
Sree Balaji Medica laji Medical College & Hospital ollege & Hospital
Upload
independentCategory
view
1download
0
This article was downloaded by:[Yan, Benedict]On: 5 July 2008Access Details: [subscription number 794752928]Publisher: Informa HealthcareInforma Ltd Registered in England and Wales Registered Number: 1072954Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
PathologyPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t713440474
TRARESA: a tissue microarray-based hospital systemfor biomarker validation and discoveryKakoli Das ab; Mohd Feroz Mohd Omar b; Chee Wee Ong c; Suhaimi Bin AbdulRashid c; Bee Keow Peh ab; Thomas Choudary Putti a; Puay Hoon Tan d; KeeSeng Chia c; Ming Teh a; Nilesh Shah b; Richie Soong ab; Manuel Salto-Tellez aba Department of Pathology,b Oncology Research Institute,c Centre for Molecular Epidemiology, National University Hospital and Yong Loo LinSchool of Medicine, National University of Singapore,d Department of Pathology, Singapore General Hospital, Singapore
Online Publication Date: 01 August 2008
To cite this Article: Das, Kakoli, Mohd Omar, Mohd Feroz, Ong, Chee Wee, BinAbdul Rashid, Suhaimi, Peh, Bee Keow, Putti, Thomas Choudary, Tan, Puay Hoon, Chia, Kee Seng, Teh, Ming,Shah, Nilesh, Soong, Richie and Salto-Tellez, Manuel (2008) 'TRARESA: a tissue microarray-based hospital systemfor biomarker validation and discovery', Pathology, 40:5, 441 — 449
To link to this article: DOI: 10.1080/00313020802198101URL: http://dx.doi.org/10.1080/00313020802198101
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article maybe used for research, teaching and private study purposes. Any substantial or systematic reproduction,re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expresslyforbidden.
The publisher does not give any warranty express or implied or make any representation that the contents will becomplete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should beindependently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings,demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with orarising out of the use of this material.

Dow
nloa
ded
By:
[Yan
, Ben
edic
t] A
t: 10
:22
5 Ju
ly 2
008
R E V I E W
TRARESA: a tissue microarray-based hospital system for biomarkervalidation and discovery
KAKOLI DAS*{, MOHD FEROZ MOHD OMAR{, CHEE WEE ONG{,SUHAIMI BIN ABDUL RASHID{, BEE KEOW PEH*{, THOMAS CHOUDARY PUTTI*,PUAY HOON TANx, KEE SENG CHIA{, MING TEH*, NILESH SHAH{,RICHIE SOONG*{ AND MANUEL SALTO-TELLEZ*{
*Department of Pathology, {Oncology Research Institute and {Centre for Molecular Epidemiology, National
University Hospital and Yong Loo Lin School of Medicine, National University of Singapore, and xDepartment
of Pathology, Singapore General Hospital, Singapore
Summary
Formalin fixed and paraffin embedded tissue (FFPE) collectionsin pathology departments are the largest resource for retro-spective biomedical research studies. Based on the literatureanalysis of FFPE related research, as well as our own technicalvalidation, we present the Translational Research Arrays(TRARESA), a tissue microarray centred, hospital based,translational research conceptual framework for both validationand/or discovery of novel biomarkers. TRARESA incorporatesthe analysis of protein, DNA and RNA in the same samples,correlating with clinical and pathological parameters from eachcase, and allowing (a) the confirmation of new biomarkers,disease hypotheses and drug targets, and (b) the postulation ofnovel hypotheses on disease mechanisms and drug targetsbased on known biomarkers. While presenting TRARESA, weillustrate the use of such a comprehensive approach. Theconceptualisation of the role of FFPE-based studies in transla-tional research allows the utilisation of this commodity, and addsto the hypothesis-generating armamentarium of existing high-throughput technologies.
Key words: Tissue microarrays, molecular pathology, translational
research.
Abbreviations: BCC, basal cell carcinoma; c-erbB-2/HER2-neu, human
epidermal growth factor receptor 2, erbB-2; DHPLC, denaturing high
performance liquid chromatography; DNA, deoxyribonucleic acid; EGFR,
epidermal growth factor receptor; ER, oestrogen receptor; FFPE, formalin
fixed and paraffin embedded; GIST, gastrointestinal stromal tumour; PCR,
polymerase chain reaction; PR, progestogen receptor; RNA, ribonucleic
acid; SHH, Sonic Hedgehog; TMA, tissue microarrays; TRARESA,
translational research arrays; TGF-b, transforming growth factor beta;
VEGF, vascular endothelial growth factor.
Received 11 February, accepted 20 February 2008
INTRODUCTION
Although there has been some interest in the literature indescribing a general system for pathology integration intothe translational research pipeline, this has been described invery general terms1 or exclusively focused in specific aspectsof this development such as tissue microarrays (TMAs)2 or
informatics in pathology.3–6 Hereby, we describe a general,comprehensive framework for the use of formalin fixed,paraffin embedded (FFPE) tissue to investigate clinicalsamples at different molecular levels and link them withclinical endpoints, illustrating the process with work fromour own laboratory and from others.
