Effects of Low Frequency Repetitive Transcranial Magnetic Stimulation (rTMS) on Gamma Frequency...
16
NeuroRehabilitation 28 (2011) 113–128 113 DOI 10.3233/NRE-2011-0640 IOS Press The effects of low frequency Repetitive Transcranial Magnetic Stimulation (rTMS) and sham condition rTMS on behavioural language in chronic non-fluent aphasia: Short term outcomes Caroline H.S. Barwood a,* , Bruce E. Murdoch a , Brooke-Mai Whelan a , David Lloyd a,b , Stephan Riek b , John O’Sullivan c , Alan Coulthard d , Andrew Wong c,e,f , Phil Aitken f ,h and Graham Hall f ,g a Centre for Neurogenic Communication Disorders Research, School of Health and Rehabilitation Sciences, University of Queensland, Australia b School of Human Movement Studies, University of Queensland, Australia c Department of Neurology and Neurosurgery, Royal Brisbane and Women’s Hospital, Queensland, Australia d Department of Medical Imaging, Royal Brisbane and Women’s Hospital, Queensland, Australia e Department of Neurology, Princess Alexandra Hospital, Queensland, Australia f Acute Stroke Unit, Princess Alexandra Hospital, Queensland, Australia g Department of Medicine, Princess Alexandra Hospital, Queensland, Australia h Department of Geriatric Medicine, Princess Alexandra Hospital, Queensland, Australia Abstract. Introduction: The application of low frequency (1 Hz) Repetitive Transcranial Magnetic Stimulation (rTMS) to right hemisphere (RH) language homologues in non-fluent aphasic populations has yielded improvements in behavioural language function, up to 43 months post stimulation 32. Functional imaging studies have demonstrated RH language homologue “overac- tivation” post left inferior frontal gyrus (IFG) damage, in chronic non-fluent aphasia. The effects of low frequency (inhibitory) rTMS are postulated to be as a result of a reduction of overactivation in RH language homologues, facilitating the reorganisation of neural language networks. Methods: Low frequency (1 Hz) rTMS was applied to the anterior portion of a Broca’s area homologue (pars triangularis), for 20 minutes per day for 10 days, using a stereotactic neuronavigational system. Twelve non-fluent aphasic patients (six real stimulation and six sham), 2–10 years post stroke were stimulated. Behavioural language outcome measures were taken at baseline and 1 week post rTMS. Results: Comparisons between the real stimulation and sham conditions indicated significant main effects between the stimulation and sham groups to 1 week post stimulation for naming accuracy, latency and repetition. Conclusions: This study indicates that rTMS has the capacity to modulate neural language networks, to facilitate improvements in behavioural language function, 1 week post TMS. Keywords: Transcranial Magnetic Stimulation (TMS), aphasia, stroke rehabilitation, language * Corresponding author: Caroline Barwood, Centre for Neuro- genic Communication Disorders Research, School of Health and Re- hab ilitation Sciences, University of Queensland, Brisbane St Lucia, QLD 4072, Australia. Tel.: +617 3365 6162; Fax: +617 3365 1877; E-mail: [email protected]. ISSN 1053-8135/11/$27.50 2011 – IOS Press and the authors. All rights reserved
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Effects of Low Frequency Repetitive Transcranial Magnetic Stimulation (rTMS) on Gamma Frequency...

NeuroRehabilitation 28 (2011) 113–128 113DOI 10.3233/NRE-2011-0640IOS Press
The effects of low frequency RepetitiveTranscranial Magnetic Stimulation (rTMS)and sham condition rTMS on behaviourallanguage in chronic non-fluent aphasia: Shortterm outcomes
Caroline H.S. Barwooda,∗, Bruce E. Murdocha, Brooke-Mai Whelana, David Lloyda,b, Stephan Riekb,John O’Sullivanc, Alan Coulthardd, Andrew Wongc,e,f , Phil Aitkenf,h and Graham Hallf,g
aCentre for Neurogenic Communication Disorders Research, School of Health and Rehabilitation Sciences,University of Queensland, AustraliabSchool of Human Movement Studies, University of Queensland, AustraliacDepartment of Neurology and Neurosurgery, Royal Brisbane and Women’s Hospital, Queensland, AustraliadDepartment of Medical Imaging, Royal Brisbane and Women’s Hospital, Queensland, AustraliaeDepartment of Neurology, Princess Alexandra Hospital, Queensland, AustraliafAcute Stroke Unit, Princess Alexandra Hospital, Queensland, AustraliagDepartment of Medicine, Princess Alexandra Hospital, Queensland, AustraliahDepartment of Geriatric Medicine, Princess Alexandra Hospital, Queensland, Australia
Abstract. Introduction: The application of low frequency (1 Hz) Repetitive Transcranial Magnetic Stimulation (rTMS) to righthemisphere (RH) language homologues in non-fluent aphasic populations has yielded improvements in behavioural languagefunction, up to 43 months post stimulation 32. Functional imaging studies have demonstrated RH language homologue “overac-tivation” post left inferior frontal gyrus (IFG) damage, inchronic non-fluent aphasia. The effects of low frequency (inhibitory)rTMS are postulated to be as a result of a reduction of overactivation in RH language homologues, facilitating the reorganisationof neural language networks.Methods: Low frequency (1 Hz) rTMS was applied to the anterior portionof a Broca’s area homologue (pars triangularis),for 20 minutes per day for 10 days, using a stereotactic neuronavigational system. Twelve non-fluent aphasic patients (six realstimulation and six sham), 2–10 years post stroke were stimulated. Behavioural language outcome measures were taken atbaseline and 1 week post rTMS.Results:Comparisons between the real stimulation and sham conditions indicated significant main effects between the stimulationand sham groups to 1 week post stimulation for naming accuracy, latency and repetition.Conclusions:This study indicates that rTMS has the capacity to modulate neural language networks, to facilitate improvementsin behavioural language function, 1 week post TMS.
Keywords: Transcranial Magnetic Stimulation (TMS), aphasia, stroke rehabilitation, language
∗Corresponding author: Caroline Barwood, Centre for Neuro-genic Communication Disorders Research, School of Health and Re-hab ilitation Sciences, University of Queensland, Brisbane St Lucia,
QLD 4072, Australia. Tel.: +617 3365 6162; Fax: +617 3365 1877;E-mail: [email protected].
ISSN 1053-8135/11/$27.50 2011 – IOS Press and the authors. All rights reserved

114 C.H.S. Barwood et al. / Effects of low frequency rTMS in chronic non-fluent aphasia
1. Introduction
In recent years, low frequency repetitive Transcra-nial Magnetic Stimulation (rTMS) has been safelyand successfully applied to patients with chronic non-fluent aphasia, modulating neural language networksto improve language performance, subsequent to lefthemisphere (LH) stroke. The resulting effects on be-havioural language function show significant improve-ments in picture naming performance up to 43 monthspost stimulation [32,39]. To date, some TMS re-searchers have proposed that the inhibition of righthemisphere (RH) language homologues using low fre-quency rTMS and the subsequent improvements innaming may be due to transcallosal disinhibition [55]where a decrease of overactivation in RH perisylviansites may promote increased LH perilesional activa-tions and function [32,38,39]. There may be additionalexplanations for functional reorganisation of languagepost rTMS nonetheless current evidence from chronicnon-fluent aphasia populations substantiates the neuro-physiological and behavioural changes associated withtranscallosal disinhibition. Current functional neu-roimaging evidence offers valuable insight into recov-ery mechanisms post LH infarction however, has failedto resolve many issues regarding the functional rolesof both the LH and RH and the integration of bilateralnetworks in recovery of language in the aphasic brain.Both the LH and RH are believed to assist languagerecovery after stroke [9,15,44,56]. Despite this, in thechronic stage of aphasia RH activations are thought tobe a maladaptive process indicating faulty recovery oflanguage systems [4].
1.1. Evidence for the modulation of language usingrTMS in normal control and aphasic populations
rTMS modulates neural activity in brain regionswhere it is applied with effects ranging from excitationto inhibition, depending on the frequency [3]. Modula-tion of language using rTMS has been demonstrated inboth normal control and aphasic populations. A previ-ous study by Thiel et al. [54] applied low frequency (in-hibitory) rTMS to the left inferior frontal gyrus (IFG) inright (R) handed normal controls demonstrating inter-ferences in semantic processing and repetition priming.Such studies involving the creation of temporal lesionsin neurologically healthy individuals using rTMS haveestablished causal links between neural language sitesand language behaviour.
rTMS has been applied to LH language sites and RHlanguage homologues to investigate the role of bothhemispheres in language processing after neurologicalinsult (e.g., stroke and brain tumour). Winhuisen etal. [63] applied 4 Hz rTMS to maximal activation sitesidentified on PET scans in L and R IFG in LH strokepatients with aphasia. Patients were stimulated within2 weeks post stroke, to elucidate the acute activationpatterns and behavioural interference using a rTMS. Bi-lateral hemispheric activations were reported for mostpatients in response to semantic based paradigm. WhenrTMS was applied to the L IFG, significantly longerlatencies were reported indicating disruptions of thebrain region responsible for language processes. Simi-lar results were reported in a follow-up investigation onthe same patient sample 8 weeks post stroke [64], fur-ther reiterating the importance of residual LH functionin the recovery of language in aphasia.
rTMS studies targeting patients with chronic non-fluent aphasia have reported significantly improved be-havioural language function post stimulation [32,37–39,64]. Such studies have demonstrated the success-ful modulation of behavioural language function insome patients following administration of low frequen-cy (1 Hz) rTMS to inhibit counterproductiveRH activa-tion. Naeser et al. [38] demonstrated significantly im-proved picture naming function in a cohort of four non-fluent aphasic patients when rTMS was applied to theanterior portion of pars triangularis, (right Brodmannarea 45 [R BA45]), for 20 minutes per day over 10days. Improvements in behavioural language functionwere reported up to 8 months post stimulation, signi-fying reorganisation of neural language networks overtime. Additionally, case study evidence substantiatesthe use of rTMS on global aphasic patients to remediateimpaired language function [39].
In more recent rTMS research, improvements in spe-cific picture naming function have been documented upto 43 months post TMS [32]. Functional magnetic res-onance imaging evidence accompanying these rTMSapplications has identified a significant reduction in RHactivation with a concurrent increase in LH perilesionalactivation, up to 46 months post rTMS stimulation [32].Such evidence verifies the long term, potentially pos-itive neuromodulatory effects of rTMS. Additionally,TMS has been postulated as an adjunct to tradition-al behavioural language therapy. A recent pilot studyby Martin et al. [33] combined 1 Hz rTMS and Con-straint Induced Language Therapy (CILT) to treat a sin-gle patient. Significant improvements were noted onsome naming outcome measures. Cumulatively, thesestudies substantiate the therapeutic potential of rTMSprotocols for patients with chronic non-fluent aphasia.

