85127.pdf - mediaTUM
43
Methods Inf Med 4/2008 279 © 2008 Schattauer GmbH Introducing Kuhn et al.’s Paper “Informatics and Medicine: From Molecules to Populations” and Invited Papers on this Special Topic C. A. Kulikowski Rutgers – The State University of New Jersey, New Brunswick, New Jersey, USA Summary Objective: To introduce the paper by Kuhn et al. “Informatics and Medicine: From Molecules to Popu- lations” and the papers that follow on this special topic in this issue of Methods of Information in Medicine, which opens a debate on the Kuhn et al. paper’s assertions by an international panel of invited researchers in biomedical informatics. Method: An introductory summary and comparative review of the Kuhn et al. paper and the debate papers, with some personal observations. Results: The Kuhn et al. paper makes a strong case for interdisciplinary education in biomedical informatics across institutions at the graduate level, which could be strengthened by analysis of previous relevant inter- disciplinary experiences elsewhere, and the challenges they have faced, which point to more pervasive and earlier-stage needs for both education and practice bridging the research and healthcare communities. Conclusions: The experts debating the Kuhn et al. paper strongly and broadly support the key recommen- dation of developing graduate education in biomedical informatics in a more comprehensive way, yet at the same time make some incisive comments about the limitations of the “positivistic” and excessively tech- nological orientation of the paper, which could benefit from greater attention to the narrative and care-giving aspects of health practice, with more emphasis on its human and social aspects. Keywords Informatics, medicine, interdisciplinary education, molecules to populations, genotype to phenotype, clinome, narrative medicine, evidence-based medicine Methods Inf Med 2008; 47: 279–282 Editorial Parallel rapid developments in both the science and technologies of biology and in- formatics are already strongly affecting the practice of medicine. They hold the promise of eventually revolutionizing our knowl- edge of how genetics, development, disease, and environment interact in affecting human health, and strongly impacting medi- cal and healthcare practices. Recently, Professor Klaus Kuhn and colleagues at Munich Technical University, the Ludwig- Maximilians University and the Munich Helmholtz Center proposed the creation of “a research-oriented interdisciplinary Grad- uate School” [1] which has now been estab- lished. This issue of Methods publishes a paper by Kuhn et al. [1] laying out the rationale for such a Graduate School, ar- guing how informatics and medicine inter- act uniquely in the study of health and dis- ease across a range of biological scales from molecules to populations, in a way that requires a much stronger interdisciplinary focus than current individual programs to prepare future leaders in the study of bio- medical systems affecting all aspects of bio- medical research, healthcare practice, and education. Because the importance of this initiative far transcends its immediate local and national contexts in Munich and Ger- many, the editor of Methods solicited com- ments on the paper from an international group of experts in biomedical and health informatics and related disciplines, with the goal of stimulating a lively debate on the challenges facing our field. I believe that our readers will agree they have succeeded in this. The paper with these commentaries [2] and one by the past editor of Methods and founder of the IMIA Yearbook [3] which follow that of Kuhn et al. include a wide range of reasoned arguments and original position statements which, while
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of 85127.pdf - mediaTUM

Methods Inf Med 4/2008
279
© 2008 Schattauer GmbH
Introducing Kuhn et al.’s Paper “Informaticsand Medicine: From Molecules to Populations”and Invited Papers on this Special TopicC. A. KulikowskiRutgers – The State University of New Jersey, New Brunswick, New Jersey, USA
SummaryObjective: To introduce the paper by Kuhn et al.“Informatics and Medicine: From Molecules to Popu-lations” and the papers that follow on this special topicin this issue of Methods of Information in Medicine,which opens a debate on the Kuhn et al. paper’sassertions by an international panel of invitedresearchers in biomedical informatics.Method: An introductory summary and comparativereview of the Kuhn et al. paper and the debate papers,with some personal observations.Results: The Kuhn et al. paper makes a strong case forinterdisciplinary education in biomedical informaticsacross institutions at the graduate level, which could bestrengthened by analysis of previous relevant inter-disciplinary experiences elsewhere, and the challengesthey have faced, which point to more pervasive andearlier-stage needs for both education and practicebridging the research and healthcare communities.Conclusions: The experts debating the Kuhn et al.paper strongly and broadly support the key recommen-dation of developing graduate education in biomedicalinformatics in a more comprehensive way, yet at thesame time make some incisive comments about thelimitations of the “positivistic” and excessively tech-nological orientation of the paper, which could benefitfrom greater attention to the narrative and care-givingaspects of health practice, with more emphasis on itshuman and social aspects.
KeywordsInformatics, medicine, interdisciplinary education,molecules to populations, genotype to phenotype,clinome, narrative medicine, evidence-based medicine
Methods Inf Med 2008; 47: 279–282
Editorial
Parallel rapid developments in both thescience and technologies of biology and in-formatics are already strongly affecting thepractice of medicine. They hold the promiseof eventually revolutionizing our knowl-edge of how genetics, development, disease,and environment interact in affectinghuman health, and strongly impacting medi-cal and healthcare practices. Recently,Professor Klaus Kuhn and colleagues atMunich Technical University, the Ludwig-Maximilians University and the MunichHelmholtz Center proposed the creation of“a research-oriented interdisciplinary Grad-uate School” [1] which has now been estab-lished. This issue of Methods publishes apaper by Kuhn et al. [1] laying out therationale for such a Graduate School, ar-guing how informatics and medicine inter-act uniquely in the study of health and dis-ease across a range of biological scales frommolecules to populations, in a way thatrequires a much stronger interdisciplinaryfocus than current individual programs toprepare future leaders in the study of bio-medical systems affecting all aspects of bio-medical research, healthcare practice, andeducation. Because the importance of thisinitiative far transcends its immediate localand national contexts in Munich and Ger-many, the editor of Methods solicited com-ments on the paper from an internationalgroup of experts in biomedical and healthinformatics and related disciplines, with thegoal of stimulating a lively debate on thechallenges facing our field. I believe thatour readers will agree they have succeededin this. The paper with these commentaries[2] and one by the past editor of Methodsand founder of the IMIA Yearbook [3]which follow that of Kuhn et al. include awide range of reasoned arguments andoriginal position statements which, while

Methods Inf Med 4/2008
280
Editorial
strongly endorsing the educational needsidentified by Kuhn and his colleagues, alsopoint out fundamental challenges that arevery specific to the unusual combination ofscientific, technological, personal and so-cial problems characterizing biomedical in-formatics. Most importantly, these point tothe ultimate objectives of managing diffi-cult human health problems which are un-likely to yield to technological solutionsalone, however effective these may prove forsolving some of the better understood andconstrained ones. The psychological, so-cietal, and environmental components ofhealth and disease are emphasized by sev-eral of the commentators, setting the stagefor further debate and constructive sugges-tions. I appreciate the opportunity to con-tribute this Guest Editorial emphasizingsome of the highlights of Kuhn et al.’s paperwith those of the expert commentators in thelight of some of my own observations andexperiences [4].
What are the major points made by Kuhnet al. to support their thesis that interdisci-plinarity is more needed than ever to makeinformatics effective in medicine? And,does the case for biomedical informatics gobeyond what is needed for other similarinterdisciplinary programs? The analyticalfoundation of the paper rests on a four-waybreakdown of how informatics has an im-pact on: 1) basic (systems) biology; 2) bio-medical engineering; 3) eHealth; and 4)public health, which is illustrated in figure 1of [1]. This breakdown gives structure to thearguments of how informatics and its math-ematical and computational underpinningswill increasingly help support the devel-opment of molecular medicine, clinicaltranslational research, clinical medicine,seamless healthcare and public health (fig-ure 2 in [1]). In defining “the overall pic-ture” early in the paper, the authors identifyeight major technical trends in computingand software technology which are likely toincrease the ability of systems to handle themassive amounts of complex, structured in-formation involved. These are then dividedinto groups in terms of their likely impact onadvancing: 1) bioinformatics methods forresearch and increasing the reliability ofremote telematics applications of eHealth,2) clinical decision support for integrating
the interpretation of complex and hetero-genous data; 3) improvements in the oppor-tunities for personalized prevention strat-egies; 4) effectiveness of the design of newmedical devices; and 5) interface to thewealth of structured knowledge in the litera-ture through the semantic web. The authorsthen argue for “structured interdisciplinaryeducation” in four areas: bioinformatics andsystems biology; informatics for biomedi-cal engineering; health informatics andeHealth, and public health informatics andpublic health. The core of this paper detailsthose aspects of each that the authors con-sider most valuable for such education, con-cluding with an observation that “traditionaluniversity systems tend to strengthen a ‘cul-tural gap’ between classical natural science(e.g. chemistry, biology, physics) and engin-eering and informatics” ([1], p 11). These inturn are considered to lead to discontinuitiesbetween “discovery, invention and inno-vation” and “widespread technology adop-tion”, which could be overcome by “chang-ing the patterns of scientific education at theMS and PhD levels where teaching and re-search meet”. Implementation suggestionsare to: 1) coordinate and combine coursesacross the disciplines; 2) encourage joint re-search projects and workshops to share ex-perience; 3) foster links at the institutionaland personal levels; and 4) encourage pro-ject-oriented teamwork spanning the differ-ing research cultures at a high scientificlevel. The paper concludes by saying thatdoing this at early graduate school levelswith “experts of one scientific disciplinewho have a profound understanding of theother disciplines’ terminology and scien-tific culture” is a major need for healthcaresystems. The case for breadth and heteroge-neity of informatics problems and solutionsacross the spectrum from “molecules topopulations” is certainly convincing. How-ever, what is not addressed are whether theremight be lessons to be learned from experi-ences in other interdisciplinary fields whereinformatics is critical – in ecological man-agement, earth and environmental scienceswhere satellite images, GPS and advancedsensor arrays are affecting all sorts ofnatural, civil and military problems, or thepolitical and economic sciences, where theweb of online information has likewise
changed the practices of political, legal,commercial and financial competition, forinstance.
The commentaries in [2] touch on manydifficult problems faced by biomedical in-formatics as it attempts to span the in-credibly wide range of differing needs frombasic biological research, through individu-al healthcare and consumer perspectives in anetworked society, to understanding publichealth implications for various populationsat risk. There is a pattern, however, to boththe praise and criticisms made by the ex-perts. No one disagrees that more interdisci-plinary education is needed and that thegraduate level is the realistic one at which todo this, once students have acquired enoughbackground in two or more contributingdisciplines. The commentators on the wholetake a positive view of the Kuhn et al. paper,suggesting ways of amplifying its content orstrengthening its arguments. What provesmore controversial is the emphasis on tech-nological solutions to research and health-care problems argued in [1]. This tends todownplay the personal and social aspects ofbiomedical informatics which often aremajor barriers to improving healthcare, andseveral commentators emphasize this as alimitation. I will next highlight some of themajor supporting and critical points madeby each commentator, and conclude with asummary.
Russ Altman of Stanford University addsto Kuhn et al.’s analysis an emphasis on the“empowered, independent and thoroughlynetworked (health) consumer” [2], whichhas transformed the world of communi-cation and social interaction so completelyin the past decade. He argues that in thefuture this trend will have a strong effect onpeople increasingly making decisions onhandling their own healthcare – whichshould dramatically change the concept andpractice of medical and health education forpractitioners and health consumers alike –and provide ample research opportunitiesfor biomedical informatics and allied fields.Rudi Balling from the Braunschweig Helm-holtz Center for Infection Control raises thevexing questions of the contrast between the“hard” vs. “soft” sciences in the cultures thatmake up biomedical informatics, and thedifficulties of trying to overcome cur-

rent disciplinary prejudices at the graduatelevel – he argues for the need to do this muchearlier in the educational process, whilerecognizing the political and societal trendsthat work against it. His plea to “merge thecoffeerooms” for students and faculty sug-gests that increasing understanding andrespect among colleagues might be asnecessary for finding constructive solutionswithin competitive environments as its moretypical opposite.
James Brinkley from the University ofWashington compares and contrasts theMunich proposal to some of the experiencesat his university, noting that differences interminology and practice in informatics be-tween the US and Europe gives the latter abroader scope which could help unify prac-tices across a broad range of biomedical ap-plications. In addition, he points out thatfigure 2 should more generally show a fullset of interconnections between core in-formatics competencies and the differentlevels of biomedical application, rather thanthe strictly horizontal ones, which are toorestrictive.
Enrico Coeira of the University of NewSouth Wales points to antecedents for themultilevel approach to informatics andmedicine and then focuses on the barriers toadoption of IT in healthcare, which he positsare mainly of a social and not technologicalnature. He argues for the need to develop anunderstanding of the unexpected inter-actions between humans and technologicalartefacts which can help bridge the differentsocial systems of bioscience, clinical medi-cine and the citizen. Fabrizio Consorti of LaSapienzia contrasts the technological andevidence-based medicine (EMB) perspec-tive of the Kuhn et al. paper to the need for anarrative-based medicine (NBM) approachwhich is more typical of the practicingclinician’s way of describing a patient’s con-dition within the clinical context. He arguesthat considering EMB and NBM as “twodifferent paired dimensions of medicalknowledge”[2] will reduce the boundariesbetween knowledge management ande-learning.
Ali Dhansay from South Africa empha-sizes the challenges for biomedical in-formatics in developing and “hybrid” coun-tries like his own where interracial differ-
ences and endemic HIV/AIDS, malaria andtuberculosis have a major daily impact onthe lives of people. He brings up a number ofeconomic, ethical and practical issues thatarise when one tries to make the scientificachievements in genomics and biomedicinemore effective and accessible through in-formatics, while, however, creating newchallenges in terms of anonymity and con-fidentiality. Antoine Geissbuhler of GenevaUniversity and Hospitals argues that the“info-bio convergence” implicit in Kuhn etal.’s proposal is challenged by the need forsemantic integration across very differentdomains, which will change the current em-phasis on hypothesis-driven research to-wards more data-driven research in the fu-ture. This certainly will require more edu-cation and new models to encourage cross-disciplinary skills for the healthcare work-force under exceptionally difficult and com-plex social conditions. William Hersh ofOregon Health and Science University sug-gests that informatics has to go beyond com-puter science and embrace the human di-mensions of information processing, andthe need to identify the core competenciesof a field which will continue to lead to awide variety of very distinct career path-ways. Yunkap Kwankam of WHO and theUniversity of Yaounde raises the importantissue of assessment of health informatics,which is underplayed in the Kuhn et al.paper. After pointing out the known finan-cial benefits from programs that improvedrinking water and sanitation worldwide, heargues that health informatics must demon-strate comparable or even greater benefits inorder to obtain more adequate funding. Heemphasizes the need to identify “commu-nities of practice” that are effective in devel-oping a “collective wisdom” that can helpWHO and other organizations to includebiomedical informatics in its “valuechain”[2]. Nancy Lorenzi, from VanderbiltUniversity, and immediate Past President ofIMIA, and developer of IMIA’s StrategicPlan Towards IMIA 2015, comments thatKuhn at al’s article supports the view that in-formatics is “the most important driver andmediator for innovation” [2] and that collab-oration is essential to achieve this. Knowl-edge is seen as the core of innovation, whichfeeds into the major components of IMIA’s
Strategic Plan that are designed to integrateand connect the science with the practice ofinformatics in biomedicine and healthcare.Publications and electronic disseminationof information are identified as the majordisseminators of knowledge, and the inter-national interdisciplinary collaborationsfostered by IMIA are seen as central toachieving the future goals for informaticsand medicine as envisioned by Kuhn et al.’spaper. Fernando Martin-Sanchez from theMinistry of Science and Innovation in Mad-rid makes the point that nanomedicine andregenerative medicine present both oppor-tunities and challenges for biomedical in-formatics. With a rapidly ageing population,many European (and other, mostly devel-oped) countries are faced with urgent needsfor management and prevention of chronicconditions in disproportionately large per-centages of their populations. This willrequire imaginative and novel approaches toprevention and rehabilitation, including theincorporation of the latest developments innanomaterials and artifacts for effective de-ployment. He lists EU initiatives, such as theACTION-Grid which is to develop health-care information systems based on the Gridcapabilities and new technologies that sup-port these novel directions. George Mihalasof Victor Babes University in Timisoarapoints to the difficulties that were faced byneuroinformatics in having an impact, andthe need to connect to systems biology withprojects like the Virtual PhysiologicalHuman and the Physiome Project – all ofwhich will require educational componentslike AMIA’s 10×10 to educate the work-force in informatics.Yuval Shahar of BenGurion University in Beer Sheva brings outa very essential point in Kuhn et al’s paper:“only through experts in one discipline whoprofoundly understand the conceptualworld of another discipline can true multi-disciplinary research develop” – he arguesfor “boundary breaking agents” [2] as rolemodels for students to meet during theirtraining in order to foster true and produc-tive interdisciplinarity. Using the specificexample of developing a “smart medicalhome” Shahar says that only by combiningthe right bioengineering and medical in-formatics will this be achieved. He arguesfor tackling a number of grand challenges,
Methods Inf Med 4/2008
281
Editorial

Methods Inf Med 4/2008
282
Editorial
including what he terms the “Human Cli-nome Project”[2] as a continuously chang-ing library of declarative and proceduralclinical knowledge that can be “representedand accessed by computational means”. Hepoints to preliminary successes in clinicalguideline structuring and representation asprecursors to this work. Two other chal-lenges Shahar identifies are the manage-ment of patients, especially those withchronic disease, and with emphasis on thetemporal aspects of their conditions and theneed to define “clinarrays” of laboratorydata (in analogy to microarrays) to suggestnew ways for subtyping diseases. In addi-tion, the need for decision support includinggenetic components is seen as a fertile areafor engaging patients to take more responsi-bility for their own decisions while tyingthis to clinical workflows. Katsuhiko Taka-bayashi, from Chiba University emphasizesthe role of clinical studies and appropriatesecurity and confidentiality needed to safe-guard the individual while yielding theknowledge that underlies how medical deci-sions are complemented by genetic data.But he warns that law and ethics are also im-portant areas of study for biomedical in-formatics given their strong impact onpeople and how they handle health informa-tion. Finally, Gio Wiederhold from StanfordUniversity gives a more detailed descriptionof the interrelated roles of biomedical in-formatics, engineering, and software engin-eering (SWE). He recognizes the bureau-cratic barriers to change, but indicates thatpractical problems of security, confidential-ity, and limitations of the state-of-the-art inSWE, and economic considerations con-strain the development of large and effectiveeHealth systems. He points out that the ratioof 25:7 :1 between research projects, theirpractical implementation, and integrationinto practice has remained unchanged de-spite new initiatives such as Service-Oriented Architectures. His commentarytouches on the social expectations whichlimit collaboration between the formalmathematically based disciplines and thoseof the biological world, where variabilityand ongoing experimentation is the norm,and concludes with an interesting commenton the nature of randomness in limitingwhat we can know about our own reasoning
processes – suggesting the need for more re-search in this direction to help improveclinician-patient interactions.
The separate paper by Jan van Bemmel[3] provides an excellent summary of Kuhnet al.’s paper and draws parallels and con-trasts to the experience at Erasmus Univer-sity Medical Center in Rotterdam, and itspioneering development of a framework forinterdisciplinary research in medical in-formatics. He quotes from Gilles Holst’s“Ten Commandments” for encouragingproductive research in a long-standing,highly successful industrial research lab(Philips Physics Research Lab in Eind-hoven). These include the need for engagingcompetent scientists when young, withouttoo much concern about their prior experi-ence, giving them a lot of freedom, but ex-pecting them to work hard and share theirwork through publications and discussions.Solving problems through multidisciplinaryteams and encouraging the free movementfrom research to development, while beingguided by academic insights as much as bymarket opportunities are also essential forsuccess.Van Bemmel identifies a number ofgrand challenges which he ties to the adher-ence to these “commandments” and illus-trates how they might be solved if there wasmore attention to aspects of human behaviorthat define needs not easily or necessarilysatisfied by technological solutions alone.The cultural aspects of “overstretched ex-pectations’ is a concern raised to caution thereaders about the need to realistically assessproposals such as the one in Kuhn et al.’spaper.
In summary, the paper “Informatics andMedicine: From Molecules to Populations”[1] has opened a timely debate through theCommentary papers [2, 3] on the nature ofbiomedical informatics and the challenges itfaces, especially in education, in this era oftranslational and personalized medicine.They highlight the urgent need to improveour understanding of how structuring andmanaging information is central to under-standing the roles of genomics and other-omics methods in contributing to the pro-motion of individual and group health as weattempt to map the complex pathways fromgenotype to phenotype [5]. Further con-siderations extending the scope of these
commentaries might well ask whether andhow the underlying basic sciences of infor-mation generation and processing in hu-mans as well as machines is likely to be ad-vanced by biomedical informatics, which isat the unique intersection of science, tech-nology, and the practice of healthcare. Help-ing alleviate suffering draws on deep emo-tional sources of shared empathy, for whichbetter cognitive and perceptual models areneeded. And, to better understand how suc-cessful nursing and medicine can interactwith the help of informatics in social situ-ations and across different cultures [6], maywell open a largely untapped and rich sourceof experience into how we can truly person-alize healthcare in ways that we as in-dividuals would wish it to be practiced whenwe ourselves need it the most.
On behalf of the editors and editorialboard of this journal I am pleased to extendan invitation to all readers to contribute tothis ongoing debate through Letters to theEditor which could be published in futureeditions of Methods of Information in Medi-cine. We look forward to your contributions.
References1. Kuhn KA, et al. Informatics and Medicine: From
Molecules to Populations. Methods Inf Med 2008;47: 283-295.
2. Altman RB, et al. Commentaries on Informaticsin Medicine: From Molecules to Populations.Methods Inf Med. 2008; 47: 296-317.
3. Van Bemmel J. Medical Informatics Is Interdisci-plinary avant la Lettre. Methods Inf Med 2008;47: 318-321.
4. Kulikowski CA. The Micro-Macro Spectrum ofMedical Informatics Challenges: From MolecularMedicine to Transforming Health Care in aGlobalizing Society. Methods Inf Med 2002: 41:20-24.
5. Strohman R. Maneuvering in the Complex Pathfrom Genotype to Phenotype. Science 2002; 296:701-703.
6. Tallberg M. 25 Years in a Nutshell – IMIA-NI,1982-2007. IMIA Yearbook of Medical Infor-matics 2008. Methods Inf Med 2008; 47 (Suppl1): 173-178.
Correspondence to:Professor Casimir A. KulikowskiDepartment of Computer ScienceRutgers – The State University of New JerseyHill Center, Busch CampusNew Brunswick, NJ 08903, USAE-mail: [email protected]

Informatics and MedicineFrom Molecules to Populations
K. A. Kuhn1, A. Knoll1, H.-W. Mewes1, M. Schwaiger1, A. Bode1, M. Broy1, H. Daniel1,H. Feussner1, R. Gradinger1, H. Hauner1, H. Höfler1, B. Holzmann1, A. Horsch1,A. Kemper1, H. Krcmar1, E. F. Kochs1, R. Lange1, R. Leidl2, U. Mansmann2, E. W. Mayr2,T. Meitinger1, M. Molls1, N. Navab1, F. Nüsslin1, C. Peschel1, M. Reiser2, J. Ring1,E. J. Rummeny1, J. Schlichter1, R. Schmid1, H. E. Wichmann2, S. Ziegler1
1Technische Universität München, Munich, Germany*2Ludwig-Maximilians-Universität, Munich, Germany*
SummaryObjectives: To clarify challenges and research topics forinformatics in health and to describe new approachesfor interdisciplinary collaboration and education.Methods: Research challenges and possible solutionswere elaborated by scientists of two universities usingan interdisciplinary approach, in a series of meetingsover several months.Results and Conclusion: In order to translate scientificresults from bench to bedside and further into anevidence-based and efficient health system, intensivecollaboration is needed between experts from medicine,biology, informatics, engineering, public health, as wellas social and economic sciences. Research challengescan be attributed to four areas: bioinformatics and sys-tems biology, biomedical engineering and informatics,health informatics and individual healthcare, andpublic health informatics. In order to bridge existinggaps between different disciplines and cultures, wesuggest focusing on interdisciplinary education, takingan integrative approach and starting interdisciplinarypractice at early stages of education.
KeywordsInformatics, bioinformatics, health informatics,biomedical engineering, biomedical informatics,public health
Methods Inf Med 2008; 47: 283–295
doi:10.3414/ME9117
1. Introduction
Medicine and the whole health care domainare undergoing substantial changes. On theone hand, advances in molecular lifesciences, biomedical sciences and engineer-ing have significantly influenced diagnosticand therapeutic options. Molecular mecha-nisms of disease are being understood betterthan ever before, and disease patterns can beunderstood with increasing granularitydown to the level of molecules. Therapeuticmethods range from drug design and in-dividualized therapy to image guided mini-mally invasive surgery. On the other hand,demographic and sociocultural changes,together with increasing costs of new diag-nostic and therapeutic procedures, have putour health systems under severe pressure.
In this complex situation, a key role hasemerged for informatics in health, in healthtechnology and in related fields, includingbiomedical engineering, bioinformatics,biotechnology, pharmacology, managementand also economics. Informatics is anunderlying core element for these fields,providing scientific methodology, key ap-plications, and the pioneering of new ser-vices. We believe that informatics will bethe most important driver and mediator forinnovation in all health-related scientificdisciplines – with even more significantimpact than previously seen in other fields,such as the automotive industry, e-com-merce, or global logistics.
The focus of informatics is information:how it is discovered, created, identified, col-lected, structured, managed, preserved, ac-cessed, processed, presented, and studied.This also includes how it is used in differentenvironments with different informationtechnologies, and how it is applied andchanges over time. The successful use ofinformatics has to be based on intimateknowledge and interaction of scientific,technological and professional practicecomponents.The term “informatics”, whichwas coined in 1957 [1], has been increas-ingly used across Europe during the lastdecades [2, 3] implying a meaning similar to“computer science” as denoted in manyEnglish speaking countries. In thesecountries, the term “informatics” was firstused in the context of “medical in-formatics”. Biomedical informatics hasbeen defined as “the scientific field thatdeals with biomedical information, data,and knowledge – their storage, retrieval, andoptimal use for problem solving and de-cision making” [4]. For a discussion ofterminology we refer to [4].
To face the challenges in medicine and inrelated fields, multidisciplinary collabora-tion between informatics, medicine, andmany other fields has become essential.Experts from the areas of biology, medicine,public health, informatics, engineering, so-cial and economic sciences need to co-operate. In this article, we aim at clarifyingchallenges and research topics. We suggestintensive collaboration, and we recommendto educate a new generation of experts withinterdisciplinary knowledge and skills, whowill be ready to work in a multidisciplinaryenvironment and to think out of the box.
283
© 2008 Schattauer GmbH
Methods Inf Med 4/2008
* See more detailed authors´ affiliations at the endof the article.