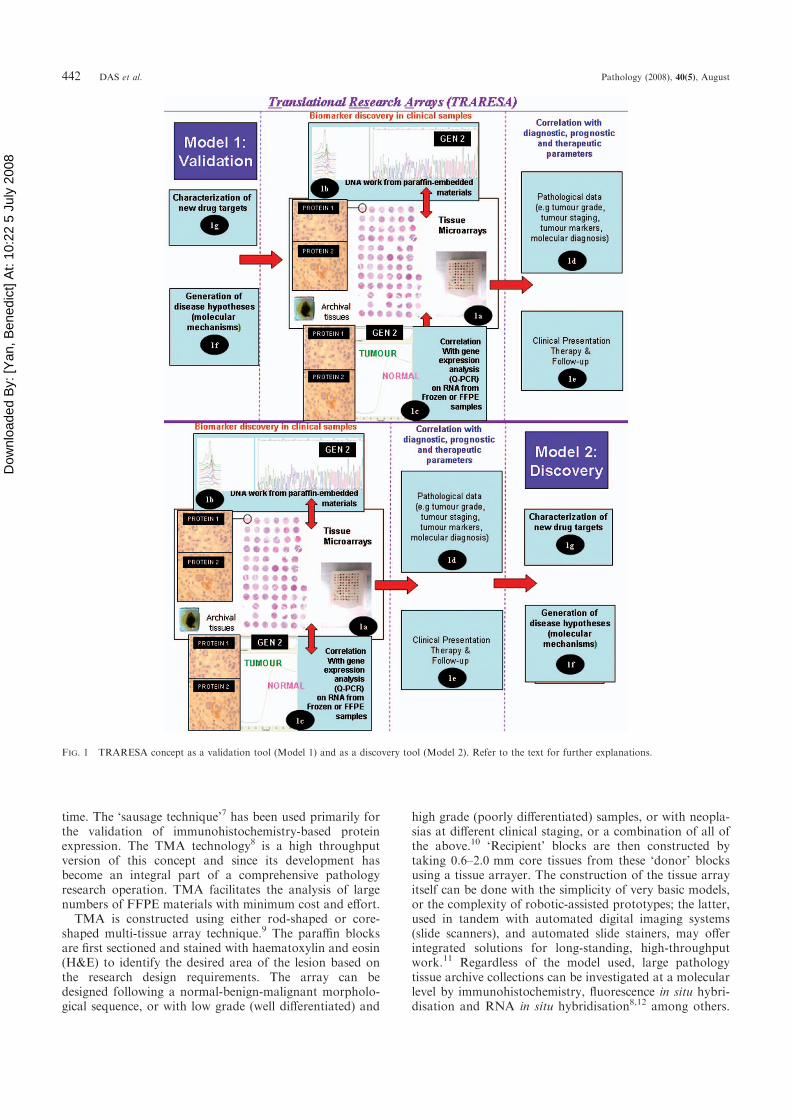
DESCRIPTION OF THE TRARESA PLATFORM
The conceptualisation of this platform is shown in (Fig. 1)under ‘Model 1: Validation’. FFPE tissues, arrayed in aTMA format, are the first step in assessing the expression ofnumerous available antibodies to known proteins (Fig. 1a).A suitable statistical analysis (unsupervised monothetichierarchical cluster analysis in our case)6 is capable ofhighlighting the importance of some of these biomarkers inthe overall re-classification of the cases studied in hier-archically organised subgroups. A correlation betweenthese subgroups and the available pathological (Fig. 1d)and clinical (Fig. 1e) information of the individual caseswould indicate if this ‘biological grouping’ has prognosticsignificance. Once this has been established, further studiesmay follow to assess if the impression of differential proteinexpression by immunohistochemistry is confirmed at a geneexpression level (Fig. 1c). Some of the results could beexplained by the presence of mutations unknown to date;this can be examined by DNA extraction (Fig. 1b). BothDNA and RNA are extracted from the FFPE blocks of thesame cases in which the TMA protein results weregenerated (see below). Eventually, these findings may leadto the generation of new hypotheses on molecularmechanisms of disease (Fig. 1f). The observations mayhave important implications in the discovery of possiblenew targets for therapy (Fig. 1g).
TECHNIQUES WHICH FORM PARTOF THE TRARESA CONCEPT
1. Tissue microarrays
Pathologists have prepared composite paraffin blocks oftissues from different patients and/or pathologies for a long
Pathology (August 2008) 40(5), pp. 441–449
Print ISSN 0031-3025/Online ISSN 1465-3931 # 2008 Royal College of Pathologists of Australasia
DOI: 10.1080/00313020802198101
Dow
nloa
ded
By:
[Yan
, Ben
edic
t] A
t: 10
:22
5 Ju
ly 2
008
time. The ‘sausage technique’7 has been used primarily forthe validation of immunohistochemistry-based proteinexpression. The TMA technology8 is a high throughputversion of this concept and since its development hasbecome an integral part of a comprehensive pathologyresearch operation. TMA facilitates the analysis of largenumbers of FFPE materials with minimum cost and effort.
TMA is constructed using either rod-shaped or core-shaped multi-tissue array technique.9 The paraffin blocksare first sectioned and stained with haematoxylin and eosin(H&E) to identify the desired area of the lesion based onthe research design requirements. The array can bedesigned following a normal-benign-malignant morpholo-gical sequence, or with low grade (well differentiated) and
high grade (poorly differentiated) samples, or with neopla-sias at different clinical staging, or a combination of all ofthe above.10 ‘Recipient’ blocks are then constructed bytaking 0.6–2.0 mm core tissues from these ‘donor’ blocksusing a tissue arrayer. The construction of the tissue arrayitself can be done with the simplicity of very basic models,or the complexity of robotic-assisted prototypes; the latter,used in tandem with automated digital imaging systems(slide scanners), and automated slide stainers, may offerintegrated solutions for long-standing, high-throughputwork.11 Regardless of the model used, large pathologytissue archive collections can be investigated at a molecularlevel by immunohistochemistry, fluorescence in situ hybri-disation and RNA in situ hybridisation8,12 among others.
FIG. 1 TRARESA concept as a validation tool (Model 1) and as a discovery tool (Model 2). Refer to the text for further explanations.
442 DAS et al. Pathology (2008), 40(5), August

Dow
nloa
ded
By:
[Yan
, Ben
edic
t] A
t: 10
:22
5 Ju
ly 2
008
TMA also helps to preserve the original blocks of tissuesamples for further use and treats different patient samplesuniformly on the same slide allowing analytical homo-geneity.9 Besides clinical specimens, TMA with paraffin-embedded human cell lines have also been constructed.10
Thus, in general, TMAs have been used primarily forconfirmation of the importance of biomarkers detectedbeforehand by other means,9,13–15 for the biologicalsubgrouping of diseases16 that may have prognosticimplications,17–18 and in the area of pharmacologicalresearch and drug discovery,19 with a special emphasis oncancer.20 FFPE tissue is by far the most common clinicalmaterial available for research. Hence, a system that wouldmake these materials easily available for studies leading tothe discovery of the biological and clinical significance ofestablished biomarkers (rather than the corroborative ortaxonomic studies mentioned above), would enhance thearmamentarium of translational researchers and open anew avenue for the use of this abundant resource.
