
Tramadol/Acetaminophen combination tablets for the treatment of chronic lower back pain: A...
19
Tramadol/Acetaminophen Combination Tablets for the Treatment of Chronic Lower Back Pain: A Multicenter, Randomized, Double-Blind, Placebo-Controlled Outpatient Study Gary E. Ruoff, MD, 1 Norman Rosenthal, MD, 2 Donna Jordan, BSN, 2 Rezaul Karim, PhD, 2 and Marc Kamin, MD, 2 on behalf of the Protocol CAPSS-112 Study Group* 1Michigan State University College of Medicine, and Westside Family Medical Center, Kalamazoo, Michigan, and 20rtho-McNeil Pharmaceutical, Inc., Raritan, New Jersey ABSTRACT Background: Tramadol and acetaminophen (APAP) have both shown efficacy in the treatment of lower back pain. The combination of these 2 agents has demonstrated synergistic analgesic action in animal models at specific ratios. Objective: This study assessed the long-term (3-month) efficacy and safety of tramadol 37.5 mg/APAP 325 mg combination tablets in the treatment of chronic lower back pain. Methods: Patients with at least moderate lower back pain (pain visual analog [PVA] score >40 mm on a 100-ram scale) were randomized to receive up to 8 tablets of tramadol/APAP per day or placebo for 91 days. Medication was titrated from 1 to 4 tablets/d by day 10. The primary efficacy measure was PVA score at the final visit. Secondary measures included scores on the Pain Relief Rating Scale (PRRS), Short-Form McGill Pain Questionnaire (SF-MPQ), Roland Disability Questionnaire (RDQ), and 36-Item Short-Form Health Survey (SF-36); the inci- dence of discontinuation due to insufficient pain relief (Kaplan-Meier analysis); and overall assessments of medication by the patients and investigators. Results: Three hundred eighteen patients (161 tramadol/APAP, 157 placebo) were included in the intent-to-treat population, defined as all patients who took >1 Data from this study were presented at the 65th Annual Meeting of the American College of Rheumatology, November 11-15, 2001, San Francisco, California. "Members of the CAPSS-112 Study Group are listed in the Acknowledgments. Accepted for publication February 3, 2003. Printed in the USA. Reproduction in whole or part is not permitted. 014%2918/03/$19.00 Copyright © 2003 Excerpta Medica,Inc. 1123
Transcript of Tramadol/Acetaminophen combination tablets for the treatment of chronic lower back pain: A...

Tramadol/Acetaminophen Combination Tablets for the Treatment of Chronic Lower Back Pain: A Multicenter, Randomized, Double-Blind, Placebo-Controlled Outpatient Study
Gary E. Ruoff, MD, 1 Norman Rosenthal, MD, 2 Donna Jordan, BSN, 2 Rezaul Karim, PhD, 2 and Marc Kamin, MD, 2 on behal f of the Protocol CAPSS-112 Study Group* 1Michigan State University College of Medicine, and Westside Family Medical Center, Kalamazoo, Michigan, and 20rtho-McNeil Pharmaceutical, Inc., Raritan, New Jersey
ABSTRACT
Background: Tramadol and acetaminophen (APAP) have both shown efficacy in the treatment of lower back pain. The combination of these 2 agents has demonstrated synergistic analgesic action in animal models at specific ratios.
Objective: This study assessed the long-term (3-month) efficacy and safety of tramadol 37.5 mg/APAP 325 mg combination tablets in the treatment of chronic lower back pain.
Methods: Patients with at least moderate lower back pain (pain visual analog [PVA] score >40 mm on a 100-ram scale) were randomized to receive up to 8 tablets of tramadol/APAP per day or placebo for 91 days. Medication was titrated from 1 to 4 tablets/d by day 10. The primary efficacy measure was PVA score at the final visit. Secondary measures included scores on the Pain Relief Rating Scale (PRRS), Short-Form McGill Pain Questionnaire (SF-MPQ), Roland Disability Questionnaire (RDQ), and 36-Item Short-Form Health Survey (SF-36); the inci- dence of discontinuation due to insufficient pain relief (Kaplan-Meier analysis); and overall assessments of medication by the patients and investigators.
Results: Three hundred eighteen patients (161 tramadol/APAP, 157 placebo) were included in the intent-to-treat population, defined as all patients who took >1
Data from this study were presented at the 65th Annual Meeting of the American College of Rheumatology, November 11-15, 2001, San Francisco, California. "Members of the CAPSS-112 Study Group are listed in the Acknowledgments.
Accepted for publication February 3, 2003. Printed in the USA. Reproduction in whole or part is not permitted. 014%2918/03/$19.00
Copyright © 2003 Excerpta Medica, Inc. 1123
CLINICAL THERAPEUTICS ~)
dose of study medication and had _>1 postrandomization efficacy measurement. The mean age of the study population was 53.9 years, 63.2% were female, 90.3% were white, and the mean baseline PVA score was 70.0 mm. There were no significant differences between groups at baseline. Tramadol/APAP significantly improved final PVA scores (P = 0.015) and final PRRS scores (P < 0.001) compared with placebo. Tramadol/APAP also significantly improved RDQ scores (P < 0.027) and scores on many subcategories of the SF-MPQ, including total score (P = 0.021). The tramadol/ APAP group had significant improvements on the role-physical (P = 0.005), bod- ily pain (P = 0.046), role-emotional (P = 0.001), mental health (P = 0.026), re- ported health transition (P = 0.038), and mental component summary (P = 0.008) subscales of the SF-36. The cumulative incidence of discontinuation due to insuf- ficient pain relief was 22.1% for tramadol/APAP and 41.0% for placebo (P < 0.001). Treatment-emergent adverse events in the tramadol/APAP group included nausea (13.0%), somnolence (12.4%), and constipation (11.2%).
Conclusions: In this study, tramadol 37.5 mg/APAP 325 mg combination tablets were effective and had a favorable safety profile in the treatment of chronic lower back pain. (Clin Ther. 2003;25:1123-1141) Copyright © 2003 Excerpta Medica, Inc.
Key words: acetaminophen, tramadol, analgesics, combination therapy, lower back pain, chronic pain.
I N T R O D U C T I O N Lower back pain and associated disabilities constitute a growing public health problem, particularly in industrialized countries. Between 60% and 80% of adults in the United States experience lower back pain at some time in their life, and estimates of the associated costs range from $24 billion to >$100 billion annu- ally. 1 Chronic lower back pain is responsible for a large proportion of those costs; a study of workers' compensation in the United States between 1988 and 1996 found that although patients with lower back pain for >_1 year represented only 4.6% to 8.8% of compensation claims, they accounted for 64.9% to 84.7% of an- nual costs. 2 Unlike acute back pain, chronic back pain is often poorly understood and difficult to treat and can have a significant influence on quality of life in nu- merous areas of everyday functioning. As underscored by a recent review, 3 many patients with chronic lower back pain have no radiculopathic or anatomic ab- normalities that could explain their symptoms. Evidence suggests that sensitiza- tion of the central nervous system (CNS) may perpetuate the perception of pain in the absence of ongoing tissue damage. 3,4
Many of the available pharmacologic treatment options for lower back pain have limited efficacy, 5 and new pharmacologic solutions are needed. Clinical trial
]124
G.E. Ruoff et al.
