ELDERLY FIRST AID HANDBOOK
59
Emergency Medicine Interest Group Presents Li Ka Shing Faculty of Medicine The University of Hong Kong Emergency Medicine Unit ELDERLY FIRST AID HANDBOOK A BOOK
-
Upload
khangminh22 -
Category
Documents
-
view
5 -
download
0
Transcript of ELDERLY FIRST AID HANDBOOK

Emergency Medicine Interest Group
Presents
Li Ka Shing Faculty of Medicine
TheUniversityof Hong Kong
Emergency Medicine Unit
ELDERLYFIRST AIDHANDBOOK
AB O O K

Foreword
Process of Aging
Basic Life SupportBasic Life SupportHands-on Bystander CPRConventional Bystander CPRRecovery PositionAutomated External Defibrillator (AED)
Bandaging and Wound DressingHead InjuryArm SlingElevation BandageElbow BandageForearm BandageWrist BandageHand Wound
Pain ManagementCommon Pain Relief Methods Musculoskeletal Pain
Lower back painNeck pain and shoulder painknee pain
Traumatic Spinal Cord InjuryHerps Zoster
Central Nervous SystemDepression and SuicideHead InjuryStrokeSyncopeSeizure
3
4
910131618
21222324252627
29
3234353637
3943464850
CO
NT
EN
T
1
Co
nte
nt

Aging is a term to describe the changes in our body functions when we get older. The changes affect every body system and are affected by environmental and genetic causes. The following are changes that appear in our body during the process of aging. Ur? Etur aut autem quia nessite mollescides est, quibus sumquunt rem repel id que volupta tempos eumquae pedigenim is ut repre volendamus ditat omnimos earum quatest, aut est lamus que pos ma qui nam erumquae nisciet quidel inveleni de dita voluptatiur, conescime odicab in res et dolut eos magnimil eum dolorit es aliti cuptae con nonecab oristius minctum lat lab in enitibus utendel iquunt eos moluptin porem quisqui sincien dandae. Ecto ipide verum id molorum a non non re quosaec aeperunt omnit, susaped maion niet voles entis eriti dolupti unducitios eius veles qui doloreptate officimincta none officiis vendae dic to volore, sequis aciam eosti ra sent que molent.Ratem. Et pel evenducita volupti usapien ditisit volo iuntibus ilitatur, quae la erum re pa doloresequi remporibus eat odigentium accae aut experibus aliquae ptassint, explab ilit, si invenim undaest andit amet eos repedit pliqui beaquatus ea nobis minctatem. Et volorer ionsed est omnime eum est ma am essinum delit quam, explibus coris reped mil et plignit eaquias essequatum alibearum acilis ipsunt voluptis sinctur?Nat velente la quiame nissinvel magnimi nctem. Parum at officit doluptium eos et anis sin cum cusam, erecae adicia nis apis eum nimodi simus.Volorum venihicae none accum quat archicium harum id quame prae moloreictat.
Ear Nose ThroatNose Bleeding
ThoraxAcute Asthmatic AttackChoking and Aspiration
Cardiovascular SystemHypertensive EmergencyAngina
AbdomenAbdominal PainVomitingDehydrationConstipation
Pelvis and PerineumAcute Retention of UrineUrinary Tract Infection
LimbsSoft Tissue InjuriesWoundsFracturesFall and Fall PreventionDislocationAcute Gout
Osteoarthritis
Acknowledgement | Disclaimer
53
5761
6567
71747780
8385
889094
101105106110
111
FO
RE
WO
RD
2 3
Co
nte
nt
Fo
rew
ord

Ph
ysi
olo
gy/A
nato
my o
f A
gin
gA
ging
is a
term
to d
escr
ibe
the
chan
ges
in o
ur b
ody
func
tions
whe
n w
e ge
t old
er. T
he c
hang
es a
ffect
ev
ery
body
sys
tem
and
are
affe
cted
by
envi
ronm
enta
l and
gen
etic
cau
ses.
The
follo
win
g ar
e ch
ange
s th
at a
ppea
r in
our b
ody
durin
g th
e pr
oces
s of
agi
ng.
Skel
eton
- Bot
h m
en a
nd w
omen
lose
bon
e m
ass
dur
ing
ag
ing
- Wom
en h
ave
fast
er lo
ss in
bon
e m
ass,
whi
ch
acce
lera
tes
afte
r men
opau
se- M
en h
ave
slow
er b
one
loss
, as
they
sta
rt lo
sing
oth
er
tissu
es a
s w
ell
- Hig
her p
reva
lenc
e of
ost
eop
oros
is in
bot
h g
end
ers
Ner
vous
sys
tem
- Slo
wer
cen
tral
pro
cess
ing
and
long
er re
actio
n tim
e- R
educ
ed s
ensi
tivity
to v
ibra
tion
esp
ecia
lly in
feet
- Les
s se
nsiti
vity
to te
mp
erat
ure
- Mod
est l
oss
of n
euro
ns- S
light
dec
reas
e in
bra
in m
ass
Eye
s- Y
ello
win
g o
f len
s- H
ighe
r pre
vale
nce
in c
atar
act
- Low
er li
ght
sen
sitiv
ity- P
oore
r dar
k ad
apta
tion
- Red
uced
tear
pro
duc
tion
- Min
imal
dec
reas
e of
vis
ual a
cuity
at r
est b
ut s
igni
fican
t d
ecre
ase
of v
isua
l acu
ity w
ith a
mov
ing
targ
et
PROCESS OF AGING
Ge
ne
ral
- D
ecre
ase
in b
od
y m
ass
- D
ecre
ase
in th
e p
rop
ortio
n of
bod
y fa
t
Skin
- W
rinkl
ing
and
sag
gin
g e
spec
ially
on
face
, nec
k an
d h
and
s-
Get
ting
thi
n an
d p
ale
- W
ound
s he
al m
ore
slow
ly o
r may
not
hea
l at
all
- R
educ
ed s
ensi
tivity
to
co
ld-
Red
uced
sw
eatin
g-
Red
uced
resi
stan
ce to
UV
light
dam
age
Mus
cle
- Red
uced
mus
cle
mas
s (3
0-40
%) a
nd
mus
cle
pow
er- B
ecom
ing
fatig
ue e
arlie
r and
mor
e ea
sily
dur
ing
exe
rtio
n- L
ower
reg
ener
ativ
e ab
ility
- Mor
e fa
t in
mus
cle
tissu
e
4 5

Res
pir
atory
sys
tem
(bre
athi
ng)
- Dec
reas
e in
dia
phr
agm
str
eng
th- D
ecre
ase
in lu
ng v
olum
e an
d a
ir flo
w
rate
- Inc
reas
e in
resi
dua
l air
in lu
ngs
Dig
est
ive
syst
em
- Mor
e st
omac
h ac
id p
rod
uctio
n- M
ore
com
mon
to h
ave
cons
tipat
ion
- Red
uced
ab
sorp
tion
of n
utrie
nts
- Dec
reas
e in
live
r mas
s
He
art
an
d b
loo
d v
ess
els
- No
chan
ge
in h
eart
rate
and
co
ntra
ctio
n fo
rce
at re
st- L
ess
incr
ease
in h
eart
rate
and
co
ntra
ctio
n fo
rce
dur
ing
exe
rcis
e- M
oder
ate
incr
ease
in h
eart
siz
e- S
tiffe
r hea
rt a
nd b
lood
ves
sel t
issu
es- I
ncre
ased
blo
od p
ress
ure
Kid
ne
y, u
rin
ary
an
d g
en
ital
syst
em
s- D
ecre
ase
in k
idne
y fil
trat
ion
func
tion,
con
cent
ratio
n ab
ility
and
dilu
tion
of u
rine
- Dec
reas
e in
kid
ney
mas
s- I
ncom
ple
te b
lad
der
em
pty
ing
lead
ing
to in
crea
se in
re
sid
ual u
rine
- Les
s in
tens
e or
gas
ms
(bot
h m
en a
nd w
omen
)- L
ong
er re
stin
g ti
me
bet
wee
n or
gas
m a
nd n
ext
erec
tion
for m
en
Imm
un
e s
yst
em
- Mor
e p
rone
to in
fect
ion
- Red
uced
resp
onse
to v
acci
natio
n
Oth
er
syst
em
s- I
mp
aire
d s
hive
ring
- Dec
reas
e in
sen
sitiv
ity o
f sm
ell
- Dec
reas
e in
thirs
t driv
e- D
eter
iora
tion
of b
alan
ce- L
oss
of h
earin
g in
hig
h-fre
que
ncy
tone
s
PROCESS OF AGING
6 7

Basic
Life
Su
pp
ort
BASIC LIFE SUPPORT
Basic Life Support (BLS)Basic Life Support is the combination of emergency procedures needed to ensure a person’s survival, including CPR, control of bleeding, treatment of shock and poisoning, stabilization of injuries and/or wounds, and basic first aid. In this chapter, we will cover CPR, recovery position, and AED.
Why Basic Life Support?It is important to learn BLS because emergencies happen! There are a lot of things you can do with little or no equipment to deal with medical emergencies, and you could potentially save a life with these simple skills.
CPRRecovery Pose
AED
Average age
71.5Witnessed
50%CPRed
15%
Why learn Bystander CPR? Because Bystander CPR is a simple and effective way to keep a person with sudden cardiac arrest alive. This is a series of actions to support the breathing and circulation of a person whose heart has stopped beating, and help maintain blood perfusion to the vital organs to a certain extent to buy time for more definitive treatment.
What is sudden cardiac arrest?Sudden cardiac arrest (SCA) is when there is a sudden failure of the heart to contract effectively, so that the delivery of oxygen by blood to the body tissues, including the brain and the heart itself, is disrupted, or even stopped. This situation is very dangerous, and is one of the leading causes of death worldwide, especially in the elderly. The mean age of SCA in Hong Kong is 71.5 years old. Two-thirds of the cases occur at home, and 50% occur witnessed. Yet, only 15% of the elderlys in Hong Kong get immediate CPR from a bystander. This is very low compared to other developed countries, and many more lives could potentially be saved if more people step out to carry out CPR on an elderly with SCA.
9

Basic
Life
Su
pp
ort
Basic
Life
Su
pp
ort
How does Bystander CPR help? Hands-only Bystander CPR
The Chain ofSurvivalThe Chain of Survival is a closely packed series of five steps to keep the chances favorable for a SCA elderly to stay alive. The steps are:1) Early access to care (e.g. calling 999)2) Early CPR3) Early defibrillation (i.e. with an AED)4) Early advanced care (by professionals)5) Good post-care
Each one of these steps must be done well and early, and with the Bystander CPR routine, you will already be covering the first 3 key steps in saving the elderly. Here is how to do it.
CPR is one of the most important first aid techniques, it’s a series of actions to support the circulation of a person whose heart has stopped beating. This helps maintain blood perfusion to the vital organs to a certain extent to buy time for more definitive treatment.
If you have not been trained in CPR, or do not wish to have mouth-to-mouth contact with a stranger, you can do hands-only CPR. It is as effective as the conventional bystander CPR.
The approach can be remembered with a mnemonic of :
Check if the environment is safe for you and the elderly
Check the elderly forResponsiveness: call the elderly; shake the elderly’s shoulders
IF the elderly is not responsive AND not breathing properly, call for help by- Dialing 999- Asking a bystander to take the nearby AED for you
Proceed to CPR (C A B)
Breathing: observe if there are chest movements; listen for any breathing sound
CPR
AED
1
1 Danger
2 Check
3 Call
4 Chest Compression2
3
Danger + Check + Call + ChestCompression
10 11

