
Use of intravenous tissue plasminogen activator ... - CDC stacks
Upload
uhhospitalsCategory
view
0download
0
Bone Marrow Transplantation (2001) 28, 187–196 2001 Nature Publishing Group All rights reserved 0268–3369/01 $15.00
www.nature.com/bmt
Graft-versus-host disease
A multicenter, randomized, double-blind comparison of different dosesof intravenous immunoglobulin for prevention of graft-versus-hostdisease and infection after allogeneic bone marrow transplantation
DJ Winston1, JH Antin2, SN Wolff3, BE Bierer4, T Small5, KB Miller6, C Linker7, H Kaizer8,HM Lazarus9, FB Petersen10, MJ Cowan7, WG Ho11, JR Wingard12, GJ Schiller1, MC Territo1,J Jiao13, MA Petrarca13, and SA Tonetta13
1UCLA Center for the Health Sciences, Los Angeles, CA; 2Brigham and Women’s Hospital, Boston, MA; 3Vanderbilt UniversityMedical Center, Nashville, TN; 4Dana Farber Cancer Institute, Boston, MA; 5Memorial Sloan-Kettering Cancer Center, New York,NY; 6Tufts-New England Medical Center, Boston, MA; 7Cancer Research Center and Department of Pediatrics, University ofCalifornia at San Francisco, San Francisco, CA; 8Rush-Presbyterian-St Luke’s Medical Center, Chicago, IL; 9Case Western ReserveUniversity Hospital, Cleveland, OH; 10University of Utah Hospital, Salt Lake City, UT; 11St Joseph’s Hospital, Orange, CA; 12EmoryUniversity Cancer Center, Atlanta, GA; and 13Alpha Therapeutic Corporation, Los Angeles, CA, USA
Summary:
Intravenous immunoglobulin is approved for use inallogeneic bone marrow transplant recipients for pre-vention of graft-versus-host disease (GVHD) and infec-tions, but the minimally effective dose has not beenestablished. In this multicenter, randomized, double-blind trial, patients undergoing allogeneic marrowtransplantation were randomized to receive 100 mg/kg,250 mg/kg, or 500 mg/kg doses of intravenous immuno-globulin. Each dose was given weekly for 90 days andthen monthly until 1 year after transplant. Six hundredand eighteen patients were evaluated. Acute GVHD(grades 2–4) occurred in 39% of the patients (80 of 206)in the 100 mg/kg group, 42% of the patients (88 of 208)in the 250 mg/kg group, and in 35% of the patients (72of 204) in the 500 mg/kg group (P = 0.344). Amongpatients with unrelated marrow donors, a higher doseof intravenous immunoglobulin (500 mg/kg) was asso-ciated with less acute GVHD (P = 0.07). The incidencesof chronic GVHD, infection and interstitial pneumoniawere similar for all three doses of intravenous immuno-globulin. The dose of intravenous immunoglobulin alsohad no effect on the types of infection, relapse of hema-tological malignancy or survival. Except for more fre-quent chills (P = 0.007) and headaches (P = 0.015) inpatients given the 500 mg/kg or 250 mg/kg dose ofimmunoglobulin, adverse events were similar for allthree doses. These results suggest that 100 mg/kg, 250mg/kg, and 500 mg/kg doses of intravenous immuno-globulin are associated with similar incidences ofGVHD and infections in most allogeneic marrow trans-plants. These results should be considered when design-
Correspondence: Dr DJ Winston, Room 42–121 CHS, Department ofMedicine, UCLA Medical Center, Los Angeles, California 90095, USAReceived 5 October 2000; accepted 7 March 2001
ing cost-effective strategies for the use of intravenousimmunoglobulin in allogeneic marrow transplantsreceiving other current regimens for prophylaxis ofGVHD and infection. Bone Marrow Transplantation(2001) 28, 187–196.Keywords: immunoglobulin; graft-versus-host disease;infection
Intravenous immunoglobulin is frequently administered toallogeneic bone marrow transplant recipients to prevent ormodify graft-versus-host disease (GVHD), interstitial pneu-monia, and infections. This use is based upon the favorableresults of several randomized, controlled trials whichprompted a National Institutes of Health (NIH) consensuspanel to endorse the efficacy of intravenous immunoglob-ulin after allogeneic bone marrow transplantation.1–9 Ameta-analysis of these trials revealed significant reductionsin fatal cytomegalovirus (CMV) infections, CMV pneu-monia, non-CMV interstitial pneumonia, and transplant-related mortality among patients receiving prophylacticintravenous immunoglobulin.10 Three trials also found areduction of acute GVHD in recipients of intravenousimmunoglobulin.1,7,8 Nevertheless, due to concerns aboutthe high cost of large doses (500 mg/kg of body weight)of prophylactic intravenous immunoglobulin, the NIH con-sensus panel and other investigators emphasized the impor-tance of a clinical trial to determine the minimally effectivedose of intravenous immunoglobulin for prevention ormodification of GVHD and infections after allogeneic bonemarrow transplantation.9 For this reason, we performed amulticenter, double-blind trial comparing the immunomod-ulating and antimicrobial efficacy of three different dosesof intravenous immunoglobulin in patients undergoingallogeneic bone marrow transplantation.

Immunoglobulin therapy after marrow transplantDJ Winston et al
188
Bone Marrow Transplantation
Methods
Patients
Patients were eligible for the study if they satisfied the fol-lowing criteria: (1) undergoing allogeneic bone marrowtransplantation for a hematological malignancy or aplasticanemia; (2) 5 years of age or older; (3) receiving a pretrans-plant preparative regimen of cytotoxic chemotherapy and/orradiation therapy. Patients positive for antibody to humanimmunodeficiency virus-I (HIV-I), patients with docu-mented viral hepatitis or CMV disease, and patients withrenal failure (serum creatinine �3.0 mg/dl) or respiratoryfailure requiring mechanical ventilation were excluded.Similarly, any patient with a history of a previous bonemarrow or stem cell transplant was excluded. Informedconsent approved by the institutional review board ateach study center was obtained from each patient orresponsible relative.
Study drugs and design
Eligible patients were randomly assigned in a double-blindfashion to receive one of three different doses of intra-venous immunoglobulin (100 mg/kg, 250 mg/kg or 500mg/kg). The 500 mg/kg dose was a dose previously shownto be effective for reducing GVHD and infections after allo-geneic bone marrow transplantation.7 At the time this studywas initiated, there was considerable evidence from otherstudies that intravenous immunoglobulin was efficaciousfor modification of GVHD and prevention of infectiouscomplications after allogeneic bone marrow transplan-tation.1–8 In addition, the use of intravenous immunoglob-ulin in bone marrow transplant recipients had beenapproved by the Federal Drug Administration.11 Intra-venous immunoglobulin was part of the standard care at allthe centers participating in this trial. Thus, a control groupnot receiving intravenous immunoglobulin was notincluded in the study. Instead, this trial was designed todetermine whether a dose–response effect is associated withintravenous immunoglobulin in bone marrow transplantrecipients and whether lower, less costly doses of intra-venous immunoglobulin (250 mg/kg, 100 mg/kg) are aseffective as higher doses of intravenous immunoglobulin(500 mg/kg).
