
Use of 201Tl SPECT imaging to assess the response to therapy in patients with high grade gliomas
10
Journal of Neuro-Oncology 59: 81–90, 2002. © 2002 Kluwer Academic Publishers. Printed in the Netherlands. Clinical Study Use of 201 201 201 Tl SPECT imaging to assess the response to therapy in patients with high grade gliomas V. Vallejos 1 , C. Bala ˜ na 2 , M. Fraile 1 , Y. Roussos 3 , J. Capellades 4 , P. Cuadras 4 , R. Ballester 5 , A. Ley 3 , A. Arellano 5 and R. Rosell 2 1 Departments of Nuclear Medicine, 2 Medical Oncology, 3 Neurosurgery, 4 Radiology, 5 Radiotherapy, Hospital Universitari Germans Trias i Pujol, Badalona, Spain Key words: high grade glioma, chemotherapy, 201 Tl SPECT, computed tomography, magnetic resonance imaging Summary Purpose. To assess the potential role of 201 Tl single photon emission tomography (201-Thallium SPECT) when compared to other imaging modalities in the evaluation of the response to therapy in high grade gliomas. Materials and methods. Twenty patients with histologically proved high grade glioma have been included: 15 with glioblastoma (GBM), 3 with anaplastic astrocytoma (AA) and 2 with anaplastic oligoastrocytoma (AOA). Patients were assessed by 201 Tl SPECT, computed tomography (CT) and magnetic resonance imaging (MRI) at (a) either at the moment of maximum response to first line chemotherapy, or after the completion of radiotherapy and chemotherapy if post-surgical residual disease was present, and (b) after the completion of second line chemotherapy if disease persisted, or either a relapse or disease progression was confirmed. Final response was evaluated according to the McDonald criteria, and by comparing SPECT, CT and MRI results. Results. According to the McDonald criteria, clinical response after first line chemotherapy was 5 partial response, 7 stable disease and 8 progressive disease. Evaluation by 201 Tl SPECT was in agreement with such criteria in nearly all patients (90%). MRI findings closely agreed with the clinical follow-up. CT findings clearly differed from those observed by SPECT and MRI. After second line therapy, 10 patients progressed, 3 had stable disease and 7 had partial response. 201 Tl SPECT agreed with the clinical status in 89% cases, whereas MRI and, specially CT, fared significantly lower. Conclusion. Compared to conventional neuroimaging, 201 Tl SPECT added valuable information in the assessment of the response to therapy in our patient population; whenever findings were not conclusive and in the case of disagreement between CT and MRI findings. Introduction Malignant gliomas of astrocytic origin account for almost half of the primary central nervous sys- tem (CNS) malignant tumors [1]. According to the World Health Organisation (WHO) classification, high grade gliomas include grade III anaplastic astrocytoma (AA) and grade IV glioblastoma (GBM) multiforme. Anaplastic forms of oligoastrocytomas and oligoden- drogliomas may also be included into grade III [2]. Despite advances in diagnostic techniques and therapy, the prognosis for patients with glioma remains poor. Multimodality therapy consists of intended maximal surgical resection, radiation therapy and nitrosoureas- based combined chemotherapy. Despite aggressive treatment, malignant gliomas almost invariably recur. Therapy for recurrent glioma is similar to that used for the intact tumor (typically re-resection, in approximately 20% of patients, and either procar- bazine, cisplatin or nitrosourea-based chemotherapy) [3]. Combination of procarbazine, CCNU and vin- cristine (PCV) has shown to be effective in patients with recurrent AA or with anaplasic oligoden- droglioma [4]. Outstanding among recent advances in chemotherapy is Temozolamide (TMZ), a promis- ing new drug for the treatment of malignant gliomas, and the first available dacarbazine-analogue to be used orally. On the basis of its in vitro activity against glioma cell-lines and good cerebrospinal fluid penetration, TMZ has been shown to produce
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Use of 201Tl SPECT imaging to assess the response to therapy in patients with high grade gliomas

Journal of Neuro-Oncology 59: 81–90, 2002.© 2002 Kluwer Academic Publishers. Printed in the Netherlands.
Clinical Study
Use of 201201201Tl SPECT imaging to assess the response to therapy inpatients with high grade gliomas
V. Vallejos1, C. Balana2, M. Fraile1, Y. Roussos3, J. Capellades4, P. Cuadras4, R. Ballester5,A. Ley3, A. Arellano5 and R. Rosell 2
1Departments of Nuclear Medicine, 2Medical Oncology, 3Neurosurgery, 4Radiology,5Radiotherapy, Hospital Universitari Germans Trias i Pujol, Badalona, Spain
Key words: high grade glioma, chemotherapy, 201Tl SPECT, computed tomography, magnetic resonance imaging
Summary
Purpose. To assess the potential role of 201Tl single photon emission tomography (201-Thallium SPECT) whencompared to other imaging modalities in the evaluation of the response to therapy in high grade gliomas.
Materials and methods. Twenty patients with histologically proved high grade glioma have been included: 15with glioblastoma (GBM), 3 with anaplastic astrocytoma (AA) and 2 with anaplastic oligoastrocytoma (AOA).Patients were assessed by 201Tl SPECT, computed tomography (CT) and magnetic resonance imaging (MRI) at (a)either at the moment of maximum response to first line chemotherapy, or after the completion of radiotherapy andchemotherapy if post-surgical residual disease was present, and (b) after the completion of second line chemotherapyif disease persisted, or either a relapse or disease progression was confirmed. Final response was evaluated accordingto the McDonald criteria, and by comparing SPECT, CT and MRI results.
