
University of Groningen Effectiveness and safety of medicines ...
212
University of Groningen Effectiveness and safety of medicines used in COPD patients Wang, Yuanyuan DOI: 10.33612/diss.123921981 IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2020 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): Wang, Y. (2020). Effectiveness and safety of medicines used in COPD patients: pharmacoepidemiological studies. University of Groningen. https://doi.org/10.33612/diss.123921981 Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license. More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne- amendment. Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 12-03-2022
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of University of Groningen Effectiveness and safety of medicines ...

University of Groningen
Effectiveness and safety of medicines used in COPD patientsWang, Yuanyuan
DOI:10.33612/diss.123921981
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2020
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Wang, Y. (2020). Effectiveness and safety of medicines used in COPD patients: pharmacoepidemiologicalstudies. University of Groningen. https://doi.org/10.33612/diss.123921981
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license.More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne-amendment.
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 12-03-2022

Effectiveness and safety of medicines used in COPD patients
Pharmacoepidemiological studies
Yuanyuan Wang

Effectiveness and safety of medicines used in COPD patientsPharmacoepidemiological studies
ISBN: 978-94-034-2555-9 (printed version)ISBN: 978-94-034-2554-2 (electric version)
Author: Yuanyuan WangCover-design: IRINA SHI (photo) & Off Page (content)Printing: Off Page (www.offpage.nl)
The studies presented in this thesis were funded by University of Groningen and the China Scholarship Council (CSC) Scholarship. This thesis was conducted within the Groningen University Institute for Drug Exploration (GUIDE). Printing of this thesis was financially supported by the University of Groningen and the Graduate School of Science and Engineering (GSSE).
Copyright ©Yuanyuan Wang, 2020, Groningen, The Netherlands.All rights reserved. No part of this book may be reproduced or transmitted in any form by any means, electronically or mechanically by photocopying, recording, or otherwise, without the written permission of the author. The copy right of previously published chapters of this thesis remains with the publisher or journal.
Paranymphs: Jurjen van der Schans Yanni Li
Effectiveness and safety of medicines used in COPD patients
Pharmacoepidemiological studies
PhDthesis
to obtain the degree of PhD at the University of Groningen on the authority of the
Rector Magnificus Prof. C. Wijmenga and in accordance with
the decision by the College of Deans.
This thesis will be defended in public on
Friday 8 May 2020 at 14.30 hours
by
YuanyuanWang
born on 15 February 1988 in Henan, China

SupervisorsProf. . Ha Prof. H.M. oe en
AssessmentCommitteeProf. T. .M. erheij Prof. . van der Palen Prof. . tienstra
TABLE OF CONTENTS
Chapter 1 General Introduction 7
Part I Effects of antibiotic use for COPD exacerbations and potential DDIs during COPD exacerbation management
Chapter 2 Effects of Prophylactic Antibiotics on Patients with Stable COPD: 21 A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Chapter 3 The influence of age on real-life effects of doxycycline for 43 acute exacerbations among COPD outpatients: a population-based cohort study
Chapter 4 Real-world short- and long-term effects of antibiotic therapy on 61 acute exacerbations of COPD in outpatients: a cohort study under the PharmLines Initiative
Chapter 5 Improving antibacterial prescribing safety in 81 the management of COPD exacerbations: systematic review of observational and clinical studies on potential drug interactions associated with frequently prescribed antibacterials among COPD Patients
Part II Neuropsychiatric safety of varenicline use for smoking cessation and the application of prescription sequence symmetry analysis in drug safety evaluation
Chapter 6 Neuropsychiatric safety of varenicline in the general and 119 COPD population with and without psychiatric disorders: a retrospective inception cohort study in a real-world setting
Chapter 7 Risk of neuropsychiatric adverse events associated with 145 varenicline treatment for smoking cessation: a prescription sequence symmetry analysis
Chapter 8 Effect estimate comparison between the prescription 165 sequence symmetry analysis and parallel group study designs: a systematic review
Chapter 9 General discussion 183
Chapter 10 Summary 197Samenvatting 201Acknowledgement 204List of publications 208About the author 211
SupervisorsProf. . Ha
Prof. H.M. oe en
AssessmentCommittee
Prof. T. .M. erheij
Prof. . van der Palen
Prof. . tienstra

C H A P T E R 1

General Introduction


General Introduction
9
1GENERAL INTRODUCTIONChronic obstructive pulmonary disease
According to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) report 2020, Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease that is characterized by persistent respiratory symptoms and airflow limitation. Such symptoms are caused by airway and/or alveolar abnormalities usually triggered by significant exposure to noxious particles or gases.1 Cigarette smoking is the main independent causal risk factor for COPD with indoor and outdoor air pollution and occupational exposure to dust and noxious particles also being the risk factors for COPD.2 Moreover, host factors that may contribute to the development of COPD include age, genetics, airway hyper responsiveness and abnormal lung development.3-5
The prevalence of COPD varies across countries as well as regions within countries. According to the findings of a global meta-analysis, the number of COPD cases increased to 384 million in 2010, with a global prevalence of 12% (ranging between 8% and 15%).6 COPD is commonly diagnosed in individuals aged 40 years or older based on the presence of associated symptoms and risk factors. However, a definitive COPD diagnosis requires the performance of spirometry. The presence of a post-bronchodilator FEV1/FVC < 0.7 confirms the presence of airflow limitation and results in a COPD diagnosis. COPD patients are currently categorized into four GOLD stages of severity of airflow limitations based on the predicted value of FEV1: mild (stage I, FEV1
≥ 80% predicted), moderate (stage II, 50% ≤ FEV1 < 80% predicted), severe (stage III, 30% ≤ FEV1 < 80% predicted) and very severe (stage IV, FEV1 < 30% predicted).1 A large prevalence study estimated that the rate of COPD for GOLD stage II and higher is around 10% in the general population, and a little higher in men than women (11.8% and 8.5%, respectively).7
COPD is one of the leading causes of morbidity and mortality worldwide.8 Its burden is predicted to increase in the coming decades as a result of continuous exposure to risk factors in developing countries and aging of the population worldwide, particularly in high-income countries.9 Smoking cessation interventions, increased physical activity, and early diagnosis and treatment of related comorbidities are considered key measures for reducing the health-economic burden of COPD. 10
Up to now, the key goals of COPD treatment have been to improve patients’ prognosis and prevent the disease from worsening. The main treatment used in the daily management of mild and moderate COPD is pharmacotherapy. Bronchodilators, including short- and long-acting β2-agonists (SABA and LABA) and short- and long-acting anticholinergics (SAMA and LAMA) are essential for managing and preventing symptoms, and combined treatment (SABA/SAMA, LABA/LAMA or LABA/ICS) may be used as appropriate. Non-

Chapter 1
10
pharmacological treatment comprises pulmonary rehabilitation (e.g., exercise training, education, and behavioral change).11 Oxygen therapy is necessary for patients with very severe COPD and lung surgery may also be necessary.
Exacerbations of COPD and antibiotic use
An exacerbation of COPD is defined as an acute worsening of respiratory symptoms that necessitates additional therapy.1 COPD patients can periodically experience acute exacerbations that may accelerate the decline in lung function, reduce the quality of life, and increase mortality and health-care costs.12,13 14 Infections, especially bacterial infections, and inflammation are thought to be an important trigger for exacerbations of COPD. Previous studies have found that bacteria are responsible for around 40% to 50% of exacerbations.15,16 S. pneumoniae, H. influenza, P. aeruginosa, M. catarrhalis, A. baumannii, and S. aureus were the most frequently reported bacteria that cause exacerbations of COPD.16-18 According to the GOLD guideline, the main goals in treatment of COPD exacerbations are minimizing the negative impact of the current exacerbation and preventing subsequent exacerbations.1 Because almost 40% of exacerbations are bacteria-caused respiratory tract infections,16 the use of antibiotics has become a common component in the management of acute exacerbations among COPD patients, both in terms of treatment and prevention.1,19
Notably, recommendations in prophylactic use of antibiotics in the management of COPD exacerbations are conditional and unspecific. Only long-term macrolides are currently mentioned as first-line therapy.1,19 Moreover, in terms of current evidence, an optimal regimen of prophylactic antibiotics for exacerbations has not been well established, and related recommendations regarding an appropriate schedule (continuous vs. intermittent) and the duration of a specific antibiotic intervention (below or equal to 6 months vs. above 6 months) are still lacking. Besides, the effects of even the most extensively researched antibiotics macrolides—let alone other potentially suitable antibiotics—on the time to the first exacerbation, changes in lung function, the bacterial load, and airway inflammation have not been adequately evaluated.20 Knowledge of these outcomes is also vital for elucidating possible mechanisms behind the reduction of exacerbations through the prophylactic use of antibiotics, and for weighing benefits and risks.21
The beneficial effects of oral corticosteroids as an effective treatment for acute exacerbations of COPD (AECOPD) in improving COPD symptoms and lung function are well established.22 However, although antibiotics have been recommended for the treatment of AECOPOD when signs of bacterial infection are present,1 there is still uncertainty regarding the beneficial effects of antibiotic treatment used in the combination with oral glucocorticoids for AECOPD, particularly in the case of outpatients in real-world settings. In 2012, a Cochrane review that pooled the results

General Introduction
11
1of five RCTs conducted among outpatients did not reveal a significantly reduced risk of treatment failure associated with antibiotics currently prescribed for outpatients.23 However, an updated version of this Cochrane review conducted in 2018 presented statistically significant beneficial effects of current antibiotics prescribed for outpatients.24 Two new RCTs were included in this later study in relation to the earlier review conducted in 2012.25,26 Notably, one of the two RCTs did not support the beneficial effects of antibiotics treatment on AECOPD, although it did contribute to almost 25% of the sample size of the updated pooled results.25
Hence, most of the available scientific evidence on the effects of antibiotics for AECOPD is basically derived from RCTs. It is widely accepted that RCTs provide solid evidence with high internal validity, however, their generalizability in the real world, especially in outpatient settings is low. COPD is a chronic disease and is mostly managed on an outpatient basis within a population that is more heterogeneous compared with populations from RCTs. Moreover, the use of antibiotics for AECOPD treatment is not always appropriate and in line with related guidelines.27,28 Therefore, the effect of antibiotic treatment for AECOPD in real-world settings may differ from those obtained in clinical trials and require further investigation.
Comorbidities of COPD and potential drug-drug interactions
COPD is a chronic disease and its prevalence increases with age; around 15% of the general population over 65 years is affected by COPD.29 Hence, age-related comorbidities frequently co-exist with COPD.30 The most common concomitant chronic conditions associated with COPD include cardiovascular disease (e.g., heart failure, ischemic heart disease, and arrhythmias), metabolic disease (e.g., diabetes), osteoporosis, depression and anxiety, lung cancer and gastroesophageal reflux (GERD).1,30
COPD itself is a complex disease that entails the need for a variety of medications to improve lung function and treat exacerbations.1 Multiple comorbidities further complicate the medical management of COPD, resulting in polypharmacy among a large section of COPD patients. Polypharmacy poses a potential risk of drug-drug interactions (DDIs) that may induce adverse events and treatment failures. Moreover, COPD is an age-related disease that generally manifests at an older age. Therefore, these older patients are more susceptible to DDIs due to gradual physiologic negative changes that may influence their pharmacokinetics and the pharmacodynamics of the drugs used.31
As most evidence about drug effects is from clinical trials, more attention should be paid to issues related to polypharmacy and to potential DDIs in the management of COPD in real-world settings.32 This is especially the case for antibiotic therapy as it includes different drug classes that vary in their mechanisms relating to absorption and metabolism, making their interaction with other medications more likely. Comprehensive information for clinicians to avoid potential DDIs, however, is lacking.
Chapter 1
12
Smoking cessation drug therapy and neuropsychiatric safety
Tobacco smoking is the main risk factor for COPD and other physical and mental disorders.33-35 This preventable behavior poses huge threats to global public health.36,37 Although in recent years, strict tobacco control policies have prompted a global decline in smoking,36 the actual numbers of smokers and smoking-related disease burden continues to increase because of the growing population worldwide.38 More than eight million people continue to die annually as a result of tobacco consumption.39
Therefore, smoking cessation strategies to prevent smoking-related diseases are imperative.40 Varenicline, which was the first non-nicotine, pharmacotherapeutic, smoking cessation product, has been found to be more efficacious than other therapies, such as single-dose bupropion and nicotine replacement therapy (NRT).41 However, following varenicline’s approval by the FDA in 2006, safety concerns were raised relating to its neuropsychiatric adverse events, which include suicidal thoughts, aggressive behavior, depression, anxiety, and sleep disorders.42 Numerous RCTs were subsequently conducted with varenicline to generate evidence on its safety.43 In light of their findings, the FDA warning was removed in 2016. However, concerns remain, given the strict inclusion and exclusion criteria applied in RCTs that result in the participation of relatively healthy individuals and the lack of consistent real-world evidence. Notably, special risk populations demonstrating increased smoking prevalence, such as COPD patients, have generally been excluded from RCTs.44
As previously noted, most COPD patients are elderly and have multi-morbidities, making them more susceptible to adverse drug events (ADEs). Similarly, there is evidence that individuals with psychiatric disorders experience relapses of psychiatric symptoms more frequently than those without these disorders.45,46 The safety of varenicline use for these specific populations has not been established. Although a few studies were conducted among patients with COPD or psychiatric disorders,47,48 the results were inconsistent. Consequently, more observational studies are still needed to generate the real-world evidence relating to the safety of varenicline use.
PSSA and observational study designs in drug safety evaluation
Most evidence regarding the effects of drugs is derived from strictly regulated clinical trials. However, the results from RCTs may not reflect the real-world situations, given that the participants are relatively healthy and because of the limited scope for detecting rare events with clinical trials. Therefore, real-world evidence derived from traditional, non-randomized, observational study designs is valuable for exploring such drug effects or toxicities within the field of pharmacoepidemiology. However, the evidence from observational studies is often inconsistent, and such designs have been criticized for their potential of bias (e.g., selection or information bias) and confounding (e.g. unmeasured confounding).49
General Introduction
13
1Prescription sequence symmetry analysis (PSSA) is increasingly being used to detect adverse effects or events associated with medications. PSSA is a self-controlled study design in which genetic and other time-invariant confounding can be well controlled, it does not entail the abovementioned bias.50,51 It compares the symmetry in the sequence of exposure medication and marker (outcome) medications as proxy for ADRs within a specific time window based on prescriptions or claims databases.52 The sequence ratio (SR) reflects the association between exposure and outcome. However, PSSA is still sensitive to time-varying variables, notably if the follow-up time is long. The overall validity of PSSA study designs has not been fully evaluated by comparing its result with those from conventional observational parallel group study designs, and such comparisons are urgently required.
AIM OF THIS THESISIn this thesis, we aim to develop a comprehensive profile on the effectiveness of antibiotic use for acute exacerbations of COPD both prescribed prophylactically and therapeutically, and to provide real-world data on neuropsychiatric safety of varenicline use for smoking cessation, particularly among high risk populations with COPD or psychiatric diseases.
OUTLINE OF THIS THESISIn part I of this thesis, we present several studies on the role of antibiotics in acute exacerbations of COPD (AECOPD).
In Chapter 2, we report the results from a meta-analysis of RCTs focusing on the beneficial effects and side effects of prophylactic antibiotic therapy in COPD patients.
In Chapter 3, we demonstrate the real-world effects of doxycycline treatment on acute exacerbations among COPD outpatients based on data extracted from the University of Groningen’s prescription database (IADB.nl) and explored the possible influence of age on the clinical outcomes.
In Chapter 4, we further explored the real-world effects of several antibiotic drugs used for acute exacerbations of COPD patients based on a linked database between the Lifelines Cohort biobank with extensive clinical information and the University of Groningen’s prescription database (IADB.nl).
In Chapter 5, we present a systematic review of drug-drug interactions associated with frequently prescribed antibiotics among COPD patients based on causal evidence obtained from observational cohort studies, case-control studies and clinical studies, aimed at improving the safety of antibacterial prescriptions.

Chapter 1
14
In part II of this thesis, we present studies on the role of varenicline for smoking cessation using different designs.
In Chapter 6, we present the results of a retrospective inception cohort study aimed at assessing the risk of neuropsychiatric adverse events (NPAEs) in starters with varenicline versus starters with nicotine replacement therapy (NRT) among both the general and COPD populations, with and without psychiatric disorders. This study was conducted using data extracted from the University of Groningen’s prescription database (IADB.nl).
In Chapter 7, we further examine the association between varenicline use and the onset of NPAEs in a real-world setting using a prescription sequence symmetry analysis (PSSA) study design.
Furthermore, in Chapter 8 we systematically compared effect estimates derived from the PSSA study with effect estimates from conventional observational parallel group study designs, to assess the validity and constraints of the PSSA study design within epidemiological research.
Last, in Chapter 9, we summarized the main findings of this thesis, discussed these findings in detail and provided suggestions for future research.

General Introduction
15
1REFERENCES
1. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease: 2020 Report. https://goldcopd.org/gold-reports/. Date last accessed: December 17, 2019.
2. Postma DS, Bush A, van den Berge M. Risk factors and early origins of chronic obstructive pulmonary disease. Lancet. 2015;385(9971):899-909.
3. Lange P, Celli B, Agusti A, et al. Lung-Function Trajectories Leading to Chronic Obstructive Pulmonary Disease. N Engl J Med. 2015;373(2):111-122.
4. Stern DA, Morgan WJ, Wright AL, Guerra S, Martinez FD. Poor airway function in early infancy and lung function by age 22 years: a non-selective longitudinal cohort study. Lancet. 2007;370(9589):758-764.
5. Tashkin DP, Altose MD, Bleecker ER, et al. The lung health study: airway responsiveness to inhaled methacholine in smokers with mild to moderate airflow limitation. The Lung Health Study Research Group. Am Rev Respir Dis. 1992;145(2 Pt 1):301-310.
6. Adeloye D, Chua S, Lee C, et al. Global and regional estimates of COPD prevalence: Systematic review and meta-analysis. J Glob Health. 2015;5(2):020415.
7. Buist AS, McBurnie MA, Vollmer WM, et al. International variation in the prevalence of COPD (the BOLD Study): a population-based prevalence study. Lancet. 2007;370(9589):741-750.
8. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095-2128.
9. Lopez AD, Shibuya K, Rao C, et al. Chronic obstructive pulmonary disease: current burden and future projections. Eur Respir J. 2006;27(2):397-412.
10. Rabe KF, Watz H. Chronic obstructive pulmonary disease. Lancet. 2017;389(10082):1931-1940.
11. Spruit MA, Singh SJ, Garvey C, et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13-64.
12. Wedzicha JA, Seemungal TAR. COPD exacerbations: defining their cause and prevention. Lancet. 2007;370(9589):786-796.
13. Soler-Cataluna JJ, Martinez-Garcia MA, Roman Sanchez P, Salcedo E, Navarro M, Ochando R. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60(11):925-931.
14. O’Reilly JF, Williams AE, Rice L. Health status impairment and costs associated with COPD exacerbation managed in hospital. Int J Clin Pract. 2007;61(7):1112-1120.
15. Sethi S, Murphy TF. Infection in the pathogenesis and course of chronic obstructive pulmonary disease. N Engl J Med. 2008;359(22):2355-2365.
16. Moghoofei M, Azimzadeh Jamalkandi S, Moein M, Salimian J, Ahmadi A. Bacterial infections in acute exacerbation of chronic obstructive pulmonary disease: a systematic review and meta-analysis. Infection. 2019.
17. Wilkinson TMA, Aris E, Bourne SC, et al. Drivers of year-to-year variation in exacerbation frequency of COPD: analysis of the AERIS cohort. ERJ Open Res. 2019;5(1).
18. Monso E, Garcia-Aymerich J, Soler N, et al. Bacterial infection in exacerbated COPD with changes in sputum characteristics. Epidemiol Infect. 2003;131(1):799-804.
19. Wedzicha JA, Calverley PMA, Albert RK, et al. Prevention of COPD exacerbations: a European Respiratory Society/American Thoracic Society guideline. Eur Respir J. 2017;50(3).
20. Ni WT, Shao XD, Cai XJ, et al. Prophylactic Use of Macrolide Antibiotics for the Prevention of Chronic Obstructive Pulmonary Disease
Chapter 1
16
Exacerbation: A Meta-Analysis. Plos One. 2015;10(3).
21. Cameron EJ, McSharry C, Chaudhuri R, Farrow S, Thomson NC. Long-term macrolide treatment of chronic inflammatory airway diseases: risks, benefits and future developments. Clin Exp Allergy. 2012;42(9):1302-1312.
22. Walters JA, Tan DJ, White CJ, Gibson PG, Wood-Baker R, Walters EH. Systemic corticosteroids for acute exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2014(9):CD001288.
23. Vollenweider DJ, Jarrett H, Steurer-Stey CA, Garcia-Aymerich J, Puhan MA. Antibiotics for exacerbations of chronic obstructive pulmonary disease. Cochrane Db Syst Rev. 2012(12).
24. Vollenweider DJ, Frei A, Steurer-Stey CA, Garcia-Aymerich J, Puhan MA. Antibiotics for exacerbations of chronic obstructive pulmonary disease. Cochrane Db Syst Rev. 2018(10).
25. van Velzen P, Ter Riet G, Bresser P, et al. Doxycycline for outpatient-treated acute exacerbations of COPD: a randomised double-blind placebo-controlled trial. Lancet Respir Med. 2017;5(6):492-499.
26. Hassan WA, Shalan I, Elsobhy M. Impact of antibiotics on acute exacerbations of COPD. Egypt J Chest Dis Tu. 2015;64(3):579-585.
27. Bathoorn E, Groenhof F, Hendrix R, et al. Real-life data on antibiotic prescription and sputum culture diagnostics in acute exacerbations of COPD in primary care. Int J Chron Obstruct Pulmon Dis. 2017;12:285-290.
28. Roede BM, Bindels PJ, Brouwer HJ, Bresser P, de Borgie CA, Prins JM. Antibiotics and steroids for exacerbations of COPD in primary care: compliance with Dutch guidelines. Br J Gen Pract. 2006;56(530):662-665.
29. Halbert RJ, Natoli JL, Gano A, Badamgarav E, Buist AS, Mannino DM. Global burden of COPD: systematic review and meta-analysis. Eur Respir J. 2006;28(3):523-532.
30. Chetty U, McLean G, Morrison D, Agur K, Guthrie B, Mercer SW. Chronic obstructive pulmonary disease and comorbidities:
a large cross-sectional study in primary care. Br J Gen Pract. 2017;67(658):e321-e328.
31. Mangoni AA, Jackson SH. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. Br J Clin Pharmacol. 2004;57(1):6-14.
32. Hanlon P, Nicholl BI, Jani BD, et al. Examining patterns of multimorbidity, polypharmacy and risk of adverse drug reactions in chronic obstructive pulmonary disease: a cross-sectional UK Biobank study. BMJ Open. 2018;8(1):e018404.
33. Banks E, Joshy G, Korda RJ, et al. Tobacco smoking and risk of 36 cardiovascular disease subtypes: fatal and non-fatal outcomes in a large prospective Australian study. BMC Med. 2019;17(1):128.
34. Gaudet MM, Carter BD, Brinton LA, et al. Pooled analysis of active cigarette smoking and invasive breast cancer risk in 14 cohort studies. Int J Epidemiol. 2017;46(3):881-893.
35. Tjora T, Hetland J, Aaro LE, Wold B, Wiium N, Overland S. The association between smoking and depression from adolescence to adulthood. Addiction. 2014;109(6):1022-1030.
36. Collaborators GBDT. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990-2015: a systematic analysis from the Global Burden of Disease Study 2015. Lancet. 2017;389(10082):1885-1906.
37. Thun MJ, Carter BD, Feskanich D, et al. 50-Year Trends in Smoking-Related Mortality in the United States. New Engl J Med. 2013;368(4):351-364.
38. The L. Progress towards a tobacco-free world. Lancet. 2018;392(10141):1.
39. World Health Organisation. WHO report on the global tobacco epidemic 2019: offer help to quit tobacco use. Geneva: World Health Organisation, 2019: 17-21.
40. Mehrotra R, Yadav A, Sinha DN, et al. Smokeless tobacco control in 180 countries across the globe: call to action for full implementation of WHO FCTC measures. Lancet Oncol. 2019;20(4):e208-e217.
41. Anthenelli RM, Benowitz NL, West R, et al. Neuropsychiatric safety and efficacy of

General Introduction
17
1varenicline, bupropion, and nicotine patch in smokers with and without psychiatric disorders (EAGLES): a double-blind, randomised, placebo-controlled clinical trial. Lancet. 2016;387(10037):2507-2520.
42. Moore TJ, Furberg CD, Glenmullen J, Maltsberger JT, Singh S. Suicidal behavior and depression in smoking cessation treatments. Plos One. 2011;6(11):e27016.
43. Thomas KH, Martin RM, Knipe DW, Higgins JP, Gunnell D. Risk of neuropsychiatric adverse events associated with varenicline: systematic review and meta-analysis. BMJ. 2015;350:h1109.
44. Lawrence D, Mitrou F, Zubrick SR. Smoking and mental illness: results from population surveys in Australia and the United States. Bmc Public Health. 2009;9.
45. Garza D, Murphy M, Tseng LJ, Riordan HJ, Chatterjee A. A double-blind randomized placebo-controlled pilot study of neuropsychiatric adverse events in abstinent smokers treated with varenicline or placebo. Biol Psychiatry. 2011;69(11):1075-1082.
46. Tonstad S, Davies S, Flammer M, Russ C, Hughes J. Psychiatric adverse events in randomized, double-blind, placebo-controlled clinical trials of varenicline: a pooled analysis. Drug Saf. 2010;33(4):289-301.
47. Kotz D, Viechtbauer W, Simpson CR, van Schayck OCP, West R, Sheikh A. Cardiovascular and neuropsychiatric risks of varenicline and bupropion in smokers with chronic obstructive pulmonary disease. Thorax. 2017;72(10):905-911.
48. Evins AE, Benowitz NL, West R, et al. Neuropsychiatric Safety and Efficacy of Varenicline, Bupropion, and Nicotine Patch in Smokers With Psychotic, Anxiety, and Mood Disorders in the EAGLES Trial. J Clin Psychopharmacol. 2019;39(2):108-116.
49. Boyko EJ. Observational research--opportunities and limitations. J Diabetes Complications. 2013;27(6):642-648.
50. Wahab IA, Pratt NL, Wiese MD, Kalisch LM, Roughead EE. The validity of sequence symmetry analysis (SSA) for adverse drug reaction signal detection. Pharmacoepidemiol Drug Saf. 2013;22(5):496-502.
51. Lai ECC, Pratt N, Hsieh CY, et al. Sequence symmetry analysis in pharmacovigilance and pharmacoepidemiologic studies. European Journal of Epidemiology. 2017;32(7):567-582.
52. Hallas J. Evidence of depression provoked by cardiovascular medication: a prescription sequence symmetry analysis. Epidemiology. 1996;7(5):478-484.

PA R T I
Effects of antibiotic use for COPD exacerbations and potential DDIs during COPD
exacerbation management
C H A P T E R 2

Yuanyuan Wang Tanja R. Zijp
Muh. Akbar Bahar Janwillem W.H. Kocks
Bob Wilffert Eelko Hak
Effects of Prophylactic Antibiotics on Patients with Stable COPD: A Systematic Review and
Meta-Analysis of Randomized Controlled Trials
Published as: Wang Y, Zijp TR, Bahar MA, Kocks JWH, Wilffert B, Hak E. Effects of prophylactic antibiotics on patients with stable COPD:
a systematic review and meta-analysis of randomized controlled trials. J Antimicrob Chemother. 2018;73(12):3231–3243.

Chapter 2
22
ABSTRACTBackground
As bacterial infections provoke exacerbations, COPD patients may benefit from prophylactic antibiotics. However, evidence regarding their overall benefit-risk is conflicting.
Objectives
To update previous evidence and systematically evaluate the beneficial and side effects of prophylactic antibiotics on stable COPD patients.
Methods
Several databases were searched up to April 26, 2017 for randomized controlled trials (RCTs) on prophylactic antibiotics in stable COPD patients. The Primary outcomes were exacerbations and quality of life. Duration and schedule of antibiotics were considered in sub-group analyses.
Results
Twelve RCTs involving 3,683 patients were included. Prophylactic antibiotics significantly reduced the frequency of exacerbations (risk ratio [RR] 0.74, 95% CI 0.60-0.92) and the number of patients with one or more exacerbations (RR 0.82, 95% CI 0.74-0.90). Erythromycin and azithromycin appeared the most effective with the number needed to treat ranging from four to seven. Quality of life was also significantly improved by prophylactic antibiotics (mean difference -1.55, 95% CI -2.59 to -0.51). Time to first exacerbation was prolonged in six studies with one conflicting result. Neither the rate of hospitalization nor the rate of adverse events was significantly changed. Furthermore, no significant changes were observed in lung function, bacterial load and airway inflammation. However, antibiotic resistant isolates were significantly increased (OR 4.49, 95% CI 2.48-8.12).
Conclusions
Prophylactic antibiotics were effective in preventing COPD exacerbations and improving quality of life among stable patients with moderate to severe COPD. The choice of prophylactic antibiotics should be analysed and considered case by case, especially for long and continuous use.

Effects of prophylactic antibiotics on COPD
23
2
INTRODUCTION COPD is an inflammatory disease that is characterized by persistent respiratory symptoms and airflow limitation.1 At present, COPD is one of the leading causes of chronic morbidity and mortality worldwide, its burden is predicted to increase in the coming decades due to continuous exposure to risk factors and aging of population globally.2 In the course of COPD, exacerbation as an acute worsening of respiratory symptoms has a profound negative impact on health oucomes.3 A vicious circle of infection and inflammation is thought as a key to trigger exacerbations of COPD, about 40-50% of exacerbations are caused by bacteria.4
The use of prophylactic antibiotic has been suggested to prevent exacerbations in COPD patients for a long time. However, a Cochrane review in 2003 concluded that antibiotics only contribute to a small 9% reduction of exacerbations and should not be part of routine treatment considering the risk of antibiotic resistance and adverse effects.5 Ten years later in 2013, the review by Herath et al. concluded a clinically significant benefit in reducing COPD exacerbations from continuous use of prophylactic antibiotics, but not from intermittent way due to only one randomized controlled trial (RCT) included in this subgroup.6 Influence of different duration of antibiotic intervention were not explored in this study. The most recent review by Ni et al. in 2015 focused on macrolides only and did not evaluate meaningful outcomes including the time to first exacerbation, change of lung function, bacterial load and airway inflammation.7 The latter outcome is important to support the hypothetical mechanism behind the reduction of exacerbations by antibiotics.8
Current recommendation from guidelines about prophylactic antibiotic use in the management of COPD exacerbations is conditional and unspecific.1,9 At present, the optimal regimen of prophylactic antibiotics for exacerbations has not been well established, and there are no advices for an appropriate schedule and duration of specific antibiotic intervention. To further enhance information on the public health benefit-risk associated with this intervention, we here aimed to provide a comprehensive overview of the positive and negative effects of prophylactic antibiotics on COPD patients.
METHODSSearch strategy
We performed an update of the previous review by Herath et al. in 20136 according to the PRISMA guidelines. Cochrane Central Register of Controlled Trials (CENTRAL), Medline, EMBASE, Web of Science, CINAHL, AMED and PsycINFO databases were systematically searched for relevant RCTs published from 29 August 2013 (when the review by Herath et al. ended) until 26 April 2017 using key elements of “COPD”,

Chapter 2
24
“RCT” and “antibiotics” (details are presented in Table S1). References from identified studies and relevant review articles were also checked manually. No language restrictions were applied. For the final analysis, we included both the new studies from this searching strategy and previous studies from the review by Herath et al.
Selection criteria
Studies included in this review met the following criteria: (1) focus on the effects of prophylactic antibiotics in COPD patients; (2) study designs must be RCTs with placebo group; (3) COPD patients should be aged over 18 years and with a well-defined diagnosis of COPD and confirmed evidence of persistent airflow limitation (the presence of a post-bronchodilator FEV1/FVC < 0.7); (4) prophylactic antibiotics must be given for a minimum period of 12 weeks; (5) patients must be clinically stable without exacerbation for at least three weeks before enrolment. Studies that focused on combined antibiotics (≥ 2) and studies of patients with other respiratory disease (e.g. bronchiectasis, asthma) or related genetic diseases such as cystic fibrosis and primary ciliary dyskinesia were excluded.
Outcomes and data analysis
The Primary outcomes were: number of patients with exacerbations; frequency of exacerbation; health-related quality of life assessed by the St Georges Respiratory Questionnaire (SGRQ).10 The Secondary outcomes were: the median time to first exacerbation; frequency of hospitalization; all-cause mortality; adverse events; antibiotic resistance; change in lung functions, bacteria load and airway inflammation. The influence of different schedules and durations of prophylactic antibiotic use on exacerbations and quality of life in COPD patients were explored. For the missing of standard deviation of SGRQ score change in two studies,11,12 we calculated it according to Cochrane guideline (see Supplement data). All analyses were done in accordance with the intention-to-treat principle using Review Manager Version 5.3. Risk ratio (RR) or OR was calculated for binary outcomes, while mean difference (MD) was for continuous outcomes. Generic inverse variance (GIV) methods were used for non-standard types of both dichotomous and continuous data. Summary measures were pooled using random-effects models. If data could not be combined, we performed a descriptive analysis. Statistical heterogeneity among studies was assessed using conventional chi-squared (X2, or Chi2) test and I2 statistic of inconsistency. Sensitivity analysis was performed by removing studies with a high risk for bias or deviation. A funnel plot was used to assess publication bias.

Effects of prophylactic antibiotics on COPD
25
2
Figure 1. Flow diagram of literature search and study selection.
data). All analyses were done in accordance with the intention‐to‐treat principle using Review
Manager Version 5.3. Risk ratio (RR) or OR was calculated for binary outcomes, while mean
difference (MD) was for continuous outcomes. Generic inverse variance (GIV) methods were
used for non‐standard types of both dichotomous and continuous data. Summary measures
were pooled using random‐effects models. If data could not be combined, we performed a
descriptive analysis. Statistical heterogeneity among studies was assessed using conventional
chi‐squared (X2, or Chi2) test and I2 statistic of inconsistency. Sensitivity analysis was
Figure 1. Flow diagram of literature search and study selection.
RESULTS Search results
From the 667 records generated by new search strategy, five new RCT studies were eligible and included (Figure 1). Together with the previous seven studies from the review by Herath et al.,6 a total of twelve RCTs were included for this systematic review. However, of all twelve studies , one was a conference abstract,13 one was not blinded,14 one did not report effect measures.15 In total, nine studies were qualified for the meta-analysis.

Chapter 2
26
Table 1. Characteristics of included studies.
Studies(1st author, year)
Study design Country
Patients(T/P)
Age(year)(T/P)
FEV1/FVC ratio (%)(T/P)
Prophylactic Antibiotics(dose)
Duration of treatment & follow up (months) Maintenance medication
Previous included studies
Albert, 2011 RCT US 570:572 65:66 42:43 Azithromycin, 250 mg daily 12 / 12 ICS, LABA, LAMAHe, 2010 RCT UK 18:18 68.8:69.3 46.9:48.6 Erythromycin, 125 mg, 3 times a day; 6 / 6 ICS,Mygind, 2010 RCT Denmark 287:288 71 (Median) NA Azithromycin, 500 mg daily, 3 days a month 36 / 36 ICS, Theophylline, inhaled
anticholinergic, inhaled β-adrenergic
Sethi, 2010 RCT US 569:580 66.1:66.6 45.0:46.3 Moxifloxacin, 400 mg daily, 5 days every 8 weeks
12 / 18 LABA, LAMA, SABA, SAMA, ICS, theophylline;
Seemungal, 2008 RCT UK 53:56 66.6:67.8 48.9:50.9 Erythromycin, 250 mg twice daily 12 / 12 LABA, LAMA, theophyllineBanerjee, 2005 RCT UK 31:36 65.1:68.1 43.8:45.5 Clarithromycin, 500 mg once daily 3 / 3 ICSSuzuki, 2001 RCT Japan 55:54 69.1:71.7 NA Erythromycin, 200-400 mg daily 12 / 12 Inhaled anticholinergic,
theophylline
New included studies
*Brill, 2015 RCT UK (25:25:25):24 (70.9:70.4:67.9): 68.7 (51:51:45):51 T1: Moxifloxacin, 400 mg, 5 times every 4 weeks; T2: Doxycycline, 100 mg daily; T3: Azithromycin, 250 mg, 3 times a week;
3.25 /3.25 ICS
†Shafuddin, 2015 RCT New Zealand 97:94 67.6:66.7 41.5:43.7 Roxithromycin, 300 mg daily 3 / 12 Not availableSimpson, 2014 RCT Australia 15:15 71.7:69.9 52.3:51.3 Azithromycin, 250 mg daily 3 / 6 ICSUzun, 2014 RCT Netherlands 47:45 64.7:64.9 38.0:40.3 Azithromycin, 500 mg, 3 times a week 12 / 12 LABA, LAMA, SABA, ICS,
PrednisoloneBerkhof, 2013 RCT Netherlands 42:42 67:68 42.2:43.2 Azithromycin, 250 mg, 3 times a week 3 / 4.5 LABA, LAMA, ICS
T/P: Treatment group versus Placebo group; ICS: inhaled corticosteroid; LABA: long-acting beta-2 agonists; LAMA: long-acting muscarinic antagonist; SABA: short-acting beta-2 agonists; SAMA: short-acting muscarinic antagonist; NA: data were not available; *This study designed
3 different treatment arms with one common placebo arm; †The study included 2 treatment arms, according to preset criteria, we only include the arm about single antibiotic use, the other arm in this study about combined antibiotic treatment is excluded;
Characteristics of included studies
The characteristics of twelve included studies are shown in Table 1, other specific baseline characteristics about COPD severity and exacerbation history were summarized in Table S2. All these studies were conducted over the last seventeen years involving 3,683 stable COPD patients, with 2932 patients involved in the meta-analysis. All included studies focused on one antibiotic arm with one placebo arm except the study by Brill et al.,16 which compared three antibiotics with one common placebo and we treated this study as three independent RCTs (Trial 1-3: T1, T2, T3). In all, six antibiotics were investigated in this review: azithromycin,11,13,16-19 erythromycin,12,14,20 moxifloxacin,16,21 clarithromycin,15 roxithromycin22 and doxycycline.16 The duration of treatment ranged from 3 to 36 months with study size ranging from 30 to 1,149 patients.

Effects of prophylactic antibiotics on COPD
27
2
Table 1. Characteristics of included studies.
Studies(1st author, year)
Study design Country
Patients(T/P)
Age(year)(T/P)
FEV1/FVC ratio (%)(T/P)
Prophylactic Antibiotics(dose)
Duration of treatment & follow up (months) Maintenance medication
Previous included studies
Albert, 2011 RCT US 570:572 65:66 42:43 Azithromycin, 250 mg daily 12 / 12 ICS, LABA, LAMAHe, 2010 RCT UK 18:18 68.8:69.3 46.9:48.6 Erythromycin, 125 mg, 3 times a day; 6 / 6 ICS,Mygind, 2010 RCT Denmark 287:288 71 (Median) NA Azithromycin, 500 mg daily, 3 days a month 36 / 36 ICS, Theophylline, inhaled
anticholinergic, inhaled β-adrenergic
Sethi, 2010 RCT US 569:580 66.1:66.6 45.0:46.3 Moxifloxacin, 400 mg daily, 5 days every 8 weeks
12 / 18 LABA, LAMA, SABA, SAMA, ICS, theophylline;
Seemungal, 2008 RCT UK 53:56 66.6:67.8 48.9:50.9 Erythromycin, 250 mg twice daily 12 / 12 LABA, LAMA, theophyllineBanerjee, 2005 RCT UK 31:36 65.1:68.1 43.8:45.5 Clarithromycin, 500 mg once daily 3 / 3 ICSSuzuki, 2001 RCT Japan 55:54 69.1:71.7 NA Erythromycin, 200-400 mg daily 12 / 12 Inhaled anticholinergic,
theophylline
New included studies
*Brill, 2015 RCT UK (25:25:25):24 (70.9:70.4:67.9): 68.7 (51:51:45):51 T1: Moxifloxacin, 400 mg, 5 times every 4 weeks; T2: Doxycycline, 100 mg daily; T3: Azithromycin, 250 mg, 3 times a week;
3.25 /3.25 ICS
†Shafuddin, 2015 RCT New Zealand 97:94 67.6:66.7 41.5:43.7 Roxithromycin, 300 mg daily 3 / 12 Not availableSimpson, 2014 RCT Australia 15:15 71.7:69.9 52.3:51.3 Azithromycin, 250 mg daily 3 / 6 ICSUzun, 2014 RCT Netherlands 47:45 64.7:64.9 38.0:40.3 Azithromycin, 500 mg, 3 times a week 12 / 12 LABA, LAMA, SABA, ICS,
PrednisoloneBerkhof, 2013 RCT Netherlands 42:42 67:68 42.2:43.2 Azithromycin, 250 mg, 3 times a week 3 / 4.5 LABA, LAMA, ICS
T/P: Treatment group versus Placebo group; ICS: inhaled corticosteroid; LABA: long-acting beta-2 agonists; LAMA: long-acting muscarinic antagonist; SABA: short-acting beta-2 agonists; SAMA: short-acting muscarinic antagonist; NA: data were not available; *This study designed
3 different treatment arms with one common placebo arm; †The study included 2 treatment arms, according to preset criteria, we only include the arm about single antibiotic use, the other arm in this study about combined antibiotic treatment is excluded;
Quality assessment
The review authors’ judgment about each risk of bias item in each study can be seen in Figure S1.1. The risk of bias items presented as percentage across all included studies were presented in Figure S1.2. There was no reporting bias in all included studies; only 2 studies14,16 have potential high risk in the blinding process. For the remaining of bias items, only a small proportion of unclear bias exists. Overall, low risk of bias dominates in all domains of bias.
Primary outcomes
Seven studies involving 2,642 participants11,12,17-21 reported the number of patients with exacerbations (Figure 2), which was significantly reduced (RR 0.82, 95% CI 0.74-0.90) by prophylactic antibiotics and there was no difference between continuous

Chapter 2
28
significance (p = 0.07) suggested that using antibiotics 6 months may achieve better
treatment effects (RR 0.59, 95% CI 0.40‐0.86) than longer time (RR 0.84, 95% CI 0.77‐0.93),
which requires further confirmation. The risk difference (RD) between antibiotic and placebo
Figure 2. Forest plot of risk ratio (antibiotics versus placebo) for total number of patients with
one or more exacerbations stratified by (a) schedule of prophylactic antibiotics and (b)
duration of prophylactic antibiotics. M‐H: Mantel‐Haenszel; *Studies reviewed by Herath et al.
in 2013.
Figure 2. Forest plot of risk ratio (antibiotics versus placebo) for total number of patients with one or more exacerbations stratified by (a) schedule of prophylactic antibiotics and (b) duration of prophylactic antibiotics. M-H: Mantel-Haenszel; *Studies reviewed by Herath et al. in 2013.
and intermittent subgroups. However, the difference between other subgroups with a distinct trend toward significance (p = 0.07) suggested that using antibiotics ≤ 6 months may achieve better treatment effects (RR 0.59, 95% CI 0.40-0.86) than longer time (RR 0.84, 95% CI 0.77-0.93), which requires further confirmation. The risk difference (RD) between antibiotic and placebo groups is presented in Figure 3, for erythromycin, the RD is substantial (RD -0.24, 95% CI -0.39 to -0.08), the corresponding number needed to treat (NNT) was 4; for azithromycin, the RD was moderate (RD -0.14, 95% CI -0.20 to -0.08), the NNT was 7; no statistically significant effect for moxifloxacin intervention.
Effects of prophylactic antibiotics on COPD
29
2
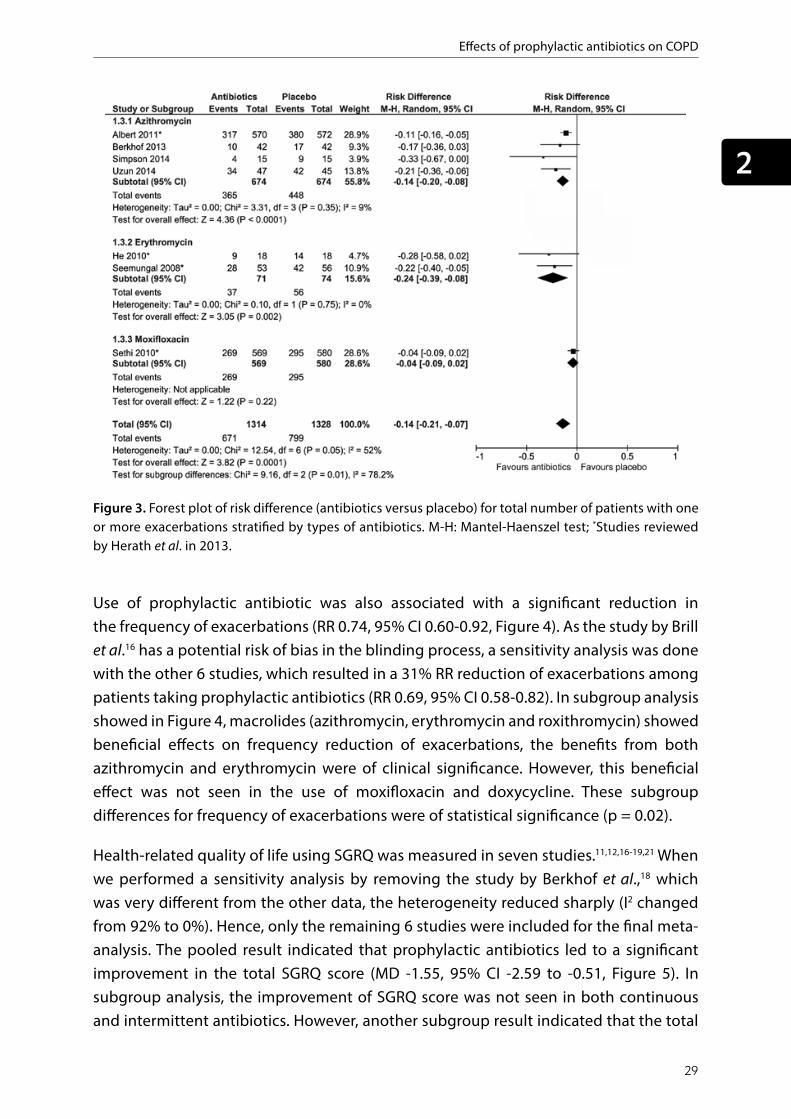
Figure 3. Forest plot of risk difference (antibiotics versus placebo) for total number of patients
with one or more exacerbations stratified by types of antibiotics. M‐H: Mantel‐Haenszel test; *Studies reviewed by Herath et al. in 2013.
groups is presented in Figure 3, for erythromycin, the RD is substantial (RD ‐0.24, 95% CI ‐0.39
to ‐0.08), the corresponding number needed to treat (NNT) was 4; for azithromycin, the RD
was moderate (RD ‐0.14, 95% CI ‐0.20 to ‐0.08), the NNT was 7; no statistically significant effect
for moxifloxacin intervention.
Use of prophylactic antibiotic was also associated with a significant reduction in the frequency
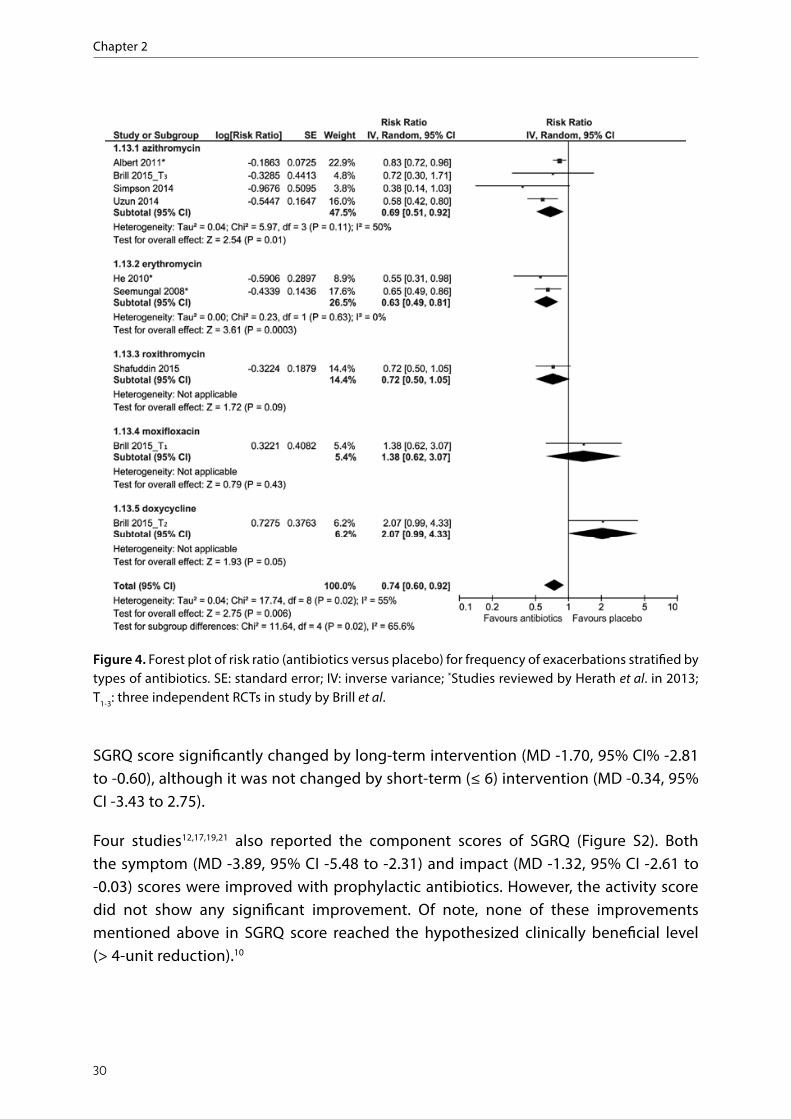
of exacerbations (RR 0.74, 95% CI 0.60‐0.92, Figure 4). As the study by Brill et al.16 has a
potential risk of bias in the blinding process, a sensitivity analysis was done with the other 6
studies, which resulted in a 31% RR reduction of exacerbations among patients taking
prophylactic antibiotics (RR 0.69, 95% CI 0.58‐0.82). In subgroup analysis showed in Figure 4,
macrolides (azithromycin, erythromycin and roxithromycin) showed beneficial effects on
frequency reduction of exacerbations, the benefits from both azithromycin and erythromycin
were of clinical significance. However, this beneficial effect was not seen in the use of
Figure 3. Forest plot of risk difference (antibiotics versus placebo) for total number of patients with one or more exacerbations stratified by types of antibiotics. M-H: Mantel-Haenszel test; *Studies reviewed by Herath et al. in 2013.
Use of prophylactic antibiotic was also associated with a significant reduction in the frequency of exacerbations (RR 0.74, 95% CI 0.60-0.92, Figure 4). As the study by Brill et al.16 has a potential risk of bias in the blinding process, a sensitivity analysis was done with the other 6 studies, which resulted in a 31% RR reduction of exacerbations among patients taking prophylactic antibiotics (RR 0.69, 95% CI 0.58-0.82). In subgroup analysis showed in Figure 4, macrolides (azithromycin, erythromycin and roxithromycin) showed beneficial effects on frequency reduction of exacerbations, the benefits from both azithromycin and erythromycin were of clinical significance. However, this beneficial effect was not seen in the use of moxifloxacin and doxycycline. These subgroup differences for frequency of exacerbations were of statistical significance (p = 0.02).
Health-related quality of life using SGRQ was measured in seven studies.11,12,16-19,21 When we performed a sensitivity analysis by removing the study by Berkhof et al.,18 which was very different from the other data, the heterogeneity reduced sharply (I2 changed from 92% to 0%). Hence, only the remaining 6 studies were included for the final meta-analysis. The pooled result indicated that prophylactic antibiotics led to a significant improvement in the total SGRQ score (MD -1.55, 95% CI -2.59 to -0.51, Figure 5). In subgroup analysis, the improvement of SGRQ score was not seen in both continuous and intermittent antibiotics. However, another subgroup result indicated that the total
Chapter 2
30
moxifloxacin and doxycycline. These subgroup differences for frequency of exacerbations
were of statistical significance (p = 0.02).
Health‐related quality of life using SGRQ was measured in seven studies.11,12,16‐19,21 When we
performed a sensitivity analysis by removing the study by Berkhof et al.,18 which was very
different from the other data, the heterogeneity reduced sharply (I2 changed from 92% to 0%).
Hence, only the remaining 6 studies were included for the final meta‐analysis. The pooled
result indicated that prophylactic antibiotics led to a significant improvement in the total
SGRQ score (MD ‐1.55, 95% CI ‐2.59 to ‐0.51, Figure 5). In subgroup analysis, the improvement
of SGRQ score was not seen in both continuous and intermittent antibiotics. However, another
Figure 4. Forest plot of risk ratio (antibiotics versus placebo) for frequency of exacerbations
stratified by types of antibiotics. SE: standard error; IV: inverse variance; *Studies reviewed by
Herath et al. in 2013; T1‐3: three independent RCTs in study by Brill et al.
Figure 4. Forest plot of risk ratio (antibiotics versus placebo) for frequency of exacerbations stratified by types of antibiotics. SE: standard error; IV: inverse variance; *Studies reviewed by Herath et al. in 2013; T1-3: three independent RCTs in study by Brill et al.
SGRQ score significantly changed by long-term intervention (MD -1.70, 95% CI% -2.81 to -0.60), although it was not changed by short-term (≤ 6) intervention (MD -0.34, 95% CI -3.43 to 2.75).
Four studies12,17,19,21 also reported the component scores of SGRQ (Figure S2). Both the symptom (MD -3.89, 95% CI -5.48 to -2.31) and impact (MD -1.32, 95% CI -2.61 to -0.03) scores were improved with prophylactic antibiotics. However, the activity score did not show any significant improvement. Of note, none of these improvements mentioned above in SGRQ score reached the hypothesized clinically beneficial level (> 4-unit reduction).10

Effects of prophylactic antibiotics on COPD
31
2
Secondary outcomes
Seven studies involving 2,803 patients reported the median time to first exacerbation (Table S3). Four studies indicated that using prophylactic antibiotics lengthened the median time to first exacerbation signficantly.12,17,19,20 Two other studies found a similar trend, but without statistical significance.18,21 Only one study showed the opposite result in antibiotic and placebo arms.22
Figure 5. Forest plot of mean difference (antibiotics versus placebo) of quality of life by SGRQ stratified by (a) schedule of prophylactic antibiotics and (b) duration of prophylactic antibiotics. SGRQ: St Georges Respiratory Questionnaire; IV: inverse variance; SE: standard error; *Studies reviewed by Herath et al. in 2013; T1-3: three independent RCTs in study by Brill et al.
Figure 5. Forest plot of mean difference (antibiotics versus placebo) of quality of life by SGRQ
stratified by (a) schedule of prophylactic antibiotics and (b) duration of prophylactic
antibiotics. SGRQ: St Georges Respiratory Questionnaire; IV: inverse variance; SE: standard
error; *Studies reviewed by Herath et al. in 2013; T1‐3: three independent RCTs in study by Brill
et al.
subgroup result indicated that the total SGRQ score significantly changed by long‐term
intervention (MD ‐1.70, 95% CI% ‐2.81 to ‐0.60), although it was not changed by short‐term (
6) intervention (MD ‐0.34, 95% CI ‐3.43 to 2.75).

