enfeksiyonlara sebep olabilir. Son yıllarda yapılan derlemelerde hastalarda ölümcül komplikasyonların tahmin edilenden daha az olduğunu yansıtmaktadır. Vakamızda da görüldüğü gibi uygun antibiyoterapi ve gözlem ile hastaların komplikasyonsuz taburculuğu mümkün olabilmektedir. Anahtar Kelimeler: Pnömomediastinum, travma, çoklu travma

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
431
P 454 VENA CAVA SUPERIOR SYNDROME OR ANGIOEDEMA Bilgen İlküplü, Özge Can, Funda Karbek Akarca Ege University School of Medicine, Department of Emergency Medicine, Izmir, Turkey Introductıon: Vena Cava Superior Syndrome (VCSS) most frequently progresses with dyspnea, cough, enlargement in neck veins, and edema in head, neck and upper extremities. Since underlying cause is mostly overlooked, the patient can be evaluated as angioedema or overload regarding chronic renal failure as in the case that we will present. Case: A 56-year-old female patient applied to emergency service with swelling in the face, low back pain continuing for several months, shortness of breath. She had a known chronic renal failure and in the dialysis programme. In her physical examination, there was diffuse edema in periorbital area, around the mouth and neck. The patient was assessed in terms of angioedema, however, there was no stenosis in stridor, hypoxia and airway. There was no remission in edema following the treatment. The patient with chronic renal failure and recurrent catheter interference was evaluated as overload, taken to dialysis, nevertheless, no remission was observed in her edema after dialysis. In thorax angio CT of the patient who had persistent shortness of breath, there were total occlusion, generalized edema on the chest wall, mass at T10 level and mediastinal axillary lymphadenopathy. The patient hospitalized in intensive care unit. Discussion: VCSS forms depending on benign or malignant diseases with external compression, trombus in lumen, direct invasion or infiltration of vein wall. Occurs due to malignant reasons like an lung cancer and lymphomas. It is mostly observed by shortness of breath and swelling in the head and neck. Therefore, it can be misjudged with overload as in our case. Diagnosis method is plain graphy of lung, thorax angio CT, upper extremity venography. Conclusion: We would like to remind vena cava superior syndrome since its differential diagnosis that can be overlooked requires urgent attention and its treatment should be arranged promptly. Keywords: Vena cava superior syndrome, angioedema mimics, shortness of breath, chronic renal failure P 455 SUPRAVENTRİKÜLER TAŞİKARDİ İLE BAŞVURAN EBSTEİN ANOMALİSİ Can Özen, Serkan Emre Eroğlu Ümraniye Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Ebstein anomalisi 1866 yılında tanımlanan nadir bir doğumsal bir kalp hastalığıdır. Her 200.000 doğumda 1 görüldüğü tahmin edilmektedir ve tüm konjenital kalp hastalıklarının %1'inden azını oluşturur. Maternal benzodiazepin ve lithium gibi ajanlaın kullanımına bağlı geliştiği düşünülen bu malformasyonda triküspit kapağın septal ve posterior kapakçıkları miyokarda yapışmış haldedir, fonksiyonal annulus aşağı yer değiştirmiştir ve sağ ventrikülün "atrialize" olarak duvarı incelmiştir. Triküspit kapak fonksiyonunıu yerine getiremez. Patent ductus arteriozus varlığı hastalığın ciddiyetini etkiler. En ciddi vakalar yaşamın ilk yıllarında kaybedilirken yaşayan en yaşlı hasta 85 olarak bildirilmiştir. Bu sunumda acil servislerde nadir görülse de supraventriküler taşikardi (SVT) ayırıcı tanısında yer alan bu malformasyonu vurgulamak hedeflenmiştir. 20 yaşında bilinen hastalığı olmayan erkek hasta acil servise hayatında ikinci defa olan çarpıntı hissi ile başvurdu. 170/dk kalp hızı dışındaki vital bulguları normal olan hastanın EKG'sinde 170/dk hızda, dar QRS'li taşikardisi tespit edildi. İntravenöz 6 mg adenozin uygulanması ardından normal sinüs ritmi görülen hastanın takiplerinde göğüs ağrısı olması ve kardiyak markerları yüksek seyretmesi üzerine kardiyoloji ile konsülte edilerek ekokardiyografisi yapıldı. Ebstein anomalisi saptanan hasta takibi için bir üst merkeze sevk edildi. 24 saat takip edilen hasta komplikasyonsuz seyretmesi üzerindepoliklinik kontrolü önerilerek taburcu edildi. Ebstein anomalisi bulguları malformasyonun ciddiyetine göre yenidoğan döneminden itibaren çeşitli yaşlarda görülebilmektedir. En sık siyanoz, dispne, çarpıntı hissi, ani kardiyak ölüm ile birliktedir. Daha az ciddi malformasyonlarda genç yaşta sağ kalp yetmezliği bulguları görülebilir. Yaşamın ilk yıllarında ölüme neden olmayan ciddiyetteki malformasyonlar genellikle ergenliğin ilk yıllarında tanı alır. Elektrokardiyografik olarak tamamen normal olabileceği gibi paroksismal SVT, uzun PR segmenti ve Wolf Parkinsonm White Sendromu, düşük voltajlı QRS görülebilir. 20 yaşında olması itibariyle nispeten geç tanı olgumuzda da görülen SVT vakaların 1/3'ünde bulunmaktadır. Genç hastalarda görülen aritmilerin ayırıcı tanısında konjenital kalp hastalıkları mutlaka değerlendirilmelidir. Anahtar Kelimeler: Ebstein anomalisi, konjenital kalp hastalıkları, supraventriküler taşikardi

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
432
P 456 ACİL SERVİSTE KIYMA MAKİNESİ
Eren Usul, Kerim Abatay, Emrah Arı, Engin Deniz Arslan Dışkapı Yıldırım Beyazıt Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Ankara Amaç: Acil serviste iş kazalarıyla sıkça karşılaşılmaktadır. Bu olgumuzda nadir görülebilecek bir iş kazası sonucu elini kıyma makinesine kaptıran ve 112 ekipleri tarafından kıyma makinesiyle beraber acil servise getirilen hastayı tartışmayı amaçladık. Olgu: On beş yaşında erkek hasta kıyma makinesinde et çekerken elini makinaya kaptırmış. 112 ekipleri tarafından kıyma makinesi ile acil servise getirildi. Sağ el 1. Parmak haricinde kıyma makinası içerisindeydi. Hastaya mayi desteği sağlandı; sedoanaljezi yapıldı, tetenoz ve profilaktik antibiyoterapi uygulandı. İtfaiye ekiplerine haber verildi. İtfaiye ekipleri yaklaşık 2 saat süren bir çalışmayla kıyma makinasını kesip motoruna ulaştılar ve motorun çalışmasının tersi yönde hareketle hastanın elini çıkardılar. Hastanın kolu çıktıktan sonra plastik cerrahi tarafından 1. Parmak haricinde diğer parmaklar güdük yapılıp ampute edildi. Sonuç: Acil servislerde beklenmedik durumlarla sıkça karşılaşılmaktadır. Acil servis doktorları olarak beklenmedik durumlarda problemlere soğukkanlı yaklaşabilmeli, bilgili ve deneyimli olmalıyız. Bu gibi durumlarda diğer kurumlarla beraber hareket etmeyi ve destek istemeyi akılda tutmalıyız. Anahtar Kelimeler: Travma, kıyma makinesi, acil servis P 457 AN UNCOMMON CAUSE OF LEG WEAKNESS: ILIOPSOAS ABSCESS DUE TO DIVERTICULITIS Hüseyin Koçyiğit, Sinan Genç, Müge Günalp Eneyli, Onur Polat, Serdar Gürler
Ankara University School of Medicine, Department of Emergency Medicine, Ankara, Turkey Iliopsoas abscess (IPA) is an uncommon condition that infection spreads from a distant septic focus or contiguous retroperitoneal structures. The clinical presentation of IPA is often variable and nonspecific. The classic triad of IPA consist of fever, back pain and anterior or groin pain, but these symptoms were present in fewer than 50% of patients. Diagnosis of IPA is usually delayed due to its atypical clinical presentation. A 67-year-old female patient presented to the emergency department with a right leg weakness complaint. Vital signs were body temperature: 37,4 C°, pulse rate: 100/bpm, blood pressure: 110/70 mmHg. Physical examination revealed right lower extremity weakness with 3/5 muscle strength, sensory examination and other examinations were normal. Blood examination showed that hemoglobin: (Hb) 8,9 g/dL, white blood cells: 16 960/μL, platelets: 657 000/μL, C-reactive protein: 148 mg/L, erythrocyte sedimentation rate: 58 mm/h. Contrast enhanced abdominopelvic computerized tomography demonstrated an abscess measuring 14x5 cm in the right iliopsoas muscle and another collection measuring 6,3x3,9 cm at rectosigmoid junction level. IPA can be primary or secondary to gastrointestinal and genitourinary infections. Aetiological factors include Crohn’s disease, appendicitis, sigmoid diverticulitis, colorectal carcinoma and tuberculosis. Clinical diagnosis is difficult because of non-specific symptoms. Common symptoms are fever, lower abdominal and inguinal pain. Laboratory results reveal leukocytosis and elevated C-reactive protein levels. Conventional radiological techniques are often unhelpful. CT imaging is most important diagnostic technique since it provides optimal sensitivity and specify. The most common microorganisms found are enteric origin, such as Escherichia coli, Klebsiella spp. and Proteus mirabilis. Staphylococcus aureus is most common in primary abscess. Early treatment with broad spectrum antibiotics as well as percutaneous drainage or surgery is necessary before sepsis becomes lethal. Bowel resection, thorough debridement and external drainage, parallel to antibiotics, are essential for IPA complicating gastrointestinal disease. Keywords: Diverticulitis, emergency medicine, iliopsoas abscess

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
433
P 458 FOODBORNE BOTULISM WITH ALLERGIC REACTION TO ANTITOXIN
Mevlana Ömeroğlu, Atıf Bayramoğlu, Ayşe Şenyurt, Safa Dönmez Atatürk University Faculty of Medicine, Department of Emergency Medicine, Erzurum, Turkey Clostridium botulinum is a gram-positive, rod-shaped, spore-forming, anaerobic bacterium. C. Botulinum spores are heat resistant and can be destroyed by heating to 120ºC for five minutes. Regardless of the route of entry into the body, the toxin binds to a specific receptor on the presynaptic sides at ganglia and neuromuscular junctions. It produces an irreversible disruption in acetylcholine release. Return of synaptic function requires approximately six months with sprouting of a new presynaptic terminal. A 41-year-old man was admitted to our service with dyspnea, diplopia, dysphagia and emesis. Previous day, at the dinner, he ate cooked beans. They were kept frozen in the deepfreeze. On examination, he was confused and had a GCS of G3M6V5. His tension arterial was 119/87 mmHg, pulse as 113/minute, respiratory rate as 20/minute, body temperature as 36.9 oC and oxygen saturation as 97% at the room air. On neurologic examination, he has no lateralization but dysphagia, dysphonia and signs of total ophthalmoplegia were obvious. The patient was unable to phonate clearly, thus communicated primarily by writing. There was bilateral ptosis and weakness on eye movements. Pupillary examination showed anisocoria and pupillary light reflex was (-/+ | -/+). Biochemical parameters were unremarkable. İmaging studies were all normal. Supplemental oxygen and antibiotic was initiated. Botulism antitoxin was began intravenously, but the patient showed signs of allergic reaction, thus infusion was stopped. He admitted to intensive care unit for respiratory support. After one month of hospitalization, his general condition returned to nearly normal gradually. He was discharged on the thirty fifth day to home. We reported foodborne botulism due to home cooked beans, and kept frozen in the deepfreeze that showed signs of allergic reaction as dyspnea and chest pain to Botulism antitoxin. Nevertheless antitoxin did not administered because of our patient showed allergic reaction, his symptoms regressed. Keywords: Antitoxin, botulism, deepfreeze P 459 GEÇ GELEN ACİL; POSTRAVMATİK 10.GÜNDE HEMOPNOMOTORAKS Erdem Aydın, Bora Kaya, Onur Karakayalı, Okay Albayrak, Serkan Yılmaz Kocaeli Derince Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, Kocaeli Giriş: Künt göğüs yaralanmaları tüm yaralanma kaynaklı ölümlerin %25’ini oluşturmaktadır. Toraks travmalarında intratorasik yaralanma nedeniyle en sık görülen patolojik bulgular hemotoraks ve/veya pnömotorakstır. Olgumuzda ciddi sonuçlara sebep olabilen, genelde hastaneye erken başvuru sebeplerinden biri olan travmatik hemopnömotoraksın daha hafif ve gecikmiş semptomlarla ve ya kot fraktürü gibi sebeplerden dolayı geç dönemde gerçekleşerek hastaneye başvurabileceğini göstermek amaçlanmıştır. Olgu: 39 yaş erkek hasta acil servise 10 gün önce yaklaşık 1,5 metre yükseklikten sağ yanı üzerine düşme, 4 gün sonra başlayan sağ yan ve göğüs ağrısı, nefes darlığı şikayeti ile başvurdu. Hastalık ve ilaç kullanım öyküsü yoktu. Vital bulguları stabil Fizik muayenesi: Sağ 5-10 kot hizası palpasyonla ciddi ağrılıydı, solunum sesleri sağ hemitoraksta alınamıyordu. Diğer sistemler normaldi. Laboratuar bulguları normal, Yapılan toraks bt incelemesinde: Sağ akciğerde üst-orta lobda pnömotoraks, kompresyon atelektazisi, 7-8 cm plevral efüzyon (hemotoraks?), 8-10 kotlarda fraktür saptandı. Travma müşahade alanında monitörize edilerek gözleme alındı. Göğüs cerrahisi ile birlikte değerlendirilen hastaya tüp torakostomi planlandı. Hastaya oksijen tedavisi altında 6. interkostal aralık orta koltuk hattı hizasından 32F tüp yerleştirildi 900 cc hemorajik sıvı ve hava gelişi oldu. Hasta göğüs cerrahisi servisine yatırıldı. Tartışma: Plevral boşluk içindeki kanın kompresyon etkisi, akciğerdeki tromboplastin, düşük pulmoner arter basıncı kanamayı sınırlandırır. Olgumuzda bu mekanizmalar ile kanamanın sınırlandığı düşünülmektedir. Göğüs travması ile başvuran hastaların <%5 tüp torakostomi gereklidir. Göğüs travmasında etkin ağrı kontrolü, akciğer fizyoterapisi ve tüp torakostomi çoğunlukla yeterlidir. Tüp torakostomiden sonra devam eden kanamalarda, hastaların monitörizasyonu ve drenajı takip edilmelidir, uygun endikasyonlar geliştiğinde torakotomi uygulanmalıdır. Olgumuzda orta düzeyde hemotoraks düşünülmüştür, bu sebeple torakotomi planlanmamıştır. Çalışmada kot fraktürlerinin sayısı; uzamış hastane yatışı, yoğun bakım yatışı, hemotoraks-pnömotoraks-hemopnöomtoraks komplikasyonları gelişmesi ile ilişkili olduğu gösterilmiştir. Literatürde travma sonrası tedavi edildikten sonra ilerleyen günlerde tekrarlayan tarzda veya protrombin sentezini engelleyen ilaç kullanan hastada geç dönemde görülen hemopnömotoraks olguları bildirildiğini gördük. Olgumuzda olduğu gibi ilaç kullanımı olmayan ve hemopnömotoraks için akut dönemde tedavi almamış vaka bildirimine rastlamadık. Anahtar Kelimeler: Toraks travması, geç hemopnomotoraks, acil servis

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
434
P 460 KOKSİKS DİSLOKASYONUNA BAĞLI REKTUM PERFORASYONU
Mehmet Can Girgin, Pınar Akhanlı, Hakan Topaçoğlu İstanbul Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Koksiksin aşırı mobilitesine bağlı olan ve bu bölgeye uygulanan basınçla koksiks çevresinde hissedilen ağrı koksidinia olarak tanımlanır. Kadınlarda sık görülen bu durumun en sık nedeni travmadır. Bu yazıda acil servise koksidinia ve hematokezya nedeni ile başvuran, koksiks dislokasyonu ve rektum perforasyonu saptanan hasta rapor edildi.54 yaşında erkek hasta rektal bölgede ağrı şikayeti ile acil servise başvurdu. Hastanın 4 gün önce kalçası üzerine düşme sonrası doktora gitmediği ve ağrısının giderek arttığı ve aralıklı kanlı dışkılama eklendiği belirtildi. Acil servise başvuru anında genel durum iyi koopere oryante idi. Hastanın vital bulguları stabil olarak saptandı. Hastanın gastrointestinal malignite tanısı aldığı ve şuan aktif ilaç tedavisi altında olmadığı belirlendi. Sistemik muayenede patolojik özellik saptanmayan hastanın yapılan rektal tuşesinde palpabl kitle veya aktif kanama saptanmadı. Prosedür esnasında hasta ağrı tanımladı. X-ray görüntülemede koksiks dislokasyonu saptandı. Hastanın tam kan sayımı, kan biyokimya ve koagulasyon tetkiklerinde anormallik saptanmadı. Hastanın çekilen rektal kontrastlı batın tomografisinde pararektal alanda kontrast madde sızıntısı görüldü. Hastaya koksiks dislokasyonuna sekonder rektal perforasyon tanısı konularak hastaneye yatırıldı. Acil servislere travma sonrası gelişen koksidinia nedeni ile başvuran hastalarda, koksiks yaralanmalarının yanında nadirde olsa yaralanmaya bağlı gelişebilecek rektum perforasyonu akılda tutulmalıdır. Özellikle hematokezya tanımlayan hastalarda mukozal değerlendirme önemlidir. Anahtar Kelimeler: Koksiks dislokasyonu, rektum perforasyonu, travma P 461 BİLİNÇ BOZUKLUĞU OLAN HASTADA NÖROLEPTİK MALİGN SENDROM Mustafa Orfi Erdede1, Aziz Vatan2, Hakan Topacoglu3
1İstanbul Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Nöroleptik malign sendrom (NMS) nöroleptik kullanan hastalarda nadir görülen, hayatı tehdit edici idiosinkratik reaksiyondur. Ateş, kas rijiditesi, bilinç değişikliği ve otonomik disfonksiyon ile kendini göstermektedir. Bu yazıda acil servise ateş nedeniyle başvuran NMS olgusu rapor edilmiştir. 43 yaşında hasta acil servise ateş yüksekliği ve ajitasyon şikayetiyle acil servise getirildi. Hastanın özgeçmişinde hipoksik beyin hasarına bağlı mental retardasyon ve epilepsi öyküsü bulunmaktaydı. Uzun dönemdir nöroleptik ilaç (levetiracetam, clomipramin, quetiapine, valproik asit) kullanan hasta yaklaşık üç gündür ateş yüksekliği olduğu son iki gündür farklı davranışlar gösterdiği bu nedenle ilaç dozunun arttırıldığı belirtildi. Genel durum kötü olan yatalak hastanın başvuru anında ölçülen vital bulguları; kan basıncı 145/95 mmHg, vücut sıcaklığı 41,5 C0, solunum sayısı 18/dk, nabız 120 atım/dk, oda havasında oksijen satürasyonu %98 olarak saptandı. Kardiyovasküler, toraks ve abdominal muayene bulgularında anormallik saptanmadı. Nörolojik muayenede nonkoopere, nonoryante, pupiller izokorik, ışık refleksi bilateral pozitif, tremor (+), kas rijiditesi (+) olan hastanın fokal nörolojik bulgusu yoktu. Meninks irritasyon bulguları saptanmadı. Tam kan sayımı normal olan hastanın ve kan biyokimyasal tetkiklerinde; glukoz 115 mg/dL, olup diğer parametrelerde anormallik saptanmadı. Beyin BT ve MRI görüntülemede akut iskemik veya hemorajik saptanmadı. NMS ön tanısı ile eksternal soğutma başlanan ve hemodinamik sıvı desteği sağlanarak yoğun bakıma yatırılan hasta ikinci gün öldü. NMS olan hastalarda erken dönemde tedavi başlanması mortalite açısından önemlidir. Özellikle bilinç değişikliği, mental retardasyon gibi kronik nedenler ile izlenen ve nöroleptik kullanan hastalarda hastanın bilincinde olan akut değişikliğin aile tarafından saptanması güçleşebilir. Bu hasta grubunda bu ilaçların kullanımında aile bireylerinin ilaç yan etkileri açısından iyi bilgilendirilmeleri gereklidir. Anahtar Kelimeler: Nöroleptik malign sendrom, acil servis, şuur bulanıklığı

