
A performance evaluation of 90Y dose-calibrator measurements in nuclear pharmacies and clinics in...
9
Applied Radiation and Isotopes 66 (2008) 252–260 A performance evaluation of 90 Y dose-calibrator measurements in nuclear pharmacies and clinics in the United States Michael K. Schultz a, , Jeffrey T. Cessna a , Tamara L. Anderson b , James A. Ponto c , Neil Petry d , Richard J. Kowalsky e , Matthew R. Palmer f , Uwe F. Beinlich g , William Baker h , George H. Hinkle i , Joseph C. Hung j , Timothy Quinton k , Peter A. Rice l , Chaitanya Divgi m , Jeffrey P. Norenberg b a The National Institute of Standards and Technology, Nuclear Medicine Standards Program, 100 Bureau Drive, MS 8462, Gaithersburg, MD 20899, USA b College of Pharmacy, University of New Mexico Health Sciences Center, New Mexico Center for Isotopes in Medicine, 2502 Marble, NE MSC09 5360, Albuquerque, NM 87131-0001, USA c Department of Radiology, Division of Nuclear Medicine, University of Iowa Hospital and Clinics, 200 Hawkins Drive, 3832 JPP, Iowa City, IA 52242, USA d Department of Radiology, Department of Nuclear Medicine, Duke University Medical Center, 133 Bell Building, Box 3304, Durham, NC 27710-3304, USA e Department of Radiology, University of North Carolina, 1312 Kerr Hall, CB 7360, Chapel Hill, NC 27599, USA f Department of Radiology, Division of Nuclear Medicine, Beth Israel Deaconess Medical Center, 330 Brookline Avenue, Boston, MA 02215-5400, USA g QSA Global, Inc., Auriga Medical Division, 40 North Avenue, Burlington, MA 01803, USA h Pharmaceutical and Diagnostic Services, 1152 West 2240 South St. E., West Valley City, UT 84119, USA i The Ohio State University Medical Center, Room 203D, Doan Hall, 410 West 10th Avenue, Columbus, OH 43210, USA j Mayo Clinic, Division of Nuclear Medicine, Department of Radiology, 200 First Street SW, Rochester, MN 55905, USA k Radiopharmacy, Inc., 1409 E. Virginia St., Evansville, IN 47711, USA l Massachusetts General Hospital, Division of Nuclear Medicine, Tilton-2, 55 Fruit Street, Boston, MA 02114, USA m Division of Nuclear Medicine and Clinical Molecular Imaging, University of Pennsylvania, Hospital of the University of Pennsylvania, 3400 Spruce Street, Room Donner 116, Philadelphia, PA 19104, USA Received 2 November 2006; received in revised form 19 July 2007; accepted 10 September 2007 Abstract A blind performance test was conducted to evaluate dose-calibrator measurements at nuclear pharmacies in the United States (US). Two test-sample geometries were chosen to represent those used for measurements of 90 Y-ibritumomab tiuxetan (ZEVALIN s ). The radioactivity concentration of test-samples was verified by the US National Institute of Standards and Technology. Forty-five results were reported by 10 participants. Eighty percent of reported values were within the US Pharmacopoeia content standard (710%) for 90 Y-ZEVALIN s . All results were within US Nuclear Regulatory Commission conformance limits (720%) for defining therapeutic misadministrations. r 2007 Elsevier Ltd. All rights reserved. Keywords: 90 Yttrium; Radiopharmacy; Ibritumomab tiuxetan; Dose calibrator; Measurement assurance 1. Introduction The application of targeted radiotherapy techniques for treatment of human cancer continues to increase. These techniques promise enhanced treatment options not only for malignancies refractory to traditional chemotherapy, but also as a primary therapeutic option (Maloney and Press, 1998; Allen et al., 2004; Connors, 2005). To ensure that the radioactivity dose administered to the patient is within prescribed limits, a radioactivity measurement is performed prior to administration of the drug. In most cases, this measurement is performed in the radiopharmacy or nuclear medicine clinic. Thus, the safety and effectiveness ARTICLE IN PRESS www.elsevier.com/locate/apradiso 0969-8043/$ - see front matter r 2007 Elsevier Ltd. All rights reserved. doi:10.1016/j.apradiso.2007.09.002 Corresponding author. Tel.: +1 319 356 4159; fax: +1 319 353 6512. E-mail address: [email protected] (M.K. Schultz).
Transcript of A performance evaluation of 90Y dose-calibrator measurements in nuclear pharmacies and clinics in...

ARTICLE IN PRESS
0969-8043/$ - se
doi:10.1016/j.ap
�CorrespondE-mail addr
Applied Radiation and Isotopes 66 (2008) 252–260
www.elsevier.com/locate/apradiso
A performance evaluation of 90Y dose-calibrator measurements innuclear pharmacies and clinics in the United States
Michael K. Schultza,�, Jeffrey T. Cessnaa, Tamara L. Andersonb, James A. Pontoc,Neil Petryd, Richard J. Kowalskye, Matthew R. Palmerf, Uwe F. Beinlichg, William Bakerh,George H. Hinklei, Joseph C. Hungj, Timothy Quintonk, Peter A. Ricel, Chaitanya Divgim,
Jeffrey P. Norenbergb
aThe National Institute of Standards and Technology, Nuclear Medicine Standards Program, 100 Bureau Drive, MS 8462, Gaithersburg, MD 20899, USAbCollege of Pharmacy, University of New Mexico Health Sciences Center, New Mexico Center for Isotopes in Medicine, 2502 Marble, NE MSC09 5360,
Albuquerque, NM 87131-0001, USAcDepartment of Radiology, Division of Nuclear Medicine, University of Iowa Hospital and Clinics, 200 Hawkins Drive, 3832 JPP, Iowa City, IA 52242, USAdDepartment of Radiology, Department of Nuclear Medicine, Duke University Medical Center, 133 Bell Building, Box 3304, Durham, NC 27710-3304, USA
eDepartment of Radiology, University of North Carolina, 1312 Kerr Hall, CB 7360, Chapel Hill, NC 27599, USAfDepartment of Radiology, Division of Nuclear Medicine, Beth Israel Deaconess Medical Center, 330 Brookline Avenue, Boston, MA 02215-5400, USA
gQSA Global, Inc., Auriga Medical Division, 40 North Avenue, Burlington, MA 01803, USAhPharmaceutical and Diagnostic Services, 1152 West 2240 South St. E., West Valley City, UT 84119, USA
iThe Ohio State University Medical Center, Room 203D, Doan Hall, 410 West 10th Avenue, Columbus, OH 43210, USAjMayo Clinic, Division of Nuclear Medicine, Department of Radiology, 200 First Street SW, Rochester, MN 55905, USA
kRadiopharmacy, Inc., 1409 E. Virginia St., Evansville, IN 47711, USAlMassachusetts General Hospital, Division of Nuclear Medicine, Tilton-2, 55 Fruit Street, Boston, MA 02114, USA
mDivision of Nuclear Medicine and Clinical Molecular Imaging, University of Pennsylvania, Hospital of the University of Pennsylvania, 3400 Spruce Street,
Room Donner 116, Philadelphia, PA 19104, USA
Received 2 November 2006; received in revised form 19 July 2007; accepted 10 September 2007
Abstract
A blind performance test was conducted to evaluate dose-calibrator measurements at nuclear pharmacies in the United States (US).
