
tugas PA.291014
8
ORIGINAL ARTIC LE Posaconazole versus fluconazole or itraconazole for prevention of invasive fungal infections in patients undergoing intensive cytotoxic therapy for acute myeloid leukemia or myelodysplasia: a cost effectiveness analysis George Dranitsaris & Haytham Khoury Received: 26 July 2010 /Accepted: 4 October 2010 /Published online: 23 October 2010 # Springer-Verlag 2010 Abstract Introduct ion Invasi ve fungal infect ions (IFI) remain a clinical concern in hematological patients with prolonged neutropenia because they are a major cause of morbidity and mortality. In a recent randomized trial, prophylaxis with posaconazole was associated with fewer IFI and related death s relat ive to a fluco nazole or itrac onazo le (Flu/ Itra) cont rol gr oup ( p <0.001) . In the current st udy , a cost effectiveness anal ysi s was conduct ed to est imate the economic value of posaconazole as an alternative to Flu/ Itra when used to prevent IFI in this patient population. Methods A decision analysis model was developed using clinical and economic data from randomized comparative trials, the economic literature, and from expert opinion. The data were then used to estimate the incremental cost per life year saved with oral posaconazole prophylaxis relative to Flu/Itra from the Canadian provinci al healt h care system perspective. The base case results were then tested with a sensit ivity analysis which evaluate d ext remes in the incidence of IFI as we ll as variations in their cost of management. Results Prophylaxis with posaconazole provides increased ef fi cacy and an overa ll cost savi ngs of app roxi mate ly $Can4,259 per patient. Despite variations in the base case parameters, the sensitivity analysis suggested stability in the primary findings. Posaconazole was associated with an overal l cost savin gs (range=$Can1,765 to $Can 4,505) in all of the scenar ios evalu ated. Optimal cost effect iven ess was obtained because the drug was able to avoid the more resource intensive Aspergillus infections. Conclusions Prophyl axis wit h posa cona zol e in cancer patients with prolong ed neutrop enia is not only cost effective but also cost saving. The economic benefits were due to the drug’s ability to reduce the incidence of high cost fungal infections, particularly Aspergillus species. Keywords Posaconazole . Fluconazole . Itraconazole . Prophylaxis . Invasive fungal infections . Cost analysis Introduction Pati ents recei ving int ensiv e cytot oxic thera py for acut e myel ogen ous leukemia (AML) or myel odys plast ic syn- drome (MDS) suf ficient to produc e severe (absol ute neutrophil count <0.5×10 9 /L) and prol onged (>7 to 10 days) neutropen ia are at increased risk for invasive fungal infec tions (IFI) [ 1,2]. The ris k for opport uni sti c yeast infections is associated wit h intestinal mucosal colonization and cytot oxic therapy-induced intestinal mucosal dama ge leading to trans loca tion and syst emic infec tion [3,4]. Risk fact ors for inv asiv e mold infections inc lud e the dur at ion of severe neutro pen ia , expos ure to increased inocula of airborne conidia due to environmental disruption prior to and during treatment, increased iron stores, treatmen t with corticostero ids, high dose cytosine arabino- side, a myel ody spl asia state before AML, and adva nced underlyi ng disease [5 – 8]. IFI is susp ect ed in the set tin g of a pers ist ent o r rec rude sce nt neutropenic fever syndrome unresponsive to the administra- G. Dranits aris : H. Khoury Princess Margaret Hospital, Toronto, ON, Canada G. Dranits aris (*) Health Economics and Biosta tistics , 283 Danforth Avenue, Suite 448, Toronto, ON M4K 1N1, Canada e-mail: [email protected] Suppor t Care Cancer (201 1) 19:1807 –1813 DOI 10.1007/s00520-010-1022-7
Transcript of tugas PA.291014

8/9/2019 tugas PA.291014
http://slidepdf.com/reader/full/tugas-pa291014 1/8
ORIGINAL ARTICLE
Posaconazole versus fluconazole or itraconazole
for prevention of invasive fungal infections in patients
undergoing intensive cytotoxic therapy for acute myeloid
leukemia or myelodysplasia: a cost effectiveness analysis
George Dranitsaris & Haytham Khoury
Received: 26 July 2010 /Accepted: 4 October 2010 /Published online: 23 October 2010# Springer-Verlag 2010
Abstract
Introduction Invasive fungal infections (IFI) remain a clinical concern in hematological patients with prolonged
neutropenia because they are a major cause of morbidity
and mortality. In a recent randomized trial, prophylaxis with
posaconazole was associated with fewer IFI and related
deaths relative to a fluconazole or itraconazole (Flu/Itra)
control group ( p<0.001). In the current study, a cost
effectiveness analysis was conducted to estimate the
economic value of posaconazole as an alternative to Flu/
Itra when used to prevent IFI in this patient population.
