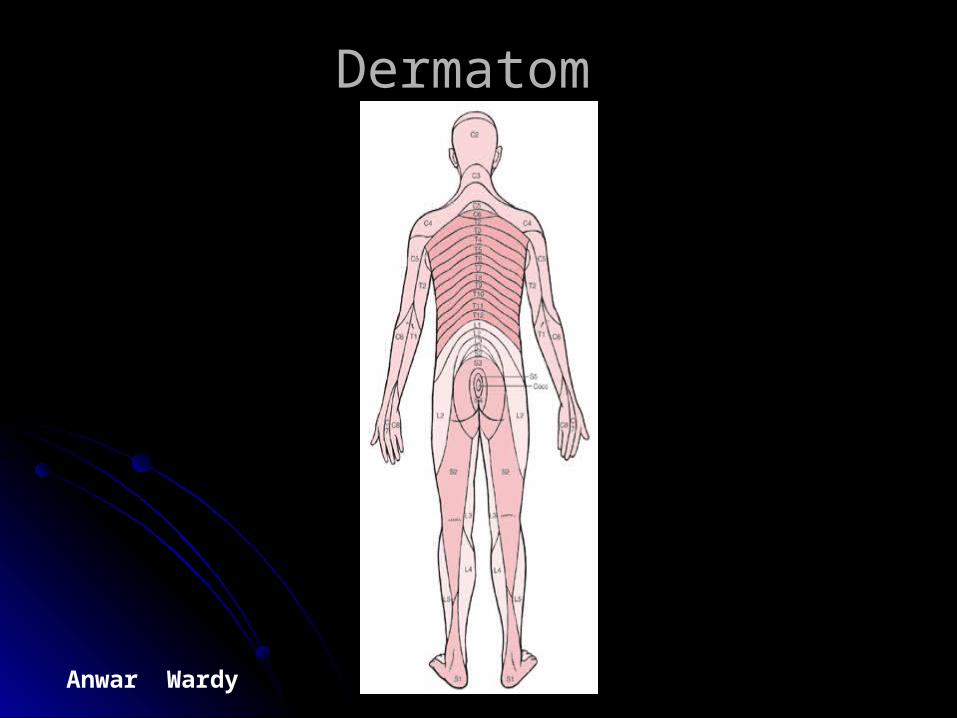

Fisik Diagnose Neuro
78
Anwar Wardy [email protected] 2007 [email protected] 2007 The Neurological The Neurological Examination Examination The goals of the neurological The goals of the neurological examination are several examination are several
-
Upload
nida-nabilah-akmal -
Category
Documents
-
view
234 -
download
4
description
info
Transcript of Fisik Diagnose Neuro
Anwar Wardy [email protected] [email protected] 2007
The Neurological The Neurological ExaminationExamination
The goals of the neurological The goals of the neurological examination are severalexamination are several
Anwar Wardy [email protected] [email protected] 2007
Independent learningIndependent learning
Case discussion during weekly didacticsCase discussion during weekly didacticsStudent presentations on a topicStudent presentations on a topicConsider some online material to Consider some online material to
supplement didactics or case discussionssupplement didactics or case discussionsGroup-study meetingGroup-study meeting? PDA use to track experiences? PDA use to track experiences
Anwar Wardy [email protected] [email protected] 2007
Major Diagnoses for clerkshipMajor Diagnoses for clerkship(Kuasai Sebelum Masuk RS)(Kuasai Sebelum Masuk RS)
*Psychosis *Psychosis Schizophrenia Schizophrenia Substance induced Substance induced In context of delirium In context of delirium
*Mood disorders *Mood disorders Depression Depression Bipolar disorder Bipolar disorder
Anxiety Anxiety *Substance abuse and *Substance abuse and
dependence dependence *Delirium *Delirium *Dementia*Dementia NeurosurgeryNeurosurgery
Head and spinal cord injuryHead and spinal cord injury Radiculopathy and myelopathyRadiculopathy and myelopathy Brief survey of neuro-oncology Brief survey of neuro-oncology
Pain Pain *Stroke *Stroke
SAH SAH Hemorrhage Hemorrhage Ischemic Ischemic
*Headache *Headache *Movement Disorders *Movement Disorders
Parkinson’s ,Essential tremor, Parkinson’s ,Essential tremor, Huntington’s Huntington’s
Neuromuscular Neuromuscular Myasthenia & ALS Myasthenia & ALS
*Dementia *Dementia *Epilepsy *Epilepsy Multiple SclerosisMultiple Sclerosis PediatricPediatric
Well child neurology examinationWell child neurology examination Static and progressive Static and progressive
encephalopathiesencephalopathies Pediatric epilepsyPediatric epilepsy

Anwar Wardy [email protected] [email protected] 2007
Didactic TopicsDidactic Topics(Umumnya di Indonesia)(Umumnya di Indonesia)
Emergency psychiatryEmergency psychiatry SchizophreniaSchizophrenia Mood DisordersMood Disorders PsychopharmacologyPsychopharmacology Confusion or memory problems Confusion or memory problems
(Dementia and delirium)(Dementia and delirium) Child psychiatryChild psychiatry Personality developmentPersonality development Substance dependence (alcohol Substance dependence (alcohol
and others)and others) Neuroscience reviewNeuroscience review Eating disordersEating disorders Personality disordersPersonality disorders PsychotherapyPsychotherapy Anxiety disordersAnxiety disorders Systems of practice in psychiatrySystems of practice in psychiatry
Weakness –Neuromuscular Weakness –Neuromuscular problemsproblems
Numbness – sensory changesNumbness – sensory changes Neurological exam and what it Neurological exam and what it
meansmeans Pediatric neurology examPediatric neurology exam Loss of consciousness differential Loss of consciousness differential
(seizure, syncope, coma)(seizure, syncope, coma) Epilepsy- Adult and pediatricEpilepsy- Adult and pediatric Sleep disordersSleep disorders Pain and headachePain and headache StrokeStroke Shaking-Movement disordersShaking-Movement disorders Disorders of intracranial pressureDisorders of intracranial pressure Head and spinal cord injuryHead and spinal cord injury Neuro-oncologyNeuro-oncology
Anwar Wardy [email protected] [email protected] 2007
Integrated Longitudinal Integrated Longitudinal CurriculumCurriculum
Disease prevention and health promotion – issues related to stroke Disease prevention and health promotion – issues related to stroke and prevention and healthand prevention and health
Stroke prevention, endarterectomy, migraine headache treatment, Stroke prevention, endarterectomy, migraine headache treatment, dementiadementia
End of life care – mgmt after stroke, ALS, Huntington’s, and neuro-End of life care – mgmt after stroke, ALS, Huntington’s, and neuro-diagnoses diagonses for quality of lifediagnoses diagonses for quality of life
Ethics – cases on informed consentEthics – cases on informed consent Nutrition- childhood developmental disordersNutrition- childhood developmental disorders Pain mgmt-Headache, back pain, neuropathy and neuropathic painPain mgmt-Headache, back pain, neuropathy and neuropathic pain Path and lab -?Path and lab -? Patient safety – head injury, topics of suicide risk prevention, Patient safety – head injury, topics of suicide risk prevention,
involuntary commitments, informed consent, drug interactions, involuntary commitments, informed consent, drug interactions, driving and epilepsydriving and epilepsy
Professional communication – working as a consultant and rolesProfessional communication – working as a consultant and roles Radiology – neuroradiology, interventional neurologyRadiology – neuroradiology, interventional neurology System based practice-systems of care in psychiatrySystem based practice-systems of care in psychiatry
Anwar Wardy [email protected] [email protected] 2007
For patients presenting with symptoms For patients presenting with symptoms suggestive of a neurological problem, the suggestive of a neurological problem, the
examination shouldexamination should
Determine, on the basis of an organized and thorough Determine, on the basis of an organized and thorough examination, whether in fact neurological dysfunction examination, whether in fact neurological dysfunction exists. exists.
Identify which component(s) of the neurological Identify which component(s) of the neurological system are affected (e.g. motor, sensory, cranial system are affected (e.g. motor, sensory, cranial nerves, or possibly several systems simultaneously). nerves, or possibly several systems simultaneously).
If possible, determine the precise location of the If possible, determine the precise location of the problem (e.g. peripheral v central nervous system; problem (e.g. peripheral v central nervous system; region and side of the brain affected etc.). region and side of the brain affected etc.).
On the basis of these findings, generate a list of On the basis of these findings, generate a list of possible etiologies. Unlikely diagnoses can be possible etiologies. Unlikely diagnoses can be excluded and appropriate testing (e.g. brain and excluded and appropriate testing (e.g. brain and spinal cord imaging) then applied in an orderly and spinal cord imaging) then applied in an orderly and logical fashion. logical fashion.
Anwar Wardy [email protected] [email protected] 2007
Screening for the presence of discrete abnormalities in Screening for the presence of discrete abnormalities in patients at risk for the development of neurological patients at risk for the development of neurological disorders. This is appropriate for individuals who disorders. This is appropriate for individuals who have no particular subjective symptoms have no particular subjective symptoms suggestive of a neurological problem, yet have suggestive of a neurological problem, yet have systemic illnesses that might put them at risk for systemic illnesses that might put them at risk for subtle dysfunction. Diabetic patients, for example subtle dysfunction. Diabetic patients, for example (particularly those with long standing poor (particularly those with long standing poor control), may develop peripheral nerve control), may develop peripheral nerve dysfunction. This may only be detected through dysfunction. This may only be detected through careful sensory testing (see Sensory Testing), careful sensory testing (see Sensory Testing), which would have important clinical implications. which would have important clinical implications.
Anwar Wardy [email protected] [email protected] 2007
1.1. Cursory screening/documentation of baseline Cursory screening/documentation of baseline function for those who are otherwise healthy. In function for those who are otherwise healthy. In patients with neither signs nor risk factors for patients with neither signs nor risk factors for neurological disease, it’s unlikely that the detailed neurological disease, it’s unlikely that the detailed exam would uncover occult problems. Simply exam would uncover occult problems. Simply observing the patient during the course of the usual observing the patient during the course of the usual H&P (i.e. watching them walk, get up and down from H&P (i.e. watching them walk, get up and down from the exam table, etc.) may well suffice. Many the exam table, etc.) may well suffice. Many examiners incorporate some aspects of the neuro examiners incorporate some aspects of the neuro exam into their standard evaluations. Cranial Nerve exam into their standard evaluations. Cranial Nerve testing, for example, can be easily blended into the testing, for example, can be easily blended into the Head and Neck evaluation. Deciding what other Head and Neck evaluation. Deciding what other aspects to routinely include is based on judgment aspects to routinely include is based on judgment and experience. and experience.
Anwar Wardy [email protected] [email protected] 2007
The major areas of the exam, covering the The major areas of the exam, covering the most testable components of the most testable components of the
neurological system, include:neurological system, include:
Mental status testing (covered in a separate Mental status testing (covered in a separate section of this web site) section of this web site)
Cranial Nerves Cranial Nerves Muscle strength, tone and bulk Muscle strength, tone and bulk Reflexes Reflexes Cerebellar Function Cerebellar Function Sensory Function Sensory Function Gait Gait
Anwar Wardy [email protected] [email protected] 2007
Real and imagined problems with Real and imagined problems with the neurological examination the neurological examination
The neurological examination is one of The neurological examination is one of the least popular and (perhaps) most the least popular and (perhaps) most poorly performed aspects of the poorly performed aspects of the complete physical. I suspect that this complete physical. I suspect that this situation exists for several reasons:situation exists for several reasons:
Anwar Wardy [email protected] [email protected] 2007
This exam is perceived as being time and labor intensive. This exam is perceived as being time and labor intensive. Students and house staff never develop an adequate level of Students and house staff never develop an adequate level of
confidence in their ability to perform the exam, nor in the accuracy confidence in their ability to perform the exam, nor in the accuracy of their findings. This, in turn, probably translates into poor of their findings. This, in turn, probably translates into poor performance later in their careers. performance later in their careers.
Exam findings are often quite subjective.Thus, particularly when the Exam findings are often quite subjective.Thus, particularly when the examiner does not have confidence in their abilities (see above), examiner does not have confidence in their abilities (see above), interpretation of the results can be problematic. interpretation of the results can be problematic.
Understanding/Interpretation of some neurological findings requires Understanding/Interpretation of some neurological findings requires an in depth understanding of neuroanatomy and pathophysiology. an in depth understanding of neuroanatomy and pathophysiology. As many clinicians do not see a large number of patients with As many clinicians do not see a large number of patients with neurological disorders, they likely maintain a limited working neurological disorders, they likely maintain a limited working understanding of this information. understanding of this information.
There is an over reliance on the utility of neuro-imaging (e.g. CT, There is an over reliance on the utility of neuro-imaging (e.g. CT, MRI). These studies provide an evaluation of anatomy but not MRI). These studies provide an evaluation of anatomy but not function. Thus, while extremely helpful, they must be interpreted function. Thus, while extremely helpful, they must be interpreted within the context of exam findings. Careful examination may make within the context of exam findings. Careful examination may make imaging unnecessary. Also, exam findings can make a strong case imaging unnecessary. Also, exam findings can make a strong case for the presence of a pathologic process, even if it is not seen on a for the presence of a pathologic process, even if it is not seen on a particular radiological study (i.e. there are limits to what can be particular radiological study (i.e. there are limits to what can be seen on even the most high tech imaging). seen on even the most high tech imaging).
Anwar Wardy [email protected] [email protected] 2007
Cranial Nerve (CN) TestingCranial Nerve (CN) Testing
CN2 CN3, 4, 5 CN6CN7CN8CN9, 10CN11CN12
Anwar Wardy [email protected] [email protected] 2007
Cranial Nerve 1 (Olfactory)Cranial Nerve 1 (Olfactory): :
Each nostril should be checked separately. Each nostril should be checked separately. Push on the outside of the nares, occluding Push on the outside of the nares, occluding the side that is not to be tested. the side that is not to be tested.
Have the patient close their eyes. Make sure Have the patient close their eyes. Make sure that the patient is able to inhale and exhale that the patient is able to inhale and exhale through the open nostril. through the open nostril.
