Co-Delivery of Eugenol and Dacarbazine by Hyaluronic Acid ...
Upload
independentCategory
view
0download
0
A new experimental model of glaucoma in rats through intracameral
injections of hyaluronic acid
Marıa Cecilia Morenoa, Hernan J. Aldana Marcosb, J. Oscar Croxattoc, Pablo H. Sandea,
Julieta Campanellia, Carolina O. Jaliffaa, Jorge Benozzia, Ruth E. Rosensteina,*
aLaboratorio de Neuroquımica Retiniana y Oftalmologıa Experimental, Departamento de Bioquımica Humana, Facultad de Medicina,
Universidad de Buenos Aires, Paraguay 2155, 5th floor, 1121 Buenos Aires, ArgentinabLaboratorio de Histologıa, Facultad de Medicina, Universidad de Moron, Pcia. de Buenos Aires, Buenos Aires, Argentina
cLaboratorio de Patologıa Ocular, Fundacion Oftalmologica Argentina ‘Jorge Malbran’, Buenos Aires, Argentina
Received 18 June 2004; accepted in revised form 13 January 2005
Available online 23 February 2005
Abstract
An experimental model of pressure-induced optic nerve damage would greatly facilitate the understanding of the cellular events leading to
ganglion cell death, and how they are influenced by intraocular pressure and other risk factors associated to glaucoma. The aim of the present
report was to study the effect of a long-term increase of intraocular pressure in rats induced by intracameral injections of hyaluronic acid with
respect to electroretinographic activity and retinal and optic nerve histology. For this purpose, hyaluronic acid was injected weekly in the rat
anterior chamber of one eye, whereas the contralateral eye was injected with saline solution. The results showed a significant decrease of
oscillatory potentials and a- and b-wave amplitude of the scotopic electroretinogram after 3 or 6 weeks of hyaluronic acid administration,
respectively. These parameters were further reduced after 10 weeks of treatment with hyaluronic acid. No significant changes in anterior
chamber angle structures from hyaluronic acid- and vehicle-injected eyes were observed, whereas a significant loss of ganglion cell layer
cells and of optic nerve axons were detected in animals that received hyaluronic acid for 10 weeks, as compared to eyes injected with saline
solution. In summary, present results indicate that the chronic administration of hyaluronic acid induced a significant decrease in the
electroretinographic activity and histological changes in the retina and optic nerve that seem consistent with some features of chronic open-
angle glaucoma. Therefore, this could be an experimental model to study the cellular mechanisms by which elevated intraocular pressure
damages the optic nerve and the retina.
q 2005 Elsevier Ltd. All rights reserved.
Keywords: hyaluronic acid; intraocular pressure; electroretinography; glaucoma; ganglion cells; optic nerve
1. Introduction
Although the pathogenesis of optic neuropathy in
glaucoma is still elusive, increased intraocular pressure
(IOP) is probably the most important risk factor in primary-
angle open glaucoma. In fact, nearly all glaucoma therapy
relies on lowering IOP. The trabecular meshwork in the
anterior chamber angle is thought to play a key role in
0014-4835/$ - see front matter q 2005 Elsevier Ltd. All rights reserved.
doi:10.1016/j.exer.2005.01.008
* Corresponding author. Dr Ruth E. Rosenstein, Laboratorio de
Neuroquımica Retiniana y Oftalmologıa Experimental, Departamento de
Bioquımica Humana, Facultad de Medicina, Universidad de Buenos Aires,
Paraguay 2155, 5th floor, 1121 Buenos Aires, Argentina.
E-mail address: [email protected] (R.E. Rosenstein).
the regulation of aqueous outflow and IOP. It is composed of
sheets of trabecular beams that contain lamellae made of
extracellular matrix materials, which comprise a significant
portion of this tissue and probably of the outflow barrier.
Among the materials of the trabecular extracellular matrix,
glycosaminoglycans (GAGs) profile (i.e. hyaluronic acid
(HA), keratan sulfate, heparan sulfate, and hybrid dermatan
sulfate–chondroitin sulfate) has been identified in rabbit
(Knepper et al., 1981), monkey, and human eyes (Acott
et al., 1985). Trabecular GAGs, particularly, have been
implicated in the modulation of outflow resistance as well as
in the development of glaucoma. In the trabecular mesh-
work obtained from patients with primary open-angle
glaucoma, several studies have noted excessive
Experimental Eye Research 81 (2005) 71–80
www.elsevier.com/locate/yexer

M.C. Moreno et al. / Experimental Eye Research 81 (2005) 71–8072
accumulation of extracellular matrix materials (Segawa,
1975; Rohen, 1983). In particular, a depletion of HA and the
accumulation of chondroitin sulfates were detected in
primary open-angle glaucoma trabecular meshwork
(Knepper et al., 1996). An abnormal accumulation of acid
mucopolysaccharides in the anterior chamber angle was
also reported in steroid-induced ocular hypertension
(Francois et al., 1984). Intense histochemical staining for
GAGs in the human trabecular meshwork suggests that a
substantial amount of HA is present in the outflow pathway
(Lerner et al., 1997) and a quantitative analysis indicated
that it is the most abundant GAG of the human trabecular
meshwork (Acott et al., 1985). In a previous report we
showed that brimonidine, a highly selective a2-adreno-
receptor agonist that decreases IOP, significantly increases
hyaluronidase activity in rabbit trabecular meshwork
(Benozzi et al., 2000). Based on these results, we suggested
that the effect of brimonidine in increasing outflow could be
mediated, at least in part, by its stimulation of hyaluronidase
activity, e.g. by increasing GAGs clearance. If a decrease of
GAGs content reduces IOP, it seems likely that an increase
of intracameral HA levels could induce the opposite effect.
