Dyslipidemia therapy update: the importance of full lipid profile assessment
8
I. B. A. Menown () Craigavon Cardiac Centre, Craigavon BT63 5QQ, Northern Ireland, UK. Email: [email protected] G. Murtagh · V. Maher · M. T. Cooney · I. M. Graham Adelaide, Meath and National Children’s Hospital (AMNCH), Tallaght, Dublin 24, Ireland G. Tomkin Diabetes Institute of Ireland, Beacon Clinic, Sandyford, Dublin 18, Ireland Adv Ther (2009) 26(7):711-718. DOI 10.1007/s12325-009-0052-3 REVIEW Dyslipidemia Therapy Update: the Importance of Full Lipid Profile Assessment I. B. A. Menown · G. Murtagh · V. Maher · M. T. Cooney · I. M. Graham · G. Tomkin Received: June 6, 2009 / Published online: July 27, 2009 / Printed: July 29, 2009 © Springer Healthcare Communications 2009 ABSTRACT Lipid guidelines typically focus on total choles- terol ± low-density lipoprotein cholesterol levels with less emphasis on high-density lipoprotein cholesterol (HDL-C) or triglyceride assessment, thus potentially underestimating cardiovascular (CV) risk and the need for lifestyle or treatment optimization. In this article, we highlight how reliance on isolated total cholesterol assessment may miss prognostically relevant lipid abnormal- ities; we describe from the European Systematic COronary Risk Evaluation (SCORE) data set how incorporation of HDL-C may improve estima- tion of CV risk; and, finally, we critically evalu- ate the evidence base surrounding triglycerides and CV risk. Keywords: cardiovascular risk; cholesterol; dyslipidemia; high-density lipoprotein choles- terol; triglycerides INTRODUCTION For the treatment of patients with, or at risk of, cardiovascular (CV) disease, some guidelines focus primarily on total cholesterol ± low-density lipoprotein cholesterol (LDL-C) levels. However, this can lead clinicians to disregard, or even fail to measure, high-density lipoprotein cholesterol (HDL-C) and triglycerides (TGs), thus poten- tially underestimating CV risk and the need for lifestyle or treatment optimization. European guidelines recommend measurement of HDL-C and TGs (although not formal treatment goals) in patients at intermediate or high risk, 1 and the North American National Cholesterol Education Program (NCEP ATP III) identifies non-HDL-C as a secondary target for treatment. 2 A practical example of how knowledge of HDL-C and TG levels may be used to guide lipid treatment is shown in Figure 1. This guide, which was based largely on the Joint British Societies (JBS)-2 rec- ommendations for primary and secondary pre- vention, 3 additionally suggests consideration of specific HDL-C and TG targets (as agreed by
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Dyslipidemia therapy update: the importance of full lipid profile assessment

I. B. A. Menown () Craigavon Cardiac Centre, Craigavon BT63 5QQ, Northern Ireland, UK. Email: [email protected]
G. Murtagh · V. Maher · M. T. Cooney · I. M. Graham Adelaide, Meath and National Children’s Hospital (AMNCH), Tallaght, Dublin 24, Ireland
G. Tomkin Diabetes Institute of Ireland, Beacon Clinic, Sandyford, Dublin 18, Ireland
Adv Ther (2009) 26(7):711-718.DOI 10.1007/s12325-009-0052-3
REVIEW
Dyslipidemia Therapy Update: the Importance of Full Lipid Profile Assessment
I. B. A. Menown · G. Murtagh · V. Maher · M. T. Cooney · I. M. Graham · G. Tomkin
Received: June 6, 2009 / Published online: July 27, 2009 / Printed: July 29, 2009© Springer Healthcare Communications 2009
ABSTRACT
Lipid guidelines typically focus on total choles-terol ± low-density lipoprotein cholesterol levels with less emphasis on high-density lipoprotein cholesterol (HDL-C) or triglyceride assessment, thus potentially underestimating cardiovascular (CV) risk and the need for lifestyle or treatment optimization. In this article, we highlight how reliance on isolated total cholesterol assessment may miss prognostically relevant lipid abnormal- ities; we describe from the European Systematic COronary Risk Evaluation (SCORE) data set how incorporation of HDL-C may improve estima-tion of CV risk; and, finally, we critically evalu-ate the evidence base surrounding triglycerides and CV risk.