Two test-sample geometries were chosen to represent those used for measurements of 90Y-ibritumomab tiuxetan (ZEVALINs). The
radioactivity concentration of test-samples was verified by the US National Institute of Standards and Technology. Forty-five results
were reported by 10 participants. Eighty percent of reported values were within the US Pharmacopoeia content standard (710%) for90Y-ZEVALINs. All results were within US Nuclear Regulatory Commission conformance limits (720%) for defining therapeutic
misadministrations.
r 2007 Elsevier Ltd. All rights reserved.
Keywords: 90Yttrium; Radiopharmacy; Ibritumomab tiuxetan; Dose calibrator; Measurement assurance
1. Introduction
The application of targeted radiotherapy techniques fortreatment of human cancer continues to increase. Thesetechniques promise enhanced treatment options not only
e front matter r 2007 Elsevier Ltd. All rights reserved.
radiso.2007.09.002
ing author. Tel.: +1319 356 4159; fax: +1 319 353 6512.
ess: [email protected] (M.K. Schultz).
for malignancies refractory to traditional chemotherapy,but also as a primary therapeutic option (Maloney andPress, 1998; Allen et al., 2004; Connors, 2005). To ensurethat the radioactivity dose administered to the patient iswithin prescribed limits, a radioactivity measurement isperformed prior to administration of the drug. In mostcases, this measurement is performed in the radiopharmacyor nuclear medicine clinic. Thus, the safety and effectiveness

ARTICLE IN PRESS
Table 1
List of participants that reported results for the NRQMP0305 perfor-
mance test
Participant Organization/location
William Baker, PhD Pharmaceutical and Diagnostic
Services, West Valley City, Utah
George H. Hinkle, RPh, BCNP,
FASHP, FAPhA
Ohio State University Medical
Center, Columbus, Ohio
Joseph C. Hung, PhD, BCNP Mayo Clinic, Rochester,
Minnesota
Richard J. Kowalsky, PharmD,
BCNP, FAPhA
University of North Carolina,
Chapel Hill, North Carolina
Jeffrey P. Norenberg, PharmD University of New Mexico,
Albuquerque, New Mexico
Matthew R. Palmer, PhD Beth Israel Deaconess Medical
Center, Boston, Massachussetts
Neil Petry, RPh, MS, BCNP,
FAPhA
Duke University Medical Center,
Durham, North Carolina
James A. Ponto, MS, RPh, BCNP,
FAPhA, FASHP
University of Iowa Hospitals and
Clinics, Iowa City, Iowa
Timothy Quinton, PharmD, MS Radiopharmacy, Inc. Evansville,
Indiana
Peter A. Rice, RPh, BCNP Massachusetts General Hospital,
Boston, Massachussetts
M.K. Schultz et al. / Applied Radiation and Isotopes 66 (2008) 252–260 253
of these radiopharmaceuticals for patients depend on,among other factors, the ability of these facilities to makeaccurate radioactivity measurements.
To promote good radioactivity measurement practice,ongoing ‘‘measurement assurance’’ programs (MAPs) arecommonly administered by regulatory and standardsorganizations. A MAP can be defined as an ongoing seriesof measurement performance tests that are administered bya recognized standards organization. For nuclear medicinefacilities, several such programs are administered outside ofthe United States (US; Oropesa et al., 2005). The purposeof these programs is to improve radioactivity measurementaccuracy and precision and provide for a linkage betweenroutine measurements and national standards (Oropesaet al., 2005). In the US, the National Institute of Standardsand Technology (NIST), under an agreement with theNuclear Energy Institute (NEI) has operated a MAP forradiopharmaceutical manufacturers since the mid-1970s(Golas, 1982, 1998; Golas and Calhoun, 1983). In the NEI/NIST Program, traceability of radioactivity measurementsto national standards is demonstrated by radiopharmaceu-tical manufacturers through ongoing-blind proficiencytesting using NIST Standard Reference Materials (SRMs;Cavallo et al., 1979; Golas, 1982, 1998). Test-samples aremanufactured, calibrated, and distributed to participatinglaboratories, where radioactivity measurements are con-ducted. To demonstrate measurement proficiency, partici-pants make required measurements and report the resultsfor each test to NEI, which evaluates the reported values(relative to NIST-certified values) and returns an officialreport to the participant. The program has operatedsuccessfully for approximately 30 years (Cavallo et al.,1979; Golas, 1982, 1998; Golas and Calhoun, 1983). On theother hand, recent efforts to monitor the proficiency ofradioactivity measurements conducted in US radiophar-macies and nuclear medicine clinics have been minimal.Prior to the current study, the most recent evaluations ofradioactivity measurements performed in these facilitieswere carried out by NIST (then known as the NationalBureau of Standards, NBS) from 1970 through 1980 at therequest of College of American Pathologists (CAP) and theUS Atomic Energy Commission (AEC; now known as theUS Department of Energy, DOE; Golas, 1982; NCRP,1985). No such ongoing MAP exists for evaluatingradioactivity measurement performance of nuclear medi-cine clinics and radiopharmacies in the United Statestoday.
In this work, a performance test (referred to as theNRQMP0305 performance test) of 90Y dose-calibratormeasurements conducted in US radiopharmacies andnuclear medicine clinics is described. The test wasadministered by the NIST in collaboration with theNational Association of Nuclear Pharmacists (NANP).Study design and an analysis of the reported results arehighlighted. The feasibility of an ongoing measurementassurance program for radioactivity measurements in USradiopharmacies and nuclear medicine clinics is examined.