In this sense, it was shown that the injection of HA into the
anterior chamber of rabbits and owl monkeys significantly
increases IOP (Harooni et al., 1998; Schubert et al., 1984).
However, while in these species the effect of HA lasts for
relatively short periods (70 and 24 hr post-injection in rabbit
and owl monkeys, respectively), we showed that a single
injection of HA maintains elevated levels of IOP for 8 days,
while an injection performed once a week induces a
sustained and significant hypertension that lasts all along
the duration of the study (10 weeks) (Benozzi et al., 2002).
The longer-lasting effect of a single injection of HA on IOP
could be attributed to the fact that the rat anterior chamber
being very shallow, the actual intracameral concentration of
HA is higher than that achieved in other species. In addition,
a poorer ability of HA washout in rats cannot be ruled out.
These results indicate that the injection of HA could be a
new model of ocular hypertension in rats.
It is well known that ocular hypertension plays a causal,
albeit not necessarily exclusive, role in glaucomatous visual
loss. In fact, not all models of ocular hypertension cause the
same disease at the level of the retina or the optic nerve.
Therefore, the aim of the present study was to examine the
effect of a long-term increase of IOP in rats induced by the
intracameral injection of hyaluronic acid (HA) on retinal
function and histology.
2. Materials and methods
2.1. Animals
Male Wistar rats (average weight 200G40 g) were
housed in a standard animal room with food and water
ad libitum under controlled conditions of humidity and
temperature (218G28C). The room was lighted by fluor-
escent lights, that were turned on and off automatically
every 12 hr, with the lights on from 6:00 a.m. to 6:00 p.m.
Rats were anaesthetized with ketamine hydrochloride
(50 mg kgK1) and xylazine hydrochloride (0.5 mg kgK1)
administered intraperitoneally. Using a Hamilton syringe
with a 30-gauge needle, 25 ml of HA (obtained from Sigma
Chemical Co., St Louis, MO, USA, catalog # H1751,
10 mg mlK1 in sterile saline solution) were injected weekly
into one eye of anaesthetized rats, while an equal volume of
vehicle (saline solution) was injected in the fellow (control)
eye. The eyes were focused under a binocular Colden
surgical microscope with coaxial light. The needle moved
through the corneoscleral limbus to the anterior chamber
with the bevel up. When the tip of the bevel reached the
anterior chamber, the liquid progressively increased the
chamber’s depth, separating the needle from the iris and
avoiding needle–lens contact. Injections were applied at the
corneoscleral limbus beginning from hour 12 and changing
the site of the next injection from hour to hour by rotating
the head to achieve better access to the limbus. The
injections and IOP assessments were performed after
applying one drop of 0.5% proparacaine hydrochloride to
each eye. Of 48 rats, three showing cataract were excluded
from the experiments. In addition, almost all the animals
developed a localized corneal edema at the site of the
injection that lasted less than 24 hr.
2.2. IOP assessment
A TonoPen XL (Mentor, Norwell, MA) tonometer was
used to assess IOP in conscious, unsedated rats as described
by Moore et al. (1995). All IOP determinations were
assessed by operators who were blind with respect to the
treatment applied to each eye. Animals were wrapped in a
small towel and held gently, with one operator holding the
animal and another making the readings. Five IOP readings
were obtained from each eye by using firm contact with the
cornea and omitting readings obtained as the instrument was
removed from the eye. Differences among reading were less
than 10% (standard error). The mean of these readings was
recorded as the IOP for this eye and this day. Mean values
from each rat were averaged, and the resultant mean value
was used to compute the groups mean IOPGSE. HA was
injected once a week in one eye, whereas the other eye was
injected with saline solution. IOP was assessed weekly,
before the new injection. IOP measurements were per-
formed at the same time each day or week (between 11:00
and 12:00 hr) to correct for diurnal variations in IOP.
2.3. Electroretinography
Electroretinographic activity was assessed in dark-
adapted rats as follows: after 6 hr of dark adaptation, rats
were anaesthetized with an intraperitoneal injection of
ketamine hydrochloride and xylazine hydrochloride under

M.C. Moreno et al. / Experimental Eye Research 81 (2005) 71–80 73
dim red illumination. Phenylephrine hydrochloride (2.5%)
and 1% tropicamide (Alcon Laboratories, Argentina) were
used to dilate the pupils, and the cornea was intermittently
irrigated with balanced salt solution (Alcon Laboratories,
Argentina) to maintain the baseline recording and to prevent
exposure keratopathy. Rats were placed facing the stimulus
at a distance of 20 cm. All recordings were completed
within 20 min of the induction of anaesthesia and animals
were kept warm during and after the procedure. A reference
electrode was placed through the ear, a grounding electrode
was attached to the tail, and a gold electrode was placed in
contact with the central cornea. A 15 W red light was used
to enable accurate electrode placement. This maneuver did
not significantly affect dark adaptation and was switched off
during the electrophysiological recordings. Electroretino-
grams (ERGs) were recorded from both eyes simultaneously
and 10 responses to flashes of unattenuated white light
(5 ms, 0.2 Hz) from a photic stimulator (light-emitting
diodes) set at maximum brightness (350 cd sec mK2 with-
out a filter) were amplified, filtered (1.5-Hz low-pass filter,
1000 high-pass filter, notch activated) and averaged (Akonic
BIO-PC, Akonic, Argentina). The a-wave was measured as
the difference in amplitude between the recording at onset
and the trough of the negative deflection and the b-wave
amplitude was measured from the trough of the a-wave to
the peak of the b-wave. Electrophysiological responses were
averaged for each run. Runs were repeated three times with
5 min intervals, to confirm consistency and the mean of
these three runs was used for subsequent analysis. The mean
peak latencies and peak-to-peak amplitudes of the responses
from each group of rats were compared. Oscillatory
potentials (OPs) were assessed as described by Bayer
et al. (2001a). Briefly, the same photic stimulator with a
0.2 Hz frequency and filters of high (300 Hz) or low
(100 Hz) frequency were used. The amplitudes of the OPs
were estimated by measuring the heights from the baseline
drawn between the troughs of successive wavelets to their
peaks. The sum of three OPs was used for statistical
analysis. ERGs were performed 3 days after the injection of
HA or vehicle and they were assessed by operators who
were blind with respect to the treatment applied to each eye.
