
Mechanisms of nuclear reprogramming by eggs and oocytes: a deterministic process?
Upload
khangminh22Category
view
2download
0
181
Vitrification of human oocytes and embryos of different development stages Ahmed Elnahas¹, Ebru Alcolak¹, Ehab Abu Marar¹, Tamer Elnahas², Kareem Elnahas², Vassili Palapelas¹, Klaus Diedrich¹, Safaa Al-Hasani1 ¹University of Schleswig-Holstein, Department of Gynecology and Obstetrics, Reproductive Medicine Unit, University of Lübeck, Ratzeburger Allee 160, 23560 Lübeck, Germany; ²Department of Reproductive Health and Family Planning, National Research Center, Cairo, Egypt. Abstract Cryopreservation of oocytes and embryos leads to increased cumulative pregnancy rates, enables the recovery of the cost of treatment for Assisted Reproductive Technology (ART), minimizes risks of ovarian hyper stimulation syndrome (OHSS) through reducing number of stimulated cycles, reduces the risks of multiple pregnancy, allows patients undergoing chemotherapy and radiotherapy to preserve their fertility. In addition it also offers hope to those with genetic diseases such as Turner Syndrome and premature ovarian failure, or both. With the high viability rates now obtained following cryopreservation by vitrification of oocytes and embryos it is no longer a concern that compliance with regulation of certain countries that requires selection of limited number of oocytes for fertilization or the transfer of single embryos will compromise the patients’ chances of achieving pregnancy. Considerable effort is now focused on optimising the vitrification technique of cryopreservation worldwide. It is recommended vitrification is used instead of slow freezing as the latter is costly necessitating the purchase of programmable freezers, tedious and time consuming. The authors have nothing to declare. J Reprod Stem Cell Biotechnol 1(2):181-192 Correspondence: Dr Safaa Al-Hasani, University of Lübeck, Department of Gynecology and Obstetrics, Ratzeburger Allee 160, 23560, Lübeck, Germany; Tel: +49 4515002155;Fax: +49 4515004746; E-mail: [email protected] Introduction Cryopreservation provides an opportunity to limit the numbers of embryos transferred while maximizing the usable embryo per oocyte retrieval ratio at each stimulation attempt (Veeck 2003; Anderson 2005). The first successful report of clinical pregnancies with frozen-thawed human embryos was in the late 1970’s and the 1980’s (Mukherjee et al., 1978; Trounson and Mohr 1983). Two methods of cryopreservation that has been in use are in the ART are the slow freezing and vitrification techniques. Vitrification (or non-equilibrium cooling) is a method of glass-like solidification with an extreme increase in viscosity without formation of intracellular or extracellular ice crystal formation at a very low temperature (-196°C). Three types of damage occur during the cooling process, namely:
Damage to the microtubules including meiotic spindle with relative high temperature (+5 to - 5) °C that occur , in the mature oocytes.
Intracellular crystal formation (-5 to -80) °C.
Damage of zona pellucida (-80 to -150) °C.
( Aman and Parks ,1994; Leibo et al., 1996; Zenzes et al., 2001 ; Rall and Meyer,1989)
Historically the initial report of Rall and Fahy (1985) suggested that vitrification holds considerable promise as a viable method of cryopreservation but that vitrification solutions are invariably toxic due to the very high concentration of solute required to achieve vitrification. This led a number of workers invest considerable effort to reduce the toxicity of vitrification solutions. Foremost amongst these were two groups, one in Japan, (Kasai et al) and the other in Australia (Ali and Shelton), which worked to reduce the toxicity of vitrification solutions. Kasai et al. (1990) reported that an ethylene glycol based solution could be used to vitrify mouse morulae with no appreciable loss of viability. At about the same time, unaware of Kasai et al’s work, Ali and Shelton embarked on an extensive and systematic investigation beginning in 1989 through 1992 at the John Curtin School of Medical Research of The Australian National University to identify the least toxic and most efficacious vitrification solution (Ali and Shelton, 1993a-c). This massive study systematically investigated 3,044 binary cryoprotectant solutions involving about 6,088 experimental permutations to identify cryoprotectant solutions that exhibit vitrification properties and that are non-chemotoxic or at least less toxic. Their efforts led to the

182
identification of a vitrification solution consisting of 5.5M ethylene glycol and 1.0M sucrose called VS14 or EG5.5 (Ali and Shelton, 1993a). Both Kasai et al and, Ali and Shelton utilized 0.25ml plastic straws as vehicles for vitrification. Improved methods of vitrification that utilized 0.25ml heat-sealed straws (Kasai et al., 1990; Ali and Shelton, 1993a-c; Ali, 1995; Ali, 1996) developed in the 1990’s resulted in survival rates with almost insignificant loss of viability in the mouse and sheep in vitro and in vivo including excellent survival in vitro survival of abnormal (1PN/3PN) human embryos. These methods offered protection from contamination as the ends of the cryostraws were heat sealed. From the mid-1990’s however and in the ensuing years the trend was in the use of an array of micro cryovehicles (cryotop, cryotip, cryoloop, cryoleaf, etc) that employed ultra micro-volumes of vitrification solutions often in the order of 0.1 to 1.0 microliter as well as different vitrification solutions. Although these techniques compromised safety as the potential for contamination was high but they appear to have been almost universally adopted. These techniques that employed microcarriers too led to excellent survival rates often with insignificant losses or survival as high as 100% and excellent pregnancy rate in the human (53%; Takahashi., 2005). The vitrification methods that employed microcarriers compromised safety as the specimen is exposed to the elements. Furthermore it also compromised safety of other specimen stored in the same Dewar tank due to cross-contamination. These techniques are now in wide use for the cryopreservation of different developmental stages of embryos and oocytes; namely at the oocyte, zygote, cleavage or blastocyst stages. It is well documented that vitrification can be performed with minimal manpower requirements in a rapid manner within a few minutes with the use of low cost equipment (Rall and Fahy, 1985; Kasai et al., 1990; Ali and Shelton, 1993a-c; Ali et al., 1995; Ali, 1996; Kuwayama et al., 2005a). The authors (Al-Hasani et al., 2007) have obtained high survival rates of 89% following vitrification of zygotes (302 of 339) that did not affect the quality of the zygotes appreciably when scored by the zygote score described by Steer at al.(Steer et al., 1992).
