
The effects of acetazolamide in albino rabbits, pigmented rabbits, and humans

9–106
The Knee 14 (2007) 9Two incision synovectomy and radiation treatment for diffuse pigmentedvillonodular synovitis of the knee with extra-articular component☆
Chia-Chun Wu e, Tamir Pritsch a,⁎, Jacob Bickels d, Tierney Wienberg a, Martin M. Malawer a,b,c
a Department of Orthopedic Oncology, C2173, Washington Cancer Institute, 110 Irving St. NW, Washington, DC 20010 United Statesb Georgetown University, Washington DC, United States
c Pediatric and Surgery Branch, National Cancer Institute, Bethesda, MD, United Statesd The National Unit of Orthopedic Oncology, Tel-Aviv Sourasky Medical Center, Israel
e Department of Orthopaedic, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan
Received 20 August 2006; received in revised form 16 October 2006; accepted 28 October 2006
Abstract
Diffuse pigmented villonodular synovitis (PVNS) of the knee is a rare, locally aggressive disease. Since 1995 the senior author has beentreating patients with diffuse intra- and extra-articular PVNS of the knee with a bimodality treatment protocol, consisting of anterior andposterior open synovectomies in conjunction with external-beam radiation. The purpose of this study was to describe the surgical technique,evaluate our protocol's efficacy in limiting local recurrences, and assess its functional implications and associated morbidities. The medicalrecords of nine consecutive patients were analyzed. Functional results were measured using the Knee Society score. The mean follow-up was67 months (range 37–103 months). Eight patients were disease free and one patient had local recurrence, which was extra-articular, localizedand non-progressive. The mean knee rating and functional rating had significantly improved from 65.2 and 70 preoperatively to 93.7 and96.6 postoperatively respectively. Maximal knee flexion ranged from 90° to 130°, and only 3 patients developed flexion contractures of 5°. Inconclusion our bimodality protocol of anterior and posterior open synovectomies, in conjunction with external-beam radiation, limited therecurrence of diffuse intra- and extra-articular PVNS of the knee. All patients showed good-to-excellent functional outcomes and were able toreturn to their previous level of activity.© 2006 Elsevier B.V. All rights reserved.
Keywords: Knee; Pigmented villonodular synovitis; Radiotherapy; Synovectomy; Adjuvant therapy
1. Introduction
Pigmented villonodular synovitis (PVNS) is a rare synovialdiseasewith an annual incidence of two cases permillion in thegeneral population [1,2]. Although the pathogenesis of PVNSis still unknown, recent karyotype chromosomal analysissuggested that it is a true neoplasm [2–6]. The knee is the mostcommonly involved anatomic location. The localized nodularform of the disease can be treated successfully with open or
☆ Investigation performed at the Department of Orthopedic Oncology,Washington Cancer Institute, Washington Hospital Center, Washington DC.⁎ Corresponding author. Tel.: +1 202 877 3970; fax: +1 202 877 8959.E-mail addresses: [email protected], [email protected]
(T. Pritsch).
0968-0160/$ - see front matter © 2006 Elsevier B.V. All rights reserved.doi:10.1016/j.knee.2006.10.014
arthroscopic synovectomies [7–9]. Conversely, the treatmentof the diffuse, aggressive form of PVNS is much moreproblematic, especiallywhen it extends extra-articularly, and isassociated with high recurrence rates of up to 46% [3,7,9–11].Schwartz et al. [9] reported a mean time to recurrence of4.9 years with the earliest recurrence occurring 31 days afterthe index operation.
The oncological principles of the treatment of most benignaggressive tumors dictate either (1) a wide resection with 1–2 cm of negative surgical margins or (2) marginal resection inconjunction with an adjuvant therapy; a wide surgicalapproach that provides adequate exposure and direct visual-ization ismandatory. Despite the locally aggressive pattern andpossible neoplastic origin, most authors did not address diffuseextra- and intra-articular PVNS according to those oncological

Fig. 1. T1-weighted MRI of a 31-year-old male with recurrent diffuse PVNSof the knee, 3 years after undergoing two arthroscopic synovectomies. Thedisease process has low signal intensity due to the high concentration ofhemosiderin. The sagittal view showing large nodular synovitis occupyingthe popliteal fossa, extending from the gastrocnemius heads into thesubcutaneous tissue (arrow).
Fig. 2. Surgical technique. Operative photos of anterior synovectomy. (A) Theanterior medial capsule is exposed and carefully separated from the mass. Athin layer of fat which outlines the plane between the anterior capsule and thesynovial membrane facilitates the dissection of the capsule. The entire grosssynovial mass is exposed en-bloc (P—patella; V-Med—vastus medialis; JTLine—joint line; Supra—suprapatellar pouch; Infra PF—infrapatellar fat pad).(B) Following the resection of the majority of the synovial mass as 1–3 largepieces, diseased synovium is resected from the intercondylar notch anddissected off the anterior cruciate ligament (solid arrow). The cruciate liga-ments are always preserved.
