Doctoral Thesis Creating and validating UML class diagrams ...
Upload
independentCategory
view
1download
0
ORIGINAL PAPER
Validating the Repetitive Behavior Scale-Revised in YoungChildren with Autism Spectrum Disorder
Pat Mirenda • Isabel M. Smith • Tracy Vaillancourt • Stelios Georgiades •
Eric Duku • Peter Szatmari • Susan Bryson • Eric Fombonne •
Wendy Roberts • Joanne Volden • Charlotte Waddell • Lonnie Zwaigenbaum •
The Pathways in ASD Study Team
Published online: 20 April 2010
� Springer Science+Business Media, LLC 2010
Abstract This study examined the factor structure of the
Repetitive Behavior Scale-Revised (RBS-R) in a sample of
287 preschool-aged children with autism spectrum disorder
(ASD). A confirmatory factor analysis was used to examine
six competing structural models. Spearman’s rank order
correlations were calculated to examine the associations
between factor scores and variables of interest. The 3- and
5-factor models were selected as preferable on the basis of
fit statistics and parsimony. For both models, the strongest
correlations were with problem behavior scores on the
Child Behavior Checklist and repetitive behavior scores on
the ADI-R. Developmental index standard scores were not
correlated with factors in either model. The results confirm
the utility of the RBS-R as a measure of repetitive
behaviors in young children with ASD.
Keywords Repetitive behavior �Autism spectrum disorder � Factor analysis �Internal validity � External validity � Preschool
Introduction
Autism spectrum disorders (ASD; also termed Pervasive
Developmental Disorders in the DSM-IV-TR) are defined
by significant difficulties with social communication and
unusual patterns of behavior (e.g. restricted interests,
repetitive activities, stereotyped movements, and/or unu-
sual responses to sensory stimuli) (American Psychiatric
Association 2000). The area of social communication has
received considerable research attention over the years;
however, systematic study of the restricted and repetitive
behaviors (RRB) domain has increased only recently. RRB
includes both behavior that has been characterized as
‘‘lower level’’ repetitive sensory motor behavior (RSMB),
such as hand flapping, rocking, and humming, motoric
compulsions, and some self-injurious behaviors; and
‘‘higher level’’ insistence on sameness behavior (ISB), such
as pursuit of narrow circumscribed interests, insistence that
routines always occur in the same way, and repetitive use
of language (Bodfish et al. 2000; Lewis and Bodfish 1998).
The distinction between RSMB and ISB has been rein-
forced in reviews (e.g., Turner 1999) and subsequently in
several factor analytic studies with both adult and child
samples (e.g., Bodfish et al. 2000; Cuccaro et al. 2003;
Lam and Aman 2007; Szatmari et al. 2006). For example,
P. Mirenda (&)
University of British Columbia, 2125 Main Mall,
V6T 1Z4 Vancouver, BC, Canada
e-mail: [email protected]
I. M. Smith � S. Bryson
IWK Health Sciences Centre, Dalhousie University,
Halifax, NS, Canada
T. Vaillancourt
University of Ottawa, Ottawa, ON, Canada
S. Georgiades � E. Duku � P. Szatmari
McMaster University, Hamilton, ON, Canada
E. Fombonne
McGill University, Montreal, QC, Canada
W. Roberts
The Hospital for Sick Children, University of Toronto, Toronto,
ON, Canada
J. Volden � L. Zwaigenbaum
University of Alberta, Edmonton, AB, Canada
C. Waddell
Simon Fraser University, Burnaby, BC, Canada
123
J Autism Dev Disord (2010) 40:1521–1530
DOI 10.1007/s10803-010-1012-0

Mooney et al. (2009) conducted an exploratory factor
analysis on RRB items in the Autism Diagnostic Interview-
Revised (ADI-R; Rutter et al. 2003), using data from 137
preschool children with ASD and 77 developmentally
delayed children without ASD. Their two-factor solution
was characterized as consisting of ‘‘lower-order’’ behaviors
(e.g., repetitive use of objects, hand and finger manner-
isms—that is, RSMB) and ‘‘higher-order’’ behaviors (e.g.,
compulsions and rituals—that is, ISB). The two factors
accounted for 43% of variance in the entire sample, and
31% of variance for the ASD group alone. Similarly, Lam
et al. (2008) conducted a factor analysis using ADI-R items
from a more heterogeneous sample of individuals with
autism aged 20 months to 29 years (mean age = 9 years)
and identified three factors—RSMB, ISB, and Circum-
scribed Interests—each of which was composed of three
items from the ADI-R. Overall, the three factors accounted
for 52% of the variance in the sample. The discrepancy
between the Mooney et al. and Lam et al. analyses might
be explained by differences in the chronological ages of the
two samples, among other possible variables; however, the
relationship between age and RRBs has not been system-
atically addressed in factor analytic studies to date.
The measurement of RSMB and ISB has been accom-
plished in a number of ways. The most common has been
to use relevant items from the ADI-R (e.g., Bishop et al.
2006; Cuccaro et al. 2003; Honey et al. 2008; Mooney
et al. 2009; Richler et al. 2007; Szatmari et al. 2006). Other
researchers have used RRB-related items from various
parent interviews and scales (e.g., Bopp et al. 2009; Mili-
terni et al. 2002), or a variety of formal questionnaires
(e.g., Bodfish et al. 2000; Cuccaro et al. 2003; Gabriels
et al. 2005). Finally, a few studies have employed direct
observations of RRB (Epstein et al. 1985; Goldman et al.
