Ultrasonic-activated micellar drug delivery for cancer treatment
17
REVIEWS Ultrasonic-Activated Micellar Drug Delivery for Cancer Treatment GHALEB A. HUSSEINI, 1,2 WILLIAM G. PITT 2 1 Chemical Engineering Department, American University of Sharjah, Sharjah, United Arab Emirates 2 Department of Chemical Engineering, Brigham Young University, Provo, Utah 84602 Received 11 November 2007; revised 21 February 2008; accepted 3 April 2008 Published online 27 May 2008 in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/jps.21444 ABSTRACT: The use of nanoparticles and ultrasound in medicine continues to evolve. Great strides have been made in the areas of producing micelles, nanoemulsions, and solid nanoparticles that can be used in drug delivery. An effective nanocarrier allows for the delivery of a high concentration of potent medications to targeted tissue while minimizing the side effect of the agent to the rest of the body. Polymeric micelles have been shown to encapsulate therapeutic agents and maintain their structural integrity at lower concentrations. Ultrasound is currently being used in drug delivery as well as diagnostics, and has many advantages that elevate its importance in drug delivery. The technique is noninvasive, thus no surgery is needed; the ultrasonic waves can be easily controlled by advanced electronic technology so that they can be focused on the desired target volume. Additionally, the physics of ultrasound are widely used and well under- stood; thus ultrasonic application can be tailored towards a particular drug delivery system. In this article, we review the recent progress made in research that utilizes both polymeric micelles and ultrasonic power in drug delivery. ß 2008 Wiley-Liss, Inc. and the American Pharmacists Association J Pharm Sci 98:795–811, 2009 Keywords: micelle; ultrasound; drug delivery; chemotherapy; cancer; surfactant; controlled release/delivery INTRODUCTION The high toxicity of potent chemotherapeutic agents limits the therapeutic window in which they can be utilized. This window can be expanded by controlling the drug delivery in both space (selective to the tumor volume) and time (timing and duration of release) such that nontargeted tissues are not adversely affected. Research in this area has focused on the synthesis of different drug depots that are capable of delivering a high concentration of chemotherapy drugs to cancerous tissues without affecting cells and organs in the systemic circulation. These depots can be broadly classified into three groups: liposomes, micelles, and shelled vesicles. In this review we focus on the use of micelles in conjunction with ultrasound (US) to treat cancerous tissues. Low frequency ultrasound refers to frequencies less than 1 MHz, while the ranges for medium and high acoustic frequencies are 1–5 and 5–10 MHz, respectively. We will present the advantages and disadvan- tages of such a drug delivery system, the recent advancements in this field, the future directions, and some unanswered questions that remain in Correspondence to: Ghaleb A. Husseini (Telephone: 971-6- 515-2970; Fax: 971-6-515-2979; E-mail: [email protected]) Journal of Pharmaceutical Sciences, Vol. 98, 795–811 (2009) ß 2008 Wiley-Liss, Inc. and the American Pharmacists Association JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009 795
Transcript of Ultrasonic-activated micellar drug delivery for cancer treatment

REVIEWS
Ultrasonic-Activated Micellar Drug Delivery forCancer Treatment
GHALEB A. HUSSEINI,1,2 WILLIAM G. PITT2
1Chemical Engineering Department, American University of Sharjah, Sharjah, United Arab Emirates
2Department of Chemical Engineering, Brigham Young University, Provo, Utah 84602
Received 11 November 2007; revised 21 February 2008; accepted 3 April 2008
Published online 27 May 2008 in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/jps.21444
Corresponde515-2970; Fax:
Journal of Pharm
� 2008 Wiley-Liss
ABSTRACT: The use of nanoparticles and ultrasound in medicine continues to evolve.Great strides have been made in the areas of producing micelles, nanoemulsions, andsolid nanoparticles that can be used in drug delivery. An effective nanocarrier allows forthe delivery of a high concentration of potent medications to targeted tissue whileminimizing the side effect of the agent to the rest of the body. Polymeric micelles havebeen shown to encapsulate therapeutic agents and maintain their structural integrity atlower concentrations. Ultrasound is currently being used in drug delivery as well asdiagnostics, and has many advantages that elevate its importance in drug delivery. Thetechnique is noninvasive, thus no surgery is needed; the ultrasonic waves can be easilycontrolled by advanced electronic technology so that they can be focused on the desiredtarget volume. Additionally, the physics of ultrasound are widely used and well under-stood; thus ultrasonic application can be tailored towards a particular drug deliverysystem. In this article, we review the recent progress made in research that utilizes bothpolymeric micelles and ultrasonic power in drug delivery. � 2008 Wiley-Liss, Inc. and the
American Pharmacists Association J Pharm Sci 98:795–811, 2009
Keywords: micelle; ultrasound; drug
delivery; chemotherapy; cancer; surfactant;controlled release/deliveryINTRODUCTION
The high toxicity of potent chemotherapeuticagents limits the therapeutic window in whichthey can be utilized. This window can be expandedby controlling the drug delivery in both space(selective to the tumor volume) and time (timingand duration of release) such that nontargetedtissues are not adversely affected. Research in thisarea has focused on the synthesis of different drug
nce to: Ghaleb A. Husseini (Telephone: 971-6-971-6-515-2979; E-mail: [email protected])
aceutical Sciences, Vol. 98, 795–811 (2009)
, Inc. and the American Pharmacists Association
JOURNAL OF
depots that are capable of delivering a highconcentration of chemotherapy drugs to canceroustissues without affecting cells and organs in thesystemic circulation. These depots can be broadlyclassified into three groups: liposomes, micelles,and shelled vesicles. In this review we focus on theuse of micelles in conjunction with ultrasound(US) to treat cancerous tissues. Low frequencyultrasound refers to frequencies less than 1 MHz,while the ranges for medium and high acousticfrequencies are 1–5 and 5–10 MHz, respectively.We will present the advantages and disadvan-tages of such a drug delivery system, the recentadvancements in this field, the future directions,and some unanswered questions that remain in
PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009 795

796 HUSSEINI AND PITT
this research topic; but first we will discuss theadvantages of ultrasound.
ULTRASOUND IN DRUG DELIVERY
Using ultrasonic power as a drug release mechan-ism is advantageous for several reasons: first, thetechnique is noninvasive. The main advantagethat renders ultrasound so useful is that noinsertion or surgery is needed; acoustic transdu-cers are placed in contact with a water-soluble gelthat is spread on the skin. In addition, ultrasonicwaves can penetrate deep into the interior of thebody, an advantage that optical (visible wave-lengths) techniques cannot provide. Ultrasonicwaves can be carefully controlled and focused onthe tumor site. Ultrasound consists of pressurewaves (with frequencies of 20 kHz or greater)generated by piezoelectric transducers thatchange an applied voltage into mechanical move-ment. Like optical and audio waves, ultrasonicwaves can be focused, reflected and refractedthrough a medium.
There appears to be a synergistic effect betweenthe pharmacological activity of some drugs andultrasound. Loverock et al.1 have shown that 1 hof exposure to ultrasound (2.6 MHz at 2.3 W/cm2)rendered Adriamycin significantly more toxictoward Chinese hamster lung fibroblasts. Whenthe cell line was exposed to ultrasound alone, thecell viability was not affected. Using flow cyto-metry, the same study found an increase inconcentration of the chemotherapeutic agentinside the cells.
Tachibana et al.2 used a clonogenic assay tostudy the effect of 0.3 W/cm2 and 48 kHzultrasound on the cytotoxicity of Cytosine Arabi-noside (Ara-C). Sonicating human Leukemia cellsfor 120 s without Ara-C, did not cause a significantdecrease in the number of colonies counted whencompared to the control. When cells were soni-cated for 60 s only in the presence of thechemotherapeutic agent, there was no significantdifference in the cell survival rate betweensonicated and nonsonicated cells. However, soni-cating for 120 s in the presence of 1� 10�7 M ofAra-C reduced the number of observed colonies100 times when compared to cells incubated withthe same concentration of the drug. This acousticenhancement was more pronounced at the lowerconcentrations of Ara-C (2� 10�9 to 2� 10�8 M)than at concentrations greater than 2� 10�8 M.
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009
This increase in cell death was not caused byhyperthermia, since the temperature increasewas less than 0.28C throughout the experiments.In their attempt to understand the mechanism ofthis ultrasonic enhanced killing, the group usedscanning electron microscopy and observed adecrease in the total number of microvilli and ‘‘aslight disrupted cell surface with flap-like wrin-kles’’ under the action of ultrasound. Theyconcluded that low intensity ultrasound alteredthe cell membrane, which resulted in the increaseof Ara-C cell uptake.
Ultrasound has been shown to increase thekilling of bacteria both in planktonic3,4 and biofilmforms5–7 in the presence of antibiotics. Thisbioacoustic effect was more pronounced at lowerfrequencies and decreased as the frequency ofinsonation increased.8,9 The effect was morepronounced in E. coli and P. aeruginosa (gramnegative bacteria) than in Staphylococcus epider-midis (gram positive bacteria). In vivo experi-ments confirmed the increased toxicity ofgentamicin against E. coli biofilms in the presenceof low frequency ultrasound (28.48 kHz and 0.3 W/cm2).4,10 The group also found that this bioacous-tic effect is operative with certain antibiotics, butis not manifest when others are used.11 Theyhypothesized that stable cavitation or sonopora-tion might be involved in increasing the transportof antibiotics into the bacteria either by reducingthe mass transfer boundary layer around the cells,or by altering the cell membrane, thus allowingthe antibiotics to diffuse through newly formedmembrane pores.
Ultrasound enhances drug transport throughtissues and across cell membranes. Severalstudies have shown that ultrasound facilitatesdrug delivery and absorption. Mitragotri et al.12
have shown that low frequency ultrasound(20 kHz) can be used in the transdermal deliveryof medium and high molecular weight proteins(including insulin, interferon, and erythropoie-tin). Three hours after the ultrasonic treatmentconcluded, the skin regained its transport resis-tance to insulin, indicating that no permanentdamage was done by ultrasound. In anotherstudy by the same group, therapeutic ultrasound(1 MHz, 1.4 W/cm2, continuous) resulted in 14-foldelevation of cell membrane permeability forseveral chemical enhancers (e.g., poly(ethyleneglycol), isopropyl myristate, 50% ethanol satu-rated with linoleic acid).13
Bommannan et al.14,15 have shown that highfrequency ultrasound (10 and 16 MHz) for a period
DOI 10.1002/jps