The first dose of intravenous immunoglobulin was givenon day −2 before transplant. After transplant, the intra-venous immunoglobulin was given every 7 days betweenday 0 and day 90 and then once monthly between day 90and day 360. Additional doses of the study intravenousimmunoglobulin were allowed during the trial only fortreatment of CMV disease or severe thrombocytopeniarefractory to platelet transfusions. The study intravenousimmunoglobulin was discontinued if one of the followingevents occurred: (1) serious adverse event definitely relatedto intravenous immunoglobulin; (2) another intravenousimmunoglobulin product was given; or (3) patient’sinability to continue in the study due to noncompliance withthe protocol or death.
Unselected lots of commercially available Venoglobulin-S (5%) (Alpha Therapeutic Corporation, Los Angeles, CA,
USA) were used in the study. The Venoglobulin-S was sup-plied as a 5% aqueous sterile solution in 50 ml glass vials(50 mg of immunoglobulin/ml). Blinding during the studywas maintained by administering each dose at the same vol-ume per patient’s weight (10 ml/kg) in three containers con-taining either intravenous immunoglobulin or 5% dextrose.
Transplantation regimen
Investigators at each study center were allowed to use pre-parative regimens of chemoradiotherapy and thoseimmunosuppressive agents for GVHD prophylaxis whichwere considered standard practice at their institution. Eachstudy center also used its own standard agents for preven-tion and treatment of infections. Cyclosporine, methotrex-ate, and corticosteroids were the most common drugs givenfor prevention of GVHD. For prophylaxis of bacterial, fun-gal, and viral infections, oral quinolones, nystatin, clotrima-zole, fluconazole, trimethoprim-sulfamethoxazole, acyclo-vir, ganciclovir, and CMV-seronegative blood productswere given. Treatment of GVHD consisted of increaseddoses of corticosteroids or cyclosporine, antithymocyteglobulin, or a combination of these agents.
Laboratory procedures
Complete blood counts with differential white blood cellcount and platelet count, blood urea nitrogen levels, serumcreatinine and uric acid determinations, and liver functionstudies (total bilirubin, aspartate aminotransferase, alanineaminotransferase, and alkaline phosphatase) were perfor-med at the time of study entry, within 24 h of the start ofeach infusion of intravenous immunoglobulin, at the timeof readmission to the hospital, and at the time of studycompletion. Serological tests for hepatitis B surface anti-gen, hepatitis C antibody (total, IgM and IgG), HIV anti-body, and CMV antibody (IgM and IgG) were obtained atthe time of enrollment into the study, and at the time ofcompletion of the study. Cultures for bacteria, fungi, andviruses, repeat serological tests for CMV IgM and IgG,chest radiographs, and tissue biopsies were done wheneverclinically indicated.
Definitions of GVHD and infections
The criteria for the diagnosis and grading of GVHD havebeen previously published.12,13 Each patient was evaluatedfor the absence (grades 0 and 1) or presence (grades 2 to4) of acute GVHD as well as chronic GVHD.
Bacteremia was defined as the isolation of a pathogenicorganism from at least one blood culture in association withfever or other signs of infection. Septicemia was diagnosedif a patient with bacteremia also had hypotension. Localinfections were defined as either microbiologically docu-mented (positive culture from a site with signs and symp-toms of infection) or clinically documented (signs andsymptoms of infection at a site with negative cultures). Thediagnosis of invasive fungal infection required either theisolation of a fungus from blood culture or the demon-stration of fungus in pulmonary secretions, lung tissue, orother organ tissue in association with signs and symptoms

Immunoglobulin therapy after marrow transplantDJ Winston et al
189of infection. A fungal infection was considered dissemi-nated if fungus was isolated from the blood or found byculture or histology in the tissues of multiple organs. Viralinfections were classified as either asymptomatic (positiveculture without signs or symptoms of infection) or sympto-matic (positive culture with clinical evidence of disease).Interstitial pneumonia was indicated by the presence ofinterstitial infiltrates on chest radiograph and hypoxemiawhich were inexplicable by pulmonary edema, septicemia,bacterial infection, or fungal infection. All classificationsof infections, GVHD, and adverse events were done in ablinded fashion.
Statistical analysis
Chi-square tests were used to compare differences in thedemographic data among the treatment groups. Compari-sons among treatment groups for the incidence of acuteGVHD were done by the Mantel–Haenszel test.14 Compari-sons of times to specific events were performed by usingKaplan–Meier estimates of survival distributions and thelog-rank test.15 Relative risks for infection and multivariateanalyses of risk factors for GVHD were done by the Coxproportional hazard model.16 Fisher’s exact test was usedto compare differences in adverse experiences among thetreatment groups. Except for nine patients who neverreceived the study intravenous immunoglobulin, all patientswere included in the efficacy analysis (intent-to-treatanalysis). An independent monitoring group evaluatedstudy data for safety.
The planned sample size for the trial was 526 patientsequally divided among the three treatment groups. Thissample size was based upon a test of treatment differencefor acute GVHD between the 100 mg/kg study group andthe 500 mg/kg study group and a test of equivalence foracute GVHD between the 250 mg/kg study group and the500 mg/kg study group.14 The sample size estimated forthe difference test was based on a two-sided test with aconfidence level of 95% and 80% power. The sample sizeestimated for the equivalence test was based on a two-sidedtest with a confidence level of 80% and 95% power. Theprocedure of Munoz and Rosner was used to obtain theseestimates.17 A sample size of 526 patients provided theopportunity to detect at sufficient power a difference in theproportion of patients without GVHD between the 100mg/kg and 500 mg/kg groups of 0.22 and a difference of0.16 between the 250 mg/kg and 500 mg/kg groups.