Methods Inf Med 4/2008
284
Kuhn et al.
In the following chapters, we will outlineour vision of collaborative research andstructured interdisciplinary education. Inorder to clarify needs, multidisciplinaryworking groups were established in 2006,involving researchers from the two MunichUniversities and the Munich HelmholtzCenter, representing five different faculties.In an iterative and interactive process, areasof collaboration were identified, and newperspectives on education were elaboratedin 2006/7. Our central aim was to lay thefoundation for a research-oriented inter-disciplinary Graduate School which hasbeen established in 2008.
2. The Overall Picture:Where Do We Standand Where Do We GoProgress in medicine, covering all areasfrom drug development to personalizeddiagnostics and therapeutics, reflects thesuccess of the most challenging disciplinesinvolved: molecular biology and informa-tion science and technology. Digital dataand information are key elements of a) basicand applied research in molecular lifesciences, clinical, and population-basedstudies, b) biomedical engineering and in-formatics, c) medical care, d) organizationand communication for efficient andseamless care, e) public health, health caremanagement, and health economics.
Dramatic developments in molecularbiology and their direct influence on theunderstanding of human diseases will havefar-reaching consequences for the wholehealthcare system, significantly influencingprevention, diagnosis, and therapy. Progressin biomedical engineering will result in newdiagnostic (e.g. devices for home monitor-ing) and therapeutic options (e.g. image-guided minimally invasive surgery). Prog-ress in biomedical informatics will result innew large-scale, pervasive and ubiquitoussystems for human-computer interaction andtransformation of scientific inquiry and tech-nological development, finally realizingwhat Wiener proposed for cybernetics morethan 50 years ago. An aging society on the
one hand, and the need for affordable health-care on the other, are more than enough rea-son that there is an urgent demand to translatethe scientific progress into clinical practiceand into new prevention strategies usingtools from informatics, economics, and manyother sciences and technologies
A number of observable technical trendsin computing and software technology willcreate significant impact on the handlingand processing of huge amounts of complexinformation:1) Computing power will continue to grow,
permitting complex tasks to be solvedsuch as local correlation of patient-related data as well as the systematicexploration of huge distributed data sets.
2) Broadband networks and reliable wire-less roaming enable access to this com-puting power from everywhere and makehigh-volume data transfers and sharingof analytical and interpretive softwaretools possible – even in real time.
3) Powerful and reliable embedded systemswill become increasingly networked andwill be able to make use of their environ-ment using a variety of data acquisitiontechniques based on complex sensorsand large sensor networks.
4) Data volumes will continue to growexponentially; database technology in-cluding integration and associationmethods will enable us to efficientlyhandle unprecedented volumes of com-plex data and to structure them into use-ful knowledge.
5) Multi-agent software systems have thepotential of becoming more and moreautonomous and federated, e.g. experi-menting with becoming self-organizingwhen performing varying tasks, as wellas self-administrating and self-healing.As a consequence, the ascription of re-sponsibility and liability can become asignificant challenge.
6) Service-oriented architectures (SOA)enable a much more flexible, integratedsoftware environment; thanks to ad-vances in middleware technology, accessto data resources and software tools willbecome increasingly seamless, enablingcomplex tasks and workflows as re-quired, e.g., for systems biology and foreHealth architectures.
7) The metaphor of new medical devicesbecoming intelligent ‘assistance sys-tems’is increasingly becoming accepted;unrealistic claims of full automationhave been abandoned. Keeping humansin the loop and using their cognitiveabilities will lead to a much higheracceptance of computer-aided systemsin health than previous approaches.
8) Advanced knowledge management andthe development of advanced semanticdata models and inference methods willenable researchers to explore the medicalknowledge in research and will supportknowledge-driven discovery and inter-pretation of complex data sets (such asstudies correlating individual geneticdisposition, physiological data, and dis-ease statistics).
In concrete terms, we anticipate the follow-ing benefits for health research and its trans-lation into medicine from the above: items1-3 will rapidly advance bioinformatics-based progress in data analysis and datamining and will also improve imaging tech-nologies; they will make reliable healthtelematics and eHealth strategies possible;items 3-8 will help to provide large amountsof knowledge for the interpretation of com-plex data, to support decision-making and toallow for new prevention concepts; withitem 4 not only triggerering the develop-ment of new (implantable, intelligent) de-vices providing direct feedback from bio-chemical or physiological data but alsomaking devices possible that close the con-trol loop, i.e. sense-compute-act, inside (ornear) the patient. Software trends may leadto completely new devices – and it seemsobvious that items 5 and 6 will enableeHealth systems via highly interactive ad-vice loops. Item 6 will make it possible toidentify, choose and manage approaches inprevention and healthcare that are cost-effective and that fit patients’ preferences;item 7 will guide the development strategiesof new medical devices, from simple (inpreventive applications) to complex (in theoperating theatre); while item 8 will supportbasic and applied research with structuredinterfaces to medical knowledge.
These developments are of relevance notonly at the scientific, but also at the indus-

285
Informatics and Medicine: From Molecules to Populations
Methods Inf Med 4/2008
trial and societal level. According to a studyby the Boston Consulting Group [5], thethree pillars of the health market, phar-maceutical industry, medical technology,and healthcare IT are growing by 5% to 12%per year, with growth rates increasingsteadily. More specifically, the overallgrowth rate for medical technology is a sus-tained 5% per year, with the total worldwidemarket having grown from 124 bn in 1980to 1109 bn in 2004 and 1133 bn in 2008 [6].The healthcare-IT market (hardware, soft-ware and related services) is growing at arate of 12% per year, with a total volume of160 bn (predicted for 2008), up from12.5 bn in 1980. In other words: in the last25 years the proportion of spending on in-formation technology has increased from10% to almost 50%. We can anticipate long-term development that will lead to a com-plete information logistics chain ‘fromsingle molecules to the entire humanpopulation’ (see Fig. 1).
From the perspective of the bio-sciences,medicine, and public health (upper part ofFig. 1), informatics plays a significant roleas a critical enabler: Research in the field ofmolecular biology requires computationalresources to make huge amounts of datagenerated at independent sites available andsubject to multiple analyses. Not only domassive datasets of biological informationneed to be handled, but so must the analysis,experimental design and process-control forheterogeneous experimental systems rang-ing from nano- and cryo-technologies to theincreasingly more precise atomic-levelprobes. Clinical research will not be re-stricted to small local patient groups, but islikely to be more frequently extendedworldwide, increasing the quality andlowering the cost of studies. The integrationof genetic information into clinical trialsand into the clinical environment willchange medicine, both in the area of clinicalresearch and in clinical practice. The corre-lation of genomic variation with individualphenotypes will make it possible to betterestimate risks, and success rates of ther-apies, leading to increasingly personalizedmedicine. Population-based studies areabout to correlate genetic variation withclinically defined phenotypes taking intoaccount environmental factors. Economic
evidence finally enables society to ration-ally decide which innovations are accept-able under financial as well as legal/ethicalconstraints. In all of these domains, digitaldata must be stored, processed and analyzed,and information models need to be built. In-tegration and multidisciplinary collabora-tion are essential. Traditionally separate dis-ciplines on both sides – informatics andmedicine – need to collaborate and shareinformation in a much more coherent way.
The lower part of Figure 1 shows themethodology and technology research areasrelevant to the application domains men-tioned above. Methodology and technologyareas overlap, and their relationships to theapplication domains are not one-to-one butmany-to-many. It is these areas that willmost directly benefit from advances in in-formatics. They will enjoy the most rapidgrowth and create the highest demand forinterdisciplinary experts. We would like topoint out that this requires more than infor-mation logistics for communicating data be-tween the application domains: these scien-tific results and concepts also need to becommunicated between application do-mains and methodological research areas –
which requires intensive cooperation be-tween application domains, biomedical in-formatics and informatics. Moreover, proto-type implementations have to be translatedsubsequently into the professional environ-ment of the participating industrial andmedical partners.
The importance of cooperation betweendisciplines, and the perspectives for thefields involved have been described beforefor a number of specific fields, e.g. for bio-medical information in clinical trials and inpublic health [7, 8]. The need for tools and anew generation of information systems hasbeen described and analyzed. [9-11]. Syner-gy between medical informatics and bioin-formatics was described in 2004 [12], Sev-eral “Grand Challenges” articles have beenpublished over the last decade [13-15],which emphasize interdisciplinary work.The need for translation is being addressedin the U.S. by the CTSA program [16]. In2002 Kulikowski characterized challengesfor medical informatics in relation to a spec-trum from molecular medicine to public andglobal health [17]. To face these challengesand the challenges outlined by us, we arguein favor of intensive transdisciplinary co-
Fig. 1 Health and interrelations with informatics (for explanation see text)
Methods Inf Med 4/2008
286
Kuhn et al.
operation and true multidisciplinary edu-cation.
3. Areas for Collaborationand CooperationIn recognition of the need for profiling andconceptual exchange, we have identifiedfour areas for collaboration and cooperationwhich are closely intertwined. No order ofimportance implied, the priority areas forcollaborative research and development,complemented by structured interdisci-plinary education are:● bioinformatics and systems biology● informatics for biomedical engineering
(BME)● health informatics and eHealth● public health informatics and public
health
The goal of bioinformatics is to understandmolecular mechanisms, their genetic frame-work for diseases and their responsivenessto therapy (e.g. expression analysis vs.tumor type) using advanced informationtechnologies.
There are relevant informatics-relatedaspects of biomedical engineering andbiomedical physics, such as bio-signal andimage processing, robotics, sensors, bio-medical imaging, modeling and simulationof biophysical processes, adaptation ofmodels to treatment strategies, and alsoanalysis of clinical outcomes.
eHealth covers the whole range of use ofinformation and communication within thehealth sector, focusing on individualcitizens and patients. eHealth is one of thecore application areas of health infor-matics which addresses biomedical andhealth information discovery and manage-ment, technology, science and their social/ethical implications.
Public Health combines science andtechnologies directed to maintaining andimproving the health of all people, empha-sizing prevention and basic health needs ofthe population as a whole and managingcare given the constraints of our health caresystems. While health informatics is mainlyoriented towards individual healthcare,public health informatics is mainlyoriented towards population measures andhealth policy.
Aiming at an evidence-based and effi-cient health system, these areas will helpto● understand molecular mechanisms of
disease based on biological networks andcomputational models, including visual-izing disease with increasing granularitydown to the molecular level,
● study and apply new fine-grained andtranslational insights into disease mech-anisms for personalized medicine, in-cluding identifying personal risks andtargeting preventive interventions (be-havioral, social and medical),
● construct sensors and devices for re-search, diagnosis, treatment,
● improve communication and coopera-tion,
● gain and apply knowledge about geneticvariation in the population,
● analyze and evaluate cost-effectivenessof health care interventions.
There is a need for a generation of scientists,who can combine knowledge and skillsfrom the areas of medicine and informaticsrelated to these areas. This would cover amultidisciplinary perspective from anunderstanding of basic research topics(“bench”) to clinical medicine (”bedside”)and to the societal environment, and con-versely, from bedside to bench. The conceptshould involve clinical and epidemiologicalresearch, as well as engineering and in-formatics research.
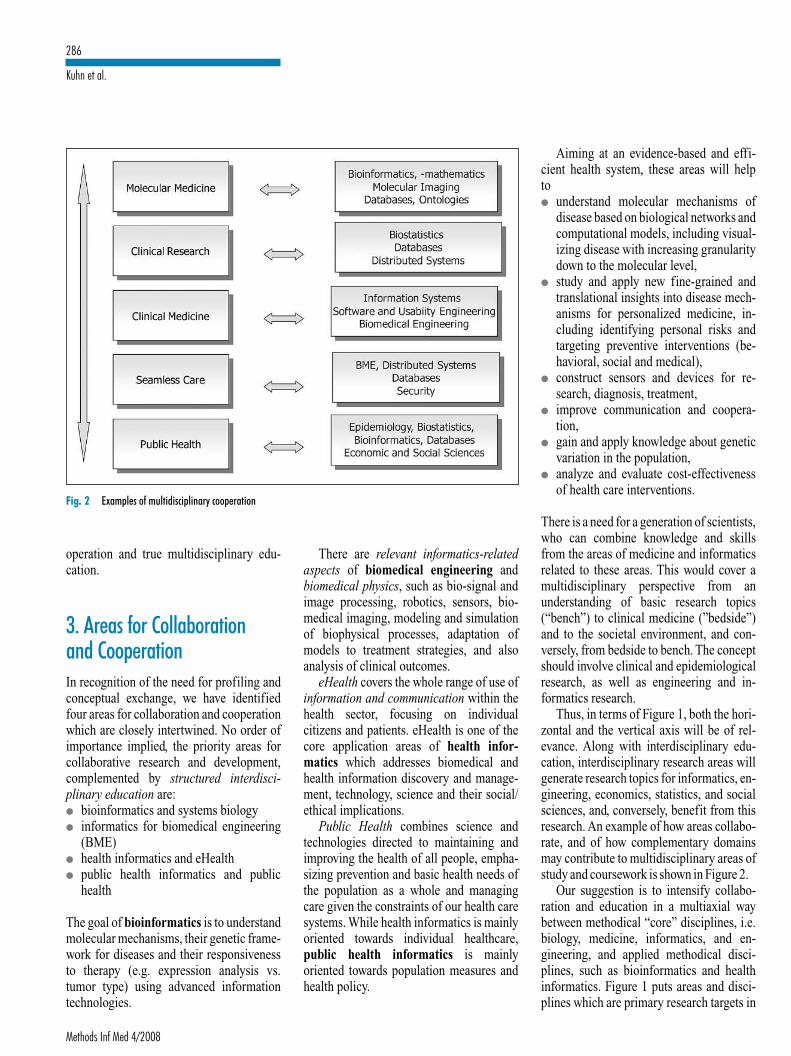
Thus, in terms of Figure 1, both the hori-zontal and the vertical axis will be of rel-evance. Along with interdisciplinary edu-cation, interdisciplinary research areas willgenerate research topics for informatics, en-gineering, economics, statistics, and socialsciences, and, conversely, benefit from thisresearch. An example of how areas collabo-rate, and of how complementary domainsmay contribute to multidisciplinary areas ofstudy and coursework is shown in Figure 2.
Our suggestion is to intensify collabo-ration and education in a multiaxial waybetween methodical “core” disciplines, i.e.biology, medicine, informatics, and en-gineering, and applied methodical disci-plines, such as bioinformatics and healthinformatics. Figure 1 puts areas and disci-plines which are primary research targets in
Fig. 2 Examples of multidisciplinary cooperation

287
Informatics and Medicine: From Molecules to Populations
Methods Inf Med 4/2008
relation to applied methodical disciplines.Biomedical informatics can be describedas a biomedical science, underlying andconnecting these applied methodical disci-plines (cf. [4]), while on the other handdrawing upon methodical core disciplines.Figure 2 illustrates this by showingexamples of how applied and underlyingbasic methodical disciplines can cooperatewith the application domains. In the follow-ing subsections, we will describe the fourareas outlined in more detail, pointing outtheir relevance to health in general and theirrole for research and education. Besides de-scribing interdisciplinary and translationalresearch challenges, we will contribute tothe discussion on education and collabora-tion [4, 18, 19, 20].
3.1 Bioinformatics and SystemsBiology3.1.1 Background and Motivation
With increasing amounts of human genomicinformation at hand, the challenge is to cor-relate medical phenotypic information withits genomic and epigenetic counterparts; inother words, with the genetic background ofthe patient and its environmental modifiersThe etiology of human diseases and theirprogression is often reflected by unexpectedpatterns of evidence at the molecular level.Monitoring such molecular states and pre-dicting the outcomes of treatments willrequire intensive research employing manyhigh-throughput technologies. These ad-vanced methods generate complex data thatare typically large in scale, high-dimen-sional and highly structured. The inter-pretation of data in the context of existingknowledge and the conversion of the resultsinto meaningful and clinically actionableknowledge is of utmost importance to theprogress of medical research.
Molecular data, in contrast to classicalbiochemical parameters, are not as directlyinterpreted clinically. Thus, therapeutic ap-proaches must rely on medical recordswhich are structured and administered insuitable, integrated databases. Research inthe past has usually focused on the computa-tional aspects of data analysis (efficiency),
on scalability to large and highly structureddatabases, and on user/computational inter-faces for data exploration. Other problemsthat have been studied include integratingdata from heterogeneous sources, correlat-ing phenomena from different views, de-tecting unusual subgroups, and probabilis-tic approaches to support medical decision-making or the design of mathematical mod-els. One of the key problems is the organi-zation of knowledge related to moleculardisease mechanisms as well as clinicalstudies (e.g., probabilistic prognosis basedon classification of tumor expression pro-files). Research aims include discoveringnew biomarkers for diagnostic purposes,correlating these markers with the clinicalcourse of disease, and choosing the “right”therapy for specific patient phenotypes.While the bioinformatics groundwork mustprovide generic workflows for the imple-mentation of such data collections and thetools to explore them, clinical and popu-lation genetics studies must generate thedata required. Such an approach is often re-ferred to as “personalized medicine”, whichcritically needs evaluation and feedback toexperimental design to close the “bench tobedside and back” loop.
3.1.2 Research Challenges
The challenges are, on the one hand, thetransformation of experimental or clinicaldata into suitable models (in the sense of thebiology of the system), and on the otherhand the professional implementation ofthese models in software systems that areaccepted by medical staff. Indeed, availablebiological measurements (e.g., differentialpatterns of gene expression) and images inthe context of medical knowledge generateinformation of a complexity far beyondwhat can currently be processed. To achievesustained progress, it is also necessary toimprove considerably on the underlyingmathematical and biological models forprocesses at many different levels, includ-ing those for cellular compartments, wholecells and their development, organs, andtheir variation across animal models andhuman populations. More powerful hybridmodels (combining discrete and continuousmodeling techniques) must be developed
and implemented. In particular, processesconcerning several (temporal and spatial)orders of magnitude have to be represented.These challenges can be addressed only byinterdisciplinary teams and researchgroups, since advanced methods from medi-cine, molecular and systems biology, bio-informatics, mathematics and computerscience are required. One example is thestudy of genetic variations, such as SNPs(single nucleotide polymorphisms) asmarkers for individual susceptibility to cer-tain diseases. The amount of data fromgenome-wide association studies with morethan 1 million SNPs per person for thou-sands of individuals provides challenges fordata management, biostatistics and bioin-formatics. And, SNPs only provide a first,simplified set of associations which do notcover the many multiple gene interactions,alternative splicings, and effects withinproteomes of different tissues and systems.
Dealing with the large data volumes to begenerated by the many such new datasets isa key research area for he database and datamanagement communities, where integra-tion, handling of large and complex data,and security are essential. Moreover, se-mantic data modelling and reasoning acrossthe semantic web – allowing the associationof rich application-specific semantics withraw and derived data – is likely to become acentral topic of research in the infor-matics community, extending translation-ally today’s methods .
Besides the modelling challenges arisingfrom high-dimensional data, there is also aneed to create and implement new IT con-cepts which allow a practical presentation aswell as manipulation not only of complexdata but also of complex concepts. A unify-ing methodological toolbox for specifica-tion and usage of high-dimensional andcomplex models is needed. On the statisticalside, this includes models with many andhigh-dimensional covariates, specificationof interaction structures and non-linearterms in functional form, or specification ofadditional information like prior distribu-tions in Bayesian models.
A challenge for translating experimentalapproaches into clinical practice is the pre-clinical evaluation of safety and efficacy.Specific and economic delivery systems

Methods Inf Med 4/2008
288
Kuhn et al.
need to be developed for drugs, genes orcells. New bioimaging techniques are re-quired to monitor effects at the molecular,cellular and organism level. Genomic, tran-scriptomic and proteomic approaches willidentify novel targets for diagnosis andtherapy and will also help to monitor con-sequences of therapeutic strategies at themolecular level. In a second and final step,candidate drugs or cell preparations must beprepared under GLP/GMP (Good Labora-tory/Manufacturing Practice) conditionsand a clinical evaluation must be undertakenin well defined groups of patients with athorough monitoring of pharmacokinetics,cell traffic, clinical side effects and efficacyparameters.
3.1.3 New Perspectives in Systems Biology
The understanding of biological systemswill be supported by formalized descrip-tions of interactions following the abstrac-tion of input/output models and various al-ternative structural and functional assump-tions about their internal composition. Awide range of complexity has to be investi-gated from simple “what if ” models to com-plex networks of differential equations withstochastic effects, allowing for the predic-tion or at least rough estimation of systemsbehavior in yet unobserved states. Subsys-tems, their stability, and their interactionshave to be characterized, modeled, andsimulated.The parameter space of the possi-ble states of any biological system is prac-tically unlimited, but, on the other hand,highly restricted in “real life” by constraintsas the result of evolution. We will never beable to span this space by experiments.However, if the parameters involved can beexperimentally derived, models can be builtand tested. Pioneering efforts in systemsbiology are introducing novel methodolo-gies for the understanding and descriptionof biological systems.
Bioinformatics has grown to an indis-pensable discipline driven by biologicalchallenges. The understanding of the organ-ism, its constituent components and theirinteractions is a prerequisite for the rationaltranslation of biological knowledge intomedicine. Within a few years, the availabil-ity of genomic and proteomic information
has revolutionized the understanding ofbiology, but it is yet far from yieldingmechanistic models of complex diseases,though new functional discoveries are madeon an ongoing basis. It is not clear whetherclassical mechanistic reductionism will beable to describe the wide range of signifi-cant epigenetic effects critical in medicine.
Bioinformatics plays a key role in inter-disciplinary education due to its profoundexperience serving as an interface betweenlife sciences and informatics. However, thegenome and proteome-based views in clini-cal research and medical diagnostics arestill in their infancy and the recent progressin the application of different omics tech-nologies is only beginning to influencemedical research, diagnostics and therapy.Yet, the successes of genomics and func-tional genomics can be found in the field ofmodel organisms, ranging from unicellulareukaryotes to model species with func-tional characteristics more directly relatedto those of human biology. Since bioin-formatics spans biology, mathematics, andinformation technologies and their appli-cations, it is ideally positioned to mediatethe interdisciplinary connections betweeninformatics and medicine. The transition,which is already taking place from the in-vestigation of single genes to complex in-teractions, is being driven by research pro-jects in many new areas involving bioin-formatics, such as monitoring of metab-olism in diabetes by high-throughput MS/MS and its correlation to susceptibility lociat the genomics level. Bioinformatics isclosely related to biomedical engineering(e.g., molecular imaging), as well as tohealth informatics and eHealth (e.g.,studies combining genetic and clinicaldata), public health informatics (e.g., newperspectives for epidemiological studies)and general informatics (e.g., handling oflarge and complex data volumes includingthe semantic web, distributed processingand knowledge representation, and themanagement of pervasively available data,which, despite attempts at de-identifica-tion, presents critical confidentiality andsecurity challenges). All related areas willbenefit from the research re-sults of the adjacent areas and, conversely,generate research topics.
3.2 Informatics for BiomedicalEngineering3.2.1 Background and Motivation
Biomedical engineering (BME) is com-monly defined as “a discipline that ad-vances knowledge in engineering, biologyand medicine, and improves human healththrough cross-disciplinary activities thatintegrate the engineering sciences with thebiomedical sciences and clinical practice”[21]. Broadly speaking, BME is the appli-cation of engineering principles and tech-niques to a large number of medical fields,ranging from materials science for simpleand complex artificial organs, by way ofmechanical and electronic devices for drugdelivery or life support functions, to themost complex machines for detecting andimaging the finest details of the humanbody [22]. The field deals with the designand use of all kinds of medical devices, in-cluding probes and sensors, as well as theirintegration within individual-level devices,or systems-level automation and informa-tion, and – often under-estimated – their in-tegration with human perception and cogni-tion [23].
As in many other engineering disci-plines, in BME product innovation and de-velopment process efficiency are facilitatedby informatics and technology. Virtually allmedical devices crucially depend on sophis-ticated software for their operation. Butpowerful software tools are also a prerequi-site for modeling, designing, testing, vali-dating and producing them. Moreover, net-working these devices, embedding theminto the work flow of hospitals and integrat-ing the data from a multitude of differentclasses of devices (in-house and outdoor)are just another few prominent applicationsof informatics and technology to BME.Closely related to BME, biomedical phys-ics (BMP) deals with all applications ofphysics and physical methods in lifesciences which are relevant to imagingtechnologies, modeling and simulation ofbiological processes, sensors, biosignalprocessing, robotics, and instrumentation.
The areas in which advanced informaticsmethods are particularly important for prog-ress in BME and BMP are, for example: im-

289
Informatics and Medicine: From Molecules to Populations
Methods Inf Med 4/2008
aging with different modalities and inter-pretation of images, recording and analysisof biosignals, computer-aided medical pro-cedures like surgery or endoscopy. Bio-medical informatics researchers then usethe output from such devices in the develop-ment of new cross-disciplinary computa-tional models to characterize not only indi-viduals, but populations of subjects or pa-tients, and their correlation with clinicalconditions and outcomes under health anddisease, as is carried out through integratedimaging architectures based on semanticmodels such as the Foundational Model ofAnatomy (FMA) and large-scale atlases ofthe brain and body [24-26].
Modern cross-sectional imaging mo-dalities such as Multi-Detector row CT(MDCT) and Magnetic Resonance Imaging(MRI) provide imaging data with sub-millimeter isotropic voxels of large bodyparts, or even the whole body. Moreover,functional, metabolic and even molecularinformation can be obtained by tracer andoptical techniques and combined with high-resolution morphological visualization inmultimodality imaging. On the one hand,this results in an enormous amount of het-erogeneous and multi-dimensional data onthe human organism; on the other hand, theclinician then has to cope with this huge datavolume. Therefore, support by adequatesoftware tools for classification and mutualregistration of these data as well as for theintegration into complex clinical decision-making processes is urgently needed inorder to fully exploit the potentials of mod-ern imaging modalities. Promising resultshave been obtained with whole-body im-aging, both in preventive care and in clinicalapplication. Instead of diagnostic imagingtargeted to particular organs and body parts,examinations tailored to specific diseaseentities and risk patterns can be set up. Thisapproach takes into account the systemicnature of various diseases, such as diabetesmellitus, atherosclerosis, immunologicaland oncological diseases.
Advances in the areas of data and signalacquisition as well as software technologieshave resulted in intelligent recording, pro-cessing, transfer and storage of a variety ofbiosignals, e.g. of neurophysiological, he-modynamic, and respiratory signals. In
order to use these signals for monitoringpurposes intraoperatively as well as duringlater treatment (in different clinical situ-ations, i.e., intensive care unit, operatingroom or home care), relevant informationhas to be extracted from highly complex sig-nals. For routine use in clinical practice theraw signals need to be analyzed, trans-formed and condensed into an easily-under-standable form of an indicator and pre-sented to the clinicians. This ambitious goalinvolves biomedical engineering, informaticsand medicine with subtasks including signalrecording and processing, information re-trieval and machine learning as well as medi-cal expertise. Specific characteristics of in-dividual patients or the time course of the in-dicator values are often neglected in this pro-cedure, particularly since this information isoften not sufficiently represented by thegiven example data.Tests must be performedin the clinical environment, to check theplausibility of the developed indicators.
As for computer-aided medical pro-cedures, more and more open operations arebeing replaced by minimally invasive,image-guided therapeutic options. Theyinclude ablation of tumor tissue by radio-frequency energy, laser, microwaves, andcryoprobes as well as photons, particle ionsand ultrasound energy (focused ultrasound).Extremely high precision in targeting thevolume to be destroyed is imperative, andadjacent normal tissues must not be dam-aged. Therefore, online registration andcorrection have to be implemented in theguiding devices. Complex data manage-ment and integration issues arise, such asimage fusion, real-time processing of largeamounts of data, and process integration[27]. Endoscopy is another field where in-creasingly complex devices are transmittingonline data from within the body, and whereone would expect that optical technologiescould be combined with nano-technologies,biosensors and maneuvering technologies.Embedding these devices into the clinicalworkflow and integrating and managingcomplex data will also be a challenge.
3.2.2 Research Challenges
As a consequence of the expected domi-nance of information and communication
technologies and their theoretical and scien-tific foundation, a focus on research on theaspects of informatics-related BME and acloser coupling to biomedical informatics isneeded. This will cover the design and opti-mization of algorithms, the study of theircomplexity, the integration of sensors ofdifferent reliabilities for on-line coupling ofthe system to a human, the need for dataintegration, real-time issues, among others.Education should cover the complete soft-ware development process, i.e. specifica-tion, verification and validation in themedical domain including all safety-relatedproblems, integration of large distributedmedical systems (including sub-systemsand devices connected via wireless broad-band networks), automatic adaptation andlearning (e.g. for personalization), and in-formation logistics, i.e. transparent andseamless bridging between and across dif-ferent modalities.
From an applications point of view, thisincludes (in arbitrary order) the use of in-formatics methodologies for systems analy-sis, medical imaging and multi-modal datafusion, high-resolution image processing,physiological signal processing, as well as3-D modeling, for tasks such as predictingtissue and tumor behavior. Concrete devicesthat profit from this research in a more orless generic way include multiphoton la-serscanning microscopes, (f)MRI scanners,X-ray machines, CT scanners, PET andultrasonic scanners, as well as any com-bination of such devices.
Beyond the classical cutting-edge chal-lenge of improving sensor resolution downto millimeter-size and lower, we are facingemerging challenges like cognitively ad-equate real-time visualization, picturearchiving and communication (PACS) andcontent-based image retrieval (CBIR) [28],e.g., based on natural language interfaces.
As mentioned above, another emergingfield that opens up completely new areas ofexciting research for many years to come ismolecular imaging, where biomarkerprobes are developed and validated to helpvisualize various targets, pathways, or sys-tems in a living organism. Future medicalapplications include early detection of dis-eases, as well as the study of the effect ofpharmaceuticals on an organism. Current