2. Materials and methods
2.1. Performance test description
The NRQMP0305 performance test was a blind test—anestimate of the activity level was provided for informa-tional purposes to each participant, but the certifiedactivities were unknown. A total of 11 facilities agreed toparticipate in this study. Ten participants reported resultsof measurements to NIST (Table 1). Measurements wereconducted using dose calibrators located within theparticipating radiopharmacies and/or within the clinicalfacilities serviced by the radiopharmacies. The intention ofthe organizers was to select a group of nuclear medicinefacilities that represents (to the extent possible) a reason-able cross-section of nuclear medicine facilities in the US.A commercial radionuclide manufacturer (QSA Global,
Inc., Burlington, MA, USA; formerly AEA Technologies,GmbH, Braunschweig, Germany) prepared and distributedall test-samples to participants for this study. Participantswere instructed to perform measurements according to‘‘routine’’ procedures for measurements of 90Y-ZEVA-LINs. In summary, participants received the materialsthrough normal channels, unpacked the samples, maderequested measurements, recorded the results, completedthe enclosed reporting forms and returned the reportforms, and test-samples to NIST for certification. No decaycorrection was required for reporting measurement results.There appeared to be some ambiguity in initial reportingforms, where the reporting field for analysis results for eachmeasurement was identified by the heading ‘‘Readout(MBq)’’. Consequently, in some cases results were reportedwithout the required multiplication factors to convert the

ARTICLE IN PRESS
Table 2
Half lives and uncertainties (Unc) used for decay corrections and activity
calculations (Kossert and Schrader, 2004; ENSDF, 2005)
Radionuclide Half life (Unc)
90Y 64.05370.020 h3H 12.3270.02 years90Sr 28.7970.06 years
M.K. Schultz et al. / Applied Radiation and Isotopes 66 (2008) 252–260254
‘‘readout’’ of the dose calibrator to actual ‘‘activity’’. Toremedy this apparent ambiguity in reporting fields, anupdated reporting form was sent to all participants. In thisupdated reporting form, the field was identified moreprecisely as the ‘‘Prescribed Activity (MBq)’’. Participantswere instructed to update the values that were originallyreported and to return the updated values to NIST(including a description of the conversion factors used toconvert the instrument readout to the activity value).
2.2. Reference time and uncertainties
All radioactivity values presented in this paper are as ofthe reference time 17 March 2005 12:00p.m. EasternStandard Time (EST). All evaluations of uncertainties adhereto accepted conventions used by the NIST RadioactivityGroup and are in concordance with those recommended bythe principal metrology standards organizations (Taylor andKuyatt, 1994; ISO, 1995). All individual uncertaintycomponents are given as estimated experimental standarddeviations (or standard deviations of the mean, if appro-priate), or quantities assumed to correspond to standarddeviations, regardless of the method used to evaluate theirmagnitude. Unless otherwise stated explicitly, all uncertain-ties cited in this paper are ‘‘standard uncertainties,’’corresponding to a one uncertainty interval.
For verification measurements conducted at NIST, allsolution transfers were performed using disposable high-density polyethylene pycnometers (Canus Plastics, Ottawa,Ont., Canada) to minimize effects of evaporation duringtransfers and mass measurements. Gravimetric measure-ments were performed by determining the difference inpycnometer weights before and after transfers of activitysolutions and diluents. A six-decimal-place microbalance(model M5, Mettler-Toledo, Toledo, OH, USA) wasemployed for all gravimetric measurements made at NIST.Appropriate air-buoyancy and balance-tare correctionswere made for each gravimetric measurement. The result-ing uncertainty from balance measurements is estimated tobe approximately 0.05%.
2.3. Test-samples
Test-samples were prepared so as to represent thecomposition and geometries provided as part of the ‘‘kit’’for preparing and dispensing the radiopharmaceutical 90Y-ibritumomab tiuxetan (ZEVALINs) at the time of thisperformance test. Half lives and nuclear data were adoptedfrom current-published sources (Kossert and Schrader,2004; ENSDF, 2005; Table 2). The test-sample geometrieswere 10mL 90Y solution in a 10-mL reaction vial (RV) anda 90Sr/90Y source designed to simulate 4mL 90Y solution ina 10-mL plastic syringe (TS). The RV is identical toreaction vials supplied as part of the 90Y-ZEVALINs kit(Witzig et al., 2003).
Individual RV solutions were prepared by dispensing1mL (nominally) of 90Y stock solution (90Y chloride,
90YCl3) in 0.1mol L�1 hydrochloric acid (HCl) to eachreaction vial and diluting to a nominal total volume of10mL with a solution of 25 mgmL�1 stable Y3+
, as YCl3, in0.1mol L�1 HCl. A precise determination of the mass ofdispensed solution was made in each case. Previouscomparisons of calibration factors for dose calibratorsreveal no apparent dependence on solution composition for90Y (whether as chloride 1mol L�1 HCl or the 90Y-ZEVALINs drug product, Zimmerman et al., 2004). Tominimize the variability in dose-calibrator response arisingfrom differences in the volume contained in each RV,dispensed-solution volumes were held constant to within0.2% (calculated as the relative standard deviation of thegrand average for all dispensed RV solutions). Theprecision of dispensed volume was controlled by auto-mated volumetric dispensing using a model Microlab 500Bauto-dispensing system (Hamilton, Inc., Bondaluz, Swit-zerland). Confirmatory mass measurements of dispensedvolumes were conducted using a digital microbalance(Sartorius model LA230S) with a readability of 0.1mg(Sartorius AG, Goettingen, Germany). The total activitydispensed to each reaction vial was approximately 1.5GBqas of the reference time.The TS is a long-lived 90Sr/90Y enclosed-sealed calibra-
tion source (model number SIM.SY2 90Sr/90Y TransferStandard, QSA Global), constructed in a 10-mL syringegeometry (in an aluminum casing, Thieme et al., 2004). Thedevice is designed to simulate the dose-calibrator responseresulting from the use of a 10-mL plastic Becton DickinsonLuer-LokTM type syringe (BD syringe, model number300192, Becton, Dickinson and Company, Franklin Lakes,NJ, USA) containing 4mL 90Y solution (approximately1.2GBq equivalent). The design utilizes the bremsstrahlungradiation produced as a result of the 90Sr/90Y beta-particleinteractions with the syringe materials, source holder, andconstruction material of the dose-calibrator ionizationchamber. Thus, the 90Y simulated-total activity is instru-ment dependant. Although the device was designedspecifically for use with the Capintec Model CRC-15Rdose calibrator (Capintec, Inc., Ramsey, NJ, USA), thecurrent study extends the use of the device to two otherdose calibrators (Capintec model CRC-12; and Biodexmodel AtomLab 100, Biodex Medical Systems, Shirley,NY, USA; Table 3). The intended purpose of the device isfor calibrations required for the 90Y-ZEVALINs proce-dure (Witzig et al., 2003; Thieme et al., 2004).