ULTRASONIC-ACTIVATED MICELLAR DRUG DELIVERY 797
of 20 min increased the transport of salicylic acidby a factor of 4 (at 10 MHz) and 2.5 (at 16 MHz).Their studies also showed that lanthanum hydro-xide penetrates human skin under the influence ofultrasound through the stratum corneum and theepidermal cell layers by an unknown intercellularmechanism.
Rapoport et al.16 investigated the increase inintracellular drug uptake by HL-60 cells as aresult of ultrasound irradiation (67 kHz and2.5 W/cm2) using fluorescence techniques. Thegroup found that that the amount of Dox (and itsparamagnetic analog Ruboxyl) that intercalatedDNA in leukemia cells increased as a result ofsonication for an hour. In another related study,Munshi et al.17 reported that the IC50 for Dox wasreduced from 2.35 to 0.9 mg/mL when HL-60 weresonicated for 1 h at 80 kHz in the presence of theantineoplastic agent. In that study, IC50 wasdefined as the concentration of (Dox) that resultedin 50% survival of the cells after 96 h ofposttreatment incubation compared to the control.
Ultrasonic waves have been used to inducehyperthermia. Saad and Hahn18 exposed Chinesehamster cells to 2.025 MHz ultrasound (averageintensities range between 0.5 and 2 W/cm2) and toseveral drugs at temperatures ranging between37 and 438C. The study showed that at lowerintensities (0.5 W/cm2) the cytotoxicity of Adria-mycin (synonymous with Doxorubicin) was sig-nificantly enhanced when the temperature wasraised from 37 to 418C. At higher ultrasonic powerdensities (1 W/cm2), the cytotoxic effect ofAdriamycin increased threefold when the tem-perature reached 418C. The study concluded thatthe ‘‘temperature threshold’’ decreases as thepower intensity of ultrasound increases.
Singer et al.19 have also shown that hyperther-mia induced by low-frequency ultrasound candecrease the number of S. epidermidis colonies. Intheir experiments, 20-kHz ultrasound wasapplied for 5 s in a 10-s cycle (5:5 duty cycle) for2 min. Two transducers were used: 1-cm cylind-rical probe and 5-cm probe. There was a differencein the temperature ranges of both probes. Thetemperatures of the 1-cm probe ranged from 31 to748C, while for the 5-cm probe the temperaturesranged between 22 and 408C. With the 5-cm probe,increasing the intensity of ultrasound causedbacterial counts to increase. However, when the1-cm transducer was used, the number of coloniesdecreased as the intensity of ultrasound increased.The effect of ultrasound was more pronounced whenthe incubation fluid temperature exceeded 458C.
DOI 10.1002/jps JOU
The study stated that ultrasound has the ability toaffect bacteria by three routes: thermal, cavitationand other ‘‘direct effects.’’ Since the bacterialcounts were only affected when the temperatureincreased above 45–508C, the group attributed theantibacterial effect of low-frequency ultrasound toultrasonic hyperthermic effects.
In summary, ultrasound can be used incombination with chemotherapy agents for sev-eral reasons. It has been shown to enhance thetransport of drugs and other chemicals into cellsand tissues. The cytotoxic efficiency of chemother-apeutic agents has been shown to increase underthe action of ultrasound. Since ultrasound increasesthe local temperature of the exposed tissues,hyperthermia can be used as an additionalultrasonic advantage. Mechanisms are not wellknown, and there is a large effect of insonationfrequency and power intensity that needs to bestudied.
Polymeric micelles have been used to improvesite-specific drug delivery in cancer therapy. Thetechnique relies on these carriers’ small size toextravasate at the tumor site where the drug candiffuse into the tumor and carry out its ther-apeutic effect.20–23 Although several groups haveinvestigated the use of polymeric carriers todeliver chemotherapeutic and other drugs,24–42
the only two groups that have reported the use ofpolymeric micelles in conjunction with US areRapoport, Pitt and colleagues at the University ofUtah and Brigham Young University, and Myhr’sgroup at the Norwegian Radium Hospital. Themicelles used in both of these groups’ studies arecomposed of polymers that belong to the Pluro-nic1 family of block copolymers.
PLURONIC1 CARRIERS
Pluronic1 polymers are triblock copolymers ofpoly(ethylene oxide) (PEO)—poly(propyleneoxide) (PPO)—poly(ethylene oxide) (PEO). Theyare soluble in water, and at sufficiently highconcentrations they form micelles. For example,the critical micellar concentration (CMC) ofPluronic1 P105 is approximately 1 wt% at roomtemperature.43 These micelles have a spherical,core–shell structure with the hydrophobic blockforming the core of the micelle and the hydrophilicPEO chains forming the corona. Alexandridiset al. have studied Pluronic1 properties inaqueous solutions.44–47 The phase state of Pluro-nic1 micelles at a desired temperature can be
RNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009
798 HUSSEINI AND PITT
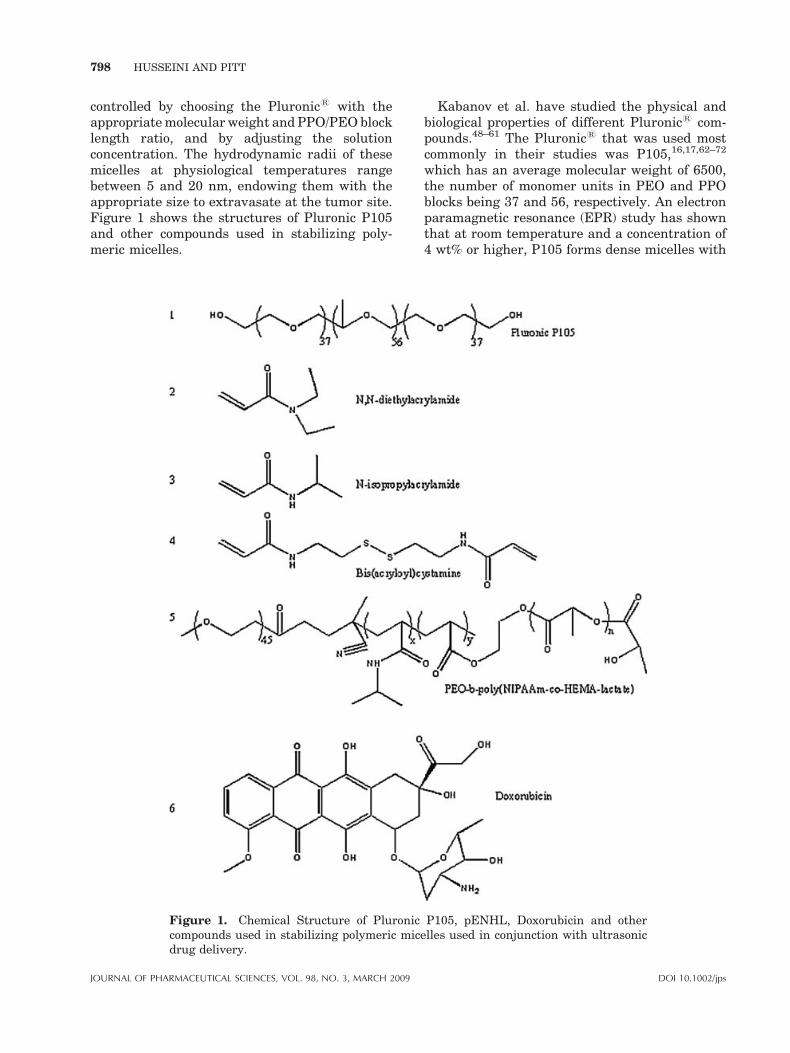
controlled by choosing the Pluronic1 with theappropriate molecular weight and PPO/PEO blocklength ratio, and by adjusting the solutionconcentration. The hydrodynamic radii of thesemicelles at physiological temperatures rangebetween 5 and 20 nm, endowing them with theappropriate size to extravasate at the tumor site.Figure 1 shows the structures of Pluronic P105and other compounds used in stabilizing poly-meric micelles.
Figure 1. Chemical Structure of Pluroniccompounds used in stabilizing polymeric micedrug delivery.
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009
Kabanov et al. have studied the physical andbiological properties of different Pluronic1 com-pounds.48–61 The Pluronic1 that was used mostcommonly in their studies was P105,16,17,62–72
which has an average molecular weight of 6500,the number of monomer units in PEO and PPOblocks being 37 and 56, respectively. An electronparamagnetic resonance (EPR) study has shownthat at room temperature and a concentration of4 wt% or higher, P105 forms dense micelles with
P105, pENHL, Doxorubicin and otherlles used in conjunction with ultrasonic
DOI 10.1002/jps

