
Ultrasonic parathyroid localisation in previously operated patients
6
ClinicalRadiology (1984) 35, 113-118 © 1984 Royal College of Radiologists 000%9260/84/0255113 $02.00 Ultrasonic Parathyroid Localisation in Previously Operated Patients ADRIAN G. KRUDY, THOMAS H. SHAWKER, JOHN L. DOPPMAN, KLARA HORVATH, PHILIP D. SCHNEIDER*, JEFFREY A. NORTON*, STEPHEN J. MARX? and ALLEN M. SPIEGELt Diagnostic Radiology Department, The Clinical Center, *Surgery Branch, National Cancer Institute, and ?Metabolic Diseases Branch, National Institute of Arthritis, Diabetes, and Digestive and Kidney Diseases, National Institutes of Health, Bethesda, Maryland, USA Sixty-two patients with hyperparathyroidism and failed prior neck surgery were examined by ultrasound before reoperation to localise abnormally enlarged glands. If mediastinal lesions are excluded, a total of 57 glands >5mm in size were removed from 48 patients. Ultrasound demonstrated only 18 of these for a true positive rate of 32%. There were 39/57 (68%) false negatives. In addition, there were 16 false positives. In our experience, the detection rate of ultrasound for enlarged parathyroid glands in patients with failed surgery is significantly less than that reported in previously unoperated patients (73%), or in the limited number of reported cases of patients with previous operations (75%). Our high false negative rate is probably partially due to the large number of posteriorly located small glands which cannot be adequately visualised by ultrasound. Nevertheless, because of its non-invasive nature, low cost and ready availability, ultrasound should be utilised as an initial screening procedure in patients with failed previous surgery. Several recent reports have described the successful detection by ultrasound of enlarged parathyroid glands in patients with hyperparathyroidism without previous surgery (Sample et al., 1978; Edis and Evans, 1979; Duffy et al., 1980; Scheible et al., 1981; Simeone et al., 1981; Reading et al., 1982) (Table 1). The sensitivity in this group varied from 70% to 100%, with an overall mean sensitivity of 73 %. The experience in patients with hyperparathyroidism and prior failed surgery is more limited (Table 2). Surprisingly, a few authors (Simeone et al., 1981; Reading et al., 1982) have claimed a higher detection rate in this particular group, although the Address for reprints: Dr Adrian G. Krudy, Diagnostic Radiology Department, Bldg 10, Rm 6S211, NIH, The Clinical Center, Bethesda, Maryland 20205, USA. overall average detection rate (75%) is not significantly different from that in non-operated patients. In this report we describe our experience with ultrasound in tocalising enlarged parathyroid glands in 62 patients with hyperparathyroidism and previous failed neck surgery. PATIENTS AND METHODS Sixty-two patients (38 females, 24 males, age 17-76 years) were evaluated. All patients had clinically and biochemically confirmed hyperparathyroidism and had had at least one prior cervical surgical procedure for parathyroid exploration. Patients who had prior neck surgery for thyroid disease alone were not included. Most of the patients were evaluated using a 5MHz real-time (ATL Mode 600 B Mark II) and a 5 MHz static B-mode scanner (Searle Pho-Sonic, Siemens Medical Systems). More recently, the patients were also examined using a Diasonics 7.5 MHz real-time small parts unit. Scanning was performed with multiple closely spaced transverse and sagittal static B-scans or con- tinuous visualisation in the transverse and sagittal planes with real-time. No water bag was utilised. Sixty-one patients were re-explored and the surgical findings were compared with the lesions seen on ultrasound. One patient had a mediastinal gland detected by arteriogra- phy and confirmed by a fall in serum calcium after contrast staining. RESULTS As described in the previous literature (Sample et al.,1978; Edis and Evans, 1979; Duffy et al., 1980; Scheible et al., 1981; Simeone et al., 1981; Reading et al., Table 1 - Reported sensitivity of ultrasound in the detection of enlarged parathyroid glands in patients not previously operated Authors Year Type of unitS; No. of abnormal Ultrasound glands true positive Sample et al. 1978 5 MHz B 21§ 19/21 (90%) Edis and Evans 1979 10 MHz RT 8 8/8 (100%) Duffy et al. 1980 5 MHz B 23 19/23 (83%) Scheible et al. 1981 10 MHz RT 14 10/14 (71%) Simeone et al. 1981 10 MHz RT 40 31/40 (77%) Reading et al. 1982 10 MHz RT 163 110/163 (70%) Totals 269 197/269 (73%) SB = B-mode static scanner; RT = real-time. § Data from this report unclear but four previously operated patients were four assumed to have one gland each.