In some slow freezing (equilibrium freezing) methods low concentrations of cryoprotectants appear to be insufficient to avoid intracellular crystal formation, leading to cell injury and low survival as well as low pregnancy rates but with high cost of cryopreservation due to higher capital outlay for expensive freezing equipment (Boldt et al., 2003; Fossan et al., 2003). It was found that the time needed for vitrification is ten times less than the slow freezing method (Kuleshova and Lapata, 2002) with total elimination of crystal formation (Rall and Fahy, 1985; Vajta and Kato et al., 2005; Mukaida et al., 2003). The interest in vitrification of human embryos, especially at early stages; is increasingly reported to be comparable if not better in clinical and laboratory outcomes, (Liebermann et al., 2002; Salumets et al., 2003; Saito et al, 2003) with better survival rates compared to slow freezing (Hredzak et al., 2005; Huang et al., 2005). Many variables in the vitrification process can profoundly influence its effectiveness and the potential to affect the survival rates of the vitrified cells. These variables are the type and concentration of cryoprotectants, the temperature of the vitrification solution at time of exposure, the duration of exposure to the final cryoprotectant before plunging into liquid nitrogen, the type of device used for vitrification and the quality of embryos. Increasing the speed of thermal conduction and decreasing the concentration of cryoprotectant is an ideal strategy to achieve higher survival rates following cryopreservation. Basic physiochemical determinants of vitrification The complete vitrification protocol involves just two steps; the vitrification and the warming processes .The primary goal in establishing an appropriate cryopreservation protocol is to avoid damage as much as possible while exposing specimens to non-physiological ultra low temperatures. Events occurring during cooling may cause lethal oocyte injury due to intracellular ice formation, uncontrolled dehydration, gas bubble formation and increase in viscosity (Coticchio et al.,2004). Re-crystallization and osmotic shock could happen during the warming process in suboptimal cooling or vitrification process, which may effectively reduce survival rates. It is essential to reduce the intracellular water of the oocyte by prior

183
partial dehydration using brief exposure to high concentrations of cryoprotectants (Bernard and Fuller, 1996). Physically there is a close link between the cooling rate and concentration of cryoprotectants; higher cooling rates require lower concentrations of cryoprotectants and vice versa (Yoon et al., 2000) to achieve vitrification. Therefore the establishment of specific balance between highest cooling and warming rates that prevent formation and growth of ice nuclei into ice crystals and a safe concentration of cryoprotectants without any toxic effect is critical for preventing cell damage (Mukida et al., 2003). Cryoprotectants Cryoprotectants are chemicals that protect cells from damage known as 'cold shock' from occurring during the cooling-warming procedure. Cryoprotectants are usually of high solubility that however oftentimes express cytotoxicity that is directly proportional to their concentration and temperature. Biochemically, it might be alcohols such as methanol, ethanol, 1,2 propanediol (PrOH) and glycerol , dimethylsulphoxide (DMSO) as well as sugars such as glucose, lactose and sucrose. Ethylene glycol (EG) has been widely used by numerous workers for the vitrification of mammalian embryos and, human oocytes and embryos due to its low toxicity and high permeability (Kasai et al., 1990; Ali and Shelton, 1993a-c; Kuleshova et al., 1999; Yoon et al., 2003). It has been reported that DMSO may cause spindle polymerization with an increased risk for polyploidy (Glenister et al., 1987). It has also been reported that cryoprotectant mixtures might have better results using a solution containing one permeable cryoprotectant (Vajta et al.,1998). Cryoprotectants can be classified into permeating such as PrOH, EG, and DMSO; and non- permeating such as sucrose, according to their capacity for penetrating the oocyte membrane. Since the oocyte membrane is permeable to certain cryoprotectants, a coupled influx of permeable cryoprotectants and the efflux of water from the oocyte following exposure to cryoprotectants results in dehydration of the oocyte. Subsequent rehydration may cause swelling of the oocyte. This shrinkage and swelling is capable of causing oocyte damage, thus, impermeable solutions such as sucrose are often added for dilution to prevent excessive osmotic swelling during thawing.