2009; Morgan et al. 2008; Watt et al. 2008) The use of such
diverse measurement approaches makes it difficult to
compare results across studies.
Papageorgiou et al. (2008) noted that, since RRBs
encompass a variety of behaviors that are not addressed in
the ADI-R, future research examining the structure of these
behaviors should make use of more comprehensive
instruments. One such measure is the Repetitive Behavior
Questionnaire-2 (Leekam et al. 2007) and its predecessor,
the Repetitive Behavior Interview (Turner 1996), both
which have been used in a few published studies to date
(Ozonoff et al. 2000; Zandt et al. 2007). Other studies (e.g.,
Bodfish et al. 2000; Esbensen et al. 2008; Gabriels et al.
2005) have examined RRB using either the original or
revised version of the Repetitive Behavior Scale (RBS;
Bodfish et al. 1999) which samples a broader array of
behaviors than either the RBQ-2 or the ADI. The RBS
comprises six subscales, each a set of discrete, observable
topographies of restricted, repetitive behaviors that were
based on a theoretical framework involving latent pro-
cesses. The subscales include: (a) Stereotyped Behavior
(i.e., movements with no obvious purpose that are repeated
in a similar manner); (b) Self-injurious Behavior (i.e.,
actions that cause or have the potential to cause redness,
bruising, or other injury to the body); (c) Compulsive
Behavior (i.e., behavior that is repeated and performed
according to a rule or involves things being done ‘‘just
so’’); (d) Ritualistic Behavior (i.e., performing activities of
daily living in a similar manner); (e) Sameness Behavior
(i.e., resistance to change, insisting that things stay the
same); and (f) Restricted Behavior (i.e., limited range of
focus, interest, or activity). Items are rated on a four-point
Likert scale ranging from (0) ‘‘behavior does not occur’’ to
(3) ‘‘behavior occurs and is a severe problem,’’ and raters
are asked to refer to the previous month when completing
the scale.
The current version, the Repetitive Behavior Scale-
Revised (RBS-R; Bodfish et al. 2000) contains 43 items
that were drawn from other instruments and grouped the-
oretically based on the authors’ clinical experience. In a
recent study, Lam and Aman (2007) conducted an
exploratory factor analysis of the RBS-R that utilized data
from 307 participants who ranged in age from 3 to 48 years
(mean = 15 years). The authors identified five factors that
accounted for 47.5% of the variance among items,
including: (a) Rituals/Sameness, (b) Self-injurious Behav-
ior, (c) Stereotypic Behavior, (d) Compulsive Behavior,
and (e) Restricted Interests. Items from two separate con-
ceptually-based subscales on the RBS-R (Ritualistic
Behavior and Sameness Behavior) were combined in a
single factor (Rituals/Sameness), while 22 of the remaining
26 items loaded onto the other four factors in a manner
consistent with the structure of the original RBS-R.
The design employed by Lam and Aman (2007) invites
consideration at several levels. First, they recruited par-
ticipants through a mailed invitation to members of a
statewide autism society, with a response rate of 32%.
Thus, the individuals with ASD who were the focus of the
study may have represented primarily those with active,
informed caregivers and/or those with high rates of RRBs
whose caregivers were highly motivated to complete the
assessment. Further, no standard approach was used for
diagnosis of participants in this study, and it was not pos-
sible to verify that their diagnoses were accurate. In addi-
tion, the broad age range of the individuals with ASD in
Lam and Aman’s study (i.e., 3–48 years) limits interpret-
ability of the findings. Perhaps the items load on factors
differently in different age groups; in particular, RRB
profiles of very young children may differ from those of
older children and adults. This is an important issue for
clarification, since the five-subscale grouping of Lam and
Aman was subsequently used in a recent study of 712
1522 J Autism Dev Disord (2010) 40:1521–1530
123

individuals aged 2–62, 74 (10.4%) of whom were 2–
4 years old (Esbensen et al. 2008). The results of this study
indicated age-related patterns of differences in RRB among
the five subscales of the RBS-R, with the most significant
age-related decreases seen for restricted interests and ste-
reotyped movements. However, if the RBS-R factor
structure differs for young children, the results of this
analysis may not apply to that age group. Indeed, RRB
patterns seen in children may differ from those in older
individuals (see Richler et al. 2007).
Because of the increasing use of the RBS-R in research,
it is important to clarify the extent to which it is applicable
to young children with ASD. Previous research suggests
that the relationship between chronological age and RRB is
not straightforward. In general, RSMBs have been found to
be less frequent among older individuals (Esbensen et al.
2008; Lam and Aman 2007; Militerni et al. 2002). In
contrast, the findings on IS have been mixed. Bishop et al.
(2006) reported that IS behaviors become more frequent
with age, while Esbensen et al. (2008) reported a decrease.
Given these mixed findings, we were interested in exam-
ining the entire range of both RSMB and IS behaviors in
young children with ASD. Thus, the primary purpose of
this study was to examine the factor structure (i.e., internal
validity; see Cantwell 1996) of the RBS-R in a large
inception cohort of young children (aged 2–5 years), using
a confirmatory factor analytic approach. A secondary goal
was to examine external validity (Cantwell 1996) of the
RBS-R by examining correlations between RBS-R factors
and several variables that have been related to repetitive
behavior in previous research. These include children’s
developmental level (Bishop et al. 2006; Honey et al.
2008), adaptive behavior (Cuccaro et al. 2003; Hus et al.
2007; Szatmari et al. 2006), autism symptoms (Watt et al.
2008), and other unusual behaviors (Zandt et al. 2007).