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Ultrasonic parathyroid localisation in previously operated patients

ClinicalRadiology (1984) 35, 113-118 © 1984 Royal College of Radiologists
000%9260/84/0255113 $02.00
Ultrasonic Parathyroid Localisation in Previously Operated Patients ADRIAN G. KRUDY, THOMAS H. SHAWKER, JOHN L. DOPPMAN, KLARA HORVATH, PHILIP D. SCHNEIDER*, JEFFREY A. NORTON*, STEPHEN J. MARX? and ALLEN M. SPIEGELt
Diagnostic Radiology Department, The Clinical Center, *Surgery Branch, National Cancer Institute, and ?Metabolic Diseases Branch, National Institute of Arthritis, Diabetes, and Digestive and Kidney Diseases, National Institutes of Health, Bethesda, Maryland, USA
Sixty-two patients with hyperparathyroidism and failed prior neck surgery were examined by ultrasound before reoperation to localise abnormally enlarged glands. If mediastinal lesions are excluded, a total of 57 glands > 5 m m in size were removed from 48 patients. Ultrasound demonstrated only 18 of these for a true positive rate of 32%. There were 39/57 (68%) false negatives. In addition, there were 16 false positives. In our experience, the detection rate of ultrasound for enlarged parathyroid glands in patients with failed surgery is significantly less than that reported in previously unoperated patients (73%), or in the limited number of reported cases of patients with previous operations (75%). Our high false negative rate is probably partially due to the large number of posteriorly located small glands which cannot be adequately visualised by ultrasound. Nevertheless, because of its non-invasive nature, low cost and ready availability, ultrasound should be utilised as an initial screening procedure in patients with failed previous surgery.
Several recent reports have described the successful detection by ultrasound of enlarged parathyroid glands in patients with hyperparathyroidism without previous surgery (Sample et al., 1978; Edis and Evans, 1979; Duffy et al., 1980; Scheible et al., 1981; Simeone et al., 1981; Reading et al., 1982) (Table 1). The sensitivity in this group varied from 70% to 100%, with an overall mean sensitivity of 73 %. The experience in patients with hyperparathyroidism and prior failed surgery is more limited (Table 2). Surprisingly, a few authors (Simeone et al., 1981; Reading et al., 1982) have claimed a higher detection rate in this particular group, although the
Address for reprints: Dr Adrian G. Krudy, Diagnostic Radiology Department, Bldg 10, Rm 6S211, NIH, The Clinical Center, Bethesda, Maryland 20205, USA.
overall average detection rate (75%) is not significantly different from that in non-operated patients.
In this report we describe our experience with ultrasound in tocalising enlarged parathyroid glands in 62 patients with hyperparathyroidism and previous failed neck surgery.
PATIENTS AND METHODS
Sixty-two patients (38 females, 24 males, age 17-76 years) were evaluated. All patients had clinically and biochemically confirmed hyperparathyroidism and had had at least one prior cervical surgical procedure for parathyroid exploration. Patients who had prior neck surgery for thyroid disease alone were not included. Most of the patients were evaluated using a 5MHz real-time (ATL Mode 600 B Mark II) and a 5 MHz static B-mode scanner (Searle Pho-Sonic, Siemens Medical Systems). More recently, the patients were also examined using a Diasonics 7.5 MHz real-time small parts unit. Scanning was performed with multiple closely spaced transverse and sagittal static B-scans or con- tinuous visualisation in the transverse and sagittal planes with real-time. No water bag was utilised. Sixty-one patients were re-explored and the surgical findings were compared with the lesions seen on ultrasound. One patient had a mediastinal gland detected by arteriogra- phy and confirmed by a fall in serum calcium after contrast staining.