Establishing the optimal exposure time of the oocyte to cryoprotectants is very critical. It has to be long enough to permit sufficient dehydration and not so long as to damage the cell through alterations in the intracellular pH or through the time dependant cytotoxicity of the cryoprotectants (Fabbri et al., 2001). The cooling and warming protocol in vitrification The complete vitrification protocol involves ice-free cooling and warming processes. Various groups have attempted to optimize the protocol by modifications to these essential steps. These include variations to the duration of equilibration to the vitrification solution or to the use of different carrier system. As a result now a number of protocol exists for the vitrification of oocytes and embryos. In the authors’ laboratory in Lübeck the protocol used is similar to that described by Katayama et al. ( Katayama et al., 2003) with some modifications ( Al-Hasani et al 2007). The equilibration solution consisted of 7.5% EG and 7.5% DMSO in Ham's F-10 media supplemented with 20% of serum albumin. The vitrification solution was made up to contain 15% EG, 15% DMSO and 0.5M sucrose. In this protocol the cells are initially maintained in an equilibration solution for 5-15 minutes (depending on the time needed for re-expansion of the vitrified material) at room temperature, after an initial shrinkage and recovery. The cells are then aspirated and placed in the vitrification solution at room temperature for a period between 50 seconds to one minute. Thereafter, having confirmed that cellular shrinkage has taken place; the cells are aspirated and placed on the tip of cryotop carrier. No more than two oocytes or embryos are placed on each carrier. Cooling of oocytes and embryos is achieved by direct contact with the liquid nitrogen, and the cryotops are stored in liquid nitrogen Dewar storage tank. The warming of the cells are performed by placing the cryotop in a warming solution (1 M sucrose), again for a period between 50 seconds and one minute at a temperature of 37°C, and then into a second warming solution (0.5 M sucrose) for three minutes. This was followed by washing the warmed cells ten times in a washing solution ( Ham's F-10 + 20% serum albumin) before incubation in a culture media (Sage, cleavage media).

184
Our previous results showed a survival rate after rehydration to be as high as 90% and a pregnancy rate of 36.8%. The majority of zygotes were of grade A quality that attained the four cell stage one day after rehydration (Al-Hasani et al., 2007). Aims and advantages of different cryocarriers A number micro cryocarriers are in use at the present moment (Table 1). The most common of these micro cryocarriers are: the hemi-straw system, Cryotop, Cryoloop, Cryoleaf ((Kuwayama et al.,2005a; Vajta et al., 2006). The Cryotop consists of a 0.4 mm wide × 20mm long × 0.1 thick polypropylene strip attached to a plastic handle and equipped with a cover straw. Individual embryos were picked up in an extremely small volume of vitrification solution, placed on the strip and submerged into filtered liquid nitrogen. Underneath the liquid nitrogen, the plastic cover was placed over the strip to provide protection during storage. For warming the cryotop the protective cover was removed in liquid nitrogen and the end of the polypropylene strip was immersed directly in 1M warming solution. It is then transferred into 0.5M thawing solution for 3 minutes then washed eight to ten times before culture. Cryoloop method uses the small volume direct contact principle. A small nylon loop is attached to a holder and equipped with a container. Using this tool, safe cryopreservation can be achieved even in the vapour of liquid nitrogen (Larman et al., 2006). Kuwayama et al. (2005b) compared the open system (cryotop) and the closed system (cryotip) over 13,000 embryos at different stages and suggested that cryotop is an efficient and reliable way to vitrify cleavage embryos, blastocysts and oocytes in daily practice. The Cryoleaf cryocarrier has likewise shown to result in high survival and hatching rates when bovine blastocysts vitrified (Huang et al., 2005). Vitrification on immature oocytes It has been assumed that immature human oocytes obtained from unstimulated and stimulated ovaries might be of poor quality, demonstrating low rates of pregnancy after IVM, IVF and embryo transfer (Toth et al., 1994). Boiso et al. (2002) reported that oocytes at prophase I are capable of surviving cryopreservation and maturation to metaphase II stage after rehydration however, the high
rate of spindle and chromosomal abnormalities in his results were attributed to the cryopreservation itself. Vitrification appears to be a promising choice in cryopreservation of immature oocyte. Cha et al. (2000) reported high rates of morphologically normal immature oocytes (83%) after vitrification. Blastocysts with normal chromosome status and biochemical pregnancies were also obtained from vitrified immature oocytes (Cha et al.,2000; Chung et al,2000).
Vitrification of mature human oocyte The oocyte is one of the largest cells in the mammalian body and because of its spherical shape it has the lowest surface area to volume ratio, compared with other cell types with irregular shapes (Smith and Silva 2004; Wright et al., 2004). Moreover, the oocyte has lower permeability to cryoprotective agents (CPA) compared to zygotes and embryos.

185
One major problem in vitrification is the deleterious effect of high (CPA) concentration. The high concentration of the CPA is usually regarded as indispensable to induce the glass-like solidification. Oocytes at MII stage are not only difficult to equilibrate with CPA, but they are also quite sensitive to physical and chemical insults because of their vulnerable spindle apparatus (Zenzes et al., 2001; Stacheki et al., 2004). Consequently, one of the most promising approaches to improve their functional survival after vitrification might be to minimize the amount of CPA added to the vitrification solution, so as to reduce possible chemical toxicity and osmotic injury. Reducing the CPA concentration of the
vitrification solution may be one reason for the improved survival rate after the vitrification procedure. The first birth of a healthy female conceived by the association of cryopreservation and intracytoplasmic sperm (ICSI) was reported by Porcu et al. (Porcu et al., 1997). Subsequenty, many studies demonstrated reproducible success with oocyte cryopreservation. Oocyte freezing instead of embryo cryopreservation were suggested for introduction in a clinical routine, since preliminary data showed similar pregnancy rates post thaw when comparing the use of frozen oocytes versus frozen embryos (Porcu et al., 2002). (Table 2).