100 C.-C. Wu et al. / The Knee 14 (2007) 99–106
principles. While many authors supported open synovec-tomies, especiallywhen the disease expanded extra-articularly,others have expressed their concern about potential negativefunctional implications and high complication rates, andattempted less invasive techniques [8,12,13]. In addition,several recently reported open surgical techniques specificallyavoid the neurovascular structures of the popliteal fossainstead of exposing and mobilizing them, and consequentlyfail to provide complete direct exposure of all anatomicstructure of the popliteal space [14–16]. Finally, despite thepopular term “radical synovectomy” all synovectomies shouldbe considered at most as marginal resections with very closesurgical margins. Nevertheless, only a few authors includedphysical adjutants in their treatment protocols [13,14,17–20].
Since 1995, the senior author (MMM) has been treatingpatients with diffuse intra- and extra-articular PVNS with auniform multimodality approach, based on the oncologicalprinciples of the treatment of benign locally aggressivetumors, consisting of anterior and posterior open synovec-tomies in conjunction with adjuvant radiation therapy. AnMRI is used for preoperative planning, outlining the number,size and location of all extra-articular foci of the disease. Inaddition, serial MRIs are routinely performed as part of thepostoperative follow-up.
The purpose of this study was to determine whether ourmultimodality treatment protocol was successful in mini-mizing local recurrence of diffuse intra- and extra-articularPVNS and to evaluate its associated complications andfunctional implications on the knee joint. We describe oursurgical technique and analyze the clinical outcomes of nineconsecutive patients.
2. Materials and methods
This study undertook a retrospective review of patients with diffuseintra- and extra-articular PVNS of the knee treated by the senior authorbetween 1995 and 2003. Following the approval of the institutional reviewboard, patients were identified through a musculoskeletal oncologydatabase. Only patients with diffuse intra- and extra-articular PVNS of theknee, which was demonstrated radiologically and intraoperatively and wasproven pathologically, were included in this study. The study groupconsisted of five males and four females, whose median age at the time ofsurgery was 31 years (range: 19 to 51 years). Four patients were referred tous after having undergone failed arthroscopic synovectomies.
2.1. Staging and imaging studies
Prior to surgery, all patients underwent AP and lateral radiographs of theinvolved knee and gadolinium-enhanced magnetic resonance imaging(MRI) in the coronal, sagital and axial planes. MRI was used to establishthe diagnosis of diffuse PVNS and to create a preoperative plan byspecifically identifying all extra-articular foci of the disease including theirnumber, location and size (Fig. 1).
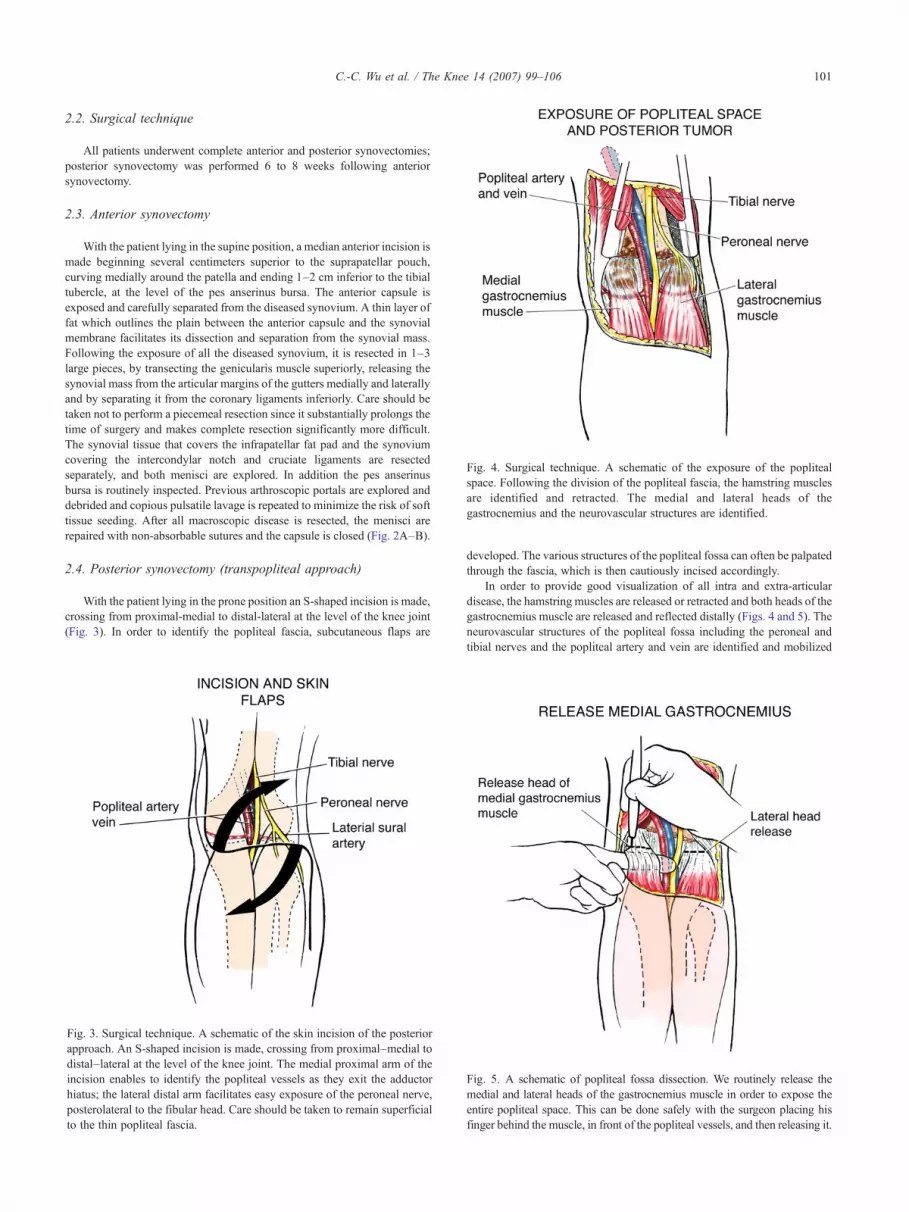
Fig. 4. Surgical technique. A schematic of the exposure of the poplitealspace. Following the division of the popliteal fascia, the hamstring musclesare identified and retracted. The medial and lateral heads of thegastrocnemius and the neurovascular structures are identified.
101C.-C. Wu et al. / The Knee 14 (2007) 99–106
