
CRYSTAL-ASSOCIATED ARTHRITIS IN THE ELDERLY
23
Crystal-Associated Arthritis in the Elderly Christopher M. Wise, MD Internal Medicine, Division of Rheumatology, Allergy, and Immunology, Medical College of Virginia, Virginia Commonwealth University Health System, 417 North 11th Street, Box 980647, Richmond, VA 23298, USA The two best-recognized forms of crystal-induced joint disease are caused by the deposition of monosodium urate (MSU) and calcium pyrophosphate dihydrate (CPPD). Although initially described by Sir Alfred Garrod in the eighteenth century, the first modern association of articular crystal deposi- tion with arthritis was established in 1961 with the identification of MSU crystals in the synovial fluid of patients who had acute gout [1]. This descrip- tion was followed shortly by the recognition of pseudogout associated with CPPD crystals [2]. Since then, a great deal has been learned about these two common types of arthritis that are seen frequently in elderly patients. In addition, the role of other crystals, particularly basic calcium phosphate (BCP) crystals, in the pathogenesis of osteoarthritis has been further explored. Gout and pseudogout usually present as acute, self-limited episodes of monoarthritis but may be associated with polyarticular attacks, chronic ar- thritis, and destructive changes in cartilage and bone. MSU and CPPD crys- tals can be found in synovial tissue and fluid from asymptomatic patients or during acute attacks of arthritis associated with a marked inflammatory response. The factors responsible for the inflammatory response to crystals are not completely understood [3]. The phlogistic properties of crystals seem to be linked to their ability to bind immunoglobulins and other proteins. These complexes bind to surface receptors on macrophages and mast cells, leading to activation and release of proinflammatory cytokines, chemotactic factors, and other mediators. An influx of phagocytic cellsdparticularly neutrophilsdfollows. Crystals are engulfed, and subsequent disruption of lysosomes releases arachidonate metabolites, collagenases, and oxygen A version of this article originally appeared in Clinics in Geriatric Medicine, 21:3, August 2005. E-mail address: [email protected] 0889-857X/07/$ - see front matter Ó 2007 Elsevier Inc. All rights reserved. doi:10.1016/j.rdc.2006.12.007 rheumatic.theclinics.com Rheum Dis Clin N Am 33 (2007) 33–55
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of CRYSTAL-ASSOCIATED ARTHRITIS IN THE ELDERLY

Rheum Dis Clin N Am
33 (2007) 33–55
Crystal-Associated Arthritisin the Elderly
Christopher M. Wise, MDInternal Medicine, Division of Rheumatology, Allergy, and Immunology,
Medical College of Virginia, Virginia Commonwealth University Health System,
417 North 11th Street, Box 980647, Richmond, VA 23298, USA
The two best-recognized forms of crystal-induced joint disease are causedby the deposition of monosodium urate (MSU) and calcium pyrophosphatedihydrate (CPPD). Although initially described by Sir Alfred Garrod in theeighteenth century, the first modern association of articular crystal deposi-tion with arthritis was established in 1961 with the identification of MSUcrystals in the synovial fluid of patients who had acute gout [1]. This descrip-tion was followed shortly by the recognition of pseudogout associated withCPPD crystals [2]. Since then, a great deal has been learned about these twocommon types of arthritis that are seen frequently in elderly patients. Inaddition, the role of other crystals, particularly basic calcium phosphate(BCP) crystals, in the pathogenesis of osteoarthritis has been further explored.
Gout and pseudogout usually present as acute, self-limited episodes ofmonoarthritis but may be associated with polyarticular attacks, chronic ar-thritis, and destructive changes in cartilage and bone. MSU and CPPD crys-tals can be found in synovial tissue and fluid from asymptomatic patients orduring acute attacks of arthritis associated with a marked inflammatoryresponse. The factors responsible for the inflammatory response to crystalsare not completely understood [3]. The phlogistic properties of crystals seemto be linked to their ability to bind immunoglobulins and other proteins.These complexes bind to surface receptors on macrophages and mast cells,leading to activation and release of proinflammatory cytokines, chemotacticfactors, and other mediators. An influx of phagocytic cellsdparticularlyneutrophilsdfollows. Crystals are engulfed, and subsequent disruption oflysosomes releases arachidonate metabolites, collagenases, and oxygen
A version of this article originally appeared in Clinics in Geriatric Medicine, 21:3, August
2005.
E-mail address: [email protected]
0889-857X/07/$ - see front matter � 2007 Elsevier Inc. All rights reserved.
doi:10.1016/j.rdc.2006.12.007 rheumatic.theclinics.com
34 WISE
radicals. Factors that contribute to the self-termination of attacks includedigestion of crystals by myeloperoxidase, increased heat and blood flowleading to dissolution and removal of crystals from the joint, alterationof the crystal properties by the inflammatory process itself, and down-reg-ulation that occurs with crystal phagocytosis by more mature macrophageslater in the attack [4,5].
Gout typically has an onset in middle-aged adults, but has an increasingprevalence in older age groups, often with unique and atypical features.Pseudogout, on the other hand, is more often associated with onset inelderly patients and has more predictable features in this population. Therecognition of crystal-induced arthritis in elderly patients should lead tothe avoidance of unnecessary diagnostic tests and therapies in many patientswho have acute and chronic arthritis and allow more optimal managementof two conditions that usually have a favorable outcome.
Gout
Epidemiology and pathogenesis of gout and hyperuricemia
Gout has been classically recognized as a disease affecting middle-agedmen, but in fact has an increasing frequency in men and women in olderage groups. The annual incidence of gout in men in most studies is in therange of 1 to 3 per 1000, but is much lower in women [6,7]. In the Framing-ham Study, for example, the 2-year incidence of gout was 3.2 per 1000 formen compared with 0.5 per 1000 for women [8]. The epidemiology ofgout may have changed in various population groups over the past 10 to20 years. For example, recent studies of gout in the United States overthe past 2 decades has suggested that the prevalence of gout may be increas-ing, with most of this increase coming in men and women over the age of 65,and now approaches 7% in men in this age group [9–11]. Conversely, theaverage age of onset of gout seems to have decreased in a recent study ofpatients in Taiwan [12].
The overall prevalence of self-reported gout in the general population is0.7% to 1.4% in men and 0.5% to 0.6% in women. In people older than65, this prevalence increases to 4.4% to 5.2% in men and 1.8% to 2.0% inwomen [6,13–15]. In male populations in particular, gout reaches a high prev-alence by the fifth decade. For example, the prevalence of gout in a study ofUnited States physicians was 5.8% among whites and 10.9% among AfricanAmericans who had been surveyed for a mean of 28 years after graduationfrommedical school [16]. Most patients who have gout are men, even in olderage groups. Among patients who have the onset of gout after the age of 60,however, the distribution between men and women is almost equal, and inthose who have onset after age 80 women seem to predominate [17,18].
The incidence and prevalence of gout is parallel to that of hyperuricemia inthe general population. Serum urate levels increase by 1 to 2 mg/dL in men at

35CRYSTAL-ASSOCIATED ARTHRITIS IN THE ELDERLY
the time of puberty, but women exhibit little change in urate levels until aftermenopause, when concentrations approach those seen in men [19]. Hyperuri-cemia is clearly associated with an increased risk for developing gout, al-though most patients who have elevated serum uric acid levels do not havegout [20]. People who have serum urate levels greater than 10 mg/dL havean annual incidence of gout of 70 per 1000 and a 5-year prevalence of 30%,whereas those who have levels less than 7 mg/dL have an annual incidenceof only 0.9 per 1000 and prevalence of 0.6%. Additional factors that correlatestrongly with serum urate levels and the prevalence of gout in the general pop-ulation include serum creatinine levels, body weight, height, and blood pres-sure. Most of the renal disease in patients who have gout is believed to be theresult of nephrosclerosis related to hypertension. A direct pathogenetic rolefor uric acid in the development of renal disease and hypertension is still pos-sible, however [21,22]. Recent studies have also demonstrated that the devel-opment of gout is associated with higher levels of alcohol, meat, and seafoodconsumption but not with higher levels of vegetable purine intake, and therisk for gout is decreased in those who have higher levels of dairy product con-sumption [23,24].
Hyperuricemia can result from decreased renal excretion or increased pro-duction of uric acid [25]. In 80% to 90% of patients who have primary gout,hyperuricemia is caused by renal underexcretion of uric acid, even though re-nal function is otherwise normal. The defect in renal excretion of uric acid inpatients who have primary gout may be attributed to reduced filtration,enhanced reabsorption, or decreased secretion, but it is unclear which of thesemechanisms is most important. Patients who have secondary gout related torenal disease are hyperuricemic because of a decreased filtered load and de-creased tubular secretion of uric acid. Patients who have lead nephropathyseem to be particularly prone to the development of gout, and recent studieshave suggested that subclinical exposure to environmental lead may contrib-ute to some of the hyperuricemia and gout seen in the general population[26,27]. The hyperuricemia associated with diuretic therapy, seen frequentlyin older populations, results from volume depletion, which leads to a de-creased filtered load and enhanced tubular reabsorption [28]. A renal mech-anism is also the cause of hyperuricemia associated with most other drugs,including low-dose aspirin and cyclosporine. About 40% of patients reporta family history of gout in most series, and the hereditary component for se-rum uric acid levels in the general population has been estimated to be ap-proximately 40% [19,29]. Most available data suggest that the geneticcomponent of hyperuricemia and gout is related to multiple genes involvingproduction and excretion of uric acid.
Typical clinical features
In typical gout, occurring most often in middle-aged men, the usual initialattack of gout occurs after years of sustained hyperuricemia and deposition

