7 2 July-December 2019 - International Journal of Physiology
138
7 2 July-December 2019
-
Upload
khangminh22 -
Category
Documents
-
view
9 -
download
0
Transcript of 7 2 July-December 2019 - International Journal of Physiology

7 2 July-December 2019

National Advisory Board1. Dr. Ruma Idnani, Principal, SIMS, Hapur
2. Prof S K Thakur, Head, Department of Surgery, Saraswathi Institute of Medical Sciences, Hapur, Uttar Pradesh
3. Prof. Ashutosh Niranjan, Department of Surgery, School of Medical Sciences & Research, Sharda University, Greater Noida (UP)
4. Dr. Ramesh G, Professor of Obstetrics and Gynaecology,M.V.J. Medical college and research hospital Bangalore
5. Dr. Deepak Chatterjee, Consultant Surgeon Gold Field Hospital & Associate Professor of Surgery, Gold Field Institute of Medical Sciences & Research, Ballabgarh, Faridabad 121004, Haryana.
6. Prof. Dr. P.S. Manoharan, Medical Superintdent, Vinayaka Mission’s Kirupananda Variyar Medical College & Hospital. Sankari Main Road( NH-47) Salem. 636008 Tamil Nadu
7. Dr. Rana A K Singh, Professor, Hepatobiliary Surgery, RML Hospital, New Delhi
8. Dr. Sanjay Pandey, Professor of Surgery, Subharati Medical College, Merrut
9. Dr. Pardeep Garg, Sr. Prof., Deptt. of Surgery, PGIMS, Rohtak
Scientific Committee1. Dr. Arati Srivarstava, Associate Professor, Department
of anesthesia, School of Medical Sciences & Research, Sharda University, Greater Noida (UP)
2. Dr. Anand Verma, Assistant Prof Ophthalmology, SMS&R,Sharda Hospital, Sharda University, Greater Noida
3. Dr. Vikrant Sharma, Associated Professor Opthalmology Muti Speciality Govt Hospital, Noida
4. Dr. Manisha Kamal Kukreja, Asstt. Prof. Deptt. of Orthodontics, PGIMS , Rohtak
International Journal of Contemporary SurgeryEditor-in-Chief
Prof (Dr) R.K. SharmaFormerly at- All-India Institute of Medical Sciences, New Delhi
E mail: [email protected]
International Journal of Contemporary Surgery is a double blind peer reviewed international journal which has commenced its publication from January 2013. The journal is half yearly in frequency. The journal covers all aspects of Surgical practice. The journal has been assigned ISSN 2320-9615 (Print Version) and ISSN 2321-1024 (Online Version). The journal is Indexed in many international data bases.
Website: www.ijocs.in
All rights reserved. The views expressed by authors in journal are not necessarily views of International Journal of Contemporary Surgery. The advertisements are purely commercial in nature and journal does not guarantee their efficacy.
ISSN 2320-9615 (Print Version) and ISSN 2321-1024(Online Version). Frequency: Half Yearly
EditorDr. R.K. Sharma
Institute of Medico-legal PublicationsLogix Office Tower, Unit No. 1704, Logix City Centre Mall,
Sector- 32, Noida - 201 301 (Uttar Pradesh)
Printed, published and owned byDr. R.K. Sharma
Institute of Medico-legal PublicationsLogix Office Tower, Unit No. 1704, Logix City Centre Mall,
Sector- 32, Noida - 201 301 (Uttar Pradesh)
Published atInstitute of Medico-legal Publications
Logix Office Tower, Unit No. 1704, Logix City Centre Mall, Sector- 32, Noida - 201 301 (Uttar Pradesh)

Contents
Volume 7, Number 2 July-December 2019
I
International Journal of Contemporary Surgery
1. A Prospective, Randomized, Controlled Study For Efficacy of Phenytoin Sodium Powder, Eusol Solution, Nanocrystalline Silver Gel in Diabetic Foot Ulcer ....................................................................................... 01 Ajay Chauhan, Bhavesh K. Patel, P. P. Sharma, F. S. Mehta
2. Efficacy and Safety of Sarclav in the Treatment of Acute Otitis Media in Children ...................................... 08 Abhay Kumar Singh, Harsimrat Singh, Himani Singh
3. Clinical Profile and Outcome of Diabetic Foot in a Tertiary Care Centre ..................................................... 14 Abhishek Gupta, Subash Chandra Sharma, Janmejai Prasad Sharma
4. Locking Versus Non-Locking Plate Fixation in the Management of Maxillofacial Fractures : A Prospective Comparative Study ......................................................................................................................................... 19 Nitin Verma, Neha Mann, Jaspreet Kaur, Supreet Gill
5. Treatment of Liver Abscess: A Comparison of Catheter Drainage and Needle Aspiration ............................ 25 Ajay Chauhan, Yashasvi Patel, P. P. Sharma, F. S. Mehta
6. A Comparative Study of Standard PCNL vs Tubeless PCNL at a Tertiary Care Hospital ............................ 31 Navneet Garg, Bindu Agrawal, Nikita Garg, Manish Agrawal
7. Choledochodudenostomy Revisited: The Present Scenario .......................................................................... 36 Alok V Mathur, Manmeet Kaur
8. Role of Diagnostic Nasal Endoscopy in Sinonasal Disease ........................................................................... 42 Abhay Kumar Singh, Pal Satyajit Singh Athwal, Harsimrat Singh, Himani Singh
9. Study on the Incidence of Salmonella Infection in Patients with Carcinoma Gall Bladder ........................... 47 Apoorva Pratap Singh, Alok Vardhan Mathur
10. Review of Clinical and Functional Result of Abdominal Rectopexy Using Proline Mesh for Complete Rectal Prolapse Over a Period of 1 Year at Tertiary Care Centre in Bihar ................................................................ 53 Nitesh Kumar, Nitesh, Vibhuti Bhushan, Ashwini Kumar, Monika Raj
11. Morbidity Pattren in Patients of Ileostomy: An Observational Study ............................................................ 59 Rao Aftab Alam, Pradeep Singhal, Anurag Bijalwan, Syed Altamash
12. Comparative Study of Chemical Sphincterotomy and Lateral Internal Sphincterotomy for Chronic Anal Fissure .............................................................................................................................................................65 Nitesh Kumar, Deepak Pankaj, Nitesh, Ashwini Kumar, Monika Raj
13. Comparative Study of Lateral Internal Sphincterotomy vs Glyceryl Trinitrate Ointment for Fissure in Ano .................................................................................................................................................73 Ravichandran Subramaniam

II
14. Assessing Pressure Ulcer Knowledge of General and Orthopedic Surgical Residents Using the Pieper Pressure Ulcer Knowledge Test .......................................................................................................................78 Sanjay Kumar Mishra, Shafaq Mahmood
15. Is Cartilage Shield Tympanoplasty better than Fascia Tympanoplasty ........................................................ 84 Shahnaz Sheikh, Anushree Bajaj,Vikrant Vaze
16. Various Presentations of Hepatic Hydatid Cystic Disease and their Management ......................................... 89 Pradeep Kumar, Sandeep Maliyan, Sohan Pal Singh, Manjul Kumar, Nitin chauhan, Anshu Tiwari
17. A Clinical Study and Management of Hypocalcemia Following Thyroid Surgery ........................................ 94 Pratima Raj, Abhilash V, Suma S, Krishna Prasad K
18. Incidence of Malignancy in Unilateral Tonsillar Enlargement Over a Period of 10 Years ............................. 99 Sushil Gaur, Vandana Singh, Prince Hirdesh, Akshay S Panakkal
19. A Prospective Comparative Study of Intestinal Anastomosis, Single Layer Extramucosal Versus Double Layer ............................................................................................................................................................. 103 Sohan Pal Singh, Divya Prakash, Dheeraj Raj Baliyan, Virendra Kumar, Vishal Saxena, Prachi
20. Intra-Peritoneal Bupivacaine Instillation for Post-Operative Pain Relief after Laparoscopic Cholecystectomy: A Prospective Study ...................................................................................................................................... 108 Suma S, Vikranth Suresh N, Nikhil M, Sreeramulu P N
21. Incidence of Differentiated Thyroid Carcinoma in Multinodular Goitre Patients in Western UP ................ 115 Yogendra Kumar, Vandana Singh, Sushil Gaur
22. Clinical Profile and Outcome of Patients Suffering from Soft Tissue Infection in Lower Limb Disease in the Department of Surgery in Tertiary Care Center .............................................................................................121 Rishabh Sharma, Ram Kumar Verma, Alok Vardhan Mathur, Rajendra Kumar Srivastava, Saurabh Kumar
23. A Clinical Study of Management of Perforative Peritonitis and Its Surgical Outcome ............................... 125 Chandra Kumar P C, Venkatesh Kharalkar, Bellara Raghavendra

A Prospective, Randomized, Controlled Study For Efficacy of Phenytoin Sodium Powder, Eusol Solution, Nanocrystalline
Silver Gel in Diabetic Foot Ulcer
Ajay Chauhan1, Bhavesh K. Patel2, P. P. Sharma3, F. S. Mehta3
1Associate Professor, 23rd year PG Resident, 3Professor, 4Professor, Department of General Surgery, Geetanjali Medical College and Hospital, Udaipur, Rajasthan
Abstract
Background: Diabetic foot is one of the most significant and devastating complications of diabetes. Not all foot complications can be prevented, but it is possible to dramatically reduce their incidence through appropriate management and prevention. Various dressings are available that fulfils a number of functions like cosmesis, haemostasis, protection, support and absorption.
Objectives: To study and compare the efficacy of different topical agents like phenytoin sodium powder, eusol solution, nanocrystalline silver gel in patient with diabetic foot ulcer by recording the mean ulcer size pre-treatment, during the course of treatment (1 week, 2 week, 3 week and 4 week follow up) and post- treatment and mean percentage of the wound size healing after treatment.
Material & Method: This prospective study was conducted in the Department of General Surgery, Geetanjali Medical College & Hospital, affiliated to Geetanjali University from January 2017 to June 2018. 90 patients with diabetic foot ulcers without any other co-morbid conditions and ulcers belonging to Grade I & II as per Wagner diabetic foot ulcers classification were compared with the efficacy of different topical agents.
Results: Out of 90 patients, there was a highly significant reduction in the mean ulcer size after 2 week, 3 week and 4 week follow up in nanocrystalline silver gel group (p<0.05) as compared to the phenytoin sodium powder and eusol solution group and the formation of granulation tissue was higher in nanocrystalline silver gel group (90%) as compared to phenytoin sodium powder (80%) and eusol solution (73.33%).
Conclusion: Dressings done with nanocrystalline silver gel was found to be more efficacious than the other topical agents in patients with diabetic foot ulcers in terms of increased rate of wound healing, greater reduction in the mean ulcer size after treatment, absence of pain, swelling and type of discharge after treatment, greater incidence of formation of granulation tissue and less duration of antibiotic therapy and hospital stay.
Keyword: Diabetic foot ulcer, phenytoin sodium powder, nanocrystalline silver gel, eusol solution.
Corresponding author:Dr. Bhavesh K. Patel 3rd year PG resident, Department of General Surgery, Geetanjali Medical College and Hospital, Udaipur, Rajasthan. Mobile- 9901341346Email- [email protected]
Introduction
Diabetic foot is one of the most significant and devastating complications of diabetes, and is defined as a foot affected by ulceration that is associated with neuropathy and ischaemia of the lower limb in a patient with diabetes (1). In India, diabetic foot
DOI Number: 10.5958/2321-1024.2019.00014.X

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 2
infection constitutes upto 10% of diabetes related hospital admissions. Furthermore, of the 40,000 legs amputated per year, the majority are due to diabetic foot ulcers.
Not all foot complications can be prevented, but it is possible to dramatically reduce their incidence through appropriate management and prevention programs (2). They must be managed by a multidisciplinary team for optimal outcome with diabetic foot ulcer. Studies have shown that a multidisciplinary team can reduce amputation rates, lower costs and lead to better quality of life for patients with diabetic foot ulcer (3). The ideal dressing should be free from contaminants, be able to remove excess exudates and toxic components, maintain a moist environment at the wound- dressing interface, be impermeable to microorganisms, allow gaseous exchange, and, finally, should be easily removed and cost-effective. Various dressings are available that are intended to prevent infection and enhance wound healing, and several studies support their effectiveness for this purpose (4). Various therapeutic methods are applied for the healing of diabetic foot ulcer such as topical Phenytoin sodium powder, Eusol solution, Nanocrystalline silver gel. Each has its own positive and negative factors.
Phenytoin powder is prepared from the capsule and promotes wound healing by neovascularisation, enhanced granulation tissue formation, increase in deposition of collagen, increase in proliferation of fibroblasts and decrease in bacterial contamination of wounds. Oral phenytoin does have dose-related side effects. The most serious of these is the hypersensitivity syndrome. However, the side effects of oral phenytoin have not been reported in the topical application of phenytoin in wound healing. The precise mechanism of phenytoin decreasing bacterial contamination of wounds is not known (5).
Eusol (Edinburgh University Solution of lime) is a commonly used solution which help faster wound healing, found most effective in pseudomonads organism and acts by releasing nascent chlorine which act as desloughing agent and dilute concentrations kills fibroblast, neutrophils and endothelial cells in tissue culture. When applied to open wound that are healing by secondary intention delays the appearance of hydroxyproline (amino acid marker of wound collagen content) and prolongs the acute inflammation response.
Side effects of eusol solution may dissolve blood clots and cause bleeding. Toxic effects on neutrophils & fibroblasts. Burn injury is possible if used without proper dilution with distilled water or normal saline (6).
Silver has antiseptic, antimicrobial, anti-inflammatory properties and is a broad spectrum antibiotic. Silver ions are active against a broad range of bacteria, fungi and viruses, including many antibiotic-resistant bacteria, such as methicillin- resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococci (VRE). Free silver cations have a potent antimicrobial effect which destroys microorganisms immediately by blocking the cellular respiration and disrupting the function of bacterial cell membranes. Nanocrystalline silver utilizes nanotechnology to release clusters of extremely small and highly reactive silver particles, the smaller the particles of silver, the greater the wound surface area that will be in contact with silver, thus increasing bioactivity and silver solubility (7).
In this study, we compared the effectiveness of different topical agents on diabetic foot ulcers for rapid growth of healthy granulation tissue, hence early closure of wound.
Materials & Method
This prospective study was conducted in the Department of General Surgery, Geetanjali Medical College & Hospital, affiliated to Geetanjali University from January 2017 to June 2018. 90 patients with diabetic foot ulcers without any other co-morbid conditions and ulcers belonging to Grade I & II as per Wagner diabetic foot ulcers classification. Patients aged 30 years and above, with a known history of diabetes and diagnosed diabetic on admission with a diabetic foot. Patients below 30 years of age, diabetic ulcer in grade 3, 4, 5, on steroids, and suffering from other condition like traumatic and burn wounds, vascular impairment, osteomyelitis, hepatic and renal diseases, gangrene, malignancy.
Diabetic foot ulcer Wagner classification: -
Grade 0- no risk
Grade1- superficial ulcer
Grade 2- deep ulcer

3 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
Grade 3- deep ulcer with abscess
Grade 4- gangrene limited
Grade 5- gangrene extensive.
Patients were then subjected for detailed clinical examination with baseline investigations, were posted for surgical procedures (debridement) if required & follow up of patients during hospital stay and at 1st, 2nd, 3rd and 4th week was done. We did dressings of patients as required until wound healing achieved and changes in wound size (area of the wound was measured in square centimeters by taking an impression of the wound on a gauze piece and tracing it on graph paper on subsequent days) was recorded when the dressing was removed and changed. phenytoin sodium powder group, eusol solution group and nanocrystalline silver gel group to compare the effectiveness of these different topical agents on patients with diabetic foot ulcer in regards of presence of pus, swelling, pain before treatment and after treatment, mean ulcer size pre-treatment, during the course of treatment (1 week,2 week, 3 week and 4 week follow up) and post-
treatment, mean percentage of the wound size healing after treatment, duration of antibiotic therapy, duration of hospital stay and formation of granulation tissue.
The quantitative data was represented as their mean ± SD. Categorical and nominal data was expressed in percentage. The t-test was used for analysing quantitative data, or else non parametric data was analyzed by Mann Whitney test and categorical data was analyzed by using chi-square test. Pearson’s correlation coefficient was used to determine the correlation between parameters. The significance threshold of p-value was set at <0.05. All analysis was carried out by using SPSS software version 20.
Results
A total of 90 patients were included in the study under the age group of 40-70 years. Males (71) were more affected than females (19). Pain after treatment- lower pain scores in the nanocrystalline silver gel group (1.20 + 1.24) as compared to the phenytoin sodium powder (2.03 + 1.45) and eusol solution group (1.87 + 1.57).
Table 1: Presence of Pain (VAS) after Treatment in all 3 groups
Pain (VAS)
Phenytoin Sodium Powder Eusol Solution
NanocrystallineSilver Gel
No. % No. % No. %
0 7 23.33% 9 30.00% 12 40.00%
1 3 10.00% 4 13.33% 7 23.33%
2 8 26.67% 6 20.00% 5 16.67%
3 6 20.00% 4 13.33% 5 16.67%
4 6 20.00% 7 23.33% 1 3.33%
Mean±SD 2.03 1.45 1.87 1.57 1.20 1.24
The mean ulcer size was significantly smaller in the nanocrystalline silver gel group (3.41 + 3.17) as compared to the phenytoin sodium powder (9.21 + 7.41) and eusol solution (7.72 + 6.65) group after 4 weeks follow up (p<0.05). Also, there was a highly
significant reduction in the mean ulcer size after 2 week, 3 week and 4 week follow up in nanocrystalline silver gel group (p<0.05) as compared to the phenytoin sodium powder and eusol solution group.

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 4
Table 2: Mean Ulcer Size Pre, During and Post Treatment in all 3 groups
Mean Ulcer Size(cm2)
Phenytoin Sodium Powder Eusol Solution
Nanocrystalli- ne Silver Gel
PvalueMean SD Mean SD Mean SD
Pre-treatment 17.08 7.72 16.66 7.52 16.94 7.78 >0.05
After 1 wk follow-up 15.68 8.27 16.16 7.52 14.38 6.38 >0.05
After 2 wk follow-up 13.58 7.58 14.16 6.54 11.02 5.46 >0.05
After 3 wk follow-up 10.12 6.52 11.18 7.48 7.16 4.51 >0.05
After 4 wk follow-up 9.21 7.41 7.72 6.65 3.41 3.17 <0.05
P value >0.05 >0.05 <0.001
The formation of granulation tissue was higher in nanocrystalline silver gel group (90%) as compared to phenytoin sodium powder (80%) and eusol solution (73.33%) groups.
Table 3: Formation of granulation tissue in all 3 groups
GranulationTissue
Phenytoin Sodium Powder
Eusol Solution
NanocrystallineSilver Gel
No. % No. % No. %
Present 24 80% 22 73.33% 27 90%
Absent 6 20% 8 26.67% 3 10%
Our study found that there more significant improvement in nanocrystalline silver gel group (83.07%) as compared to the phenytoin sodium powder (57.98%) and eusol solution (63.69%) groups. Also the mean wound size healed in nanocrystalline silver gel group was much more 13.53 ± 5.74 cm2 as compared to phenytoin sodium powder 7.87 ± 0.89 cm2 and eusol solution group 8.94 ± 1.58 cm2.
Table 4: Mean percentage of wound size healing in all 3 groups
Wound Size Healed (cm2)
Phenytoin Sodium PowderSodium Powder
Eusol Solution Nanocrystalline silver Gel
Mean SD Mean SD Mean SD
Improvement 57.98% 28.46 63.69% 24.64 83.07% 13.31
Size Healed (Sq. cm) 7.87 0.89 8.94 1.58 13.53 5.74
The duration of hospital stay (in days) was shorter in the nanocrystalline silver gel group (10.27 + 5.27)
as compared to the phenytoin sodium powder (14.97+ 5.73) and eusol solution (13.30+4.48) groups.

Table 5: Duration of hospital stay in all 3 groups
Phenytoin Sodium Powder Eusol Solution Nanocrystalline Silver Gel
Mean SD Mean SD Mean SD
Duration (days) 14.97 5.73 13.30 4.48 10.27 5.27
Table 6: No. of Weeks and Dressings Required for Wound Healing in all 3 groups
Phenytoin Sodium Powder Eusol Solution Nanocrystalline Silver Gel
No. % No. % No. %
1 week 1 3.33% 0 0.00%2
6.67%
2 weeks 6 20.00% 6 20.00%8
26.67%
3 weeks 8 26.67% 8 26.67%11
36.67%
4 weeks 9 30.00% 8 26.67%6
20.00%
Total 24 80.00% 22 73.33%27
90.00%
Discussion
Diabetic foot ulcer is one of the most devastating complications of diabetes mellitus and early effective management can reduce the severity of complications such as preventable amputations and possible mortality and can also improve the quality of life. Topical phenytoin is a known inexpensive therapeutic agent in wound healing as it induces growth of granulation tissue, angiogenesis and decreases the wound size. Eusol is a commonly used solution for wound healing as it is a desloughing agent and helps in effective healing. Nanocrystalline silver gel also promotes wound healing through the antiseptic, antimicrobial and anti-inflammatory properties of silver.
In our study, after treatment and follow-up of 4 weeks pain scores in all the three groups reduced, however, there was much lower pain scores in the nanocrystalline silver gel group (1.20 + 1.24) as compared to the phenytoin sodium powder (2.03 + 1.45) and eusol solution group (1.87 + 1.57). Ramanaiah et al (8) also found a significant reduction in the pain scores in the nanocrystalline silver gel group post treatment in their study. Similarly, in a study done by Jayalal et al
(9) on efficacy of topical phenytoin sodium powder
in diabetic foot ulcer, pain scores were found to be significantly lower in the study group as compared to the control group.
Our study showed that the mean ulcer size after 1 week, 2 week and 3 week follow up in silver group reduced more as compared to the phenytoin sodium powder and eusol solution group. Similarly, Ramanaiah et al
(8) found significant reduction in the wound size in their study after treatment with nanocrystalline silver gel dressings. Sharma et al
(10) also found a significant
reduction in the wound size with an effective wound healing with nanocrystalline silver gel dressings as compared to the conventional dressings.
In a study done by Jayalal et al(9) on the efficacy
of topical application of phenytoin sodium powder in diabetic foot ulcer, there was a significant reduction in the slough and wound size area after treatment. Charne et al
(11) demonstrated nanocrystalline silver gel had
a much higher rate of healing ulcer size compared to other applications.
In our study, mean percentage of wound size healing of ulcer with nanocrystalline silver gel dressing is 83.07% as compared to the phenytoin sodium powder (57.98%) and eusol solution (63.69%).
5 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 6
In the study done by Miller et al(11)
, a comparison of the number of wounds that healed within each treatment group was explored for the wound duration and wound size segmentations. Beele et al
(12) had similar findings to ours showing ulcer healing rate at 6 months significantly increased from 49% to 54% between 2008 and 2011.
Our study found that the duration of hospital stay (in days) was shorter in the nanocrystalline silver gel group (10.27 + 5.27) as compared to the phenytoin sodium powder (14.97+ 5.73) and eusol solution (13.30+4.48) groups. Similarly, Ramanaiah et al
(8)
found that the duration of hospital stay was shorter in the nanocrystalline silver gel group. Sharma et al (10)
also found shorter duration of hospital stay with nanocrystalline silver gel dressings as compared to the conventional dressings.
In our study number of nanocrystalline silver gel dressings required per patient is significantly less compared to conventional dressing group. In the study done by Miller et al
(11), it was concluded by the results
that the time taken and number of dressings taken for healing of ulcers in both cases with nanocrystalline silver gel and betadine were similar.
Further studies with larger population will be needed in the future before topical nanocrystalline silver gel dressing can be added to the wide spectrum of treatment modalities available in the management of diabetic ulcers and ulcers of other etiologies. A unique, nationwide quality improvement initiative should be established among diabetic foot clinics, covering ulcer healing, lower limb amputation and many other aspects of diabetic foot care.
Conclusion
Nanocrystalline silver gel dressings in the treatment of diabetic foot ulcers were found to be safe, effective, higher rate of wound healing, promotes epithelization, accelerates healing, eliminates anaerobes and breaks microbial synergy more effectively than conventional dressing. Hence nanocrystalline silver gel prove to be more effective in the management of diabetic foot ulcers.
Conflict of Interest – Nil
Source of Funding – Self
Ethical Clearance – Human Research Ethics Committee (HREC) on 28th Feb. 2017.
References
1. Abbott CA, Carrington AL, Ashe H, Bath S, Every LC, Griffiths J, Hann AW, Hussein A, Jackson N, Johnson KE, Ryder CH. The North‐West Diabetes Foot Care Study: incidence of, and risk factors for, new diabetic foot ulceration in a community‐based patient cohort. Diabetic medicine. 2002 May;19(5):377-84.
2. Pendsey SP. Understanding Diabetic Foot. Int J Diabetes Dev ctries. 2010; 30 (2): 75-9.
3. Yazdanpanah L, Nasiri M, Adarvishi S. Literature review on the management of diabetic foot ulcer. World journal of diabetes. 2015 Feb 15;6(1):37.
4. Katsilambros N, Dounis E, Makrilakis K, Tentolouris N, Tsapogas P. Atlas of the diabetic foot, Second edition. 2011; 10.1002/9781444317589.
5. Steed DL. Clinical evaluation of recombinant human platelet-derived growth factor for the treatment of lower extremity ulcers. Plast Reconstr Surg. 2006; 117 (7): 143-9.
6. Okeniyi JAO, Olubanjo OO, Ogunlesi TA, Oyelami OA. Comparison of healing of incised abscess wounds with honey and EUSOL dressing. Journal of Alternative and complementary Medicine. 2005; 11 (3): 511-3.
7. Fong J, Wood F, Fowler B. A silver coated dressing reduces the incidence of early burn wound cellulitis and associated costs of inpatient treatment: Comparative patient care audits. Burns. 2005; 31: 562-7.
8. Ramanaiah N. V., Saikrishna, Chandrasekhar, Vamshidhar, Ramanaiah G. V., K. Lokesh. “A Clinical Study on Efficacy of Nanocrystalline Silver Dressing in Diabetic Foot Ulcers”. Journal of Evidence based Medicine and Healthcare; November 05, 2015; 2 (45): 8160-8170, DOI: 10.18410/jebmh/2015/1097.
9. Jayalal JA, Kumar SJ, Dhinesh DT, Kadar JM. Efficiency of topical phenytoin on healing in diabetic foot ulcer: A randomized controlled trial.

7 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
International journal of scientific study. 2015; 3(3): 84-9.
10. Sharma R, Rajkamal, Kumar R, Mittal S, Kaur A. Study of effect of topical nano silver gel on wound healing. J Adv Med Dent Sci Res 2016; 4(5): 59-61.
11. Charne N Miller, Nelly Newall RN, Suzanne E. Kapp BN, Gill Lewin. A randomized controlled trial comparing cadexomer iodine and nanocrystalline
silver on the healing of leg ulcers. The Intern J Tissue Repair and Regeneration. July/August 2010; 18, (4): 359-367
12. Beele H, Doggen K, Van Acker K, Dumont I, Félix P, Lauwers P, Lavens A, Implementation of a quality improvement initiative in Belgian diabetic foot clinics: feasibility and initial results. Diabetes Metab Res Rev. 2014 Jul; 30(5):435-43.

Efficacy and Safety of Sarclav in the Treatment of Acute Otitis Media in Children
Abhay Kumar Singh1, Harsimrat Singh2, Himani Singh2
1Assistant Professor, 2Post Graduate, Department of ENT Saraswathi Institute of Medical Sciences Hapur (U.P)
Abstract
Background: Acute otitis media (AOM) is a community-acquired respiratory tract infection in childhood frequently encountered by primary-care physicians and can cause a significant morbidity. Increasing bacterial resistance has led to concern about the current options for empirical antibiotic treatment and has prompted a search for effective treatments.
Objectives: To evaluate the clinical efficacy and safety of Sarclav (cefpodoxime proxetil) in the treatment of children with acute otitis media.
Patients and Method: A prospective, multicenter study was conducted on 1380 children aged from 1 to 13 years with AOM who were prescribed a 5–10 day course of Sarclav (cefpodoxime proxetil) (8 mg/kg/day). Patients were followed-up after 7–14 days from baseline visit. Efficacy was assessed by the percentage of patients with clinical cure, improvement or failure at the follow-up visit. Safety was evaluated by recording the occurrence and severity of any adverse events and by the physicians’ and patients’ assessment of overall tolerability.
Results: Clinically, 82.5% of patients were cured, 16.4% were improved and there was failure of therapy in 1.1% of the patients. The overall combined cure and improvement rate of all related signs and symptoms was 98.9%. Adverse events, diarrhea and skin rash, were reported by only 16 patients (1.2%). The overall tolerability according to the physicians’ and patients’ assessment was excellent in 93.9% and 88.9%, respectively. Compliance was attained in 99.5% of patients.
Conclusion: Sarclav (cefpodoxime proxetil) is an effective, safe, well-tolerated antimicrobial agent for treatment of acute otitis media in children. It can be considered as an excellent choice for the empirical treatment of bacterial AOM.
Keywords: Acute otitis media, Sarclav (cefpodoxime) , Children, Efficacy.
Corresponding Author: Dr Abhay Kumar SinghAssistant Professor, Department of ENT, Saraswathi Institute of Medical Sciences, Hapur (U.P)E-mail: [email protected]
Introduction
Acute otitis media (AOM) is one of the most frequent diseases in early infancy and childhood. It is defined as the presence of middle ear effusion and a rapid onset of signs or symptoms of middle-ear inflammation, such as ear pain, otorrhea or fever.1It is estimated that
more than two-thirds of children experience one or more attacks of AOM by the age of 3 years.2, 3, 4 The peak age of incidence is 6–24 months and decreases with age.5
The pathogenesis of AOM is multifactorial, involving the adaptive and native immune system, eustachian tube dysfunction, viral and bacterial load, in addition to genetic and environmental factors.2 Bacteria are believed to play a predominant role in the causation of AOM-related symptoms.
Streptococcus pneumoniae has been reported as the predominant pathogen causing AOM for many years, next to Moraxella catarrhalis and non-typeable Haemophilus
DOI Number: 10.5958/2321-1024.2019.00015.1

9 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
influenzae. The implementation of vaccination programs for pneumococcal infection changed the etiology of AOM over time resulting in H. influenzae to be the main pathogen in AOM.7, 8 Moreover, increasing bacterial resistance, particularly beta-lactamase producing strains of H. influenzae and M. catarrhalis as well as penicillin and macrolide resistance among S. pneumoniae, has raised the concern about the current options for empirical antibiotic treatment and has prompted a search for effective treatments.1, 6, 9
Sarclav is an oral third generation cephalosporin of choice for the treatment of AOM.1 In vitro studies show that it has activity against many common Gram-positive and Gram-negative pathogens associated with common pediatric infections including AOM, making it a useful option for Sarclav empirical therapy.1,6, 11 Moreover, in vivo sensitivity studies assessing the bacteriological efficacy by examining middle-ear fluid before and a few days after the start of treatment and retrospective analyses of treatment failures, have shown a good bacteriological efficacy for Sarclav (cefpodoxime) against H. influenzae and penicillin-susceptible S. pneumoniae.7, 8 It is highly stable to hydrolysis by the most commonly found plasmid-mediated β-lactamases.10 Its relatively long half-life and sustained tissue concentrations support twice daily dosing, representing an advantage over many other antibiotics with comparable clinical efficacy and features that may encourage patient compliance.11
Finally, physicians’ familiarity with dosing schedules and potential side effects may reduce prescribing errors.12
Aim
The aim of the study was to evaluate the clinical efficacy and safety of Sarclav (cefpodoxime proxetil) in the treatment of children with acute otitis media.
Patients and method
Study design
This prospective, multicentre study was conducted in SARASWATHI MEDICAL COLLEGE, Hapur, U.P from May 2017 to December 2018. The study was approved by the local Ethics Committee. A written informed parental/guardians’ consent was obtained prior to enrollment in the study.
Study population
A total of 1380 children aged 1–13 years, presenting with clinically diagnosed AOM suspected to be of bacterial origin were eligible for the study. Patients were not on any antibiotic therapy when enrolled in the study. The exclusion criteria were restricted to the contraindications to Sarclav (cefpodoxime) given in the summary of the product characteristics, i.e. patients with known hypersensitivity to cephalosporin antibiotics.
Method
Study procedure
The study was conducted in 2 visits, baseline visit at clinical evaluation and treatment initiation, and follow-up visit (day 7–14) following the routine practice of the trained physician.
Baseline visit
All candidates were subjected to comprehensive history-taking and clinical evaluation. The diagnosis of purulent AOM was based on a triad of recent clinical symptoms including otalgia, fever and irritability; tympanic membrane (TM) signs of AOM such as middle ear effusion characterized by bulging, limited or absent mobility of the TM or air-fluid level behind membrane; and otoscopic evidence of TM inflammation indicated by erythema, perforation or otorrhea in at least one ear were eligible for the study.13 Patients fulfilling the eligibility criteria were prescribed Sarclav (cefpodoxime proxetil) 8 mg/kg/day in two divided doses for 5–10 days. Additional medications for symptom relief were prescribed and documented.
Evaluation visit
The physician examined the patient and recorded their adherence to therapy, any drug adverse events and the clinical response to treatment. Symptoms of otalgia, fever and irritability were assessed and recorded. Otoscopy was performed to assess the tympanic membrane for severity of erythema, opacification, loss of light reflex, fullness or bulging, drainage, perforation, mobility and middle ear effusion. Patients were also monitored for any complications. Patients were considered to be compliant with the study medication if at least 80% of the antimicrobial course were taken according to the prescribed regimen; otherwise the

patient was considered to be non-compliant.
Study endpoints
Primary and secondary endpoints were the efficacy and safety assessment of Sarclav (cefpodoxime), respectively.
Efficacy assessment
According to the physicians’ assessment, efficacy was defined by the percentage of patients with either clinical cure: absence of fever, otalgia, irritability, and otoscopic signs of AOM; clinical improvement: clinical signs and symptoms including otoscopic findings diminished but did not completely resolve; or failure: unsatisfactory resolution of tympanic membrane signs or symptoms of AOM, or worsening of the patients’ condition.
Safety assessment
Safety was monitored by recording the Sarclav (cefpodoxime) related-adverse events (AEs) during the observational period and by the physicians’ and patients’ assessment of overall tolerability at the end of the study. The recorded clinical AEs likely to be related to the use of antibiotics are vomiting, diarrhea or rash.4, 14 The severity was assessed by the physicians as mild, moderate or severe. Necessary treatment, outcome at time of report and serious criteria of AEs were recorded. The assessment of the overall tolerability was rated either: excellent, fair or poor.
Statistical analysis
Data were analyzed using Statistical Package for Social Sciences software version 17.0 (SPSS, Inc., Chicago, IL, USA). Numerical data were expressed as mean and standard deviation. Qualitative data were expressed as frequency and percentage. Chi-square test was used to examine the relation between the qualitative variables. p-value <0.05 was considered statistically significant.
Results
Two patients out of the enrolled 1380 patients did not show up at the follow-up visit and were excluded. Of the 1378 patients who completed the study, 788 (57.2%) were males and 590 (42.8%) were females, with a mean age of 3.8 ± 2.5 years. Their mean weight and length/height measured at the initial visit were 17.1 ± 7.1 kg
and 94.4 ± 19.0 cm respectively.
At baseline visit
The mean temperature was 38.3 ± 0.7 °C. All children had one or more pre-treatment AOM related signs and symptoms; the most frequent were otalgia (93.6%), spontaneous otorrhea (51%), purulent discharge (49.7%), fever (21.6%) and erythematous tympanic membrane (1.7%). In addition, nasal discharge was found in 3.3% of patients, sore throat in 2.4%, cough in 2.2%, and pharyngitis in 1.4% (Fig. 1). The onset of the first symptom occurred at less than 4 days prior to the baseline visit in 87.9% of the patients.
Figure 1. Signs and symptoms of acute otitis media at baseline visit (n = 1378).
The most frequently reported prescription durations were five days in 783 (56.8%), seven days in 326 (23.7%) and ten days in 269 (19.5%) of the patients, with a mean duration of 6.5 ± 2.0 days. Other symptomatic medications were prescribed in 66.4% of the patients, ncluding: antipyretics (24.7%), analgesics (22.1%), decongestants (14.6%), cough preparations (2.2%) and anti-inflammatory agents(8.3%).
At the follow-up visit
There was marked improvement of all AOM-related signs and symptoms. Seven patients (0.5%) were non-compliant. Among the remaining 1371 patients – according to physicians’ assessment – 1131 patients (82.5%) were cured, 225 (16.4%) improved, and 15 (1.1%) failed to respond to therapy; with one reported worsening of patient’s condition. Cure or improvement rate was 100% in all symptoms and signs except spontaneous otorrhea (98.0%), purulent discharge (98.5%) and nasal discharge (93.5%).
Patients that received a 5-day course of Sarclav (cefpodoxime) had a significantly higher cure rate of 84.6% (659/779) compared to those taking Sarclav
International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 10

11 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
(cefpodoxime) for a duration of more than 5 days (472/592, 79.7%) (χ2 = 5.515, p = 0.019).
Adverse events of Sarclav (cefpodoxime) were reported by only 16 patients (1.2%), which included diarrhea (n = 9) and skin rash (n = 7). The nature of AEs were mild to moderate and did not require any dose reduction or discontinuation of the prescribed course; while none of the AEs reported were serious and all resolved without sequelae (Table 1).
Table 1. Sarclav (cefpodoxime) related-adverse events (n = 1371).
Number Percentage
Adverse event
Diarrhea 9 0.7
Skin rash 7 0.5
Severity
Mild 8 0.6
Moderate 8 0.6
Treatment
No 8 0.6
Yes 8 0.6
Outcome at time of report
Resolved 16 1.2
Serious criteria of adverse events
No 16 1.2
Yes 0 0.0
The overall tolerability of Sarclav (cefpodoxime) according to the physicians’ assessment was excellent in 1287 (93.9%) of patients, fair in 73 (5.3%) and poor in 11 (0.8%); while according to the patients’ assessment, it was excellent in 1219 (88.9%), fair in 142 (10.4%) and poor in 10 (0.7%) (Fig. 2).
Figure 2. Tolerability assessment from the physicians’ and patients’ perspectives (n = 1371).
Discussion
Acute otitis media is a community-acquired respiratory tract infection, frequently encountered by primary-care physicians. The selection of the most effective antimicrobial to treat AOM has become more difficult in recent years because of increasing antibiotic resistance among all AOM pathogens to the standard first-line recommended antibiotics.15,16 . Empirical treatment by cephalosporin with beta lactamase stability should be preferred especially in cases with penicillin allergy. Sarclav (cefpodoxime) is one of three oral third generation cephalosporins recommended for empiric antibiotic treatment of AOM as designated by the AAP guidelines.1
Findings of this study indicate that Sarclav (cefpodoxime) is an effective antimicrobial agent for AOM. The 5–10 day treatment course resulted in an excellent response in signs and symptoms. Clinical cure was achieved in 82.5% of patients; and improvement in 16.4%, with an overall combined cure and improvement rate of 98.9%. The clinical efficacy of Sarclav (cefpodoxime) in this study was found to be in line with earlier clinical studies for Sarclav (cefpodoxime) who found that the overall combined cure and improvement rate ranged from 86% to 95%.19
The optimal duration of antibiotic therapy for patients with AOM is uncertain.1 In the present study it was found that Sarclav (cefpodoxime) , in the 5-day treatment regimen, seems to be a suitable drug for AOM in children, with a significantly higher cure rate (84.6%) than an extended treatment course (79.7%) (p = 0.019).
Regarding safety, Sarclav (cefpodoxime) was well tolerated by most patients. It has a tolerability profile similar to that of other oral cephalosporins, with

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 12
gastrointestinal related symptoms and skin rash being the most frequently reported AEs.21 The twice daily regimen was acceptable to the majority of patients and accordingly compliance to treatment regimen was excellent (99.5%). It has been noted that patient compliance is inversely related to the frequency of drug administration and is directly related to the efficacy of the drug.22 Moreover, the less frequent dosing schedule of Sarclav (cefpodoxime) (BD) compared with either amoxicillin–clavulanate or cefaclor (TDS), would be an added advantage for treatment with Sarclav (cefpodoxime).21
As a consequence, the efficacy and safety of Sarclav (cefpodoxime) reported in this multicenter study is likely to be a true reflection of the effectiveness in actual clinical paediatric practice.
Conclusion
Sarclav (Cefpodoxime proxetil) is an effective, safe, well-tolerated antimicrobial agent for treatment of acute otitis media in children. It is an excellent choice for the empirical treatment of bacterial AOM, with a recommended twice-daily regimen for an optimum duration of 5 days.
Acknowledgment- The authors are thankful to chairman and managing member of Saraswathi institute of medical sciences, Hapur, U.P for their encouragement.
Ethical Clearance- Taken from ethical committee of institute
Source of Funding- Self
Conflict of Interest – Nil
References
1. Lieberthal, A.E. Carroll, T. Chonmaitree, T.G. Ganiats, A. Hoberman, M.A. Jackson,et al.The diagnosis and management of acute otitis media Paediatrics, 131 (3) (2013), pp. e964-e999 CrossRefView Record in ScopusGoogle Scholar
2. Rovers, A.G. Schilder, G.A. Zielhuis, R.M. Rosenfeld Otitis media Lancet, 363 (9407) (2004), pp. 465-473 ArticleDownload PDFView Record in ScopusGoogle Scholar
3. Taylor, P. Marchisio, A. Vergison, W.P. Hausdorrf, M. HaggardImpact of pneumococcal conjugate vaccination on otitis media: a systematic review
Clin Infect Dis, 54 (12) (2012), pp. 1765-1773 CrossRefView Record in ScopusGoogle Scholar
4. Venekamp, S.L. Sanders, P.P. Glasziou, C.B. Del Mar, M.M. RoversAntibiotics for acute otitis media in children Cochrane Database Syst Rev (6) (2015), Article CD000219,10.1002/14651858.CD000219.pub4 [P. 2, 6, 19] Google Scholar
5. CherpillodAcute otitis media in children Int J Gen Med, 4 (2011), pp. 421-423 CrossRefView Record in ScopusGoogle Scholar
6. Hoberman, J.L. Paradise, H.E. Rockette, N. Shaikh, E.R. Wald, D.H. Keamey, et al.Treatment of acute otitis media in children under 2 years of age N Engl J Med, 364 (2) (2011), pp. 105-115 CrossRefView Record in ScopusGoogle Scholar
7. Casey, R. Kaur, V.C. Friedel, M.E. PichicheroAcute otitis media otopathogens during 2008 to 2010 in Rochester, New York Pediatr Infect Dis J, 32 (8) (2013), pp. 805-809 View Record in ScopusGoogle Scholar
8. Coker, L.S. Chan, S.J. Newberry, M.A. Limbos, M.J. Suttorp, P.G. Shekelle, et al.Diagnosis, microbial epidemiology, and antibiotic treatment of acute otitis media in children: a systematic review JAMA, 304 (19) (2010), pp. 2161-2169 CrossRefView Record in ScopusGoogle Scholar
9. Pichichero, M.D. ReedVariations of pharmacokinetic/pharmacodynamic (PK/PD) parameters of amoxicillin may explain treatment failure in acute otitis media Pediatr Drugs, 11 (4) (2009), pp. 243-249 CrossRefView Record in ScopusGoogle Scholar
10. Sader, M.R. Jacobs, T.R. FritscheReview of the spectrum and potency of orally administered cephalosporins and amoxicillin/clavulanate Diagn Microbiol Infect Dis, 57 (Suppl. 3) (2007 Mar), pp. S5-S12 ArticleDownload PDFView Record in ScopusGoogle Scholar
11. Fulton, C.M. PerryCefpodoxime proxetil: a review of its use in the management of bacterialinfections in paediatric patients Paediatr Drug, 3 (2) (2001), pp. 137-158 CrossRefView Record in ScopusGoogle Scholar
12. AronovitzAntimicrobial therapy of acute otitis media: review of treatment recommendations Clin Ther, 22 (2000), pp. 29-39 ArticleDownload

13 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
PDFView Record in ScopusGoogle Scholar
13. Casselbrant, E.M. MandelAcute otitis media and otitis media with effusion P.W. Flint, B.H. Haughey, V.J. Lund, J.K. Niparko, M.A. Richardson, K.T. Robbins, et al.(Eds.), Cummings otolaryngology: head and neck surgery (5th ed.), Mosby Elsevier,Philadelphia PA (2010), pp. 2761-2777 View Record in Scopus Google Scholar
14. Tapiainen, T. Kujala, M. Renko, P. Koivunen, T. Kontiokari, A. Kristo, et al.Effect of antimicrobial treatment of acute otitis media on the daily disappearance of middle ear effusion: a placebo-controlled trial JAMA Pediatr, 168 (7) (2014), pp. 635-641 CrossRefView Record in ScopusGoogle Scholar
15. PichicheroOtitis media Pediatr Clin North Am, 60 (2) (2013), pp. 391-407 ArticleDownload PDFView Record in ScopusGoogle Scholar
I6. BrookUse of oral cephalosporins in the treatment of acute otitis media in children Int J Antimicrob Agents, 24 (1) (2004 Jul), pp. 18-23 ArticleDownload PDFView Record in ScopusGoogle Scholar
17. Cohen, F. de LRocque, M. Boucherat, C. Levy, J. Langue, A. BourrillonRandomized trial comparing 5-day cefpodoxime proxetil and 8-day amoxicillin–clavulanate treatment of acute otitis media in children Med Mal Infect, 27 (1997), pp.
596-602 ArticleDownload PDFView Record in ScopusGoogle Scholar
18. Gehanno, B. Barry, S. Bobin, C. SafranTwice daily cefpodoxime proxetil compared with thrice daily amoxicillin/clavulanic acid for treatment of acute otitis media in children Scand J Infect Dis, 26 (5) (1994), pp. 577-584 CrossRefView Record in ScopusGoogle Scholar
19. Mendelman, M.A. Del Beccaro, S.E. McLinn, W.M. ToddCefpodoxime proxetil compared with amoxicillin–clavulanate for the treatment of otitis media J Pediatr, 121 (3) (1992 Sep), pp. 459-465 ArticleDownload PDFView Record in ScopusGoogle Scholar
20. Cohen, F. de Rocque, M. Boucherat, Ph. Grandsenne, F. Corrard, Ch.A. Bouhanna,et al.Cefpodoxime proxetil vs cefixime for painful febrile acute otitis media in children Med Mal Infect, 24 (1994), pp. 844-851 ArticleDownload PDFView Record in ScopusGoogle Scholar
21. Cohen Clinical efficacy of cefpodoxime in respiratory tract infection J Antimicrob Chemother, 50 (Suppl. 1) (2002), pp. 23-27 CrossRefView Record in ScopusGoogle Scholar
22. Sackett, R.B. HaynesCompliance with therapeutic regimens Johns Hopkins University Press, Baltimore, MD (1976), p. 293 Google Scholar

Original Research Article
Clinical Profile and Outcome of Diabetic Foot in a Tertiary Care Centre
Abhishek Gupta1, Subash Chandra Sharma2, Janmejai Prasad Sharma3
1 Post Graduate Resident, 2Associate Professor, 3Professor, Department of Surgery, Shri Guru Ram Rai Institute of Medical & Health Sciences, Dehradun, UK, India
Abstract
Background: This study attempted to determine the disease burden in terms of clinical profile and outcome of diabetic foot admissions at a tertiary care hospital in a developing country.
Method: This study was done in Department of Surgery at Shri Guru Ram Rai Institute of Medical and Health Sciences and Shri Mahant Indiresh Hospital, Dehradun. Duration of the study was 1 year. The demographic characteristic, type of foot lesion, etiology, isolated micro-organism, treatment, and outcome were reviewed.
Results: A total of 49 patient were diagnosed with Diabetic Foot. All patients had type 2 diabetes with no gender predominance. Majority of the patient were above age of 40 years and diabetes control was very poor. Before admission, the ulcers had already developed for 4.7 ± 2.9 weeks; however, the majority of patients were unaware of the preceding causes. More than 70% of ulcers were in Wagner grade≥3 with infection event in nearly all patients. The most common isolates from culture were Gram-negative bacteria. A total of 8 patient required lower extremity amputations (LEAs) at various level of the foot were carried out, including major LEA.
Conclusions: Diabetic foot problems constitute a source of morbidity, a reason for LEA surgery as well as being a cause of death among patients with diabetes mellitus
Keywords – Diabetic Foot, Clinical Profile, Amputation
Introduction
Patients with lower limb diseases are commonly seen in surgical wards 7% to 10% of hospitalized patients are affected by soft tissue infections in the United States. The most common cause of soft tissue infections is Staphylococcus aureus.1 Frequently these patients are diabetic, immune compromised, etc. Establishing the diagnosis of Necrotizing Soft Tissue Infection (NSTI) can be the main challenge in treating patients with NSTI, and knowledge of all available tools is the key for early and accurate diagnosis.2
The skin is the largest organ of the body and, with the underlying soft tissue, which includes the fat layers, fascia and muscle, represents the majority of the tissue in the body. It acts as a tough, flexible, structural barrier
to invasion.3 Failure to do so result in an extremely high mortality rate (80 to 100%), and even with rapid recognition and intervention, current mortality rates remain approximately 30 to 50%.4
In the USA, diabetes mellitus (DM) affects 9.9 % of the population over 40 years of age, of which 30 % suffer from lower extremity diseases.5 It is estimated that the annual population-based incidence of a diabetic foot ulcer (DFU) ranges from 1.0% to 4.1%. The lifetime incidence may be as high as 25%.6
Foot problems in diabetics can frequently be life or limb threatening, yet have not received the same level of attention as other diabetes complications.7
DOI Number: 10.5958/2321-1024.2019.00016.3

15 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
Our hospital is tertiary care centre in the capital of Uttarakhand state. So this study is undertaken with an aim to evaluate clinical profile and outcome of patients suffering from Diabetic foot.
Aim was to evaluate clinical profile and outcome of patients suffering from lower limb diseases in Department of Surgery at Shri Guru Ram Rai Institute of Medical and Health Sciences and Shri Mahant Indiresh Hospital, Dehradun. Duration of study was 1 year.
Materials and Method
The present study was conducted in the Department of Surgery at Shri Guru Ram Rai Institute of Health and Medical Sciences, Dehradun. The duration of the study was 1 year with follow-up of up to 6 months.
Inclusion Criteria
All patient admitted in Department of Surgery with Diabetes Mellitus having foot problem.
Exclusion Criteria
Patients with traumatic pathology to bone and soft tissue have been excluded
Patients suffering from central nervous system diseases as paraplegia, hemiplegia have been soft tissue infection (non-diabetic) and peripheral vascular disease were excluded.
A written informed consent from the patient was obtained. The study was conducted after approval from the Institutional Ethics Committee.
Patients were evaluated by proper history, examination and necessary investigations as per proforma enclosed. Treatment was given as per standard treatment guidelines and the result of treatment has been noted. The data collected has been evaluated to see the outcome of treatment.
Result
49 patients were diagnosed as diabetic foot. I n diabetic foot, the age of patients ranged from 22 to 86 years. No patient was less than 20 years. 10 (20.4%) patients were between 21 to 40 years; 20 (40.8%) patients were between 41 to 60 years and 19 (38.7%) patients were above 60 years.
Majority of the patients with diabetic foot were above 40 years of age.
Table 1 - Age distribution of patients with diabetic foot
Age(in years) Diabetic foot (n=49) Percentage
<20 0 0%
21-40 10 20.4%
41-60 20 40.8%
>60 19 38.7%
Out of 49 patients with diabetic foot, 41 patients were treated by debridement, in which 16 patients had deranged lipid profile and 25 had normal lipid profile.
Out of 49 patients with diabetic foot, 8 patients were treated by amputation, out of which 7 patients had deranged lipid profile and 1 had normal lipid profile. It’s significant p value is 0.03 (fisher exact test = 4.519).
Patients with deranged lipid profile had increased chances of amputation.
Table 2: Distribution of patients according to the treatment and lipid profile
Treatment ( n=49) Deranged lipid profile
Normal lipid profile
Amputation (n=8) 7 1
Debridement (n=41) 16 25
Out of 49 patients with diabetic foot, 33 patients had HbA1c more than 8.5 and 16 patients had HbA1c <8.5.
Mean hospital stay of patients with HbA1c> 8.5 was 10.24 days. Mean hospital stay with HbA1c<8.5 was 6days.
Mean serum creatinine of patients with HbA1c >8.5 was 1.86 mg/dl. Mean serum creatinine of patients with HbA1c< 8.5 was 1.19 mg/dl.
The hospital stay and serum creatinine values were significantly higher in patients with HbA1c>8.5 (p valve >0.05).

