Sma Et Polio

of 21
-
Upload
kent-ado-almodin -
Category
Documents
-
view
222 -
download
0
Transcript of Sma Et Polio
-
8/12/2019 Sma Et Polio
1/21
1
ST. PAUL UNIVERSITY ILOILO
College of Physical Therapy
2014
Seminar 2
SPINAL MUSCULAR ATROPHY and POLIOMYELITIS
Group # 2
Section A:
Leaders: Dariza Badeo & Mitchell Teodosio
Members: Trisha Jane Wong
Jahanne Rafio
John Xand Acuros
Rustom John Ordaniel
Ervin Sales
Eduardo Montinola
Section B:
Leaders: Floyd Juatas & Justine Vee Guardapavo
Members: Jethro Von Guardapavo
Cirille JuarezKent Lauro Almodin
Stella Tingson
BSPT IV
January 6, 2014
-
8/12/2019 Sma Et Polio
2/21
2
Table of Contents
Definition of Terms -------------------- 3
Anatomy et Physiology -------------------- 4-5
SPINAL MUSCULAR ATROPHY
Definition of Condition -------------------- 6
Etiology -------------------- 6
Epidemiology -------------------- 6-7
Classification -------------------- 7-8
Pathomechanism -------------------- 8
Signs and Symptoms -------------------- 8
Differential Diagnosis -------------------- 8-9
Diagnostic Tools -------------------- 9-10
Medical Management -------------------- 10
Surgical Management -------------------- 10-11
PT Management -------------------- 11
Prognosis -------------------- 12
POLIOMYELITIS
Definition of Condition -------------------- 13
Etiology -------------------- 13
Epidemiology -------------------- 13
Classification -------------------- 14-15
Pathomechanism -------------------- 16
Signs and Symptoms -------------------- 16
Differential Diagnosis -------------------- 17
Diagnostic Tools -------------------- 17-18
Medical Management -------------------- 18
Surgical Management -------------------- 18-19
PT Management -------------------- 19
Prognosis -------------------- 20
References -------------------- 21
-
8/12/2019 Sma Et Polio
3/21
3
I. Definition of terms
Apoptosis programmed cell death
Bulbar motor nuclei involvement or Bulbar palsy refers to impairment of functionof the cranial nerves IX, X, XI and XII, which occurs due to a lower motor neuron
lesion either at nuclear or fascicular level in the medulla oblongata or from lesions of
the lower cranial nerves outside the brainstem. It is characterized by dysarthria.
ConusMedullaris - is the tapered, lower end of the spinal cord.
Encephalomeningitis is a fatal medical condition that is characterised by an
inflammation of the meninges of the brain and spinal cord. It may be caused by apathogenic infection by a disease vector that can penetrate the barriers of the
Central Nervous System.
FilumTerminale - the slender threadlike prolongation of the spinal cord below the
origin of the lumbar nerves : the last portion of the pia mater.
Hypotonia - is a medical term that describes decreased muscle tone.
Motor unit -The muscle fibers innervated by a single anterior horn cell.
Myasthenia gravis is an autoimmune neuromuscular disease leading to fluctuating
muscle weakness and fatigue.
Spinal Cord - is a long, thin, tubular bundle of nervous tissue and support cells that
extends from the brain
Somatotopically - point-for-point correspondence of an area of the body to aspecific point on the central nervous system.
Viraemia is a medical condition where viruses enter the bloodstream and hence
have access to the rest of the body.
-
8/12/2019 Sma Et Polio
4/21
4
II. ANATOMY AND PHYSIOLOGY
Spinal Cord
- Approximately 42-45 cm in length
- Spinal Column approx 72 cm in length.
- Begins at the Foramen Magnum
- Terminates at L1-L2, L2-L3
- Tapers off into CONUS MEDULLARIS and forms an apex called FILIUM TERMINALE
- Attached are 31 spinal nerves
A. Anterior Gray Matter
a. MEDIAL
-present in most segments
-for the innervation of skeletal muscles, trunk, intercostal and abdominal muscles
b. LATERAL
-present in CERVICAL and LUMBOSACRAL seg.
