14 03 28 Histo-Patofisiologi Saraf (A-B) ---
89
PATOFISIOLOGI SISTEM SARAF dr. Darma Satria, M.Si Bagian Patologi Anatomi Fakultas Kedokteran Universitas Syiah Kuala
Transcript of 14 03 28 Histo-Patofisiologi Saraf (A-B) ---
PATOFISIOLOGI
SISTEM SARAFdr. Darma Satria, M.SiBagian Patologi Anatomi
Fakultas Kedokteran Universitas Syiah Kuala
Topik Pembahasan• Edema otak, Herniasi otak dan Hydrocephalus– Cerebral edema– Cerebral Herniation– Hydrocephalus
• Kelainan kongenital pada Sistem Saraf– Neural Tube Defects– Malformasi terkait Hydrocephalus
• Vascular disease• Infection of the nervous system• Central Nervous System Trauma
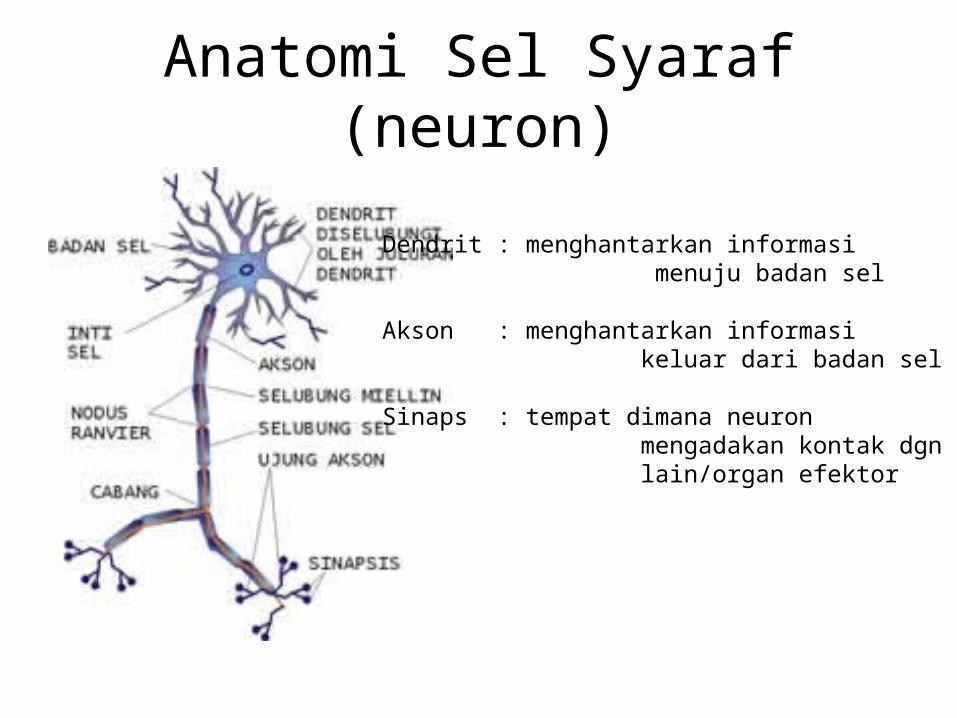
Anatomi Sel Syaraf (neuron)
Dendrit : menghantarkan informasi menuju badan sel
Akson : menghantarkan informasi keluar dari badan sel
Sinaps : tempat dimana neuron mengadakan kontak dgn neuron lain/organ efektor
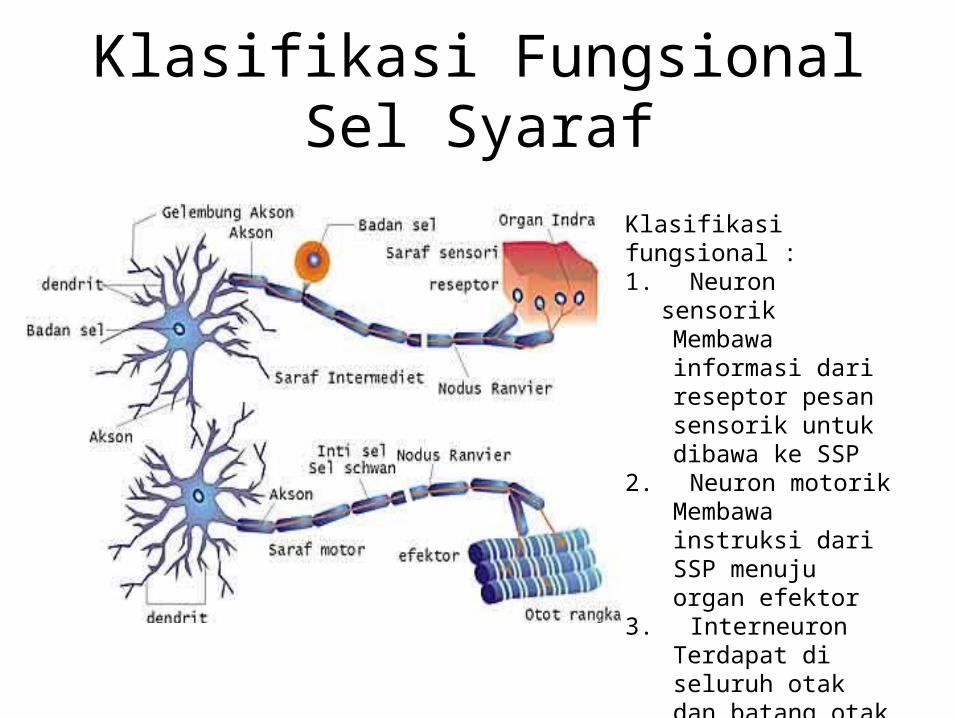
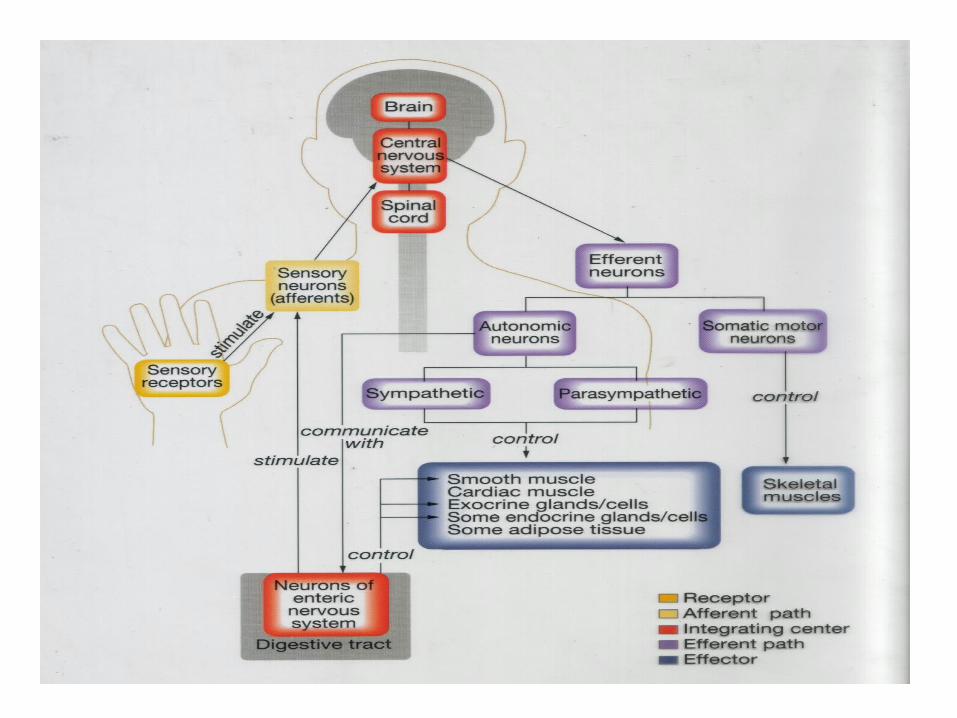
Klasifikasi Fungsional Sel Syaraf
Klasifikasi fungsional : 1. Neuron
sensorikMembawa informasi dari reseptor pesan sensorik untuk dibawa ke SSP
2. Neuron motorik Membawa instruksi dari SSP menuju organ efektor
3. InterneuronTerdapat di seluruh otak dan batang otak
Cara komunikasi neuron :
• Impuls Listrik • Neurotransmitter (zat kimiawi) : ACh, Adneralin, Noradrenalin, Dopamin, Serotonin, GABA
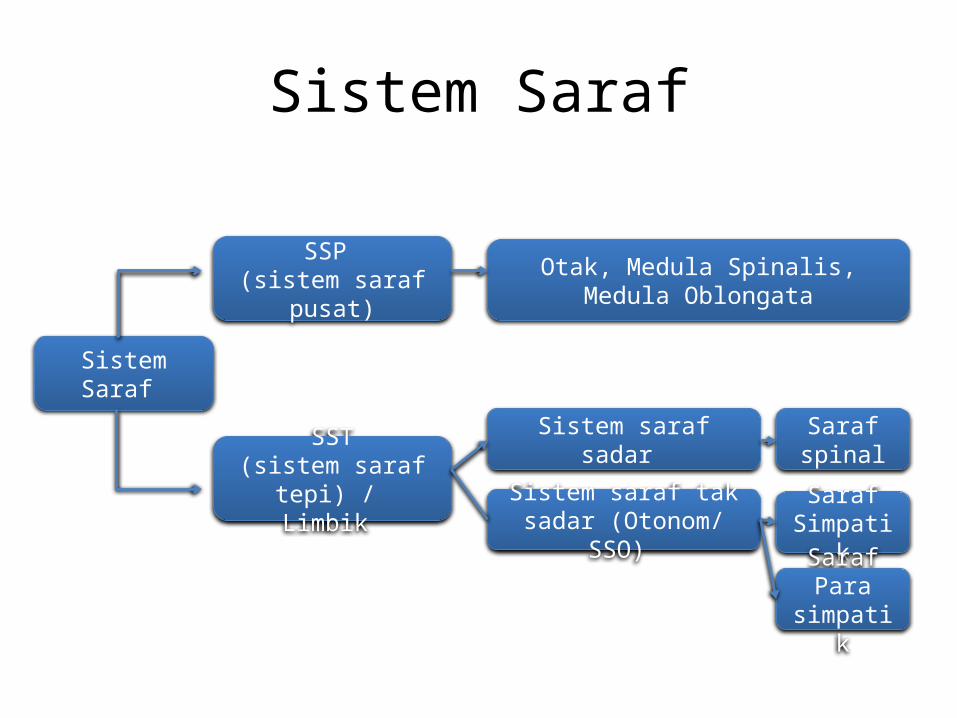
Sistem Saraf
Sistem Saraf
SSP (sistem saraf
pusat)
SST(sistem saraf
tepi) / Limbik
Sistem saraf sadar
Sistem saraf tak sadar (Otonom/
SSO)
Saraf spinalSaraf Simpati
kSaraf Para
simpatik
Otak, Medula Spinalis, Medula Oblongata
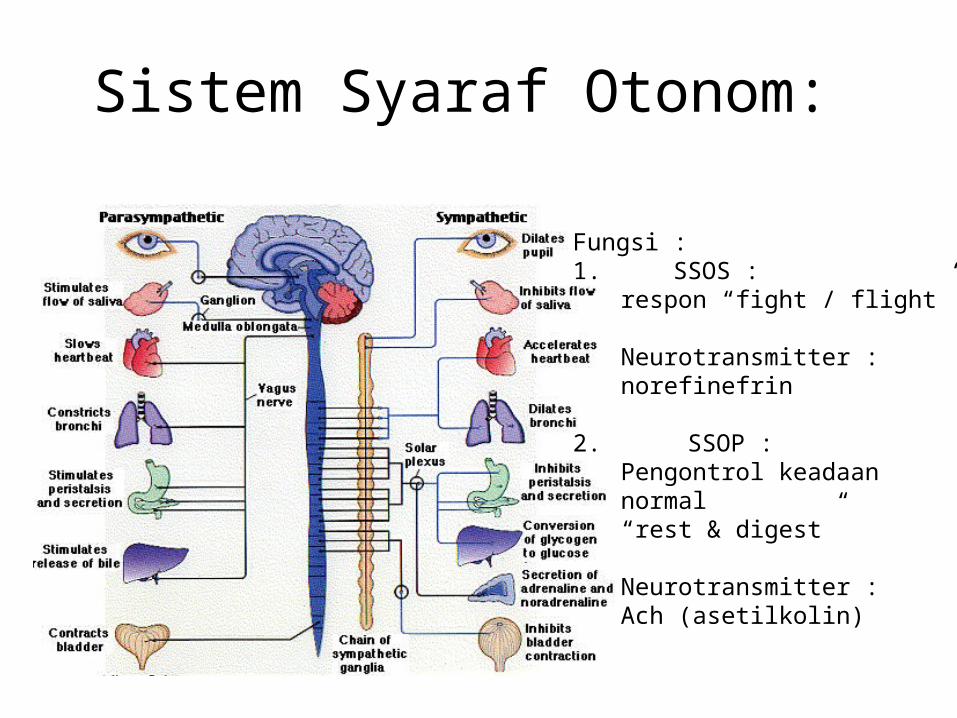
Sistem Syaraf Otonom:
Fungsi : 1. SSOS :
respon “fight / flight”
Neurotransmitter : norefinefrin
2. SSOP : Pengontrol keadaan normal“rest & digest”
Neurotransmitter : Ach (asetilkolin)
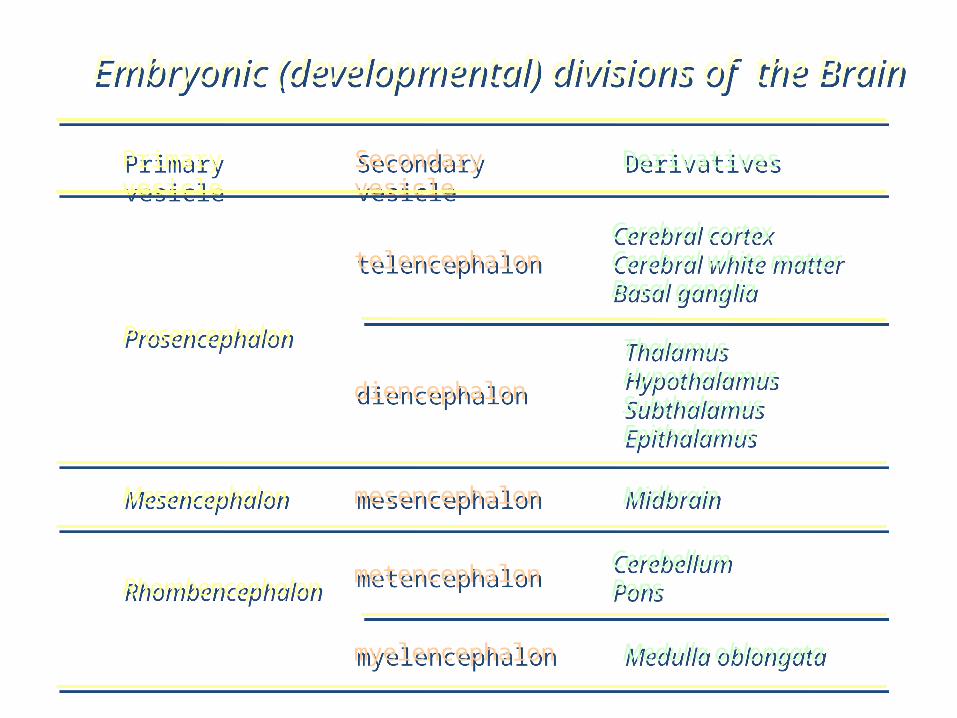
telencephalonCerebral cortexCerebral white matterBasal ganglia
metencephalon CerebellumPons
Primary vesicle
Secondary vesicle
Derivatives
Prosencephalon
diencephalonThalamusHypothalamusSubthalamusEpithalamus
Mesencephalon mesencephalon Midbrain
Rhombencephalon
