
HUMAN GLOMERULAR BASEMENT MEMBRANE: CHEMICAL COMPOSITION IN DIABETES MELLITUS
Upload
independentCategory
view
1download
0
Type 2 diabetes mellitus and Alzheimer’s disease:from physiopathology to treatment implications
Rodrigo O. Moreira1,2*Stella C. Campos1,2
Ana L. Soldera1,2
1Instituto Estadual de Diabetes eEndocrinologia (IEDE), Rio deJaneiro, Brazil2Pontifícia Universidade Católica doRio de Janeiro (PUC-RJ), Rio deJaneiro, Brazil
* Correspondence to:Rodrigo O. Moreira, InstitutoEstadual de Diabetes eEndocrinologia, Rua Moncorvo Filho90, CEP 20211–340, Rio de Janeiro,Brazil.E-mail: [email protected]
Abstract
Alzheimer’s disease (AD) is the most common cause of dementia worldwide. Type2 diabetesmellitus (T2DM) is a disease characterized by insulin resistance (IR) andprogressive β-cell failure, and affected individuals are at increased risk to developseveral forms of cognitive dysfunction, including AD. Different mechanisms havealready been identified linking visceral obesity, IR and AD. IR is associated witha decrease in glucose uptake by neurons, an increase in amyloid β productionand secretion, in the formation of senile plaques, and also in tau protein phosphor-ylation. Othermechanisms also include a decrease in insulin-degrading enzyme ac-tivity and an increase in oxidative stress secondary to hyperglycemia. Takentogether, these mechanisms suggest that drugs used to ameliorate hyperglycemiaand IR may also have beneficial effects in diabetic patients with AD. Indeed,manuscripts investigating the effects of metformin, thiazolidinedione, leptin,GLP-1 therapies, insulin and bariatric surgery in cognition, and AD have beenpublishedwith very promising results, whichmay indicate an alternative approachfor these patients. Copyright © 2013 John Wiley & Sons, Ltd.
Keywords Cognition; Alzheimer´s Disease; Diabetes Mellitus
Introduction
Alzheimer’s disease (AD) is themost common cause of dementia, and it is currentlyresponsible for up to 4 million cases worldwide. The risk of AD increases exponen-tially with age and doubles every 5 years after 65 years old. Nowadays, AD can befound in up to 50% of the population older than 85 years old [1,2]. The conceptthat dementia is a common and an unpreventable consequence of ageing is widelydisseminated. However, this is not always true. The diagnosis and treatment areusually inadequate because most of the times symptoms are recognized neitherby the physicians nor by the patients (or their families). Recent data suggest thatless than 50% of the patients with dementia receive a formal diagnosis, and thenumber of individuals who receive adequate treatment is even lower [3].
Type 2 diabetes mellitus (T2DM) is a disease characterized by insulinresistance (IR) and progressive β-cell failure. IR is defined as an inadequateresponse by insulin target tissues, such as skeletal muscle, liver and adiposetissue, to the physiological effects of circulating insulin. In the early stages ofT2DM, there is a compensatory increase in insulin levels (hyperinsulinemia)in response to IR [4]. As the disease progress, insulin levels begin to dropand diabetic patients, particularly those with long-term disease, have very
REVIEW ARTICLE
Received: 06 August 2012Revised: 14 February 2013Accepted: 03 June 2013
Copyright © 2013 John Wiley & Sons, Ltd.
DIABETES/METABOLISM RESEARCH AND REVIEWSDiabetes Metab Res Rev 2013.Published online in Wiley Online Library (wileyonlinelibrary.com) DOI: 10.1002/dmrr.2442
low levels of circulating insulin. Recent studies haveindicated that elderly people with T2DM have a higherrisk of cognitive dysfunction and dementia [5], includingthe clinical diagnosis of AD-type dementia [6]. The aimof this review is to discuss the possible mechanismslinking T2DM to AD and also to discuss the effects ofanti-diabetic medication in cognitive function.
Basic concepts in AD – Aβ depositionand tau protein phosphorylation
Alzheimer’s disease is a neurodegenerative diseasecharacterizedbyaprogressivedestructionofneurons.Severalmechanismshave alreadybeen implied in thedevelopmentofAD, and two of the most important are amyloid β (Aβ)depositionand tauproteinhyperphosphorylation.
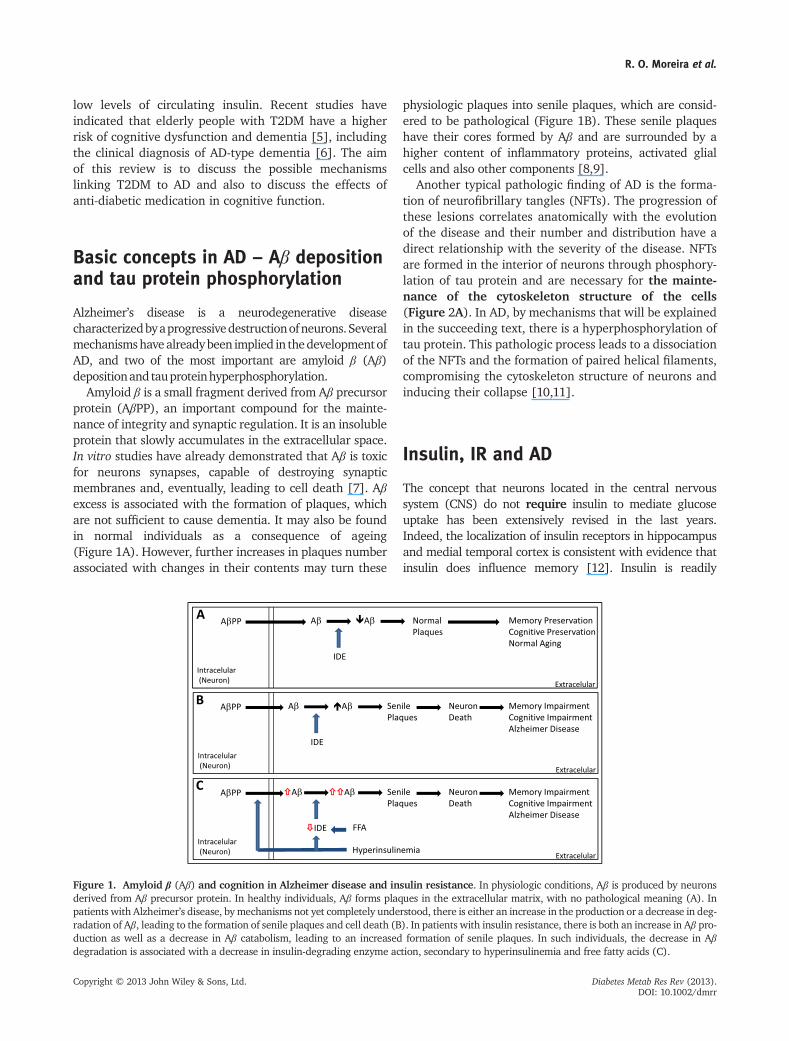
Amyloid β is a small fragment derived from Aβ precursorprotein (AβPP), an important compound for the mainte-nance of integrity and synaptic regulation. It is an insolubleprotein that slowly accumulates in the extracellular space.In vitro studies have already demonstrated that Aβ is toxicfor neurons synapses, capable of destroying synapticmembranes and, eventually, leading to cell death [7]. Aβexcess is associated with the formation of plaques, whichare not sufficient to cause dementia. It may also be foundin normal individuals as a consequence of ageing(Figure 1A). However, further increases in plaques numberassociated with changes in their contents may turn these
physiologic plaques into senile plaques, which are consid-ered to be pathological (Figure 1B). These senile plaqueshave their cores formed by Aβ and are surrounded by ahigher content of inflammatory proteins, activated glialcells and also other components [8,9].