Results
Patient characteristics
From September 1991 to September 1995, a total of 627patients at 13 bone marrow transplant centers were enrolledin the study. Nine patients never received the study intra-venous immunoglobulin and were excluded from analysis.The characteristics of the other 618 patients who receivedone or more infusions of the study intravenous immuno-globulin are summarized in Table 1. Two hundred and sixpatients received the 100 mg/kg dose, 208 patients were
Bone Marrow Transplantation
given the 250 mg/kg dose, and 204 patients were given ahigh dose of 500 mg/kg. The three groups of patients weresimilar in terms of age, underlying disease, disease prog-nosis, marrow source, pretransplant preparative regimens,the types and doses of agents used for GVHD prophylaxis,and recipient/donor CMV antibody status. A greater num-ber of male patients were in the group given the 100 mg/kgdose (71%) than in the groups receiving the 250 mg/kgdose (56%) or the 500 mg/kg dose (58%) (P = 0.003).There were also more male/male donor/recipient sexmatches in the 100 mg/kg group (41% vs 32%, P = 0.05).Other donor/recipient sex matches were similar among thethree study groups. Approximately 80% of the patientswere 20 years of age or older, while about one-fourth of thepatients had unrelated donors. Advanced underlying diseasewas present in about one-half of the patients in eachtreatment group. Fifty-two to 56% of the patients wereseropositive for CMV antibody before transplant.
GVHD
Table 2 shows the incidences and severity of acute GVHDin the three treatment groups. Acute GVHD developed in39% of the patients in the 100 mg/kg group, 42% of thepatients in the 250 mg/kg group, and in 35% of the patientsin the 500 mg/kg group. These differences were not sig-nificant (P = 0.344). Kaplan–Meier estimates of the per-centage of patients in each group who did not have acuteGVHD also showed no significant differences among thethree treatment groups (Figure 1, P = 0.29). The incidencesof grades 3 and 4 GVHD were lowest among patientsreceiving the 500 mg/kg dose (18%), but these incidenceswere not significantly different from the incidences ofgrades 3 and 4 GVHD in the 100 mg/kg group (23%) andthe 250 mg/kg group (24%) (P = 0.33).
The effects of different doses of intravenous immuno-globulin on the development of acute GVHD were analyzedfurther in a Cox proportional hazards regression model inorder to adjust for other potential confounding factorsinfluencing the incidence of acute GVHD. The factorsincluded in the analysis were dose of intravenous immuno-globulin, age, sex, underlying disease, disease prognosis,marrow source (related, unrelated, HLA-identical, HLA-non-identical), donor–recipient sex match, pretransplantpreparative regimen, and method of GVHD prophylaxis (Tcell depletion, other regimens). The model demonstrated anincreased risk of developing acute GVHD in male patients(risk ratio = 1.461, P = 0.009), patients 20 years of age orolder (risk ratio = 1.509, P = 0.027), patients with an unre-lated donor (risk ratio = 2.125, P = 0.0001), and patientsnot receiving a T cell-depleted bone marrow transplant (riskratio = 3.037, P = 0.015). The dose of intravenous immuno-globulin was not a significant covariate in this model (riskratio = 0.925, P = 0.331). Similarly, when the Cox pro-portional hazards regression model was used to determinefactors influencing only grades 3 and 4 GVHD, male sex(risk ratio = 2.34, P = 0.0002), an unrelated donor (riskratio = 3.73, P = 0.0001), and transplantation withoutT cell depletion (risk ratio = 3.96, P = 0.036) were thesignificant risk factors.
Figure 2 shows the effects of different doses of intra-

Immunoglobulin therapy after marrow transplantDJ Winston et al
190
Bone Marrow Transplantation
Table 1 Patient characteristics
Characteristics Dose of intravenous immunoglobulin
100 mg/kg 250 mg/kg 500 mg/kg
Total No. of patients 206 208 204Median age (range), years 32 (5–58) 33 (5–61) 33 (5–57)Age groups
�20 years 41 (20%) 37 (18%) 40 (20%)�20 years 165 (80%) 171 (82%) 164 (80%)
SexMale 147 (71%)* 117 (56%) 119 (58%)Female 59 (29%) 91 (44%) 85 (42%)
Disease at transplantAcute leukemia 87 (42%) 86 (41%) 72 (36%)Chronic myelogenous leukemia 73 (35%) 70 (34%) 70 (34%)Lymphoma 10 (5%) 10 (5%) 16 (8%)Aplastic anemia 4 (4%) 17 (8%) 17 (8%)Other 28(14%) 25 (12%) 29 (14%)
Disease prognosisStandard riska 92 (45%) 94 (45%) 91 (44.5%)Advanced
Acute leukemia or lymphoma in second remission 29 (14%) 31 (15%) 21 (10%)Acute leukemia or lymphoma in third or greater remission 15 (7%) 17 (8%) 17 (8%)Refractory or relapsed acute leukemia or lymphoma 29 (14%) 31 (15%) 31 (15%)Chronic myelogenous leukemia in accelerated phase 8 (4%) 15 (7%) 15 (7%)Chronic myelogenous leukemia in blast crisis 5 (2%) 0 4 (2%)Myelodysplasia 18 (9%) 13 (6%) 16 (8%)Other 6 (3%) 4 (2%) 8 (4%)
Unknown 4 (2%) 3 (2%) 1 (0.5%)Marrow source
Related, HLA-identical 138 (67%) 144 (69%) 130 (64%)Related, HLA-nonidentical 13 (6%) 15 (7%) 24 (12%)Unrelated 55 (27%) 49 (24%) 50 (24%)
Donor/recipient sexMale/Male 85 (41%)** 66 (32%) 66 (32%)Male/Female 31 (15%) 43 (20.5%) 42 (21%)Female/Female 28 (14%) 48 (23%) 43 (21%)Female/Male 62 (30%) 50 (24%) 53 (26%)Unknown 0 1 (0.5%) 0
Preparative regimenChemotherapy + radiation 154 (75%) 152 (73%) 140 (68.5%)Chemotherapy alone 52 (25%) 56 (27%) 63 (31%)Radiation alone 0 0 1 (0.5%)
GVHD prophylaxisCyclosporine + methotrexate 94 (45%) 90 (43%) 91 (45%)Cyclosporine + methotrexate + corticosteroids 59 (29%) 75 (36%) 65 (32%)Cyclosporine + corticosteroids 18 (9%) 15 (7%) 20 (10%)Cyclosporine alone 24 (12%) 18 (9%) 19 (9%)T cell depletion 9 (4%) 8 (4%) 9 (4%)Other 2 (1%) 2 (1%) 0
CMV antibody status (patient/donor)Negative/negative 58 (28%) 65 (31%) 53 (26%)Negative/positive 32 (15%) 29 (14%) 31 (15%)Positive/negative 49 (24%) 48 (23%) 45 (22%)Positive/positive 61 (30%) 60 (29%) 70 (34%)Unknown 6 (3%) 6 (3%) 5 (3%)
GVHD = graft-versus-host disease; CMV = cytomegalovirus.*P = 0.003 vs 250 mg/kg and 500 mg/kg groups; **P = 0.05 vs 250 mg/kg and 50 mg/kg groups.aStandard risk: acute leukemia in first remission, chronic myelogenous leukemia in chronic phase, aplastic anemia.
venous immunoglobulin in patients with each of those riskfactors for acute GVHD identified in the Cox proportionalhazards regression model. These Kaplan–Meier estimatesof the percentage of patients without GVHD show thatpatients with unrelated donors had a lower incidence ofGVHD when receiving a higher dose of intravenousimmunoglobulin (500 mg/kg). Similarly, in very high-risk
marrow transplant patients with all four risk factors associa-ted with acute GVHD (male, 20 years of age or older, unre-lated marrow donor, marrow graft without T cell depletion),the 500 mg/kg dose of intravenous immunoglobulin is asso-ciated with the lowest incidence of GVHD (Figure 3).These differences, however, did not achieve statistical sig-nificance (P values of 0.07 and 0.06, respectively).