myelencephalon Medulla oblongata
Embryonic (developmental) divisions of the Brain
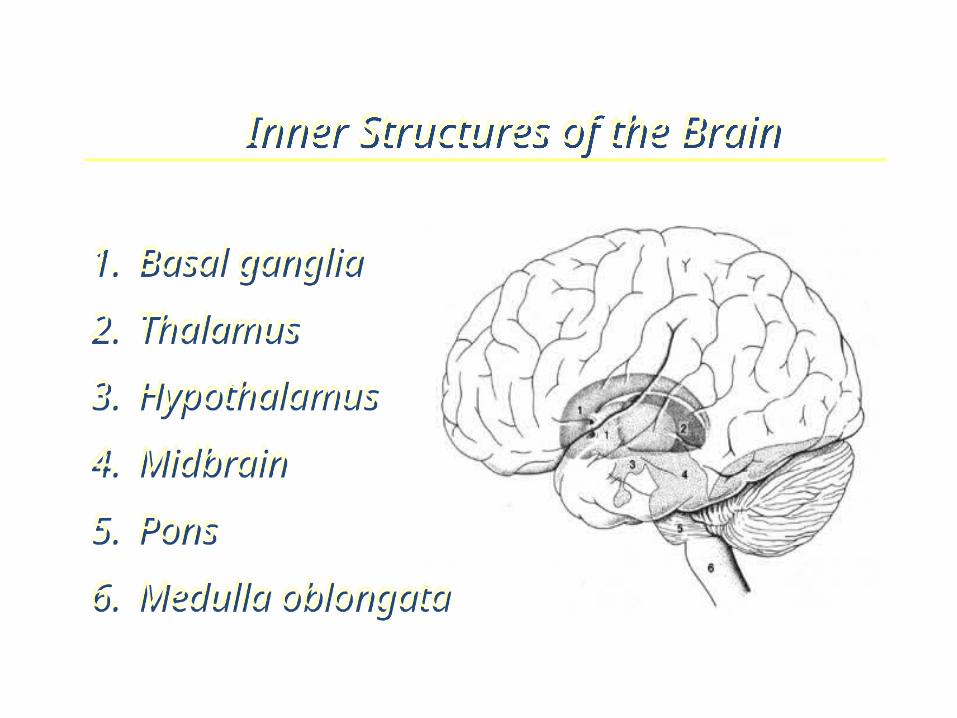
Inner Structures of the Brain
1. Basal ganglia2. Thalamus3. Hypothalamus4. Midbrain5. Pons6. Medulla oblongata
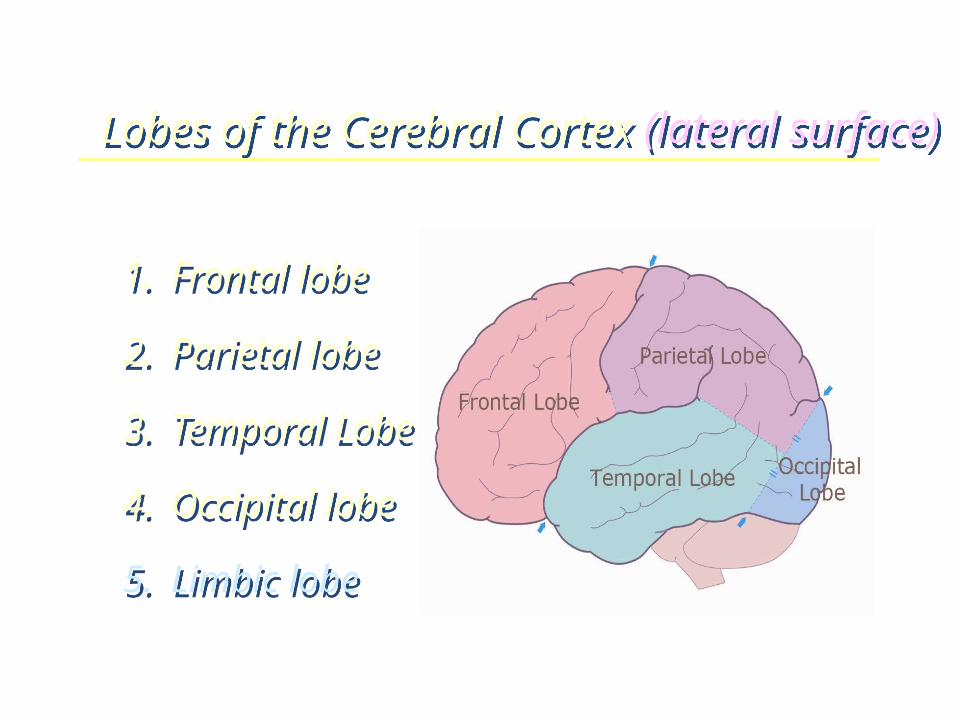
Lobes of the Cerebral Cortex (lateral surface)
1. Frontal lobe
2. Parietal lobe
3. Temporal Lobe
4. Occipital lobe
5. Limbic lobe
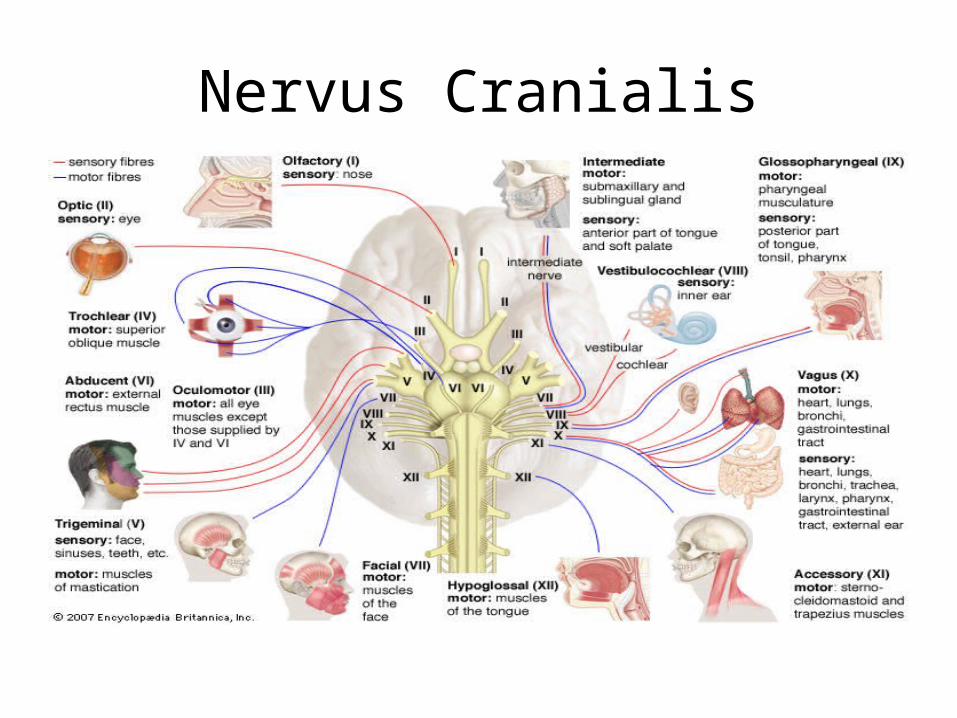
Nervus Cranialis
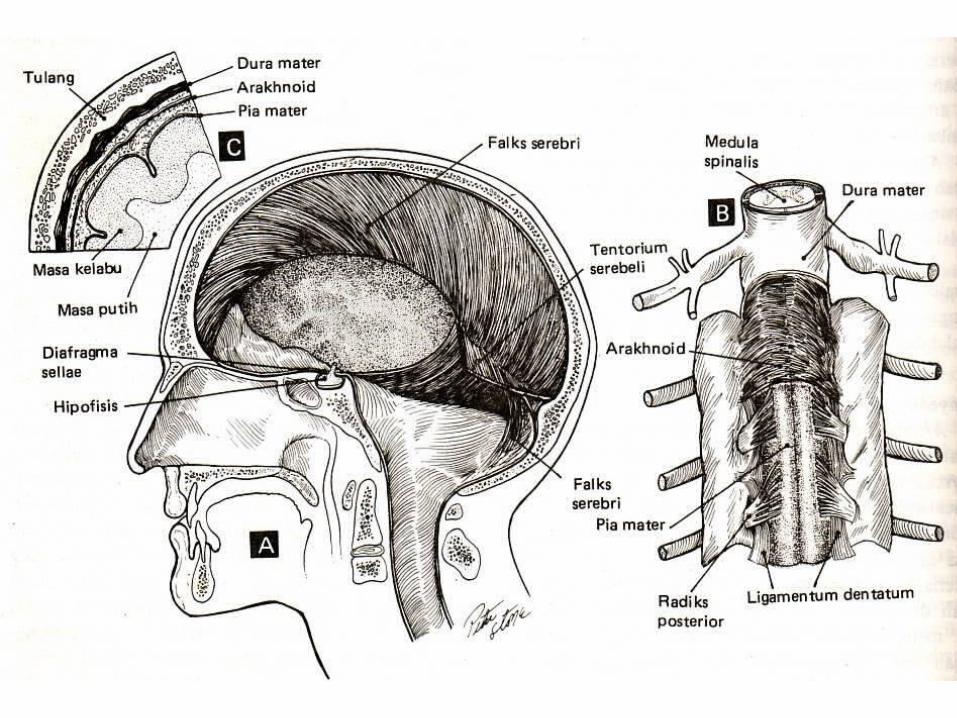
Susunan saraf pusat• Dilindungi tulang tengkorak dan tulang belakang
• Dilindungi suspensi cairan serebrospinalis
• Ditutupi tiga lapis jaringan dinamakan meningen : duramater (pachymeninx) selaput tebal dan keras, arachnoid dan piamater (leptomeninx) selaput yang halus dan tipis
EDEMA, HERNIASI DAN HIDROSEFALUS
• Otak dan medulla spinalis terdapat didalam struktur kaku, yaitu tengkorak, corpus vertebrae, dan duramater. Fungsi : pelindung
• Kerugiannya : ruang expansi dari parenkim otak sangat kecil
16
Increased intracranial pressure (IICP)
• Normal intracranial pressure is 5-15 mm Hg
• May be due to:– Tumor growth– Edema– Excess cerebrospinal fluid– Hemorrhage
Monro-Kellie Doctrine• The ICP within the skull is directly related to the volume of the contents.– Defined as the Monro-Kellie Doctrine– This doctrine states that any increase in volume of the contents within the brain must be met with a decrease in the other cranial contents
– v.intracranial (constant) = v.brain + v.CSF + v.blood + v.mass lesion
– Normally: brain 80%, CSF 10%, Blood 10%
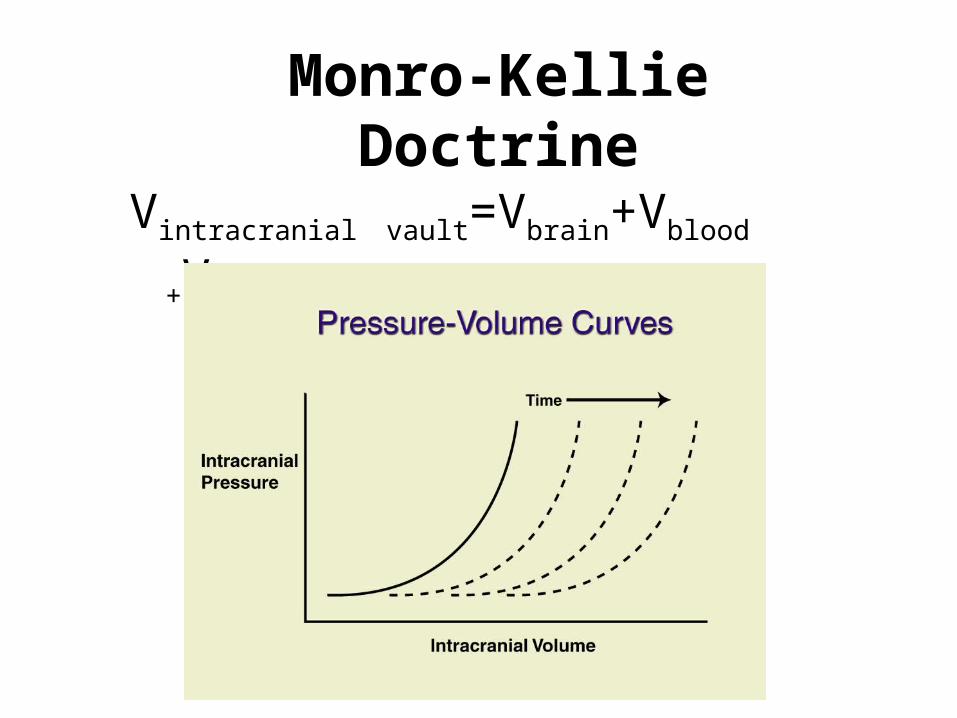
Monro-Kellie Doctrine
Vintracranial vault=Vbrain+Vblood
+Vcsf

Edema Cerebri• Definisi : peningkatan cairan pada parenkim otak
• Pengelompokan : Vasogenic edema dan Cytotoxic edema
Cerebral EdemaVasogenic Edema
• Kerusakan dari blood brain barrier, cairan masuk dari vascular ke interstial space otak (interstitial edema)
• Tidak adanya drainase limfatik pada otak mengakibatkan terganggunya reabsorpsi kembali cairan ekstraseluler yang berlebihan
• Edema dapat bersifat lokal misalnya pada kerusakan pembuluh darah pada tumor dan abses otak ataupun general