Present a small test tube filled with Present a small test tube filled with something that has a distinct, common odor something that has a distinct, common odor (e.g. ground coffee) to the open nostril. The (e.g. ground coffee) to the open nostril. The patient should be able to correctly identify patient should be able to correctly identify the smell.the smell.
Anwar Wardy [email protected] [email protected] 2007
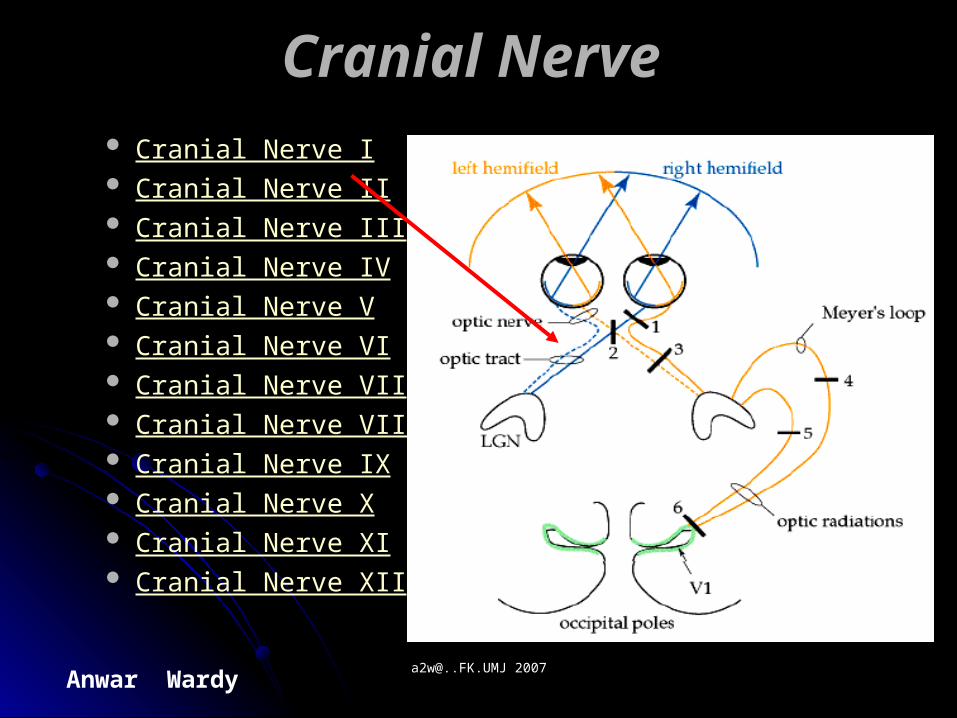
Cranial Nerve 2 (Optic)Cranial Nerve 2 (Optic)
Acuity:Acuity: Each eye is tested separately. If the patient uses glasses to view Each eye is tested separately. If the patient uses glasses to view
distant objects, they should be permitted to wear them (referred distant objects, they should be permitted to wear them (referred to as best corrected vision). to as best corrected vision).
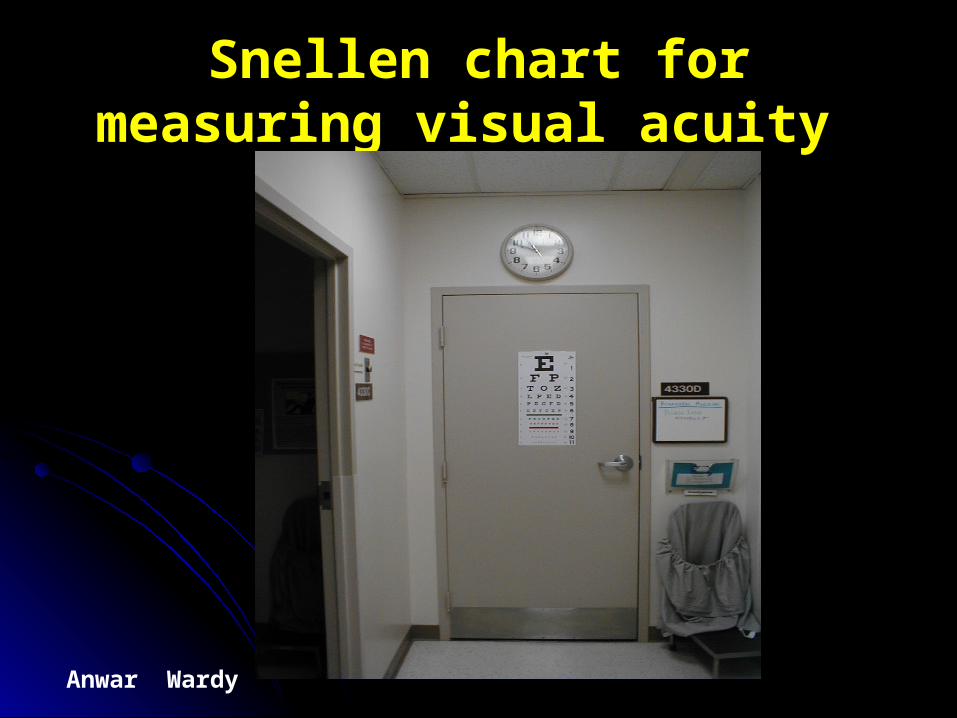
A Snellen Chart is the standard, wall mounted device used for A Snellen Chart is the standard, wall mounted device used for this assessment. Patients are asked to read the letters or this assessment. Patients are asked to read the letters or numbers on successively lower lines (each with smaller images) numbers on successively lower lines (each with smaller images) until you identify the last line which can be read with 100% until you identify the last line which can be read with 100% accuracy. Each line has a fraction written next to it. 20/20 accuracy. Each line has a fraction written next to it. 20/20 indicates normal vision. 20/400 means that the patient's vision indicates normal vision. 20/400 means that the patient's vision 20 feet from an object is equivalent to that of a normal person 20 feet from an object is equivalent to that of a normal person viewing the same object from 400 feet. In other words, the larger viewing the same object from 400 feet. In other words, the larger the denominator, the worse the vision. the denominator, the worse the vision.
Anwar Wardy [email protected] [email protected] 2007
Snellen chart for measuring Snellen chart for measuring visual acuity visual acuity
Anwar Wardy [email protected] [email protected] 2007
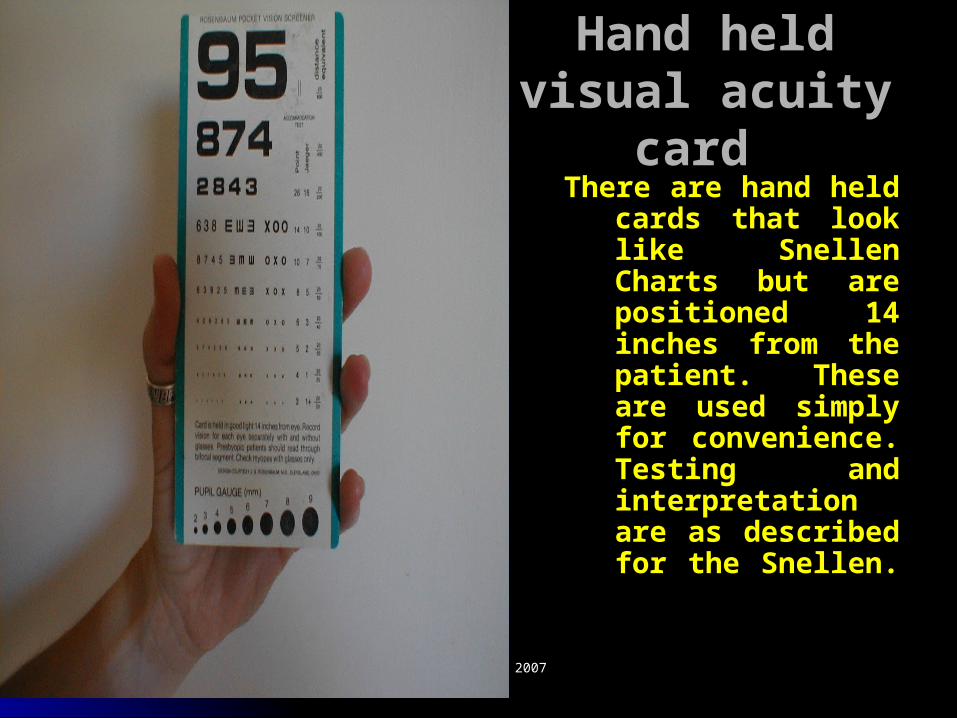
Hand held visual Hand held visual acuity cardacuity card There are hand held There are hand held
cards that look cards that look like Snellen like Snellen Charts but are Charts but are positioned 14 positioned 14 inches from the inches from the patient. These are patient. These are used simply for used simply for convenience. convenience. Testing and Testing and interpretation are interpretation are as described for as described for the Snellen. the Snellen.
Anwar Wardy [email protected] [email protected] 2007
If neither chart is available and the patient has If neither chart is available and the patient has visual complaints, some attempt should be visual complaints, some attempt should be made to objectively measure visual acuity. This made to objectively measure visual acuity. This is a critically important reference point, is a critically important reference point, particularly when trying to communicate the particularly when trying to communicate the magnitude of a visual disturbance to a magnitude of a visual disturbance to a consulting physician. Can the patient read news consulting physician. Can the patient read news print? The headline of a newspaper? print? The headline of a newspaper? Distinguish fingers or hand movement in front Distinguish fingers or hand movement in front of their face? Detect light?Failure at each level of their face? Detect light?Failure at each level correlates with a more severe problem. correlates with a more severe problem.
Anwar Wardy [email protected] [email protected] 2007
Visual fields can be crudely Visual fields can be crudely assessed as follows assessed as follows
The examiner should be nose to nose with the patient, The examiner should be nose to nose with the patient, separated by approximately 8 to 12 inches. separated by approximately 8 to 12 inches.
Each eye is checked separately. The examiner closes one eye Each eye is checked separately. The examiner closes one eye and the patient closes the one opposite. The open eyes and the patient closes the one opposite. The open eyes should then be staring directly at one another. should then be staring directly at one another.
The examiner should move their hand out towards the The examiner should move their hand out towards the periphery of his/her visual field on the side where the eyes are periphery of his/her visual field on the side where the eyes are open. The finger should be equidistant from both persons. open. The finger should be equidistant from both persons.
The examiner should then move the wiggling finger in towards The examiner should then move the wiggling finger in towards them, along an imaginary line drawn between the two them, along an imaginary line drawn between the two persons.The patient and examiner should detect the finger at persons.The patient and examiner should detect the finger at more or less the same time. more or less the same time.
The finger is then moved out to the diagonal corners of the The finger is then moved out to the diagonal corners of the field and moved inwards from each of these directions. field and moved inwards from each of these directions. Testing is then done starting at a point in front of the closed Testing is then done starting at a point in front of the closed eyes. The wiggling finger is moved towards the open eyes. eyes. The wiggling finger is moved towards the open eyes.
The other eye is then tested. The other eye is then tested.
Anwar Wardy [email protected] [email protected] 2007
Pupils Pupils The pupil has afferent (sensory) nerves The pupil has afferent (sensory) nerves
that travel with CN2. These nerves carry that travel with CN2. These nerves carry the impulse generated by the light back the impulse generated by the light back towards the brain. They function in towards the brain. They function in concert with efferent (motor) nerves that concert with efferent (motor) nerves that travel with CN 3 and cause pupillary travel with CN 3 and cause pupillary constriction. Seen under CN 3 for constriction. Seen under CN 3 for specifics of testing. specifics of testing.
Anwar Wardy [email protected] [email protected] 2007
CN 3 (Occulomotor):CN 3 (Occulomotor): This nerve is responsible for most of the eyeball’s This nerve is responsible for most of the eyeball’s
mobility, referred to as extra-occular movement. CN mobility, referred to as extra-occular movement. CN 3 function is assessed in concert with CNs 4 and 6, 3 function is assessed in concert with CNs 4 and 6, the other nerves responsible for controlling eyeball the other nerves responsible for controlling eyeball movement. CN 4 controls the Superior Oblique movement. CN 4 controls the Superior Oblique muscle, which allows each eye to look down and muscle, which allows each eye to look down and medially. CN 6 controls the Lateral Rectus muscle, medially. CN 6 controls the Lateral Rectus muscle, which allows each eye to move laterally. CN 3 which allows each eye to move laterally. CN 3 controls the muscles which allow motion in all other controls the muscles which allow motion in all other directions. The pneumonic “S O 4 – L R 6 – All The directions. The pneumonic “S O 4 – L R 6 – All The Rest 3” may help remind you which CN does what Rest 3” may help remind you which CN does what ((SSuperior uperior OOblique CN blique CN 44 – – LLateralateralRRectus CN ectus CN 66 – – AAll ll TThe he RRest of the muscles innervated by CN est of the muscles innervated by CN 33). ).
Anwar Wardy [email protected] [email protected] 2007
Inspeksi diskus optikusInspeksi diskus optikus papiledema, atau atrofi Nn papiledema, atau atrofi Nn Optikus.Optikus.
3.Nn. Optikus dan Okulomotoris,3.Nn. Optikus dan Okulomotoris, reaksi pupil reaksi pupil terhadap cahaya, jika hasil AbN, Uji reaksi sampai terhadap cahaya, jika hasil AbN, Uji reaksi sampai maksimalmaksimal Kebutaan, paralisis Nn.III, Sindroma Kebutaan, paralisis Nn.III, Sindroma Horner’sHorner’s
4. 4. Nn.III, IV, VI;Nn.III, IV, VI; gerakan ekstraokuler gerakan ekstraokulerstrabismus strabismus atau nistagmus akibat paralisis.atau nistagmus akibat paralisis.