Immunoglobulin therapy after marrow transplantDJ Winston et al
191Table 2 Incidence of acute graft-versus-host disease (GVHD)
Characteristic Dose of intravenous immunoglobulin
100 mg/kg 250 mg/kg 500 mg/kg
Total No. of patients 206 208 204Patients with GVHD 80 (39%) 88 (42%) 72 (35%)*
Grade 2 33 (16%) 37 (18%) 34 (17%)Grade 3–4 47 (23%) 51 (24%) 38 (18%)
*P = 0.344 vs 100 mg/kg and 250 mg/kg groups.
���
��
��
��
��
������������������
�� ������������������
���
�����
����
�����
��
�� !
"
�!��!�!
�����#����$%&'%� ��#����"�����#����$%&'%� ��#����"�����#�����$%&'%� ��#����" ��#��(��
Figure 1 Time to development of acute graft-versus-host disease (grades2–4). Kaplan–Meier product limit estimates of survival distributions todevelopment of acute graft-versus-host disease (GVHD) in the 500 mg/kg,250 mg/kg and 100 mg/kg groups.
���
��
��
��
��
�� �� �� � �� � �� �� �� ��
�� ������������������
���
�����
����������
��
�� !
"
�����#����$%&'%� ��#����"�����#����$%&'%� ��#����"�����#�����$%&'%� ��#���" ��#��(��
���
��
��
��
��
�� �� �� � �� � �� �� �� ��
�� ������������������
���
�����
����������
��
�� !
"
�����#����$%&'%� ��#��"�����#����$%&'%� ��#���"�����#�����$%&'%� ��#�" ��#��(��
���
��
��
��
��
�� �� �� � �� � �� �� �� ��
�� ������������������
���
�����
����������
��
�� !
"
�����#����$%&'%� ��#����"�����#����$%&'%� ��#����"�����#�����$%&'%� ��#����" ��#��(��
���
��
��
��
��
�� �� �� � �� � �� �� �� ��
�� ������������������
���
�����
����������
��
�� !
"
�����#����$%&'%� ��#����"�����#����$%&'%� ��#����"�����#�����$%&'%� ��#����" ��#��(��
)������������
*�������+�+����� ,��-�.����+��������
��!�!��!
�!
��!��!
�!
�!�!
��!��!�!
/��� �������+
Figure 2 Time to development of acute graft-versus-host disease (grades 2–4) among patients with increased risk for acute graft-versus-host disease(male patients, age �20 years old, unrelated donors, or non T cell-depleted marrow graft). Kaplan–Meier product limit estimates of survival distributionsto development of acute graft-versus-host disease (GVHD) in the 500 mg/kg, 250 mg/kg and 100 mg/kg groups.
Bone Marrow Transplantation
���
��
��
��
��
������������������
�� ������������������
!
�!
��!
���
�����
����������
��
�� !
"
�����#����$%&'%� ��#���"�����#����$%&'%� ��#��"�����#�����$%&'%� ��#���" ��#��(��
Figure 3 Time to development of acute graft-versus-host disease (grades2–4) among patients with multiple risk factors for acute graft-versus-hostdisease (male patient, age �20 years old, unrelated donor, and non T cell-depleted marrow graft). Kaplan–Meier product limit estimates of survivaldistributions of time to development of acute graft-versus-host disease(GVHD) in the 500 mg/kg, 250 mg/kg and 100 mg/kg groups.
The incidence of chronic GVHD among the three treat-ment groups was also compared by both Kaplan–Meier sur-vival distributions and the Cox proportional hazards model.Only the 349 patients free of chronic GVHD before day100 after transplant and surviving 100 or more days wereincluded in these analyses. The factors included in the pro-portional hazards model were dose of intravenous immuno-globulin, age, sex, underlying disease, disease prognosis,marrow source, HLA identity, donor–recipient sex match,pretransplant preparative regimen, method of GVHDprophylaxis (T cell depletion, other regimens), and prior

Immunoglobulin therapy after marrow transplantDJ Winston et al
192
Bone Marrow Transplantation
���
��
��
��
��
�������������������
�� ������������������
���
�����
����������
��
�� !
"
�����#����$%&'%� ��#����"�����#����$%&'%� ��#���"�����#�����$%&'%� ��#����" ��#��(�
�!�!
��!
Figure 4 Time to development of chronic graft-versus-host disease.Kaplan–Meier product limit estimates of survival distributions of time todevelopment of chronic graft-versus-host disease (GVHD) in the 500mg/kg, 250 mg/kg and 100 mg/kg groups.
grade 2–4 acute GVHD. As shown in Figure 4, the cumulat-ive incidences of chronic GVHD in the 500 mg/kg group(42%) and 250 mg/kg group (42%) were lower than the53% incidence in the 100 mg/kg group, but this differencewas not statistically significant (P = 0.15). In the Cox pro-portional hazards model, the dose of intravenous immuno-globulin was not a significant covariate for development ofchronic GVHD (risk ratio = 0.85, P = 0.142). An increasedrisk for chronic GVHD was found in patients 20 years orolder (risk ratio = 1.88, P = 0.011) and in patients with anunrelated donor (risk ratio = 1.90, P = 0.002). Prior grade2–4 acute GVHD was not found to be a significant riskfactor (risk ratio = 1.14, P = 0.504).