C.H.S. Barwood et al. / Effects of low frequency rTMS in chronic non-fluent aphasia 115
1.2. Theories to explain low frequency rTMSmodulation of language
Inhibitory forms of rTMS may be used to decreaseoveractivity in RH language homologues [38]. Previ-ous research has identified unusually high RH corti-cal activation patterns in the superior temporal gyrus(STG) [62] and the IFG [41,50,53] in association witha variety of experimental language paradigms in strokepatients. High levels of activation found in R homolo-gous language centres post stroke suggest an interhemi-spheric shift in neural language networks, to recruitundamaged neural resources in the unaffected hemi-sphere [27,57]. There is little doubt that the RH may as-sume a compensatory role in the presence of damage toLH language centres [13,63], however, the capacity towhich the RH is significant for language recovery overtime remains controversial. Paramount to the restora-tion of language function in aphasia is the reintegrationof damaged left fronto-temporal areas into functionallanguage networks [3].
Altered RH activation patterns are postulated in somestudies to be a significant compensatory mechanism tolanguage recovery in aphasia [7,36,47,49]. Compara-tively, other studies have indicated that reactivation ofipsilateral, perilesional sites is frequently a marker ofbetter recovery [4,6]. This suggests that RH integrationinto language networks may impede overall languagerecovery in some patients. Time post stroke, lesionlocation and the specific language tasks examined mayinfluence reported results and the mechanisms control-ling language recovery [44,55]. Some studies have in-dicated that high activation in RH language regions maynot be correlated with improvements in behaviourallanguage performance on specific language tasks. Ev-idence provided by Belin et al. [4] indicated abnormalactivation in homologousRH language regions in apha-sic patients compared to normal controls in response toword repetition tasks. Additionally, improvementsdur-ing the Melodic Intonation Therapy using word repeti-tion tasks accompanied increased activation in Broca’sarea and the L prefrontal cortex [4]. Similarly, Naeseret al. [37] identified increased RH activation comparedto control subjects during overt speech on a story tellingtask, suggesting that RH contribution may influenceagrammatic speech in aphasia. Contralateral areas inthe non-dominant hemisphere may have only limitedcompensatorycapabilities for language processing [47]however, a lack of consistency in the language tasksinvestigated hinders the interpretation of results in thisresearch area.
Low frequency rTMS is used to create a transient“virtual lesion” in RH language homologues (e.g., RBA45). Evidence suggests that this facilitates downregulation of overactive RH sites and the potential up-regulation of perilesional sites in the damaged LH [55].This theory is consistent with the principle of Para-doxical Functional Facilitation (PFF) which proposesthat direct or indirect damage to a particular part ofthe central nervous system may result in facilitationof behavioural outcomes [12,25]. The application of1 Hz rTMS may result in a decrease of overactivationin R BA45, promoting reduced inhibition by R BA45on adjacent and distant neural sites, resulting in modu-lation of bilateral neural networks responsible for pic-ture naming. Previous studies have verified the in-hibitory effects of 1 Hz frequency rTMS on corticalbrain tissue in humans [8,31] and the inhibitory effecton event related brain potentials after stimulation of atleast 15 minutes [18].
Abnormally high RH activation patterns in someaphasic patients post stroke may be due in part totranscallosal disinhibition, where persisting languagedeficits are caused by incomplete or faulty recov-ery mechanisms. According to Heiss and Thiel [20]changes in excitability inipsilateral andcontralateralhomologousregions of a cortical lesion occur as a re-sult of a reduction incollateral andtranscallosal inhi-bition. In normal processing, specialised neural areas(e.g. those specific to language function) inhibit regionsipsilateral, contralateral, or those in bilateral networksthat do not participate in any specialised language func-tion [40] When a specialised neural area is damaged,adaptive processes (plasticity) facilitate functional re-organisation and a cessation of disinhibitive processingto draw on resources perilesional (collateral Disinhibi-tion) and contralateral (transcallosal Disinhibition) tothe damage [65]. With respect to damage in LH lan-guage areas, transcallosal disinhibition may facilitate afunctional shift in language processes from LH to theRH language homologue. Some residual function maystill remain in the LH. Secondary to this, a reductionin collateral disinhibition is thought to allow recruit-ment of areas ipsilateral to the lesion site (in the LH) toassume compensatory language function. In patientswith extensive lesions not limited to language dedicat-ed neural sites (e.g. Broca’s area), the theory of mutualinhibition by transcallosal disinhibition in homologousareas may be less applicable. It is unlikely that suchwide areas of homologous brain tissue are participat-ing in mutual inhibitive processes instigated by a sin-gle neural site (e.g. R Broca’s area). In spite of this,previous case study evidence from global aphasia has

116 C.H.S. Barwood et al. / Effects of low frequency rTMS in chronic non-fluent aphasia
demonstrated improved language skills post rTMS sug-gesting that theories of inhibition may be one compo-nent at work in a complex interconnected bilateral lan-guage network, in the presence of extensive areas ofneural damage [39]. Current theories have promptedthe exploration of alternative therapeutic interventionswhich may directly target neural activity in contralater-al language homologues to induce transient or lastingcognitive and behavioural change [45].
Overactivation of RH language homologues has beenthe target of many neuroimaging investigations and ishypothesised to be a form of neural plasticity to pro-mote recovery. Despite this, evidence still suggeststhat activation and recruitment of perilesional neuronalresources in the LH remain critical to patient recov-ery [20,26,30,47], regardless of the amount of RH ac-tivation [14,63]. Recruitment of the available undam-aged areas ipsilateral to language areas in the LH e.g.STG and the supplementary motor area (SMA), appearsto facilitate better overall aphasia recovery [6,19,26,35,62]. Many factors must be considered when interpret-ing the extent of RH activation such as lesion size andsite [46] as well as time frame post stroke [23,49] Ithas also been hypothesised that the RH may have aninitial compensatory significance in the acute recoveryphase of aphasia, thus, RH activations are present at 10days and remain for up to 8 weeks after stroke [64,65].Furthermore, persisting RH activations are postulatedto be maladaptive processes, marking failed or faultyrecovery and/or a breakdown in inter-hemispheric con-trol [4].
The present study aims to investigate and charac-terise the short term behavioural language changes, 1week post stimulation, associated with a protocol ofinhibitory rTMS as defined by Naeser et al. [38,39].Specifically, it aims to improve on previous rTMS pro-tocols by incorporating a sham condition to investigatethe placebo effects of rTMS and will utilise neuronavi-gational techniques to ensure the accurate identificationof cortical targets. This study will provide a compar-ison of the short term behavioural language effects ofrTMS between stimulation and sham stimulation (con-trol) conditions based on larger sample sizes than thosepreviously published, and test current hypotheses re-garding the ability of low frequency rTMS to inhibitoveractivation in RH language homologues and inducebehavioural language improvements in picture namingfunction.
2. Methods
Twelve (12) right-handed, chronic aphasic patientsreceived rTMS. Handedness was assessed using the Ed-
inburgh Handedness Inventory (EHI) [42]. All patientshad suffered a L middle cerebral artery (MCA) strokebetween 2–10 years previously and had residual lan-guage impairments, including deficits in picture nam-ing. Patient severities ranged from mild to severe. Ta-ble 1 provides detailed biographical information aboutthe patients who participated in the present study. Ap-pendices A-D detail the language profiles of all pa-tients prior to stimulation and 1 week post stimulation.Patients were recruited through two major metropoli-tan hospitals and university research databases in theGreater Brisbane Region, Australia. Ethical clearancewas granted from hospital and university review boards.All patients gave informed consent to participate in thisresearch. A rigorous medical screening procedure (as-sisted by neurologists) was implemented to ensure thatpatients were suitable to receive rTMS.
Exclusion criteria for rTMS were derived fromguidelines published by Wasserman [61]. These in-clude: patients with a personal or family history ofepilepsy or seizures, the presence of: metal anywherein the head, cardiac pacemakers, implanted medica-tion pumps, intracardiac lines, other serious medicalconditions including serious heart disease, any medi-cations which lower neural thresholds (tricyclic anti-depressants, neuroleptic agents etc.). Patients whowere identified as having an increased risk of adverseside effects from receiving rTMS were excluded fromparticipating. A full medical history was compiled forall patients. Patients who had suffered multiple strokeswere excluded due to increased risk of adverse reac-tions to stimulation. Exclusion was on the basis of theneuroradiological report and medical history. Thosepatients who had severe visual or hearing impairmentswere also excluded.
Patients did not receive speech therapy services dur-ing their participation in this research study. Due to thechronic nature of language deficits, none of the patientcohort were receiving speech therapy immediately pri-or to participating in the study. Therefore, no thera-peutic interventions were interrupted to receive rTMS.All patients received comprehensive speech therapy in-tervention up to 4 months post stroke however, all pa-tients in the current cohort had residual language (in-cluding naming) impairments that were not alleviatedby behavioural therapy.
A double blind methodologywas employed wherebypatients were randomly assigned to one of two groupseither receivingreal conditionTMS (n = 6, aged be-tween 54 and 67 years; mean age (SD)= 60.8 (5.98)years, mean time post stroke (SD)= 3.49 (1.27) years)