2.4. Light microscopy
At 10 weeks of treatment with HA or vehicle, eight
eyes/group were analyzed by light microscopy. Eyes were
enucleated after anaesthetic overdose and immersed
immediately in a fixative containing 4% paraformaldehyde
and 1% glutaraldehyde in 0.1 M phosphate buffer (pH 7.2)
for 1 hr. The nictitans membrane was maintained in each
eye to facilitate orientation. The cornea and the lens were
carefully removed, and the posterior portions were fixed for
an additional 12-hr period in the same fixative. A cross-
section of the optic nerve from control and HA-treated eyes
was removed 1.5 mm posterior to the globe and post-fixed in
1% osmium tetroxide in phosphate buffer. Nerves were
processed into epoxy resin, sectioned at 1 mm, and stained
with 1% toluidine blue. Eyecups were dehydrated in an
alcohol series, and embedded in paraffin. Sections (4 mm
thick) were cut along the horizontal meridian through the
optic nerve head and stained with haematoxylin and eosin.
In addition, three whole eyes were fixed for 12 hr in B4-G
(6% HgCl2 and 0.1% glutaraldehyde in 1% sodium acetate).
The latter mixture was considered to be a good fixative for
tissues containing glycoconjugates (Spicer and Schulte,
1992). The eyes were routinely processed with paraffin for
histological and histochemical studies of the anterior
segment. For histological details Masson trichrome staining
was used. The histochemical characterization of HA was
performed using Alcian Blue 8G stain (Kiernan, 2003). A
hyaluronidase digestion technique was used to detect HA.
For the hyaluronidase digestion procedure, 50 mg of bovine
testicular hyaluronidase (Sigma Chemical Co., St Louis,
MO, USA) were diluted in 100 ml phosphate-buffered
saline solution. Each section was incubated in this solution
for 1 hr at 378C. Then, sections were stained with Alcian
Blue (pH 2.5). HA was detected by comparing the sections
without digestion with those with digestion.
2.5. Image analysis
Microscopic images were digitally captured with a Nikon
Eclipse E400 microscope (illumination: 6-V halogen lamp,
20 W, equipped with a stabilized light source) via a Sony
SSC-DC50 camera. The microscope was set up properly for
Koehler illumination. The camera output was digitized into
a 520!390 pixel matrix (each pixel with 0–255 grey levels)
with a Leadteckw WinView 601 video capture card,
displayed on a computer monitor and saved as an image
of 24 bit RGB in BMP format. The digitalized images were
transferred to a Scion Image for Windows analysis system
(Scion Corporation Beta 4.0.2).
2.6. Eye cups analysis
Retinal morphometry was evaluated as described by
Takahata et al. (2003) with minor modifications. Three
sections were randomly selected from each eye. Nine
microscopic images at 1 mm from the temporal edge of the
optic disc were digitally analyzed. The light microscope was
adjusted to level 4 and a 40! CF E achromat objective was
used. At the magnification utilized, each pixel of the image
corresponds to 0.31 mm, and each field in the monitor
represented a tissue area of 19 318.7 mm2. The thickness
(in mm) of the inner plexiform layer (IPL), inner nuclear
layer (INL), outer nuclear layer (ONL), and total retina was
measured. The number of cells in the ganglion cell layer
(GCL) was calculated by linear cell density (cells per
100 mm). For each eye, results obtained from three separate
sections were averaged and the mean of five eyes was
recorded as the representative value for each group. No
attempt was made to distinguish cell types in the GCL for

0
5
10
15
20
25
intr
aocu
lar
pre
ssu
re (
mm
Hg
)
vehicle HA
6 weeks 10 weeks
vehicle vehicleHA HA
3 weeks
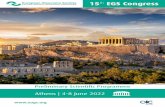
Fig. 1. Tonopen measurements of IOP in rats injected with HA in one eye
and vehicle in the contralateral eye for 3, 6, or 10 weeks. At all these
intervals, HA induced a significant increase in this parameter. No
differences were observed in control eyes among 3, 6, and 10 weeks of
treatment (ANOVA). Data are meanGSE (n, 20 eyes/group), **p!0.01,
by Student’s test.
M.C. Moreno et al. / Experimental Eye Research 81 (2005) 71–8074
enumeration of cell number. The morphometric analysis
was performed by observers masked to the protocol used in
each eye.
2.7. Optic nerve morphometry
Optic nerve axon counting was evaluated as described by
Levkovitch-Verbin et al. (2002) with minor modifications.