2.2. Surgical technique
All patients underwent complete anterior and posterior synovectomies;posterior synovectomy was performed 6 to 8 weeks following anteriorsynovectomy.
2.3. Anterior synovectomy
With the patient lying in the supine position, a median anterior incision ismade beginning several centimeters superior to the suprapatellar pouch,curving medially around the patella and ending 1–2 cm inferior to the tibialtubercle, at the level of the pes anserinus bursa. The anterior capsule isexposed and carefully separated from the diseased synovium. A thin layer offat which outlines the plain between the anterior capsule and the synovialmembrane facilitates its dissection and separation from the synovial mass.Following the exposure of all the diseased synovium, it is resected in 1–3large pieces, by transecting the genicularis muscle superiorly, releasing thesynovial mass from the articular margins of the gutters medially and laterallyand by separating it from the coronary ligaments inferiorly. Care should betaken not to perform a piecemeal resection since it substantially prolongs thetime of surgery and makes complete resection significantly more difficult.The synovial tissue that covers the infrapatellar fat pad and the synoviumcovering the intercondylar notch and cruciate ligaments are resectedseparately, and both menisci are explored. In addition the pes anserinusbursa is routinely inspected. Previous arthroscopic portals are explored anddebrided and copious pulsatile lavage is repeated to minimize the risk of softtissue seeding. After all macroscopic disease is resected, the menisci arerepaired with non-absorbable sutures and the capsule is closed (Fig. 2A–B).
2.4. Posterior synovectomy (transpopliteal approach)
With the patient lying in the prone position an S-shaped incision is made,crossing from proximal-medial to distal-lateral at the level of the knee joint(Fig. 3). In order to identify the popliteal fascia, subcutaneous flaps are
ig. 3. Surgical technique. A schematic of the skin incision of the posteriorpproach. An S-shaped incision is made, crossing from proximal–medial toistal–lateral at the level of the knee joint. The medial proximal arm of thecision enables to identify the popliteal vessels as they exit the adductoriatus; the lateral distal arm facilitates easy exposure of the peroneal nerve,osterolateral to the fibular head. Care should be taken to remain superficial
Fig. 5. A schematic of popliteal fossa dissection. We routinely release themedial and lateral heads of the gastrocnemius muscle in order to expose theentire popliteal space. This can be done safely with the surgeon placing his
Fadinhp
to the thin popliteal fascia.developed. The various structures of the popliteal fossa can often be palpatedthrough the fascia, which is then cautiously incised accordingly.
In order to provide good visualization of all intra and extra-articulardisease, the hamstring muscles are released or retracted and both heads of thegastrocnemius muscle are released and reflected distally (Figs. 4 and 5). Theneurovascular structures of the popliteal fossa including the peroneal andtibial nerves and the popliteal artery and vein are identified and mobilized
finger behind the muscle, in front of the popliteal vessels, and then releasing it.