Vitrification has been suggested to improve the viability and quality of vitrified-thawed oocytes. Some researchers have suggested that the inclusion of macromolecules in the vitrification solution facilitates vitrification and protected the zona pellucida (Bergers et al.,1993). The addition of cytoskeletal stabilizers such as taxol and cytochalasin B in the vitrification solution is suggested to improve the post thaw development (Dobrinsky et al., 2000; Park et al., 2001). The authors group reported the first twin pregnancy from embryos generated following injection of vitrified oocytes with cryopreserved testicular sperm ( Youssry et al., 2007) Vitrification of cleavage stage embryos embryos The first birth from vitrified human embryos was a case report by Ohta et al.(1996). Subsequently Mukaida et al. reported successful vitrification of human 4-8 cell embryos by use of the method developed for
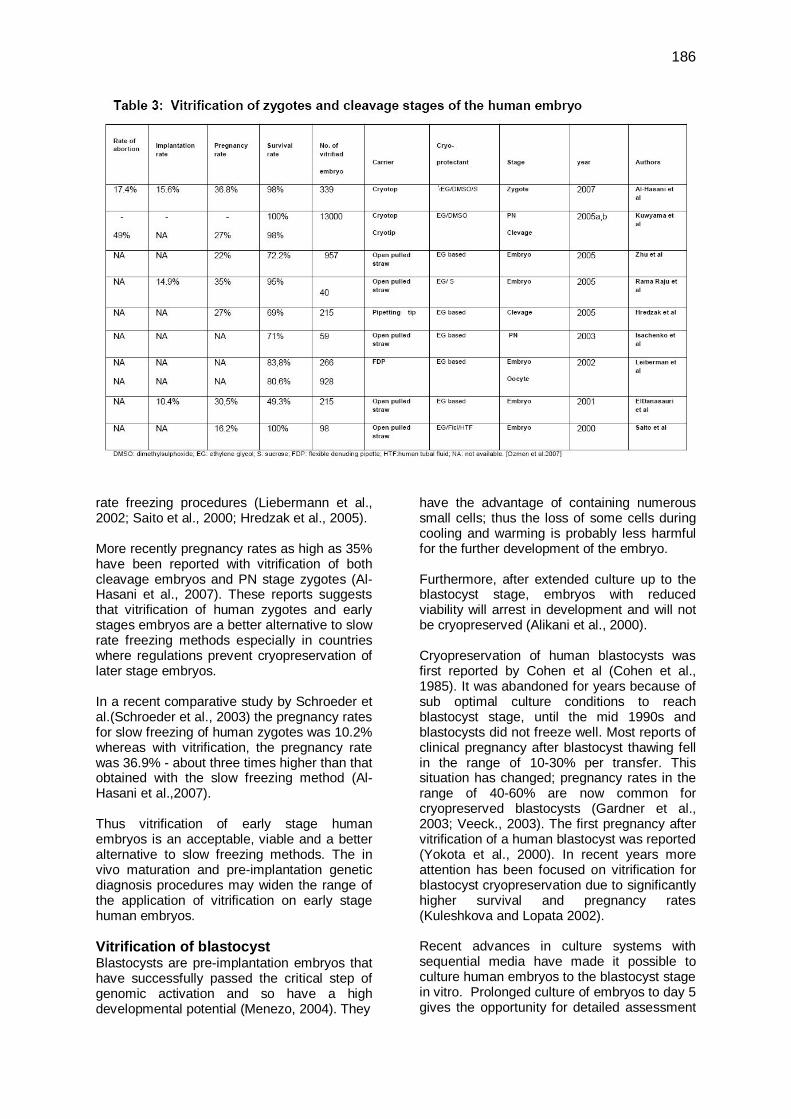
mouse embryos using the plastic cryopreservation 0.25ml straw (Mukaida et al., 1998) with live births. In subsequent years a number workers stopped using the 0.25ml plastic straws and chose to use much smaller vehicles in vitrification procedures that utlized microvolumes of the vitrification solution, such as the cryoloop, cryotop, cryotip, cryoleaf, etc., with good survival and pregnancy rates (Kuwayama et al., 2005b; Vajta and Nagy, 2006). Pronuclear stage embryos could survive with high survival rates after vitrification and warming procedures (Kuwayama et al., 2005b). This might be due to the hardening of the zona pellucida after the cortical reaction that occurs with and after the process of fertilization, which gives the ooplasmic membrane more stability to cope with the low temperature and osmotic changes. The majority of studies comparing vitrification of early stage embryos reported high survival rates of over 80% and pregnancy rates in the range of 22-30%; (Table 3) much higher than the survival rates reported for slow
186
rate freezing procedures (Liebermann et al., 2002; Saito et al., 2000; Hredzak et al., 2005). More recently pregnancy rates as high as 35% have been reported with vitrification of both cleavage embryos and PN stage zygotes (Al-Hasani et al., 2007). These reports suggests that vitrification of human zygotes and early stages embryos are a better alternative to slow rate freezing methods especially in countries where regulations prevent cryopreservation of later stage embryos. In a recent comparative study by Schroeder et al.(Schroeder et al., 2003) the pregnancy rates for slow freezing of human zygotes was 10.2% whereas with vitrification, the pregnancy rate was 36.9% - about three times higher than that obtained with the slow freezing method (Al-Hasani et al.,2007). Thus vitrification of early stage human embryos is an acceptable, viable and a better alternative to slow freezing methods. The in vivo maturation and pre-implantation genetic diagnosis procedures may widen the range of the application of vitrification on early stage human embryos. Vitrification of blastocyst Blastocysts are pre-implantation embryos that have successfully passed the critical step of genomic activation and so have a high developmental potential (Menezo, 2004). They
have the advantage of containing numerous small cells; thus the loss of some cells during cooling and warming is probably less harmful for the further development of the embryo. Furthermore, after extended culture up to the blastocyst stage, embryos with reduced viability will arrest in development and will not be cryopreserved (Alikani et al., 2000). Cryopreservation of human blastocysts was first reported by Cohen et al (Cohen et al., 1985). It was abandoned for years because of sub optimal culture conditions to reach blastocyst stage, until the mid 1990s and blastocysts did not freeze well. Most reports of clinical pregnancy after blastocyst thawing fell in the range of 10-30% per transfer. This situation has changed; pregnancy rates in the range of 40-60% are now common for cryopreserved blastocysts (Gardner et al., 2003; Veeck., 2003). The first pregnancy after vitrification of a human blastocyst was reported (Yokota et al., 2000). In recent years more attention has been focused on vitrification for blastocyst cryopreservation due to significantly higher survival and pregnancy rates (Kuleshkova and Lopata 2002). Recent advances in culture systems with sequential media have made it possible to culture human embryos to the blastocyst stage in vitro. Prolonged culture of embryos to day 5 gives the opportunity for detailed assessment

187