Basic
Life
Su
pp
ort
Basic
Life
Su
pp
ort
Hands-only Bystander CPR Conventional Bystander CPR
Chest Compression(Optional) If you have been trained and confident in doing pulse check, check if there is a neck (carotid) pulse by placing two fingers on the side of the prominence at the front of the neck.
A. PositionPlace the heel of a hand on the breastbone at the center of the elderly’s chest.
C. DepthUsing your body weight, press the elderly’s chest down hard for 5-6 cm (at least 2 inches).
E. RecoilAfter each press, make sure you allow the chest of the elderly to recoil.
B. PosturePlace the other hand on top of the first hand, and make your fingers interlock. Move your shoulders so that they are directly above your hands, keep your arms vertical and straight throughout. Do not bend them even as you apply pressure.
D. FrequencyPress repeatedly and fast with the same posture at a frequency of 100-120 per minute. As a rule of thumb, run the song “Ha, ha, ha, ha, staying alive, staying alive…” in your head. Each beat roughly corresponds to one press.
2
x 100 - 120/mins
Check if the environment is safe for you and the elderly
Check the elderly forResponsiveness: call the elderly; shake the elderly’s shoulders
IF the elderly is not responsive AND not breathing properly, call for help by- Dialing 999- Asking a bystander to take the nearby AED for you
Proceed to CPR (C A B)
Breathing: observe if there are chest movements; listen for any breathing sound
1 Danger
2 Check
3 Call
4 CAB (CPR)
C - CirculationA - AirwayB - Rescue Breaths
This is a series of actions to support the breathing and circulation of a person whose heart has stopped beating. The approach can be remembered with a mnemonic of :
Danger + Check + Call + C A B
Repeat the procedure until- the elderly regains consciousness with normal breathing and heart rate
- an ambulance has arrived- the AED has arrived- you are exhausted and cannot carry on.
12 13

Basic
Life
Su
pp
ort
Basic
Life
Su
pp
ort
C A
B
Hands-only Bystander CPR
C for Circulation - Chest Compression(Optional) If you have been trained and confident in doing pulse check, check if there is a neck (carotid) pulse by placing two fingers on the side of the prominence at the front of the neck.
B for Rescue BreathsAfter 30 chest compressions, give 2 breaths.
Place your mouth on the elderly’s mouth so that it is airtight, and blow steadily into his/her mouth.
Each breath must last at least 1 second.
Observe to see if his/her chest rises. If so, the rescue breath is effective.
In conventional bystander CPR, the cycle between chest compressions and rescue breaths in a 30:2 ratio, in which 30 chest compressions are followed by 2 rescue breaths.
If neck injury is suspected, jaw thrust can be performed instead.
A for AirwayIf neck injury is not suspected, head-tilt and chin-lift can be performed: Tilt the head back, and lift the chin up.
Repeat the procedure until- the elderly regains consciousness with normal breathing and heart rate
- an ambulance has arrived- the AED has arrived- you are exhausted and cannot carry on.
A. PositionPlace the heel of a hand on the breastbone at the center of the elderly’s chest.
C. DepthUsing your body weight, press the elderly’s chest down hard for 5-6 cm (at least 2 inches).
E. RecoilAfter each press, make sure you allow the chest of the elderly to recoil.
B. PosturePlace the other hand on top of the first hand, and make your fingers interlock. Move your shoulders so that they are directly above your hands, keep your arms vertical and straight throughout. Do not bend them even as you apply pressure.
D. FrequencyPress repeatedly and fast with the same posture at a frequency of 100-120 per minute. As a rule of thumb, run the song “Ha, ha, ha, ha, staying alive, staying alive…” in your head. Each beat roughly corresponds to one press.
2
x 100 - 120/mins
14 15

Basic
Life
Su
pp
ort
Basic
Life
Su
pp
ort
Recovery Position
If the elderly is unconscious without any suspected neck injuries and breathes spontaneously, he/she should be placed in the recovery position. The recovery position keeps the airway patent, and prevents the elderly from choking with any fluid.
Stay with the person and monitor the elderly’s ABC continuously until an ambulance arrives.If the injuries are not too severe, turn the person to the other side after 30 minutes.
1. Kneel by the right side of the elderly. 2. Place the right arm of the elderly at right angle with his/her palm facing up.
3. Hold the left hand of the elderly and place the back of the hand against his/her right cheek.
4. Grasp his/her left leg and bend to a right angle.
5. Keep his/her left hand on the right cheek. Pull the bent leg towards you to make the elderly roll to your side. His/her left arm should prevent the elderly from rolling too far.
6. Gently tilt the head back, and lift the chin (head-tilt and chin-lift), and perform the airway check of ABC again if you have not done so.
90̊
16 17

Basic
Life
Su
pp
ort
Basic
Life
Su
pp
ort
Automated External Defibrillator (AED)
Commonly called AED, the device has a daunting full name. However, its principles and use are actually not difficult to grasp.
Sudden cardiac arrest, in which the heart stops beating suddenly, can cause death within minutes if untreated. The 2 major causes of sudden cardiac arrest, both triggering irregular heartbeats, are ventricular fibrillation and ventricular tachycardia. The commoner cause is ventricular fibrillation, in which the lower chambers (ventricles) of the heart quiver quickly and irregularly. The other cause is ventricular tachycardia, in which the ventricles have regular, fast beats that lasts for a short period of time.
The AED can be used in this condition to assess the heart rhythm and restore it to normal by administering electric shocks to the heart. CPR also helps the chance of survival.
AED sets usually come with spoken or visual instructions for the untrained user and are easy to use, hence they are not detailed here. An important point, though, would be to make sure that no one is touching the elderly when the shock is being administered.
AED
ON-OFF
1
2
3
It’s important for the local EMS system to know where AEDs are located in the community. In the event of a sudden cardiac arrest emergency, you can find AED quickly.
There are many different brands of AEDs, but the same basic steps apply to all of them.
STEPS in using AED 1. Turn on the AED
2. Attach defibrillation pads to the chest (Right side upper chest , Left side lower chest, wipe the chest dry if it’s wet)
3. Push the analyze button and the AED analyze heart rhythm
If AED advises you to shock the person:4. Make sure no one, including you, is
touching the personTell everyone to “STAND CLEAR!”
5. Push the “shock” button
AEDs can be found in many public places, such as shopping malls, airports, hotels and schools. You can find them directly under these signs
ON-OFF
ON-OFF
1
2
3
18 19

BANDAGING AND WOUND DRESSING
Apply a dressing to the wound.
Materials
Steps
front
Fold the base (longest edge) of the bandage inwards, and put it at the centre of the forehead, above the eyebrows.
Cross the ends of the bandage behind the head.
Take the ends over the forehead and tie them.
Triangular Bandage X 1 Dressing X 1
1
3
4
2
Pull and tuck the bandage behind the head.
5
front
front side back
front back
Head Injury
21
Ban
dag
ing
an
d W
ou
nd
Dre
ssing

1 1 2 3
Ask the victim to support his injured arm. Place the triangular bandage. The point of the bandage should be at the elbow of the injured side. Slide the upper end of the bandage under the injured arm, and wrap around the neck to the shoulder of the injured side.
Ask the victim to support his injured arm. The fingers of the injured side should be on the opposite shoulder.
Place the triangular bandage. The point of the bandage should be at the elbow of the injured side, and the edge along the injured arm.
Ask the victim to stop supporting the arm. Tuck the base of the bandage under the injured arm.
Point
2
3 4
Bring the lower end of the bandage over the forearm to the shoulder of the injured side.
Tie the ends with a knot at the collar bone of the injured side, and tuck the ends under the knot.
Twist the point and tuck it above his elbow.
Arm Sling
Triangular Bandage X 1 Triangular Bandage X 1
5
Final position
Elevation Bandage
4 5 6
Bring the lower end of the bandage up across his back, meeting the other end at his shoulder.
Tie the ends with a knot at the collar bone of the opposite side, and tuck the ends under the knot.
Twist the point and tuck it above his elbow.
back back
MaterialsMaterials
StepsSteps
22 23
Ban
dag
ing
an
d W
ou
nd
Dre
ssing
Ban
dag
ing
an
d W
ou
nd
Dre
ssing
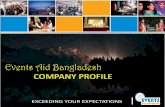
Elbow Bandage
2-inch gauze roll bandage X 1Dressing x 1
2-inch gauze roll bandage X 1Dressing x 1
Forearm Bandage
1 1
3
2 2
4
Elevate the wound above heart level. Cover it with a dressing.
Elevate the wound above heart level. Cover it with a dressing.
Wrap around the elbow at level slightly below and above the wound alternately
Using a 2-inch gauze roll bandage, wrap it around the elbow from the level of dressing, from inside to outside of the limb
Wrap with a 2-inch gauze roll bandage. Wrap twice at the bottom end of the wound from inside to outside of the limb.
x 2
Fasten the end of the bandage with pins or tape
3 4
Wrap continuously in spiral turns up towards the elbow covering the dressing, rolling over 2/3 of previous turn each time.
Wrap until the entire dressing is covered. Fasten the bandage with pins or tape.
MaterialsMaterials
StepsSteps
24 25
Ban
dag
ing
an
d W
ou
nd
Dre
ssing
Ban
dag
ing
an
d W
ou
nd
Dre
ssing

Wrist Bandage Hand Wound
2-inch gauze roll bandage X 1Dressing x 1
1 1 2a
b
c
2 3
4 5 6
Elevate the wound above heart level. Cover it with a dressing.
For severe bleeding of the palm, elevate the wound above heart level and ask the elderly to hold the dressing in a fist to cover the wound. Using a partially unfolded triangular bandage, place the center of bandage against the top of the fist.
Cross the two ends of bandage at the wrist.
Using a 2-inch gauze roll bandage, wrap it around the wrist twice from inside to outside of the limb.
Wrap the bandage from the inside of the wrist, diagonally across the back of hand up to the nail of little finger
Straight across underneath the fingers, and diagonally back across the back of the hand to the outside of the wrist.
Pass the bandage under their wrist and repeat the diagonal over the back of the hand like a figure-of-eight, each time covering 2/3 of previous layer.
Once the entire hand is covered, wrap straight around the wrist twice.
Triangular Bandage X 1 Dressing X 1
3 4 5
Wrap each end of bandage around the wrist to the back of hand and cover 3 fingers for each end before reaching back to the wrist.
After crossing the two ends over the wrist again.
Wrap around the wrist and tie on the back of hand.
back
MaterialsMaterials
StepsSteps
26 27
Ban
dag
ing
an
d W
ou
nd
Dre
ssing
Ban
dag
ing
an
d W
ou
nd
Dre
ssing

PAINMANAGEMENT
Common Pain Relief Methods
Medication
Cold pad
Heat pad
40̊C
Simple analgesics can be used to relieve pain.
a / Paracetamol should be started with dose of 500-1000mg (1-2 tablets). If instructed by doctor, higher dose can be taken.
b / Alternatively, NSAIDs such as ibuprofen can be
used. However, some NSAIDs may cause stomach bleeding and should be avoided for people who have bleeding disorders or gastrointestinal symptoms.
Cold pad is used to decrease inflammation. Used first during injury. Avoid direct contact with ice to prevent frostbite.
To increase circulation in the area, so that tissue repair and heal can take place more efficiently. Hot towel (40 degrees) can be applied on the affected surface. For trauma, it is best used after inflammation has subsided (use when the affected area is no longer hot).
29
Pain
Man
ag
em
en
t

Stretching With the help of an elastic band anchoring the knee of one leg and mid shin, separate the two legs against resistance to train the muscle of the leg.
Lying down with your face down, slowly raise your leg up as shown in the picture above slowly. After 5-10 cycles, switch side and raise the leg of the opposite leg.
Sitting with your face facing upward, slowly flex your thigh up to your chest as shown above. Then slowly return to the original position. Repeat for 5-10 times according to your physique.
Aerobic exercises
Resistanceexercises
Transcutaneous electrical nerve stimulation (TENS)
Examples include swimming and fast walking. Aerobic exercise is the best for relieving chronic pain.
Resistance exercises increase muscle strength, which can help stabilise joints. This can be good for joint pain (consult phyiotherapist for exercises that can prevent further damage of joint).
By stimulating the nerve using electric current, pain signals in your brain can be modulated or suppressed to relieve pain.
1
1
1
2
2
2
x 5-10
x 5-10
x 5-10
99 99
150
CH1 CH2
bps
30 31
Pain
Man
ag
em
en
t
Pain
Man
ag
em
en
t