C.H.S. Barwood et al. / Effects of low frequency rTMS in chronic non-fluent aphasia 117
Tabl
e1
Pat
ient
Sex
Age
Edi
nbur
ghH
ande
d-Y
ears
ofL
esio
nsi
teT
ime
post
stro
keH
emip
ar-
Aph
asia
Stim
ulat
ion
hand
edne
ssne
ssed
ucat
ion
toin
itial
esis
diag
nosi
sgr
oup
inve
ntor
yte
stin
g(y
ears
;(E
HI)
scor
em
onth
s)
rTM
S1
F65
80R
18L
ong
stan
ding
LM
CA
terr
itory
infa
rct
with
exvacu
odi
lata
tion
ofth
ele
ftla
tera
lven
tric
le.
4;5
No
Mild
-mod
erat
eno
n-flu
ent
Rea
l
rTM
S3
M59
50R
12L
MC
Ain
farc
twith
exva
cuo
dilta
tion
ofth
eleftla
tera
lven
tric
lean
den
ceph
alom
acia
inth
ele
ftin
sula
and
left
parie
to-o
ccip
ital
regi
on.
3;3
No
Mod
erat
e-se
vere
non-
fluen
t/glo
bal
Rea
l
rTM
S4
F66
100
R14
LM
CA
infa
rct
with
ence
phal
omac
iaan
dex
vac
uodi
lata
tion
ofth
ele
ftla
tera
lven
tric
le.
The
sylv
ian
fissu
reis
enla
rged
.T
heence
phal
o-m
alac
iaex
tend
ssu
perio
rlyan
dm
edia
llyto
invo
lve
the
med
ial
aspe
ctof
the
left
mot
orst
rip.
5;8
Yes
Mod
erat
eno
n-flu
ent
Rea
l
rTM
S9
M67
100
R16
Sig
nific
ant
LM
CA
terr
itory
infa
rct
with
enc
epha
lom
alac
iaan
dex
-va
cuo
dila
tatio
nof
the
left
late
ral
vent
ricle
.T
heB
asal
nucl
eiar
ela
rgel
ysp
ared
.
2;6
No
Sev
ere
non-
fluen
t/glo
bal
Rea
l
rTM
S10
M54
60R
10M
atur
eL
MC
Ain
farc
text
endi
ngla
tera
llyfr
omth
epo
ster
ior
horn
ofth
ele
ftla
tera
lven
tric
lew
ithen
ceph
alom
alac
iaan
dex
-va
cuo
dila
ta-
tion
ofth
eve
ntric
le.
Sm
alll
acun
arty
pein
farc
tsbi
late
rally
.N
orm
alpo
ster
ior
foss
ast
ruct
ures
.
3;5
Yes
Sev
ere
non-
fluen
t/glo
bal
Rea
l
rTM
S13
M54
100
R10
LM
CA
terr
itory
infa
rct
with
asi
gnifi
cant
are
aof
ence
phal
omac
iain
the
left
fron
tall
obe
and
asso
ciat
edex
vacu
odi
lata
tion
of
the
left
vent
ricle
and
left
cere
bral
pedu
ncle
redu
ctio
n.
2;5
Yes
Mild
-mod
erat
eno
n-flu
ent
Rea
l
rTM
S2
M72
100
R14
Lin
ferio
rdiv
isio
nM
CA
infa
rctw
ithac
com
panyi
ng
tem
pero
-par
ieta
len
ceph
alom
acia
.4;
0N
oM
ild-m
oder
ate
non-
fluen
tS
ham
rTM
S5
F51
100
R13
LC
VA,
tota
lan
terio
rci
rcul
atio
nin
farc
t,exte
nsiv
ele
fthe
mis
pher
eM
CA
/str
oke
with
gros
sen
ceph
alom
alac
ia.
The
reis
ahy
perin
tens
eco
llect
ion
over
the
left
hem
isph
ere
whi
chis
assu
med
tore
pres
ent
asu
bacu
tesu
bdur
alha
emat
oma.
The
right
hem
isph
ere
appe
ars
nor-
mal
.T
here
isat
roph
yof
the
left
cere
bral
pedu
ncle
and
left
sid
eof
the
pons
,in
keep
ing
with
Wal
leria
nde
gene
ratio
n.
3;4
Yes
Mod
erat
eno
n-flu
ent
Sha
m
rTM
S8
M77
100
R13
LM
CA
terr
itory
infa
rctw
ithsu
bacu
terig
htocci
pita
l(po
ster
iorc
ere-
bral
arte
ry)
terr
itory
infa
rct.
Aco
uple
ofsm
allg
lobu
larfoc
iare
seen
inth
ede
epw
hite
mat
ter
ofbo
thce
rebr
alhe
mis
pher
esco
nsis
tent
with
chro
nic
isch
emia
rela
ted
tom
icro
vasc
ular
dise
ase.
2;2
No
Mild
-Mod
erat
eno
n-flu
ent
Sha
m
rTM
S11
M66
80R
12L
MC
Ate
rrito
ryin
frac
tw
ithen
ceph
alom
ala
cia
invo
lvin
gth
ele
ftfr
onta
llo
bean
dm
oder
ate
ex-
vacu
odi
lata
tion
ofth
ele
ftla
tera
lve
ntric
le.
The
right
hem
isph
ere
and
the
post
erio
rfo
ssa
str
uctu
res
appe
arre
lativ
ely
norm
al(W
alle
rian
dege
nera
tion
note
dle
ftup
per
brai
nst
em).
2;3
Yes
Mod
erat
eno
n-flu
ent
Sha
m
rTM
S14
M71
100
R10
Sig
nific
antL
MC
Ate
rrito
ryin
farc
twith
mode
rate
exva
cuo
dila
tatio
nof
the
left
vent
ricle
and
tem
pero
-par
ieta
lenc
epha
lom
acia
.2;
9Y
esM
oder
ate-
seve
reno
n-flu
ent
Sha
m
0rT
MS
15M
6310
0R
15L
arge
LM
CA
terr
itory
infa
rct
with
sign
ificant
tissu
elo
ssw
ithex
vacu
odi
lata
tion
ofth
ele
ftve
ntric
le.
The
right
hem
isph
ere
and
post
erio
rfo
ssa
stru
ctur
esap
pear
norm
al.
6;3
Yes
Sev
ere
non-
fluen
t/glo
bal
Sha
m