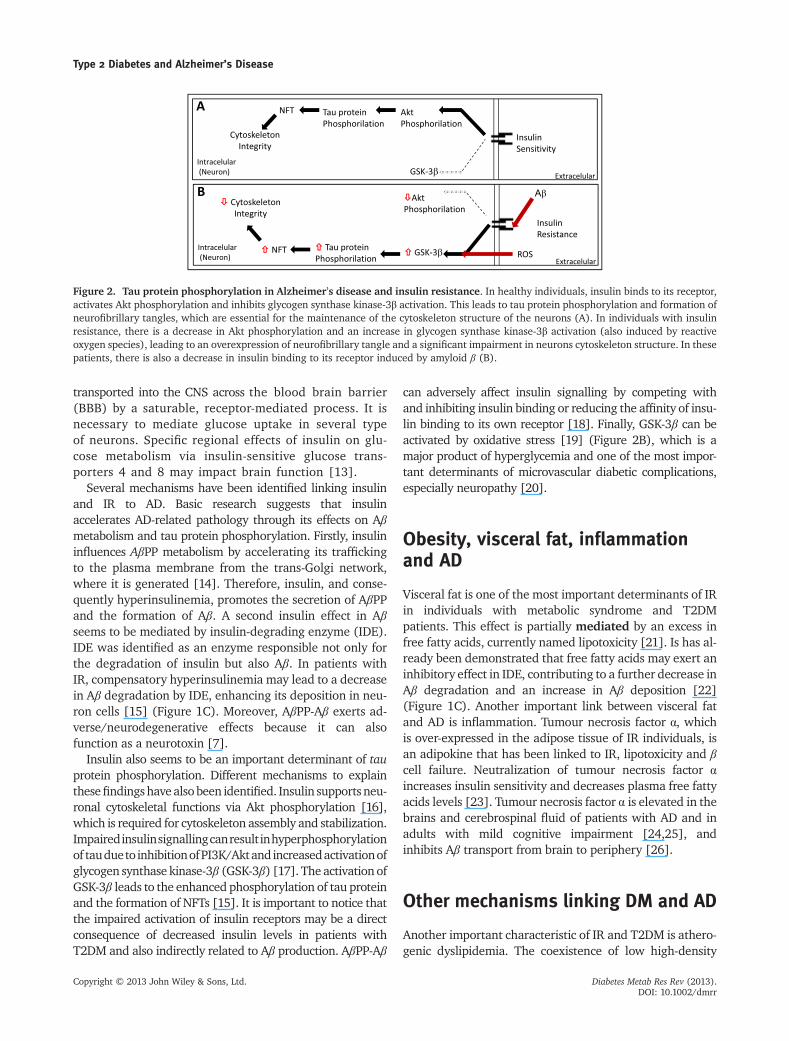
Another typical pathologic finding of AD is the forma-tion of neurofibrillary tangles (NFTs). The progression ofthese lesions correlates anatomically with the evolutionof the disease and their number and distribution have adirect relationship with the severity of the disease. NFTsare formed in the interior of neurons through phosphory-lation of tau protein and are necessary for the mainte-nance of the cytoskeleton structure of the cells(Figure 2A). In AD, by mechanisms that will be explainedin the succeeding text, there is a hyperphosphorylation oftau protein. This pathologic process leads to a dissociationof the NFTs and the formation of paired helical filaments,compromising the cytoskeleton structure of neurons andinducing their collapse [10,11].
Insulin, IR and AD
The concept that neurons located in the central nervoussystem (CNS) do not require insulin to mediate glucoseuptake has been extensively revised in the last years.Indeed, the localization of insulin receptors in hippocampusand medial temporal cortex is consistent with evidence thatinsulin does influence memory [12]. Insulin is readily
Figure 1. Amyloid β (Aβ) and cognition in Alzheimer disease and insulin resistance. In physiologic conditions, Aβ is produced by neuronsderived from Aβ precursor protein. In healthy individuals, Aβ forms plaques in the extracellular matrix, with no pathological meaning (A). Inpatients with Alzheimer’s disease, by mechanisms not yet completely understood, there is either an increase in the production or a decrease in deg-radation of Aβ, leading to the formation of senile plaques and cell death (B). In patients with insulin resistance, there is both an increase in Aβ pro-duction as well as a decrease in Aβ catabolism, leading to an increased formation of senile plaques. In such individuals, the decrease in Aβdegradation is associated with a decrease in insulin-degrading enzyme action, secondary to hyperinsulinemia and free fatty acids (C).
R. O. Moreira et al.
Copyright © 2013 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2013).DOI: 10.1002/dmrr
transported into the CNS across the blood brain barrier(BBB) by a saturable, receptor-mediated process. It isnecessary to mediate glucose uptake in several typeof neurons. Specific regional effects of insulin on glu-cose metabolism via insulin-sensitive glucose trans-porters 4 and 8 may impact brain function [13].
Several mechanisms have been identified linking insulinand IR to AD. Basic research suggests that insulinaccelerates AD-related pathology through its effects on Aβmetabolism and tau protein phosphorylation. Firstly, insulininfluences AβPP metabolism by accelerating its traffickingto the plasma membrane from the trans-Golgi network,where it is generated [14]. Therefore, insulin, and conse-quently hyperinsulinemia, promotes the secretion of AβPPand the formation of Aβ. A second insulin effect in Aβseems to be mediated by insulin-degrading enzyme (IDE).IDE was identified as an enzyme responsible not only forthe degradation of insulin but also Aβ. In patients withIR, compensatory hyperinsulinemia may lead to a decreasein Aβ degradation by IDE, enhancing its deposition in neu-ron cells [15] (Figure 1C). Moreover, AβPP-Aβ exerts ad-verse/neurodegenerative effects because it can alsofunction as a neurotoxin [7].