Methods A decision analysis model was developed using
clinical and economic data from randomized comparative
trials, the economic literature, and from expert opinion. Thedata were then used to estimate the incremental cost per life
year saved with oral posaconazole prophylaxis relative to
Flu/Itra from the Canadian provincial health care system
perspective. The base case results were then tested with a
sensitivity analysis which evaluated extremes in the
incidence of IFI as well as variations in their cost of
management.
Results Prophylaxis with posaconazole provides increased
efficacy and an overall cost savings of approximately
$Can4,259 per patient. Despite variations in the base case
parameters, the sensitivity analysis suggested stability in the
primary findings. Posaconazole was associated with an
overall cost savings (range=$Can1,765 to $Can4,505) inall of the scenarios evaluated. Optimal cost effectiveness
was obtained because the drug was able to avoid the more
resource intensive Aspergillus infections.
Conclusions Prophylaxis with posaconazole in cancer
patients with prolonged neutropenia is not only cost
effective but also cost saving. The economic benefits were
due to the drug’s ability to reduce the incidence of high cost
fungal infections, particularly Aspergillus species.
Keywords Posaconazole . Fluconazole . Itraconazole .
Prophylaxis . Invasive fungal infections . Cost analysis
Introduction
Patients receiving intensive cytotoxic therapy for acute
myelogenous leukemia (AML) or myelodysplastic syn-
drome (MDS) sufficient to produce severe (absolute
neutrophil count <0.5×109/L) and prolonged (>7 to
10 days) neutropenia are at increased risk for invasive
fungal infections (IFI) [1,2]. The risk for opportunistic
yeast infections is associated with intestinal mucosal
colonization and cytotoxic therapy-induced intestinal
mucosal damage leading to translocation and systemic
infection [3,4]. Risk factors for invasive mold infections
include the duration of severe neutropenia, exposure to
increased inocula of airborne conidia due to environmental
disruption prior to and during treatment, increased iron stores,
treatment with corticosteroids, high dose cytosine arabino-
side, a myelodysplasia state before AML, and advanced
underlying disease [5 – 8].
IFI is suspected in the setting of a persistent or recrudescent
neutropenic fever syndrome unresponsive to the administra-
G. Dranitsaris : H. Khoury
Princess Margaret Hospital,
Toronto, ON, Canada
G. Dranitsaris (*)
Health Economics and Biostatistics,
283 Danforth Avenue, Suite 448,
Toronto, ON M4K 1N1, Canada
e-mail: [email protected]
Support Care Cancer (2011) 19:1807–1813
DOI 10.1007/s00520-010-1022-7
8/9/2019 tugas PA.291014
http://slidepdf.com/reader/full/tugas-pa291014 2/8
tion of broad-spectrum antibacterial therapy over 4 – 7 days [9].
This risk is significantly higher during remission-induction or
salvage re-induction therapy compared to post-remission
consolidation. Anti-fungal prophylaxis may reduce the event
rates for IFI and the need for empirical anti-fungal therapy
[10,11]. The possible outcomes for anti-fungal prophylaxis
include a breakthrough IFI, an unexplained persistent
neutropenic syndrome, an adverse drug reaction that mayrequire discontinuance, and prophylaxis success defined by
avoidance of IFI or the need to administer systemic anti-
fungal therapy [12,13].
The agents that are used for anti-fungal prophylaxis
include posaconazole, micafungin, fluconazole, and intra-
conazole. Micafungin is only in an intravenous formula-
tion and is impractical for all patients. Posaconazole is
available at a higher drug acquisition cost relative to
fluconazole and intraconazole. All of these three agents
are available in an orally administered suspension.