ULTRASONIC-ACTIVATED MICELLAR DRUG DELIVERY 799
relatively little water in the core.73 That studyalso showed that depending on concentration, thiscopolymer associates as unimers, loose aggre-gates, and dense micelles. When associated asaggregates and micelles, chemotherapy drugs canaccumulate in the hydrophobic PPO core while thePEO chains extend into the aqueous solution, thuspreventing proteins from adsorbing on the surfaceof these drug carriers and identifying them to thereticulo-endothelial system.
In addition to the advantages of polymericmicelles, several studies have reported the effectof Pluronic1 surfactants in overcoming multidrugresistance (MDR). Alakhov et al.48 investigatedthe hypersensitization effect of Pluronic1 P85block copolymer on MDR human ovarian carci-noma cells. This study showed a substantialincrease in the activity of Daunorubicin in thepresence of 0.01–1 wt% copolymer. Venne et al.51
have also shown that the use of Pluronic1 micellesare effective in overcoming multi-drug resistance.That group studied the effect of Dox- (Fig. 1) onMDR-hamster ovarian and breast cancer cells andobserved a 290- and 700-fold increase respectivelyon the cytotoxic action of Dox in the presence ofPluronic1 L61.
IN VITRO AND IN VIVO EXAMPLES
The feasibility of using ultrasound in associationwith polymeric micelles to deliver antineoplasticagents to cancer cell in vitro was first reported byMunshi et al.17 They reported that a combinationof US and Pluronic1 P105-encapsulated Doxsynergistically lowered the drug’s IC50 from 2.35to 0.19 mg/mL.
The same group then investigated the amountof DNA damage induced by Dox delivered toHuman leukemia (HL-60) cells from Pluronic1
P105 micelles with and without the application ofUS.65 Their results indicated that there was nosignificant DNA damage observed when the cellswere exposed to 10mg/mL of Dox in the presence of10 wt% P105 for up to 9 h of incubation. However,when US was applied, a rapid and significantincrease in DNA damage and cell death wasobserved.
To understand the mechanism of this enhancedacoustic delivery, an ultrasonic exposure chamberwith real-time fluorescence detection was used tomeasure acoustically triggered Dox and Ruboxylrelease from Pluronic1 P105 micelles.69 Theresults showed that more drug was released at
DOI 10.1002/jps JOU
lower frequencies (20, 40, 70 kHz) and higherpower densities, and that there was a powerdensity threshold below which no release wasobserved.74 The threshold apparently corre-sponded to the onset of collapse cavitation. Thedata were further corroborated by EPR using 5,5-dimethyl-1-pyrroline-N-oxide (DMPO) as a radi-cal trap.69 The ultrasonic intensity at onset ofdrug release coincided with the formation ofDMPO-OH adducts formed upon the ultrasonica-tion of a micellar solution containing 10 wt% P105.The OH radicals are generated as the temperatureinside cavitating bubbles raises to several 1000 K.These radicals are then trapped using DMPO.Thus the collapse cavitation was implicated in thisdrug release phenomenon.
A subsequent study investigated the kinetics ofultrasonic drug delivery and reported that bothrelease and reencapsulation is completed within0.6 s of initiation and cessation of ultrasound.66
Their report indicated that when insonationceased, the chemotherapeutic agent is reseques-tered inside the micelle, thus potentiallyminimizing interaction with the aqueous sur-roundings, which may be beneficial to anynontargeted cells downstream of the ultrasonicfocal volume. Several proposed physical modelswere analyzed mathematically to see which if anyfit the observed kinetic data. The zero-orderrelease with first order reencapsulation appearedto represent this system better than the otherproposed models.66
Recently the kinetics of ultrasonic drug releasefrom Pluronic1 micelles were revisited.75 Theobserved triphasic nature of the release and thebiphasic nature of reencapsulation were repre-sented by a more comprehensive mathematicalmodel. This newer model assumed that micelleswere of different sizes (five different sizes) andthat the larger micelles were destroyed first, thuscausing an initial fast release phase. Smallermicelles were then destroyed which caused aslower release phase. A third phase was alsoobserved, and this was attributed to smallerfragments and smaller micelles coalescing intolarger micelles. This new model, based uponexperiments employing continuous US, was vali-dated by its accurate prediction of drug releaseobserved in a totally different data set in whichpulsed US was used to release Dox from unsta-bilized Pluronic1 P105 polymeric micelles.75
Using fluorescent microscopy and flow cytome-try, Marin et al.76 reported that exposure toultrasound enhanced the intracellular uptake of
RNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009

800 HUSSEINI AND PITT
Pluronic1 micelles loaded with Dox and theirinternalization into the nucleus of HL-60 cells.Under exposure to US, more drug was presentinside the cell in free form than was retainedinside the micelles, which suggested that US hadreleased the agent from the micelle core. Theyreported that US enhanced the intracellularuptake of the drug by HL-60 cells and attributedthis increase to US-induced cellular change.Exposure to US has also been shown to changethe intracellular distribution of the drug fromacidic compartments (endosomes or lysosomes) toneutral compartments (in the cytoplasm and thenucleus).71,77,78 The characteristic times of micel-lar drug release and cellular uptake were both onthe order of 1–2 s, confirming the important roleplayed by US in the transport of Dox into HL-60cells.79
The main challenge facing the use of micelles todeliver chemotherapy drugs is that the concen-tration of the polymer must be above the CMC toguarantee that the multimeric micellar structuresremain intact and do not dissolve and release thedrug before reaching the target site. An EPRstudy found that at low concentrations (less than0.1 wt% P105), the polymer forms unimericmicellar structures at 378C; at intermediateconcentrations, hydrophobic micellar cores areneeded to effectively sequester hydrophobic che-motherapeutic agents. However, the body may nottolerate these required high concentrations of thesurfactant. For this reason, a method for stabiliz-ing the micelle and its hydrophobic core of wasrequired.
Pruitt et al.80 stabilized Pluronic1 micelles bypolymerizing an interpenetrating network of N,N-diethylacrylamide (see Fig. 1) within the hydro-phobic core to form stabilized micelles calledNanoDelivTM. The size of these stabilized micellesranges from 150 to 500 nm at 258C and 50 to400 nm at 378C. The thermally responsive net-work expands at room temperature, allowing thedrug to accumulate inside its hydrophobic core,and contracts above 318C, thus trapping the drugmolecules when injected at body temperature. Thepolymerization employed bis(acryloyl)cystamine(BAC) as a crosslinker, and 2,20-azobis(isobutyr-onitrile) (AIBN) as an initiator. The hydrophobicNIPAAm monomers and crosslinkers polymerizeinside the core of the P105 micelles, thus formingan interpenetrating network. Upon dilution,the network prevents the quick degradation ofthe micellar structure and keeps the therapeuticagent encapsulated, which in turn minimizes the
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009
drug’s side effects. As the temperature surround-ing the micelle increases, the association of waterwith the PEO blocks decreases (due to decreasedhydrogen bonding), and the stabilized micelleshrinks, as evidenced by a decrease in itsmeasured size.80 The network-micellar structureis eventually degraded after several days (thein vitro half-life is approximately 17 h). As withPluronic1 micelles, NanoDelivTM micelles havebeenshowntoreleaseDoxuponexposuretoUS.81,82
Recently, Zeng and Pitt83 synthesized a newmicellar vehicle using a block of polyethyleneoxide, N-isopropyl acrylamide (NIPAAm), andpolylactate ester of hydroxyl-ethyl methacrylate(pENHL) (see Fig. 1). Due to the presence of thePEO block, this pENHL micelle retained itsstealth characteristics, while the hydrophobiccore provided a nonpolar nano-environmentwhere hydrophobic drugs can accumulate spon-taneously. The main advantage of this carrier isthe controlled degradability of the NIPAAm-HEMA-lactate block; thus its lifetime in thesystemic circulation can be tailored by choosingthe appropriate composition of NIPAAm, PEO andHEMA-lactate. This renders the synthesizedpolymer more versatile with respect to timedrelease and ultimate degradation in variousapplications. Like its predecessors, this pENHLmicelle released Dox upon the application of70 kHz ultrasound.84
Recently, in vivo studies examined the feasi-bility of acoustically activated drug delivery fromthe NanoDelivTM carrier. Nelson et al.85 showedthat exposure to 20- and 70-kHz US for 1 h in thepresence 2.67 mg/kg of Dox encapsulated inNanoDelivTM significantly decreased (p¼ 0.0061)the size of subcutaneous tumors in the hind leg ofBDIX rats compared to control tumors on thecontralateral leg. The Dox sequestered in Nano-DelivTM was administered systemically via tailvein injection, so both tumors were equivalentlyexposed to Dox, but only one tumor received US.
In similar experiments, Staples exposed thetumor to Dox in NanoDelivTM to 20- and 500-kHzUS for 15 min.86 The insonated tumors grew moreslowly than the contra lateral controls (p¼0.0047). Both frequencies were equally effectivein treating the tumor.
Staples also investigated the distribution of Doxin several organs at various times after the Dox/NanoDelivTM injection and insonation.87 He foundthat both the insonated and control tumors hadDox concentrations that were not statisticallydifferent 6 or more hours following drug injection
DOI 10.1002/jps

ULTRASONIC-ACTIVATED MICELLAR DRUG DELIVERY 801
(p¼ 0.988). However, at the 30-min time point,the concentration of Dox in the insonated tumorwas higher (p¼ 0.055). The tumors receiving Doxand NanoDelivTM with insonation grew moreslowly (p¼ 0.0047). Dox concentrations found inthe heart, kidneys, liver, and muscle decreased toundetectable levels within a week, but a slightlymeasurable amount persisted in the tumorsbeyond 1 week.
Gao et al.88 studied the intracellular distribu-tion in mice of fluorescently labeled unstabilizedPluronic1 P105 and Pluronic1 P105 stabilizedusing PEG-diacylphospholipid. The study showedthat 1 MHz insonation for times as short as 30 swere able to enhance the accumulation of theselabeled micelles at the tumor site in ovariancancer-bearing nu-nu mice. Employing flow cyto-metry to the tumor tissues excised from inocu-lated mice, Rapoport et al.89 showed that micelleaccumulation was significantly higher in theultrasonicated tumor than in the noninsonatedtumor of the same mouse. The study also reportedthat encapsulated Dox did not accumulate in theheart, which would ameliorate the well-documen-ted cardiotoxicity of this antineoplastic agent.Although low frequency US (20–100 kHz)66,69 wasable to release more Dox from Pluronic1 micellesthan high frequency US (1 and 3 MHz),70
Rapoport’s in vivo research efforts used 1 MHzUS because it can be focused more precisely on thetumor site and causes less sonolysis.
Recently, Myhr et al. have shown that acombination of NanoDelivTM-encapsulated fluor-ouracil (5-FU) combined with ultrasound signifi-cantly reduced the tumor (human colon cancer)volume in Balb/c nude mice, when compared to thecontrol group (p¼ 0.0034). The authors reported amore significant tumor volume reduction athigher drug concentrations.
MECHANISMS
The mechanisms of this acoustically activatedmicellar drug delivery system are still underinvestigation, and in vitro there is a strongcorrelation with insonation frequency and powerdensity that suggests a strong role of cavitation.Here we will discuss the two main mechanismsthat render this micellar drug delivery systemeffective. Ultrasound appears to disrupt the coreof polymeric micelles, allowing the drug to bereleased in the volume of the ultrasonic field.Additionally, ultrasonic waves have been shown
DOI 10.1002/jps JOU
to cause the formation of micropores in cellmembranes, which in turn allows for the passivediffusion of drugs into cell.
Disruption of Micelles
After proving that Dox and Rb were released frommicelles under the action of ultrasound,69 Hus-seini et al. embarked on a study of the mechanismunderlying this release. They improved theirpreviously designed ultrasonic exposure chamberwith fluorescence detection,66,69 so as to recordacoustic emissions at 70 kHz while simulta-neously recording the decrease in fluorescence.This in vitro study showed that there is athreshold value of about 0.38 W/cm2 below whichno measurable release occurred. Furthermore theonset of Dox release from P105 micelles corre-sponded to the emergence of a subharmonic peakin acoustic spectra at this same threshold. Theexistence of a threshold at this intensity tends topoint toward a strong role of cavitation, particu-larly inertial or collapse cavitation, in this releasephenomenon. Several groups have reported theexistence of a threshold for the onset of inertialcavitation.90–94 Daniels et al.90 reported aninertial cavitation threshold between 0.036 and0.141 W/cm2 at 750 kHz insonation, while Hillshowed the thresholds to occur below 1 W/cm2 forfrequencies ranging between 0.25 and 4 MHz.91
Obviously there is a wide range of intensitiesreported for the onset of inertial cavitation. Weattribute this to two factors. First, the thresholdshould in general decrease as the frequencydecreases. But this does not explain all of thevariation in reported thresholds. We attribute agood deal of the remaining variation to the variousexperimental conditions under which the thresh-olds were measured. For example, the thresholdswill be sensitive to the state of degassing of theliquid employed, to the temperature of the experi-ment, to the presence of surfactants or othersubstances that can serve as a nidus for hetero-geneous bubble nucleation, and to the equipmentand analytical procedures employed to detect thecavitation events. To date there is no standardmethod for the measurement of thresholds.
Several publications have reported ultrasonicintensity thresholds for an observed biologicaleffect in cells and tissues.91,95–104 Mitragotri et al.were the first to show the existence of an ultra-sonic threshold for enhancing skin permeabil-ity.99,103,105–107 This threshold is a strong function
RNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009