Other studies that have examined the measurement model
of the RBS were not able to examine correlates from as
wide an array of clinical characteristics.
Method
Participants and Procedure
The participants were children participating in a Canadian
multi-site longitudinal study (Pathways in ASD) examining
the developmental trajectories of children with ASD. All
participants met the following inclusion criteria: (a) recent
(i.e., within 4 months) clinical diagnosis of ASD, con-
firmed by both the Autism Diagnostic Observation Sche-
dule (ADOS; Lord et al. 2002) and the Autism Diagnostic
Interview-Revised (ADI-R; Rutter et al. 2003), and by a
diagnosis assigned by a clinician using DSM-IV criteria
(American Psychiatric Association 2000); and (b) chrono-
logical age between 24 and 60 months at the time of
diagnosis. Children were excluded from the study if they
had: (a) cerebral palsy or other neuromotor disorders
interfering with study assessments; (b) a known genetic or
chromosomal abnormality; or (c) a severe vision or hearing
impairment. Invitation to participate in the study was
extended to all eligible families from five regional ASD
referral centres across Canada. To ensure independence of
observations, only one child per family was recruited to the
study. The study was approved by the local Research
Ethics Boards at participating sites.
The present sample consisted of 287 preschool children
with ASD (242 boys and 45 girls) with a mean age of
40.72 months at completion of the RBS-R (range =
24.1–64.0 months; SD = 9.27). Additional descriptive
statistics for the children at entry into the study are pre-
sented in Table 1.
Measures
Five measures were used in the present study as indices of
repetitive behavior, autism symptoms, adaptive behavior,
problem behavior, and cognitive development.
Repetitive Behavior Scale-Revised (Bodfish et al. 2000)
This is an empirically derived clinical rating scale for
measuring the presence and severity of a variety of forms
of restricted, repetitive behavior that are characteristic of
persons with ASD. The Repetitive Behavior Scale-Revised
(RBS-R) is designed to provide a quantitative, continuous
Table 1 Descriptive statistics for sample
Characteristic N % Mean SD Min–Max
Sex 287
Male 242 84.3
Female 45 15.7
Child’s age at assessment
(months)
287 40.7 9.3 24.1–64.0
Child’s age group
2-year-olds 105 36.6
3-year-olds 125 43.6
4-year-olds 57 19.9
Merrill-Palmer-Revised
Developmental Index age
equivalent (months)
272 23.1 11.4 5–68
Ethnicity
Caucasian 206 71.8
Other 81 28.2
J Autism Dev Disord (2010) 40:1521–1530 1523
123

measure of the spectrum of repetitive behaviors. The RBS-
R consists of 43 items distributed across six conceptually
derived subscales: Stereotyped Behavior, Self-injurious
Behavior, Compulsive Behavior, Routine Behavior,
Sameness Behavior, and Restricted Behavior. This scale
was completed by parent informants.
Autism Diagnostic Interview: Revised (Rutter et al. 2003)
The Autism Diagnostic Interview: Revised (ADI-R) is a
standardized semi-structured interview used in the differ-
ential diagnosis of the ASDs. It is designed to be used with
a parent or caregiver who is familiar with the develop-
mental history and current behavior of individuals over the
age of 2. It consists of three major domains: (1) language
and communication, (2) reciprocal social interaction, and
(3) restricted, repetitive, and stereotyped behaviors and
interests. The ADI-R uses a cut-off point for each of the
three domains, which provides a reliable diagnostic algo-
rithm that is accurate in differentiating autism from other
developmental disorders.
Autism Diagnostic Observation Schedule (Lord et al. 2002)
The Autism Diagnostic Observation Schedule (ADOS) is a
semi-structured assessment that consists of activities that
provide interesting, standard contexts in which interactions
can occur. The activities allow the assessor to observe
social and communication behaviors related to the diag-
nosis of ASD. Ratings for the behaviors are entered into a
reliable diagnostic algorithm that differentiates both autism
and the broader category of ASD from other developmental
disorders.
Vineland Adaptive Behavior Scales Second Edition
(Sparrow et al. 2005)
The Vineland Adaptive Behavior Scales Second Edition
(VABS II) assesses child adaptive behavior in the com-
munication, socialization, daily living skills, and motor
domains, and expresses overall functioning in the Adap-
tive Behavior Composite (ABC) score. The VABS II is
administered to a parent or caregiver using a semi-
structured interview format. Open-ended questions gather
in-depth information and promote rapport between the
interviewer and respondent.
Child Behavior Checklist (Achenbach and Rescorla 2000)
The Child Behavior Checklist (CBCL 1.5-5) obtains par-
ents’ ratings of 99 problem items, and is a well-standardized
measure of externalizing and internalizing behavior prob-
lems in preschool children.
Merrill-Palmer-Revised Scales of Development
(Roid and Sampers 2004)
This is an individually administered measure of develop-
ment that is appropriate for children ages 2–78 months of
age. The Developmental Index is comprised of the cogni-
tive, receptive language, and fine motor scales.
Data Analysis
Baseline data were used in a confirmatory factor analysis
(CFA; Muthen and Muthen 2007) to describe the structure
of the RBS-R. CFA was applied to test the six competing
structural models proposed in the literature (APA 2000;
Bodfish et al. 2000; Lam and Aman; 2007; Lam et al.
