
Cardiac sympathetic activity pre and post resynchronization therapy evaluated by 123I-MIBG...
8
Cardiac sympathetic activity pre and post resynchronization therapy evaluated by 123I-MIBG myocardial scintigraphy Silvana A. D’Orio Nishioka, MD, PhD, a Martino Martinelli Filho, MD, PhD, a Simone C. Soares Brandão, MD, b Maria Clementina Giorgi, MD, PhD, b Marcelo L.C. Vieira, MD, PhD, c Roberto Costa, MD, PhD, a Wilson Mathias, MD, PhD, c and José Cláudio Meneghetti, MD, PhD b Background. Imaging with 123 I-metaiodobenzylguanidine (MIBG) is used for the assessment of cardiac sympathetic activity (CSA). We analyzed CSA before and after cardiac resynchro- nization therapy (CRT), and correlated these data with CRT response. Methods and Results. Thirty patients with chronic heart failure and classic indications for CRT were prospectively studied before and at least 3 months after CRT. The variables analyzed were: QRS width, left-ventricular ejection fraction (LVEF), left-ventricular end-diastolic diameter (LVEDD), heart/mediastinum MIBG uptake ratio (H/M), and washout rate (WR). After CRT, patients were divided into two groups: group 1 (21 patients), responders improving to functional class (FC) I or II; and group 2 (9 patients), nonresponders remaining in FC III or IV. After CRT, only group 1 showed favorable changes in QRS width (P .003), LVEF (P .01), LVEDD (P .04), and H/M ratio (P .003). The H/M ratio and WR were associated with CRT response (P .005 and P .04, respectively). The H/M ratio was the only independent predictor of CRT response (P .01). Receiver operating characteristic curves showed that the optimal H/M ratio cutoff point was 1.36 (sensitivity, 75%; specificity, 71%). Conclusions. Improvement in CSA correlated with a positive CRT response. Lower MIBG uptake before therapy was associated with CRT nonresponse. The H/M ratio could be helpful in selecting patients for CRT. (J Nucl Cardiol 2007;14:852-9.) Key Words: Cardiac resynchronization therapy • chronic heart failure • cardiac MIBG scintigraphy • prognosis Cardiac resynchronization therapy (CRT) has proven beneficial in patients with advanced chronic heart failure (HF) and QRS duration greater than 120 milliseconds (ms) in addition to optimal medical therapy. 1-4 Much improvement has been achieved in the pharmacologic treatment of HF. 1-6 However, in patients with chronic HF whose symptoms remain severe, CRT can improve clinical manifestations and quality of life, and reduce complications and risk of death. 4 Despite initial enthusiasm about providing this ther- apy to patients who fulfilled current CRT guidelines, 3,6 a lack of response was observed in about one third of patients who did not benefit clinically or who experi- enced left-ventricular reverse remodeling after biven- tricular stimulation. 7 Furthermore, the invasive nature and costs of CRT have highlighted the need to identify optimal candidates. Therefore, selection criteria to detect the most suitable candidates for CRT are crucial. 7-11 In patients with chronic HF, various neurohor- monal alterations contribute to the progression of the disease, and are associated with an unfavorable prog- nosis. 5 Increased levels of catecholamines have a direct cardiotoxic effect and are important predictors of HF mortality and morbidity. Cardiac imaging From the Department of Arrhythmia and Cardiac Stimulation, a Depart- ment of Nuclear Medicine, b and Department of Echocardiography, c Heart Institute, InCor, University of São Paulo Medical School, São Paulo, Brazil. This study was supported by grants from the Research Support Foundation of the State of São Paulo, Brazil. Received for publication June 24, 2007; final revision accepted Aug 6, 2007. Reprint requests: Silvana A. D’Orio Nishioka, MD, PhD, Assistant of Cardiology, Unidade Clínica de Estimulação Cardíaca Artificial do Instituto do Coração do Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo, Av. Dr. Enéas de Carvalho Aguiar 44, CEP 05403000 São Paulo, São Paulo, Brazil; silvanadorio@ uol.com.br. 1071-3581/$32.00 Copyright © 2007 by the American Society of Nuclear Cardiology. doi:10.1016/j.nuclcard.2007.08.004 852
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Cardiac sympathetic activity pre and post resynchronization therapy evaluated by 123I-MIBG...
Cardiac sympathetic activity pre and postresynchronization therapy evaluated by 123I-MIBGmyocardial scintigraphy
Silvana A. D’Orio Nishioka, MD, PhD,a Martino Martinelli Filho, MD, PhD,a
Simone C. Soares Brandão, MD,b Maria Clementina Giorgi, MD, PhD,b
Marcelo L.C. Vieira, MD, PhD,c Roberto Costa, MD, PhD,a
Wilson Mathias, MD, PhD,c and José Cláudio Meneghetti, MD, PhDb
Background. Imaging with 123I-metaiodobenzylguanidine (MIBG) is used for the assessmentof cardiac sympathetic activity (CSA). We analyzed CSA before and after cardiac resynchro-nization therapy (CRT), and correlated these data with CRT response.
Methods and Results. Thirty patients with chronic heart failure and classic indications forCRT were prospectively studied before and at least 3 months after CRT. The variables analyzedwere: QRS width, left-ventricular ejection fraction (LVEF), left-ventricular end-diastolicdiameter (LVEDD), heart/mediastinum MIBG uptake ratio (H/M), and washout rate (WR).After CRT, patients were divided into two groups: group 1 (21 patients), responders improvingto functional class (FC) I or II; and group 2 (9 patients), nonresponders remaining in FC III orIV. After CRT, only group 1 showed favorable changes in QRS width (P � .003), LVEF (P �.01), LVEDD (P � .04), and H/M ratio (P � .003). The H/M ratio and WR were associated withCRT response (P � .005 and P � .04, respectively). The H/M ratio was the only independentpredictor of CRT response (P � .01). Receiver operating characteristic curves showed that theoptimal H/M ratio cutoff point was 1.36 (sensitivity, 75%; specificity, 71%).