data suggest that centrally acting antidepressants and tramadol are effective in some patients with chronic back pain, 6-1° whereas peripherally acting non- steroidal anti-inflammatory drugs (NSAIDs) are not. 5,11 Tramadol exhibits com- plementary mechanisms of action (mu-opioid receptor agonism and norepinephrine/ serotonin reuptake inhibition) 12 and has demonstrated efficacy in the treatment of lower back pain, 9 as well as in the treatment of other forms of nociceptive 13q6 and neuropathic pain. a7,1s
For years, acetaminophen (APAP) has been a first-choice analgesic for the phar- macologic treatment of chronic pain, 19 but its mechanisms of action remain un- clear. Although initial studies suggested that the analgesic effects of APAP could be attributed to selective inhibition of prostaglandin synthesis in the C N S , 20-23
more recent studies have identified other potential centrally mediated mecha- nisms of action, including inhibition of N-methyl-D-aspartate- or substance P- mediated nitric oxide synthesis 24-26 and inhibition of prostaglandin-E 2 release in the spinal cord. 27
A promising pharmacologic strategy for analgesia is to combine medications that have multiple mechanisms of action within the CNS. Tablets containing tramadol 37.5 mg/APAP 325 mg* combine multiple analgesic mechanisms12,28,29; combina- tions using similar ratios have demonstrated synergistic analgesic action in animal models, 3° as well as a more rapid onset of action than tramadol alone and a longer duration of action than APAP alone in a single-dose study in acute dental pain. 31 The combination of tramadol 37.5 mg/APAP 325 mg showed comparable analge- sia to the combination of APAP/codeine in a longer study (4 weeks) in patients with chronic nonmalignant pain. 32 This same combination of tramadol/APAP used as add-on therapy was effective in controlling osteoarthritis flare pain not con- trolled by ongoing therapy with NSAIDs or cyclooxygenase-2-selective inhibitors. 33
The purpose of the present study was to assess the long-term (3-month) effi- cacy and safety of tramadol 37.5 mg/APAP 325 mg combination tablets in the treatment of chronic lower back pain.
P A T I E N T S A N D M E T H O D S
Patients To be eligible for the study, patients were required to be between the ages of
25 and 75 years, be in general good health, be ambulatory, and have lower back pain such that daily medication was needed for >3 months before entry into the study screening/washout phase. All patients were required to be able to read and comprehend written instructions and be able to complete the pain assessment forms. Women had to be postmenopausal, surgically sterile, or practicing an ac- ceptable method of contraception; in the latter case, they were required to have
*Trademark: ULTRACET M (Ortho-McNeil Pharmaceutical, Inc., Raritan, New Jersey).
1125

CLINICAL THERAPEUTICS ~'
a negative result on a urine pregnancy test i week before study entry. Patients who completed the screening/washout phase were required to have a pain visual analog (PVA) score >40 mm on a scale from 0 to t00 ram.
Patients were excluded from the study if they had previously discontinued tra- madol therapy due to adverse effects or if they had undergone therapy with tra- madol within 30 days before study entry. They were also excluded if they had taken antidepressants, cyclobenzaprine, or antiepileptic drugs for pain, or if they had received transcutaneous electrical nerve stimulation, chiropractic adjust- ments, or acupuncture within 3 weeks of the double-blind phase. Patients were also excluded if they had taken sedative-hypnotics, short-acting analgesics, topi- cal anesthetics, or muscle relaxants for a period of <5 half-lives of the specific medication before the double-blind phase. Patients could not have received in- jections of corticosteroids in the lower back region or have used systemic steroids within the 3 months before the screening/washout phase. Patients were not per- mitted to enroll if they had severe pain in a location other than the lower back or had neurologic deficits in the lower extremities. Patients with known con- traindications to opioids or APAP, major psychiatric disorders, or a history of at- tempted suicide or substance abuse were excluded. Patients who were pregnant or lactating were excluded, as were those who had received an investigational drug or used an investigational device within 30 days before study entry.
All patients (or their legal representatives) provided written informed consent. The study was conducted in accordance with the Declaration of Helsinki (as amended in 1989), and an independent institutional review board approved the study protocol.
Study Design and Intervention This was a 91-day, multicenter (29 sites), randomized, double-blind, placebo-
controlled, parallel-group outpatient study comparing tramadol 37.5 mg/APAP 325 mg oral tablets with placebo for the long-term treatment (3 months) of chronic lower back pain. After a 3-week screening and washout phase, patients with at least moderate lower back pain (PVA score >40 mm) were randomly as- signed to receive either tramadol/APAP or placebo (Figure 1). Randomization was performed using SAS version 8 (SAS Institute Inc., Cary, North Carolina). Block randomization was by site. Patients, investigators, clinical staff, and study moni- tors remained blinded to treatment assignments until therapy was complete and the database was finalized.
Study medication was titrated over a 10-day period from 1 to 4 tablets/d. Thereafter, the dosage was adjusted according to each patient's requirement to a maximum of 8 tablets/d. Rescue medication was allowed only on days 1 to 6 of the double-blind phase and consisted of up to 2000 mg APAP (provided the patient was not taking >6 tablets of study medication per day).
1126

1 ta
blet
hs
Was
hout
ph
ase
1 ta
blet
hs
1
tabl
et
BID
1
tabl
et
TID
1 ta
blet
T
ID
1 ta
blet
B
ID
Tram
adol
/AP
AP
1
or 2
tab
lets
QID
(m
axim
um 8
tab
lets
/d)
Pla
cebo
1
or 2
tab
lets
QID
(m
axim
um 8
tab
lets
/d)
I
-21 I
Scr
eeni
ng/W
asho
ut
Pha
se
Dou
ble-
Blin
d P
hase
Day
I 10
I 91
~J
Figu
re
I.
Stu
dy d
esig
n. A
PA
P =
ace
tam
inop
hen.
m
;o
O .=_
..
CLINICAL THERAPEUTICS ~
Outcome Measures The primary efficacy variable was a comparison of PVA scores at the final visit
using the baseline score as covariate. To generate PVA scores, patients indicated the amount of back pain they had experienced within the previous 48 hours by making a mark on a line from "no pain" (0 ram) to "extreme pain" (100 mm) during study visits on days 1, 14, 28, 56, and 91. A categorical responder analy- sis was conducted based on PVA scores.
Secondary outcomes included Pain Relief Rating Scale (PRRS) scores (scale: 4 = complete, 3 = a lot, 2 = moderate, 1 = slight, 0 = none, -1 = worse), Short-Form McGill Pain Questionnaire (SF-MPQ) scores, Roland Disability Questionnaire (RDQ) scores, 36-Item Short-Form Health Survey (SF-36) scores, overall assess- ments of medication by both patients and physicians, and the incidence of dis- continuation due to insufficient pain relief (Kaplan-Meier analysis). These out- comes were assessed at various time points from day 1 through the final visit.
The SF-MPQ was administered on day 1 of the double-blind phase and at the final visit. Patients rated 15 pain descriptors (including sensory and affective com- ponents) as follows: 0 = none, 1 = mild, 2 = moderate, and 3 = severe. Present pain intensity was rated on the following 6-point index: 0 = no pain, 1 = mild, 2 = discomforting, 3 = distressing, 4 = horrible, and 5 = excruciating.