Musculoskeletal Pain
Symptoms and signs
See further medical attention immediately if there is any of the following warning signs.
Serious cause of lower back pain
Cancer
Pott’s disease (tuberculosis of spine)
Compressed nerve
Fracture
Infection
Cauda equina syndrome (compression of the nerve in spinal cord)
Warning sign
- Previous history of cancer- Unintentional weight loss
- Low grade fever- Chronic cough with red sputum- Night sweat
- Muscle weakness / wasting- Lost of tendon reflex- Positive Babinski reflex
- Severe trauma: fall from height- Corticosteroid use- Osteoporosis (woman in
menopause)- Pain in spine relieved by lying
down
- Severe pain after surgery in nearby site
- Fever- Urinary tract infection- Immunosuppression- Intravenous drug user- Previous cancer
- Urinary and faecal incontinence- Weakness in muscle and
or sensory abnormalities- Loss of sensation in the
inner thigh buttocks
Lower back painAs a first aider
Paracetamol and NSAIDs may be beneficial. Use cautiously as instructed by the doctor.
There is a common misconception that lower back pain requires bed rest. However, if the pain is not due to trauma, active lifestyle is actually what the patient needs. Yoga, stretching and core strength building exercises may also be useful.
Do’s
Don’ts
32 33
Pain
Man
ag
em
en
t
Pain
Man
ag
em
en
t

Muscle strains, degeneration, incorrect postures or even cancer can lead to neck and shoulder pain. In severe cases, the neck and shoulder pain may radiate to the head, causing headache.
Knee pain is extremely common in the elderly population. However the causes of knee pain may vary.
Causes- Bursitis- Torn ligaments or tendons- Bleeding into the joint- Gout- Septic arthritis (infected knee joint)- Soft tissue damage/ inflammation
Neck pain and shoulder pain Knee pain
Background Background
! Numbness and tingling sensation
! Traumatic injury! Weakness in the limbs! Unexplained weight loss! Previous cancer! Dysphagia
! An extremely painful red hot knee may indicate septic arthritis, which is a medical emergency. Medical advice must be sought immediately or the knee joint may risk being damaged by the bacteria.
! Inability to walk may also indicate serious problems and urgent medical advice should also be sought.
!
! ! ! ! !
!
As a first aider
- Apply heat pads and cold pads to relieve pain- Exercise and correction of positioning may treat the neck and
shoulder pain- Consult doctor or physiotherapist for further radiography check-up
- Avoid over-twisting the neck to prevent further injury- Avoid further over-straining the neck and the shoulder
Do’s
Don’ts
!
Remarks
TreatmentsSimple analgesics may be helpful.
34 35
Pain
Man
ag
em
en
t
Pain
Man
ag
em
en
t

TraumaticSpinal Cord Injury
Symptoms and signs
- Numbness (loss of sensation) in any part of the body- Weakness of muscle after trauma- Urinary or faecal incontinence with loss of feeling around the anus.- Neck pain elicited by touching
! Be extremely gentle when touching the spinal cord of the patient with suspected spinal cord injury
!
As a first aider
Call for help to fix the patient’s spinal cord.
Do’s
Unless the patient is in a dangerous place, do not move the patient.
Don’ts
Symptoms and signs
- Reddening of skin with vesicles along one dermatome - Common in weak elders with poor immunity.
As a first aider
- Seek medical help for anti-viral medication as soon as possible- Over the counter medication like paracetamol may be able to
relieve mild pain- Vaccination- After the acute episode has resolved, the affected area may be
painful. Seek medical advice from pain specialist to relieve the neuropathic pain caused by the virus
- Avoid contact with the vesicles to prevent infection- Advise the patient not to rub the affected area and contact
pregnant woman and young children
Do’s
Don’ts
Herpes Zoster
This condition is caused by a virus called herpes zoster virus. After an episode of chickenpox, the virus will remain inactive in the nerve cells. When the immune system becomes weak, the virus reactivates and causes the red rash in the same dermatome.Background
vesicles
36 37
Pain
Man
ag
em
en
t
Pain
Man
ag
em
en
t

CENTRAL NERVOUS SYSTEM
Depression and SuicideDepression is one of the commonest psychiatric disorders in old age. Yet, it is frequently unrecognized. In Hong Kong, the prevalence of depressive disorders in elderly is 9.7%, compared to 8.4% in adults aged 18-65 years old.
Depression is a known risk factor of suicide, and suicide risk increases with age. The suicide rate in the general population of Hong Kong is around 10 to 13 per 100 000, whereas the rate in the age group of 65 and above is around 30 per 100 000, and in the age group of 75 or above is 50 per 100 000. The ratio of the male to the female suicide rate in the elderly is 1.3 to 1. Compared to other countries, the elderly suicide rate in Hong Kong is relatively high.
Background
39
Ce
ntra
l Ne
rvo
us S
yste
m

The most important red flag in a depressed elderly is suicidal tendency. It is commonly found in those institutionalized, or those with chronic illness or disability. The elderly suffering from depression may think that the future is so hopeless that suicide is the only way out. Following an attempted suicide, further attempts — and successful suicide — are common.
Suicidal tendency may be overt or covert.Overt manifestations include: ! Intentional drug overdoses (opiates, antidepressants,
paracetamol, benzodiazepines; more common in women)
! Self-injury (hanging, shooting, jumping, drowning; more common in men)
Covert features are especially common in older people, and include:! Social withdrawal! Severe self-neglect! Refusal of food, fluid,
or medication
! !!
!
!
Symptoms and signs
According to the Diagnostic and Statistical Manual of Mental Disorders (DSM-V) of the American Psychiatric Association, the definition of depression is:
Anyone who has 5 or more of the following symptoms, including at least one of the first two symptoms, nearly every day for at least 2 weeks- An usually sad mood- Loss of enjoyment and interest in activities that used to be enjoyable- Lack of energy and tiredness- Feeling worthless or feeling guilty when they are not really at fault- Thinking about death a lot or wishing to be dead- Difficulty concentrating or making decisions- Moving more slowly or sometimes becoming agitated and unable
to settle- Having sleeping difficulties or sometimes sleeping too much- Loss of interest in food or sometimes eating too much
Risk factors- Family history- Being female- Disability and illness (especially if serious) - Old age home residents- Bereavement- Social isolation- Chronic pain - Sensory impairment (e.g. hearing or sight)
40 41
Ce
ntra
l Ne
rvo
us S
yste
m
Ce
ntra
l Ne
rvo
us S
yste
m

Head Injury
Falls account for the majority of head injury cases in elderly. Serious head injuries are often a result of traffic accidents. In the elderly, an apparently trivial head trauma may lead to complications not commonly seen in the young. Intracranial bleeding is the most worrisome complication. What’s more important to note is the onset of the intracranial bleeding may be delayed and may go unrecognized for months until the elderly suddenly deteriorates or becomes symptomatic.
Background
As a first aider
1. Listen non-judgmentally.2. Express empathy to the elderly.3. Take every suicidal idea or expression seriously4. Seek professional help whenever possible
1. Leave the elderly with suicidal risk alone. If you cannot stay with them, you must arrange someone else to do so, for example, a family member or friend who has agreed to help.
2. Ignore any idea of suicide, no matter how casual the elderly expresses it.
- Approach the depressed elderly and assess whether there is any immediate suicidal risk. Immediate suicidal risk is suggested by strong and frequent suicidal ideation or presence of a suicide plan. However, the absence of which is not equivalent to a lower risk. If the person has an immediate risk of committing suicide or the situation is beyond control, seek medical help immediately, or simply call 999.
- Provide emotional support to the person and encourage him or her to get appropriate professional help if there is no immediate risk.
- Whatever the situation is, always ensure that support and attention is readily available to the elderly.
Do’s
Don’ts
Symptoms and signs
It is usually not difficult to recognize the symptoms and signs of an acute head injury. There may be a wound or swelling on the scalp and the elderly may complain of pain. For those elderly who cannot express themselves properly, very often the injury is only incidentally noted.
The elderly with acute complication as a result of the head injury almost always appear unwell and may appear different from their usual status. On the other hand, those with delayed complication are difficult to recognize. Sometimes, they may be able to recall that there was a head injury or the injury was so trivial that they forget it. One of the most well-known delayed complication in the elderly is called ‘subdural hematoma’. It means there is blood collection beneath the dura covering the brain surface. The symptoms and signs are often subtle. For example, the elderly may appear more and more forgetful, with unexplained personality change or non-specific dizziness and headache. A high index of suspicion is needed.
42 43
Ce
ntra
l Ne
rvo
us S
yste
m
Ce
ntra
l Ne
rvo
us S
yste
m

As a first aider
For those with red flags or you are not sure about the clinical status of the injured elderly:1. Seek emergency medical help immediately 2. Provide BLS if needed3. Provide basic wound care if there is a wound 4. Regularly monitor the vital signs including responsiveness,
breathing and pulse until medical help is available
For those without red flags and you are confident that the injured elderly is stable and well:1. Observe for at least 24 hours from time of injury for any
abnormal symptoms (refer to the A&E head injury card)
Common Head Injury Symptoms / Post-Concussion Syndrome (PCS)
2. Ensure there is a responsible adult who can observe the elderly Whenever there is doubt, seek medical consultation as soon as possible.
Give food and drink to the injured elderly with red flags.
- Look for the red flag signs - Protect the elderly from further injury
Do’s
Don’ts
One of the objectives of first aid for an elderly with acute head injury is to look for clues suggestive of post-injury complication, in particular, intracranial bleeding.
! Clear fluid or watery blood from nose or ear! Bruise around eyes ! Increasing drowsiness! Confusion! Impaired consciousness! Memory impairment! Weakness ! Numbness! Worsening headache! Repeated vomiting ! Convulsion! Irregular breathing
!
!! !!!!!! !! !
Physical Symptoms:- Headache,
Dizziness- Sensitive to noise &
visual disturbance- Fatigue
Cognitive Symptoms:- Memory problems- Poor concentration- Judgement problems
Behavioural Symptoms:- Depression- Anxiety & Stress- Irritability
44 45
Ce
ntra
l Ne
rvo
us S
yste
m
Ce
ntra
l Ne
rvo
us S
yste
m