Conclusions. Improvement in CSA correlated with a positive CRT response. Lower MIBGuptake before therapy was associated with CRT nonresponse. The H/M ratio could be helpfulin selecting patients for CRT. (J Nucl Cardiol 2007;14:852-9.)
Key Words: Cardiac resynchronization therapy • chronic heart failure • cardiac MIBG
scintigraphy • prognosisCardiac resynchronization therapy (CRT) has provenbeneficial in patients with advanced chronic heart failure(HF) and QRS duration greater than 120 milliseconds(ms) in addition to optimal medical therapy.1-4 Much
From the Department of Arrhythmia and Cardiac Stimulation,a Depart-ment of Nuclear Medicine,b and Department of Echocardiography,c
Heart Institute, InCor, University of São Paulo Medical School, SãoPaulo, Brazil.
This study was supported by grants from the Research SupportFoundation of the State of São Paulo, Brazil.
Received for publication June 24, 2007; final revision accepted Aug 6,2007.
Reprint requests: Silvana A. D’Orio Nishioka, MD, PhD, Assistant ofCardiology, Unidade Clínica de Estimulação Cardíaca Artificial doInstituto do Coração do Hospital das Clínicas da Faculdade deMedicina da Universidade de São Paulo, Av. Dr. Enéas de CarvalhoAguiar 44, CEP 05403000 São Paulo, São Paulo, Brazil; [email protected].
1071-3581/$32.00Copyright © 2007 by the American Society of Nuclear Cardiology.
doi:10.1016/j.nuclcard.2007.08.004852
improvement has been achieved in the pharmacologictreatment of HF.1-6 However, in patients with chronic HFwhose symptoms remain severe, CRT can improveclinical manifestations and quality of life, and reducecomplications and risk of death.4
Despite initial enthusiasm about providing this ther-apy to patients who fulfilled current CRT guidelines,3,6 alack of response was observed in about one third ofpatients who did not benefit clinically or who experi-enced left-ventricular reverse remodeling after biven-tricular stimulation.7 Furthermore, the invasive natureand costs of CRT have highlighted the need to identifyoptimal candidates. Therefore, selection criteria to detectthe most suitable candidates for CRT are crucial.7-11
In patients with chronic HF, various neurohor-monal alterations contribute to the progression of thedisease, and are associated with an unfavorable prog-nosis.5 Increased levels of catecholamines have adirect cardiotoxic effect and are important predictors
of HF mortality and morbidity. Cardiac imaging
Journal of Nuclear Cardiology D’Orio Nishioka et al 853Volume 14, Number 6;852-9 MIBG imaging and cardiac resynchronization therapy
with123I-metaiodobenzylguanidine (MIBG), an ana-logue of norepinephrine, is an important tool fordetecting abnormalities in the myocardial adrenergicnervous system, and has useful prognostic value inpatients with chronic HF.12-15
Some studies showed that the pharmacologic treatmentof HF improves cardiac sympathetic activity, as demon-strated by cardiac MIBG scintigraphy.16-21 A small clinicalstudy also suggested that CRT could induce favorablechanges in the neurohumoral system, as evaluated byplasma brain natriuretic peptide concentration and car-diac MIBG imaging, in patients with HF and a left-ventricular ejection fraction of �35%,22 but no data havedescribed the ability of cardiac MIBG scintigraphy topredict the efficacy of CRT. The aims of the presentstudy were to analyze cardiac sympathetic activity,comparing MIBG imaging before and after CRT, and tocorrelate these data with clinical results after therapy.
METHODS
Study Patients
Thirty patients with symptomatic chronic HF, referred forimplantation of a CRT device, were included in the presentstudy after written, informed consent was obtained. The EthicsCommittee of our institution approved the study protocol. Thisinvestigation conforms to the principles outlined in the Decla-ration of Helsinki.
The mean age of patients was 59 � 12 years (range, 37 to79 years), and 17 (57%) patients were men. Heart failure wasdue to idiopathic dilated cardiomyopathy in 23 (77%) patients,and ischemic heart disease in 7 (23%). Their pharmacologictherapy (Table 1) was unchanged for 6 weeks before CRT andduring a follow-up of at least 3 months. Patients enrolled forCRT had left-ventricular systolic dysfunction with a left-ventricular ejection fraction of �35%, the presence of leftbundle-branch block with QRS equal to or wider than 120 ms,and chronic HF in New York Heart Association (NYHA)functional classes III and IV with optimized clinical treat-ment.3,6 Patients were excluded from the study if they hadatrial fibrillation, an atrioventricular block, a permanent pace-maker, end-stage renal failure, insulin-dependent diabetes mel-litus, or autonomic neuropathy.
Study Protocol
Before and at least 3 months after CRT, patientsunderwent electrocardiography, echocardiography, and car-diac MIBG scintigraphy. Three months after CRT, thesepatients were divided into two groups according to theirresponses to CRT: group 1 (G1), responders who improved tofunctional class (FC) I or II; and group 2 (G2), nonresponders
who remained in FC III or IV.Electrocardiography
The duration of QRS was measured on a surface 12-leadelectrocardiogram, using the widest QRS complex from the DIIlead. Electrocardiograms were recorded at a speed of 25mm/second, and were evaluated by two observers withoutknowledge of the clinical status of the patient.