802 HUSSEINI AND PITT
of ultrasound frequency; as the frequencyincreases so does the threshold. Tang et al.108
showed that low-frequency sonophoresis (LFS)was able to permeabilize pig skin using 20 kHzultrasound. They postulated that the key mechan-ism involved in LFS is cavitation bubbles inducedby US. Copious research has been conducted onincreased cell membrane permeability under theaction of ultrasound.95,96,104,109,110 For example,there is a reported threshold for DNA delivery torabbit endothelial cells of about 2000 W/cm2 at apulse average intensity 0.85 MHz (short pulseaverage intensity).96 Another example is thethreshold of 0.06 W/cm2 at 20 kHz reported byRapoport et al.89 for HL-60 lysis. The rangereported for biological thresholds is obviously verylarge, and thus provides little guidance for a prioriprediction of threshold values for biologicalevents. One must remember that in biologicalsystems, the observed event is not the threshold ofinertial cavitation; there is usually an ultrasonicintensity beyond the simple inertial cavitationthreshold that is required to provide sufficientnumbers and sufficient intensities of damagingcavitation events. Biological systems are muchmore complicated. In addition to the experimentalfactors mentioned above (e.g., level of gas satura-tion and heterogeneous nucleation materials), onemust also consider the cells involved. For exam-ple, biological manifestations will be related tothings such as the proximity of the cells to thecollapse events, the presence of microjets fromcollapse events, the cell membrane strength andintegrity, the requirements following cell mem-brane permeation (transport only to the cytosol orall the way to the nucleus) to produce a biologicalresponse, and much more. Obviously, muchresearch remains to be done in this area ofpredicting thresholds for cellular response.
In this review, we will devote some discussion tothe origin of the subharmonic acoustic peak,inertial cavitation, and its relation to the releasephenomena. As bubbles oscillate with increasingamplitude in an ultrasonic field (of frequency f),they start to generate higher harmonic (2f, 3f,etc.), ultraharmonic (3/2f, 5/2f, etc.), and sub-harmonic ( f/2, f/3, etc.) emissions. There arereports that correlate the subharmonic emissionwith certain indicators of inertial cavitation,including sonoluminescence, acoustic white noise,and iodine generation.91,111–113 Leighton114 usedmathematical modeling of cavitating bubbles tosimulate a signal at f/2 (the subharmonic) andcame to the conclusion that a subharmonic occurs
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009
due to a prolonged expansion phase immediatelypreceding a delayed collapse phase of the bubbleimplosion event. However, modeling by othersshow that the f/2 signal can be produced(mathematically at least) without collapse cavita-tion occurring,92,115–117 albeit the definition of‘‘collapse’’ is difficult to define in a mathematicalmodel.118
Sundaram et al.105 clearly show that themembrane permeability of 3T3 mouse cellscorrelates with an increase in background noisein acoustic spectra. The group came to theconclusion that ultrasound-induced permeabiliza-tion of cell membranes is caused by collapsecavitation events. On the other hand, Liu et al.109
found a strong dependence of the degree ofhemolysis (permeabilization of red blood cells asmeasured by the degree of hemoglobin release) onthe intensities of the subharmonic and ultrahar-monic frequencies, but not on the broadbandnoise. The group concluded that the best correla-tion between ultrasonic parameters and hemoly-sis was the product of the total ultrasonicexposure time and the subharmonic pressure.Accordingly, there are varied opinions as towhether the subharmonic emission always corre-lates with biological phenomena, or even withcollapse cavitation.
As to the relationship between the mechanismof release and inertial cavitation, Husseini et al.postulated that as the shock wave caused bycollapse cavitation propagates through the vici-nity of a micelle, the abrupt compression andexpansion of fluid in the shock wave is able toshear open the micelle so that the drug is releasedor at least exposed to the aqueous environment.Oscillating bubbles, even in stable cavitation,create very strong shear forces near the surface ofthe bubble. The shearing velocity of fluid near a10 mm (diameter) bubble, with a 1 mm oscillationamplitude and 70 kHz oscillation frequency isapproximately 1 m/s.119 Additionally, it importantto keep in mind that the extremely high viscousshear rates near the surface of 10-mm bubbles areon the order of 105/s. Furthermore, this rate isequivalent to shearing water in a 1 mm gapbetween parallel plates in which plate is sta-tionary and the other moving at 100 m/s. Thus, thegroup speculated that these shear forces may bestrong enough to open up a P105 micelle, exposingthe hydrophobic drug inside its core to thesurrounding aqueous environment.
The group also extended their study of therelease mechanism to stabilized and unstabilized
DOI 10.1002/jps

ULTRASONIC-ACTIVATED MICELLAR DRUG DELIVERY 803
micelles.84 In this study they compared therelease of Dox from the core of unstabilizedPluronic1 105 micelles to the release fromstabilized micelles such as NanoDelivTM micellesand micelles of pENHL described previously inPluronic1 Carriers Section. They found that therelease of Dox at 378C from Pluronic1 micellesappeared to be several times higher than therelease from the more stabilized micelles. Inter-estingly, the onset of release occurred at about thesame power density for all carriers investigated intheir study, whether stabilized or not. Similarly,the threshold of Dox release from all threemicelles correlated with the emergence of sub-harmonic peaks in the acoustic spectra.
Apparently the structures of the stabilized andnonstabilized micelles are perturbed by cavitationevents that cause the release of Dox. The grouphypothesized that stabilized micelles are lesssusceptible to disruption by the shearing forcesof shock waves produced by cavitation events.84
Since the threshold of release also correlates withthe subharmonic peak in all micellar systemsinvestigated, discovering the origin of the sub-harmonic peak is vital in understanding drugrelease from micelles under the action of ultra-sound.
Disruption of Cell Membrane
Although Pitt’s group has focused on studying thepossible mechanisms by which the P105 micellesand ultrasound drug delivery system induce druguptake by the cancer cells, is has also studied thebiological mechanism involved here. The cometassay was used to quantify the amount of DNAdamage in HL-60 cells by measuring the fractionand length of broken nuclear DNA strands.120–122
Large amounts of DNA damage as measured bythe comet assay is indicative of cell death, eitherby necrosis or by apoptosis.123,124 Results of thecomet assay show that Dox eventually binds to theDNA and causes it to fragment.65 In a separatebut related study, Husseini et al.65,125 reported onthe mode of cell death exhibited by cells exposed toa combination of Pluronic1 micelles, ultrasoundand Dox. Using the comet assay, the groupobserved the electrophoretic pattern of thenuclear DNA from HL-60 cells insonated at70 kHz in a solution of P105 micelles containing10 mg/mL Dox for 30 min, 1 and 2 h. The pattern ofthe DNA fragments as well as the gradual damageobserved after 2 h of ultrasonic exposure were
DOI 10.1002/jps JOU
consistent with apoptosis as a mode of cell deathrather than necrosis. However, the questionremains as to if and how ultrasound enhancesuptake of Dox by the cell. In this section, we willdiscuss three postulated mechanisms that havebeen tested in an attempt to answer the abovequestion. These mechanisms are (1) ultrasonicrelease of the drug from micelles is followed bynormal transport into the cell; (2) ultrasoundupregulates endocytosis of the micelles (withdrug) into the cell; (3) ultrasound perturbs thecell membrane which increases passive transportof the drug and Pluronic1 molecules into the cell.
The first hypothesis proposes that the drug isreleased from micelles outside the cancer cells,followed by normal penetration of the polymer anddrug into the cells by simple diffusion or normalcellular uptake mechanisms. To test this postu-lated mechanism, the hydroxyl groups at the endsof P105 chains were labeled with a fluoresceinderivative.70,71,126 HL-60 cells were then incu-bated or sonicated with the fluorescein-labeledP105 micelles containing Dox, which fluoresces ata different wavelength. Results showed that Doxin 10 wt% P105 appeared inside the cells.
The next question was whether the fluores-cently labeled P105 entered the cells along with orindependent of the Dox. The experiments revealedthe presence of P105 inside the cells whenincubated or insonated for 20 min. Because thelabeled P105 molecules themselves were foundinside the HL-60 cells, they rejected the firsthypothesis of external drug release followed bypassive drug diffusion without the polymericdiffusion into the cells. Although their experimentshowed that the P105 entered the cells, it was notpossible to determine whether the copolymerentered the cells through holes punched in thecell membrane or through endo-/pino-cytoticroutes.
Next they turned their attention to the secondhypothesis whereby entire micelles (with drug)are endocytosed into the cells. Since it is unlikelythat HL-60 cells express a receptor for Pluronic1
micelles, receptor-induced endocytosis was con-sidered to be very unlikely. However, pinocytosisinvolves vesicles that nonspecifically engulf smallvolumes of extracellular fluid and any materialcontained therein. To test the postulate that thecells were taking up the drug and P105 in byendocytosis, a model drug that fluoresces morestrongly in acidic environments was used, namelyLysosensor Green. This probe has a pKa of 5.2,which causes it to fluoresce more strongly in an
RNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009