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 16
Table 3: Mean parameters of patient according to HbA1c
Mean Parameters HbA1c> 8.5 (n= 33)
HbA1c <8.5 (n= 16)
Mean hospital stay 10.24 6
Mean creatinine 1.86 1.19
Out of 49 patients with diabetic foot; 14 (29%) patients had pseudomonas; 12 (25%) patients had E. Coli; 11 (22%) patients had Klebsiella; 10 (20%) patients had staphylococci and 2 (4%) patients had no growth on aerobic culture media
Table 4 : Organism in Diabetic Foot
Organism Diabetic foot (n= 49) Percentage
Pseudomonas 14 29%
E. coli 12 25%
Klebsiella 11 22%
Staphylococci 10 20%
No growth 2 4%
Fig 1:- Image showing WAGNER grade 4 Diabetic Foot Ulcer
Discussion
Abbott et al. reported that more than 2% of diabetic patients will develop new foot ulcers annually.8 The prevalence of DFU varied between 4% and 20.4% among hospital-based studies in individuals with
diabetes.9,10 According to some authorities, diabetic foot problems are responsible for 23–50% of the hospital bed occupancies by diabetic patients.11,12
Diabetic foot usually presents as infections, ulcers and charcot foot along with peripheral neuropathy and peripheral arterial disease in diabetic patients. According to a study by Schaper et al and another similar study conducted by Mendes et al diabetic foot remains the single most important precursor for lower limb amputations.13,14
In our study, majority of patient were of middle-age group. Due to lack of education on nature of illness, they presented to the hospital after 4 weeks after the ulcers had developed. In a study by Lavery et al. duration of ulcers > 30 days was a factor related to development of a wound infection.15 In our report, infection was present invariably in nearly all patients and Gram-negative bacteria were the most commonly isolated.
With regards to diabetes control, 67.3% of patients had poor glycemic control, i.e. HbA1c > 8.5. For a variety of reasons, good glucose control is not easily obtained in many Indian patients; poor drug compliance, lack of financial resources, and poor access to medical facilities may all compound this problem.16 Overall mean HbA1c in this study was 11.2%, higher than what Hartemann-Heutier et al. and Ozkara et al. have shown (mean HbA1c 8.7% and 10.3%, respectively).17,18 The patients with diabetic foot having HbA1c levels> 8.5 showed increased serum creatinine levels and increased duration of hospital stay. Christman et al demonstrated that patients with HbA1c >7 have poor wound healing as compared to patient with HbA1c < 7.19
It was observed that the mean duration of hospital stay for diabetic foot problem was 10.24 days in poor glycemic control patient and 6 days in patient whose HbA1c was less than 8.5%, comparable with Ozkara et al.’s report of an average of 17.2 days. In studies from England, Tanzania, and Nigeria, the mean duration of hospital stay was 22.2, 36.2 days, and 60.3 days, respectively.20-22 The variation from study to study might be related to differences in clinical practice, severity of illness, and availability of supportive care in their hospital. However, the relatively lower duration of hospitalization in the present study may be a result of death at early date or discharge from the hospital. Meanwhile, our rate is longer than the reported rate for

17 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
patients who routinely examined and attend outpatient diabetic foot service (mean length of stay of only 7.1 days) when hospitalization is required.23 This is a persuasive argument for the provision of diabetic foot care at a very early stage to reduce both the necessity and length of hospital admission and also improve patient’s outcome.
Conclusion
Diabetic foot pathologies are common in diabetics and pose serious health problems for developing countries. They seem to affect both sexes equally. The present study highlights the significance of patients with DFU in tertiary care hospital in India context where diabetes is poorly controlled, there was also little awareness for foot care and delay in seeking treatment, as this will worsens the extent of tissue destruction. Our center is a tertiary referral center in which patients referred have- rather advanced diseases. Many patients fail to receive timely and optimal care once present in the hospital. In the end, Lower Extremity Amputation is a common outcome of Diabetic Foot who are admitted to our hospital, as well as being a notable cause of morbidity and mortality.
Funding: Self
Conflict of Interest: None
Ethical approval: Approved from Institutional Ethical Commitee.
References
1. Vinh DC, Embil JM. Rapidly progressive soft tissue infections. Lancet Infectious Disease. 2005; 5:501-13.
2. Mishra SP, Singh S, Gupta SK. Necrotizing Soft Tissue Infections: Surgeon’s Prospective. Int J Inflam. 2013;2013:609-28.
3. Mims C, Playfair J, RoittI, et al. Medical Microbiology London Mosby Int Ltd, ISBN 0 7234 2781 X
4. Charles Brunicardi F. Surgical Infections. In: Schwartz Principles of Surgery. Chapter 5. 8th edition. USA: Mc Graw Hill; 2006:93.
5. Gregg EW, Gu Q, Williams D, de Rekeneire N, Cheng YJ, GeissL, et al. Prevalence of lower extremity diseases associated with normal glucose.
6. Reiber GE. Epidemiology of foot ulcers and amputation in the diabetic foot. In: Bowker J, Pfeifer M, editors. The diabetic foot. St. Louis: Mosby; 2001. p. 12–32.
7. Waspadji S. Kaki diabetik: kaitannya dengan neuropati diabetik. In: Djokomoeljanto R, Darmono Suhartono T, editors. Kaki diabetik: patogenesis dan penatalaksanaan. Semarang: Diponegoro University Press; 1996. p. E1 –E23.
8. Abbott CA, Carrington AL, Ashe H, et al. The north-west diabetes foot care study: incidence of, and risk factors for, new diabetic foot ulceration in a community-based patient cohort. Diabet Med.2002;19:377–384. DOI:10.1046/j.1464-5491.2002.00698.x
9. Bouter KP, Storm AJ, de Groot AJ, et al. The diabeticfoot in Dutch hospital: epidemiological features andclinical outcome. Eur J Med.1993;2:215–218.
10. Benotmane A, Mohammedi F, Ayad F, et al. Diabetic foot lesions: etiologic and prognostic factors. Diabetes Metab (Paris).2000;26:113–117.
11. Smith DM, Weinberger M, Katz BP. Predicting non elective hospitalization: a model based on risk factors associated with diabetes mellitus. J Gen Intern Med.1987;2:168–173. DOI:10.1007/BF02596146
12. Waugh NR. 1988. Amputations in diabetic patients – a review of rates, relative risks and resource use. Comm Med.;10:279–288. DOI:10.1093/ oxfordjournals. pubmed.a042420
13. Schaper NC, Van Netten JJ, Apelqvist J, Lipsky BA, Bakker K, International Working Group on the Diabetic Foot Prevention and management of foot problems in diabetes: a Summary Guidance for Daily Practice 2015, based on the IWGDF Guidance Documents. Diabetes Metab Res Rev. 2016;32(Suppl 1):7–15.
14. Martins-Mendes D, Monteiro-Soares M, Boyko EJ, Ribeiro M, Barata P, Lima J, et al. The independent contribution of diabetic foot ulcer on lower extremity amputation and mortality risk. J Diabetes Complications. 2014;28(5):632–638.
15. Lavery LA, Armstrong DG, Wunderlich RP, et al. Risk factors for foot infections in individuals with diabetes. Diabetes Care.2006;29:1288–1293. DOI:10.2337/dc05-2425

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 18
16. Sutanegara D. Darmono, Budhiarta AAG. The epidemiology and management of diabetes mellitus in Indonesia. Diabetes Res Clin Pract.2000;50(Suppl.2):S9–S16. DOI:10.1016/S0168-8227(00)00173-X
17. Hartemann-Heutier A, Ha Van G, Danan JP, et al. Outcome of severe diabetic foot ulcers after standardized management in a specialized unit. Diabetes Metab (Paris).2002;28:477–484.
18. Ozkara A, Delibasi T, Selcoki Y, et al. The major clinical outcomes of diabetic foot infections: one center experience. Cent Eur J Med.2008;3:464–469.DOI:10.2478/s11536-008-0018-x
19. Christman A, Selvin E, Margolis D, Lazarus G, Garza L. Hemoglobin A1c Predicts Healing Rate in Diabetic Wounds. Journal of Investigate Dermatology. 2011;131(10):2121-2127.
20. Coles DR, Coppini DV. Survey of hospital admissions related to diabetic foot disease. J Diabetes Nurs.2005;9:33–35.
21. Chalya PL, Mabula JS, Dass RM, et al. Surgical management of diabetic foot ulcers: a Tanzanian university teaching hospital experience. BMC Res Notes.2011;4:365. DOI:10.1186/1756-0500-4-365
22. Ogbera OA, Osa E, Edo A, et al. Common clinical features of diabetic foot ulcers: perspectives from a developing nation. Int J Low Extrem Wounds.2008;7:93–98. DOI:10.1177/1534734608318236
23. Jessup RL, Spring AA, Grollo A. Current practice in the assessment and management of acute diabetes-related foot complications. Aust Health Rev.2007;31:217–222. DOI:10.1071/AH070217.

Locking Versus Non-Locking Plate Fixation in the Management of Maxillofacial Fractures : A Prospective
Comparative Study
Nitin Verma1, Neha Mann2, Jaspreet Kaur2, Supreet Gill3
1Associate Professor, 2Junior Resident, Punjab Government Dental College and Hospital, Amritsar, 3Shri Guru Ramdas Institute of Dental Sciences and Research, Amritsar
Abstract
Introduction: Various methods of fixation have been advocated for the treatment of maxillofacial fractures. A new type of plating system, initially developed by Raveh et al. is locking plate/screw system. This system has various advantages over conventional non locking plating system like better stability, ease of plate adaptation, early restoration of function, internal locking system which decreases the chance of screw loosening and infection.
Objectives: A comparative evaluation of locking plates system versus conventional miniplates in maxillofacial fractures.
Method: Twenty patients presenting with maxillofacial fractures were treated with locking plates and conventional non locking plates in two years from 2014 to 2016. Ten patients were treated with locking plate system in group A and 10 patients with conventional non locking plates in group B. Patients were evaluated on clinical and radiographic parameters during three months follow up.
Results: Postoperative outcomes for both groups were extremely favorable with a relatively small number of complications. There was no case of postoperative wound dehiscence, infection, damage to tooth roots, plate exposure and plate removal, malunion and any other complication in both the groups. Postoperative occlusion disturbance was seen in 20% cases in both group A as well as group B in mandible fractures. In maxillary fractures postoperative occlusion disturbance was seen in one case (20%) in group B.
Conclusion: This study concluded that despite the significant theoretical advantages of locking system seen in biomechanical studies, no statistical significant results were found between these two systems. The postoperative outcomes for both groups were almost similar with a relatively small number of complications.
Keywords: Locking Plate System, Mandibular Fractures, Maxillary Fractures, Locking Versus Non Locking System
Corresponding Author:Jaspreet Kaur, Junior Resident, Punjab Government Dental College and Hospital, Amritsar.
Introduction
The treatment of facial fractures has evolved greatly over the years, from supportive bandages, splints, circum-mandibular wiring and extraoral pins. Then eventually, the treatment modality changed from closed reduction
to open reduction and direct fixation using trans-osseous wiring, bone plates and screws. Traditionally, stainless steel wire was used for osteosynthesis in maxillofacial surgery until the seminal work of Michelet (1970) and the modifications given by Champy (1978), which led to wide acceptance of monocortical miniplates, thus improving the standards of patient safety, rehabilitation and recovery. Mini plate osteosynthesis, developed by Champy in 19751 is today’s standard for the treatment of facial fractures. More recently, resorbable plates screws and three dimensional miniplating systems have been widely used for the fixation of facial fractures.
DOI Number: 10.5958/2321-1024.2019.00017.5

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 20
A major disadvantage of the conventional bone plate is that it must be perfectly adapted to the underlying bone to prevent alterations in the alignment of the segments and changes in the occlusal relationship. The loosening of one or more screws in miniplate ostesynthesis is a problem especially during convalescent period where loosening of screws may require removal of the fixation appliance. Currently, modifications in miniplates, like the locking plate/screw system have been developed to overcome these problems.2-4
Locking miniplates utilize double threaded screws, which lock to the bone and the plate, creating a mini-internal fixator. This results in a more rigid construction with less distortion of the fracture or osteotomy, less screw loosening and less interference with bone circulation since the plate is not too tightly pressed against the bone5. It also reduces compressive forces between the undersurface of the plate and lateral bony cortex compared with a conventional plate. This limits stress shielding and creates a more stable fixation over time6. The purpose of this study is to evaluate the efficacy of locking miniplate/screw system compared with conventional non locking miniplate/screw system in the management of maxillofacial fractures.
Materials and Method
This prospective study was undertaken in twenty randomly selected patients reporting to the department of oral and maxillofacial surgery of Punjab government dental college and hospital, Amritsar. The patients presenting with maxillofacial fractures were treated with locking plates and conventional non locking plates in two years from 2014 to 2016. In group A ten patients were treated with locking plate system (figure 1) in which 5 patients treated with 1.8 mm titanium locking plate for mid facial fractures and 5 patients with 2.0 mm locking plate for mandibular fractures. In group B ten patients were treated with conventional non locking plates, in which 5 patients were treated with 1.5 mm non locking conventional plates for mid facial fractures and 5 patients with 2.0 mm non locking conventional plates for mandibular fractures. The patients meeting the following criteria were included 1) Patients above 14 years of age 2) Patients with associated fractures of other regions of mandible like ramus, condyle 3) Patients who agreed to give consent for this study. Approval from institutional ethical committee and consent from the patient was obtained. Clinical follow up of treated
cases was done first after a period of 1 week, then 15 days, 6 weeks and thereafter done for a minimum period of 3 months and maximum period of 6 months postoperatively. Radiographic examination was done six weeks postoperatively (figure 2). During the follow-up, evaluation was done regarding the restoration of function, postoperative occlusion discrepancy, postoperative infection, wound dehiscence, exposure of plate and need for plate removal, malunion, postoperative paraesthesia, other complications, etc.
Observations and Results
The present study was carried out on patients between the age group of 15-64 years. In mandibular fractures maximum number of patients were in the age group of 15-24 years. In maxillary fractures, age predilection was bimodal i.e., 15-24 years and 45-54 years. Road side accident was the main cause of maxillofacial fractures (60%) in our study followed by physical assault (35%) and fall (5%). Most common site of mandibular fractures was found to be parasymphysis followed by symphysis and in maxillary fractures le-fort 1 fracture was seen as most common type of fracture. Variables like sex, age, etiology, time interval, post-traumatic occlusion status, status of overlying soft tissue, infection, site of fracture, pattern of tooth injuries and postoperative complications like wound dehiscensce, infection, paraesthesia, disturbance in occlusion, malunion, plate exposure and need for plate removal and others were analysed statistically using chi square test. P-value < 0.05 was taken as statistically significant, and a value of < 0.01 was taken as highly significant. Any value of p > 0.05 was taken as statistically insignificant.
In this present study, post-operative outcomes for both the groups were extremely favourable with a relatively small number of complications. There were no cases of post-operative wound dehiscence, infection, damage to tooth roots, plate exposure and need for plate removal or malunion in both the groups. No statistically significant difference was found between the two groups regarding loosening of plate and screw. In case of mandibular fractures, transient postoperative paraesthesia was reported in one case in each group (20%), which improved during subsequent follow up (p-value = 0.370, non significant). While in case of maxillary fractures, transient paraesthesia occurred in 2 cases (40%) in group A and 1 case (20%) in group B, which improved subsequently.

21 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
Figure 1 – Locking plate fixed
Figure 2 – Post operative OPG
Discussion
The objective of maxillofacial fracture management includes the restoration of existing anatomical form, function, occlusion, facial aesthetics and control of
Occlusion of the patient was evaluated preoperatively and postoperatively at 1 week, 6 week and 3 months. Chi square test was applied to compare the results between the two groups. Statistical analysis did not show significant difference of incidence of malocclusion between the two groups. Postoperative occlusion disturbance was seen in only one case (20%) in each of the group in mandibular fractures, with no functional disturbance. It was not found to be statistically significant (P-value = 1.00). In maxillary fractures, no case of occlusion disturbance was seen in locking group, while 20% cases of occlusion disturbance was seen in non locking group and it was found to be statistically insignificant (P-value = 0.292) [table]. Only one case in mandibular as well as in maxillary fractures needed additional maxillomandibular fixation in case of locking group, whereas, the conventional non locking system showed two cases of both mandibular as well as maxillary fractures, in which additional maxillomandibular fixation was required.
Table : Status of post-traumatic occlusion
LocationStatus of occlusion m= malocclusion n= normal
GroupsTotal P-Value
Group A Group B
Mandible
M5100%
480%
990%
0.292 NSN00%
120%
110%
Total5100%
5100%
10100%
Maxilla
M 480%
5100%
990%
0.292NSN
120%
00%
110%
Total5100%
5100%
10100%
NS: p > 0.05; Not significant

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 22
postoperartive infection. To obtain other objectives, plate osteosynthesis came as a breakthrough in maxillofacial surgery. Various methods of fixation have been advocated for the treatment of maxillofacial fractures. A new type of plating system is locking plate/screw system, which was initially developed by Raveh et al.7,8
The locking plate/screw system does not need a friction lock between plate and bone for stability.9 These plates have an advantage that they do not compress the undersurface of the bone plate to the cortical bone as in conventional plates.10-12 This result in less disturbance of perfusion of underlying bone and decreased chances of bone necrosis which further leads to increased bony healing and regeneration.
Another advantage of this system is that the screws lock to the plates and are unlikely to loosen further decreasing the incidence of inflammatory complications.13 Ellis & Graham (2002) also proposed that this locking system provides greater stability than the standard conventional miniplate.10
It is observed that as the screw locks with the plate in locking system, the degree of plate adaptation does not affects its mechanical behavior. To ensure the proper assembly of screw with plate especially perpendicular placement of screw, one should always use a drill guide to center the drill hole in the center of bone plate.5, 9
The present study was carried out on patients between the age group of 15-64 years. In mandibular fractures maximum number of patients were in the age group of 15-24 years. In maxillary fractures, age predilection was bimodal i.e 15-24 years and 45-54 years. There was predominance of male in this study.
In this present study, post-operative outcomes for both the groups were extremely favourable with a relatively small number of complications. There were no cases of post-operative wound dehiscence, infection, damage to tooth roots, plate exposure and need for plate removal or malunion in both the groups.
No statistically significant difference was found between the two groups regarding loosening of plate and screw. Haugh (1996) had similar experience with titanium conventional bone plates.15 Ellis conducted a study on locking plates and described the incidence of surgical infections were less and plate removal was minimal.10
In our study, in case of mandibular fractures, transient postoperative paraesthesia was reported in one case in each group (20%), which improved during subsequent follow up ( p-value = 0.370, non significant). Halpern, Kaban & Dodson (2004) found that inferior alveolar nerve neurosensory disturbances were unchanged or improved immediately after treatment in most patients.16
In case of maxillary fractures, transient paraesthesia occurred in 2 cases (40%) in group A and 1 case (20%) in group B, which improved subsequently.
One unique advantage of locking plate/screw system is that it is not necessary for the plate to have an intimate contact with underlying bone, making its adaptation easier than conventional plates.17 During the placement of locking plates, a drill guide is necessary to both center the drill hole and to ensure a perpendicular placement of the screw. In our study, this was found to be a cumbersome procedure in maxillary fractures, due to lack of sufficient exposure with intraoral incisions.
In mandibular fractures, postoperative occlusion disturbance was seen in only one case (20%) in each of the group, with no functional disturbance. It was not found to be statistically significant (P-value = 1.00). In maxillary fractures, no case of occlusion disturbance was seen in locking group, while 20% cases of occlusion disturbance was seen in non locking group in case of maxillary fractures. Locking plates in maxillary fractures seemed to show better stability than conventional mini plates. But this was not found to be statistically significant (P-value = 0.292).
In this study, maxillomandibular fixation was removed after 7 days. Any discrepancy was further managed with additional 1 week maxillomandibular fixation or guiding elastics. Additional need for maxillomandibular fixation was found to be less in locking screw and plate system i.e only in one case for mandibular fractures as well as in maxillary fractures. Whereas, the conventional non locking system showed two cases of both mandibular as well as maxillary fractures, in which additional maxillomandibular fixation was required. Collins et al assessed the complication rate to be approximately 5% for both locking and non locking group after keeping the intermaxillary fixation for 4 weeks.17 Our study found similar results and showed no statistically significant difference between the two groups regarding postoperative complications.

23 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
Despite the theoretical advantages of locking system over non locking system reported in various biomechanical studies, our study did not show any statistical significant result between them, in both maxilla and mandible. Also the postoperative outcomes for both groups were extremely favourable with a relatively small number of complications. These findings were in concurrence with the results of Singh, Kumar & Bhagol 2011, Chritah, Lazow & Berger 2005, Chrcanovic 2014.18,19
Limitations of this study included small sample size and limited follow up period. As this study was carried out in 20 patients only (10 patients in each group), the sample size was suggested to be small for reaching a final conclusion. Large number of patients and multicenter approach is required to prove it to be more authentic and conclusive. High cost of titanium locking plate is another deterrent for its wider use in developing countries like India with low income group.
Conclusion
Despite the theoretical advantages of locking system over non locking system reported in various biomechanical studies, our study did not show any statistical significant result between them, in both maxilla and mandible. Also the postoperative outcomes for both groups were extremely favourable with a relatively small number of complications. Hence, keeping in mind the cost factor and parameters of our study, non locking plating system are more economical with almost similar mechanical benefits as locking plating system.
Conflict of Interest: None
Source of Funding: Self
Ethical Clearance: The faculty of Dental Sciences in its meeting held at Punjab Government Dental College and Hospital, Amritsar has approved the study and ethical clearance has been given.
References
1. Champy M, Lodde JP, Schmitt R, Jaeger JH, Muster D. Mandibular osteosynthesis by miniaturescrewed plates via a buccal approach. Journ of maxfac surg. 1978;6 (1):14-21.
2. Erdmann D, Follmar KE, DeBruijn M, Bruno AD, Jung SH, Edelman D, Mukundan S, Marcus JR. A
retrospective analysis of facial fracture etiologies. Annals of plastic surg. 2008;60(4):398-403.
3. Frigg R. Development of the locking compression plate. Injury. 2003;34:6-10.
4. Alpert B, Gutwald R, Schmelzeisen R. New innovations in craniomaxillofacial fixation: the 2.0 lock system. The Keio journ of med. 2003;52(2):120-7.
5. Gutwald R, Alpert B, Schmelzeisen R. Principle and stability of locking plates. The Keio journ of med. 2003;52(1):21-4.
6. Chiodo TA, Ziccardi VB, Janal M, Sabitini C. Failure strength of 2.0 locking versus 2.0 conventional Synthes mandibular plates: a laboratory model. Journ of oral and maxfac surg. 2006;64(10):1475-9.
7. Potter J, Ellis E. Treatment of mandibular angle fractures with a malleable noncompression miniplate. Journ of oral and maxfac surgery. 1999;57(3):288-92.
8. Seward, G.R., Foreman, B.G. Quick-release locking plates. Br Dent J. 1972;132:366.
9. Haug RH, Street CC, Goltz M. Does plate adaptation affect stability? A biomechanical comparison of locking and nonlocking plates. Journ of oral and maxfac surg. 2002;60(11):1319-26.
10. Ellis E, Graham J. Use of a 2.0-mm locking plate/screw system for mandibular fracture surgery. Journ of oral and maxfac surg. 2002;60(6):642-5.
11. Sikes JW, Smith BR, Mukherjee DP, Coward KA. Comparison of fixation strengths of locking head and conventional screws, in fracture and reconstruction models. Journ of oral and maxfac surg. 1998;56(4):468-73.
12. Villarreal PM, Junquera LM, Martínez A, García-Consuegra L. Study of mandibular fracture repair using quantitative radiodensitometry: a comparison between maxillomandibular and rigid internal fixation. Journ of oral and maxfac surg. 2000;58(7):776-81.
13. Schmidt BL, Kearns G, Gordon N, Kaban LB. A financial analysis of maxillomandibular fixation versus rigid internal fixation for treatment of

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 24
mandibular fractures. Journ of oral and maxfac surg. 2000;58(11):1206-10.
14. Natu SS, Pradhan H, Gupta H, Alam S, Gupta S, Pradhan R, Mohammad S, Kohli M, Sinha VP, Shankar R, Agarwal A. An epidemiological study on pattern and incidence of mandibular fractures. Plast surg intern. 2012;2012.
15. Haug RH. Retention of asymptomatic bone plates used for orthognathic surgery and facial fractures. Journ of oral and maxfac surg. 1996;54(5):611-7.
16. Halpern LR, Kaban LB, Dodson TB. Perioperative neurosensory changes associated with treatment of mandibular fractures. Journ of oral and maxfac surg. 2004;62(5):576-81..
17. Collins CP, Pirinjian-Leonard G, Tolas A, Alcalde R. A prospective randomized clinical trial comparing 2.0-mm locking plates to 2.0-mm standard plates in treatment of mandible fractures. Journ of oral and maxfac surg 2004;62(11):1392-5.
18. Singh V, Kumar I, Bhagol A. Comparative evaluation of 2.0-mm locking plate system vs 2.0-mm nonlocking plate system for mandibular fracture: a prospective randomized study. Intern journ of oral and maxfac surg. 2011;40(4):372-7.
19. Chrcanovic BR. Locking versus non-locking plate fixation in the management of mandibular fractures: a meta-analysis. Intern journ of oral and maxfac surg. 2014;43(10):1243-50.

Treatment of Liver Abscess: A Comparison of Catheter Drainage and Needle Aspiration
Ajay Chauhan1, Yashasvi Patel2, P. P. Sharma3, F. S. Mehta3
1Associate Professor, 23rd Year PG Resident, 3Professor, Department of General Surgery, Geetanjali Medical College and Hospital, Udaipur, Rajasthan
Abstract
Background: The aim of the study was to evaluate the clinical presentation, and to investigate the effectiveness of continuous catheter drainage in comparison to needle aspiration in the treatment of liver abscesses.
Method: This is a comparative study of 50 patients, presented in outpatient and emergency department at the hospital,equally into two groups,
percutaneous needle aspiration and pigtail catheter drainage. The effectiveness of either treatment was measured in terms of duration of hospital stay, days to achieve clinical improvement, 50% reduction in abscess cavity size and total/near total resolution of abscess cavity.
Results: The success rate was significantly better in catheter drainage group. The patients in pigtail catheter drainage group showed earlier clinical improvement and decrease in abscess cavity volume as compared to those who underwent percutaneous needle aspiration.
Conclusions: Percutaneous catheter drainage is a better modality as compared to percutaneous needle aspiration especially in larger abscesses which are partially liquefied or with thick pus.
Keywords: Liver abscess, Catheter drainage, Needle aspiration
Corresponding author: Dr. Yashasvi Patel 3rd year PG resident, Department of General Surgery, Geetanjali Medical College and Hospital, Udaipur, Rajasthan. Mobile- 7230088277Email- [email protected]
Introduction
Liver abscess has been recognized since hippocrates (400 B.C.)who speculated that the prognosis of patients were related to the type of fluid within the abscess cavity(1). A liver abscess is a suppurative cavity in the liver resulting from the invasion and multiplication of microorganisms, entering through the blood vessels or by the way of the biliary ductal system. It is the commonest infection affecting liver. Liver comprises 48% of all the visceral abscesses(2). Liver abscess is
the constant source of mortality in developing country. India being a developing country, a large proportion of population living under poverty line, a good amount of people are predisposed to liver abscess. It is common in India with 2nd highest incidence due to poor sanitation, overcrowding and inadequate nutrition(3). Prevalence of infection is higher than 5%-10% in endemic areas(4).
Liver abscess is a major tropical disease of the gastrointestinal system which is mainly classified into amoebic and pyogenic. Pyogenic liver abscess which used to be mainly tropical in location. Majority of liver abscess cases from developing country are of amoebic etiology. (5)
Liver abscess is found more commonly in men between 20 and 40 years of age but can occur at any age. Approximately 60% of the abscesses are solitary and mainly located in the right lobe of the liver, as a result of the streaming of the portal blood flow secondary to
DOI Number: 10.5958/2321-1024.2019.00018.7

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 26
fact that the right lobe is predominantly supplied by the superior mesenteric vein and because most of the hepatic volume is in the right lobe. Liver abscesses continue to be an important cause of morbidity and mortality in tropical countries, especially among lower socioeconomic class living with poor hygienic sanitary conditions. Percutaneous drainage of liver abscess has been an important advancement in the treatment of liver abscesses(6,7).
In recent years, image-guided percutaneous drainage has been increasingly used to treat liver abscesses with reported success rates ranging from 70-100%(8,9). Although the primary mode of treatment of liver abscess is medical and may need needle aspiration but in abscess cavity larger then 5cms in size catheter drainage is treatment of choice. Percutaneous catheter drainage, under USG guidance, is safe and effective mode of treatment of liver abscess with low morbidity and no mortality. It results in an early relief of symptoms and faster resolution of abscess cavity(10). So Modern treatment has shifted the treatment of liver abscess toward IV broad-spectrum antibiotics and imaging-guided percutaneous needle aspiration (PNA) or percutaneous catheter drainage (PCD)(11,12).
Various studies done in the recent past have not given a concrete conclusion as to which treatment of liver abscess is better. Hence the present study was planned to compare the above mentioned treatment modalities and identify the better option for treating patients suffering from liver abscess.
Materials & Method
This was a single-center prospective comparative study conducted by the departments of Surgery at Geetanjali Medical College and Hospital Udaipur Rajasthan. A total of 50 patients were included in the study, divided into two
groups, percutaneous needle aspiration (n=25) and pigtail catheter drainage (n=25). The patients were studied from September 2016 to September
2018. The protocol was approved by institutional ethical committee. Written informed consent was obtained from all participants. All the patients who had liver abscess clinically and radio logically [USG / CT scan] were included in the study. The patients had prior intervention, ruptured liver abscess, biliary tract
malignancy, uncorrectable coagulopathy were excluded from the study. In all patients complete blood count, liver function test, PT/INR, X-ray chest, abdominal sonography and C.T. scan as & when required were performed and antibiotics were started, as soon as diagnosis was made. Abscess less than 5cm managed by needle aspiration. Abscess more than 5 cm managed by percutaneous catheter drainage.
Percutaneous Needle Aspiration: The patient was subjected to USG of the abdomen and the characteristics of the abscess cavities were recorded. Local anesthesia was infiltrated at the proposed puncture site using a 18 G needle. Under real-time USG guidance using 18/20 G spinal needle the abscess cavity was entered and pus was aspirated till no more pus could be aspirated further. A sample of pus was sent for culture and sensitivity. A dressing was applied.
Percutaneous Catheter Drainage: Seldinger technique used for catheter drainage. Abscess localised by USG, The site of drainage marked under all aseptic condition where minimum depth from skin noted. The site infiltrated with 2%
xylocaine and 4 mm skin incision made and through which 18G guide wire introducer needle passed under USG guidance till it will reach the centre of cavity. A Guide wire introduced through the needle and position inside the cavity following which the needle removed keeping the guide wire in situ. Serial dilator then passed over the wire to dilate track up to 12 to 14 F sizes. A PCN MELECOTS catheter of size equal to the size of dilator passed over the wire and positioned in the center of cavity under USG guidance. The guide wire than withdrawn and PCN melecots catheter fixed to the skin with suture and connect with drainage bag and pus sent for cytology and bacteriology. Amount of pus drainage in 24 hours monitored and catheter flushed daily to prevent blockage with 10ml normal saline. The drainage catheter removed when drainage become less than 20ml to 30ml/24 hours.
The effectiveness of treatment was measured in terms of parameters like duration of hospital stay, days to achieve clinical improvement, days to achieve 50% reduction in abscess cavity size and days to achieve total/near total resolution of abscess cavity. The data was measured in numbers (percentage) and mean±SD.

27 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
Results
In presenting study the age group of the patients ranged from the 20-72 years.
Highest incidence(66%) was found between 3rd - 4th decades. In this study
45 patients were male and 5 patients were female and ratio being, male : female was 9:1. 40 patients were from rural and 10 were from urban population and the incidence of alcohol consumption was 72%.
In present study, all patients gave history of right upper quadrant dull aching pain associated with anorexia and Fever. (Table 1)
Table 1: Symptoms & signs of liver abscesses (n=50)
Characteristic Percutaneous needle aspiration(n=25) Percutaneous catheter drainage (n=25)
Right upper quadrant pain 100% 100%
Right hypochondruim tenderness 100% 100%
Anorexia 100% 100%
Fever 96% 96%
Nausea & vomiting 60% 60%
Hepatomegaly 52% 88%
Respiratory symptoms 12% 32%
Jaundice 08% 12%
Diarrhoea 0% 0%
It was observed that 96% had leucocytosis (Table 2).
Table 2: Laboratory Data of all patients (N=50)
Investigation Percutaneous needle aspiration (n=25) Percutaneous catheter drainage (n=25)
Leucocytosis (>11000) 84% 100%
Elevated S. Bilirubin Total 12% 24%
Elevated SGOT 64% 84%
Elevated SGPT 64% 100%
Hypoalbuminemia 52% 96%
Elevated Alkaline phosphatase 64% 92%
Elevated INR 64% 88%
In the present study, 38(76%) patients had solitary abscess and 12(24%) patients showed multiple abscesses. 41(82%) had right lobe involvement, 6(12%) had left lobe involvement and 3(6%) had both lobes involved. Volume of abscess was measured, the smallest was 65 cc and the largest was 1200cc. It was observed that the volume of the abscess cavities was mostly between
150-350cc. Pus aspirated from all abscesses was sent for culture and sensitivity. Cultures were found to be positive in 16(32%) cases. The rest were sterile. Amoebic liver abscesses were encountered more frequently (68%) compared to pyogenic (30%). Only 1 ( 2% ) case was encountered with mixed of liver abscess.

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 28
A total of 50 patients underwent either of the two percutaneous procedures and their response to treatment was recorded and analyzed (Table 3). Percutaneous needle aspiration was successful in 22 of 25 patients. Out of these 22 patients, 13 patients required one aspiration, 9 required two aspirations. The 3 patients who did not show clinical improvement or decrease in cavity size despite 2 aspirations were taken as failure.
Pigtail percutaneous drainage was successful in all the 25 cases. Out of these patients, in 1(4%) patient three melecot catheters were inserted at a single time
while in remaining all 24 (96%) patients one catheter was inserted. In 9( 36% ) patients tube was removed on the 4th or less than 4th postoperative day while in 13( 52% ) patients tube was removed on the 5th day. Only in 3( 12% ) patient’s tube was removed on 6th or more than 6th postoperative day. It was also effective in those patients who fail to respond with needle aspiration twice. The patients in PCD group showed earlier clinical improvement and 50% decrease in abscess cavity volume as compared to those who underwent PNA. However, there was no significant difference between the duration of hospital stay or the time required for total or near-total resolution of cavity.
Table 3: Intervention and their Results
Parameters Percutaneous needle aspiration (n=25)
Percutaneous catheter drainage (n=25)
Mean ± SD Mean ± SD P value
Mean volume cavity (cc) 177.32 ± 46.93 363 ±216.4 <0.005
Clinical improvement (Days) 5.5 ±1.9 4.5± 1.55 <0.005
Time taken to reduce cavity up to 50% (Days) 7.1 ±2.3 4.9 ±1.6 <0.005
Time taken to total or near totoal resolution of abscess cavity (week) 10.1 ±4.2 10.9± 4.1 >0.005
Average hospital stays (Days) 5.96±1.17 6.96±1.37 >0.005
Discussion
Amoebiasis affects approximately 10% of the population all over world. Amoebic liver abscess is the most common(3-9%) extra intestinal manifestation of Amoebiasis, with the pathognomonic anchovy sauce color of abscess(13). Amoebic abscesses are commonly confused with pyogenic abscesses. The clinical distinction between the two is difficult since both can have similar clinical features and investigations. If amoebic abscess is suspected clinically, needle aspiration may be necessary for confirmation. The fluid will often have an “anchovy sauce” and color and amoebae can be found in at least 30% of aspirates(14).
In our study we found the male to female ratio to be 9 : 1. The most frequently affected age group was in the 30 to 40 year and compared with the study of Singh et al(15). Liver abscess is the disease among the lower socioeconomic class living with poor hygienic sanitary conditions. In this study 80% patients were from rural
and 20%were from urban population.
The common sign and symptom in our study were right upper quadrant pain and tenderness associated with anorexia, fever, nausea & vomiting, respiratory symptoms. On examination hepatomegaly and Jaundice was seen which were similar to those described in previous studies(16).
In our study alcohol was the single most consistent etiological factor of liver abscess, compared to Choudhary et al(17).
Leucocytosis, elevated Serum alkaline phosphatase, elevated SGOT & SGPT, hypoalbiminemia were found & similar finding was reported by Ghosh et al.
Ultrasonography revealed solitary abscesses and multiple abscesses. In our study the number and location of abscesses were comparable with the studies of Christopher et al, Choudhary et al. So Solitary & right

29 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
lobe abscesses were more common.
Amoebic abscesses were more common finding than pyogenic abscesses in our study. These findings were comparable with Singh et al study.
We performed image-guided percutaneous intervention in 50 patients. Their response to treatment was recorded and analyzed. Same results of PNA and PCD were reported by Bansal et al(18).
The time required for 50% reduction in the cavity size was significantly less in the PCD compared to PNA group. However, time required for total or near-total resolution of the abscess cavity did not show any significant difference in the two group. It can be concluded that the abscess cavities showed faster collapse during the initial period in the PCD group but it did not have an advantage as far as total or near-total resolution of cavity is concerned. Similar result were recorded by other researcher as Rajak et al(19).
Needle aspiration is simple, safe & acceptable treatment of choice in liver abscess less than 5cm in diameter under US guidance. The major advantages of PNA are easy to perform as a outdoor procedure, less invasive, less expensive with medical & nursing care, avoids problems related to catheter care, multiple abscess cavities can be aspirated easier in the same setting(20). Inability to completely evacuate the Large ( >5 cm) abscesses, thick viscous pus and rapid re-accumulation of pus are the important reasons for failure of needle aspiration(21). Placement of an indwelling drainage catheter addresses all of these issues. This explains the higher success rates of PCD treatment group observed in our study and several previous studies(22).
Conclusion
Our study concludes that the percutaneous catheter drainage is a better and effective percutaneous treatment modality as compared to percutaneous needle aspiration in view of greater volume of pus drained in first sitting, in respect to clinical improvement, resolution of cavity, success rate but there was no significant morbidity - mortality occur during both the procedure.
Ethical Clearance- Taken from Human Research Ethics Committee
Source of Funding- Self
Conflict of Interest- Nil
References
1. Hippocrates. The genuine works of Hippocrates, Translation (from the Greek with a preliminary discourse and annotations). In: Hippocrates, eds. A Book. New York: William Wood & Co.; 1886: 57, 58, 266, 267.
2. Braunwald E, Fauci AS, Kasper DL, Hauser SL, Longo DL, Jameson JL. Harrison’s principles of internal medicine. McGraw Hill; 2001.
3. Channanna C, Rehman FU, Choudhuri B, Patil A. A clinical study, diagnosis and management of LiverAbscess at VIMS, Bellary. Journal of Evidence Based Medicine and Health Care. 2014;1:668-85.
4. Stanley SL., Jr. Amoebiasis. Lancet. 2003; 361:1025–34.
5. Kapoor OP. surgical amebiasis – Treatment is often conservative. Bombay Hospital J 1990; 32; 128-133.
6. Singh S, Chaudhary P, Saxena N, Khandelwal S, Poddar DD, Biswal UC. Treatment of liver abscess: prospective randomized comparison of catheter drainage and needle aspiration. Annals of Gastroenterology: Quarterly Publication of the Hellenic Society of Gastroenterology. 2013;26(4):332.
7. Saraswat VA, Agarwal DK, Baijal SS, Roy S, Choudhuri G, Dhiman RK, Bhandari L, Naik SR. Percutaneous catheter drainage of amoebic liver abscess. Clinical radiology. 1992 Mar 1;45(3):187-9.
8. Gerzot SG, Johnson WC, Robbins AH, Nabseth DC. Intrahepatic pyogenic abscesses: treatment by percutaneous drainage. The American journal of surgery. 1985 Apr 1;149(4):487-94.
9. Attar B, Levendoglu H, Cuasay NS. CT--guided Percutaneous Aspiration and Catheter Drainage of Pyogenic Liver Abscesses. American Journal of Gastroenterology. 1986 Jul 1;81(7).
10. Balogun BO, Olofinlade OO, Igetei R, Onyekwere CA. Ultrasound-guided percutaneous drainage of liver abscess: 6 years experience in Lagos State university teaching hospital, Lagos. Nigerian Journal of Surgical Research. 2013 Jan 1;15(1):13.
11. Seeto RK, Rockey DC. Pyogenic liver abscess. Changes in etiology, management, and outcome.

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 30
Medicine. 1996 Mar;75(2):99-113.
12. Bornman PC, Beckingham IJ. ABC of diseases of liver, pancreas, and biliary system: chronic pancreatitis. Bmj. 2001 Mar 17;322(7287):660-3.
13. Mueller PR, VanSonnenberg E, Ferrucci Jr JT. Percutaneous drainage of 250 abdominal abscesses and fluid collections. Part II: Current procedural concepts. Radiology. 1984 May;151(2):343-7.
14. Kumawat JL, Udawat HS, Mehta FS, Bhatnagar PK, Saxena P, Saxena R. Liver abscess in tribal population of south Rajasthan; management by sonography guided percutaneous tube drainage in 61 cases in four years. J Evid Based Med. 2015;2(20):2992-3000.
15. Christopher S, Kumar A, Achar S. Liver abscess-various modalities of treatment and its clinical outcome. International Surgery Journal. 2016 Dec 10;3(4):1868-74.
16. Ghosh S, Sharma S, Gadpayle AK, Gupta HK, Mahajan RK, Sahoo R, Kumar N. Clinical, laboratory, and management profile in patients of liver abscess from northern India. Journal of tropical medicine. 2014;2014.
17. Choudhary V, Chaudhary A. Clinico-pathological profile of liver abscess: a prospective study of 100
cases. International Surgery Journal. 2016 Dec 13;3(1):266-70.
18. Bansal A, Bansal AK, Bansal V, Kumar A. Liver abscess: catheter drainage v/s needle aspiration. International Surgery Journal. 2016 Dec 11;2(1):20-5.
19. Rajak CL, Gupta S, Jain S, Chawla Y, Gulati M, Suri S. Percutaneous treatment of liver abscesses: needle aspiration versus catheter drainage. AJR. American journal of roentgenology. 1998 Apr;170(4):1035-9.
20. Agarwal DK, Baijal SS, Roy S, Mittal BR, Gupta R, Choudhuri G. Percutaneous catheter drainage of amebic liver abscesses with and without intrahepatic biliary communication: a comparative study. European journal of radiology. 1995 May 1;20(1):61-4.
21. Dietrick RB. Experience with liver abscess. Am J Surg. 1984;147:288-91.
22. Gupta SS, Singh O, Sabharwal G, Hastir A. Catheter drainage versus needle aspiration in management of large (> 10 cm diameter) amoebic liver abscesses. ANZ journal of surgery. 2011 Jul;81(7‐8):547-51.