Methods Inf Med 4/2008
290
Kuhn et al.
research challenges are the qualitative andquantitative assessment of the significanceof observed changes for disease devel-opment. Simulation and modeling of theprobe’s kinetic behavior yield new insightsin complex biological processes, but posemany challenges in the areas of imagegeneration algorithms and image process-ing. In vivo images will be correlated withmicroscopic images and high throughputmolecular analyses obtained from the verysame neoplastic or non-neoplastic tissue todemonstrate sensitivity and specificity.
Among the research challenges resultingfrom embedding BME into health infor-matics is the handling of streaming data inaddition to (conventional) persistent data.Tasks that can benefit from processing datastreams on-the-fly include traditional taskssuch as bedside patient monitoring as wellas new applications like mobile devices formonitoring patients at home or ad-hoc net-works for data acquisition, data sharing, anddata analysis, e.g., in the context of disastermanagement. Such processing may includealerting responsible physicians or an ambu-lance whenever certain vital signs reachcritical values. It may also comprise filter-ing and delivering incoming information torelevant recipients among the physicians,authorities, and coordinators working at thescene of a disaster. Distributed sensor net-works in general provide for monitoring,archiving, and presentation of correspond-ing data. Streaming applications will con-tinue to gain importance since they allowquick reaction time to various kinds ofevents and are also able to efficiently pro-cess large volumes of data online.
3.3 Health Informaticsand eHealth3.3.1 Background and Motivation
Due to demographic development, socio-cultural changes, increasing mobility ofcitizens, the globalization of markets, in-creasing costs of new examination and ther-apy methods, and the growing demands ofthe health services consumer, modernhealth systems are under significant pres-sure. There is a broad consent among stake-
holders worldwide that eHealth is one of themost important tools for meeting the chal-lenge. eHealth has been defined by theWHO as the use of information and com-munication technology (ICT) for health atthe local site and from a distance [29]. Thedriving force behind eHealth from thecitizens’ and patients’ perspective is theneed for seamless, high quality, and effi-cient care, and the opportunity to empowercitizens to manage their own health by im-proved access to knowledge and to personalmedical data. On the level of healthcare sys-tems, coordination of activities via informa-tion logistics is essential. Especially in thecase of scarce resources, coordination andcollaboration are necessary to bridge inter-faces between all agents involved in health-care delivery and prevention.
eHealth is already the third largest pillarof the healthcare industry (after pharma-ceutical and medical devices industries),and its market is expected to grow to 5% ofhealthcare expenditure within the next tenyears [30]. A large number of possibleeHealth applications have shown their po-tential for various application scenarios, in-cluding: i) management of trauma, emer-gency and disaster, ii) prevention and self-management, iii) healthcare at home (e.g.tele-monitoring), iv) integrated care, v) sur-veillance and early warning.
All components of healthcare systemsaccording to WHO, i.e., service delivery,financing, resource generation and stew-ardship [31], are likely to become the targetof informatics applications and services inthe following areas [32]: eCare, mainly ad-dressing the delivery of health servicesfrom healthcare providers to personsfacing a health problem, utilizing ICT forthe delivery: eLearning, addressing profes-sional education, but also the education ofpatients (especially for chronic con-ditions), and also the education of healthycitizens on prevention and lifestyle-relatedhealth threats; eSurveillance, supportinghealth reporting, acquisition and analysesof epidemiological data, including obser-vation satellite data, for early warning onepidemics and public health developmentand monitoring; eGovernance /eAdminis-tration, to streamline and enhance the effi-ciency of activities such as electronic reim-
bursement, checking of insurance status ofpatients, and decision-making of stake-holders; eResearch, aiming at the supportof biomedical research in all its aspects,with electronic source data interchangeand bridging clinical and research informa-tion systems being the major challenge.The increasing importance of informationtechnology in medicine has been describedrecently [33]. Studies evaluating the im-pact of informatics on medical care havebeen carried out [34, 35], demonstratingpositive effects on access to care, on pre-ventive health, and on surveillance andmonitoring.
3.3.2 Research Challenges
For more than a decade, advances in in-formatics and in health informatics havebroadened the scope of information systemsand have contributed to the comprehensivescope of eHealth. Hospitals, regions, andcountries are being networked, health careprofessionals’ decisions are being sup-ported by information systems and knowl-edge bases, patients and citizens are beingempowered, and concepts of ubiquitouscomputing are being transformed into realsystems. Electronic patient records andhealth records are being implemented morewidely. Many old challenges still exist,however, and new ones add to the com-plexity of the emerging picture [36-38].
Further research is needed on architec-tures, interoperability, ontologies, and stan-dards. In order to build modular, dynami-cally adapting systems that can guaranteeadequate quality of service, research shouldfocus on distributed information systemsand databases, on interoperability on thetechnical and semantic level, but also on theorganizational and political level. eHealthrequires data integration and the handling oflarge and complex data volumes, especiallywhen existing islands of information are tobe combined, and when genomic data are tobe added to the electronic health records.Moreover, functional and process inte-gration is needed. Service-oriented archi-tectures (SOAs), which are a current in-formatics research topic, provide a meansfor enabling the integration of hetero-geneous information systems on a global

291
Informatics and Medicine: From Molecules to Populations
Methods Inf Med 4/2008
scale via loosely coupled subsystems, whileat the same time preserving their local au-tonomy. Maturing standards are supportingcommunication and cooperation [39], butfor knowledge management and for devel-oping the full potential of decision support,further research on their underlying seman-tics and ontologies is essential.
Often seen as a major barrier in gainingbroad acceptance of eHealth among pro-fessionals and citizens, the need for safestorage and communication of confidentialdata requires research on innovative com-binations of technologies and their smoothincorporation into the eHealth infrastruc-ture and processes. Current security re-search topics in the database domain com-prise efficient and secure execution ofworkflows and fine-grained access control,e.g., as needed in the context of patientempowerment. Incorporation of currentinformatics research topics is a relevantoption. These include concepts such ask-anonymity or new approaches followingthe Heisenberg principle, as well as researchon trusted pseudonymity services that areresistant to unauthorized access, taking intoaccount that most security-critical incidentsare due to human error or neglect.At presentthere are no guaranteed methods for secur-ing the privacy of health (or other) informa-tion on systems, and the resulting lack oftrust presents a major challenge to wide-spread voluntary adoption of these systemsfor health-and-security critical information.
Acceptance research, impact researchand human factors analyses are needed.Thefactors contributing to the acceptance ofnew, eHealth-enhanced, services and work-flows among professionals, patients andcitizens have to be researched and related tospecific impacts, such as the time-savingfactor, the costs-savings potential, and im-proved medical service quality. In spite ofpromising perspectives, it has become in-creasingly clear over the last few years thatcost savings and improvements in medicalquality, e.g. by decision support and guide-lines, are difficult to achieve and hard to ver-ify. Moreover, failures are not uncommonand even adverse consequences were ob-served. Failure analyses and evaluationshave shown the need for advances in humanfactors analyses, cognitive science, and
change management involving health risksunder the wide range of uncertainty char-acteristic of these problems [40]. Researchon workflows and related socio-technicalaspects is essential in order to build success-ful, effective, and efficient eHealth services,with a focus on patients and health care pro-fessionals as well as on organizations on theintra- and cross-enterprise level. Innovativemethods and systems for information logis-tics and information management, includ-ing risk management, are needed.
For the management of eHealth services,considerable research on logistic and eco-nomic models is necessary in order to sup-port informed decision making for investorsin this fragmented market.
For full deployment of eHealth services,existing regulations and legal frameworkshave to be revised. Research is needed onhow to break down the requirements ofeHealth service categories with their spe-cific technological, organizational, socialand political constraints into broader work-able principles that can form the core ofamendments and extensions to existing actsand rules, while at the same time coveringemerging technologies as widely as possi-ble.
Digital data have become a core elementof research, knowledge generation andknowledge management. Data organizationhas become critical due to the known com-plexity of clinical data as well as the increas-ing volume of genomic data and its avail-ability through public databases. Varioustypes of information (literature, clinicalguidelines, clinical pathways) are publiclyavailable and appropriate to support evi-dence-based medicine (EBM). Biomedicalinformatics methods are needed to find newways to synthesize information and knowl-edge from diverse data sources and to carryout coordinated research efforts that spanmultiple institutions [9-17]. A commonvision is the integration of various datasources and types into a comprehensive in-frastructure in order to accelerate the com-plete translational cycle, from genomic,molecular, and clinical data collection, toindividualized and tailored treatment, andfurther to evaluation, and new hypotheses.Three perspectives need to be combined tosupport both high-quality patient care, and
clinical as well as translational researchfrom bench to bedside to bench:1) Information flow needs to be adapted to
the work practice of healthcare profes-sionals, providing access to data fromdifferent sources and locations, includ-ing imaging devices, biosignals, text, andmolecular data. Decisions need to bebased on comprehensive data and on thebest available evidence. Among the chal-lenges are seamless integration at thesemantic and ontological level, data se-curity, workflow management, andknowledge management which supportsevidence-based medicine.
2) Clinical trials need to be supported bysophisticated systems which are in com-pliance with regulatory requirements.The interchange of clinical trial data andsemantic interoperability with clinicalsystems will improve recruitment, fol-low-up, scheduling, adverse event re-porting, and individual feedback to pa-tients, but requires research and develop-ment efforts. Among the challenges areissues such as access right management,de- and re-identification of patient data,pseudonymization, separation of per-sonal and research data, informationalself-determination (patient view), andintellectual property rights (IPR) (re-searcher view), as well as their closerelationships to legal issues.
3) Systematic tissue collection has to becombined with use of molecular-basedtechnologies. Tissue, serum, and bodyfluid banks provide access to biomedicalphenotype data which needs to be com-bined with higher clinical data.
Health informatics is a discipline which fo-cuses on the complete spectrum of appliedinformatics in medicine and health, so inter-relationships and overlaps exist with allthree other areas, as well as with informaticsas the underlying core discipline. As in theother three areas, knowledge discovery, dataintegration, data visualization and datamanagement are essential for analyzingdifferent biomedical data (e.g., gene ex-pression, sequence, signal transductionpathways, gene signature, clinical data, im-aging data, sensor data) and for integrating awide variety of data on all levels of research,

Methods Inf Med 4/2008
292
Kuhn et al.
health care, and prevention. Scientific chal-lenges such as limitations of today’s earlyontological efforts are accompanied bytechnological challenges like, for instance,difficulties with multimodal data fusion andnetwork security. With public health itshares the ubiquitous problems of defininghealth risk and hazard for individuals asopposed to groups, and related challengesin accounting for genetic versus environ-mental factors.
3.4 Public Health, Life Sciences,and Public Health Informatics3.4.1 Background and Motivation
Improving human health is one of the keygoals of society from a global perspective.In particular, demographic changes repre-sent an extraordinary challenge with therapidly growing number of elderly peoplerequiring adequate healthcare. However, thefinancial resources for large-scale socialcoverage are decreasing, and it appears un-avoidable that decisions in the healthcaresystems of developed nations will be deter-mined by the effectiveness of all medicalservices and their cost-effectiveness. In anaging society, effective prevention is there-fore of the highest priority, in particular forthose chronic diseases that are becoming amajor burden to societies, in conjunctionwith the rapidly declining number ofyounger people who are active members ofthe work force. It is mandatory to obtain abetter understanding of the determinantsunderlying those diseases that can developeven at a young age, and, more importantly,to develop new measures to mitigate or con-trol them. And, learning about the cost-effectiveness of such new prevention strat-egies is essential [41, 42]. Efficient preven-tion strategies need to be embedded into in-novative solutions for healthcare, whichwill become available through progress inbiomedicine and information technologies.
Genome research and genetic medicineare core disciplines driving technologicalprogress in medicine. A basic requirementfor successful applications in healthcare isknowledge about the genetic variation in theentire population. In addition, population-
wide patterns of metabolic states, images,and disease phenotypes in general, arerequired to study disease predisposition,disease course and treatments in the contextof different lifestyles and environments on apopulation level. We must also understandthe economic boundary conditions underwhich novel technologies can be developedand implemented in the healthcare system.Information technology is central to suchapplications – in order to improve targeteddiagnosis and treatment, and also for devel-oping new forms of early intervention. Thisleads to new challenges on how health is-sues are communicated and how increasingmanagement needs can be met. A high de-gree of multidisciplinarity is required, in-cluding input from clinical and geneticmedicine, epidemiology, health economicsand the public area for providing and devel-oping new strategies and putting them intoaction.
At present, the incidence and prevalenceof several important chronic disorders is in-creasing. This applies, e.g., to obesity andmetabolic disorders such as diabetes, to al-lergies, and to neurological disorders suchas dementia. In addition, the high load ofcancer morbidity and mortality is especiallyburdensome. The prevention and control ofsuch conditions pose specific challenges forpublic health and related basic, clinical andpopulation sciences. Many of these diseasesare a consequence of an aging population incombination with sedentary lifestyles, char-acterized by hypernutrition and a lack ofexercise.
There are two levels of interaction withpopulations in the context of future health-care systems: i) recording and describingdisease and disease courses in targetedpopulations, and ii) choosing, implement-ing, and evaluating treatments and preven-tion strategies. The first level includes theassessment of comprehensive biomarkerprofiles derived from genomic applications.The second level includes interventionstudies, interactive counselling and the im-plementation of lifestyle modifications. Forboth levels there will be overlaps with bio-informatics and with the health informaticsactivities.
Extensive databases and informationplatforms combined with powerful profil-
ing technologies will enable the devel-opment of new health care tools with mani-fold applications, for instance, to identifypopulation groups at risk, to detect environ-mental cancerogenic factors, to designcancer prevention campaigns, and to estab-lish public information centers.
3.4.2 Research Challenges
With the wealth of genomic information andhigh-throughput profiling technologies fora wide range of biological organisms andsystems, medical research is able for thefirst time to define on a molecular basis thesusceptibility, course and outcome of dis-ease within the context of different environ-ments and treatments. For metabolic dis-orders for instance, diet and food com-ponents are prime environmental factorsthat interact with the genome, transciptome,proteome and metabolome. This life-longinteraction defines the health or diseasestate of an organism. Profiling technologiesare also used in cancer and age-related neu-rological disorders to guide clinical sciencesin developing evidence-based recommen-dations and health-promoting strategies.Hence, this research area needs to focus oni) developing new health-care supportingtools (e.g. tele-monitoring devices) to allowthe assessment and reporting of health-related parameters in targeted populations;ii) developing new avenues of interactionbetween healthcare providers and customersin order to obtain high levels of informationand to ensure consent on a population level;iii) developing the information/communi-cations technology structure for studycenters in the area of nutrition and chronicdiseases; iv) developing web-based infor-mation and interactive counselling tools forprevention and the promotion of healthylifestyles.
Epidemiological study platforms withbiobanks form a good example for the needof combining advanced methods from epi-demiology, genetics, clinical medicine,bioinformatics, and informatics. Pseudo-nymization services are necessary, and phe-notype data need to be managed togetherwith data from genetic and molecularstudies. The genetic and molecular data arehigh-dimensional and pose the challenge of

293
Informatics and Medicine: From Molecules to Populations
Methods Inf Med 4/2008
integrating data coming from differentsources and different experimental tech-niques. Current databases contain 1 billiondatasets and more, while an increase with afactor of ten is realistic within the next fewyears.
Research in health economics is needed.The care of chronically ill people may sig-nificantly benefit from technical devicesthat support monitoring of functioning andof clinical parameters, as well as preventiveand treatment interventions (e.g., by in-creasing adherence to in-time and in-dosedrug treatment) or that are endowed withemergency help capabilities. The questionof how effectively health can be improved,and with what cost-effectiveness this can beaccomplished, is of relevance to publichealth and to social security systems. Evalu-ations of various types of health care inter-ventions regarding medical and economiccriteria, and studies on the optimization ofhealth care management are a highly rel-evant research focus in this context.
In summary, challenges in public healthinformatics and life sciences are closely re-lated to all other areas, e.g. the challenge ofintegrating genetic and telemetry data intoepidemiological studies, and of buildingeResearch and eHealth infrastructures. Atthe same time, relevant aspects of currentinformatics research need to be addressed,such as the handling of large and com-plex data sets, integration, ontologies, andsecurity concepts.
4. InterdisciplinaryCollaboration and EducationOur suggestion is to strengthen collabora-tion and structured interdisciplinary edu-cation in the four priority areas en-compassing medicine, informatics, bio-informatics, biology and system biology,engineering, health informatics and publichealth. As mentioned before, each of thesedisciplines has developed its own domesticculture. These cultures have proven to behighly resilient to change and, for many rea-sons, have resisted, to a large extent, all at-tempts to become integrated. In some dis-ciplines, subcultures have emerged that
obstruct communication even betweenmembers of the same discipline, e.g. be-tween clinical and basic medical research.
In our opinion, it is only through achange in the attitude of scientists that thesecultures will merge, and this change willcome about only in new generations ofscientists that are educated in (at least) twoof these cultures. Moreover, while the scien-tific core of each discipline will remainstable, interdisciplinary education is neededto provide a firm structure for permanentand effective exchange of people and ideas.This will encourage the networking of prac-ticing scientists and engineers or tech-nologists, and, in a very natural way, alsoencourage more integration with industry.
The fact that scientists and students areobliged to act and to learn together acrossdisciplines will also refute the entrenchedbelief that integration is not feasible. Inother words, historical structures need to berethought: an innovative type of education isneeded that will have structural impact, notby trying to dilute the disciplines or researchareas, but by providing its scholars with aninterwoven approach to applying in-formatics in health. While excelling in their“home disciplines”, members of such aschool can also serve as “boundary-break-ing” agents to other research areas and thusempower innovation. In our opinion, thisconcept will offer a high potential for sub-stantial and sustainable change in thesestructures because of its long-term bottom-up approach.
In the traditional university system, therehas been a cultural gap between classicalnatural sciences (e.g., chemistry, biology,physics) and engineering and informatics.While the former are primarily dedicated tobasic research, engineers and informati-cians consider themselves closer to tech-nological applications, which frequently re-sults in gaps or avoidable discontinuities be-tween discovery, invention, innovation, andwidespread technology adoption. It wouldbe desirable to overcome such gaps or dis-continuities, to translate research resultsinto applications, and to take steps thatwould encourage various disciplines towork together much more closely. From ourperspective, the most effective way ofchanging the patterns of scientific edu-
cation is to address the level where teachingand research meet: MSc and PhD programs.Accordingly, the operational objectives ofsuch programs would be:i) to coordinate and combine advanced
courses and research training for ad-vanced students in medicine, scienceand engineering/informatics therebypromoting their interaction across dis-ciplines;
ii) to create added value for individual keyresearch areas through structural pro-visions, e.g., definition of joint researchprojects, focused and targeted work-shops;
iii) to foster links at the institutional andpersonal levels;
iv) to encourage project-oriented teamworkat a high scientific level, covering differ-ent research cultures.
All students in such a program should re-ceive true interdisciplinary tuition in at leasttwo previously distinct fields while per-forming their research work.
5. ConclusionThe relevance of informatics in health hascontinuously grown over the last decade. Wehave outlined the urgent need to translatescientific progress into clinical practice andinto new prevention strategies. In order tohandle the massive complexity of medicineand health care, and to build affordable andefficient health care systems, true multidis-ciplinary collaboration has become essen-tial over a broad spectrum of disciplines. Inour opinion, the ‘top-down’ approach of de-fining joint research programs which try tocombine scientists from applied sciences,engineering and life sciences in order toachieve progress in health has not alwayslived up to its promise. Our suggestion is totake an integrative approach by starting in-terdisciplinary practice at early stages ofeducation, and to build common groundearly and in a structured way. It is onlythrough having experts in one scientific dis-cipline who have a profound understandingof the other disciplines’ terminology andscientific culture, that true interdisciplin-

References1. Steinbuch K. Informatik: Automatische Informa-
tionsverarbeitung. SEG-Nachrichten 1957; 4.2. Dreyfus P. L’informatique. Paris: Gestion; 1962.
pp 240-241.3. Mikhailov AI, Chernyl AI, Gilyarevskii RS. In-
formatika – novoe nazvanie teorii nauãnoj infor-macii. Nauãno tehniãeskaja informacija 1966; 12:35-39.
4. Shortliffe EH (ed), Cimino JJ (assoc ed). Bio-medical Informatics (3rd ed). New York; 2006.
5. Boston Consulting 2006. Internationales Bench-marking der Innovationsleistung für Pharma,Medizintechnik und Healthcare-IT. Berlin: Bos-ton Consulting Group; March 2006. www.amcham.de/fileadmin/templates/main/pdf/bcg-benchmark-study.pdf. Accessed 2008-05-14.
6. ESPICOM 2005. ESPICOM World MedicalMarket Report 2005.
7. MaojoV, Garcia-Remesal M, Billhardt H,Alonso-Calvo R, Perez-Rey D, Martin-Sanchez F. Design-ing New Methodologies for Integrating Biomedi-cal Information in Clinical Trias. Methods InfMed 2006; 45: 180-185.
8. Maojo V, Martin-Sanchez F. Bioinformatics: To-wards New Directions for Public Health. MethodsInf Med 2004; 43: 208-214.
9. Martin-Sanchez F, Maojo V, Lopez-Campos G.Integrating Genomics into Health InformationSystems. Methods Inf Med 2002; 41: 25-30.
10. Oliveira IC, Oliveira JL, Sanchez JP, López-Alonso V, Martin-Sanchez F, Maojo V, SousaPereira A. Grid Requirements for the Integrationof Biomedical Information Resources for HealthApplications. Methods Inf Med 2005; 44 (2):161-167.
11. Anderson NR, Lee ES, Brockenbrough JS, MinieME, Fuller S, Brinkley J, Tarczy-Hornoch P. Is-sues in Biomedical Research Data Managementand Analysis: Needs and Barriers. J Am Med In-form Assoc 2007; 14 (4): 478-488.
12. Martin-Sanchez F, Iakovidis I, Norager S, MaojoV, de Groen P, Van der Lei, J, Jones T, Abraham-Fuchs K, Apweiler R, Babic A, Baud R, Breton V,Cinquin P, Doupi P, Dugas M, Eils R, EngelbrechtR, Ghazal P, Jehenson P, Kulikowski C, Lampe K,De Moor G, Orphanoudakis S, Rossing N, Sara-chan B, Sousa A, Spekowius G, Thireos G, Zahl-mann G, Zvarova J, Hermosilla I, Vicente FJ.Synergy Between Medical Informatics and Bio-informatics: Facilitating Genomic Medicine forFuture Health Care. J Biomed Inform 2004; 37(1): 30-42.
Methods Inf Med 4/2008
294
Kuhn et al.
arity can develop, which is exactly what isnow needed for our health care systems.
AcknowledgementThe authors would like to thank all cooperationpartners of the initiative “Graduate School of Infor-mation Science in Health” for their support. We addspecial thanks to the reviewers of Methods of Infor-mation in Medicine.
Authors´ AffiliationsKlaus A. Kuhn – Chair of Medical Informatics, Tech-nische Universität München; Alois Knoll – Chair ofRobotics and Embedded Systems,Technische Univer-sität München; Hans-Werner Mewes – Chair of Ge-nome Oriented Bioinformatics, Technische Universi-tät München, and Bioinformatics and Systems Biol-ogy, Helmholtz Center Munich; Markus Schwaiger –Nuklearmedizinische Klinik und Poliklinik, Tech-nische Universität München; Arndt Bode – Chair ofComputer Organisation and Parallel Computer Archi-tecture, Technische Universität München; ManfredBroy – Chair of Software and Systems Engineering,Technische Universität München; Hannelore Daniel –Molecular Nutrition Unit, Technische UniversitätMünchen; Hubertus Feussner – Chirurgische Klinikund Poliklinik, Technische Universität München;Reiner Gradinger – Orthopädische und Sportortho-pädische Klinik und Poliklinik, Technische Universi-tät München; Hans Hauner – Klinik für Ernährungs-medizin, Technische Universität München; HeinzHöfler – Institut für Allgemeine Pathologie undpathologische Anatomie, Technische UniversitätMünchen, and Institute of Pathology, HelmholtzCenter Munich; Bernhard Holzmann – ChirurgischeKlinik und Poliklinik, Technische UniversitätMünchen; Alexander Horsch – Medical Informatics,Technische Universität München; Alfons Kemper –Chair of Database Systems, Technische UniversitätMünchen; Helmut Krcmar – Lehrstuhl für Wirt-schaftsinformatik, Technische Universität München;Eberhard F. Kochs – Klinik für Anästhesiologie,Technische Universität München; Rüdiger Lange –Chair of Cardiovascular Surgery, Technische Univer-sität München; Reiner Leidl – Chair of Health Eco-nomics and Health Care Management, UniversitätMünchen, and Helmholtz Center Munich; UlrichMansmann – Chair of Biometry and Bioinformatics,Universität München; Ernst W. Mayr – Chair of Effi-cient Algorithms, Technische Universität München;Thomas Meitinger – Chair of Human Genetics, Tech-nische Universität München and Helmholtz CenterMunich; Michael Molls – Klinik und Poliklinik fürStrahlentherapie und Radiologische Onkologie,Technische Universität München; Nassir Navab –Chair of Computer Aided Medical Procedures andAugmented Reality, Technische UniversitätMünchen; Fridtjof Nüsslin – Klinik und Poliklinik fürStrahlentherapie und Radiologische Onkologie,Technische Universität München; Christian Peschel –III. Medizinische Klinik und Poliklinik, TechnischeUniversität München; Maximilian Reiser – Chair ofClinical Radiology, Universität München; JohannesRing – Klinik und Poliklinik für Dermatologie undAllergologie, Technische Universität München; Ernst
13. Haux R. Aims and Tasks of Medical Informatics.Int J Med Inform 1997; 44: 9-87.
14. Greenes RA, Lorenzi NM. Audacious Goals forHealth and Biomedical Informatics in the NewMillennium. J Am Med Inform Assoc 1998; 5:395-400.
15. Musen MA, van Bemmel JH (eds). Challenges forMedical Informatics as an Academic Discipline.Methods Inf Med 2002; 41: 1-3.
16. http://www.ncrr.nih.gov/clinical_research_resources/clinical_and_translational_science_awards/. Accessed 2008-05-14.
17. Kulikowski CA. The Micro-Macro Spectrum ofMedical Informatics Challenges: From MolecularMedicine to Transforming Health Care in aGlobalizing Society. Methods Inf Med 2002; 41:20-24.
18. Hersh W, Williamson J. Educating 10,000 in-formaticians by 2010: theAMIA 10 × 10 program.Int J Med Inform 2007; 76: 377-382.
19. Hersh WR. Who are the informaticians? What weknow and should know. JAMIA 2006; 13:166-170.
20. Ash JS, Anderson NR, Tarczy-Hornoch P. Peopleand Organizational Issues in Research SystemsImplementation. JAMIA PrePrint: Acceptedarticle. Published February 28, 2008 asdoi:10.1197/jamia.M2582.
21. Imperial College London, Department of Bio-engineering. http://www3.imperial.ac.uk/pls/portallive/docs/1/51182.PDF. Accessed 2008-05-14.
22. Bronzino J. The Biomedical Engineering Hand-book. CRC Press; 2000.
23. Bronzino J. Medical Devices and Systems. Taylorand Francis; 2006.
24. Rosse C, Mejino JL Jr. A reference ontology forbiomedical informatics: the Foundational Modelof Anatomy. J Biomed Inform 2003; 36 (6):478-500.
25. Rosse C.Anatomy atlases. Clin Anat 1999; 12 (4):293-299. Review.
26. MacKenzie-Graham A, Boline J, Toga AW. Brainatlases and neuroanatomic imaging. Methods MolBiol 2007; 401: 183-194.
27. Gering DT, Nabavi A, Kikinis R, Hata N, O’Don-nell LJ, Grimson WE, Jolesz FA, Black PM, WellsWM 3rd. An Integrated Visualization System forSurgical Planning and Guidance Using ImageFusion and an Open MR. J Magn Reson Imaging2001; 13 (6): 967-975.
28. Deserno TM,Antani S, Long R. Ontology of Gapsin Content-Based Image Retrieval. J Digit Im-aging 2008 (Epub ahead of print).
29. WHO 2004. eHealth for Health Care DeliveryDraft Strategy. Geneva, World Health Organiza-tion, Department of Essential Health Technol-ogies; 2004.
30. Iakovidis I. EMBEC ’05, Prague November 23,2005. http://ec.europa.eu/information_society/activities/health/docs/events/embec05/iakovidis-embec05–0.pdf. Accessed 2008-05-14.
31. WHO 2000. The World Health Report 2000.Health Systems: Improving Performance. Gene-va: World Health Organization; 2000
J. Rummeny – Institut für Röntgendiagnostik,Technische Universität München; Johann Schlichter –Chair of Applied Informatics – Cooperative Systems,Technische Universität München; Roland Schmid –II. Medizinische Klinik und Poliklinik, TechnischeUniversität München; H.-Erich Wichmann – Chair ofEpidemiology, Universität München and HelmholtzCenter Munich; Sibylle Ziegler – Nuklearmedizi-nische Klinik und Poliklinik, Technische UniversitätMünchen