118 C.H.S. Barwood et al. / Effects of low frequency rTMS in chronic non-fluent aphasia
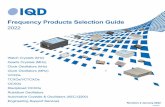
Fig. 1. Structural 3T MRI scans for two patients of the twelvepatient cohort, demonstrating the range of lesion severities A) PatientrTMS 15;left extensive middle cerebral (MCA) territory infarct with ex vacuo dilatation of the left ventricle. Patient has a severe non-fluent/ global aphasia.B) PatientrTMS 13; L MCA territory infarct with a significant area of encephalomacia in the left frontal lobe and associated ex vacuo dilatationof the left ventricle and left cerebral peduncle reduction.Patient has a mild- moderate non-fluent aphasia.
or a placeboTMS (using a SHAM coil) (n =6, agedbetween 51 and 77 years; mean age (SD)= 66.6 (9.09)years, mean time post stroke (SD)= 3.46 (1.53) years).All recorded language measures were scored by an ex-ternal researcher who was not aware of the conditionor testing occasion of each patient, to reduce observerbias. The sham stimulation group in this study served asa placebo condition to measure the effects of real con-dition stimulation. The sham coil employed (Magstim,Carmarthenshire, Wales, UK) was identical in shapeand size to the real stimulation coil and produced nomagnetic field. Thus it is hypothesised that the place-bo TMS condition does not induce neuro-physiologicalchanges to influence behavioural language function.Each patient only received ONE type of stimulation.Sham stimulation was utilised to verify the effects ofthe real stimulation protocol as a control condition.
Prior to stimulation, all subjects were required to un-dertake a 3-Tesla structural magnetic resonance imag-ing (MRI) scan, to aid target localisation and provideadditional information on the size, extent and compo-sition of the lesion. Figure 1 shows examples of MRIsfrom two of the stimulated patients. Acquisition pa-rameters were as follows: TR= 19, TE= 4.92, ma-
trix size = 256× 256, number of slices= 128, slicethickness= 2 mm. The study neuroradiologist pro-vided a radiological report to specify affected neuralregions. A computerised MRI visualisation and anal-ysis system [51] was then employed to visually marktarget areas (R BA45 and the motor hand knob) witha crosshair (i.e., +). This software program permits aTalairach transformation of each subject’s brain, gen-erating voxel and Talairach co-ordinates in referenceto general neuroanatomical landmarks and Brodmannareas within designated “hot spots,” which may then bemarked for future reference. In this research study, suchmarkings assist in defining the orientation of the TMScoil on the skull using the neuronavigational system.
The language related cortical area in the contralater-al (right) hemisphere (i.e., homologue R BA) was es-tablished as the stimulation target. The foot of the 3rdfrontal convolution represents the classical definitionof Broca’s area [5]. Within the L IFG, this region in-corporates the structures pars triangularis and pars op-ercularis, also known as Brodmann areas 45 (BA 45)and 44 (BA 44), respectively. The cytoarchitecture ofBroca’s area was informed by papers from Amunts etal. [1,2]. Previous studies have revealed TMS of BA

C.H.S. Barwood et al. / Effects of low frequency rTMS in chronic non-fluent aphasia 119
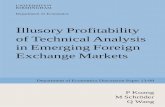
Fig. 2. A 3D brain surface reconstruction from 3T StructuralMRI scan of patientrTMS 5. The target for stimulation has been marked in theunaffected, healthy right hemisphere. The target is definedas the apical portion of R Brodmann area 45, delimited ventrally by the horizontalramus of the Sylvian fissure and laterally by the vertical ramus of Sylivan fissure.
45 (pars triangularis) and not BA 44 (pars opercularis)significantly increases the accuracy and decreases re-action time of picture naming in aphasic patients [37,38]. The apical portion of right BA 45 was thereforeselected as the specific stimulation point for the presentstudy, delimited ventrally by the horizontal ramus ofthe Sylvian fissure [11], and laterally by the verticalramus of Sylivan fissure. Figure 2 shows the stimula-tion target marked on 3D reconstruction of the patient’sbrain.
The resting motor threshold (rMT) for stimulationwas determined using one of the hand muscles. TheTMS coil (bi-phasic stimulation) was placed on themotor “hot spot” for the first dorsal interosseous (FDI)muscle in the left hand (i.e. knob within pre-centralgyrus) in the contralateral hemisphere as determinedby MRI marking and Stealthstation software (Medtron-ic, USA). Motor evoked potentials (MEPs) were thenelicited via TMS and surface EMG recorded fromFDI via Ag/AgCl electrodes (1 cm in diameter), posi-tioned over the belly of the muscle and the metacarpo-phalangeal joint of the index finger, respectively. Theground electrode was attached over a bony prominenceon a distal region of the radius. The coil was posi-tioned tangentially to the skull above the left M1 withthe handle pointing backward and laterally at an angleof about 45◦ to the sagittal plane inducing an electricalcurrent in the brain tissue with a posterior–lateral toanterior–medial direction roughly perpendicular to thecentral sulcus. This current orientation is known to beoptimal for evoking a motor response in the contralat-eral hand [34]. The location and exact orientation atwhich stimuli was applied at suprathreshold intensityconsistently yielded maximal MEPs in the contralat-eral FDI muscle. rMT was defined as the minimumstimulus intensity eliciting 5 responses of about 50µV
out of 10 consecutive trials (50% successful MEPS) inthe relaxed contralateral FDI [48]. Trials commencedwith a suprathreshold value and subsequent TMS in-tensities were decreased in steps of 2% until no reliableMEPs were recorded. For the present research studyon lesioned stroke patients, stimulation was applied at90% of the rMT attained [37]. Patient stimulation in-tensities in the present study ranged between 35–55%of maximum stimulator output.
Once the target was marked on the image, the MRIswere imported into theStealthstation Treon(Medtron-ic, USA), a frameless stereotactic image guidance sys-tem designed for neurosurgical application but adaptedfor our purposes via several custom software modifica-tions. Within the Stealthstation, the “hot spots” wereconverted to target plans. In brief, reflective markersattached to the subject’s head were detected via an in-frared tracking camera, subsequently logging the po-sition of the head in space. The software then co-registered the position of the subject’s head with theMRI data set and target plans were established. Eachplan consists of a perpendicular line from the “hot spot”to the external skull surface. It is reported that the max-imum electric field produced by a figure of eight coilcan be measured at the point of the cortex lying perpen-dicular to the midline of the centre of the coil [21]. A3D model of the head was then constructed with rele-vant target plans depicted. Reflective markers were al-so attached to the TMS coil, subsequently allowing thecoil to be positioned on the head and tracked, relevantto these predetermined target plans.
Low frequency, 1 Hz rTMS was applied to patientsfor 20 minutes per day (1200 pulses), for 2 weeks (10sessions) as defined by Naeser et al. [38] and used instudies to remediate depression [28]. The stimulationprotocol aimed to down regulate RH overactivation in

120 C.H.S. Barwood et al. / Effects of low frequency rTMS in chronic non-fluent aphasia
homologous language sites. The TMS target was theanterior portion of the homologue of pars triangularis(R Brodmann area 45), in the Broca’s homologue ascited in previous rTMS studies [32,37,39]. A figure ofeight, 70 mm diameter rTMS coil and identical shamcoil were utilised (Magstim, Carmarthenshire, Wales,UK). The coil was placed over the marked region ofinterest on the MRI scan (on the gyrus immediatelyrostral to the anterior (vertical) ascending ramus of thesylvian fissure). The coil was held by hand and positionrelative to the head was maintained using realtime feed-back from the stereotatic guidance system, the StealthStation Treon. As the Stealth Station gives continuousfeedback of coil position relative to head position, therewas no need to fixate the participant’s head. Accordingto Naeser et al. [38], the approximate size of the corticalarea stimulated utilising a 70 mm coil is 1 cm× 1 cm.
Standardised language assessments were utilised tomeasure changes in behavioural language function as-sociated with rTMS treatment. 1 week prior to stim-ulation (baseline), and 1 week post stimulation pa-tients were tested using the standard form of the BostonNaming Test (BNT) [24] and selected subtests of theBoston Diagnostic Aphasia Examination (BDAE) [17]were administered according to a protocol outlined byNaeser et al. [38]. Receptive and expressive languageabilities were tested. The subtests administered were:picture description (Cookie Theft Picture) (analysis ofcomplexity index and longest number of words perphrase length), word comprehension,word comprehen-sion by category, commands, complex ideational ma-terials, repetition (single words, non-words and sen-tences), responsive naming, naming screening of spe-cial categories, naming colours, naming actions, nam-ing animals, naming tools and implements. The overallscore on the above BDAE was also collated. Thosesubtests containing culturally sensitive materials wereomitted from the testing battery. This was a com-prehensive language battery that provided a detailedoverview of each patient’s language profile. Appen-dices A-D outline individual patient assessment results.
Additionally, a set of 144 black and white line draw-ings of objects, taken from a previously published com-mon object picture inventory [52] were used to measurechanges in lexical-semantic function at baseline and 1week post stimulation. Pictures were administered inlists of 48 words, balanced for average response la-tency, syllable length, frequency and visual complexi-ty and percentage agreement from normal control sin-gle pulse TMS studies previously administered in ourlaboratory. Norms pertaining to these variables were
obtained from the online International Picture Nam-ing Database. The entire picture set was randomisedeach time it was presented and patients were given restbreaks during administration. Pictures were present-ed on a 20” LCD computer monitor where the patientsat approximately 30 cm from the screen. Each pic-ture was preceded by a preparatory dot on screen for200 msec. The picture appeared for 5 sec, with an ad-ditional 5 sec recording for responses and a 1sec inter-stimulus interval. Verbal responses were recorded via amicrophone positioned approximately 10 cm from thesubject’s mouth. Responses was digitised via a custommadeSound Detectprogram (Matlab version 6.5) at a16 bit resolution and a sampling rate of 22kHz, whichproduced acoustic waveforms on a computer screen foranalysis. As per Topper’s [57] methodology, an ampli-tude filter was used to remove all acoustic signals withan amplitude of less than 7.5% of the maximum soundlevel. Acoustic onset time/naming latency (i.e., time inmsec from presentation of picture to acoustic onset ofaccurate response) was calculated.
Using the digitised naming responses, the mean re-action time and accuracy of naming (i.e., no. of pic-tures named correctly) for the picture set at baselineand 1 week post stimulation was calculated. Accordingto Naeser et al. [38] the learning and priming effects onresponse times for the Snodgrass and Vanderwart [52]pictures are negligible, thus, the repeated exposure ofpatients to the same picture set was justified.
3. Results
A comparison of performance between the stimula-tion and sham groups across baseline and 1 week postrTMS is shown in Fig. 3. A series of two-way re-peated measures analysis of variances (ANOVA) wereconducted for all BDAE subsets, BNT, picture namingaccuracy and latency, by time of testing (baseline, priorto TMS vs. 1 week post TMS) and group (real stimu-lation vs. sham). Table 2 outlines mean values, stan-dard deviations, significant main effects and effect sizedemonstrated on the ANOVA statistical analyses. Sig-nificant differences in the interactions between groupand time were found on the following subtests: BDAEnaming actions (p < 0.05), BDAE naming tools andinstruments (p < 0.05), BDAE repetition of sentences(p < 0.05), Cookie Theft picture description complex-ity index (p < 0.05), Cookie Theft picture descrip-tion longest words per phrase (p < 0.01), Commands(p < 0.05), the overall score calculated from the BDAE