102 C.-C. Wu et al. / The Knee 14 (2007) 99–106
medially or laterally (Fig. 6A). For adequate mobilization of the poplitealvessels, all geniculate branches need to be ligated.
The exposed posterior capsule is completely excised. No attempt is madeto preserve the posterior capsule since unlike the anterior capsule we find ittechnically impossible to separate from the abnormal synovial tissue. Theposterior aspect of the knee joint including the intercondylar notch, theposterior horns of both menisci and the posterior cruciate ligament (PCL), isthen thoroughly inspected and any abnormal tissue is excised. When theposterior horns of the menisci are intentionally detached for exploration andresection of the diseased synovium, they are later sutured back with No. 1Ethibond sutures. In addition, possible extra-articular locations of thedisease are routinely explored including both heads of the gastrocnemius
Fig. 6. Surgical technique. Posterior resection of extra and intra-articularPVNS. (A) A schematic of the resection. The posterior joint capsule isidentified and excised to expose both femoral condyles. No attempt is madeto preserve the posterior capsule since we find it very difficult to separatefrom the diseased synovium. The geniculate branches are ligated foradequate medial or lateral mobilization of the popliteal vessels in order topermit complete resection of all the diseased synovium. (B) Intraoperativephoto. All macroscopic disease was resected. This is the typical surgicalappearance following complete resection. The posterior cruciate ligament isalways preserved (pop a/v — popliteal artery and vein).
Fig. 7. Surgical technique. A schematic of the posterior capsulereconstruction. The medial and lateral heads of the gastrocnemius muscleare tenodesed to each other and to the deep fascia of the hamstring muscles.
muscle, the popliteal tendon sheath, the recess anterior to the poplitealmuscle, the semimembranosus bursa, the sheath overlying the poplitealvessels and popliteal lymph nodes. The number and location of extra-articular foci of the disease are verified against the findings of thepreoperative MRI (Fig. 6B).
On completion of resection, the posterior capsule is reconstructed bytenodesing the medial and lateral heads of the gastrocnemius to each otherand to the deep fascia of the medial and lateral hamstring muscles (Fig. 7).
Following the second operation, all nine patients underwent external-beam radiation therapy, with total dosages ranging from 4000–4500 cGy.The delivery dose covered the lining of the joint with small margins of 0.5 to1.5 cm, and involved the entire circumference of the knee. The treatmentregimen consisted of a single fraction of radiation per treatment session onconsecutive weekdays for 3 weeks.
All patients underwent several sessions of physical therapy between thetwo surgical procedures focusing on active and passive range of motion.Following the second procedure the operated knees were immobilized in aknee immobilizer in 15° of flexion to relieve tension from the posteriorsurgical wound; physical therapy was resumed 10 days later focusing onactive and passive range of motion and muscle strengthening. Physicaltherapy continued throughout the time period of the adjuvant radiotherapy inorder to maintain knee range of motion and to counteract the potential hazardof developing flexion contractures.
All study patients were followed for a minimum of 3 years (mean67 months, range 37–103 months). For the first 2 years, patients wereevaluated every 3 months. On each visit, a physical examination and an MRIof the operated limb were performed. Patients were evaluated semiannuallyfor an additional 3 years and annually thereafter. An orthopedic oncologistanalyzed the clinical records, imaging studies and operative and pathologicreports.
Patients' medical history including pre- and postoperative data regardingrange of motion, walking capacity and postoperative complications werereviewed and analyzed. Functional outcomes were evaluated using the twocomponents of the Knee Society score namely, the knee rating andfunctional score [21].
The differences between pre- and postoperative Knee Society scoreswere assessed using the Wilcoxon signed-ranks test for paired continuous

Table 1Clinical data of nine consecutive patients with diffuse intra- and extra- articular PVNS of the knee treated in our institution between 1995 and 2003
Patient Age(years)
Gender Previoussurgery
Preoperativerange of motion(degrees)
Postoperativerange of motion(degrees)
Preoperative Knee Societyscores (knee rating/functional score) ⁎
Postoperative Knee Societyscores (knee rating/functional score) ⁎
Recurrence
1 21 M Yes:arthroscopy
0°–90° 0°–135° 63/75 98/100 No
2 28 M No 10°–90° 0°–135° 41/50 98/100 No3 43 F Yes: 2
arthroscopies10°–90° 0°–130° 63/45 88/80 No
4 19 F Yes:arthroscopy
10°–100° 0°–120° 76/90 98/100 Yes(asymptomatic)
5 31 F No 20°–80° 5°–120° 37/60 98/100 No6 31 M No 10°–90° 5°–120° 68/70 86/90 No7 51 M No 5°–90° 0°–90° 86/80 93/100 No8 40 F No 5°–90° 0°–100° 82/80 95/100 No9 31 M Yes:
arthroscopy10°–90° 5°–90° 71/70 93/100 No
⁎ A statistically significant difference was found between the pre- and post-operative results of both the knee rating (pb0.005) and the functional score(pb0.005).