36 WISE
of monosodium urate in the synovial tissue (Table 1). The initial attack ofgout is monoarticular in 85% to 90% of patients [19]. Lower-extremityjoints are usually affected, with approximately 60% of first attacks involvingthe first metatarsophalangeal (MTP) joints. Attacks may last from a fewdays to 2 to 3 weeks, with a gradual resolution of all inflammatory signsand a return to apparent normalcy. An intercritical period lasting weeksto months may elapse before a new attack occurs in the same or anotherjoint. Without specific therapy, a second attack occurs in 78% of patientswithin 2 years, and in 93% within 10 years. Over subsequent years, attacksoccur more frequently and may be polyarticular and associated with feverand constitutional symptoms [30–32]. Tophaceous deposits become appar-ent over the elbows, fingers, or other areas over the years, and chronic poly-articular arthritis may develop, sometimes resembling rheumatoid arthritisor degenerative joint disease.
Clinical features of gout in the elderly
The recognition of gout in elderly patients may be complicated by a ten-dency for patients in this age group to present differently than younger pa-tients (see Table 1). Clinical observations have suggested several areas inwhich gout in elderly patients differs from gout in younger age groups, asfollows:
Polyarticular gout is more common in older patients and appears earlierin disease.
Women make up a larger proportion of older patients who have gout.Gout involves the small joints of the fingers in older patients more
frequently.Tophi occur earlier in the course of gout in older patients, often in atyp-
ical locations.
Table 1
Clinical features of gout: typical versus elderly onset gout
Feature Typical gout Elderly onset gout
Age of onset Peak in mid-40s Over 65
Sex distribution Men OO women Men ¼ women
Presentation Acute monoarthritis Polyarticular onset more often
Lower extremity
(podagra 60%)
Upper extremity more often
Finger involvement more often
Tophi After years of attacks May occur early or without history
of prior attacks
Elbows O fingers Possibly more often over fingers
Associated features Obesity Renal insufficiency
Hyperlipidemia Diuretic use, especially in women
Hypertension Alcohol use less common
Alcohol use, heavy

37CRYSTAL-ASSOCIATED ARTHRITIS IN THE ELDERLY
Diuretic use and renal disease are more frequent in older people who havegout.
Polyarticular gout
Patients who have polyarticular gout tend to be older than those whohave monoarticular attacks, with a mean age of 60 to 64 years reported inprevious series [30–32]. About 10% to 39% of these patients give a historyof a polyarticular onset of their disease. One series of 36 patients who hadonset of gout after the age of 60 noted a polyarticular onset in 18 (50%),a much higher incidence than that seen in typical middle-aged patientswho have gout [18]. The higher frequency of polyarticular involvement inolder patients is likely to result from multiple factors. Elements that likelycontribute to this phenomenon include more patients who have chronicconcomitant cardiac and renal disease, and medications, such as low-doseaspirin and diuretics, that contribute to the development of chronic hyper-uricemia. A delay in diagnosis and treatment of gout in younger age groupsmay result in more older patients who have a more indolent inflammatorycomponent that may be difficult to distinguish from rheumatoid arthritis[18,33,34]. In such patients, the history of illness at onset is often difficultto obtain, and a prior history of acute intermittent arthritis or podagramay not be recalled.
Increased female frequency
An increased frequency of female patients is noted among older patientswho have gout, particularly in those with elderly onset gout. Most women,possibly up to 85%, have the onset of disease after menopause [35]. In a re-cent series of Korean women who had gout, 75% developed the first symp-tomatic episode of gout after the onset of menopause, and most of thosewho had gout before menopause had renal disease or were taking cyclospor-ine for renal transplantation [36]. The mean age of women who have gout inmost series tends to be about 7 to 10 years older than in men, with a shorterduration of disease at the time of study [35,37]. Women constitute about50% to 60% of patients who have the onset of gout over the age of 60[17,38,39] and almost all of the patients who have the onset of diseaseover the age of 80 [17,40].
Small-joint finger involvement
Gouty inflammation of the small joints of the fingers in elderly patientshas been noted more frequently in recent years (Fig. 1). Osteoarthritis ofthe distal and proximal interphalangeal (IP) joints is common in elderlypatients, particularly women, and the typical inflammatory exacerbationsseen in this condition are attributed to BCP crystals or other factors. Thefirst convincing series of patients experiencing acute gout in previously

38 WISE
osteoarthritic distal IP joints was reported by Simkin and colleagues in 1983[41]. In this series of five patients (four women and one man, aged 67 to 77),attacks of acute inflammation occurred in previously osteoarthritic joints,with urate crystals demonstrated in four of the involved joints. Most of thesepatients had a history of previous attacks of gout and obvious tophaceous de-posits in the involved joints or elsewhere. Subsequent series have describeda predilection for involvement of the small joints of the hands in elderly pa-tients who had gout, particularly women [17,18,35,38,39]. In one of the largerseries of patients who had elderly onset gout, initial symptoms beginning inthe fingers was noted in 25% of women but none of the men [18]. Anotherseries of women who had gout noted upper extremity involvement, usually inthe finger joints, in about 30% [35]. Two larger series of patients who hadgouty involvement of the proximal and distal IP joints have been published[38,39]. In both studies, most patients were women with a mean age in the70s. Distal IP joint involvement was a little more common than proximalIP involvement. Roentgenographic differentiation from the typical changesof erosive osteoarthritis was sometimes difficult, but the presence of soft tissuedensities, large intra-articular and nonmarginal erosions, and osteolysis weremore characteristic of gouty involvement. In addition, both series noteda high frequency of diuretic use in patients who had IP joint involvementwith gout.
Early atypical tophaceous gout
The early development of tophi, often in atypical locations, has been de-scribed frequently in elderly patients who have gout, again particularly inwomen (Fig. 2). One early series reported that 44% of elderly womenwho had gout had tophi compared with 8% of men, even though the womenhad a shorter duration of illness and fewer previous attacks [17]. In addition,
Fig. 1. Acute gout in the distal interphalangeal joints, mimicking a flare of osteoarthritis.
(Courtesy of the Clinical Slide Collection on the Rheumatic Diseases, American College of
Rheumatology, 1996; with permission.)