DOI
0052-3Issue Number:
7
Keywords: cardiovascular risk; cholesterol; dyslipidemia; high-density lipoprotein choles- terol; triglycerides
INTRODUCTION
For the treatment of patients with, or at risk of, cardiovascular (CV) disease, some guidelines focus primarily on total cholesterol ± low-density lipoprotein cholesterol (LDL-C) levels. However, this can lead clinicians to disregard, or even fail to measure, high-density lipoprotein cholesterol (HDL-C) and triglycerides (TGs), thus poten-tially underestimating CV risk and the need for lifestyle or treatment optimization. European guidelines recommend measurement of HDL-C and TGs (although not formal treatment goals) in patients at intermediate or high risk,1 and the North American National Cholesterol Education Program (NCEP ATP III) identifies non-HDL-C as a secondary target for treatment.2 A practical example of how knowledge of HDL-C and TG levels may be used to guide lipid treatment is shown in Figure 1. This guide, which was based largely on the Joint British Societies (JBS)-2 rec-ommendations for primary and secondary pre-vention,3 additionally suggests consideration of specific HDL-C and TG targets (as agreed by
712 Adv Ther (2009) 26(7):711-718.
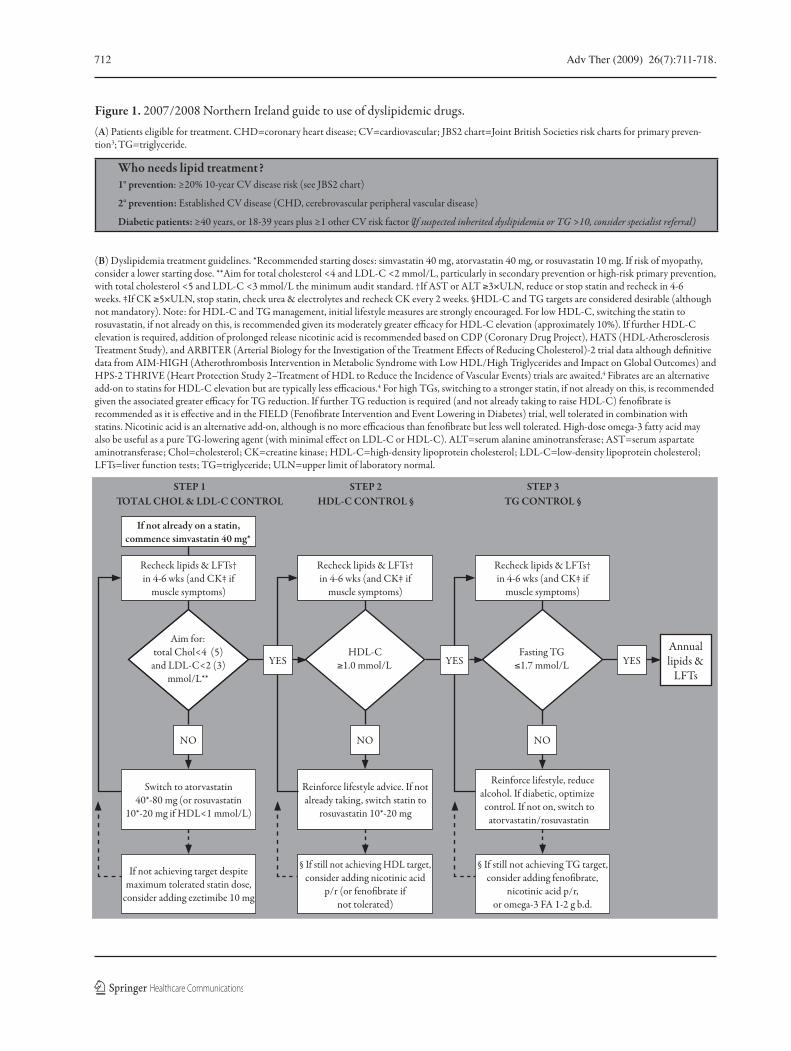
Figure 1. 2007/2008 Northern Ireland guide to use of dyslipidemic drugs.(A) Patients eligible for treatment. CHD=coronary heart disease; CV=cardiovascular; JBS2 chart=Joint British Societies risk charts for primary preven-tion3; TG=triglyceride.