Taking breast cancer biology as a paradigm, wedemonstrated that the TMA format is highly reliable foranalysis of the biology of cancer.21 Using the same cases asZhang et al.,21 we aimed to establish the effect that a rangeof variables may have in the concordance of results, such astumour heterogeneity, effect of time in preservation of theantigenicity and the epitope stability, use of differentantibodies (except for ER) and the use of a differentarrayer (ATA100, Advanced Tissue Arrayer; Chemicon,USA) in a different laboratory environment. Ninety-eighttumour and matched normal blocks were recalled from ourarchives to construct a new TMA and H&E was preparedto verify the availability of cancer tissues in each core.Subsequently, sections were stained with oestrogen receptoralpha (ERa; clone 1D5, dilution 1:250; DakoCytomation,Denmark), progestogen receptor (PR; clone PgR 636,1:250; DakoCytomation) and c-erbB-2 oncoprotein(1:250; DakoCytomation) according to the manufacturer’sprotocols. The new TMA constructed in 2006 showed aconcordance of 92% for ER, 97% for PR and 87% for c-erbB-2 stains when compared with full sections and 91%for ER, 96% for PR and 92% for c-erbB-2 when comparedwith the TMA constructed in 2003. This suggests that theTMA technology can be reliably utilised in the course oftime and subsequent TMAs constructed from the samecases maintain a constant biological profile, allowingcomparisons of biological, diagnostic and therapeuticnature.
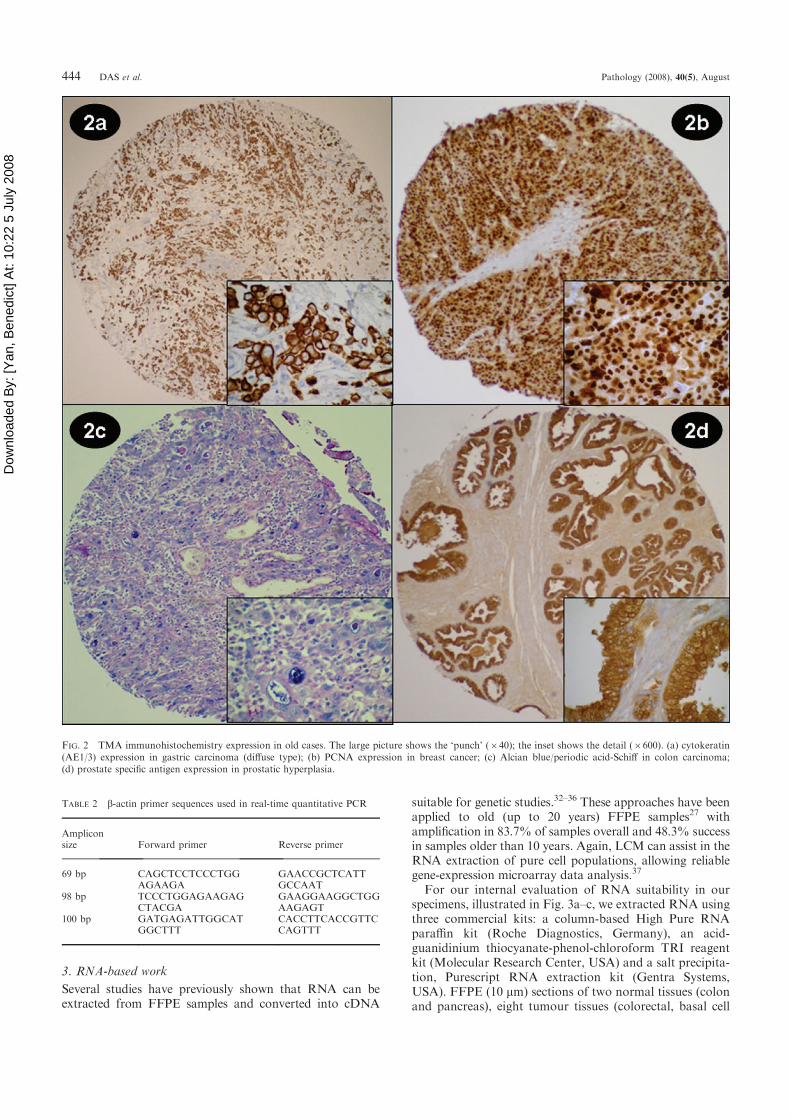
In another study, we constructed a TMA of 0.6 mm usingthe Advanced Tissue Arrayer ATA100 (Chemicon) con-sisting of 90 tumour and 13 matched normal tissues [tonsil(1), thyroid (1), brain (1), bone (1), lung (1), bladder (1),kidney (2), ligament tissue (1), gall bladder (1), prostate (2),nasopharynx (2), liver (3), cervix (4), uterus (4), ovary (4),lymph node (6), skin (7), stomach (15), colorectal (16),breast (17)] representing samples from 1956 to 1984 (so-called ‘old legacy TMA’) from two hospitals in Singapore,NUH and SGH. The mean age of these blocks was 34.5(range 22–47) years. Immunohistochemistry was performedusing 10 antibodies used in routine pathology diagnostics(Table 1) as well as the special stain Alcian blue/periodicacid-Schiff. Analysis was carried out annotating the natureof all the tissues present in the sections and their expectedpositivity with the antibodies analysed. The expected
expression was present in all samples (100%; Fig. 2). Therewas no lack of epitope specificity or sensitivity in relation toage of paraffin blocks.