103C.-C. Wu et al. / The Knee 14 (2007) 99–106
data (Version 9.1; SPS). A two-tailed p value of less than 0.05 wasconsidered significant.
3. Results
All nine study patients presented with diffuse extensive intra-articular disease that involved the anterior and posterior compart-ments of the knee and expended extra-articularly, involving variousstructures of the popliteal fossa. The preoperative radiographs ofone patient demonstrated moderate degenerative changes whichwere also observed intraoperatively.
Only one patient (patient 4) in our series developed localrecurrence, which was completely asymptomatic and was detectedon routine MRI 5 years after the operation. The eight other patients inour series remained disease free (Table 1). The single recurrence waslocated extra-articularly, posterior to the PCL, measuring 2×1 cm.Since the patient was completely asymptomatic and her recurrentdisease was localized and did not involve the knee joint, no surgicalintervention was required. The patient was followed closely by serialMRIs, and over a time period of 24months, the PVNS nodule had notincreased in size and the patient remained completely asymptomatic.
Both knee range of motion and functional results hadsubstantially improved as compared to the preoperative state.Table 1 details the pre- and postoperative range of motion and KneeSociety score of the nine study patients. The serial postoperativeradiographs did not demonstrate any new development orprogression of degenerative changes.
All patients showed relief of pain and stiffness and were able toreturn to their previous level of activity. According to the results ofthe Knee Society score, both the knee rating and the functionalrating had significantly improved as compared to the preoperativestate (pb0.005 for both). The mean knee rating improved from65.2 points (range, 37 to 86 points) to 93.7 points (range, 86 to98 points) and the mean functional rating improved from 70 points(range, 45 to 90 points) to 96.6 points (range, 80 to 100 points).
One patient (patient 6) developed severe stiffness of the knee6 weeks after his second operation and prior to the beginning ofradiation therapy. This patient underwent a closed manipulation of hisknee followed by intensive physical therapy; on the final evaluationhis arc of flexion to the extension of the knee joint was 5° to 120°.
All surgical wounds healed uneventfully and none of thepatients experienced any superficial or deep infection. In addition,none of the patients sustained peroneal or tibial nerve palsies ordeveloped deep vein thrombosis.
4. Discussion
Diffuse pigmented villonodular synovitis is a benign,locally aggressive disease of the synovium [22,23]. Thepathogenesis of PVNS is unknown; however, recentkaryotype chromosomal analysis suggested that it is a trueneoplasm [2–6]. While the nodular, non-aggressive form ofthe disease can be successfully treated with arthroscopicsynovectomy, the aggressive diffuse PVNS of the knee posesa much more difficult surgical and oncological challenge,especially when it extends extra-articularly, and is associatedwith reported recurrence rates of up to 46% [3,5–7,24].
Our surgical technique provided an excellent exposure,facilitated the removal of all macroscopic disease, andpermitted a clear identification and mobilization of theneurovascular structures of the popliteal fossa. Only one ofnine patients (11.1%) developed local recurrence, which waslocalized, extra-articular, asymptomatic, and non-progres-sive. The Knee Society scores showed statistically signifi-cant clinical improvement, and all patients demonstratedgood-to-excellent functional results and most importantlywere able to return to their previous level of activity.
This study has two obvious limitations: it is a non-controlled retrospective study and the sample size isrelatively small. Due to the rarity of PVNS, it is difficultfor one institution to perform a large controlled study,especially when focusing on a specific aggressive subtype ofthe disease (diffuse PVNS of the knee with extra-articularcomponent). Nevertheless, to our knowledge, only one otherstudy specifically addressed the problem of treating diffuseintra- and extra-articular PVNS of the knee, and only five

104 C.-C. Wu et al. / The Knee 14 (2007) 99–106
patients in that study were treated with anterior and posteriorsynovectomies in conjunction with external-beam radiationtherapy [14]. Moreover, a search of the English literaturefailed to uncover previous descriptions of the surgicaltechniques described in this study for the complete resectionof the diseased synovium.
Several authors advocated less extensive approaches forthe treatment of diffuse PVNS of the knee [8,13,15]. Twoauthors reported good results and low recurrence rates usingarthroscopic synovectomies; however, it is unclear whethertheir series included patients with extra-articular disease, andsince postoperative MRIs were not performed in bothstudies, the true local recurrence rate cannot be determined[8,13]. Flandry et al. [15] reported on two clinicalrecurrences in a group of 25 patients with diffuse PVNStreated with combined limited anterior and posteriorsynovectomies; however, since serial postoperative MRIswere not performed and only plain radiographs and clinicalsymptoms were used to identify recurrences, the truerecurrence rate in their study may have been underestimatedas well. Similar to other authors, we believe that thearthroscopic and limited open synovectomies often provideinsufficient visualization and do not permit resection of allaffected synovial tissue, especially when extra-articulardisease is present [12,14,25].