A Comparative Study of Standard PCNL vs Tubeless PCNL at a Tertiary Care Hospital
Navneet Garg1, Bindu Agrawal2, Nikita Garg3, Manish Agrawal4
1Associate Professor, Department of Surgery, Rama Medical College, Hapur, 2Associate Professor, Department of Radiodiagnosis, Muzaffarnagar Medical College, Muzaffarnagar,
3Junior Resident, Department of Obst. & Gynecology, LLRM Medical College, Meerut, 4Professor & Head, Department of Pediatrics, Saraswathi Medical College, Hapur
Abstract
Introduction: The role of percutaneous nephrostomy tube for drainage after percutaneous nephrolithotomy (PCNL) procedure has come under scrutiny in recent years. The procedure has been modified to use of small diameter tubes and tubeless PCNL.
Aim & Objectives: This study was done to evaluate perioperative characteristics, postoperative analgesic requirement, length of hospital stay and post-surgical complications between standard PCNL and tubeless PCNL.
Methodology: This prospective comparative study was conducted in department of surgery and radiodiagnosis of Rama Medical College, Hapur from June 2017 to September 2018 on 80 patients of nephrourolithiasis, who were randomly divided into two groups of 40 patients each, group A underwent standard PCNL while group B underwent tubeless PCNL. Post operatively, the efficacy of the operative procedure was analyzed based on the outcome of the procedure, duration of patient stay and post-operative complications.
Result: Majority of patient who had underwent PCNL were in age group of 21-60 years (mean age- 36.78 years) with a male predominance (M:F= 69:11). Operative time for tubeless PCNL (mean time ± SD = 59.97 ± 26.40 minutes) was shorter than for standard PCNL (mean time ± SD = 67.55 ± 28.00 minutes) but it was statistically insignificant (p value = 0.73462). 26 patients (65 %) of tubeless PCNL were discharged within 48 hours while 33 patients (82.5 %) of standard PCNL had to stay in hospital for a longer duration of 3-4 days. Post-operative analgesia requirement (Inj. Diclofenac) was significantly high in standard PCNL group (mean dose ± SD = 136.84 mg ± 39.12 mg) than in tubeless PCNL group (mean dose ± SD = 119.74 mg ± 36.13 mg, p value = 0.0026). Post-operative complications such as hematuria, urosepsis and leakage were also much less in tubeless PCNL (n=11, 27.5 %) than in standard PCNL (n= 17, 42.5 %).
Conclusion: Tubeless PCNL is a safe and effective technique and is associated with decreased pain, low analgesic requirement, less operating time and faster recovery. However it has its own limitation that precludes secondary procedure for the treatment, removal of internal stent, dysuria and need to visit hospital for subsequent removal of internal stent.
Keywords: Kidney stones, percutaneous nephrolithotomy, PCNL, tubeless PCNL
Corresponding author: Dr. Bindu AgrawalAssociate Professor, Department of Radiodiagnosis, Muzaffarnagar Medical College, Muzaffarnagar E-mail: [email protected]
Introduction
Renal calculus is solid concretion or crystal aggregation formed in the kidneys from dietary minerals in the urine. The diagnosis of kidney stones is made on the basis of information obtained from the history,
DOI Number: 10.5958/2321-1024.2019.00019.9

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 32
physical examination, urinalysis and radiographic studies including x-ray & ultrasound KUB.1,2,3
Percutaneous nephrolithotomy completely changed the approach to large and complex renal calculi, first introduced in the early 1980s. PCNL decreased morbidity and minimized invasiveness progressively replacing the open surgical approach. The standard PCNL procedure consists of a tiny percutaneous access to the kidney and the formation of a working tract connecting the flank surface with the intra-renal collecting system to allow endoscopic stone disintegration and removal. A temporary nephrostomy tube is usually left in place at the end of the procedure to allow drainage, tamponade of bleeding and delayed second look nephroscopy. This tube and the persistent urinary leakage after its removal cause significant inconvenience to both patient and medical personal in addition to increasing analgesic requirement, and prolonging hospitalization and recovery time.1,2,3
To obviate these problems, a tubeless approach was devised in 1997 and was reportedly successful in selected groups of patients. The tubeless PCNL involves internalization of the postoperative renal drainage by placement of an internal stent and bladder catheter instead of the traditional nephrostomy tube.3
Aims and Objectives
To Analyze Overall Experience Of Pcnl At Our Institute
To Compare Post-Operative Outcomes – Safety, Effectiveness, Post-Operative Complications, Time Taken To Revert To Daily Activities, Analgesic Requirement In Standard Pcnl And Tubeless Pcnl.
Material and Method
Study Design: A prospective comparative study
Study Place: RAMA Medical College, Hapur
Study Population: 80 patients of nephrourolithiasis, who met inclusion criteria
Period of Study: 12 months from June 2017 to May 2018
Inclusion Criteria:
Stones of 1 – 5 cms in size
Renal calculi , upper 1/3rd ureteric calculi , PUJ
calculi
Exclusion Criteria:
• Congenital anomalies of urogenital tract
• Patients unfit for surgery and anesthesia
• Stones below 1 cm and above 5cms in size
• Body Habitus that excludes prone position
Methodology
Documentation of patients including identification data, history, clinical findings, renal function test, USG KUB region, XRAY KUB, IVP and/or CT urography scan at the presentation in the hospital and the final outcome were recorded in the predefined proforma. 80 patients of radiologically confirmed renal calculus were divided into two groups of 40 patients each, group A underwent standard PCNL while group B underwent tubeless PCNL. Post-operatively, the efficacy of the operative procedure was analyzed based on the outcome of the procedure, analgesic requirement, duration of patient stay and post-operative complications.
Observations and Result
Table 1: Age Distribution
Age group (Years) Group-A Group-B
Range Number Percentage Number Percen-tage
< 20 6 15.0 410.0
21-40 20 50.0 16 40.0
41-60 13 32.5 18 45.0
> 60 1 2.5 2 5.0
Total 40 100 40 100
Table 1 depicts that majority of patient who had underwent PCNL were in age group of 21-60 years with a mean age of 36.78 years. Group A had 34 male (85 %) and 6 females (15 %) patients while group B had 35 male (87.5 %) and 5 female (12.5 %) patients. In Group A, out of 40 patients, 31 had single stone and rest 9 had multiple stones while in group B, there were 28 patients with single stone and rest 12 had multiple stones.

33 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
Table 2: Comparison According to Operative Time
Operating Time (minutes) Group A Group B
Range Number Percentage Number Percentage
0-40 4 10.0 6 15.0
41-80 28 70.0 27 67.5
81-120 6 15.0 6 15.0
121-160 2 5.0 1 2.5
Total 40 100 40 100
Mean 67.55 59.97
SD 28.00 26.40
p value = 0.73462
As evident from table 2, mean and standard deviation of operative time for tubeless PCNL were 59.97 minutes and 26.40 minutes respectively and for standard PCNL were 67.55 minutes and 28 minutes, but it was statistically insignificant (p value = 0.73462).
Table 3: Length of Hospitalization
Hospitalization (Stay in days) Group A Group B
Range Number Percentage Number Percentage
0-2 2 5.0 26 65.0
3-4 33 82.5 13 32.5
> 4 5 12.5 1 2.5
Total 40 100 40 100
Mean 67.55 59.97
SD 28.00 26.40
p value = 0.73462
26 patients (65 %) of tubeless PCNL were discharged within 48 hours while 33 patients (82.5 %) of standard PCNL had to stay in hospital for a longer duration of 3-4 days.
Table 4: Analgesia Requirement
Analgesic Dose Group A Group B
Inj. Diclofenac Number Percentage Number Percentage
50-100 mg 10 25.0 24 60.0
100-150 mg 30 75.0 16 40.0
Total 40 100 40 100
As evident from table 4, the post-operative analgesia requirement was much less in tubeless PCNL group than standard PCNL group.

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 34
Table 5: Comparison of Post-Operative Complications
Post-Operative Complications Group A (n= 40) Group B (n= 40)
Number Percentage Number Percentage
Hematuria 5 12.5 3 7.5
Urosepsis 6 15.0 4 10.0
Leakage 6 15.0 2 5.0
Urinoma/ Hematoma 0 0 1 2.5
Hydrothorax 0 0 1 2.5
Total 17 42.5 11 27.5
Table 5 depicts that post-operative complications were also much less in tubeless PCNL (n=11, 27.5 %) than in standard PCNL (n= 17, 42.5 %). Haematoma or urinoma was seen in only 1 patients of tubeless PCNL group, which was managed conservatively. One patient of tubeless PCNL developed hydrothorax for which intercostal tube placement was done.
Discussion
In a study by Hemendra Shah, Amit Khankar, Hiran Sodha et al, mean age of patients who underwent tubeless PCNL was 41.4 years and male to female ratio was 295:159. In comparison of this study, our study patients were younger. It may be due to that in our area preponderance of kidney stone is more common in younger age group and female patients were relatively very less in our study.10
Sung II yun et all in 2012 reported that the mean operation time was slightly longer in the standard group (148.5 minutes) than in the totally tubeless group (128.7 minutes) but there was no statistically significant difference. This was in accordance of our study but mean operative time was significantly shorter in our study which may be due to person to person expertise and good assistance.4
In our study mean hospital stay for patients those underwent tubeless PCNL was significantly shorter than standard PCNL. This was in accordance of previous studies by Bellman et al, Kwon and Kim, Karami and Ghoamrezaie, Bdesha et al and Crook et al.3,5,6,7,8
Post-operative analgesia requirement (Inj. Diclofenac) was significantly high in standard PCNL group (mean dose ± SD = 136.84 mg ± 39.12 mg) than in tubeless PCNL group (mean dose ± SD = 119.74 mg ± 36.13 mg, p value = 0.0026). This was in accordance to the studies done by Karami and Ghoamrezaie, Aghamir et al, Ni S & Qiyin et al, and Hemendra Shah et al.2,6,9,10
In our study, post-operative complications such as fever, leakage and haematuria were less in tubeless PCNL group in comparison with standard PCNL. Similar observation was also done by Hemendra Shah et al, Sichani et al and Zheo et al in their study. Hydrothorax, requiring intervention and urinoma/ haemotoma were seen in one patient each in tubeless PCNL group although this result was not statistically proven.1,10,11,12
Conclusion
Tubeless PCNL is a safe and effective technique and is associated with decreased pain, low analgesic requirement, less operating time and faster recovery. However it has its own limitation that precludes secondary procedure for the treatment, removal of internal stent, dysuria and need to visit hospital for subsequent removal of internal stent.
Financial Support & Sponsorship: Nil
Conflict of Interest: None
Ethical Clearence: Was taken from Institutional Ethical Committee and informed consent from the participating patients.

35 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
Acknowledgement: I am grateful to faculties and resident doctors of Surgery and Radiodiagnosis department for their support in this study. I also appreciate my enrolled patients for their co-operation.
References
1. Agrawal MS, Agrawal M. Percutaneous Nephrolithotomy: Large tube, small tube, tubeless, or totally tubeless?. Indian J Urol. 2013 Jul-Sep; 29(3): 219-224
2. Aghamir S.M.K. et al. Totally tubeless Percutaneous nephrolithotomy. J Endourol. 2004; 18:647-648.
3. Bellman G.C. et al. Tubeless percutaneous renal surgery. J Urol. 1997; 157:1578-1582.
4. Sung Il Yun et al. Comparative study between Standard and Totally Tubeless Percutaneous Nephrolithotomy. Korean J Urol. 2012 Nov; 53(11):7857-89
5. Kwon S, Kim HG. A comparitive study between standard and tubeless Percutaneous Nephrolithotomy, Korean J Urol. 2017; 48:45-48.
6. Karami H, Gholamrezaie HR. Totally Tubeless Percutaneous Nephrolithotomy in selected patients. J Endourol 2004; 18:475-476.
7. Bdesha AS et al. Routine placement of nephrostomy tube is necessary after pertutaneous nephrolithotomy. Br J Urol 1997; 79 Suppl 4:1.
8. Crook TJ et al. A randomized controlled trial of nephrostomy placement versus tubeless percutaneous nephrolithotomy. J Urol 2008; 180:612-614.
9. Ni S, Qiyin C et al. Tubeless percutaneous nephrolithotomy is associated with less pain and shorter hospitalization compared with standard or small bore drainage: a mata analysis of randomized, controlled trials; Urology. 2011 Jun; 77(6):12938.
10. Hemendra Shah et al. Tubeless percutaneous nephrolithotomy: 3 years of experience with 454 patients; BJU international 2009, 104;840-846.
11. Sichani MM et al. Is it necessary to perform Nephrostomy before Tube removal after Percutaneous Nephrolithotomy?. Adv Biomed Res. 2017; 6:35
12. Zhao PT et al. A Randomized Controlled Comparison of Nephrostomy Drainage vs Ureteral Stent following Percutaneous Nephrolithotomy using Wisconsin StoneQOL. J Endourol. 2016 Dec; 30(12): 1275-1284.

Original Research Article
Choledochodudenostomy Revisited: The Present Scenario
Alok V Mathur1 , Manmeet Kaur2
1Professor, Department of Surgery, Shri Guru Ram Rai Medical and Health Institute, Dehradun, Uttrakhand,
2Assistant Professor Department of Surgery, GMC, Kathua, J&K
Abstract
Background- Choledochoduodenostomy as a surgical management of common bile duct obstruction aims at free flow of bile to duodenum, being more physiological, relatively quick, simple and with fewer anastomotic sites. Objectives: investigate the safety and long term outcome of this procedure and to access its uses in present era of endoscopy and interventional radiology.. Material and methods- Study was conducted in the Department of Surgery at Shri Guru Ram Rai Institute of Health and Medical Sciences, Dehradun. Over a period of 7 years retrospectively until 2015 and prospectively from then on till december 2017. A total of 34 patients who underwent Choledochoduodenostomy(CDD) were evaluated by going through their hospital records and regular OPD follow up. Results – the results were encouraging with 33 of our patients did well in the long term follow up. Average duration of surgery was 115 minutes. Postoperatively one patient had haematemesis, later on she went to develop recurrent stricture. She later also developed long-term impairment of hepatic functions. No case of feared sump syndrome, or reflux cholangitis was observed. Conclusions - Authors are of the view that Side to side choledochoduodenostomy, should be considered by surgeons, as a simpler , less technically demanding and physiologically better procedure. It does not carry the problems usually feared with it. The excellent long term results of this series allow us to have more frequent but indicated use of this procedure, even in the young patients.
Keywords- choledochoduodenostomy, cholecystectomy, obstructive jaundice
Introduction
Surgeons in general practice often encounter the problem of Obstructive jaundice requiring surgical management. Approximately 10–18% of patients who undergo cholecystectomy for gallstones also have common bile duct stones.1 At present, endoscopic sphincterotomy is widely accepted as the treatment of choice for patients with common bile duct stones.2 Subsequent laparoscopic cholecystectomy is indicated in patients with concomitant gallstones. There have been many studies on the recurrence of bile duct stones after endoscopic sphincterotomy; however, the reported frequency of stone recurrence ranged from 4% to 24%
and failure of endoscopic management occurred in patients with large stones, multiple stones, impacted stones, multiple intra-hepatic stones and peripapillary diverticula.3,4,5,6 Choledochoduodenostomy as surgical management of obstructive jaundice had been described long back by Riedel7 in 1888 but, though done infrequently, this technique has been standardized and has yielded good results.8 Choledochoduodenostomy(CDD), choledochojejunostomy, or sphincteroplasty are used in the treatment of selected patients with retained, recurrent, and impacted bile duct stones; strictures of the bile ducts; stenosis of the sphincter of Oddi; pancreatitis associated with biliary disease; choledochal cysts; fistulas of the bile duct; and biliary obstruction, either benign or malignant. The main principle of the CDD is that a side-to-side anastomosis is designed to allow free flow of bile from the common bile duct to the duodenum. It offers some advantages over choledochojejunostomy:
Corresponding author:Dr. Manmeet kaurAssistant Professor Department of Surgery, GMC, Kathua, J&K, Mobile) No.: 09419236928Email: [email protected]
DOI Number: 10.5958/2321-1024.2019.00020.5

37 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
• A more physiologic conduit
• Relatively quick and simple, with fewer anastomotic sites
• Ease of access for future endoscopic interventions
However, its use remains debatable because of the risk of complications such as reflux cholangitis, sump syndrome and alkaline reflux gastritis. Sump syndrome is the development of cholangitis, hepatic abscess or pancreatitis after CDD, owing to stones, sludge or debris being lodged in the pool of the terminal common bile duct.9 However, the true incidence and resultant morbidity of these complications are not well defined and have not yet been thoroughly examined. Encouraged by our early results, we set out to, investigate the safety and long term outcome of this procedure.
Material and Method
The study was carried out in Post Graduate, Department of Surgery, Shri Guru Ram Rai Medical and Health Institute, Dehradun. Over a period of 7 years retrospectively until 2015 and prospectively from then on till december 2017. A total of 34 patients who underwent Choledochoduodenostomy were evaluated by going through their hospital records and regular OPD followup plus telephonic conversations. All patients included in this series were evaluated and operated upon by one or more of the authors or under his direct guidance, for a uniform set of criteria to the decision-making process. Indications for surgery are summarised in table no.1. Out of 34 patients 19 (55.9%)were females and 15(44.1%) males with age ranging from 35- 68 years.
Table no. 1- Indications of Choledochoduo-denostomy
INDICATION MALE TOTAL
Common bile duct stones in which endoscopic clearancewas difficult or
failed(including impacted stone)
8 12 20
Gross Bile duct dilatation (with biliary sludge) 1 1 2
Recurrent stones after endoscopic clearance 2 1 3
Bile duct stricture 1 2 3
Bile duct injury 3 2 5
Ampullary stenosis(benign) 0 1 1
Total 15 19 34
All the patients underwent routine investigative protocol. Diagnosis of bile duct pathology was established primarily by Liver Function Test (LFT) and Ultrasonography (USG) followed by MRCP in all cases for detailed evaluation before surgery. Size of CBD ranged from 8 mm to 24 mm. 5 patients had the GB removed in the past, these patients presented with recurrent/retained stones in the bile ducts plus jaundice. The duodenum was widely mobilized by a generous kocher maneuver for approximation to common bile duct without tension. A longitudinal choledochotomy(as close as possible) and a longitudinal duodenostomy were made each of about 2 to 2.5cm, A single or a two –layered anastomosis between the incised bile duct and the adjacent duodenum was accomplished by beginning posteriorly using simple interrupted sutures with round bodied atraumatic needle with 3-0 vicryl sutures making a triangulated stoma size of about 2- 2.5cm. (fig. 1,2,3)
Fig. 1,2-. diagrammatic representation of longitudinally placed incisions in the bile duct and duodenum and construction of two layered anastomosis.20
Fig. 3-intraoperative picture showing longitudinal choledochotomy.

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 38
Average duration of surgery was 115 minutes. Postoperatively 2 patients developed wound infection, one patient had haematemesis. Later on she went to develop recurrent stricture ( treated with percutaneous transhepatic biliary stenting, possibly secondary to vascular injury at time of CBD injury). She later also developed long-term impairment of hepatic functions. No case of feared sump syndrome, or reflux cholangitis was observed, the other complications are summarised in table no.2, all were managed conservatively. No mortality was observed in our study.
Table 2- Postoperative complications
COMPLICATION NO. OF PATIENTS
Immediate post operative complications
Haematemesis in one patient with CBD injury
Wound infection 2
Bile leak 3
Sump syndrome 0
Long term impairment of hepatic function 1
Reflux cholangitis 0
Pancreatitis 1
Stone recurrence/ residual stones 0
Anastomotic stricture 1
Gastroduodenal ulcers 2
Alkaline reflux gastritis 0
Bile duct carcinoma, post. surgical 0
Discussion
Choledochoduodenostomy was first performed by Riedel, in 1888,7who intended to cut across the common duct and implant the severed end into the duodenum, but abandoned this idea and united by lateral anastomosis the dilated common duct to the duodenum. Though that patient died as a result of leakage of infected bile into the peritoneal cavity, but the main principle of the procedure was that a side-to-side anastomosis is designed to allow free flow of bile from the common bile duct to the duodenum as intra luminal pressure between biliary tree and intestinal tract appears to be equalized.
Sprengel,10 in 1891, reported the first recovery following choledochoduodenostomy; the patient was a woman on whom he had previously performed a
cholecystectomy.
W. J. Mayo,12 in 1905, reported successful treatment of stricture of the common duct following cholecystectomy and choledochotomy by suturing the end of the dilated portion of the duct to the duodenum.
The first criteria of operation is that the duct must be sufficiently large to permit an adequate stoma. Second, the duct must be of ample length above the obstruction to permit anastomosis without tension, or, one must be able to mobilize the duodenum to a sufficient extent. Side-tracking operations for obstruction of the bile ducts are fraught with many difficulties and dangers. The abdomen is frequently filled with adhesions, hemorrhage may be troublesome, and identification of the ducts and vessels is often a time-consuming process. Added to this, patients with a long history of duct obstruction usually present a deep jaundice with an alteration in the blood clotting time, loss of weight and strength, and advanced renal and hepatic changes.12 Sanders R. L. was impressed with the results of choledochoduodenostomy, when feasible, as a means of relieving obstructions of the common duct. The procedure is not only comparatively simple from the standpoint of technique, but is physiologic in principle and, thus, offers a wide margin of safety. All the bile is immediately made available in that portion of the intestinal tract where it normally empties, intestinal function is soon restored, and the patient’s convalescence is thereby facilitated.12
Numerous complications specific to the procedure have been described classically including ascending cholangitis, alkaline reflux gastritis, and sump syndrome, which may be the reason of this procedure being performed less frequently over the years. Several studies on the long-term follow-up of CDD had good outcomes, with an incidence of sump syndrome and/or cholangitis of <5%. Most of these complications can be readily dealt with endoscopic treatment.8,13,14 Our study confirms the same. There has been a renewed interest in CDD in the last three decades, with several publications carefully evaluating the results, indications, advantages, complications, and shortcomings of CDD. The consensus is that CDD is a very satisfactory surgical procedure to treat a variety of obstructing lesions of the distal CBD. Most of these authors stipulate that the diameter of the CBD should be at least 16 mm for good outcomes of CDD.13,15,16,17 There is a thought that CDD should be avoided in younger patients who have a life expectancy

39 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
of 10 or more years due to long-term complication of cholangitis and the “sump syndrome.” This is a rare and late, albeit overemphasized, complication of CDD. Its prevalence has been reported widely varying from as low as 0% to as high as 10%8,14 which is in accordance to our study with 0% incidence of “sump syndrome”. CDD virtually eliminates the chance of residual or recurrent stones is evident from our study and the findings of studies done earlier.8,9,17,18 In a study done by gupta BS all the patients selected for CDD had a dilated common duct of at least 1.5 cm diameter and 71% of them had multiple stones, only one patient suffered from recurrent cholangitis because of inadequate stoma size. No case of “sump syndrome” was observed in this series.19
An extensive literature review showed that the absence of this complication could be explained based on at least two important factors. Firstly, a wide tension-free anastomosis provides effective drainage of enteric contents that may enter the CBD through the CDD site. Secondly, the narrow part of CBD distal to the anastomosis prevents the entry and stasis of duodenal contents. Also in patients who have undergone a preoperative ERCP with papillotomy, the contents easily pass through the ampulla, preventing this complication altogether. Choledochoduodenostomy has its own technical advantages; for instance, it maintains the normal anatomy. As compared with a routine Roux-en-Y hepaticojejunostomy, CDD is technically easier, faster, requires less manipulation of the CBD, and is more physiological. Subsequent endoscopic intervention is possible following CDD. Choledochoduodenostomy bypasses the narrowed/strictured area and is amenable to subsequent surgical intervention (hepaticojejunostomy) in case required. It is suitable for patients with multiple surgeries and interventions. Roux-en-Y hepaticojejunostomy in comparison requires construction of two anastomoses, is more time consuming, is technically more demanding, and alters the normal anatomy.
Scarring of the duodenum and impending obstruction of the duodenum are contraindications for CDD; under these circumstances, hepaticojejunostomy is performed.20 Madden et al.8 have suggested that “descending” cholangitis is a more accurate term than “ascending” cholangitis. They demonstrated experimentally that cholangitis did not occur, even when the bile duct was anastomosed to the colon, if 1) an adequate stoma was
created and 2) stricture did not develop. In Madden’s collected series of 1255 patients, the incidence of cholangitis was 0.4%. An adequate sphincteroplasty also allows reflux of duodenal contents into the biliary system, therefore, it is not reflux of duodenal contents but anastomotic stricture and subsequent stasis that are responsible for cholangitis. This is equally true for sphincteroplasty, choledochoduodenostomy, and choledochojejunostomy.8 In a study of 125 cases by H Okomoto et al. reflux cholangitis and stone recurrence was 1.6% (2/125) and 0% (0/125) of cases by CDD. There is no therapeutic related pancreatitis in CDD. Sump syndrome was not also observed in side-to-side CDD.21 Recurrent bile duct stones after endoscopic sphincterotomy have been suggested to be caused by inflammation of the bile duct, a bile duct diameter greater than 15 mm, papillary stenosis, peripapillary diverticula, reflux of the duodenal contents into the bile duct, parasites or foreign bodies within the bile duct.22,23 At present, the combination of endoscopic sphincterotomy and laparoscopic cholecystectomy is the gold standard therapy and is often used as a first choice for the treatment of cholecysto- and choledocho-lithiasis to minimise invasive surgery.24 However, the incidence of related complications, such as pancreatitis, reflux cholangitis and stone recurrence and failed stone removal were reported to be approximately 10 –20% of follow-up cases.22,25,26The high incidence was attributed to the existence of a dilated common bile duct and peripapillary diverticulum. In such recurrent or difficult cases, CDD would be the best therapeutic option. Accordingly, the indication of endoscopic sphincterotomy is currently thought to be a first choice in choledocholithiasis in regard to minimally invasive therapy. We consider that the indication of CDD is the cases of recurrent stone after endoscopic sphincterotomy or the cases of difficult and failed endoscopic sphincterotomy. Furthermore, choledochojejunostomy is an alternative therapy to CDD in difficult cases such as duodenal ulceration or scar. Minimally invasive techniques, such as laparoscopic side-to-side CDD, have been increasingly adapted for use and have been reported to be clinically useful.27,28
Conclusion -Authors are of the view that Side to side choledochoduodenostomy, should be considered by surgeons, as a simpler , less technically demanding and physiologically better procedure. It does not carry the problems usually feared with it. The excellent long term results of this series allow us to have more frequent

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 40
but indicated use of this procedure, even in the young patients.
Funding: None
Conflict of Interest: None
Ethical Approval: Yes
References
1. Soltan HM, Kow L, Toouli JA. A simple scoring system for predicting bile duct stones in patients with cholelithiasis. J Gastrointest Surg 2001; 5: 434–437
2. Cotton PB, Geenen JE, Sherman , et al. Endoscopic sphincterotomy for stones by experts is safe, even in younger patients with normal ducts. Ann Surg 1998;227: 201–204.
3. Bergman JJ, van der Mey S, Rauws EA et al. Long-term follow-up after endoscopic sphincterotomy for bile duct stones in patients younger than 60 years of age. Gastrointest Endosc 1996; 44: 643–649.
4. Prat F, Malak NA, Pelletier G et al. Biliary symptoms and complications more than 8 years after endoscopic sphincterotomy for choledocholithiasis.Gastroenterology 1996; 110: 894–899.
5. Tanaka M, Takahata S, Konomi H et al. Long-term consequence of endoscopic sphincterotomy for bile duct stones. Gastrointest Endosc 1998; 48: 465–469.
6. Pereira-Lima JC, Jakobs R, Winter UH et al. Long-term results (7 to 10 years) of endoscopic papillotomy for choledocholithiasis. Multivariate analysis of prognostic factors for the recurrence of biliary symptoms. Gastrointest Endosc1998; 48: 457–464.
7. Riedel H.:Uber den Zungenfoermigen fortstz des rechten Lebberlappens und seine pathognostiche bedentung fur die erkrankungen der Gallenblase nebst bemerkungen uber Gallensteinoperationen. Ben.Kim.Wschr.1888; 25:577-602
8. Madden JL, Chun JY, Kandalaft S, Parekh M. Choledocho-duodenostomy: an unjustly maligned surgical procedure? Am J Surg 1970 Jan;119(1):45-54
9. Srivengadesh G et al. Evaluation of long term results of choledochoduodenostomy for benign biliary obstruction. Trop. Gastroenterol. 2003, 24(4): 205-7
10. Sprengel O. Uber einen Fall Von Extripation der Gallenblase mit Anlegung einer Communication Zwischen Ductus Choledochus und Duodenum. Arch Klin Chir 1891;42:550
11. Mayo WJ. VI. Some remarks on cases involving operative loss of continuity of the common bile duct:With the report of a case of anastomosis between the hepatic duct and the duodenum. Ann Surg. 1905; 42:90-96.
12. Sanders R. L. M.D.Indications For And Value CholedochoduodenostomyAnnals of Surgery: May 1946 - Volume 123 - Issue 5 - ppg 847-858
13. Malik AA, Rather SA, Bari SUL, Wani KA. Long-term results of choledochoduodenostomy in benign biliary obstruction. World J Gastrointest Surg 2012 Feb;4(2):36-40.
14. Baker AR, Neoptolemos JP, Leese T, James DC, Fossard DP. Long term follow-up of patients with side to side choledo-choduodenostomy and transduodenal sphincteroplasty. Ann Roy Coll Surg Engl 1987 Nov;69(6):253-257
15. Escudero-Fabre A, Escallon A Jr, Sack J, Halpern NB, Aldrete JS. Choledochoduodenostomy. Analysis of 71 cases followed for 5 to 15 years. Ann Surg 1991 Jun;213(6):635-644.
16. Blankenstein JD, Terpstra OT. Early and late results following choledochoduodenostomy and choledochojejunostomy. HPB Surg 1990;2(3):151-158.
17. Dagenshein G.A. Choledochoduodenostomy: An 18 yr study of 175 consecutive cases.Surgery. 1974, 76: 319-24
18. Florcken H. Zentralbi.Chir. No3. 1928 cited by Dagenshein G.A.Choledochoduodenostomy: An 18 yr studyof 175 consecutive cases. Surgery. 1974, 76:319-24
19. Gupta BS. Choledochoduodenostomy: a study of 28 consecutive cases. Kathmandu Univ Med J (KUMJ). 2004 Jul-Sep;2(3):193-7.
20. Vogt DP, Hermann RE. Choledochoduodenostomy, choledochojejunostomy or sphincteroplasty for biliary and pancreatic disease. Ann Surg 1981 Feb;193(2):161-168
21. Okamoto H, Miura K, Itakura J, Fujii H. Current assessment of choledochoduodenostomy: 130

41 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
consecutive series. Ann R Coll Surg Engl. 2017;99(7):545-549.
22. Kim DII, Kim M-H, Lee SK et al. Risk factors for recurrence of primary bile duct stones after endoscopic biliary sphincterotomy. Gastrointest Endosc2001;54:42–48.
23. Sugiyama M, Suzuki Y, Abe Net al. Endoscopic retreatment of recurrent choledocholithiasis after sphincterotomy.Gut2004;53: 1,856–1,859.
24. Lauter DM, Froines EJ. Laparoscopic common duct exploration in the management of choledocholithiasis.Am J Surg2000;179: 372–374.
25. Pereira-Lima JC, Rynkowski CB, Rhoden EL. Endoscopic treatment of choledocholithiasis in the era of laparoscopic cholecystectomy:prospective
analysis of 386 patients. Hepatogastroenterology 2001;48:1,271–1,274.
26. Contractor QQ, Dubian MK, Boujemla Met al. Endoscopic therapy after laparoscopic cholecystectomy.J Clin Gastroenterol2001;33: 218–222.
27. Khajanchee YS, Cassera MA, Hammill CWet al. Outcomes following laparoscopic choledochoduodenostomy in the management of benign biliary obstruction.J Gastrointest Surg 2012;16: 801–805.
28. Okamoto H, Maruyama S, Takahashi Ket al. Laparoscopic choledochoduodenostomy for biliary alleviation.Surg Sci 2017;8:65–72.

Role of Diagnostic Nasal Endoscopy in Sinonasal Disease
Abhay Kumar Singh1, Pal Satyajit Singh Athwal2, Harsimrat Singh3, Himani Singh3
1Assistant Professor, Department of E.N.T, 2MBBS, 3Post graduate, Department of E.N.T, Saraswathi Institute of Medical Sciences Hapur (U.P)
Abstract
Objective- To study the extent of disease by DNE in case of sinonasal diseases as compared to patients’ symptoms and CT finding as well as surgical findings.
Method- Study was conducted at Saraswathi institute of medical sciences, Hapur from may 2017 to October 2018. Study consists of hundred patients who underwent DNE and CT scan. DNE findings were scored using Lanza and Kennedy scoring and patients were also staged using CT. We used the current definition of CRS.
Observation and Results- In our study 16 patients had paradoxical middle turbinate (16%), Septal deviation in 70 patients (70%), 50 had polys (50%), 68 patients had the nasal discharge (68%), 24 patients had mucosal abnormality (24%), 26 with inferior turbinate hypertrophy (26%), 18 patients had concha bullosa (18%).
Conclusion- Nasal endoscopy can diagnose sinonasal diseases accurately regardless of CT scan.
Keywords- Diagnostic nasal endoscopy, Sinonasal diseases.
Introduction
Otolaryngologists have traditionally considered chronic sinusitis to be a progressive condition associated with an escalating degree of treatment difficulty related to the extent of sinus involvement. The majority of reports of the results of sinus surgery, until recently, have emphasized techniques, but have generally lacked specificity as to the extent and nature of the disease process and the criteria for a successful outcome. The need for classifying and accurately evaluating the treatment of sinusitis has been driven by the burgeoning interest in surgery of the paranasal sinuses coupled with the recognition that sinusitis is now one of the most common medical diagnosis. It is no longer sufficient for a surgeon to report excellent results in treating sinusitis without describing the degree of disease treated, a treatment protocol, and an assessment of results based on the extent of the disease process.
Corresponding Author: Pal Satyajit Singh Athwal MBBS Saraswathi Institute of Medical Sciences, Hapur (U.P), E-mail: [email protected]
Previously there had been no organised format for the documentation of these. In 1994, the Committee on Rhinology and Paranasal Sinus Disease of the American Academy of Otolaryngology, Head and Neck Surgery established an international protocol to evaluate CT staging systems for sinus disease. Later scoring systems for endoscopy by Lanza and Kennedy (16) were also developed, the symptoms were evaluated in the clinical practice and research by the 20 item Sinonasal Outcome Test (SNOT 20), (7) Rhinosinusitis Disability Index, Quality of Life Questionnaire, Chronic Rhinosinusitis Quality of Life Questionnaire and Chronic Sinusitis.
Among all the recent advances, the development of the nasal endoscopy has been most efficient, and useful advance made in evaluation and treatment of sinonasal disorders. It has afforded the otolaryngologist unparalleled access to paranasal structures and site of disease. It allows for precision of instrumentation and surgery in the region of osteo-meatal complex and beyond, in restoring anatomic continuity, mucociliary clearance, ventilation, and reversing Sinunasal disorders more effectively. It has also encroached into the field of Ophthalmology and Neurosurgery. Use of endoscope reduces the morbidity and the length of hospital stay and surgery is also cosmetically more acceptable.
DOI Number: 10.5958/2321-1024.2019.00021.7

43 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
Messerklinger(19) is credited with being the first to develop and establish a systematic endoscopic diagnostic approach to the lateral wall of the nose and the PNS.
In our study we have made an attempt to correlate symptoms, DNE findings, CT scan finding and operative findings in patients of chronic rhinosinusitis and other Sino-nasal disorders.
Aims
The study aimed to assess extent of disease by DNE in cases of sinonasal disorders & compare them with CT findings and patient symptoms. They were also compared with surgical finding.
Materials and Method
This study was conducted in the Department of Otolaryngology, Saraswathi medical college, hapur, U.P. Hundred patients who presented to the OPD with features suggestive of sinonasal disorders like CRS, DNS, ANGIOFIBROMA etc. After obtaining Informed consent of all the patient suffering from sinonasal disorders, confirmed by their history symptoms and clinical findings, patients were taken for DNE and CT Scan. We used the current definition of CRS which is based upon the persistence for more than twelve weeks of 2 or more major Signs and symptoms or at least one major or 2 minor symptoms with adequate treatment.
Exclusion criteria were patients who had undergone FESS previously or had associated debilitating disease like HlV, DM, HTN.
All patients were treated with the steroid nasal spray and course of antihistamine. If there was evidence of infection or purulent discharge or PND, patients were given course of antibiotic. All patients were followed up in OPD for 6 months. Non-responders were taken up for DNE and CT Scan & SNAQ was filled (based on clinical history proforma).
On DNE presence of any DNS, Spur, Paradoxical middle turbinate polyp and mucosal abnormality was made. DNE findings were scored using Lanza & Kennedy. A maximum of 12 points and a minimum of 0 points is given.
0 1 2
Secretion Absent Watery/clear Dense/Purulent
Oedema Absent Minor Massive
Polyp Absent In middle meatus
Massive Polyposis
Both Sides would be assessed individually and their sum would represent the endoscopy score.
CT as an essential prerequisite was done in each patient. All patients underwent optimal (3 weeks) medical therapy prior to proceeding for CT examination. 3mm coronal cuts were taken from the frontal to the sphenoid sinus. 3mm axial cuts were taken from roof of the frontal sinus to the floor of nasal cavity. A bone window width of +2000 HU with a level of ~2000 HU was chosen.
Patient were staged in accordance with the following computed tomography staging system. This is a point-based system which stage the disease on basis of number of points scored. It has also taken into account any bony changes along with. Total of maximum 24 points can be score 12 for each side sinus system.
LEFT RIGHT
Maxillary Sinus
Anterior Ethmoid Sinus
Posterior Ethmoid Sinus
Sphenoid Sinus
Frontal Sinus
Osteo-meatal complex
TOTAL
Scoring: For all sinus systems except osteomeatal complex, 0= no abnormalities, 1= partial opacification, 2= complete opacification. For osteomeatal complex, 0= not occluded, 2= occluded.
Observations and Results
Our study group comprised of patients in age group of 18-60 years with 60 males and 40 females. Overall median age was 30.58 years.The duration of disease ranged. between 2 months to 13 years, with a mean being 3.24 years. Maximum number of patients presented within 1 year from of the first symptom (34%). The most

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 44
prominent symptom in our study was nasal blockage (88%) and nasal congestion, nasal discharge (74%) Other signs and symptoms including headache (66%), excessive sneezing (56%), pus on anterior rhinoscopy (38%), post nasal drip (36%), anosmia / hyposmia (22%), cough (14 %) and facial pain (8%). Most of the patients presented with more than two major symptoms, only two patients presented with one major symptom. Only two patients each with ear fullness, Chronic suppurative Otitis Media and complaint of decreased hearing.According to SNAQ scoring,0 patients had score <10, 8 patients had score 10 -20 (16%) 26 Patients had score 21-30 [52%] 3 patients had score 41-50 [6%] and no patients had score >51 Maximum score was 45 & minimum total score was 15.On anterior rhinoscopic examination, 4 patients {4%} were found to be normal among the positive findings, septal deviation were seen in 68 patients [68%] The other findings were turbinate hypertrophy in 38 patients [38%], polyp in 36 patients [36%], M/P Ds in 44 patients {44%}, nasal mucosal abnormality in 24 patients [24%].
The routine Investigations were normal in all patients. Diagnostic endoscopy was done in all the patients. In our study group,16 patients had paradoxical middle turbinate [16%], septal deviation in 70 patients [70%], 50 patient had polyp [50%],68 patients had nasal discharge [68%],24 patients had mucosal abnormalities [24%],26 patients had inferior turbinate hypertrophy [26%] and 18 patients had concha bullosa [18%].On the basis of computed tomography findings patients were scored in accordance with the sinus Score. findings were recorded. Maximum number belong to score 7-12 (14 patients) followed by 14 patients in Score 0-6, 12 patients in Score 13-18, and 6 patients in Score 19-24. Maximum score obtained was 24 and minimum being 4; mean LM score was 11. In all the patients, who underwent surgery was done under endoscopic control or septoplasty or excision. Operative findings were recorded based on surgical procedure performed in 40 patients, data was recorded mucosal abnormalities seen in 6 patients [15%], polyposis was recorded in 24 (60%) patients, pus was drained from 12 [30%] patients, turbinate changes were found in 8 [20%] patients and septal deviations was seen in 12 [30%].
Our findings were extremely interesting and conclusive in this aspect of our study and we were able to draw a hypothesis based on this finding.
Discussion
In our study we have correlated symptoms, DNE findings, CT scan findings and operative findings in patients of chronic rhinosinusitis and other Sinonasal disorders.
Our study group comprised of patients in age group of 18-60 years with more than 50% of the patient were in age range of 20-40 years. The mean age was 30.6 years. Unlike the finding of Dudvarski(8) in whose study mean age was 45 years. In our study there was a predominance of males (60%) as compared to Dudvarski(7), whose study included 52% males and 48% females,
The duration of disease ranged. between 2 months to 13 years, with a mean being 3.24 years. Maximum number of patients presented within 1 year from of the first symptom (34%).
The most commonly reported signs and symptoms in order of decreasing severity were nasal blockage, nasal congestion, nasal discharge, fatigue, headache, facial pressure, and dysosmia as found by N. Bhattacharya (3,4). Most of the patients presented with more than two major symptoms, only one patient presented with one major symptom. Only one patient each with ear fullness, Chronic suppurative Otitis Media and complaint of decreased hearing. Many patients also complained of fatigue and nasal bleeding.
All the patients were examined clinically before being taken up for nasal endoscopy and CT scanning. 42 patients (42%) had discharge in nasal cavity, 68 patients (68%) had septal deviations and 34 patients (34%) had polyp on clinical examination. However, on DNE examination 50 patients (50%) were diagnosed having polyp and 70 patients (70%) had septal deviation.
Each patient was treated with maximal medical therapy prior to being considered for DNE. Diagnostic Nasal Endoscopy was done in all patient 100 patients,70 were found to have septal deviation and nasal polyps were found in 50 patients while paradoxical middle turbinate was found in 16 patients. Anatomical variants such as-medially bent uncinate process and paradoxical middle turbinate were visualised on CT scan as well as on endoscopy but were not included in staging of disease, although they are known to affect the disease prognosis. Rationale given was to have a simplified system and to make it more comprehensive and broaden

45 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
its application. Patient DNE score was in range of 2 to 12 (mean being 4.03). in Z. Dudvarski’s study DNE score was 9.03 in the polyposis group and 2.43 in non-polyposis group (mean of 6.833) (7).
Patients filled Sinoasal Assessment Questionnaire and were accordingly scored. Score was in the range of 15 to 45 (mean being 27.1) as compared to S. Basu(2) study where SNAQ Score assessed was in range of 25 to 60 (mean of 47.2).Our patient group complained of more than one major symptom(except one) yet our scoring was very less in comparison to S.Basu(2). Probably because our study’ group was small and as infections are more common in tropical areas patients observed more relief during the initial 3 weeks treatment thereby having a lesser score of SNAQ.In our study polyps were seen in 20 patients (40%), in comparison to Jerry W Sonkens (1991)(3,5) study of sinus CT cans of 500 patients in which he saw polyposis in 49 patients (10%). Our staging system has been deliberately reduced to its simplest form to minimize individual variation in interpretation of the degree of opacification.
May and Levine’s staging system was very time efficient but as it only gave a single score per patient it did not allow comparisons of extent. of disease at different anatomical sites. The division of osteomeatal complex into anatomical subdivisions as in Jorgenson’s system, resulted in a reduced level of inter-observer agreement when compared with assessment of the osteomeatal complex as a single entity in Lund and Mackay’s scoring. Lund-Mackay (CT scan) Score was in range of 4 to 24 (mean being 11). As compared to Lund-Mackay score in S. Basu’s study which was in range of 5.5 to 24 (mean being 14.5). In its comparison N. Bhattacharya’s (3,4) study showed a Lund-Mackay score of 3.79 in patients of CRS.
In this study a 68% of the patient had septal deviation in DNE in comparison to 40% on CT
scan & 30% at surgery. Polyps were seen in 36%patients in comparison to 40% on CT scan & 60% at surgery. Such difference can be attributed to a small study group and much smaller number of patients undergoing surgery. Those patients who underwent surgery mostly had more extensive disease.
Statistical analysis confirmed there was correlation between SNAQ & LUND-MACKAY SCORE (CT
SCAN) Pearson Correlation Coefficient being 0.66. As compared to S.Basu(2) study where no correlation, was found correlation coefficient being 0.152. Correlation coefficient between SNAQ score and LANZA-KENNEDY SCORE (DNE) was 0.64 showing positive correlation. Correlation Coefficient between LANZA-KENNEDY SCORE (DNE) and LUNDMACKAY SCORE (CT SCAN) was 0.75; in comparison to Z.Liu(22) study where a much stronger correlation was found correlation coefficient being 0.88. Positive predictive value of DNE was 0.762; and negative predictive value was 0.5.
Conclusions
Due to better illumination, magnified view and deflected angles of the endoscopes every nook and corner of the, otherwise inaccessible areas of the nasal cavity can be examined with great accuracy by nasal endoscopy.
Photo documentation is possible in nasal endoscopy.
Nasal endoscopy can diagnose sinonasal diseases accurately regardless of CT scan.
Nasal endoscopy and CT scan are complimentary to each other.
Extensive polyposis with any intra cranial extension should always be confirmed by CT SCAN.
Haller cells, Onodi cells and other anatomical variations need to be confirmed by CT scan.
CT scan is mandatory before a patient is taken up for FESS to confirm the diagnosis and to know the extent of disease.
Follow up endoscopy gives an idea about the response to medical as well as surgical treatment. It also helps to find out recurrence and synechiae formation.
Acknowledgment- The authors are thankful to the chairman and managing member of Saraswathi institute of medical sciences, Hapur, U.P for their encouragement.
Ethical Clearance- Taken from the ethical committee of institute
Source of Funding- Self
Conflict of Interest - Nil

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 46
References
1). Arslan, Auris, Nasus,: Anatomic variations of the paranasal sinuses CT 1) examination sinus surgery. Larynx 1999: Jan (1)
2). Basu S. Georglas C, Kumar B N, Desai 8. :Correlation between symptoms & radiological findings in patients with chronic rhinosinusitis:an evaluation study using the sinonasai assessment questionnaire & Lund-Mackay grading system. European Archieve Otorhinoiaryngol 2005;p.751-754:262
3) Bhattacharya N .Computed tomographic staging and the fate of the dependent sinuses revision endoscopic sinus surgery. Arch Otolaryngol Head Neck Surg 1999. p.994-99. 125
4) Bhattacharya N, Lee K H .Chronic recurrent sinusitis: disease severity and clnical characterization.Laryngoscope;2005.p.306-10.115.
5) Chambers. DW : Long term outcome analysis of functional endoscopic sinus surgery:; Correlation of symptoms with endoscopic examination, Findings and potential prognosis variables. Laryngoscope, 1997.p.504-510.vol.107.
6) Chow J M , Stankiewicz JA. A diagnostic dilemma for chronic rhinosinusitis: definition accuracy and validity .Am JRhinol;2002.p.199-202.vol.16.
7) Dudvarski Z, Pendjer I, Djukic V, Janosevic L, Mikic A:The analysis of clinical characteristics of the chronic rhinosinusitis: complicated and uncomplicated form ; European Archives of Oto-Rhino-Laryngology, 2008.p.923-927.voi.265.
8) Fahamy FF, McCombe A, Mckierrnan D C : Sino nasal outcome quiestionnaire, a patient focused, rhinosinusitis specific outcome measure. Rhinology ;2002.p.195-197.vol40.
9) Virgin F, Ling FTK, Kountakis, SE. Radiology and endoscopy findings of silent maxillary sinus atelectasis and enophthalmos. American Journal of Otolaryngology – Head and Neck Medicine and Surgery. 2008 May 1;29(3):167-170.
10) Friedman W.H.: Staging of chronic hyperplastic rhinosinusitis treatment strategies Otolaryngology Head and Neck Surgery,1995; 112:21 0-14.
11) Freidman W H : Staging system for chronic sinus
disease, ENT Joumal.1994;73:480-84.
12) Garacia D P ‘. Quoted by 8. James Zinreich in Rhinosinusitis Radiological diagnosis. Otolaryngology Head and Neck Surgery,1997.527-34.117.
13) Gaskins R E :A surgical staging system for chronic rhinosinusitis.Am J Rhinol,1992.5-12.6.
14) Jorgenson : Endoscopic and computed tomographic findings in ostiomeatal sinus disease. Arch. Otolaryngolog Head and Neck Surgew.1991-P.279‘ 87.117(3).
15) Jianetto D F: Correlation between pre-operative computed tomography and operative findings in functional endoscopic sinus surgery. Laryngoscope 105:924-27,1995.
16) Lanza DC, Kennedy DW: Nose and sinus mucosal inflammation and infection, including medical therapy, Curr Opin Otolaryngol Head and NNeck; 1994. 27’ 32. 2. Quoted by David W Kennedy, William E Bolger: Diseases of the sinuses: diagnosis and management; 2001: 119-128.
17) Levine & May : Quoted by V.J. Lund-Staging for rhinosinusitis, Otolaryngology. Head and Neck Surgery:1997.p.35-40.117.
18) Liu Z, Wang H, Lu X, You XG, Gao Q, Cui Y. Correlation between rhinosinusitis symptoms and objective sinus examinations; 2007 Jun.483-5.vol.21(11).
19) O|uwole M,A comparison of computerized tomographic staging system inn chronic sinusitis. Clin Otolaryngol 1996,91-95.12: Quoted by David W Kennedy, William E Bolger: Diseases of the sinuses: diagnosis and management;2001:119-128.
20) Vining EM, Yanagisawa K, Yanagisawa E: The importance of preoperative nasal endoscopy in patients with sinonasal disease. Laryngoscope.1993 May.p.5129.103((5).
21) V.F.H. Chong : Pictorial review functional endoscopic sinus surgery 1 what radiologist need to know. Clinical Radiology: 1998;53 2650-58.
22) Liu Z, Wang H, Lu X, You XG, Gao Q, Cui Y. Correlation between rhinosinusitis symptoms and objective sinus examination; 2007 Jun.483-5 vol.21(11)

