
A CHILD WITH UNDIFFERENTIATED SARCOMA OF THE LIVER COMPLICATED WITH BRONCHOBILIARY FISTULA AND...
7
Pediatric Hematology and Oncology, 21: 427–433, 2004 Copyright C Taylor & Francis Inc. ISSN: 0888-0018 print / 1521-0669 online DOI: 10.1080/08880010490457150 A CHILD WITH UNDIFFERENTIATED SARCOMA OF THE LIVER COMPLICATED WITH BRONCHOBILIARY FISTULA AND DETECTED BY HEPATOBILIARY SCINTIGRAPHY Funda C ¸ orapc ¸ıoglu, Nazan Sarper, Hakan Demir, B. Haluk G ¨ uvenc ¸, Selami S ¨ oz¨ ubir, G ¨ ur Akansel, and Fatma Sen Berk ✷ Undifferentiated (embryonal) sarcoma of the liver (USL) is a rare malignant mesenchymal tu- mor principally affecting patients of pediatric age. Bronchobiliary fistula is a very rare complication in patients with liver tumor. To the authors’ knowledge, this is the first report of a bronchobiliary fistula resulting from tumor invasion in a child with liver sarcoma. A 12-year-old boy was diag- nosed to have USL of the right liver lobe, invading the diaphragm. An extended right hepatectomy and total resection of the mass was performed, leaving patchy tumoral invasion of the anterior di- aphragmatic surface followed by combined chemotherapy regimen. Six months after the operation, the presence of bilious sputum suggested a bronchobiliary fistula, which was confirmed by hepa- tobiliary scintigraphy. The patient underwent a right thoracotomy and fistula division. Although bronchobiliary fistula is a very rare complication in patients with hepatic tumors, suspicion in the appropriate clinical setting is necessary to recognize this problem. Hepatobiliary scintigraphy is the useful diagnostic procedure to define bronchobiliary fistula in children with liver tumor and clinical suspicion of bronchobiliary fistula. Keywords. bronchobiliary fistula, hepatobiliary scintigraphy, undifferentiated liver sar- coma Undifferentiated (embryonal) sarcoma of the liver (USL) is a rare pri- mary malignant mesenchymal hepatic tumor that occurs in elder children [1–3]. Surgical resection remains the mainstay of treatment [4, 5]. Thoraco- biliary communications in the form of either pleurobiliary or bronchocobil- iary fistulas are reported complications of malignant primary or metastatic liver tumors in adulthood [6]. To our knowledge, this is the first report of a bronchobiliary fistula in a child with liver sarcoma. CASE REPORT A 12-year-old boy was admitted to our center with a 3-month history of malaise and mild abdominal pain. On physical examination, a solid, painless abdominal mass in the upper right quadrant was found. His complete blood count, liver function test, and AFP level were within normal range. Abdomi- nal ultrasonography, computerized tomography, and MRI findings revealed Received 2 October 2003; accepted 8 March 2004. Address correspondence to Funda C ¸ orapc ¸ioglu, Cumhuriyet Mah. Misir Sok, EKAS yapi koop, B blok, Kat:1, Da:1, Izmit-Kocaeli, Turkey. E-mail: [email protected] 427
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of A CHILD WITH UNDIFFERENTIATED SARCOMA OF THE LIVER COMPLICATED WITH BRONCHOBILIARY FISTULA AND...