Cardiac MIBG Scintigraphy
After thyroid blockade with 100 mg of potassium iodidegiven orally, patients received an intravenous injection of 185MBq of 123I-MIBG. Fifteen minutes (early imaging) and 3hours (delayed imaging) after MIBG administration, a two-million count planar anterior image of the chest was acquiredby using a gamma camera (ORBITER, Siemens MedicalSystems, Hoffmann Estates, Ill) equipped with a low-energy,all-purpose collimator and stored in a 128 � 128 matrix. TheMIBG activity was measured using a manually drawn region ofinterest around the left ventricle (LV) and in the uppermediastinum. Mediastinal and myocardial values were ex-pressed as mean counts per pixel. To evaluate MIBG myocar-dial uptake, the heart/mediastinum count (H/M) ratio wasdetermined from the delayed anterior planar MIBG image. Thewashout rate (WR) was calculated by using the followingformula: [(H/T � M/T) early � (H/T � M/T) delayed]/(H/T �M/T) early � 100(%), where H � mean count per pixel in LV,M � mean count per pixel in the mediastinum, and T � imageacquisition times, with values undergoing correction for 123Iphysical decay.
Echocardiography
Transthoracic echocardiographic studies were performedbefore and 3 months after CRT, with a Philips HDI-5000 model(Philips, Andover, Mass) equipped with a 2 to 4 MHz trans-ducer, following American Society of Echocardiography rec-ommendations.23 Two experienced, independent observerswho had no knowledge of the clinical data measured the
Table 1. Baseline patient characteristics (N � 30)
Age (y) 59 � 12Male sex, n (%) 17 (57)Cause of CHF – n (%)
Idiopathic 23 (77)Ischemic 7 (23)
Drugs, n (%)ACE inhibitor or ARB 30 (100)Beta-blocker 29 (97)Spironolactone 26 (87)Diuretic 26 (87)Digoxin 18 (60)Amiodarone 7 (23)
ACE, Angiotensin-converting enzyme; ARB, angiotensin receptorblocker; CHF, chronic heart failure.
left-ventricular end-diastolic diameter and the left-ventricular

854 D’Orio Nishioka et al Journal of Nuclear CardiologyMIBG imaging and cardiac resynchronization therapy November/December 2007
ejection fraction. The left-ventricular end-diastolic diameterwas obtained from the parasternal long-axis view, and theleft-ventricular ejection fraction was calculated by using thebiplane method (Simpson’s rule).
Atriobiventricular Device Implantation
Commercially available biventricular pacemakers wereused (Insync III 8042/Medtronic, Minneapolis, Minn; StratosLV/Biotronik, Berlin, Germany; and Frontier/St. Jude Medical,Memphis, Tenn). The right atrial lead was positioned in theright atrial appendix, and the ventricular lead was positioned inthe right ventricular outflow. The LV pacing lead was posi-tioned in a posterior or lateral branch of the coronary sinus inall patients. An atriobiventricular system was used in allpatients.
Statistical Analysis
Data are expressed as the mean � 1 standard deviation.For the comparison of qualitative variables, the chi-square test,the Fisher exact test, and the likelihood ratio chi-square testwere used. For the comparison of parametric variables beforeand after CRT, we used the paired t test and analysis ofvariance for repeated measures. The comparison of parametersbetween groups was analyzed with an unpaired t test, and astepwise logistic model was used to identify predictive param-eters. The sensitivity and specificity of the H/M ratio beforetreatment for predicting response to CRT was determined byreceiver-operating characteristic curves. Statistical significance
Table 2. Clinical and functional changes in relationto CRT
Pre-CRT(N � 30)
Post-CRT(N � 30)
Pvalue
NYHA class (n)I/II 0 13/8III/IV 26/4 8/1
ElectrocardiographyQRS duration (ms) 163 � 22 147 � 26 .0002
EchocardiographyLVEDD (mm) 79 � 11 76 � 16 .07LVEF (%) 0.22 � 0.05 0.27 � 0.09 .02
123I-metaiodoben-zylguanidine
H/M ratio 1.42 � 0.26 1.53 � 0.27 .005WR (%) 44 � 25 42 � 30 .7
NYHA, New York Heart Association; CRT, cardiac resynchronizationtherapy; ms, milliseconds; LVEDD, left-ventricular end diastolicdiameter; LVEF, left-ventricular ejection fraction; H/M ratio, heartto mediastinum count; WR, washout rate.
was defined at P � .05.
RESULTS
Clinical and Functional Follow-Up
Before CRT, 26 (87%) patients were in FC III, and4 (13%) were in FC IV. After CRT, 12 (40%) patientschanged from FC III to FC I, 8 (27%) patients changedfrom FC III to FC II, 1 (3%) patient changed from FC IVto FC I, 6 patients (20%) remained in FC III, 2 (7%)patients changed from FC IV to FC III, and 1 patient(3%) remained in FC IV. After CRT, the QRS widthchanged from 163 � 22 milliseconds to 147 � 26milliseconds (P � .0002), the mean left-ventricularejection fraction increased from 0.22 � 0.05 to 0.27 �0.09 (P � .02), and the mean left-ventricular end-diastolic diameter changed from 79 � 11 mm to 76 � 16mm (P � .07). The H/M ratio increased significantlycompared with the baseline value (from 1.42 � 0.26 to1.53 � 0.27; P � .005), but the change of in WR was notstatistically significant (Table 2).
Characteristics of Groups
After CRT, patients were classified into two groups:G1, 21 (70%) patients in FC I or II; and G2, 9 (30%)
Table 3. Baseline characteristics of patientsaccording to CRT response: Group 1 (responders,improvement to functional class II or I) or group 2(nonresponders, remaining in class III or IV)
Group 1(N � 21)
Group 2(N � 9)
Pvalue
Age (y) 57 � 11 64 � 15 NSMale sex (%) 57 43 NSCause of CHF, n (%) NS
Idiopathic 17 (81) 6 (67)Ischemic 4 (19) 3 (33)
NYHA class, n (%)III 20 (95) 6 (67)IV 1 (5) 3 (33)
Drugs, n (%)ACE inhibitor or
ARB21 (100) 9 (100) NS
Beta-blocker 21 (100) 8 (89) NSSpironolactone 19 (90) 7 (78) NSDiuretic 18 (86) 8 (89) NSDigoxin 12 (57) 6 (67) NSAmiodarone 4 (19) 3 (33) NS
ACE, Angiotensin-converting enzyme; ARB, angiotensin receptorblocker; CHF, chronic heart failure; CRT, cardiac resynchronizationtherapy; NS, not significant; NYHA, New York Heart Association.
patients in FC III or IV. There were no differences in age,
Journal of Nuclear Cardiology D’Orio Nishioka et al 855Volume 14, Number 6;852-9 MIBG imaging and cardiac resynchronization therapy
sex, cause of cardiomyopathy, and medical treatmentsbetween groups. The baseline characteristics of bothgroups and medical treatments are shown in Table 3.