-for the innervation of skeletal muscles.
c. CENTRAL
-smallest
-present in CERVICAL and LUMBOSACRAL seg
B. Posterior Gray Matter
a. Substantia Gelatinosa
-found along the ENTIRE length of the cord-for Pain, Touch and Temperature
b. Nucleus Propius
-found along the ENTIRE length of the cord
-for 2 point discrimination
c. Clarke's Column-found on C8-L4
-for proprioception
d. Visceral Afferent Nucleus
-
8/12/2019 Sma Et Polio
5/21
5
-found on T1-L3
-for Visceral Sensation
C. Lateral Gray Matter
a. Preganglionic Sympathetic Fibers
-found on T1 to L3
b. Preganglionic Parasympathetic Fibers
-found on S2-S4
Motor neurons
- Also called efferent nerves and effector neurons, that carry signals from the spinal cordto the muscles to produce movement.
Anterior horn cell
- also called the anterior cornu, anterior column or ventral horn is the ventral (front) greymatter section of the spinal cord.
- It is one of the three grey columns and it contains motor neurons that affect the axialmuscles while the posterior horn receives information regarding touch and sensation.
- It is where the cell bodies of alpha motor neurons are located.
SMN1 gene
- provides instructions for making the survival motor neuron (SMN) protein.
SMN protein
- is a 294 amino acid polypeptide that is expressed in all cell types of vertebrateorganisms which is necessary for the survival of motor neurons.
- it is localized in the cytoplasm and play a crucial role in the assembly of spliceosomaluridine-rich small nuclear ribonucleoprotein (U snRNP) complexes.
SnRNPs
- are made up of small nuclear RNA (snRNA) and a group of seven proteins that areknown as Sm ribonucleoproteins. These seven proteins are what make the core of snRNPextremely stable.
- are essential to the job of splicing introns in pre-mRNA during the post-transcriptionalmodification of RNA that occurs after transcription.
In cells, the SMN protein plays an important role in processing molecules called messengerRNA (mRNA), which serve as genetic blueprints for making proteins. Messenger RNA beginsas a rough draft (pre-mRNA) and goes through several processing steps to become a final,mature form. The SMN protein helps to assemble the cellular machinery needed to processpre-mRNA.
-
8/12/2019 Sma Et Polio
6/21
6
SPINAL MUSCULAR ATROPHY
III. Definition of Condition
Spinal muscular atrophy (SMA) is an autosomal recessive disease caused by a
genetic defect in the SMN1 gene, which encodes SMN (Survival Motor Neuron) a protein
widely expressed in all eukaryotic cells. SMN1 is apparently selectively necessary for
survival of motor neurons, as diminished abundance of the protein results in death of
neuronal cells in the anterior horn of the spinal cord and subsequent system-wide muscle
wasting.
IV. Etiology:
SMA is caused by a missing or abnormal (mutated) gene known as survival motor
neuron gene 1 (SMN1). In a healthy person, this gene produces a protein in the body called
survival motor neuron (SMN) protein. In a person with mutated genes, this protein is absent
or significantly decreased, and causes severe problems for motor neurons. Motor neurons
are nerve cells in the spinal cord which send out nerve fibers to muscles throughout the
body. Since SMN protein is critical to the survival and health of motor neurons, nerve cellsmay shrink and eventually die without this protein, resulting in muscle weakness. As a child
with SMA grows, it is difficult for his/her weakened muscles to keep up with the demands of
daily activities. The resulting weakness can also lead to bone and spine changes that may
cause breathing problems and further loss of function.
V. Epidemiology:
Frequency
U.S., SMA are the 2nd most common autosomal-recessive inherited disorder after cystic
fibrosis.
SMA type 1 affects approximately 1 per 10,000 live births.
SMA type 2&3 affects approximately 1 per 24,000 births.
SMA type 1&3 each account for about of cases, whereas,
SMA type 2 is the largest group and accounts for of all cases.