Chin et al. [14] described a different technique ofcombined anterior and posterior synovectomies for diffuseintra and extra-articular PVNS of the knee. Instead ofidentifying and mobilizing all neurovascular structures tofully expose the popliteal fossa and posterior capsule, theychose to avoid the vessels and nerves by alternativelyapproaching the posterior aspect of the knee through twoseparate medial and lateral fascial incisions. We believe thisapproach provides inferior direct visualization of theposterior elements (posterior cruciate ligament, posteriorhorns of both menisci, posterior joint line, and the extra-articular structures within the popliteal space) and that smallhidden PVNS foci can consequently be missed. In addition,according to the description of their technique, the posteriorcapsule is either primarily repaired or left partially openedwhen primary repair is expected to cause flexion contracture.Since we found separating the diseased synovium from theposterior capsule very difficult, we routinely resect themajority of the posterior capsule and subsequently recon-struct it with the gastrocnemius and hamstring muscles.
Ohnuma et al. [16] reported on 5 patients with diffusePVNS extending to periarticular bursae around the knee.Their posterior approach consisted of two medial and lateralskin incisions through which all periarticular bursae of theknee as well as the posterior aspect of the joint wereaccessed. Of the five patients in their series, one patientdeveloped a symptomatic recurrence and another patient hadan asymptomatic, non-progressive recurrence which wasnoted on MRI. We disagree with the authors' assumption thatall periarticular bursae cannot be approached by one curvedposterior incision. By ligating the geniculate branches, the
popliteal vessels can be mobilized medially or laterally andthereby facilitate complete exposure of the posterior aspectof the knee and popliteal space. The pes anserinus bursa isroutinely explored as part of our anterior approach.
Because of the destructive and progressive nature ofdiffuse PVNS, especially when it expands extra-articularly,and due to its probable neoplastic pathogenesis, we believethat its management should follow the oncological principlesof the treatment of benign locally aggressive neoplasms.Attaining good local control of most benign aggressivetumors necessitates either a wide resection with 1–2 cm ofnegative surgical margins, or a marginal resection combinedwith an adjuvant therapy. Since conservation of the kneejoint and its intra-articular structures limits the extensivenessof resection, we consider a physical adjuvant necessary forthe eradication of microscopic disease. External-beamradiation, which is also used as an adjuvant for the treatmentof other benign locally aggressive processes such as desmoidtumor, is our adjuvant treatment of choice [26–28]. Bycombining radiotherapy with an extensive surgical approach,we managed to limit the recurrences in our series to oneasymptomatic case, which was localized, extra-articular, andnon-progressive. It should be noted that because of thepotential hazards of radiation therapy, we limit this approachto the most aggressive form of PVNS, namely, diffuse intra-and extra-articular disease.
External-beam radiation has been used successfully as anadjuvant treatment in other case series of diffuse PVNS [17,18].Radiation synovectomy using intra-articular injection ofYttrium 90 or Dysprosium-165-Ferric hydroxide macroaggre-gates has also been reported to limit recurrences of the disease[14,19,20]; however, the use of thismethod carries the hazard ofleakage and resultant radionecrosis of periarticular soft tissues[25,29]. O'Sullivan et al. [18] concluded that external-beamradiation is an effective adjuvant therapy for the aggressiveforms of PVNS, provided that all gross disease is surgicallyresected. Accordingly, incomplete resection of all macroscopicdisease might explain the results of a few authors who did notfind adjuvant radiation therapy beneficial [9,10]. Because of thepotential risk of postradiation arthrofibrosis, swelling, andwound breakdown, Chin et al., [14] recommended radiationtherapy only for patients with symptomatic recurrences.Conversely, none of the patients in our series experiencedwound complications and the only case of severe arthrofibrosisoccurred before the beginning of radiation therapy.
MRI was utilized in our series for the diagnosis of PVNS,for preoperative planning, and as part of the routinepostoperative follow-up. Several authors found MRI to bethe most effective tool for preoperative detection andpostoperative monitoring of diffuse PVNS of the knee[30–35]. The benefit of MRI is highlighted by the fact thatthe only recurrence in our series was asymptomatic andwould not have been detected otherwise. Similarly, in a caseseries of diffuse PVNS by Chin et al. [14], three of the sevenrecurrences were asymptomatic and were only discovered byroutine postoperative MRIs.