39CRYSTAL-ASSOCIATED ARTHRITIS IN THE ELDERLY
at least three patients in this series had developed tophi on the fingers with-out any history of previous gouty attacks. The potential for the developmentof tophi without a prior history of gout was reported in another series offour elderly women who had finger pad tophi seen over a 1-year period oftime [40] and in a subsequent series of larger numbers of patients [42].Another series of mostly postmenopausal women noted the presence of tophiin 27%, with localization to the fingers in 90% and no tophi noted on theelbows [35]. A more recent series of 22 women and 18 men who had elderlyonset gout did not demonstrate a tendency for an atypical distribution oftophi, however [18], and another series did not find any difference in age orsex between patients who had finger pad tophi compared with those whodid not [43]. Observations of frequent atypical tophi in older patients thusmay be the result of some element of observer bias.
Increased association with diuretic use
A high association with diuretic use and renal insufficiency has beennoted in most elderly populations with gout [28]. Diuretic use has been re-ported in more than 75% of patients who have elderly onset gout, with a fre-quency of 95% to 100% in women [17,18,35]. In addition, most small seriesof elderly patients who have atypical finger joint disease or tophaceous de-posits report a consistent majority of patients taking diuretics [38–41]. A re-cent retrospective cohort study documented an almost twofold increase inthe risk for initiating antigout therapy in patients within 2 years of startingthiazide diuretics for hypertension compared with nonthiazide therapy [44].The association of gout with diuretic use may be confounded by the associ-ation of gout with cardiovascular disease in general [45]. The recent increas-ing prevalence of gout in older populations in one recent study did not findthat this increase was associated with diuretic use, however [9]. The
Fig. 2. A tophaceous gouty deposit over the index finger, with early ulceration. (Courtesy of the
Clinical Slide Collection on the Rheumatic Diseases, American College of Rheumatology, 1996;
with permission.)
40 WISE
association of gout and alcohol use seems to be less in elderly patients, par-ticularly among women. Finally, some degree of renal insufficiency seems tobe a regular phenomenon in most series of elderly patients who have gout.Because of a lack of direct comparison to other elderly patients, it is unclearwhether this decrease in renal function is peculiar to patients who have goutor merely reflects the trend seen in elderly populations in general.
Diagnosis and differential diagnosis
In younger patients, gout is often suspected on the basis of a typical at-tack of podagra in a man, or the development of tophi after many years ofrecurring attacks. In elderly patients, many of the presenting elements oftenrelied on as surrogates for diagnosis are not present, and identification ofcrystals in synovial fluid or tissue becomes even more important in confirm-ing a diagnosis.
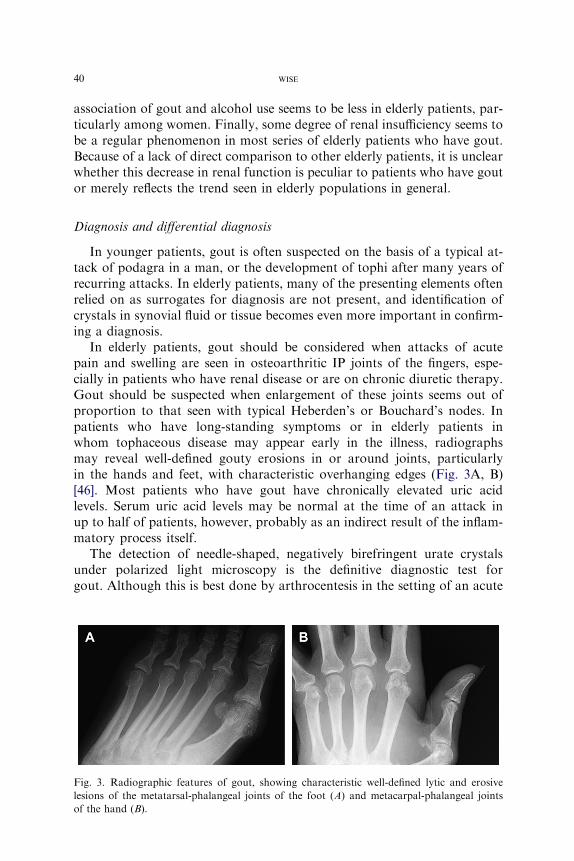
In elderly patients, gout should be considered when attacks of acutepain and swelling are seen in osteoarthritic IP joints of the fingers, espe-cially in patients who have renal disease or are on chronic diuretic therapy.Gout should be suspected when enlargement of these joints seems out ofproportion to that seen with typical Heberden’s or Bouchard’s nodes. Inpatients who have long-standing symptoms or in elderly patients inwhom tophaceous disease may appear early in the illness, radiographsmay reveal well-defined gouty erosions in or around joints, particularlyin the hands and feet, with characteristic overhanging edges (Fig. 3A, B)[46]. Most patients who have gout have chronically elevated uric acidlevels. Serum uric acid levels may be normal at the time of an attack inup to half of patients, however, probably as an indirect result of the inflam-matory process itself.
The detection of needle-shaped, negatively birefringent urate crystalsunder polarized light microscopy is the definitive diagnostic test forgout. Although this is best done by arthrocentesis in the setting of an acute
Fig. 3. Radiographic features of gout, showing characteristic well-defined lytic and erosive
lesions of the metatarsal-phalangeal joints of the foot (A) and metacarpal-phalangeal joints
of the hand (B).
41CRYSTAL-ASSOCIATED ARTHRITIS IN THE ELDERLY
attack, aspiration of synovial fluid from previously affected joints or aspi-ration of a subcutaneous nodule suspected of being a tophus is often help-ful [47,48]. An examiner experienced in crystal identification shouldexamine the synovial fluid, because inexperienced observers may miss theirpresence.
Alternative diagnoses should be considered in all patients suspected ofgout. Acute arthritis can be caused by infection or other crystal-induced ar-thropathies, particularly pseudogout (CPPD deposition disease). Becauseof a tendency for polyarticular attacks, sometimes associated with fever,gout should be considered in patients who have suspected acute bacterialarthritis with negative cultures [30–32]. In addition, gout and infectioncan coexist in the same joints, making therapeutic decisions difficult in in-dividual cases [49]. Synovial fluid cultures are essential in any patient whohas suspected gout having fever, comorbid conditions, or purulent-appear-ing synovial fluid.
Management
The goals of therapy in gout include termination of the acute attack, pre-vention of further attacks in the subsequent several weeks, assessment forassociated and contributing factors, and consideration of long-term hypour-icemic therapy (Table 2) [50–52]. The therapy for gout in older patients isoften influenced by the presence of comorbid conditions, which dictate dif-ferent approaches to the acute and chronic therapy [53].
Management of acute gout
Treatment of acute gout should be initiated as early into the attack aspossible to achieve optimal results. Agents available for terminating acutegout include colchicine, nonsteroidal antiinflammatory drugs (NSAIDs),corticotropin (ACTH), and corticosteroids. Because of the variable toxic-ities of these therapies, the choice among agents should be based on the pa-tient’s age and overall health, with underlying renal and gastrointestinaldisease often limiting factors for NSAID and colchicine use. In recent years,corticosteroids have been used more often in older patients who have mul-tiple comorbid conditions because of their low toxicity profile.
Colchicine has been used for centuries to treat acute attacks of gout. Un-fortunately, most patients experience nausea, vomiting, abdominal cramps,and diarrhea when given doses needed to control severe attacks. Colchicineshould be given more cautiously in elderly patients (at the minimal dose re-quired to control the acute attack) and avoided in those who have renal orhepatic insufficiency or in patients already on chronic maintenance colchi-cine [54]. Intravenous colchicine was used more in the past for acute gout,but increasing recognition of the potential for bone marrow suppressionand other systemic toxicities has resulted in guidelines for restricting dosage
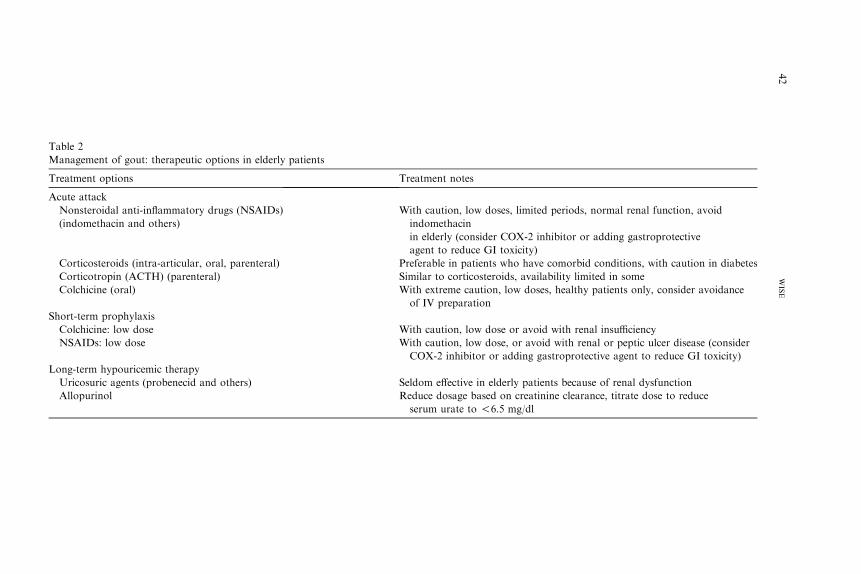
Table 2
Management
Treatment op
Acute attack
Nonsteroida
(indometha
s, limited periods, normal renal function, avoid
OX-2 inhibitor or adding gastroprotective
oxicity)
Corticostero ho have comorbid conditions, with caution in diabetes
Corticotrop ds, availability limited in some
Colchicine ( low doses, healthy patients only, consider avoidance
Short-term pr
Colchicine: or avoid with renal insufficiency
NSAIDs: lo , or avoid with renal or peptic ulcer disease (consider
dding gastroprotective agent to reduce GI toxicity)
Long-term hy
Uricosuric a rly patients because of renal dysfunction
Allopurinol n creatinine clearance, titrate dose to reduce
mg/dl
42
WISE
of gout: therapeutic options in elderly patients
tions Treatment notes
l anti-inflammatory drugs (NSAIDs)
cin and others)
With caution, low dose
indomethacin
in elderly (consider C
agent to reduce GI t
ids (intra-articular, oral, parenteral) Preferable in patients w
in (ACTH) (parenteral) Similar to corticosteroi
oral) With extreme caution,
of IV preparation
ophylaxis
low dose With caution, low dose
w dose With caution, low dose
COX-2 inhibitor or a
pouricemic therapy
gents (probenecid and others) Seldom effective in elde
Reduce dosage based o
serum urate to !6.5