Correspondence to:Prof. Dr. Klaus A. KuhnChair of Medical InformaticsKlinikum rechts der IsarTechnische Universität MünchenIsmaninger Str. 2281675 MünchenGermanyE-mail: [email protected]
32. Mitchell J. From Telehealth to e-Health: the Un-stoppable Rise of e-Health. Canberra: NationalOffice for the Information Economy, Dept ofCommunications, Information Technology andthe Arts; 1999.
33. Chaudry B, Wang J, Shinyi W, Maglione M, Mo-jica W, Roth E, Morton SC, Shekelle PG. System-atic Review: Impact of Health Information Tech-nology on Quality, Efficiency, and Costs of Medi-cal Care. Ann Intern Med 2006; 144: 742-752.
34. Cleland JGF, LouisA, RigbyAS, Janssens U, BalkAHMM, on behalf of the TEN-HMS Investi-gators. Noninvasive Home Telemonitoring forPatients with Heart Failure at High Risk of Re-current Admission and Death. J Am Coll Cardiol2005; 45: 1654-1664.
35. Blumenthal D, Glaser JP. Information TechnologyComes to Medicine. N Engl J Med 2007; 356; 24:2527-2534.
36. Kuhn KA, Giuse DA. From Hospital InformationSystems to Health Information Systems. Prob-lems, Challenges, Perspectives. Methods Inf Med2001; 40 (4): 275-287.
37. Kuhn KA, Giuse DA, Lapão L, Wurst SH. Ex-panding the Scope of Health Information Sys-tems – From Hospitals to Regional Networks, toNational Infrastructures, and Beyond. MethodsInf Med 2007; 46 (4): 500-502.
38. Lehmann CU, Altuwaijri MM, Li YC, Ball MJ,Haux R. Editorial: Translational Research inMedical Informatics or fromTheory to Practice.ACall for an Applied Informatics Journal. MethodsInf Med 2008; 47 (1): 1-3.
39. Lenz R, Beyer M, Kuhn KA. Semantic Integrationin Healthcare Networks. Int J Med Inform 2007;76 (2-3): 201-207.
40. Ball MJ, Silva JS, Bierstock S, Douglas JV, NorcioAF, Chakraborty J, Srini J. Failure to ProvideClinicians Useful IT Systems: Opportunities toLeapfrog Current Technologies. Methods Inf Med2008; 47 (1): 4-7.
41. Leidl R, Stratmann D. Economic Evaluation Is Es-sential in Health Care for the Elderly: A View-point. Drugs and Aging 1998, 13 (5): 255-262.
42. von der Schulenburg JM, Greiner W, Jost F,Klusen N, Kubin M, Leidl R, Mittendorf T,
Rebscher H, Schoeffski O, Vauth C, Volmer T,Wahler S, Wasem, J, Weber C, and the HanoverConsensus Group. German recommendations onhealth economic evaluation – Third and updatedversion of the Hanover Consensus. Value inHealth 2008, online January 11th, doi:10.1111/j.1524-4733.2007.00301.x
295
Informatics and Medicine: From Molecules to Populations
Methods Inf Med 4/2008

Commentaries on “Informatics and Medicine:From Molecules to Populations”R. B. Altman1, R. Balling2, J. F. Brinkley3, E. Coiera4, F. Consorti5, M. A. Dhansay6,A. Geissbuhler7, W. Hersh8, S. Y. Kwankam9, N. M. Lorenzi10, F. Martin-Sanchez11,G. I. Mihalas12, Y. Shahar13, K. Takabayashi14, G. Wiederhold1
1Stanford University, Stanford, CA, USA2Helmholtz Centre for Infection Research, Braunschweig, Germany3University of Washington, Seattle, WA, USA4University of New South Wales, Sydney, NSW, Australia5University of Rome “Sapienza”, Rome, Italy6South African Medical Research Council, Cape Town, South Africa7Geneva University and University Hospitals, Geneva, Switzerland8Oregon Health and Science University, Portland, OR, USA9World Health Organization, Geneva, Switzerland and University of Yaounde I, Cameroon10Vanderbilt University, Nashville, TN, USA11Institute of Health “Carlos III”, Madrid, Spain12Victor Babes University of Medicine and Pharmacy, Timisoara, Romania13Ben Gurion University, Beer Sheva, Israel14Chiba-University, Chiba, Japan
SummaryObjective: To discuss interdisciplinary research andeducation in the context of informatics and medicine bycommenting on the paper of Kuhn et al. “Informaticsand Medicine: From Molecules to Populations”.Method: Inviting an international group of experts inbiomedical and health informatics and relateddisciplines to comment on this paper.Results and Conclusions: The commentaries include awide range of reasoned arguments and original posi-tion statements which, while strongly endorsing theeducational needs identified by Kuhn et al., also pointout fundamental challenges that are very specific to theunusual combination of scientific, technological, per-sonal and social problems characterizing biomedicalinformatics. They point to the ultimate objectives ofmanaging difficult human health problems, which areunlikely to yield to technological solutions alone. Thepsychological, societal, and environmental componentsof health and disease are emphasized by several of thecommentators, setting the stage for further debate andconstructive suggestions.
KeywordsMedical informatics, biomedical informatics,health informatics, interdisciplinarity
Methods Inf Med 2008; 47: 296–317
With these comments on the paper “In-formatics and Medicine: From Molecules toPopulations”, written by Prof. Klaus Kuhnand others [1], Methods of Information inMedicine wants to stimulate an urgentlyneeded broad discussion for further inter-disciplinary research and education of in-formatics and medicine, and beyond. An in-ternational group of experts in biomedicaland health informatics and related disci-plines have been invited by the editor ofMethods to comment on this paper. Each ofthe invited commentaries forms one sectionof this paper.
1. Informatics for the“Networked” Generation(by Russ B. Altman)The paper by Kuhn et al. [1] offers an excit-ing and comprehensive vision of how in-formatics can be a unifying force for inte-grative research in biology and medicine.They make a convincing case that the physi-cal spectrum from atoms and molecules topopulations and global health has a parallel
“informatics spectrum” from bioinfor-matics to public health informatics. Whatcan be added to their comprehensive andconvincing analysis? I would like to stressone important emerging phenomenon: theempowered, independent, and thoroughly“networked” consumer.
Modern youth have access to technologythat arguably makes their intellectual, socialand economic development radically differ-ent from not only their parents, but from anygeneration of humans that have yet lived.Young adults have grown up in a world withroutine access to information around theglobe via the internet (news sites, blogs,wikis, chat rooms, social networking sites,and more). They have and expect rapid ac-cess to volumes of information that couldhardly be imagined 25 years ago. They man-age this information with novel strategiesthat emerge by necessity: some use fairlystatic trusted sources (in the form of blogsites, wikipedia or even traditional newsagencies) to aggregate information anddistill it to something more consumable.Others have increased their communicationbandwidth through apparently constant, un-interrupted use of e-mail, instant mes-saging, and text messaging to create multi-
Methods Inf Med 4/2008
296
© 2008 Schattauer GmbH

plexed conversations that allow them to“sense” their environment and make deci-sions about how to respond. Of course, mostuse combinations of these strategies. Therevolutionary nature of these changes isclear to anyone who speaks to a young per-son: “Why do we even have libraries? Whatare newspapers for? Why would I use e-mailwhen I can ‘text’? Why should I pay formusic?”
What does this have to do with biologyand medicine? I think we are already seeingchanges in the fabrics of both disciplinesthat we can attribute to these trends. Inscience, there is great interest among youngscientists in open access publications, opensource software, and open data sharing. Thetraditional silos that provided protection andcontrolled access to information are not ac-ceptable anymore. This creates not onlymajor social and economic challenges(which I will not address here), but createsfascinating informatics research problems.Indeed, the availability of all these datasources creates a market for innovative in-formatics tools that can connect people tothe information they want, when they wantit, and in the (integrated) form they want itin. Research about how these tools shouldwork will transcend any division betweenbioinformatics, engineering informatics,eHealth and public health informatics, be-cause the best tools are likely to be generalpurpose.
In medicine, the effects of this transitionare likely to have an even larger impact.Health care consumers are increasingly re-jecting a model of parentalistic healthcare,where the physician is a parent-figure whomakes independent decisions based on ac-cess to specialized information and as aproxy decision-maker for the patient. Con-sumers now have access to massive amountsof information on the web, and access toother consumers with similar health issues,and a willingness to share their experiences,treatments, and opinions. Even access totests of potential medical relevance, such aslarge-scale genotyping of an individual’s ge-nome, is now available “direct to consumer”along with web resources to assist in theinterpretation. The implications of all theseactivities for the informatics research agen-da are tremendous: How can we support
decision-making by healthcare consumersin partnership with their physician, as wellas in partnership with their social network?How can we help them best use the networkof health information and health providersto manage their health? How can we createmethods for helping consumers gauge thecredibility of an information source, and in-tegrate information sources dynamically fora given health-related query? Finally, howcan we ensure that the overall outcome ofthis new health-information economy is im-proved health?
One approach to these challenges may beto radically reconsider the structure of howwe train scientists and medical students, andhow we model the interaction between phy-sicians and patients. In both cases, I thinkthat the principles of informatics can be theactual basis of the “curriculum”. We shouldacknowledge to young researchers andphysicians-in-training that there is too muchknowledge for them to master in theirbrains, and so we will present a frameworkfor knowledge and information use thatstresses how to gather, organize and use in-formation in their professional life, withmuch less stress on large amounts of con-tent. Through problem-based learning, andresearch projects, they will get experiencecollecting and using detailed information tosolve problems, but the curriculum will beentirely about collecting and managing in-formation for the purposes of research andproviding healthcare.
For patients, we should acknowledge thathealth-related information is overwhelm-ing, and their physician is a collaboratorwho will help them navigate through this in-formation, formulate questions and poten-tial actions, and help them make decisionsabout how to proceed. The primary phys-ician will be a “general contractor” forhealth information, who will work with thepatient to find “subcontractors” that canprovide specialized services and informa-tion that the patient needs.
In summary, current trends indicate thatan information-processing metaphor forscientists, healthcare providers and patientsis a more realistic model as we move for-ward. If this is true, the research oppor-tunities for bringing it to reality are ex-tremely exciting.
2. Let´s Merge Coffeerooms(by Rudi Balling)My first reaction to the article by Klaus A.Kuhn and his colleagues was asking myself,whether the first author was related toThomas S. Kuhn, the author of the famousbook “The Structure of Scientific Revolu-tions”, published in 1962. In this book T.Kuhn describes the development of newparadigms in the course of the history ofscience stating: “Conversions will occur afew at a time until, after the last holdoutshave died, the whole profession will againbe practicing under a single, but now a dif-ferent, paradigm” (p 151).
I think there is no doubt that we are cur-rently in the midst of a scientific revolution.The question is which one: The revolutiontriggered by the progress in information andcommunication technology, where we havedevelopments such as the Turing-machine,the invention of the transistor, integratedcircuits and the computer? Or the revolutionin genetics and genomics providing com-pletely new insights into the complexity,emergence and regulation of biologicalsystems?
The article by K. A. Kuhn et al. “In-formatics and Medicine” reminds us that weare already at the next phase, which is char-acterized by the merger of these two fieldsand how they influence each other. The au-thors provide an impressive description ofthe “application space” of these new tech-nologies and one wonders if their outline ofthe convergence of informatics and medi-cine is already an indicator of a 6th “Kon-dratieff-cycle”.
Being excited and enthusiastic about thescientific and economic potential, or skepticand reflective about the social and ethicalrisks involved is one side of the story.Equally interesting is the question of howwe, as a scientific community, cope with thechallenges of interdisciplinary research.Kuhn et al. argue for a strengthening of in-terdisciplinary collaboration and education.
It is much easier to talk about interdisci-plinarity than to practice it. There is nodoubt that, quoting Leland H. Hartwell [3]:“The next generation of students shouldlearn how to look for amplifiers and logic
Methods Inf Med 4/2008
297
Commentaries on Kuhn et al.́ s Article

circuits, as well as to describe and look formolecules and genes.” But how do we teachthe ability to work in an interdisciplinaryenvironment? How should future curriculafor biology and informatics look like?“Depth or breadths?”
Kuhn et al. describe the cultural gap be-tween classical natural sciences (e.g. chem-istry, biology, physics) and engineering andinformatics. I spent some time during thelast years in talking to engineers, physicists,mathematicians and computer science/informatics professionals trying to enticethem for joint research programs tacklingthe complexity of biological systems. I hadto learn that many of these colleagues wereas scared of biology as biologists are oftenscared of mathematics. Nevertheless, theinterest and the excitement to bridge the gapof disciplines and go beyond one’s own“domestic culture” was enourmous.
It is not so long ago, that mathematicians,computer scientists and physicists werelooked down upon by their colleagues ifthey devoted their research to biologicalproblems. Apparently they didn’t make it intheir own hard and stringent discipline. Thishas changed. The grand challenges of thefuture have been recognized to lie, notexclusively but increasingly, in understand-ing the complexities of biological systems.And this is recognized by the best and thebrightest in these “hard and stringent” dis-ciplines.
My suggestion is to put the emphasis onour ability to talk with each other across thevarious disciplines. Talking to each otherrequires either the same language or at leastsome basic knowledge in the foreign lan-guage. Mathematics is THE language if wewant to tackle the issue of predicting howbiological systems will behave in case theyare perturbed. Information science andtechnology could not exist witout mathe-matics at the heart of it.
I am not sure whether I agree with thesuggestion made by Kuhn et al. that “… themost effective way of changing the patternsof scientific education is to address the levelwhere teaching and research meet: MSc andPhD programs”. I fully support their propo-sal to set up coordinated and combinedcourses and research training for advancedstudents in medicine, science and engineer-
ing/informatics. I am also a great fan defin-ing joint research projects and workshops,to foster links at the institutional and per-sonal level and to encourage team-work at ahigh scientific level.
I am worried that all of this will comewill come too late. We need to start muchearlier. There are a lot of complaints fromour colleagues teaching first year biologyabout a declining level of the students pro-fiency (and interest) in mathematics. Atleast in German highschools one can ob-serve a dramatic degradation in the import-ance given to mathematics, physics and bi-ology. Parents are more worried about get-ting their children through highschool at all,opening the doors to soft(er) disciplines anda lack of appreciation for a solid educationin natural sciences.
Unfortunately this trend is amplified bymany of our leading politicians. We areheading for a disaster, and our politicalleadership still braggs about how little theyunderstand about mathematics and genetics.The waters might be muddy and the logicmight be fuzzy, but the message is clear:Informatics and medicine will converge.Kuhn et al. give us a valuable orientation onhow to structure the bewildering hetero-geneity and opportunities of cooperation ofthese fields. As a first step I suggest tomerge the coffeerooms for our students andfaculties. Then all the rest will follow.
3. Towards BiomedicalInformatics as a Scientific Field(by James F. Brinkley)This paper by Kuhn et al. [1] is the result ofa set of meetings among leaders of two uni-versities in Munich, the goal being to imple-ment an interdisciplinary graduate school inbiomedical informatics. Members of thegroup, who are the authors of this paper, aregenerally the leaders of biomedical, techni-cal and management departments at the twouniversities. Specific fields represented in-clude medical informatics, bioinformaticsand systems biology, robotics, computerarchitecture, software engineering, data-bases, algorithms, augmented reality, nu-
clear medicine, molecular biology, cardio-vascular surgery, genetics, radiology, inter-nal medicine, dermatology, orthopedics,biometry, and epidemiology. The particularlist of fields is relevant because much of thepaper can be seen as an attempt to discoverand classify the common biomedical in-formatics activities already ongoing in theseseparate disciplines. In fact the recognitionof this commonality, along with the increas-ing relevance of informatics to biomedicine,is undoubtedly the major impetus for thecreation of the interdisciplinary graduateschool. Such an endeavor is truly visionary,going far beyond most academic biomedicalinformatics programs, many of which arestruggling to achieve departmental status,let alone the status of an entire graduateschool.Yet the shear breadth of activities de-scribed in the paper makes it clear that thereare enough biomedical research problems tojustify the creation of an entire graduateschool, so it is likely that this effort will notbe the last of its kind.
In order to create a graduate school themany activities need to be organized intoseparate but overlapping units. In the USsuch units would be called departments.Thus, the four classifications in the papersuggest separate departments of bioin-formatics and systems biology, bioengi-neering informatics, health informatics andeHealth, and public health informatics. Thisclassification is similar to one that we use inour University of Washington (UW) Bio-medical and Health Informatics graduateprogram (BHI): biology informatics, clini-cal informatics, and public health in-formatics. We never considered includingbioengineering informatics in our programbecause the UW already has a very strongbioengineering department, many membersof which are involved in some aspect ofcomputing. On the other hand we do collab-orate with faculty in bioengineering, bring-ing expertise in information and knowledgemanagement, which the bioengineering fac-ulty are generally not experts in. Thus, acase could certainly be made for includingbioengineering informatics, especially ifthere is not already a separate bioengineer-ing department.
One difference in terminology appears tocome from the use of the term “bioin-
Methods Inf Med 4/2008
298
Altman et al.

formatics”. In the paper it is stated that “thegoal of bioinformatics is to understand themolecular mechanisms, their genetic frame-work for diseases and their responsivenessto therapy…”, yet many of the researchproblems described in section 3.1 involvecorrelating genotype with phenotype,which often means dealing with informa-tion at all structural levels ranging fromgenes to the whole organism. Although it istrue that the common understanding ofbioinformatics is that it deals with the mo-lecular level, the need to correlate genotypewith phenotype has led many researchers tomove beyond the molecular level. With thecompletion of the various genome projectsthis migration will only become moreprominent, and in fact several groups haveattempted to extend the definition of bio-informatics to include all of basic biology,thereby automatically including such fieldsas physiological simulation and systemsbiology (which many would argue are thesame thing). One reason we chose not to usethe term “bioinformatics” in our program isto avoid this ambiguity.
A second difference in terminology is inthe use of the word “informatics”. In the in-troduction it is stated that the European useof this word corresponds more or less to theterm “computer science” in English speak-ing countries. Yet the many research prob-lems described in the paper go beyond whatis generally taught in most US computerscience departments, including activitieslike imaging, signal processing and com-putational modeling, which are generallytaught in electrical engineering or bioengi-neering departments. Thus, the impressionis that the use of the term “informatics” inthe title of the paper implies all these activ-ities applied to biomedicine. Such a broaddefinition is appealing because it helps tounify many activities under one umbrella –although such a unification would not occurin the US given our more narrow definitionof computer science.
Given the broad definition of informaticsas defined in the paper, it might be useful tolist the informatics research issues that aredescribed under the four categories. Theseissues include but are not limited to: signaland image processing, simulation and mod-eling, data and knowledge representation,
data management and integration, visuali-zation, information retrieval, and sociotech-nical issues. As noted several times in thepaper these informatics issues occur inmany if not all of the four fields described inthe paper, which is where the commonalityof these fields is seen to lie. Thus, in someways figure 2 is misleading: in fact arrowsshould be drawn between each box on theleft side and every box on the right side, notjust those on the same level.
This commonality leads to the notionthat there is a core set of informaticsmethodologies that underlies all four of theareas. Thus, in the BMI program we wouldcall the areas in the paper application do-mains (which in our case are basic biology,clinical medicine and public health), and wedefine core informatics domains as thoseareas that underlie biomedical informaticsresearch in all the application domains.These areas are generally drawn from andinclude pre-requisites from underlying dis-ciplines such as computer science or electri-cal engineering, but the courses that teachthem are tailored to the biomedical domain.Thus, as the new graduate school is devel-oped it might be worthwhile considering theaddition of a unit that could teach these coreinformatics areas. Such a unit would for-malize the commonality that is already evi-dent in the descriptions seen in the paper,and would help transform the field of bio-medical informatics from a collection ofloosely connected application areas to ascientific or engineering field in its ownright, with its own core principles andmethodology distinct from any other field.
4. Systems Informatics and theSocio-technology of Bioscience(by Enrico Coiera)The agenda of informatics researchers al-most inevitably returns to technology, andfor good reason. Information and com-munication systems are transforming ourworld in a powerful way. We would not beable to anticipate climate change withouthighly sophisticated computational modelsto alert us to its risks. We would not be able
to more robustly deal with international fi-nancial shocks than we did in past centurieswithout the web of economic data shared bycentral banks globally.And we would not beable to anticipate the now palpable revol-utions in systems biology and genomescience that foreshadow truly personalisedmedicine, without IT. The human genomeproject after all, in the end hinged on com-puters to pull together shot-gunned geneticfragments into a plausible pastiche of awhole genome.
The technological challenge in bringingtogether systems biology and clinical medi-cine, what we now seem to be calling trans-lational bioinformatics [4], is huge. Thisunion “from cell to system” has been longanticipated, and Blois back in the 1980s al-ready then wrote of the nature of ‘verticalreasoning’ that takes place in clinical deci-sions, from low-level biology through toclinical and organisational levels [5]. Kuhnand his colleagues paint us a broad and ex-citing picture of many of the informationtechnology challenges that we face in thatjourney [1]. Not least of these is the hugerepresentational and inferential challengesof build knowledge structures at differentscales and expecting them all to effectivelyinteract and generate meaningful informa-tion [6]. They also note in passing that hu-mans themselves are part of the big picture,and that there are cultural barriers to bebreached if we are to bring bioscientists andclinicians together.
I have said in the past that health in-formatics is “the study of how clinicalknowledge is created, shaped, shared andapplied. Ultimately, it is the study of how weorganise ourselves to create and run health-care organisation” [7]. In other words, wecannot separate the cognitive and the socialfrom the technical, and this lesson is as trueof the challenges for e-health at the clinicallevel as it will be for translational bio-informatics. Indeed, if we are to imagine aninformatics which is all about integratingdifferent biomedical, clinical and organisa-tional systems – let us call it a systems in-formatics – then I want to argue again thatwe must put ourselves into the middle ofthat system as primary actors whose be-haviour needs to be modelled, along withmolecules and medicines.
Methods Inf Med 4/2008
299
Commentaries on Kuhn et al.́ s Article