-
8/12/2019 Sma Et Polio
7/21
7
Mortality/Morbidity
The mortality rates of SMA are inversely correlated with the age at onset. High death rates
are associated with early onset disease. In patients with SMA type 1, the median survival
is 7 months, with a mortality rate of 95% by age 18 months.
Respiratory infections account for most deaths.
In type 2 SMA, the age of death varies, but death is most often due to respiratory
complications.
Age - According to the ISMAC system, the age of onset for SMA is as follows:
SMA type 1 : onset is from birth to 6 months
SMA type 2 : onset is between 6 and 18 months
SMA type 3 : onset is after 18 months
SMA type 4 : onset in adulthood (mean onset, mid 30s).
VI. CLASSIFICATION
SMA Type I( Acute infantile or Werdnig-Hoffman disease)
They have severe, progressive mm weakness and flaccid or reduced muscle tone
(hypotonia). Bulbar dysfunction includes poor suck ability, reduced swallowing, and
respiratory failure. Patients have no involvement of the extraocular muscles, and
facial weakness is often minimal or absent. They have no evidence of cerebral
involvement, and infants appear alert.
SMA Type II ( Chronic infantile form )
The most common form of SMA, and some experts believe that SMA Type II may
overlap types I and III. Patients may have developmental motor delay. Infants with
SMA type II often have difficulties with sitting independently or failure to stand by 1
year of age. An unusual feature of the disease is a postural tremor affecting the
fingers. This is thought to be related to fasciculation in the skeletal muscles.
SMA Type III (Chronic juvenile or Kugelberg-Welander syndrome)
This is a mild form of autosomal recessive SMA that appears after age 18 months. It
is characterized by slowly progressive proximal weakness. Most children with SMA
III can stand and walk but have trouble with motor skills, such as going up and down
-
8/12/2019 Sma Et Polio
8/21
8
the stairs. The diseases progresses slowly, and the overall course is mild. Many
patients have normal life expectancies.
SMA Type IV (Adult-onset form)
Onset is typically in the mid 30s. the disease mimics the symptoms of type III.
Overall, the course of the disease is benign, and patients have a normal life
expectancy.
VII. Pathomechanism et Signs and Symptoms:
Signs et Symptoms
Often, weakness is first felt in the shoulder and leg muscles. Weakness gets worse
over time and eventually becomes severe.
Symptoms in an infant:
Breathing difficulty, leading to a lack of oxygen
Feeding difficulty (food may go into the windpipe instead of the stomach)
Floppy infant (poor muscle tone)
Lack of head control
Little movement
Weakness that gets worse
Symptoms in a child:
Frequent, increasingly severe respiratory infections
Nasal speech
Posture that gets worse
V. Differential Diagnosis:
Condition Differentialing S/Sx SimilaritiesAmyotrophic LateralSclerosis
ALS involves upper andlower motor neurons andpresents as an idiopathic,
Both SMA and ALS have astheir cardinal feature theloss of spinal motor
Mutation or Absence in the survival motor neuron gene
(telomeric SMN1 gene found in arm 5q - bands q11.2-13.3 )
Programmed Cell Death (Apoptosis)
Progressive Hypotonia or Muscle Weakness
-
8/12/2019 Sma Et Polio
9/21
9
progressive degeneration ofanterior horn cells and theirassociated neurons,resulting in progressivemuscle weakness, atrophy,
and fasciculations.
Neurons.
Congenital MuscularDystrophy
Autosomal recessivediseases resulting in severeproximal weakness at birth(or within the first 12 mo oflife) that is either slowlyprogressive ornonprogressive.Contractures are common,and CNS abnormalities canoccur.
Both caused by faulty gene
Congenital Myopathies Hypotonia is the clinicalhallmark of congenitalmyopathies. It presents inthe neonatal period as headlag; lack of flexion of thehips, knees, and elbows;external rotation of the hips;diffuse weakness in facial,limb, and axial muscles;and reduced muscle mass.