804 HUSSEINI AND PITT
acidic compartment such as a lysosome.126 Thegreat majority of endosomes fuse with a primarylysosome to form a secondary lysosome, which hasa pH of about 4.8 while the pH outside thesecompartments is about 7.1. Cells exposed to USand P105 micelles with Lysosensor Green wereexamined by flow cytometry, which showed nodifference in fluorescence between cells incubatedand insonated for 1 h at 70 kHz. Thus, ultrasonicexposure did not cause the probe to partition to amore acidic environment anymore than it didwithout ultrasound, and the hypothesis wasrejected that US induces upregulation of endo-/pino-cytosis. The observation that US enhancedthe uptake of both drug and labeled Pluronic1
supported the third hypothesis that drug-ladenmicelles entered through holes in the membranesof insonated cells in these studies.
It is relevant that Rapoport77 reported that US-assisted micellar drug delivery enhances the rateof endocytosis into cells. Furthermore, Sheikovet al.127 showed that US induced pinocytosis in theendothelial cells lining arterioles and capillariesof the brain. Thus the role of US in promotingendocytosis and pinocytosis is unresolved. It maybe that different cells respond differently toultrasonic exposure such that a general andsimplified rule cannot be applied.
The ability of carefully controlled US to createnonlethal and repairable holes in cell membranesis gaining support. For example, Schlicher et al.128
have shown that the accumulation of the modeldrug calcein in prostate cancer cells was caused byUS-induced membrane disruptions.
In a similar study of US-induced calcein uptakeinto colon cancer cells, Stringham et al. proved theinvolvement of collapse cavitation in cell mem-brane disruption. The calcein uptake was sup-pressed by increasing the hydrostatic pressure atconstant ultrasonic intensity at 500 kHz. It is wellknown that increasing hydrostatic pressure sup-presses collapse cavitation, although stable cavi-tation still occurs. In these experiments lowermembrane permeability correlated directly withhigher hydrostatic pressure.129
Tachibana et al. has reported the increase in cellmembrane permeability and skin porosity causedby ultrasound.2,130–135 His group has shown thatthe exposure of HL-60 cells to 255 kHz ofultrasound and MC 540 (an anticancer drug) for30 s formed pores in the cell membrane.2 Thecytoplasm of some cells seemed to have extrudedthrough the pores formed in the cell membrane asa result of sonoporation. When cells were exposed
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009
to ultrasound alone, the cell membrane showedonly minor disruptions. Saito et al.136 demonstratedthat exposure to ultrasound increased the perme-ability of corneal endothelium cells. The increase inpermeability appeared to be reversible and the cellsregained their membrane integrity after severalminutes. Thus there is ample evidence thatultrasonic cavitation events create transient holesin the cell membrane, which in the case of micellardrug delivery would increase the passive diffusionof micelles and drugs into the cells.
FUTURE
Remaining Questions on Mechanism
Before examining the remaining questions on themechanism of acoustically activated micellar drugdelivery, we need to review the origin andcharacteristics of the two modes of cavitation asthey affect biological tissues.
This discussion leads us to the main mechan-istic question remaining: Which type of cavitationis mainly involved in acoustically activated drugdelivery from micelles?
Future studies should focus on distinguishingbetween these two mechanisms. This may beaccomplished by listening to acoustic emissions orby measuring the sonoluminescence emittedduring insonation, keeping in mind that stablecavitation produces no broadband acoustic emissionand generates little if any luminescent emissions.Another characteristic that can be employed todistinguish between the two modes of cavitation isthe measurement of free radicals that are producedby the high temperatures of bubble collapse.
Another interesting technique that has not beenfully utilized in micellar drug delivery is math-ematical modeling of bubble behavior and none-quilibrium thermodynamics. These techniquesmight help in resolving the questions surroundingthe role of cavitation in micellar drug delivery. Toachieve this goal a better understanding of bubbledynamics, the physics of microbubble oscillationand collapse, the parameters controlling micro-bubble size, the internal gas composition, as wellas acoustic frequency and pressure amplitude areneeded prior to initiating the model.
Therapeutics
The agents that have been encapsulated innanoparticles for ultrasonic delivery have been
DOI 10.1002/jps

ULTRASONIC-ACTIVATED MICELLAR DRUG DELIVERY 805
primarily hydrophobic drugs. Future work shouldinclude other drug delivery vehicles, such asliposomes, which have hydrophilic volumes andare able to sequester and deliver hydrophilicdrugs, DNA or RNA.
Other Targeting Techniques
The micellar drug delivery system developed byPitt et al. shows strong promise. First, it is able toeffectively sequester a potent chemotherapeuticagent inside the core of stabilized micelles andsuccessfully release Dox upon application of US.They also reported success in using a secondgeneration of nanocapsules in vivo using a ratmodel of colorectal cancer. Although this noveldrug delivery system is an excellent start, it mostprobably can be improved.
One way of improving this micellar deliverysystem is to decorate the surface with a targetingmoiety, thus creating a double targeting system.There are many reports of the attachment ofantibodies to solid particles and gas bubbles.137,138
Often this is done by covalent attachment via theavailable –SH groups in Fab fragments of specificantibodies.139 Other techniques employ attach-ment of short peptide sequences (e.g., RGD140,141)or larger biomolecules (e.g., folic acid andbiotin141,142).
Folic acid derivatives (folated molecules) havebeen shown to be endocytosed into humancancerous cells via pinocytosis. Various cancercells over-express the folate receptor on theirsurface.143,144 Thus, the conjugation of folatemolecules to drug delivery carriers gained specialattention in recent years since it minimizes theinteraction between healthy cells and chemother-apeutic agents which will in turn reduce theside effects of conventional chemotherapy.Folate molecules display a high affinity for thefolate receptor which facilitates the binding of thefolated-drug to the its receptor.145–147 This leadsto the internalization of the drug carrier bythe cell. A folate-poly(ethylene glycol)-Pt(II) con-jugate has been synthesized by Steenis et al.,148
while two other groups succeeded in synthesizingother folate-drug conjugates.149,150 More recently,the attachment of the folate molecule to micellarstructures has been reported.29,151–153 The aim ofconjugating the folate onto micelles is to reducethe amount of the drug in the systemic circulationuntil the drug loaded micelle is taken up by thecancerous target cell via endocytosis.
DOI 10.1002/jps JOU
There are several aspects that still need to beexplored in order to understand the role ofultrasound in acoustically activated drug deliveryfrom micelles: the role of ultrasonic-inducedcavitation in releasing drug from the micellarcarrier, the use of ultrasound to specifically targetdrug release to a specific tissue without releasingdrug in nontargeted tissues, and the ability ofultrasound to cause cells to take up the drug.
One of the most important aspects that need tobe explored is the role of the nature of the carrierin ultrasonic-activated tumor regression. Toanswer this question, several different carriersshould be examined for their efficiency in deliver-ing chemotherapeutic agents to diseased tissues.These include micelles, liposomes, and othertargeted vesicles. Additionally, the concentrationof the therapeutic agent in the tumor should beinvestigated as a function of the carrier whenultrasound is applied.
Most importantly, the aspect that warrants themost attention in the future of micellar drugdelivery by US is the optimization of acousticparameters. This includes elucidating the effect offrequency and the total energy delivered upondrug release and cellular penetration/retention.Additionally, the length of insonation time andthe intervals between acoustic treatments shouldbe optimized to maximize drug efficiency.
SUMMARY
This article has reviewed the recent advances inthe use of ultrasound and polymeric micelles incancer therapy. This area of drug delivery isanticipated to experience considerable technolo-gical growth in the next 10 years for manyreasons. Ultrasound is an extremely usefulmodality in drug delivery because of its non-invasive nature and the ease with which ultra-sonic waves can be controlled. Additionally, highfrequency ultrasound can be used both as adiagnostic technique and as a delivery mechan-ism. Stabilized polymeric micelles have beensynthesized to increase the vehicle’s circulationtime, its loading capacity and the hydrophobicityof its core in order to meet the needs of theparticular delivery system being investigated.
Thus, the combination of micelles and ultra-sound has a strong potential for the future of drugdelivery in the treatment of malignancies.
RNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009