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
435
P 462 IMPLEMENTING AN ONLINE TRAINING FOR EMERGENCY MANAGEMENT AND DISASTER PREPAREDNESS
Erkan Gunay1, Patricia Roblin2, Bonnie Arquilla2
1Şişli Hamidiye Etfal Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey 2SUNY Downstate Medical Center, Department of Emergency Medicine, New York, USA Free, Open Access Medical Education (FOAM) is a teaching modality that include blogs, podcasts, social media, web based applications, online videos and have been an effective instructional medical training method. Computer and lecture based training interventions found to be effective in increasing disaster related knowledge for out of hospital providers. Interest on these online modalities is evident in Turkey with an increased number of users of Turkish FOAM websites. ITunes University, an online training modality with downloadable educational podcasts, is proved to be an effective for medical training. Main purpose of this abstract is to introduce an online training modality for Turkish emergency physicians on emergency preparedness training. Emergency preparedness topics were categorized and prioritized based on a previously published needs assessment survey by the research team and ITunes University was used for content administration. Based on the needs assessment survey, residency lectures were described as the number one source of training on emergency preparedness but participants evaluated their residency training on various topics as inadequate. Itunes course is prepared to introduce basic disaster management knowledge for the emergency physicians. First phase of the course consists of five lectures; 1-introduction to disaster management, 2-disaster management organizations, 3- healthcare disaster management in Turkey, 4-hospital disaster planning, 5- emergency department during disasters. Important publicly available documents on disaster management such as hospital disaster planning guidelines and hyperlinks to government websites on the topics were included to the course content as well as other FOAM materials.Increased conflicts around its borders, and terror attacks within the country demonstrated the importance of disaster management in Turkey. This training modality can be used as an additional tool for residency lectures and training programs should be encouraged to use these types of teaching modalities in order to fulfill the interests on disaster management within the specialty. Keywords: Disaster, emergency preparedness, medical education, Itunes university, FOAM P 463 EFOR ANJİNA: AKUT KORONER SENDROM? BRONKOPNÖMONİ? Mustafa Orfi Erdede, Aziz Vatan, Hakan Topacoglu İstanbul Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Akciğer parankiminin enfeksiyonu olan pnomonilerde en sık etken bakteri ve viral kaynaklardır. Klinik olarak en sık rastlanan bulgu ve semptomlar ateş, öksürük, takipne, nefes darlığı, balgam çıkarma, plöretik göğüs ağrısı, hipoksidir. Hastanın immun durumuna ve etkene bağlı olarak atipik prezentasyon ile başvuran olgular literatürde bildirilmiştir. Bu yazıda acil servise atipik bulgular ile gelen bronkopnomoni olgusu rapor edildi. 40 yaşında erkek hasta sternum alt tarafında baskı tarzında ağrı ile acil servise başvurdu. Hasta yaklaşık bir hafta öncesinde göğüs orta alt kısmında başlayan ve efor ile artan istirahat ile geçen sıkıştırıcı, baskı tarzında ağrı tanımladı. Hasta bu bir haftalık dönem içerisinde öksürük balgam çıkarma, ateş olmadığını belirtti. Özgeçmişinde bir hastalık ve ilaç kullanımı öyküsü olmayan hastanın 20 yıl sigara kullanımı öyküsü mevcuttu. Hastanın genel durumu iyi, koopere oryante idi. Geliş vitallerinde kan basıncı 134/84 mmHg, vücut ısısı 36,7 C0, nabız 86 atım/dk, solunum sayısı 16 soluk/dk, oda havasında oksijen satürtasyonu %98 idi. Hastanın acil servise başvuru anında çekilen EKG’de sağ aks deviasyonuna ait bulgular dışında anormallik iskemik değişiklik gözlenmedi. Hastanın toraks, kardiyovasküler ve abdominal muayeneleri normaldi. Akciğer röntgeninde anormal bulgu saptanmayan hastaya yapılan ekokardikardiyografi ve efor EKG’de iskemi lehine anlamlı bulgu saptanmadı. Baskı tarzında ağrısı devam eden ve o anda çekilen EKG’lerinde değişiklik saptanmayan hasta kardiyak olarak izleme alındı. Kan biyokimya testlerinde ve kardiyak testlerinde anormallik saptanmayan hastanın göğüs ağrısının azalmaması nedeniyle çekilen toraks BT’sinde sol alt parakardiyak alanda milimetrik atelektazi sahaları, sol lingula ve alt lob segmentleri hizasında kistik ve tübüler bronşiektazi alanları ile beraber bronkopnomoni alanları görüldü. Bronkopnomoni tanısıyla hastaneye yatırılan ve antibiyotik tedavisi ile ağrısı gerileyen hasta 10 gün sonrasında taburcu edildi. Acil servise akut koroner sendrom düşündüren iskemik ağrı benzeri şikayet ile gelen olgularda klinik ve röntgen bulguları olmasa dahi bronkopnomoni açısından ayrıcı tanıya gidilmelidir. Anahtar Kelimeler: Bronkopnomoni, anjina, acil servis

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
436
P 464 MAYBE NOT FAST, BUT FURIOUS: SPINAL CORD ISCHEMIA
Elif Dilek Cakal, Ilhan Uz Ege University Medical School, Department of Emergency Medicine, Izmir, Turkey Introduction: Spinal cord ischemia (SCI), a rare condition in children, is only limitedly discussed in emergency medicine literature. We present a case of SCI. Case: A previously healthy 7-year-old male presented with weakness in the legs. His family explained he had hit his back 9 hours earlier. He had no bruise. Physical examination revealed no point tenderness to palpation on his cervical, thoracic, or lumbar spine. While muscle strength in upper extremities was normal, it was grade 1 in lower extremities. Sensory examination was normal. His whole-body computed tomography showed no vertebral fractures or traumatic injuries. Non-enhanced MRI of his thoracic and lumber spine demonstrated diffuse but mainly central edema from T7 to the end of conus medullaris. Diffusion-weighted imaging confirmed the central spinal cord ischemia. The patient was admitted to neurosurgical ward. After approximately 1.5 year of physical therapy, the patient can crawl on his knees but he has no sensation in his legs. He applies clean intermittent catheterization. Discussion: SCI is rare and represents only 1.2% of strokes. Currently, aortic surgery is emphasized the most common etiology of SCI in adults. In children, a spectrum of etiologies causing decreased blood flow may lead to SCI; such as hypotension, vascular injury, compression, thrombosis or embolization. Minor trauma, a well-known cause of SCI in children, is arguably caused by reactive vasospasm of spinal cord arteries secondary to hyperflexion injuries of the relatively less elastic spinal cord inside the more flexible spinal column. Presentation of neurological impairment may delay hours to days after trauma and clinical syndromes seen in spinal cord ischemia are dependent on which vessel is affected. Treatment of SCI is based on prevention of secondary injury or repeat infarctions. Conclusion: Emergency physicians should be able to consider SCI in cases with delayed neurological impairment after minor trauma. Keywords: Spinal cord ischemia, minor trauma, pediatric patient, emergency department P 465 THE FRONTAL BONE FRACTURE RELATED TO A CRAMPON Serife Ozdinc, Emel Gokalp Afyon Kocatepe University School of Medicine, Department of Emergency Medicine, Afyonkarahisar, Turkey Major causes of maxillofacial injuries are traffic accidents, falling and violence. Sports and exercise are also important causes of maxillofacial injuries. Different types of sports might differ in frequency and type of fractures. We present the case of frontal bone fracture related to football. A 31-year-old man was admitted to our emergency room with complaints of pain and wound on the frontal area. He incurred a forehead injury by an opponent’s crampon impact during a football match about half an hour ago. He is a footballer who played in the amateur league. There were no remarkable features in either his personal medical history or that of his family. On his physical examination, his vital signs were stable. There was 3 * 1 cm laceration and tenderness on the right frontal area. Examination of all other systems disclosed no abnormalities. A computed brain tomography scan showed displaced, comminuted, compression fracture of right frontal sinus anterior wall. There is no pathology in the brain parenchyma. The patient was consulted with clinic of plastic surgery and hospitalized. We learned that, patient who underwent open reduction and internal fixation of right frontal sinus anterior wall was discharged on the third day of the hospitalization. Training of soccer players about trauma and its serious results and also adherence to the rules of sports can prevent sports injuries. Keywords: Sports injuries, frontal bone fracture, emergency room

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
437
P 466 PNEUMATOSIS INTESTINALIS IN A HAEMODIALYSIS PATIENT
Serife Ozdinc, Burcu Coker Afyon Kocatepe University School of Medicine, Department of Emergency Medicine, Afyonkarahisar, Turkey Pneumatosis intestinalis (PI) is a process characterized by submucosal and subserosal gas cysts in the wall of the intestine. Not only PI can be seen alone, but also it may be accompanied with other diseases such as chronic obstructive pulmonary disease, collagen vascular diseases, ischemic and inflammatory bowel disease, hemodialysis patients... It is generally associated in hemodialysis patients with hypovolaemia, low blood pressure and mesenteric vasoconstriction with advanced atherosclerotic disease. We report the case of an 62 year old man on chronic hemodialysis with PI. A 62-year-old man was admitted to our emergency room with complaints of abdominal pain, diarrhea, dizziness. Three days prior to his visit, he experienced progressive abdominal pain accompanied by nausea, bloodless watery diarrhea. The last day, weakness dizziness and deterioration of general condition were added to his other complaints. He had been chronic renal failure for 3 years and he had dependent on hemodialysis in a three days a weak for 4 months. On his physical examination, arterial blood pressure was 90/ 50 mmHg, pulse was 100 /min, axillary temperature was 360C. His Glasgow coma scale was 15. His general condition was slightly impaired and dehydrated. On abdominal examination, increased bowel sounds and diffuse tenderness without defence and rebound were detected. Examination of all other systems disclosed no abnormalities. An unenhanced abdominal computed tomography scan showed gas-filled cystic images related to pneumatosis intestinalis within the small intestinal wall. The patient was consulted with clinic of general surgery and transfered to the intensive care unite. We learned that, total abdominal ischemia was detected in patient who underwent abdominal exploration. It was decided not to do any surgical intervention to the patient. It was learned that the next day the patient died. PI should be considered in hemodialysis patients presenting with abdominal pain and diarrhea Keywords: Pneumatosis intestinalis, haemodialysis, abdominal pain, chronic renal failure, emergency medicine P 467 EID AL-ADHA IN EMERGENCY ROOM Musa Adanç, Serhat Ömercikoğlu, Burak Özcan, Kerem Ali Kabaroğlu, Arzu Denizbaşı Marmara University Pendik Training and Research Hospital, Department of Emergency Medicine, Istanbul, Turkey Introduction: The feast of sacrifice is a Muslim tradition. Every year during the month of pilgrimage to Mecca (Hajj), it is celebrated. During this feast, thousands of animals, like cows, camels, sheep or goats, are sacrificed and their meat donated to poor people. Many injuries occur especially because of the non-professionals who perform this Islamic ritual without proper precautions during the sacrifice.(1,2) Thus, the aim of this study was to determine the demographic characteristics of patients, injury types and most effected extremities and evaluation of the surgical management and the orthopedic consultations. Materials-Methods: This retrospective study was conducted in Emergency Department (ED) of Marmara University Pendik Training and Research Hospital. Patients who admitted ED between 12-14 September 2016; first 3 days of feast of sacrifice were included. Patients classified and evaluated according to gender, effected extremities, injury type, need of consultation and surgery. Results: Total of 44 patients admitted to ED in the first three days of the feast of sacrifice. 37(84.1%) of them was male. 28(63.6%) patients needed orthopedic consultation. 4(9.1%) of these patients have tendon injury and 4(9.1%) of them have fracture. 36(81.8%) people have upper extremity injuries. Discussion: Injuries in the feast of sacrifice are mostly related with tools which are used by slaughters. Most injuries seen as hand injuries, skin incisions, tendon injuries and finger amputations. (3) In our study most of the injuries are located in upper extremities. There was also a scapula fracture, a subarachnoid bleeding and a tibia fracture in our study. Our data was similar as other studies. Many inexperienced people, sacrifice animals themselves, leading numerous injuries. Consequently, in order to reduce these injuries, animals should only sacrificed by professionals and protective equipments must be used. This will reduce the unnecessary crowd in ED and also prevent the health problems. Keywords: Eid al-Adha, emergency room, trauma

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
438
P 468 ISONIAZID INTOXICATION: 1-YEAR CASE SERIES
Funda Karbek Akarca, Gizem Söyler, İlhan Uz, Murat Ersel Ege University School of Medicine, Department of Emergency Medicine, Izmir, Turkey Introduction: The so-called reborn of tuberculosis has led to an increase in consumption and acute or chronic intoxication of isoniazid. We present 5 cases of isoniazid poisonings in the last year. Cases: One of cases visited emergency department twice so 4 cases are presented. Three of four cases are 18 years old; the other is 22 years old. While one patient took his own medication, the others took drugs of their close relatives. The amount ranges between 2.1 and 15 grams (Mean: 10.0 grams). Glascow Coma Scale (GCS) Score at the admission time were 9 in one patient and 15 in the others. All patients had seizures in ED. Four patients developed metabolic (lactic) acidosis. Benzodiazepine, first line drug, was given to patients. Pyridoxine (5 grams-3 patients, 1 grams-2 patients) was required because benzodiazepine was unable to terminate seizures. Pyridoxine successfully ended the seizures. At the time of discharge, GCS Score of each patient was 15 and patients were discharged after psychiatry consultations. Conclusion: Tuberculosis is a recently increasing global public health issue, especially in developing countries. Isoniazid, the main therapeutic agent, is frequently used in the treatment. Acute intoxication causes status epilepticus resistant to treatment, coma and metabolic acidosis. Undertreatment may lead to fatal consequences. Pyridoxine should not be forgotten and should be available in every hospital Keywords: Pyridoxine, isoniazid intoxication, lactic asidosis P 469 HİDROKSİZİNE BAĞLI GELİŞEN PARKİNSON BENZERİ BELİRTİLER
Attila Aydın1, Sedat Bilge1, Cemile Aydın3, Meltem Bilge2
1Gülhane Eğitim ve Araştırma Hastanesi, Acil Tıp Anabilim Dalı, Ankara 2Dışkapı Eğitim ve Araştırma Hastanesi, Anestezi ve Reanimasyon Kliniği, Ankara 3Etimesgut Devlet Hastanesi, İç Hastalıkları Kliniği, Ankara Hidroksizin, özellikle psikonörozlara bağlı anksiyete ve gerginliğin semptomatik tedavisinde ve anksiyetenin ortaya çıktığı organik hastalıklarda yardımcı tedavi olarak kullanılır. Vakamızda anksiyete ve uyku bozukluğu için verilmiş olup, klasik yan etkilerinden farklı bir yan etki ile prezente olmuştur. 61 yaşında erkek hasta bilinen HT dışında başka hastalık öyküsü yok. 10 günden beri devam eden uyuyamama şikayeti olan hastaya hidroksizin (Atarax®) tablet 2*1 başlanmış. İlacı kullanmaya başladıktan 2 gün sonra hareketlerinde ve konuşmasında yavaşlama şikayeti olması üzerine Acil Servisimize başvurdu. Muayenesinde; genel durumu iyi, oryantasyon ve zaman bozuk, solda belirgin iki taraflı olmak üzere, aktivasyonla belirginleşen rijidite, maske yüz ve bradikinezi mevcuttu. Aciıldı. l servis'te alınan görüntüleme yöntemlerinde akut iskemi-hemorajiyi düşündürür bulgu saptanmadı. Hasta mevcut klinik durumu ile Nöroloji Kliniğinde hospitalize edildi. Hidroksizin tedavisi kesilen hastanın iki gün içinde tüm şikayetleri geriledi. Özellikle bu tip ilaçları reçete eden doktorların ilk bir haftada hastayı yakın takibe alması gerektiği ve farklı yan etkileri olabileceği akılda tutulmalıdır. Anahtar Kelimeler: Hidroksizin, parkinsonizm, rijidite

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
439
P 470 CELIAC ARTERY THROMBOSIS MASQUERADING AS RENAL COLIC IN THE EMERGENCY SETTING Tahir Telat Yurttaş, Sarper Yılmaz, Fulya Temizsoy Korkmaz, Hakan Topaçoğlu, Özgür Karcıoğlu Istanbul Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey Introduction: Thrombosis of the celiac artery trunk is a rare cause of acute abdominal pain. Angiography is the gold standard diagnostic modality. The main goal of treatment is to reestablish blood flow in the mesenteric vessels and to prevent end-organ ischemic damage and infarction. Celiac artery thrombosis is usually associated with other cardiovascular diseases. Successful treatment depends on expedient diagnoses and effective intervention -either surgically or endovascularly - to reestablish blood flow and surgical resection of necrotic parts and intensive care unit management as required. Case: A 55 year-old woman was admitted to the Urology outpatient clinic because of right lumbar pain lasting for two days just similar to the colicky attacks she had suffered before. Following examination, she was directed to the emergency department for analgesia. Tenderness in the right costovertebral angle and whole abdominal area was noted on examination. Nonetheless, there were no rebound tenderness and guarding. Her abnormal laboratory tests were as follows: WBC: 30980/mm3, PLT:220.000/mm3 AST: 546 IU, ALT: 511 IU, lactate:5,18 mmol/L, INR:1,8, PT:41,4 sn, aPTT:36,1. There were nearly complete obstruction in the celiac and superior mesenteric artery and accompanying cholecystitis. Cholecystitis was thought to be related to vascular insufficiency resulting from celiac thrombosis. After consultation with related departments stenting and intravascular thrombolysis were performed endovascularly. But the symptoms of the patient did not regress. Then the patient were taken to the surgery and small bowel resection and cholecystectomy were performed. Conclusion: As a rule, every single patient directed from other departments for symptomatic treatment needs to be examined and evaluated thoroughly again in the emergency department. Further investigation and treatment may be necessary as warranted by the patient’s condition. Also celiac arter thrombosis may mimic all kinds of acute abdominal pathologies because of its wide vascular network. Keywords: Celiac artery thrombosis, renal colic, superior mesenteric artery thrombosis P 471 SPONTANEOUS PNEUMOMEDIASTINUM: A CASE REPORT Elif Kılıçlı Doğanay, Meliha Fındık, Cemil Kavalcı, Afşin Emre Kayıpmaz, Ayşegül Akçebe Aydın Başkent University Hospital, Ankara, Turkey Introduction: Pneumomediastinum is defined by the presence of air in the mediastinum and first described by Laennec in 1819. The diagnosis is based on imaging techniques and clinical symptoms. The standard radiography diagnostic procedure chest x-ray; showing a double line outlining the mediastinum. Diagnosis can be confirmed by chest CT when not apparent on radiography. Once confirmed the diagnosis, patient should be admitted for monitoring and treatment: avoidance of the trigger factor, oxygen and bed rest. Here we describe a patient with spontaneous pneumomediastinum and extensive subcutaneous emphysema. Case Report: An 18 year old woman presented to the emergency department complaining of cough and pain of the neck. A postero-anterior chest X-ray showed a slight layer of air surrounding the cardiac silhouette. Chest CT was performed, which confirmed the existence of pneumomediastinum with further issection of air into the neck; there was no signs of pneumothorax, parenchymal and/or pleural abnormalities. Discussion: Spontaneous pneumomediastinum or spontaneous mediastinal emphysema was officially described for the first time by Louis Hamman in 1939. This case shares many aspects with most cases reported in the literature, particularly regarding the form of presentation, therapeutic approach and clinical evolution. Regarding the diagnostic investigation, chest X-ray is the method of choice; however, the postero-anterior view establishes the diagnosis in only half of the cases, making it important to obtain a profile view, allowing for the diagnosis in approximately 100% of cases. Conclusion: Pneumomediastinum is a rare and generally benign condition. As larger and larger case reports are published in the future, we will be able to more diagnosed spontaneous pneumomediastinum. Keywords: Spontaneous pneumomediastinum, Hamman’s syndrome, pulmonary diseases