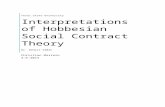
2008; Szatmari et al. 2006). The specific models ranged
from 1 to 6 factors (Fig. 1). Five statistical indices,
including the model chi-square/degrees of freedom
(v2/df), the Comparative Fit Index (CFI), the Tucker-
Lewis Index (TLI), the Root Mean Square Error of
Approximation (RMSEA), and the Standardized Root
Mean Square Residual (SRMR), were used to evaluate the
goodness-of-fit of each model to the data. In general, a
v2/df value less than 3.0, CFI and TLI values greater than
0.90, SRMR values below 0.08, and RMSEA values of
0.06 or less indicate a good model fit (Briggs and Cheek
1986; Hu and Bentler 1999). The Akaike Information
Criterion (AIC) was also used as a criterion of model fit,
with lower values indicating a better fit (Akaike 1987).
Figure 1 depicts the six competing models tested in the
analyses. The internal consistency for each unique factor
from the six models was assessed using Cronbach’s alpha
(a). A Cronbach’s a value of 0.70 or higher indicates a
scale with acceptable internal consistency (Heppner et al.
1999).
In addition, non-parametric Spearman’s rank correla-
tions were calculated to examine the association between
factor scores and other variables of interest. Spearman’s
rank correlation coefficients were used because the dis-
tribution of the three factors was not normal. The vari-
ables of interest included the child’s age at diagnosis,
developmental level (as indexed by the Merrill-Palmer-
Revised Scales of Development (M-P-R) Developmental
Index), adaptive behavior ability (as indexed by the
VABS II Adaptive Behavior Composite), autistic symp-
toms (as indexed by the ADI-R and the ADOS), and other
problem behaviors (as indexed by raw scores on the
CBCL 1.5-5).
1524 J Autism Dev Disord (2010) 40:1521–1530
123

Results
The CFA results for all six factor models are presented in
Table 2.
The CFA results indicate that the 3-, 4-, 5-, and 6-factor
models were all reasonably good fits for the data, based on
the fit statistics guidelines described previously. Models III
and V were selected as the preferable models on the basis
of both fit statistics and parsimony. Model III is comprised
of Factor I: Compulsive Ritualistic Sameness Behaviors
(CRSB), including RBS-R items 15–39 (a = 0.909); Fac-
tor II: Self Injurious Behaviors (SIB), items 7–14
(a = 0.811); and Factor III: Restricted Stereotyped
Behaviors (RSB), items 1–6 and 40–43 (a = 0.816). Model
V comprises Factor I: Stereotyped Behaviors (STEREO),
items 1–6 (a = 0.733); Factor II: Self Injurious Behaviors
(SIB), items 7–14 (a = 0.811); Factor III: Compulsive
Behaviors (COMP), items 15–22 (a = 0.720); Factor IV:
Ritualistic Sameness Behaviors (RITUAL/SAME), items
22–39 (a = 0.898); and Factor V: Restricted Behaviors
(RESTR), items 40–43 (a = 0.787). The primary differ-
ence between the two models was that Compulsive and
Ritualistic behaviors comprised one factor in Model V but
were separate in Model III; this was also the case for
Stereotypic and Restricted behaviors.
Table 3 presents correlations between the three factors
from Model III and the variables of interest, and Table 4
presents the same set of correlations for the five factors in
Model V.
For both models, the strongest correlations were with the
CBCL total and subscale raw scores. In addition, all factors
in Model III and all factors except SIB in Model V were
Model I(1-factor)
Stereotypy
Self-Injurious
Compulsive
RitualisticSameness
Restricted
Model II(2-factors)
Stereotypy
Restricted
Self-Injurious
Compulsive
Ritualistic
Sameness
Model III(3-factors)
Stereotypy
Restricted
Self-Injurious
Compulsive
Ritualistic
Sameness
Model IV(4-factors)
Stereotypy
Restricted
Self-Injurious
Compulsive
Ritualistic
Sameness
Model V(5-factors)
Stereotypy
Self-Injurious
Compulsive
Ritualistic
Sameness
Restricted
Model VI(6-factors)
Stereotypy
Self-Injurious
Compulsive
Ritualistic
Sameness
Restricted
Fig. 1 Six competing hypothesized models of the RBS-R factor structure
Table 2 Goodness-of-fit indices of the hypothesized latent-factor models of the RBS-R (N = 287)
Model v2 df v2/df CFI TLI RMSEA SRMR AIC
Model I (one factor) 2536.92* 860 2.94 0.629 0.610 0.082 0.082 25423.755
Model II (two factors) 2183.74* 859 2.54 0.707 0.692 0.073 0.075 25072.572
Model III (three factors) 1998.62* 857 2.33 0.747 0.734 0.068 0.071 24891.456
Model IV (four factors) 1923.89* 854 2.26 0.763 0.750 0.066 0.068 24822.718
Model V (five factors) 1840.61* 850 2.17 0.781 0.767 0.064 0.066 24747.436
Model VI (six factors) 1830.61* 845 2.17 0.782 0.767 0.064 0.066 24747.439
Note: RBS-R repetitive behavior scale-revised, CFI comparative fit index, TLI Tucker Lewis index, RMSEA Root-mean square error of
approximation, SRMR standardized root mean square residual, AIC Akaike information criterion; numbers in bold meet the criterion set for good
model fit
* p \ .001
J Autism Dev Disord (2010) 40:1521–1530 1525
123

strongly correlated with the ADI-R repetitive behaviors
total score. However, only the RSB factor in Model III and
the Restricted and Stereotypy factors in Model V were
correlated with scores on the ADOS. All factors in both
models were negatively correlated with the VABS II total
score, most strongly for RSB (Model III) and Stereotypy
(Model V). The only factors that were strongly correlated
with chronological age were those related to compulsive
ritualistic sameness behaviors (CRSB). Developmental
index standard scores as measured by the M-P-R were not
correlated with any factors in either model.