43CRYSTAL-ASSOCIATED ARTHRITIS IN THE ELDERLY
or availability, and this form of colchicine should not be used in elderlypatients or should be used with extreme caution [55,56]. Because of thesemultiple limitations, colchicine has a limited role in the therapy of acutecrystal-induced arthritis in elderly patients.
NSAIDs remain the agents of choice for acute gout in young, healthy pa-tients who do not have comorbid diseases. The use of all NSAIDs is limitedby the risks of NSAID gastropathy (eg, gastric ulceration and gastritis),other GI bleeding, acute renal failure, fluid retention, interference with an-tihypertensive therapy, and, in older patients, problems with mentation. Therisks for toxicity of all types are increased in elderly patients, particularlythose who have renal dysfunction [50,57,58]. Indomethacin, in particular,although notorious for its efficacy, is also notorious for its poor tolerabilityin elderly patients. In most elderly patients who have acute gout, indometh-acin should be avoided and other NSAIDs should be used only in low dosesfor short periods of time. Careful monitoring of renal function is particu-larly important in patients who have decreased renal function or edematousstates before starting therapy. The newly available selective cyclo-oxygen-ase-2 (COX-2) inhibitory NSAID (celecoxib) has potential as safer therapyfor acute gout, as these agents have a decreased risk for serious gastrointes-tinal toxicity and do not inhibit platelet function [59]. Selective COX-2 in-hibitors still have potential to interfere with renal function and causeedema, however, and should be used with caution in patients who have renalinsufficiency, hypertension, or edema.
Corticosteroids have become increasingly popular in acute gout in recentyears in elderly patients [60–66]. Intra-articular steroids after arthrocentesisare extremely useful in providing relief, particularly in large effusions inwhich the aspiration of as much fluid as possible results in rapid improve-ment in pain and tightness of the affected joint. The dose of steroid variesdepending on the size of the joint, ranging from 5 to 10 mg of triamcinolonefor small joints of the hands or feet to 40 to 60 mg for larger joints such asthe knee [67]. Systemic corticosteroids may also be useful in patients forwhom colchicine or NSAIDs are inadvisable, or in patients who have poly-articular attacks. Tapered doses of oral prednisone, starting at 40 to 60 mgdaily, and single intramuscular injections of ACTH (40 units) or triamcino-lone (40 to 60 mg) have all been shown to be as effective as NSAIDs in acutegout. In most studies of systemic steroids for acute gout, only a small pro-portion of patients have required repeat therapy or experienced rebound at-tacks in the first several days after therapy.
Intercritical gout
Patients remain at increased risk for another attack for several weeks af-ter resolution of an acute attack of gout. For this reason, prophylaxis withsmall doses of colchicine or NSAIDs may be considered to prevent furtherattacks in selected patients. Colchicine in a dose of 0.6 mg twice daily

44 WISE
prevents attacks in more than 80% of patients. Prophylaxis should be con-tinued for 1 to 2 months after an acute attack or for several months in pa-tients who have a history of frequent attacks and when urate-lowering drugsare initiated. The dose of colchicine should be reduced to 0.6 mg every dayto every other day, or duration limited in patients who have reduced renalfunction, because bone marrow suppression and myoneuropathy havebeen reported in patients on chronic low-dose colchicine with a creatinineclearance of less than 50 mL/min [68,69].
A 24-hour urine collection or spot urinary urate/creatinine determinationto determine whether a patient is an overproducer or underexcretor of uricacid is seldom useful in elderly patients [70,71]. Because most elderly patientswho have gout have decreased renal function and many have tophaceous dis-ease, uricosuric drugs would not be indicated in management, and informa-tion obtained from this determination is usually of no help in makingdecisions regarding long-term hypouricemic therapy. Dietary factors arenot likely to have a major impact on elderly patients who have gout, andeven a strict purine-free diet has only a small effect on serum urate levels. Re-cent epidemiologic data suggest that it may be useful to reduce meat and sea-food intake and increase dairy product intake to lower risks for gout in thegeneral population [72]. In addition, some patients may have amild reductionin serum urate levels with dietary restrictions designed to improve lipid pro-files [73,74]. Heavy alcohol use seems to be less common in elderly women,but may be a correctable factor in older men. A history of homemade whiskey(moonshine) ingestion and possible chronic lead intoxication should be con-sidered in male gout patients who have renal insufficiency [75]. A review ofconcomitant medications, with special attention to diuretic use, is essentialin all elderly patients who have gout. In patients who have tophaceous diseaseor recurrent attacks, the need for diuretics should be assessed and discontin-uation considered in those patients for whom alternatives are available formanaging comorbid hypertension and cardiac disease. In addition, the effectof low-dose aspirin on urate excretion in this population should be consid-ered when treatment is initiated in elderly patients who have gout [76].
Chronic hypouricemic therapy
Therapy with drugs to lower urate levels should be considered in patientswho have had crystal-proven gout with recurrent attacks and in those whohave tophaceous gout. In addition, patients who have a history of gout andrenal insufficiency may have improvement in renal function with hypourice-mic therapy, possibly because of reduction in renal urate deposition or re-duced use of NSAIDs [77]. Because of the high frequency of comorbidconditions and decreased life expectancy in elderly patients, it may be lessimportant to institute urate-lowering therapy than in younger patientswho have many years of cumulative attacks and joint damage in their future[78].

45CRYSTAL-ASSOCIATED ARTHRITIS IN THE ELDERLY
Most patients who have had more than two to three attacks, those whohave coexistent renal disease, or those who have tophi and evidence ofradiographic joint damage should be treated with hypouricemic therapy.Reduction of serum urate levels well into the normal range (ie, less than6.0 mg/dL) eventually leads to prevention of further attacks and resorptionof tophi [79]. As noted previously, low-dose colchicine or NSAIDs may beused to prevent attacks that can occur for several months after beginningtherapy, but still should be used with caution in older patients who havereduced renal function [80].
Uricosuric drugs are seldom used in elderly patients because of the highfrequency of renal insufficiency in this population, but may be considered inpatients who have a creatinine clearance greater than 50 mL/min, no historyof nephrolithiasis, and a 24-hour excretion of urate less than 700 mg daily.Probenecid in doses of 1 to 2 g daily is the most commonly used agent in thisclass but carries a risk for precipitating renal stones, which may be reducedby high urine volume and alkalinization with bicarbonate intake. Overall,up to 25% of patients are not well controlled on currently available urico-suric drug therapy. Benzbromarone, a uricosuric agent currently availablein Europe, has been shown to be comparable to allopurinol in lowering ur-ate levels in patients who have moderate renal insufficiency, but has alsobeen associated with severe hepatoxicity in some patients [15,81]. In addi-tion, recent studies demonstrating a uricosuric effect with the lipid-loweringagent fenofibrate and the angiotensin receptor blocker losartan suggest thatthese agents could be used in selected patients to lower serum urate levels[82,83].
Allopurinol, the only currently available inhibitor of xanthine oxidase,reduces serum urate levels in almost all compliant patients [51,84]. In prac-tice, the dosage of allopurinol prescribed is often inappropriately high orlow in elderly patients, but compliance among elderly patients tends to bebetter than in younger patients [85,86]. A dosage of 300 mg daily is standardin younger patients who have normal renal function, but this should be re-duced to 200 mg in patients who have glomerular filtration rates (GFR) lessthan 60 mL per minute, and to 100 mg in those who have a GFR less than30 mL per minute. After initiation of allopurinol, dosage should be adjustedto lower serum urate levels well into the normal range, because a fixed dosebased on estimated GFR may lead to underdosing and suboptimal controlof urate levels [87]. Patients who have a GFR less than 10 mL per minutecan be treated with 100 mg every 2 to 3 days. The dose of some other drugs,particularly azathioprine, needs to be reduced in patients on allopurinolbecause of common pathways of metabolism. Approximately 2% of patientstaking allopurinol develop a hypersensitivity rash that can progress to a severeexfoliative dermatitis in a small number of patients [84]. This rash is morelikely to occur in patients taking ampicillin or in those who have renal insuf-ficiency. Severe rashes may be accompanied by a syndrome of vasculitis, hep-atitis, and interstitial renal disease, with a risk for mortality of 20% in some