Insulin also seems to be an important determinant of tauprotein phosphorylation. Different mechanisms to explainthesefindingshave also been identified. Insulin supports neu-ronal cytoskeletal functions via Akt phosphorylation [16],which is required for cytoskeleton assembly and stabilization.Impairedinsulinsignallingcanresultinhyperphosphorylationof taudueto inhibitionofPI3K/Aktandincreasedactivationofglycogen synthase kinase-3β (GSK-3β) [17]. The activation ofGSK-3β leads to the enhanced phosphorylation of tau proteinand the formation of NFTs [15]. It is important to notice thatthe impaired activation of insulin receptors may be a directconsequence of decreased insulin levels in patients withT2DM and also indirectly related to Aβ production. AβPP-Aβ
can adversely affect insulin signalling by competing withand inhibiting insulin binding or reducing the affinity of insu-lin binding to its own receptor [18]. Finally, GSK-3β can beactivated by oxidative stress [19] (Figure 2B), which is amajor product of hyperglycemia and one of the most impor-tant determinants of microvascular diabetic complications,especially neuropathy [20].
Obesity, visceral fat, inflammationand AD
Visceral fat is one of the most important determinants of IRin individuals with metabolic syndrome and T2DMpatients. This effect is partially mediated by an excess infree fatty acids, currently named lipotoxicity [21]. Is has al-ready been demonstrated that free fatty acids may exert aninhibitory effect in IDE, contributing to a further decrease inAβ degradation and an increase in Aβ deposition [22](Figure 1C). Another important link between visceral fatand AD is inflammation. Tumour necrosis factor α, whichis over-expressed in the adipose tissue of IR individuals, isan adipokine that has been linked to IR, lipotoxicity and βcell failure. Neutralization of tumour necrosis factor αincreases insulin sensitivity and decreases plasma free fattyacids levels [23]. Tumour necrosis factor α is elevated in thebrains and cerebrospinal fluid of patients with AD and inadults with mild cognitive impairment [24,25], andinhibits Aβ transport from brain to periphery [26].
Other mechanisms linking DM and AD
Another important characteristic of IR and T2DM is athero-genic dyslipidemia. The coexistence of low high-density
Figure 2. Tau protein phosphorylation in Alzheimer’s disease and insulin resistance. In healthy individuals, insulin binds to its receptor,activates Akt phosphorylation and inhibits glycogen synthase kinase-3β activation. This leads to tau protein phosphorylation and formation ofneurofibrillary tangles, which are essential for the maintenance of the cytoskeleton structure of the neurons (A). In individuals with insulinresistance, there is a decrease in Akt phosphorylation and an increase in glycogen synthase kinase-3β activation (also induced by reactiveoxygen species), leading to an overexpression of neurofibrillary tangle and a significant impairment in neurons cytoskeleton structure. In thesepatients, there is also a decrease in insulin binding to its receptor induced by amyloid β (B).
Type 2 Diabetes and Alzheimer’s Disease
Copyright © 2013 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2013).DOI: 10.1002/dmrr

lipoprotein cholesterol with increased levels of triglycer-ides, and small and dense low-density lipoprotein choles-terol is often associated with both subclinical and clinicalatherosclerosis, including cerebrovascular disease [4].Recent studies have suggested that these modifications inthe vascular wall may also influence cognitive status,including the development of AD. It has been hypothesizedthat even small increases in carotid intima media thicknessmay produce diffuse hypoperfusion with chronic hypoxia,which might ultimately trigger neurodegenerative changes[27]. An altered cerebral hemodynamic might also favourthe cognitive decline by producing a detrimental effect onthe neurovascular unit. A deregulation of the neurovascularunitwould reduce the clearance of products of inflammation,oxidative stress and of Aβ promoting neurodegeneration[28]. In line with this hypotheses, Silvestrini et al. demon-strated that the progression of subclinical carotid disease(measured through intima media thickness) is directlyassociated with the decline in cognitive function (measuredwith mini-mental state examination) after 1 year of followup in patients previously diagnosed with dementia [29].
Is there a role for anti-diabeticmedication in Alzheimer’s treatment?
The relationship among IR, T2DM and AD seemsundoubtedly. However, it still needs to be determinedwhether the use of anti-diabetic medications, particularlyinsulin sensitizers and insulin, could have any beneficialeffects in cognition and memory. Although there is onlya few manuscript published in this topic, results suggesta promising effect of insulin sensitizers and intranasalleptin, among others, in the treatment of AD.
Insulin sensitizer – metformin
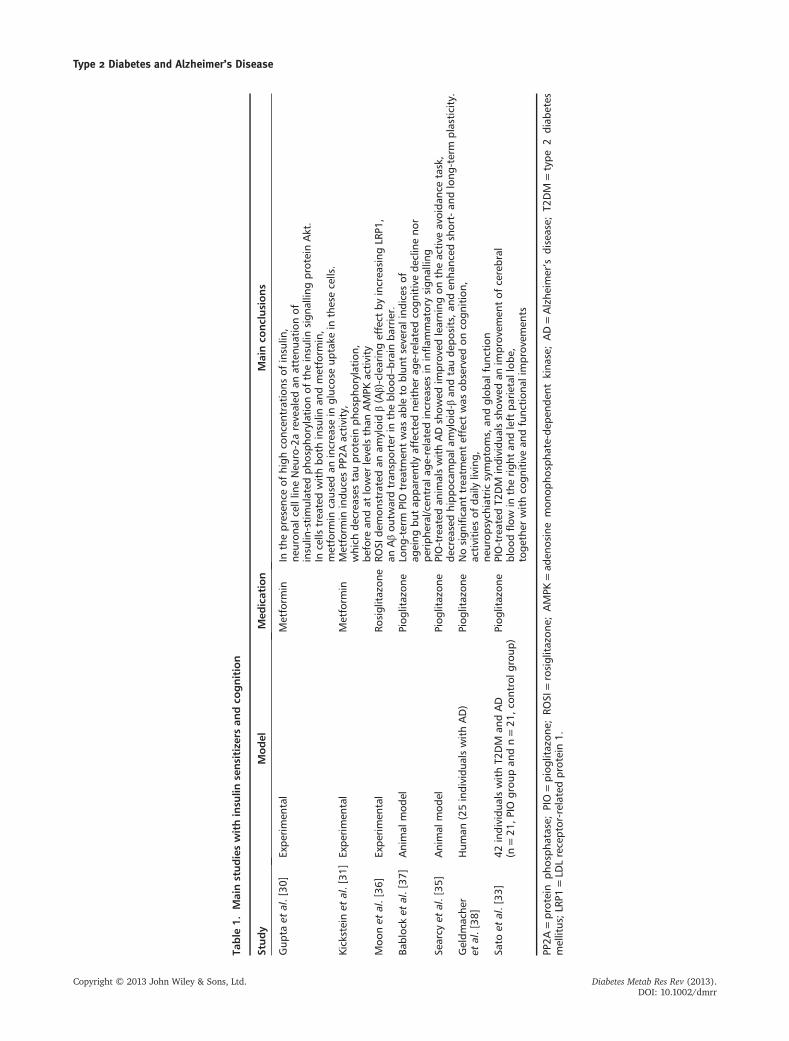
The effects of metformin in cognition and AD have beenstudied both in vitro and in animal models. Gupta et al.studied metformin effects on neuronal IR andAD-associated characteristics in an in vitro model of ‘type3 diabetes’ by differentiating neuronal cell line Neuro-2aunder prolonged presence of insulin. A time-coursedanalysis with 100 nM insulin revealed an attenuation ofinsulin-stimulated phosphorylation of the key insulinsignalling protein Akt (Table 1). It should be noticed thata decrease in Akt phosphorylation is associated with anincrease in tau protein phosphorylation. They alsoobserved a marked reduction in insulin-stimulated tyro-sine phosphorylation of IRß in cells under prolongedpresence of insulin. The results from this study thussuggest that metformin could effectively ameliorate theimpaired glucose uptake in insulin-resistant neuronal
cells. Treatment with metformin did not affect cellmorphology, growth rates or caused cell death. Finally,metformin effect on adenosine monophosphate-dependentkinase (AMPK) activation was tested and an enhancementin AMPK phosphorylation, as compared with respectiveuntreated controls, was demonstrated. These results suggestthat the use of insulin sensitizer drugmetformin, well-knownfor its action in peripheral tissues, could also directly sensitizethe impaired insulin action in neuronal IR [30].