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
440
P 472 A FATAL PROPAFENONE POISONING
Elif Dilek Cakal, Yusuf Ali Altunci, Guclu Selahattin Kiyan Ege University Medical School, Department of Emergency Medicine, Izmir, Turkey Introduction: Suicidal attempts by oral intake of pharmaceuticals are common in emergency department. Thankfully, in most cases, the amount and the type of drug are innocuous and patients can be discharged after observation or minor interventions. We present a case of mortal suicidal propafenone intoxication. Case: A 22-year-old female presented to emergency department approximately thirty minutes after oral intake of 3750 milligrams of propafenone, 5000 miligrams of acetaminophen, 2000 milligrams of trimebutine and unknown amount of alcohol. Initially, patient was normotensive, minimally tachycardic in sinus rhythm and asymptomatic. Gastric lavage and activated charcoal were applied. Hydration was started. Arterial blood gases showed compensated metabolic acidosis. Thirty minutes later, she became hypotensive and tachycardic and had a tonic-clonic seizure, which was terminated by diazepam. She was intubated and ventilated. Cardiac arrest occurred and she had first-degree atrioventricular block with prolonged QRS after return of spontaneous circulation (ROSC). Femoral venous catheter and transient pacemaker were placed. She had two more seizures and cardiac arrests with ROSC. Resuscitation efforts remained unsuccessful after fourth cardiac arrest despite intravenous lipid, sodium bicarbonate, hypertonic saline, calcium and inotrope therapies and a cardiopulmonary resuscitation effort of total 92 minutes. Discussion: Propafenone poisoning is rare but life-threatening. Propafenone is a class Ic antidysrhythmic agent that has weak beta-blocking effects. A spectrum of cardiac effects like hypotension, bradycardia, sinoatrial blocks, left ventricular failure, atrioventricular junctional, ventricular tachycardia, coma or sudden cardiac arrest may be seen in the course. While fatal results due to 3 grams of propafenone were reported, doses over 4 grams are usually lethal. Decontamination, supportive therapies, transient heart pacing, acidosis treatment are essential in the treatment. The efficacy of intravenous lipids, insulin glucagon therapy, sodium bicarbonate, hypertonic saline is unknown but the literature reports successful results. Conclusion: Emergency physicians should master possibly life-threatening intoxications like propafenone. Keywords: Propafenone intoxication, toxicology, intravenous lipid, emergency department P 473 YILDIRIM ÇARPMASINA BAĞLI KULAK AĞRISI: İKİ OLGU SUNUMU Sinem Çelik, Halil Doğan, Dogac Niyazi Ozucelik, Sezgin Sarikaya
Bakırköy Dr. Sadi Konuk Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Yıldırımlara bağlı yıllık mortalitenin milyonda 0.2–1.7 arasında değiştiği bildirilmektedir (2). Mortalite sebepleri arasında kardiyovasküler nedenler ön plandadır. Yazımızda yakın mesafeye düşen yıldırımdan etkilenme sonrasında kulakta ağrı ve dengesizlik şikayeti ile gelen iki olgu sunulmuştur. Olgu sunumları: Acil kliniğine dolaylı yoldan yıldırım çarpması sonrası getirilen 26 ve 29 yaşlarında iki erkek hasta havaalanında pistte çalışırken kulaklıkla uçağın yanında olup kokpitle iletişim halinde olduğu esnada uçağa yıldırım çakması ile kulaklık takılı olan sağ kulakta ağrı ve sersemlik şikayeti ile acil servise başvurdular. Hastaların başvuru anında bilinci açık, oryantasyonu ve kooperasyonu tam, sağ kulakta ağrı, sersemlik hissi ve dengesizlik mevcut idi. İki hastanın da vital bulguları stabil. Hastaların yapılan bilateral otoskobik muayenesinde bilateral dış kulak yolu ve kulak zarı normal idi, fasiyal sinir muayenesi doğaldı. Elektrokardiyografi normal sinüs ritminde. Yapılan odyometrik değerlendirme sonucu sağ: 13/10 sol: 12/8 bilateral işitme normal sınırlardaydı. Yapılan tetkiklerinde; elektrolit bozukluğu yoktu, karaciğer ve böbrek fonksiyon testleri normaldi. Kreatin Kinaz (CK):210 U/L olarak ölçüldü. Hastanın Beyin BT’si normaldi. Hemodinamik yönden stabil bulunan hastaya 1000cc % 0.9 NaCl infüzyonu başlandı. Şikayetleri 4 saat sonra gerileyen hasta taburcu edildi. Yıldırım çarpmasına bağlı geniş timpanik membran perforasyonu, sensörinöral işitme kaybı ve dengesizlik karşılaşılan bulgulardandır. Literatürde yıldırım çarpması sonrası hayatta kalan hastaların çoğunda odiyovestibüler anormallik bildirilmiştir. Yıldırım çarpmasına bağlı en sık rapor edilen kulak hasarı iletim tipi işitme kaybınında eşlik ettiği timpanik membran perforasyonudur. Bizim her iki olgumuzda da yıldırımın yan sıçrama etkisi ile mağdurlar denge kaybı ve kulakta ağrı hissetmişlerdir. Mağdurlar dışarıda açık alanda çalışan yıldırım çarpmasından en çok etkilenebilecek kesimdendirler. Ve her iki mağdurda yıldırım çarpma insidansının en yüksek olduğu aylardan olan ağustos ayında etkilenmişlerdir. Her iki olguda da denge kaybı olmuş olup, iletim tipi veya sensörinöral işitme kaybı gözlenmemiştir. Kulaklık ve benzeri aparatlar dolaylı olarak yıldırım'ın kulak üzerine olan etkilerini artışına zemin hazırlayabilir. Anahtar Kelimeler: Yıldırım çarpması, kulak ağrısı, hava alanı, kulaklık

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
441
P 474 STERNUM FRACTURE DIAGNOSIS WITH ULTRASOUND
Taygun Baykal, Tanju Biçer, Muharrem Doğan, Demet Devrimsel Doğan, Ecem Deniz Kırkpantur Fatih Sultan Mehmet Training and Research Hospital, Istanbul, Turkey Introduction: Tenderness on the sternum is a strong clue for sternum fracture. Sternal fractures generally occurs at the body or the manibrium. Computed tomography is the gold standard for diagnosis. Ultrasound imaging is a useful headboard choice and showed that, it’s more effective than conventional radiography. Nowadays we believe that sternal fractures are, approximately, only %1 mortal, and barely related with cardiac injury. Case: In our case a 27-year-old man was admitted our emergency department because of assault. He had mild head, abdominal and thoracal trauma. He was complaining about a sternal pain. His Glasgow coma score was 15 and vital signs were stabile. Physical examination revealed tenderness on the sternum and sundry dermal abrassions at the extremities. His cardiac and respiratory sounds were normal. There was no confusion or abdominal tenderness. His laboratory was completely normal. We performed focuses sonography of abdominal trauma (FAST) to the patient. The FAST was normal, there was no free abdominal fluid or pericardiac fluid. In this point, because of sternal tenderness, we performed a sternal USG with a view to sternal fracture. There was a hypoechoic area on the sternum, some cortical irregularities, and a collapsing area. Sternal fracture diagnosis was made. After that we confirmed this diagnosis with thorax computed tomography. His electrocardiography and other imaging modalities were normal. So patient discharged with NSAID treatment and cardiovascular surgery appointment. Discussion: Sternal fractures should be considered for patients who has chest trauma and sternal tenderness. Gold standard for stenal fracture diagnosis is computed tomography. Ultrasound is another useful method for sternal imaging and it is non-invasive, fast, and reliable with no side effects. Cortical irregularity, dislocated fragments, collapsing areas, hypoechoic areas are enough for making a sternal fracture diagnosis. İt can be used safely and confidently for especially radiation sensitive patients. Keywords: Sternum fracture, trauma, ultrasound P 475 THALASSEMIA RELEATED PULMONARY EMBOLISM Taygun Baykal, Tanju Biçer, Muharrem Doğan, Demet Devrimsel Doğan, Abdullah Taşcı Fatih Sultan Mehmet Training and Research Hospital, Istanbul, Turkey Introduction: Thalassemia, also called Mediterranean anemia, is a form of inherited autosomal recessive blood disorder characterized by abnormal formation of hemoglobin. Thalassemia can cause complications, including iron overload, bone deformities, and cardiovascular illness Although the life expectancy of thalassemia patients has markedly improved over the last few decades, patients still suffer from many complications of this congenital disease. Venous thromboembolism (VTE) occurs in approximately 10% of patients after splenectomy, particularly splenectomy performed for hematologic abnormalities. Clinicians often fail to recognize this potential complication in the postoperative period approximately 10% of symptomatic VTE cases occur within 3 months of hospital discharge Case: In our case a 34-year-old woman presented our clinic with progressive dyspnea and palpitation worsened at last 3 days. She was also complaining about stabbing chest pain. She experienced no fever, cough or any infectious symptoms. Her medical history contains beta thalassemia major, splenectomy 3 years earlier and no other specialties. Her body temperature was 36.6 C, heart rate was 89 bpm, blood pressure was 90/50 mm/Hg and oxygen saturation was 95%. Her physical examination were normal. Her revised Geneva score for Pulmonary Embolism was 3, low risk score. Her laboratory reveals Hb:10.6 mg/dl, Troponin:0.484(0-0.30), d-dimer:10.92(0-0.05), platelet:1.000.000 and other values were normal. So we performed an thorax computed tomography pulmonary angiography and it revealed hypodense filling defects at the both of lobary and segmental arteries. So a pulmonary embolism (PE) diagnosis was made. Discussion: In the present article, we offer a case report and clinical situation that highlight morbidity associated with PE after splenectomy procedures of the patients who has thalassemia. Our objective is to raise physician awareness of the unique PE risks that splenectomy surgical procedures pose to patients. Keywords: Pulmonary embolism, respiratory emergency, Thallasemiae

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
442
P 476 TRAVMATİK RENAL ARTER DİSEKSİYONU: OLGU SUNUMU
Halil Doğan, Sinem Çelik, Dogac Niyazi Ozucelik, Ayca Ayaz Şahin, Sezgin Sarikaya Bakırköy Dr. Sadi Konuk Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Giriş ve Amaç: Travma sonrası renal arter diseksiyonu çok nadir bir durum olup acil tedavisi gereken bir durumdur. Olgumuzda araç içi trafik kazası sonrası renal arter diseksiyonu gelişen olgunun tanı ve tavisi literatür eşliğinde tartışılmıştır. Olgu: 18 yaşında erkek hasta araç içi trafik kazası sebebiyle acil servise getirildi. Öyküsünde yüksek enerjili bir kaza olduğu ve hava yastığının açıldığı öğrenildi. Hastanın bilinen hastalık öyküsü yok. Fizik muayenesinde, kan basıncı: 130/65 mmHg, kalp tepe atımı:96 atım/dk, solunum sayısı: 17/dk, SpO2: % 97 idi. sol frontoparietalde minimal scalp kanaması, sağ el üstünde 4. parmak ekstansör tendon kesisi, sağ patella üzerinde 10 cm açık yarası mevcut, batın sol üst kadranda hassasiyet. Labratuar tetkiklerinde Hbg: 15,1 g/dl Hct: %43,6 Wbc: 11.9, CK: 233, lipaz: 66, CK-MB: 183, karaciğer ve böbrek fonksiyon testleri normal idi. Kan gazında laktat: 3,2 olan hastanın kontrol biyokimyasında ve kontrol hemogram tetkikinde anlamlı değişiklik olmadı. Kontrastlı batın BT’de; sol böbrekte de kontrast fiksasyonu göstermeyen hipodansiteler izlendi. Girişimsel radyoloji ile hastanın sol renal arterinde disseksiyon saptanıp, stent uygulaması yapıldı. Tetenoz profilaksisi ve Sefazol 1 gr, Gentamisin 80 mg, Metronidazol 500 mg tedavisi başlandı. Hastanın takiplerinde 1 hafta sonra yapılan değerlendirilmede sol böbreğin %50 oranında kanlanmasının sağlandığı görüldü.Gençlerde arteriyal diseksiyonun en sık nedeni travmadır. En sık karotis arterde görülür. Travma sonrası renal arter diseksiyonu gelişebilecek nadir bir durumdur. Özellikle gençlerde acil müdahale gerektiren bir durumdur. Endo vasikuler stent yerleştirilmesi ile başarılı bir şekilde tedavi edilebilir. Anahtar Kelimeler: Renal arter diseksiyonu, travma, endo vasküler stent P 477 EFFECTS OF ANTIARRYTHMIC DRUG THERAPY ON PERFUSION INDEX IN PATIENTS WITH ATRIAL FIBRILLATION PRESENTING TO EMERGENCY DEPARTMENT Muge Surmeli, Hakan Topacoglu, Sila Sadillioglu Istanbul Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey Objective: The aim of the study was to evaluate the relationship between the perfusion index (PI) and the changes in heart rate of the patients with acute symptomatic atrial fibrillation (AF) Method: The study was conducted as prospective cross-sectional study. A total of 51 patients with acute symptomatic AF, ventricular rate >110 bpm were included in the study during a period of four months. Vital signs including arterial hypertension, pulse, respiratory rate, temperature, blood oxygen saturation and PI values were measured at the admission time and after heart rate management. Rate control was defined as decrease in ventricular rate to less than 100 bpm. In addition, the relationship between the PI and the patient’s demographics and vital signs were analyzed. Results: Fifty-one patients were included in the study, 36 of them were female (70.6%) and 15 male (29.4%) with median age 70.3±13.2 (range 44-100 years). The mean PI of the patients with AF measured on admission to ER was 2.9±2.7 (range 0.18-13), while it was 4.6±3.6 (range 0.14-14) after heart rate management. (Spearman’s correlation test, p=0.108). There was no statistically significant difference in the vital parameters and PI values of the patients at the presenting time to ER (p>0.05). There was statistically significant difference between in PI mean values of the patients achieving normal ventricular rate (34 patients, mean PI: 5.2±3.8) and those who still had heart rate over 100 bpm despite antiarrhythmic drug therapy (17 patients, mean PI 3.2±3.7) (p:0,035). Conclusion: Reducing the heart rate to below 100 bpm in patients with AF has positive effect on perfusion index. Thus, in patients with AF, heart rate below 100 bpm can be taken as limiting value for PI. Keywords: Perfusion index, atrial fibrillation, emergency department

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
443
P 478 ACİL SERVİS'TE NADİR BİR TRAVMA: LUXATIO ERECTA
Attila Aydın1, Sedat Bilge1, Meltem Bilge2, Cemile Aydın3
1Gülhane Eğitim ve Araştırma Hastanesi, Acil Tıp Anabilim Dalı, Ankara 2Dışkapı Eğitim ve Araştırma Hastanesi, Anestezi ve Reanimasyon Kliniği, Ankara 3Etimesgut Devlet Hastanesi, İç Hastalıkları Kliniği, Ankara Glenohumeral eklemin inferior dislokasyonu veya luxatio erecta acil serviste nadir görülen bir yaralanmadır. Genellikle kolun hiperabdüksiyonu sırasında gelişen travma etkisiyle ortaya çıkar. Omuz çıkıkların %95 kadarı anterior olup sadece %0.5’i inferior lokalizasyondadır. Oldukça nadir görülmesinden dolayı luxatio erecta olgusunun tanı, yönetimi ve tedavisini literatür eşliğinde tartışmayı amaçladık.26 yaşında erkek hasta ağırlık kaldırırken yere düşmesi sonucunda sağ omuzda şiddetli ağrı ve hareket kısıtlılığı nedeniyle Acil servise başvurdu. Yaklaşık 3 gün önce travmaya sekonder anterior omuz çıkığı öyküsü olduğu ve velpoue bandajı önerilmesine rağmen kullanmadığı bilinmektedir. Fizik muayenesinde; sağ omuz yaklaşık 130 derece abdüksiyonda ve eksternal rotasyonda, ön kol pronasyonda ve dirsek fleksiyon pozisyondaydı. Humerus başı aksiller bölgede palpe edildi. Sağ omuzda belirgin hareket kısıtlılığı mevcuttu. Ön kol, dirsek ve parmakları hareket ettiriyor, radial ve ulnar nabazanlar palpabldı. Duyusal defisiti yoktu. Aksiller bölgede belirgin şişlik yoktu ve yatak başı doppler usg’de axiller arter ve vende akım alındı. AP radyografide humerus başı glenoid fossanın altında görüldü. Glenohumeral eklemin inferior dislokasyonu (luxatio erecta) tanısı konuldu. Hastaya sedasyon analzeji eşliğinde kapalı redüksiyon işlemi uygulandı. Birçok luxatio erecta vakaları yanlışlıkla subglenoid anterior dislokasyon gibi yanlış tanı ile tedavi edilmeye çalışılır. Bu sebeple, hastaların yönetimi zorlaşır, hastanın ağrısı artar ve komplikasyonlar gelişir. Luxatio erecta vakalarını ayırt ederken hastanın tipik klinik görüntüsü ve radyografi bulguları önem kazanır Anahtar Kelimeler: İnferior, humerus, dislokasyon P 479 PRION DISEASE AT THE EMERGENCY DEPARTMENT Tahir Telat Yurttaş, Ahmet Faruk Orhan, İncifer Kanbur, Hakan Topaçoğlu, Özgür Karcıoğlu Istanbul Training and Research Hospital, Emergency Medicine Clinic, Istanbul, Turkey Introduction: Prion diseases are neurodegenerative disorders with long incubation periods that progress irreversibly as they start to cause clinical symptoms. Prion diseases are rare and mortal disorders that may be observed both in humans and animals. They affect 1-2 people/million around the world in a year. There are five different forms observed in human beings: Kuru, Creutzfeldt-Jacob disease, Gerstmann-Straussler-Scheinker syndrome, fatal familial insomnia and bovine spongioform encephalopathies. The most common one is Creutzfeldt-Jacob disease. Case: A 53 year-old male was admitted to the emergency department with symptoms of headache, dizziness and gait disorder for approximately one month. He had hypertension in the medical history and his vitals were as follows: BP: 176/84 mmHg, HB: 92/min, temp: 36.4 C, SpO2: 98%. He was fully conscious, oriented and cooperated; PIR +/+, isocoric; glob movements of the eyes were normal on both four directions; the speech was slow. Muscle strength was normal on both upper and lower extremities. However, cerebellar tests were awkward, walking was leery, oscillation and stepping phases were irregular and tandem walking was disarranged. Deep tendon reflexes were all normoactive. Hyperdense areas were detected on both caudate nuclei and also on the right putamen in the diffusion MRI. BOS cultures and HSV type 1 and 2, Tbc PCR were all negative. However, protein 14-3-3 was positive. Severe deceleration of strata activities and periodically sharp, slow waves were detected in electroencephalogram performed at 3-day intervals. He was diagnosed as Creutzfeldt-Jacobs disease according to the investigations. Then, fever and wheezing was attended and cooperation and orientation was distorted. As the clinical condition deteriorated, he died due to respiratory failure in four weeks after hospitalization. Conclusion: Neurological complaints like headache and dizziness are common causes of admission to the emergency department. Rare causes such as prion diseases sould be kept in mind in such patients. Keywords: Prion disorders, vertigo, emergency department