46 WISE
series. Because of this, allopurinol should be discontinued in any patient de-veloping a rash, and reinstitution considered only in patients who have mildrashes and a clear-cut need for allopurinol therapy. In addition, a regimenof slow oral desensitization, starting with doses of 50 mcg daily and increas-ing to 100 mg daily over a 4-week period, has been shown to be safe andsuccessful in allowing most patients who had prior hypersensitivity reac-tions to restart allopurinol therapy [88]. Other nonpurine agents capableof inhibiting xanthine oxidase and thereby lowering uric acid are in develop-ment (eg, febuxostat) [89].
Calcium pyrophosphate dihydrate deposition disease (pseudogout)
The term pseudogout was first used to describe patients who had goutlikeattacks of arthritis, CPPD crystals found in synovial fluids, and radiographicintra-articular cartilage calcification (chondrocalcinosis) [2]. Since that time,other clinical presentations and patterns of joint disease have been associatedwith CPPD crystals, and the term CPPD deposition disease has been used.
CPPD deposition disease is generally a disease of the elderly with an av-erage age of patients in most series of around 70 years. The metabolic basisfor CPPD formation and deposition is less well understood than that for ur-ate crystals. CPPD crystal formation occurs almost exclusively in the artic-ular and periarticular tissue, usually near the surface of chondrocytes [90].Crystal formation is enhanced by locally elevated levels of either calciumor pyrophosphate (PPi) or factors in the cartilage matrix that promote crys-tal formation. An abnormal substrate of matrix collagen and proteoglycanand variations in mineral content may promote crystal deposition. Localelevations of PPi levels seem to be related to overactivity of a cell surface en-zyme (ectoenzyme) known as nucleoside triphosphate pyrophosphohydrolase(NTPPH), which catalyzes the extracellular hydrolysis of ATP, and the extra-cellular transport of PPi by a transmembrane protein (ANK) [91]. In addition,some of the excess PPi production may take place intracellularly throughNTPPH or as a byproduct of cellular proteoglycan and protein synthesis.Other factors that may contribute to excess PPi and crystal formation includedecreased activity of pyrophosphatase, degenerating cellular debris, abnor-malmatrix collagen, and even the local influence of growth factors (transform-ing growth factor and insulin-like growth factor). The mechanisms by whichCPPD crystals induce inflammation are believed to be similar to those ob-served in gout.
The role of calcium-containing crystals (both CPPD and BCP) in the de-velopment of osteoarthritis has been supported by clinical observations andby experimental evidence of the effects of these crystals on cartilage in vitro[92–94]. Both crystals have been associated with exaggerated forms ofosteoarthritis and are more commonly seen in osteoarthritic joints than innormal joints or those affected by inflammatory forms of arthritis. Inaddition, calcium-containing crystals have been shown to promote synovial

47CRYSTAL-ASSOCIATED ARTHRITIS IN THE ELDERLY
hyperplasia, induce collagenase and metalloproteases, and lead to the gener-ation of proinflammatory prostaglandins and cytokines [95].
The radiographic correlate of CPPD deposition disease (chondrocalcino-sis) is a common finding in older individuals; it may be an incidental findingor associated with arthritis. The prevalence of chondrocalcinosis in the gen-eral population is as high as 10% to 15% in those aged 65 to 75, and in-creases to more than 40% in patients more than 80 years of age[33,96,97]. In most of these older individuals, concomitant osteoarthritis ispresent. Because osteoarthritis is common in the elderly, the role each pro-cess plays in the pathogenesis of the other is not completely understood.Most cases of CPPD are idiopathic. Familial occurrence has been reported,however. Most of the familial forms have shown an autosomal dominanttransmission but have displayed various clinical presentations, and mostseem to involve single gene mutations [98]. An association with various en-docrine and metabolic conditions is well accepted (Box 1). These includehyperparathyroidism in up to 5% of cases, hypophosphatasia, hypomagne-semia, and hemochromatosis. Schumacher [99] first described a distinctform of arthritis in association with hemochromatosis in 1964. This arthrop-athy has some similarities to osteoarthritis and rheumatoid arthritis andmay be the initial presenting feature in some patients [100]. Arthritis isa common clinical feature at the time of diagnosis of hemochromatosis,and patients who have arthropathy tend to be older [101].
Clinical features
CPPD deposition disease may have many clinical presentations mimick-ing gout, rheumatoid arthritis, osteoarthritis, or neuropathic joint disease[102]. In addition, CPPD may coexist in symptomatic or asymptomaticform with any of these conditions. The three most common clinical forms
Box 1. Clinical associations with calcium pyrophosphatedihydrate deposition disease
Aging� Asymptomatic chondrocalcinosis or associated with
osteoarthritis
IdiopathicFamilialEndocrine and metabolic diseases� Hyperparathyroidism� Hemochromatosis� Hypophosphatasia� Hypomagnesemia

48 WISE
of the disease present as acute attacks of mono- or polyarthritis (pseudog-out), a chronic arthropathy associated with osteoarthritis, or an incidentalasymptomatic process. The joints most frequently involved in pseudogoutare the knee, wrist, shoulder, and hip. In fact, knee involvement is so char-acteristic of CPPD deposition that it is often said that the knee joint is topseudogout what the MTP joint is to gout.
Acute pseudogout is similar to acute gout, with acute monoarticularswelling, particularly prominent in the knee, wrist, or over the dorsum ofthe hand and wrist. Attacks may be precipitated by trauma and havebeen noted to occur after acute medical illness or after surgery [103]. Poly-articular attacks have been reported, but are not as well described, and areprobably not as common as in gout. Other systemic features, such as fever,confusion, disorientation, nuchal rigidity, and leucocytosis, have been re-ported in individual cases [104].
Diagnosis and differential diagnosis
Themain differential diagnosis is with other crystal-induced processes, pri-marily gout, and with infection, which should always be included in the differ-ential diagnosis. Synovial fluid aspiration and examination for crystals arethus essential to the diagnosis. The synovial fluid in pseudogout is usually in-flammatory and may occasionally be hemorrhagic. A leucocyte count of10,000 to 20,000/mL cells is the rule, but in the small joints, as in the wrist,high counts may be seen. CPPD crystals are pleomorphic, and may be intra-cellular or extracellular. These crystals can be visualized under regularmicros-copy as square or rectangular intracellular inclusions, and give a weaklypositive birefringence under polarized microscopy. Because of this weak bire-fringence, many laboratories may miss CPPD crystals, emphasizing the im-portance for an observer experienced in crystal identification to examine thefluid.
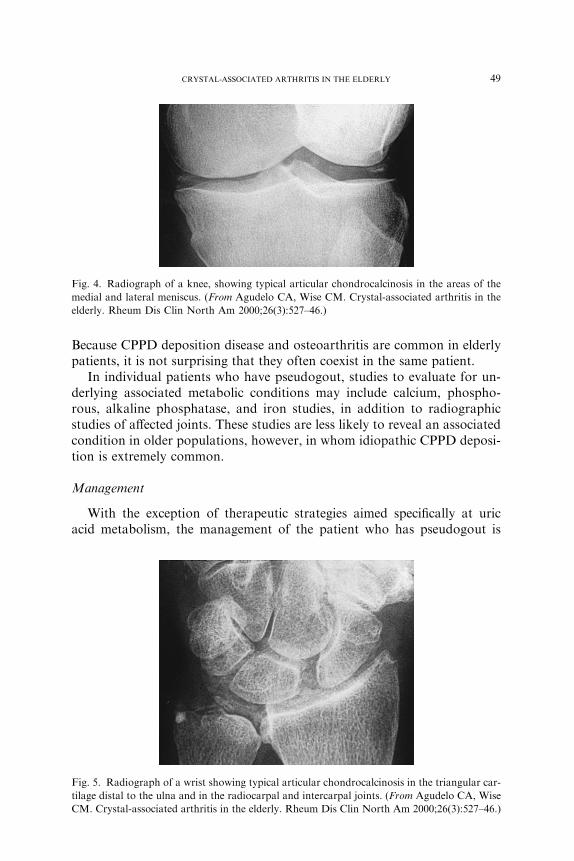
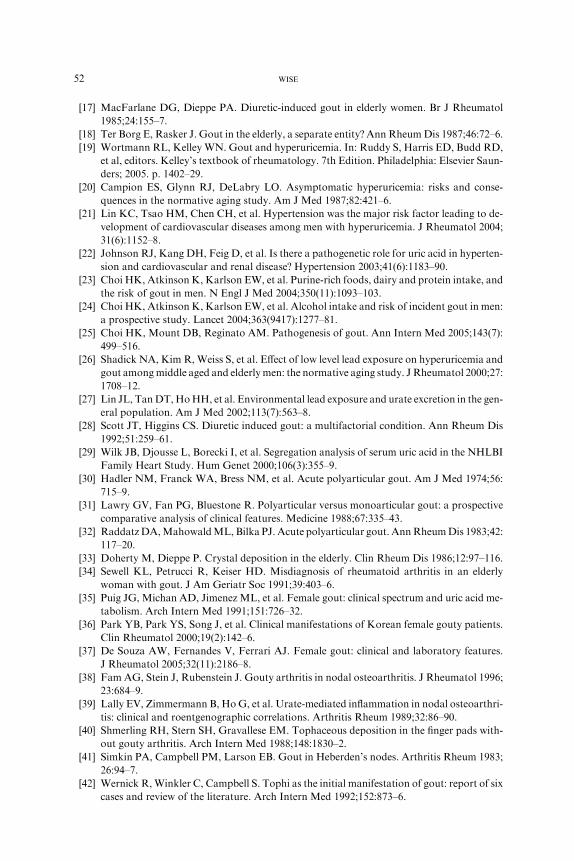
Occasionally, infection or other crystals, such as MSU or BCP, may co-exist with CPPD. Radiographic studies of affected joints often reveal chon-drocalcinosis of the articular cartilage (Figs. 4 and 5). Bilateral calcificationsof the menisci in the knees or of the triangular ligament at the radioulnarjoint at the wrist are characteristic. Other features include narrowing andsclerosis of the radiocarpal and patellofemoral joints. Rarely, extra-articularcalcifications involving tendons or tophaceous deposits occur. Other clinicalpresentations include a pseudorheumatoid type with polyarticular jointswelling, morning stiffness, pain, and high sedimentation rate. Because ofthe high prevalence of wrist involvement in CPPD and the increased preva-lence of positive rheumatoid factor tests in older populations, it may be dif-ficult to distinguish a patient who has CPPD arthropathy from a patient whohas early rheumatoid arthritis. The radiologic findings of chondrocalcinosis,the absence of erosive disease, and the synovial fluid findings of CPPD crys-tals help differentiate CPPD deposition from true rheumatoid arthritis.
49CRYSTAL-ASSOCIATED ARTHRITIS IN THE ELDERLY
Because CPPD deposition disease and osteoarthritis are common in elderlypatients, it is not surprising that they often coexist in the same patient.
In individual patients who have pseudogout, studies to evaluate for un-derlying associated metabolic conditions may include calcium, phospho-rous, alkaline phosphatase, and iron studies, in addition to radiographicstudies of affected joints. These studies are less likely to reveal an associatedcondition in older populations, however, in whom idiopathic CPPD deposi-tion is extremely common.
Management
With the exception of therapeutic strategies aimed specifically at uricacid metabolism, the management of the patient who has pseudogout is
Fig. 5. Radiograph of a wrist showing typical articular chondrocalcinosis in the triangular car-
tilage distal to the ulna and in the radiocarpal and intercarpal joints. (From Agudelo CA, Wise
CM. Crystal-associated arthritis in the elderly. Rheum Dis Clin North Am 2000;26(3):527–46.)
Fig. 4. Radiograph of a knee, showing typical articular chondrocalcinosis in the areas of the
medial and lateral meniscus. (From Agudelo CA, Wise CM. Crystal-associated arthritis in the
elderly. Rheum Dis Clin North Am 2000;26(3):527–46.)