Original Research Article
Study on the Incidence of Salmonella Infection in Patients with Carcinoma Gall Bladder
Apoorva Pratap Singh1, Alok Vardhan Mathur2
1Post Graduate Resident, 2Professor, Department of Surgery, Shri Guru Ram Rai Institute of Medical & Health Sciences, Dehradun, UK, India
Abstract
Objectives- This study was conducted to study the association of salmonella infection with carcinoma gall bladder.
Materials and Method- A total of 36 radiologically or histologically proven cases of Carcinoma Gall Bladder were included in the study and their thorough clinical history was taken and WIDAL titres were recorded using the ‘Stained Salmonella’ Antigen set.
Results- The ratio of male to females among salmonella positive and salmonella negative patient were 1:3 & 1:2.2 respectively.
Keywords - Carcinoma gall bladder, Salmonella.
Introduction
Carcinoma of the gallbladder (CaGB) is the fifth most common cancer of the gastrointestinal tract and is one of the commonest biliary tract (BT) malignancies[1].It is seen that for the majority of patients, late diagnosis and lack of effective treatment is a typical feature of the disease even today[2-4]. Carcinoma of the gallbladder is an aggressive disease with poor prognosis and it’s incidence has marked ethnic and geographical variations. Ca GB is more common in females than in males, except in countries like Japan and China. The highest rates of incidence were documented in women from Delhi, India (21.5/100 000)[5]. . In India, carcinoma of gall bladder is much more common among women in the northern and central part. In Kashmir, it is the third most common cancer in females after cancer cervix and
Corresponding author:Dr . Alok Vardhan MathurProfessor, Department of Surgery, Shri Guru Ram Rai Institute of Medical & Health Sciences, Patel Nagar, Dehradun, UK, India, Contact No.-+91 9412195558..Email id: [email protected]
breast cancer. In Delhi, gall bladder carcinoma is the fourth commonest malignancy, and the most frequent gastrointestinal cancer in women [6]. A number of factors, such as genetics, infections, and life style have been reported to be associated with Ca GB.[7]
Understanding bacteria-induced carcinogenesis might enable us to prevent and cure some forms of cancers [8]. The involvement of bacteria in carcinogenesis is still not without controversy because no clear agreement has been achieved on the molecular mechanism/s by which they might promote carcinogenesis. In the 21st century, scientists started hypothesizing that: (1) Chronic inflammation caused by persistent bacterial infections might lead to carcinogenesis [9-11]; and (2) Bacterial toxins and secondary metabolites produced by the chronic bacterial infection might induce carcinogenesis [10].
Objectives- To study the association of salmonella infection with carcinoma gall bladder.
Materials and Method
This study was conducted at Shri Guru Ram Rai Institue of Medical and Health sciences and Shri Mahant Indresh Hospital (SMIH), Dehradun Uttarakhand over
DOI Number: 10.5958/2321-1024.2019.00022.9

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 48
a period of 24 months. Patients attending the in-patient or out-patient department in Shri Guru Ram Rai Institue of Medical and Health sciences and Shri Mahant Indresh Hospital (SMIH), Dehradun who were a radiologically or histologically proven case of Carcinoma Gall Bladder were included in the study. A total of 36 patients were included in the study and their thorough clinical history was taken and WIDAL titres were recorded using the ‘Stained Salmonella’ Antigen set by ARKRAY Healthcare Pvt. Ltd.
Results and Observation
The male to female ratio among the patients suffering from carcinoma gall bladder in our study was 1 : 2.6.
Table 1: Baseline characteristics of study group according to age in %
Age group No. %
<40yrs 6 16.7
41 – 50yrs 10 27.8
51 – 60yrs 7 19.4
61 – 70yrs 8 22.2
>70yrs 5 13.9
TABLE 1 shows the distribution of carcinoma gall bladder in accordance with the age group. There were 6 patients below the age of 40 years which presented with aggressive disease, and 5 cases were above the age of 70years. Maximum number of cases i.e. 10 cases were found in 5th decade followed by 8 patients in the age group of 60-70years and 7 patients among 50-60 years of age.
Chart 1: Graphical representation of distribution of study subjects according to symptoms
TABLE 2: Total number of salmonella positive subjects in study group in %
Salmonella No. %
Positive 4 11.11
Negative 32 88.89
Total 36 100.0
TABLE 2 shows salmonella infection detected by significant widal titres ( the agglutinin titre greater than 1:80 for anti “O” antibodies and titre 1:160 for anti “H” antibody) which was positive in only 4(11%) patients
out of the total 36 patients of carcinoma gall bladder.
TABLE 3: Association of chronic salmonella infection with carcinoma gall bladder
Observed Proportion 11.11%
Point prevalence of Salmonella in Dehradun district 1.78%
Z statistic 4.23
95 % CI 3.11% - 26.06%
p Value 0.0001*

49 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
TABLE 3 It shows association using Z score of salmonella infection with carcinoma gall bladder based on point prevalence in Dehradun district i.e 1.78% which was derived from data given by a survey report “Burden of diseases on hospitals in selected districts of Uttarakhand” by Directorate of Economics and
Statistics Uttarakhand for CENTRE FOR RESEARCH, PLANNING AND ACTION, NEW DELHI 110001 in May – 2017. According to 95% CI (confidence interval) the association of chronic salmonella infection was found to be highly significant with p value <0.05( p value of 0.0001*)
CHART 2: Compares clinical features among salmonella positive and negative cases
TABLE 4: Correlation of Liver Function Tests with salmonella positive and negative cases of carcinoma gall bladder
Variable
Salmonella
p ValuePositive Negative
Mean SD Mean SD
Total bilirubin 13.70 9.92 6.87 6.33 0.06
Conjugated bilirubin 10.30 8.71 4.63 4.47 0.04*
unconjugated bilirubin 2.00 1.44 1.26 0.96 0.18
SGOT 164.5 131.0 78.0 58.98 0.02*
SGPT 179.0 157.65 72.98 71.28 0.02*
ALP 592.75 516.63 288.50 319.67 0.10
Serum Total Protein 6.47 0.54 6.56 1.51 0.90
Serum Albumin 3.27 0.26 3.44 0.96 0.72
Serum Globulin 3.27 0.65 3.08 0.66 0.59
SGOT-serum glutamic oxaloacetic transaminase, SGPT- serum glutamic pyruvate transaminase, ALP- alkaline phosphate
TABLE 4 shows correlation of liver function tests among salmonella positive and salmonella negative cases among the study group. Independent sample t test was applied to calculate the p value . Conjugated bilirubin, SGOT & SGPT had p values < 0.05 which were
(0.04,0.02 & 0.02 respectively) statistically significant .
Discussion
In a period of two years, a total of 36 cases of confirmed CAGB were studied ,out of which 72.22%

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 50
were females and 27.78% were males. . There were 6 patients below the age of 40 years which presented with aggressive disease, and 5 cases were above the age of 70years while the peak incidence of GBC in the present study was observed in the age group of 41-50 years (27.8%). Similar results were seen in other studies from India (Shukla et al., [12]; Pandey et al., [13]; Kapoor et al., [14]; Nissar Hussain et al., [15]; Imran et al., [16]). In stark contrast, studies from west reported the mean age of 67 years (Beltz et al., [17]) and the peak age of incidence in the seventh decade of life (Perpetuo et al., [3]). In our study, the female to male ratio was 2.6, with the mean age for females (mean 55.36 years) being higher than in males(mean 53.63636 years) . Females usually present at a younger age at diagnosis compared to their male counterparts. The above findings were in contrast with that of other studies (Beltz et al., [17]; Shukla et al., [12]; Pandey et al., [13]) where the female to male ratio was reported to be 3, 3 and 2.5 respectively. Based on the review of literature of the worldwide incidence of GBC, the average female to male ratio was reported between 2 and 3 [18] while it was more decisively skewed toward the female sex in our study. This pattern of distribution of GBC in females is more strikingly observed in countries and regions with the highest incidence rates of GBC, such as northern India [19]. This marked gender bias for GBC—which to some extent reflects a gender bias for cholelithiasis and the distinct geographic and genetic factors involved in pathogenesis—warrants the need for a more detailed evaluation of the role of hormonal (estrogen/progesterone) receptors in the pathogenesis of GBC.
Clinical predilection
Pain is a presenting feature in nearly all the cases (97 %) followed by weight loss (77 %), hepatomegaly (65 %) and nausea and vomiting (64 %) [20]. Shukla reviewed 315 patients and reported pain to be the commonest symptom (85 %) followed by icterus (60.3 %), lump(40 %) and loss of appetite(40 %) [12]. They noted hepatomegaly in 85.7 % and a palpable gall bladder in 47 %. Al– Hadeedi reported Pain abdomen, anorexia, jaundice, weight loss, right upper quadrant mass in 47.3 %, 39.4 %, 36.4 %, 39.4 % and 34.2 % respectively out of 38 patients of gall bladder carcinoma from Queen Mary Hospital, Hong Kong [21]. In our study, lump and anorexia were the commonest complaints (94.44 %), followed by jaundice, right upper quadrant
pain, fever and nausea & vomiting in 63.88 %, 30.55 %, 27.77%, 25 % patients, respectively.
Laboratory Findings
The baseline liver parameters of the study group were as follows. Total bilirubin 7.62±6.98 mg/dl with conjugated bilirubin and unconjugated 5.26±5.24 mg/dl and 1.34±1.02 mg/dl respectively. Transaminases levels in the study ,SGOT and SGPT were found to be 87.61±72.89U/L and 84.76±88.16 U/L respectively. Serum alkaline phosphatase level were 322.3±350.42 U/L. Total serum protein were 6.55±1.43 gm/dl of which serum albumin and serum globulin were 3.42±0.91 gm/dl and 3.10±0.66 gm/dl respectively .Independent sample t test was applied to calculate the p value . Conjugated bilirubin, SGOT & SGPT had p values < 0.05 which were (0.04,0.02 & 0.02 respectively) statistically significant .
Baseline renal function test among the study group showed that serum urea was 38.59±36.76mg/dl , serum creatinine 1.03±1.18mg/dl, serum sodium 134.64±4.36 mmol/L , serum potassium 3.96±0.72mmol/L and serum calcium was 8.48±0.84mg/dl.
Salmonella typhi has been frequently associated with gall bladder carcinoma. The relationship of typhoid carrier state and gall bladder carcinoma was first reported by Axelord in 1978 [22]. It was also reported by Mellemgaard that a six times higher risk for hepatobiliary cancer exists among typhoid carriers [23]. In our study, WIDAL test was performed to assess the carrier status of Salmonella typhi using ‘Stained Salmonella’ Antigen set for Widal Test by ARKRAY Healthcare Pvt. Ltd which was positive in 4 patients out of the 36 patients of gall bladder carcinoma(11.11%) ,in accordance to the findings of the study carried out by Nath et.al. at Banaras Hindu University,Varanasi[24]
Of the 4 patients positive for Salmonella, 75% were females and 25% male.(a difference in male to female ratio among salmonella positive and salmonella negative patient being 1:3 & 1:2.2 respectively )Thus showing a greater percentage of female preponderance among salmonella positive patients of carcinoma gall bladder. Right upper quadrant pain was a presenting feature of all salmonella negative patients whereas all 4 salmonella positive patients of carcinoma gallbladder were inconsistent with pain as a symptom. While jaundice was present in 75% of salmonella positive patients compared

51 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
to 62.5% patients in salmonella negative group. Fever was absent in all of salmonella positive patients whereas 10 patients presented with fever of salmonella negative group. Among all patients of the study group, loss of appetite was a consistent clinical feature with no significant difference in either of the two groups. Lump was also a consistent finding among both the groups, with all four salmonella positive patient presenting with abdominal lump. Vomiting was not a consistent clinical feature among both the groups, only 28.1% patients presented with vomiting, all of which belonged to the salmonella negative group
Conclusion
Our study draws a strong association between chronic salmonella infection and carcinoma gall bladder, thus favoring a strategy of advocation of prophylactic cholecystectomy for all individuals with silent gall stones in this geographical area. This is because Salmonella is an endemic infection, and itself represents a significant risk factor for gall bladder cancer, besides the additional risk from gall stones.
Funding: Self
Conflict of Interest: None
Ethical approval: Approved from Institutional Ethical Commitee
References
1. Piehler JM, Crichlow RW. Primary carcinoma of the gallbladder. SurgGynecolObstet 1978; 147(6): 929-942
2. Nevin JE, Moran TJ, Kay S, King R. Carcinoma of the gallbladder: staging, treatment, and prognosis. Cancer 1976; 37(1): 141-148
3. Perpetuo MD, Valdivieso M, Heilbrun LK, Nelson RS, Connor T, Bodey GP. Natural history study of gallbladder cancer: a review of 36 years experience at M. D. Anderson Hospital and Tumor Institute. Cancer 1978; 42(1): 330-335
4. Gupta SK, Shukla VK. Gallbladder cancer: etiopathology and treatment. Health Administrator 2004; XVII (1): 134-142
5 Lazcano-Ponce EC, Miquel JF, Muñoz N, Herrero R, Ferrecio C, Wistuba II, Alonso de Ruiz P, AristiUrista G, Nervi F. Epidemiology and
molecular pathology of gallbladder cancer. CA Cancer J Clin 2001; 51: 349-364
6 Nandakumar A (ed). National Cancer Registry Programme. Consolidated Report of the Population Based Cancer Registries. Incidence and Distribution of Cancer:1990–96. Indian Council of Medical Research, New Delhi; pp 52–53.
7 Walsh N, Qizilbash A, Banerjee R, Waugh GA. Biliary neoplasia in Gardner’s syndrome. Arch Pathol Lab Med 1987; 111(1): 76-77
8 Malfertheiner P, Sipponen P, Naumann M, Moayyedi P, Mégraud F, Xiao SD, Sugano K, Nyrén O. Helicobacter pylori eradication has the potential to prevent gastric cancer: a stateof-the-art critique. Am J Gastroenterol 2005; 100: 2100-2115
9 Lax AJ, Thomas W. How bacteria could cause cancer: one step at a time. Trends Microbiol 2002; 10(6): 293-299
10 Karin M, Greten FR. NF-kappaB: linking inflammation and immunity to cancer development and progression. Nat Rev Immunol 2005; 5: 749-759
11. Travaglione S, Fabbri A, Fiorentini C. The Rho-activating CNF1 toxin from pathogenic E. coli: a risk factor for human cancer development? Infect Agent Cancer 2008; 3: 4
12. Shukla VK, Khandelwal C, Roy SK, Vaidya MP. Primary carcinomaofthegallbladder:areviewofa16-yearperiodattheUniversity hospital. J Surg Oncol. 1985;28:32–5.
13. Pandey M, Pathak AK, Gautam A, Aryya NC, Shukla VK. Carcinoma of the gallbladder: a retrospective review of 99 cases. Digest Dis and Sci. 2001;46:1145–51.
14. Kapoor VK, Mc Michael AJ. Gallbladder cancer: an ‘Indian’ disease. Natl Med J Ind. 2003;16:209–13.
15. Hamdani NH, Qadri SK, Aggarwalla R, Bhartia VK, Chaudari S, Pal NK. Clinicopathology of gallbladder carcinoma with reference to gallstones in eastern India. Asian Pacific Journal of Cancer Prevention. 2012;13:5613–7.
16. KhanI, PandaN, Banerjee M.Epidemiological factorsingall bladder cancer in eastern India-a

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 52
single centre study. Indian J Surg Oncol. 2013;4(1):67–72.
17. Beltz WR. Condon RE (1974). Primary carcinoma of the gallbladder. Ann Surg. 1974;180(2):180–4.
18. Randi G, Franceschi S, La Vecchia C. Gallbladder cancer worldwide: geographical distribution and risk factors. Int J Cancer. 2006;118(7):1591–602.
19. Flavio Nervi F, Wistuba II, de Ruiz PA, Gerardo Aristi Urista Eduardo C, Lazcano P, et al. Epidemiology and molecular pathology of gallbladder cancer. CA Cancer J Clin. 2001;51:349–64
20. Shekhar Pal et al. Baseline Widal Titre in Hilly Areas of Garhwal Region of Uttarakhand, India.Journal of Clinical and Diagnostic Research.2013; 7(3): 437-440
21. Alok Vardhan Mathur. Need for Prophylactic Cholecystectomy in Silent Gall Stones in North India. Indian J Surg Oncol .2015; 6(3):251–255
22. Axelord L, Munster AM, O’Brian. TFTyphoid cholecystitis and gall bladder cancer after interval of 61 years. JAMA . 1978;217:83
23. Mellemgard A, Gaarslev K .Risk of hepatobiliary cancer in carriers of Salmonella typhi. J Natl Cancer Inst.1988; 80(4):288
24. Nath,G et al. Association of the carcinoma of the gall bladder with typhoid carriage in a typhoid endemic area using a nested PCR. The Journal of Infection in Developing Countries.2008; 2(04):302-307.

Review of Clinical and Functional Result of Abdominal Rectopexy Using Proline Mesh for Complete Rectal Prolapse
Over a Period of 1 Year at Tertiary Care Centre in Bihar
Nitesh Kumar1, Nitesh2, Vibhuti Bhushan3, Ashwini Kumar2, Monika Raj4 1Assistant Professor, 2Senior Resident, 3Additional Professor, 4Intern,
Department of General Surgery IGIMS, Patna
Abstract
Background and Objectives: There are many surgical procedures for treating complete rectal prolapse ranging from complex abdominal interventions to simple perineal procedures with varying results. The ideal procedure suitable in all cases is still an enigma. Many surgeons believe that abdominal rectopexy has become the operation of choice not only in the young but even in the elderly patients, resulting in a low recurrence rate and restoration of continence in significant number of patients. The present study to evaluate clinical and functional results of abdominal rectopexy using prolene mesh for complete rectal prolapse in our centre.
Method: Fifteen patients with complete rectal prolapse underwent abdominal rectopexy using prolene mesh. They were followed up for a mean period of 7.3 months and was analysed for postoperative complications like haemorrhage, operative mortality, wound infection, bladder and erectile dysfunction recurrence of rectal prolapse, changes in bowel frequency and restoration or deterioration in continence were noted.
Results: There was no mortality or recurrence in any patient and (100%) improvement in continence in a lone patient with incontinence and decrease in bowel frequency in 2 patients (13%), postoperatively but this did not result in clinical constipation in any of the patient.
Conclusion: Abdominal rectopexy using prolene mesh is a simple operation with satisfactory low recurrence rate, good functional out come with low morbidity and mortality. This procedure can be considered in all patients who are considered fit to undergo an abdominal procedure.
Keywords: Complete Rectal Prolapse; Abdominal Rectopexy; Prolene Mesh; Incontinence; Constipation.
Introduction
When an internal organ persists in an endeavor to become an external organ, it generally causes a great deal of trouble. The rectum is occasionally an offender in this respect1. W. Ernest Miles, 1993. Complete rectal prolapse or procidentia is a protrusion beyond the anal verge which secretes mucus and may bleed
Corresponding authorDr. Nitesh Kumar, Assistant Professor, Department of General Surgery IGIMS, Patna, Mobile no. 9971060788, Email id- [email protected]
and associated with incontinence either because there is an underlying weakness in the sphincter mechanism or because of the presence of the prolapse protruding through the anal canal leads to poor sphincter function2,3. The multitude of methods that have been devised for its relief. Abdominal rectopexy has a low morbidity and mortality rate. The recurrence rate is usually less than 4% with improvement in incontinence and constipation6,7.
This clinical study of abdominal rectopexy using prolene mesh was done.
To study recurrence and post-operative complications of complete rectal prolapse.
DOI Number: 10.5958/2321-1024.2019.00023.0

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 54
To study the functional results (bowel frequency and incontinence).
Methodology
This prospective clinical study included 15 cases of complete rectal prolapse who underwent abdominal rectopexy using prolene mesh. These patients were admitted to Department of General Surgery, IGIMS Patna during the period from January 2017 to December 2017.The patients coming with a history of protrusion of mass per anus were interviewed and a diagnosis of complete rectal prolapse was made essentially on clinical examination.
For assessing functional results, continence was classified after Browning and Park’s as follows8:
Classification of continence (Browning and parks)
Grade 1 Fully continent for flatus & stool
Grade 2 Continent for Stool but not for Flatus
Grade 3 Incontinent for liquid stool
Grade 4 Incontinent for solid stool
Grade 3 and 4 were considered unacceptable. No distinction was made between occasional and regular episodes of incontinence.
Following investigations were done in all cases.
• Blood: Hb%, TC, DC and ESR.
• Urine: sugar, albumin, microscopy.
• FBS, serum creatine, HIV, HbsAg, Anti HCV
• Chest x-ray and ECG.
• Sigmoidoscopy.
All patients were subjected to abdominal rectopexy using prolene mesh
Inclusion Criteria: Patients with complete rectal prolapse who underwent abdominal rectopexy using prolene mesh.
Exclusion Criteria:
1. Complete rectal prolapse where sigmoidectomy or colectomy was combined with abdominal rectopexy.
2. Cases which could not be followed up for a
minimum period of 6 months.
In all, 18 cases of complete rectal prolapse were admitted during the period. 3 patients refused to undergo surgery. Only 15 cases who underwent abdominal rectopexy were followed up for a minimum period of 6 months and were included in the study.
Figures 1 to 3 shown complete rectal prolapse and operative details
Figure 1
Figure 2

55 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
Figure 3
Results
Table 1: Age distribution
Age in Years No. of Cases Percentage
21-30 1 6
31-40 4 27
41-50 7 47
51-60 3 20
Total 15 100
Table 2: Sex distribution
Sex No. of Cases Percentage
Male 12 80
Female 3 20
Total 15 100
Table 3: Symptoms with duration
Symptoms No of cases with percentage
Mean duration
Rectal prolapse 15 (100%) 7.3 months
Mucus discharge 15 (100%) 7.3 months
Occasional bleeding 9 (60%) 3.2 months
Loose stools 2 (13%) 2.6 months
Constipation 4(27%) 18 months
Straining at stools 4 (27%) 18 months
Incontinence to stool/flatus 1 (7%) 3 months
Uterine prolapse Nil Nil
Interpretation: The predominant symptoms seen in all patients were prolapse and mucus discharge form anal canal with a mean duration of 7.3 months. The next common symptom was occassional bleeding seen in 9 (60%) patients with mean duration of 3.2 months. Constipation with straining at stool was seen in four (27%) cases. Only two patients (13%) had bowel frequency of more than 3 times per day and one among them complained of incontinence for liquid stools. Four (25%) patients had undergone previous anorectal surgery. Haemorrhoidectomy (three), Thiersch stitch (one). One female patient had undergone vaginal hysterectomy with pelvic repair for uterine prolapse 3 years prior to noticing prolapse of rectum.
Table 4: Signs at presentation
Signs No of cases Percentage
Complete prolapse + manually reducible with no ulceration or bleeding
6 40
Complete prolapse + manually reducible + with bleeding ulceration
9 60
Total 15 100
Interpretation: In 6 (40%) patients presented with complete prolapse which was manually reducible and there was no ulceration or bleeding. Nine patients (60%) presented with complete prolapse with ulceration and bleeding. There was no cystocele, rectocele or uterine prolapse in female patients. The anal canal was patulous in all cases. On sigmoidoscopy distal proctitis was noticed in 9 (60%) cases
Table 5: Post-operative complications
Complications No of cases Percentage
Haemorrhage Nil 0
Prolonged ileus 1 7
Mesh infection Nil 0
Wound infection Nil 0
Bladder dysfunction Nil 0
Erectile dysfunction Nil 0
Mortality Nil 0

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 56
Interpretation: There was no mortality. Only one case of prolonged ileus was seen extending for seven days which resolved on conservative treatment. The average duration of hospital stay was 8 days and the average time taken by patient to return to normal daily activities was 7 days. There was no recurrence of rectal prolapse either partial or complete. Bowel frequency of more than 3 times per day seen in 2 patients pre operatively improved to 1-2 times per day post operatively. Out of 4 patients with preoperative constipation, improvement was seen in only one patient.
Table 6: Fecal Continence
No of cases
Pre Operative Post Operative
Grade I fully continent for flatus and stools 14 15
Grade II continent for stool but not flatus Nil Nil
Grade III incontinent to liquid stools 1 Nil
Grade IV incontinent for solid stool Nil Nil
Total 15 100
Interpretation: One patient who had incontinence to liquid stools had improvement after rectopexy and was fully continent after wards.
Discussion
Complete rectal prolapse, a distressing condition is more common in adults than in children. In our study that this condition is seen predominantly after the age of 40 nearly in 67% of cases shown in Table-1 did not have any paediatric case with complete rectal prolapse in our series1,2. In West with female to male ratio of 6:1. in India and other Asian countries slight male preponderance is reported .However in our series there is male preponderance with male to female ratio being 4:1 shown in Table -2. All females were parous.
Constipation with straining is considered to be one of the predisposing factors in the aetiology of prolapse. We have found constipation only in 4 (27%) patients preoperatively.
Incontinence of various grades reported in different studies in West range from 30% to 80%. But our series had only one patient (7%) who complained of incontinence for liquid stools only. Probably this is because of the fact that we may be seeing the patients at much younger age than in the West3,4. Over the past 30 to 35 years, abdominal rectopexy has become the accepted management of complete rectal prolapse in patients fit enough for an abdominal procedure. Several series report no mortality following operation.
Keighley MRB, Shouler P.J. (1983) in their series of 100 cases of abdominal rectopexy using marlex mesh reported no mortality19. Hilsabeck (1981) reported no mortality in their series of 17 cases. Notarus (1979) reported nil mortality in their series of 32 cases20.We also did not encounter any mortality in our series.
We did not experience any technical difficulty in performing the abdominal rectopexy using prolene mesh. Mean operating time was 1 hour 33 minutes. Practically we did not have in our patients post operative complications like haemorrhage, bladder or erectile dysfunction, mesh infection or abdominal wound infection. Except in one patient who had prolonged paralytic ileus.
Recurrence: Keighley et al (1983) reported no recurrence in their series of 100 cases19. Hilsabeck (1981) reported no recurrence in 17 patients20. Kim D.S, Tsang CB, Wong WD, Lowry Ae, Gold berg SM, Madoff RD (1999) found recurrence in 5% of 161 patients23. Hiltunen KM and Matikainen M (1991) show recurrence rate to be 1.8% in their series of 54 cases24. In our study did not have recurrence either partial or full thickness for a mean follow up period of 7.3 months. The shorter follow up period (7.3 months) and small number of patients (total 15) are the limitations of our study.
Functional results:
Constipation: Abdominal rectopexy is shown by many to produce post operative constipation in 10% to 47% of patients. Hiltunen KM and Matikainen M (1991) found post operative constipation in 31% of cases in their series of 54 consecutive marlex mesh abdominal rectopexy24. G S Duthie and DCC Bartolo (1992) reported no evidence of significant post operative constipation in their series of 20 patients followed up for a period of 6 months21. Bowel frequency in two of our patients

57 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
(13%) who had bowel frequency of more than 3 times per day preoperatively decreased to 1 to 2 times per day postoperatively. We did not observe development of post operative constipation in previously normal patients.We had in our present study, 4 patients who complained of constipation with straining preoperatively. The symptom of constipation continued in 3 of them postoperatively and it disappeared in the fourth patient. Those who had continued constipation postoperatively were treated with bulk laxatives and were satisfied with the treatment.
Incontinence: The incidence of restored continence associated with successful abdominal rectopexy is generally high12,25. G S Duthie and D C C Bartolo (1992) reported improved continence in 67% following Marlex mesh abdominal rectopexy21. Hiltunen K M and Matikainen M (1991) found improvement in continence in 75%.24
We did not observe incontinence in majority of our patients. It was observed only in one (7%) patient who was incontinent for liquid stools only became fully continent postoperatively resulting in 100% improvement in incontinence. This remarkable (100%) improvement in incontinence has to be interpreted with caution as the number of incontinent patients was too low in our study.
Conclusion
The abdominal rectopexy using prolene mesh produced no mortality or recurrence in our hands and this operation easy to learn and master. There were no significant postoperative complications including intractable troublesome constipation, mesh infection etc. Functional result in the form of improvement in incontinence was also excellent. Therefore, we considered the abdominal rectopexy using prolene mesh an ideal operation for complete rectal prolapse for patients who are fit for an abdominal procedure.
Source of Funding: Self
Conflict of Interest: None
Ethical Clearance: Taken
References
1. J.C. Goligher. Prolapse of the Rectum. In Surgery of Colon, Rectum Anus. 463-478.
2. Robin K.S. Phillips. Rectal prolapse. In A Companion
to Specialist Surgical Practice. Colorectal Surgery 2nd edition. W.B. Saunders. Co. Ltd. Philadelphia. 250-266.
3. Robert. J. Fitz Gibbons, Jr A. Gerson Greenburg, Prolapse of Rectum. In HERNIA, 4th edition, 455-464.
4. Michael R.B. Keighley and Norman S. Williams, Rectal Prolapse. In Surgery of the Anus, Rectum, and Colon. W.B. Saunders Co. Philadelphia 1997, 794-860.
5. Joshi P.N. “Prolapse of Rectum”. In ASI Text book of Surgery. Ahamad A. Hai and Rabindra B, Shrivastava (eds), New Delhi, Tata McGraw Hill Publishing Company Ltd., 2003; 484-488.
6. Boccasanta P, Rosati R, Venturi M, Montorsi M, Cioffic U, Demone M. Comparison of Laparoscopic Rectopexy with Open Technique in Treatment of Complete Rectal Prolapse. Clinical and Functional Results. Surg Laparosc. Endosc 1998; 8: 460-5.
7. Cuschieri A, Shimi, Vander Varder Velpen, Bantings, Wood RA, Lapacoscopic Prosthesis Fixation Rectopexy for Complete Rectal Prolapse. Br. J.Surg 1994; 81: 138-9.
8. McCue JL and Thomson JPS. Clinical and Functional Results of Abdominal Rectopexy for Complete Rectal Prolapse. Br J Surg 1991; 78: 921-923.
9. Lloyd M. Nyhus, Robert E. Condon. Prolapse of the Rectum. In HERNIA 4th edition 455-464.
10. Patrick. W. Mazier, David.H. Levien, Martin A. Luchtefeld, Anthony J. Senagore, Rectal Prolapse. In Surgery of the Colon, Rectum and Anus. W.B. Saunders Co. 1995:515-537.
11. Norman S. Williams. “The Rectum”. In Bailey and Love’s Short Practice of Surgery, RCG Russel, Norman S Williams and Chirstopher JK Bulstrode (eds), London: Arnold, 2014; 1097-1101.
12. Frank J. Theuerkauf, jr, Iraj. Kodner, Mark J. Hoffmann, Robert Dean Fry, Rectal Prolapse and Internal Intussusception of the Rectum: Diagnosis and Surgical Treatment. In Colon, Rectum and Anal Surgery. Current Techniques and Controversies 76-90.
13. Keighley MRB, Shouler PJ. Results of Marlex Mesh Abdominal Rectopexy for Rectal Prolapse. Br J Surg 1983; 78: 229-232.

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 58
14. Hilsabeck JR. Transabdominal Posterior Rectopexy using an Inverted T of Synthetic Material. Arch Surg 1981; 116: 41-44.
15. Duthie GS, Bartolo DCC. Abdominal Rectopexy for Rectal Prolapse: A Comparison of Techniques. Br J Surg 1992; 79: 107-113.
16. Boccasanta P, Rosati R, Venturi M, Cioffi U, De simone, Montorsi: Surgical Treatment of Complete Rectal Prolapse: Results of Abdominal and Perineal Procedures. J Laparoendosc Adv Surg Tech 1999; 9 (3): 235-238.
17. Kim D.S, Tsang C.B, Wong W.D, Lowry A.C, Goldburg S.M, Madoff R.D. Complete Rectal Prolapse: Evolution of Management and Results. Dis Colon Rectum 1999; 42 (4): 460-466.
18. Hiltunen KM, Matikainen M. Clinical Results of Abdominal Rectopexy for Rectal Prolapse. Ann Chir Gynaecol 1991; 80 (3): 263-266.
19. Marvin L. Corman, M.D. Rectal Prolapse, Solitary Rectal Ulcer, Syndrome of the Descending Perineum and Rectocele. In Colon and Rectal Surgery 4th edition Lippincott- Raven Company New York 1998. 401-448.
20. Eukw, Seow-choen F. Funtional Problems in Adult Rectal Prolapse and Controversies in Surgical Treatment. (Review) (140 refs) Br. J.Surg 1997: 84:904-11.
21. Keighley MRB, Makuria T, Alexander-Williams J, Arabi Y Clinical and Manometric Evaluation of Rectal Prolapse and Incontinence. Br. J. Surg 1998: 67: 54-6.
22. Yoshioka K, Hyland G, Keighley MRB, Functional Results after Posterior Abdominal Rectopexy. Parameters of Predictive Value in Identifying Return of Continence. Br J Surg 1989; 76: 64.
23. Marvin L. Corman, Herand Abcarian, AR Denison, Larry C. Carey, Rectal Prolapse Surgical Techniques. In Surg. Clin. North Amer. 1988 December; 68 (6): 1255-1265.
24. Thandin Kosi E. Madiba, Mirza K. Baig, Steven D. Wexmer, Surgical Management of Rectal Prolapse. Review Article Arch Surg2005; 140: 63-73.
25. Fang CB, Candelária P de A, Klug WA, Capelhuchnik P. “Surgical treatment of rectal prolapse by the Delorme technique and rectopexy” Rev Assoc Med Bras. 2008;54(2):142–5.
26. Tou S, Brown SR, Malik AI, Nelson RL. Surgery for complete rectal prolapse in adults. Cochrane Database of Systematic Reviews. 2008;4
27. Senapati A, Gray RG, Middleton LJ, Harding J, Hills RK, Armitage NC, et al. PROSPER. Collaborative Group Colorectal Dis. 2013 Jul;15(7):858–68.

Morbidity Pattren in Patients of Ileostomy: An Observational Study
Rao Aftab Alam1, Pradeep Singhal2, Anurag Bijalwan3, Syed Altamash4
1Postgraduate Resident, 2Assistant Professor, 3Professor, 4Senior Resident, Department of General Surgery, Shri Guru Ram Rai Institute of Medical and Health Sciences
Abstract
Introduction: An ileostomy is an opening constructed between the small intestine and the abdominal wall usually by using distal ileum but sometimes more proximal small intestine. It is a lifesaving surgery that enables the individuals with co-morbidities to recover from the acute stress of a major surgery. An ileostomy may be permanent or temporary depending upon the reason for surgery. An ileostomy is associated with multiple morbidities.
Aims & Objectives: To study the morbidity in patients with ileostomy.
Material and Method: The present study was a prospective and descriptive study which was conducted on patients admitted in general surgery department of Shri Guru Ram Rai Institute of Medical and Health Sciences in patients who underwent ileostomy as a part of abdominal surgery.Total number of 50 patients were studied. The parameters studied were site of ileostomy, dermatitis, abdominal pain, stomal complications, odour, wound infection, nutritional status, anaemia, diarrhoea, electrolyte imbalance and psychological problems at 2wk, 1mth, 2mth, 3mth post-operative period.
Conclusion : The study shows significant morbidity like electrolyte abnormalities (52%), skin problems(32%), stoma diarrhoea(54%), psychosocial disturbances(50%) in first 2 week post surgery.It also shows that Typhoid and tubercular pathology is the commonest indication for loop ileostomy.It is of paramount importance that ileostomies are properly sited, improper siting may increase the incidence of dermatitis, leakage, foul odour and other complications.Whenever possible ileostomy should not be located too proximal to the terminal ileum, to avoid high output, electrolyte abnormalities and malnutrition.Despite of ileostomy, proper care of peristomal skin, nutritional status, taking food with high residue and proteins, electrolyte and fluid requirements of patients can be managed and can lead to near normal life style of patient.
Keywords: Ileostomy, Morbidity pattern, Electrolyte abnormalities, Skin complications, Stoma diarrhoea, psychological disturbances.
Introduction
An ileostomy is an opening constructed between the small intestine and the abdominal wall usually by using distal ileum but sometimes more proximal small
Corresponding Author :Dr. Rao Aftab Alam PG Resident, Dept. of General Surgery SGRRIM & HS Patelnagar Dehradun. E-Mail [email protected] No.- 7017971542
intestine. [1] It is a lifesaving surgery that enables the individuals with co-morbidities to recover from the acute stress of a major surgery. However, the surgical construction of an ileostomy must be precise because the content is liquid, high volume and corrosive to the peristomal skin.[2] Ileostomy is needed to be performed for many different disease and conditions such as abdominal surgery done for intestinal perforation with co-morbid conditions, ulcerative colitis, familial adenomatosis coli. [3] An ileostomy may be permanent or temporary depending upon the reason for surgery. There
DOI Number: 10.5958/2321-1024.2019.00024.2

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 60
are many types of ileostomy like end-ileostomy, loop ileostomy, loop-end ileostomy, continent ileostomy. [4] An ileostomy is associated with many morbidities. Due to the electrolyte rich and corrosive nature of ileostomy content, it is associated with multiple morbidities.
Materials and Method
The present study was a cross-sectional study which was conducted on patients admitted in general surgery department of Shri Guru Ram Rai Institute of Medical and Health Sciences in patients who underwent ileostomy as a part of abdominal surgery. Total number of 60 patients were studied. The study period was from October 2016 to march 2018. The source of data are patients with associated abdominal conditions admitted as in patients, in various surgical wards in Shri Mahant Indresh Hospital and Shri Guru Ram Rai Institute of Medical and Health Sciences, Dehradun who underwent laparotomy and ileostomy
Inclusion criteria: Patients who underwent ileostomy in general surgery department of SGRRIM & HS Dehradun and were willing to be a part of study after giving proper consent.
Exclusion criteria : Patients not willing to participate in the study. Patients who do not report for follow-up. In our study out of total 60 patients, 6 patients who did not turn up for follow up were excluded from the study and 4 patients who died in post-operative period (due to other co-morbid conditions like cardiac or other systemic pathologies) were also excluded from the study, hence they were excluded from the study.
Table 1: Distribution of cases on type of stoma created, indication of stoma, disease etiology and intraoperative findings.
Parameter No. (%)
Types of stoma
Loop ileostomy 39 (78)
Double barrel ileostomy09 (18)
End ileostomy 02 (4)
Indication of stoma
Perforation 26 (32)
Obstruction 14 (28)
Blunt trauma abdomen (gangrenous bowel) 04 (8)
Strangulated hernia 02 (4)
Ca colon 01 (2)
volvulus 01 (2)
Ca rectum (inoperable) 01 (2)
Faecal fistula due to R.A. leak 01 (2)
Etiology/HPE
Enteric perforation 18 (36)
Tubercular 12 (24)
Appendicular abscess 02 (4)
Non-specific inflammation 16 (32)
Malignancy 02 (4)
Intra-operative findings
Ileal perforation 16 (32)
Gangrenous gut 08 (16)
Adhesions 08 (16)
Inflammatory lump 04 (8)
Strictures’ 04 (8)
Other’s 10 (20)
Table 2: Distribution of cases with hypoalbuminemia in relation to distance of stoma from i-c junction
Distance from i-c junction
Cases No. (%)
Hypoalbuminemia (<3.5 mg/dl) (%)
<1 feet 05 (10) 01 (2)
2-3 feet 30 (60) 07 (14)
>3 feet 15 (30) 12 (24)
Cont... Table 1: Distribution of cases on type of stoma created, indication of stoma, disease etiology and intraoperative findings.

61 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
Table 3: Distribution of complications according to duration of follow up visits.
Complications/ condition Duration of follow up
N= 502 weekNo.(%)
1 monthNo.(%)
2 monthNo.(%)
3 monthNo.(%)
Electrolyte abnormality
Hyponatremia 16 (32) 12 (24) 02 (04)
Hypokalemia 5 (10) 5 (10) 01 (02)
Hypocalcaemia10 (20) 4 (08) 0 (0)
Dermatitis/skin ailments
Irritation 08 (16) 08 (16) 05 (10) 1 (2)
Parastomal site Itching 06 (12) 4 (8) 1 (2) 0 (0)
Necrosis 0 (0) 01 (2) 0 (0) 0 (0)
Excoriation 02 (4) 0 (0) 0 (0) 0 (0)
Stoma Diarrhorea
With Flatulent dyspepsia 16 (32) 3 (6) 0 (0) 0 (0)
Without flatulent dyspepsia 11 (22) 01 (2) 0 (0) 0 (0)
Nutritional status (albumin level)
Healthy (>3.5) mg/dl 45 (90) 30 (60) 35 (70) 0 (0)
Undernourished (<3.5) mg/dl 05 (10) 20 (40) 15 (30) 0 (0)
Malnourished (<2) mg/dl 0 (0) 0 (0) 0 (0) 0 (0)
Anemia
Hb level <11(mild) 18 (36) 14 (28) 06 (12) 1 (2)
Hb level 8-10(moderate) 12 (24) 11 (22) 4 (8) 1 (2)
Hb level <8(severe) 5 (10) 03 (06) 1 (2) 0 (0)
Psychological problems
Insomnia 06 (12) 02 (4) 01 (2) 0 (0)
Depression 18 (36) 15 (30) 08 (16) 2 (4)
Poor social acceptance 1 (2) 0 (0) 0 (0) 0 (0)
Stomal complications
Retraction 02 (4) 02 (4) 02 (4) 2 (4)
In our study out of total 50 patients only 2 patients i.e. 4% suffered stoma retraction. Both cases were managed by refashioning of stoma
Discusion
In our study electrolyte imbalance is more in first month post-op. 26 patients (52%) in first 2 weeks and 17 patients (34%) in first month suffer hyponatremia

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 62
and hypokalemia. 20% suffer hypocalcemia in 2 weeks and 8% in 1 month. Hyponatremia was more prevalent i.e.21 patients (42%) then hypocalcemia and hypokalemia. Electrolyte imbalance shows improving trend as time progresses most likely due to improved diet and physiological adaptations of body. According to review of literature[5] electrolyte imbalance occurred in 0.8 to 16.7 % cases but in our study it occurred in 52% cases, it may be largely due to high incidence of emergency laparotomy patients in our set-up as most of these patients were in shock and dehydrated with poor nutritional status. They were presented in hospital quite late post bowel injury/bowel disease. Shellito PC et al
[6] stated in their study that electrolyte imbalance is more during 3rd to 8th post-op day but in our study it was found immediately from post-op day one to 2-4 week and it was also largely attributed to emergency laparotomies and condition of dehydration and shock at time of presentation in our hospital.
Others studies[7,8] said that skin complication occur in 18% to 55 % cases, this large number in their study was more attributed to poor siting of stoma, difficult to fit stomas & frequent appliance change but in our study it was not mechanical but chemical dermatitis due to high output/effluent and acidic nature of stoma output. The decreasing trend of skin complications in our study as time progress post-ileostomy is largely due to better ileostomy care provided both by stoma therapist and trained medical/paramedical staff who regularly counsel and also trains family members about stoma care, change of ileostomy bag, how to use adhesives, zinc paste and silver preparation ointments for peristomal skin care.
Fig-1 Ileostomy (skin necrosis)
Fig-2 Ileostomy (skin excoriation)
Some other studies[8] stated that stoma diarrhoea occurs in only 3.98% of cases, which may be due to the fact that author did not mention the time of observation in post-op period whereas our study was conducted on a regular basis and in post-op period gradual decline from 54% to zero percent in 2 months was observed. Large number of stomal diarrhorea in our study may be attributed largely to variation in dietary pattern. Patients were used to of taking more fluid and less roughage in their diet responsible for diarrhoea. Also as most of our cases were emergency laparotomy with patients presenting in dehydrated and electrolyte imbalance state. A recent study[8] suggested a wound infection rate of 9.21 %. In our study low stoma site infection may be attributed to proper pre-op siting of stoma by surgeons, classical surgical techniques adopted by surgeon and traditional spigot configuration adopted by them. Moreover, patient care and education provided to them regarding stoma bag changing and peristomal skin care is responsible for low stoma site infection. In our study out of total 50 patients only 2 patients i.e. 4% suffered stoma retraction(fig.3).
Chaudhary CR et al [9] stated retraction in 22 % cases.In our study a low stoma complication rate would be attributed largely due to classical surgical skills like proper pre-op siting of stoma, proper fixing of the ileostomy at sheath and skin, spigot configuration and proper stoma-care education to nursing staff and patient’s attendant
Fig – 3 Ileostomy retraction

63 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
In our study 25 patients have some psychosocial problem 18 patients i.e. 36% had depressive thought and distress and 12 % had insomnia in first 2 weeks, while 30 % (15 cases) were suffering from depressive thought and distress at 1 month and 4 % from insomnia at 1 month. A recent western study[10] stated stated that psychological distress is common in 21-70% cases. An indian study[11] stated psychological distress in 16 to 26 % cases. Liao & Qin et al [12] stated that individual with stoma have to cope with sensitive issues such as loss of control over their elimination of faeces, they also may experience changes to body image, sexual function, social isolation, stigma, embarrassment and decreased mood. In our study psychiatric disturbances are also high but low in comparison to western studies. It is largely due to proper emotional support to patient and his attendant by our team of medical and paramedical staff, education of stoma-care and access to stoma-therapist. It was observed that in our Indian set-up, due to financial constraints and lack of awareness people tend to suffer from depression and other psychosocial problems but also they are habitual of hardships and receive better family support, so less likelihood of psychiatric disturbances than their western counterparts.A good social and emotional support by the patient’s families and stable social environment may also be responsible for the lower number of affected patients than in western countries
In our study 05 patients suffer from hypoalbuminemia at 2 weeks i.e. 10% but at 1 month 20 patient i.e. 40% and at 2 months 15 patient i.e. 30% were suffering from hypoalbuminemia, but condition shows a bell-shaped curve and again improve at third month with no case featuring hypoalbuminemia
BELL- shaped curve in hypoalbuminemia
Distance of I-C junction from ileostomy and relation with hypoalbuminemia
Total 35 patients, had their ileostomy within 3 feet from ileocaecal junction. Only 8 (22.9%) cases, out of
35 developed hypoalbuminemia whereas, it was seen in 12 patients (80%) out of 15, who had their ileostomies at more than 3 feet from ileocaecal junction. This may be attributed to less absorptive surface area of ileum being available and increased absorption of nutrients towards terminal ileum. Previous similar studies by other researchers have not commented upon nutritional status in relation to distance from ileocaecal junction.
In our study 18 cases present with mild anaemia (Hb<11gm/dl) and only 5 cases (10%) present with moderate anaemia (Hb 8-10 gm/dl) during first 2 weeks in post-op period. Kennedy H.J. et al [13] said that 38% cases show mild anaemia, this discrepancy arises as in their study most cases were due to ulcerative colitis and crohn’s disease and absorption of vit-B12 was hampered but in our setup as emergency surgeries are more, malnourishment is the most likely cause which got improved in 2-3 week post-operatively when the patients started taking a balanced nutritious diet and absorption gradually improved.
Conclusion
This cross sectional study was conducted in Dept. of General surgery, Shri Mahant Indiresh Hospital & Shri Guru Ram Rai Institute of Medical and Health Sciences, Patel nagar, Dehradun from October 2016 to march 2018. Total 50 patients who underwent ileostomy in this institute was studied for morbidity in a patient of ileostomy in a 3 month follow-up period. Findings are shown in the table
Our study shows significant morbidity like electrolyte abnormalities (52%), skin problems (32%), stoma diarrhoea (54%), psychosocial disturbances (50%) in first 2 weeks post-surgery.
It also shows that:
Typhoid and tubercular pathology is the commonest indication for loop ileostomy
There is an increasing trend of performing ileostomy in emergency situations, although being bothersome, ileostomy is still a life-saving procedure.
It is of paramount importance that ileostomies are properly sited, improper siting may increase the incidence of dermatitis, leakage, foul odour and other complications.