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
444
P 480 GULLIAN BARRE SENDROMU VARYANTI: MILLER FISCHER SENDROMU
Sedat Bilge1, Attila Aydın1, Derya Can1, Ayhan Acar1, Meltem Bilge2, Cemile Aydın3
1Gülhane Eğitim ve Araştırma Hastanesi, Acil Tıp Anabilim Dalı, Ankara 2Dışkapı Eğitim ve Araştırma Hastanesi, Anestezi ve Reanimasyon Kliniği, Ankara 3Etimesgut Devlet Hastanesi, İç Hastalıkları Kliniği, Ankara Gullian Barre Sendromu (GBS) sıklıkla akut ve hızlı ilerleyen inflamatuar demiyelizan polinöropatidir. GBS varyantları arasında Miller Fischer sendromu (MFS) yer almaktadır. Otoimmün kökenli hastalığın karakteristik klinik bulguları; alt ekstremiteden başlayan arefleksi ve asendan ilerleyen simetrik motor zayıflıktır. İlk olarak çift görme ile başlayan, daha sonra GBS tipik bulguları eşlik eden MFS olgusunu paylaşmak istedik.32 yaşında bayan hasta acil servise başvurmadan üç gün önce çift görme şikayeti ile dış merkeze başvurmuş. Dış merkezde yapılan laboratuvar, görüntüleme ve elektrofizyolojik incelemelerde herhangi patoloji saptanmamış. Çift görme şikayetinden yaklaşık 24 saat sonra denge kaybı, dizlerde güçsüzlük, ayak ve el parmaklarda uyuşma şikayeti başlamış. Bu semptomlara konuşma bozukluğu ve dilde peltekleşme semptomları eklenince acil servisimize başvurmuş. Anamnezinde; 2 hafta önce gribal enfeksiyon öyküsü mevcut olup, kronik ilaç kullanım ve hastalık öyküsü yoktu. Vital bulguları; TA:122/78 mmHg, Ateş:36.1 derece, nabız:88 vuru/dakika, SaO2:99%. Nörolojik muayenesinde; GKS:15, şuuru açık oryantasyon ve kooperasyon tamdı. Göz hareketleri bilateral dışa ve yukarı bakış kısıtlı, bilateral içe ve aşağı bakış kısıtlıydı. İndirekt ve direk ışık refleksi bilateral normaldi. GAG refleksi alınmıyor, taban deri yanıtı bilateral fleksör, DTR’leri alınamıyor, yürüyüş ataksik olup, romberg testi ve ense sertliği negatifti. Yapılan Beyin BT ve Difüzyon MR görüntülemelerinde herhangi bir kanama, kitle, iskemiye ait bulguya rastlanmadı. Hasta Gullian Barre (Miller Fisher?) ön tanısı ile Nöroloji Kliniğine ileri tetkik ve tedavi amacıyla yatırıldı. Acil serviste görevli hekimlerin nörolojik semptomlarla gelen hasta gruplarında Miller Ficher Sendromunu akılda tutmaları gerekmektedir. Anahtar Kelimeler: Miller Fischer, Gullian Barre, polinöropati P 481 NEFREKTOMİ İLE SONUÇLANAN BASİT BİR EV KAZASI Bilge Ercan, Zeynep Konyar, Fatma Sarı Doğan, Özlem Güneysel İstanbul Dr. Lütfi Kırdar Kartal Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Giriş: Renal travma tüm travma olgularının %1-5’inde görülür ve en sık nedeni motorlu taşıt kazalarıdır. Bu olgu sunumunda basit bir ev kazası sonucu yan ağrısı ile başvuran hastada meydana gelen izole renal hasardan bahsedilmektedir. Travma, dünyada ölüm nedenleri arasında altıncı sırada yer almaktadır. Genitoüriner ve renal travmalar ise tüm travmaların %5’ini, tüm batın travmalarının ise %10’unu oluşturur. Genitoüriner travmaların %5’i künt, %20’si penetran travmaya bağlı gelişir. Düşük enerjili künt travma ile oluşan ve nefrektomi gereken bir olgu sunuyoruz. Olgu: 25 yaşında kadın hasta künt travma sonrası oluşan sol yan ağrısı ile acil servise başvurdu. Başvuru sırasında GKS:15, TA:120/80 mmHg, KTA:86/dk, SS:16/dk, SO2:%98 idi. Anamnezde perde takarken düştüğünü ve düşerken karın bölgesini sandalyeye çarptığını ifade etti. Hastanın fizik muayenesinde batında sol alt ve üst kadranda hassasiyet mevcuttu, diğer sistem muayeneleri doğaldı. Yapılan FAST sonucu sol splenorenal lojda mayi tespit edildi. Kanama odağı açısından çekilen kontrastlı BT’de sol renal grade 4-5 yaralanma ve etrafında kontrast tutulumu görüldü. hgb:13 gr/dl htc:%37,7, olan hastanın yaklaşık 1 saat sonra bakılan hemogramda hgb:12,1 gr/dl htc:%36,2 saptandı. Künt travmaya bağlı renal yaralanma olan hasta üroloji ile konsülte edildi ve nefrektomi uygulandı. Sonuç: Acil servislerde sıkça karşılaştığımız ev kazalarına yaklaşımda dikkatli olmalıyız, çünkü organ kaybıyla sonuçlanan olgumuzda olduğu gibi, atlanması halinde yaşamı tehdit eden durumlara yol açabilirler. Kolay ulaşılabilen, dakikalar içinde hasta hakkında bize bilgi veren, hastanın tanı ve tedavi sürecini hızlandıran USG, acil servislerde hekimlerin vazgeçilmezleri arasında yerini almalıdır. Anahtar Kelimeler: Düşme, ev kazası, renal travma, nefrektomi

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
445
P 482 EXPERIENCES OF DIGIFAB; TWO CASES
Özge Can, Elif Dilek Çakal, Murat Ersel Ege University School of Medicine, Department of Emergency Medicine, Izmir, Turkey Introduction: Digoxin is a drug commonly used in the treatment of atrial fibrillation (AF) with rapid ventricular response to control the rate. Therapeutic range of drug is narrow and life threatening acute and chronic toxicity is occur. In our two cases, chronic digoxin intoxication were treated with digoxin antibody (DigiFab). Case: Two digoxin user patients were admitted to the emergency department with altered mental status nausea and vomiting. Vitally unstable patients had bradycardia. EKG showed third-degree atrioventricular (AV) block. Hyperkalemia was occur in two patient. Treatment of hyperkalemia was ineffective for AV block. Digoxin levels determined above to normal range and digiFab treatment was started. Rhythm back to sinus rhythm and patient consciousness was improved. Vital signs were stable. One patient discharged, the other extubed. Discussion: DigiFab is digoxin antidote. Indications are arrhythmias with hemodynamically unstable, hyperkalemia (>5 mEq/L), end-organ damage is accompanied by hypoperfusion. In our case digoxin intoxication with third-degree AV block were treated with digiFab. Conclusion: The digiFab is rarely used antidote but necessary to remember the effect of fatal arrhythmias. Keywords: DigiFab, digoxin intoxication, third-degree AV block P 483 ACİL SERVİS'TE KULLANILAN YENİ PROSEDÜR: SUPRAKONDİLER RADİAL BLOK Sedat Bilge1, Attila Aydın1, Cemile Aydın3, Meltem Bilge2, Ayhan Acar1
1Gülhane Eğitim ve Araştırma Hastanesi, Acil Tıp Anabilim Dalı, Ankara 2Dışkapı Eğitim ve Araştırma Hastanesi, Anestezi ve Reanimasyon Kliniği, Ankara 3Etimesgut Devlet Hastanesi, İç Hastalıkları Kliniği, Ankara Distal radius kırıkları (DRF) tüm popülasyonda üst ekstremite kırıklarının en çoğunu oluşturmaktadır. Acil servislerde redüksiyonda ağrı kontrolünde çoğunlukla Prosedürel sedasyon analjezi (PSA) uygulanmaktadır. Ancak PSA prosedüründe kullanılan ilaçların çoğunda ciddi yan etkileri olması ve her hastanın yakın monitorizasyon ve gözlem gerekliliği gibi dezavantajları nedeniyle acil servislerde alternatif yöntemlere ihtiyaç duyulmaktadır. Bu amaçla Suprakondiler radial bloğun (SKRB) iyi bir alternatif olabileceği düşünülmüştür. 65 yaşında bayan hasta acil servise trafik kazası sonrasında sol el bileğinde ağrı ve şişlik nedeniyle başvurdu. Kronik kullandığı bir ilaç yoktu. Çekilen el bileği direk grafide radius distal uç kırığı tespit edildi. Acil serviste redüksiyon öncesinde ağrı yönetiminde SKRB kullanıldı. USG eşliğinde Acil serviste uygulandı. Yaklaşık 10-15 dakika sonra redüksiyon uygulanan hastanın VAS skorunda ciddi derecede azalma sağlandı. Bu sonuçlar ışığında DRF redüksiyonunda; SKRB'nin acil servislerde USG eşliğinde kolay uygulanabilmesi, redüksiyon esnasındaki VAS skorlarının sedasyon analjeziye benzer şekilde başarılı olması, hastanede kalış süresi açısından avantajlı olması, hasta-hekim memnuniyetinde fark olmaması ve komplikasyonlar açısından oldukça güvenli olması sebebi ile PSA’ya önemli bir alternatif olduğu düşünülmektedir. Anahtar Kelimeler: Suprakondiler, radial, blok, periferik

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
446
P 484 A RARE EMERGENCY MEDICINE CASES: ORF
Özge Can, Yusuf Ali Altuncı, Funda Karbek Akarca Ege University School of Medicine, Department of Emergency Medicine, Izmir, Turkey Introduction: Human orf is an uncommon disease. History of direct contact with infected sheep, goats or wild animals is a diagnostic tool. Skin lesions appears mostly on hands. In our last religious days patients was admitted to emergency room with typically skin lesions. Case: Five patients were admitted to the emergency department with necrotizing skin lesions on the hands and arms. One patient was a butcher, had a history of use of colchicine. Lymphadenopathy and fever detected in this patient and was hospitalized for observation and discharged healthy after five days. The other patients, both with the same family members, had no immunocompromised status. Treatment was started in ED with the diagnosis of ORF. Patient referred to infection desaese physicians to follow up. Discussion: Orf is a viral skin disease. Direct contact history is helpful for diagnosis. Papular rash begins and proceeds with a sequence similar to the iris image, exudative and papillomatous lesions. The most common seen in farmers and shepherd in dealing with the animals, veterinarians are rarely seen. Treatment of lesions is kept clean and protect from secondary infection with antibiotics. Conclusion: We would like to remind benign self-limiting desease and the skin incision is contraindicated. Keywords: Orf, papillomatous skin lesions, viral infection of skin P 485 LANSOPRAZOLE BAĞLI ANAFLAKSI
Sedat Bilge1, Attila Aydın1, Erdem Cevik4, Cemile Aydın3, Meltem Bilge2, Güçlü Aydın1
1Gülhane Eğitim ve Araştırma Hastanesi, Acil Tıp Anabilim Dalı, Ankara 2Dışkapı Eğitim ve Araştırma Hastanesi, Anestezi ve Reanimasyon Kliniği, Ankara 3Etimesgut Devlet Hastanesi, İç Hastalıkları Kliniği, Ankara 4Haydarpaşa Eğitim ve Araştırma Hastanesi, Acil Tıp Kliniği, İstanbul Proton pompa inhibitörleri tüm hekimler tarafından mide ağrısı ile ilişkili hastalıklarda sık olarak reçete edilen bir ilaçtır. Bu gruptaki ilaçların reçete edilme sıklığı giderek artarken, lansoprazole bağlı yan etkiler %1 veya daha az sayıda hastalarda bildirilmiştir. Ayrıca bildiğimiz kadarıyla lansoprazole bağlı anaflaktoid reaksiyon nadir görülen bir yan etki olup çok az sayıda olgu tanımlanmıştır. Biz lansoprazol aldıktan sonra anaflaksi gelişen ve başarı bir şekilde tedavi edilen olgumuzu sunduk. Ayrıca lansoprazolün güvenli ve rahatlıkla reçete edilecek bir ilaç olduğu bilinmesine rağmen, hayatı tehdit eden durumlara yol açabileceğini vurgulamaktayız.61 yaşında bayan hasta 1 haftadan beri devam eden mide ağrısı nedeni ile acil servis polikliniğine başvurdu. Hikayesinde; kronik hastalık, ilaç kullanma ve allerji öyküsü yok. Acil servis triyaj bölümünde vital bulguları alınırken nefes alamadığını ve tüm vücudunda kaşınmalar olduğunu ifade etti. Hasta yakını tarafından acil servise gelmeden yaklaşık 30 dakika önce lansoprazole 30 mg oral tablet aldığı bilgisi verildi. Fizik muayenede; Vital bulguları; T.A. 70/40mmHg, sat %92, nabız:77, ateş:36 dereceydi. Uvula, müköz membranlarda ve dudakta hafif ödem mevcuttu. Yüzde ve gövde üst kısımlarında raşları mevcuttu. Ac sesleri bilateral azalmıştı. Hastada anaflaksi düşünüldü ve uyluk lateral bölgeden 0.5 mg IM epinephrin uygulandı. Hasta supin pozisyonuna getirildi ve damar yolundan 100 mg metilprednisolon IV, 50 mg difenhidramin IV uygulandı. Sıvı resüsitasyonu devam edilen hastanın yaklaşık 15 dakika sonra hipoperfüzyon bulguları düzeldi. Kontrol vital değerleri; TA:110/80 mmHg, sat %96, nabız:98/dk, ateş:37 dereceydi. Hasta acil serviste yaklaşık 24 saat boyunca hemodinamik monitorizasyon altında takip edildi. Takipleri sırasında herhangi bir komplikasyon gelişmedi. Alerji uzmanınca takip edilmek üzere hastaneden oral antihistaminik ve prednisolon tablet verilerek taburcu edildi. Lansoprazole halen güvenle kullanılan ve çekinmeden reçete edilebilecek bir ilaçtır. Fakat hastalarda ortaya çıkabilecek ve ciddi mortal seyreden yan etkiler açısından hasta değerlendirilmeli ve tedavi öncesi risk faktörü olan hastalar tespit edilerek hastaların uygun yönetimi sağlanmalıdır Anahtar Kelimeler: Lansoprazol, anaflaksi, proton pompa

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
447
INDEX

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
448
A
Abacı, A. 21 Abanoz, B. 30, O-120 / 168, O-121 / 169 Abatay, K. P-326 / 367, P-327 / 367, P-329 / 368, P-330 / 369, P-331 / 369, P-333 / 370, P-335 / 371, P-338 / 373,
P-389 / 398, P-456 / 432 Aboshanb, R. O-048 / 132 Abuşka, D. 32, O-135 / 176, P-049 / 228, P-198 / 303 Acar, A. P-480 / 444, P-483 / 445 Acar, F. P-405 / 406 Acar, N. 34, 97, O-033 / 125, O-072 / 144, O-117 / 167, O-133 / 175, O-134 / 175, O-147 / 182, O-148 / 182, P-128 / 267,
P-201 / 304, P-252 / 330, P-340 / 374, P-346 / 377, P-348 / 378, P-358 / 383, P-402 / 405, / 23 Acar, Y. A. O-185 / 202, P-205 / 306, P-268 / 338, P-272 / 340 Açıkalın Akpınar, A. O-104 / 160, O-180 / 199, P-202 / 305 Açıkalın, A. 16, 32, O-061 / 139, O-138 / 177, O-168 / 193 Açıkgözlü, V. O-075 / 146 Açıksarı, K. P-119 / 263, P-120 / 263, P-442 / 425 Adanc, M. P-139 / 273, P-168 / 287, P-169 / 288 Adanç, M. P-467 / 437 Afacan, G. 19, O-067 / 142, O-123 / 170, P-005 / 206, P-006 / 206, P-007 / 207, P-008 / 207, P-009 / 208, P-010 / 208,
P-011 / 209, P-135 / 271, P-224 / 316 Ağaçkıran, İ. O-034 / 125, P-056 / 231 Ağar, İ. G. P-308 / 358, P-446 / 427 Ağı, İ. P-255 / 331 Ağır, İ. O-149 / 183 Ak, A. P-215 / 311 Ak, H. O-157 / 187 Ak, R. P-095 / 251, P-096 / 251, P-108 / 257, P-109 / 258, P-110 / 258, P-121 / 264, P-149 / 278, P-150 / 278,
P-152 / 279, P-163 / 285, P-164 / 285, P-165 / 286, P-167 / 287, P-170 / 288, P-171 / 289, P-172 / 289, P-173 / 290, P-174 / 290, P-176 / 291, P-177 / 292, P-178 / 292, P-180 / 293, P-181 / 294, P-191 / 299, P-256 / 332, P-258 / 333, P-260 / 334, P-261 / 334, P-262 / 335, P-267 / 337, P-373 / 390, P-378 / 392, P-400 / 404, P-412 / 410
Akalın, L. E. O-068 / 142 Akarca, F. K. 19, 23, O-040 / 128, P-366 / 387, P-386 / 396, P-454 / 431, P-484 / 446 Akay, A. O-040 / 128 Akay, H. P-363 / 385 Akay, S. O-075 / 146, P-362 / 385, P-365 / 386, P-368 / 388, P-371 / 389 Akbal Kahraman, H. P-018 / 212 Akbay, D. O-026 / 121 Akbuga Özel, B. O-016 / 116, P-057 / 232 Akbulut, M. U. P-159 / 283, P-231 / 319 Akcaci Baran, E. O-133 / 175 Akça, I. O-180 / 199 Akçay, D. P-003 / 205 Akçebe Aydın, A. P-471 / 439 Akçimen, M. O-009 / 113 Akday, U. P-138 / 272 Akdeniz, Y. S. P-320 / 364, P-347 / 377, P-359 / 383, P-425 / 416, P-426 / 417 Akdoğan, A. O-083 / 150 Akdoğan, H. İ. P-441 / 424 Akdur, G. P-220 / 314 Akdur, O. 24 Akgöl Gür, S. T. O-123 / 170, P-006 / 206, P-008 / 207, P-011 / 209 Akgün, F. S. P-098 / 252 Akgün, T. O-082 / 149 Akhanlı, P. P-076 / 241, P-460 / 434 Akın, Ü. P-207 / 307 Akıncı, E. O-119 / 168, O-152 / 184 Akkaş, M. O-034 / 125, P-056 / 231 Akkaya, A. P-361 / 384, P-367 / 387, P-372 / 390 Akkaya,, A. P-370 / 389 Akkoyunlu, R. U. P-382 / 394, P-407 / 407 Akkuş, Ş. O-152 / 184 Akman, C. P-217 / 312, P-245 / 326, P-249 / 328, P-304 / 356, P-306 / 357 Akoglu, H. O-029 / 123, O-051 / 134, O-069 / 143, O-155 / 186, O-181 / 200, P-131 / 269, P-133 / 270, P-134 / 270,
P-136 / 271, P-137 / 272, P-139 / 273, P-140 / 273, P-141 / 274, P-142 / 274, P-145 / 276, P-147 / 277, P-148 / 277, P-159 / 283, P-160 / 283, P-162 / 284, P-162 / 284, P-166 / 286, P-168 / 287, P-169 / 288, P-229 / 318, P-230 / 319, P-231 / 319

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
449
Akoğlu, H. 9, 15, 17, 31, 32, 46 Akova, S. P-017 / 212 Akoz, A. O-041 / 129, P-204 / 306 Aköz, A. 24, 28, O-094 / 155, O-156 / 186, P-135 / 271, P-224 / 316 Akpancar, M. P-235 / 321 Akpınar, E. 7 Akpınar, G. O-164 / 191 Akpınar, M. O-109 / 163 Akpınar, O. O-061 / 139 Akpolat, B. P-049 / 228 Aksay, E. 14, 24, O-020 / 118, O-057 / 137, O-065 / 141, P-242 / 325, P-269 / 338, P-277 / 342, P-284 / 346,
P-406 / 407 Aksel, G. O-011 / 114, P-018 / 212, P-419 / 413 Aktas, C. P-022 / 214 Aktaş, A. P-084 / 245 Aktaş, H. P-282 / 345 Aktepe, M. P-347 / 377, P-359 / 383, P-425 / 416, P-426 / 417 Aktürk, Ö. E. P-361 / 384, P-362 / 385, P-372 / 390 Akyol, C. O-009 / 113, O-028 / 122 Akyol, P. Y. O-015 / 116, O-086 / 151, O-103 / 160, O-130 / 173, O-146 / 181, O-178 / 198, P-023 / 215, P-077 / 242,
P-212 / 310, P-228 / 318, P-281 / 344, P-325 / 366 Alakuş, Ü. P-012 / 209 Alaska, Y. 8, 35 Alatlı, T. P-441 / 424 Albayrak, D. P-194 / 301, P-344 / 376, P-352 / 380 Albayrak, O. P-357 / 382, P-360 / 384, P-459 / 433 Aleksandrowicz, S. P-040 / 223, P-041 / 224 Algan Kaya, H. P-114 / 260 Algın, A. O-149 / 183 Alışık, M. O-113 / 165 Alkandari, F. O-048 / 132 Alkaş, G. P-334 / 371 Almajed, A. O-048 / 132 Almalki, M. 10, 20, 74 Alomar, M. O-048 / 132, / 8 Altınsoy, G. O-144 / 180 Altıntop, İ. 12, O-017 / 117, P-421 / 414, P-423 / 415, P-424 / 416 Altun, İ. P-047 / 227, P-153 / 280, P-158 / 282 Altunbas, E. O-029 / 123 Altuncı, Y. A. 8, 42, O-071 / 144, P-273 / 340, P-484 / 446 Altunci, Y. A. P-321 / 364, P-472 / 440 Altuntaş, G. O-120 / 168, O-121 / 169, P-113 / 260, P-116 / 261, P-157 / 282, P-203 / 305, / 30 Altuntaş, M. 23, O-066 / 141, O-084 / 150, O-089 / 153, O-097 / 157, O-132 / 174, P-117 / 262, P-118 / 262, P-209 / 308,
P-210 / 309, P-307 / 357 Alyamaç, M. P-257 / 332, P-283 / 345 Alyesil, C. P-219 / 313 Alyeşil, C. O-068 / 142, P-064 / 235, P-124 / 265 Anıl, M. 10, 23, 50, O-082 / 149 Aracı, Ç. E. P-278 / 343 Ararat, E. O-032 / 124 Araz, C. P-017 / 212 Ardıç, Ş. 17, 35, O-027 / 122, O-120 / 168, O-121 / 169, P-047 / 227, P-085 / 246, P-113 / 260, P-116 / 261, P-153 / 280,
P-158 / 282, / 104 Arı, E. P-330 / 369, P-456 / 432 Arık, Ö. P-127 / 267 Arık, Y. E. O-004 / 110, P-381 / 394 Arık, Y.E. 6 Arikan, S. O-096 / 156 Armağan, H. H. O-024 / 120, O-078 / 147, P-332 / 370 Arquilla, B. P-462 / 435 Ars, E. P-022 / 214 Arsava, M. 21 Arslan Turan, C. O-127 / 172 Arslan, A. P-265 / 336 Arslan, C. O-038 / 127, P-313 / 360 Arslan, E. O-072 / 144, O-117 / 167, O-134 / 175, O-148 / 182, P-201 / 304, / 32 Arslan, E. D. P-302 / 355, P-303 / 355, P-309 / 358, P-316 / 362, P-333 / 370, P-338 / 373, P-456 / 432