To measure the density and fibre diameter distributions,
images were captured with a 100! achromat objective from
10 spaced nerve regions (two central and eight peripheral in
a clockwise manner). The light microscope was adjusted to
level 6. At the magnification utilized, each pixel of the
image corresponds to 0.123 mm, and each field in the
monitor represented a tissue area of 3090.99 mm2. These
captured images were edited to eliminate non-axonal
images, and the size of each axon with its myelin sheath
(diameter) and the density of axons per square millimetre
were calculated for each image. The axon number/field in
the HA-treated groups was compared with the control
fellow eye. The number of axons counted in 10 images from
each nerve was approximately 10.6% of the total optic nerve
area. The counting process was performed by observers
masked to the protocol used in each nerve.
2.8. Statistical analysis
Statistical analysis of results was made by a Student’s
t-test or by a two-way analysis of variance (ANOVA)
followed by Student’s t-test or Dunnett’s test, as stated.
All animal use procedures were in strict accordance with
the ARVO Statement for the Use of Animals in Ophthalmic
and Vision Research.
3. Results
Fig. 1 shows the average IOP of 20 rats injected weekly
with HA (in one eye) or vehicle in the other during 3, 6, or
10 weeks. At all these intervals, a significant increase of IOP
was observed in eyes injected with HA, as compared with
the respective controls. The injection itself did not affect
IOP (data not shown), and no differences in the IOP of
vehicle-injected eyes were detected among these time-
points. In order to analyze the functional state of the retinas
from HA-injected eyes, scotopic ERGs were performed.
Representative scotopic ERG traces from rats injected with
vehicle or HA for 6 weeks are shown in the left panel of
Fig. 2A. The average amplitudes of scotopic ERG a- and
b-waves of 20 rats injected with vehicle in one eye and with
HA in the contralateral eye during the same interval are
depicted in the right panel of the same figure. These
parameters were significantly reduced in eyes receiving HA.
Similar studies were performed after 10 weeks of treatment
with HA or vehicle (Fig. 2B). Also in this case, a significant
reduction of ERG a- and b-waves amplitude was observed in
the eyes injected with HA. The treatment with HA for 6 or
10 weeks did not affect a- and b-wave latencies, as
compared with animals injected with vehicle. After
3 weeks of HA or vehicle treatment, no changes in ERG
a- and b-waves amplitude were detected (data not shown).
In contrast, the sum of the scotopic ERG OP amplitudes was
significantly reduced at all times of treatment with HA, as
shown in Fig. 3. The injection itself did not affect
the electroretinographic response, since no changes in
ERG a- and b-waves or OPs amplitude were observed
between vehicle-injected and intact eyes (Figs. 2 and 3).
Fig. 4A shows a light microscopy analysis of a
representative anterior chamber angle from rats treated
during 10 weeks with HA. The anterior chamber angle and
outflow structures were conserved and looked similar in
both HA-injected and control animals. In all eyes, the
anterior chamber angle was open. No significant differences
in the morphology of the iris, ciliary body, and ciliary
processes were observed between HA-injected and control
eyes. The histochemical staining method for HA revealed
the presence of irregular granular masses alcian blue
positive associated with the trabecular meshwork in the
eyes of rats treated with HA (Fig. 4B) but not in vehicle-
injected eyes (data not shown). The positive reaction in the
granular masses was abolished with the previous digestion
treatment with hyaluronidase, indicating the presence
of HA.
The only significant changes were observed in the retina
and the optic nerve from rats injected with HA for 10 weeks.

Fig. 2. Scotopic ERGs in rats injected with HA or vehicle. (A) Animals were weekly injected with HA in one eye or saline solution in the contralateral eye
during 6 weeks. (B) Effect of a 10-weeks treatment with HA or vehicle. In both cases left panels, representative scotopic ERG traces; right panels, average
amplitudes of scotopic ERG a- and b-waves. A significant reduction in the amplitude of both scotopic ERG a- and b-wave amplitude was observed in eyes
injected with HA for 6 and 10 weeks. No changes between intact and vehicle injected eyes were observed. Data are meanGSE (n, 20 eyes/group), *p!0.05,
**p!0.01 by Student’s test.
M.C. Moreno et al. / Experimental Eye Research 81 (2005) 71–80 75
Although total retinal, IPL, INL and ONL thickness did not
change between vehicle- or HA-injected eyes (control
132G7, 32.2G5, 22.2G3.5, 37.1G3; HA 123G12, 30.6G3.5, 19.4G2.3, 33.5G4.7 for total retinal, IPL, INL and
ONL width, respectively) a significant loss of GCL cells in
HA-injected eyes for 10 weeks was observed (Fig. 5). The
mean number/100 mmGSE of GCL cells from the control
group was 8.7G0.7, whereas in HA-injected eyes, it was
5.2G0.6 (p!0.01). The optic nerve from eyes treated with
HA for 10 weeks exhibited an overall loss of staining
uniformity and integrity (Fig. 6). Axons in control optic
nerve were generally uniform in shape (rounded) and
showed a variable size. In contrast, in HA-treated eyes,
spacing between bundles of axons increased by an apparent
development of glial profiles, glial nuclei, and axon loss.
Individual axons of treated optic nerve also exhibited
distention and distortion that resulted in a departure from the
circular morphology of normal axons. This loss of
uniformity at the level of individual axons and the
prominence of glial profiles and nuclei probably underlies
the overall loss of staining uniformity and nerve integrity.
To compare the loss of axons by diameter, the number of

Fig. 3. OPs in intact rats or injected with HA or vehicle for 3, 6, or 10 weeks. Left panels, representative OPs traces; right panels, average amplitudes of OPs in
intact animals or injected with HA or vehicle. The differences in sum of scotopic ERG OP amplitudes between vehicle and HA-injected eyes were significant at
all times of measurement. No changes between intact and vehicle injected eyes were observed. Data are meanGSE (n, 10 eyes/group), *p!0.05, **p!0.01 by
Student’s test.