At present the cross-systems informaticsresearch agenda is driven largely by thetechnical challenges of information inte-gration, and an analysis based upon an as-sumption about the way scientists “dothings around here”. In many ways the bio-science informatics agenda is where clinicalinformatics was in the eighties, where weused idealised models of what work shouldbe, and were blind to how things actuallywere. The last 20 years have seen a growingsociotechnical critique, for example frominfluential commentators like Berg [8], whobegan to highlight how often seeminglywell-designed IT failed when it was finallyput into the clinical workplace, because it’sdesigners fundamentally misunderstoodhow clinical work was done. The mantra of‘re-engineering’ clinical work for efficien-cy, and of clinicians and not technologistsneeding to change their attitudes was theinitial informatics response to this clinicalpush-back.
But we now know a little better. Clini-cians usually resist change for very goodreasons – we still build systems that help ad-ministrators more than clinicians. We stillbuild electronic record systems that on theface of it take longer to use than pen andpaper, even if there is a big downstreampayoff in safety, quality and efficiency. Andwe build systems that still ignore the fun-damentally complex nature of healthcare.Clinical work is not like work in a factory, isnot like a pilot’s cockpit nor like a bank, andmany of the models of workflow automationthat work so well in other settings ill-fitclinical practice, which is fluid, multi-tasking, interrupt-driven [9], complex, andwhere treatment is often necessarily be-spoke because of patient differences.
We should therefore already intuitivelyunderstand that bioscientists do more thananalyse complex data sets. Before the ex-periment, before the analysis, there is acomplex social process, in some way similarto the processes that clinicians undertakebefore a treatment plan is agreed upon. Andonce an analysis is done, its meaning is de-bated and shaped socially, because of the in-herent ambiguity and incompleteness of ourknowledge, and the various perspectivesscientists bring to such discussions. Forexample, co-expression of cellular proteins
does not strictly imply co-regulation or acausal relationship in biochemical pro-cesses. Scientists employ additional back-ground knowledge to make assessmentsabout the weight of evidence behind knownrelationships, or the likely causal relationsthat might be implied through associa-tional studies. Whose background know-ledge triumphs in a research team’s debate isstill no doubt often a tribal affair.
Latour has written vividly about such so-cial aspects of science [10] and our newchallenge is to embrace a richer sociotech-nical agenda so that we can craft systemsthat truly link bench to bedside [11]. The‘secret’ work that gives rise to biosciencedata and its interpretation is something wereally need to understand, because whatbioscientists do today, clinicians will do to-morrow. The clinicians of the near futurewill be awash with genetic and biomarkerdata from their patients, and they will oftenhave little concrete information to guidethem to what they all really mean. As ever,we have much more data than we haveknowledge about what those data mightmean.
Socio-technical systems science hasarisen in response to the challenges ofunderstanding complex technical systemsthat are embedded in a human world [12]. Ithas arisen most strongly because the unex-pected interactions between humans and ar-tefacts often produce unanticipated errors,system failures, cost overruns and break-downs.The socio-technical view attempts tounderstand the contribution of phenomenaat the human social level to the performanceof technical systems, and vice versa. It isthus the missing system in any bold re-con-ceptualisation of our field as a systems in-formatics. What is therefore needed is a wayof describing events at the socio-technicallevel, connecting them to system behavioursand thence to artefact design. We need to get‘technical’ about what we mean when wedescribe socio-technical events, ‘technical’about what we want from system design,and we need to work both alongside technol-ogists to shape technology, as well as withthe processes, organizations and cultureswithin which they will be embedded [13].
Socio-technical systems thinking is anessential prerequisite to the process of de-
veloping new, safer and more effective ICTsystems that span different social systemslike bioscience, clinical medicine and thecitizen. Each is its own universe, and tech-nology will not ‘normalise’ these universesinto one. Instead it must help bridge theseuniverses, which are ever evolving, ever dif-ferent, ever new.
5. Enhancing the “HumanFactor” into the Framework(by Fabrizio Consorti)Multidisciplinary integration at researchand educational level is surely the right wayto proceed and face the relevant challengesthat the inner complexity of healthcare do-main put forward, especially when the man-agement of information is concerned. Thepaper of Klaus Kuhn and co-workers [1]represents a powerful effort toward a com-prehensive framework for an inter-profes-sional curriculum in health informatics.Nevertheless, to the taste of a physician –like I am – an essential ingredient is stillscarce in the recipe, in its dual flavor of“caregiver” and “patient”: the human factor.
In the paper, social sciences are quoted inconjunction with economics, ethics or withpassive concepts like “acceptance” or “im-pact”, along with functional expressions as“time-saving” or “cost-saving”. Moreover,topics like the Internet or the web, intendedas social environments, are never explicitlymentioned. Maybe these remarks come justfrom a wrong feeling, based on a misunder-standing of the sense of some sentences, butall the same it’s a worth discussing the di-mensions of the “human factor” in deeperdetails.
Multi-professionalism is not just amatter of exchange of competencies butmainly an encounter of professional para-digms, aimed at the definition of a commonmeta-paradigm, bridging cultural gaps. Mu-tual awareness of the different points ofview is as important as the acknowledgmentof the different, specific technical com-petencies. Then my contribution to the dis-cussion will bring an up-to-date clinicalpoint of view, by briefly summarizing the
Methods Inf Med 4/2008
300
Altman et al.

role of the web-based social cooperativeenvironments in the evolution of current“master narratives” related to the healthcaredomain. Concepts like wellness and illness,process of care, patient-caregiver relation-ship are changing in their social represen-tation and ICT is a factor of the process.Thistrend will be framed in the context of the twoconflicting paradigms of evidence-basedmedicine (EBM) and narrative-based medi-cine (NBM).
Narrative has always been the main wayto communicate knowledge about facts inthe world. Even scientific knowledgeneeds the support of narrative to be com-municated: a scientific paper is the “story”of an experiment, even if it is expressed ina rather formalized structure. More spe-cifically, narrative knowledge is focusedabout understanding the situation of a sin-gular person through cognitive, symbolicand affective means. A master narrative (ormeta-narrative) “is a global or totalizingcultural narrative schema which orders andexplains knowledge and experience” [14].It acts as an organizing principle whichprovides sense to every-day experienceand synthesizes shared ideas in an arche-typical way. Examples of master narrativesare myths and popular tales, the narrationof national historical events, masterpiecesof literature. Personal identities too arenarratively constituted [15], as complexnetworks made by self-narration and by thestories told by others about ourselves. Inthis context, identity is then a social con-struct and every mean affecting in someway socially shared narratives has a rel-evant consequence for everyone [16].Technological innovations such as the In-ternet have increased the interconnected-ness of groups. The web has contributed tothe erosion of traditional community lifeby decreasing the importance of proximal,local sites of social influence with respectto the global community [17]. Basic con-cepts like health, illness and risk con-ditions are evolving in their meaning [18]and the evolution is strongly influencednot only by the great availability of health-care-related information on the web butalso by social environments like virtualcommunities [19, 20]. As a matter of fact,the largest part of knowledge present on
the web – in forums and blogs – has a nar-rative format.
The term “narrative based medicine”was born by the end of nineties, in a series ofpapers on the British Medical Journal [21],based on an original book by Katrin Hunter[22]. NBM is a novel approach to medicalpractice, as a reaction to a technology-driven practice lacking empathy. It has beenoften opposed to the other raising profes-sional paradigm of the evidence-basedmedicine (EBM), even if the competitionhas in fact no foundation, because NBM andEBM simply define two different, paireddimensions of medical knowledge.
However, since its more known defini-tion by Sackett in 1996 [23] as “the con-scientious, explicit and judicious use ofcurrent best evidence in making decisionsabout the care of individual patients, in-tegrating individual clinical expertise withthe best available external clinical evi-dence” EBM produced an uninterruptedflow of discussion, which reveals how sensi-tive is the topic of representing medicalknowledge among physicians.
EBM as intended nowadays would bevirtually impossible without the availabilityof digital libraries. This last point, togetherwith the diffusion of systems for at-distancelearning based on a constructivist approach,highlights the importance of considering theongoing shift from a static representation ofknowledge as a “content” (accurate and uni-versal representation of some prior reality)to a concept of knowledge as an enactmentof “knowing” in a given context [24]. Focus-ing on the contextualized act of knowledgerather than on the content in fact stronglyreduces the difference between “knowing”and “learning” and it blurs the boundariesbetween knowledge management systemsand e-learning systems [25, 26].
Which consequences for research andeducation can we drive from all of theseconsiderations?1) There should be an explicit involvement
of anthropology, sociology, social psy-chology and education sciences in theblend of multi-professionalism, for aneffective curriculum and a creative re-search environment.
2) Attention should be devoted not only totechnologic development (technology in
itself is not inherently empowering) andto quantitative research aimed to maxi-mize/minimize a parameter but also toqualitative research, aimed to “know-ing”, also in terms of personal commit-ment of the intended users of ICT sys-tems.
3) From an educational point of view, a sys-temic approach should be adopted, al-ways keeping in mind the whole whilediscussing the detail and highlighting thelinks and the relationships among di-mensions and contexts.
4) A particular attention should be de-voted to emerging topics for researchand education like the management ofnarrative knowledge, also in consider-ing that in a few years the generation of“digital natives” will be adult and willhave an active role in society. Forthem, booking an appointment or ac-cessing personal health data by the In-ternet will be just a routinary task,while probably they will be demandingfor much more sophisticated possibil-ities of interaction.
6. Informatics and Medicinefrom a Developing WorldPerspective (by Ali Dhansay)When I was invited to write a commentaryon the paper by Kuhn et al. [1], I was uncer-tain since I saw myself as being ‘informaticsnaïve’. On the other hand, I thought I couldbring to the discussion a multidisciplinarymedical background (pediatrics and childhealth with research experience in the samefields), as well as nutrition research and re-search management experience at a seniorlevel in a developing country setting – SouthAfrica. Some might argue, justifiably to mymind, that SA is a ‘hybrid’ of a developing(major part) and developed country, whichlends itself to novel research opportunitiesand challenges. I consider the invitation as alearning (for myself in the area of in-formatics) and a sharing opportunity (froma South African, research and medical per-spective).
Methods Inf Med 4/2008
301
Commentaries on Kuhn et al.́ s Article

6.1 Introduction“Knowledge of what is, does not directlyopen the door to what should be.”– AlbertEinstein
The above quote, in effect, exhorts one tomove towards action, i.e. translating knowl-edge into outcomes beneficial for the healthand well-being of populations [27, 28]. Itcaptures the essence of what Kuhn andcolleagues from two Munich universitiesand the Munich Heimholz Center haveachieved, with the establishment of a ‘re-search-oriented interdisciplinary GraduateSchool’. Their paper neatly captures the‘knowledge of what is’, as well as the ‘whatshould be’ parts of the above quote. Theyhave moved from theory to practice in asense and should be commended for this.The bottom line, of course, will be theevaluation of whether the graduate schoolreached its intended goals – a keenlyawaited result in light of the dearth of docu-mentation of such experiences [29].
6.2 Interdisciplinary Research(IDR)A definition of IDR is appropriate at thistime: “Interdisciplinary research is a modeof research by teams or individuals that in-tegrates information, data, techniques,tools, perspectives, concepts, and/or the-ories from two or more disciplines orbodies of specialized knowledge to ad-vance fundamental understanding or tosolve problems whose solutions arebeyond the scope of a single discipline orarea of research practice” [30].
“It took an ex-physicist – Francis Crick –and a former ornithology student – JamesWatson – to crack the secret of life. Theyshared certain wanderlust, an indifferenceto boundaries.”– Robert Wright
It is refreshing to see that informatics re-searchers are looking at concrete ways ofcontributing, nay, being part of the currentmovement towards translating knowledgeto practice. The paper reflects, on onehand, the universal call for employing in-
terdisciplinary research to tackle the com-plex nature of disease and ill health intoday’s globalized society, and on theother, seeks to specifically establish therole of informatics and its disciplines aspart of this important challenge. There isno doubting the role of ID health research[30-35]. ID health research is based uponthe recognition of diversity/differences,yet agreeing upon the ultimate objective ofa unitary outcome, viz. improvement ofhealth and well-being for individuals andpopulations. Interdisciplinary thinking israpidly becoming an integral feature of re-search as a result of four powerful“drivers” [30]:1) the inherent complexity of nature and so-
ciety;2) the desire to explore problems and ques-
tions that are not confined to a single dis-cipline;
3) the need to solve societal problems;4) the power of new technologies.
It is encouraging to note that Kuhn and col-leagues have moved beyond the bedside, tothe community and population level. Thekeywords that stand out in the paper are col-laborative research and structured interdis-ciplinary education. While somewhat ‘lost’within figure 1 and not repeated again in thetext, the critical phrase ‘Informatics in Sup-port of Translational Research’ captures theessence of their paper.
Kuhn et al. have also traversed the inter-section of bioinformatics and medical in-formatics (biomedical informatics)[36-39] and cogently address the issues ofpublic health informatics and publichealth, with prevention as an ultimate tar-get. They present a practical framework ofhow informatics can act as driver/enabler/interlocker in the continuum from mol-ecules to population via the fields of bios-ciences, medicine and public health. Theauthors call for collaborative research andstructured interdisciplinary education infour priority areas: bioinformatics and sys-tems biology; informatics for biomedicalengineering; health informatics ande-Health; and public health informaticsand public health.
6.3 The Challenges of IDRWhen setting up their graduate school, oneaccepts that the authors would have takeninto account the comments of the NationalAcademy of Sciences [30] and others[40-43] regarding IDR, viz. (not in order ofimportance)● need for structures to support interdisci-
plinary research;● job opportunities for IDR;● evaluation of IDR and scientists and out-
puts will need modification of the peer-review process to include researcherswith interdisciplinary expertise in addi-tion to researchers with expertise in therelevant disciplines;
● funders’ views on IDR and its support;● role of professional and academic so-
cieties;● shortage of health workers and scientists/
researchers in developing countries;● the success of IDR groups depends on in-
stitutional commitment and leadership;● promotion, tenure, and resource allo-
cation;● institutions are impeded by traditions
and policies that govern hiring practices;● the success of IDR groups depends on in-
stitutional commitment and researchleadership;
● new modes of organization and a modi-fied reward structure to facilitate inter-disciplinary interactions;
● professional societies have the opportun-ity to facilitate IDR by producing state-of-the-art reports on recent research de-velopments and on curriculum, assess-ment, and accreditation methods; en-hancing personal interactions; buildingpartnerships among societies; publish-ing interdisciplinary journals [44] andspecial editions of disciplinary journalsand promoting mutual understanding ofdisciplinary methods, languages, andcultures;
● learning from collaborative interdisci-plinary research partnerships among uni-versities, industry, and government.
The above points immediately present abigger challenge to researchers in devel-oping countries, faced with problems ofrudimentary health systems, poor infra-
Methods Inf Med 4/2008
302
Altman et al.

structure and human resources for health,and low spending on research and devel-opment. Table 1 and Figure 1 below illus-trate the situation well.
6.4 IDR Leading to TranslationalResearchWhile the lack of funding, health infrastruc-ture and resources can be seen as added im-pediments to IDR in developing countries,this makes it even more important to ‘worksmartly’ in multidisciplinary and interdisci-plinary collaborations than ever. Similarly,the need to fast track knowledge translationin these countries is just as urgent – inter-ventions which are cost-effective need to beimplemented. In this regard, the frameworkfor the integration of informatics withhealth as presented by Kuhn et al. needs tobe tested and implemented in developingcountry settings as a matter of urgency.
6.5 Context Is ImportantWhile there are many similarities in healthchallenges facing developing countriescompared to developed countries (e.g.health and nutrition transition to ‘diseasesof lifestyle’), there are also major differ-ences, e.g. the massive burden of HIV andAIDS, tuberculosis and malaria in Africa.Health information systems are not effi-cient, impacting on resource allocation andevaluations of the health system. Develop-ing countries including South Africa areexperiencing severe shortages of healthcare personnel in the public sector to Eu-rope and North America, as well as to theWHO! Poverty and inequity (in generaland in health) are inexorably linked, andthis is reflected in the not unexpected dif-ferentials in morbidity and mortality foundin South Africa (skewed unfavorably to-wards blacks). Inequality and inequity atall levels and sectors present many chal-lenges to the goal of improving the healthof nations [45].
In South Africa, 93% of the majorityblack African population (80% of SA popu-lation) has no medical aid (insurance) and isdependent on the public health sector, while
58% of the minority white population (9%of SA population) has no private medicalcover. These differences in health care fi-nancing are important in the context offunding of ‘high tech’ innovations. A recentsurvey of the role of genomics medicine indeveloping country contexts, which in-cluded South Africa, argues that there is arole for investing in genomic sciences in de-veloping countries.They posit that investingin the field, identifying niche areas within itand within areas of local interest, and build-ing life sciences-based capacity aroundsuch knowledge could contribute to improv-ing local health, as well as potentially stimu-lating economic development. The role ofprivate partnerships in this regard is alsohighlighted [46]
The area of personalized medicine wasalso mentioned by Kuhn et al. in the con-text of public health and genomics. Again,in the South African context, issues such asrace and ethnicity and the medicalizationof race are issues that numerically and ethi-cally assume much greater importancethan the BiDil debate in the USA [47].These are fertile areas of potential researchfor interdisciplinary teams, including in-formaticians.
6.6 What Are the Implicationsof the Paper for DevelopingCountries?
1) There is a need to embrace the call for in-terdisciplinary research and education,and to highlight the role of informatics asan enabler in the whole process frombench to bedside to the community.
2) Collaboration with developing countrieson an equal footing should be encour-aged.
3) Realization that there are context-spe-cific issues that have to be considered,e.g. local technological, funding, popu-lation dynamics. Recognition of diver-sity and differences.
4) Foster debate around ethics (of genomicmedicine and personalized medicine),information access, education and socialissues in developing country settings.
5) Personalized medicine also raises thequestion of identification of patients whoare most likely to benefit.
6) Ensure partnerships with, for exampleprivate sector are conducted ethicallyand openly for the benefit of publichealth.
Table 1Researchers and GERD indeveloping and developedcountries
Fig. 1 Researchers per million inhabitants – year 2000 (source: National Research Foundation, South Africa)
Worldpopulation
Developing countries 79%
Developed countries 21%
GERD=gross expenditure on research and development
Worldresearchers
28%
72%
WorldGDP
42%
58%
WorldGERD
20%
80%
Methods Inf Med 4/2008
303
Commentaries on Kuhn et al.́ s Article

6.7 ConclusionOne trusts that new synergies will beforged between the various disciplines,e.g. medical informatics and bioin-formatics, based on the promise outlined inthe paper by Kuhn et al. To quote the pres-ent director of the National Institutes ofHealth, Dr. E. A. Zerhouni: “It is the re-sponsibility of all of us who are involved inhealth research to translate the remarkablescientific achievements/innovations weare witnessing into health gains for thenation” [28]. Of course, this should be ex-tended to the global community, and es-pecially the developing nations with theirgreater burden of disease.
The authors have taken a bold step in es-tablishing the Graduate School in Munich– in effect demonstrating the move fromtheory to practice. To my mind, there is adearth of information on such initiatives;little has been documented about how re-searchers experience interdisciplinaryhealth research in practice. Furthermore,factors such as career path opportunities,reward and recognition, evaluation crite-ria, long-term future etc. are all important.It is therefore imperative that they docu-ment and share their experiences, whichwill be keenly awaited by the scientific,academic, medical, and informatics frater-nity.
Both the medical and informatics com-munities need to extend the discourseinitiated by Kuhn et al. to the challengesposed by developing country settings. Itis only proper that those areas of theworld most beset by ill health should bepart of the move towards working smartlyand in an interdisciplinary fashion. SouthAfrica has the unenviable reputation ofbeing the world leader in many diseaseareas such as HIV and AIDS, tuberculosisand fetal alcohol syndrome. With its di-versity of populations (exemplified by itsrainbow nation tag) and in burden of dis-ease patterns, the country lends itself toopportunities for collaborative researchon informatics and health between northand south [48, 49].
7. On Global Trendsand Challenges (by AntoineGeissbuhler)
Enabling information and knowledge toflow and grow from molecular scale to pa-tients and populations is one of our ambi-tious goals and grand challenges. This“info-bio convergence” has an enormouspotential to improve our fundamentalknowledge in life sciences, the ability totranslate it into better and individualizedpatient care, and will open new ways of stu-dying and steering our pressured health andhealthcare systems. Further down the road,many foresee the additional convergencewith nanotechnologies and cognitive sci-ences, thus realizing an unprecedented syn-ergy of skills and knowledge [50].
Although the way seems clear and thefuture bright, there are many obstacles thatneed to be overcome, many of which liepartly within the scope of biomedical in-formatics, and most of which will requirenew forms of collaboration, of research, andprobably of education.
We must be able to connect informationfrom these various knowledge domains.Connectivity of the infrastructure frommultiple, heterogeneous, and distributed re-sources is likely to evolve from the currentdata and computational grids. Connectingthe physical and the information world willrequire new abilities to identify, track, andlink objects from both worlds. But the mainconnection challenge will be the semanticintegration of these mostly distinct do-mains, as exemplified by the IUPS Physi-ome Project [51].
With the advent of our knowledge so-ciety, we need to rethink the way we designresearch. Digging in the massive amount ofdata that is made available on the Web, willneed new research paradigms, potentiallymoving away from hypothesis-driven re-search (whether in vivo, in vitro or in silico)into data-driven research [52]. At the sametime, citizens of our knowledge society willhave the opportunity to reshape the waytheir information can be used for research,potentially displacing the centers of knowl-edge production away from the academic
environments [53]. Furthermore, the newinteractions between humans and machinesthat are currently appearing will require newresearch disciplines, such as the Webscience, coined by the Web inventor, TimBerners-Lee [54].
In this interconnected, highly complexlandscape, multidisciplinary collaborationwill indeed be the rule for progress. A chal-lenge will be to foster the right mix of hardsciences, life sciences and social sciencesnecessary to apprehend the problems at hand.The collaborative tools of the social Web willhelp to some extent, as will the knowledgeengineering tools brought by informatics re-search. It is however likely that the currenteducational models will not be able to copewith the increased needs for cross-disciplin-ary skills and will have to be revisited.
Finally, we must realize that the knowl-edge society is becoming global, bringingnew challenges and new opportunities. Inorder to limit the progress of the digital di-vide between those who have access to thesenew tools and those who don’t, we will haveto learn how to better share knowledge, andmake it relevant to multiple contexts, inorder to solve real and urgent problems, andin particular those of the health systems. Forexample, it is likely that biomedical in-formatics, e-health and telemedicine will en-able new solutions for the current healthcareworkforce crisis, helping to train, inform andsupport healthcare professionals and pa-tients in the poorest and most remote parts ofthe world, where they are most needed [55].
Enthused by these new promises, weshould always keep in mind that the overarch-ing goal of our efforts, from fundamental re-search to the bedside activities, from mol-ecules to populations, is to improve the healthand quality of life of the people of the world.
8. From Molecules to Popula-tions Is Only One Dimensionof Health and Biomedical In-formatics (by William Hersh)
The paper by Kuhn et al. [1] describing thespectrum of health and biomedical in-
Methods Inf Med 4/2008
304
Altman et al.

formatics provides an excellent elucidationof the subject domains that describe ourfield. But the subject domain is only one di-mension of informatics, and other importantdimensions must be described and explored.In my commentary, I will set forth my ownview of informatics, health and biomedicalinformatics, and the dimensions that thefield covers.
First, what exactly is informatics? Thepaper discusses this only briefly, noting butexpressing some dissent the European viewthat informatics is fundamentally computerscience. I am glad to see this view changingin Europe and beyond. My view of in-formatics is that it is fundamentally aboutinformation, in particular what humans dowith it and how they apply technology to im-prove its use for improving the human con-dition. Informatics is an integrative disci-pline, drawing upon areas such as informa-tion and computational sciences, businessand management, and other fields, but alsodeeply rooted in a subject domain. In thefield of health and biomedical informatics,the subject domains range from biology tomedicine to personal and public health.
All branches of health and biomedical in-formatics are heterogeneous yet have a com-mon intellectual core. The bioinformaticianwho analyzes gene expression microarraydata may seem to have little in common withthe clinical informatician who is trying toreconcile with highly interrupted workflowof clinical care with collecting high-qualityinformation that can be used not only forbetter patient care, but also to drive decisionsupport systems and quality assessment.Likewise, a consumer health informaticianmight be focused on helping an individualmaintain optimal health, while the publichealth informatician is likely to be focusedon monitoring risk factors for disease in acommunity.
Yet all of these areas of health and bio-medical informatics have common underly-ing themes. All are focused on the optimalcollection and use of information.All wouldbenefit from technology systems that haveoptimal usability, facilitate collection anduse of high-quality data, and aim for inter-operability based on the best standards. Allrequire attention to the larger contexts andhuman organizations in which they are used,
whether biomedical research organizations,health care delivery systems, or publichealth agencies.
The paper by Kuhn et al. acknowledgesthat all subject domains of biomedical in-formatics have related areas, whether thestatistical methods of bioinformatics, thepeople and organizational issues of medicalinformatics, or the social and economic as-pects of public health. I would argue thatthese related areas are not necessarily lim-ited to any particular subject domain.Examples include the application of quali-tative methods to bioinformatics [56] andthe need to be cognizant of genomics (e.g.,single-nucleotide polymorphisms or SNPs)and clinical data quality issues in genome-wide association studies [57].
It is thus imperative for us to movebeyond arguing what adjective should pre-cede informatics (e.g., bio-, medical, con-sumer health, etc.) and instead focus on thecore attributes that unite all aspects of in-formatics and how we apply them in healthand biomedical informatics. Our disciplineis indeed interdisciplinary, and some of itskey attributes reflect that. Informatics is in-tegrative, drawing on computational and in-formation sciences as well as business andmanagement sciences, yet firmly rooted in adeep understanding of the discipline inwhich it is applied, be it biology, medicine,or health.
Our academic departments must recog-nize this fundamental undercurrent of allinformatics. Our educational programsshould teach from this perspective. Notevery health and biomedical informatics de-partment or degree program must cover theentire domain perspective, but they shouldperform their research, teaching, and ser-vice from the viewpoint of informatics.Likewise, their educational programsshould recognize there is no single careerpathway within the field. What an in-formatician does as a job is a function bothof what he or she did before entering train-ing and what knowledge and skills he or shegained from that training.
The 21st century provides exciting op-portunities in health and biomedical in-formatics. Improvements in informationtechnology provide us a growing ability touse information to improve human health at
the personal, health care, and public healthlevels. This will require research and edu-cational programs that acknowledge thecore similarities across the subject domainsof health and biomedical informatics andtrain new practitioners and academicians inthis point of view.
9. The Value Chain“from Bench to Bedside”(by Yunkap Kwankam)The paper of Dr. Klaus Kuhn et al. [1] is welldocumented (researched) and clearlywritten. It captures the essence of the broadspectrum of issues spanning the continuumfrom molecular genetics to public healthpolicy.The fact that it elaborates on the quiteintuitive value of interdisciplinary researchin health informatics, is itself indicative ofthe imperviousness of the silos into whichresearch has fallen. The reaffirmation isthus very welcome.
And although the consultation on creat-ing the graduate program was local – limitedto Germany – the challenges discussedcover a variety of socio-political and eco-nomic contexts, and thus the paper is ofmuch broader relevance than to single atypology of health system context.
9.1 Assessment of HealthInformaticsThe paper mentions the importance of as-sessment and the dearth of robust methodol-ogies for such assessments. This is the cruxof the matter. Methodological improve-ments in the assessment of informatics areneeded to convincingly chart influencepathways from health informatics interven-tions to health intermediate and final out-comes. This is the key to unlocking fundingfor the very promising research describedand support for the marketing, deploymentand use of the fruits of such research. Untilthe return on investment, or return on value,is demonstrated, the funding levels neededto sustain interdisciplinary efforts will con-tinue to be a challenge and thus an inhibitor
Methods Inf Med 4/2008
305
Commentaries on Kuhn et al.́ s Article