Infection
Tables 3 and 4 summarize the types of infection in the threetreatment groups from day 0 to day 100 after transplant and
Table 3 Infections from day 0 to day 100 after transplant
100 mg/kg (n = 206) 250 mg/kg (n = 208) 500 mg/kg (n = 204)
No. of No. of Rate per 100 No. of No. of Rate per 100 No. of No. of Rate per 100patients infections patient days patients infections patient days patients infections patient days
Patient-days at risk 15681 15499 15099Any type of infection 157 (76%) 422 2.69 146 (70%) 428 2.76 163 (80%) 378 2.50Disseminated infection
Gram-negative bacteremia 20 (10%) 25 0.16 22 (11%) 25 0.16 24 (12%) 27 0.18Gram-positive bacteremia 34 (17%) 45 0.29 51 (25%) 66 0.42 47 (23%) 57 0.38Fungal 19 (9%) 21 0.13 27 (13%) 32 0.21 23 (11%) 28 0.18Total 62 (30%) 91 0.58 81 (39%) 123 0.79 79 (39%) 112 0.74
Local infectionGram-negative 33 (16%) 55 0.35 33 (16%) 50 0.32 33 (16%) 44 0.29Gram-positive 58 (28%) 106 0.67 51 (25%) 92 0.59 41 (20%) 68 0.45Fungal 60 (29%) 101 0.64 56 (27%) 102 0.66 58 (28%) 86 0.57Viral 27 (13%) 28 0.18 25 (12%) 25 0.16 22 (11%) 27 0.18Culture-negative 11 (5%) 14 0.09 18 (9%) 23 0.15 17 (8%) 19 0.12Total 102 (50%) 304 1.93 98 (47%) 292 1.88 103 (50%) 244 1.61
CMV infection 25 (12%) 27 0.17 12 (6%) 13 0.08 17 (8%) 22 0.14Sepsis syndrome 9 (4%) 10 0.06 8 (4%) 8 0.05 15 (7%) 15 0.10CMV disease 20 (10%) 21 0.13 10 (5%) 10 0.06 18 (9%) 18 0.12Interstitial pneumonia 5 (2%) 5 0.03 1 (0.5%) 1 0.01 2 (1%) 2 0.01Death from infection 23 (11%) 23 0.15 20 (10%) 20 0.13 24 (12%) 24 0.16
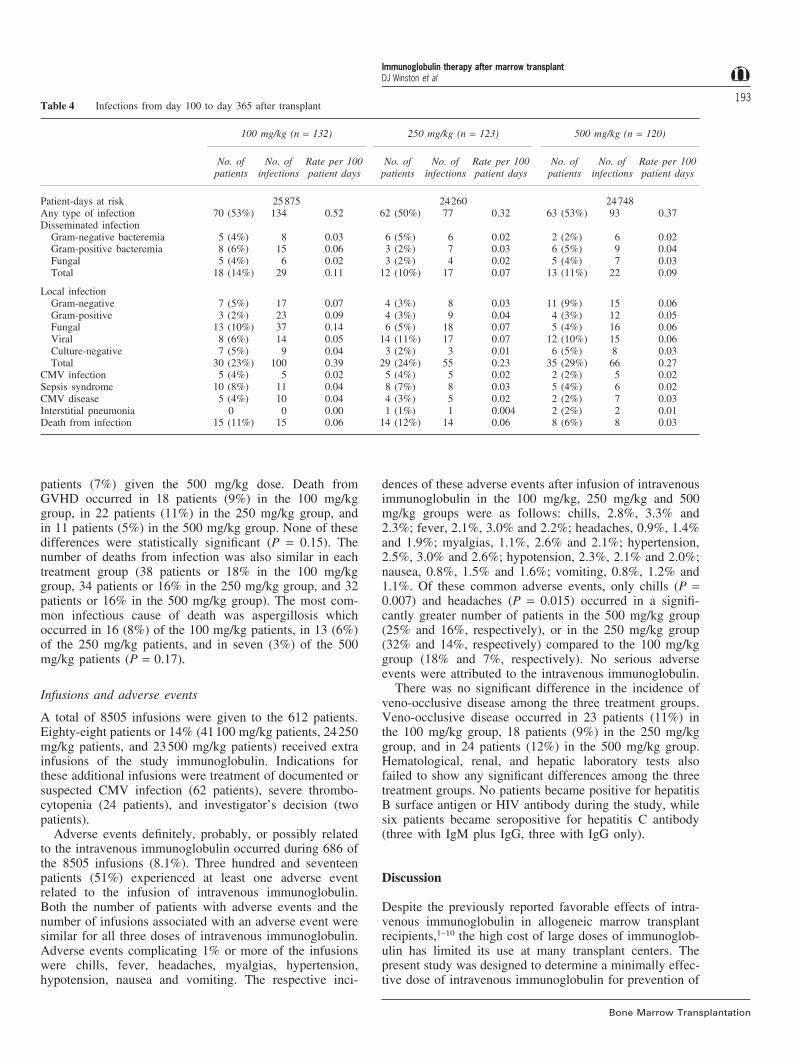
between days 100 and 365 after transplant. The overallrates of infection, the types of infection, and the numberof deaths from infection were similar for all three dosesof intravenous immunoglobulin both before day 100 aftertransplant and between days 100 and 365 after transplant.Of note, the incidence of CMV disease was 10% or less ineach treatment group before day 100 and between 2% and4% after day 100. There was a very low incidence of inter-stitial pneumonia (2% or less) associated with all threedoses of intravenous immunoglobulin. The rates and typesof infections during the early period of neutropenia (�500cells/mm3) immediately after transplant were also notsignificantly different among the three treatment groups.
Survival, relapse and mortality
All patients were followed for at least 1 year after enteringthe study or until the time of their death. Overall survivalat 1 year after transplant was 52% (107 of 206 patients) inthe 100 mg/kg group, 51% (106 of 208 patients) in the 250mg/kg group, and 52% (106 of 204 patients) in the 500mg/kg group (P = 0.997). Further analyses of survival ratesstratified by age (�20 years, �20 years), marrow source(related or unrelated), HLA-identity, disease prognosis, pre-transplant preparative regimen, and method of GVHDprophylaxis (T cell depletion, other regimens) also revealedno significant differences among the three treatment groups.