Results. According to the McDonald criteria, clinical response after first line chemotherapy was 5 partial response,7 stable disease and 8 progressive disease. Evaluation by 201Tl SPECT was in agreement with such criteria in nearlyall patients (90%). MRI findings closely agreed with the clinical follow-up. CT findings clearly differed from thoseobserved by SPECT and MRI. After second line therapy, 10 patients progressed, 3 had stable disease and 7 hadpartial response. 201Tl SPECT agreed with the clinical status in 89% cases, whereas MRI and, specially CT, faredsignificantly lower.
Conclusion. Compared to conventional neuroimaging, 201Tl SPECT added valuable information in the assessmentof the response to therapy in our patient population; whenever findings were not conclusive and in the case ofdisagreement between CT and MRI findings.
Introduction
Malignant gliomas of astrocytic origin account foralmost half of the primary central nervous sys-tem (CNS) malignant tumors [1]. According to theWorld Health Organisation (WHO) classification, highgrade gliomas include grade III anaplastic astrocytoma(AA) and grade IV glioblastoma (GBM) multiforme.Anaplastic forms of oligoastrocytomas and oligoden-drogliomas may also be included into grade III [2].Despite advances in diagnostic techniques and therapy,the prognosis for patients with glioma remains poor.
Multimodality therapy consists of intended maximalsurgical resection, radiation therapy and nitrosoureas-based combined chemotherapy. Despite aggressive
treatment, malignant gliomas almost invariably recur.Therapy for recurrent glioma is similar to thatused for the intact tumor (typically re-resection, inapproximately 20% of patients, and either procar-bazine, cisplatin or nitrosourea-based chemotherapy)[3]. Combination of procarbazine, CCNU and vin-cristine (PCV) has shown to be effective in patientswith recurrent AA or with anaplasic oligoden-droglioma [4]. Outstanding among recent advancesin chemotherapy is Temozolamide (TMZ), a promis-ing new drug for the treatment of malignant gliomas,and the first available dacarbazine-analogue to beused orally. On the basis of its in vitro activityagainst glioma cell-lines and good cerebrospinalfluid penetration, TMZ has been shown to produce

82
objective tumor regression after the first relapse[5,6].
Unfortunately, recurrence is the main problem inthe management of patients with glioma. When clin-ical recurrence is suspected, radiological diagnosis(computed tomography (CT) or magnetic resonanceimaging (MRI)) may not be fully reliable for the dif-ferential diagnosis between tumor necrosis, scar oractual recurrence [7,8]. In such cases, radionuclideimaging with 201-Thallium single photon emissiontomography (201Tl SPECT) may be used to separateresponse to therapy from tumoral growth [9,10].
The unique functional properties of this tracer haveprompted its use in clinical oncology, specially in glialtumors [9–12]. Thallium uptake depends on cell mem-brane ATP-ase pump activity, tumoral vascularizationand cell proliferation. Unlike tumor viable cells, reac-tive glial cells are not accompanied by increasedATP-ase activity [13–14]. Although blood–brain bar-rier breakdown is the most important mechanismleading to contrast-enhancement in CT scans and MRI,it is much less important for 201Tl uptake [15].
Here we report on a prospective study which wasdesigned to establish the role of 201Tl SPECT inthe assessment of the response to chemotherapy inpatients with high grade gliomas as compared withother imaging modalities (CT and MRI).
Patients and methods
Twenty consecutive patients (aged 36–74 years, 17male) admitted to the neurosurgery department ofour hospital with a suspicion of CNS high gradeglioma were included in the study. Patients had eitherundergone surgery with intended total tumor resection(n = 10) or partial resection (n = 9), or had been diag-nosed by stereotactic biopsy (n = 1). Final histopatho-logic diagnosis was: 15 GBM, 3 AA, and 2 anaplasticoligoastrocytoma (AOA). Patients were imaged by CTscan, MRI and SPECT before surgery and within thefirst five days post-surgery.
Post-operatively, follow-up of the patients wascarried out within the setting of a multidisciplinaryNeuro-oncology committee. Patients received differ-ent chemotherapy regimes: (a) BCNU (carmustine)was used in 11 patients with GBM and withoutmeasurable residual post-surgical disease; in 10 ofthem it was given in association with radiotherapy,(b) BCNU plus CDDP (cisplatin) and radiother-apy was used in one case of GBM with measurable
residual disease; both as first line therapy, (c) PCV(procarbazine, CCNU, vincristine) was used in 5cases (3 AA and 2 AOA) as primary line combinedwith radiotherapy, and (d) TMZ plus CDDP (cis-platin) was used as primary treatment in 3 GBMcases.
A second line of treatment was required in 17patients in whom tumor persisted, relapsed or hadprogressed at the end of first line therapy: (a) TMZwas used in 13 patients with relapse (10 GBM,3 AA), (b) TMZ combined with CCDP was given toone patient with GBM showing progressive diseaseafter completion of first line with BCNU, and (c)VP16 (etoposide)+ CDDP was used in two patientswith AOA who did no show response to a firstcourse with PCV. TMZ was also used in one of suchpatients with AOA after failure of both first line (PCV)and second line therapy (VP16+ CDDP).
As previously described, 17 patients received 3-Dplanned external beam radiotherapy (60 Gy) eitherbefore or concurrently with chemotherapy.
During the course of adjuvant therapy, patientswere reassessed by SPECT, MRI and CT. Intervalamong techniques was less than two weeks. Assess-ment was done at the moment of maximal clinicalresponse, which could be either (a) after 3–4 cyclesof chemotherapy or completion of radiotherapy, or (b)after chemotherapy if residual post-surgical diseasewas still present. Similarly, response was evaluatedafter second line chemotherapy. Patients with partialresponse to first line therapy were evaluated every threemonths by SPECT, MRI and CT.