June 9, 2004 11:54 PHO TJ1131-09
Generated by TechBooks Automated Layout System
Pediatric Hematology and Oncology, 21: 427–433, 2004Copyright ©C Taylor & Francis Inc.ISSN: 0888-0018 print / 1521-0669 onlineDOI: 10.1080/08880010490457150
A CHILD WITH UNDIFFERENTIATED SARCOMA OF THE LIVERCOMPLICATED WITH BRONCHOBILIARY FISTULA AND DETECTEDBY HEPATOBILIARY SCINTIGRAPHY
Funda Corapcıoglu, Nazan Sarper, Hakan Demir, B. Haluk Guvenc,Selami Sozubir, Gur Akansel, and Fatma Sen Berk
� Undifferentiated (embryonal) sarcoma of the liver (USL) is a rare malignant mesenchymal tu-mor principally affecting patients of pediatric age. Bronchobiliary fistula is a very rare complicationin patients with liver tumor. To the authors’ knowledge, this is the first report of a bronchobiliaryfistula resulting from tumor invasion in a child with liver sarcoma. A 12-year-old boy was diag-nosed to have USL of the right liver lobe, invading the diaphragm. An extended right hepatectomyand total resection of the mass was performed, leaving patchy tumoral invasion of the anterior di-aphragmatic surface followed by combined chemotherapy regimen. Six months after the operation,the presence of bilious sputum suggested a bronchobiliary fistula, which was confirmed by hepa-tobiliary scintigraphy. The patient underwent a right thoracotomy and fistula division. Althoughbronchobiliary fistula is a very rare complication in patients with hepatic tumors, suspicion in theappropriate clinical setting is necessary to recognize this problem. Hepatobiliary scintigraphy is theuseful diagnostic procedure to define bronchobiliary fistula in children with liver tumor and clinicalsuspicion of bronchobiliary fistula.
Keywords. bronchobiliary fistula, hepatobiliary scintigraphy, undifferentiated liver sar-coma
Undifferentiated (embryonal) sarcoma of the liver (USL) is a rare pri-mary malignant mesenchymal hepatic tumor that occurs in elder children[1–3]. Surgical resection remains the mainstay of treatment [4, 5]. Thoraco-biliary communications in the form of either pleurobiliary or bronchocobil-iary fistulas are reported complications of malignant primary or metastaticliver tumors in adulthood [6]. To our knowledge, this is the first report of abronchobiliary fistula in a child with liver sarcoma.
CASE REPORT
A 12-year-old boy was admitted to our center with a 3-month history ofmalaise and mild abdominal pain. On physical examination, a solid, painlessabdominal mass in the upper right quadrant was found. His complete bloodcount, liver function test, and AFP level were within normal range. Abdomi-nal ultrasonography, computerized tomography, and MRI findings revealed