of the embryonic development parameters (Fisch et al.,2003). In an extended embryo culture program, blastocyst transfer on day 5 increased implantation rates (32%) in comparison to day 3 transfer (23%) with a significant increase in pregnancy rates. Such high pregnancy rates could be obtained in spite of the lower numbers of blastocysts transferred (Marek et al.,1999). Blastocysts appear to be better suited to the uterine environment and blastocyst formation selects for a more viable outcome (Gardner et al., 1998). As more and more centers opt for blastocyst transfer the need to develop techniques for blastocysts has likewise increased. Excellent survival has been achieved after vitrification of blastocysts using novel micro volume cryo carriers such as the cryotop (Kuwayama and Kato, 2000), cryoloop (Mukaida et al., 2001), or the hemi straw (Vanderzwalmen et al., 2003). In addition, survival rates of expandable blastocysts after cryopreservation increased (Motoishi, 2000; Son et al., 2003). Troup et al. reported that at the extended blastocyst stage, only 38% of embryos survived when frozen/thawed. A significantly lower proportion of patients had embryo replacement at the extended blastocyst stage (52.9%), no pregnancies were achieved following the replacement of frozen/thawed expanded blastocysts (Troup et al., 1990). Therefore the results of slow freezing of blastocysts are not satisfactory. Good results were obtained by Reed et al. following vitrification using the cryoloop method, where 15 out of 54 blastocysts were warmed. All (100%) were recovered, yielding an implantation rate of (15.4%) with two clinical pregnancies. One of them resulted in the live term birth of a healthy male infant (Reed et al., 2002). Subsequently studies by Mukaida et al. and by Huang et al. supported cryopreservation of human blastocysts using the cryoloop as a simple and effective method with a satisfactory survival rate (79%) and pregnancy rate (53%). This technique is simple, easy and quick, yielding the same high pregnancy and implantation rates as fresh blastocyst transfer (Mukaida et al., 2003; Huang et al., 2005). Vitrification has been successfully applied to human blastocysts using open and closed
straws. The open pulled straw (OPS) method, which renders very high cooling and warming rates and brief contact with concentrated cryoprotective additives, offer the possibility to circumvent chilling injury and to decrease toxic and osmotic damage. The OPS has been used for vitrifying mammalian oocytes and embryos, (Vajta et al.,1999) giving better success rates than those obtained with normal straws (Silvestre et al., 2003). This method has also been applied to human oocytes and early embryos (Lieberman et al., 2002). Blastocyst and further stages of human embryos have different requirements than the early stage embryos, which affect the chance of survival after being subjected to non-physiological situations such as ultra rapid cooling (Veeck, 2003). A major factor that affects the survival rate of the blastocyst is the fluid filled cavity called the blastocoele. As expected, the formation of intracellular ice crystals is directly proportional to the volume of this blastocoele. Vanderzwalmen et al. (2002) postulated that a large blastocoele might disturb the cryopreservative potential due to ice crystal formation during the cooling step. Therefore they analyzed the effectiveness of reducing the volume of the blastocoelic cavity before vitrification (collapse of blastocyst). Initially they encountered low survival rates after vitrification of blastocyst (20.3% expanded blastocyst, 54.4% with morulae and 58.5% with early blastocyst). They were able to overcome the problem by reducing the blastocoelic cavity and puncturing it with a special pipette before cryopreservation. Thereafter an increase in survival rates up to 70.6% was noted. The pregnancy rate improved after the artificial shrinkage procedure (20.5%) compared with the control intact blastocyst group (4.5%). After the reduction of the blastocoelic cavity a significant increase in the implantation rates per vitrified blastocyst was observed (12% versus 1.4%). They also concluded that survival rates in cryopreserved expanded blastocysts could be improved by reducing the fluid content (Table 4). Assisted hatching (AH) was later incorporated to the cryopreservation protocol and performed prior to transfer of vitrified embryos. AH was shown to have beneficial effects in vitrification cycles by increasing pregnancy and implantation rates (Vanderzwalmen et al., 2003 ).

188
They concluded that artificially opening the zona pellucida after warming vitrified blastocyst significantly improved the rate of transfers with hatched blastocysts and the implantation and pregnancy rates. Some studies report survival rates of more than 90% on the average; with 50-70% pregnancy rates, after cryopreservation of human blastocysts using different vitrification protocols. It appears that the vitrification protocol published by Kuwayama et al. had the highest survival and pregnancy rates (Kuwayama et al., 2005a,b) . From the results of studies in Table 4, it can be concluded that early blastocysts on day 5 seem to be the most suitable in terms of stage and age for cryopreservation. However fully developed and day 6 blastocysts can also be cryopreserved. Vitrification of human blastocysts yield the same or even better
results than slow freezing in regard to survival, implantation and pregnancy rates. Conclusion Today vitrification appears on the verge of replacing the slow freezing protocols due to improved survival rates and clinical outcomes. Although different stages of human oocytes and embryos show different physiological requirements that affect the survival rate but without doubt the outcomes of vitrification of human embryos and oocytes are encouraging. Therefore vitrification should be accepted as a viable, safe and a more efficient alternative to slow freezing method of cryopreservation of human embryos and oocytes. It is recommended vitrification be used instead of slow freezing as the latter is costly necessitating the purchase of programmable freezers, tedious and time consuming.