RESULTS
As described in the previous literature (Sample et al.,1978; Edis and Evans, 1979; Duffy et al., 1980; Scheible et al., 1981; Simeone et al., 1981; Reading et al.,
Table 1 - Reported sensitivity of ultrasound in the detection of enlarged parathyroid glands in patients not previously operated
Authors Year Type o f unitS; No. o f abnormal Ultrasound glands true positive
Sample et al. 1978 5 MHz B 21§ 19/21 (90%) Edis and Evans 1979 10 MHz RT 8 8/8 (100%) Duffy et al. 1980 5 MHz B 23 19/23 (83%) Scheible et al. 1981 10 MHz RT 14 10/14 (71%) Simeone et al. 1981 10 MHz RT 40 31/40 (77%) Reading et al. 1982 10 MHz RT 163 110/163 (70%)
Totals 269 197/269 (73%)
SB = B-mode static scanner; RT = real-time. § Data from this report unclear but four previously operated patients were four assumed to have one gland each.
114 CLINICAL RADIOLOGY
Table 2 - Reported sensitivity of ultrasound in the detection of enlarged parathyroid glands in patients previously operated
Authors Year Type of unit* No. of abnormal glands
Ultrasound true positive
Sample et al. 1978 5 MHz B 4? Edis and Evans 1979 10 MHz RT 2 Simeone et al. 1981 10 MHz RT 45 Reading et al. 1982 10 MHz RT 20§
Totals 30
2/4 (50%) 2/2 (100%) 4/4 (100%)
16/20 (80%)
24/30 (75%)
*B = B-mode static scanner; RT = real-time. ? Total glands not stated in article but assumed to be four glands in four patients. $ Excluding mediastinal glands. § Includes five patients with prior thyroid surgery.
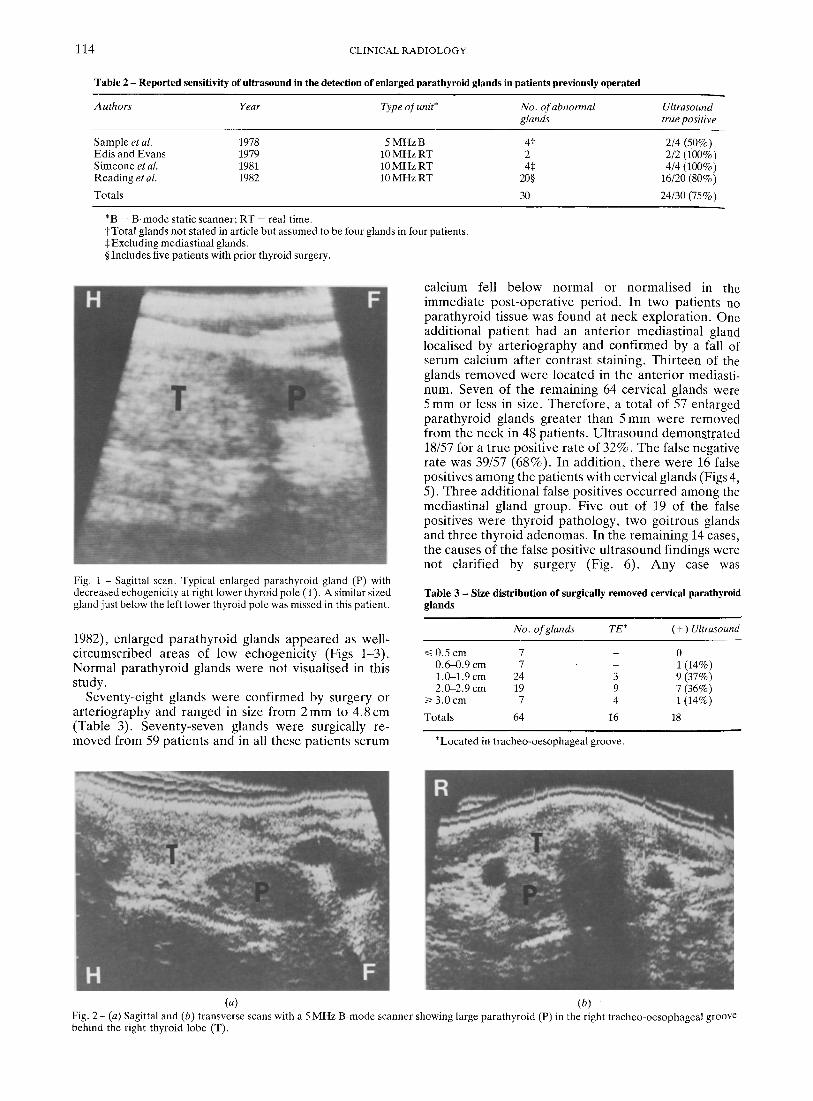
Fig. 1 - Sagittal scan. Typical enlarged parathyroid gland (P) with decreased echogenicity at right lower thyroid pole (T). A similar sized gland just below the left lower thyroid pole was missed in this patient.