Final response for each branch (summarized inTable 1) was evaluated by (a) the McDonald criteria,which were used as the standard, (b) 201Tl SPECT and(c) TC and MRI.
McDonald criteria
McDonald et al. [16] postulated the response crite-ria for citotoxic agents in supratentorial malignantgliomas based on clinical status, need of steroid ther-apy, and radiological findings. Today this system iswidely accepted among neuro-oncologists.
The scheme includes four response categories: com-plete response (CR): disappearance of all enhancinglesion by MRI or CT, off steroids, or neurologicallystable or improved. Partial response (PR): evidenceof �50% reduction in tumor size (by RMI or CT),steroids stable or reduced, patient neurologically stable

Tabl
e1.
Sum
mar
yof
final
resp
onse
afte
rfir
stan
dse
cond
line
ther
apy
IdT
umor
loca
tion
His
tolo
gySu
rger
y1s
tlin
eth
erap
yR
espo
nse
Res
pons
e(M
cDon
ald)
(m)
TT
P(m
onth
s)(m
)
2nd
line
ther
apy
Res
pons
eFi
nal
Res
pons
e(M
c-D
onal
d)(m
)
Exi
tus
(m)
CT
MR
ISP
EC
TC
TM
RI
SPE
CT
1Fr
onta
lRG
BM
Part
ial
BC
CN
U+
RT
SDSD
SDSD
(6m
)P
(12
m)
TM
ZP
PP
P(1
4m
)14
m2
Fron
talR
GB
MC
ompl
ete
BC
CN
U+
RT
PP
PP
(4m
)P
(4m
)T
MZ
P∗P∗
PRPR
(16
m)
∗20
m3
Fron
toba
salR
GB
MPa
rtia
lB
CC
NU
+C
CD
PSD
SDSD
SD(5
m)
P(6
m)
RT
PRP
PP
(8m
)9
m
4C
orpu
sca
llosu
mA
APa
rtia
lPC
V+
RT
SDSD
SDSD
(6m
)SD
(6m
)T
MZ
PRPR
PR+
PR(1
2m
)—
5Fr
onta
lLG
BM
Part
ial
TM
Z+
CC
DP
+R
TPR
PRPR
PR(9
m)
PR(9
m)
/PR
PRPR
PR(1
3m
)—
6Fr
onto
pari
etal
LA
AB
iops
yPC
V+
RT
PRSD
SDSD
(9m
)P
(18
m)
TM
ZP∗
P∗P
P(2
2m
)23
m7
Fron
talL
GB
MC
ompl
ete
BC
NU
+R
T+/
−+/
−P
P(5
m)
P(5
m)
TM
ZPR
PRPR
PR(1
0),
P(1
3m
)13
m
8Te
mpo
ralR
GB
MC
ompl
ete
TM
Z+
CC
DP
+R
T+/
−+/
−PR
PR(6
m)
//
(−)
SDSD
SD(1
2m
),P
(16
m)
16m
9Te
mpo
ropa
riet
alL
GB
MC
ompl
ete
BC
NU
+R
T(−
)P
PP
(3m
)P
(3m
)T
MZ
PP
PP
(5m
)5
m10
Fron
tal
para
sagi
talL
Olig
oAA
Part
ial
PCV
+R
T+/
−+/
−PR
SD(4
m)
P(1
2m
)V
P16+
CC
DP
PP
PP
(18
m)
18m
11Te
mpo
ralR
GB
MPa
rtia
lB
CN
U+
RT
PP
PP
(8m
)P
(8m
)T
MZ+
CC
DP
SDSD
SDSD
(11
m),
P(1
3m
)13
m
12Pa
riet
alR
GB
MC
ompl
ete
BC
NU
+R
T/
PP
P(5
m)
P(5
m)
TM
Z/
P∗PR
P∗(9
m)
15m
13Fr
onta
lLG
BM
Com
plet
eB
CN
U+
RT
PRPR
PRPR
(5m
)P
(13
m)
TM
ZPR
PRPR
PR(1
7m
),¿
14Fr
onta
lRA
APa
rtia
lPC
V+
RT
SDSD
SDSD
P(4
m)
TM
Z/
PSD
SD¿
15Te
mpo
ralL
Olig
oAA
Com
plet
e1-
PCV
+R
TSD
SDSD
SD(4
m)
P(8
m)
P(1
2m
)2-
CC
DP+
VP1
63-
TM
Z
Pvs
.RN
/
Pvs
.RN
PRP PR
P(1
2m
)PR
(20
m)
—
16Fr
onta
lLG
BM
Part
ial
TM
Z+
CC
DP
+R
TPR
PRPR
PR(3
m)
P(5
m)
TM
ZP
PP
P(7
m)
7m
(¿)
17Te
mpo
ralR
GB
MC
ompl
ete
BC
NU
+R
TP
PP
P(4
m)
P(4
m)
TM
ZP∗
P∗PR
P∗(8
m),
SD(1
3m
)20
m
18Te
mpo
ralL
GB
MPa
rtia
lB
CN
U.