Cytotoxic Edema• Peningkatan cairan intraseluler (intraseluler edema) sekunder karena jejas sel, misalnya pada pasien dengan hipoxia-iskemik. Terjadi abnormalitas transport ion, sehingga terjadi peningkatan cairan dalam sel
• Ditandai dengan edema general
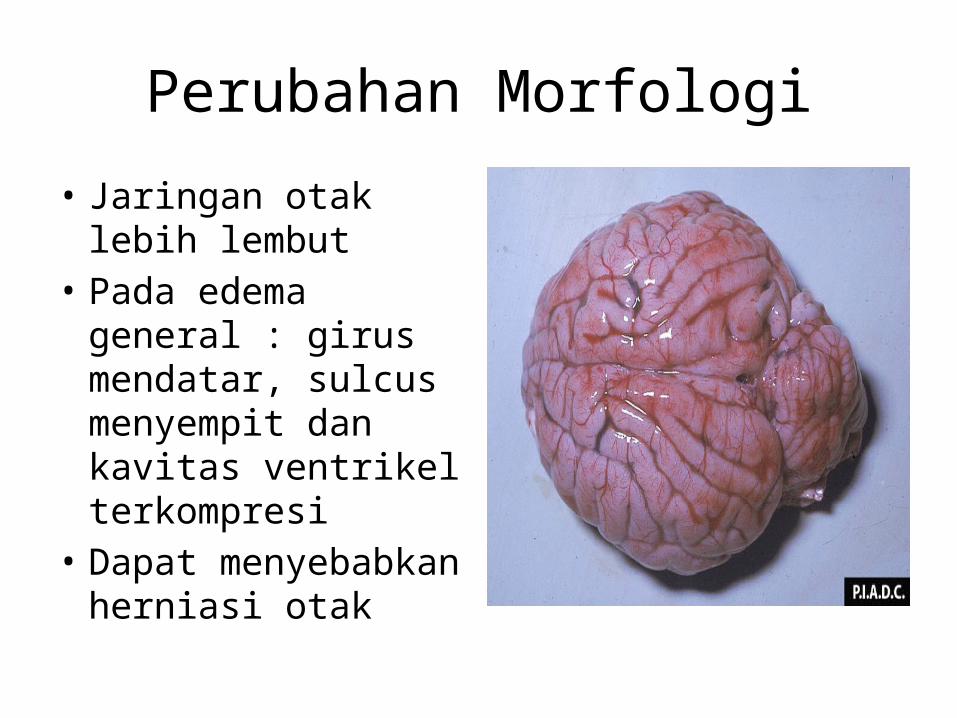
Perubahan Morfologi• Jaringan otak lebih lembut
• Pada edema general : girus mendatar, sulcus menyempit dan kavitas ventrikel terkompresi
• Dapat menyebabkan herniasi otak
Herniasi• Pada bayi: sutura masih belum menutup menyebabkan adanya akomodasi dari peningkatan tekanan intrakranial
• Pada anak dan dewasa : peningkatan TIK sulit diakomodasi akibat cranium yang kaku
• Tekanan akan diteruskan ke sisi lain seperti dural reflextion atau foramen magnum herniasi
Bentuk Herniasi1.Transtentorial (uncal gyral, mesial temporal)
herniation : bila aspek medial lobus temporal terkompresi tentorium Cerebelli. Terjadi kompresi dari N.Cranialis III dan serabut simpatisnya sehingga menyebabkan pupil dilatasi dan gangguan pergerakan bola mata sisi lesi. Arteri serebral posterior terkompresi menyebabkan iskemia korteks visual
2.Subfalcine (cingulate gyrus) herniation : ekspansi asimetris/unilateral dari hemisfer cerebral mendorong cingulate gyrus kebawah falx cerebri. Berhubungan dengan kompresi cabang arteri cerebri anterior kelemahan dan atau abnormalitas sensorik pada kaki karena iskemik pada korteks sensorik/motorik

Bentuk Herniasi• Tonsillar Herniation :
displacement dari tonsil cerebellar melewati foramen magnum.– Mengancam nyawa karena kompresi
batang otak dan pusat pernapasan di medulla oblongata.
– Disertai dengan lesi perdarahan di otak tengah dan pons disebut secondary brain stem/Duret Hemorrhages
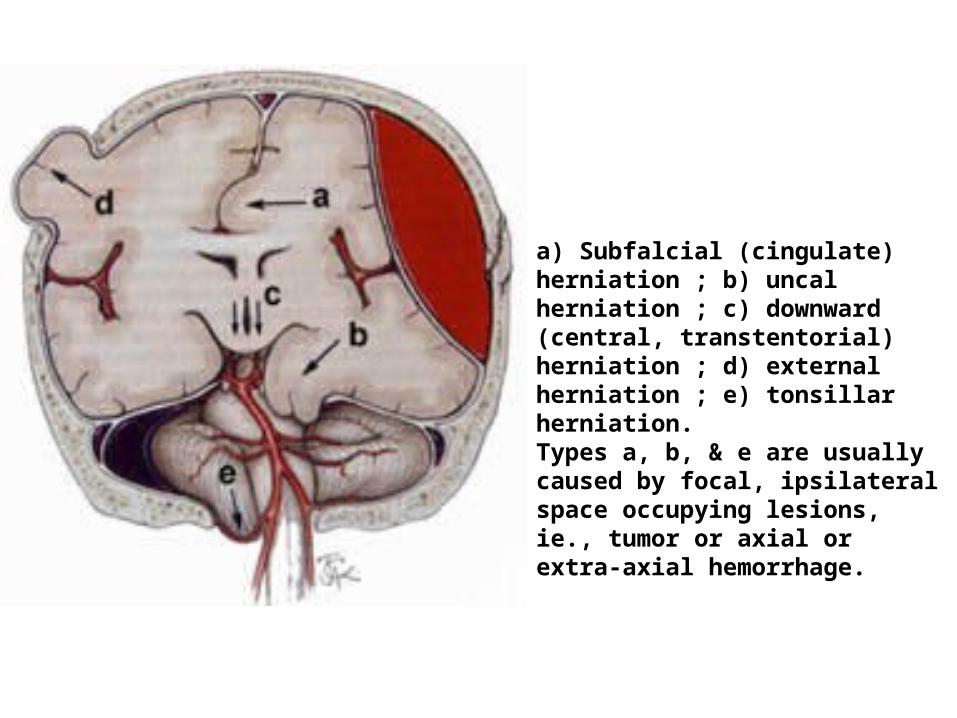
a) Subfalcial (cingulate) herniation ; b) uncal herniation ; c) downward (central, transtentorial) herniation ; d) external herniation ; e) tonsillar herniation.Types a, b, & e are usually caused by focal, ipsilateral space occupying lesions, ie., tumor or axial or extra-axial hemorrhage.

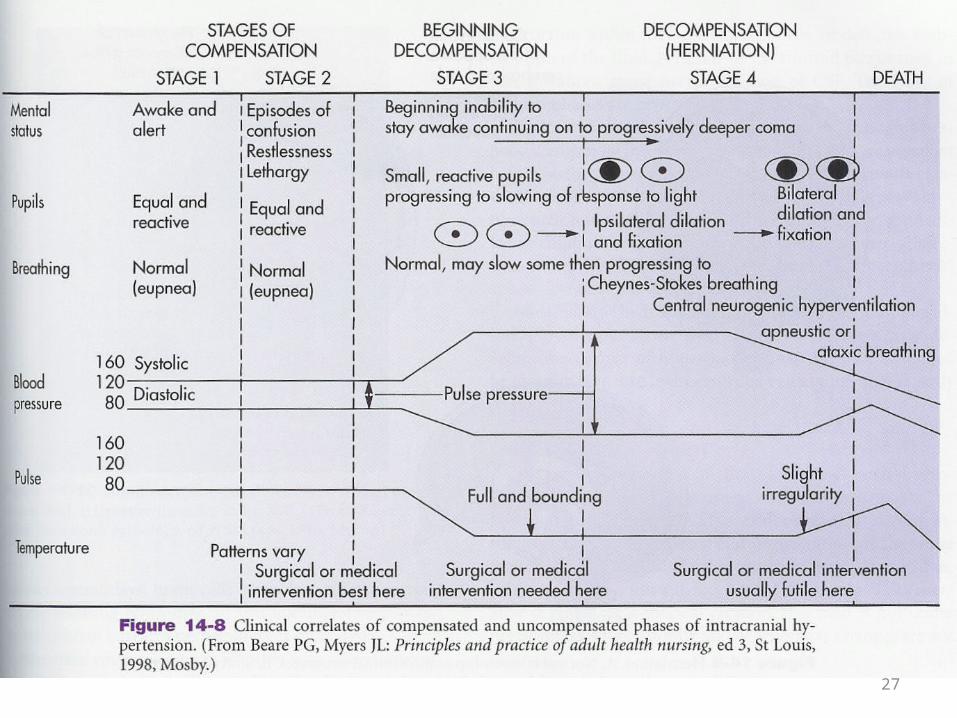
Cushing Reflex
• Bradycardia• Hypertension• Altered respiratory status OFTEN A VERY LATE CLINICAL FINDING!