2. DNA-based work
The suitability of DNA extracted from FFPE tissues forboth research and diagnostic purposes has been firmlyestablished throughout the years.22 DNA extraction fromFFPE tissues (normal or malignant) can be assisted by theidentification of the area of interest by either manual(scraping with scalpel) or laser capture-assisted microdis-section (LCM).23–25 Interestingly, at the time of TMAconstruction, parallel tissue cores can be used for DNAextraction of neighbouring areas, minimising the effect ofheterogeneity in protein-DNA correlations.26
DNAhas been extracted fromarchival FFPEby a plethoraof different protocols throughout the years.27,28 Someof theseprotocols can be applied to many samples in large scalepopulations29 or to samples archived for a long time.30
To test the robustness of these approaches in the contextof our challenging analytic environment (a FFPE old tissuelegacy collection of more than 40 years, stored in damagingtropical weather conditions and hence prone to significantDNA degradation), we analysed the quality of DNA usingthe Gentra Pure Gene DNA extraction kit (GentraSystems, USA). DNA was quantified and amplified by Q-PCR using b-actin primers of different amplicon sizes(Table 2). The PCR reaction components included 100 ngof DNA, 1 mL (10 mM) each of forward and reverseprimers, 0.5 mL of 10 mM dNTPs, 0.4 mL of Taqpolymerase in a final volume of 25 mL. The PCR cyclingconditions were 40 cycles at 948C, 568C and 728C for 1 mineach and a further extension at 728C for 10 min. PCRproduct analysed in gel electrophoresis showed bands in 38/90 (42%) of the samples. Quantitative real-time PCRanalysis of these 38 PCR products showed amplification in33 of 38 (87%) samples. Combined, the qualitative andquantitative data confirmed the suitability of the legacytissue DNA for molecular analysis in our tropical environ-ment (Fig. 1b).
However, the use of DNA from FFPE tissues may besuboptimal for other genomic approaches. For instance, itssuitability for DNA profiling by array comparativegenomic hybridisation (CGH) was clearly suboptimal whencompared with fresh-frozen samples.31
TABLE 1 Antibodies with dilution used in immunostaining the tumourtissues
No. Antibody Dilution Manufacturer
1 AE1/3 1:100 Dako, Denmark2 CD30 1:200 Dako, Denmark3 CD31/PECAM-1 1:100 BD Pharmingen, USA4 CD34 1:1000 Dako, Denmark5 CD45/LCA 1:100 BD Pharmingen, USA6 PSA 1:50 Dako, Denmark7 SMA 1:1000 Dako, Denmark8 Ki-67 1:100 Dako, Denmark9 PCNA 1:1000 Dako, Denmark
10 S-100 (polyclonal) 1:1000 Dako, Denmark
PCNA, proliferating cell nuclear antigen; PSA, prostate specific antigen;SMA, smooth muscle actin.
TRARESA 443
Dow
nloa
ded
By:
[Yan
, Ben
edic
t] A
t: 10
:22
5 Ju
ly 2
008
3. RNA-based work
Several studies have previously shown that RNA can beextracted from FFPE samples and converted into cDNA
suitable for genetic studies.32–36 These approaches have beenapplied to old (up to 20 years) FFPE samples27 withamplification in 83.7% of samples overall and 48.3% successin samples older than 10 years. Again, LCM can assist in theRNA extraction of pure cell populations, allowing reliablegene-expression microarray data analysis.37
For our internal evaluation of RNA suitability in ourspecimens, illustrated in Fig. 3a–c, we extracted RNA usingthree commercial kits: a column-based High Pure RNAparaffin kit (Roche Diagnostics, Germany), an acid-guanidinium thiocyanate-phenol-chloroform TRI reagentkit (Molecular Research Center, USA) and a salt precipita-tion, Purescript RNA extraction kit (Gentra Systems,USA). FFPE (10 mm) sections of two normal tissues (colonand pancreas), eight tumour tissues (colorectal, basal cell
FIG. 2 TMA immunohistochemistry expression in old cases. The large picture shows the ‘punch’ (640); the inset shows the detail (6600). (a) cytokeratin(AE1/3) expression in gastric carcinoma (diffuse type); (b) PCNA expression in breast cancer; (c) Alcian blue/periodic acid-Schiff in colon carcinoma;(d) prostate specific antigen expression in prostatic hyperplasia.
TABLE 2 b-actin primer sequences used in real-time quantitative PCR
Ampliconsize Forward primer Reverse primer
69 bp CAGCTCCTCCCTGGAGAAGA
GAACCGCTCATTGCCAAT
98 bp TCCCTGGAGAAGAGCTACGA
GAAGGAAGGCTGGAAGAGT
100 bp GATGAGATTGGCATGGCTTT
CACCTTCACCGTTCCAGTTT
444 DAS et al. Pathology (2008), 40(5), August

Dow
nloa
ded
By:
[Yan
, Ben
edic
t] A
t: 10
:22
5 Ju
ly 2
008
carcinoma, synovial sarcoma, breast carcinoma), two celllines (colorectal adenocarcinoma DLD-1 and breastadenocarcinoma MDA-MB-231) and a mouse xenograftwith RUNX3 transfected MDA-MB-231 cells were used forthis purpose. Total RNA was isolated and quantified usingND-1000 spectrophotometer (NanoDrop Technologies,USA). The High Pure RNA paraffin kit provided betterRNA yields than the other two kits.