Discussion
The primary purpose of this study was to examine the
RBS-R factor structure proposed by Bodfish et al. (1999),
Bodfish and Lewis (2002) in a carefully selected sample of
Table 3 Spearman’s rank order correlation coefficients for Model III and variables of interest
Variable RBS-R Factor
CRSB SIB RSB
RBS-R age at assessment (in months) .210** -.029 .084
VABS II adaptive behavior composite -.153* -.222** -.247**
ADI-R social domain total .194** .194** .232**
ADI-R communication domain nonverbal/verbal total .137* .143* .156**
ADI-R repetitive behaviors domain total .377** .129* .374**
ADOS repetitive behaviors total (modules 1, 2, 3) .064 .075 .236**
M-P-R developmental index standard score .054 -.096 -.035
CBCL internalizing problems total raw score .629** .384** .550**
CBCL externalizing problems total raw score .531** .437** .517**
CBCL total problems raw score .648** .497** .608**
CBCL pervasive developmental problems raw score .521** .300** .497**
Note: RBS-R repetitive behavior scale-revised, VABS II Vineland adaptive behavior scale second edition, ADI-R Autism diagnostic interview-
revised, M-P-R Merrill-Palmer-revised, CRSB compulsive ritualistic sameness behaviors, SIB self injurious behaviors, RSB restricted stereotyped
behaviors
* p \ .05 level (2-tailed) ** p \ .01 level (2-tailed)
Table 4 Spearman’s rank order correlation coefficients for Model V and variables of interest
Variable RBS-R Factor
STEREO SIB COMP RITUAL/SAME RESTR
RBS-R age at assessment (in months) .037 -.029 .139* .207** .104
VABS II adaptive behavior composite -.306** -.222** -.167** -.141* -.127*
ADI-R social domain total .222** .194** .159** .196** .169**
ADI-R Communication domain nonverbal/verbal total .120* .143* .040 .169** .152*
ADI-R repetitive behaviors domain total .297** .129* .330** .362** .351**
ADOS repetitive behaviors total (modules 1, 2, 3) .270** .075 .092 .031 .148*
MP-R developmental index standard score -.099 -.096 -.032 .083 .044
CBCL internalizing problems total .455** .384** .476** .619** .494**
CBCL externalizing problems total .452** .437** .394** .531** .444**
CBCL total problems .528** .497** .491** .639** .519**
CBCL pervasive developmental problems raw score .448** .300** .415** .509** .415**
Note: RBS-R repetitive behavior scale-revised, VABS II Vineland adaptive behavior scale second edition, ADI-R Autism diagnostic interview-
revised, M-P-R Merrill-Palmer-revised, STEREO stereotyped behaviors, SIB self injurious behaviors, COMP compulsive behaviors, RITUAL/SAME ritualistic/sameness behaviors, RESTR restricted behaviors
* p \ .05 level (2-tailed) ** p \ .01 level (2-tailed)
1526 J Autism Dev Disord (2010) 40:1521–1530
123

young children with ASD, using data gathered soon after
diagnosis. Because the RBS-R was based on a theoretical
framework involving latent processes, a confirmatory fac-
tor analysis was deemed appropriate to assess internal
validity for the present analysis (Brown 2006; Tabachnick
and Fidell 2007). The results confirm the utility of the
RBS-R as a measure of a wide range of RRBs seen in
young children with ASD.
The issue of how many factors to select following CFA
is complex and is typically addressed from multiple per-
spectives. In this study, Cronbach’s a was at least 0.72 for
the factors in all six models, indicating adequate or better
internal consistency (see Appendix). Factors with a values
between .70 and .80 are not less internally consistent than
those with a[ .80. Rather, the finding that even these
factors, which contain only a few item indicators, have
acceptable a values confirms the robustness of the
instrument overall. The fit indices for Model I, the single
factor solution, were the least acceptable, with a RMSEA
value of .082 that was well over the recommended value
of .06. This confirms previous reports indicating that the
structure of RRBs in children with ASD is not uni-
dimensional (e.g., Lam et al. 2008; Mooney et al. 2009).
The fit index results (Table 2) indicate that the 5- and
6-factor solutions were almost identical, but the 5-factor
model is more parsimonious. We propose adopting this
model when a detailed measure of RRB is required. For
example, the 5-factor model might be especially appro-
priate when assessing the extent to which specific types of
RRBs are affected by treatments that are specifically
designed for this purpose, as well as interventions that
target other areas but might have collateral effects on
RRBs. Advantages of using a measure such as the RBS-R
in such circumstances include the brief completion time;
the ability to quantify subtle differences in the degree of
impairment; and weak or no correlation with IQ, as evi-
denced by the results of our correlational analyses (see
Tables 3, 4). With regard to the latter issue, it should be
noted that we found slight variations in the size and
direction of correlations between IQ and RRB factors for
the 2-, 3-, and 4-year-olds in our sample, but none of
these differences were significant.