Most deaths in each treatment group were caused byrelapse of hematological malignancy, GVHD or infection.Among patients with a hematological malignancy, therelapse rate at 1 year after transplant was 10% (19 of 200patients) in the 100 mg/kg group, 9% (17 of 197 patients)in the 250 mg/kg group, and 9% (18 of 197 patients) inthe 500 mg/kg group. Relapsed disease was the cause ofdeath in 19 patients (9%) receiving the 100 mg/kg dose, in17 patients (8%) receiving the 250 mg/kg dose, and in 14
Immunoglobulin therapy after marrow transplantDJ Winston et al
193Table 4 Infections from day 100 to day 365 after transplant
100 mg/kg (n = 132) 250 mg/kg (n = 123) 500 mg/kg (n = 120)
No. of No. of Rate per 100 No. of No. of Rate per 100 No. of No. of Rate per 100patients infections patient days patients infections patient days patients infections patient days
Patient-days at risk 25875 24260 24748Any type of infection 70 (53%) 134 0.52 62 (50%) 77 0.32 63 (53%) 93 0.37Disseminated infection
Gram-negative bacteremia 5 (4%) 8 0.03 6 (5%) 6 0.02 2 (2%) 6 0.02Gram-positive bacteremia 8 (6%) 15 0.06 3 (2%) 7 0.03 6 (5%) 9 0.04Fungal 5 (4%) 6 0.02 3 (2%) 4 0.02 5 (4%) 7 0.03Total 18 (14%) 29 0.11 12 (10%) 17 0.07 13 (11%) 22 0.09
Local infectionGram-negative 7 (5%) 17 0.07 4 (3%) 8 0.03 11 (9%) 15 0.06Gram-positive 3 (2%) 23 0.09 4 (3%) 9 0.04 4 (3%) 12 0.05Fungal 13 (10%) 37 0.14 6 (5%) 18 0.07 5 (4%) 16 0.06Viral 8 (6%) 14 0.05 14 (11%) 17 0.07 12 (10%) 15 0.06Culture-negative 7 (5%) 9 0.04 3 (2%) 3 0.01 6 (5%) 8 0.03Total 30 (23%) 100 0.39 29 (24%) 55 0.23 35 (29%) 66 0.27
CMV infection 5 (4%) 5 0.02 5 (4%) 5 0.02 2 (2%) 5 0.02Sepsis syndrome 10 (8%) 11 0.04 8 (7%) 8 0.03 5 (4%) 6 0.02CMV disease 5 (4%) 10 0.04 4 (3%) 5 0.02 2 (2%) 7 0.03Interstitial pneumonia 0 0 0.00 1 (1%) 1 0.004 2 (2%) 2 0.01Death from infection 15 (11%) 15 0.06 14 (12%) 14 0.06 8 (6%) 8 0.03
patients (7%) given the 500 mg/kg dose. Death fromGVHD occurred in 18 patients (9%) in the 100 mg/kggroup, in 22 patients (11%) in the 250 mg/kg group, andin 11 patients (5%) in the 500 mg/kg group. None of thesedifferences were statistically significant (P = 0.15). Thenumber of deaths from infection was also similar in eachtreatment group (38 patients or 18% in the 100 mg/kggroup, 34 patients or 16% in the 250 mg/kg group, and 32patients or 16% in the 500 mg/kg group). The most com-mon infectious cause of death was aspergillosis whichoccurred in 16 (8%) of the 100 mg/kg patients, in 13 (6%)of the 250 mg/kg patients, and in seven (3%) of the 500mg/kg patients (P = 0.17).
Infusions and adverse events
A total of 8505 infusions were given to the 612 patients.Eighty-eight patients or 14% (41100 mg/kg patients, 24250mg/kg patients, and 23500 mg/kg patients) received extrainfusions of the study immunoglobulin. Indications forthese additional infusions were treatment of documented orsuspected CMV infection (62 patients), severe thrombo-cytopenia (24 patients), and investigator’s decision (twopatients).
Adverse events definitely, probably, or possibly relatedto the intravenous immunoglobulin occurred during 686 ofthe 8505 infusions (8.1%). Three hundred and seventeenpatients (51%) experienced at least one adverse eventrelated to the infusion of intravenous immunoglobulin.Both the number of patients with adverse events and thenumber of infusions associated with an adverse event weresimilar for all three doses of intravenous immunoglobulin.Adverse events complicating 1% or more of the infusionswere chills, fever, headaches, myalgias, hypertension,hypotension, nausea and vomiting. The respective inci-
Bone Marrow Transplantation
dences of these adverse events after infusion of intravenousimmunoglobulin in the 100 mg/kg, 250 mg/kg and 500mg/kg groups were as follows: chills, 2.8%, 3.3% and2.3%; fever, 2.1%, 3.0% and 2.2%; headaches, 0.9%, 1.4%and 1.9%; myalgias, 1.1%, 2.6% and 2.1%; hypertension,2.5%, 3.0% and 2.6%; hypotension, 2.3%, 2.1% and 2.0%;nausea, 0.8%, 1.5% and 1.6%; vomiting, 0.8%, 1.2% and1.1%. Of these common adverse events, only chills (P =0.007) and headaches (P = 0.015) occurred in a signifi-cantly greater number of patients in the 500 mg/kg group(25% and 16%, respectively), or in the 250 mg/kg group(32% and 14%, respectively) compared to the 100 mg/kggroup (18% and 7%, respectively). No serious adverseevents were attributed to the intravenous immunoglobulin.
There was no significant difference in the incidence ofveno-occlusive disease among the three treatment groups.Veno-occlusive disease occurred in 23 patients (11%) inthe 100 mg/kg group, 18 patients (9%) in the 250 mg/kggroup, and in 24 patients (12%) in the 500 mg/kg group.Hematological, renal, and hepatic laboratory tests alsofailed to show any significant differences among the threetreatment groups. No patients became positive for hepatitisB surface antigen or HIV antibody during the study, whilesix patients became seropositive for hepatitis C antibody(three with IgM plus IgG, three with IgG only).
Discussion
Despite the previously reported favorable effects of intra-venous immunoglobulin in allogeneic marrow transplantrecipients,1–10 the high cost of large doses of immunoglob-ulin has limited its use at many transplant centers. Thepresent study was designed to determine a minimally effec-tive dose of intravenous immunoglobulin for prevention of

Immunoglobulin therapy after marrow transplantDJ Winston et al
194
Bone Marrow Transplantation
GVHD and infections and thereby establish a more cost-effective dosing regimen. We found no significant differ-ences in the overall incidence of acute GVHD among thethree dosing groups. Acute GVHD developed in 39% ofpatients in the 100 mg/kg group, 42% in the 250 mg/kggroup, and 35% in the 500 mg/kg group. These incidencesof acute GVHD are all comparable to the incidences of34% reported in intravenous immunoglobulin recipientsparticipating in earlier trials at UCLA and Seattle whereimmunoglobulin at doses of 1000 mg/kg or 500 mg/kg onceweekly were associated with less GVHD compared to notreatment.1,7 Of note, among patients with unrelated donors,especially if they were male, 20 years of age or older, anddid not receive a T cell-depleted graft, the higher dose ofintravenous immunoglobulin (500 mg/kg) appeared to beassociated with the lowest incidence of acute GVHD(Figures 2 and 3). A multicenter randomized trial is furtherevaluating the efficacy of intravenous immunoglobulin inmarrow transplant recipients with unrelated donors.18
The inability of this study to demonstrate any clearrelationship between the dose of intravenous immunoglob-ulin and the incidence of acute GVHD or infections mightbe interpreted as a lack of benefit of intravenous immuno-globulin in marrow transplants that receive other moreupdated regimens for prevention of infection and GVHD.Generally, the number of serious infections, especiallyCMV disease and interstitial pneumonia, were considerablylower in this trial than in earlier studies of prophylacticintravenous immunoglobulin in marrow transplants.1–4,7,10
Fluoroquinolones, fluconazole, and ganciclovir are effec-tive agents for prophylaxis of infection and were commonlyused in this study.19–23 Such drugs were either unavailableor not used in previous trials of prophylactic intravenousimmunoglobulin. The current availability of these moreeffective antimicrobial drug regimens for prevention ofinfection suggests a lesser need to use intravenous immuno-globulin for prophylaxis of infection after marrowtransplantation.