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 64
Early referral to tertiary hospital, early diagnosis, proper pre-op management like I.V. fluids, antibiotics, early detection and prevention of hypotension, reduction of time consumption for emergency laparotomy, close post-operative monitoring reduces the morbidity in a patient of ileostomy.
Despite of ileostomy, proper care of peristomal skin, nutritional status, taking food with high residue and proteins, electrolyte and fluid requirements of patients can be managed and can lead to near normal life style of patient.
Whenever possible ileostomy should not be located too proximal to the terminal ileum, to avoid high output, electrolyte abnormalities and malnutrition.
A proper siting of the stoma, better pre and post-operative care and patient education about diet and stomal care can significantly reduce the physiological and psychological effects of ileostomy
Patient should also be given mental and emotional support to keep him mentally healthy.
This information reinforces earlier studies and suggests interventions that will improve care and quality of life for individuals living with an ileostomy.
Funding : No funding sources
Conflict of Interest : None Declared
Ethical Approval : The study was approved by the institutional ethics committee
References
1. Irving MH, Hulme O. Intestinal stomas. Br Med J 1992; 304: 1679-81
2. Shirley F, Kodner IJ, Fry RD. Loop ileostomy: techniques and indications. Dis_Colon Rectum. 1984;27:382
3. Burch J. _e pre- and postoperative nursing care for patients with a stoma.
4. Br J Nurs. 2005;14(6):310–318
5. Crile G Jr, Turnbull RB Jr. Mechanism and prevention of ileostomy dysfunction. Ann Surg. 1954;140:459
6. Formijne Jonkers H A, Draaisma W A, Roskott A M, van Overbeeke A J, Broeders I A, Consten E C. Early complications after stoma formation: a prospective cohort study in 100 patients with 1-year follow-up. Int J Colorectal Dis. 2012;27(8):1095–1099.
7. Shellito PC: Complications of Abdominal stoma surgery. Dis Colon Rectum 41:1562-1572, 1998
8. Arumugam P J, Bevan L, Macdonald L. et al. A prospective audit of stomas—analysis of risk factors and complications and their management. Colorectal Dis. 2003;5(1):49–52.
9. Ahmad Z etal. Int J Res Med Sci.2013 NOV; 1(4) : 536-540
10. Choudhury CR et al. Int Surg J. 2018 Oct;5(10):3265-3272
11. Colorectal Dis.2010 July ; 12(7 online) : e88-92. doi : 10.1111/J 1463-1318
12. BMC Res Notes.2016 Dec 5; 9(1) :500
13. LIAO & QIN IJN sciences 1(2) June 2014 doi:10.1016/J.IJnss
14. Kennedy HJ, Al-Dujaili EA, Edwards CR, et al. Water and electrolyte balance in subjects with a permanent ileostomy. Gut 1983;24(8):702-5.

Comparative Study of Chemical Sphincterotomy and Lateral Internal Sphincterotomy for Chronic Anal Fissure
Nitesh Kumar1, Deepak Pankaj1, Nitesh2, Ashwini Kumar2, Monika Raj3
1Assistant Professor, 2Senior Resident, 3Intern, Department of General Surgery IGIMS, Patna
Abstract
Introduction : Fissure-in-ano is a very common problem which causes considerable morbidity and affects the patient’s quality of life to a great extent. This warrants prompt treatment of the condition with appropriate methods. In this study, we assess and compare the efficacy and adverse effects of topical application of 2% Diltiazem gel with that of Lateral internal sphincterotomy.
Method: 100 patients with chronic fissure in ano were divided into Diltiazem gel and Lateral internal sphincterotomy groups and followed up at regular intervals for symptomatic relief and healing.
Results: Fissure was completely healed in 42 (89.36%) out of 47 patients by 8 weeks in the Diltiazem group, 3 patients experienced mild headache , 2 local irritation, 13 patients were pain-free at the end of 4 weeks, 26 patients were 8 weeks and 3 patients by 14 weeks. 5 patients were not relieved of pain at the end of 14 weeks. Completely healed in 48 (100%) out of 48 patients by 4 weeks in the Lateral Internal Sphincterotomy group.21 patients experienced post-operative pain and incontinence for flatus in 1 patient. 32 patients were pain-free by 4 weeks and all the patients were free of pain by 8 weeks.
Conclusion: The current study shows results in favour of lateral internal sphincterotomy with a healing rate of 100% with a faster pain-relief and minimal complications if performed by the experienced surgeon. However topical 2% diltiazem gel is an effective agent can be safely prescribed for patients having contraindications for surgery . With a healing rate close to 90%, topical 2% Diltiazem therapy can be advised as the first line of treatment for the treatment of chronic anal fissure.
Keywords: Anal Fissure; Diltiazem; Internal Sphincterotomy
Corresponding authorDr. Nitesh Kumar, Assistant Professor, Department of General Surgery IGIMS, Patna, Mobile no. 9971060788, Email id- [email protected]
Introduction
Anal fissure, a common disease was first described by Recamier2 in 1829. It is a vertically ulceration in the squamous lining of the anal canal between the pectinate line and anal verge and associated with pain on defecation, bleeding per anum and anal sphincter spasm. All age groups particularly in young and adults can affect but shows no sex preponderance. Most of the
anal fissures are acute, resolving spontaneously or with increased dietary fibres intake and stool softeners where appropriate. Those lesions which fail to heal despite lifestyle modifications and persist beyond six weeks are designated as Chronic anal fissures. It is usually deeper and has exposed internal sphincter fibers in its base. It is frequently associated with a hypertrophic anal papilla at its upper aspect and with a Sentinel pile at its distal aspect. Painful fissures are generally associated with spasm of the internal sphincter.
Surgical techniques like manual anal dilatation or lateral internal sphincterotomy, effectively heal most fissures within a few weeks, but may result in permanently impaired anal continence. ‘Chemical Sphincterotomy’ (Topical nitroglycerine ointment,
DOI Number: 10.5958/2321-1024.2019.00025.4

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 66
Topical calcium channel blockers and Topical 2% diltiazem gel) are being investigated and used as the first line of treatment for chronic anal fissure.
Objectives of the Study
1. To assess and compare the efficacy and adverse effects of topical application of 2% Diltiazem gel with that of Lateral internal sphincterotomy in patients diagnosed with chronic anal fissure.
2. To compare the complications associated with both the modalities of treatment.
3. To decide on the better treatment for chronic anal fissure based on the findings of the study,
Methodology
The material for the study is taken from the cases attending the surgery OPD of all the units of the Department of General Surgery, IGIMS Patma, who are diagnosed to have chronic analfissure.
This study includes 100 patients presenting with chronic anal fissure from April 2016 to October 2017. These patients are randomly selected and classified into two groups each consisting of 50 patients.
Group A: 50 patients who are subjected to chemical sphincterotomy using topical application of 2% Diltiazem gel.
Group B: 50 patients who are subjected to Lateral Internal Sphincterotomy.
Both the groups are advised plenty of oral fluids, high fibre diet, laxatives and seitz bath. Follow-up of the patients is done by history and per-rectal examination to assess the efficacy of the treatment and the complications like pain, bleeding, sphincter spasm, discharge per anum and incontinence.
Inclusion Criteria:
All with complaints of painful passage of stool, with or without bleeding of more than 6 weeks duration, diagnosed to be having chronic anal fissure based on the history and on clinical examination.
Exclusion Criteria
a. Tuberculosis
b. Haemorrhoids
c. Ano rectal abscesses
d. Anal malignancies
e. Immunocompromised patients
f. Previous history of faecal incontinence or anal stenosis
g. Patients who have undergone previous anal surgeries
Follow up: Patients are followed up at 2,4,6,8,14 weeks and 6 months. During each visit enquiries are made regarding the expected complications using a questionnaire. Patients are also examined. Results of the follow-up are tabulated and analysed.
Method of application of 2% Diltiazem gel: Informed consent from the patient was taken prior to the study. Patients were advised to apply 1.5 to 2 cms length of gel thrice daily at least 1.5 cm into the anus.
Figure 1: Lateral Internal Sphincterotomy- Closed method
Figure 2: Lateral Internal Sphincterotomy- Open method

67 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
Results
Table 1: Age and Sex
Age group (years)Males Females Total
No. % No. % No. %
11-20 06 11.1 03 6.5 9 9
21-30 20 37 16 34.8 36 36
31-40 19 35.2 12 26 31 31
41-50 05 9.3 10 21.8 15 15
51-60 04 7.4 05 10.9 9 9
Total 54 100 46 100 100 100
Table 2: Symptomatology of Chronic anal fissure
SymptomsMales Females Total
No. % No. % No. %
Pain 50 100 50 100 100 100
Bleeding 41 82 35 70 76 76
Discharge 06 12 03 06 09 09
Constipation 39 78 43 86 82 82
Pruritus 04 08 08 16 12 12
Table 3: Site of Fissure-in-ano
Sex Site Number of patients Percentage
Males
Anterior 01 1.9
Posterior 52 96.2
Both 01 1.9
Females
Anterior 05 10.9
Posterior 40 86.9
Both 01 2.2

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 68
Presence of Sentinel pile: Out of the 100 patients in our study, Sentinel pile was present in 78% of the patients.
Figure3 : Chronic anal fissure
Figure 4: Healed Anal Fissure

69 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
Table 4: Duration for healing and postoperative findings in Diltiazem and LIS Group
Pain relief
Diltiazem group LIS group
No. % No. %
At the end of 4 Weeks 13 27.7 32 66.7
At the end of 8 Weeks 26 55.3 16 33.3
At the end of 14 Weeks 03 6.4 - -
No relief 05 10.6 - -
The p value from above table is <0.001 which is heighly significant
Table 5: Healing
Healing No. of patients Percentage
Diltiazem group 42 89.36
LIS group 48 100
The p value from the above table is 0.02 which is significant
Loss of follow-up: A total of 5 patients were lost to follow-up at various stages of the study, 3 from the Diltiazem-group and 2 from the LIS group.
Complications
Table 6: Complications in Diltiazem group
Side effects Number of patients Percentage
Headache 03 6.4
Vertigo -- --
Local irritation 02 4.3
Table 7: Complications in LIS Group
Complications Number of patients Percentage
Post-operative pain 21 43.8
Bleeding -- --
Infection -- --
Incontinence 1 2.1

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 70
Recurrence: Recurrence was seen in 1(2.1%) patient in the Diltiazem group and none in the LIS group.
Discussion
Fissure-in-ano is a common problem the rationale of treating this condition lies in reducing the internal anal sphincter tone, relieving the spasm and thereby improving the circulation. Among surgical modalities, the gold standard procedure is lateral internal sphincterotomy. Chemical sphincterotomy, which is a medical line of treatment has now been accepted as the first line of treatment of chronic anal fissures at various centers.
In the present study, a comparative analysis of topical application of 2% diltiazem gel and lateral sphincterotomy has been done with regards to efficacy, adverse effects and complications in patients with chronic anal fissure. The current study included a total of 100 patients of chronic fissure in ano who presented to the surgery OPD at IGIMS Patna between April2016 to October 2017. The patients were randomly allocated into two groups of chemical (group A) and surgical (group B) sphincterotomy, comprising 50 patients each.
In the study the age group most affected was 21-30 years (36%) and least affected was 11-20 and 51-60 years (9%) as shown in Table -1. According to J.C. Goligher27 the disease is usually encountered in middle aged adults. In Udwadia T.E54 series maximum incidence was seen in 31-40 years age group.
There was only a slight male preponderance (54%) compared to females (46%) in our study shown in Table -1. It is similar to the study from Bennett and Goligher7 (1962) which says anal fissure is equally common in both sexes.
Painful defecation was the most common symptom (100%) followed by constipation and bleeding per anum in 82% and 76% of the patients respectively. Local pruritus was present in 12% and discharge per anum in 9% of the study group shown in Table -2.
The presence of posterior anal fissure was noted 96.2% (52 out of 54 patients) in males and 86.9% (40 out of 46 patients) in females. The posterior anal fissure was found to be 92% making it the most common site involved. Anterior anal fissure was noted in 1.9% of male and 10.9% of female patients. The incidence of
concomitant anterior and posterior fissure-in-ano is seen in 1.9% and 2.2% of males and females respectively shown in Table -3 . This is in conjunction with the study from Boulous55 which says posterior fissure (85.7%) is more common than anterior fissure (14.2%).
The sentinel pile which was present in 78% of the patients.
In group A, with 2% Diltiazem gel 42 (89.36%) fissures healed completely between 4-8 weeks, while 3 patients were lost to follow-up.
In group B, who underwent internal sphincterotomy, 48 (100%) patients healed completely at the end of 4 weeks and 2 patients were lost to follow-up shown in Table-5.
In the diltiazem group, 13(27.7%) patients were pain-free at the end of 4 weeks, 26 (55.3%) by 8 weeks and 3(6.4%) were pain free by 14 weeks. 5 patients (10.6%) were not relieved of pain even at the end of 14 weeks.shown in Table -5 Fissure was completely healed in 42 (89.36%) out of 47 patients by 8 weeks. Study conducted by Knight9 et al (2001) reported a healing rate of 89.4% after treatment with Diltiazem gel. U. K. Shrivastava15 (2007) reported a healing rate of 80% with Diltiazem gel in 12weeks.
Scouten W.R. et al33 reported pain relief in 98% of cases after undergoing internal sphincterotomy. Adriano Tocchhiet al56 (2004) reported a healing rate of 100% with internal sphincterotomy at the end of 6 weeks post-sphincterotomy review. Jensen et al have reported a healing rate of 100% and Evans et al and Wiley et al have reported healing rate of 97% with lateral internalsphincterotomy.
In our study, out of the 47 patients that were followed up in the Diltiazem group 3(6.2%) patients experienced mild headache and local irritation was present in 2(4.3%) patients shown in Table- 6. Study conducted by U. K. Shrivastava reports no side effects in patients treated with Diltiazem gel.15
In a study conducted by G. F. Nash et al47 112 patients were treated with 2% Diltiazem gel for 6 weeks and were followed up over 2 years. The success rate and satisfaction of topical Diltiazem were each over two thirds. Nearly 80% of patients reported no adverse effects.

71 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
Of the 48 patients that were followed up in the LIS group 21(43.8%) patients experienced post-operative pain and transient incontinence for flatus was present in 1(2.1%) patient. Adriano Tocchhi et al. report no long-term complication after internal sphincterotomy and patient satisfaction was96%.56
Recurrence was seen in 1(2.1%) patient in the Diltiazem group and none in the LIS group. Comparison between Diltiazem gel therapy and internal sphincterotomy showed a difference in pain relief (P<0.001) and fissure healing (P= 0.02) which is statistically significant.
The follow up period after treatment with Diltiazem gel was short and therefore no long-term conclusions can be drawn. Long term follow up is needed to assess the risk of recurrence after initial healing with Diltiazem gel therapy.
Conclussion
The current study shows results in favour of lateral internal sphincterotomy with a healing rate of 100% with faster pain-relief and minimal or no complications.
Topical 2% diltiazem gel is an effective agent in the treatment of chronic fissure-in-ano. Though there is latency in the clearance of symptoms and lesions when compared to surgical sphincterotomy, this has shown minimal and insignificant adverse effect. Topical diltiazem can be safely prescribed for patients who are unfit or unwilling for surgery. Healing rate is slower compared to surgery but the need for hospital stay is abolished and it reduces the psychological and financial burden on the patient. With a healing rate close to 90%, topical 2% Diltiazem therapy can be advised as the first line treatment of chronic anal fissure.
By comparing the above two modalities of treatment for chronic anal fissure, we conclude that Lateral internal sphincterotomy appears to be the better line of treatment as there is 100% healing rate.
Source of Funding: Self
Conflict of Interest: None
Ethical Clearance: Taken
References
1. Carapeti EA, Kamm MA, Phillips RKS. Topical
diltiazem and bethanechol decrease anal sphincter pressure and heal anal fissures without side effects. Dis Colon Rectum. 1999: 45; 719-22.
2. Jone OM, Bradig AF, Mortensons. The physiology, pharmacology and therapeutic manipulation of the internal anal sphincter. Can J Gastrenterology. 2002; 16: 249-57.
3. Aziz A, Sheikh L, et al. Lateral subcutaneous internal sphincterotomy in chronic anal fissure. Pakistan Journal of Surgery. 2009; 26: 92-94.
4. Knight JS, Birks M, Farouk R. Topical diltiazem ointment in the treatment of chronic anal fissure. Br J Surg. 2001; 88(4): 553-6.
5. Ward DI, Miller BJ, Schahe PJ, et al. The use of glyceryltrinitrate in the treatment of acute and chronic anal fissure. Aust N Z J Surg. 2000; 70: 19-21.
6. Leong APK. Pharmacological Treatment of Anal Fissure A Future Role in Primary Care. Singapore Med J. 2003;44(3):136-7.
7. Bhardwaj R, Vaizey CJ, Bulos PB, et al. Neuromyogenic properties of the internal anal sphincter: therapeutic rationale for anal fissures. Gut2000;46:861-8.
8. Marion Jonas, William Speake, John H. Scholefield, Diltiazem heals Glyceryltrinitrate resistant chronic anal fissures: a prospective study. Diseases of the colon and Rectum. 2002; 45 (8):1091-1095.
9. Jonas Marion, Scholefield J.H., Anal fissure and chemical sphincterotomy. Taylor I. Johnson C.D., Recent advances in Surgery. Churchill Livingstone, 24th Edition, 2001: 115.
10. Bannister H.L., Muscle System, Soames R. Gray’s Anatomy, Churchill Livingstone, Harcourt Publishers, 2007:737.
11. Kodner IJ, Fry RD, Fleshman JW, Birnbaum EH, Read TE. Colon, Rectum and Anus. In: Schwartz Seymour I, et al. Principles of Surgery. 7th ed. Mac Grow- Hill: 1999. p. 1265-1382.
12. Charles Orsay, Jan Rakinic, Brian Perry W, et al. Practice Parameters for the Management of Anal Fissures (Revised). Dis Colon rectum2004;47:2003-7.
13. Peter J. Lunniss, The anus and anal canal, Norman S. Williams, Christopher J.K. Bulstrode& P. Roman

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 72
O’Connell. Bailey & Love’s Short Practice of Surgery, Hodder Arnold, 25th edition, 2008: 1251-1253.
14. Collins EE, Lund JN. A review of chronic anal fissure management. Techniques in Coloproctology Vol.11, No.3, 2007:209-223.
15. Marion Jones Jolm R. Scholefield. Anal fissure and chemicalsphincterotomy. Recent Advances in Surgery 2001; 24.
16. Michael E, Friscia MD and Robert D. Anal pain: office diagnosis and treatment. 2008; 48:1-3.
17. Harry T. Papa Constantinou, Philip Huber, Jr., & Clifford L. Simmang, Fissure-in ano, Charles J. Yea, Daniel T. Dempsey, Andrew S. Klein, John H. Pemberton, Jeffrey H. Peters. Shackelford’s Surgery of the Alimentary Tract, Elsevier, 6thedition, 2007:2038-2044.
18. R. Bhardwaj, M. C. Parker, Modern perspectives in the treatment of chronic anal fissures. Annals of the Royal College of Surgeons of England. 2007; 89 (5): 472- 478.
19. Z. Haq, M. Rahman, R. A. Chowdhury, M. A. Baten, M. Khatun, Chemical sphincterotomy – first line of treatment for chronic anal fissure. Mymensingh Medical Journal.2005;14(1):88-90.
20. K. Bielecki, M. Kolodziejczak, A prospective randomized trial of Diltiazem and Glyceryltrinitrate ointment in the treatment of chronic anal fissure. Colorectal disease the official journal of the Association of Coloproctology of Great Britain and Ireland. 2003; 5(3):256-257.
21. M. S. Sajid, J. Rimple, E. Cheek, M. K. Baig, The efficacy of Diltiazem and glyceryltrinitrate for the medical management of chronic anal fissure: a meta- analysis. International Journal of Colorectal Disease. 2008; 23(1):1-6.
22. Griffin N, Acheson AG, Jonas M, et al. The role of topical diltiazem in the treatment of chronic anal fissures that have failed glyceryltrinitrate therapy. Colorectal Dis 2002 Nov;4(6):430-5.
23. G. F. Nash, K. Kapoor, K. Saeb-Parsy, T. Kunanadam, P. M. Dawson, The long term results of Diltiazem treatment for anal fissure. International Journal of Clinical Practice. 2006; 60(11):1411-1413.
24. Eveline B. Boeker, M. J. P. Marjan Kruijer, Paul C. M. Verbeek, Treatment of chronic anal fissures: Diltiazem or Isosorbidedinitrate as first choice? Nedherlands Tijdschrift Voor Geneeskunde. 2011;155:A2594.
25. A. M. Saad, A. Omer, Surgical treatment of chronic fissure in ano: a prospective randomized study. East African Medical Journal. 1992; 69(11):613-615.
26. P.B. and Araujo J.G.C.34 (1984) Boulos P. B., Araujo J. G. C., Adequate internal sphincterotomy for chronic anal fissure: subcutaneous or open technique? British Journal of Surgery. 1984; 71 (5):360-362.
27. Wiley M, Day P, Rieger N, Stephens J, Moore J. Open vs. closed lateral internal sphincterotomy for idiopathic fissurein- ano: a prospective, randomized, controlled trial. Dis Colon Rectum 2004; 47:847-852.

Comparative Study of Lateral Internal Sphincterotomy vs Glyceryl Trinitrate Ointment for Fissure in Ano
Ravichandran Subramaniam
Associate Professor, Department of General Surgery, Melmaruvathur Adhi Parasakthi Institute of Medical Sciences And Research, Melmaruvathur, Tamil Nadu
Abstract
Aim: To compare and find out the effectiveness of lateral internal sphincterotomy as well as glyceryl trinitrate in the treatment of anal fissure.
Materials & Method : A prospective study of 100 patients at the surgery department of a medical college and tertiary health care centre, over a period of 6 months that included cases of fissure in ano in the age group of 18 yrs and 70 years. They were randomly assigned to two different groups. One for surgery and the other for medical management with GTN.Each group had 50 patients in it .
Results: The pain relief of the patients after the surgical operation was fast and very satisfactory. On follow up at 2 weeks post operatively, pain and other symptoms were present in only 10patients (20 %) . Whereas the pain relief in medical management group was not fully satisfactory and it took more time.. and it was only temporary and how ever on follow up at 2 weeks, 15 patients came with recurrent pain and other symptoms.( 30% ). On follow up at 8 weeks , in both groups ,all the 100 patients were symptoms free (100%) in this study. The complications that were observed during this study were soiling in 5 patients (10 %) and incontinence to flatus in 2 patients (4%) in the surgical group and headache in 10 patients ( 20% ) and peri anal itching in 4 patients (8% ) in the medical management group.. how ever there was no recurrence of anal fissure observed in this study group.
Conclusion: From the above study, it is proved that lateral internal sphincterotomy is by far the best operation for pain relief and rapid cure for fissure in ano
Keywords : Fissure in ano, lateral sphincterotomy, chemical sphincterotomy, glyceryl trinitrate.
Introduction
Perianal pain forms large volume of patients in any surgical OPD. Fissure in ano is a common surgical problem . It causes a lot of pain. It cases loss of many functioning man – hours. Anal fissure is an ulcer in the long axis of lower anal canal.
Young individuals of both sexes are equally affected. Patient present with severe anal pain during defection and / or rectal bleeding. Chronicity of a fissure relates to duration of greater than 6 weeks.
Most fissures occur in the posterior midline, this my be anatomically related as there is a lack of tissue support posteriorly within the anal canal. Fissures associated with pregnancy are commonly located anteriorly. Other causes of fissures include crohn’s disease, syphilis, human immune – deficiency virus. (HIV) or tuberculosis. These are secondary fissures.
The exact aetiology of primary anal fissure is unknown. High resting anal pressure and reduced vascular perfusion at the base caused by increased internal sphincter tone appears to be the underlying pathological factor.
We manage large number of patients of anal fissure. Many patients are fearing for surgery and want to try newly emerging non surgical procedures.. like GTN
Corresponding author:Ravichandran SubramaniamE-mail: [email protected]
DOI Number: 10.5958/2321-1024.2019.00026.6

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 74
ointment and calcium channel blockers and botulinum injection .
Materials and Method
Inclusion Criteria
Study was carried out on patients aged 18 yrs and above, who were diagnosed clinically as anal fissure and attended the surgery outpatient clinic.
Exclusion Criteria
Age less than 18 yrs
Important secondary changes in the anal fissure such as cicatricial deformation, large sentinel pile and subfissural infiltration.
Any previous anal surgery
Patient with systemic diseases (Diabetes Mellitus, chronic liver disease and collagen vascular diseases)
Patients under treatment with diltiazem or nitroglycerine for other diseases such as ischemic heart diseases.
Pregnant women were also excluded from the study.
Study of anal fissure associated with other local diseases such as internal piles, fistula and with diseases like inflammatory bowel disease and rectal cance.
Methodology
The study was carried out as a prospective observational study of 100 patients at surgery department of a medical college and tertiary health care centre, over a period of 6 months that included cases of anal fissure in the age group of 18 yrs and above for conservative and surgical management. In this study the case definition of anal fissure was:
Evidence of posterior circumscribed ulcer with a large sentinel tag of skin.
Induration at the edges
Exposure of horizontal fibres of the internal anal sphincter (IAS)
Symptoms such as : post defecatory or nocturnal pain, bleeding or both and pruritus ani lasting for more than 2 months and constipation
Each patient in the study was informed in detail about the aim of the study and the type of the procedure.
A fully informed written consent was obtained from him / her prior to the study.
Appropriate ethical committee approval was taken.
All patients subjected to lateral internal sphincterotomy were treated by the same surgeons using uniform method of lateral sphincterotomy in the lithotomy position. (surgical procedure is mentioned later)
All patients received stool softeners, daily sitz bath and fibre supplement diet.
All the patient were followed up at 2 weeks interval for 8 weeks. In each follow up visit, the patients were evaluated for the criteria mentioned later.
All the patients were informed to report SOS in case of any side effects or adverse effects.
All patients were followed up for three months for evidence of recurrence of the fissure and the presence of possible side effects.
The complications of surgery in relation to incontinence & recurrence were observed only within the time frame of this study. The other post operative complications e.g. soilage, pain, bleeding were studied.
All patients who underwent surgery received spinal or general anaesthesia
Operative procedure (Lateral Internal Anal Sphincterotomy)
This procedure was carried out under spinal anaesthesia or general anaesthesia in all the patients. Once in lithotomy position, 5ml of 2 % lignocaine + adrenaline was injected at the proposed site of incision at either 3 or 9’o clock position in the intersphincteric plane. This facilitated bloodless dissection. A transverse incision was made at 3 or 9’o clock position and blunt dissection was carried out in the plane between internal and external sphincters. The internal sphincter was dissected away from anal mucosa. Once free in both planes, the sphincter was grasped between two haemostats and was brought on to the surface of wound. The haemostats were kept for 30 seconds and lower half of sphincter (approximately 1cm) was divided with

75 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
the help of scissors. The wound was left open and a small wick was placed to control oozing. The dressing was removed on first post operative day after sitz bath. Patients were discharged on second post operative day with advice to have sitz bath for next two weeks.
Results
Patients between the age of 31 to 40 yrs (47.5 %) were affected commonly by anal fissure. The overall incidence of posterior anal fissure in all age groups was as follow: 60 male (60%) and 40 female (40%) patients.
Pain was the commonest symptom observed (100%) in all the patients. Bleeding was associated in 80% of patients. 70% of patients complained constipation and 50 % complained of pruritus –ani.
Local examination revealed posterior circumscribed ulcer and induration in all the patients (100%) followed by sentinel (skin) tag in 60%.
The recovery of the patient after the operation was fast and the pain relief was dramatic. , When compared with medically managed group
. In follow up at 2 weeks post operatively pain and other symptoms were present only in 14 patients (28 %). On follow up at 8 weeks post operatively all 100 patients (100%) were symptom free in this study.
The fissure healing after lateral internal sphincterotomy was very fast with 85 % fissure healing (43 patients) with in 4 weeks post operatively and
97.5% fissure healing 49 patients at 8 weeks post operatively.
The defects of continence were minimal after lateral internal sphincterotomy. Soiling of undergarments was seen in 5 patients (10%) and incontinence to flatus was seen in 2 patients (4 %).
Discussion
The Anal fissure is an ulcer in the skin lined part of the anal canal. It occurs most frequently in young adults and affects both sexes equally9. The great majority of fissures occur in the posterior midline, although anterior midline fissures are seen in 25% if affected women and 8 % if affected men 1. About 3% of patients have both anterior and posterior fissures.
Anal fissure is probably secondary to over stretching of the anoderm during the passage of a large or hard stool2, 10. W.E. Miles had postulated the passage of a scybalum over that part of the anal canal, which was relatively immobile, i.e. the part situated over the so called pectin Band, developed as a result of constipation, just above Hilton’s line.
In our study we found that average age incidence was 39 yrs and the patients in the age of 31-40 yrs were the commonest sufferers. Anal fissure produces pain out of proportion to its size and thus causes much discomfort.
Out of 100 patients studies 60 were males (60%) and 40 were female (40%) patients. Posterior fissure was the inclusion criteria of this study. James G. Petros et al 13have found that chronic fissures were equally common in males and females and that in both sexes most fissures were located posteriorly.
Pain was the most common symptom (100%), often associated with bleeding per rectally (80%) followed by constipation (70%) and pruritus ani (50%). While studying the clinical presentations of anal fissures James G. Petros et al 13have found that pain, bleeding and pruritus were the commonest symptoms. Patients who presented with bleeding were significantly younger than those without bleeding. In this study bleeding was most commonly seen in the age group of 31 to 40 yrs (48%).
The operative management of anal fissure was aimed to cause permanent functional changes in the internal sphincter, it has been shown that the resting tone of internal anal sphincter is higher in patients of chronic anal fissure. The computerized profiles of anal canal with the aid of manometry 3has shown that operative intervention significantly reduces the tone of internal anal sphincter, but still remains higher than normal making such persons prone to develop fissure. Xynos et al6 observed that increased anal sphincter activity was a major factor in anal fissure pathogenesis, and that successful internal sphincterotomy helps to heal fissure and improve the manometric performance of sphincter.
Chemical sphincterotomy is the technical term for application of Glyceryl trinitrate over the region.. Here it is used once in three hours for three to four days and to be continued accoordingly for a reasonable length of time.

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 76
Sphincterotomy was initiated with the idea of decreasing the spasm of pectin band which was shown to be nothing but internal sphincter, Notaras 7,11developed the technique of lateral subcutaneous sphincterotomy. It was simpler and quick procedure which produced a small wound. Postoperative wound infection were negligible.
The reduction in the symptoms occurred immediately after lateral sphincterotomy. On follow up at 2 weeks post operatively the symptoms of pain, bleeding and pruritus ani were present in 14 patients (28%) this number reduced significantly throughout the study period and on follow up at 8 weeks post operatively all the 100 patients (100%) were symptom free. Garcea ET all reported persistence of symptoms after conservative sphincterotomy in 11.9% with only 9.2% needing topical analgesia.
In this study complete healing of fissures occurred in 85% within 4 weeks post operatively and by the end of 8 weeks fissures healed in 98% patients. The average time taken for fissure healing after lateral internal sphincterotomy was 3 and half weeks in P.R. Hawley’s series18 and 3 weeks in Notaras’ series 11.
In our study the post operative complications that occurred were soiling of undergarments in 5(10%) patients and incontinence to flatus in 2(4%)..
Collopy and Ryan found that on the basis of fewer recurrences and less incontinence, sphincterotomy appeared superior to manual stretch 14,20.
Jensen suggested that lateral sphincterotomy was superior to manual stretch on the basis of fewer persistence / recurrent fissures19,20, the pain relief and minimal complications were the same as was the healing time.
Hoffman and goligher16,17 compared posterior sphincterotomy, lateral sphincterotomy and sphincter stretch and favoured lateral sphincterotomy.
There was no recurrence of anal fissure observed in this study group within the time frame of this study. According to reports, after lateral internal sphincterotomy, the long term results were excellent and the recurrence rate was low6,11,15.
Conclusion
From the above study it has been proved that a
simple ‘ Lateral internal sphincterotomy’ can cure the extremely painful chronic anal fissure., much better than the chemical sphincterotomy by GTN.
In patients not fit for surgery and in patients not willing for surgery, GTN may be considered.
Ethical Clearance: Taken from the Institute ethical committee
Source of Funding: Self
Conflict of Interest: Nil
References
1. Lund JN, scholefield JH. Aetiology and treatment of anal fissure. Br J surg 1996: 83;1335-44.
2. Goligher JC. Surgery of the Anus Rectum and colon, 4th ed, chapters 1 and 5.1980
3. Keck JO, Remond J, Coller, et al. Computer generated pro files of anal canal in fissure. Dept of colon and rectal surgery Lahey clinic, Massachusetts. Dis colon rectum 1995; 38: 72-9.
4. Nothmann BJ. Schuster MM. Internal anal sphincter derangement with anal fissures. Gastroenterology, 1974, 67,216-20
5. Hancock BD. The internal sphincter and anal fissure. Br J surg. 1977; 64: 92-5.
6. Xynos E, Chrysos E, et al. Anal manometry in patients with fissure in ano before and after internal sphincterotomy. Colorectal disease. 1993: 8(3): 125-8.
7. Notaras MJ. Fissure in ano – lateral subcutaneous sphincterotomy. 3rd ed. Todd IP(Ed) colon rectum and anus 354-60.
8. Garcea G, Sutton C, Mansoori S, Lioyed T, Thomas M, Results following conservative lateral sphincterotomy for the treatment of chronic anal fissures. Colorectal Dis. 2003;5: 311-4.
9. Schouten WR, Briel JW, Auwerda JJ, De Graaf EJ. Ischemic peture of anal fissure. Br J surg 1996; 83; 63-5.
10. Hughes ESR. Anal fissure. BMJ. 1970; 3: 673.
11. Notaras MJ. The treatment of anal fissure by lateral subcutaneous internal sphincterotomy a technique and results. Br J Surg. 1971; 58: 96-100.

77 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
12. Miles WE. Observations upon internal piles. Surg Gyn Obstet. 1919; 29; 497.
13. James GP, Eric B Rimm, Renne JR. Clinical presentation of chronic anal fissure. Dept of surgery, Harward school of public health Boston. American surgeon 1993; 59: 666-
14. Collopy B, Ryan P. Comparison of lateral sphincterotomy with anal dilation. Med J Australia. 1979; 2: 461-2
15. Abcarian HMD. Lateral internal sphincterotomy. A new technique for treatment of chronic fissure in ano SCNA. 1975; 55-143
16. Hoffman DC. Lateral subcutaneous sphincterotomy in treatment of anal fissure. Br. Med J. 1970; 3: 673-75.
17. Goligher JC. An evaluation of internal sphincterotomy and simple sphincter stretching in the treatment of anal fissure. Surg clin North Am. 42: 1299, 1965
18. Howley PR. Treatment of chronic anal fissure. A trial of methods. Br J surg. 1969; 56: 915 -8.
19. Jensen SL, Lund E, Neilsen OV, Tange G. Lateral subcutaneous sphincterotomy versus anal dilatation in the treatment of fissure in ano in out patients, a prospective randomized study. BMJ (Clin Res ED) 1984; 289: 528-30
20. Anorectal surgery – Jerome J Decosse, Ian P Todd. Clinical surgery international. 15: 1-8, 20-43,56-93.

Assessing Pressure Ulcer Knowledge of General and Orthopedic Surgical Residents Using the Pieper Pressure
Ulcer Knowledge Test
Sanjay Kumar Mishra1, Shafaq Mahmood2
1Assistant Professor, Department of Surgery, Saraswathi Institute of Medical Sciences, Hapur, India, 2Post-graduate Resident, Community Medicine, Health Services Academy, Islamabad
Abstract
Objective: To determine the knowledge of postgraduate and non-postgraduate general and orthopedic surgical residents regarding pressure ulcer (PU) prevention, staging and wound description.
Study Design: Cross sectional, descriptive survey.
Place and Duration of Study: Six major tertiary care hospitals in India, from Sep-2018 to Nov-2018.
Methodology: All consenting postgraduate and non-postgraduate general and orthopedic surgical residents were included in the study using convenience sampling. An adapted version of Pressure Ulcer Knowledge Test (PUKT) comprising of 47-true/false items was used as a research tool. For every correct response, 1 point was awarded. Whereas, an incorrect or NK response was scored as 0. All the data was entered and analyzed using SPSS version 21.
Results: A total of 126 trainees comprising 120 (95.23%) males and 6 (4.76%) females participated in the study. The average PUKT score obtained by the surgical residents was 30.2+3.7 (65.65%), thus indicating a “low” level of knowledge.
Conclusion: The current levels of knowledge regarding PU prevention among the surgical residents in our study was “low”. The authors recommend continuous education for PU prevention in a hospital care setting.
Keywords: pressure ulcers, pressure ulcer knowledge, surgical residents.
Corresponding author: Sanjay Kumar MishraAssistant Professor, Department of Surgery, Saraswathi Institute of Medical Sciences, Hapur, India. Email: [email protected]
Introduction
Pressure ulcers (PUs) are defined as localized injuries to the skin and/or underlying soft tissue, usually over a bony prominence or related to a medical device as a result of pressure and/or shear.1 An estimated 1.7 million people develop PUs each year.2 Worldwide, it has an incidence rate between 0.4% to 38% in hospital setting and 0 to 17% in nursing homes.3 The development of PUs is associated with a poor quality of life, imposing
a substantial psychological and social burden on patients and their families.4 Moreover, PUs have also been ranked as the third most expensive disorder owing to a prolonged hospitalization and costly treatment.3
In order to minimize the occurrence of PUs in vulnerable patients, preventive strategies in compliance with the international guidelines must be implemented at the right time.4 It has been established that prompt recognition, accurate staging and timely treatment of a PU can reduce the morbidity and mortality associated with this devastating disorder.5 Despite the availability of evidence-based and internationally accepted guidelines, various studies have highlighted an extreme knowledge deficit among healthcare professionals towards PUs prevention.2,6,7,8 Vanderwee et al assessed the adequacy
DOI Number: 10.5958/2321-1024.2019.00027.8

79 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
of PU prevention in a hospital care setting with only 10% of the patients receiving preventive treatment in accordance with the approved guidelines.9 Thus, to optimize the preventive care being practiced in the hospitals, a frequent evaluation of the knowledge and understanding of the healthcare professionals regarding PU management is recommended.
Various cognitive theories have established knowledge and education as the two most important factors influencing one’s behavior and practices. It has been postulated that in order to achieve adherence to the proposed guidelines, it is necessary to improve the knowledge and skills of the entire concerned disciplines.4 Till now, most of the studies have focused and assessed knowledge, attitude and skills about PU prevention among nurses and nursing students.2,10,11 Very little literature is available regarding this topic in general and orthopedic surgical residents, despite of the fact that they are predominantly involved in the management of the complications of PUs.7 We found only a few studies demonstrating limited PU knowledge among geriatric fellows, internal medicine residents and general physicians, however, surgical residents’ understanding of PU prevention and care still needs to be explored.6,7,8
In light of the above facts, we conducted this study with an objective to determine the knowledge of postgraduate and non-postgraduate general and orthopedic surgical residents regarding PU prevention, staging and wound description. To our knowledge, this is probably the first study being carried out in India targeting surgical trainees to see whether or not they are well-informed and proficient at the clinical practice guidelines about PUs. The findings of this study would be useful to get an accurate picture of the preventive PU care being provided in the Indian surgical and orthopedic units. Moreover, the conclusions drawn from this study would enable us to identify and fill the knowledge gaps through various educational incentive programs.
Materials and Method
A cross sectional descriptive survey was conducted at six tertiary care hospitals in India between Sep-2018 to Nov-2018. The study population comprised of all the postgraduate and non-postgraduate general and orthopedic surgical residents recruited from each hospital using the convenience sampling method. All eligible participants were approached during their free
time in their break rooms and the outline of the study was explained to them verbally by the researchers. An informed oral consent was taken from all the participants after explaining the study objectives. Confidentiality of participant’s information was maintained properly where the participant had the choice to refuse and withdraw from the interview. The study was approved by the Ethical review board of the hospital.
To measure the knowledge of surgical residents, an adapted version of Pressure Ulcer Knowledge Test (PUKT) was used. This tool was developed by Pieper and Mott in 1995 to examine the knowledge of healthcare staff on PU prevention.12 It comprises of 47-true/false items with 3 subscales: risk and prevention (33 items), pressure ulcer staging (7 items), and wound description (7 items). In the present study, one question regarding the assignment of a government committee to investigate PU risk was deleted from the original version as it did not relate with the current study conditions. For each of the remaining questions, participants had to choose one true response from among True (T), False (F), or I don’t know (NK) options. For every correct response, 1 point was awarded. Whereas, an incorrect or NK response was scored as 0. The maximum achievable score on the test was 46.
In the original study, participants with a score of 90% or above were considered to have an adequate level of knowledge.12 In our study, the range of scores was categorized as follows: <60%: very low; 60-69.99%: low; 70-79.99%: moderate; 80-89.99%: high and 90-100%: very high. All the data was entered and analyzed using SPSS version 21. For categorical variables, frequencies and proportions were calculated and for continuous variables, means and standard deviations were calculated. The descriptive analysis of data was presented in the form of tables and graphs. Respondents with missing data were omitted from specific analyses.
Results
A total of 126 trainees of general surgery and orthopedics participated in the study comprising 120 (95.23%) males and 6 (4.76%) females. Their age ranged from 28-32 years with a mean age of 28+2.3 years.
The average PUKT score obtained by the surgical residents was 30.2+3.7 (65.65%) with a range of 16-41, thus indicating a “low” level of knowledge regarding PU prevention (Table I).

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 80
When measured on sub-scales, 53% participants demonstrated a “moderate” level of knowledge (72.6%) about pressure ulcer staging. Whereas, the performance of the residents in providing a correct wound description was very poor with only 19.2% participants scoring “high” on this scale. Regarding risk assessment and PU prevention, a mean score of 31.3+4.1 was observed, thus exhibiting a “low” level of knowledge (68.04%) in this area. None of the participant was able to score >90% on any of the sub-scales (Fig 1).
A detailed assessment of resident’s knowledge for each item on PUKT revealed that the majority of the participants (58%-73%) considered massaging bony prominences, repositioning a bed-bound person every 3 hours and using heel protectors to relieve pressure as important measures of PU prevention. Although these techniques have now become obsolete. Similarly, only 32.5% surgical residents considered fitting a chair cushion beneficial to avoid the development of PU in a chair bound person. However, most participants (82.53%) correctly identified elevating the heels off the bed as a good measure to reduce pressure. Surgical residents scored high (>80% correct) in identifying immobility, incontinence, impaired nutrition, and altered level of consciousness as risk factors for PU development, maintaining an adequate dietary intake of proteins and calories during illness, keeping the skin dry and clean, and recognizing the role of educational programs in reducing the incidence of PU (Table II and III).
Table I: Summary of knowledge scores
Level of knowledge N %
Very low (<60%) 33 26.19
Low (60-69.99%) 57 45.23
Moderate (70-79.99%) 22 17.46
High (80-89.99%) 12 9.52
Very High (90-100%) 2 1.58
Table II: PUKT items answered correctly by >80% of the residents
Item N %
Risk factors for development of pressure ulcers are immobility, incontinence, impaired nutrition, and altered level of consciousness. (T)
101 80.15
All individuals should be assessed on admission to a hospital for risk of pressure ulcer development. (T)
103 81.17
Cornstarch, creams, transparent dressings, and hydrocolloid dressings do not protect against the effects of friction. (F)
106 84.12
An adequate dietary intake of protein and calories should be maintained during illness. (T)
119 94.44
The epidermis should remain clean and dry. (T) 126 100
A low-humidity environment may predispose a person to pressure ulcers. (T) 124 98.41
To minimize the skin’s exposure to moisture on incontinence, underpads should be used to absorb moisture. (T)
110 87.30
A good way to decrease pressure on the heels is to elevate them off the bed. (T) 104 82.53
Friction may occur when moving a person up in bed. (T) 102 80.95
Educational programs may reduce the incidence of pressure ulcers. (T) 126 100

81 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
Table III: PUKT items answered correctly by <50% of the residents
Item N %
It is important to massage bony prominences. (F) 18 14.28
Persons confined to bed should be repositioned every 3 hours. (F) 11 8.73
Heel protectors relieve pressure on the heels. (F) 13 10.31
Donut devices/ring cushions help to prevent pressure ulcers. (F) 20 15.87
In a side lying position, a person should be at a 30 degree angle with the bed unless inconsistent with the patient’s condition and other care needs that take priority. (T)
8 6.34
A person who cannot move him or herself should be repositioned every 2 hours while sitting in a chair. (F)
6 4.76
A pressure redistribution surface reduces tissue interface pressure below capillary closing pressure. (T) 39 30.95
A low Braden score is associated with increased pressure ulcer risk. (T) 28 22.22
Eschar is good for wound healing. (F) 45 35.71
Undermining is the destruction that occurs under the skin. (T) 54 42.85
Chair-bound persons should be fitted for a chair cushion. (T) 41 32.53
Figure 1
Discussion
The occurrence of PUs has become a universally validated indicator of quality of care in the hospital setting.2 Despite of the availability of appropriate guidelines and modern preventative technology, a high prevalence rate of PUs in Indian hospitals is an indicator of poor quality of preventive care being provided by the healthcare professionals.13 According to the literature, physicians and surgeons often neglect crucial matters related to wound recognition and PU care, considering
it as a “nursing issue”.6 This anecdotal assertion is common among the surgical residents too, which has resulted in an inadequately prepared team with a below average knowledge to deal with PUs.
In our study, the average PUKT score for general and orthopedic surgical residents was 65.65%, which is lower than the scores of general physicians (69%) and nurses (75.0%) reported in the literature.2,6 However, our results are consistent with the low scores of geriatric fellows (58+18%) reported from New York state.7

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 82
In a study by Levine et al, the authors designed a photograph based wound identification test to examine the knowledge of medical residents about PU staging. It was found that the residents faced most difficulty in identifying stage III ulcers and suspected deep tissue injury. Whereas, stage I and stage IV ulcers were correctly identified by majority of the participants. 6 Likewise, Odierna et al also reported somewhat similar results with more than half of the geriatric fellows identifying stage I and stage IV ulcers accurately.7 In our study as well, the percentage of times that surgical residents correctly identified PU stages was 72.21%.
Kohta et al in his cross sectional survey reported a moderate level of knowledge (78.6%) among social welfare professionals about PU prevention. In his study, the repositioning schedules and pressure reducing techniques were known by 100% of the care managers.1 On the other hand, only 67% of the geriatric fellows were aware of the role of pressure modifying surfaces in reducing the incidence of PUs.7 Similarly, in our study, majority were not able to answer questions related to pressure reduction and minimizing shearing force. This highlights a significant knowledge deficit among clinicians as compared to the social welfare workers, thus emphasizing a need for behavior specific educational campaigns targeting residents in various surgical and medical specialties.
It is important to understand that once developed, PUs rapidly progress to an advanced stage requiring an enormous amount of time and energy for their management. Moreover, the treatment of PUs is extremely costly placing a substantial financial burden on hospitals.14 Previous studies have shown that preventing PUs is 2.5 times cheaper than its treatment.15 In 2008, the Centers for Medicare and Medicaid Services (CMS) published guidelines related to hospital-acquired conditions (HACs). They reported PUs as the most frequently acquired HAC. Afterwards, they refused to bear any additional charges incurred for hospital acquired ulcers. This new policy led to an intensified effort on developing strategies and action plans aiming at reducing the incidence of PUs in hospitalized patients.16
In addition, the incidence of PUs in Indian surgical wards is considerably higher (12-66%) than the other long-term care facilities (2.2-23.9%).17 Current study reported an extreme lack of awareness prevailing among surgical residents about the recommended PU care.
Therefore, educating surgical and orthopedic residents on this topic is of immense significance. According to the latest CMS guidelines about PUs, documentation for wound identification and staging is required by the healthcare providers and physicians.6 Thus, in order to fulfill this task accurately, an extensive training program on risk assessment, prevention, and PU staging is required for the residents in all hospital care settings.
Few limitations of this study should be considered. Firstly, the study only determined the knowledge of surgical residents regarding PU prevention without assessing their attitude and practices which the authors plan to investigate in future. Secondly, although the sample size was small but it may represent surgical residents’ knowledge in other hospitals settings of India as well.
Conclusion
Through the results of this questionnaire survey, we concluded that the current levels of knowledge regarding PU prevention among the surgical residents was “low”. The authors recommend continuous education and practical training enabling the residents to intervene positively in the process to prevent and treat PUs. Moreover, specific curricular guidelines are required to improve the overall compliance with the international recommendations of PU prevention and care.
Conflict of Interest: None.
Funding Disclosure: None.
References
1. Kohta M, Kameda Y, Morita S. Knowledge and practice for pressure injury prevention among care managers in a home care setting: a cross-sectional study. Chronic wound care manag. res. 2017 Aug 9; 2017:4: p. 99-105.
2. Kaddourah B, Abu-Shaheen AK, Al-Tannir M. Knowledge and attitudes of health professionals towards pressure ulcers at a rehabilitation hospital: a cross-sectional study. BMC Nurs. 2016; 15(17).
3. Agrawal K, Chauhan N. Pressure ulcers: Back to the basics. Indian J Plast Surg. 2012; 45(244): p. 244-54.
4. Demarré L, Vanderwee K, Defloor T, Verhaeghe S, Schoonhoven L, Beeckman D. Pressure ulcers:

83 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
knowledge and attitude of nurses and nursing assistants in Belgian nursing homes. J Clin Nurs. 2012 May; 21(9-10): p. 1425-34.
5. Delmore B, Ayello E, Smart H, Sibbald R. Assessing Pressure Injury Knowledge Using the Pieper-Zulkowski Pressure Ulcer Knowledge Test. Adv Skin Wound Care. 2018 Sep; 31(9): p. 406-412.
6. Levine J, Ayello E, Zulkowski K, Fogel J. Pressure ulcer knowledge in medical residents: an opportunity for improvement. Adv Skin Wound Care. 2012 Mar; 25(3): p. 115-7.
7. Odierna E, Zeleznik J. Pressure ulcer education: a pilot study of the knowledge and clinical confidence of geriatric fellows. Adv Skin Wound Care 2003;16:26-30.
8. Suen W, Parker V, Harney L, Nevin S, Jansen J, Alexander L, et al. Internal medicine interns’ and residents’ pressure ulcer prevention and assessment attitudes and abilities: results of an exploratory study. Ostomy Wound Manage. 2012 Apr; 58(4): p. 28-35.
9. Vanderwee K, Defloor T, Beeckman D, Demarre L, Verhaeghe S, Van Durme T, et al. Assessing the adequacy of pressure ulcer prevention in hospitals: a nationwide prevalence survey. BMJ Qual Saf. 2011 Mar; 20(3): p. 260-7.
10. Ilesanmi R, Ofi B, Adejumo P. Nurses’ knowledge of pressure ulcer prevention in ogun state, Nigeria: results of a pilot survey. Ostomy Wound Manage. 2012 Feb; 58(2): p. 24-32.
11. Larcher Caliri M, Miyazaki M, Pieper B. Knowledge of pressure ulcers by undergraduate nursing students in Brazil. Ostomy Wound Manage. 2003 Mar; 49(3): p. 54-63.
12. Pieper B, Mott M. Nurses’ knowledge of pressure ulcer prevention, staging, and description. Adv Wound Care 1995;8:34-48.
13. Chauhan V, Goel S, Kumar P, Srivastava S, Shukla V. The prevalence of pressure ulcers in hospitalised patients in a university hospital in India. J Wound Care. 2005 Jan; 14(1): p. 36-7.
14. Cooper K. Evidence-based prevention of pressure ulcers in the intensive care unit. Crit Care Nurse. 2013 Dec; 33(6): p. 57-66.
15. Gelfand JM et al (2003) In: Freedberg IM et al (eds) Fitzpatrick’s dermatology in general medicine. McGraw-Hill Professional, New York, p 1256
16. VanGilder C, Amlung S, HarrisonP, Meyer S. Results of the 2008-2009 International Pressure Ulcer Prevalence Survey and a three year acute care unit specific analysis. Ostomy Wound Manage. 2009;55(11):39-55.
17. Kumari S, Sharma D, Rana A, Pathak R, Lal R, Kumar A, et al. Risk Assessment Tool for Pressure Ulcer Development in Indian Surgical Wards. Indian J Surg. 2015 Jun; 77(3): p. 206-12.