ARTICLE IN PRESS
Table 3
Summary of dose calibrators employed, number of results submitted for
reaction vial and transfer standard measurements and NIST determined
dial settings for available dose calibrators for the NRQMP0305
comparison test
Dose calibrator No. of resultsa NIST dial settingb
Reaction vial—RV (10-mL fill volume)
CRC-4c 1 NAd
CRC-5Rc 2 NAd
CRC-7c 1 NAd
CRC-12c 2 (3971)� 10
CRC-15Rc 16 (3971)� 10
CRC-15Wc 1 NAd
CRC-30BCc 1 NAd
CRC-127Rc 2 NAd
Transfer Standard—TS (4-mL fill volume)
CRC-12c 2 (5871)� 10
CRC-15Rc 16 (5271)� 10
Atomlab 100e 1 38272
aNo. of reported results submitted by participants for each model.bDial setting determined by NIST.cManufactured by Capintec, Inc.dNA signifies that the model was not available at NIST.eManufactured by Biodex Medical Systems.
(RV2) (RV5) (RV11)
Transfer 0.10 g
Transfer 0.15 g
DF~50
5 g
Tran
Dilution
Two sets of five for each RV
LS Vials
Blanks5 mL glass ampoules
Two
2 5 11
0
50
(1)
(2)
(1)
(2)
L
Fig. 1. Flow diagram depicting preparation of 90Y, 3H, and Blank (B) sourc
Material 3H in water (H2O) SRM 4927E. Two sample sets were prepared for 90Y
employed (Set 1: ReadySafeTM; Set 2: Opti-FluorTM). Arrows indicate transfe
diluted by a factor (DF) of 50. Matrix matching of liquid-scintillation source
hydrochloric acid (0.1M HCl) fractions as shown. Effect of quench was monito
(CH3NO2, diluted to 10% volume:volume concentration with ethanol) to all s
M.K. Schultz et al. / Applied Radiation and Isotopes 66 (2008) 252–260 255
2.4. Test-sample activity certifications
All test-samples were returned to NIST for radioactivitycertification and verification following measurements at theparticipants’ facilities. The CIEMAT (Centro de Investi-gaciones Energeticas, Medioambientales y Tecnologicas deEspana)/NIST method of tritium (3H) efficiency tracing ofmatrix-matched liquid-scintillation (LS) counting sourceswas employed for activity determination of the RVsolution (Fig. 1; Zimmerman et al., 2004). LS sources wereprepared from a secondary dilution of three randomlyselected RV’s (RV2, RV5, RV11). Two separate LS-samplesets were prepared using ReadySafeTM (Beckman–Coulter,Inc., Fullerton, CA, USA) and Opti-FluorTM (Perkin-Elmer Life Sciences, Inc., Shelton, CT, USA) LS cocktails.Five LS-sources were prepared for each cocktail for RV’sand 3H samples (Fig. 1). Two blanks were prepared foreach cocktail. Sources (n ¼ 44 total) were counted for 10cycles, in 10min count-time intervals, using a modelnumber LS7800 liquid-scintillation counter (Beckman–Coulter) for a total count time of approximately 3 days.After allowing sufficient time (460 days) for the decay ofunsupported 90Y, the level of 90Sr impurity present in the
NIST SRM
4927E
Transfer 0.02 g
Quench
0.15 g
Two sets of five
sfer 0.02 g
LS Vials
sets of two
0.15 g
.1 M HCl
µg mL-1
Y3+
3H
(1)
(2)
H2O
10%CH3NO2
B B
B B
S Vials
es for liquid-scintillation (LS) counting using NIST Standard Reference
, 3H, and Blank (signified by nos. 1, 2). Sample sets differed in LS cocktail
r of solutions. Masses shown are approximate values. RV solutions were
s was accomplished by matching H2O, stable yttrium (Y3+) carrier, and
red by addition of known amounts (1–8 drops per sample) of nitromethane
amples.
ARTICLE IN PRESSM.K. Schultz et al. / Applied Radiation and Isotopes 66 (2008) 252–260256
RV solutions was determined in a separate experimentusing the same LS measurement approach. The 90Y activityvalue (as determined by LS counting) was then used todetermine dial settings for two dose-calibrator modelsavailable at NIST (Capintec models CRC-12 and CRC-15R), according to previously published methods (Thiemeet al., 2004; Zimmerman et al., 2004). Reagents wereAmerican Chemical Society (ACS) grade or equivalent.High-purity acids were used for preparation of carriersolution (Fisher Scientific International, Hampton, NJ,USA). Stable Y3+ carrier solution was prepared byvolumetric dilution of NIST SRM 3167a (NIST, Gaithers-burg, MD, USA).