27

Overview of CSF production
• The CSF volume of an average adult ranges from 80 to 160 ml
• The ventricular system holds approximately 20 to 50 ml of CSF
• CSF is produced in the choroid plexuses at a daily rate of 14-36 ml/hr
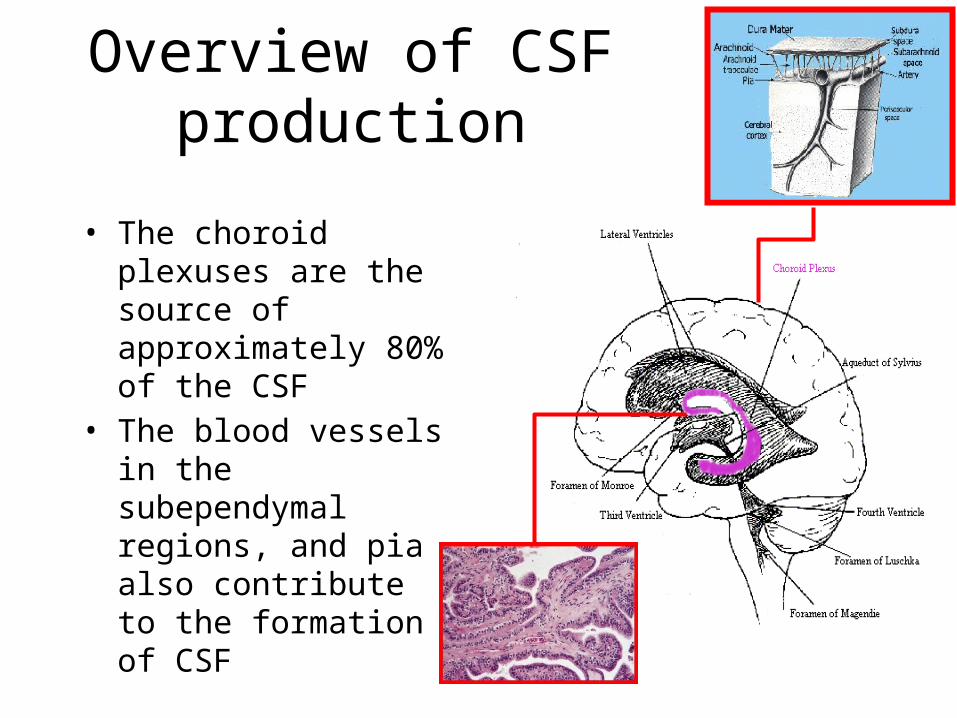
Overview of CSF production
• The choroid plexuses are the source of approximately 80% of the CSF
• The blood vessels in the subependymal regions, and pia also contribute to the formation of CSF
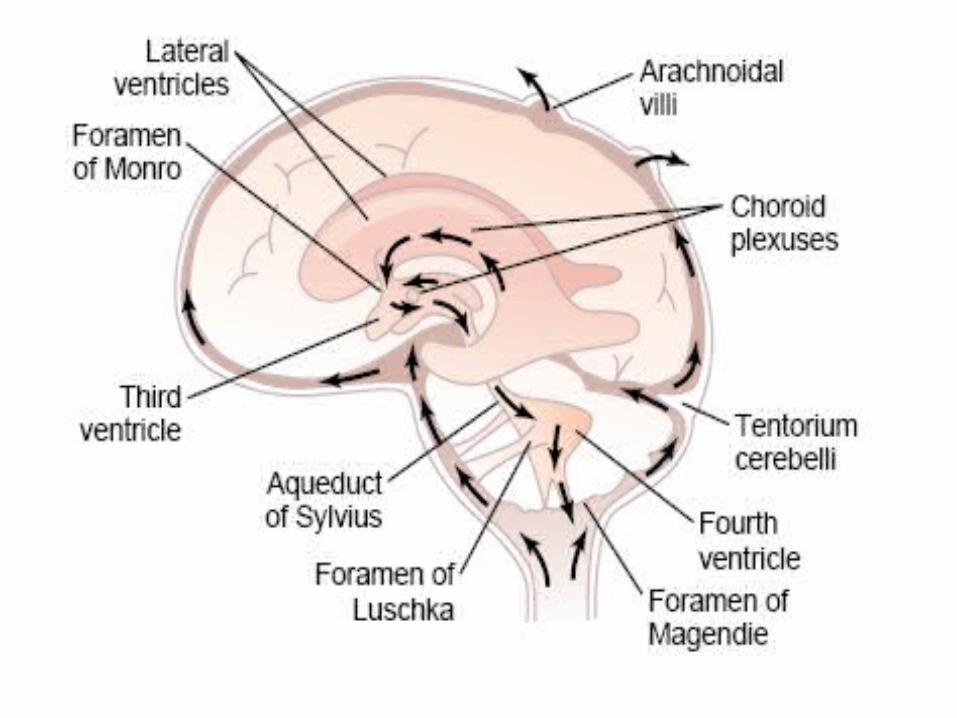
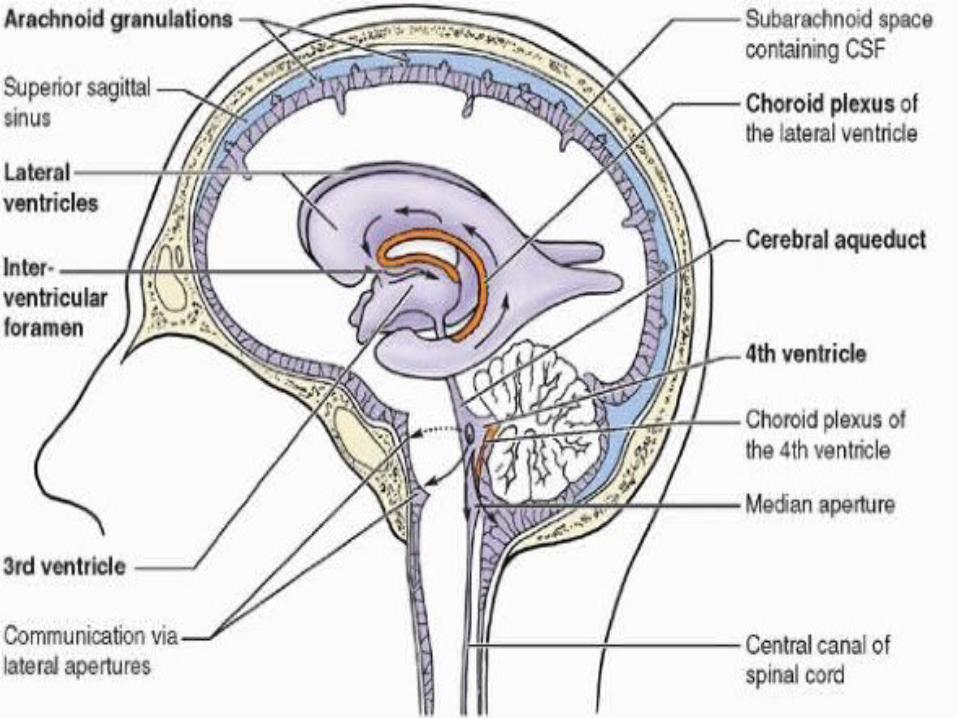
CIRCULATION OF CSFLateral ventricleForamen of Monro
[Interventricular foramen]
Third ventricle
Subarachnoid space
Fourth ventricle:Cerebral aqueduct
Foramen of megendie , luschka
The function of the CSF
• The CSF acts as a “water jacket” for the brain and spinal cord
• The 1300 g adult brain weighs approximately 45 g when suspended in CSF
The function of the CSF• The CSF acts like a
“sink”, effectively flushing waste products as new fluid is secreted reabsorbed
• A constant CSF electrolyte composition helps maintain a stable medium for excitable cells (neurons)
FUNCTIONS OF CSFA shock absorberA mechanical bufferAct as cushion between the brain and craniumAct as a reservoir and regulates the contents of the craniumServes as a medium for nutritional exchange Transport hormones and hormone releasing factors
Mechanisms of increase intracranial pressure
• Brain, Blood and CSF are held in an inelastic container (cranium, vertebral canal and dura)
• Changes in volume of either element (Brain,CSF, Blood) is at the expense of the other two
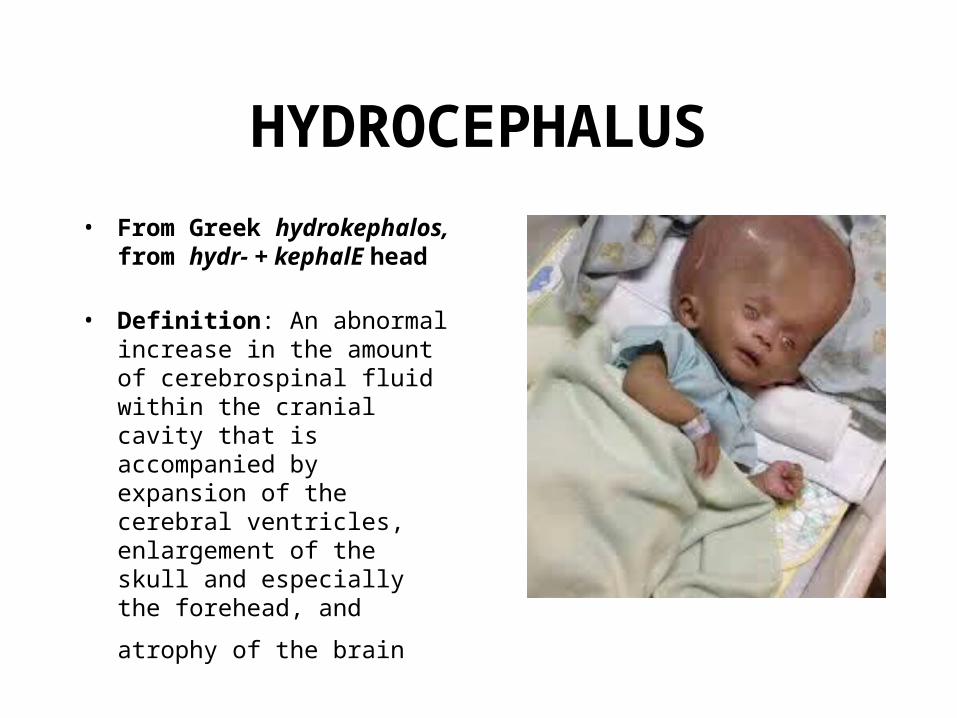
HYDROCEPHALUS• From Greek hydrokephalos,
from hydr- + kephalE head
• Definition: An abnormal increase in the amount of cerebrospinal fluid within the cranial cavity that is accompanied by expansion of the cerebral ventricles, enlargement of the skull and especially the forehead, and atrophy of the brain
Hidrosefalus•Penyebab :1. Peningkatan produksi LCS : sering2. Penurunan reabsorpsi LCS : jarang, misalnya pada tumor
pada plexus choroideus3. Obstruksi aliran keluar LCS
•Peningkatan volume LCS menyebabkan pelebaran ventrikel dan peningkatan tekanan intrakranial•Bila hidrosefalus terjadi sebelum masa penutupan sutura cranium, maka terjadi pelebaran lingkar kepala•Hidrosefalus yang terjadi setelah penutupan sutura cranium : pelebaran ventrikel otak dan peningkatan tekanan intrakranial tanpa pembesaran lingkar kepala
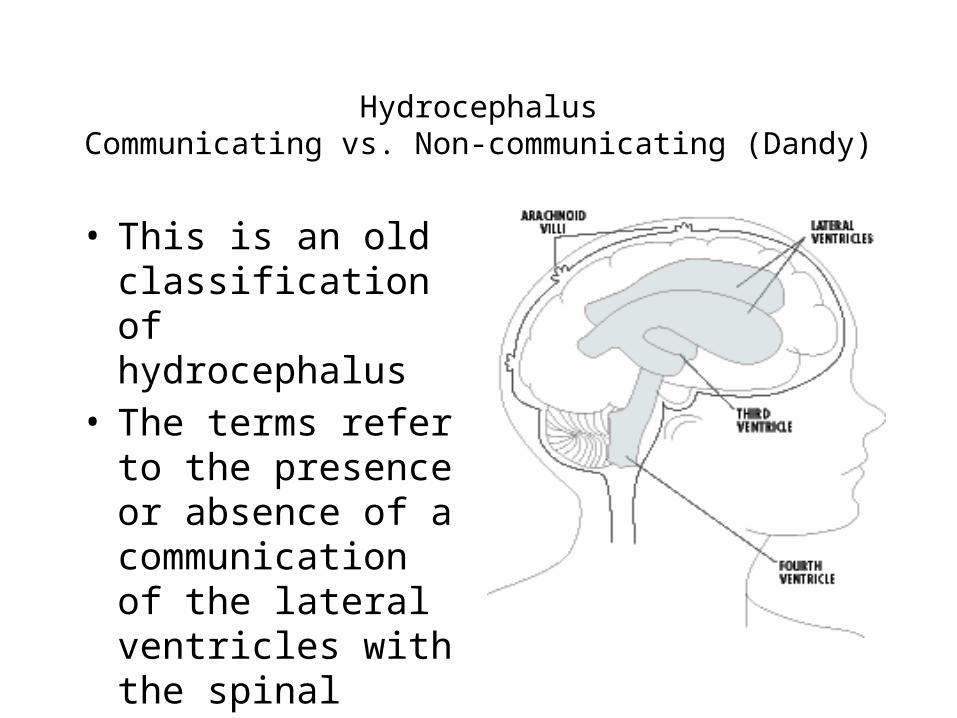
HydrocephalusCommunicating vs. Non-communicating (Dandy)
• This is an old classification of hydrocephalus
• The terms refer to the presence or absence of a communication of the lateral ventricles with the spinal subarachnoid space
Non-communicating hydrocephalus
•There is no communication between the ventricular system and the subarachnoid space. The commonest cause of this category is aqueduct blockage or stenosis.