Who needs lipid treatment?1° prevention: ≥20% 10-year CV disease risk (see JBS2 chart)
2° prevention: Established CV disease (CHD, cerebrovascular peripheral vascular disease)
Diabetic patients: ≥40 years, or 18-39 years plus ≥1 other CV risk factor (If suspected inherited dyslipidemia or TG >10, consider specialist referral)
(B) Dyslipidemia treatment guidelines. *Recommended starting doses: simvastatin 40 mg, atorvastatin 40 mg, or rosuvastatin 10 mg. If risk of myopathy, consider a lower starting dose. **Aim for total cholesterol <4 and LDL-C <2 mmol/L, particularly in secondary prevention or high-risk primary prevention, with total cholesterol <5 and LDL-C <3 mmol/L the minimum audit standard. †If AST or ALT ≥3×ULN, reduce or stop statin and recheck in 4-6 weeks. ‡If CK ≥5×ULN, stop statin, check urea & electrolytes and recheck CK every 2 weeks. §HDL-C and TG targets are considered desirable (although not mandatory). Note: for HDL-C and TG management, initial lifestyle measures are strongly encouraged. For low HDL-C, switching the statin to
elevation is required, addition of prolonged release nicotinic acid is recommended based on CDP (Coronary Drug Project), HATS (HDL-Atherosclerosis
data from AIM-HIGH (Atherothrombosis Intervention in Metabolic Syndrome with Low HDL/High Triglycerides and Impact on Global Outcomes) and HPS-2 THRIVE (Heart Protection Study 2–Treatment of HDL to Reduce the Incidence of Vascular Events) trials are awaited.4 Fibrates are an alternative
4 For high TGs, switching to a stronger statin, if not already on this, is recommended
aminotransferase; Chol=cholesterol; CK=creatine kinase; HDL-C=high-density lipoprotein cholesterol; LDL-C=low-density lipoprotein cholesterol; LFTs=liver function tests; TG=triglyceride; ULN=upper limit of laboratory normal.
STEP 1 TOTAL CHOL & LDL-C CONTROL
STEP 2 HDL-C CONTROL §
STEP 3 TG CONTROL §
If not already on a statin, commence simvastatin 40 mg*
Annual lipids &
LFTs
Recheck lipids & LFTs† in 4-6 wks (and CK‡ if
muscle symptoms)
Fasting TG ≤1.7 mmol/L
NO
Reinforce lifestyle, reduce alcohol. If diabetic, optimize
control. If not on, switch to atorvastatin/rosuvastatin
§ If still not achieving TG target, consider adding feno�brate,
nicotinic acid p/r, or omega-3 FA 1-2 g b.d.