As a first aider
The FAST test could be used to recognize stroke.1. A Chinese mnemonic to remember the test is “微笑殭屍會說話“
a / Face (Facial weakness)- Ask the casualty to smile- If he has a stroke, he may only be able to smile on one
side and his face may look unevenb / Arm (Arm weakness)
- Ask the casualty to close his eyes and raise both arms- If he has a stroke, he may only be able to move one arm or
has weakness on one armc / Speech (Speech problems)
- Find out if the casualty can speak clearly and understand your words
- If he has a stroke, he may not be able to speak clearly or respond appropriately
d / Time- If any of the signs are present, call 999 for emergency help- If possible, record the time the symptoms first appear
2. Reassure the elderly and keep him or her comfortable3. Monitor the level of responsiveness, breathing and pulse
until help arrives4. If the patient becomes unconscious, check for pulse and
breathing and start CPR if necessary
Give the elderly anything to eat or drink
- Recognize the symptoms and signs of stroke and arrange emergency help
- Reassure and comfort the elderly to keep him or her calm
Do’s
Don’ts
Remarks
Transient Ischemic Attack (TIA) is commonly known as a mini stroke by the lay public. The symptoms and signs are similar to those of stroke. However, the symptom and signs are often transient and the elderly may recover within 24 hours. TIA is associated with a high risk of stroke in the subsequent days and weeks. Those elderly with features suggestive of TIA should obtain immediate medical consultation despite the recovery from the symptoms and signs.
Stroke
Stroke is a medical emergency. It occurs when the blood supply to the brain is disrupted, causing oxygen starvation and loss of function of the affected area. Strokes could be caused by either a clot in a blood vessel stopping blood passing to the brain or a burst blood vessel bleeds into the brain.
Stroke is more common in old age. It is associated with circulatory system disorders, such as high blood pressure.
Early recognition and hospital care (within 3 hours) may improve the chance of recovery.
In Hong Kong, nearly 3,000 people die of stroke each year. At present, it is the 4th fatal disease in Hong Kong. In general, people who suffer a stroke are at the age over 50.
Background
Symptoms and signs
A characteristic of acute stroke is that the symptoms and signs often come suddenly.- Facial weakness- Limb weakness- Speech problems like slurring or inability to comprehend or express- Difficulty to swallow, maybe associated with drooling and easy choking- Headache, especially new or sudden- Nausea not accountable by other apparent causes- Reduced level of responsiveness- Numbness and tingling in face, arms or legs- Dizziness especially persistent, severe or unrelated to posture change- Loss of balance or inability to walk steadily- Blurred vision especially only one eye is affected- Loss of bladder or bowel control
46 47
Ce
ntra
l Ne
rvo
us S
yste
m
Ce
ntra
l Ne
rvo
us S
yste
m

! Prolonged loss of consciousness! Irregular pulse! Chest pain or palpitation
before or after the syncope! Prolonged seizure or confusion! Incomplete recovery of
consciousness! Recurrent syncope within
a short period of time
!!!
!!
!
As a first aider
1. Allow the syncopal elderly to lie supine until he or she is fully conscious
2. Consider raising the elderly’s legs above heart level if postural hypotension is suspected
3. Maintain airway patency and smooth breathing when the elderly is unconscious
4. Loosen belts, collars or other constrictive clothing5. Check for any injuries 6. For almost all elderly with syncope, medical consultation
should be obtained as soon as possible
1. Sit the syncopal elderly up2. Give the elderly food and drinks unless fully conscious
- Look for red flags and manage as medical emergency- Stay with the elderly and prevent further injury until the elderly
has regained full consciousness
Do’s
Don’ts
Syncope
Syncope is a sudden, transient loss of consciousness due to reduced and inadequate cerebral perfusion. The incidence of syncope increases with age. Some studies showed that as many as a quarter of institutionalized elderly had this problem and the recurrence rate could be as high as 30%. The elderly is unresponsive with a loss of postural tone (ie slumps or falls). In the majority of cases, they would regain consciousness spontaneously. Secondary injury like hip fracture may occur as the elderly loses consciousness and fall. Syncope is not a disease by itself. It is a manifestation of an underlying disorder that causes reduced cerebral perfusion. Some of the important causes are:
1.Transient hypotension caused by the upright posture, straining, or coughing which is exacerbated by low circulating volume (dehydration or bleeding somewhere), hypotensive drugs or concurrent illnesses. Orthostatic hypotension (lower blood pressure on standing than lying down) is the most common cause of syncope.
2. Vasovagal response to pain, fright, emotion leading to slowing of heart beat and then hypotension.
3. Heart diseases such as myocardial infarction, arrhythmia, and aortic stenosis (narrow aortic valve opening)
Background
Symptoms and signs
- Loss of consciousness - Pale, sweaty, absent or very weak carotid pulse- Reduced muscle tone- Possible tongue biting- Possible incontinence - Brief (few seconds) seizure activity - Brief (minutes) period of confusion may occur- Recovery is usually brisk and spontaneous
48 49
Ce
ntra
l Ne
rvo
us S
yste
m
Ce
ntra
l Ne
rvo
us S
yste
m

! Repeated seizures within a short time
! Having the first seizure! Seizure lasts for > 5mins! Loss of consciousness for
>10mins! Limb weakness or paralysis
after the seizure has stopped
!
!!!
!
As a first aider
1. Seek emergency medical help as soon as possible2. Protect the elderly - clear away any potentially dangerous
objects to prevent injury of the elderly, pad the area with clothing or pillows if the elderly is close to wall or hard objects, ask bystanders to keep clear
3. Protect the head and loosen tight clothing around neck4. Lie the elderly down in recovery position (if not suspecting a
spinal injury)5. Monitor closely the responsiveness level and breathing; open
airway6. Note the time of onset and duration of seizure 7. Check for any injuries and apply necessary first aid
1. Move the elderly unnecessarily 2. Put anything in his mouth or attempt to restrain him or her
during a seizure so as to prevent from inducing injuries3. Give food and drinks unless the elderly is fully conscious
- Look for red flags and manage as medical emergency - Protect the seizing elderly from injury- Maintain a patent airway and smooth breathing during and after
the seizure when the elderly is not fully conscious
Do’s
Don’ts
Seizure
Seizure consists of involuntary muscle contractions due to disturbance in electrical activity of the brain. It presents with sudden loss of consciousness and jerking of the extremities in most cases. In rare cases, consciousness is preserved.
In elderly, the most common causes of seizure include epilepsy, Alzheimer’s disease, stroke and medication. Seizure can also be caused by head injury, brain-damaging disease (neurodegenerative diseases, tumor, and infection), and lack of nutrients in brain (hypoglycemia, acute alcohol intoxication or drug withdrawal)
Background
Symptoms and signs
- Sudden unconsciousness - Rigid and aching back- Breathing difficulty (grey-bluish lips, red and puffy face/neck)- Convulsive movements (clenched jaw with noisy breathing, facial
twitching, tongue-biting, drooling/foaming saliva) - Possible loss of bladder or bowel control- Tiredness and sleepy after seizure
The elderly may have brief warning period (aura) just before seizure, for example, strange feeling, and special smell/taste. He/she may regain consciousness in a few minutes, and may be unaware of the actions.
50 51
Ce
ntra
l Ne
rvo
us S
yste
m
Ce
ntra
l Ne
rvo
us S
yste
m

EAR NOSE THROAT
Nose BleedingBleeding can arise from any part of the nasal cavity. The most common site of bleeding is from the anterior part of the nasal septum. The so-called Little’s area.
It bleeds when tiny blood vessels on the mucosal surface of the nostrils rupture. Very often, it is a result of trauma like nose pricking or forceful sneezing. Sometimes it is a symptom of another disorder. For instance, nose bleeding may be a manifestation of high blood pressure. Of course, the most worrisome cause is malignancy. Among southern Chinese, nasopharyngeal cancer is a
Background
diagnosis every doctor would consider.
Elderly commonly experience nasal bleeding. Some statistics showed that they accounted for 29-50% of cases of nasal bleeding. In the elderly with nasal bleeding, a secondary cause must be sought especially if the bleeding is unprovoked.
Nose bleeding becomes an emergency when it is not controlled by simple pressure or it is prolonged and massive. An elderly may become very ill if a lot of blood is lost from nasal bleeding. Massive blood loss from the nose can lead to death.
Anterior ethmoid artery
Posteriorethmoid artery
Little area(Kiesselbach plexus)
Greaterpalatine artery
Superior labial artery
Sphenopalatine artery
53
Ear, N
ose
, Th
roat

Local causes- A blow to the nose- Sneezing, picking or blowing the nose - Rhinitis - Rarely tumor
Systemic causes- Bleeding disorder, use of anti-clotting drugs (eg: aspirin, NSAIDs,
warfarin, Plavix)
It is associated with older age, hypertension and dry weather.
Below are some of the causes of nose bleeding:
Symptoms and signs
- Bleeding from nostril, on one side or both- Blood stained sputum and saliva when blood from the nose drips
down to the pharynx posteriorly- Nausea and vomiting if a lot blood is swallowed- Bloody tear because of the communication between the nose and
eyes via the nasolacrimal duct- Dizziness and other signs of blood loss, especially the amount of
blood loss is great
! Nasal bleeding that is unprovoked, prolonged, recurrent, or massive
! Associated symptoms of abnormal nasal discharge, hearing impairment, headache and neck swelling
!
!
As a first aider
1. Reassure and keep the elderly calm2. Sit the elderly up and tilt the head forward to allow the blood
to drain from nostrils3. Ask the elderly to breathe through mouth and pinch the soft
parts ( just below the nasal bridge) of nose for up to 10mins. Do it by the first aider if the elderly is unable to pinch his or her nose
Let the elderly tip the head back since blood may then run down the throat and induce vomiting or choking
- Stop or reduce blood loss- Maintain a patent airway and avoid aspiration of blood
Do’s
Don’ts
4. Use a clean cloth or tissue to mop up any dribbling5. If bleeding continues, re-apply pressure for another 10 minutes6. Once bleeding stops, patient remains leaning forward and
cleans around the nose with lukewarm water7. Seek medical help if bleeding cannot be stopped by local
pressure for around 20 minutes 8. Arrange medical consultation if there are associated symptoms
mentioned above
2 3
54 55
Ear, N
ose
, Th
roat
Ear, N
ose
, Th
roat

THORAX Acute Asthmatic AttackAsthma is a small airway disease that causes airway obstruction due to bronchoconstriction (constriction of the airway) and increased sputum production. It is most commonly triggered by allergens exposure.
Asthma among older adults are common and can be serious. Although many people have their first episode of asthma at young age, asthma can happen in any ages including elderly. Unlike their younger counterparts, the elderly are more likely to develop severe health problems
(for example, respiratory failure) even during mild asthma attack. The condition rarely resolves itself and remains as a disabling disorder to the advanced age.
Diagnosis of asthma in elderly may be missed due to the masking effect from other illnesses, such as heart disease and emphysema. The less active lifestyle of elderly compared to a young person also lowers the chance of provoking acute asthmatic symptoms (e.g. wheezing and breathing problems).
Mild AsthmaMinimal fibrosis
Minimal muscle thickness
Minimal mucus
Chronic Asthma with Airway RemodelingIncresed fibrosis
Increased muscle thickness
Increased mucus
Increased inflammatory cells(CD4 and eosinophils)
Effect of Inhibiting NF-kB on Airway RemodelingDecreased fibrosis
Decreased muscle thickness
Decreased mucus
Decreased inflammatory cells(CD4 and eosinophils)
Background
57
Th
ora
x

! Breathing very fast or very slow
! Unilateral chest pain! Excessive sweating! Unable to speak in full
sentences! Altered mental status
!
! ! !
!
Symptoms and signs
As a first aider
Remarks
- Productive cough with sputum, especially recurrent- Wheezing or noisy breathing- Shortness of breath- Insucking chest wall- Use of accessory muscles
Allergens- Dust mites- Pollen- Animal Dander- Perfume- Medication such as aspirinExacerbation Factors- Cold Weather- Air Pollutants- Smoking- Emotional Stress- Infection
The precipitants of acute asthmatic attack include:
ComplicationsAcute- Pneumothorax- Acute Respiratory FailureChronic- Increase chances of infection
of the lung
1. Administer bronchodilator if the elderly has one2. Keep the elderly calm and comfortable3. Position the patient upright and loosen all tight clothing4. Seek emergency medical help if there is no bronchodilator or
the elderly does not respond to the bronchodilator
Emergency medicationShort Acting Bronchodilator (Salbutamol—blue bottle)
Dosage - Emergency ReliefGive 4-6 puff of bronchodilator, take 4-6 breaths between each puff
If the patient is still having asthma attack, repeat the above step after 4-6 minutes.
1. Leave the elderly unattended2. Delay medical consultation if the elderly does not improve
promptly
- Provide symptomatic relief to alleviate bronchoconstriction- Monitor closely to detect any deterioration
Do’s
Don’ts
Canister
Mouthpiece
58 59
Th
ora
x
Th
ora
x

