34 Dyslipidemia in the elderly Clin Lipidol11
12
339 ISSN 1758-4299 10.2217/CLP.11.20 © 2011 Future Medicine Ltd Clin. Lipidol. (2011) 6(3), 339–350 REVIEW Dyslipidemias in the older subject: features, significance and treatment dilemmas Indications for chronic disease preventive strate- gies blur with advancing age, throwing up new challenges. Treating high cholesterol levels in older persons requires a preliminary insight into the role that lipids play in this age-group, followed by a risk/benefit analysis. As more people live longer these issues have become highly critical. Cardiovascular guidelines generally assume that hypercholesterolemia may be detrimental to every- one, independent of age [1], but epidemiological data and hypolipidemic trials are not unequivocal on this aspect. Besides old-age is a heterogeneous term broadly including people more than 65 years of age; it is different dealing with individuals in their sixties and seventies than with octogenar- ians. For instance, oldest old subjects are more likely to experience frailty, illness with comorbid- ity, disability and physical dependence compared with younger old people [2–4]; moreover, they are often treated with multiple medications, and this increases the risk of harmful interactions [5] if a new drug (e.g., a statin) is added. Heart disease and stroke represent the first and third leading causes of death in Europe and North America, respectively. Cumulatively they may be the most common reasons for hos- pitalization and are responsible for more than 40% total mortality in older persons. In the last 50 years mortality rates for these conditions dropped by more than 50%, a decline highly apparent in the groups of old (65–75 years), very old (75–85 years) and oldest old (85+ years) individuals [2] . Among several causes, these changes may also be related to therapeu- tic interventions addressing cardiovascular risk factor control in general, and cholesterol reduc- tion (both total cholesterol [TC] and LDL-C) in particular. Cholesterol, cardiovascular events & mortality While no reasonable doubts exist on the causal relationships between high plasma TC and LDL-C and ischemic coronary heart disease (IHD) in middle-aged population and younger- old persons [6,7] , this link weakens progres- this link weakens progres- sively with advancing age. A paradoxical asso- ciation has been reported between low TC and increased risk for all-cause mortality in elderly subjects [8–10] , while several epidemiological Almost two thirds of major coronary events take place in subjects over 65 years of age. Old (65–75 years), very old (75–85 years), and oldest old (85+ years) individuals should be considered separately when addressing cardiovascular (CV) risk. Several observational investigations have shown that the relationship between plasma cholesterol and CV events is less stringent with advancing age, especially in the very old and oldest old subject. In this context, both a decrease in total cholesterol and low HDL-C levels may be linked to coronary morbidity and total mortality through an independent association with disability and frailty. On the other hand, although elevated plasma LDL-C might still represent a CV risk factor in older people, the potential benefits originating from its reduction may exceed those obtained in younger ages, given the higher prevalence of CV disease in late life. At present statins, which represent the most effective hypocholesterolemic drugs, have been shown to significantly reduce CV events up to 82 years of age in randomized controlled trials and epidemiological surveys. The occurrence of multiple chronic conditions (comorbidity), decreased life expectancy and polypharmacotherapy suggest the need for a careful assessment of indications for aggressive hypolipidemic treatment. Drug interactions and low-pharmacological adherence may concur, causing a failure of preventive measure or side effects. Specific guidelines do not always recommend special caution or prudence in the elderly, but the selection of older patients for hypolipidemic treatment requires a high grade of clinical judgment. KEYWORDS: cardiovascular risk n dyslipidemia n elderly n hydroxymethyl-glutaryl coenzyme A reductase inhibitors n hypercholesterolemia n hypolipidemic drugs n lipoproteins Giovanni Battista Vigna †1 , Giovanni Zuliani 1 & Renato Fellin 1 1 Section of Internal Medicine, Gerontology and Clinical Nutrition, Department of Clinical & Experimental Medicine, University of Ferrara, via Savonarola, 9 44100, Ferrara, Italy † Author for correspondence: [email protected] For reprint orders, please contact: [email protected]
Transcript of 34 Dyslipidemia in the elderly Clin Lipidol11

339ISSN 1758-429910.2217/CLP.11.20 © 2011 Future Medicine Ltd Clin. Lipidol. (2011) 6(3), 339–350
Review
Dyslipidemias in the older subject: features, significance and treatment dilemmas
Indications for chronic disease preventive strate-gies blur with advancing age, throwing up new challenges. Treating high cholesterol levels in older persons requires a preliminary insight into the role that lipids play in this age-group, followed by a risk/benefit ana lysis. As more people live longer these issues have become highly critical.
Cardiovascular guidelines generally assume that hypercholesterolemia may be detrimental to every-one, independent of age [1], but epidemio logical data and hypolipidemic trials are not unequivocal on this aspect. Besides old-age is a heterogeneous term broadly including people more than 65 years of age; it is different dealing with individuals in their sixties and seventies than with octogenar-ians. For instance, oldest old subjects are more likely to experience frailty, illness with comorbid-ity, disability and physical dependence compared with younger old people [2–4]; moreover, they are often treated with multiple medications, and this increases the risk of harmful interactions [5] if a new drug (e.g., a statin) is added.
Heart disease and stroke represent the first and third leading causes of death in Europe and North America, respectively. Cumulatively
they may be the most common reasons for hos-pitalization and are responsible for more than 40% total mortality in older persons. In the last 50 years mortality rates for these conditions dropped by more than 50%, a decline highly apparent in the groups of old (65–75 years), very old (75–85 years) and oldest old (85+ years) individuals [2]. Among several causes, these changes may also be related to therapeu-tic interventions addressing cardiovascular risk factor control in general, and cholesterol reduc-tion (both total cholesterol [TC] and LDL-C) in particular.
Cholesterol, cardiovascular events & mortalityWhile no reasonable doubts exist on the causal relationships between high plasma TC and LDL-C and ischemic coronary heart disease (IHD) in middle-aged population and younger-old persons [6,7], this link weakens progres- this link weakens progres-sively with advancing age. A paradoxical asso-ciation has been reported between low TC and increased risk for all-cause mortality in elderly subjects [8–10], while several epidemiological
Almost two thirds of major coronary events take place in subjects over 65 years of age. Old (65–75 years), very old (75–85 years), and oldest old (85+ years) individuals should be considered separately when addressing cardiovascular (CV) risk. Several observational investigations have shown that the relationship between plasma cholesterol and CV events is less stringent with advancing age, especially in the very old and oldest old subject. In this context, both a decrease in total cholesterol and low HDL-C levels may be linked to coronary morbidity and total mortality through an independent association with disability and frailty. On the other hand, although elevated plasma LDL-C might still represent a CV risk factor in older people, the potential benefits originating from its reduction may exceed those obtained in younger ages, given the higher prevalence of CV disease in late life. At present statins, which represent the most effective hypocholesterolemic drugs, have been shown to significantly reduce CV events up to 82 years of age in randomized controlled trials and epidemiological surveys. The occurrence of multiple chronic conditions (comorbidity), decreased life expectancy and polypharmacotherapy suggest the need for a careful assessment of indications for aggressive hypolipidemic treatment. Drug interactions and low-pharmacological adherence may concur, causing a failure of preventive measure or side effects. Specific guidelines do not always recommend special caution or prudence in the elderly, but the selection of older patients for hypolipidemic treatment requires a high grade of clinical judgment.