Economic value is the ability of a drug to avoid down
stream health care costs. In the face of increasing drugexpenditures, comparative economic data to identify
which agent provides optimal economic value would be
of benefit to drug formulary committees. In this study, a
cost effectiveness analysis was conducted to measure the
economic value of mold-active posaconazole as an
alternative to fluconazole or itraconazole when used to
prevent IFI in patients with AML or MDS undergoing
intensive chemotherapy.
Methods
Decision model
The target patient population focused upon those receiving
intensive induction or re-induction cytotoxic therapy for AML
or MDS. Using the commercially available DATA™ software
program, we created a decision analysis model representingthe clinical outcomes and the economic consequences of
prophylaxis with oral posaconazole compared to fluconazole
or itraconazole. Since fluconazole is the primary alternative
used in Canada, it was the comparator in the base case
analysis. The face and content validity of the model was then
evaluated by an infectious disease specialist.
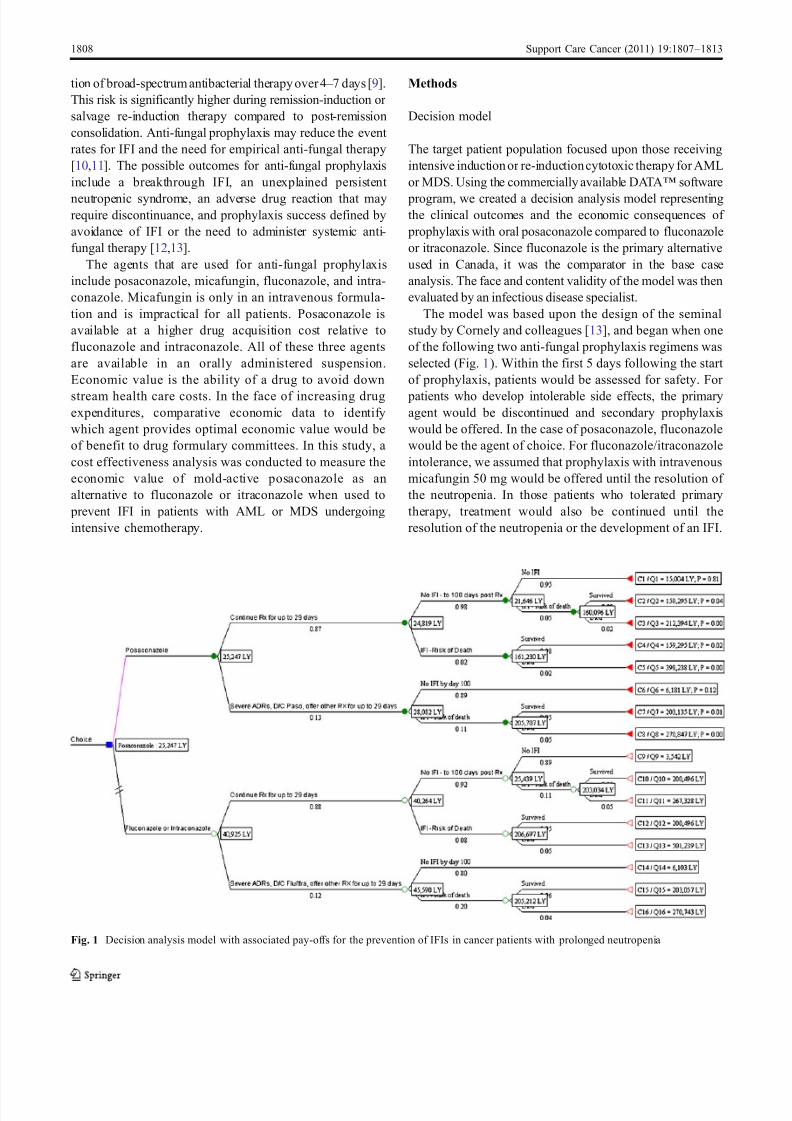
The model was based upon the design of the seminal
study by Cornely and colleagues [13], and began when one
of the following two anti-fungal prophylaxis regimens was
selected (Fig. 1). Within the first 5 days following the start
of prophylaxis, patients would be assessed for safety. For
patients who develop intolerable side effects, the primaryagent would be discontinued and secondary prophylaxis
would be offered. In the case of posaconazole, fluconazole
would be the agent of choice. For fluconazole/itraconazole
intolerance, we assumed that prophylaxis with intravenous
micafungin 50 mg would be offered until the resolution of
the neutropenia. In those patients who tolerated primary
therapy, treatment would also be continued until the
resolution of the neutropenia or the development of an IFI.