Non
RT
PP
PP
(2m
)P
(2m
)T
MZ
SD PPR P
PR PPR
(7m
)P
(9m
)11
m
19Te
mpo
ralL
GB
MPa
rtia
lB
CN
U+
RT
PP
PP
(3m
)P
(3m
)—
3m
20Te
mpo
ropa
riet
alR
GB
MC
ompl
ete
BC
NU
+R
T+/
−PR
CR
PR∗
(5m
)P
(12
m)
TM
Zin
cour
se—
(+/−)
:non
-con
clus
ive
(non
-spe
cific
infla
mm
ator
ypo
st-t
reat
men
trea
ctio
n);P
∗ :mas
sef
fect
and
incr
ease
ded
ema
with
outc
hang
esin
tum
orsi
ze;R
EC
:rec
urre
nce;
CR
:com
plet
ere
spon
se;
PR:p
artia
lres
pons
e;P:
prog
ress
ion;
(PR
+)si
gnifi
cant
decr
ease
ofth
alliu
mup
take
intu
mor
area
;TM
Z:t
emoz
olam
ide;
BC
NU
:car
mus
tine;
CC
DP:
cisp
latin
;PC
V:C
CN
U,p
roca
rbaz
ine
and
vinc
rist
ine;
VP1
6:et
opos
ide;
RT
:rad
ioth
erap
y;R
N:r
adio
necr
osi;
L:l
eft;
R:r
ight
.

84
or improved. Progressive disease (PD): 25% increasein tumor size or any new tumor, steroids stable orincreased, neurologically worse. Stable disease (SD):all other situations.
201Tl SPECT
Thallium SPECT imaging [9,14] was performed inevery patient. Patients were injected with 4 mCi(148 MBq) 201Tl chloride and 2 h later delayed SPECTwas acquired using a single-head rotating gammacam-era (GE camstar) equipped with a LEAP (low energy allpurpose) collimator; 64 views were obtained for 25 seceach on 64×64 word matrix. A 57–80 KeV energy win-dow was selected. Acquired images were reconstructedby filtered backprojection (ramp filter) and a Butter-worth filter (0.4 cicles/pixel of cut-off frequency, order10) without attenuation correction. Transaxial, coronaland saggital slices were visually inspected on a colourscale display, slice thickness being 6.4 mm.
SPECT images were evaluated by visual analysis. Inorder to meet correlation with the clinical and radiolog-ical findings, consensus criteria for therapy responsewere as follows: CR was suggested if images did notshow any abnormal uptake at the tumor area. PR wasconsidered if uptake had decreased to at least 50% com-pared with the baseline study, and SD if no changes hadbeen observed. Tumor progression (P) was defined ifuptake was increased, even if only slightly so (25%),compared with the baseline study.
Computed Tomography
Imaging included scans obtained both prior to and afterintravenous injection of iodinated contrast material.Axial slices of the pre-contrast scan provided a base-line density for the lesion relative to the normal brain,which was used to determine the degree of contrastenhancement.
CT follow-up examinations were assessed forresponse, stability or progression taking into accountchanges in tumor size, extent and degree of contrastenhancement, mass effect and edema. Unfortunately,not every patient could be evaluated for response byCT: 2 patients after the first line and 4 cases after thesecond line of chemotherapy were not imaged.
Magnetic Resonance Imaging
Magnetic resonance imaging studies included spin–echo T1–T2-weighted axial images which were
obtained before the intravenous administration ofgadolinium-DTPA. Post-contrast T1-weighted axialslices were also performed.
Like with CT, the status of the disease defined byMRI was as overall progression or regression as judgedby tumor size and/or degree of gadolinium enhance-ment, mass effect or surrounding edema.
Four response categories were established here alsoaccording to the McDonald criteria, on both CT andMRI studies: CR: disappearance of all enhancinglesion. PR: evidence of �50% reduction in tumor sizeor enhancing lesion. PD: 25% increase in tumor sizeor any new tumor. SD: all other situations. New tumormasses or new hemorrhagic focus, adjoining or at a dis-tance from post-operative cavities were defined as PDon both CT and MRI scans.
The time interval for the CT, MRI and SPECTexaminations did not exceed two weeks.
Results
Evaluation after first line chemotherapy
Response to therapy could be evaluated in all patients(see Table 2). 201Tl SPECT agreed with the clinicalstatus in 18 out of 20 assessed patients (90%). Also,MRI findings closely agreed with the clinical follow-up, whereas CT findings clearly differed from theother modalities, as follows: (a) 201Tl SPECT correctly
Table 2. SPECT 201Tl versus TC and/or MRI findings after firstline chemotherapy
SPECT CT MRI McDonald
Progressive disease 8 P 5 P 7 P 8 P1 nc 1 nc(−2)
Stable disease 6 SD 5 SD 6 SD 6 SD1 PR
Partial response 5 PR 3 PR 3 PR 4 PR1 SD 1 SD 1 SD1 nc 1 nc
Complete response 1 CR 1 nc 1 PR 1 PR∗
Non conclusive — 2 2(n = 20) 20 18 20 20
CT: computed tomography; MRI: magnetic resonance imag-ing; SPECT: Single photon emission tomography; SD: stabledisease; PR: partial response; CR: complete response; nc: non-conclusive; P: progression. (∗) patient 20 (Figure 2) had partialresponse by MRI (tumor size decreased more than 50% and aresidual nodule persisted). 201Tl SPECT showed disappearanceof tumor uptake. Symptoms improved and anti-edema therapywas not needed.

85
identified all patients (n = 8) with progression accord-ing to the McDonald criteria (see Figure 1), whereasMRI could only identified seven. In the remainingpatient, MRI imaging was non-conclusive because ofpost-treatment changes (patient 7). As for CT scans,progression was seen in 5 patients, and the result wasuncertain in another patient (patient 7). In two cases CTwas not performed. (b) Six patients had stable disease,and both 201Tl SPECT and MRI findings agreed withthe McDonald criteria. Five patients were classified asstable disease by CT scan, and one patient was thoughtto have partial response (patient 6). (c) Five patientshad partial response as judged by 201Tl SPECT. Infour such patients the McDonald criteria establisheda partial response. Stable disease was found in theremaining case. MRI and CT findings showed partialresponse in 3 of the patients, and stable disease in onepatient, respectively. In one case, both MRI and CTwere non conclusive for partial response (patient 8).(d) A complete response was defined by 201Tl SPECTeven though it was considered as partial responseby clinical criteria an MRI (patient 20, Figure 2). Inthis patient tumor size had decreased more than 50%although persisted as a residual nodule. CT scan couldnot determine the degree of response. Thallium uptakehad totally disappeared.