Another important study suggests that metforminactivates a kinase implicated in tau protein phosphoryla-tion [31]. The enzyme named protein phosphatase 2A(PP2A) seems to be the major tau phosphatase, andefficiently dephosphorylates tau in vitro and in vivo[31,32]. The authors demonstrated that metformin has adirect effect on the association between PP2Ac, theregulatory subunit of PP2A-α4, and the ubiquitin ligaseMID1, which targets microtubule-associated PP2A fordegradation via the proteasome. The study demonstrateda significant insulin-independent influence of metforminon the phosphorylation pattern of the AD-related tau pro-tein. It also suggests a potential beneficial effect of long-term metformin treatment and raises the expectation thatmetformin would have a neuroprotective and prophylacticeffect in patients with the predisposition for AD [31].
Insulin Sensitizer – PPAR-γ Agonists
Thiazolidinedione (TZD) activate peroxisome proliferator-activated receptor gamma (PPAR-γ) and are used toimprove peripheral insulin sensitivity in T2DM. PPAR-γmay offer some therapeutic relief for AD by loweringperipheral insulin and enhancing insulin sensitivity,including in substantia nigra pars compacta neurons. Inaddition, PPAR-γ agonists have been shown to inhibitinflammatory gene expression [33], alter Aß and exhibitneuroprotective effects [34]. A few mechanisms have al-ready been proposed to explain these neuroprotectiveeffects. As shown in Table 1, TZDs may directly decreaseAβ deposition and tau protein hyperphosphorylation[35], or act indirectly through an Aβ-clearing effect [36].
As ageing is a common risk factor for both AD andT2DM, Blalock et al. investigated whether pioglitazonecould alter brain ageing under non-pathological condi-tions. Male rats were treated for 4–5 months with eithera control or a pioglitazone-containing diet and a reductionin the Ca2+�dependent afterhyperpolarization was seenin aged animals, with no significant change in long-termpotentiation maintenance or learning and memory perfor-mance. Finally, a combination of microarray analyses ofhippocampal tissue and serum-based multiplex cytokineassays revealed that age-dependent inflammatory increases
R. O. Moreira et al.
Copyright © 2013 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2013).DOI: 10.1002/dmrr
Table
1.Mainstudieswithinsu
linsensitize
rsan
dco
gnition
Study
Model
Med
ication
Mainco
nclusions
Gup
taet
al.[30
]Expe
rimen
tal
Metform
inIn
thepresen
ceof
high
conc
entrations
ofinsulin
,ne
uron
alcelllin
eNeu
ro-2arevealed
anattenu
ationof
insulin
-stimulated
phosph
orylationof
theinsulin
sign
allin
gproteinAkt.
Incells
trea
tedwithbo
thinsulin
andmetform
in,
metform
incaused
anincrea
sein
gluc
oseup
take
inthesecells.
Kicksteinet
al.[31
]Expe
rimen
tal
Metform
inMetform
inindu
cesPP
2Aactivity,
which
decrea
sestauproteinph
osph
orylation,
before
andat
lower
levelsthan
AMPK
activity
Moo
net
al.[36
]Expe
rimen
tal
Rosiglitazon
eRO
SIde
mon
stratedan
amyloidβ(Aβ)-clearingeffect
byincrea
sing
LRP1
,an
Aβou
twardtran
sporterin
thebloo
d–brainba
rrier.
Babloc
ket
al.[37
]Animal
mod
elPiog
litazon
eLo
ng-term
PIO
trea
tmen
twas
able
toblun
tseveralind
ices
ofag
eing
butap
parently
affected
neithe
rag
e-relatedco
gnitivede
clineno
rpe
riph
eral/cen
tral
age-relatedincrea
sesin
inflam
matorysign
allin
gSe
arcy
etal.[35
]Animal
mod
elPiog
litazon
ePIO-treated
anim
alswithADshow
edim
prov
edlearning
ontheactive
avoida
ncetask,
decrea
sedhipp
ocam
pala
myloid-βan
dtaude
posits,a
nden
hanc
edshort-an
dlong
-term
plasticity.
Geldm
ache
ret
al.[38
]Hum
an(25individu
alswithAD)
Piog
litazon
eNosign
ificant
trea
tmen
teffect
was
observed
onco
gnition,
activities
ofda
ilyliving,
neurop
sych
iatric
symptom
s,an
dglob
alfunc
tion
Sato
etal.[33
]42
individu
alswithT2
DM
andAD
(n=21
,PIO
grou
pan
dn=21
,con
trol
grou
p)Piog
litazon
ePIO-treated
T2DM
individu
alsshow
edan
improv
emen
tof
cerebral
bloo
dflow
intherigh
tan
dleft
parietal
lobe
,toge
ther
withco
gnitivean
dfunc
tion
alim
prov
emen
ts
PP2A
=protein
phosph
atase;
PIO=piog
litazon
e;RO
SI=rosiglitazon
e;AMPK
=ad
enosine
mon
opho
spha
te-dep
ende
ntkina
se;AD=Alzhe
imer’s
disease;
T2DM
=type
2diab
etes
mellitus;L
RP1=LD
Lreceptor-related
protein1.
Type 2 Diabetes and Alzheimer’s Disease
Copyright © 2013 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2013).DOI: 10.1002/dmrr

were not reversed by the PPAR-γ [37]. Conclusions for thisstudy are presented in Table 1.