Received 2 October 2003; accepted 8 March 2004.Address correspondence to Funda Corapcioglu, Cumhuriyet Mah. Misir Sok, EKAS yapi koop,
B blok, Kat:1, Da:1, Izmit-Kocaeli, Turkey. E-mail: [email protected]
427

June 9, 2004 11:54 PHO TJ1131-09
Generated by TechBooks Automated Layout System
428 F. Corapcioglu et al.
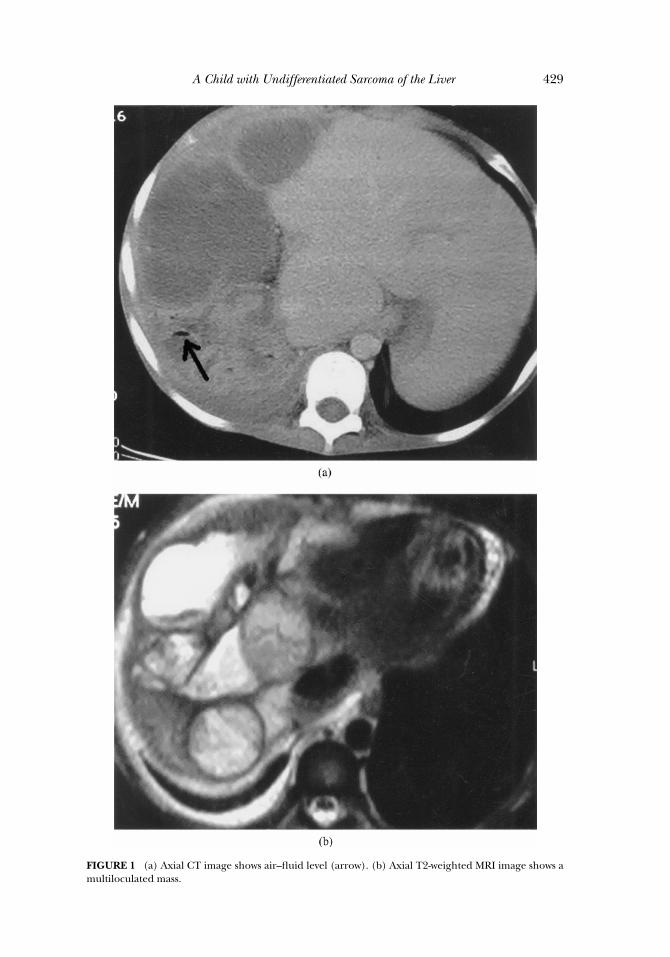
a large mass originating from the right liver lobe, which had a cystic ap-pearance resembling hydatid disease. An extended right hepatectomy andtotal resection of the mass was performed, leaving patchy tumoral invasionof the anterior diaphragmatic surface. Histologically, the tumor was com-posed of diffuse, large, spindle-shaped cells in a myxoid stroma. Immuno-histochemically, the tumor cells reacted with antibodies against vimentin,cytokeratin, and desmin. The pathological examination of the mass revealedUSL. An adjuvant chemotherapy with ifosphamide, vincristin, and etoposidewas given. The patient was lost to follow-up for 4 months following his firstcourse of chemotherapy, and was readmitted to our center with abdominaldistention and jaundice. On physical examination, a large solid mass wasfound in the upper right abdominal quadrant. CT and MRI scan revealedprogression of the residual mass extending to the thoracic cavity but therewas no lung metastasis or invasion and left hepatic lobe was normal. A sec-ond chemotherapy course with ifosphamide, carboplatin, and etoposide wasgiven. Ten days after the chemotherapy, he presented a febrile neutropenicepisode, which was successfully treated with antimicrobial therapy. On thepostoperative sixth month, he was admitted to the hospital with complaintsof bilious expectoration. CT and MRI scan of the thorax revealed a multi-loculated right upper quadrant mass extending into the chest, with air bron-chograms and air–fluid levels (Figure 1) These findings suggested the pres-ence of a bronchobiliary communication.
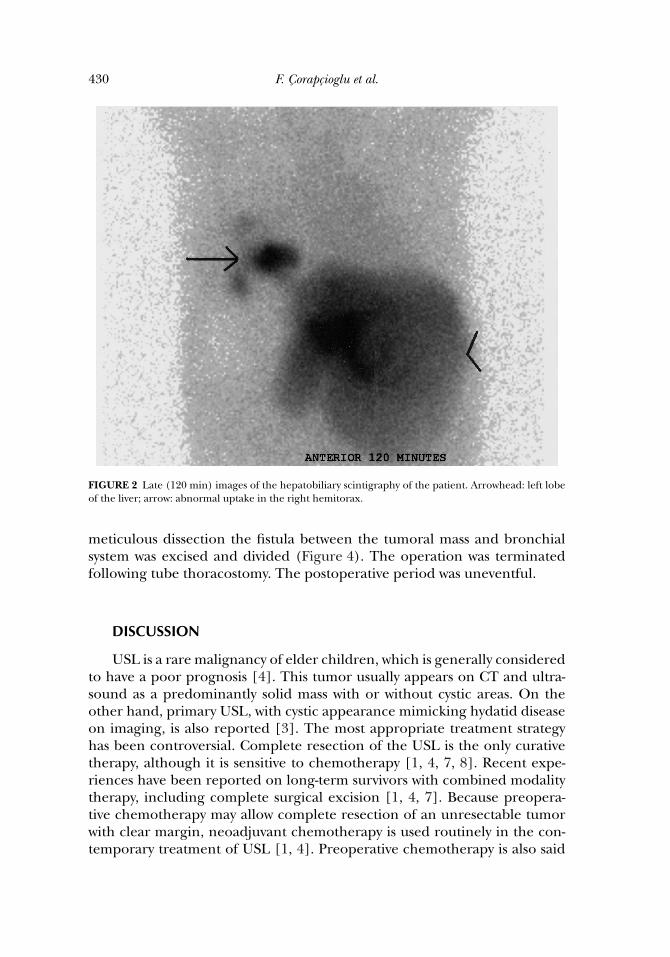
Hepatobiliary scintigraphy (HBS) was performed after intravenous in-jection of 74 MBq (2 mCi) 99mTc N-3-bromo-2,4,6 trimethylphenylcar-bamoylmethyl iminodiacetic acid (Mebrofenin), following 4 h of fast-ing. After perfusion images (1 s/frame for 1 min in anterior position),functional images (1 min/frame for 30 min in anterior position),and late images (3–5 min static images in anterior, lateral, andposterior positions, every 20–30 min until 4 h) were obtained with asingle-head gamma camera (ADAC Argus, Epic) using a low-energy, high-resolution, parallel-hole collimator in a 64 × 64 matrix at 20% energy win-dow and 140 keV peak energy.