RNA extraction was followed by cDNA synthesis usingtwo reverse transcriptase PCR kits, high capacity cDNAarchive kit (ABI, USA) and SuperScript III first strandsynthesis (Invitrogen, USA) to evaluate the optimal cDNAnecessary for quantitative real-time RT-PCR. The PCRefficiency of three common house keeping genes (GAPDH,18S RNA and b-actin) and two genes (p53 and EGFR)using templates synthesised from both the kits was found to
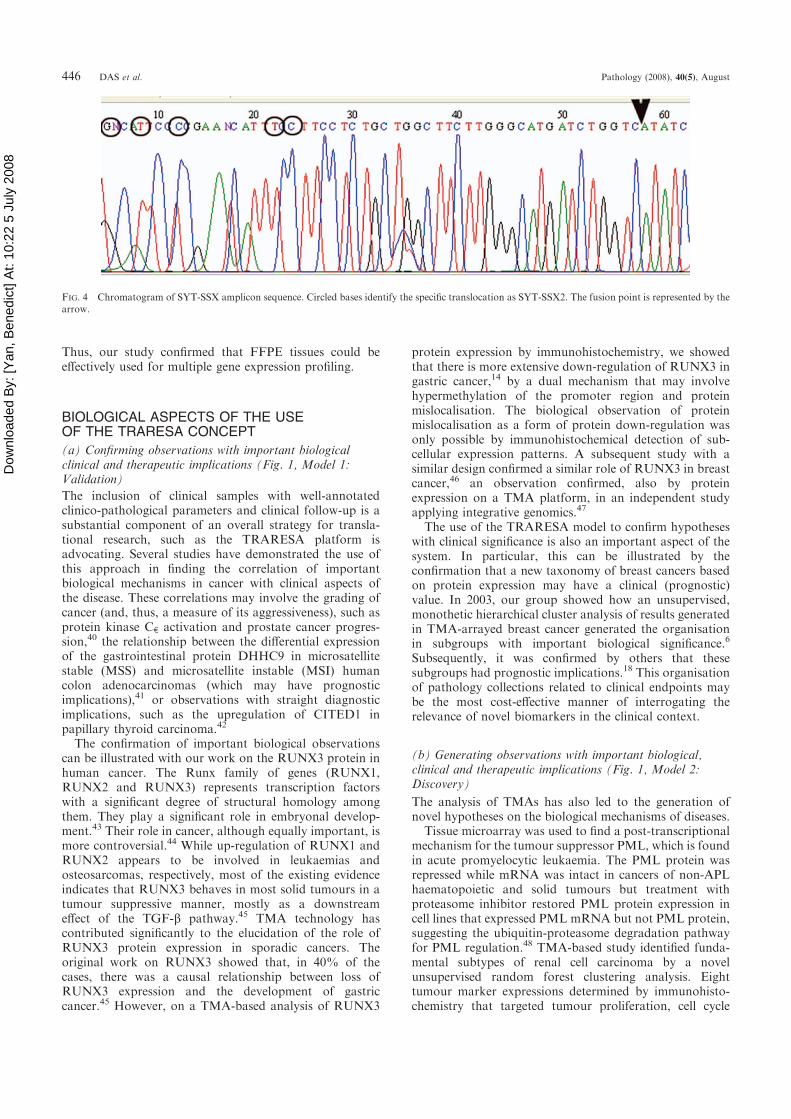
be similar (Fig. 3a). We then analysed the templatesobtained from the synovial sarcoma samples by PCRamplification, agarose gel electrophoresis and sequencing.Adequate amplification was observed with a fragment sizeof 98 bp38 and 86 bp.39 Additionally, synovial sarcomatranslocation was also identified and confirmed by sequen-cing (Fig. 4) suggesting that the RNA quality from ourFFPE samples was optimum to detect genetic instability incancer research. Finally, we looked at the expression of b-actin, EGFR and RUNX3 genes in all of the samples; 33%of the samples showed amplification of all three genes. Therelative quantitation of EGFR as compared with b-actinremained relatively constant (Fig. 3b) in these sampleswhich were then run on a 96-gene Low Density ArrayPlatform (Applied Biosystems, USA). Eighty-six of 96genes (each gene in quadruples) amplified well (Fig. 3c).
FIG. 3 Validation of RNA extraction and gene expression analysis in FFPE tissue. (a) Comparison of DNA extraction efficiency with different commerciallyavailable kits. (b) Relation of housekeeping gene versus target gene in two cell lines and four treatment samples: fresh, frozen, FFPE for 3 hours and FFPE for12 hours, for each sample, respectively. (c) Relative gene expression on RNA extracted from two FFPE basal cell carcinoma samples, normalised againstexpression on a FFPE sample of normal skin; detail of expression of 29 genes of a total of 384 (96 genes, each gene in quadruples).
TRARESA 445
Dow
nloa
ded
By:
[Yan
, Ben
edic
t] A
t: 10
:22
5 Ju
ly 2
008
Thus, our study confirmed that FFPE tissues could beeffectively used for multiple gene expression profiling.
BIOLOGICAL ASPECTS OF THE USEOF THE TRARESA CONCEPT
(a) Confirming observations with important biologicalclinical and therapeutic implications (Fig. 1, Model 1:Validation)
The inclusion of clinical samples with well-annotatedclinico-pathological parameters and clinical follow-up is asubstantial component of an overall strategy for transla-tional research, such as the TRARESA platform isadvocating. Several studies have demonstrated the use ofthis approach in finding the correlation of importantbiological mechanisms in cancer with clinical aspects ofthe disease. These correlations may involve the grading ofcancer (and, thus, a measure of its aggressiveness), such asprotein kinase Ce activation and prostate cancer progres-sion,40 the relationship between the differential expressionof the gastrointestinal protein DHHC9 in microsatellitestable (MSS) and microsatellite instable (MSI) humancolon adenocarcinomas (which may have prognosticimplications),41 or observations with straight diagnosticimplications, such as the upregulation of CITED1 inpapillary thyroid carcinoma.42
The confirmation of important biological observationscan be illustrated with our work on the RUNX3 protein inhuman cancer. The Runx family of genes (RUNX1,RUNX2 and RUNX3) represents transcription factorswith a significant degree of structural homology amongthem. They play a significant role in embryonal develop-ment.43 Their role in cancer, although equally important, ismore controversial.44 While up-regulation of RUNX1 andRUNX2 appears to be involved in leukaemias andosteosarcomas, respectively, most of the existing evidenceindicates that RUNX3 behaves in most solid tumours in atumour suppressive manner, mostly as a downstreameffect of the TGF-b pathway.45 TMA technology hascontributed significantly to the elucidation of the role ofRUNX3 protein expression in sporadic cancers. Theoriginal work on RUNX3 showed that, in 40% of thecases, there was a causal relationship between loss ofRUNX3 expression and the development of gastriccancer.45 However, on a TMA-based analysis of RUNX3
protein expression by immunohistochemistry, we showedthat there is more extensive down-regulation of RUNX3 ingastric cancer,14 by a dual mechanism that may involvehypermethylation of the promoter region and proteinmislocalisation. The biological observation of proteinmislocalisation as a form of protein down-regulation wasonly possible by immunohistochemical detection of sub-cellular expression patterns. A subsequent study with asimilar design confirmed a similar role of RUNX3 in breastcancer,46 an observation confirmed, also by proteinexpression on a TMA platform, in an independent studyapplying integrative genomics.47
The use of the TRARESA model to confirm hypotheseswith clinical significance is also an important aspect of thesystem. In particular, this can be illustrated by theconfirmation that a new taxonomy of breast cancers basedon protein expression may have a clinical (prognostic)value. In 2003, our group showed how an unsupervised,monothetic hierarchical cluster analysis of results generatedin TMA-arrayed breast cancer generated the organisationin subgroups with important biological significance.6
Subsequently, it was confirmed by others that thesesubgroups had prognostic implications.18 This organisationof pathology collections related to clinical endpoints maybe the most cost-effective manner of interrogating therelevance of novel biomarkers in the clinical context.