Both the 5- and 6-factor models show evidence of a
better statistical fit than the 3- and 4-factor models; how-
ever, the latter two models also have acceptable (and
similar) fit statistics and might be useful in some circum-
stances. In particular, the 3-factor model, consisting of
Self-injurious Behavior, Compulsive/Ritualistic/Sameness
behaviors, and Restricted Stereotypic behaviors, might be
appropriate in studies requiring broad descriptors of RRB
symptomatology, such as those that are used in genetic
quantitative trait locus (QTL) analyses. QTL is especially
useful for complex, neurobehavioral phenotypes such as
autism, the characteristics of which can be measured and
quantified along continua. It links two types of informa-
tion—phenotypic data (i.e., trait measurements) and
genotypic data (usually molecular markers)—in order to
explain the genetic basis of variation in complex traits
(Miles and Wayne 2008). This requires a tool that can
measure the trait of interest along a continuum, in a manner
that is parsimonious yet sufficiently precise to capture the
entire spectrum of variability, including subclinical mani-
festations. Recent QTL analyses in ASD have examined
nonverbal communication (Chen et al. 2006), social
responsiveness (Duvall et al. 2007), and both language
delay and RRB (Alarcon et al. 2002) as potential compo-
nent phenotypes (Szatmari et al. 2006). Interestingly, the
Alarcon et al. study found no QTL for RRB, although four
chromosomal regions were identified that may harbor
QTLs for age-at-first-word and age-at-first-phrase. The
authors noted that use of the ADI-R for measurement of
RRB might have affected the results, and suggested that
more comprehensive examination of the RRB construct is
warranted. The 3-factor RBS-R model might be useful in
this regard, since all three factors were correlated with the
ADI-R (suggesting that they measure the same construct)
but provide additional specificity.
Correlational analyses indicated moderately strong
relationships between all RBS-R factors and both inter-
nalizing and externalizing problem behaviors on the
CBCL. There were also significant correlations between
the Pervasive Developmental Disorders-oriented subscale
of the CBCL and all RBS-R factors, providing evidence
of concurrent validity. Associations were also evident
between VABS II adaptive behavior scores and all factors
in both Models III and V. The strongest of these corre-
lations was with the Stereotypic behavior factor, which
echoes the results of previous studies that have also found
correlations between RSMBs and adaptive behavior (e.g.,
Cuccaro et al. 2003; Hus et al. 2007; Szatmari et al.
2006). The relationships between RBS-R factors and
chronological age were less straightforward, with low,
positive correlations across all factors except SIB, for
which a negative correlation was evident. With the
exception of the SIB result, this supports previous work
suggesting that RRBs occur more frequently in older than
in younger children (e.g., Bishop et al. 2006; Cox et al.
1999), although our age range was admittedly narrow
(2–5 years).
The limitations of this study include our inability to
examine measurement equivalence across genders, given
the low number of girls in the study. The strengths of our
J Autism Dev Disord (2010) 40:1521–1530 1527
123

approach include the fact that we recruited an inception
cohort within a specific age range, ascertained our sample
in a systematic manner using gold standard instruments to
confirm diagnoses, and examined several correlates drawn
from previous work. We were also able to examine cor-
relates with one observational measure (the ADOS) in
addition to those that rely on parent reports (i.e., the ADI-
R, VABS II, and CBCL). In the future, we plan to use
longitudinal data to examine RRB differences of individ-
uals in various age groups as well as the progression of
RRBs as children with ASD develop over time.
In summary, the CFA results provide support for use of
the RBS-R to measure a range of RRBs in young children
with ASD. When parsimony is the primary consideration,
Model III would be an appropriate choice; and when a
more detailed examination of RRB is required, Model V
could also be used. Both are theoretically sound, with
evidence of good fit indices and high internal consistency.
From a clinical perspective, this instrument appears to be
psychometrically sound and has several advantages over
measures such as the ADI-R that were developed for other
purposes. That is, the RBS-R covers a broader range of
repetitive behaviors and was designed as a quantitative
index of RRB, whereas the ADI-R was developed to aid in
categorical diagnostic decision-making. As such, the use of
three or five RBS-R factors to measure response to treat-
ment or quantify RRBs for other purposes should provide
sufficient coverage of the domain. Moreover, more wide-
spread adoption of a broad-based instrument such as the
RBS-R to measure RRBs would enable efficient compari-
son of research results across samples of different ages,
genders, levels of development, and autism symptom
severity.
Acknowledgments This study was supported by the Canadian
Institutes of Health Research, Autism Speaks, the Government of
British Columbia, the Alberta Heritage Foundation for Medical
Research, and the Sinneave Family Foundation. The authors thank
all the families who participated in the Pathways in ASD study. The
authors also acknowledge the members of the Pathways in ASDStudy Team. These members had equal contribution to the study and
are listed here alphabetically: Liliana Abruzzese, Susan Bauld, Terry
Bennett, Ainsley Boudreau, Colin Andrew Campell, Mike Chalupka,
Lorna Colli, Melanie Couture, Bev DaSilva, Natalie Dinsdale,
Vikram Dua, Lindsay Fleming, Kristin Fossum, Nancy Garon,
Shareen Holly, Karen Kalynchuk, Kathryne MacLeod, Wendy
Mitchell, Julianne Noseworthy, Irene O’Connor, Sarah Peacock,
Teri Phillips, Sara Quirke, Jennifer Saracino, Cody Shepherd,
Rebecca Simon, Mandy Steiman, Benjamin Taylor. Ann Thompson,
Lee Tidmarsh, Larry Tuff, Stephen Wellington, Isabelle Yun, and Li
Hong Zhong.
Appendix
See Table 5.