to the change in culture within disciplinesthat the paper calls for.
Funding for public health informatics isin competition with other priorities, and thiscompetition is especially fierce in resource-challenged health systems. Health, as aproduction function, shows a number ofvariables, water and sanitation, for example,accounting for nearly 10% of the globalburden of disease. A 2008 WHO report esti-mates the economic benefits of investing indrinking-water and sanitation in severalforms: “health-care savings of US$ 7 billiona year for health agencies and US$ 340 mil-lion for individuals; 320 million productivedays gained each year in the 15- to 59-yearage group, an extra 272 million school at-tendance days a year, and an added 1.5 bil-lion healthy days for children under fiveyears of age, together representing produc-tivity gains of US$ 9.9 billion a year; timesavings resulting from more convenientdrinking-water and sanitation services, to-taling 20 billion working days a year, givinga productivity payback of some US$ 63billion a year.“ [58]. The above figures aretaken from a study which shows a totalpayback of US$ 84 billion a year from theUS$ 11.3 billion per year investment neededto meet the drinking-water and sanitationtarget of the Millennium DevelopmentGoals [59].
Health informatics would need to showsimilar, or better benefits, in order to get afare share of limited budgets.
9.2 Translating Knowledgeinto Policy and ActionThe paper lays heavy emphasis on greaterlevels of sophistication in research forscientific discovery. However, one couldargue that the weakest link in the researchcontinuum from discovery to disseminationand deployment, is perhaps in the latterphases of this chain. Therefore, there needsto be a balance between efforts aimed at dis-covery and those targeted at the so called“know-do gap” – the gulf between what isknown and what is done in policy and prac-tice. Again, interdisciplinary training,which the paper advocates, wouldstrengthen research into “technology en-
hanced knowledge translation” [60]. Thefield examines the role that ICT can play inthe actions of individuals, as well as sys-temic factors that militate in favor of suc-cessful transformation of available informa-tion and knowledge into action. It also looksat what informatics tools need to be devisedfor capturing and sharing experiential (ortacit) knowledge, which unfortunately iscompartmentalized in individuals. Canhealth informatics networks in support ofcommunities of practice serve as a modelfor breaking down these silos, so as to pro-mote sharing of available tacit knowledge?Can such networks improve the use of ex-periential knowledge on a systematic basiswithin health systems?
ICT can remove distance and time bar-riers to the flow of information and knowl-edge for health and help ensure that ourcollective knowledge is brought to bear ef-fectively on health problems in individualcountries, as well as globally. It would re-quire a system where all decision-making inhealth is supported by an ICT-mediatedknowledge-coupling system which buildson Weed’s vision [61] as adapted by Kwan-kam et al. [62] and ensures that: a) allrelevant options known to the healthsciences are readily available for consider-ation; b) specific features of the situation athand that bear on the discrimination amongthese options are taken into account; c) ap-propriate associations are made between thespecific features of the situation and themany options; and d) the right technology isdeployed and local capacity developed topermit access to the information.
9.3 Building on the CollectiveWisdomSeveral recent meetings have raised theissue of an international registry for in-formatics research/trials – to provide a re-pository of research information/experienceand the potential to build on successes whilelearning from the errors of one and all.
The paper’s broad scope also covers therole that informatics can play in empower-ing citizens to contribute to their health. Theauthors thus encourage one to hope thatsuch thinking also offers an opportunity to
focus less on health as the absence of dis-ease, and the attendant emphasis on diseasemechanisms, and more on the WHO visionof an ecological balance between the physi-cal, mental and social dimensions of life.
The paper concludes that “it is onlythrough having experts in one scientific dis-cipline who have a profound understandingof the other disciplines’ terminology andscientific culture, that true inter-disciplinar-ity can develop ...”. Such interdisciplinaryunderstanding would greatly facilitate vis-ualizing and understand the big picture.Then the boundary conditions that arenecessary for information and knowledgeexchange between disciplines, and betweensub-disciplines within disciplines, in thevalue chain that leads from bench to im-proved health, may be better understood andmanaged.
10. Envisioning the Future –Informatics and Collaboration(by Nancy Lorenzi)
In Lewis Carroll’s classic book, Alice inWonderland [63], Alice comes to a fork inthe road with two paths leading in differentdirections. Confronted by a Cheshire cat sheasks: “Which path should I take.” The re-sponse from the Cheshire cat is: “Well, thatdepends on where you want to end up?”Alice said she did not know. The Cheshirecat responds: “If you don’t know where youwant to go, it doesn’t matter which path youtake.”
Without vision we are both unclear aboutour direction and at times have conflictingdirections. This makes it difficult to formu-late plans, objectives, goals, actions, and noway to measure results. Unless we knowwhere we need to go, we cannot create thepath to the future
The Informatics and Medicine: FromMolecules to Population article presents anoutstanding overview of the current prog-ress in medicine, bioinformatics and biol-ogy informatics, biomedical engineeringhealth informatics and eHealth, and publichealth, life sciences, public health, life
Methods Inf Med 4/2008
306
Altman et al.

sciences and public health informatics. Thisarticle will become an instant cornerstoneclassic article not only for its overview, butfor its challenges and directions. Congratu-lations to the multiple authors for creatingthis article that is a world-wide guide.
I titled my commentary “Envisioning theFuture – Informatics and Collaboration”.The phrase “envisioning the future” char-acterizes the challenge that we face inachieving the overall picture painted in thevision the Informatics and Medicine: FromMolecules to Population article creates. Thesub-title “Informatics and Collaboration”not only supports that informatics will be“the most important driver and mediator forinnovation” as stated in the article, butstresses that we need collaboration to besuccessful.
One organization that is prepared to sup-port collaboration is the International Medi-cal Informatics Association (IMIA). Threeof IMIA’s goals include:● promote informatics in health care and
research in health, bio and medical in-formatics;
● advance and nurture international co-operation;
● further the dissemination and exchangeof knowledge, information and technol-ogy.
IMIA created a strategic plan (TowardsIMIA 2015 [64-67]). Knowledge is the cen-tral core of IMIA’s strategies, interactionsand efforts. The plan next focuses onscience, portraying IMIA members’ con-nection and integration with the science anddiscovery of informatics. The next connec-tion is the application of scientific dis-coveries, including the multiple questionsand issues that are created and disseminatedin informatics. This is followed by IMIA’simpact, referring to the potential impact thatIMIA and its members can have on govern-ments, nations, outcomes, health profes-sionals, and all other stakeholders. The lastmajor focus represents IMIA’s interactionswith individuals, citizen organizations, per-sonal health involvement, disseminationand acceptance, enabling personal responsi-bility, and public/personal health.
The second dimension of IMIA’s Stra-tegic Plan represents six key sectors that
IMIA as an international association is pre-pared to facilitate or work with others to ef-fectively address. The six sectors are:1) health improvement;2) research/science (including how we
understand and create evidence to sup-port health);
3) the behavioral responsibility (ethics) thatrefers to our ethical and social responsi-bility;
4) education (including best practices ineducating ourselves and others);
5) the multiple types of relationships (com-munications and connections to buildrelationships among stakeholders); and
6) the equity of IMIA, our obligation toshare, distribute and disseminate.
We stand at the crossroads of tomorrow,compelled to address the challenges out-lined in the article and impact of ourmultiple efforts and the visions they enable.
Inherent in IMIA’s role is to bring to-gether, from a global perspective, scien-tists, researchers, users, vendors, devel-opers, consultants and suppliers in an en-vironment of cooperation and sharing toresearch and develop the concepts neededto support the organizations of the worldseeking technology as transformational.Through its many publications (Methods ofInformation in Medicine, InternationalJournal of Medical Information and Year-book of Medical Informatics) and elec-tronic communication mechanisms IMIAcan be a major disseminator of the know-ledge created. As an organization com-mitted to promoting best practice in the useof information and communication tech-nologies within biomedical informaticsand in health and healthcare, IMIA will en-sure that it uses and promotes best practicein its own use of technology as a trans-formational strategic asset.
We stand looking at the future portrayedby the Informatics and Medicine article. Wehave a vision. If we work independently to-ward various isolated goals we will lose theopportunity to work together to create thesynergy needed for reaching the desiredstate. This is an excellent time for inter-national cooperation.
11. Nanomedicine andRegenerative Medicine PoseNew Challenges forBiomedical Informatics(by Fernando Martin-Sanchez)The reading and study of the paper of Kuhn etal. [1] has represented a particularly motivat-ing and scientifically enriching task. Afterseveral years of working on aspects relatedwith the analysis and implementation of thesynergy between medical informatics andbioinformatics, this document represents themost complete updated review of the researchchallenges in each of the four areas that areaccepted as constituent of biomedical in-formatics (BMI). Furthermore, these four dis-ciplines are not described independently, in-stead a thorough analysis of their mutual re-lations is provided. The analysis of the con-nections between BMI and biomedical engi-neering results especially interesting becausethis is a topic that has given rise to some con-troversial opinions in the past. The authorsprovide here a framework that can be veryuseful to facilitate a reciprocal collaborationbetween experts in both fields and to definesome common ground (such as image pro-cessing or modeling and simulation of bio-logical entities and processes).
It is also very valuable the effort made bythe authors to provide a model for interdisci-plinary education that it is clearly orientedtowards facilitating translational research. Ifully agree with their claim that the newgeneration of scientists should have to beexposed to (at least) two of the core disci-plines at early stages of education. Fur-thermore, I believe that the integrativeapproach that has inspired the authors to de-sign the new Graduate School will become areference and will be followed by other aca-demic centers.
Indeed, there is no a major criticism tothe paper from my side, however, taking intoaccount that several outstanding bioengi-neers have participated in the work leadingto this paper, I believe that it would havebeen important to raise the issue of nano-technology and regenerative medicine sincethey pose new challenges for BMI. It is not
Methods Inf Med 4/2008
307
Commentaries on Kuhn et al.́ s Article

my intent to consider these issues in depth inthis brief commentary. Rather, I will pointout some considerations and let the readerbecome more informed and interested aboutthese topics, particularly with reference totheir complementarity with the paper au-thors’ design of educational programs.
11.1 Nanomedicine and Regener-ative Medicine Represent NewTrends beyond Genomic Medicine
Although the paper only mentions nano-technology on one occasion in section 2, na-nomedicine and regenerative medicine arerecognized to be among the most promisingtrends in medicine for the future. Nano-medicine is defined as the use of nanoscaletools and components for the diagnosis, pre-vention and treatment of diseases and forunderstanding their pathophysiology (Euro-pean Science Foundation, Nov. 2005). Re-generative medicine seeks to develop func-tional cell, tissue, and organ substitutes torepair, replace or enhance biological func-tion that has been lost due to congenital ab-normalities, injury, disease, or aging (NIHDefinition, NIBIB, June 2004).
Interestingly, while genomic medicine isbased on the use of molecular information todesign new approaches to promote health,and prevent, diagnose, cure and treat dis-ease, nanomedicine and regenerative medi-cine go beyond that point, in the sense thatthey can entail an intervention on the bio-logical structure of the human being. It is mybelief that these two fields pose new chal-lenges for informatics beyond those ad-dressed under the realm of genomic medi-cine.
11.2 Impacts of these New Trendsthat Can Be Envisioned in EveryFacet of Healthcare
Nowadays the number of clinical appli-cations of nanotechnology is increasingwith research at the nanoscale providing im-portant information prior to clinical appli-cation. Just as mentioned above, we are
likely to see nanomedicine impacting onareas such as biomedical research, preven-tion, diagnosis and therapy [68].● Prevention and diagnosis – All the new
advances in nanotechnology are en-couraging the scientific community, es-pecially in biomedicine, to use the ‘na-noscope’ that will allow them to see anew scale of genomic, phenotypic andenvironmental data to integrate with theinformation already available. As anexample, the next generation of DNAsequencers makes use of beads andother nanotechnologies. Nanosensorsand nanodevices will permit to assessthe different positive and negative envi-ronmental factors that affect an individ-ual’s risk to suffer from a disease. Newin vitro diagnostic tests and miniatur-ized imaging systems will provide moresensitive detection methods.
● Therapy – New nanostructures will beused as drugs. Novel methods of drug de-livery systems consisting of anti-cancerproducts bound to nanoparticles such asbuckyballs, nanocapsules and den-drimers are already a reality. Imagingtechniques will be used to monitor drugrelease or for patient’s follow-up. Stemcells may provide tissue for transplants inthe context of degenerative diseases. Fi-nally regenerative medicine will allowthe manufacture of new artificial tissuesor organs, or the use of nanotubes andnanofibers to build scaffolds where cellsfrom different organs can grow.
Nevertheless, some of the recently devel-oped nanoparticles may have negative sideeffects. For instance, an article in NatureNanotechnology has recently reported thatsome forms of carbon nanotubes could be asharmful if inhaled in sufficient quantities[69]. This fact justifies the need of carefuldata handling in clinical trials in this area.
11.3 Nanoinformatics CouldRepresent a New Subdisciplinewithin Biomedical Informatics
Nanotechnology requires the contributionof informatics to process all the knowledge
that is being generated at the nano level andto integrate it with the biomedical (pheno-typic, genotypic and environmental) data.Nanomedicine gathers and deals with largevolumes of complex data, linked with ex-ternal sources and usually distributed inheterogeneous locations.
Nanoinformatics involves the researchand development of effective tools/technol-ogies for collecting, standardizing, sharing,analyzing and visualizing the vast amountsof data and information relevant to thenanoscale science in several areas such asliterature, physico-chemical properties, bio-logical and toxicological interactions andclinical effects [70].
Several requirements for BMI come fromthe need of improved tools for designing,modeling, and visualizing the new nano-materials and scaffolds for tissue engineer-ing. Also, new databases will have to bedesigned to store physical, chemical and bio-logical properties of nanotechnology devel-opments. Semantic interoperability willhave to be granted not only between nanoresources, but also between them and theexisting medical terminology and codingsystems. Biomedical informatics can sup-port regenerative medicine through the ap-plication of tools and information systems tocharacterize the molecules involved in dif-ferentiation mechanisms, including growthfactors, hormones, cytokines or integrins.
ACTION-Grid is a new research projectfunded by the European Commission(2008-2009) on healthcare information sys-tems based on grid capabilities and nano/bio/medical informatics. This project, co-ordinated by Prof. Maojo from the Univer-sidad Politécnica de Madrid and our owngroup has as its main objectives to analyzesynergies between biomedical informaticsand nanoinformatics and to combine theseresults with data from an inventory of grid/nano/bio/medical methods and services de-veloped by the consortium [71].
11.4 In ConclusionNanomedicine and regenerative medicineopen new avenues for research in biomedi-cal informatics methods and tools. Just asthe advances in “-omics” research brought
Methods Inf Med 4/2008
308
Altman et al.

about the connection of medical informaticswith the molecular domain, is BMI readynow for addressing the nano world and ex-panding its scope down to the atomic levelas shown in Figure 2?
None of my views expressed in this com-mentary should be interpreted as a critic to thepaper by Kuhn et al. On the contrary, an edu-cational program such as the one described inthe paper by our colleagues from Munich, thatis based on interdisciplinarity and with a cleartranslational vocation, is placed in the bestposition to face the new challenges related toinformation processing in medicine, whetherthey come from the side of nanotechnology orfrom any other new development that mayarise in the future.
In this regard, a new generation of scien-tists knowledgeable about nanotechnologywill be essential to manage this new infor-mation and efficiently integrate it with bio-medical data from the atomic to the popu-lational level to translate all these findingsinto better healthcare.
12. The Need to Createthe Frame for InterdisciplinaryCollaboration (by GeorgeMihalas)
Biomedical informatics is today a fieldwith one of the highest rates of devel-opment. New techniques or devices, newapproach or methods, new applications orsolutions are reported every day [1]. Suchan avalanche of news needs a systematicwork for classifying and stratifying all ac-cumulated data and knowledge. The mostnatural approach in classification wouldstart from the structural level of the studiedsystem [72]. And this approach has beenadopted also by Kuhn and his collaborators[1] who emphasized this view even in thetitle: “From Molecules to Population”.Their excellent paper is fully comprehen-sive by counting all topics of research,brings some refinement in description andupdates the actual trends. It is worth tomake here some short comments concern-ing the research challenges on each level.
12.1 Bio-silico InterfacingI would start my comments by noting theoriginal approach in the second chapter“The Overall Picture: Where Do We Standand Where Do We Go”, with a detailed listof technical trends in computer science andadjacent domains which will bring a signifi-cant impact biomedical informatics. We canadd here the interdisciplinary research (bio-physics and computer science) on the directinformation transfer between biologicalsystem and computers [73]. The potentialapplications are tremendous and still seemclose to “science-fiction”.
12.2 NeuroinformaticsDuring the nineties most prospective viewsabout medical informatics research used toconsider bioinformatics and neuroin-formatics as most promising [74]. Theprevisions on bioinformatics turned out tobe true. However, the chapters on neuroin-formatics are now rarely present.The reasonmight be that the impact of neuroin-formatics research would rather be on cog-nitive sciences than on medical sciences.And the same might be true about “affectivecomputing” [75]. However, applications inneurosciences and psychology, with their“medical” shadows – neurology and psy-chiatry – , show that the connections to bio-
medical informatics are strong enough andthe integrative view, which has been re-peatedly mentioned by the authors, wouldbecome even more consistent by includingthese items too.
12.3 Simulations in SystemBiology and VirtualPhysiological Human
Another welcomed feature in the article isthe specific reference and the detailedpresentation of “Informatics for Biomedi-cal Engineering”, a topic often left on asecond place or treated superficially. Theresearch challenges cover, indeed, severaldirections, requiring various tools. Andwhen we talk about new informatics toolsin cell biology we must mention the workof Masaru Tomita and his co-workers [76]on the “virtual cell” – a package for com-puter simulation of cellular processes,dedicated software developed for this pur-pose [77]. We can expect that specializedsoftware or even new theoretical modelswill be developed for each level. On thenext structural level we have to mentionthe Physiome Project, initiated by PeterHunter [78], followed by the Euro-physiome Project, and continued by theVirtual Physiological Human Project of theEuropean Commission [79].
Fig. 2 Information and medicine: from atom to population
Methods Inf Med 4/2008
309
Commentaries on Kuhn et al.́ s Article

12.4 Integration and the Roleof Professional Organizations
Various aspects of integration have beendiscussed in the paper and there are also sev-eral other studies dedicated to integration(refs. 9, 10, 12, 17, 37, 39 of [1]). The em-phasis on integration is understandable: theproperties of a level are different from asimple sum of the properties of lower com-ponent levels! Some recent events organ-ized by the European Federation for Medi-cal Informatics EFMI had topics dedicatedto integration of biomedical information[80, 81].
Actually the integrative view supposes aquite complex approach and here it is the ori-gin of the need to create the frame for inter-disciplinary collaboration and provide aneducation which crosses the boundaries – asso well is presented in the paper in chapter 4.I fully share the view of the authors and doconsider that biomedical and health in-formatics professional organizations, likeEFMI or IMIA (International Medical In-formatics Association) should get involvedin creating the appropriate collaborativeframe and contribute to educational pro-grams, following the good example of the10×10 program of theAmerican Medical In-formaticsAssociationAMIA (ref. 18 of [1]).
13. The Need for a HumanClinome Project(by Yuval Shahar)The “Molecules to Populations” paper byKuhn et al. is a highly commendable effortat a through, in-depth analysis of the needfor multidisciplinary collaboration in the21st century between informatics, as an areaof scientific endeavor, and several specificsubareas of medicine and biology, as othersuch areas. I would like to comment onsome of its key strengths as well as on sev-eral important key challenges to be facedthat should be added to its research chal-lenges list.
First, regarding the key strengths andmain significance of the paper: I had found
both the descriptive insights provided fromthis analysis, and the specific educationalstructural recommendations implied bythese insights, to be quite invigorating, andpotentially highly beneficial. In particular,the authors emphasize that only throughexperts in one discipline who profoundlyunderstand the conceptual world of anotherdiscipline can true multidisciplinary re-search develop. This emphasis is very im-portant, and is certainly evident to multidis-ciplinary researchers, but unfortunately isnot as obvious to decision makers in edu-cation as one would like it to be. One oftenencounters the view that, for example, hav-ing a well trained computer scientist or in-formatician work with biologists or clini-cians is sufficient for bringing about newbreakthroughs in bioinformatics or medicalinformatics; similar views are often held inthe case of other disciplines. But, as the au-thors point out, the various sub-cultures ofthe disciplines studied by Kuhn et al. havebeen highly resilient to change or to inte-gration. Only by what the authors term“boundary breaking agents”, i.e., personalexamples of multidisciplinary researchersthat the students meet during their training,can true interdisciplinary understandingand research exist.
A particularly good example out of theseveral potential interdisciplinary collab-orations suggested by the authors, is, in myopinion, the need to strengthen the linksamong bioengineering and medical infor-matics. A specific example, not explicitlydiscussed by the authors but probably ontheir mind, is the possibility of developing a“smart medical home”, which monitors itsresidents, alerts them or specific carecenters when unusual patterns are detected(e.g., an elderly person falls, or seems tohave a heart attack). Developing such asmart home requires understanding of boththe multiple sophisticated (and possiblyquite new) sensors involved, as well asdevelopment of intelligent computationalmethods for analyzing the huge volumes ofdata emerging from these sensors, and forcontinuously integrating these data withup-to-date clinical and epidemiologicalknowledge.
Second, regarding several of the areas Iwould like to see more strongly emphasized
as part of the key research challenges, atleast as a part of any interdisciplinary re-search program that includes as one of itscomponents the area of medical infor-matics: I would like list three such chal-lenges, although they are somewhat linked.
1) The first grand challenge for a multi-disciplinary collaboration is the creation ofa universal, formal, computationally acces-sible medical knowledge base. Much of thecollaboration among areas such as clinicalmedicine, clinical research, public health,and medical informatics, can and should bedistilled into a set of formal representationsof declarative and procedural knowledgethat would be stored in a universally acces-sible (to humans and machines) knowledgebase. That is, insights regarding meaningful[declarative] patterns of both individual(clinical) or population (epidemiological)data, and, most importantly, the best state-of-the-art [procedural] methods, protocols,guidelines, and care plans, to deal with suchpatterns, can and should be organized,specified, stored, and maintained within auniversally accessible digital library, using amachine-comprehensible format (includingthe use of a set of ontological and termino-logical standards) that supports mainten-ance, use, reuse, and sharing of the knowl-edge.
I call such a continuously changing li-brary of declarative and procedural clinicalknowledge “the Human Clinome Project”,in homage to the Human Genome project –or perhaps it should be termed the HumanCli-Knowme project, since it would en-compass all currently known declarativeand procedural human knowledge that canbe represented within and accessed by com-putational means.
A particular section of the Human Cli-nome project that I have in mind as a goodspecific starting point is a worldwide ma-chine-comprehensible digital library of pro-cedural knowledge, namely, clinical guide-lines and their somewhat more rigorous ver-sion, clinical protocols. These guidelineshave been shown to be highly beneficialwith respect to both improving the quality ofcare [82] and reducing its cost; it is alsoclear that to be effective, the guidelines mustbe integrated within the clinician’s work-flow [83]. Free-text and even somewhat
Methods Inf Med 4/2008
310
Altman et al.

structured guideline libraries exist and areaccessible through the World-Wide Web.However, to be truly effective, guidelinesmust be continuously updated and univer-sally accessible in a machine-comprehen-sible way, so that they can be automaticallyapplied to the relevant patient (or patientpopulation). One such attempt at a digitalguideline architecture is the DeGeL project[84], which includes a comprehensivemethodology for specification, mainte-nance, search, retrieval, and application ofclinical guidelines, using a hybrid method-ology that support several intermediateformats on the way from a free-text-basedrepresentation to a completely formal, exe-cutable format.The collaborative methodol-ogy for guideline specification was recentlyevaluated in a multinational collaborationand found to be feasible [85]. Of course,many sub-parts of such an architecturerequire further research and enhancement;multiple researchers throughout the medi-cal informatics community are working onvarious aspects of this challenging problem,such as how to expressively represent theguidelines, or how to automatically verifyand validate the knowledge expressed with-in them.
Such a grand challenge would bring to-gether many of the disciplines mentioned bythe authors of Kuhn et al.’s paper, and en-force true collaboration to be successful.
2) Much of the declarative biomedicalknowledge necessary for better manage-ment of patients, in particular, chronic pa-tients (the care of which is responsible forabout 80% of the health care costs in devel-oped countries), such as might be part of theHuman Clinome project, should be acquiredfrom analysis of massive amounts of data ofpatients monitored longitudinally for sig-nificant amounts of time (i.e., often, manyyears), to mine meaningful patterns fromthe data, using pre-existing clinical knowl-edge. In other words, we need to continu-ously perform massive, distributed, intelli-gent temporal data mining. Indeed, it hasbeen recently suggested, although withoutmuch emphasis on the temporal aspect, that“clinarrays” (influenced by microarrays)might be constructed from analyzing largeamounts of population-based laboratorydata, possibly correlating it with biological
data, so as to suggest new ways for diseasesubtyping [86]. However, adding the tem-poral dimension as well as the effect ofusing existing medical ontologies andknowledge bases to better interpret the datawould shift the emphasis towards a massive,large scale, continuous clinical trial thatuses and reuses the world's increasinglyvoluminous electronic medical record database. Needless to say, ontological and ter-minological standards are an absolute pre-requisite in the case of accessing clinicaldata as they are in the case of accessingmedical knowledge.
Such an analysis would better identifymeaningful [temporal] patterns and associ-ations within and among features of dis-eases such as diabetes, hypertension, cer-ebral stroke, AIDS, etc. The goal would beto discover the “natural” course of suchdiseases, to identify meaningful temporalclusters and patient types, to detect patternspredictive of certain intermediate and finaloutcomes, to improve best practice guide-lines (i.e., affect also the procedural aspectof the Human Clinome library), and to en-hance our epidemiological knowledge andpreventive care understanding.
Such a challenge requires and fostersclose collaboration among clinicians, epi-demiologists, informaticians, mathema-ticians, computer scientists, biomedical en-gineers (consider the effect of a “smartmedical home” technology on the source ofdata available for such a project), biologists,and other disciplines.
3) One aspect I would like to see betterrepresented in the context of both individualand public health care (and it could be even-tually part of the universal proceduralknowledge base) is an emphasis on medicaldecision support that considers individual,customizable, patient preferences as an in-herent part of each decision that might in-clude an option for deliberative thinking.
Examples include genetic consultation(e.g., the value of early knowledge of poten-tial serious disabilities of the baby, versusthe risk of spontaneous abortion of a healthybaby), therapy of hypercholesterolemia,hypertension, and depression, oncologicalcare (e.g., weighing the benefits and costs ofsurgery, chemotherapy, and irradiation), andmany other situations that are not life-
threatening in an immediate fashion, enablea certain amount of deliberation on the sideof the patient and care provider, and mightbe potentially affected by patient prefer-ences. Such an endeavor is not only useful;it is ethically imperative, even if some of thepatients might elect to not use it, delegatingthe responsibility of deciding on the bestcourse of action to their care provider [87].
Again, effective solution of such a chal-lenging problem requires and fosters thecollaboration and deep mutual understand-ing of care providers, decision analysts,game theorists, behavioral scientists, econo-mists, computational scientists, and othermedical, engineering, and computationaldisciplines. Typical challenging researchtasks include finding and developing in-creasingly effective ways to elicit patientpreferences [88], and efficiently integratingsuch preferences within the overall clinicaland public health care workflow [89].
In summary, I welcome the discussionstarted by Kuhn et al. and its stimulatingeducational implications, while suggestinga particular set of challenges that we mightfocus on, especially in the area of enhancingour understanding of individual and popu-lation-based patient care.
14. Collaboration of SpecialistsIs more Practical than to Finda Genius (by KatsuhikoTakabayashi)
Current medical and health care domainscan be divided into several fields from mo-lecular medicine to public health and in eachfield informatics plays a significant role.Kuhn et al. described precisely each rela-tionship and explained the importance of in-terdisciplinary collaboration and educationin their review. Kuhn realized the substantialchange from hospital information systemsto electric health records (EHRs) in the earlydays with distinguished ability [90]. Here heclassified informatics into four areas forcorresponding medicine and health care;bioinformatics and systems biology, in-formatics for biomedical engineering,
Methods Inf Med 4/2008
311
Commentaries on Kuhn et al.́ s Article