Chapter 2
32
Figure 7. Forest plot of risk ratio (antibiotics versus placebo) for adverse events. M‐H: Mantel‐
Haenszel test; *Studies reviewed by Herath et al. in 2013.
show significant difference between two arms (RR 0.93, 95% CI 0.83‐1.05, I2 = 2%). In
subgroups, gastrointestinal disorders were more frequent in the intervention group than
control group (RR 1.87, 95 CI 0.98‐3.59, Figure S4) with a boundary statistical significance (p =
0.06). However, no statistical significant difference for respiratory and cardiovascular
disorders were found.
Eight studies had the bacteriological assessments (see Table S4),12,15‐21 however, only three
studies with five RCTs reported the quantitative results for antibiotic resistance.16,17,19 Due to
the different definition about bacterial resistant outcome in study by Uzun et al, only the other
homogeneous studies involving four RCTs were included for pooled results (OR 4.49, 95% CI
2.48‐8.12, Figure 8), long‐term (versus short‐term) and continuous (versus intermittent)
antibiotic intervention seems to cause more antibiotic resistance, although these subgroup
difference did not reach statistical significant level. Antibiotic resistance appeared in all types
of antibiotics involved (Figure 9), although the result from moxifloxacin did not reach
statistical significance. No subgroup differences about this outcome were seen among
azithromycin, moxifloxacin and doxycycline (p = 0.63).
Eight studies11,13,16‐18,20‐22 provided the data on changes of lung function (Table S5). However,
no study found significant increase by antibiotic intervention compared with placebo. Mygind
et al. did not compare the lung function change directly, but measured and compared the lung
function in both groups at enrolment and endpoint separately, they also did not find any
significant difference.13
Figure 6. Forest plot of risk ratio (antibiotics versus placebo) for frequency of hospitalization. M-H: Mantel-Haenszel test; *Studies reviewed by Herath et al. in 2013.
Four studies12,17,19,21 also reported the component scores of SGRQ (Figure S2). Both the
symptom (MD ‐3.89, 95% CI ‐5.48 to ‐2.31) and impact (MD ‐1.32, 95% CI ‐2.61 to ‐0.03) scores
were improved with prophylactic antibiotics. However, the activity score did not show any
significant improvement. Of note, none of these improvements mentioned above in SGRQ
score reached the hypothesized clinically beneficial level (> 4‐unit reduction).10
Secondary outcomes
Seven studies involving 2,803 patients reported the median time to first exacerbation (Table
S3). Four studies indicated that using prophylactic antibiotics lengthened the median time to
first exacerbation signficantly.12,17,19,20 Two other studies found a similar trend, but without
statistical significance.18,21 Only one study showed the opposite result in antibiotic and placebo
arms.22
The frequency of hospitalization related to COPD was pooled from five studies with 2,576
participants,17‐21 no significant difference was observed between antibiotic and placebo
groups (RR 0.94, 95% CI 0.83‐1.06, Figure 6). Also, no difference in the rate of all‐cause
mortality were found between the two arms (Figure S3).
Eight studies involving 2,833 participants reported adverse events related to antibiotic
use.11,12,17‐22 Overall, there was no significant difference between two comparison arms in the
rate of adverse events (RR 1.09, 95% CI 0.84‐1.42, Figure 7). As there was a lack of uniform
definition about adverse events, the heterogeneity was substantial (I2 = 73%). Considering that
the result by Shafuddin et al.22 was deviant from the other seven studies, a sensitivity analysis
was, therefore, performed after removal of this study. The homogeneous result also did not
Figure 6. Forest plot of risk ratio (antibiotics versus placebo) for frequency of hospitalization.
M‐H: Mantel‐Haenszel test; *Studies reviewed by Herath et al. in 2013.
Figure 7. Forest plot of risk ratio (antibiotics versus placebo) for adverse events. M-H: Mantel-Haenszel test; *Studies reviewed by Herath et al. in 2013.
The frequency of hospitalization related to COPD was pooled from five studies with 2,576 participants,17-21 no significant difference was observed between antibiotic and placebo groups (RR 0.94, 95% CI 0.83-1.06, Figure 6). Also, no difference in the rate of all-cause mortality were found between the two arms (Figure S3).
Eight studies involving 2,833 participants reported adverse events related to antibiotic use.11,12,17-22 Overall, there was no significant difference between two comparison arms in the rate of adverse events (RR 1.09, 95% CI 0.84-1.42, Figure 7). As there was a lack of uniform definition about adverse events, the heterogeneity was substantial (I2 = 73%). Considering that the result by Shafuddin et al.22 was deviant from the other seven studies, a sensitivity analysis was, therefore, performed after removal of this study. The homogeneous result also did not show significant difference between two arms (RR 0.93, 95% CI 0.83-1.05, I2 = 2%). In subgroups, gastrointestinal disorders were more frequent in the intervention group than control group (RR 1.87, 95 CI 0.98-3.59,

Effects of prophylactic antibiotics on COPD
33
2
Three studies reported the change of bacterial load.11,15,16 Although both Brill et al. and
Simpson et al. have found the more reduction of bacterial load by prophylactic antibiotic
compared with placebo, the results did not reach the level of statistical significance, even both
quantitative culture and 16S qPCR methods were used by Brill et al. Benerjee et al. also did
not find a significant difference between pre‐and post‐ sputum cfu numbers/bacterial (PPM)
isolates in two arms.
Figure 8. Forest plot of odds ratio (antibiotics versus placebo) for antibiotic resistance
stratified by (a) schedule of prophylactic antibiotics and (b) duration of prophylactic
antibiotics. IV: inverse variance; *Studies reviewed by Herath et al. in 2013; T1‐3: three
independent RCTs in study by Brill et al.
Figure 8. Forest plot of odds ratio (antibiotics versus placebo) for antibiotic resistance stratified by (a) schedule of prophylactic antibiotics and (b) duration of prophylactic antibiotics. IV: inverse variance; *Studies reviewed by Herath et al. in 2013; T1-3: three independent RCTs in study by Brill et al.
Figure S4) with a boundary statistical significance (p = 0.06). However, no statistical significant difference for respiratory and cardiovascular disorders were found.
Eight studies had the bacteriological assessments (see Table S4),12,15-21 however, only three studies with five RCTs reported the quantitative results for antibiotic resistance.16,17,19 Due to the different definition about bacterial resistant outcome in study by Uzun et al, only the other homogeneous studies involving four RCTs were included for pooled results (OR 4.49, 95% CI 2.48-8.12, Figure 8), long-term (versus short-term) and continuous (versus intermittent) antibiotic intervention seems to cause more antibiotic resistance, although these subgroup difference did not reach statistical significant level. Antibiotic resistance appeared in all types of antibiotics involved (Figure 9), although the result

Chapter 2
34
Figure 9: Forest plot of odds ratio (antibiotics versus placebo) for antibiotic resistance
stratified by types of antibiotics. SE: standard error; IV: inverse variance; *Studies reviewed by
Herath et al. in 2013; T1‐3: three independent RCTs in study by Brill et al.
The change of airway inflammation was only reported in two studies.11,16 The study by Brill et
al. showed that no significant changes were seen in cytokines IL‐6, IL‐8 and IL‐1 in any of
three antibiotic arms compared with placebo.16 Similarly, Simpson et al. also did not report a
significant reduction in sputum neutrophil proportion level of IL‐8 in those who received
azithromycin compared to placebo group.11
Figure 9. Forest plot of odds ratio (antibiotics versus placebo) for antibiotic resistance stratified by types of antibiotics. SE: standard error; IV: inverse variance; *Studies reviewed by Herath et al. in 2013; T1-3: three independent RCTs in study by Brill et al.
from moxifloxacin did not reach statistical significance. No subgroup differences about this outcome were seen among azithromycin, moxifloxacin and doxycycline (p = 0.63).
Eight studies11,13,16-18,20-22 provided the data on changes of lung function (Table S5). However, no study found significant increase by antibiotic intervention compared with placebo. Mygind et al. did not compare the lung function change directly, but measured and compared the lung function in both groups at enrolment and endpoint separately, they also did not find any significant difference.13
Three studies reported the change of bacterial load.11,15,16 Although both Brill et al. and Simpson et al. have found the more reduction of bacterial load by prophylactic antibiotic compared with placebo, the results did not reach the level of statistical significance, even both quantitative culture and 16S qPCR methods were used by Brill et al. Benerjee et al. also did not find a significant difference between pre-and post- sputum cfu numbers/bacterial (PPM) isolates in two arms.
The change of airway inflammation was only reported in two studies.11,16 The study by Brill et al. showed that no significant changes were seen in cytokines IL-6, IL-8 and IL-1β in any of three antibiotic arms compared with placebo.16 Similarly, Simpson et al. also did not report a significant reduction in sputum neutrophil proportion level of IL-8 in those who received azithromycin compared to placebo group.11

Effects of prophylactic antibiotics on COPD
35
2
DISCUSSIONThis update of previous systematic reviews demonstrates that prophylactic antibiotic use could significantly lower the risk of exacerbations by 26% and prevent stable COPD patients from getting exacerbations by 18%, which is consistent with the result by Herath et al.,6 but the difference is that our review with more RCTs suggest that intermittent antibiotics may also be effective in preventing exacerbations, although the result is of boundary significance. Moreover, in contrast with the result by Ni et al.,7 we found both short-term (≤ 6 months) and long-term (> 6 months) treatments can prevent patients from exacerbations significantly. A short-term treatment even had better prevention effects than long-term treatment. Considering all included patients are clinically stable without exacerbation before enrolment, the above benefit from short therapy is likely due to the benefits of less resistance and adverse events or shorter follow-up time to detect related exacerbations compared with long therapy.
Besides duration and schedule of antibiotics, the types of antibiotics also have a profound influence on preventing exacerbations of COPD. In our pre-specified subgroup analysis, we did not find significant effect from moxifloxacin and doxycycline intervention on preventing exacerbations, although a previous study showed moxifloxacin is equivalent and bacteriologically superior to other antibiotic regimens routinely used.23 However, our results confirmed the superiority of macrolides (azithromycin, erythromycin) in preventing exacerbations of COPD. This benefit of macrolides has also been confirmed previously in patients with cystic fibrosis and non-cystic fibrosis bronchiectasis.24,25
Although the optimal treatment using macrolide for preventing exacerbation was already conditional recommended by related guidelines,1,9 the mechanisms behind are not totally clear.8 Many studies have confirmed that macrolides with 14 and 15-membered macrocyclic lactone ring have properties such as anti-inflammatory, anti-viral and potential immune-modulation,26 which were proved to be beneficial for COPD patients.27 Therefore, some researchers hypothesized that prevention of exacerbation by macrolides may due to its antimicrobial effects or anti-inflammatory effects or both. However, neither of the above mechanisms could be supported by evidence in our review,11,15,16,20 More studies are needed in future to explore the answers to this question.
Regarding the health-related quality of life, our review showed a significant reduction in the total score of SGRQ with no heterogeneity. This is consistent with the association study by Martin et al.28 From our study, duration longer than 6 months of antibiotic intervention can significantly improve the total score of SGRQ. As the health-related quality of life is influenced largely by the frequency of exacerbations in COPD patients,29 it will be an ideal therapy if both the exacerbation and quality of life change towards the same positive direction. Our subgroup analysis in both exacerbation and quality of life showed the positive results in longer duration (above 6 months) of prophylactic

Chapter 2
36
antibiotics. However, as the improvements of total SGRQ score did not reach a clinical significant level, further research were still in need to explore the influence of prophylactic antibiotic use on quality of life in the real world.
The benefits achieved by prophylactic antibiotics always came at the expense of a variety of adverse events according to the earlier reviewers.30 However, we did not find significant differences in the overall rate of adverse events between antibiotic and placebo arms. It is worth noting that the heterogeneity was substantial due to the variety of definition and measurement methods, thus much consistent definition is needed for future study. Furthermore, much attention should be given to the gastrointestinal disorder by antibiotic use as this disorder was also observed in patients with cystic fibrosis.24 Although not established as an endpoint in our review, hearing loss caused by azithromycin also should draw much attention.19
Along the use of prophylactic antibiotics, another growing concern regarding the development of antibiotic resistance also appears. In this review, the increased resistant isolates were seen during the intervention of prophylactic antibiotics, which involved macrolides (azithromycin), tetracycline (doxycycline), and quinolones (moxifloxacin).16,19 At the same time, as lots of conflicting reports existed with heterogeneous definitions,15,17,18,20,21 much related evidence from studies of uniform criteria is needed for further exploration. Before that, clinicians should pay much attention especially to long and continuous use of antibiotics considering potential risk of bacterial resistance for future treatment of infections.4 Furthermore, although the use of macrolides in preventing exacerbations was considered as a cost-effective strategy31, the rather quick bacterial resistance induced by macrolides should not be ignored.32 Its use should at best be limited to high-risk populations based on consideration of age, exacerbation frequency in previous year, COPD severity and comorbidity conditions. The choice of antibiotics should be based on the community resistant pattern and their benefits and potential risks must be weighted by analysing the specific situation case by case.
Although the obvious benefits of antibiotics in prevention of exacerbations, we did not find any reduction in the rate of hospital admission by antibiotic intervention, which are in contrast with the result by Donath et al.33 Moreover, as hospitalization for exacerbation is always associated with poor prognosis and increased mortality in COPD patients,34 there was also no difference in the rate of all-cause mortality between antibiotic and placebo groups. Besides, the lung function was not improved in any of the included studies after the antibiotic intervention. There is still no conclusive clinical trial evidence up to now that any existing medication for COPD could modify the long-term decline in lung function.1

Effects of prophylactic antibiotics on COPD
37
2
Study limitations and future perspectives
There were several limitations in this review. Firstly, there were some notable heterogeneous results between studies. On the one hand, due to limited information available, we could not totally analysis and exclude the influence of potential difference in distribution of baseline characteristics especially like COPD severity, exacerbation history and bacterial colonization on outcomes, although all included patients were relative stable with similar COPD severity (GOLD 2-4). On the other hand, heterogeneity also existed between antibiotic therapies, as regimen, dosages, durations and follow-up time of antibiotic intervention were different. Secondly, the included patients may concomitantly take other therapies such as influenza vaccines, bronchodilators or inhaled corticosteroid, which could also have a potential impact on related outcomes if these factors are not comparable between antibiotic and placebo groups. For example, LABA/LAMA combination as a maintenance therapy of COPD could reduce the rate of exacerbation.35,36 Thirdly, the definitions and measurements of some outcomes were different, like the varying definitions of adverse events and varying methods for identifying antibiotic resistance. Finally, due to limited studies included, we could not evaluate the effects of the different doses of a specific antibiotic on COPD patients.
In the future, more RCTs of high quality are needed to explore a more personalized therapy by studying the optimal dose, duration and schedule of specific antibiotic use, preferably macrolides, with therapeutic drug monitoring on more homogenous COPD patients. Besides, uniform standards for evaluating the effects of antibiotic use should be made. Considering the safety of antibiotics, how to avoid or reduce the side effects such as gastrointestinal events and bacterial resistance during long-term use of antibiotic is still a problem that needs to be tackled.
CONCLUSIONSThis updated systematic review confirms the benefit of prophylactic antibiotics in preventing exacerbations in stable patients with moderate to severe COPD, this benefit existed in all subgroups ignoring the different duration and schedules of antibiotic intervention. The overall quality of life was also significantly increased by prophylactic antibiotics. However, this benefit was only observed in long-term (above 6 months) subgroup of antibiotics. At the same time, considering the possible risk of bacterial resistance, long-term and continuous prophylactic antibiotics are at best limited to high risk of population with severe COPD and history of frequent exacerbations and the choice of antibiotic should be based on local bacterial resistance pattern. Furthermore, much attention should be paid to some adverse effects like gastrointestinal disorders and hearing loss.

Chapter 2
38
SUPPLEMENTARY MATERIALSTable S1-S5 and Figures S1-S4 are available as Supplementary data at JAC Online (https://doi.org/10.1093/jac/dky326)

Effects of prophylactic antibiotics on COPD
39
2
REFERENCES 1. Global Strategy for the Diagnosis,
Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2017. Available from: http://goldcopd.org.
2. Lopez AD, Shibuya K, Rao C, et al. Chronic obstructive pulmonary disease: current burden and future projections. Eur Respir J. 2006;27(2):397-412.
3. Wedzicha JA, Seemungal TAR. COPD exacerbations: defining their cause and prevention. Lancet. 2007;370(9589):786-796.
4. Sethi S, Murphy TF. Infection in the pathogenesis and course of chronic obstructive pulmonary disease. N Engl J Med. 2008;359(22):2355-2365.
5. Staykova T, Black PN, Chacko EE, Poole P. Prophylactic antibiotic therapy for chronic bronchitis. Cochrane Database Syst Rev. 2003(1):CD004105.
6. Herath SC, Poole P. Prophylactic antibiotic therapy for chronic obstructive pulmonary disease (COPD). Cochrane Database Syst Rev. 2013(11):CD009764.
7. Ni W, Shao X, Cai X, et al. Prophylactic use of macrolide antibiotics for the prevention of chronic obstructive pulmonary disease exacerbation: a meta-analysis. Plos One. 2015;10(3):e0121257.
8. Cameron EJ, McSharry C, Chaudhuri R, Farrow S, Thomson NC. Long-term macrolide treatment of chronic inflammatory airway diseases: risks, benefits and future developments. Clin Exp Allergy. 2012;42(9):1302-1312.
9. Wedzicha JA, Calverley PMA, Albert RK, et al. Prevention of COPD exacerbations: a European Respiratory Society/American Thoracic Society guideline. Eur Respir J. 2017;50(3):1602265.
10. Jones P. St George’s Respiratory Questionnaire Manual. Version 2.3. 2009: 1-6.
11. Simpson JL, Powell H, Baines KJ, et al. The effect of azithromycin in adults with
stable neutrophilic COPD: a double blind randomised, placebo controlled trial. Plos One. 2014;9(8):e105609.
12. He ZY, Ou LM, Zhang JQ, et al. Effect of 6 months of erythromycin treatment on inflammatory cells in induced sputum and exacerbations in chronic obstructive pulmonary disease. Respiration. 2010;80(6):445-452.
13. Mygind LH, Pedersen C, Vestbo J et al. A randomized, placebo-controlled 3 years study of prophylactic azithromycin in 575 patients with chronic obstructive pulmonary disease (COPD). Abstract 36 Suppl 54: 1018s. In: Abstracts of the European Respiratory Society Annual Congress, Barcelona, Spain, 2010. European Respiratory Society.
14. Suzuki T, Yanai M, Yamaya M, et al. Erythromycin and common cold in COPD. Chest. 2001;120(3):730-733.
15. Banerjee D, Khair OA, Honeybourne D. The effect of oral clarithromycin on health status and sputum bacteriology in stable COPD. Respir Med. 2005;99(2):208-215.
16. Brill SE, Law M, El-Emir E, et al. Effects of different antibiotic classes on airway bacteria in stable COPD using culture and molecular techniques: a randomised controlled trial. Thorax. 2015;70(10):930-938.
17. Uzun S, Djamin RS, Kluytmans JA, et al. Azithromycin maintenance treatment in patients with frequent exacerbations of chronic obstructive pulmonary disease (COLUMBUS): a randomised, double-blind, placebo-controlled trial. Lancet Respir Med. 2014;2(5):361-368.
18. Berkhof FF, Doornewaard-ten Hertog NE, Uil SM, Kerstjens HA, van den Berg JW. Azithromycin and cough-specific health status in patients with chronic obstructive pulmonary disease and chronic cough: a randomised controlled trial. Respir Res. 2013;14:125.
19. Albert RK, Connett J, Bailey WC, et al. Azithromycin for prevention of exacerbations of COPD. N Engl J Med. 2011;365(8):689-698.

Chapter 2
40
20. Seemungal TA, Wilkinson TM, Hurst JR, Perera WR, Sapsford RJ, Wedzicha JA. Long-term erythromycin therapy is associated with decreased chronic obstructive pulmonary disease exacerbations. Am J Respir Crit Care Med. 2008;178(11):1139-1147.
21. Sethi S, Jones PW, Theron MS, et al. Pulsed moxifloxacin for the prevention of exacerbations of chronic obstructive pulmonary disease: a randomized controlled trial. Respir Res. 2010;11:10.
22. Shafuddin E, Mills GD, Holmes MD, Poole PJ, Mullins PR, Black PN. A double-blind, randomised, placebo-controlled study of roxithromycin and doxycycline combination, roxithromycin alone, or matching placebo for 12 weeks in adults with frequent exacerbations of chronic obstructive pulmonary disease. J Negat Results Biomed. 2015;14:15.
23. Liu KX, Xu B, Wang J, et al. Efficacy and safety of moxifloxacin in acute exacerbations of chronic bronchitis and COPD: a systematic review and meta-analysis. J Thorac Dis. 2014;6(3):221-229.
24. Florescu DF, Murphy PJ, Kalil AC. Effects of prolonged use of azithromycin in patients with cystic fibrosis: a meta-analysis. Pulm Pharmacol Ther. 2009;22(6):467-472.
25. Figueiredo Bde C, Ibiapina Cda C. The role of macrolides in noncystic fibrosis bronchiectasis. Pulm Med. 2011;2011:751982.
26. Rubin BK. Immunomodulatory properties of macrolides: overview and historical perspective. Am J Med. 2004;117 Suppl 9A:2S-4S.
27. Martinez FJ, Curtis JL, Albert R. Role of macrolide therapy in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2008;3(3):331-350.
28. Martin AL, Marvel J, Fahrbach K, Cadarette SM, Wilcox TK, Donohue JF. The association of lung function and St. George’s respiratory questionnaire with exacerbations in
COPD: a systematic literature review and regression analysis. Respir Res. 2016;17:40.
29. Miravitlles M, Ferrer M, Pont A, et al. Effect of exacerbations on quality of life in patients with chronic obstructive pulmonary disease: a 2 year follow up study. Thorax. 2004;59(5):387-395.
30. Yamaya M, Azuma A, Takizawa H, Kadota J, Tamaoki J, Kudoh S. Macrolide effects on the prevention of COPD exacerbations. Eur Respir J. 2012;40(2):485-494.
31. Simoens S, Laekeman G, Decramer M. Preventing COPD exacerbations with macrolides: a review and budget impact analysis. Respir Med. 2013;107(5):637-648.
32. Serisier DJ. Risks of population antimicrobial resistance associated with chronic macrolide use for inflammatory airway diseases. Lancet Resp Med. 2013;1(3):262-274.
33. Donath E, Chaudhry A, Hernandez-Aya LF, Lit L. A meta-analysis on the prophylactic use of macrolide antibiotics for the prevention of disease exacerbations in patients with Chronic Obstructive Pulmonary Disease. Respir Med. 2013;107(9):1385-1392.
34. Soler-Cataluna JJ, Martinez-Garcia MA, Roman Sanchez P, Salcedo E, Navarro M, Ochando R. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60(11):925-931.
35. Wedzicha JA, Decramer M, Ficker JH, et al. Analysis of chronic obstructive pulmonary disease exacerbations with the dual bronchodilator QVA149 compared with glycopyrronium and tiotropium (SPARK): a randomised, double-blind, parallel-group study. Lancet Respir Med. 2013;1(3):199-209.
36. Wedzicha JA, Banerji D, Chapman KR, et al. Indacaterol-Glycopyrronium versus Salmeterol-Fluticasone for COPD. N Engl J Med. 2016;374(23):2222-2234.

C H A P T E R 3
Yuanyuan Wang Jens H. Bos
H. Marike Boezen Jan-Willem C. Alffenaar
Job F.M. van Boven Catharina C.M. Schuiling-Veninga
Bob Wilffert Eelko Hak
The influence of age on real-life effects of doxycycline for acute exacerbations among COPD outpatients:
a population-based cohort study
Publisher as: Wang Y, Bos JH, Boezen HM, et al. Influence of age on real-life effects of doxycycline for acute exacerbations among COPD outpatients:
a population-based cohort study. BMJ Open Respiratory Research 2020;7:e000535. doi: 10.1136/bmjresp-2019-000535.
Chapter 3
44
ABSTRACTIntroduction
Although bacteria contribute significantly to acute exacerbations of COPD (AECOPD), the added value of antibiotics remains controversial, especially in outpatient settings. Age may affect antibiotic effectiveness, but real-world evidence is lacking. We aimed to assess the influence of age on the effectiveness of doxycycline for AECOPD.
Methods
A retrospective cohort study among outpatients with the first recorded AECOPD treated with oral corticosteroids was conducted using a large pharmacy dispensing database. The primary outcome was treatment failure within 15 to 31 days after treatment start. Secondary outcome was time to second exacerbation. All analyses were stratified by age groups.
Results
We identified 6300 outpatients with the first AECOPD. 2261 (36%) received doxycycline and 4039 (64%) did not receive any antibiotic (reference group). Overall, there was no difference in treatment failure (adjusted OR 0.97, 95% CI 0.84 to 1.12) between two groups. Similarly, no difference in treatment failure was observed in younger groups. However, in patients with advanced age (≥ 75 years), treatment failure was significantly reduced by doxycycline compared with reference (16% vs 20%, adjusted OR 0.77, 95% CI 0.62 to 0.97). Overall, median time to second exacerbation was 169 days (95% CI 158 to 182 days) in doxycycline group compared with 180 days (95% CI 169 to 191 days) in reference group (adjusted HR 1.06, 95% CI 0.99 to 1.12), Although in older patients there was a trend within 3 months towards longer time of next exacerbation by doxycycline, it did not achieve statistical significance.
Conclusions
Our findings showed short-term treatment benefit of doxycycline added to oral corticosteroids for COPD patients with advanced age. This value remains unclear for persons aged under 75 years in current primary care. Long-term preventive benefits of doxycycline for the next exacerbation were not observed, irrespective of age.

Age Influence on Effects of Doxycycline for AECOPD
45
3
INTRODUCTIONChronic obstructive pulmonary disease (COPD) is a chronic, progressive, inflammatory disease and a leading cause of death worldwide.1 Acute exacerbations of COPD (AECOPD) characterized by the sudden worsening of respiratory symptoms may accelerate the progress of COPD and contribute significantly to worsened patients’ health status, mortality and medical costs.2,3 As about 50% of AECOPD are triggered by bacterial infections,4 the use of antibiotics has become a common component in the therapeutic management of AECOPD.5,6
The evidence on the benefits of oral corticosteroids for AECOPD is of high quality.6,7 However, the effects of antibiotics in addition to corticosteroids are still uncertain, especially in an outpatient setting. A Cochrane review in 2012 did not show a significant reduced risk of treatment failure by antibiotics.8 Although treatment guidelines in 2017 conditionally recommended antibiotics for AECOPD among outpatients,6 this recommendation was based on synthesized evidence from only two earlier RCTs.9,10 In the same year, a new large RCT concluded that antibiotics for AECOPD in an outpatient setting are not effective.11 Later in 2018, an updated Cochrane review included two more RCTs than in 201211,12 and showed statistically significant beneficial effects of antibiotics.13 Of note, while most RCTs focused on the short-term effect of antibiotics, the long-term effect in outpatient settings also remains unclear due to conflicting results.11,14,15
The majority of AECOPD is treated in primary care and establishing a bacterial infection diagnosis with sputum cultures is not always feasible in routine practice due to technical reasons.5,16 Therefore, accurate prescribing of antibiotics according to guidelines is still low.17-19 Notably, many studies indicate that the susceptibility to infections increases with age.20,21 According to a large population-based observational study, the protective effect of antibiotics against pneumonia is more pronounced in older patients.22 23 Thus, we hypothesized that older patients may benefit more from empirical antibiotic treatment for AECOPD than younger patients.
In addition to prednisone or prednisolone, doxycycline is one of the first-choice oral antibiotics for AECOPD if antibiotic treatment is indicated.24 5,16 Since only one RCT studied doxycycline, we conducted a cohort study to evaluate if doxycycline has meaningful value added to oral corticosteroids on AECOPD in both the short- and longer-term for outpatients, and examined the potential effect modification across age groups.
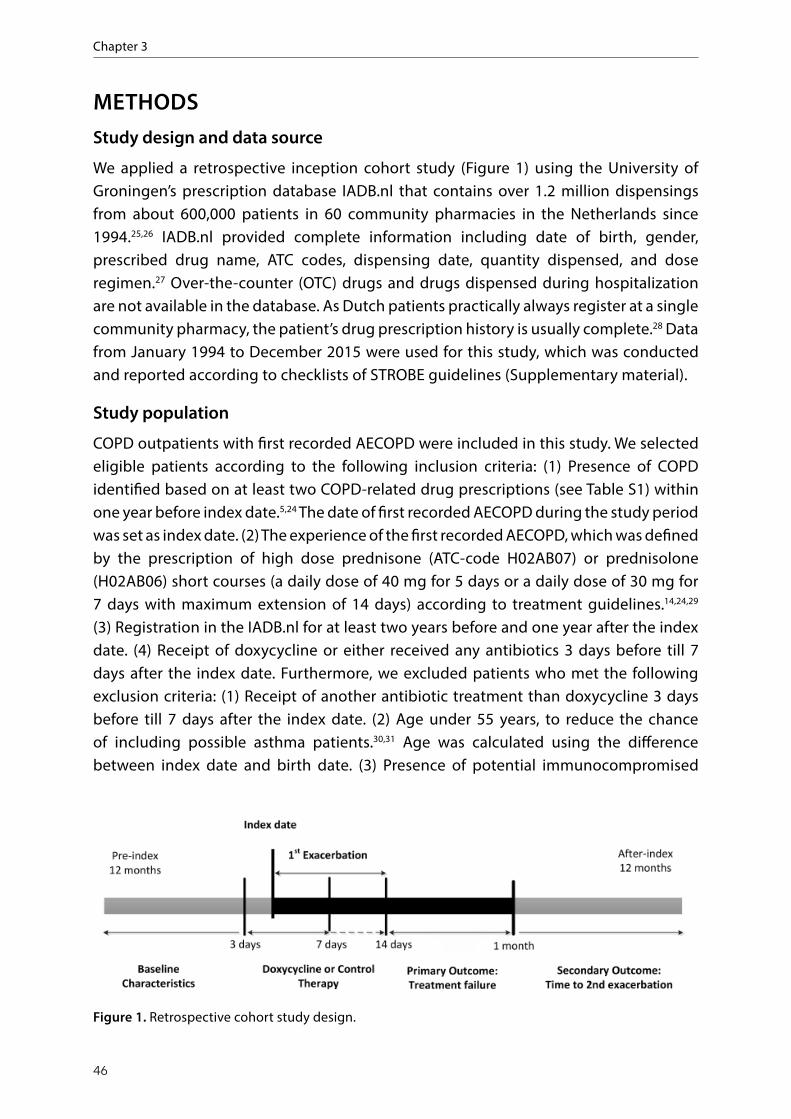
Chapter 3
46
METHODSStudy design and data source
We applied a retrospective inception cohort study (Figure 1) using the University of Groningen’s prescription database IADB.nl that contains over 1.2 million dispensings from about 600,000 patients in 60 community pharmacies in the Netherlands since 1994.25,26 IADB.nl provided complete information including date of birth, gender, prescribed drug name, ATC codes, dispensing date, quantity dispensed, and dose regimen.27 Over-the-counter (OTC) drugs and drugs dispensed during hospitalization are not available in the database. As Dutch patients practically always register at a single community pharmacy, the patient’s drug prescription history is usually complete.28 Data from January 1994 to December 2015 were used for this study, which was conducted and reported according to checklists of STROBE guidelines (Supplementary material).
Study population
COPD outpatients with first recorded AECOPD were included in this study. We selected eligible patients according to the following inclusion criteria: (1) Presence of COPD identified based on at least two COPD-related drug prescriptions (see Table S1) within one year before index date.5,24 The date of first recorded AECOPD during the study period was set as index date. (2) The experience of the first recorded AECOPD, which was defined by the prescription of high dose prednisone (ATC-code H02AB07) or prednisolone (H02AB06) short courses (a daily dose of 40 mg for 5 days or a daily dose of 30 mg for 7 days with maximum extension of 14 days) according to treatment guidelines.14,24,29 (3) Registration in the IADB.nl for at least two years before and one year after the index date. (4) Receipt of doxycycline or either received any antibiotics 3 days before till 7 days after the index date. Furthermore, we excluded patients who met the following exclusion criteria: (1) Receipt of another antibiotic treatment than doxycycline 3 days before till 7 days after the index date. (2) Age under 55 years, to reduce the chance of including possible asthma patients.30,31 Age was calculated using the difference between index date and birth date. (3) Presence of potential immunocompromised
corticosteroids on AECOPD in both the short‐ and longer‐term for outpatients, and examined the
potential effect modification across age groups.
Methods
Study design and data source
We applied a retrospective inception cohort study (Figure 1) using the University of Groningen’s
prescription database IADB.nl that contains over 1.2 million dispensings from about 600,000
patients in 60 community pharmacies in the Netherlands since 1994.25,26 IADB.nl provided
complete information including date of birth, gender, prescribed drug name, ATC codes,
dispensing date, quantity dispensed, and dose regimen.27 Over‐the‐counter (OTC) drugs and
drugs dispensed during hospitalization are not available in the database. As Dutch patients
practically always register at a single community pharmacy, the patient's drug prescription history
is usually complete.28 Data from January 1994 to December 2015 were used for this study, which
was conducted and reported according to checklists of STROBE guidelines (Supplementary
material).
Figure 1. Retrospective cohort study design.
Study population
COPD outpatients with first recorded AECOPD were included in this study. We selected eligible
patients according to the following inclusion criteria: (1) Presence of COPD identified based on at
least two COPD‐related drug prescriptions (see Table S1) within one year before index date.5,24
The date of first recorded AECOPD during the study period was set as index date. (2) The
Figure 1. Retrospective cohort study design.

Age Influence on Effects of Doxycycline for AECOPD
47
3
diseases, which were defined by the prescription of antiviral drugs for HIV infection, immunosuppressant drugs or antineoplastic agents within one year before index date and one month after index date.
Exposure and outcomes
Among patients with a first identified AECOPD, during their treatment period of oral prednisone or prednisolone (3 days before till 7 days after the index date), those who were also prescribed doxycycline and no other antibiotics were classified as treatment exposure group. Those who did not receive doxycycline (or any other antibiotic) were classified as reference group. The primary outcome was treatment failure defined as a new prescription of prednisone or prednisolone or an antibiotic treatment within a period of 15 to 31 days after index date according to Dutch NHG guidelines for COPD management. Secondary outcome was time to the second exacerbation within a follow-up period of 12 months. As the first exacerbation may last for a longer time, and to avoid counting it as second exacerbation, we limited the minimum time from first exacerbation to second one to 21 days.32 A few patients could be included in the treatment failure outcome and the second exacerbation outcome if the drugs appeared within 21 and 31 days after index date.
Covariates
The following covariates were included as potential confounders: age; gender; frequently used maintenance drugs for COPD treatment within 365 days before index date including SABA, SAMA, LABA, LAMA, SABA/SAMA, LABA/LAMA, LABA/ICS and theophylline. Comorbidities in COPD patients were defined on the basis of at least two prescriptions of related drugs within 365 days prior to index date: diabetes (A10), heart failure (C01AA05 or C03C), ischemic heart disease (C01DA), other cardiovascular disease (C02 or C03 or C07 or C08 or C09, but not for C01AA05, C03C and C01DA), dyslipidaemia (C10), osteoporosis (M05B), anxiety (N05B, N05C), dementia (N06D), depression (N06A), rheumatic arthritis (M01 or M02), hypothyroid disease (H03).30
Statistical methods
The differences in distribution of baseline characteristics of COPD outpatients between two exposure groups were compared using t-test and Chi-square test for continuous and categorical variables, respectively. We applied logistic regression to estimate the odds ratio (OR) with 95% confidence interval (CI) for treatment failure and adjusted for possible covariates. The time to second exacerbation was compared by Kaplan-Meier survival analysis. Cox proportional hazards regression was applied to estimate the hazard ratio (HR) and 95% CI for risk of second exacerbation. For all tests, p-values were 2-sided. A p-value < 0.05 was considered statistically significant. All analyses were performed using IBM SPSS statistics 22 (IBM Corp., Armonk, NY, USA).
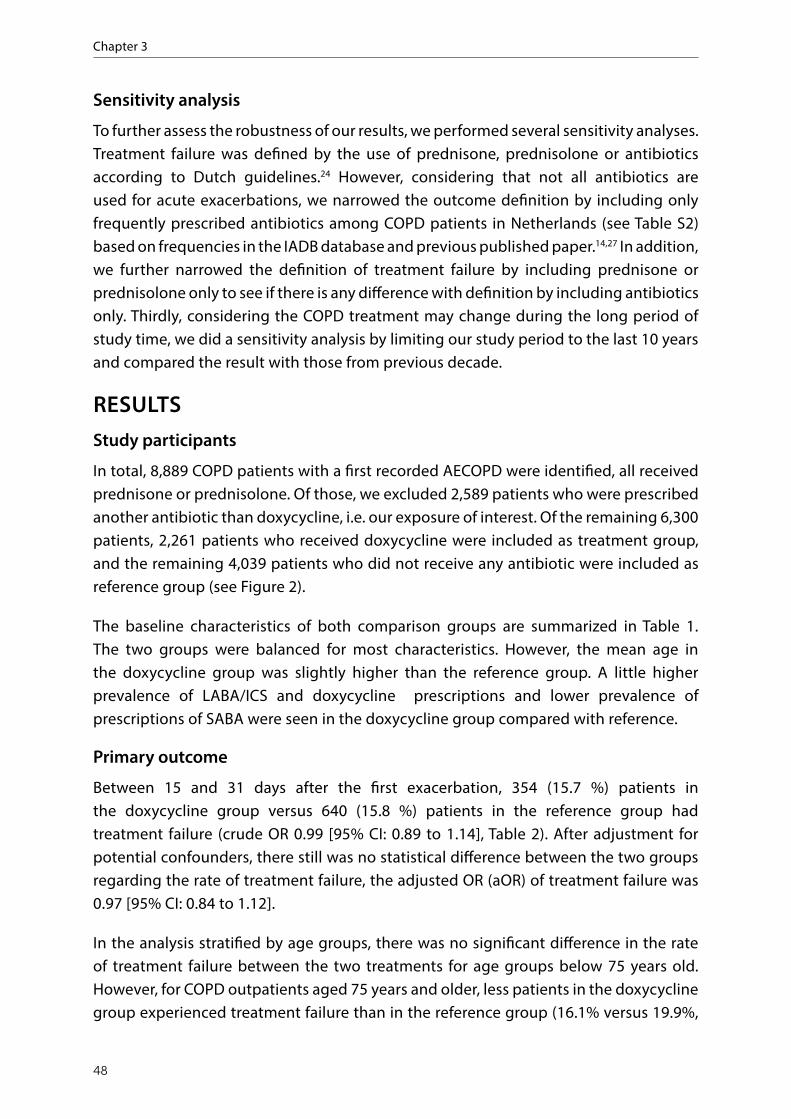
Chapter 3
48
Sensitivity analysis
To further assess the robustness of our results, we performed several sensitivity analyses. Treatment failure was defined by the use of prednisone, prednisolone or antibiotics according to Dutch guidelines.24 However, considering that not all antibiotics are used for acute exacerbations, we narrowed the outcome definition by including only frequently prescribed antibiotics among COPD patients in Netherlands (see Table S2) based on frequencies in the IADB database and previous published paper.14,27 In addition, we further narrowed the definition of treatment failure by including prednisone or prednisolone only to see if there is any difference with definition by including antibiotics only. Thirdly, considering the COPD treatment may change during the long period of study time, we did a sensitivity analysis by limiting our study period to the last 10 years and compared the result with those from previous decade.
RESULTSStudy participants
In total, 8,889 COPD patients with a first recorded AECOPD were identified, all received prednisone or prednisolone. Of those, we excluded 2,589 patients who were prescribed another antibiotic than doxycycline, i.e. our exposure of interest. Of the remaining 6,300 patients, 2,261 patients who received doxycycline were included as treatment group, and the remaining 4,039 patients who did not receive any antibiotic were included as reference group (see Figure 2).
The baseline characteristics of both comparison groups are summarized in Table 1. The two groups were balanced for most characteristics. However, the mean age in the doxycycline group was slightly higher than the reference group. A little higher prevalence of LABA/ICS and doxycycline prescriptions and lower prevalence of prescriptions of SABA were seen in the doxycycline group compared with reference.
Primary outcome
Between 15 and 31 days after the first exacerbation, 354 (15.7 %) patients in the doxycycline group versus 640 (15.8 %) patients in the reference group had treatment failure (crude OR 0.99 [95% CI: 0.89 to 1.14], Table 2). After adjustment for potential confounders, there still was no statistical difference between the two groups regarding the rate of treatment failure, the adjusted OR (aOR) of treatment failure was 0.97 [95% CI: 0.84 to 1.12].
In the analysis stratified by age groups, there was no significant difference in the rate of treatment failure between the two treatments for age groups below 75 years old. However, for COPD outpatients aged 75 years and older, less patients in the doxycycline group experienced treatment failure than in the reference group (16.1% versus 19.9%,

Age Influence on Effects of Doxycycline for AECOPD
49
3
Study participants
In total, 8,889 COPD patients with a first recorded AECOPD were identified, all received
prednisone or prednisolone. Of those, we excluded 2,589 patients who were prescribed another
antibiotic than doxycycline, i.e. our exposure of interest. Of the remaining 6,300 patients, 2,261
patients who received doxycycline were included as treatment group, and the remaining 4,039
patients who did not receive any antibiotic were included as reference group (see Figure 2).
Figure 2. Flow chart of participation selection. Figure 2. Flow chart of participation selection.
OR 0.78 [95% CI: 0.62, 0.97]). After adjustments for possible confounders, the value of OR did not change much, and results were compatible with a 23% relative risk reduction of treatment failure observed by doxycycline treatment compared with reference group (aOR 0.77 [95% CI: 0.62 to 0.97]).
Secondary outcome
After a follow-up of 12 months, 71.4% and 67.9% COPD outpatients experienced the next exacerbation in doxycycline and reference groups, respectively. The median time to next exacerbation was 169 days [95% CI 156-182] in the doxycycline group compared with 180 days [95% CI 169-191] in the reference group (p=0.07, Figure 3). However, if we included only those patients who experienced a second exacerbation within 12 months follow up, the median time was longer in the doxycycline group than in the reference

Chapter 3
50
Table 1. Baseline characteristics of COPD outpatients with first exacerbation in treatment groups.
Doxycycline (n=2261)
Reference(n= 4039) P-value
Gender, no. (%) Men 1085 (48.0) 1999 (49.5) 0.252Female 1176 (52.0) 2040 (50.5)
Age, years, no. (%) Mean age (SD) 71.08 (9.6) 70.30 (9.4) 0.002#
55-64 667 (29.5) 1285 (31.8) 0.018*
65-74 733 (32.4) 1357 (33.6)≥75 861 (38.1) 1397 (34.6)
Year of index date (%)1996-2004 893 (39.5) 1676 (41.5) 0.1212005-2015 1368 (60.5) 2363 (58.5)
PrescriberGP 2147 (95.0) 3424 (84.8) <0.001Specialist 114 (5.0) 615 (15.2)
Maintenance medicines, no. (%)SABA 775 (34.3) 1579 (39.1) <0.001LABA 494 (21.8) 847 (21.0) 0.414SAMA 689 (30.5) 1216 (30.1) 0.761LAMA 555 (24.5) 1020 (25.3) 0.534SABA/SAMA 80 (3.5) 173 (4.3) 0.149LABA/LAMA 0 (0) 1 (0) 0.454LABA/ICS 1093 (48.3) 1846 (45.7) 0.044Theophylline 124 (5.5) 159 (3.9) 0.004
Comorbidity, no. (%) Diabetes mellitus 301 (13.3) 504 (12.5) 0.341Disorders of lipid metabolism 629 (27.8) 1093 (27.1) 0.517Heart failure 363 (16.1) 676 (16.7) 0.484Ischemic heart disease 206 (9.1) 336 (8.3) 0.282Other cardiovascular disorders 843 (37.3) 1493 (37.0) 0.801Thyroid disease 115 (5.1) 192 (4.8) 0.556Rheumatic arthritis 355 (15.7) 660 (16.3) 0.508Osteoporosis 117 (5.2) 232 (5.7) 0.343Anxiety 392 (17.3) 649 (16.1) 0.193Depression 274 (12.1) 438 (10.8) 0.125Dementias 9 (0.4) 10 (0.2) 0.296
#Student’s t-test; SD: standard deviation; *Pearson Chi-Square test;
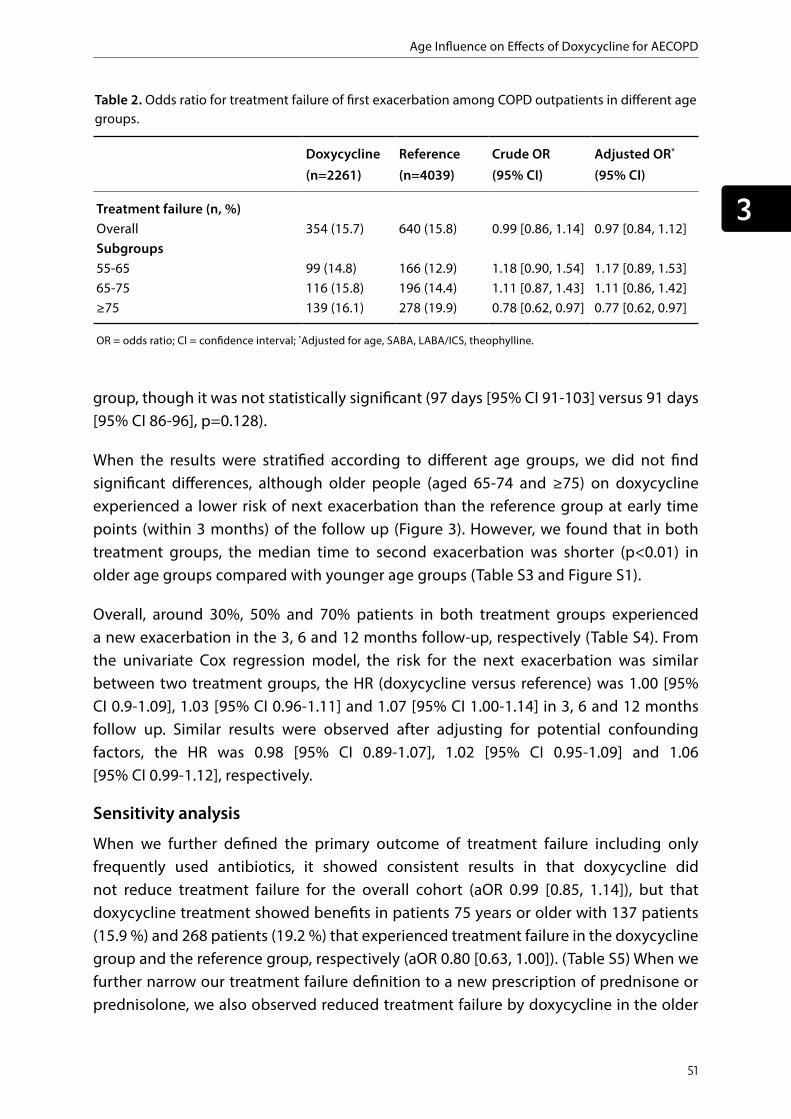
Age Influence on Effects of Doxycycline for AECOPD
51
3
group, though it was not statistically significant (97 days [95% CI 91-103] versus 91 days [95% CI 86-96], p=0.128).
When the results were stratified according to different age groups, we did not find significant differences, although older people (aged 65-74 and ≥75) on doxycycline experienced a lower risk of next exacerbation than the reference group at early time points (within 3 months) of the follow up (Figure 3). However, we found that in both treatment groups, the median time to second exacerbation was shorter (p<0.01) in older age groups compared with younger age groups (Table S3 and Figure S1).
Overall, around 30%, 50% and 70% patients in both treatment groups experienced a new exacerbation in the 3, 6 and 12 months follow-up, respectively (Table S4). From the univariate Cox regression model, the risk for the next exacerbation was similar between two treatment groups, the HR (doxycycline versus reference) was 1.00 [95% CI 0.9-1.09], 1.03 [95% CI 0.96-1.11] and 1.07 [95% CI 1.00-1.14] in 3, 6 and 12 months follow up. Similar results were observed after adjusting for potential confounding factors, the HR was 0.98 [95% CI 0.89-1.07], 1.02 [95% CI 0.95-1.09] and 1.06 [95% CI 0.99-1.12], respectively.
Sensitivity analysis
When we further defined the primary outcome of treatment failure including only frequently used antibiotics, it showed consistent results in that doxycycline did not reduce treatment failure for the overall cohort (aOR 0.99 [0.85, 1.14]), but that doxycycline treatment showed benefits in patients 75 years or older with 137 patients (15.9 %) and 268 patients (19.2 %) that experienced treatment failure in the doxycycline group and the reference group, respectively (aOR 0.80 [0.63, 1.00]). (Table S5) When we further narrow our treatment failure definition to a new prescription of prednisone or prednisolone, we also observed reduced treatment failure by doxycycline in the older
Table 2. Odds ratio for treatment failure of first exacerbation among COPD outpatients in different age groups.
Doxycycline (n=2261)
Reference (n=4039)
Crude OR(95% CI)
Adjusted OR*
(95% CI)
Treatment failure (n, %)Overall 354 (15.7) 640 (15.8) 0.99 [0.86, 1.14] 0.97 [0.84, 1.12] Subgroups 55-65 99 (14.8) 166 (12.9) 1.18 [0.90, 1.54] 1.17 [0.89, 1.53]65-75 116 (15.8) 196 (14.4) 1.11 [0.87, 1.43] 1.11 [0.86, 1.42] ≥75 139 (16.1) 278 (19.9) 0.78 [0.62, 0.97] 0.77 [0.62, 0.97]
OR = odds ratio; CI = confidence interval; *Adjusted for age, SABA, LABA/ICS, theophylline.

Chapter 3
52
age group compared with reference (aOR 0.72 [0.55, 0.95], Table S6), while no significant difference was observed between groups for the narrow definition of treatment failure by a new prescription of antibiotics. When we limit the study period to the last decade (2005-2015) and the previous decade (1994-2004) separately, the treatment failure was also less among patients with advanced age in doxycycline group than reference group. (aOR 0.75 [0.55, 1.01] and aOR 0.84 [0.60, 1.18], separately, Table S7).
DISCUSSIONMain findings
In a real-world population of primary care patients with AECOPD of any age, doxycycline did not appreciably reduce the failure rate, nor prolong time to next exacerbation. However, when stratified by age, we found a statistically significant 23% relative
Figure 3. Kaplan-Meier curves showing the proportion of patients free of 2nd exacerbation in COPD outpatients up to 12 months’ follow up: a) all-age group patients (p = 0.07); b) patients aged 55-64 (p=0.252); c) patients aged 65-74 (p=0.564); d) patients aged ≥75 (p=0.421).
Figure 3. Kaplan‐Meier curves showing the proportion of patients free of 2nd exacerbation in
COPD outpatients up to 12 months' follow up: a) all‐age group patients (p = 0.07); b) patients
aged 55‐64 (p=0.252); c) patients aged 65‐74 (p=0.564); d) patients aged 75 (p=0.421).
Sensitivity analysis
When we further defined the primary outcome of treatment failure including only frequently
used antibiotics, it showed consistent results in that doxycycline did not reduce treatment failure
for the overall cohort (aOR 0.99 [0.85, 1.14]), but that doxycycline treatment showed benefits in
patients 75 years or older with 137 patients (15.9 %) and 268 patients (19.2 %) that experienced

Age Influence on Effects of Doxycycline for AECOPD
53
3
reduction in treatment failure by doxycycline for AECOPD in outpatients aged 75 years and older. These benefits were not seen in younger age groups. In the long-term, we observed that the protective effect of doxycycline for the subsequent exacerbations was only present in the first 3 months among older patients. After that, the protective effect wanes over time.
The observed short-term effect regarding reduction rate in treatment failure for older patients (≥75 years) is compatible with a previous RCT which found that short-term treatment non-response rates are significantly lower in the doxycycline group compared to placebo (OR 0.77, 95% CI [0.63, 0.94]).11 Our sub-group result is also consistent with a recent Cochrane review that showed that the current available antibiotics reduce the risk for treatment failure between seven days and one month after treatment initiation (OR 0.72, 95% CI [0.56, 0.94]).13
The benefit of doxycycline in older patients may be primarily due to their increased susceptibility to infection.20 With increasing age, not only the lung function changes, the natural defense mechanisms of the lungs also decrease gradually.33 Intercellular communications become less effective which could contribute to immune-senescence.34 Additionally, mucocilliary clearance is also compromised with age.35 All these changes with age contribute to the greater possibility of bacterial infection and inflammation in elderly.20 Therefore, the elderly seem to benefit more from antibiotic treatment than younger patients.
The average age of study patients (about 70 years) was comparable with previous studies.36 We did not find a short-term benefit of doxycycline in the younger age group (< 75), which may be explained by the fact that the overall rate of appropriate antibiotic use in practice is rather low.17-19 According to GOLD, general practitioners should only consider antibiotics for patients when signs of bacterial infection are present.5 However, in reality, guidelines regarding the prescription of antibiotics are poorly followed,17,19 on average in only 25% of AECOPD antibiotics were prescribed properly according to the GOLD criteria.18 For AECOPD with other etiology like viral infection and environmental pollution, antibiotics may not have been effective. Of note, a complicating factor in the outpatient setting is that sputum cultures are not feasible as they take at least two days and frequently do not give reliable results.5 Identification of bacterial exacerbation still relies on clinical assessment rather than laboratory biomarkers.37 As infection is the most treatable cause of breathlessness, it is not surprising that many patients continue to receive antimicrobials in the absence of clinical, pathological or radiological evidence of infection.38 Therefore, if the proportion of patients who were prescribed doxycycline but in fact should not be given antibiotics is large, it will be difficult to find significant beneficial effects of doxycycline treatment.
Chapter 3
54
Observed long-term effects from this study for all patients independent of age were also consistent with the findings of two previous RCTs that antibiotics did not prolong time to next exacerbation.11,39 However, two observational studies showed different results in that the time to next exacerbation was significantly extended if the exacerbation was treated with antibiotics.14,15 Similarly, one RCT also showed a pronged time to next exacerbation by antibiotic treatment.9 In this study, the prolonged time to next exacerbation by doxycycline was only seen in older outpatients within 3 months. Of note, as different definitions for subsequent exacerbation and different types of antibiotics were used in these studies when evaluating the long-term effect of antibiotics, these may led to the inconsistent results.
Besides the effects of ageing on bacterial susceptibility,22 we should also realize that COPD itself is an age-related chronic inflammatory disorder. After the lungs reach their maximum function around the age of 25 years, its function progressively declines as a sequence of structural and physiological changes to the lung.33 With ageing, severity and comorbidities of COPD usually also increase. These factors could further influence the frequency of exacerbations in primary care patients with COPD.40 A higher frequency also means a shorter time to experience the next exacerbation. In this study we have found that the time to next exacerbation was shorter in older than younger patients, and it was consistent in both doxycycline and reference groups.
Strengths and limitations
This study has several strengths. One strength is that this study was based on a large real-life prescription database which enabled us to evaluate the effects of doxycycline in a large COPD population. Another strength is that both short-term and long-term effects of additional doxycycline were evaluated, which may offer more comprehensive support for decision making in clinical practice. Additionally, we chose the first recorded exacerbation as investigated event for all COPD outpatients, which could exclude the influence of historical exacerbation frequency as a risk factor on targeted outcomes to a large extent. In addition, as oral steroids and antibiotics cannot be bought over the counter in the Netherlands, the study population from the IADB database represents a generalizable population for AECOPD outpatients treated with doxycycline.
Limitations to observational studies also need to be discussed. First, due to the characteristics of the prescription database, there was no diagnostic information available. Therefore, the definition of COPD, comorbidities and outcomes were defined using related drugs as proxies, which may result in potential misclassification bias. Secondly, although the relevant measured baseline characteristics of the two groups were similar in this study, other clinical information like lung function, GOLD stages (I-IV) of COPD and severity of exacerbations were lacking, which may influence our outcome to some extent if these unknown characteristics were not balanced between the two

Age Influence on Effects of Doxycycline for AECOPD
55
3
study groups. In clinical practice, antibiotics may be prescribed to those who in fact did not have enough indication of infection due to limitation of outpatients setting or to those with more severe COPD,5 which may have led to underestimation of the efficacy of additional doxycycline treatment in all age groups compared to corticosteroids only. Thirdly, there were overlap for a few patients within 21 days and 31 days between the short- and long- term outcome definitions by a new prescription of corticosteroids due to lack of clinical information to distinguish and classify the outcomes. Finally, although we set the age limitation of 55 years older to exclude potential asthma, asthma-COPD overlap patients may still existed as we did not exclude the patients who use asthma drugs at the stage of study design. However, these patients were very few and unlikely to influence the overall results based on the fact that no patients were prescribed leukotriene receptor antagonists and only 11 patients were prescribed cromoglycates within one year before index date among all the AECOPD patients in our study.
Implications for future research and clinical practice
The tendency towards better effects of antibiotics in the elderly COPD patients may offer clues for clinicians and researchers for more targeted management of AECOPD. In particular, decision making about empirical antibiotic therapy for AECOPD should take the age of patients into consideration. However, before that, more prospective, well-designed studies with more accurate diagnostic information are needed to further confirm the finding from this study.
Although related guideline and GOLD report about antibiotic use for AECOPD were basically based on secondary care RCT evidence,5,6 decision making in daily practice is influenced by many factors making AECOPD treatment more challenging in outpatient settings.5 Therefore, identifying high risk populations for infection may improve management and clinical decisions about antibiotic use in COPD outpatients. The high risk of infection and beneficial effects from antibiotics for AECOPD in elderly outpatients should warrant a personalized approach towards antibiotic treatment.
CONCLUSIONDoxycycline in addition to oral corticosteroid treatment was associated with a reduced risk of treatment failure for AECOPD in patients 75 years or older, but not in younger patients. Long-term effects of doxycycline treatment on subsequent exacerbations was not observed, though among older persons there was a non-statistically significant beneficial trend within 3 months after doxycycline treatment. Clinicians should take the age of patients into consideration in empirical antibiotic therapy for AECOPD. More real-world studies with high quality, preferably prospective clinical data collections, should be recommended to confirm the influence of age on effects of antibiotics and

Chapter 3
56
to further explore which patient groups could benefit most from antibiotic treatment for AECOPD.
SUPPLEMENTARY DATATable S1 to S7 and Figure S1 are available as Supplementary data at BMJ Open Respiratory Research online (https://bmjopenrespres.bmj.com/content/7/1/e000535)

Age Influence on Effects of Doxycycline for AECOPD
57
3
REFERENCES
1. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095-2128.
2. Soler-Cataluna JJ, Martinez-Garcia MA, Roman Sanchez P, Salcedo E, Navarro M, Ochando R. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60(11):925-931.
3. O’Reilly JF, Williams AE, Rice L. Health status impairment and costs associated with COPD exacerbation managed in hospital. International journal of clinical practice. 2007;61(7):1112-1120.
4. Sethi S, Murphy TF. Infection in the pathogenesis and course of chronic obstructive pulmonary disease. N Engl J Med. 2008;359(22):2355-2365.
5. Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD). Global Strategy for the Diagnosis, Management and Prevention of COPD. 2019. Available from: http://goldcopd.org.
6. Wedzicha JAEC-C, Miravitlles M, Hurst JR, et al. Management of COPD exacerbations: a European Respiratory Society/American Thoracic Society guideline. Eur Respir J. 2017;49(3).
7. Walters JA, Tan DJ, White CJ, Gibson PG, Wood-Baker R, Walters EH. Systemic corticosteroids for acute exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2014(9):CD001288.
8. Vollenweider DJ, Jarrett H, Steurer-Stey CA, Garcia-Aymerich J, Puhan MA. Antibiotics for exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;12:CD010257.
9. Llor C, Moragas A, Hernandez S, Bayona C, Miravitlles M. Efficacy of antibiotic therapy for acute exacerbations of mild to moderate chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186(8):716-723.
10. Anthonisen NR, Manfreda J, Warren CP, Hershfield ES, Harding GK, Nelson NA. Antibiotic therapy in exacerbations of chronic obstructive pulmonary disease. Ann Intern Med. 1987;106(2):196-204.
11. van Velzen P, Ter Riet G, Bresser P, et al. Doxycycline for outpatient-treated acute exacerbations of COPD: a randomised double-blind placebo-controlled trial. Lancet Respir Med. 2017;5(6):492-499.
12. Hassan WA, Shalan I, Elsobhy M. Impact of antibiotics on acute exacerbations of COPD. Egypt J Chest Dis Tu. 2015;64(3):579-585.
13. Vollenweider DJ, Frei A, Steurer-Stey CA, Garcia-Aymerich J, Puhan MA. Antibiotics for exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2018;10:CD010257.
14. Roede BM, Bresser P, Bindels PJ, et al. Antibiotic treatment is associated with reduced risk of a subsequent exacerbation in obstructive lung disease: an historical population based cohort study. Thorax. 2008;63(11):968-973.
15. Roede BM, Bresser P, Prins JM, Schellevis F, Verheij TJ, Bindels PJ. Reduced risk of next exacerbation and mortality associated with antibiotic use in COPD. Eur Respir J. 2009;33(2):282-288.
16. Team NGU. National Institute for Health and Care Excellence: Clinical Guidelines. Chronic obstructive pulmonary disease in over 16s: diagnosis and management. London: National Institute for Health and Care Excellence (UK). Copyright (c) NICE 2018.; 2018.
17. Bathoorn E, Groenhof F, Hendrix R, et al. Real-life data on antibiotic prescription and sputum culture diagnostics in acute exacerbations of COPD in primary care. Int J Chron Obstruct Pulmon Dis. 2017;12:285-290.
18. Dietrich E, Klinker KP, Li J, Nguyen CT, Quillen D, Davis KA. Antibiotic Stewardship for Acute Exacerbation of Chronic Obstructive Pulmonary Disease. Am J Ther. 2018.
19. Roede BM, Bindels PJ, Brouwer HJ, Bresser P, de Borgie CA, Prins JM. Antibiotics and

Chapter 3
58
steroids for exacerbations of COPD in primary care: compliance with Dutch guidelines. Br J Gen Pract. 2006;56(530):662-665.
20. Brandsma CA, de Vries M, Costa R, Woldhuis RR, Konigshoff M, Timens W. Lung ageing and COPD: is there a role for ageing in abnormal tissue repair? Eur Respir Rev. 2017;26(146).
21. Gardner ID. The Effect of Aging on Susceptibility to Infection. Rev Infect Dis. 1980;2(5):801-810.
22. Petersen I, Johnson AM, Islam A, Duckworth G, Livermore DM, Hayward AC. Protective effect of antibiotics against serious complications of common respiratory tract infections: retrospective cohort study with the UK General Practice Research Database. BMJ. 2007;335(7627):982.
23. Stone RA, Lowe D, Potter JM, Buckingham RJ, Roberts CM, Pursey NJ. Managing patients with COPD exacerbation: does age matter? Age Ageing. 2012;41(4):461-468.
24. Snoeck-Stroband JB, Schermer TRJ, Van Schayck CP, et al. NHG-Werkgroep Astma bij volwassenen en COPD. NHG-Standaard COPD (derde herziening). Huisarts Wet 2015; 58(4):198-211.
25. Bahar MA, Wang Y, Bos JHJ, Wilffert B, Hak E. Discontinuation and dose adjustment of metoprolol after metoprolol-paroxetine/fluoxetine co-prescription in Dutch elderly. Pharmacoepidemiol Drug Saf. 2018;27(6):621-629.
26. Mulder B, Pouwels KB, Schuiling-Veninga CC, et al. Antibiotic use during pregnancy and asthma in preschool children: the influence of confounding. Clinical and experimental allergy : journal of the British Society for Allergy and Clinical Immunology. 2016;46(9):1214-1226.
27. Visser ST, Schuiling-Veninga CC, Bos JH, de Jong-van den Berg LT, Postma MJ. The population-based prescription database IADB.nl: its development, usefulness in outcomes research and challenges. Expert Rev Pharmacoecon Outcomes Res. 2013;13(3):285-292.
28. Monster TB, Janssen WM, de Jong PE, de Jong-van den Berg LT, REnal PSGPo, Vascular ENTSD. Pharmacy data in epidemiological
studies: an easy to obtain and reliable tool. Pharmacoepidemiol Drug Saf. 2002;11(5):379-384.
29. Woods JA, Wheeler JS, Finch CK, Pinner NA. Corticosteroids in the treatment of acute exacerbations of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2014;9:421-430.
30. van Boven JF, van Raaij JJ, van der Galien R, et al. Impact of multiple-dose versus single-dose inhaler devices on COPD patients’ persistence with long-acting beta(2)-agonists: a dispensing database analysis. NPJ Prim Care Respir Med. 2014;24:14069.
31. Penning-van Beest F, van Herk-Sukel M, Gale R, Lammers JW, Herings R. Three-year dispensing patterns with long-acting inhaled drugs in COPD: a database analysis. Respir Med. 2011;105(2):259-265.
32. Seemungal TA, Donaldson GC, Bhowmik A, Jeffries DJ, Wedzicha JA. Time course and recovery of exacerbations in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2000;161(5):1608-1613.
33. Rojas M, Meiners S, Le Saux CJ. Molecular aspects of aging : understanding lung aging. Hoboken, New Jersey: John Wiley & Sons, Inc.; 2014.
34. Lopez-Otin C, Blasco MA, Partridge L, Serrano M, Kroemer G. The hallmarks of aging. Cell. 2013;153(6):1194-1217.
35. Bailey KL, Bonasera SJ, Wilderdyke M, et al. Aging causes a slowing in ciliary beat frequency, mediated by PKCepsilon. Am J Physiol Lung Cell Mol Physiol. 2014;306(6):L584-589.
36. Balcells E, Anto JM, Gea J, et al. Characteristics of patients admitted for the first time for COPD exacerbation. Respir Med. 2009;103(9):1293-1302.
37. Jacobs DM, Pandit U, Sethi S. Acute exacerbations in chronic obstructive pulmonary disease: should we use antibiotics and if so, which ones? Curr Opin Infect Dis. 2019.
38. Taverner J, Ross L, Bartlett C, et al. Antimicrobial prescription in patients dying from chronic obstructive pulmonary disease. Internal medicine journal. 2019;49(1):66-73.