(b) Generating observations with important biological,clinical and therapeutic implications (Fig. 1, Model 2:Discovery)
The analysis of TMAs has also led to the generation ofnovel hypotheses on the biological mechanisms of diseases.
Tissue microarray was used to find a post-transcriptionalmechanism for the tumour suppressor PML, which is foundin acute promyelocytic leukaemia. The PML protein wasrepressed while mRNA was intact in cancers of non-APLhaematopoietic and solid tumours but treatment withproteasome inhibitor restored PML protein expression incell lines that expressed PML mRNA but not PML protein,suggesting the ubiquitin-proteasome degradation pathwayfor PML regulation.48 TMA-based study identified funda-mental subtypes of renal cell carcinoma by a novelunsupervised random forest clustering analysis. Eighttumour marker expressions determined by immunohisto-chemistry that targeted tumour proliferation, cell cycle
FIG. 4 Chromatogram of SYT-SSX amplicon sequence. Circled bases identify the specific translocation as SYT-SSX2. The fusion point is represented by thearrow.
446 DAS et al. Pathology (2008), 40(5), August

Dow
nloa
ded
By:
[Yan
, Ben
edic
t] A
t: 10
:22
5 Ju
ly 2
008
abnormality, cell mobility and hypoxia pathway were usedto detect classes of low and high grade patients and asubgroup with distinct molecular profile that survived clearcell carcinoma.49
A novel biomarker, CEACAM6 was identified inpancreatic adenocarcinoma and intraepithelial neoplasiaby TMA immunostaining. Tumoral CEACAM6 expres-sion was detected in 92% of pancreatic adenocarci-noma specimens and was over-expressed in high graderather than low grade intraepithelial neoplasias. Patients atlow cancer stage without lymph node metastases andsurviving at post-operative stage showed no expression ofthis protein.50
In line with these studies, we decided to analyse theprotein expression of RUNX3 in a type of cancerinvariably controlled by the Sonic Hedgehog (SHH)pathway, the basal cell carcinoma (BCC). In view of theevidence of Sonic Hedgehog dysregulation in BCC,particularly at the level of the Patch1 gene, and therelationship of RUNX3 with the TGF-b pathway, wethought that the BCC model would provide a naturalframework to study TGF-b/RUNX3/SHH interactions.Interestingly, we reported that there is up-regulation ofRUNX3, thus functioning as a bona fide oncogene inBCC,51 as opposed to all the solid neoplasms analysed todate. Again, this new hypothesis (the oncogenic role ofRUNX3) could be established by the systematic analysis ofmany samples from many different tumour types, asfacilitated by the TRARESA system.
The role of TRARESA to generate observations withimportant clinical implications (in this case with bothprognostic value and generating possible new targets forexisting drugs) can be illustrated by the use of TMA in thestudy of gastrointestinal stromal tumours (GIST).52 In thisstudy, 50 paraffin blocks were characterised clinically andpathologically. A TMA was constructed with these cases,which allowed the expression analysis of 22 proteins andthe analysis with an unsupervised, hierarchical monotheticcluster statistical method. Those biomarkers with strongclinical significance were tested for mutation status by bothPCR-denaturing high performance liquid chromatography(DHPLC) and direct sequencing. This analysis charac-terised a VEGF protein overexpression signature, includingboth VEGF-A ligand and VEGF receptor proteins, as astatistically significant discriminator of prognosis in GIST.Furthermore, the analysis of the VEGF-A gene allowed thediscovery of novel DNA variants. VEGF-A is a major anti-angiogenic therapeutic target.53 Recently anti-VEGF-Atherapy has been successful in the treatment of GIST54
with drugs such as Sutent and sorafenib. The results of thisstudy may prove a biological explanation for the success ofthis therapeutic approach.
CONCLUSION
Here we present TRARESA, a conceptual frameworkmaking use of established technology, which through arigorous preliminary analysis, allows analysis of DNA,RNA and protein in the largest available repository ofclinical samples, the FFPE samples from pathologyarchives.
TRARESA is based on an initial high throughput proteinexpression analysis by TMA, followed by exploratory or
confirmatory RNA- or DNA-based analyses in all cases ora subset of them. This has two primary advantages: (a) thefirst analysis is based on the interrogation of hundreds ofsamples; and (b) the results are based on the expression ofprotein, the determinant of biological function. These areclear advantages when compared with other high through-put technologies based on analyses at a DNA or RNA levelalone; invariably, these technologies must be applied to asignificantly smaller number of cases and to achieve fullmeaning must be confirmed at a protein level withtechnologies such as TMA.
The importance of allowing full biological interrogationof large sample collections for basic and translationalresearch cannot be over-emphasised. The Cancer GenomeAtlas is one of the most ambitious ongoing projects in thestudy of disease genomics. In 2006, it was suspected thatnot enough samples are available in the conventional,frozen tissue repositories, to develop this program.55 In2007, this suspicion was clearly substantiated.56 Thus, it isimportant to develop the technical capability to be able toinvestigate FFPE tissue collections from all possible angles,in a biologically satisfactory manner, following similarmodels to the one we present here.
This development highlights a leading research role forhospitals. Until now, hospitals were primarily providers ofadequate healthcare to the population, taking care of thepresent needs. However, it is mandatory that they modifytheir operations to allow, as much as possible, theirfunction as facilitators of translational research and, assuch, taking care of the future.
Pathology departments will have to play a central role inthis development into translational research facilitators,allowing the treatment of diagnostic samples in such waythat their use for research purposes can be maximised. Thisrole, together with the necessary role of pathologists asproviders of molecular diagnostics,57 may transform theway in which pathology is practised in hospitals in the nearfuture. In addition, as indicated by the TRARESA concept,analyses of clinical samples will only have full meaningwhen correlated with clinical endpoints, suggesting aprominent role for those that keep clinical records in thehospital setting. This may change the way we organiseclinical operations in hospitals in general.