calcium fell be low no rma l or n o r m a l i s e d in the i m m e d i a t e p o s t - o p e r a t i v e pe r iod . In two pa t ien t s no p a r a t h y r o i d t issue was found at neck exp lo ra t ion . One addi t iona l pa t i en t had an an te r io r med ias t ina l gland local ised by a r t e r i o g r a p h y and con f i rmed by a fall of se rum calc ium af te r con t ras t s taining. Th i r t een of the glands r e m o v e d were l oca t ed in the an t e r io r medias t i - num. Seven of t he r ema in ing 64 cervical glands were 5 m m or less in size. The re fo r e , a to ta l of 57 enlarged p a r a t h y r o i d g lands g rea te r than 5 m m were r emoved f rom the neck in 48 pa t ien ts . U l t r a s o u n d d e m o n s t r a t e d 18/57 for a t rue pos i t ive ra te of 32%. T h e false negat ive ra te was 39/57 (68%) . In add i t ion , t he re were 16 false posi t ives a m o n g the pa t ien ts wi th cervical g lands (Figs 4, 5). Th ree add i t i ona l false pos i t ives occu r r ed among the med ias t ina l g land group. F ive out of 19 of the false posi t ives were t hy ro id pa tho logy , two goi t rous glands and th ree t hy ro id a d e n o m a s . In the r ema in ing 14 cases, the causes of the false pos i t ive u l t r a sound f indings were not c lar i f ied by surgery (Fig. 6). A n y case was
Table 3 - Size distribution of surgically removed cervical parathyroid glands
1982), en la rged p a r a t h y r o i d g lands a p p e a r e d as well- c i rcumscr ibed a reas of low echogen ic i ty (Figs 1-3). N o r m a l p a r a t h y r o i d glands were not v isual ised in this s tudy.
Seventy-e igh t g lands were con f i rmed by surgery or a r t e r iog raphy and r anged in size f rom 2 m m to 4 . 8 c m (Table 3). Seven ty - seven glands were surgical ly re- m o v e d f rom 59 pa t i en t s and in all these pa t i en t s s e rum
No. o f glands TE* (+) Ultrasound
~< 0.5 cm 7 - 0 0.6-0.9 cm 7 - 1 (14%) 1.0-1.9 cm 24 3 9 (37%) 2.0-2.9 cm 19 9 7 (36%)
/> 3.0 cm 7 4 1 (14%)
Totals 64 16 18
*Located in tracheo-oesophageal groove.
(a) (b) Fig. 2 - (a) Sagittal and (b) transverse scans with a 5 MHz B-mode scanner showing large parathyroid (P) in the right tracheo-oesophageal groove behind the right thyroid lobe (T).

ULTRASONIC PARATHYROID LOCALISATION 115
(a) (b)
Fig. 3 - (a) Sag ittal and (b) transverse scans showing a typical posteriorly located enlarged parathyroid gland (P). Carotid artery (C) and thyroid (T).
considered a false positive where a lesion consistent with parathyroid was described by ultrasound and was surgically accounted for by non-parathyroid tissue or was not elucidated and parathyroid was removed from another site, accompanied by a post-operative fall in serum calcium.