50 WISE
similar to the management of the patient who has acute gout (see discus-sion under gout), with the main goal of therapy being control of the acuteinflammatory reaction [51]. Rest of the inflamed joints, NSAIDs, or intra-articular corticosteroid preparations are the mainstay of therapy. Becausemany attacks are of short duration, complete aspiration of the joint maybe sufficient to significantly relieve pain and discomfort in some patients.Colchicine is effective in acute pseudogout but should be used with cautionbecause of the risk for toxicity in elderly patients at the doses required tocontrol the acute attack (see discussion under gout). At lower doses of0.6 mg once or twice daily, colchicine can be helpful in preventing furtherattacks [105]. In some patients, intramuscular or subcutaneous ACTH (40units) or intramuscular triamcinolone (60 mg) can control the acute inflam-matory reaction [65]. For those who have chronic pain and inflammation,physiotherapy, analgesics, colchicine, and NSAIDs are alternatives formanagement. For patients who have chronic pseudorheumatoid CPPD de-position disease, hydroxychloroquine in dosages of 200 to 400 mg/d hasbeen shown to be superior to placebo in one small controlled study [106].
Basic calcium phosphate hydroxyapatite deposition disease
A group of apatite-like (BCP) crystals has been identified in pathologicsynovial fluids and articular and periarticular tissues in various musculoskel-etal disorders [107]. Because of their smaller size and lack of easily availabledetection methods, the identification of these crystals is much more difficultthan for CPPD crystals. For these reasons, most of the information on therole of BCP crystals in arthritis is based on the use of x-ray diffraction orinfrared spectroscopy. BCP crystals may be found in 30% to 60% of syno-vial fluids from patients who have osteoarthritis and may contribute to thelow-grade inflammatory process and cartilage destruction seen in typical os-teoarthritis; BCPs seem to be associated with more severe osteoarthritis[93,95]. In other patients, periarticular soft tissue calcifications may be asso-ciated with an acute inflammatory reaction, clinically recognized as acutecalcific periarthritis-tendinitis-bursitis. Shoulder involvement is common,and involvement of the first metatarsophalangeal joint (pseudopodagra),primarily affecting young women, has been described. Subcutaneous or peri-articular calcifications have been found also in patients who have chronicrenal failure and secondary to connective tissue disorders, such as in patientswho have inflammatory myopathies.
A severe destructive arthropathy of the shoulder and of the knee associ-ated with BCP crystals has been described primarily in older women [108–111]. This entity, the Milwaukee shoulder–knee syndrome, is often bilateraland in most patients leads to significant functional impairment and pain. Itis associated with rotator cuff degeneration and glenohumeral joint instabil-ity. Radiologic changes include glenohumeral degeneration, periarticular