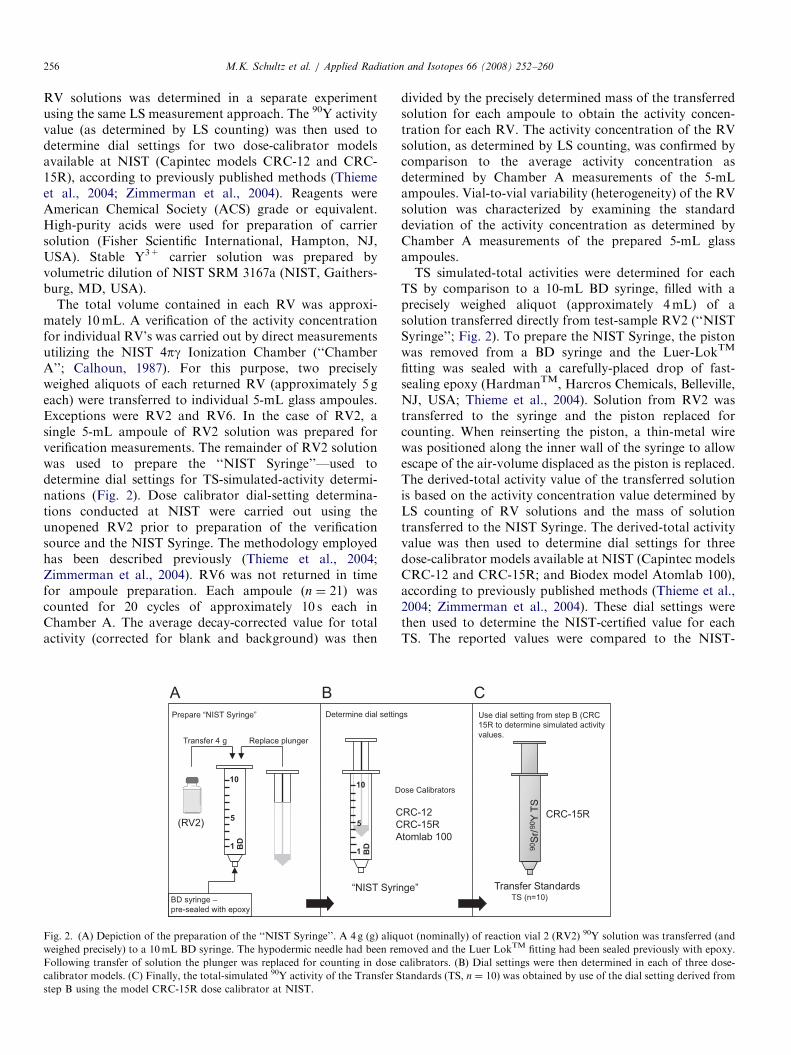
The total volume contained in each RV was approxi-mately 10mL. A verification of the activity concentrationfor individual RV’s was carried out by direct measurementsutilizing the NIST 4pg Ionization Chamber (‘‘ChamberA’’; Calhoun, 1987). For this purpose, two preciselyweighed aliquots of each returned RV (approximately 5 geach) were transferred to individual 5-mL glass ampoules.Exceptions were RV2 and RV6. In the case of RV2, asingle 5-mL ampoule of RV2 solution was prepared forverification measurements. The remainder of RV2 solutionwas used to prepare the ‘‘NIST Syringe’’—used todetermine dial settings for TS-simulated-activity determi-nations (Fig. 2). Dose calibrator dial-setting determina-tions conducted at NIST were carried out using theunopened RV2 prior to preparation of the verificationsource and the NIST Syringe. The methodology employedhas been described previously (Thieme et al., 2004;Zimmerman et al., 2004). RV6 was not returned in timefor ampoule preparation. Each ampoule (n ¼ 21) wascounted for 20 cycles of approximately 10 s each inChamber A. The average decay-corrected value for totalactivity (corrected for blank and background) was then
(RV2)
“NIST Syri
1
5
10
BD
Transfer 4 g Replace plunger
Determine dial settin
C
C
A
1
5
10
BD
Prepare “NIST Syringe”
BD syringe –
pre-sealed with epoxy
D
Fig. 2. (A) Depiction of the preparation of the ‘‘NIST Syringe’’. A 4 g (g) aliq
weighed precisely) to a 10mL BD syringe. The hypodermic needle had been re
Following transfer of solution the plunger was replaced for counting in dose
calibrator models. (C) Finally, the total-simulated 90Y activity of the Transfer S
step B using the model CRC-15R dose calibrator at NIST.
divided by the precisely determined mass of the transferredsolution for each ampoule to obtain the activity concen-tration for each RV. The activity concentration of the RVsolution, as determined by LS counting, was confirmed bycomparison to the average activity concentration asdetermined by Chamber A measurements of the 5-mLampoules. Vial-to-vial variability (heterogeneity) of the RVsolution was characterized by examining the standarddeviation of the activity concentration as determined byChamber A measurements of the prepared 5-mL glassampoules.TS simulated-total activities were determined for each
TS by comparison to a 10-mL BD syringe, filled with aprecisely weighed aliquot (approximately 4mL) of asolution transferred directly from test-sample RV2 (‘‘NISTSyringe’’; Fig. 2). To prepare the NIST Syringe, the pistonwas removed from a BD syringe and the Luer-LokTM
fitting was sealed with a carefully-placed drop of fast-sealing epoxy (HardmanTM, Harcros Chemicals, Belleville,NJ, USA; Thieme et al., 2004). Solution from RV2 wastransferred to the syringe and the piston replaced forcounting. When reinserting the piston, a thin-metal wirewas positioned along the inner wall of the syringe to allowescape of the air-volume displaced as the piston is replaced.The derived-total activity value of the transferred solutionis based on the activity concentration value determined byLS counting of RV solutions and the mass of solutiontransferred to the NIST Syringe. The derived-total activityvalue was then used to determine dial settings for threedose-calibrator models available at NIST (Capintec modelsCRC-12 and CRC-15R; and Biodex model Atomlab 100),according to previously published methods (Thieme et al.,2004; Zimmerman et al., 2004). These dial settings werethen used to determine the NIST-certified value for eachTS. The reported values were compared to the NIST-
nge”
90S
r/90Y
TS
gs
RC-12
RC-15R
tomlab 100
TS (n=10)
Use dial setting from step B (CRC
15R to determine simulated activity
values.
CRC-15R
Transfer Standards
ose Calibrators
uot (nominally) of reaction vial 2 (RV2) 90Y solution was transferred (and
moved and the Luer LokTM fitting had been sealed previously with epoxy.
calibrators. (B) Dial settings were then determined in each of three dose-
tandards (TS, n ¼ 10) was obtained by use of the dial setting derived from

ARTICLE IN PRESSM.K. Schultz et al. / Applied Radiation and Isotopes 66 (2008) 252–260 257
certified value to assess the accuracy of the reported result.The approach allowed the direct comparison of each TS toa NIST-certified radioactivity solution in the geometry theTS is designed to simulate.
2.5. Statistical analyses
Reported results for this study were compared to aNIST-certified value as a measure of the accuracy of themeasurements at the individual laboratories. Bias in ameasurement result is defined by the percent differencefrom the NIST value (relative to the NIST value). Themean, standard deviation, and range of measurementresults are reported separately for RV and TS results. Astatistical test was employed to confirm that the use ofmean-centered statistics was reasonable (i.e., that the dataare normally distributed). The test employed was a normalprobability regression technique, which uses the correlationcoefficient (R) as a test statistic (Filliben, 1975). Theapproach entails ranking the submitted values (in thepresent study, normalized to the NIST value) in ascendingorder, plotting the data versus the normal order statisticmedians (NORM), performing a least-squares regression,and comparing the resulting regression coefficient (R) to anumerically determined ‘‘critical value’’ (Vc). The Vc
represents a theoretical-threshold for testing the hypothesisof normality (within familiar confidence levels). For thisstudy, all comparisons of Vc’s to calculated values for R
were made at the 95% confidence level. Critical values wereobtained from published tables (Filliben, 1975). Calculatedvalues for R were obtained using the PEARSON functionin the software program Microsofts ExcelTM (Version2002 SP2, Microsoft Corporation, Redman, WA, USA)and confirmed by comparison to values obtained usingNIST internally developed software. Comparisons of R
values obtained from these two sources agreed to within70.1%. For a given confidence level, the Vc approachesunity as the population size increases. In the assessment ofthe ‘‘normality’’ of a given dataset, the value of R iscompared to the numerically determined Vc. For a givendistribution of related numbers (such as normalizedreported measurement results), a value of R that is greaterthan the numerically determined Vc indicates that thedistribution of reported results appears to be ‘‘normal’’ andmean-centric statistical analysis is reasonable (Filliben,1975). On the other hand, a value of R that is less than theVc is an indication that the dataset has ‘‘non-normal’’characteristics (e.g., presence of outliers).