The RDQ was administered on day 1 of the double-blind phase and at the fi- nal visit. The 25-item questionnaire assessed the components of health status be- lieved to be most affected by lower back pain. Patients answered the first 24 items, which included physical function, feelings of well-being, and difficulty per- forming activities of daily living, as "yes" or 'no" they rated bothersomeness on a scale from 0 = not at all bothersome to 10 = extremely bothersome.
The 5F-36 was administered on day 1 of the double-blind phase and at the fi- nal visit to assess physical, social, and mental well-being. Scores were transformed to a scale of 0 to 100, with a higher score indicating better quality of life, except in the case of reported health transition, for which a higher score reflected poorer quality of life.
Data on vital signs (resting heart rate, blood pressure, and body weight), phys- ical examination, serum chemistry, hematology, urinalysis, and adverse events (re- ported spontaneously by patients or in response to general, nondirected ques- tioning) were collected throughout the double-blind phase at protocol-specified visits. All laboratory tests were processed at a central facility.
Statistical Analysis It was calculated that a sample size of 143 patients per group would have 80%
power to detect a mean difference of 10 mm on the PVA scale score, assuming a common SD of 30 mm using a 2-group t test. Therefore, a sample size of >150 patients per group was chosen for this study
1128
G.E. Ruoff et al,
For the primary efficacy variable (PVA score), the statistical significance of any difference in mean scores was assessed using an analysis of covariance (ANCOVA) of the final score, with the baseline score as covariate and treatment and center as qualitative factors. With the exception of the PRRS score and the patient's and investigator's overall medication assessments, for which the baseline PVA score was the covariate, secondary measures were analyzed using ANCOVA with score as a dependent variable, treatment as a qualitative factor, and the corresponding baseline score as the covariate. Kaplan-Meier estimates were determined for the distribution of time to discontinuation due to insufficient pain relief; the statisti- cal significance of any difference between treatment groups was analyzed using the Cox proportional hazards regression model, with treatment and center as qualitative factors and baseline PVA score as covariate.
All statistical tests were 2-sided, and the level of significance was set at P = 0.05. No interim analyses were planned or conducted.
R E S U L T S Demographic and Baseline Pain Characteristics
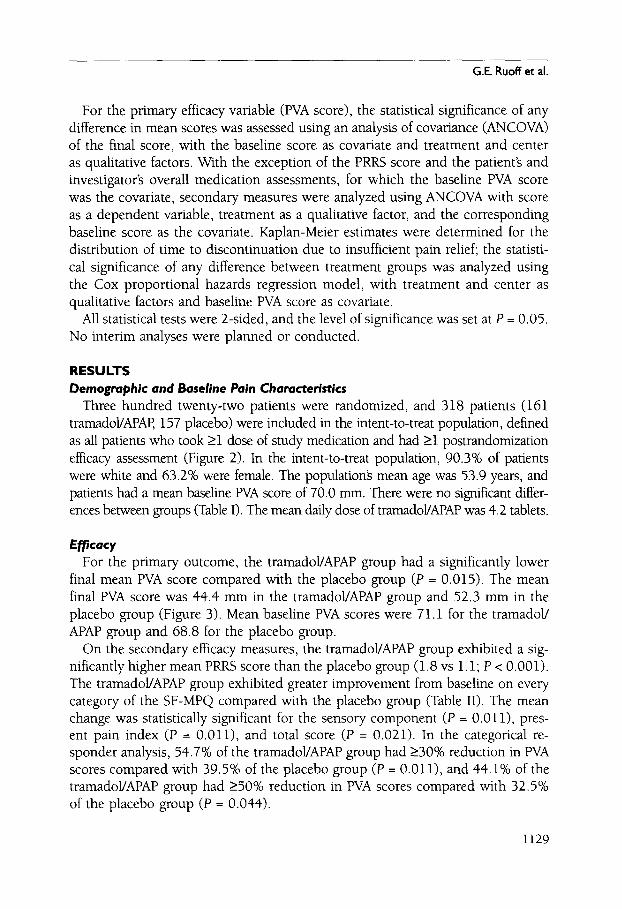
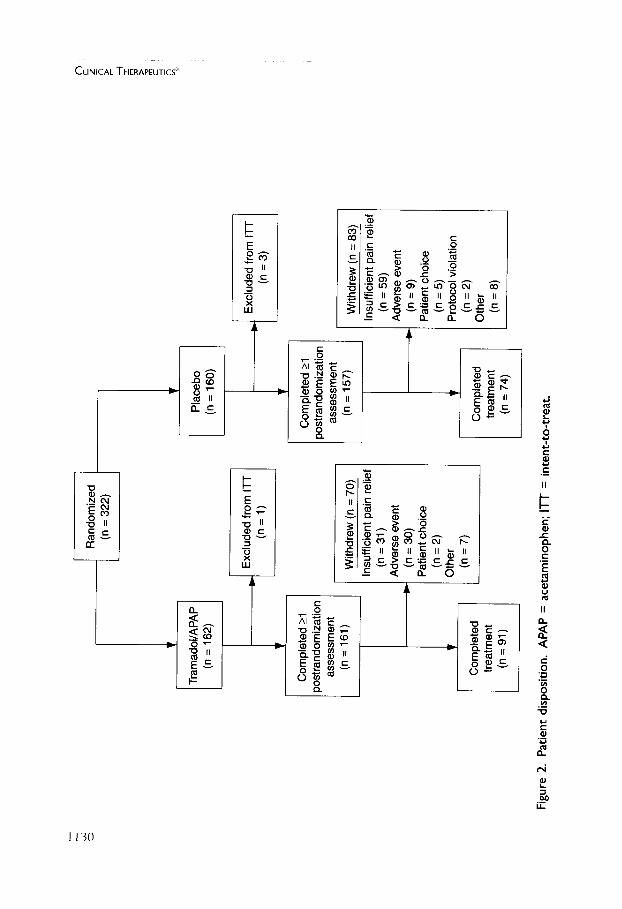
Three hundred twenty-two patients were randomized, and 318 patients (161 tramadol/APAP, 157 placebo) were included in the intent-to-treat population, defined as all patients who took >1 dose of study medication and had >1 postrandomization efficacy assessment (Figure 2). In the intent-to-treat population, 90.3% of patients were white and 63.2% were female. The populationg mean age was 53.9 years, and patients had a mean baseline PVA score of 70.0 ram. There were no significant differ- ences between groups (Table I). The mean daily dose of tramadol/APAP was 4.2 tablets.
Efficacy For the primary outcome, the tramadol/APAP group had a significantly lower
final mean PVA score compared with the placebo group (P = 0.015). The mean final PVA score was 44.4 mm in the tramadol/APAP group and 52.3 mm in the placebo group (Figure 3). Mean baseline PVA scores were 71.1 for the tramadol/ APAP group and 68.8 for the placebo group.