5.Nn.V(Trigeminal)5.Nn.V(Trigeminal); raba, konraksi temporal dan ; raba, konraksi temporal dan otot2 maseter, hilangnya sensorik atau motorik otot2 maseter, hilangnya sensorik atau motorik karena lesi Nuvleus atau UMNkarena lesi Nuvleus atau UMN refleks kornea refleks kornea dan sentuhan ringan-nyeri pada wajahdan sentuhan ringan-nyeri pada wajah
Anwar Wardy [email protected] [email protected] 2007
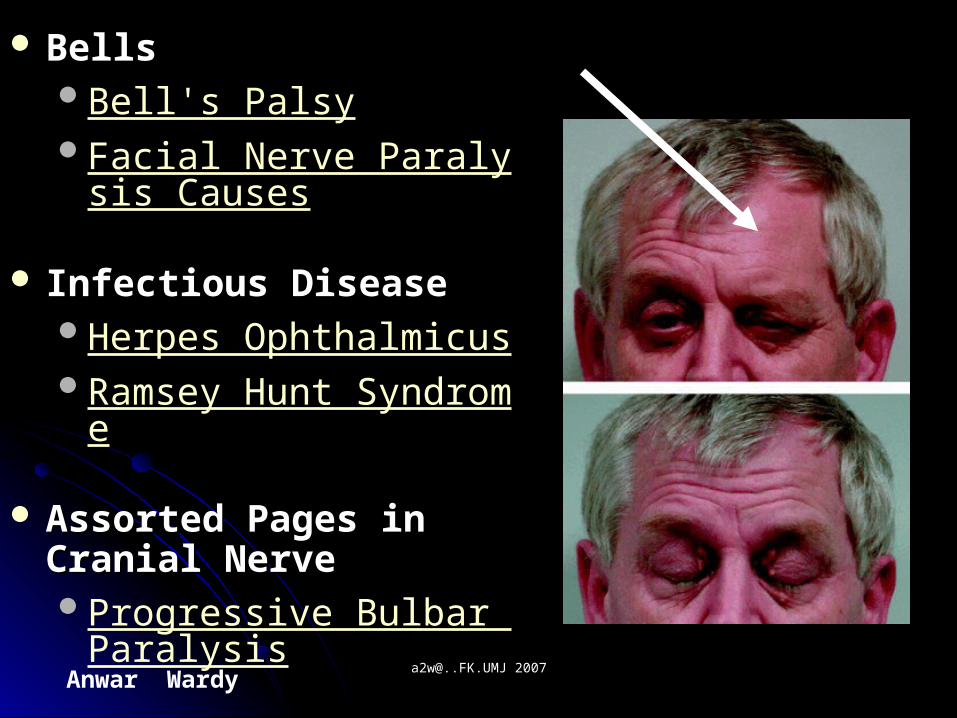
BellsBells Bell's Palsy Facial Nerve Paralysis Ca
uses
Infectious DiseaseInfectious Disease Herpes Ophthalmicus Ramsey Hunt Syndrome
Assorted Pages in Assorted Pages in Cranial NerveCranial Nerve Progressive Bulbar Paraly
sis
Trigeminal Neuralgia
Anwar Wardy [email protected] [email protected] 2007
6.6. Nn.VII. (Fasialis);Nn.VII. (Fasialis); angkat kedua alis angkat kedua alis mata, cemberut, menutup mata dengan mata, cemberut, menutup mata dengan rapat, perlihatkan gigi, tersenyum.rapat, perlihatkan gigi, tersenyum.
7.7. Nn.VIII(Akustik);Nn.VIII(Akustik); jika pendengaran jika pendengaran menurun, uji lateralisasi (Weber / Rinne).menurun, uji lateralisasi (Weber / Rinne).
8.8. Nn.Glossopharungeus & Vagus Nn.Glossopharungeus & Vagus ( IX, X);( IX, X); amati kesulitan menelan, amati kesulitan menelan, dengar suara serak atau hidung. Amati dengar suara serak atau hidung. Amati naiknya langit2 lunak dengan “Ah”naiknya langit2 lunak dengan “Ah” paralisis palatum.paralisis palatum.
Uji refleks gag pada kedua sisi hilang Uji refleks gag pada kedua sisi hilang refleks.refleks.
Anwar Wardy [email protected] [email protected] 2007
9. 9. Nn Asesori (XI); Nn Asesori (XI); Otot trapezius, kekuatan Otot trapezius, kekuatan angkat bahu. Mm Sternokleidomastoideus; angkat bahu. Mm Sternokleidomastoideus; uji berpaling kekiri / kekanan terhadap tahan uji berpaling kekiri / kekanan terhadap tahan tangan pemeriksa.tangan pemeriksa.
10. Nn.XII (Hypoglosal); dengarkan artikulasi 10. Nn.XII (Hypoglosal); dengarkan artikulasi pasien, inspeksi seluruh lidah dan bila pasien, inspeksi seluruh lidah dan bila dijulurkan apakah ada deviasi ke kiri / dijulurkan apakah ada deviasi ke kiri / kekanankekanan ada kelemahan atau disartri, atau ada kelemahan atau disartri, atau fasikulasi, serta atrofi lidah.fasikulasi, serta atrofi lidah.
Anwar Wardy [email protected] [email protected] 2007
SISTEM MOTORIKSISTEM MOTORIK
Posisi : Hemiplegi / Hemiparese!Posisi : Hemiplegi / Hemiparese!Gerakan involenter; amati letak, Gerakan involenter; amati letak,
kualitas, frekwensi, irama, amplitudokualitas, frekwensi, irama, amplitudo tremor, fasikulasi, tiks, chorea, tremor, fasikulasi, tiks, chorea, atetosis, diskinesis oro-fasial.atetosis, diskinesis oro-fasial.
Bulk otot; inspeksi kontur ototBulk otot; inspeksi kontur ototatrofi.atrofi.Tonus otot; amati tahanan dari Tonus otot; amati tahanan dari
kekuatan pasif lengan atau kekuatan pasif lengan atau tungkaitungkaispastis, kekakuan atau flasid.spastis, kekakuan atau flasid.
Anwar Wardy [email protected] [email protected] 2007
Lanjutan; periksa rentang gerakLanjutan; periksa rentang gerak Fleksi Fleksi pada pinggul dan lutut,pada pinggul dan lutut, fleksi dari tungkai yang fleksi dari tungkai yang
berlawanan mengisyaratkan deformitas pada pinggul berlawanan mengisyaratkan deformitas pada pinggul tersebut.tersebut.
Rotasi Rotasi pada pinggul, baik internal dan pada pinggul, baik internal dan eksternal,eksternal,keterbatasan pada artritis.keterbatasan pada artritis.
AbduksiAbduksi pada pinggul pada pinggul keterbatasan pada artritis. keterbatasan pada artritis. PalpasiPalpasi; sendi pinggul dan bursa ileopektinal, lateral ; sendi pinggul dan bursa ileopektinal, lateral
terhadap denyut femoralis,terhadap denyut femoralis,nyeri pada sinovitis.nyeri pada sinovitis. Bursa trochanter mayor pada femurBursa trochanter mayor pada femurbursitisbursitis Bursa iskial,Bursa iskial,nyeri pada bursitis.nyeri pada bursitis. Amati Amati lutut dan kaki saat berdiri; pembengkakan popliteal lutut dan kaki saat berdiri; pembengkakan popliteal
(kista Baker’s,& kaki datar)(kista Baker’s,& kaki datar)
Anwar Wardy [email protected] [email protected] 2007
VERTEBRA (T.BELAKANG)VERTEBRA (T.BELAKANG) InspeksiInspeksi dari ventral dan dorsal;perhatikan setiap dari ventral dan dorsal;perhatikan setiap
kurvatura abnormal (kurvatura abnormal (perhatikan asimetris; bahu, krista perhatikan asimetris; bahu, krista iliaka atau bokongiliaka atau bokong)) Kifosis, Skoliosis, Lordosis, Gibbus. Kifosis, Skoliosis, Lordosis, Gibbus.
Posisi berdiriPosisi berdiri amati bentuk asimetris bahu, krista iliaka amati bentuk asimetris bahu, krista iliaka atau bokong; pelvik mendongakatau bokong; pelvik mendongak
Periksa rentang gerak pada; fleksi, gerakan kelateral, Periksa rentang gerak pada; fleksi, gerakan kelateral, ekstensi dan rotasiekstensi dan rotasi
Konkavitas lumbal yang menetap dan keterbatasan gerak Konkavitas lumbal yang menetap dan keterbatasan gerak karena spasme otot, penyakit diskus, atau ankilosing karena spasme otot, penyakit diskus, atau ankilosing spondilitis.spondilitis.
PalpasiPalpasi terhadap nyeri tekan terhadap nyeri tekan kelaianan diskus, spasme kelaianan diskus, spasme otot, fraktur kompresi atau kondisi lain.otot, fraktur kompresi atau kondisi lain.
Anwar Wardy [email protected] [email protected] 2007
SISTEM MOTORIKSISTEM MOTORIK
Posisi : Hemiplegi / Hemiparese!Posisi : Hemiplegi / Hemiparese!Gerakan involenter; amati letak, Gerakan involenter; amati letak,
kualitas, frekwensi, irama, amplitudokualitas, frekwensi, irama, amplitudo tremor, fasikulasi, tiks, chorea, tremor, fasikulasi, tiks, chorea, atetosis, diskinesis oro-fasial.atetosis, diskinesis oro-fasial.
Bulk otot; inspeksi kontur ototBulk otot; inspeksi kontur ototatrofi.atrofi.Tonus otot; amati tahanan dari Tonus otot; amati tahanan dari
kekuatan pasif lengan atau kekuatan pasif lengan atau tungkaitungkaispastis, kekakuan atau flasid.spastis, kekakuan atau flasid.
Anwar Wardy [email protected] [email protected] 2007
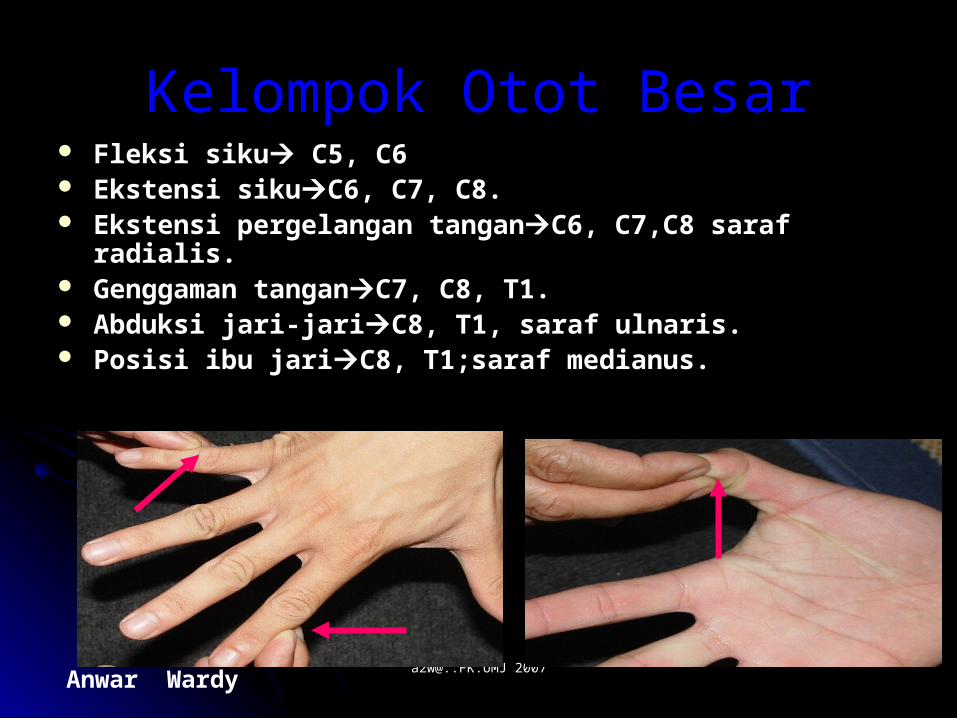
Kelompok Otot BesarKelompok Otot Besar Fleksi sikuFleksi siku C5, C6 C5, C6 Ekstensi sikuEkstensi sikuC6, C7, C8.C6, C7, C8. Ekstensi pergelangan tanganEkstensi pergelangan tanganC6, C7,C8 saraf radialis.C6, C7,C8 saraf radialis. Genggaman tanganGenggaman tanganC7, C8, T1.C7, C8, T1. Abduksi jari-jariAbduksi jari-jariC8, T1, saraf ulnaris.C8, T1, saraf ulnaris. Posisi ibu jariPosisi ibu jariC8, T1;saraf medianus.C8, T1;saraf medianus.
Anwar Wardy [email protected] [email protected] 2007
GARIS BESAR PEMERIKSAAN GARIS BESAR PEMERIKSAAN GEJALA SENDIGEJALA SENDI
Kepala & LeherKepala & Leher: : (Posisi Pasien Duduk)(Posisi Pasien Duduk)Palpasi Palpasi sendi temporomandibula ketika pasien sendi temporomandibula ketika pasien
membuka dan menutup mulut;membuka dan menutup mulut; Pembengkakan, Nyeri Tekan, Hambatan gerakan Pembengkakan, Nyeri Tekan, Hambatan gerakan
pada artritis.pada artritis.InspeksiInspeksi leher untuk mengetahui adanya leher untuk mengetahui adanya
deformitas;deformitas;Tortikolis; immobilitas pada ankilosis spondilitis,Tortikolis; immobilitas pada ankilosis spondilitis,Palpasi Palpasi Columna Vetebra Servikal dan ototnya dari Columna Vetebra Servikal dan ototnya dari
belakang pasien;belakang pasien;Nyeri tekan setempat.Nyeri tekan setempat.
Anwar Wardy [email protected] [email protected] 2007
UJI BATAS GERAK LEHERUJI BATAS GERAK LEHER::
FLEKSIFLEKSIEKSTENSIEKSTENSIROTASIROTASIGERAKAN KEARAH LATERAL KIRI GERAKAN KEARAH LATERAL KIRI
& KANAN.& KANAN.