KEYWORDS: cardiovascular risk n dyslipidemia n elderly n hydroxymethyl-glutaryl coenzyme A reductase inhibitors n hypercholesterolemia n hypolipidemic drugs n lipoproteins
Giovanni Battista Vigna†1, Giovanni Zuliani1 & Renato Fellin1
1Section of Internal Medicine, Gerontology and Clinical Nutrition, Department of Clinical & Experimental Medicine, University of Ferrara, via Savonarola, 9 44100, Ferrara, Italy†Author for correspondence: [email protected]
For reprint orders, please contact: [email protected]

Clin. Lipidol. (2011) 6(3)340 future science groupClin. Lipidol. (2011) 6(3)
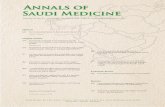
studies showed no definite relationship between high TC and cardiovascular disease (CVD) [11–13], particularly when octogenarians are con-sidered (Figure 1) [14]. For example, Iversen and colleagues in a survey considering more than 10,000 men and women before statin intro-duction in Denmark [15], recently dealt with the effects of TC levels on cardiovascular risk according to age in a healthy population from the Copenhagen City Heart Study. They con-cluded that the association between high TC and incident IHD event rate declined progressively with advancing age and seemed to disappear above 80 years of age.
On the other hand Curb et al. described a U-shaped risk distribution in a sample of 2424 Japanese-American (from the Honolulu Heart Program) men aged 71–93 years [16] without pre-vious CVD and not on lipid-lowering treatment; subjects with either low or high TC and LDL-C had a greater risk of incident IHD over a 6-year follow-up than those with TC and LDL-C in intermediate ranges (200–219 mg/dl for TC and 120–139 mg/dl for LDL-C). The authors sug-gest that frailty (i.e., the multi system deteriora-tion and loss of physio logical reserve frequently occurring later in life), poor health status and dietary intake partially explain the changing
relationship between TC and coronary heart disease with advancing age. Moreover published data in this same group of men disclosed intrigu-ing findings [10]. TC levels were compared in two different surveys 20 years apart: those subjects ranking low-levels in both investigations showed significantly higher mortality than the interme-diate/intermediate group. While the reasons for this are rather obscure, it may indicate that long-term persistence of low cholesterol concentration actually increases the risk of death (exerting a patho genetic effect), but it may also simply be due to selective mortality (i.e., those individuals who are susceptible to biological effects of high TC die prematurely).
The Established Populations for Epidemio-logic Studies of the Elderly (EPESE) study [17] related the apparent adverse effects associated with low TC levels in very old patients (aver-age baseline age of 79 years) to comorbidity and frailty. After adjusting this heterogeneous population for potential confounders (IHD risk factors, indicators of poor health such as serum iron and albumin levels and excluding first year events), the direct relationship between TC and IHD was restored, indicating that the burden of disease may alter the association linking plasma cholesterol and IHD in older individuals.
Data from a recent meta-ana lysis of 61 pro-spective observational studies, consisting of almost 900,000 adults without previous disease and more than 55,000 vascular deaths [18], could not find any independent association of choles-terol with stroke mortality, especially at older ages, but disclosed that 1 mmol/l lower TC was associated with a statistically significant hazard ratio (HR) of 0.44, 0.58, 0.72, 0.82 and 0.85 lower IHD mortality in both sexes at ages 40–49, 50–59, 60–69, 70–79 and 80–89 years, respec-tively. Accordingly, age appeared to substantially attenuate the proportional differences in IHD risk decrease, but cholesterol still remained a strong positive risk factor for IHD mortality throughout the range of measured plasma levels (~4–8 mmol/l) both in middle age and in old age. Given that IHD incidence and mortality rates highly increase with advancing age, the absolute difference in the annual risk of IHD death for a 1 mmol/l difference in TC was much greater at older than at younger ages, reaching a figure ten times higher at 80–89 years than at 40–49 years of age. This comprehensive collaborative investi-gation also showed that HDL-C was a sensitive coronary death predictive parameter but that the TC/HDL-C ratio was more informative than
Figure 1. Observational cohort study of 65,020 postmyocardial infarction subjects aged more than 65 years. Adjusted hazard ratio (HR) of 3‑year mortality in patients prescribed statins versus patients not prescribed statins at discharges from hospital. Bar graph (HR and CI 95%) represent subjects overall (A), dichotomized according to age 80 years (B) and by 5‑year age increments (C). HR >1 indicates excess risk of death for statin prescription versus no statin prescription; HR <1 indicates lesser risk of death. Statin therapy is associated with lower mortality in older patients less than 80 years but not in those aged 80 years and older. Adapted with permission from [14].
0.25 0.50 0.75 1 1.25 1.50
65–69
70–74
75–79
80–84
>85
Hazard ratio
>80
<80
Ag
e
All
Review | Vigna, Zuliani & Fellin

www.futuremedicine.com 341future science group
TC, HDL-C and non-HDL-C alone. Other related lipid measurements (LDL-C, apolipopro-tein A1, apolipoprotein B) might also have been useful but were not available and therefore were not considered in this meta-ana lysis.
Previous studies [19] and the experience of our investigational group [20] suggests a promi-nent effect related to HDL-C, showing that free-living healthy octo–nonagenarians (with-out IHD and stroke) were not characterized by high HDL-C or low LDL-C levels, but by a very small prevalence of low HDL-C car-riers (3.9%) [21]. In a different population [22] we found that low HDL-C was independently associated with disability and, most important, it predicted a worsening in functional status. The strength of the association between HDL-C and health status was successively confirmed in larger populations of community-dwelling nondisabled older persons [23], finding that among individu-als with hypocholesterolemia and normal serum albumin, HDL-C level further identified sub-groups of subjects with different risks of death. In another survey we found a strong and graded relationship between plasma HDL-C levels and several objective measures of physical perfor-mance [24]. On the whole, these data suggest the existence of a direct relationship between HDL-C and successful aging (defined as aging with a good health status and without disability) (Box 1), even if a causal relationship has not yet been demonstrated.
A working hypothesis may be outlined as fol-lows: proatherogenic dyslipidemias are under-represented in old people owing to selective mor-tality of those individuals who are susceptible to the biological effects of high TC or who manifest lipoprotein abnormalities that have been related to IHD [25]. The remaining subjects would rep-resent a selected group characterized by a ‘shift to left’ of the cholesterol distribution curve, and a rather atheroprotective genetic background. The links between TC and IHD in this context appear more complex to define, weakened but not erased, also depending on other risk param-eters (e.g., HDL-C and/or lipoprotein dimension and/or apolipoprotein content). Epidemiological
investigations cannot disclose whether chronic diseases and frailty, by lowering plasma choles-terol, simply hide the main-actor role of TC in atherogenesis or exert a direct pathophysiologic effect favoring heart attacks (e.g., by promoting a hypercoagulant-inflammatory state, coronary flow decrease, stressful stimuli) [26,27]. Likewise, when considering the relationship between low-TC or HDL-C and overall mortality, it is diffi-cult to explain if decreased lipid levels are merely the effect of illness and frailty (a reverse causality mechanism in which the disease itself directly or indirectly affects plasma constituents) or if low plasma lipids have an active causative role (e.g., by modulating the aging process [28] or by increasing cancer incidence or death [29,30]). Recent investi-gations do not support the latter hypothesis and some clues suggest that low cholesterol levels may even protect from some types of neoplastic diseases [30,31].