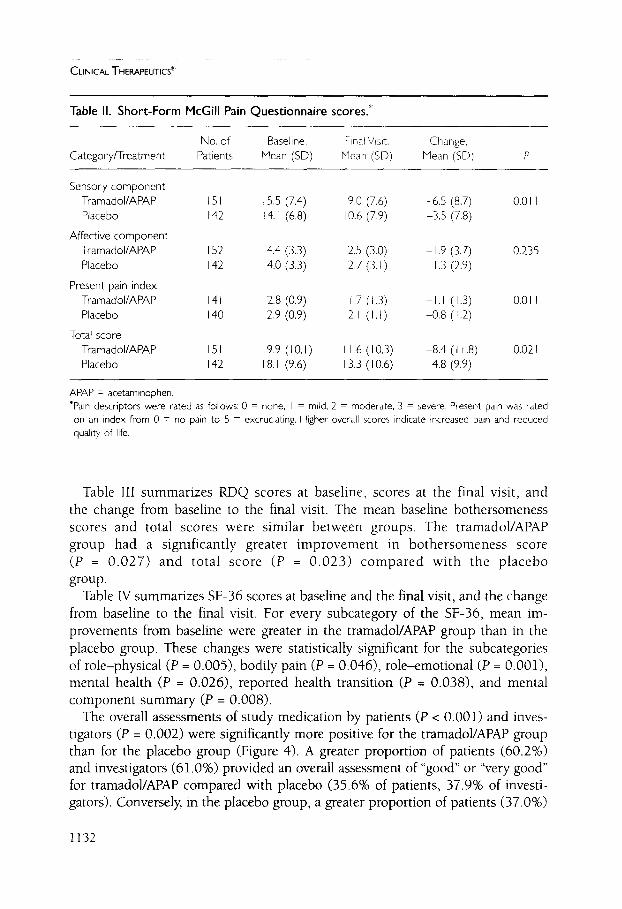
On the secondary efficacy measures, the tramadol/APAP group exhibited a sig- nificantly higher mean PRRS score than the placebo group (1.8 vs 1.1; P < 0.001). The tramadol/APAP group exhibited greater improvement from baseline on every category of the SF-MPQ compared with the placebo group (Table II). The mean change was statistically significant for the sensory component (P = 0.011), pres- ent pain index (P = 0.011), and total score (P = 0.021). In the categorical re- sponder analysis, 54.7% of the tramadol/APAP group had >30% reduction in PVA scores compared with 39.5% of the placebo group (P = 0.011), and 44.1% of the tramadol/APAP group had >50% reduction in PVA scores compared with 32.5% of the placebo group (P = 0.044).
1129
0
Tram
adol
/APA
P (n
= 1
62)
Ran
dom
ized
(n
= 3
22)
Com
plet
ed _
>1
post
rand
omiz
atio
n as
sess
men
t (n
= 1
61)
Com
plet
ed
treat
men
t (n
= 9
1)
Exclu
ded(
n =fr°
ml)
Il-r
With
drew
(n
= 70
) In
suffi
cien
t pa
in r
elie
f (n
= 3
1)
Adv
erse
eve
nt
=-
(n =
30)
Pa
tient
cho
ice
(n =
2)
Oth
er
(n =
7)
Pla
cebo
(n
= 1
60)
Com
plet
ed >
1 )o
stra
ndom
izat
ion
asse
ssm
ent
(n =
157
)
Com
plet
ed
treat
men
t (n
= 7
4)
Excl
uded
fro
m I
-IF
(n =
3)
I W
ithdr
ew (
n =
83)
Insu
ffici
ent
pain
rel
ief
(n =
59)
A
dver
se e
vent
-~
(n
= 9
) Pa
tient
cho
ice
(n =
5)
Prot
ocol
vio
latio
n (n
= 2
) O
ther
(n
= 8
)
r-
N -H
"r
C
-H %
Figu
re 2
. P
atie
nt d
ispo
sitio
n.
AP
AP
= a
ceta
min
ophe
n;
ITT
= in
tent
-to-
trea
t.

G.E. Ruoff et al.
Table I. Demographic and baseline pain characteristics.
Tramadol/APAP Placebo (n-- 161) (n = 157)
Age <65 years, no. (%) 128 (79.5) 123 (78.3) >_65 years, no. (%) 33 (20.5) 34 (21.7) Mean (SD) 53.6 (I 1.9) 54.1 (I 2.0)
Sex, no. (%) Female 108 (67.1) 93 (59.2) Male 53 (32.9) 64 (40.8)
Race, no. (%) White 148 (91.9) 139 (88.5) Black 13 (8. I) 17 (I 0.8) Asian 0 (0) I (0.6)
PVA scale score, mean (SD), mm 7 I. I (14.5) 68.8 (I 4.9)
APAP -- acetaminophen; PVA = pain visual analog (scale from 0 to 100 mm).
• Tramadol/APAP (n = 158) [ ] Placebo (n = 153)
80-
71.1
E E
v
0
r -
¢)
70-
60-
50-
40-
30
~ Q Q
44.4
52.3
I I Baseline Final Visit
Figure 3. Mean pain visual analog (PVA) scale scores (scale from 0 to 100 mm) at base- line and the final visit. APAP = acetaminophen. *P = 0.015 versus placebo.
1131
CLINICAL THERAPEUTICS ~
Table II. Short-Form McGill Pain Questionnaire scores.*
No. of Baseline, Final Visit, Change, Category/Treatment Patients Mean (SD) Mean (SD) Mean (SD) P
Sensory component Tramadol/APAP 151 15,5 (7.4) Placebo 142 14. I (6,8)
Affective component Tramadol/APAP 152 4.4 (3,3) Placebo 142 4.0 (3.3)
Present pain index Tramadol/APAP 141 2.8 (0.9) Placebo 140 2,9 (0,9)
Total score Tramadol/APAP 151 19,9 ( t 0, I Placebo 142 18. I (9.6)
9.0 (7,6) -6.5 (8.7) 0.011 10.6 (7.9) -3,5 (7,8)
2.5 (3.0) -I,9 (3.7) 0.235 2.7 (3.1) 1.3 (2.9)
1.7 (I.3) - I . I ( I .3) 21 ( I , t ) -0.8 (t.2)
O.Oll
) I 1.6 (10.3) 8.4 (I t.8) 0.021 13.3 (I 0.6) 4 . 8 (9.9)
APAP = acetaminophen. "Pain descriptors were rated as follows: 0 = none, I = mild, 2 = moderate, 3 = severe. Present pain was rated on an index from 0 = no pain to 5 = excruciating. Higher overall scores indicate increased pain and reduced quality of life.