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
450
Arslan, H. Ç. P-020 / 213, P-094 / 250 Arslan, İ. F. O-165 / 192 Arslan, Ü. P-217 / 312, P-245 / 326, P-249 / 328, P-304 / 356, P-306 / 357 Arslan, V. 5 Artuk, H. P-039 / 223 Asik, O. P-354 / 381 Aslan, Ş. O-011 / 114 Aslaner, M. A. 23, 84 Aslanov, A. O-092 / 154 Aslanyavrusu, M. P-403 / 405 Aşık, O. P-266 / 337 Aşık, Ö. P-043 / 225 Atabay, D. P-085 / 246 Atalay, H. I. P-131 / 269, P-133 / 270, P-134 / 270, P-139 / 273, P-140 / 273, P-141 / 274, P-142 / 274, P-145 / 276,
P-147 / 277, P-148 / 277, P-166 / 286, P-230 / 319 Ataman, A. K. P-151 / 279 Atay, S. P-453 / 430 Ateş, F. O-170 / 194 Atik, İ. P-300 / 354 Atilla, D. Ö. 13 Atilla, R. 7, 20, 39, 72 Atlı, B. O-164 / 191 Atmaca Temrel, T. P-374 / 390 Atmaca, Y. 20 Avcı Dönmez, D. P-002 / 204 Avcı, A. 16 Avcı, H. O-140 / 178 Avcı, M. 18, O-037 / 127, P-300 / 354 Avcı, S. P-067 / 237, P-071 / 239 Avcı, V. P-103 / 255, P-104 / 255 Avci, A. O-057 / 137, O-063 / 140 Avci, M. O-032 / 124 Avci, V. P-100 / 253 Avcil, M. O-041 / 129, O-056 / 136, P-204 / 306 Avcu, N. O-068 / 142 Avşaroğulları, L. 7, 17, 38 Ay Altıntop, Y. O-017 / 117 Ay, D. O-111 / 164, P-014 / 210, P-015 / 211, P-016 / 211, P-119 / 263, P-120 / 263, P-216 / 312, P-218 / 313,
P-291 / 349, P-442 / 425, P-444 / 426 Ay, M. O. O-032 / 124, O-128 / 172 Ay, O. M. 17, 31 Ayaz, G. O-028 / 122 Aydemir, O. P-076 / 241 Aydın Altay, D. P-266 / 337 Aydın, A. 8, 9, O-010 / 113, O-046 / 131, P-239 / 323, P-296 / 352, P-469 / 438, P-478 / 443, P-480 / 444, P-483 / 445,
P-485 / 446 Aydın, C. O-010 / 113, O-046 / 131, P-239 / 323, P-296 / 352, P-469 / 438, P-478 / 443, P-480 / 444, P-483 / 445,
P-485 / 446 Aydın, E. P-459 / 433 Aydın, G. P-485 / 446 Aydın, İ. 32, O-149 / 183 Aydın, İ. E. P-101 / 254, P-388 / 397 Aydın, K. P-432 / 420 Aydın, M. P-085 / 246, P-432 / 420 Aydın, Ö. F. O-114 / 165, P-042 / 224 Aydın, S. O-043 / 130 Aygün, A. O-150 / 183 Aygün, C. P-083 / 245 Aygün, K. P-313 / 360 Ayhan, H. O-039 / 128 Aykal, G. O-009 / 113 Aykut, A. P-102 / 254, P-105 / 256, P-173 / 290, P-236 / 322 Ayrık, C. 13, 15, 59, O-170 / 194, O-171 / 195, P-308 / 358, P-446 / 427 Ayvacı, B. M. 5, 16, 25, 88 Azapoğlu Kaymak, B. P-256 / 332, P-313 / 360, P-394 / 401, P-444 / 426 Azapoğlu, B. P-447 / 427

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
451
B
Bağdiden, S. P-291 / 349 Bahadır, M. O-013 / 115 Bahadur, H. P-100 / 253 Bal, A. O-082 / 149 Bal, U. P-058 / 232, P-257 / 332 Balcı, D. E. P-113 / 260 Balcı, P. O-025 / 121 Baloglu Kaya, F. P-348 / 378 Baloğlu Kaya, F. O-117 / 167, O-134 / 175, P-346 / 377 Barış, M. M. O-025 / 121 Barut, P. P-371 / 389 Bas, B. O-106 / 161, P-227 / 317 Baskın Embleton, D. P-356 / 382 Basol, N. O-143 / 180 Baş, S. S. P-275 / 341 Başara Akın, I. O-025 / 121 Başçı, O. O-020 / 118 Başol, N. 20, 28, 32, 69, O-059 / 138, O-079 / 148, O-101 / 159, P-146 / 276, P-233 / 320 Baştuğ, B. T. 15 Batur, A. O-070 / 143, P-080 / 243, P-081 / 244, P-082 / 244, P-086 / 246 Bayır, A. 13, 58 Bayir, A. P-215 / 311 Baykal, T. P-090 / 248, P-170 / 288, P-183 / 295, P-184 / 295, P-240 / 324, P-241 / 324, P-394 / 401, P-396 / 402,
P-474 / 441, P-475 / 441 Baykan, N. P-046 / 226 Bayoğlu Tekin, Y. P-187 / 297 Bayrak, Ö. P-277 / 342, P-406 / 407 Bayram, B. O-020 / 118, O-036 / 126, O-184 / 201, P-242 / 325, P-269 / 338, P-376 / 391, / 3, / 10, / 13, / 26 Bayram, N. P-162 / 284, P-166 / 286, P-230 / 319 Bayramoğlu, A. P-393 / 400, P-437 / 422, P-458 / 433 Beceren, N. G. 54, O-024 / 120, P-332 / 370 Beden, S. O-075 / 146, P-155 / 281, / 21 Beğenen, M. P-025 / 216 Bekgöz, B. O-011 / 114 Bektaş, T. O-140 / 178 Belen, N. O-075 / 146 Benli, A. R. O-164 / 191 Berberoğlu, M. P-285 / 346 Berikol, B. G. 9 Berikol, G. O-007 / 112, P-222 / 315 Berksoy, E. O-082 / 149 Beser, F. P-350 / 379 Beştemir, A. P-222 / 315 Beydilli, I. O-032 / 124 Beydilli, İ. O-037 / 127, O-122 / 169, P-300 / 354 Beykoz Çetin, E. P-157 / 282 Bıcılıoğlu, Y. O-082 / 149 Bıçakçı, N. O-077 / 147 Bıçakçı, S. 33, O-076 / 146, O-173 / 196, P-250 / 329 Biberoğlu, S. O-164 / 191 Biçer, T. P-090 / 248, P-170 / 288, P-183 / 295, P-184 / 295, P-240 / 324, P-241 / 324, P-394 / 401, P-396 / 402,
P-474 / 441, P-475 / 441 Bildik, F. O-055 / 136, O-062 / 139, P-044 / 225 Bilge İpek, A. O-074 / 145 Bilge, M. O-010 / 113, O-046 / 131, P-239 / 323, P-296 / 352, P-469 / 438, P-478 / 443, P-480 / 444, P-483 / 445,
P-485 / 446 Bilge, S. O-010 / 113, O-046 / 131, P-239 / 323, P-296 / 352, P-469 / 438, P-478 / 443, P-480 / 444, P-483 / 445,
P-485 / 446 Bilgi, Z. O-042 / 129 Bilgili, H. P-320 / 364, P-347 / 377, P-359 / 383, P-425 / 416, P-426 / 417 Bilgin, M. O-033 / 125, O-072 / 144, O-147 / 182, P-128 / 267 Bilgin, S. 32, O-015 / 116, O-086 / 151, O-103 / 160, O-130 / 173, O-146 / 181, O-178 / 198, P-077 / 242, P-228 / 318,
P-281 / 344 Bilir, Ö. O-066 / 141, O-089 / 153, O-097 / 157, O-132 / 174, P-059 / 233, P-060 / 233, P-118 / 262, P-210 / 309,
P-307 / 357 Biricik, S. 33, O-170 / 194, P-274 / 341 Bol, O. 21, O-076 / 146, O-077 / 147, P-250 / 329

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
452
Bora, S. E. O-075 / 146 Boz, M. 19, O-070 / 143, O-074 / 145 Bozan, Ö. P-018 / 212 Bozdereli Berikol, G. O-007 / 112, P-222 / 315 Bozkurt Babuş, S. O-170 / 194, P-274 / 341 Bozkurt, G. O-056 / 136 Bozkurt, Y. C. P-075 / 241 Bozkus, G. O-001 / 109 Bozkuş, G. 6 Bucak, A. P-087 / 247 Bulajic, R. P-088 / 247, P-092 / 249 Bulandere, N. P-439 / 423, P-452 / 430 Bulut, B. O-142 / 179 Bulut, S. P-155 / 281, P-199 / 303, P-365 / 386 Büyüksütcü, C. O-111 / 164, P-014 / 210, P-015 / 211, P-216 / 312 C - Ç
Cabioglu, E. P-417 / 412, P-448 / 427 Cabioglu, S. P-417 / 412, P-448 / 427 Cakal, E. D. O-008 / 112, P-287 / 347, P-289 / 348, P-409 / 408, P-464 / 436, P-472 / 440 Can, D. P-480 / 444 Can, N. O. P-436 / 422, P-437 / 422 Can, Ö. 10, 18, / O-040 / 128, O-144 / 180, P-273 / 340, P-343 / 375, P-435 / 421, P-454 / 431, P-482 / 445,
P-484 / 446 Can, S. P-008 / 207, P-009 / 208, P-135 / 271, P-224 / 316 Canakci, M. E. O-133 / 175, P-348 / 378 Candan Aydın, F. P-206 / 307 Candemir, H. P-131 / 269, P-133 / 270, P-137 / 272, P-139 / 273 Catal, E. O-133 / 175 Cebe, İ. H. O-149 / 183 Cehreli, O. B. O-184 / 201 Celik, A. P-159 / 283, P-229 / 318 Cenker, E. O-028 / 122 Cerit, Ö. P-220 / 314 Cevik, A. A. P-128 / 267 Cevik, E. O-010 / 113, O-046 / 131, P-239 / 323, P-296 / 352, P-485 / 446 Cevik, Y. P-083 / 245 Ceylan, E. P-131 / 269, P-133 / 270, P-136 / 271, P-137 / 272 Ceylan, S. R. P-284 / 346 Choudhary, K. S. 6 Choudhary, S. K. O-005 / 111 Cıcek, M. P-350 / 379, P-354 / 381 Cicek, M. P-345 / 376 Cimilli Öztürk, T. O-127 / 172, O-129 / 173, O-131 / 174, P-095 / 251, P-096 / 251, P-121 / 264, P-149 / 278, P-150 / 278,
P-152 / 279, P-163 / 285, P-164 / 285, P-165 / 286, P-167 / 287, P-171 / 289, P-172 / 289, P-173 / 290, P-174 / 290, P-177 / 292, P-178 / 292, P-180 / 293, P-181 / 294, P-256 / 332, P-258 / 333, P-260 / 334, P-261 / 334, P-262 / 335, P-267 / 337, P-373 / 390, P-378 / 392, P-384 / 395, P-400 / 404
Cinar, O. Y. O-051 / 134, P-136 / 271, P-140 / 273, P-147 / 277, P-160 / 283 Ciran, E. P-148 / 277 Coban, K. P-354 / 381 Coker, B. P-466 / 437 Copcuoğlu, Z. P-349 / 378, P-353 / 380, P-355 / 381 Coskun, F. O-160 / 188 Coşkun, A. 14, O-022 / 119, O-060 / 138, P-157 / 282, P-209 / 308 Coşkun, F. O-166 / 192, P-111 / 259 Coşkun, F. F. P-254 / 331, P-380 / 393 Cömertpay, E. P-114 / 260 Çağlar, B. O-075 / 146 Çağlayan, T. 19, O-072 / 144, O-117 / 167, O-134 / 175 Çakal, E. D. 9, P-482 / 445 Çakır, U. O-028 / 122 Çakmak, O. P-208 / 308 Çakmak, S. O-087 / 152, O-099 / 158, P-264 / 336, / 28 Çalbay, A. P-390 / 398, P-436 / 422, P-437 / 422, P-438 / 423 Çalışkan, D. P-334 / 371 Çalışkan, F. O-006 / 111 Çalışkan, M. P-325 / 366 Çamcı, M. P-388 / 397

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
453
Çanakçı, M. E. 30, O-033 / 125, O-072 / 144, O-117 / 167, O-134 / 175, P-128 / 267, P-252 / 330, P-346 / 377, P-358 / 383, P-402 / 405
Çanakçı, S. E. O-056 / 136, P-204 / 306 Çatal, E. P-358 / 383 Çavumirza Ergül, G. P-326 / 367 Çavumirza, G. P-067 / 237 Çavuş, U. Y. O-141 / 179 Çavuşoğlu, M. P-355 / 381 Çelebi Yamanoğlu, N. G.
P-264 / 336
Çelik, B. 33, O-171 / 195 Çelik, C. P-427 / 417 Çelik, E. 14, O-058 / 137, P-382 / 394 Çelik, G. K. O-004 / 110, O-102 / 159 Çelik, S. P-427 / 417, P-473 / 440, P-476 / 442 Çelik, Ş. P-403 / 405 Çelikel, E. 12, O-016 / 116, P-057 / 232, P-058 / 232, P-061 / 234, P-093 / 250, P-122 / 264, P-255 / 331, P-257 / 332,
P-259 / 333, P-263 / 335, P-283 / 345 Çete, Y. 6, 8, 13,15, 21, P-278 / 343 Çetin, B. P-407 / 407 Çetin, E. P-407 / 407 Çetin, G. 12 Çetin, M. 12, 57 Çetinkaya, H. O-160 / 188 Çetinkurşun, S. P-356 / 382 Çevik, N. 6 Çevik, Y. O-053 / 135, O-119 / 168, O-124 / 170, O-152 / 184 Çevrim, Ö. O-064 / 140, / 26 Çığşar, G. O-042 / 129, O-108 / 162, P-179 / 293, P-182 / 294, P-185 / 296 Çıldır, H. P-269 / 338, P-376 / 391 Çınar, O. 10, / 15, / 22 Çınaroğlu, S. O. P-307 / 357 Çıvgın, E. P-058 / 232, P-061 / 234, P-093 / 250, P-122 / 264 Çiftçi, H. 18, O-042 / 129, O-108 / 162, P-179 / 293, P-182 / 294, P-185 / 296 Çil Direk, E. O-168 / 193 Çiloğlu, Ü. P-290 / 349 Çim, E. P-213 / 310 Çimen, T. O-088 / 152 Çinaroğlu, O. S. P-232 / 320 Çoban, K. P-270 / 339 Çoker, B. O-080 / 148, P-349 / 378, P-353 / 380, P-355 / 381 Çokluk, M. P-195 / 301, P-307 / 357 Çolak Oray, N. P-151 / 279, P-242 / 325 Çolak, B. O-115 / 166, O-176 / 197, P-062 / 234, P-063 / 235, P-099 / 253 Çopuroğlu, G. P-020 / 213, P-078 / 242, P-094 / 250 Çorbacıoğlu, Ş. K. 9, 30, 32, / O-053 / 135, O-124 / 170, O-152 / 184, P-083 / 245 Çorbacıoğluu, Ş. K. O-011 / 114 Çorbacıoğu, Ş. K. O-119 / 168 Çoskun, G. O-024 / 120 Çoskun, S. O-113 / 165 Çoşkun, A. 28, O-097 / 157, P-059 / 233 Çoşkun, S. O-031 / 124 Çöllü, M. O-111 / 164, P-216 / 312 D
Dag, N. O-126 / 171 Dagli, B. O-041 / 129 Dağ, N. 31 Dağ, S. G. 15 Dağar, S. O-053 / 135 Dağlı, B. O-056 / 136 Dağlı, S. P-332 / 370 Dağlıoğlu, G. O-061 / 139 Dağtekin, Ö. P-192 / 300 Daltaban, İ. S. O-157 / 187 De Geyter, L. P-001 / 204 Degirmenci, E. P-022 / 214

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
454
Değerli, V. 25, 86, P-155 / 281, P-194 / 301, P-196 / 302, P-344 / 376, P-352 / 380, P-362 / 385, P-363 / 385, P-365 / 386, P-368 / 388, P-371 / 389
Delice, O. O-067 / 142, P-005 / 206, P-080 / 243, P-082 / 244, P-086 / 246 Delice, Y. O-110 / 163 Delikanlı, M. O-024 / 120 Demir, A. P-053 / 230, P-169 / 288 Demir, C. M. 17 Demir, E. P-414 / 411 Demir, H. O-129 / 173, O-131 / 174, P-176 / 291, P-412 / 410 Demir, H. A. O-062 / 139, P-044 / 225, P-045 / 226, P-197 / 302 Demir, M. C. O-034 / 125, P-056 / 231 Demir, O. P-139 / 273, P-168 / 287, P-199 / 303, P-229 / 318 Demir, Ö. F. 16, P-068 / 237, P-432 / 420 Demir, S. O-120 / 168, O-121 / 169 Demirbaş, H. P-349 / 378 Demircan, A. 9, 28, O-055 / 136, P-197 / 302, P-334 / 371 Demirdöven, B. T. P-123 / 265 Demirel, B. P-024 / 215, P-065 / 236, P-066 / 236, P-067 / 237, P-068 / 237, P-069 / 238, P-070 / 238, P-071 / 239,
P-072 / 239, P-221 / 314, P-451 / 429 Demirel, C. O-143 / 180 Demirel, M. P-065 / 236 Demirkan, A. O-100 / 158 Denizbasi, A. O-029 / 123, O-051 / 134, O-155 / 186, O-181 / 200, P-131 / 269, P-133 / 270, P-134 / 270, P-136 / 271,
P-137 / 272, P-139 / 273, P-140 / 273, P-141 / 274, P-142 / 274, P-145 / 276, P-147 / 277, P-148 / 277, P-159 / 283, P-160 / 283, P-166 / 286, P-168 / 287, P-169 / 288, P-229 / 318, P-230 / 319, P-231 / 319
Denizbaşı, A. 15, 20, 34, 35, 96, 107, P-467 / 437, Devrimsel Doğan, D. P-097 / 252, P-183 / 295, P-184 / 295, P-240 / 324, P-241 / 324, P-394 / 401, P-396 / 402, P-474 / 441,
P-475 / 441 Dılaver, E. P-350 / 379 Di Somma, S. 10, 19, 35, 47 Dikme, O. O-096 / 156, O-137 / 177, O-137 / 177, O-177 / 198, O-177 / 198, O-182 / 200, O-182 / 200, P-022 / 214,
P-129 / 268, P-129 / 268, P-130 / 268, P-130 / 268, P-132 / 269, P-132 / 269 Dikme, Ö. 13, 18, 23, 27, 32, 82, O-035 / 126, P-227 / 317 Dinç, Y. O-072 / 144 Diri, U. 16 Dişel, N. R. O-061 / 139, O-104 / 160, O-138 / 177, O-168 / 193, O-180 / 199, P-202 / 305, / 33 Dogan, B. O-096 / 156 Dogan, N. O. P-219 / 313 Dogan, S. O-162 / 189, P-318 / 363, P-397 / 402, P-398 / 403 Dogan, T. O-128 / 172 Doganay, M. P-139 / 273 Doğan, B. P-244 / 326, P-248 / 328, P-301 / 354, P-302 / 355, P-309 / 358, P-383 / 395, P-387 / 397 Doğan, D. P-090 / 248 Doğan, D. D. P-170 / 288 Doğan, F. S. 22, 25, 81 Doğan, H. P-413 / 410, P-414 / 411, P-417 / 412, P-427 / 417, P-448 / 427, P-473 / 440, P-476 / 442, / 24 Doğan, M. P-090 / 248, P-156 / 281, P-170 / 288, P-183 / 295, P-184 / 295, P-240 / 324, P-241 / 324, P-394 / 401,
P-396 / 402, P-474 / 441, P-475 / 441 Doğan, N. Ö. 13,16,19,24, 63, O-052 / 134, O-068 / 142, P-064 / 235, P-124 / 265 Doğan, S. 26, 32, 94, O-142 / 179, P-312 / 360 Doğanay, F. P-163 / 285, P-164 / 285, P-165 / 286, P-167 / 287, P-171 / 289, P-172 / 289, P-173 / 290, P-174 / 290,
P-176 / 291, P-177 / 292, P-178 / 292, P-180 / 293, P-181 / 294, P-256 / 332, P-258 / 333, P-260 / 334, P-261 / 334, P-262 / 335, P-373 / 390, P-400 / 404
Doğanlı, S. O. O-159 / 188 Dolgun, H. O-072 / 144, O-117 / 167, O-134 / 175 Domanovits, H. P-088 / 247, P-092 / 249 Donertas, E. O-032 / 124 Dölek, M. O-023 / 120 Dönmez, D. P-342 / 375 Dönmez, S. P-458 / 433 Dubus, T. O-096 / 156, P-049 / 228 Duman Atilla, Ö. O-006 / 111, P-094 / 250 Duman, A. 18, O-041 / 129, O-056 / 136, O-094 / 155, O-156 / 186, P-135 / 271, P-204 / 306, P-224 / 316, P-276 / 342 Dumanlı, E. O-135 / 176 Durak, V. A. P-220 / 314 Duran, E. O-091 / 154 Duran, Ö. P-363 / 385, P-365 / 386, P-368 / 388, P-370 / 389, P-371 / 389 Durdu, T. P-058 / 232, P-259 / 333