189
Acknowledgement The authors gratefully acknowledge the assistance of N. Ali in amending the language in the manuscript. References Al-Hasani S, Ozmen B, Koutlaki N et al. (2007)
Three year experience on routine vitrification of human zygote: Is it still fair to advocate slow rate freezing? Reprod Biomed Online. 14:288-93.
Ali, J. and Shelton, J.N. (1993a) Design of vitrifcation solutions for the cryopreservation of embryos J. Reprod. Fertil. 99:471-477
Ali, J. and Shelton, J.N. (1993b) Vitrification of preimplantation stages of mouse embryos J. Reprod. Fertil. 98:459-465
Ali, J. and Shelton, J.N. (1993c) Successful vitrification of sheep day-6 embryos J. Reprod. Fertil. 99:65-70
Ali, J., Bongso, A., Ratnam, S.S. (1995) Chromosomal analysis of day-2 human embryos vitrified with VS14. Med. Sci. Res.(UK) 23:539-540
Ali, J. (1996) Developmental competence of unipronuclear and triploid day-2 human embryos after vitrification with VS14. Med. Sci. Res. (UK) 24:377-378
Alikani M, Calderon G, Tomkin G et al. (2005) Cleavage anomalies in early embryos and survival after prolonged culture in-vitro Human Reprod 15:2634-2643.
Aman PR, Parks JE (1994) Effects of cooling and rewarming of the meiotic spindle and chromosomes in vitro matured bovine oocytes, Biol Reprod 50:103-110
Antinori M, Licata E, Dani G et al. (2007) Cryotop vitrification of human oocytes results in high survival rate and healthy deliveries. Reprod Biomed Online 14:72-79
Salumets A, Maria A, Mäkinen S et al. (2006) Frozen embryo transfers: implications of clinical and embryological factors on the pregnancy outcome. Human Reprod 21: 2368-2374
Anderson AR (2005) Reduction of high order multiples in frozen embryo transfers. Reprod Biomed Online 10: 402-405.
Bergers J, Dumulin J, Bras M et al. (1993) The effect of polymers on the cryopreservation of mouse embryos. Human Reprod 8:148.
Bernard A, Fuller B (1996) Cryopreservation of human oocytes: a review of current problems and perspectives Human Reprod Update 2:193-207.
Boiso I, Veiga A, Edwards RG (2002) Fundamentals of human embryonic growth in vitro and the selection of high-quality embryos for transfer. Reprod BioMed Online 5:328-350
Boldt J, Cline D, Mclaughlin D (2003) Human oocyte cryopreservation as an adjunct to IVF-embryo transfer cycles. Human Reprod 18:1250-1255.
Cha K, Chung H, Lim J et al. (2000) Freezing immature oocytes. Mol Cell Endocrinol 169:43-47.
Chen SU, Lien YR, Cheng YY et al. (2001) Vitrification of mouse oocytes using closed pulled straws (CPS) achieves a high survival and preserve good patterns of meiotic spindles, compared with conventional straws, open pulled straws (OPS) and grids. Human Reprod 11: 2350-2356.
Cho HG, Son WY, Yoon SH et al. (2002) An improved protocol for dilution of cryoprotectants from vitrified human blastocyst. Human Reprod 17:2419-2422.
Chung H, Hong S, Lim J et al. (2000) In vitro blastocyst formation of human oocytes obtained from unstimulated and stimulated cycles after vitrification at various maturation stages. Fertil Steril 73:545-551.
Cobo A, Domingo J, Perez S et al.(2008) Vitrification: an effective new approach to oocyte banking and preserving fertility in cancer patients,J Clin Transl Oncol12094:268-27
Cohen J, Simons RF, Edwards RG et al. (1985) Pregnancies following the frozen storage of expanding human blastocysts. J In Vitro Fertil Emb Transf 2:59-64.
Coticchio G, Bonu M, Borini A, Flamigni C. (2004) Oocyte cryopreservation: a biological prespective. Eur J Obstet Gynecol Reprod Biol 115:2-7.
Dobrinsky J, Pursel V, Long C et al. (2000) Birth of piglets after transfer of embryos cryopreserved by cytoskeletal stabilization and vitrification. Biol Reprod 62:564-570
El-Danasouri I, Selman H. (2001) Successful pregnancies and deliveries after a simple vitrification protocol for day 3 human embryos. Fertil Steril 76: 400-402.
Fabbri R, Porcu E, Marsella T et al. (2001) Human oocyte cryopreservation: new perspectives regarding oocyte survival. Human Reprod 16: 411-416

190
Fisch JD, Sher G, Adamowicz M, et al. (2003) The graduated embryo score predicts the outcome of assisted reproductive technologies better than a single day 3 evaluation and achieves results associated with blastocyst transfer from day 3 embryo transfer. Fertil Steril 80:1352-1358.
Fossas N, Marina F, Torres PJ et al. (2003) The births of five Spanish babies from cryopreserved donated oocytes. Human Reprod 18:1417-1421.