Comparison of Findings Between Groups
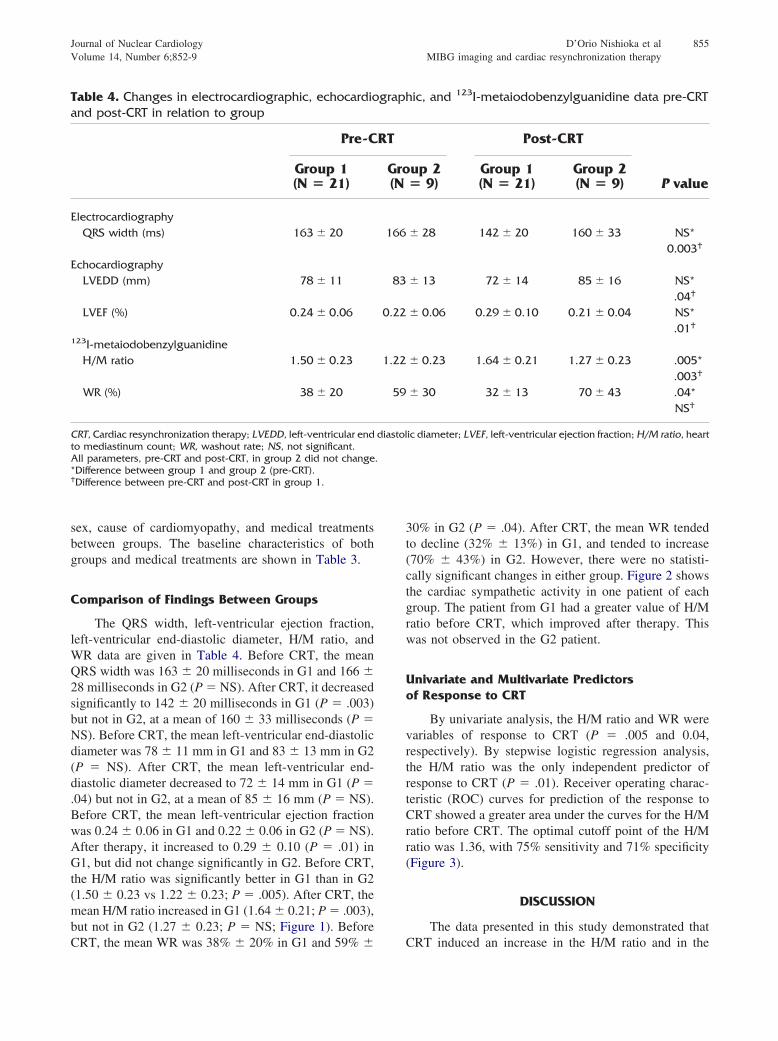
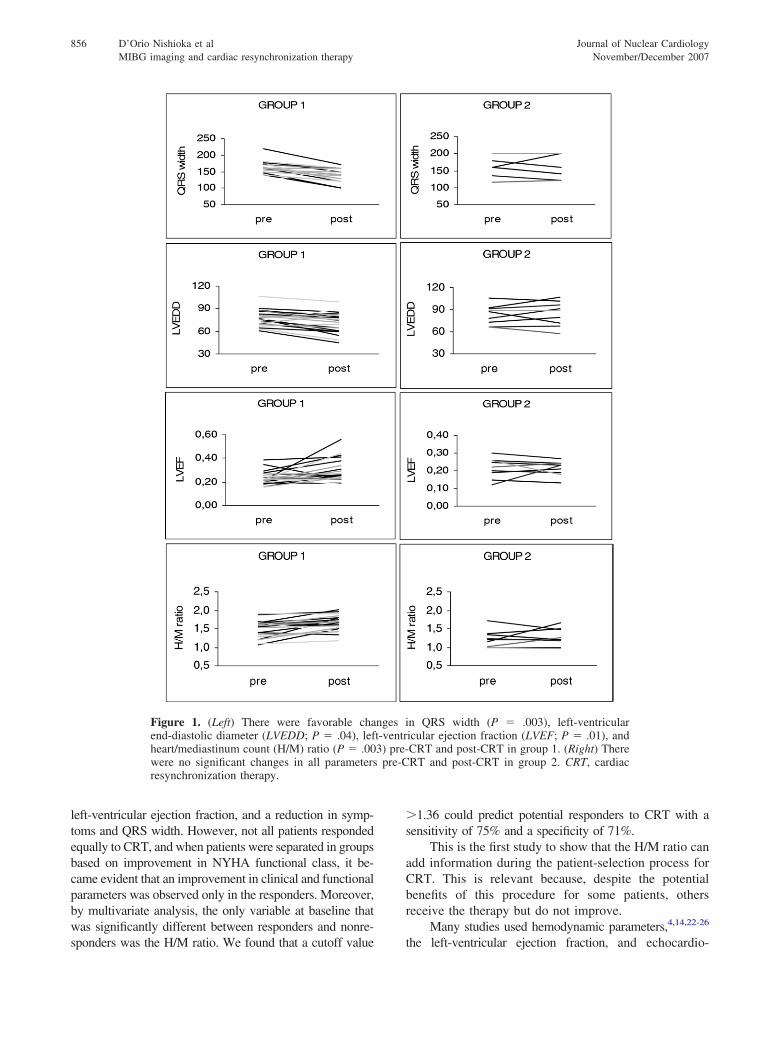
The QRS width, left-ventricular ejection fraction,left-ventricular end-diastolic diameter, H/M ratio, andWR data are given in Table 4. Before CRT, the meanQRS width was 163 � 20 milliseconds in G1 and 166 �28 milliseconds in G2 (P � NS). After CRT, it decreasedsignificantly to 142 � 20 milliseconds in G1 (P � .003)but not in G2, at a mean of 160 � 33 milliseconds (P �NS). Before CRT, the mean left-ventricular end-diastolicdiameter was 78 � 11 mm in G1 and 83 � 13 mm in G2(P � NS). After CRT, the mean left-ventricular end-diastolic diameter decreased to 72 � 14 mm in G1 (P �.04) but not in G2, at a mean of 85 � 16 mm (P � NS).Before CRT, the mean left-ventricular ejection fractionwas 0.24 � 0.06 in G1 and 0.22 � 0.06 in G2 (P � NS).After therapy, it increased to 0.29 � 0.10 (P � .01) inG1, but did not change significantly in G2. Before CRT,the H/M ratio was significantly better in G1 than in G2(1.50 � 0.23 vs 1.22 � 0.23; P � .005). After CRT, themean H/M ratio increased in G1 (1.64 � 0.21; P � .003),but not in G2 (1.27 � 0.23; P � NS; Figure 1). Before
Table 4. Changes in electrocardiographic, echocardioand post-CRT in relation to group
Pre-C
Group 1(N � 21)
ElectrocardiographyQRS width (ms) 163 � 20
EchocardiographyLVEDD (mm) 78 � 11
LVEF (%) 0.24 � 0.06