The beneficial effects of TZD in cognition have alreadybeen demonstrated in humans. However, results are stillcontradictory. For instance, Sato et al. decided to test theeffects of pioglitazone on cognition, regional cerebralblood flow and plasma levels of Aß40 and Aß42. To reachthis goal, a controlled trial in T2DM patients with mild ADwas performed. The pioglitazone group showed animprovement of regional cerebral blood flow in the rightand left parietal lobe and some regions of the frontal lobe.In contrast, the control group showed no improvement ofregional cerebral blood flow in any brain regions. Animprovement in insulin action in the brain was alsodemonstrated, resulting in cognitive improvement [33].On the other hand, Geldmacher et al. failed to demon-strate any significant effect of pioglitazone on cognition,activities of daily living, neuropsychiatric symptoms andglobal function of patients with AD [38].
Leptin
Leptin is a protein that was originally discovered as anadipocyte-derived hormone that controls feeding behaviourthrough receptors in the hypothalamus [39]. It has beenshown that it has some important physiological roles in thecontrol of fat storage and mobilization, the reproductivesystem, the immune system, bone homeostasis, insulinsensitivity, and neuronal activity and protection.
Leptin receptors have been identified in peripheral tissues,and in neurons in the brain, including the hippocampus,which is particularly vulnerable in AD [16,40–42]. Leptinhas been shown to reduce the amount of extracellular Aβ,both in vitro and in vivo models of AD, as well as to reducetau protein phosphorylation in neuronal cells. One of themost important activities of leptin is the control of AMPK.In addition to maintaining lipid levels, AMPK may also beof great relevance to AD, because its activation may directlydecrease tau protein phosphorylation, at least in vitro. Asecond mechanism attributed to leptin involves theAMPK-mediated down regulation of GSK-3β, which is an im-portant activator of tau hyperphosphorylation. Importantly,chronic administration of leptin resulted in a significantimprovement in the cognitive performance of transgenicanimal models of AD.
On the basis of the available data, select neuronalpopulations may have a deficient/defective AMPK systemfor one or more of the following reasons: low leptin/insu-lin levels, low leptin/insulin sensitivity, abnormal choles-terol and fatty acid membrane composition, and lowglucose uptake. These pathways can then lead to changesin synaptic properties, to an increase in Aβ deposition, to
an increase in tau protein phosphorylation and finallydeath. These intriguing biological activities of leptin holda promise for long-term therapeutic benefit for ADpatients. Its unique mode of action in the CNS canpositively sway disease pathways and may be used as adesirable complementation to other strategies [19].
Insulin
Insulin has a profound effect in the CNS where it entersthrough the BBB. It is responsible for many key processesin the brain, such as food intake, energy homeostasis, repro-ductive endocrinology, synaptic activity, peripheral insulinactions, learning andmemory. It also regulates neural prolif-eration, apoptosis and synaptic transmission [43,44].
The importance of insulin in the pathogenesis of AD seemsto be a paradox. In the early stages of IR, hyperinsulinemiaassociated with an impaired transport of insulin throughthe BBB leads to an impaired activation of insulin receptorin neurons, to an increase in tau protein phosphorylationand in Aβ deposition. As disease progress, insulin levels beginto fall. It should be noted that T2DM is characterized by lowinsulin levels, particularly in those patients with long-termdisease. Consequently, insulin levels in the CNS should alsobe low. Therefore, although insulin excess may contributeto the development of AD in the early stages of disease,insulin deficient seems to aggravate cognitive impairmentin patients with long-term disease. This hypothesis suggeststhat insulin replacement may be of some benefit in specificpopulations of diabetic patients with AD.
Plastino et al. developed a study to evaluate cognitiveimpairment patients with AD and T2DM with either oralanti-diabetic drugs or combination of insulin with othermedications. Medications for AD were kept unchanged. Atthe end of the study, authors evaluated cognitive functionand memory ability in 104 patients. A significant slowingin cognitive decline was demonstrated in the group ofpatients treated with a combination of insulin and oralanti-diabetic medications (group B) in comparison withthe group treated only with oral medications (group A).Among group B patients, more than 76.8% were found tobe stabilized over 12 months on mini-mental state scores[45]. Another important study, the Honolulu–Asia AgingStudy, demonstrated that the effect of high levels of insulinon the risk of dementia was independent of diabetes andblood glucose level [46]. Conversely, some studies supportedthat intranasal insulin improves memory and cognitiveabilities in patients with early AD [47].
Insulin therapy could have an independent effect on cog-nitive performance, and this could be explained throughdifferent mechanisms. For instance, insulin promotes cellmembrane expression of N-Methyl-D-aspartate receptors,
R. O. Moreira et al.
Copyright © 2013 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2013).DOI: 10.1002/dmrr
which increases neuronal Ca2+ influx [48]. Ca2+ influxpresumably activates Ca2+-dependent enzymes, includingα-dependent enzymes and, strengthens neuronal synapticassociation [49]. Low doses of exogenous insulin mayincrease cerebral glucose metabolism, and then modulateselective brain functions, such as memory [50], and alsoneurotransmitter synthesis and secretion, reversing theamnestic effects of cholinergic blockade [51]. However,these studies did not take into account glycemic controland the overall effects of hyperglycemia in cognition.
Intranasal insulin
Intranasal delivery is a non-invasive mean of bypassingthe BBB and introduces this hormone to the brain withouta significant rise in its circulating levels. Shemesh et al.systematically reviewed and analysed existing clinicaltrials that assessed the potential beneficial effects of intra-nasal insulin administration on cognitive functions. Eightstudies (328 participants) were analysed. In healthypeople, Cohen’s effect size calculations suggest that only160 IU/d intranasal insulin induced potential beneficialeffects [52]. Among cognitively impaired patients, onlylower doses of insulin were assessed, and 20 IU revealedpotential beneficial effects on cognitive function. Thiswas significant in a single study assessing long-termintranasal insulin administration, whereas acute adminis-tration of 20 IU intranasal insulin tended to show abeneficial effect on immediate recall in APOE ε 4(�),but not APOE ε 4(+) patients [53]. The current limitedclinical experience suggests potential benefit on cognitiveeffects of intranasal insulin but more analyses should beprovided for clinical considerations for the future.