Gardner DK, Lane M, Stevens J et al (2003) Changing the start temperature and cooling rate in a slow-freezing protocol increases human blastocyst viability. Fertil Steril 79:407-410.
Gardner DK, Vella P, Lane M et al. (1998) Culture and transfer of human blastocysts increase implantation rates and reduces the need for multiple embryo transfers. Fertil Steril 69:84-88.
Glenister PH, Wood MJ, Kirby C, Whittingham DG (1987) Incidence of chromosome anomalies in first cleavage mouse embryos obtained from frozen thawed oocytes fertilized in vitro. Gamete Res 16:205-216.
Hredzak R, Ostra A, Zdilova V et al. (2005) Clinical experience with a modified method of human embryo vitrification. Ceska Gynekologie 70:99-103.
Huang CC, Lee TH, Chen SU et al. (2005) Successful pregnancy following blastocyst cryopreservation using super cooling ultra-rapid vitrification, Human Reprod 20:122-128.
Isachenko V, Selman H, Isachenko E et al. (2003) Modified vitrification of human pronuclear oocytes: efficacy and effects on ultrastructure. Reprod BioMed Online 7:211-216.
Katayama K, Stehlik J, Kuwayama M et al (2003) High survival rate of vitrified human oocytes results in clinical pregnancy. Fertil Steril 80:223-224.
Kong IK, Lee SI, Cho SG et al (2000) Comparison of open pulled straw (OPS) vs glass micropipette (GMP) vitrification in mouse blastocysts.Theriogenology 53: 1817-1826.
Kuleshova LL, Ginaroli L, Magli C, Trounson (1999) A Birth following vitrification of a small number of human oocytes. Human Reprod 14:3077-3079.
Kuleshova LL, Lopata A. (2002) Vitrification can be more favourable than slow cooling. Fertil Steril 78:449-454.
Kuwayama M, Kato O. (2000) All round vitrification of human oocytes and embryos. J Assist Reprod Genetics17: 477.
Kuwayama M, Vajta G, Kato O et al (2005a) Highly efficient vitrification method for cryopreservation of human oocytes. Reprod BioMed Online 11:300-308
Kuwayama M, Vajta G, Leda S, Kato O. Vitrification of human embryos using the cryotip method. Reproductive BioMedicine Online 2005b; 11:608-614.
Kartberg A-J, Hambiliki F , Arvidsson1 T, Stavreus-Evers A, Svalander P (2008) Vitrification with DMSO protects embryo membrane integrity better than solution without DMSO Reprod BioMed Online 17:378–384
Larman MG, Sheenan CB, Gardner D (2006) Vitrification of mouse pronuclear oocyte with no direct liquid nitrogen contact. Reprod BioMed Online 12: 66-69.
LeiboSP, Martino A, Kobayashi S, Pollard JW (1996) Stage dependent sensitivity of oocytes and embryos to low tempratures. Anim Reprod Sci 42:45-53.
Lieberman J, Tucker MJ. (2002) Effect of carrier system on the yield of human oocyte and embryos as assessed by survival and developmental potential after vitrification. Reproduction 124:483-489.
Lieberman J, Tucker MJ. (2006) Comparison of vitrification and conventional cryopreservation of day 5 and day 6 blastocysts during clinical application, Fertil Steril 84:88-92.
Marek D, Langley M, Gardner DK et al (1999) Introduction of blastocyst culture and transfer for all patient in an in vitro fertilization program. Fertil Steril 72:1035-1040.
Martino A, Songsasen N, Leibo SP (1996) Development into blastocysts of bovine oocytes cryopreserved by rapid cooling Biol Reprod 54:1059-1069.
Matsumoto H, Jiang JY, Tanaka T et al (2001) Vitrification of large quantities of immature bovine oocyte using nylon mesh. Cryobiology 42:139-144.
Menezo YJR (2004) Blastocyst freezing. Eur J Obstet Gynecol Reprod Biol 1158:12-15.
Motoishi M (2000) Cryopreservation of human blastocysts. J Clin Embryol 5:6-14.

191
Mukaida T, Takahashi K, Kasai M (2003) Blastocyst cryopreservation: ultra rapid vitrification using cryoloop technique. Reproduct BioMed Online 6: 221-225.
Mukaida T, Nakamara S, Tomiyama T et al. (2001) Successful birth after transfer of vitrified human blastocysts with use of cryoloop containerless technique. Fertil Steril 76: 618-620.
Mukaida T, Wada M, Takahashi K et al (1998) Vitrification of human embryos based on the assessment of suitable conditions for 8-cell mouse embryos. Human Reprod 13: 2874-2879.
Mukherjee S, Mukherjee S, Bhattacharya SK. (1978) The feasibility of long term cryogenic storage of viable human embryos- a breief pilot study report. Indian J. Cryogenics 3:80
Ohta N, Nohara M, Kojimara T et al. (1996) Ultrarapid freezing of human embryos by vitrification method. [Case report in Japanese]. Jpn J Fertil. Steril. 41:276-279
Ozmen B, Schultze A, Yousri M et al (2007) Vitrification of human embryos: which one is the best? Zygote and Cleavage and Blastocyst stage. J Turkish German Gynecol Assoc 8:218-226.
Park S, Chung H, Cha K et al. Cryopreservation of ICR mouse oocytes: improved post thawed pre implantation development after vitrification using taxol, a cytoskeleton stabilizer. Fertility and Sterility 2001; 75:1177-1184.
Porcu E, Fabbri R, Giotti PM et al (2002) Oocytes or embryo storage? Fertil Steril 78:15.