123I-metaiodobenzylguanidineH/M ratio 1.50 � 0.23
WR (%) 38 � 20
CRT, Cardiac resynchronization therapy; LVEDD, left-ventricular endto mediastinum count; WR, washout rate; NS, not significant.All parameters, pre-CRT and post-CRT, in group 2 did not change*Difference between group 1 and group 2 (pre-CRT).†Difference between pre-CRT and post-CRT in group 1.
CRT, the mean WR was 38% � 20% in G1 and 59% �
30% in G2 (P � .04). After CRT, the mean WR tendedto decline (32% � 13%) in G1, and tended to increase(70% � 43%) in G2. However, there were no statisti-cally significant changes in either group. Figure 2 showsthe cardiac sympathetic activity in one patient of eachgroup. The patient from G1 had a greater value of H/Mratio before CRT, which improved after therapy. Thiswas not observed in the G2 patient.
Univariate and Multivariate Predictorsof Response to CRT
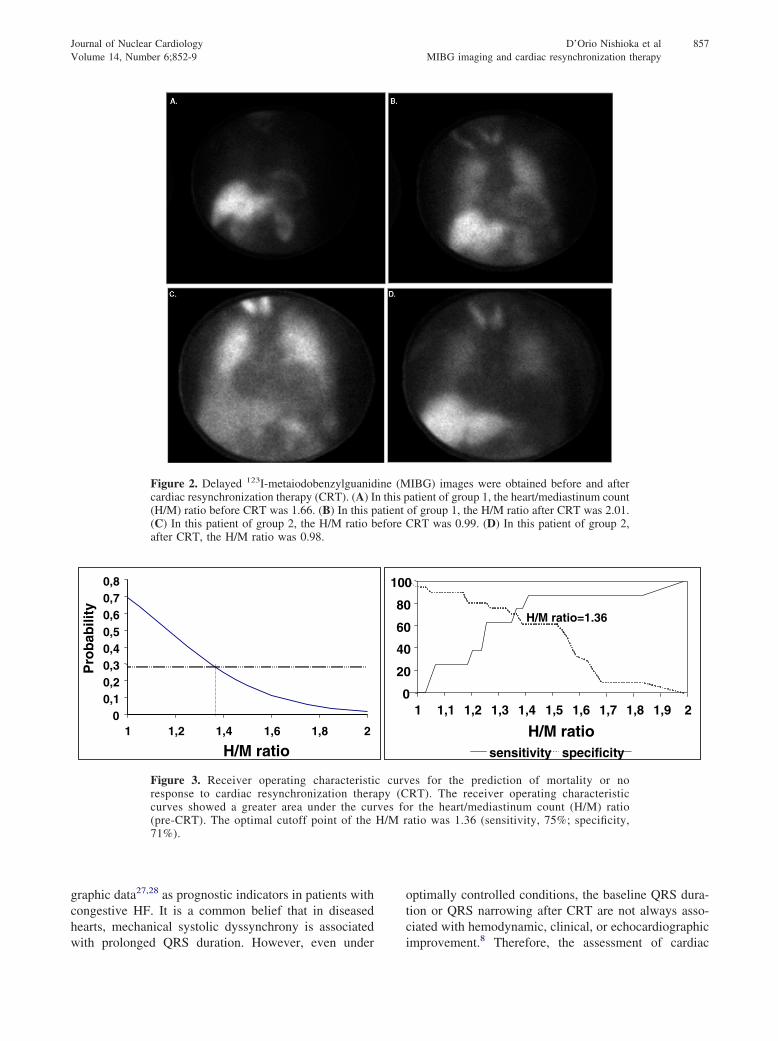
By univariate analysis, the H/M ratio and WR werevariables of response to CRT (P � .005 and 0.04,respectively). By stepwise logistic regression analysis,the H/M ratio was the only independent predictor ofresponse to CRT (P � .01). Receiver operating charac-teristic (ROC) curves for prediction of the response toCRT showed a greater area under the curves for the H/Mratio before CRT. The optimal cutoff point of the H/Mratio was 1.36, with 75% sensitivity and 71% specificity(Figure 3).