Fourteen glands were found in the anterior mediasti- num. Thirteen were demonstrated by operation and one by a fall in the calcium on staining with contrast material. Two patients had both cervical and mediastinal glands and in neither ~of these were the cervical glands detected. Of the remaining 12 mediastinal glands, eight patients were called negative by ultrasound and could be
classified as true negatives. A total of eight patients had multiple cervical glands greater than 5 mm in size. In only one case was more than one gland correctly identified, indicating a poor detection rate (16%) for hyperplasia.
Of the 57 cervical parathyroid glands greater than 5mm, 16 (28%) were located in the tracheo- oesophageal groove of the posterior mediastinum. Only three out of 16 (19%) were detected. Of the other glands less than l cm in size, only one (0.7cm) gland was detected. One 1.5 cm gland in the left carotid sheath was not visualised in spite of the foreknowledge of the exact location by arteriographic localisation.
(a) (b) Fig. 4. - Potential false positive. Sagittal scan (a) shows structure of cystic appearance at lower pole of right thyroid (T), Slightly lateral scan (b) shows this to be a tortuous innominate artery in this older patient. Enlarged parathyroid gland (P) is now visible at right superior thyroid pole.

116 CLINICAL RADIOLOGY
Fig. 5 - False positive study. Sagittal scan of right lobe of thyroid showing thyroid gland of irregular consistency with two low-echogenic lesions (arrowheads) at upper and lower thyroid pole. Calcification (arrow) with shadowing is also noted. At surgery two thyroid adenomas were found in a goitrous gland on the right. An enlarged parathyroid was removed on the left but was not found by ultrasound.
(a)
Fig. 6 - False positive study. Sagittal view of right thyroid lobe (T) with a small area of decreased echogenicity (arrow) in the right lobe. Abnormal parathyroid gland (not seen by ultrasound) was removed from low left neck and calcium reverted to normal. Surgical confirmation of this lesion is not available but this is presumed to be a small thyroid cyst.
(b)
Fig. 7 - False negative study. (a) CT showing enlarged par~ithyroid gland (arrow) in typical location in the right tracheo-oesophageal groove, partly behind the trachea. (b) Parathyroid is not visualised on transverse ultrasound due to tracheal shadowing (TS). Carotid artery (c).
DISCUSSION
The detection rate (32%) for abnormal parathyroid glands in this series of previously operated patients is considerably less than that (50-100%) reported by others in either non-operated or previously operated patients (Tables 1, 2). Experience with previously operated patients, however, is limited and no large series other than the present one has appeared in the literature.
A partial explanation for this difference is probably the location of parathyroid glands in these two groups of patients. In non-operated patients abnormal parathyr- oid glands are most often in close proximity to the thyroid gland (Wang, 1976). In a previously operated group, the most common site of an overlooked
parathyroid gland is in the posterior superior mediasti- num, in the tracheo-oesophageal groove or adjacent to the oesophagus (Brennan etal . , 1978; Wang, 1977). This region is not well visualised by ultrasound due to the shadowing by the trachea and the oesophagus and, in our experience, even larger glands can escape detection, especially when they extend behind the trachea or the oesophagus. Reading et al. (1982) also reported difficulty in visualising glands in this location. We have been unable to visualise some glands in this region, even knowing their location beforehand by computed tomography (CT) or angiography (Fig. 7). Techniques such as angling the transducer or attempts to displace the trachea manually have not been successful. In this series, approximately 16 out of 50 (32%) glands greater than 1.0 cm were in this location and only three out of 16 (19%) of these were seen by ultrasound.

ULTRASONIC PARATHYROID LOCALISATION 117
Fig. 8 - Intrathyroidal parathyroid gland shown by ultrasound. Sagittal scan showing abnormal parathyroid (P) at right lower thyroid (T) pole with surrounding rim of thyroid tissue. At surgery, parathyroid was completely within the right thyroid lobe.