C.H.S. Barwood et al. / Effects of low frequency rTMS in chronic non-fluent aphasia 121
Table 2Overview of significant results baseline to 1 week post stimulation
Language subtest Baseline Pre- 1 week ANOVA ANOVA Group Effect sizerTMS post rTMS × Time Cohen’s
Stim Sham Stim Sham f df (P) (d)
BDAE naming actions Mean 5.50 6.66 7.50 6.17 5.95 10 0.035 0.393SD 4.72 5.27 5.43 4.87
BDAE Naming tools and Mean 5.83 6.67 7.66 6.67 9.31 10 0.012 0.469instruments SD 3.54 4.17 4.23 4.27BDAE repetition of sentences Mean 2.83 4.0 4.67 4.0 9.31 10 0.012 0.502
SD 3.19 3.58 4.08 3.41Picture description complexity Mean 1.21 1.12 1.55 1.12 5.13 10 0.043 0.777index SD 0.39 0.30 0.58 0.26Picture description longest Mean 4.17 4.00 5.00 3.83 18.00 10 0.002 0.392word per phrase SD 2.23 2.61 2.00 2.40Commands Mean 7.67 5.83 9.5 5.83 7.857 10 0.019 0.378
SD 5.16 1.72 4.50 1.72BDAE overall score Mean 147.83 156 166.33 156.17 23.00 10 0.001 0.319
SD 58.33 45.93 57.65 44.88Boston Naming Test (BNT) Mean 29.17 28.33 36.00 28.67 5.107 10 0.047 0.283
SD 23.27 22.20 25.12 22.54Snodgrass and Vanderwart Mean 1770.76 1838.89 1469.96 1914.45 8.14 10 0.005 0.543picture naming latency (msec) SD 558.83 165.72 549.96 154.79Snodgrass and Vanderwart Mean 88.33 79.50 94.50 80.00 5.93410 0.035 0.107picture naming accuracy SD 56.97 61.73 58.36 61.53
subtests administered (p < 0.01), Snodgrass and Van-derwart [52] picture naming latency (p < 0.01) andSnodgrass and Vanderwart [52] picture naming accu-racy (p < 0.05). No significant results within the shamgroup across time were found.
Post Hoc analyses were conducted between the twogroups (independent samples) at baseline and 1 weekpost rTMS and within sample groups across baseline to1 week post rTMS (repeated measures t-test). All anal-yses at baseline demonstrated no significant differencesbetween the real stimulation and sham conditions. At 1week post stimulation, significant differences betweenthe stimulation and sham groups were found for somepicture naming and repetition subtests. Within the re-al stimulation group significant differences across time(baseline to 1 week post stimulation) were found for:BDAE naming of tools and instruments (t = −3.379,p = 0.020), BDAE overall score (t = −4.959,p =
0.004), BDAE repetition of sentences (t = −3.379,p = 0.020), Commands (t = −2.803,p = 0.038), theSnodgrass and Vanderwart [52] picture naming laten-cy (t = 4.073,p = 0.015) and Snodgrass and Van-derwart [52] picture naming accuracy (t = 2.750,p =
0.04).
4. Discussion
The present study incorporated a sample size oftwelve patients, including a sham (control) group to in-
vestigate the behavioural language effects of rTMS onlanguage function 1 week post stimulation in a popula-tion of chronic non-fluent aphasic patients. To date, thisis the largest chronic aphasic sample population whichrTMS has been applied to, with a placebo stimulationgroup as a comparative control measure. Comparisonbetween the real stimulation and sham conditions in-dicated significant main effects between the stimula-tion and sham group one week post-stimulation, withthe former group, but not the sham group, demonstrat-ing significantly improved performance on the picturenaming and repetition subtests of the BDAE [17] andnaming accuracy and latency on a standardised pictureinventory [52]. Results from the present study indicatethat low frequency, 1 Hz rTMS to R BA 45 (pars trian-gularis) has a positive effect on behavioural languagefunction 1 week post stimulation. The improvementsreported 1 week post stimulation are noteworthy, withsignificant differences between the means of the realstimulation and sham groups at 1 week post stimulationfor many subtests, directly relating to picture namingfunction. These results are consistent with those pre-viously reported by Naeser et al. [38,39] and Martinet al. [32], which exemplify improvements in picturenaming function associated with PFF effects inducedby low frequency rTMS.
It is hypothesised that the effect of rTMS on the LIFG lesioned brain is due to down-regulation of overactivity in R Broca’s homologue in chronic aphasic pa-tients, and potential up regulation of LH perilesional

122 C.H.S. Barwood et al. / Effects of low frequency rTMS in chronic non-fluent aphasia
Fig. 3. Graphs showing means at baseline and 1 week post stimulation for real and sham stimulation groups across subtestsadministered fromBoston Diagnostic Aphasia Examination [17] and Snodgrass and Vanderwart [52] picture naming inventory.
resources. The present study proposes that the sup-pression of R pars triangularis using rTMS will mod-ulate prefrontal and temporo-parietal neural connec-tions responsible for naming processes, to facilitate be-havioural improvements in naming function. Semanticbased experimental paradigms have previously elicitedactivations in L Broca’s area, (including pars opercu-laris (BA 44) and pars triangularis (BA 45)) and theL posterior temporal lobe structures in normal controlsubjects [15,44] and in aphasic patients [44]. rTMScan facilitate decreased RH activations in the R SMAand increased LH in the L SMA compared to baselinemeasures [32]. This study demonstrates the potentialneuromodulatory advantage of rTMS over time.
The theory of compensatorybrain responses in apha-sia recovery provides a beneficial framework on whichto base further experimental rTMS research. Howev-er, some pertinent issues within the present stimulationand sham patient samples must be addressed. Patientsin both samples were in the stable, chronic phase ofaphasia, and were well past the spontaneous recoveryperiod of 3–6 months post stroke [10]. As a result ofstrict randomisation procedures, differences were not-ed into the mean age of each group (the sham meanage was higher than the stimulation group mean). Ad-
ditionally, the variability of ages within the sham sam-ple was much greater than that in the stimulation sam-ple which may impact the capacity for neural and ul-timately behavioural language change (e.g., as a resultof age related atrophic changes). Heterogeneity, par-ticularly in small sample populations is also a majorconfounding factor to results obtained in all rTMS re-search, including the present study. A widely diverserange of: lesions sites, lesion size, aging effects onbrain tissue, time post stroke, severity of language im-pairment and neurobiological factors such as tissue dis-tribution affecting stimulation parameters [58] cautionthe interpretation of results. Many of these differencesbetween groups and within groups in the present studycan be attributed to randomisation of the sample pop-ulation. Particularly noteworthy are individual patientresponses to rTMS, which in this study and have beenreported previously to be linked to the severity of lan-guage impairment. Those patients with severe non-fluent or global aphasia have shown the least capacityfor neurological or behavioural change in response torTMS [32]. This may be due to an inability to rerecruitresources within the LH or adequately integrate RHsites in bilateral language networks. Despite the limi-tations discussed the capacity of behavioural language