Ta
ble
5In
tern
alco
nsi
sten
cy(C
ron
bac
h’s
a)fo
rfa
cto
rsfr
om
the
six
com
pet
ing
mo
del
s
Fac
tors
RB
S-R
Item
sC
ron
bac
h’s
aM
od
elI
Mo
del
IIM
od
elII
IM
od
elIV
Mo
del
VM
od
elV
I
Ste
reo
typ
y1
–6
.73
3X
X
Sel
f-in
juri
ou
s7
–1
4.8
11
XX
XX
Co
mp
uls
ive
15
–2
2.7
20
XX
X
Rit
ual
isti
c2
3–
29
.70
8X
Sam
enes
s3
0–
39
.87
9X
Res
tric
ted
40
–4
3.7
87
XX
Rit
ual
isti
c/sa
men
ess
23
–3
9.8
98
XX
Ste
reo
typ
y/r
estr
icte
d1
–6
,4
0–
43
.81
6X
X
Co
mp
uls
ive/
ritu
alis
tic/
sam
enes
s1
5–
39
.90
9X
X
Ste
reo
typ
y/r
estr
icte
d/s
elf
Inju
rio
us
1–
14
,4
0–
43
.85
8X
Ste
reo
typ
y/r
estr
icte
d/s
elf
inju
rio
us/
com
pu
lsiv
e/ri
tual
isti
c/sa
men
ess
1–
43
.93
0X
1528 J Autism Dev Disord (2010) 40:1521–1530
123

References
Achenbach, T. M., & Rescorla, L. A. (2000). Manual for ASEBApreschool forms & profiles. Burlington, VT: University of
Vermont, Research Center for Children, Youth, & Families.
Akaike, H. (1987). Factor analysis and AIC. Psychometrika, 52, 317–
322.
Alarcon, M., Cantor, R. M., Liu, J., Gilliam, T. C., the Autism
Genetic Resource Exchange Consortium, & Geschwind, D. H.
(2002). Evidence for a language quantitative trait locus on
chromosome 7q in multiplex autism families. American Journalof Human Genetics, 70, 60–71.
Association, American. Psychiatric. (2000). Diagnostic and statisticalmanual of mental disorders (4th ed.). Washington, DC: Amer-
ican Psychiatric Association. text revision.
Bishop, S., Richler, J., & Lord, C. (2006). Association between
restricted and repetitive behaviors and nonverbal IQ in children
with autism spectrum disorders. Child Neuropsychology, 12,
247–267.
Bodfish, J. W., & Lewis, M. H. (2002). Repetitive behavior in autism.Paper presented at the International Meeting for Autism
Research. (IMFAR), Orlando, FL.
Bodfish, J. W., Symons, F., & Lewis, M. (1999). The RepetitiveBehavior Scale: Test manual. Morganton: Western Carolina
Center Research Reports.
Bodfish, J. W., Symons, F. J., Parker, D. E., & Lewis, M. H. (2000).
Varieties in repetitive behavior in autism. Journal of Autism andDevelopmental Disorders, 30, 237–243.
Bopp, K., Mirenda, P., & Zumbo, B. (2009). Behavior predictors of
language development over two years in children with autism
spectrum disorders. Journal of Speech, Language, and HearingResearch, 52, 1106–1120.
Briggs, S. R., & Cheek, J. M. (1986). The role of factor analysis in the
development and evaluation of personality scales. Journal ofPersonality, 54, 106–148.
Brown, T. A. (2006). Confirmatory factor analysis for appliedresearch. New York: Guilford.
Cantwell, D. P. (1996). Classification of child and adolescent
psychopathology. Journal of Child Psychology and Psychiatry,37, 3–12.
Chen, G. K., Kono, N., Geschwind, D. H., & Cantor, R. M. (2006).
Quantitative trait locus analysis of nonverbal communication in
autism spectrum disorder. Molecular Psychiatry, 11, 214–220.
Cox, A., Klein, K., Charman, T., Baird, G., Baron-Cohen, S.,
Swettenham, J., et al. (1999). Autism spectrum disorders at 20
and 42 months of age: Stability of clinical and ADI-R diagnosis.
Journal of Child Psychology and Psychiatry, 40, 719–732.
Cuccaro, M. L., Shao, Y., Grubber, J., Slifer, M., Wolpert, C. M.,
Donnelly, S. L., et al. (2003). Factor analysis of restricted and
repetitive behaviors in autism using the Autism Diagnostic
Interview-Revised. Child Psychiatry and Human Development,1, 3–17.
Duvall, J. A., Lu, A., Cantor, R. M., Todd, R. D., Constantino, J. N.,
& Geschwind, D. H. (2007). A quantitative trait locus analysis of
social responsiveness in multiplex autism families. AmericanJournal of Psychiatry, 164, 656–662.
Epstein, L. J., Taubman, M. T., & Lovaas, O. I. (1985). Changes in
self-stimulatory behaviors with treatment. Journal of AbnormalPsychology, 13, 281–294.
Esbensen, A., Seltzer, M., Lam, K., & Bodfish, J. (2008). Age-related
differences in restricted repetitive behaviors in autism spectrum
disorders. Journal of Autism and Developmental Disorders, 39,
57–66.
Gabriels, R. L., Cuccaro, M. L., Hill, D. E., Ivers, B. J., & Goldson, E.
(2005). Repetitive behaviors in autism: Relationships with
associated clinical features. Research in Developmental Disabil-ities, 26, 169–181.
Goldman, S., Wang, C., Salgado, M., Green, P., Kim, M., & Rapin, I.
(2009). Motor stereotypies in children with autism and other
developmental disorders. Developmental Medicine and ChildNeurology, 51, 30–38.
Heppner, P. P., Kivlighan, D., Jr., & Wampold, B. E. (1999).
Research design in counseling (2nd ed.). Pacific Grove, CA:
Brooks/Cole.