Lipid-lowering treatment in old subjects�n Indications from clinical trials
From the aforementioned considerations, hypo-lipidemic treatment in old subjects would require much more consideration and caution than for younger patients.
Statins (lovastatin, simvastatin, pravastatin, f luvastatin, atorvastatin, rosuvastatin and pitavastatin) or, more properly, hydroxymethyl-glutaryl coenzyme A (HMG-CoA) reductase inhibitors, represent the most effective and most prescribed drugs that lower plasma TC and LDL-C [32]. Although their use has been mainly in middle-aged hypercholesterolemic men, some randomized controlled trials (RCTs) [33–42] and a few comprehensive meta-analyses [43–45], reaffirming that cardiovascular mortality and morbidity were diminished both in treated individuals as a whole and separately in sub-jects with or without previous IHD or stroke, showed that statin treatment may also be effec-tive in old individuals (>65 years of age), at least until their early eighties, but with some ambi-guities (Table 1). It should be recognized that most elderly individuals have manifest CVD or
Box 1. The reported association between HDL plasma levels and longevity/successful aging.
�n High plasma levels of HDL‑C are associated with longevity in family studies.�n Low HDL‑C is very frequent in older individuals with disability.�n HDL‑C is positively associated with physical function.�n Low HDL‑C predicts the worsening of functional status in older individuals.�n HDL‑C is inversely correlated with total mortality in older individuals with low total cholesterol levels.
Dyslipidemias in the older subject: features, significance & treatment dilemmas | Review

Clin. Lipidol. (2011) 6(3)342 future science group
have a high prevalence of hidden atherosclerotic lesions: therefore it seems particularly hard to discriminate between primary and secondary vascular prevention, mainly in the very-old or oldest-old subjects.
Among the most relevant trials, the Heart Protection Study (HPS), published in 2002 [40], randomized 20,536 men and women aged 40–80 years with nonfasting blood total cho-lesterol concentrations of at least 3.5 mmol/l (135 mg/dl), and a high cardiovascular risk pre-disposing to IHD, stroke, lower-limb vascular disease or diabetes. Treatment with simvastatin 40 mg once daily decreased all-cause mortality by 14.7% and cardiovascular events by about one-quarter; these effects were irrespective of age, and even among the 1263 individuals aged 75–80 years at entry, and so aged about
80–85 years by the end of the study, the reduc-tion in the event rate was substantial (-30%, p < 0.001).
In the same year another investigation, the Prospective Study of Pravastatin in the Elderly at Risk (PROSPER) study [41], evaluated the effects of 40 mg pravastatin in an elderly cohort of men and women (5804 subjects, 70–82 years) at high risk of developing CVD and stroke. After a follow-up of 3.2 years, the primary end point (coronary death, myocardial infarction [MI] and stroke) was significantly reduced by 15%, but treatment had little effect on decreasing cerebro-vascular events alone, in women and in those individuals without previous CVD manifesta-tion (i.e., in primary prevention). The PROSPER trial raised some concern about a potential increase in cancer diagnoses (25%, p < 0.02,
Table 1. Major primary, secondary and mixed cardiovascular prevention trials with statins: event rate reductions (primary end point) by age.
Trial (year) Description Statin Age range (year)
Event rate reduction Ref.
Primary prevention trials
ASCOT‑LLA (2003) 19,342 hypertensive patients, TC <260 mg/dl
Atorvastatin 40–80 ≤60 years: HR 0.66, p = n.s.>60 years: HR 0.64, p < 0.01
[33]
CARDS (2004) 2838 diabetic patients with RF (smoking, hypertension, microangiopathy), LDL‑C <160 mg/dl
Atorvastatin 40–75 <65 years: RRR 37%, p < 0.05≥65 years: RRR 38%, p < 0.05
[34]
MEGA (2006) 3966 healthy men and women, TC 220–270 mg/dl
Pravastatin 40–70 <60 years: HR 0.81, p = n.s.≥60 years: HR 0.59, p < 0.01
[35]
JUPITER (2008) 17,802 healthy subjects, LDL‑C <130 mg/dl, CRP >2mg/dl
Rosuvastatin Men >50, Women >60
All: HR 0.56, p < 0.001≥70 years: HR 0.61, p < 0.001
[36]
Secondary and mixed prevention trials
4S (1994) 4444 patients with angina pectoris or previous myocardial infarction, TC 220–320 mg/dl
Simvastatin 35–70 <65 years: RRR 28%, p < 0.01≥65 years: RRR 34%, p < 0.001
[37]
CARE (1996) 4159 patients with myocardial infarction, TC <240 mg/dl
Pravastatin 21–75 <60 years: RRR 20%, p < 0.05≥60 years: RRR 27%, p < 0.001
[38]
LIPID (1998) 9014 patients with a history of myocardial infarction or unstable angina, TC 155–271 mg/dl
Pravastatin 31–75 <55 years: RRR 32%, p < 0.05≥70 years: RRR 15%, p = n.s.
[39]
HPS (2002) 20,536 high‑risk individuals (diabetics, hypertensive, patients with CHD or PAD), TC >135 mg/dl
Simvastatin 40–80 <65 years: RRR 23%, p < 0.05≥70 years: RRR 18%, p < 0.05
[40]
PROSPER (2002) 5804 patients with a history of (or risk factors for) vascular disease, TC 160–360 mg/dl
Pravastatin 70–82 All: HR 0.85, p < 0.05 [41]
GISSI‑HF (2008) 4574 heart failure patients (40% from ischemic cause)
Rosuvastatin >18 <70 years: HR 1.08, p = n.s.≥70 years: HR 0.97, p = n.s.
[42]
CHD: Coronary heart disease; CRP: C‑reactive protein; CVD: Cardiovascular disease; HR: Hazard ratio; n.s.: Not significant; PAD: Peripheral arterial disease; RF: Risk factors; RRR: Relative risk reduction; TC: Total cholesterol. AFCAPS/TexCAPS: Air Force/Texas Coronary Atherosclerosis Prevention Study; ASCOT‑LLA: Anglo–Scandinavian Cardiac Outcomes Trial–Lipid Lowering Arm; CARDS: Collaborative Atorvastatin Diabetes Study; CARE: Cholesterol And Recurrent Events; JUPITER: Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin; LIPID: Long–term Intervention with Pravastatin in Ischemic Disease; MEGA: Management of Elevated Cholesterol in the Primary Prevention Group of Adult Japanese Study Group; PROSPER: Prospective Study of Pravastatin in the Elderly at Risk.
Review | Vigna, Zuliani & Fellin

www.futuremedicine.com 343future science group
mainly breast and gastrointestinal tract tumors), but incorporation of this finding into a meta-ana lysis of all pravastatin and all statin trials did not confirm the results, relating them to chance alone [41].
The Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER) trial [46] was a multi-center investigation designed to assess the ben-efits of rosuvastatin treatment in healthy subjects with normal cholesterol levels and increased C reactive protein plasma levels (≥2 mg/l). After a follow-up of almost 2 years this study was pre-maturely stopped by an interim efficacy analysis, which disclosed a significant reduction of car-diovascular events among statin-treated partici-pants. HR for the primary cardiovascular end point in treated subjects was 0.56 and was similar and significant in subjects less than 65 years and in elderly men and women separately [47].