The detection of glands smaller than i cm (maximal dimension) was also quite poor and one out of 14 (7%) was seen. Reading et al. (1982) found the detection of glands less than 200mg considerably less successful (35%) than those weighing more than 1000mg (95%). The fact that tissue planes had been interrupted, and that partial or total thyroid lobectomies had been performed in this group of patients, almost certainly contributed significantly to the poorer visualisation of glands. Parathyroids in other ectopic locations were also poorly seen. Two glands (0.4 and 2.0cm) in a high ectopic location near the hyoid bone were also not seen. Considerable artefact is caused by the hyoid bone and by air shadowing in this region.
Intrathyroidal parathyroid glands are a rare, but important, cause of failed operation (Spiegel et al., 1975; Bainbridge and Barnes, 1982). Of the three intrathyroidal glands in this series, one normal-sized gland was not seen but a 1.8 and 0.7cm gland were detected (Fig. 8). The detection of multiple enlarged glands was also poor, similar to the experience of Simeone et al. (1981) and only one out of eight glands (16%) in cases of multiglandular enlargement was demonstrated ultrasonographically. This indicates a poor differentiation of hyperplasia from single gland adenoma.
The specificity for this series was not estimated for several reasons. First, the false negative rate was very high (68%) which rendered the predictive value of the negative examination useless. Second, although other authors (Simeone et al., 1981; Reading et al., 1982) have calculated specificity by assuming four glands as the denominator in unoperated patients we feel that this figure is misleading and often is of no practical clinical value. For example, in a series of hyperparathyroid patients with a single abnormal gland each, if all abnormal glands were missed a specificity of 75% could still be claimed, yet the examinations are 100% worthless from a clinical standpoint. In this series, due to
the high incidence of false negatives, abnormal para- thyroid tissue cannot be excluded from the neck by a negative examination. Furthermore, in patients with a single positive gland shown by ultrasound, lack of visualisation of other glands doe~ not exclude multi- glandular disease.
While it can be argued that another reason for our poor results is the fact that higher frequency (10 MHz) equipment was not used, we do not think this is the entire answer. Although the resolution for millimetre- sized objects would improve with a 10 MHz as against a 5 MHz or 7.5 MHz transducer, the penetration would decrease. Since many of the glands that were missed were actually in a posterior location, a high-frequency transducer would not be of more help in this area. Probably more important than an inability to visualise an abnormal gland based on resolution was an ability to visualise it due to lack of tissue contrast. With prior surgery, partial or total lobectomies, the anatomically normal thyroid is no longer present to contrast with adjacent enlarged glands. Post-operative areas of fibrosis, shift in vascular structures and skin scarring not only make actual visualisation of abnormal glands difficult but cause difficulty in identifying a parathyroid gland. It is probable that in many of these cases the gland was visible but could not be distinguished from post-surgical changes.
A significant number of false positive studies (16 cases) was encountered in patients with cervical glands and three additional false positives were noted in the mediastinal group. The cause of these in most cases could not be determined from the operative report. In five out of 19 cases some type of thyroid pathology (adenoma, three cases; colloid goitre, two cases) was noted.
In spite of our experience demonstrating the low sensitivity of ultrasound for abnormal parathyroid glands in previously operated patients, we still strongly recommend the ultrasonic examination of such patients. The method is inexpensive and non-invasive and any additional yield in these difficult-to-manage patients is highly beneficial. In addition, the ultrasound examina- tion is complementary to both angiography and CT of the neck. Ultrasound is most accurate in showing glands that are either adjacent to the thyroid or intrathyroidal, areas which both CT and angiography have more difficulty in demonstrating. Conversely, CT more readily detects parathyroid glands that lie in the posterior superior mediastinum (Doppman et al., 1982). Angiography and digital arteriography can define more easily lesions which are not obscured by the adjacent thyroid stain.