Communicating hydrocephalus
• In communicating or non-obstructive hydrocephalus there is communication between the ventricular system and the subarachnoid space
• Obstruksi terjadi diluar sistem ventrikel, misalnya diryang subaarachnoid, atau di arachnoid granulations
• The commonest cause of this group is post-infectious and post-hemorrhagic hydrocephalus
• Terjadi organisasi dari eksudat inflamasi dan darah menyebabkan parut pada arachnoid granulations
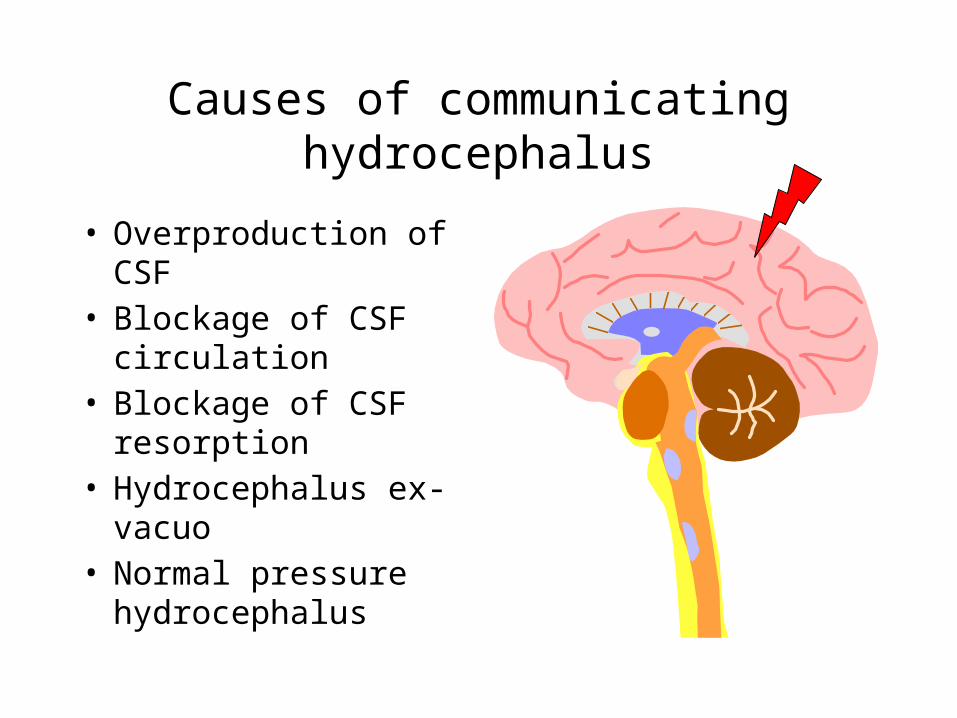
Causes of communicating hydrocephalus
• Overproduction of CSF
• Blockage of CSF circulation
• Blockage of CSF resorption
• Hydrocephalus ex-vacuo
• Normal pressure hydrocephalus
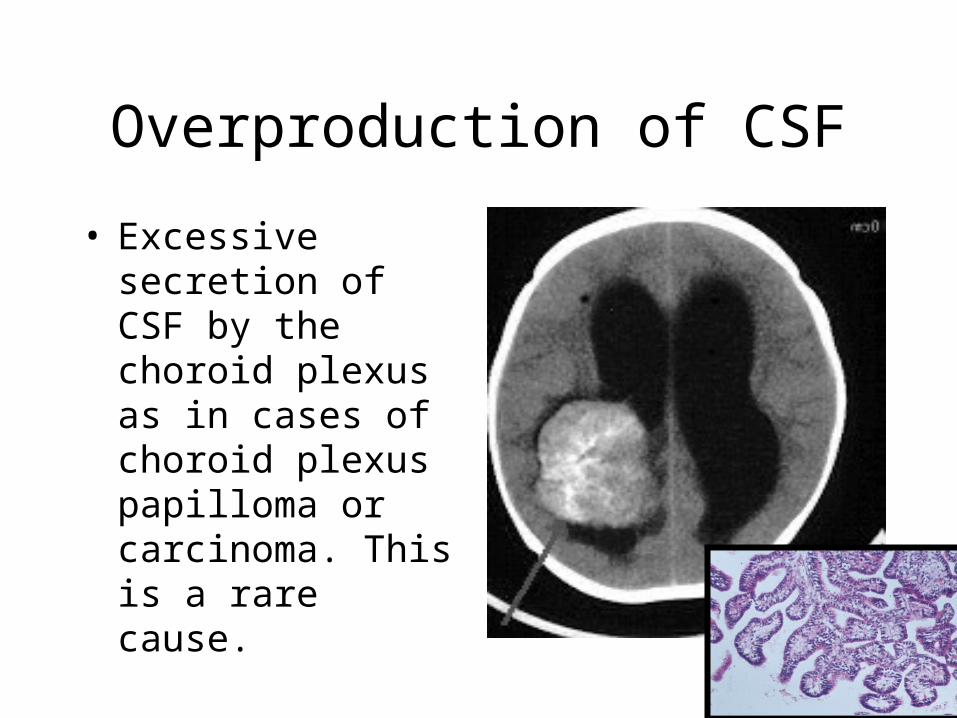
Overproduction of CSF• Excessive secretion of CSF by the choroid plexus as in cases of choroid plexus papilloma or carcinoma. This is a rare cause.
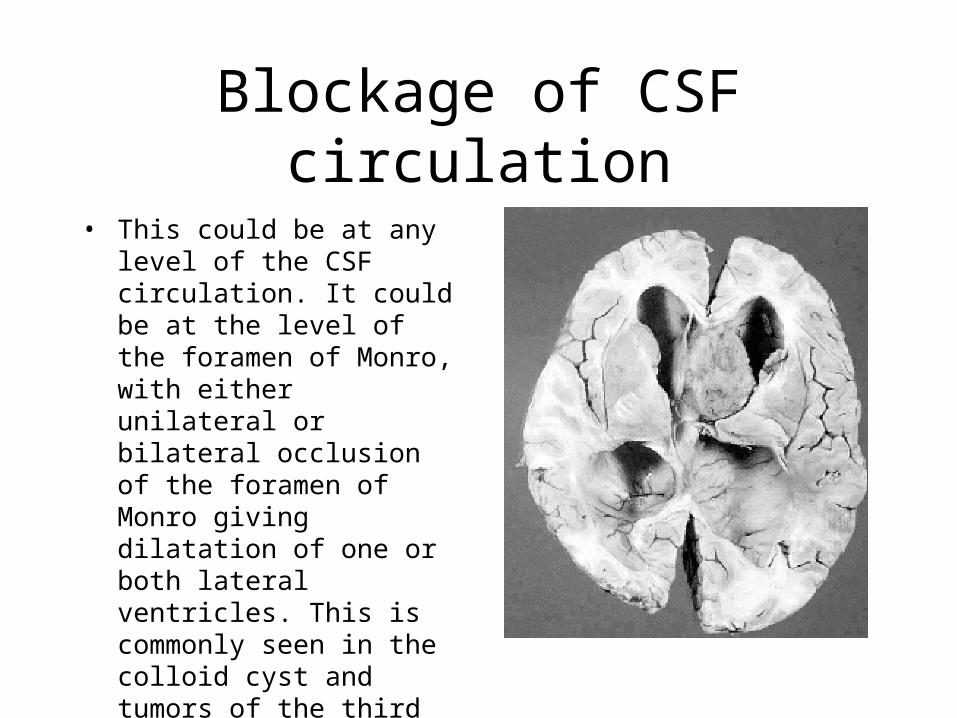
Blockage of CSF circulation
• This could be at any level of the CSF circulation. It could be at the level of the foramen of Monro, with either unilateral or bilateral occlusion of the foramen of Monro giving dilatation of one or both lateral ventricles. This is commonly seen in the colloid cyst and tumors of the third ventricle.
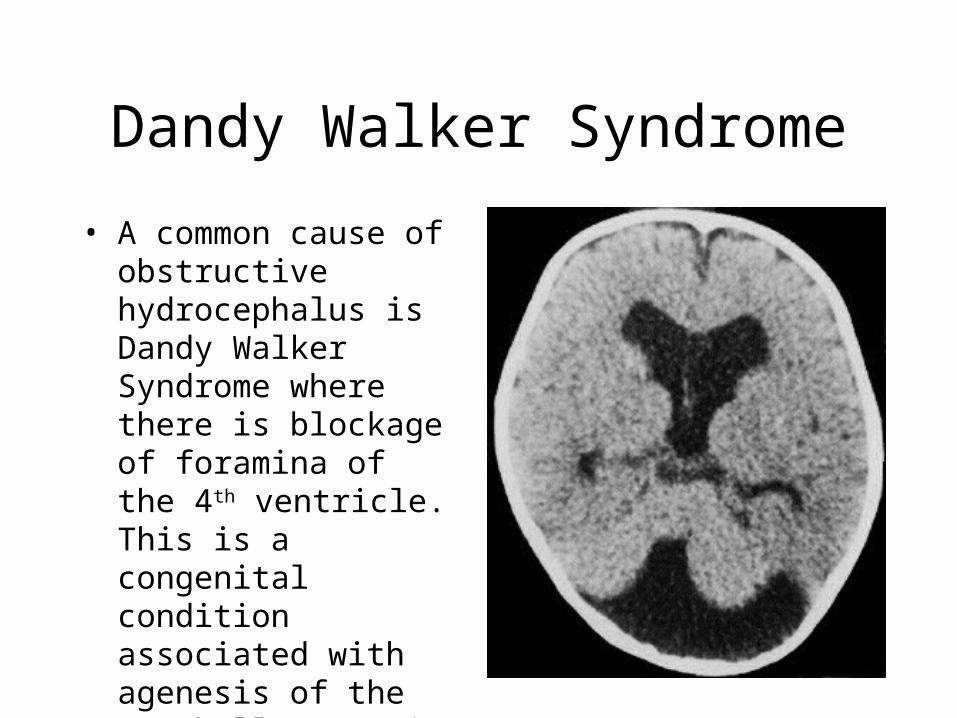
Dandy Walker Syndrome• A common cause of obstructive hydrocephalus is Dandy Walker Syndrome where there is blockage of foramina of the 4th ventricle. This is a congenital condition associated with agenesis of the cerebellar vermis
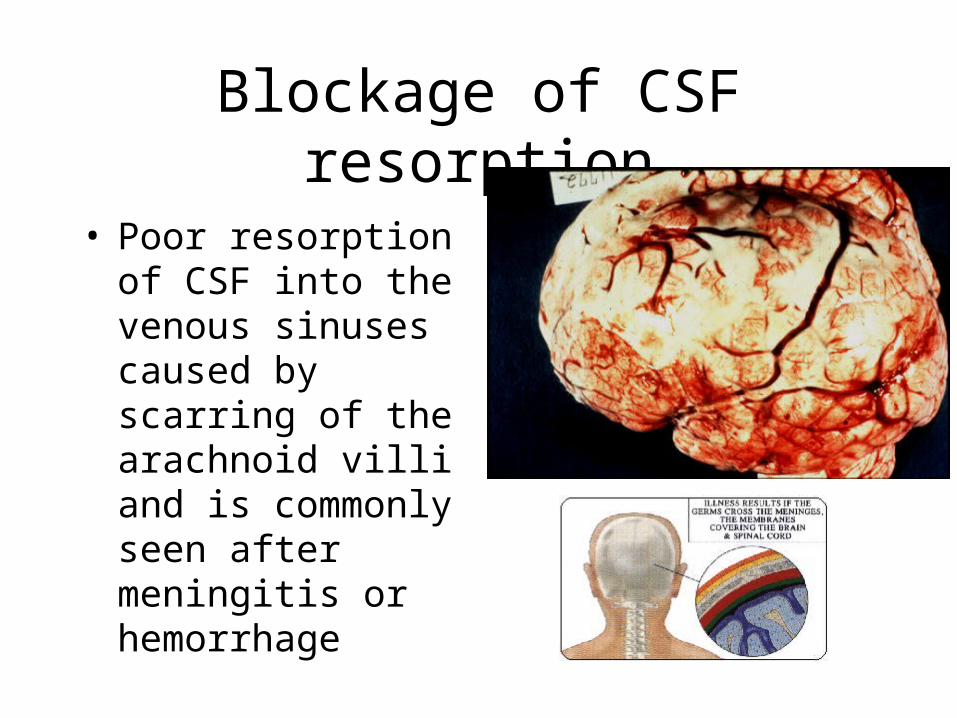
Blockage of CSF resorption
• Poor resorption of CSF into the venous sinuses caused by scarring of the arachnoid villi and is commonly seen after meningitis or hemorrhage
Treatment of hydrocephalus
• The two most commonly used shunt systems are the ventriculoatrial (VA) and ventriculoperitoneal (VP) shunts. The VP shunt is most commonly used as it is simpler to place, extra tubing may be placed in the peritoneum and the consequences of infection are less.