Anwar Wardy [email protected] [email protected] 2007
Neuro-OphthalmologyNeuro-Ophthalmology Eye Neurologic Exam Oculocephalic Reflex Nystagmus
Face ExamFace Exam Cranial Nerve Exam Exam Palpebral fissures equal Palpebral fissures equal Facial symmetry Facial symmetry Tongue midline with no fasciculations midline with no fasciculations Jaw symmetric Jaw symmetric
Anwar Wardy [email protected] [email protected] 2007
Cranial NerveCranial Nerve Cranial Nerve I Cranial Nerve II Cranial Nerve III Cranial Nerve IV Cranial Nerve V Cranial Nerve VI Cranial Nerve VII Cranial Nerve VIII Cranial Nerve IX Cranial Nerve X Cranial Nerve XI Cranial Nerve XII

Anwar Wardy [email protected] [email protected] 2007
Oropharynx ExamOropharynx Exam Gag Reflex Swallow reflex Swallow reflex Regurgitation (nasal or liquid) Regurgitation (nasal or liquid)
Larynx and LanguageLarynx and Language Voice quality Voice quality Speech Exam Dysarthria (explosive or nasal) (explosive or nasal) Aphasia (writing) (writing)
Anwar Wardy [email protected] [email protected] 2007
SensorySensory Two Point Discrimination Sharp and dull discrimination Sharp and dull discrimination Proprioception (finger up or down?) Proprioception (finger up or down?) Stereography Stereography
Motor ExamMotor Exam Motor Strength Motor Strength Tone (flaccid, rigid, or cogwheel) Tone (flaccid, rigid, or cogwheel) Atrophy Atrophy Fasciculations Fasciculations Muscle tenderness Muscle tenderness Tremor Tremor
Anwar Wardy [email protected] [email protected] 2007
Sensory ExamSensory Exam
AgnosiaAgnosia; ketidaksanggupan ; ketidaksanggupan mengenali benda dan artinyamengenali benda dan artinya
Diabetic Neuropathy Testing Diabetic Neuropathy Testing Two Point DiscriminationTwo Point Discrimination
Anwar Wardy [email protected] [email protected] 2007
Motor ExamMotor Exam : :
Movement Disorder Movement Disorder Reflex Exam Reflex Exam Tetany Tetany Acute Motor Weakness Causes Acute Motor Weakness Causes Hemiplegia Hemiplegia Left Hemiplegia Left Hemiplegia Right Hemiplegia Right Hemiplegia
Anwar Wardy [email protected] [email protected] 2007
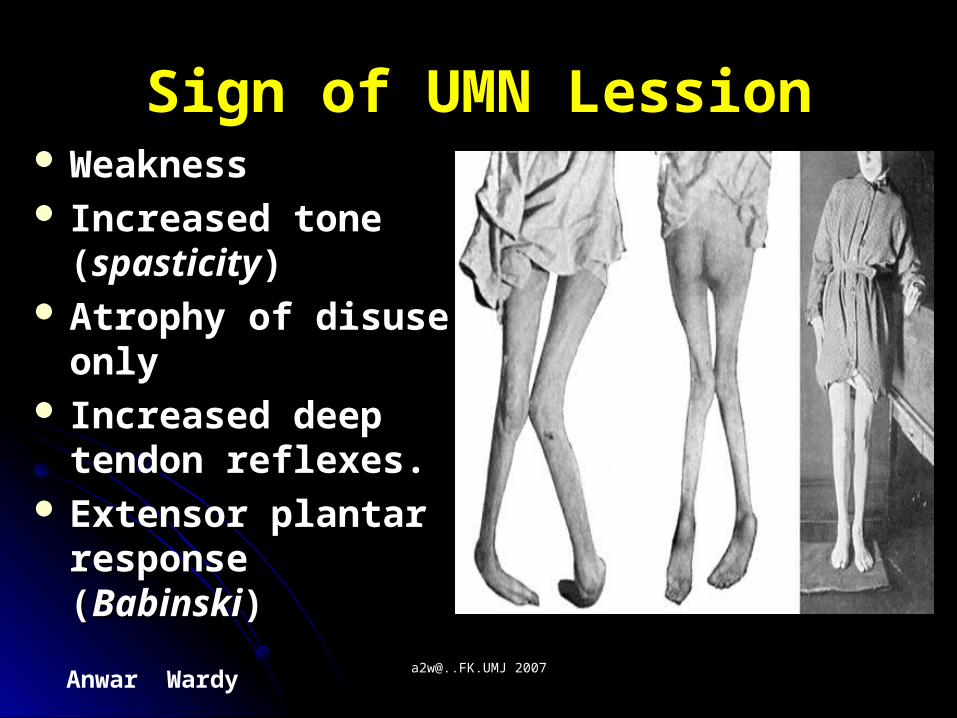
Sign of UMN LessionSign of UMN Lession WeaknessWeakness Increased tone Increased tone
((spasticityspasticity)) Atrophy of disuse Atrophy of disuse
onlyonly Increased deep Increased deep
tendon reflexes.tendon reflexes. Extensor plantar Extensor plantar
response (response (BabinskiBabinski))
Anwar Wardy [email protected] [email protected] 2007
Sign of LMN LessionSign of LMN Lession
WeaknessWeaknessDecreased tone (flaccidity)Decreased tone (flaccidity)AtrophyAtrophyFasciculationsFasciculationsDecreased to absent deep Decreased to absent deep
tendon reflexestendon reflexes
Anwar Wardy [email protected] [email protected] 2007
ReflexesReflexes
Deep Tendon Reflexes Deep Tendon Reflexes Primitive Reflexes Primitive Reflexes
Babinski Reflex Babinski Reflex Grasp Reflex Grasp Reflex Suck Reflex Suck Reflex Glabellar Reflex Glabellar Reflex Hoffman ReflexHoffman Reflex
Anwar Wardy [email protected] [email protected] 2007
PERGELANGAN TANGAN & PERGELANGAN TANGAN & TANGANTANGAN
Instrusikan pasienInstrusikan pasien membuat kepalan tangan pada membuat kepalan tangan pada kedua tangan;kedua tangan;
Perhatikan signifikansi fungsi dan arti diagnosis dari Perhatikan signifikansi fungsi dan arti diagnosis dari keterbatasan gerakan.keterbatasan gerakan.
-Meluruskan jari-jari;-Meluruskan jari-jari;--Fleksi dan ekstensiFleksi dan ekstensi pergelangan tangan. pergelangan tangan.-Membalikkan tangan (dgn telapak tangan menghadap -Membalikkan tangan (dgn telapak tangan menghadap
kebawah) kearah lateral dan medial (penyimpangan lateral kebawah) kearah lateral dan medial (penyimpangan lateral dan medial)dan medial)
--InspeksiInspeksi tangan dan pergelangan tangan; tangan dan pergelangan tangan; Deformitas, pembengkakan atau atrofi muskularDeformitas, pembengkakan atau atrofi muskular
Anwar Wardy [email protected] [email protected] 2007
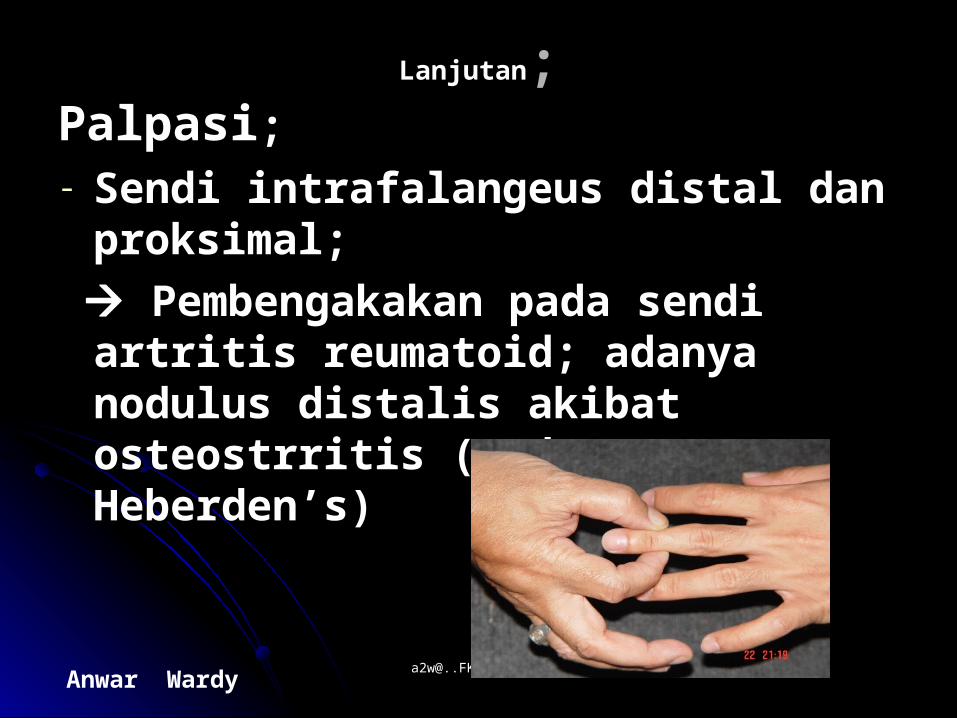
LanjutanLanjutan;;PalpasiPalpasi; ; - Sendi intrafalangeus distal dan Sendi intrafalangeus distal dan
proksimal;proksimal;
Pembengakakan pada sendi artritis Pembengakakan pada sendi artritis reumatoid; adanya nodulus distalis reumatoid; adanya nodulus distalis akibat osteostrritis (akibat osteostrritis (nodus nodus Heberden’sHeberden’s))
Anwar Wardy [email protected] [email protected] 2007
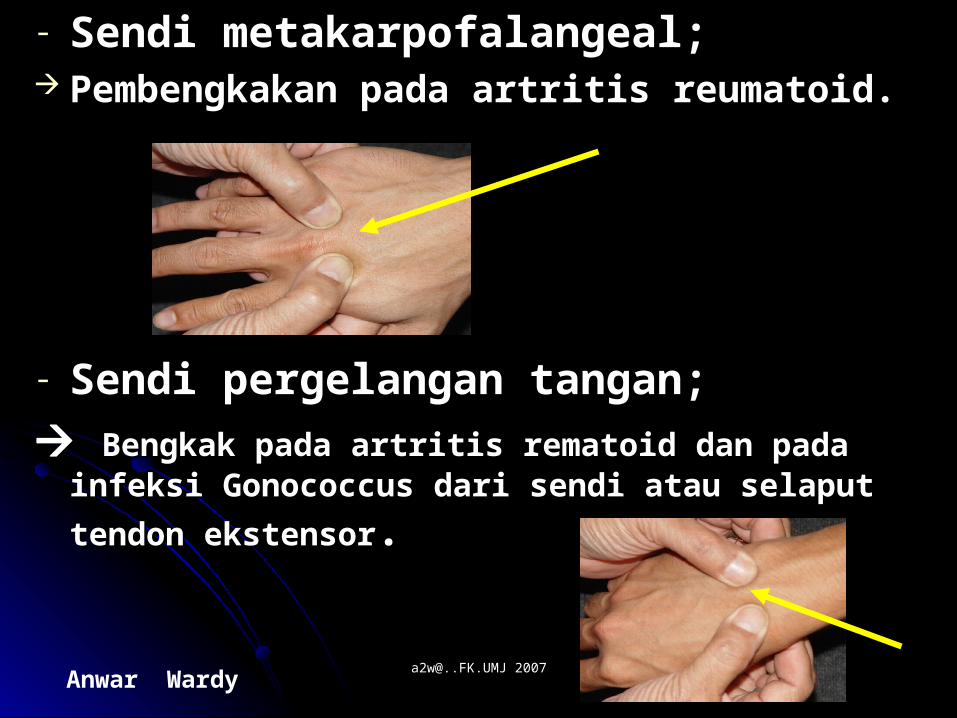
- Sendi metakarpofalangeal;Sendi metakarpofalangeal; Pembengkakan pada artritis reumatoid.Pembengkakan pada artritis reumatoid.
- Sendi pergelangan tangan;Sendi pergelangan tangan;
Bengkak pada artritis rematoid dan pada infeksi Bengkak pada artritis rematoid dan pada infeksi
Gonococcus dari sendi atau selaput tendon ekstensorGonococcus dari sendi atau selaput tendon ekstensor..
Anwar Wardy [email protected] [email protected] 2007
S I K US I K U Pasien dianjurkan menekuk dan meluruskan Pasien dianjurkan menekuk dan meluruskan
siku.siku. Membalikkan telapak tangan keatas dan Membalikkan telapak tangan keatas dan
kebawah (kebawah (supinasi dan pronasisupinasi dan pronasi) dari lengan ) dari lengan bawah.bawah.
Inspeksi dan PalpasiInspeksi dan Palpasi Siku, temasuk; Siku, temasuk;-Prosessus olekranon; adanya bursitis olekranon.-Prosessus olekranon; adanya bursitis olekranon.-Lekukan pada sendi siku; nyeri tekan pada -Lekukan pada sendi siku; nyeri tekan pada
artritis.artritis.-Epikondile medial dan lateral; nyeri tekan pada -Epikondile medial dan lateral; nyeri tekan pada
epikondilitis.epikondilitis.-Permukaan ekstensor dari ulna; adanya nodulus -Permukaan ekstensor dari ulna; adanya nodulus
rematoid.rematoid.
Anwar Wardy [email protected] [email protected] 2007
B A H UB A H U((Perhatikan adanya Hambatan PergerakanPerhatikan adanya Hambatan Pergerakan))
Mengangkat kedua tangan kearah vertikal keatas / bebawah.Mengangkat kedua tangan kearah vertikal keatas / bebawah.Letakkan kedua tangan dibelakang leher dengan siku ke arah Letakkan kedua tangan dibelakang leher dengan siku ke arah luar (luar (abduksi dan rotasi eksternalabduksi dan rotasi eksternal))
Letakkan kedua tangan dibelakang punggung atas (Letakkan kedua tangan dibelakang punggung atas (rotasi rotasi internalinternal).).
InspeksiInspeksi bahu dan pangkal bahu dari depan dan belakang; bahu dan pangkal bahu dari depan dan belakang; adanya Atropi muskular.adanya Atropi muskular.