DISCUSSION
The data presented in this study demonstrated that
ic, and 123I-metaiodobenzylguanidine data pre-CRT
Post-CRT
P valueup 2� 9)
Group 1(N � 21)
Group 2(N � 9)
� 28 142 � 20 160 � 33 NS*0.003†
� 13 72 � 14 85 � 16 NS*.04†
� 0.06 0.29 � 0.10 0.21 � 0.04 NS*.01†
� 0.23 1.64 � 0.21 1.27 � 0.23 .005*.003†
� 30 32 � 13 70 � 43 .04*NS†
ic diameter; LVEF, left-ventricular ejection fraction; H/M ratio, heart
graph
RT
Gro(N
166
83
0.22
1.22
59
diastol
.
CRT induced an increase in the H/M ratio and in the
856 D’Orio Nishioka et al Journal of Nuclear CardiologyMIBG imaging and cardiac resynchronization therapy November/December 2007
left-ventricular ejection fraction, and a reduction in symp-toms and QRS width. However, not all patients respondedequally to CRT, and when patients were separated in groupsbased on improvement in NYHA functional class, it be-came evident that an improvement in clinical and functionalparameters was observed only in the responders. Moreover,by multivariate analysis, the only variable at baseline thatwas significantly different between responders and nonre-
Figure 1. (Left) There were favorable chaend-diastolic diameter (LVEDD; P � .04), lefheart/mediastinum count (H/M) ratio (P � .00were no significant changes in all parametersresynchronization therapy.
sponders was the H/M ratio. We found that a cutoff value
�1.36 could predict potential responders to CRT with asensitivity of 75% and a specificity of 71%.
This is the first study to show that the H/M ratio canadd information during the patient-selection process forCRT. This is relevant because, despite the potentialbenefits of this procedure for some patients, othersreceive the therapy but do not improve.
Many studies used hemodynamic parameters,4,14,22-26
n QRS width (P � .003), left-ventricularicular ejection fraction (LVEF; P � .01), andCRT and post-CRT in group 1. (Right) ThereRT and post-CRT in group 2. CRT, cardiac
nges it-ventr3) pre-
pre-C
the left-ventricular ejection fraction, and echocardio-
Journal of Nuclear Cardiology D’Orio Nishioka et al 857Volume 14, Number 6;852-9 MIBG imaging and cardiac resynchronization therapy
graphic data27,28 as prognostic indicators in patients withcongestive HF. It is a common belief that in diseasedhearts, mechanical systolic dyssynchrony is associated
Figure 2. Delayed 123I-metaiodobenzylguanidcardiac resynchronization therapy (CRT). (A) I(H/M) ratio before CRT was 1.66. (B) In this p(C) In this patient of group 2, the H/M ratio bafter CRT, the H/M ratio was 0.98.
00,10,20,30,40,50,60,70,8
1 1,2 1,4 1,6 1,8 2
H/M ratio
Pro
bab
ility
Figure 3. Receiver operating characteristiresponse to cardiac resynchronization theracurves showed a greater area under the cur(pre-CRT). The optimal cutoff point of the71%).
with prolonged QRS duration. However, even under
optimally controlled conditions, the baseline QRS dura-tion or QRS narrowing after CRT are not always asso-ciated with hemodynamic, clinical, or echocardiographic
IBG) images were obtained before and afteratient of group 1, the heart/mediastinum countof group 1, the H/M ratio after CRT was 2.01.CRT was 0.99. (D) In this patient of group 2,
1 1,1 1,2 1,3 1,4 1,5 1,6 1,7 1,8 1,9 2
H/M ratiosensitivity specificity
H/M ratio=1.36
es for the prediction of mortality or noRT). The receiver operating characteristicr the heart/mediastinum count (H/M) ratioatio was 1.36 (sensitivity, 75%; specificity,
ine (Mn this patientefore
0
20
40
60
80
100
c curvpy (Cves foH/M r
improvement.8 Therefore, the assessment of cardiac

858 D’Orio Nishioka et al Journal of Nuclear CardiologyMIBG imaging and cardiac resynchronization therapy November/December 2007
sympathetic activity by MIBG scintigraphy may contrib-ute to a more appropriate patient selection and predictionof response to this therapy.
Merlet et al.29 assessed MIBG uptake and othervariables in patients with dilated cardiomyopathy, andverified that MIBG uptake, as assessed with the H/Mratio, was the best predictor of survival. Suwa et al.17
used MIBG imaging to predict the response to bisoprololtherapy, identifying an H/M ratio �1.7 as a goodpredictor. In this study, CRT increased cardiac MIBGuptake in patients who benefited from therapy, reflectingimprovement in the balance of cardiac adrenergic func-tion. Furthermore, one study indicated that MIBG pa-rameters correlate with inflammatory cytokines such asinterleukin.30 Gerson et al.31 showed that using MIBG tofurther classify severe heart-failure patients by risk typecan effectively contribute to establishing indications forheart transplantation.
The degree of sympathetic nervous-system derange-ment measured by MIBG scintigraphy is related tocardiac remodeling during the evolution of HF, reflectingthe degree of cardiac dysfunction. Kasama et al.18 foundgreater values of H/M ratio in a population with conges-tive heart failure and preserved left-ventricular ejectionfraction. It is possible that lower values of H/M ratiosrepresent hearts with more severe myocardial damageand without conditions to improve function despite anytherapeutic approach. Thus, the lowest H/M values insome patients represent advanced and irreversible intra-cellular derangement.
A misbalance of adrenergic function is a hallmark ofchronic HF, and cardiac MIBG imaging seems to be auseful tool in the evaluation of prognosis13-15 and re-sponse to treatment.16-22 To distinguish respondersamong patients at both ends of the HF spectrum repre-sents a major problem. Considering the procedural risks,the use of CRT in end-stage HF is even more trouble-some, because little evidence of HF improvement existsin this population.32,33
We can state that the baseline cardiac sympatheticactivity evaluated by MIBG scintigraphy offers addi-tional information to that of ventricular dyssynchrony,thus leading to a better definition of HF outcome aftertherapy. This assessment is also useful in evaluating thecardiac sympathetic activity response in patients whoundergo CRT.