YES
Recheck lipids & LFTs† in 4-6 wks (and CK‡ if
muscle symptoms)
HDL-C ≥1.0 mmol/L
NO
Reinforce lifestyle advice. If not already taking, switch statin to
rosuvastatin 10*-20 mg
§ If still not achieving HDL target, consider adding nicotinic acid
p/r (or feno�brate if not tolerated)
YES
Recheck lipids & LFTs† in 4-6 wks (and CK‡ if
muscle symptoms)
Aim for: total Chol<4 (5)
and LDL-C<2 (3) mmol/L**
NO
Switch to atorvastatin 40*-80 mg (or rosuvastatin
10*-20 mg if HDL<1 mmol/L)
If not achieving target despite maximum tolerated statin dose,
consider adding ezetimibe 10 mg
YES

Adv Ther (2009) 26(7):711-718. 713
consensus opinion of a Northern Ireland lipid advisory group, in keeping with the NCEP ATP III guideline) and suggests logical strategies on how to attain such targets if thought clini-cally desirable, most typically in a secondary prevention setting. In this review, we first quan-tify the incidence of lipid abnormalities identifi-able on full lipid profile, which may be missed if relying on isolated total cholesterol assessment. Then, from the European Systematic COronary Risk Evaluation (SCORE) data set we describe how incorporation of HDL-C may improve esti-mation of CV risk, in particular by reclassifying some patients into higher clinical risk groups. Finally, we critically evaluate the evidence base surrounding TGs and CV risk and lay out both sides of the complex debate on whether elevated TGs act as a risk marker or as an independent risk factor.
Isolated Cholesterol Measurements Hide Significant Lipid Abnormalities
In current practice, isolated total cholesterol measurements are frequently used and, if low, subjects are reassured. However, low total chol- esterol levels may hide HDL-C and TG abnormal- ities. Ginsburg et al., in a study of patients with angiographically established coronary artery disease,5 found that 32% had total cholesterol <5.17 mmol/L, of whom 59% had low HDL-C <0.90 mmol/L. Subsequent analysis of those admitted for elective angiography (to exclude the effects of hospitalization per se on serum lipids) revealed a similar pattern. In a 12-year follow-up of patients in the Framingham study,6 29% of those in the lowest total cho-lesterol subgroup (<4.9 mmol/L in men and <5.4 mmol/L in women) were found to have low levels of HDL-C (<0.92 mmol/L in men and <1.18 mmol/L in women), which was associ-ated with a marked increase in incidence of
myocardial infarction. In a recent study pre-sented by Murtagh,7 from 45,200 laboratory lipid profiles performed at a tertiary Dublin hos-pital over 1 year, a cohort of n=9417 individual patients were identified with a fasting full lipid profile and glucose level (48% male, median age 57 years). In those with total cholesterol <5 mmol/L, up to 20% had an abnormal fasting TG level >1.7 mmol/L and up to 40% had an abnormal HDL-C level ≤1.0 mmol/L.
These findings show that an isolated total cholesterol measurement, even when <5 mmol/L, may be associated with significant HDL-C and TG abnormalities. Isolated total cholesterol is thus not sufficient for the accu-rate prediction of CV risk, and indeed may give false reassurance to some patients.
HDL-C and Estimation of CV Risk
Multiple statin intervention trials,4 while confirming the benefit of reduction of LDL-C, have also demonstrated an increase in risk asso-ciated with low levels of HDL-C (Figure 2). In the Prospective Cardiovascular Münster (PROCAM) study, men with HDL-C <0.9 mmol/L had four times the risk of coronary heart disease com-pared to those with HDL-C ≥0.9 mmol/L.8
European guidelines on CV disease preven-tion stress the importance of estimating absolute CV risk; therefore, the most aggressive risk fac-tor modification can be directed towards those at highest risk.1 SCORE is the recommended risk estimation system9 and estimates a 10-year risk of CV mortality based on age, gender, country of origin, systolic blood pressure, smoking status, and either total cholesterol or the total/HDL-C ratio. Counterintuitively, in a previous study, the ratio version was not shown to provide superior risk estimation, despite the fact that HDL-C is known to be an important protective factor.10 However, the authors commented that the