PalpasiPalpasi terhadap nyeri tekan dibeberapa daerah sendi bahu; terhadap nyeri tekan dibeberapa daerah sendi bahu; adanya tendinitis manset rotator adalah penyebab umum dari adanya tendinitis manset rotator adalah penyebab umum dari nyeri tekan subakromial(B); lht- gambar/ nyeri tekan subakromial(B); lht- gambar/ Tendinitis bisipital (A)Tendinitis bisipital (A)
Anwar Wardy [email protected] [email protected] 2007
PERGELANGAN KAKI DAN PERGELANGAN KAKI DAN TUNGKAI.TUNGKAI.
InspeksiInspeksi sendi pergelangan sendi pergelangan kaki;kaki;Hallus valgus, corns, calluses.Hallus valgus, corns, calluses.
PalpasiPalpasi setiap sendi setiap sendinyeri pada nyeri pada artritis; nyeri ligamen pada saat terkilir.artritis; nyeri ligamen pada saat terkilir.
Raba sepanjang tendon Raba sepanjang tendon AchillesAchillesnodulus rematoidnodulus rematoid
Anwar Wardy [email protected] [email protected] 2007
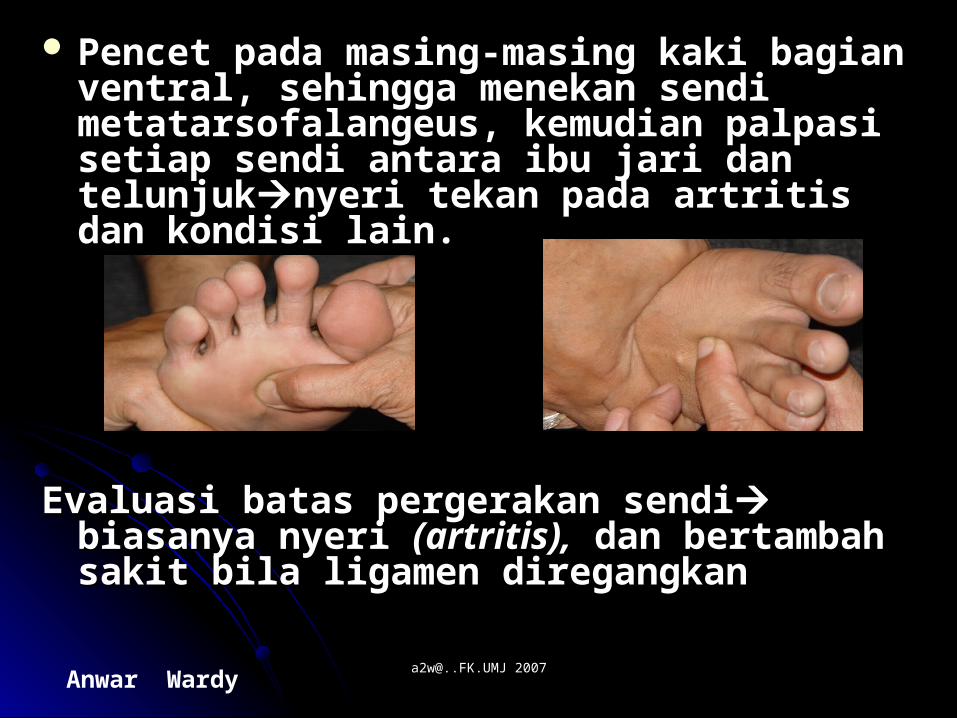
Pencet pada masing-masing kaki bagian Pencet pada masing-masing kaki bagian ventral, sehingga menekan sendi ventral, sehingga menekan sendi metatarsofalangeus, kemudian metatarsofalangeus, kemudian palpasipalpasi setiap setiap sendi antara ibu jari dan telunjuksendi antara ibu jari dan telunjuknyeri tekan nyeri tekan pada artritis dan kondisi lain.pada artritis dan kondisi lain.
Evaluasi batas pergerakan sendiEvaluasi batas pergerakan sendi biasanya biasanya nyeri nyeri (artritis),(artritis), dan bertambah sakit bila dan bertambah sakit bila ligamen diregangkanligamen diregangkan
Anwar Wardy [email protected] [email protected] 2007
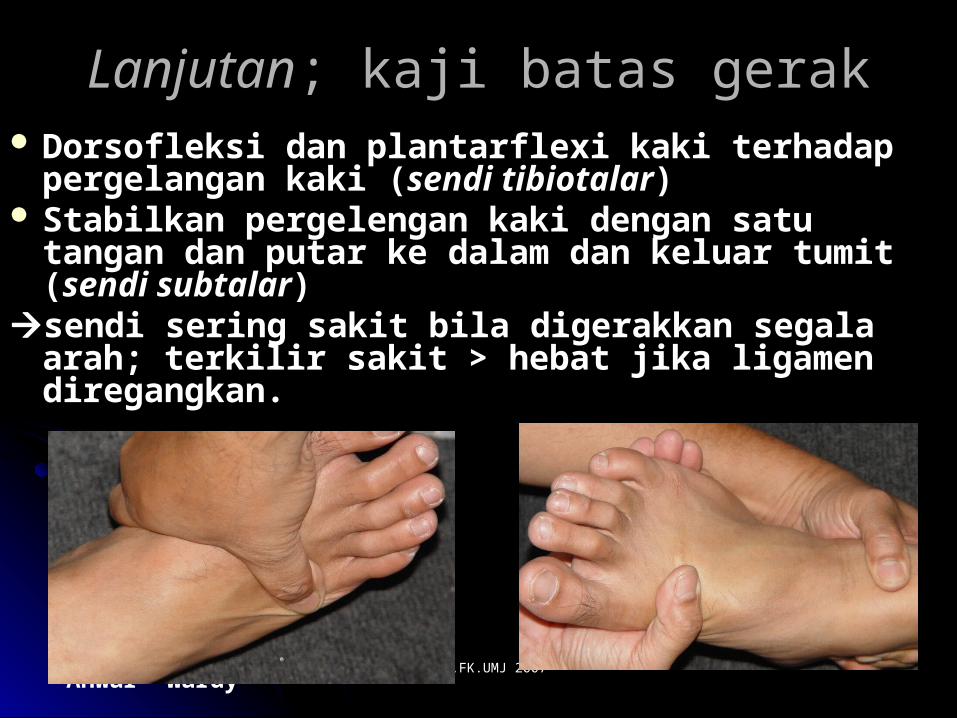
LanjutanLanjutan; kaji batas gerak; kaji batas gerak Dorsofleksi dan plantarflexiDorsofleksi dan plantarflexi kaki terhadap kaki terhadap
pergelangan kaki (pergelangan kaki (sendi tibiotalarsendi tibiotalar)) Stabilkan pergelengan kaki dengan satu tangan Stabilkan pergelengan kaki dengan satu tangan
dan putar ke dalam dan keluar tumit (dan putar ke dalam dan keluar tumit (sendi sendi subtalarsubtalar))
sendi sering sakit bila digerakkan segala arah; sendi sering sakit bila digerakkan segala arah; terkilir sakit > hebat jika ligamen diregangkan.terkilir sakit > hebat jika ligamen diregangkan.
Anwar Wardy [email protected] [email protected] 2007
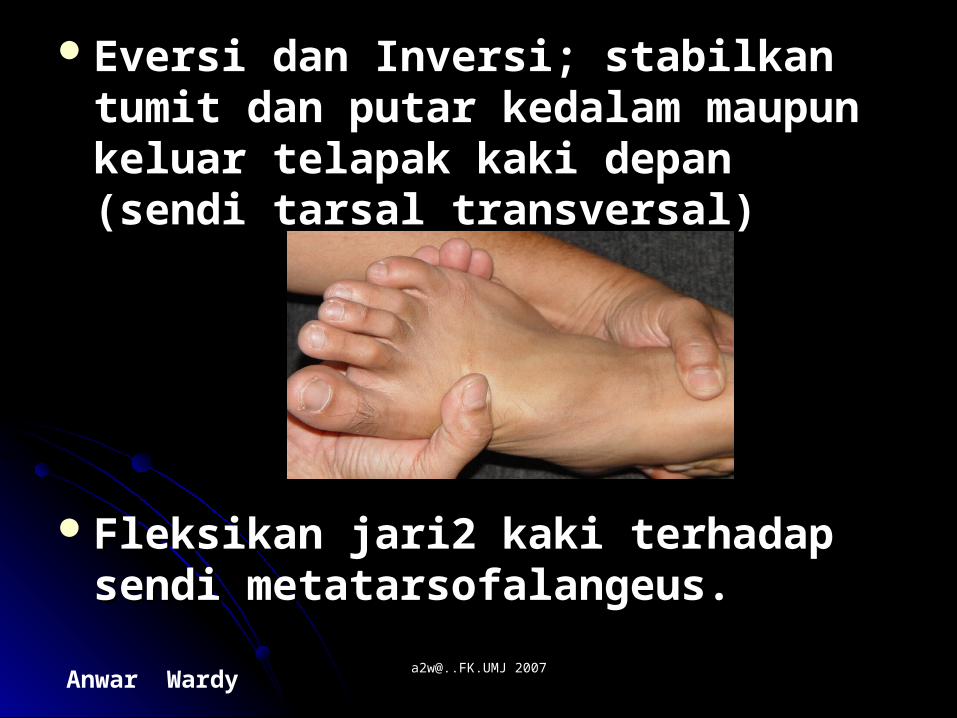
Eversi dan InversiEversi dan Inversi; stabilkan tumit ; stabilkan tumit dan putar kedalam maupun keluar dan putar kedalam maupun keluar telapak kaki depan (sendi tarsal telapak kaki depan (sendi tarsal transversal)transversal)
FleksikanFleksikan jari2 kaki terhadap sendi jari2 kaki terhadap sendi metatarsofalangeus.metatarsofalangeus.
Anwar Wardy [email protected] [email protected] 2007
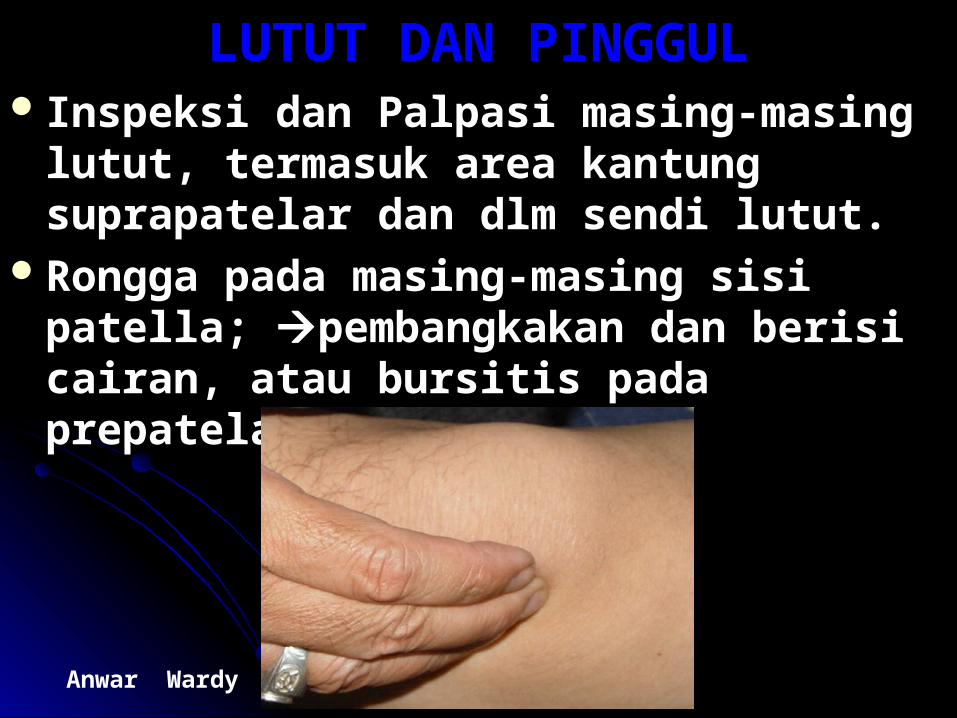
LUTUT DAN PINGGULLUTUT DAN PINGGUL Inspeksi dan PalpasiInspeksi dan Palpasi masing-masing masing-masing
lutut, termasuk area kantung suprapatelar lutut, termasuk area kantung suprapatelar dan dlm sendi lutut.dan dlm sendi lutut.
Rongga pada masing-masing sisi patella; Rongga pada masing-masing sisi patella; pembangkakan dan berisi cairan, atau pembangkakan dan berisi cairan, atau bursitis pada prepatelar.bursitis pada prepatelar.
Anwar Wardy [email protected] [email protected] 2007
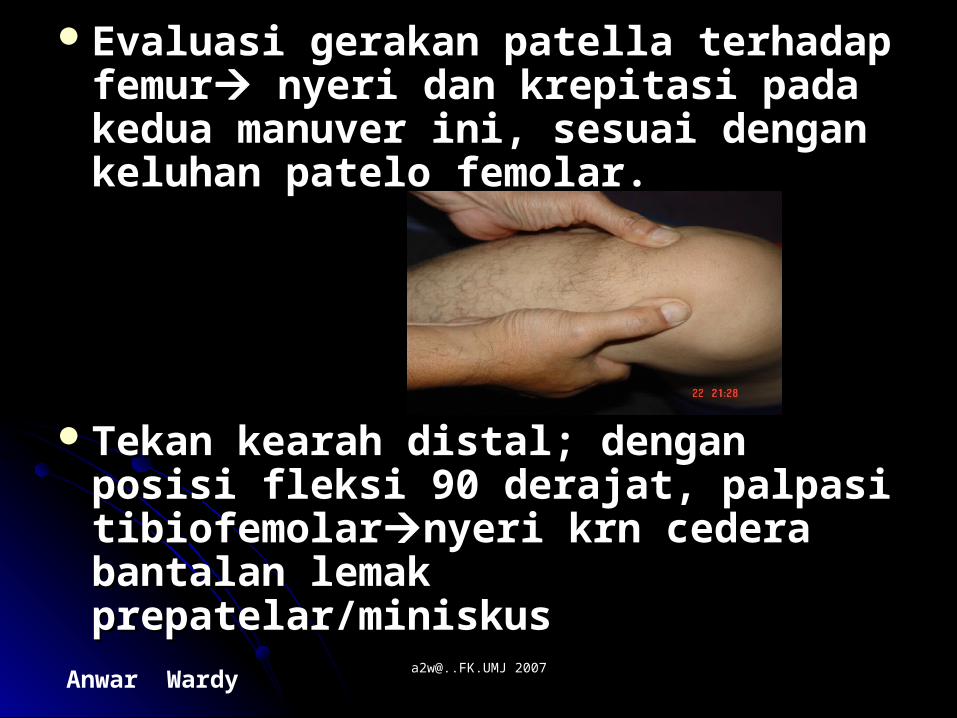
Evaluasi gerakan patella terhadap Evaluasi gerakan patella terhadap femurfemur nyeri dan krepitasi pada kedua nyeri dan krepitasi pada kedua manuver ini, sesuai dengan keluhan manuver ini, sesuai dengan keluhan patelo femolar.patelo femolar.