Generalized muscleweakness and poor musclebulk.
Myasthenia Gravis A reduction in the number
of ACh receptors results ina characteristic pattern ofprogressively reducedmuscle strength. The bulbarmuscles are affected mostcommonly and mostseverely, but most patientsalso develop some degreeof fluctuating generalizedweakness.
progressive weakness,
muscle wasting, andmuscle fasciculations
Primary lateral sclerosis progressive, degenerative
disease of upper motorneurons characterized byprogressive spasticity (ie,stiffness). It affects thelower extremities, trunk,upper extremities, andbulbar muscles (usually inthat order).
VI. Diagnostic tools: 1. Genetic Testing
Although we do not fully understand how the gene abnormality produces the disease,
the discovery of the SMN gene has proved extremely helpful in both establishing a
diagnosis of SMA, and offering precise genetic counseling.
-
8/12/2019 Sma Et Polio
10/21
10
confirms the diagnosis
2. Clinical Tests
Typically, the child with SMA Type I and II will exhibit his or her most dramatic
weakness in the proximal muscles of the legs and arms.
Most children with SMA lose their deep tendon reflexes (the reflexes physicians check
when they strike the knees or ankles with a rubber hammer).
3. Electromyography Testing (EMG)
4. Muscle Biopsy
VII. Medical management:
NO cure
Supportive treatment should be aimed at improving the patients' quality of life and
minimizing disability, particularly in patients with slow progression.
The goals are to maximize the patient's independence and quality of life at each stage
of the disease.
Respiratory muscle weakness - Assisted ventilation also can help children and adults
with different forms of SMA. Many physicians advise starting out with noninvasive
ventilation, which generally means that air (usually room air, not enriched with oxygen) is
delivered under pressure through a mask or mouthpiece. This kind of system comes in
many forms and can be used as many hours of the day and/or night as necessary. It can
easily be removed for eating, drinking and talking.
Swallowing muscle weakness - Babies with severe swallowing and sucking weakness
can be fed by alternative methods, such as a feeding tube, often called a gastrostomy tube
or g-tube. A feeding tube is a small, flexible tube, about the diameter of a pencil, that allows
liquid nutrition (homemade or commercially prepared) to enter the stomach directly,
bypassing the mouth, throat and esophagus.
VIII. Surgical management:
Surgical revision may provide stable correction of the spine, and early orthopedic
intervention may be indicated in patients in whom prolonged survival is anticipated. Hip
-
8/12/2019 Sma Et Polio
11/21
11
subluxations and dislocations are common. Nonsurgical treatment is generally preferred
unless pain is severe, owing to the high rate of repeated dislocation.
Noninvasive ventilation and percutaneous gastrostomy reportedly improves the quality
of life with no effect on survival. These modalities may be most effective in prolonginglifespan in patients with slowly progressive disease, whereas they may provide comfort
care in rapidly progressive infantile forms.
If scoliosis develops in a patient with spinal muscular atrophy, spinal instrumentation
and fusion may be necessary. Some upper extremity function can be lost after fusion.
Tendon lengthenings may be needed to improve joint position.
IX. PT management:
Physical Therapy is the treatment of disease and injury by mechanical means such as
exercise, heat, light, massage and electricity.
Goals: Maximize function, mobility, safety, and comfort
Aquatic therapy is an excellent way to maintain mobility, strength, and flexibility.
PT assists you in walking, transfers from one place to another, exercise, pain relief and
education for you and your family.
Exercise: helps maintain joint movement (Maintaining the patient's joint mobility is very
important, because the goal is to decrease the incidence of contractures. Plantar flexion
contractures are the most common), mood elevation and improves sleep patterns.
Stretching: to preserve or increase flexibility
o Active
o Active assistedo Passive
Ankle-foot orthotics worn at night may help to provide prolonged, passive stretching to
prevent worsening of ankle plantar flexion contractures.
Strengthening: does not change the progression of the disease. Too much can actually
over fatigue the muscle. Active exercise within the limits of your disease in important to
maximize your ability and prevent disuse and contractures.