Findings at the completion of second linechemotherapy
Second line chemotherapy was given to 16 patients (seeTable 3): 15 with progression due to relapse or pro-gressive residual disease (11 GBM, 2 AA, 2 oligoAA)and one patient with stable disease (1 AA). One patientreceived radiotherapy at progression. Mean time to pro-gression was 7.5 months (range 3–18 months).
Temozolamide was used in 14 patients: 12 with pro-gression, one with stable disease, and one case of AOAafter failure of CDDP + VP16. Temozolamide in asso-ciation with CDDP was proposed in another case ofGBM with progression.
Follow-up evaluation was available for 15 patientsafter completion of chemotherapy (18 studies). Whilewriting the manuscript, one patient was still in thecourse of therapy. After second line therapy, 201TlSPECT agreed with clinical status in 89% cases (16 outof 18 evaluated studies).
Three patients did not receive second line therapy:two of them had partial response after first line therapy,and the remaining patient died 3 months after surgery.A clinical status of partial response was maintained in
Table 3. 201Tl SPECT compared to TC and/or MRI duringfollow-up in second line therapy
SPECT CT MRI McDonald
Progressive 8 P 5 P 6 P 8 Pdisease 1 P∗ 1 P∗
1 P vs.RN
1 P vs.RN
1 PRStable 2 SD 1 SD 1 SD 2 SD
disease (−1) 1 P∗
Partial 7 PR 3 PR 5 PR 7 PRresponse 1 PR+ 2 P∗ 3 P∗ 21 P∗
1 SD(−2)
Completeresponse
— — — —
Non-conclusive — — — —(n = 18) 18 16 18 18
Refer footnote of Table 2 for explanation of symbols; (∗)patients with increased perilesional edema without tumorsize changes. (PR+) significant decrease of thallium uptakein tumor area.
these two patients (patients 5 and 8) for a long time (13and 12 months respectively).
If all follow-up studies are considered, overall agree-ment between SPECT and McDonald criteria was 90%(19/21 studies). MRI and, specially, CT differed sig-nificantly from 201Tl SPECT findings, as follows: (a)eight patients had clinical symptoms of progressionand were consistent with SPECT images. Radiologicalimaging was discordant as follows. One of the patientshad confusing CT and MRI findings and a differentialdiagnosis between progression versus radionecrosiscould not be established (patient 15 after CDDP+VP16therapy). A partial response was observed by CT inone patient with clinical progression. In two patients,CT and MRI showed radiological signs of progres-sion, such as increased edema and mass effect. Thesetwo patients, with tumor stability by 201Tl SPECTimproved significantly after steroid therapy (patients2 and 6). (b) 201Tl SPECT images did not change fromthe previous study in two patients, who were con-sidered as having stable disease. These two patientskept clinically stable and one of them did not showchanges in MRI. The remaining patient initially hadneurological worsening caused by increased edemaaround a tumor which did not increase in size. Patientimproved after steroid therapy (patient 14). Unfortu-nately, CT scan was performed in only one patient andrevealed stable disease. (c) Partial response with faintto moderate decreased thallium uptake in the tumor
86
A B
C D
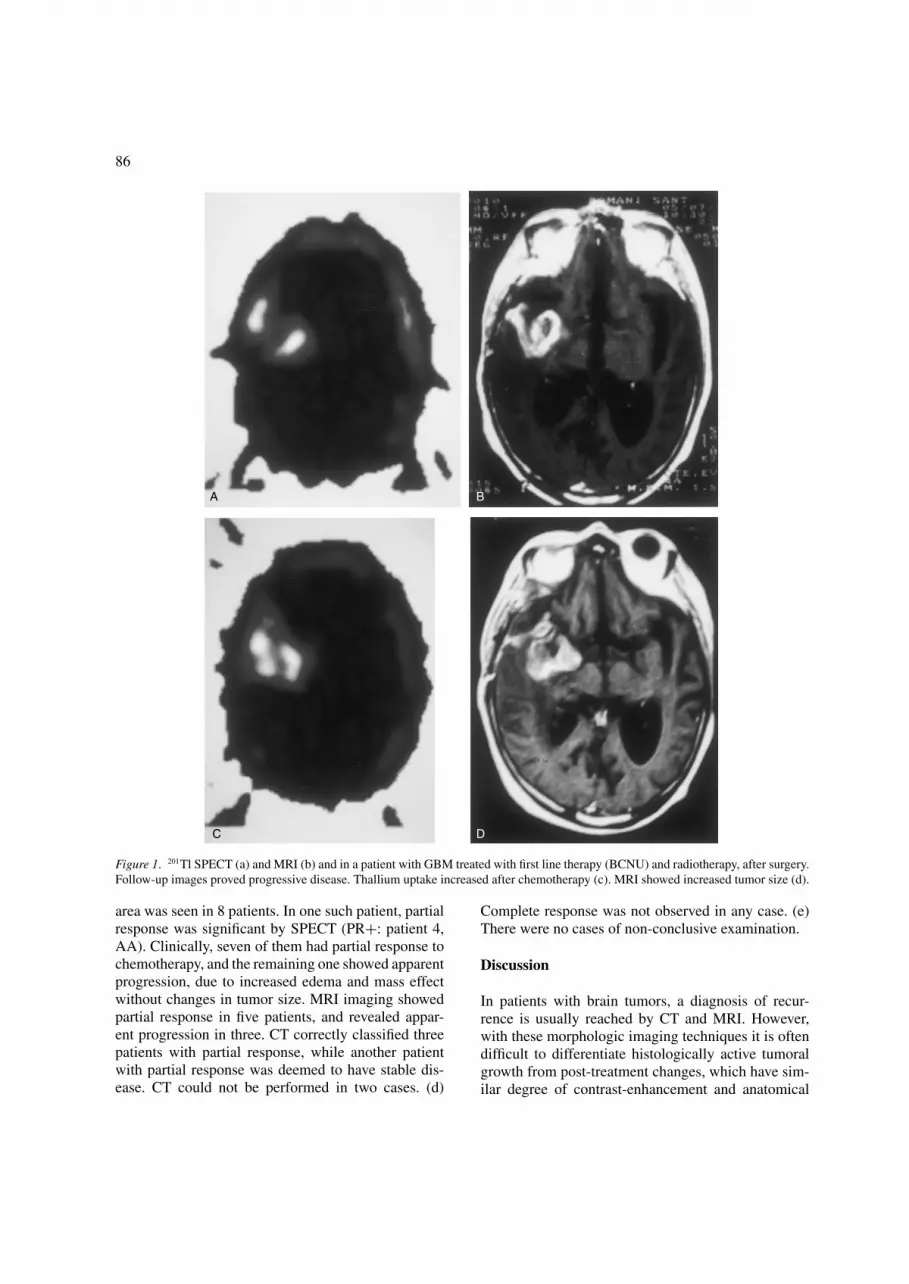
Figure 1. 201Tl SPECT (a) and MRI (b) and in a patient with GBM treated with first line therapy (BCNU) and radiotherapy, after surgery.Follow-up images proved progressive disease. Thallium uptake increased after chemotherapy (c). MRI showed increased tumor size (d).
area was seen in 8 patients. In one such patient, partialresponse was significant by SPECT (PR+: patient 4,AA). Clinically, seven of them had partial response tochemotherapy, and the remaining one showed apparentprogression, due to increased edema and mass effectwithout changes in tumor size. MRI imaging showedpartial response in five patients, and revealed appar-ent progression in three. CT correctly classified threepatients with partial response, while another patientwith partial response was deemed to have stable dis-ease. CT could not be performed in two cases. (d)