How to use a bronchodilator1. Remove cap and shake the canister thoroughly2. Hold the canister upright3. Breathe out fully4. Place mouthpiece between lips5. Press the inhaler and inhale slowly and deeply simultaneously6. Hold the breath for 10 seconds or more7. Wait at least 1 minute before taking second dose
How to use a bronchodilator (with spacer)1. Remove cap and shake the canister thoroughly2. Insert the bronchodilator inhaler into the spacer3. Breathe out fully4. Place mouthpiece of the spacer between lips, ensure air tight5. Press the inhaler and breathe normally for 5 breaths
Choking and AspirationChoking occurs when the elderly’s airway is partially or completely blocked by a foreign body. The foreign body causing choking is commonly a food bolus, though it can be anything like a broken denture. The elderly is prone to choking for various reasons. Their chewing mechanism may be impaired because of dental problem. Swallowing is also affected because of pre-existing stroke. A demented elderly is also at risk because of loss of coordination of mastication and swallowing.
Symptoms and signs
During a meal,- Sudden coughing- Sudden shortness of breath - Difficulty speaking- Making high-pitched noise while breathing- Clutching the throat with one or both hands
Background
60 61
Th
ora
x
Th
ora
x

As a first aider 1. Call for help
2. If the elderly is conscious and able to cough:- Encourage the elderly to cough- Stay with the elderly and monitor
3. If the patient is conscious but unable to cough or speak, or begins to exhaust:a / Back blows
1 Position yourself behind the elderly, place one arm diagonally across the chest
2 Bend the elderly forward by 90 degrees3 Strike the back between shoulder blades with heel of the
hand4 Repeat the above steps 5 times
1. Give the elderly any food or drink2. Give the elderly vinegar to drink3. Do finger sweep blindly
Apply standard maneuver to remove the foreign body
Do’s
Don’ts
b / Abdominal thrusts1. Position yourself behind the elderly2. Locate the elderly’s navel3. Make a fist and place it below breastbone tip and
above navel4. Grab the fist and give a quick upward thrust into
the abdomen5. Repeat the above steps 5 times
1 2 3
c / Perform the above 2 maneuver consecutively4. If the patient is unconscious:
a / Lower the patient to the groundb / Try to look for object obstructing the airway, if it can be
seen, try to remove it with fingersc / If it cannot be seen, tilt the patient head and give 2 rescue
breaths while checking chest rised / Perform chest compression 30 times to a depth at least 2
inches at 100 compress /mine / Look for foreign object again, if it can be seen, remove itf / Repeat the above 3 steps until help arrives
1 2 3
navel
breastbone tip
! Unable to speak or cough! Impaired consciousness! Appear exhausted and
unable to stand! Cyanosis
! ! !
!
62 63
Th
ora
x
Th
ora
x

Hypertensive EmergencyHypertension is one of the most common chronic illnesses in elderly in Hong Kong. A study by the School of Public Health of the University of Hong Kong in 2012 revealed that about 1 in 3 adults in Hong Kong has hypertension, and almost 50% of elderly are suffering from the disease.
When the heart beats, blood is pumped into arteries. Blood pressure is the pressure against which blood pushes the arterial walls. Blood pressure readings are given in two numbers, written as 120/80 mmHg. The first number is called the “systolic pressure” or “upper pressure”, which is the pressure exerted on the arterial walls when the heart contracts. The second number called the “diastolic pressure” or “lower pressure” is the pressure exerted on the arterial walls when the heart relaxes.
Hypertension is a reading of blood pressure greater than 140 (higher pressure) over 90 (lower pressure) mmHg with repeated
measurements when the person is resting. Systolic hypertension is a common condition in elderly.
When blood pressure spikes to a dangerous level that can potentially cause organ damage and other complications in the body, it is a hypertensive emergency. The blood pressure has to be lowered to avoid imminent organ damage. High blood pressure can have adverse effects on the brain, heart, kidneys and eyes.
Hypertensive emergencies generally occur at blood pressure levels exceeding 180 systolic OR 120 diastolic, but can occur at even lower levels in people whose blood pressure has not been previously high.
In elderly, forgetting to take blood pressure medication and interactions between medications are the common scenarios to trigger hypertensive emergencies. Some, however, do not have any underlying causes.
Background
CARDIOVAS-CULAR SYSTEM
65
Card
iov
asc
ula
r Syste
m

Symptoms and signs
In some cases of hypertension, there are no symptoms present. However, in cases of hypertensive emergencies, the following signs and symptoms may occur:- Severe chest pain- Shortness of breath, that may be increasing- Intense headache- Nausea and vomiting- Blurred vision- Increasing confusion- Numbness/weakness- Difficulty speaking- Seizures- Tinnitus- Fainting episodes- Unresponsiveness
As a first aider
1. If the elderly has BP > 180/120 mm Hg and with the above symptoms and signs:- Seek emergency medical help
2. If the elderly is unconscious:- Check for airway, breathing and pulse and perform CPR if
necessary3. If the elderly is conscious:
- Help the elderly into a comfortable position, usually sitting- Calm and reassure the elderly
4. If the elderly is vomiting or having seizures: - Put the elderly in recovery position to prevent aspiration
5. If the elderly complains of difficulty in breathing:- Prop him/her up using pillows behind upper back
Wait for the blood pressure to drop down on its own when symptoms occur
- Recognize the signs and symptoms of hypertensive emergency - Seek emergency medical help
Do’s
Don’ts
Angina
Heart disease is the 2nd killer disease in Hong Kong after cancer. Coronary heart disease is a major type of heart disease.
Incidence and prevalence of ischemic heart disease rise with age. More than 30% people aged >65 years in the developed world have angina or myocardial infarction (MI) and a further 30% have covert (asymptomatic) disease.
Angina is a sensation of chest pain typically squeezing or pressure liked due to ischemic heart disease. When the coronary vessels become narrowed, the blood supply of heart muscle may impaired. This is aggravated on exertion when oxygen demand increases.
Heart attack occurs with severe occlusion of coronary vessel leading to heart muscle death. However, it is not unusual for the elderly to have silent ischemia.
Risk factors for cardiovascular diseases include hypertension, hyperlipidemia, diabetes mellitus, smoking and family history of angina or cardiac muscle infarction. The untreated ischemic chest pain can cause cardiac muscle infarction, complicated by sudden cardiac death, shock, acute decompensated heart failure or congestive heart failure.
Background
66 67
Card
iov
asc
ula
r Syste
m
Card
iov
asc
ula
r Syste
m
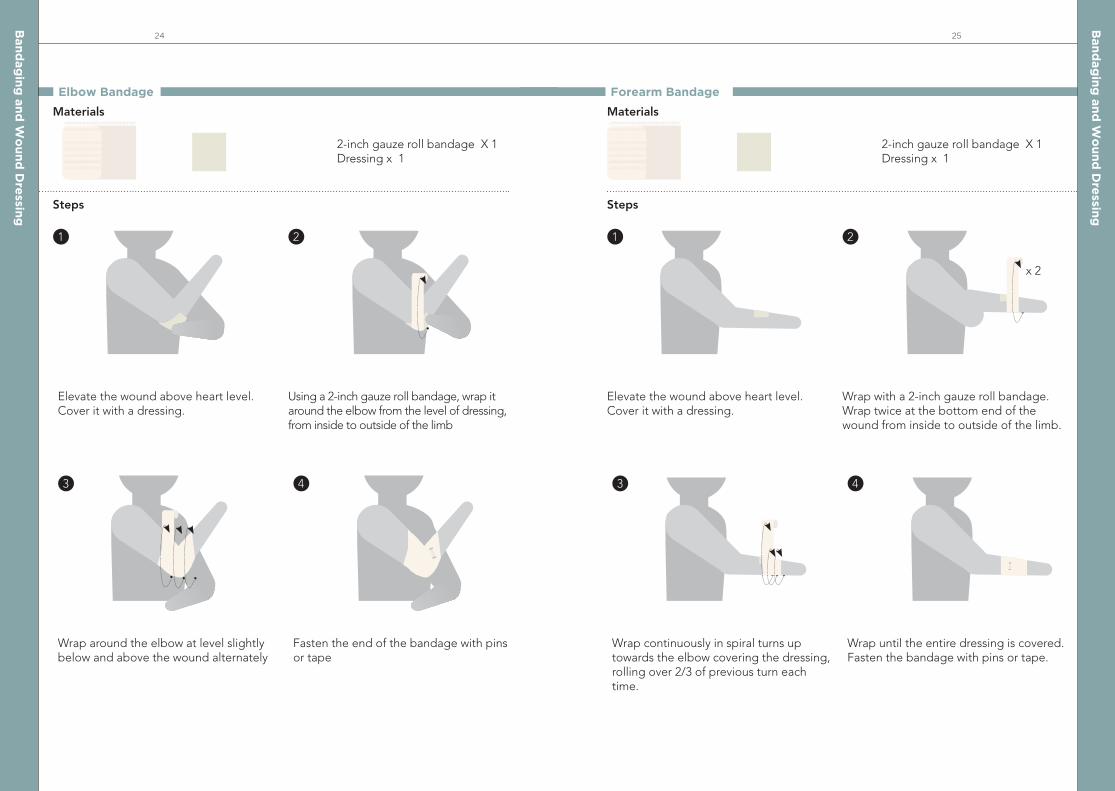
! Sudden onset! Exertional! Intensive pain! Sweating ! Shortness of breath ! Fainting or loss of
consciousness
! ! ! ! !
!
Symptoms and signs
Ischemic chest pain (severe and prolonged)
Atypical chest pain
Angina Symptoms
- Sharp or knife-stabbing like pain brought on by re-spiratory movements or cough
- Primary or sole location of discomfort in the middle or lower abdominal region
- Pain that may be localized at the tip of one finger, particularly over the left ventricular apex
- Pain reproduced with movement or palpation of the chest wall or arms
- Constant pain that persists for many hours- Very brief episodes of pain that last a few seconds
or less- Pain that radiates to lower extremities
Site
Onset
Characteristics
Radiation
Associated Symptoms
Duration
Exacerbating Factors
Relieving Factors
Severity
Central Midline Chest Pain
Acute
Crushing or stabbing discomfort, chest tight, squeezing/pressure feelings
Left Arm, Jaw, Neck
Shortness of breath, sweating, tachycardia, anxiety, nausea and vomiting
Gradually increasing but usually fading away in 10 minutes
Exercise, stress and coldness
Resting and nitrate (antianginal medication )
Variable, from little pain to severe pain
As a first aider
1. If the elderly is consciousa / Assist the elderly in half-sitting position with support for the
back and head. b / Assist the elderly to take sublingual nitrates (Nitroglycerin) c / Loosen any tight clothing d / Get the elderly to hospital
2. If the elderly is unconscious a / Rest the elderly lying on his/ her side b / Call 999 c / Loosen any tight clothingd / Re-place elderly lying on his/ her back and perform CPR
until ambulance arrive3. When in doubt, always call 999 in case the patient suddenly
collapse
- Assist the elderly to rest- Seek emergency medical help- Monitor the condition closely
Do’s
1. Leave the elderly alone2. Wait to see if the symptoms subside3. Give any medication (except cardiovascular medications) by mouth
Don’ts
68 69
Card
iov
asc
ula
r Syste
m
Card
iov
asc
ula
r Syste
m

ABDOMEN Abdominal Pain Abdominal pain in an elderly can be caused by a variety of conditions. Most of the time, it is caused by simple food poisoning, gastroenteritis or cramps.
However, “acute abdominal pain”, defined as an abdominal pain of less than 6 hours of onset, must be treated with caution. Elderly with acute
Background
abdominal pain often presents late to a hospital. Also, they usually present at a more severe stage and require hospitalization (50-60%) or surgical treatments (20-33%).
The following table shows the most common diseases causing acute abdominal pain in a person above 55 years of age:
By Location
Upper Right Quadrant- Biliary Tract Disease
Upper Left Quadrant- Gastric Ulce Disease
Lower Right Quadrant- Appendicitis
Lower Left Quadrant- Diverticulitis - Intestinal Obstruction
71
Ab
do
me
n