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
455
Durmus, E. P-117 / 262 Durmuş, E. P-157 / 282 Duzok, E. P-272 / 340 Dübüş, T. 28 Dündar, G. A. 59, O-171 / 195, P-446 / 427 Düzkel, T. O-111 / 164, P-291 / 349 Düzok, E. O-185 / 202 E
Ece, I. 29, O-049 / 133, O-093 / 155, O-115 / 166, O-136 / 176, O-161 / 189, O-176 / 197, P-028 / 217, P-029 / 218, P-030 / 218, P-031 / 219, P-032 / 219, P-033 / 220, P-034 / 220, P-035 / 221, P-048 / 227, P-050 / 228, P-051 / 229, P-052 / 229, P-054 / 230, P-062 / 234, P-063 / 235, P-099 / 253, P-411 / 409
Ece, İ. O-105 / 161 Ecmel Onur, Ö. O-129 / 173, P-095 / 251, P-096 / 251, P-108 / 257, P-109 / 258, P-110 / 258, P-121 / 264, P-149 / 278,
P-150 / 278, P-152 / 279, P-163 / 285, P-164 / 285, P-165 / 286, P-167 / 287, P-171 / 289, P-172 / 289, P-173 / 290, P-174 / 290, P-176 / 291, P-177 / 292, P-178 / 292, P-180 / 293, P-181 / 294, P-183 / 295, P-184 / 295, P-256 / 332, P-258 / 333, P-260 / 334, P-261 / 334, P-262 / 335, P-267 / 337, P-373 / 390, P-378 / 392, P-384 / 395, P-394 / 401, P-396 / 402, P-400 / 404
Eden, A. O. O-037 / 127 Efe, M. P-287 / 347, P-366 / 387, P-375 / 391 Efeoglu Sacak, M. O-155 / 186 Efeoglu, M. P-168 / 287 Ege, D. P-019 / 213 Eke, Ş. Z. P-149 / 278, P-150 / 278 Ekinci, B. P-253 / 330 Elçin, A. E. O-151 / 184 Elçin, Y. M. O-151 / 184 Eldali, A. O-048 / 132 Elgörmüş, Ç. P-324 / 366 Elverici, E. P-282 / 345 Emecan, A. 18, O-038 / 127, P-095 / 251, P-096 / 251, P-149 / 278, P-150 / 278, P-152 / 279, P-163 / 285, P-164 / 285,
P-165 / 286, P-167 / 287, P-171 / 289, P-172 / 289, P-174 / 290, P-261 / 334, P-267 / 337, P-384 / 395 Emecen, A. O-098 / 157, O-127 / 172, P-089 / 248, P-191 / 299, P-236 / 322, P-412 / 410, / 31 Emektar, E. 11, 24, 31, O-053 / 135, O-124 / 170, P-083 / 245 Eneyli, M. G. 6, 7, O-014 / 115, P-445 / 426 Engin, Ö. P-123 / 265 Engin, S. P-115 / 261 Er, E. O-011 / 114 Eraybar, S. O-081 / 149 Erbil, B. 21, O-074 / 145 Ercan Haydar, G. P-451 / 429 Ercan, B. P-420 / 414, P-481 / 444 Erdede, M. O. P-461 / 434, P-463 / 435 Erdem Sultanoğlu, T. O-158 / 187, P-294 / 351, P-297 / 352, P-392 / 400, P-395 / 401, P-416 / 412 Erdem, E. O-118 / 167, O-145 / 181, P-078 / 242, P-339 / 373 Erdem, M. N. O-047 / 132, O-077 / 147 Erdem, N. P-250 / 329 Erdem, N. M. 21 Erdoğan, A. P-367 / 387 Erdoğan, S. O-170 / 194 Erdoğan, T. P-232 / 320 Erdur, B. 23, 26, O-140 / 178, O-159 / 188, P-314 / 361, P-317 / 362 Erel, O. P-217 / 312 Erel, Ö. O-113 / 165, P-103 / 255 Eren, Ş. H. O-022 / 119, O-060 / 138 Erenler, A. K. O-128 / 172 Ergin, M. O-004 / 110, O-102 / 159, O-172 / 195, P-322 / 365, P-324 / 366, P-377 / 392, P-388 / 397 Ergün, H. O-099 / 158 Erkek, A. O-058 / 137 Ermete, E. P-212 / 310 Eroğlu, O. O-166 / 192, P-111 / 259, P-114 / 260, / 33 Eroğlu, S. E. 13, 61, P-018 / 212, P-021 / 214, P-419 / 413, P-453 / 430, P-455 / 431 Erol, T. O-073 / 145 Erol, Y. P-265 / 336, P-350 / 379 Ersel, M. 7, 19, 30, 32, 68, O-008 / 112, O-071 / 144, O-110 / 163, O-144 / 180, P-043 / 225, P-343 / 375,
P-415 / 411, P-431 / 419, P-468 / 438, P-482 / 445 Ersöz Genç, E. P-266 / 337 Ersöz, N. O-091 / 154, O-092 / 154, P-012 / 209 Ersunan, G. 25, O-066 / 141, O-089 / 153, O-097 / 157, O-132 / 174, P-157 / 282, P-209 / 308, P-307 / 357

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
456
Ertan, C. P-098 / 252, / 40, / 7, / 13, / 32 Ertürk, K. Z. O-172 / 195 Ertürk, Z. K. P-310 / 359, P-322 / 365 Eryılmaz, M. O-010 / 113, O-046 / 131, P-239 / 323 Eryigit, U. O-150 / 183 Eryiğit, H. O-111 / 164, P-014 / 210, P-015 / 211, P-016 / 211, P-119 / 263, P-120 / 263, P-216 / 312, P-218 / 313,
P-442 / 425 Eryiğt, H. P-291 / 349 Esen, M. O-101 / 159, P-235 / 321 Eşfer, B. P-255 / 331 Eşfer, S. P-208 / 308 Ethemoğlu, F. B. P-217 / 312 Etienne, A. P-013 / 210, P-055 / 231 Evirgen, O. O-100 / 158 Evrin, T. 33, O-172 / 195, P-041 / 224, P-310 / 359, P-322 / 365, P-440 / 424 Eyinç, Y. O-038 / 127 Eyler, Y. 16, O-065 / 141, P-002 / 204, P-078 / 242, P-192 / 300, P-342 / 375 F
Fares, S. 22 Fatihoğlu, E. O-043 / 130 Fındık, M. O-085 / 151, P-471 / 439 Filipiak, K. J. P-040 / 223, P-440 / 424 Foggle, J. L. 8, 20, 35, 43, 72, 101 Forth, M. 34, 98, P-280 / 344 Fowler, J. 7, 22 G
Gaffari, E. O-095 / 156, P-036 / 221, P-037 / 222, P-038 / 222, P-073 / 240, / 28 Garda, E. B. P-384 / 395 Genç, E. P-252 / 330, P-358 / 383 Genç, S. O-099 / 158, O-151 / 184, O-153 / 185, P-206 / 307, P-432 / 420, P-457 / 432 Gençbay, H. P-113 / 260 Gevrek, F. O-143 / 180 Geyik, A. P-213 / 310 Geyik, M. N. P-213 / 310 Gezer, N. S. 17, O-025 / 121 Ghanaim, M. 7, 20, 41 Giden, R. P-100 / 253, P-103 / 255, P-104 / 255 Girgin, M. C. P-246 / 327, P-460 / 434 Giritli, Ö. P-018 / 212 Gizli, G. P-125 / 266 Gokalp, E. P-465 / 436 Goksu, E. P-115 / 261 Gonenc Cekic, O. O-174 / 196 Göğebakan, A. O-009 / 113 Gök, F. P-259 / 333 Gök, P. G. P-128 / 267 Gökalp, E. O-080 / 148, P-349 / 378, P-353 / 380, P-355 / 381 Gökalp, G. O-082 / 149 Gökcek, I. P-058 / 232 Gökçek, İ. P-259 / 333 Gökdağ, E. 30, O-114 / 165, P-042 / 224 Gökdemir, M. T. 24, P-100 / 253, P-103 / 255, P-104 / 255 Gökel, Y. O-138 / 177 Gökhan, Ş. 25, / O-004 / 110, O-031 / 124, O-102 / 159, P-101 / 254, P-324 / 366, P-374 / 390, P-377 / 392, P-381 / 394 Gökharman, F. D. 8, O-043 / 130 Göksu, A. P-079 / 243 Göksu, E. 3, 5, 6, 10, 34, 52, O-030 / 123, O-050 / 133, P-091 / 249 Göktaş, M. U. 31, O-130 / 173 Gönenc Cekic, O. P-345 / 376 Gören, N. Z. 18, O-036 / 126 Görüroğlu Öztürk, Ö. O-061 / 139 Gregor, P. 10, 18 Gucuyener, M. B. P-130 / 268 Gulen, B. O-001 / 109, O-125 / 171, O-126 / 171 Gulsen, B. P-238 / 323 Gumusel, M. P-162 / 284

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
457
Gunay, E. P-462 / 435 Gunduz, A. O-145 / 181 Gunes, H. O-179 / 199, P-200 / 304, P-337 / 372 Gunes, M. O-139 / 178 Guneysel, O. O-139 / 178 Gurgun, S. O-143 / 180 Gurmen, E. S. P-398 / 403 Güçlü, S. P-436 / 422 Gül, S. S. O-018 / 117, O-167 / 193 Gülalp, B. 11, 13, 20, 21, 25, 65, O-073 / 145, O-090 / 153, P-226 / 317, P-271 / 339, P-323 / 365 Gülcan, G. P-121 / 264 Güleç, T. P-074 / 240 Gülen, B. 12, 30, 56, O-026 / 121, O-112 / 164 Gülen, M. O-057 / 137, O-063 / 140, / 14 Gülen, N. O-087 / 152, / 25 Gülenç, K. P-196 / 302 Güler, A. O-071 / 144, P-043 / 225, P-409 / 408 Güler, B. P-332 / 370 Güler, S. O-011 / 114 Güllüpınar, B. P-361 / 384, P-362 / 385, P-363 / 385, P-364 / 386, P-365 / 386, P-367 / 387, P-368 / 388, P-370 / 389,
P-371 / 389, P-372 / 390 Güloğlu, C. 16 Gülöksüz, U. O-062 / 139 Gülşen, B. P-037 / 222, P-038 / 222 Gülünay, B. P-403 / 405 Gümrükçü, A. P-153 / 280 Günal, E. O-042 / 129, O-108 / 162, P-179 / 293, P-182 / 294, P-185 / 296, / 29 Günal, N. P-114 / 260 Günalp Eneyli, M. O-087 / 152, O-099 / 158, O-151 / 184, O-153 / 185, P-206 / 307, P-457 / 432 Günalp, M. O-100 / 158, / 20, / 28 Günay, M. P-290 / 349 Günaydın, G. P. O-031 / 124, O-113 / 165 Günaydın, O. O-062 / 139, / 16 Gündoğan, F. Ç. P-205 / 306 Gündoğdu, Ö. L. P-188 / 298 Gündüz, E. O-111 / 164, P-014 / 210, P-015 / 211, P-016 / 211, P-119 / 263, P-120 / 263, P-218 / 313 Güner, N. G. P-336 / 372, P-346 / 377 Güneş, H. O-107 / 162, P-351 / 379, / 27, / 29 Güneş, M. O-165 / 192, / 32 Güney, H. P-233 / 320 Güney, S. P-064 / 235 Güneysel, Ö. O-027 / 122, O-114 / 165, P-042 / 224, P-098 / 252, P-420 / 414, P-481 / 444, / 13 Güngör, F. O-009 / 113, O-028 / 122, O-030 / 123, / 5, / 17 Güngör, H. P-123 / 265 Güngör, I. P-057 / 232, P-255 / 331, P-257 / 332, P-259 / 333, P-263 / 335, P-283 / 345 Gür, A. S. T. 30 Gürbilek, Ü. P-276 / 342 Gürler, S. O-099 / 158, O-100 / 158, O-151 / 184, O-153 / 185, P-206 / 307, P-457 / 432 Gürman, G. O-151 / 184 Gürsoy, O. P-094 / 250 Gürü, S. P-208 / 308 Güven, D. S. O-030 / 123 Güven, R. O-122 / 169 Güven, Ş. P-017 / 212 Güvenç, E. P-123 / 265 H
Hacar, S. O-006 / 111, P-193 / 300 Haedar, A. 22, 34, 77 Hakbilir, O. P-057 / 232, P-257 / 332 Halhallı, H. C. O-083 / 150 Halıcı, A. P-326 / 367, P-327 / 367, P-330 / 369, P-331 / 369, P-335 / 371, P-338 / 373, P-391 / 399 Hasgül, B. O-079 / 148, P-146 / 276, P-233 / 320, P-235 / 321, / 23 Hastas, E. P-060 / 233 Hastürkoglu, S. P-057 / 232 Hatip, A. Y. O-024 / 120, / 15 Haydar, G. E. O-113 / 165

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
458
Hayırlı, E. N. O-100 / 158 Hizmetçi, A. P-274 / 341 Hodgdon, A. 9, 7, 45 Horozoğlu, H. O-047 / 132 Höbel, A. P-314 / 361 Höke, M. H. P-293 / 350 Humaid. A. 20 Hussein, S. K. P-132 / 269 Hünük, A. O-098 / 157, P-089 / 248, / 28 Hür, I. P-432 / 420 Hür, İ. P-068 / 237 Hyun, K. L. 7, / 20 I - İ
Imamoglu, M. P-354 / 381 Ince, A. P-134 / 270, P-145 / 276, P-147 / 277, P-148 / 277 Ince, L. P-012 / 209 Incealtın, O. P-016 / 211, P-119 / 263, P-120 / 263 Ipek, A. P-345 / 376 Iscanlı, M. D. P-058 / 232 Işık, S. O-111 / 164, P-014 / 210, P-015 / 211, P-016 / 211, P-119 / 263, P-120 / 263, P-218 / 313, P-291 / 349,
P-442 / 425 İbze, S. P-091 / 249 İlhan, A. O-044 / 130 İlhan, D. O-082 / 149 İlhan, G. T. O-086 / 151 İlküplü, B. P-410 / 409, P-434 / 421, P-454 / 431 İmamoğlu, M. P-116 / 261, P-265 / 336 İnan, S. P-259 / 333 İnce, L. O-091 / 154, P-003 / 205, / 28 İnce, M. O-091 / 154, O-092 / 154, P-003 / 205, P-012 / 209, / 28 İpekci, A. P-320 / 364, P-347 / 377, P-425 / 416, P-426 / 417 İşcanlı, E. P-282 / 345 İşcanlı, M. D. P-263 / 335 İşkorur, C. P-278 / 343 İşler, Ş. O-081 / 149 İşler, Y. O-081 / 149, / 23 J - K
Jacobus, C. 10, 49 Kabaroglu, K. P-230 / 319 Kabaroğlu, K. A. P-467 / 437 Kablan, A. O-059 / 138, / 14 Kaçmaz, Ö. P-100 / 253, P-103 / 255, P-104 / 255 Kadı, G. P-044 / 225, P-045 / 226, P-208 / 308, / 16 Kadıoğlu, E. O-163 / 190, P-127 / 267, P-295 / 351 Kadioglu, E. O-003 / 110 Kafalı, M. E. P-430 / 419 Kahraman Çetin, N. O-094 / 155 Kahraman, F. A. O-157 / 187, / 32 Kahramanca, Ş. O-108 / 162, P-185 / 296 Kahriman, N. P-220 / 314 Kahveci, U. P-327 / 367, P-329 / 368, P-330 / 369, P-331 / 369, P-333 / 370, P-335 / 371, P-338 / 373,
P-389 / 398 Kala, F. P-216 / 312 Kala, I. P-057 / 232 Kala, İ. P-255 / 331, P-283 / 345 Kalafat, A. F. P-318 / 363 Kalafat, U. M. O-142 / 179, P-318 / 363, P-397 / 402, P-398 / 403 Kalcan, S. P-059 / 233 Kalkan, A. O-132 / 174, P-154 / 280 Kalyon, Z. P-136 / 271, P-160 / 283 Kan, E. O-124 / 170 Kanbakan, A. P-320 / 364 Kanbur, I. O-106 / 161, P-211 / 309, P-237 / 322, P-247 / 327 Kanbur, İ. P-234 / 321, P-238 / 323, P-246 / 327, P-479 / 443 Kantar, Y. P-046 / 226 Kantekin, B. P-019 / 213, P-204 / 306