C.H.S. Barwood et al. / Effects of low frequency rTMS in chronic non-fluent aphasia 123
change over time (as a result of neuromodulation) canbe accurately measured through repeated behaviouralassessments in which patients act as their own control.
The sham group in the present study showed no sig-nificant improvements across baseline to 1 week poststimulation for any subtests on the BDAE or picturenaming inventories. Some minor improvements werenoted in individual patient’s data e.g. BNT. Further lon-gitudinal research on this sham population will deter-mine the effects of sham stimulation over time. Insome cognitive and motor cortex TMS studies, im-provements in sham group performance are reported.These are postulated to be a result of “activation” ofneurons rather than stimulation, whereby, sham formsof TMS may induce neuronal activity to modulate cor-tical activity through somatosensory input e.g. audito-ry click [60]. This may explain any minor individualchanges in language function in the present study how-ever, the results of the present sham group are not sig-nificant when compared to the real stimulation groupon a number of behavioural language outcome mea-sures. Reproducibility of these sham results on dif-ferent aphasic populations is paramount to verify thatsham conditions may be employed as a reliable con-trol measure of TMS neuromodulation, particularly inmodulation of cognitive measures such as language.
Clearly, further research to investigate the capaci-ty of rTMS to modulate neural language networks tofacilitate long-term improvements in behavioural lan-guage function post-stroke is warranted. Future re-search however, needs to address a number of inherentinadequacies in many of the studies reported to date.Firstly, by far the majority of previous studies involveonly very small numbers. Indeed, the present study isthe largest study of rTMS in relation to language func-tion completed to date. Further, many studies have notutilised appropriate and accurate techniques to identi-fy cortical targets for rTMS stimulation. Neuronavi-gational approaches to TMS coil placement have beenrecognised as essential to localise cortical targets withbenchmark precision [22]. Finally few studies haveexamined the longer-term effects of rTMS on languagefunction. The current research represents an unprece-dented attempt to study the effects of rTMS on word re-trieval processes in a larger cohort of aphasic individu-als using a state-of-the-art neuronavigational guidancesystem (Stealthstation) for stimulus target localisation.Future studies applying rTMS to patients with aphasiashould incorporate larger sample sizes, further longi-tudinal data collection and test variations of stimula-tion protocols (intensity and length of stimulation) andbrain sites to establish the most efficacious methods ofneuromodulation for the greatest number of patients.
5. Conclusions
The present research provides evidence to show thatrTMS can be utilised to facilitate improved behaviourallanguage function, in particular picture naming perfor-mance, in patients with non-fluent aphasia through thesuppression of RH language homologues. As indicat-ed by the results, the short term effects of real con-dition rTMS are significant across baseline to 1 weekpost stimulation, when compared to a sham stimula-tion group. The incorporation of a sham control groupverified the positive behavioural effects of real condi-tion stimulation. The effects of sham stimulation onbehavioural language function are postulated to be low,however, the results may be specific to this sampleaphasic population and impacted by the small samplesize. Further longitudinal research on both the realstimulation and sham groups is necessary to charac-terise the long term effects of TMS on behavioural lan-guage measures and clarify its role in neurorehabilita-tion of post stroke aphasia. Future research incorpo-rating electrophysiological measures may be advanta-geous to identify subtle changes in language process-ing in chronic non-fluent aphasia associated with rTMSapplications.
Acknowledgement
We acknowledge the assistance of the Communica-tion Disability Centre’s Aphasia Registry, in recruitingparticipants for this project.
References
[1] K. Amunts, A. Schleicher, U. Burgel, H. Mohlberg, H.B.Uylings and K. Zilles, Broca’s region revisited: Cytoarchitec-ture and intersubject variability,The Journal of ComparativeNeurology412 (1999), 319–341.
[2] K. Amunts, P.H. Weiss, H. Mohlberg, P. Pieperhoff, S. Eick-hoff, J.M. Gurd, J.C. Marshall, N.J. Shah, G.R. Fink and K.Zilles, Analysis of neural mechanisms underlying verbal flu-ency in cytoarchitectonically defined stereotaxic space – theroles of Brodmann areas 44 and 45,Neuroimage22 (2004),42–56.
[3] J. Andoh and J.L. Martinot, Interhemispheric compensation: ahypothesis of TMS-induced effects on language-related areas,European Psychiatry23 (2008), 281–288.
[4] P. Belin, P. Van Eeckhout, M. Zilbovicius, P. Remy, C. Fran-cois, S. Guillaume, F. Chain et al., Recovery from nonflu-ent aphasia after melodic intonation therapy: a PET study,Neurology47 (1996), 1504–1511.

124 C.H.S. Barwood et al. / Effects of low frequency rTMS in chronic non-fluent aphasia
[5] P. Broca, Remarques sur le sie‘ge de la faculte’ du langagearticule, suivies dune observation daphe’mie (perte de laparole),Bulletin de la Socie’te’ Anatomique de Paris6 (1861),330–357.
[6] Y. Cao, E.M. Vikingstad, K.P. George, A.F. Johnson and K.M.Welch, Cortical language activation in stroke patients recov-ering from aphasia with functional MRI,Stroke; a Journal ofCerebral Circulation30 (1999), 2331–2340.
[7] S.F. Cappa, D. Perani, F. Grassi, S. Bressi, M. Alberoni,M. Franceschi, V. Bettinardi, S. Todde and F. Fazio, A PETfollow-up study of recovery after stroke in acute aphasics,Brain and Language56 (1997), 55–67.
[8] R. Chen, J. Classen, C. Gerloff, P. Celnik, E.M. Wassermann,M. Hallett and L.G. Cohen, Depression of motor cortex ex-citability by low-frequency transcranial magnetic stimulation,Neurology48 (1997), 1398–1403.
[9] B. Crosson, K. McGregor, K.S. Gopinath, T.W. Conway, M.Benjamin, Y.-L. Chang, A.B. Moore, A.M. Raymer, R.W.Briggs, M.G. Sherod, C.E. Wierenga and K.D. White, Func-tional MRI of language in aphasia: a review of the literatureand the methodological challenges,Neuropsychology Review17 (2007), 157–177.
[10] G. Demeurisse and A. Capon, Language recovery in aphasicstroke patients: Clinical, CT and CBF studies,Aphasiology1(1987), 301–315.
[11] J.T. Devlin, P.M. Matthews and M.F.S. Rushworth, Semanticprocessing in the left inferior prefrontal cortex: A combinedfunctional magnetic resonance imaging and transcranial mag-netic stimulation study,Journal of Cognitive Neuroscience15(2003), 71–84.
[12] S. Fecteau, A. Pascual-Leone and H. Theoret, Paradoxical fa-cilitation of attention in healthy humans,Behavioral Neurol-ogy17 (2006), 159–162.
[13] B. Fernandez, D. Cardebat, J.-F.O. Demonet, P.A. Joseph,J.-M. Mazaux, M. Barat and M.L. Allard, Functional MRIfollow-up study of language processes in healthy subjects andduring recovery in a case of aphasia,Stroke; a Journal ofCerebral Circulation35 (2004), 2171–2176.
[14] G. Gainotti, The riddle of the right hemisphere’s contributionto the recovery of language,European Journal of Disordersof Communication: The Journal of The College of Speech andLanguage Therapists, London28 (1993), 227–246.
[15] B.T. Gold and A. Kertesz, Right hemisphere semantic pro-cessing of visual words in an aphasic patient: an fMRI study,Brain and Language73 (2000), 456–465.
[16] B.T. Gold and R.L. Buckner, Common prefrontal regions coac-tivate with dissociable posterior regions during controlled se-mantic and phonological tasks,Neuron35 (2002), 803–812.
[17] H. Goodglass, E. Kaplan and B. Barresi,The assessment ofaphasia and related disorders(3rd ed.), Philadelphia: Lippin-cott, Williams and Wilkins, 2001.
[18] M. Hansenne, O. Laloyaux, S. Mardaga and M. Ansseau,Impact of low frequency transcranial magnetic stimulationon event-related brain potentials,Biological Psychology67(2004), 331–341.
[19] W.D. Heiss, J. Kessler, H. Karbe, G.R. Fink and G. Pawlik,Cerebral glucose metabolism as a predictor of recovery fromaphasia in ischemic stroke,Archives of Neurology50 (1993),958–964.
[20] W.D. Heiss and A. Thiel, A proposed regional hierarchy in re-covery of post-stroke aphasia,Brain and Language98 (2006),118–123.
[21] U. Herwig, C. Schonfeldt-Lecuona, A.P. Wunderlich, C.VonTiesenhausen, A. Thielscher, H. Walter and M. Spitzer, The
navigation of transcranial magnetic stimulation,PsychiatryResearch108 (2001), 123–131.
[22] P. Herwig, P. Satrapi and C. Schonfeldt-Lecuona, Usingtheinternational 10-20 EEG system for positioning of transcranialmagnetic stimulation,Brain topography16 (2003), 95–99.
[23] A.E. Hillis, Aphasia: Progress in the last quarter of a century,Neurology69 (2007), 200–213.
[24] E. Kaplan, H. Goodglass and S. Weintraub,The Boston Nam-ing Test. Philadelphia: Lippincott, Williams and Wilkins,2001.
[25] N. Kapur, Paradoxical functional facilitation in brain-behaviour research. A critical review,Brain119 (1996), 1775–1790, 1996.
[26] H. Karbe, A. Thiel, G. Weber-Luxenburger, K. Herholz, J.Kessler and W.D. Heiss, Brain plasticity in poststroke aphasia:what is the contribution of the right hemisphere?Brain andLanguage64 (1998), 215–230.
[27] Y.-H. Kim, M.-H. Ko, T.B. Parrish and H.-G. Kim, Reorga-nization of cortical language areas in patients with aphasia:a functional MRI study,Yonsei Medical Journal43 (2002),441–445.
[28] E. Klein, I. Kreinin, A. Chistyakov, D. Koren, L. Mecz, S.Marmur, D. Ben-Shachar et al., Therapeutic efficacy of rightprefrontal slow repetitive transcranial magnetic stimulation inmajor depression: A double-blind controlled study,Archivesof General Psychiatry56 (1999), 315–320.
[29] E. Klein, Y. Kolsky, M. Puyerovsky, D. Koren, A. Chistyakovand M. Feinsod, Right prefrontal slow repetitive Transcranialmagnetic stimulation in schizophrenia: A double-blind sham-controlled pilot study,Biological Psychiatry46 (1999), 1451–1454.
[30] A. Leger, J.F. Demonet, S. Ruff, B. Aithamon, B. Touyeras,M. Puel, K. Boulanouar and D. Cardebat, Neural substrates ofspoken language rehabilitation in an aphasic patient: an fMRIstudy,Neuroimage17 (2002), 174–183.
[31] F. Maeda, J.P. Keenan, J.M. Tormos, H. Topka and A. Pascual-Leone, Modulation of corticospinal excitability by repetitivetranscranial magnetic stimulation,Clinical Neurophysiology:official Journal of The International Federation of ClinicalNeurophysiology111 (2000) 800-805.
[32] P.I. Martin, M.A. Naeser, M. Ho, K.W. Doron, J. Kurland,J.Kaplan, Y. Wang, M. Nicholas, E.H. Baker, F. Fregni and A.Pascual-Leone, Overt naming fMRI pre- and post-TMS: Twononfluent aphasia patients, with and without improved namingpost-TMS,Brain and Language111 (2009a), 20–35.
[33] P.I. Martin, M.A. Naeser, M. Ho, E. Treglia, E. Kaplan, E.H.Baker and A. Pascual-Leone, Research with transcranial mag-netic stimulation in the treatment of aphasia,Current Neurol-ogy and Neuroscience Reports9 (2009b), 451–458.
[34] K.R. Mills, S.J. Boniface and M. Schubert, Magnetic brainstimulation with a double coil: the importance of coil orienta-tion, Electroencephalography and Clinical Neurophysiology85 (1992), 17–21.
[35] K. Miura, Y. Nakamura, F. Miura, I. Yamada, M. Takahashi, A.Yoshikawa and T. Mizobata, Functional magnetic resonanceimaging to word generation task in a patient with Broca’saphasia,Journal of Neurology246 (1999), 939–942.
[36] M. Musso, C. Weiller, S. Kiebel, S.P. Muller, P. Bulau and M.Rijntjes, Training-induced brain plasticity in aphasia,Brain:A Journal of Neurology122 (Pt 9) (1999), 1781–1790.
[37] M.A. Naeser, P.I. Martin, E.H. Baker, S.M. Hodge, S.E. Scz-erzenie, M. Nicholas, C.L. Palumbo et al., Overt propositionalspeech in chronic nonfluent aphasia studied with the dynamic