Age Influence on Effects of Doxycycline for AECOPD
59
3
39. Wilson R, Jones P, Schaberg T, et al. Antibiotic treatment and factors influencing short and long term outcomes of acute exacerbations of chronic bronchitis. Thorax. 2006;61(4):337-342.
40. Westerik JA, Metting EI, van Boven JF, Tiersma W, Kocks JW, Schermer TR. Associations between chronic comorbidity and exacerbation risk in primary care patients with COPD. Respir Res. 2017;18(1):31.

C H A P T E R 4

Yuanyuan Wang Victor Pera
H. Marike Boezen Jan-Willem C. Alffenaar
Bob Wilffert Rolf H.H. Groenwold
Eelko Hak
Real-world short- and long-term effects of antibiotic therapy on acute
exacerbations of COPD in outpatients: a cohort study under the PharmLines Initiative
Submitted for publication.

Chapter 4
62
ABSTRACTIntroduction
Although antibiotic treatment is recommended for acute exacerbations of COPD (AECOPD) under specific circumstances, the treatment’s value in an outpatient setting is unclear. We aim to evaluate the real-world short- and long-term effects of antibiotic treatment on AECOPD outpatients.
Methods
This retrospective inception cohort study was conducted under the PharmLines Initiative that linked the Lifelines cohort study database with IADB.nl, the University of Groningen’s medication prescription database during the period 2005-2017. We included participants with a first recorded diagnosis of COPD who underwent systemic glucocorticoids treatment for an AECOPD episode. The exposed and reference group was defined as patients who received and not received any antibiotic prescriptions during AECOPD treatment. The short-term outcome was AECOPD treatment failure within 14-30 days after the index date. The long-term outcome was the time to the next exacerbation within a one-year follow-up period. Binary logistic regression analysis combined with propensity scores (PS) were used to estimate the association between antibiotic use and treatment failure. The risk of another exacerbation was assessed using Kaplan-Meier survival and Cox regression analyses. Several subgroup and sensitivity analyses were also performed.
Results
We analyzed linked data for 1,105 AECOPD patients. Antibiotics were prescribed for 518 patients (46.9%) while 587 patients (53.1%) received no antibiotics. The overall antibiotic use was associated with a significant relative risk reduction of AECOPD treatment failure by 33%-37% compared with the risk for the reference group (adjusted odds ratio [aOR]: 0.67 [95% CI: 0.42-1.04] and 0.63 [95% CI: 0.40-0.99] by regression and PS analyses, respectively). Similar protective effects were observed for doxycycline, macrolides and co-amoxiclav, but not for amoxicillin, and only the effects of doxycycline were statistically significant (aOR 0.53 [95% CI: 0.28-0.99] by PS analysis). There was no difference between the exposure and reference groups regarding the risk of and time to the next exacerbation, irrespective of the follow-up duration.
Conclusion
Our finding that antibiotics treatment supplementing systemic glucocorticoids treatment reduces short-term AECOPD treatment failure in real-world settings concurs with those of clinical trials. Larger studies of high quality are needed to confirm the beneficial effects for specific classes of antibiotics. Our results after controlling for confounding suggest that in observational studies on AECOPD, unmeasured confounding may induce underestimated beneficial antibiotic treatment effects.

Effects of Antibiotic Therapy on AECOPD
63
4
INTRODUCTIONChronic obstructive pulmonary disease (COPD), which is characterized by persistent respiratory symptoms and airflow limitation is one of the leading causes of morbidity and mortality worldwide.1,2 COPD patients frequently experience acute exacerbations of COPD (AECOPD), defined as acute worsening of respiratory symptoms, necessitating additional therapy.3 AECOPD has major impacts on patients’ health status, accelerates the disease progression and increases health-care costs.4,5 Therefore, reducing the symptoms of current exacerbations and preventing further exacerbations are essential aspects of sound pharmaceutical management of AECOPD. Because AECOPD is associated with increased airway inflammations, systemic glucocorticoids treatment is recommended to shorten the recovery time, improve lung function and promote oxygenation, given its proven beneficial effects.3,6
The majority of AECOPD episodes are caused by respiratory infections, especially bacterial infections, which account for around 50% of all exacerbations.7,8 The most widely reported bacteria associated with exacerbations are S. pneumoniae, H. influenza, P. aeruginosa, M. catarrhalis, A. baumannii, and S. aureus.7,9,10 Accordingly, antibiotics have been recommended for the management of AECOPD when signs of bacterial infection are present.3 However, the beneficial effects of antibiotic treatment in addition to oral glucocorticoids for AECOPD are still uncertain among outpatients. The pooled results from five randomized controlled trials (RCTs) examined in a Cochrane meta-analysis conducted in 2012 did not show a significant reduced risk of treatment failure associated with currently prescribed antibiotics among outpatients.11 However, an updated (2018) version of this Cochrane review that included two new RCTs, presented statistically significant beneficial effects of current prescribed antibiotics among outpatients.12,13 Especially the RCT conducted by van Velzen et al in 2017 contributed a large proportion (24%) of the updated pooled results.13 This RCT itself was not statistically significant. The limited external validity of RCTs prompts questions about the effects of antibiotics treatment for AECOPD in real-world settings.
Primary care of patients with COPD is mostly managed on an outpatient basis. This population from real-world setting is more heterogeneous than those of RCTs.14 Additionally, antibiotic treatment for AECOPD is often not in accordance with current guidelines.15,16 Therefore, the real-world treatment effects of antibiotics for AECOPD may differ from those obtained from clinical trials and merit further investigation. So far, only few observational studies were conducted to evaluate the treatment effects of antibiotics for AECOPD. Two of these studies focused exclusively on the long-term effects of antibiotics used for AECOPD and lacked any adjustments for potential differences in lung function and smoking history.17,18 Two other cohort studies were conducted among inpatients.19,20 The PharmLines Initiative presented a unique opportunity to retrieve precise information on many previously unmeasured confounders. Using an
Chapter 4
64
inception cohort design, we assessed the short- and long-term effects of antibiotics used in addition to systemic glucocorticoids treatment for AECOPD in outpatients.
METHODSStudy setting and data sources
This retrospective cohort study was conducted as part of the PharmLines Initiative,21 which linked the Lifelines Cohort Study database (https://www.lifelines.nl) and the IADB.nl prescription database (http://www.iadb.nl) affiliated to the University of Groningen. Individuals included in these two databases are representative for the population in the northern Netherlands.22,23
Lifelines is a multi-disciplinary prospective population-based cohort study involving 167,729 participants across three generations from 2006 to 2017. A broad range of investigative procedures were used to assess the biomedical, socio-demographic, behavioural, physical and psychological factors contributing to the health and disease status of the general population, with a particular focus on multi-morbidity and complex genetics.24,25 Following baseline assessments, participants underwent physical examinations at the Lifelines location every 5 years and completed extensive questionnaires every 1.5 years. IADB.nl is an evolving drug prescription database since 1996 that currently covers prescription data for 730,000 participants from 72 community pharmacies.23 Each patient is individually tracked throughout the database’s operational period and their prescription records contain information on the date of dispensing, the quantity of medication dispensed, the dose regimen, the number of days for which the prescription is valid, the prescribing physician and the anatomical therapeutic chemical code (ATC code). Each patient, whose date of birth and gender are recorded, is assigned a unique anonymous identifier. Because of the strong patient-pharmacy commitment in the Netherlands, the medication records for each patient are virtually complete, except for over the counter drugs and medication dispensed during hospitalization.
The Lifelines cohort study was approved by the medical ethical committee of the University Medical Center Groningen, and all participants signed informed consent forms confirming their permission for their (anonymized) data and material to be used for scientific purposes. IADB.nl data are collected in accordance with the national and European guidelines on privacy requirements for handling human data.
Study population
Patients with a first recorded diagnosis of COPD who took systemic glucocorticoids for an acute exacerbation were selected for this study according to the following inclusion criteria: (1) patients were entered in both the Lifelines and IADB.nl databases. (2) Patients had spirometrically-confirmed COPD with a forced expiratory volume in 1

Effects of Antibiotic Therapy on AECOPD
65
4
second/forced volume capacity (FEV1/FVC) < 70% according to lung function test or had general practitioner (GP)-confirmed COPD according to the self-reported questionnaire in the Lifelines Cohort Study. The date of first recorded COPD diagnosis was set as enrolment date of this study. (3) Patients had the first recorded acute exacerbation after enrolment date, which was indicated by the prescription of prednisone or prednisolone push treatments (3-4 defined daily doses for 3-14 days) recorded in the IADB.nl database in line with Dutch College of GPs guideline for COPD management.26 The date of the first prescriptions for acute exacerbation was set as the index date. (4) Patients were 18 years or older on the index date.
Exposure and outcomes
During the treatment for first recorded acute exacerbation with systemic corticosteroid treatment, patients who also received antibiotics (ATC code: J01) within 3 days before and 7 days after the index date were defined as the exposed group. Those patients who were not prescribed any antibiotics during the same period were defined as the reference group. The short-term outcome was treatment failure defined as any new prescription of prednisolone, prednisone or antibiotics between 14 and 30 days after index date. The long-term outcome was the time to the next exacerbation defined as a new prescription of prednisone or prednisolone within a one-year follow-up period. As the first exacerbation may last for a long time, to avoid counting its following treatment as a second exacerbation, we restricted the minimum time from the first to the second exacerbation to 21 days.27 The study design for the exposure and outcome measurements is described in Figure 1.
Data collection and covariates
Age was calculated as the difference in years between the date of birth and the index date. On the enrolment date, the following information was extracted as covariates from the Lifelines database to describe the characteristics of cohort members with AECOPD: smoking history, the global initiative for chronic obstructive lung disease (GOLD) stages of COPD, lung function parameters and related comorbidities including cardiovascular diseases, diabetes, depression and other disorders. If information concerning the risk status of AECOPD (e.g., smoking history and chronic comorbidities) was not documented on the enrolment date, we used information from the closest follow-up assessment in the Lifelines, if available. Additionally, information on the frequency of AECOPD and maintenance drugs for COPD in the previous year before the index date was retrieved as covariates from the IADB.nl database.
Subgroup and sensitivity analysis
Given that different antibiotics may have different effects on AECOPD, we conducted a subgroup analysis to explore the effects of four most frequently used antibiotics (doxycycline, macrolides, co-amoxiclav and amoxicillin). As COPD patients with an

Chapter 4
66
asthma component may respond differently to antibiotics, we conducted a sensitivity analysis by excluding these patients to verify the robustness of our study.
Statistical analysis
Continuous variables were presented as means with standard deviations (SDs) or median with interquartile ranges (IQRs) and Student’s t-test or Mann-Whitney U Test was performed, as appropriate, to examine their difference between the two patient groups. Categorical variables were presented as percentages with 95% confidence intervals (95% CI) and compared using a Chi-square test or Fisher’s exact test, as appropriate. Binary logistic regression was performed to estimate the odds ratio (OR) with a 95% CI for treatment failure and adjusted for possible covariates. To better control the differences of characteristics between groups, propensity score (PS) analysis was also conducted by including the PS as a single covariate in the binary logistic regression model. A Kaplan-Meier survival analysis and log-rank test were conducted to compare the times to the next exacerbations between exposure and reference groups. A cox proportional hazards regression was performed to estimate the hazard ratio (HR) and 95% CI for the risk of the next exacerbation. A p-value < 0.05 was considered as statistically significant. All analyses were performed using the IBM SPSS statistics version 22 (IBM Corp., Armonk, NY, USA).
RESULTSBaseline characteristics
The linkage of the IADB.nl and Lifelines database provided 7,760 adults who were prescribed a prednisone or prednisolone treatment (Figure 2). Of these adults, 2,614 (34%) had a diagnosis of COPD. Of these COPD patients, 1,105 with a first acute exacerbation recorded after their enrolment dates according to pre-set definitions were eligible for our study. In all, 518 patients were enrolled in the exposed group, receiving both systemic glucocorticoids and an antibiotic. 587 patients were enrolled in the reference group, only receiving systemic glucocorticoids. The baseline characteristics of the study population are summarized in Table 1. Overall, the measured covariates were very similar for both exposed and reference groups. The number of previous exacerbations and antibiotic courses as well as the prevalence of heart failures were higher in the exposure group compared with the reference group.
Short-term outcome
Within 14-30 days after treatment of the index exacerbation, 56 (10.8%) patients in the antibiotic exposed group versus 62 (10.6%) patients in the reference group experienced treatment failure (crude OR: 1.03 [95% CI: 0.70-1.50], Table 2). After adjusting for potential confounders through regression and PS analysis, the OR decreased in the direction of a beneficial effect of antibiotics (aOR: 0.67 [95% CI: 0.42-

Effects of Antibiotic Therapy on AECOPD
67
4
1.04] in the regression analysis), which was statistically significant in the PS analysis (aOR 0.63 [95%CI: 0.40-0.99]).
Long-term outcome
Within a year of follow-up after the index date, 153 (29.5%) patients in the exposure group and 147 (25.0 %) patients in the reference group experienced a next exacerbation (crude HR: 1.19 [95% CI: 0.95-1.49], see Table 3). After adjusting for confounders, the point estimate of the HR for subsequent exacerbation did not change substantially (adjusted HR 1.14 [95% CI: 0.87-1.49]). There was also no difference between the two comparison groups for the time to the next exacerbation (Figure 3), which applied to the short follow-up period of 3 and 6 months (Table 3).
Subgroup and sensitivity results
The findings of both the logistic regression and PS analyses indicated that the risk of treatment failure was reduced significantly by 47% by doxycycline compared to the reference treatments (aOR 0.53 [95% CI: 0.28-1.00] and 0.53 [95% CI: 0.28-0.99] by regression and PS analyses, respectively, Table 1). Although not statistically significant, similar beneficial trends were seen for the macrolides exposed group (aOR 0.49 [95% CI: 0.22-1.11] and 0.58 [95% CI: 0.26-1.29] by regression and PS analyses, respectively) and co-amoxicillin exposed group (aOR 0.50 [95% CI: 0.19-1.32] and 0.46 [95% CI: 0.17-1.24] by regression and PS analyses, respectively) compared to the results in the reference group. No statistical difference was observed between the amoxicillin exposed group and the reference group (aOR 1.56 [95% CI: 0.81-3.00] and 1.49 [95% CI: 0.78-2.84] by regression and PS analyses, respectively) and the point estimate of aOR was in the opposite direction.
Even when we excluded self-reported COPD and focused only on spirometrically-confirmed COPD, the protective effect of antibiotics on treatment failure continued (aOR 0.56 [95% CI: 0.32-0.97] and 0.52 [95% CI: 0.29-0.90] by regression and PS analyses,
minimum time from the first to the second exacerbation to 21 days.27 The study design for the
exposure and outcome measurements is described in Figure 1.
Data collection and covariates
Age was calculated as the difference in years between the date of birth and the index date.
On the enrolment date, the following information was extracted as covariates from the
Lifelines database to describe the characteristics of cohort members with AECOPD: smoking
history, the global initiative for chronic obstructive lung disease (GOLD) stages of COPD, lung
function parameters and related comorbidities including cardiovascular diseases, diabetes,
depression and other disorders. If information concerning the risk status of AECOPD (e.g.,
smoking history and chronic comorbidities) was not documented on the enrolment date, we
used information from the closest follow‐up assessment in the Lifelines, if available.
Additionally, information on the frequency of AECOPD and maintenance drugs for COPD in the
previous year before the index date was retrieved as covariates from the IADB.nl database.
Figure 1. Retrospective cohort study design.
Subgroup and sensitivity analysis
Given that different antibiotics may have different effects on AECOPD, we conducted a
subgroup analysis to explore the effects of four most frequently used antibiotics (doxycycline,
macrolides, co‐amoxiclav and amoxicillin). As COPD patients with an asthma component may
respond differently to antibiotics, we conducted a sensitivity analysis by excluding these
patients to verify the robustness of our study.
Figure 1. Retrospective cohort study design.

Chapter 4
68
Figure 2. Flow chart of study subject selection.
LifeLines participants from 2007(n 167.000)
IADB participants from 1994 to 2017(n 600.000)
Databases overlap(n=7760)
Prednisone or prednisolone users
COPD patients(n=2614)
Inclusion:1. Clinical COPD diagnosis (FEV1/FVC<0.70) n=15962. Self‐reported COPD diagnosis: n=1635
Patients 18 years(n=152.728)
COPD patients, using corticosteroids (n=1594)
COPD patients with exacerbations(n=1105)
Exposed group: corticosteroids & antibiotic use
(n=518)
Reference group: corticosteroids
use only (n=587)
Inclusion:Using 3 or 4 DDDs daily corticosteroids for 3‐14 days
Figure 2. Flow chart of study subject selection.
Statistical analysis
Continuous variables were presented as means with standard deviations (SDs) or median with
interquartile ranges (IQRs) and Student’s t‐test or Mann‐Whitney U Test was performed, as
appropriate, to examine their difference between the two patient groups. Categorical
variables were presented as percentages with 95% confidence intervals (95% CI) and
compared using a Chi‐square test or Fisher’s exact test, as appropriate. Binary logistic
regression was performed to estimate the odds ratio (OR) with a 95% CI for treatment failure
and adjusted for possible covariates. To better control the differences of characteristics
between groups, propensity score (PS) analysis was also conducted by including the PS as a
single covariate in the binary logistic regression model. A Kaplan‐Meier survival analysis and
respectively; Table 4). Similarly, after excluding COPD patients with asthma, the aOR (exposure vs reference) for treatment failure was further reduced towards a protective effect (aOR 0.58 [95% CI: 0.32-1.01] and 0.57 [0.32, 1.02] by regression and PS analyses) with a boundary statistical significance.
DISCUSSIONPrimary findings
In this study of COPD outpatients with mostly mild to moderate GOLD stages, antibiotics prescription, notably doxycycline, in addition to systemic prednisone or prednisolone therapy, appeared to reduce the treatment failure of AECOPD substantially. The supplementation of antibiotic treatment to systemic glucocorticoids did not prolong the time to the next exacerbation for up to one follow-up year compared with

Effects of Antibiotic Therapy on AECOPD
69
4
Table 1. Baseline characteristics of COPD patients included in this study (N=1,105).
Patient characteristicsExposed (n=518)N (%)
Reference (n=587)N (%) P-value
Age (yr.)Median 55 (18) 54 (18) 0.24<= 50 185 (35.7) 222 (37.8) 0.7750-65 189 (36.5) 208 (35.4)>=65 144 (27.8) 157 (26.7)
Gender 0.68Male 211 (40.7) 232 (39.5)Female 307 (59.3) 355 (60.5)
BMI (kg/m2)Median 26.85 (6.5) 26.40 (5.9) 0.24<= 24.9 171 (33.0) 203 (34.6) 0.3525.0-29.9 195 (37.6) 239 (40.7) >= 30 152 (29.3) 145 (24.7)
Lung functionFEV1 (L) 2.59 (1.0) 2.68 (1.0) 0.24FEV1 (% predicted) 83.91 (23.25) 84.28 (22.29) 0.76FVC (L) 3.86 (1.0) 3.96 (1.0) 0.13FVC (% predicted) 65.54 (18.72) 66.45 (17.16) 0.72FEV1 to FVC ratio 0.68 (0.11) 0.67 (0.09) 0.77
GOLD stage 0.43I: Mild 266 (59.1) 307 (59.4)II: Moderate 160 (35.6) 193 (37.3)III and IV: Severe/very severe 24 (5.4%) 17 (3.3)
Smoking status 0.25Current smoker 169 (35.6) 167 (30.8)Former smoker 190 (40.0) 227 (41.9)Non smoker 116 (24.4) 148 (27.3)
No. of AECOPD in previous yr. 0.010 472 (91.1) 557 (94.9)1 17 (3.3) 17 (2.9)2 or more 29 (5.6) 13 (2.2)
No. of antibiotics prescription in previous yr. <0.010 20 (3.9) 322 (54.9)1 228 (44.0) 139 (23.7)2 or more 270 (52.1) 126 (21.5)
ComorbiditiesA. Cardiovascular diseases
Heart failure 22 (4.2) 12 (2.0) 0.03Heart attack 23 (4.4) 18 (3.1) 0.23Stroke < 10 11 (1.9) 0.87Arrhythmia 74 (14.4) 78 (13.3) 0.63Hypertension 165 (31.9) 180 (30.7) 0.67

Chapter 4
70
treatment with only glucocorticoids. Our results, after limiting to the COPD patients to those who had spirometrically-confirmed COPD, were robust. Similar robust results were also obtained after excluding COPD patients with self-reported asthma.
The beneficial treatment effects of antibiotic use for AECOPD observed in this study were consistent with the updated pooled results by Vollenweider et al. for outpatients.12 The finding that additional antibiotic treatment for AECOPD did not produce long-term beneficial effects is also consistent with results of a previous RCT conducted in COPD outpatients.13 Conversely, two previous observational studies reported that antibiotic treatment is associated with a reduced risk of a subsequent exacerbation.17,18 However,
Table 1. (continued)
Patient characteristicsExposed (n=518)N (%)
Reference (n=587)N (%) P-value
B. other major disordersAsthma 169 (32.6) 200 (34.1) 0.62Pulmonary fibrosis < 10 < 10 0.99Diabetes 28 (5.4) 34 (5.8) 0.78Cancer < 10 < 10 0.79Osteoporosis 27 (5.2) 21 (3.6) 0.18Renal impairment 16 (3.1) 22 (3.7) 0.55Depression 83 (16.0) 87 (14.8) 0.58Anxiety < 10 < 10 0.26Anemia 72 (13.9) 78 (13.3) 0.77
C. other minor disordersUlcerative colitis < 10 < 10 0.03Stomach ulcer 24 (4.6) 23 (3.9) 0.56Irritable bowel syndrome 61 (11.8) 62 (10.6) 0.52Hepatic impairment 13 (2.5) 10 (1.7) 0.35
COPD maintenance medications in previous yr.SABA 169 (32.6) 183 (31.2) 0.61LABA 22 (4.2) 31 (5.3) 0.42SAMA 12 (2.3) 14 (2.4) 0.94LAMA 72 (13.9) 61 (10.4) 0.07ICS 67 (12.9) 70 (11.9) 0.61LABA/ICS 190 (36.7) 194 (33) 0.21Theophylline < 10 < 10 0.67
Note: Data are presented as mean (standard deviation [SD]) or median with interquartile range (IQR) or numbers with percentage. Due to privacy protection of patients according to contract, the number below 10 was not permitted to present. Abbreviations: BMI: body mass index; SABA: short-acting β agonist; SAMA: short-acting muscarinic antagonist; LABA: long-acting β agonist; LAMA: long-acting muscarinic antagonist; ICS: inhaled corticosteroid; GOLD: global initiative for chronic obstructive lung disease; FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; AECOPD: acute exacerbation of chronic obstructive pulmonary disease;

Effects of Antibiotic Therapy on AECOPD
71
4
insufficient information in these studies on, for example, lung function, smoking history and related comorbidities, which are important risk factors associated with exacerbation events, could have accounted for these discrepancies.28
GOLD guidelines recommend amoxicillin with clavulanic acid, macrolide and tetracycline as the first-line antibiotics treatment for AECOPD.3 The Dutch primary care guidelines recommend amoxicillin or doxycycline as first-line antibiotics in AECOPD treatment.26 The combined results of seven RCTs examined in the updated Cochrane review showed that the antibiotics were generally effective in treating AECOPD in outpatients.12 However, three of these studies examined combined antibiotics29-31 and only four focused on the specific antibiotics recommended in the above-mentioned guidelines: one on doxycycline, two on co-amoxiclav and one on amoxicillin.13,32-34 Therefore, no scientifically sound conclusion could be drawn about the effects of these specific antibiotics used for AECOPD. Regarding specific antibiotics in our study, doxycycline had significant beneficial treatment effects on AECOPD, we observed similar trends towards beneficial effects for macrolides and amocillin-clavunalate, though non-significant, which may be due to the limited power of our study size to detect effects in subgroup analysis, or there were no effects at all, and more qualified studies are needed
Table 2. Odds ratio for treatment failure of index exacerbation among COPD outpatients with adjustment by logistic regression and propensity score weighted analysis.
Treatment groups(No.)
Treatment failure No. (%)
Crude OR (95% CI)
Adjusted OR (95% CI)a
PS adjusted OR (95% CI)b
Reference (587) 56 (10.8) 1 1 1All antibiotics (518) 56 (10.8) 1.03 (0.70-1.50) 0.67 (0.42-1.04) 0.63 (0.40-0.99)*
Doxycycline (214) 19 (8.9) 0.83 (0.48-1.42) 0.53 (0.28-1.00)* 0.53 (0.28-0.99)*
Macrolides (102) 11 (10.8) 1.02 (0.52-2.02) 0.49 (0.22-1.11) 0.58 (0.26-1.29)Amoxicillin (100) 18 (18.0) 1.86 (1.05-3.30) 1.56 (0.81-3.00) 1.49 (0.78-2.84)Co-amoxicillin (87) < 10 0.74 (0.33-1.68) 0.50 (0.19-1.32) 0.46 (0.17-1.24)
Abbreviation: OR: odds ratio; CI: confidence interval; PS: propensity score weighted analysis; No.: number; aAdjusted result by logistic regression; bAdjusted result by propensity score weighted analysis; *P<0.05;
Tables 3. Hazard ratio for next exacerbation with follow-up of 1 year among COPD outpatients.
Follow-up time Antibiotics group Reference group Crude HR (95% CI) Adjusted HR (95% CI)a
3 months 57 (11.0) 60 (10.2) 1.10 [0.76, 1.58] 1.11 [0.71, 1.71]6 months 109 (21.0) 119 (20.3) 1.06 [0.81, 1.37] 1.05 [0.77, 1.42]12 months 153 (29.5) 147 (25.0) 1.19 [0.95, 1.49] 1.14 [0.87, 1.49]
Abbreviation: HR: hazard ratio; CI: confidence interval; aAdjusted baseline characteristics by using cox hazard logistic regression.

Chapter 4
72
to explore these effects further. Regarding the short-term effects of doxycycline, the resistance of common pathogens for AECOPD like Haemophilus influenzae and Streptococcus pneumonia to doxycycline is reported to be rare in the Netherlands,35 this may contribute to its successful short-term treatment effects.
There is a general consensus that exacerbation frequency increases with COPD severity.36 Because the COPD severity of patients in our study was generally mild (around 60%) compared with that of patients in previous studies (10%-20%),12,13 the rate of next exacerbations in our study was relatively low. About 30% of patients experienced re-exacerbation after index exacerbation within one year of follow-up. After adjusting for possible confounders, we observed similar rates of next exacerbations between antibiotic users and non-antibiotic users, a finding that is consistent with that of a previous RCT report.13
Although the presence of purulent sputum is widely deemed to be the sole determinant of antibiotic treatment of AECOPD,3 its accuracy and reproducibility as an indicator of bacterial infection is limited,37 especially for outpatients. Consequently, guidelines on antibiotics prescriptions are not stringently adhered to for treating AECOPD.15 Moreover, antibiotics were unusually overprescribed for patients, notably for patients between 18 and 65 years of age in general practice.16,38 Accordingly, we could not exclude
Figure 3. Kaplan-Meier curves showing the proportion of patients free of next exacerbation in COPD outpatients up to follow-up of 1 year.
Figure 3. Kaplan‐Meier curves showing the proportion of patients free of next exacerbation in
COPD outpatients up to follow‐up of 1 year.
Subgroup and sensitivity results
The findings of both the logistic regression and PS analyses indicated that the risk of treatment
failure was reduced significantly by 47% by doxycycline compared to the reference treatments
(aOR 0.53 [95% CI: 0.28‐1.00] and 0.53 [95% CI: 0.28‐0.99] by regression and PS analyses,
respectively, Table 1). Although not statistically significant, similar beneficial trends were seen
for the macrolides exposed group (aOR 0.49 [95% CI: 0.22‐1.11] and 0.58 [95% CI: 0.26‐1.29]
by regression and PS analyses, respectively) and co‐amoxicillin exposed group (aOR 0.50 [95%
CI: 0.19‐1.32] and 0.46 [95% CI: 0.17‐1.24] by regression and PS analyses, respectively)
compared to the results in the reference group. No statistical difference was observed
between the amoxicillin exposed group and the reference group (aOR 1.56 [95% CI: 0.81‐3.00]
and 1.49 [95% CI: 0.78‐2.84] by regression and PS analyses, respectively) and the point
estimate of aOR was in the opposite direction.
Even when we excluded self‐reported COPD and focused only on spirometrically‐confirmed
COPD, the protective effect of antibiotics on treatment failure continued (aOR 0.56 [95% CI:

Effects of Antibiotic Therapy on AECOPD
73
4Ta
ble
4. S
ensi
tivity
ana
lyse
s: od
ds ra
tio fo
r tre
atm
ent f
ailu
re o
f ind
ex e
xace
rbat
ion
amon
g CO
PD o
utpa
tient
s.
Lim
ited
stud
y po
pula
tion
(Num
ber)
Trea
tmen
t fai
lure
N
o. (%
)Cr
ude
OR
(95%
CI)
Adju
sted
ORa
(95%
CI)
PS a
djus
ted
ORb
(95%
CI)
Antib
iotic
sRe
fere
nce
COPD
with
out a
sthm
a (7
36)
36 (1
0.3)
)39
(10.
1)1.
03 [0
.64,
1.6
6]0.
58 [0
.32,
1.0
1]0.
57 [0
.32,
1.0
2]CO
PD w
ith a
sthm
a (3
69)
20 (1
1.8)
23 (1
1.5)
1.03
[0.5
5, 1
.95]
0.81
[0.3
9, 1
.67]
0.71
[0.3
5, 1
.48]
Spiro
met
rical
ly c
onfir
med
CO
PD (7
07)
30 (9
.4)
43 (1
.1)
0.83
[0.5
1, 1
.36]
0.56
[0.3
2, 0
.97]
0.52
[0.2
9, 0
.90]
Self-
repo
rted
CO
PD (3
98)
26 (1
3.1)
19 (9
.5)
1.42
[0.7
6, 2
.67]
1.03
[0.4
6, 2
.32]
0.94
[0.4
3, 2
.06]
Abbr
evia
tion:
OR:
odd
s rat
io; C
I: co
nfide
nce
inte
rval
; PS:
pro
pens
ity sc
ore
wei
ghte
d an
alys
is; N
o.: n
umbe
r; a ad
just
ed re
sult
by lo
gist
ic re
gres
sion
; b Adju
sted
resu
lt by
pro
pens
ity sc
ore
wei
ghte
d an
alys
is; * P<
0.05
;
Chapter 4
74
the possibility that antibiotic treatment for some of patients were improperly prescribed. The general implication of our finding is that contrasting with an ideal situation in which all patients’ prescriptions adhere to the guidelines, effects of antibiotics for a bacterially caused AECOPD were underestimated in our study.
Clinical implications
Although improper use of antibiotics may occur within the COPD outpatient population in a real-world setting, our findings supported the beneficial effect of antibiotics used for AECOPD. Valid antibiotics prescription could further improve the effects of antibiotic treatments on AECOPD. According to the latest GOLD guideline, the sputum colour can be used to avoid unnecessary antibiotic therapy safely with cream, white or clear sputum indicating very low bacterial infections.3,14 If applicable, a procalcitonin-guided algorithm or C-reactive protein (CPR) test can also be considered before making decisions for GP to reduce the unnecessary administration of antibiotics .39,40
Given significant variability between GP practices of prescribing antibiotics to COPD patients experiencing exacerbations,41 we recommend doxycycline as the mainstay based on our findings that are consistent with the Dutch guidelines.26 Though estimates indicate similar beneficial effects for some specific antibiotics, larger studies of high quality with extensive control for potential confounders are needed to explore their role in AECOPD management. Importantly, the final antibiotic choice should also be based on the local bacterial resistance patterns, and sputum cultures of high-risk patients with frequent exacerbations and severe airflow limitations should be performed, given the possible presence of resistant pathogens.3
Strengths and limitations
Our study had several strengths. Firstly, the population included in this study was representative of COPD outpatients. Hence our findings reflect the real-world effects of antibiotic treatment for AECOPD. Secondly, properly diagnosed COPD patients and their complete background information , for example, lung function, smoking status and related comorbidities that were lacking in previous observational studies were included in this study. Moreover, the outcomes were adjusted for possible confounders using both logistic regression and PS analyses. Sensitivity analyses by further narrowing study population by excluding different sources of uncertainty were also conducted to test the robustness of the results.
There were, however, several limitations. Firstly, an acute exacerbation was defined by the prescriptions of systemic glucocorticoids as a proxy according to Dutch guideline for AECOPD and this may have led to some misclassifications. In addition, we lacked clinical information on the severity of AECOPD at the time of diagnosis. Moreover, the severity of exacerbations may not have been evenly distributed between the two comparison

Effects of Antibiotic Therapy on AECOPD
75
4
groups. Secondly, antibiotics may have been prescribed improperly in the absence of confirmed bacterial infections, this could lead to an underestimated effect of antibiotics on AECOPD. Thirdly, the low power of subgroup analyses in this study hindered us to make a definitive conclusion regarding the effects of some specific antibiotics on AECOPD. Finally, the IADB.nl did not include prescriptions during a hospitalization. However, given the relatively mild outpatient group, we expect only few patients to have such a serious outcome in our study.
CONCLUSIONThe results of this study support the use of antibiotic therapy, notably doxycycline, for AECOPD in addition to systematic glucocorticoids treatment among outpatients. Further larger qualified studies with prospective designs and extensive control of confounders are required to explore the effects of other specific antibiotics in a real-world settings. No further long-term beneficial effects of antibiotics treatment on AECOPD were found for subsequent exacerbations.
Chapter 4
76
REFERENCES1. Lozano R, Naghavi M, Foreman K, et al.
Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095-2128.
2. Lopez AD, Shibuya K, Rao C, et al. Chronic obstructive pulmonary disease: current burden and future projections. Eur Respir J. 2006;27(2):397-412.
3. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease: 2020 Report. https://goldcopd.org/gold-reports/. Date last accessed: December 17, 2019.
4. Donaldson GC, Seemungal TAR, Bhowmik A, Wedzicha JA. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax. 2002;57(10):847-852.
5. Anzueto A. Impact of exacerbations on COPD. Eur Respir Rev. 2010;19(116):113-118.
6. Walters JAE, Tan DJ, White CJ, Gibson PG, Wood-Baker R, Walters EH. Systemic corticosteroids for acute exacerbations of chronic obstructive pulmonary disease. Cochrane Db Syst Rev. 2014(9).
7. Moghoofei M, Azimzadeh Jamalkandi S, Moein M, Salimian J, Ahmadi A. Bacterial infections in acute exacerbation of chronic obstructive pulmonary disease: a systematic review and meta-analysis. Infection. 2019.
8. Sethi S, Murphy TF. Infection in the pathogenesis and course of chronic obstructive pulmonary disease. N Engl J Med. 2008;359(22):2355-2365.
9. Wilkinson TMA, Aris E, Bourne SC, et al. Drivers of year-to-year variation in exacerbation frequency of COPD: analysis of the AERIS cohort. ERJ Open Res. 2019;5(1).
10. Monso E, Garcia-Aymerich J, Soler N, et al. Bacterial infection in exacerbated COPD with changes in sputum characteristics. Epidemiol Infect. 2003;131(1):799-804.
11. Vollenweider DJ, Jarrett H, Steurer-Stey CA, Garcia-Aymerich J, Puhan MA. Antibiotics for exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;12:CD010257.
12. Vollenweider DJ, Frei A, Steurer-Stey CA, Garcia-Aymerich J, Puhan MA. Antibiotics for exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2018;10:CD010257.
13. van Velzen P, Ter Riet G, Bresser P, et al. Doxycycline for outpatient-treated acute exacerbations of COPD: a randomised double-blind placebo-controlled trial. Lancet Respir Med. 2017;5(6):492-499.
14. Kurisu K, Yoshiuchi K, Ogino K, Okada Y, Oda T. Peak C-reactive protein levels do not predict 30-day mortality for bacteremia: A retrospective cohort study. J Infect Chemother. 2020;26(1):23-27.
15. Bathoorn E, Groenhof F, Hendrix R, et al. Real-life data on antibiotic prescription and sputum culture diagnostics in acute exacerbations of COPD in primary care. Int J Chron Obstruct Pulmon Dis. 2017;12:285-290.
16. Roede BM, Bindels PJ, Brouwer HJ, Bresser P, de Borgie CA, Prins JM. Antibiotics and steroids for exacerbations of COPD in primary care: compliance with Dutch guidelines. Br J Gen Pract. 2006;56(530):662-665.
17. Roede BM, Bresser P, Prins JM, Schellevis F, Verheij TJM, Bindels PJE. Reduced risk of next exacerbation and mortality associated with antibiotic use in COPD. Eur Respir J. 2009;33(2):282-288.
18. Roede BM, Bresser P, Bindels PJE, et al. Antibiotic treatment is associated with reduced risk of a subsequent exacerbation in obstructive lung disease: an historical population based cohort study. Thorax. 2008;63(11):968-973.
19. Stefan MS, Rothberg MB, Shieh MS, Pekow PS, Lindenauer PK. Association between antibiotic treatment and outcomes in patients hospitalized with acute

Effects of Antibiotic Therapy on AECOPD
77
4
exacerbation of COPD treated with systemic steroids. Chest. 2013;143(1):82-90.
20. Petite SE, Murphy JA. Systemic Corticosteroid and Antibiotic Use in Hospitalized Patients With Chronic Obstructive Pulmonary Disease Exacerbation. Ann Pharmacother. 2019;53(2):144-150.
21. Sediq R, van der Schans J, Dotinga A, et al. Concordance assessment of self-reported medication use in the Netherlands three-generation Lifelines Cohort study with the pharmacy database iaDB.nl: The PharmLines initiative. Clin Epidemiol. 2018;10:981-989.
22. Klijs B, Scholtens S, Mandemakers JJ, Snieder H, Stolk RP, Smidt N. Representativeness of the LifeLines Cohort Study. Plos One. 2015;10(9).
23. Visser ST, Schuiling-Veninga CCM, Bos JHJ, de Jong-van den Berg LTW, Postma MJ. The population-based prescription database IADB.nl: its development, usefulness in outcomes research and challenges. Expert Rev Pharm Out. 2013;13(3):285-292.
24. Scholtens S, Smidt N, Swertz MA, et al. Cohort Profile: LifeLines, a three-generation cohort study and biobank. Int J Epidemiol. 2015;44(4):1172-1180.
25. Stolk RP, Rosmalen JGM, Postma DS, et al. Universal risk factors for multifactorial diseases - LifeLines: a three-generation population-based study. Eur J Epidemiol. 2008;23(1):67-74.
26. Snoeck-Stroband JB ST, Van Schayck CP, Muris JW, Van der Molen T, In ’t Veen JCCM, Chavannes NH, Broekhuizen BDL, Barnhoorn MJM, Smeele I, Geijer RMM, Tuut MK. NHG-Werkgroep Astma bij volwassenen en COPD. NHG-Standaard COPD (derde herziening). Huisarts Wet 2015;58(4):198-211.
27. Seemungal TA, Donaldson GC, Bhowmik A, Jeffries DJ, Wedzicha JA. Time course and recovery of exacerbations in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2000;161(5):1608-1613.
28. Mullerova H, Shukla A, Hawkins A, Quint J. Risk factors for acute exacerbations
of COPD in a primary care population: a retrospective observational cohort study. Bmj Open. 2014;4(12):e006171.
29. Hassan WA, Shalan I, Elsobhy M. Impact of antibiotics on acute exacerbations of COPD. Egypt J Chest Dis Tu. 2015;64(3):579-585.
30. Sachs APE, Koeter GH, Groenier KH, Vanderwaaij D, Schiphuis J, Meyboomdejong B. Changes in Symptoms, Peak Expiratory Flow, and Sputum Flora during Treatment with Antibiotics of Exacerbations in Patients with Chronic Obstructive Pulmonary-Disease in General-Practice. Thorax. 1995;50(7):758-763.
31. Anthonisen NR, Manfreda J, Warren CP, Hershfield ES, Harding GK, Nelson NA. Antibiotic therapy in exacerbations of chronic obstructive pulmonary disease. Ann Intern Med. 1987;106(2):196-204.
32. Llor C, Moragas A, Hernandez S, Bayona C, Miravitlles M. Efficacy of antibiotic therapy for acute exacerbations of mild to moderate chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186(8):716-723.
33. Brusse-Keizer M, VanderValk P, Hendrix R, Kerstjens H, van der Palen J. Necessity of amoxicillin clavulanic acid in addition to prednisolone in mild-to-moderate COPD exacerbations. Bmj Open Respir Res. 2014;1(1):e000052.
34. Jorgensen AF, Coolidge J, Pedersen PA, Petersen KP, Waldorff S, Widding E. Amoxicillin in treatment of acute uncomplicated exacerbations of chronic bronchitis. A double-blind, placebo-controlled multicentre study in general practice. Scand J Prim Health Care. 1992;10(1):7-11.
35. Greeff SC, Mouton JW, eds. NethMap 2015. Consumption of antimicrobial agents and antimicrobial resistance among medically important bacteria in the Netherlands. Bilthoven: National Institute for Public Health and the Environment, 2015.
36. Donaldson GC, Wedzicha JA. COPD exacerbations 1: Epidemiology. Thorax. 2006;61(2):164-168.

Chapter 4
78
37. Siddiqi A, Sethi S. Optimizing antibiotic selection in treating COPD exacerbations. Int J Chron Obstruct Pulmon Dis. 2008;3(1):31-44.
38. Dekker AR, Verheij TJ, van der Velden AW. Inappropriate antibiotic prescription for respiratory tract indications: most prominent in adult patients. Fam Pract. 2015;32(4):401-407.
39. Chan HP, Lim TK. Procalcitonin and antibiotics in moderate-severe acute exacerbation of chronic obstructive
pulmonary disease: to use or not to use. Curr Opin Pulm Med. 2019;25(2):150-157.
40. Butler CC, Gillespie D, White P, et al. C-Reactive Protein Testing to Guide Antibiotic Prescribing for COPD Exacerbations. N Engl J Med. 2019;381(2):111-120.
41. Boggon R, Hubbard R, Smeeth L, et al. Variability of antibiotic prescribing in patients with chronic obstructive pulmonary disease exacerbations: a cohort study. Bmc Pulm Med. 2013;13:32.


C H A P T E R 5

Yuanyuan Wang Muh. Akbar Bahar
Anouk M.E. Jansen Janwillem W.H. Kocks
Jan-Willem C. Alffenaar Eelko Hak
Bob Wilffert Sander D. Borgsteede
Improving antibacterial prescribing safety in the management of COPD exacerbations:
systematic review of observational and clinical studies on potential drug interactions associated
with frequently prescribed antibacterials among COPD Patients
Published as: Wang Y, Bahar MA, Jansen AME, Kocks JWH, Alffenaar JC, Hak E, Wilffert B, Borgsteede SD. Improving antibacterial prescribing safety in
the management of COPD exacerbations: systematic review of observational and clinical studies on potential drug interactions associated with
frequently prescribed antibacterials among COPD patients. J Antimicrob Chemother. 2019;74(10):2848–2864.

Chapter 5
82
ABSTRACTBackground
Guidelines advice the use of antibacterials (ABs) in the management of COPD exacerbations. COPD patients often have multiple comorbidities like diabetes mellitus and cardiac diseases leading to polypharmacy. Consequently, drug-drug interactions (DDIs) may frequently occur, cause serious adverse events and treatment failure.
Objective
(i) To review DDIs related to frequently prescribed ABs among COPD patients from observational and clinical studies. (ii) To improve AB prescribing safety in clinical practice by structuring DDIs according to comorbidities of COPD.
Methods
We conducted a systematic review by searching Pubmed and Embase up to Feb 8, 2018 for clinical trials, cohort and case-control studies reporting DDIs of ABs used for COPD. Study design, subjects, sample size, pharmacological mechanism of DDI, and effect of interaction were extracted. We evaluated level of DDIs and quality of evidence according to established criteria and structured the data by possible comorbidities.
Results
In all, 318 articles were eligible for review describing a wide range of drugs used for comorbidities and their potential DDIs with ABs. DDIs between ABs and co-administered drugs could be subdivided into: (1) co-administered drugs alter the pharmacokinetics of ABs; and (2) ABs interfere with the pharmacokinetics of co-administered drugs. The DDIs could lead to therapeutic failures or toxicities.
Conclusion
DDIs related to ABs with clinical significance may involve a wide range of indicated drugs to treat comorbidities in COPD. The evidence can support (computer supported) decision-making by health practitioners when prescribing ABs during COPD exacerbations in the case of co-medication.

DDIs Associated with Antibacterials for COPD
83
5
INTRODUCTIONChronic obstructive pulmonary disease (COPD) is a complex respiratory disorder characterized by persistent respiratory symptoms and airflow limitation.1 The chronic and progressive course of COPD is frequently aggravated by exacerbation defined as an acute worsening of respiratory symptoms like increased cough, dyspnea and production of sputum.2 Exacerbations of COPD can be triggered by respiratory tract infections, 40% to 60% of exacerbations are caused by bacteria, especially by Haemophilus influenzae, Streptococcus pneumoniae and Moraxella catarrhalis.3 Evidence from randomized controlled trials (RCTs) indicated that use of antibacterials (ABs) may reduce the frequency and severity of COPD exacerbations.4-6 Therefore, guidelines have recommended involving ABs in the therapeutic and preventive management of COPD exacerbations.1,7
Patients with COPD often suffer from multiple morbidities.8 Hence, polypharmacy is common and contributes to drug-drug interactions (DDIs). Adverse drug reactions (ADRs) or therapeutic failure may be the result of ABs and co-administered drugs interactions. Besides, COPD is an age-related disease and elderly are more susceptible to the effect of DDIs because of gradual physiologic changes affecting pharmacokinetics and pharmacodynamics.9
The objective of this study was to (1) systematically review DDIs related to frequently prescribed ABs among COPD patients from observational and clinical studies and (2) improve AB prescribing safety in clinical practice by structuring DDIs according to comorbidities of COPD. Studies without comparison groups, and therefore have low quality of the causal evidence, like case reports about QT-interval prolonging interactions are not included in this review. Hence, a DDI handbook like Stockley’s Drug Interactions and the official product information can be referred to see the clinical impact of those kinds of interactions.
METHODSSearching strategy
We conducted a systematic review following PRISMA guideline. PubMed and Embase databases were searched for related articles published in English up to Feb 8, 2018 using key terms of “drug interactions,” “pharmacokinetics”, “pharmacodynamics”, and a list of most frequently used ABs for COPD (see Table 1). The ABs were selected based on two related Cochrane reviews and their prescription frequency by the University of Groningen prescription database IADB.nl (http://www.iadb.nl/) covering drug prescriptions of approximately 700,000 people.4,5 Additionally, we checked the primary sources of signals from Dutch DDI alert systems: G-Standard and Pharmabase.10

Chapter 5
84
Reference lists from eligible studies were also tracked for additional qualified papers. Searching details are provided in supplementary data.
Study selection criteria
Eligible studies met the following criteria: (1) DDIs in humans; (2) involving the targeted ABs; (3) being clinical trials, RCTs, cohort, or case-control study. We excluded case reports or other descriptive studies. We further excluded studies with subjects whose pharmacokinetics and pharmacodynamics were not comparable to the general COPD patients, e.g. newborn babies, pregnant women and patients with severe renal/hepatic impairment. Other exclusion criteria were: (1) unregistered drugs (by FDA or EMA); (2) involving three or more drug interactions; (3) not DDIs (food-drug, gene-drug); (4) not original studies (reviews, letters and editorials). Besides, pharmacodynamic interactions were beyond the scope of this review and then, excluded.
Data extraction and quality assessment
All records were exported to Refworks; title and abstracts were screened by Y.W. and A.M.E.J. independently. Full-text papers were obtained for records that were considered of potential relevance by at least one of the reviewers. Final decisions were made by consensus between two reviewers according to the preset criteria. Discrepancies between reviewers were resolved by discussion, a third reviewer (E.H.) was asked if no consensus was reached. Information about name of ABs and related interacting drug, study design, study subjects, sample size, interacting mechanism, effects of interaction, recommendation by study authors were extracted by the same reviewers (Y.W., A.M.E.J.)
Table 1. Antibacterials (ABs) of study that are frequently prescribed among COPD patients.*
Category Sub-category ABs included
Beta-lactam Penicillins Amoxicillin/clavulanic acid (co-amoxiclav), Amoxicillin, Flucloxacillin, Pheneticillin, phenoxymethylpenicillin (penicillin V),
Cephalosporins Cefaclor, Cefuroxime, Ceftriaxone, Cephradine, CeftazidimeMacrolides Erythromycin, Clarithromycin, Azithromycin, Roxithromycin,
Clindamycin,Tetracycline Tetracycline, Doxycycline, Minocycline, Quinolones Fluoroquinolone Ciprofloxacin, Moxifloxacin, Levofloxacin,
Ofloxacin, Norfloxacin, Other quinolone Pipemidic acid
Sulfonamides Sulfamethoxazole Others Nitrofurantoin, Methenamine, Trimethoprim
*based on two Cochrane reviews4 and use within the University Groningen prescription database IADB.nl from Netherlands (http://www.iadb.nl/)

DDIs Associated with Antibacterials for COPD
85
5
Table 2. Quality of Evidence for DDIs11,12
Definition Score
Clinical researches with appropriate control group and relevant pharmacokinetics and/or pharmacodynamics parameters. The studies meet all of the criteria below:
The interacting effect of concomitant medication with investigated drugs is reported in the manuscript.All of potential confounders are mentioned and taken into account (for example smoking behavior or renal function).The results of interaction are built on the ‘steady-state kinetics’.- Variation in dose was adjusted.
4
Clinical researches with appropriate control group and relevant pharmacokinetics and/or pharmacodynamics parameters which do not meet one or more pre-defined criteria above.
3
Complete observational studies with clinically relevant results. 2Incomplete observational studies. (e.g. without controlling confounders or presence of other explanation factors for the adverse reaction), case reports, SmPc.
1
In vitro studies, in vivo animal studies, prediction modelling studies. 0
Table 3. Description for level of DDIs10
Definition Score*
Involving inhibitor = > 200% ↑AUC; clearance ↓ > 67%Involving inducer = > 90% ↓ AUC; clearance ↑ ≥ 900%For observational studies, RR/OR ≥ 10
111
Involving inhibitor = 75-200% ↑AUC; clearance ↓ ≥ 43% to < 67%Involving inducer = 60-90% ↓ AUC; clearance ↑ ≥ 150% to < 900%For observational studies, RR/OR = 3~9
222
Involving inhibitor = 25-75% ↑AUC; clearance ↓ ≥ 20% to < 43%Involving inducer = 25-60% ↓AUC; clearance ↑ ≥ 33 % to < 150%For observational studies, RR/OR = 1.5~2.9
333
<25% change in AUC; clearance ↓ < 20% or ↑ < 33 %For observational studies, RR/OR < 1.5
44
a. For the Interacting drugs with narrow therapeutic index, the degree of DDIs will be improved to the one higher degree of level. b. If the DDIs level cannot be judged by the above criteria, we assess it by discussion based on available data and evidence.
ExceptionException
*definition: 1 = strong interaction, 2 = substantial interaction, 3 = moderate interaction, and 4 = weak/no interaction
and checked by another reviewer (M.A.B.). Quality of evidence was evaluated by grade 0 to 4 based on criteria (Table 2) used by previous studies.11,12
The strength of the DDIs were classified into four levels (1= strong /2 = substantial /3 = moderate /4 = weak/no) according to the preset published criteria (Table 3).12 In case

Chapter 5
86
of several studies on the same DDI combination, we categorized the DDI based on the highest level of severity. Considering that narrow therapeutic index (NTI) drugs are more vulnerable to DDIs, the strength of the DDI was upgraded one level.12
RESULTSPublications identified by literature search
Our search yielded 1,412 and 1,734 studies from Pubmed and Embase, respectively (Figure 1). After removing duplicates, 2,560 articles were screened by title and abstracts, of which 630 papers were included for full-text screening, resulting in 282 eligible articles. With 36 studies identified from other resources, we got 318 studies finally for assessment in this review.
The interacting drugs, underlying mechanisms, levels and practice recommendations of the DDIs are presented in Table 4. Details on individual studies of DDIs with a potential clinical significance (level 1 to 3) were presented in Supplementary Table S1 and S2 and the data of studies with a low level (weak or no) of DDIs were presented in Table S3.
Prescribing AB in COPD: step-by-step approach
1. Check if comorbidity is present (Table 4).2. A quick overview on AB and its interacting medication, possible interacting mechanism,
level of interaction, and practical recommendations is provided in Table 4.3. Detailed explanation about related interacting mechanism and recommendation to
manage related DDIs is provided in main text.
Mechanisms of DDI
AB can act as an inhibitor/inducer and/or a substrate producing moderate to strong DDI with other co-administered medication. There are two scenarios: (1) co-administered drug alters the pharmacokinetics parameters of AB; and (2) AB influences the pharmacokinetics parameters of co-administered medication. The main mechanisms of these DDIs are complex-forming, inhibition/ induction of drug metabolizing enzymes and alteration of drug transporters (Table 4). The ability to inhibit CYP3A4 makes the ABs prone to interact with many different drugs as CYP3A4 metabolizes more than 50% of the clinically prescribed drugs.13
Information structured according to drugs for comorbidities
The presentation of information on potential clinically significant DDIs with moderate to strong level of interaction is according to the most frequent comorbidities that

DDIs Associated with Antibacterials for COPD
87
5
have been reported in COPD patients.8,14 Potential mechanisms of DDIs and actionable recommendation to manage the DDIs are provided in Table 4.
1. Diabetes
Patients with COPD have a 50% higher risk to develop diabetes than persons without COPD.15 Some antidiabetic drugs are substrates of enzymes like CYP3A4 (glipizide, tolbutamide), CYP2C9 (glipizide, glyburide) and CYP2C8 (repaglinide); and substrates of drug transporter like P-gp transporter (glipizide, glyburide).16-26 ABs may inhibit the function of those metabolic enzymes and transporters such as clarithromycin (CYP3A4 and P-gp inhibitor), trimethoprim–sulfamethoxazole (CYP2C8/2C9 inhibitor) and levofloxacin (P-gp inhibitor). These medicines can potentially increase the blood concentration of those antidiabetic agents.16-26 Consequently, patients may develop hypoglycemia. Therefore, it is suggested to avoid these combinations by replacing related AB or adjusting the dose of antidiabetic agents as well as monitoring the patients’ blood glucose.
Figure 1. Flowchart of study selection.
Information structured according to drugs for comorbidities
The presentation of information on potential clinically significant DDIs with moderate to
strong level of interaction is according to the most frequent comorbidities that have been
reported in COPD patients.8,14 Potential mechanisms of DDIs and actionable
recommendation to manage the DDIs are provided in Table 4.
1. Diabetes
Patients with COPD have a 50% higher risk to develop diabetes than persons without
COPD.15 Some antidiabetic drugs are substrates of enzymes like CYP3A4 (glipizide,
tolbutamide), CYP2C9 (glipizide, glyburide) and CYP2C8 (repaglinide); and substrates of drug
transporter like P‐gp transporter (glipizide, glyburide).16‐26 ABs may inhibit the function of
those metabolic enzymes and transporters such as clarithromycin (CYP3A4 and P‐gp
inhibitor), trimethoprim–sulfamethoxazole (CYP2C8/2C9 inhibitor) and levofloxacin (P‐gp
Figure 1. Flowchart of study selection.