Fig. 1 Decision analysis model with associated pay-offs for the prevention of IFIs in cancer patients with prolonged neutropenia
1808 Support Care Cancer (2011) 19:1807–1813

8/9/2019 tugas PA.291014
http://slidepdf.com/reader/full/tugas-pa291014 3/8
The primary endpoint in the model was the development of
a breakthrough IFI during the neutropenic period and while
the patient was receiving active prophylaxis. The break-
through IFI was documented and categorized as proven or
probable. Proven IFI may be due to a mold such as Aspergillus
fumigatus or a yeast such as Candida glabrata [13].
Following the development of these infections or even in
patients non-responsive to empiric antibiotic therapy, appro- priate systemic anti-fungal therapy would be given consisting
of an echinocandin such as caspofungin, an extended spectrum
azole or liposomal amphotericin B for invasive candidiasis
[14,15]. Treatment would be continued until the resolution of
signs and symptoms of infections or until death (Fig. 1).
Clinical outcomes data
The clinical data required for the model, which consisted of
rates for the development of IFIs while on active prophy-
laxis or within the first 100 days, treatment discontinuations
because of adverse events and overall mortality wereobtained from a review of the literature. A computer
literature search of Medline, Pubmed, and Google Scholar
was performed from 2000 through 2010. Keywords for the
search consisted of prophylaxis, posaconazole, fluconazole,
itraconazole, micafungin, neutropenia, and randomized
trial. Care was taken to avoid inclusion of duplicate
publications. An additional literature search was performed
to identify systematic reviews and meta-analyses that would
provide pooled clinical endpoints that could be used in
cases where data was missing and for the planned
sensitivity analysis of the base case results.
Estimation of treatment costs
This evaluation assumed a Canadian health care system
perspective. The analytic time period was the first 100 days
following the start of anti-fungal prophylaxis. Patient
survival was not simulated to 5 years because we did not
want to go beyond the clinical trial horizon. Secondly,
limited data was available on the shape of the hazard
function for AML or MDS related relapse and death
beyond 100 days. Relevant costs for the model included
resources for drugs, a baseline electrocardiogram in the
case of posaconazole, and systemic therapy in cases where
IFIs develop. These were obtained from the Princess
Margaret Hospital in Toronto. The costs of managing IFIs
secondary to invasive aspergillosis and candidiasis species
were obtained from the Canadian and international eco-
nomic literature. For the base case analysis, the cost of
treating an IFI was weighted based on the incidence of
invasive aspergillus and invasive candidiasis reported in the
pivotal trial [13]. It was also assumed that the anti-fungal
prophylaxis regimen would be discontinued during that
treatment period and that the prophylaxis drug costs would
be reconciled accordingly. Costs from non-Canadian sour-
ces were converted and updated into 2010 Canadian dollars
using the consumer price index for health care as reported
by Statistics Canada. All costs are reported in 2010
Canadian dollars (1$ Can=1$ US, as of May 2010).
Cost effectiveness analysis
The clinical, economic, and survival estimates were then used
to conduct a cost effectiveness comparing the following: (1)
posaconazole to fluconazole; and (2) posaconazole to
itraconazole. The primary outcome was the incremental cost
per life year saved (LYS) with posaconazole, which was
calculated by dividing the difference in cost relative to
fluconazole or itraconazole (numerator) by the difference in
LYS (denominator). Future costs and benefits were not
discounted because of the short time periods involved.
However, the robustness of the base case results was tested
through a one-way sensitivity analyses. This procedureincluded re-analyzing the data using the upper and lower
bound of the 95% confidence intervals (CI) for rates of drug
discontinuations due to adverse events, the trial reported
incidence of IFIs, and costs to treat specific infections due to
Aspergillus and Candida species. Lastly, the duration of
posaconazole and fluconazole prophylaxis was also varied
based on results from the randomized trial [13].