Incretins hormones
The incretins glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) have very simi-lar properties in protecting neurons from toxic effects, andare capable of reversing the detrimental effects that Aβ frag-ments have on synaptic plasticity. GLP-1 is an endogenous30-amino acid peptide hormone, which is released by intesti-nal L-cells and binds to the GLP-1 receptor (GLP-1R) coupledto the cyclic AMP second messenger pathway [54]. GLP-1Rstimulation enhances β -cell proliferation, glucose-dependentinsulin secretion and lowers blood glucose in T2DM patients[55]. GLP-1R is found in neurons in brains of rodents andhumans [56]. Moreover, GLP-1 and exendin-4, a more stableanalogue of GLP-1, have been shown to reduce endogenouslevels of Aβ in the mouse brain and AβPP in neurons [57].GIP is also a gastrointestinal hormone that is secreted in
response to food intake. It has modulating effects on bloodsugar levels similar to GLP-1 or insulin [58,59]. Recently, ithas been found that GIP receptors are also expressed in neu-rons in the CNS [60]. Furthermore, GIP receptors are foundin neuronal progenitor cells [61]. These two hormones havea half-time of minutes in the blood stream and for thetreatment of T2DM, long-lasting analogues have been devel-oped not to be broken down by the endogenous proteasedipeptidyl peptidase-4.
The same biochemical mechanisms that control neuro-transmitters release into the synaptic cleft via cyclic AMPlevel regulation are found in neurons [62–64]. Bindingsites for GLP-1Rs have been found in the hypothalamus,striatum, brain stem, substantia nigra and subventricularzone among other structures [65–67]. Moreover, it hasbeen hypothesized that GLP-1 can influence brain metab-olism. In fact, a small human study with positron emissiontomography with 18-fluorodeoxyglucose has shown a pos-sible effect of GLP-1 in brain glucose metabolism. The au-thors hypothesized that GLP-1 may exert a neuroprotectiveeffect by limiting intracerebral glucose fluctuation in post-prandial periods, when plasma glucose is increased [68].GLP-1R expression has also been observed in specific cellularsubtypes, which are crucial for memory and learningfunctions [69]. GLP-1R activation has been shown to reverseneuronal insulin receptor desensitization [70]. An importantadvantage of administering incretins over insulin is the factthat incretins only affect high glucose level triggered insulinrelease but show little effect in normoglycaemic situations.This opens the possibility to administer incretins to peoplewho do not have T2DM [71]. However, further studies arenecessary to confirm these hypotheses.
Bariatric surgery
Ghanim et al. hypothesized that AβPP, expressed inthe peripheral blood mononuclear cells, diminishes af-ter marked caloric restriction and weight loss associ-ated with Roux-en-Y gastric bypass surgery. FifteenT2DM patients with morbid obesity underwent Roux-en-Y gastric bypass, and the expression of inflamma-tory and AD-related genes was examined before andafter 6 months in plasma and in mononuclear cells.The expression of APP mRNA fell by 30%, and thatof protein fell by 36%. In addition, there was a reduc-tion in the expression of other AD-related genesincluding presinilin-2, ADAM-9, GSK-3ß, PICALM,SORL-1 and clusterin. They conclude that obesityand caloric intake modulate the expression of AβPPin mononuclear cells. And it is relevant that cognitivefunction has been shown to improve with weight lossfollowing bariatric surgery [71].
Type 2 Diabetes and Alzheimer’s Disease
Copyright © 2013 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2013).DOI: 10.1002/dmrr

ConclusionsIn the last years, the importance of insulin in memoryformation, cognition and neuron function has been exten-sively revised. The former concept that neurons do notrequire insulin for glucose transport has been provenwrong, and insulin has been shown to modulate severalother actions in the CNS. Therefore, diseases that compro-mise either insulin levels and/or insulin function may leadto neurological damage, including neurodegenerative dis-eases. In line with this hypothesis, IR and T2DM wereidentified as major pathogenic determinants of AD. Thisrelationship has been demonstrated in vivo, in vitro andalso in epidemiological studies. Moreover, other compo-nents of these diseases, such as atherogenic dyslipidemia,inflammation, micro and macrovascular disease, andoxidative stress may contribute, or even exacerbate,neuron dysfunction.
The concept that IR, T2DM and AD share common patho-physiological features suggests that drugs that improve gly-cemic levels and IR might have additional benefits in T2DMpatients with cognitive dysfunction, including patients with
AD. A few studies have already been performed but resultsare still preliminary and, in some cases, contradictories.Larger, randomized, double-blind trials are necessary toelucidate the effects of some anti-diabetic medications,including metformin, pioglitazone, dipeptidyl peptidase-4inhibitors and GLP-1 analogues/agonists in the preventionand/or progression of cognitive dysfunction, particularly inpatients with T2DM. Because of the impact of AD inmortal-ity and quality of life, treatment should be initiated as soonas possible to prevent the progression of the disease.Therefore, it should be also considered that these studiesshould evaluate the effects of these medications in combi-nation and in early stages of IR, and not only after the diag-nosis of T2DM.
Conflict of interest
Rodrigo O. Moreira received Speaker fees from Novartis,Novo Nordisk, Abbott, Merck Serono, Servier and MSD.Stella C. Campos and Ana L. Soldera have no conflicts ofinterest to declare.
References
1. Blennow K, de Leon MJ, ZetterbergH. Alzheimer’s disease. Lancet 2006;368: 387–403.
2. Hebert LE, Scherr PA, Bienias JL,Bennett DA, Evans DA. Alzheimerdisease in the US population: prevalenceestimates using the prevalence estimatesusing the 2000 census. Arch Neurol2003; 60(8): 1119–22.
3. Lopez OL. The growing burden ofAlzheimer’s disease. Am J Manag Care2011; 17(Suppl 13): S339–45.
4. DeFronzo RA. Insulin resistance,lipotoxicity, type 2 diabetes and athero-sclerosis: the missing links. The ClaudeBernard Lecture 2009. Diabetologia2010; 53(7): 1270–87.
5. Stewart R, Liolitsa D. Type 2 diabetesmellitus, cognitive impairment anddementia. Diabet Med 1999; 16: 93–112.
6. Li L, Hölscher C. Common pathologicalprocesses in Alzheimer disease and type2 diabetes: a review. Brain Res Rev 2007;56: 384–402.
7. Dore S, Kar S, Quirion R. Insulin-likegrowth factor I protects and rescues hippo-campal neurons against beta-amyloid- andhuman amylin-induced toxicity. Proc NatlAcad Sci USA 1997; 94: 4772–4777.
8. LaFerla FM, Green KN, Oddo S. Intracel-lular amyloid-beta in Alzheimer’s disease.Nat Rev Neurosci 2007; 8(7): 499–509.
9. Selkoe DJ. Alzheimer’s disease results fromthe cerebral accumulation and cytotoxicityof amyloid beta-protein. J Alzheimers Dis-ease 2001; 3: 75–80.
10. Braithwaite SP, Stock JB, Lombroso PJ,Nairn AC. Protein phosphatases andAlzheimer’s disease. Prog Mol Biol TranslSci2012;106: 343–79.
11. Boutajangout A, Sigurdsson EM,Krishnamurthy PK. Tau as a therapeutictarget for Alzheimer’s disease. CurrAlzheimer Res 2011; 8(6): 666–77.
12. Craft S. The Role of metabolic disordersin Alzheimer’s disease and vasculardementia: two roads converged? ArchNeurol 2009; 66(3): 300–305.