Because of the clinical tissue availability, and theimportance of proteins as the ultimate ‘actors’ in biologyfunction, the TMA technology (which combines both)appears as a central tool for translational research. TheTRARESA conceptualisation framework, allowing discov-ery and validation with immediate clinical relevance,provides a hospital-based environment for clinical applica-tions of biological sciences. In a way, such framework putshospitals settings ‘at the service’ of translational research.In essence, TRARESA moves the focus of TMA from aresearch tool into a research system.
ACKNOWLEDGMENT MST receives funding support fromSCS Grants MN-005 and MN-077, awarded by theSingapore Cancer Syndicate, Agency for Science,Technology and Research, Singapore.
Address for correspondence: Professor M. Salto-Tellez, Department ofPathology, Yong Loo Lin Faculty of Medicine, National University ofSingapore, 5 Lower Kent Ridge Road, Singapore 119074. E-mail:[email protected]
TRARESA 447
Dow
nloa
ded
By:
[Yan
, Ben
edic
t] A
t: 10
:22
5 Ju
ly 2
008
References1. Crawford JM, Tykocinski ML. Pathology as the enabler of human
research. Lab Invest 2005; 85: 1058–64.2. Kajdacsy-Balla A, Geynisman JM, Macias V, et al. Cooperative
Prostate Cancer Tissue Resource. Practical aspects of planning,building, and interpreting tissue microarrays: the CooperativeProstate Cancer Tissue Resource experience. J Mol Histol 2007; 38:113–21.
3. Sinard JH, Morrow JS. Informatics and anatomic pathology: meetingthe challenges and charting the future. Hum Pathol 2001; 32: 143–8.
4. Drake TA, Braun J, Marchevsky A, et al. A system for sharing routinesurgical pathology specimens across institutions: the Shared PathologyInformatics Network. Hum Pathol 2007; 38: 1212–25.
5. Mohanty SK, Parwani AV, Crowley RS, et al. The importance ofpathology informatics in translational research. Adv Anat Pathol 2007;14: 320–2.
6. Zhang DH, Salto-Tellez M, Chiu LL, et al. Tissue microarraystudy for classification of breast tumors. Life Sciences 2003; 73:3189–99.
7. Battifora H. The multitumor (sausage) tissue block: novel method forimmuno-histochemical antibody testing. Lab Invest 1986; 55: 244–8.
8. Kononen J, Bubendorf L, Kallioniemi A, et al. Tissue microarrays forhigh-throughput molecular profiling of tumor specimens. Nat Med1998; 4: 844–7.
9. Eguiluz C, Viguera E, Millan L, et al. Multitissue array review: achronological description of tissue array techniques, applications andprocedures. Pathol Res Pract 2006; 202: 561–8.
10. Hoos A, Cordon-Cardo C. Tissue microarray profiling of cancerspecimens and cell lines: opportunities and limitations. Lab Invest 2001;81: 1331–8.
11. Manley S, Mucci NR, De Marzo AM, et al. Rubin relational databasestructure to manage high-density tissue microarray data and images forpathology studies focusing on clinical outcome. Am J Pathol 2001; 159:837–43.
12. Takikita C, Chung JY, Hewitt SM. Tissue microarrays enablinghigh-throughput molecular pathology. Curr Opin Biotech 2007; 18:318–25.
13. Hans CP, Weisenburger DD, Greiner TC, et al. Confirmation of themolecular classification of diffuse large B-cell lymphoma byimmunohistochemistry using a tissue microarray. Blood 2004; 103:275–82.
14. Mousses S, Bubendorf L, Wagner U, et al. Clinical validation ofcandidate genes associated with prostate cancer progression in theCWR22 model system using tissue microarrays. Cancer Res 2002; 62:1256–60.
15. Ito K, Liu Q, Salto-Tellez M, et al. Frequent cytoplasmic retention ofRUNX3 in gastric cancer cells: A novel mechanism of inactivation.Cancer Res 2005; 65: 7743–50.
16. Huang BH, Laban M, Leung CHW, et al. Inhibition of histonedeacetylase 2 increases apoptosis and p21Cip1/WAF1 expression,independent of histone deacetylase 1. Cell Death Differ 2005; 12:395–404.
17. Makretsov NA, Huntsman DG, Nielsen TO, et al. Hierarchicalclustering analysis of tissue microarray immunostaining data identifiesprognostically significant groups of breast carcinoma. Clin Cancer Res2004; 10: 6143–51.
18. Jacquemier J, Ginestier C, Rougemont J, et al. Protein expressionprofiling identifies subclasses of breast cancer and predicts prognosis.Cancer Res 2005; 65: 767–79.
19. Sauter G, Simon R, Hillan K. Tissue microarrays in drug discovery.Nat Rev Drug Discov 2003; 2: 962–72.
20. Horvath L, Henshall S. Timely Topic: The application of tissuemicroarrays to cancer research. Pathology 2001; 33: 125–9.
21. Zhang DH, Salto-Tellez M, Putti TC, et al. Reliability of tissuemicroarrays in detecting protein expression and gene amplification inbreast cancer. Mod Pathol 2003; 16: 79–84.
22. Shibata D, Martin WJ, Arnheim N. Analysis of DNA sequences inforty-year old paraffin-embedded thin-tissue sections: a bridge betweenmolecular biology and classical histology. Cancer Res 1988; 48: 4564–6.
23. Zhuang Z, Bertheau P, Emmert-Buck MR, et al. A microdissectiontechnique for archival DNA analysis if specific cell populations inlesions 51 mm in size. Am J Pathol 1995; 146: 620–5.
24. Emmert-Buck MR, Bonner RF, Smith PD, et al. Laser capturemicrodissection. Science 1996; 274: 998–1001.
25. Rubin MA. Tech.Sight. Understanding disease cell by cell. Science2002; 296: 1329–30.
26. Prince ME, Ubell ML, Castro J, et al. Tissue preserving approach toextracting DNA from paraffin-embedding specimens using tissuemicroarray technology. Head Neck 2007; 29: 465–71.
27. Coombs NJ, Gough AC, Primrose JN. Optimisation of DNA andRNA extraction from archival formalin-fixed tissue. Nucleic Acids Res1999; 27: e12–7.
28. Shi SR, Cote RJ, Wu L, et al. DNA extraction from archival formalin-fixed, paraffin-embedded tissue sections based on the antigen retrievalprinciple: heating under the influence of pH. J Histochem Cytochem2002; 50: 1005–11.