714 Adv Ther (2009) 26(7):711-718.
inclusion of HDL-C as a separate variable, which is possible as part of the electronic interactive ver-sion of SCORE, HeartScore, may improve risk esti-mation.9 Cooney recently presented work from a data set of 57,302 men and 47,659 women, from which was derived a SCORE function (Cox pro-portional hazards method) containing HDL-C as a separate variable to assess whether its incor-poration improved risk estimation.11 The per-formance of this function was compared with that of an identical function without HDL-C, using area under receiver operating character- istic curve (AUROC) and net reclassification indices.12 Using AUROC analysis, inclusion of HDL-C resulted in a statistically significant although modest improvement in risk estima-tion (0.814 vs. 0.808; P<0.0001 for the func-tions with and without HDL-C, respectively). The improvement was greatest in women from high-risk countries (0.829, improved from 0.796; P=0.0001). However, using the net reclassifica-tion index analysis, addition of HDL-C resulted in a significant and sizeable proportion being reclassified to a more appropriate category. The net reclassification index was 0.022 (P=0.006) in the overall group, and was again greatest in women from high-risk countries at 0.115 (P=0.015). Thus in summary, inclusion of HDL-C as a separate variable in the SCORE function appeared to improve CV risk estimation, par-ticularly when considering the more clinically relevant method of examining which patients are reclassified. Inclusion of HDL-C may be par-ticularly useful in women from high-risk coun-tries and individuals with unusually high or low HDL-C levels.
Triglycerides: a ‘Risk Marker?’
There has been much debate regarding the role of elevated TGs in atherosclerosis because of their clear association with vascular risk. The
Figure 2. Low HDL-C levels associated with increased risk in statin trials. 4S=Scandinavian Simvastatin Survival Study; HDL-C=high-density lipoprotein cholesterol; HPS=Heart Protection Study; PPPP=Prospective Pravastatin Pooling Project.
Firs
t maj
or va
scul
ar ev
ent (
%)
19
17
21
23
27
25
15<0.90
Simvastatin(n=10,269)
≥0.90-<1.1 ≥1.1
HDL-C (mmol/L)
HPS study
Maj
or co
rona
ry ev
ents
(%)
19
17
21
23
27
25
15<1.0
Simvastatin(n=2221)
1.0-1.14 1.15-1.34 1.35
HDL-C (mmol/L)
4S study
Even
t rat
e (%
)
19
17
21
23
27
25
15<0.78
Pravastatin(n=6593)
0.9-0.980.8-0.88 1.0-1.14 >1.14
HDL-C (mmol/L)
PPPP study

Adv Ther (2009) 26(7):711-718. 715
NCEP ATP III guidelines recommend a non-HDL-C goal (which varies according to a patient’s risk) if fasting TGs are >200 mg/dL (2.3 mmol/L); this reflects the concern that the TG-rich remnant lipoproteins, such as small particles of very-low-density lipoprotein (VLDL) and intermediate-density lipoprotein (IDL), may be particularly atherogenic.2 However, the body of evidence to date supporting TGs as a causative factor in ath-erosclerosis has been inconclusive.1,2 If TGs are directly implicated in atherogenesis, it would be anticipated that primary forms of hypertrig-lyceridemia (which result in extremely elevated plasma TGs) would increase CV risk; however, the majority of TG-raising genetic abnormali-ties are not associated with increased CV risk. Disorders such as type I or type V hyperlipi-demia, in which TG-rich chylomicron (CM) particles are in abundance, are not associated with CV disease but rather with pancreatitis.13 Type III hyperlipidemia is associated with an increased CV risk, but this is not due to a TG abnormality per se; rather, it is due to defec-tive binding of apolipoprotein (apo) E2 to the LDL receptor, and as apoE reacts with the LDL receptor,14 defective apoE2 results in reduced clearance and raised levels of atherogenic rem-nant particles. Individuals susceptible to raised TG levels are particularly prone to developing quite marked increases in TG levels following alcohol. Subjects with such disorders who are also alcohol-addicted develop recurrent severe hypertriglyceridemia yet have less coronary artery disease.15
Epidemiological studies have shown an association between elevated TGs and CV risk. In a 10-year follow-up of 7531 Japanese men in the Honolulu Heart Study,16 nonfasting TG >3 mmol/L was associated with a 2.1-fold increased CV mortality, although significance was lost when adjusted for HDL-C and LDL-C. In the PROCAM study,17 TG >2.3 mmol/L was
associated with a doubling of CV risk when the LDL-C/HDL-C ratio was >5, but had no impact on vascular risk when the LDL-C/HDL-C ratio was <5.