Symptoms and signs
- Acute pain in abdomen- Severe pain that may persist for hours Abdominal pain can be accompanied by other symptoms in different diseases:
- Severe pain in the URQ a few hours after meal, pain may radiate to the right scapula
- Nausea- Vomiting- Tea colour urine - Fever - Shaking
- Colicky pain around the belly button that shifts to the lower right quadrant after 6 hours
- Nausea and vomiting- Constipation- Fever
- Colicky abdominal pain- Abdominal distension- Constipation- Vomiting
- Pain in upper central/left abdomen
- Pain comes and goes, lasts for days to weeks
- Pain aggravated by spicy food & relieved by milk
- Pain starts about 2 hours after meal
- Acute onset abdominal pain that shifts from below to umbilicus to the left lower quadrant
- Vomiting- Fever
Symptoms
Biliary tract infection (e.g. cholecystitis, cholangitis)
Appendicitis
Intestinal obstruction
Peptic ulcer disease
Diverticulitis
Diseases
! Persistent pain! Worsening pain! Pain in a few hours after meal! Abdominal distension! Fever! Nausea! Vomiting! Constipation
! Shaking! Reluctant to eat or drink! Inability to tolerate any food or drink by mouth! Abnormal urination or defecation
! ! ! ! ! !!!
! ! ! !
As a first aider 1. Reassure the elderly and help him into a comfortable position
2. Sit him or her up if there is severe vomiting3. Heat pad or a hot water bottle wrapped in a towel may help
ease the pain 4. Seek emergency medical help in case of red flag symptoms or
you are in doubt of the elderly’s condition
Recognize red flag signs and manage as medical emergency
Do’s
Offer food or drinks if medical emergency is suspected (the elderly may require an emergency surgery)
Don’ts
Remarks
Generally speaking, abdominal pain is a non-specific symptom. It can be caused by benign and serious conditions. Atypical presentation is not uncommon in the elderly. Abdominal pain is no exception. For example, an elderly harboring a serious pathology may only experience mild abdominal pain initially and then suddenly deteriorates. The advice is that we should never underestimate the seriousness of the symptom of abdominal pain in the elderly.
72 73
Ab
do
me
n
Ab
do
me
n

Vomiting
Vomiting is commonly caused by gastroenteritis, food poisoning and motion sickness. However, some conditions such as outbreak of norovirus in institutions, gastroesophageal reflux disease, appendicitis, intestinal obstruction, metabolic
Background
disturbance, head injury, cancer and many others can also cause vomiting. Drugs such as opioids and chemotherapy can induce vomiting. When caring for a vomiting elderly, it is important to prevent dehydration and look out for underlying causes.
Symptoms and signs
Vomiting can be accompanied by various symptoms of different diseases:
- Watery diarrhea (usually non-bloody – bloody diarrhea may indicate a more severe infection)
- Abdominal cramps and pain- Nausea- Fever
- Severe pain in the URQ a few hours after meal, pain may radiate to the right scapula
- Nausea- Tea colour urine - Fever - Shaking
- Uneasiness- Cold sweat- Dizziness
- Acute onset abdominal pain that shifts from below to umbilicus to the left lower quadrant
- Fever
- Abdominal pain- Nausea- Diarrhea- Constipation- Inability to have a bowel movement or
pass gas- Abdominal distension
- Vomiting of blood (may be red or black)- Dark blood in stools or tarry stool- Nausea - Unexplained weight loss- Change in appetite
Symptoms
Symptoms
Viral gastroenteritis, food poisoning
Biliary tract infection
Motion sickness
Diverticulitis
Intestinal obstruction
Peptic ulcer
Diseases
Diseases
- Colicky pain around the belly button that shifts to the lower right quadrant after 6 hours
- Nausea and vomiting- Constipation- Fever
- Acid regurgitation- Heartburn sensation- Chest pain- Difficulty in swallowing- Dry cough- Hoarseness or sore throat
- Excessive thirst- Frequent urination- Nausea- Abdominal pain- Fruity breath- Shortness of breath- Confusion
- Loss of consciousness- Confusion or disorientation- Headache- Nausea- Fatigue or drowsiness- Dizziness or loss of balance- Sensory changes (e.g. blurring of
vision, ringing in ears, changed smell or taste, increased sensitivity to light or sound)
- Memory or mood changes
Appendicitis
Gastroesophageal reflux disease
Diabetic acidosis
Head injury
74 75
Ab
do
me
n
Ab
do
me
n

! Pain in right lower quadrant
! Signs of central nervous system involvement (confusion, stiff neck, photophobia)
! Bloody vomit or stool! Severe dehydration ! Inability to take
medication
! !
! ! !
As a first aider
1. Seek emergency medical help 2. In case red flag signs occur
a / Advise the elderly to restb / Give clear fluid (water, unsweetened fruit juice) frequently in small amount c / Give easy-to-digest food (congee, banana, potato)
- Recognize red flag signs and manage as medical emergency - Check if any stomach contents are aspirated- Relieve the patient’s symptoms by antiemetic medication and
maintain hydration - Consult family doctor for work up
Do’s
Give solid food
Don’ts
Dehydration
If the excess water loss from vomiting and diarrhea is not promptly replenished, an elderly may develop dehydration. Dehydration can begin to develop when a person losses as little as 1% of his body weight through fluid loss. Without prompt treatment, the elderly will go into heat exhaustion and shock.
Background
Common causes of dehydration include excessive sweating (exercise, fever, hot weather), diarrhea, vomiting and excessive urine output due to medical conditions. Elderly with chronic diseases such as diabetes, heart failure, and kidney diseases is prone to dehydration. Hot humid weather, physical disability and negligence by caretaker are also risk factors.
Symptoms and signs
- Dry mouth & dry eyes- Dry and/or cracked lips- Thirst- Headache (lightheadedness)- Dark urine- Reduced urine output- Cramping
76 77
Ab
do
me
n
Ab
do
me
n

As a first aider
1. Give plenty of fluid to drink. Water is usually sufficient but oral rehydration solutions can help with salt replacement.
Oral Rehydration SaltOral rehydration therapy is the administration of fluid by mouth to prevent or correct the dehydration that is a consequence of diarrhoea. In addition to water replenishment, oral rehydration solution is designed to replace the lost ions and correct any underlying acid-base imbalance due to excess water loss. Oral rehydration salts are available commercially for purchase. Alternatively, they can be prepared at home with simple ingredients. When preparing oral rehydration solution, you MUST follow the instructions on the packet. Adding too much or too little water may worsen the patient’s condition.
- Recognize red flag signs and manage as medical emergency- Rehydrate and monitor hydration status
Do’s
Consume milk or milk products, alcohol and caffeine
Don’ts
! Irritability and confusion! Dizziness! Low blood pressure! Palpitation ! Rapid breathing ! Fever
! ! ! ! ! !
In severe dehydration, the following symptoms may occur:
How to make Oral Rehydration Solution from Salt & Sugara / Wash your handsb / Measure 1 litre of drinking water into a clean containerc / Measure 1 levelled teaspoon of SALT and 8 levelled
teaspoons of SUGAR into the water. (A levelled teaspoon is where the salt or sugar is FLAT in the spoon, NOT piled up)
d / Mix the salt and sugar into the water well until you cannot see the salt or sugar at the bottom of the container
e / Taste the solution. It should never taste very salty. DO NOT boil up this solution once it is made up
f / Give the drink to the elderly with diarrhoea
levelledteaspoon
1 LitreDRINKINGWATER
SALTx1 x8SUGAR
Treatment should continue until the diarrhea stops. Patients should be allowed to drink freely as they need. Rehydration is generally adequate when the person no longer feels thirsty and has a normal urine output
2. Perform stretching & massage to relieve muscle cramps3. Monitor the input output balance and hydration status of the elderly4. Seek medical attention immediately if the condition does not
improve
78 79
Ab
do
me
n
Ab
do
me
n
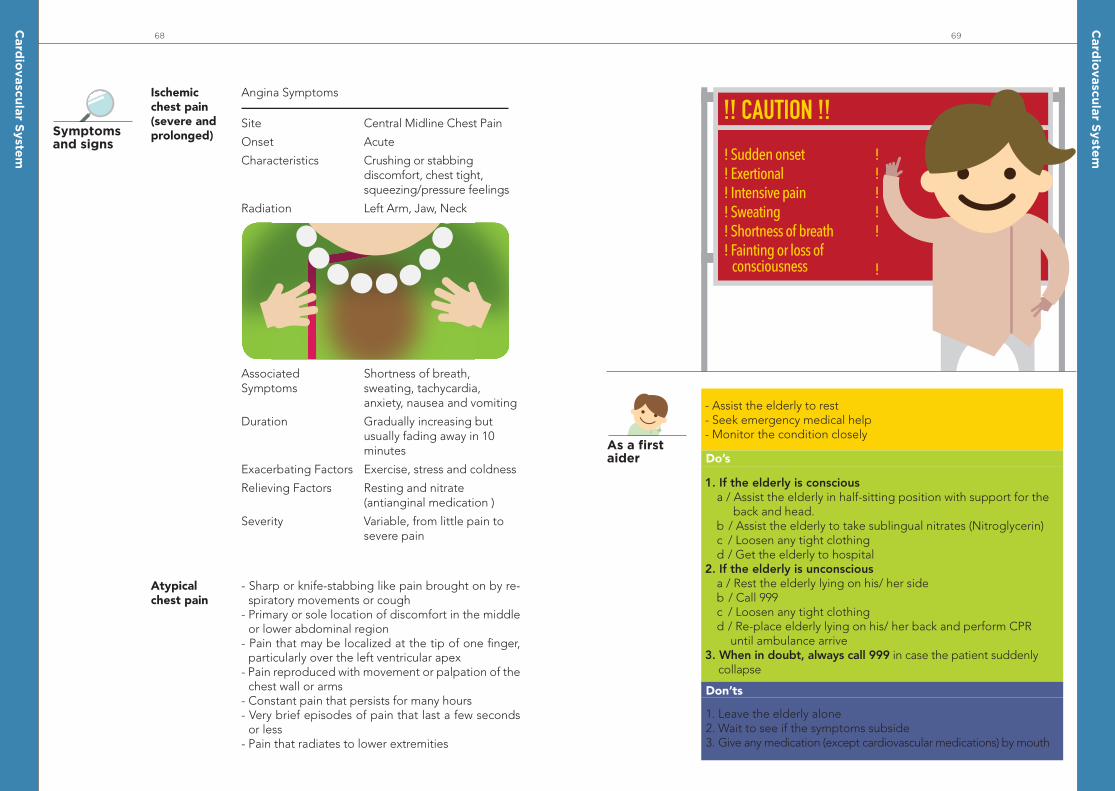
Constipation
Constipation refers to infrequent passage of hard stools. It can be caused by lack of fiber or fluid intake, inadequate physical activities, intestinal diseases or diseases such as overactive parathyroid, scleroderma (a connective tissue disease), Parkinsonism, stroke and diabetes. Medications such as antacid and overuse of laxatives can also cause constipation.
Background
Constipation can be complicated by fecal impaction, in which the rectum becomes filled with large, dried and hardened masses of stool that cannot be passed. It may be further complicated by injury to the rectal wall, bleeding and even perforation.
Symptoms and signs
- Sense of incomplete evacuation- Hard and small stool- Swollen abdomen- Abdominal pain
! Bloody stool! Severe abdominal pain! Bloating! Constipation of more
than 2 weeks! Watery overflow diarrhea! Weight loss
! ! ! !
! !
As a first aider
1. Increase fluid intake (extra 2 to 4 glasses of water per day)2. Drink warm liquid in the morning3. Increase fiber intake (fruit, vegetables and cereal)4. Use mild stool softener or laxatives for NO LONGER than 2 weeks
- Recognize red flag signs as well as fecal impaction and manage as medical emergency - Relieve the patient’s symptom by laxative for simple case
Do’s
Attempt to dislodge an impacted stool with your fingers at home
Don’ts
80 81
Ab
do
me
n
Ab
do
me
n