Complete response was not observed in any case. (e)There were no cases of non-conclusive examination.
Discussion
In patients with brain tumors, a diagnosis of recur-rence is usually reached by CT and MRI. However,with these morphologic imaging techniques it is oftendifficult to differentiate histologically active tumoralgrowth from post-treatment changes, which have sim-ilar degree of contrast-enhancement and anatomical

87
A B
C D
Figure 2. Follow-up in a patient with GBM treated after surgery with first line chemotherapy (BCNU) and RT. 201Tl SPECT (a) and MRI(b) after surgery. At the completion of chemotherapy, 201Tl SPECT (c) showed a complete response (absence of tracer uptake in the tumorarea), while partial response was considered by the McDonald criteria (reduction in tumor size on MRI (d) and decrease of dexametasonedose).
appearance [14]. Radiation necrosis is known to mimictumor recurrence [17]. Therefore, findings of CT orMRI are not always conclusive. In such cases SPECTwith 201Tl may provide useful information. Thalliumis taken up by neoplastic glial cells [9–12]. Uptake isnot only dependent on the breakdown of blood–brain
barrier, as is the case with contrast agents, but is alsorelated to cell growth.
Knowledge of specific structural changes asrevealed by CT and MRI is necessary for surgicalplanning and other therapeutic decision-making[18–20]. Furthermore, neuroimaging evaluation during

88
treatment is needed to identify the cause of clinicalworsening such as true tumor progression, develop-ment of hydrocephalus or other causes of mass effect.However, conventional imaging methods do not alwaysallow for a distinction between tumor progression andside effects such as inflammatory or glial reaction, orradionecrosis [20]. In this context, it has been sug-gested that 201Tl SPECT may be clinically useful andreliable for the differential diagnosis between viabletumor and necrotic tissue or post-surgical changes[18,19]. Moreover, 201Tl SPECT results are compara-ble to PET (position emission tomography) [21,22],but PET is not widely available.
In our study, the final response to therapy was evalu-ated according to the McDonald criteria [16], which arebased both on clinical and radiological findings. Wors-ening of the clinical status in many of these patientslimit the availability of histological confirmation.
A comparison of radiological and nuclear medicinediagnostic modalities for the assessment of theresponse to therapy in patients with high grade gliomashas not been widely reported. Specifically, the use of201Tl SPECT has seldom been reported to our knowl-edge for the evaluation of therapy in high grade gliomas[20,25]. Roesdi et al. [25] studied ten patients using201Tl SPECT findings as a response parameter forPCV chemotherapy in recurrent glioma. Kallen et al.[20] published a preliminary study comparing 201TlSPECT, MRI and MR spectroscopy during astrocy-toma chemotherapy. Also, 201Tl SPECT was shown tobe useful for the diagnosis of suspected astrocytomarecurrence [10,28–30] and to differentiate radiationnecrosis from tumor regrowth [31].
Contrary to the opinion of Kallen et al. [27], we sup-port the use of 201Tl SPECT during the course of therapyto help establish the degree of response, in accordancewith MRI and clinical status in most cases, speciallywhen MRI is non conclusive (patient 7). In our experi-ence, 201Tl SPECT changes are in agreement with MRIresults, both in cases of regression (partial or complete)or progression. In addition, our data suggest that treat-ment induces thallium tumor uptake variations that mayprecede anatomic changes on MRI. Sometimes, neu-roimaging studies may not be conclusive because ofpost-surgery or post-treatment changes in brain tissue.In any case, for those patients with suspected recurrentglioma after therapy, 201Tl SPECT detected tumoralgrowth better than TC or even MRI.