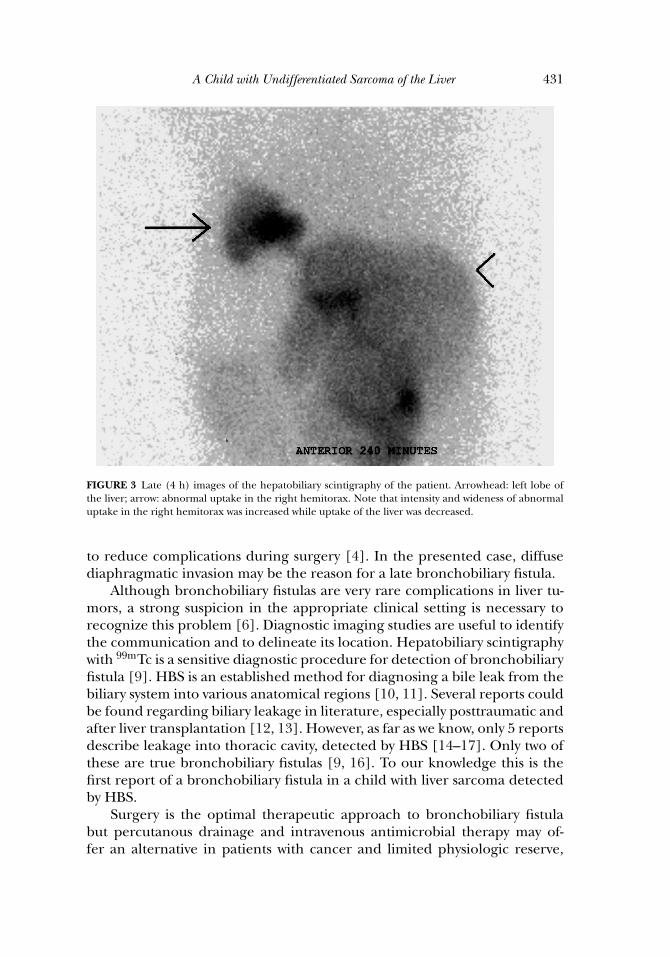
Hepatic perfusion was normal. In functional images the left lobe ofthe liver was located slightly superiorly and its dimensions were abnormallyincreased and had irregular shape. Uptake in the right lobe couldn’t beobserved because of partial lobectomy. Left lobe uptake was slightly de-creased. Normal transit of radiopharmaceutical to the gut was observed atnormal time. Yet, from the first hour an unusual uptake had been seen inthe right inferior hemithorax. The intensity and wideness of the abnormaluptake increased by the time (Figures 2 and 3). HBS confirmed broncobil-iary fistula.
A right thoracotomy revealed multiple adhesions and large tumoralmass invading the diaphragm adjacent to the base of right lung. Under
June 9, 2004 11:54 PHO TJ1131-09
Generated by TechBooks Automated Layout System
A Child with Undifferentiated Sarcoma of the Liver 429
FIGURE 1 (a) Axial CT image shows air–fluid level (arrow). (b) Axial T2-weighted MRI image shows amultiloculated mass.
June 9, 2004 11:54 PHO TJ1131-09
Generated by TechBooks Automated Layout System
430 F. Corapcioglu et al.
FIGURE 2 Late (120 min) images of the hepatobiliary scintigraphy of the patient. Arrowhead: left lobeof the liver; arrow: abnormal uptake in the right hemitorax.