29. Tos-Gillo A, Marco LD, Fiano V, et al. Efficient DNA extraction from25 year old paraffin-embedded tissues: studies of 365 samples.Pathology 2007; 39: 345–8.
30. Sjoholm MIL, Hoffmann G, Lindgren S, et al. Comparison of archivalplasma and formalin-fixed paraffin-embedded tissue for genotyping inhepatocellular carcinoma. Cancer Epidemiol Biomarkers Prev 2005; 14:251–5.
31. Mc Sherry EA, McGoldrick A, Kay EW, et al. Formalin fixed paraffinembedded clinical tissues show spurious copy number changes in array-CGH profiles. Clin Genet 2007; 72: 441–7.
32. Rupp GM, Locker J. Purification and analysis of RNA from paraffin-embedded tissues. Biotechniques 1988; 6: 56–60.
33. Finke J, Fritzen R, Temes P, et al. An improved strategy and auseful housekeeping gene for RNA analysis from formalin-fixed, paraffin-embedded tissues by PCR. Biotechniques 1993; 14:448–53.
34. Stanta G, Bonin S. RNA quantitative analysis from fixed and paraffin-embedded tissues: membrane hybridization and capillaryelectrophoresis. Biotechniques 1998; 24: 271–6.
35. Godfrey TE, Kim SH, Chavira M, et al. Quantitative mRNAexpression analysis from formalin-fixed paraffin-embedded tissuesusing 5’ nuclease quantitative reverse transcription-polymerase chainreaction. J Mol Diagn 2000; 2: 84–91.
36. Specht K, Richter T, Muller U, et al. Quantitative gene expressionanalysis in microdissected archival formalin-fixed and paraffin-embedded tumour tissue. Am J Pathol 2001; 158: 419–29.
37. Coudry RA, Meireles SI, Stoyanova R, et al. Successful application ofmicroarray technology to microdissected formalin-fixed, paraffin-embedded tissue. J Mol Diagn 2007; 9: 70–9.
38. Tsuji S, Hisaoka M, Morimitsu Y, et al. Detection of SYT-SSX fusiontranscripts in synovial sarcoma by reverse transcription-polymerasechain reaction using archival paraffin-embedded tissues. Am J Pathol1998; 153: 1807–12.
39. Tvrdik D, Povysil C, Svatosova J, et al. Molecular diagnosis ofsynovial sarcoma: RT-PCR detection of SYT-SSX1/2 fusiontranscripts in paraffin-embedded tissue. Med Sci Monit 2005; 11:MT1–7.
40. Aziz MH, Manoharan HT, Church DR, et al. Protein kinase Ce
interacts with signal transducers and activators of transcription 3(Stat3), phosphorylates Stat3ser727 and regulates its constitutiveactivation in prostate cancer. Cancer Res 2007; 67: 8828–38.
41. Mansilla F, Birkenkamp-Demtroder K, Kruhoffer M, et al.Differential expression of DHHC9 in microsatellite stable andinstable human colorectal cancer subgroups. Br J Cancer 2007; 96:1896–903.
42. Prasad ML, Pellegata NS, Kloos RT, Barbacioru C, Huang Y,Chapelle de la A. CITED1 protein expression suggests papillarythyroid carcinoma in high throughput tissue microarray based study.Thyroid 2004; 14: 169–75.
43. Ito Y, Miyazono K. RUNX transcription factors as key targetsof TGF-beta superfamily signaling. Curr Opin Genet Dev 2003; 132:43–7.
44. Blyth K, Cameron ER, Neil JC. The RUNX Genes: gain or loss offunction in cancer. Nat Rev Cancer 2005; 5: 76–87.
45. Li QL, Ito K, Sakakura C, et al. Causal relationship between theloss of RUNX3 expression and gastric cancer. Cell 2002; 109:113–24.
46. Lau QC, Raja E, Salto-Tellez M, et al. RUNX3 is frequentlyinactivated by dual mechanisms of protein mislocalization andpromoter hypermethylation in breast cancer. Cancer Res 2006; 66:6512–20.
47. Chen W, Salto-Tellez M, Palanisamy N, et al. Targets of genome copynumber reduction in primary breast cancers identified by integrativegenomics. Genes Chromosomes Cancer 2007; 46: 288–301.
48. Gurrieri C, Capodieci P, Bernardi R, et al. Loss of tumor suppressorPML in human cancers of multiple histologic origins. J Natl CancerInst 2004; 96: 269–79.
49. Shi T, Seligson D, Belldegrun AS, et al. Tumor classification by tissuemicroarray profiling: random forest clustering applied to renal cellcarcinoma. Mod Pathol 2005; 18: 547–57.
50. Duxbury MS, Matros E, Clancy T, et al. CEACAM6 is a novelbiomarker in pancreatic adenocarcinoma and panIN lesions. Ann Surg2005; 241: 491–6.
448 DAS et al. Pathology (2008), 40(5), August

Dow
nloa
ded
By:
[Yan
, Ben
edic
t] A
t: 10
:22
5 Ju
ly 2
008
51. Salto-Tellez M, Peh BK, Ito K, et al. Runx3 protein is overexpressed inhuman basal cell carcinomas. Oncogene 2006; 25: 7646–9.
52. Salto-Tellez M, Nga ME, Han HC, et al. Tissue microarrayscharacterize the clinical significance of a VEGF-A protein expressionsignature in gastro-intestinal stromal tumors. Br J Cancer 2007; 96:776–82.
53. Ferrara N, Kerbel RS. Angiogenesis as a therapeutic target. Nature2005; 438: 967–74.
54. Marx J. Medicine: Cancer-suppressing enzyme adds a link to type 2diabetes. Science 2005; 310: 1259.
55. Waltz E. Informed consent issues hobble cancer genome scheme. NatMed 2006; 12: 719.
56. Waltz E. Pricey cancer genome project struggles with sample shortage.Nat Med 2007; 13: 391.
57. Salto-Tellez M. A case for integrated morphomolecular pathologists.Clin Chem 2007; 53: 1188–90.
TRARESA 449
Copyright © 2022 FDOKUMEN




