Tekan kearah distal; dengan posisi Tekan kearah distal; dengan posisi fleksi 90 derajat, palpasi fleksi 90 derajat, palpasi tibiofemolartibiofemolarnyeri krn cedera bantalan nyeri krn cedera bantalan lemak prepatelar/miniskuslemak prepatelar/miniskus
Anwar Wardy [email protected] [email protected] 2007
Lanjutan; periksa rentang gerakLanjutan; periksa rentang gerak Fleksi Fleksi pada pinggul dan lutut,pada pinggul dan lutut, fleksi dari tungkai yang fleksi dari tungkai yang
berlawanan mengisyaratkan deformitas pada pinggul berlawanan mengisyaratkan deformitas pada pinggul tersebut.tersebut.
Rotasi Rotasi pada pinggul, baik internal dan pada pinggul, baik internal dan eksternal,eksternal,keterbatasan pada artritis.keterbatasan pada artritis.
AbduksiAbduksi pada pinggul pada pinggul keterbatasan pada artritis. keterbatasan pada artritis. PalpasiPalpasi; sendi pinggul dan bursa ileopektinal, lateral ; sendi pinggul dan bursa ileopektinal, lateral
terhadap denyut femoralis,terhadap denyut femoralis,nyeri pada sinovitis.nyeri pada sinovitis. Bursa trochanter mayor pada femurBursa trochanter mayor pada femurbursitisbursitis Bursa iskial,Bursa iskial,nyeri pada bursitis.nyeri pada bursitis. Amati Amati lutut dan kaki saat berdiri; pembengkakan popliteal lutut dan kaki saat berdiri; pembengkakan popliteal
(kista Baker’s,& kaki datar)(kista Baker’s,& kaki datar)
Anwar Wardy [email protected] [email protected] 2007
VERTEBRA (T.BELAKANG)VERTEBRA (T.BELAKANG) InspeksiInspeksi dari ventral dan dorsal;perhatikan setiap dari ventral dan dorsal;perhatikan setiap
kurvatura abnormal (kurvatura abnormal (perhatikan asimetris; bahu, krista perhatikan asimetris; bahu, krista iliaka atau bokongiliaka atau bokong)) Kifosis, Skoliosis, Lordosis, Gibbus. Kifosis, Skoliosis, Lordosis, Gibbus.
Posisi berdiriPosisi berdiri amati bentuk asimetris bahu, krista iliaka amati bentuk asimetris bahu, krista iliaka atau bokong; pelvik mendongakatau bokong; pelvik mendongak
Periksa rentang gerak pada; fleksi, gerakan kelateral, Periksa rentang gerak pada; fleksi, gerakan kelateral, ekstensi dan rotasiekstensi dan rotasi
Konkavitas lumbal yang menetap dan keterbatasan gerak Konkavitas lumbal yang menetap dan keterbatasan gerak karena spasme otot, penyakit diskus, atau ankilosing karena spasme otot, penyakit diskus, atau ankilosing spondilitis.spondilitis.
PalpasiPalpasi terhadap nyeri tekan terhadap nyeri tekan kelaianan diskus, spasme kelaianan diskus, spasme otot, fraktur kompresi atau kondisi lain.otot, fraktur kompresi atau kondisi lain.
Anwar Wardy [email protected] [email protected] 2007
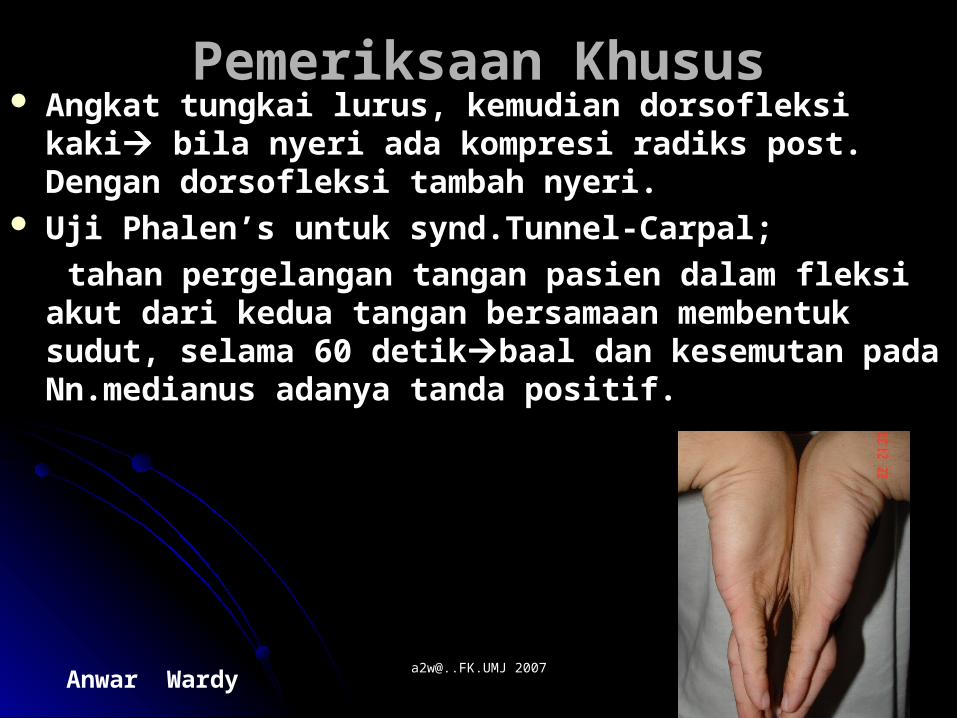
Pemeriksaan KhususPemeriksaan Khusus Angkat tungkai lurus, kemudian dorsofleksi kakiAngkat tungkai lurus, kemudian dorsofleksi kaki bila bila
nyeri ada kompresi radiks post. Dengan dorsofleksi nyeri ada kompresi radiks post. Dengan dorsofleksi tambah nyeri.tambah nyeri.
Uji Phalen’sUji Phalen’s untuk synd.Tunnel-Carpal; untuk synd.Tunnel-Carpal;
tahan pergelangan tangan pasien dalam fleksi akut dari tahan pergelangan tangan pasien dalam fleksi akut dari kedua tangan bersamaan membentuk sudut, selama 60 kedua tangan bersamaan membentuk sudut, selama 60 detikdetikbaal dan kesemutan pada Nn.medianus adanya baal dan kesemutan pada Nn.medianus adanya tanda positif.tanda positif.
Anwar Wardy [email protected] [email protected] 2007
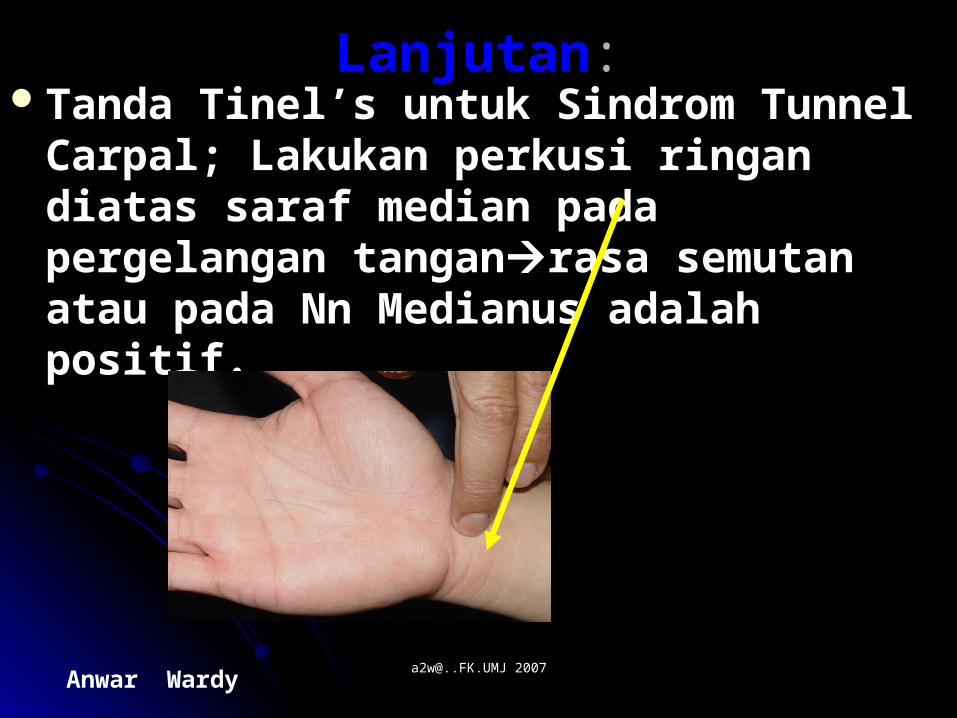
LanjutanLanjutan::Tanda Tinel’sTanda Tinel’s untuk Sindrom Tunnel untuk Sindrom Tunnel
Carpal; Lakukan perkusi ringan diatas saraf Carpal; Lakukan perkusi ringan diatas saraf median pada pergelangan tanganmedian pada pergelangan tanganrasa rasa semutan atau pada Nn Medianus adalah semutan atau pada Nn Medianus adalah positif.positif.
Anwar Wardy [email protected] [email protected] 2007
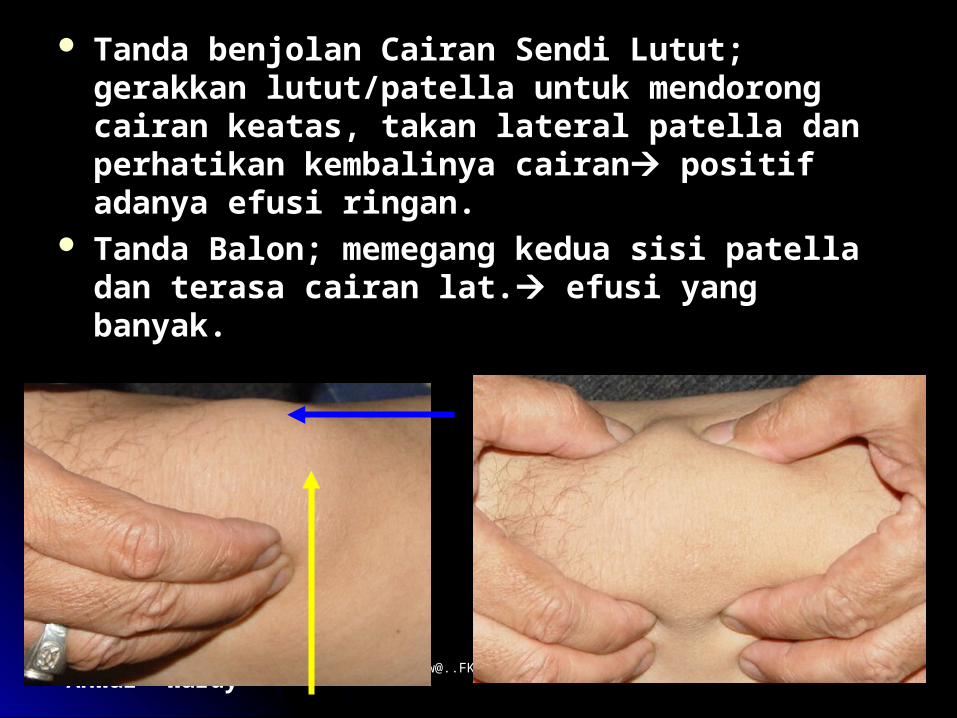
Tanda benjolanTanda benjolan Cairan Sendi Lutut; gerakkan Cairan Sendi Lutut; gerakkan lutut/patella untuk mendorong cairan keatas, takan lutut/patella untuk mendorong cairan keatas, takan lateral patella dan perhatikan kembalinya cairanlateral patella dan perhatikan kembalinya cairan positif adanya efusi ringan.positif adanya efusi ringan.
Tanda Balon; Tanda Balon; memegang kedua sisi patella dan memegang kedua sisi patella dan terasa cairan lat.terasa cairan lat. efusi yang banyak. efusi yang banyak.

Anwar Wardy [email protected] [email protected] 2007
Lanjutan:Lanjutan:
Mengukur panjang tungkai; tungkai Mengukur panjang tungkai; tungkai lurus simetris, dengan meter/plester lurus simetris, dengan meter/plester dari spina iliaka sup/anterior ke dari spina iliaka sup/anterior ke maleolus medialia melalui lutut maleolus medialia melalui lutut dibagian medialdibagian medial bila tdk sama adanya bila tdk sama adanya skoliosis.skoliosis.
Mengukur rentang gerak; tangan fleksi Mengukur rentang gerak; tangan fleksi dan ektensi; 0 – dan ektensi; 0 – 45- 9045- 90 dan 160 dan 160 derajat.derajat.
Anwar Wardy [email protected] [email protected] 2007
Cara BerjalanCara BerjalanBerjalan hemiparesis spastikBerjalan hemiparesis spastik; lengan ; lengan
tertahan rapat pada sisi tubuh dengan tertahan rapat pada sisi tubuh dengan persendian fleksi. Tungkai ekstensi dan kaki persendian fleksi. Tungkai ekstensi dan kaki fleksi plantar. Saat berjalan, jari-jari kaki fleksi plantar. Saat berjalan, jari-jari kaki mencengkram dan tungkai circumduksi.mencengkram dan tungkai circumduksi.