Chapter 5
88
2. Heart and circulatory system diseases
2.1. Antihypertensive agents
Hypertension is associated with COPD with relative risk of 1.6.15 Antihypertensive calcium channel blocker (CCB) like diltiazem and verapamil are CYP3A4 substrates.27-29 Therefore, macrolides (CYP3A4 inhibitors) can enhance the pharmacologic activity of CCB.30 Avoiding the combination by substitution of macrolides or CCB to another group of drugs or adjusting the dose of CCB while monitoring the blood pressure is recommended. Erythromycin and clarithromycin are the most potent CYP3A4 inhibitors, while azithromycin and roxithromycin are weak inhibitors.30,31 Hence, if prescribing macrolides, choosing macrolides with minimal inhibitory capacity to be co-prescribed with CCB may minimize the risk of DDI.
Spironolactone, a potassium sparing diuretic, is used to lower blood pressure. Spironolactone and trimethoprim–sulfamethoxazole combination may produce hyperkalemia because both drugs can inhibit renal excretion of potassium.32 Therefore, avoiding combination by selecting an alternative AB or adjusting the dose of spironolactone and closely monitoring potassium plasma levels is strongly recommended.
2.2. Lipid-lowering drugs
Lipid metabolism problem is one of the most prevalent comorbidities in COPD patients.14 The main pharmacologic approach to manage blood cholesterol levels is by statin therapy.33 Some ABs increase the plasma concentration of statins by several mechanisms. Statins like simvastatin and atorvastatin are bio-degraded by CYP3A4.34,35 Therefore, potent CYP3A4 inhibitors (erythromycin and clarithromycin) increase the risk for statin related side effects like rhabdomyolysis.34,35 Other statins like rosuvastatin, pravastatin and fluvastatin are not CYP3A4 substrates.36 Yet, the hepatic clearance of these statins are facilitated by anion–transporting polypeptides.37 These influx transporters facilitate the transportation of statins from systemic blood to liver cells to be metabolized or subsequently delivered into the bile for elimination.37 Clarithromycin and erythromycin have been reported to be inhibitors of these transporters.38 Therefore, replacing erythromycin and clarithromycin with other ABs, temporarily stopping statins, or adjusting the dose of statins while monitoring statin related side effects is recommended.
2.3. Oral anticoagulants
Both coumarins and direct oral anticoagulants (DOACs) may interact with ABs. Multiple studies reported that DDIs between ABs with coumarins (warfarin, phenprocoumon, acenocoumarol) led to increased risks of hemorrhage.39-58 Several interacting mechanisms were proposed.59,60 One mechanism is by disruption of intestinal flora

DDIs Associated with Antibacterials for COPD
89
5
that synthesizes vitamin K, as many ABs could alter the balance of gut flora.59 Another mechanism is that ABs (e.g. trimethoprim–sulfamethoxazole and macrolide) alter coumarins’ metabolism which mainly involves CYP2C9 and CYP3A4, respectively.60 Therefore, to choose alternative AB or if not possible, to monitor INR values and adjust the dose of coumarins is recommended.
DOACs are regarded as a safe alternative to replace coumarins.61 However, since some DOACs (edoxaban, rivaroxaban, dabigatran) are substrates of CYP3A4 and/or P-gp transporter, their AUC values can be increased by ABs like macrolides.62,63 Therefore, when macrolides and DOACs are required in combination, careful monitoring the signs of bleeding is needed, and adjusting the dose of DOACs should be done if it is necessary.
2.4. Antiarrhythmic agents
Some antiarrhythmic agents like digoxin, quinidine, lignocaine, and procainamide potentially interact with ABs.64-75 Quinidine and lignocaine are CYP3A4 substrates, and therefore, macrolides may inhibit their degradation and increase their bioavailabilities.64,65 Meanwhile, the renal clearance of procainamide and digoxin were inhibited by trimetophrim.66,67,72,73 Mechanism of interaction is inhibition of tubular secretion via inhibition of renal organic cation transporter because they are substrates of the transporter.66,67,72,73 Consequently, blood concentrations of these drugs are increased.66,67,72,73 Digoxin is a substrate of P-gp transporter.68-71 Accordingly, AUC of digoxin is elevated by clarithromycin and therefore, may cause toxicities.68-71 Since quinidine, lignocaine, digoxin, and procainamide are drugs with NTI, avoiding ABs that can lead to DDIs with these drugs is recommended.76,77 However, if they are necessary to be co-prescribed, therapeutic drug monitoring (TDM) of these antiarrhythmic agents is strongly recommended.77
3. Respiratory diseases
3.1. Medication for obstructive airways diseases
One of the most prevalent comorbidities in COPD is asthma.14 Some anti-asthma drugs such as methylprednisolone, montelukast, loratadine, roflumilast and theophylline were substrates of CYP3A4 and/or P-gp transporter and therefore, evidenced to interact with macrolides.78-87 Hence, one might consider other ABs to be combined with asthma drugs, or closely monitor patients, especially in case of theophylline which is a NTI drug.88 As theophylline is also metabolized by CYP1A2,89 ciprofloxacin (a CYP1A2 potent inhibitor) should be avoided.90-97
3.2. Anti-mycobacterial agents
Tuberculosis and COPD diseases share comparable risk factors and therefore, can coincide in individuals, particularly elderly patients.98 Rifampicin and rifabutin (anti-mycobacterial agents) work as potent inducers of hepatic and intestinal CYP enzymes.99

Chapter 5
90
Table 4. DDI of antibacterials (ABs) for COPD exacerbation and other drugs for treating its comorbidities
Comorbidity Medication Interacting AB Mechanism Management suggestionLevel of interaction Ref.
1. DiabetesAntidiabetic medication
Glipizide, glyburide TMP-SMX Inhibition of CYP2C9 Consider alternative, adjusted dose of substrate or used cautiously by monitoring patients’ blood glucose.
2 16-19Glyburide Clarithromycin Inhibition of P-gp
Glipizide, glyburide Levofloxacin Inhibition of P-gp Monitor patients’ blood glucose and if necessary, adjusted dose of substrate.
3 16, 20-26Tolbutamide Clarithromycin Inhibition of CYP3A4 &
P-gpTMP-SMX Inhibition of CYP2C9
Glipizide, repaglinide Clarithromycin Inhibition of CYP3A4Repaglinide, rosiglitazone TMP-SMX Inhibition of CYP2C8Metformin TMP-SMX Inhibition of OCT2 &
MATE12. Heart and circulatory system diseases2.1 Antihypertensive agents
Spironolactone TMP-SMX Inhibition of potassium secretion
Avoid combination or adjusted dose of substrates & closely monitoring potassium plasma levels.
1 32
Calcium channel blocker Erythromycin, clarithromycin Inhibition of CYP3A4 Consider alternative/adjusted dose of substrate or used cautiously by monitoring side effects.
2 27-29
Azithromycin Inhibition of CYP3A4 Monitor side effects and if necessary, adjusted dose of substrate.
3 27
2.2 Lipid-lowering drugs
Simvastatin Erythromycin Inhibition of CYP3A4 Avoid combination or adjusted dose of substrates & closely monitoring side effects.
1 34
Atorvastatin Clarithromycin Inhibition of CYP3A4 Consider alternative/adjusted dose of substrate or used cautiously by monitoring side effects.
2 35
Erythromycin Inhibition of CYP3A4 Monitor side effects and if necessary, adjusted the dose of substrate.
3 36, 204Rosuvastatin/pravastatin/fluvastatin Clarithromycin Inhibition of OAT
2.3 Oral anticoagulants Warfarin, phenprocoumon /acenocoumarol
TMP-SMX Inhibition of CYP2C9 Avoid combination or closely monitor the change of INR routinely and adjusted the dose if needed.
1 39-58
Amoxicillin/co-amoxiclav, ceftriaxone Alterations in normal gut flora
Choose alternative AB or if not possible, monitor the change of INR routinely.
2
Clarithromycin, azithromycin, ciprofloxacin, levofloxacin, ofloxacin, doxycycline
Inhibition of CYP3A4 or alterations in normal gut flora
Edoxaban, dabigatran, rivaroxaban Erythromycin, clarithromycin Inhibition of CYP3A4 &/or P-gp
Consider alternative/adjusted dose of substrate or monitor the signs of excessive anticoagulant effect.
2 62, 63
Warfarin Moxifloxacin Inhibition of CYP3A4 or alterations in normal gut flora
Monitor the change of INR routinely 3 41

DDIs Associated with Antibacterials for COPD
91
5
Table 4. DDI of antibacterials (ABs) for COPD exacerbation and other drugs for treating its comorbidities
Comorbidity Medication Interacting AB Mechanism Management suggestionLevel of interaction Ref.
1. DiabetesAntidiabetic medication
Glipizide, glyburide TMP-SMX Inhibition of CYP2C9 Consider alternative, adjusted dose of substrate or used cautiously by monitoring patients’ blood glucose.
2 16-19Glyburide Clarithromycin Inhibition of P-gp
Glipizide, glyburide Levofloxacin Inhibition of P-gp Monitor patients’ blood glucose and if necessary, adjusted dose of substrate.
3 16, 20-26Tolbutamide Clarithromycin Inhibition of CYP3A4 &
P-gpTMP-SMX Inhibition of CYP2C9
Glipizide, repaglinide Clarithromycin Inhibition of CYP3A4Repaglinide, rosiglitazone TMP-SMX Inhibition of CYP2C8Metformin TMP-SMX Inhibition of OCT2 &
MATE12. Heart and circulatory system diseases2.1 Antihypertensive agents
Spironolactone TMP-SMX Inhibition of potassium secretion
Avoid combination or adjusted dose of substrates & closely monitoring potassium plasma levels.
1 32
Calcium channel blocker Erythromycin, clarithromycin Inhibition of CYP3A4 Consider alternative/adjusted dose of substrate or used cautiously by monitoring side effects.
2 27-29
Azithromycin Inhibition of CYP3A4 Monitor side effects and if necessary, adjusted dose of substrate.
3 27
2.2 Lipid-lowering drugs
Simvastatin Erythromycin Inhibition of CYP3A4 Avoid combination or adjusted dose of substrates & closely monitoring side effects.
1 34
Atorvastatin Clarithromycin Inhibition of CYP3A4 Consider alternative/adjusted dose of substrate or used cautiously by monitoring side effects.
2 35
Erythromycin Inhibition of CYP3A4 Monitor side effects and if necessary, adjusted the dose of substrate.
3 36, 204Rosuvastatin/pravastatin/fluvastatin Clarithromycin Inhibition of OAT
2.3 Oral anticoagulants Warfarin, phenprocoumon /acenocoumarol
TMP-SMX Inhibition of CYP2C9 Avoid combination or closely monitor the change of INR routinely and adjusted the dose if needed.
1 39-58
Amoxicillin/co-amoxiclav, ceftriaxone Alterations in normal gut flora
Choose alternative AB or if not possible, monitor the change of INR routinely.
2
Clarithromycin, azithromycin, ciprofloxacin, levofloxacin, ofloxacin, doxycycline
Inhibition of CYP3A4 or alterations in normal gut flora
Edoxaban, dabigatran, rivaroxaban Erythromycin, clarithromycin Inhibition of CYP3A4 &/or P-gp
Consider alternative/adjusted dose of substrate or monitor the signs of excessive anticoagulant effect.
2 62, 63
Warfarin Moxifloxacin Inhibition of CYP3A4 or alterations in normal gut flora
Monitor the change of INR routinely 3 41
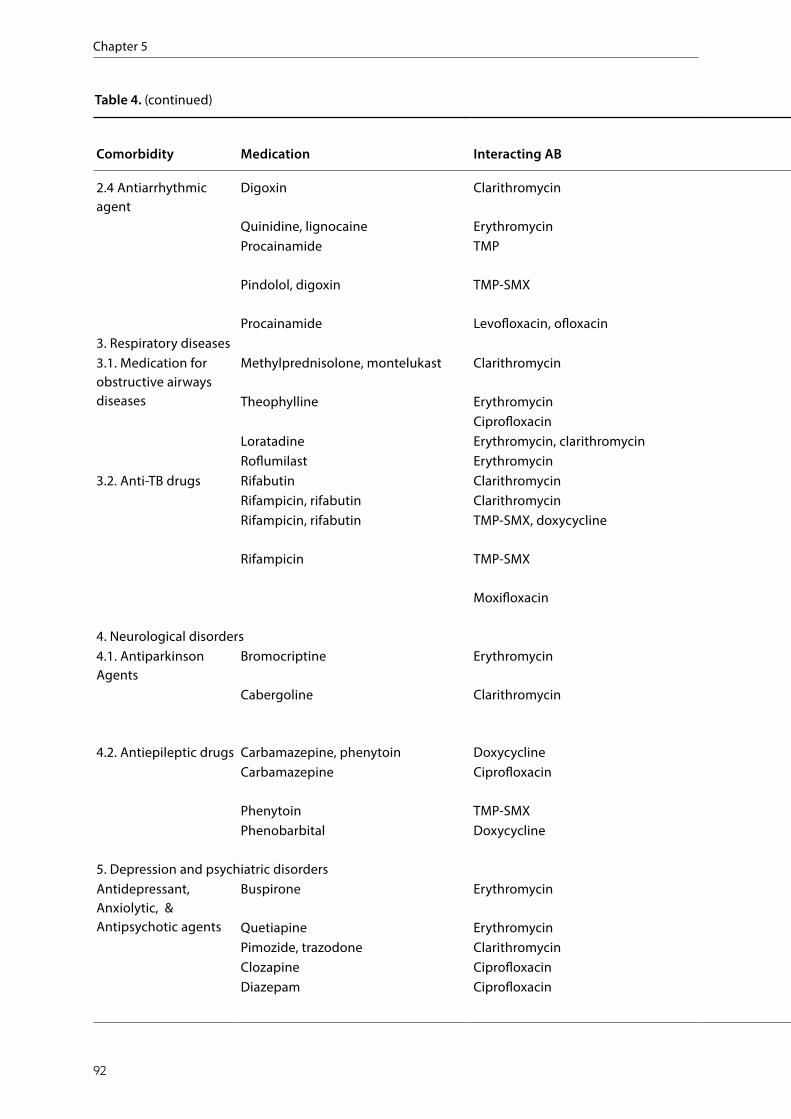
Chapter 5
92
Table 4. (continued)
Comorbidity Medication Interacting AB Mechanism Management suggestionLevel of interaction Ref.
2.4 Antiarrhythmic agent
Digoxin Clarithromycin Inhibition of P-gp Avoid combination or perform TDM and if necessary, adjusted dose of substrate.
1 68-71
Quinidine, lignocaine Erythromycin Inhibition of CYP3A4 Consider alternative or perform TDM and if necessary, adjusted dose of substrate.
2 64-67Procainamide TMP Inhibition of tubular
secretionPindolol, digoxin TMP-SMX Inhibition of tubular
secretionPerform TDM and if necessary, adjusted dose of substrate.
3 72-75
Procainamide Levofloxacin, ofloxacin Inhibition of OCT3. Respiratory diseases3.1. Medication for obstructive airways diseases
Methylprednisolone, montelukast Clarithromycin Inhibition of CYP3A4 & P-gp
Consider alternative/adjusted dose of substrate or used cautiously by monitoring side effects. For theophylline, perform TDM.
2 78-85, 90-97
Theophylline Erythromycin Inhibition of CYP3A4Ciprofloxacin Inhibition of CYP1A2
Loratadine Erythromycin, clarithromycin Inhibition of CYP3A4 Monitor side effects and if necessary, adjusted dose of substrate.
3 86, 87Roflumilast Erythromycin Inhibition of CYP3A4
3.2. Anti-TB drugs Rifabutin Clarithromycin Inhibition of CYP3A4 Avoid combination 1 101, 110, 111Rifampicin, rifabutin Clarithromycin Induction of CYP3A4 Consider alternative AB for COPD 2 100, 101Rifampicin, rifabutin TMP-SMX, doxycycline Induction of CYP3A4/
CYP2C9 Consider alternative AB for COPD or monitor the effectiveness of AB and if necessary, adjusted dose of AB.
3 102-104, 106-109
Rifampicin TMP-SMX Inhibition of mixed oxidases
Moxifloxacin Inducing phase II enzymes
4. Neurological disorders4.1. Antiparkinson Agents
Bromocriptine Erythromycin Inhibition of CYP3A4 Avoid combination or adjusted dose of substrates & closely monitoring side effects.
1 112
Cabergoline Clarithromycin Inhibition of CYP3A4 & P-gp
Consider alternative/adjusted dose of substrate or used cautiously by monitoring side effects.
2 113
4.2. Antiepileptic drugs Carbamazepine, phenytoin Doxycycline Induction of CYP3A4 Consider alternative or perform TDM 2 117, 116Carbamazepine Ciprofloxacin Inhibition of
CYP3A4/1A2Consider alternative or perform TDM 2 118
Phenytoin TMP-SMX Inhibition of CYP2C8 Consider alternative or perform TDM 2 116, 119Phenobarbital Doxycycline Induction of CYP3A4 Monitor side effects and if necessary, adjusted
dose of substrate.3 115
5. Depression and psychiatric disordersAntidepressant, Anxiolytic, & Antipsychotic agents
Buspirone Erythromycin Inhibition of CYP3A4 Avoid combination or adjusted dose of substrates & closely monitoring side effects.
1 125
Quetiapine Erythromycin Inhibition of CYP3A4 Consider alternative/adjusted dose of substrate or used cautiously by monitoring side effects. For clozapine, perform TDM.
2 122-124, 129Pimozide, trazodone Clarithromycin Inhibition of CYP3A4Clozapine Ciprofloxacin Inhibition of CYP1A2Diazepam Ciprofloxacin Inhibition of CYP3A4 Monitor side effects and if necessary, adjusted
the dose of substrate.3 127

DDIs Associated with Antibacterials for COPD
93
5
Table 4. (continued)
Comorbidity Medication Interacting AB Mechanism Management suggestionLevel of interaction Ref.
2.4 Antiarrhythmic agent
Digoxin Clarithromycin Inhibition of P-gp Avoid combination or perform TDM and if necessary, adjusted dose of substrate.
1 68-71
Quinidine, lignocaine Erythromycin Inhibition of CYP3A4 Consider alternative or perform TDM and if necessary, adjusted dose of substrate.
2 64-67Procainamide TMP Inhibition of tubular
secretionPindolol, digoxin TMP-SMX Inhibition of tubular
secretionPerform TDM and if necessary, adjusted dose of substrate.
3 72-75
Procainamide Levofloxacin, ofloxacin Inhibition of OCT3. Respiratory diseases3.1. Medication for obstructive airways diseases
Methylprednisolone, montelukast Clarithromycin Inhibition of CYP3A4 & P-gp
Consider alternative/adjusted dose of substrate or used cautiously by monitoring side effects. For theophylline, perform TDM.
2 78-85, 90-97
Theophylline Erythromycin Inhibition of CYP3A4Ciprofloxacin Inhibition of CYP1A2
Loratadine Erythromycin, clarithromycin Inhibition of CYP3A4 Monitor side effects and if necessary, adjusted dose of substrate.
3 86, 87Roflumilast Erythromycin Inhibition of CYP3A4
3.2. Anti-TB drugs Rifabutin Clarithromycin Inhibition of CYP3A4 Avoid combination 1 101, 110, 111Rifampicin, rifabutin Clarithromycin Induction of CYP3A4 Consider alternative AB for COPD 2 100, 101Rifampicin, rifabutin TMP-SMX, doxycycline Induction of CYP3A4/
CYP2C9 Consider alternative AB for COPD or monitor the effectiveness of AB and if necessary, adjusted dose of AB.
3 102-104, 106-109
Rifampicin TMP-SMX Inhibition of mixed oxidases
Moxifloxacin Inducing phase II enzymes
4. Neurological disorders4.1. Antiparkinson Agents
Bromocriptine Erythromycin Inhibition of CYP3A4 Avoid combination or adjusted dose of substrates & closely monitoring side effects.
1 112
Cabergoline Clarithromycin Inhibition of CYP3A4 & P-gp
Consider alternative/adjusted dose of substrate or used cautiously by monitoring side effects.
2 113
4.2. Antiepileptic drugs Carbamazepine, phenytoin Doxycycline Induction of CYP3A4 Consider alternative or perform TDM 2 117, 116Carbamazepine Ciprofloxacin Inhibition of
CYP3A4/1A2Consider alternative or perform TDM 2 118
Phenytoin TMP-SMX Inhibition of CYP2C8 Consider alternative or perform TDM 2 116, 119Phenobarbital Doxycycline Induction of CYP3A4 Monitor side effects and if necessary, adjusted
dose of substrate.3 115
5. Depression and psychiatric disordersAntidepressant, Anxiolytic, & Antipsychotic agents
Buspirone Erythromycin Inhibition of CYP3A4 Avoid combination or adjusted dose of substrates & closely monitoring side effects.
1 125
Quetiapine Erythromycin Inhibition of CYP3A4 Consider alternative/adjusted dose of substrate or used cautiously by monitoring side effects. For clozapine, perform TDM.
2 122-124, 129Pimozide, trazodone Clarithromycin Inhibition of CYP3A4Clozapine Ciprofloxacin Inhibition of CYP1A2Diazepam Ciprofloxacin Inhibition of CYP3A4 Monitor side effects and if necessary, adjusted
the dose of substrate.3 127

Chapter 5
94
Table 4. (continued)
Comorbidity Medication Interacting AB Mechanism Management suggestionLevel of interaction Ref.
6. DyspepsiaAntidyspepsia medications
Aluminum hydroxide, sucralfat Quinolone, tetracyclines Complex-forming Avoid combination or administer quinolone at least 2 hours before or 6 hours after co-agents.
1 131-142
Lansoprazole Clarithromycin Inhibition of CYP3A4 Consider alternative/adjusted dose of substrate or used cautiously by monitoring side effects.
2 147
Calcium carbonate Quinolone, tetracyclines Complex-forming Avoid co-administration or administration interval of at least 2 h or more
2 131, 139
Bismuth subsalicylate Quinolone, tetracyclines Complex-forming Administration interval of at least 2 h or more 3 143, 2057. HIVAnti-HIV drugs Didanosine Ciprofloxacin Complex-forming Avoid combination or administer quinolone at
least 2 hours before or 6 hours after the co-agents.1 149, 150
Saquinavir Erythromycin Inhibition of CYP3A4 Consider alternative/adjusted dose of substrate or used cautiously by monitoring side effects.
2 151
Lamivudine, didanosine TMP-SMX Inhibition of tubular secretion
Monitor side effects and if necessary, adjusted dose of substrate.
3 152, 153
8. OtherPulmonary arterial hypertension medications
Bosentan Clarithromycin Inhibition of CYP3A4 & P-gp
Avoid combination or adjusted dose of substrates & closely monitoring side effects.
1 206
Ambrisentan Clarithromycin Inhibition of CYP3A4 & P-gp
Monitor side effects and if necessary, adjusted the dose of substrate.
3 207
Insomnia medications Brotizolam, triazolam, zopiclone Erythromycin Inhibition of CYP3A4 Consider an alternative AB or other hypnotic drugs (not a CYP3A4 substrate)
2 208-210
Zolpidem Ciprofloxacin Inhibition of CYP3A4 Monitor side effects and if necessary, choose alternative AB or other hypnotic drugs (not a CYP3A4 substrate)
3 211
Antifungal agents Voriconazole Erythromycin Inhibition of CYP3A4 Consider alternative/adjusted dose of substrate or used cautiously by monitoring side effects. For voriconazole, perform TDM and adjust the dose if needed.
2 154, 155Itraconazole Ciprofloxacin Inhibition of CYP3A4
Antineoplastic drugs Vinorelbine Clarithromycin Inhibition of CYP3A4 & P-gp
Avoid combination or adjusted dose of substrates & closely monitoring side effects.
1 179
Anti-gout drugs Colchicine Clarithromycin Inhibition of CYP3A4 Avoid combination or perform TDM and adjust the dose if needed.
1 180
Azithromycin Inhibition of CYP3A4 Consider alternative/adjusted dose of substrate or used cautiously by monitoring side effects.
2 180
Probenecid Ciprofloxacin Inhibition of OAT Monitor side effects and if necessary, adjusted dose of substrate.
3 194, 195
Anesthesia drugs Midazolam Clarithromycin, erythromycin Inhibition of CYP3A4 Avoid combination or adjusted dose of substrates & closely monitoring side effects.
1 156-160
Ketamine Clarithromycin Inhibition of CYP3A4 Consider alternative or perform TDM and adjust the dose if needed.
2 161

DDIs Associated with Antibacterials for COPD
95
5
Table 4. (continued)
Comorbidity Medication Interacting AB Mechanism Management suggestionLevel of interaction Ref.
6. DyspepsiaAntidyspepsia medications
Aluminum hydroxide, sucralfat Quinolone, tetracyclines Complex-forming Avoid combination or administer quinolone at least 2 hours before or 6 hours after co-agents.
1 131-142
Lansoprazole Clarithromycin Inhibition of CYP3A4 Consider alternative/adjusted dose of substrate or used cautiously by monitoring side effects.
2 147
Calcium carbonate Quinolone, tetracyclines Complex-forming Avoid co-administration or administration interval of at least 2 h or more
2 131, 139
Bismuth subsalicylate Quinolone, tetracyclines Complex-forming Administration interval of at least 2 h or more 3 143, 2057. HIVAnti-HIV drugs Didanosine Ciprofloxacin Complex-forming Avoid combination or administer quinolone at
least 2 hours before or 6 hours after the co-agents.1 149, 150
Saquinavir Erythromycin Inhibition of CYP3A4 Consider alternative/adjusted dose of substrate or used cautiously by monitoring side effects.
2 151
Lamivudine, didanosine TMP-SMX Inhibition of tubular secretion
Monitor side effects and if necessary, adjusted dose of substrate.
3 152, 153
8. OtherPulmonary arterial hypertension medications
Bosentan Clarithromycin Inhibition of CYP3A4 & P-gp
Avoid combination or adjusted dose of substrates & closely monitoring side effects.
1 206
Ambrisentan Clarithromycin Inhibition of CYP3A4 & P-gp
Monitor side effects and if necessary, adjusted the dose of substrate.
3 207
Insomnia medications Brotizolam, triazolam, zopiclone Erythromycin Inhibition of CYP3A4 Consider an alternative AB or other hypnotic drugs (not a CYP3A4 substrate)
2 208-210
Zolpidem Ciprofloxacin Inhibition of CYP3A4 Monitor side effects and if necessary, choose alternative AB or other hypnotic drugs (not a CYP3A4 substrate)
3 211
Antifungal agents Voriconazole Erythromycin Inhibition of CYP3A4 Consider alternative/adjusted dose of substrate or used cautiously by monitoring side effects. For voriconazole, perform TDM and adjust the dose if needed.
2 154, 155Itraconazole Ciprofloxacin Inhibition of CYP3A4
Antineoplastic drugs Vinorelbine Clarithromycin Inhibition of CYP3A4 & P-gp
Avoid combination or adjusted dose of substrates & closely monitoring side effects.
1 179
Anti-gout drugs Colchicine Clarithromycin Inhibition of CYP3A4 Avoid combination or perform TDM and adjust the dose if needed.
1 180
Azithromycin Inhibition of CYP3A4 Consider alternative/adjusted dose of substrate or used cautiously by monitoring side effects.
2 180
Probenecid Ciprofloxacin Inhibition of OAT Monitor side effects and if necessary, adjusted dose of substrate.
3 194, 195
Anesthesia drugs Midazolam Clarithromycin, erythromycin Inhibition of CYP3A4 Avoid combination or adjusted dose of substrates & closely monitoring side effects.
1 156-160
Ketamine Clarithromycin Inhibition of CYP3A4 Consider alternative or perform TDM and adjust the dose if needed.
2 161

Chapter 5
96
Antimalarial agent Halofantrine Tetracycline Probably by CYP3A4 inhibition
Avoid combination or perform TDM and adjust the dose if needed.
1 177
Muscle relaxant Tizanidine Ciprofloxacin Inhibition of CYP1A2 Avoid combination or perform TDM and adjust the dose if needed.
1 183
Anti-diarrheal Loperamid TMP-SMX Inhibition of CYP2C8 Consider alternative/adjusted dose of substrate or used cautiously by monitoring side effects.
2 186
Anemia medications Iron supplements Quinolone, tetracyclines Complex-forming Avoid co-administration or administration interval of at least 2 hours or more
2 212-220
Other metal cations Zinc sulfate Quinolone, tetracyclines Complex-forming Avoid co-administration or administration interval of at least 2 h or more
2 144, 188, 189
Calcium acetate, calcium carbonate, calcium polycarbophil, patiromer, lanthanum carbonate, sevelamer
Quinolone, tetracyclines Complex-forming Administration interval of at least 2 h or more 3 139, 190-193
Other ABs Linezolid Clarithromycin Inhibition of P-gp Consider alternative or perform TDM and adjust the dose if needed.
2 196
Dapson Trimethoprim Inhibition of CYP2C8 Monitor side effects and if necessary, adjusted the dose of substrate.
3 187
Neomycin Penicillin V NA Consider alternative or adjusted the dose of penicillin.
3 221
Definition of level of interaction: 1 = strong interaction, 2 = substantial interaction, 3 = moderate interaction, and 4 = weak/no interaction; Ref. = reference; h = hour; OCT= organic cation transporter; OAT= Organic anion transporter; MATE=
multidrug and toxin extrusion 1; P-gp: P-glycoprotein; TMP-SMX= Trimethoprim and Sulfonamides; TDM = therapeutic drug monitoring; NA = not available yet. All detailed supported information about each DDI were available in Table S1 and S2.
Table 4. (continued)
Comorbidity Medication Interacting AB Mechanism Management suggestionLevel of interaction Ref.
Alfentanil Erythromycin Inhibition of CYP3A4 Monitor side effects and if necessary, adjusted the dose of substrate.
3 162-166Ropivacaine Clarithromycin Inhibition of CYP3A4
Ciprofloxacin Inhibition of CYP1A2Midazolam Roxithromycin Inhibition of CYP3A4
Analgesics Oxycodone Clarithromycin Inhibition of CYP3A4 Avoid combination or adjusted dose of substrates & closely monitoring side effects.
1 167
Immunosuppressant drugs
Cyclosporine Erythromycin Inhibition of CYP3A4 Avoid combination or adjusted dose of substrates & perform TDM.
1 168, 169, 181, 182Everolimus Erythromycin Inhibition of CYP3A4
and/ P-gpTacrolimus Levofloxacin Inhibition of CYP3A4 or
P-gpConsider alternative/adjusted dose of substrate or used cautiously by monitoring side effects.
2 170
Cyclosporine Ciprofloxacin Inhibition of CYP3A4 Monitor side effects and if necessary, adjusted the dose of substrate.
3 171, 172
Vasoactive agent Sildenafil Clarithromycin, erythromycin, ciprofloxacin
Inhibition of CYP3A4 Consider alternative/adjusted dose of substrate or used cautiously by monitoring side effects.
2 173, 174
Appetite suppressant Sibutramine Clarithromycin Inhibition of CYP3A4 & P-gp
Avoid combination or adjusted dose of substrates & closely monitoring side effects.
1 175, 176
Emergency birth control
Ulipristal acetate Erythromycin Inhibition of CYP3A4 Avoid combination or adjusted dose of substrates & closely monitoring side effects.
1 178

DDIs Associated with Antibacterials for COPD
97
5
Antimalarial agent Halofantrine Tetracycline Probably by CYP3A4 inhibition
Avoid combination or perform TDM and adjust the dose if needed.
1 177
Muscle relaxant Tizanidine Ciprofloxacin Inhibition of CYP1A2 Avoid combination or perform TDM and adjust the dose if needed.
1 183
Anti-diarrheal Loperamid TMP-SMX Inhibition of CYP2C8 Consider alternative/adjusted dose of substrate or used cautiously by monitoring side effects.
2 186
Anemia medications Iron supplements Quinolone, tetracyclines Complex-forming Avoid co-administration or administration interval of at least 2 hours or more
2 212-220
Other metal cations Zinc sulfate Quinolone, tetracyclines Complex-forming Avoid co-administration or administration interval of at least 2 h or more
2 144, 188, 189
Calcium acetate, calcium carbonate, calcium polycarbophil, patiromer, lanthanum carbonate, sevelamer
Quinolone, tetracyclines Complex-forming Administration interval of at least 2 h or more 3 139, 190-193
Other ABs Linezolid Clarithromycin Inhibition of P-gp Consider alternative or perform TDM and adjust the dose if needed.
2 196
Dapson Trimethoprim Inhibition of CYP2C8 Monitor side effects and if necessary, adjusted the dose of substrate.
3 187
Neomycin Penicillin V NA Consider alternative or adjusted the dose of penicillin.
3 221
Definition of level of interaction: 1 = strong interaction, 2 = substantial interaction, 3 = moderate interaction, and 4 = weak/no interaction; Ref. = reference; h = hour; OCT= organic cation transporter; OAT= Organic anion transporter; MATE=
multidrug and toxin extrusion 1; P-gp: P-glycoprotein; TMP-SMX= Trimethoprim and Sulfonamides; TDM = therapeutic drug monitoring; NA = not available yet. All detailed supported information about each DDI were available in Table S1 and S2.
Table 4. (continued)
Comorbidity Medication Interacting AB Mechanism Management suggestionLevel of interaction Ref.
Alfentanil Erythromycin Inhibition of CYP3A4 Monitor side effects and if necessary, adjusted the dose of substrate.
3 162-166Ropivacaine Clarithromycin Inhibition of CYP3A4
Ciprofloxacin Inhibition of CYP1A2Midazolam Roxithromycin Inhibition of CYP3A4
Analgesics Oxycodone Clarithromycin Inhibition of CYP3A4 Avoid combination or adjusted dose of substrates & closely monitoring side effects.
1 167
Immunosuppressant drugs
Cyclosporine Erythromycin Inhibition of CYP3A4 Avoid combination or adjusted dose of substrates & perform TDM.
1 168, 169, 181, 182Everolimus Erythromycin Inhibition of CYP3A4
and/ P-gpTacrolimus Levofloxacin Inhibition of CYP3A4 or
P-gpConsider alternative/adjusted dose of substrate or used cautiously by monitoring side effects.
2 170
Cyclosporine Ciprofloxacin Inhibition of CYP3A4 Monitor side effects and if necessary, adjusted the dose of substrate.
3 171, 172
Vasoactive agent Sildenafil Clarithromycin, erythromycin, ciprofloxacin
Inhibition of CYP3A4 Consider alternative/adjusted dose of substrate or used cautiously by monitoring side effects.
2 173, 174
Appetite suppressant Sibutramine Clarithromycin Inhibition of CYP3A4 & P-gp
Avoid combination or adjusted dose of substrates & closely monitoring side effects.
1 175, 176
Emergency birth control
Ulipristal acetate Erythromycin Inhibition of CYP3A4 Avoid combination or adjusted dose of substrates & closely monitoring side effects.
1 178

Chapter 5
98
They could markedly reduce the ABs activities of clarithromycin, doxycycline, and trimethoprim–sulfamethoxazole by rapidly elimination.100-104 Since, rifampicin also exhibits other ABs activities such as treating methicillin-resistant staphylococcus aureus (MRSA) in combination with other drugs, rationalizing antimicrobial therapy should be considered accordingly.105 Alternative AB for treating COPD is also recommended to reduce the risk of treatment failures.
Moxifloxacin might be an alternative AB as the evidence of moxifloxacin interaction with rifampicin was not consistent with moderate or weak interactions.106-109 Moxifloxacin is not metabolized by CYP450 and its interacting mechanisms with rifampicin might be facilitated by induction of other enzymes like uridine diphosphate-glucuronosyltransferases and sulfotransferases.106-109
Rifabutin and rifampicin are CYP substrates. Rifabutin is a CYP3A4 substrate, and therefore, macrolides may increase its serum concentration and enhance the risk of related ADR.101,110,111 Another study reported rifampicin concentration in blood is moderately elevated by co-trimoxazole.104 It was assumed that the interaction was facilitated by inhibition of the mixed function oxidases, which is responsible for metabolizing rifampicin.104 Thus, considering alternative AB or monitoring the clinical and biochemical parameters for rifampicin related hepatotoxicity is suggested when rifampicin and co-trimoxazole are combined.
What need to be mentioned is that not all the drugs for atypical mycobacterium spp were included in this review due to the selection limitation of ABs that used frequently among COPD patients. For drugs outside the scope of this review, other references (e.g. SPCs) need to be considered.
4. Neurological disorders
4.1. Anti-Parkinson drugs
Bromocriptine and cabergoline (dopamine agonists) are substrates of CYP3A4 and/or P-gp transporter.112,113 Co-prescription of these drugs with clarithromycin and erythromycin may produce major interactions and therefore, might lead to toxicities.112,113 Thus, avoiding combination is recommended. However, if it is not possible, adjusting the dose of those Parkinson medication and closely monitoring side effects are needed.
4.2. Antiepileptic drugs
Carbamazepine, phenytoin, and phenobarbital could stimulate the activity of a variety of CYP (CYP1A2/2C9/3A4) and glucuronyl transferase enzymes, which results in multiple DDIs with other substrates for these enzymes.114-116 Carbamazepine and phenytoin were reported to reduce t1/2 of doxycycline by stimulating the hepatic metabolism of
DDIs Associated with Antibacterials for COPD
99
5
doxycycline.117 It is suggested to consider an alternative AB or to adjust the dose of antiepileptic drugs while monitoring the AB activity of doxycycline.
Moreover, carbamazepine and phenytoin are substrates of CYP1A2/3A4 and CYP2C8, respectively. A CYP1A2/3A4 inhibitor (ciprofloxacin) and a CYP2C8 inhibitor (trimethoprim) were reported to increase the bioavailability of carbamazepine and phenytoin, respectively.116-119 Moreover, phenytoin is a NTI drug and therefore, avoiding using trimethoprim concomitantly or performing TDM of phenytoin is recommended when this DDI is not avoidable.120
Meanwhile, ciprofloxacin was reported to increase AUC of carbamazepine by more than 50%.118 Although it is not clear whether carbamazepine can be included as a NTI drug, the rise of carbamazepine plasma concentration because of this DDI needs special caution.121 Dose adjustment and TDM of carbamazepine are suggested to diminish potential toxicities.
5. Depression and psychiatric disorders
Depression and psychiatric disorders are common among COPD patients.14 Some antidepressant (trazodone), anxiolytic (buspirone), and antipsychotic (quetiapine, and pimozide) drugs are CYP3A4 substrates and therefore, might trigger clinically relevant DDIs with ABs.122-125 Erythromycin and clarithromycin increased AUCs of these drugs substantially.122-125 Considering alternative AB or adjusting the dose of substrates and monitoring related side effects is the way to control potential ADR.
CYP3A4 is also responsible for metabolizing diazepam, in addition to CYP2C19.126 Ciprofloxacin was reported to decrease diazepam clearance moderately by inhibiting CYP3A4 activity.127 Monitoring diazepam-related side effects can therefore be considered when this combination is prescribed.
Ciprofloxacin is also a potent CYP1A2 inhibitor.128 Therefore, metabolism of an atypical antipsychotic clozapine, a CYP1A2 substrate with NTI, can be relevantly altered by ciprofloxacin which produces a significant increase of clozapine serum concentration.129,130 Replacing ciprofloxacin or TDM of clozapine is option that can be chosen in managing this DDI.
6. Dyspepsia
Drugs containing metal cations (e.g. antacids, sucralfate and bismuth salts) produced chemical interactions with some ABs like oral tetracyclines (e.g. tetracycline, doxycycline) and fluoroquinolones (e.g. ciprofloxacin, moxifloxacin).131-144 Tetracyclines have a high affinity to form chelates due to their structural features with lots of chelation sites.145

Chapter 5
100
Meanwhile, fluoroquinolones have two main sites of metal chelation: 4-keto oxygen and 3-carboxylic acid groups.146
The formation of metal ion chelation complexes decreased absorption of tetracycline and fluoroquinolones, the reduced bioavailability may lead to ineffectiveness of these ABs.131-144 Therefore, it is recommended to avoid combination by replacing tetracyclines and fluoroquinolones with another AB, e.g. amoxicillin or amoxicillin/clavulanic acid. It was reported that antacids did not affect the bioavailability of amoxicillin and amoxicillin/clavulanic acid when they were co-administered.136 If replacement of the AB is not possible, substitution of antacids, sucralfate or bismuth salts to PPI is also favored. Another alternative is to separate administration by using quinolone or tetracycline at least 2 hours before and 6 hours after the dyspepsia drugs.
When considering a PPI, lansoprazole may not be the best alternative as it is partly metabolized by CYP3A4 and found to interact with clarithromycin.147
7. HIV
HIV-positive patients have about 50% higher risk to develop COPD than HIV-negative patients.148 Then, the risk of co-prescriptions for treating those chronic conditions is also possibly high. A protease inhibitor (saquinavir) and nucleoside reverse transcriptase inhibitors (didanosine and lamivudine) were found to clinically interact with ABs.149-153
Didanosine is very acid sensitive, and therefore, the didanosine formulations are supplemented by buffering mixtures containing magnesium hydroxide, dihydroxyaluminum sodium carbonate, and sodium citrate to prevent hydrolysis by gastric acid.149 These metal ions may form chelation complexes with quinolones and reduce their serum concentration.149,150 Two studies confirmed the didanosine and ciprofloxacin interaction, and recommended that when co-administration cannot be avoided, ciprofloxacin must be given at least 2 hours before didanosine.149,150
Trimethoprim–sulfamethoxazole may inhibit clearances of didanosine and lamivudine by competitively hinder their renal secretion.152,153 Consequently, AUCs of didanosine and lamivudine elevate moderately.152,153 Monitoring of the presumed side effects should be performed.
Saquinafir is metabolized by CYP3A4 and the presence of erythromycin increased its AUC by almost 100%.151 Choosing an alternative AB or adjusting the dose of saquinafir while monitoring toxicities can be considered to manage this DDI.
8. Other potential clinically significant DDI
Some other drugs that have indications for comorbidities in COPD patients were found to interact with ABs. Some individual drugs of different classes (e.g. voriconazole and

DDIs Associated with Antibacterials for COPD
101
5
vinorelbine) are metabolized by CYP3A4.154-182 Therefore, their metabolism is interfered by CYP3A4 inhibitors (macrolides).154-182 Other drugs are CYP1A2 substrates (e.g. ropivacaine and tizanidine) and therefore, CYP1A2 potent inhibitors like quinolones significantly alter their metabolism and elevate their bioavailabilities.164,183-185 Others are CYP2C8 substrates (e.g. loperamid for diarrhea) and therefore, trimethoprim (a CYP2C8 potent inhibitor) inhibits their clearance and increases their AUC values.186,187 Some drugs containing metal cations (e.g. Fe, Zn, Ca) should be avoided or administered separately at least 2 hours or more with quinolones and tetracyclines.139,144,188-193 Other interactions were facilitated by drug transporters. An uricosuric agent (probenecid) interacts moderately with ciprofloxacin via competitive inhibition of organic anion transporters in renal tubules.194,195 Meanwhile, linezolid (other AB), which is a substrate of P-gp transporter, can potentially produce clinically significant interaction with P-gp inhibitors (macrolides).196
DDI related to NTIs
Some ABs may interact with NTI drugs and therefore, can produce serious ADRs. The NTI drugs in this review includes CYP3A4 substrates (theophylline, ketamine, everolimus, tacrolimus, halofantrine, lignocaine, quinidine, voriconazole, carbamazepine, warfarin, cyclosporine, colchicine, phenprocoumon/acenocoumarol); CYP1A2 substrates (theophylline, carbamazepine, clozapine, tizanidine); CYP2C9 substrates and sensitive to alterations in normal gut flora (warfarin, phenprocoumon/acenocoumarol); a CYP2C8 substrate (phenytoin); substrates of P-gp transporter (digoxin, linezolid); and a substrate of organic cation transporter (procainamide).76,77,88,120,197
DISCUSSIONIncluded articles
This study outlined the possible DDIs related to frequently prescribed ABs in COPD patients from clinical and observational studies. We only included well-designed studies (2 points or higher) since they provide more valid evidence than studies without a control or comparison group (0 or 1 point). DDIs based on case-reports or hypotheses may lead to unnecessary warnings if these are not confirmed by well-designed studies. One classic example at this point is ABs and oral contraceptive interactions; lots of cases reported unintended pregnancies after ABs were prescribed to women on oral contraceptives, which attracted much attention from health practitioners.198,199 After scientific evidence from clinical and pharmacokinetic studies has consistently and repeatedly failed to support such interaction, the warning about DDIs between hormonal contraception and non-rifampicin ABs were finally canceled by related guidelines.199

Chapter 5
102
Mechanisms of DDI
The DDI of potential clinical significance between AB and co-administered medication may occur in two situations: (1) co-administered drug influences the absorption, distribution, metabolism, and elimination (ADME) of AB; and (2) AB influences the ADME of co-administered medication. When AB acted as substrates, some co-administered drugs reduced the blood concentration of AB and led to treatment failure of AB in reducing exacerbations. Other co-administered drugs increased the blood concentration of AB, which could result in the termination of AB use because of an ADR, and therefore acted against the control of infections. As inhibitors, the blood concentrations of co-administered drugs were increased by AB which may also produce an ADR and lead to termination of co-administered drugs, and therefore, may produce a treatment failure of comorbidities. In all, DDIs related to ABs may hinder effective infection control and exacerbation management among COPD patients as well as treatment of comorbidities in COPD.
Comorbidities among COPD patients
The impact of comorbidities on quality of life in COPD patients are well reported, however, potential drug interactions between drugs for these comorbidities and ABs used for COPD has received little specific attention. From this review, we found that many drugs (e.g. those used for heart and circulatory system disease) should not be co-administered with related AB and other actions such as dose adjustment, choosing an alternative drug and monitoring ADRs are necessary. These drug interactions could not only influence treatment options of clinical practitioner but also influence treatment effects for both COPD and comorbidities.
Information collected from this review can be used as input to improve the sensitivity and specificity of drug-drug interaction alert systems. Moreover, this study may also be attractive for researchers in this field who may take into account the availability of high-quality studies when evaluating the evidence for many potential interactions.
Special warning for NTI drugs
We found that some NTI drugs might potentially interact with ABs. Because of the narrow separation between effective and toxic dosing of these drugs, small alteration on their pharmacokinetics parameters can produce fatal consequences.88,120 Therefore, combination of particular AB which have an ability to inhibit their clearance pathways should be avoided if it is possible. However, if the benefits of combination outweigh the potential side effects, dose adjustment and performing TDM of the NTI drugs are strongly recommended.

DDIs Associated with Antibacterials for COPD
103
5
Limitations
Some limitations to this review are worth to be mentioned. First, although we reviewed a significant part of the literature, we did not include all sources that might indicate relevant DDIs such as case reports, summary of product characteristics or theoretical hypotheses. As a result, we did not find some DDIs that are considered serious and clinically highly relevant, such as QT-interval prolonging interactions for combinations of macrolides with other QT-prolonging drugs or the risk for pseudotumor cerebri in case of combination of doxycycline with vitamin-A analogs.200,201 Such interactions are commonly found as case reports, as it is unethical to design studies to confirm these serious risks in clinical studies. However for some DDIs, it is possible to study the clinical manifestation of a potential DDI in an observational study using a real world drug utilization data.202 Secondly, selection of ABs included in this review was based on their frequent use in COPD and therefore, information for other ABs used for COPD comorbidities such as atypical Mycobacterium spp is limited and therefore, may restrict the application scope of this review. Thirdly, due to limited comparative analyses for several specific DDIs included in this review, it may be difficult to make recommendations for a specific situation. Our classification of DDIs levels just offers a general consideration. The specific impact of a DDI is decided by many variables like different doses and formulations, the comorbidities of patients, etc. Therefore, case-by-case analysis is important in clinical practice and a drug interaction handbook like Stockley’s Drug Interactions further expands on these issues.203
CONCLUSIONClinically significant DDIs related to ABs may involve a wide range of indicated drugs to treat comorbidities in COPD. Clinicians should pay attention to these drug interactions when prescribing AB to reduce the frequency and severity of exacerbations in COPD patients and take necessary actions to ensure therapeutic effect and safety of patients. This study may contribute to better prescribing of ABs to COPD patients with comorbidities using potentially interacting combination. Furthermore, the information may be used to point at gaps in scientific knowledge about potential adverse effects from DDIs.
SUPPLEMENTARY DATATable S1 to S3 are available as Supplementary data at JAC Online (https://doi.org/10.1093/jac/dkz221)

Chapter 5
104
REFERENCES
1. Vogelmeier CF, Criner GJ, Martinez FJ et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med 2017; 195: 557-82.
2. Decramer M, Janssens W, Miravitlles M. Chronic obstructive pulmonary disease. Lancet 2012; 379: 1341-51.
3. Sethi S, Murphy TF. Infection in the pathogenesis and course of chronic obstructive pulmonary disease. N Engl J Med 2008; 359: 2355-65.
4. Vollenweider DJ, Jarrett H, Steurer-Stey CA et al. Antibiotics for exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2012; 12: CD010257.
5. Herath SC, Poole P. Prophylactic antibiotic therapy for chronic obstructive pulmonary disease (COPD). Cochrane Database Syst Rev 2013; CD009764.
6. Wang Y, Zijp TR, Bahar MA et al. Effects of prophylactic antibiotics on patients with stable COPD: A systematic review and meta-analysis of randomized controlled trials. J Antimicrob Chemother 2018; 73: 3231-43.
7. Wedzicha JA, Calverley PMA, Albert RK et al. Prevention of COPD exacerbations: A european respiratory Society/American thoracic society guideline. Eur Respir J 2017; 50: 10.1183/13993003.02265,2016. Print 2017 Sep.
8. Chetty U, McLean G, Morrison D et al. Chronic obstructive pulmonary disease and comorbidities: A large cross-sectional study in primary care. Br J Gen Pract 2017; 67: e321-8.
9. Mangoni AA, Jackson SH. Age-related changes in pharmacokinetics and pharmacodynamics: Basic principles and practical applications. Br J Clin Pharmacol 2004; 57: 6-14.
10. Bahar MA, Hak E, Bos JH et al. The burden and management of cytochrome P450 2D6 (CYP2D6)‐mediated drug–drug interaction (DDI): Co‐medication of metoprolol and paroxetine or fluoxetine in the elderly. Pharmacoepidemiol Drug Saf 2017; 26: 752-65.
11. van Roon EN, Flikweert S, le Comte M et al. Clinical relevance of drug-drug interactions : A structured assessment procedure. Drug Saf 2005; 28: 1131-9.
12. Bahar MA, Setiawan D, Hak E et al. Pharmacogenetics of drug-drug interaction and drug-drug-gene interaction: A systematic review on CYP2C9, CYP2C19 and CYP2D6. Pharmacogenomics 2017; 18: 701-39.
13. Zhou S, Chan E, Li X et al. Clinical outcomes and management of mechanism-based inhibition of cytochrome P450 3A4. Ther Clin Risk Manag 2005; 1: 3-13.
14. Divo M, Cote C, de Torres JP et al. Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2012; 186: 155-61.
15. Mannino DM, Thorn D, Swensen A et al. Prevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPD. Eur Respir J 2008; 32: 962-9.
16. Schelleman H, Bilker WB, Brensinger CM et al. Anti-infectives and the risk of severe hypoglycemia in users of glipizide or glyburide. Clin Pharmacol Ther 2010; 88: 214-22.
17. Lilja JJ, Niemi M, Fredrikson H et al. Effects of clarithromycin and grapefruit juice on the pharmacokinetics of glibenclamide. Br J Clin Pharmacol 2007; 63: 732-40.
18. Tan A, Holmes HM, Kuo YF et al. Coadministration of co-trimoxazole with sulfonylureas: Hypoglycemia events and pattern of use. J Gerontol A Biol Sci Med Sci 2015; 70: 247-54.
19. Kradjan WA, Witt DM, Opheim KE et al. Lack of interaction between glipizide and co-trimoxazole. J Clin Pharmacol 1994; 34: 997-1002.
20. Jayasagar G, Dixit AA, Kishan V et al. Effect of clarithromycin on the pharmacokinetics of tolbutamide. Drug Metabol Drug Interact 2000; 16: 207-15.
21. Wing LM, Miners JO. Cotrimoxazole as an inhibitor of oxidative drug metabolism: Effects

DDIs Associated with Antibacterials for COPD
105
5
of trimethoprim and sulphamethoxazole separately and combined on tolbutamide disposition. Br J Clin Pharmacol 1985; 20: 482-5.
22. Niemi M, Neuvonen PJ, Kivisto KT. The cytochrome P4503A4 inhibitor clarithromycin increases the plasma concentrations and effects of repaglinide. Clin Pharmacol Ther 2001; 70: 58-65.
23. Niemi M, Kajosaari LI, Neuvonen M et al. The CYP2C8 inhibitor trimethoprim increases the plasma concentrations of repaglinide in healthy subjects. Br J Clin Pharmacol 2004; 57: 441-7.
24. Hruska MW, Amico JA, Langaee TY et al. The effect of trimethoprim on CYP2C8 mediated rosiglitazone metabolism in human liver microsomes and healthy subjects. Br J Clin Pharmacol 2005; 59: 70-9.
25. Grun B, Kiessling MK, Burhenne J et al. Trimethoprim-metformin interaction and its genetic modulation by OCT2 and MATE1 transporters. Br J Clin Pharmacol 2013; 76: 787-96.
26. Muller F, Pontones CA, Renner B et al. N(1)-methylnicotinamide as an endogenous probe for drug interactions by renal cation transporters: Studies on the metformin-trimethoprim interaction. Eur J Clin Pharmacol 2015; 71: 85-94.
27. Wright AJ, Gomes T, Mamdani MM et al. The risk of hypotension following co-prescription of macrolide antibiotics and calcium-channel blockers. CMAJ 2011; 183: 303-7.
28. Gandhi S, Fleet JL, Bailey DG et al. Calcium-channel blocker-clarithromycin drug interactions and acute kidney injury. JAMA 2013; 310: 2544-53.
29. Fraser LA, Shariff SZ, McArthur E et al. Calcium channel blocker-clarithromycin drug interaction did not increase the risk of nonvertebral fracture: A population-based study. Ann Pharmacother 2015; 49: 185-8.
30. Westphal JF. Macrolide–induced clinically relevant drug interactions with cytochrome P‐450A (CYP) 3A4: An update focused on clarithromycin, azithromycin and dirithromycin. Br J Clin Pharmacol 2000; 50: 285-95.
31. Yamazaki H, Shimada T. Comparative studies of in vitro inhibition of cytochrome P450 3A4-dependent testosterone 6beta-hydroxylation by roxithromycin and its metabolites, troleandomycin, and erythromycin. Drug Metab Dispos 1998; 26: 1053-7.
32. Antoniou T, Hollands S, Macdonald EM et al. Trimethoprim-sulfamethoxazole and risk of sudden death among patients taking spironolactone. CMAJ 2015; 187: E138-43.
33. Parhofer KG. The treatment of disorders of lipid metabolism. Dtsch Arztebl Int 2016; 113: 261-8.
34. Kantola T, Kivisto KT, Neuvonen PJ. Erythromycin and verapamil considerably increase serum simvastatin and simvastatin acid concentrations. Clin Pharmacol Ther 1998; 64: 177-82.
35. Amsden GW, Kuye O, Wei GC. A study of the interaction potential of azithromycin and clarithromycin with atorvastatin in healthy volunteers. J Clin Pharmacol 2002; 42: 444-9.
36. Li DQ, Kim R, McArthur E et al. Risk of adverse events among older adults following co-prescription of clarithromycin and statins not metabolized by cytochrome P450 3A4. CMAJ 2015; 187: 174-80.
37. Kalliokoski A, Niemi M. Impact of OATP transporters on pharmacokinetics. Br J Pharmacol 2009; 158: 693-705.
38. Seithel A, Eberl S, Singer K et al. The influence of macrolide antibiotics on the uptake of organic anions and drugs mediated by OATP1B1 and OATP1B3. Drug Metab Dispos 2007; 35: 779-86.
39. Glasheen JJ, Fugit RV, Prochazka AV. The risk of overanticoagulation with antibiotic use in outpatients on stable warfarin regimens. J Gen Intern Med 2005; 20: 653-6.
40. Lane MA, Zeringue A, McDonald JR. Serious bleeding events due to warfarin and antibiotic co-prescription in a cohort of veterans. Am J Med 2014; 127: 657.
41. Ghaswalla PK, Harpe SE, Tassone D et al. Warfarin-antibiotic interactions in older adults of an outpatient anticoagulation clinic. Am J Geriatr Pharmacother 2012; 10: 352-60.
Chapter 5
106
42. Mergenhagen KA, Olbrych PM, Mattappallil A et al. Effect of azithromycin on anticoagulation-related outcomes in geriatric patients receiving warfarin. Clin Ther 2013; 35: 425-30.
43. McCall KL, Anderson HG,Jr., Jones AD. Determination of the lack of a drug interaction between azithromycin and warfarin. Pharmacotherapy 2004; 24: 188-94.
44. Fischer HD, Juurlink DN, Mamdani MM et al. Hemorrhage during warfarin therapy associated with cotrimoxazole and other urinary tract anti-infective agents: A population-based study. Arch Intern Med 2010; 170: 617-21.
45. Washington C, Hou SY, Hughes NC et al. Ciprofloxacin prolonged-release tablets do not affect warfarin pharmacokinetics and pharmacodynamics. J Clin Pharmacol 2007; 47: 1320-6.
46. Israel DS, Stotka J, Rock W et al. Effect of ciprofloxacin on the pharmacokinetics and pharmacodynamics of warfarin. Clin Infect Dis 1996; 22: 251-6.
47. Bianco TM, Bussey HI, Farnett LE et al. Potential warfarin-ciprofloxacin interaction in patients receiving long-term anticoagulation. Pharmacotherapy 1992; 12: 435-9.
48. Abdel-Aziz MI, Ali MA, Hassan AK et al. Warfarin-drug interactions: An emphasis on influence of polypharmacy and high doses of amoxicillin/clavulanate. J Clin Pharmacol 2016; 56: 39-46.
49. Schelleman H, Bilker WB, Brensinger CM et al. Warfarin with fluoroquinolones, sulfonamides, or azole antifungals: Interactions and the risk of hospitalization for gastrointestinal bleeding. Clin Pharmacol Ther 2008; 84: 581-8.
50. Baillargeon J, Holmes HM, Lin YL et al. Concurrent use of warfarin and antibiotics and the risk of bleeding in older adults. Am J Med 2012; 125: 183-9.
51. O’Reilly RA, Motley CH. Racemic warfarin and trimethoprim-sulfamethoxazole interaction in humans. Ann Intern Med 1979; 91: 34-6.
52. Mercadal Orfila G, Gracia Garcia B, Leiva Badosa E et al. Retrospective assessment of
potential interaction between levofloxacin and warfarin. Pharm World Sci 2009; 31: 224-9.
53. Liao S, Palmer M, Fowler C et al. Absence of an effect of levofloxacin on warfarin pharmacokinetics and anticoagulation in male volunteers. J Clin Pharmacol 1996; 36: 1072-7.
54. Stroud LF, Mamdami MM, Kopp A et al. The safety of levofloxacin in elderly patients on warfarin. Am J Med 2005; 118: 1417.
55. Penning-van Beest, van Meegen E, Rosendaal FR et al. Drug interactions as a cause of overanticoagulation on phenprocoumon or acenocoumarol predominantly concern antibacterial drugs. Clin Pharmacol Ther 2001; 69: 451-7.
56. Jobski K, Behr S, Garbe E. Drug interactions with phenprocoumon and the risk of serious haemorrhage: A nested case-control study in a large population-based german database. Eur J Clin Pharmacol 2011; 67: 941-51.
57. Abbas S, Ihle P, Harder S et al. Risk of bleeding and antibiotic use in patients receiving continuous phenprocoumon therapy. A case-control study nested in a large insurance- and population-based german cohort. Thromb Haemost 2014; 111: 912-22.
58. Penning-van Beest, Koerselman J, Herings RM. Risk of major bleeding during concomitant use of antibiotic drugs and coumarin anticoagulants. J Thromb Haemost 2008; 6: 284-90.
59. Juurlink DN. Drug interactions with warfarin: What clinicians need to know. CMAJ 2007; 177: 369-71.
60. Ufer M. Comparative pharmacokinetics of vitamin K antagonists - warfarin, phenprocoumon and acenocoumarol. Clin Pharmacokinet 2005; 44: 1227-46.
61. Thachil J. The newer direct oral anticoagulants: A practical guide. Clin Med (Lond) 2014; 14: 165-75.
62. Parasrampuria DA, Mendell J, Shi M et al. Edoxaban drug-drug interactions with ketoconazole, erythromycin, and cyclosporine. Br J Clin Pharmacol 2016; 82: 1591-600.
63. Gouin-Thibault I, Delavenne X, Blanchard A et al. Interindividual variability in dabigatran

DDIs Associated with Antibacterials for COPD
107
5
and rivaroxaban exposure: Contribution of ABCB1 genetic polymorphisms and interaction with clarithromycin. J Thromb Haemost 2017; 15: 273-83.
64. Damkier P, Hansen LL, Brosen K. Effect of diclofenac, disulfiram, itraconazole, grapefruit juice and erythromycin on the pharmacokinetics of quinidine. Br J Clin Pharmacol 1999; 48: 829-38.
65. Isohanni MH, Neuvonen PJ, Olkkola KT. Effect of erythromycin and itraconazole on the pharmacokinetics of oral lignocaine. Pharmacol Toxicol 1999; 84: 143-6.
66. Kosoglou T, Rocci ML,Jr., Vlasses PH. Trimethoprim alters the disposition of procainamide and N-acetylprocainamide. Clin Pharmacol Ther 1988; 44: 467-77.
67. Vlasses PH, Kosoglou T, Chase SL et al. Trimethoprim inhibition of the renal clearance of procainamide and N-acetylprocainamide. Arch Intern Med 1989; 149: 1350-3.
68. Zapater P, Reus S, Tello A et al. A prospective study of the clarithromycin-digoxin interaction in elderly patients. J Antimicrob Chemother 2002; 50: 601-6.
69. Chan AL, Wang MT, Su CY et al. Risk of digoxin intoxication caused by clarithromycin-digoxin interactions in heart failure patients: A population-based study. Eur J Clin Pharmacol 2009; 65: 1237-43.
70. Tanaka H, Matsumoto K, Ueno K et al. Effect of clarithromycin on steady-state digoxin concentrations. Ann Pharmacother 2003; 37: 178-81.
71. Rengelshausen J, Goggelmann C, Burhenne J et al. Contribution of increased oral bioavailability and reduced nonglomerular renal clearance of digoxin to the digoxin-clarithromycin interaction. Br J Clin Pharmacol 2003; 56: 32-8.
72. Petersen P, Kastrup J, Bartram R et al. Digoxin-trimethoprim interaction. Acta Med Scand 1985; 217: 423-7.
73. Bauer LA, Black DJ, Lill JS et al. Levofloxacin and ciprofloxacin decrease procainamide and N-acetylprocainamide renal clearances. Antimicrob Agents Chemother 2005; 49: 1649-51.
74. Martin DE, Shen J, Griener J et al. Effects of ofloxacin on the pharmacokinetics and pharmacodynamics of procainamide. J Clin Pharmacol 1996; 36: 85-91.
75. Ujhelyi MR, Bottorff MB, Schur M et al. Aging effects on the organic base transporter and stereoselective renal clearance. Clin Pharmacol Ther 1997; 62: 117-28.
76. Raebel MA, Carroll NM, Andrade SE et al. Monitoring of drugs with a narrow therapeutic range in ambulatory care. Am J Manag Care 2006; 12: 268-75.
77. Campbell T, Williams K. Therapeutic drug monitoring: Antiarrhythmic drugs. Br J Clin Pharmacol 2001; 52: 21-33.
78. Fost DA, Leung DY, Martin RJ et al. Inhibition of methylprednisolone elimination in the presence of clarithromycin therapy. J Allergy Clin Immunol 1999; 103: 1031-5.
79. Hegazy SK, Mabrouk MM, Elsisi AE et al. Effect of clarithromycin and fluconazole on the pharmacokinetics of montelukast in human volunteers. Eur J Clin Pharmacol 2012; 68: 1275-80.
80. Branigan TA, Robbins RA, Cady WJ et al. The effects of erythromycin on the absorption and disposition of kinetics of theophylline. Eur J Clin Pharmacol 1981; 21: 115-20.
81. Reisz G, Pingleton SK, Melethil S et al. The effect of erythromycin on theophylline pharmacokinetics in chronic bronchitis. Am Rev Respir Dis 1983; 127: 581-4.
82. Prince RA, Wing DS, Weinberger MM et al. Effect of erythromycin on theophylline kinetics. J Allergy Clin Immunol 1981; 68: 427-31.
83. May DC, Jarboe CH, Ellenburg DT et al. The effects of erythromycin on theophylline elimination in normal males. J Clin Pharmacol 1982; 22: 125-30.
84. Maddux MS, Leeds NH, Organek HW et al. The effect of erythromycin on theophylline pharmacokinetics at steady state. Chest 1982; 81: 563-5.
85. Pfeifer HJ, Greenblatt DJ, Friedman P. Effects of three antibiotics on theophylline kinetics. Clin Pharmacol Ther 1979; 26: 36-40.