C.H.S. Barwood et al. / Effects of low frequency rTMS in chronic non-fluent aphasia 125
susceptibility contrast fMRI method,Neuroimage22 (2004),29–41.
[38] M.A. Naeser, P.I. Martin, M. Nicholas, E.H. Baker, H. Seekins,M. Kobayashi, H. Theoret et al., Improved picture naming inchronic aphasia after TMS to part of right Broca’s area: anopen-protocol study,Brain and Language93 (2005a), 95–105.
[39] M.A. Naeser, P.I. Martin, M. Nicholas, E.H. Baker, H. Seekins,N. Helm-Estabrooks, C. Cayer-Meade, M. Kobayashi, H.Theoret, F. Fregni, J.M. Tormos, J. Kurland, K.W. Doronand A. Pascual-Leone, Improved naming after tms treatmentsin a chronic, global aphasia patient-case report,Neurocase:Case Studies in Neuropsychology, Neuropsychiatry, and Be-havioural Neurology11 (2005b), 182–193.
[40] J. Netz, U. Ziemann and V. Homberg, Hemispheric asymme-try of transcallosal inhibition in man, Experimental BrainRe-search,Experimentelle Hirnforschung104 (1995), 527–533.
[41] M. Ohyama, M. Senda, S. Kitamura, K. Ishii, M. Mishina andA. Terashi, Role of the nondominant hemisphere and undam-aged area during word repetition in poststroke aphasics. A petactivation study,Stroke; A Journal of Cerebral Circulation27(1996), 897–903.
[42] R.C. Oldfield, The assessment and analysis of handedness:The Edinburgh inventory,Neuropsychololgia9, 97–113.
[43] D. Perani, S.F. Cappa, M. Tettamanti, M. Rosa, P. Scifo,A.Miozzo, A. Basso and F. Fazio, A fMRI study of word retrievalin aphasia,Brain and Language85 (2003), 357–368.
[44] C.J. Price and J. Crinion, The latest on functional imagingstudies of aphasic stroke,Current Opinion In Neurology18(2005), 429–434.
[45] M.C. Ridding and J.C. Rothwell, Is there a future for therapeu-tic use of transcranial magnetic stimulation,Nature ReviewsNeuroscience8 (2007), 559–567.
[46] M. Rijntjes, Mechanisms of recovery in stroke patientswithhemiparesis or aphasia: New insights, old questions andthe meaning of therapies,Current Opinion In Neurology19(2006), 76–83.
[47] H.J. Rosen, S.E. Petersen, M.R. Linenweber, A.Z. Snyder,D.A. White, L. Chapman, A.W. Dromerick, J.A. Fiez and M.D.Corbetta, Neural correlates of recovery from aphasia afterdamage to left inferior frontal cortex,Neurology55 (2000),1883–1894.
[48] P.M. Rossini, A.T Barker, A. Berardelli, M.D. Caramia,G.Caruso, R.D. Cracco, M.R. Dimitrijevic et al., Non-invasiveelectrical and magnetic stimulation of the brain, spinal cordand roots: basic principles and procedures for routine clin-ical application. Report of an IFCN committee,Electroen-cephalography and Clinical Neurophysiology91(2) (1994),79–92.
[49] D. Saur, R.D. Lange, A. Baumgaertner, V. Schraknepper,K.Willmes, M. Rijntjes and C. Weiller, Dynamics of languagereorganization after stroke,Brain: A Journal of Neurology129 (2006), 1371–1384.
[50] R.Schlosser, S. Hunsche, J. Gawehn, P. Grunert, G. Vucurevic,T. Gesierich, B Kaufmann et al., Characterization of bold-fmrisignal during a verbal fluency paradigm in patients with intrac-erebral tumors affecting the frontal lobe,Magnetic ResonanceImaging20 (2002), 7–16.
[51] Singh K. Mri3dx.Aston University. Available at: http://www.aston.ac.uk/lhs/staff/singhkd/mri3dx/features. Accessed 21November, 2007.
[52] J.G. Snodgrass and M. Vanderwart, A standardized set of260pictures: Norms for name agreement, image agreement, fa-miliarity, and visual complexity,Journal of Experimental Psy-chology. Human Learning and Memory6 (1980), 174–215.
[53] A. Thiel, K. Herholz, A Koyuncu, M Ghaemi, L.W. Kracht, BHabedank and W.D. Heiss, Plasticity of language networks inpatients with brain tumors: A positron emission tomographyactivation study,Annals of Neurology50 (2001), 620–629.
[54] A. Thiel, B. Habedank, L. Winhuisen, K. Herholz, J. Kessler,W.F. Haupt and W.-D. Heiss, Essential language function ofthe right hemisphere in brain tumor patients,Annals of Neu-rology 57 (2005), 128–131.
[55] A. Thiel, B. Schumacher, K. Wienhard, S. Gairing, L.W.Kracht, R. Wagner, W.F. Haupt and W.-D. Heiss, Directdemonstration of transcallosal disinhibition in languagenet-works,Journal of Cerebral Blood Flow and Metabolism: of-ficial Journal of The International Society of Cerebral BloodFlow and Metabolism26 (2006), 1122–1127.
[56] C.K. Thompson, The neurobiology of language recovery inaphasia,Brain and Language71 (2000), 245–248.
[57] K.R. Thulborn, P.A. Carpenter and M.A. Just, Plasticity oflanguage-related brain function during recovery from stroke,Stroke; A Journal of Cerebral Circulation30 (1999), 749–754.
[58] R. Topper,F.M. Mottaghy, M. Brugmann, J. Noth and W. Hu-ber, Facilitation of picture naming by focal transcranial mag-netic stimulation of Wernicke’s area,Experimental Brain Re-search121 (1998), 371–378.
[59] N. Toschi, T. Welt, M. Guerrisi and M.E. Keck, A reconstruc-tion of the conductive phenomena elicited by Transcranialmagnetic stimulation in heterogeneous brain tissue,MedicalPhysics24 (2008), 80–86.
[60] N. Toschi, T. Welt, M. Guerrisi and M.E. Keck, Transcranialmagnetic stimulation in heterogeneous brain tissue: clinicalimpact on focality, reproducibility and true sham stimulation,Journal of Psychiatric Research43 (2009), 255–264.
[61] E.M. Wassermann, Risk and safety of repetitive transcranialmagnetic stimulation: Report and suggested guidelines fromthe international workshop on the safety of repetitive tran-scranial magnetic stimulation, June 5–7, 1996,Electroen-cephalography and Clinical Neurophysiology108 (1998), 1–16.
[62] C. Weiller, C. Isensee, M. Rijntjes, W. Huber, S. Muller, D.Bier, K. Dutschka, R.P. Woods, J. Noth and H.C. Diener, Re-covery from Wernicke’s aphasia: a positron emission tomo-graphic study,Annals of Neurology37 (1995), 723–732.
[63] L. Winhuisen, A. Thiel, B. Schumacher, J. Kessler, J. Rudolf,W.F. Haupt and W.D. Heiss, Role of the contralateral infe-rior frontal gyrus in recovery of language function in post-stroke aphasia: a combined repetitive transcranial magneticstimulation and positron emission tomography study,Stroke;A Journal of Cerebral Circulation36 (2005), 1759–1763.
[64] L. Winhuisen, A. Thiel, B. Schumacher, J. Kessler, J. Rudolf,W.F. Haupt and W.D. Heiss, The right inferior frontal gyrusand poststroke aphasia: a follow-up investigation,Stroke; AJournal of Cerebral Circulation38 (2007), 1286–1292.
[65] O.W. Witte, I. Buchkremer-Ratzmann, K. Schiene, T. Neu-mann-Haefelin, G. Hagemann, M. Kraemer, K. Zilles and H.J.Freund, Lesion-induced network plasticity in remote brainareas,Trends In Neurosciences20 (1997), 348–349.