Honey, E., McConachie, H., Randle, V., Shearer, H., & Le Couteur,
A. (2008). One-year change in repetitive behaviors in young
children with communication disorders including autism. Jour-nal of Autism and Developmental Disorders, 38, 1439–1450.
Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in
covariance structure analysis: Conventional criteria versus new
alternatives. Structural Equation Modeling, 6, 1–55.
Hus, V., Pickles, A., Cook, E., Jr., Risi, S., & Lord, C. (2007). Using
the Autism Diagnostic Interview-Revised to increase phenotypic
homogeneity in genetic studies of autism. Biological Psychiatry,61, 438–448.
Lam, K. S. L., & Aman, M. G. (2007). The Repetitive Behavior
Scale-Revised: Independent validation in individuals with autism
spectrum disorders. Journal of Autism and DevelopmentalDisorders, 37, 855–866.
Lam, K., Bodfish, J., & Piven, J. (2008). Evidence for three subtypes
of repetitive behavior in autism that differ in familiality and
association with other symptoms. Journal of Child Psychologyand Psychiatry, 49, 1193–1200.
Leekam, S., Tandos, J., McConachie, H., Meins, E., Parkinson, K.,
Wright, C., et al. (2007). Repetitive behaviours in typically
developing 2-year-olds. Journal of Child Psychology andPsychiatry, 48, 1131–1138.
Lewis, M. H., & Bodfish, J. W. (1998). Repetitive behavior disorders
in autism. Mental Retardation and Developmental DisabilitiesResearch Reviews, 4, 80–89.
Lord, C., Rutter, M., DiLavore, P. C., & Risi, S. (2002). ADOS: TheAutism Diagnostic Observation Scale. Los Angeles, CA:
Western Psychological Services.
Miles, C., & Wayne, M. (2008). Quantitative trait locus (QTL) analysis.
Nature Education, 1(1). Retrieved from http://www.nature.
com/scitable/topicpage/Quantitative-Trait-Locus-QTL-Analysis-
53904.
Militerni, R., Bravaccio, C., Falco, C., Fico, C., & Palermo, M. T.
(2002). Repetitive behaviors in autistic disorder. European Childand Adolescent Psychiatry, 11, 210–218.
Mooney, E., Gray, K., Tonge, B., Sweeney, D., & Taffe, J. (2009).
Factor analytic study of repetitive behaviors in young children
with pervasive developmental disorders. Journal of Autism andDevelopmental Disorders, 39, 765–774.
Morgan, L., Wetherby, A., & Barber, A. (2008). Repetitive and
stereotyped movements in children with autism spectrum
disorders late in the second year of life. Journal of ChildPsychology and Psychiatry, 49, 826–837.
Muthen, L. K., & Muthen, B. O. (2007). M-plus user’s guide (5th ed
ed.). Los Angeles, CA: Muthen & Muthen.
Ozonoff, S., South, M., & Miller, J. (2000). DSM-IV-defined
Asperger syndrome: Cognitive, behavioral and early history
differentiation from high-functioning autism. Autism: The Inter-national Journal of Research and Practice, 4, 29–46.
Papageorgiou, V., Georgiades, S., & Mavreas, V. (2008). Brief report:
Cross-cultural evidence for the heterogeneity of the restricted,
repetitive behaviours and interest domain of autism: A Greek
study. Journal of Autism and Developmental Disorders, 38, 558–
561.
Richler, J., Bishop, S., Klienke, J., & Lord, C. (2007). Restricted and
repetitive behaviors in young children with autism spectrum
J Autism Dev Disord (2010) 40:1521–1530 1529
123

disorders. Journal of Autism and Developmental Disorders, 37,
73–85.
Roid, G., & Sampers, J. (2004). Merrill-Palmer-Revised Scales ofDevelopment. Wood Dale, IL: Stoelting Co.
Rutter, M., LeCouteur, A., & Lord, C. (2003). ADI-R: The AutismDiagnostic Interview-Revised. Los Angeles, CA: Western Psy-
chological Services.
Sparrow, S. S., Cicchetti, D. V., & Balla, D. A. (2005). VinelandAdaptive Behavior Scales: Second edition (Vineland II), Surveyinterview form/caregiver rating form. Livonia, MN: Pearson
Assessments.
Szatmari, P., Georgiades, S., Bryson, S., Zwaigenbaum, L., Roberts,
W., Mahoney, W., et al. (2006). Investigating the structure of the
restricted, repetitive behaviors and interests domain of autism.
Journal of Child Psychology and Psychiatry, 47, 582–590.
Tabachnick, B., & Fidell, L. (2007). Using multivariate statistics (5th
ed.). Boston: Pearson Education.
Turner, M. (1996). Repetitive behaviour and cognitive functioning inautism. Unpublished doctoral dissertation, University of Cam-
bridge, UK.
Turner, M. (1999). Repetitive behaviors in autism: A review of
psychological research. Journal of Child Psychology andPsychiatry and Allied Disciplines, 40, 839–849.
Watt, N., Wetherby, A., Barber, A., & Morgan, L. (2008). Repetitive
and stereotyped behaviors in children with autism spectrum
disorders in the second year of life. Journal of Autism andDevelopmental Disorders, 38, 1518–1533.
Zandt, F., Prior, M., & Kyrios, M. (2007). Repetitive behavior in children
with high functioning autism and obsessive compulsive disorder.
Journal of Autism and Developmental Disorders, 37, 251–259.
1530 J Autism Dev Disord (2010) 40:1521–1530
123
Copyright © 2022 FDOKUMEN