13. Jolivalt CG, Lee CA, Beiswenger KK, et al.Defective insulin signaling pathway andincreased glycogen synthase kinase-3activity in the brain of diabetic mice:parallels with Alzheimer’s disease andcorrection by insulin. J Neurosci Res2008; 86(15): 3265–3274.
14. de la Monte SM. Insulin resistance andAlzheimer’s disease.BMBRep2009;42(8):475–81.
15. Umegaki H. Pathophysiology of cognitivedysfunction in older people with type 2diabetes: vascular changes or neurodege-neration? Age Ageing 2010; 39: 8–10.
16. Hong M, Lee VM. Insulin and insulin-like growth factor-1 regulate tauphosphorylation in cultured humanneurons. J Biol Chem 1997; 272:19547–19553.
17. Schubert M, Brazil DP, Burks DJ, et al.Insulin receptor substrate-2 deficiencyimpairs brain growth and promotes tauphosphorylation. J Neurosci 2003; 23:7084–7092.
18. Xie L,Helmerhorst E,Taddei K,PlewrightB, VanBronswijkW,MartinsR.Alzheimer’sbeta-amyloid peptides compete for insulinbinding to the insulin receptor. J Neurosci2002;22:RC221.
19. Tezapsidisa N, Johnstona JM, Smith MA,et al. Leptin: a novel therapeutic strategyfor Alzheimer’s disease. J Alzheimers Dis2009; 16(4): 731–740.
20. Tesfaye S, Selvarajah D. Advances inthe epidemiology, pathogenesis andmanagement of diabetic peripheralneuropathy. Diabetes Metab Res Rev2012; 28(Suppl 1): 8–14.
21. Luchsinger JA, Gustafson DR. Adiposity,type 2 diabetes and Alzheimer’s disease.J Alzheimers Dis 2009; 16(4): 693–704.
22. Bravata DM, Wells CK, Concato J,Kernan WN, Brass LM, Gulanski BI.Two measures of insulin sensitivity pro-vided similar information in a U.S. pop-ulation. J Clin Epidemiol 2004; 57(11):1214–1217.
23. Piers LS, Walker KZ, Stoney RM,Soares MJ, O’Dea K. The influence ofthe type of dietary fat on postprandialfat oxidation rates: monounsaturated(olive oil) vs saturated fat (cream).Int J Obes Relat Metab Disord 2002;26(6): 814–821.
24. Proietto J, Filippis A, Nakhla C, Clark S.Nutrient-induced insulin resistance.Mol Cell Endocrinol 1999; 151(12):143–149.
25. Vessby B, Unsitupa M, Hermansen K,et al. Substituting dietary saturated for
R. O. Moreira et al.
Copyright © 2013 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2013).DOI: 10.1002/dmrr
monounsaturated fat impairs insulinsensitivity in healthy men and women:the KANWU study. Diabetologia 2001;44(3): 312–319.
26. López SBB, Pacheco YM, Villar J,Abia R, Muriana FJ. Distinctive post-prandial modulation of beta cellfunction and insulin sensitivity by di-etary fats: monounsaturated com-pared with saturated fatty acids. AmJ Clin Nut 2008; 88(3): 638–644.
27. Viticchi G, Falsetti L, Vernieri F, et al. Vascu-lar predictors of cognitive decline in patientswith mild cognitive impairment. NeurobiolAging 2012; 33: 1127.e1–1127.e9.
28. Iadecola C. Neurovascular regulation inthe normal brain and in Alzheimer’s dis-ease. Nat Rev Neurosci 2004; 5: 347–360.
29. Silvestrini M, Gobbi B, Pasqualetti P,et al. Carotid atherosclerosis and cog-nitive decline in patients withAlzheimer’s disease. Neurobiol Aging2009; 30: 1177–1183.
30. Gupta A, Bisht B, Dey CS. Peripheralinsulin-sensitizer drug metformin ame-liorates neuronal insulin resistance andAlzheimer’s-like changes. Neuropharma-cology 2011; 60: 910–920.
31. Kickstein E, Krauss S, Thornhill P, et al.Biguanide metformin acts on tau phos-phorylation via mTOR/protein phospha-tase 2A (PP2A) signaling. Proc Natl AcadSci USA 2010; 107(50): 21830–5.
32. Janssens V, Goris J. Protein phosphatase2A: A highly regulated family of serine/threonine phosphatases implicated in cellgrowth and signalling. Biochem J 2001;353: 417–439.
33. Sato T, Hanyu H, Hirao K, Kanetaka H,Sakurai H, Iwamoto T. Efficacy of PPAR-#x0194; agonist pioglitazone in mildAlzheimer disease. Neurobiol Aging 2011;32: 1626–1633.
34. Landreth G. Therapeutic use of agonistsof the nuclear receptor PPAR inAlzheimer’s disease. Curr Alzheimer Res2007; 4: 159–164.
35. Searcy JL, Phelps JT, Pancani T, et al.Long-term pioglitazone treatment im-proves learning and attenuates patho-logical markers in a mouse model ofAlzheimer’s disease. J Alzheimers Dis2012; 30(4): 943–61.
36. Moon JH, Kim HJ, Yang AH, et al. Theeffect of rosiglitazone on LRP1 expressionand amyloid β uptake in human brain mi-crovascularendothelialcells:apossibleroleof a low-dose thiazolidinedione fordemen-tia treatment. Int J Neuropsychopharmacol2012;15: 135–42.
37. Blalock EM, Phelps JT, Pancani T,et al. Effects of long-term pioglitazonetreatment on peripheral and centralmarkers of aging. PLoS ONE 2010;5(4): e104–05.
38. Geldmacher DS, Fritsch T, McClendonMJ,Landreth G. A randomized pilot clinicaltrial of the safety of pioglitazone in treat-ment of patients with Alzheimer disease.Arch Neurol 2011; 68(1): 45–50.
39. Zhang Y, Proenca R, Maffei M, Barone M,Leopold L, Friedman JM. Positional clon-ing of themouse obese gene and its humanhomologue. Nature 1994; 372: 425–432.
40. Shimomura I, Hammer RE, Ikemoto S,Brown MS, Goldstein JL. Leptin reversesinsulin resistance and diabetes mellitusin mice with congenital lipodystrophy.Nature 1999; 401: 73–76.
41. Harvey J. Leptin: a diverse regulator ofneuronal function. J Neurochem 2007;100: 307–313.
42. Terry RD, Davies P. Dementia of theAlzheimer type. Annu Rev Neurosci1980; 3: 77–95.
43. Zhao WQ, Alkon DL. Role of insulinand insulin receptor in learning andmemory. Mol Cell Endocrinol 2001;177: 12–e134.
44. Van der Heide LP, Ramakers GM, SmidtMP. Insulin signaling in the centralnervous system: learning to survive.Prog Neurobiol 2006; 79: 205–221.