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
459
Kapar Yavasi, S. P-190 / 299 Kara, D. O-064 / 140, / 16 Kara, E. O-097 / 157 Kara, H. P-215 / 311 Karabağ, H. P-103 / 255 Karabay, O. P-198 / 303 Karabıyık Gözkaya, M. O-002 / 109 Karabulut, A. E. O-053 / 135 Karabulut, H. O-014 / 115, P-445 / 426 Karabulut, N. P-207 / 307 Karaca, B. P-257 / 332, P-283 / 345 Karaca, M. A. 16, 24, 27, 66, 85, O-074 / 145 Karaca, Y. O-145 / 181, O-150 / 183, O-174 / 196, P-265 / 336, P-270 / 339, P-354 / 381, / 27 Karaca, Z. I. O-143 / 180 Karacabey, S. O-069 / 143, O-157 / 187 Karadana, G. A. P-154 / 280 Karadaş, A. P-161 / 284 Karagün, Ö. O-073 / 145 Karakaş, H. M. P-412 / 410 Karakaya, Z. 25, 27, 90, O-015 / 116, O-086 / 151, O-103 / 160, O-130 / 173, O-146 / 181, O-175 / 197,
O-178 / 198, P-023 / 215, P-077 / 242, P-212 / 310, P-228 / 318, P-281 / 344, P-325 / 366 Karakayalı, B. P-017 / 212 Karakayalı, O. 23, 26, 93, O-052 / 134, P-360 / 384, P-382 / 394, P-407 / 407, P-459 / 433 Karakayali, O. O-083 / 150, P-357 / 382, P-429 / 418 Karakılıç, E. M. P-058 / 232 Karakılıç, M. E. P-255 / 331 Karakoç, E. O-138 / 177 Karakuş Yılmaz, B. P-106 / 256 Karakuş, A. P-087 / 247, P-112 / 259, P-223 / 315, P-399 / 403, P-408 / 408, P-418 / 413, P-449 / 427 Karakuş, M. P-217 / 312, P-245 / 326, P-249 / 328, P-304 / 356, P-306 / 357 Karakükçü, Ç. O-017 / 117 Karaman, K. P-026 / 216, P-027 / 217 Karaman, S. 12, / O-018 / 117, O-059 / 138, O-079 / 148, O-167 / 193, P-127 / 267, P-146 / 276, P-233 / 320, P-295 / 351 Karamercan, M. A. O-160 / 188, P-208 / 308 Karamişe, G. P-353 / 380 Karaoğlu, E. P-451 / 429 Karapınarlı, B. P-283 / 345 Karataş, S. 15 Karbek Akarca, F. O-008 / 112, O-071 / 144, O-144 / 180, P-043 / 225, P-287 / 347, P-289 / 348, P-409 / 408, P-434 / 421,
P-443 / 425, P-468 / 438 Karcıoglu, Ö. P-227 / 317 Karcıoğlu, Ö. P-036 / 221, P-037 / 222, P-038 / 222, P-073 / 240, P-198 / 303, P-470 / 439, P-479 / 443, / 10, / 13, / 19 Karcioglu, O. P-049 / 228 Karsandı, A. P-329 / 368 Kartal, M. 13 Katırcı, Y. O-160 / 188 Katipoglu, B. O-150 / 183 Kavak, N. O-141 / 179, O-158 / 187, P-243 / 325, P-244 / 326, P-248 / 328, P-251 / 329, P-282 / 345, P-286 / 347,
P-288 / 348, P-292 / 350, P-294 / 351, P-297 / 352, P-299 / 353, P-301 / 354, P-302 / 355, P-303 / 355, P-305 / 356, P-309 / 358, P-316 / 362, P-379 / 393, P-383 / 395, P-385 / 396, P-387 / 397, / 32
Kavak, R. O-141 / 179, P-243 / 325, P-244 / 326, P-248 / 328, P-251 / 329, P-282 / 345, P-286 / 347, P-288 / 348, P-292 / 350, P-302 / 355, P-383 / 395, P-385 / 396
Kavaklı, H. Ş. P-217 / 312, P-245 / 326, P-249 / 328, P-306 / 357 Kavalcı, C. O-022 / 119, P-471 / 439, / 25 Kavalci, C. O-016 / 116, O-085 / 151, P-039 / 223 Kaya, A. E. O-088 / 152, O-183 / 201, / 27 Kaya, B. P-459 / 433 Kaya, F. B. O-033 / 125, O-072 / 144, O-147 / 182, O-148 / 182, P-128 / 267, P-201 / 304, P-252 / 330, P-336 / 372,
P-340 / 374 Kaya, H. O-081 / 149 Kaya, M. P-296 / 352 Kaya, U. B. P-263 / 335 Kayacı Yıldız, M. P-021 / 214, P-419 / 413 Kayacı, S. P-195 / 301 Kayalı, A. O-146 / 181 Kayayurt, K. O-066 / 141, O-132 / 174 Kayıpmaz, A. E. O-022 / 119, O-085 / 151, P-471 / 439 Kayipmaz, A. E. O-016 / 116

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
460
Kaykısız, E. O-103 / 160, / 29 Kazzi, A. A. 7, / 10, / 34 Kececi, E. P-397 / 402 Keçecioğlu, A. O-055 / 136 Kefal, D. P-278 / 343 Keha Kurt, N. O-174 / 196 Keha Kurt, N. B. O-150 / 183 Kekeç, Z. O-138 / 177, P-087 / 247, P-112 / 259, P-138 / 272, P-223 / 315, P-279 / 343, P-399 / 403, P-408 / 408,
P-418 / 413, P-449 / 427, / 8, / 13 Keleş, A. O-055 / 136, O-062 / 139, P-334 / 371 Keser, İ. P-175 / 291 Keskin, C. P-085 / 246 Keşaplı, M. O-009 / 113, / 9 Kıdak, S. P-374 / 390, P-377 / 392 Kılıç, A. P-079 / 243, P-152 / 279, P-178 / 292, P-184 / 295, P-396 / 402, P-447 / 427 Kılıç, D. O-050 / 133, P-091 / 249, P-278 / 343, / 11 Kılıç, M. P-095 / 251, P-163 / 285, P-164 / 285, P-165 / 286, P-167 / 287, P-171 / 289, P-172 / 289, P-174 / 290 Kılıç, R. O-045 / 131, / 8 Kılıç, T. 17, 26, 92, O-009 / 113, O-028 / 122, O-030 / 123, P-278 / 343 Kılıç, T. Y. O-006 / 111, P-078 / 242, P-094 / 250 Kılıçaslan, İ. P-045 / 226 Kılıçaslan, Ö. P-351 / 379 Kılıçlı Doğanay, E. P-471 / 439 Kılıçlı, E. O-085 / 151 Kır, E. P-263 / 335 Kıray, C. P-317 / 362 Kırkpantur, E. D. O-131 / 174, P-102 / 254, P-110 / 258, P-121 / 264, P-177 / 292, P-240 / 324, P-260 / 334, P-474 / 441, / 31 Kırpat, V. P-300 / 354 Kıyak, S. K. P-253 / 330 Kıyan, G. S. O-110 / 163 Kıyan, S. P-415 / 411, P-435 / 421 Kızılay, E. P-270 / 339 Kilic, D. P-115 / 261 Kim, G. B. P-004 / 205 Kirkpantur, E. D. P-109 / 258 Kitapçıoğlu, G. O-144 / 180, P-043 / 225 Kiyan, G. S. P-472 / 440 Koca Tanrıverdi, A. P-206 / 307 Koca Tanriverdi, A. O-151 / 184 Koca, C. P-217 / 312 Kocabas, R. O-128 / 172 Kocabay, K. P-351 / 379 Kocalar, Ü. O-016 / 116 Kockan, S. P-404 / 406 Kocyigit, A. O-112 / 164 Koçak, A. O. P-390 / 398 Koçyiğit, H. P-457 / 432 Kodik, M. S. O-110 / 163, P-431 / 419 Kokkoz, Ç. O-006 / 111 Koldaş, M. P-143 / 275, P-207 / 307 Konyar, Z. P-420 / 414, P-481 / 444 Koptur, P. P-217 / 312, P-245 / 326, P-249 / 328, P-304 / 356, P-306 / 357 Korcak, M. F. P-141 / 274, P-142 / 274, P-159 / 283, P-169 / 288 Korgan, M. B. P-343 / 375, P-409 / 408 Korkmaz, E. P-269 / 338, P-376 / 391 Korkmaz, F. T. P-073 / 240 Korol, G. O-175 / 197 Korucu, O. O-124 / 170 Koruk, R. O-033 / 125, O-147 / 182, P-358 / 383, / 32 Koşar, P. N. O-043 / 130 Koyuncu, M. O-164 / 191, / 33 Koyuncu, S. O-018 / 117, O-164 / 191, O-164 / 191, O-167 / 193, P-146 / 276, P-233 / 320, P-235 / 321, / 33 Kozacı, N. O-037 / 127, O-122 / 169, P-300 / 354 Kozaci, N. O-032 / 124 Kozak, O. O-092 / 154 Köksal, A. P-336 / 372

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
461
Köksal, M. O-166 / 192, P-111 / 259 Köksal, Ö. P-025 / 216, P-084 / 245, P-125 / 266, P-126 / 266, P-220 / 314, P-315 / 361, / 35 Köksal, T. P-382 / 394 Köksal, V. O-066 / 141, P-188 / 298 Kömürcü, Ö. O-063 / 140 Köse, A. O-170 / 194, P-274 / 341 Köse, B. O-121 / 169, P-047 / 227, P-116 / 261, P-153 / 280 Köse, Ş. O-006 / 111 Köstekçi, Ş. K. O-164 / 191 Kuas, Ç. P-402 / 405 Kucur, D. O-034 / 125, P-056 / 231 Kuday Kaykisiz, E. P-023 / 215 Kum, S. O-094 / 155 Kunt, M. M. 8, 22, 79, O-070 / 143 Kupcuk, O. P-354 / 381 Kurgun Girgin, D. P-314 / 361 Kurt, E. P-149 / 278, P-150 / 278, P-373 / 390 Kurtoğlu Çelik, G. P-381 / 394 Kuseyri, M. A. P-412 / 410 Kutur, A. P-225 / 316 Kuvandık, G. P-112 / 259, P-449 / 427 Küçükkapdan, M. P-278 / 343 Küpçük, O. P-270 / 339 L
Ladny, J. R. P-040 / 223 Laggner, A. P-088 / 247, P-092 / 249 Larkin, G. L. 7, / 18, / 21 Larkin, S. Y. 35 Lisar, H. O-125 / 171, / 31 M
Maharani, T. 20, / 22 Majzoub, I. 7 Mamak, T. O-051 / 134, P-142 / 274, P-162 / 284, P-166 / 286, P-230 / 319, / 11 Manap, A. M. P-102 / 254, P-105 / 256, P-108 / 257, P-156 / 281, P-173 / 290, P-180 / 293, P-241 / 324, P-256 / 332,
P-262 / 335, P-400 / 404 Manap, M. O-098 / 157, P-089 / 248 Maralcan, G. P-353 / 380 Matyar, S. O-061 / 139, O-138 / 177, O-168 / 193 Meels, D. P-001 / 204 Mehmet, A. O-028 / 122 Memiş, M. B. P-096 / 251 Menteşe, A. O-120 / 168, O-121 / 169 Menteşe, S. Ö. P-113 / 260 Meral, G. P-116 / 261 Metin Aksu, N. O-034 / 125, O-070 / 143, O-087 / 152, P-056 / 231 Metin, H. O-026 / 121 Metin, Y. P-186 / 297, P-187 / 297 Metiner, Y. P-267 / 337, P-412 / 410 Mıdık, Ş. O-144 / 180, P-443 / 425 Midik, A. C. O-137 / 177 Milenkovic, D. P-088 / 247, P-092 / 249 Motov, S. 9, 22, 44 Mulligan, T. 8, / 10 Muratoğlu, M. O-085 / 151 Müderris, E. P-257 / 332 N
Nakış, B. O-038 / 127, O-127 / 172, P-191 / 299 Nalbant, E. P-203 / 305 Narcı, H. O-171 / 195, P-274 / 341, P-308 / 358, P-446 / 427 Nikovic, V. P-088 / 247, P-092 / 249 Nizamoğlu, M. P-017 / 212 Nogay, S. O-021 / 119 O - Ö
Ocak, N. Y. 30 Ocak, T. O-142 / 179, O-162 / 189, P-312 / 360, P-318 / 363, P-397 / 402, P-398 / 403 Oğuzlar, F. Ç. O-024 / 120, O-078 / 147, P-332 / 370

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
462
Oktar, D. P-402 / 405 Oktay, C. / 37, / 7, / 18, / 22 Oktay, M. O-084 / 150, P-060 / 233, P-157 / 282, P-189 / 298, P-232 / 320 Okur, N. P-356 / 382 Okur, O. M. O-022 / 119, O-060 / 138, / 15 Olgaç, V. P-143 / 275 Omercikoglu, S. O-029 / 123 Ongar, M. P-259 / 333 Onur, O. O-029 / 123, O-051 / 134, O-155 / 186, O-181 / 200, P-134 / 270, P-137 / 272, P-139 / 273, P-140 / 273,
P-141 / 274, P-142 / 274, P-145 / 276, P-147 / 277, P-148 / 277, P-160 / 283, P-162 / 284, P-166 / 286, P-168 / 287, P-169 / 288, P-229 / 318, P-230 / 319, P-231 / 319
Onur, O. E. P-131 / 269, P-133 / 270, P-136 / 271 Onur, Ö. P-144 / 275, P-240 / 324, P-241 / 324 Onur, Ö. E. O-038 / 127, O-127 / 172, O-131 / 174, P-105 / 256, P-156 / 281, P-191 / 299, P-412 / 410, P-447 / 427 Orak, M. 25 Oray, Ç. N. 5, 13, 27, 62, O-020 / 118, O-025 / 121, O-184 / 201 Orhan Metin, N. P-187 / 297 Orhan, A. F. P-479 / 443 Orun, S. O-041 / 129 Oskay, A. O-003 / 110 Otal, Y. O-113 / 165, P-101 / 254 Ozakin, E. O-133 / 175, P-348 / 378 Ozakyol, A. H. P-201 / 304 Ozaydin, V. O-139 / 178 Ozdinc, S. P-465 / 436, P-466 / 437 Ozgan, A. Y. O-133 / 175 Ozpolat, C. O-181 / 200, P-140 / 273, P-141 / 274, P-142 / 274, P-159 / 283, P-160 / 283, P-162 / 284, P-166 / 286,
P-230 / 319, P-231 / 319 Ozucelik, D. N. P-427 / 417, P-448 / 427, P-473 / 440, P-476 / 442 Öktem, B. P-197 / 302, P-208 / 308 Ölmez, Ü. O-111 / 164, P-015 / 211, P-119 / 263, P-218 / 313 Ömercikoğlu, E. P-156 / 281 Ömercikoğlu, S. P-467 / 437 Ömeroğlu, M. P-393 / 400, P-458 / 433 Önal, Ç. P-116 / 261 Öner, E. O-100 / 158 Önge, T. P-222 / 315 Örük, C. P-253 / 330 Örün, S. O-156 / 186, P-008 / 207, P-135 / 271, P-224 / 316, / 32 Özakın, E. O-033 / 125, O-072 / 144, O-117 / 167, O-134 / 175, O-147 / 182, O-148 / 182, P-128 / 267, P-201 / 304,
P-252 / 330, P-336 / 372, P-340 / 374, P-346 / 377, P-358 / 383, P-402 / 405, / 17, / 21, / 24 Özakyol, A. H. O-148 / 182 Özalp, D. S. O-131 / 174 Özaydın, V. O-165 / 192, P-216 / 312, P-218 / 313, P-442 / 425, P-444 / 426, / 33 Özbay, S. O-022 / 119, O-060 / 138 Özbek, A. E. O-052 / 134, P-369 / 388, P-407 / 407 Özbek, B. P-217 / 312 Özbülbül, N. I. O-033 / 125 Özcan, B. P-467 / 437 Özcan, İ. O-017 / 117 Özcan, N. P-252 / 330 Özçete, E. O-110 / 163, P-401 / 404, P-422 / 415 Özdamar, Y. O-034 / 125, P-056 / 231 Özdemir, A. P-189 / 298 Özdemir, A. Ö. O-072 / 144, P-346 / 377 Özdemir, B. O-066 / 141, P-186 / 297 Özdemir, F. P-276 / 342, P-315 / 361 Özdemir, M. O-042 / 129, O-108 / 162, P-179 / 293, P-182 / 294, P-185 / 296 Özdemir, S. P-310 / 359 Özdinç, Ş. O-175 / 197 Özel Sönmez, A. P-071 / 239, P-450 / 429 Özel, A. B. 25, 87 Özel, M. O-095 / 156 Özel, M. F. P-214 / 311 Özel, R. P-153 / 280 Özen, A. P-268 / 338 Özen, C. 21, 75, P-453 / 430, P-455 / 431
5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
463
Özen, M. O-003 / 110, O-140 / 178, O-159 / 188, P-314 / 361, P-317 / 362 Özer Ünal, E. P-432 / 420 Özer, B. P-263 / 335 Özer, H. P-061 / 234, P-093 / 250, P-122 / 264 Özer, Ö. F. O-026 / 121 Özer, T. P-003 / 205 Özer, V. P-265 / 336, P-270 / 339 Özeroğlu, E. P-352 / 380 Özgan, A. Y. 31 Özgenç, E. P-270 / 339 Özhasenekler, A. 20, 70, O-004 / 110, O-031 / 124, O-102 / 159, P-101 / 254, P-388 / 397 Özkan, B. P-340 / 374 Özkan, S. O-088 / 152, O-158 / 187, O-183 / 201, P-293 / 350, P-294 / 351, P-299 / 353, P-301 / 354, P-305 / 356,
P-326 / 367, P-327 / 367, P-329 / 368, P-330 / 369, P-331 / 369, P-335 / 371, P-379 / 393, P-387 / 397, P-389 / 398, P-391 / 399, P-392 / 400, P-416 / 412, P-450 / 429
Özkök Koz, N. P-451 / 429 Özkula, U. O-102 / 159, P-374 / 390, / 29 Özlem, M. P-057 / 232, P-283 / 345 Özlüer, Y. E. P-019 / 213 Özlük, Ö. P-109 / 258 Özmert Toplu, A. Ç. P-191 / 299 Özpolat, Ç. 27 Özselçuk, S. P-138 / 272 Özsoy, A. P-282 / 345 Özşahin, F. O-120 / 168 Öztekin, İ. O-013 / 115, / 12 Öztermeli, A. D. P-447 / 427 Öztoprak, A. O-153 / 185 Özturan, I. U. O-052 / 134, P-064 / 235 Özturan, İ. U. P-124 / 265, P-161 / 284, P-219 / 313 Özturan, U. İ. 11 Öztürk, E. O-070 / 143, O-074 / 145, / 21 Öztürk, P. O-020 / 118, / 15 Öztürk, T. P-361 / 384, P-362 / 385, P-364 / 386, P-367 / 387, P-370 / 389, P-372 / 390 Öztürk, T. C. P-412 / 410 Öztürk, U. P-362 / 385 Özucelik, D. N. P-413 / 410, P-417 / 412 Özüçelik, N. 13 Özyurt, S. O-132 / 174 P - R
Pala, E. P-017 / 212 Pamukçu, G.G. P-374 / 390, P-451 / 429 Parlak, İ. O-075 / 146 Parlak, S. P-061 / 234, P-093 / 250, P-122 / 264, / 12 Parlar, T. P-087 / 247 Paslı, S. P-266 / 337, P-354 / 381 Patan, T. O-098 / 157, P-079 / 243, P-089 / 248, P-105 / 256, P-170 / 288, P-313 / 360 Patlakoğlu, M. S. O-163 / 190 Paydaş, S. O-168 / 193 Payza, U. O-015 / 116, O-086 / 151, O-103 / 160, O-130 / 173, O-146 / 181, O-175 / 197, O-178 / 198, P-023 / 215,
P-077 / 242, P-212 / 310, P-228 / 318, P-281 / 344, / 12 Pekdemir, M. O-052 / 134, O-068 / 142, / 15 Peker Seçim, A. P-019 / 213 Peker, G. P-153 / 280, P-158 / 282 Pergel, A. P-203 / 305 Pirhan, A. D. S. O-055 / 136 Pişkin, S. O-002 / 109, / 6 Poh, K. C. 21, 76 Polat, M. A. P-402 / 405 Polat, O. O-087 / 152, O-099 / 158, O-100 / 158, O-151 / 184, O-153 / 185, P-206 / 307, P-457 / 432 Polattaş, P. P-061 / 234, P-093 / 250, P-122 / 264 Poyraz, B. P-151 / 279 Poyraz, M. K. O-149 / 183 Preseau, T. P-013 / 210 Prosen, G. 53 Qureshi, N. 10, 19 Radny, J. P-440 / 424
5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
464
Ramadan, S. O-124 / 170 Roblin, P. P-462 / 435 Ruetzler, K. P-041 / 224 S - Ş
Sabak, M. O-021 / 119, O-169 / 194 Sabbe, M. 9, 10, 48 Sadıllıoglu, S. P-132 / 269 Sadillioglu, S. O-106 / 161, P-211 / 309, P-234 / 321, P-237 / 322, P-238 / 323, P-247 / 327, P-404 / 406, P-477 / 442 Sadoğlu, D. P-085 / 246, P-116 / 261, P-158 / 282 Safi, Y. O-021 / 119, O-169 / 194, / 15 Saglam, B. P-345 / 376 Saglık, A. O-142 / 179 Saglik, A. P-312 / 360 Sağlam, C. O-075 / 146, P-364 / 386, P-367 / 387, P-370 / 389, P-371 / 389, P-372 / 390 Sağlam, Ö. P-451 / 429 Sağlamol, G. P-279 / 343 Sahin, A. O-145 / 181, O-150 / 183, O-174 / 196, P-345 / 376 Sahin, E. O-150 / 183, O-174 / 196 Sahin, G. K. P-199 / 303 Sahin, O. O-182 / 200 Sakal, C. P-144 / 275 Salman, N. O-185 / 202, P-205 / 306, P-268 / 338, P-272 / 340 Salt, Ö. O-109 / 163, P-275 / 341 Sancak, Ö. P-108 / 257, P-258 / 333 Sanrı, E. 19 Sanri, E. O-051 / 134, O-069 / 143, P-131 / 269, P-133 / 270, P-134 / 270, P-136 / 271, P-137 / 272, P-139 / 273,
P-142 / 274, P-145 / 276, P-147 / 277, P-148 / 277, P-166 / 286, P-230 / 319, P-231 / 319 Sapmaz, B. P-289 / 348, P-431 / 419 Saraç, F. P-143 / 275, P-207 / 307 Sarbay, İ. P-413 / 410 Sarı Doğan, F. O-165 / 192, P-042 / 224, P-420 / 414, P-481 / 444 Sarıaydın, T. O-119 / 168 Sarıkaya, R. P-299 / 353, P-301 / 354, P-303 / 355, P-305 / 356, P-309 / 358, P-316 / 362, P-379 / 393, P-387 / 397 Sarıkaya, S. P-413 / 410, P-417 / 412, / 12 Sarıtaş, A. O-107 / 162, P-351 / 379, / 11 Sari Dogan, F. O-139 / 178 Sarikaya, S. P-448 / 427, P-473 / 440, P-476 / 442 Saritas, A. O-054 / 135, O-179 / 199, P-200 / 304, P-337 / 372 Sarsu, S. B. P-143 / 275 Satar, S. O-057 / 137, O-063 / 140 Savaşer, D. 34 Sayhan, M. B. 13, 29, 64, O-109 / 163, P-275 / 341 Sayraç, H. N. K. O-030 / 123 Sebe, A. O-104 / 160, O-138 / 177, O-168 / 193, O-180 / 199, P-202 / 305, / 27, / 29 Selçok, K. P-382 / 394 Sener, S. P-272 / 340 Sert, E. O-162 / 189, P-312 / 360, P-397 / 402, / 33 Sertbas, I. P-350 / 379 Sesigur, S. I. P-159 / 283, P-168 / 287 Sever, M. O-065 / 141, O-118 / 167, P-002 / 204 Sevim, E. P-368 / 388 Seviner, M. O-011 / 114 Seyit, M. O-003 / 110, O-140 / 178, / 6 Sezer, A. A. P-217 / 312, P-245 / 326, P-249 / 328, P-304 / 356, P-306 / 357 Sezgin, S. B. P-132 / 269 Sharma, R. 22, 78 Silcan, M. P-364 / 386, P-367 / 387 Simsek, Y. P-199 / 303 Sisman, M. P-350 / 379 Sivil, R. P-115 / 261 Smereka, J. P-040 / 223, P-041 / 224, P-440 / 424 Solak, S. P-214 / 311, P-225 / 316, P-311 / 359, P-319 / 363 Solgun, B. 6 Songür Kodik, M. P-401 / 404, P-415 / 411 Sonmez, E. O-001 / 109, O-125 / 171, O-126 / 171 Soykan, E. P-321 / 364, P-328 / 368, P-435 / 421