Acute Retention of UrineUrinary retention is the inability to empty the bladder. Urinary retention can be acute, chronic or acute on chronic.
Acute urinary retention in men becomes more common with age and peaks at their 50s-60s. In men 40 to 83 years old, the overall incidence of urinary retention is 4.5 to 6.8 per 1,000 men. For men in their 70s and 80s, the overall incidence increases to 100 per 1,000 men and 300 per 1,000 men. The risk factors for male urinary retention are kidney stones, prostatitis, benign prostate hypertrophy, and prostate cancer.
In female, acute urinary retention is less common. It can happen if the bladder sags or moves out of the normal position (cystocele) or is pulled out of position by a sagging of the lower part of the colon (rectocele). The risk factors for female urinary retention are history of kidney stones, history of urinary tract infections, and those with recent gynecological surgery.
The causes of acute urinary retention can be classified into extramural, mural and intraluminal.
Background
Extramural obstruction can be caused by an enlarged prostate in male, any pelvic masses pressing against the bladder or urethra and constipation.
Mural can point to weak bladder muscle. Intraluminal causes include stones in urethra, urethral stricture and tumor at bladder neck or urethra. Acute urinary retention can also be caused by urinary tract infections leading swelling or irritation, nervous problems interfering with signals between the brain and the bladder, spinal cord problems and medications such as those used in flu, cough or nausea and vomiting.
In most cases, the bladder has to be drained by passing a small catheter through the urethra in the emergency department. At the same time, any known precipitating factors have to be corrected, like the medications mentioned above have to be stopped. In other cases where a reversible factor is found, a catheter may not be required. For example, if the urinary retention is caused by fecal impaction, the elderly should be able to pass urine once he or she opens the bowel.
PELVIS AND PERINEUM
83
Pe
lvis a
nd
Pe
rine
um

Symptoms and signs
- Inability to urinate- Painful, urgent need to urinate- Dribbling of urine- Pain or discomfort in the lower abdomen- Bloating of the lower abdomen
! Blood in urine! Loin pain! Fever ! Back pain or prior history of back trauma! Lower limb weakness or numbness
! ! ! ! !
As a first aider 1. Help the elderly to take a posture most comfortable to him or her
2. Seek emergency medical help
Recognize the condition and manage it as medical emergency
Do’s
1. Continue medication that might worsen the retention2. Drink plenty of water 3. Try to urinate forcefully
Don’ts
Urinary Tract InfectionA urinary tract infection (UTI) is an infection in any part of the urinary system — kidneys, ureters, bladder and urethra. Most infections involve the lower urinary tract — the bladder and the urethra.Women are at greater risk of developing a UTI than men. Infection limited to bladder can be painful and annoying. However, serious consequences can occur if a UTI spreads to kidneys and blood stream.
Background
The annual incidence of UTIs in the elderly is around 10% and it may be as high as 30% for those living in nursing homes and other institutions.The mortality rate in bacteremic elderly patients with UTI is as high as 33%.
In severe urinary tract infection, other systemic manifestations may arise, including high fever, shaking and chills, nausea, vomiting, palpitation, dizziness and even collapse. It can also be complicated by kidney damage and renal failure.
Symptoms and signs
Different types of UTI may result in different signs and symptoms, depending on the part of urinary tract affected.
Urinary tract infections don’t always cause signs and symptoms, but when they do they may include:- A strong, persistent urge to urinate- A burning sensation when urinating- Passing frequent, small amounts of urine- Urine that appears cloudy- Urine that appears red, bright pink or cola-colored — a sign of blood in the urine- Smelly urine- Pelvic pain, in women
- Pain at upper back and flank
- Pelvic pressure- Lower abdomen discomfort
- Burning with urination
Signs & Symptoms
Kidneys (acute pyelonephritis)
Bladder (cystitis)
Urethra (urethritis)
Part of urinary tract affected
84 85
Pe
lvis a
nd
Pe
rine
um
Pe
lvis a
nd
Pe
rine
um

! High or persistent fever! Chills or rigors! Loin pain
! ! !
As a first aider
1. Seek emergency medical help call 999 in case of severe infection with systemic symptoms. For a severe UTI, you may need treatment with intravenous antibiotics in a hospital
2. Give paracetamol as indicated to lower body temperature and decrease pain
3. Take the entire course of antibiotics prescribed by doctor to ensure that the infection is completely gone
4. Drink plenty of water to dilute urine and help flush out5. Wipe from front to back after urinating and after a bowel
movement. This helps to prevent bacteria in the anal region from spreading to the vagina and urethra
- Recognize red flags and manage it as medical emergency - Consult family doctor early if there is symptom of UTI
Do’s
1. Use potentially irritating feminine products. Using deodorant sprays or other feminine products, such as douches and powders, in the genital area can irritate the urethra
2. Drink coffee, alcohol, and soft drinks containing citrus juices and caffeine until your infection has cleared
Don’ts
LIMBS86
Pe
lvis a
nd
Pe
rine
um

Soft Tissue InjuriesSoft tissue injuries can be classified into bruises, strains and sprains. Injuries can either be acute, which happens suddenly, or overuse injury, which is caused by repetitive tasks over a long period of time or bad postures. Ankle sprain and back strain are the most common soft tissue injury as a result of improper physical activity.
Bruises can be resulted from an injury by a blunt force leading to bleeding in the soft tissue. Strains can be due to overstretching of muscles and tendons leading to tearing of muscles & tendons. Sprains can be caused by forcing joints beyond normal range of motion leading to overstretching of ligaments.
Background
Symptoms and signs
- Bruise - Pain- Swelling- Limited movement in injured part
! Severe pain & swelling! Unable to move, walk or bear weight on injured limb
! !
As a first aider
1. Soft tissue injuries should be treated with “RICE”:Rest Rest the injured part and avoid moving itIce Apply ice or cold compress (wrapped in a towel)
on the injured partCompression Provide comfortable supportElevation Elevate the injured limb
2. Simple painkillers such as paracetamol could be used to relieve pain as instructed by doctor
- Relieve symptoms by medication and physical method
Do’s
1. Move the injured part unnecessarily2. Apply heat to the injured part3. Apply herbs without prior medical consultation
Don’ts
88 89
Lim
bs
Lim
bs

Wounds
Good wound dressing is especially important for elderly with chronic diseases, as they have an increased risk of wound infection. Common types of wound are minor cuts, scratches, deep cuts/penetrating wounds, and skin tear.Background
! Wounds that are large or deep
! Wounds contaminated by foreign bodies
! Wounds caused by animal bite
! Wound occurring over joints! Wound with large skin loss! Wounds not treated for 8 or
more hours
!
! !
!!!
As a first aider
1. Stop bleeding (if any), using gauze for compression2. Clean wound3. For minor injuries, rinse the wound surface with running water4. For deep injuries, rinse the wound with running water, then
disinfect the wound5. For skin tear, disinfect both the wound surface and the
underside of the skin tear using Hibitane, then rinse with saline6. Cover and dress wound7. The preferred method is open method. Non-waterproof
adhesive dressing is the most convenient to use8. For large skin tear, lay the skin flap back on the wound and
cover the entire area with gauze. Seek medical attention IMMEDIATELY
- Stop bleeding from the wound- Prevent wound infection- Recognize red flags as they require medical attention, for
example, tetanus prophylaxis
Do’s
1. Cover wound with emulsifying ointment (豬油膏), toothpaste, vinegar or soy sauce
2. Clean wound with alcohol or hydrogen peroxide3. Rip off a bandage too quickly, which may reopen a healed wound
Don’ts
Remarks
Types of disinfectants
Solution
Ingredient: Chlorhexidine gluconateEffect: Disinfectant effect
Hibitane
Ingredient: Cetrimide in addition to chlorhexidine gluconateEffect:Detergent effect
Cetrimide
90 91
Lim
bs
Lim
bs

Remarks
Types of dressings
Fine tulles have smaller holes. Cover the wound with a single layer
Coarse tulles are more common on the market and they have larger holes. Cover the wound with two layers
It can be changed every 7 days because the dressing has holes that allow exudate to flow away
Change the dressing every 2-3 days to avoid infection and allow any exudate to leave
Open Method
Closed Method
Fine Tulles
This is the preferred method for most wounds. The dressings (besides silicon) should be changed after showering or after coming in contact with water
Non-adhesive dressings
Non-waterproof adhesive dressings
Silicon dressings
Waterproof adhesive dressings
CoarseTulles
Dry powder spray
It is sprayed over the wound and forms a protective layerIngredient: Povidone iodineEffect: Disinfect the wound and absorb any exudate that comes from the wound
Betadane
92 93
Lim
bs
Lim
bs

Fractures
Fractures usually occur in acute events such as falls and accidents. It can also be a form of overuse injury. Elderly is prone to fracture even in trivial injuries due to brittle bones. Common fracture sites include the hip, upper arm, wrist, spine and ribs.
Elderly are prone to fall as a result of reduced muscle power and balancing ability. With aging, the density of bone drops (osteoporosis) and the bones become brittle. Elderly
Background
can fracture their upper end of thigh bone from a simple move or minor injury. Hip fracture is one of the top injuries in elderly. Wrist fracture is another common injury from a fall on to an outstretched hand resulting in a forced backward displacement of hand and fracture of the bone in forearm.
Osteoporosis, physical inactivity, smoking, drinking and steroid therapy are risk factors of fractures.
Symptoms and signs
- Snap sound heard as bone breaks- Pain- Swelling- Deformity at fractured site- Inability to move the injured limb- For an open fracture, a wound, possibly with bone visible
Triangular bandage Fold the top edge down so that it touches the base – Cravat (2-folded)
Fold the of the triangle down so that the tip of the triangle touches the base – Cravat (1-fold)
As a first aider
1. Immobilize the injured limb with a splint if available2. If no splint is available, use a triangular bandage to support the
injured limb3. Cover the wound, if present, with a clean dressing
- Recognize that there is a fracture and seek medical consultation as soon as possible
- Prevent further injury
Do’s
1. Move the injured limb unnecessarily2. Apply heat locally3. Apply herbs locally4. Try to reduce any deformity5. Try to push back any visible bone if it is an open fracture
Don’ts
Remarks
Things to check beforehand1. Locate site of possible fracture2. Check circulation below fracture site
Symptoms & signs of Poor circulation- Weak/absent of pulse of the elderly below the fracture site, e.g. radial pulse. - Pale, white or bluish skin color - Cooler temperature of the injured limb - Numb or tingling of limbs
1 2 3
Upper Limb Splint
Lie downthe victim supine with the injured arm resting next to the trunk.
1
Folding method of triangular bandage into longitudinal bandages
Steps
Materials
Triangular bandage x 3 Splints: rigid boards, sticks x 2Padding: blankets, clothes x 1
94 95
Lim
bs
Lim
bs