A meta-ana lysis from the Cholesterol Treatment Trialists’ (CTT) Collaboration including 26 major statin trials [45], showed that, compared with placebo, statin treatment decreased the 5-year incidence of major coronary events, coronary revascularization and stroke per 1 mmol/l reduction in LDL-C by 22%; indi-viduals aged more than 75 years of age (a rather small percentage of the total) seemed to benefit slightly less than subjects 75 years of age or less (16 vs 22% risk reduction, respectively). Another meta-ana lysis including nine trials [48], investi-gated whether statins reduced all-cause mortal-ity in 19,569 elderly IHD patients. The results were similar to those previously described with a relative risk reduction of 22% for overall deaths, 30% for IHD mortality, 26% for non-fatal MI, 30% for revascularization and 25% for stroke.
The MIRACL Study was an interesting short-term (16-weeks), randomized, double blind investigation, evaluating atorvastatin effects in a setting of recent acute coronary syndrome [49]; post hoc ana lysis also assessed if statin therapy was beneficial and safe in older patients [50]. Overall treated subjects (n = 3086) showed 16% risk reduction (p = 0.05) in a composite cardio-vascular end point (death, nonfatal acute MI, resuscitated cardiac arrest or hospitalization for symptomatic myocardial ischemia), while those aged more than 65 years (n = 1672) had a 14% decrease (p was not statistically significant) and those 80 years of age and older (n = 314) a 34% risk reduction (p = 0.05). Another unusual statin trial is the Study Assessing Goals in the Elderly (SAGE) trial [51], which demonstrated that older
men and women (65–85 years of age) with coronary heart disease, benefited from statin treatment (reduced total duration of myocar-dial ischemia on 48-h Holter monitoring) and, if intensively treated, also had a trend towards fewer cardiovascular events and a reduction in all-cause mortality.
There has been much interest in the potential therapeutic role of statins in heart failure (HF) since HF is a highly prevalent condition in elderly subjects (in the Framingham study, 10% of peo-ple in their 80s had HF) [52]. The CORONA trial [53] is an investigation recruiting subjects with HF of ischemic cause, who were random-ized between rosuvastatin 10 mg or placebo; mean patient age was 73 years and more than 40% of these subjects were at least 75 years old. Basal LDL-C levels were 3.6 mmol/l (137 mg/dl) and dropped to 2 mmol/l (76 mg/dl) in treated individuals. Cardiovascular death, MI and stroke incidence were not significantly reduced in the latter subjects compared with controls during a median follow-up of approximately 33 months, and outcomes did not differ in patients after subdivision using a cutoff age of 77 years. These unfavorable results were replicated in another large statin trial published the following year: the GISSI-HF study [54]. Once more observa-tional studies indicated that in patients with HF, lower rather than higher levels of TC were associated with worse outcomes [55]. A reverse causality (frailty) or pathogenic effects (e.g., low lipoprotein removal of endotoxin entering cir-culation through the intestinal wall) might have been the cause, and potential statin benefits in these RCTs were perhaps balanced by the unfa-vorable effects of lowering cholesterol levels in this population [56].
The issue of low HDL-C and high plasma triglyceride has not been addressed by previous trials: other hypolipidemic drugs such as fibrates, niacin and omega-3 fatty acids may prove more effective than statins in ameliorating these dys-lipidemias [32]. However, whether the benefits of these treatments extend to old subjects or are additive to statins and also safe in later life is not known.
Cost–effectiveness of statin therapy is accept-able for a wide range of individuals. Ganz et al. estimated an incremental cost–effectiveness of statin therapy versus usual care of US$18,800 per quality-adjusted life-year gained by extra-polating results from published RCTs to patients 75–84 years of age with previous MI [57]. Cost of preventing a major vascular event with
Dyslipidemias in the older subject: features, significance & treatment dilemmas | Review

Clin. Lipidol. (2011) 6(3)344 future science group
sim vastatin in subjects aged more than 70 years from the HPS investigation (and a 30% cardio-vascular risk at 5 years) has been shown to be about $15,000, while cost per vascular death avoided is about $75,000 [58]: they are compa-rable to those of other commonly accepted treat-ments. Since cost–effectiveness ratio depends chiefly on the underlying risk of vascular events, it seems particularly favorable in the elderly patient population on secondary prevention.
�n Observational studies: indications & confoundersLittle experimental data are available on hypo-lipidemic drug effects in octogenarians or older individuals, and also statin-ascribed benefits in the extreme ages covered by some RCTs is only tentative and risky, given the limited number of patients evaluated.
However, observational investigations may provide some additional indications. A 7.3 year follow-up in the Cardiovascular Health Study, found that the use of hypolipidemic drugs was associated with a decreased risk of incident cardio vascular events among subjects 65 years and older (multivariate HR 0.53; 95% CI, 0.36–0.76) and risk estimates were similar in those more than 74 years of age at baseline (HR 0.42; 95% CI, 0.15–1.14) [59]. Aronow et al. documented that at 3-year follow-up of a group of 1410 older patients with prior MI, LDL-C of at least 125 mg/dl and mean age of 81 years, the use of statins significantly reduced MI or IHD-related death by 50%, stroke by 60% and HF by 48% [60]. Also, subjects older than 90 years of age exhibited coronary event reduction. A large study in patients with angiographically proven IHD showed that statin therapy was associated with decreased overall mortality in the following 40 months up to 97 years of age [61]. Old subjects were significantly less likely to receive statins than younger patients but death rate decreased among statin recipients in all age groups; the relative risk reductions in mortality reached 50% for those ≥80 years, compared with 44 and 30% for indi-viduals 65–79 years old and those <65 years of age, respectively, even after adjusting for various potentially confounding factors. Several limita-tions to this study can be noted; among them frailty indices were not considered and cause-specific mortality was unavailable while, as the authors recognize, there were less diabetics and less subjects with HF among patients receiv-ing statins, thus, these subjects may represent a healthier group explaining lower mortality rates;
moreover, statin therapy was evaluated at hospital discharge but no data was collected concerning long-term drug compliance.
Prescription and adherence to statin treat-ment have distinct but complementary roles in the beneficial effects due to preventive interven-tions. We evaluated these parameters in sub-jects affected by MI, trying to correlate them to mortality rates in a prospective investigation carried out in the province of Ferrara (Italy) [62]. Preliminary ana lysis of clinical administrative and prescriptive databases of the whole resi-dent population during a 3-year period allowed the identification of 1529 MI subjects, aged 72.6±13.0 years. Statin-treated individuals compared with not-treated ones were younger, more frequently males and more often taking other cardiovascular drugs. After adjusting for several confounders (age, gender, cohort, drugs, comorbidity) total mortality HR reduction was 56% in statin not-adherent and 81% in statin adherent subjects compared with not-treated individuals (p < 0.001), while HR for individuals aged more than 80 years showed a reduction of 57 and 78%, respectively (Figure 2) [Satta E et al.,
Unpublished Data]. Of course we cannot exclude that these data represent, at least in part, the results of inverse causality or a ‘healthy user bias’, but we adjusted our ana lysis for the number of concomitant diseases and excluded events that occurred during the first 6 months after hospi-talization in order to uncover their independent role on mortality rates.