Chapter 5
108
86. Carr RA, Edmonds A, Shi H et al. Steady-state pharmacokinetics and electrocardiographic pharmacodynamics of clarithromycin and loratadine after individual or concomitant administration. Antimicrob Agents Chemother 1998; 42: 1176-80.
87. Brannan MD, Reidenberg P, Radwanski E et al. Loratadine administered concomitantly with erythromycin: Pharmacokinetic and electrocardiographic evaluations. Clin Pharmacol Ther 1995; 58: 269-78.
88. Blix HS, Viktil KK, Moger TA et al. Drugs with narrow therapeutic index as indicators in the risk management of hospitalised patients. Pharm Pract (Granada) 2010; 8: 50-5.
89. Ha HR, Chen J, Freiburghaus A et al. Metabolism of theophylline by cDNA‐expressed human cytochromes P‐450. Br J Clin Pharmacol 1995; 39: 321-6.
90. Nix DE, DeVito JM, Whitbread MA et al. Effect of multiple dose oral ciprofloxacin on the pharmacokinetics of theophylline and indocyanine green. J Antimicrob Chemother 1987; 19: 263-9.
91. Wijnands WJ, Vree TB, van Herwaarden CL. The influence of quinolone derivatives on theophylline clearance. Br J Clin Pharmacol 1986; 22: 677-83.
92. Loi CM, Parker BM, Cusack BJ et al. Individual and combined effects of cimetidine and ciprofloxacin on theophylline metabolism in male nonsmokers. Br J Clin Pharmacol 1993; 36: 195-200.
93. Robson RA, Begg EJ, Atkinson HC et al. Comparative effects of ciprofloxacin and lomefloxacin on the oxidative metabolism of theophylline. Br J Clin Pharmacol 1990; 29: 491-3.
94. Prince RA, Casabar E, Adair CG et al. Effect of quinolone antimicrobials on theophylline pharmacokinetics. J Clin Pharmacol 1989; 29: 650-4.
95. Raoof S, Wollschlager C, Khan FA. Ciprofloxacin increases serum levels of theophylline. Am J Med 1987; 82: 115-8.
96. Antoniou T, Gomes T, Mamdani MM et al. Ciprofloxacin-induced theophylline
toxicity: A population-based study. Eur J Clin Pharmacol 2011; 67: 521-6.
97. Batty KT, Davis TM, Ilett KF et al. The effect of ciprofloxacin on theophylline pharmacokinetics in healthy subjects. Br J Clin Pharmacol 1995; 39: 305-11.
98. Inghammar M, Ekbom A, Engström G et al. COPD and the risk of tuberculosis-a population-based cohort study. PloS One 2010; 5: e10138.
99. Baciewicz AM, Chrisman CR, Finch CK et al. Update on rifampin, rifabutin, and rifapentine drug interactions. Curr Med Res Opin 2013; 29: 1-12.
100. Wallace Jr RJ, Brown BA, Griffith DE et al. Reduced serum levels of clarithromycin in patients treated with multidrug regimens including rifampin or rifabutin for mycobacterium avium-M. intracellulare infection. J Infect Dis 1995; 171: 747-50.
101. Hafner R, Bethel J, Power M et al. Tolerance and pharmacokinetic interactions of rifabutin and clarithromycin in human immunodeficiency virus-infected volunteers. Antimicrob Agents Chemother 1998; 42: 631-9.
102. Colmenero JD, Fernandez-Gallardo LC, Agundez JA et al. Possible implications of doxycycline-rifampin interaction for treatment of brucellosis. Antimicrob Agents Chemother 1994; 38: 2798-802.
103. Winter HR, Trapnell CB, Slattery JT et al. The effect of clarithromycin, fluconazole, and rifabutin on sulfamethoxazole hydroxylamine formation in individuals with human immunodeficiency virus infection (AACTG 283). Clin Pharmacol Ther 2004; 76: 313-22.
104. Bhatia RS, Uppal R, Malhi R et al. Drug-interaction between rifampicin and cotrimoxazole in patients with tuberculosis. Hum Exp Toxicol 1991; 10: 419-21.
105. Garske L, Kidd T, Gan R et al. Rifampicin and sodium fusidate reduces the frequency of methicillin-resistant staphylococcus aureus (MRSA) isolation in adults with cystic fibrosis and chronic MRSA infection. J Hosp Infect 2004; 56: 208-14.

DDIs Associated with Antibacterials for COPD
109
5
106. Weiner M, Burman W, Luo CC et al. Effects of rifampin and multidrug resistance gene polymorphism on concentrations of moxifloxacin. Antimicrob Agents Chemother 2007; 51: 2861-6.
107. Nijland HM, Ruslami R, Suroto AJ et al. Rifampicin reduces plasma concentrations of moxifloxacin in patients with tuberculosis. Clin Infect Dis 2007; 45: 1001-7.
108. Manika K, Chatzika K, Papaioannou M et al. Rifampicin-moxifloxacin interaction in tuberculosis treatment: A real-life study. Int J Tuberc Lung Dis 2015; 19: 1383-7.
109. Naidoo A, Chirehwa M, McIlleron H et al. Effect of rifampicin and efavirenz on moxifloxacin concentrations when co-administered in patients with drug-susceptible TB. Antimicrob Chemother 2017; 72: 1441-9.
110. Apseloff G, Foulds G, LaBoy-Goral L et al. Comparison of azithromycin and clarithromycin in their interactions with rifabutin in healthy volunteers. Eur Respir J 1998; 38: 830-5.
111. Jordan MK, Polis MA, Kelly G et al. Effects of fluconazole and clarithromycin on rifabutin and 25-O-desacetylrifabutin pharmacokinetics. J Clin Pharmacol 2000; 44: 2170-2.
112. Nelson MV, Berchou RC, Kareti D et al. Pharmacokinetic evaluation of erythromycin and caffeine administered with bromocriptine. Clin Pharmacol Ther 1990; 47: 694-7.
113. Nakatsuka A, Nagai M, Yabe H et al. Effect of clarithromycin on the pharmacokinetics of cabergoline in healthy controls and in patients with parkinson’s disease. J Pharmacol Sci 2006; 100: 59-64.
114. Perucca E. Clinically relevant drug interactions with antiepileptic drugs. Br J Clin Pharmacol 2006; 61: 246-55.
115. Neuvonen PJ, Penttila O. Interaction between doxycycline and barbiturates. Br Med J 1974; 1: 535-6.
116. Hansen JM, Kampmann JP, Siersbaek-Nielsen K et al. The effect of different sulfonamides on phenytoin metabolism in man. Acta Med Scand Suppl 1979; 624: 106-10.
117. Penttila O, Neuvonen PJ, Aho K et al. Interaction between doxycycline and some antiepileptic drugs. Br Med J 1974; 2: 470-2.
118. Shahzadi A, Javed I, Aslam B et al. Therapeutic effects of ciprofloxacin on the pharmacokinetics of carbamazepine in healthy adult male volunteers. Pak J Pharm Sci 2011; 24: 63-8.
119. Antoniou T, Gomes T, Mamdani MM et al. Trimethoprim/sulfamethoxazole-induced phenytoin toxicity in the elderly: A population-based study. Br J Clin Pharmacol 2011; 71: 544-9.
120. Greenberg RG, Melloni C, Wu H et al. Therapeutic index estimation of antiepileptic drugs: A systematic literature review approach. Clin Neuropharmacol 2016; 39: 232-40.
121. Bialer M, Rene’H L, Perucca E. Does carbamazepine have a narrow therapeutic plasma concentration range? Ther Drug Monit 1998; 20: 56-9.
122. Li KY, Li X, Cheng ZN et al. Effect of erythromycin on metabolism of quetiapine in chinese suffering from schizophrenia. Eur J Clin Pharmacol 2005; 60: 791-5.
123. Desta Z, Kerbusch T, Flockhart DA. Effect of clarithromycin on the pharmacokinetics and pharmacodynamics of pimozide in healthy poor and extensive metabolizers of cytochrome P450 2D6 (CYP2D6). Clin Pharmacol Ther 1999; 65: 10-20.
124. Farkas D, Volak LP, Harmatz JS et al. Short-term clarithromycin administration impairs clearance and enhances pharmacodynamic effects of trazodone but not of zolpidem. Clin Pharmacol Ther 2009; 85: 644-50.
125. Kivisto KT, Lamberg TS, Kantola T et al. Plasma buspirone concentrations are greatly increased by erythromycin and itraconazole. Clin Pharmacol Ther 1997; 62: 348-54.
126. Dean L. Diazepam therapy and CYP2C19 genotype. In: Pratt V, McLeod H, Rubinstein W et al eds. Medical Genetics Summaries. US: National Center for biotechnology information, 2012. Available from: https://www.ncbi.nlm.nih.gov/books/NBK379740/.
Chapter 5
110
127. Kamali F, Thomas SH, Edwards C. The influence of steady-state ciprofloxacin on the pharmacokinetics and pharmacodynamics of a single dose of diazepam in healthy volunteers. Eur J Clin Pharmacol 1993; 44: 365-7.
128. Fuhr U, Anders EM, Mahr G et al. Inhibitory potency of quinolone antibacterial agents against cytochrome P450IA2 activity in vivo and in vitro. Antimicrob Agents Chemother 1992; 36: 942-8.
129. Raaska K, Neuvonen PJ. Ciprofloxacin increases serum clozapine and N-desmethylclozapine: A study in patients with schizophrenia. Eur J Clin Pharmacol 2000; 56: 585-9.
130. Meyer JM, Proctor G, Cummings MA et al. Ciprofloxacin and clozapine: A potentially fatal but underappreciated interaction. Case Rep Psychiatry 2016; 2016: .
131. Nix DE, Wilton JH, Ronald B et al. Inhibition of norfloxacin absorption by antacids. Antimicrob Agents Chemother 1990; 34: 432-5.
132. Garty M, Hurwitz A. Effect of cimetidine and antacids on gastrointestinal absorption of tetracycline. Clin Pharmacol Ther 1980; 28: 203-7.
133. Van Slooten AD, Nix DE, Wilton JH et al. Combined use of ciprofloxacin and sucralfate. DICP 1991; 25: 578-82.
134. Parpia SH, Nix DE, Hejmanowski LG et al. Sucralfate reduces the gastrointestinal absorption of norfloxacin. Antimicrob Agents Chemother 1989; 33: 99-102.
135. Lehto P, Kivisto KT. Effect of sucralfate on absorption of norfloxacin and ofloxacin. Antimicrob Agents Chemother 1994; 38: 248-51.
136. Deppermann KM, Lode H, Hoffken G et al. Influence of ranitidine, pirenzepine, and aluminum magnesium hydroxide on the bioavailability of various antibiotics, including amoxicillin, cephalexin, doxycycline, and amoxicillin-clavulanic acid. Antimicrob Agents Chemother 1989; 33: 1901-7.
137. Nix DE, Watson WA, Lener ME et al. Effects of aluminum and magnesium antacids and ranitidine on the absorption of ciprofloxacin. Clin Pharmacol Ther 1989; 46: 700-5.
138. Stass H, Bottcher MF, Ochmann K. Evaluation of the influence of antacids and H2 antagonists on the absorption of moxifloxacin after oral administration of a 400mg dose to healthy volunteers. Clin Pharmacokinet 2001; 40 Suppl 1: 39-48.
139. Frost RW, Lasseter KC, Noe AJ et al. Effects of aluminum hydroxide and calcium carbonate antacids on the bioavailability of ciprofloxacin. Antimicrob Agents Chemother 1992; 36: 830-2.
140. Motoya T, Shimozono T, Yamaguchi T et al. Effects of milk and aluminum hydroxide on the absorption of norfloxacin, ciprofloxacin and tosufloxacin in healthy volunteers. J Appl Ther 1997; 1: 213-7.
141. Nguyen VX, Nix DE, Gillikin S et al. Effect of oral antacid administration on the pharmacokinetics of intravenous doxycycline. Antimicrob Agents Chemother 1989; 33: 434-6.
142. Nix DE, Watson WA, Handy L et al. The effect of sucralfate pretreatment on the pharmacokinetics of ciprofloxacin. Pharmacotherapy 1989; 9: 377-80.
143. Albert KS, Welch RD, DeSante KA et al. Decreased tetracycline bioavailability caused by a bismuth subsalicylate antidiarrheal mixture. J Pharm Sci 1979; 68: 586-8.
144. Mapp RK, McCarthy TJ. The effect of zinc sulphate and of bicitropeptide on tetracycline absorption. S Afr Med J 1976; 50: 1829-30.
145. Chopra I, Roberts M. Tetracycline antibiotics: Mode of action, applications, molecular biology, and epidemiology of bacterial resistance. Microbiol Mol Biol Rev 2001; 65: 232,60 ; second page, table of contents.
146. Kamberi M, Nakashima H, Ogawa K et al. The effect of staggered dosing of sucralfate on oral bioavailability of sparfloxacin. Br J Clin Pharmacol 2000; 49: 98-103.
147. Miura M, Tada H, Yasui-Furukori N et al. Effect of clarithromycin on the enantioselective disposition of lansoprazole in relation to CYP2C19 genotypes. Chirality 2005; 17: 338-44.

DDIs Associated with Antibacterials for COPD
111
5
148. Crothers K, Butt AA, Gibert CL et al. Increased COPD among HIV-positive compared to HIV-negative veterans. Chest 2006; 130: 1326-33.
149. Sahai J, Gallicano K, Oliveras L et al. Cations in the didanosine tablet reduce ciprofloxacin bioavailability. Clin Pharmacol Ther 1993; 53: 292-7.
150. Knupp CA, Barbhaiya RH. A multiple-dose pharmacokinetic interaction study between didanosine (videx) and ciprofloxacin (cipro) in male subjects seropositive for HIV but asymptomatic. Biopharm Drug Dispos 1997; 18: 65-77.
151. Grub S, Bryson H, Goggin T et al. The interaction of saquinavir (soft gelatin capsule) with ketoconazole, erythromycin and rifampicin: Comparison of the effect in healthy volunteers and in HIV-infected patients. Eur J Clin Pharmacol 2001; 57: 115-21.
152. Srinivas NR, Knupp CA, Batteiger B et al. A pharmacokinetic interaction study of didanosine coadministered with trimethoprim and/or sulphamethoxazole in HIV seropositive asymptomatic male patients. Br J Clin Pharmacol 1996; 41: 207-15.
153. Moore KH, Yuen GJ, Raasch RH et al. Pharmacokinetics of lamivudine administered alone and with trimethoprim-sulfamethoxazole. Clin Pharmacol Ther 1996; 59: 550-8.
154. Shi HY, Yan J, Zhu WH et al. Effects of erythromycin on voriconazole pharmacokinetics and association with CYP2C19 polymorphism. Eur J Clin Pharmacol 2010; 66: 1131-6.
155. Sriwiriyajan S, Samaeng M, Ridtitid W et al. Pharmacokinetic interactions between ciprofloxacin and itraconazole in healthy male volunteers. Biopharm Drug Dispos 2011; 32: 168-74.
156. Olkkola KT, Aranko K, Luurila H et al. A potentially hazardous interaction between erythromycin and midazolam. Clin Pharmacol Ther 1993; 53: 298-305.
157. Yeates RA, Laufen H, Zimmermann T. Interaction between midazolam and clarithromycin: Comparison with azithromycin. Int J Clin Pharmacol Ther 1996; 34: 400-5.
158. Quinney SK, Haehner BD, Rhoades MB et al. Interaction between midazolam and clarithromycin in the elderly. Br J Clin Pharmacol 2008; 65: 98-109.
159. Zimmermann T, Yeates RA, Laufen H et al. Influence of the antibiotics erythromycin and azithromycin on the pharmacokinetics and pharmacodynamics of midazolam. Arzneimittelforschung 1996; 46: 213-7.
160. Mattila MJ, Vanakoski J, Idanpaan-Heikkila JJ. Azithromycin does not alter the effects of oral midazolam on human performance. Eur J Clin Pharmacol 1994; 47: 49-52.
161. Hagelberg NM, Peltoniemi MA, Saari TI et al. Clarithromycin, a potent inhibitor of CYP3A, greatly increases exposure to oral S-ketamine. Eur J Pain 2010; 14: 625-9.
162. Backman JT, Aranko K, Himberg JJ et al. A pharmacokinetic interaction between roxithromycin and midazolam. Eur J Clin Pharmacol 1994; 46: 551-5.
163. Bartkowski RR, Goldberg ME, Larijani GE et al. Inhibition of alfentanil metabolism by erythromycin. Clin Pharmacol Ther 1989; 46: 99-102.
164. Jokinen MJ, Olkkola KT, Ahonen J et al. Effect of ciprofloxacin on the pharmacokinetics of ropivacaine. Eur J Clin Pharmacol 2003; 58: 653-7.
165. Jokinen MJ, Ahonen J, Neuvonen PJ et al. Effect of clarithromycin and itraconazole on the pharmacokinetics of ropivacaine. Pharmacol Toxicol 2001; 88: 187-91.
166. Jokinen MJ, Ahonen J, Neuvonen PJ et al. The effect of erythromycin, fluvoxamine, and their combination on the pharmacokinetics of ropivacaine. Anesth Analg 2000; 91: 1207-12.
167. Liukas A, Hagelberg NM, Kuusniemi K et al. Inhibition of cytochrome P450 3A by clarithromycin uniformly affects the pharmacokinetics and pharmacodynamics of oxycodone in young and elderly volunteers. J Clin Psychopharmacol 2011; 31: 302-8.
168. Gupta SK, Bakran A, Johnson RW et al. Cyclosporin-erythromycin interaction in renal transplant patients. Br J Clin Pharmacol 1989; 27: 475-81.
Chapter 5
112
169. Freeman DJ, Martell R, Carruthers SG et al. Cyclosporin-erythromycin interaction in normal subjects. Br J Clin Pharmacol 1987; 23: 776-8.
170. Federico S, Carrano R, Capone D et al. Pharmacokinetic interaction between levofloxacin and ciclosporin or tacrolimus in kidney transplant recipients - ciclosporin, tacrolimus and levofloxacin in renal transplantation. Clin Pharmacokinet 2006; 45: 169-75.
171. Wrishko RE, Levine M, Primmett DR et al. Investigation of a possible interaction between ciprofloxacin and cyclosporine in renal transplant patients. Transplantation 1997; 64: 996-9.
172. Tan KK, Trull AK, Shawket S. Co-administration of ciprofloxacin and cyclosporin: Lack of evidence for a pharmacokinetic interaction. Br J Clin Pharmacol 1989; 28: 185-7.
173. Hedaya MA, El-Afify DR, El-Maghraby GM. The effect of ciprofloxacin and clarithromycin on sildenafil oral bioavailability in human volunteers. Biopharm Drug Dispos 2006; 27: 103-10.
174. Muirhead GJ, Faulkner S, Harness JA et al. The effects of steady-state erythromycin and azithromycin on the pharmacokinetics of sildenafil in healthy volunteers. Br J Clin Pharmacol 2002; 53 Suppl 1: 37S-43S.
175. Shinde DD, Kim HS, Choi JS et al. Different effects of clopidogrel and clarithromycin on the enantioselective pharmacokinetics of sibutramine and its active metabolites in healthy subjects. J Clin Pharmacol 2013; 53: 550-8.
176. Pan W, Bae SK, Shim EJ et al. Effects of clopidogrel and clarithromycin on the disposition of sibutramine and its active metabolites M1 and M2 in relation to CYP2B6*6 polymorphism. Xenobiotica 2013; 43: 211-8.
177. Bassi PU, Onyeji CO, Ukponmwan OE. Effects of tetracycline on the pharmacokinetics of halofantrine in healthy volunteers. Br J Clin Pharmacol 2004; 58: 52-5.
178. Pohl O, Osterloh I, Gotteland JP. Effects of erythromycin at steady-state concentrations on the pharmacokinetics of ulipristal acetate. J Clin Pharm Ther 2013; 38: 512-7.
179. Yano R, Tani D, Watanabe K et al. Evaluation of potential interaction between vinorelbine and clarithromycin. Ann Pharmacother 2009; 43: 453-8.
180. Terkeltaub RA, Furst DE, Digiacinto JL et al. Novel evidence-based colchicine dose-reduction algorithm to predict and prevent colchicine toxicity in the presence of cytochrome P450 3A4/P-glycoprotein inhibitors. Arthritis Rheum 2011; 63: 2226-37.
181. Kovarik JM, Beyer D, Bizot MN et al. Effect of multiple-dose erythromycin on everolimus pharmacokinetics. Eur J Clin Pharmacol 2005; 61: 35-8.
182. Kovarik JM, Hsu CH, McMahon L et al. Population pharmacokinetics of everolimus in de novo renal transplant patients: Impact of ethnicity and comedications. Clin Pharmacol Ther 2001; 70: 247-54.
183. Granfors MT, Backman JT, Neuvonen M et al. Ciprofloxacin greatly increases concentrations and hypotensive effect of tizanidine by inhibiting its cytochrome P450 1A2-mediated presystemic metabolism. Clin Pharmacol Ther 2004; 76: 598-606.
184. Tan KK, Allwood MC, Shawket S. Effect of ciprofloxacin on the pharmacokinetics of antipyrine in healthy volunteers. J Clin Pharm Ther 1990; 15: 151-4.
185. Ludwig E, Szekely E, Csiba A et al. The effect of ciprofloxacin on antipyrine metabolism. J Antimicrob Chemother 1988; 22: 61-7.
186. Kamali F, Huang ML. Increased systemic availability of loperamide after oral administration of loperamide and loperamide oxide with cotrimoxazole. Br J Clin Pharmacol 1996; 41: 125-8.
187. Lee BL, Medina I, Benowitz NL et al. Dapsone, trimethoprim, and sulfamethoxazole plasma levels during treatment of pneumocystis pneumonia in patients with the acquired immunodeficiency syndrome (AIDS). evidence of drug interactions. Ann Intern Med 1989; 110: 606-11.
188. Piccolo ML, Toossi Z, Goldman M. Effect of coadministration of a nutritional

DDIs Associated with Antibacterials for COPD
113
5
supplement on ciprofloxacin absorption. Am J Hosp Pharm 1994; 51: 2697-9.
189. Penttila O, Hurme H, Neuvonen PJ. Effect of zinc sulphate on the absorption of tetracycline and doxycycline in man. Eur J Clin Pharmacol 1975; 9: 131-4.
190. Kays MB, Overholser BR, Mueller BA et al. Effects of sevelamer hydrochloride and calcium acetate on the oral bioavailability of ciprofloxacin. Am J Kidney Dis 2003; 42: 1253-9.
191. Kato R, Ueno K, Imano H et al. Impairment of ciprofloxacin absorption by calcium polycarbophil. J Clin Pharmacol 2002; 42: 806-11.
192. Lesko LJ, Offman E, Brew CT et al. Evaluation of the potential for drug interactions with patiromer in healthy volunteers. J Cardiovasc Pharmacol Ther 2017; 22: 434-46.
193. How PP, Fischer JH, Arruda JA et al. Effects of lanthanum carbonate on the absorption and oral bioavailability of ciprofloxacin. Clin J Am Soc Nephrol 2007; 2: 1235-40.
194. Landersdorfer CB, Kirkpatrick CM, Kinzig M et al. Competitive inhibition of renal tubular secretion of ciprofloxacin and metabolite by probenecid. Br J Clin Pharmacol 2010; 69: 167-78.
195. Jaehde U, Sorgel F, Reiter A et al. Effect of probenecid on the distribution and elimination of ciprofloxacin in humans. Clin Pharmacol Ther 1995; 58: 532-41.
196. Bolhuis MS, van Altena R, van Soolingen D et al. Clarithromycin increases linezolid exposure in multidrug-resistant tuberculosis patients. Eur Respir J 2013; 42: 1614-21.
197. Mitchell PB. Therapeutic drug monitoring of psychotropic medications. Br J Clin Pharmacol 2000; 49: 303-12.
198. Dickinson BD, Altman RD, Nielsen NH et al. Drug interactions between oral contraceptives and antibiotics. Obstet Gynecol 2001; 98: 853-60.
199. Taylor J, Pemberton MN. Antibiotics and oral contraceptives: New considerations for dental practice. Br Dent J 2012; 212: 481-3.
200. Albert RK, Schuller JL, Network CCR. Macrolide antibiotics and the risk of cardiac arrhythmias. Am J Respir Crit 2014; 189: 1173-80.
201. Tabibian JH, Gutierrez MA. Doxycycline-induced pseudotumor cerebri. South Med J 2009; 102: 310-1.
202. Berger FA, Monadian N, Groot N et al. QTc prolongation during ciprofloxacin and fluconazole combination therapy: Prevalence and associated risk factors. Br J Clin Pharmacol 2018; 84: 369-78.
203. Baxter K, Preston C. Stockley’s Drug Interactions. London: Pharmaceutical Press, 2010.
204. Siedlik PH, Olson SC, Yang BB et al. Erythromycin coadministration increases plasma atorvastatin concentrations. J Clin Pharmacol 1999; 39: 501-4.
205. Ericsson CD, Feldman S, Pickering LK et al. Influence of subsalicylate bismuth on absorption of doxycycline. JAMA 1982; 247: 2266-7.
206. Markert C, Schweizer Y, Hellwig R et al. Clarithromycin substantially increases steady-state bosentan exposure in healthy volunteers. Br J Clin Pharmacol 2014; 77: 141-8.
207. Markert C, Hellwig R, Burhenne J et al. Interaction of ambrisentan with clarithromycin and its modulation by polymorphic SLCO1B1. Eur J Clin Pharmacol 2013; 69: 1785-93.
208. Tokairin T, Fukasawa T, Yasui-Furukori N et al. Inhibition of the metabolism of brotizolam by erythromycin in humans: In vivo evidence for the involvement of CYP3A4 in brotizolam metabolism. Br J Clin Pharmacol 2005; 60: 172-5.
209. Phillips JP, Antal EJ, Smith RB. A pharmacokinetic drug interaction between erythromycin and triazolam. J Clin Psychopharmacol 1986; 6: 297-9.
210. Aranko K, Luurila H, Backman JT et al. The effect of erythromycin on the pharmacokinetics and pharmacodynamics of zopiclone. Br J Clin Pharmacol 1994; 38: 363-7.
211. Vlase L, Popa A, Neag M et al. Pharmacokinetic interaction between zolpidem and ciprofloxacin in healthy volunteers. Eur J Drug Metab Pharmacokinet 2011; 35: 83-7.

Chapter 5
114
212. Polk RE, Healy DP, Sahai J et al. Effect of ferrous sulfate and multivitamins with zinc on absorption of ciprofloxacin in normal volunteers. Respir Care 1989; 33: 1841-4.
213. Kara M, Hasinoff BB, McKay DW et al. Clinical and chemical interactions between iron preparations and ciprofloxacin. Br J Clin Pharmacol 1991; 31: 257-61.
214. Lehto P, Kivisto KT, Neuvonen PJ. The effect of ferrous sulphate on the absorption of norfloxacin, ciprofloxacin and ofloxacin. Br J Clin Pharmacol 1994; 37: 82-5.
215. Gothoni G, Neuvonen PJ, Mattila M et al. Iron-tetracycline interaction: Effect of time interval between the drugs. Acta Med Scand 1972; 191: 409-11.
216. Leyden JJ. Absorption of minocycline hydrochloride and tetracycline hydrochloride. effect of food, milk, and iron. J Am Acad Dermatol 1985; 12: 308-12.
217. Neuvonen PJ, Penttila O. Effect of oral ferrous sulphate on the half-life of doxycycline in man. Eur J Clin Pharmacol 1974; 7: 361-3.
218. Neuvonen PJ, Turakka H. Inhibitory effect of various iron salts on the absorption of tetracycline in man. Eur J Clin Pharmacol 1974; 7: 357-60.
219. Venho VM, Salonen RO, Mattila MJ. Modification of the pharmacokinetics of doxycycline in man by ferrous sulphate or charcoal. Eur J Clin Pharmacol 1978; 14: 277-80.
220. Stass H, Kubitza D. Effects of iron supplements on the oral bioavailability of moxifloxacin, a novel 8-methoxyfluoroquinolone, in humans. Clin Pharmacokinet 2001; 40 Suppl 1: 57-62.
221. Cheng SH, White A. Effect of orally administered neomycin on the absorption of penicillin V. N Engl J Med 1962; 267: 1296-7.


PA R T I I
Neuropsychiatric safety of varenicline use for smoking cessation and the application of prescription sequence symmetry analysis in
drug safety evaluation
C H A P T E R 6
Yuanyuan Wang Jens H. Bos
Catharina C.M. Schuiling-Veninga H. Marike Boezen
Job F.M. van Boven Bob Wilffert
Eelko Hak
Neuropsychiatric safety of varenicline in the general and COPD population with and without
psychiatric disorders: a retrospective inception cohort study in a real-world setting
Submitted for publication.

Chapter 6
120
ABSTRACTBackground
Although varenicline is an effective treatment for smoking cessation, evidence on its real-world neuropsychiatric safety is inconsistent, notably for high-risk populations.
Objectives
To evaluate the association between varenicline use and major neuropsychiatric adverse events (NPAEs) in the general and COPD population with and without psychiatric disorders compared with nicotine replacement therapy (NRT) in a real-world setting.
Methods
A retrospective inception cohort study was conducted among new users of varenicline or NRT using the University of Groningen pharmacy database IADB.nl. The primary outcome was the incidence of any drug-treated NPAEs including depression, anxiety and insomnia within 24 weeks after treatment initiation. Subgroup and sensitivity analyses were also conducted.
Results
In the general population without psychiatric disorders, the incidence of total NPAEs in varenicline and NRT groups was 13.7% and 18.3%, respectively (adjusted OR [aOR] 0.78, 95% confidence interval [CI]: 0.67 to 0.90). In the general population with psychiatric disorders, the incidence of total NPAEs was much higher, 81.3% and 84.3% for varenicline and NRT groups, respectively (aOR 0.81, 95% CI: 0.65 to 0.99). In the COPD population, there were no differences in the incidence of NPAEs between comparison groups in both the psychiatric cohort (aOR 1.01, 95% CI [0.65, 1.58]) and the non-psychiatric cohort (aOR 0.75, 95% CI [0.53, 1.05]). Results from subgroup or sensitivity analyses did not reveal increased risks of varenicline compared to NRT.
Conclusion
Varenicline does not increase the risk for NPAEs in both general and COPD populations compared with NRT, irrespective of the presence of psychiatric disorders. Our results provide reassurance for the patients and physicians and may be of help to enhance the use of varenicline for smoking cessation by weighing its risks and benefits.

Neuropsychiatric Safety of Varenicline by Cohort
121
6
INTRODUCTIONTobacco smoking is the leading preventable risk factor for a range of physical and mental illnesses1-4 which poses enormous threats to global public health.5 Although average global smoking rates have declined since 1990 through tobacco control policies,6 the actual number of smokers and disease burden related to smoking continues to increase owing to population growth.7 More than 8 million people are killed by tobacco use each year.8 Therefore, more intensified efforts are needed to fight this deadly epidemic. Smoking cessation strategies as key interventions to prevent smoking-related diseases are therefore urgently needed.9 Varenicline was the first non-nicotine pharmacotherapy for smoking cessation and has greater efficacy than single bupropion, nicotine replacement therapy (NRT) or placebo.10,11 However, substantial concerns regarding its neuropsychiatric safety (e.g. suicidal thoughts, aggressive behavior) have been raised since its approval in the United States in 2006.12 Therefore, after the first safety communication and public health advisory in 2008, the FDA released a black box warning on July 1, 2009.13 Of note, these reports could not establish the causality because of a lack of control or comparator. Afterwards, many randomized controlled trials (RCTs) were conducted to evaluate the possible risk of neuropsychiatric adverse events (NPAEs). Notably, pooled evidence of these RCTs did not indicate an association between varenicline and NPAEs.14 Neither did the Evaluating Adverse Events in a Global Smoking Cessation Study (EAGLES) show a significant increase in NPAEs with varenicline relative to NRT or placebo.10
Although the FDA warning was removed in 2016, concerns regarding the external validity of the RCT evidence remained. Indeed, due to the strict inclusion and exclusion criteria of RCTs, trial participants were generally healthy. Special risk populations with increased smoking prevalence, such as those with COPD and psychiatric disorders, were usually excluded.15 Importantly, COPD patients are older and suffer from many comorbidities making these patients more susceptible to drug-drug interactions potentially leading to related adverse drug events (ADEs).16 Similarly, it has been reported that individuals with psychiatric disorders are prone to experience relapse of psychiatric symptoms.17,18 Varenicline safety in these specific populations is not well explored. Only few studies assessed the neuropsychiatric safety of varenicline in patients with COPD or psychiatric disorders,10,19,20 yet results were inconsistent and related evidence from real-world setting is still lacking.
We therefore conducted this cohort study based on real-life data to assess the risk of NPAEs in starters with varenicline versus NRT starters in both the general and the COPD population with and without psychiatric disorders.

Chapter 6
122
METHODSStudy design and setting
We conducted a retrospective inception cohort study based on the University of Groningen pharmacy dispensing database IADB.nl (http://www.iadb.nl/) which has been widely used for various drug utilization studies.21 IADB.nl contains information of prescribed medications from 70 community pharmacies covering a representative population of approximately 700,000 persons of the Netherlands, regardless of insurance type. It provides both patient information (e.g. date of birth, gender) and complete prescription records including the date of dispensing, quantity dispensed, dose regimen, the number of days the drug will be used, and the related Anatomical Therapeutic Chemical (ATC) codes.
Study population
We included adult patients (>18 years) who started with varenicline or NRT. The individuals only prescribed varenicline (ATC code: N07BA03) or NRT (N07BA01) were included as anti-smoking drug users from the general population. Individuals that were prescribed drugs for obstructive airway disease (R03) at least 3 times within 1 year since 1st prescription after the age of 40 years were defined as COPD patients. COPD patients who were prescribed varenicline or NRT were included as COPD anti-smoking drug users.
For both the general and COPD population with anti-smoking drug use, the first prescription date of varenicline and NRT was set as entry date (index date) of participants for exposure and control groups, respectively. Those who were prescribed other smoking cessation drugs including bupropion (N06AX12), nortriptyline (N06AA10) and cytisine (N07BA04) rather than the studied drugs (varenicline, NRT) within 180 days before or 180 days after index date were excluded. Those who were registered in IADB.nl less than 24 weeks before or after index date were also excluded. For individuals who were prescribed both varenicline and NRT and met criteria of both groups (see Figure 1), we allocated the study subject to the group with the first index date according to the intention-to-treat principle.
In both the general and the COPD population, we classified the individuals into a psychiatric cohort and non-psychiatric cohort according to the presence of psychiatric disorders defined by the prescription of two or more drugs from the neurological ATC group, i.e. N02, N03, N04, N05, N06 within 6 months before index date. In all, our study population covered four separate cohorts (1. General population with psychiatric disorders, 2. General population without psychiatric disorders, 3. COPD population with psychiatric disorders and 4. COPD population without psychiatric disorders) in which the association between exposure and outcomes were assessed (Figure 1).

Neuropsychiatric Safety of Varenicline by Cohort
123
6
Figure 1. Flow chart of population selection. NRT: nicotine replacement therapies; ATC: anatomical therapeutic chemical.
Exposure and outcomes
We defined individuals using varenicline as the exposure group and those using NRT as the reference group. The primary outcome was incidence of any drug-treated neuropsychiatric adverse event (NPAE) including depression (drugs with ATC-codes N06A, N06CA), anxiety (N05B) and insomnia (N05C), defined as one or more prescriptions of the specified drugs within 24 weeks after the first prescription of varenicline or NRT.

Chapter 6
124
Covariates
The following covariates were included as possible confounders: age, gender, social economic status (SES) based on postal codes, previous psychiatric disorders and other comorbidities including heart failure, ischemic heart disease, hypertension, cancer, diabetes, osteoporosis, peptic ulcer and gastroesophageal reflux disease (GERD), rheumatic arthritis, thyroid disorder, anemia, glaucoma, gout, and allergic rhinitis. All the comorbidities were defined by at least two prescriptions of related drugs within 6 months prior to index date (see detailed ATC codes in supplementary Table S1), The ATC codes used to define the comorbidities in this study were consistent with those in previous published papers.22-26
Statistical methods
The continuous and categorical variables are presented as means with standard deviations (SD) and numbers with percentages, respectively. The differences of characteristics between two groups were compared using student’s t-tests and chi-square tests for continuous and categorical variables, respectively. Binary logistic regression modeling was used to obtain the odds ratio (OR) and corresponding 95% confidence interval (CI) after adjustment for the potential confounders. A two-sided p ≤ 0.05 was considered to be statistically significant for all tests. All analyses were performed using IBM SPSS statistics 25 (IBM Corporation, Armonk, NY, USA) for Windows.
Subgroup and sensitivity analyses
Considering the possible influence of age and gender on the association between NPAEs and varenicline use, we further analyzed the primary outcome in the four cohorts (general and COPD populations with or without psychiatric disease, separately) by stratifying the results by age groups and gender. To further test the robustness of the results, we performed several sensitivity analyses. First, because the common treatment duration of varenicline is 12 weeks, we explored the outcome occurring within 12 weeks after treatment initiation. Second, to exclude an active psychiatric status, we further selected subjects who were not prescribed any drugs for psychiatric disorders within 30 days before index date. Finally, considering the influence of policy changes about reimbursement of smoking cessation treatment on the use of anti-smoking drugs,27 we also performed a sensitivity analysis by excluding the patients whose prescription date of varenicline or NRT may be in the period of Dutch smoking policy changes (i.e. from July 1st 2011 to June 30, 2013).
RESULTSBaseline characteristics
In total, we included 9077 subjects who initiated varenicline or NRT from the general population, of which 2627 had psychiatric disorders. For the COPD population, we

Neuropsychiatric Safety of Varenicline by Cohort
125
6
included 1598 individuals, of which 649 had psychiatric disorders. In both the general and COPD population, individuals treated with varenicline were younger than those treated with NRT (Table 1). Drug use for heart failure and ischemic heart disease was lower in the varenicline-treated than the NRT-treated group. In patients without psychiatric disorders, drug use for other comorbidities (e.g. diabetes and osteoporosis) was also less in individuals treated with varenicline than in those with NRT.
Primary outcome in the general and COPD population
In the general population with psychiatric disorders, the incidence of overall NPAEs within 24 weeks was lower in the varenicline group than the NRT group (81.3% vs 84.3%, OR 0.81 [0.66, 0.99], Table 2). After adjusting for potential confounders, the association did not substantially change (adjusted OR (aOR) 0.81, 95% CI [0.65, 0.99]). All the specific NPAEs were also less in the varenicline group than the NRT group, although the difference between the two comparison groups for depression and insomnia events did not reach statistical significance.
In the general population without psychiatric disorders, the incidence rates of NPAEs were lower than among those with psychiatric disorders. The incidence of overall NPAEs within 24-weeks in the varenicline group was lower than those in the NRT group (13.7% and 18.3%, respectively; aOR 0.78, 95% CI [0.67, 0.90]). No difference was observed between the two treatment groups for depression and anxiety, however, less insomnia was seen for varenicline than NRT (aOR was 0.63, 95% CI [0.49, 0.82]).
In the COPD population, we did not see a statistical significant difference for incidence of overall NPAEs between the varenicline and NRT groups for both the psychiatric cohort (OR 1.01, 95% CI [0.65, 1.58], Table 3) and the non-psychiatric cohort (OR 0.75, 95% CI [0.53, 1.05]). There were also no differences for specific NPAEs between treatment groups in these two cohorts except for anxiety, which was observed significantly less in the varenicline group compared with the NRT group (aOR 0.68, 95% CI [0.49, 0.94] for the psychiatric cohort and aOR 0.69, 95% CI [0.50, 0.96] for the non- psychiatric cohort, respectively).
Subgroup analysis
In the general population with psychiatric disorders, the risk of overall NPAEs was even lower among varenicline than NRT users for younger patients (aOR 0.54, 95% CI [0.28, 1.04] for age < 40, aOR 0.78, 95% CI [0.63, 0.98] for age 40-65, Table S2) and females (aOR 0.74, 95% CI [0.57, 0.97]). However, in the general population without psychiatric disorders, a lower risk of overall NPAE by varenicline treatment compared with NRT was seen in older patients (aOR 0.52, 95% CI [0.33, 0.82]) and male subjects (aOR 0.78, 95% CI [0.61, 0.99]).

Chapter 6
126
Tabl
e 1.
Bas
elin
e ch
arac
teris
tics o
f gen
eral
and
CO
PD p
opul
atio
n w
ith a
nd w
ithou
t psy
chia
tric
dis
orde
rs b
y tr
eatm
ent g
roup
s.
Char
acte
ristic
s
Gen
eral
pop
ulat
ion
(n =
907
7)CO
PD p
opul
atio
n (1
598)
Psyc
hiat
ric c
ohor
t(n
= 2
627)
Non
-psy
chia
tric
coh
ort
(n =
645
0)Ps
ychi
atric
coh
ort
(n =
649
)N
on-p
sych
iatr
ic c
ohor
t(n
= 9
49)
Vare
nicl
ine
(N=1
427)
NRT
(N=1
200)
Vare
nicl
ine
(N=4
480)
NRT
(N=
1970
)Va
reni
clin
e (N
=327
)N
RT(N
=322
)Va
reni
clin
e (N
=608
)N
RT(N
= 34
1)
Age
(yea
rs)
Mea
n (S
D)
54.5
(9.6
)*55
.8 (1
2.3)
52.1
(9.7
)*53
.4 (1
2.5)
59.2
(8.6
)*62
.4 (1
0.2)
58.9
(8.9
)*62
.7 (9
.8)
Age
rang
e32
- 87
25 -
9232
- 10
222
- 90
41 -
8741
- 92
40 -
102
42 -8
9G
ende
r (n,
%)
Men
541
(37.
9)*
523
(43.
6)24
06 (5
3.7)
1100
(55.
8)11
1 (3
3.9)
126
(39.
1)31
0 (5
1.0)
184
(54.
0)Fe
mal
e 88
6 (6
2.1)
677
(56.
4)20
74 (4
6.3)
870
(44.
2)21
6 (6
6.1)
196
(60.
9)29
8 (4
9.0)
157
(46.
0)Ye
ar o
f ind
ex d
ate
(n, %
)19
94-2
010
519
(36.
4)*
492
(41.
0)14
97 (3
3.4)
*89
5 (4
5.4)
135
(41.
3)13
5 (4
1.9)
211
(34.
7)12
4 (3
6.4)
2011
-201
790
8 (6
3.6)
708
(59.
0)29
83 (6
6.6)
1075
(54.
6)19
2 (5
8.7)
187
(58.
1)39
7 (6
5.3)
217
(63.
6)So
cial
eco
nom
ic s
tatu
s (n
, %)
Low
714
(50.
0)*
655
(54.
6)21
17 (4
7.3)
*10
80 (5
4.8)
170
(52.
0)17
2 (5
3.4)
287
(47.
2)17
5 (5
1.3)
Hig
h71
3 (5
0.0)
545
(45.
4)23
63 (5
2.7)
890
(45.
2)15
7 (4
8.0)
150
(46.
6)32
1 (5
2.8)
166
(48.
7)Co
mor
bidi
ties
(n, %
)H
eart
failu
re41
(2.9
)*82
(6.8
)47
(1.0
)*53
(2.7
)23
(7.0
)*42
(13.
0)20
(3.3
)*27
(7.9
)Is
chem
ic h
eart
dis
ease
25 (1
.8)*
39 (3
.3)
36 (0
.8)*
31 (1
.6)
9 (2
.8)*
20 (6
.2)
9 (1
.5)*
12 (3
.5)
Hyp
erte
nsio
n50
8 (3
5.6)
465
(38.
8)10
39 (2
3.2)
*54
7 (2
7.8)
146
(44.
6)16
7 (5
1.9)
234
(38.
5)14
5 (4
2.5)
Canc
ers
9 (0
.6)*
0 (0
.0)
9 (0
.2)
9 (0
.5)
0 (0
.0)
0 (0
.0)
0 (0
.0)
2 (0
.6)
Dia
bete
s mel
litus
162
(11.
4)12
9 (1
0.8)
260
(5.8
)*14
6 (7
.4)
53 (1
6.2)
40 (1
2.4)
47 (7
.7)*
43 (1
2.6)
Ost
eopo
rosi
s39
(2.7
)32
(2.7
)25
(0.6
)*26
(1.3
)17
(5.2
)20
(6.2
)6
(1.0
)*14
(4.1
)Pe
ptic
ulc
er a
nd G
ERD
436
(30.
6)40
7 (3
3.9)
474
(10.
6)*
253
(12.
8)13
4 (4
1.0)
142
(44.
1)12
3 (2
0.2)
82 (2
4.0)
Rheu
mat
ic a
rthr
itis
170
(11.
9)17
2 (1
4.3)
204
(4.6
)*12
3 (6
.2)
45 (1
3.8)
41 (1
2.7)
40(6
.6)
21 (6
.2)

Neuropsychiatric Safety of Varenicline by Cohort
127
6
Tabl
e 1.
(con
tinue
d)
Char
acte
ristic
s
Gen
eral
pop
ulat
ion
(n =
907
7)CO
PD p
opul
atio
n (1
598)
Psyc
hiat
ric c
ohor
t(n
= 2
627)
Non
-psy
chia
tric
coh
ort
(n =
645
0)Ps
ychi
atric
coh
ort
(n =
649
)N
on-p
sych
iatr
ic c
ohor
t(n
= 9
49)
Vare
nicl
ine
(N=1
427)
NRT
(N=1
200)
Vare
nicl
ine
(N=4
480)
NRT
(N=
1970
)Va
reni
clin
e (N
=327
)N
RT(N
=322
)Va
reni
clin
e (N
=608
)N
RT(N
= 34
1)
Thyr
oid
diso
rder
55 (3
.9)
40 (3
.3)
96 (2
.1)
49 (2
.5)
18 (5
.5)
13 (4
.0)
18 (3
.0)
5 (1
.5)
Anem
ia49
(3.4
)52
(4.3
)49
(1.1
)*38
(1.9
)11
(3.4
)20
(6.2
)4
(0.7
)*12
(3.5
)G
lauc
oma
13 (0
.9)
12 (1
.0)
17 (0
.4)*
23 (1
.2)
4 (1
.2)
4 (1
.2)
3 (0
.5)*
7 (2
.1)
Gou
t 4
(0.3
)9
(0.8
)16
(0.4
)*24
(1.2
)1
(0.3
)3
(0.9
)3
(0.5
)*10
(2.9
)Al
lerg
ic rh
initi
s76
(5.3
)47
(3.9
)10
4 (2
.3)
34 (1
.7)
28 (8
.6)
24 (7
.5)
33 (5
.4)
15 (4
.4)
*p<0
.05;
GER
D: G
astr
oeso
phag
eal R
eflux
Dis
ease
. N
RT: N
icot
ine
repl
acem
ent t
hera
py.

Chapter 6
128
Tabl
e 2.
Inci
denc
e of
neu
rops
ychi
atric
adv
erse
eve
nts
(NPA
Es) a
nd a
ssoc
iatio
n w
ith v
aren
iclin
e co
mpa
red
with
NRT
in g
ener
al p
opul
atio
n w
ith a
nd w
ithou
t ps
ychi
atric
dis
orde
rs w
ith fo
llow
up
of 2
4 w
eeks
.
NPA
Es
Psyc
hiat
ric c
ohor
tVa
reni
clin
e vs
NRT
(142
7 vs
120
0)
Non
-psy
chia
tric
coh
ort
Vare
nicl
ine
vs N
RT(4
480
vs 1
970)
Even
ts (n
, %)
Crud
e O
R (9
5% C
I)Ad
just
ed O
R*
(95%
CI)
Even
ts (n
, %)
Crud
e O
R (9
5% C
I)Ad
just
ed O
R**
(95%
CI)
Ove
rall
1160
(81.
3): 1
012
(84.
3)0.
81 [0
.66,
0.9
9]0.
81 [0
.65,
0.9
9]61
2 (1
3.7)
: 360
(18.
3)0.
71 [0
.61,
0.8
2]0.
78 [0
.67,
0.9
0]De
pressio
n62
9 (4
4.1)
: 548
(45.
7)0.
94 [0
.80,
1.0
9]0.
90 [0
.77,
1.0
5]
148
(3.3
): 57
(2.9
)1.
15 [0
.84,
1.5
6]1.
15 [0
.84,
1.5
7]
Anxiety
456
(32.
0): 4
72 (3
9.3)
0.72
[0.6
2, 0
.85]
0.71
[0.6
1, 0
.84]
215
(4.8
): 11
0 (5
..6)
0.85
[0.6
7, 1
.08]
0.90
[0.7
1, 1
.15]
Insomnia
372
(26.
1): 3
52 (2
9.3)
0.85
[0.7
2, 1
.01]
0.89
[0.7
5, 1
.06]
147
(3.3
): 10
5 (5
.3)
0.60
[0.4
7, 0
.78]
0.63
[0.4
9, 0
.82]
NPA
Es: n
euro
psyc
hiat
ric a
dver
se e
vent
s; N
RT: n
icot
ine
repl
acem
ent t
hera
py; O
R: o
dds
ratio
; CI:
confi
denc
e in
terv
al; *
Adju
sted
for a
ge, g
ende
r, so
cioe
cono
mic
sta
tus,
hear
t fai
lure
, isc
hem
ic
hear
t dis
ease
and
can
cer;.
**A
djus
ted
for a
ge, s
ocio
econ
omic
sta
tus,
hear
t fai
lure
, isc
hem
ic h
eart
dis
ease
, hyp
erte
nsio
n, d
iabe
tes,
oste
opor
osis
, pep
tic u
lcer
and
GER
D, R
heum
atic
art
hriti
s, an
emia
, gla
ucom
a an
d go
ut;

Neuropsychiatric Safety of Varenicline by Cohort
129
6
Tabl
e 3.
Inci
denc
e of
neu
rops
ychi
atric
adv
erse
eve
nts
(NPA
Es) a
nd a
ssoc
iatio
n w
ith v
aren
iclin
e co
mpa
red
with
NRT
in C
OPD
pop
ulat
ion
with
and
with
out
psyc
hiat
ric d
isor
ders
with
follo
w u
p of
24
wee
ks.
NPA
Es
Psyc
hiat
ric c
ohor
tVa
reni
clin
e vs
NRT
(327
vs
322)
Non
-psy
chia
tric
coh
ort
Vare
nicl
ine
vs N
RT(6
08 v
s 34
1)
Even
ts (n
, %)
Cru
de O
R (9
5% C
I)Ad
just
ed O
R*
(95%
CI)
Even
ts (n
, %)
Crud
e O
R (9
5% C
I)Ad
just
ed O
R**
(95%
CI)
Ove
rall
276
(84.
4): 2
78 (8
6.3)
0.86
[0.5
5, 1
.33]
1.01
[0.6
5, 1
.58]
104
(17.
1): 7
9 (2
3.2)
0.68
[0.4
9, 0
.95]
0.75
[0.5
3,1.
05]
Dep
ress
ion
146
(44.
6): 1
45 (4
5.0)
0.99
[0.7
2, 1
.34]
0.90
[0.6
5, 1
.24]
22 (3
.6):
10 (2
.9)
1.24
[0.5
8, 2
.66]
1.37
[0.6
2, 3
.03]
Anxi
ety
110
(33.
6): 1
36 (4
2.2)
0.69
[0.5
0, 0
.95]
0.68
[0.4
9, 0
.94]
38 (6
.3):
25 (7
.3)
0.84
[0.5
0, 1
.42]
0.69
[0.5
0, 0
.96]
Inso
mni
a10
2 (3
1.2)
: 124
(38.
5)0.
72 [0
.52,
1.0
0]0.
84 [0
.60,
1.1
8]25
(4.1
): 21
(6.2
)0.
65 [0
.36,
1.1
9]0.
83 [0
.59,
1.1
6]
NPA
Es: n
euro
psyc
hiat
ric a
dver
se e
vent
s; N
RT: n
icot
ine
repl
acem
ent t
hera
py; O
R: o
dds
ratio
; CI:
confi
denc
e in
terv
al; * Ad
just
ed fo
r age
, hea
rt fa
ilure
, isc
hem
ic h
eart
dis
ease
; **Ad
just
ed fo
r age
, he
art f
ailu
re, i
sche
mic
hea
rt d
isea
se, d
iabe
tes,
oste
opor
osis
, ane
mia
, gla
ucom
a an
d go
ut;

Chapter 6
130
In the COPD population, in both the psychiatric and non-psychiatric cohorts, there was no difference for overall NPAEs between the varenicline and NRT groups in each age group and gender group (aOR 0.99, 95% CI [0.53,1.87]; aOR 0.76, 95% CI [0.44, 1.31]; respectively for men and women, Table S2).
Sensitivity analysis
In the general population, considering a follow-up of 12 weeks, the risk of overall NPAEs was less for varenicline compared with NRT in both the psychiatric and non-psychiatric cohorts (aOR 0.78, 95% CI: 0.64 to 0.94; aOR 0.74, 95% CI: 0.62 to 0.89; respectively, Table S3). After limiting the study population to those who were not prescribed drugs for any psychiatric disorder or those who were not prescribed drugs for depression, anxiety and insomnia within 1 month before index date, there was no statistical significant difference for overall NPAEs, irrespective of presence of psychiatric disorders in the previous year (Table S4). The result was similar when we limited our cohort to individuals whose study period was not in the period of Dutch smoking policy change; the aOR for varenicline compared with NRT was 0.86, 95% CI [0.69, 1.07] in the psychiatric cohort and 0.86, 95% CI [0.71, 1.03] in non-psychiatric cohort.
In the COPD population, there were no statistical significant differences for overall and subgroup NPAEs within follow-up of 12 weeks between the two treatments except for anxiety in the psychiatric cohort (aOR 0.64, 95% CI [0.46, 0.90], Table S5). After limiting the study population to those who were not prescribed drugs for any psychiatric disorder or those who were not prescribed drugs for depression, anxiety and insomnia within 1 month before index date, there was no statistical significant difference for overall NPAEs, irrespective of presence of psychiatric disorders (Table S6). Similar results were seen when limiting individuals to those whose study period was not in the period of Dutch smoking policy change (OR 0.97, 95% CI: 0.62 to 1.51; OR 1.00, 95% CI: 0.64 to 1.58; respectively for the psychiatric and non-psychiatric cohorts, Table S6)
DISCUSSIONMain findings and interpretation
Within 24 weeks following initiation of varenicline treatment, we found no significantly increased risk of NPAEs in both the general and COPD population compared with those using NRT, irrespective of the presence of psychiatric disorders. These findings are consistent with the results of previous RCTs and large observational studies,10,28,29 Considering the fact that the smoking cessation treatment may last for only 12 weeks without further treatment,30 we also explored the NPAEs in this shorter time period and observed no increased risk in overall and specific NPAEs for varenicline compared with NRT.

Neuropsychiatric Safety of Varenicline by Cohort
131
6
In contrast to the concerns about a possible increased risk of NPAEs among varenicline users, we found a 19% and 22% relative decrease in NPAEs in varenicline users of the general population with and without psychiatric disorders, respectively, compared with NRT. Regarding the safety of varenicline for specific NPAEs, we recorded a 29% reduced risk of anxiety by varenicline (vs NRT) in the psychiatric cohort, and a 37% reduced risk of insomnia in the non-psychiatric cohort. Rates of depression events were comparable between the two groups in both psychiatric and non-psychiatric cohorts among the general population. These results were consistent with the pooled results of 39 RCTs in a meta-analysis,14 which indicated that less anxiety (hazard ratio (HR) 0.75, 95% CI: 0.61, 0.93) was also observed in the varenicline group (vs NRT), and depression episodes were also evenly distributed among two treatments (HR 0.96, 95% CI: 0.75, 1.22). Compared with our study, the difference is that in this review an increased risk of insomnia was observed in the varenicline group (HR 1.56, 95% CI: 1.36, 1.78).14 Of note, the aforementioned review did not explore the risk of varenicline on NPAEs separately in those with and without psychiatric disorders, which may contribute to the observed differences in this review compared to our results. Of note, our result is consistent with another cohort study based data from the general practice that no increased depression were observed to be associated with varenicline (HR 0.88 [0.77-1.00]). 31
COPD patients are considered a high-risk population with high prevalence of smoking and relatively older age, making these persons more susceptible for possible adverse drug reactions (ADEs).16,32 Of note, in our study we did not observe an increased risk of overall NPAEs among COPD patients using varenicline in both the psychiatric and non-psychiatric cohorts. Of note, regarding the occurrence of specific NPAEs, less anxiety was seen in the varenicline group than in the NRT group in both cohorts. The safety of varenicline was not fully explored among COPD patients in previous studies. To the best of our knowledge, only two studies (one RCT and one cohort study) were previously conducted.19,33 Similar to our results, both of these two studies did not find an increased risk of NPAEs for varenicline. Notably, in the cohort study even a reduced risk of depression was observed in varenicline users compared with users of NRT among COPD patients.19 This may be misled by unmeasured confounders, however, after modelling the effects of possible unmeasured confounders, the author concluded that an increased risk of these adverse events was very unlikely.19
It is notable that there is a large heterogeneity in the definition of NPAEs across studies. In some studies, the investigators focused on moderate to serious adverse events like depression, suicide or mental disorders that require hospitalization or an emergency department visit.19,29,34,35 While other studies included all adverse symptoms (e.g. angry, nervousness) or adverse events such as traffic offences.10,30 In this study, we used prescriptions to define neuropsychiatric outcomes for the most commonly reported NPAEs including depression, anxiety and insomnia during the study period.

Chapter 6
132
Despite differences in clinical definitions, the observed 24-week event rates of specific NPAEs (3%-9%) for depression, anxiety or insomnia in our general population without psychiatric disorders were similar to previous studies.14 However, the rate of NPAEs was substantially higher in participants with psychiatric disorders than those without such illness, which was also consistent with findings from previous studies.35-37 When we further limited our study population to those who did not experience any psychiatric disorder or not experienced any depression, anxiety and insomnia within 1 month of enrollment, we found that both the overall NPAEs and specific NPAE reduced substantially.
Although the rates of NPAEs are different between psychiatric and non-psychiatric cohorts in this study, the presence of psychiatric disorders did not influence the risk of NPAEs by varenicline compared with NRT which was also consistent with previous studies.10,38 In a prospective longitudinal study among psychiatric patients, there was no exacerbation of psychiatric symptoms detected except gastrointestinal adverse events.39 However, although it is not within the scope of this study, what need to be mentioned is that an increased rate of outpatient visits for schizophrenia was previously reported to be present only in patients with a pre-existing mental health disorder.34 This may be explained by mediation through individual genetic liability.40
In interpreting the absence of increased risks by varenicline (vs NRT) observed in the general population, we can only speculate that the positive effect from varenicline may result from its effect of consistently reducing withdrawal-related symptoms of negative affect and raised levels of positive affect.41 It has been reported that varenicline yields higher abstinence rates than NRT,10,11 irrespective of smoker characteristics.42 The successful quitting of smoking by varenicline may offer more benefits to the psychiatric status compared with NRT. Moreover, there is evidence that quitting smoking is associated with recovery in stress, anxiety and depression in smokers.43,44 A significant and progressive improvement of anxiety and depression was also reported in an observational study, and the protective effect was observed regardless of the presence of psychiatric pathology.38
Many studies demonstrated gender differences in varenicline efficacy for smoking cessation,45,46 some studies also found a difference in neuropsychiatric events between genders.47 In this study, we found less risk of NPAEs by varenicline for females in the psychiatric cohort compared with NRT. This may be explained by the better therapeutic response to varenicline in women compared with men. 45 However, in the non-psychiatric cohort, we observed less risk of NPAEs in males by varenicline (vs NRT) which we cannot explain and more research needs to be done on gender disparities. Similarly, there are some indications for age group-dependent NPAEs risk by varenicline (vs NRT) in two cohorts of this study. In the psychiatric cohort, there were

Neuropsychiatric Safety of Varenicline by Cohort
133
6
lower event rates in the varenicline group than the NRT group in younger age groups. Contrary, in the non-psychiatric cohort, lower event rates were seen in older users of varenicline than NRT. The age-specific effectiveness of varenicline relative to NRT patch or gum were also reported that only younger smokers achieved greater likelihood of abstinence than NRTs.48As such, age disparities also need to be studied more closely.
Strengths and limitations
A major strength of this study is that we evaluated the safety of varenicline in both the general and COPD population with and without psychiatric disorders based on large real-life population data making the results representative and more applicable to daily clinical practice. Both short- (12 weeks) and long-term (24 weeks) NPAEs after treatment initiation were explored in this study. Besides the influence of current or previous psychiatric disorders, we also evaluated the influence of age and gender on the NPAEs between treatment groups. Additionally, to test the robustness of our study results, several sensitivity analyses were conducted.
There are several potential limitations in our study that need to be discussed. First, as no diagnostic information was available in this study, outcome events and comorbidities were defined by prescriptions of related drugs as proxies. Although we used similar ATC codes as in previous studies and it’s reported that pharmacy data can be used to provide reliable prevalence estimates of several chronic conditions,26 it may still have led to some misclassification. Second, the prescription of medication may not always lead to intake of the drugs (non-adherence) and such misclassification, if random, may have caused associations to be biased towards the null value. Third, some serious behavioral changes like self-harm or suicide could not be evaluated in this study due to the limitation of the prescription database, although we included the most frequently reported NPAEs that are commonly drug treated. Similarly, some minor symptoms like fatigue could not be evaluated. Fourth, although we tried our best to exclude the influence of baseline differences between exposure groups by adjusting for potential confounders, possible unmeasured confounding may still exist. From the baseline characteristics, we could see that the prevalence of comorbidity in varenicline users was lower than in NRT users which may have been the result of the reluctance of prescribing varenicline by clinicians considering its possible risk of related adverse events for high-risk populations. Such potential channeling bias may have caused a relatively better profile of varenicline. However, this kind of bias may not be large, as most associations (OR) between varenicline and specific NPAEs observed in this study were still below 1 and such bias should be large enough to contradict our conclusion. Additionally, the difference in characteristics could also be attributable to a disparity in the cumulative cigarette exposure between treatment groups,49 however, it’s pity that smoking history was not available in this study.

Chapter 6
134
CONCLUSIONFrom this population-based real-life inception cohort study, we conclude that varenicline is not associated with a significant increased risk of NPAEs in both general and COPD patients with or without psychiatric disorders following its initiation compared with NRT. These results provide further support for the safety of varenicline to quit smoking in both the general and COPD populations.