Fig. 4. (A) Section of the anterior portion of an eye injected with HA for 10 weeks showing the cornea (C), iris (I), ciliary body with ciliary processes (CB) and
zonule filaments (Z). Note that the anterior chamber including the trabecular meshwork had not signs of damage. Masson trichrome. (B) The histochemical
staining method for HA revealed the presence of irregular granular masses alcian blue positive associated with the fine connective strands of the trabecular
meshwork (arrows). Alcian blue.
Fig. 5. Light micrographs of transverse sections of a retina from a rat, in which one eye was injected with saline solution (A) and the contralateral eye was
injected with HA during 10 weeks (B). Note the diminution of ganglion cell layer (GCL) cells in the eye injected with HA. The other retinal layers showed a
normal appearance. IPL, inner plexiform layer; INL, inner nuclear layer; OPL, outer plexiform layer; ONL, outer nuclear layer. Haematoxylin and eosin.
M.C. Moreno et al. / Experimental Eye Research 81 (2005) 71–8076

Fig. 6. Low- and high-magnification images of optic nerve cross-sections in control eye (A, C) and HA-treated eye (B, D). (A) Healthy, intact optic nerve. Note
the homogeneity of the staining. In (C) individual axons were generally uniform in shape (arrowhead), generally rounded and packed together tightly to form
the fibres of the healthy nerve. In the nerve of the treated eye (B) a less stained area (arrowhead) indicates a nerve alteration. At high-magnification (D) this area
is characterized by a prominence of glial profiles. Disease in individual axons was characterized by axonal distention and distortion that resulted in a departure
from the circular morphology of normal axons (arrowheads). There is a predominance of small-diameter axons. Toluidine blue.
M.C. Moreno et al. / Experimental Eye Research 81 (2005) 71–80 77
axons in each size group from 0.2 to 5 mm was compared in
both experimental groups (Fig. 7). A significant loss of large
and medium but not of small-diameter axons was observed.
4. Discussion
The foregoing results indicate that chronic injections of
HA in the rat anterior chamber induced significant retinal
changes both at functional and histological level, as
compared with the contralateral eye injected with vehicle.
In this sense, a significant decrease in the scotopic ERG
activity as well a significant damage confined to the GCL
and optic nerve axons were observed in HA-injected eyes.
In a previous report, we postulated that the intracameral
injection of HA could be a new model of ocular
hypertension in rats (Benozzi et al., 2002). Several groups
have developed different ways to increase IOP in the rat eye:
by injection of hypertonic saline into aqueous humour
collecting veins (Moore et al., 1993), by cautery and
occlusion of two or three of the episcleral/extraorbital veins
(Shareef et al., 1995), or by blockage of aqueous pathway
caused by photocoagulation after injection of India ink into
anterior chamber of the eye (Ueda et al., 1998). Several
advantages support the usefulness of our model: (1) it is
inexpensive and easy to perform, (2) a highly consistent
intraocular hypertension may be achieved, (3) it may have a
reasonably long course, and (4) daily variations in IOP
persisted in HA-injected eyes. In contrast to the model of
veins cautery, in all likelihood, HA does not impede the
blood flow out of the eye. Furthermore, we have demon-
strated that this model may also be useful for pharmaco-
logical studies with drugs that affect aqueous outflow,
formation, or a combination of both (Benozzi et al., 2002).
Although multiple injections of HA may be needed to obtain
a sustained hypertension, we have demonstrated that the
procedure of injection itself does not affect IOP.
To assess retinal function, scotopic flash ERGs were
performed in the eyes from animals injected chronically
with HA or vehicle since the rat has a predominantly

0
200
400
600
nu
mb
er o
f ax
on
s
axon diameter (µm)
0.05 - 0.2 0.2 - 0.4 0.4- 0.6
vehicle HA vehicle HA vehicle HA
Fig. 7. Axonal diameter distribution in eyes injected with vehicle or HA
during 10 weeks. A significant decrease in the number of middle and large
but not small axons was observed in HA-injected eyes. Data are meanGSE
(n, 8 eyes/group), **p!0.01, by Student’s test.
M.C. Moreno et al. / Experimental Eye Research 81 (2005) 71–8078
rod-retina. As shown herein, a significant reduction of OPs
as well as the a- and b-wave amplitude but not of their
latencies was observed in HA-injected eyes. The pattern
electroretinogram (PERG), a direct indicator of retinal
ganglion cell function, has become accepted as a sensitive
test for detecting early functional changes in glaucoma. In
contrast to the PERG, the flash ERG has been viewed
traditionally as reflecting activity of retinal neurons distal to
the ganglion cells and to be relatively unaffected in
glaucoma (Korth, 1997; Graham and Klistorner, 1998).
However, more recently, flash ERG was successfully
introduced as a non-invasive procedure to monitor the
progression of pathophysiology in a rat glaucoma model
(Bayer et al., 2001a). From a practical standpoint, the
uniform field ERG is easier to record than the PERG,
because it does not require refractive correction or exact
foveal placement. Together with similar reports on ERG
findings in subjects with advanced open-angle glaucoma
(Fazio et al., 1986; Holopigian et al., 1990; Korth et al.,
1994; Velten et al., 2001a,b), several observations support
the fact that in experimental models of glaucoma some
components of the flash ERG, such as scotopic ERG
amplitude, can be affected. In this sense, in the three-vein
episcleral/limbal vein occlusion model for inducing glau-
comatous pathology in the rat eye, a significant decrease of
OPs and the a- and b-wave amplitude was observed (Bayer
et al., 2001a). Similar changes in ERG a- and b-waves were
described in DBA/2 mouse with angle-closure glaucoma
(Bayer et al., 2001b). Furthermore, Viswanathan et al.