Results
Clinical outcome data
A large randomized trial which compared posaconazole to
either fluconazole or itraconazole in patients undergoing
remission-induction therapy for AML or MDS was identified
and provided the bulk of the clinical outcomes data required to
populate the model [13]. In that study, a total of 602 patients
were randomly allocated to receive oral anti-fungal prophy-
laxis with posaconazole (200 mg three times daily, n=304)
or fluconazole (400 mg daily, n =240)/itraconazole (200 mg
twice daily, n=58) for up to 12 weeks or until myeloid
reconstitution beginning upon completion of induction
chemotherapy. The primary endpoint was the development
of proven or probable IFI during the active treatment phase.
Secondary analyses included the incidences of invasive
aspergillosis , invasive candidiasis, and total IFI within
100 days after randomization.
During the treatment phase, a total of seven of 304
patients (2.3%) developed an IFI in the posaconazole group
compared to 25 of 298 (8.4%) in the control, with the
difference between statistically significant ( p <0.001). Dur-
ing the 100-day period after randomization, 4.6% and
Support Care Cancer (2011) 19:1807–1813 1809

8/9/2019 tugas PA.291014
http://slidepdf.com/reader/full/tugas-pa291014 4/8
11.1% of posaconazole and fluconazole/itraconazole devel-
oped an IFI ( p=0.003). Of the 116 deaths that occurred
during the study period, 21 were considered to be related to
the fungal infection; approximately 2% and 5% of these
deaths occurred in the posaconazole and fluconazole/
itraconazole groups ( p=0.01), respectively [13]. Treatments
were reasonably well tolerated with 13.1% and 12.4% of
patients requiring discontinuations in the posaconazole andfluconazole/itraconazole groups because of adverse events.
Clinical outcomes data following prophylaxis with mica-
fungin were obtained from a randomized trial of hemato-
logical patients receiving stem cell transplantation [16]. All
of the data inputs for the model are summarized in Table 1.
The cost of treating invasive fungal infections
A highly relevant economic driver in this study was the
cost treatment an IFI. Upon review of the economic
literature, a cost-of-illness study by Wilson et al. was
identified and provided the relevant costs for treatingIFIs secondary to candidiasis and aspergillosis [17].
Using large hospital discharge databases from the USA,
the investigators estimated that the incremental cost of
treating invasive candidiasis and aspergillosis in cancer
patients was $17,763 and $47,915 respectively (1998
$US). These data were then converted into Canadian
dollars and adjusted to 2010 values using the consumer
price index for health care as reported by Statistics
Canada. A second cost estimate ($40,583) for treatingIFIs as reported by O’Sullivan and colleagues was also
used in the sensitivity analysis [18].
Cost effectiveness analysis
The life-year outcomes for each branch of the model
were combined with the clinical and economic data for a
cost effectiveness analysis. The average cost effective-
ness ratios were the most favorable with posaconazole
prophylaxis (Table 2). Furthermore, the incremental cost
per LYS indicated a cost savings with posaconazole and
improved efficacy relative to fluconazole/itraconazole(Table 2). Therefore, this is a situation of economic
Parameter Estimate Source
Cost of drugs
Posaconazole $141/day Princess Margaret
Hospital, TorontoFluconazole $40.43/day
Itraconazole $32.48/day
Micafungin $96/daya
Cost of invasive fungal infections (IFI) Wilson et al. [17]
Candidiasis $22,884
Aspergillosis $61,729
Weighted cost of an IFI in the posaconazole trial arm b $39,532 Cornely et al. [13]
Weighted cost of an IFI in the Flu/Itra trial arm b $53,960
Cost of an IFI reported in the literature $40,583 O’Sullivan et al. [18]
Clinical data (95% CI): posaconazole Cornely et al. [13]
Duration of prophylaxis in days 29 (26.6 – 31.4)
Development of IFI while on therapy 2.3% (0.93 – 4.7)
Development of IFI by day 100 4.6% (2.5 – 7.6)
Risk of death secondary to an IFI 2%
Discontinuations due to side effects 13.1% (9.6 – 17.5)
Clinical data (95% CI): Flu/Itra c
Duration of prophylaxis in days 24 (21.8 – 26.2)
Development of IFI while on therapy 8.4% (5.5 – 12.1)
Development of IFI by day 100 11.1% (7.7 – 15.2)
Risk of death secondary to an IFI 5%
Discontinuations due to side effects 12.4% (8.9 – 16.7)
Development of IFI while on micafungin 20.0%
Risk of death secondary to an IFI while on micafungin 4.2% van Burik et al . [16]
Table 1 Costs and clinical
parameters used in the econom-
ic model
a
Includes cost of preparation, ad-ministration, and supplies b
Weighted by the incidence of
candidiasis and aspergillosis
reported in the posaconazole and
control arm from the randomized
trial [13]. All costs were converted
to 2010 Canadian dollarsc Flu/Itra refers to the control
group receiving either fluconazole
or itraconazole
1810 Support Care Cancer (2011) 19:1807–1813

8/9/2019 tugas PA.291014
http://slidepdf.com/reader/full/tugas-pa291014 5/8
dominance with an average savings of approximately
$4,259 per patient.