126 C.H.S. Barwood et al. / Effects of low frequency rTMS in chronic non-fluent aphasia
App
endi
xA
.Pat
ient
resu
ltson
audi
tory
com
preh
ensi
onsu
btes
tsad
min
iste
red
from
the
Bos
ton
Dia
gnos
ticA
phas
iaE
xam
ina
tion
(BD
AE
)2n
dE
ditio
n[1
7]
Pat
ient
resu
ltson
audi
tory
com
preh
ensi
onsu
btes
ts-
BD
AE
Wor
dco
mpr
ehen
sion
Wor
dco
mpr
ehen
sion
Wor
dco
mpr
ehen
sion
-W
ord
com
preh
ensi
on-
Wor
dco
mpr
ehen
sion
-W
ord
com
preh
ens
ion-
Com
man
dsC
ompl
exId
eatio
nal
Tota
l=37
byca
tego
ryTo
ols
and
impl
emen
tsF
ood
Tota
l=
10A
nim
als
Tota
l=10
Bod
yP
arts
Tota
l=15
Mat
eria
lTo
tal=
50To
tal=
10To
tal=
20To
tal=
12
ST
IMB
asel
ine
Pos
tTM
SB
asel
ine
Pos
tTM
SB
asel
ine
Pos
tTM
SB
ase
line
Pos
tTM
SB
asel
ine
Pos
tTM
SB
asel
ine
Pos
tTM
SB
asel
ine
Pos
tTM
SB
asel
ine
Pos
tTM
SrT
MS
137
3750
5010
1010
1010
1020
2015
1512
12rT
MS
336
3750
5010
1010
1010
1020
205
93
7rT
MS
437
3747
5010
1010
1010
1017
2010
137
12rT
MS
931
3439
3910
1010
1010
109
96
87
8rT
MS
1013
1822
277
79
86
90
30
21
3rT
MS
1335
3750
5010
1010
1010
1020
2010
108
12
SH
AM
rTM
S2
3234
4441
99
88
1010
1714
66
1011
rTM
S5
3737
5050
1010
1010
1010
2020
77
108
rTM
S8
3436
5048
1010
1010
1010
2018
66
107
rTM
S11
3637
4849
1010
1010
1010
1819
88
1112
rTM
S14
2627
3839
88
88
88
1415
33
01
rTM
S15
3131
4243
1010
1010
78
1515
55
12
App
endi
xB
.Pat
ient
resu
ltson
repe
titio
nan
dpi
ctur
ede
scr
iptio
nsu
btes
tsfr
omth
eB
osto
nD
iagn
ostic
Aph
asia
Exa
min
atio
n(B
DA
E)
2nd
Edi
tion
[17]
Pat
ient
resu
ltson
repe
titio
nan
dpi
ctur
ede
scrip
tion
subt
ests
-B
DA
E
Pat
ient
Rep
etiti
onof
sing
leR
epet
ition
ofno
nsen
se-
Rep
etiti
onof
sent
ence
sP
ictu
rede
scrip
tion
Pic
ture
desc
riptio
n-w
ords
Tota
l=10
wor
dsTo
tal=
5To
tal=
10co
mpl
exity
inde
x-C
ooke
long
estw
ords
per
The
ftpi
ctur
eph
rase
Tota
l=7
ST
IMB
asel
ine
Pos
tTM
SB
asel
ine
Pos
tTM
SB
asel
ine
Pos
tTM
SB
ase
line
Pos
tTM
SB
asel
ine
Pos
tTM
SrT
MS
19
93
38
101.
11.
56
6rT
MS
38
83
31
21.
11.
15
6rT
MS
48
83
53
51.
12.
03
4rT
MS
97
72
30
21.
01.
11
2rT
MS
100
00
00
01.
01.
13
4rT
MS
138
92
45
92.
02.
56
7S
TIM
Bas
elin
eP
ostT
MS
Bas
elin
eP
ostT
MS
Bas
elin
eP
ostT
MS
Ba
selin
eP
ostT
MS
Bas
elin
eP
ostT
MS
rTM
S2
99
12
87
1.4
1.6
76
rTM
S5
99
22
45
1.1
1.1
66
rTM
S8
88
52
44
1.25
1.4
55
rTM
S11
99
43
88
1.1
1.1
44
rTM
S14
45
11
00
0.9
1.0
22
rTM
S15
00
00
00
0.7
0.7
22

C.H.S. Barwood et al. / Effects of low frequency rTMS in chronic non-fluent aphasia 127
App
endi
xC
.R
esul
tsof
expr
essi
vena
min
gsu
btes
tsad
min
ist
ered
from
the
Bos
ton
Dia
gnos
ticA
phas
iaE
xam
inat
ion
(BD
AE
)2n
dE
ditio
n[1
7],
incl
udin
gth
eov
eral
lsc
ore
obta
ined
onth
eco
mpl
ete
batte
ryof
subt
ests
adm
inis
tere
d.
Pat
ient
resu
ltson
nam
ing
subt
ests
-BD
AE
Pat
ient
Scr
eeni
ngof
Spe
cial
Scr
eeni
ngof
Spe
cial
Scr
eeni
ng
ofS
peci
alN
amin
gin
Nam
ing
inN
amin
gin
Nam
ing
inB
osto
nN
aming
BD
AE
Ove
rall
Cat
egor
ies-
Let
ters
Cat
egor
ies-
Num
bers
Cat
egor
ies-
Col
ors
cate
gorie
s-C
olor
sca
tego
ries-
Act
ions
cate
gorie
s-A
nim
als
cate
gorie
s-To
ols
Test
(BN
T)
scor
e(e
xclu
des
Tota
l=4
Tota
l=4
Tota
l=4
Tota
l=8
Tota
l=12
Tota
l=12
and
Impl
emen
tsTo
tal=
60B
NT
)To
tal=
12To
tal=
195
ST
IMB
asel
ine
Pos
tB
asel
ine
Pos
tB
asel
ine
Pos
tB
asel
ine
Pos
tB
asel
ine
Pos
tB
asel
ine
Pos
tB
asel
ine
Pos
tB
asel
ine
Pos
tB
ase
line
Pos
tT
MS
TM
ST
MS
TM
ST
MS
TM
ST
MS
TM
ST
MS
rTM
S1
44
44
44
88
1011
1111
811
4452
183
189
rTM
S3
44
44
44
88
1111
1212
811
5757
157
170
rTM
S4
44
44
44
88
611
1112
78
2442
159
181
rTM
S9
33
44
22
44
01
89
36
59
116
130
rTM
S10
12
12
01
00
00
00
00
44
3852
rTM
S13
44
44
33
48
611
1011
910
4556
158
182
SH
AM
rTM
S2
44
44
32
68
119
76
87
3138
133
150
rTM
S5
44
44
44
88
1111
1212
1212
5457
174
173
rTM
S8
44
44
44
44
88
1010
77
4548
158
153
rTM
S11
44
44
44
88
109
1212
910
3736
175
177
rTM
S14
21
22
00
00
00
21
44
33
122
125
rTM
S15
11
00
00
00
00
11
11
33
8284

128 C.H.S. Barwood et al. / Effects of low frequency rTMS in chronic non-fluent aphasia
Appendix D. Patient results of picture naming accuracy and la-tency measured on 144 pictures selected from the Snodgrass andVanderwart, (1980) picture naming inventory
Snodgrass and Vanderwart Picture Naming Inventory
Patient Naming accuracy Naming latencyTotal= 144 (msec)
STIM Baseline Post TMS Baseline Post TMS
rTMS 1 118 132 1823.76 1256.14rTMS 3 123 134 1233.02 1099.76rTMS 4 124 124 1568.64 1344.31rTMS 9 25 32 2695.38 2441.31rTMS 10 6 8 2765.90 2513.54rTMS 13 134 137 1522.87 1209.68
SHAM Baseline Post TMS Baseline Post TMS
rTMS 2 86 88 1636.46 1629.70rTMS 5 138 136 1491.20 1601.53rTMS 8 112 112 1420.39 1480.59rTMS 11 134 136 1237.63 1289.36rTMS 14 6 7 2386.94 2298.22rTMS 15 1 1 2880.22 3004.11