We have been evaluating recently the use of fine-needle aspiration of parathyroid glands (Doppman et al., 1983). Our initial experience indicates that cervical glands can be definitively identified as para- thyroid tissue in aspirate by measuring high concentra- tions of parathyroid hormone. Although our prelimin- ary work was carried out under CT guidance, needle aspiration can also be performed using real-time ultrasonic guidance.
In summary, our series indicates that ultrasound in previously operated patients appears to be less sensitive in localising abnormal glands than has been reported in unoperated cases but is, nevertheless, potentially

118 CLINICAL RADIOLOGY
helpful and should be per formed . We remain uncon- vinced of the necessity for any local isat ion studies pr ior to initial surgery, which cures 90-95% of all pat ients . Al though ul t rasonic local isat ion in this group can be very successful, exper ienced surgeons a re .unconv inced of its usefulness (Van H e e r d e n et al., 1982).
REFERENCES
Bainbridge, E. T. & Barnes, A. D. (1982). Primary hyperparathyroid- ism due to overactive intrathyroid parathyroid glands: a potential cause of failed exploration. British Journal of Surgery, 69,200-202.
Brennan, M. F., Doppman, J. L., Marx, S. J., Spiegel, A. M., Brown, E. M. & Aurbach, G. D. (1978). Reoperative parathyroid surgery for persistent hyperparathyroidism. Surgery, 83, 669-676.
Doppman, J. L., Krudy, A. G., Brennan, M. F., Schneider, P., Lasker, R. D. & Marx, S. J. (1982). CT appearance of enlarged parathyroid glands in the posterior superior mediastinum. Journal of Computer Assisted Tomography, 6, 1099-1102.
Doppman, J. L., Krudy, A. G., Marx, S. J., Saxe, A., Schneider, P., Norton, J., Spiegel, A. M., Downs, R., Schaaf, M., Brennan, M. F. & Aurbach, G. (1983). Aspiration of enlarged parathyroid glands for parathyroid hormone assay. Radiology, 148, 31-35.
Duffy, P., Picker, R. H., Duffield, S., Reeve, T. & Hewlet, S. (1980). Parathyroid sonography: a useful aid to preoperative localization. Journal of Clinical Ultrasound, 8, 113-116.
Edis, A. J. • Evans, T. C. (1979). High-resolution, real-time ultrasonography in the preoperative location of parathyroid tumours: pilot study. New England Journal of Medicine, 301, 532-534.
Reading, C. C., Charboneau, J. W., James, E. M., Karsell, P. R., Purnell, D. C., Grant, C. S. & van Heerden, J. A. (1982). High-resolution parathyroid sonography. American Journal of Roentgenology, 139, 539-546.
Sample, F. W., Mitchell, S. P. & Bledsoe, R. C. (1978). Parathyroid ultrasonography. Radiology, 127, 485-490.
Scheible, W., Deutsch, A. L. & Leopold, G. R. (1981). Parathyroid adenoma: accuracy of preoperative localization by high-resolution real-time sonography. Journal of Clinical Ultrasound, 9, 325-330.
Simeone, J. F., Mueller, P. R., Ferrucci, J. T., van Sonnenberg, E., Wang, C. A., Hall, D. A. & Wittenburg, J. (1981). Real-time sonography of the parathyroid. Radiology, 141,745-751.
Spiegel, A. M., Marx, S. J., Doppman, J. L., Beazley, R. M., Ketcham, A. S,, Kasten, B. & Aurbach, G. D. (1975). Intrathyroid parathyroid adenoma or hyperplasia. An occasionally overlooked cause of surgical failure in primary hyperparathyroid- ism. Journal of the American Medical Association, 234, 1029-1033.
Van Heerden, J. A., James, E. M., Karsell, P. R., Charboneau, J. W., Grant, C. S. & Purnell, D. C. (1982). Small-part ultrasonography in primary hyperparathyroidism. Annals of Surgery, 195, 774.
Wang, C. A. (1976). The anatomic basis of parathyroid surgery. Annals of Surgery, 183, 271-275.
Wang, C. A. (1977). Parathyroid re-exploration: a clinical and pathological study of 112 cases. Annals" of Surgery, 186, 140-145.




