health informatics and eHealth, and publichealth informatics in order from the point ofmicro to the mass world. In fact it is in-credible to do without informatics in allfields nowadays and he also provided theirperspectives respectively.
As for bioinformatics and systems biol-ogy, there are large amounts of data in omic(genomics, transcriptomics, proteomics andphenomics) world [91, 92]. Because genomicand proteomic data will explode to astro-nomical numbers of information in the verynear future, researchers cannot work withoutinformatics to handle these data and to knowtheir relations. Since even SNPs which justexpress point mutations exist in one millionper person, or there are 22,000 genes andmore than 100,000 proteomes, it is quite easyto imagine numerous combinations existingbetween them to be explored. Thus sophis-ticated and useful information technologyand powerful software will contribute to agreat progress in molecular medicine. Es-pecially data mining techniques [93] will bevery useful tools for translational research toconnect omic data and clinical phenomenonor contribution to diagnosis and selection oftreatment with omics data. Therefore wemust provide suitable environments to usethem [94]. As it will bring reasonable profitsin this field, many industries will emerge todeal with them as venture companies as inSilicon valley.
Healthcare information is also a fieldfor blue chip industries, because eHealthprovides a large portion of healthcare ex-penditure [95] in this decade as Kuhn men-tioned. Electronic medical records(EMRs) will certainly advance in the nearfuture, and EHRs hold many dreams as in-tegration of not only EMR but also withmany other health areas or even other in-formation not related to health. Some gov-ernments consider an electronic postoffice box or an ATM card system for theintegration of pensions, EMR of severalhospitals, health checkup data, health in-surance and so on. This personal healthrecords (PHR) concept [96] is also open toindustries as well, and all data of one indi-vidual about not only PHR but also variousinformation would be stored. Of coursedata of PHR must be strictly limited to per-sonal use because it includes confidential
information. However, when some com-mon parts can be utilized as EHR in broadterms, it will be reutilized in many otherways apart from personal use. To achieveit, preparing the rules and guidelines suchas access control [97] and protection sys-tems of privacy as well as many sophis-ticated systems in compliance with regula-tory requirements are crucial. Additionallyeven after de-identification, proprietary ofthe data to use is not clearly defined in law,though it is very important in the near fu-ture for transverse study. If someone wouldnot accept one’s data to be used for such astudy, it will make some bias in results.Therefore all data should be enrolled forspecial studies, which is controversial inregard to individual rights.
As Kuhn emphasized, digital data havebecome a core element of research, knowl-edge generation and knowledge manage-ment. EMRs and EHRs are ultimate targetsfor automated research like text mining[98]. We would find drug interactions orpotential effects and side effects quiteeasily from medical records with them.Sometimes we need the tools to transformoriginal data into other expressions inorder to use them more easily. Forexample, time-oriented clinical data suchas laboratory findings or prescriptions willbe perhaps transformed into other ex-pressions for easy manipulation and accu-rate enhancement of clinical assessmentsuch as temporal abstraction [99]. Thereare only few practical tools at the momentbut we will obtain universal tools after trialand error in the future. Moreover, for thesetrials, we also need long data storagebeyond facilities. With them we can com-plete one’s whole life data for PHR andalso to compare with or integrate withomic (genome or proteome) data, whichwill be a very strong method for trans-lational studies. In these days retrospectivestudies are not well estimated in medicaljournals. However when we expect the ef-fects or outcome of some treatment overthe long term such as ten years or more, wehave to wait for the results many years, andexpected results would not be obtained be-cause of changes of treatment or other cir-cumstances in that period. From this pointof view, the retrospective study is very im-
portant and efficient when informatics canprovide enough huge data to be analyzed.
Public health informatics seems to havemore weight than any informatics in otherfields of medicine or health care, becausethe results of analysis of information in thisfield directly affects critical politics such asglobal warming, biofuels, or global foodshortage, which relates to the fate of hu-manity. Since public health informaticsshould include all information comprehen-sively with absolute accuracy, it is expensiveto create and maintain vital information.Even though, we cannot completely entrustindustries with these works, because theresults might be crucial in deciding ourdestiny.
Finally, in all informatics fields, datavalue increases when integrated under theguarantee of their credibility in quality andthey are now showing their whole appear-ance as the name of truth in front of us by in-tegrating. However they might be so hugelike an ocean or a big forest. Unless we havestrong tools to discover their relations andoffer them before us, we cannot say that wecan really see them, though it might be avicious cycle between the data and datamining tools.
Kuhn mentioned how vital it is for gen-erations of scientists who can combineknowledge and skills from both medicineand informatics and emphasized the im-portance of the interdisciplinary edu-cation in early phases as well as interdis-ciplinary collaboration. He started tostrengthen the collaboration and struc-tured interdisciplinary education in en-compassing medicine, informatics, bioin-formatics, biology and system biology,engineering, health informatics and pub-lic health in Munich. In eastern Asiancountries like Japan, different environ-ments from those of the European coun-tries, most researches in clinical medicinehave been proceeding in the departmentsof medical informatics at national univer-sity hospitals. They consist of medicaldoctors and specialists of informatics orcomputer sciences and there were few de-partments for bioinformatics in other fac-ulties. This might mean that they are stillin the course of western countries in theold days where bioinformatics was not in-
Methods Inf Med 4/2008
312
Altman et al.

dependent of medical school, or it mightbe as a result of different historical per-spectives. At any rate they can worktogether without any restraint in the hos-pital at the moment. Some engineeringstudents work together with medical doc-tors in our department at the hospital. Inother fields of medicine such as molecu-lar medicine, however, specialists forinformatics come from school of engi-neering or physics. In summary, in east-ern Asia, there is no strict boundarybetween specialties originated fromMeister system and they seem to have lessdifficulty to collaborate in clinical medi-cine. Nevertheless it is not ideal becausethis is not intended systematized interdis-ciplinary collaboration.
Even in medicine or in informatics,there are no specialists in all fields, andtherefore we need teamwork collaborationbetween medical doctors and specialistsfor the informatics field and others in vari-ous fields if necessary. There are a fewpeople who are familiar with both fieldsbecause of graduation from both medicalschool and faculty of engineering orphysics. However they are rare cases andeven if one knows well in both fields, hecannot surpass two specialists who collab-orate well unless he is a real genius. Thereis a proverb in Japan that god gives us onlyone talent. According to this proverb andtaking into account of the very smallnumbers of geniuses in the world, good andsuccessful collaboration of specialists ofdifferent disciplines will be more practicalthan to find a genius. One of the purposesof multidisciplinary education is under-standing one’s colleagues’ work as well asknowing the position of one’s specialtycomprehensively in the beginning of one’seducation. It is also important to learnabout laws and ethics in the fields as gen-eral matters in this education. Thus I be-lieve most importantly that a key to successto collaborate in information and medicineis mutual respectability and generosity totheir colleagues in different discipline.This spirit will be cultivated in early inter-disciplinary education that Kuhn pro-posed.
15. Strategic Thinking IsNeeded, Cost when theResearch Results Are Trans-ferred to Practice Is an Issueto Be Addressed(by Gio Wiederhold)
The article by Kuhn et al. [1] is impressivein its comprehensiveness. It also is frighten-ing.The number of problems that require re-search, the multi-disciplinary cooperationsneeded to be successful in the interaction ofinformatics and medicine, the difficulties ofdemonstrating effectiveness, and the bar-riers to beneficial implementations areshown to be massive. While there may in-deed be an urgent need to transfer researchresults to practice, strategic thinking isneeded as well, as has been shown insimpler settings [100]. Cost is one issue tobe addressed. We expected in the past ratiosof research projects efforts to practical im-plementation to integration into practice of1 :7 :25 [101], and little has been changed toimprove this ratio. Medical informatics willhave to depend on progress in software en-gineering to create usable software. We ex-pect that new initiatives cited, as service-oriented architectures, will improve soft-ware development, but an early reliance on atechnology that is not yet mature is current-ly frustrating efforts at the US VeteransHealth Administration systems to updatetheir medical record system (VistA) [102].It is purely a coincidence, but also an illus-tration, that other Vistas are encounteringdevelopment and acceptance problems aswell [103]. Medical informatics cannot sup-plant computer software engineering(SWE) efforts but must take care in under-standing when and what to exploit as part ofbiomedical engineering (BME).
The total cost of software-based sol-utions in any setting has to be budgetedproperly. Computer science educationserves us poorly there. Software mainten-ance costs run at about 15% of prior soft-ware investment costs and are due primarilyto keep the software up-to-date as the exter-nal world changes around us [104]. These
maintenance costs over time exceed initialdevelopment costs, and after some furthertime, exceed the benefits that software pro-vides. This fact is the major reason for clos-ing down apparently successful medical in-formatics projects, often surprising andfrustrating the participants. Unfortunately,we do not teach our SWE students how toplan for these costs, nor do we teach themhow to assess the potential economic bene-fits of the software [105].
Replicating successful local systems hasbeen difficult in the past and remains hard.Early systems were tied to obsolescing tech-nology, but more recent systems, as seen atVanderbilt and the Palo Alto Medical Foun-dation have not spawned successors either[106]. There is more involved than technol-ogy, leadership is certainly one issue.
The hard issues of economics are cited inthe beginning and the end of the paper, butdo not pervade the discussions. The growthof IT spending at 12% year is taken as indi-cation of importance, but is also a rate whichis unsustainable in relation to nationalexpenses in any country, especially as thesupport base of working taxable individualsdecreases [1, Sec. 2 and Sec. 3.4.1]. At thesame time the industrial tax base is di-minishing, as companies find ways to movetheir intellectual property and the profits de-rived from that IP to tax havens with no orsmall health care costs [107]. Given the highcost of implementation, it is important tofocus on large and costly populations whereactual cost reductions are possible, an issuenot always covered by cost-effectivenessarguments. Some disease-based categoriesare well recognized now, as diabetes. How-ever most diabetics present multiple prob-lems, are seen in diverse settings, and theirrecords at each site tend to be incomplete.For information integration there is a bene-fit in that members of that patient grouptend to travel less, so that local and regionalintegration can proceed before national andglobal record integration is achieved, andeconomic benefits can be realized as well asimproved care [108]. The same patternholds for many of the elderly population,who require a substantial fraction of ourhealth care services. Cost-effectiveness isstressed in the paper, but transfer to practicerequires a cost-benefit as well. That benefits
Methods Inf Med 4/2008
313
Commentaries on Kuhn et al.́ s Article

are hard to demonstrate is recognized in thepaper, but must be sought.
Moving to the opposite direction, per-sonalized diagnoses and therapies, is an ex-tremely attractive goal. But given financialconstraints, systems to bring research re-sults will require very careful strategies.How does one conduct clinical trials to de-termine efficacy of personalized care proto-cols? Presenting findings to clinicians willrequire innovation. Phrasing findings interms of statistical evidence based on simi-lar populations, as done now for medicalversus surgical treatment choices conveyslittle insight or trust. Can the findings beconveyed using a “mechanistic” metabolicmodel, showing affected pathways [1, Sect.3.1.3]? How can we present patient-specificinformation from probes [1, Sect. 3.2.1]?And how should patients be informed ofconditions for which no known interventionexists? In general unfettered access to thepatients’ own medical information has beenshown to be beneficial, but customizationhas been recommended as well [109]. Anyapproach supporting personalized treatmentdecisions requires novel software, incor-porating experience from many disciplines.Such software will require regular updating,since our knowledge is bound to change formany years to come. How will software bemaintained when personalized experiencediffers? Who will maintain the software at areasonable cost?
Cooperative approaches are recom-mended in Section 3. Bureaucrats indeedfeel safer when topics and funding can beconstrained to recognized disciplines. Onlyif scientists and the public experiencebenefits will existing regulations and legalframeworks that limit interdisciplinarywork be removed [1, Sec. 3.3.2]. Practicaland beneficial examples will be important.Figure 2 only links abstract concepts; les-sons learned from actual projects are neededas well. The gap between the “bench” and“bedside’ communities is recognized. So-cial expectations limit collaboration as well.There is a serious, but largely unrecognizedgap between the mathematically-baseddisciplines, where proofs, once validated,should stand forever, and the biological dis-ciplines, where experiments have to be re-peated to cover ever more of the variations
that the living world presents. Scientistshave at times disparaged scientific ap-proaches used by others as being eithernaïve or imprecise. Engendering sympathyto the problems that both communities facein their research is a prerequisite to achievecooperation at the individual level, creatinga model that can then move up the organi-zational ladders. My personal sense is thatdirectives imposed from above, mandatingcooperation, do not create effective long-term collaborations.
One barrier, recognized in the paper, totransition of research to practice are pri-vacy concerns [110]. Expecting guaranteedmethods for securing privacy is too much toask for [1, Sec. 3.3.1].Approaches as k-ano-nymity, while already problematic, assumethat there is no external information that canbe exploited by an intruder. Lack of trustand the resulting rules will continue tohinder beneficial applications of health careinformation systems [Ness]. Involuntaryadoption of EHR, as implied here, willcause politicians and the administratingbureaucrats to mandate approaches to pri-vacy protection that are based on worst casescenarios, and give little choice to the pa-tients. Questions posed in motivating sur-veys often reveal a bias by the questioner.How questions are phrased makes a greatdeal of difference, i.e. asking “Are you con-cerned about others accessing your privatemedical records?” will elicit a different re-sponse than “Are you willing to share infor-mation from your medical records so thatothers with similar problems can benefit?”.Some indication about patients’ attitudesabout privacy will be gleaned from the ac-ceptance of web-based voluntary personalmedical data systems, as Dossia, GoogleHealth, and MS Healthvault. While all ofthese promise privacy, individual with deepconcerns are sure not to participate. The im-mediate reason not to join is of course thatwith few participating health care providersthe benefits of entering data and links areminimal.
In conclusion, even Norbert Wiener,cited in [1, Sect. 2], will probably agree thatwe don’t have the capability to move most ofour research results into practice, and notonly because of economic constraints. Ourgenetic and environmental history, even if it
could be fully captured, does not fully deter-mine who we are. For instance, what ourbrains do with all the inputs is yet quite un-known, and randomness remains [111]. Re-search is required to open up possibilities.On the horizon are systems that help theclinicians and the patients to interact effec-tively, to which research into the issueslisted in this paper will contribute.
References1. Kuhn KA, Knoll A, Mewes HW, Schwaiger M, et
al. Informatics and medicine: from molecules topopulations. Methods Inf Med 2008; 47: 283-295.
2. Kuhn TS. The Structure of Scientific Revolutions.Chicago: Univ of Chicago Press; 1962.
3. Hartwell LH, Hopfield JJ, Leibler S, Murray AW.From molecular to modular cell biology. Nature1999; 402 (6761 Suppl): C47-52.
4. Butte AJ, Chen R. Finding disease-related ge-nomic experiments within an international reposi-tory: first steps in translational bioinformatics.AMIA Annu Symp Proc 2006. pp 106-110.
5. Blois MS. Medicine and the nature of vertical rea-soning. N Engl J Med 1988; 318: 847-851.
6. Tsafnat G. The Field Representation Language.J Biomed Inform 2008; 40: 46-57.
7. Coiera E. Guide to Health Informatics. 2nd Edi-tion. London: Hodder Arnold; 2003.
8. Berg M, Langenberg C, v d Berg I, Kwakkernaat J.Considerations for sociotechnical design: experi-ences with an electronic patient record in a clinicalcontext. Int J Med Inform 1998; 52: 243-251.
9. Coiera E. When conversation is better than com-putation. J Am Med Inform Assoc 2000; 7:277-286.
10. Latour B WS, Salk J. Laboratory Life: The Con-struction of Scientific Facts. Princeton, NJ:Princeton University Press; 1986.
11. Ash JS, Anderson NR, Tarczy-Hornoch P. Peopleand Organizational Issues in Research SystemsImplementation. J Am Med Inform Assoc. 2008;15: 283-289.
12. Trist EL. The evolution of sociotechnical systemsas a conceptual framework and as an action re-search program. In: Van de Ven AH, Joyce WF,editors. Perspectives on organization design andbehavior. New York: John Wiley, Wiley-Inter-science; 1981. pp 19-75.
13. Coiera E. Getting technical about socio-technicalsystems science. Int J Med Inform 2007; 76:S98-S103.
14. Stephens J. Retelling stories, framing culture:traditional story and metanarratives in children’sliterature. New York: Routledge Publ.; 1998.
15. Lindemann Nelson H. Damaged identities, nar-rative repair. Ithaca, NY: Cornell Univ. Press;2001.
16. Roesler C. The self in cyberspace. Identityformation in postmodern societies and Jung’s Selfas an objective psyche. J Anal Psychol 2008; 53:421-436.
Methods Inf Med 4/2008
314
Altman et al.

17. Arnett JJ. The psychology of globalization.American Psychologist 2002; 57, 774–783.
18. Harter LM, Japp PM, Beck CS. Narratives, health,and healing: communication theory, research, andpractice. New York: Routledge Publ.; 2005.
19. Wald HS, Dube CE, Anthony DC. Untangling theWeb – the impact of Internet use on health careand the physician-patient relationship. PatientEduc Couns 2007; 68: 218-224.
20. Demiris G. The diffusion of virtual communitiesin health care: concepts and challenges. PatientEduc Couns 2006; 62: 178-188.
21. Greenhalgh T, Hurwitz B. Narrative based medi-cine: why study narrative? BMJ 1999: 318: 48-50.
22. Hunter KM. Doctors’stories.The narratrive struc-ture of medical knowledge. Princeton, NJ: Prince-ton University Press; 1991.
23. Sackett DL, Rosenberg WC, Gray JAM, HaynesRB, Richardson WS. Evidence based medicine:What it is and what it isn’t. BMJ 1996; 312: 71-72.
24. Thomas P. General medical practitioners need tobe aware of the theories on which our work de-pend. Ann Fam Med 2006; 4: 450-454.
25. Revere D, Turner AM, Madhavan A, Rambo N,Bugni PF, Kimball A, Fuller SS. Understandingthe information needs of public health practi-tioners: a literature review to inform design of aninteractive digital knowledge management sys-tem. J Biomed Inform 2007; 40: 410-421.
26. Le Beux P, Fieschi M. Virtual biomedical univer-sities and e-learning. Int J Med Inform 2007; 76:331-335.
27. Hiatt R, Samet J, Ness RB for the American Col-lege of Epidemiology Policy Committee. The roleof the epidemiologist in clinical and translationalscience. Ann Epidemiol 2006; 16: 409-410.
28. Zerhouni EA. Translational and clinical science –time for a new vision. N Engl J Med 2005; 353:1621-1623.
29. van Mulligen EM, Cases M, Hettne K, et al.Train-ing multidisciplinary biomedical informatics stu-dents: three years of experience. JAm Med InformAssoc 2008; 15: 246-254.
30. National Academy of Sciences. Facilitating Inter-disciplinary Research. Washington, DC: TheNational Academic Press; 2005.
31. Aboelela SW, Larson E, Bakken S, et al. Defininginterdisciplinary research: conclusions from acritical review of the literature. Health Serv Res2007; 42: 329-346.
32. Rhoten D. Interdisciplinary Research: Trend orTransition. Items and Issues 2004; 5 (1-2): 6-11.
33. Choi BC, Pak AW. Multidisciplinarity, interdisci-plinarity and transdisciplinarity in health re-search, services, education and policy: 1. Defini-tions, objectives, and evidence of effectiveness.Clin Invest Med 2006; 29: 351-364.
34. Choi BC, Pak AW. Multidisciplinarity, interdisci-plinarity, and transdisciplinarity in health re-search, services, education and policy: 2. Promo-tors, barriers, and strategies of enhancement. ClinInvest Med 2007; 30: E224-232.
35. Choi BC, Pak AW. Multidisciplinarity, interdisci-plinarity, and transdisciplinarity in health re-search, services, education and policy: 3. Disci-
pline, inter-discipline distance, and selection ofdiscipline. Clin Invest Med 2008; 31: E41-48.
36. Martin-Sanchez F, Iakovidis I, Nørager S, et al.Synergy between medical informatics and bioin-formatics: facilitating genomic medicine for fu-ture health care. J Biomed Inform 2004; 37:30-42.
37. Maojo V, Kulikowski C. Medical informatics andbioinformatics: integration or evolution throughscientific crises? Methods Inf Med 2006; 45:474-482.
38. Kulikowski CA. The micro-macro spectrum ofmedical informatics challenges: from molecularmedicine to transforming health care in a global-izing society. Methods Inf Med 2002; 41: 20-24.
39. Maojo V, Martin-Sanchez F. Bioinformatics: to-wards new directions for public health. MethodsInf Med 2004; 43: 208-214.
40. Lynch J. It’s not easy being interdisciplinary. Int JEpidemiol 2006; 35: 1119-1122.
41. Smith JA, Carey GE. What is the role of an inter-disciplinary researcher? Int J Epidemiol 2007; 36:690.
42. PaytonA, Zoback M. Crossing boundaries, hittingbarriers: interdisciplinary research may be lauded,but it’s not yet rewarded. Nature 2007; 445: 950.
43. Carey G, Smith J. Jack of all-trades, master ofnone: postgraduate perspectives of interdisci-plinary health research in Australia. BMC HealthServices Res 2007; 7: 1-15.
44. Lehmann CU, Altuwaijri MM, Li YC, Ball MJ,Haux R. Translational research in medical in-formatics or from theory to practice. A call for anapplied informatics journal. Methods Inf Med2008; 47: 1-3.
45. Dhansay MA. The need for context-specific nutri-tion and health policies and interventions: thereality of disparities in socio-economic, healthand nutritional status. S Afr J Clin Nutr 2006; 19:142-145.
46. Séguin B, Hardy B-J, Singer PA, Daar AS. Ge-nomic medicine and developing countries: creat-ing a room of their own. Nat Rev Genet 2008; 9:487-493.
47. Séguin B, Hardy B, Singer PA, Daar AS. Bidil:recontextualizing the race debate. Pharmacoge-nomics J 2008; 8: 169-173.
48. Eriksson N, Pachter L, Mitsuya Y, et al. Viralpopulation estimation using pyrosequencing.PLoS Comput Biol 2008; 4: e1000074.
49. Lengauer T, Sander O, Sierra S, et al. Bioinfor-matics prediction of HIV coreceptor usage. NatBiotechnol 2007; 25: 1407-1410.
50. Rocco MC. Science and technology integrationfor increased human potential and societal out-comes. Ann N Y Acad Sci 2004; 1013: 1-16.
51. Hunter PJ, Crampin EJ, Nielsen PM. Bioinfor-matics, multiscale modeling and the IUPS physi-ome project. Brief Bioinform 2008; 9: 333-343.
52. Anderson C. The end of theory: the data delugemakes the scientific method obsolete. WiredMagazine 23.06.2008, http://www.wired.com/science/discoveries/magazine/16-07/pb_theory.Last accessed July 10, 2008.
53. Mandl KD, Kohane IS. Tectonic shifts in thehealth information economy. New Engl J Med2008; 358: 1732-1737.
54. Berners-Lee T, Hall W, Hendler JA, O’Hara K,Shadbolt N, Weitzner DJ. A framework for webscience. Foundations and Trends in Web Science2006; 1: 1-130.
55. Crisp N, Gawanas B, Sharp I, Task force for scal-ing up education and training for health workers.Training the health workforce: scaling up, savinglives. The Lancet 2008; 371: 689-691.
56. Anderson NR,Ash JS,Tarczy-Hornoch P.A quali-tative study of the implementation of a bioin-formatics tool in a biological research laboratory.Int J Med Inform 2007; 76: 821-828.
57. Pearson TA, Manolio TA. How to interpret a ge-nome-wide association study. J Am Med Assoc2008; 299: 1335-1544.
58. Prüss-Üstün A, Bos R, Gore F, Bartram J. Saferwater, better health: Costs, benefits and sustain-ability of interventions to protect and promotehealth. Geneva: WHO; 2008.
59. Fewtrell L, Kaufmann RB, Kay D, Enanoria W,Haller L, Colford JM Jr. Water, sanitation, andhygiene interventions to reduce diarrhoea in lessdeveloped countries: a systematic review andmetaanalysis. Lancet Infect Dis 2005; 5: 42-52.
60. BC Workshop, March 27-28, Morris J. WoskCenter for Dialogue, Vancouver, BC.
61. Weed LL. New connections between medicalknowledge and patient care. BMJ 1997; 315:231-235.
62. Kwankam SY, Pablos-Mendez A, Kay M.eHealth. In: Unwin T, editor. ICT for Devel-opment. In press.
63. Carroll L. Alice’s adventures in wonderland.1865.
64. The IMIA Strategic Plan: Towards IMIA 2015.Available online at http://www.imia.org/strategic/index.lasso Last accessed July 10, 2008.
65. Murray PJ. The IMIA strategic plan – towardsIMIA 2015. Geissbuhler A, Kulikowski CA, edi-tors. IMIA Yearbook of Medical Informatics2008. Methods Inf Med 2008; 47 (Suppl 1): 7-15.
66. Lorenzi NM, Murray PJ, Moura L, Goh HM,Huesing S, Martin-Sanchez F, Eisenberg F,Strachan H (The IMIA Strategic Planning TaskForce). Strategy in a fishbowl: An invitation to de-termine the shape of IMIA in 2015. Methods InfMed 2006; 45: 235-239.
67. Murray PJ, Haux R, Lorenzi NM. Let a thousandflowers bloom: Transition towards implemen-tation of the IMIA strategic plan. Methods InfMed 2007; 46: 625-628.
68. Schmidt KF. Nanofrontiers: Visions for the futureof Nanotechnology. Woodrow Wilson Interna-tional Center for Scholars. Project on EmergingNanotechnologies; 2007.
69. Poland CA, et al. Carbon nanotubes introducedinto the abdominal cavity of mice show asbestos-like pathogenicity in a pilot study. Nature Nano-technology 2008; 3: 423-428.
70. NNN – National Nanomanufacturing Network.NSF. Workshop on nanoinformatics strategies.Arlington, VA, June 2007. http://128.119.56.118/
Methods Inf Med 4/2008
315
Commentaries on Kuhn et al.́ s Article