Is Cartilage Shield Tympanoplasty better than Fascia Tympanoplasty
Shahnaz Sheikh1, Anushree Bajaj2,Vikrant Vaze3
1Senior Resident, 2Associate Professor, 3Senior Resident, DUPMC Jalgoan
Abstract
Background: Temporalis fascia and cartilage are the most commonly used graft materials, though contradictory reports are available in literature as regards their efficacy in Tympanoplasty. The aim of the study was to compare the graft uptake rates and hearing results in case of temporalis fascia and cartilage in type 1 tympanoplasty
Material and Method: A total of 400 cases with large, subtotal and total perforation were considered in the study. All the selected patients were divided into two groups . Group A in which temporalis fascia graft was used and including 200 cases and cartilage graft was used in group B patients including 200 cases. Pure tone audiometry was performed preoperatively and postoperatively at 3 months, 6 months and 12 months.
Results : The graft uptake rate were more than 90 percent and more than 80 percent in group B respectively at the end of 14 week
Conclusion: From our study we came to the conclusion that both cartilage shield graft and temporalis fascia graft can be used as graft materials independently in Tympanoplasty. But the results of our study suggest that cartilage shield Tympanoplasty can be considered as the first line treatment in chronic otitis media especially with moderate/large/subtotal perforations with good success rate and hearing improvement.
Keywords : Tympanoplasty, fascia, cartilage, audiometry.
Introduction
Chronic otitis media is the chronic inflammation of mucoperiosteal lining of the middle ear cleft characterized by ear discharge, a permanent perforation of the tympanic membrane and impairment in hearing .In India including other developing countries chronic otitis media is one of the common diseases due to poor socioeconomic status ,poor nutrition, lack of health education and unhygienic habits.1,2,3It is a major cause of deafness in india.4Tympanoplasty is a commonly performed surgical procedure by otolaryngologists for the repair of tympanic membrane perforations.5 Autologous graft materials like temporalis facia, cartlage, perichondirum, fat and fascia can be used as graft materials. Temporalis fascia because of its close proximity , translucency, close
Corresponding Author: Dr. Anushree BajajAssociate Professor, DUPMC Jalgoan
proximity and suppleness is most commonly used graft in primary Tympanoplasties. Failure rates are higher in larger perforations with temporalis facia as a graft material.6,7Displacement of graft, improperly placed graft ,autolysis , infection, hemorrhage, Eustachian tube dusfunction are the known contributory factors for the failure of closure of tympanic membrane perforation8.Cartilage on the other hand has a constant shape, is firm than fascia and does not contain fibrous tissue so postoperative dimensions are predictable.9 Therefore cartilage shield graft is preferred in cases with large perforations, revision surgery, tympanosclerosis, tympanic membrane ,atelactesis and Eustachian tube dysfunction. Being rigid and thicker cartilage can affect the pliability of the tympanic membrane and result in inferior hearing outcome as compared to temporalis fascia graft which is thinner and moré pliable. The greatest advantage of the cartilage graft has been thought to be its very low metabolic rate and it can resist
DOI Number: 10.5958/2321-1024.2019.00028.X

85 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
deformation from pressure variation.
Material and Method
This prospective study was conducted in the department of ENT at dr ulhas patil medical college jalgaon from October 2015 to December 2018. A total of 400 patients were selected for the study. All the patients underwent type 1 tympanoplasty . Cartilage was used in 200 patients and temporalis fascia graft in were used in 200 patients. All the selected patients had moderate/subtotal/large size perforations.
Inclusion criteria were patients of age group between 10 to 50 years. Patients with CSOM mucosal and safe type, with intact ossicular chain and pure conductive hearing loss . Exclusion criteria were patients with age less than 10 years, chronic otitis media with active squamous disease, actively discharging ears. Patients having sensorineural loss and ossicular chain erosion. Surgical approach.
Cartilage Tympanoplasty was performed through endaural approach and Tympanoplasty using temporalis fascia graft was performed through post aural approach because of easy availability of respective grafts . Both of these procedures were performed under local anesthesia and if required under general anesthesia. One ampule of promethazine and one ampule of pentazocin were mixed together. Half of the mixture were given 30 minutes before surgery and half were given intravenously just before the surgery in case of local anesthesia. For local infiltration adrenaline and lignocaine were used in the ratio of 1:100000.2ml of the solution was injected in the four quadrants of external auditory canal . Cartilage graft were harvested from tragal cartilage. Cases selected for cartilage Tympanoplasty were done through the endaural approach and the cases selected for Tympanoplasty using temporalis fascia were done through postauricular approach. In all the cases type 1 TP was done through underlay technique.All the patients were called for regular follow up once weekly for 1 month and fortnightly for 3 months, then after 6 months and 1 year. Hearing assessment using tunning fork tests and pure tune audiometry was done to access the auditory status after 8th week, 3 month,6months and one year to see if there are any changes. Statistical analysis with the students t test, chi-square test, and F-test for large sample size was used to examine these parameters with regards to graft take up and hearing outcome. Figure 1
and 2 show the intraop picture of temporalis fascia graft placed and fig 3 and 4 show the intra operative picture of tragal cartilage graft placed
Figure 1: Elevatuion and reposition of tympanomaetal flap
Figure 2: Temporalis fascia graft
Figure 3: Reposition of tympanomaetal flap in cartilage Tympanoplasty
Results
Out of 200 patients 60 percent 120 were females and 40 percent 80 were males
Table 1: Number of patients in both the groups
Sex Number of patients percentage
Males 160 40
Females 240 60
Total 400 100

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 86
Table 2: Size of perforation in both the groups
Size of perforation
Number of patients percentage
Moderate 140 70
large 48 24
subtotal 12 6
total 200 100
In cartilage shield Tympanoplasty complete graft uptake was seen in more than 90% of cases with partial failure in more than 9 percent of cases. Similarly in group B, graft uptake rate in patients in the temporalis fascia Tympanoplasty complete graft uptake was seen in more than 84 percent of cases and graft failure in more than 15 percent of cases.
Table 3: Graft uptake rate in both the group.
Graft status Numbers in cartilage tympanoplasty Percentage Numbers in temporalis
fascia tympanoplasty percentage
Complete graft uptake 186 93 174 87
Residual perforation 14 7 26 13
Total 200 100 200 100
This signifies that postoperative graft uptake in cartilage shield Tympanoplasty and temporalis fascia graft Tympanoplasty group was insignificant. The mean preoperative ABGs in moderate,large ,subtotal perforations were 39.7,41.6,45.2in group A compared with group B where where corresponding values38.8,40.1,44.6 dB. Similarly mean postoperative
ABGs were 18.1,19.4,19.8 dB in group A and 17.3,18.9,19.4 in group B respectively. The mean improvement in ABG was >10 dB in both the groups. Hearing gain signifies use of cartilage shield or temporalis fascia graft does not affect postoperative hearing gain which was also proved statistically insignificant(p>0.05)
Table 4: Mean AB GAP( in dB) both the groups
Group A Group B
Size of perforation Number of patients Mean ABGAP(in db) Number of patients Mean ABGAP(in db)
Moderate 140 18.1 140 17.3
Large 40 19.4 40 18.9
Subtotal 20 19.8 20 19.4
Discussion
This study was designed to evaluate the graft uptake rates and hearing results in case of temporalis facia and cartilage graft in type 1 Tympanoplasty using modified Ducket technique.10Mohamad et al. have concluded that Tympanoplasty using cartilage with or without
perichondrium has better morphological outcome than Tympanoplasty using the temporalis fascia.11 However there was no significant differences in in hearing outcomes between the two grafts.Khan and Prab hav shown good anatomical and functional results using sliced cartilage for Tympanoplasty technique. 12Chapola and Matta have mentioned that cartilage thickness of

87 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
<0.5 mm seen to have similar acoustic properties as the tympanic membrane.13 The current study shows better graft uptake rates with the use of cartilage shield method and hearing improvement comparable with temporalis fascia as a graft material. Other popular methods for cartilage Tympanoplasty are the grafting procedures like Island technique, Wheel technique, Inlay butterfly technique, shield technique and palisade technique.14,15Cartilage is prefered over temporalis fascia especially for moderate/large/subtotal perforations which shows better graft uptake. A review of literature by Onal et al and Demirpehlivan et al studies reveals previously conducted demonstrating the effectiveness of cartilage graft over the temporalis fascia for type -1 tympanoplasty.16 In the current study, we obtained the encouraging postoperative results of tragal cartilage grafting over temporalis fascia in type-1 tympanoplasty in terms of graft uptake rates in patients with tragal cartilage which was 93 percent in contrast with the fascia which had an uptake rate of 87 at the 10th week. The mean postoperative ABG in the fascia group was was 15 dB, in contrast with the cartilage Tympanoplasty group in which it was found to be 11 dB. In both the groups 100 percent of patients showed significant improvement in hearing which is consistent with the previous study by Yetiser et al.17 All these results are suggestive of that the tragal cartilage graft is a good graft material because of its stability and more resistant to negative middle ear pressure and but sufficiently elastic for good sound conduction. Furthermore it has a constant shape, firmer than fascia and it does not contain fibrous tissue so that the postoperative dimension are predictable, and it is easily accessible, well tolerated resistant to resorption, inflammatory reactions to or rejection are rare. Cartilage is also nourished by diffusion and incorporated into the tympanic membrane , and also not involved into the additional costs. All the patients presented with significant improvement in hearing>10dB in the postoperative period, which is consistent with a study conducted by Dornhofferl comparing the cartilage island and cartilage palisade technique for type-1 and type-2 tympanoplasties and demonstrated that the anatomical and functional outcomes were similar in both the groups. Guneri et al , Ozbek et al and Wielgosz et al have also claimed a better graft uptake rate and hearing outcome in cartilage Tympanoplasty compared with temporalis fascia in type _1 tympanoplasty.18
Conclusion
Tragal cartilage graft can be used in cartilage Tympanoplasty especially in moderate,large andsubtotal perforations. The graft has better uptake rate, less partial failure and hearing improvement results were comparable to temporalis fascia graft. From our study we came to the conclusion that both cartilage shield graft and temporalis fascia graft can be used as graft materials independently in Tympanoplasty. But the results of our study suggest that cartilage shield Tympanoplasty can be considered as the first line treatment in chronic otitis media especially with moderate/large/subtotal perforations with good success rate and hearing improvement.
Ethical Clearance – the ethical clearance was taken from the ethical committee of DUPMC .
Conflict of Interest – none
Funding –None
References
1. Jung TT, Hanson JB. Classification of otitis media and surgical principles. Otolaryngol Clin North Am 1992;32:369-83.
2. Saha AK, Munshi DM, Ghosh SN. Evaluation of improvement of hearing in type 1 tympanoplasty and its influencing factors. Indian J Otolaryngol Head Neck Surg 2006;58:253-7.
3. Chandra KS. Combined effect of Eustachian tube function and middle ear mucosa on Tympanoplasty. Indian J Otol 2006;12:26-7.
4. Singh M, Rai A , Bandyopadhyay S, Middle ear microsurgery in India; A retrospective audit study. Indian J Otolaryngol Heads Neck Surg2006;58:133-6.
5. Sade J, Berco E, Brown M , Weinberg J , Avraham S , Myringoplasty; short and long –term results in a training program. J Laryngol Otol 1981;95:653-65.
6. Gibb AG, Chang SK. Myringoplasty( A review of 365 operations). J Laryngol Otol 1982:96:915-30
7. Dabholkar JP, Vora K , Skidar A . Comparative study of underlay Tympanoplasty with temporalis fascia and tragal perichondrium. Indian J Otolaryngol Head Neck Surg 2007;59:116-9.

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 88
8. Herman MK. Tang: The perforated ear drum: To repair or not . Hong Kong J Online 1989;11:124-5
9. Nissen AJ, Nissen RL, Yonkers AJ. A historical review of the use of bone and cartilage in otologic surgery. Ear Nose Throat J. 1986;65:493-6.
10. Duuckert LG . Muller J , Makielski KH, Helms J . Compositye autograft shield reconstruction of remnant tympanic membranes . Am J Otol. 1995;16:21-6.
11. S.h. Mohamad , I . Khan, and S.S. M. Hussain, Is cartilage Tympanoplasty more effective than fascia Tympanoplasty. A systematic review . Otology and Neurotology, vol.33, no.5, pp.699-705,2012.
12. M.M.Khan and S. R . Parab . Primary cartilage Tympanoplasty : our technique and results, American journal of otolaryngology- Head and Neck medicine and Surgery, vol.32,no.5 pp. 381-387,2011.
13. S. Chhapola and I. Matta, Cartilage-perichondrium: an ideal graft material. Indian Jourrnal of Otolaryngology and Head and neck surgery,vol.64,no.3,pp.208-213,2012.
14. Vashishth A. Mathur NN, Choudhary SR, Bhardwaj A. Clinical advantages of cartilage palisades over temporalis facia in type 1 tympanoplasty. Auris Nasus Larynx . 2014;41950;422-7.
15. Guneri EA, Ikiz AO. Erdag Tk .Sutay S. Cartilage Tympanoplasty: indications, techniques, and results. J Otolaryngol Head Neck Surg. 2009;38(3):362-8.
16. Demirpehlivan IA, Onal K, Arslanoglu S , Songu M, Ciger E, Can N. Comparision of different tympanic mem,brane reconstruction techniques in type 1. Eur Arch Otorhinolaryngol. 2011;268(3):471-4.
17. Yetiser S , Hidir Y. Temporalis fascia and cartilage-perichondrium composite shield grafts for reconstruction of the tympanic membrane. Annals Otol Rhinol Laryngol. 2009;118:570-4.
18. Ozbek C , Ciftci O, Tuna EE, Yazkan O, Ozdem C.A. comparision of cartilage palisades and fascia in type 1 tympanoplasty in children: anatomic and functional results . Otol Neurotol . 2008:29(5): 679-83.
Original Article
Various Presentations of Hepatic Hydatid Cystic Disease and their Management
Pradeep Kumar1, Sandeep Maliyan2, Sohan Pal Singh3, Manjul Kumar4, Nitin chauhan5, Anshu Tiwari6
1Associate Professor, 2Senior Resident, 3Professor,, Department of Surgery, LLRM Medical College, Meerut,
4Senior Resident, Department of Surgery, Teerthanker Mahaveer Medical College, Moradabad, 5Junior Resident, Department of Surgery, LLRM Medical College, Meerut, 6Senior Resident, Teerthanker Mahaveer Medical College,
Moradabad
Abstract
Introduction: Hydatidosis, a zoonotic infection, is due to the larval stage of the tapeworm Echinococcus (E.). Two of the recognised species, E. granulosus and E. multilocularis, are of importance for humans. The disease has a world-wide distribution.Biological diagnosis relies on serological tests. CT-scan of abdomen and chest, while not usually essential for diagnosis, gives a better definition of cysts content, number, size and calcification together with relation to vessels or other organs. With this information this study aims to analyze the different clinical presentations, complications and available various management options available for hydatid cyst of liver.
Method & Materials: This is a prospective observational study of 30 patients with hydatid cyst of liver included the patients admitted in the Department of General Surgery, L.L.R.M. Medical College, Meerut and S.V.B.P. Hospital, Meerut between jan 2018 to august 2018. All patients of either sex, male or female admitted with the diagnosis of hepatic hydatid cyst. There were no exclusion criteria. The data was analyzed by SPSS 21.0 version.
Result: In our series we analysed 30 patients. M:F ratio was 1.3:1. Most commonly involved age group was 40-49 yrs. Pain abdomen was the most common presenting symptom seen in 22 patients. Hepatomegaly was seen in 22 patients, Jaundice seen in 16 patients. Right lobe of liver was involve in 20 patients while both lobes were involved in 10 patients. Isolated left lobe involvement was not seen.ELISA for Echinococcal Antibody was performed in all 30 patients. Sensitivity was 100% while specificity was 99%. Deroofing with omentoplasty and wound drainage was the most commonly performed procedure and was performed in 12 patients
Concluson: This study was conducted to highlight the different modes of presentations of hydatid cyst of liver and effective management techniques. For symptomatic hydatid cyst of liver, open surgical approach is the best modality of management. Although majority of patients were treated surgically, importance of antihelminthics chemotherapy pre and post operatively is immense. As there are less number of patients presented in our study this data can be meta analyzed in other higher institutions.
Keywords: hydatid cyst, pericystectomy , zoonotic infections
Corresponding author : Dr. Sandeep Maliyan Senior Resident, (Deptt of surgery , LLRM , medical college Meerut, UP , India)Email: dr.sandeep02@gmail .com
Introduction
Hydatidosis, a zoonotic infection, is due to the larval stage of the tapeworm Echinococcus (E.). Two of the recognised species, E. granulosus and E. multilocularis, are of importance for humans. The disease has a world-
DOI Number: 10.5958/2321-1024.2019.00029.1

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 90
wide distribution. It is endemic in the Mediterranean and Baltic areas, Middle and Far East, South America and South Africa. Sheep-rearing European regions and central North America are also affected. E. granulosus producing unilocular hydatid disease (cystic echinococcosis - CE) is cosmopolitan whereas E. multilocularis producing alveolar hydatid disease (alveolar echinococcosis - AE) is limited to restricted areas of the northern hemisphere. Although less common, AE poses a far more serious problem due to the infiltrative nature of its cysts and its greater ability to metastasise; it has to be regarded as a malignant disease carrying a mortality of up to 90% in untreated cases. Unless otherwise stated in text we refer to E. granulosus and CE. Most patients will have a single organ involvement in primary echinococcosis. In adults the liver represents the prevalent site (50–70%) and lungs are the second commonest site (10–30%). In children the lungs are the prevalent location. Although primary extra-hepatic locations are less common (or even rare in AE), any other organ may be involved. After an asymptomatic phase of variable length, clinical manifestations depending on cysts localization and size appear as a result of compression or complication (rupture or infection). Cyst rupture can result in dissemination and hypersensitivity or anaphylactic reaction. Rupture into the biliary tree is the commonest complication (up to 25% of cases) and can be associated with biliary obstruction by daughter cysts. There is no specific clinical peculiarity for the disease although right upper quadrant pain, liver enlargement or a palpable mass with weight loss, fever or jaundice in endemic areas are strongly suggestive of hydatidosis.
Biological diagnosis relies on serological tests. Complement fixation test has poor sensitivity and specificity. Indirect hemagglutination (IHA) has good sensitivity but false positives do occur. Immunoelectrophoresis (IE), especially if arc 5 is present (precipitation for antigen (Ag) 5), and enzyme-linked immunosorbent assay (ELISA) for IgG against Ag 5 or Ag B yield the best results. Their association may detect up to 90% and 80% of hepatic and pulmonary locations respectively. Immunodiagnostic tests been studied and reviewed extensively by Gottstein B. and Schantz P. Co-agglutination for circulating antigen and latex agglutination are well suited for diagnosis in field conditions[1]. Hydatid antigen dot immunobinding assay[2] and dot-ELISA are aimed at the same use.
Serological tests such IHA and IE for the diagnosis of AE have used E. granulosus antigens for long. At present, more specific tests such as Emc- or Em2-ELISA are probably better choices [3].
Chest x-ray may give diagnostic images in a few typical situations whereas plain abdominal film has very low specificity. Ultrasound due to its wide availability, moderate cost and high diagnostic rate (90%) is first of the diagnostic tools. It is equally important for follow-up. Gharbi’s classification into types I to V perfectly describes the different presentations as well as the likely evolution of the lesions with time. CT-scan of abdomen and chest, while not usually essential for diagnosis, gives a better definition of cysts content, number, size and calcification together with relation to vessels or other organs. It is therefore fundamental in planing for surgery. It is similarly important in assessing complications or for follow-up. MRI, beside failing to demonstrate calcifications, is of questionable use as its superiority over CT-scan has yet to be established. Immunoscintigraphy is under evaluation [4]. With this information this study aims to analyze the different clinical presentations , complications and available various management options available for hydatid cyst of liver.
Materials and Method
This is a prospective observational study of 30 patients with hydatid cyst of liver included the patients admitted in the Department of General Surgery, L.L.R.M. Medical College, Meerut and S.V.B.P. Hospital, Meerut between jan 2018 to august 2018. All patients of either sex, male or female admitted with the diagnosis of hepatic hydatid cyst. There were no exclusion criteria. Detailed History was taken as per the prepared proforma and then complete clinical examination was done. The data was analyzed by SPSS 21.0 version.
Observation & Result
Total 30: patients were included in this study. Most commonly involved age group was 40-49 yrs.(table:1)

91 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
Table: 1 showing age groups of patients presented with hydatid cyst of liver
Age group No. of patients
10 -19 years 1
20 -29 years 4
30-39 years 7
40 -49 years 12
50- 59 years 5
>70 years 1
Total 30
Out of 30 patients 17 patients were male & 13 patients were female .M:F ratio was 1.3:1 .Pain abdomen was the most common presenting symptom seen in 22 patients.(table:2)
Table:2 showing presenting symptoms of patients with hydatid cyst of liver.
Presenting symptoms No.Of patients
Pain abdomen 22
Abdominal lump 16
jaundice 2
Fever 18
Cholangitis 5
Constitutional 2
Total 30
Hepatomegaly was seen in 22 patients, Jaundice seen in 16 patients ,Pallor in 30 patients & Poor nutritional states in 16 patients.
Right lobe of liver was involve in 20 patients while both lobes were involved in 10 patients. Isolated left lobe involvement was not seen.
ELISA for Echinococcal Antibody was performed in all 30 patients. Sensitivity was 100% while specificity was 99%.
Deroofing with omentoplasty and wound drainage was the most commonly performed procedure and was performed in 12 patients.Partial pericystectomy
was performed in 9 patients, Pericystic cystectomy was performed in 6 patients , Marsupialization was performed in 2 patients while one patient managed conservatively.
Post operative complications were seen in 7 patients. (table:3)
Table 3: Showing post operative complications.
Complications n
Retained cyst 1
Biliary fistula 2
Post operative cholangitis 2
Surgical site infection 2
TOTAL 7
Treatment related factors:
A) Modality of treatment Surgery-29 Preoperative Chemotherapy -30 Postoperative Chemotherapy - 30
B) Scolicidal agents: Combination of 0.5 % Cetrimide and 0.05% Chlorhexididine (SAVLON) TM Hypertonic Saline 20% and 10%.

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 92
Discussion
In our study most common age group involved was 5th decade (40%) which differs from other studies of Akhter et al[4], Md.Khader Faheem N. et al[5] (12%) and Kayal et al[6] (21%) who concluded as 3rd decade as the most common presenting age group in patients of hepatic hydatid cyst. In our study male population had 57% incidence compared to 43% incidence of females (ratio = 1.3 : 1). It is comparable to study of Khader Faheem N. et al[5] (2.5:1) but opposite to Kayal et al[6] (1:2) and Akhter et al[4] (1:1.5). Most common presenting complaint in our group of patients was pain in abdomen (34%) followed by fever (28%).this is in accordance to study of Khader Faheem N. et al[5] (16.7%) where pain was chief presenting complaint. While lump was most common presentation in other studies of Kayal et al (67.8%) & Akhter et al (78.7%). Most common sign elicited on examination in our observations was hepatomegaly (73.33%), which is comparable to study of Akhter et al (66.6%), and also comparable to study of Khader Faheem N. et al. Discussion 51 In our study, about 66.6% had involvement of right lobe only while in 33.4%, both lobes were involved. This was in concordance to study of Akhter et al (62.6%-right, 11.3% - B/L), right lobe was also most commonly involved in
Kayal et al (58.7%). We did deroofing with omentoplasty and drainage in 40% pateints and partial pericyctectomy in 30% of patients. In study of Akhter et al, omentoplast was done in 10.2% and external darianage was done in 68.3%. Biliary fistula and surgical site infection were the most common complication in our study with incidence of 6.67 %.in study of Akhtar et al, most common complication was wound infection (18.7) followed by biliary fistula (1.17%). Biliary leak was seen in 7% of patients in study of Kayal et al.
These may be conservative or radical. Conservative procedures aim at sterilization and evacuation of cyst content, including the hydatid membrane (hydatidectomy), and partial removal of the cyst. The evacuation and hydatidectomy consist of puncture of cyst and aspiration of part of the content to permit introduction of scolicidal agent and total aspiration thereafter. The risks are anaphylactic shock, chemical cholangitis, if the cyst communicates with the biliary tree, and spillage of the cyst contents and secondary hydatidosis. Relapse rates of up to 20% are reported after surgery of LHCs.[7,8,9] After partial removal of the cyst, a residual cavity remains, bearing the risk of secondary bacterial infection and abscess formation. Radical procedures aim at complete removal of the cyst with or without hepatic resection. Radical procedures bear greater intraoperative risks, with less postoperative complications and relapses.
Laparoscopic management of LHCs has gained ground despite the initial exaggerated fear of complications such as anaphlaxis. Various techniques such as total pericystectomy, puncture and aspiration of contents followed by marsupialization, unroofing and drainage, unroofing and omentoplasty, and omentoplasty using helical fasteners have been described.16,17 One of the problems faced in laparoscopic treatment of liver hydatid cysts is the difficulty in evacuating the particulate contents of the cyst, the daughter cysts, and laminated membrane. Bickel et al initially advocated the use of a large transparent beveled cannula. 18 Saglam described a perforator-grinder-aspirator apparatus designed specifically for the evacuation of hydatid cysts.19Palanivelu developed the “Palanivelu Hydatid System” (PHS) consisting of a complex system of fenestrated trocar and cannulas to avoid peritoneal spillage. PHS not only prevents any spillage of hydatid fluid but also assists complete evacuation of the cyst

93 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
content and allows intracystic magnified visualization for cyst-biliary communication.20
Conclusion
This study was conducted to highlight the different modes of presentations of hydatid cyst of liver and effective management techniques. During the course of this study, abdominal USG & CT scan demonstrated accurate characterization of this hydatid cyst - single /multiple cyst, living / dead, whether there is any calcification etc. And USG is an effective tool in the follow up period following surgery. For symptomatic hydatid cyst of liver, open surgical approach is the best modality of management. Although majority of patients were treated surgically, importance of antihelminthics chemotherapy pre and post operatively is immense. As there are less number of patients presented in our study this data can be meta analyzed in other higher institutions.
Source of Funding : Self
Ethical Clearance : Not required
Conflict of Inetrest : Nil
References
1. Parija S C. A review of some simple immunoassays in the serodiagnosis of cystic hydatid disease. Acta Trop. (1998);70:17–24. [PubMed]
2. Mistrello G, Gentili M, Falagiani P, Roncarolo D, Riva G, Tinelli M. Dot immunobinding assay as a new diagnostic test for human hydatid disease. Immunol Lett. (1995);47:79–85. [PubMed]
3. Bresson-Hadni S, Laplante J J, Lenys D, Rohmer P, Gottstein B, Jacquier P. et al. Seroepidemiologic screening of Echinococcus multilocularis infection in a European area endemic for alveolar echinococcosis. Am J Trop Med Hyg. (1994);51:837–846. [PubMed]
4. Akhter, Tselentis, J, Karpathios, T, Fretzayas, A (1983) Hydatid disease in asymptomatic young carriers in northern Greece. Am. J. Trop. Med. Hyg. 32: pp. 1462-1463
5. Md.Khader Faheem N. et al ,Bchir, A, Hamdi, A, Jemni, L (1988) Serological screening for
hydatidosis in households of surgical cases in central Tunisia. Ann. Trop. Med. Parasitol. 82: pp. 271-273
6. Kayal et al ,Anderson FL. Introduction to cystic ecchinococcosis and description of cooperative research project in Morocco. In Anderson FL, Ouhelli H, Kachani M, editors, Compendium on Cystic Ecchinococcosis in Africa and Middle Eastern Countries with Special Reference to Morocco, Provo, UT, Brigham Young University,, 1997;1–17
7. Vaquerizo A., Sola J.L., Bondia A., Opla J.M., Madariaga M.J. Intraoperative hydatid anaphylactic shock. Rev Esp Anestesiol Reanim. 1994;41:113–116. [PubMed]
8. 14. Belghiti J., Benhamou J.P., Houry S., Grenier P., Huguier M., Fekete F. Caustic sclerosing cholangitis. A complication of the surgical treatment of hydatid disease of the liver. Arch Surg. 1986;121:1162–1165.[PubMed]
9. 15. Atmatzidis K.S., Pavlidis T.E., Papaziogas B.T., Mirelis C., Papaziogas T.B. Recurrence and long-term outcome after open cystectomy with omentoplasty for hepatic hydatid disease in an endemic area. Acta Chir Belg. 2005;105:198–202. [PubMed]
10. Khoury G., Geagea T., Hajj A. Laparoscopic treatment of hydatid cysts of the liver. Surg Endosc. 1994;8(9):1103–1104. [PubMed]
11. Manterola C., Fernandez O., Munoz S. Laparoscopic pericystectomy for liver hydatid cysts. Surg Endosc. 2002;16(3):521–524. [PubMed]
12. Bickel A., Eitan A. The use of a large transparent cannula, with a beveled tip, for safe laparoscopic management of hydatid cysts of liver. Surg Endosc. 1995;9:1304–1305. [PubMed]
13. Saglam A. Laparoscopic treatment of liver hydatid cysts. Surg Laparosc Endosc. 1996;6(1):16–21.[PubMed]
14. Palanivelu C., Jani Kalpesh, Malladi Vijaykumar. Laparoscopic management of hepatic hydatid disease. JSLS. 2006;10(1):56–62. [PMC free article] [PubMed.

Original Research Article
A Clinical Study and Management of Hypocalcemia Following Thyroid Surgery
Pratima Raj1, Abhilash V2, Suma S3, Krishna Prasad K4
1Assistant Professor, Department of Obstetrics and Gynaecology, 2Assistant Professor, Department of General Surgery, 3Post-graduate (PGY3)Department of Surgery, 4Professor, Department of General Surgery,
Sri Devaraj Urs Medical College, Kolar, Karnataka, India
Abstract
Background: Post-thyroidectomy hypocalcaemia is a serious complication. Hypocalcaemia may occur secondarily to surgical trauma, devascularisation, unintentional removal of parathyroid glands, reoperation. Surgery has been seen as a risk factor, as in total thyroidectomy there is potential blood supply involvement resulting from bilateral surgical manipulation. This study aims to prospectively study and analyse the incidence and possible causes of hypocalcaemia following thyroid surgery, and its management.
Method and Materials: Data was collected from the patients undergoing subtotal and near total thyroidectomies from November 2012 to October 2014 by evaluating and investigating meticulous and planned for surgery. They were follow-up on day one after surgery, at the time of discharge and 6 months after surgery for post-operative hypocalcaemia.
Observation: 6 out of 50 patients (12%) developed postoperative hypocalcaemia, there was no incidence of permanent hypocalcaemia. Near total thyroidectomy was performed in 35(70%) patients, 1 from them (2.86%) developed hypocalcaemia and the other 5 out of 14 cases (35.71%) underwent total thyroidectomy. The hypocalcaemia was 9% in multinodular goitre (3 out of 33 patients), 20% in papillary carcinoma (1 out of 5 patients) and 40 % in follicular neoplasm (2 out of 5 patients).
Conclusion: When preservation of parathyroid glands and their blood supply is enforced during thyroidectomy, the incidence of postoperative hypocalcaemia and permanent hypoparathyroidism can be consistently deceased.
Keywords: Thyroidectomy, Hypocalcaemia, post-operative complications, management, hypo parathyroid
Introduction
Chronic hypoparathyrodism is a serious and potentially debilitating disorder that results from a variety of causes. It most commonly occurs as a complication of thyroid surgery, severity depends on the extent of thyroid
Corresponding Author: Dr. Abhilash V Assistant Professor, Department of Surgery, Sri Devaraj Urs Medical College, Kolar, Karnataka, India. Phone No.:9886456626, e-mail ID: [email protected]
surgery and parathyroid damaged. A postoperative decrease of serum calcium is frequently observed within 1 to 5 days after a total or subtotal thyroidectomy, requiring exogenous replacement therapy to alleviate clinical symptoms. In patients experiencing significant hypocalcaemia, the most probable cause is certainly hypoparathyroidism secondary to trauma which usually results from intentional or inadvertent extirpation of the parathyroid glands during thyroidectomy or from interruption of the blood supply to the glands with subsequent infarction. Permanent hypocalcaemia is common cause of malpractice litigation after endocrine surgery. In this study we prospectively evaluate the
DOI Number: 10.5958/2321-1024.2019.00030.8

95 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
incidence and assess the risk factors and management of temporary and permanent hypoparathyrodism following thyroidectomy.
Aim
• To determine the incidence of hypocalcemia following thyroid surgery
• To determine the causes and management of postoperative hypocalcemia following thyroid surgery.
Method
This prospective study was conducted in tertiary centre, Study was conducted for 20 months between November 2012 to October 2014, on 50 patients by meticulous history taking, careful clinical examination, and appropriate radiological, hematological investigations. Other investigations included serum calcium, serum albumin and parathyroid hormone, operative findings and follow-up of the cases day one after surgery, at the time of discharge and 6 months after surgery was done for postoperative hypocalcaemia.
Results
A prospective study was carried out in the Department of General Surgery, during the period from October 2012 to September 2014 in 50 patients undergoing subtotal and near total thyroidectomy. All surgeries were performed by the same surgeon. Observations and analysis of all the parameters studies are as follows.
Table 1 : Age incidence
Age Group No. of Patients Percentage (%)
20-29 11 22 %
30-39 17 34 %
40-49 11 22 %
50-59 8 16 %
60-69 2 4 %
70-80 1 2 %
Total 50 100 %
The mean age in this study was 32 years. The age group of the patients ranged from 20 to 80 years. The maximum incidence is seen in the age group of 30-39 years followed by 20-29 and 40-49 years of age.
Table 2 : Sex Incidence
Gender No. of Patients Percentage (%)
Male 5 10 %
Female 45 90 %
In 50 cases, 5 were males and 45 were females. The ratio of males to females 1:9. The above sex distribution shows that thyroid diseases have a higher frequency in female than in males.
Table 3: Pre-operative diagnosis
Pre-operative diagnosis No. of cases Percentage (%)
Multi-nodular goiter 33 66 %
Solitary nodule thyroid 7 14 %
Papillary carcinoma 5 10 %
Follicular neoplasm 5 10 %
Total 50 100 %
Out of 50 patients, 33 patients (66%) were diagnosed pre-operatively for multinodular goiter, 7 patients (14%) presented with solitary nodule thyroid, 5 patients (10%) were diagnosed as papillary carcinoma thyroid and the remaining 5 patients (10%) with follicular neoplasm.
Table 4: Surgical procedure
Surgical procedure Number of patients
Percen-tage
Near total thyroidectomy(total lobectomy + isthmusectomy +
subtotal lobectomy)35 70 %
Total thyroidectomy(2 x total lobectomy +
isthmusectomy)14 28 %
Bilateral subtotal thyroidectomy(2 x subtotal lobectomy +
isthmusectomy)1 2 %
Total 50 100 %
Out of 50 patients, 35 patients (70%) underwent near-total throidectomy, 14 patients (28%) total thyroidectomy and 1 patient underwent bilateral subtotal

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 96
thyroidectomy.
Table 5: Duration of hypocalcemia treatment with IV calcium
Duration of Post-operative hospital stay
No. of cases Percentage (%)
Upto 3 days 1 16.66 %
4 – 6 days 3 50.0 %
More than 6 days 2 33.33.0 %
The average duration of treatment of hypocalcemic patients with IV calcium was 5.33 days. 1 patient received IV calcium for less than 3 days, 3 patients was administered it for 4-6 days and 2 patients received it for more than 6 days.
Table 6: Number of parathyroid glands identified and incidence of hypocalcemia
Number of Incidence of Percentage incidence
parathyroid glands Number of patients
hypocalcemia in this
of hypocalcemia in
identified group the group
All 4 glands identified 23 0 0 %
3 glands identified 21 1 4.7 %
2 glands idetified 5 4 80 %
1 gland identified 1 1 100 %
Out of 50 patients, all four parathyroid glands were identified in 23 patients of whom none developed post-op hypocalcemia. Three parathyroid glands were identified in 21 patients among whom only 1 patient developed hypocalcemia (4.7%). Two parathyroid glands were identified in 5 patients and 4 among them developed hypocalcemia (80%). One gland was identified in just one patient who also developed hypocalcemia (100%).
Hypocalcemia
Near total thyroidectomy was the procedure in
35(70%) patients ,1 from them (2.86%) devoloped hypocalcaemia and the other 5 out of 14 cases( 35.71%) were after total thyroidectomy. Hypocalcaemia was found in 9% in multinodular goitre (3 out of 33 patients), 20% in papillary carcinoma (1 out of 5 patients) and 40 % in follicular neoplasm (2 out of 5 patients). Hypocalcemia was found in 11.1% in females (5 out of 45 patients), and 20% in males (1 out of 5 patients).
In the present study, there were 50 thyroid surgeries performed. 6 cases with temporary hypocalcemia and no cases with permanent hypocalcemia were documented. The mortality in this series was zero. All patients with hypocalcemia were appropriately managed with IV and oral calcium with satisfactory patient outcome.
Discussion
The successful thyroid surgery requires detailed knowledge of anatomy, skill and patience from the surgeon, the good anesthetic team, and all others involved in giving holistic healthcare to the patient.
In our study, sex distribution shows that thyroid diseases have a higher frequency in female than in males. There was no statistical difference in the age and sex of the patients who had temporary hypocalcaemia, permanent hypocalcaemia. This supports the findings of Glinoer et al.3 but contrasts with the study by Prim et al.1 who found hypocalcaemia was statistically more common in females.
The mean age in our study was 32 years. Lin DT et al2 concluded that younger age was considered as risk factors in the incidental parathyroid removal. However, in our study age was not found to carry any risk for the incidental parathyroid removal.
The incidence of hypocalcemia was noticed in the first post-operative day among our patients. The patients mainly complained of circum-oral numbness and tingling sensation. On examination carpo-pedal spasm was seen in 1 patient. Serum calcium was decreased in all the 6 patients. Although Lin et al2 did not find any association between hypocalcemia and incidental parathyroid removal (IPE), Sippel et al3 reported that the incidental parathyroid removal group had significantly lower postoperative calcium levels, and this is in line with our findings.
Injury, devascularization, and unintentional excision

97 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
of the parathyroids have all been cited as the causes of postoperative hypocalcemia. Although other specific factors have been studied, the cause of postoperative hypocalcemia remains to be multifactorial4. Although hypocalcemia reverses spontaneously in most patients, it can remain permanent when caused by an injury or removal of the parathyroid glands.5-8 The overall incidence of temporary hypocalcemia among our patients was 12%.
In the present study, risk factors for the incidental parathyroid removal included total thyroidectomy. As expected in total thyroidectomy fact that dissection bilaterally puts all four glands at risk. In addition, in the current study, total thyroidectomy was done mainly for MNG and malignancy was reported to be a strong predictor of IPE in earlier studies,9,10. In the present as well as earlier studies,9,11,12 total thyroidectomy was found to be a risk factor for the incidental parathyroid removal. Near total thyroidectomy can also be a risk factor for IPE but lesser than total thyroidectomy. Although extrathyroid extension was not found to be a risk factor in a recent study,13 in the present study, we found it to be another strong predictor of IPE. All the cases were temporary hypoparathyroidism because subsequent follow up showed normal serum calcium levels. This was attributed to temporary spasm of the vessels supplying the parathyroid glands and hence the resulting tetany.
In our study, The incidence of transient hypoparathyroidism increased when less than 2 parathyroid gland was preserved and there was no permanent hypoparathyroidism. Hence, our data suggest that the preservation of at least one viable parathyroid gland prevents permanent hypoparathyroidism. In addition to preserving as many viable parathyroid glands as possible, the blood supply of parathyroid gland should be preserved with great care and careful dissection of tissue to maintain the viability of the parathyroid glands
In our study, auto transplantation of parathyroid glands were not associated with increased risk of either transient or permanent hypocalcaemia. Judging the viability of the parathyroid glands to predict postoperative insufficiency of the gland in situ is very difficult. Khuhel et al14 found that the absence of discoloration is not reliable to determine whether the parathyroid blood supply is in intact. It is therefore recommended to leave as many parathyroid glands in situ as possible. Similar
results were reported in a study by Ohman et al in 1978, where an increased risk of permanent hypocalcaemia in patients with auto transplanted parathyroid glands were noted. The authors suggested that all efforts should be made to leave the parathyroid glands in situ15.
In our study, All the patients who developed hypocalcemia were administered IV calcium till serum calcium was normal and oral calcium and vitamin-D supplements were given for maintenance. The average duration of IV calcium treatment was 5.33 days. All the patients recovered satisfactorily. Our patients with a corrected serum calcium of <8 mg/dl received calcium with additional vitamin D prescribed for 4 weeks initially.
Conclusion
Post-operative hypocalcemia is the most complication following thyroid surgery. Although multifactorial, total thyroidectomy is the most important risk factor for hypocalcemia. Other factors are related to the chosen surgical procedure and its impact on devascularization or accidental removal of the parathyroid glands. The re-commended surgical strategy is meticulous dissection and preservation of atleast one parathyroid gland and their blood supply. Parathyroid auto transplantation seems to be warranted as a way of minimizing the risk of permanent hypoparathyroidism. IV and oral calcium supplementation is effective in treating hypoparathyroidism
Conflict of Interest: Authors & Co-authors declare that no conflict of interest was there, during the conduct of the study.
Funding: Authors & Co-authors declare that no funding or financial support was provided by any sources, during the conduct of the study.
Ethical Committee Approval: Ethical committee clearance from Institutional Ethical Committee (IEC) was taken prior to the start of the study.
References
1. Prim MP, de Diego JI, Hardisson D, Madero R, Gavilan J. Factors related to nerve injury and hypocalcaemia in thyroid gland surgery. Otolaryngol Head Neck Surg. 2001;124:111–4
2. Lin DT, Patel SG, Shaha AR, Singh B, Shah JP. Incidence of inadvertent parathyroid removal during

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 98
thyroidectomy. Laryngoscope. 2002;112:608–11.
3. Sippel RS, Ozgul O, Hartig GK, Mack EA, Chen H. Risks and consequences of incidental parathyroidectomy during thyroid resection. ANZ J Surg. 2007;77:33–6.
4. Schawrtz AE, Friedman EW. Preservation of the parathyroid glands in total thyroidectomy. Surg Gynecol Obstet. 1987;165:327–32.
5. Thompson NW, Reeve T. Complications of thyroid surgery: How to avoid them, how to manage them, and observations on their possible effect on the whole patient. World J Surg. 2000;24:971–5.
6. Thomusch O, Mchens A, Sekulla C, Ukkat J, Lippert H, Gastinger I, et al. Multivariate analysis of risk factors for postoperative complications in benign goiter surgery: Prospective multicenter study in Germany. World J Surg. 2000;24:1335–42.
7. Bellamy RJ, Kendall-Taylor P. Unrecognized hypocalcemia diagnosed 36 years after thyroidectomy. J R Soc Med. 1985;88:690–1. [PMC free article] [PubMed]
8. Gourgiotis S, Moustafellos P, Dimopoulos N, Papaxoinis G, Baratsis S, Hadjiyannakis E. Inadvertent parathyroidectomy during thyroid surgery: The incidence of a complication of thyroidectomy. Langenbecks Arch Surg.
2006;391:557–60.
9. Bergmaschi R, Becouarn G, Ronceray J, Arnaud JP. Morbidity of thyroid surgery. Am J Surg. 1998;176:715.
10. Pelizzo MR, Bernante P, Toniato A, Piotto A, Grigoletto R. Hypoparathyroidism after thyroidectomy. Analysis of a consecutive recent series [in Italian] Minerva Chir. 1998;53:239–44.
11. De Pasquale L, Schubert L, Bastagli A. Post-thyroidectomy hypocalcaemia and feasibility of short-stay thyroid surgery. Chir Ital. 2000;52:549–54.
12. Tartaglia F, Sgueglia M, Muhaya A, Cresti R, Mulas MM, et al. Complications in total thyroidectomy: our experience and a number of considerations. Chir Ital. 2003;55:499–510.
13. Akerstrom G, Malmaeus J, Bergstrom R. Surgical anatomy of human parathyroid glands. Surgery. 1984;95:14–21.
14. Pattou, F., et al., Hypocalcemia following thyroid surgery: incidence and prediction of outcome. World J Surg, 1998. 22(7): p. 718-24.
15. Edafe, O., et al., Systematic review and meta-analysis of predictors of post-thyroidectomy hypocalcaemia. Br J Surg, 2014.