Avoid activities that cause muscle or joint pain and excessive fatigue either during orafter your exercise program. Energy conservation is needed so that you do not over
work body areas of increased weakness and cause overuse syndromes and more pain,
weakness etc.
-
8/12/2019 Sma Et Polio
12/21
12
X. Prognosis:
There is no cure for SMA. Treatment consists of managing the symptoms and preventing
complications.
The prognosis is poor for babies with SMA Type I. Most die within the first two years, because
of respiratory problems and infections. For children with SMA Type II, the prognosis for life
expectancy or for independent standing or walking roughly correlates with how old they are
when they first begin to experience symptoms - older children tend to have less severe
symptoms Life expectancy is reduced but some individuals live into adolescence or young
adulthood. Children with type III disease may survive into early adulthood. However, people
with all forms of the disease have weakness and debility that gets worse over time. May beprone to respiratory infections but with care may have a normal lifespan.
-
8/12/2019 Sma Et Polio
13/21
13
POLIOMYELITIS
I. Definition of Condition
Poliomyelitis is an acute infectious virus disease caused by the poliovirus,
characterized by fever, motor paralysis, and atrophy of skeletal muscles often withpermanent disability and deformity, and marked by inflammation of nerve cells in the
ventral horns of the spinal cord called also infantile paralysis, polio.
II. Etiology:
Poliomyelitis is a disease caused by infection with the poliovirus. A human enterovirus
and member of the family of Picornaviridae. Poliovirus is composed of an RNA genome
and a protein capsid. The viral particle is about 30 nanometres in diameter with icosahedralsymmetry. Because of its short genome and its simple composition, poliovirus is widely
regarded as the simplest significant virus.
The virus spreads by:
Direct person-to-person contact
Contact with infected mucus or phlegm from the nose or mouth
Contact with infected feces
The virus enters through the mouth and nose, multiplies in the throat and intestinal tract,
and then is absorbed and spread through the blood and lymph system. The time from being
infected with the virus to developing symptoms of disease (incubation) ranges from 5 - 35
days (average 7 - 14 days).
III. Epidemiology:
affects children > 5 y.o.
1 in 200 infections leads to irreversible paralysis. Paralysed, 5% to 10% die when
their breathing muscles become immobilized.
Polio cases have decreased by over 99% since 1988,
In 2013, only three countries (Afghanistan, Nigeria and Pakistan) remain polio-
endemic, down from more than 125 in 1988.
Children in all countries are at risk of contracting polio. Failure to eradicate polio
from these last remaining strongholds could result in as many as 200 000 new cases
every year, within 10 years, all over the world.
In most countries, the global effort has expanded capacities to tackle other
infectious diseases by building effective surveillance and immunization systems.
-
8/12/2019 Sma Et Polio
14/21
14
IV. Classification
STAGES
1. Acute Stage
Variable incubation period
6-20 days (1-3 weeks)
Reflects virus ingestion & multiplication
Increased physical activity late in incubation period leads to poorer prognosis
Acute disease reflects viraemia
Varies from mild malaise to encephalomeningitis & paralysis
Children may have initial malaise & fever followed by several days of well -being
Then recurrence with sore throat, d iarrhoea & meningism
Older children & adults lack prodrome Spinal anterior horn cell involvement
Onset of patchy asymmetric paralysis
Spasm of opposing muscles produces pain
DTR disappear
Flexor posturing = Lie with curled up joints
Muscles tender t o palpation
Reflex spasm with stretching
No sensory changes
Bulbar motor nuclei involvement
Fulminant encephalitis
Speech & swallowing problems
Sudden respiratory failure from resp centre involvement
Clinical diagnosis with no laboratory tests
Cons idered infective for 4 weeks
2. Convalescent Stage