Sensitivity analysis on the incremental cost per life year
saved
A series of one-way sensitivity analyses were conducted
on the key clinical and economic drivers. Extreme
variations, all against posaconazole, were evaluated. This
included using the upper 95% CI for the posaconazole
IFIs during therapy (4.7%) and at 100 days (7.6%) as
well as variations in the drug discontinuation rates and
the duration of therapy. Under all of the unfavorable
posaconazole scenarios evaluated, the cost-saving poten-
tial remained and economic dominance was sustained
(Table 3). Variations in the cost of treating IFIs were also
evaluated. The data suggested that cost savings would be
maximized if posaconazole were able to avoid more
invasive aspergillosis relative to fluconazole or itracona-
zole or if the duration of therapy was reduced to 27 days,
which is the lower limit of the 95% CI (Table 3). In
contrast, cost savings would be minimized to $1,765 per
patient if only invasive candidiasis was avoided. In
summary, the findings of the sensitivity analysis revealed
that the base case results were stable and supported the
conclusion of economic dominance.
Discussion
The cost effectiveness analysis indicated that posacona-
zole prophylaxis is a cost-effective and cost-saving
alternative to fluconazole and itraconazole in cancer
patients with prolonged neutropenia. This is a rare
occurrence in oncology because most of the newer
phar maceutical interventions are associated with an
increase in the overall cost of care [19,20]. The cost-
saving potential was maintained under every scenario
Outcome Posaconazole Fluconazole Itraconazole
Reference casea
Average cost/patient $6,913 $11,172 $10,957
Number of life years saved 0.28 0.27 0.27
Incremental cost vs. posaconazole – $4,259 $4,044
Average cost – effectiveness ratio b $25,000 $41,000 $40,000
Incremental cost per life year savedc
Dominatedc
Dominatedc
Table 2 Results of cost effec-
tiveness analysis for the base
case
a All ratios were rounded to the
nearest thousand b
Average cost divided by the
number of life years savedc Posaconazole provides at least as
much benefit in terms of life yearssaved and is also cost saving
Table 3 One-way sensitivity analysis on cost per life year saved with posaconazole
Parameter variationsa Cost savings Cost per l ife year saved
Base case b $4,259 Dominateda
Upper 95% CI for IFI during posaconazole therapy (4.7%) $3,480 Dominateda
Lower 95% CI for IFI during Flu/Itra therapy (5.5%) $3,041 Dominateda
Upper 95% CI for IFI with posaconazole at day 100 (7.6%) $3,253 Dominateda
Lower 95% CI for IFI with Flu/Itra at day 100 (7.7%) $2,788 Dominateda
Upper 95% CI for severe side effects with posaconazole (17.5%) $4,221 Dominateda
Lower 95% CI for severe side effects with Flu/Itra (8.9%) $4,208 Dominateda
Using the cost of treating an aspergillosis infection ($61,729) $4,292 Dominateda
Using the cost of treating an candidiasis infection ($39,532) $1,765 Dominateda
Using the cost of treating an IFI as reported by O’Sullivan et al. [18] — ($40,583) $1,885 Dominateda
Upper 95% CI of the posaconazole treatment duration (31 days) $4,014 Dominateda
Lower 95% CI of the posaconazole treatment duration (22 days) $4,505 Dominateda
a Posaconazole provides at least as much benefit in terms of life years saved and is also cost saving
bRelative to fluconazole
IFI invasive fungal infections
Support Care Cancer (2011) 19:1807–1813 1811

8/9/2019 tugas PA.291014
http://slidepdf.com/reader/full/tugas-pa291014 6/8
evaluated in the sensitivity analysis. It was primarily
driven by the drug’s ability to lower to incidence of