However, the benefit of TG intervention is less clear. In the Helsinki Heart Study,18 a 35% reduction in TGs had a relatively small impact on vascular events compared with the impact of raising HDL-C or reducing LDL-C. This may suggest that high TGs are not directly associated with CV disease, although they may aggravate disease if subjects have concomitant elevated LDL-C and/or low HDL-C. The underlying mech-anism may be that raised TGs are associated with reductions in LDL particle size and altered HDL metabolism with reduced HDL-C. Raised TGs are also an integral component of the insu-lin resistance syndrome,19 itself associated with glucose intolerance, hypertension, and diabetes, which compounds the vascular risk in the pres-ence of LDL-C and HDL-C abnormalities.
In summary, it can be argued that the above data indicate elevated TGs are a risk marker rather than risk factor. One analogy is that TGs are important energy molecules that are transported via lipoprotein particles to a site of action as fuel, or to a site of storage when energy requirements are low. If these lipoprotein trans-port vehicles are defective (apoprotein abnor-malities) or encounter road blocks, eg, receptor or enzyme defects, TGs, although bystanders, may indirectly contribute to obstructions in our vascular roadways.
Triglycerides: a ‘Risk Factor’ for Atherosclerosis?
Is there additional evidence to suggest that ele-vated TGs might be more than just a risk marker, ie, be acting as an independent CV risk factor? The CM is the main TG-carrying protein and is defined by the solubilizing protein apoB48.

716 Adv Ther (2009) 26(7):711-718.
The particle is not only a TG-carrying particle but carries absorbed cholesterol and choles-terol synthesized in the intestine to the liver, where it is reprocessed and the lipid excreted as VLDL, losing apoB48 and gaining apoB100 as a solubilizing protein.13 Though the CM par-ticle has little cholesterol per particle, it carries a large amount of cholesterol as its turnover is minutes rather than days (LDL half life is ~4 days); therefore, potentially, CM cholesterol is as important as LDL-C in delivering choles-terol to the atherosclerotic plaque. The Hoorn Study demonstrated that in the presence of high non-HDL particles, patients with abnor-mal glucose metabolism had a much higher CV event rate with high TGs compared with low TGs.20 The Women’s Health Study 200721
demonstrated that nonfasting rather than fast-ing TGs were associated with CV events. In that study, >26,000 initially healthy US women were examined, of whom >6000 had a nonfasting TG level measured. The nonfasting TG levels had a strong independent relationship to CV events and in particular, TG levels measured 2-4 hours postprandially had the strongest cor-relation to CV events, demonstrating the dan-gers of the postprandial TG-rich lipoproteins. The Copenhagen Heart Study,22 a prospective cohort study of >7000 women and >6000 men followed for >25 years, demonstrated nonfasting TGs to be a significant risk in relation to myo-cardial infarction, ischemic heart disease, and death (independent of smoking, hypertension, inactivity, and diabetes), particularly noting the dangers of nonfasting TG >5 mmol/L. The authors suggested that it was not the TG per se that caused the problem but rather the choles-terol content of the remnant lipoproteins. In the Diabetes Atherosclerosis Intervention Study, fenofibrate was associated with a reduc-tion in progression of angiographically defined coronary atherosclerosis.23
Raised postprandial blood glucose is a risk factor for coronary artery disease whether it is in the diabetes or the prediabetes range, and as blood glucose rises so do free fatty acids. Even when fasting blood glucose is normal, postprandial abnormalities in free fatty acids and postprandial TG-rich lipoproteins occur in the presence of postprandial hyperglycemia, in both apoB48- or apoB100-containing particles. Improvement in blood glucose control can improve this postprandial excursion.24 Many studies have demonstrated that apoB48 is associated with atherosclerosis. The macrophage has a specific apoB48 receptor and preferentially takes up CM particles as compared with apoB100-containing VLDL or LDL particles (Figure 3). Proctor and Mamo25 have demonstrated that when they perfused normal rabbit arteries with LDL and CMs, the CMs were preferentially taken up by the intima and at higher levels than the LDL particles, confirming the potential atherogenicity of the apoB48-containing CMs.