Berjalan seperti guntingBerjalan seperti gunting (paresis (paresis spastik bilateral);cara berjalan yang kaku, spastik bilateral);cara berjalan yang kaku, paha menyilang ke depan satu sama lain paha menyilang ke depan satu sama lain setiap kali melangkah. Langkahnya pendek.setiap kali melangkah. Langkahnya pendek.
Anwar Wardy [email protected] [email protected] 2007
Berjalan TimplangBerjalan Timplang (Gangguan saraf (Gangguan saraf Perifer); karena Perifer); karena foot drop, tampak foot drop, tampak menyeret kaki atau mengangkatnya tinggi-menyeret kaki atau mengangkatnya tinggi-tinggi dan menghentakkan kebawah.tinggi dan menghentakkan kebawah.
Ataksia sensoris; Ataksia sensoris; tidak tegap cara tidak tegap cara berjalan dengan ancang yang melebar, berjalan dengan ancang yang melebar, secara sepihak dapat diperbaiki dengan secara sepihak dapat diperbaiki dengan memperhatikan lantai. Kaki diajunkan memperhatikan lantai. Kaki diajunkan kedepan dan keluar dan dijatuhkan pada kedepan dan keluar dan dijatuhkan pada tumid dan kemudian jari-jari kaki. Dengan tumid dan kemudian jari-jari kaki. Dengan test Romberg positif.test Romberg positif.
Anwar Wardy [email protected] [email protected] 2007
Berjalan Atasia Serebral; Berjalan Atasia Serebral; tidak tidak mantap saat berjalan dengan ancang lebar mantap saat berjalan dengan ancang lebar dan mengalami kesulitan bila berbalik dan mengalami kesulitan bila berbalik arah.Saat test arah.Saat test RombergRomberg, tidak tegap , tidak tegap dengan mata terbuka atau terpejam. Tanda dengan mata terbuka atau terpejam. Tanda lain serebral berkaitan.lain serebral berkaitan.
Jalan Parkinsonisme;Jalan Parkinsonisme; postur postur membungkuk dengan siku dan membungkuk dengan siku dan pergelengan tangan fleksi. Cara berjalan pergelengan tangan fleksi. Cara berjalan lambat, melayang dengan langkah pendek lambat, melayang dengan langkah pendek dan kaku saat berbalik.dan kaku saat berbalik.
Anwar Wardy [email protected] [email protected] 2007
Daerah PinggulDaerah Pinggul
Fleksi pinggulFleksi pinggul L2, L3, L4 L2, L3, L4Adduksi pinggulAdduksi pinggulL2,L3,L4L2,L3,L4Abduksi pinggulAbduksi pinggulL2, L5, S1L2, L5, S1Ekstensi pinggulEkstensi pinggulS1.S1.Ekstensi lututEkstensi lututL2,L3,L4L2,L3,L4Fleksi lututFleksi lututL4,L5, S1,S2.L4,L5, S1,S2.Dorsofleksi pergelangan kakiDorsofleksi pergelangan kakiL4, L5.L4, L5.Plantar pergelangan kakiPlantar pergelangan kakiS1.S1.
Anwar Wardy [email protected] [email protected] 2007
Skala Kekuatan OtotSkala Kekuatan Otot..
0; Tidak terdapat konraksi otot yang 0; Tidak terdapat konraksi otot yang terlihat.terlihat.
1; Kontraksi dapat terlihat.1; Kontraksi dapat terlihat.2.Gerakan aktif penghilangan gravitasi.2.Gerakan aktif penghilangan gravitasi.3.Gerakan aktif terhadap gravitasi.3.Gerakan aktif terhadap gravitasi.4.Gerakan aktif dengan tahanan.4.Gerakan aktif dengan tahanan.5.Gerakan aktif terhadap tahanan 5.Gerakan aktif terhadap tahanan
penuh.penuh.
Anwar Wardy [email protected] [email protected] 2007
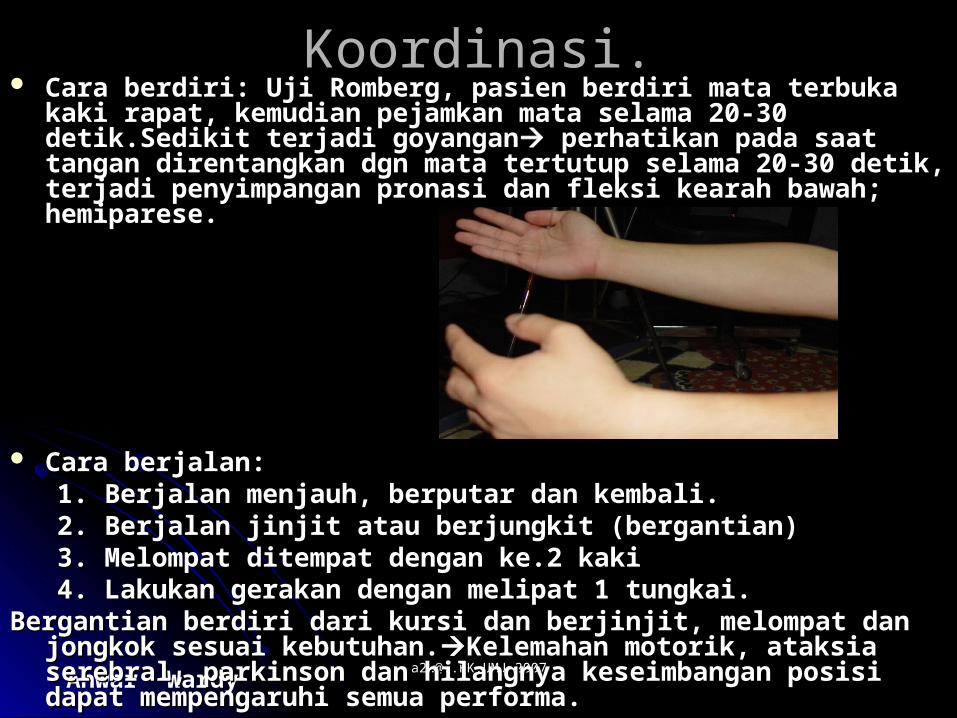
KoordinasiKoordinasi.. Cara berdiriCara berdiri: : Uji RombergUji Romberg, pasien berdiri mata terbuka kaki rapat, , pasien berdiri mata terbuka kaki rapat,
kemudian pejamkan mata selama 20-30 detik.Sedikit terjadi kemudian pejamkan mata selama 20-30 detik.Sedikit terjadi goyangangoyangan perhatikan pada saat tangan direntangkan dgn mata perhatikan pada saat tangan direntangkan dgn mata tertutup selama 20-30 detik, terjadi penyimpangan pronasi dan fleksi tertutup selama 20-30 detik, terjadi penyimpangan pronasi dan fleksi kearah bawah; kearah bawah; hemiparese.hemiparese.
Cara berjalanCara berjalan:: 1. Berjalan menjauh, berputar dan kembali.1. Berjalan menjauh, berputar dan kembali. 2. Berjalan jinjit atau berjungkit (bergantian)2. Berjalan jinjit atau berjungkit (bergantian) 3. Melompat ditempat dengan ke.2 kaki3. Melompat ditempat dengan ke.2 kaki 4. Lakukan gerakan dengan melipat 1 tungkai. 4. Lakukan gerakan dengan melipat 1 tungkai. Bergantian berdiri dari kursi dan berjinjit, melompat dan jongkok sesuai Bergantian berdiri dari kursi dan berjinjit, melompat dan jongkok sesuai
kebutuhan.kebutuhan.Kelemahan motorik, ataksia serebral, parkinson dan Kelemahan motorik, ataksia serebral, parkinson dan hilangnya keseimbangan posisi dapat mempengaruhi semua performa.hilangnya keseimbangan posisi dapat mempengaruhi semua performa.
Anwar Wardy [email protected] [email protected] 2007
Lanjutan:Lanjutan:
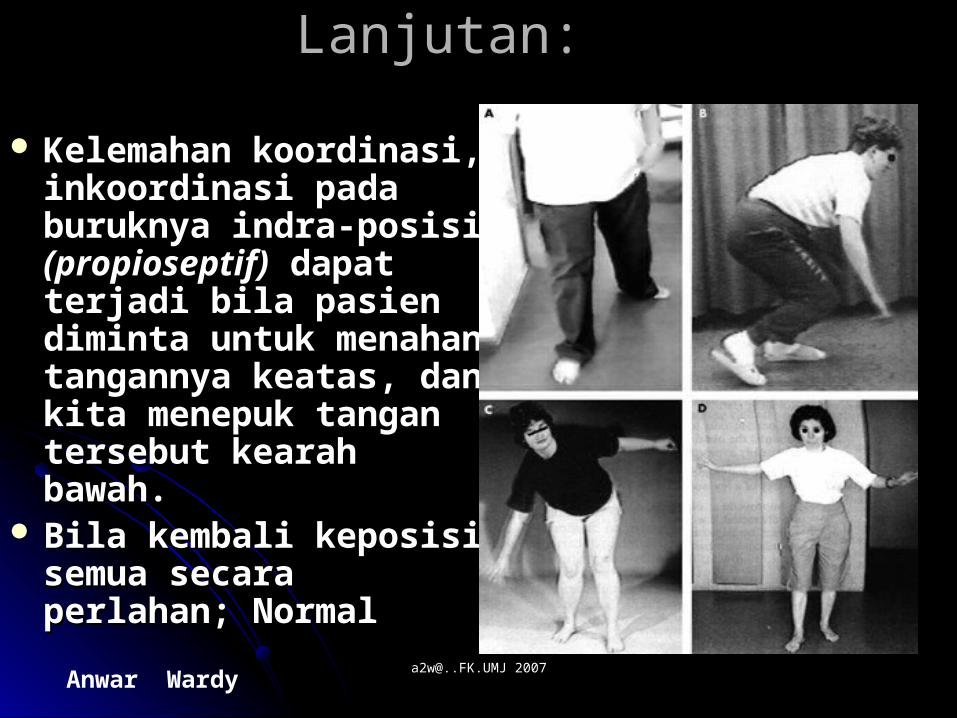
Kelemahan Kelemahan koordinasi, koordinasi, inkoordinasiinkoordinasi pada pada buruknya indra-posisi buruknya indra-posisi (propioseptif)(propioseptif) dapat dapat terjadi bila pasien terjadi bila pasien diminta untuk menahan diminta untuk menahan tangannya keatas, dan tangannya keatas, dan kita menepuk tangan kita menepuk tangan tersebut kearah bawah.tersebut kearah bawah.
Bila kembali keposisi Bila kembali keposisi semua secara perlahan; semua secara perlahan; NormalNormal
Anwar Wardy [email protected] [email protected] 2007
Types of ParalysisTypes of Paralysis FlaccidFlaccid paralysis occurs with damage to ventral root paralysis occurs with damage to ventral root
or anterior horn, resulting in no stimulation of or anterior horn, resulting in no stimulation of voluntary and involuntary movement.voluntary and involuntary movement.
SpasticSpastic paralysis from damage of upper motor paralysis from damage of upper motor neurons of primary motor cortex, causes loss of neurons of primary motor cortex, causes loss of voluntary movements, but spinal reflex activity still voluntary movements, but spinal reflex activity still occurs.occurs.
ParaplegiaParaplegia is a term used to indicate loss of lower is a term used to indicate loss of lower limb control due to damage to cord in thoracic region.limb control due to damage to cord in thoracic region.
QuadraplegiaQuadraplegia refers to damage at cervical region, refers to damage at cervical region, which affects all limbs.which affects all limbs.
Anwar Wardy [email protected] [email protected] 2007
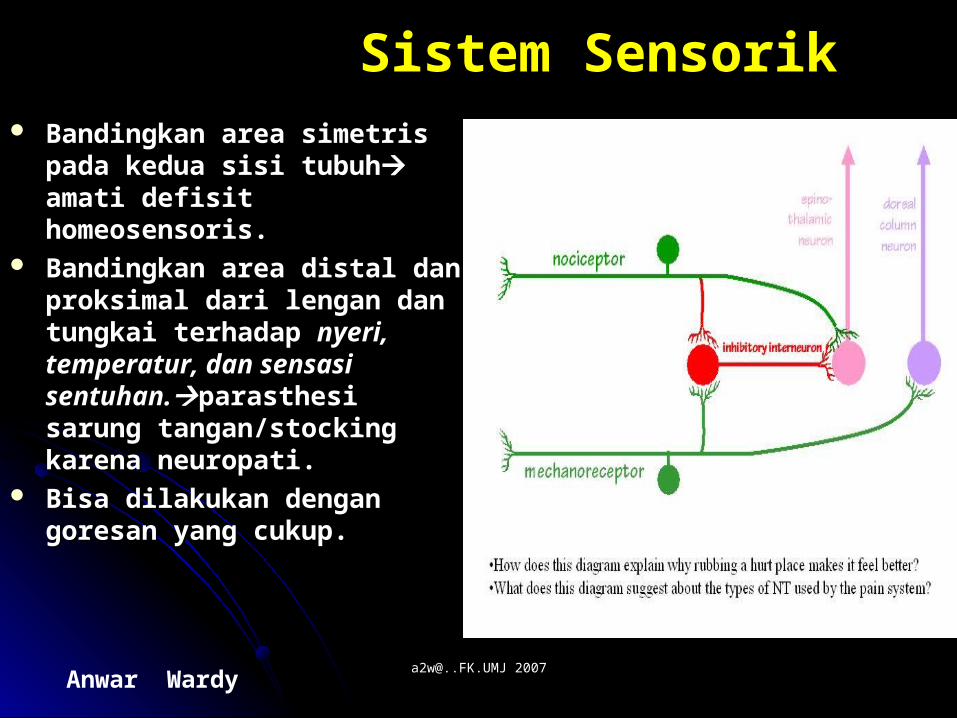
Sistem SensorikSistem Sensorik Bandingkan area simetris pada Bandingkan area simetris pada
kedua sisi tubuhkedua sisi tubuh amati defisit amati defisit homeosensoris.homeosensoris.