Methods Inf Med 4/2008
316
Altman et al.
~nnn01/Workshop.html. Last accessed July 10,2008.
71. Martin-Sanchez F, Lopez-Alonso V, Hermosilla-Gimeno I, Lopez-Campos G. A primer in knowl-edge management for Nanoinformatics in Medi-cine. (Accepted as oral communication in the 12thInternational Conference on Knowledge-Basedand Intelligent Information and Engineering Sys-tems). KES 2008. Zagreb, Croatia. September2008.
72. Mihalas GI, Lungeanu D, Vernic C, Kigyosi A,Focsa M. Criteria for classification of medicalinformation. In: Baud R, Fieschi M, Le Beux P,Ruch P, editors. The new navigators: from profes-sionals to patients (Proc MIE 2003, St. Malo).Amsterdam: IOS Press; 2003. pp 358-363.
73. Hafizovic S, Heer F, Ugniwenko T, Frey U, BlauA, Ziegler C, Hirlemann. A CMOS-based micro-electrode array for interaction with neuronal cul-tures. J Neurosci Methods 2007; 164: 93-106.
74. Information workshop in neuroinformatics.http://cordis.europa.eu/search/, (Brussels,09.06.2000). Last accessed July 10, 2008.
75. Picard RW. Affective computing. CambridgeMass: MIT Press; 2000.
76. http://ecell3d.iab.keio.ac.jp. Last accessed July10, 2008.
77. http://www.e-cell.org. Last accessed July 10,2008.
78. http://www.physiome.org.nz. Last accessed July10, 2008.
79. http://www.biomedtown.org. Last accessed July10, 2008.
80. Engelbrecht R, Geissbuhler A, Lovis C, MihalasGI, editors. Connecting Medical Informatics andBioinformatics (Proc. MIE 2005, Geneva). Am-sterdam: IOS Press; 2005
81. Reichert A, Mihalas GI, Stoicu-Tivadar L, SchulzS, Engelbrecht R, editors. Integrating biomedicalinformation: From e-Cell to e-Patient. (Proc. STC2006, Timisoara). Amsterdam: IOS Press; 2006.
82. Grimshaw JM, Russel IT. Effect of clinicalguidelines on medical practice: a systematic re-view of rigorous evaluations. Lancet 1993: 342:1317-1322.
83. Quaglini S, Stefanelli M, Lanzola G, CaporussoV,Panzarasa S. Flexible guideline-based patientcareflow systems. Artif Int Med 2001; 22: 65-80.
84. Shahar Y, Young O, Shalom E, et al. A frameworkfor a distributed, hybrid, multiple-ontology clini-cal-guideline library and automated guideline-support tools. J Biomed Inform 2004; 37:325-344.
85. Shalom E, Shahar Y, Taieb-Maimon M., Lunen-feld E, Bar G, Yarkoni A, Young O, Martins SB,Vaszar LT, Goldstein MK, Liel, Y, Leibowitz A,Marom T., Lunenfeld E. A quantitative evaluationof a methodology for collaborative specificationof clinical guidelines at multiple representationlevels. J BioMed Inform 2008; in press.
86. Chen DP, Weber SC, Constantinu PS, Ferris TA,Lowe HJ, Butte AJ. Clinical arrays of laboratorymeasures, or “clinarrays”, built from an electronichealth record enable disease subtyping by sever-ity. Proceedings of the 2007 American Medical
Informatics Fall meeting (AMIA 2007). pp115-199.
87. Doyal L. Informed consent: moral necessity orillusion? Quality in Health Care 2002; 10 (Suppli): i29-i33.
88. Bowling A, Ebrahim S. Measuring patients’ pref-erences for treatment and perceptions of risk.Quality in Health Care 2001; 10 (Suppl i): i2-i8.
89. Woolf SH, Chan ECH, Harris R, Sheridan SL,Braddock BH, Kaplan RM, Krist A, O’ConnorAM, Tunis S. Promoting informed choice: trans-forming health care to dispense knowledge fordecision making. Annals of Internal Medicine2005; 143: 293-300.
90. Kuhn KA, Giuse DA. From hospital informationsystems to health information systems. Problems,challenges, perspectives. Methods Inf Med 2001;40: 275-287.
91. Bhave SV, Hornbaker C, Phang TL, Saba L, Lapa-dat R, Kechris K, Gaydos J, McGoldrick D,Dolbey A, Leach S, Soriano B, Ellington A, El-lington E, Jones K, Mangion J, Belknap JK, Wil-liams RW, Hunter LE, Hoffman PL, Tabakoff B.The PhenoGen informatics website: tools foranalyses of complex traits. BMC Genet 2007; 30:8-59.
92. Vivona S, Gardy JL, Ramachandran S, BrinkmanFS, Raghava GP, Flower DR, Filippini F. Com-puter-aided biotechnology: from immuno-infor-matics to reverse vaccinology. Trends Biotechnol2008; 26: 190-200.
93. HawkinsT, Chitale M, Kihara D. New paradigm inprotein function prediction for large scale omicsanalysis. Mol Biosyst. 2008; 4: 223-231.
94. Borisjuk L, Hajirezaei MR, Klukas C, Rollet-schek H, Schreiber F. Integrating data from bio-logical experiments into metabolic networks withthe DBE information system. In Silico Biol 2005;5: 93-102.
95. Olsson S, Hofmann I, Brambilla PM, JacobssonU, Kennedy P, Roca J, Schmitt KJ, Wyke A. Newsolutions for personalised health management:citizens’ needs, healthcare changes, and marketperspectives round table debate. Stud HealthTechnol Inform 2004; 108: 305-312.
96. Ball MJ, Costin MY, Lehmann C. The personalhealth record: consumers banking on their health.Stud Health Technol Inform 2008; 134: 35-46.
97. Ferreira A, Cruz-Correia R, Antunes L, ChadwickD. Access control: how can it improve patients’healthcare? Stud Health Technol Inform 2007;127: 65-76.
98. Hazlehurst B, Sittig DF, Stevens VJ, Smith KS,Hollis JF, Vogt TM, Winickoff JP, Glasgow R,Palen TE, Rigotti NA. Natural language process-ing in the electronic medical record: assessingclinician adherence to tobacco treatment guide-lines. Am J Prev Med 2005; 29: 434-439.
99. Post AR, Harrison JH Jr. Temporal data mining.Clin Lab Med 2008; 28 (1): 83-100.
100. Haux R, et al. Strategic information manage-ment in hospitals. New York: Springer; 2004.
101. Shortliffe EH, et al. Medical informatics: Com-puter applications in health care and biomedi-cine. 1st edition. Addison-Wesley; 1990. p 164.
102. Brown B. VHA eyes open-source replacementfor VistA. Government HealthIT, June 2006.
103. Ricadela A. Closing the door to Microsoft Vista.Business Week 2008, March 13, .
104. Cusumano MA. The business of software. FreePress; 2004.
105.Wiederhold, G. What is Your Software Worth.Comm ACM 2006; 49 (9): 65-75.
106. Reid PP, et al. Building a better delivery system,a new engineering/healthcare partnership. Was-hinton DC: National Academy Press; 2005.
107. The Economist: Places in the Sun. 2007, Febru-ary 2.
108. Commission on Systemic Interoperability: End-ing the Document Game, Connecting and Trans-forming Your Healthcare Through InformationTechnology. Washington, DC: U.S. GovernmentPrinting Office; 2005.
109. Institute of Medicine: Crossing the QualityChasm, A New Health System for the 21st Cen-tury. Washington DC: National Academy Press;2001.
110. Ness RB. Influence of the HIPAA privacy rule onhealth research. JAMA 2007; 298: 2164-2170.
111. Wiener N. Perspectives in cybernetics, 1964;published 1965 and in Masanti: Norbert Wiener,collected works. Boston, MA: MIT Press; 1985.pp 360-369.
Addresses of the authors:Prof. Russ B. Altman, MD, PhDStanford UniversityChair, Department of BioengineeringStanford, CAUSAE-mail: [email protected]
Prof. Rudi Balling, PhDScientific DirectorHelmholtz Centre for Infection ResearchBraunschweigGermanyE-mail: [email protected]
Prof. James F. Brinkley, MD, PhDUniversity of WashingtonDepartment of Biological StructureSeattle, WAUSAE-mail: [email protected]
Prof. Enrico Coiera, MB BS, PhDUniversity of New South WalesDirector, Centre for Health InformaticsSydney, NSWAustraliaE-mail: [email protected]
Prof. Fabrizio Consorti, MDDept. of Surgery “Francesco Durante”University of Rome “Sapienza”RomeItalyE-mail: [email protected]

Methods Inf Med 4/2008
Muhammad Ali Dhansay, MDVice-President for ResearchSouth African Medical Research CouncilTygerberg, Cape TownSouth AfricaE-mail: [email protected]
Prof. Antoine Geissbuhler, MDGeneva University and University HospitalsChair, Department of Radiology and Medical InformaticsGenevaSwitzerlandE-mail: [email protected]
Prof. William Hersh, MDOregon Health and Science UniversitySchool of MedicineProfessor and Chair, Department of Medical Informatics andClinical EpidemiologyPortland, ORUSAE-mail: [email protected]
S. Yunkap Kwankam, PhDWorld Health OrganizationCoordinator eHealthDepartment of Health Statistics and InformaticsGenevaSwitzerlandProfessor and Director EmeritusUniversity of Yaounde ICenter for Health TechnologyYaoundeCameroonE-mail: [email protected]
Prof. Nancy M. Lorenzi, PhDPast-President, International Medical Informatics Association(IMIA)Vanderbilt UniversityMedical CenterThe Informatics CenterNashville, TennesseeUSAE-mail: [email protected]
Fernando J. Martin-Sanchez, PhDMinistry of Science and InnovationInstitute of Health “Carlos III”Head, Medical Bioinformatics DepartmentMadridSpainE-mail: [email protected]
Prof. George Mihalas, PhDPast President, European Federation for Medical Informatics(EFMI)Victor Babes University of Medicine and PharmacyChair, Department of Medical InformaticsTimisoaraRomaniaE-mail: [email protected]
Prof. Yuval Shahar, MD, PhDBen Gurion UniversityDepartment of Information Systems EngineeringHead, Medical Informatics Research CenterBeer ShevaIsraelE-mail: [email protected]
Prof. Katsuhiko Takabayashi, MDChiba-UniversitySchool of MedicineDirector, Division of Medical Informatics and ManagementChibaJapanE-mail: [email protected], [email protected]
Prof. Gio Wiederhold, PhDStanford UniversityProfessor Emeritus, Depts. of Computer Science,Electrical Engineering and MedicineStanford, CAUSAE-mail: [email protected]
317
Commentaries on Kuhn et al.́ s Article
Medical Informatics Is Interdisciplinaryavant la LettreJ. H. van BemmelErasmus Medical Center and Erasmus University Rotterdam, Rotterdam, the Netherlands
SummaryObjective: To discuss the elements of interdisciplinaryresearch and to analyze its contribution to (bio)medicalinformatics.Method: Commenting on ‘Informatics and Medicine –From Molecules to Populations‘ from K. A. Kuhn et al.in this issue of Methods of Information in Medicine.Referring to examples of successfully established inter-disciplinary research.Results and Conclusions: Medical informatics is an in-terdisciplinary field avant la lettre. Experience with suc-cessful interdisciplinary research already exists for manydecades: Interdisciplinary research is not a category ofresearch but a consequence of addressing a complexproblem in society, involving the collaboration betweenand methods drawn from multiple disciplines. Becauseresearch is people, personal interactions are critical forinterdisciplinary research. Collaboration takes extratime to develop, to build consensus and to understandnew methodologies, languages, and each other‘s cul-ture. Interdisciplinary research requires leaders withvision and expressive skills. Effective scientific and in-stitutional leadership is critical to the success of inter-disciplinary groups. Interdisciplinarity begins in theclassroom. Interdisciplinary research cannot be effectivewithout interdisciplinary education. Researchers andteachers should immerse themselves in the culture ofother disciplines, learning to explain their work in termsunderstood by people outside their own discipline.Teams that perform interdisciplinary research shouldpromote collaboration, meet regularly, and recognizethat it requires a commitment toward good communi-cation and clear goals. Although much progress isachieved by interdisciplinary research, basic mono-disciplinary research is still required to advance thefrontiers of scientific knowledge, such as in physics orbiology.
KeywordsMedical informatics, biomedical informatics,interdisciplinarity
Methods Inf Med 2008; 47: 318–321
doi:10.3414/ME9119
On several occasions researchers in(bio)medical informatics have presentedtheir visions on the expected contributionsof informatics to health care. Klaus Kuhnand his colleagues from two universities inMunich have added their views to the al-ready existing body of opinions on thissubject [1]. Probably, one of the very firstworkshops on the challenges in MedicalInformatics took place during an earlySCAMC congress in Baltimore, in 1984 [2,3]. Since then, several meetings were heldand articles published on the subject of thefuture direction of (bio)medical infor-matics, health informatics, nursing in-formatics and the like (e.g. [4]).
1. The Core Messageof the ArticleKuhn et al. [1] observe substantial changesin health care. The main changes they seeare the impact of molecular biology, con-tributions by engineering, design of newdrugs, minimally invasive surgery, and so-ciocultural changes in the structure of healthcare provision. They notice a central role forinformatics in all such domains, consider-ing it to be the key element and the most im-portant driving force for all developments.They conclude that there is a need to educatea new generation of experts who can work ina multidisciplinary team. Their commongoal was to establish in 2008 a research-oriented Graduate School in Munich, sup-ported by the two universities they repre-sent.
Some elements for the future researchthat they envisage are the following: Newsystems for man-machine interaction alongthe lines predicted by Wiener in the 1950s; asystematic exploration of large databases ofpatient-related data; embedded systems for
the acquisition of data from sensor net-works; useful knowledge to be derived fromlarge data sets; the realization of autono-mous and self-healing software systems;seamless access to software and data by ad-vances in middleware technology; intelli-gent medical assist devices, while keepinghumans in the loop; knowledge-driven dis-covery and interpretation of complex bio-medical data. In short, they foresee a com-plete information logistics chain, fromsingle molecules to the entire human popu-lation.
To meet such challenges, multidisci-plinary collaboration is a must. Four appli-cation domains are indicated by the authors:1) bioinformatics and systems biology;2) informatics and biomedical engineering;3) health informatics and eHealth; and4) public health informatics and publichealth. The article of Kuhn et al. [1] thenenlarges on these four areas and makessuggestions for future research, such as theunderstanding of molecular mechanisms toget insight in the development of diseases;the translation of newly obtained knowledgefor personalized health care; the construc-tion of new sensors for data acquisition; theapplication of knowledge on genetic varia-tion in the population; and the assessment ofhealth care interventions. In pursuing thismultidisciplinary research they hope to con-tribute to an evidence-based and efficienthealth system.
2. CommentaryFirst of all, I applaud the initiative of the col-leagues in Munich to found this multidis-ciplinary Graduate School, for which appar-ently the agenda has been set in the docu-ment contained in their article. Their initi-ative is very far-reaching indeed, and covers
318
© 2008 Schattauer GmbH
Methods Inf Med 4/2008

virtually all the challenging developmentswe see in biomedicine, from biomolecularresearch up to the social aspects of healthcare. In a way, this plan is paralleled bymany similar initiatives around the world. Inmy commentary I will make a few support-ing and also some mildly critical remarks.
2.1 Graduate SchoolsThe idea of Graduate Schools is very timelyand has proven to be highly beneficial forthe advancement of science. Many re-searchers have noted that the future progressin science will come from research at thecrossroads of different disciplines. Since thebeginning of the 1990s, in the Netherlandswe have also seen the establishment of manysuch schools. These schools are in principlemulti-departmental research institutions.Many of them have an interdisciplinarycharacter. The task of the schools is 1) theadvancement of disciplinary or multidis-ciplinary research, and 2) education andtraining of young researchers at the MScand PhD level. One of the schools in the bio-medical domain, operational since the early1990s, is the Netherlands Institute forHealth Sciences (NIHES) at Erasmus Medi-cal Center Rotterdam, where researchers inepidemiology, medical informatics, andpublic health research collaborate aroundmajor and challenging research projects andwhere both MSc and PhD students aretrained [5]. NIHES has around 200 PhD stu-dents. It is hoped that the Munich initiativewill be equally successful. It is our experi-ence that both high-quality leadership andthe ability to attract talented PhD studentsare key factors for success. I have no doubtthat the colleagues in Munich are well awareof these factors.
2.2 InterdisciplinarityAs said, taking a multidisciplinary approachtowards the solution of major scientificproblems is often the right way to go. Itshould be mentioned at the same time, thatfundamental monodisciplinary research isstill of utmost importance, such as the re-search in the Large Hadron Collider in
Geneva or the ITER project in Grenoble.Nevertheless, for large problems in society,such as the changing climate, the energy cri-sis, or the provision of advanced health care,a multidisciplinary approach is the properdirection to take.
A few years ago I was a member of aCommittee on Interdisciplinary Research(IDR) of the NationalAcademy of Sciences,the Institute of Medicine, and the NationalAcademy of Engineering in the UnitedStates. The Committee consisted of re-searchers from a wide range of differentdisciplines, from the natural sciences to thesocial sciences and from engineering tophilosophy and ethics. I was privileged togive input from medical informatics andalso to provide a bridge to similar devel-opments in Europe. For the results of thisIDR Committee see [6], which also includesmany references to interdisciplinary re-search. One of the results of the work of theCommittee was a definition for this newtype of research, which was phrased asfollows:
‘Interdisciplinary research in scienceand engineering is a mode of research byteams or individuals that uses information,techniques, tools, perspectives, and/or the-ories from two or more established disci-plines to solve problems whose solutions arebeyond the scope of a single scientific disci-pline or area of scientific practice.’
2.3 Early InitiativeWhen diving into the history of interdisci-plinary research it is interesting to see that avery early initiative in this sense was takenin the 1930s by Gilles Holst at PhilipsPhysics Research Laboratory near Eind-hoven, the Netherlands. Hendrik Casimir,the famous Dutch physicist, who was formany years the Research Director of thePhysics Research Lab, documented thispioneering initiative in a publication, inwhich he summarized Holst’s principles inthe form of ‘Ten Commandments’ [7]:11) Engage competent scientists, if possible
young, yet with academic research ex-perience.
12) Do not pay too much attention to the de-tails of their previous experience.
13) Give them a good deal of freedom andgive a good deal of leeway to their par-ticular idiosyncrasies.
14) Let them publish and take part in inter-national scientific activities.
15) Steer a middle course between individu-alism and strict regimentation; baseauthority on real competence; in case ofdoubt prefer anarchy.
16) Do not divide a laboratory according todifferent disciplines but create multidis-ciplinary teams.
17) Give the research laboratories indepen-dence in choice of subjects but see to itthat leaders and staff are thoroughlyaware of their responsibility for the fu-ture of the company.
18) Do not try to run the research labora-tories on a detailed budget system andnever allow product divisions budgetarycontrol over research projects.
19) Encourage transfer of competent seniorpeople from the research laboratories tothe development laboratories of productdivisions.
10) In choosing research projects, be guidednot only by market possibilities, but alsoby the state of development of academicscience.
The history of the Philips Company wasdocumented in 2001 in a book by Prof. Marcde Vries from Delft University of Technol-ogy [8]. From his book I cite the followingobservation: ‘The fact that the Philips Re-search Lab survived until today, in contrastto the research labs of many of its competi-tors, is most probably rooted in its multidis-ciplinary character. The directors of thiscompany always understood the importanceof the collaboration between different disci-plines. This was also reflected in the organ-ization of the lab. The structure of the labhas always been project-oriented. On itsnew large research campus, which is nowbeing realized south of Eindhoven, manydisciplines will be present, including the so-cial sciences, e.g., to conduct research forthe realization of the intelligent home.’Thisconclusion is a very stimulating one for theinitiative phrased by the colleagues fromMunich.
319
Medical Informatics Is Interdisciplinary avant la Lettre
Methods Inf Med 4/2008

2.4 RecommendationsComing back to the IDR Committee that Imentioned, I want to cite some of its mainconclusions and recommendations, relevantand supportive for the Munich initiative andsimilar endeavors elsewhere [6]:● Interdisciplinary research is not a cat-
egory of research but a consequence ofaddressing a complex question, withmethods drawn from multiple disciplines.
● Research is people, and personal interac-tions are critical to interdisciplinary re-search. Collaboration takes extra time todevelop, to build consensus and under-stand new methodologies, language, andculture.
● Interdisciplinary research requiresleaders with vision and ‘expressive’skills. Effective scientific and institu-tional leadership are critical to the suc-cess of interdisciplinary groups.
● Interdisciplinarity begins in the class-room. Interdisciplinary research cannotbe effective without interdisciplinaryeducation.
● Researchers and teachers should im-merse themselves in the culture of otherdisciplines, learning to explain theirwork in terms understood by people out-side their own discipline.
● Teams that perform interdisciplinary re-search should promote collaboration,meet regularly, and recognize that itrequires a commitment toward goodcommunication and clear goals.
I dare to say that medical informatics is aninterdisciplinary field avant la lettre. In ourown institute in Rotterdam, we have re-search teams with very different back-grounds: physicists and medical doctors,engineers and informaticians, epidemiol-ogists and biologists. For such teams, therecommendations by Holst and the onesfrom the US Committee on IDR are veryrelevant.
After the paragraphs above, much in sup-port of the Munich initiative, I also take theopportunity to make some critical com-ments. These remarks pertain to the largelypositivistic and technological approach thatis described in [1] and the minimal descrip-tion of the grand challenges in modern
health care. Last, I want to mention some ofthe over-optimistic expectations of the pastthat – regretfully – were not fulfilled. Thequestion then is, why was there a lack of suc-cess? This is most important, becausepeople who do not know their history runthe risk of repeating the errors of the past.
2.5 Technology-driven ApproachThe type of research that is described in [1]to advance biomedicine is characterized bythe authors as ‘a complete logistics chain,from single molecules to the entire humanpopulation’. The way in which they want toaccomplish this ‘logistics chain’ is sum-marized as exploration of large patient data-bases; acquisition of data from sensors;knowledge derivation from databases; self-healing software systems; seamless accessto software and data; intelligent medicaldevices; and knowledge-driven discovery.This is, indeed, a long-term research agendafor a large institute, mainly oriented towardstechnology-driven research. And this is atthe same time one of the ‘mild’ criticismsthat I have about this proposal: the authorsgive the impression that they do not basetheir research agenda on needs in health careor society, but to start from possible con-tributions of technology.
Of course, all research in the natural andbiomedical sciences is a compromise be-tween needs and possibilities; the needs arethe driving forces and the methods offeredby science are the vehicles to reach thegoals. I have the feeling that the balance in[1] is too much tilted towards technologicalpossibilities, although even in this respect,much basic research is still to be done. Hav-ing said that, I am still missing a few areas ofexciting ‘technology-driven’ research, suchas imaging and image interpretation, arapidly expanding field. Perhaps, this typeof research is meant to have been incor-porated in one of the areas that are men-tioned, but I consider imaging and 4-Dimage processing, let alone image inter-pretation, both at the level of organs andcells, as a most important research field initself. More examples can be given, butperhaps it is more appropriate to discusssome health care challenges themselves.
2.6 Health Care Grand ChallengesThe field of (bio)medical informatics is atbest an ancillary discipline, only existing forthe benefit of health care. It is not an inde-pendent, ‘stand-alone’ domain, such as as-tronomy, geology or biology. Because medi-cine itself is a melting pot of many differentdisciplines, also medical informatics bearsthe same characteristics. As said, it is amultidisciplinary domain avant la lettre.For every different research challenge inmedicine and health care, multidisciplinaryresearch teams are composed to solve aspecific problem. For the computer inter-pretation of medical images one needs dif-ferent people than for the construction ofelectronic health records. For the develop-ment of modern hospital networks, givingseamless access to patient data, again differ-ent disciplines are required. For research onsystems for intensive patient care, the teamis again differently composed.
Thus, each research team is brought to-gether in such a way that it can tackle thespecific problem to be solved.The problemsare most often not defined by the researchteams themselves, but presented by healthcare in its widest sense. In this, typical dis-eases of modern society play a key role,such as cardiac and lung diseases, cancer,and – in general – the multiple diseases ofthe elderly, including stroke and Alz-heimer’s disease. Many chronic diseases,such as diabetes and hypertension, arecaused by our lifestyle. But we should alsonot forget, that ‘old’ diseases, such as tuber-culosis and many other infectious and viraldiseases, such as HIV, can also be the con-sequence of human behavior, impure watersanitation, unhealthy food, smoking, unsafepersonal behavior, global travel and some-times also the mismanagement of anti-biotics. Besides, there is a growing insightin the genetic causes of diseases. To enlargethe list of challenges a bit further, we seethat modern societies are confronted withexponentially rising costs of health care andeven in rich countries one is sometimes con-fronted with inequities in the distribution ofmedical services for different social groups.In addition, patients and consumer groupsare, because of the Internet, increasinglyinvolved in their own health care and want to
Methods Inf Med 4/2008
320
van Bemmel

321
Medical Informatics Is Interdisciplinary avant la Lettre
Methods Inf Med 4/2008
have insight in the effectiveness and thequality of care. Lastly, in most countries,health care provision is very much scatteredand improperly coordinated, even in coun-tries with a prominent primary health caresystem. Implicitly and explicitly the articleby Kuhn and colleagues addresses all theseexternal factors on health and our healthcare system (the needs), but – as said – Ihave the impression that the balance issomewhat tilted towards potential tech-nological possibilities instead of needs.
Finally, I would like to make a remark re-garding lessons from the past. In the past,there have been several overoptimistic ex-pectations regarding the contributions frommedical technology to health care. I vividlyremember the predictions in the 1970s onthe impact of medical decision-support sys-tems, expert systems etcetera on medicalcare. Well – to put it in a friendly way – theircontributions were only very modest. Thesame applies to the overoptimistic expec-tations of the realization of electronic healthrecords. All of this appears to be far morecomplex than ever expected, although thetechnology is widely available. Anotherexample pertains to medical image process-ing. Image boundary detection in often
noisy medical images appears to be ex-tremely difficult. A last example is the pro-cessing of free text in medical records. Notonly from the viewpoint of a natural lan-guage processing is this most difficult, butthe nature and culture of medicine itself,with its many traditions and continuouslychanging knowledge, appears to be a hin-drance to a generalized approach.This is notthe proper place to discuss the reasons forthese overstretched expectations, but it ismost important to take this experience intoaccount when setting the research agendafor the future.
3. ConclusionI repeat that I am most impressed by theMunich initiative and therefore I congratu-late the colleagues with the founding oftheir Graduate School. I have made somepositive and some mildly critical remarks.Looking at their very comprehensive re-search agenda, I would like to phrase a verylast remark in German: In der Beschrän-kung zeigt sich der Meister (In the restric-tion the master appears).
References1. Kuhn KA, et al. Informatics and Medicine: From
Molecules to Populations. Methods Inf Med 2008;47: 283-295.
2. Van Bemmel JH. The structure of medical in-formatics. Med Inform 1984; 9: 175-180.
3. Shortliffe EH. The science of biomedical com-puting. Med Inform 1984; 9: 185-193.
4. Musen MA, Van Bemmel JH. Challenges formedical informatics as an academic discipline.Methods Inf Med 2002; 41: 1-3.
5. http://www.nihes.nl6. Facilitating Interdisciplinary Research. Washing-
ton DC: National Academies Press; 2004.7. Casimir HBG. G. Holst and his ideas in industrial
research. Eindhoven: Philips Research Reports1969: 24 (3); 161-167.
8. De Vries MJ. 80 Years of Research at the PhilipsNatuurkundig Laboratorium (1914-1994). TheRole of the Nat. Lab. at Philips. Eindhoven: Foun-dation for the History of Technology; 2001.
Address of the author:Jan H. van BemmelInstitute of Medical InformaticsErasmus MC /Erasmus UniversityP.O. Box 20403000 CA RotterdamThe NetherlandsE-mail: [email protected]