At the time of recurrence, all our patients showedincreased 201Tl uptake in the surgical area as aundeniable sign of tumoral growth, while this could
not be established in three patients on CT and intwo patients on MRI. In two patients, 201Tl SPECTshowed partial response while on clinical progression.However, such patients improved after anti-edematherapy. Edema may cause neurological deteriorationthat leads to an underestimation of the response bythe McDonald criteria. Steroids used in these patientsas an anti-edema treatment do not modify thalliumuptake, although their influence on MRI findings iswell known [32]. Also, it is important to underline thatsome patients, even with partially controlled tumor (bySPECT) may develop progressive brain damage at theend stage of their disease due to demyelinization (asobserved by RMI and CT). In such patients, it is likelythat polytherapy lengthens survival at the expense ofprogressive cognitive and neurological worsening thatmay mimic progression.
Temozolamide, which seems prolong survival inhigh grade glioma patients when other therapy modal-ities have failed, has not been assessed by 201TlSPECT. In our limited number of patients, temozo-lamide showed promising results.
Our preliminary study is limited by the few numberof patients, and by the fact that not all patients wereevaluated simultaneously by CT along with SPECT andMRI. For the purpose of glioma treatment evaluation,MRI offers higher sensitivity and specificity than CT,and nowadays MRI is the key follow-up examination.Nevertheless, both CT and MRI, have limitations thatleave an important role for 201Tl SPECT.
We conclude that thallium SPECT adds valuableinformation in the evaluation of the response to ther-apy in high grade gliomas, specially compared to CTscan, in cases where it is not fully reliable or in thecase of disagreement with MRI. Intensity of responseaccording to 201Tl SPECT correlates with the clinicalfollow-up and the McDonald criteria. We believe that201Tl SPECT is useful because it provides an estimationof the outcome after therapy in these patients. Never-theless, a large number of patients will be necessary tostrengthen these statements. The study continues.
References
1. Fleury A, Manegoz F, Grosclaude P, Daures JP, Henry-Amar M, Raverdy N, Schaffer P, Poisson M, Delattre JY:Descriptive epidemiology of cerebral gliomas in France.Cancer 79: 1195–1202, 1997
2. Kleihues P, Burger PC, Scheithauer BW: The new WHOclassification of brain tumours. Brain Pathol 3: 255–268,1993

89
3. Fine HA, Dear KB, Loeffler JS, Black PM, Canellos GP:Meta-analysis of radiation therapy with and without adju-vant chemotherapy for malignant gliomas in adults. Cancer71: 2585–2597, 1993
4. Levin VA: Chemotherapy for brain tumors of astrocytic andoligodendroglial lineage: the past decade and where we areheading. Neuro-Oncol 1: 69–80, 1999
5. Yung WK, Prados M, Yaya-Tur R, Rosenfeld SS, Brada M,Friedman HS, Albright R, Olson J, Chang SM, O’Neill AM,Friedman AH, Bruner J, Yue N, Dugan M, Z, Levin VA:Multicenter phase II trial of temozolomide in patients withanaplastic astrocytoma or anaplastic oligoastrocytoma atfirst relapse. Temodal Tumor Group. J Clin Oncol 17:2762–2771, 1999
6. Yung WK, Albright RE, Olson J, Fredericks R, Fink K,Prados MD, Brada M, Spence A, Hohl RJ, Shapiro W,Glantz M, Greenberg H, Selker RG, Vick NA, Rampling R,Friedman H, Phillips P, Bruner J, Yue N, Osoba D,Zaknoen S, Levin VA: A phase II study of temozolamidevs. procarbazine in patients with glioblastoma multiformeat first relapse. Br J Cancer 83: 588–593, 2000
7. Kosuda S, Fujii H, Aoki S, Suzuki K, Tanaka Y,Nakamura O, Shitara N: Prediction of survival in patientswith suspected recurrent cerebral tumors by quantitativeThallium-201 single photon emission computed tomogra-phy. Int J Radiat Oncol Biol Phys 30: 1201–1206, 1994
8. Vertosick FT, Seiker RG, Grossman SJ, Joyce JM:Correlation of thallium-201 single photon emission com-puted tomography and survival after treatment failure inpatients with glioblastoma multiforme. Neurosurgery 34:396–401, 1994
9. Oriuchi N, Tamura M, Shibazaki T, Ohye C, Watanabe N,Tateno M, Tomiyoshi K, Hirano T, Inoue T, Endo K: Clin-ical evaluation of thallium-201 SPECT in supratentorialgliomas: relationship to histologic grade, prognosis, and pro-liferative activities. J Nucl Med 34: 2085–2089, 1993
10. Yoshii Y, Satou M, Yamamoto T, Yamada Y, Hyodo A,Nose T, Ishikawa H, Hatakeyama R: The role of thallium-201 single photon emission tomography in the investiga-tion and characterisation of brain tumours in man and theirresponse to treatment. Eur J Nucl Med 20: 39–45, 1993