KELAINAN KONGENITAL• Neural Tube Defect• Kelainan terkait Hidrosefalus• Neurocutaneus syndrome
Neural Tube Defects• Otak dan Medula Spinalis berasal dari lapisan ektoderm yang berproliferasi dan diferensiasi membentuk neural tube
• Penutupan neural tube dimulai pada hari ke-28 gestasi s/d hari ke 26-28
• Kelainan kongenital terkait penutupan neural tube (otak dan atau medula spinalis) Neural tube defects
• Contoh : anencephali, cranial meningocele dan encephalocele, berbagai bentuk spina bifida
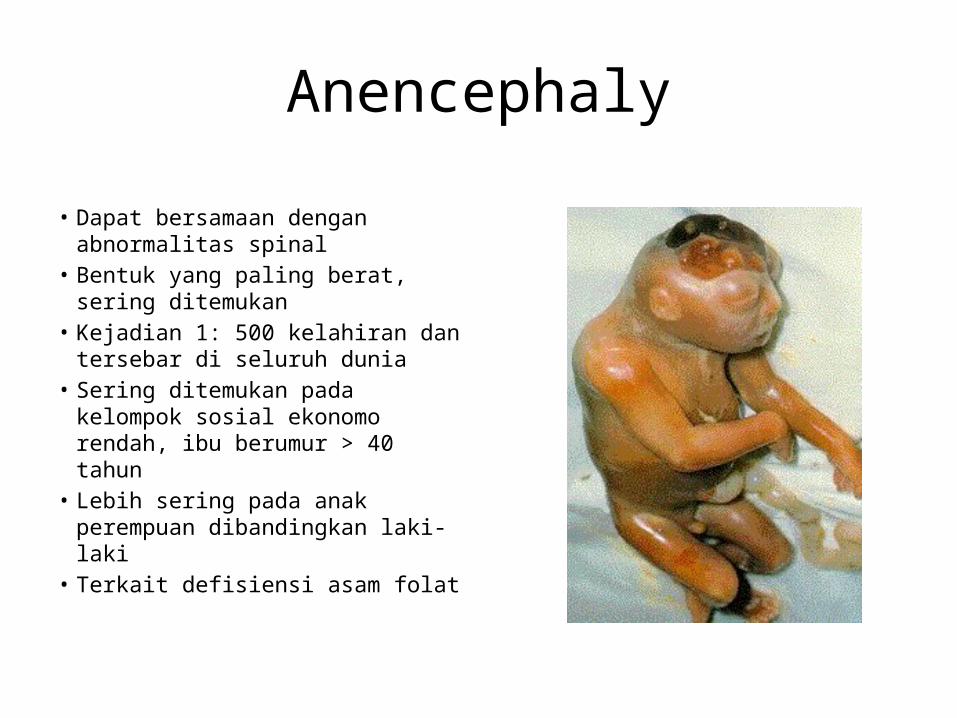
Anencephaly• Dapat bersamaan dengan abnormalitas spinal
• Bentuk yang paling berat, sering ditemukan
• Kejadian 1: 500 kelahiran dan tersebar di seluruh dunia
• Sering ditemukan pada kelompok sosial ekonomo rendah, ibu berumur > 40 tahun
• Lebih sering pada anak perempuan dibandingkan laki-laki
• Terkait defisiensi asam folat
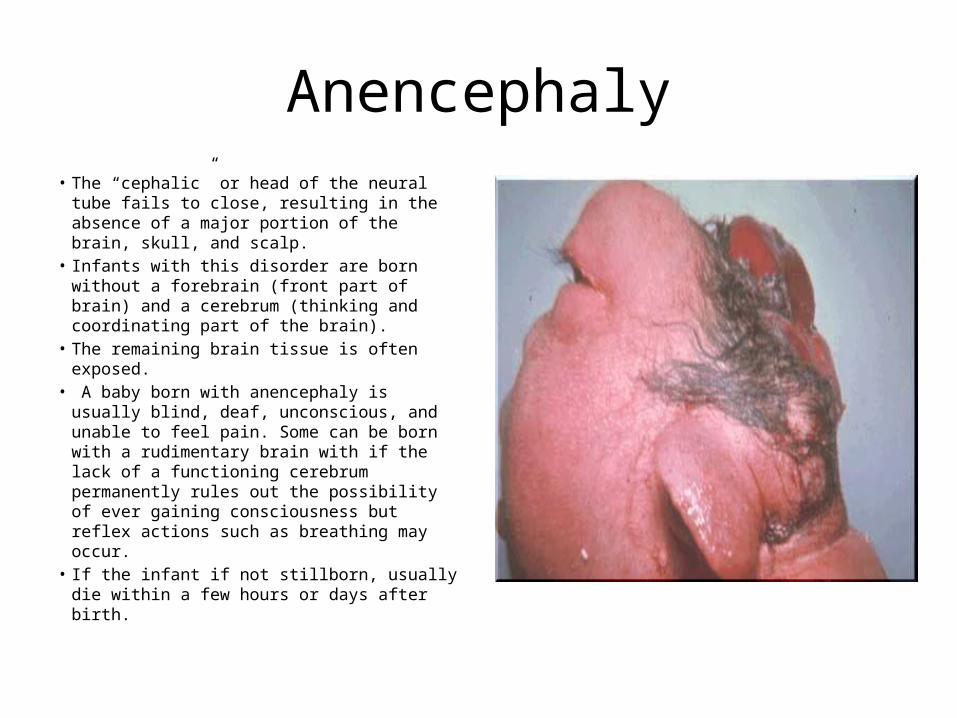
Anencephaly• The “cephalic” or head of the neural tube fails to close, resulting in the absence of a major portion of the brain, skull, and scalp.
• Infants with this disorder are born without a forebrain (front part of brain) and a cerebrum (thinking and coordinating part of the brain).
• The remaining brain tissue is often exposed.
• A baby born with anencephaly is usually blind, deaf, unconscious, and unable to feel pain. Some can be born with a rudimentary brain with if the lack of a functioning cerebrum permanently rules out the possibility of ever gaining consciousness but reflex actions such as breathing may occur.
• If the infant if not stillborn, usually die within a few hours or days after birth.
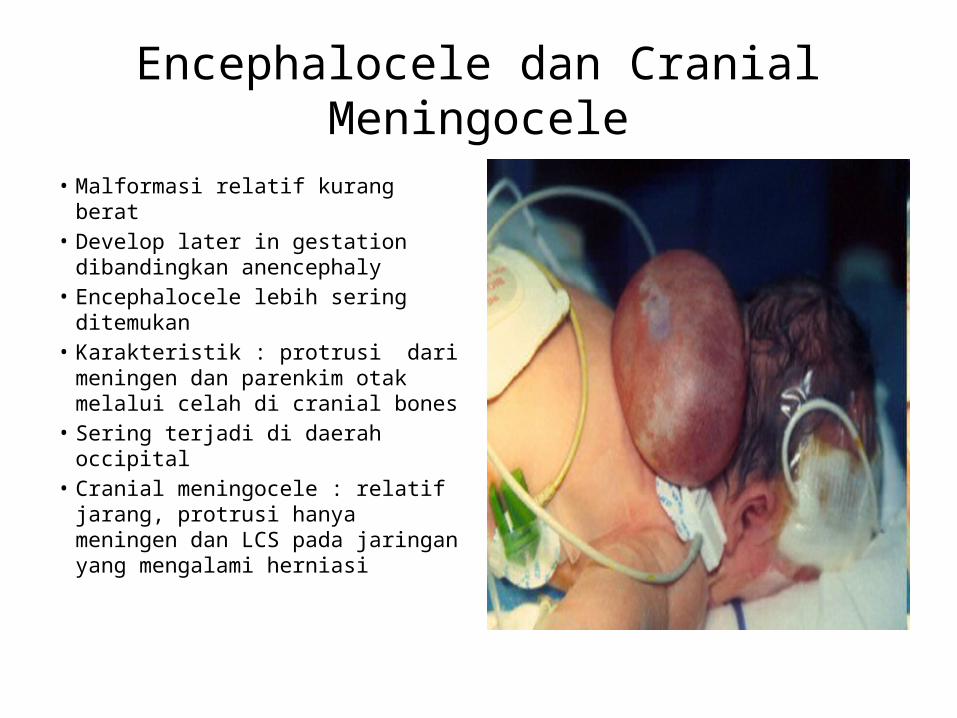
Encephalocele dan Cranial Meningocele
• Malformasi relatif kurang berat
• Develop later in gestation dibandingkan anencephaly
• Encephalocele lebih sering ditemukan
• Karakteristik : protrusi dari meningen dan parenkim otak melalui celah di cranial bones
• Sering terjadi di daerah occipital
• Cranial meningocele : relatif jarang, protrusi hanya meningen dan LCS pada jaringan yang mengalami herniasi

Spina Bifida• Spina Bifida: “Split spine”
• Dapat terjadi pada semua segmen spinal
• Paling sering di regio lumbosacral
• Tidak adanya/hipoplasia dari satu atau lebih arcus vertebral dengan berbagai abnormalitas pada meningen dan atau medulla spinalis
TIPE :
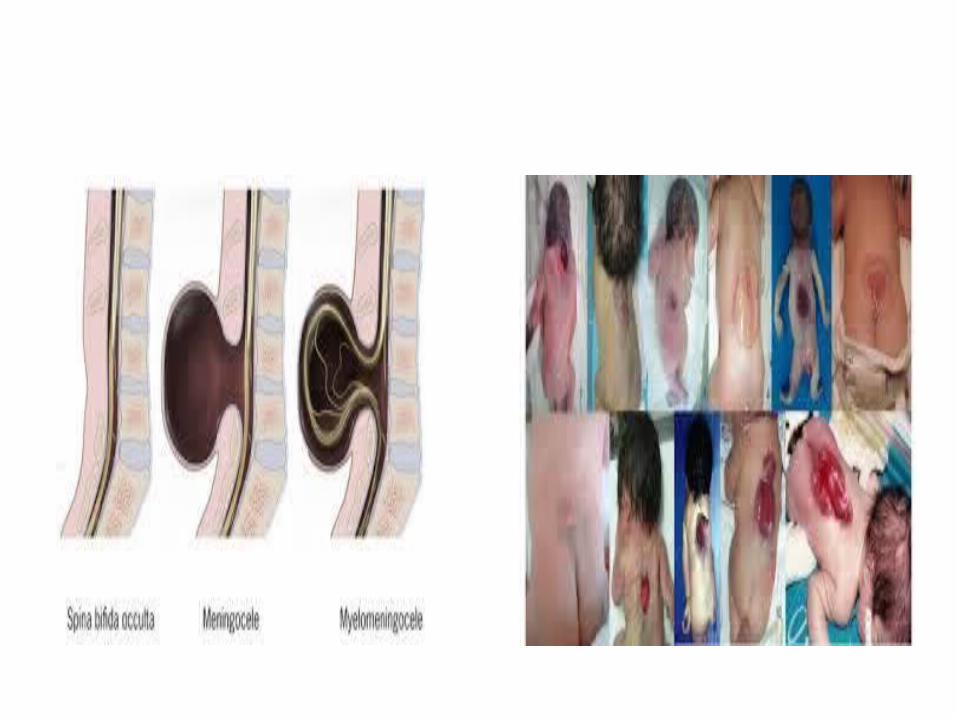
• Spina Bifida Aperta/Occulta Osseous fusion of one or more vertebral arches is lacking, without involvement of the underlying meninges or neural tissue
• Spina Bifida Cystica Sac like casing is filled with cerebrospinal fluid (CSF), spinal cord, and nerve roots that have herniated through a posterior defect in the vertebral arches and duramater spinal
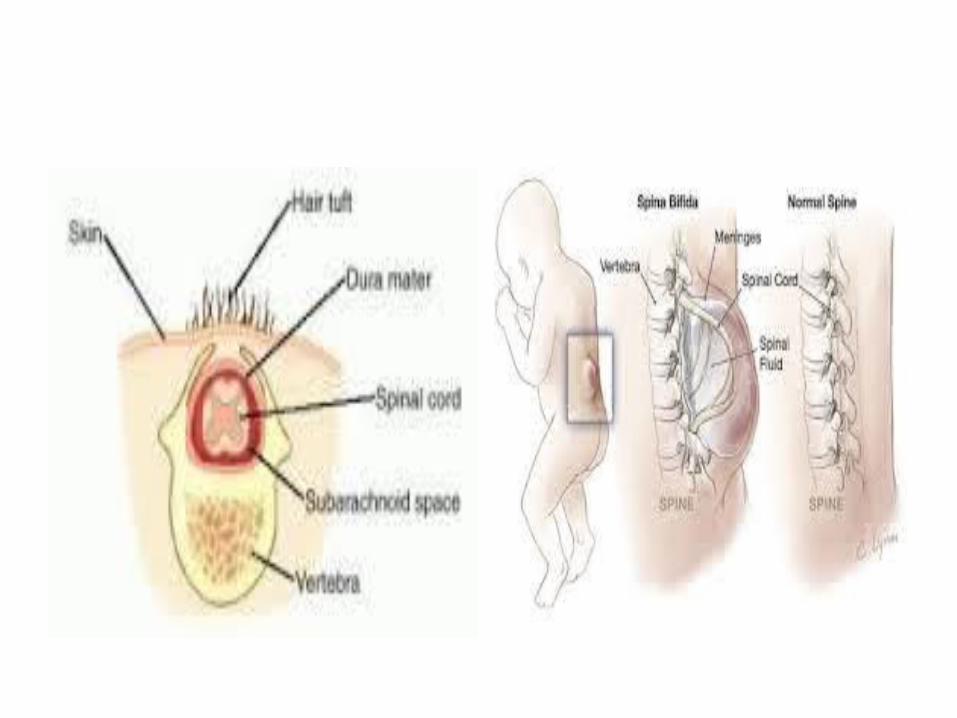
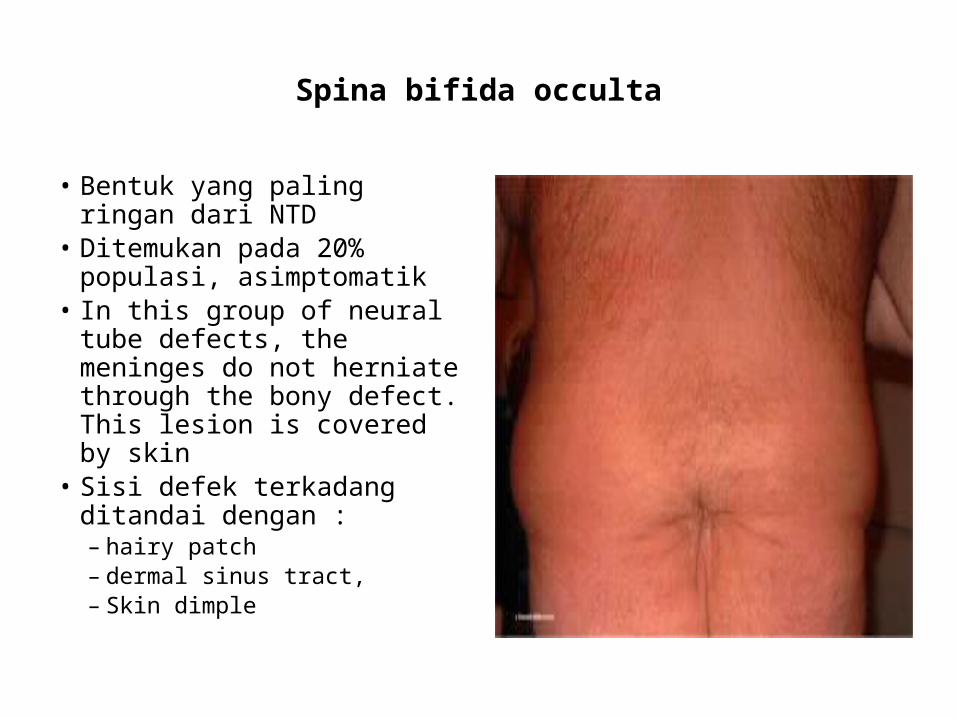
Spina bifida occulta
• Bentuk yang paling ringan dari NTD
• Ditemukan pada 20% populasi, asimptomatik
• In this group of neural tube defects, the meninges do not herniate through the bony defect. This lesion is covered by skin
• Sisi defek terkadang ditandai dengan :– hairy patch– dermal sinus tract,– Skin dimple

Spina bifida cysticamyelomeningoceles meningoceles
Cervical and thoracic regions are the least common sites, and lumbar and lumbosacral regions are the most common sites for these lesions
Malformasi Terkait Hidrosefalus
Arnold Chiari-Malformation
• Pendangkalan abnormal fossa cranium posterior dikarenakan caudal extension dari medulla oblongata, vermis serebelum sampai dengan foramen magnum
• Batang Otak bawah menjadi elongasi dan terkompresi, dengan herniasi sedikit, parenkim gliotik serebelum melapisi sisi dorsal dari medulla
• Aquaductus serebelum stenosis, bagian dorsal otak tengah malformasi
• Sering bersamaan dengan hidrosefalus
Dandy-Walker Malformation
• Aplasia/hipoplasia dari vermis cerebellum
• Terjadi dilatasi “balloon-like “ pada ventrikel empat dan pelebaran fossa posterior
• Lesi ini bersamaan dengan terjadinya hidrosefalus
• Abnormalitas lainnya seperti : agenesis corpus callosum, occipital meningocele, lesi terkait abnormalitas migrasi neuron selama embriogenesis
Chiari Malformation
• The deformity consists of displacement of the cerebellar tonsils into the cervical canal.