105C.-C. Wu et al. / The Knee 14 (2007) 99–106
The hypothesis that open surgical approach to the kneewill carry negative functional implications and high infectionrates has led several surgeons to attempt minimally invasivetechniques for the resection of diffuse PVNS of the knee[8,12,13]. This hypothesis was found to be untrue in our caseseries. None of the patients developed any superficial or deepinfection; all patients demonstrated good-to-excellent func-tional results and all returned to their previous level ofactivity. Although one patient developed knee stiffness andunderwent closed manipulation 6 weeks after surgery, at theend evaluation, all patients displayed satisfactory knee rangeof motion. These results are in agreement with the results ofother studies where open synovectomies were performed[14–16]. We believe that the intense physical therapyprogram that focused on early range of motion largelycontributed to the prevention of arthrofibrosis in mostpatients.
In order to shorten the operative time and avoidsubsequent potential complications we chose to performthe anterior and posterior synovectomies as separateprocedures, 6–8 weeks apart; however, during the past3 years, we treated two patients with diffuse intra- and extra-articular PVNS of the knee with a single operation thatincluded anterior and posterior synovectomies. The rehabil-itation of both patients was uneventful, and neitherdemonstrated postoperative complications. Currently, wetreat young healthy patients with a combined one stageprocedure and reserve the two stage approach for potentiallyproblematic patients such as morbidly obese patients andpatients with multiple unrelated comorbidities.
In summary, based on our experience, we suggest openanterior and posterior complete synovectomies in conjunc-tion with adjuvant radiation therapy for the treatment ofdiffuse intra- and extra-articular PVNS of the knee. Webelieve this subtype of PVNS should be managed accordingto the same oncological principles as the treatment of benignlocally aggressive neoplasms. The extensiveness of thedisease necessitates a wide surgical approach, and itsaggressiveness and limited surgical margins require theaddition of adjuvant radiation therapy. MRI is useful forpreoperative planning, outlining the number, size andlocation of all extra-articular foci of the disease. It isextremely important that all macroscopic disease becompletely resected. All patients should be assigned to anintensive physiotherapy program and postoperative follow-up should include serial MRIs for better and earlier detectionof recurrences. This therapeutic approach has resulted in alow recurrence rate and good-to-excellent functional results.
References
[1] Myers BW, Masi AT, Freigenbaum SL. Pigmented villonodularsynovitis and tenosynovitis: a clinical epidemiological study of 166cases and literature review. Medicine (Baltimore) 1980;59:223–38.
[2] Ohjimi Y, Iwasaki H, Ishiguro M, Kaneko Y, Tashiro H, Emoto G, et al.Short arm of chromosome 1 aberration recurrently found in pigmentedvillonodular synovitis. Cancer Genet Cytogenet 1996;90:80–5.
[3] Rao AS, Virgorita VJ. Pigmented villonodular synovitis (giant-celltumor of the tendon sheath and synovial membrane). A review ofeighty-one cases. J Bone Joint Surg Am 1984;66:76–94.
[4] Choong PF, Willen H, Nilbert M, Mertens F, Mandahi N, Carlen B, et al.Pigmented villonodular synovitis. Monoclonality and metastasis — acase for neoplastic origin? Act Orhop Scand 1995;66:64–8.
[5] Kalil RK, Unni KK. Malignancy in pigmented villonodular synovitis.Skeletal Radiol 1998;27:392–5.
[6] Sakkers RJ, de Jong D, van der Heul RO. X-chromosome inactivationin patients who have pigmented villonodular synovitis. J Bone JointSurg Am 1991;73:1532–6.
[7] Granowitz SP, D'Antonio J, Mankin HJ. The pathogenesis and long-term end results of pigmented villonodular synovitis. Clin Orthop RelatRes 1976;114:335–51.
[8] Ogilvie-Harris DJ, McLean J, Zarnett ME. Pigmented villonodularsynovitis of the knee: the results of total arthroscopic synovectomy,partial arthroscopic synovectomy and arthroscopic local excision.J Bone Joint Surg Am 1992;74:119–23.
[9] Schwartz HS, Unni KK, Pritchard DJ. Pigmented villonodularsynovitis. Clin Orthop Relat Res 1989;247:243–55.
[10] Byers PD, Cotton RE, Deacon OW, Lowy M, Newman PH, SissonsHA, et al. The diagnosis and treatment of pigmented villonodularsynovitis. J Bone Joint Surg Br 1968;50(2):290–305.
[11] Johansson JE, Ajjoub S, Coughlin LP, Wener JA, Cruess RL. Pigmentedvillonodular synovitis of joints. ClinOrthopRelat Res 1982;163:159–66.
[12] De Ponti A, Sansone V, Malchere M. Result of arthroscopic treatment ofpigmented villonodular synovitis of the knee. Arthroscopy 2003;19:602–7.
[13] Zvijac JE, Lau AC, Hechtman KS, Uribe JW, Tjin-A-Tsoi EW.Arthroscopic treatment of pigmented villonodular synovitis of theknee. Arthroscopy 1999;15:613–7.