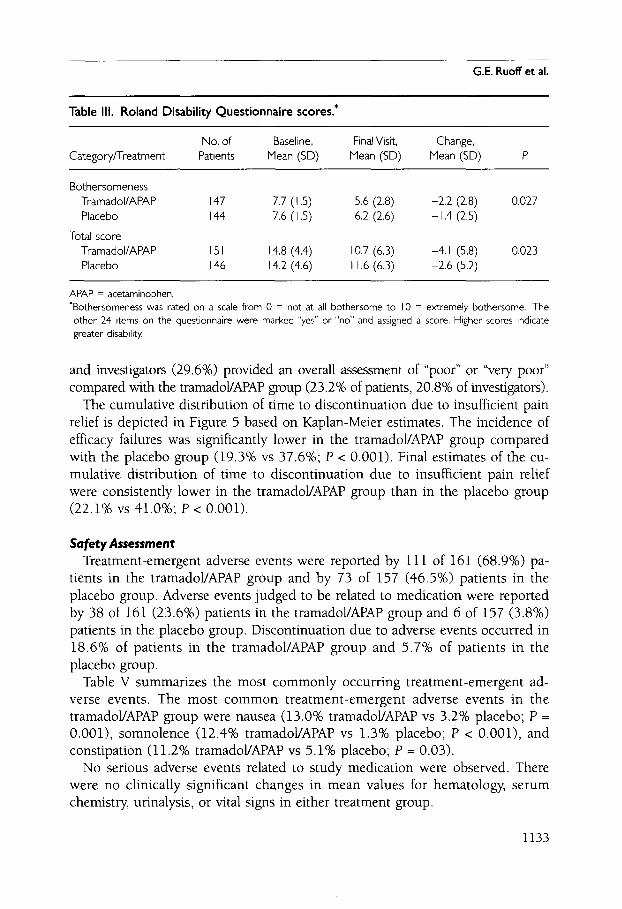
Table III summarizes RDQ scores at baseline, scores at the final visit, and the change from baseline to the final visit. The mean baseline bothersomeness scores and total scores were similar between groups. The tramadol/APAP group had a significantly greater improvement in bothersomeness score (P = 0.027) and total score (P = 0.023) compared with the placebo group.
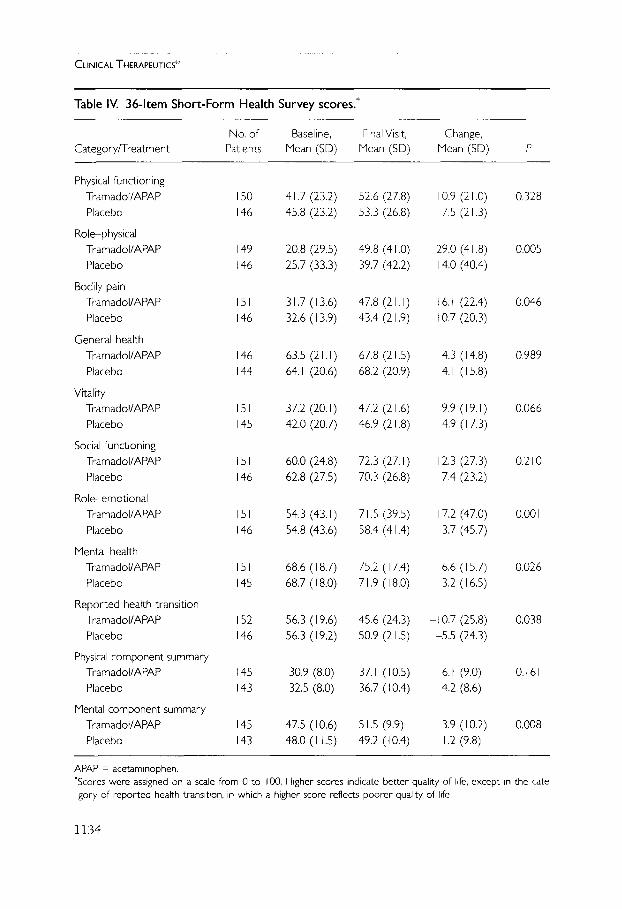
Table 1V summarizes SF-36 scores at baseline and the final visit, and the change from baseline to the final visit. For every subcategory of the SF-36, mean im- provements from baseline were greater in the tramadol/APAP group than in the placebo group. These changes were statistically significant for the subcategories of role-physical (P = 0.005), bodily pain (P = 0.046), role-emotional (P = 0.001), mental health (P = 0.026), reported health transition (P = 0.038), and mental component summary (P = 0.008).
The overall assessments of study medication by patients (P < 0.001) and inves- tigators (P = 0.002) were significantly more positive for the tramadol/APAP group than for the placebo group (Figure 4). A greater proportion of patients (60.2%) and investigators (61.0%) provided an overall assessment of "good" or "very good" for tramadoVAPAP compared with placebo (35.6% of patients, 37.9% of investi- gators). Conversely, in the placebo group, a greater proportion of patients (37.0%)
1132
G.E. Ruoff et al.
Table III. Roland Disability Questionnaire scores.*
No. of Baseline, Final Visit, Change, Category/Treatment Patients Mean (SD) Mean (SD) Mean (SD) P
Bothersomeness Tramadol/APAP 147 7.7 (I.5) 5.6 (2.8) -2.2 (2.8) Placebo 144 7.6 (I .5) 6.2 (2.6) -1.4 (2.5)
Total score Tramadol/APAP 151 14.8 (4.4) 10.7 (6.3) -4. I (5.8) Placebo 146 14.2 (4.6) 11.6 (6.3) -2.6 (5.2)
0.027
0.023
APAP = acetaminophen. "Bothersomeness was rated on a scale from 0 = not at all bothersome to 10 = extremely bothersome. The other 24 items on the questionnaire were marked "yes" or "no" and assigned a score. Higher scores indicate greater disability.
and investigators (29.6%) provided an overall assessment of "poor" or "very poor" compared with the tramadol/APAP group (23.2% of patients, 20.8% of investigators).
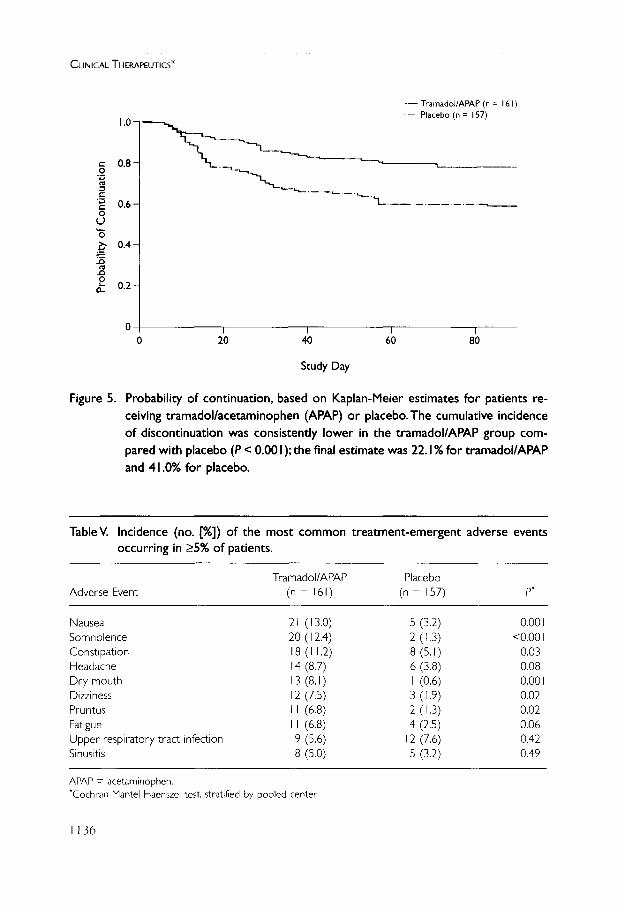
The cumulative distribution of time to discontinuation due to insufficient pain relief is depicted in Figure 5 based on Kaplan-Meier estimates. The incidence of efficacy failures was significantly lower in the tramadol/APAP group compared with the placebo group (19.3% vs 37.6%; P < 0.001). Final estimates of the cu- mulative distribution of time to discontinuation due to insufficient pain relief were consistently lower in the tramadol/APAP group than in the placebo group (22.1% vs 41.0%; P < 0.001).