(2000) showed changes in the uniform field ERG that
correlate with PERG responses produced by a laser-induced
glaucoma in monkeys. More recently, a significant
reduction of scotopic b-wave amplitude was described in
Brown Norway rats with hypertonic saline injection into an
episcleral vein (Chauhan et al., 2002). The retinal dysfunc-
tion described herein seems to be time of hypertension-
dependent. Only OPs decreased at 3 weeks of ocular
hypertension, whereas changes in a- and b-wave amplitude
began at 6 weeks of treatment with HA. In both cases, a
higher decrease in these parameters was observed at 10
weeks as compared to 6 weeks of ocular hypertension. It
should be noted that before the injections of HA or vehicle,
in control experiments we had ascertained that flash ERGs
in the two eyes of the rats were very similar. Thus, the
different records between treated and control eyes are valid
indicators of the effects of the chronic ocular hypertension.
The present findings on flash ERG changes in rats with
chronic ocular hypertension strengthens the suggestions
from previous studies that the full-field ERG could serve as
a useful alternative in the assessment of glaucomatous
neuropathy, particularly in experimental models. Moreover,
in agreement with Bayer et al. (2001a) these results further
support that OPs constitute the earliest significant change,
and therefore it probably could be the best predictor of
glaucomatous neuropathy.
As for the histological analysis, the eye’s general
architecture was relatively unaffected by the treatment
with HA. Conceivably, chronic intracameral injections per
se could cause some degree of chamber angle constriction.
However, the histopathologic examination indicated that
it was not the case in our experimental setting, since a
normal angle was observed in both HA- and vehicle-
injected eyes. In contrast, differences were observed at
retinal level at 10 weeks of treatment with HA. While no
changes were observed in IPL, INL, and ONL, a significant
loss (y40%) was observed in GCL cells. These data on
ganglion cell loss are in agreement with results obtained by
other groups using different methodologies to induce
experimental glaucoma (Naskar et al., 2002; Grozdanic
et al., 2003).
In control eyes, morphology compatible with a healthy,
intact optic nerve was observed. Individual axons were
generallyuniforminshapeandpackedtogether tightly toform
the fibres of the nerve. In contrast, an overall loss of nerve
integrity as well as an alteration of axons shape was observed
in hypertensive eyes. In addition, a significant decrease in
axon number was evident, being large axons significantly
more vulnerable than small-diameter fibres. Since no shift of
axonal diameter distribution to smaller sizes was evident in
HA-injected eyes, it seems unlikely that this result may be
attributable to axons shrinkage. This loss of uniformity at the
levelof individual axons probablyunderlies the overall loss of
uniformity and nerve integrity. In agreement, a preferential
loss of large optic nerve axons was demonstrated in other
modelsof rat andmonkeyexperimentalglaucoma(Glovinsky
et al., 1991; Levkovitch-Verbin et al., 2002).

M.C. Moreno et al. / Experimental Eye Research 81 (2005) 71–80 79
The correlation between retinal histology and ERG
response in the eyes injected with HA is not completely well
understood. The a-wave of the flash ERG is classically
thought to represent photoreceptor activity, whereas the
b-wave reflects bipolar and Muller cells function. Although
glaucoma is known to cause primary death of ganglion cells,
there is also morphological evidence for damage to the outer
retina (Panda and Jomas, 1992). Swelling and loss of
photoreceptors were found in human and monkey glauco-
matous eyes (Nork et al., 2000). In addition, changes in
Muller cells in glaucomatous eyes were reported (Wang
et al., 2002). Since, as mentioned before, the components of
the ERG have been shown to be affected in some patients
with glaucoma, it seems possible either that, at least in some
cases, glaucoma affects retinal cells besides ganglions cells
or that there is a component of the ERG that reflects the
activity of these cells. Although no significant major
morphological changes of photoreceptors were found in
the eyes injected with HA, this evidence does not detract the
possibility of a functional impairment in these cells that
could explain the ERG findings described herein. Glutamate
is the main excitatory neurotransmitter in the retina but it
can be toxic to retinal ganglion cells in animal models when
administered at non-physiological concentrations (Vorwerk
et al., 1996). Several lines of evidence support that
abnormalities of glutamate metabolism play a causal role
in glaucomatous neurotoxicity (Dreyer et al., 1996; Brooks
et al., 1997). Since glutamate is necessary for light-elicited
signalling between photoreceptors and their target cells, it
seems likely that an alteration of glutamatergic neurotrans-
mission may affect other retinal layers besides its effect on
retinal ganglion cells. This hypothesis is under current
investigation. Moreover, since measuring the scotopic
threshold response (STR) in addition to the standard
a- and b-waves could provide information on the magnitude
of functional damage to third-order retinal neurons, the
assessment of this parameter in HA-treated eyes will be
performed in the near future.
Whether the histologic and functional retinal changes
observed are merely consequence of a toxic effect of HA per
se or, alternatively, they are a hypertension triggered
process is not clear. However, while HA was detected in
the anterior chamber of HA-injected eyes, no histological
evidences were found that support the possibility that this
GAG injected in the anterior chamber may reach the retina
or the optic nerve head. In addition, since no loss of the
midretinal architecture (the area supplied by retinal arteries)
was evident, it seems improbable that the HA-induced
hypertension could provoke a significant retinal ischaemia.