Neuropsychiatric Safety of Varenicline by Cohort
135
6
REFERENCES
1. Banks E, Joshy G, Korda RJ, et al. Tobacco smoking and risk of 36 cardiovascular disease subtypes: fatal and non-fatal outcomes in a large prospective Australian study. BMC Med. 2019;17(1):128.
2. Gaudet MM, Carter BD, Brinton LA, et al. Pooled analysis of active cigarette smoking and invasive breast cancer risk in 14 cohort studies. Int J Epidemiol. 2017;46(3):881-893.
3. Tjora T, Hetland J, Aaro LE, Wold B, Wiium N, Overland S. The association between smoking and depression from adolescence to adulthood. Addiction. 2014;109(6):1022-1030.
4. Evins AE, Korhonen T, Kinnunen TH, Kaprio J. Prospective association between tobacco smoking and death by suicide: a competing risks hazard analysis in a large twin cohort with 35-year follow-up. Psychol Med. 2017;47(12):2143-2154.
5. Thun MJ, Carter BD, Feskanich D, et al. 50-Year Trends in Smoking-Related Mortality in the United States. New Engl J Med. 2013;368(4):351-364.
6. Collaborators GBDT. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990-2015: a systematic analysis from the Global Burden of Disease Study 2015. Lancet. 2017;389(10082):1885-1906.
7. The L. Progress towards a tobacco-free world. Lancet. 2018;392(10141):1.
8. World Health Organisation. WHO report on the global tobacco epidemic 2019: offer help to quit tobacco use. Geneva: World Health Organisation, 2019: 17-21.
9. Mehrotra R, Yadav A, Sinha DN, et al. Smokeless tobacco control in 180 countries across the globe: call to action for full implementation of WHO FCTC measures. Lancet Oncol. 2019;20(4):e208-e217.
10. Anthenelli RM, Benowitz NL, West R, et al. Neuropsychiatric safety and efficacy of varenicline, bupropion, and nicotine patch in smokers with and without psychiatric
disorders (EAGLES): a double-blind, randomised, placebo-controlled clinical trial. Lancet. 2016;387(10037):2507-2520.
11. Ebbert JO, Hughes JR, West RJ, et al. Effect of varenicline on smoking cessation through smoking reduction: a randomized clinical trial. JAMA. 2015;313(7):687-694.
12. Moore TJ, Furberg CD, Glenmullen J, Maltsberger JT, Singh S. Suicidal behavior and depression in smoking cessation treatments. PLoS One. 2011;6(11):e27016.
13. US Food and Drug Administration. Public health advisory: FDA requires new boxed warnings for the smoking cessation drugs Chantix and Zyban. http://wayback.archive -it.org/7993/20170112005513/h t t p : / / w w w . f d a . g o v / D r u g s /DrugSafety/Postmarket Drug SafetyInformationforPatientsandProviders/ucm169988.htm. Published July 1, 2009. Accessed June 7, 2019. .
14. Thomas KH, Martin RM, Knipe DW, Higgins JP, Gunnell D. Risk of neuropsychiatric adverse events associated with varenicline: systematic review and meta-analysis. BMJ. 2015;350:h1109.
15. Lawrence D, Mitrou F, Zubrick SR. Smoking and mental illness: results from population surveys in Australia and the United States. BMC Public Health. 2009;9:285.
16. Wang Y, Bahar MA, Jansen AME, et al. Improving antibacterial prescribing safety in the management of COPD exacerbations: systematic review of observational and clinical studies on potential drug interactions associated with frequently prescribed antibacterials among COPD patients. J Antimicrob Chemother. 2019;74(10):2848-2864.
17. Garza D, Murphy M, Tseng LJ, Riordan HJ, Chatterjee A. A double-blind randomized placebo-controlled pilot study of neuropsychiatric adverse events in abstinent smokers treated with varenicline or placebo. Biol Psychiatry. 2011;69(11):1075-1082.

Chapter 6
136
18. Tonstad S, Davies S, Flammer M. Psychiatric Adverse Events in Randomized, Double-Blind, Placebo-Controlled Clinical Trials of Varenicline: A Pooled Analysis (vol 33, pg 298, 2010). Drug Safety. 2010;33(6):522-522.
19. Kotz D, Viechtbauer W, Simpson CR, van Schayck OCP, West R, Sheikh A. Cardiovascular and neuropsychiatric risks of varenicline and bupropion in smokers with chronic obstructive pulmonary disease. Thorax. 2017;72(10):905-911.
20. Evins AE, Benowitz NL, West R, et al. Neuropsychiatric Safety and Efficacy of Varenicline, Bupropion, and Nicotine Patch in Smokers With Psychotic, Anxiety, and Mood Disorders in the EAGLES Trial. J Clin Psychopharmacol. 2019;39(2):108-116.
21. Visser ST, Schuiling-Veninga CC, Bos JH, de Jong-van den Berg LT, Postma MJ. The population-based prescription database IADB.nl: its development, usefulness in outcomes research and challenges. Expert Rev Pharmacoecon Outcomes Res. 2013;13(3):285-292.
22. Kronig M, Haverkamp C, Schulte A, et al. Diabetes and beta-adrenergic blockage are risk factors for metastatic prostate cancer. World J Surg Oncol. 2017;15(1):50.
23. van Boven JF, van Raaij JJ, van der Galien R, et al. Impact of multiple-dose versus single-dose inhaler devices on COPD patients’ persistence with long-acting beta(2)-agonists: a dispensing database analysis. NPJ Prim Care Respir Med. 2014;24:14069.
24. Huber CA, Szucs TD, Rapold R, Reich O. Identifying patients with chronic conditions using pharmacy data in Switzerland: an updated mapping approach to the classification of medications. Bmc Public Health. 2013;13.
25. Monte S, Macchia A, Romero M, D’Ettorre A, Giuliani R, Tognoni G. Antidepressants and cardiovascular outcomes in patients without known cardiovascular risk. Eur J Clin Pharmacol. 2009;65(11):1131-1138.
26. Chini F, Pezzotti P, Orzella L, Borgia P, Guasticchi G. Can we use the pharmacy
data to estimate the prevalence of chronic conditions? a comparison of multiple data sources. Bmc Public Health. 2011;11.
27. van Boven JF, Vemer P. Higher Adherence During Reimbursement of Pharmacological Smoking Cessation Treatments. Nicotine Tob Res. 2016;18(1):56-63.
28. Kotz D, Viechtbauer W, Simpson C, van Schayck OC, West R, Sheikh A. Cardiovascular and neuropsychiatric risks of varenicline: a retrospective cohort study. Lancet Respir Med. 2015;3(10):761-768.
29. Thomas KH, Martin RM, Davies NM, Metcalfe C, Windmeijer F, Gunnell D. Smoking cessation treatment and risk of depression, suicide, and self harm in the Clinical Practice Research Datalink: prospective cohort study. BMJ. 2013;347:f5704.
30. Molero Y, Lichtenstein P, Zetterqvist J, Gumpert CH, Fazel S. Varenicline and risk of psychiatric conditions, suicidal behaviour, criminal offending, and transport accidents and offences: population based cohort study. BMJ. 2015;350:h2388.
31. Gunnell D, Irvine D, Wise L, Davies C, Martin RM. Varenicline and suicidal behaviour: a cohort study based on data from the General Practice Research Database. BMJ. 2009;339:b3805.
32. Mangoni AA, Jackson SH. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. Br J Clin Pharmacol. 2004;57(1):6-14.
33. Tashkin DP, Rennard S, Hays JT, Ma W, Lawrence D, Lee TC. Effects of varenicline on smoking cessation in patients with mild to moderate COPD: a randomized controlled trial. Chest. 2011;139(3):591-599.
34. Cunningham FE, Hur K, Dong D, et al. A comparison of neuropsychiatric adverse events during early treatment with varenicline or a nicotine patch. Addiction. 2016;111(7):1283-1292.
35. Pasternak B, Svanstrom H, Hviid A. Use of varenicline versus bupropion and risk of psychiatric adverse events. Addiction. 2013;108(7):1336-1343.

Neuropsychiatric Safety of Varenicline by Cohort
137
6
36. Kanner AM, Wuu J, Faught E, et al. A past psychiatric history may be a risk factor for topiramate-related psychiatric and cognitive adverse events. Epilepsy Behav. 2003;4(5):548-552.
37. Croce Nanni R, Troisi A. Maternal attachment style and psychiatric history as independent predictors of mood symptoms in the immediate postpartum period. J Affect Disord. 2017;212:73-77.
38. Pacheco VA, Fernandez APGB, Morales AV, Crespo EL, Garcia SM, Rubio TM. Anxiety, Depression and Tobacco Abstinence. Adicciones. 2017;29(4):233-244.
39. Raich A, Ballbe M, Nieva G, et al. Safety of Varenicline for Smoking Cessation in Psychiatric and Addicts Patients. Subst Use Misuse. 2016;51(5):649-657.
40. Agerbo E, Sullivan PF, Vilhjalmsson BJ, et al. Polygenic Risk Score, Parental Socioeconomic Status, Family History of Psychiatric Disorders, and the Risk for Schizophrenia: A Danish Population-Based Study and Meta-analysis. JAMA Psychiatry. 2015;72(7):635-641.
41. Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD) 2019 Report. Available from: http://goldcopd.org.
42. Walker N, Gainforth H, Kiparoglou V, Robinson H, van Woerden H, West R. Factors moderating the relative effectiveness of varenicline and nicotine replacement
therapy in clients using smoking cessation services. Addiction. 2018;113(2):313-324.
43. Zarghami M, Taghizadeh F, Sharifpour A, Alipour A. Efficacy of Smoking Cessation on Stress, Anxiety, and Depression in Smokers with Chronic Obstructive Pulmonary Disease: A Randomized Controlled Clinical Trial. Addict Health. 2018;10(3):137-147.
44. Taylor G, McNeill A, Girling A, Farley A, Lindson-Hawley N, Aveyard P. Change in mental health after smoking cessation: systematic review and meta-analysis. BMJ. 2014;348:g1151.
45. McKee SA, Smith PH, Kaufman M, Mazure CM, Weinberger AH. Sex Differences in Varenicline Efficacy for Smoking Cessation: A Meta-Analysis. Nicotine Tob Res. 2016;18(5):1002-1011.
46. Smith PH, Kasza KA, Hyland A, et al. Gender differences in medication use and cigarette smoking cessation: results from the International Tobacco Control Four Country Survey. Nicotine Tob Res. 2015;17(4):463-472.
47. The Lancet P. Sex and gender in psychiatry. Lancet Psychiatry. 2016;3(11):999.
48. Chang PY, Shiu MN, Yuan YT, Chang HC, Su PY, Lan TH. Comparative Effectiveness of Varenicline and Nicotine Replacement Therapy for Smoking Cessation in Older and Younger Smokers: A Prospective Cohort in Taiwan. Nicotine Tob Res. 2019;21(2):149-155.
49. Fidler L, Anand A, Stanbrook M. Cardiovascular and neuropsychiatric risks of varenicline.
Lancet Respir Med. 2016;4(3):e9-e10.

Chapter 6
138
SUPPLEMENTARY MATERIALS
Table S1. List of ATC codes used for identification of related diseases and outcome events.
Variables ATC codes
COPD R03General psychiatric disorders N02, N03, N04, N05, N06Depression N06A, N06CA, Anxiety N05BInsomnia N05CHeart failure C01AA, C03CIschemic heart disease C01DAHypertension C02, C03 (except C03C), C07, C08, C09Cancers L01Diabetes mellitus A10Osteoporosis M05BPeptic ulcer and GERD A02BRheumatic arthritis M01, M02Thyroid disorders H03Anemia B03Glaucoma S01EGout M04Allergic rhinitis R01AD
ATC: anatomical therapeutic chemical; GERD: gastroesophageal reflux disease;
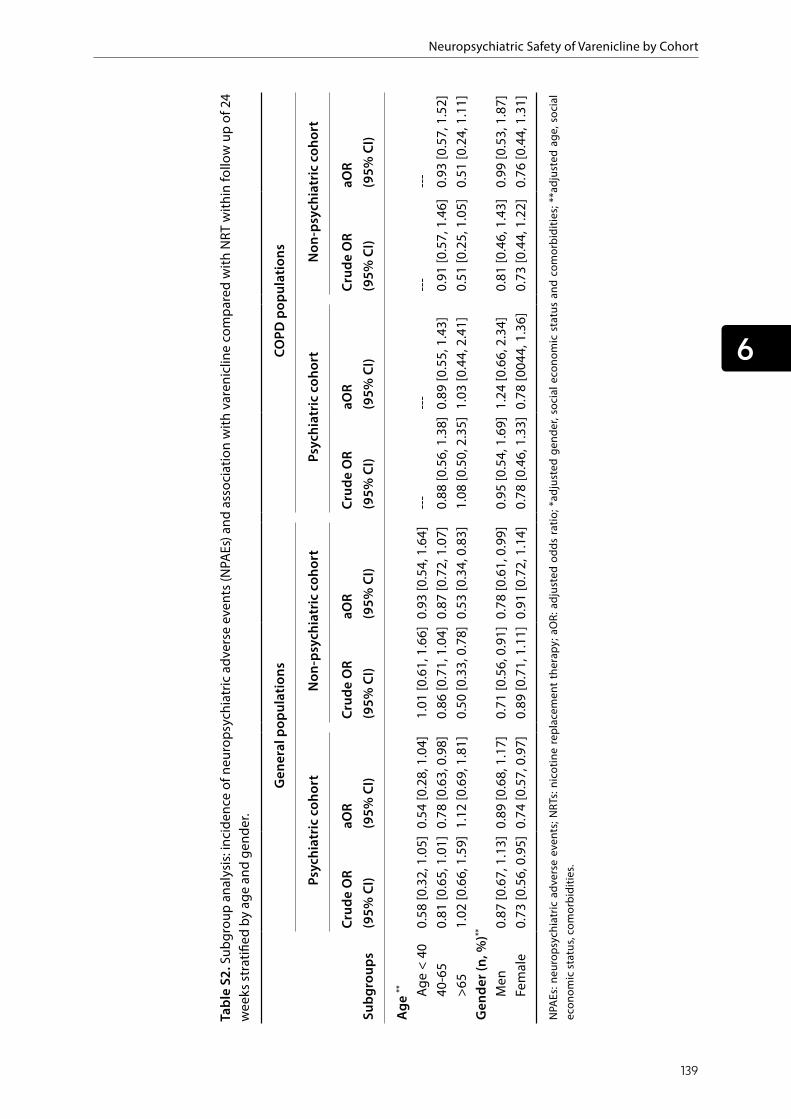
Neuropsychiatric Safety of Varenicline by Cohort
139
6
Tabl
e S2
. Sub
grou
p an
alys
is: i
ncid
ence
of n
euro
psyc
hiat
ric a
dver
se e
vent
s (N
PAEs
) and
ass
ocia
tion
with
var
enic
line
com
pare
d w
ith N
RT w
ithin
follo
w u
p of
24
wee
ks st
ratifi
ed b
y ag
e an
d ge
nder
.
Subg
roup
s
Gen
eral
pop
ulat
ions
COPD
pop
ulat
ions
Psyc
hiat
ric c
ohor
tN
on-p
sych
iatr
ic c
ohor
tPs
ychi
atric
coh
ort
Non
-psy
chia
tric
coh
ort
Crud
e O
R (9
5% C
I)aO
R (9
5% C
I)Cr
ude
OR
(95%
CI)
aOR
(95%
CI)
Crud
e O
R (9
5% C
I)aO
R (9
5% C
I)Cr
ude
OR
(95%
CI)
aOR
(95%
CI)
Age
**
Ag
e <
400.
58 [0
.32,
1.0
5]0.
54 [0
.28,
1.0
4]1.
01 [0
.61,
1.6
6]0.
93 [0
.54,
1.6
4]--
---
---
---
-40
-65
0.81
[0.6
5, 1
.01]
0.78
[0.6
3, 0
.98]
0.86
[0.7
1, 1
.04]
0.87
[0.7
2, 1
.07]
0.88
[0.5
6, 1
.38]
0.89
[0.5
5, 1
.43]
0.
91 [0
.57,
1.4
6]0.
93 [0
.57,
1.5
2]>6
51.
02 [0
.66,
1.5
9] 1
.12
[0.6
9, 1
.81]
0.50
[0.3
3, 0
.78]
0.53
[0.3
4, 0
.83]
1.08
[0.5
0, 2
.35]
1.03
[0.4
4, 2
.41]
0.51
[0.2
5, 1
.05]
0.
51 [0
.24,
1.1
1]G
ende
r (n,
%)**
Men
0.87
[0.6
7, 1
.13]
0.8
9 [0
.68,
1.1
7]0.
71 [0
.56,
0.9
1]0.
78 [0
.61,
0.9
9]0.
95 [0
.54,
1.6
9] 1
.24
[0.6
6, 2
.34]
0.81
[0.4
6, 1
.43]
0.99
[0.5
3, 1
.87]
Fem
ale
0.73
[0.5
6, 0
.95]
0.7
4 [0
.57,
0.9
7]0.
89 [0
.71,
1.1
1]0.
91 [0
.72,
1.1
4]0.
78 [0
.46,
1.3
3]0.
78 [0
044,
1.3
6]0.
73 [0
.44,
1.2
2]0.
76 [0
.44,
1.3
1]
NPA
Es: n
euro
psyc
hiat
ric a
dver
se e
vent
s; N
RTs:
nico
tine
repl
acem
ent
ther
apy;
aO
R: a
djus
ted
odds
rat
io; *
adju
sted
gen
der,
soci
al e
cono
mic
sta
tus
and
com
orbi
ditie
s; **
adju
sted
age
, soc
ial
econ
omic
stat
us, c
omor
bidi
ties.

Chapter 6
140
Tabl
e S3
. Sen
sitiv
ity a
naly
sis:
inci
denc
e of
neu
rops
ychi
atric
adv
erse
eve
nts (
NPA
Es) a
nd a
ssoc
iatio
n w
ith v
aren
iclin
e co
mpa
red
with
NRT
in g
ener
al p
opul
atio
n w
ith a
nd w
ithou
t psy
chia
tric
dis
orde
rs w
ithin
follo
w u
p of
12
wee
ks.
NPA
Es
Psyc
hiat
ric c
ohor
tVa
reni
clin
e vs
NRT
s(1
427
vs 1
200)
Non
-psy
chia
tric
coh
ort
Vare
nicl
ine
vs N
RTs
(448
0 vs
197
0)
Even
ts (n
, %)
Crud
e O
R (9
5% C
I)Ad
just
ed O
R#
(95%
CI)
Even
ts (n
, %)
Crud
e O
R (9
5% C
I)Ad
just
ed O
R#(9
5% C
I)
Follo
w-u
p of
12
wee
ksO
vera
ll10
62 (7
4.4)
: 948
(79.
0)0.
77 [0
.64,
0.9
3]0.
78 [0
.64,
0.9
4]36
3 (8
.1):
223
(11.
3)0.
69 [0
.58,
0.82
]0.
74 [0
.62,
0.8
9]D
epre
ssio
n56
0 (3
9.2)
: 491
(40.
9)0.
93[0
.80,
1.0
9]0.
89 [0
.76,
1.0
5]86
(1.9
): 30
(1.5
)1.
27 [0
.83,
1.9
2]1.
29 [0
.84,
1.9
7]
Anxi
ety
367
(25.
7): 4
23 (3
5.3)
0.64
[0.5
4, 0
.75]
0.63
[0.5
3, 0
.74]
119
(2.7
): 61
(3.1
)0.
85 (0
.62,
1.1
7)0.
90 [0
.65,
1.2
4]In
som
nia
321
(22.
5): 3
11 (2
5.9)
0.83
[0.6
9, 0
.99]
0.88
[0.7
3, 1
.05]
82 (1
.8):
61 (3
.1)
0.58
[0.4
2, 0
.82]
0.62
[0.4
4, 0
.88]
NPA
E: n
euro
psyc
hiat
ric a
dver
se e
vent
s; O
R: o
dds r
atio
; NRT
s: ni
cotin
e re
plac
emen
t the
rapy
; # a
djus
ted
for a
ge, g
ende
r, so
cial
eco
nom
ic st
atus
and
rela
ted
com
orbi
ditie
s.

Neuropsychiatric Safety of Varenicline by Cohort
141
6
Tabl
e S4
. Sen
sitiv
ity a
naly
sis:
inci
denc
e of
neu
rops
ychi
atric
adv
erse
eve
nts (
NPA
Es) a
nd a
ssoc
iatio
n w
ith co
mpa
red
with
NRT
in g
ener
al p
opul
atio
n w
ithin
follo
w
up o
f 24
wee
ks.
Lim
itatio
ns
Gen
eral
pop
ulat
ions
Psyc
hiat
ric c
ohor
t (va
reni
clin
e vs
NRT
s)N
on-p
sych
iatr
ic c
ohor
t (va
reni
clin
e vs
NRT
s)
Even
ts
OR
(95%
CI)
aOR
(95%
CI)*
Even
tsO
R (9
5% C
I)aO
R (9
5% C
I)*
Excl
ude
part
icip
ants
pre
scrib
ed d
rugs
for a
ny N
SP w
ithin
1 m
onth
bef
ore
inde
x da
teO
vera
ll25
4 (5
7.6)
: 157
(60.
4)0.
89 [0
.65,
1.2
2]0.
87 [0
.63,
1.2
1]41
8 (9
.6):
192
(10.
4)0.
91 [0
.76,
1.1
0]0.
93 [0
.78,
1.1
2]
Dep
ress
ion
158
(35.
8): 8
2 (3
1.5)
1.21
[0.8
8, 1
.68]
1.18
[0.8
4, 1
.67]
139
(3.2
): 50
(2.7
)1.
18 [0
.85,
1.6
4]1.
16 [0
.84,
1.6
2]An
xiet
y78
(17.
7): 6
2 (2
3.8)
0.69
[0.4
7, 0
.10]
0.68
[0.4
6, 1
.01]
197
(4.5
): 85
(4.6
)0.
98 [0
.76,
1.2
7]1.
02 [0
.78,
1.3
3]In
som
ina
75 (1
7.0)
: 48
(18.
5)0.
94 [0
.74,
1.2
0]0.
94 [0
.62,
1.4
3]13
1 (3
.0):
91 (4
.9)
0.60
[0.4
6, 0
.79]
0.61
[0.4
6, 0
.80]
Excl
ude
part
icip
ants
pre
scrib
ed d
rugs
for d
epre
ssio
n, a
nxie
ty a
nd in
som
nia
with
in 1
mon
th b
efor
e in
dex
date
Ove
rall
314
(48.
9): 2
01 (4
6.1)
1.12
[0.8
8, 1
.43]
1.05
[0.8
2, 1
.36]
424
(9.6
): 20
3 (1
0.6)
0.90
[0.7
5, 1
.07]
0.92
[0.7
7, 1
.11]
Dep
ress
ion
191
(29.
8): 1
04 (2
3.9)
1.35
[1.0
2, 1
.79]
1.
25 [0
.93,
1.6
6]14
3 (3
.3):
52 (2
.7)
1.20
[0.8
7, 1
.66]
1.19
[0.8
6, 1
.65]
Anxi
ety
99 (1
5.4)
: 81
(18.
6)0.
80 [0
.58,
1.1
0]0.
75 [0
.54,
1.0
5]19
9 (4
.5):
92 (4
.8)
0.94
[0.7
3, 1
.21]
0.
98 [0
.75,
1.2
6]In
som
nia
92 (1
4.3)
: 63
(14.
4)0.
99 [0
.70,
1.4
0]
1.03
[0.7
2, 1
.47]
132
(3.0
): 94
(4.9
)0.
60 [0
.46,
0.7
8]0.
61 [0
.47,
0.8
1]Ex
clud
e pa
rtic
ipan
ts w
hose
stu
dy p
erio
d in
clud
es p
olic
ies
chan
ges
Ove
rall
797
(76.
0): 7
33 (7
7.7)
0.91
[0.7
4, 1
.12]
0.86
[0.6
9, 1
.07]
352
(11.
1): 2
05 (1
2.9)
0.85
[0.7
0, 1
.02]
0.86
[0.7
1, 1
.03]
Dep
ress
ion
468
(44.
7): 4
11 (4
3.6)
1.04
[0.8
8, 1
.25]
0.98
[0.8
2, 1
.18]
11
5 (3
.6):
45 (2
.8)
1.30
[0.9
1, 1
.84]
1.28
[0.9
0, 1
.82]
Anxi
ety
343
(32.
7): 3
72 (3
9.4)
0.75
[0.6
2, 0
.90]
0.72
[0.6
0, 0
.87]
169
(5.3
): 95
(6.0
)0.
89 [0
.69,
1.1
5]0.
91 [0
.70,
1.1
9]In
som
nia
273
(26.
0): 2
80 (2
9.7)
0.83
[0.6
9, 1
.02]
0.87
[0.7
1, 1
.07]
109
(3.4
): 83
(5.2
)0.
65 [0
.48,
0.8
7]0.
66 [0
.49,
0.8
8]
NPA
Es: n
euro
psyc
hiat
ric a
dver
se e
vent
s; N
RTs:
nico
tine
repl
acem
ent t
hera
py; a
OR:
adj
uste
d od
ds ra
tio; * ad
just
ed a
ge, g
ende
r, so
cial
eco
nom
ic s
tatu
s an
d co
mor
bidi
ties.
We
set t
he in
dexd
ate
was
with
in p
erio
d be
twee
n Ju
ly 1
st, 2
011
and
June
30,
201
3; P
olic
y ch
ange
: In
the
Net
herla
nds,
phar
mac
olog
ic S
mok
ing
Cess
atio
n Tr
eatm
ents
(pSC
Ts) w
ere
reim
burs
ed in
201
1. In
201
2 th
e re
imbu
rsem
ent w
as d
isco
ntin
ued.
As o
f 201
3, p
SCTs
wer
e ag
ain
reim
burs
ed, p
rovi
ded
they
are
acc
ompa
nied
by
beha
vior
al c
ouns
elin
g.
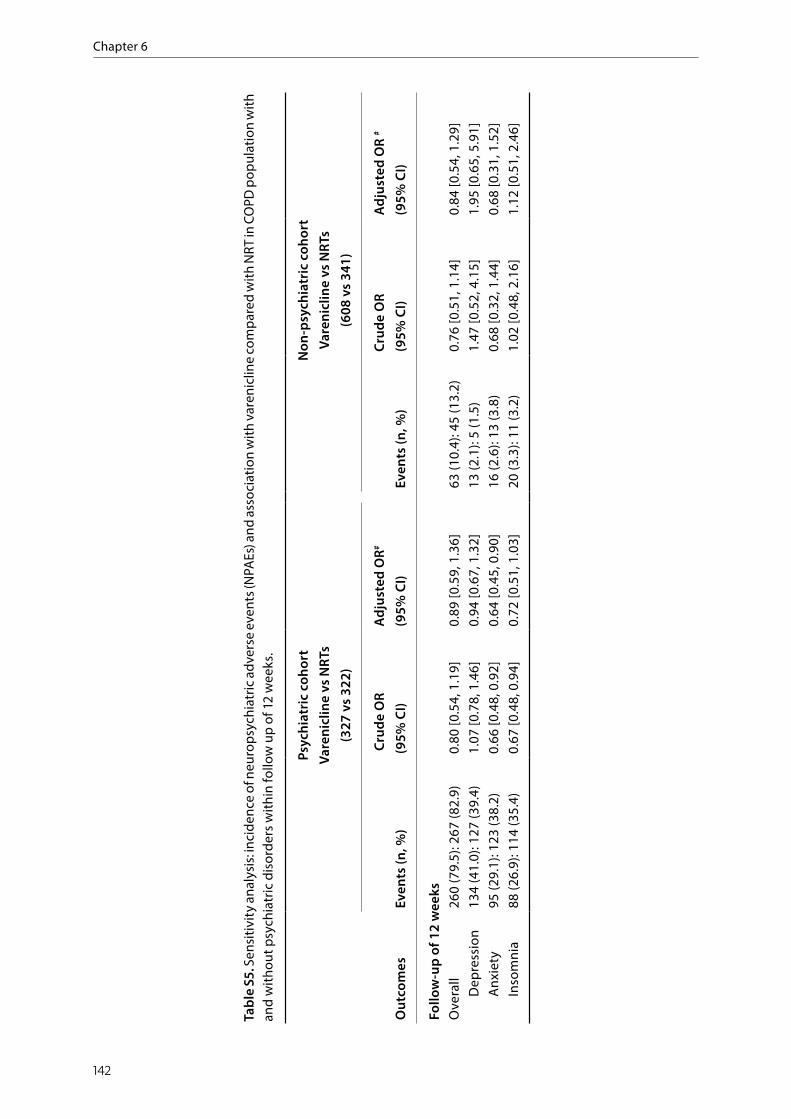
Chapter 6
142
Tabl
e S5
. Sen
sitiv
ity a
naly
sis:
inci
denc
e of
neu
rops
ychi
atric
adv
erse
eve
nts (
NPA
Es) a
nd a
ssoc
iatio
n w
ith v
aren
iclin
e co
mpa
red
with
NRT
in C
OPD
pop
ulat
ion
with
an
d w
ithou
t psy
chia
tric
dis
orde
rs w
ithin
follo
w u
p of
12
wee
ks.
Out
com
es
Psyc
hiat
ric c
ohor
tVa
reni
clin
e vs
NRT
s(3
27 v
s 32
2)
Non
-psy
chia
tric
coh
ort
Vare
nicl
ine
vs N
RTs
(608
vs
341)
Even
ts (n
, %)
Cru
de O
R (9
5% C
I)Ad
just
ed O
R#
(95%
CI)
Even
ts (n
, %)
Crud
e O
R (9
5% C
I)Ad
just
ed O
R #
(95%
CI)
Follo
w-u
p of
12
wee
ksO
vera
ll26
0 (7
9.5)
: 267
(82.
9)0.
80 [0
.54,
1.1
9]0.
89 [0
.59,
1.3
6]63
(10.
4): 4
5 (1
3.2)
0.76
[0.5
1, 1
.14]
0.84
[0.5
4, 1
.29]
Dep
ress
ion
134
(41.
0): 1
27 (3
9.4)
1.07
[0.7
8, 1
.46]
0.94
[0.6
7, 1
.32]
13 (2
.1):
5 (1
.5)
1.47
[0.5
2, 4
.15]
1.95
[0.6
5, 5
.91]
Anxi
ety
95 (2
9.1)
: 123
(38.
2)0.
66 [0
.48,
0.9
2]
0.64
[0.4
5, 0
.90]
16 (2
.6):
13 (3
.8)
0.68
[0.3
2, 1
.44]
0.68
[0.3
1, 1
.52]
Inso
mni
a88
(26.
9): 1
14 (3
5.4)
0.67
[0.4
8, 0
.94]
0.72
[0.5
1, 1
.03]
20 (3
.3):
11 (3
.2)
1.02
[0.4
8, 2
.16]
1.12
[0.5
1, 2
.46]

Neuropsychiatric Safety of Varenicline by Cohort
143
6
Tabl
e S6
. Sen
sitiv
ity a
naly
sis:
inci
denc
e of
neu
rops
ychi
atric
adv
erse
eve
nts (
NPA
Es) a
nd a
ssoc
iatio
n w
ith c
ompa
red
with
NRT
in C
OPD
pop
ulat
ion
with
in fo
llow
up
of 2
4 w
eeks
.
Lim
itatio
ns
COPD
pop
ulat
ions
Psyc
hiat
ric c
ohor
t (va
reni
clin
e vs
NRT
s)N
on-p
sych
iatr
ic c
ohor
t (va
reni
clin
e vs
NRT
s)
Even
ts
OR
(95%
CI)
aOR
(95%
CI)*
Even
tsO
R (9
5% C
I)aO
R (9
5% C
I)*
Excl
ude
part
icip
ants
pre
scrib
ed d
rugs
for a
ny N
SP w
ithin
1 m
onth
bef
ore
inde
x da
teO
vera
ll54
(60.
0): 3
9 (6
1.9)
0.92
[0.4
8, 1
.79]
0.85
[0.4
1, 1
.77]
72 (1
2.1)
: 40
(12.
7)0.
95 [0
.63,
1.4
3]0.
92 [0
.60,
1.4
3]
Dep
ress
ion
29 (3
2.2)
: 19
(30.
2)1.
10 [0
.55,
2.2
1]0.
88. [
0.39
, 1.9
7]20
(3.4
): 10
(3.2
)1.
06 [0
.49,
2.2
9]1.
12 [0
.50,
2.5
2]An
xiet
y22
(24.
4): 2
0 (3
1.7)
0.70
[0.3
4, 1
.42]
0.87
[0.4
0, 1
.90]
38 (6
.4):
19 (6
.0)
1.06
[0.6
0, 1
.87]
1.10
[0.6
0, 2
.01]
Inso
min
a15
(16.
7): 1
6 (2
5.4)
0.59
[0.2
7, 1
.30]
0.60
[0.2
4, 1
.49]
25 (4
.2):
16 (5
.1)
0.82
[0.4
3, 1
.56]
0.71
[0.3
6, 1
.37]
Excl
ude
part
icip
ants
pre
scrib
ed d
rugs
for d
epre
ssio
n, a
nxie
ty a
nd in
som
nia
with
in 1
mon
th b
efor
e in
dex
date
Ove
rall
68 (5
1.1)
: 48
(47.
5)1.
16 [0
.69,
1.9
4]1.
29 [0
.73,
2.2
6]73
(12.
1): 4
3 (1
3.0)
0.92
[0.6
2, 1
.38]
0.93
[0.6
1, 1
.42]
Dep
ress
ion
35 (2
6.3)
: 23
(22.
8)1.
21 [0
.66,
2.2
2]
1.08
[0.5
6, 2
.08]
21 (3
.5):
10 (3
.0)
1.16
[0.5
4, 2
.49]
1.33
[0.6
0, 2
.99]
Anxi
ety
27 (2
0.3)
: 23
(22.
8)0.
86 [0
.46,
1.6
2]0.
97 [0
.49,
1.9
1]38
(6.3
): 21
(6.4
)0.
99 [0
.57,
1.7
2]
1.00
[0.5
6, 1
.79]
Inso
mni
a21
(15.
8): 2
0 (1
9.8)
0.76
[0.3
9, 1
.49]
0.
87 [0
.42,
1.8
2]25
(4.2
): 17
(5.2
)0.
80 [0
.43,
1.5
0]0.
72 [0
.37,
1.3
9]Ex
clud
e pa
rtic
ipan
ts w
hose
stu
dy p
erio
d in
clud
es p
olic
ies
chan
ges
Ove
rall
203
(78.
1): 2
11 (8
0.2)
0.88
[0.5
8, 1
.34]
0.97
[0.6
2, 1
.51]
63 (1
4.2)
: 41
(15.
1)0.
93 [0
.61,
1.4
3]1.
00 [0
.64,
1.5
8]D
epre
ssio
n11
4 (4
3.8)
: 110
(41.
8)1.
09 [0
.77,
1.5
4]0.
96 [0
.66,
1.4
0]
18 (4
.1):
7 (2
.6)
1.60
[0.6
6, 3
.89]
1.73
[0.6
8, 4
.42]
Anxi
ety
89 (3
4.2)
: 109
(41.
4)0.
74 [0
.52,
1.0
5]0.
72 [0
.49,
1.0
5]35
(7.9
): 20
(7.4
)1.
08 [0
.61,
1.9
1]1.
21 [0
.66,
2.2
4]In
som
nia
81 (3
1.2)
: 106
(40.
3)0.
67 [0
.47,
0.9
6]0.
75 [0
.51,
1.1
0]19
(4.3
): 15
(5.5
)0.
77 [0
.38,
0.5
3]0.
71 [0
.34,
1.4
5]
NPA
Es: n
euro
psyc
hiat
ric a
dver
se e
vent
s; N
RTs:
nico
tine
repl
acem
ent t
hera
py; * aO
R: a
djus
ted
odds
ratio
; adj
uste
d ag
e, g
ende
r, so
cial
eco
nom
ic s
tatu
s an
d co
mor
bidi
ties.
We
set t
he in
dexd
ate
was
with
in p
erio
d be
twee
n Ju
ly 1
st, 2
011
and
June
30,
201
3; P
olic
y ch
ange
: In
the
Net
herla
nds,
phar
mac
olog
ic S
mok
ing
Cess
atio
n Tr
eatm
ents
(pSC
Ts) w
ere
reim
burs
ed in
201
1. In
201
2 th
e re
imbu
rsem
ent w
as d
isco
ntin
ued.
As o
f 201
3, p
SCTs
wer
e ag
ain
reim
burs
ed, p
rovi
ded
they
are
acc
ompa
nied
by
beha
viou
ral c
ouns
ellin
g.

C H A P T E R 7
Yuanyuan Wang Job F.M. van Boven
Jens H. Bos Catharina C.M. Schuiling-Veninga
H. Marike Boezen Bob Wilffert
Eelko Hak
Risk of neuropsychiatric adverse events associated with varenicline treatment for smoking cessation:
a prescription sequence symmetry analysis
Submitted for publication (under review).
Chapter 7
146
ABSTRACTBackground
Varenicline is an effective treatment for smoking cessation. While clinical trials among selected patients did not confirm a causal role, spontaneous reports from daily practice have suggested a possible risk of neuropsychiatric adverse events (NPAEs) by varenicline.
Objectives
To investigate the risk of NPAEs associated with varenicline initiation among the general population in a real-world setting.
Methods
We conducted a prescription sequence symmetry analysis (PSSA) using data from 2007 to 2018 from the University of Groningen IADB.nl prescription database. We selected incident users of both varenicline and marker drugs for NPAEs, including depression, anxiety and sleep disorder within different time-intervals (30, 60, 90, 180, 365 days). Adjusted sequence ratios (aSR) were calculated for each time-interval.
Results
Within 365-days’ time-interval 1,066 patients were incident users of both varenicline and NPAE marker drugs. In total, 505 patients were prescribed varenicline before NPAE marker drugs and 561 vice versa (crude sequence ratio (cSR) 0.90, 95% CI: 0.80-1.02). After adjustments for trends in prescriptions, overall a null association was found (aSR 1.00, 95% CI: 0.89-1.13). Regarding specific NPAEs, no increased risks were found for depression nor anxiety within any time-interval. A small transient increased risk was found for sleep disorders, particularly in earlier time-intervals 3 months and 6 months (aSRs 1.52, [1.10, 2.11] and 1.45, [1.15, 1.83], respectively). The results were robust in stratified analyses by age and gender, and several sensitivity analyses.
Conclusions
Findings from this real-world study were generally consistent with the evidence from clinical trials. Varenicline initiation was not associated with an increased risk of taking anti-depressants nor anti-anxiety drugs, yet a small, but statistically significant, transient association with drugs for sleep disorders was noticed, possibly associated with withdrawal symptoms caused by smoking cessation.
NAPEs Associated with Varenicline by PSSA
147
7
INTRODUCTIONAlthough in many countries the prevalence of tobacco use has been declining in recent years,1 the tobacco epidemic is still one of the largest global public health threats, related to more than 8 million deaths worldwide each year.2 Smoking-related health problems, including cardiovascular and respiratory disease, are associated with a high burden for both family and society.3 To help halt this burden, several pharmacological and non-pharmacological treatments are available. Varenicline, a first-line pharmacological smoking cessation treatment (PSCT), which was approved by the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA) in 2006. It has a unique mechanism of action compared with other PSCTs by acting as a partial agonist/antagonist with affinity and selectivity for α4β2 nicotinic acetylcholine receptors.4 In several randomized clinical trials (RCTs), varenicline was more effective for smoking cessation than bupropion, nicotine replacement therapy (NRT) or placebo.5-7
However, subsequent post-marketing reports related to neuropsychiatric adverse events (NPAEs), such as depression, anxiety, sleep disorder but also suicide, among varenicline users raised concerns about the neuropsychiatric safety of varenicline.8 Based on the post-marketing surveillance reports, the FDA placed a black box warning on varenicline about its risk of NPAEs in 2009.9 The spontaneous case-reports and the FDA warning may have confused both smokers and physicians regarding the causal role of varenicline in inducing NPAEs.10 Such misunderstanding undoubtedly has led to the underutilization of varenicline for smoking cessation.11-13
Although case reports are important signals of drug safety, causality could not be established without using an adequate control group.14 Therefore, to identify the causal association between varenicline and risk of NPAEs, several large cohort studies were conducted after the safety warning15-19 as well as RCTs.7,20,21 Notably, the synthesized evidence did not confirm the earlier suggestions from case reports about severe neuropsychiatric risk from varenicline use.22-24 Therefore, the warning about possible suicidal risk from varenicline was removed by FDA in 2016. In subsequent years, doubts remained regarding the decision to lift the FDA warning. In particular, considering the relatively healthy population and limited power to detect rare events in clinical trials, results from RCTs may not reflect the situation in the real-world setting. Moreover, evidence from available observational cohort studies is inconsistent, and these studies were criticized for their potential bias (e.g. selection bias) and confounding (e.g. residual confounding).25
To overcome this bias, the prescription sequence symmetry analysis (PSSA) has been proposed to investigate acute adverse effects of medications, with moderate sensitivity, high specificity and robust performance.26-28 Unlike spontaneous reporting systems, it uses individual prescription or hospitalization data to assess the association between

Chapter 7
148
a medication and an adverse drug reaction (ADR) by examining the symmetry in the sequence of index medication and marker medications as proxy for ADRs within a specific time window.27,29 Compared with traditional observational studies (i.e. cohort or case-control), PSSA controls genetic and other time-invariant confounding effectively due to its self-controlled study design. Of note, the relationship between varenicline and NPAEs has not been studied before by using PSSA.
The aim of this study was to examine whether there is an association between varenicline use and onset of NPAEs in the real-world setting using PSSA.
METHODSData source and setting
This study was conducted using the widely researched University of Groningen’s pharmacy prescription database IADB.nl, a growing database that comprises a population of approximately 730,000 people from 72 community pharmacies in the northern Netherlands since 1994, regardless of type of health insurance.30 The individuals are representative of the Dutch population with respect to drug use. Detailed prescription information includes date of prescription, name of dispensed drug, dosage, duration and related Anatomical Therapeutic Chemical (ATC) code of prescribed drug, but also year of birth and gender. As Dutch patients usually register at one single community pharmacy, the prescription information from pharmacies are relatively complete. Of note, over-the-counter drugs and prescriptions during hospital stay are not included in IADB.nl. Data after registration of varenicline from 2007 to 2018 were used for this study. The IADB.nl has been used in several previous PSSAs.31,32
Study design
The applied PSSA design compares the frequency of initiation of a marker drug (as proxy for an ADR) before and after initiation of an index drug within the same individual. The individuals who were prescribed the index drug (i.e. varenicline) before marker drugs for NPAEs were labeled the “causal group”. Conversely, those who were prescribed varenicline after the marker drugs were labeled the “non-causal group”. The crude sequence ratio (cSR) was defined by the number of patients in the causal group divided by the number of patients in the non-causal group which reflects the association between exposure and outcome. If there is no association, the distribution of sequence orders is expected to be symmetrical and the SR is close to 1. Of note, the PSSA design is sensitive to changing trends in drug prescriptions over time, which could be caused by factors like reimbursement policy changes and safety warnings. Therefore, a null-effect sequence ratio (nSR) was used to adjust for the temporal prescription trends of varenicline and marker drugs for ADRs.29 This trend can be used to estimate the probability of varenicline

NAPEs Associated with Varenicline by PSSA
149
7
to be prescribed first, in the absence of any causal relationship. The adjusted sequence ratio (aSR) was calculated by dividing the cSR by the nSR.
Run-in period
As the goal of PSSA is to evaluate the relation between two incident events, we needed to identify the incident users of both index and marker drugs. As our index drug, i.e. varenicline, was authorized for use by EMA on 26 September 2006, no varenicline was prescribed in the database IADB.nl before 2007. Therefore, in theory, patients with the first recorded prescription of varenicline during the study period were all incident users. Since the marker drugs have long been used for chronic treatment of NPAEs, most of their current users will be captured at the beginning of the study period. To exclude the current users and identify incident users of NPAEs marker drugs, we used the waiting time distribution to determine the run-in period.33
Study population and time interval
This study included all individuals who were incident users of both varenicline (ATC: N07BA03) and any marker drugs as potential treatment for NPAEs including depression (N06B, N06CA), anxiety (N05B) and sleep disorder (N05C) from 1 January 2007 to 31 December 2018 in IADB.nl. The first prescription of varenicline was the index date of varenicline, the first prescription of any of the marker drugs for NPAEs was set as index date of any NPAEs. The first prescription of specific marker drugs for depression, anxiety and sleep disorder were set as index date of specific NPAE. Those who were prescribed the index and marker drug on the same day were excluded.
We defined different time-intervals (365 days, 180 days, 90 days, 60 days and 30 days) between the initiation of the varenicline and NPAEs marker drugs to explore their association. Therefore, incident users of both varenicline and marker drugs, irrespective of dose and duration, within pre-set time intervals of each other were included for the PSSA.
Statistical analysis
The crude sequence ratio (cSR) was calculated by dividing the number of individuals in the causal group with the number of individuals in the non-causal group. The adjusted SR (aSR) was calculated by adjusting the time trend of the crude SR. A null-effect SR (nSR) is the expected SR without any causal associations. Therefore, the aSR is calculated as the ratio of crude SR to null-effect SR (cSR/nSR). The detailed formula were as follows:
(1) cSR = number of patients in the causal group/number of patients in the non-causal group.
(2)
any of the marker drugs for NPAEs was set as index date of any NPAEs. The first prescription
of specific marker drugs for depression, anxiety and sleep disorder were set as index date of
specific NPAE. Those who were prescribed the index and marker drug on the same day were
excluded.
We defined different time‐intervals (365 days, 180 days, 90 days, 60 days and 30 days)
between the initiation of the varenicline and NPAEs marker drugs to explore their association.
Therefore, incident users of both varenicline and marker drugs, irrespective of dose and
duration, within pre‐set time intervals of each other were included for the PSSA.
Statistical analysis
The crude sequence ratio (cSR) was calculated by dividing the number of individuals in the
causal group with the number of individuals in the non‐causal group. The adjusted SR (aSR)
was calculated by adjusting the time trend of the crude SR. A null‐effect SR (nSR) is the
expected SR without any causal associations. Therefore, the aSR is calculated as the ratio of
crude SR to null‐effect SR (cSR/nSR). The detailed formula were as follows:
(1) cSR = number of patients in the causal group/number of patients in the non‐causal group.
(2) nSR= 𝑃𝑃�/1‐𝑃𝑃�, 𝑃𝑃� = ∑ ����∑ �������������� ��∑ ������� �∑ �����
����� �∑ ������������
In the above formula, u is the last day of the research period, m and n are the consecutive
days of the survey period, d is the time interval between index and marker drugs. Am is the
number of individuals being prescribed the index drug first on the m day. Bn is the number of
individuals being prescribed marker drugs first on the n day.
(3) aSR = cSR/nSR
Confidence intervals (95% CI) of cSR and aSR were calculated by using the binomial distribution
as follows:
95% CI =𝑒𝑒��������.����,
where standard error
(SE) = � ������� �� ������ ����� �
������� �� ����������� �����
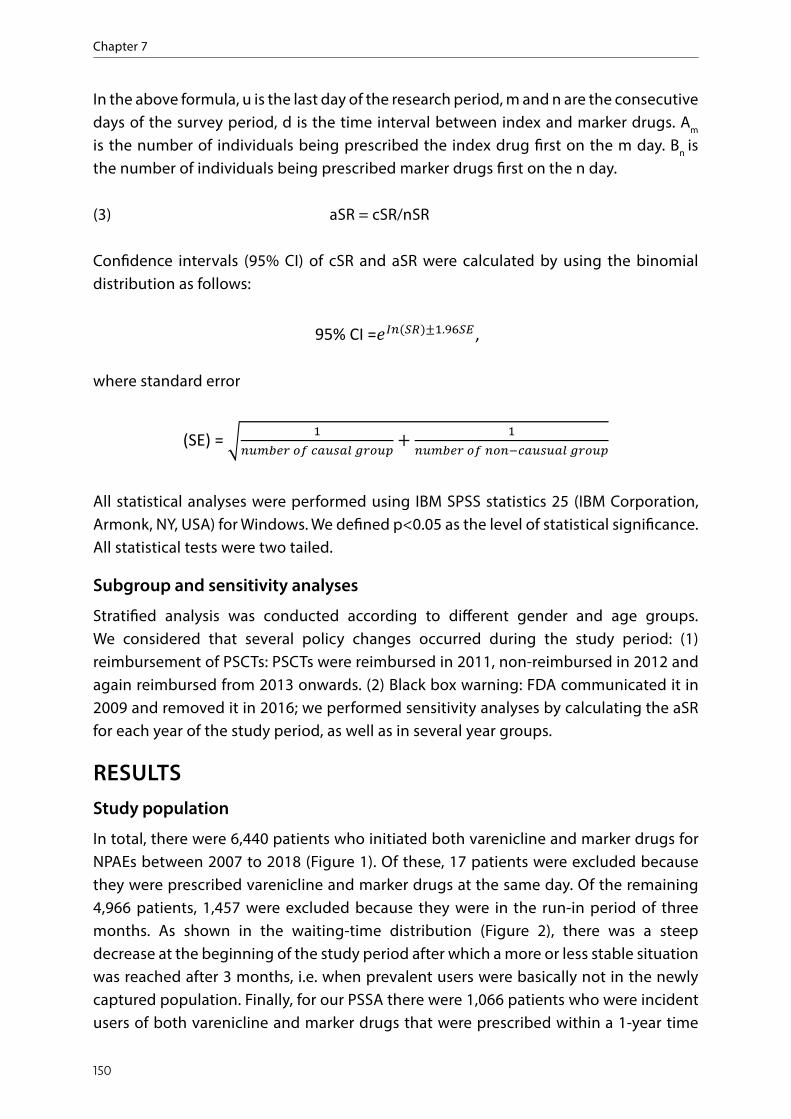
Chapter 7
150
In the above formula, u is the last day of the research period, m and n are the consecutive days of the survey period, d is the time interval between index and marker drugs. Am is the number of individuals being prescribed the index drug first on the m day. Bn is the number of individuals being prescribed marker drugs first on the n day.
(3) aSR = cSR/nSR
Confidence intervals (95% CI) of cSR and aSR were calculated by using the binomial distribution as follows:
where standard error
All statistical analyses were performed using IBM SPSS statistics 25 (IBM Corporation, Armonk, NY, USA) for Windows. We defined p<0.05 as the level of statistical significance. All statistical tests were two tailed.
Subgroup and sensitivity analyses
Stratified analysis was conducted according to different gender and age groups.We considered that several policy changes occurred during the study period: (1) reimbursement of PSCTs: PSCTs were reimbursed in 2011, non-reimbursed in 2012 and again reimbursed from 2013 onwards. (2) Black box warning: FDA communicated it in 2009 and removed it in 2016; we performed sensitivity analyses by calculating the aSR for each year of the study period, as well as in several year groups.
RESULTSStudy population
In total, there were 6,440 patients who initiated both varenicline and marker drugs for NPAEs between 2007 to 2018 (Figure 1). Of these, 17 patients were excluded because they were prescribed varenicline and marker drugs at the same day. Of the remaining 4,966 patients, 1,457 were excluded because they were in the run-in period of three months. As shown in the waiting-time distribution (Figure 2), there was a steep decrease at the beginning of the study period after which a more or less stable situation was reached after 3 months, i.e. when prevalent users were basically not in the newly captured population. Finally, for our PSSA there were 1,066 patients who were incident users of both varenicline and marker drugs that were prescribed within a 1-year time
any of the marker drugs for NPAEs was set as index date of any NPAEs. The first prescription
of specific marker drugs for depression, anxiety and sleep disorder were set as index date of
specific NPAE. Those who were prescribed the index and marker drug on the same day were
excluded.
We defined different time‐intervals (365 days, 180 days, 90 days, 60 days and 30 days)
between the initiation of the varenicline and NPAEs marker drugs to explore their association.
Therefore, incident users of both varenicline and marker drugs, irrespective of dose and
duration, within pre‐set time intervals of each other were included for the PSSA.
Statistical analysis
The crude sequence ratio (cSR) was calculated by dividing the number of individuals in the
causal group with the number of individuals in the non‐causal group. The adjusted SR (aSR)
was calculated by adjusting the time trend of the crude SR. A null‐effect SR (nSR) is the
expected SR without any causal associations. Therefore, the aSR is calculated as the ratio of
crude SR to null‐effect SR (cSR/nSR). The detailed formula were as follows:
(1) cSR = number of patients in the causal group/number of patients in the non‐causal group.
(2) nSR= 𝑃𝑃�/1‐𝑃𝑃�, 𝑃𝑃� = ∑ ����∑ �������������� ��∑ ������� �∑ �����
����� �∑ ������������
In the above formula, u is the last day of the research period, m and n are the consecutive
days of the survey period, d is the time interval between index and marker drugs. Am is the
number of individuals being prescribed the index drug first on the m day. Bn is the number of
individuals being prescribed marker drugs first on the n day.
(3) aSR = cSR/nSR
Confidence intervals (95% CI) of cSR and aSR were calculated by using the binomial distribution
as follows:
95% CI =𝑒𝑒��������.����,
where standard error
(SE) = � ������� �� ������ ����� �
������� �� ����������� �����
any of the marker drugs for NPAEs was set as index date of any NPAEs. The first prescription
of specific marker drugs for depression, anxiety and sleep disorder were set as index date of
specific NPAE. Those who were prescribed the index and marker drug on the same day were
excluded.
We defined different time‐intervals (365 days, 180 days, 90 days, 60 days and 30 days)
between the initiation of the varenicline and NPAEs marker drugs to explore their association.
Therefore, incident users of both varenicline and marker drugs, irrespective of dose and
duration, within pre‐set time intervals of each other were included for the PSSA.
Statistical analysis
The crude sequence ratio (cSR) was calculated by dividing the number of individuals in the
causal group with the number of individuals in the non‐causal group. The adjusted SR (aSR)
was calculated by adjusting the time trend of the crude SR. A null‐effect SR (nSR) is the
expected SR without any causal associations. Therefore, the aSR is calculated as the ratio of
crude SR to null‐effect SR (cSR/nSR). The detailed formula were as follows:
(1) cSR = number of patients in the causal group/number of patients in the non‐causal group.
(2) nSR= 𝑃𝑃�/1‐𝑃𝑃�, 𝑃𝑃� = ∑ ����∑ �������������� ��∑ ������� �∑ �����
����� �∑ ������������
In the above formula, u is the last day of the research period, m and n are the consecutive
days of the survey period, d is the time interval between index and marker drugs. Am is the
number of individuals being prescribed the index drug first on the m day. Bn is the number of
individuals being prescribed marker drugs first on the n day.
(3) aSR = cSR/nSR
Confidence intervals (95% CI) of cSR and aSR were calculated by using the binomial distribution
as follows:
95% CI =𝑒𝑒��������.����,
where standard error
(SE) = � ������� �� ������ ����� �
������� �� ����������� �����
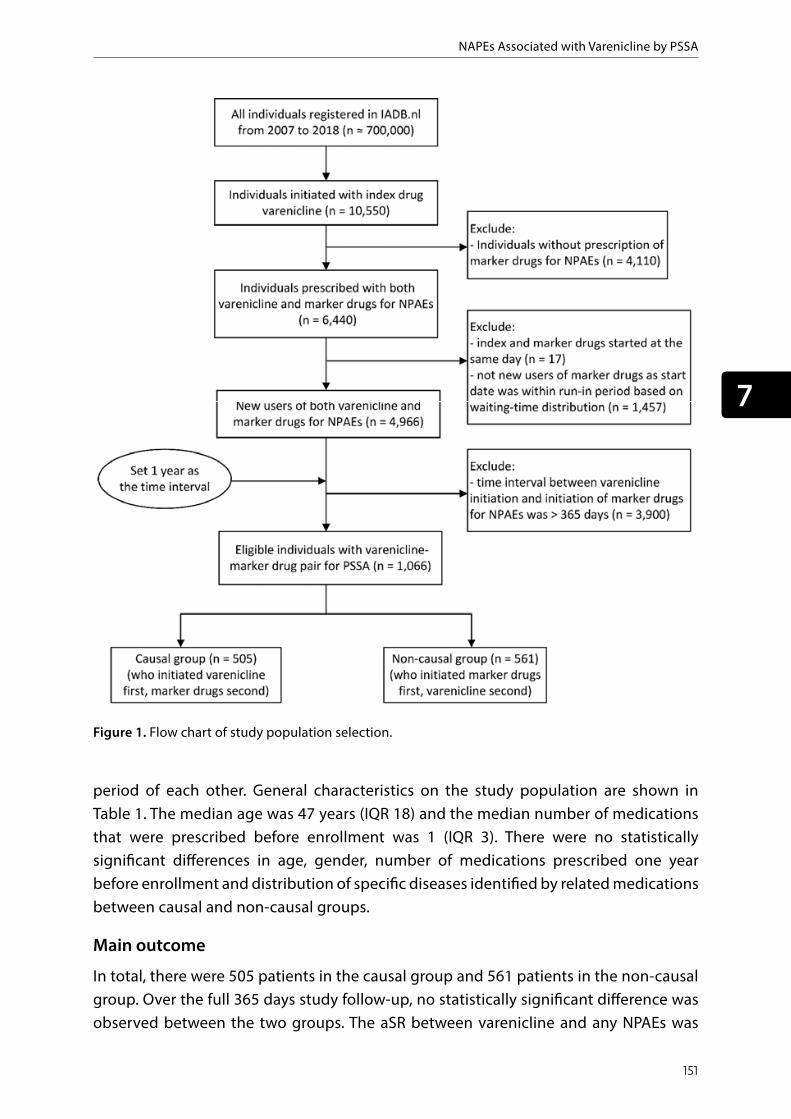
NAPEs Associated with Varenicline by PSSA
151
7
Subgroup and Sensitivity analyses
Stratified analysis was conducted according to different gender and age groups.We
considered that several policy changes occurred during the study period: (1) reimbursement
of PSCTs: PSCTs were reimbursed in 2011, non‐reimbursed in 2012 and again reimbursed from
2013 onwards. (2) Black box warning: FDA communicated it in 2009 and removed it in 2016;
we performed sensitivity analyses by calculating the aSR for each year of the study period, as
well as in several year groups.
Figure 1. Flow chart of study population selection.
Figure 1. Flow chart of study population selection.
period of each other. General characteristics on the study population are shown in Table 1. The median age was 47 years (IQR 18) and the median number of medications that were prescribed before enrollment was 1 (IQR 3). There were no statistically significant differences in age, gender, number of medications prescribed one year before enrollment and distribution of specific diseases identified by related medications between causal and non-causal groups.
Main outcome
In total, there were 505 patients in the causal group and 561 patients in the non-causal group. Over the full 365 days study follow-up, no statistically significant difference was observed between the two groups. The aSR between varenicline and any NPAEs was

Chapter 7
152
Table 1. Characteristics of the study population in the prescription sequence symmetry analysis.
CharacteristicsTotal population(N = 1066)
Causal groupa
(n = 505)Non-casual groupb
(n = 561) P-value*
Gender (n, %) 0.677Male 529 (49.6) 254 (50.3) 275 (49.0)Female 537 (50.4) 251 (49.7) 286 (51.0)
Age groups (n, %)Median (IQR) 47 (18) 48 (19) 47 (17)<= 40 323 (30.3) 152 (30.1) 171 (30.5) 0.29940 - 50 307 (28.8) 135 (26.7) 172 (30.7)50 - 60 290 (27.2) 150 (29.7) 140 (25.0) > 60 146 (13.7) 68 (13.5) 78 (13.9)
Number of total medications 1 year before enrolment# (n, %)Median (IQR) 1 (3) 1 (3) 1 (3)0 406 (38.1) 189 (37.4) 217 (38.7) 0.9241 197 (18.5) 95 (18.8) 102 (18.2)2-3 249 (23.4) 116 (23.0) 133 (23.7)>= 4 214 (20.1) 105 (20.8) 109 (19.4)
Number of patients with specific medication use (n, %)For obstructive airway diseases (ATC codes: R03)
198 (18.6) 100 (19.8) 98 (17.5) 0.328
For cardiac diseases (C01) 27 (2.5) 16 (3.2) 11 (2.0) 0.210For diabetes (A10) 52 (4.9) 27 (5.3) 25 (4.5) 0.500
Note: ATC: The Anatomical Therapeutic Chemical (ATC); aCausal group: patients prescribed varenicline first following by marker drugs for NPAEs.bNon-causal group: patients prescribed marker drugs for NPAEs first, following by varenicline. *Chi-square test; #Enrollment: the original prescribing date of varenicline of patients in causal group or the original prescribing date of marker drugs for NPAEs of patients in non-causal group.
1.00 [95% CI: 0.89, 1.13, Table 2]. Also, no statistical significant association was observed between varenicline and the occurrence of depression (aSR 1.09 [95% CI: 0.94, 1.26]) nor anxiety (aSR 0.98 [0.85, 1.14]). There was, however, a small statistically significant increased risk of sleep disorders observed associated with varenicline (aSR 1.25 [95% CI: 1.05, 1.48]).
Impact of time intervals
When we considered different time-intervals between initiation of varenicline and any NPAE marker drugs, we also did not find significant associations (Table 2) within 30 days (aSR 0.96, [0.66, 1.39]) and 60 days (aSR 1.10, [0.84, 1.44]. However, there was a boundary significant increased risk of NPAEs observed with varenicline within 90 and 180 days.