Low statin use in elderly subjects may be related to incompletely defined advantages. However, old patients often present multiple chronic conditions and it has been shown that subjects with comorbidities are also less likely to receive effective treatment than healthier patients with lower illness burden and sever-ity [63]. A retrospective cohort study by Ko et al. found a treatment paradox in high-risk elderly subjects [64]: while prescription of statins should ideally correlate with the future probability of death, conversely the authors described a dimin-ished likelihood of receiving hypolipidemic therapy with increasing age and baseline car-diovascular risk, even after adjustment for sex, socioeconomic status and rural versus urban resi-dence. Perhaps the reason is that patients may be reluctant to accept multiple interventions, or that clinicians try to keep care simple, or fear that supplementary medications alter patient’s adherence to prescriptions or increase the risk of unwanted drug interactions and harmful effects.
Review | Vigna, Zuliani & Fellin

www.futuremedicine.com 345future science group
�n Adverse events & lipid-loweringPotential benefits of statin treatment must be weighed against severity and possibly adverse drug reactions to these agents. Muscular com-plaints are relatively frequent (up to 10–15% of treated subjects), generally of minor impor-tance and related to statin type and dosage [65]. Rhabdomyolysis, on the other hand, is a rare but potentially fatal complication (less than 1:10,000 person-years). Muscle tenderness or minor mus-cle aches (myalgias) are very rarely a prodromal of rhabdomyolysis, being highly prevalent in the general population and related to a variety of widespread condition (e.g., exercise, alcoholism or drug addiction, osteo muscular disease, infec-tions). Myopathy with mild creatine phosphoki-nase elevation (<5–10 × upper limit of normal) is an intermediate condition that deserves follow-up and statin dose lowering or tapering-off and, on a patient basis, rechallenge [66]. Asymptomatic mild to moderate plasma liver transaminase elevation has been noticed in 1–3% of treated patients, while actual hepatic damage seems an exceptional finding [67]. Statins have been claimed to cause untoward effects on the nervous system, but case reports and clinical studies suggesting change in cognition and hemorrhagic stroke were not confirmed and even some benefits have been suggested [68,69]. Altogether such conditions and diseases are rather common in the elderly, and older individuals may be reluctant to report pain and symptoms often aspecifically related to aging. It has been observed that advanced age (particu-larly >80 years), female sex and small body frame increase the myopathic effect of statins [70]. Also frailty and underlying chronic systemic diseases
(in particular renal failure and liver dysfunc-tion) may represent non-modifiable risk factors that decrease statin metabolism and excretion in elderly individuals, thus promoting toxicity. Statin-induced myopathy may cause two negative consequences. First, it diminishes drug adherence even in cases of slight discomfort; second, due to aches or weakness, it may partially or completely compromise patient’s independence in perform-ing routine daily activities, with a substantial unfavorable impact on the quality of life.
An additional factor contributing to adverse drug reactions in old subjects may be the simul-taneous use of multiple medications: it has been estimated that two drugs cause an interaction in about one fifth of cases, four drugs in 50% and eight drugs in almost all cases [71]. This is particularly true in elderly individuals, often on polypharmacotherapy [72], and with some statins (simvastatin, lovastatin and atorvastatin) that have a common metabolic pathway with other drugs (e.g., fibrates, cyclosporin, macro-lides, antifungal drugs, calcium antagonists and warfarin) at the level of cytochrome P450 isoen-zyme 3A4 [5,73,74]. Surprisingly there is shortage of investigational data on this relevant topic: in the PRIMO study [65] concomitant medication per se was associated with a borderline increased risk of muscular symptoms (odds ratio 1.15; 95% CI 0.98–1.34, p = 0.081), while starting a new medication was identified as a triggering factor for muscular symptoms by 30% of patients who reported potential factors.
Prevention and early recognition are the best approaches to managing statin-related adverse drug reactions and averting serious sequelae
543210
1.0
0.8
0.6
0.4
0.2
Time (years)
543210
1.0
0.9
0.8
0.7
0.6
Time (years)Time (years)543210
1.0
0.9
0.8
0.7
0.6
0.5
Su
rviv
al
TATNANT
TATNANT
TATNANT
Su
rviv
al
Su
rviv
al
Figure 2. ALARM2 trial. Kaplan–Meier survival curves according to statin treatment. (A) All myocardial infarction patients, (B) younger myocardial infarction patients (< 80 years) and (C) myocardial infarction patients 80 years of age or older. NT: Not treated; TA: Treated, adherent; TNA: Treated, not‑adherent.
Dyslipidemias in the older subject: features, significance & treatment dilemmas | Review

Clin. Lipidol. (2011) 6(3)346 future science group
in elderly individuals. Statin treatment should begin with low doses that are progressively increased; patients should be counseled on the risk of myopathy and on the possibility of drug interactions, while any unexplained muscle symptoms should be reported immediately to the attending physician.
Older populations & cardiovascular guidelinesWhile the European guidelines on CVD pre-vention in clinical practice [75] do not particu-larly underline the old patient issue, and a recent Consensus Conference Report on cardiometa-bolic risk considers elderly subjects as a subset of patients that needs more investigation [76], more accurate indications derive from the National Cholesterol Education Program Expert Panel (Adult treatment Panel III) [1]. On the premise that older persons benefit from LDL-lowering therapy similarly to middle-aged individuals, the ATP-III considers several major problems limiting potential indications to treatment, such as statin prices (prohibitive for many subjects in several countries), the low reliability of avail-able techniques to assess absolute cardiovascular risk in the elderly and the use of noninvasive methods to detect subclinical atherosclerosis and more properly select good candidates for intensive LDL-lowering therapy.
Dietary interventions and changes in life-style, including smoking cessation and physical activity, are regarded as main treatment options for dyslipidemic older individuals similarly to younger subjects (especially if cardiovascular risk is not particularly high) and emphasis is put on managing other risk conditions (e.g., hypertension and diabetes). On the other hand it must be recognized that many elderly people are attached to personal lifestyle habits and not easily persuaded to change behaviors; further-more, strict dietary advice may produce undue food restriction and risk of malnutrition (e.g., for milk and dairy products, whose adequate ingestion may prevent osteoporosis).
Clinical judgment assumes increasing impor-tance in the choice of LDL-lowering therapies in older persons: physicians must use special caution. Coexisting diseases, biological and functional age, life expectancy, cognitive sta-tus, social and economic issues, and risk, all rep-resent modulating factors in the final decision to treat the patient with hypolipidemic drugs (Figure 3). An update of ATP-III instructions suggests more intense statin treatment in very
high CV risk patients (i.e., a LDL-C target less than 70 mg/dl [1.8 mmol/l]) [77]. Among patients aged more than 70 years, with acute coronary syndrome and prescribed high-dose statins at hospital discharge [78], reaching this new NCEP goal appears safe and may pre-vent four times as many events than in their younger counterparts.