51CRYSTAL-ASSOCIATED ARTHRITIS IN THE ELDERLY
calcification, rotator cuff degeneration and rupture, and superior displace-ment of the humeral head.
The synovial fluid may be serosanguineous and contains few cells. Underregular light microscopy, hydroxyapatite crystals may appear as clumps oras intracellular ‘‘shiny coins’’ and are not birefringent under polarized mi-croscopy. Radiograph diffraction and biochemical analysis may be neededfor definitive identification of these crystals. The treatment of these patientsis frequently unsatisfactory. Joint aspirations and intra-articular corticoste-roid injections have been helpful in some. For those patients who have acuteperiarthritis, analgesics, NSAIDs, corticosteroid injections, and physiother-apy are the choices in therapy.
References
[1] McCarty DJ, Hollander JL. Identification of urate crystals in gouty synovial fluids. Ann
Intern Med 1961;54:452–60.
[2] McCarty DJ, Kohn NN, Faires JS. The significance of calcium phosphate crystals in the
synovial fluid of arthritis patients: the ‘‘pseudogout syndrome.’’ I. Clinical aspects. Ann
Intern Med 1962;56:711–37.
[3] Schiltz C, Liote F, Prudhommeaux F, et al. Monosodium urate monohydrate crystal-in-
duced inflammation in vivo: quantitative histomorphometric analysis of cellular events.
Arthritis Rheum 2002;46(6):1643–50.
[4] Landis RC, Yagnik DR, Florey O, et al. Safe disposal of inflammatory monosodium urate
monohydrate crystals by differentiated macrophages. Arthritis Rheum 2002;46(11):
3026–33.
[5] Yagnik DR, Hillyer P, Marshall D, et al. Noninflammatory phagocytosis of monosodium
urate monohydrate crystals by mouse macrophages. Implications for the control of joint
inflammation in gout. Arthritis Rheum 2000;43:1779–89.
[6] Roubenoff R. Gout and hyperuricemia. Rheum Dis Clin North Am 1990;16:539–50.
[7] Mikuls TR, Saag KG. New insights into gout epidemiology. Curr Opin Rheumatol 2006;
18(2):199–203.
[8] Abbott RD, Brand FN,KannelWB, et al. Gout and coronary artery disease. The Framing-
ham study. J Clin Epidemiol 1988;41:237–42.
[9] Arromdee E, Michet CJ, Crowson CS, et al. Epidemiology of gout: is the incidence rising?
J Rheumatol 2002;29(11):2403–6.
[10] Wallace KL, Riedel AA, Joseph-Ridge N, et al. Increasing prevalence of gout and hyper-
uricemia over 10 years among older adults in a managed care population. J Rheumatol
2004;31(8):1582–7.
[11] Mikuls TR, Farrar JT, Bilker WB, et al. Gout epidemiology: results from the UK General
Practice Research Database, 1990-1999. Ann Rheum Dis 2005;64(2):267–72.
[12] Yu KH, Luo SF. Younger age of onset of gout in Taiwan. Rheumatology (Oxford) 2003;
42(1):166–70.
[13] Lawrence RC, Hochberg MC, Kelsey JL, et al. Estimates of the prevalence of selected
arthritic and musculoskeletal diseases in the United States. J Rheumatol 1989;16:427–41.
[14] Lawrence RC, Helmick CG, Arnett FC, et al. Estimates of the prevalence of arthritis and
selected musculoskeletal disorders in the United States. Arthritis Rheum 1998;41(5):
778–99.
[15] Bieber JD, Terkeltaub RA. Gout: on the brink of novel therapeutic options for an ancient
disease. Arthritis Rheum 2004;50(8):2400–14.
[16] Hochberg MC, Thomas J, Thomas DJ, et al. Racial differences in the incidence of gout.
Arthritis Rheum 1995;38:628–32.
52 WISE
[17] MacFarlane DG, Dieppe PA. Diuretic-induced gout in elderly women. Br J Rheumatol
1985;24:155–7.
[18] Ter Borg E, Rasker J. Gout in the elderly, a separate entity? Ann RheumDis 1987;46:72–6.
[19] Wortmann RL, Kelley WN. Gout and hyperuricemia. In: Ruddy S, Harris ED, Budd RD,
et al, editors. Kelley’s textbook of rheumatology. 7th Edition. Philadelphia: Elsevier Saun-
ders; 2005. p. 1402–29.
[20] Campion ES, Glynn RJ, DeLabry LO. Asymptomatic hyperuricemia: risks and conse-
quences in the normative aging study. Am J Med 1987;82:421–6.
[21] Lin KC, Tsao HM, Chen CH, et al. Hypertension was the major risk factor leading to de-
velopment of cardiovascular diseases among men with hyperuricemia. J Rheumatol 2004;
31(6):1152–8.
[22] Johnson RJ, Kang DH, Feig D, et al. Is there a pathogenetic role for uric acid in hyperten-
sion and cardiovascular and renal disease? Hypertension 2003;41(6):1183–90.
[23] Choi HK, Atkinson K, Karlson EW, et al. Purine-rich foods, dairy and protein intake, and
the risk of gout in men. N Engl J Med 2004;350(11):1093–103.
[24] Choi HK, Atkinson K, Karlson EW, et al. Alcohol intake and risk of incident gout in men:
a prospective study. Lancet 2004;363(9417):1277–81.
[25] Choi HK, Mount DB, Reginato AM. Pathogenesis of gout. Ann Intern Med 2005;143(7):
499–516.
[26] Shadick NA, Kim R,Weiss S, et al. Effect of low level lead exposure on hyperuricemia and
gout amongmiddle aged and elderlymen: the normative aging study. J Rheumatol 2000;27:
1708–12.
[27] Lin JL, TanDT,HoHH, et al. Environmental lead exposure and urate excretion in the gen-
eral population. Am J Med 2002;113(7):563–8.
[28] Scott JT, Higgins CS. Diuretic induced gout: a multifactorial condition. Ann Rheum Dis
1992;51:259–61.
[29] Wilk JB, Djousse L, Borecki I, et al. Segregation analysis of serum uric acid in the NHLBI
Family Heart Study. Hum Genet 2000;106(3):355–9.
[30] Hadler NM, Franck WA, Bress NM, et al. Acute polyarticular gout. Am J Med 1974;56:
715–9.
[31] Lawry GV, Fan PG, Bluestone R. Polyarticular versus monoarticular gout: a prospective
comparative analysis of clinical features. Medicine 1988;67:335–43.
[32] RaddatzDA,MahowaldML, Bilka PJ. Acute polyarticular gout. AnnRheumDis 1983;42:
117–20.
[33] Doherty M, Dieppe P. Crystal deposition in the elderly. Clin Rheum Dis 1986;12:97–116.
[34] Sewell KL, Petrucci R, Keiser HD. Misdiagnosis of rheumatoid arthritis in an elderly
woman with gout. J Am Geriatr Soc 1991;39:403–6.
[35] Puig JG, Michan AD, Jimenez ML, et al. Female gout: clinical spectrum and uric acid me-
tabolism. Arch Intern Med 1991;151:726–32.
[36] Park YB, Park YS, Song J, et al. Clinical manifestations of Korean female gouty patients.
Clin Rheumatol 2000;19(2):142–6.
[37] De Souza AW, Fernandes V, Ferrari AJ. Female gout: clinical and laboratory features.
J Rheumatol 2005;32(11):2186–8.
[38] Fam AG, Stein J, Rubenstein J. Gouty arthritis in nodal osteoarthritis. J Rheumatol 1996;
23:684–9.
[39] Lally EV, Zimmermann B, HoG, et al. Urate-mediated inflammation in nodal osteoarthri-
tis: clinical and roentgenographic correlations. Arthritis Rheum 1989;32:86–90.
[40] Shmerling RH, Stern SH, Gravallese EM. Tophaceous deposition in the finger pads with-
out gouty arthritis. Arch Intern Med 1988;148:1830–2.
[41] Simkin PA, Campbell PM, Larson EB. Gout in Heberden’s nodes. Arthritis Rheum 1983;
26:94–7.
[42] Wernick R,Winkler C, Campbell S. Tophi as the initial manifestation of gout: report of six
cases and review of the literature. Arch Intern Med 1992;152:873–6.

53CRYSTAL-ASSOCIATED ARTHRITIS IN THE ELDERLY
[43] Holland NW, Jost D, Beutler A, et al. Finger pad tophi in gout. J Rheumatol 1996;23(4):
690–2.
[44] Gurwitz JH, Kalish SC, Bohn RL, et al. Thiazide diuretics and the initiation of anti-gout
therapy. J Clin Epidemiol 1997;50(8):953–9.
[45] Janssens HJ, van de Lisdonk EH, JanssenM, et al. Gout, not induced by diuretics? A case-
control study from primary care. Ann Rheum Dis 2006;65(8):1080–3.
[46] Nakayama DA, Barthelemy C, Carrera G, et al. Tophaceous gout: a clinical and radio-
graphic assessment. Arthritis Rheum 1984;27:468–71.
[47] Agudelo CA, Weinberger A, Schumacher HR, et al. Definitive diagnosis of gout by identi-
fication of urate crystals in asymptomatic metatarsophalangeal joints. Arthritis Rheum
1979;22:559–60.
[48] Pascual E, Batlle-Gualda E,Martinez A, et al. Synovial fluid analysis for diagnosis of inter-
critical gout. Ann Intern Med 1999;131(10):756–9.
[49] Yu KH, Luo SF, Liou LB, et al. Concomitant septic and gouty arthritisdan analysis of 30
cases. Rheumatology (Oxford) 2003;42(9):1062–6.
[50] Emmerson BT. The management of gout. N Engl J Med 1996;334:445–51.
[51] Agudelo CA, Wise CM. Crystal deposition diseases. In: Weisman MH, Weinblatt ME,
Louie J, editors. Treatment of rheumatic disease. Philadelphia: Saunders; 2001. p. 447–60.
[52] Terkeltaub RA. Clinical practice. Gout. N Engl J Med 2003;349(17):1647–55.
[53] FamAG.Gout in the elderly. Clinical presentation and treatment.DrugsAging 1998;13(3):
229–43.
[54] RobertsWN, LiangMH, Stern SH.Colchicine in acute gout: reassessment of risks and ben-
efits. JAMA 1987;257:1920–2.
[55] Wallace SL, Singer JZ. Systemic toxicity associated with the intravenous administration of
colchicinedguidelines for use. J Rheumatol 1988;15:495–9.
[56] Bonnel RA, Villalba ML, Karwoski CB, et al. Deaths associated with inappropriate intra-
venous colchicine administration. J Emerg Med 2002;22(4):385–7.
[57] Griffen MR, Piper JM, Daugherty JR, et al. Nonsteroidal anti-inflammatory drug use and
increased risk for peptic ulcer disease in elderly persons. Ann InternMed 1991;114:257–63.
[58] Gurwitz JH, Avorn J, Ross-Degnan D, et al. Nonsteroidal anti-inflammatory drug-associ-
ated azotemia in the very old. JAMA 1990;264:471–5.
[59] Fam AG. Treating acute gouty arthritis with selective COX 2 inhibitors. BMJ 2002;
325(7371):980–1.
[60] Alloway JA, Moriarty MJ, Hoogland YT, et al. Comparison of triamcinolone acetonide
with indomethacin in the treatment of acute gouty arthritis. J Rheumatol 1993;20:111–3.
[61] Axelrod D, Preston S. Comparison of parenteral adrenocorticotropic hormone with oral
indomethacin in the treatment of acute gout. Arthritis Rheum 1988;31:803–5.
[62] FamAG.Current therapy of acutemicrocrystalline arthritis and the role of corticosteroids.
J Clin Rheumatol 1997;3:35–40.
[63] Groff GD, Franck WA, Raddatz DA. Systemic steroid therapy for acute gout. Semin
Arthritis Rheum 1990;19:329–36.
[64] Ritter J, Kerr JD, Valeriano-Marcet J, et al. ACTH revisited: effective treatment for acute
crystal induced synovitis in patients with multiple medical problems. J Rheumatol 1994;21:
696–9.
[65] Roane DW, Harris MD, Carpenter MT, et al. Prospective use of intramuscular triamcin-
olone acetonide in pseudogout. J Rheumatol 1997;24:1168–70.
[66] Siegel LB, Alloway JA, Nashel DJ. Comparison of adrenocorticotropic hormone and tri-
amcinolone acetonide in the treatment of acute gouty arthritis. J Rheumatol 1994;21:
1325–7.
[67] Fernandez C, Noguera A, Gonzalez JA, et al. Treatment of acute attacks of gout with
a small dose of intraarticular triamcinolone acetonide. J Rheumatol 1999;26(10):2285–6.
[68] Kuncl RW, Duncan G, Watson D, et al. Colchicine myopathy and neuropathy. N Engl J
Med 1987;316:1562–8.