NAPEs Associated with Varenicline by PSSA
153
7
Figure 2. W
aitin
g tim
e distrib
ution of th
e first prescrip
tions of m
arker d
rugs fo
r NPA
Es with
the 1s
t year o
f study
period.
Figu
re 2
. Wai
ting
time
dist
ribut
ion
of th
e fir
st p
resc
riptio
ns o
f mar
ker d
rugs
for N
PAEs
with
the
1st y
ear o
f stu
dy p
erio
d.

Chapter 7
154
Table 2. Results of the prescription sequence symmetry analysis for the association between varenicline use and marker drugs use for NPAEs by different time periods.
NPAEsPopulation*
(n)Causal group (n)
Non-causal group (n) cSR (95% CI) nSR aSR (95% CI)
Within 365 daysOverall 1066 505 561 0.90 [0.80, 1.02] 0.900 1.00 [0.89, 1.13]
depression 727 364 363 1.00 [0.87, 1.16] 0.924 1.09 [0.94, 1.26]anxiety 716 335 381 0.88 [0.76, 1.02] 0.893 0.98 [0.85, 1.14]sleepdisorder 532 286 246 1.16 [0.98, 1.38] 0.931 1.25 [1.05, 1.48]
Within 180 daysOverall 603 322 281 1.15 [0.98, 1.34] 0.949 1.21 [1.03, 1.42]
depression 389 208 181 1.15 [0.94, 1.40] 0.964 1.19 [0.98, 1.45]anxiety 394 206 188 1.10 [0.90, 1.34] 0.943 1.16 [0.95, 1.42]sleepdisorder 295 172 123 1.40 [1.11, 1.76] 0.965 1.45 [1.15, 1.83]
Within 90 daysOverall 315 173 142 1.22 [0.98,1.52] 0.975 1.25 [1.00, 1.56]
depression 209 110 99 1.11 [0.85, 1.46] 0.984 1.13 [0.86, 1.48]anxiety 189 99 90 1.10 [0.83, 1.46] 0.971 1.13 [0.85, 1.51]sleepdisorder 150 90 60 1.50 [1.08, 2.08] 0.984 1.52 [1.10, 2.11]
Within 60 daysOverall 212 110 102 1.08 [0.82, 1.41] 0.982 1.10 [0.84, 1.44]
depression 138 62 76 0.82 [0.58, 1.14] 0.989 0.83 [0.59, 1.15]anxiety 137 72 65 1.11 [0.79, 1.55] 0.979 1.13 [0.81, 1.58]sleepdisorder 101 56 45 1.24 [0.84, 1.84] 0.990 1.26 [0.85, 1.86]
Within 30 daysOverall 111 54 57 0.95 [0.65,1.37] 0.988 0.96 [0.66, 1.39]
depression 74 31 43 0.72 [0.45, 1.14] 0.993 0.73 [0.46, 1.15]anxiety 73 32 41 0.76 [0.47, 1.21] 0.986 0.77 [0.48, 1.22]sleep disorder 50 25 25 1.00 [0.57, 1.74] 0.993 1.01 [0.58, 1.77]
NPAEs: neuropsychiatric adverse events. cSR: crude sequence ratio; aSR: adjusted sequence ratio; nSR: null-effect sequence ratio; CI: confidence interval;
For the specific NPAEs, similar to the results observed within 365 days, no significant associations were observed between varenicline and specific NPAEs. Again, sleep disorder was the exception with an aSR of 1.52 [95% CI: 1.10, 2.11] and 1.45 [95% CI: 1.15, 1.83] within 90 and 180 days, respectively. Frequency distributions of patients with any NPAE or specific NPAE (depression, anxiety and sleep disorder) are shown in Figure 3.
Subgroup and sensitivity analyses
In stratified analyses by gender and age groups (Table S1), a significant association between varenicline and sleep disorder was only seen in female and older age groups. Of note, a boundary significant risk of depression associated with varenicline was also

NAPEs Associated with Varenicline by PSSA
155
7
Figure 3. Frequ
ency distrib
ution of patients w
ith (a) all N
PAEs; (b) dep
ression; (c) anxiety; (d) sleep disorder by n
umbe
r of m
onths b
efore or afte
r
the initiation of varen
icline with
in 1 year.
Figu
re 3
. Fre
quen
cy d
istr
ibut
ion
of p
atie
nts w
ith (a
) all
NPA
Es; (
b) d
epre
ssio
n; (c
) anx
iety
; (d)
slee
p di
sord
er b
y nu
mbe
r of m
onth
s bef
ore
or a
fter
the
initi
atio
n of
var
enic
line
with
in 1
yea
r.

Chapter 7
156
observed in older age groups (aSR 1.23, 95% CI: 1.01-1.50]). As shown in Figure S1, there were three main fluctuations in the curve for the number of patients newly prescribed varenicline by years of study period. There was a high rise in newly prescribed varenicline in 2011 and a drop in 2012, followed by a sharp increase in 2013. Also, there was a small increase in newly prescribed varenicline from 2015 to 2016. In the results of sensitivity analysis by year groups or each year for the aSR between varenicline and overall NPAEs, we did not observe any statistical significant difference for the order of causal and non-causal-groups, except for year 2011 (aSR 1.72, 95% CI: 1.27, 2.32, Table S2).
DISCUSSIONMain findings
This is the first study to assess the risk of NPAEs associated with varenicline by applying a PSSA design. Based on the results of this study, we further confirm that no statistical significant increased risk of anti-anxiety and anti-depressant drug prescription was associated with varenicline prescription in all different time-intervals. However, within 3, 6 and 12 months, there was a small, but statistically significant, increased risk of sleep disorder. We did not observe significant risk of sleep disorder associated with varenicline within shorter time-intervals (1 or 2 months).
Interpretation
The results of this study are consistent with a large meta-analysis of RCTs published in 2015,22 regarding mood change and sleeping disorders. In this systematic review involving 39 studies, there was no evidence of an increased risk of depression and anxiety among varenicline users, compared with placebo users. Oppositely, a higher risk of sleep problems (e.g. insomnia, abnormal dreams) was observed, which was also seen in our study. Of note, different from PSSA as a self-controlled design, most previous observational cohort studies used nicotine replacement therapy (NRTs) as the reference group to explore the risk of NPAEs associated with varenicline. In two large cohort studies, there was also no increased depression risk observed among varenicline users.15,16 However, in a third cohort study, varenicline was found to be associated with a small increase in the risk of anxiety and mood conditions, but this was only observed in people with previous psychiatric disorders.17
Sleep disorder is well recognized as a commonly reported ADR associated with varenicline in clinical trials with an incidence ranging from 14.0% to 37.2%.4 It was also the most frequently reported psychiatric event (1.6%) according to a prescription-event monitoring study based in general practice in England.8 However, it is difficult to identify whether sleeping problems are due to side effects of PSCTs or related to withdrawal from nicotine. Indeed, difficulty falling asleep and increased number of awakenings are also common symptoms of nicotine withdrawal.34 Although sleep disorder is not
NAPEs Associated with Varenicline by PSSA
157
7
a serious ADR, it may result in poor adherence to varenicline and therefore potentially affect the possibility of quitting successfully. As such, clinicians should pay particular attention to this kind of side effect among varenicline users.
Of note, there was a traditional self-controlled analysis conducted by Gershon et al. in 2018,35 that compared the relative incidence of hospitalizations and emergency department visits during the period of varenicline use compared to the period without varenicline use. The relative incidence (RI) of NPAEs was significantly increased (RI 1.06; 95%CI: 1.00-1.13). Considering that the boundary significant result was not robust in sensitivity analyses and subgroup analyses stratified by age groups, the authors did not come to a firm conclusion about the risk of NPAEs associated with varenicline. Compared with this previous study that focused on inpatients, we focused more on NPAEs that happened among outpatients by using a different self-controlled study design (i.e. PSSA). Combining the results from our study and the study by Gershon et al, provides complimentary varenicline safety evidence for the general population among different real-world settings.
Considering PSSA is sensitive to fluctuation of medication prescriptions, we did sensitivity analyses by calculating the aSR in each year of the study period. We observed fairly consistent results except for the year 2011, which may be biased by PSCT reimbursement policy changes in the Netherlands since PSCTs were reimbursed in 2011 and the reimbursement was temporarily discontinued in 2012.36 Before the cancellation of reimbursement, more varenicline was prescribed in 2011, the sharp increase of varenicline may have led to more people falling in the causal group (varenicline first and maker drugs second) and less people falling into the non-causal group, which might have led to the aSR above 1. It’s reported that females and older people are more sensitive to NPAEs.37-39 However, we did not find a significant risk of any NPAEs associated with varenicline in these sub-groups except for sleep disorders, which is consistent with our original outcomes and showed the robustness of our results.
Strengths and limitations
Our study has several strengths. The major strength of PSSA design is that it inherently controls for time-invariant, patient-specific confounders (e.g., sociodemographic characteristics, genetic and lifestyle-related factors) compared with other observational study designs such as cohort or case-control.26 Second, we used a large prescription database with information about medicines dispensed in community pharmacies in the Netherlands, which is representative for a general, unselected, population. Third, due to our design we went beyond the question whether varenicline-related ADRs occurred, and could also provide in-depth analysis of their timing. Our study also has several potential limitations. First, PSSA is sensitive to time-varying confounding like disease severity, which could possibly affect the prescription of sequence of the index

Chapter 7
158
and marker drugs. To minimize this time-varying bias, we limited the time window between index and marker drugs to a maximum of 12 months. Furthermore, due to absence of diagnostic data, marker drugs were used as proxy for NPAEs. Lastly, some severe NPAEs like suicide, neuropsychiatric hospitalizations and emergency department visits could not be evaluated. Despite these limitations are inherent to PSSA methods and common in real-world data sources, this study provides good supplementary evidence for the risk of NPAEs associated with varenicline use in a real-word setting.
Recommendations for future research, policy and clinical practice
Our results re-assure the safety of varenicline and may help further minimizing the doubt regarding potential severe adverse drug reactions related to varenicline and support the removal of FDA’s black box warning. Clinicians and users of varenicline should however remain aware of increased occurrence of sleep disorder, especially in the first three to six months after varenicline initiation. Proper education on expected timing of this event and personalized coping strategies is particularly required. Eventually, this may result in increased smoking cessation treatment uptake, adherence and, ultimately, cessation rates. Future research should focus on whether this sleep disorder is caused by varenicline itself or more related to withdrawal of nicotine.
CONCLUSIONSOur PSSA results suggest that real-world use of varenicline is not associated with any serious risk of NPAEs. However, consistent with previous evidence, there was a transient increased risk of sleep disorder associated with varenicline initiation, particularly in the first three to six months. Whether sleep disorder was caused by the adverse effects of varenicline or related to withdrawal symptoms needs further study.
NAPEs Associated with Varenicline by PSSA
159
7
REFERENCES
1. Collaborators GBDT. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990-2015: a systematic analysis from the Global Burden of Disease Study 2015. Lancet. 2017;389(10082):1885-1906.
2. World Health Organization. Tobacco fact sheet. 2019 [cited 2019 Nov. 3]. Available from: http://www.who.int/mediacentre/fact sheets/fs339/en.
3. Goodchild M, Nargis N, Tursan d’Espaignet E. Global economic cost of smoking-attributable diseases. Tob Control. 2018;27(1):58-64.
4. Garrison GD, Dugan SE. Varenicline: a first-line treatment option for smoking cessation. Clin Ther. 2009;31(3):463-491.
5. Cahill K, Stevens S, Perera R, Lancaster T. Pharmacological interventions for smoking cessation: an overview and network meta-analysis. Cochrane Database Syst Rev. 2013(5):CD009329.
6. Ebbert JO, Hughes JR, West RJ, et al. Effect of varenicline on smoking cessation through smoking reduction: a randomized clinical trial. JAMA. 2015;313(7):687-694.
7. Anthenelli RM, Benowitz NL, West R, et al. Neuropsychiatric safety and efficacy of varenicline, bupropion, and nicotine patch in smokers with and without psychiatric disorders (EAGLES): a double-blind, randomised, placebo-controlled clinical trial. Lancet. 2016;387(10037):2507-2520.
8. Kasliwal R, Wilton LV, Shakir SA. Safety and drug utilization profile of varenicline as used in general practice in England: interim results from a prescription-event monitoring study. Drug Saf. 2009;32(6):499-507.
9. US Food and Drug Administration. Information for healthcare professionals: varenicline (marketed as Chantix) and bupropion (marketed as Zyban, Wellbutrin and generics). FDA Drug Safety Newsletter, 2009.
10. Davies NM, Thomas KH. The Food and Drug Administration and varenicline: should risk communication be improved? Addiction. 2017;112(4):555-558.
11. Gaballa D, Drowos J, Hennekens CH. Smoking Cessation: The Urgent Need for Increased Utilization of Varenicline. Am J Med. 2017;130(4):389-391.
12. Sheals K, Tombor I, McNeill A, Shahab L. A mixed-method systematic review and meta-analysis of mental health professionals’ attitudes toward smoking and smoking cessation among people with mental illnesses. Addiction. 2016;111(9):1536-1553.
13. Desai RJ, Good MM, San-Juan-Rodriguez A, et al. Varenicline and Nicotine Replacement Use Associated With US Food and Drug Administration Drug Safety Communications. Jama Network Open. 2019;2(9).
14. Shakir SA, Layton D. Causal association in pharmacovigilance and pharmacoepidemiology: thoughts on the application of the Austin Bradford-Hill criteria. Drug Saf. 2002;25(6):467-471.
15. Kress CM, Obi NU, Prochazka AV. In smokers with COPD, neither varenicline nor bupropion was linked to increased CV or neuropsychiatric risk vs NRT. Ann Intern Med. 2017;167(6):JC31.
16. Kotz D, Viechtbauer W, Simpson CR, van Schayck OCP, West R, Sheikh A. Cardiovascular and neuropsychiatric risks of varenicline and bupropion in smokers with chronic obstructive pulmonary disease. Thorax. 2017;72(10):905-911.
17. Molero Y, Lichtenstein P, Zetterqvist J, Gumpert CH, Fazel S. Varenicline and risk of psychiatric conditions, suicidal behaviour, criminal offending, and transport accidents and offences: population based cohort study. BMJ. 2015;350:h2388.
18. Kotz D, Viechtbauer W, Simpson C, van Schayck OC, West R, Sheikh A. Cardiovascular and neuropsychiatric risks of varenicline: a retrospective cohort study. Lancet Respir Med. 2015;3(10):761-768.
19. Thomas KH, Martin RM, Davies NM, Metcalfe C, Windmeijer F, Gunnell D. Smoking cessation treatment and risk of depression,

Chapter 7
160
suicide, and self harm in the Clinical Practice Research Datalink: prospective cohort study. Bmj-Brit Med J. 2013;347.
20. Garza D, Murphy M, Tseng LJ, Riordan HJ, Chatterjee A. A double-blind randomized placebo-controlled pilot study of neuropsychiatric adverse events in abstinent smokers treated with varenicline or placebo. Biol Psychiatry. 2011;69(11):1075-1082.
21. Smith RC, Amiaz R, Si TM, et al. Varenicline Effects on Smoking, Cognition, and Psychiatric Symptoms in Schizophrenia: A Double-Blind Randomized Trial. PLoS One. 2016;11(1):e0143490.
22. Thomas KH, Martin RM, Knipe DW, Higgins JP, Gunnell D. Risk of neuropsychiatric adverse events associated with varenicline: systematic review and meta-analysis. BMJ. 2015;350:h1109.
23. Lancaster T, Cahill K. ACP Journal Club. Review: Varenicline does not differ from placebo for adverse neuropsychiatric events. Ann Intern Med. 2015;163(2):JC6.
24. Gibbons RD, Mann JJ. Varenicline, smoking cessation, and neuropsychiatric adverse events. Am J Psychiatry. 2013;170(12):1460-1467.
25. Boyko EJ. Observational research--opportunities and limitations. J Diabetes Complications. 2013;27(6):642-648.
26. Lai EC, Pratt N, Hsieh CY, et al. Sequence symmetry analysis in pharmacovigilance and pharmacoepidemiologic studies. Eur J Epidemiol. 2017;32(7):567-582.
27. Wahab IA, Pratt NL, Wiese MD, Kalisch LM, Roughead EE. The validity of sequence symmetry analysis (SSA) for adverse drug reaction signal detection. Pharmacoepidemiol Drug Saf. 2013;22(5):496-502.
28. Park SK, Baek YH, Pratt N, Kalisch Ellett L, Shin JY. The Uncertainty of the Association Between Proton Pump Inhibitor Use and the Risk of Dementia: Prescription Sequence Symmetry Analysis Using a Korean Healthcare Database Between 2002 and 2013. Drug Saf. 2018;41(6):615-624.
29. Hallas J. Evidence of depression provoked by cardiovascular medication:
a prescription sequence symmetry analysis. Epidemiology. 1996;7(5):478-484.
30. Visser ST, Schuiling-Veninga CC, Bos JH, de Jong-van den Berg LT, Postma MJ. The population-based prescription database IADB.nl: its development, usefulness in outcomes research and challenges. Expert Rev Pharmacoecon Outcomes Res. 2013;13(3):285-292.
31. Pouwels KB, Visser ST, Bos HJ, Hak E. Angiotensin-converting enzyme inhibitor treatment and the development of urinary tract infections: a prescription sequence symmetry analysis. Drug Saf. 2013;36(11):1079-1086.
32. van Boven JF, de Jong-van den Berg LT, Vegter S. Inhaled corticosteroids and the occurrence of oral candidiasis: a prescription sequence symmetry analysis. Drug Saf. 2013;36(4):231-236.
33. Hallas J, Gaist D, Bjerrum L. The waiting time distribution as a graphical approach to epidemiologic measures of drug utilization. Epidemiology. 1997;8(6):666-670.
34. Ashare RL, Lerman C, Tyndale RF, et al. Sleep Disturbance During Smoking Cessation: Withdrawal or Side Effect of Treatment? J Smok Cessat. 2017;12(2):63-70.
35. Gershon AS, Campitelli MA, Hawken S, et al. Cardiovascular and Neuropsychiatric Events after Varenicline Use for Smoking Cessation. Am J Respir Crit Care Med. 2018;197(7):913-922.
36. van Boven JF, Vemer P. Higher Adherence During Reimbursement of Pharmacological Smoking Cessation Treatments. Nicotine Tob Res. 2016;18(1):56-63.
37. Li SH, Graham BM. Why are women so vulnerable to anxiety, trauma-related and stress-related disorders? The potential role of sex hormones. Lancet Psychiat. 2017;4(1):73-82.
38. Riecher-Rossler A. Sex and gender differences in mental disorders. Lancet Psychiat. 2017;4(1):8-9.
39. Vasiliadis HM, Lamoureux-Lamarche C, Gontijo Guerra S. Gender and age group differences in suicide risk associated with co-morbid physical and psychiatric disorders in older adults. Int Psychogeriatr. 2017;29(2):249-257.
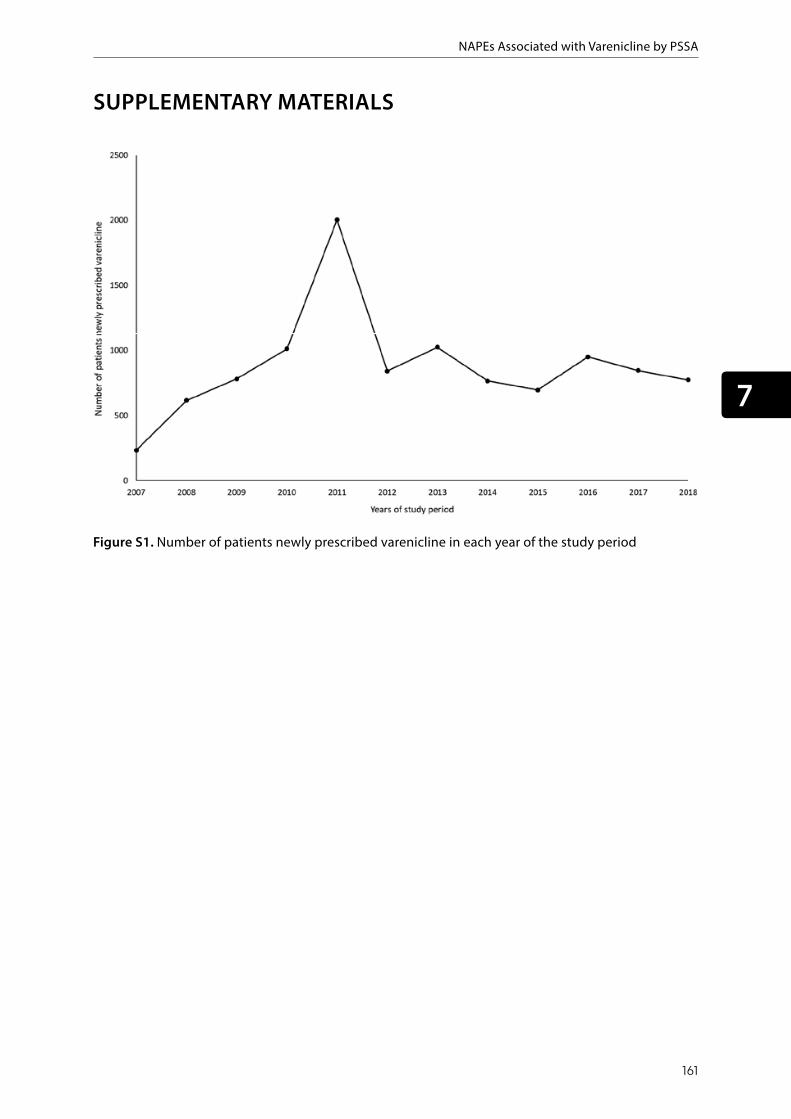
NAPEs Associated with Varenicline by PSSA
161
7
SUPPLEMENTARY MATERIALSSupplementary materials
Figure S1. Number of patients newly prescribed varenicline in each year of the study period
Figure S1. Number of patients newly prescribed varenicline in each year of the study period

Chapter 7
162
Table S1. Prescription sequence symmetry results of the association between varenilcine use and marker drugs for NPAEs within a time window of 1 year, stratified by year.
Time periodsNumber of patients*
Sequence ordera Crude SR
Null-effect SR Adjusted SR
Year groups2007-2010 430 164/266 0.62 [0.51, 0.75] 0.75 0.82 [0.67, 1.00]2011-2013 345 199/146 1.36 [1.10, 1.69] 1.10 1.23 [1.00, 1.53]2014-2018 291 142/149 0.95 [0.76, 1.20] 0.96 0.99 [0.79, 1.25]
Year2007 75 19/56 0.34 [0.20, 0.57] 0.62 0.55 [0.33, 0.93]2008 122 41/81 0.51 [0.35, 0.74] 0.70 0.72 [0.49, 1.05]2009 103 42/61 0.69 [0.46, 1.02] 0.97 0.71 [0.48, 1.06]2010 130 62/68 0.91 [0.65, 1.29] 0.98 0.93 [0.66, 1.32]2011 173 99/74 1.34 [0.99, 1.81] 0.78 1.72 [1.27, 2.32]#
2012 73 44/29 1.52 [0.95, 2.42] 1.06 1.43 [0.89, 2.28]2013 99 56/43 1.30 [0.88, 1.94] 1.27 1.02 [0.69, 1.52]2014 67 30/37 0.81 [0.50, 1.31] 0.98 0.83 [0.51, 1.34]2015 58 25/33 0.76 [0.45, 1.27] 0.92 0.83 [0.49, 1.39]2016 65 36/29 1.24 [0.76, 2.02] 0.83 1.50 [0.92, 2.44]2017 69 35/34 1.03 [0.64, 1.65] 1.08 0.95 [0.59, 1.52]2018 32 16/16 1.00 [0.50, 2.00] 1.11 0.90 [0.45, 1.80]
*Patients with initial prescription of both index drug varenicline and marker drugs for NPAEs. #p<0.05, with statistical significance. a the number of patients who initiated marker drugs for NPAEs after index drug varenicline divided by the number of patients who initiated varenicline after marker drugs for NPAEs. NPAEs: neuropsychiatric adverse events; SR: sequence ratio;

NAPEs Associated with Varenicline by PSSA
163
7
Table S2. Prescription sequence symmetry results of the association between varenicline use and marker drugs for NPAEs within a time window of 365 days, stratified by gender and age groups.
VariablesNumber of patients*
Sequence ordera Crude SR
Null-effect SR Adjusted SR
GenderMale
Any NPAEs 529 254/275 0.92 [0.78, 1.10] 0.91 1.02 [0.86,1.21]Depression 307 149/158 0.94 [0.75, 1.18] 0.92 1.02 [0.82, 1.28]Anxiety 333 151/182 0.83 [0.67, 1.03] 0.90 0.92 [0.74, 1.15]Sleep disorder 254 136/118 1.15 [0.90, 1.47] 0.94 1.22 [0.95, 1.56]
FemaleAny NPAEs 537 251/286 0.88 [0.74, 1.04] 0.90 0.98 [0.83, 1.16]Depression 420 215/205 1.05 [0.87, 1.27] 0.93 1.13 [0.94, 1.37]Anxiety 383 184/199 0.92 [0.76, 1.13] 0.89 1.04 [0.85, 1.27]Sleep disorder 278 150/128 1.17 [0.93, 1.48] 0.92 1.27 [1.00, 1.61]#
Age groups< = 45 years
Any NPAEs 476 214/262 0.82 [0.68, 0.98] 0.91 0.89 [0.75, 1.07]Depression 326 151/175 0.86 [0.69, 1.07] 0.93 0.93 [0.75, 1.15]Anxiety 323 136/187 0.73 [0.58, 0.91] 0.90 0.81 [0.65, 1.01]Sleep disorder 234 116/118 0.98 [0.76, 1.27] 0.95 1.04 [0.80, 1.34]
> 45 yearsAny NPAEs 590 291/299 0.97 [0.83, 1.14] 0.89 1.10 [0.93, 1.29]Depression 401 213/188 1.13 [0.93, 1.38] 0.92 1.23 [1.01, 1.50]Anxiety 393 199/194 1.03 [0.84, 1.25] 0.89 1.16 [0.95, 1.41]Sleep disorder 298 170/128 1.33 [1.06, 1.67] 0.92 1.44 [1.15, 1.82]#
*Patients with initial prescription of both index drug varenicline and maker drugs for NPAEs. a the number of patients who initiated marker drugs for NPAEs after index drug varenicline divided by the number of patients who initiated varenicline after marker drugs for NPAEs. #P<0.05; NPAEs: neuropsychiatric adverse events; SR: sequence ratio;

C H A P T E R 8

Demy L. Idema Yuanyuan Wang
Michael Biehl Peter L. Horvatovich
Eelko Hak
Effect estimate comparison between the prescription sequence symmetry analysis and parallel group
study designs: a systematic review
Published as: Idema DL, Wang Y, Biehl M, Horvatovich PL, Hak E. Effect estimate comparison between the prescription sequence symmetry analysis (PSSA) and
parallel group study designs: A systematic review. PLoS One. 2018 Dec 6;13(12):e0208389.

Chapter 8
166
ABSTRACT Prescription sequence symmetry analysis (PSSA), a case-only design introduced in 1996, has been increasingly used to identify unintentional drug effects, and has potential applications as a hypothesis-testing and a hypothesis-generating method, due to its easy application and effective control of time-invariant confounders. The aim of this study is to systematically compare effect estimates from the PSSA to effect estimates from conventional observational parallel group study designs, to assess the validity and constraints of the PSSA study design. We reviewed the MEDLINE®, EMBASE®, and Web of Science® databases until February 2016 to identify studies that compared PSSA to a parallel group design. Data from the eligible articles was extracted and analyzed, including making a Bland-Altman plot and calculating the number of discrepancies between the designs. 63 comparisons (from two studies) were included in the review. There was a significant correlation (p < 0.001) between the effect estimates of the PSSA and the parallel group designs, but the bias indicated by the Bland-Altman plot (0.20) and the percentage of discrepancies (70-80%) showed that this correlation was not accompanied by a considerable similarity of the effect estimates. Overall, the effect estimates of the parallel group designs were higher than those of the PSSA, not necessarily further away from 1, and the parallel group designs also generated more significant signals. However, these results should be approached with caution, as the effect estimates were only retrieved from two separate studies. This review indicates that, even though PSSA has a lot of potential, the effect estimates generated by the PSSA are usually lower than the effect estimates generated by parallel group designs, and PSSA mostly has a lower power than the conventional study designs, but this is based on limited comparisons, and more comparisons are needed to make a proper conclusion.

Comparison between PSSA and Parallel Group Study
167
8
INTRODUCTIONConventional observational parallel group studies, such as the cohort study and the case-control study, are still predominantly used to determine causal effects of risk factors and to assess drug safety 1. An important limitation of these designs is that they use an exposed- and a reference group which are (frequently) not readily comparable. This can lead to biased results 2. Case-only designs, such as the case-crossover study design and the self-controlled case-series are alternatives to parallel group designs, and they aim to decrease the possibility of introducing bias 3,4. These designs are particularly useful to control for time-invariant confounders, even when these confounders are generally not recorded in the databases, such as genetic disposition, diet, and over-the-counter drug use 2,5.
In 1996, Hallas introduced another case-only study design: the prescription sequence symmetry analysis (PSSA) 6. A key advantage of PSSA is that it can be used when there is an extensive amount of prescription data available, but no information is given for diagnoses, co-morbidities, and other possible confounders. In this study design, only patients who filled incident prescriptions for both the index drug (the drug under investigation) and the marker drug (the drug prescribed as a proxy/indicator for the outcome of interest, usually an unintentional effect of the index drug) during a predefined risk period are included in the analysis. The crude sequence ratio (SR) is calculated by dividing the number of patients who filled the prescription for the index drug first and the prescription for the marker drug second, by the number of patients with their prescriptions in the reverse order 7. Since PSSA can be sensitive to temporal prescribing trends, the null-effect sequence ratio is also calculated. This is the expected SR in absence of a causal relationship between the index- and marker drug. A more detailed explanation of the originally proposed method to calculate the null-effect SR is given by Hallas 6. In a study by Tsiropoulos et al. an adjustment to this calculation method is proposed, that takes into account risk periods that are shorter than the total study period 8. By dividing the crude SR by the null-effect SR, the adjusted sequence ratio (ASR) is determined 9. An ASR (including its confidence interval [CI]) above 1 indicates that the index drug may cause the adverse event for which the marker drug is prescribed, while an ASR (including its CI) below 1 suggests a possible protective effect 10. A schematic representation of the cohort-, case-control, and PSSA study design is shown in Fig 1. Variations on the PSSA, such as (event) sequence symmetry analysis ((E)SSA), are also described in literature, and these variations also look at index- and marker events instead of drugs, such as surgeries or behavioral interventions 11.
PSSA has been used less frequently than other, more conventional, pharmacoepidemiologic study designs, and comparisons of PSSA to these designs are lacking 7-10, 12-26. In this systematic review, we aim to compare PSSA to conventional study designs. In a previous study, the correlation between effect estimates from different designs has been
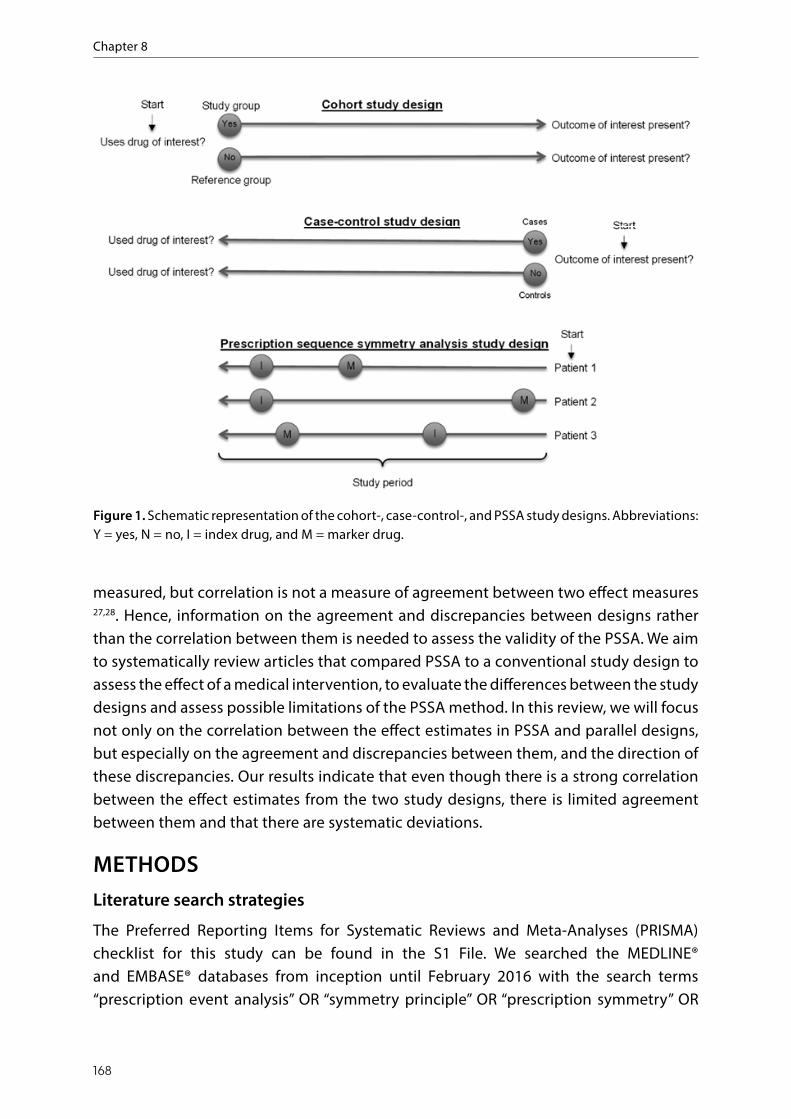
Chapter 8
168
measured, but correlation is not a measure of agreement between two effect measures 27,28. Hence, information on the agreement and discrepancies between designs rather than the correlation between them is needed to assess the validity of the PSSA. We aim to systematically review articles that compared PSSA to a conventional study design to assess the effect of a medical intervention, to evaluate the differences between the study designs and assess possible limitations of the PSSA method. In this review, we will focus not only on the correlation between the effect estimates in PSSA and parallel designs, but especially on the agreement and discrepancies between them, and the direction of these discrepancies. Our results indicate that even though there is a strong correlation between the effect estimates from the two study designs, there is limited agreement between them and that there are systematic deviations.
METHODSLiterature search strategies
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist for this study can be found in the S1 File. We searched the MEDLINE® and EMBASE® databases from inception until February 2016 with the search terms “prescription event analysis” OR “symmetry principle” OR “prescription symmetry” OR
below 1 suggests a possible protective effect [10]. A schematic representation of the cohort‐,
case‐control, and PSSA study design is shown in Fig 1. Variations on the PSSA, such as (event)
sequence symmetry analysis ((E)SSA), are also described in literature, and these variations also
look at index‐ and marker events instead of drugs, such as surgeries or behavioral interventions
[11].
Fig. 1. Schematic representation of the cohort‐, case‐control‐, and PSSA study designs.
Abbreviations: Y = yes, N = no, I = index drug, and M = marker drug.
PSSA has been used less frequently than other, more conventional, pharmacoepidemiologic
study designs, and comparisons of PSSA to these designs are lacking [7‐10, 12‐26]. In this
systematic review, we aim to compare PSSA to conventional study designs. In a previous study,
the correlation between effect estimates from different designs has been measured, but
correlation is not a measure of agreement between two effect measures [27,28]. Hence,
information on the agreement and discrepancies between designs rather than the correlation
Figure 1. Schematic representation of the cohort-, case-control-, and PSSA study designs. Abbreviations: Y = yes, N = no, I = index drug, and M = marker drug.

Comparison between PSSA and Parallel Group Study
169
8
“proximate clinical event ratio*” OR “sequence symmetry” OR “sequence-symmetry” OR “symmetry analys*” OR “sequence rat*” OR “prescription sequence”. We also performed a Web of Science® cited reference search (also from inception until February 2016) for the article in which the PSSA method was introduced: “Hallas J”, “1996”, “Epidemiology”. All search results were limited to studies on humans, articles in English, and articles for which the abstract was available.
Selection criteria
All identified articles were exported to RefWorks (ProQuest, Michigan). Title and abstract screening were performed and the full text of the relevant studies was reviewed for eligibility by two independent reviewers (D.L.I. and Y.W.). Disagreement between the reviewers was solved by consensus. Studies were eligible for inclusion in the review if they met the following criteria: the article compares (P)SSA to a conventional study design, the data for both study designs comes from the same data source and the definitions for the exposure(s) (index drug/event), outcome(s) (marker drug/event) and risk period(s) are equal for both study designs. Articles were excluded if they were systematic reviews, methodological studies, or studies with simulated data.
Data extraction and analysis
For all articles that used (P)SSA as a study design identified by our search, whether the article was eligible for the review or not, the publication year was extracted to examine trends of application of this study design in time. These articles were split up into articles that used PSSA and articles that used another type of SSA, such as event sequence symmetry analysis. If both PSSA and SSA were used, the article was classified according to the principal study design, as identified by the article’s author.
From the eligible articles, we extracted the following data: author(s), year of publication, journal name, type of conventional study design and risk measure, exposure (index drug/event), outcome (marker drug/event), comparator used in the conventional study design, risk period(s), the conventional effect estimate and the PSSA effect estimate. If the study investigated multiple drug pairs, and there was not both a conventional effect estimate and a PSSA effect estimate for all of them, only the data for the drug pairs for which both effect estimates were reported was extracted.
As we compared multiple study designs to each other, rather than using different quality assessment tools for each study design, a method of quality assessment that we employed was to assess the reporting of potential confounders in the eligible articles. We based our assessment on the checklist by Pouwels et al., derived from the “Strengthening the Reporting of Observational Studies in Epidemiology” (STROBE) statement 29,30.

Chapter 8
170
The effect estimates were exported to SPSS (IBM, New York, version 23), where they were analyzed using several approaches. First, a scatterplot was made of the effect estimates from the conventional study designs against the effect estimates from the PSSA study design to qualitatively examine potential differences in effect estimates. Second, the Spearman’s correlation coefficients were determined to evaluate the correlation between the effect estimates. Third, we examined whether the different study designs found the same significant associations. Fourth, because correlation may not be ideal to measure agreement between two types of study design, a Bland-Altman plot was made to assess this 28. Moreover, the discrepancies between the effect estimates were evaluated, as previously done by Ioannidis et al: results were found to be discrepant if there was an absolute difference of 50% or more between the PSSA effect estimate and the parallel group design effect estimate on the natural logarithmic scale 31.
RESULTSArticle identification
The search identified 183 unique articles. Based on the title and abstract screening, 85 potentially relevant articles were selected for full-text screening. After reviewing for eligibility, two articles were included into the review (Fig 2). The first article compared PSSA to both cohort- and nested case-control studies and the second article compared PSSA solely to a cohort study 27,32. The data extracted from both articles is presented in Table 1.
types of study design, a Bland‐Altman plot was made to assess this [28]. Moreover, the
discrepancies between the effect estimates were evaluated, as previously done by Ioannidis et
al: results were found to be discrepant if there was an absolute difference of 50% or more
between the PSSA effect estimate and the parallel group design effect estimate on the natural
logarithmic scale [31].
Fig. 2. PRISMA flow diagram of the study selection process.
Results
Article identification
The search identified 183 unique articles. Based on the title and abstract screening, 85
potentially relevant articles were selected for full‐text screening. After reviewing for eligibility,
two articles were included into the review (Fig 2). The first article compared PSSA to both
cohort‐ and nested case‐control studies and the second article compared PSSA solely to a
cohort study [27,32]. The data extracted from both articles is presented in Table 1.
There were 50 articles (S2 File) that used (P)SSA to determine the effect of a medical
intervention, and Fig 3 shows the number of these articles published per year. Even though the
Figure 2. PRISMA flow diagram of the study selection process.
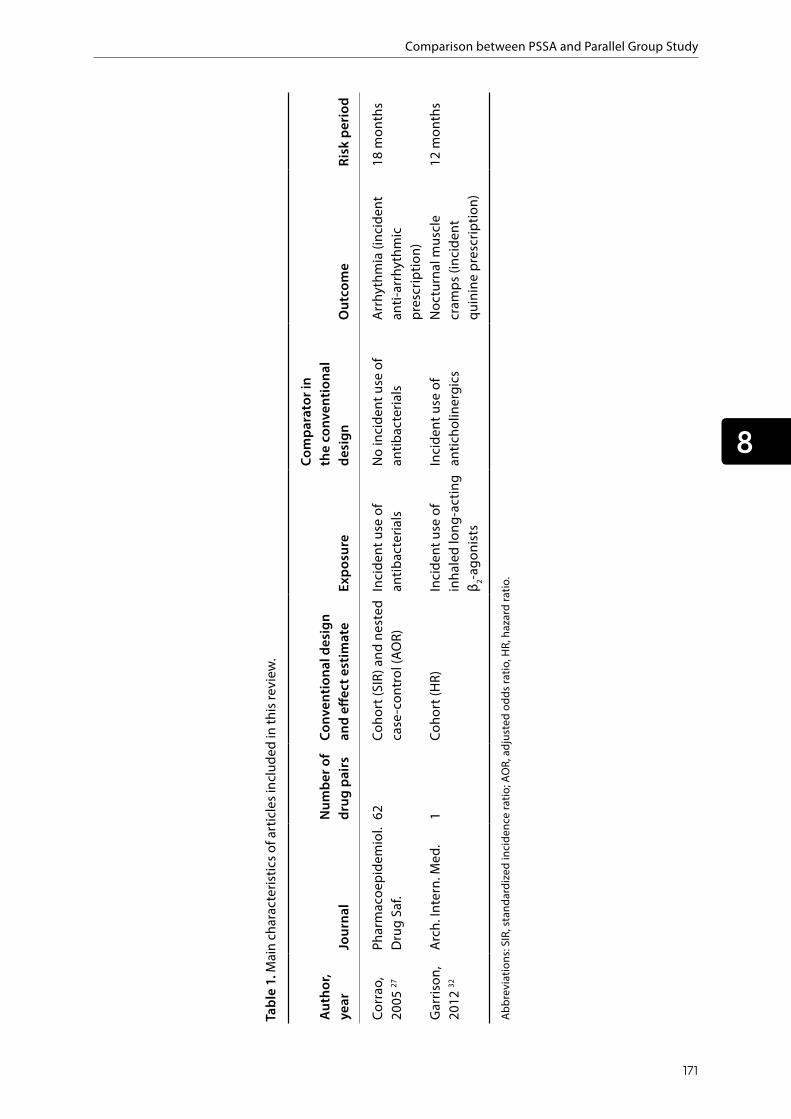
Comparison between PSSA and Parallel Group Study
171
8
Tabl
e 1.
Mai
n ch
arac
teris
tics o
f art
icle
s inc
lude
d in
this
revi
ew.
Auth
or,
year
Jour
nal
Num
ber o
f dr
ug p
airs
Conv
entio
nal d
esig
n an
d eff
ect e
stim
ate
Expo
sure
Com
para
tor i
n th
e co
nven
tiona
l de
sign
Out
com
eRi
sk p
erio
d
Corr
ao,
2005
27
Phar
mac
oepi
dem
iol.
Dru
g Sa
f.62
Coho
rt (S
IR) a
nd n
este
d ca
se-c
ontr
ol (A
OR)
Inci
dent
use
of
antib
acte
rials
No
inci
dent
use
of
antib
acte
rials
Arrh
ythm
ia (i
ncid
ent
anti-
arrh
ythm
ic
pres
crip
tion)
18 m
onth
s
Gar
rison
, 20
12 32
Arch
. Int
ern.
Med
.1
Coho
rt (H
R)In
cide
nt u
se o
f in
hale
d lo
ng-a
ctin
g β 2-a
goni
sts
Inci
dent
use
of
antic
holin
ergi
csN
octu
rnal
mus
cle
cram
ps (i
ncid
ent
quin
ine
pres
crip
tion)
12 m
onth
s
Abbr
evia
tions
: SIR
, sta
ndar
dize
d in
cide
nce
ratio
; AO
R, a
djus
ted
odds
ratio
, HR,
haz
ard
ratio
.

Chapter 8
172
There were 50 articles (S2 File) that used (P)SSA to determine the effect of a medical intervention, and Fig 3 shows the number of these articles published per year. Even though the method was rarely used after its introduction in 1996, there is a clear increasing trend in the number of (published) PSSA studies during the last three to four years. For reference, the total number of articles indexed by MEDLINE® per year has also been added to the figure 33. The increase in the number of articles using the (P)SSA study design is relatively larger than the increase in total number of articles.
Number of PSSA articles (black bar) and number of SSA articles (grey bar) published per year and the total number of articles indexed in MEDLINE (black line) per year after the introduction of the method in 1996 (first bar in the graph).
Correlation analysis
A scatterplot was made of the conventional effect estimates against the PSSA effect estimates (S3 Fig). This scatterplot showed that there was a visible correlation between the effect estimates, but that for most of the investigated drug-pairs, the effect estimate from the conventional study designs was higher than the effect estimate from the PSSA study design, i.e. most of the data points were above the y = x reference line.
Spearman Rank-Order Correlation tests were performed (Table 2), first for all results taken into consideration, and followed by tests of the subsets of the results PSSA vs. cohort and PSSA vs. nested case-control designs. Their Spearman’s correlation coefficients were 0.621, 0.553, and 0.676, respectively. All results were highly statistically significant, with p ≤ 0.001.
Fig. 3. Number of (P)SSA articles published per year.
Spearman Rank‐Order Correlation tests were performed (Table 2), first for all results taken into
consideration, and followed by tests of the subsets of the results PSSA vs. cohort and PSSA vs.
nested case‐control designs. Their Spearman’s correlation coefficients were 0.621, 0.553, and
0.676, respectively. All results were highly statistically significant, with p 0.001.
Table 2. Summary of the Spearman‐Rank Order Correlation analysis.
Dataset N Spearman’s correlation coefficient p‐value
All results 63 0.621 5.521�10‐8
PSSA vs. cohort 35 0.553 0.001
PSSA vs. nested case‐control 28 0.676 7.900�10‐5
Figure 3. Number of (P)SSA articles published per year.
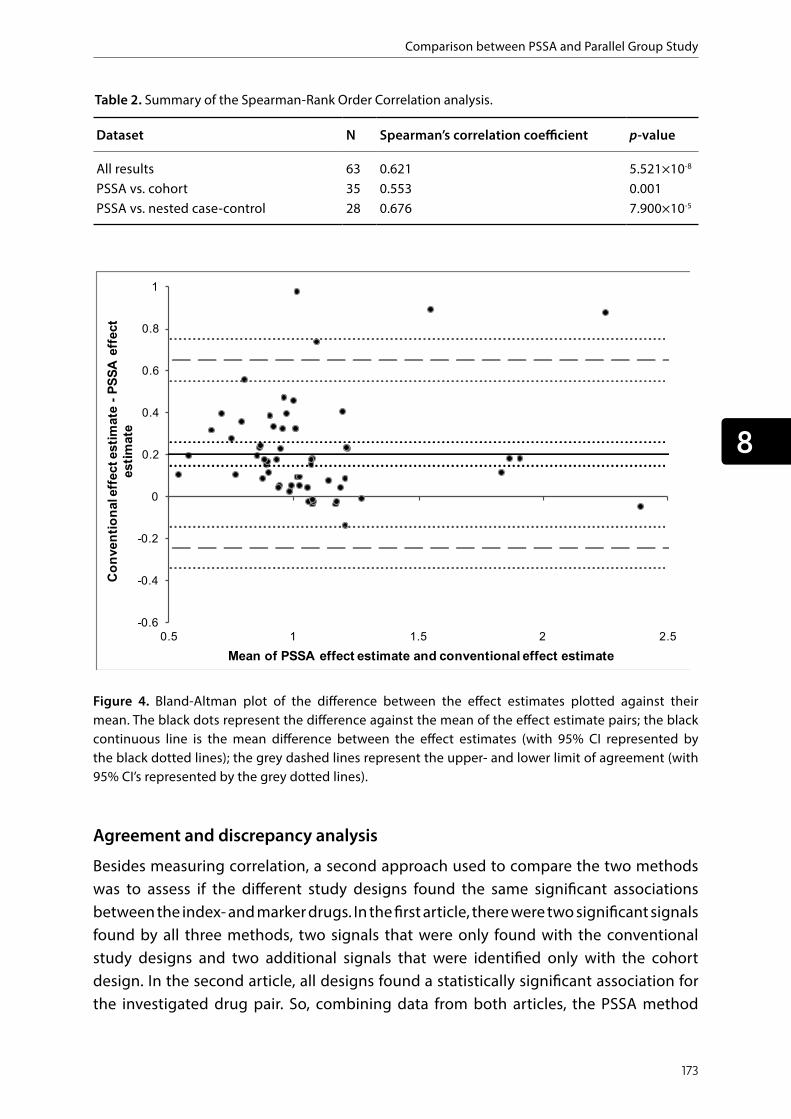
Comparison between PSSA and Parallel Group Study
173
8
Table 2. Summary of the Spearman-Rank Order Correlation analysis.
Dataset N Spearman’s correlation coefficient p-value
All results 63 0.621 5.521×10-8
PSSA vs. cohort 35 0.553 0.001PSSA vs. nested case-control 28 0.676 7.900×10-5
Figure 4. Bland-Altman plot of the difference between the effect estimates plotted against their mean. The black dots represent the difference against the mean of the effect estimate pairs; the black continuous line is the mean difference between the effect estimates (with 95% CI represented by the black dotted lines); the grey dashed lines represent the upper- and lower limit of agreement (with 95% CI’s represented by the grey dotted lines).
Fig 4. Bland‐Altman plot of the difference between the effect estimates plotted against their
mean. The black dots represent the difference against the mean of the effect estimate pairs;
the black continuous line is the mean difference between the effect estimates (with 95% CI
represented by the black dotted lines); the grey dashed lines represent the upper‐ and lower
limit of agreement (with 95% CI’s represented by the grey dotted lines).
Agreement and discrepancy analysis
Besides measuring correlation, a second approach used to compare the two methods was to
assess if the different study designs found the same significant associations between the index‐
and marker drugs. In the first article, there were two significant signals found by all three
methods, two signals that were only found with the conventional study designs and two
additional signals that were identified only with the cohort design. In the second article, all
designs found a statistically significant association for the investigated drug pair. So, combining
data from both articles, the PSSA method identified less significant, potentially causal,
associations between the index‐ and the marker drug than the two parallel group designs.
Co
nve
nti
on
al e
ffec
t est
imat
e -
PS
SA
eff
ect
esti
mat
e
Mean of PSSA effect estimate and conventional effect estimate
Agreement and discrepancy analysis
Besides measuring correlation, a second approach used to compare the two methods was to assess if the different study designs found the same significant associations between the index- and marker drugs. In the first article, there were two significant signals found by all three methods, two signals that were only found with the conventional study designs and two additional signals that were identified only with the cohort design. In the second article, all designs found a statistically significant association for the investigated drug pair. So, combining data from both articles, the PSSA method

Chapter 8
174
identified less significant, potentially causal, associations between the index- and the marker drug than the two parallel group designs.
The third approach used to compare the effect estimates from the different study designs was to make a Bland-Altman plot to assess the degree of agreement between them (Fig 4). This figure shows that the mean difference between the conventional study design effect estimates and the PSSA study design effect estimates is 0.20 (95% CI [0.15, 0.26]), with the limits of agreement ranging from the lower limit of -0.24 (95% CI [-0.34, -0.14]) to the upper limit of 0.65 (95% CI [0.55, 0.75]). The Bland-Altman analysis shows that there is a degree of bias because the line of equality (the x-axis, y = 0) is not included in the confidence interval of the mean difference.
A fourth approach to compare the effect estimates is by determining discrepancies between them, as described before. The number and percentage of discrepancies are shown in Table 3. Even though the effect estimates were highly correlated, many results were characterized as discrepant when looking at the difference between them. Around 70-80% of all results were found to be discrepant, irrespective of whether it is a comparison to a cohort design or a comparison to a nested case-control design. Looking at these discrepancies, 92% of the cohort effect estimates and 96% of the nested case-control effect estimates were larger than the corresponding PSSA effect estimates. When assessing for the discrepancies whether the conventional effect estimate or the PSSA effect estimate was further away from 1, it was found that 33% of the cohort effect estimates and 36% of the nested case-control effect estimates were further away from 1 than the PSSA effect estimates.
Table 3. Number of discrepancies between PSSA and parallel group designs.
DatasetNumber (%) of discrepanciesa
Number (%) of discrepancies for which the conventional effect estimate is largerb
Number (%) of discrepancies for which the conventional effect estimate is further away from 1c
All results (n=63) 46 (73) 43 (94) 16 (35)PSSA vs. cohort (n=35) 24 (69) 22 (92) 8 (33)PSSA vs. nested case-control (n=28)
22 (79) 21 (96) 8 (36)
aDiscrepancies were characterized by the natural logarithm of the PSSA effect estimate being ≥50% larger or smaller than the natural logarithm of the conventional study design effect estimate. bThe fraction of the total number of discrepancies for which the conventional effect estimate is larger than the PSSA effect estimate. cThe fraction of the total number of discrepancies for which the conventional effect estimate is further away from 1 than the PSSA effect estimate.

Comparison between PSSA and Parallel Group Study
175
8
DISCUSSIONThis study aimed to assess and quantify the correlation, agreement, and discrepancies between effect estimates from the PSSA and two conventional pharmacoepidemiologic study designs, the cohort- and nested case-control study design. We found that there was a significant correlation between the effect estimates of the PSSA and effect estimates of the conventional studies, but this strong correlation was not accompanied by similar effect estimates; there were systematic differences between the effect estimates generated by the two types of design. The Bland-Altman analysis showed significant bias between the effect estimates, with the effect estimates from the conventional study designs being, on average, 0.20 higher than the effect estimates from the PSSA.
The difference in effect size between the two types of design could originate from the use of a reference group in the conventional study designs, while the PSSA is a case-only design. Time-invariant confounders, whether registered or unregistered, such as advanced age, female gender, and hypochondriasis, may result in bias in parallel group designs (if they are not adjusted for) but not in the case-only PSSA 8. Most comparisons (all apart from one) used in this review were derived from the study by Corrao et al. 27, and in this study, the comparisons from the cohort design were only adjusted for gender, age and month of observation, and the comparisons from the nested case-control design for gender, age, cumulative number of antibiotic prescriptions, and date of cohort entry. The PSSA method may inherently control for more confounders than this, and better confounder control could account for the difference in effect estimates.
However, this may not be the reason for the discrepancies if important assumptions for the validity of PSSA are not met. The assumptions of PSSA, based on the strengths and limitations of the method, are: there is an appropriate and specific indicator/proxy for the outcome, the proxy can be prescribed independently of the sequence of the exposure to the index drug and the occurrence of the outcome (e.g. if the outcome is fatal, the proxy could only be prescribed after incident index drug use), the outcome of interest has no effect on subsequent treatment, the effect of the exposure is transient, and the drug-induced symptom is relatively unknown to the prescribing physician 2,10,34-36. Both articles discussed in this review mostly meet all assumptions, indicating that the differences between the effect estimates do not originate from invalid use of the PSSA design. The only possible problem is that the use of proxies for the outcomes may miss some cases, such as patients with unrecognized symptoms or patients who are hospitalized because of them, or it may include subjects taking the drug who do not have the outcome of interest.
The included articles used relatively long risk periods; 12- and 18 months. These are quite wide time-windows since exposure to the index drug shortly before the onset of the adverse event is more likely to be causal for the investigated exposures, especially for

Chapter 8
176
the antibacterials exposures from the study by Corrao et al. 27. Here, more accurate effect estimates could be obtained if the risk window would be chosen more appropriately, i.e. would be shorter, based on the expected time that is needed for the manifestation of the adverse event. Also, to reduce the possibility of time-variant confounding, the risk period should be relatively small and should generally not exceed a couple of months to a year maximum. Note that for other drugs that are used for more extensive periods of time, and outcomes that may not be reported right away, longer risk periods may be appropriate.
Additionally, the underestimation of the effect size by the PSSA compared to the conventional study designs could be caused by the use of the relatively long risk periods in the PSSA. Using a longer risk period than necessary, especially in the case of the antibacterials exposure, could have diluted the signal by including more nonspecific sequences in the calculation of the adjusted sequence ratio. If the use of a longer risk period has more effect on the PSSA study design than on the other two designs, this could account (in part) for the lower effect estimates generated in this study design.
More differences were observed when assessing the number of adverse event signals (i.e. statistically significant results). There were cases where adverse event signals were only measured in the cohort- and nested case-control designs, but not in the PSSA. Since PSSA is only performed on subjects that filled incident prescriptions for both the index- and the marker drug, the sample size of the PSSA is smaller, and therefore the power lower, compared to that of the conventional designs. A possible solution for this was used by Pratt et al. in 2013, when they used a distributed network model to investigate the risk of acute hyperglycemia with antipsychotic use 17. Using data from multiple countries increases the size of the population and the power of the analysis, and PSSA can therefore also detect rarer adverse events.
In general, for all arguments made above, it must be noted that our results are only based on two separate studies, and that it is therefore not possible to generalize these results to all studies that use PSSA and/or conventional study designs. A large part of our results (62 of the 63 comparisons included, 98%) are derived from a single study, and therefore these comparisons cannot be considered independent, and the results of our review are greatly dependent on the methodology and results used in that particular study. It may be the case that some part of the methodology of this study caused a systematic underestimation of the effect size of the PSSA study design compared to a conventional study design, and that application of the PSSA methodology is the cause of the discrepancy rather than the PSSA methodology itself. To be able to draw any generalizable conclusion from comparisons between the PSSA study design and conventional study designs, more independent comparisons between the two are greatly needed.