Starts 2 days after normal temp & cessation of paralytic disease
Continues for 2 years
Spontaneous improvement in muscle power
Most rapid in first 4/12
Almost complete after 6/12
Average improvement is 2 grades above assessment at 1/12 following onset
1 grade above assessment at 6/12
3. Chronic Stage
-
8/12/2019 Sma Et Polio
15/21
15
AKA Stage of Residual Paralysis
After 2 years
No further recovery
Characteristic features
Limb bluish
Wasted
Deformed
Disease in childhood = shortened limb (hence LLD)
Limb has floppy feel
Normal sensation
If trunk affected then see scoliosis or respiratory insufficiency
Problems include Deformity due to unbalanced paralysis
Instability from balanced paralysis
Deformity contributed to by growth & worse in earlier disease
4. Post-Polio Syndrome
Return of:
Pain
Fatigue
Muscle weakness
Functional impairment
30 -35 years after original polio
Late onset > 10 years
Severe disease
Four extremities involved
Ventilator dependence
Hospitalisation during acute illness
Onset of 2 or more of following
-Fatigue -Muscle weakness -New weakness -New atrophy
-Functional loss -Cold intolerance -No other cause
-
8/12/2019 Sma Et Polio
16/21
16
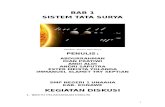
V. Pathomechanism et Signs and Symptoms:
-
8/12/2019 Sma Et Polio
17/21
17
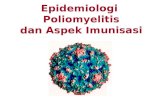
VI. Differential Diagnosis:
VII. Diagnostic Tools
1. Throat and stool culture
2. Urine culture3. Test for polio antibodies levels
4. Lumbar puncture or spinal tap : performed to collect a sample of cerebrospinal
fluid (CSF) for biochemical, microbiological, and cytological analysis, or very
Disease Similarities Rule-outGuillain-Barr syndrome Muscle contractions or
muscle spasms in the calf,neck, or backMuscle weakness that isonly on one side or worseon one side comes onquickly
And may go worst intoparalysis
loss of reflexes, andnumbness or tingling inyour arms, legs, face, andother parts of your body.
Spinal Cord lesions
urinate Muscle contractions ormuscle spasms in the calf,neck, or back
Medical Hx.
Neuropathies
spasm in any area of thebody
neckstiffness of the
back, arms, legs,abdomen
Physical trauma,repetitive injury,metabolic problems andexposure to toxins andsome drugs
Myasthenia Gravis Fluctuating muscleweakness andfatigue
Possitive acetylcholinereceptor antibodies
West nile virus infection Skin rashSwollen lymph glandsStiff neck
Disorientation or confusionStupor or comaTremors or muscle jerkingLack of coordinationEye pain
-
8/12/2019 Sma Et Polio
18/21
18
rarely as a treatment ("therapeutic lumbar puncture") to relieve increased
intracranial pressure.
VIII. Medical Management
There is no cure for polio, only treatment to alleviate the symptoms. Heat and physical
therapy is used to stimulate the muscles and antispasmodic drugs are given to relax the
muscles. While this can improve mobility, it cannot reverse permanent polio paralysis.
Polio can be prevented through immunization. Polio vaccine, given multiple times,
almost always protects a child for life.
IX. Surgical management:
1. Hip and knee contractures of over 30
Souttars release involves the soft tissue release on the anterolateral aspect of the hip
joint, whereby the tensor fascia lata and gluteus maximus are released from their origins,
as they contribute to the formation of the iliotibial band.
Younts releas e involves reexcision of the thickened anterolateral fascia lata so that the
knee contracture is better corrected.
The subcutaneous method of division is very satisfactory for less severe contractures,
provided it is done correctly and as extensively as necessary. Care must be taken to avoid
damaging the femoral and popliteal arteries, as well as the common peroneal nerve. The
biceps, however, should always be divided under direct vision because of the risk of
damaging the adjacent lateral popliteal nerve.
2. Tendon transfer to reestablish muscle power
In selecting a tendon to transfer, the muscle should be sufficiently strong to supplement
the power of a paralyzed muscle. The nerve and blood supply of the transferred muscle
should be preserved in order to avoid iatrogenic weakness.