Safety Assessment Treatment-emergent adverse events were reported by 111 of 161 (68.9%) pa-
tients in the tramadol/APAP group and by 73 of 157 (46.5%) patients in the placebo group. Adverse events judged to be related to medication were reported by 38 of 161 (23.6%) patients in the tramadol/APAP group and 6 of 157 (3.8%) patients in the placebo group. Discontinuation due to adverse events occurred in 18.6% of patients in the tramadol/APAP group and 5.7% of patients in the placebo group.
Table V summarizes the most commonly occurring treatment-emergent ad- verse events. The most common treatment-emergent adverse events in the tramadol/APAP group were nausea (13.0% tramadol/APAP vs 3.2% placebo; P = 0.001), somnolence (12.4% tramadol/APAP vs 1.3% placebo; P < 0.001), and constipation (11.2% tramadol/APAP vs 5.1% placebo; P = 0.03).
No serious adverse events related to study medication were observed. There were no clinically significant changes in mean values for hematology, serum chemistry, urinalysis, or vital signs in either treatment group.
1133
CLINICAL THERAPEUTICS ~":
Table IV. 36-Item Short-Form Health Survey scores.*
No. of Baseline, Final Visit, Change, Category/Treatment Patients Mean (SD) Mean (SD) Mean (SD) P
Physical functioning Tramadol/APAP 150 41.7 (23.2) 52.6 (27.8) Placebo 146 45.8 (23.2) 53.3 (26.8)
Role-physical Tramadol/APAP 149 20.8 (29.5) 49.8 (41.0) Placebo t46 25.7 (33.3) 39.7 (42.2)
Bodily pain Tramadol/APAP 151 31.7 (I 3.6) 47.8 (2 I. I) Placebo 146 32.6 (I 3.9) 43.4 (21.9)
General health Tramadol/APAP 146 63.5 (21,1) 67.8 (21.5) Placebo 144 64.1 (20.6) 68.2 (20.9)
Vitality Tramadol/APAP 151 37.2 (20. I) 47.2 (21.6) Placebo 145 42.0 (20.7) 46.9 (21.8)
Social functioning Tramadol/APAP 151 60.0 (24.8) 72.3 (27. I) Placebo 146 62.8 (27.5) 70,3 (26.8)
Role-emotional Tramadol/APAP 151 54,3 (43. l) 71.5 (39.5) Placebo 146 54.8 (43.6) 58.4 (41.4)
Mental health Tramadol/APAP 151 68.6 (I 8.7) 75.2 (17.4) Placebo 145 68.7 (I 8.0) 71.9 (18.0)
Reported health transition Tramadol/APAP 152 56.3 (I 9.6) 45.6 (24.3) Placebo 146 56.3 (I 9.2) 50.9 (21.5)
Physical component summary Tramadol/APAP 145 30.9 (8.0) 37.1 (10.5) Placebo 143 32.5 (8.0) 36.7 (10.4)
Mental component summary Tramadol/APAP 145 47.5 (I 0.6) 51.5 (9.9) Placebo 143 48.0 (I 1.5) 49.2 (I 0.4)
i0.9 (21.0) 75 (21,3)
29.0 (41.8) 4.0 (40.4)
6.1 (22.4) 0.7 (20.3)
4.3 (I 4.8) 4.1 (15.8)
9.9 (19.1) 419 (I 7.3)
2.3 (27,3) 7,4 (23.2)
7.2 (47.0) 3.7 (45.7)
6,6 (I 5.7) 3.2 (I 6.5)
--1017 (25 '8) -5.5 (24.3)
6. I (9.0) 4.2 (8.6)
3.9 (10.2) 1.2 (9.8)
0,328
0.005
0.046
0,989
0.066
0.210
0.001
0.026
0.038
0.161
0.008
APAP -- acetaminophen. "Scores were assigned on a scale from 0 to 100, Higher scores indicate better quality of life, except in the cate gory of reported health transition, in which a higher score reflects poorer quality of life.
1134

G.E. Ruoff et al.
A 401 3O
.= t- O o.
24.0
Very Poor Poor
27.4
N o Change
99 1
• Tramadol/APAP (n = I 5 I) [ ] Placebo (n = 146)
31.1
Good Very Good
o£
40 t 3O
.= t-
O 20 17.9
10- 11.7
32.4
0 - I I Very Poor Poor N o Change
29.5
• Tramadol/APAP (n = 149) [ ] Placebo (n = 145)
31.5
t Good Very Good
Figure 4. Overall assessments of medication by (A) patients and (B) investigators in the intent-to-treat population.Tramadol/APAP was superior to placebo based on the proportions assessing medication "good" or "very good" (patients' assess- ment, P < 0.001 ; investigators' assessment, P = 0.002). APAP = acetaminophen.
D I S C U S S I O N In this long-term (3-month) study of the treatment of chronic lower back pain, tramadol/APAP combination therapy was associated with a significant reduction in pain, a significant increase in pain relief, and a favorable assessment of treat- ment by both patients and physicians. Additionally, fewer patients in the tramadol/ APAP group compared with the placebo group withdrew due to insufficient pain relief (31 vs 59, respectively). Furthermore, the favorable responder analyses
1135
C L I N I C A L THERAPEUTICS '~
1.0-
= 0.8- 0
c
~ o . s - 0 u
"6 ~ o.4-
. .o
2 0.2-
Figure 5.
- - T ramado l /APAP (n = 161 )
- - - - Placebo (n = 157)
I I I I 0 20 40 60 80
Study Day
Probability of continuation, based on Kaplan-Meier estimates for patients re- ceiving tramadol/acetaminophen (APAP) or placebo.The cumulative incidence of discontinuation was consistently lower in the tramadol/APAP group com- pared with placebo (P < 0.00 I); the final estimate was 22. 1% for tramadol/APAP and 41.0% for placebo.
TableV. Incidence (no. [%]) of the most common treatment-emergent adverse events occurring in >5% of patients.
Tramadol/APAP Placebo Adverse Event (n -- 161) (n -- 157) P"
Nausea 21 (13.0) 5 (3.2) 0.001 Somnolence 20 (I 2.4) 2 (I.3) <0,001 Constipation 18 (I 1.2) 8 (5, I) 0.03 Headache 14 (8.7) 6 (3.8) 0.08 Dry mouth 13 (8.1) I (0.6) 0.001 Dizziness 12 (7.5) 3 (I .9) 0.02 Pruritus II (6.8) 2 (I.3) 0.02 Fatigue II (6.8) 4 (2.5) 0,06 Upper respiratory tract infection 9 (5.6) 12 (7.6) 0.42 Sinusitis 8 (5.0) 5 (3.2) 0.49
APAP = acetaminophen. "Cochran-ManteI-Haenszel test, stratified by pooled center.
1136
G.E. Ruoff et al.
based on PVA scores are consistent with a clinically meaningful response, as de- scribed by Farrar et al. 34 To our knowledge, this is the first report to demonstrate that tramadol 37.5 mg/APAP 325 mg combination tablets are an effective long- term treatment for chronic lower back pain. Combining 2 centrally acting anal- gesics having multiple mechanisms of action that address both nociceptive and non-nociceptive pain successfully reduced lower back pain, a condition that can have an imprecise pathophysiology and can be refractory to treatment.