806 HUSSEINI AND PITT
ACKNOWLEDGMENTS
The authors gratefully acknowledge funding fromthe National Institutes of Health (CA 98138)which supported portions of this research.
REFERENCES
1. Loverock P, Ter Haar G, Ormerod MG, Imrie PR.1990. The effect of ultrasound on the cytoxicity ofAdriamycin. Br J Radiol 63:542–546.
2. Tachibana K, Uchida T, Tamura K, Eguchi H,Yamashita N, Ogawa K. 2000. Enhanced cytotoxiceffect of Ara-C by low intensity ultrasound to HL-60 cells. Cancer Lett 149:189–194.
3. Rediske AM, Hymas WC, Wilkinson R, Pitt WG.1998. Ultrasonic enhancement of antibiotic actionon several species of bacteria. J Gen Appl Microbiol44:283–288.
4. Rediske AM, Rapoport N, Pitt WG. 1999. Reducingbacterial resistance to antibiotics with ultrasound.Lett Appl Microbiol 28:81–84.
5. Qian Z. 1996. Antibiotic and ultrasonic treatmentof bacterial biofilm. MS Thesis, Brigham YoungUniversity, Provo, UT.
6. Qian Z, Sagers RD, Pitt WG. 1997. The role ofinsonation intensity in acoustic-enhanced antibio-tic treatment of bacterial biofilms. Colloids Surf BBiointerfaces 9:239–245.
7. Qian Z, Sagers RD, Pitt WG. 1999. Investigation ofthe mechanism of the bioacoustic effect. J BiomedMater Res 44:198–205.
8. Qian Z, Sagers RD, Pitt WG. 1997. The effect ofultrasonic frequency upon enhanced killing ofP. aeruginosa biofilms. Ann Biomed Eng 25:69–76.
9. Johnson LL, Peterson RV, Pitt WG. 1998. Treat-ment of bacterial biofilms on polymeric implantsusing antibiotics and ultrasound. J Biomater SciPolym Ed 9:1177–1185.
10. Rediske AM, Roeder BL, Brown MK, Nelson JL,Robison RL, Draper DO, Schaalje GB, Robison RA,Pitt WG. 1999. Ultrasonic enhancement of anti-biotic action on Escherichia coli biofilms: Anin vivo model. Antimicrob Agents Chemother43:1211–1214.
11. Rediske AM, Roeder BL, Nelson JL, Robison RL,Schaalje GB, Robison RA, Pitt WG. 2000. Pulsedultrasound enhances the killing of E. coli biofilmsby aminoglycoside antibiotics in vivo. AntimicrobAgents Chemother 44:771–772.
12. Mitragotri S, Blankschtein D, Langer R. 1995.Ultrasound-mediated transdermal protein deliv-ery. Science 269:850–853.
13. Johnson ME, Mitragotri S, Patel A, BlankschteinD, Langer R. 1996. Synergistic effects of chemical
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009
enhancers and therapeutic ultrasound on trans-dermal drug delivery. J Pharm Sci 85:670–677.
14. Bommannan D, Okuyama H, Stauffer P, Guy RH.1992. Sonophoresis. I. The use of high-frequencyultrasound to enhance transdermal drug delivery.Pharm Res 9:559–564.
15. Bommannan D, Menon GK, Okuyama H, Elias PM,Guy RH. 1992. Sonophoresis. II. Examination of themechanism(s) of ultrasound-enhanced transdermaldrug delivery. Pharm Res 9:1043–1047.
16. Rapoport NY, Herron JN, Pitt WG, Pitina L. 1999.Micellar delivery of doxorubicin and its paramag-netic analog, ruboxyl, to HL-60 cells: Effect ofmicelle structure and ultrasound on the intracel-lular drug uptake. J Control Release 58:153–162.
17. Munshi N, Rapoport N, Pitt WG. 1997. Ultrasonicactivated drug delivery from Pluronic P-105micelles. Cancer Lett 117:1–7.
18. Saad AH, Hahn GM. 1989. Ultrasound enhanceddrug toxicity on Chinese hamster ovary cells invitro. Cancer Res 49:5931–5934.
19. Singer AJ, Coby CT, Singer AH, Thode HC Jr.,Tortora GT. 1999. The effects of low-frequencyultrasound on Staphylococcus epidermidis. CurrMicrobiol 38:194–196.
20. Yokoyama M, Okano T, Sakurai Y, Fukushima S,Okamoto K, Kataoka K. 1999. Selective delivery ofAdriamycin to solid tumor using a polymericmicelle carrier system. J Drug Target 7:171–186.
21. Kwon G, Naito M, Yokoyama M, Okano T, SakuraiY, Kataoka K. 1997. Block copolymer micelles fordrug delivery: Loading and release of doxorubicin.J Control Release 48:195–201.
22. Kwon GS, Naito M, Yokoyama M, Okano T,Sakurai Y, Kataoka K. 1995. Physical entrapmentof Adriamicin in AB block copolymer micelles.Pharm Res 12:192–195.
23. Kwon GS, Kataoka K. 1995. Block copolymermicelles as long circulating drug vehicles. AdvDrug Deliv Rev 16:295–309.
24. Gutowska A, Bae YH, Jacobs H, Feijen J, Kim SW.1994. Thermosensitive interpenetrating polymernetworks: Synthesis, characterization, and macro-molecular release. Macromolecules 27:4167–4175.
25. Vernon B, Gutowska A, Kim SW, Bae YH. 1996.Thermally reversible polymer gels for biohybridartificial pancreas. Macromol Symp 109:155–167.
26. Jeong B, Bae YH, Lee DS, Kim SW. 1997. Biode-gradable block copolymers as injectable drug-delivery systems. Nature 388:860–862.
27. Jeong B, Bae YH, Kim SW. 2000. Drug releasefrom biodegradable injectable thermosensitivehydrogel of PEG-PLGA-PEG triblock copolymers.J Control Release 63:155–163.
28. Gao ZG, Lee DH, Kim DI, Bae YH. 2005. Doxor-ubicin loaded pH-sensitive micelle targeting acidicextracellular pH of human ovarian A2780 tumor inmice. J Drug Target 13:391–397.
DOI 10.1002/jps

ULTRASONIC-ACTIVATED MICELLAR DRUG DELIVERY 807
29. Lee ES, Na K, Bae YH. 2003. Polymeric micellesfor tumor pH and folate mediated targeting.J Control Release 91:103–113.
30. Bae Y, Jang WD, Nishiyama N, Fukushima S,Kataoka K. 2005. Multifunctional polymericmicelles with folate-mediated cancer cell targetingand pH-triggered drug releasing properties foractive intracellular drug delivery. Mol Biosystems1:242–250.
31. Lee ES, Na K, Bae YH. 2005. Doxorubicin loadedpH-sensitive polymeric micelles for reversal ofresistant MCF-7 tumor. J Control Release 103:405–418.
32. Bae Y, TA TAD, Zhao A, Kwon GS. 2007. Mixedpolymeric micelles for combination cancer che-motherapy through the concurrent delivery ofmultiple chemotherapeutic agents. J ControlRelease 122:324–330.
33. Bae Y, Buresh RA, Williamson TP, Chen THH,Furgeson DY. 2007. Intelligent biosynthetic nano-biomaterials for hyperthermic combinationchemotherapy and thermal drug targeting ofHSP90 inhibitor geldanamycin. J Control Release122:16–23.
34. Leroux JC. 2007. Injectable nanocarriers for bio-detoxification. Nat Nanotechnol 2:679–684.
35. Le Garrec D, Ranger M, Leroux JC. 2004. Micellesin anticancer drug delivery. Am J Drug Deliv 2:15–42.
36. Leroux JC. 2007. Injectable nanocarriers for bio-detoxification. Nat Nanotechnol 2:679–684.
37. Rossi J, Giasson S, Khalid MN, Delmas P, Allen C,Leroux JC. 2007. Long-circulating poly(ethyleneglycol)-coated emulsions to target solid tumors.Eur J Pharm Biopharm 67:329–338.
38. Torchilin VP. 2005. Lipid-core micelles for tar-geted drug delivery. Curr Drug Deliv 2:319–327.
39. Lukyanov AN, Elbayoumi TA, Chakilam AR,Torchilin VP. 2004. Tumor-targeted liposomes:Doxorubicin-loaded long-circulating liposomesmodified with anti-cancer antibody. J ControlRelease 100:135–144.
40. Kale AA, Torchilin VP. 2007. ‘‘Smart’’ drug car-riers: PEGylated TATp-modified pH-sensitiveliposomes. J Liposome Res 17:197–203.
41. Elbayoumi TA, Torchilin VP. 2007. Enhancedcytotoxicity of monoclonal anticancer antibody2C5-modified doxorubicin-loaded PEGylated lipo-somes against various tumor cell lines. Eur JPharm Sci 32:159–168.
42. Torchilin VP. 2007. Nanocarriers. Pharm Res24:2333–2334.
43. Rapoport NY, Christensen DA, Fain HD, BarrowsL, Gao Z. 2004. Ultrasound-triggered drug target-ing of tumors in vitro and in vivo. Ultrasonics42:943–950.
44. Alexandridis P, Holzwarth JF, Hatton TA. 1994.Micellization of Poly(ethylene oxide)-Poly(propy-
DOI 10.1002/jps JOU
lene oxide)-Poly(ethylene oxide) Triblock Copoly-mer in Aqueous Solutions: Thermodynamicsof Copolymer Association. Macromolecules 27:2414–2425.
45. Alexandridis P, Nivaggioli T, Hatton TA. 1995.Temperature effects on structural properties ofPluronic P104 and F108 PEO-PPO-PEO blockcopolymer solutions. Langmuir 11:1468–1476.
46. Alexandridis P, Athanassiou V, Hatton TA. 1995.Pluronic-P105 PEO-PPO-PEO block copolymer inaqueous urea solutions: Micelle formation, struc-ture, and microenvironment. Langmuir 11:2442–2450.
47. Alexandridis P, Hatton TA. 1995. Poly(ethyleneox-ide)-poly(propyleneoxide)-Poly(ethyleneoxide) blockcopolymer surfactants in aqueous solutions and atinterfaces: Thermodynamics, structure, dynamics,and modeling. Colloids Surf A: Physicochem EngAspects 96:1–46.
48. Alakhov VY, Moskaleva EY, Batrakova E, Kaba-nov AV. 1996. Hypersensitization of multidrugresistant human ovarian carcinoma cells by Pluro-nic P85 block copolymer. Bioconjug Chem 7:209–216.
49. Kabanov AV, Nazarova IR, Astafieva IV, Batra-kova EV, Alakhov VY, Yaroslavov AA, KabanovVA. 1995. Micelle formation and solubilization offluorescent probes in poly(oxyethylene-b-oxypro-pylene-b-oxyethylene) solutions. Macromolecules28:2303–2314.
50. Kabanov AV, Batrakova EV, Melik-NubarovNS, Fedoseev NA, Dorodnich TY, Alakhov VY,Nazarova IR, Kabanov VA. 1992. A new class ofdrug carriers: Micelles of poly(oxyethylene)-poly(oxypropylene) block copolymers as microcontai-ners for targeting drugs from blood to brain.J Control Release 22:141–158.
51. Venne A, Li S, Mandeville R, Kabanov A, AlakhovV. 1996. Hypersensitizing effect of Pluronic L61 oncytotoxic activity, transport, and subcellular dis-tribution of doxorubicin in multiple drug-resistantcells. Cancer Res 56:3626–3629.
52. Batrakova EV, Dorodnych TY, Klinskil EY,Kliushnenkova EN, Shemchukova OB, Goncha-rova ON, Arjakov SA, Alakov VY, Kabanov AV.1996. Anthracycline antibiotics non-covalentlyincorporated into the block copolymer micelles:In vivo evaluation of anti-cancer activity. Br JCancer 74:1545–1552.
53. Miller DW, Batrakova EV, Waltner TO, AlakhovVY, Kabanov AV. 1997. Interaction of Pluronicblock copolymer with brain microvessel endothe-lial cells: Evidence of two potential pathways fordrug absorption. Bioconjug Chem 8:649–657.
54. Kabanov AV, Chekhonin VP, Alakhov VYu, Batra-kova EV, Lebedev AS, Melik-Nubarov NS, Arzha-kov SA, Levashov AV, Morozov GV, Severin ES,Kabanov VA. 1989. The neuroleptic activity of
RNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009