For efficiency, the transferred tendon should be securely attached (with tension) close
to the insertion of a paralyzed tendon and should be routed in a direct line between its
origin and the new insertion. The transferred tendon loses its power by one grade.
3. Muscle transplantation to replace a paralyzed muscle
In muscle transplant procedures, unlike in tendon transfer, both the origin and the
insertion of a muscle are detached along with its neurovascular pedicle. This procedure is
-
8/12/2019 Sma Et Polio
19/21
19
not as popular as tendon transfer, because of the difficulty in finding a normal muscle to
transplant.
4. Arthrodesis
5. Limb lengthening6. Joint replacement surgery
X. PT management:
Physical therapy plays an important role in
rehabilitation for patients with poliomyelitis.
Patients with muscle paralysis benefit from
frequent passive range of motion (PROM)
and splinting of joints to prevent contracture
and joint ankylosis.
Chest physical therapy (CPT) helps
patients with bulbar involvement prevent any
pulmonary complications, such asatelectasis.
Frequent repositioning of paralyzedpatients helps to prevent bedsores.
Strengthening exercises should benonfatiguing. A specific suggestion is toexercise every other day, and the perceivedrate of exertion should be less than "veryhard." Loads should be held for only 4-5
seconds, and there should be a 10-second rest between bouts and a 5-minute restbetween sets. The patient should perform about 3 sets of 5-10 repetitions.
Electrical stimulation has been used to strengthen weakened muscles or to reeducatemuscles weakened through disuse, as well as to decrease pain.
For myofascial pain , consider heat, electrical stimulation, trigger point injections,stretching exercises, biofeedback, muscle relaxation exercises, or static magnetic fieldsfor trigger points.
For gait disturbances , assistive devices can be used, but sometimes patients refuse
because of the philosophy of "not giving in." Treatment also can involve limitation of
ambulation to shorter distances and the use of orthotics for joint protection.
Exercise therapy and training programs in PPS patients should be carefully
customized and planned by physiotherapists to avoid both overuse and disuse, and the
level of physical activity should be modified to decrease pain.
-
8/12/2019 Sma Et Polio
20/21
20
XI. Prognosis:
People with minor illness and nonparalytic forms of polio recover completely, and most
people with major illness who were paralyzed also recover completely. Fewer than 25% of
people with polio are disabled for life.
Even though you can recover completely from polio symptoms, polio leaves behind
some damage. As you age, your nervous system may become less able to compensate for
the damage that polio caused, so symptoms may gradually reappear. This can happen 15
or 30 years after the polio infection was active. Recurring symptoms from polio are called
post-polio syndrome.
-
8/12/2019 Sma Et Polio
21/21
21
REFERENCES:
A. Online Sources
Guillain-Barre Syndrome. (2012, August 29). Retrieved December 29, 2013, fromhttp://emedicine.medscape.com/article/315632-overview
Salinas, J., Jr. (2012, January 18). West Nile Virus. Retrieved December 29, 2013,
from http://emedicine.medscape.com/article/312210-overview
Polio. (2011, March 5). Retrieved January 4, 2013, from http://www.mayoclinic.org/
diseases-conditions/polio/basics/tests-diagnosis/CON-20030957