The results of this study also indicate that in addition to relieving pain, treatment with tramadol/APAP had a positive effect on patients' quality of life. One of the most common reasons for repeated office visits in patients with chronic lower back pain is their difficulty in performing daily tasks. 35 The tramadol/APAP group had significantly better scores on the RDQ, which measures improvements in function, compared with the placebo group. Results on several subcategories of the SF-MPQ and SF-36 also in- dicated that the tramadol/APAP group had significant improvements in emotional and mental health. Both physical and psychological factors such as these can play an im- portant role in chronic lower back pain 4,36 and can determine the rapidity with which patients are able to return to normal activities, both at work and at home. In spite of the broad range of outcomes measured and the clinically important benefits observed, the well-defined population included in this study may limit the ability to generalize from the results. Studies that include patients with associated neurologic deficits (eg, in their lower extremities) would further explore the clinical utility of this medication.
By combining 2 centrally acting analgesics, it was possible to keep the dosage of each medication relatively low (mean 4.2 tramadol/APAP tablets/d = 157.5 mg tramadol/1365 mg APAP). Efficacy at these dosages may be attributable to the synergistic effects of tramadol on mu-opioid receptors and monoamine trans- porters, 37 the "self-synergistic" effects of APAP on spinal and supraspinal pain pathways, 38 or the combination of these mechanisms. The observed improve- ments in quality of life reflect the low incidence of medication-related adverse events with the tramadol 37.5 mg/APAP 325 mg combination tablets. No serious adverse events related to study medication were reported; the most commonly re- ported adverse events were nausea, somnolence, and constipation.
The safety profile observed in this study is consistent with the results of previ- ous studies of tramadol/APAP in which the combination demonstrated a favor- able safety profile, as well as a favorable efficacy profile, in both acute and chronic pain. 31-33'39--43 In a recent study, 39 the combination also showed comparable effi- cacy to hydrocodone/APAP (10 mg/650 mg) for moderate to severe dental pain, with reduced rates of nausea (18% tramadol/APAP vs 36% hydrocodone/APAP) and vomiting (12% tramadol/APAP vs 30% hydrocodone/APAP). Tramadol/APAP has also shown comparable efficacy to codeine/APAP for chronic lower back pain and/or joint pain, with reduced rates of constipation (11% tramadol/APAP vs 21% codeine/APAP) and somnolence (17% tramadol/APAP vs 24% codeine/APAP). 32
1137

CLINICAL THERAPEUTICS :~
C O N C L U S I O N S Additional pharmacologic options for the treatment of chronic lower back pain are needed. NSAIDs may be effective for short-term treatment of acute lower back pain; however, there is insufficient evidence of their efficacy in chronic back pain. The results of this randomized, double-blind, placebo-controlled study suggest that the tramadol 37.5 mg/APAP 325 mg combination tablet is an effective ther- apy for the treatment of chronic lower back pain with a favorable safety profile. In the population studied, it relieved pain and improved scores on measures of functioning and quality of life.
A C K N O W L E D G M E N T S Members of the CAPSS-112 Study Group were: David Gilbert Borenstein, MD, Washington, DC; Jennifer Jericho Capezio, MD, Lake Forest, Illinois; Robert G. Cesarec, MD, Wauwatosa, Wisconsin; Mark P. Ettinger, MD, FACR, Stuart and Lake Worth, Florida; Darrell N. Fiske, MD, Stuart and Lake Worth, Florida; W. Thomas Garland, Jr., MD, FACC, Lawrenceville, New Jersey; Ellen J. Gelles, MD, Chicago, Illinois; Larry I. Gilderman, DO, Pembroke Pines, Florida; Geoffrey 5. Gladstein, MD, Stamford, Connecticut; Oscar S. Gluck, MD, FACE FACR, Phoenix, Arizona (replaced by John Tesser, MD, Phoenix, Arizona); William L. Gray, MD, Spokane, Washington; Warren E. Greth, MD, West Reading, Pennsyl- vania; Rodney J. Johnson, MD, Bellevue, Washington; Shelly P. Kafka, MD, Rochester, New York (replaced by Keith G. Pryhuber, MD, Rochester, New York); Alan Kivitz, MD, Duncansville, Pennsylvania; Michael D. Kohen, MD, South Day- tona, Florida; John Claude Krusz, MD, PhD, Dallas, Texas; Lawrence V. Larsen, MD, PhD, Salt Lake City, Utah; Michael 5. Maehara, MD, Long Beach, California; Robert B. Nett, Jr., MD, RPh, San Antonio, Texas; Howard L. Offenberg, Daytona Beach, Florida; Robert Zorba Paster, MD, Oregon, Wisconsin; Dianne Lynn Petrone, MD, Dallas, Texas; Bruce G. Rankin, DO, DeLand, Florida; Sanford H. Roth, MD, Phoenix, Arizona; Gary E. Ruoff, MD, Kalamazoo, Michigan; Cynthia Schloss-Guy, MD, St. Louis, Missouri; Stuart L. Silverman, MD, FACE FACR, Bev- erly Hills, California; Sheldon Solomon, MD, FACE Cherry Hill, New Jersey; and Barbara A. Tyler, MD, Bryan, Texas.
REFERENCES 1. Frymoyer JW, Cats-Baril WL. An overview of the incidences and costs of low back
pain. Orthop Clin North Am. 1991;22:263-271. 2. Hashemi L, Webster BS, Clancy EA. Trends in disability duration and cost of workers'
compensation low back pain claims (1988-1996).J Occup Environ Med. 1998;40:1110-1119. 3. Deyo RA, Weinstein JN. Low back pain. N Engl J Med. 2001;344:363-370. 4. Borenstein DG. Epidemiology, etiology, diagnostic evaluation, and treatment of low
back pain. Curt Opin Rheumatol. 2001;13:128-134.
1138
G.E. Ruoff et al.
5. Deyo RA. Drug therapy for back pain: Which drugs help which patients? Spine. 1996;21:2840-2850.
6. Atkinson JH, Slater MA, Williams RA, et al. A placebo-controlled randomized clini- cal trial of nortriptyline for chronic low back pain. Pain. 1998;76:287-296.
7. Pheasant H, Bursk A, Goldfarb J, et al. Amitriptyline and chronic low-back pain. A randomized double-blind crossover study. Spine. 1983;8:552-557.
8. Ward NG. Tricyclic antidepressants for chronic low-back pain. Mechanisms of action and predictors of response. Spine. 1986;11:661-665.
9. Muller FO, Odendaal CL, Muller FR, et al. Comparison of the efficacy and tolerabil- ity of a paracetamol/codeine fixed-dose combination with tramadol in patients with refractory chronic back pain. Arzneimittelforschung. 1998;48:675-679.
10. Schnitzer TJ, Gray WL, Paster RZ, Kamin M. Efficacy of tramadol in treatment of chronic low back pain. J Rheumatol. 2000;27:772-778.
11. van Tulder MW, Scholten RJ, Koes BW, Deyo RA. Nonsteroidal anti-inflammatory drugs for low back pain: A systematic review within the framework of the Cochrane Collaboration Back Review Group. Spine. 2000;25:2501-2513.