Porcu E, Fabbri R, Seracchioli R et al (1997) Birth of healthy female after intracytoplasmic sperm injection of cryopreserved human oocytes. Fertil Steril 68:724-726.
Rall WF, Fahy GM (1985) Ice free cryopreservation of mouse embryos at -196°C by vitrification. Nature 1985; 313:573-575.
Rall WF, Mayer TK (1989) Zona fracture damage and its avoidance during the cryopreservation of mammalian embryos. Theriogenology 31:683-692.
Rama Raju GA, Haranath Gb Krishna KM et al (2005) Vitrification of human 8 cell embryos as a modified protocol for better pregnancy rates. Reprod BioMed Online 11:434-437.
Reed ML, Lane M, Gardner DK et al. (2002) Vitrification of human blastocysts
using the cryoloop method: successful clinical application and birth of offspring. J Assist Reprod Genet 19:304-306.
Saito H, Ishida GM, Kaneko T et al (2000) Application of vitrification to human embryo freezing. Gynecol Obstet Invest 49:145-149.
Smith GD, Silva C(2004) Developmental consequences of cryopreservation of mammalian oocytes and embryos. Reprod BioMed Online 9:171-178.
Schroeder AK, Banz C, Katalinic A et al (2003) Counseling on cryopreservation of pronucleated oocytes. Reprod BioMed Online 6:69-74.
Silvestre MA, Saeed AM, Escriba MJ et al (2003)Vitrification of invitro cultured rabbit morulae. Anim Reprod Sci 76:113-124.
Son WY, Yoon SH, Yoon HG (2003) Pregnancy outcome following transfer of human blastocysts vitrified on electron microscopy grids after introduce collapse of the blastocoele. Human Reprod 18:137-139.
Steer CV, Mills CL, Tan SL et al (1992) The cumulative embryo score: a predictive embryo scoring technique to select the optimal number of embryos to transfer in an in-vitro fertilization and embryo transfer programme. Hum. Reprod 7:117–119
Stachecki JJ, Cohen J (2004) An overview of oocyte cryopreservation. Reprod BioMed Online 9:152-163.
Takahashi K, Mukaida T, Goto T et al (2005) Perinatal outcome of blastocys transfer with the vitrification using cryoloop: a 4 year follow-up study. Fertil Steril 46:268-272.
Toth T, Baka S, Veek L et al (1994) Fertilization and in vitro development of cryopreserved human prophase I oocytes. Fertil Steril 61:891-894
Tominaga K, Hamada Y (2001) Gel loading
tips as container for vitrification in vitro-produced bovine embryos. J Reprod Dev 47:267–27
Trounson A, Mohr L (1983) Human pregnancy following cryopreservation, thawing and transfer of an eight cell embryo Nature 1983; 305:707-709.
Troup SA, Matson PL Critchlow JD et al (1990) Cryopreservation of human embryos at the pronucleate, early cleavage or expanded blastocyst stages. Eur J Obstet Gynecol Reprod Biol 38:133-139

192
Vaita G, Holm P, Kuwayama M et al. (1998)
Open pulled straw (OPS) vitrification: a new way to reduce cryo injuries of bovine ova and embryos. Mol Reprod Dev 51:53-58
Vajta G, Murphy C N, Macháty Z, Prather R S, Greve T, Callesen H (1999) In-straw dilution of bovine blastocysts after vitrification with the open-pulled straw method. Vet Record144:180-181
Vaita G, and Nagy ZP (2006) Are programmable freezers still needed in the embryo laboratory? Review on vitrification. Reprod BioMed Online 12:779-796
Vajta G, Kato O, Leibo SP (2005) Highly efficient vitrification method for cryopreservation of human oocytes. Reprod BioMed Online 11:300-308
Vanderzwalmen P, Bertin G, Debauche C et al. Births after vitrification at morula and blastocyst stages: effect of artificial reduction of the blastocoelic cavity before vitrification. Human Reprod 2002; 17:744-751
Vanderzwalmen P, Bertin G, Debauche CH et al (2003) Vitrification of human blastocysts with the Hemi-Straw carrier: application of assisted hatching after thawing. Hum Reprod 18:1504-11.
Veeck L. Does the developmental stage at freeze impact clinical results post thaw? Reprod BioMed Online 6:367-74
Wright DL, Eroglu A, Toner M et al (2004) Use of sugars in cryopreserving human oocytes. Reprod BioMed Online 9:179-186
Yoon TK, Kim TJ, Park SE et al (2003) Live birth after vitrification of oocytes in a stimulated in vitro fertilization embryo-transfer program. Fertil Steril 79: 1323–1326
Yoon TK, Chung HM, Lim JM et al (2000) Pregnancy and delivery of healthy infants developed from vitrified oocytes in a stimulated in vitro fertlization embryo transfer program. Fertil Steril 74: 180-181.
Yokota Y, Sato S, Yokota M et al (2000) Successful pregnancy following blastocysts vitrification Human Reprod 15:1802-1803
Youssry M, Ozmen B, Zohni K et al (2008) Current aspects of blastocyst cryopreservation. Reprod BioMed Online 16: 31 1-20.
Zenzes MT, Bielecki R, Casper RF et al (2001) Effects of chilling to 0ºC on the morphology of meiotic spindles in human metaphase II oocytes. Fertil Steril 75: 769-777
Zhu GJ, Jin L, Zhang HW et al (2005) Vitrification of human cleaved embryos in vitro fertilizedation embryo transfer. Zhonghua Fu Chan KE Za Zhi 40: 682-684.
Copyright © 2022 FDOKUMEN




