These evidences together with the fact that the changes
described herein are similar to those observed in other
glaucoma experimental models strongly suggest that they
are mostly attributable to the HA-induced hypertension.
Although considered the major risk factor for glaucoma
neuropathy, the cellular mechanisms by which elevated IOP
damages the optic nerve remain unknown. Acquiring this
knowledge relies heavily on the use of animal models of
chronically elevated IOP. The use of rodents allows
experimentation with sufficient number of animals and
could provide a complete picture of both ultrastructural
consequences and cell biology of pressure-induced optic
nerve damage. Based on both functional and histomorpho-
logic evidences, present results indicate that the intracam-
eral injection of HA appears to mimic some features of
primary open-angle glaucoma, and therefore it may be a
useful tool for understanding this ocular disease.
Acknowledgements
The authors wish to thank Drs Rafael Iribarren and Diego
Golombek, for the helpful discussion of this manuscript.
This research was supported by grants from Agencia
Nacional de Promocion Cientıfica y Tecnologica
(ANPCyT), Sigma Xi, Fight for Sight Research Division
of Prevent Blindness America, and by the ‘Ramon Carrillo-
Arturo Onativia’ fellowship from the National Health
Office, Argentina.
References
Acott, T.S., Westcott, M., Passo, M.S., Van Buskirk, E.M., 1985.
Trabecular meshwork glycosaminoglycans in human and cynomolgus
monkey eye. Invest. Ophthalmol. Vis. Sci. 26, 1320–1329.
Bayer, A.U., Danias, J., Brodie, S., Maag, K.P., Chen, B., Shen, F.,
Podos, S.M., Mittag, T.W., et al., 2001a. Electroretinographic
abnormalities in a rat glaucoma model with chronic elevated intraocular
pressure. Exp. Eye Res. 72, 667–677.
Bayer, A.U., Neuhardt, T., May, A.C., Martus, P., Maag, K.P., Brodie, S.,
Lutjen-Drecoll, E., Podos, S.M., Mittag, T., et al., 2001b. Retinal
morphology and ERG response in the DBA/2NNia mouse model of
angle-closure glaucoma. Invest. Ophthalmol. Vis. Sci. 42, 1258–1265.
Benozzi, J., Jaliffa, C.O., Firpo Locoste, F., Weinberg Llomovatte, D.,
Keller Sarmiento, M., Rosenstein, R.E., 2000. Effect of brimonidine on
rabbit hyaluronidase activity. Invest. Ophthalmol. Vis. Sci. 41,
2268–2272.
Benozzi, J., Nahum, L.P., Campanelli, J.L., Rosenstein, R.E., 2002. Effect
of hyaluronic acid on intraocular pressure in rats. Invest. Opthalmol.
Vis. Sci. 43, 2196–2200.
Brooks, D.E., Garcia, G.A., Dreyer, E.B., Zurakowski, D., Franco-
Bourland, R.E., 1997. Vitreous body glutamate concentration in dogs
with glaucoma. Am. J. Vet. Res. 58, 864–867.
Chauhan, B.C., Pan, J., Archibald, M.L., LeVatte, T.L., Kelly, M.E.,
Tremblay, F., 2002. Effect of intraocular pressure on optic disc
topography, electroretinography, and axonal loss in a chronic pressure-
induced rat model of optic nerve damage. Invest. Ophthalmol. Vis. Sci.
43, 2969–2976.
Dreyer, E.B., Zurakowski, D., Schumer, R.A., Podos, S.M., Lipton, S.A.,
1996. Elevated glutamate levels in the vitreous body of humans and
monkeys with glaucoma. Arch. Ophthalmol. 114, 299–305.
Fazio, D.T., Heckenlively, J.R., Martin, D.A., Christensen, R.E., 1986. The
electroretinogram in advanced open-angle glaucoma. Doc. Ophthalmol.
63, 45–54.
Francois, J., Benozzi, J., Victoria-Troncoso, V., Bohyn, W., 1984.
Ultraestructural and morphometric study of corticosteroid glaucoma
in rabbits. Ophthalmic Res. 16, 168–178.

M.C. Moreno et al. / Experimental Eye Research 81 (2005) 71–8080
Glovinsky, Y., Quigley, H.A., Dunkelberger, G.R., 1991. Retinal ganglion
cell loss is size dependent in experimental glaucoma. Invest.
Ophthalmol. Vis. Sci. 32, 484–491.
Graham, S.L., Klistorner, A., 1998. Electrophysiology. A review of signal
origins and applications to investigating glaucoma. Aust. NZ
J. Ophthalmol. 26, 71–85.
Grozdanic, S.D., Betts, D.M., Sakaguchi, D.S., Allbaugh, R.A.,
Kwon, Y.H., Kardon, R.H., 2003. Laser-induced mouse model of
chronic ocular hypertension. Invest. Ophthalmol. Vis. Sci. 44,
4337–4346.
Harooni, M., Freilich, J.M., Abelson, M., Refojo, M., 1998. Efficacy of
hyaluronidase in reducing increases in intraocular pressure related to
the use of viscoelastic substances. Arch. Ophthalmol. 116, 1218–1221.
Holopigian, K., Seiple, W., Mayron, C., Koty, R., Lorenzo, M., 1990.
Electrophysiological and psychophysical flicker sensitivity in patients
with primary open-angle glaucoma and ocular hypertension. Invest.
Ophthalmol. Vis. Sci. 31, 1863–1868.
Kiernan, J.A., 2003. Carbohydrate histochemistry, Third Ed., In: Histo-
logical and Histochemical Methods: Theory and Practice Arnold,
London pp. 213–242.