808 HUSSEINI AND PITT
haloperidol increases after its solubilization insurfactant micelles. Micelles as microcontainersfor drug targeting. FEBS Lett 258:343–345.
55. Kabanov AV, Nametkin SN, Klyachko NL, Leva-shov AV. 1990. The principal difference in regula-tion of the catalytic activity of water soluble andmembrane forms of enzymes in reversed micelles.g-Glutamyltransferase and aminopeptidase.FEBS Lett 267:236–238.
56. Kozlov MY, Melik-Nubarov NS, Batrakova EV,Kabanov AV. 2000. Relationship between Pluronicbock copolymer structure, critical micellizationconcentration and partitioning coefficients of lowmolecular mass solutes. Macromolecules 33:3305–3313.
57. Batrakova E, Lee S, Li S, Venne A, Alakhov V,Kabanov A. 1999. Fundamental relationshipsbetween the composition of Pluronic block copoly-mers and their hypersensitization effect in MDRcancer cells. Pharm Res 16:1373–1379.
58. Kozlov MY, Melik-Nubarov NS, Batrakova EV,Kabanov AV. 2000. Relationship between Pluronicblock copolymer structure, critical micellizationconcentration and partitioning coefficients of lowmolecular mass solutes. Macromolecules 33:3305–3313.
59. Kabanov AV, Alakhov VY. 2002. Pluronic blockcopolymers in drug delivery: From micellar nano-containers to biological response modifiers. CritRev Ther Drug Carrier Syst 19:1–73.
60. Batrakova EV, Li S, Li Y, Alakhov VY, ElmquistWF, Kabanov AV. 2004. Distribution kinetics of amicelle-forming block copolymer Pluronic P85.J Control Release 100:389–397.
61. Batrakova E, Li S, Li Y, Alkhov VY, Elmquist W,Kabanov AV. 2004. Distribution kinetics ofmicelle-forming bock copolymer Pluronic 185.J Control Release 100:389–397.
62. Rapoport N, Munshi N, Pitt WG. 1998. 3rd Inter-national Symposium on Polymer Therapeutics,London, pp 32.
63. Rapoport N, Munshi N, Pitina L, Pitt WG. 1997.Pluronic micelles as vehicles for tumor-specific deliv-ery of two anti-cancer drugs to HL-60 cells usingacoustic activation. Polym Preprints 38:620–621.
64. Rapoport N, Pitina L, Munshi N, Pitt WG. 1997.8th International Symposium on Recent Advancesin Drug Delivery Systems, Salt Lake City, Utah,pp 260–261.
65. Husseini GA, El-Fayoumi RI, O’Neill KL, Rapo-port NY, Pitt WG. 2000. DNA damage induced bymicellar-delivered doxorubicin and ultrasound:Comet assay study. Cancer Lett 154:211–216.
66. Husseini GA, Rapoport NY, Christensen DA, PruittJD, Pitt WG. 2002. Kinetics of ultrasonic release ofdoxorubicin from Pluronic P105 micelles. ColloidsSurf B Biointerfaces 24:253–264.
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009
67. Husseini G, Christensen DA, Pitt WG, RapoportN. 1999. Twenty-Fifth Annual Meeting of theSociety For Biomaterials, Providance, RhodeIsland, USA, April 28–May 2, 1999, pp 429.
68. Husseini GA, Pitt WG, Fayoumi RYA, O’Neill KL,Rapoport NY. 1999. AICHE 1999 Annual Meeting,Dallas, Texas, USA, October 31–November 5,1999.
69. Husseini GA, Myrup GD, Pitt WG, ChristensenDA, Rapoport NY. 2000. Factors affecting acous-tically-triggered release of drugs from polymericmicelles. J Control Release 69:43–52.
70. MarinA,SunH,HusseiniGA,PittWG,ChristensenDA, Rapoport NY. 2002. Drug delivery in pluronicmicelles: Effect of high-frequency ultrasound ondrugrelease frommicellesand intracellularuptake.J Control Release 84:39–47.
71. Muniruzzaman MD, Marin A, Luo Y, PrestwichGD, Pitt WG, Husseini G, Rapoport NY. 2002.Intracellular uptake of Pluronic copolymer:Effects of the aggregation state. Colloids Surf BBiointerfaces 25:233–241.
72. Rapoport N, Pitt WG, Sun H, Nelson JL. 2003.Drug delivery in polymeric micelles: From in vitroto in vivo. J Control Release 91:85–95.
73. Rapoport N, Caldwell K. 1994. Structural transi-tions in micellar solutions of Pluronic P-105 andtheir effect on the conformation of dissolved Cyto-chrome C: An electron paramagnetic resonanceinvestigation. Colloids Surf B Biointerfaces3:217–228.
74. Husseini GA, Diaz MA, Richardson ES, Christen-sen DA, Pitt WG. 2005. The role of cavitation inacoustically activated drug delivery. J ControlRelease 107:253–261.
75. Stevenson-Abouelnasr D, Husseini GA, Pitt WG.2007. Further investigation of the mechanism ofDoxorubicin release from P105 micelles usingkinetic models. Colloids Surf B Biointerfaces55:59–66.
76. Marin A, Muniruzzaman M, Rapoport N. 2001.Mechanism of the ultrasonic activation of micellardrug delivery. J Control Release 75:69–81.
77. Rapoport N. 2004. Combined cancer therapy bymicellar-encapsulated drug and ultrasound. Int JPharm 227:155–162.
78. Rapoport N, Marin A, Luo Y, Prestwich GD,Munirzzaman M. 2002. Intracellular uptake andtrafficking of Pluronic micelles in drug-sensitiveand MDR cells: Effect on the intracellular druglocalization. J Pharm Sci 91:157–170.
79. Marin A, Muniruzzaman M, Rapoport N. 2001.Acoustic activation of drug delivery from poly-meric micelles: Effect of pulsed ultrasound.J Control Release 71:239–249.
80. Pruitt JD, Husseini G, Rapoport N, Pitt WG. 2000.Stabilization of Pluronic P-105 micelles with an
DOI 10.1002/jps