ConclusionThe relationship between cholesterol and CVD is rather complex in the elderly. However, in older individuals small differences in choles-terol-related relative IHD risk is associated with a striking increase in the absolute risk, given the high prevalence of IHD later in life. This sug-gests that excluding older persons from choles-terol screening may be inappropriate, but also that a comprehensive lipid profile (in particular HDL-C in addition to TC and LDL-C), and in-depth clinical evaluation is essential for deciding if pharmacological treatment is needed. Because of heightened risks of drug–drug interactions, the prevalence of polypharmacy in seniors, and issues of tolerability and convenience, monother-apy with low doses of one efficacious statin may be preferable to other therapeutical strategies. Nevertheless, from the available limited expe-rience with high-dose regimens, statins seem safe. Treatment should be checked periodically as nonadherence to therapy negatively influences health costs by increasing the number of future CV events. We therefore believe that, aiming to optimize patient outcomes, clinicians should consider not only the real need for treatment, and the specific drug or dose to use, but also the clinical and social factors that impact the adherence to therapy.
Frailty/disabilityNo Yes
65–8
5 ye
ars
≥85
year
s
Ag
e cl
ass
Figure 3. Indications for hypolipidemic drug treatment according to age and disease burden in high-risk elderly subjects. White area: treatment indicated; gray area: not univocal indication to treatment; black area: treatment not‑indicated.
Review | Vigna, Zuliani & Fellin

www.futuremedicine.com 347future science group
Future perspectiveThe implications of an altered lipid profile in the extreme ages of life need better clarification. In particular, it is not clear which are the mecha-nisms relating aging and possible modifications of lipoprotein levels and functions, and how HDLs might influence specific aging processes, frailty and disability.
Upcoming investigations are required to fur-ther discriminate the older population necessitat-ing treatment with hypolipidemic drugs, and to evaluate if oldest old people have an advantage from statin use. Longer follow-up of cohort stud-ies and increased life duration make it possible to implement existing cardiovascular risk charts by adding data from senior subjects. On the other hand, new tools for correct risk stratification and widely applying not-invasive tests for investigat-ing subclinical vascular disease will probably permit the identification of older patients who require aggressive hypolipidemic therapy.
AcknowledgementsThe authors would like to thank Luca Degli Esposti, Stefano Buda and Chiara Veronesi (Health Economics and Outcomes Research, CliCon s.r.l., Ravenna, Italy), and Emidia Vagnoni (Department of Economia Istituzioni Territorio, University of Ferrara, Italy) for the permission to use some preliminary data and figures from the Adherence to Long-term therapies: Assessment and Real practice Management-2 (ALARM-2) study, carried out in the province of Ferrara (Italy).
Financial & competing interests disclosureThe authors have no relevant affiliations or financial involvement with any organization or entity with a finan-cial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Executive summary
Cholesterol, cardiovascular events & mortality�n In the elderly, dyslipidemias represent significant risk, strengthened by the high prevalence of cardiovascular disease late in life. High
total cholesterol, but also hypocholesterolemia and HDL‑C levels may be associated with atherosclerosis and increased total mortality and cardiovascular morbidity.
Lipid-lowering treatment in old subjects�n Observational investigations and clinical trials have shown the efficacy of hypolipidemic therapy, particularly statins, in lowering the
risk of coronary events and stroke in old and very old subjects; nevertheless, beyond 85 years of age the effects of cholesterol‑lowering therapy have yet to be assessed.
Adverse events & lipid lowering�n When deciding on drug treatment, several factors have to be considered: age, frailty/disability and comorbidity, life expectancy,
concomitant drug consumption, social and economic context, presence of subclinical atherosclerosis and cardiovascular risk level.Older populations & cardiovascular guidelines�n Statin therapy must be undertaken prudently in the elderly and generally necessitates lower drug dosage; patients should be informed of
the risk of myopathy and pharmacological interactions are of special concern, since both conditions may adversely impact on adherence.
Dyslipidemias in the older subject: features, significance & treatment dilemmas | Review
BibliographyPapers of special note have been highlighted as:n of interestnn of considerable interest
1 Expert Panel: Third report of the National Cholesterol Education Program (NCEP) Expert Panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III) final report. Circulation 106, 3143–3421 (2002).
2 Guralnik JM, Ferrucci L: Demography and epidemiology. In: Principles of Geriatric Medicine and Gerontology. Hazard WR, Blass JP, Halter JB, Ouslander JG, Tinetti ME (Eds). McGraw Hill, NY, USA, 53–75 (2003).
3 Lang PO, Michel JP, Zekry D: Frailty syndrome: a transitional state in a dynamic process. Gerontology 55, 539–549 (2009).
4 Maraldi C, Ble A, Zuliani G et al.: Association between anemia and physical disability in older patients: role of comorbidity. Aging Clin. Exp. Res. 18, 485–492 (2006).
5 Klotz U: Pharmacokinetics and drug metabolism in the elderly. Drug Metab. Rev. 41, 67–76 (2009).
6 Neaton JD, Wentworth D: Serum cholesterol, blood pressure, cigarette smoking, and death from coronary heart disease. Overall findings and differences by age for 316,099 white men. Multiple Risk Factor Intervention Trial Research Group. Arch. Intern. Med. 152, 56–64 (1992).
7 Castelli WP, Anderson K, Wilson PW, Levy D: Lipids and risk of coronary heart disease. The Framingham Study. Ann. Epidemiol. 2, 23–28 (1992).
8 Brescianini S, Maggi S, Farci G et al.: Low total cholesterol and increased risk of dying: are low levels clinical warning signs in the elderly? Results from the Italian longitudinal study on aging. J. Am. Geriatr. Soc. 51, 991–996 (2003).
9 Spada RS, Toscano G, Cosentino FI et al.: Low total cholesterol predicts mortality in the nondemented oldest old. Arch. Gerontol. Geriatr. 44(Suppl. 1), 381–384 (2007).
10 Schatz IJ, Masaki K, Yano K, Chen R, Rodriguez BL, Curb JD: Cholesterol and all-cause mortality in elderly people from the Honolulu Heart Program: a cohort study. Lancet 358, 351–355 (2001).
nn� A survey from an important investigation performed in Japanese/American men living in Hawaii; among elderly subjects,

Clin. Lipidol. (2011) 6(3)348 future science group
long-term persistence of low plasma cholesterol shows a significant association with increased mortality.
11 Kozarevic D, McGee D, Vojvodic N et al.: Serum cholesterol and mortality. The Yugoslavia Cardiovascular Disease Study. Am. J. Epidemiol. 114, 21–28 (1981).
12 Raiha I, Marniemi J, Puukka P et al.: Effect of serum lipids, lipoproteins, and apolipoproteins on vascular and nonvascular mortality in the elderly. Arterioscler. Thromb. Vasc. Biol. 17, 1224–1232 (1997).
13 Simons LA, Simons J, Friedlander Y, McCallum J: Cholesterol and other lipids predict coronary heart disease and ischemic stroke in the elderly, but only in those below 70 years. Atherosclerosis 159, 201–208 (2001).
14 Foody JM, Rathore SS, Galusha D et al.: Hydroxymethylglutaryl-CoA reductase inhibitors in older persons with acute myocardial infarction: evidence for an age-statin interaction. J. Am. Geriatr. Soc. 54, 421–430 (2006).
15 Iversen A, Jensen JS, Scharling H, Schnohr P: Hypercholesterolemia and risk of coronary heart disease in the elderly. Impact of age. The Copenhagen City Heart Study. Eur. J. Int. Med. 20, 139–144 (2009).