4 5 12 13
18
3
6
Placing bandagesFold three cravats into longitudinal bandages, and push them under natural body curvature.a / above the fracture siteb / below the fracture sitec / at the site wrapping from the wrist to the contralateral pelvis.(Avoid pressing directly on the suspected fracture site)
Apply paddingPlace paddings between the fractured upper limb and the trunk that are going to be splinted.
Tie knotsTie the ends of each cravat in a non slip knot on the contralateral side of trunk and away from the causality. The cravat should be tight enough to hold the fracture upper limb securely in place, but not tight enough to interfere with blood circulation.
Wrap aroundWrap the cravats from the injured limb to the contralateral side of the trunk one by one.
Check circulationObserve the limb below the cravats for signs of impaired circulation after securing all the three cravats.
Finish! Dial 999 to call for ambulance
Signs and symptoms of poor circulation- Cooler temperature - Bluish color change of skin- Pain - Numbness or tingling sensation- Reduced or absent of movement- Weaker or absence of pulse
Upper Limb Splint
2
ab
c
7 8 11109
14
19 19
15 16 17
96 97
Lim
bs
Lim
bs

Lower Limb Splint
Before splinting1. Avoid moving the fractured limb2. Check for a / Touch sensation b / Ability to move c / Pulse
Materials
Steps
Triangular bandage x 4 Splints: rigid boards, sticks x 2Padding: blankets, clothes x 1
Slide three triangular bandages under both legs: a / above the site of fracture, b / below the site of fracturec / under the knees.
Place a splint or padding between the legs. It should be long enough to extend from the thigh to the ankles.
Bring the two ends of the triangular bandage under the knee together.
Tie the knot of the triangular bandage over the knee of the uninjured leg. Make sure the bandage is tight enough so that no movement is possible.
Take another triangular bandage and fold it in half three times, so that it is half the width of the other triangular bandages. Slide this bandage under the ankles.
1
2
3
4
a
b
c
5
6 Next, tie a figure of eight bandage around the ankle.
Tie the triangular bandage around the feet and cross over at the dorsum of the feet. Wrap the bandage around the feet one more time.
98 99
Lim
bs
Lim
bs

7
8
9
Lower Limb Splint
Tie the knot of the triangular bandage over the uninjured foot.
Tie the remaining two triangular bandages, tying knots over the uninjured leg.
After tying all four bandages, check for touch sensation, ability to move and pulses again. Note the color and temperature of the skin.
Fall
Fall Prevention
Falls are the most common cause of injury in the elderly. It can cause significant immobility, morbidity, and mortality. The outcome of the fall may be determined more by the underlying reasons (such as existing diseases, or compromised body functions) than the actual injuries.
Risk factors for fall include history of fall, gait and balance problems, impaired mental status, drugs (more than four types, or antihypertensive, pain-killing, diuretic, psychotropic drugs), neurological diseases and weakness of legs (e.g. stroke, Parkinson’s, etc.), impaired sight (e.g. glaucoma, cataract, etc.), problems with foot (calluses, nail disease, joint problems), alcohol, low blood pressure and environmental hazards.
There are two approaches to preventing falls. Primary fall prevention concerns itself with avoiding fall, and secondary fall prevention focuses on detecting the risk of fall. Both preventions have been intensively studied, and secondary prevention has been shown to be the most efficient. It is difficult to prevent falls completely, and repeated falls are more dangerous to the patient than the risk of falls alone.
An efficient secondary prevention involves the education to the elderly and their caregiver. All elderly with the age above 70 should be counseled for the specific measures of fall prevention if they have one of more risk factors as above. They are encouraged to exercise at the level compatible with their physical fitness.
Background
Background
100 101
Lim
bs
Lim
bs

The most successful preventive approach is to assess multiple factors and take measures targeting the risk factors in the elderly. It encompasses the following aspects:- Medications: review and reduction (esp. psychotropic drugs)- Balance and gait training- Exercise to strengthen muscles- Postural blood pressure monitoring- Home hazards modifications
Reduce your risk of falling at home
Particular attention must also be paid to these items, and they should be corrected as soon as possible:- Inappropriate footwear inducible to slipping and loss of balance- Inappropriate use of walking aids- Uncorrected vision impairments
For elderly living alone, it is helpful to install an emergency alarm system (see Section 5 - Call for help). On the other hand, there is evidence that a supplement of vitamin D can help prevent falls and fractures in older people. Consider asking a doctor for advice.
Exercise is an effective method of countering certain aging effects, preventing falls, and enhancing quality of life in general, and is beneficial no matter the person falls or not. Some of the other benefits include, but are not limited to:- Slowing bone and muscle loss- Decrease cognitive impairment and improve function- Decrease constipation and incontinence- Improve blood sugar control- Enhance sleep
The amount of exercise can vary according to the relative fitness of the person. For a high-fitness elderly, 30-60 minutes of moderate activity (such as brisk walking, light cycling or badminton) 5-7 days per week may be suitable. For low-fitness elders, moderate activity of less than 10 minutes may be permitted, but a gradual increase in duration is recommended.
There is also a large amount of evidence pointing to the importance of balance training in fall prevention, such as dancing or Tai-Chi. Other simpler balance exercises also exist. Consult your doctor or physiotherapist for more information.
1
2
3
4
56
7
8
9 10 11 14
15
12 13
Bedroom1. Keep a light - a lamp, light
switch or night light - near your bed
2. Sit down to get dressed.3. Keep loose items off the floor
Bathroom4. Install grab bars near toilet
and shower5. Put a riser seat on the toilet6. Use a shower chair and
handheld shower head while bathing
Stairs and Hallways7. add handrails on both sides of
the stairs8. Install anti-slip strips on each
stair9 make sure pathways are well-lit
and clear of tripping hazards
Livingroom10. Move cords and other
objects out of walkways11. Remove rugs or securely
tape down their edges12. Use a cushion or a seat riser
if your favorite chair is too low to easily stand from
Kitchen13. Use dinning chairs that have
arnrests and no wheels14. Don’t clean with high-gloss
wax floor protector15. Move things so they’re within
easy reach
102 103
Lim
bs
Lim
bs

Dislocation
Dislocations are caused by a force (from falls, collisions, accidents) resulting the bone being moved into an abnormal position. Anterior shoulder dislocation, which is resulted from fall on outstretched hand or direct impact to shoulder, is the most common site of dislocation. Closed reduction must be done quickly by experienced personnel.
Background
Symptoms and signs
- Snap sound heard as bone breaks- Pain- Swelling- Deformity in the injured area- Unable to move the joint
! Loss of sensation, motion or circulation beyond injured part
!
As a first aider
1. Seek emergency medical help immediately for reduction 2. Advise the casualty to stay still3. Support the injured limb in position of comfort
- Recognize the condition and seek orthopedic help immediately
Do’s
Attempt to reduce the joint if not trained
Don’ts
Steps to Get Up After Fall
After fall, try to find a chair for facilitating you to climb up. If possible, try to crawl near the chair.
Use one hand to hold the chair as supporting for lifting up your body.
Then use both hands to grab the chair. Try to lift up on leg stepping on the ground while the other leg knees on the ground.
Try to stand up with both legs.
Sit on the chair and take a rest.
1
2
3
4
5
104 105
Lim
bs
Lim
bs

Acute Gout
Acute gout is a condition of acute inflammatory arthritis — a red, tender, hot, swollen pint. It affects 5% of Hong Kong population and the hospitalization rate is significantly higher among elderly patient.
Acute gout is induced by excess uric acid in blood leading to crystals forming in joints. It could happen in over uric acid production, excess consumption of high-purine foods like meat and fish, consumption of alcohol, medications such as diuretics, under excretion of uric acid, and renal failure.
Background
Under-excretion of uric acid by the kidney is the primary cause of hyperuricemia in about 90% of cases, while overproduction is the cause in less than 10%. However, only 10% hyperuricemia patient develop gouty arthritis.
The risk factors for acute gout include overweight, high blood pressure, purine rich diet (like meat and fish), consumption of alcohol, and medications such as diuretics.
Symptoms and signs
During a gout attack:- Sudden burning pain and stiffness in a joint (affects the big toe in
50% of cases, may also happen in ankle and knee) - Redness Pain and swelling are worst at the beginning of gout attack. Most occur during night time
! Affecting a joint not usually involved
! High fever with chills and rigors
! History of diabetes mellitus or any compromised states
!
! !
As a first aider 1. Rest the affected joint until the attack subsides and for the next
24 hours2. Elevate affected joint3. Use ice to reduce swelling4. Seek further medical help if it is the first attack5. For recurrent attack medications (for example, NSAIDs,
colchicine and steroid) may be taken as instructed by doctor. Treatment should start as soon as possible for more rapid and complete resolution of symptoms
6. Stick to a low purine diet
- Symptomatic relief by medication and physical method- Bring the patient to consult family doctor early for definitive care
Do’s
1. Apply warm pad to affected joint2. Discontinue allopurinol if taking it regularly3. Delay medical consultation if symptoms do not respond
promptly to standard treatment of gout
Don’ts
All these suggest it may not be a simple gouty attack but infection of the joint.
106 107
Lim
bs
Lim
bs

Remarks
Dietary control is important to reduce the risk of gout. It should contain vegetables, fruits and low-fat dairy products. Drink at least 8 glasses of water daily to keep body well-hydrated. Consumption of fish, poultry and lean meat should be kept to 4-6 ounces per day.
High-purine food and beverage that should be avoided:
Food and beverage that are safe to consume (low in purines):
Meat – especially fatty red meat, goose and organ meats
Green vegetables and tomatoes
High fructose corn syrup-sweetened sodas, beverages, or foods
Coffee, tea, and carbonated beverages
Shellfishes – Mussels, clams, scallops, shrimps
Breads and cereals that are not whole-grain
Yeast
Chocolate and cocoa
Fishes – sardines, mackerel, salmon
Fruits
Mushrooms, asparagus, cauliflower, spinach
Butter, buttermilk, cheese, and eggs
Alcohol
Peanut butter and nuts
Dairy products that may lower your risk of gout:- Low-fat or nonfat milk- Low-fat yogurt
108 109
Lim
bs
Lim
bs

Osteoarthritis
Osteoarthritis is a common disease among the elderly population with 1 in 3 people aged 70 and older being affected. It is also one of the leading causes of disability particularly in elderly population.
Osteoarthritis is caused by degeneration of joints. It usually affects knees, hips, lower back, neck, joints of fingers and toes.
In the early stage, cartilages that help reduce friction between
Background
the bones begin to break down, causing pain and swelling upon joint movement.
In the later stage, bone spurs may form on the joint causing further inflammation and damage to the joint.
The risk factors for osteoarthritis include age, overweight, trauma to joint due to repetitive movements. In particular, squatting and kneeling are common risk factors of knee osteoarthritis.
Symptoms and signs
- Limited range of motion due to pain and stiff joints- Clicking / cracking sound when moving a joint- Mild swelling around the affected joint
! Affecting a joint not usually involved
! High fever with chills and rigors
! History of diabetes mellitus or any compromised states
!
!
!
As a first aider 1. For swelling in joints:
a / Rest the jointb / Apply cold pad to affected joint for 20 minutes every few hoursc / Compress the joint with elastic bandaged / Elevate the limb
2. For stiffness in joints:a / Apply hot pad to affected joint for 20 minutes every few hours
3. Lifestyle changes such as light exercise (e.g. Tai Chi, stretching) and weight reduction may help in managing in osteoarthritis
4. Physiotherapy – for suitable exercise routines5. Occupational therapy – for assistive devices to improve mobility6. Simple pain killer and anti-inflammatory medication can be
used as instructed by doctor
- Relieve the patient’s symptoms by medication and physical method- Consult family doctor for persistent symptom
Do’s
Delay medical consultation if symptoms do not respond promptly to standard treatment
Don’ts
110 111
Lim
bs
Lim
bs

Disclaimer Every effort has been made to ensure that all the information contained in this book is correct and accurate. Readers are, nevertheless, advised that the statements and opinions expressed in this book are provided as guidelines. The publisher, editors and authors disclaims any liability or responsibility for the consequences of any actions taken in reliance on those statements or opinions.
112
Ackn
ow
led
ge
me
nt | D
iscla
ime
r