Consists of two major subgroups:1.Type I
• Produces symptoms during adolescence or adult life and is usually not associated with hydrocephalus.
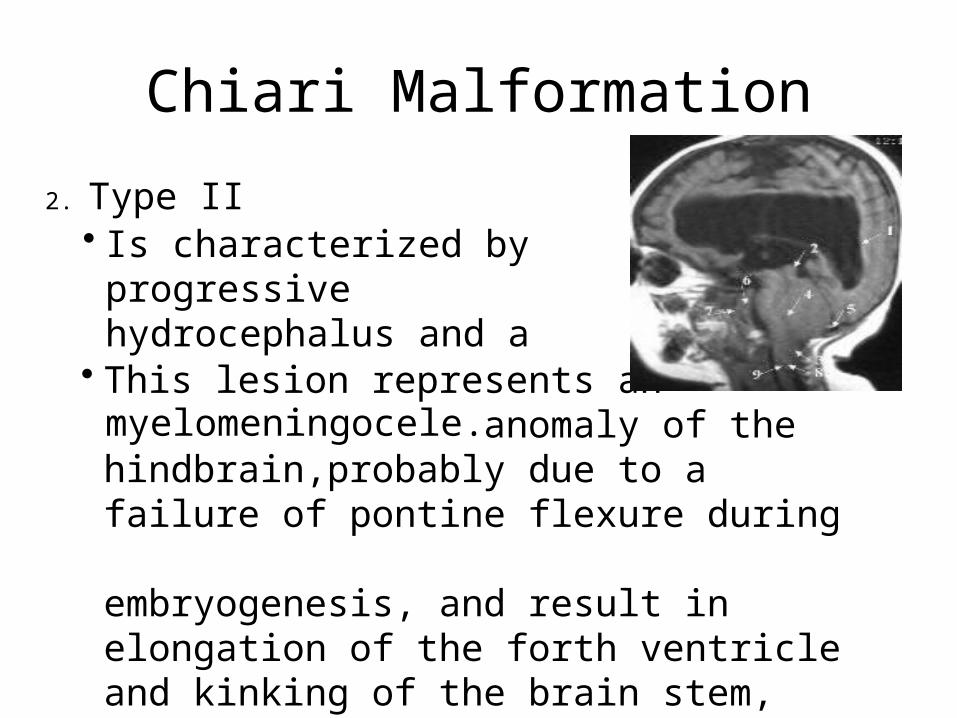
Chiari Malformation
• This lesion represents an anomaly of the hindbrain,probably due to a failure of pontine flexure during embryogenesis, and result in elongation of the forth ventricle and kinking of the brain stem, with displacement of the inferior vermis, pons, and medulla into the cervical canal.
2. Type II• Is characterized by progressive hydrocephalus and a myelomeningocele.
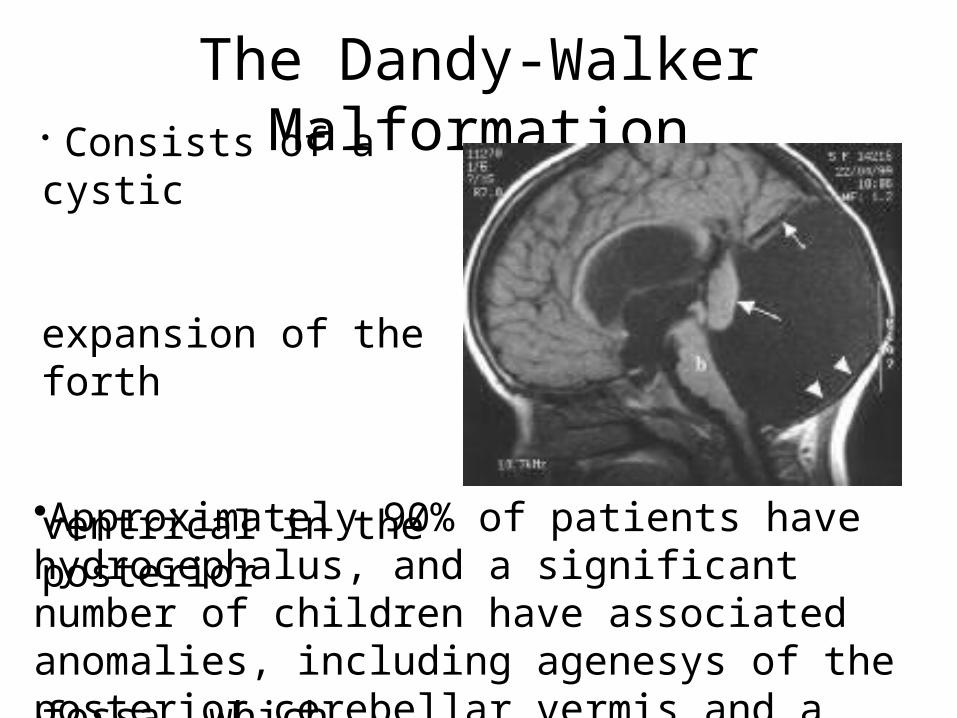
The Dandy-Walker Malformation
•Approximately 90% of patients have hydrocephalus, and a significant number of children have associated anomalies, including agenesys of the posterior cerebellar vermis and a corpus callosum.
• Consists of a cystic expansion of the forth ventrical in the posterior fossa, which results from a developmental failure of the roof of the forth ventrical during embryogenesis .
Infeksi pada Sistem Saraf
• Rute penyebaran: hematogen, implantasi langsung, malformasi kongenital, perluasan infeksi lokal struktur didekatnya (infeksi telinga tengah, sinusitis), penyebaran dari saraf perifer (rabies)
• Meningitis (leptomeningitis) : inflamasi dari leptomeningen dan rongga subarachnoid
• Meningitis : akut purulenta (bakteria), akut limfositik (virus) dan meningitis kronis
Meningitis Akut Purulen• Penyebab tersering : bakteri terutama dari nasofaring
• Etiologi :– Neonatus : Streptococcus group B, Escherichia coli
– Anak > 6 bulan : Haemophillus influenzae, streptococcus pneumonia
– Young adult, dewasa : Neisseria meningitidis– Dewasa tua : S. pneumonia– Pasien immunokompromise : Listeria monocytogenes– Staphylococcus aureus dan batang gram negatif patogen setelah tindakan VP shunt
Meningitis Akut Purulen• Morfologi otak :
– Makros : kongesti pada meningen, eksudat pada rongga subarachnoid
– Mikros : kongesti, netrofil >>, fibrin• Gejala klinis ;
– Demam, nyeri kepala, kaku kuduk, perubahan status mental
– CSF dominasi netrofil, kadar protein meningkat, kadar glukosa menurun
– Tampak bakteri pada pewarnaan gram
Meningitis Akut Limfositik
• Disebut juga aseptik meningitis, self limited disease, prognosis baik
• Agen utama : echovirus, coxsackie virus, mumps virus, dab HIV
• Klinis mirip dengan meningitis bakterial, tapi lebih ringan.
• CSF predominan limfosit, protein meningkat, glukosa normal
Meningitis Kronik• Penyebabnya : bakteri dan jamur• Mycobacterium tuberkulosa, Cryptococcus neoforman, Brucella spesies dan Treponema pallidum
• Meningitis kriptococcus terutama ditemukan pada pasien HIV
• Klinis : nyeri kepala, kaku kuduk dan tanda rangsang meningeal lainnya
Encephalitis• Infeksi pada parenkim otak• Abses otak : staphylococcus dan streptococcus
– Penyebaran infeksi ke otak : hematogen, contigous spread from adjacent foci (sinusitis, OMSK), direct implantation during trauma.