Bandingkan area distal dan Bandingkan area distal dan proksimal dari lengan dan proksimal dari lengan dan tungkai terhadap tungkai terhadap nyeri, nyeri, temperatur, dan sensasi temperatur, dan sensasi sentuhan.sentuhan.parasthesi sarung parasthesi sarung tangan/stocking karena tangan/stocking karena neuropati.neuropati.
Bisa dilakukan dengan goresan Bisa dilakukan dengan goresan yang cukup.yang cukup.
Anwar Wardy [email protected] [email protected] 2007
Lanjutan:Lanjutan:
Periksa jari tangan dan kaki kearah distal Periksa jari tangan dan kaki kearah distal terhadap vibrasi dan indra posisi terhadap vibrasi dan indra posisi (propioseptif);(propioseptif); jika respons abnormal periksa jika respons abnormal periksa kearah proksimalkearah proksimalhilangnya rasa vibrasi hilangnya rasa vibrasi dan propioseptif terjadi pada kelainan tulang dan propioseptif terjadi pada kelainan tulang belakangbelakangbuat mapping pada respons abN.buat mapping pada respons abN.((pasien diperiksa dgn mata tertutup)pasien diperiksa dgn mata tertutup)
Anwar Wardy [email protected] [email protected] 2007
NyeriNyeri;; gunakan ujung runcing peniti/jarum dan gunakan ujung runcing peniti/jarum dan ujung lainya tumpul sebagai ujung lainya tumpul sebagai pembandingpembandinganalgesia, hipalgesia, hiperalgesia.analgesia, hipalgesia, hiperalgesia.
TemperaturTemperatur;(jika ada indikasi) gunakan uji tabung ;(jika ada indikasi) gunakan uji tabung dgn air panas dan dingin dgn temp.yang sesuai(+/- dgn air panas dan dingin dgn temp.yang sesuai(+/- 20 derajat tbh).20 derajat tbh).
Sentuhan Sentuhan ringan dengan ujung kapas.ringan dengan ujung kapas. VibrasiVibrasi;; garpu-tala 128 Hz – 256 Hz letakkan pada garpu-tala 128 Hz – 256 Hz letakkan pada
tonjolan tulangtonjolan tulang Vibrasi dan posisi keduanya Vibrasi dan posisi keduanya melalui cornu posterior C.Vertebra, sering melalui cornu posterior C.Vertebra, sering berhubungan satu dengan lainnya.berhubungan satu dengan lainnya.
Anwar Wardy [email protected] [email protected] 2007
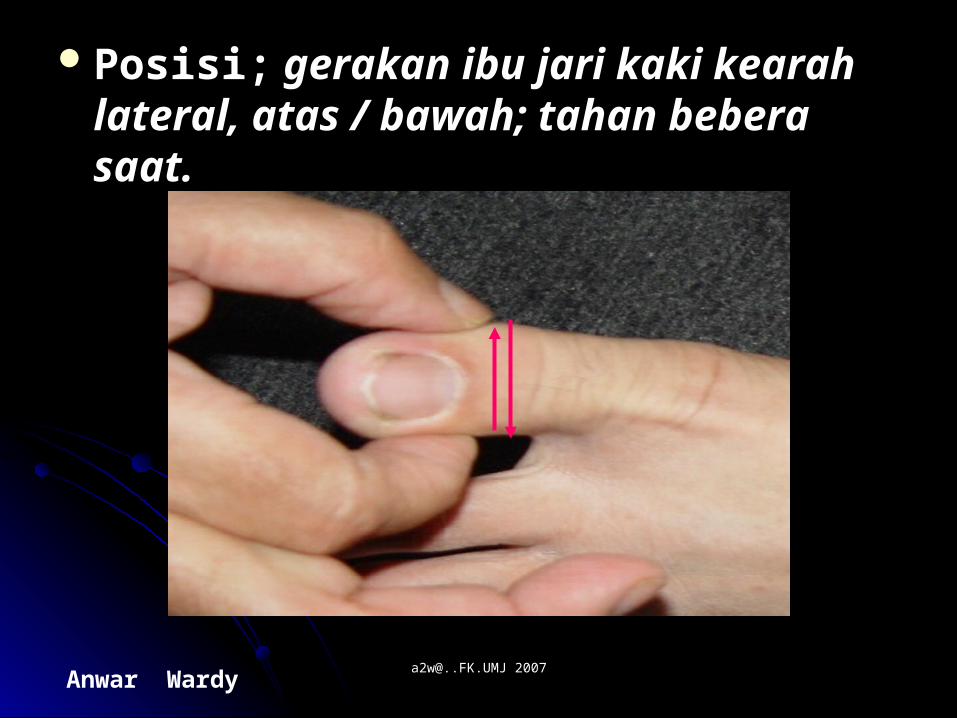
Posisi;Posisi; gerakan ibu jari kaki kearah gerakan ibu jari kaki kearah lateral, atas / bawah; tahan bebera saat.lateral, atas / bawah; tahan bebera saat.
Anwar Wardy [email protected] [email protected] 2007
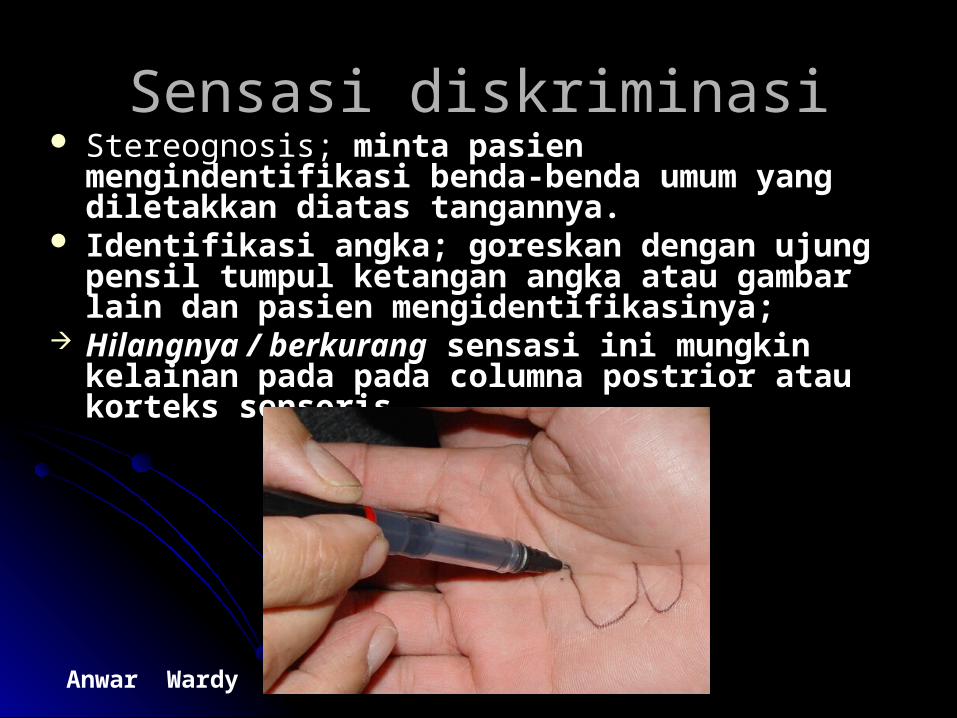
Sensasi diskriminasiSensasi diskriminasi Stereognosis; Stereognosis; minta pasien mengindentifikasi minta pasien mengindentifikasi
benda-benda umum yang diletakkan diatas benda-benda umum yang diletakkan diatas tangannya.tangannya.
Identifikasi angka;Identifikasi angka; goreskan dengan ujung pensil goreskan dengan ujung pensil tumpul ketangan angka atau gambar lain dan pasien tumpul ketangan angka atau gambar lain dan pasien mengidentifikasinya;mengidentifikasinya;
Hilangnya / berkurangHilangnya / berkurang sensasi ini mungkin sensasi ini mungkin kelainan pada pada columna postrior atau korteks kelainan pada pada columna postrior atau korteks sensoris.sensoris.
Anwar Wardy [email protected] [email protected] 2007
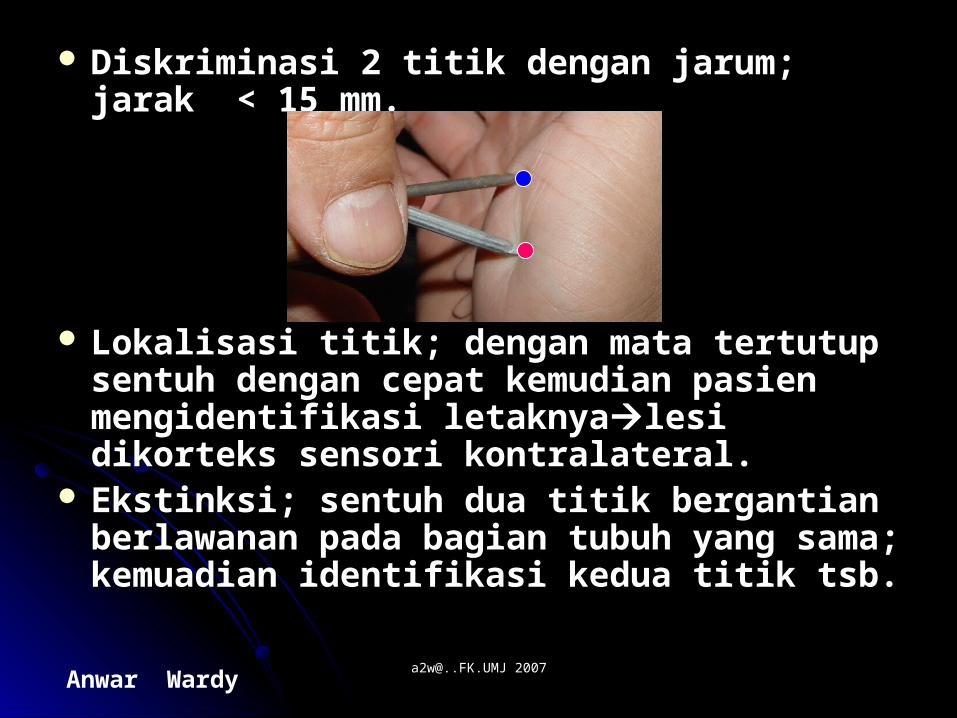
Diskriminasi 2 titikDiskriminasi 2 titik dengan jarum; jarak < dengan jarum; jarak < 15 mm.15 mm.
Lokalisasi titikLokalisasi titik; dengan mata tertutup ; dengan mata tertutup sentuh dengan cepat kemudian pasien sentuh dengan cepat kemudian pasien mengidentifikasi letaknyamengidentifikasi letaknyalesi dikorteks lesi dikorteks sensori kontralateral.sensori kontralateral.
EkstinksiEkstinksi; sentuh dua titik bergantian ; sentuh dua titik bergantian berlawanan pada bagian tubuh yang sama; berlawanan pada bagian tubuh yang sama; kemuadian identifikasi kedua titik tsb.kemuadian identifikasi kedua titik tsb.
Anwar Wardy [email protected] [email protected] 2007
REFLEKS-REFLEKSREFLEKS-REFLEKS
Biceps (C5, C6)Biceps (C5, C6)Triceps (C6, C7)Triceps (C6, C7)Supinator( brachioradialis; C5, C6).Supinator( brachioradialis; C5, C6).Abdominal; gores kearah umbilikus dengan Abdominal; gores kearah umbilikus dengan
pensil tumpul.pensil tumpul.
Refleks hiperaktif, Abdominal Reflek (-), Refleks hiperaktif, Abdominal Reflek (-), Babinsky + adalah lesi UMN.Babinsky + adalah lesi UMN.
Anwar Wardy [email protected] [email protected] 2007
Anggota bawah:Anggota bawah:
Refleks LututRefleks Lutut (L 2, L3, L4); ketok (L 2, L3, L4); ketok tendo patella inferior.tendo patella inferior.
Pergelangan kakiPergelangan kaki (S1); ketok tendo (S1); ketok tendo AchilesAchiles..
Plantar (L5, S1)-fleksorPlantar (L5, S1)-fleksor; gores dari ; gores dari lateral kemediallateral kemedial Refleks BabinskiRefleks Babinski bila positif; Periksa klonus otot kaki.bila positif; Periksa klonus otot kaki.
Anwar Wardy [email protected] [email protected] 2007
Skala Peringkat Refleks:Skala Peringkat Refleks:
+ 4 hiperaktif dengan klonus+ 4 hiperaktif dengan klonusAbN.AbN.+ 3 Lebih cepat dari biasanya; jangan + 3 Lebih cepat dari biasanya; jangan
cepat mengambil kesimpulan AbN.cepat mengambil kesimpulan AbN.+ 2 rata-rata Normal.+ 2 rata-rata Normal.+ 1 Penurunan normal rendah.+ 1 Penurunan normal rendah.0 Tak ada respons.0 Tak ada respons.
Anwar Wardy [email protected] [email protected] 2007
Buku bacaan wajib:Buku bacaan wajib:
1.1. Medical Neurology, Gylroy/Meyer 2005.Medical Neurology, Gylroy/Meyer 2005.2.2. Handbook of Neurophysiology, Stalberg 2005.Handbook of Neurophysiology, Stalberg 2005.3.3. Principles of Neurology, Edisi 8, Adam and Principles of Neurology, Edisi 8, Adam and
Victors, 2005.Victors, 2005.4.4. Gambar; erossyahGambar; erossyah (Buku diatas ada pada Penulis)(Buku diatas ada pada Penulis)Tidak semua pointer (85) diberikan pada Tidak semua pointer (85) diberikan pada
Mahasiswa; diwajibkan kembangkan dari buku Mahasiswa; diwajibkan kembangkan dari buku teks dan online.teks dan online.
Anwar Wardy [email protected] [email protected] 2007
Jakarta, 12 Desember 2007Jakarta, 12 Desember 2007
FKK-UMJFKK-UMJ
Wassalamu’Alaikum Wr, Wassalamu’Alaikum Wr, Wbr.Wbr.