3. Results
3.1. NIST certifications and dial settings
The NIST-certified value of 90Y activity concentration ofthe RV solution was determined (as of the reference timeby LS measurements) to be 1.54E+8Bq g�171.10E+6Bq g�1, where the uncertainty is an expanded uncertainty,
which represents an approximate 95% confidence interval(coverage factor of k ¼ 2). Included component uncertain-ties are: LS counting (90Y) source to source (0.10%); LScounting cycle to cycle (0.10%); half-life propagation (90Y,0.28%); effect of the background standard deviation on90Y count rate (0.002%); live time (LS counting, 0.10%);possible impurities (0.01%); gravimetric measurements (LSsources, 0.05%, vial preparation, 0.05%); and dilutions(0.09%). The certified activity concentration is correctedfor minimal 90Sr impurity. The ratio of 90Sr Bq g�1:90YBq g�1 at the reference time was determined by a separateliquid-scintillation counting procedure to be approximately3.4E-7.Based on these results, dial settings of (3971)� 10 and
(3971)� 10 were determined for dose-calibrator modelsCRC-12 and CRC-15R, respectively (Table 3). Theuncertainties are the combined standard uncertaintiesarising from instrument readout instability, curve fitting,and the results of replicate measurements.Results of the Chamber A measurements of the prepared
ampoules confirm the liquid-scintillation results. Theaverage activity concentration, based on Chamber Aresults is 1.52E+08Bq g�171.67E+6Bq g�1, representingan average difference of �1.3% from the value determinedby LS measurements. The uncertainty is an expandeduncertainty (k ¼ 2). Included component uncertainties are:gravimetric measurements (0.05%); radium referencesource ratio (0.10%); source positioning uncertainty(0.10%); and the relative standard deviation of the averageactivity concentration obtained from counting 21 ampoules(0.53%). Based on the relative standard deviation of theaverage activity of ampoule counting results, solutionheterogeneity can be characterized as negligible.The NIST-certified value of 90Y total activity of the
NIST Syringe was determined to be 6.45E+8Bq g�1
74.68E+6Bq g�1, where the uncertainty is an expandeduncertainty (k ¼ 2). The value is based on the results of theRV solution 90Y activity-concentration determination byLS counting and the mass measurement of the solutiontransferred to the plastic syringe (4.197199 g; Fig. 2). Theuncertainty comprises all uncertainties arising from thedetermination of the NIST-certified value for the RVsolution activity concentration as well as uncertaintyarising from gravimetric measurement (0.05%) of thesolution transferred to the NIST Syringe.Based on the NIST-certified value for the NIST Syringe,
dial settings of (5871)� 10, (5271)� 10, and 38272 weredetermined for dose-calibrator models CRC-12, CRC-15R,and Atomlab100, respectively, where the uncertainties arethe combined standard uncertainties arising from instru-ment readout instability, curve fitting, and the results ofreplicate measurements (Table 3).
3.2. Reported results
Ten laboratories submitted a total of 45 individualmeasurement results for this exercise (26 RV, 19 TS). All

ARTICLE IN PRESS
-15
-10
-5
0
5
10
0 10 15 20 25 30
Reported Result
Diffe
rence F
rom
NIS
T (
%)
Range: -12 to +3%
Reaction Vial Results Relative to NIST (n=26)
AverageReported
Value (-6%)
NIST Value
5
Fig. 3. Comparison of reported results (n ¼ 26) of the reaction vials to the
‘‘NIST-certified value’’ for the NRQMP0305 comparison test. An overall
average bias of �6% was observed with a standard deviation of 4% and
range of �12% to +3%.
-20
-15
-10
-5
0
5
10
15
20
0 10 15 20
Reported Result
Diffe
rence F
rom
NIS
T (
%)
Range: -17 to +17%
Transfer Standard Results Relative to NIST (n=19)
AverageReported
Value (-4%)
NIST Value
5
Fig. 4. Comparison of reported results (n ¼ 19) of the Transfer Standards
to the ‘‘NIST-certified value’’ for the NRQMP0305 comparison test. An
overall average bias of �4% was observed with a standard deviation of
8% and range of �17% to +17%.
M.K. Schultz et al. / Applied Radiation and Isotopes 66 (2008) 252–260258
reported results were within conformance limits of 720%published by the US NRC for defining misadministrationof therapeutic doses (NRC, 2005). The average bias for allreported RV results, when compared to the NIST-certifiedvalue at the reference time is �6% with a standarddeviation of 4%, and a range of �12% to +3% (Fig. 3).An examination of the results (normalized to the NISTvalue) by normal probability regression analysis indicatesthat the distribution is not non-normal (R ¼ 0.9834Vc ¼ 0.956). Of the 26 RV measurement results reportedto NIST, four values (approximately 15%) fall outsideof the content standard published by USP (710%) for90Y-ZEVALINs (USP, 2005).
A similar distribution of results was obtained throughthe analysis of the reported TS measurements compared tothe NIST-certified values. The average bias for all reportedTS results is �4%, with a standard deviation of 8%, andrange of �17% to +17% (Fig. 4). The results appear to benormally distributed (R ¼ 0.9544Vc ¼ 0.948). Five re-ported results (26% of submitted values), lie outsideof the content standard published by USP (710%) for90Y-ZEVALINs (USP, 2005).