ULTRASONIC-ACTIVATED MICELLAR DRUG DELIVERY 809
interpenetrating network of N,N-diethylacryla-mide. Macromolecules 33:9306–9309.
81. Pruitt JD, Pitt WG. 2002. Sequestration and ultra-sound-induced release of doxorubicin fromstabilized Pluronic P105 micelles. Drug Deliv 9:253–259.
82. Husseini GA, Christensen DA, Rapoport NY, PittWG. 2002. Ultrasonic release of doxorubicin fromPluronic P105 micelles stabilized with an inter-penetrating network of N,N-diethylacrylamide.J Control Release 83:302–304.
83. Zeng Y, Pitt WG. 2005. Poly(ethylene oxide)-b-poly(N-isopropylacrylamide) nanoparticles withcrosslinked cores as drug carriers. J BiomaterSci Polym Ed 16:371–380.
84. Husseini GA, Diaz de la Rosa MA, Gabuji T, ZengY, Christensen DA, Pitt WG. 2007. Release ofdoxorubicin from unstabilized and stabilizedmicelles under the action of ultrasound. J NanosciNanotech 7:1–6.
85. Nelson JL, Roeder BL, Carmen JC, Roloff F, PittWG. 2002. Ultrasonically activated chemothera-peutic drug delivery in a rat model. Cancer Res62:7280–7283.
86. Staples BJ, Roeder BL, Pitt WG. 2006. AnnualMeeting of the Society for Biomaterials, Pitts-burgh, PA, USA, April 26–29, 2006, pp 476.
87. Staples BJ. 2007. Pharmacokinetics of Ultrasoni-cally-Released, Micelle-Encapsulated Doxorubicinin the Rat Model and its Effect on Tumor Growth.Chemical Engineering Department, M.S. Thesis,Provo, UT: Brigham Young University.
88. Gao Z, Fain HD, Rapoport N. 2004. Ultrasound-enhanced tumor targeting of polymeric micellardrug carriers. Mol Pharm 1:317–330.
89. Rapoport N, Christensen DA, Fain HD, Barrows L,Gao Z. 2004. Ultrasound-triggered drug targetingof tumors in vitro and in vivo. Ultrasonics 42:943–950.
90. Daniels S, Blondel D, Crum LA, ter Haar GR,Dyson M. 1987. Ultrasonically induced gas bubbleproduction in agar based gels: Part I, experimentalinvestigation. Ultrasound Med Biol 13:527–539.
91. Hill CR. 1971. Ultrasonic exposure thresholds forchanges in cells and tissues. J Acoust Soc Am52:667–672.
92. Brennen CE. 1995. Cavitation and bubble dyna-mics. New York: Oxford University Press. p 282.
93. Urick RJ. 1983. Principles of underwater sound,3rd edition. San Francisco: McGraw-Hill BookCompany. p 423.
94. Kuijpers MWA, van Eck D, Kemmere MF, Keur-entjes JTF. 2002. Cavitation-induced reactions inhigh-pressure carbon dioxide. Science 298:1969–1971.
95. Barnett S. 1998. Thresholds for nonthermal biofef-fects: Theoretical and experimental basis for athreshold index. Ultrasound Med Biol 24:S41–S49.
DOI 10.1002/jps JOU
96. Huber PE, Mann MJ, Melo LG, Ehsan A, Kong D,Zhang L, Rezvani M, Peschke P, Jolesz F, Dzau VJ,Hynynen K. 2003. Focused ultrasound (HIFU)induces localized enhancement of reporter geneexpression in rabbit carotid artery. Gene Therapy10:1600–1607.
97. Hynynen K, McDannold N, Martin H, Jolesz FA,Vykhodtseva N. 2003. The threshold for braindamage in rabbits induced by bursts of ultra-sound in the presence of an ultrasound contrastagent (Optison (R)). Ultrasound Med Biol29:473–481.
98. Miller DL, Thomas RM. 1995. Thresholds forhemorrhages in mouse skin and intestine inducedby Lithotripter shock waves. Ultrasound Med Biol21:249–257.
99. Mitragotri S, Farrell J, Tang H, Terahara T, KostJ, Langer R. 2000. Determination of thresholdenergy dose for ultrasound-induced transdermaldrug transport. J Control Release 63:41–52.
100. Mitragotri S, Ray D, Farrell J, Tang H, Yu B, KostJ, Blankschtein D, Langer R. 2000. Synergisticeffect of low-frequency ultrasound and sodiumlauryl sulfate on transdermal transport.J Pharm Sci 89:892–900.
101. Saad AH, Williams AR. 1982. Effects of therapeu-tic ultrasound on clearance rate of blood bornecolloidal particles in vivo. Br J Cancer 45:202–205.
102. Tachibana K, Tachibana S. 1995. Albumin micro-bubble echo-contrast material as an enhancer forultrasound accelerated thrombolysis. Circulation92:1148–1150.
103. Tezel A, Sens A, Tuchscherer J, Mitragotri S.2001. Frequency dependence of sonophoresis.Pharm Res 18:1694–1700.
104. Nyborg WL. 2001. Biological Effects of Ultra-sound: Development of Safety Guidelines. PartII: General Review. Ultrasound Med Biol27:301–333.
105. Sundaram J, Mellein BR, Mitragotri S. 2003.An experimental and theoretical analysis of ultra-sound-induced permeabilization of cell mem-branes. Biophys J 84:3087–3101.
106. Tezel A, Sens A, Mitragotri S. 2002. Investigationsof the role of cavitation in low-frequency sonophor-esis using acoustic spectroscopy. J Pharm Sci91:444–453.
107. Mitragotri S. 2000. Synergistic effect of enhancersfor transdermal drug delivery. Pharm Res17:1354–1357.
108. Tang H, Wang CCJ, Blankschtein D, Langer R.2002. An investigation of the role of cavitation inlow-frequency ultrasound-mediated transdermaldrug transport. Pharm Res 19:1160–1169.
109. Liu J, Lewis TN, Prausnitz MR. 1998. Non-inva-sive assessment and control of ultrasound-mediated membrane permeabilization. PharmRes 15:918–924.
RNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009
810 HUSSEINI AND PITT
110. Rooney JA. 1970. Hemolysis near an ultrasoni-cally pulsating gas bubble. Science 169:869–871.
111. Gudra T, Opielinski KJ. 2004. Applying spectrumanalysis and cepstrum analysis to examine thecavitation threshold in water and in salt solution.Ultrasonics 42:621–627.
112. Johri GK, Singh D, Johri M, Saxena S, Iernetti G,Dezhkunov N, Yoshino K. 2002. Measurement ofthe intensity of sonoluminescence, subharmonicgeneration and sound emission using pulsed ultra-sonic technique. Jpn J Appl Phys 41:5329–5331.
113. Neppiras EA. 1968. Subharmonic and other low-frequency emission from bubbles in sound-irra-diated liquids. J Acoust Soc Am 46:187–601.
114. Leighton TG. 1994. The acoustic bubble. London:Academic Press. p 613.
115. Flynn HG, Church CC. 1988. Transient pulsationsof small gas bubbles in water. J Acoust Soc Am84:1863–1876.
116. Eller A, Flynn HG. 1969. Generation of subhar-monics of order one-half by bubbles in a soundfield. J Acoust Soc Am 46:722–727.
117. Neppiras EA. 1969. Subharmonic and other low-frequency emission from bubbles in sound-irra-diated liquids. J Acoust Soc Am 46:587–601.
118. Diaz-De-La-Rosa MA. 2007. High-FrequencyUltrasound Drug Delivery and Cavitation Chemi-cal Engineering Department. MS Thesis, BrighamYoung University, Provo, UT.
119. Nyborg WL. 1982. Ultrasonic microstreaming andrelated phenomena. Br J Cancer 45:156–160.
120. Fairbairn DW, Olive PL, O’Neill KL. 1995. Thecomet assay: A comprehensive review. Mutat Res339:37–59.
121. Fairbairn DW, O’Neill KL. 1995. Letter to theEditor: Necrotic DNA degradation mimics apopto-tic nucleosomal fragmentation comet tail length.In Vitro Cell Dev Biol 31:171–173.
122. Fairbairn JJ, Khan MW, Ward KJ, Loveridge BW,Fairbairn DW, O’Neill KL. 1995. Induction ofapoptotic cell DNA fragmentation in human cellsafter treatment with hyperthermia. Cancer Lett89:183–188.
123. Fairbairn DW, Neill KLO. 1996. The neutral cometassay is sufficient to identify an apoptotic ‘window’by visual inspection. Apoptosis 1:91–94.
124. Fairbairn DW, Walburger DK, Fairbairn JJ,O’Neill KL. 1996. Key morphologic changes andDNA strand breaks in human lymphoid cells:Discriminating apoptosis from necrosis. Scanning18:407–416.
125. Husseini GA, O’Neill KL, Pitt WG. 2005. Thecomet assay to determine the mode of cell deathfor the ultrasonic delivery of doxorubicin to humanleukemia (HL-60 cells) from pluronic P105micelles. Technol Cancer Res Treat 4:707–711.
126. Husseini GA, Runyan CM, Pitt WG. 2002. Inves-tigating the mechanism of acoustically activated
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009
uptake of drugs from Pluronic micelles. BMCCancer 2:1–6.
127. Sheikov N, McDannold N, Jolesz F, Zhang YZ,Tam K, Hynynen K. 2006. Brain arterioles showmore active vesicular transport of blood-bornetracer molecules than capillaries and venules afterfocused ultrasound-evoked opening of the blood-brain barrier. Ultrasound Med Biol 32:1399–1409.
128. Schlicher RK, Radhakrishna H, Tolentino TP,Apkarian RP, Zarnitsyn V, Prausnitz MR. 2006.Mechanism of intracellular delivery by acousticcavitation. Ultrasound Med Biol 32:915–924.
129. Stringham SB, Murray BK, O’Neill KL, Ohmine S,Gaufin TA, Pitt. WG. 2005. 96th Annual Meeting ofthe American Association for Cancer Research, Ana-heim, CA, USA, April 16–20, 2005, pp 1415.
130. Yamashita N, Tachibana K, Ogawa K, Tsujita N,Tomita A. 1997. Scanning electron microscopicevaluation of the skin surface after ultrasoundexposure. Anat Rec 247:455–461.
131. Tachibana K, Uchida T, Ogawa K, yamashita N,Tamura K. 1999. Induction of cell-membrane por-osity by ultrasound. Lancet 353:1409.
132. Ogawa K, Tachibana K, Uchida T, Tai T, Yama-shita N, Tsujita N, Miyauchi R. 2001. High-reso-lution scanning electron microscopic evaluation ofcell-membrane porosity by ultrasound. Med Elec-tron Microsc 34:249–2253.
133. Miura S, Tachibana K, Okamoto T, Saku K. 2002.In vitro transfer of antisense oligodeoxynucleotidesinto coronary endothelial cells by ultrasound. Bio-chem Biophys Res Commun 298:587–590.
134. Taniyama Y, Tachibana K, Hiraoka K, Aoki M,Yamamoto S, Matsumoto K, Nakamura T, Ogi-hara T, Kaneda Y, Morishita R. 2002. Develop-ment of safe and efficient novel nonviral genetransfer using ultrasound: Enhancement of trans-fection efficiency of naked plasmid DNA in skeletalmuscle. Gene Ther 9:372–380.
135. Sivakumar M, Tachibana K, Pandit AB, Yasui K,Tuziuti T, Towata A, IIDA Y. 2005. Transdermaldrug delivery using ultrasound-theory, under-standing and critical analysis. Cell Mol Biol 51:OL767–OL784.
136. Saito K, Miyake K, McNeil PL, Kato K, Yago K,Sugai N. 1999. Plasma membrane disruptionunderlies injury of the corneal endothelium byultrasound. Exp Eye Res 68:421–427.
137. Schrama D, Reisfeld RA, Becker JC. 2006. Anti-body targeted drugs as cancer therapeutics. NatRev Drug Discov 5:147–159.
138. Datta SK, Takabayashi K, Raz E. 2003. The ther-apeutic potential of antigen-oligonucleotide con-jugates. Ther Oligonucleotides 1002:105–111.
139. Jeong JH, Lee M, Kim WJ, Yockman JW, Park TG,Kim YH, Kim SW. 2005. Anti-GAD antibody tar-geted non-viral gene delivery to islet beta cells.J Control Release 107:562–570.
DOI 10.1002/jps

ULTRASONIC-ACTIVATED MICELLAR DRUG DELIVERY 811
140. Lathia JD, Leodore L, Wheatley MA. 2004. Poly-meric contrast agent with targeting potential.Ultrasonics 42:763–768.
141. Kim WJ, Yockman JW, Lee M, Jeong JH, Kim YH,Kim SW. 2005. Soluble Flt-1 gene delivery usingPEI-g-PEG-RGD conjugate for anti-angiogenesis.J Control Release 106:224–234.
142. Lum AFH, Borden MA, Dayton PA, Kruse DE,Simon SI, Ferrara KW. 2006. Ultrasound radia-tion force enables targeted deposition of modeldrug carriers loaded on microbubbles. J ControlRelease 111:128–134.
143. Weitman SD, Lark RH, Coney LR, Fort DW,Frasca V, Zurawski VR. 1992. Distribution offolate receptors GP38 in normal malignant celllines and tissues. Cancer Res 52:3396–3401.
144. Coney LR, Tomassetti A, Carayannopoulos L,Frasca V, Kamen BA, Colnaghi MI, ZurawskiVR. 1991. Cloning of a tumor associated antigen:MOv18 and MOv19 antibody recognize a folate-binding protein. Cancer Res 51:6125–6132.
145. Lu JY, Lowe DA, Kennedy MD, Low PS. 1999.Folate-targeted enzyme prodrug cancer therapyutilizing penicillin-V amidase and a doxorubicinprodrug. J Drug Target 7:43–53.
146. Lu JY, Low PS. 2002. Folate-mediated delivery ofmacromolecular anticancer therapeutic agents.Adv Drug Deliv Rev 54:675–693.
DOI 10.1002/jps JOU
147. Lu Jy, Low PS. 2003. Immunotherapy of folatereceptor-expressing tumors: Review of recentadvances and future prospects. J Control Release91:17–29.
148. Steenis JH, Maarseveen EM, Verbaan FJ, VerrijkR, Crommelin DJA, Storm G, Hennink WE. 2003.Preparation and characterization of folate-tar-geted PEG-coated PDMAEMA-based polyplexes.J Control Release 87:167–176.
149. Lee D, Lockey R, Mohapatra S. 2006. Folate recep-tor-mediated caner cell specific gene deliveryusing folic acid-conjugated oligochitosans.J Nanosci Nanotechnol 6:2860–2866.
150. Hofland HE, Masson C, Iginla S, Osetinsky I,Reddy JA, Leamon CP, Scherman D, BessodesM, Wils P. 2002. Folate-targeted gene transferin vivo. Mol Ther 5:739–744.
151. Park EK, Lee SB, Lee YM. 2005. Preparation andcharacterization of methoxy poly(ehtylene glycol)/poly(caprolactone) amphiphilic block copolymericnanospheres for tumor-specific folate-mediatedtargeting of anticancer drugs. Biomaterials 26:1053–1061.
152. Leamon CP, Reddy JA. 2004. Folated-targeted che-motherapy. Adv Drug Deliv Rev 56:1127–1141.
153. Torchilin VP. 2001. Structure and design of poly-meric surfactant-based drug delivery systems.J Control Release 73:137–172.
RNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009




