11. Diercks RA, Martin JJ, Dobbeleir A, Crols R, Neetens I,De Deyn PP: Sensitivity and specificity of thallium-201single-photon emission tomography in the functional detec-tion and differential diagnosis of brain tumours. Eur J NuclMed 21: 621–633, 1994
12. Ishibashi M, Taguchi A, Sugita Y, Morita S, Kawamura S,Umezaki N, Shigemori M, Hayabuchi N: Thallium-201 inbrain tumors: relationship between tumor cell activity inastrocytic tumor and proliferating cell nuclear antigen. JNucl Med 36: 2201–2206, 1995
13. Arbab A, Koizumi K, Toyama K, Arai T, Araki T: Uptakeof thechnetioum-99m-tetrofosmin, technetium-99m-MIBIand Thallium-201 in tumor cell lines. J Nucl Med 37:1551–1556, 1996
14. Taki S, Kakuda K, Kakuma K, Kobayashi K, Ohashi M,Ito S, Yokoyama M, Annen Y, Tonami N: 201Tl SPET in thedifferential diagnosis of brain tumours. Nucl Med Commun20: 637–645, 1999
15. Tonami N. Thallium-201 SPECT in the evaluation ofgliomas. J Nucl Med 34: 2085–2089, 1993
16. McDonald DR, Cascino Tl, Schold Jr SC, Cairncross JG:Response criteria for phase II studies of supratentorialmalignant glioma. J Clin Oncol 8: 1277–1280, 1990
17. Doom GC, Hecht S, Brant-Zawadzki M, Berthiaume Y,Norman D, Newton TH: Brain radiation necrosis: MR imag-ing. Radiology 158: 149–155, 1986
18. Kallen K, Heiling M, Andersson AM, Brun A, Holtas S,Ryding E: Preoperative grading of glioma malignancy withThallium-201 single-photon emission CT: comparison withconventional CT. AJNR Am J Neuradiol 17: 925–932, 1996
19. Bloom M, Jacobs S, Pile-Spellman J, Pozniakoff A,Mabutas MI, Fawwaz RA: Cerebral SPECT imaging: effecton clinical management. J Nucl Med 37: 1070–1073, 1993
20. Kallen K, Burtscher IM, Holtas S, Ryding E, Rosen I:201Thallium SPECT and 1H-MRS compared with MRI inchemotherapy monitoring of high-grade malingnant astro-cytomas. J Neuro-Oncol 46: 173–185, 2000
21. Black KL. Emerick T, Hoh CK, Hawkins RA, Mazziota J,Becker DP: Thallium-201 SPECT and positron emissiontomography equal predictors of glioma grade and recur-rence. Neurol Res 16: 93–96, 1994
22. Kahn D, Follett KA, Bushnell DL, Nathan MA, Piper JG,Madsen M, Kirchner PT: Diagnosis of recurrent brain tumor:value of 201Tl SPECT vs. 18F-fluorodeoxyglucose PET.AJR Am J Roentgenol 163: 1459–1462, 1994
23. Sasaki M, Kuwabara Y, Yoshida T, Nakagawa M,Fukumura T, Mihara F, Morioka T, Fukui M, Masuda K:A comparative study of thallium-201 SPET, Carbon-11-methionine PET and fluorine-18 fluorodeoxyglucose PETfor the differentiation of astrocytic tumours. Eur J Nucl Med25: 1261–1269, 1998
24. Loberboym M, Mandell LR, Mosesson RE, Germano I,Lou W, DaCosta M, Linzer DG, Machac J: The role ofThallium-201 uptake and retention in intracranial tumorsafter radiotherapy. J Nucl Med 38: 223–226, 1997
25. Roesdi MF, Postma TJ, Hoekstra OS, Van Groeningen CJ,Wolbers JG, Heimans JJ: Thallium-201 SPECT as responseparameter for PCV chemotherapy in recurrent glioma. JNeuro-Oncol 40: 251–255, 1998
26. Staffen W, Hondl N, Trinka E, Iglseder B, Unterrainer J,Ladurner G: Clinical relevance of 201Tl-chloride SPECT inthe differential diagnosis of brain tumours. Nucl Med Com-mun 19: 335–340, 1998
27. Kallen K, Geijer B, Malmstrom P, Andersson AM, Holtas S,Ryding E, Rosen I: Quantitative 201Tl SPECT imaging inthe follow-up of treatment for a sensitive tool for the earlyidentification of response to chemotherapy. Nucl Med Com-mun 21: 259–267, 2000
28. Carvalho PA, Schwartz RB, Alexander E 3rd, Garada BM,Aimmerman RE, Loeffler JS, Holman BL: Detectionof recurrent gliomas with quantitative thallium-201/technetium-99m HMPAO single-photon emissioncomputerized tomography. J Neurosurg 77(4): 565–570,1992
29. Zhang JJ, Park CH, Kim SM, Ayyangar KM, Haghbin M:Dual Isotope SPECT in the evaluation of recurrent braintumor. Clin Nucl Med 17: 663–664, 1992

90
30. Moustafa HM, Omar WM, Ezzat I, Ziada GA,el-Ghonimy EG: 201Tl single photon emission tomogra-phy in the evaluation of residual and recurrent astrocytoma.Nucl Med Commun 15: 140–143, 1994
31. Schwartz RB, Carvalho PA, Alexander E 3rd, Loeffler JS,Folkerth R, Holman BL: Radiation necrosis vs. high-grade recurrent glioma: differentiation by using dual-isotopeSPECT WITH 201Tl and 99mTc-HMPAO. AJNR Am JNeuroradiol 12: 1187–1192, 1991
32. Namba H, Togawa T, Yui N, Yanagisawa M, Kinoshita F,Iwadate Y, Ohsato K, Sueyoshi K: The effect of steroid onthallium-201 uptake by malignant gliomas. Eur J Nucl Med23: 991–992, 1996
Address for offprints: Virginia Vallejos, Nuclear Medicine Depart-ment, Hospital Universitari Germans Trias i Pujol, Cra. Canyet s/n,Badalona 08916. Spain; E-mail: [email protected]




