12. Raffa RB, Friderichs E, Reimann W, et al. Opioid and nonopioid components inde- pendently contribute to the mechanism of action of tramadol, an 'atypical' opioid an- algesic. J Pharmacol Exp Ther. 1992;260:275-285.
13. Roth SH. Efficacy and safety of tramadol HC1 in breakthrough musculoskeletal pain attributed to osteoarthritis. J Rheumatol. 1998;25:1358-1363.
14. Fleischmann RM, Caldwell JR, Roth SH, et al. Tramadol for the treatment of joint pain associated with osteoarthritis: A randomized, double-blind, placebo-controlled trial. Curr Ther Res Clin Exp. 2001;62:113-128.
15. Tarradell R, Pol O, Farre M, et al. Respiratory and analgesic effects of meperidine and tramadol in patients undergoing orthopedic surgery. Methods Find Exp Clin Pharma- col. 1996;18:211-218.
16. Moore PA, Crout RJ, Jackson DL, et al. Tramadol hydrochloride: Analgesic efficacy compared with codeine, aspirin with codeine, and placebo after dental extraction. J Clin Pharmacol. 1998;38:554-560.
17. Harati Y, Gooch C, Swenson M, et al. Double-blind randomized trial of tramadol for the treatment of the pain of diabetic neuropathy. Neurology. 1998;50:1842- 1846.
18. Harati Y, Gooch C, Swenson M, et al. Maintenance of the long-term effectiveness of tramadol in treatment of the pain of diabetic neuropathy. J Diabetes Complications. 2000; 14:65-70.
19. American Medical Directors Association. Chronic Pain Management in the Long-Term Care Setting: Clinical Practice Guideline. Baltimore, Md: American Medical Directors Association; 1999.
20. Flower RJ, Vane JR. Inhibition of prostaglandin synthetase in brain explains the anti- pyretic activity of paracetamol (4-acetamidophenol). Nature. 1972;240:410-411.
1139
CLINICAL THERAPEUTICS ~
21. Bjorkman R. Central antinociceptive effects of non-steroidal anti-inflammatory drugs and paracetamol. Experimental studies in the rat. Acta Anaesthesiol Stand Suppl. 1995; 103:1-44.
22. Ferrari RA, Ward SJ, Zobre CM, et al. Estimation ot the in vivo effect of cyclooxygen- ase inhibitors on prostaglandin E 2 levels in the mouse brain. EurJ Pharmacol. 1990; 179:25-34.
23. Bannwarth B, Demotes-Mainard E Schaeverbeke T, et al. Central analgesic effects of aspirin-like drugs. Fundarn Clin Pharmacol. 1995;9:1-7.
24. Bjorkman R, Hallman KM, Hedner J, et al. Acetaminophen blocks spinal hyperalge- sia induced by NMDA and substance P Pain, 1994;57:259-264.
25. Hunskaar S, Fasmer OB, Hole K. Acetylsalicylic acid, paracetamol and morphine in- hibit behavioral responses to intrathecally administered substance P or capsaicin. Life Sci. 1985;37:1835-1841.
26. Walker JS. NSAID: An update on their analgesic effects. Clin Exp Pharmacol Physiol. 1995;22:855-860.
27. Muth-Selbach US, Tegeder 1, Brune K, Geisslinger G. Acetaminophen inhibits spinal prostaglandin E 2 release after peripheral noxious stimulation. Anesthesiology. 1999;91: 231-239.
28. Raffa RB, Friderichs E. The basic science aspect of tramadol hydrochloride. Pain Rev. 1996;3:249-271.
29. Raffa RB. Pharmacology of oral combination analgesics: Rational therapy for pain. ] Clin Pharm Ther. 2001;26:257-264.
30. Tallarida RJ, Raffa RB. Testing for synergism over a range of fixed ratio drug combi- nations: Replacing the isobologram. Life Sci. 1996;58:PL23-PL28.
31. Medve RA, Wang J, Karim R. Tramadol and acetaminophen tablets for dental pain. Anesth Prog. 2001;48:79-81.
32. Mullican WS, Lacy JR. Tramadol/acetaminophen combination tablets and codeine/ acetaminophen combination capsules for the management of chronic pain: A compara- tive trial. Clin The~ 2001;23:1429-1445.
33. Silverfield JC, Kamin M, Wu SC, Rosenthal N. Tramadol/acetaminophen combination tablets for the treatment of osteoarthritis flare pain: A multicenter, outpatient, ran- domized, double-blind, placebo-controlled, parallel-group, add-on study. Clin Ther 2002;24:282-297.
34. Farrar JT, Portenoy RK, Berlin JA, et al. Defining the clinically important difference in pain outcome measures. Pain. 2000;88:287-294.
35. McPhillips-Tangum CA, Cherkin DC, Rhodes LA, Markham C. Reasons for repeated medi- cal visits among patients with chronic back pain. J Gen Intern Med. 1998; 13:289-295.
36. Spengler DM, Bigos SJ, Martin NA, et al. Back injuries in industry: A retrospective study. I. Overview and cost analysis. Spine. 1986; 11:241-245.
37. Raffa RB, Friderichs E, Reimann W, et al. Complementary and synergistic antinoci- ceptive interaction between the enantiomers of tramadol. J Pharmacol Exp Ther. 1993;267:331-340.
1140
G.E. Ruoff et al.
38. Raffa RB, Stone DJ Jr, Tallarida RJ. Discovery of "self-synergistic" spinal/supraspinal antinociception produced by acetaminophen (paracetamol). J Pharmacol Exp Thee 2000;295:291-294.
39. Fricke JR Jr, Karim R, Jordan D, Rosenthal N. A double-blind, single-dose comparison of the analgesic efficacy of tramadol/acetaminophen combination tablets, hydrocodone/ acetarninophen combination tablets, and placebo after oral surgery. Clin Ther. 2002;24: 953-968.
40. Bennett RM, Kamin M, Karim R, Rosenthal N. Tramadol and acetaminophen combi- nation tablets in the treatment of fibromyalgia pain: A double-blind, randomized, placebo-controlled study. Am J Med. In press.
41. Peloso P, Fortin L, Beaulieu A. Tramadol and acetaminophen combination tablets (ULTRACET TM) for the treatment of chronic lower back pain: A multicenter, outpatient, randomized, double-blind, placebo-controlled study. J Pain. 2002;3(Suppl 1): 14. Abstract.
42. Rosenthal N, Kamin M, Jordan D, Wu S-C. Efficacy and safety of tramadol/acetaminophen tablets (ULTRACET TM) as add-on therapy for osteoarthritis in patients taking COX-2 NSAIDs: A multicenter, outpatient, randomized, double-blind, placebo-controlled study. J Pain. 2002;3(Suppl 1): 10. Abstract.
43. Rosenthal N, Wu S, Jordan D. Combination tramadol and acetaminophen tablets (ULTRACET TM) for the treatment of pain associated with osteoarthritis flare in an el- derly population. J Am Geriatr Soc. 2002;50:$145. Abstract.
Address correspondence to: Gary E. Ruoff, MD, Medical Director, Clinical Research, Westside Family Medical Center, 6565 West Main Street, Kalamazoo, MI 49009.
1141




