54 WISE
[69] Wallace SL, Singer JZ,DuncanGL, et al. Renal function predicts colchicine toxicity; guide-
lines for the prophylactic use of colchicine in gout. J Rheumatol 1992;18:264–9.
[70] Gonzalez EB, Miller SB, Agudelo CA. Optimal management of gout in older persons.
Drugs Aging 1994;4:128–34.
[71] Simkin PA.When, why, and how should we quantify the excretion rate of urinary uric acid?
J Rheumatol 2001;28(6):1207–10.
[72] Choi HK, Liu S, Curhan G. Intake of purine-rich foods, protein, and dairy products and
relationship to serum levels of uric acid: the Third National Health and Nutrition Exami-
nation Survey. Arthritis Rheum 2005;52(1):283–9.
[73] Fam AG. Gout, diet, and the insulin resistance syndrome. J Rheumatol 2002;29(7):
1350–5.
[74] Snaith ML. Gout: diet and uric acid revisited. Lancet 2001;358(9281):525.
[75] Bautman V,Maesako JK, Haddad B, et al. The role of lead in gout nephropathy. N Engl J
Med 1981;304:520–3.
[76] Caspi D, Lubart E, Graff E, et al. The effect of mini-dose aspirin on renal function and uric
acid handling in elderly patients. Arthritis Rheum 2000;43:103–8.
[77] Perez-Ruiz F, CalabozoM,Herrero-Beites AM, et al. Improvement of renal function in pa-
tients with chronic gout after proper control of hyperuricemia and gouty bouts. Nephron
2000;86(3):287–91.
[78] Michet CJ, Evans JM, Fleming KC, et al. Common rheumatologic diseases in the elderly.
Mayo Clin Proc 1995;70:1205–14.
[79] Shoji A, Yamanaka H, Kamatani N. A retrospective study of the relationship between se-
rum urate level and recurrent attacks of gouty arthritis: evidence for reduction of recurrent
gouty arthritis with antihyperuricemic therapy. Arthritis Rheum 2004;51(3):321–5.
[80] Bull PW, Scott JT. Intermittent control of hyperuricemia in the treatment of gout. J Rheu-
matol 1989;16:1246–8.
[81] Perez-Ruiz F, Calabozo M, Fernandez-Lopez MJ, et al. Treatment of chronic gout in pa-
tients with renal function impairment: an open, randomized, actively controlled study.
J Clin Rheumatol 1999;5:49–55.
[82] FeherMD, Hepburn AL, HogarthMB, et al. Fenofibrate enhances urate reduction in men
treated with allopurinol for hyperuricaemia and gout. Rheumatology (Oxford) 2003;42(2):
321–5.
[83] Takahashi S,Moriwaki Y, Tamamoto T, et al. Effects of combination treatment using anti-
hyperuricaemic agents with fenofibrate and/or losartan on uric acid metabolism. Ann
Rheum Dis 2003;62(6):572–5.
[84] Hande KR, Noone RM, Stone WJ. Severe allopurinol toxicity: description and guidelines
for prevention in patients with renal insufficiency. Am J Med 1984;76:47–56.
[85] Smith P, Karlson N, Nair BR. Quality use of allopurinol in the elderly. J Qual Clin Pract
2000;20(1):42–3.
[86] Riedel AA, NelsonM, Joseph-Ridge N, et al. Compliance with allopurinol therapy among
managed care enrollees with gout: a retrospective analysis of administrative claims. J Rheu-
matol 2004;31(8):1575–81.
[87] Dalbeth N, Kumar C, Stamp L, et al. Dose adjustment of allopurinol according to creati-
nine clearance does not provide adequate control of hyperuricemia in patients with gout.
J Rheumatol 2006;33(8):1646–50.
[88] Fam AG, Dunne SM, Iazzetta J, et al. Efficacy and safety of desensitization to allopurinol
following cutaneous reactions. Arthritis Rheum 2001;44:231–8.
[89] Becker MA, Schumacher HR, Wortmann RL, et al. Febuxostat, a novel nonpurine selec-
tive inhibitor of xanthine oxidase: a twenty-eight-day, multicenter, phase II, randomized,
double-blind, placebo-controlled, dose-response clinical trial examining safety and efficacy
in patients with gout. Arthritis Rheum 2005;52(3):916–23.
[90] Terkeltaub R. Diseases associated with articular deposition of calcium pyrophosphate de-
hydrate and basic calcium phosphate crystals. In: Harris ED, Budd RD, Genovese MC,

55CRYSTAL-ASSOCIATED ARTHRITIS IN THE ELDERLY
et al, editors. Kelley’s textbook of rheumatology. 7th edition. Philadelphia: Elsevier Saun-
ders; 2005. p. 1430–48.
[91] Hirose J, RyanLM,Masuda I.Up-regulated expression of cartilage intermediate-layer pro-
tein and ANK in articular hyaline cartilage from patients with calcium pyrophosphate
dihydrate crystal deposition disease. Arthritis Rheum 2002;46(12):3218–29.
[92] Ryan LM, Cheung HS. The role of crystals in osteoarthritis. Rheum Dis Clin North Am
1999;25:257–67.
[93] Jaovisidha K, Rosenthal AK. Calcium crystals in osteoarthritis. Curr Opin Rheumatol
2002;14(3):298–302.
[94] Nalbant S,Martinez JA,KitumnuaypongT, et al. Synovial fluid features and their relations
to osteoarthritis severity: new findings from sequential studies. Osteoarthritis Cartilage
2003;11(1):50–4.
[95] Morgan MP, McCarthy GM. Signaling mechanisms involved in crystal-induced tissue
damage. Curr Opin Rheumatol 2002;14(3):292–7.
[96] Wilkins E, Dieppe P, Maddison P. Osteoarthritis and articular chondrocalcinosis in the
elderly. Ann Rheum Dis 1983;42:280–4.
[97] Neame RL, Carr AJ, Muir K, et al. UK community prevalence of knee chondrocalcinosis:
evidence that correlation with osteoarthritis is through a shared association with osteo-
phyte. Ann Rheum Dis 2003;62(6):513–8.
[98] Timms AE, Zhang Y, Russell RG, et al. Genetic studies of disorders of calcium crystal
deposition. Rheumatology (Oxford) 2002;41(7):725–9.
[99] Schumacher HRJ. Hemochromatosis and arthritis. Arthritis Rheum 1964;7:41–50.
[100] Tanglao EC, Stern MA, Agudelo CA. Arthropathy as the presenting symptom in heredi-
tary hemochromatosis. Am J Med Sci 1996;312:306–9.
[101] Faraawi R, HarthM,KerteszA, et al. Arthritis in hemochromatosis. J Rheumatol 1993;20:
448–52.
[102] McCarty DJ. Diagnostic mimicry in arthritis: patterns of joint involvement associated with
calcium pyrophosphate dihydrate crystals. Bull Rheum Dis 1975;25:1438–40.
[103] Ho GJ, DeNuccio M. Gout and pseudogout in hospitalized patients. Arch Intern Med
1993;153:2787–90.
[104] Bona D, Bennett R. Pseudogout mimicking systemic disease. JAMA 1981;246:1438–40.
[105] Alvarellos A, Spilberg I. Colchicine prophylaxis in pseudogout. J Rheumatol 1986;13:
804–5.
[106] Rothschild B, Yakaobov LE. Prospective 6 month double blind trial of hydroxychloro-
quine treatment of CPPD. Compr Ther 1997;23:327–30.
[107] Molloy ES, McCarthy GM. Hydroxyapatite deposition disease of the joint. Curr Rheuma-
tol Rep 2003;5(3):215–21.
[108] Halverson PB, CarreraGF,McCartyDJ.Milwaukee shoulder syndrome: fifteen additional
cases and a description of contributing factors. Arch Intern Med 1990;150:677–82.
[109] McCarty DL,Halverson PB, Carrera CF, et al. ‘‘Milwaukee shoulder’’dassociation of mi-
crospheroids containing hydroxyapatite crystals, active collagenase, and neutral protease
with rotator cuff defects. I. Clinical aspects. Arthritis Rheum 1981;24:464–73.
[110] Halverson PB. Crystal deposition disease of the shoulder (including calcific tendonitis and
Milwaukee shoulder syndrome). Curr Rheumatol Rep 2003;5(3):244–7.
[111] Antoniou J, Tsai A, Baker D, et al. Milwaukee shoulder: correlating possible etiologic vari-
ables. Clin Orthop 2003;407:79–85.




