Limitations
The number of patients in the present study limitsthe power of its findings. The results shown here seem tobe very promising. However, further studies with a large
patient population, using this cutoff value H/M ratio inthe selection of candidates for CRT, will be necessary tovalidate these results.
Another limitation may involve the fact that onlyplanar images were used. Maybe the use of MIBGtomographic images would allow a better separation ofthe heart from other thoracic structures. This couldcontribute to the achievement of a more precise numberof counts in the heart and mediastinum regions of interestand more accurate indices.
Possible interobserver and intraobserver variabilitymay also have interfered with the results, because pa-tients with severe HF have a low cardiac concentration ofMIBG, which increases statistical errors during calcula-tions.
Conclusions
In conclusion, these results show that an improve-ment in cardiac sympathetic activity correlated with apositive response to CRT, and that the H/M ratio ofMIBG uptake could help in selecting patients for CRT. Alow value for cardiac MIBG uptake seems to be a markerof end-stage chronic HF and nonresponse to CRT.
References
1. Cazeau S, Leclercq C, Lavergne T, Walker S, Varma C, Linde C,et al. Multisite Stimulation in Cardiomyopathies (MUSTIC) StudyInvestigators. Effects of multisite biventricular pacing in patientswith heart failure and intraventricular conduction delay. N EnglJ Med 2001;344:873-80.
2. Abraham WT, Fisher WG, Smith AL, Delurgio DB, Leon AR, LohE, et al. MIRACLE Study Group. Multicenter In Sync RandomizedClinical Evaluation. Cardiac resynchronization in chronic heartfailure. N Engl J Med 2002;346:1845-53.
3. Swedberg K, Cleland J, Dargie H, Drexler H, Follath F, KomajdaM, et al. Guidelines for the diagnosis and treatment of chronicheart failure: executive summary (update 2005); the Task Force forthe Diagnosis and Treatment of Chronic Heart Failure of theEuropean Society of Cardiology. Eur Heart J 2005;26:1115-40.
4. Cleland JG, Daubert JC, Erdmann E, Freemantle N, Gras D,Kappenberger L, et al. The effect of cardiac resynchronization onmorbidity and mortality in heart failure. N Engl J Med 2005;352:1539-49.
5. Khand A, Gemmel J, Clark AL, Cleland JGF. Is the prognosis ofheart failure improving? J Am Coll Cardiol 2000;36:2284-6.
6. Bonow RO, Bennett S, Casey DE, Ganiats TG, Hlatky MA,Konstam MA, et al. ACC/AHA clinical performance measures foradults with chronic heart failure: a report of the American Collegeof Cardiology/American Heart Association Task Force on Perfor-mance Measures (Writing Committee to Develop Heart FailureClinical Performance Measures) endorsed by the Heart FailureSociety of America. J Am Coll Cardiol 2005;46:1144-78.
7. Yu CM, Zhang Q, Fung JW, Chan HC, Chan YS, Yip GW, et al.A novel tool to assess systolic asynchrony and identify respondersof cardiac resynchronization therapy by tissue synchronizationimaging. J Am Coll Cardiol 2005;45:677-84.
8. Rosanio S, Schwarz ER, Ahmad M, Jammula P, Vitarelli A,
Uretsky BF, et al. Benefits, unresolved questions, and technical
Journal of Nuclear Cardiology D’Orio Nishioka et al 859Volume 14, Number 6;852-9 MIBG imaging and cardiac resynchronization therapy
issues of cardiac resynchronization therapy for heart failure. Am JCardiol 2005;96:710-7.
9. Strickberger SA, Conti J, Daoud EG, Havranek E, Mehra MR, PiñaIL, Young J. Patient selection for cardiac resynchronization ther-apy: from the Council on Clinical Cardiology Subcommittee onElectrocardiography and Arrhythmias and the Quality of Care andOutcomes Research Interdisciplinary Working Group, in collabo-ration with the Heart Rhythm Society. Circulation 2005;111:2146-50.
10. Bax JJ, Abraham T, Barold SS, Breithardt OA, Fung JW, GarrigueS, et al. Cardiac resynchronization therapy. Part 1—issues beforedevice implantation. J Am Coll Cardiol 2005;46:2153-67.
11. Marcassa C, Campini R, Verna S, Ceriani L, Giannuzzi P.Assessment of cardiac asynchrony by radionuclide phase analysis:correlation with ventricular function in patients with narrow orprolonged QRS interval. Eur J Heart Fail 2007;9:484-90.
12. Ogita H, Shimonagata T, Fukunami M, Kumagai K, Yamada T,Asano Y, et al. Prognostic significance of cardiac 123I metaiodo-benzylguanidine imaging for mortality and morbidity in patientswith chronic heart failure: a prospective study. Heart 2001;86:656-60.
13. Flotats A, Carrió I. Cardiac neurotransmission SPECT imaging.J Nucl Cardiol 2004;11:587-602.
14. Anastasiou-Nana MI, Terrovitis JV, Athanasoulis T, Karaloizos L,Geramoutsos A, Pappa L, et al. Prognostic value of iodine-123-metaiodobenzylguanidine myocardial uptake and heart rate vari-ability in chronic congestive heart failure secondary to ischemic oridiopathic dilated cardiomyopathy. Am J Cardiol 2005;96:427-31.
15. Matsui T, Tsutamoto T, Maeda K, Kusukawa J, Kinoshita M.Prognostic value of repeated 123I-metaiodobenzylguanidine imag-ing in patients with dilated cardiomyopathy with congestive heartfailure before and after optimized treatments—comparison withneurohumoral factors. Circ J 2002;66:537-43.
16. Agostini D, Belin A, Amar MH, Darlas Y, Hamon M, Grollier G,et al. Improvement of cardiac neuronal function after carvediloltreatment in dilated cardiomyopathy: a 123I-MIBG scintigraphicstudy. J Nucl Med 2000;41:845-51.