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
465
Soyudoğru, S. P-359 / 383 Söğüt, Ö. P-154 / 280, / 35 Sönmez, B. M. O-122 / 169, P-257 / 332, / 30 Sönmez, E. O-026 / 121 Sönmez, E. 17 Sönmez, G. O-172 / 195 Sönmez, L. Ö. O-172 / 195, P-310 / 359, P-322 / 365 Sönmez, M. B. P-058 / 232 Söyler, G. O-071 / 144, P-468 / 438 Sucu Dağ, G. O-002 / 109, O-023 / 120 Sultanoğlu, H. O-141 / 179, O-158 / 187, P-243 / 325, P-244 / 326, P-248 / 328, P-293 / 350, P-294 / 351, P-297 / 352,
P-299 / 353, P-301 / 354, P-302 / 355, P-303 / 355, P-305 / 356, P-309 / 358, P-316 / 362, P-379 / 393, P-383 / 395, P-387 / 397, P-392 / 400, P-395 / 401, P-416 / 412, P-450 / 429, / 32
Suman, E. P-232 / 320 Suner, S. 7, 10, 19, 20, 51, 73 Surmeli, M. P-477 / 442 Susur, Ö. P-193 / 300 Sutaşır, N. P-107 / 257 Suveren Artuk, D. P-039 / 223 Süğüt, Ö. P-264 / 336 Süner, S. O-052 / 134 Süygün, H. P-101 / 254 Szarpak, L. P-040 / 223, P-041 / 224, P-322 / 365, P-440 / 424 Şadıllıoğlu, S. 29 Şahan, M. P-449 / 427 Şahan, Ö. O-104 / 160 Şahin, A. P-270 / 339, P-326 / 367, P-327 / 367, P-335 / 371, P-391 / 399 Şahin, A. A. P-476 / 442 Şahin, B. O-078 / 147, P-332 / 370 Şahin, H. O-047 / 132, O-076 / 146, O-173 / 196, P-250 / 329, / 8 Şahin, M. P-281 / 344 Şahin, Ö. F. P-205 / 306 Şahin, Y. P-212 / 310, P-325 / 366 Şahiner, A. P-109 / 258, P-163 / 285, P-164 / 285, P-165 / 286, P-167 / 287, P-171 / 289, P-172 / 289, P-173 / 290,
P-174 / 290, P-176 / 291, P-177 / 292, P-178 / 292, P-180 / 293, P-181 / 294, P-256 / 332, P-258 / 333, P-260 / 334, P-261 / 334, P-262 / 335, P-267 / 337, P-400 / 404
Şakar, Ş. P-406 / 407 Şancı, E. P-151 / 279, P-254 / 331, P-380 / 393 Şeker Eren, E. P-094 / 250 Şen, C. O-021 / 119, O-169 / 194, / 33 Şen, İ. A. O-169 / 194 Şendağ, R. P-446 / 427 Şener, A. P-053 / 230, P-377 / 392 Şener, S. O-185 / 202, P-268 / 338, / 100, / 34 Şenyurt, A. P-393 / 400, P-438 / 423, P-458 / 433 Şimşek, A. O-078 / 147, P-332 / 370, / 21 Şükün, A. O-030 / 123 T
Tan, G. C. O-086 / 151 Tanrıverdi, A. K. 32 Tanrıverdi, F. O-004 / 110, O-102 / 159, P-324 / 366, P-374 / 390, P-381 / 394 Tanrıverdi, S. P-329 / 368 Tapkan, R. B. O-162 / 189, P-318 / 363, P-397 / 402, P-398 / 403 Tarhan, N. P-259 / 333 Taskin, B. P-140 / 273, P-229 / 318 Tasyurek, T. P-134 / 270, P-145 / 276 Taş, M. P-213 / 310 Taşcı, A. P-090 / 248, P-109 / 258, P-144 / 275, P-176 / 291, P-181 / 294, P-183 / 295, P-258 / 333, P-373 / 390,
P-394 / 401, P-433 / 420, P-475 / 441 Taşcı, U. P-192 / 300, P-193 / 300 Taşçı, A. O-129 / 173, P-097 / 252, P-170 / 288, P-236 / 322 Tatlı, M. O-017 / 117, P-421 / 414, P-423 / 415, P-424 / 416 Tatlı, Ö. 12, 32, 55, O-120 / 168, / O-145 / 181, O-174 / 196, O-150 / 183, P-266 / 337, P-345 / 376,
P-350 / 379 Teberik, K. O-054 / 135 Teke, C. P-388 / 397 Tekgül, Z. T. P-196 / 302
5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
466
Tel, M. R. P-285 / 346 Temel, T. O-148 / 182, P-201 / 304 Temiz, G. O-147 / 182 Temizkan, R. C. P-351 / 379 Temizsoy Korkmaz, F. P-470 / 439 Temrel, T. A. P-324 / 366 Tezel, O. 34, 99, O-185 / 202, P-205 / 306, P-268 / 338, P-272 / 340 Tiryaki Baştuğ, B. O-019 / 118 Togan, S. P-281 / 344 Toker, İ. O-006 / 111, O-118 / 167, P-078 / 242, P-094 / 250, P-339 / 373 Tokgoz, D. O-184 / 201 Tokgöz, D. O-020 / 118, P-242 / 325 Toklucu, M. Ö. P-017 / 212 Tokocin, O. O-044 / 130, P-074 / 240, P-075 / 241, P-076 / 241 Tokoçin, O. 8 Toksul, İ. H. O-122 / 169 Toktaş, R. P-339 / 373, P-342 / 375 Tomruk, Ö. O-024 / 120 Top, A. A. O-120 / 168 Topacoglu, H. O-044 / 130, O-106 / 161, O-137 / 177, O-182 / 200, P-049 / 228, P-074 / 240, P-075 / 241, P-076 / 241,
P-130 / 268, P-132 / 269, P-211 / 309, P-234 / 321, P-237 / 322, P-246 / 327, P-247 / 327, P-404 / 406, P-461 / 434, P-463 / 435, P-477 / 442
Topaçoğlu, H. 6, / 8, / 13, / O-013 / 115, O-095 / 156, O-116 / 166, O-135 / 176, P-073 / 240, P-460 / 434, P-470 / 439, P-479 / 443
Topal, F. O-146 / 181 Topal, F. E. O-015 / 116, O-086 / 151, O-103 / 160, O-130 / 173, O-146 / 181, O-175 / 197, O-178 / 198 TOPAL, F. E. P-023 / 215 Topal, F. E. P-077 / 242, P-212 / 310, P-228 / 318, P-325 / 366 Topaloğlu, E. O-089 / 153, P-059 / 233, P-060 / 233, P-118 / 262, P-203 / 305 Topcu, H. P-106 / 256, P-107 / 257 Toprak, D. O-064 / 140 Toptaş, M. P-143 / 275, P-154 / 280, P-414 / 411 Topuk, S. P-382 / 394, P-429 / 418 Tortum, F. P-390 / 398, P-393 / 400, P-438 / 423 Torun, O. E. P-215 / 311 Tosun, E. O. P-373 / 390, P-378 / 392 Tosun, O. P-413 / 410 Tözüm, H. P-444 / 426 Truszewski, Z. P-040 / 223, P-041 / 224, P-440 / 424 Tuna, K. Ç. O-025 / 121 Tunay, K. 35 Tuncer, A. A. P-356 / 382 Turan Sonmez, F. O-179 / 199, P-200 / 304, P-337 / 372 Turan Sönmez, F. O-107 / 162, P-351 / 379 Turedi, S. O-145 / 181, O-174 / 196 Turgut, A. O-065 / 141 Turhan, S. O-032 / 124, O-037 / 127 Turkdogan, K. A. O-041 / 129, O-056 / 136, O-094 / 155, P-204 / 306 Turkmen, S. O-145 / 181, O-150 / 183, O-174 / 196 Tünay, K. 102 Türe, M. O-094 / 155 Türedi, S. 14, / 15, / 32, / O-120 / 168, O-121 / 169, P-085 / 246, P-113 / 260, P-116 / 261, P-153 / 280, P-158 / 282 Türkçüer, İ. O-140 / 178, O-159 / 188, P-314 / 361, P-317 / 362, / 13 Türkdoğan, K. A. 14 Türkeli, A. O-153 / 185, / 32 Türker, G. 4 Türkmen, S. P-047 / 227 Tüten, G. P-116 / 261 Tyndall, A. 9, / 10 U - Ü
Uçar, A. B. O-129 / 173, / 31 Uçar, F. O-088 / 152 Uğraş, E. O-066 / 141, O-132 / 174, P-186 / 297 Ulubay, H. G. P-263 / 335 Uncugil, C. F. P-217 / 312 Unlu, E. N. P-337 / 372 Urnal, R. O-178 / 198, / 27

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
467
Us Altay, D. O-174 / 196 User, N. N. O-080 / 148, P-349 / 378, P-353 / 380, P-355 / 381, P-356 / 382, / 23 Uslu, Z. P-116 / 261 Ustaalioğlu, İ. P-097 / 252, P-108 / 257 Usul, E. 25, O-088 / 152, O-183 / 201, P-329 / 368, P-333 / 370, P-338 / 373, P-389 / 398, P-391 / 399, P-456 / 432 Uyanık, A. Y. P-369 / 388 Uyar, Y. P-290 / 349 Uysal, E. P-214 / 311, P-225 / 316, P-311 / 359, P-319 / 363 Uysal, P. P-255 / 331, P-283 / 345 Uysal, Y. O-170 / 194 Uz, I. P-464 / 436 Uz, İ. 29, O-110 / 163, O-144 / 180, P-321 / 364, P-328 / 368, P-401 / 404, P-422 / 415, P-434 / 421, P-439 / 423,
P-452 / 430, P-468 / 438 Uz, Y. P-433 / 420 Uzel Şener, M. P-053 / 230 Uzun, S. P-205 / 306 Uzun, Y. P-373 / 390, P-378 / 392 Uzun, Z. P-126 / 266, P-315 / 361 Uzundurukan, A. P-350 / 379 Uzunget, S. C. P-310 / 359 Uzunosmanoğlu, H. O-124 / 170, O-152 / 184, P-083 / 245 Ülker Dörttepe, Z. P-175 / 291 Ünal Akoğlu, E. O-098 / 157, O-129 / 173, P-089 / 248, P-097 / 252, P-105 / 256, P-108 / 257, P-152 / 279, P-378 / 392 Ünal, A. 23 Ünal, İ. O-168 / 193 Ünaldı, M. 30, O-111 / 164, P-014 / 210, P-015 / 211, P-016 / 211, P-119 / 263, P-120 / 263, P-216 / 312, P-218 / 313,
P-291 / 349, P-442 / 425 Ünaldı, Y. C. P-202 / 305 Ünek, O. O-006 / 111, O-118 / 167, / 6 Ünlü, A. P-390 / 398 Ünlüer, E. E. O-175 / 197, P-310 / 359 V - W
Vatan, A. P-036 / 221, P-461 / 434, P-463 / 435 Vural, M. P-436 / 422, P-438 / 423 Walton, L. M. 8, 18, 22, 67, 80 Y
Yadigaroğlu, M. P-265 / 336, P-266 / 337 Yaka, E. O-052 / 134, O-068 / 142 Yakar, Ş. P-046 / 226 Yalcınlı, S. P-410 / 409 Yalcinli, S. O-069 / 143, P-434 / 421 Yalçın Ocak, N. O-118 / 167, P-002 / 204, P-078 / 242, P-192 / 300, P-193 / 300, P-339 / 373, P-342 / 375 Yalçın, N. O-065 / 141 Yalçınkaya, S. O-163 / 190, / 33 Yalçınlı, S. O-040 / 128, P-273 / 340, P-366 / 387, P-375 / 391, P-386 / 396, P-443 / 425 Yamanoğlu, A. 23, 83, P-264 / 336 Yanıker, M. P-250 / 329 Yanıker, R. M. O-076 / 146, O-173 / 196 Yanturalı, S. P-380 / 393 Yapakçı, Z. T. O-163 / 190 Yardım, O. O-053 / 135 Yarkaç, A. P-308 / 358 Yaşar, E. O-153 / 185 Yavası, O. P-117 / 262 Yavasi, O. O-132 / 174, P-186 / 297, P-187 / 297, P-188 / 298, P-189 / 298, P-190 / 299, P-195 / 301 Yavaş, G. C. O-015 / 116, O-103 / 160, O-130 / 173, O-178 / 198, P-077 / 242, P-228 / 318 Yavaşi, Ö. O-066 / 141, O-097 / 157, P-203 / 305, / 16, / 31, / 35 Yazıcı, M. P-189 / 298, P-195 / 301, P-210 / 309 Yazıcı, M. M. P-059 / 233, P-060 / 233, P-203 / 305 Yazıcı, R. P-318 / 363, P-398 / 403 Yazıcıoğlu, M. 5, P-207 / 307 Yelli, S. O-143 / 180 Yenigün, H. P-091 / 249 Yenilmez, Ç. O-117 / 167 Yeniocak, S. O-116 / 166, P-143 / 275, P-154 / 280, P-207 / 307, / 30 Yeniova, A. Ö. P-146 / 276

5th Eurasian Congress on Emergency Medicine & 12th Turkish Emergency Medicine Congress
November 10 – 13, 2016, Titanic Deluxe Belek Hotel, Antalya / Turkey
468
Yeşil, O. P-095 / 251, P-096 / 251, P-156 / 281, P-161 / 284, P-384 / 395 Yeşilaras, M. O-006 / 111, O-065 / 141, P-020 / 213 Yeşilkaya, İ. O-100 / 158 Yetim, M. O-128 / 172 Yılar, S. P-437 / 422 Yıldırım, A. C. P-182 / 294 Yıldırım, C. O-021 / 119, O-169 / 194, / 12, / 13 Yıldırım, Ç. O-031 / 124, O-113 / 165, P-374 / 390, P-377 / 392, P-381 / 394, / 17 Yıldırım, H. P-194 / 301, P-344 / 376, P-352 / 380 Yıldırımer, Y. P-068 / 237 Yıldız, F. P-097 / 252, P-108 / 257 Yıldız, N. O-014 / 115, P-445 / 426, / 12 Yıldız, Y. P-021 / 214, P-419 / 413 Yılmaz Aydın, Y. P-071 / 239 Yılmaz Duran, F. P-194 / 301, P-196 / 302, P-344 / 376, P-352 / 380 Yılmaz, A. 32, O-122 / 169, O-140 / 178, O-142 / 179, O-159 / 188, O-162 / 189, P-314 / 361, P-317 / 362 Yılmaz, B. P-111 / 259 Yılmaz, D. O-164 / 191 Yılmaz, E. P-363 / 385 Yılmaz, F. O-012 / 114, O-037 / 127, O-122 / 169, P-300 / 354, P-341 / 374 Yılmaz, G. O-075 / 146, P-235 / 321, P-253 / 330 Yılmaz, H. O-012 / 114, P-217 / 312, P-245 / 326, P-249 / 328, P-298 / 353, P-306 / 357, P-341 / 374, P-428 / 418 Yılmaz, M. S. P-255 / 331, P-263 / 335 Yılmaz, O. P-320 / 364 Yılmaz, S. O-052 / 134, O-068 / 142, O-080 / 148, O-083 / 150, P-047 / 227, P-369 / 388, P-459 / 433, P-470 / 439 Yılmaz, S. M. P-058 / 232 Yılmaz, Ş. E. P-113 / 260 Yımaz, H. P-304 / 356 Yigit, H. P-215 / 311 Yiğit, M. 26, 95 Yiğit, Ö. 4, 9, 19, 24 Yiğit, Y. 18, O-039 / 128, O-083 / 150, P-369 / 388 Yildiz, I. P-345 / 376 Yilmaz, S. P-219 / 313, P-407 / 407 Yormaz, B. O-012 / 114, O-049 / 133, O-093 / 155, O-115 / 166, O-136 / 176, O-161 / 189, O-176 / 197, P-028 / 217,
P-029 / 218, P-030 / 218, P-031 / 219, P-032 / 219, P-033 / 220, P-034 / 220, P-035 / 221, P-048 / 227, P-050 / 228, P-051 / 229, P-052 / 229, P-054 / 230, P-062 / 234, P-063 / 235, P-099 / 253, P-298 / 353, P-341 / 374, P-405 / 406, P-411 / 409, P-428 / 418, P-430 / 419, / 9, / 11, / 27, / 28, / 30, / 32, / 33
Yormaz, S. 32, O-049 / 133, O-093 / 155, O-115 / 166, O-154 / 185, O-161 / 189, O-176 / 197, P-028 / 217, P-029 / 218, P-030 / 218, P-031 / 219, P-032 / 219, P-033 / 220, P-034 / 220, P-035 / 221, P-048 / 227, P-050 / 228, P-051 / 229, P-052 / 229, P-054 / 230, P-062 / 234, P-063 / 235, P-099 / 253, P-411 / 409
Yönak, H. P-419 / 413 Yurdakul, M. S. P-222 / 315 Yurtsever, S. P-157 / 282 Yurttaş, T. T. P-470 / 439, P-479 / 443 Yüceer, Ö. P-276 / 342 Yücetaş, E. P-143 / 275, P-207 / 307 Yüksel, A. O-140 / 178 Yüzbaşıoğlu, Y. O-113 / 165, O-160 / 188, / 30, / 33 Yüzgeç, Z. O-055 / 136, / 14 Z
Zafer, N. P-078 / 242 Zehir, E. P-331 / 369 Zengin, S. O-021 / 119, O-169 / 194 Zengin, Y. 35, 106 Zeren, C. P-312 / 360



www.TurkJEmergMed.comsubmit your articles @