S Vidyadhara, MBBS, MD, MS(Ortho), DNB(Ortho), FNB(Spine Surgery), MNAMS Consultant, Department of Spine Surgery, Manipal Hospital, India (2012, May 11) .Poliomyelitis treatment and management. Retrieved on Jan 3 2014 fromhttp://emedicine.medscape.com/article/1259213-treatment#a1128
Spinal Muscular Atrophy-Wikipedia, the free encyclopedia. (n.d.).Retrieved onDecember 10, 2013 from http://en.wikipedia.org/wiki/Spinal_muscular_atrophy Motorneuron.(n.d.). Retrieved on December 10, 2013 fromhttp://www.princeton.edu/~achaney/tmve/wiki100k/docs/Motor_neuron.html
SMN1-Genetics Reference. (2012). Retrieved on December 10, 2013 fromhttp://ghr.nlm.nih.gov/gene/SMN1 What causes Spinal Muscular Atrophy? (n.d.).Retrieved December 5, 2013, from FSMA website:http://www.fsma.org/FSMACommunity/understandingsma/WhatCausesSMA/
What causes Spinal Muscular Atrophy? (n.d.). Retrieved December 5, 2013, fromFSMA website:
http://www.fsma.org/FSMACommunity/understandingsma/WhatCausesSMA/ Tsao, B. (2013, May 8) Retrieved January 4, 2014, from
http://emedicine.medscape.com/article/1181436-differential
(2013) MDA's disease information centers. Retrieved January 5, 2014, fromhttp://mda.org/disease/spinal-muscular-atrophy/medical-management
Endgame PR ( 2000, February 24 ) FightSMA. Retrieved January 5, 2014, fromhttp://www.fightsma.org/sma-guidebook/spinal-muscular-atrophy-diagnosis-tests/
Tsao, B (2013, May 8 ) Retrieved January 5, 2014, fromhttp://emedicine.medscape.com/article/1181436-treatment
The Spinal Cord. Retrieved January 4, 2013, from http://biology.about.com/od/Nervous-System/ss/spinal-cord.htm
Meninges of the Brain and Spinal Cord. Retrieved January 4, 2013, from
http://www.nlm.nih.gov/medlineplus/ency/imagepages/19080.htm Spinal Cord. Retrieved January 4 2013, from
http://www.getbodysmart.com/ap/nervoussystem/cns/spinalcord/grayfunction/tutorial.html
http://emedicine.medscape.com/article/1259213-treatment#a1128http://en.wikipedia.org/wiki/Spinal_muscular_atrophyhttp://www.princeton.edu/~achaney/tmve/wiki100k/docs/Motor_neuron.htmlhttp://ghr.nlm.nih.gov/gene/SMN1http://www.fsma.org/FSMACommunity/understandingsma/WhatCausesSMA/http://emedicine.medscape.com/article/1181436-differentialhttp://mda.org/disease/spinal-muscular-atrophy/medical-managementhttp://www.fightsma.org/sma-guidebook/spinal-muscular-atrophy-diagnosis-tests/http://emedicine.medscape.com/article/1181436-treatmenthttp://biology.about.com/od/Nervous-System/ss/spinal-cord.htmhttp://biology.about.com/od/Nervous-System/ss/spinal-cord.htmhttp://www.nlm.nih.gov/medlineplus/ency/imagepages/19080.htmhttp://www.getbodysmart.com/ap/nervoussystem/cns/spinalcord/grayfunction/tutorial.htmlhttp://www.getbodysmart.com/ap/nervoussystem/cns/spinalcord/grayfunction/tutorial.htmlhttp://www.getbodysmart.com/ap/nervoussystem/cns/spinalcord/grayfunction/tutorial.htmlhttp://www.getbodysmart.com/ap/nervoussystem/cns/spinalcord/grayfunction/tutorial.htmlhttp://www.nlm.nih.gov/medlineplus/ency/imagepages/19080.htmhttp://biology.about.com/od/Nervous-System/ss/spinal-cord.htmhttp://biology.about.com/od/Nervous-System/ss/spinal-cord.htmhttp://emedicine.medscape.com/article/1181436-treatmenthttp://www.fightsma.org/sma-guidebook/spinal-muscular-atrophy-diagnosis-tests/http://mda.org/disease/spinal-muscular-atrophy/medical-managementhttp://emedicine.medscape.com/article/1181436-differentialhttp://www.fsma.org/FSMACommunity/understandingsma/WhatCausesSMA/http://ghr.nlm.nih.gov/gene/SMN1http://www.princeton.edu/~achaney/tmve/wiki100k/docs/Motor_neuron.htmlhttp://en.wikipedia.org/wiki/Spinal_muscular_atrophyhttp://emedicine.medscape.com/article/1259213-treatment#a1128