The last piece of supporting evidence is the finding that there is an inverse correlation between LDL size and large TG-rich particles.26
Small, dense LDL is particularly atherogenic
Figure 3. Schematic diagram of the macrophage illustrating preferential uptake of chylomicron particles compared with apoB100-containing particles via the apoB48 receptor. apo=apolipoprotein; LDL=low-density lipoprotein; VLDL=very-low-density lipoprotein.
B/E receptorLDLVLDL
B48 receptor
Chylomicrons
Macrophage

Adv Ther (2009) 26(7):711-718. 717
and the demonstration that TG-rich lipoprotein particles influence LDL atherogenicity is further evidence of the importance of the TG-rich lipoprotein particle in the genesis of atherosclerosis.
In summary, there is overwhelming evidence to confirm that atherosclerosis develops due to abnormalities in the postprandial TG-rich lipo-proteins, both through their effect in deliv-ery of cholesterol to the atherosclerotic plaque and by their influence on the formation of atherogenic LDL.
CONCLUSIONS
It is clear that multiple lipid factors contri- bute to overall CV risk and an isolated total chol- esterol measurement is inadequate. Although we await results of ongoing randomized clinical trials testing the value of intervention with HDL- C-raising agents, incorporation of HDL-C as part of CV risk assessment has been proven to be of independent predictive value, and in particular may appropriately guide classification of some patients from a lower to a higher risk grouping. The debate surrounding TGs contin-ues, with their place as a CV risk marker well established, but with emerging data—particu-larly in the postprandial setting—raising the possibility of a direct atherogenic role.
ACKNOWLEDGMENTS
No relevant conflicts of interest declared. All authors contributed to the writing of this paper and are in agreement with the submission.
REFERENCES
Graham I, Atar D, Borch-Johnsen K, et al. 1. Europe-an guidelines on cardiovascular disease prevention in clinical practice. Eur J Cardiovasc Prev Rehabil. 2007;14(suppl. 2):S1-S113.
Third Report of the National Cholesterol Education 2. Program (NCEP) Expert Panel on Detection, Evalu-ation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106:3143-3421.
British Cardiac Society, British Hypertension Society, 3. Diabetes UK, HEART UK, Primary Care Cardiovas-cular Society, Stroke Association. JBS 2: Joint British Societies’ guidelines on prevention of cardiovas- cular disease in clinical practice. Heart. 2005; 91(suppl. 5):1-52.
Menown IBA. HDL cholesterol – a new target 4. for cardiovascular intervention. Cardiol News. 2006;9:11-13.
Ginsburg GS, Safran C, Pasternak RC. Frequency of 5. low serum high-density lipoprotein cholesterol lev-els in hospitalized patients with “desirable” total cholesterol levels. Am J Cardiol. 1991;68:187-192.
Abbott R6. D, Wilson PW, Kannel WB, Castelli WP. High density lipoprotein cholesterol, total chol- esterol screening, and myocardial infarction. The Framingham study. Arteriosclerosis. 1988;8: 207-211.
Murtagh G, Kiernan TJ, Tekle S, Boran G, Maher V. 7. Isolated cholesterol measurements hide significant lipid abnormalities. Paper presented at: Irish Athero-sclerosis Society; October 11, 2008; Galway, Ireland.
Assmann 8. G, Schulte H, von Eckardstein A, Huang Y. High-density lipoprotein cholesterol as a predic-tor of coronary heart disease risk. Atherosclerosis. 1996;124:S11-S20.