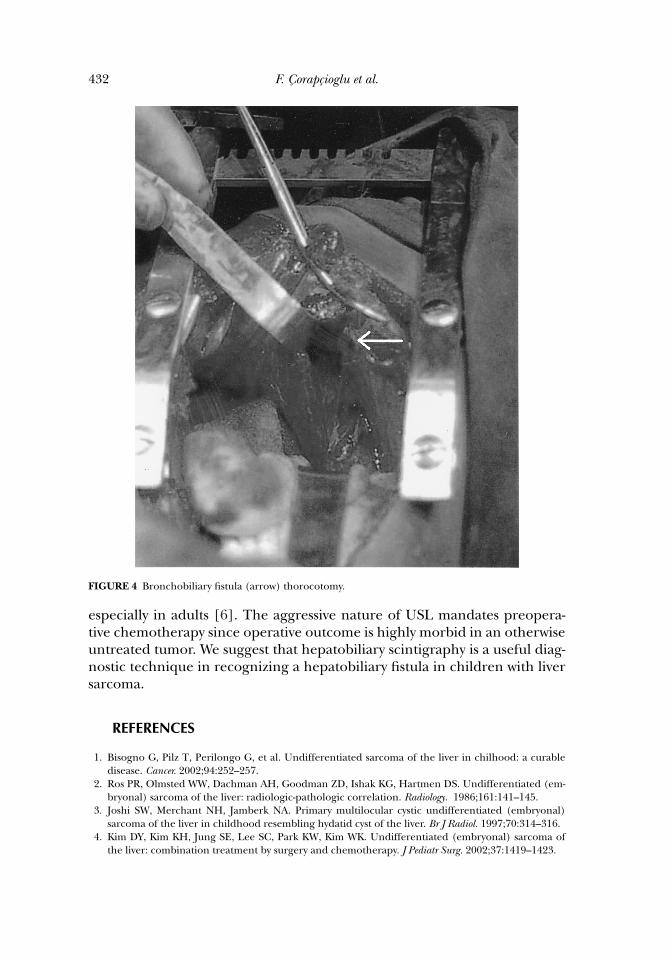
meticulous dissection the fistula between the tumoral mass and bronchialsystem was excised and divided (Figure 4). The operation was terminatedfollowing tube thoracostomy. The postoperative period was uneventful.
DISCUSSION
USL is a rare malignancy of elder children, which is generally consideredto have a poor prognosis [4]. This tumor usually appears on CT and ultra-sound as a predominantly solid mass with or without cystic areas. On theother hand, primary USL, with cystic appearance mimicking hydatid diseaseon imaging, is also reported [3]. The most appropriate treatment strategyhas been controversial. Complete resection of the USL is the only curativetherapy, although it is sensitive to chemotherapy [1, 4, 7, 8]. Recent expe-riences have been reported on long-term survivors with combined modalitytherapy, including complete surgical excision [1, 4, 7]. Because preopera-tive chemotherapy may allow complete resection of an unresectable tumorwith clear margin, neoadjuvant chemotherapy is used routinely in the con-temporary treatment of USL [1, 4]. Preoperative chemotherapy is also said
June 9, 2004 11:54 PHO TJ1131-09
Generated by TechBooks Automated Layout System
A Child with Undifferentiated Sarcoma of the Liver 431
FIGURE 3 Late (4 h) images of the hepatobiliary scintigraphy of the patient. Arrowhead: left lobe ofthe liver; arrow: abnormal uptake in the right hemitorax. Note that intensity and wideness of abnormaluptake in the right hemitorax was increased while uptake of the liver was decreased.
to reduce complications during surgery [4]. In the presented case, diffusediaphragmatic invasion may be the reason for a late bronchobiliary fistula.
Although bronchobiliary fistulas are very rare complications in liver tu-mors, a strong suspicion in the appropriate clinical setting is necessary torecognize this problem [6]. Diagnostic imaging studies are useful to identifythe communication and to delineate its location. Hepatobiliary scintigraphywith 99mTc is a sensitive diagnostic procedure for detection of bronchobiliaryfistula [9]. HBS is an established method for diagnosing a bile leak from thebiliary system into various anatomical regions [10, 11]. Several reports couldbe found regarding biliary leakage in literature, especially posttraumatic andafter liver transplantation [12, 13]. However, as far as we know, only 5 reportsdescribe leakage into thoracic cavity, detected by HBS [14–17]. Only two ofthese are true bronchobiliary fistulas [9, 16]. To our knowledge this is thefirst report of a bronchobiliary fistula in a child with liver sarcoma detectedby HBS.