4. Discussion
4.1. Laboratory performance
The size and scope of this pilot performance test is smallwhen compared to the size of the entire population ofnuclear medicine clinics and radiopharmacies in the US.Further, the instructions provided with the performancetesting samples (although intended to represent ‘‘routine’’procedures) may not reflect precisely the standard operat-ing procedures of individual laboratories. Nonetheless, theresults of this test can be considered as guidelines, withinwhich the value of an on-going MAP can be examined.The calculated average of reported results (relative to the
NIST values) for the RV and TS measurements are withinthe acceptable limits (720% of prescribed dose) codified inNRC Regulations (NRC, 2005). However, a substantialnumber (n ¼ 9) of the combined measurements (n ¼ 45)result in an activity determination that is beyondthe content standard limits of 710% outlined in USP for90Y-ibritumomab tiuxetan (USP, 2005). The cause forerrant reported values is unclear. Reporting forms dis-tributed with the test-samples for this exercise included afield, in which a description of the instrument quality-control procedure employed by the participant wasrequested. The field requested a description of the qualityassurance procedures, including check-source identifica-tion, radionuclide employed, and the procedure used forchecking the instrument used. All participants reported theuse of an instrument quality-control procedure (prior tomeasurements) using a 137Cs check source. Two of the 10participants reported the use also of a 57Co source formonitoring the daily stability of the instrument. Allparticipants reported that quality-control limits were metprior to conducting measurements for this study. Althoughthese quality-control measurements may be appropriate assystem checks or calibrations for certain radionuclides, norelationship can be established between the accuracy of 90Y(in the measurement geometries of the test) and the resultsof these system performance checks conducted prior tomeasurements for this test.The results showed no statistically significant relation-
ship to the dose-calibrator model employed for measure-ments in this performance test. All results submitted toNIST for RV measurements were conducted using instru-ments manufactured by the same company (Capintec,Inc.). Sixteen of 26 reported reaction-vial measurementresults were obtained by use of a single dose-calibratormodel (Table 3). The number of results reported forremaining dose-calibrator models employed was small.Similarly, of the 19 results submitted for TS measurements,16 values were obtained by participants using the samemodel dose calibrator (Table 3).Perhaps the most obvious characteristic of the reported
results is the persistent negative bias when compared to theNIST value. Participants indicated that the manufacturerof the ZEVALINs drug product (Biogen IDEC, Inc.)

ARTICLE IN PRESSM.K. Schultz et al. / Applied Radiation and Isotopes 66 (2008) 252–260 259
provided instructions for carrying out calibrations of dosecalibrators prior to distributing the radiopharmaceutical topharmacies. Although it is possible that the persistentnegative bias is the result of an error introduced by themanufacturer during the initial calibration of dosecalibrators for the ZEVALIN product, quantification ofthe relationship is not possible based on the results of thistest. Further, the average bias of results for each of thegeometries is within acceptable limits found in USP andNRC regulations. On the other hand, a significant numberof experimental results (20%) fell outside of contentstandards published by USP for preparing and dispensing90Y-ibritumomab tiuxetan.
4.2. Pilot test evaluation
MAPs are an effective tool for monitoring the radio-analytical-measurement performance of medical labora-tories (Herrera and Paras, 1983; Debertin and Schrader,1992; Woods et al., 1996; Szorenyi et al., 1998; Iwaharaet al., 2002; dos Santos et al., 2004; Oropesa et al., 2005).The technique has been demonstrated to be effective inevaluating individual laboratory performance and identify-ing the presence of variances related to instrumentperformance and technical procedures. The test describedin this paper represents a pilot exercise designed not only toassess the current state-of-the-art in measurement capabil-ities of nuclear medicine facilities in the US, but also toevaluate the feasibility of implementing an ongoingprogram for these institutions. In evaluating the successof the present pilot test, certain drawbacks in the designand implementation (and possible solutions to the difficul-ties) must be pointed out.
Based on an analysis of the current test, definiteimprovements to the reporting format would be necessaryfor a successful ongoing program. For example, althoughan attempt was made to capture the procedures used todetermine the reported values, the actual calibrationprocedure used for obtaining the dial settings used foractivity estimation by the participants was not asked forexplicitly. This hinders the ability of the organizers to assistparticipants in making necessary adjustments to calibrationprocedures on a timely basis. Successful MAPs demon-strate the need for continuous communication with theadministrators of the program (Herrera and Paras, 1983;Debertin and Schrader, 1992; Woods et al., 1996; Szorenyiet al., 1998; Iwahara et al., 2002; dos Santos et al., 2004;Oropesa et al., 2005). Most importantly, the infrastructurefor delivering a timely response to the participants must beimproved in order to rapidly identify difficulties inmeasurements and offer timely guidance for improvementsto be implemented.
5. Conclusions
A blind proficiency test was conducted to evaluate theperformance of nuclear medicine facilities in making dose-
calibrator measurements. The study was conducted byNIST in collaboration with the NANP, a commercialradioisotope manufacturer and 10 nuclear medicine facil-ities. Test-sample geometries were chosen to representtypical geometries used in preparing and dispensing theradiopharmaceutical 90Y-ZEVALINs. All test-sampleswere returned to NIST for activity verification andcertification. All reported values were within the 720%conformance limits published by the US NRC for definingtherapeutic dose misadministration. On the other hand,20% of reported values fell outside of the 710% contentlimits specified by USP for 90Y-ZEVALINs. An identifi-able negative bias was revealed for measurements of 90Y inthe syringe (�4%) and reaction vial (�6%) geometries.Participants indicated that calibration instructions wereprovided by the radiopharmaceutical manufacturer, butdetails for the precise method for determination of dialsetting (at individual sites) were not obtained. The averagebias of the reported results (RV and TS) fall withinacceptable limits (NRC and USP). All participantsreported that quality-control radioactivity standardsources (137Cs and 57Co) were measured prior to measure-ments performed for this test. Reporting forms indicatedthat quality-control acceptance criteria were met in allcases. Based on these results, no relationship can beestablished between the accuracy of 90Y radioactivitydeterminations (in the measurement geometries of the test)and the results of system performance tests conducted priorto measurements. Instructions provided for theNRQMP0305 performance test were prescriptive. It ispossible that unintended bias may have been introduceddue to instructed deviations from normal operatingprocedures of the participants. Future tests are to includea more detailed questionnaire that will enable theorganizers to evaluate more effectively the differencebetween routine procedures and performance testingsample measurements.This performance test can be considered a guide, within
which the value of an ongoing MAP for nuclear medicinepharmacies and clinics can be evaluated. Within thiscontext, clearly improvements can be made to the accuracyand precision of the composite of measurements conductedfor this test. An ongoing MAP, whereby measurementperformance of facilities is monitored on an ongoing basis(e.g., quarterly), may provide the necessary feedback forlaboratories to maintain accurate calibrations for theradionuclides and measurement geometries performed intheir labs. On the other hand, for such a program to beeffective, the responsiveness of the administering organiza-tion must be rapid.