45. Plastino M, Fava A, Pirritano D, et al.Effects of insulinic therapy on cognitiveimpairment in patients with Alzheimerdisease and diabetes mellitus type-2. JNeurol Sci 2010; 288: 112–116.
46. CraftS,NewcomerJ,KanneS,Dagogo-JackS,CryerP,ShelineY.Memoryimprovementfollowing induced hyperinsulinemia inAlzheimer’s disease.Neurobiol Aging 1996;17: 123–30.
47. Reger MA, Watson GS, Green PS, et al.Intranasal insulin improves cognitionand modulates beta-amyloid in earlyAD. Neurology 2008; 70(6): 440–8.
48. Skeberdis VA, Lan J, Zheng X, Zukin RS,Bennett MV. Insulin promotes rapiddelivery of N-methyl-D-aspartate recep-tors to the cell surface by exocytosis. ProcNatl Acad Sci USA 2001; 98: 3561–6.
49. Byme JH. Learning and memory: basicmechanism. In Fundamental neurosci-ence, Squire LR, Bloom FE, Mc ConnelSK, Roberts JL, Spitzer NC, ZigmondMJ (eds). Academic Press: San Diego(CA), 2003; 1276–98.
50. Bingham EM, Hopkins D, Smith D,Pernet A, Hallett W, Reed L. The role of in-sulin in human brain glucose metabolism:an 18fluoro-deoxyglucose positron emis-sion tomography study. Diabetes 2002; 51:3384–90.
51. Blanchard JG, Duncan PM. Effect in combi-nations of insulin, glucose and scopolamineon radial armmazeperformance.PharmacolBiochem Behav 1997; 58: 209–14.
52. Shemesh E, Rudich A, Harman-Boehm I,Cukierman-Yaffe T. Effect of intranasalinsulin on cognitive function: a system-atic review. J Clin Endocrinol Metab2012; 97: 366–376.
53. Reger MA, Watson GS, Frey WH II, et al.Effects of intranasal insulin on cognitionin memory-impaired older adults: modu-lation by APOE genotype. NeurobiolAging 2006; 27: 451–458.
54. Green BD, Gault VA, Flatt PR, Harriott P,Greer B, O’Harte FP. Comparative effectsof GLP-1 and GIP on cAMP production,
insulin secretion, and in vivo antidiabeticactions following substitution of Ala8/Ala2 with 2-aminobutyric acid. ArchBiochem Biophys 2004; 428: 136–143.
55. Green BD, Lavery KS, Irwin N, et al. NovelGLP-1 analogue (Val8)GLP-1 results insignificant improvements of glucosetolerance and pancreatic beta cell functionafter 3weeks daily administration in obesediabetic (ob/ob) mice. J Pharmacol ExpTher 2006; 318: 914–921.
56. Perry T, Greig NH. Enhancing centralnervous system endogenous GLP-1 re-ceptor pathways for intervention inAlzheimer’s disease. Curr Alzheimer Res2005; 2: 377–385.
57. Perry T, Lahiri DK, Sambamurti K,et al. Glucagon-like peptide-1 de-creases endogenous amyloid- betapeptide (Abeta) levels and protectshippocampal neurons from death in-duced by Abeta and iron. J NeurosciRes 2003; 72: 603–612.
58. Gault VA, O’Harte FP, Flatt PR. Glucose-de-pendent insulinotropic polypeptide (GIP):anti-diabetic and anti-obesity potential?Neuropeptides 2003; 37: 253–263.
59. Gault VA, McClean PL, Irwin N,Power GJ, McCluskey JT, Flatt PR. Ef-fects of subchronic treatment withthe long-acting glucose- dependentinsulinotropic polypeptide receptoragonist, N-AcGIP, on glucose homeo-stasis in treptozotocin induced diabe-tes. Pancreas 2007; 35: 73–79.
60. Nyberg J, Anderson MF, Meister B, et al.Glucose-dependent insulinotropic poly-peptide is expressed in adult hippocampusand induces progenitor cell proliferation. JNeurosci 2005; 25: 1816–1825.
61. Nyberg J, Jacobsson C, Anderson MF,Eriksson PS. Immunohistochemical distri-bution of glucose-dependent insulinotropicpolypeptide in the adult rat brain. JNeurosci Res 2007; 85: 2099–2119.
62. Winder DG, Conn PJ. Activation ofmetabotropic glutamate receptors increasescAMP accumulation in hippocampus by po-tentiating responses to endogenous adeno-sine. J Neurosci 1993; 13: 38–44.
63. Okamoto N, Hore S, Akazawa C,et al. Molecular characterization of anew metabotropic glutamate receptormGluR7 coupled to inhibitory cyclicAMP signal transduction. J Biol Chem1994; 269: 1231–1236.
64. Hölscher C, Li L. New roles for insulin-like hormones in neuronal signallingand protection: New hopes for noveltreatments of Alzheimer’s disease?Neurobiol Aging 2010; 31(9): 1495–502.
65. Campos RV, Lee YC, Drucker DJ. Diver-gent tissue-specific and developmentalexpression of receptors for glucagon andglucagon- like peptide-1 in the mouse.Endocrinology 1994; 134: 2156–2164.
66. Merchenthaler I, Lane M, ShughrueP. Distribution of pre-pro-glucagonand glucagon-like peptide-1 receptormessenger RNAs in the rat centralnervous system. J Comp Neurol1999; 403: 261–280.
Type 2 Diabetes and Alzheimer’s Disease
Copyright © 2013 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2013).DOI: 10.1002/dmrr

67. Harkavyi A, Whitton PS. Glucagon-likepeptide 1 receptor stimulation as a meansof neuroprotection. Brit J Pharmacol2010; 159: 495–501.
68. Lerche S, Brock B, Rungby J, et al.Glucagon-like peptide-1 inhibits blood–brain glucose transfer in humans.Diabetes 2008; 57(2): 325–331.
69. Iwai T, Ito S, Tanimitsu K, UdagawaS, Oka S. Glucagon-like peptide-1inhibits LPS-induced IL-1β productionin cultured rat astrocytes. Neurosci-ence Res 2006; 55(4): 352–360.
70. Gao H, Wang X, Zhang Z, et al. GLP-1amplifies insulin signaling by up-regulation of IR beta IRS-1 and Glut4
in 3 T3-L1 adipocytes. Endocrine2007; 32: 90–95.
71. GhanimH,Monte SV, Sia CL, et al. Reduc-tion in Inflammation and the Expressionof Amyloid Precursor Protein and OtherProteins Related to Alzheimer’s diseasefollowing gastric bypass surgery. J ClinEndocrin Metab 2012; 97(7): E1197–201.
R. O. Moreira et al.
Copyright © 2013 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2013).DOI: 10.1002/dmrr
Copyright © 2022 FDOKUMEN




