Surgery is the optimal therapeutic approach to bronchobiliary fistulabut percutanous drainage and intravenous antimicrobial therapy may of-fer an alternative in patients with cancer and limited physiologic reserve,
June 9, 2004 11:54 PHO TJ1131-09
Generated by TechBooks Automated Layout System
432 F. Corapcioglu et al.
FIGURE 4 Bronchobiliary fistula (arrow) thorocotomy.
especially in adults [6]. The aggressive nature of USL mandates preopera-tive chemotherapy since operative outcome is highly morbid in an otherwiseuntreated tumor. We suggest that hepatobiliary scintigraphy is a useful diag-nostic technique in recognizing a hepatobiliary fistula in children with liversarcoma.
REFERENCES
1. Bisogno G, Pilz T, Perilongo G, et al. Undifferentiated sarcoma of the liver in chilhood: a curabledisease. Cancer. 2002;94:252–257.
2. Ros PR, Olmsted WW, Dachman AH, Goodman ZD, Ishak KG, Hartmen DS. Undifferentiated (em-bryonal) sarcoma of the liver: radiologic-pathologic correlation. Radiology. 1986;161:141–145.
3. Joshi SW, Merchant NH, Jamberk NA. Primary multilocular cystic undifferentiated (embryonal)sarcoma of the liver in childhood resembling hydatid cyst of the liver. Br J Radiol. 1997;70:314–316.
4. Kim DY, Kim KH, Jung SE, Lee SC, Park KW, Kim WK. Undifferentiated (embryonal) sarcoma ofthe liver: combination treatment by surgery and chemotherapy. J Pediatr Surg. 2002;37:1419–1423.
June 9, 2004 11:54 PHO TJ1131-09
Generated by TechBooks Automated Layout System
A Child with Undifferentiated Sarcoma of the Liver 433
5. Aggarwal S, Guleria S, Dinda AK, Kumar L, Tarique S. Embryonal sarcoma of the liver mimicking ahydatid cyst in an adult. Trop Gastroenterol. 2001;22:141–142.
6. Johson MM, Chin R Jr, Haponik EF. Thoracobiliary fistula. South Med J. 1996;89:335–339.7. Rosito P, Mancini AF, Semeraro M, et al. Malignant primary tumors of the liver in chilhood. Pediatr
Med Chir. 2002;24:200–207.8. Chuang WY, Lin JN, Hung IJ, Hsueh C. Undifferentiated sarcoma of the liver. Chang Gung Med J.
2002;25:399–404.9. Velchik MG, Roth GM, Wegener W, Alavi A. Bronchobiliary fistula detected by cholescintigraphy.
J Nucl Med. 1991;32:136–138.10. Roca I, Ciofetta G. Hepatobiliary scintigraphy in current pediatric practice. Q J Nucl Med.
1998;42:113–118.11. Nadel HR. Hepatobiliary scintigraphy in children. Semin Nucl Med. 1996;26:25–42.12. Kim JS, Moon DH, Lee SG, et al. The usefulness of hepatobiliary scintigraphy in the diagnosis of
complications after adult-to-adult living donor liver transplantation. Eur J Nucl Med Mol Imaging.2002;29:473–479.
13. Colletti PM, Barakos JA, Ralls PW, Siegel ME, Halls JM. Hepatobiliary scintigraphy and scintiangiog-raphy in abdominal trauma. Clin Nucl Med. 1987;12:901–909.
14. Lee JK. Tc-99m DISIDA hepatobiliary scintigraphy showing bile leakage into the thoracic cavity. ClinNucl Med. 2001;26:861–862.
15. Suehiro M, Ishimura J, Fukuchi M. Detection of bile leakage into the thoracic cavity by hepatobiliaryscintigraphy. Ann Nucl Med. 1991;5:167–169.
16. Rubin RH, Livni E, Babich J, et al. Pharmacokinetics of fleroxacin as studied by positron emissiontomography and [18F]fleroxacin. Am J Med. 1993;94:31–37.
17. Marlatt SW, Caride VJ, Prokop EK. Incidental demonstration of pericardial fistula during hepatobil-iary scintigraphy. J Nucl Med. 1991;32:518–522.




