Incidence of Malignancy in Unilateral Tonsillar Enlargement Over a Period of 10 Years
Sushil Gaur1, Vandana Singh2, Prince Hirdesh3, Akshay S Panakkal3
1Associate Professor, 2Professor and Head, 3Post Graduate Residents; Dept. of ENT, Santosh Medical College, Ghaziabad, U.P.
Abstract
Objective: To determine the incidence of carcinoma in patients with unilateral tonsillar enlargement. Study Design: A clinical retrospective case series based on medical records of our medical college.
Results: During a ten-year period, 495 patients underwent tonsillectomy at various medical colleges in western Uttar Pradesh. 29(5.9) of those patients had asymmetrical enlargement of their tonsils, three of whom had suspicious clinical findings at presentation. The latter were found to have tonsillar malignancy on histopathological testing. Malignancy was excluded in all other specimen.
Conclusions: Since the incidence of malignancy in asymmetrical tonsils is negligible in the absence of other associated risk factors, watchful waiting may be appropriate prior to any surgical intervention. Diagnostic tonsillectomy is indicated in patients with asymmetrical tonsillar enlargement with associated suspicious clinical findings, including cervical lymphadenopathy and rapid tonsillar enlargement.
Keywords: Tonsil, Asymmetry, Enlargement, Malignancy, Tonsillectomy
Introduction
Tonsils are lymphoid tissue collections located at either side of the oropharynx. They are primarily made of B lymphocytes and are lined by stratified squamous epithelium. They lack afferent lymphatic channels. Their main function is to produce antibodies, lymphokines and gamma interferon. There are several aetiologies behind unilateral tonsillar enlargement, including tuberculosis, actinomycoses, syphilis and sarcoidosis [1], chronic inflammatory response, papilloma [2], reactive immunological response to a nearby primary tumour in cervical lymph node and malignancy. Furthermore, asymmetric tonsils could be a normal variant due to varying depth of tonsillar fossa or asymmetry in anterior pillars.
Tonsillectomy is among the most commonly performed operations in otorhinolaryngology. The indications are classified into absolute and relative indications. Malignant tumours of the tonsil are one of the definitive indications for tonsillectomy. Suspected tonsillar malignancy cannot be confirmed
except by histopathological examination usually after tonsillectomy. Tonsillar malignancy has different presentations. It could present as ulcerated tonsillar mucosa as in squamous cell carcinoma of the tonsil. However, a normal tonsillar mucosa does not exclude tonsillar malignancy. For example, nonepidermoid malignancy of the tonsil can present with asymmetrical tonsillar enlargement with normal mucosa. The aim of this study is to determine the incidence of malignancy in patients with unilateral tonsillar enlargement.
Patients and Method
Patients who underwent tonsillectomy during the period of ten years between January 2009 and March 2019 were included in the study. We conducted a clinical retrospective review of our institution’s experience with unilateral tonsillar enlargement in the above-mentioned period. All the preoperative clinical findings were reviewed. The size of each tonsil was documented in patients’ medical records using a clinical assessment scale (CAS) of 0, +1, +2, +3, +4. This scale evaluates tonsillar hypertrophy relative to the midline (0 = absent,
DOI Number: 10.5958/2321-1024.2019.00031.X

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 100
1+ = small within the tonsillar fossa, 2+ =extends beyond the tonsillar pillar, 3+ = enlarged tonsils but not touching the midline, 4+ = enlarged tonsils touching the midline). Asymmetric tonsils included all tonsils with different CAS between the right and left sides. The patient’s age, gender, tonsil size, associated symptoms, suspicious findings and pathology results were entered for all patients. Tonsil size was measured in histopathology laboratory postoperatively, the three-dimensional volume being calculated. Ethical clearance to review the medical records of our patients was approved by the Santosh Medical college ethical committee. There were no missing data or data outliers for our subjects. Limitations for our study included small sample size and ethnicity; since all the patients were from western UP, our findings may not translate to patients of other ethnicities.
Data was recorded and analysed using SPSS version 20 software.
Results
During the ten-year period, 495 patients underwent tonsillectomy at different medical colleges in western UP. 30 (6%) of those patients had asymmetrical enlargement of their tonsils. Of the 30 patients, 17 were male and 13 were female patients (Table 1). Five (1.01%) out of the 30 patients did not have a diagnosis of asymmetry on histopathological testing as compared to the CAS. All the patients had CAS difference between tonsils. 10 patients had a difference of 1+, 14 patients had a difference of 2+ and 6 patients had a difference of 3+ between the CAS for each tonsil (Table 2).
Table 1. Gender distribution of patients with tonsil asymmetry
Tonsillar size (CAS)
Frequency Percent Valid percent Cumulative percentage
+1 10 33.3 33.3 33.3
+2 14 46.7 46.7 66.7
+3 6 20 20 100
Total 30 100 100
Two (6.6%) of the 30 patients had benign lesions on their unilaterally-enlarged tonsil (Table 3 and Figure 1). Two patients had papillomatous hyperplasia of the squamous epithelium on histopathology and were diagnosed with papilloma. The third patient was diagnosed with neurofibroma of the tonsil on histopathological examination. All of them had suspicious clinical findings on examination, including papillomatous lesions over the tonsil and greyish tonsillar discoloration, respectively. In addition, 2 (6.6%) of the 30 patients were found to have malignant changes of their tonsils (Table 3 and Figure 1). All those patients had preoperative signs raising the possibility of malignancy. The first patient was a 44-year-old male of Meerut, U.P., found to have ulcer over his left unilaterally-enlarged tonsil. Histopathology testing showed that the tonsil was completely replaced by diffuse lymphoid infiltrate composed of sheets of pleomorphic large cells with
nucleoli and occasional tangible body macrophages. He was diagnosed with large cell diffuse B cell lymphoma. The second patient was a 65-year-old male who also had ulcerative lesions over both tonsils associated with cervical lymphadenopathy. On histopathological examination, the tonsil showed loss of follicular architecture with monotonous sheets of lymphoid cells, oval nuclei and prominent nucleoli. Mitosis figures and foci of necrosis were noted. Immunohistochemistry was strongly positive for B cells (CD 20). He was diagnosed with B-cell type low-grade non-Hodgkin lymphoma. The third patient was a 60 year-old female from Hapur, U.P. who had palpable cervical lymphadenopathy. She had subepithelial infiltration of her tonsil by clumps and sheets of large neoplastic cells composed of vesicular nuclei, multiple nucleoli and considerable pleomorphism with occasional mitotic figures. She was diagnosed with invasive poorly-differentiated nonkeratinizing squamous

101 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
cell carcinoma.
Table 2. Tonsil size difference (CAS).
Gender
Frequency Percent Valid% Cumulative%
Male 17 56.6 56.6 56.6
Female 13 43.3 43.3 100
Total 30 100 100
Table 3. Histopathology of asymmetrically-enlarged tonsils
Histopathology
frequency percent Valid% Cumulative%
Lymphoid hyperplasia 26 86.7 86.7 86.7
Malignant tumour 2 6.6 6.6 10.1
Benign tumor 2 6.7 6.7 100
Total 30 100 100
Discussion
According to the American Academy of Otolaryngology-Head and Neck Surgery Clinical Indicator Compendium [3], unilateral hypertrophy of the tonsil presumed to be neoplastic is an indication for tonsillectomy. Otolaryngologists must weigh the risks and complications of doing tonsillectomy versus the possibility of missing a diagnosis of malignancy. In patients with unilateral tonsillar hypertrophy associated with other signs pointing towards malignancy, the possibility of cancerous changes is high, and tonsillectomy is usually done. However, patients who have normal physical examination findings including absent ulceration on the tonsils, absent cervical lymphadenopathy and other systemic symptoms, the decision whether to do tonsillectomy or not becomes more challenging.
In a similar study [4], 70 patients underwent tonsillectomy to rule out malignancy in asymmetrically-enlarged tonsils. Histopathology was unremarkable except in one, B-cell lymphoma. This patient did not
have cervical lymphadenopathy or other associated systemic symptoms.
Another study [5] included 49 patients whose only indications for tonsillectomy was asymmetrical enlargement. Only 2 of the patients were diagnosed with cancerous changes. According to the study, there is no alternative modality to tonsillectomy in such patients; for instance, “the sensitivities and specificities for fine-needle aspiration in the tonsil have not been reported”. Overall, the results of our study as well as similar studies could be interpreted to mean that a significant percentage of patients have undergone a “needless” surgery. But up till now, tonsillectomy is still necessary and is the only definitive way to confirm tonsillar malignancy.
Furthermore, 5 (17%) of the patients did not have actual asymmetry after the pathology test results were known (Table 4). CAS is the clinical evaluation of the hypertrophy of the tonsils in relation to the midline. This means that the physician could notice asymmetry of the tonsils while being of the same size.
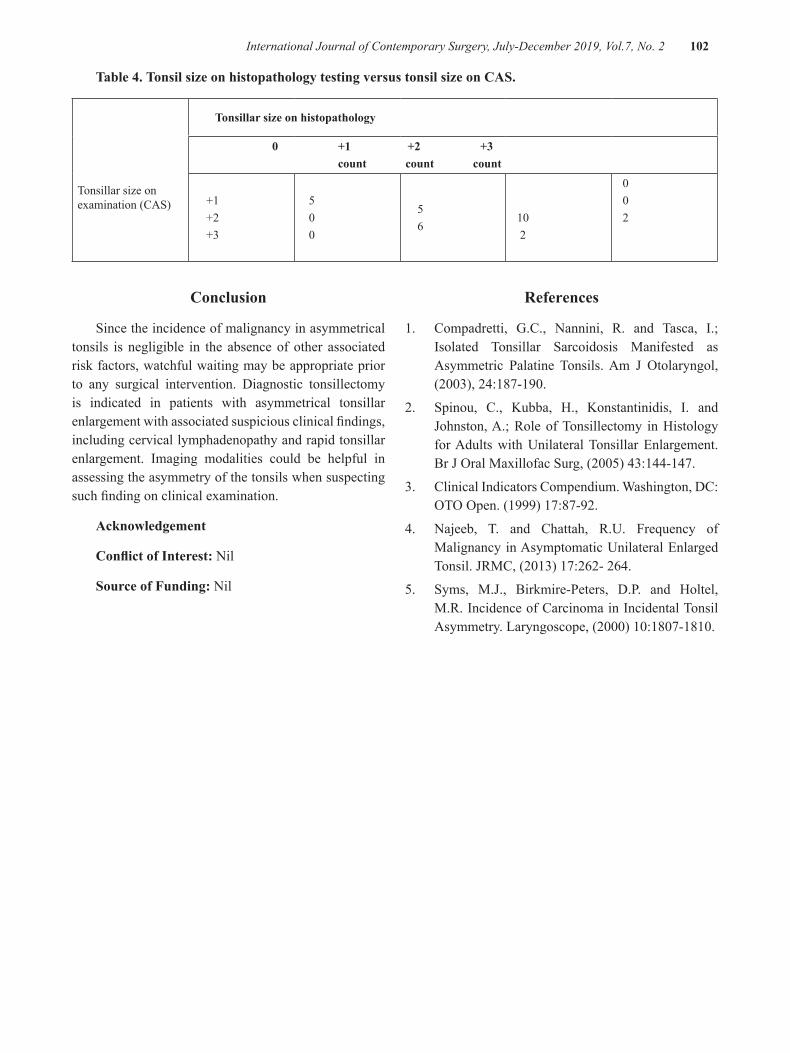
International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 102
Table 4. Tonsil size on histopathology testing versus tonsil size on CAS.
Tonsillar size on examination (CAS)
Tonsillar size on histopathology
0 +1 +2 +3 count count count
+1 +2 +3
5 0 0
5 6
10 2
0 0 2
Conclusion
Since the incidence of malignancy in asymmetrical tonsils is negligible in the absence of other associated risk factors, watchful waiting may be appropriate prior to any surgical intervention. Diagnostic tonsillectomy is indicated in patients with asymmetrical tonsillar enlargement with associated suspicious clinical findings, including cervical lymphadenopathy and rapid tonsillar enlargement. Imaging modalities could be helpful in assessing the asymmetry of the tonsils when suspecting such finding on clinical examination.
Acknowledgement
Conflict of Interest: Nil
Source of Funding: Nil
References
1. Compadretti, G.C., Nannini, R. and Tasca, I.; Isolated Tonsillar Sarcoidosis Manifested as Asymmetric Palatine Tonsils. Am J Otolaryngol, (2003), 24:187-190.
2. Spinou, C., Kubba, H., Konstantinidis, I. and Johnston, A.; Role of Tonsillectomy in Histology for Adults with Unilateral Tonsillar Enlargement. Br J Oral Maxillofac Surg, (2005) 43:144-147.
3. Clinical Indicators Compendium. Washington, DC: OTO Open. (1999) 17:87-92.
4. Najeeb, T. and Chattah, R.U. Frequency of Malignancy in Asymptomatic Unilateral Enlarged Tonsil. JRMC, (2013) 17:262- 264.
5. Syms, M.J., Birkmire-Peters, D.P. and Holtel, M.R. Incidence of Carcinoma in Incidental Tonsil Asymmetry. Laryngoscope, (2000) 10:1807-1810.
Original Article
A Prospective Comparative Study of Intestinal Anastomosis, Single Layer Extramucosal Versus Double Layer
Sohan Pal Singh1, Divya Prakash2, Dheeraj Raj Baliyan1, Virendra Kumar3, Vishal Saxena4, Prachi2
1Professor, 2Resident, 3Associate Professor, 4Assistant Professor, Department of Surgery, LLRM Medical College Meerut
Abstract
Background: Intestinal perforation peritonitis is a common surgical emergency in the Indian subcontinent and in tropical countries. Formation of an intestinal stoma is frequently a component of surgical intervention for diseases of the small bowel. The technique for stoma reversal has remained controversial in the use of single layer or two layers of anastomosis. Method: 30 patients for stoma closure were taken for study. These patients divided in two groups A and B, 20 and 10 each. These patients were taken up for ileostomy closure in single layer group A n-20 & double layer group B n-10. Results: 30 Patients of ileostomy were studied, divided in 2 groups, both groups were found to be comparatively equal in outcome with no any significant difference in complications. Conclusion: Double-layer anastomosis for ileostomy closure offers no definite advantage over single layer anastomosis in terms of postoperative leak and other complications. Single layer ileostomy closure technique is safe, easy to perform and simply to taught. Considering duration of the closure procedure and cost benefits, single-layer intestinal anastomosis may prove the choice of procedure for most of the surgeons.
Key words: Ileostomy closure, Acute abdomen, Peritonitis, Anastomosis, Stoma reversal
Corresponding author : Divya Prakash JR-III E-mail: [email protected]
Introduction
The intestinal anastomosis is a surgical procedure to restore intestinal continuity after removal of a pathological condition affecting the bowel. Intestinal anastomosis is one of the most commonly performed surgical procedures, especially in emergency setting and is also commonly performed in elective setting when the resection are carried out for benign or malignant lesions of the gastrointestinal tract.
The basic principles of intestinal suture were established more than 100 years ago by Travers, Lembert and Halsted1, and have since undergone little modification. One aspect of intestinal suturing technique that has remained controversial is the use of either one or two layers of sutures for anastomosis.
Historically, two-layer anastomosis using interrupted silk sutures for an outer inverted seromuscular layer and a running absorbable suture for a transmural inner layer has been standard for most surgical situations. Some recent reports have described single-layer continuous anastomosis using monofilament sutures as requiring less time and cost than any other method, without incurring any added risk of leakage2-5. Many surgeons probably now use single-layer suturing due to reductions in ischemia, tissue necrosis or narrowing of the lumen compared to the two-layer method.
Leakage from an anastomosis in the gastrointestinal tract that is often associated with increased morbidity, mortality rate6 and adversely affect length of hospital stay and cost7. The cause of the leakage may be multifactorial, including contribution from faulty technique, ischemia of the intestine at the suture line, excessive tension across anastomosis and mesentery, the presence of local sepsis, presence of obstruction distal to the anastomosis. Among other factors are male gender, smoking, obesity,
DOI Number: 10.5958/2321-1024.2019.00032.1

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 104
alcohol abuse, long duration of operation, preoperative blood transfusion and timing during duty hours8. The mortality rate for an anastomotic leak in the literature typically is in the 6 to 39% range and a 10- 100% rise of permanent stoma9. So the aim of this prospective study is to define the risk factors, comparison of single layer Vs double layer technique in patient outcome, morbidity and cost effectiveness.
Theory
It has been stated that “the key to a successful anastomosis is the accurate union of two viable bowel ends with complete avoidance of tension”10. Thus, the most important factors in the creation of a bowel anastomosis are1: meticulous technique2; good blood supply; and no tension3.
In addition various patient and technical factors can influence anastomotic healing are-
Patient factors affecting anastomotic healing
Positive factors: Good nutritional status11 - low pre-operative albumen and recent weight loss of over 5 kg are independent risk factors for anastomotic leakage12 Haemodynamic stability14 Healthy bowel ends and microvasculature14
Negative factors : High-dose steroids11 Old age11 Anaemia - haemoglobin < 11g/dL is an independent risk factor for anastomotic leakage11 Uraemia11 Diabetes mellitus11 Smoking12 Alcohol abuse12 High risk site of anastomosis e.g., low colorectal anastomoses12 Male sex in colorectal anastomoses - presumably as the narrow pelvis results in poor visualisation and a more challenging operation12
Technical factors affecting anastomotic healing
Positive factors : Accurate seromuscular apposition3, No distal obstruction14, Closure of the mesenteric window3
Negative factors : Faecal contamination12, Haematoma formation12
Method
Patients and Method
The study was approved by the Ethics Committee of the CCS University Meerut. All patients who were
admitted for closure of ileostomy to the SVBP Hospital Meerut from Sept 2017 to August 2018 were included in the study. The following information was extracted from the patient admitted at hospital: patient demographics, indication for ileostomy, comorbidity status, length of hospital stay, duration of stoma, time taken to achieve bowel movement after closure, time taken or passage of flatus and feces, time taken for orally allowed performance status of the patient, experience level of surgeon performing the operation junior resident or consultants, duration of the surgery, duration of hospital say and morbidity, and whether the patient required re-operation or not.
The complications observed were divided into 3 main groups, major, minor and medical complications. The major complications included reoperation and anastomotic leaks, the occurrence of wound site dehiscence, fever >3 days, chest infection. Minor complications included surgical site infection, bleeding per rectum and occurrence of a stitch granuloma. Medical complications included pneumonia, UTI, line sepsis, cardiac complications, renal failure, anemia, DVT and allergic reaction to medication. The frequency of these complications was then recorded for each patient.
Surgical Technique
All patients had a radiological contrast study loopogram done prior to closure to rule out any distal bowel obstruction and leaks. All patients receive bowel preparation prior to closure. At the operation all patients received a single dose of prophylactic antibiotics Ceftriaxone 1g IV about 30 minutes prior to the skin incision. A peristomal skin incision was used and none of the patients needed a laparotomy for the closure. Standard loop ileostomy closure was performed using either a single layer hand sewn end to end anastomosis or double layer in form of continuous simple or interrupted simple or connell or alternate simple and connell. All operations were performed by a senior resident under the supervision of a senior consultant
Data Analysis
Data was analyzed after taking mean of various outcomes.
Inclusion Criteria
1. All patients undergoing stomach closure

105 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
coming to SVBP Hospital between a period of Sept 2017 to August 2018.
2. Age between 6 years and 65 years.
Exclusion Criteria
1. Esophageal, Duodenal, Jejunal, Anastomosis
2. Age <6 years and >65 years
Technique
Technique: the bowel loop of stoma was mobilized from surrounding skin, minor adhesions were separated using blunt dissection. The bowel ends were cleaned and freshened using 15 no. blade for fresh bleeding points and approximated. Double layer anastomosis: The inner layer was constructed in a continuous manner using silk 3-0 suture, or full thickness interrupted simple suture with silk 3-0. The outer seromuscular sutures were taken in an interrupted manner, inverting the inner layer using 3–0 silk suture. Single layer anastomosis: All the single layered intestinal anastomoses were performed using an interrupted 4–0 silk that began at the mesenteric border, incorporating outer seromuscular layer. Each bite included 4–6 mm of the wall from the edge and about 5 mm from each other. The larger bites were used at the mesenteric border to ensure an adequate seal. Only enough pressure was applied to the suture to avoid ischemia of the anastomosis. The edges of the mesentery were closed to prevent any internal herniation. The patency of the anastomosed segment was confirmed by gently palpating the anastomosis between the thumb and the index finger.
Each case was analyzed with respect to duration required to perform intestinal anastomosis & post-operative complications like anastomotic leak. The duration of anastomosis begins with patient being taken on operation table and ended when the last stitch was cut. All single layer anastomoses were done with silk 3-0 pack which had a suture material of 60 cm length. For double layer, 3-0 silk was used taking through all layers and seromuscular layer with 3-0 Silk pack which had suture material measuring 60 cm.
Anastomotic leak was defined as fecal discharge in the drain or from the wound. On discharge, the patients were followed up at 1st week thereafter. The patients were evaluated for gastrointestinal complaints and other complaints, if any.
Table 1: Showing site of anastomosis
Disease Group No. of Cases n%
FUC of ileostomy 28 93.3%
FUC of Colostomy 2 6.6%
Table 2: Comparison between site of anastomosis
Site of anastomosis
This Study Previous study Burch et al study9
Group A Group B Group A Group B
Ileo ileal 18 9 37% 28%
Ileo colic 2 1 29% 40%
Table 3: Comparison between single Vs double layer anastomosis
Groups This Study Previous study
Burch et al study9
Silk Vicryl Silk Prolene
Single layer Group A 14 6 1
Double layer Group B 6 4 3 0
Table 4: Comparison between duration of anastomosis
Groups Mean duration of Anastomosis
My Study Burch et al9
Khan et al12
Single layer Group A 46.0 min 20.8 20
Double layer Group B 86.5 min 30.7 35
Table 5: Comparison between hospital stay
Groups Hospital stay
My Study Burch et al 9
Garude et al 10
Single layer Group A 8.45 days 7.9 12
Double layer Group B 8.2 days 9.9 12

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 106
Table 6 : Postop characteristics of patients
Groups
ICU
ICU Stay
Oral sips allowed
Flatus Passed
Single layer Group A 3.8 3.7 2.05
Double layer Group B 4.8 3.2 2.4
Results
Twenty patients were selected in single layer group, and 10 patients in double layer group. in single layer 66.6 % of the patients were male while in double layer 80% were male. The mean age for single layer was 27.2 years and in double layer was 31.9 year. all of procedures were performed in elective settings with proper bowel wash. In maximum cases 18 in single layer and 9 in double layer end to end type of anastomosis was done (Table 2). Single pack of suture material silk used in single layer and two pack of silk used in double layer anastomosis(Table 3). Mean duration required for single layer anastomosis was 46.0 minutes and for double layer anastomosis was 86.5 minutes (Table 4). The mean duration of hospital stay in single layer was 8.45 days and in double layer 8.2 days (Table 5). None of the patients in either group developed anastomotic leak. So when the data was compared, hospital stay and the number of patients developing complication anastomotic leak rate in the single-layered group was not found to be significant, whereas the mean time required for construction of anastomosis and no. of sutures used was found to be highly significant when compared with the double-layered group.
Discussion
This study assessed the efficacy and safety of single layer anastomosis in comparison with double layer anastomosis in stoma closure. The study included two groups: Group A-Single layer and Group B-Double layer, with a total of 30 cases. technique of single Vs double layer was surgeons choice depending on comfort zone. Anastomosis was done at stoma site between bowel loops and delivered into peritoneal cavity. The efficacy of both groups was compared in terms of duration required to perform intestinal anastomosis, cost effectiveness and post-operative complications like anastomotic leak. In our study majority of procedures
involved were of ileo-ileal type of anastomosis Single layer-90 % and Double layer-90%. In our study the mean duration required to construct a single layer anastomosis was 46.0 minutes and 86.5 minutes for double layered anastomosis. Therefore there is significant difference in time taken between both groups Single layered found to economical compare to double anastomosis as the total number of suture silk packs required in double-layered anastomosis was 2, whereas in single-layer anastomosis only one pack of silk was used. In our study we used silk as suture material because it is cheap and easily available. In our comparative study the mean duration of hospital stay in single layer was 8.45 days and in double layer it is 8.2 days which almost equal to mean duration of stay in Niyaz Ahmed study 7.32 and 7.92 where as in Garude et al. study duration of stay is equal in each group 12 and 12 and in Burch et al study 7.9 and 9.9, 2 days more in double layer was noted. But in our study, no significant change noted on duration of hospital stay (Table 5). The number of anastomotic leak in our study was nil in both groups. Whereas in Khan et al. study 1 6% leak in single layer and 2 12% in double layer while in Niyaz Ahmed study 1 4% leak was present in single layer and 2 8% in double layer. However in our study, anastomotic leak rate is nil as all the patients were electively chosen for stoma closure, with negligible comorbidities and proper bowel preparation
Intestinal anastomosis has been intensely studied and many comparisons between alternative techniques and suture materials have been made. Double-layered intestinal anastomosis was first performed by Travers and Lembert6 in the early 19th century. Since then double layer technique was used widely over the years. The single-layered interrupted anastomosis was first described by Hautefeuille8 in 1976. Outcome of any intestinal anastomosis depends upon its ability to heal without leakage. Healing process in gastrointestinal tract proceeds through same stages as wound healing elsewhere in body. Several factors like blood supply is less compromise, less damage to submucosal venous plexus, excessive inversion of tissue or very less narrowing, may responsible for good outcome in single layer anastomosis. In our institute like government hospitals where large number of emergency procedures perform and most of patients are poor with economic problems, single layer anastomosis method is beneficial as it reduces operative time, time of anesthesia and less suture material required so economical and equally safe.

107 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
Permission from ethical committee -taken
Source of Funding - Self
Conflict Interest - None
References
1. Brooks DC, Zinner MJ. Surgery of the Small and Large Bowel. In: Zinner MJ, editor. Maingot’s Abdominal operations. 10. Vol. 2. Stamford: Appleton & Lange; 1997. pp. 1309–1310.
2. Thomson WHF, Robinson MHE. One-layer continuously sutured colonic anastomosis. Br J Surg. 1993;80:1450–1451.
3. AhChong AK, Chiu KM, Law IC, Chu MK, Yip AW. Single-layer continuous anastomosis in gastrointestinal surgery: a prospective audit. Aust NZ J Surg. 1996; 66:34–36.
4. Brodsky JT, Dadian N. Single-layer continuous suture for gastrojejunostomy. Am Surg. 1997;63:395–398.
5. Law WL, Bailey HR, Max E, Butts DR, Smith KW, Thompson DA, Skakun GB, Graves E. Single-layer continuous colon and rectal anastomosis using monofilament absorbable suture Maxon: study of 500 cases. Dis Colon Rectum. 1999;42:736–740. doi:10.1007/BF02236928
6. Bruce J, Krukowski ZH, Al-Khairy G et al 2001. Systematic review of the definition and measurement of anastomotic leak after gastrointestinal surgery. Br J Surg. 889: 1157- 68.
7. Sultan R, Chawla T and Zaidi M 2014. Factors affecting anastomotic leak after colorectal anastomosis in patients without protective stoma in tertiary care hospital.J Pak Med Assoc. 642:166-70.
8. Gorissen KJ, Benning D, Berghmans T et al 2012. Risk of anastomotic leakage with nonsteroidal anti-inflammatory drugs in colorectal surgery. Br J Surg. 995:721-7.
9. Brisinda G, Vanella S, Cadeddu F et al 2009. End-to-end versus end-to-side stapled anastomoses after anterior resection for rectal cancer. J Surg Oncol. 991:75-9.
10. Kirk RM, Winslet M. Essential General Surgical Operations. Edinburgh: Churchill Livingstone; 2001.
11. Paterson-Brown S, Beck DE, Whitlow CB. A Companion to Specialist Surgical Practice: Core Topics in General and Emergency Surgery. 4th ed.Philadelphia: Elsevier Saunders; 2009. pp. 167–192.
12. Taflampas P, Christodoulakis M, Tsiftsis DD. Anastomotic leakage after low anterior resection for rectal cancer: facts, obscurity, and fiction. Surg Today. 2009;39:183–188.
13. Saha AK, Tapping CR, Foley GT, Baker RP, Sagar PM, Burke DA, Sue-Ling HM, Finan PJ. Morbidity and mortality after closure of loop ileostomy. Colorectal Dis. 2009;11:866–871.
14. Scott-Conner CEH. Chassin’s Operative Strategy in General Surgery. Heidelberg: Springer; 2002.

Original Research Article
Intra-Peritoneal Bupivacaine Instillation for Post-Operative Pain Relief after Laparoscopic Cholecystectomy:
A Prospective Study
Suma S1, Vikranth Suresh N2, Nikhil M3, Sreeramulu P N4
1Post-graduate (PGY3),2Assistant Professor, Department of Surgery, 3Assistant Professor, Department of Anaesthesia, 4Professor, Department of Surgery, Sri Devaraj Urs Medical College, Kolar, Karnataka, India
Abstract
Background: Pain relief remains milestone achievement ascribed to laparoscopic cholecystectomy. Post laparoscopic cholecystectomy patient still complains of port site/incisional pain, shoulder pain and vague upper abdominal pain. A simple method of portal or incisional infiltration and intra-peritoneal spraying of a local anesthetic agent over gall bladder fossa can reduce postoperative pain.
Method: This study was conducted to determine whether Bupivacaine wash at gall bladder fossa and infiltration of local anesthetic at trocar sites has any effect in postoperative pain relief. This prospective study was conducted on 68 patients, where 20 ml of normal saline wash was given in group A and 20ml of 0.25% bupivacaine wash was given in group B at the gall bladder fossa and in both the groups, the same local anesthetic was infiltrated at the port sites and the outcomes was studied.
Results: Pulse rate and blood pressure were significantly low in group B than group A. The median pain score was significantly low in group B than group A. Also, the total number of analgesic doses used in group B was significantly less than the group A.
Conclusions: Instillation at gall bladder fossa and infiltration to the port sites using 0.25% bupivacaine is an effective method of postoperative pain relief after laparoscopic cholecystectomy.
Keywords: Bupivacaine wash, Normal saline wash, Post-operative analgesia, Laparoscopic cholecystectomy.
Corresponding Author: Dr. Vikranth Suresh N, Assistant Professor, Department of Surgery, Sri Devaraj Urs Medical College, Kolar, Karnataka, India. Phone No.: 7022528219, e-mail ID: [email protected]
Introduction
Laparoscopic cholecystectomy has become the procedure of choice for symptomatic cholelithiasis. This procedure returns the patient to full activity within 1 week when compared to open cholecystectomy where the return to full activity is around 1 month. It has improved surgical outcome in terms of reduced pain
and early return to activity compared to conventional cholecystectomy.1,2 In laparoscopic cholecystectomy, pain is derived from multiple sites, port site pain (somatic), deep intra-abdominal pain (visceral), and shoulder pain (due to phrenic nerve irritation). 5,6 Pain management with multiple analgesic and opioids has been reported with variable success.1,2,4
The various methods used with variable success are NSAID’S7, infiltration of wound with local anaesthetics8 and intermittent intramuscular narcotics9. Considering the variable results obtained by various authors and availability of few studies, 11,12,13,14 the present study was conducted in patients undergoing laparoscopic cholecystectomy where 20 ml of normal saline wash was given in group A and 20ml of 0.25% bupivacaine wash
DOI Number: 10.5958/2321-1024.2019.00033.3

109 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
was given in group B at the gall bladder fossa and both in the groups, the same local anesthetic was infiltrated at the port sites and the outcomes were studied.
Aims and Objectives
1. To study the post-operative pain relief in patients undergoing laparoscopic cholecystectomy for symptomatic gall stone disease, who have received intra-peritoneal lavage with 20 ml of normal saline at the gall bladder fossa and port site infiltration with the local anaesthetic.
2. To study the post-operative pain relief in patients undergoing laparoscopic cholecystectomy for symptomatic gall stone disease, who have received intra-peritoneal lavage with 20 ml of 0.25% bupivacaine at the gall bladder fossa and port site infiltration with local anaesthetic.
3. To compare the outcomes between two set of patients.
Method
Study design
This prospective study was conducted in tertiary centre, R.L Jalappa Hospital, Kolar, Karnataka, India. Study was conducted for 12 months between January 2018 to December 2018, on 68 patients undergoing laparoscopic cholecystectomy after obtaining the consent.
Inclusion criteria
Patients with gallstone disease who underwent standard 4 port laparoscopic cholecystectomy above 18 years of age who were willing to participate in the study.
Exclusion criteria
Documented allergy to bupivacaine or after skin testing, history of cardiovascular disease which required treatment, history of chronic pain disease other than that related to gallstone, and pregnant patients
Method
Two 10mm ports, umbilical and epigastric port and two 5mm working ports were inserted after induction of general anesthesia. Patient was placed in head up and slight tilt on left side. A Veress needle was used to create pneumoperitoneum with CO2 insufflator to create a pressure of 10mmHg at a flow rate of 1litre/min.
The patients were randomized into 2 groups of 34 cases each. In group A, 20ml of normal saline was instilled at gall bladder fossa. In group B, 20ml of 0.25% bupivacaine was instilled in gallbladder fossa after removal of gall bladder. In both the groups the same local anesthetic was infiltrated at port sites. 15 ml of 0.5% bupivacaine was taken and diluted with 15 ml of distilled water to make it 30 ml of 0.25% concentration. 20 ml was used for intra-peritoneal lavage and 10 ml was used for infiltration at port sites.
Postoperatively the patients were assessed for pain using Wong Baker Faces pain rating scale as shown in figure 1, also other parameters like heart rate, blood pressure, and total number of analgesic doses used were assessed. The above parameters were assessed at 1, 3, 6, 12 and 24 hours in post-operative period. First dose (rescue) analgesia was used when the pain score was above 6. The analgesic used was, injection diclofenac sodium 75mg intramuscularly, given after test dose.
Figure 1

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 110
Results
Statistical analysis:
Data was entered into Microsoft excel data sheet and was analyzed using SPSS 22 version software. Categorical data was represented in the form of Frequencies and proportions. Chi-square test was used as test of significance for qualitative data. Continuous data was represented as mean and standard deviation. Independent t test or Mann Whitney U test was used as test of significance to identify the mean difference between two quantitative variables and qualitative variables respectively. Paired t test or Wilcoxon
Signed rank test is the test of significance for paired data such as before and after surgery for quantitative and qualitative data respectively.
Graphical representation of data: MS Excel and MS word was used to obtain various types of graphs such as bar diagram.
p value (Probability that the result is true) of <0.05 was considered as statistically significant after assuming all the rules of statistical tests.
Statistical software: MS Excel, SPSS version 22 (IBM SPSS Statistics, Somers NY, USA) was used to analyze data.
Table 1: General profile of subject’s comparison between two groups
Group
P value Bupivacaine wash Normal Saline wash
Count % Count %
Age
<30 years 10 29.4% 5 14.7%
0.363
31 to 40 years 13 38.2% 14 41.2%
41 to 50 years 2 5.9% 4 11.8%
51 to 60 years 6 17.6% 5 14.7%
61 to 70 years 3 8.8% 3 8.8%
>70 years 0 0.0% 3 8.8%
SexFemale 21 61.8% 27 79.4%
0.110Male 13 38.2% 7 20.6%
Diagnosis
Calculous cholecystitis 3 8.8% 1 2.9%
0.587Cholelithiasis 30 88.2% 32 94.1%
Chronic cholecystitis 1 2.9% 1 2.9%
In Bupivacaine wash group, majority were in the age group 31 to 40 years (38.2%), 61.8% were female, 88.2% had Cholelithiasis. Similarly in Normal saline wash, majority were in the age group 31 to 40 years (41.2%), 79.4% were female, 94.1% had Cholelithiasis.
There was no significant difference in age, sex and diagnosis between two groups. This ensures age and sex matching between two groups.
Table 2: Vital signs comparison between two groups
Group
P value Bupivacaine wash Normal Saline wash
Mean SD Mean SD
PR 85.29 6.40 92.18 6.41 <0.001*
SBP 126.06 10.12 134.35 12.65 0.004*
DBP 81.00 7.73 86.24 9.30 0.014*

111 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
In Bupivacaine wash group, mean Pulse rate was 85.29 ± 6.40 bpm, mean SBP was 126.06 ± 10.12 mmhg, mean DBP was 81.00 ± 7.73 mmhg.
In Normal Saline wash group, mean Pulse rate was 92.18 ± 6.41 bpm, mean SBP was 134.35 ± 12.65 mmhg,
mean DBP was 86.24 ± 9.30 mmhg.
The pulse rate and blood pressure were significantly lower in group B than in group A.
Table 3: Pain Score at operative site comparison between two groups at different time intervals
Pain score at operative site
Group
P value Bupivacaine wash Normal Saline wash
Mean SD Median Mean SD Median
1 hour 7 1 6 7 1 8 0.034*
3 hours 6 1 6 7 1 8 0.006*
6 hours 6 2 6 7 1 7 0.033*
12 hours 4 1 4 5 1 4 0.013*
24 hours 2 1 2 3 1 4 <0.001*
In the Bupivacaine wash, pain score at operative site, at baseline was 6, at 3 hours was 6, at 6 hours was 6, at 12 hours was 4 and at 24 hours was 2.
In Normal Saline wash, Median pain score at baseline was 8, at 3 hours was 8, at 6 hours was 7, at 12 hours was 4 and at 24 hours was 4.
The Median pain score was significantly less in Bupivacaine wash (group B) as compared to normal saline wash (group A)
Table 4: Pain score at Shoulder Site comparison between two groups at different time intervals
Pain score at Shoulder Site
Group
P value Bupivacaine wash Normal Saline wash
Mean SD Median Mean SD Median
3 hours 0 1 0 1 1 0 0.023*
6 hours 0 1 0 1 1 0 0.023*
12 hours 0 1 0 0 1 0 0.102
24 hours 0 0 0 0 1 0 0.079
In the study, the Median Shoulder pain score was significantly low in group B as compared to group A at 3 hours and 6 hours. At 12 hours and 24 hours there was no significant difference in Shoulder pain score between two groups.
Table 5: First dose of Analgesic and Number of Doses comparison between two groups
Group
P valueBupivacaine wash Normal Saline wash
Mean SD Median Mean SD Median
First dose of Analgesic 3.2 0.8 3 1.4 0.6 1 <0.001*
No of doses 1.8 0.4 2 3.1 0.3 3 <0.001*

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 112
In group B, mean first dose of analgesic used was 3.2 hours and in group A was 1.4 hours. There was significant difference in mean first dose of analgesic used between two groups.
In group B, mean number of analgesic doses used was 1.8 and in group A was 3.1. The total number of analgesics used was significantly high in group A as compared to group B.
Discussion
Laparoscopic cholecystectomy is one of the most common elective laparoscopic surgeries done in our institute. We observed that post-operatively majority of the patients complain of abdominal pain, incisional pain at port sites and right shoulder tip pain. Often there is need of intravenous and intramuscular analgesic.
In present study the pulse rate and blood pressure were significantly lower in group B than group A. The increase in heart rate and blood pressure in group A during early post-operative period could be due to pain.
These findings are comparable to the findings of study conducted by Rajesh kumar meena et al, where the heart rates were low in patients received 0.75% ropivacaine in comparison to the group who received 0.25% bupivacaine whereas the blood pressures were statistically insignificant in both the groups.16
In our study, the analgesic effect was sustained upto 6 hours with the median pain score of 6 in group B, in comparison with the group A which was 7 at 6 hours and significantly reduced, with the pain score of 2 and 4 at 24hours respectively. Thus the median pain score in group B was significantly low in group B as compared to group A in first 24 hours.
This was comparable to the study by Devalkar and Salgaonkar who found mean VAS score readings to be lower in Bupivacaine group as compared to Normal saline group and were statistically significant at 2, 4, 8, and 12 h.17
In present study, there was significant difference in the mean shoulder pain in the initial 6 hours, but no significant difference noted at 12 and 24 hours.
Bisguard et al has also shown that combination of local and intra-peritoneal anaesthetic is effective in decreasing incisional pain but not in visceral or shoulder
pain.18
In Our study, mean First dose of analgesic used was 3.2 hours in group B and in group A was 1.4 hours. The mean first dose of analgesic requirement in group B was significantly lower as compared to group A.
A similar study by Sulekha et al showed on an average the frequent dosing of rescue analgesia were highest in patients who received normal saline wash as compared to those receiving 0.5% bupivacaine wash.19
In Our study, mean number of analgesic doses used was 1.8 in group B and 3.1 in group A. There was significant difference in mean number of analgesic doses between two groups.
A study done by Rafaei et al revealed that the number of patients who needed postoperative analgesia with bupivacaine was significantly lower than control.20 Goldstein et al recorded that morphine consumption at wake-up and over the first 24 hours, was significantly lower with bupivacaine and ropivacaine when compared with normal saline.21
Scheinin et al conducted a study, they found that while using 10ml of 0.15% bupivacaine with adrenaline (150mg) intra-peritoneally, there were no side effects such as circumoral numbness, tinnitus, muscle twitches or cardiac arrhythmias.22
In our study also there was no incidence of these above mentioned side effects.
Conclusion
From our study, the pain score and the total number of analgesic doses used was significantly low in patients receiving bupivacaine wash as compared to those receiving normal saline wash. Thus, we conclude that intra-peritoneal instillation and port site infiltration of 0.25% bupivacaine is a safe and effective method of achieving post-operative analgesia after laparoscopic cholecystectomy.
Conflict of Interest: Authors & Co-authors declare that no conflict of interest was there, during the conduct of the study.
Funding: Authors & Co-authors declare that no funding or financial support was provided by any sources, during the conduct of the study.

113 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
Ethical Committee Approval: Ethical committee clearance from Institutional Ethical Committee (IEC) was taken prior to the start of the study.
References
1. Downs SH, Black NA, Devlin HB, et al. Systematic review of the effectiveness and safety of laparoscopic cholecystectomy. Ann R Coll Surg Engl 1996 ;78:241–323.
2. Lau H, Brooks DC. Predictive factors for unanticipated admissions after ambulatory laparoscopic cholecystectomy. Arch Surg. 2001; 136:1150–1153.
3. Fiorillo MA, Davidson PG, Fiorillo M, et al. 149 ambulatory laparoscopic cholecystectomies. Surg Endosc. 1996; 10:52–56.
4. Callesen T, Klarskov B, Mogensen, et al. Day case laparoscopic cholecystectomy: feasibility and convalescence. Ugeskr Laeger. 1998; 160: 2095–2100.
5. Bisgaard T, Klarskov B, Rosenberg J, et al. Characteristics and prediction of early pain after laparoscopic cholecystectomy. Pain. 2001; 90: 261–269.
6. David CW. Analgesic treatment after laparoscopic cholecystectomy. Anesthesiology. 2006; 104:835–846.
7. Lord Mc Coll. Laparoscopic cholecystectomy. Am R coll Surg Engl: 1992; 74:231
8. Rees BI, Williams HR. Laparoscopic Cholecystectomy the first 155 patients. Am R Coll Surg Eng 1992; 74:233- 6.
9. Scott AND, Greville AC, Mc Millan L, Wellwood J Mc K. Laparoscopic laser cholecystectomy results of the technique in 210 patients Am R Coll Surg; 1992; 74: 237 – 241.
10. Joris J, Cigarini, I, Legrand M, Jacquet N, De GD, Franchiment P, Lamy M. Metabolic and respiratory changes after cholecystectomy performed via laparotomy or laparoscopy. Brit J Anaesth 1992; 69: 341-345.
11. Paras K Pandove, Nitish Arora, Arun Garg, Lovelesh Pandove,Ashwani kumar. Intraperitoneal instillation of gallbladder fossa and at trocar sites in reduction of post-operative pain after laparoscopic cholecystectomy: a prospective randomized
controlled double blind trial. International Surgery Journal 2017 Apr; 4(4); 1204-8.
12. Neerja Bhardwaj, Vikas Sharma, Pramila Chari. Intraperitoneal bupivacaine instillation for postoperative pain relief after laparoscopic cholecystectomy. Indian journal of Anesthesia 2002; 46(1): 49-52.
13. Gerardo Castillo-Garza, MD, Jose A. Diaz-Elizondo, MD, Carloa A. Cuello-Garcia, MD, Oscar Villegas-Cabello, MD. Irrigation with bupivacaine at the surgical bed for post-operative pain relief after laparoscopic cholecystectomy. Journal of the society of Laparoendoscopic Surgeons 2012; 16:105-111.
14. Saurabh Agarwal, Srinivas Pai. Evaluation of postoperative pain relief with intraperitoneal bupivacaine instillation in laparoscopic cholecystectomy-a randomized control study. International Surgery Journal 2017 Apr; 4(4):1195-1200.
15. Il-Ok Lee MD PhD, Sun-Han Kim MD, Myung-Hoon Kong MD PhD, Mi-Kyung Lee MD PhD. Pain After Laparoscopic cholecystectomy: the effect and timing of incisional and intraperitoneal bupivacaine. Canadian Journal Of Anesthesia 2012: 545-50.
16. Meena RK, Meena K, Loha S, Prakash S. A comparative study of intraperitoneal ropivacaine and bupivacaine for postoperative analgesia in laparoscopic cholecystectomy: A randomized controlled trial. Anaesth Pain Intensive Care 2016; 20: 295‐300.
17. Devalkar PS, Salgaonkar SV. Intraperitoneal instillation of 0.25% bupivacaine for laparoscopic cholecystectomy: Effect on postoperative pain. IJCMAAS 2016; 12: 91‐5.
18. Bisgaard T, Kehlet H, Rosenberg J. Pain and convalescence after laparoscopic cholecystectomy. Eur J Surg. 2001; 167: 84-96.
19. Sulekha. The Effect Of Intraperitoneal Bupivacaine For Post-Operative Pain Management In Patients Undergoing Laparoscopic Cholecystectomy- A Prospective Double-Blind Randomized Control Study. IOSR Journal of Dental and Medical Sciences 2013; 4: 64-69.
20. Rafaie AMN, Khatab MM. Reduction of early postoperative pain after diagnostic laparoscopy

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 114
with local bupivacaine: a randomized placebo controlled study. J Middle East Fertility Society. 2005; 10(3):244-49.
21. Goldstein A, Grimault P, Henique A, Keller M, Fortin A, Darai E. Preventing postoperative pain by local anesthetic instillation after laparoscopic gynecologic surgery: a placebo-controlled
comparison of bupivacaine and ropivacaine. Anesth Analg. 2000 Aug; 91(2):403-7.
22. Scheinin B, Kellokumpu I, Lindgren L. effect of intraperitoneal bupivacaine on pain after laparoscopic cholecystectomy. Act Anaesthesiol Scand. 1995; 39:195-8.