[14] Chin KR, Barr SJ, Winalski C, Zurakowski D, Brick GW. Treatment ofadvanced primary and recurrent diffuse pigmented villonodularsynovitis of the knee. J Bone Joint Surg Am 2002;84:2192–202.
[15] Flandry FC, Hughston JC, Jacobson KE, Barrack RL, McCann SB,Kurtz DM. Surgical treatment of diffuse pigmented villonodularsynovitis of the knee. Clin Orthop Relat Res 1994;300:183–92.
[16] Ohnuma M, Sugita T, Kawamata T, Hosaka M, Yoshizumi Y, UmeharaJ. Pigmented villonodular synovitis of the knee with lesions of thebursae. Clin Orthop Relat Res 2003;414:212–8.
[17] Blanco CE, Leon HO, Guthrie TB. Combined partial arthroscopicsynovectomy and radiation therapy for diffuse pigmented villonodularsynovitis of the knee. Arthroscopy 2001;17:527–51.
[18] O'Sullivan B, Cummings B, Catton C, Bell R, Davis A, FornasierV, et al. Outcome following radiation treatment for high-riskpigmented villonodular synovitis. Int J Radiat Oncol Biol Phys1995;32:777–86.
[19] Shabat S, Kollender Y, Merimsky O, Isakov J, Flusser G, Nyska M,et al. The use of surgery and yttrium 90 in the management of extensiveand diffuse pigmented villonodular synovitis of large joint. Rheuma-tology (Oxford) 2002;41:1113–8.
[20] Wiss DA. Recurrent villonodular synovitis of the knee. Successfultreatment with yttrium-90. Clin Othop Relat Res 1982;169:139–44.
[21] Insall JN, Dorr LD, Scott RD, Scott WN. Rationale of the knee society:clinical rating system. Clin Orthop Relat Res 1989;248:13–4.
[22] Bertoni F, Unni KK, Beabout JW, Sim FH. Malignant giant cell tumorof tendon sheath and joint (malignant pigmented villonodularsynovitis). Am J Surg Pathol 1997;21:153–63.
[23] Lu KH. Subcutaneous pigmented villonodular synovitis caused byportal contamination during knee arthroscopy and open synovectomy.Arthroscopy 2004;20:e9–e13.
[24] Jones G. Yttrium synovectomy: a meta-analysis of the literature. AustN Z J Med 1993;23:272–5.
[25] Chin KR, Brick GW. Extraarticular pigmented villonodular synovitis: acause for failed knee arthroscopy.ClinOrthopRelat Res 2002;404:330–8.
[26] Hosalkar HS, Fox EJ, Delaney T, Torbert JT, Ogilvie CM, LackmanRD. Desmoid tumors and current status of management. Orthop ClinNorth Am 2006;37(1):53–63.

106 C.-C. Wu et al. / The Knee 14 (2007) 99–106
[27] McCollough WM, Parsons JT, van der Griend R, Enneking WF, HeareT. Radiation therapy for aggressive fibromatosis. The experience at theUniversity of Florida. J Bone Joint Surg Am 1991;73(5):717–25.
[28] Suit H, Spiro I. Radiation treatment of benign mesenchymal disease.Semin Radiat Oncol 1999;9(2):171–8.
[29] Sojan S, Bartholomeusz D. Cutaneous radiation necrosis as a complica-tion of yttrium-90 synovectomy. Hell J Nucl Med 2005;8(1):58–9.
[30] Bassett LW, Gold RH. Magnetic resonance imaging of the musculo-skeletal system. An overview. Clin Orthop Relat Res 1989;244:17–28.
[31] Jelinek JS, Kransdorf MJ, Utz JA, Berrey Jr BH, Thomson JD, HeekinRD, et al. Imaging of pigmented villonodular synovitis. Am JRoentgenol1989;152:337–42.
[32] Mandelbaum BR, Grant TT, Hartzman S, Reicher MA, Flannigan B,Bassett LW, et al. The use of MRI to assist in diagnosis of pigmented
villonodular synovitis of the knee joint. Clin Orthop Relat Res1988;231:135–9.
[33] Musculo DL, Makino A, Costa-Paz M, Ayerza MA. Localizedpigmented villonodular synovitis of the posterior compartment of theknee: diagnosis with magnetic resonance imaging. Arthroscopy1995;11:482–5.
[34] Poletti SC, Gates III HS, Martinez SM, Richardson WJ. The use ofmagnetic resonance imaging in the diagnosis of pigmented villonod-ular synovitis. Orthopedics 1990;13:185–90.
[35] Steinbach LS, Neumann CH, Stoller DW, Mills CM, Crues III JV,Lipman JK, et al. MRI of the knee in diffuse pigmented villonodularsynovitis. Clin Imaging 1989;13:305–16.
Copyright © 2022 FDOKUMEN




