invasive aspergillosis infections, which are highly costly
to manage and are associated with a high risk of mortality
[13,17,21]. Notwithstanding, reducing the number of
patients developing systemic candidiasis infections would
also result in an overall cost savings as indicated in the
sensitivity analysis.The findings of this study are consistent with those of
a similar cost effectiveness evaluation conducted from
the US health care perspective [18]. In that study, which
included a 5-year relative survival extension in AML and
MDS patients receiving chemotherapy, a cost savings was
reported in most of the scenarios evaluated. The only case
where the cost per LYS with posaconazole was relatively
high was when the incidence of IFI was raised to 8.83%
(vs. 4.6%) on the posaconazole prophylaxis arm. Under
this scenario, the cost per LYS with posaconazole was
$48,600 [18]. However, an IFI rate of 8.83% with
posaconazole is unlikely and is beyond the upper 95%CI reported in the trial (i.e., 7.6%) [13]. Given the external
validity of our findings, posaconazole should be the drug
of choice when prophylaxis is indicated in AML and MDS
patients who are expected to have a prolonged episode of
neutropenia.
There are several limitations in the current study that
need to be acknowledged. The principal limitation relates
to the use of a decision model rather than actual resource
use data from the randomized trial that compared
posaconazole to fluconazole and itraconazole. Secondly,
the cost of treating an IFI was obtained from a study
conducted in the USA. This data may not be fully
generalizable to the Canadian setting. IFIs can have a
major impact on patient quality of life secondary to their
severe clinical consequences. In economic evaluations,
impact on patient quality of life is typically captured via
measurements of health state utilities. Therefore, another
limitation in the current study was the failure to measure
and include utilities in the economic model. This would
be a bias against posaconazole because the drug is able
to reduce the incidence of IFIs. The clinical data for
micafungin were from a randomized prophylaxis trial in
patients undergoing hematopoietic stem cell transplanta-
tion. This data may not be fully generalizable in patients
with AML/MDS receiving intensive chemotherapy. The
cost of IFI-related morbidity was not considered due to
limited Canadian cost data. This may be an important
economic component particularly for patients that need to
have surgical debridement, which is a common procedure
for refractory mold infections [21]. Not all AML/MDS
patients in Canada receive anti-fungal prophylaxis. How-
ever, our model did not include a “no prophylaxis” arm
due to the lack of good quality data. We acknowledge this
as a limitation but given the magnitude of the savings with
posaconazole, it is likely that a “no prophylaxis” arm will
also be economically dominated by posaconazole. Finally,
the current study considered only direct hospital and drug-
related expenditures; indirect costs (e.g., loss of produc-
tivity) secondary to IFI complications were not included in
the analysis.
Conclusions
Posaconazole prophylaxis in AML and MDS patients with
prolonged neutropenia is a cost-effective and cost-saving
alternative to fluconazole or itraconazole in Canada. Given
the practical advantages of this drug in terms of safety,
improved efficacy, and cost-saving potential, it is a
clinically and economically attractive alternative to fluco-
nazole and itraconazole for the prevention of IFIs in this
patient population.
Acknowledgment This study was funded by Merck Canada Inc.