Incidence of Differentiated Thyroid Carcinoma in Multinodular Goitre Patients in Western UP
Yogendra Kumar1, Vandana Singh2, Sushil Gaur3
1Assistant Professor, SIMS Hapur, 2Professor, 3Associate Professor, SMC Ghaziabad
Abstract
Background: The prevalence of multinodular goitre in all over the world is high, commonly in developing countries. Incidence of differentiated thyroid carcinoma among patients with multinodular goitre is increased in recent literature.
Aim of Study: To determine the incidence rate of differentiated thyroid carcinoma among patients with multinodular goitre.
Patients and Method: This study is a cross sectional study carried out in Surgical Ward of Saraswati Institute Of Medical Sciences,Hapur, during the period from September 2016 to July 2017 on convenient sample of 60 patients with multinodular goitre.
Clinical history and examination, fine needle aspiration and postoperative histopathology examination was done to confirm the diagnosis.
Results: Mean age of patients was 43.9 years, with 5 males and 55 females. Fine needle aspiration test showed that 13 (21.7%) multinodular goitre patients had differentiated thyroid carcinoma, while 47 (78.3%) patients had benign goitre. The histopathology of multinodular goitre patients revealed that 41.7% of them had colloid goitre, 16.7% of them had micro-papillary carcinoma and 38.3% of them had follicular adenoma. Differentiated thyroid carcinoma among multinodular goitre patients was significantly associated with smoking and exposure to ionizing radiation.
Conclusions: The incidence of differentiated thyroid carcinoma among multinodular goitre patients is high.
Keyword - Multinodular goitre, malignancy, differentiated thyoid carcinoma
Corresponding author:E-mail: [email protected]
Introduction
Multi-nodular goitre
Goitre, or the enlargement of the thyroid gland, comprises a variety of conditions. Goitres can be classified as toxic or non toxic, diffuse or nodular and solitary or multiple. Multi is a commonly used term describing an enlarged thyroid gland with multiple areas of nodularity [4]. Histologically, MNG is defined as a thyroid enlargement with follicles that are morphologically and functionally grossly altered,it usually develops over years Goitre, or
the enlargement of the thyroid gland, comprises a variety of conditions. Goitres can be classified as toxic or non toxic, diffuse or nodular. Multi-nodular goitre term describing an enlarged thyroid gland with multiple areas of nodularity, MNG is defined as a thyroid enlargement with follicles that are morphologically and functionally grossly altered: it usually develops over years [5]. MNG is endemic in certain regions of world, mostly in regions of Iodine deficient diet [3]. Various factors are implicated in the development of MNG 6.
Epidemiology
MNG is the most common endocrine disorder affecting 500 to 600 million people worldwide7. In India about 54 million people have goitre and the number
DOI Number: 10.5958/2321-1024.2019.00034.5

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 116
at risk is estimated to be about 167 million6. MNG is said to be endemic when it affects more than 10% of a given population3. Non endemic goitre is more common in women and elderly 8. An average figure for sex distribution in both endemic and non endemic regions is 3:1 (Female: Male)3. Nodules appear early in endemic goitre and later in sporadic goitres although patient may be unaware of the goitre until he or she in their late 40s and 50s9. In India, main endemic goitre belt is sub Himalayan region and pockets of endemic goitre are present in many states6.
In study conducted in western UP, there were 64.6% with multinodular goitre, 22% were with diffuse goitre and 12.6% were solitary nodules. Thyrotoxicosis was noticed in 21.5%. Thyroid malignancy was diagnosed in 6.3% with a female predominance (80%). Papillary carcinoma was among 80% of patients with malignancy. Hashimoto’s thyroiditis was observed in 6.3%, all of them were females10.
Diagnosis of differentiated thyroid cancer
The most common clinical sign of thyroid cancer is a solid,rapid growing and painless nodule, discovered by the patient or at a clinical examination. The diagnosis of thyroid cancer is based on U/ S and FNAC. FNAC is performed under U/S guidance and is indicated in cases of clinical or U/S suspicion of a malignancy11.
Differentiated thyroid cancer and multi-nodular goitre
The prevalence of incidental thyroid cancer (ITC) in multinodular goitre (MNG) has been previously estimated to be 5-10%12,13; however, recent studies have reported higher ITC prevalence rates, ranging from 8.6 to 22% 14,15 The optimal surgical procedure for MNG patents remains a subject of debate, due to not only the increasing prevalence of ITC among these patients but also the incidence of TC in recurrent goitre15. In this particular study, the authors observed the patients for approximately 180 months.
Statistical Analysis
All patients’ data entered using computerized statistical software; Statistical Package for Social Sciences (SPSS) version 20 was used. Descriptive statistics presented as (mean ± standard deviation) and frequencies as percentages. Multiple contingency tables
conducted and appropriate statistical tests performed, Chi-square used for categorical variables (Fishers exact test was used when expected variables were less than 5) and Independent samplet test was used to compare between two means. In all statistical analysis, level of significance (p value) set at 0.05 and the result presented as tables and/or graphs. Statistical analysis of the study was done by the community medicine specialist.
Result
This study included 60 patients with multi-nodular goitre (MNG) with mean age of 43.9 ± 11.6 years; 6.7% of them were less than 30 years age, 22.5% of them were in age group 30-39 years, 39.2% of them were in age group 40-49 years, 20.8% of them were in age group 50-59 years and 10.8% of them were 60 years of age and more. Female patients with MNG were more than males with female to male ratio of 11:1. All these findings were shown in Table 1. More than two thirds (76.7%) of studied MNG patients were living in urban areas while 23.3% of them were living in rural areas. The educational level of MNG patients was distributed as followings;28.4% illiterate, 56.6% primary level, 10% secondary level and 5% higher education. All (100%) of studied MNG patients were Indians, Hindu and Muslims. All these findings were shown in Table 2. About two thirds (66.6%) of MNG patients were non-smokers, while 15.1% of them were current smokers and 18.3% of them were ex-smokers. The family history of thyroid malignant diseases was positive among 15% of MNG patients while the family history of exposure to ionizing radiation was positive among only 2 MNG patients. All these findings were shown in Table 3. All studied MNG patients had euthyroid status at diagnosis. Fine needle aspiration test revealed that 13(21.7%) MNG patients had differentiated thyroid carcinoma, while 47 (78.3%) patients had benign MNG. The histopathology of MNG patients revealed that 41.7% of them had colloid goiter, 38.3% follicular adenoma, 16.7% micro-papillary carcinoma and 3.3% follicular carcinoma. All these findings were shown in Table 4. No significant difference was observed between MNG patients with differentiated carcinoma and those with benign MNG regarding their age and gender. All these findings were shown in Table 5.

117 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
Table 1 : Demographic characteristics of MNG patients
Variable No. Percent%
Age mean +sd(43.9+116 years)
<30years 4 6.7
30-39 years 13 22.5
40-49 years 24 39.2
50-59 13 20.8
>60 6 10.8
Total 60 100.0
Gender
Male 5 8.3
Female 55 91.7
Total 60 100.0
Table 2: Social characteristics of MNG patients
Variable No. Percentage%
Residence
Urban 46 76.7
Rural 14 23.3
Total 60 100
Education Level
Illiterate 17 28.4
Primary 34 56.6
Secondary 6 10
Higher Education 3 5
Total 60 100
Religion
Hindu 27 45
Muslim 33 55
Total 60 100
Table 3: Clinical history of MNG patients.
Variable No. Percentage %
Smoking status
Smoking 9 15.1
Ex-smoking 11 18.3
Non-smoking 40 66.6
Total 60 100
Family history of Thyroid malignant disease
Positive 9 15
Negative 51 85
Total 60 100
History of exposure to ionizing radiation
Positive 2 3.3
Negative 58 96.6
Total 601 100
Table 4: Investigations findings of MNG patients
Variable No. Percentage%
TFT at the time of diagnosis
Euthyroid 60 100
total 60 100
FNAC findings
Differentiated carcinoma 13 21.7
Benign 47 78.3
Total 60 100
Histopathological Findings
Colloid goitre 25 41.7
Micro papillary carcinoma 10 16.7
Follicular adenoma 23 38.3
Follicular carcinoma 2 3.3
Total 60 100

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 118
No significant difference was observed between MNG patients with differentiated carcinoma and those with benign MNG regarding their residence and educational level. All these findings were shown in Table 6. There was a highly significant association between current smoking status of MNG patients and differentiated carcinoma (p < 0.001). No significant difference was observed between MNG patients with differentiated carcinoma and those with benign MNG
regarding family history of thyroid diseases. MNG patients with positive exposure to ionizing radiation history were significantly associated with differentiated carcinoma (p ¼ 0.02). All these findings were shown in Fig. 6. A highly significant association was observed between histopathology findings and FNA findings (p < 0.001), all MNG patients detected by FNAC as carcinoma were diagnosed by histopathology as carcinoma (p < 0.001).
Table 5: Distribution of demographic characteristics according to FNAC findings.
VariableCarcinomaNo. %
BenignNo. %
p
Age 0.1aNS
<30 2 15.3 3 6.3
30-39 1 7.6 12 25.5
40-49 5 38.4 18 38.2
50-59 4 30.7 8 17.0
>60 1 7.6 6 12.7
Mean +SD 45.1 + 12.6 43.5+11.3 0.5bNS
Gender 0.5aNS
Male 2 15.3 4 8.5
Female 11 84.7 43 91.5
NS ¼ Not significant.
a. Fishers exact test.
b. Independent sample t-test.
Discussion
Multi-nodular goitre (MNG) is still epidemic in areas with iodine deficiency especially among women; however, most of these nodules diagnosed are benign but the possibility of malignancy is present especially for differentiated thyroid carcinoma as both conditions share the same risk factors16. Present study showed by FNAC and histopathology that 21.7% of patients with MNG had differentiated thyroid carcinoma decades and all over world, there was an increase in thyroid cancer incidence related to changing in lifestyle, increased
obesity prevalence, higher exposure to ionizing radiation, in addition to increased MNG prevalence related to iodine deficiency. Scopa study in Greece stated that the incidence of differentiated carcinoma among MNG goiter patients was 4-17% worldwide and the papillary carcinoma accounts for about 80% thyroid carcinomas19. Preoperative diagnosis of differentiated thyroid carcinoma with different diagnostic materials is always not accurate even with use of fine needle aspiration before surgery particularly for MNG patients25. The incidental thyroid carcinoma is common postoperative finding among MNG patients detected by histopathology investigation. It was proved that incidence of differentiated thyroid carcinoma among patients with MNG is lower than incidence among patients with

119 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
single nodule20, but the diagnosis of carcinoma among MNG patients is difficult than single nodule17. Current study showed that the common histopathology type of differentiated carcinoma was micro-papillary carcinoma. This finding is consistent with results of Tas¸ova et al.21 Study in Turkey which revealed that incidence of thyroid carcinoma among MNG patients after thyroidectomy was 14% with prevalence of papillary carcinoma as 84%. Our histopathology findings showed also that common benign finding of MNG patients was follicular adenoma. These findings are similar to results of Matar et al.18
Our study showed no significant difference between carcinoma and benign thyroid MNG patients regarding educational level of patients. This finding is in consistent with results of AschebrookKilfoy et al.22
Our study found a highly significant association between current smoking status of MNG patients and differentiated carcinoma (p < 0.001). This is consistent with results of Sawicka-Gutaj et al.23 In present study, MNG patients with positive exposure to ionizing radiation history were significantly associated with differentiated carcinoma (p ¼ 0.02). This finding is in agreement with reports of Nikiforovetal24study in USA which documented that long exposure to ionizing radiation is significantly risk factor for development of thyroid carcinoma. Another American study by Aschebrook-Kilfoy et al25 stated that occupation hazard for thyroid carcinoma is prominent risk factor especially occupations with exposure tom ionizing radiation.. Present study showed that FNA findings of MNG patients were significantly associated with histopathology findings (p < 0.001). This finding is similar to results of Sharma study in India 26 which stated that FNA is an invasive highly accurate diagnostic technique for diagnosis of thyroid cancer among MNG patients with significant correlation to histopathology findings. Gupta et al.27 revealed that FNAC is the first line diagnostic technique for solitary nodular thyroid diseases but not for multinodular. However, due to its cost-effectiveness and non-invasiveness, FNAC with ultrasound imaging is the first line diagnosis of thyroid cancer in Iraq 10,18
Conclusions
- The incidence of differentiated thyroid carcinoma among multinodular goitre patients is high.
The common thyroid malignant tumour type among
multinodular goitre patients was papillary carcinoma.
- The common thyroid benign tumour type among multinodular goitre patients was follicular adenoma.
- The prevalent risk factors for differentiated thyroid carcinoma among multinodular goitre patients were illiteracy, cigarette smoking and exposure to ionizing radiation.
- The fine needle aspiration test for differentiated thyroid is relatively accurate and reliable.
Conflict of Interest: Nil
Ethical Clearance: Taken from ethical committee of Saraswati Institute of medical sciences,Hapur
Source of Funding: Self
References
[1] Ass. Prof. Dr. Basim Rassam Ghadhban,
[2] DR. Satar M kadam, and Dr. Hanan Abdullatif sultan
[3] Burnicardi FC, Andersen DK, Billiar TR, Dunn DL, Hunter JG, Matthews JB, et al. ABSITE and board review. In: Schwartz’s principles of surgery. tenth ed. USA: McGraw & Hill Education; 2016.
[4] Day TA, Chu A, Hoang K. Multinodular goitre. Otolaryngol Clin N Am 2003;36: 35e54.
[5] Frilling A, Hertl M. Endemic goitre and benign multinodular goitre. In: Doherty GM, Skogseid B, editors. Surgical endocrinology. Philadelphia: Lippincott Williams and Wilkins; 2001. p. 37e45.
[6] Poulose KP, Krishna Das KV. Thyroid and its disorders. In: Krishna Das KV, Bahuleyan CG, Haridas KK, Jayakumar PV, Visweswaran K, Krishna Kutty K, et al., editors. Text book of medicine. fourth ed. New Delhi: Jaypee Brothers; 2002. p. 490e501.
[7] Ganly I, Ricarte Filho J, Eng S, Ghossein R, Morris LG, Liang Y, et al. Genomic dissection of Hurthle cell carcinoma reveals a unique class of thyroid malignancy. J Clin Endocrinol Metabol 2013;98(5):962e72.
[8] Khatawkar AV, Awati SM. Multi-nodular goiter: epidemiology, etiology, pathogenesis

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 120
and pathology. Int Arch Integrated Med 2015;2(9):152e6.
[9] Krukowski ZH. The thyroid and the thyroglossal tract. In: Russell RCG, WilliamsNS, Bulstrode CJK,editors. Bailey andLove’s short practice of surgery. 24th edition. London: Arnold; 2004. p. 776e803.
[10] Al-Hashimi AM. Thyroid nodules in Baghdad, Iraq: a personal experience. Int J Sci Res (IJSR) 2015;4(7):588e9.
[11] Pacini F,Castagna MG,Brilli L,Pentheroudekis G,ESMO guidelines working group.Thyroid Cancer: ESMO clinical Practice guidelines for diagnosis,treatment and follow up .Ann oncol 2010 .21(suppl 5):214-9
[12] Miccoli P, Minuto MN, Galleri D, D’Agostino J, Basolo F, Antonangeli L, et al. Incidental thyroid carcinoma in a large series of consecutive patients operated on for benign thyroid disease. ANZ J Surg 2006;76:123e6.
[13] Cerci C, Cerci SS, Eroglu E, Dede M, Kapucuoglu N, Yildiz M, et al. Thyroid cancer in toxic and non-toxic multinodular goiter. J Postgrad Med 2007;53: 157e60.
[14] Bahl M, Sosa JA, Nelson RC, Esclamado RM, Choudhury KR, Hoang JK.Trends in incidentally identified thyroid cancers over a decade: a retrospective analysis of 2,090 surgical patients. World J Surg 2014;38:1312e7.
[15] Slijepcevic N, Zivaljevic V, Marinkovic J, Sipetic S, Diklic A, Paunovic I. Retrospective evaluation of the incidental finding of 403 papillary thyroid microcarcinomas in 2466 patients undergoing thyroid surgery for presumed benign thyroid disease. BMC Cancer 2015;15:330.
[16] Ríos A, Rodríguez JM, Canteras M, Galindo PJ, Tebar FJ, Parrilla P. Surgical management of multinodular goiter with compression symptoms. Arch Surg 2005;140:49e53.
[17] Pellegriti G, Frasca F, Regalbuto C, Squatrito S, Vigneri R. Worldwide increasing incidence of thyroid cancer: update on epidemiology and risk factors. J Cancer Epidemiol 2013;2013:965212.
[18] Al-Katib AA, Al-Fallouji SKH, Jassim AH. Thyroid malignancy (incidence and management): a three-year study in Al-Hilla surgical hospitals retrospective study. Med J Babylon 2009;6(1):186e200.
[19] Scopa CD. Histopathology of thyroid tumors an over view. Hormones 2004;3(2):100e10.
[20] Liu Q, Djuricin G, Prinz RA. Total thyroidectomy for benign thyroid disease. Surgery 2000;123:2e7.
[21] Tasova V, Kilicoglu B, Tuncal S, Uysal E, Sabuncuoglu MZ, Tanrikulu Y, et al. Evaluation of incidental thyroid cancer in patients with thyroidectomy. W Indian Med J 2013;62(9):844e8.
[22] Aschebrook-Kilfoy B, Shu X-O, Gao Y-T. Thyroid cancer risk and dietary nitrate and nitrite intake in the Shanghai Women’s Health Study. Int J Cancer J Int du Cancer 2013;132(4):897e904.
[23] Sawicka-Gutaj N, Gutaj P, Sowinski J, Wender-O_zegowska E, Czarnywojtek A, Bra ˛zert J, et al. Influence of cigarette smoking on thyroid gland–an update. Endokrynol Pol 2014;65(1):54e62.
[24] Nikiforov YE. Is ionizing radiation responsible for the increasing incidence of thyroid cancer? Cancer 2010;116(7):1626e8.
[25] Aschebrook-Kilfoy B, Ward MH, Valle CTD, Friesen MC. Occupation and thyroid cancer. Occup Environ Med 2014;71(5):366e80.
[26] Sharma C. Diagnostic accuracy of fine needle aspiration cytology of thyroid and evaluation of discordant cases. J Egypt Natl Canc Inst 2015;27(3):147e53.
[27] Gupta M, Gupta S, Gupta VB. Correlation of fine needle aspiration cytology with histopathology in the diagnosis of solitary thyroid nodule. J Thyroid Res 2010;2010:379051.

Research Article
Clinical Profile and Outcome of Patients Suffering from Soft Tissue Infection in Lower Limb Disease in the Department of
Surgery in Tertiary Care Center
Rishabh Sharma1, Ram Kumar Verma2, Alok Vardhan Mathur2, Rajendra Kumar Srivastava2, Saurabh Kumar3
1Post Graduate Resident, 2Professor, 3Associate Professor, Department of Surgery, SGGRRIM&HS, Dehradun, UK
Abstract
Background: Patients with lower limb diseases are commonly seen in surgical wards 7% to 10% of hospitalized patients are affected by soft tissue infections in the United States. The most common cause of soft tissue infections is Staphylococcus aureus.[1] Frequently these patients are diabetic, immune compromised, etc. Establishing the diagnosis of Necrotizing Soft Tissue Infection (NSTI) can be the main challenge in treating patients with NSTI, and knowledge of all available tools is the key for early and accurate diagnosis[2]
The skin is the largest organ of the body and, with the underlying soft tissue, which includes the fat layers, fascia and muscle, represents the majority of the tissue in the body. It acts as a tough, flexible, structural barrier to invasion.[3] Failure to do so result in an extremely high mortality rate (80 to 100%), and even with rapid recognition and intervention, current mortality rates remain approximately 30 to 50%.[4]
Corresponding author:Dr. Rishabh SharmaSenior Resident, Department of Surgery, SGRRIM&HS, Patel Nagar, Dehradun(248001)Uttarakhand, Ph.: +91-99974 55005
Aims and Objectives
To evaluate clinical profile and outcome of patients suffering from soft tissue infection in lower limb diseases in Department of Surgery at Shri Guru Ram Rai Institute of Medical and Health Sciences and Shri Mahant Indresh Hospital, Dehradun.
Duration of study has been 1 year.
Materials and Method
The present study has been conducted in the Department of Surgery at Shri Guru Ram Rai Institute of Health and Medical Sciences, Dehradun. The duration of the study was 1 year with follow-up of upto 6 months . [2015-2016]
Inclusion Criteria
All patients admitted in Department of Surgery with lower limb pathology including soft tissue have been included.
Exclusion Criteria
Patients with traumatic pathology to bone and soft tissue have been excluded.
Patients suffering from central nervous system diseases as paraplegia, hemiplegia have been excluded.
A well informed consent from the patient has been taken.
The study has been conducted after approval from the Institutional Ethics Committee.
Soft Tissue Infection
Out of 226 patients, 103 patients were diagnosed as Soft tissue infections.
DOI Number: 10.5958/2321-1024.2019.00035.7

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 122
All the 103 patients 103 (100%) patients had pain, swelling, redness, tenderness, increased local temperature, erythema and edema. 75 (73%) patient had cellulitis; 55 (53%) patients had necrosis; 40 (39%) patients had abscess; 36 (35%) patients had blisters; 32 (31%) patients had purulent discharge from wound; 6 (6%) patients had crepitus. No patients had folliculitis, furuncles and carbuncles were nil as these patients receive treatment on OPD basis.
Table 1: Clinical manifestations of soft tissue infections.
Clinical features Present (n=103)
Percentage
Pain 103 100%
Swelling 103 100%
Redness 103 100%
Erythema 103 100%
Edema 103 100%
Tenderness 103 100%
Warmth 97 94%
Cellulitis 75 73%
Necrosis 55 53%
Abscess 40 39%
Bulla/ Blister 36 35%
Purulent discharge from wound 32 31%
Crepitus 6 6%
Furuncles 0 0%
Carbuncles 0 0%
Folliculitis 0 0%
Gangrene 0 0%
Out of 103 patients with soft tissue infections, total leucocyte count was normal in 31 (30.1%) patients and raised in 72 (69.9%) patients.The rise in total leucocyte count was statistically significant ( p value >0.05)
Serum creatinine level was normal in 94 (91.3%) patients and raised in 9 (8.7%) patients. Serum creatinine was not statistically significant.
HbA1c was normal in 95 (92.2%) patients and raised in 8 (7.8%) patients. HbA1c was not statistically significant.
Table 2: Blood parameters of patients with soft tissue infections
Intervention Normal High Total
TLC 31(30.1%) 72(69.9%) 103
Creatinine 94(91.3%) 9(8.7%) 103
HbA1c 95(92.2%) 8(7.8%) 103
Out of 103 patients with soft tissue infections, 50 (48.5%) patients had beta haemolytic streptococci; 26 (25.2%) patients had staphylococci; 13 (12.6%) patients had klebsiella; 6 (5.8%) patients had enterococcus faecalis; 5 (4.8%) patients had pseudomonas and 3 (2.9%) patients had no growth on aerobic culture media.
Beta haemolytic streptococci was the most common organism in patients with soft tissue infections.
Table 3: Distribution of microbial infection in Soft tissue infections
Organism Soft tissue infections (n= 103) Percentage
Beta-hemolytic streptococci 50 48.5%
Staphylococci 26 25.2%
Klebsiella 13 12.6%
Enterococcus faecalis 6 5.8%
Pseudomonas 5 4.8%
No growth 3 2.9%
Out of 103 patients with soft tissue infections; 50(48.5%) patients were treated by debridement; 27 (26.2%) patients were treated by fasciotomy; 21 (20.4%) patients were treated by incision and drainage; 3 (2.9%) patients were treated by amputations and 2 (1.9%) patients were treated conservatively.

123 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
Table 4:- Mode of treatment in Soft tissue infections
Intervention Soft tissue infections
n= 103 Percentage
Debridement 50 48.5%
Fasciotomy 27 26.2%
Incision and drainage 21 20.4%
Amputation 3 2.9%
Conservative 2 1.9%
Out of 103 patients with soft tissue infections, 5 patients developed septicaemia.
Out of 5 patients with septicaemia 3 progressed to acute renal failure. Out of those 3 patients with septicaemia and acute renal failure one expired due to multi organ dysfunction syndrome.
Table 5: Septicaemia in Soft tissue infections
Complications Septicemia (n=5) %
Septicemia 2 40%
Septicaemia+ARF 2 40%
Death 1 20%
Discussion
Soft tissue infections came out to be the most common (45.6%) cause of lower limb diseases in our study. The patients with soft tissue infections had a significantly increased level of total leucocyte count. Majeski et al also noted increased level of leucocyte count in patient with soft tissue infection.
The patients with soft tissue infections had increased serum creatinine and diabetes, but it wasn’t statistically significant finding in our study .However according to Majeski et al serum creatinine>2mg/dl was associated with increased mortality.[5]
Beta hemolytic streptococci were seen in 48.5% of all soft tissue infections, being the most common organism. This correlates with the study conducted by Bjornsdottir et al in which it was seen that skin soft
tissue infection in lower limbs is due to staphylococcus aureus and/or beta hemolytic streptococcus.[6]
Most patients of soft tissue infections responded well to early debridement and fasciotomy. Similar outcomes were seen in a study conducted by Freischlag et al which concluded that the appropriate treatment of NSTIs was found to be early and wide surgical debridement. Increased time from admission to debridement and inadequate initial debridement was associated with increased mortality. [7]
Conclusion
• Soft tissue infections was the commonest (45.6%) cause of the lower limb diseases.
• Patient with soft tissue infections had statistically significantly increased total leucocyte count. (P value is > 0.05.) However serum creatinine was not statistically significant raised.
• Patients with soft tissue infections who had diabetes mellitus also were not statistically significant.
• Most common presentation of soft tissue infection was pain, swelling, redness, tenderness, increased temperature and erythema seen in all patients.
• Presence of necrosis and blisters were uncommon features of soft tissue infection seen in 53% and 35% patient respectively.
• Beta hemolytic streptococci (48.5%) was the most common organism of soft tissue infection.
• Most soft tissue infection responded to debridement and fasciotomy.
Funding: No funding sources
Conflict of Interest: None declared
Ethical approval: The study was approved by the institutional ethics committee
References
1. Vinh DC, Embil JM. Rapidly progressive soft tissue infections. Lancet Infectious Disease. 2005; 5:501-13.
2. Mishra SP, Singh S, Gupta SK. Necrotizing Soft Tissue Infections: Surgeon’s Prospective. Int J Inflam. 2013;2013:609-28.

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 124
3. Mims C, Playfair J, RoittI, et al. Medical Microbiology London Mosby Int Ltd, ISBN 0 7234 2781 X
4. Charles Brunicardi F. Surgical Infections. In: Schwartz Principles of Surgery. Chapter 5. 8th edition. USA: Mc Graw Hill; 2006:93.
5. Majeski JA, John JF Jr. Necrotizing soft tissue infections: a guide to early diagnosis and initial therapy. South Med J. 2003;96(9):900-905.
6. Björnsdóttir S, Gottfredsson M, Thórisdóttir AS, et al. Risk factors for acute cellulitis of the lower limb: A prospective case-control study. Clin Infect Dis. 2005;41:1416–22.
7. Freischlag J, Ajalat G, Busuttil R. Treatment of necrotizing soft-tissue infections. Am J Surg.1985;149:751–755.

Original Research Article
A Clinical Study of Management of Perforative Peritonitis and Its Surgical Outcome
Chandra Kumar P C1, Venkatesh Kharalkar2, Bellara Raghavendra3 1Associate Professor, 2Junior Resident, Department of General Surgery, 3Professor, Department of Community
Medicine, Vijayanagara Institute of Medical Sciences, Bellary, Karnataka
Abstract
Background: Secondary peritonitis presents common life-threatening conditions associated with high mortality and morbidity. Management of perforative peritonitis poses significant challenges to the treating surgeons with respect to surgical outcome thereby demanding thorough evaluation and appropriate management in such cases.
Objectives: To study the clinical profile, management of perforative peritonitis and its surgical outcomes. Methodology: A case series study of 513 patients with Perforative Peritonitis was studied in setting of tertiary care hospital in the department of general surgery at Vijayanagara Institute of Medical Sciences, Ballari, Karnataka during the period of June 2015 to January 2018. Among the selected patients the clinical profile, etiological profile and the surgical interventions were undertaken and the outcome were noted. Appropriate descriptive statistics were used to analyse the findings and to draw the inferences. Results: There were 390 males and 123 females. The mean age of patients was 35.95 ± 24.87 years. Common cause of perforative peritonitis were acid peptic disease (35.7%), infectious disease (23%), trauma (13%) and malignancy (2.3%). Complication rate and mortality among the patients was 47.2% and 9.6% respectively. Elderly age, comorbid condition, infectious disease etiology and malignancy and site of perforation were the important determinants of mortality among the patients. Conclusion: GI perforations are one of the most common surgical emergencies. Mortality depends on the age and general condition of the patient, associated pre-operative co-morbidities, site of perforation and etiology.
Keywords: Perforative peritonitis, surgical outcome, etiology, complication, mortality
Corresponding Author:Dr. Bellara Raghavendra, Associate Professor, Department of Community Medicine, Vijayanagara Institute of Medical Sciences, Bellary, Karnataka. Email ID: [email protected] #: +91 9901301830
Background
Even today, secondary peritonitis presents common life-threatening conditions associated with high mortality and morbidity. Management of perforative peritonitis poses significant challenges to the treating surgeons with respect to surgical outcome thereby
demanding thorough evaluation and appropriate management in such cases. In our current study, we will be evaluating the disease to know the various clinical presentations, epidemiology, general principals of surgical management and its surgical outcomes.
Objectives
To study the clinical profile, management of perforative peritonitis and its surgical outcomes.
Methodology
Study design: A case series study design.
Study setting: The study was carried out in the setting of tertiary care hospital in the department of
DOI Number: 10.5958/2321-1024.2019.00036.9

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 126
general surgery, Vijayanagar Institute of Medical Sciences, Ballari, Karnataka
Study subjects: All patients admitted with perforative peritonitis were included in the study. A total of 513 patients with perforative peritonitis were included in the study admitted from the year 2015 to 2018.
Sampling: Non-random purposive sampling was adopted to select patients
Study period: Study was done by collecting data retrospectively from the year 2015 to 2018
Data variables: Among the selected patients socio demographic profile, the clinical profile, surgical interventions undertaken and the outcome including complications was noted. All the patients were followed for 6 months.
Analysis: The collected data with respect to various variables was entered into an excel sheet and after appropriate data filtering , the data was transferred and analysed using SPSS version 2.0.appropriate descriptive descriptive statistics was used to analyse the findings and to draw the inferences.
Ethical Clearance: Due ethical clearance for the conduct of the study was issued by Institutional Ethical Committee of Vijayanagara Institute of Medical Sciences, Ballari, Karnataka.
Results
A total of 513 patients with perforative peritonitis were included in the study. Two thirds of the patients were in the age group of 20 to 40 years age group. Majority of the patients were males (76%) compared to females (24%).
Almost every patient had pain abdomen (98.8%) and other predominant symptom were vomiting (78.2%), fever (49.9%) followed by constipation (40.9%) and abdominal distension (38.4%).
Tachycardia was observed in majority of the patients and other signs of shock such as hypotension (42.3%), low urine output (22.2%) and tachypnoea (46%) were also observed in the patients.
Presence of co-morbid conditions was assessed among the patients where in hypertension (13.1%) was the common co-morbid condition followed by
respiratory disease (9.9%), diabetes mellitus (7.2%), renal disease (5.3%) and cardiac disease (4.1%).
More than half of the patients were alcoholic (52.8%) and nearly 5% of the patients had history of NSAID abuse.
Table no. 01:
Clinical profile of the patients (n=513)
Parameter Frequency Percent
Etiology
Acid peptic disease 183 35.7
Trauma 67 13.1
Malignancy 12 2.3
Obstruction 57 11.1
Typhoid 83 16.2
Tuberculosis 33 6.4
Not defined 78 15.2
Perforation site
Gastric 24 4.7
Duodenal 185 36.1
Jejunal 71 13.8
Ileal 85 16.6
Appendicular 107 20.9
Large bowel 41 8.0
Investigative findings
Pneumoperitoneum on xray 477 93.0
Air fluid level on xray(>4) 87 17.0
Dyselectrolytemia 241 47.0
Raised leucocyte count >14k 426 83.0
Raised renal function tests 213 41.5
Low hemoglobin 65 12.7
The underlying etiology of the perforative peritonitis among the patients was evaluated and it was observed that acid peptic disease was the common cause accounting for 35.7% of the patients, followed by typhoid (16.2%), trauma (13.1%), obstruction (11.1%) and tuberculosis (6.4%). Malignancy accounted for 2.3% of the cases in our study. In about 15% of the cases the etiology was not defined.

127 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
The commonest site of perforation was found to be duodenum accounting for 36.1% of the cases followed by appendicular (20.9%), Ileum (16.6%), Jejunal (13.8%), large bowel (8%) and gastric (4.7%).
After stabilizing the patients’ operative management was done where in Grahams modified patch repair
was done in 35.7%, appendectomy in 20.9%, simple closure of the perforation was done in 19.9%, resection and anastomosis was done in 10.5% and resection and diversion was done in 9.4% of the patients. Billroth 1 operative procedure was done in one case and Billroth 2 procedure was done in 18 cases.
Table no. 02:
Surgical outcome among the patients (n=513)
Outcome Frequency Percent
Complication 242 47.2 Mortality 49 9.6 Recovered 222 43.3 Type of complication (n=242) Wound infection 78 32.2 Dyselectrolemia 21 8.7
Respiratory complication 57 23.6
Abdominal collection 25 10.3
Obstruction 34 14.0 Burst abdomen 13 5.4 Anastomotic leak 14 5.8
All the patients were followed up for a period of 6 months and the surgical outcome of the patients was assessed where in the mortality rate among the patients was at 9.6% and the rate of complication was at 47.2% and remaining 43.3% of the patients recovered completely. Among the complications wound infection (32.2%) and respiratory complication (23.6%) were common, followed by abdominal collection (10.3%), Obstruction (14%), dyselectrolemia (8.7%), burst abdomen (5.4%) and anostomotic leak (5.8%).
Table no. 02:
Factors influencing mortality among the patients
Variable N Mortality P Value
age group
<20 years 45 3(6.6%) 0.71
20-40 years 345 26(7.5%) 0.02
40-60 years 67 8(11.9%) 0.47
>60 years 56 12(21.4%) 0.0013
Sex
Male 390 40(10.2%) 0.32
Female 123 9(7.3%)
Etiology
Acid Peptic Disease 183 14 (7.6%) 0.27
Trauma 67 1 (1.4%) 0.013
Malignancy 12 2 (16.6%) 0.64

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 128
Obstruction 57 5 (8.7%) 0.83
Typhoid 83 4 (4.8%) 0.14
Tuberculosis 33 11 (33%) <0.001
not defined 78 12 (15.3%) 0.05
Pre-existing medical condition
Hypertension 67 2 (2.9%) 0.06
diabetes mellitus 37 2 (5.4%) 0.58
respiratory disease 51 9 (17.6%) 0.03
cardiac disease 21 2 (9.5%) 0.99
renal disease 27 4 (14.81%) 0.5
No disease 310 30 (9.6%) 0.9
Site
Gastric 24 4 (16.6%) 0.37
Duodenal 185 10 (5.4%) 0.016
Jejunal 71 4 (5.6%) 0.32
Ileal 85 22 (25.8%) <0.001
Appendicular 107 1 (0.93%) <0.001
large bowel 41 8 (19.55%) 0.023
Operative procedures
Simple closure 102 23 (22.5%) <0.001
Grahams modified patch repair 183 10 (5.4%) 0.019
Resection with anastomosis 54 11 (20.3%) 0.004
Appendectomy 107 1 (0.9%) <0.001
Resection with diversion 48 3 (6.2%) 0.6
Billroth 1 1 0 (0.0%) >0.99
Billroth 2 18 2 (11.1%) >0.99
The mortality was high among elderly patients (21.4%) and 40-60 years age groups (11.9%) compared to rest of the age groups and this difference in the mortality rates was found to be statistically significant. Male patients had higher mortality (10.2%) compared to females (7.3%).
Patients with Tuberculosis (33%), Malignancy (16.7%) and ill-defined etiology (15.3%) had higher mortality rates compared to other etiology and this difference in the mortality rates with respect to etiology was found to be statistically significant.
Patients with co-morbid condition of respiratory disease (17.6%) and renal disease (14.8%) had higher mortality rates compared to other co-morbid conditions and this was found to be statistically significant.
Cont... Table no. 02:
Site of perforation as an influencing factor of mortality was assessed; it was found that patients with Ileum (25.8%) and large bowel (19.5%) had higher mortality compared to other sites. Patients with appendicular perforation had the lowest mortality (0.93%). This difference in the mortality rates with respect to the site of perforation was found to be statistically significant.
Patients who underwent simple closure (22.5%) and resection and anastomosis (20.3%) had higher mortality rates compared to patients who underwent other operative procedures. Patients who underwent appendectomy had the least mortality (0.93%). This difference in the mortality rates with respect to the type of operative procedures was found to be statistically significant.

129 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
Discussion
One of the most common surgical emergencies is perforation peritonitis. It is commonly seen in a younger age group in the tropical countries (mean age in our study was 37.8 years) as compared to the studies in the West.1,2
More commonly the perforations involve the proximal part of the gastrointestinal tract;3,4 this being in contrast to studies from the western countries, where perforations are common in the distal part.5,6 Etiological factors also show a wide geographical variation. According to a study from India, infections formed the most common cause of perforation peritonitis.7 In our study 23% of the cases were due to typhoid and tuberculosis. In contrast to this, Noon et al.8 from Texas in their study reported only 2.7% cases due to infections. Also studies from the west have shown that around 15–20% cases are due to malignancy,9,10 this being in stark
contrast to our study where malignancy was ascertained to be the cause of perforation peritonitis in only 3% of the cases. This shows that malignancy is not a common cause of perforation peritonitis in our setup as compared to our western counterparts.
In our study; surgical outcome of the patients was assessed where in the mortality rate among the patients was at 9.6% and the rate of complication was at 47.2% and remaining 43.3% of the patients recovered completely. [Table 05] Among the complications wound infection (32.2%) and respiratory complication (23.6%) were common, followed by abdominal collection (10.3%), Obstruction (14%), dyselectrolemia (8.7%), burst abdomen (5.4%) and anostomotic leak (5.8%).
The rates of common complications were comparable with other studies in India and neighbouring countries.11-16(table no. 04).
Table no. 04:
Comparison of post-op complications with other studies Author
Study series Wound infection (%)
Wound dehiscence (%)
Pulmonary complications (%)
Electrolyte imbalance (%)
Septi-caemia (%)
Thammegowda K etal[11](N=369) 30 12 21 19 16
PrajaktVPatil,etal[12](N=150) 20 20 20 - -
Shyamkumargupta,etal[13](N=400) 16 3.5 6 4 3
Memon AA, et al[14] (N=311) 10.2 4.5 - 6.7 10.6
ShahidaPAfridi etal [15] (N=300) 42 26 20 - 20
RajenderSJhobta[16] (N=504) 25 9 28 17 18
Presentstudy (N=513) 32.3 - 23.6 8.7 -
The overall mortality due to perforation peritonitis ranges between 6 and 27%.17 The mortality rate in our study was 9.6%. Comparison of mortality rates with respect to other studies has been shown below.11-1(table no. 05).
Table no. 05:
Comparison of mortality rates with other studies
Study Year Mortality (%)
Thammegowda K etal[11](N=369) 2001-2010 13.8
PrajaktVPatil,etal[12](N=150) 2006 13

International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2 130
Shyamkumargupta,etal[13](N=400) 2006-2008 6
Memon AA, et al[14] (N=311) 2008-2010 16.7
ShahidaPAfridi etal [15] (N=300) 2008 10.6
RajenderSJhobta[16] (N=504) 2006 10
Ramachandra ML, et al[18]. (N=50) 2003-2004 14
Nuhu ali, etal[19]. (N=153) 2010 26.1
Present study (N=513) 2013-2016 9.6
Cont... Table no. 05:
The mortality was high among elderly patients (21.4%) and 40-60 years age groups (11.9%) compared to rest of the age groups and this difference in the mortality rates was found to be statistically significant. Male patients had higher mortality (10.2%) compared to females (7.3%). Results were similar to study conducted by Parwez Sajad Khan et al, 20 and Rajender Singh Jhobta et al.16
Patients with Tuberculosis (33%), Malignancy (16.7%) and ill-defined etiology (15.3%) had higher mortality rates compared to other etiology and this difference in the mortality rates with respect to etiology was found to be statistically significant. Patients with co-morbid condition of respiratory disease (17.6%)
and renal disease (14.8%) had higher mortality rates compared to other co-morbid conditions and this was found to be statistically significant. Study done by NBG Prasad et al, 21 also gave similar results.
Site of perforation as an influencing factor of mortality was assessed; it was found that patients with Ileum (25.8%) and large bowel (19.5%) had higher mortality compared to other sites. Patients with appendicular perforation had the lowest mortality (0.93%). This difference in the mortality rates with respect to the site of perforation was found to be statistically significant. These study results are in consonance with other studies done elsewhere.20,22,23 (table no. 06).
Table no. 06:
Comparison of site of perforation and Mortality with other studies
Study series Tripathi et al.22 N=160) Khan S et al.20 (N=54) Rao DCM et al.23 (N=46) Present study. (N=513)
Gastroduodenal 15.0% 38.8% 56.5% 40.7%
Small bowel 35.6% 25.9% 39.1% 30.4%
Appendicular 10.0% 11.1% 4.3% 20.8%
Colorectal NA 7.4% 0.0% 7.9%
Mortality 23.7% NA 26.1% 9.6%
Patients who underwent simple closure (22.5%) and resection and anastomosis (20.3%) had higher mortality rates compared to patients who underwent other operative procedures. Patients who underwent appendectomy had the least mortality (0.93%). This difference in the mortality rates with respect to the type of operative procedures was found to be statistically significant.
Peritonitis is one of the commonest surgical emergencies in our country. Despite advancements
in surgical techniques, anti–microbial therapy and intensive care, management of peritonitis continues to be highly demanding, complex and its outcome is mainly determined by the age of the patient, site of perforation, etiology, comorbid conditions and the type of surgical procedure done.
Conclusion
GI perforations are one of the most common surgical emergencies. Duodenal perforations are most common. Ileal perforations have the highest morbidity

131 International Journal of Contemporary Surgery, July-December 2019, Vol.7, No. 2
and mortality. Mortality depends on the age and general condition of the patient, associated pre-operative co-morbidities, site of perforation and etiology.
Conflict of Interest: None
Source of Funding: None
References
1. A. Uccheddu, G. Floris, M. L. Altana, A. Pisanu, A. Cois, and S. L. F. Farci. Surgery for perforated peptic ulcer in the elderly: Evaluation of factors influencing prognosis. Hepato-Gastroenterology Jour, 2003; vol. 50 (54):1956–1958.
2. C. Svanes, H. Salvesen, B. Espehaug, O. Soreide, and K. Svanes. A multifactorial analysis of factors related to lethality after treatment of perforated gastroduodenal ulcer 1935–1985. Annals of Surgery, 1989; 209 (4): 418–423, 1989.
3. N. Agarwal, S. Saha, A. Srivastava, S. Chumber, A. Dhar, and S.Garg. Peritonitis: 10 years’ experience in a single surgical unit. Tropical Gastroenterology, 2007; 28(3): 117–120.
4. M. A.Malangoni and T. Inui. Peritonitis—theWestern experience. World Journal of Emergency Surgery, 2006; 1 (1): article 25.
5. S. Gupta, R. Kaushik, R. Sharma, and A. Attri. The management of large perforations of duodenal ulcers. BMC Surgery, 2005; 5: article 15.
6. B. di Venere, M. Testini, S. Miniello et al. Rectal perforations. Personal experience and literature review. Minerva Chirurgica, 2002; 57(3): 357–362.
7. A.K.Khanna and M.K.Misra. Typhoid perforation of the gut. Postgraduate Medical Journal, 1984; 60: 523–525.
8. G. P. Noon, A. C. Beall, and G. L. Jorden. Clinical evaluation of peritoneal irrigation with antibiotic solution. Surgery, 1967. 67: 73–78.
9. S. Breitenstein, A. Kraus, D. Hahnloser, M. Decurtins, P. A.Clavien, and N. Demartines. Emergency left colon resection for acute perforation. Primary anastomosis or hartmann’s procedure? A case-matched control study. World Journal ofSurgery, 2007; 31(11): 2117–2124.
10. F. Roviello, S. Rossi, D. Marrelli et al. Perforated gastric carcinoma: a report of 10 cases and review
of the literature. World Journal of Surgical Oncology, 2006; 4(19).
11. Thammegowda Kemparaj, Syed Iqbalulla Sha Khadri. Gastrointestinal Perforations - Our Experience. The Internet Journal of Surgery, 2012; 28(2).
12. Prajakt V. Patil, Manmohan M. Kamat, Milan M. Hindalekar. Spectrum of Perforative Peritonitis- A Prospective Study of 150 Cases. Bombay Hospital Journal, 2012; 54(1).
13. Shyam Kumar Gupta, Rajan Gupta, Gurdev Singh, Sunil Gupta. Perforation Peritonitis: A Two Year Experience. JK Science, 2010; 12(3): 141-144.
14. Memon AA, Siddique FG, Abro AH, Agha AH, Lubina Shahazadi, Memon AS. An audit of secondary peritonitis at a tertiary care university hospital of Sindh, Pakistan. World J Emerg Surg. 2012 Mar; 7:6.
15. Shahida P Afridi, Faiza Malik, Shafiq Ur-Rahman, Shahid Shamim and Khursheed A Samo. Spectrum of perforation peritonitis in Pakistan: 300 cases Eastern experience. World Journal of Surgery, 2008; 3(31).
16. Rajender Singh Jhobta, Ashok Kumar Attri, Robin Kaushik, Rajeev Sharma, and Anupam Jhobta. Spectrum of perforation peritonitis in India-review of 504 consecutive cases. World J Emerg Surg. 2006; 1: 26.
17. M. Oheneh-Yeboah. Postoperative complications after surgery for typhoid ileal perforation in adults in Kumasi. West African Journal of Medicine, 2007; 26(1): 32–36.
20. Khan S, Khan IU, Aslam S, Haque A. Retrospective analysis of abdominal surgeries at Nepalgunj Medical College, Nepalgunj, Nepal: 2years’ experience. Kathmandu University Medical Journal. 2004; 2: 336-43.
21. N. Baba Guru Prasad, KV Bhaskar Reddy. A study of acute peritonitis: evaluation of its mortality and morbidity. Int Surg J. 2016 May; 3(2): 663-668.
22. Tripathi MD, Nagar AM, Srivastava RD, PartapVK. Peritonitis- study of factors contributing tomortality. Indian J Surg. 1993; 55: 342-9.
23. Rao DCM, Mathur JC, Ramu D, Anand D.Gastrointestinal tract perforations. Indian Journal Surg.1984; 46: 94-6.

Call for Papers/Article Submission
International Journal of Contemporary Surgery is a double blind peer reviewed international journal
The following guidelines should be noted:
• The article must be submitted by e-mail only. Hard copy not needed. Send article as attachment in e-mail.
• The article should be accompanied by a declaration from all authors that it is an original work and has not been sent to any other journal for publication.
• As a policy matter, journal encourages articles regarding new concepts and new information.
• Article should have a Title
• Names of authors
• Your Affiliation (designations with college address), e-mail id.
• Abstract
• Key words
• Introduction or back ground
• Material and Methods
• Findings
• Discussion
• Conclusion
• Ethical Clearance
• Interest of Conflict
• References in Vancouver style.
• Please quote references in text by superscripting
• Word limit 2500-3000 words, MSWORD Format, single file
All articles should be sent to : [email protected]
Our Contact Info:
Institute of Medico-Legal PublicationsLogix Office Tower, Unit No. 1704, Logix City Centre Mall
Sector- 32, Noida - 201 301 (Uttar Pradesh) Ph. +91 120 429 4015, Mob: 09971888542,
Email: [email protected], Website: www.ijocs.in

International Journal of Contemporary Surgery
Institute of Medico-Legal PublicationsLogix Office Tower, Unit No. 1704, Logix City Centre MallSector- 32, Noida - 201 301 (Uttar Pradesh) Mob: 09971888542, Email: [email protected], Website: www.ijocs.in
CALL FOR SUBSCRIPTIONS
ISSN 2320-9615 (Print Version) ISSN 2321-1024 (Online Version) Frequency Half yearly International Journal of Contemporary Surgery is a double blind peer reviewed international journal which has commenced its publication from January 2013. The journal is half yearly in frequency. The journal covers all aspects of medical practice. The journal has been assigned ISSN 2320-9623 (Print Version) and ISSN 2321-1032 (Online Version). The journal is indexed in many international data bases.
Journal Title Print Only
International Journal of Contemporary Surgery INR 9000
NOTE FOR SUBSCRIBERS
• Advance payment required by cheque/demand draft in the name of “Institute of Medico-Legal Publications“ payable at Noida, Uttar Pradesh.
• Cancellation not allowed except for duplicate payment.• Claim must be made within six months from issue date.• A free copy can be forwarded on request.
Bank DetailsName of account : Institute of Medico-Legal Publications Pvt Ltd
Bank: HDFC Bank
Branch Sector-50, Noida-201 301
Account number: 09307630000146
Type of Account: Current Account
MICR Code: 110240113
RTGS/NEFT/IFSC Code: HDFC0000728
Please quote reference number.Send all payment to :
Institute of Medico-Legal PublicationsLogix Office Tower, Unit No. 1704, Logix City Centre Mall, Sector- 32, Noida - 201 301 (Uttar Pradesh)
Mob: 09971888542, Email: [email protected], Website: www.ijocs.in








![[Volume 23], July - December 1925 - FRASER - St. Louis Fed](https://static.fdokumen.com/doc/165x107/63389ed1283e1abca203decf/volume-23-july-december-1925-fraser-st-louis-fed.jpg)