17. Suwa M, Otake Y, Moriguchi A, et al. Iodine-123 metaiodoben-zylguanidine myocardial scintigraphy for prediction of response tobeta-blocker therapy in patients with dilated cardiomyopathy. AmHeart J 1997;133:352-8.
18. Kasama S, Toyama T, Kumakura H, Takayama Y, Ichikawa S,Suzuki T, et al. Effects of candesartan on cardiac sympatheticnerve activity in patients with congestive heart failure and pre-served left ventricular ejection fraction. J Am Coll Cardiol 2005;45:661-7.
19. Toyama T, Hoshizaki H, Seki R, Isobe N, Adachi H, Naito S, et al.Efficacy of carvedilol treatment on cardiac function and cardiacsympathetic nerve activity in patients with dilated cardiomyopa-thy: comparison with metoprolol therapy. J Nucl Med 2003;44:1604-11.
20. Choi JY, Lee KH, Hong KP, Kim BT, Seo JD, Lee WR, Lee SH.
Iodine-123 MIBG imaging before treatment of heart failure withcarvedilol to predict improvement of left ventricular function andexercise capacity. J Nucl Cardiol 2001;8:4-9.
21. Gerson MC, Craft LL, McGuire N, Suresh DP, Abraham WT,Wagoner LE. Carvedilol improves left ventricular function in heartfailure patients with idiopathic dilated cardiomyopathy and a widerange of sympathetic nervous system function as measured byiodine 123 metaiodobenzylguanidine. J Nucl Cardiol 2002;9:608-15.
22. Erol-Yilmaz A, Verberne HJ, Schrama TA, Hrudova J, De WinterRJ, Van Eck-Smit BL, et al. Cardiac resynchronization inducesfavorable neurohumoral changes. Pacing Clin Electrophysiol 2005;28:304-10.
23. Schiller NB, Shah PM, Crawford M, DeMaria A, Devereux R,Feigenbaum H, et al. Recommendations for quantitation of the leftventricle by two-dimensional echocardiography. American Societyof Echocardiography Committee on Standards, Subcommittee onQuantification of Two-Dimensional Echocardiograms. J Am SocEchocardiogr 1989;2:358-67.
24. Wieland DM, Wu J, Brown LE, Mangner TJ, Swanson DP,Beierwaltes WH. Radiolabeled adrenergic neuron-blocking agents:adrenomedullary imaging with (131I)iodobenzylguanidine. J NuclMed 1980;21:349-53.
25. Dae MW, O’Connell JW, Botvinick EH, Ahearn T, Yee E,Huberty JP, et al. Scintigraphic assessment of regional cardiacinnervation. Circulation 1989;79:634-44.
26. Merlet P, Benvenuti C, Moyse D, Pouillart F, Dubois-Randé JL,Duval AM, et al. Prognostic value of MIBG imaging in idiopathicdilated cardiomyopathy. J Nucl Med 1999;40:917-23.
27. Unverferth DV, Magorien RD, Moeschberger ML, Baker PB,Fetters JK, Leier CV. Factors influencing the one-year mortality ofdilated cardiomyopathy. Am J Cardiol 1984;54:147-52.
28. Florea VG, Henein MY, Cicoira M, Anker SD, Doehner W,Ponikowski P, et al. Echocardiographic determinants of mortalityin patients �67 years of age with chronic heart failure. Am JCardiol 2000;86:158-61.
29. Merlet P, Valette H, Dubois-Randé JL, Moyse D, Duboc D, DoveP, et al. Prognostic value of cardiac metaiodobenzylguanidineimaging in patients with heart failure. J Nucl Med 1992;33:471-7.
30. Parthenakis FI, Patrianakos A, Prassopoulos V, Papadimitriou E,Nikitovic D, Karkavitsas NS, et al. Relation of cardiac sympatheticinnervation to proinflammatory cytokine levels in patients withheart failure secondary to idiopathic dilated cardiomyopathy. Am JCardiol 2003;91:1190-4.
31. Gerson MC, McGuire N, Wagoner LE. Sympathetic nervoussystem function as measured by I-123 metaiodobenzylguanidinepredicts transplant-free survival in heart failure patients withidiopathic dilated cardiomyopathy. J Card Fail 2003;9:384-91.
32. Greenberg B, Mehra MR. All patients with heart failure andintraventricular conduction defect or dyssynchrony should notreceive cardiac resynchronization therapy. Circulation 2006;114:2685-91.
33. Yamashina S, Yamazaki J-I. Role of MIBG myocardial scintigra-phy in the assessment of heart failure: the need to establish
evidence. Eur J Nucl Med Mol Imaging 2004;31:1353-5.

![A new approach in the treatment of stage IV neuroblastoma using a combination of [ 131I]meta-iodobenzylguanidine (MIBG) and cisplatin](https://static.fdokumen.com/doc/165x107/631dc56e4265d1c0f1072023/a-new-approach-in-the-treatment-of-stage-iv-neuroblastoma-using-a-combination-of.jpg)







![Somatostatin receptor scintigraphy with [111In-DTPA-d-Phe1]- and [123I-Tyr3]-octreotide: the Rotterdam experience with more than 1000 patients](https://static.fdokumen.com/doc/165x107/63360adfb5f91cb18a0ba76f/somatostatin-receptor-scintigraphy-with-111in-dtpa-d-phe1-and-123i-tyr3-octreotide.jpg)



![Striatal amphetamine-induced dopamine release in patients with schizotypal personality disorder studied with single photon emission computed tomography and [123I]iodobenzamide](https://static.fdokumen.com/doc/165x107/631cb9a45a0be56b6e0e579d/striatal-amphetamine-induced-dopamine-release-in-patients-with-schizotypal-personality.jpg)