Disclaimer
This document summarizes a comparison test conductedby the National Institute of Standards and Technology(NIST) of 90Y measurements in two measurement geome-tries. The purpose of comparison testing is to foster

ARTICLE IN PRESSM.K. Schultz et al. / Applied Radiation and Isotopes 66 (2008) 252–260260
understanding of cross-laboratory variability of measure-ments and in no way implies recommendation of thematerials and methods included in this paper by NIST, nordoes it imply that the materials and methods identified arenecessarily the best available for the intended purpose.Participation in a single comparison test, such as the onedescribed in this paper, does not constitute traceability ofan institution or company to NIST, but rather representspart of an overall quality management system that relatesmeasurements to national standards.
References
Allen, B., Raja, C., Rizvi, S., et al., 2004. Targeted alpha therapy for
cancer. Phys. Med. Biol. 49 (16), 3703–3712.
Calhoun, J.M., 1987. Radioactivity calibrations with the 4p gamma
ionization chamber and other radioactivity calibration capabilities.
NBS Special Publication 250-10. National Bureau of Standards.
Library of Congress Catalog No. 87-619870.
Cavallo, L.M., Golas, D.B., Mann, W.B., 1979. The traceability program
for radiopharmaceuticals at the National Bureau of Standards. Atomic
Energy, 55–57.
Connors, J.M., 2005. Radioimmunotherapy—a hot new treatment for
lymphoma. N. Engl. J. Med. 352 (5), 496–498.
Debertin, K., Schrader, H., 1992. Intercomparisons for quality assurance
of activity measurements with radionuclide calibrators. Nucl. Instrum.
Methods A 312, 241–245.
dos Santos, J.A., Iwahara, A., de Oliveira, A.E., et al., 2004. National
intercomparison program for radiopharmaceutical activity measure-
ments. Appl. Radiat. Isot. 60, 523–527.
ENSDF, 2005. Evaluated Nuclear Structure Data File, /www.nndc.
bnl.gov/nndc/nudatS. United States Department of Energy National
Nuclear Data Center, Brookhaven National Laboratory, Upton, NY,
US.
Filliben, J.J., 1975. The probability plot correlation coefficient test for
normality. Technometrics 17 (1), 111–117.
Golas, D.B., 1982. Traceability programs for nuclear medicine. In:
Proceedings of a Meeting on Traceability for Ionizing Radiation
Measurements. National Bureau Standards Special Publication 609.
Library of Congress Catalog No. 81-600197, 99-110.
Golas, D.B., 1998. NIST Radiopharmaceutical Standard Reference
Materials and the NEI/NIST Radiopharmaceutical Measurement
Assurance Program. Appl. Radiat. Isot. 49 (4), 329–334.
Golas, D.B., Calhoun, J.M., 1983. US National Bureau of Standards
Atomic Industrial Forum Radioactivity Measurements Assurance
Program. Int. J. Nucl. Med. Biol. 10 (2–3), 163–168.
Herrera, N.E., Paras, P., 1983. Q-Series. The College of American
Pathologists Surveillance of activity (dose) calibrators. Int. J. Nucl.
Med. Biol. 10 (1-2), 107–110.
ISO, International Standards Organization, 1995. Guide to the Expression
of Uncertainty in Measurement. ISO, Geneva, Switzerland.
Iwahara, A., de Oliveira, A.E., Tauhata, L., et al., 2002. Performance of
dose calibrators in Brazilian hospitals for activity measurements. Appl.
Radiat. Isot. 56, 361–367.
Kossert, K., Schrader, H., 2004. Activity standardization by liquid
scintillation counting and half-life measurements of 90Y. Appl. Radiat.
Isot. 60, 741–749.
Maloney, D.G., Press, O.W., 1998. New treatments for non-Hodgkins
lymphoma: monoclonal antibodies. Oncology 12 (10), 63–76.
NCRP, 1985. Measurement assurance, standards, traceability and the
statement of uncertainty. A Handbook of Radioactivity Measure-
ments Procedures. NCRP Report No. 58. ISBN: 0-913392-71-5,
pp. 332–349.
NRC, 2005. US Nuclear Regulatory Commission, Code of Federal
Regulations. Medicinal Use of Bioproduct Material 10CFR (Part 35),
562–609.
Oropesa, P., Hernadez, A.T., Serra, R., Varela, C., 2005. Comparisons of
activity measurements with radionuclide calibrators—a tool for quality
assessment and improvement in nuclear medicine. Appl. Radiat. Isot.
63, 493–503.
Szorenyi, A., Vagvilgyi, J., Zsinka, A., 1998. Experiences of fifteen years
on metrological supervision of radionuclide calibrators used in nuclear
medicine. Appl. Radiat. Isot. 49 (9-11), 1459–1461.
Taylor, B.N., Kuyatt, C.E., 1994. Guidelines for evaluating and expressing
the uncertainty of NIST measurement results. NIST Technical Note
1297.
Thieme, K., Beinlich, U., Fritz, E., 2004. Transfer standard for beta
decay radionuclides in radiotherapy. Appl. Radiat. Isot. 60,
519–522.
USP, 2005. United States Pharmacopoeia. Yttrium Y-90 Ibritumomab
Tiuxetan Injection. USP28, Official Monograph, pp. 2044–2045.
Witzig, T.E., White, C.A., Gordon, L.I., Wiseman, G.A., Emmanoulides,
C., Murray, J.L., Lister, J., Multani, P.S., 2003. Safety of Yttrium-90
Ibritumomab Tiuxetan Radioimmunotherapy for relapse low-grade,
follicular, or transformed Non-Hodgkin’s lymphoma. J. Clin. Oncol.
21 (7), 1263–1270.
Woods, M.J., Keightley, J.D., Ciocanel, M., 1996. Intercomparison of67Ga solution sources in UK hospitals. National Physical Laboratory
Report CIRA(EXT)012. National Physical Laboratory, Centre for
Ionizing Radiation, Teddington, UK.
Zimmerman, B.E., Cessna, J.T., Millican, M.A., 2004. Experimental
determination of calibration settings for plastic syringes containing
solutions of 90Y using commercial dose calibrators. App. Radiat. Isot.
60, 511–517.

















![Understanding the solvatochromism of 10-hydroxybenzo[h]quinoline. An appraisal of a polarity calibrator](https://static.fdokumen.com/doc/165x107/63174024bc8291e22e0e2a62/understanding-the-solvatochromism-of-10-hydroxybenzohquinoline-an-appraisal-of.jpg)