Knepper, P.A., Farbman, A.I., Telser, A., 1981. Aqueous outflow pathway
glycosaminoglycans. Exp. Eye Res. 32, 265–277.
Knepper, P.A., Goossens, W., Palmberg, P.F., 1996. Glycosaminoglycan
stratification of the juxtacanalicular tissue in normal and primary open-
angle glaucoma. Invest. Ophthalmol. Vis. Sci. 37, 2414–2425.
Korth, M., 1997. The value of electrophysiological testing in glaucomatous
diseases. J. Glaucoma 6, 331–343.
Korth, M., Nguyen, N.X., Horn, F., Martus, P., 1994. Scotopic threshold
response and scotopic PII in glaucoma. Invest. Ophthalmol. Vis. Sci.
35, 619–625.
Lerner, L.E., Polansky, J.R., Howes, E.L., Stern, R., 1997. Hyaluronan in
the human trabecular meshwork. Invest. Ophthalmol. Vis. Sci. 38,
1222–1228.
Levkovitch-Verbin, H., Quigley, H.A., Martin, K.R., Valenta, D.,
Baumrind, L.A., Pease, M.E., 2002. Translimbal laser photocoagulation
to the trabecular meshwork as a model of glaucoma in rats. Invest.
Ophthalmol. Vis. Sci. 43, 402–410.
Moore, C., Milne, S., Morrison, J.C., 1993. A rat model of pressure-induced
optic nerve damage [ARVO Abstract]. Invest. Ophthalmol. Vis. Sci. 34,
1141 (Abstract nr 2158).
Moore, C.G., Epley, D., Milne, S.T., Morrison, J.C., 1995. Long-term non-
invasive measurement of intraocular pressure in the rat eye. Curr. Eye
Res. 14, 711–717.
Naskar, R., Wissing, M., Thanos, S., 2002. Detection of early neuron
degeneration and accompanying microglial responses in the retina of a
rat model of glaucoma. Invest. Ophthalmol. Vis. Sci. 43, 2962–2968.
Nork, T.M., Ver Hoeve, J.N., Poulsen, G.L., Nickells, R.W.,
Davis, M.D., Weber, A.J., Vaegan, Sarks, S.H., Lemley, H.L.,
Millecchia, L.L., et al., 2000. Swelling and loss of photoreceptors in
chronic human and experimental glaucomas. Arch. Ophthalmol. 118,
235–245.
Panda, S., Jonas, J.B., 1992. Inner nuclear layer of the retina in eyes with
secondary angle-block glaucoma. Ophthalmologe 89, 468–471.
Rohen, J.W., 1983. Why is intraocular pressure elevated in chronic simple
glaucoma? Ophthalmology 90, 758–769.
Schubert, H.D., Denlinger, J.L., Balazs, E.A., 1984. Exogenous Na-
hyaluronate in the anterior chamber of the owl monkey and its effect on
the intraocular pressure. Exp. Eye Res. 39, 137–152.
Segawa, K., 1975. Ultraestructural changes of the trabecular meshwork in
primary open glaucoma. Jpn. J. Ophthalmol. 19, 317–322.
Shareef, S.R., Garcia-Valenzuela, E., Salierno, A., Walsh, J., Sharma, S.C.,
1995. Chronic ocular hypertension following episcleral venous
occlusion in rats. Exp. Eye Res. 61, 379–382.
Spicer, S.S., Schulte, B.A., 1992. Diversity of cell glycoconjugates shown
histochemically: a perspective. J. Histochem. Cytochem. 40, 1–38.
Takahata, K., Katsuki, H., Kume, T., Nakata, D., Ito, K., Muraoka, S.,
Yoneda, F., Kashii, S., Honda, Y., Akaike, A., et al., 2003. Retinal
neuronal death induced by intraocular administration of a nitric oxide
donor and its rescue by neurotrophic factors in rats. Invest. Ophthalmol.
Vis. Sci. 44, 1760–1766.
Ueda, J., Sawaguchi, S., Hanyu, T., Yaoeda, K., Fukuchi, T., Abe, H.,
Ozawa, H., et al., 1998. Experimental glaucoma model in the rat
induced by laser trabecular photocoagulation after an intracameral
injection of India ink. Jpn. J. Ophthalmol. 42, 337–344.
Velten, I.M., Horn, F.K., Korth, M., Velten, K., 2001a. The b-wave of the
dark adapted flash electroretinogram in patients with advanced
asymmetrical glaucoma and normal subjects. Br. J. Ophthalmol. 85,
403–409.
Velten, I.M., Korth, M., Horn, F.K., 2001b. The a-wave of the dark adapted
electroretinogram in glaucomas: are photoreceptors affected? Br.
J. Ophthalmol. 85, 397–402.
Viswanathan, S., Frishman, L.J., Robson, J.G., 2000. The uniform field and
pattern ERG in macaques with experimental glaucoma: removal of
spiking activity. Invest. Ophthalmol. Vis. Sci. 41, 2797–2810.
Vorwerk, C.K., Lipton, S.A., Zurakowski, D., Hyman, B.T., Sabel, B.A.,
Dreyer, E.B., 1996. Chronic low dose glutamate is toxic to retinal
ganglion cells: toxicity blocked by memantine. Invest. Ophthalmol.
Vis. Sci. 37, 1618–1624.
Wang, X., Tay, S.S., Ng, Y.K., 2002. An electron microscopic study of
neuronal degeneration and glial cell reaction in the retina of
glaucomatous rats. Histol. Histopathol. 17, 1043–1052.
Copyright © 2022 FDOKUMEN