On the other hand, acute GVHD continues to be a verycommon complication after allogeneic bone marrow trans-plantation despite current combination regimens ofimmunosuppressive drugs. Furthermore, with expansion ofthe application of allogeneic marrow transplantation to nowinclude older patients and more patients with HLAnon-identical or unrelated donors, the incidence andseverity of GVHD has actually increased in certain typesof patients.24–26 Acute GVHD still develops in approxi-mately 35% to 60% of recipients of HLA-identical, relatedmarrow allografts and in more than half of patients whoreceive unmanipulated marrow grafts from HLA non-ident-ical or unrelated donors.27 Thus, the present indications forintravenous immunoglobulin may be stronger for patientsat high risk for severe GVHD than for prevention of infec-tions.28 Additional randomized trials comparing differentdoses of intravenous immunoglobulin to placebo in patientsreceiving more effective immunosuppressive drugs for pre-vention of GVHD could be undertaken to further clarifythe role of intravenous immunoglobulin in recipients ofallogeneic marrow or stem cell grafts.
One of the potential limitations of this multicenter trialis the diversity of immunosuppressive drug regimens given
to prevent GVHD. Approximately 75% of the patientsreceived cyclosporine in combination with methotrexateand/or corticosteroids. However, the use of a single uniformimmunosuppressive drug regimen for GVHD prophylaxisin all patients may have provided a greater opportunity todetect any potential differences in the efficacy of the differ-ent doses of intravenous immunoglobulin for preventionof GVHD.
Patients with chronic GVHD have persistent defects inboth cellular and humoral immune responses. Thesepatients are particularly susceptible to many types of infec-tion, especially infections caused by encapsulated bac-teria.29 Nevertheless, a previous trial evaluating the effectsof monthly administration of intravenous immunoglobulinon chronic GVHD and associated infections showed nosubstantial benefits.30 In the present study, the overall inci-dence of chronic GVHD and late infections between days100 and 360 after transplantation was similar in all threedosing groups. Due to a significant fall in serum IgG levelswhen intravenous immunoglobulin dosing is changed fromweekly to monthly in marrow transplants,30 a weeklyinstead of a monthly schedule of intravenous immunoglob-ulin administration could still be beneficial in those patientswith chronic GVHD who also have severe hypogamma-globulinemia.
Two other randomized, unblinded clinical trials evaluat-ing the effects of different doses of intravenous immuno-globulin on complications after allogeneic bone marrowtransplantation have been reported recently. In a multicen-ter trial comparing a 250 mg/kg dose of intravenousimmunoglobulin with a 500 mg/kg dose each given onceweekly from day 8 before transplant to day 111 after trans-plant, the incidence of acute GVHD was less in patientsreceiving the higher dose (44% vs 58%, P = 0.03).31 Similarrates of infection and survival were observed with bothdoses. In a single-center trial, adult patients given related-donor marrow grafts were randomized to receive or not toreceive prophylactic intravenous immunoglobulin adminis-tered at a loading dose of 500 mg/kg per day from day 6to day 1 before transplant and then at a lower maintenancedose of 100 mg/kg every 3 days from day 3 to day 90after transplant.18 The incidences of acute GVHD, CMVinfection, interstitial pneumonia, bacteremia, and mortalitywere similar in the recipients of intravenous immunoglob-ulin and the control patients. Interpretation of these results,however, is clouded by the administration of intravenousimmunoglobulin to control patients who developed hypo-gammaglobulinemia (IgG level �500 mg/dl). Indeed, acuteGVHD was less frequent among patients achievingmaximum serum IgG levels �3000 mg/dl after the admin-istration of intravenous immunoglobulin. Trough serumIgG levels �1200 mg/dl were associated with less severeacute GVHD in another study of intravenous immunoglob-ulin.32 Serum IgG levels were not routinely followed inour study.
The intravenous immunoglobulin in this study was well-tolerated. There were no serious adverse events attributedto the intravenous immunoglobulin. An increase in mor-tality from veno-occlusive disease of the liver has beenreported in allogeneic marrow transplants receiving prophy-lactic intravenous immunoglobulin at a dose of 500 mg/kg

Immunoglobulin therapy after marrow transplantDJ Winston et al
195once per week.33 However, we found no relationshipbetween the dose of intravenous immunoglobulin and theincidence or severity of veno-occlusive disease whichoccurred in about 10% of all patients in each study group.
In summary, for most allogeneic bone marrow transplantrecipients, 100 mg/kg, 250 mg/kg, and 500 mg/kg dosesof intravenous immunoglobulin are associated with similarincidences of GVHD, infection, interstitial pneumonia,relapse, and survival. These results should be considered inthe development of cost-effective strategies for the use ofintravenous immunoglobulin in allogeneic marrow trans-plants. Since this study was not designed to demonstratethe efficacy of intravenous immunoglobulin compared totreatment without immunoglobulin, another randomizedtrial of different doses of intravenous immunoglobulincompared to placebo may be indicated as other more effec-tive agents for prevention of GVHD and infection aredeveloped.
Acknowledgements
We thank Dr Frank Norton of Alpha Therapeutic Corporation forassistance in preparation of the manuscript. We are also gratefulto the following study coordinators for their valuable assistanceduring the study: Kathy Bartoni, RN, UCLA Center for the HealthSciences, Los Angeles, CA; Sharon Manson, RN, MS, Rush-Pres-byterian-St Luke’s Medical Center, Chicago, Illinois. We thankKatharine Fry for typing the manuscript. This work was supportedby research grants from Alpha Therapeutic Corporation, LosAngeles, California.
References
1 Winston DJ, Ho WG, Lin CH et al. Intravenous immuneglobulin for prevention of cytomegalovirus infection and inter-stitial pneumonia after bone marrow transplantation. AnnIntern Med 1987; 106: 12–18.
2 Bowden RA, Sayers M, Flournoy N et al. Cytomegalovirusimmune globulin and seronegative blood products to preventprimary cytomegalovirus infection after marrow transplan-tation. New Engl J Med 1986; 314: 1006–1010.
3 Condie RM, O’Reilly RJ. Prevention of cytomegalovirusinfection by prophylaxis with an intravenous, hyperimmune,native, unmodified cytomegalovirus globulin. Randomizedtrial in bone marrow transplant recipients. Am J Med 1984;76: 134–141.