16 Curb JD, Abbott RD, Rodriguez BL et al.: Prospective association between low and high total and low-density lipoprotein cholesterol and coronary heart disease in elderly men. J. Am. Geriatr. Soc. 52, 1975–1980 (2004).
17 Corti MC, Guralnik JM, Salive ME et al.: Clarifying the direct relation between total cholesterol levels and death from coronary heart disease in older persons. Ann. Int. Med. 126, 753–760 (1997).
n� This multicenter, longitudinal study with 5-year follow-up, relates high total cholesterol to cardiovascular mortality also in older adults; the apparent adverse effects associated with hypocholesterolemia seem secondary to comorbidity and frailty.
18 Prospective Study Collaboration: Blood cholesterol and vascular mortality by age, sex, and blood pressure: a meta-ana lysis of individual data from 61 prospective studies with 55000 vascular deaths. Lancet 370, 1829–1839 (2007).
nn� Almost 900,000 participants in 61 epidemiological studies were included in this meta-ana lysis, disclosing that total cholesterol was positively associated with ischemic heart disease mortality in both middle and old age (until 89 years) but not with stroke mortality.
19 Corti MC, Guralnik JM, Salive ME et al.: HDL cholesterol predicts coronary heart disease mortality in older persons. JAMA 274, 539–544 (1995).
20 Volpato S, Leveille SG, Corti MC, Harris TB, Guralnik JM: The value of serum albumin and high-density lipoprotein cholesterol in defining mortality risk in older persons with low serum cholesterol. J. Am. Geriatr. Soc. 49, 1142–1147 (2001).
21 Zuliani G, Palmieri E, Volpato S et al.: High-density lipoprotein cholesterol strongly discriminates between healthy free-living and disabled octo-nonagenarians: a cross sectional study. Aging 9, 335–341 (1997).
22 Zuliani G, Romagnoni F, Bollini C, Leoci V, Soattin L, Fellin R: Low levels of high-density lipoprotein cholesterol are a marker of disability in the elderly. Gerontology 45, 317–322 (1999).
23 Volpato S, Leveille SG, Corti MC, Harris TB, Guralnik JM: The value of serum albumin and high-density lipoprotein cholesterol in defining mortality risk in older persons with low serum cholesterol. J. Am. Geriatr. Soc. 49, 1142–1147 (2001).
24 Volpato S, Ble A, Metter EJ et al.: High-density lipoprotein cholesterol and objective measures of lower extremity performance in older nondisabled persons: the InChianti study. J. Am. Geriatr. Soc. 56, 621–629 (2008).
25 Vigna GB, Zuliani G, Fellin R: Hypercholesterolemia and the ageing subject. Eur. J. Intern. Med. 21, e19 (2010).
26 Afilalo J, Karunananthan S, Eisenberg MJ, Alexander KP, Bergman H: Role of frailty in patients with cardiovascular disease. Am. J. Cardiol. 103, 1616–1621 (2009).
27 Kanapuru B, Ershler WB: Inflammation, coagulation, and the pathway to frailty. Am. J. Med. 122, 605–613 (2009).
28 Walter M: Interrelationships among HDL metabolism, aging and atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 29, 1244–1250 (2009).
29 Nago N, Ishikawa S, Goto T, Kayaba K: Low cholesterol is associated with mortality from stroke, heart disease, and cancer: the Jichi medical school cohort study. J. Epidemiol. 21(1), 67–74 (2011).
30 Brown AJ: Cholesterol, statins and cancer. Clin. Exp. Pharmacol. Physiol. 3, 135–141 (2007).
31 Di Vizio D, Solomon KR, Freeman MR: Cholesterol and cholesterol-rich membranes in prostate cancer: an update. Tumori 94, 633–639 (2008).
32 Vigna GB, Fellin R: Pharmacotherapy of dyslipidemias in the adult population. Expert Opin. Pharmacother. 11, 3041–3052 (2010).
33 Sever PS, Dahlöf B, Poulter NR et al.: Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial-Lipid Lowering Arm (ASCOT-LLA): a multicentre randomised controlled trial. Lancet 361, 1149–1158 (2003).
34 Neil HA, DeMicco DA, Luo D et al.: Analysis of efficacy and safety in patients aged 65–75 years at randomization. Diabetes Care 29, 2378–2384 (2006).
35 Nakamura H, Arakawa K, Itakura H et al.: Primary prevention of cardiovascular disease with pravastatin in Japan (MEGA Study): a prospective randomised controlled trial. Lancet 368, 1155–1163 (2006).
36 Glynn RJ, Koenig W, Nordestgaard BG, Shepherd J, Ridker PM: Rosuvastatin for primary prevention in older persons with elevated C-reactive protein and low to average low-density lipoprotein cholesterol levels: exploratory ana lysis of a randomized trial. Ann. Intern. Med. 152, 488–496 (2010).
37 Miettinen TA, Pyörälä K, Olsson AG et al.: Cholesterol-lowering therapy in women and elderly patients with myocardial infarction or angina pectoris. findings from the Scandinavian Simvastatin Survival Study (4S). Circulation 96, 4211–4218 (1997).
38 Sacks FM, Pfeffer MA, Moye LA et al.: The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels. N. Engl. J. Med. 335, 1001–1009 (1996).
39 The Long-term Intervention with Pravastatin in Ischemic Disease (LIPID) Study Group: Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N. Engl. J. Med. 339, 1349–1357 (1998).
40 Heart Protection Study Collaborative Group: MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20 536 high-risk individuals: a randomised placebo-controlled trial. Lancet 360, 7–22 (2002).
41 Shepherd J, Blaw GJ, Murphy MB et al.: Pravastatin in elderly individuals at risk of vascular disease (PROSPER): a randomised controlled trial. Lancet 360, 1623–1630 (2002).
Review | Vigna, Zuliani & Fellin

www.futuremedicine.com 349future science group
42 GISSI-HF Investigators: Effect of rosuvastatin in patients with chronic heart failure (the GISSI-HF trial): a randomised, double-blind, placebo-controlled trial. Lancet 372, 1231–1239 (2008).
43 Thavendiranathan P, Bagai A, Brookhart MA, Choudhry NK: Primary prevention of cardiovascular diseases with statin therapy. A meta-ana lysis of randomized controlled trials. Arch. Intern. Med. 166, 2307–2313 (2006).
44 Brugts JJ, Yetgin T, Hoeks SE et al.: The benefits of statins in people without established cardiovascular disease but with cardiovascular risk factors: meta-ana lysis of randomised controlled trials. BMJ 338, b2376 (2009).
45 Cholesterol Treatment Trialists’ (CTT) Collaborators: Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-ana lysis of data from 170000 participants in 26 randomised trials. Lancet 376, 1670–1681 (2010).
nn� A comprehensive recent meta-ana lysis considering the most relevant statin trials (both drug-treated versus controls and more intensive versus standard statin regimens) with the purpose to determine whether large reductions in LDL-C safely produce reductions in major vascular events.
46 Ridker PM, Danielson E, Fonseca FAH et al.: Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N. Engl. J. Med. 359, 2195–2207 (2008).
47 Mora S, Glynn RJ, Hsia J, MacFadyen JG, Genest J, Ridker PM: Statins for the primary prevention of cardiovascular events in women with elevated high-sensitivity C-reactive protein or dyslipidemia: results from the Justification for the Use of statins in prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER) and meta-ana lysis of women from primary prevention trials. Circulation 121, 1069–1077 (2010).