Conroy RM, Pyörälä K, Fitzgerald AP, et al. Esti-9. mation of ten-year risk of fatal cardiovascular dis-ease in Europe: the SCORE project. Eur Heart J. 2003;24:987-1003.
Ingelsson E, Schaefer EJ, Contois JH, et al. Clinical 10. utility of different lipid measures for prediction of coronary heart disease in men and women. JAMA. 2007;298:776-785.
Cooney MT, Dudina A, Graham I. SCORE HDL – 11. incorporation of HDL into risk estimation. Paper presented at: Irish Atherosclerosis Society; October 11, 2008; Galway, Ireland.
Pencina MJ, D’Agostino RB Sr, D’Agostino RB Jr, 12. Vasan RS. Evaluating the added predictive ability of a new marker: from area under the ROC curve to reclassification and beyond. Stat Med. 2008;27: 157-172.

718 Adv Ther (2009) 26(7):711-718.
Durrington PN. Lipid and lipoprotein disorders. In: 13. Weatherall DJ, Ledingham JGG, Warrell DA, eds. Oxford Textbook of Medicine. Oxford: Oxford Uni-versity Press; 1996:1399-1415.
Maher VMG, Gallagher JJ, Myant NB. The binding 14. of very-low-density lipoprotein remnants to the low-density lipoprotein receptor in patients with familial defective apolipoprotein B-100. Athero-sclerosis. 1993;102:51-61.
Kokolis 15. S, Marmur JD, Clark LT, et al. Effects of al-coholism on coronary artery disease and left ven-tricular dysfunction in male veterans. J Invasive Cardiol. 2006;18:304-307.
Rhoads GG, Feinleib M. Honolulu Heart Study. 16. Arteriosclerosis. 1983;3:316-322.
Assmann G, Schulte H. Prospective Cardiovas-17. cular Münster Study. Am J Cardiol. 1992;70: 733-737.
Manninen 18. V, Elo MO, Frick MH, et al. Lipid al-terations and decline in the incidence of coronary heart disease in the Helsinki Heart Study. JAMA. 1988;260:641-651.
Balkau B, Deanfield JD, Despres J-P, et al. Inter- 19. national day for the evaluation of abdominal obesity (IDEA). Circulation. 2007;116:1941-1951.
Bos G, Dekker JM, Nijpels G, et al. A combina-20. tion of high concentrations of serum triglyceride and non-high-density-lipoprotein-cholesterol is a risk factor for cardiovascular disease in subjects
with abnormal glucose metabolism – the Hoorn study. Diabetologia. 2003;46:910-916.
Bansal S, Buring JE, Rifai N, et al. Fasting com-21. pared with nonfasting triglycerides and risk of cardiovascular events in women. JAMA. 2007;298: 309-316.
Nordestgaard BG, Benn M, Schnohr P, Tybjaerg- 22. Hansen A. Nonfasting triglycerides and risk of myocardial infarction, ischemic heart disease, and death in men and women. JAMA. 2007;298: 299-308.
Diabetes Atherosclerosis Intervention Study In-23. vestigators. Effect of fenofibrate on progression of coronary-artery disease in type 2 diabetes: the Diabetes Atherosclerosis Intervention Study, a randomised study. Lancet. 2001;357:905-909.
Muragasu G, Phillips C, Owens D, Collins P, John-24. son A, Tomkin GH. Effect of improvement in glycaemic control on apo B48 and post-prandial lipoproteins in non-insulin-dependent diabetes. Diabet Med. 1998;15:S3.
Proctor SD, Mamo JC. Retention of fluorescent- 25. labelled chylomicron remnants within the intima of the arterial wall – evidence that plaque choles-terol may be derived from post-prandial lipopro-teins. Eur J Clin Invest. 1998;28:497-503.
Taskinen MR. Diabetic dyslipidaemia: from basic 26. research to clinical practice. Diabetologia. 2003;46:733-749.