4 Kubanek B, Ernst P, Ostendorf P et al. Preliminary data of acontrolled trial of intravenous hyperimmune globulin in theprevention of cytomegalovirus infection in bone marrow trans-plant recipients. Transplant Proc 1985; 17: 468–469.
5 Petersen FB, Bowden RA, Thornquist M et al. The effect ofprophylactic intravenous immune globulin on the incidenceof septicemia in marrow transplant recipients. Bone MarrowTransplant 1987; 2: 141–148.
6 Graham-Pole J, Camitta B, Casper J et al. Intravenousimmunoglobulin may lessen all forms of infection in patientsreceiving allogeneic bone marrow transplantation for acutelymphoblastic leukemia: a Pediatric Oncology Group study.Bone Marrow Transplant 1988; 3: 559–566.
7 Sullivan KM, Kopecky KJ, Jocom J et al. Immunomodulatoryand antimicrobial efficacy of intravenous immunoglobulin inbone marrow transplantation. New Engl J Med 1990; 323:705–712.
Bone Marrow Transplantation
8 Winston DJ, Ho WG, Bartoni K, Champlin RE. Intravenousimmunoglobulin and CMV-seronegative blood products forprevention of CMV infection and disease in bone marrowtransplant recipients. Bone Marrow Transplant 1993; 12:283–288.
9 Consensus on IVIG. Lancet 1990; 336: 470–472.10 Bass EB, Powe NR, Goodman SN et al. Efficacy of immune
globulin in preventing complications of bone marrow trans-plantation: a meta-analysis. Bone Marrow Transplant 1993;12: 273–282.
11 Package Insert. Gaminune N 5% (Immune Globulin Intra-venous (Human), 5%, Solvent/Detergent Treated). Bayer Cor-poration, Pharmaceutical Division, Elkhart, Indiana, USA.
12 Thomas ED, Storb R, Clift RA et al. Bone-marrow transplan-tation. New Engl J Med 1975; 292: 832, 895–902.
13 Sullivan KM, Shulman HM, Storb R et al. Chronic graft-ver-sus-host disease in 52 patients: adverse natural course and suc-cessful treatment with combination immunosuppression.Blood 1981; 57: 267–276.
14 Mantel N, Haenszel W. Statistical aspects of the analysis ofdata from retrospective studies of disease. J Natl Cancer Inst1959; 22: 719–748.
15 Kaplan EL, Meier P. Nonparametric estimation from incom-plete observation. J Am Stat Assoc 1958; 53: 457–481.
16 Cox PR. Regression models and life-tables. JR Statist Soc1972; 34: 187–220.
17 Munoz A, Rosner B. Power and sample size for a collectionof 2 × 2 tables. Biometrics 1984; 40: 995–1004.
18 Feinstein LC, Seidel K, Jocum J et al. Reduced dose intra-venous immunoglobulin does not decrease transplant-relatedcomplications in adults given related donor marrow allografts.Biol Blood Marrow Transplant 1999; 5: 369–378.
19 Winston DJ. Use of quinolone antimicrobial agents inimmunocompromised patients. In: Hooper DC, Wolfson JS(eds). Quinolone Antimicrobial Agents, 2nd edn. AmericanSociety for Microbiology: Washington, DC, 1993, pp 435–471.
20 Goodman JL, Winston DJ, Greenfield RA et al. A controlledtrial of fluconazole to prevent fungal infections in patientsundergoing bone marrow transplantation. New Engl J Med1992; 326: 845–851.
21 Slavin MA, Osborne B, Adams R et al. Efficacy and safetyof fluconazole prophylaxis for fungal infections after marrowtransplantation – a prospective, randomized, double-blindstudy. J Infect Dis 1995; 171: 1545–1552.
22 Winston DJ, Ho WG, Bartoni K et al. Ganciclovir prophylaxisof cytomegalovirus infection and disease in allogeneic bonemarrow transplants: results of a placebo-controlled, double-blind trial. Ann Intern Med 1993; 118: 179–184.
23 Goodrich JM, Bowden RA, Fisher L et al. Ganciclovirprophylaxis to prevent cytomegalovirus disease after allog-eneic marrow transplant. Ann Intern Med 1993; 118: 173–178.
24 Bross DS, Tutschka PJ, Farmer ER et al. Predictive factorsfor acute graft-versus-host disease in patients transplantedwith HLA-identical bone marrow. Blood 1984; 63: 1265–1270.
25 Nash RA, Pepe MS, Storb R et al. Acute graft-versus-hostdisease: analysis of risk factors after allogeneic marrow trans-plantation and prophylaxis with cyclosporine and methotrex-ate. Blood 1992; 80: 1838–1845.
26 Nademanee A, Schmidt GM, Parker P et al. The outcome ofmatched unrelated donor bone marrow transplantation inpatients with hematologic malignancies using moleculartyping for donor selection and graft-versus-host diseaseprophylaxis regimen of cyclosporine, methotrexate, andprednisone. Blood 1995; 86: 1228–1234.

Immunoglobulin therapy after marrow transplantDJ Winston et al
196
Bone Marrow Transplantation
27 Lazarus HM, Vogelsang, GB, Rowe JM. Prevention and treat-ment of acute graft-versus-host disease: the old and the new.A report from The Eastern Cooperative Oncology Group(ECOG). Bone Marrow Transplant 1997; 19: 577–600.
28 Guglielmo BJ, Wong-Beringer A, Linker CA. Immune globu-lin therapy in allogeneic bone marrow transplant: a criticalreview. Bone Marrow Transplant 1994; 13: 499–510.
29 Sullivan KM, Agura E, Anasetti C et al. Chronic graft-versus-host disease and other late complications of bone marrowtransplantation. Semin Hematol 1991; 28: 250–259.
30 Sullivan KM, Storek J, Kopecky KJ et al. A controlled trialof long-term administration of intravenous immunoglobulin toprevent late infection and chronic graft-vs.-host disease aftermarrow transplantation: clinical outcome and effect on sub-
sequent immune recovery. Biol Blood Marrow Transplant1996; 2: 44–53.
31 Abdel-Mageed A, Graham-Pole J, Del Rosario MLU et al.Comparison of two doses of intravenous immunoglobulin afterallogeneic bone marrow transplants. Bone Marrow Transplant1999; 23: 929–932.
32 Cottler-Fox M, Lynch M, Pickle LW et al. Some but not allbenefits of intravenous immunoglobulin therapy after marrowtransplantation appear to correlate with IgG trough levels.Bone Marrow Transplant 1991; 8: 27–33.
33 Klaesson S, Ringden O, Ljungman P et al. Does high-doseintravenous immune globulin treatment after bone marrowtransplantation increase mortality in veno-occlusive disease ofthe liver. Transplantation 1996; 60: 1225–1230.
Copyright © 2022 FDOKUMEN




