48 Afilalo J, Duque G, Steele R, Jukema JW, de Craen AJM, Eisenberg MJ: Statins for secondary prevention in elderly patients. A hierarchical Bayesan meta-ana lysis. J. Am. Coll. Cardiol. 51, 37–45 (2008).
n� This analysis specifically addressed to elderly people: the evaluation of nine statin trials showed that hypocholesterolemic treatment reduces all-cause mortality in subjects 65–82 years of age, and that the magnitude of this effect is larger than previously believed.
49 Schwartz GG, Olsson AG, Ezekowitz MD et al.: Effects of atorvastatin on early recurrent ischemic events in acute coronary
syndromes the MIRACL Study: a randomized controlled trial. JAMA 285, 1711–1718 (2001).
50 Olsson AG, Schwartz GG, Szarek M, Luo D, Jamieson MJ: Effects of high-dose atorvastatin in patients >65 years of age with acute coronary syndrome (from the Myocardial Ischemia Reduction with Aggressive Cholesterol Lowering [MIRACL] Study). Am. J. Cardiol. 99, 632–635 (2007).
51 Deedwania P, Stone PH, Bairey Merz CN et al.: Effects of intensive versus moderate lipid-lowering therapy on myocardial ischemia in older patients with coronary heart disease: results of the Study Assessing Goals in the Elderly (SAGE). Circulation 115, 700–707 (2007).
52 Ho KK, Pinsky JL, Kannel WB et al.: The epidemiology of heart failure: the Framingham Study. J. Am. Coll. Cardiol. 22, A6–A13 (1993).
53 Kjekshus J, Apetrei E, Barrios V et al.: Rosuvastatin in older patients with systolic heart failure. N. Engl. J. Med. 357, 2248–2261 (2007).
54 GISSI-HF investigators: Effect of rosuvastatin in patients with chronic heart failure (the GISSI-HF trial): a randomised, double-blind, placebo-controlled trial. Lancet 372, 1231–1239 (2008).
55 Horwich TB, Hamilton MA, MacLellan WR, Fonarow GC: Low serum total cholesterol is associated with marked increase in mortality in advanced heart failure. J. Card. Fail. 8, 216–224 (2002).
56 Fonarow GC: Statins and n-3 fatty acid supplementation in heart failure. Lancet 372, 1195–1196 (2008).
57 Ganz DA, Kuntz KM, Jacobson GA, Avorn J: Cost–effectiveness of 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitor therapy in older patients with myocardial infarction. Ann. Intern. Med. 132, 780–787 (2000).
58 Heart Protection Study Collaborative Group: Cost–effectiveness of simvastatin in people at different levels of vascular disease risk: economic ana lysis of a randomised trial in 20536 individuals. Lancet 365, 1779–1785 (2005).
59 Lemaitre RN, Psaty BM, Heckbert SR, Kronmal RA, Newman AB, Burke GL: Therapy with hydroxymethylglutaryl coenzyme a reductase inhibitors (statins) and associated risk of incident cardiovascular events in older adults. Evidence from the Cardiovascular Health Study. Arch. Intern. Med. 162, 1395–1400 (2002).
60 Aronow WS, Frishman WH: Management of hypercholesterolemia in older persons for the prevention of cardiovascular disease. Cardiol. Rev. 18, 132–140 (2010).
61 Allen Maycock CA, Muhlestein JB, Horne BD et al.: Statin therapy is associated with reduced mortality across all age groups of individuals with significant coronary disease, including very elderly patients. J. Am. Coll. Cardiol. 40, 1777–1785 (2002).
62 Satta E, Vigna GB, Veronesi C, Vagnoni E, Buda S, Degli Esposti L: Secondary prevention of myocardial infarction and long-term adherence to statin therapy: data from the ALARM2 investigation. Presented at: Congresso Nazionale SISA. Rome, Italy 24–27 November 2010 (Abstract XXIV).
63 Redelmeier DA, Tan SH, Booth GL: The treatment of unrelated disorders in patients with chronic medical diseases. N. Engl. J. Med. 338, 1516–1520 (1998).
64 Ko DT, Mamdani M, Alter DA: Lipid-lowering therapy with statins in high-risk elderly patients. The treatment-risk paradox. JAMA 291, 1864–1870 (2004).
n� A retrospective cohort study in Ontario (GOLD), including 1.44 million residents aged 66 years or older, surprisingly observing that prescription of statins diminishes progressively as cardiovascular risk and probability of death incresase.
65 Bruckert E, Hayem G, Dejager S et al.: Mild to moderate muscular symptoms with high-dosage statin therapy in hyperlipidemic patients - The PRIMO Study. Cardiovasc. Drugs Ther. 19, 403–414 (2005).
66 McKenney JM, Davidson MH, Jacobson TA, Guyton JR: Final conclusions and recommendations of the National Lipid Association statin safety assessment Task Force. Am. J. Cardiol. 97(Suppl.), C89–C94 (2006).
67 Kinman N, Hultcrantz R: Lipid lowering medications and hepatotoxicity. J. Intern. Med. 250, 183–185 (2001).
68 Kandiah N, Feldman HH: Therapeutic potential of statins in Alzheimer’s disease. J. Neurol. Sci. 283, 230–234 (2009).
69 Amarenco P, Labreuche J: Lipid management in the prevention of stroke: review and updated meta-ana lysis of statins for stroke prevention. Lancet Neurol. 8, 453–463 (2009).
70 Schech S, Graham D, Staffa J et al.: Risk factors for statin-associated rhabdomyolysis. Pharmacoepidemiol. Drug Saf. 16, 352–358 (2007).
71 Weideman RA, McKinney WP, Bernstein IH: Predictors of potential drug interactions. Hosp. Pharm. 33, 835–840 (1998).
Dyslipidemias in the older subject: features, significance & treatment dilemmas | Review

Clin. Lipidol. (2011) 6(3)350 future science group
72 Steinman MA, Hanlon JT: Managing medications in clinically complex elders. There’s got to be a happy medium. JAMA 304, 1592–1601 (2010).
73 Corsini A: The safety of HMG-CoA reductase inhibitors in special populations at high cardiovascular risk. Cardiovasc. Drugs Ther. 17, 265–285 (2003).
74 Bottorff MB: Statin safety and drug interactions: clinical implications. Am. J. Cardiol. 97(Suppl.), C27–C31 (2006).
75 Graham I, Atar D, Borch-Johnsen K et al.: European guidelines on cardiovascular disease prevention in clinical practice: executive summary. Atherosclerosis 194, 1–45 (2007).
76 Brunzell JD, Davidson M, Furberg CD et al.: Lipoprotein management in patients with cardiometabolic risk: consensus conference report from the American Diabetes Association and the American College of Cardiology Foundation. J. Am. Coll. Cardiol. 51, 1512–1524 (2008).
77 Grundy SM, Cleeman JI, Merz CN et al.: Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelines. Circulation 110, 227–239 (2004).
78 Ray KK, Bach RG, Cannon CP et al.: Benefits of achieving the NCEP optional LDL-C goal among elderly patients with ACS. Eur. Heart J. 27, 2310–2316 (2006).
Review | Vigna, Zuliani & Fellin