Comparison between PSSA and Parallel Group Study
177
8
To assess the reporting of potential confounding in the articles used for this review, we used the checklist by Pouwels et al, derived from the “Strengthening the Reporting of Observational Studies in Epidemiology” (STROBE) statement 29,30. In this checklist, there are eight items for the reporting of confounding. The first article in our review reported seven out of eight items from this checklist, while the second article reported six out of eight 27,32. This is a high reporting quality compared to other articles, as demonstrated in the review by Pouwels et al, which found a median of four out of eight items reported 29.
One important advantage of PSSA is that it eliminates time-invariant confounders, but PSSA may still be sensitive to other types of confounding. Both articles calculated the adjusted sequence ratio to eliminate confounding by temporal prescribing trends and one article also adjusted for age and seasonal trends in drug prescription. Contra-indication was identified as a potential confounder, but this confounder is hard to control. A large part of the results of this review originates from a study that aimed to determine the effect of antibacterials on arrhythmia. The study split up the antibacterials into many subgroups and this division could have introduced confounding by contra-indication: physicians might only prescribe certain antibacterials to patients who are known to be at risk of arrhythmia. While this bias would not be the cause of the difference between the study designs, because this same division was made for the conventional study designs, it is an important confounder to take into consideration when using PSSA to compare subgroups of drugs prescribed for a similar indication. This is especially true when prescribing physicians are already aware of the potential adverse event, and may let this influence their prescribing behavior in choosing a specific drug for high-risk patients.
Also, when subjects consult their physician when they present with symptoms of an adverse event, some physicians may discontinue the index drug instead of prescribing the marker drug. In this case, these subjects would be missed by the PSSA, resulting in an underestimation of the effect estimate. Furthermore, it would also reduce the sample size, which further decreases the power of PSSA. However, most of the effect estimates from the conventional designs were also based on drug dispensing data, so this would not cause discrepancies between the effect estimates of both types of design studied in this review. Besides, it was demonstrated that even fairly well known adverse events are often treated by prescribing additional drugs, rather than discontinuing the drug that might have caused it 21.
Strengths and limitations
This is the first systematic review that assesses the performance of PSSA compared to conventional study designs by reporting on the agreement and the discrepancies between the effect estimates and the direction of the discrepancies. A challenge that we have faced was the limited data available since empirical comparisons between

Chapter 8
178
PSSA and conventional designs are rare, and therefore it is hard to draw any definite conclusions from our results. We recognize that this could be due to the fact that researchers may perform both types of study and then publish the study with the most relevant results. This would underestimate the discrepancies between the study designs. Another possibility is that the results for both types of study were so similar that researchers only chose to publish the results of one of the two study designs. This would result in an overestimation of the difference between the study designs. Also, because the study designs use different effect measures, they may not be readily comparable, causing inconsistencies that are based on the different effect measures used rather than the different study designs. Therefore, there is a need for a quantitative statistical test that compares effect estimates from different risk measures.
CONCLUSIONSPSSA, due to its simple and quick implementation and its ability to eliminate time-invariant confounding has a lot of potential in assessing drug safety. However, our results indicate that PSSA lacks power in many situations, and its results often significantly deviate from effect estimates generated by conventional parallel group study designs. PSSA might, therefore, be more suitable as a hypothesis-generating design, that should be followed by a more conventional parallel group design for hypothesis-testing and confirmation. Our results should be approached with some caution, though, as they are only based on two independent studies. To get a better understanding of the practical differences between the two types of designs, and to be able to make any generalizations, more comparisons between PSSA and parallel group designs are required. Future studies should also compare PSSA to randomized controlled trials, to assess how PSSA performs against the study design considered to be the golden standard.
SUPPLEMENTARY MATERIALSFile S1-S2 are available as Supplementary data at PLOS ONE Online (https://doi.org/10.1371/journal.pone.0208389)

Comparison between PSSA and Parallel Group Study
179
8
REFERENCES 1. Consiglio GP, Burden AM, Maclure M,
McCarthy L, Cadarette SM. Case-crossover study design in pharmacoepidemiology: systematic review and recommendations. Pharmacoepidemiol Drug Saf. 2013;22: 1146-1153. doi: 10.1002/pds.3508
2. Hallas J, Pottegård A. Use of self-controlled designs in pharmacoepidemiology. J Intern Med. 2014;275: 581-589. doi: 10.1111/joim.12186
3. Maclure M. The case-crossover design: a method for studying transient effects on the risk of acute events. Am J Epidemiol. 1991;133: 144-153.
4. Farrington P, Pugh S, Colville A, Flower A, Nash J, Morgan-Capner P, et al. A new method for active surveillance of adverse events from diphtheria/tetanus/pertussis and measles/mumps/rubella vaccines. Lancet. 1995;345: 567-569.
5. Newsom JT, Jones RN, Hofer SM. Longitudinal data analysis: a practical guide for researchers in aging, health, and social sciences. New York: Routledge; 2012.
6. Hallas J. Evidence of depression provoked by cardiovascular medication: a prescription sequence symmetry analysis. Epidemiology. 1996;7: 478-484.
7. Hersom K, Neary MP, Levaux HP, Klaskala W, Strauss JS. Isotretinoin and antidepressant pharmacotherapy: a prescription sequence symmetry analysis. J Am Acad Dermatol. 2003;49: 424-432.
8. Tsiropoulos I, Andersen M, Hallas J. Adverse events with use of antiepileptic drugs: a prescription and event symmetry analysis. Pharmacoepidemiol Drug Saf. 2009;18: 483-491. doi: 10.1002/pds.1736
9. Lai EC, Hsieh CY, Kao Yang YH, Lin SJ. Detecting potential adverse reactions of sulpride in schizophrenic patients by prescription sequence symmetry analysis. PLoS One. 2014;9: e89795. doi: 10.1371/journal.pone.0089795
10. Bytzer P, Hallas J. Drug-induced symptoms of functional dyspepsia and nausea. A symmetry
analysis of one million prescriptions. Aliment Pharmacol Ther. 2000;14: 1479-1484.
11. Cole JA, Farraye FA, Cabral HJ, Zhang Y, Rothman KJ. Irritable bowel syndrome and hysterectomy: a sequence symmetry analysis. Epidemiology. 2007;18: 837-838. doi: 10.1097/EDE.0b013e3181571f1b
12. Caughey GE, Roughead EE, Pratt N, Shakib S, Vitry AI, Gilbert AL. Increased risk of hip fracture in the elderly associated with prochlorperazine: is a prescribing cascade contributing? Pharmacoepidemiol Drug Saf. 2010;19: 977-982. doi: 10.1002/pds.2009
13. Fujimoto M, Higuchi T, Hosomi K, Takada M. Association of statin use with storage lower urinary tract symptoms: data mining of claims database. J Pharmacovigilance. 2014;2: 147. doi: 10.4172/2329-6887.1000147
14. Hallas J, Bytzer P. Screening for drug-related dyspepsia: an analysis of prescription symmetry. Eur J Gastroenterol Hepatol. 1998;10: 27-32.
15. Lai EC, Yang YH, Lin SJ, Hsieh CY. Use of antiepileptic drugs and risk of hypothyroidism. Pharmacoepidemiol Drug Saf. 2013;22: 1071-1079. doi: 10.1002/pds.3498
16. Pouwels KB, Visser ST, Bos HJ, Hak E. Angiotensin-converting enzyme inhibitor treatment and the development of urinary tract infections: a prescription sequence symmetry analysis. Drug Saf. 2013;36: 1079-1086. doi: 10.1007/s40264-013-0085-z
17. Pratt N, Andersen M, Bergman U, Choi NK, Gerhard T, Huang C, et al. Multi-country rapid adverse drug event assessment: the Asian Pharmacoepidemiology Network (AsPEN) antipsychotic and acute hyperglycaemia study. Pharmacoepidemiol Drug Saf. 2013;22: 915-924. doi: 10.1002/pds.3440
18. Rasmussen L, Hallas J, Madsen KG, Pottegård A. Cardiovascular drugs and erectile dysfunction - a symmetry analysis. Br J Clin Pharmacol. 2015;80: 1219-1223. doi: 10.1111/bcp.12696
19. Roughead EE, Kalisch LM, Pratt NL, Killer G, Barnard A, Gilbert AL. Managing glaucoma
Chapter 8
180
in those with co-morbidity: not as easy as it seems. Ophthalmic Epidemiol. 2012;19: 74-82. doi: 10.3109/09286586.2011.638743
20. Van Boven JF, De Jong-van den Berg LT, Vegter S. Inhaled corticosteroids and the occurrence of oral candidiasis: a prescription sequence symmetry analysis. Drug Saf. 2013;36: 231-236. doi: 10.1007/s40264-013-0029-7
21. Vegter S, De Jong-van den Berg LT. Misdiagnosis and mistreatment of a common side-effect – angiotensin-converting enzyme inhibitor-induced cough. Br J Clin Pharmacol. 2010;69: 200-203. doi: 10.1111/j.1365-2125.2009.03571.x
22. Fujimoto M, Higuchi T, Hosomi K, Takada M. Association between statin use and cancer: data mining of a spontaneous reporting database and a claims database. Int J Med Sci. 2015;12: 223-233. doi: 10.7150/ijms.10656
23. Kalisch Ellett LM, Pratt NL, Barratt JD, Rowett D, Roughead EE. Risk of medication-associated initiation of oxybutynin in elderly men and women. J Am Geriatr Soc. 2014;62: 690-695. doi: 10.1111/jgs.12741
24. Pouwels KB, Kalkman GA, Schagen D, Visser ST, Hak E. Is combined use of SSRIs and NSAIDs associated with an increased risk of starting peptic ulcer treatment? Br J Clin Pharmacol. 2014;78: 192-193. doi: 10.1111/bcp.12300
25. Takada M, Fujimoto M, Yamazaki K, Takamoto M, Hosomi K. Association of statin use with sleep disturbances: data mining of a spontaneous reporting database and a prescription database. Drug Saf. 2014;37: 421-431. doi: 10.1007/s40264-014-0163-x
26. Takeuchi Y, Kajiyama K, Ishiguro C, Uyama Y. Atypical antipsychotics and the risk of hyperlipidemia: a sequence symmetry analysis. Drug Saf. 2015;38: 641-650. doi: 10.1007/s40264-015-0298
27. Corrao G, Botteri E, Bagnardi V, Zambon A, Carobbio A, Falcone C et al. Generating signals of drug-adverse effects from prescription databases and application to the risk of arrhythmia associated with antibacterials. Pharmacoepidemiol Drug Saf. 2005;14: 31-40.
28. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1: 307-310.
29. Pouwels KB, Widyakusuma NN, Groenwold RH, Hak E. Quality of reporting of confounding remained suboptimal after the STROBE guideline. J Clin Epidemiol. 2016;69: 217-224. doi: 10.1016/j.jclinepi.2015.08.009
30. Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 2007;4: 1623-1627. doi: 10.1371/journal.pmed.0040296
31. Ioannidis JPA, Haidich AB, Pappa M, Pantazis N, Kokori SI, Tektonidou MG, et al. Comparison of evidence of treatment effects in randomized and nonrandomized studies. JAMA. 2001;286: 821-830.
32. Garrison SR, Dormuth CR, Morrow RL, Carney GA, Khan KM. Nocturnal leg cramps and prescription use that precedes them: a sequence symmetry analysis. Arch Intern Med. 2012;172: 120-126. doi: 10.1001/archinternmed.2011.1029
33. U.S. National Library of Medicine. National Institutes of Health. Detailed indexing statistics: 1965-2014. 2015. Available from: https://www.nlm.nih.gov/bsd/index_stats_comp.html. Accessed March 11 2016.
34. Wahab IA, Pratt NL, Kalisch LM, Roughead EE. Comparing time to adverse drug reaction signals in a spontaneous database and a claims database: a case study of rofecoxib-induced myocardial infarction and rosiglitazone-induced heart failure signals in Australia. Drug Saf. 2014;37: 53-64. doi: 10.1007/s40264-013-0124-9
35. Kubota K. Symmetry analysis for monitoring safety of newly marketed drugs. Pharmacoepidemiol Drug Saf. 2016;25: 349-351. doi: 10.1002/pds.3886
36. Thacker EL, Schneeweiss S. Initiation of acetylcholinesterase inhibitors and complications of chronic airways disorders in elderly patients. Drug Saf. 2006; 29:1077-1085.

C H A P T E R 9

General discussion


General Discussion
185
9
GENERAL DISCUSSIONThe objective of this thesis was to provide a comprehensive profile about the effectiveness and safety of some drugs commonly used by COPD patients, based on a range of pharmacoepidemiological studies. In the first part of this thesis, we evaluated the effects of several antibiotics for the prevention and treatment of acute exacerbations of COPD (AECOPD), and the potential for drug-drug-interactions (DDIs) during antibiotic therapeutic management. We conducted a systematic review and meta-analysis to provide a benefit-risk profile of prophylactic antibiotics for AECOPD. The influence of the drug schedule (continuous vs intermittent) and treatment duration of prophylactic antibiotics (<=6 months vs > 6months) on clinical outcomes were also explored (Chapter 2). The effects of doxycycline in addition to oral corticosteroids in AECOPD and possible influence of age were explored in Chapter 3. To further reduce the influence of possible unmeasured confounding bias as potentially present in Chapter 3, a cohort study with complete information on COPD clinical diagnosis and lung function was conducted to explore the effects of therapy with any or a specific first-line antibiotic in AECOPD (Chapter 4). Considering the frequent occurrence of polypharmacy in COPD drug management, we presented a systematic DDI review focused on frequently used antibiotics among COPD patients to optimize drug treatment (Chapter 5). In the second part of this thesis, we assessed the neuropsychiatric safety of varenicline for smoking cessation in a real-world setting. Using a traditional cohort study, we especially explored the neuropsychiatric safety in COPD patients and those with previous psychiatric disorders as these are high-risk populations for psychiatric events (Chapter 6). Since conventional cohort studies may be vulnerable to potential for confounding bias, we further explored the neuropsychiatric safety of varenicline by use of a self-controlled study design, called Prescription Sequence Symmetry Analysis (PSSA, Chapter 7). Finally, we performed a systematic review comparing the effect estimates between PSSA and traditional parallel group studies with correlation analysis, agreement and discrepancy analysis (Chapter 8).
Antibiotics in management of COPD exacerbations
As respiratory bacterial infection is a major risk factor of COPD exacerbations,1,2 antibiotics can be part of the drug management of COPD according to recent guidelines.3 However, these recommendations are based on a limited body of evidence from randomized controlled trials (RCTs) and lack of consistent results from studies in a real-world setting. Therefore, we conducted four separate scientific studies to provide more evidence for the optimal use of antibiotics among COPD patients.
Effects of antibiotics for preventive use
In Chapter 2, we conducted a systematic review to evaluate all possible beneficial and side effects of prophylactic antibiotics in stable COPD patients. Pooled results from
Chapter 9
186
twelve RCTs showed that the frequency of AECOPD and the number of patients with AECOPD were significantly reduced, independent of the drug schedule (continuous vs intermittent) and duration of treatment (<=6 months vs >6 months). However, when we examined specific antibiotics, we could only confirm the superiority of macrolides in preventing exacerbations of COPD and erythromycin and azithromycin appeared the most effective, a finding which is in line with clinical recommendations.4,5 Previous research suggested properties of anti-inflammation and immune-modulation by macrolides,6,7 however, this was not supported by findings from our review, where we observed changes in neither bacterial load nor airway inflammation. Despite the direct beneficial effects of prophylactic antibiotics regarding the reduction of exacerbations, the patients’ quality of life was only improved by longer use (> 6 months) of prophylactic antibiotics. There were no differences in the rate of hospitalization, adverse events and the time to next exacerbation between patients with prophylactic antibiotics and those on placebo.
Of note, antibiotic resistance problems always come along with antibiotic use, especially for macrolides, for which the review data showed an increase in resistance.8 Weighing benefits and risks of prophylactic antibiotic therapy, the long and continuous use of such therapy should be advised carefully, and it should be used preferably by the high-risk patient population who are at risk for development of severe infections such as patients who are older, with high-risk comorbidities and with higher frequency of exacerbations in the previous year, and those with more severe AECOPD.
Effects of antibiotics for therapeutic use
According to the GOLD guideline, amino-penicillin with clavulanic acid, macrolide, or tetracycline antibiotics are recommended as the initial empirical choice of antibiotic treatment for AECOPD.3 In the Netherlands, according to the Dutch primary care guideline, doxycycline or amoxicillin are recommended as the first choice in AECOPD treatment.9 These recommendations were basically based on results of RCTs. Real-world evidence from observational studies is valuable to evaluate the applicability of the findings from RCTs for the real-world setting, and these were presented in chapter 3 and 4.
In chapter 3, we conducted a cohort study including the outpatient population from the University of Groningen’s prescription database IADB.nl, to explore the real-world effects of doxycycline for AECOPD and the influence of age. We found a 23% reduced risk of treatment failure by doxycycline in addition to systemic corticosteroids among COPD outpatients aged 75 years and older; a finding consistent with results from few previous RCTs about doxycycline for AECOPD among outpatients.10 However, in younger patients with COPD, we did not find any difference between additional antibiotic use and oral corticosteroids use only, which is consistent with our hypothesis that older people may
General Discussion
187
9
benefit more from antibiotics due to their susceptibility to bacterial infections and inflammations. The fact that the natural lung function, the natural defense mechanism and mucocilliary clearance are reduced with increasing age is also in line with this hypothesis.11-13
However, due to a lack of detailed clinical diagnostic information, the identification of COPD and other comorbidities in the study reported in chapter 3 were based on drug prescriptions as proxies for these diseases, which may have biased the results. Moreover, important baseline information on GOLD stages of severity of airway limitations in COPD and smoking history was also absent, though these are vital risk factors for the prognosis of AECOPD and this may have led to unmeasured confounding.3 Accordingly, in Chapter 4, we further explored the effects of both any antibiotic and some specific antibiotics in the treatment of AECOPD among outpatients based on the “PharmLines Initiative”, which linked extensive clinical information from both the Lifelines Cohort Study and drug information from the IADB.nl prescription database. Within the Lifelines Cohort information on clinical diagnosis of almost all possible chronic diseases and information on parameters of physical examinations like spirometry of lung function is obtained on a regular basis.14 Largely in line with with findings in chapter 3, overall the prescription of any antibiotic was associated with a statistically significant reduction of treatment failure of AECOPD. Similar trends towards protective effects were also observed for the specific antibiotics doxycycline, co-amoxiclav, and macrolides, separately, except for amoxicillin which was associated with no effect. The doxycycline treatment was even associated with a statistically significant 47% reduced risk of treatment failure of AECOPD, after adjustments in both conventional logistic regression and propensity score analysis. Indeed, in Chapter 4, information about the actual severity of the presented first AECOPD according to signs and symptoms at diagnosis was absent. However, we believe that antibiotics will most likely be given to more severe AECOPD, which may have biased our result towards a null finding. Further, severe exacerbations that resulted in hospitalizations were not included, but we believe that in an outpatient setting the chance of such severe cases is low.
Although previously two observational studies indicated long-term benefits from short use of antibiotics for next exacerbations,15,16 we did not observe this in both Chapter 3 and Chapter 4. A long-term effect is also doubtful given the fact that re-infections are not substantially affected by a short-course of antibiotics. Our results about the absence of long-term effects of antibiotic treatment are in line with findings from a more recent RCT reported by van Velzen et al. in 2017.10
Management of DDIs in AECOPD
In chapter 3 and 4, it has been shown that antibiotics play a vital role in the management of patients with AECOPD. However, in COPD patients many comorbidities like

Chapter 9
188
cardiovascular disease, diabetes, and lung cancer coexist.17 These comorbidities may contribute to polypharmacy and result in potential DDIs when antibiotics are prescribed simultaneously.
In chapter 5, based on the causal evidence from clinical trials and observational studies with a control group, we found that many drugs interact with commonly used antibiotics in the treatment of COPD. Some co-administered drugs can alter the pharmacokinetics of antibiotics, while other antibiotics can also interfere with the pharmacokinetics of co-administered drugs. DDIs may result in treatment failures of disease or lead to adverse events. For example, clarithromycin as inhibitor of CYP3A4 can increase the risk of hypoglycemia among diabetes patients by inhibition of the metabolic enzymes of related anti-diabetic drugs (e.g. glipizide, glyburide), which are substrates of CYP3A4.
We presented details of potential clinical significant DDIs with moderate to strong levels of interaction in this review according to highly prevalent comorbidities, and such information may be used to improve the sensitivity and specificity of drug-drug interaction alert systems. Importantly, it may help physicians to improve the prescription of antibiotics to COPD patients with comorbidities.
Varenicline intervention for smoking cessation
Pharmaceutical smoking cessation treatment (PSCT) is an important intervention for tobacco smoking. Varenicline as first-line drug of PSCTs has been proven effective for smoking cessation.18 However, concerns about neuropsychiatric adverse events (NPAEs) were raised since the spontaneous reports about such events and the related warning from the FDA.19 Due to strict selection criteria for participants in RCTs, high-risk populations of smokers like those with COPD and psychiatric disorders were usually excluded which hinders making conclusions for a real-world setting.
Neuropsychiatric safety of varenicline for smoking cessation
In chapter 6, the association between varenicline use and major NPAEs was explored among general and COPD patients with or without psychiatric disorder. However, we did not observed a significant association between varenicline use and the occurrence of any NPAE in high-risk populations and the general population. Although COPD patients are considered more susceptible for possible adverse drug reactions (ADEs), in our study we did not observe an increased risk of any NPAE among COPD patients using varenicline in the psychiatric and non-psychiatric cohorts. This finding was consistent with the findings from two earlier studies.20,21
When we examined specific NPAEs, we observed a significantly reduced risk of anxiety among varenicline users in those with psychiatric disorders compared with NRTs users, which may be due to the combined effects of reduced withdrawal-related symptoms

General Discussion
189
9
and raised level of positive affect on mood due to varenicline treatment for smoking cessation. As varenicline users have higher abstinence rates and successful quitting rates than NRT users, quitting of smoking is associated with recovery in psychiatric status for smokers.22
Of note, although the NPAEs observed in earlier studies were defined in different ways, the incidence rates of specific NPAEs related to depression, anxiety and insomnia defined by the occurrence of prescriptions of related drugs in our study were similar to these reports.23 Much higher rates of NPAEs were observed in the specific high-risk population with psychiatric disorders in this study, which was also consistent with previous reports.24,25
Role of PSSA in drug safety evaluations
To overcome the limitations of traditional cohort studies regarding the control of confounding in chapter 6, we conducted a PSSA study described in chapter 7 using the same IADB.nl prescription database. PSSA has been increasingly used for detecting adverse events of medication. Due to its self-controlled study design, the PSSA design may control genetic and other time-invariant confounding effectively.
Consistent with results from chapter 6, results in chapter 7 also showed that varenicline was not associated with increased risks for depression or anxiety. However, it was associated with a small significant, but transient, increase in sleep disorders, which was a well-known side effect of varenicline from RCTs and other previous studies.23,26 However, it is difficult to identify whether sleeping problems are due to side effects of PSCTs or related to withdrawal from nicotine as difficulty falling asleep and increased number of awakenings are also common symptoms of nicotine withdrawal.27
Of note, most observational studies (e.g. the cohort study described in chapter 6) used NRT as the reference group to explore the risk of NPAEs associated with varenicline to make sure the baseline characteristics of study subjects in the comparison groups are more similar. In the PSSA all patients used varenicline and only the sequence orders of prescriptions of varenicline and marker drugs for NPAEs were compared due to its self-controlled design. The difference in outcomes between study designs may be due to either missing a transient risk in the cohort study or by the absence of a reference group in the PSSA.
Although we found consistent findings in Chapter 6 and 7, the validity and constraints of the PSSA study design regarding the effect estimate of drug use are never compared with conventional observational parallel group study designs (e.g. cohort, case-control), which has already been proven to be an effective design to obtain causal evidence from real-world data.
Chapter 9
190
Therefore, in chapter 8, we compared the effect estimates from two study designs, by systematically searching for publications that explored the effects of the same drug use by applying both of these study designs. Based on the correlation analysis, agreement and discrepancy analysis, this review indicated that the effect estimates generated by the PSSA are usually lower than the effect estimates generated by parallel group designs, and PSSA usually has a lower power than the conventional study designs. However, these results should be interpreted with caution, as the effect estimates were only retrieved from two separate studies. More comparisons are needed to confirm our conclusion.
FUTURE PERSPECTIVESAlthough prophylactic antibiotics, especially macrolides, were shown to be effective for preventing exacerbations of COPD in chapter 2, the optimal regimen of antibiotics regarding dose, duration and schedule has not been well established yet, and such treatment is still far from more personalized therapy. For the long and continuous use of antibiotics, it is still an issue how to balance its advantages towards COPD exacerbations and the development of antibacterial resistance in both the individual and the community. It is wise for clinical practitioners to limit their prescription to high-risk populations in order to reduce unnecessary bacterial resistance. Better understanding of the yet unclear mechanisms behind macrolides preventing exacerbations could help develop targeted treatment for AECOPD in the future.
Regarding the antibiotic treatment for ongoing AECOPD, related guidelines were basically depend on the evidence from RCTs.3,28 However, in reality, it is more complicated to make decisions about antibiotic use considering the heterogeneous characteristics in outpatients and various factors that may influence the final treatment outcome. The tendency towards beneficial effects of antibiotics in the elderly COPD patients shown in chapter 3 may offer clues for clinicians and researchers to use antibiotics in more targeted populations by considering age. A personalized specific antibiotic treatment could further improve the therapeutic effects in AECOPD, but such evidence is currently lacking.
Of note, antibiotics were not always properly prescribed in line with the guidelines.29,30 Some antibiotics could have been used in AECOPD without actual bacterial infection. Hence, the beneficial effects as reported in chapter 4 may underestimate the true effects in bacterially confirmed AECOPD. In the future, how to improve the appropriate personalized use of antibiotics is a problem that needs to be studied. From a pragmatic perspective, clinicians may reduce unnecessary antibiotic therapy for AECOPD by using sputum color as a predictor of potentially pathogenic bacterial infection in practice.3 A procalcitonin-guided algorithm or C-reactive protein (CPR) test can also be considered,

General Discussion
191
9
if applicable, as a way to better instruct antibiotic use.31 However, both application and accuracy of bacterial tests come with limitations for the outpatient setting, and more practical tests should be developed.
Consistent with the Dutch primary guideline,9 the findings in chapter 4 confirmed the beneficial effect of doxycycline treatment for AECOPD among outpatients. However, no definite conclusion can be drawn for other antibiotics from this study. Considering the variability between GP practices in the prescriptions of antibiotics to patients with AECOPD,32 larger studies of high quality with extensive control for confounding by indication are needed to confirm and support their role in the management of AECOPD. Notably, the final antibiotic choice for AECOPD treatment should always consider the local bacterial resistance patterns and possibility of resistant pathogens by performing culture of sputum especially among high risk patients with frequent exacerbations and severe airflow limitations.3
Chapter 5 showed that there is a variety of clinically significant DDIs between antibiotics and a wide range of drugs that are used to treat related comorbidities in COPD. Clinicians should pay attention to these drug interactions when prescribing antibiotics by assessing the present comorbidities and polypharmacy of patients to ensure therapeutic effect and reduce the possibility of adverse effects. However, the evidence base for clinical adverse outcomes due to DDIs is still weak, and warrants further study in larger cohorts.
Based on previous evidence and the results from our studies in both cohort and PSSA study design in chapter 6 and 7, varenicline is safe to use for smoking cessation among general and COPD populations. Although there was no increased risk of NPAEs by varenicline compared with NRTs among patients with psychiatric disorders, considering the relatively high rate of NPAEs in smokers with psychiatric disorders, these patients should be instructed carefully. Notably, sleeping disorder is a well-recorded and common adverse event of varenicline, especially in the first three to six months after varenicline initiation. Although sleep disorders do not belong to the “severe” adverse events, it could influence the uptake and adherence of varenicline. As a result, it may finally result in the failure of smoking cessation. However, up to now, it is still not clear whether sleep disorders are caused by varenicline itself or are more related to withdrawal of nicotine. The distinction between these causes is important for pharmacists and clinicians to take appropriate actions to improve compliance and adherence of varenicline use.
Based on the findings from chapter 8, the lack of a wider variety of comparisons between PSSA and parallel group designs that cover more topics make it difficult to make definite conclusions about the validity of PSSA in establishing associations between drug use and related events. Thus, more studies that explore the association between drug use and adverse events by using both of these study designs based on

Chapter 9
192
the same database or populations are needed. Ideally, comparisons with high-quality pragmatic trials with similar populations, exposure and outcomes could help to specify the validity of the PSSA design even better.
CONCLUSIONIn the first part of this thesis, we confirmed the beneficial effects of antibiotics both in the prevention and treatment of AECOPD. Macrolides should be prescribed as the first-line antibiotic to prevent recurrence of exacerbations and doxycycline appeared the best choice for preventing treatment failure of a current exacerbation. Those with a higher risk of bacterial infections such as older patients among COPD outpatients benefit the most and personalizing therapy for these patients may possibly reduce the development of antibiotic resistance. Considering the polypharmacy among COPD patients, clinicians should pay attention to related DDIs while prescribing antibiotics to avoid treatment failure or adverse events. In the second part of our thesis, neither traditional cohort nor prescription sequence symmetry analysis showed a potential neuropsychiatric risk of varenicline use for smoking cessation among general and COPD patients. Attention should be given to patients with psychiatric disorders. The PSSA design has shown significant promise in detecting related drug adverse events, however, due to the limited available comparisons between PSSA and other traditional studies, it is still necessary to test its validity by comparisons with parallel controlled studies and clinical trials.
General Discussion
193
9
REFERENCES
1. Sethi S, Murphy TF. Infection in the pathogenesis and course of chronic obstructive pulmonary disease. N Engl J Med. 2008;359(22):2355-2365.
2. Moghoofei M, Azimzadeh Jamalkandi S, Moein M, Salimian J, Ahmadi A. Bacterial infections in acute exacerbation of chronic obstructive pulmonary disease: a systematic review and meta-analysis. Infection. 2019.
3. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease: 2020 Report. https://goldcopd.org/gold-reports/. Date last accessed: December 17, 2019.
4. Ni WT, Shao XD, Cai XJ, et al. Prophylactic Use of Macrolide Antibiotics for the Prevention of Chronic Obstructive Pulmonary Disease Exacerbation: A Meta-Analysis. Plos One. 2015;10(3).
5. Wedzicha JA, Calverley PMA, Albert RK, et al. Prevention of COPD exacerbations: a European Respiratory Society/American Thoracic Society guideline. Eur Respir J. 2017;50(3).
6. Rubin BK. Immunomodulatory properties of macrolides: overview and historical perspective. Am J Med. 2004;117 Suppl 9A:2S-4S.
7. Martinez FJ, Curtis JL, Albert R. Role of macrolide therapy in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2008;3(3):331-350.
8. Serisier DJ. Risks of population antimicrobial resistance associated with chronic macrolide use for inflammatory airway diseases. Lancet Resp Med. 2013;1(3):262-274.
9. Snoeck-Stroband JB, Schermer TRJ, Van Schayck CP, et al. NHG-Werkgroep Astma bij volwassenen en COPD. NHG-Standaard COPD (derde herziening). Huisarts Wet 2015; 58(4):198-211.
10. van Velzen P, Ter Riet G, Bresser P, et al. Doxycycline for outpatient-treated acute exacerbations of COPD: a randomised double-blind placebo-controlled trial. Lancet Respir Med. 2017;5(6):492-499.
11. Brandsma CA, de Vries M, Costa R, Woldhuis RR, Konigshoff M, Timens W. Lung ageing and COPD: is there a role for ageing in abnormal tissue repair? Eur Respir Rev. 2017;26(146).
12. Lopez-Otin C, Blasco MA, Partridge L, Serrano M, Kroemer G. The Hallmarks of Aging. Cell. 2013;153(6):1194-1217.
13. Wilkinson TMA, Aris E, Bourne SC, et al. Drivers of year-to-year variation in exacerbation frequency of COPD: analysis of the AERIS cohort. ERJ Open Res. 2019;5(1).
14. Scholtens S, Smidt N, Swertz MA, et al. Cohort Profile: LifeLines, a three-generation cohort study and biobank. Int J Epidemiol. 2015;44(4):1172-1180.
15. Roede BM, Bresser P, Prins JM, Schellevis F, Verheij TJM, Bindels PJE. Reduced risk of next exacerbation and mortality associated with antibiotic use in COPD. Eur Respir J. 2009;33(2):282-288.
16. Roede BM, Bresser P, Bindels PJE, et al. Antibiotic treatment is associated with reduced risk of a subsequent exacerbation in obstructive lung disease: an historical population based cohort study. Thorax. 2008;63(11):968-973.
17. Chetty U, McLean G, Morrison D, Agur K, Guthrie B, Mercer SW. Chronic obstructive pulmonary disease and comorbidities: a large cross-sectional study in primary care. Br J Gen Pract. 2017;67(658):e321-e328.
18. Anthenelli RM, Benowitz NL, West R, et al. Neuropsychiatric safety and efficacy of varenicline, bupropion, and nicotine patch in smokers with and without psychiatric disorders (EAGLES): a double-blind, randomised, placebo-controlled clinical trial. Lancet. 2016;387(10037):2507-2520.
19. US Food and Drug Administration. Public health advisory: FDA requires new boxed warnings for the smoking cessation drugs Chantix and Zyban. http://wayback.archive-it.org/7993/20170112005513/http://www.fda.gov/Drugs/DrugSafety/Postmarket Drug Safety Information for Patients and Providers/
Chapter 9
194
ucm169988.htm. Published July 1, 2009. Accessed June 7, 2019.
20. Kotz D, Viechtbauer W, Simpson CR, van Schayck OCP, West R, Sheikh A. Cardiovascular and neuropsychiatric risks of varenicline and bupropion in smokers with chronic obstructive pulmonary disease. Thorax. 2017;72(10):905-911.
21. Tashkin DP, Rennard S, Hays JT, Ma W, Lawrence D, Lee TC. Effects of Varenicline on Smoking Cessation in Patients With Mild to Moderate COPD A Randomized Controlled Trial. Chest. 2011;139(3):591-599.
22. Taylor G, McNeill A, Girling A, Farley A, Lindson-Hawley N, Aveyard P. Change in mental health after smoking cessation: systematic review and meta-analysis. BMJ. 2014;348:g1151.
23. Thomas KH, Martin RM, Knipe DW, Higgins JP, Gunnell D. Risk of neuropsychiatric adverse events associated with varenicline: systematic review and meta-analysis. BMJ. 2015;350:h1109.
24. Kanner AM, Wuu J, Faught E, et al. A past psychiatric history may be a risk factor for topiramate-related psychiatric and cognitive adverse events. Epilepsy Behav. 2003;4(5):548-552.
25. Nanni RC, Troisi A. Maternal attachment style and psychiatric history as independent predictors of mood symptoms in the immediate postpartum period. J Affect Disorders. 2017;212:73-77.
26. Kasliwal R, Wilton LV, Shakir SAW. Safety and Drug Utilization Profile of Varenicline as
Used in General Practice in England Interim Results from a Prescription-Event Monitoring Study. Drug Safety. 2009;32(6):499-507.
27. Ashare RL, Lerman C, Tyndale RF, et al. Sleep Disturbance During Smoking Cessation: Withdrawal or Side Effect of Treatment? J Smok Cessat. 2017;12(2):63-70.
28. Wedzicha JAEC-C, Miravitlles M, Hurst JR, et al. Management of COPD exacerbations: a European Respiratory Society/American Thoracic Society guideline. Eur Respir J. 2017;49(3).
29. Bathoorn E, Groenhof F, Hendrix R, et al. Real-life data on antibiotic prescription and sputum culture diagnostics in acute exacerbations of COPD in primary care. Int J Chron Obstruct Pulmon Dis. 2017;12:285-290.
30. Roede BM, Bindels PJ, Brouwer HJ, Bresser P, de Borgie CA, Prins JM. Antibiotics and steroids for exacerbations of COPD in primary care: compliance with Dutch guidelines. Br J Gen Pract. 2006;56(530):662-665.
31. Butler CC, Gillespie D, White P, et al. C-Reactive Protein Testing to Guide Antibiotic Prescribing for COPD Exacerbations. N Engl J Med. 2019;381(2):111-120.
32. Boggon R, Hubbard R, Smeeth L, et al. Variability of antibiotic prescribing in patients with chronic obstructive pulmonary disease exacerbations: a cohort study. BMC Pulm Med. 2013;13:32.


C H A P T E R1 0
C H A P T E R1 0 Summary
Samenvatting
Acknowledgement
List of publication
About the author


Summary
199
10
SUMMARYChronic obstructive pulmonary disease (COPD) is a very common chronic progressive disease that affects millions of middle-aged and older smokers. COPD patients frequently suffer from exacerbations (worsening of their respiratory symptoms). As bacterial infection is the primary trigger of exacerbations, antibiotics can be given to those patients with potential infections. However, the effects of antibiotics on COPD exacerbations in both treatment and prevention have not been consistently reported and are especially unclear in real-world settings. Smoking is an important risk factor for COPD. Stopping smoking, especially by means of pharmaceutical treatment with varenicline, is a vital intervention to improve the quality of life and reduce smoking-related disease among COPD patients. However, concerns about varenicline’s neuropsychiatric safety for patients still exist due to conflicting evidence obtained from randomized controlled trials and case-report systems. It is necessary to evaluate the risk of the neuropsychiatric adverse events (NPAEs) due to varenicline by studies based on a large observational database.
The aim of the first part of this thesis was to evaluate the effectiveness of antibiotic use to treat COPD exacerbations and explore the potential drug-drug interactions (DDIs) related to antibiotics use among COPD patients. The results from a systematic review described in Chapter 2 show that prophylactic antibiotics are effective in preventing COPD exacerbations and improve the quality of life of stable COPD patients. Concerning the effects of antibiotics treatment for COPD exacerbations, however, the cohort study based on the prescription database described in Chapter 3 shows that the short-term benefits of doxycycline in addition to oral corticosteroids are only observed in COPD patients of advanced age. No long-term benefits were observed. Clinicians should take the patients’ age into consideration when prescribing antibiotics to patients with acute exacerbation of COPD (AECOPD). Another cohort study, described in Chapter 4 and concerning clinically diagnosed COPD, confirmed the short-term protective effects of doxycycline use with AECOPD. However, the treatment effects of other antibiotics in real-world settings are still unclear and need to be explored further in more extensive research. In general practice, physicians may prescribe antibiotics erroneously or improperly, which may underestimate the real-world effects of antibiotic use on AECOPD. In addition, since comorbidities and polypharmacy are common among COPD patients, associated DDIs– of which there are many and which are summarized in a systematic review described in Chapter 5 – may also influence the effects of antibiotics by directly altering their pharmacokinetics or by indirectly influencing patient compliance due to adverse drug reactions (ADRs) due to DDIs.
The second part of this thesis focused on the neuropsychiatric safety of varenicline to aid smoking cessation among patients in general and COPD patients in particular.

Chapter 10
200
The findings from a cohort study described in Chapter 6 do not indicate an increased risk of NPAEs associated with varenicline in either the general or the COPD population, irrespective of the psychiatric status of the patients. Considering the limitation for controlling of time-invariant confounders in traditional observational research, Chapter 7 reports a self-controlled study of a prescription sequence symmetry analysis (PSSA) to explore the varenicline’s risk of NPAEs further. The PSSA results also confirm the neuropsychiatric safety of varenicline use. Remarkably, a transient increased risk of varenicline-induced sleep disorder was observed, which clinicians should take into account to reduce its influence on the adherence of patients taking varenicline. In the last chapter of the thesis, the effect estimate of the PSSA was compared with parallel group study designs, showing that the effects estimated by the PSSA may be lower than those in the parallel group study designs. However, since only two studies were included, more comparisons are necessary to draw solid conclusions.
In this thesis, we confirm the beneficial effects of prophylactic antibiotic use to prevent COPD exacerbations. However, the antibiotic treatment effects on AECOPD were only seen with doxycycline. Although other antibiotics also showed benefits, these were not statistically significant and need be investigated further. We confirm the safety of varenicline use for smoking cessation, varenicline as an effective treatment should be used widely to reduce the burden of smoking-related diseases. However, patients with neuropsychiatric disease in their history must be monitored closely considering their higher risk of NPAEs. Since the PSSA is an effective tool for identifying ADRs, it could be applied more widely to better evaluate the effectiveness and safety of medications. Other study designs and methodologies should be explored to achieve better control of related confounders in observational studies based on real-world data.

Samenvatting
201
10
SAMENVATTING Chronic Obstructive Pulmonary Disease, oftewel COPD, is een veelvoorkomende chronische en progressieve ziekte waar miljoenen rokers op middelbare en hogere leeftijd last van krijgen. COPD-patiënten lijden regelmatig aan exacerbaties (verergering van hun ademhalingsklachten). Omdat bacteriële infecties vaak de hoofdoorzaak zijn van exacerbaties, kunnen antibiotica toegediend worden bij patiënten met potentiële infecties. De effecten van antibiotica op COPD exacerbaties bij zowel behandeling als preventie zijn echter niet nauwkeurig geschat en zijn met name onduidelijk in de praktijk. Roken is een belangrijke risicofactor voor COPD. Stoppen met roken, vooral met behulp van farmaceutische behandeling met varenicline, is een essentiële ingreep om de kwaliteit van leven te verbeteren en om ziektes die verband houden met roken te verminderen bij COPD-patiënten. Echter, bezorgdheid om de neuropsychiatrische veiligheid van varenicline voor de patiënten blijft bestaan door tegenstrijdig bewijs dat voortkomt uit randomized controlled trials en case-reports. Het is van belang om het risico op neuropsychiatrische bijwerkingen bij vareniclinegebruik te evalueren met behulp van grootschalige observationele databases.
Het doel van het eerste deel van deze thesis is het evalueren van de effectiviteit van antibiotica voor de behandeling van COPD-exacerbaties, en om de potentiële interacties tussen geneesmiddelen (drug-drug interactions ofwel DDI’s) in relatie tot antibioticagebruik bij COPD-patiënten te onderzoeken. De resultaten van een systematisch onderzoek in hoofdstuk 2 laten zien dat profylactische antibiotica effectief zijn in het voorkomen van COPD-exacerbaties en de kwaliteit van leven bij stabiele COPD-patiënten kan verbeteren. We kijken verder naar van de effecten van antibioticabehandelingen tijdens COPD-exacerbaties in hoofdstuk 3 met behulp van een cohort onderzoek dat gebaseerd is op een prescriptie-database. Dit onderzoek toont aan dat naast het gebruik van orale corticosteroïden de voordelen van doxycycline op korte termijn alleen zichtbaar zijn bij COPD-patiënten op hogere leeftijd. Er werden geen voordelen op de lange termijn gevonden. Clinici zouden daarom de leeftijd van de patiënten in acht moeten nemen als zij antibiotica voorschrijven aan patiënten met acute exacerbatie van COPD (AECOPD). Een vervolgstudie met klinisch gediagnostiseerde COPD, beschreven in hoofdstuk 4, bevestigt dat er kortdurende beschermende effecten van doxycyclinegebruik bij AECOPD zijn. De effecten van andere antibiotica in de praktijk zijn echter nog steeds onduidelijk en moeten nader onderzocht worden in een uitgebreider onderzoek. In het dagelijks leven kan het voorkomen dat artsen antibiotica onterecht of onjuist voorschrijven, wat ervoor kan zorgen dat de effecten van antibiotica op AECOPD in de praktijk onderschat worden. Daar komt nog bij dat comorbiditeiten en polyfarmacie gebruikelijk zijn bij COPD-patiënten. Daardoor kunnen geassocieerde DDI’s – die in groten getale voorkomen en zijn samengevat in een systematisch overzicht in hoofdstuk 5 – ook invloed hebben
Samenvatting

202
Chapter 10
op de effecten van antibiotica door directe veranderingen te induceren in hun farmacokinetiek of door het indirect beïnvloeden van de therapietrouw van patiënten door bijwerkingen ten gevolge van de DDI.
Het tweede gedeelte van deze scriptie focust op de neuropsychiatrische veiligheid van varenicline als geneesmiddel om patiënten te helpen stoppen met roken, met name bij COPD-patiënten. De bevindingen van een cohortstudie, zoals beschreven in hoofdstuk 6, tonen niet aan dat er een verhoogd risico van NPAE’s geassocieerd is met varenicline in zowel de algemene als de COPD-populatie, ongeacht wat hun psychiatrische status is. In hoofdstuk 7 houden we rekening met zogenaamde tijd ongebonden verstorende factoren (confounding) die in traditioneel observatieonderzoek kunnen optreden. Hiertoe pasten we de zogenaamde prescription sequence symmetry analysis (PSSA) toe om het risico op neuropsychiatrische bijwerkingen van varenicline verder te onderzoeken. De PSSA-resultaten bevestigen ook de neuropsychiatrische veiligheid van vareniclinegebruik. Opmerkelijk is dat een kortstondig verhoogd risico op slaapstoornis werd gerapporteerd bij vareniciline gebruik, waar clinici rekening mee zouden moeten houden om de invloed van varenicline op de therapietrouw van de patiënten te verminderen. In het laatste hoofdstuk van deze scriptie wordt het geschatte effect van de PSSA vergeleken met een parallelgroep-studie, die aantoont dat de geschatte effecten bij de PSSA lager zouden kunnen zijn dan die in de parallelgroep-studie. Maar omdat dit slechts twee onderzoeken omvat, zijn er meer vergelijkingen nodig om betrouwbare conclusies te trekken.
In deze scriptie bevestigen we de positieve effecten van profylactisch antibioticagebruik om COPD-exacerbaties te voorkomen. Echter, de effecten van de antibioticabehandelingen op AECOPD kwamen alleen voor bij doxycycline. Hoewel andere antibiotica ook voordelen toonden, waren deze resultaten niet statistisch significant en zullen daarom verder onderzocht moeten worden. We bevestigen de veiligheid van vareniclinegebruik voor het stoppen met roken, en varenicline als een effectieve behandeling zou veelal ingezet moeten worden om de last van ziektes die met roken verband houden te verminderen. Desalniettemin moeten patiënten met een verleden van neuropsychiatrische aandoeningen nauwlettend in de gaten gehouden worden omdat bij hen een hoger risico van neuropsychiatrische bijwerkingen bestaat. Omdat de PSSA een effectief hulpmiddel is om bijwerkingen te identificeren, zou deze techniek ook wijder verbreid toegepast kunnen worden om de effectiviteit en veiligheid van medicatie beter te kunnen inschatten. Andere methodologieën moeten onderzocht worden om betere beheersing te hebben over de verstorende factoren (confounders) in observationele onderzoeken gebaseerd op data uit de praktijk.

Acknowledgement
204
ACKNOWLEDGEMENTI am very excited at this moment to defend my PhD degree after four years of study at the University of Groningen. Since 2007, I have been studying in the field of Public Health for approximately twelve years, when I was so young and had never imagined to go so far towards reaching my dream as being an epidemiologist and an academic researcher. What surprised me most is that I met my Mr. Right and had my adorable son during my PhD study in the Netherlands. I am so grateful for all wonderful things that happened to me and I know that I could not achieve these without the kind help and support from many people, whom I would like to thank sincerely.
First and foremost, I would like to express my deepest gratitude to my supervisor Prof. Eelko Hak. Dear Eelko, thank you for providing me the great opportunity to study in your fantastic group. You always give the continuous support for my studies and life during my PhD trajectory. Although the research did not go smoothly at the beginning of my research, your patience and guidance with professional knowledge helped me to continue the projects in the right direction. For me, you are not only an easy-going supervisor, but also a good friend. Thanks for visiting my family after my son was born and I also enjoyed visiting your family members together with our colleagues in Giethoorn, which is a beautiful memory for me.
In addition, I would like to express my sincere gratitude to my second supervisor Prof. H. Marike Boezen. Dear Marike, thank you very much for your valuable suggestions and discussions on my projects, especially in the vital stage of organizing my thesis. You dedicated lots of time revising my chapters, even when it was close to the Christmas holiday. Through the discussion in our regular meetings, I got lots of insightful comments and encouragement. I benefited a lot from your professional feedback and points of view.
Many thanks also go to my assessment committee members: Prof. T.J.M. Verheij, Prof. J. van der Palen and Prof. Y. Stienstra for taking valuable time in reading and assessing my thesis.
I would like to thank my co-authors Prof. Bob Willffert, Dr. C.C.M.(Nynke) Schuiling-veninga, Mr. Jens. H.J. Bos from our department and Dr. Job J.M.D. van Boven, Dr. Jan-willem C. Alffenaar, Prof. Rolf H.H. Groenwold from other institutes, who gave me enormous support to finish my projects listed in my thesis. Dear Bob, thank you for lots of support at the beginning of my PhD study and good feedback. As co-author, you always provided detailed revisions to improve my manuscripts. Dear Nynke, I’m very grateful for your help in the stage of protocol writing and study design by providing professional suggestions about drug prescriptions. Dear Jens, thank you for your continuous technical support in working with the prescription database. I have learned

Acknowledgement
205
10
a lot from you about SQL-coding. Dear Job, you always show passion in research and are glad to offer any help that you could. I am really grateful for the help about calculation of null-effect sequence ratio in PSSA project, which speeded up the completion of that project. Dear Jan-willem, you really offered many valuable suggestions, based on your research background, in the projects on antibiotic use for COPD exacerbations. Dear Rolf, thank you so much for your statistical support in the PharmLines project. You always offered detailed explanations for our questions, I learned a lot from you.
Special thanks also to prof. W.J. (Wim) Quax. Dear Wim, thank you for introducing me to the pharmacoepidemiological research at the University of Groningen in November 2014 in Beijing. I still remember that morning when we met each other at the PhD workshop. Without the informal but sweet conversation, my story in Groningen would not have happened.
I would like to show gratitude here to my MS supervisor at the Peking University, Prof. dr. Aiguo Ren. Your previous support made it possible for me to pursue my PhD study abroad. In fact, your words that “Do not label yourself” gave me much courage to explore the possibility of myself in the academic field. You always show respect and understanding to me, even though I have left our institute for several years. Each contact with you makes me feel warm and full of strength.
I also would like to give my gratitude to my colleagues in the department of PharmcoTherapy, -Epidemiology & Economics (PTEE). Dear Jannie, Anja and Felicia, thank you for dealing with all kinds of things for conferences, Dutch translation and more during my PhD study. Dear Bert and Jugo, thank you for solving all the problems related to my computer and software. Dear Sylvi, Akbar and Ivan, as officemates, your encouragement and support means a lot to me, I will never forget the joyful moments we shared together in the past four years. Dear Jurjen (My paranymph), Heleen, Linda, Eva, Pieter, Christiaan, Simon and Thea, as typical Dutch, you are so kind and nice to offer any help during my stay in Groningen. I really enjoyed the time that we spent together. Dear Sofa, Ira, Taichi, Fajri, Abrham, Monik, Tia, Lusi, Afifah, yunyu and all other members in PTEE, I have many beautiful memories of all of you. I benefited from our regular meetings and PhD workshop to discuss projects and exchange ideas.
Next, I would like to acknowledge the master students I supervised in the PTEE group: Victor, Tanja, Demy, Anouk and Yingxuan. You are very smart students and I learned a lot by routine discussions with you about the details of our projects. Victor, thank you so much for helping me preparing the protocol forms for the PharmLines project during my maternity leave. Without your help, I could not finish that project smoothly.
I have met many fantastic Chinese friends during my PhD study in Groningen, they are the precious possessions in my life. Dear Qi, I am so happy for you that you got

Acknowledgement
206
a new wonderful job in MSD and found your true love Jia. Without you, I would not have met the wonderful friends that I would like to thank below. Dear Jun, thank you for introducing me to my Mr. Right and helping me know him well. Dear Jiacong, Xiaohong, you are the friends that I could always share with freely and safely, the trip together with you in Gran Canaria is really a wonderful memory. Dear Haoxiao & Bing, Yi & Ting, Yingruo & Qihui, Tiantian & Siqi, Jiaying & Jing, Baojie & Xiaodong, Yifei & Yihui, Changsen & Yingying, Yuanyuan (Shen) & Yanji, Jingjing & Yuanze, Qingkai & Mengmeng, Wangli & Jianjun, Jiapan & Chenyu, Beibei & Jiawen, Ping & Yegang, Rui & Robert and Ying’s family, you are the fantastic couples that I have met and you helped me to understand how to support each other in the marriage that is full of love and understanding. I will not forget the wonderful times that we spent together while enjoying dinners and sharing our stories. Dear Xiaoming, Huatang, Yanan, Zhenchen (& Shilin), Hongyan, Shuai, Cong and Jing (Wu) thank you for the nice meals and especially the kind help offered in my first half year in Groningen, I really had a wonderful time with you. Dear Yanni (my paranymph), , Xiaojing, Fangfang, Si, Jing (Li), Yizhou, Keni, Huala, Yehan, Yichen, Yuzhen, Mingming, Kai, Bin (UMCG) & Lin, Bin (Zernike), Haigen, Chao, Hao, Chengtao, Jielin, Surigula, Chan, Jing (Du), Tian (Xie), Qingqing (Cai), Qing (Chen), Lianhong, Cancan & Shixian, Lianmin, Yuntao, Yihui and all other friends that I forgot to mention here, I am so lucky to know you in this wonderful place. It is really amazing that we shared our lives and dreams together and helped each other to overcome difficulties here thousands miles away from our home. I could not appreciate it more. Wish you all a bright future.
Besides, I also got lots of support from my friends far away from Groningen for my PhD. Dear Pei Qin in China, We have known each other for twelve years and faced difficulties in our life together. I really miss the time we spent together during our bachelor and master study. Wish your daughter Ruoxi grows up happily and will have a wonderful friendship in her future. Dear You Li in UK, thank you for your kind help offering all the possible positions for me, you are really smart and kind person, wish you have more achievements in the field of Public Health. Dear Xue Li in UK, thanks for your kind help on the way of my study, especially for sharing me the PhD workshop in Beijing 2014, where I had a chance by surprise with a better choice of my PhD study. Looking forward to seeing your lovely baby. Dear Helen (Ying He) in UK, thank you for your encouragement and support all the time, you are the girl with passion and dreams always. I learned a lot from you.
I would like to thank the China Scholarship Committee (CSC) for offering the funding for my PhD study, I am lucky to benefit from the fast development of China. China is now experiencing a fight towards the novel coronavirus (2019-nCoV). I wish the 2019-nCoV will be controlled early and the Public Health System in China will be getting better and better.
Acknowledgement
207
10
Finally, I would like to give my great gratitude to my parents, Guoyin and Fengli. Dear dad and mom, thank you for your love and support all the time. In my last year of my PhD, you even take a long trip from China to the Netherlands to help me get over difficulties in my life. You are the best friends and teachers in my life, I love you. Dear brother Yuanpeng, thank you for taking care of our parents when I study abroad, I know it is a little hard for you this year, there are always ups and downs in life, but you will definitely embrace a bright future in another way. I am grateful for my parents-in-law, thank you for your love and understanding, although we have not yet known each other well. But through your son, I know where the bright sides of him come from. Wish you be healthy and happy in Jinan. Particularly, I would like to express my gratitude to my deeply loved husband, Liqiang. Meeting you is the most unexpected surprise for me in The Netherlands. We have so much differences in many aspects, but these help me to see the beautiful world in other ways and make my life complete. Thank you for your understanding, support and encouragement all the time. My lovely son, Youran, I love you so much, you are my sunshine, bringing me lots of happiness and helping me to understand love deeper and comprehensively, I really enjoy reading books with you every night. Wish you could grow up happily just like your name.
Finishing the PhD is the end of my education, but it is also a new beginning of my academic career. Knowledge is infinite. I really enjoy exploring and swimming in the sea of knowledge. I may have lots of regret and lost times in my past, but I will hold it tightly in my future to pursue my dreams without any regret.
Yuanyuan Wang February 2020
Groningen
List of publications
208
LIST OF PUBLICATIONSYuanyuan Wang, Tanja R. Zijp, Muh. Akbar Bahar, Janwillem W.H. Kocks, Bob Wilffert, Eelko Hak. Effects of prophylactic antibiotics on patients with stable COPD: a systematic review and meta-analysis of randomized controlled trials. Journal of Antimicrobial Chemotherapy. 2018 Dec 1; 73(12): 3231-3243.
Yuanyuan Wang, Muh. Akbar Bahar, Anouk M.E. Jansen, Janwillem W.H. Kocks, Jan-Willem C. Alffenaar, Eelko Hak, Bob Wilffert, Sander D. Borgsteede. Improving antibacterial prescribing safety in the management of COPD exacerbations: systematic review of observational and clinical studies on potential drug interactions associated with frequently prescribed antibacterials among COPD patients. Journal of Antimicrobial Chemotherapy. 2019 Oct 1; 74(10):2848-2864.
Yuanyuan Wang, Jens H. Bos, H. Marike Boezen, Jan-Willem C. Alffenaar, Job F.M. van Boven, Catharina C.M. Schuiling-Veninga, Bob Wilffert, Eelko Hak. The influence of age on real-life effects of doxycycline for acute exacerbations among COPD outpatients: a population-based cohort study. BMJ Open Respiratory Research. 2020 Feb; 7(1). pii: e000535. doi: 10.1136/bmjresp-2019-000535.
Yuanyuan Wang, Jens H. Bos, Catharina C.M. Schuiling-Veninga, Job F.M. van Boven, Bob Wilffert, Eelko Hak. Neuropsychiatric safety of varenicline in the general and COPD population with and without psychiatric disorders: a retrospective inception cohort study in a real-world setting. European Addiction Research. Submitted on 2020 Jan 27. (Under review)
Yuanyuan Wang, Job F.M. van Boven, Jens H. Bos, Catharina C.M. Schuiling-Veninga, H. Marike Boezen, Eelko Hak. Risk of Neuropsychiatric Adverse Events Associated with Varenicline Treatment for Smoking Cessation in Outpatients: A prescription Sequence Symmetry Analysis. Drug Safety. Submitted on 2020 Feb 4. (Under review)
Yuanyuan Wang, Yingxuan Feng, H. Marike Boezen, Bob Wilffert, Eelko Hak. Pharmaceutical Smoking Cessation Treatment and Risk of Neuropsychiatric Adverse Events: A Systematic Review of Evidence from Observational Studies. (In submission)
Yuanyuan Wang, Victor Pera, Jens H. Bos, H. Marike Boezen, Jan-Willem C. Alffenaar, Bob Wilffert, Rolf H.H. Groenwold, Hans Wouters, Marco Grzegorczyk, Eelko Hak. Real-world short- and long-term effects of antibiotic therapy on acute exacerbations of COPD in outpatients: a cohort study under the PharmLines Initiative jointed database. (In submission)
Muh. Akbar Bahar, Yuanyuan Wang, Jens H. Bos, Bob Wilffert, Eelko Hak. Discontinuation and dose adjustment of metoprolol after metoprolol-paroxetine/fluoxetine co-
List of publications
209
10
prescription in Dutch elderly. Pharmacoepidemiology and Drug Safety. 2018 Jun; 27(6):621-629.
Demy L. Idema, Yuanyuan Wang, Michael Biehl, Peter L. Horvatovich, Eelko Hak. Effect estimate comparison between the prescription sequence symmetry analysis (PSSA) and parallel group study designs: A systematic review. PloS One. 2018 Dec 6; 13(12): e0208389.
Before Groningen
Shanshan Lin, Aiguo Ren, Linlin Wang, Yun Huang, Yuanyuan Wang, Caiyun Wang, Nicholas Greene. Oxidative stress and apoptosis in benzo[a]pyrene-induced neural tube defects. Free Radical Biology and Medicine. 2018 Feb 20; 116: 149-158.
Yuanyuan Wang, Lei Jin, Jufen Liu, Yali Zhang, Zhiwen Li, Aiguo Ren. Autopsy findings of 95 cases of neural tube defects and a comparison with clinical reports. Chinese Journal of Reproductive Health. 2015, 26(3): 207-210. (In Chinese)
International Conference
Yuanyuan Wang, Jens H. Bos, Catharina C.M. Schuiling-Veninga, et al. The effects of amoxicillin on acute COPD exacerbations in the outpatient setting: a retrospective cohort study based on real-world data. Poster session presented in 35th International Conference of Pharmacoepidemiology and Therapeutic Risk Management (ICPE), August 24-28, 2019. Philadelphia, Pennsylvania, US.
Yuanyuan Wang, Jens H. Bos, Catharina C.M. Schuiling-Veninga, et al. Real-world data on the effect of doxycycline plus prednisone/prednisolone on COPD exacerbations compared with prednisone/prednisolone alone: a retrospective cohort study among COPD outpatients. Poster session presented in 34th International Conference of Pharmarcoepidemiolgy and Therapeutic Risk Management (ICPE). August 22-26. 2018. Prague, Czech Republic.
Yuanyuan Wang, Tanja Zijp, Muh Akbar Bahar, et al. The clinical effect of prophylactic antibiotics on COPD patients: an updated systematic review and meta-analysis. Poster session presented in 33rd International Conference of Pharmarcoepidemiolgy and Therapeutic Risk Management (ICPE). August 26-30. 2017. Montreal, Canada.
Yuanyuan Wang, Anouk M.E. Jansen, Sander D. Borgsteede, et al. Drug-drug interactions and clinical significance of frequently prescribed antibiotics for treating exacerbations in COPD patients with other co-administered agents: a systematic review. Poster session presented in 33rd International Conference of Pharmarcoepidemiolgy and Therapeutic Risk Management (ICPE). August 26-30. 2017. Montreal, Canada.

List of publications
210
Yuanyuan Wang, Anouk J.M. Jansen, Jens Bos, Eelko Hak. Drug interactions as a potential instrumental variable: the example of effectiveness of antibiotic therapy in exacerbated COPD patients. Poster session presented in 32nd International Conference of Pharmarcoepidemiolgy and Therapeutic Risk Management (ICPE). August 25-28. 2016. Dublin, Ireland.

About the author
211
10
ABOUT THE AUTHORYuanyuan Wang was born on February 15th, 1988 in Henan, China. She studied Preventive Medicine at the School of Public Heath for five years in Zhengzhou University, and obtained her Bachelor of Medicine degree in July 2012. Meanwhile, she was awarded another degree of Bachelor of Arts from Zhengzhou University due to her personal interest and study of the English literature. After that, she continued her master studies in the School of Public Health at the Peking University and achieved the degree of Master of Public Health with a research direction in Reproductive Epidemiology in July 2015. During her master programme, she established her research interest in the field of Epidemiology. In October of the same year, she then came to the Netherlands to pursue her PhD studies in the department of PharmacoTherapy, -Epidemiology and –Economics (PTEE) at the Groningen Research Institute of Pharmacy (GRIP) of the University of Groningen under the primary supervision of Prof. dr. Eelko Hak. Her doctoral research focused on the effectiveness and safety of medications used in COPD patients, which as described in this thesis.
ABOUT THE AUTHOR
Yuanyuan Wang was born on February 15th, 1988 in Henan, China. She
studied Preventive Medicine at the School of Public Heath in
Zhengzhou University, and obtained her Bachelor of Medicine degree in
July 2012. Meanwhile, she was awarded another degree of Bachelor of Arts
from Zhengzhou University due to her personal interest and study of the
English literature. After that, she continued her master studies in the
School of Public Health at the Peking University and achieved the degree
of Master of Public Health with a research direction in Reproductive Epidemiology in July 2015.
During her master programme, she established her research interest in the field of Epidemiology. In
October of the same year, she then came to the Netherlands to pursue her PhD studies in the
department of PharmacoTherapy, -Epidemiology and –Economics (PTEE) at the Groningen Research
Institute of Pharmacy (GRIP) of the University of Groningen under the primary supervision of Prof. dr.
Eelko Hak. Her doctoral research focused on the effectiveness and safety of medications used in
COPD patients, which as described in this thesis.




