– Penyebab hematogen : endokarditis bakteria, abses paru, bronkiektasis
– Klinis : demam, TIK meningkat, defisit neurologi fokal
– CSF : normal glukosa, protein meningkat, sedikit cell
– Komplikasi : pecah abses ke ruang ventrikel, subarachnoid, herniasi otak
Encephalitis• Tuberculosis dan Toxoplasmosis
Pada tuberculosis : asal bakteri dari lesi paru aktif
– Tuberculoma : nodul kecil, single atau multipel dengan nekrosis kaseosa sentral
Pada toxoplasma : Toxoplasma gondii, area nekrosiss dengan sel mononuklear
• Encephalitis viral
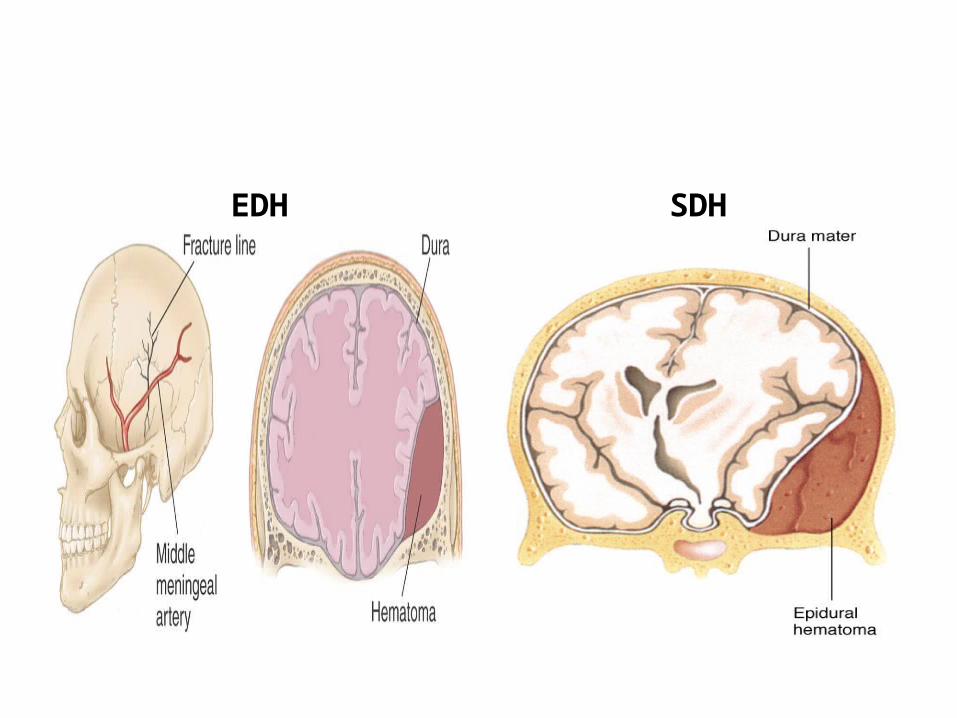
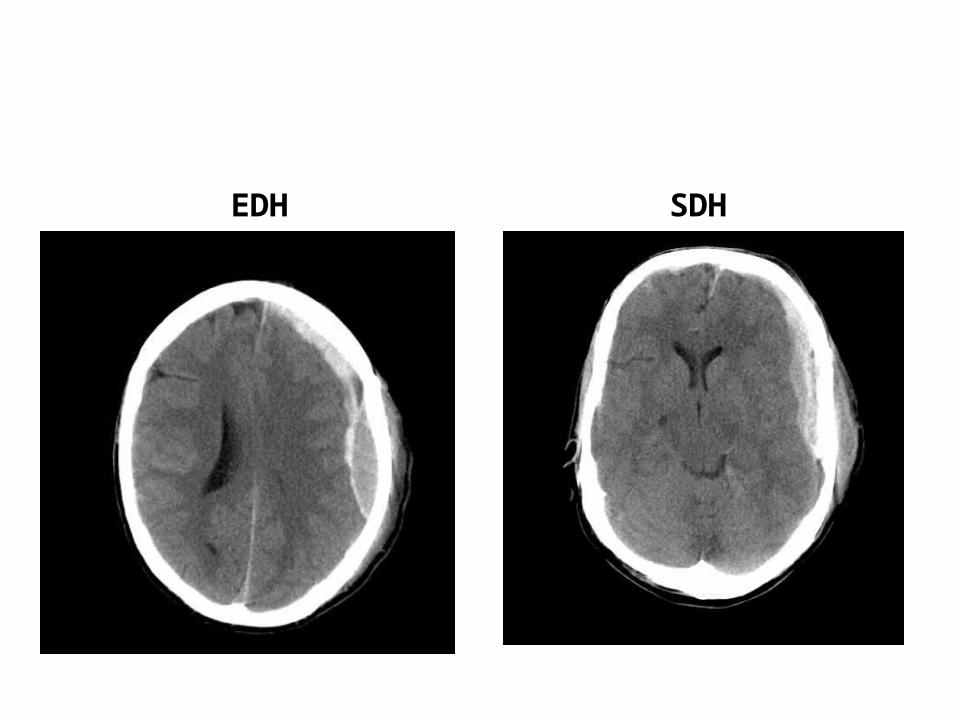
Trauma/ Cedera KepalaEpidural Hematoma :
– Ruptur a. meningea media akibat fraktur tengkorak (temporal) dikarenakan arteri melekat pada periosteum tulang temporal
– EDH mengkompresi duramater dan flatten the gyral crests of underlying brain
– Bila tidak di evakuasi : herniasi gyrus uncal dan tonsiler serebellar, kompresi batang otak dan kematian
– Biasanya ditemukan “Lucid Interval” ; penurunan kesadaran setelah trauma, kemudian hilang kesadaran kembali akibat pelebaran hematoma, edema cerebri
Trauma/ Cedera Kepala• Subdural Hematoma :
– Darah terkumpul pada rongga subdural (duramater dan arachoid mater)
– Robeknya bridging veins dari permukaan otak ke dural sinus
– Paling sering di daerah frontotemporal– Pada SDH, darah terkumpul pada sulcus dan gyrus sehingga tekanan terdistribusi merata
– Perdarahan vena, sehingga lebih lambat dibandingkan EDH
EDH SDH
EDH SDH
Trauma/ Cedera Kepala• Traumatic Parenchymal Injuries
– Terbagi menjadi : concussio, contusio dan laserasi, diffuse axonal injury, traumatic intracerebral hemorrhage dan edema cerebri
– Concussio : hilangnya kesadaran sementara, paralisis, terkadang disertai kejang, sembuh setelah beberapa jam sampai hari, sembuh tanpa sequelae, tanpa amnesia tentang kejadian.
– Diffuse axonal Injury : penyebab demensia post traumatik, hipoxic-ischemic injury, vegetatif state.
Trauma/ Cedera Kepala• Contusio : perdarahan pada permukaan superficial parenkim otak akibat trauma tumpul
• Coup-contusion : hemoragi pada area tepat dibawah area terkena ruda paksa
• Contrecoup contusion : hemoragi pada sisi berseberangan area ruda paksa
Vascular Disease• Otak menerima 15% cardiac output, mengkonsumsi 20% oksigen tubuh
• Berhentinya aliran darah ke otak dan medula spinalis akan menyebabkan jejas sel irreversibel dalam hitungan menit
• Autoregulasi : menjaga suplai O2 dan nutrisi• Cerebrovascular disease terbagi tiga :
– Jejas parenkim yang diakibatkan penurunan aliran darah, termasuk global hipoxic-ischemic encephalopathy
– Infarct yang disebabkan obstuksi vascular– Hemorrhages dalam parenkim otak atau rongga subarachnoid
Global Hypoxic-Ischemic Encephalopathy
• Tekanan darah naik, terjadi vasokontriksi pembuluh darah otak dan sebaliknya
• Bila TD< 50mmHg mekanisme autoregulasi tidak mampu mengkompensasipenurunan aliran darah injury pada parenkim otak
• Hypoxia O2 turun• Iskemia perfusi darah ke jaringan turun• Sel neuron lebih sensitif terhadap iskemia dibandingkan sel glia
• Sel piramidal di hipocampus, sel purkinje di cerebellum dan neuron di globus pallidus dari ganglia basal paling sensitif
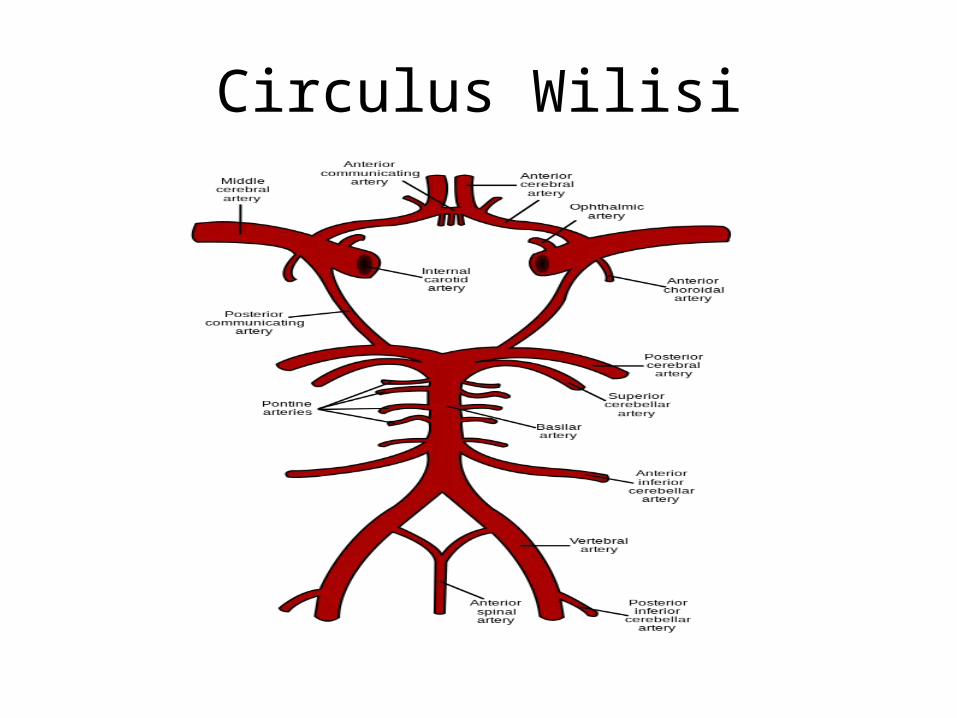
Circulus Wilisi
Global Hypoxic-Ischemic Encephalopathy
• Etiologi :– Disritmia jantung– Shock– Peningkatan TIK
• Faktor-faktor yang menentukan beratnya jejas parenkim :– Usia : dewasa muda lebih mampu mentoleransi dibandingkan orang tua
– Lamanya gangguan sirkulasi– Suhu(hipotermia meningkatkan resistensi dan sebaliknya)
Infark Cerebri• Penyebab infark : terhentinya aliran darah dikarenakan penyakit cerebrovascular (stroke)
• Atherosklerosis cerebral dan faktor predisposisinya (hipertensi, DM dan merokok)
• Trombosis segmen arteri yang atherosklerosis, emboli (dari jantung atau plak atherosklerotik)
Infark Cerebri• Terjadi tiba-tiba, defisit neurologis:
– beberapa menit s/d 24 jam TIA (transient ischemic attck). Episode self-limited obstruksi akibat emboli atheromatous dan atau agregasi platelet-fibrin.
– I/3 pasien TIA akan mengalami infarct dalam 5 tahun
• Defisit neurologis tergantung pada daerah dan luasnya infark
• Dapat terjadi edema disekitar lokasi infark yang memperberat defisit neurologis
• Pada kasus infark luas efek massa dan herniasi otak
Infark Cerebri• Infark paling paling sering terjadi pada area yang disuplai oleh percabangan a.cerebri media (tersering akibat emboli)
• Manifestasi klinis:– Hemiparesis kontralateral– Spastisitas– Hilangnya sensorik kontralateral– Gangguan lapang pandang– Aphasia
Infark Cerebri• Infark akibat oklusi a.carotis interna (trombosis) jarang
• Manifestasi klinis :– Infark luas ipsilateral hemisfer cerebral– Kebutaan monookuler sekunder akibat aliran ke a.optalmica hilang
• Atherosklerosis percabangan sistem vertebrobasiler (oklusi trombosis) :– Bisa fatal, mengenai area batang otak– Bisa tidak bergejala
Perdarahan Intrakranial• Perdarahan pada parenkim dapat diakibatkan oleh jejas iskemik (infark), nekrosis jaringan reperfusi
• Pasien dengan terapi antikoagulan• Pasien dengan infark akibat oklusi vena• Perdarahan primer pada rongga epidural dan subdural biasanya disebabkan oleh trauma
• Perdarahan primer pada parenkim otak dan rongga subarachnoid disebabkan oleh penyakit cerebrovascular
Perdarahan Primer pada Parenkim Otak
• Terjadi pada usia 60 tahun, paling sering akibat pecahnya pembuluh darah kecil intraparenkimal
• Hipertensi paling sering (>50%)• Perdarahan intrakranial merupakan salah satu penyebab kematian pada pasien hipertensi (15%)
• Hipertensi menyebabkan kelainan dinding pembuluh darah; aterosklerosis pembuluh darah besar, hyaline aterosklerosis pada pembuluh darah kecil, perubahan proliferatif dan nekrosis pada arteriol
• Hipertensi menyebabkan terjadinya aneurisma Charcot-Bouchard Microaneurysms (pembuluh darah kecil, terutama area ganglia basal)
Perdarahan Primer pada Parenkim Otak
• Peningkatan tekanan intrakranial :– Nyeri kepala hebat– Muntah-muntah– Hilang kesadaran– Bila progresif : kompresi batang otak, koma dalam, nafas Cheyne-Stokes, pupil dilatasi dan unrespon dan spastisitas
Perdarahan Subarachnoid• Penyebab tersering : ruptur saccular aneurysm (Berry Aneurysm).
• 1% populasi• 80% saccular aneurysm berasal dari percabangan a.carotis interna
• Penyebab aneurisma : – kongenital, defek pada tunica media arteri– Didapat, lesi degeneratif, terkait jejas hemodinamik pada dinding pembuluh darah
• Resiko ruptur aneurisma : ukuran 6-10mm• >25mm: giant aneurisma
Perdarahan Subarachnoid• Wanita lebih sering, sebelum usia 50 tahun
• Gejala klinis sama dengan perdarahan intraparenkimal
• Lainnya : tanda rangsang meningeal(kaku kuduk)
• LCS mengandung darah• 50% meninggal dalam bebebapa hari• Resiko lainnya: infark serebral setelah beberapa hari (4-9 hari), akut/kronik hidrosefalus, dan herniasi
Kepustakaan1.Vinay Kumar, Ramzi S.Cotran,
Stanley L.Robbins. Nervus System. In Robbins Basic Pathology. 7th ed. Philadelphia: Saunders; 2003. p. 79-102.
Ada Pertanyaan ???