References
1. Bow EJ (2008) Considerations in the approach to invasive fungal
infection in patients with haematological malignancies. Br J
Haematol 140:133 – 152
2. Bow EJ, Wingard JR, Bowden RA (2003) Infectious complications
in patients receiving cytotoxic therapy for acute leukemia: history,
background and approaches to managment. Management of infec-
tion in oncology patients. Martin Dunitz, London, pp 71 –
1043. Nucci M, Anaissie E (2001) Revisiting the source of candidemia:
skin or gut? Clin Infect Dis 33:1959 – 1967
4. Blijlevens NM, Donnelly JP, De Pauw BE (2002) Impaired gut
function as risk factor for invasive candidiasis in neutropenic
patients. Br J Haematol 117:259 – 264
5. Bow EJ, Meddings JB (2006) Intestinal mucosal dysfunction and
infection during remission-induction therapy for acute myeloid
leukaemia. Leukemia 20:2087 – 2092
6. Gerson SL, Talbot GH, Hurwitz S et al (1984) Prolonged granulocy-
topenia: the major risk factor for invasive pulmonary aspergillosis in
patients with acute leukemia. Ann Intern Med 100:345 – 351
7. Burwen DR, Lasker BA et al (2001) Invasive aspergillosis
outbreak on a hematology – oncology ward. Infect Control Hosp
Epidemiol 22:45 – 48
8. Herbrecht R, Natarajan-Amé S, Letscher-Bru V, Canuet M (2004)Invasive pulmonary aspergillosis. Semin Respir Crit Care Med
25:191 – 202
9. Bow EJ (2009) Neutropenic fever syndromes in patients under-
going cytotoxic therapy for acute leukemia and myelodysplastic
syndromes. Semin Hematol 46:259 – 268
10. Bow EJ, Laverdiere M, Lussier N et al (2002) Antifungal prophylaxis
for severely neutropenic chemotherapy recipients: a meta analysis of
randomized-controlled clinical trials. Cancer 94:3230 – 3246
11. Robenshtok E, Gafter-Gvili A, Goldberg E et al (2000) Antifungal
prophylaxis in cancer patients after chemotherapy or hematopoi-
etic stem-cell transplantation: systematic review and meta-
analysis. J Clin Oncol 25:5471 – 5489
1812 Support Care Cancer (2011) 19:1807–1813

8/9/2019 tugas PA.291014
http://slidepdf.com/reader/full/tugas-pa291014 7/8
12. Nucci M, Biasoli I, Akiti T, et al. (2000) A double-blind,
randomized, placebo-controlled trial of itraconazole capsules as
antifungal prophylaxis for neutropenic patients. Clin Infect Dis
30:300 – 305.
13. Cornely OA, Maertens J, Winston DJ et al (2007) Posaconazole
vs. fluconazole or itraconazole prophylaxis in patients with
neutropenia. N Engl J Med 356:348 – 359
14. Morrissey CO, Bardy PG, Slavin MA et al (2008) Diagnostic and
therapeutic approach to persistent or recurrent fevers of unknown
origin in adult stem cell transplantation and haematologicalmalignancy. Intern Med J 38:477 – 95
15. Martino R, Viscoli C (2006) Empirical antifungal therapy in
patients with neutropenia and persistent or recurrent fever of
unknown origin. Br J Haematol 132:138 – 54
16. van Burik JA, Ratanatharathorn V, Stepan DE et al (2004)
Micafungin versus fluconazole for prophylaxis against invasive
fungal infections during neutropenia in patients undergoing
hematopoietic stem cell transplantation. Clin Infect Dis
39:1407 – 16
17. Wilson LS, Reyes CM, Stolpman M et al (2002) The direct cost and
incidence of systemic fungal infections. Value Health 5:26 – 34
18. O’Sullivan AK, Pandya A, Papadopoulos G et al (2009) Cost
effectiveness of posaconazole versus fluconazole or intraconazole
in the presention of invasive fungal infections among neutropenic
patients in the United States. Value Health 12:666 – 673
19. Hillner BE, Smith TJ (2009) Efficacy does not necessarily translate
to cost effectiveness. A case study in the challenges associated with21st century cancer drug pricing. J Clin Oncol 27:2111 – 3
20. Fojo T, Grandy C (2009) How much is a life worth: cetuximab,
non small cell lung cancer, and the $440 billion question. J Natl
Cancer Inst 101:1044 – 48
21. Walsh TJ, Anaissie EJ, Denning DW et al (2008) Treatment of
aspergillosis: clinical practice guidelines of the Infectious Diseases
Society of America. Clin Infect Dis 46:327 – 60
Support Care Cancer (2011) 19:1807–1813 1813

8/9/2019 tugas PA.291014
http://slidepdf.com/reader/full/tugas-pa291014 8/8
Reproducedwithpermissionof thecopyrightowner. Further reproductionprohibitedwithoutpermission.




















